
JBP - Volume 42, number 3, May-June 2016
86
www.jbp.org.br ISSN 1806-3713 Volume 42, Number 3 May | June 2016 HIGHLIGHT Volume 42, Number 3 May | June 2016 COPD and cardiovascular disease Spontaneous pneumothorax Videoassisted thoracoscopy: the Brazilian experience
-
Upload
jornal-brasileiro-pneumologia -
Category
Documents
-
view
287 -
download
16
description
JBP - Volume 42, number 3, May-June - 2016. The Brazilian Journal of Pulmonology publishes scientific articles that contribute to the improvement of knowledge in the field of the lung diseases and related areas
Transcript of JBP - Volume 42, number 3, May-June 2016

www.jbp.org.br
ISSN 1806-3713
Volume 42, Number 3May | June2016
HIGHLIGHT
Vo
lum
e 4
2, N
um
be
r 3
M
ay | J
un
e
2
016
COPD andcardiovascular disease
Spontaneous pneumothorax
Videoassisted thoracoscopy: the
Brazilian experience

ISSN 1806-3713
Published once every two months J Bras Pneumol. v.42, number 3, p. 163-236 May/June 2016
Publicação Indexada em:Latindex, LILACS, Scielo Brazil, Scopus, Index Copernicus, ISI Web ofKnowledge, MEDLINE ePubMed Central (PMC)
Disponível eletronicamente nas versões português e inglês:www.jornaldepneumologia.com.br e www.scielo.br/jbpneu
Associação Brasileirade Editores Científicos
I N T E R N A T I O N A L
EDITOR-IN-CHIEFRogerio Souza - Universidade de São Paulo, São Paulo - SP
EXECUTIVE EDITORSBruno Guedes Baldi - Universidade de São Paulo, São Paulo - SPCaio Júlio Cesar dos Santos Fernandes - Universidade de São Paulo - São Paulo - SPCarlos Roberto Ribeiro de Carvalho - Universidade de São Paulo, São Paulo - SPCarlos Viana Poyares Jardim - Universidade de São Paulo, São Paulo - SP
ASSOCIATE EDITORSAfrânio Lineu Kritski - Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJÁlvaro A. Cruz - Universidade Federal da Bahia, Salvador, BAAndre Luis Pereira de Albuquerque - Universidade de São Paulo - São Paulo - SPAscedio Jose Rodrigues - Universidade de São Paulo - São Paulo - SPBruno Hochhegger - Universidade Federal do Rio Grande do Sul - Porto Alegre – RSEdson Marchiori - Universidade Federal Fluminense, Niterói - RJFernanda Carvalho de Queiroz Mello - Universidade Federal do Rio de Janeiro - Rio de Janeiro - RJGilberto de Castro Junior - Universidade de São Paulo, São Paulo - SPGiovanni Battista Migliori - Director WHO Collaborating Centre for TB and Lung Diseases, Fondazione S. Maugeri, Care and Research Institute, Tradate, ItalyIrma de Godoy - Universidade Estadual Paulista, Botucatu - SPMarcelo Alcântara Holanda - Universidade Federal do Ceará - Fortaleza - CEOliver Augusto Nascimento - Universidade Federal de São Paulo - São Paulo - SPPedro Caruso - Universidade de São Paulo - São Paulo - SPPedro Rodrigues Genta - Universidade de São Paulo - São Paulo - SPRenato Tetelbom Stein - Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre - RSRicardo de Amorim Corrêa - Universidade Federal de Minas Gerais - Belo Horizonte - MGRicardo Mingarini Terra - Universidade de São Paulo - São Paulo - SPSimone Dal Corso - Universidade Nove de Julho - São Paulo - SPUbiratan de Paula Santos - Universidade de São Paulo, São Paulo - SPVeronica Amado - Universidade de Brasília, Brasília - DF
EDITORIAL COUNCILAlberto Cukier - Universidade de São Paulo, São Paulo - SPAna C. Krieger - New York School of Medicine, New York - USAAna Luiza Godoy Fernandes - Universidade Federal de São Paulo, São Paulo - SPAntonio Segorbe Luis - Universidade de Coimbra, Coimbra - PortugalBrent Winston - Department of Critical Care Medicine, University of Calgary, Calgary - CanadaCarlos Alberto de Assis Viegas - Universidade de Brasília, Brasília - DFCarlos Alberto de Castro Pereira - Universidade Federal de São Paulo, São Paulo - SPCarlos M. Luna - Hospital de Clinicas, Universidad de Buenos Aires, Buenos Aires - ArgentinaCarmen Silvia Valente Barbas - Universidade de São Paulo, São Paulo - SPCelso Ricardo Fernandes de Carvalho - Universidade de São Paulo, São Paulo - SPChris T. Bolliger - University of Stellenbosch, Stellenbosch - South AfricaDany Jasinowodolinski - Universidade Federal de São Paulo, São Paulo - SPDenis Martinez - Universidade Federal do Rio Grande do Sul, Porto Alegre - RSDouglas Bradley - University of Toronto, Toronto, ON - CanadáEmílio Pizzichini - Universidade Federal de Santa Catarina, Florianópolis - SCFábio Biscegli Jatene - Universidade de São Paulo, São Paulo - SPFrank McCormack - University of Cincinnati School of Medicine, Cincinnati, OH - USAGeraldo Lorenzi - Filho - Universidade de São Paulo, São Paulo - SPGustavo Rodrigo - Departamento de Emergencia, Hospital Central de las Fuerzas Armadas, Montevidéu - UruguayIlma Aparecida Paschoal - Universidade de Campinas, Campinas - SPIsabela C. Silva - Vancouver General Hospital, Vancouver, BC - CanadáJ. Randall Curtis - University of Washington, Seattle, Wa - USAJohn J. Godleski - Harvard Medical School, Boston, MA - USAJosé Alberto Neder - Universidade Federal de São Paulo, São Paulo - SPJosé Antonio Baddini Martinez - Universidade de São Paulo, Ribeirão Preto - SPJosé Dirceu Ribeiro - Universidade de Campinas, Campinas - SPJosé Miguel Chatkin - Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre - RSJosé Roberto de Brito Jardim - Universidade Federal de São Paulo, São Paulo - SPJosé Roberto Lapa e Silva - Universidade Federal do Rio de Janeiro, Rio de Janeiro - RJKevin Leslie - Mayo Clinic College of Medicine, Rochester, MN - USALuiz Eduardo Nery - Universidade Federal de São Paulo, São Paulo - SPMarc Miravitlles - Hospital Clinic, Barcelona - EspañaMarisa Dolhnikoff - Universidade de São Paulo, São Paulo - SPMarli Maria Knorst - Universidade Federal do Rio Grande do Sul, Porto Alegre - RSMauro Musa Zamboni - Instituto Nacional do Câncer, Rio de Janeiro - RJNestor Muller - Vancouver General Hospital, Vancouver, BC - CanadáNoé Zamel - University of Toronto, Toronto, ON - CanadáPaul Noble - Duke University, Durham, NC - USAPaulo Francisco Guerreiro Cardoso - Universidade de São Paulo, São Paulo - SPPaulo Pego Fernandes - Universidade de São Paulo, São Paulo - SPPeter J. Barnes - National Heart and Lung Institute, Imperial College, London - UKRenato Sotto - Mayor - Hospital Santa Maria, Lisboa - PortugalRichard W. Light - Vanderbili University, Nashville, TN, USARik Gosselink - University Hospitals Leuven - BélgicaRobert Skomro - University of Saskatoon, Saskatoon - CanadáRubin Tuder - University of Colorado, Denver, CO - USASérgio Saldanha Menna - Barreto - Universidade Federal do Rio Grande do Sul, Porto Alegre - RSSonia Buist - Oregon Health & Science University, Portland, OR - USATalmadge King Jr. - University of California, San Francisco, CA - USAThais Helena Abrahão Thomaz Queluz - Universidade Estadual Paulista, Botucatu - SPVera Luiza Capelozzi - Universidade de São Paulo, São Paulo - SP
ISSN 1806-3713
Expe
dien
teBRAZILIAN THORACIC SOCIETYOffice: SCS Quadra 01, Bloco K, Asa Sul, salas 203/204. Edifício Denasa, CEP 70398-900, Brasília, DF, Brazil. Tel. +55 61 3245-1030/+55 0800 616218. Website: www.sbpt.org.br. E-mail: [email protected]
The Brazilian Journal of Pulmonology (ISSN 1806-3713) is published once every two months by the Brazilian Thoracic Society (BTS). The statements and opinions contained in the editorials and articles in this Journal are solely those of the authors thereof and not of the Journal’s Editor-in-Chief, peer reviewers, the BTS, its officers, regents, members, or employees. Permission is granted to reproduce any figure, table, or other material published in the Journal provided that the source for any of these is credited.
BTS Board of Directors (2015-2016 biennium):President: Dr. Renato Maciel - MGSecretary-General: Dr. Paulo Henrique Ramos Feitosa - DFDirector, Professional Advocacy: Dr. Jose Eduardo Delfini Cançado - SPCFO: Dr. Saulo Maia Davila Melo - SEScientific Director: Dr. Miguel Abidon Aide - RJDirector, Education and Professional Practice: Dr. Clystenes Odyr Soares Silva - SPDirector, Communications: Dra. Simone Chaves Fagondes - RSPresident, BTS Congress 2016: Marcus Barreto Conde - RJPresident Elect (2017/2018 biennium): Fernando Luiz Cavalcanti Lundgren - PEChairman of the Board: Jairo Sponholz Araújo (PR)
AUDIT COMMITTEE:Active Members: Clóvis Botelho (MT), Benedito Francisco Cabral Júnior (DF), Rafael de Castro Martins (ES)Alternates: Maurício Meireles Góes (MG), Alina Faria França de Oliveira (PE), Paulo Cesar de Oliveira (MG)
COORDINATORS, BTS DEPARTMENTS:Programmatic Initiatives – Alcindo Cerci Neto (PR)Thoracic Surgery – Darcy Ribeiro Pinto Filho (RS)Sleep–disordered Breathing – Marcelo Fouad Rabahi (GO)Respiratory Endoscopy – Mauro Musa Zamboni (RJ)Pulmonary Function – John Mark Salge (SP)Imaging – Bruno Hochhegger (RS)Lung Diseases – Ester Nei Aparecida Martins Coletta (SP)Clinical Research – Oliver Augusto Nascimento (SP)Pediatric Pulmonology – Paulo Cesar Kussek (PR)Residency – Alberto Cukier (SP)
COORDINATORS, BTS SCIENTIFIC COMMITTEES:Asthma – Emilio Pizzichini (SC)Lung Cancer – Teresa Yae Takagaki (SP)Pulmonary Circulation – Carlos Viana Poyares Jardim (SP)Advanced Lung Disease – Dagoberto Vanoni de Godoy (RS)Interstitial Diseases – José Antônio Baddini Martinez (SP)Environmental and Occupational Respiratory Diseases – Ana Paula Scalia Carneiro (MG)COPD – Roberto Stirbulov (SP)Epidemiology – Frederico Leon Arrabal Fernandes (SP)Cystic Fibrosis – Marcelo Bicalho of Fuccio (MG)Respiratory Infections and Mycoses – Mauro Gomes (SP)Pleura – Roberta Karla Barbosa de Sales (SP)International Relations – José Roberto de Brito Jardim (SP)Smoking – Luiz Carlos Corrêa da Silva (RS)Intensive Care – Marco Antônio Soares Reis (MG)Tuberculosis – Fernanda Carvalho de Queiroz Mello (RJ)
ADMINISTRATIVE SECRETARIAT OF THE BRAZILIAN JOURNAL OF PULMONOLOGYAddress: SCS Quadra 01, Bloco K, Asa Sul, salas 203/204. Edifício Denasa, CEP 70398-900, Brasília, DF, Brazil. Tel. +55 61 3245-1030/+55 0800 616218. Assistant Managing Editor: Luana Maria Bernardes Campos. E-mail: [email protected]: 3.500 copiesDistribution: Free to members of the BTS and librariesPrinted on acid-free paper
SUPPORT:

ISSN 1806-3713
Published once every two months J Bras Pneumol. v.42, number 3, p. 163-236 May/June 2016
Con
tent
sEDITORIAL
163 - Corticosteroids for the prevention of ventilator-induced lung injury?Marcelo Alcantara Holanda
CONTINUING EDUCATION: IMAGING
164 - Multiple calcified nodulesEdson Marchiori, Gláucia Zanetti, Bruno Hochhegger
CONTINUING EDUCATION: SCIENTIFIC METHODOLOGY
165 - Choosing wisely between randomized controlled trials and observational designs in studies about interventionsJuliana Carvalho Ferreira, Cecilia Maria Patino
ORIGINAL ARTICLE
166 - Pre-treatment with dexamethasone attenuates experimental ventilator-induced lung injuryFernando Fonseca dos Reis, Maycon de Moura Reboredo, Leda Marília Fonseca Lucinda, Aydra Mendes Almeida Bianchi, Maria Aparecida Esteves Rabelo, Lídia Maria Carneiro da Fonseca, Júlio César Abreu de Oliveira, Bruno Valle Pinheiro
174 - Evaluating bronchodilator response in pediatric patients with post-infectious bronchiolitis obliterans: use of different criteria for identifying airway reversibilityRita Mattiello, Paula Cristina Vidal, Edgar Enrique Sarria, Paulo Márcio Pitrez, Renato Tetelbom Stein, Helena Teresinha Mocelin, Gilberto Bueno Fischer, Marcus Herbert Jones, Leonardo Araújo Pinto
179 - Risk factors for cardiovascular disease in patients with COPD: mild-to-moderate COPD versus severe-to-very severe COPDLaura Miranda de Oliveira Caram, Renata Ferrari, Cristiane Roberta Naves, Liana Sousa Coelho, Simone Alves do Vale, Suzana Erico Tanni, Irma Godoy
185 - Robotic pulmonary lobectomy for lung cancer treatment: program implementation and initial experienceRicardo Mingarini Terra, Pedro Henrique Xavier Nabuco de Araujo, Leticia Leone Lauricella, José Ribas Milanez de Campos, Herbert Felix Costa, Paulo Manuel Pego-Fernandes
191 - Bronchoscopic diagnostic procedures and microbiological examinations in proving endobronchial tuberculosisAbdullah Şimşek, İlhami Yapıcı, Mesiha Babalık, Zekiye Şimşek, Mustafa Kolsuz
196 - Viability of gait speed test in hospitalized elderly patientsBruno Prata Martinez, Anne Karine Menezes Santos Batista, Isis Resende Ramos, Júlio Cesar Dantas, Isabela Barboza Gomes, Luiz Alberto Forgiarini Júnior, Fernanda Rosa Warken Camelier, Aquiles Assunção Camelier

ISSN 1806-3713
Published once every two months J Bras Pneumol. v.42, number 3, p. 163-236 May/June 2016C
onte
nts
203 - The value of antibody-coated bacteria in tracheal aspirates for the diagnosis of ventilator-associated pneumonia: a case-control studyOtavio Tavares Ranzani, Daniel Neves Forte, Antonio Carlos Forte, Igor Mimica, Wilma Carvalho Neves Forte
BRIEF COMMUNICATION
211 - Analysis of the stability of housekeeping gene expression in the left cardiac ventricle of rats submitted to chronic intermittent hypoxiaGuilherme Silva Julian, Renato Watanabe de Oliveira, Sergio Tufik, Jair Ribeiro Chagas
SPECIAL ARTICLE
215 - Anatomic pulmonary resection by video-assisted thoracoscopy: the Brazilian experience (VATS Brazil study)Ricardo Mingarini Terra, Thamara Kazantzis, Darcy Ribeiro Pinto-Filho, Spencer Marcantonio Camargo, Francisco Martins-Neto, Anderson Nassar Guimarães, Carlos Alberto Araújo, Luis Carlos Losso, Mario Claudio Ghefter, Nuno Ferreira de Lima, Antero Gomes-Neto, Flávio Brito-Filho, Rui Haddad, Maurício Guidi Saueressig, Alexandre Marcelo Rodrigues Lima, Rafael Pontes de Siqueira, Astunaldo Júnior de Macedo e Pinho, Fernando Vannucci
PICTORIAL ESSAY
222 - Etiology of primary spontaneous pneumothoraxRoberto de Menezes Lyra
IMAGING IN PULMONARY MEDICINE
227 - Implications of a tracheal bronchus in a patient with thymomaLuis Gorospe, Ana Paz Valdebenito-Montecino, Ana Patricia Ovejero-Díaz
CASE REPORT
228 - Impact of long-term treatment with inhaled corticosteroids and bronchodilators on lung function in a patient with post-infectious bronchiolitis obliteransCecilia Calabrese, Nadia Corcione, Gaetano Rea, Francesco Stefanelli, Ilernando Meoli, Alessandro Vatrella
LETTER TO THE EDITOR
232 - Reversed halo sign in invasive fungal infectionsEdson Marchiori, Bruno Hochhegger, Gláucia Zanetti
233 - An old risk factor for COPD: rest in peace, 15%Paulo César Rodrigues Pinto Corrêa
CORRESPONDENCE
235 - Inhalation therapy in mechanical ventilationÂngelo Roncalli Miranda Rocha,, Caio Henrique Veloso da Costa
236 - Authors’ replyJuçara Gasparetto Maccari, Cassiano Teixeira

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562016000300001
Corticosteroids for the prevention of ventilator-induced lung injury?Marcelo Alcantara Holanda1
1. Departamento de Medicina Clínica, Universidade Federal do Ceará, Fortaleza (CE) Brasil.
Numerous pharmacological therapies for acute respiratory distress syndrome (ARDS) have failed to demonstrate a benefit in multicenter clinical trials.(1) Given that dysregulated inflammation is a prominent feature of ARDS, systemic corticosteroids are thought to represent a potentially beneficial therapy.(2)
Meta-analyses of the use of corticosteroid therapy in ARDS have yielded inconsistent conclusions. That is primarily because ARDS is a heterogeneous disease with various etiologies and clinical courses. Other factors include different outcome measures and the fact that patients are usually enrolled within 48 h after meeting the criteria for a diagnosis of ARDS, while already on mechanical ventilation, which could delay the initiation of treatment until several days after the onset of lung injury.(2)
In this issue of the JBP, Reis et al.(3) publish a very well-designed experimental study that assessed the effects of dexamethasone pre-treatment on ventilator-induced lung injury (VILI), a well-recognized and important aspect of the physiopathology of ARDS. Experimental VILI was induced in Wistar rats by means of mechanical ventilation at a high tidal volume. The rats were divided into two groups according to the previous intraperitoneal administration of dexamethasone or saline at 30 min before VILI induction. The main result of the study was
that dexamethasone administration was able to attenuate the inflammatory response caused by VILI, as measured by a histopathological lung injury score, by counting the leukocytes and neutrophils in the BAL fluid, and by assessing its impact on oxygenation at 4 h and 24 h after the initial insult (injurious ventilation). One drawback of the investigation is the lack of data on the molecular mechanisms involved in the dexamethasone-induced attenuation of experimental VILI.(4)
Corticosteroids continue to be one of the most widely investigated pharmacological treatments for ARDS. One recent publication showed that short-term, low-dose corticosteroid therapy can have an impact on survival in aspiration-related ARDS.(5) It is plausible that the timing (either prophylactic or after the initial insult), the dose, and the duration of the therapy, as well as the etiology of the lung injury, are all important factors in determining the response of patients with ARDS to the administration of systemic corticosteroids. Future clinical trials must take all of these issues into account. The controversy regarding the possible benefits of this class of drugs in ARDS is therefore still “alive and kicking”. The work of Reis et al.(3) generates even more interest in pharmacological approaches to prevent or treat VILI, especially in the role of corticosteroids in such injury, mainly as a preventive measure in patients at risk for ARDS.
REFERENCES
1. Levitt JE, Matthay MA. Clinical review: Early treatment of acute lung injury--paradigm shift toward prevention and treatment prior to respiratory failure. Crit Care. 2012;16(3):223. http://dx.doi.org/10.1186/cc11144
2. Ruan SY, Lin HH, Huang CT, Kuo PH, Wu HD, Yu CJ. Exploring the heterogeneity of effects of corticosteroids on acute respiratory distress syndrome: a systematic review and meta-analysis. Crit Care. 2014;18(2):R63. http://dx.doi.org/10.1186/cc13819
3. Reis FF, Reboredo MM, Lucinda LM, Bianchi AM, Rabelo MA, Fonseca LM, et al. Dexamethasone pre-treatment attenuates experimental
ventilator-induced lung injury. J Bras Pulmonol. 2016;42(3):166-173.4. Hegeman MA, Hennus MP, Cobelens PM, Kavelaars A, Jansen NJ, et
al. Dexamethasone attenuates VEGF expression and inflammation but not barrier dysfunction in a murine model of ventilator–induced lung injury. PLoS One. 2013;8(2): e57374. http://dx.doi.org/10.1371/journal.pone.0057374
5. Zhao JN, Liu Y, Li HC. Corticosteroids in treatment of aspiration-related acute respiratory distress syndrome: results of a retrospective cohort study. BMC Pulm Med. 2016;16:29. http://dx.doi.org/10.1186/s12890-016-0194-4
J Bras Pneumol. 2016;42(3):163-163
163
EDITORIAL

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562016000000094
Multiple calcified nodulesEdson Marchiori1,2, Gláucia Zanetti2,3, Bruno Hochhegger4,5
1. Universidade Federal Fluminense, Niterói (RJ) Brasil. 2. Universidade Federal do Rio de Janeiro, Rio de Janeiro (RJ) Brasil.3. Faculdade de Medicina de Petrópolis, Petrópolis (RJ) Brasil.4. Santa Casa de Misericórdia de Porto Alegre, Porto Alegre (RS) Brasil.5. Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre (RS) Brasil.
A 22-year-old male patient previously diagnosed with osteosarcoma in the right leg, which was amputated in 2011, sought medical attention. The patient had multiple pulmonary nodules with calcifications (Figure 1). The final diagnosis was calcified metastases from osteosarcoma.
Multiple pulmonary nodules can have numerous etiol-ogies. However, when these lesions have calcifications, the diagnostic possibilities are considerably reduced. Calcified metastases, amyloidosis, hyalinizing granulomas, epithelioid hemangioendothelioma, rheumatoid nodules, and multiple chondromas can be listed as the major causes of the pattern consisting of multiple nodules and/or masses of various sizes and with calcifications. The tumors that most commonly give rise to calcified metastases are sarcomas, especially osteosarcomas; synovial sarcomas; chondrosarcomas; and carcinomas, particularly mucinous or papillary adenocarcinomas.
Amyloidosis, in its nodular form, is more common in patients over 60 years of age, and these patients are usually asymptomatic. The nodules grow slowly, over years, without regression. The definitive diagnosis is made by histopathology, on the basis of the finding of deposition of amyloid, which stains with Congo red and shows apple-green birefringence in polarized light. Hyalinizing granulomas are rare fibrotic pulmonary lesions, usually associated with autoimmune phenomena mainly related to exposure to mycobacterial or fungal antigens. These lesions can remain stable or grow slowly for years. Epithelioid hemangioendothelioma is a rare multifocal pulmonary neoplasm of endothelial origin. It is considered a sarcoma of low aggressiveness. Although it does not usually exhibit growth, it eventually grows slowly and can lead to respiratory failure. In addition, it can develop calcification within 10-20 years of diagnosis. Necrobiotic nodules can develop in patients with pneumoconiosis associated with rheumatoid arthritis. The onset of these nodules characterizes Caplan’s syndrome. Calcification in pulmonary chondromas is a common radiological finding. The association of these chondromas with gastrointestinal stromal tumors and extra-adrenal paragangliomas is known as the Carney triad. In all these diseases, patients can be asymptomatic or present with nonspecific chest symptoms. Therefore, the lesions are often incidental radiological findings. The association between clinical and radiological findings can significantly improve the accuracy of the diagnosis. However, in most cases, lung biopsy with immunohistochemical staining is required to establish the correct diagnosis. In the case of the patient in question, the history of osteosarcoma resection associated with the presence of calcified pulmonary nodules led to the final diagnosis of metastases from osteosarcoma. This diagnosis is facilitated, in the vast majority of cases, because the primary bone tumor is already known before the onset of metastases.
RECOMMENDED READING1. Webb WR, Muller NL, Naidich DP, editors. High-resolution CT of the
lung. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2008.
Figure 1. Coronal CT section (mediastinal window settings) showing multiple partially calcified nodules and masses, of various sizes, in both lungs.
J Bras Pneumol. 2016;42(3):164-164
164
CONTINUING EDUCATION: IMAGING
ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562016000000152
Choosing wisely between randomized controlled trials and observational designs in studies about interventionsJuliana Carvalho Ferreira1,2, Cecilia Maria Patino2,3
1. Divisão de Pneumologia, Instituto do Coração – InCor – Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo (SP) Brasil.2. Methods in Epidemiologic, Clinical and Operations Research–MECOR–program, American Thoracic Society/Asociación Latinoamericana del Tórax.3. Department of Preventive Medicine, Keck School of Medicine, University of Southern California, Los Angeles (CA) USA.
Randomized controlled trials (RCTs) are the gold standard for evaluating the efficacy of interventions, because they avoid key sources of bias by randomly allocating participants to the treatment or control. That feature of the study design makes RCTs the highest ranked type of study within the Evidence-Based Medicine framework grading system. However, not all questions about health interventions can be answered with an RCT. Observational studies may be more appropriate to study certain aspects about interventions and thus complement RCTs.
In some situations, it is unfeasible or unethical to randomize patients to a treatment, such as a surgical intervention, if surgeons are uncomfortable performing an unfamiliar procedure. In addition, observational studies are better suited to evaluate the incidence of adverse events of interventions because they have less strict inclusion and exclusion criteria, which allows a broader spectrum of the target population to be included. While RCTs are usually the best option to test efficacy (the effect of the intervention under ideal conditions), observational studies are a valuable option to evaluate effectiveness (the effect of an intervention in real life).
Some advantages of observational studies include the following: they are usually less expensive than RCTs, they have no ethical roadblocks in assigning participants to treatment or control groups, and placebos are rarely used (Table 1).
CHOOSING WISELY
The choice between an observational study and an RCT should be based on the specific research question. Observational designs are appropriate when it is reasonable to assume that characteristics that influence clinicians to choose a given intervention are not related to the study outcome. For example, in a comparison between the impact of radiosurgery and that of surgical lung resection on the survival of lung cancer patients, an observational study would not be appropriate, because the choice between radiosurgery and lung resection is influenced by tumor size and patient performance status, which also influence survival independently of the treatment option. In contrast, observational studies are often used to study the effectiveness of vaccination to protect against
infectious diseases, because the characteristics that influence the decision to get vaccinated are not major determinants of the risk of being infected.
MINIMIZING BIAS
When conducting observational studies to test inter-ventions, the investigator needs to design strategies to minimize bias resulting from imbalances in competing risk factors (confounders) across the intervention and control groups. In the design phase, a typical strategy involves measuring known confounders at baseline and later adjusting for those confounders during the analysis phase by using multivariable models. Another strategy includes combining confounding variables associated with the intervention and creating a new variable, called a propensity score, that can be used, for example, to match participants at baseline or adjust for confounders during analysis. However, the efficiency of such methods is limited to known and adequately measured confounders.
BEYOND STUDY DESIGN
When evaluating the medical literature, clinicians should consider not only the design (RCT or observational) but also the quality of a given study. RCTs and observational trials both contribute to advancing knowledge in health care, which can guide clinical decision-making and public health policy.
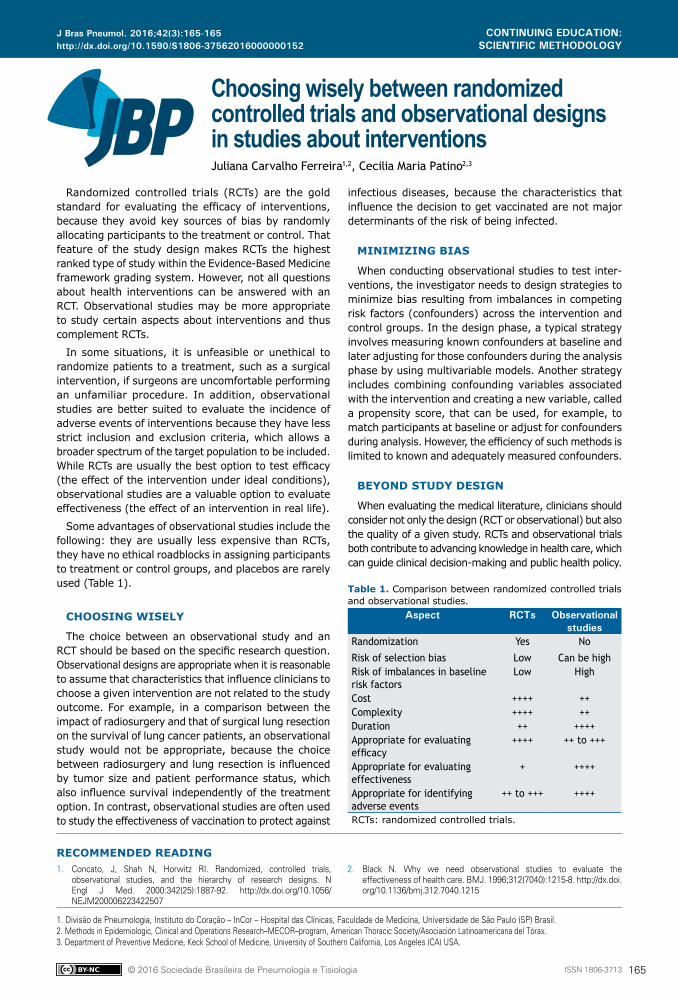
Table 1. Comparison between randomized controlled trials and observational studies.
Aspect RCTs Observational studies
Randomization Yes No
Risk of selection bias Low Can be highRisk of imbalances in baseline risk factors
Low High
Cost ++++ ++Complexity ++++ ++Duration ++ ++++Appropriate for evaluating efficacy
++++ ++ to +++
Appropriate for evaluating effectiveness
+ ++++
Appropriate for identifying adverse events
++ to +++ ++++
RCTs: randomized controlled trials.
RECOMMENDED READING1. Concato, J, Shah N, Horwitz RI. Randomized, controlled trials,
observational studies, and the hierarchy of research designs. N Engl J Med. 2000:342(25):1887-92. http://dx.doi.org/10.1056/NEJM200006223422507
2. Black N. Why we need observational studies to evaluate the effectiveness of health care. BMJ. 1996;312(7040):1215-8. http://dx.doi.org/10.1136/bmj.312.7040.1215
J Bras Pneumol. 2016;42(3):165-165
165
CONTINUING EDUCATION: SCIENTIFIC METHODOLOGY

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000350
ABSTRACTObjective: To evaluate the effects that administering dexamethasone before the induction of ventilator-induced lung injury (VILI) has on the temporal evolution of that injury. Methods: Wistar rats were allocated to one of three groups: pre-VILI administration of dexamethasone (dexamethasone group); pre-VILI administration of saline (control group); or ventilation only (sham group). The VILI was induced by ventilation at a high tidal volume. Animals in the dexamethasone and control groups were euthanized at 0, 4, 24, and 168 h after VILI induction. We analyzed arterial blood gases, lung edema, cell counts (total and differential) in the BAL fluid, and lung histology. Results: At 0, 4, and 24 h after VILI induction, acute lung injury (ALI) scores were higher in the control group than in the sham group (p < 0.05). Administration of dexamethasone prior to VILI induction decreased the severity of the lung injury. At 4 h and 24 h after induction, the ALI score in the dexamethasone group was not significantly different from that observed for the sham group and was lower than that observed for the control group (p < 0.05). Neutrophil counts in BAL fluid were increased in the control and dexamethasone groups, peaking at 4 h after VILI induction (p < 0.05). However, the neutrophil counts were lower in the dexamethasone group than in the control group at 4 h and 24 h after induction (p < 0.05). Pre-treatment with dexamethasone also prevented the post-induction oxygenation impairment seen in the control group. Conclusions: Administration of dexamethasone prior to VILI induction attenuates the effects of the injury in Wistar rats. The molecular mechanisms of such injury and the possible clinical role of corticosteroids in VILI have yet to be elucidated.
Keywords: Ventilator-induced lung injury; Dexamethasone; Respiratory distress syndrome, adult.
Pre-treatment with dexamethasone attenuates experimental ventilator-induced lung injuryFernando Fonseca dos Reis1,2, Maycon de Moura Reboredo1,2, Leda Marília Fonseca Lucinda1,2, Aydra Mendes Almeida Bianchi1,2, Maria Aparecida Esteves Rabelo1, Lídia Maria Carneiro da Fonseca1,2, Júlio César Abreu de Oliveira1, Bruno Valle Pinheiro1,2
Correspondence to:Fernando Fonseca dos Reis. Laboratório de Pesquisa Pulmonar, Universidade Federal de Juiz de Fora, Avenida Eugênio do Nascimento, s/n, Dom Bosco, CEP 36038-330, Juiz de Fora, MG, BrasilTel.: 55 32 99977-6584. E-mail: [email protected] support: This study was supported by research grants from the Rede Mineira de Ensaios Toxicológicos e Farmacológicos de Produtos Terapêuticos (Rede Mineira TOXIFAR, Minas Gerais [State] Network of Toxicological and Pharmacological Trials of Therapeutic Products), the Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG, Foundation for the Support of Research in the State of Minas Gerais), and the Centro de Biologia da Reprodução da Universidade Federal de Juiz de Fora (Reproductive Biology Center of the Federal University of Juiz de Fora).
INTRODUCTION
Although necessary in various types of respiratory failure, mechanical ventilation (MV) can be harmful, especially if its parameters are adjusted incorrectly, because that can result in so-called ventilator-induced lung injury (VILI).(1) VILI can also worsen established lung injury, such as the acute respiratory distress syndrome (ARDS), and delay its healing.(2) The clinical relevance of VILI has been determined by studies conducted in patients with ARDS, in which adjusting protective parameters during MV, mainly limiting the tidal volume and plateau pressure, has been found to decrease mortality.(3,4) In addition, studies involving patients at risk of developing ARDS have shown that those same measures decrease the occurrence of the syndrome and are currently recommended in such patients.(5,6)
VILI occurs when the transpulmonary pressure (i.e., the difference between the pressure level in the alveolus
and that in the pleural space) is above safe levels and generates high tidal volumes. The pulmonary structures exposed to this high pressure react by generating forces with the same intensity, creating a situation known as lung stress. A high tidal volume induces deformation of the alveolus, which is described as a change in a linear dimension over its initial value, creating a situation known as lung strain.(7,8) VILI can occur even with stress and strain levels lower than those necessary for disruption of alveolar structures, although sufficient to release proinflammatory cytokines and recruit neutrophils, leading to inflammatory lung injury.(9) This biological reaction to mechanical injury is designated biotrauma, and studies have been carried out to establish the mechanisms involved and to test strategies (ventilatory and pharmacological) that could avert or attenuate VILI.(10,11)
Glucocorticoids exert anti-inflammatory effects by binding to their receptors in the cytoplasm, forming
1. Laboratório de Pesquisa em Pneumologia, Universidade Federal de Juiz de Fora, Juiz de Fora (MG) Brasil.
2. Centro de Biologia da Reprodução, Universidade Federal de Juiz de Fora, Juiz de Fora (MG) Brasil.
Submitted: 17 January 2016. Accepted: 9 May 2016.
Study carried out at the Universidade Federal de Juiz de Fora, Juiz de Fora (MG) Brasil.
J Bras Pneumol. 2016;42(3):166-173
166
ORIGINAL ARTICLE

Reis FF, Reboredo MM, Lucinda LMF, Bianchi AMA, Rabelo MAE, Fonseca LMC, Oliveira JCA, Pinheiro BV
glucocorticoid-receptor complexes that migrate to the cellular nucleus, where they inhibit the transcription rates of many inflammatory elements, including nuclear factor-kappa B.(12) This decreases the production of proinflammatory cytokines, such as TNF-α, IL-1α, IL-1β, IL-2, IL-3, IL-5, IL-6, IL-8, IL-12, IFN-γ, and GM-CSF. (13) By modulating those cytokines, glucocorticoids can suppress granulocyte recruitment and activation, as well as preserving alveolar-capillary barrier integrity and controlling vascular permeability. Glucocorticoids can also inhibit fibroblast proliferation and collagen deposition, both of which are important features in the later phases of ARDS.(14,15)
Despite the potentially beneficial effects of gluco-corticoids against the mechanisms involved in ARDS and VILI, their clinical usefulness in these conditions is still under debate.(16-20) For instance, in the specific context of the effects of glucocorticoids on mortality, some meta-analyses have shown that they reduce mortality,(17,19) whereas other have failed to show a convincing effect of glucocorticoid treatment in ARDS.(20) Hypotheses to explain these dissonant results include lack of an optimal corticosteroid dose, as well as the timing and duration of the therapy.(21)
Studies employing experimental models of VILI have obtained promising results with glucocorticoids. However, such studies have evaluated the effect of dexamethasone only in the acute phase of VILI.(22-25) Therefore, the aim of this study was to evaluate the effects that administering dexamethasone before the induction of VILI has on the temporal evolution of the injury. We hypothesized that pre-treatment with dexamethasone would not only attenuate VILI in the acute phase but also accelerate the healing process thereafter.
METHODS
Animal preparationThis study was approved by the Animal Research
Ethics Committee of the Federal University of Juiz de Fora, in the state of Minas Gerais, Brazil. The animals were cared for in accordance with the guidelines established by the Brazilian National Council for the Monitoring of Animal Experimentation. Sixty-three adult male Wistar rats (mean weight, 286 ± 15 g) were obtained from the animal facility of the Reproductive Biology Center of the Federal University of Juiz de Fora. Over the week prior to the experiment, groups of three animals each were housed in clear plastic cages, with stainless steel wire lids and pinewood shavings as bedding, in a temperature-controlled environment on closed, ventilated shelves, on a 12/12-h light/dark cycle. The animals were fed standard rat chow (mean, 25 g/day) and had ad libitum access to drinking water.
Experimental protocolAnimals were allocated to one of three groups (Figure
1): dexamethasone, comprising rats that received an
intraperitoneal injection of dexamethasone (6 mg/kg) at 30 min before the induction of VILI(24,25); control, comprising rats that received an intraperitoneal injection of the same volume of saline, also at 30 min before the induction of VILI; and sham, comprising rats that received neither dexamethasone nor saline, were submitted to normal (non-injurious) ventilation for 10 min, and underwent the same experimental procedures performed in the first two groups.
The rats were anesthetized with intraperitoneal injections of xylazine (8 mg/kg) and ketamine (80 mg/kg). After confirmation of the depth of anesthesia by paw clamp, the animals were intubated with a 16-gauge intravenous catheter and ventilated in the volume-controlled mode with a small animal ventilator (Inspira ASV; Harvard Apparatus, Holliston, MA, USA). To induce VILI (in the dexamethasone and control group rats), the ventilator parameters were set as follows: tidal volume of 35 mL/kg; respiratory rate of 18 breaths/min; inspiratory to expiratory ratio of 1:2; FiO2 of 1; and positive end-expiratory pressure (PEEP) of 0 cmH2O. After 1 h of this injurious MV, the animals were extubated and kept under observation to recover from the anesthesia.
After VILI induction, animals in the dexamethasone and control groups were euthanized (n = 23 in each group): immediately after VILI induction (0 h, n = 6 in each group); at 4 h after VILI induction (n = 6 in each group); at 24 h after VILI induction (n = 6 in each group); and at 168 h (7 days) after VILI induction (n = 5 in each group). At each of those time points, the animals were again anesthetized with intraperitoneal injections of xylazine (8 mg/kg) and ketamine (80 mg/kg), after which a surgical tracheostomy was performed and a 14-gauge cannula was inserted. An arterial catheter was inserted into the left carotid to obtain blood samples for arterial blood gas analysis (ABL90 FLEX; Radiometer, Copenhagen, Denmark). The rats were then paralyzed with an intra-arterial injection of rocuronium (1 mg/kg) and mechanically ventilated at the following settings: tidal volume of 6 mL/kg; respiratory rate of 80 breaths/min; inspiratory to expiratory ratio of 1:2; FiO2 of 1; and PEEP of 2 cmH2O. After 10 min of ventilation, an arterial blood gas analysis was performed. Subsequently, a laparotomy was performed; the animals were euthanized by exsanguination and sectioning of the diaphragm. The trachea was clamped at end-expiration, with a PEEP of 2 cmH2O, and the lungs were extracted for further analysis. The animals in the sham group (n = 6) were euthanized 10 min after non-injurious MV.
MeasurementsBlood samples for arterial blood gas analysis were
obtained after 10 min of protective ventilation, imme-diately before euthanasia. The lungs were removed en bloc, after which the right lower lobes were separated, fixed in 10% buffered formaldehyde, and processed for paraffin embedding. Slices (4 µm in thickness) were cut and stained with hematoxylin-eosin. Morphological examinations were performed by an investigator who
167J Bras Pneumol. 2016;42(3):166-173
Pre-treatment with dexamethasone attenuates experimental ventilator-induced lung injury
was blinded to the groups, using a conventional light microscope (Carl Zeiss, Hallbergmoos, Germany).
The acute lung injury score, which was the primary outcome measure, was determined by using a weighted scoring system, as described elsewhere.(26) In brief, 20 random fields at a magnification of ×400 were scored independently. Values of 0, 1, or 2 were used in order to represent the severity based on the following findings: neutrophils in the alveolar space, neutrophils in the interstitial space, hyaline membranes, proteinaceous debris filling the airspaces, and alveolar septal thickening. To generate an acute lung injury score, the sum of the five variables was weighted according to the relevance ascribed to each one. The resulting score was a continuous value between 0 (normal) and 1 (the most severe injury). In addition, the extent of each acute lung injury score component was calculated on the basis of the sum of the severity values (0, 1, or 2) for the 20 fields analyzed.
To obtain a BAL fluid sample, the left lung was washed three times via a tracheal tube with 4 mL of PBS containing 10 nM of EDTA. Each sample was
centrifuged for 10 min at 1,500 rpm to separate it into its cellular and non-cellular components. The samples were diluted in Türk solution (2% acetic acid), and total leukocyte counts were determined in a Neubauer chamber under light microscopy. The cell pellet was resuspended in PBS and stained with May-Grünwald-Giemsa for differential cell counts, which were performed with a minimum of 300 cells.
The lung wet-to-dry weight ratio was determined in the right upper lobe, as previously described.(27) In brief, the right upper lobe was isolated and weighed (wet weight) using a precise balance (Ohaus Adventurer; Toledo do Brasil, São Bernardo do Campo, Brazil). It was then dried in a microwave at low power (200 W) for 5 min. The drying process was repeated until the difference between two consecutive measurements was less than 0.002 g. The last weight determined was considered the dry weight.
Statistical analysisThe distribution of the data was tested for normality
using the Kolmogorov-Smirnov test. Values are
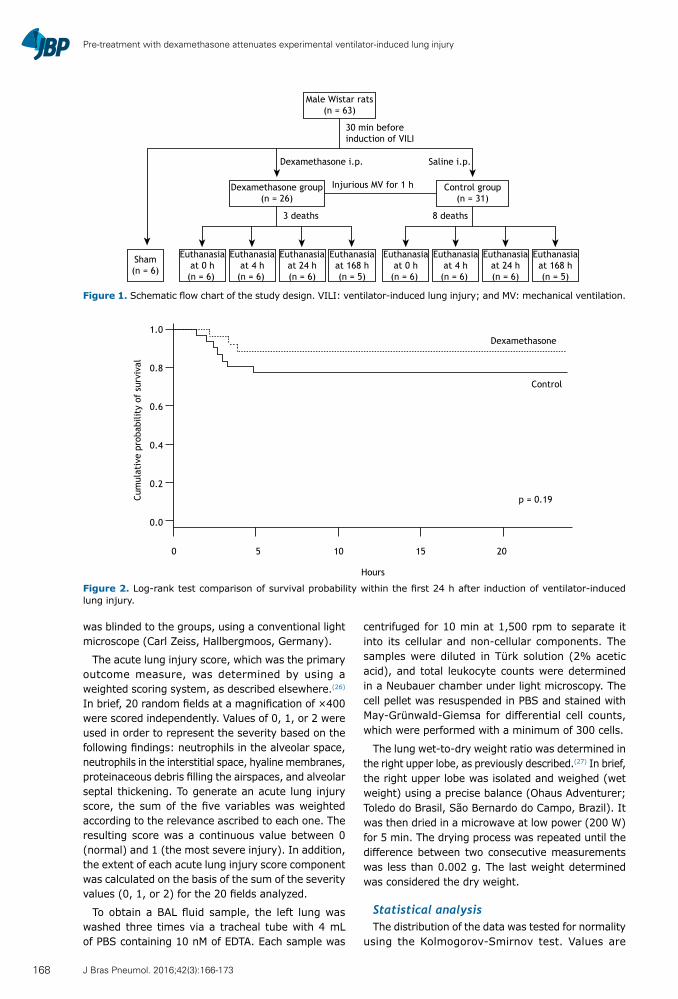
Figure 2. Log-rank test comparison of survival probability within the first 24 h after induction of ventilator-induced lung injury.
Male Wistar rats(n = 63)
30 min beforeinduction of VILI
Dexamethasone i.p. Saline i.p.
Dexamethasone group(n = 26)
Injurious MV for 1 h Control group(n = 31)
3 deaths 8 deaths
Sham(n = 6)
Euthanasiaat 168 h(n = 5)
Euthanasiaat 0 h
(n = 6)
Euthanasiaat 4 h
(n = 6)
Euthanasiaat 24 h(n = 6)
Euthanasiaat 168 h(n = 5)
Euthanasiaat 0 h
(n = 6)
Euthanasiaat 4 h
(n = 6)
Euthanasiaat 24 h(n = 6)
Cum
ulat
ive
prob
abili
ty o
f su
rviv
al
0 5 10 15 20
Hours
1.0
0.8
0.6
0.4
0.2
0.0
Dexamethasone
Control
p = 0.19
Figure 1. Schematic flow chart of the study design. VILI: ventilator-induced lung injury; and MV: mechanical ventilation.
168 J Bras Pneumol. 2016;42(3):166-173
Reis FF, Reboredo MM, Lucinda LMF, Bianchi AMA, Rabelo MAE, Fonseca LMC, Oliveira JCA, Pinheiro BV
expressed as mean ± standard deviation or median (interquartile range), as appropriate. Data for each group were analyzed by one-way ANOVA followed by the Dunnett’s test or by the Kruskal-Wallis test followed by the Mann-Whitney test, as appropriate. Adjustments for repeated measures were performed with Bonferroni correction. Comparisons between the dexamethasone and control groups at each time point were made by unpaired t-test or the Mann-Whitney test, as appropriate. The log-rank test was used for comparison of survival between the dexamethasone and control groups. Values of p < 0.05 were considered significant. All statistical analyses were performed with the Statistical Package for the Social Sciences, version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
SurvivalSurvival was not initially an objective of this study,
and the animals were therefore not followed for a pre-determined period of time specifically for the study of that outcome. However, some deaths were observed in the dexamethasone and control groups during the period between the post-induction anesthesia recovery and the time of euthanasia. Death occurred in 3 (12%) of the 26 animals in the dexamethasone group and in 8 (26%) of the 31 animals in the control group (p = 0.19). Of those 11 deaths, 10 occurred within the first 6 h after VILI induction, and 1 occurred more than 6 h but less than 24 h after VILI induction (Figure 2).
Lung histology and BALAt 0, 4, and 24 h after VILI induction, the rats in the
control group showed greater lung injury, as determined by the acute lung injury score, than did those in the
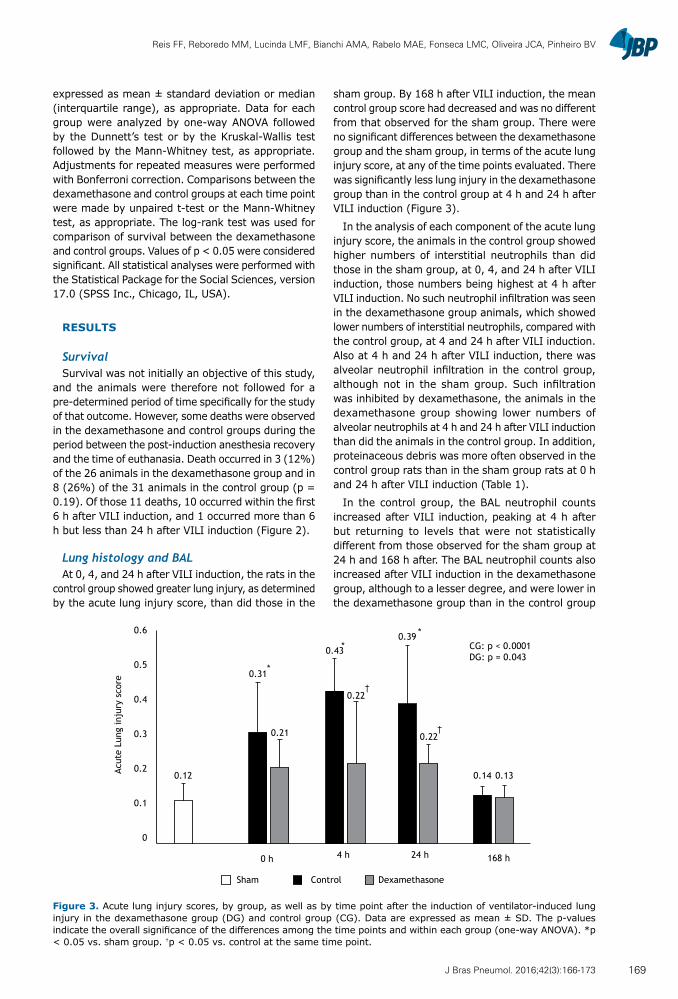
sham group. By 168 h after VILI induction, the mean control group score had decreased and was no different from that observed for the sham group. There were no significant differences between the dexamethasone group and the sham group, in terms of the acute lung injury score, at any of the time points evaluated. There was significantly less lung injury in the dexamethasone group than in the control group at 4 h and 24 h after VILI induction (Figure 3).
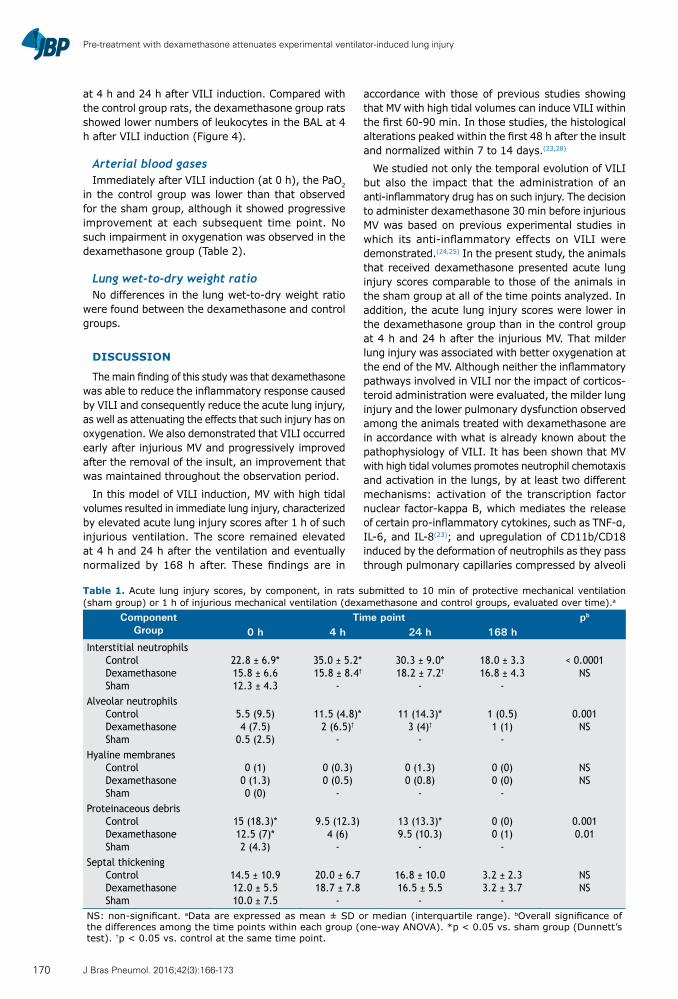
In the analysis of each component of the acute lung injury score, the animals in the control group showed higher numbers of interstitial neutrophils than did those in the sham group, at 0, 4, and 24 h after VILI induction, those numbers being highest at 4 h after VILI induction. No such neutrophil infiltration was seen in the dexamethasone group animals, which showed lower numbers of interstitial neutrophils, compared with the control group, at 4 and 24 h after VILI induction. Also at 4 h and 24 h after VILI induction, there was alveolar neutrophil infiltration in the control group, although not in the sham group. Such infiltration was inhibited by dexamethasone, the animals in the dexamethasone group showing lower numbers of alveolar neutrophils at 4 h and 24 h after VILI induction than did the animals in the control group. In addition, proteinaceous debris was more often observed in the control group rats than in the sham group rats at 0 h and 24 h after VILI induction (Table 1).
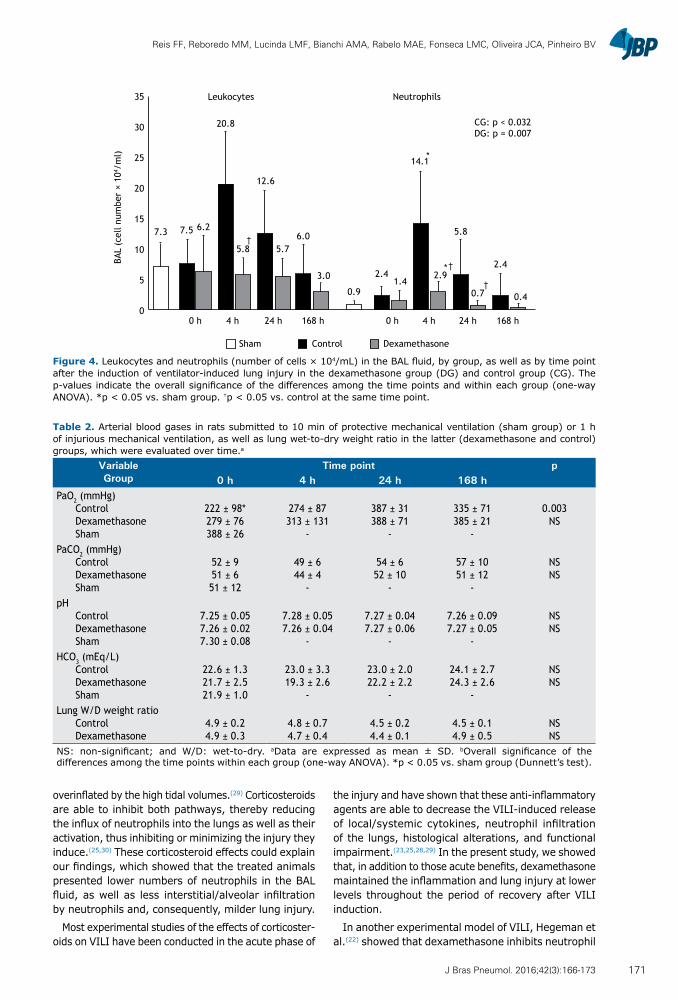
In the control group, the BAL neutrophil counts increased after VILI induction, peaking at 4 h after but returning to levels that were not statistically different from those observed for the sham group at 24 h and 168 h after. The BAL neutrophil counts also increased after VILI induction in the dexamethasone group, although to a lesser degree, and were lower in the dexamethasone group than in the control group
0.6
0.5
0.4
0.3
0.2
0.1
0
0 h 4 h 24 h 168 h
†
†
CG: p < 0.0001DG: p = 0.043
DexamethasoneControlSham
Acut
e Lu
ng in
jury
sco
re
0.12
0.31
0.21
0.43
0.22
0.39
0.22
0.14 0.13
**
*
Figure 3. Acute lung injury scores, by group, as well as by time point after the induction of ventilator-induced lung injury in the dexamethasone group (DG) and control group (CG). Data are expressed as mean ± SD. The p-values indicate the overall significance of the differences among the time points and within each group (one-way ANOVA). *p < 0.05 vs. sham group. †p < 0.05 vs. control at the same time point.
169J Bras Pneumol. 2016;42(3):166-173
Pre-treatment with dexamethasone attenuates experimental ventilator-induced lung injury
at 4 h and 24 h after VILI induction. Compared with the control group rats, the dexamethasone group rats showed lower numbers of leukocytes in the BAL at 4 h after VILI induction (Figure 4).
Arterial blood gasesImmediately after VILI induction (at 0 h), the PaO2
in the control group was lower than that observed for the sham group, although it showed progressive improvement at each subsequent time point. No such impairment in oxygenation was observed in the dexamethasone group (Table 2).
Lung wet-to-dry weight ratioNo differences in the lung wet-to-dry weight ratio
were found between the dexamethasone and control groups.
DISCUSSION
The main finding of this study was that dexamethasone was able to reduce the inflammatory response caused by VILI and consequently reduce the acute lung injury, as well as attenuating the effects that such injury has on oxygenation. We also demonstrated that VILI occurred early after injurious MV and progressively improved after the removal of the insult, an improvement that was maintained throughout the observation period.
In this model of VILI induction, MV with high tidal volumes resulted in immediate lung injury, characterized by elevated acute lung injury scores after 1 h of such injurious ventilation. The score remained elevated at 4 h and 24 h after the ventilation and eventually normalized by 168 h after. These findings are in
accordance with those of previous studies showing that MV with high tidal volumes can induce VILI within the first 60-90 min. In those studies, the histological alterations peaked within the first 48 h after the insult and normalized within 7 to 14 days.(23,28)
We studied not only the temporal evolution of VILI but also the impact that the administration of an anti-inflammatory drug has on such injury. The decision to administer dexamethasone 30 min before injurious MV was based on previous experimental studies in which its anti-inflammatory effects on VILI were demonstrated.(24,25) In the present study, the animals that received dexamethasone presented acute lung injury scores comparable to those of the animals in the sham group at all of the time points analyzed. In addition, the acute lung injury scores were lower in the dexamethasone group than in the control group at 4 h and 24 h after the injurious MV. That milder lung injury was associated with better oxygenation at the end of the MV. Although neither the inflammatory pathways involved in VILI nor the impact of corticos-teroid administration were evaluated, the milder lung injury and the lower pulmonary dysfunction observed among the animals treated with dexamethasone are in accordance with what is already known about the pathophysiology of VILI. It has been shown that MV with high tidal volumes promotes neutrophil chemotaxis and activation in the lungs, by at least two different mechanisms: activation of the transcription factor nuclear factor-kappa B, which mediates the release of certain pro-inflammatory cytokines, such as TNF-α, IL-6, and IL-8(23); and upregulation of CD11b/CD18 induced by the deformation of neutrophils as they pass through pulmonary capillaries compressed by alveoli
Table 1. Acute lung injury scores, by component, in rats submitted to 10 min of protective mechanical ventilation (sham group) or 1 h of injurious mechanical ventilation (dexamethasone and control groups, evaluated over time).a
ComponentGroup
Time point pb
0 h 4 h 24 h 168 hInterstitial neutrophils
ControlDexamethasoneSham
22.8 ± 6.9*15.8 ± 6.612.3 ± 4.3
35.0 ± 5.2*15.8 ± 8.4†
-
30.3 ± 9.0*18.2 ± 7.2†
-
18.0 ± 3.316.8 ± 4.3
-
< 0.0001NS
Alveolar neutrophilsControlDexamethasoneSham
5.5 (9.5)4 (7.5)
0.5 (2.5)
11.5 (4.8)*2 (6.5)†
-
11 (14.3)*3 (4)†
-
1 (0.5)1 (1)
-
0.001NS
Hyaline membranesControlDexamethasoneSham
0 (1)0 (1.3)0 (0)
0 (0.3)0 (0.5)
-
0 (1.3)0 (0.8)
-
0 (0)0 (0)
-
NSNS
Proteinaceous debrisControlDexamethasoneSham
15 (18.3)*12.5 (7)*2 (4.3)
9.5 (12.3)4 (6)
-
13 (13.3)*9.5 (10.3)
-
0 (0)0 (1)
-
0.0010.01
Septal thickeningControlDexamethasoneSham
14.5 ± 10.912.0 ± 5.510.0 ± 7.5
20.0 ± 6.718.7 ± 7.8
-
16.8 ± 10.016.5 ± 5.5
-
3.2 ± 2.33.2 ± 3.7
-
NSNS
NS: non-significant. aData are expressed as mean ± SD or median (interquartile range). bOverall significance of the differences among the time points within each group (one-way ANOVA). *p < 0.05 vs. sham group (Dunnett’s test). †p < 0.05 vs. control at the same time point.
170 J Bras Pneumol. 2016;42(3):166-173
Reis FF, Reboredo MM, Lucinda LMF, Bianchi AMA, Rabelo MAE, Fonseca LMC, Oliveira JCA, Pinheiro BV
overinflated by the high tidal volumes.(29) Corticosteroids are able to inhibit both pathways, thereby reducing the influx of neutrophils into the lungs as well as their activation, thus inhibiting or minimizing the injury they induce.(25,30) These corticosteroid effects could explain our findings, which showed that the treated animals presented lower numbers of neutrophils in the BAL fluid, as well as less interstitial/alveolar infiltration by neutrophils and, consequently, milder lung injury.
Most experimental studies of the effects of corticoster-oids on VILI have been conducted in the acute phase of
the injury and have shown that these anti-inflammatory agents are able to decrease the VILI-induced release of local/systemic cytokines, neutrophil infiltration of the lungs, histological alterations, and functional impairment.(23,25,28,29) In the present study, we showed that, in addition to those acute benefits, dexamethasone maintained the inflammation and lung injury at lower levels throughout the period of recovery after VILI induction.
In another experimental model of VILI, Hegeman et al.(22) showed that dexamethasone inhibits neutrophil
Table 2. Arterial blood gases in rats submitted to 10 min of protective mechanical ventilation (sham group) or 1 h of injurious mechanical ventilation, as well as lung wet-to-dry weight ratio in the latter (dexamethasone and control) groups, which were evaluated over time.a
VariableGroup
Time point p0 h 4 h 24 h 168 h
PaO2 (mmHg)ControlDexamethasoneSham
222 ± 98*279 ± 76388 ± 26
274 ± 87313 ± 131
-
387 ± 31388 ± 71
-
335 ± 71385 ± 21
-
0.003NS
PaCO2 (mmHg)ControlDexamethasoneSham
52 ± 951 ± 651 ± 12
49 ± 644 ± 4
-
54 ± 652 ± 10
-
57 ± 1051 ± 12
-
NSNS
pHControlDexamethasoneSham
7.25 ± 0.057.26 ± 0.027.30 ± 0.08
7.28 ± 0.057.26 ± 0.04
-
7.27 ± 0.047.27 ± 0.06
-
7.26 ± 0.097.27 ± 0.05
-
NSNS
HCO3 (mEq/L)ControlDexamethasoneSham
22.6 ± 1.321.7 ± 2.521.9 ± 1.0
23.0 ± 3.319.3 ± 2.6
-
23.0 ± 2.022.2 ± 2.2
-
24.1 ± 2.724.3 ± 2.6
-
NSNS
Lung W/D weight ratioControlDexamethasone
4.9 ± 0.24.9 ± 0.3
4.8 ± 0.74.7 ± 0.4
4.5 ± 0.24.4 ± 0.1
4.5 ± 0.14.9 ± 0.5
NSNS
NS: non-significant; and W/D: wet-to-dry. aData are expressed as mean ± SD. bOverall significance of the differences among the time points within each group (one-way ANOVA). *p < 0.05 vs. sham group (Dunnett’s test).
35
30
25
20
15
10
5
00 h 4 h4 h 24 h 168 h
CG: p < 0.032DG: p = 0.007
DexamethasoneControlSham
BAL
(cel
l num
ber
× 10
4 /m
l)
Leukocytes Neutrophils
†
†
7.3
0 h
7.5 6.2
168 h
6.0
3.0
†
20.8
5.8
24 h
12.6
5.7
*
*
0.9
2.41.4
14.1
2.9
5.8
0.7
2.4
0.4
Figure 4. Leukocytes and neutrophils (number of cells × 104/mL) in the BAL fluid, by group, as well as by time point after the induction of ventilator-induced lung injury in the dexamethasone group (DG) and control group (CG). The p-values indicate the overall significance of the differences among the time points and within each group (one-way ANOVA). *p < 0.05 vs. sham group. †p < 0.05 vs. control at the same time point.
171J Bras Pneumol. 2016;42(3):166-173

Pre-treatment with dexamethasone attenuates experimental ventilator-induced lung injury
influx and inflammatory mediator expression, as well as preventing vascular endothelial growth factor expression in the lungs. The authors found such expression to be associated with vascular leakage and with regulation of vascular permeability. However, they did not observe a protective effect of dexamethasone against alveolar-cap-illary barrier dysfunction, finding that glucocorticoid treatment had no effect on protein levels in the BAL fluid or on the lung wet-to-dry weight ratio. (22) The same result in relation to the lung wet-to-dry weight ratio was observed in our study. It has been shown that dexamethasone can increase extravascular lung water in animals exposed to hyperoxia, countering its positive effects on pulmonary injury so that the overall effect is neutral or even deleterious.(31)
We observed a lower mortality rate among the animals treated with dexamethasone than among those in the control group, although the difference was not statistically significant. This might have occurred because the number of animals studied was insufficient, given that survival was not an outcome for which we had planned. The study design prevented us from determining the cause of death in the 11 animals that died. Nevertheless, because those deaths occurred within the first hours after VILI induction, a period during which the levels of lung inflammation and injury were highest, we can hypothesize that they were related to the lung injury. We can also infer that dexamethasone had a positive effect on survival. Another possible hypothesis, based on the results of other studies, is that VILI could have generated a systemic inflammatory response, with hemodynamic instability, that might have been improved by the administration of dexamethasone.(32) This hemodynamic effect was demonstrated by Nin et al.,(25) who showed, in another experimental model of VILI, that the administration of dexamethasone attenuated the lung injury and avoided the hemodynamic instability seen among the animals that did not receive pre-treatment.
We chose to ventilate rats at a tidal volume of 35 mL/kg, on the basis of previous studies that have used the same settings to study VILI and the effects of therapeutic strategies.(25,33,34) Although that tidal volume might seem quite distant from what is employed in clinical practice, it should be borne in mind that, in ARDS, the alveolar area available to ventilation is highly limited (the so-called “baby lung” concept), and the tidal volume (which is set according to the ideal body weight) delivered to those available areas can be extremely high.(35)
Our study has some limitations that should be con-sidered. The analyses carried out at the different time points were performed only with the surviving animals, which constitutes a bias. The results obtained at each time point within the dexamethasone and control groups were compared with those obtained for the sham group, in which the animals were ventilated for only 10 min with a protective strategy. A more precise comparison would have included intubation and extubation of the sham group animals, euthanasia being performed at the same time points as in the other groups.
The design of this study, with induction of VILI followed by extubation and observation for a period of time, does not necessarily correlate with clinical practice. However, it furthers understanding of the course of VILI and of how the use of corticosteroids can alter that course. Although we have demonstrated the temporal evolution of VILI and its inflammatory nature, mainly by showing the capacity of dexamethasone to attenuate the injury, we did not evaluate the pathways involved. In conclusion, we have described the course of VILI induced by high tidal volumes and demonstrated that pre-treatment with dexamethasone is able to attenuate this injury in Wistar rats. The molecular mechanisms and the possible clinical role of corticosteroid therapy in VILI remain to be elucidated.
REFERENCES
1. Dreyfuss D, Saumon G. Ventilator-induced lung injury: lessons from experimental studies. Am J Respir Crit Care Med. 1998;157(1):294-323. http://dx.doi.org/10.1164/ajrccm.157.1.9604014
2. Pinhu L, Whitehead T, Evans T, Griffiths M. Ventilator-associated lung injury. Lancet. 2003;361(9354):332-40. http://dx.doi.org/10.1016/S0140-6736(03)12329-X
3. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342(18):1301-8. http://dx.doi.org/10.1056/NEJM200005043421801
4. Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho GP, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338(6):347-54. http://dx.doi.org/10.1056/NEJM199802053380602
5. Serpa Neto A, Simonis FD, Schultz MJ. How to ventilate patients without acute respiratory distress syndrome? Curr Opin Crit Care. 2015;21(1):65-73. http://dx.doi.org/10.1097/MCC.0000000000000165
6. Mechanical Ventilation Committee of the Brazilian Intensive Care Medicine Association; Commission of Intensive Therapy of the Brazilian Thoracic Society. Brazilian recommendations of mechanical
ventilation 2013. Part I. J Bras Pneumol. 2014;40(4):327-63. http://dx.doi.org/10.1590/S1806-37132014000400002
7. Gattinoni L, Protti A, Caironi P, Carlesso E. Ventilator-induced lung injury: the anatomical and physiological framework. Crit Care Med. 2010;38(10 Suppl):S539-48. http://dx.doi.org/10.1097/CCM.0b013e3181f1fcf7
8. Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013;369(22):2126-36. http://dx.doi.org/10.1056/NEJMra1208707
9. Tremblay LN, Slutsky AS. Ventilator-induced injury: from barotrauma to biotrauma. Proc Assoc Am Physicians. 1998;110(6):482-8.
10. De Prost N, Dreyfuss D. How to prevent ventilator-induced lung injury? Minerva Anestesiol. 2012;78(9):1054-66.
11. Uhlig S, Uhlig U. Pharmacological interventions in ventilator-induced lung injury. Trends Pharmacol Sci. 2004;25(11):592-600. http://dx.doi.org/10.1016/j.tips.2004.09.002
12. Barnes PJ. Corticosteroid effects on cell signalling. Eur Respir J. 2006;27(2):413-26. http://dx.doi.org/10.1183/09031936.06.00125404
13. Rhen T, Cidlowski JA. Antiinflammatory action of glucocorticoids--new mechanisms for old drugs. N Engl J Med. 2005;353(16):1711-23. http://dx.doi.org/10.1056/NEJMra050541
14. Sessler CN, Gay PC. Are corticosteroids useful in late-stage acute
172 J Bras Pneumol. 2016;42(3):166-173
Reis FF, Reboredo MM, Lucinda LMF, Bianchi AMA, Rabelo MAE, Fonseca LMC, Oliveira JCA, Pinheiro BV
respiratory distress syndrome? Respir Care. 2010;55(1):43-55.15. Thompson BT. Glucocorticoids and acute lung injury. Crit Care
Med. 2003;31(4 Suppl):S253-7. http://dx.doi.org/10.1097/01.CCM.0000057900.19201.55
16. Agarwal R, Nath A, Aggarwal AN, Gupta D. Do glucocorticoids decrease mortality in acute respiratory distress syndrome? A meta-analysis. Respirology. 2007;12(4):585-90. http://dx.doi.org/10.1111/j.1440-1843.2007.01060.x
17. Lamontagne F, Briel M, Guyatt GH, Cook DJ, Bhatnagar N, Meade M. Corticosteroid therapy for acute lung injury, acute respiratory distress syndrome, and severe pneumonia: a meta-analysis of randomized controlled trials. J Crit Care. 2010;25(3):420-35. http://dx.doi.org/10.1016/j.jcrc.2009.08.009
18. Meduri GU, Marik PE, Chrousos GP, Pastores SM, Arlt W, Beishuizen A, et al. Steroid treatment in ARDS: a critical appraisal of the ARDS network trial and the recent literature. Intensive Care Med. 2008;34(1):61-9. http://dx.doi.org/10.1007/s00134-007-0933-3
19. Tang BM, Craig JC, Eslick GD, Seppelt I, McLean AS. Use of corticosteroids in acute lung injury and acute respiratory distress syndrome: a systematic review and meta-analysis. Crit Care Med. 2009;37(5):1594-603. http://dx.doi.org/10.1097/CCM.0b013e31819fb507
20. Peter JV, John P, Graham PL, Moran JL, George IA, Bersten A. Corticosteroids in the prevention and treatment of acute respiratory distress syndrome (ARDS) in adults: meta-analysis. BMJ. 2008;336(7651):1006-9. http://dx.doi.org/10.1136/bmj.39537.939039.BE
21. Steinberg KP, Hudson LD, Goodman RB, Hough CL, Lanken PN, Hyzy R, et al. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N Engl J Med. 2006;354(16):1671-84. http://dx.doi.org/10.1056/NEJMoa051693
22. Hegeman MA, Hennus MP, Cobelens PM, Kavelaars A, Jansen NJ, Schultz MJ, et al. Dexamethasone attenuates VEGF expression and inflammation but not barrier dysfunction in a murine model of ventilator-induced lung injury. PLoS One. 2013;8(2):e57374. http://dx.doi.org/10.1371/journal.pone.0057374
23. Nin N, Lorente JA, de Paula M, El Assar M, Vallejo S, Peñuelas O, et al. Rats surviving injurious mechanical ventilation show reversible pulmonary, vascular and inflammatory changes. Intensive Care Med. 2008;34(5):948-56. http://dx.doi.org/10.1007/s00134-007-0959-6
24. Nin N, Lorente JA, Fernández-Segoviano P, De Paula M, Ferruelo A, Esteban A. High-tidal volume ventilation aggravates sepsis-induced multiorgan dysfunction in a dexamethasone-inhibitable manner. Shock. 2009;31(4):429-34. http://dx.doi.org/10.1097/SHK.0b013e318188b720
25. Nin N, Peñuelas O, de Paula M, Lorente JA, Fernández-Segoviano
P, Esteban A. Ventilation-induced lung injury in rats is associated with organ injury and systemic inflammation that is attenuated by dexamethasone. Crit Care Med. 2006;34(4):1093-8. http://dx.doi.org/10.1097/01.CCM.0000205663.92384.E7
26. Matute-Bello G, Downey G, Moore BB, Groshong SD, Matthay MA, Slutsky AS, et al. An official American Thoracic Society workshop report: features and measurements of experimental acute lung injury in animals. Am J Respir Cell Mol Biol. 2011;44(5):725-38. http://dx.doi.org/10.1165/rcmb.2009-0210ST
27. Peterson BT, Brooks JA, Zack AG. Use of microwave oven for determination of postmortem water volume of lungs. J Appl Physiol Respir Environ Exerc Physiol. 1982;52(6):1661-3.
28. Curley GF, Contreras M, Higgins B, O’Kane C, McAuley DF, O’Toole D, et al. Evolution of the inflammatory and fibroproliferative responses during resolution and repair after ventilator-induced lung injury in the rat. Anesthesiology. 2011;115(5):1022-32. http://dx.doi.org/10.1097/ALN.0b013e31823422c9
29. Ohta N, Shimaoka M, Imanaka H, Nishimura M, Taenaka N, Kiyono H, et al. Glucocorticoid suppresses neutrophil activation in ventilator-induced lung injury. Crit Care Med. 2001;29(5):1012-6. http://dx.doi.org/10.1097/00003246-200105000-00027
30. Held HD, Boettcher S, Hamann L, Uhlig S. Ventilation-induced chemokine and cytokine release is associated with activation of nuclear factor-kappaB and is blocked by steroids. Am J Respir Crit Care Med. 2001;163(3 Pt 1):711-6. http://dx.doi.org/10.1164/ajrccm.163.3.2003001
31. Ramsay PL, Smith CV, Geske RS, Montgomery CA, Welty SE. Dexamethasone enhancement of hyperoxic lung inflammation in rats independent of adhesion molecule expression. Biochem Pharmacol. 1998;56(2):259-68. http://dx.doi.org/10.1016/S0006-2952(98)00138-5
32. Imai Y, Parodo J, Kajikawa O, de Perrot M, Fischer S, Edwards V, et al. Injurious mechanical ventilation and end-organ epithelial cell apoptosis and organ dysfunction in an experimental model of acute respiratory distress syndrome. JAMA. 2003;289(16):2104-12. http://dx.doi.org/10.1001/jama.289.16.2104
33. Dreyfuss D, Basset G, Soler P, Saumon G. Intermittent positive-pressure hyperventilation with high inflation pressures produces pulmonary microvascular injury in rats. Am Rev Respir Dis. 1985;132(4):880-4.
34. Eyal FG, Hamm CR, Parker JC. Reduction in alveolar macrophages attenuates acute ventilator induced lung injury in rats. Intensive Care Med. 2007;33(7):1212-8. http://dx.doi.org/10.1007/s00134-007-0651-x
35. Gattinoni L, Pesenti A. The concept of “baby lung”. Intensive Care Med. 2005;31(6):776-84. http://dx.doi.org/10.1007/s00134-005-2627-z
173J Bras Pneumol. 2016;42(3):166-173
ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000065
ABSTRACTObjective: Post-infectious bronchiolitis obliterans (PIBO) is a clinical entity that has been classified as constrictive, fixed obstruction of the lumen by fibrotic tissue. However, recent studies using impulse oscillometry have reported bronchodilator responses in PIBO patients. The objective of this study was to evaluate bronchodilator responses in pediatric PIBO patients, comparing different criteria to define the response. Methods: We evaluated pediatric patients diagnosed with PIBO and treated at one of two pediatric pulmonology outpatient clinics in the city of Porto Alegre, Brazil. Spirometric parameters were measured in accordance with international recommendations. Results: We included a total of 72 pediatric PIBO patients. The mean pre- and post-bronchodilator values were clearly lower than the reference values for all parameters, especially FEF25-75%. There were post-bronchodilator improvements. When measured as mean percent increases, FEV1 and FEF25-75%, improved by 11% and 20%, respectively. However, when the absolute values were calculated, the mean FEV1 and FEF25-75% both increased by only 0.1 L. We found that age at viral aggression, a family history of asthma, and allergy had no significant effects on bronchodilator responses. Conclusions: Pediatric patients with PIBO have peripheral airway obstruction that is responsive to treatment but is not completely reversible with a bronchodilator. The concept of PIBO as fixed, irreversible obstruction does not seem to apply to this population. Our data suggest that airway obstruction is variable in PIBO patients, a finding that could have major clinical implications.
Keywords: Bronchiolitis obliterans; Infection/complications; Airway obstruction; Bronchodilator agents.
Evaluating bronchodilator response in pediatric patients with post-infectious bronchiolitis obliterans: use of different criteria for identifying airway reversibilityRita Mattiello1, Paula Cristina Vidal2, Edgar Enrique Sarria3, Paulo Márcio Pitrez1, Renato Tetelbom Stein1, Helena Teresinha Mocelin4, Gilberto Bueno Fischer4, Marcus Herbert Jones1, Leonardo Araújo Pinto1
Correspondence to:Leonardo A. Pinto. Instituto de Pesquisas Biomédicas, Centro Infant, Avenida Ipiranga, 6690, 2º andar, CEP 90610-000, Porto Alegre, RS, Brasil.Tel.: 55 51 3320-3000 or 55 51 3320-2221. Fax: 55 51 3320-3000. E-mail: [email protected] support: This study received financial support from the Brazilian Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq, National Council for Scientific and Technological Development), the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, Office for the Advancement of Higher Education), and the Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS, Foundation for the Support of Research in the State of Rio Grande do Sul).
INTRODUCTION
Bronchiolitis obliterans is a form of chronic obstructive lung disease secondary to a severe insult to the lower respiratory tract. The disease is characterized by the narrowing of the distal airways, which leads to a chronic obstructive disorder. In children, the most common form is post-infectious bronchiolitis obliterans (PIBO). (1,2) There are reports of PIBO secondary to infection with influenza, parainfluenza, respiratory syncytial virus, and Mycoplasma pneumonia; however, certain adenovirus serotypes seem to be the infectious agents most likely linked with PIBO. (2-4) Although PIBO has been reported in several different regions in the world, South American countries have historically reported the highest numbers of cases. (1) In most of those reports, PIBO has been classified as constrictive airway disease, presenting some degree of luminal occlusion by fibrous tissue, together with chronic inflammation. Total obliteration of the lumen by fibrotic tissue has been observed in up to 23% of patients.(4,5)
A diagnosis of PIBO should be made not only on the basis of a suggestive clinical history and characteristic HRCT findings but also on that of spirometric evidence of moderate to severe obstructive impairment.(6,7) Some authors consider PIBO a disorder involving fixed obstruction. However, there is some controversy in the aspect of pulmonary function in PIBO patients, which calls for further research at various levels.
The question of the response to the use of a broncho-dilator in patients with PIBO is an important one, given its potential impact in the clinical management of PIBO. Most authors believe that PIBO patients would not show a significant bronchodilator response, since there is considerable evidence that these subjects present with fixed airway obstruction.(1,6-9) However, in one previous study, it was reported that patients diagnosed with PIBO showed such a response.(7) In the present study, we evaluated bronchodilator responses in a large sample of pediatric patients diagnosed with PIBO, comparing different criteria to define the significance of the response.
1. Centro Infant, Instituto de Pesquisas Biomédicas, Pontifícia Universidade Católica do Rio Grande do Sul – PUCRS – Porto Alegre (RS) Brasil.
2. Universidade Regional Integrada do Alto Uruguai e das Missões – URI – Erechim (RS) Brasil.
3. Curso de Medicina, Universidade de Santa Cruz do Sul – UNISC – Santa Cruz do Sul (RS) Brasil.
4. Universidade Federal de Ciências da Saúde de Porto Alegre – UFCSPA – Porto Alegre (RS) Brasil.
Submitted: 6 April 2015. Accepted: 30 November 2015.
Study carried out at the Instituto de Pesquisas Biomédicas, Centro Infant, Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre (RS), Brasil.
J Bras Pneumol. 2016;42(3):174-178
174
ORIGINAL ARTICLE

Mattiello R, Vidal PC, Sarria EE, Pitrez PM, Stein RT, Mocelin HT, Fischer GB, Jones MH, Pinto LA
METHODS
Patients and proceduresThis was a cross-sectional study involving children
and adolescents with PIBO, all of whom had previously been diagnosed with PIBO and were under follow-up treatment at pediatric pulmonology outpatient clinics at one of two university hospitals in the city of Porto Alegre, Brazil: the Hospital São Lucas, operated by the Pontifical Catholic University of Rio Grande do Sul; or the Santo Antônio Children’s Hospital, which is part of the Santa Casa Hospital Complex. The mean age of the patients was 10 years (range, 4-17 years). The medical staff at both hospitals have clinical expertise in diagnosing PIBO in pediatric patients. For the purposes of this study, we included spirometry results for all of the patients. All of the spirometry tests performed at the two hospitals met the American Thoracic Society/European Respiratory Society (ATS/ERS) requirements for acceptability and reproducibility.(10)
The diagnosis of PIBO was based on a combination of clinical, epidemiologic, and imaging data, as previously described.(1) All diagnoses of PIBO were made on the basis of the following criteria: having had acute, severe bronchiolitis or viral pneumonia during the first two years of life after having previously been healthy; presenting with evidence of persistent airway obstruction after the acute event (identified either by physical examination or by pulmonary function testing); presenting with chest X-ray findings indicative of chronic lung disease (e.g., hyperinflation, atelectasis, airway wall thickening, and bronchiectasis); presenting with chest CT findings of a mosaic pattern and air trapping. A diagnosis of PIBO was ruled out if the patient had any other condition that progresses to permanent respiratory symptoms, including chronic lung diseases such as cystic fibrosis and bronchopulmonary dysplasia, as well as immunodeficiency disorders. Family histories of asthma and allergy (rhinitis, eczema, etc.) were taken at regular clinical visits.
Spirometric parameters (FVC, FEV1, FEF25-75%, and the FEV1/FVC ratio) were measured in accordance with international recommendations for acceptability and reproducibility.(10) The pulmonary function parameters were measured only if patients had been free of res-piratory exacerbations and clinically stable for at least two weeks. Prior to the tests, short- and long-acting β2 agonists were withheld for 12 and 48 h, respectively, although inhaled corticosteroids were maintained as prescribed. Spirometric values were chosen from the best three acceptable, reproducible FVC maneuvers, and the one with the greatest sum of FVC and FEV1 was selected. Reference values and equations employed for spirometry were those described by Stanojevic et al.(11) All pulmonary function data are expressed as z-score values. The severity of functional impairment was defined on the basis of the FEV1, in accordance with the ATS/ERS recommendations.(10) The main methods for analyzing bronchodilator responses are
described in Chart 1. In addition, we analyzed factors that could have influenced the bronchodilator response.
Statistical analysisContinuous variables are expressed as mean ±
standard deviation or as median and interquartile range, whereas categorical variables are expressed as absolute and relative frequencies. Each pulmonary function parameter was expressed as a z-score, using the regression equation and variance derived from ref-erence population values.(8,11) To analyze bronchodilator response data, we used the generalized estimating equation procedure(10-13) of a generalized linear model, which allows the analysis of repeated measures; the working correlation matrix was autoregressive.(14) A linear mixed model was used to determine whether bronchodilator responses (outcomes) were affected by patient age at the time of viral aggression, by a family history of asthma, or by allergy. For all analyses, the level of statistical significance was set at p < 0.05. Data processing and analysis were performed with IBM SPSS Statistics software package, version 18.0 (IBM Corporation, Armonk, NY, USA).
The study was approved by the local research ethics committees of both institutions. All participating patients verbally consented to be included in the study, and the parents or legal guardians of the participants gave written informed consent.
RESULTS
We evaluated a total of 72 pediatric patients with PIBO. The patients had been monitored periodically, from infancy, at outpatient clinics. The characteristics of the study sample are shown in Table 1. Of the 72 patients evaluated, 55 (76.4%) were male. Most of the patients had been diagnosed with PIBO during the first year of life.
The pulmonary function parameters of the patients, expressed as z-score values, are presented in Table 2. The mean pre- and post-bronchodilator values for all parameters were abnormal, especially those for FEF25-75%. There were significant post-bronchodilator improvements in expiratory flows, although the values did not reach normality for age. As can be seen in Table 3, the improvements were significant when the mean percent variation from the previous measurement was calculated (increases of 11% and 20% for FEV1 and FEF25-75%, respectively). However,
Chart 1. Description of different methods (equations) for calculating a bronchodilator response.Percent variation from the previous (pre-bronchodilator)
measurement:(FEV1post − FEV1pre)/(FEV1pre × 100)
Percent change in the percentage of the predicted value:
(FEV1post − FEV1pre)/(FEV1 predicted × 100)Absolute volume change from the previous
(pre-bronchodilator) measurement:FEV1post − FEV1pre
Post: post-bronchodilator; and pre: pre-bronchodilator.
175J Bras Pneumol. 2016;42(3):174-178
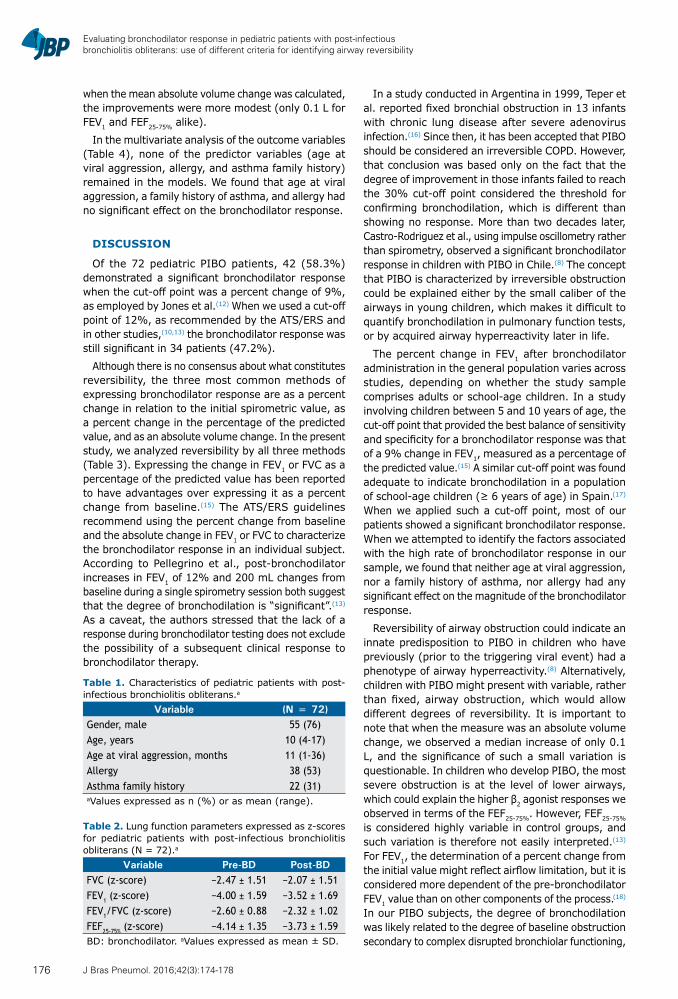
Evaluating bronchodilator response in pediatric patients with post-infectious bronchiolitis obliterans: use of different criteria for identifying airway reversibility
when the mean absolute volume change was calculated, the improvements were more modest (only 0.1 L for FEV1 and FEF25-75% alike).
In the multivariate analysis of the outcome variables (Table 4), none of the predictor variables (age at viral aggression, allergy, and asthma family history) remained in the models. We found that age at viral aggression, a family history of asthma, and allergy had no significant effect on the bronchodilator response.
DISCUSSION
Of the 72 pediatric PIBO patients, 42 (58.3%) demonstrated a significant bronchodilator response when the cut-off point was a percent change of 9%, as employed by Jones et al.(12) When we used a cut-off point of 12%, as recommended by the ATS/ERS and in other studies,(10,13) the bronchodilator response was still significant in 34 patients (47.2%).
Although there is no consensus about what constitutes reversibility, the three most common methods of expressing bronchodilator response are as a percent change in relation to the initial spirometric value, as a percent change in the percentage of the predicted value, and as an absolute volume change. In the present study, we analyzed reversibility by all three methods (Table 3). Expressing the change in FEV1 or FVC as a percentage of the predicted value has been reported to have advantages over expressing it as a percent change from baseline.(15) The ATS/ERS guidelines recommend using the percent change from baseline and the absolute change in FEV1 or FVC to characterize the bronchodilator response in an individual subject. According to Pellegrino et al., post-bronchodilator increases in FEV1 of 12% and 200 mL changes from baseline during a single spirometry session both suggest that the degree of bronchodilation is “significant”.(13) As a caveat, the authors stressed that the lack of a response during bronchodilator testing does not exclude the possibility of a subsequent clinical response to bronchodilator therapy.
In a study conducted in Argentina in 1999, Teper et al. reported fixed bronchial obstruction in 13 infants with chronic lung disease after severe adenovirus infection.(16) Since then, it has been accepted that PIBO should be considered an irreversible COPD. However, that conclusion was based only on the fact that the degree of improvement in those infants failed to reach the 30% cut-off point considered the threshold for confirming bronchodilation, which is different than showing no response. More than two decades later, Castro-Rodriguez et al., using impulse oscillometry rather than spirometry, observed a significant bronchodilator response in children with PIBO in Chile.(8) The concept that PIBO is characterized by irreversible obstruction could be explained either by the small caliber of the airways in young children, which makes it difficult to quantify bronchodilation in pulmonary function tests, or by acquired airway hyperreactivity later in life.
The percent change in FEV1 after bronchodilator administration in the general population varies across studies, depending on whether the study sample comprises adults or school-age children. In a study involving children between 5 and 10 years of age, the cut-off point that provided the best balance of sensitivity and specificity for a bronchodilator response was that of a 9% change in FEV1, measured as a percentage of the predicted value.(15) A similar cut-off point was found adequate to indicate bronchodilation in a population of school-age children (≥ 6 years of age) in Spain. (17) When we applied such a cut-off point, most of our patients showed a significant bronchodilator response. When we attempted to identify the factors associated with the high rate of bronchodilator response in our sample, we found that neither age at viral aggression, nor a family history of asthma, nor allergy had any significant effect on the magnitude of the bronchodilator response.
Reversibility of airway obstruction could indicate an innate predisposition to PIBO in children who have previously (prior to the triggering viral event) had a phenotype of airway hyperreactivity.(8) Alternatively, children with PIBO might present with variable, rather than fixed, airway obstruction, which would allow different degrees of reversibility. It is important to note that when the measure was an absolute volume change, we observed a median increase of only 0.1 L, and the significance of such a small variation is questionable. In children who develop PIBO, the most severe obstruction is at the level of lower airways, which could explain the higher β2 agonist responses we observed in terms of the FEF25-75%. However, FEF25-75% is considered highly variable in control groups, and such variation is therefore not easily interpreted.(13) For FEV1, the determination of a percent change from the initial value might reflect airflow limitation, but it is considered more dependent of the pre-bronchodilator FEV1 value than on other components of the process. (18) In our PIBO subjects, the degree of bronchodilation was likely related to the degree of baseline obstruction secondary to complex disrupted bronchiolar functioning,
Table 1. Characteristics of pediatric patients with post-infectious bronchiolitis obliterans.a
Variable (N = 72)Gender, male 55 (76)Age, years 10 (4-17)Age at viral aggression, months 11 (1-36)Allergy 38 (53)Asthma family history 22 (31)aValues expressed as n (%) or as mean (range).
Table 2. Lung function parameters expressed as z-scores for pediatric patients with post-infectious bronchiolitis obliterans (N = 72).a
Variable Pre-BD Post-BDFVC (z-score) −2.47 ± 1.51 −2.07 ± 1.51FEV1 (z-score) −4.00 ± 1.59 −3.52 ± 1.69FEV1/FVC (z-score) −2.60 ± 0.88 −2.32 ± 1.02FEF25-75% (z-score) −4.14 ± 1.35 −3.73 ± 1.59BD: bronchodilator. aValues expressed as mean ± SD.
176 J Bras Pneumol. 2016;42(3):174-178
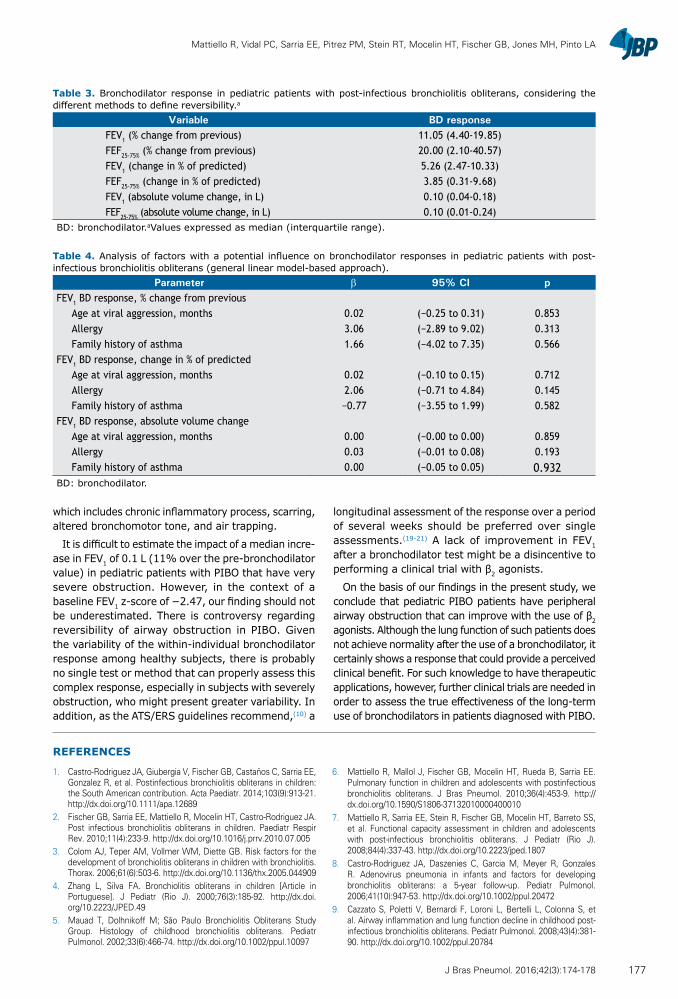
Mattiello R, Vidal PC, Sarria EE, Pitrez PM, Stein RT, Mocelin HT, Fischer GB, Jones MH, Pinto LA
which includes chronic inflammatory process, scarring, altered bronchomotor tone, and air trapping.
It is difficult to estimate the impact of a median incre-ase in FEV1 of 0.1 L (11% over the pre-bronchodilator value) in pediatric patients with PIBO that have very severe obstruction. However, in the context of a baseline FEV1 z-score of −2.47, our finding should not be underestimated. There is controversy regarding reversibility of airway obstruction in PIBO. Given the variability of the within-individual bronchodilator response among healthy subjects, there is probably no single test or method that can properly assess this complex response, especially in subjects with severely obstruction, who might present greater variability. In addition, as the ATS/ERS guidelines recommend,(10) a
longitudinal assessment of the response over a period of several weeks should be preferred over single assessments.(19-21) A lack of improvement in FEV1 after a bronchodilator test might be a disincentive to performing a clinical trial with β2 agonists.
On the basis of our findings in the present study, we conclude that pediatric PIBO patients have peripheral airway obstruction that can improve with the use of β2 agonists. Although the lung function of such patients does not achieve normality after the use of a bronchodilator, it certainly shows a response that could provide a perceived clinical benefit. For such knowledge to have therapeutic applications, however, further clinical trials are needed in order to assess the true effectiveness of the long-term use of bronchodilators in patients diagnosed with PIBO.
Table 4. Analysis of factors with a potential influence on bronchodilator responses in pediatric patients with post-infectious bronchiolitis obliterans (general linear model-based approach).
Parameter β 95% CI pFEV1 BD response, % change from previous
Age at viral aggression, months 0.02 (−0.25 to 0.31) 0.853Allergy 3.06 (−2.89 to 9.02) 0.313Family history of asthma 1.66 (−4.02 to 7.35) 0.566
FEV1 BD response, change in % of predictedAge at viral aggression, months 0.02 (−0.10 to 0.15) 0.712Allergy 2.06 (−0.71 to 4.84) 0.145Family history of asthma −0.77 (−3.55 to 1.99) 0.582
FEV1 BD response, absolute volume changeAge at viral aggression, months 0.00 (−0.00 to 0.00) 0.859Allergy 0.03 (−0.01 to 0.08) 0.193Family history of asthma 0.00 (−0.05 to 0.05) 0.932
BD: bronchodilator.
REFERENCES
1. Castro-Rodriguez JA, Giubergia V, Fischer GB, Castaños C, Sarria EE, Gonzalez R, et al. Postinfectious bronchiolitis obliterans in children: the South American contribution. Acta Paediatr. 2014;103(9):913-21. http://dx.doi.org/10.1111/apa.12689
2. Fischer GB, Sarria EE, Mattiello R, Mocelin HT, Castro-Rodriguez JA. Post infectious bronchiolitis obliterans in children. Paediatr Respir Rev. 2010;11(4):233-9. http://dx.doi.org/10.1016/j.prrv.2010.07.005
3. Colom AJ, Teper AM, Vollmer WM, Diette GB. Risk factors for the development of bronchiolitis obliterans in children with bronchiolitis. Thorax. 2006;61(6):503-6. http://dx.doi.org/10.1136/thx.2005.044909
4. Zhang L, Silva FA. Bronchiolitis obliterans in children [Article in Portuguese]. J Pediatr (Rio J). 2000;76(3):185-92. http://dx.doi.org/10.2223/JPED.49
5. Mauad T, Dolhnikoff M; São Paulo Bronchiolitis Obliterans Study Group. Histology of childhood bronchiolitis obliterans. Pediatr Pulmonol. 2002;33(6):466-74. http://dx.doi.org/10.1002/ppul.10097
6. Mattiello R, Mallol J, Fischer GB, Mocelin HT, Rueda B, Sarria EE. Pulmonary function in children and adolescents with postinfectious bronchiolitis obliterans. J Bras Pneumol. 2010;36(4):453-9. http://dx.doi.org/10.1590/S1806-37132010000400010
7. Mattiello R, Sarria EE, Stein R, Fischer GB, Mocelin HT, Barreto SS, et al. Functional capacity assessment in children and adolescents with post-infectious bronchiolitis obliterans. J Pediatr (Rio J). 2008;84(4):337-43. http://dx.doi.org/10.2223/jped.1807
8. Castro-Rodriguez JA, Daszenies C, Garcia M, Meyer R, Gonzales R. Adenovirus pneumonia in infants and factors for developing bronchiolitis obliterans: a 5-year follow-up. Pediatr Pulmonol. 2006;41(10):947-53. http://dx.doi.org/10.1002/ppul.20472
9. Cazzato S, Poletti V, Bernardi F, Loroni L, Bertelli L, Colonna S, et al. Airway inflammation and lung function decline in childhood post-infectious bronchiolitis obliterans. Pediatr Pulmonol. 2008;43(4):381-90. http://dx.doi.org/10.1002/ppul.20784
Table 3. Bronchodilator response in pediatric patients with post-infectious bronchiolitis obliterans, considering the different methods to define reversibility.a
Variable BD responseFEV1 (% change from previous) 11.05 (4.40-19.85)FEF25-75% (% change from previous) 20.00 (2.10-40.57)FEV1 (change in % of predicted) 5.26 (2.47-10.33)FEF25-75% (change in % of predicted) 3.85 (0.31-9.68)FEV1 (absolute volume change, in L) 0.10 (0.04-0.18)FEF25-75% (absolute volume change, in L) 0.10 (0.01-0.24)
BD: bronchodilator.aValues expressed as median (interquartile range).
177J Bras Pneumol. 2016;42(3):174-178

Evaluating bronchodilator response in pediatric patients with post-infectious bronchiolitis obliterans: use of different criteria for identifying airway reversibility
10. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319-38. http://dx.doi.org/10.1183/09031936.05.00034805
11. Stanojevic S, Wade A, Cole TJ, Lum S, Custovic A, Silverman M, et al. Spirometry centile charts for young Caucasian children: the Asthma UK Collaborative Initiative. Am J Respir Crit Care Med. 2009;180(6):547-52. http://dx.doi.org/10.1164/rccm.200903-0323OC
12. Jones M, Castile R, Davis S, Kisling J, Filbrun D, Flucke R, et al. Forced expiratory flows and volumes in infants. Normative data and lung growth. Am J Respir Crit Care Med. 2000;161(2 Pt 1):353-9. http://dx.doi.org/10.1164/ajrccm.161.2.9903026
13. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948-68. http://dx.doi.org/10.1183/09031936.05.00035205
14. Edwards LJ. Modern statistical techniques for the analysis of longitudinal data in biomedical research. Pediatr Pulmonol. 2000;30(4):330-44. http://dx.doi.org/10.1002/1099-0496(200010)30:4<330::AID-PPUL10>3.0.CO;2-D
15. Dundas I, Chan EY, Bridge PD, McKenzie SA. Diagnostic accuracy of bronchodilator responsiveness in wheezy children. Thorax. 2005;60(1):13-6. http://dx.doi.org/10.1136/thx.2004.029934
16. Teper AM, Kofman CD, Maffey AF, Vidaurreta SM. Lung function in infants with chronic pulmonary disease after severe adenoviral illness. J Pediatr. 1999;134(6):730-3. http://dx.doi.org/10.1016/S0022-3476(99)70289-1
17. Pardos Martínez C, Fuertes Fernández-Espinar J, Nerín De la Puerta I, González Pérez-Yarza E. Cut-off point for a positive bronchodilation test [Article in Spanish]. An Esp Pediatr. 2002;57(1):5-11. http://dx.doi.org/10.1016/S1695-4033(02)77885-5
18. Brand PL, Quanjer PH, Postma DS, Kerstjens HA, Koëter GH, Dekhuijzen PN, et al. Interpretation of bronchodilator response in patients with obstructive airways disease. The Dutch Chronic Non-Specific Lung Disease (CNSLD) Study Group. Thorax. 1992;47(6):429-36. http://dx.doi.org/10.1136/thx.47.6.429
19. O’Donnell DE. Assessment of bronchodilator efficacy in symptomatic COPD: is spirometry useful? Chest. 2000;117(2 Suppl):42S-7S. http://dx.doi.org/10.1378/chest.117.2_suppl.42S
20. Wang W, Shen KL, Zeng JJ. Clinical studies of children with bronchiolitis obliterans [Article in Chinese]. Zhonghua Er Ke Za Zhi. 2008;46(10):732-8.
21. Wang YT, Thompson LM, Ingenito EP, Ingram RH Jr. Effects of increasing doses of beta-agonists on airway and parenchymal hysteresis. J Appl Physiol (1985). 1990;68(1):363-8.
178 J Bras Pneumol. 2016;42(3):174-178
ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000121
ABSTRACTObjective: To assess and compare the prevalence of comorbidities and risk factors for cardiovascular disease (CVD) in COPD patients according to disease severity. Methods: The study included 25 patients with mild-to-moderate COPD (68% male; mean age, 65 ± 8 years; mean FEV1, 73 ± 15% of predicted) and 25 with severe-to-very severe COPD (males, 56%; mean age, 69 ± 9 years; mean FEV1, 40 ± 18% of predicted). Comorbidities were recorded on the basis of data obtained from medical charts and clinical evaluations. Comorbidities were registered on the basis of data obtained from medical charts and clinical evaluations. The Charlson comorbidity index was calculated, and the Hospital Anxiety and Depression Scale (HADS) score was determined. Results: Of the 50 patients evaluated, 38 (76%) had been diagnosed with at least one comorbidity, 21 (42%) having been diagnosed with at least one CVD. Twenty-four patients (48%) had more than one CVD. Eighteen (36%) of the patients were current smokers, 10 (20%) had depression, 7 (14%) had dyslipidemia, and 7 (14%) had diabetes mellitus. Current smoking, depression, and dyslipidemia were more prevalent among the patients with mild-to-moderate COPD than among those with severe-to-very severe COPD (p < 0.001, p = 0.008, and p = 0.02, respectively). The prevalence of high blood pressure, diabetes mellitus, alcoholism, ischemic heart disease, and chronic heart failure was comparable between the two groups. The Charlson comorbidity index and HADS scores did not differ between the groups. Conclusions: Comorbidities are highly prevalent in COPD, regardless of its severity. Certain risk factors for CVD, themselves classified as diseases (including smoking, dyslipidemia, and depression), appear to be more prevalent in patients with mild-to-moderate COPD.
Keywords: Pulmonary disease, chronic obstructive; Spirometry; Cardiovascular diseases; Risk factors.
Risk factors for cardiovascular disease in patients with COPD: mild-to-moderate COPD versus severe-to-very severe COPDLaura Miranda de Oliveira Caram1, Renata Ferrari1, Cristiane Roberta Naves1, Liana Sousa Coelho1, Simone Alves do Vale1, Suzana Erico Tanni1, Irma Godoy1
Correspondence to:Laura Miranda de Oliveira Caram. Departamento de Medicina Interna, Área de Pneumologia, Faculdade de Medicina de Botucatu, Universidade Estadual Paulista, Distrito de Rubião Junior, s/n, CEP 18618-970, Botucatu, SP, Brasil. Tel.: 55 14 3880-1171. Fax: 55 14 3882-2238. E-mail: [email protected] support: This study received financial support from the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP, São Paulo Research Foundation, grant no. 2010/10312-1). Laura Miranda de Oliveira Caram is the recipient of a research grant from the Brazilian Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, Office for the Advancement of Higher Education).
INTRODUCTION
COPD is characterized by chronic airflow limitation, a range of pathological changes in the lungs, significant extrapulmonary effects, and major comorbidities that can contribute to increasing the severity of the disease. (1) Common comorbidities in patients with COPD include cardiovascular disease (CVD), anemia, lung cancer, diabetes, osteoporosis, anxiety, and depression.(2) Among COPD patients, CVDs are responsible for approximately 50% of all hospitalizations and 20% of all deaths.(3)
The majority (94%) of all COPD patients have at least one comorbidity and up to 46% have three or more,(4) the most prevalent being high blood pressure (HBP), coronary artery disease (CAD), congestive heart failure (CHF), dyslipidemia, and diabetes mellitus (DM).(2,5) Two previous studies evaluated the prevalence of comorbid-ities according to COPD severity,(5,6) although neither evaluated all of the risk factors for CVD. Therefore, the aim of the present study was to assess the prevalence of
comorbidities and risk factors for CVD in COPD patients, comparing them by COPD severity—mild-to-moderate versus severe-to-very severe.
METHODS
Seventy patients with COPD were recruited from the Pulmonary Outpatient Unit at the Botucatu Hospital das Clínicas of the São Paulo State University Botucatu School of Medicine. Patients were included if they met the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria for a diagnosis of COPD(1): a post-bronchodilator FEV1/FVC ratio < 0.70 and a < 15% or 200-mL increase in FEV1 following inhalation of a β2 agonist; age ≥ 40 years; and a ≥ 10 pack-year smoking history. Patients with a primary diagnosis of another respiratory disease, such as asthma, a restrictive disorder (tuberculosis sequelae or interstitial fibrosis), obstructive sleep apnea-hypopnea syndrome, and lung cancer, were excluded, as were those with a primary diagnosis of unstable angina, CHF (New
1. Departamento de Medicina Interna, Área de Pneumologia, Faculdade de Medicina de Botucatu, Universidade Estadual Paulista, Botucatu (SP) Brasil.
Submitted: 20 May 2015. Accepted: 3 January 2016.
Study carried out in the Departamento de Medicina Interna, Área de Pneumologia, Faculdade de Medicina de Botucatu, Universidade Estadual Paulista, Botucatu (SP) Brasil.
J Bras Pneumol. 2016;42(3):179-184
179
ORIGINAL ARTICLE

Risk factors for cardiovascular disease in patients with COPD: mild-to-moderate COPD versus severe-to-very severe COPD
York Heart Association functional class III or IV), or any other chronic disease, such as uncontrolled DM, kidney failure, liver failure, and cancer. We took into consideration the post-bronchodilator values of FEV1 (% of the predicted value) and arterial blood gas parameters. We categorized the severity of COPD according to the GOLD stages,(1) as mild-to-moderate (GOLD stage I or II) or severe-to-very severe (GOLD stage III or IV).
The study was approved by the Research Ethics Committee of the Botucatu Hospital das Clínicas. All participating patients gave written informed consent.
Laboratory tests, pulmonary function tests, and pulse oximetry
Laboratory tests included complete blood counts, as well as determination of the following: lipid profile; total and fractional protein levels; fasting glucose level; hepatic function; and renal function. The biochemical tests were performed according to the methods applied by the Clinical Analysis Laboratory of the institution.
Pre- and post-bronchodilator spirometry were performed with a portable spirometer (Koko; Ferraris Respiratory, Louisville, CO, USA), in accordance with the American Thoracic Society criteria.(7) Values of FEV1 were expressed in liters, as percentages of the FVC, and as percentages of the reference values.(8) The SpO2 was assessed with an oximeter (Onyx 9500; Nonin Medical Inc., Plymouth, MN, USA) while the patients were breathing room air.
ComorbiditiesComorbidities were identified in medical records
and confirmed at clinical evaluation. Current smoking was considered a comorbidity, in accordance with the International Statistical Classification of Diseases, 10th Revision, in which nicotine dependence is coded as F17. The smoking status was confirmed by measuring carbon monoxide (CO) in exhaled air with a CO analyzer (Micro CO Meter, Cardinal Health, Chatham, UK). An exhaled CO level > 6.0 ppm was considered indicative of current smoking.(9)
For each patient, we calculated the Charlson comor-bidity index.(10) The Hospital Anxiety and Depression Scale (HADS), which has been translated to Portuguese and validated for use in Brazil,(11) was used in order to evaluate symptoms related to anxiety and depression.
Nutritional assessmentWe determined body weight and height using a
calibrated platform scale with a stadiometer (Filizola, São Paulo, Brazil). The body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m2). Body composition was evaluated by bioelectrical impedance (BIA 101A; RJL Systems Inc., Clinton Township, MI, USA), in accordance with the guidelines established by the European Society for Parenteral and Enteral Nutrition.(12) Fat-free mass (FFM, in kg) was calculated through the use of a group-specific regression equation developed by Kyle
et al.(13) We also calculated the FFM index (FFMI), using the following equation:FFMI = FFM/height2
Statistical analysesDescriptive statistics were calculated for the features
of all participants. Data are expressed as mean ± standard deviation or as median and interquartile range (25-75%), depending on their distribution. Categorical variables are expressed as absolute and relative frequency. The chi-square test and Fisher’s exact test were used in order to compare categorical variables. For comparisons between the two groups, an unpaired t-test was used for continuous variables and the Mann-Whitney test was used for ordinal variables. The level of significance was set at 5%. All analyses were performed with the SigmaStat program, version 3.2 (Systat Software Inc., San Jose, CA, USA).
RESULTS
Twenty patients were excluded from the final analysis, 15 because their primary diagnosis was not COPD and 5 because they did not complete the protocol. Therefore, 50 patients were included in the final analysis: 25 with mild-to-moderate COPD and 25 with severe-to-very severe COPD. Age, gender, smoking history (pack-years), BMI, and FFMI were not statistically different between the groups (Table 1). Of the 50 patients evaluated, 9 (18%) were obese (BMI ≥ 30 kg/m2), 3 in the mild-to-moderate COPD group and 6 in the severe-to-very severe COPD group (p = 0.39).(14) Five patients had very severe COPD and were on long-term oxygen therapy. Figure 1 shows the maintenance medications used by the patients.
Thirty-eight patients (76%) presented with at least one comorbidity, 21 (42%) presenting with at least one cardiovascular comorbidity: HBP, in 40% of the sample; CAD, in 10%; or New York Heart Association functional class I CHF, in 6%. Twenty-four patients (48%) presented more than one CVD. Of the 50 patients evaluated, 18 (36%) were classified as active smokers, 10 (20%) were diagnosed with depression, 7 (14%) were diagnosed with dyslipidemia, 7 (14%) were diagnosed with DM, and 4 (8%) were diagnosed with alcoholism.
Of the 25 patients in the mild-to-moderate COPD group, 14 (56%) were classified as current smokers, 5 (20%) had been diagnosed with dyslipidemia, and 7 (28%) had been diagnosed with depression. Of the 25 patients in the severe-to-very severe COPD group, only 4 (16%) were classified as current smokers, only 2 (8%) had been diagnosed with dyslipidemia, and only 3 (12%) had been diagnosed with depression.
Current smoking and dyslipidemia were more prevalent in the mild-to-moderate COPD group than in the severe-to-very severe COPD group (p < 0.001 and p = 0.02, respectively), whereas the prevalence of HBP, DM, alcoholism, CAD, and CHF was comparable between the two groups (Table 2). Although the
180 J Bras Pneumol. 2016;42(3):179-184
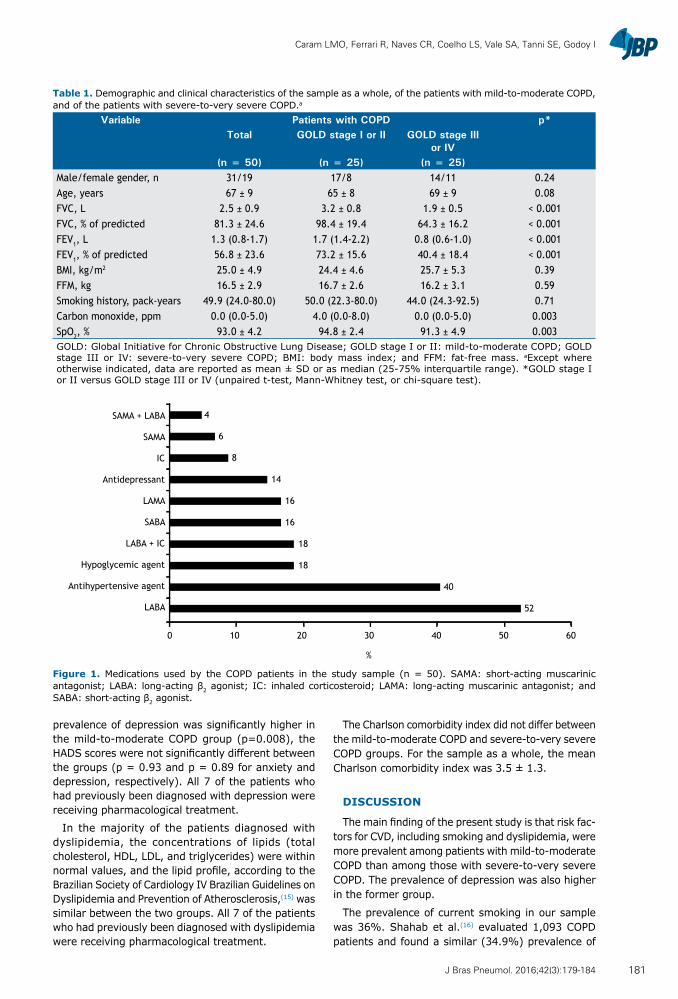
Caram LMO, Ferrari R, Naves CR, Coelho LS, Vale SA, Tanni SE, Godoy I
prevalence of depression was significantly higher in the mild-to-moderate COPD group (p=0.008), the HADS scores were not significantly different between the groups (p = 0.93 and p = 0.89 for anxiety and depression, respectively). All 7 of the patients who had previously been diagnosed with depression were receiving pharmacological treatment.
In the majority of the patients diagnosed with dyslipidemia, the concentrations of lipids (total cholesterol, HDL, LDL, and triglycerides) were within normal values, and the lipid profile, according to the Brazilian Society of Cardiology IV Brazilian Guidelines on Dyslipidemia and Prevention of Atherosclerosis,(15) was similar between the two groups. All 7 of the patients who had previously been diagnosed with dyslipidemia were receiving pharmacological treatment.
The Charlson comorbidity index did not differ between the mild-to-moderate COPD and severe-to-very severe COPD groups. For the sample as a whole, the mean Charlson comorbidity index was 3.5 ± 1.3.
DISCUSSION
The main finding of the present study is that risk fac-tors for CVD, including smoking and dyslipidemia, were more prevalent among patients with mild-to-moderate COPD than among those with severe-to-very severe COPD. The prevalence of depression was also higher in the former group.
The prevalence of current smoking in our sample was 36%. Shahab et al.(16) evaluated 1,093 COPD patients and found a similar (34.9%) prevalence of
Table 1. Demographic and clinical characteristics of the sample as a whole, of the patients with mild-to-moderate COPD, and of the patients with severe-to-very severe COPD.a
Variable Patients with COPD p*Total GOLD stage I or II GOLD stage III
or IV(n = 50) (n = 25) (n = 25)
Male/female gender, n 31/19 17/8 14/11 0.24Age, years 67 ± 9 65 ± 8 69 ± 9 0.08FVC, L 2.5 ± 0.9 3.2 ± 0.8 1.9 ± 0.5 < 0.001FVC, % of predicted 81.3 ± 24.6 98.4 ± 19.4 64.3 ± 16.2 < 0.001FEV1, L 1.3 (0.8-1.7) 1.7 (1.4-2.2) 0.8 (0.6-1.0) < 0.001FEV1, % of predicted 56.8 ± 23.6 73.2 ± 15.6 40.4 ± 18.4 < 0.001BMI, kg/m2 25.0 ± 4.9 24.4 ± 4.6 25.7 ± 5.3 0.39FFM, kg 16.5 ± 2.9 16.7 ± 2.6 16.2 ± 3.1 0.59Smoking history, pack-years 49.9 (24.0-80.0) 50.0 (22.3-80.0) 44.0 (24.3-92.5) 0.71Carbon monoxide, ppm 0.0 (0.0-5.0) 4.0 (0.0-8.0) 0.0 (0.0-5.0) 0.003SpO2, % 93.0 ± 4.2 94.8 ± 2.4 91.3 ± 4.9 0.003GOLD: Global Initiative for Chronic Obstructive Lung Disease; GOLD stage I or II: mild-to-moderate COPD; GOLD stage III or IV: severe-to-very severe COPD; BMI: body mass index; and FFM: fat-free mass. aExcept where otherwise indicated, data are reported as mean ± SD or as median (25-75% interquartile range). *GOLD stage I or II versus GOLD stage III or IV (unpaired t-test, Mann-Whitney test, or chi-square test).
Figure 1. Medications used by the COPD patients in the study sample (n = 50). SAMA: short-acting muscarinic antagonist; LABA: long-acting β2 agonist; IC: inhaled corticosteroid; LAMA: long-acting muscarinic antagonist; and SABA: short-acting β2 agonist.
4
6
8
14
16
16
18
18
40
52
0 10 20 30 40 50 60
SAMA + LABA
SAMA
IC
Antidepressant
LAMA
SABA
LABA + IC
Hypoglycemic agent
Antihypertensive agent
LABA
%
181J Bras Pneumol. 2016;42(3):179-184
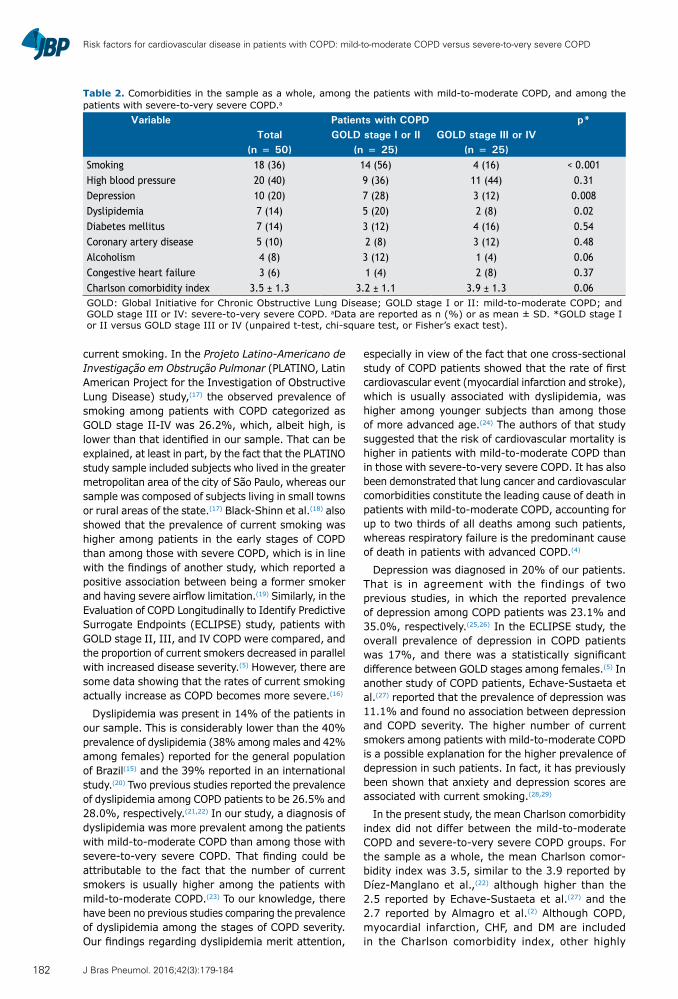
Risk factors for cardiovascular disease in patients with COPD: mild-to-moderate COPD versus severe-to-very severe COPD
current smoking. In the Projeto Latino-Americano de Investigação em Obstrução Pulmonar (PLATINO, Latin American Project for the Investigation of Obstructive Lung Disease) study,(17) the observed prevalence of smoking among patients with COPD categorized as GOLD stage II-IV was 26.2%, which, albeit high, is lower than that identified in our sample. That can be explained, at least in part, by the fact that the PLATINO study sample included subjects who lived in the greater metropolitan area of the city of São Paulo, whereas our sample was composed of subjects living in small towns or rural areas of the state.(17) Black-Shinn et al.(18) also showed that the prevalence of current smoking was higher among patients in the early stages of COPD than among those with severe COPD, which is in line with the findings of another study, which reported a positive association between being a former smoker and having severe airflow limitation.(19) Similarly, in the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study, patients with GOLD stage II, III, and IV COPD were compared, and the proportion of current smokers decreased in parallel with increased disease severity.(5) However, there are some data showing that the rates of current smoking actually increase as COPD becomes more severe.(16)
Dyslipidemia was present in 14% of the patients in our sample. This is considerably lower than the 40% prevalence of dyslipidemia (38% among males and 42% among females) reported for the general population of Brazil(15) and the 39% reported in an international study.(20) Two previous studies reported the prevalence of dyslipidemia among COPD patients to be 26.5% and 28.0%, respectively.(21,22) In our study, a diagnosis of dyslipidemia was more prevalent among the patients with mild-to-moderate COPD than among those with severe-to-very severe COPD. That finding could be attributable to the fact that the number of current smokers is usually higher among the patients with mild-to-moderate COPD.(23) To our knowledge, there have been no previous studies comparing the prevalence of dyslipidemia among the stages of COPD severity. Our findings regarding dyslipidemia merit attention,
especially in view of the fact that one cross-sectional study of COPD patients showed that the rate of first cardiovascular event (myocardial infarction and stroke), which is usually associated with dyslipidemia, was higher among younger subjects than among those of more advanced age.(24) The authors of that study suggested that the risk of cardiovascular mortality is higher in patients with mild-to-moderate COPD than in those with severe-to-very severe COPD. It has also been demonstrated that lung cancer and cardiovascular comorbidities constitute the leading cause of death in patients with mild-to-moderate COPD, accounting for up to two thirds of all deaths among such patients, whereas respiratory failure is the predominant cause of death in patients with advanced COPD.(4)
Depression was diagnosed in 20% of our patients. That is in agreement with the findings of two previous studies, in which the reported prevalence of depression among COPD patients was 23.1% and 35.0%, respectively.(25,26) In the ECLIPSE study, the overall prevalence of depression in COPD patients was 17%, and there was a statistically significant difference between GOLD stages among females.(5) In another study of COPD patients, Echave-Sustaeta et al.(27) reported that the prevalence of depression was 11.1% and found no association between depression and COPD severity. The higher number of current smokers among patients with mild-to-moderate COPD is a possible explanation for the higher prevalence of depression in such patients. In fact, it has previously been shown that anxiety and depression scores are associated with current smoking.(28,29)
In the present study, the mean Charlson comorbidity index did not differ between the mild-to-moderate COPD and severe-to-very severe COPD groups. For the sample as a whole, the mean Charlson comor-bidity index was 3.5, similar to the 3.9 reported by Díez-Manglano et al.,(22) although higher than the 2.5 reported by Echave-Sustaeta et al.(27) and the 2.7 reported by Almagro et al.(2) Although COPD, myocardial infarction, CHF, and DM are included in the Charlson comorbidity index, other highly
Table 2. Comorbidities in the sample as a whole, among the patients with mild-to-moderate COPD, and among the patients with severe-to-very severe COPD.a
Variable Patients with COPD p*Total GOLD stage I or II GOLD stage III or IV
(n = 50) (n = 25) (n = 25)Smoking 18 (36) 14 (56) 4 (16) < 0.001High blood pressure 20 (40) 9 (36) 11 (44) 0.31Depression 10 (20) 7 (28) 3 (12) 0.008Dyslipidemia 7 (14) 5 (20) 2 (8) 0.02Diabetes mellitus 7 (14) 3 (12) 4 (16) 0.54Coronary artery disease 5 (10) 2 (8) 3 (12) 0.48Alcoholism 4 (8) 3 (12) 1 (4) 0.06Congestive heart failure 3 (6) 1 (4) 2 (8) 0.37Charlson comorbidity index 3.5 ± 1.3 3.2 ± 1.1 3.9 ± 1.3 0.06GOLD: Global Initiative for Chronic Obstructive Lung Disease; GOLD stage I or II: mild-to-moderate COPD; and GOLD stage III or IV: severe-to-very severe COPD. aData are reported as n (%) or as mean ± SD. *GOLD stage I or II versus GOLD stage III or IV (unpaired t-test, chi-square test, or Fisher’s exact test).
182 J Bras Pneumol. 2016;42(3):179-184

Caram LMO, Ferrari R, Naves CR, Coelho LS, Vale SA, Tanni SE, Godoy I
prevalent diseases observed in our study, including current smoking, HBP, dyslipidemia, alcoholism, and depression, are not. Therefore, the exclusive use of the Charlson comorbidity index could result in an underestimation of the prevalence of comorbidities and of their influence on the prognosis of COPD patients. After age and chronic symptoms, comorbidities are the most important predictive factors of the future health care costs and direct costs of COPD.(4) In addition, our findings underscore the need for a new comorbidity index to be applied in patients with COPD, given that some highly prevalent comorbidities are not included in the index currently available.
Our study has certain limitations. Although the comorbidities observed in our study are similar to those
identified in the current literature, the prospective design and characteristics of the patient sample could explain some of our findings. In addition, the small size of our sample might impose some limitations on the interpretation of our data.
In conclusion, the prevalence of comorbidities is high among patients with COPD, regardless of disease severity. In addition, smoking and dyslipidemia appear to be more prevalent in mild-to-moderate COPD. Therefore, controlling these comorbidities might be a key measure in the early phases of the disease, in order to decrease mortality due to cardiovascular events. Our findings show the importance of therapeutic measures to promote smoking cessation and of early diagnosis to prevent the progression of airflow obstruction.
REFERENCES
1. Global Initiative for Chronic Obstructive Lung Disease [homepage on the Internet]. Bethesda: Global Initiative for Chronic Obstructive Lung Disease. [cited 2014 Oct 1]. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD Executive Summary, update 2014. Available from: http://www.goldcopd.org/
2. Almagro P, López García F, Cabrera F, Montero L, Morchón D, Díez J, et al. Comorbidity and gender-related differences in patients hospitalized for COPD. The ECCO study. Respir Med. 2010;104(2):253-9. http://dx.doi.org/10.1016/j.rmed.2009.09.019
3. Sin DD, Man SF. Impact of cancers and cardiovascular disease in chronic obstructive pulmonary disease. Curr Opin Pulm Med. 2008;14(2):115-21. http://dx.doi.org/10.1097/MCP.0b013e3282f45ffb
4. Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95-109. http://dx.doi.org/10.2147/COPD.S54473
5. Agusti A, Calverley PM, Celli B, Coxson HO, Edwards LD, Lomas DA, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11:122. http://dx.doi.org/10.1186/1465-9921-11-122
6. Pedone C, Scarlata S, Sorino C, Forastiere F, Bellia V, Antonelli Incalzi R. Does mild COPD affect prognosis in the elderly? BMC Pulm Med. 2010;10:35. http://dx.doi.org/10.1186/1471-2466-10-35
7. Standardization of spirometry--1987 update. Statement of the American Thoracic Society. Am Rev Respir Dis. 1987;136(5):1285-98. http://dx.doi.org/10.1164/ajrccm/136.5.1285
8. Pereira CA, Barreto SP, Simões JG, Pereira FW, Gerstler JG, Nakatani J. Valores de referência para a espirometria em uma amostra da população brasileira adulta. J Pneumol. 1992;18(1):10-22.
9. Middleton ET, Morice AH. Breath carbon monoxide as an indication of smoking habit. Chest. 2000;117(3):758-63. http://dx.doi.org/10.1378/chest.117.3.758
10. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245-51. http://dx.doi.org/10.1016/0895-4356(94)90129-5
11. Botega NJ, Bio MR, Zomignani MA, Garcia C Jr, Pereira WA. Mood disorders among medical in-patients: a validation study of the hospital anxiety and depression scale (HAD) [Article in Portuguese]. Rev Saude Publica. 1995;29(5):359-63.
12. Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Gómez JM, et al. Bioelectrical impedance analysis--part I: review of principles and methods. Clin Nutr. 2004;23(5):1226-43. http://dx.doi.org/10.1016/j.clnu.2004.06.004
13. Kyle UG, Pichard C, Rochat T, Slosman DO, Fitting JW, Thiebaud D. New bioelectrical impedance formula for patients with respiratory insufficiency: comparison to dual-energy X-ray absorptiometry. Eur Respir J. 1998;12(4):960-6. http://dx.doi.org/10.1183/09031936.98.12040960
14. World Health Organization [homepage on the Internet]. Geneva: World Health Organization; c2015 [cited 2015 May 10]. Overweight and obesity fact sheet 2015. Available from: http://www.searo.who.int/linkfiles/non_communicable_diseases_obesety-fs
15. Sposito AC, Caramelli B, Fonseca FA, Bertolami MC, Afiune Neto A, Souza AD, et al. IV Brazilian Guideline for Dyslipidemia and Atherosclerosis prevention: Department of Atherosclerosis of Brazilian Society of Cardiology [Article in Portuguese]. Arq Bras Cardiol. 2007;88 Suppl 1:2-19. http://dx.doi.org/10.1590/S0066-782X2007000700002
16. Shahab L, Jarvis MJ, Britton J, West R. Prevalence, diagnosis and relation to tobacco dependence of chronic obstructive pulmonary disease in a nationally representative sample. Thorax. 2006;61(12):1043-47. http://dx.doi.org/10.1136/thx.2006.064410
17. Menezes AM, Jardim JR, Pérez-Padilla R, Camelier A, Rosa F, Nascimento O, et al. Prevalence of chronic obstructive pulmonary disease and associated factors: the PLATINO Study in São Paulo, Brazil. Cad Saude Publica. 2005;21(5):1565-73. http://dx.doi.org/10.1590/S0102-311X2005000500030
18. Black-Shinn JL, Kinney GL, Wise AL, Regan EA, Make B, Krantz MJ, et al. Cardiovascular disease is associated with COPD severity and reduced functional status and quality of life. COPD. 2014;11(5):546-51. http://dx.doi.org/10.3109/15412555.2014.898029
19. Mitsiki E, Bania E, Varounis C, Gourgoulianis KI, Alexopoulos EC. Characteristics of prevalent and new COPD cases in Greece: the GOLDEN study. Int J Chron Obstruct Pulmon Dis. 2015;10:1371-82. http://dx.doi.org/10.2147/COPD.S81468
20. Leiter LA, Lundman P, da Silva PM, Drexel H, Jünger C, Gitt AK, et al. Persistent lipid abnormalities in statin-treated patients with diabetes mellitus in Europe and Canada: results of the Dyslipidemia International Study. Diabet Med. 2011;28(11):1343-51. http://dx.doi.org/10.1111/j.1464-5491.2011.03360.x
21. Nagorni-Obradovic LM, Vukovic DS. The prevalence of COPD co-morbidities in Serbia: results of a national survey. NPJ Prim Care Respir Med. 2014;24:14008. http://dx.doi.org/10.1038/npjpcrm.2014.8
22. Díez-Manglano J, Bernabeu-Wittel M, Escalera-Zalvide A, Sánchez-Ledesma M, Mora-Rufeti A, Nieto-Martín D, et al. Comorbidity discapacity and mortality in patients with multiple conditions and chronic obstructive pulmonary disease [Article in Spanish]. Rev Clin Esp. 2011;211(10):504-10. http://dx.doi.org/10.1016/j.rce.2011.04.006
23. Forti N, Diament J. High-density lipoproteins: metabolic, clinical, epidemiological and therapeutic intervention aspects. An update for clinicians. Arq Bras Cardiol. 2006;87(5):671-9. http://dx.doi.org/10.1590/S0066-782X2006001800019
24. Feary JR, Rodrigues LC, Smith CJ, Hubbard RB, Gibson JE. Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary care. Thorax. 2010;65(11):956-62. http://dx.doi.org/10.1136/thx.2009.128082
25. Schneider C, Jick SS, Bothner U, Meier CR. COPD and the risk of depression. Chest. 2010;137(2):341-7. http://dx.doi.org/10.1378/chest.09-0614
26. Wagena EJ, Arrindell WA, Wouters EF, van Schayck CP. Are patients with COPD psychologically distressed? Eur Respir J. 2005;26(2):242-8. http://dx.doi.org/10.1183/09031936.05.00010604
183J Bras Pneumol. 2016;42(3):179-184

Risk factors for cardiovascular disease in patients with COPD: mild-to-moderate COPD versus severe-to-very severe COPD
27. Echave-Sustaeta JM, Comeche Casanova L, Cosio BG, Soler-Cataluña JJ, Garcia-Lujan R, Ribera X. Comorbidity in chronic obstructive pulmonary disease. Related to disease severity? Int J Chron Obstruct Pulmon Dis. 2014;9:1307-14. http://dx.doi.org/10.2147/COPD.S71849
28. Northrop-Clewes CA, Thurnham DI. Monitoring micronutrients in
cigarette smokers. Clin Chim Acta. 2007;377(1-2):14-38. http://dx.doi.org/10.1016/j.cca.2006.08.028
29. Saravanan C, Heidhy I. Psychological problems and psychosocial predictors of cigarette smoking behavior among undergraduate students in Malaysia. Asian Pac J Cancer Prev. 2014;15(18):7629-34. http://dx.doi.org/10.7314/APJCP.2014.15.18.7629
184 J Bras Pneumol. 2016;42(3):179-184

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000212
ABSTRACTObjective: To describe the implementation of a robotic thoracic surgery program at a public tertiary teaching hospital and to analyze its initial results. Methods: This was a planned interim analysis of a randomized clinical trial aimed at comparing video-assisted thoracoscopic surgery and robotic surgery in terms of the results obtained after pulmonary lobectomy. The robotic surgery program developed at the Instituto do Câncer do Estado de São Paulo, in the city of São Paulo, Brazil, is a multidisciplinary initiative involving various surgical specialties, as well as anesthesiology, nursing, and clinical engineering teams. In this analysis, we evaluated the patients included in the robotic lobectomy arm of the trial during its first three months (from April to June of 2015). Results: Ten patients were included in this analysis. There were eight women and two men. The mean age was 65.1 years. All of the patients presented with peripheral tumors. We performed right upper lobectomy in four patients, right lower lobectomy in four, and left upper lobectomy in two. Surgical time varied considerably (range, 135-435 min). Conversion to open surgery or video-assisted thoracoscopic surgery was not necessary in any of the cases. Intraoperative complications were not found. Only the first patient required postoperative transfer to the ICU. There were no deaths or readmissions within the first 30 days after discharge. The only postoperative complication was chest pain (grade 3), in two patients. Pathological examination revealed complete tumor resection in all cases. Conclusions: When there is integration and proper training of all of the teams involved, the implementation of a robotic thoracic surgery program is feasible and can reduce morbidity and mortality.
Keywords: Pneumonectomy; Robotic surgical procedures; Thoracic surgery; Minimally invasive surgical procedures; Lung neoplasms.
Robotic pulmonary lobectomy for lung cancer treatment: program implementation and initial experienceRicardo Mingarini Terra1, Pedro Henrique Xavier Nabuco de Araujo2, Leticia Leone Lauricella2, José Ribas Milanez de Campos1, Herbert Felix Costa2, Paulo Manuel Pego-Fernandes1
Correspondence to:Ricardo Mingarini Terra. Avenida Dr. Enéas de Carvalho Aguiar, 44, bloco II, 2º andar, sala 9, CEP 05403-900, São Paulo, SP, Brasil. Tel./fax: 55 11 2661-5248. E-mail: [email protected] Financial support: None.
INTRODUCTION
Over the past 20 years, minimally invasive surgery has developed rapidly. Beginning in the 1990s, video-assisted technology came to be widely used for surgery, thus playing a decisive role in increasing the prominence of minimally invasive surgery. Video-assisted technology also had an impact on thoracic surgery, pleural procedures and easily performed resections having rapidly come to be performed by means of video-assisted thoracoscopic surgery (VATS) in many countries, including Brazil.(1,2)
Studies published in the last decade contributed to consolidating the role of VATS in resections that are more complex, such as lobectomy and pneumonectomy.(3,4) More recently, robotic surgery has emerged as an alternative to video-assisted surgery, its objective being to increase the amplitude and accuracy of intracavitary maneuvers and movements, as well as to provide better visualization via three-dimensional imaging. Studies have shown that robotics can be applied to thoracic surgery, being particularly useful for mediastinal tumors and anatomic lung resections, such as pulmonary lobectomy.(5-8)
The real role of robotics in thoracic surgery has yet to be defined. Although large case series have shown good results regarding intraoperative morbidity, intraoperative mortality, and length of hospital stay,(9) retrospective studies involving databases have raised questions regarding the costs and complications of the new method.(10) The results of an analysis of a US hospital database including 15,502 patients undergoing lung resection via VATS or robot-assisted thoracic surgery showed that the latter had significantly higher costs and longer operative times.(10)
In this setting of uncertainty, the implementation of a robotic surgery program is particularly challenging, and, in addition to risk minimization, attention should be given to structural issues and costs. The objectives of the present study were to describe the implementation of a robotic thoracic surgery program at the University of São Paulo School of Medicine Hospital das Clínicas Instituto do Câncer do Estado de São Paulo (ICESP, São Paulo State Cancer Institute), in the city of São Paulo, Brazil, and to analyze its initial results.
1. Disciplina de Cirurgia Torácica, Instituto do Coração, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
2. Instituto do Câncer do Estado de São Paulo – ICESP – Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
Submitted: 1 September 2015.Accepted: 25 February 2016.
Study carried out in the Disciplina de Cirurgia Torácica and at the Instituto do Câncer do Estado de São Paulo – ICESP – Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil.
J Bras Pneumol. 2016;42(3):185-190
185
ORIGINAL ARTICLE

Robotic pulmonary lobectomy for lung cancer treatment: program implementation and initial experience
METHODS
This was a planned interim analysis of a randomized clinical trial that is currently under way at our institution and that is aimed at comparing VATS and robotic surgery in terms of the results obtained after pulmonary lobectomy. In this analysis, we evaluated the patients included in the robotic lobectomy arm of the trial during its first three months (from April to June of 2015), i.e., after the surgical team had been certified (in March of 2015). All of the patients who were included in the study gave written informed consent, and the study was approved by the local research ethics committee.
In addition to the presence of primary lung cancer or lung metastasis and written informed consent, the criteria for inclusion in the randomized clinical trial were as follows, having been evaluated during the clinical staging phase:
• eligibility for the treatment of lung cancer or lung metastasis by pulmonary lobectomy
• presence of a tumor of less than 5 cm in diameter at its widest point
• absence of hilar or mediastinal lymphadenopathy • absence of tumor invasion of the chest wall, the
mediastinum, or another lung lobe • absence of tumor invasion of a main bronchus
or a lobar bronchus less than 1 cm from the secondary carina
• Clinical and anesthetic evaluation results showing that the patient was able to undergo the proposed procedure
The exclusion criteria were as follows: • having previously undergone a thoracic surgical
procedure in the hemithorax that was to be operated on
• being unable to remain on single-lung ventilation during the procedure
In the present analysis, the following variables were evaluated: operative time; length of hospital stay; complications; patient-reported pain; extent of lymph node dissection; and number of lymph nodes removed during lymph node dissection. Intraoperative and postoperative complications (up to postoperative day 30) were recorded and classified on the basis of the Common Terminology Criteria for Adverse Events, version 4.0.(11) The magnitude of the systemic inflammatory response was assessed by measuring serum creatine phosphokinase and C-reactive protein levels on postoperative day 2. Pain was assessed by a visual analog pain scale (a Likert scale)—which was administered in the morning on postoperative days 1, 2, and 3 and during follow-up visits on postoperative days 15 and 30—and by the duration of use and dose of opioids. In the early postoperative period, opioids were administered at fixed times; subsequently, they were administered as needed. The date of opioid discontinuation was defined as the day on which patients received their last dose of opioids. The extent of lymph node dissection was determined by counting the resected lymph nodes. The resected lymph nodes were counted by using a procedure that
has been standardized by the ICESP Department of Anatomic Pathology and that is consistent with the current literature.
The robotic surgery program developed at the ICESP is a multidisciplinary initiative involving various surgical specialties, as well as anesthesiology, nursing, and clinical engineering teams. All involved received specific training in operating the robot. The thoracic surgery team training consisted of an online course on how the robotic surgical system works; 20 hours of virtual reality simulation in order to familiarize participants with the movements of the robot; and lobectomy simulation in animal models. The process of certification lasted 2 days, having taken place in a specialized center abroad and having involved animal models and human cadavers. After certification, we participated as observers in various procedures performed at centers of excellence in robotic surgery. Before the first procedure, simulations were performed with the participation of the entire multidisciplinary team.
All surgical procedures were performed with the use of selective intubation and an epidural catheter for postoperative analgesia. We used a slightly modified version of a robotic lobectomy technique that was originally described by Dylewski et al.(12) Patients are placed in the lateral decubitus position with pads under their axillae, the robot being placed over their heads. A total of four ports are used: three for the robotic arms and one for the assistant surgeon (Figure 1). The first incision is made in the 6th intercostal space at the anterior axillary line. After insertion of a 5-mm trocar, carbon dioxide insufflation is initiated. With the aid of a 5-mm endoscope, the locations of the remaining ports are determined. Initially, the diaphragm insertion on the chest wall at the level of the 10th intercostal space is identified, and a 12-mm trocar is inserted at that site, the trocar being used by the assistant surgeon for exposure, aspiration, stapling, introduction/removal of materials (such as gauze), and removal of specimens for pathological examination. Subsequently, two other ports are placed in the 7th or 8th intercostal space at the midaxillary and posterior axillary lines, respectively. The robotic camera is introduced through the midaxillary line trocar, and the robotic graspers are introduced through the remaining two ports. It is extremely important that these ports are caudal to the oblique fissure.
The surgical procedure was systematized in order to minimize intraoperative lung manipulation. In all cases, the first step was to section the pulmonary ligament. Next, in a posterior and superior direction, paraesophageal and subcarinal lymph nodes were dissected. Right interlobar lymph nodes or those located between the pulmonary artery and the left main bronchus were then resected. In cases of right or left lower lobectomy, the oblique fissure is divided and the pulmonary artery is exposed and sectioned with a stapler. In cases of right or left upper lobectomy, dissection is performed cranially, the right main bronchus, the right pulmonary artery, and left pulmonary artery branches being sectioned. Pulmonary
186 J Bras Pneumol. 2016;42(3):185-190
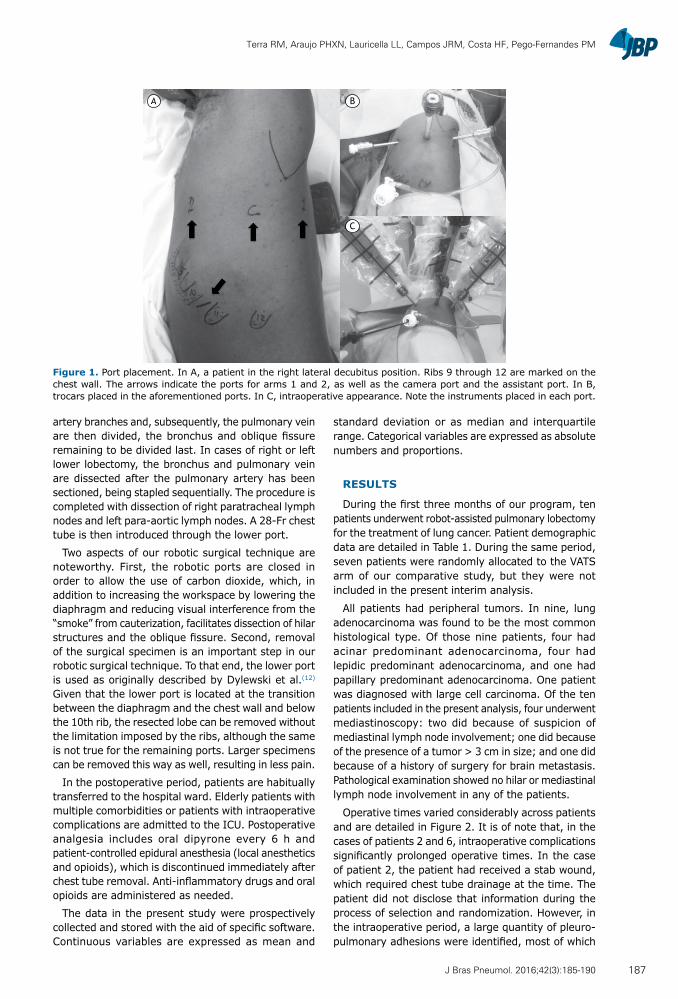
Terra RM, Araujo PHXN, Lauricella LL, Campos JRM, Costa HF, Pego-Fernandes PM
artery branches and, subsequently, the pulmonary vein are then divided, the bronchus and oblique fissure remaining to be divided last. In cases of right or left lower lobectomy, the bronchus and pulmonary vein are dissected after the pulmonary artery has been sectioned, being stapled sequentially. The procedure is completed with dissection of right paratracheal lymph nodes and left para-aortic lymph nodes. A 28-Fr chest tube is then introduced through the lower port.
Two aspects of our robotic surgical technique are noteworthy. First, the robotic ports are closed in order to allow the use of carbon dioxide, which, in addition to increasing the workspace by lowering the diaphragm and reducing visual interference from the “smoke” from cauterization, facilitates dissection of hilar structures and the oblique fissure. Second, removal of the surgical specimen is an important step in our robotic surgical technique. To that end, the lower port is used as originally described by Dylewski et al.(12) Given that the lower port is located at the transition between the diaphragm and the chest wall and below the 10th rib, the resected lobe can be removed without the limitation imposed by the ribs, although the same is not true for the remaining ports. Larger specimens can be removed this way as well, resulting in less pain.
In the postoperative period, patients are habitually transferred to the hospital ward. Elderly patients with multiple comorbidities or patients with intraoperative complications are admitted to the ICU. Postoperative analgesia includes oral dipyrone every 6 h and patient-controlled epidural anesthesia (local anesthetics and opioids), which is discontinued immediately after chest tube removal. Anti-inflammatory drugs and oral opioids are administered as needed.
The data in the present study were prospectively collected and stored with the aid of specific software. Continuous variables are expressed as mean and
standard deviation or as median and interquartile range. Categorical variables are expressed as absolute numbers and proportions.
RESULTS
During the first three months of our program, ten patients underwent robot-assisted pulmonary lobectomy for the treatment of lung cancer. Patient demographic data are detailed in Table 1. During the same period, seven patients were randomly allocated to the VATS arm of our comparative study, but they were not included in the present interim analysis.
All patients had peripheral tumors. In nine, lung adenocarcinoma was found to be the most common histological type. Of those nine patients, four had acinar predominant adenocarcinoma, four had lepidic predominant adenocarcinoma, and one had papillary predominant adenocarcinoma. One patient was diagnosed with large cell carcinoma. Of the ten patients included in the present analysis, four underwent mediastinoscopy: two did because of suspicion of mediastinal lymph node involvement; one did because of the presence of a tumor > 3 cm in size; and one did because of a history of surgery for brain metastasis. Pathological examination showed no hilar or mediastinal lymph node involvement in any of the patients.
Operative times varied considerably across patients and are detailed in Figure 2. It is of note that, in the cases of patients 2 and 6, intraoperative complications significantly prolonged operative times. In the case of patient 2, the patient had received a stab wound, which required chest tube drainage at the time. The patient did not disclose that information during the process of selection and randomization. However, in the intraoperative period, a large quantity of pleuro-pulmonary adhesions were identified, most of which
A B
C
Figure 1. Port placement. In A, a patient in the right lateral decubitus position. Ribs 9 through 12 are marked on the chest wall. The arrows indicate the ports for arms 1 and 2, as well as the camera port and the assistant port. In B, trocars placed in the aforementioned ports. In C, intraoperative appearance. Note the instruments placed in each port.
187J Bras Pneumol. 2016;42(3):185-190
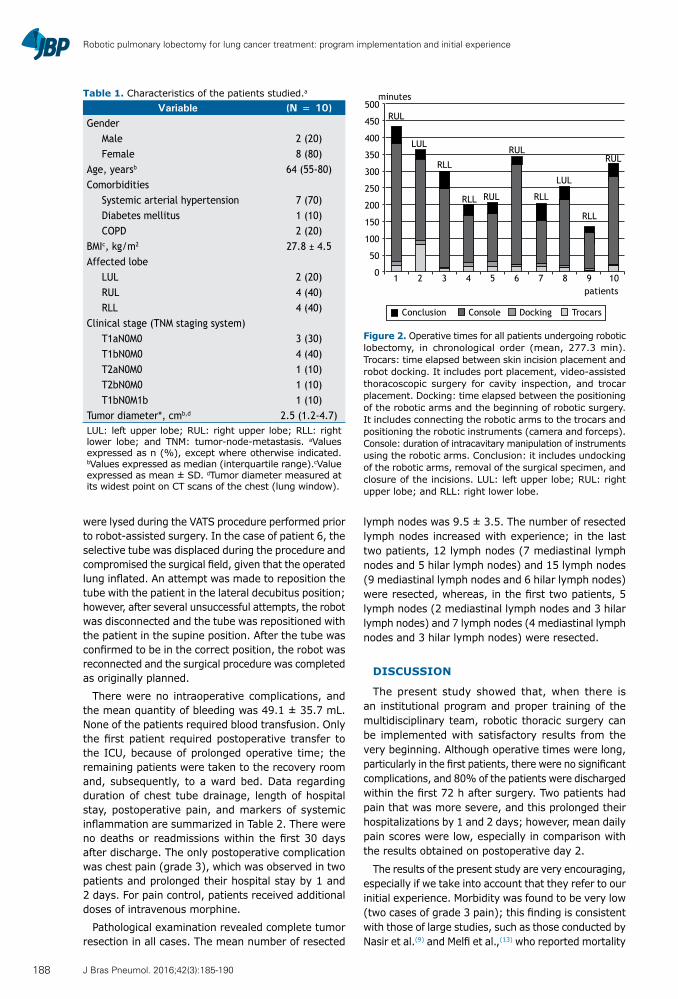
Robotic pulmonary lobectomy for lung cancer treatment: program implementation and initial experience
were lysed during the VATS procedure performed prior to robot-assisted surgery. In the case of patient 6, the selective tube was displaced during the procedure and compromised the surgical field, given that the operated lung inflated. An attempt was made to reposition the tube with the patient in the lateral decubitus position; however, after several unsuccessful attempts, the robot was disconnected and the tube was repositioned with the patient in the supine position. After the tube was confirmed to be in the correct position, the robot was reconnected and the surgical procedure was completed as originally planned.
There were no intraoperative complications, and the mean quantity of bleeding was 49.1 ± 35.7 mL. None of the patients required blood transfusion. Only the first patient required postoperative transfer to the ICU, because of prolonged operative time; the remaining patients were taken to the recovery room and, subsequently, to a ward bed. Data regarding duration of chest tube drainage, length of hospital stay, postoperative pain, and markers of systemic inflammation are summarized in Table 2. There were no deaths or readmissions within the first 30 days after discharge. The only postoperative complication was chest pain (grade 3), which was observed in two patients and prolonged their hospital stay by 1 and 2 days. For pain control, patients received additional doses of intravenous morphine.
Pathological examination revealed complete tumor resection in all cases. The mean number of resected
lymph nodes was 9.5 ± 3.5. The number of resected lymph nodes increased with experience; in the last two patients, 12 lymph nodes (7 mediastinal lymph nodes and 5 hilar lymph nodes) and 15 lymph nodes (9 mediastinal lymph nodes and 6 hilar lymph nodes) were resected, whereas, in the first two patients, 5 lymph nodes (2 mediastinal lymph nodes and 3 hilar lymph nodes) and 7 lymph nodes (4 mediastinal lymph nodes and 3 hilar lymph nodes) were resected.
DISCUSSION
The present study showed that, when there is an institutional program and proper training of the multidisciplinary team, robotic thoracic surgery can be implemented with satisfactory results from the very beginning. Although operative times were long, particularly in the first patients, there were no significant complications, and 80% of the patients were discharged within the first 72 h after surgery. Two patients had pain that was more severe, and this prolonged their hospitalizations by 1 and 2 days; however, mean daily pain scores were low, especially in comparison with the results obtained on postoperative day 2.
The results of the present study are very encouraging, especially if we take into account that they refer to our initial experience. Morbidity was found to be very low (two cases of grade 3 pain); this finding is consistent with those of large studies, such as those conducted by Nasir et al.(9) and Melfi et al.,(13) who reported mortality
Table 1. Characteristics of the patients studied.a Variable (N = 10)
GenderMale 2 (20)Female 8 (80)
Age, yearsb 64 (55-80)Comorbidities
Systemic arterial hypertension 7 (70)Diabetes mellitus 1 (10)COPD 2 (20)
BMIc, kg/m2 27.8 ± 4.5Affected lobe
LUL 2 (20)RUL 4 (40)RLL 4 (40)
Clinical stage (TNM staging system)T1aN0M0 3 (30)T1bN0M0 4 (40)T2aN0M0 1 (10)T2bN0M0 1 (10)T1bN0M1b 1 (10)
Tumor diameter*, cmb,d 2.5 (1.2-4.7)LUL: left upper lobe; RUL: right upper lobe; RLL: right lower lobe; and TNM: tumor-node-metastasis. aValues expressed as n (%), except where otherwise indicated. bValues expressed as median (interquartile range).cValue expressed as mean ± SD. dTumor diameter measured at its widest point on CT scans of the chest (lung window).
1 2 3 4 5 6 7 8 9 10
500
450
400
350
300
250
200
150
100
50
0
minutes
RUL
RUL
RULRUL
LUL
LUL
RLL
RLL
RLLRLL
patients
Conclusion DockingConsole Trocars
Figure 2. Operative times for all patients undergoing robotic lobectomy, in chronological order (mean, 277.3 min). Trocars: time elapsed between skin incision placement and robot docking. It includes port placement, video-assisted thoracoscopic surgery for cavity inspection, and trocar placement. Docking: time elapsed between the positioning of the robotic arms and the beginning of robotic surgery. It includes connecting the robotic arms to the trocars and positioning the robotic instruments (camera and forceps). Console: duration of intracavitary manipulation of instruments using the robotic arms. Conclusion: it includes undocking of the robotic arms, removal of the surgical specimen, and closure of the incisions. LUL: left upper lobe; RUL: right upper lobe; and RLL: right lower lobe.
188 J Bras Pneumol. 2016;42(3):185-190
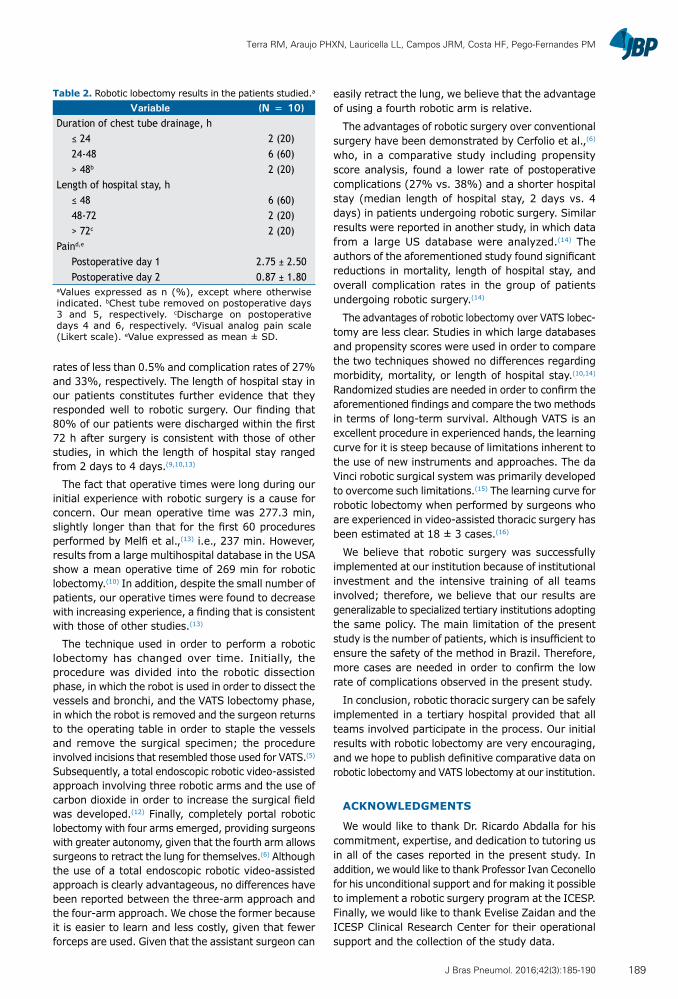
Terra RM, Araujo PHXN, Lauricella LL, Campos JRM, Costa HF, Pego-Fernandes PM
rates of less than 0.5% and complication rates of 27% and 33%, respectively. The length of hospital stay in our patients constitutes further evidence that they responded well to robotic surgery. Our finding that 80% of our patients were discharged within the first 72 h after surgery is consistent with those of other studies, in which the length of hospital stay ranged from 2 days to 4 days.(9,10,13)
The fact that operative times were long during our initial experience with robotic surgery is a cause for concern. Our mean operative time was 277.3 min, slightly longer than that for the first 60 procedures performed by Melfi et al.,(13) i.e., 237 min. However, results from a large multihospital database in the USA show a mean operative time of 269 min for robotic lobectomy.(10) In addition, despite the small number of patients, our operative times were found to decrease with increasing experience, a finding that is consistent with those of other studies.(13)
The technique used in order to perform a robotic lobectomy has changed over time. Initially, the procedure was divided into the robotic dissection phase, in which the robot is used in order to dissect the vessels and bronchi, and the VATS lobectomy phase, in which the robot is removed and the surgeon returns to the operating table in order to staple the vessels and remove the surgical specimen; the procedure involved incisions that resembled those used for VATS.(5) Subsequently, a total endoscopic robotic video-assisted approach involving three robotic arms and the use of carbon dioxide in order to increase the surgical field was developed.(12) Finally, completely portal robotic lobectomy with four arms emerged, providing surgeons with greater autonomy, given that the fourth arm allows surgeons to retract the lung for themselves.(6) Although the use of a total endoscopic robotic video-assisted approach is clearly advantageous, no differences have been reported between the three-arm approach and the four-arm approach. We chose the former because it is easier to learn and less costly, given that fewer forceps are used. Given that the assistant surgeon can
easily retract the lung, we believe that the advantage of using a fourth robotic arm is relative.
The advantages of robotic surgery over conventional surgery have been demonstrated by Cerfolio et al.,(6) who, in a comparative study including propensity score analysis, found a lower rate of postoperative complications (27% vs. 38%) and a shorter hospital stay (median length of hospital stay, 2 days vs. 4 days) in patients undergoing robotic surgery. Similar results were reported in another study, in which data from a large US database were analyzed.(14) The authors of the aforementioned study found significant reductions in mortality, length of hospital stay, and overall complication rates in the group of patients undergoing robotic surgery.(14)
The advantages of robotic lobectomy over VATS lobec-tomy are less clear. Studies in which large databases and propensity scores were used in order to compare the two techniques showed no differences regarding morbidity, mortality, or length of hospital stay.(10,14) Randomized studies are needed in order to confirm the aforementioned findings and compare the two methods in terms of long-term survival. Although VATS is an excellent procedure in experienced hands, the learning curve for it is steep because of limitations inherent to the use of new instruments and approaches. The da Vinci robotic surgical system was primarily developed to overcome such limitations.(15) The learning curve for robotic lobectomy when performed by surgeons who are experienced in video-assisted thoracic surgery has been estimated at 18 ± 3 cases.(16)
We believe that robotic surgery was successfully implemented at our institution because of institutional investment and the intensive training of all teams involved; therefore, we believe that our results are generalizable to specialized tertiary institutions adopting the same policy. The main limitation of the present study is the number of patients, which is insufficient to ensure the safety of the method in Brazil. Therefore, more cases are needed in order to confirm the low rate of complications observed in the present study.
In conclusion, robotic thoracic surgery can be safely implemented in a tertiary hospital provided that all teams involved participate in the process. Our initial results with robotic lobectomy are very encouraging, and we hope to publish definitive comparative data on robotic lobectomy and VATS lobectomy at our institution.
ACKNOWLEDGMENTS
We would like to thank Dr. Ricardo Abdalla for his commitment, expertise, and dedication to tutoring us in all of the cases reported in the present study. In addition, we would like to thank Professor Ivan Ceconello for his unconditional support and for making it possible to implement a robotic surgery program at the ICESP. Finally, we would like to thank Evelise Zaidan and the ICESP Clinical Research Center for their operational support and the collection of the study data.
Table 2. Robotic lobectomy results in the patients studied.a
Variable (N = 10)Duration of chest tube drainage, h
≤ 24 2 (20)24-48 6 (60)> 48b 2 (20)
Length of hospital stay, h≤ 48 6 (60)48-72 2 (20)> 72c 2 (20)
Paind,e
Postoperative day 1 2.75 ± 2.50Postoperative day 2 0.87 ± 1.80
aValues expressed as n (%), except where otherwise indicated. bChest tube removed on postoperative days 3 and 5, respectively. cDischarge on postoperative days 4 and 6, respectively. dVisual analog pain scale (Likert scale). eValue expressed as mean ± SD.
189J Bras Pneumol. 2016;42(3):185-190

Robotic pulmonary lobectomy for lung cancer treatment: program implementation and initial experience
REFERENCES1. Terra RM, Waisberg DR, Almeida JJ, Devido MS, Pego-Fernandes
PM, Jatene FB. Does videothoracoscopy improve clinical outcomes when implemented as part of a pleural empyema treatment algorithm? Clinics (Sao Paulo). 2012;67(6):557-64. http://dx.doi.org/10.6061/clinics/2012(06)03
2. Cirino LM, Milanez de Campos JR, Fernandez A, Samano MN, Fernandez PP, Filomeno LT, et al. Diagnosis and treatment of mediastinal tumors by thoracoscopy. Chest. 2000;117(6):1787-92. http://dx.doi.org/10.1378/chest.117.6.1787
3. McKenna RJ Jr, Houck W, Fuller CB. Video-assisted thoracic surgery lobectomy: experience with 1,100 cases. Ann Thorac Surg. 2006;81(2):421-5; discussion 425-6. http://dx.doi.org/10.1016/j.athoracsur.2005.07.078
4. Flores RM, Park BJ, Dycoco J, Aronova A, Hirth Y, Rizk NP, et al. Lobectomy by video-assisted thoracic surgery (VATS) versus thoracotomy for lung cancer. J Thorac Cardiovasc Surg. 2009;138(1):11-8. http://dx.doi.org/10.1016/j.jtcvs.2009.03.030
5. Gharagozloo F, Margolis M, Tempesta B, Strother E, Najam F. Robot-assisted lobectomy for early-stage lung cancer: report of 100 consecutive cases. Ann Thorac Surg. 2009;88(2):380-4. http://dx.doi.org/10.1016/j.athoracsur.2009.04.039
6. Cerfolio RJ, Bryant AS, Skylizard L, Minninch DJ. Initial consecutive experience of completely portal robotic pulmonary resection with 4 arms. J Thorac Cardiovasc Surg. 2011;142(4):740-6. http://dx.doi.org/10.1016/j.jtcvs.2011.07.022
7. Louie BE, Farivar AS, Aye RW, Vallières E. Early experience with robotic lung resection results in similar operative outcomes and morbidity when compared with matched video-assisted thoracoscopic surgery cases. Ann Thorac Surg. 2012;93(5):1598-604; discussion 1604-5. http://dx.doi.org/10.1016/j.athoracsur.2012.01.067
8. Park BJ, Melfi F, Mussi A, Maisonneuve P, Spaggiari L, Da Silva RK, et al. Robotic lobectomy for non-small cell lung cancer (NSCLC): long-term oncologic results. J Thorac Cardiovasc Surg. 2012;143(2):383-9.
http://dx.doi.org/10.1016/j.jtcvs.2011.10.0559. Nasir BS, Bryant AS, Minnich DJ, Wei B, Cerfolio RJ. Performing
robotic lobectomy and segmentectomy: cost, profitability, and outcomes. Ann Thorac Surg. 2014;98(1):203-8; discussion 208-9. http://dx.doi.org/10.1016/j.athoracsur.2014.02.051
10. Swanson SJ, Miller DL, McKenna RJ Jr, Howington J, Marshall MB, Yoo AC, et al. Comparing robot-assisted thoracic surgical lobectomy with conventional video-assisted thoracic surgical lobectomy and wedge resection: results from a multihospital database (Premier). J Thorac Cardiovasc Surg. 2014;147(3):929-37. http://dx.doi.org/10.1016/j.jtcvs.2013.09.046
11. National Cancer Institute [homepage on the Internet]. Bethesda: National Institutes of Health [cited 2014 Oct 6]. Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 [Adobe Acrobat document, 196p.]. Available from: http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf
12. Dylewski MR, Ohaeto AC, Pereira JF. Pulmonary resection using a total endoscopic robotic video-assisted approach. Semin Thorac Cardiovasc Surg. 2011;23(1):36-42. http://dx.doi.org/10.1053/j.semtcvs.2011.01.005
13. Melfi FM, Fanucchi O, Davini F, Romano G, Lucchi M, Dini P, et al. Robotic lobectomy for lung cancer: evolution in technique and technology. Eur J Cardiothorac Surg. 2014;46(4):626-30; discussion 630-1. http://dx.doi.org/10.1093/ejcts/ezu079
14. Kent M, Wang T, Whyte R, Curran T, Flores R, Gangadharan S. Open, video-assisted thoracic surgery, and robotic lobectomy: review of a national database. Ann Thorac Surg. 2014;97(1):236-42; discussion 242-4. http://dx.doi.org/10.1016/j.athoracsur.2013.07.117
15. Kumar A, Asaf BB, Cerfolio RJ, Sood J, Kumar R. Robotic lobectomy: The first Indian report. J Minim Access Surg. 2015;11(1):94-8. http://dx.doi.org/10.4103/0972-9941.147758
16. Meyer M, Gharagozloo F, Tempesta B, Margolis M, Strother E, Christenson D. The learning curve of robotic lobectomy. Int J Med Robot. 2012;8(4):448-52. http://dx.doi.org/10.1002/rcs.1455
190 J Bras Pneumol. 2016;42(3):185-190

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000134
ABSTRACTObjective: To determine the proportional distribution of endobronchial tuberculosis (EBTB) subtypes and to evaluate the types of bronchoscopic diagnostic procedures that can prove granulomatous inflammation. Methods: This was a retrospective study of 18 HIV-negative patients with biopsy-proven EBTB treated between 2010 and 2014. Results: The most common EBTB subtypes, as classified by the bronchoscopic features, were tumorous and granular (in 22.2% for both). Sputum smear microscopy was performed in 11 patients and was positive for AFB in 4 (36.3%). Sputum culture was also performed in 11 patients and was positive for Mycobacterium tuberculosis in 10 (90.9%). Smear microscopy of BAL fluid (BALF) was performed in 16 patients and was positive for AFB in 10 (62.5%). Culture of BALF was also performed in 16 patients and was positive for M. tuberculosis in 15 (93.7%). Culture of BALF was positive for M. tuberculosis in 93.7% of the 16 patients tested. Among the 18 patients with EBTB, granulomatous inflammation was proven by the following bronchoscopic diagnostic procedures: bronchial mucosal biopsy, in 8 (44.4%); bronchial brushing, in 7 (38.8%); fine-needle aspiration biopsy, in 2 (11.1%); and BAL, in 2 (11.1%). Bronchial anthracofibrosis was observed in 5 (27.7%) of the 18 cases evaluated. Conclusions: In our sample of EBTB patients, the most common subtypes were the tumorous and granular subtypes. We recommend that sputum samples and BALF samples be evaluated by smear microscopy for AFB and by culture for M. tuberculosis, which could increase the rates of early diagnosis of EBTB. We also recommend that bronchial brushing be employed together with other bronchoscopic diagnostic procedures in patients suspected of having EBTB.
Keywords: Tuberculosis, pulmonary; Mycobacterium tuberculosis; Diagnostic techniques and procedures; Bronchoscopy.
Bronchoscopic diagnostic procedures and microbiological examinations in proving endobronchial tuberculosisAbdullah Şimşek1, İlhami Yapıcı1, Mesiha Babalık1, Zekiye Şimşek2, Mustafa Kolsuz1
Correspondence to:Abdullah Şimşek. Department of Chest Diseases, Prof. Dr. Türkan Akyol Chest Diseases Hospital, Çamlıca Mah Gümüşyıldız Sit, 48/A, Nilüfer/Bursa, Turkey.Tel. 90 505 7130294. E-mail: [email protected] support: None.
INTRODUCTION
Pulmonary tuberculosis is one of the major health problems worldwide. There has recently been a resurgence of pulmonary tuberculosis, and that resurgence is related to the HIV epidemic, the emergence of multidrug-resistant strains of Mycobacterium tuberculosis, poverty, and immi-gration, as well as to a lack of resources in the prevention and treatment system.(1-3) Endobronchial tuberculosis (EBTB) is defined as tuberculosis of the tracheobronchial tree with microbial and histopathological evidence, with or without parenchymal involvement.(4) EBTB is a special form of pulmonary tuberculosis. Previous studies have reported that 10-40% of patients with active pulmonary tuberculosis have EBTB.(5,6) EBTB can mimic a variety of pulmonary diseases such as bronchogenic carcinoma, pneumonia, and bronchial asthma. The diagnosis of typical pulmonary tuberculosis is easily confirmed by bacteriological means and on the basis of radiological findings. However, EBTB is more difficult to diagnose because of its variable clinical manifestations. Chung
et al.(7) divided EBTB into seven subtypes according to the features observed during bronchoscopy: actively caseating, fibrostenotic, edematous-hyperemic, tumorous, ulcerative, granular, and nonspecific. Other authors have found that classification system to be valuable in predicting the therapeutic outcome of EBTB.(8) In the present study, we aimed to determine the proportional distribution of the EBTB subtypes, to evaluate the types of bronchoscopic diagnostic procedures that can prove granulomatous inflammation, and to compare bronchoscopic features with positivity for M. tuberculosis in BAL fluid and sputum samples. Thus, we wanted to show what kinds of procedures are especially needed in order to prove granulomatous inflammation and to define the relationship between bronchoscopic features and positivity for M. tuberculosis.
METHODS
The Türkan Akyol Chest Diseases Public Hospital, in the city of Bursa, Turkey, is one of several referral
1. Department of Chest Diseases, Prof. Dr. Türkan Akyol Chest Diseases Hospital, Bursa, Turkey
2. Department of Radiology, Bursa Çekirge Public Hospital, Bursa, Turkey.
Submitted: 13 June 2015. Accepted: 14 March 2016.
Study carried out in the Department of Chest Diseases, Prof. Dr. Türkan Akyol Chest Diseases Hospital, and in the Department of Radiology, Bursa Çekirge Public Hospital, Bursa, Turkey.
J Bras Pneumol. 2016;42(3):191-195
191
ORIGINAL ARTICLE

Bronchoscopic diagnostic procedures and microbiological examinations in proving endobronchial tuberculosis
hospitals for tuberculosis in the country. This was a retrospective study of 18 HIV-negative patients with biopsy-proven EBTB treated at the hospital between 2010 and 2014. The diagnosis of EBTB was confirmed histopathologically in all 18 of the patients. Some patients were initially unable to expectorate sputum and others were sputum smear-negative according to AFB staining (sputum induction tests with hypertonic saline were not used at our hospital during the study period). Fiberoptic bronchoscopy was performed in the case of suspected tuberculosis or for the differential diagnosis of tuberculosis. Some patients expectorated sputum after fiberoptic bronchoscopy. A flexible bronchoscope was inserted through the nasal passage. Forceps were advanced through the bronchoscope and airway to obtain biopsies from bronchial lesions. The characteristics of the patients, including demographic data, as well as radiological, bronchoscopic, and microbiological features, were reviewed, evaluated, and recorded retrospectively, as were the types of bronchoscopic diagnostic procedures employed in order to prove granulomatous inflammation, such as bronchial mucosal biopsy, fine-needle aspiration biopsy, bronchial brushing, and BAL. Bronchoscopic findings were categorized according to the classification system devised by Chung et al.(7) Bronchial anthracofibrosis was also recorded as a bronchoscopic finding. The results are presented as means ± standard deviations or as absolute and relative frequencies.
RESULTS
Between 2010 and 2014, a total of 1,380 patients were diagnosed with pulmonary tuberculosis at our hospital. Among those 1,380 patients, endobronchial lesions were observed in 34 (2.46%), of whom 18 (52.9%) were histopathologically diagnosed with EBTB. During the study period, 3,325 patients had been examined with fiberoptic bronchoscopy because of suspicion of pulmonary tuberculosis. Among the patients with EBTB, the female-to-male ratio was 1.57:1; ages ranged from 16 to 83 years; the mean age was 53.1 ± 20.1 years; and 38.8% of the patients were under 45 years of age.
Anatomically, the bronchoscopic findings were located primarily in the right upper lobe bronchus, in 5 (27.8%) of the 18 patients with EBTB, followed by the right lower lobe bronchus, in 4 (22.2%). Bilateral pulmonary involvement was observed in 5 patients (27.8%), right middle lobe involvement was observed in 1 (5.6%), right middle/upper lobe involvement was observed in 1 (5.6%), left upper lobe involvement was observed in 1 (5.6%), and left main bronchus involvement was observed in 1 (5.6%). Bronchoscopic features, as classified with the Chung et al. system,(7) are listed in Table 1.
Radiologic alterations were observed in 14 patients: heterogeneous infiltration in 7 cases (50%); nodular infiltration in 7 cases (50%); ground-glass appearance
in 5 cases (35.7%); consolidation in 5 cases (35.7%); atelectasis in 5 cases (35.7%); mass lesion in 4 cases (27.5%); lymphadenopathy in 3 cases (21.4%); pleural effusions in 2 cases (14.3%); and cavitary infiltration in 1 case (7.1%). Middle lobe syndrome was seen in 1 case (7.1%), and miliary tuberculosis was seen in 2 cases (14.3%). The lesions were mostly unilateral, being found in the right lung in 11 cases (78.5%). Multilobar involvement was observed in 9 cases (64.3%).
Table 2 shows the results of the microbiological and smear examinations of sputum samples evaluated in 11 cases. In some cases, the patients were unable to produce sputum, and some sputum samples were collected after fiberoptic bronchoscopy. Of the 11 samples submitted to staining, 4 (36.3%) were positive for AFB. The highest smear positivity for AFB (100%) was found in the patients with tumorous EBTB. None of the patients with edematous-hyperemic EBTB or nonspecific EBTB were sputum smear-positive for AFB. Ten (90.9%) of the 11 patients had a positive sputum culture for M. tuberculosis, and the remaining patient had nonspecific EBTB.
In two cases (one case of caseating EBTB and one case of nonspecific EBTB), the BAL fluid had not been sent for AFB staining. Therefore, microbiological and smear examinations of BAL fluid for M. tuberculosis were evaluated in only 16 patients (Table 3). Of those 16 patients, 10 (62.5%) were positive for AFB from BAL. The highest BAL smear positivity for AFB (100%) was found in the patients with tumorous EBTB. The BAL fluid culture was positive for M. tuberculosis in 15 (93.7%) of the patients, and the remaining patient had fibrostenotic EBTB.
Among the 18 patients with EBTB, granulomatous inflammation was proven by the following bronchoscopic diagnostic procedures (Table 4): bronchial mucosal biopsy, in 8 cases (44.4%); bronchial brushing, in 7 cases (38.8%); fine-needle aspiration biopsy, in 2 cases (11.1%); and BAL, in 2 cases (11.1%). In one case of nonspecific EBTB, fine-needle aspiration biopsy and bronchial brushing both revealed granulomatous inflammation. Bronchial anthracofibrosis was identified in 5 cases (27.7%): in 2 patients with tumorous EBTB (11.1%); in 2 with granular EBTB (11.1%); and in 1 with caseating EBTB (5.5%).
Table 1. Classification of endobronchial tuberculosis, by bronchoscopic features.a
EBTB subtypeb (n = 18)Tumorous 4 (22.2)Granular 4 (22.2)Caseating 3 (16.7)Edematous-hyperemic 3 (16.7)Nonspecific 2 (11.1)Fibrostenotic 1 (5.6)Ulcerative 1 (5.6)EBTB: endobronchial tuberculosis.Results expressed as n (%). bClassification system devised by Chung et al.(7)
192 J Bras Pneumol. 2016;42(3):191-195
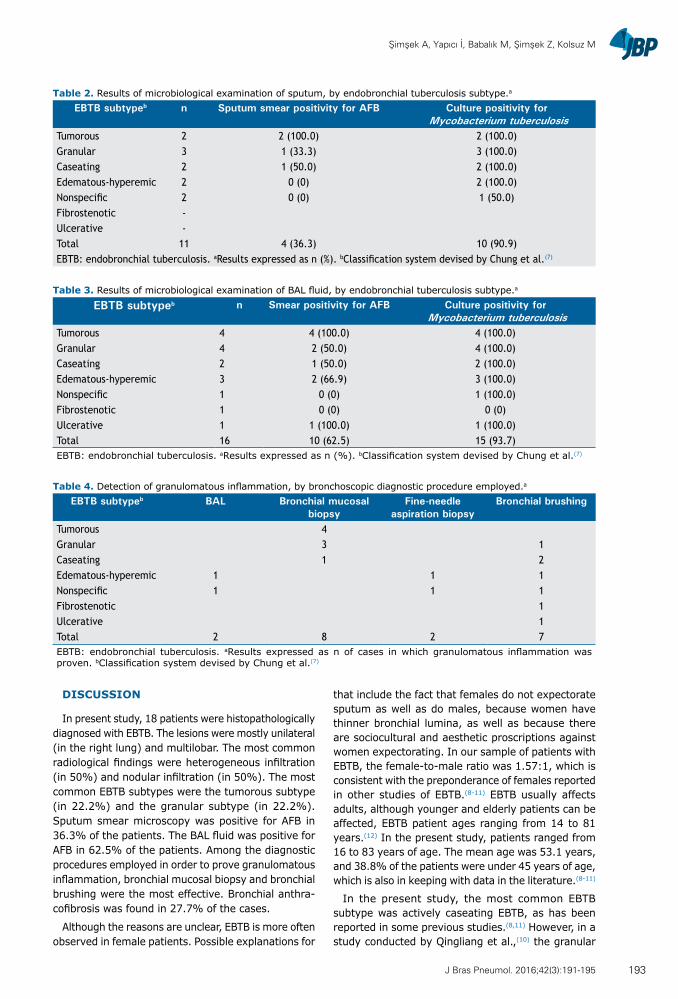
Şimşek A, Yapıcı İ, Babalık M, Şimşek Z, Kolsuz M
DISCUSSION
In present study, 18 patients were histopathologically diagnosed with EBTB. The lesions were mostly unilateral (in the right lung) and multilobar. The most common radiological findings were heterogeneous infiltration (in 50%) and nodular infiltration (in 50%). The most common EBTB subtypes were the tumorous subtype (in 22.2%) and the granular subtype (in 22.2%). Sputum smear microscopy was positive for AFB in 36.3% of the patients. The BAL fluid was positive for AFB in 62.5% of the patients. Among the diagnostic procedures employed in order to prove granulomatous inflammation, bronchial mucosal biopsy and bronchial brushing were the most effective. Bronchial anthra-cofibrosis was found in 27.7% of the cases.
Although the reasons are unclear, EBTB is more often observed in female patients. Possible explanations for
that include the fact that females do not expectorate sputum as well as do males, because women have thinner bronchial lumina, as well as because there are sociocultural and aesthetic proscriptions against women expectorating. In our sample of patients with EBTB, the female-to-male ratio was 1.57:1, which is consistent with the preponderance of females reported in other studies of EBTB.(8-11) EBTB usually affects adults, although younger and elderly patients can be affected, EBTB patient ages ranging from 14 to 81 years.(12) In the present study, patients ranged from 16 to 83 years of age. The mean age was 53.1 years, and 38.8% of the patients were under 45 years of age, which is also in keeping with data in the literature.(8-11)
In the present study, the most common EBTB subtype was actively caseating EBTB, as has been reported in some previous studies.(8,11) However, in a study conducted by Qingliang et al.,(10) the granular
Table 2. Results of microbiological examination of sputum, by endobronchial tuberculosis subtype.a
EBTB subtypeb n Sputum smear positivity for AFB Culture positivity for Mycobacterium tuberculosis
Tumorous 2 2 (100.0) 2 (100.0)Granular 3 1 (33.3) 3 (100.0)Caseating 2 1 (50.0) 2 (100.0)Edematous-hyperemic 2 0 (0) 2 (100.0)Nonspecific 2 0 (0) 1 (50.0)Fibrostenotic -Ulcerative -Total 11 4 (36.3) 10 (90.9)EBTB: endobronchial tuberculosis. aResults expressed as n (%). bClassification system devised by Chung et al.(7)
Table 3. Results of microbiological examination of BAL fluid, by endobronchial tuberculosis subtype.a
EBTB subtypeb n Smear positivity for AFB Culture positivity for Mycobacterium tuberculosis
Tumorous 4 4 (100.0) 4 (100.0)Granular 4 2 (50.0) 4 (100.0)Caseating 2 1 (50.0) 2 (100.0)Edematous-hyperemic 3 2 (66.9) 3 (100.0)Nonspecific 1 0 (0) 1 (100.0)Fibrostenotic 1 0 (0) 0 (0)Ulcerative 1 1 (100.0) 1 (100.0)Total 16 10 (62.5) 15 (93.7)EBTB: endobronchial tuberculosis. aResults expressed as n (%). bClassification system devised by Chung et al.(7)
Table 4. Detection of granulomatous inflammation, by bronchoscopic diagnostic procedure employed.a
EBTB subtypeb BAL Bronchial mucosal biopsy
Fine-needle aspiration biopsy
Bronchial brushing
Tumorous 4Granular 3 1Caseating 1 2Edematous-hyperemic 1 1 1Nonspecific 1 1 1Fibrostenotic 1Ulcerative 1Total 2 8 2 7EBTB: endobronchial tuberculosis. aResults expressed as n of cases in which granulomatous inflammation was proven. bClassification system devised by Chung et al.(7)
193J Bras Pneumol. 2016;42(3):191-195

Bronchoscopic diagnostic procedures and microbiological examinations in proving endobronchial tuberculosis
subtype was the most common (in 31.8% of the patients), whereas the edematous-hyperemic type was the most common (in 34.7% of the patients) in a study conducted by Ozkaya et al.(9) In our study, the tumorous and granular subtypes were both seen in 22.2% of the patients, which differs from that reported in other studies.(10) The ulcerative and fibrostenotic subtypes were the least common in our study, both being seen in 5.6% of the patients.
The yield of sputum smear microscopy for AFB is not as high in EBTB as it is in parenchymal involvement, even in an optimal laboratory set up for meticulous sputum examination. In recent studies, sputum positivity in EBTB has been demonstrated to range from 16.0% to 53.3%.(7,13,14) In an even more recent study,(9) sputum smear microscopy for AFB was negative in all patients. In the present study, sputum smear microscopy for AFB was positive in 36.3% of the patients and the M. tuberculosis culture positivity rate was very high (90.9%). Therefore it can be said that, when it is possible to collect sputum samples (before or after bronchoscopy), it is worthwhile to send those samples for microbiological examination for AFB.
Direct sputum smear microscopy remains a funda-mental tool in the diagnosis of tuberculosis. Alternative methods of obtaining sputum specimens, including sputum induction, BAL, and gastric lavage, are frequently called for in patients with radiological suspicion of tuberculosis who are unable to expectorate or are smear-negative. In a study conducted by McWilliams et al.,(15) the yield of induced sputum (96.3%) was superior to that of BAL fluid (51.9%) and the overall cost of BAL was found to be three times that of performing sputum induction. In comparison with BAL, sputum induction has several advantages(16): it is less invasive; it has a higher diagnostic yield; it provides greater patient comfort and safety; it is a low-cost procedure; there is no age restriction on its use; it does not require patient fasting; it is an outpatient procedure; it can be performed without the involvement of an expert; and it is less time-consuming. Unfortunately, sputum induction was not employed at our hospital during the study period.
The second step in the clinical evaluation of EBTB is bronchoscopy, in order to examine bronchial structures and obtain specimens for diagnosis. In the study conducted by Ozkaya et al.,(9) the BAL fluid was positive for AFB in 26.0% of the cases and the BAL fluid culture was positive for M. tuberculosis in 39.1%. The authors found that positivity for AFB was highest (75.0%) among the patients with the granular subtype of EBTB. They also found mycobacterial culture positivity to be highest (also 75.0%) among the patients with the granular subtype.(9) In our study, microbiological and smear examinations of BAL fluid for AFB were both positive in 62.5% of the patients. Cultures of BAL fluid for M. tuberculosis were positive in 93.7% of our patients. According to our data, microbiological and smear examinations of BAL fluid have high rates of positivity of staining for AFB and culture for M.
tuberculosis. It is therefore worthwhile to send BAL fluid samples for AFB analysis in order to facilitate the early diagnosis of EBTB.
Various bronchoscopic specimens, including those obtained through biopsy, bronchial brushing, or BAL, can be evaluated.(12) A bronchoscopic biopsy is the most reliable method for diagnosing EBTB, because a needle aspiration biopsy sample can provide only a cytological diagnosis. The reported rate of positivity in bronchial biopsy samples ranges from 30% to 84%.(13,17) We found it surprising that, in our study, the diagnostic yield of bronchial brushing was nearly equal to that of bronchial mucosal biopsy in detecting granulomas (38.8% and 44.4%, respectively). In a clinical analysis of 90 cases of EBTB in China,(13) bronchial brushing yielded variable results, ranging from 10% to 85%. In the present study, bronchial mucosal biopsy was especially effective in diagnosing EBTB in patients with the tumorous or granular subtypes (positivity rate of 100% and 75%, respectively), bronchial brushing proving diagnostic in patients with any of the other subtypes.
Tuberculosis is one of the most common diseases associated with bronchial anthracofibrosis.(18,19) Bronchial anthracofibrosis is typically induced by the long-term inhalation of biomass smoke.(18) Previous studies have reported high rates of tuberculosis in patients with bronchial anthracofibrosis.(18,20-25) In the present study, bronchial anthracofibrosis was found in 5 cases (27.7%): in 2 patients with tumorous EBTB (11.1%); in 2 with granular EBTB (11.1%); and in 1 with caseating EBTB (5.5%). These findings differ from those reported by Kim et al.,(26) who found actively caseating, edematous-hyperemic, and ulcerative EBTB to be the most common EBTB subtypes, respectively occurring in 49%, 21%, and 20% of their patients.
The results of the present study show the value of staining for AFB and culture for M. tuberculosis in sputum and BAL fluid samples for the early diagnosis of EBTB. In addition, because of its high diagnostic power, we can state that bronchial brushing is a recommended bronchoscopic diagnostic procedure in patients with suspected EBTB.
Our study has certain limitations. Primarily, due to the retrospective nature of the study, we relied on electronic medical records as our source of patient data.
In conclusion, the tumorous and granular subtypes were the EBTB subtypes most commonly seen in our study. Because of the high positivity rates, we recom-mend that sputum samples and BAL fluid samples be evaluated by smear microscopy for AFB and by culture for M. tuberculosis, which could collectively increase the rates of early diagnosis of EBTB. On the basis of our findings, we also recommend that bronchial brushing be employed together with other bronchoscopic diagnostic procedures, in order to increase the diagnostic yield, in patients suspected of having EBTB.
194 J Bras Pneumol. 2016;42(3):191-195
Şimşek A, Yapıcı İ, Babalık M, Şimşek Z, Kolsuz M
REFERENCES
1. Millard PS, Cegielski JP, Wing S, Silver A. Rurality and tuberculosis incidence trends in North and South Carolina, 1980 to 1992. J Rural Health. 1994;10(4): 226-36. http://dx.doi.org/10.1111/j.1748-0361.1994.tb00236.x
2. Glynn JR. Resurgence of tuberculosis and the impact of HIV infection. Br Med Bull. 1998;54(3):579-93. http://dx.doi.org/10.1093/oxfordjournals.bmb.a011712
3. Lerner BH. Catching patients: tuberculosis and detention in the 1990s. Chest. 1999;115(1):236-41. http://dx.doi.org/10.1378/chest.115.1.236
4. Lee JH, Park SS, Lee DH, Shin DH, Yang SC, Yoo BM. Endobronchial tuberculosis. Clinical and bronchoscopic feature in 121 cases. Chest. 1992;102(4): 990-4. http://dx.doi.org/10.1378/chest.102.4.990
5. Calpe JL, Chiner E, Larramendi CH. Endobronchial tuberculosis in HIV-infected patients. AIDS. 1995;9(10):1159-64. http://dx.doi.org/10.1097/00002030-199510000-00007
6. Han JK, Im JG, Park JH, Han MC, Kim YW, Shim YS. Bronchial stenosis due to endobronchial tuberculosis: successful treatment with self-expanding metallic stent. AJR Am J Roentgenol. 1992;159(5):971-2. http://dx.doi.org/10.2214/ajr.159.5.1414809
7. Chung HS, Lee JH, Han SK, Shim YS, Kim KY, Han YC, et al. Classification of endobronchial tuberculosis by the bronchoscopic features. Tuberc Respir Dis. 1991;38:108-15.
8. Chung HS, Lee JH. Bronchoscopic assessment of the evolution of endobronchial tuberculosis. Chest. 2000;117(2):385-92. http://dx.doi.org/10.1378/chest.117.2.385
9. Ozkaya S, Bilgin S, Findik S, Kök HC, Yuksel C, Atıcı AG. Endobronchial tuberculosis: histopathological subsets and microbiological results. Multidiscip Respir Med. 2012;7(1):34. http://dx.doi.org/10.1186/2049-6958-7-34
10. Qingliang X, Jianxin W. Investigation of endobronchial tuberculosis diagnoses in 22 cases. Eur J Med Res. 2010;15:309-13. http://dx.doi.org/10.1186/2047-783X-15-7-309
11. Sahin F, Yıldız P. Characteristics of endobronchial tuberculosis patients with negative sputum acid-fast bacillus. J Thorac Dis. 2013;5(6):764-70.
12. Kashyap S, Mohapatra PR, Saini V. Endobronchial tuberculosis. Indian J Chest Dis Allied Sci. 2003;45(4):247-56.
13. Yu W, Rong Z. Clinical analysis of 90 cases with endobronchial tuberculosis [Article in Chinese]. Zhonghua Jie He He Hu Xi Za Zhi. 1999;22(27):396-8.
14. Aggarwal AN, Gupta D, Joshi K, Behera D, Jindal SK. Endobronchial
involvement in tuberculosis: a report of 24 cases diagnosed by fibreoptic bronchoscopy. J Bronchol. 1999;6:247-50. http://dx.doi.org/10.1097/00128594-199910000-00004
15. McWilliams T, Wells AU, Harrison AC, Lindstrom S, Cameron RJ, Foskin E. Induced sputum and bronchoscopy in the diagnosis of pulmonary tuberculosis. Thorax. 2002;57(12):1010-4. http://dx.doi.org/10.1136/thorax.57.12.1010
16. Anderson C, Inhaber N, Menzies D. Comparison of sputum induction with fiber-optic bronchoscopy in the diagnosis of tuberculosis. Am J Respir Crit Care Med. 1995;1525 Pt 1):1570-4.
17. Altin S, Cikrikçioğlu S, Morgül M, Koşar F, Ozyurt H. 50 endobronchial tuberculosis cases based on bronchoscopic diagnosis. Respiration. 1997;64(2):162-4. http://dx.doi.org/10.1159/000196662
18. Kim YJ, Jung CY, Shin HW, Lee BK. Biomass smoke induced bronchial anthracofibrosis: presenting features and clinical course. Respir Med. 2009;103(5):757-65. http://dx.doi.org/10.1016/j.rmed.2008.11.011
19. Hwang J, Puttagunta L, Green F, Shimanovsky A, Barrie J, Long R. Bronchial anthracofibrosis and tuberculosis in immigrants to Canada from the Indian subcontinent. Int J Tuberc Lung Dis. 2010;14(2):231-7.
20. Chung MP, Lee KS, Han J, Kim H, Rhee CH, Han YC, et al. Bronchial stenosis due to anthracofibrosis. Chest. 1998;113(2):344-50. http://dx.doi.org/10.1378/chest.113.2.344
21. Mirsadraee M, Saeedi P. Anthracosis of lung: evaluation of potential underlying causes. J Bronchol. 2005;12(2):84-7. http://dx.doi.org/10.1097/01.laboratory.0000150873.99404.53
22. Pérez-Padilla R, Pérez-Guzmán C, Báez-Salda-a R, Torres-Cruz A. Cooking with biomass stoves and tuberculosis: a case control study. Int J Tuberc Lung Dis. 2001;5(5):441-7.
23. Pokhrel AK, Bates MN, Verma SC, Joshi HS, Sreeramareddy CT, Smith KR. Tuberculosis and indoor biomass and kerosene use in Nepal: a case-control study. Environ Health Perspect. 2010;118(4):558-64. http://dx.doi.org/10.1289/ehp.0901032
24. Kolappan C, Subramani R. Association between biomass fuel and pulmonary tuberculosis: a nested case-control study. Thorax. 2009;64(8):705-8. http://dx.doi.org/10.1136/thx.2008.109405
25. Rajagopalan S. Tuberculosis and aging: a global health problem. Clin Infect Dis. 2001;33(7):1034-9. http://dx.doi.org/10.1086/322671
26. Kim HJ, Kim SD, Shin DW, Bae SH, Kim AL, Kim JN, et al. Relationship between bronchial anthracofibrosis and endobronchial tuberculosis. Korean J Intern Med. 2013;28(3):330-8. http://dx.doi.org/10.3904/kjim.2013.28.3.330
195J Bras Pneumol. 2016;42(3):191-195

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000058
ABSTRACTObjective: The gait speed test (GST) is a physical test that can predict falls and aid in the diagnosis of sarcopenia in the elderly. However, to our knowledge, there have been no studies evaluating its reproducibility in hospitalized elderly patients. The objective of this study was to evaluate the safety and reproducibility of the six-meter GST (6GST) in hospitalized elderly patients. Methods: This repeated measures study involved hospitalized elderly patients (≥ 60 years of age) who underwent the 6GST by the fifth day of hospitalization, were able to walk without assistance, and presented no signs of dyspnea or pain that would prevent them from performing the test. The 6GST was performed three times in sequence, with a rest period between each test, in a level corridor. Gait speed was measured in meters/second. Reproducibility was assessed by comparing the means, intraclass correlation coefficients (ICCs) and Bland-Altman plots. Results: We evaluated 110 elderly patients in a total of 330 tests. All participants completed all of the tests. The comparisons between the speeds obtained during the three tests showed high ICCs and a low mean bias (Bland-Altman plots). The correlation and accuracy were greatest when the mean maximum speed was compared with that obtained in the third test (1.26 ± 0.44 m/s vs. 1.22 ± 0.44 m/s; ICC = 0.99; p = 0.001; mean bias = 0.04; and limits of agreement = −0.27 to 0.15). Conclusions: The 6GST was proven to be safe and to have good reproducibility in this sample of hospitalized elderly patients. The third measurement seems to correspond to the maximum speed, since the first two measurements underestimated the actual performance.
Keywords: Disability evaluation; Reproducibility of results; Hospitalization; Mobility limitation; Health of the elderly.
Viability of gait speed test in hospitalized elderly patientsBruno Prata Martinez1,2, Anne Karine Menezes Santos Batista3, Isis Resende Ramos3, Júlio Cesar Dantas3, Isabela Barboza Gomes3, Luiz Alberto Forgiarini Júnior4, Fernanda Rosa Warken Camelier1, Aquiles Assunção Camelier1,5
Correspondence to: Bruno Prata Martinez. Rua Silveira Martins, 2555, Departamento DCV I - Fisioterapia, Cabula, CEP 41150-010, Salvador, BA, Brasil.Tel.: 55 71 3117-2200. Email: [email protected] support: None.
INTRODUCTION
The elderly population is considered a high-risk group for experiencing worsening health over the years; this worsening health is usually associated with decreased physical performance in activities of daily living, such as walking.(1) However, this is a heterogeneous population, and early identification of individuals who are at high risk for future health problems is necessary.(2) To that end, it is vital that physical tests that are reliable and that do not pose risk to the elderly be conducted, and that such tests be carried out in a hospital setting.
Some physical tests have been used in the elderly and are able to indicate an increased risk of hospitalization, worsening health status, and even an increased risk of mortality,(3-5) as well as being one of the parameters required for the diagnosis of sarcopenia.(1) The six-meter gait speed test (6GST) is one such assessment tool and is considered a rapid, inexpensive measure that is highly reproducible in the noninstitutionalized elderly.(5)
During hospitalization, the elderly population is at even more significant risk of a decrease in their ability to perform activities of daily living and in their cognitive function.(4,6) Among all individuals over 60 years of
age and hospitalized for external causes in Brazil, falls account for 19.3% of all hospitalizations.(7) This finding is a cause for concern because of possible associated negative outcomes, such as nosocomial pneumonia, exacerbation of cardiorespiratory disease, and even death.(8,9) Identifying elderly individuals at risk of falls and screening them while they are still in the hospital setting, by using tests such as the 6GST, may be a feasible approach to enable referral of such individuals for specific treatment interventions to prevent the occurrence of such outcomes.
We found no studies evaluating the safety and repro-ducibility of the GST in elderly Brazilians in the hospital setting. Therefore, the objective of the present study was to evaluate the safety and reproducibility of the 6GST in hospitalized elderly patients. A secondary objective was to categorize the elderly and to compare the test results among the different categories.
METHODS
This was a repeated measures study conducted between August of 2013 and January of 2014 in the ICU and Inpatient Unit (IU) of the Hospital da Cidade, located
1. Universidade do Estado da Bahia – UNEB – Salvador (BA) Brasil.
2. Unidade de Terapia Intensiva, Hospital Aliança, Salvador (BA) Brasil.
3. Hospital da Cidade, Salvador (BA) Brasil.4. Curso de Fisioterapia, Programa de Pós-
Graduação em Reabilitação e Inclusão e Biociências e Reabilitação, Centro Universitário Metodista – IPA – Porto Alegre (RS) Brasil.
5. Programa de Pós-Graduação em Medicina e Saúde, Escola Bahiana de Medicina e Saúde Pública, Salvador (BA) Brasil.
Submitted: 19 March 2015.Accepted: 19 September 2015.
Study carried out at the Universidade do Estado da Bahia and at the Hospital da Cidade, Salvador (BA) Brasil.
J Bras Pneumol. 2016;42(3):196-202
196
ORIGINAL ARTICLE
Martinez BP, Batista AKMS, Ramos IR, Dantas JC, Gomes IB, Forgiarini LA Jr, Camelier FRW, Camelier AA
in the city of Salvador, Brazil. We included patients who were 60 years of age or older, were admitted to either of those units between the first and the fifth day of their hospital stay, were not on vasoactive or inotropic drugs, could move about independently (self-report of being ambulatory without external aids) in the period prior to hospitalization, had no dyspnea or cardiorespiratory changes (systolic blood pressure ≥ 180 mmHg or < 90 mmHg, heart rate > 100 bpm, and SpO2 ≤ 90%), and experienced no pain that would make the measurements impossible, as well as having physician approval to walk daily. To evaluate and increase safety during the 6GST, we considered the following test interruption criteria: precordial pain; SpO2 ≤ 90%; dizziness; pallor; nausea; sweating; palpitations; presyncope, dyspnea; accidental removal of invasive devices; falling; pain; etc.(10)
The primary variable measured was gait speed, and secondary data, such as age, gender, length of hospital stay before data collection (before the test), and the Charlson comorbidity index,(11) were obtained from medical records. In addition, cognitive function was measured with the Mini-Mental State Examination.(12) Patients were selected for inclusion in the study by the physical therapy staff, who checked the medical records in the electronic medical record system of the aforementioned hospital on a daily basis. The study project was approved by the Research Ethics Committee of the Escola Bahiana de Medicina e Saúde Pública (Protocol no. 567.937/14). All of the patients included in the study gave written informed consent.
After having been selected and having been instructed on how to perform the test, the individuals were taken to the corridors of each unit so that they could undergo the test. Patients were asked to walk ten meters as fast as possible without running. Time, in seconds, was measured between the second meter and the eighth meter, since the first two meters (acceleration period) and the last two meters (deceleration period) were not included in the calculation.(13) Speed was calculated by dividing six meters by the time to walk this distance in seconds, and a speed of ≤ 0.8 m/s was considered poor physical performance.(5) Time in relation to distance covered was measured with a digital stopwatch (CASIO HS-3V-1; CASIO, São Paulo, Brazil), which was started when one of the legs crossed the second meter and was stopped when one of the legs crossed the eighth meter. To ensure data accuracy, markings were placed on the floor of the corridor, at zero, two, eight, and ten meters.
The total time between explanation about the test and completion of the test, including the three measurements, did not exceed 20 min, and the rest period between each gait speed measurement was 1 min, so that patients would return to their pretest condition. If the patients did not return to their baseline condition, the rest period could be increased. However, none of the patients required that. All of the patients underwent three tests. A fourth test was not required in any of the cases, because neither a lack of patient
understanding nor failures during the measurements were observed.
The sample size was calculated on the basis of two studies that reported a high correlation for the test-retest reproducibility of gait speed (intraclass correlation, 0.94-0.99).(14,15) On this basis, we estimated, assuming a confidence interval greater than 95%, a significance level of 5%, and an accuracy of 10 percentage points, that the final sample size would have to be at least 73 patients.
Numerical variables were expressed as means and standard deviations, whereas categorical variables were expressed as proportions with confidence intervals. Gait speed was expressed as absolute values and was also expressed dichotomously—good physical performance vs. poor physical performance (gait speed ≤ 0.8 m/s). To compare the means of the fastest gait speeds, the elderly patients were categorized according to the following variables: gender; Charlson index (≤ 4 or > 4); length of pretest hospital stay (1-3 days or 4-5 days), and collection site (ICU or IU). Subsequently, the Student’s t-test for independent samples was used. Repeated-measures ANOVA was used to compare the gait speeds obtained in the three tests and in the three age groups (60-69, 70-79, and > 80 years). In addition, for the gait speeds obtained in the three tests and the maximum speed, we calculated the intraclass correlation coefficients (ICCs) using a two-way random effects consistency model. The measurement error was determined by dividing the standard deviation of the mean difference between the measurements by the square root of two (Bland-Altman plots for absolute reliability).(16,17) The analyses were performed with the Statistical Package for the Social Sciences, version 14.0 (SPSS Inc., Chicago, IL, USA). Values of p < 0.05 were considered statistically significant.
RESULTS
The sample consisted of 110 elderly patients. The mean age was 71.0 ± 8.5 years, and the mean Charlson index was 5.4 ± 1.8. There was a predominance of clinical patients (n = 65; 59.1%). The main reason for admission was abdominal surgery (n = 38; 34.5%), followed by cardiovascular changes (n = 22; 20.0%), pneumonia (n = 15; 13.6%), and skin infections (n = 10; 9.1%). A total of 330 6GSTs were performed, and none of the interruption criteria described in the 6GST methodology was met in any of those tests. Most measurements took place in the IU (n = 75; 68.2%) and between the first and third days of hospitalization (n = 71; 64.5%), the mean hospital stay before the test being 2.7 ± 1.6 days (Table 1).
The mean maximum gait speed was 1.26 ± 0.44 m/s, and 15 patients (13.6%) were classified as having poor physical performance (gait speed ≤ 0.8 m/s). Comparison of gait speed among the three age categories in the present study showed that values trended downward with increasing age. Intergroup comparison showed that gait speed was fastest in
197J Bras Pneumol. 2016;42(3):196-202
Viability of gait speed test in hospitalized elderly patients
the patients admitted for surgery, in those who were male, and in those with a Charlson index ≤ 4 (Table 2).
In analyzing the three gait speed measurement results in each patient, we observed a progressive increase between the first and third measurements—the mean values for the first, second, and third measurements were 1.12 ± 0.38 m/s, 1.16 ± 0.38 m/s, and 1.22 ± 0.44 m/s, respectively—with a significant difference between the third and first measurements (mean difference of 0.1 m/s; p = 0.001; Table 3). Paired comparisons among the three measurements showed that all ICCs were high—for the comparison between the first and second measurements (ICC = 0.92; p = 0.001); for that between the first and third measurements (ICC = 0.94; p = 0.001); and for that between the second and third measurements (ICC = 0.94; p = 0.001). In the analysis of correlation between the maximum gait speed attained and the three measurements performed, the highest correlation was that with the third measurement (mean = 1.22 ± 0.44 m/s; maximum = 1.26 ± 0.44 m/s; ICC = 0.99; p = 0.001; Figure 1).
The Bland-Altman plots showed low mean bias values between the measurements, as can be seen in Figure 2. In comparing all gait speed measurements, we observed that the lowest bias values (−0.04 m/s) and the lowest limits of agreement (−0.25 to 0.17 m/s) occurred for the comparison between the third measurement and the maximum gait speed attained,
which demonstrates that the third measurement was more accurate relative to the maximum speed than were the first and second measurements. Measure-ment variability was determined by calculating the measurement error between the tests (0.08 s).
DISCUSSION
The present study showed that using the 6GST in hospitalized elderly patients was safe and feasible, given that no test interruptions were required and no test-related adverse events were observed in the elderly population in the hospital setting under study. In addition, we found that, despite the high ICCs between the measurements, the third measurement was proven to be the most reliable, because its correlation with the maximum speed was the highest and because it resulted in the lowest mean bias and lowest limits of agreement. This was the first study aimed at evaluating unexpected events during the 6GST in an elderly population in the hospital setting, including some stable patients in the ICU, in Brazil.
We should also highlight the importance of using the 6GST for the diagnosis of sarcopenia, since sarcopenia is a condition that is associated with physical disability and mortality over the years in the noninstitutionalized elderly.(18,19) Although only 20 (18.1%) of the elderly patients evaluated had been hospitalized for lung problems, the 6GST, being rapid and easy to perform, can be used in patients with stable lung disease in the hospital setting(20) and even in COPD patients undergoing pulmonary rehabilitation.(21) In the future, the 6GST may serve as a tool for the identification of respiratory morbidity (nosocomial pneumonia and exacerbation of cardiorespiratory disease) during and
Table 2. Comparison of means and standard deviations for fastest gait speed among relevant variables/categories.a
Variable GS, m/s pType of admission 0.049
Clinical 1.23 ± 0.50Surgical 1.31 ± 0.34
Gender 0.014Female 1.14 ± 0.50Male 1.36 ± 0.40
Charlson index 0.012≤ 4 1.42 ± 0.50> 4 1.20 ± 0.40
Length of pretest hospital stay, days 0.8631-3 1.26 ± 0.444-5 1.28 ± 0.44
Collection site 0.317ICU 1.20 ± 0.43Inpatient Unit 1.30 ± 0.45
Age group, years < 0.0560-69 1.41 ± 0.43**/***
70-79 1.25 ± 0.31*/***
> 80 0.86 ± 0.44*/**
GS: gait speed. aValues expressed as mean ± SD. *p = 0.002; **p = 0.001; and ***p = 0.24.
Table 1. Demographic and clinical characteristics of the study sample of 110 elderly patients.a
Variable ResultAge, years 71.0 ± 8.5Cause of hospitalizationAbdominal surgery 38 (34.5)
Cardiologic 22 (20.0)Respiratory 15 (13.6)Dermatologic 10 (9.1)Gastrointestinal 8 (7.3)Neurologic 5 (4.5)Urinary 3 (2.7)Others 9 (8.2)
BMI, classification 25.4 ± 4.7Underweight 3 (2.7)Normal weight 51 (46.4)Overweight/obesity 56 (50.9)
GenderMale 64 (58.2)Female 46 (41.8)
Length of pretest hospital stay, days 2.7 ± 1.6Type of admission
Clinical 65 (59.1)Surgical 45 (40.9)
Charlson index 5.4 ± 1.8Mini-Mental State Examination 23.7 ± 5.0Gait speed, m/s 1.26 ± 0.44BMI: body mass index. aValues expressed as mean ± SD or as n (%).
198 J Bras Pneumol. 2016;42(3):196-202
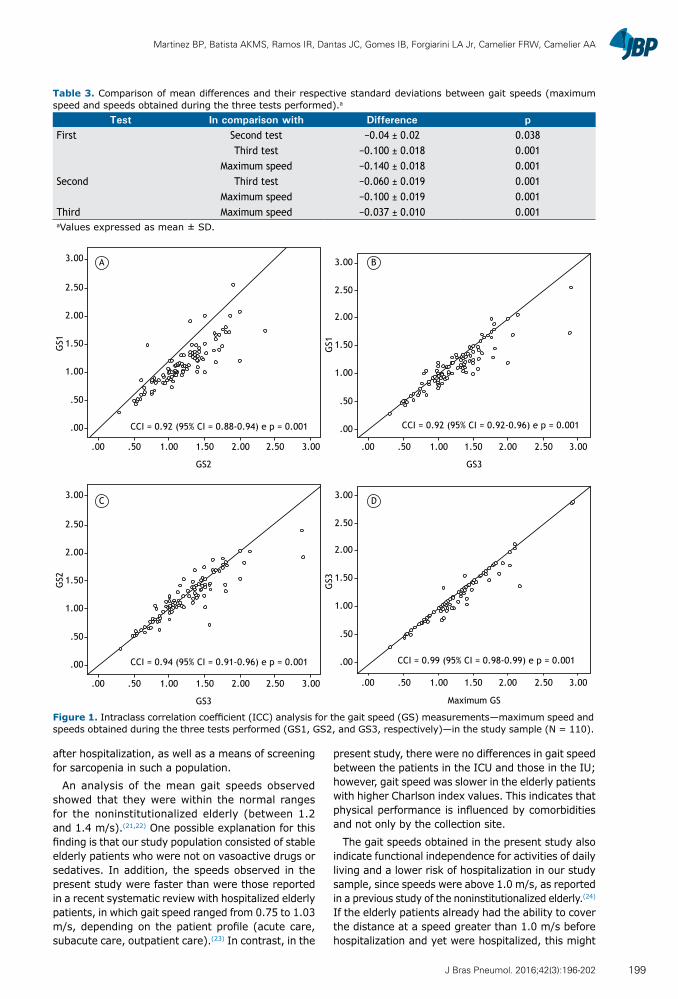
Martinez BP, Batista AKMS, Ramos IR, Dantas JC, Gomes IB, Forgiarini LA Jr, Camelier FRW, Camelier AA
after hospitalization, as well as a means of screening for sarcopenia in such a population.
An analysis of the mean gait speeds observed showed that they were within the normal ranges for the noninstitutionalized elderly (between 1.2 and 1.4 m/s).(21,22) One possible explanation for this finding is that our study population consisted of stable elderly patients who were not on vasoactive drugs or sedatives. In addition, the speeds observed in the present study were faster than were those reported in a recent systematic review with hospitalized elderly patients, in which gait speed ranged from 0.75 to 1.03 m/s, depending on the patient profile (acute care, subacute care, outpatient care).(23) In contrast, in the
present study, there were no differences in gait speed between the patients in the ICU and those in the IU; however, gait speed was slower in the elderly patients with higher Charlson index values. This indicates that physical performance is influenced by comorbidities and not only by the collection site.
The gait speeds obtained in the present study also indicate functional independence for activities of daily living and a lower risk of hospitalization in our study sample, since speeds were above 1.0 m/s, as reported in a previous study of the noninstitutionalized elderly.(24) If the elderly patients already had the ability to cover the distance at a speed greater than 1.0 m/s before hospitalization and yet were hospitalized, this might
Table 3. Comparison of mean differences and their respective standard deviations between gait speeds (maximum speed and speeds obtained during the three tests performed).a
Test In comparison with Difference pFirst Second test −0.04 ± 0.02 0.038
Third test −0.100 ± 0.018 0.001Maximum speed −0.140 ± 0.018 0.001
Second Third test −0.060 ± 0.019 0.001Maximum speed −0.100 ± 0.019 0.001
Third Maximum speed −0.037 ± 0.010 0.001aValues expressed as mean ± SD.
Figure 1. Intraclass correlation coefficient (ICC) analysis for the gait speed (GS) measurements—maximum speed and speeds obtained during the three tests performed (GS1, GS2, and GS3, respectively)—in the study sample (N = 110).
3.00
2.50
2.00
1.50
1.00
.50
.00
GS1
3.00
2.50
2.00
1.50
1.00
.50
.00
GS1
.00 .50 1.00 1.50 2.00 2.50 3.00
GS2
.00 .50 1.00 1.50 2.00 2.50 3.00
GS3
3.00
2.50
2.00
1.50
1.00
.50
.00
.00 .50 1.00 1.50 2.00 2.50 3.00
Maximum GS
C D
A B
CCI = 0.92 (95% CI = 0.88-0.94) e p = 0.001
3.00
2.50
2.00
1.50
1.00
.50
.00
GS2
GS3
.00 .50 1.00 1.50 2.00 2.50 3.00
GS3
CCI = 0.94 (95% CI = 0.91-0.96) e p = 0.001 CCI = 0.99 (95% CI = 0.98-0.99) e p = 0.001
CCI = 0.92 (95% CI = 0.92-0.96) e p = 0.001
199J Bras Pneumol. 2016;42(3):196-202
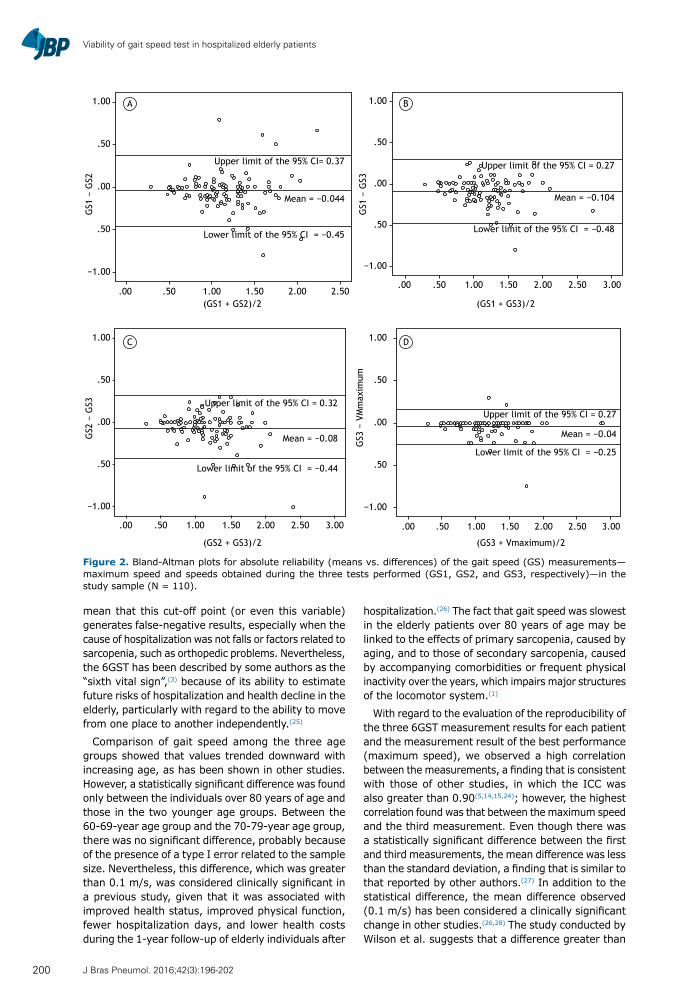
Viability of gait speed test in hospitalized elderly patients
mean that this cut-off point (or even this variable) generates false-negative results, especially when the cause of hospitalization was not falls or factors related to sarcopenia, such as orthopedic problems. Nevertheless, the 6GST has been described by some authors as the “sixth vital sign”,(3) because of its ability to estimate future risks of hospitalization and health decline in the elderly, particularly with regard to the ability to move from one place to another independently.(25)
Comparison of gait speed among the three age groups showed that values trended downward with increasing age, as has been shown in other studies. However, a statistically significant difference was found only between the individuals over 80 years of age and those in the two younger age groups. Between the 60-69-year age group and the 70-79-year age group, there was no significant difference, probably because of the presence of a type I error related to the sample size. Nevertheless, this difference, which was greater than 0.1 m/s, was considered clinically significant in a previous study, given that it was associated with improved health status, improved physical function, fewer hospitalization days, and lower health costs during the 1-year follow-up of elderly individuals after
hospitalization.(26) The fact that gait speed was slowest in the elderly patients over 80 years of age may be linked to the effects of primary sarcopenia, caused by aging, and to those of secondary sarcopenia, caused by accompanying comorbidities or frequent physical inactivity over the years, which impairs major structures of the locomotor system.(1)
With regard to the evaluation of the reproducibility of the three 6GST measurement results for each patient and the measurement result of the best performance (maximum speed), we observed a high correlation between the measurements, a finding that is consistent with those of other studies, in which the ICC was also greater than 0.90(5,14,15,24); however, the highest correlation found was that between the maximum speed and the third measurement. Even though there was a statistically significant difference between the first and third measurements, the mean difference was less than the standard deviation, a finding that is similar to that reported by other authors.(27) In addition to the statistical difference, the mean difference observed (0.1 m/s) has been considered a clinically significant change in other studies.(26,28) The study conducted by Wilson et al. suggests that a difference greater than
Figure 2. Bland-Altman plots for absolute reliability (means vs. differences) of the gait speed (GS) measurements—maximum speed and speeds obtained during the three tests performed (GS1, GS2, and GS3, respectively)—in the study sample (N = 110).
Upper limit of the 95% CI= 0.37
Upper limit of the 95% CI = 0.32
Lower limit of the 95% CI = −0.45
Lower limit of the 95% CI = −0.44
Mean = −0.044
Mean = −0.08
Upper limit of the 95% CI = 0.27
Lower limit of the 95% CI = −0.48
Mean = −0.104
Upper limit of the 95% CI = 0.27
Lower limit of the 95% CI = −0.25
Mean = −0.04
.00 .50 1.00 1.50 2.00 2.50
1.00
.50
.00
.50
−1.00.00 .50 1.00 1.50 2.00 2.50 3.00
1.00
.50
.00
.50
−1.00
1.00
.50
.00
.50
−1.00
.00 .50 1.00 1.50 2.00 2.50 3.00.00 .50 1.00 1.50 2.00 2.50 3.00
1.00
.50
.00
.50
−1.00
C D
A B
(GS1 + GS2)/2
GS1
− G
S2G
S2 −
GS3
GS1
− G
S3G
S3 −
VM
max
imum
(GS1 + GS3)/2
(GS2 + GS3)/2 (GS3 + Vmaximum)/2
200 J Bras Pneumol. 2016;42(3):196-202

Martinez BP, Batista AKMS, Ramos IR, Dantas JC, Gomes IB, Forgiarini LA Jr, Camelier FRW, Camelier AA
0.05 m/s, a value that was obtained when comparing gait speed among tests, is clinically significant.(28)
In addition to having shown the highest correlation with the maximum gait speed attained, the third measurement showed the highest accuracy, as can be observed in the Bland-Altman plots. This absolute reliability analysis is relevant, given that it addresses the proximity of values, unlike ICC analysis, which deals with the linear association between measurements. Although the accuracy and mean bias were less than 0.05 m/s, a value considered clinically significant in a previous study,(27) the limits of agreement (−0.25 to 0.17 m/s) were greater than 0.1 m/s, a value considered predictive of well-being.(26) The measurement variability of 0.08 observed in the present study was also greater than the 0.05 value reported in the Wilson et al. study.w(28) One possible explanation for this is the effect of learning and motivation to perform the test, since the third measurement showed smaller differences between means, a higher ICC, and a lower mean bias than did the first two measurements.
Poor physical performance, which is predictive of adverse outcomes, was observed for only a small proportion of the total sample (n = 15; 13.6%), and that might have accounted for the absence of complications, such as falls and cardiorespiratory instability, during the test. However, despite being stable, all of the elderly patients showed some level of disease severity, since the mean Charlson index was > 5 and some patients were in the ICU.
In addition to being easily reproducible, because of its short duration and its minimal requirement of space, the 6GST is found to be safe and may be able to identify patients at risk for poor outcomes, as well
as being useful in predicting the prognosis of such patients. In the future, the 6GST should be routinely used in hospital units, including ICUs, in elderly patients who are stable and fit to undergo the test, since there is an association between gait speeds and referral to units that can treat clinical and functional complications. (29,30) In addition, values obtained at hospital discharge may have some association with prognosis over time.
Our study has some limitations, such as the fact that gait speed was not compared with any measure of physical performance considered to be the gold standard in the hospital setting. However, this can be justified by the lack of physical tests that can be used in this setting. Another test that could be used is the six-minute walk test. However, the purpose of the six-minute walk test is different from that of GSTs, since the former measures individual aerobic capacity and the latter measure mobility. Another limitation is that the study was conducted at a single center. In addition, gait speed was measured in individuals who were ambulatory without external aids, which limits the external validity of the results to such patients. Future studies, evaluating patients at discharge and thereafter, are warranted in order to allow the analysis of medium- and long-term outcomes.
The 6GST was proven to be a safe measure of physical performance and to have good reproducibility in our sample of elderly patients evaluated in the hospital setting. Of the three gait speed measurements performed for each elderly patient, the third one seems to correspond to the maximum speed, since the first two measurements underestimated the actual physical performance in most cases.
REFERENCES
1. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412-23. http://dx.doi.org/10.1093/ageing/afq034
2. Cesari M, Kritchevsky SB, Penninx BW, Nicklas BJ, Simonsick EM, Newman AB, et al. Prognostic value of usual gait speed in well-functioning older people--results from the Health, Aging and Body Composition Study. J Am Geriatr Soc. 2005;53(10):1675-80. http://dx.doi.org/10.1111/j.1532-5415.2005.53501.x
3. Fritz S, Lusardi M. White paper: “walking speed: the sixth vital sign”. J Geriatr Phys Ther. 2009;32(2):46-9. http://dx.doi.org/10.1519/00139143-200932020-00002
4. Cawthon PM, Marshall LM, Michael Y, Dam TT, Ensrud KE, Barrett-Connor E, et al. Frailty in older men: prevalence, progression, and relationship with mortality. J Am Soc Geriatr. 2007;55(8):1216-23. http://dx.doi.org/10.1111/j.1532-5415.2007.01259.x
5. Abellan van Kan G, Rolland Y, Andrieu S, Bauer J, Beauchet O, Bonnefoy M, et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J Nutr Health Aging. 2009;13(10):881-9. http://dx.doi.org/10.1007/s12603-009-0246-z
6. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Fraity in older adults: evidence for a phenotype. J Gerontol A Sci Med Sci. 2001;56(3):M146-56.
7. Departamento de Informática do SUS - DATASUS [homepage on the Internet]. Brasília: Ministério da Saúde [cited 2014 May 29]. Available from: http://www2.datasus.gov.br/
8. Iglesias CP, Manca A, Torgerson DJ. The health-related quality of life and cost implications of falls in elderly women. Osteoporos Int. 2009;20(6):869-78. http://dx.doi.org/10.1007/s00198-008-0753-5
9. Fhon JR, Rosset I, Freitas CP, Silva AO, Santos JL, Rodrigues RA. Prevalence of falls among frail elderly adults. Rev Saude Publica. 2013;47(2):266-73. http://dx.doi.org/10.1590/S0034-8910.2013047003468
10. Stiller K. Safety issues that should be considered when mobilizing critically ill patients. Crit Care Clin. 2007;23(1):35-53. http://dx.doi.org/10.1016/j.ccc.2006.11.005
11. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-83. http://dx.doi.org/10.1016/0021-9681(87)90171-8
12. Lourenço RA, Veras RP. Mini-mental State Examination: psychometric characteristics in elderly outpatients [Article in Portuguese]. Rev Saude Publica. 2006;40(4):712-9. http://dx.doi.org/10.1590/S0034-89102006000500023
13. Ostir GV, Volpato S, Fried LP, Chaves P, Guralnik JM; Women’s Health and Aging Study. Reliability and sensitivity to change assessed for a summary measure of lower body function: results from the Women’s Health and Aging Study. J Clin Epidemiol. 2002;55(9):916-21. http://dx.doi.org/10.1016/S0895-4356(02)00436-5
14. Kon SS, Patel MS, Canavan JL, Clark AL, Jones SE, Nolan CM, et al. Reliability and validity of 4-metre gait speed in COPD. Eur Resp J. 2013;42(3):333-40. http://dx.doi.org/10.1183/09031936.00162712
15. Flansbjer U, Holmbäck AM, Downham D, Patten C, Lexell J. Reliability of gait performance tests in men and women with hemiparesis after stroke. J Reahabil Med. 2005;37(2):75-82. http://
201J Bras Pneumol. 2016;42(3):196-202

Viability of gait speed test in hospitalized elderly patients
dx.doi.org/10.1080/1650197041001721516. Altman DG, Bland JM. Measurement in medicine: the analysis of
method comparison studies. Statistician. 1983;32:307-17. http://dx.doi.org/10.2307/2987937
17. Lexell JE, Downham DY. How to assess the reliability of measurements in rehabilitation. Am J Phys Med Rehabil. 2005;84(9):719-23. http://dx.doi.org/10.1097/01.phm.0000176452.17771.20
18. da Silva Alexandre T, de Oliveira Duarte YA, Ferreira Santos JL, Wong R, Lebrão ML. Sarcopenia according to the european working group on sarcopenia in older people (EWGSOP) versus Dynapenia as a risk factor for disability in the elderly. J Nutr Health Aging. 2014;18(5):547-53. http://dx.doi.org/10.1007/s12603-014-0465-9
19. Martinez BP, Batista AK, Gomes IB, Olivieri FM, Camelier FW, Camelier AA. Frequence of sarcopenia and associated factors among hospitalized elderly patients. BMC Musculoskelet Disord. 2015;16:108. http://dx.doi.org/10.1186/s12891-015-0570-x
20. Jones SE, Maddocks M, Kon SS, Canavan JL, Nolan CM, Clark AL, et al. Sarcopenia in COPD: prevalence, clinical correlates and response to pulmonary rehabilitation. Thorax. 2015;70(3):213-8. http://dx.doi.org/10.1136/thoraxjnl-2014-206440
21. Lernier-Frankiel M, Vargas S, Brown M, Krusell L, Schoneberger W. Functional community ambulation: what are your criteria? Clin Manag Phys Ther. 1986;6:12-5.
22. Bohannon RW, Williams Andrews AW. Normal walking speed: a descriptive meta-analysis. Physiotherapy. 2011;97(3):182-9. http://dx.doi.org/10.1016/j.physio.2010.12.004
23. Peel NM, Kuys SS, Klein K. Gait speed as a measure in geriatric assessment in clinical settings: a systematic review. J Gerontol A
Biol Sci Med Sci. 2013;68(1):39-46. http://dx.doi.org/10.1093/gerona/gls174
24. Studenski SA, Perera S, Wallace D, Chandler JM, Duncan PW, Rooney E, et al. Physical performance measures in the clinical setting. J Am Geriatr Soc. 2003;51(3):314-22. http://dx.doi.org/10.1046/j.1532-5415.2003.51104.x
25. Rosa TE, Benício MH, Latorre Mdo R, Ramos LR. Determinant factors of functional status among the elderly [Article in Portuguese]. Rev Saude Publica. 2003;37(1):40-8.
26. Purser JL, Weinberger M, Cohen HJ, Pieper CF, Morey MC, Li T, et al. Walking speed predicts health status and hospital costs for frail elderly male veterans. J Rehabil Res Dev. 2005;42(4):535-46. http://dx.doi.org/10.1682/JRRD.2004.07.0087
27. Wilson CM, Kostsuca SR, Boura JA. Utilization of a 5-Meter Walk Test in Evaluating Self-selected Gait Speed during Preoperative Screening of Patients Scheduled for Cardiac Surgery. Cardiopulm Phys Ther J. 2013;24(3):36-43.
28. Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc. 2006;54(5):743-9. http://dx.doi.org/10.1111/j.1532-5415.2006.00701.x
29. Hardy SE, Perera S, Roumani YF, Chandler JM, Studenski SA. Improvement in usual gait speed predicts better survival in older adults. J Am Geriatr Soc. 2007;55(11):1727-34. http://dx.doi.org/10.1111/j.1532-5415.2007.01413.x
30. Rabadi MH, Blau A. Admission ambulation velocity predicts length of stay and discharge disposition following stroke in an acute rehabilitation hospital. Neurorehabil Neural Repair. 2005;19(1):20-6. http://dx.doi.org/10.1177/1545968304272762
202 J Bras Pneumol. 2016;42(3):196-202

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000244
The value of antibody-coated bacteria in tracheal aspirates for the diagnosis of ventilator-associated pneumonia: a case-control studyOtavio Tavares Ranzani1, Daniel Neves Forte2, Antonio Carlos Forte3, Igor Mimica3, Wilma Carvalho Neves Forte3
Correspondence to:Otavio T Ranzani. Laboratório de Pneumologia, Avenida Dr. Arnaldo, 455, 2º andar, sala 2144, CEP 01246-903, São Paulo, SP, Brasil.Tel.: 55 11 3061-7361. Fax: 55 11 3061-2492. E-mail: [email protected] support: None.
INTRODUCTION
Ventilator-associated pneumonia (VAP) affects approximately 25% of patients submitted to mechanical ventilation, with an incidence of 2-16 episodes/1,000 hospital admissions.(1,2) Although VAP is associated with high mortality, the attributable mortality can be low depending on the case mix and adjustments.(3-6) In addition, VAP contributes to multiple organ failure in debilitated patients, prolonged hospitalization and increased health-associated costs.(7,8)
The diagnosis of VAP is challenging, and guidelines suggest that a clinical approach, a microbiologic approach, or both should be employed.(4,9-11) Clinical criteria alone have been shown to have low specificity, because several other pathologies seen in the ICU can mimic VAP,(11-13) although their high sensitivity is useful for raising the suspicion of pneumonia.(9,12) Conversely, clinicians cannot rely only on microbiologic results, because it can be difficult to deal with false-positives (e.g., to differentiate between tracheal colonization and infection)(9) and false-negatives (e.g., culture-negative
results due to previous antibiotic use) when interpreting a respiratory tract culture result.(4,6,9) Combining the two approaches (clinical and microbiological) seems to improve the diagnostic accuracy.(4,9,14)
In medical practice, invasive and noninvasive techniques are used in order to obtain samples from the lower respiratory tract for microbiological evaluation. Recently, a clinical trial(15) and a meta-analysis both showed that there are no differences between invasive and noninva-sive techniques regarding main outcomes. (16) Although invasive methods have higher specificity than does the collection of endotracheal aspirate (EA), the former are more expensive and usually require bronchoscopic guidance.(14,17)
Worldwide, EA is used in order to diagnosis VAP and can be more cost-effective, making it especially useful in low-resource settings. In order to improve its speci-ficity, there is a need for a method able to differentiate between colonization and infection. The evaluation of antibody-coated bacteria (ACB) is a promising candidate that has already been applied in other areas.(18) Therefore,
ABSTRACTObjective: Ventilator-associated pneumonia (VAP) is the leading type of hospital-acquired infection in ICU patients. The diagnosis of VAP is challenging, mostly due to limitations of the diagnostic methods available. The aim of this study was to determine whether antibody-coated bacteria (ACB) evaluation can improve the specificity of endotracheal aspirate (EA) culture in VAP diagnosis. Methods: We conducted a diagnostic case-control study, enrolling 45 patients undergoing mechanical ventilation. Samples of EA were obtained from patients with and without VAP (cases and controls, respectively), and we assessed the number of bacteria coated with FITC-conjugated monoclonal antibodies (IgA, IgM, or IgG) or an FITC-conjugated polyvalent antibody. Using immunofluorescence microscopy, we determined the proportion of ACB among a fixed number of 80 bacteria. Results: The median proportions of ACB were significantly higher among the cases (n = 22) than among the controls (n = 23)—IgA (60.6% vs. 22.5%), IgM (42.5% vs. 12.5%), IgG (50.6% vs. 17.5%), and polyvalent (75.6% vs. 33.8%)—p < 0.001 for all. The accuracy of the best cut-off points for VAP diagnosis regarding monoclonal and polyvalent ACBs was greater than 95.0% and 93.3%, respectively. Conclusions: The numbers of ACB in EA samples were higher among cases than among controls. Our findings indicate that evaluating ACB in EA is a promising tool to improve the specificity of VAP diagnosis. The technique could be cost-effective and therefore useful in low-resource settings, with the advantages of minimizing false-positive results and avoiding overtreatment.
Keywords: Pneumonia, ventilator-associated/diagnosis; Immunohistochemistry; Fluorescent antibody technique; Antibodies, bacterial/analysis; Trachea/microbiology; Intensive care units.
1. Unidade de Terapia Intensiva Respiratória, Divisão de Pneumologia, Instituto do Coração, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
2. Unidade de Terapia Intensiva, Disciplina de Emergências Clínicas, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
3. Disciplina de Imunologia, Departamento de Ciências Patológicas, Faculdade de Ciências Médicas da Santa Casa de São Paulo, São Paulo (SP) Brasil.
Submitted: 28 September 2015.Accepted: 19 April 2016.
Study carried out in the Intensive Care Unit, Santa Casa de Misericórdia de São Paulo, São Paulo (SP) Brasil.
J Bras Pneumol. 2016;42(3):203-210
203
ORIGINAL ARTICLE
The value of antibody-coated bacteria in tracheal aspirates for the diagnosis of ventilator-associated pneumonia: a case-control study
our hypothesis was that ACB would be more prevalent in EA samples from patients with VAP than in those from patients without. In addition, we sought to investigate whether this difference could be used to increase the specificity of the VAP diagnosis.
METHODS
We conducted a diagnostic case-control study(19) in the general ICU of the Santa Casa de Misericórdia de São Paulo, an academic tertiary care hospital in the city of São Paulo, Brazil. The study was approved by the local research ethics committee. Family members or legal guardians of all of the participating patients gave written informed consent.
Eligible patients were adults (> 18 years of age) who were admitted to the ICU, were undergoing orotracheal intubation with mechanical ventilation, and had neither been diagnosed with nor were under suspicion of having pneumonia at ICU admission.
Case definitionWe defined cases of VAP as those meeting clinical
and microbiological criteria. The clinical criteria were signs or symptoms suggestive of pneumonia—new or progressive radiographic infiltrate plus at least two of the following after 48 h of mechanical ventilation: temperature > 38°C or < 36°C; leukocytosis or leukopenia; and purulent secretions—without any signs or symptoms of other infections. The microbiological criterion was a positive quantitative culture (≥ 105 CFU/mL) of an EA sample collected with the standard technique.(9) The EA samples were collected before the introduction of a new antibiotic. Samples were considered representative of lower respiratory tract secretions if they contained > 25 polymorphonuclear neutrophils and < 10 squamous epithelial cells/low-power field.
Control definitionPatients to compose a control group were selected on
a 1:1 basis, with concurrent sampling.(20) We selected mechanically ventilated patients who showed no clinical, biochemical, or microbiological evidence of infection at the time of diagnosis and enrolment of the cases. Patients eligible for enrolment in the control group were followed for one week and were selected only if they were not under suspicion of infection during that time. After selection, an EA sample (for culture and ACB evaluation) was collected from each patient in the control group. We then categorized the control group EA culture results as colonization or negative, depending on whether the cultures grew ≥ 105 CFU/mL or < 105 CFU/mL.
Respiratory sample preparationThe EA samples were collected into two sterile tubes.
One tube was delivered to the microbiology laboratory, and the other was delivered to the immunology labora-tory. To perform the ACB evaluation, one milliliter of the
aspirate from each sample was utilized. The samples were washed at 300 g for 15 min, the supernatant was discarded, and the sediment was washed twice with 0.9% saline solution. After the final wash, 100 µL of the sediment was diluted to 1:5 with 0.9% saline solution, because excessive mucus could hinder the visualization of bacteria and the reading of the culture.
To investigate the ACB, four assays were performed: with three monoclonal antibodies, against IgA (anti-IgA), IgM (anti-IgM), and IgG (anti-IgG), respectively; and with one polyvalent antibody, against all three. All of the antibodies were conjugated with FITC (Sigma BioSciences, St. Louis, MO, USA). A 1:20 dilution of the antibodies was prepared with Hanks balanced salt solution. The samples obtained were then placed in microtubes: 100 µL of the tracheal secretion plus 20 µL of the antibody (anti-IgA, anti-IgM, anti-IgG, or the polyvalent antibody). The assays were incubated at 37°C for 15 min in total darkness, after which they were washed twice, by centrifugation, with Hanks balanced salt solution. Subsequently, we pipetted 15 µL of the solution, using pipettes with sterile tips, and spread the solution over an area corresponding to one coverslip (24 × 24 mm). The slides were previously sterilized in a Bunsen burner and covered with sterile cover glass. For the staining, the conventional Gram technique was utilized. All assays were performed in duplicate, and the readers were blinded to whether the sample was from a case or a control.
Each assay was standardized to allow the reader to count 80 bacteria in three or four fields. To detect ACB coated with the FITC-conjugated monoclonal or polyvalent antibodies (four ACB classes), immuno-fluorescence microscopy was used. The proportion of ACB, among the fixed number of 80 bacteria, was then determined. The unspecific immunofluorescence in microorganisms was determined from bacterial incubation with unrelated FITC-conjugated antibodies.
Statistical analysisContinuous data are presented as mean ± standard
deviation or as median and interquartile range, as appropriate. Categorical variables are presented as absolute and relative frequencies. To compare the characteristics of the cases and controls, we used the Mann-Whitney test or unpaired t-tests for continuous variables, whereas we used Fisher’s exact test or chi-square tests for dichotomous variables. For comparisons among the categories of culture results (negative, colonization, and VAP), we used the Kruskal-Wallis test, with post-hoc comparison by the Mann-Whitney test with Bonferroni correction. Sensitivity, specificity, the positive likelihood ratio, and the negative likelihood ratio were calculated using the standard formulas. We did not calculate positive or negative predictive values, because of the case-control design. To evaluate the overall performance of ACB quantification in the diagnosis of VAP, we used an interactive dot diagram, and the best cut-off for the ACB proportion was established by maximizing the
204 J Bras Pneumol. 2016;42(3):203-210
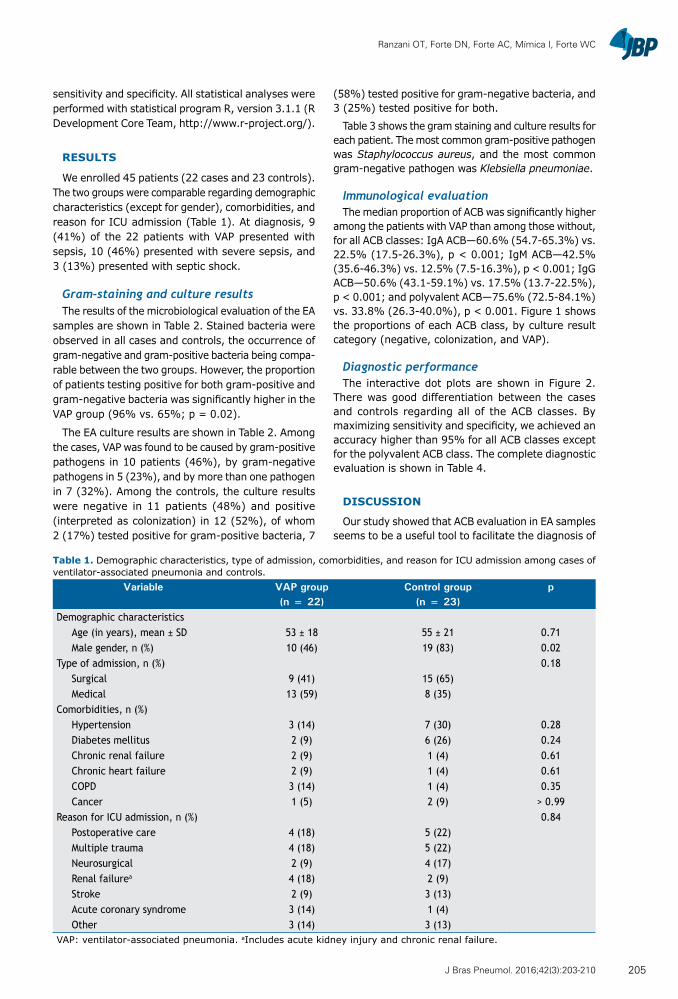
Ranzani OT, Forte DN, Forte AC, Mímica I, Forte WC
sensitivity and specificity. All statistical analyses were performed with statistical program R, version 3.1.1 (R Development Core Team, http://www.r-project.org/).
RESULTS
We enrolled 45 patients (22 cases and 23 controls). The two groups were comparable regarding demographic characteristics (except for gender), comorbidities, and reason for ICU admission (Table 1). At diagnosis, 9 (41%) of the 22 patients with VAP presented with sepsis, 10 (46%) presented with severe sepsis, and 3 (13%) presented with septic shock.
Gram-staining and culture resultsThe results of the microbiological evaluation of the EA
samples are shown in Table 2. Stained bacteria were observed in all cases and controls, the occurrence of gram-negative and gram-positive bacteria being compa-rable between the two groups. However, the proportion of patients testing positive for both gram-positive and gram-negative bacteria was significantly higher in the VAP group (96% vs. 65%; p = 0.02).
The EA culture results are shown in Table 2. Among the cases, VAP was found to be caused by gram-positive pathogens in 10 patients (46%), by gram-negative pathogens in 5 (23%), and by more than one pathogen in 7 (32%). Among the controls, the culture results were negative in 11 patients (48%) and positive (interpreted as colonization) in 12 (52%), of whom 2 (17%) tested positive for gram-positive bacteria, 7
(58%) tested positive for gram-negative bacteria, and 3 (25%) tested positive for both.
Table 3 shows the gram staining and culture results for each patient. The most common gram-positive pathogen was Staphylococcus aureus, and the most common gram-negative pathogen was Klebsiella pneumoniae.
Immunological evaluationThe median proportion of ACB was significantly higher
among the patients with VAP than among those without, for all ACB classes: IgA ACB—60.6% (54.7-65.3%) vs. 22.5% (17.5-26.3%), p < 0.001; IgM ACB—42.5% (35.6-46.3%) vs. 12.5% (7.5-16.3%), p < 0.001; IgG ACB—50.6% (43.1-59.1%) vs. 17.5% (13.7-22.5%), p < 0.001; and polyvalent ACB—75.6% (72.5-84.1%) vs. 33.8% (26.3-40.0%), p < 0.001. Figure 1 shows the proportions of each ACB class, by culture result category (negative, colonization, and VAP).
Diagnostic performanceThe interactive dot plots are shown in Figure 2.
There was good differentiation between the cases and controls regarding all of the ACB classes. By maximizing sensitivity and specificity, we achieved an accuracy higher than 95% for all ACB classes except for the polyvalent ACB class. The complete diagnostic evaluation is shown in Table 4.
DISCUSSION
Our study showed that ACB evaluation in EA samples seems to be a useful tool to facilitate the diagnosis of
Table 1. Demographic characteristics, type of admission, comorbidities, and reason for ICU admission among cases of ventilator-associated pneumonia and controls.
Variable VAP group Control group p(n = 22) (n = 23)
Demographic characteristicsAge (in years), mean ± SD 53 ± 18 55 ± 21 0.71Male gender, n (%) 10 (46) 19 (83) 0.02
Type of admission, n (%) 0.18Surgical 9 (41) 15 (65)Medical 13 (59) 8 (35)
Comorbidities, n (%)Hypertension 3 (14) 7 (30) 0.28Diabetes mellitus 2 (9) 6 (26) 0.24Chronic renal failure 2 (9) 1 (4) 0.61Chronic heart failure 2 (9) 1 (4) 0.61COPD 3 (14) 1 (4) 0.35Cancer 1 (5) 2 (9) > 0.99
Reason for ICU admission, n (%) 0.84Postoperative care 4 (18) 5 (22)Multiple trauma 4 (18) 5 (22)Neurosurgical 2 (9) 4 (17)Renal failurea 4 (18) 2 (9)Stroke 2 (9) 3 (13)Acute coronary syndrome 3 (14) 1 (4)Other 3 (14) 3 (13)
VAP: ventilator-associated pneumonia. aIncludes acute kidney injury and chronic renal failure.
205J Bras Pneumol. 2016;42(3):203-210
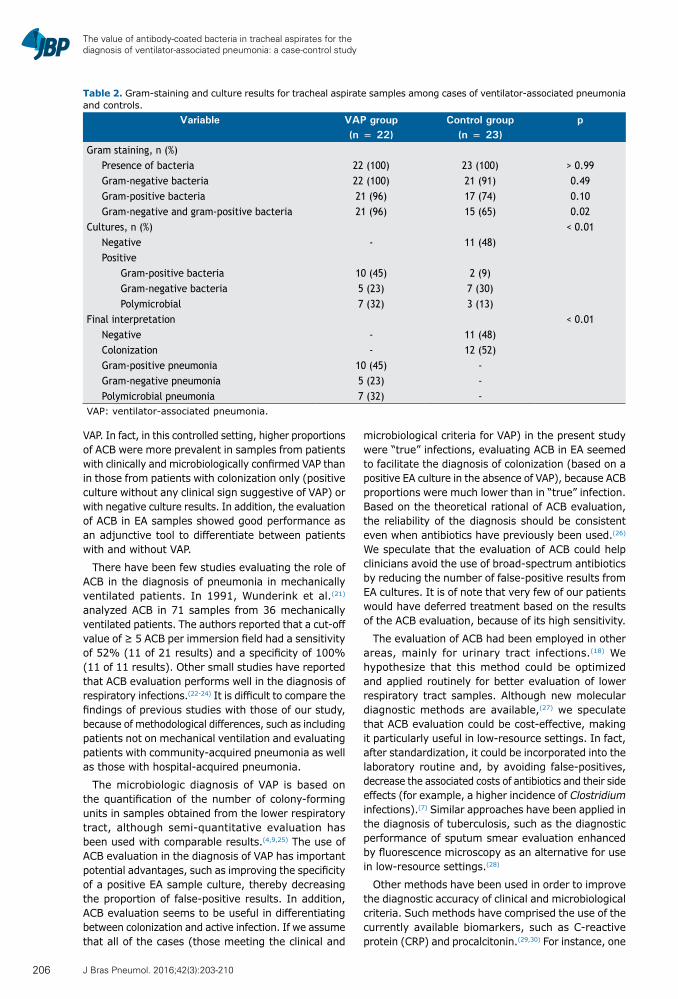
The value of antibody-coated bacteria in tracheal aspirates for the diagnosis of ventilator-associated pneumonia: a case-control study
VAP. In fact, in this controlled setting, higher proportions of ACB were more prevalent in samples from patients with clinically and microbiologically confirmed VAP than in those from patients with colonization only (positive culture without any clinical sign suggestive of VAP) or with negative culture results. In addition, the evaluation of ACB in EA samples showed good performance as an adjunctive tool to differentiate between patients with and without VAP.
There have been few studies evaluating the role of ACB in the diagnosis of pneumonia in mechanically ventilated patients. In 1991, Wunderink et al.(21) analyzed ACB in 71 samples from 36 mechanically ventilated patients. The authors reported that a cut-off value of ≥ 5 ACB per immersion field had a sensitivity of 52% (11 of 21 results) and a specificity of 100% (11 of 11 results). Other small studies have reported that ACB evaluation performs well in the diagnosis of respiratory infections.(22-24) It is difficult to compare the findings of previous studies with those of our study, because of methodological differences, such as including patients not on mechanical ventilation and evaluating patients with community-acquired pneumonia as well as those with hospital-acquired pneumonia.
The microbiologic diagnosis of VAP is based on the quantification of the number of colony-forming units in samples obtained from the lower respiratory tract, although semi-quantitative evaluation has been used with comparable results.(4,9,25) The use of ACB evaluation in the diagnosis of VAP has important potential advantages, such as improving the specificity of a positive EA sample culture, thereby decreasing the proportion of false-positive results. In addition, ACB evaluation seems to be useful in differentiating between colonization and active infection. If we assume that all of the cases (those meeting the clinical and
microbiological criteria for VAP) in the present study were “true” infections, evaluating ACB in EA seemed to facilitate the diagnosis of colonization (based on a positive EA culture in the absence of VAP), because ACB proportions were much lower than in “true” infection. Based on the theoretical rational of ACB evaluation, the reliability of the diagnosis should be consistent even when antibiotics have previously been used.(26) We speculate that the evaluation of ACB could help clinicians avoid the use of broad-spectrum antibiotics by reducing the number of false-positive results from EA cultures. It is of note that very few of our patients would have deferred treatment based on the results of the ACB evaluation, because of its high sensitivity.
The evaluation of ACB had been employed in other areas, mainly for urinary tract infections.(18) We hypothesize that this method could be optimized and applied routinely for better evaluation of lower respiratory tract samples. Although new molecular diagnostic methods are available,(27) we speculate that ACB evaluation could be cost-effective, making it particularly useful in low-resource settings. In fact, after standardization, it could be incorporated into the laboratory routine and, by avoiding false-positives, decrease the associated costs of antibiotics and their side effects (for example, a higher incidence of Clostridium infections).(7) Similar approaches have been applied in the diagnosis of tuberculosis, such as the diagnostic performance of sputum smear evaluation enhanced by fluorescence microscopy as an alternative for use in low-resource settings.(28)
Other methods have been used in order to improve the diagnostic accuracy of clinical and microbiological criteria. Such methods have comprised the use of the currently available biomarkers, such as C-reactive protein (CRP) and procalcitonin.(29,30) For instance, one
Table 2. Gram-staining and culture results for tracheal aspirate samples among cases of ventilator-associated pneumonia and controls.
Variable VAP group Control group p(n = 22) (n = 23)
Gram staining, n (%)Presence of bacteria 22 (100) 23 (100) > 0.99Gram-negative bacteria 22 (100) 21 (91) 0.49Gram-positive bacteria 21 (96) 17 (74) 0.10Gram-negative and gram-positive bacteria 21 (96) 15 (65) 0.02
Cultures, n (%) < 0.01Negative - 11 (48)Positive
Gram-positive bacteria 10 (45) 2 (9)Gram-negative bacteria 5 (23) 7 (30)Polymicrobial 7 (32) 3 (13)
Final interpretation < 0.01Negative - 11 (48)Colonization - 12 (52)Gram-positive pneumonia 10 (45) -Gram-negative pneumonia 5 (23) -Polymicrobial pneumonia 7 (32) -
VAP: ventilator-associated pneumonia.
206 J Bras Pneumol. 2016;42(3):203-210
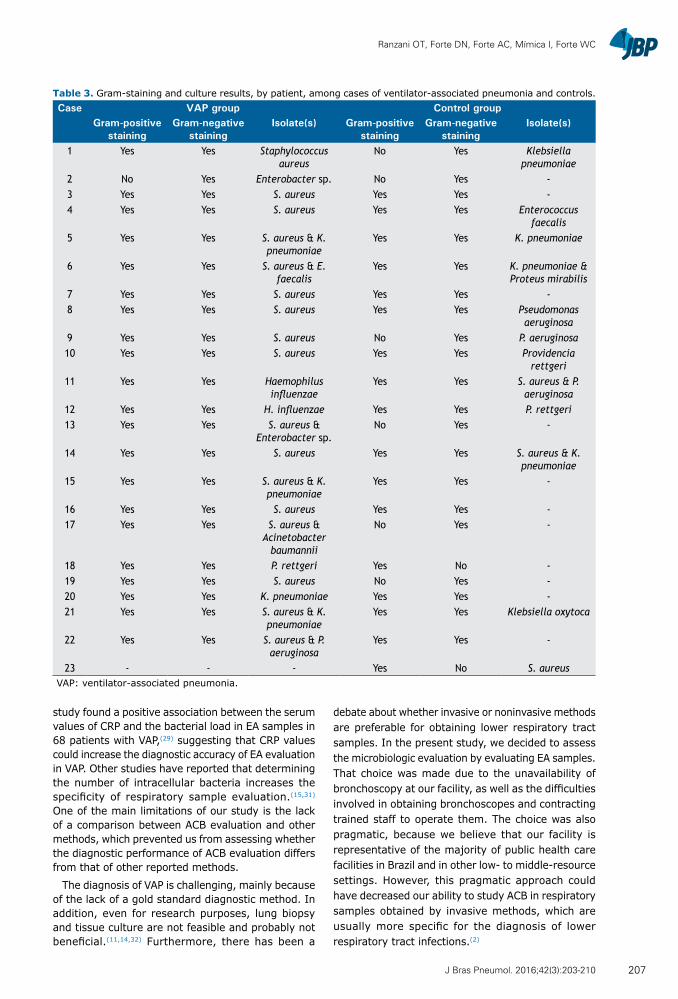
Ranzani OT, Forte DN, Forte AC, Mímica I, Forte WC
study found a positive association between the serum values of CRP and the bacterial load in EA samples in 68 patients with VAP,(29) suggesting that CRP values could increase the diagnostic accuracy of EA evaluation in VAP. Other studies have reported that determining the number of intracellular bacteria increases the specificity of respiratory sample evaluation.(15,31) One of the main limitations of our study is the lack of a comparison between ACB evaluation and other methods, which prevented us from assessing whether the diagnostic performance of ACB evaluation differs from that of other reported methods.
The diagnosis of VAP is challenging, mainly because of the lack of a gold standard diagnostic method. In addition, even for research purposes, lung biopsy and tissue culture are not feasible and probably not beneficial.(11,14,32) Furthermore, there has been a
debate about whether invasive or noninvasive methods are preferable for obtaining lower respiratory tract samples. In the present study, we decided to assess the microbiologic evaluation by evaluating EA samples. That choice was made due to the unavailability of bronchoscopy at our facility, as well as the difficulties involved in obtaining bronchoscopes and contracting trained staff to operate them. The choice was also pragmatic, because we believe that our facility is representative of the majority of public health care facilities in Brazil and in other low- to middle-resource settings. However, this pragmatic approach could have decreased our ability to study ACB in respiratory samples obtained by invasive methods, which are usually more specific for the diagnosis of lower respiratory tract infections.(2)
Table 3. Gram-staining and culture results, by patient, among cases of ventilator-associated pneumonia and controls.Case VAP group Control group
Gram-positive staining
Gram-negative staining
Isolate(s) Gram-positive staining
Gram-negative staining
Isolate(s)
1 Yes Yes Staphylococcus aureus
No Yes Klebsiella pneumoniae
2 No Yes Enterobacter sp. No Yes -3 Yes Yes S. aureus Yes Yes -4 Yes Yes S. aureus Yes Yes Enterococcus
faecalis5 Yes Yes S. aureus & K.
pneumoniaeYes Yes K. pneumoniae
6 Yes Yes S. aureus & E. faecalis
Yes Yes K. pneumoniae & Proteus mirabilis
7 Yes Yes S. aureus Yes Yes -8 Yes Yes S. aureus Yes Yes Pseudomonas
aeruginosa9 Yes Yes S. aureus No Yes P. aeruginosa10 Yes Yes S. aureus Yes Yes Providencia
rettgeri11 Yes Yes Haemophilus
influenzaeYes Yes S. aureus & P.
aeruginosa12 Yes Yes H. influenzae Yes Yes P. rettgeri13 Yes Yes S. aureus &
Enterobacter sp.No Yes -
14 Yes Yes S. aureus Yes Yes S. aureus & K. pneumoniae
15 Yes Yes S. aureus & K. pneumoniae
Yes Yes -
16 Yes Yes S. aureus Yes Yes -17 Yes Yes S. aureus &
Acinetobacter baumannii
No Yes -
18 Yes Yes P. rettgeri Yes No -19 Yes Yes S. aureus No Yes -20 Yes Yes K. pneumoniae Yes Yes -21 Yes Yes S. aureus & K.
pneumoniaeYes Yes Klebsiella oxytoca
22 Yes Yes S. aureus & P. aeruginosa
Yes Yes -
23 - - - Yes No S. aureusVAP: ventilator-associated pneumonia.
207J Bras Pneumol. 2016;42(3):203-210
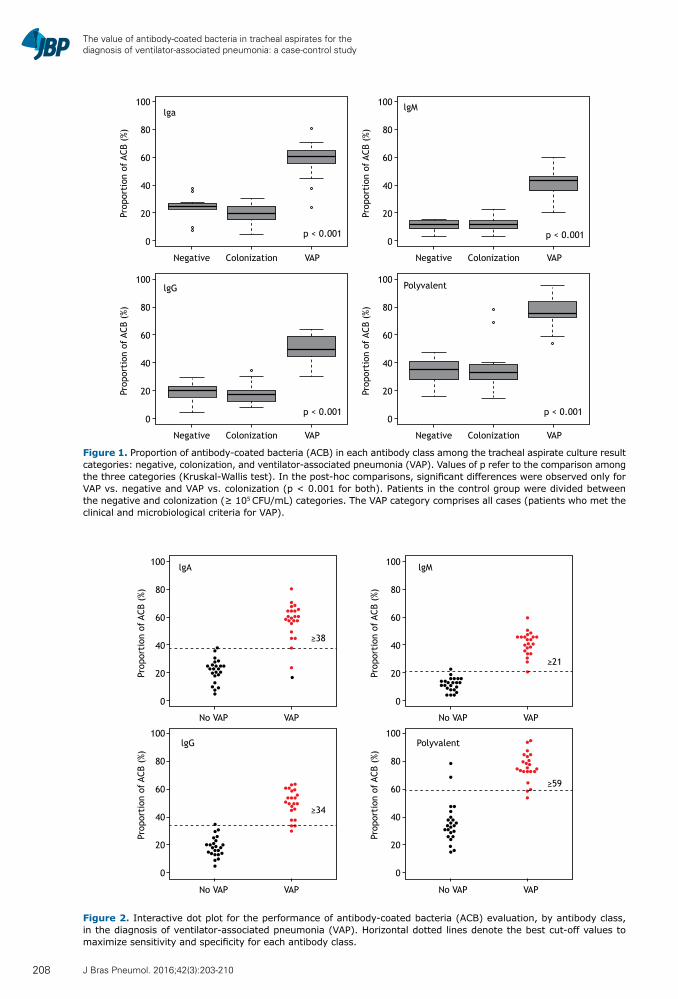
The value of antibody-coated bacteria in tracheal aspirates for the diagnosis of ventilator-associated pneumonia: a case-control study
100
80
60
40
20
0
Negative Colonization VAP
Prop
orti
on o
f AC
B (%
)
100
80
60
40
20
0
Negative Colonization VAP
Prop
orti
on o
f AC
B (%
)
100
80
60
40
20
0
Negative Colonization VAP
Prop
orti
on o
f AC
B (%
)
100
80
60
40
20
0
Negative Colonization VAP
Prop
orti
on o
f AC
B (%
)
lga
lgG Polyvalent
lgM
p < 0.001
p < 0.001
p < 0.001
p < 0.001
100
80
60
40
20
0
100
80
60
40
20
0
100
80
60
40
20
0
100
80
60
40
20
0
No VAP VAP
No VAP VAP
No VAP VAP
No VAP VAP
≥34
≥38
≥21
≥59
lgA
lgG Polyvalent
lgM
Prop
orti
on o
f AC
B (%
)
Prop
orti
on o
f AC
B (%
)
Prop
orti
on o
f AC
B (%
)
Prop
orti
on o
f AC
B (%
)
Figure 2. Interactive dot plot for the performance of antibody-coated bacteria (ACB) evaluation, by antibody class, in the diagnosis of ventilator-associated pneumonia (VAP). Horizontal dotted lines denote the best cut-off values to maximize sensitivity and specificity for each antibody class.
Figure 1. Proportion of antibody-coated bacteria (ACB) in each antibody class among the tracheal aspirate culture result categories: negative, colonization, and ventilator-associated pneumonia (VAP). Values of p refer to the comparison among the three categories (Kruskal-Wallis test). In the post-hoc comparisons, significant differences were observed only for VAP vs. negative and VAP vs. colonization (p < 0.001 for both). Patients in the control group were divided between the negative and colonization (≥ 105 CFU/mL) categories. The VAP category comprises all cases (patients who met the clinical and microbiological criteria for VAP).
208 J Bras Pneumol. 2016;42(3):203-210
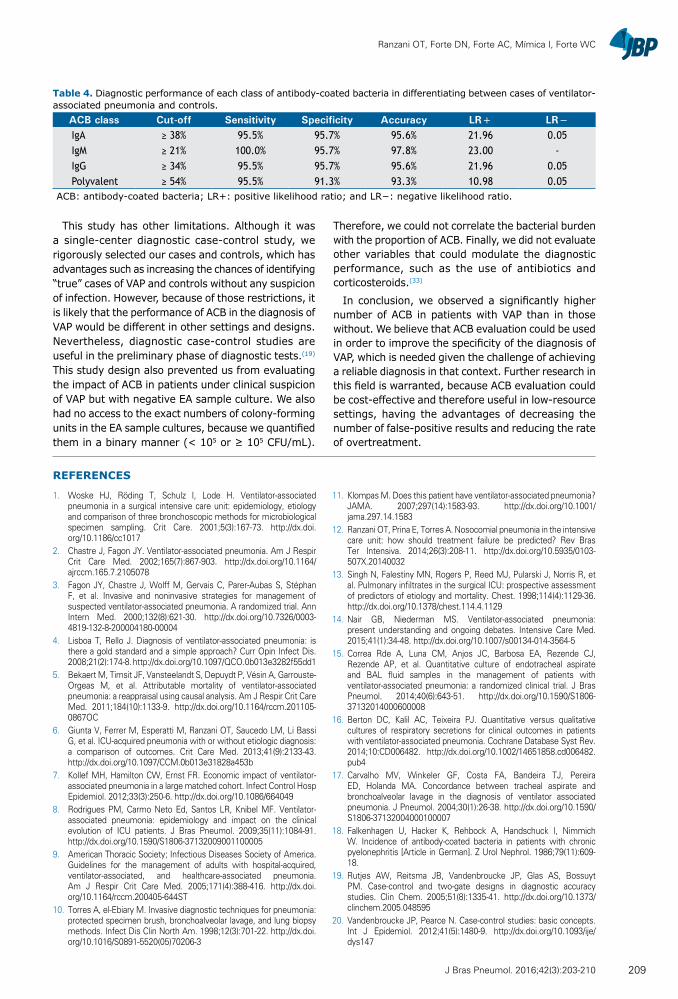
Ranzani OT, Forte DN, Forte AC, Mímica I, Forte WC
This study has other limitations. Although it was a single-center diagnostic case-control study, we rigorously selected our cases and controls, which has advantages such as increasing the chances of identifying “true” cases of VAP and controls without any suspicion of infection. However, because of those restrictions, it is likely that the performance of ACB in the diagnosis of VAP would be different in other settings and designs. Nevertheless, diagnostic case-control studies are useful in the preliminary phase of diagnostic tests.(19) This study design also prevented us from evaluating the impact of ACB in patients under clinical suspicion of VAP but with negative EA sample culture. We also had no access to the exact numbers of colony-forming units in the EA sample cultures, because we quantified them in a binary manner (< 105 or ≥ 105 CFU/mL).
Therefore, we could not correlate the bacterial burden with the proportion of ACB. Finally, we did not evaluate other variables that could modulate the diagnostic performance, such as the use of antibiotics and corticosteroids.(33)
In conclusion, we observed a significantly higher number of ACB in patients with VAP than in those without. We believe that ACB evaluation could be used in order to improve the specificity of the diagnosis of VAP, which is needed given the challenge of achieving a reliable diagnosis in that context. Further research in this field is warranted, because ACB evaluation could be cost-effective and therefore useful in low-resource settings, having the advantages of decreasing the number of false-positive results and reducing the rate of overtreatment.
Table 4. Diagnostic performance of each class of antibody-coated bacteria in differentiating between cases of ventilator-associated pneumonia and controls.
ACB class Cut-off Sensitivity Specificity Accuracy LR+ LR−IgA ≥ 38% 95.5% 95.7% 95.6% 21.96 0.05IgM ≥ 21% 100.0% 95.7% 97.8% 23.00 -IgG ≥ 34% 95.5% 95.7% 95.6% 21.96 0.05Polyvalent ≥ 54% 95.5% 91.3% 93.3% 10.98 0.05
ACB: antibody-coated bacteria; LR+: positive likelihood ratio; and LR−: negative likelihood ratio.
REFERENCES
1. Woske HJ, Röding T, Schulz I, Lode H. Ventilator-associated pneumonia in a surgical intensive care unit: epidemiology, etiology and comparison of three bronchoscopic methods for microbiological specimen sampling. Crit Care. 2001;5(3):167-73. http://dx.doi.org/10.1186/cc1017
2. Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165(7):867-903. http://dx.doi.org/10.1164/ajrccm.165.7.2105078
3. Fagon JY, Chastre J, Wolff M, Gervais C, Parer-Aubas S, Stéphan F, et al. Invasive and noninvasive strategies for management of suspected ventilator-associated pneumonia. A randomized trial. Ann Intern Med. 2000;132(8):621-30. http://dx.doi.org/10.7326/0003-4819-132-8-200004180-00004
4. Lisboa T, Rello J. Diagnosis of ventilator-associated pneumonia: is there a gold standard and a simple approach? Curr Opin Infect Dis. 2008;21(2):174-8. http://dx.doi.org/10.1097/QCO.0b013e3282f55dd1
5. Bekaert M, Timsit JF, Vansteelandt S, Depuydt P, Vésin A, Garrouste-Orgeas M, et al. Attributable mortality of ventilator-associated pneumonia: a reappraisal using causal analysis. Am J Respir Crit Care Med. 2011;184(10):1133-9. http://dx.doi.org/10.1164/rccm.201105-0867OC
6. Giunta V, Ferrer M, Esperatti M, Ranzani OT, Saucedo LM, Li Bassi G, et al. ICU-acquired pneumonia with or without etiologic diagnosis: a comparison of outcomes. Crit Care Med. 2013;41(9):2133-43. http://dx.doi.org/10.1097/CCM.0b013e31828a453b
7. Kollef MH, Hamilton CW, Ernst FR. Economic impact of ventilator-associated pneumonia in a large matched cohort. Infect Control Hosp Epidemiol. 2012;33(3):250-6. http://dx.doi.org/10.1086/664049
8. Rodrigues PM, Carmo Neto Ed, Santos LR, Knibel MF. Ventilator-associated pneumonia: epidemiology and impact on the clinical evolution of ICU patients. J Bras Pneumol. 2009;35(11):1084-91. http://dx.doi.org/10.1590/S1806-37132009001100005
9. American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416. http://dx.doi.org/10.1164/rccm.200405-644ST
10. Torres A, el-Ebiary M. Invasive diagnostic techniques for pneumonia: protected specimen brush, bronchoalveolar lavage, and lung biopsy methods. Infect Dis Clin North Am. 1998;12(3):701-22. http://dx.doi.org/10.1016/S0891-5520(05)70206-3
11. Klompas M. Does this patient have ventilator-associated pneumonia? JAMA. 2007;297(14):1583-93. http://dx.doi.org/10.1001/jama.297.14.1583
12. Ranzani OT, Prina E, Torres A. Nosocomial pneumonia in the intensive care unit: how should treatment failure be predicted? Rev Bras Ter Intensiva. 2014;26(3):208-11. http://dx.doi.org/10.5935/0103-507X.20140032
13. Singh N, Falestiny MN, Rogers P, Reed MJ, Pularski J, Norris R, et al. Pulmonary infiltrates in the surgical ICU: prospective assessment of predictors of etiology and mortality. Chest. 1998;114(4):1129-36. http://dx.doi.org/10.1378/chest.114.4.1129
14. Nair GB, Niederman MS. Ventilator-associated pneumonia: present understanding and ongoing debates. Intensive Care Med. 2015;41(1):34-48. http://dx.doi.org/10.1007/s00134-014-3564-5
15. Correa Rde A, Luna CM, Anjos JC, Barbosa EA, Rezende CJ, Rezende AP, et al. Quantitative culture of endotracheal aspirate and BAL fluid samples in the management of patients with ventilator-associated pneumonia: a randomized clinical trial. J Bras Pneumol. 2014;40(6):643-51. http://dx.doi.org/10.1590/S1806-37132014000600008
16. Berton DC, Kalil AC, Teixeira PJ. Quantitative versus qualitative cultures of respiratory secretions for clinical outcomes in patients with ventilator-associated pneumonia. Cochrane Database Syst Rev. 2014;10:CD006482. http://dx.doi.org/10.1002/14651858.cd006482.pub4
17. Carvalho MV, Winkeler GF, Costa FA, Bandeira TJ, Pereira ED, Holanda MA. Concordance between tracheal aspirate and bronchoalveolar lavage in the diagnosis of ventilator associated pneumonia. J Pneumol. 2004;30(1):26-38. http://dx.doi.org/10.1590/S1806-37132004000100007
18. Falkenhagen U, Hacker K, Rehbock A, Handschuck I, Nimmich W. Incidence of antibody-coated bacteria in patients with chronic pyelonephritis [Article in German]. Z Urol Nephrol. 1986;79(11):609-18.
19. Rutjes AW, Reitsma JB, Vandenbroucke JP, Glas AS, Bossuyt PM. Case-control and two-gate designs in diagnostic accuracy studies. Clin Chem. 2005;51(8):1335-41. http://dx.doi.org/10.1373/clinchem.2005.048595
20. Vandenbroucke JP, Pearce N. Case-control studies: basic concepts. Int J Epidemiol. 2012;41(5):1480-9. http://dx.doi.org/10.1093/ije/dys147
209J Bras Pneumol. 2016;42(3):203-210

The value of antibody-coated bacteria in tracheal aspirates for the diagnosis of ventilator-associated pneumonia: a case-control study
21. Wunderink RG, Russell GB, Mezger E, Adams D, Popovich J Jr. The diagnostic utility of the antibody-coated bacteria test in intubated patients. Chest. 1991;99(1):84-8. http://dx.doi.org/10.1378/chest.99.1.84
22. Sala-Mateus C, Lloveras P, Barber E, Puig de la Bellacasa J, Torres A, Jiménez de Anta MT, et al. Antibody-coated bacteria and quantitative culture in sputum samples from patients with bronchiectasis [Article in Spanish]. Enferm Infecc Microbiol Clin. 1990;8(9):568-71.
23. Winterbauer RH, Hutchinson JF, Reinhardt GN, Sumida SE, Dearden B, Thomas CA, et al. The use of quantitative cultures and antibody coating of bacteria to diagnose bacterial pneumonia by fiberoptic bronchoscopy. Am Rev Respir Dis. 1983;128(1):98-103. http://dx.doi.org/10.1164/arrd.1983.128.1.98
24. Matsumoto T, Kaku M, Tateda K, Furuya N, Hirakata Y, Yamaguchi K. Detection of antibody-coated bacteria in expectorated sputum for diagnosis of lower respiratory infections. Microbiol Immunol. 1994;38(4):287-93. http://dx.doi.org/10.1111/j.1348-0421.1994.tb01778.x
25. Camargo LF, De Marco FV, Barbas CS, Hoelz C, Bueno MA, Rodrigues M Jr, et al. Ventilator associated pneumonia: comparison between quantitative and qualitative cultures of tracheal aspirates. Crit Care. 2004;8(6):R422-30. http://dx.doi.org/10.1186/cc2965
26. Torres A, González J, Ferrer M. Evaluation of the available invasive and non-invasive techniques for diagnosing nosocomial pneumonias in mechanically ventilated patients. Intensive Care Med. 1991;17(8):439-48. http://dx.doi.org/10.1007/BF01690764
27. Lung M, Codina G. Molecular diagnosis in HAP/VAP. Curr Opin Crit Care. 2012;18(5):487-94. http://dx.doi.org/10.1097/MCC.0b013e3283577d37
28. Steingart KR, Henry M, Ng V, Hopewell PC, Ramsay A, Cunningham J, et al. Fluorescence versus conventional sputum smear microscopy for tuberculosis: a systematic review. Lancet Infect Dis. 2006;6(9):570-81. Erratum in: Lancet Infect Dis. 2006;6(10):628. http://dx.doi.org/10.1016/S1473-3099(06)70578-3
29. Lisboa T, Seligman R, Diaz E, Rodriguez A, Teixeira PJ, Rello J. C-reactive protein correlates with bacterial load and appropriate antibiotic therapy in suspected ventilator-associated pneumonia. Crit Care Med. 2008;36(1):166-71. http://dx.doi.org/10.1097/01.CCM.0000297886.32564.CF
30. Ramirez P, Garcia MA, Ferrer M, Aznar J, Valencia M, Sahuquillo JM, et al. Sequential measurements of procalcitonin levels in diagnosing ventilator-associated pneumonia. Eur Respir J. 2008;31(2):356-62. http://dx.doi.org/10.1183/09031936.00086707
31. Torres A, El-Ebiary M, Fábregas N, González J, de la Bellacasa JP, Hernández C, et al. Value of intracellular bacteria detection in the diagnosis of ventilator associated pneumonia. Thorax. 1996;51(4):378-84. http://dx.doi.org/10.1136/thx.51.4.378
32. Torres A, Fàbregas N, Ewig S, de la Bellacasa JP, Bauer TT, Ramirez J. Sampling methods for ventilator-associated pneumonia: validation using different histologic and microbiological references. Crit Care Med. 2000;28(8):2799-804. http://dx.doi.org/10.1097/00003246-200008000-00020
33. Ranzani OT, Ferrer M, Esperatti M, Giunta V, Bassi GL, Carvalho CR, et al. Association between systemic corticosteroids and outcomes of intensive care unit-acquired pneumonia. Crit Care Med. 2012;40(9):2552-61. http://dx.doi.org/10.1097/CCM.0b013e318259203d
210 J Bras Pneumol. 2016;42(3):203-210

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000133
ABSTRACTObstructive sleep apnea (OSA) has been associated with oxidative stress and various cardiovascular consequences, such as increased cardiovascular disease risk. Quantitative real-time PCR is frequently employed to assess changes in gene expression in experimental models. In this study, we analyzed the effects of chronic intermittent hypoxia (an experimental model of OSA) on housekeeping gene expression in the left cardiac ventricle of rats. Analyses via four different approaches—use of the geNorm, BestKeeper, and NormFinder algorithms; and 2−ΔCt (threshold cycle) data analysis—produced similar results: all genes were found to be suitable for use, glyceraldehyde-3-phosphate dehydrogenase and 18S being classified as the most and the least stable, respectively. The use of more than one housekeeping gene is strongly advised.
Keywords: Cell hypoxia; Reference standards; Sleep apnea, obstructive; Cardiovascular diseases; Models, animal; Polymerase chain reaction.
Analysis of the stability of housekeeping gene expression in the left cardiac ventricle of rats submitted to chronic intermittent hypoxiaGuilherme Silva Julian1, Renato Watanabe de Oliveira1, Sergio Tufik1, Jair Ribeiro Chagas1,2
Correspondence to: Jair Ribeiro Chagas. Rua Napoleão de Barros, 925, 3º andar, CEP 04024-002, São Paulo, SP, Brasil.Tel./fax: 55 11 2149-0144. E-mail: [email protected] support: This study received financial support from the Associação Fundo de Incentivo à Pesquisa (AFIP, Association for the Incentive Funding of Research), the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq, National Council for Scientific and Technological Development; Fellowship Grant nos. 301974/2011-0 and 310040/2011-6 to ST and JRC, respectively), the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, Office for the Advancement of Higher Education), and the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP, São Paulo Research Foundation; Grant nos. 2011/15060-4 and 2011/16011-6 to GSJ and RWO, respectively).
Obstructive sleep apnea (OSA), which is a sleep-related breathing disorder with a high worldwide prevalence,(1,2) causes various metabolic, oxidative, and sympathetic disturbances, increasing the risk of cardiovascular disease. (3) The most widely used animal model of OSA, particularly when the focus is on its cardiovascular consequences, is the chronic intermittent hypoxia (CIH) model.(3) The CIH model mimics many of the putative pathological effects of OSA, such as increased blood pressure and sympathetic activity.(4)
Real-time PCR is the most commonly used tool to study gene expression of specific targets. In order to obtain reliable results in quantitative real-time PCR, it is necessary to use appropriate reference genes, or housekeeping genes (HKGs),(5) as internal controls for gene expression normalization, which is essential to the evaluation of relative gene expression. However, using certain unstable genes as HKGs can strongly compromise data reliability.(6,7) Therefore, each experimental condition should have an HKG selection step in order to obtain good quality data. The three most widely used algorithms for HKG selection are those provided by the computer programs geNorm,(8) BestKeeper,(9) and NormFinder.(10)
To our knowledge, there have been no studies assessing the stability of HKG expression in the left ventricle, or any other cardiac structure, using in vivo models of
hypoxia, most such studies having been performed in vitro. Therefore, the objective of the present study was to report the selection of HKGs in the left cardiac ventricle of rats submitted to CIH, using the geNorm, BestKeeper, and NormFinder algorithms to analyze the expression stability of five commonly used HKGs. Our results provide important information for HKG selection in future studies employing a CIH model.
Twenty-two adult male Wistar Hannover rats were submitted to CIH (8 h/day) as described previously.(11) All experimental procedures were performed in accordance with current ethical and practical guidelines for the use of laboratory animals.(12) This study was approved by the Animal Research Ethics Committee of the Federal University of São Paulo (Protocol no. 2025/11).
Animals were assigned to one of three experimental groups: control (n = 6); CIH (six weeks of CIH, n = 7); and CIH+N (six weeks of CIH, followed by two weeks of recovery in normoxia, n = 8). The CIH protocol is described in detail elsewhere,(11) as is the rationale behind the use of a two-week recovery period in the CIH+N group.(13)
After six weeks (the end of the CIH protocol) or eight weeks (the end of the CIH+N protocol), animals were euthanized by rapid decapitation. Subsequently, the heart was rapidly removed and washed with saline, after which the left ventricle was dissected. All tissues
1. Departamento de Psicobiologia, Universidade Federal de São Paulo, Escola Paulista de Medicina – UNIFESP-EPM – São Paulo (SP) Brasil.
2. Departamento de Biociências, Universidade Federal de São Paulo – UNIFESP-Baixada Santista – Santos (SP) Brasil.
Submitted: 4 June 2015. Accepted: 11 October 2015.
Study carried out in the Departamento de Psicobiologia, Universidade Federal de São Paulo, Escola Paulista de Medicina – UNIFESP-EPM – São Paulo (SP) Brasil; and in the Departamento de Biociências, Universidade Federal de São Paulo –UNIFESP-Baixada Santista – Santos (SP) Brasil.
J Bras Pneumol. 2016;42(3):211-214
211
BRIEF COMMUNICATION

Analysis of the stability of housekeeping gene expression in the left cardiac ventricle of rats submitted to chronic intermittent hypoxia
were rapidly dissected on dry ice and stored at −80°C until extraction.
Total RNA was extracted using TRIzol reagent (Thermo Fisher Scientific Inc., Waltham, MA, USA) and treated with DNase. Quantitative real-time PCR was performed with SYBR Green, as described previously.(11) For our HKG evaluation, we chose five of the most commonly used genes, from different gene pathways: eukaryotic 18S ribosomal RNA (rRNA); beta-actin (ACTB); beta-2-microglobulin (β2M); glyceraldehyde-3-phosphate dehydrogenase (GAPDH); and hypoxanthine guanine phosphoribosyl transferase (HPRT). The primer sequences for all of those HKGs are described elsewhere.(11)
Gene expression stability was evaluated using the pro-grams geNorm (Gene Quantification: http://download.gene-quantification.info/), NormFinder (Department of Molecular Medicine, Aarhus University Hospital, Aarhus, Denmark: http://moma.dk/normfinder-software), and BestKeeper (Gene Quantification: http://download.gene-quantification.info/). The geNorm program calculates the average expression stability (M-value) for each gene, lower M-values indicating greater stability. (8) The NormFinder program provides a stability value number for each gene, lower stability values indicating less stability. (10) The BestKeeper program calculates a Pearson’s correlation coefficient for each gene, values of p closer to 1.0 indicating greater stability. (9) We also analyzed all of the 2−ΔCt (threshold cycle) data by one--way ANOVA.(14) To test for normality and homogeneity, we employed the Kolmogorov-Smirnov test and Levene’s test, respectively. The level of statistical significance was set at p < 0.05.
Our evaluation of RNA quality and integrity demons-trated intact 18S and 28S rRNA. Optimization of primer conditions and cDNA concentrations was performed and described previously.(11) The 2−ΔCt values, analyzed independently, did not achieve significance (p > 0.05 for all), although 18S expression trended toward significance (p = 0.076 vs. p > 0.4 for the remaining genes; data not shown). These data indicate that, although all five HKG candidates are suitable for use, the expression of 18S demonstrates a tendency to show greater variability between groups.
In our BestKeeper analysis to identify the best HKGs in CIH models, all five candidate genes presented values that were acceptable (p < 0.01). According to the BestKeeper ranking, GAPDH was the best candidate, followed by ACTB. In addition, 18S presented the lowest Pearson’s correlation coefficient, indicating that it was the least stable of the five HKG candidates. All BestKeeper Pearson’s correlation coefficients are described in Table 1 and depicted in Figure 1A.
In our geNorm analysis, all five candidate genes presented M-values lower than 1.5, which is considered to be the cut-off value for suitability,(8) in all analyses. According to the geNorm ranking, GAPDH was the best candidate gene, followed by β2M. In addition, 18S presented the highest M-value and was ranked as the
least stable gene. All geNorm M-values are described in Table 1 and depicted in Figure 1B. The BestKeeper and geNorm algorithms produced very similar results, the only difference being in terms of the second best HKG candidate.
In our NormFinder analysis, all five candidate genes presented stability values below 0.15, the cut-off value for suitability.(10) Similar although not identical to the BestKeeper results, the NormFinder algorithm identified GAPDH as the best candidate gene, followed by β2M. In addition, 18S presented the highest stability value and was therefore ranked as the least stable gene. All NormFinder stability values are described in Table 1 and depicted in Figure 1C.
The NormFinder HKG ranking was identical to that of BestKeeper, GAPDH and ACTB being ranked as the most stable genes, whereas 18S was ranked as the least stable. However, the geNorm ranking showed a slight difference—ACTB in third position and β2M in second position. The data from all three algorithms corroborate those reported in a previous study involving cardiosphere-derived cells (endogenous cardiac stem cells, candidates for restoring lost tissue) and evaluating the influence of aging on gene stability. The authors found that ACTB, GAPDH, and β2M were the most stable HKGs in both adult or neonatal cardiosphere-derived cells under conditions of normoxia or hypoxia. (15) Although our study involved the left ventricle portion of the heart, which is composed of several cell types, the tissue origin is the same as that of the cardiosphere-derived cells analyzed by those authors. Conversely, in a study employing an animal model of left ventricular diastolic dysfunction, GAPDH was found to be the second most stable gene, underscoring its stability in vivo.(16) In addition, ACTB presents good stability in models using different hypoxia stimuli, such as various cell types submitted to hypoxia in vitro(7,15) and various brain structures submitted to hypoxia in vivo.(11)
Although analyses of β2M have shown it to be unstable in some brain structures and cell lines,(7,11) our analysis of tissue from the left ventricle ranked β2M among the most stable candidate genes. Our data underscore those of several other studies, which classified β2M as one of the most stable candidate genes, in cardiosphere-derived cells under hypoxic conditions(15) and in human chondrocytes cultured at oxygen concentrations of 5% and 1%.(17)
In the present study, HPRT was found to be among the least stable candidate genes. However, it can be considered suitable for use because it presented acceptable stability in the geNorm and BestKeeper analyses. Our data are in conflict with those of some previous studies, in which HPRT has been reported to be one of the most stable genes, in cultures of cells submitted to acute hypoxia(7) and in an in vivo model of ischemia in the right ventricle.(18) Nevertheless, our data corroborate those of another previous study involving cardiosphere-derived cells, in which HPRT was found to be among the least stable genes under conditions of hypoxia.(19) The discrepancies among these studies might be due to differences in the origin of the
212 J Bras Pneumol. 2016;42(3):211-214
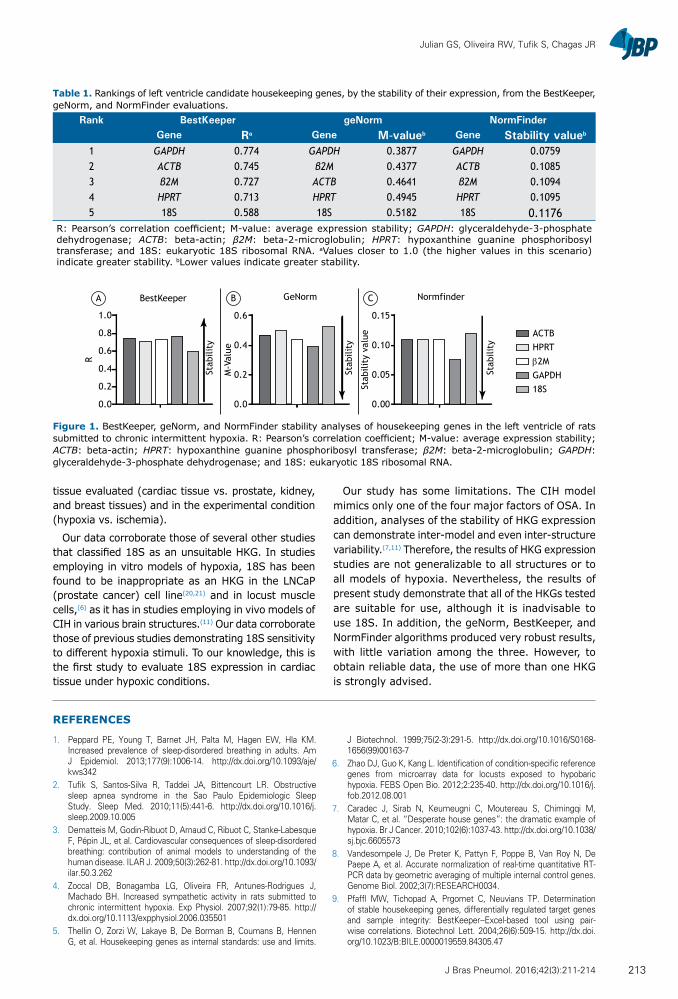
Julian GS, Oliveira RW, Tufik S, Chagas JR
tissue evaluated (cardiac tissue vs. prostate, kidney, and breast tissues) and in the experimental condition (hypoxia vs. ischemia).
Our data corroborate those of several other studies that classified 18S as an unsuitable HKG. In studies employing in vitro models of hypoxia, 18S has been found to be inappropriate as an HKG in the LNCaP (prostate cancer) cell line(20,21) and in locust muscle cells,(6) as it has in studies employing in vivo models of CIH in various brain structures.(11) Our data corroborate those of previous studies demonstrating 18S sensitivity to different hypoxia stimuli. To our knowledge, this is the first study to evaluate 18S expression in cardiac tissue under hypoxic conditions.
Our study has some limitations. The CIH model mimics only one of the four major factors of OSA. In addition, analyses of the stability of HKG expression can demonstrate inter-model and even inter-structure variability.(7,11) Therefore, the results of HKG expression studies are not generalizable to all structures or to all models of hypoxia. Nevertheless, the results of present study demonstrate that all of the HKGs tested are suitable for use, although it is inadvisable to use 18S. In addition, the geNorm, BestKeeper, and NormFinder algorithms produced very robust results, with little variation among the three. However, to obtain reliable data, the use of more than one HKG is strongly advised.
Table 1. Rankings of left ventricle candidate housekeeping genes, by the stability of their expression, from the BestKeeper, geNorm, and NormFinder evaluations.
Rank BestKeeper geNorm NormFinderGene Ra Gene M-valueb Gene Stability valueb
1 GAPDH 0.774 GAPDH 0.3877 GAPDH 0.07592 ACTB 0.745 β2M 0.4377 ACTB 0.10853 β2M 0.727 ACTB 0.4641 β2M 0.10944 HPRT 0.713 HPRT 0.4945 HPRT 0.10955 18S 0.588 18S 0.5182 18S 0.1176
R: Pearson’s correlation coefficient; M-value: average expression stability; GAPDH: glyceraldehyde-3-phosphate dehydrogenase; ACTB: beta-actin; β2M: beta-2-microglobulin; HPRT: hypoxanthine guanine phosphoribosyl transferase; and 18S: eukaryotic 18S ribosomal RNA. aValues closer to 1.0 (the higher values in this scenario) indicate greater stability. bLower values indicate greater stability.
Figure 1. BestKeeper, geNorm, and NormFinder stability analyses of housekeeping genes in the left ventricle of rats submitted to chronic intermittent hypoxia. R: Pearson’s correlation coefficient; M-value: average expression stability; ACTB: beta-actin; HPRT: hypoxanthine guanine phosphoribosyl transferase; β2M: beta-2-microglobulin; GAPDH: glyceraldehyde-3-phosphate dehydrogenase; and 18S: eukaryotic 18S ribosomal RNA.
A B C
1.0
0.0
0.2
0.4
0.6
0.8
R
0.0
0.2
0.4
0.6
0.00
0.05
0.10
0.15
M-V
alue
Stab
ility
val
ue
GeNorm NormfinderBestKeeper
Stab
ility
Stab
ility
Stab
ility
ACTBHPRT
β2MGAPDH18S
REFERENCES
1. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006-14. http://dx.doi.org/10.1093/aje/kws342
2. Tufik S, Santos-Silva R, Taddei JA, Bittencourt LR. Obstructive sleep apnea syndrome in the Sao Paulo Epidemiologic Sleep Study. Sleep Med. 2010;11(5):441-6. http://dx.doi.org/10.1016/j.sleep.2009.10.005
3. Dematteis M, Godin-Ribuot D, Arnaud C, Ribuot C, Stanke-Labesque F, Pépin JL, et al. Cardiovascular consequences of sleep-disordered breathing: contribution of animal models to understanding of the human disease. ILAR J. 2009;50(3):262-81. http://dx.doi.org/10.1093/ilar.50.3.262
4. Zoccal DB, Bonagamba LG, Oliveira FR, Antunes-Rodrigues J, Machado BH. Increased sympathetic activity in rats submitted to chronic intermittent hypoxia. Exp Physiol. 2007;92(1):79-85. http://dx.doi.org/10.1113/expphysiol.2006.035501
5. Thellin O, Zorzi W, Lakaye B, De Borman B, Coumans B, Hennen G, et al. Housekeeping genes as internal standards: use and limits.
J Biotechnol. 1999;75(2-3):291-5. http://dx.doi.org/10.1016/S0168-1656(99)00163-7
6. Zhao DJ, Guo K, Kang L. Identification of condition-specific reference genes from microarray data for locusts exposed to hypobaric hypoxia. FEBS Open Bio. 2012;2:235-40. http://dx.doi.org/10.1016/j.fob.2012.08.001
7. Caradec J, Sirab N, Keumeugni C, Moutereau S, Chimingqi M, Matar C, et al. “Desperate house genes”: the dramatic example of hypoxia. Br J Cancer. 2010;102(6):1037-43. http://dx.doi.org/10.1038/sj.bjc.6605573
8. Vandesompele J, De Preter K, Pattyn F, Poppe B, Van Roy N, De Paepe A, et al. Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol. 2002;3(7):RESEARCH0034.
9. Pfaffl MW, Tichopad A, Prgomet C, Neuvians TP. Determination of stable housekeeping genes, differentially regulated target genes and sample integrity: BestKeeper--Excel-based tool using pair-wise correlations. Biotechnol Lett. 2004;26(6):509-15. http://dx.doi.org/10.1023/B:BILE.0000019559.84305.47
213J Bras Pneumol. 2016;42(3):211-214

Analysis of the stability of housekeeping gene expression in the left cardiac ventricle of rats submitted to chronic intermittent hypoxia
10. Andersen CL, Jensen JL, Ørntoft TF. Normalization of real-time quantitative reverse transcription-PCR data: a model-based variance estimation approach to identify genes suited for normalization, applied to bladder and colon cancer data sets. Cancer Res. 2004;64(15):5245-50. http://dx.doi.org/10.1158/0008-5472.CAN-04-0496
11. Julian GS, de Oliveira RW, Perry JC, Tufik S, Chagas JR. Validation of Housekeeping genes in the brains of rats submitted to chronic intermittent hypoxia, a sleep apnea model. PLoS One. 2014;9(10):e109902. http://dx.doi.org/10.1371/journal.pone.0109902
12. Andersen M, Tufik S. Animal models as ethical tools in biomedical research. São Paulo: Universidade Federal de São Paulo; 2010. 563 pp.
13. Veasey SC, Davis CW, Fenik P, Zhan G, Hsu YJ, Pratico D, et al. Long-term intermittent hypoxia in mice: protracted hypersomnolence with oxidative injury to sleep-wake brain regions. Sleep. 2004;27(2):194-201.
14. Silver N, Best S, Jiang J, Thein SL. Selection of housekeeping genes for gene expression studies in human reticulocytes using real-time PCR. BMC Mol Biol. 2006;7:33. http://dx.doi.org/10.1186/1471-2199-7-33
15. Tan SC, Carr CA, Yeoh KK, Schofield CJ, Davies KE, Clarke K. Identification of valid housekeeping genes for quantitative RT-PCR analysis of cardiosphere-derived cells preconditioned under hypoxia or with prolyl-4-hydroxylase inhibitors. Mol Biol Rep. 2012;39(4):4857-67. http://dx.doi.org/10.1007/s11033-011-1281-5
16. Nachar W, Busseuil D, Shi Y, Mihalache-Avram T, Mecteau M, Rhéaume E, et al. Optimisation of reference genes for gene-expression analysis in a rabbit model of left ventricular diastolic dysfunction. PLoS One. 2014;9(2):e89331. http://dx.doi.org/10.1371/journal.pone.0089331
17. Foldager CB, Munir S, Ulrik-Vinther M, Søballe K, Bünger C, Lind M. Validation of suitable house keeping genes for hypoxia-cultured human chondrocytes. BMC Mol Biol. 2009;10:94. http://dx.doi.org/10.1186/1471-2199-10-94
18. Vesentini N, Barsanti C, Martino A, Kusmic C, Ripoli A, Rossi A, et al. Selection of reference genes in different myocardial regions of an in vivo ischemia/reperfusion rat model for normalization of antioxidant gene expression. BMC Res Notes. 2012;5:124. http://dx.doi.org/10.1186/1756-0500-5-124
19. Yao L, Chen X, Tian Y, Lu H, Zhang P, Shi Q, et al. Selection of housekeeping genes for normalization of RT-PCR in hypoxic neural stem cells of rat in vitro. Mol Biol Rep. 2012;39(1):569-76. http://dx.doi.org/10.1007/s11033-011-0772-8
20. Caradec J, Sirab N, Keumeugni C, Revaud D, Loric S. Reply: 18S is an appropriate housekeeping gene for in vitro hypoxia experiments. Br J Cancer. 2010;103(4):591-2. http://dx.doi.org/10.1038/sj.bjc.6605755
21. Nagelkerke A, Mujcic H, Wouters B, Span PN. 18S is an appropriate housekeeping gene for in vitro hypoxia experiments. Br J Cancer. 2010;103(4):590; author reply 591-2. http://dx.doi.org/10.1038/sj.bjc.6605754
214 J Bras Pneumol. 2016;42(3):211-214

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000337
ABSTRACTObjective: The objective of this study was to describe the results of anatomic pulmonary resections performed by video-assisted thoracoscopy in Brazil. Methods: Thoracic surgeons (members of the Brazilian Society of Thoracic Surgery) were invited, via e-mail, to participate in the study. Eighteen surgeons participated in the project by providing us with retrospective databases containing information related to anatomic pulmonary resections performed by video-assisted thoracoscopy. Demographic, surgical, and postoperative data were collected with a standardized instrument, after which they were compiled and analyzed. Results: The surgeons provided data related to a collective total of 786 patients (mean number of resections per surgeon, 43.6). However, 137 patients were excluded because some data were missing. Therefore, the study sample comprised 649 patients. The mean age of the patients was 61.7 years. Of the 649 patients, 295 (45.5%) were male. The majority—521 (89.8%)—had undergone surgery for neoplasia, which was most often classified as stage IA. The median duration of pleural drainage was 3 days, and the median hospital stay was 4 days. Of the 649 procedures evaluated, 598 (91.2%) were lobectomies. Conversion to thoracotomy was necessary in 30 cases (4.6%). Postoperative complications occurred in 124 patients (19.1%), the most common complications being pneumonia, prolonged air leaks, and atelectasis. The 30-day mortality rate was 2.0%, advanced age and diabetes being found to be predictors of mortality. Conclusions: Our analysis of this representative sample of patients undergoing pulmonary resection by video-assisted thoracoscopy in Brazil showed that the procedure is practicable and safe, as well as being comparable to those performed in other countries.
Keywords: Thoracic surgery, video-assisted; Thoracoscopy; Pneumonectomy.
Anatomic pulmonary resection by video-assisted thoracoscopy: the Brazilian experience (VATS Brazil study)Ricardo Mingarini Terra1, Thamara Kazantzis1, Darcy Ribeiro Pinto-Filho2, Spencer Marcantonio Camargo3, Francisco Martins-Neto4,5, Anderson Nassar Guimarães6, Carlos Alberto Araújo7, Luis Carlos Losso8, Mario Claudio Ghefter9, Nuno Ferreira de Lima10, Antero Gomes-Neto5, Flávio Brito-Filho10, Rui Haddad11, Maurício Guidi Saueressig12, Alexandre Marcelo Rodrigues Lima13, Rafael Pontes de Siqueira5, Astunaldo Júnior de Macedo e Pinho14, Fernando Vannucci15
Correspondence to: Ricardo Mingarini Terra. Avenida Dr. Enéas de Carvalho Aguiar, 44, Bloco II, 2º Andar, Sala 9, CEP 05403-900, São Paulo, SP, Brasil.Tel.: 55 11 2661-5000. E-mail: [email protected] support: None.
INTRODUCTION
In the last 20 years, the development of minimally invasive surgery has evolved constantly. This technique minimizes trauma response and optimizes patient recovery without compromising surgical results.(1-5) Thoracic surgery has followed this same path, which means that anatomic pulmonary resections by video-assisted thoracoscopy are routinely performed in hospitals around the world, and the number of studies that report increasingly complex surgeries, such as video-assisted thoracoscopic lobectomy with bronchoplasty for the treatment of hilar lymph node enlargement and large tumors, has increased in recent years.(6-11)
Despite the proven advantages of the minimally invasive approach, technical and financial limitations make its implementation difficult, especially in developing countries, such as India, Mexico, and Brazil. Therefore, to date, we do not yet have data from studies conducted in Brazil that can confirm the applicability and safety of the technique in our country, taking into account the particular characteristics of the patients and centers that provide care to them.(1,2,4,12)
The primary objective of the present study was to analyze the results of anatomic pulmonary resections performed by video-assisted thoracoscopy in Brazil, including
1. Departamento de Cardiopneumologia, Disciplina de Cirurgia Torácica, Instituto do Coração, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
2. Serviço de Cirurgia Torácica, Hospital Geral de Caxias do Sul, Fundação Universidade de Caxias do Sul (RS) Brasil.
3. Serviço de Cirurgia Torácica, Pavilhão Pereira Filho, Complexo Hospitalar da Santa Casa de Porto Alegre, Porto Alegre (RS) Brasil.
4. Hospital Monte Klinikum, Fortaleza (CE) Brasil.
5. Hospital de Messejana Doutor Carlos Alberto Studart Gomes, Fortaleza (CE) Brasil.
6. Casa de Saúde São José, Rio de Janeiro (RJ) Brasil.
7. Universidade Federal do Rio Grande do Norte, Natal (RN) Brasil.
8. Hospital Professor Edmundo Vasconcelos, São Paulo (SP) Brasil.
9. Hospital do Servidor Público Estadual de São Paulo, São Paulo (SP) Brasil.
10. Hospital de Base do Distrito Federal, Brasília (DF) Brasil.
11. Hospital Samaritano, Rio de Janeiro (RJ) Brasil.
12. Serviço de Cirurgia Torácica, Hospital de Clínicas de Porto Alegre, Faculdade de Medicina, Universidade Federal do Rio Grande do Sul, Porto Alegre (RS) Brasil.
13. Hospital Geral César Cals, Fortaleza (CE) Brasil.
14. Instituto Mário Penna, Hospital Luxemburgo, Belo Horizonte (MG) Brasil.
15. Hospital Naval Marcílio Dias, Rio de Janeiro (RJ) Brasil.
Submitted: 16 December 2015.Accepted: 6 April 2016.
Study carried out in the Departamento de Cardiopneumologia, Disciplina de Cirurgia Torácica, Instituto do Coração, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, and Sociedade Brasileira de Cirurgia Torácica, São Paulo (SP) Brasil.
J Bras Pneumol. 2016;42(3):215-221
215
SPECIAL ARTICLE
Anatomic pulmonary resection by video-assisted thoracoscopy: the Brazilian experience (VATS Brazil study)
intraoperative complications, postoperative complica-tions, and 30-day mortality. As a secondary objective, we sought to determine predictors of postoperative complications and 30-day mortality in our current scenario.
METHODS
This was a retrospective study commissioned by the Sociedade Brasileira de Cirurgia Torácica (SBCT, Brazilian Society of Thoracic Surgery), including data provided by 14 thoracic surgery groups in Brazil. The participating groups volunteered to donate data to the present study after an invitation was sent via e-mail to all members of the SBCT. To participate, interested parties should provide data related to anatomic pulmonary resections performed by video-assisted thoracoscopy. The minimum number of cases required for a group to be eligible for participation was 20 complete cases. The study project was approved by the Research Ethics Committee of the University of São Paulo School of Medicine (CAAE no. 40434414.6.0000.0065).
Cases of patients who underwent anatomic pulmonary resection by video-assisted thoracoscopy were included. Anatomic resections are those in which dissection and ligation is carried out regardless of the hilar structures, consisting of segmentectomy, lobectomy, or pneumonectomy. Video-assisted thoracoscopic procedures were defined as those in which there was no intercostal separation and incisions were < 8 cm.(13) Cases in which data on preoperative comorbidities, length of hospital stay, and postoperative complications were missing were excluded. The absence of only one of these data sets was not considered to be an exclusion criterion.
After accepting the invitation from the SBCT, the interested parties contacted the corresponding author and received a standardized instrument for data collection. The instrument contained closed-ended response fields and definitions for each variable.
The variables collected consisted of patient demo-graphics (age, gender, diagnosis, and comorbidities), surgery-related data (date, type of procedure, and intraoperative complications), and surgical results (duration of drainage, length of hospital stay, and morbidity). Below are the definitions used for the various postoperative variables collected(14-17):
Respiratory complications• Pneumonia: presence of persistent or progressive
pulmonary infiltrates on chest X-ray and at least two of the following clinical criteria: temperature ≥ 38°C; leukocytosis > 12,000 cells/μL or leukopenia < 3,000 cells/μL; or purulent tracheal secretions with ≥ 25 neutrophils and ≤ 10 squamous epithelial cells per field (magnification, ×100)
• Pulmonary thromboembolism diagnosed by CT angiography
• Atelectasis requiring bronchoscopic intervention
• Respiratory failure: prolonged intubation (> 48 h or need for orotracheal reintubation in the postoperative period)
• ARDS: hypoxemia and diffuse pulmonary infiltrates with a PaO2/FiO2 < 200
Cardiac complications• Acute myocardial infarction within 14 days after
surgery: as determined on the basis of creatine phosphokinase > 30 ng/mL (5 times above normal), troponin I > 5 ng/mL within 72 h after surgery, the presence of new pathological Q waves, or the medical record entry
• Arrhythmia requiring intervention or delaying hospital discharge
Infectious complications• Sepsis: suspected infection associated with at
least two of the following variables(18-20):• Temperature > 38°C or < 36°C• Heart rate > 90 bpm• Respiratory rate > 20 breaths/min• Blood workup showing leukocytosis (>12,000
cells/µL), leukopenia (< 4,000 cells/µL), or more than 10% of immature forms
• Signs of organ dysfunction, such as systolic blood pressure < 90 mmHg, mean arterial pressure < 70 mmHg, PaO2/FiO2 < 300, diuresis < 0.5 mL/kg/h, creatinine elevation > 0.5 mg/dL, international normalized ratio > 1.5 or prothrombin time > 60 s, platelets < 100,000/µL, or plasma total bilirubin > 4 mg/dL
• Pleural empyema• Surgical wound infection
Renal and metabolic complications• Kidney injury: creatinine >1.5 mg/dL or
creatinine elevation > 0.5 mg/dL within 24 h
Hematological complications• Deep vein thrombosis (confirmed by Doppler)
Neurological complications• Stroke• Delirium
Surgical complications• Need for blood transfusion• Prolonged drainage (longer than 7 days)• Prolonged air leaks (longer than 7 days)• Inadvertent injury to intrathoracic structures• Bronchial stump fistula• Reoperation
Other definitionsReadmission within 60 days and 30-day mortality,
regardless of their cause
All complications were recorded individually; however, the number of patients/cases with complications is what was used for analysis, given that various patients had more than one complication.
216 J Bras Pneumol. 2016;42(3):215-221
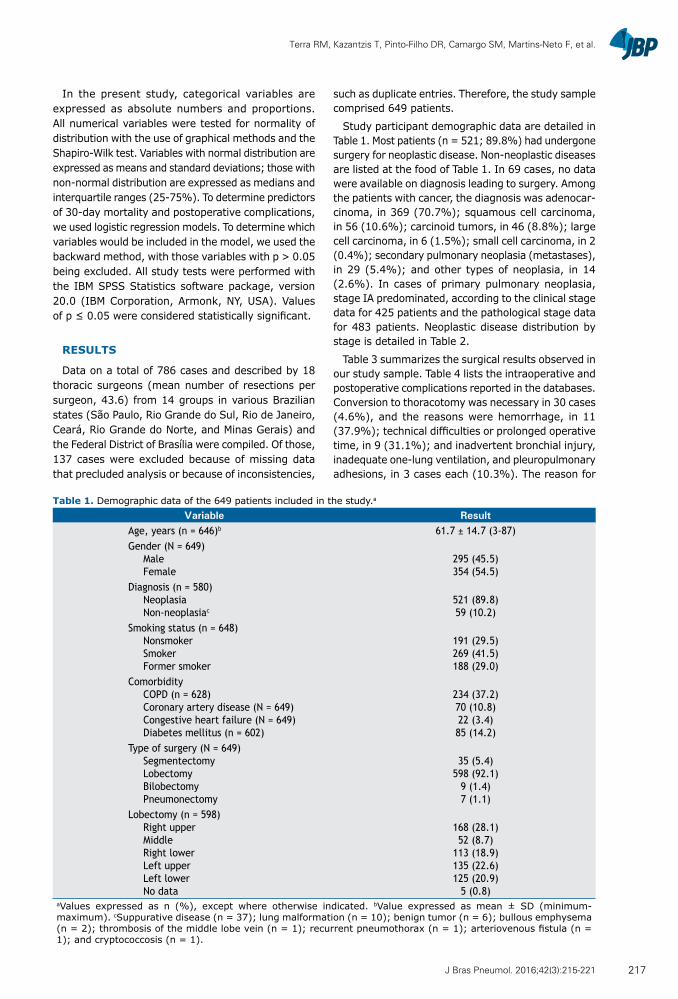
Terra RM, Kazantzis T, Pinto-Filho DR, Camargo SM, Martins-Neto F, et al.
In the present study, categorical variables are expressed as absolute numbers and proportions. All numerical variables were tested for normality of distribution with the use of graphical methods and the Shapiro-Wilk test. Variables with normal distribution are expressed as means and standard deviations; those with non-normal distribution are expressed as medians and interquartile ranges (25-75%). To determine predictors of 30-day mortality and postoperative complications, we used logistic regression models. To determine which variables would be included in the model, we used the backward method, with those variables with p > 0.05 being excluded. All study tests were performed with the IBM SPSS Statistics software package, version 20.0 (IBM Corporation, Armonk, NY, USA). Values of p ≤ 0.05 were considered statistically significant.
RESULTS
Data on a total of 786 cases and described by 18 thoracic surgeons (mean number of resections per surgeon, 43.6) from 14 groups in various Brazilian states (São Paulo, Rio Grande do Sul, Rio de Janeiro, Ceará, Rio Grande do Norte, and Minas Gerais) and the Federal District of Brasília were compiled. Of those, 137 cases were excluded because of missing data that precluded analysis or because of inconsistencies,
such as duplicate entries. Therefore, the study sample comprised 649 patients.
Study participant demographic data are detailed in Table 1. Most patients (n = 521; 89.8%) had undergone surgery for neoplastic disease. Non-neoplastic diseases are listed at the food of Table 1. In 69 cases, no data were available on diagnosis leading to surgery. Among the patients with cancer, the diagnosis was adenocar-cinoma, in 369 (70.7%); squamous cell carcinoma, in 56 (10.6%); carcinoid tumors, in 46 (8.8%); large cell carcinoma, in 6 (1.5%); small cell carcinoma, in 2 (0.4%); secondary pulmonary neoplasia (metastases), in 29 (5.4%); and other types of neoplasia, in 14 (2.6%). In cases of primary pulmonary neoplasia, stage IA predominated, according to the clinical stage data for 425 patients and the pathological stage data for 483 patients. Neoplastic disease distribution by stage is detailed in Table 2.
Table 3 summarizes the surgical results observed in our study sample. Table 4 lists the intraoperative and postoperative complications reported in the databases. Conversion to thoracotomy was necessary in 30 cases (4.6%), and the reasons were hemorrhage, in 11 (37.9%); technical difficulties or prolonged operative time, in 9 (31.1%); and inadvertent bronchial injury, inadequate one-lung ventilation, and pleuropulmonary adhesions, in 3 cases each (10.3%). The reason for
Table 1. Demographic data of the 649 patients included in the study.a
Variable ResultAge, years (n = 646)b 61.7 ± 14.7 (3-87)Gender (N = 649)
MaleFemale
295 (45.5)354 (54.5)
Diagnosis (n = 580)NeoplasiaNon-neoplasiac
521 (89.8)59 (10.2)
Smoking status (n = 648)NonsmokerSmokerFormer smoker
191 (29.5)269 (41.5)188 (29.0)
ComorbidityCOPD (n = 628)Coronary artery disease (N = 649)Congestive heart failure (N = 649)Diabetes mellitus (n = 602)
234 (37.2)70 (10.8)22 (3.4)85 (14.2)
Type of surgery (N = 649)SegmentectomyLobectomyBilobectomyPneumonectomy
35 (5.4)598 (92.1)
9 (1.4)7 (1.1)
Lobectomy (n = 598)Right upperMiddleRight lowerLeft upperLeft lowerNo data
168 (28.1)52 (8.7)
113 (18.9)135 (22.6)125 (20.9)
5 (0.8)aValues expressed as n (%), except where otherwise indicated. bValue expressed as mean ± SD (minimum-maximum). cSuppurative disease (n = 37); lung malformation (n = 10); benign tumor (n = 6); bullous emphysema (n = 2); thrombosis of the middle lobe vein (n = 1); recurrent pneumothorax (n = 1); arteriovenous fistula (n = 1); and cryptococcosis (n = 1).
217J Bras Pneumol. 2016;42(3):215-221
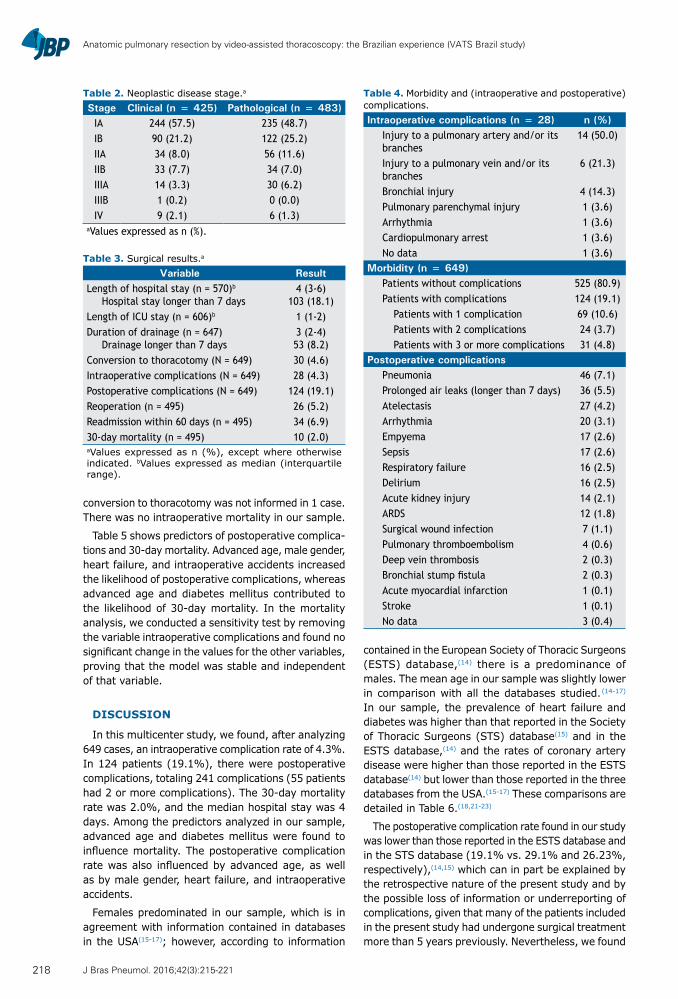
Anatomic pulmonary resection by video-assisted thoracoscopy: the Brazilian experience (VATS Brazil study)
conversion to thoracotomy was not informed in 1 case. There was no intraoperative mortality in our sample.
Table 5 shows predictors of postoperative complica-tions and 30-day mortality. Advanced age, male gender, heart failure, and intraoperative accidents increased the likelihood of postoperative complications, whereas advanced age and diabetes mellitus contributed to the likelihood of 30-day mortality. In the mortality analysis, we conducted a sensitivity test by removing the variable intraoperative complications and found no significant change in the values for the other variables, proving that the model was stable and independent of that variable.
DISCUSSION
In this multicenter study, we found, after analyzing 649 cases, an intraoperative complication rate of 4.3%. In 124 patients (19.1%), there were postoperative complications, totaling 241 complications (55 patients had 2 or more complications). The 30-day mortality rate was 2.0%, and the median hospital stay was 4 days. Among the predictors analyzed in our sample, advanced age and diabetes mellitus were found to influence mortality. The postoperative complication rate was also influenced by advanced age, as well as by male gender, heart failure, and intraoperative accidents.
Females predominated in our sample, which is in agreement with information contained in databases in the USA(15-17); however, according to information
contained in the European Society of Thoracic Surgeons (ESTS) database,(14) there is a predominance of males. The mean age in our sample was slightly lower in comparison with all the databases studied. (14-17) In our sample, the prevalence of heart failure and diabetes was higher than that reported in the Society of Thoracic Surgeons (STS) database(15) and in the ESTS database,(14) and the rates of coronary artery disease were higher than those reported in the ESTS database(14) but lower than those reported in the three databases from the USA.(15-17) These comparisons are detailed in Table 6.(18,21-23)
The postoperative complication rate found in our study was lower than those reported in the ESTS database and in the STS database (19.1% vs. 29.1% and 26.23%, respectively),(14,15) which can in part be explained by the retrospective nature of the present study and by the possible loss of information or underreporting of complications, given that many of the patients included in the present study had undergone surgical treatment more than 5 years previously. Nevertheless, we found
Table 4. Morbidity and (intraoperative and postoperative) complications.Intraoperative complications (n = 28) n (%)
Injury to a pulmonary artery and/or its branches
14 (50.0)
Injury to a pulmonary vein and/or its branches
6 (21.3)
Bronchial injury 4 (14.3)Pulmonary parenchymal injury 1 (3.6)Arrhythmia 1 (3.6)Cardiopulmonary arrest 1 (3.6)No data 1 (3.6)
Morbidity (n = 649)Patients without complications 525 (80.9)Patients with complications 124 (19.1)
Patients with 1 complication 69 (10.6)Patients with 2 complications 24 (3.7)Patients with 3 or more complications 31 (4.8)
Postoperative complicationsPneumonia 46 (7.1)Prolonged air leaks (longer than 7 days) 36 (5.5)Atelectasis 27 (4.2)Arrhythmia 20 (3.1)Empyema 17 (2.6)Sepsis 17 (2.6)Respiratory failure 16 (2.5)Delirium 16 (2.5)Acute kidney injury 14 (2.1)ARDS 12 (1.8)Surgical wound infection 7 (1.1)Pulmonary thromboembolism 4 (0.6)Deep vein thrombosis 2 (0.3)Bronchial stump fistula 2 (0.3)Acute myocardial infarction 1 (0.1)Stroke 1 (0.1)No data 3 (0.4)
Table 2. Neoplastic disease stage.a
Stage Clinical (n = 425) Pathological (n = 483)IA 244 (57.5) 235 (48.7)IB 90 (21.2) 122 (25.2)IIA 34 (8.0) 56 (11.6)IIB 33 (7.7) 34 (7.0)IIIA 14 (3.3) 30 (6.2)IIIB 1 (0.2) 0 (0.0)IV 9 (2.1) 6 (1.3)
aValues expressed as n (%).
Table 3. Surgical results.a
Variable ResultLength of hospital stay (n = 570)b
Hospital stay longer than 7 days4 (3-6)
103 (18.1)Length of ICU stay (n = 606)b 1 (1-2)Duration of drainage (n = 647)
Drainage longer than 7 days3 (2-4)53 (8.2)
Conversion to thoracotomy (N = 649) 30 (4.6)Intraoperative complications (N = 649) 28 (4.3)Postoperative complications (N = 649) 124 (19.1)Reoperation (n = 495) 26 (5.2)Readmission within 60 days (n = 495) 34 (6.9)30-day mortality (n = 495) 10 (2.0)aValues expressed as n (%), except where otherwise indicated. bValues expressed as median (interquartile range).
218 J Bras Pneumol. 2016;42(3):215-221
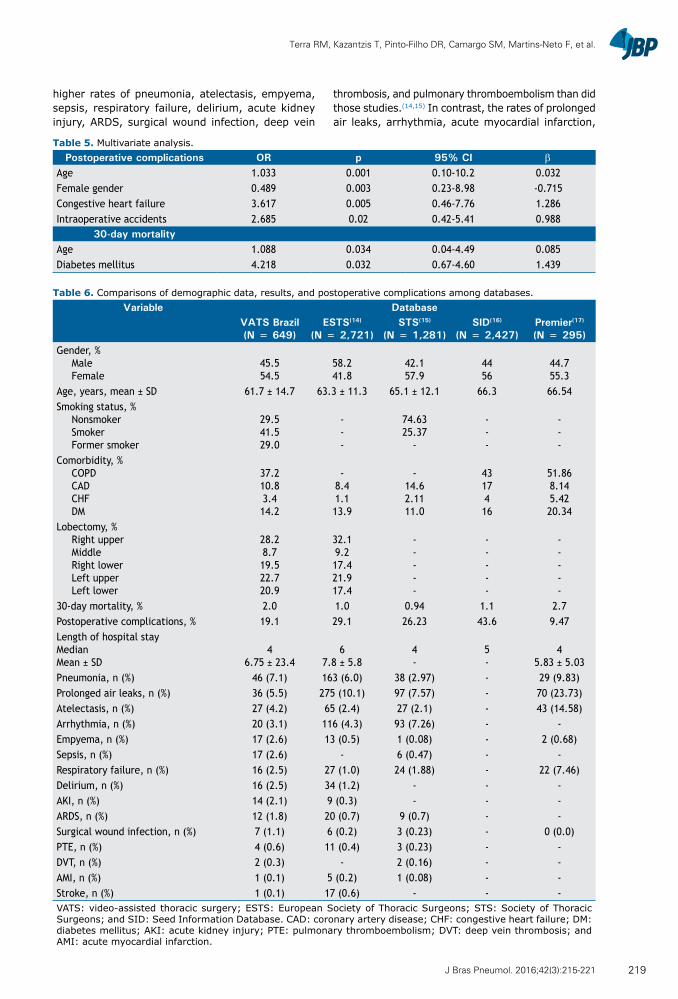
Terra RM, Kazantzis T, Pinto-Filho DR, Camargo SM, Martins-Neto F, et al.
higher rates of pneumonia, atelectasis, empyema, sepsis, respiratory failure, delirium, acute kidney injury, ARDS, surgical wound infection, deep vein
thrombosis, and pulmonary thromboembolism than did those studies.(14,15) In contrast, the rates of prolonged air leaks, arrhythmia, acute myocardial infarction,
Table 5. Multivariate analysis.Postoperative complications OR p 95% CI β
Age 1.033 0.001 0.10-10.2 0.032Female gender 0.489 0.003 0.23-8.98 -0.715Congestive heart failure 3.617 0.005 0.46-7.76 1.286Intraoperative accidents 2.685 0.02 0.42-5.41 0.988
30-day mortalityAge 1.088 0.034 0.04-4.49 0.085Diabetes mellitus 4.218 0.032 0.67-4.60 1.439
Table 6. Comparisons of demographic data, results, and postoperative complications among databases.Variable Database
VATS Brazil (N = 649)
ESTS(14) (N = 2,721)
STS(15) (N = 1,281)
SID(16)
(N = 2,427)Premier(17)
(N = 295)Gender, %
MaleFemale
45.554.5
58.241.8
42.157.9
4456
44.755.3
Age, years, mean ± SD 61.7 ± 14.7 63.3 ± 11.3 65.1 ± 12.1 66.3 66.54Smoking status, %
NonsmokerSmokerFormer smoker
29.541.529.0
---
74.6325.37
-
---
---
Comorbidity, %COPDCADCHFDM
37.210.83.414.2
-8.41.113.9
-14.62.1111.0
4317416
51.868.145.4220.34
Lobectomy, %Right upperMiddleRight lowerLeft upperLeft lower
28.28.719.522.720.9
32.19.217.421.917.4
-----
-----
-----
30-day mortality, % 2.0 1.0 0.94 1.1 2.7Postoperative complications, % 19.1 29.1 26.23 43.6 9.47Length of hospital stayMedianMean ± SD
46.75 ± 23.4
67.8 ± 5.8
4-
5-
45.83 ± 5.03
Pneumonia, n (%) 46 (7.1) 163 (6.0) 38 (2.97) - 29 (9.83)Prolonged air leaks, n (%) 36 (5.5) 275 (10.1) 97 (7.57) - 70 (23.73)Atelectasis, n (%) 27 (4.2) 65 (2.4) 27 (2.1) - 43 (14.58)Arrhythmia, n (%) 20 (3.1) 116 (4.3) 93 (7.26) - -Empyema, n (%) 17 (2.6) 13 (0.5) 1 (0.08) - 2 (0.68)Sepsis, n (%) 17 (2.6) - 6 (0.47) - -Respiratory failure, n (%) 16 (2.5) 27 (1.0) 24 (1.88) - 22 (7.46)Delirium, n (%) 16 (2.5) 34 (1.2) - - -AKI, n (%) 14 (2.1) 9 (0.3) - - -ARDS, n (%) 12 (1.8) 20 (0.7) 9 (0.7) - -Surgical wound infection, n (%) 7 (1.1) 6 (0.2) 3 (0.23) - 0 (0.0)PTE, n (%) 4 (0.6) 11 (0.4) 3 (0.23) - -DVT, n (%) 2 (0.3) - 2 (0.16) - -AMI, n (%) 1 (0.1) 5 (0.2) 1 (0.08) - -Stroke, n (%) 1 (0.1) 17 (0.6) - - -VATS: video-assisted thoracic surgery; ESTS: European Society of Thoracic Surgeons; STS: Society of Thoracic Surgeons; and SID: Seed Information Database. CAD: coronary artery disease; CHF: congestive heart failure; DM: diabetes mellitus; AKI: acute kidney injury; PTE: pulmonary thromboembolism; DVT: deep vein thrombosis; and AMI: acute myocardial infarction.
219J Bras Pneumol. 2016;42(3):215-221

Anatomic pulmonary resection by video-assisted thoracoscopy: the Brazilian experience (VATS Brazil study)
and stroke found in our study were low, which in part can be explained by the lower incidence of COPD and chronic arterial disease in our population (Table 6).
The number of infectious complications—empyema, pneumonia, or sepsis—in our sample is of note. One of the likely explanations is the fact that more than 15% of the patients included in our study had diseases associated with lung infections, such as bronchiectasis or tuberculosis, which could predispose to such complications and are less common in studies conducted in the USA and in Europe.(24) We were unable to statistically establish this correlation; however, the statistical power is low for this analysis. In any case, this is an indicator that should be paid attention to in the future.
In Brazil, there have been no studies describing complications of video-assisted thoracoscopic lobectomy; however, a study conducted at the Santa Casa Hospital Complex in Porto Alegre, located in the state of Rio Grande do Sul, Brazil, describes complications related to traditional lobectomy in lung donors.(25) In that study, 31.25% of the patients had one or more complications, the most common being pleural effusion.(25) Another study conducted in the same state, also regarding lobectomy via thoracotomy, reported a complication rate of 44%, in addition to an intraoperative mortality rate of 2.9%.(26) The mean age of those patients, 63.7 ± 9.7 years, was similar to that found in our sample; however, most of those patients (83.9%) had one or more comorbidities, and 90% had a history of smoking. The most common complication was air leaks.(26) A lower complication rate, 18.6%, was documented in a study conducted by the State University at Campinas; however, in the study, there were other procedures that did not involve resection of lung parenchyma.(27)
Our study has limitations, and the most significant is its retrospective design. As previously mentioned, we may have underestimated the actual number of complications occurring in the cases studied. In addition, we cannot classify the severity of the complications observed, since the definition of which was determined
a posteriori and the data in the medical records were very heterogeneous. The present study included cases on the learning curve of most participating surgeons (with up to 50 cases per surgeon)(28); therefore, if, on one hand, less experience might lead to a greater number of complications, on the other, favorable cases are likely to have been selected. In addition, the participation of surgeons was voluntary, so it is possible that the surgeons participating in the study do not fully represent all thoracic surgery groups in Brazil. Furthermore, although the data were collected and organized by only one researcher, each surgeon was responsible for their database and there may therefore be heterogeneity in the data provided.
As shown in the present study, anatomic pulmonary resections by video-assisted thoracoscopy have been performed at several centers throughout Brazil. The results of these surgeries, which represent the results for the learning curve of the several centers and therefore constitute the critical mass regarding video-assisted resections in our country, are consistent with the results observed in large international databases. Since the technique has been safely and successfully implemented in the participating institutions, strategies should be developed to increase access to this minimally invasive alternative. Advanced age and heart failure, which are preoperative predictors of complications, should be taken into account when considering this type of surgery.
ACKNOWLEDGMENTS
We would like to thank the thoracic surgeons who participated indirectly in this study by providing us with cases that were computed as part of institutional databases: Pedro Henrique Xavier Nabuco de Araujo, Letícia Leone Lauricella, Alberto Jorge Monteiro Dela Veja, and Benoit Jacques Bibas (University of São Paulo); José Jesus Camargo, José Carlos Felicetti, and Fabíola Perin (Santa Casa Hospital Complex in Porto Alegre); and Daniel Bonomi (Mário Penna Institute).
REFERENCES
1. Taioli E, Lee DS, Lesser M, Flores R. Long-term survival in video-assisted thoracoscopic lobectomy vs open lobectomy in lung-cancer patients: a meta-analysis. Eur J Cardiothorac Surg. 2013;44(4):591-7. http://dx.doi.org/10.1093/ejcts/ezt051
2. Cao C, Manganas C, Ang SC, Yan TD. A meta-analysis of unmatched and matched patients comparing video-assisted thoracoscopic lobectomy and conventional open lobectomy. Ann Cardiothorac Surg. 2012;1(1):16-23. http://dx.doi.org/ 10.3978/j.issn.2225-319X.2012.04.18
3. Swanson SJ, Herndon JE 2nd, D’Amico TA, Demmy TL, McKenna RJ Jr, Green MR, et al. DJ. Video-assisted thoracic surgery lobectomy: report of CALGB 39802--a prospective, multi-institution feasibility study. J Clin Oncol. 2007;25(31):4993-7. http://dx.doi.org/10.1200/JCO.2007.12.6649
4. Flores RM, Park BJ, Dycoco J, Aronova A, Hirth Y, Rizk NP, et al. Lobectomy by video-assisted thoracic surgery (VATS) versus thoracotomy for lung cancer. J Thorac Cardiovasc Surg. 2009;138(1):11-8. http://dx.doi.org/10.1016/j.jtcvs.2009.03.030
5. Lewis RJ, Caccavale RJ, Sisler GE, Mackenzie JW. Video-assisted thoracic surgical resection of malignant lung tumors. J Thorac
Cardiovasc Surg. 1992;104(6):1679-85; discussion 1685-7.6. Chin CS, Swanson SJ. Video-assisted thoracic surgery lobectomy:
centers of excellence or excellence of centers? Thorac Surg Clin. 2008;18(3):263-8. http://dx.doi.org/10.1016/j.thorsurg.2008.04.001
7. Brunelli A, Falcoz PE, D’Amico T, Hansen H, Lim E, Massard G, et al. European guidelines on structure and qualification of general thoracic surgery. Eur J Cardiothorac Surg. 2014;45(5):779-86. http://dx.doi.org/10.1093/ejcts/ezu016
8. Cooke DT, Wisner DH. Who performs complex noncardiac thoracic surgery in United States academic medical centers? Ann Thorac Surg. 2012;94(4):1060-4. http://dx.doi.org/10.1016/j.athoracsur.2012.04.018
9. Terra RM, Waisberg DR, Almeida JL, Devido MS, Pêgo-Fernandes PM, Jatene FB. Does videothoracoscopy improve clinical outcomes when implemented as part of a pleural empyema treatment algorithm? Clinics (Sao Paulo). 2012;67(6):557-64. http://dx.doi.org/10.6061/clinics/2012(06)03
10. Cirino LM, Milanez de Campos JR, Fernandez A, Samano MN, Fernandez PP, Filomeno LT, et al. Diagnosis and treatment of mediastinal tumors by thoracoscopy. Chest. 2000;117(6):1787-92.
220 J Bras Pneumol. 2016;42(3):215-221
Terra RM, Kazantzis T, Pinto-Filho DR, Camargo SM, Martins-Neto F, et al.
http://dx.doi.org/10.1378/chest.117.6.178711. McKenna RJ Jr, Houck W, Fuller CB. Video-assisted thoracic
surgery lobectomy: experience with 1,100 cases. Ann Thorac Surg. 2006;81(2):421-5; discussion 425-6. http://dx.doi.org/10.1016/j.athoracsur.2005.07.078
12. Paul S, Altorki NK, Sheng S, Lee PC, Harpole DH, Onaitis MW, Stiles BM, Port JL, D’Amico TA. Thoracoscopic lobectomy is associated with lower morbidity than open lobectomy: a propensity-matched analysis from the STS database. J Thorac Cardiovasc Surg. 2010;139(2):366-78. http://dx.doi.org/10.1016/j.jtcvs.2009.08.026
13. Rocco G, Internullo E, Cassivi SD, Van Raemdonck D, Ferguson MK. The variability of practice in minimally invasive thoracic surgery for pulmonary resections. Thorac Surg Clin. 2008;18(3):235-47. http://dx.doi.org/10.1016/j.thorsurg.2008.06.002
14. Falcoz PE, Puyraveau M, Thomas PA, Decaluwe H, Hürtgen M, Petersen RH, et al. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: a propensity-matched analysis of outcome from the European Society of Thoracic Surgeon database. Eur J Cardiothorac Surg. 2016;49(2):602-9. http://dx.doi.org/10.1093/ejcts/ezv154
15. Paul S, Altorki NK, Sheng S, Lee PC, Harpole DH, Onaitis MW, et al. Thoracoscopic lobectomy is associated with lower morbidity than open lobectomy: a propensity-matched analysis from the STS database. J Thorac Cardiovasc Surg. 2010;139(2):366-78. http://dx.doi.org/10.1016/j.jtcvs.2009.08.026
16. Kent M, Wang T, Whyte R, Curran T, Flores R, Gangadharan S. Open, video-assisted thoracic surgery, and robotic lobectomy: review of a national database. Ann Thorac Surg. 2014;97(1):236-42; discussion 242-4. http://dx.doi.org/10.1016/j.athoracsur.2013.07.117
17. Swanson SJ, Miller DL, McKenna RJ Jr, Howington J, Marshall MB, Yoo AC, et al. Comparing robot-assisted thoracic surgical lobectomy with conventional video-assisted thoracic surgical lobectomy and wedge resection: results from a multihospital database (Premier). J Thorac Cardiovasc Surg. 2014;147(3):929-37. http://dx.doi.org/10.1016/j.jtcvs.2013.09.046
18. Lever A, Mackenzie I. Sepsis: definition, epidemiology, and diagnosis. BMJ. 2007;335(7625):879-83. http://dx.doi.org/10.1136/bmj.39346.495880.AE
19. Kaukonen KM, Bailey M, Pilcher D, Cooper DJ, Bellomo R. Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med. 2015;372(17):1629-38. http://dx.doi.org/10.1056/
NEJMoa141523620. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA,
et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644-55. http://dx.doi.org/10.1378/chest.101.6.1644
21. Boffa DJ, Gangadharan S, Kent M, Kerendi F, Onaitis M, Verrier E, et al. Self-perceived video-assisted thoracic surgery lobectomy proficiency by recent graduates of North American thoracic residencies. Interact Cardiovasc Thorac Surg. 2012;14(6):797-800. http://dx.doi.org/10.1093/icvts/ivr098
22. Piwkowski C, Gabryel P, Gałęcki B, Roszak M, Dyszkiewicz Wl. High costs as a slow down factor of thoracoscopic lobectomy development in Poland - an institutional experience. Wideochir Inne Tech Maloinwazyjne. 2013;8(4):334-41. http://dx.doi.org/10.5114/wiitm.2011.35633
23. Swanson SJ, Meyers BF, Gunnarsson CL, Moore M, Howington JA, Maddaus MA, et al. Video-assisted thoracoscopic lobectomy is less costly and morbid than open lobectomy: a retrospective multiinstitutional database analysis. Ann Thorac Surg. 2012;93(4):1027-32. http://dx.doi.org/10.1016/j.athoracsur.2011.06.007
24. World Health Organization [homepage on the Internet]. Geneva: WHO [cited 2015 Dec 1]. Tuberculosis country profiles. Available from: http://who.int/tb/country/data/profiles/en/
25. Camargo SM, Camargo Jde J, Schio SM, Sánchez LB, Felicetti JC, Moreira Jda S, et al. Complications related to lobectomy in living lobar lung transplant donors. J Bras Pneumol. 2008;34(5):256-63.
26. Sánchez PG, Vendrame GS, Madke GR, Pilla ES, Camargo Jde J, Andrade CF, et al. Lobectomy for treating bronchial carcinoma: analysis of comorbidities and their impact on postoperative morbidity and mortality. J Bras Pneumol. 2006;32(6):495-504. http://dx.doi.org/10.1590/S1806-37132006000600005
27. Saad IA, De Capitani EM, Toro IF, Zambon L. Clinical variables of preoperative risk in thoracic surgery. Sao Paulo Med J. 2003;121(3):107-10. http://dx.doi.org/10.1590/S1516-31802003000300004
28. Yan TD, Cao C, D’Amico TA, Demmy TL, He J, Hansen H, Swanson SJ, et al. Video-assisted thoracoscopic surgery lobectomy at 20 years: a consensus statement. Eur J Cardiothoracic Surg. 2014;45(4):633-9. http://dx.doi.org/10.1093/ejcts/ezt463
221J Bras Pneumol. 2016;42(3):215-221

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562015000000230
ABSTRACTWith the advent of HRCT, primary spontaneous pneumothorax has come to be better understood and managed, because its etiology can now be identified in most cases. Primary spontaneous pneumothorax is mainly caused by the rupture of a small subpleural emphysematous vesicle (designated a bleb) or of a subpleural paraseptal emphysematous lesion (designated a bulla). The aim of this pictorial essay was to improve the understanding of primary spontaneous pneumothorax and to propose a description of the major anatomical lesions found during surgery.
Keywords: Pneumothorax; Pulmonary emphysema; Tomography, X-ray computed.
Etiology of primary spontaneous pneumothoraxRoberto de Menezes Lyra1,2
Correspondence to: Roberto de Menezes Lyra. Rua Pedro de Toledo, 1800, 10º andar, Serviço de Cirurgia Torácica, CEP 04039-901, São Paulo, SP, Brasil. Tel.: 55 11 4573-8144. E-mail: [email protected] Financial support: None.
INTRODUCTION
Primary spontaneous pneumothorax is usually quantified and diagnosed in the ER by means of routine chest X-rays.(1,2) However, it is not always easy to identify emphysematous bullae on routine chest X-rays. Emphysematous bullae are found in approximately 15% of cases and are primarily located on the apical margins of the affected lung lobes.(3)
Currently, HRCT is more sensitive than routine chest X-rays for the diagnosis of apical emphysematous lesions, which are found in approximately 80% of all patients with primary spontaneous pneumothorax.(4,5) In contrast, the prevalence of paraseptal emphysema in such patients is only 3%.(6)
PATHOGENESIS
The pathogenesis of primary spontaneous pneumothorax can be best understood by understanding emphysematous lung lesions.
The anatomical lesion known as a bleb was first described in 1947 by Miller, who established an anatomical distinction between a bleb and a bulla (bullous emphysema).(7)
Later, in 1967, Reid divided bullous emphysema, which causes bullae, into three types: type I, a small amount of hyperinflated lung tissue that is narrow (pedunculated) and contains no lung parenchyma; type II, a relatively smaller amount of hyperinflated lung tissue that is broad (sessile) and usually contains vanishing lung; and type III, a large amount of hyperinflated lung tissue extending to the pulmonary hilum, with ill-defined margins and vanishing parenchyma in each bulla.(8)
Chest CT has greatly contributed to the description of lung disease.(9)
For a better description of the aforementioned emphy-sematous lung lesions, a glossary of terms for thoracic imaging is required.
Bleb
The word bleb is translated to Portuguese as vesícula enfisematosa subpleural (i.e., subpleural emphysematous vesicle). A bleb is caused by alveolar rupture, which allows air to travel through the interlobular septum that divides the secondary pulmonary lobules to the subpleural region. The subpleural region is displaced, and a subpleural emphysematous vesicle (i.e., a bleb) is thus formed. Unlike a bulla, which is a distal acinar (or paraseptal) emphysematous lung lesion, the displacement caused by subpleural interstitial emphysema is generally small in size, i.e., 1-2 cm in diameter (Figure 1).
On chest CT scans, a bleb appears as a thin-walled cystic air space contiguous with the pleura. However, the use of the term bleb by radiologists is discouraged because the distinction between a bleb and a bulla is arbitrary and of little clinical importance.
PULMONARY EMPHYSEMA
Pulmonary emphysema is characterized by irreversible enlargement of the airspaces distal to the terminal bronchiole, accompanied by alveolar wall destruction.
On CT scans, emphysema appears as focal areas or regions of low attenuation, usually without visible walls. In the case of panacinar emphysema, decreased attenuation is more diffuse. Emphysema is usually classified according to the part of the acinus that is predominantly affected, being didactically divided into centriacinar (centrilobular) emphysema, panacinar (panlobular) emphysema,
1. Serviço de Cirurgia Torácica, Hospital do Servidor Público Estadual de São Paulo, São Paulo (SP) Brasil.
2. Instituto de Assistência Médica ao Servidor Público Estadual – IAMSPE – São Paulo (SP) Brasil.
Submitted: 12 September 2015. Accepted: 18 December 2015.
Study carried out in the Serviço de Cirurgia Torácica do Hospital do Servidor Público Estadual de São Paulo and at the Instituto de Assistência Médica ao Servidor Público Estadual – IAMSPE – São Paulo (SP) Brasil.
J Bras Pneumol. 2016;42(3):222-226
222
PICTORIAL ESSAY
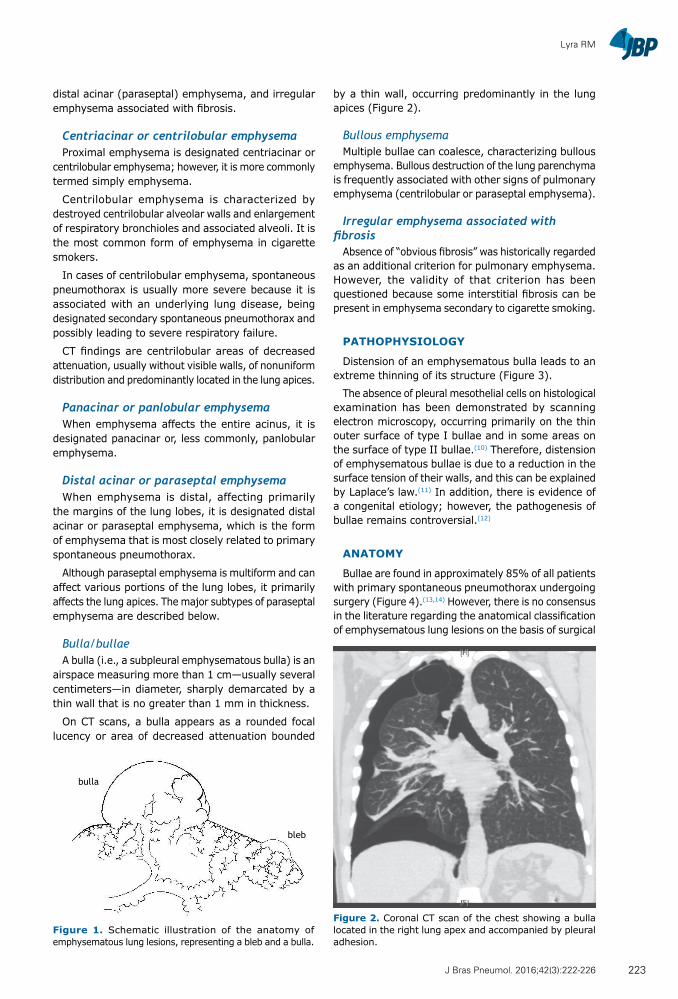
Lyra RM
distal acinar (paraseptal) emphysema, and irregular emphysema associated with fibrosis.
Centriacinar or centrilobular emphysemaProximal emphysema is designated centriacinar or
centrilobular emphysema; however, it is more commonly termed simply emphysema.
Centrilobular emphysema is characterized by destroyed centrilobular alveolar walls and enlargement of respiratory bronchioles and associated alveoli. It is the most common form of emphysema in cigarette smokers.
In cases of centrilobular emphysema, spontaneous pneumothorax is usually more severe because it is associated with an underlying lung disease, being designated secondary spontaneous pneumothorax and possibly leading to severe respiratory failure.
CT findings are centrilobular areas of decreased attenuation, usually without visible walls, of nonuniform distribution and predominantly located in the lung apices.
Panacinar or panlobular emphysemaWhen emphysema affects the entire acinus, it is
designated panacinar or, less commonly, panlobular emphysema.
Distal acinar or paraseptal emphysemaWhen emphysema is distal, affecting primarily
the margins of the lung lobes, it is designated distal acinar or paraseptal emphysema, which is the form of emphysema that is most closely related to primary spontaneous pneumothorax.
Although paraseptal emphysema is multiform and can affect various portions of the lung lobes, it primarily affects the lung apices. The major subtypes of paraseptal emphysema are described below.
Bulla/bullaeA bulla (i.e., a subpleural emphysematous bulla) is an
airspace measuring more than 1 cm—usually several centimeters—in diameter, sharply demarcated by a thin wall that is no greater than 1 mm in thickness.
On CT scans, a bulla appears as a rounded focal lucency or area of decreased attenuation bounded
by a thin wall, occurring predominantly in the lung apices (Figure 2).
Bullous emphysemaMultiple bullae can coalesce, characterizing bullous
emphysema. Bullous destruction of the lung parenchyma is frequently associated with other signs of pulmonary emphysema (centrilobular or paraseptal emphysema).
Irregular emphysema associated with fibrosis
Absence of “obvious fibrosis” was historically regarded as an additional criterion for pulmonary emphysema. However, the validity of that criterion has been questioned because some interstitial fibrosis can be present in emphysema secondary to cigarette smoking.
PATHOPHYSIOLOGY
Distension of an emphysematous bulla leads to an extreme thinning of its structure (Figure 3).
The absence of pleural mesothelial cells on histological examination has been demonstrated by scanning electron microscopy, occurring primarily on the thin outer surface of type I bullae and in some areas on the surface of type II bullae.(10) Therefore, distension of emphysematous bullae is due to a reduction in the surface tension of their walls, and this can be explained by Laplace’s law.(11) In addition, there is evidence of a congenital etiology; however, the pathogenesis of bullae remains controversial.(12)
ANATOMY
Bullae are found in approximately 85% of all patients with primary spontaneous pneumothorax undergoing surgery (Figure 4).(13,14) However, there is no consensus in the literature regarding the anatomical classification of emphysematous lung lesions on the basis of surgical
bulla
bleb
Figure 2. Coronal CT scan of the chest showing a bulla located in the right lung apex and accompanied by pleural adhesion.
Figure 1. Schematic illustration of the anatomy of emphysematous lung lesions, representing a bleb and a bulla.
223J Bras Pneumol. 2016;42(3):222-226
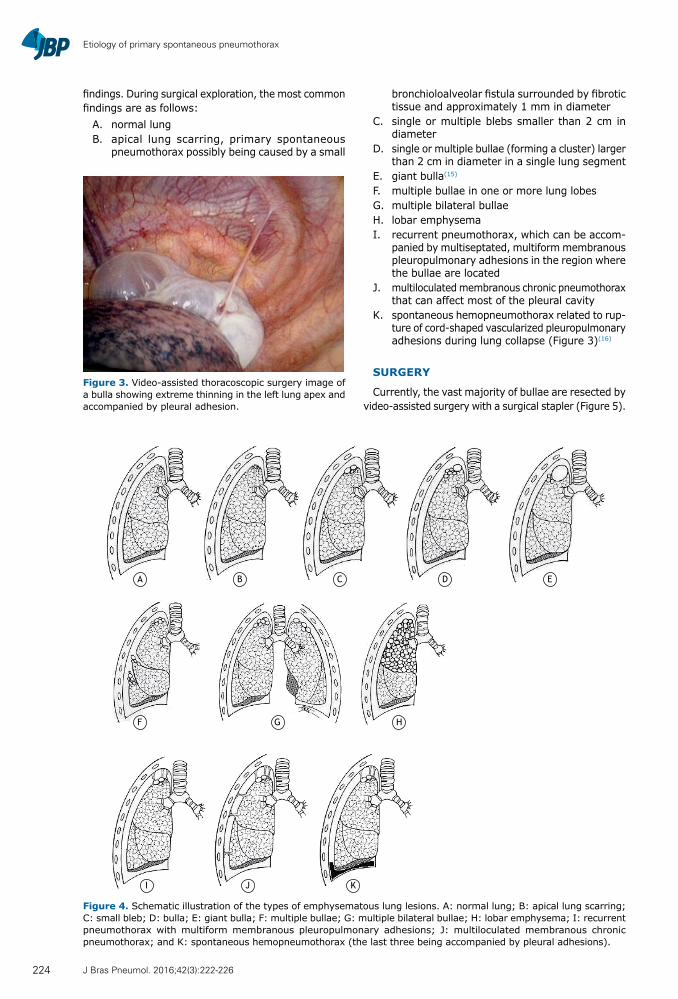
Etiology of primary spontaneous pneumothorax
findings. During surgical exploration, the most common findings are as follows:
A. normal lung B. apical lung scarring, primary spontaneous
pneumothorax possibly being caused by a small
bronchioloalveolar fistula surrounded by fibrotic tissue and approximately 1 mm in diameter
C. single or multiple blebs smaller than 2 cm in diameter
D. single or multiple bullae (forming a cluster) larger than 2 cm in diameter in a single lung segment
E. giant bulla(15) F. multiple bullae in one or more lung lobes G. multiple bilateral bullae H. lobar emphysema I. recurrent pneumothorax, which can be accom-
panied by multiseptated, multiform membranous pleuropulmonary adhesions in the region where the bullae are located
J. multiloculated membranous chronic pneumothorax that can affect most of the pleural cavity
K. spontaneous hemopneumothorax related to rup-ture of cord-shaped vascularized pleuropulmonary adhesions during lung collapse (Figure 3)(16)
SURGERY
Currently, the vast majority of bullae are resected by video-assisted surgery with a surgical stapler (Figure 5).
A
F G H
I J K
B C D E
Figure 4. Schematic illustration of the types of emphysematous lung lesions. A: normal lung; B: apical lung scarring; C: small bleb; D: bulla; E: giant bulla; F: multiple bullae; G: multiple bilateral bullae; H: lobar emphysema; I: recurrent pneumothorax with multiform membranous pleuropulmonary adhesions; J: multiloculated membranous chronic pneumothorax; and K: spontaneous hemopneumothorax (the last three being accompanied by pleural adhesions).
Figure 3. Video-assisted thoracoscopic surgery image of a bulla showing extreme thinning in the left lung apex and accompanied by pleural adhesion.
224 J Bras Pneumol. 2016;42(3):222-226
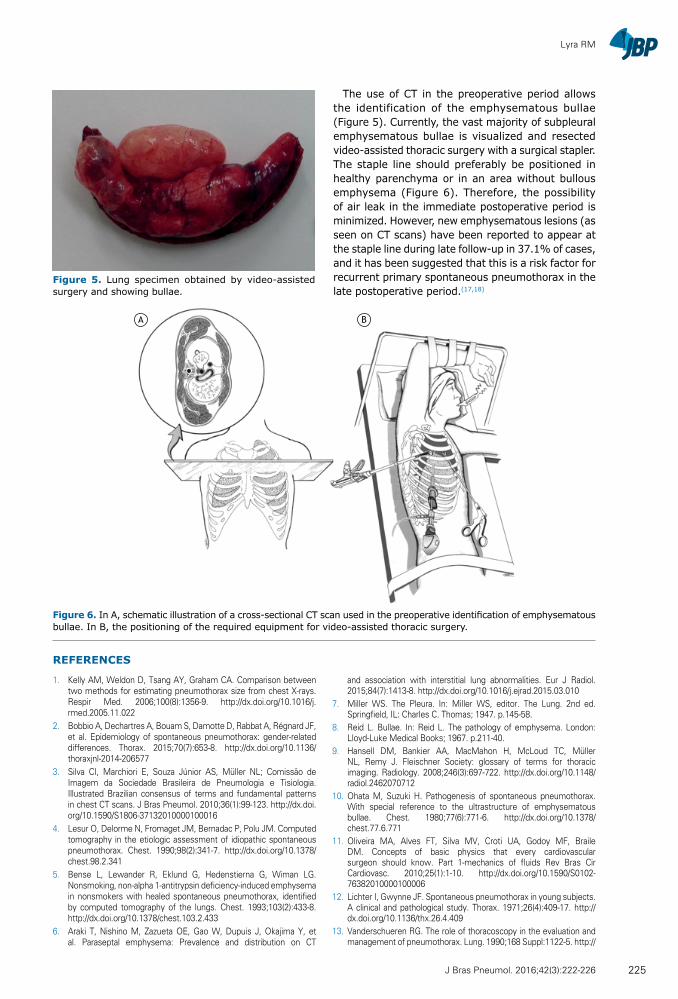
Lyra RM
The use of CT in the preoperative period allows the identification of the emphysematous bullae (Figure 5). Currently, the vast majority of subpleural emphysematous bullae is visualized and resected video-assisted thoracic surgery with a surgical stapler. The staple line should preferably be positioned in healthy parenchyma or in an area without bullous emphysema (Figure 6). Therefore, the possibility of air leak in the immediate postoperative period is minimized. However, new emphysematous lesions (as seen on CT scans) have been reported to appear at the staple line during late follow-up in 37.1% of cases, and it has been suggested that this is a risk factor for recurrent primary spontaneous pneumothorax in the late postoperative period.(17,18)
REFERENCES
1. Kelly AM, Weldon D, Tsang AY, Graham CA. Comparison between two methods for estimating pneumothorax size from chest X-rays. Respir Med. 2006;100(8):1356-9. http://dx.doi.org/10.1016/j.rmed.2005.11.022
2. Bobbio A, Dechartres A, Bouam S, Damotte D, Rabbat A, Régnard JF, et al. Epidemiology of spontaneous pneumothorax: gender-related differences. Thorax. 2015;70(7):653-8. http://dx.doi.org/10.1136/thoraxjnl-2014-206577
3. Silva CI, Marchiori E, Souza Júnior AS, Müller NL; Comissão de Imagem da Sociedade Brasileira de Pneumologia e Tisiologia. Illustrated Brazilian consensus of terms and fundamental patterns in chest CT scans. J Bras Pneumol. 2010;36(1):99-123. http://dx.doi.org/10.1590/S1806-37132010000100016
4. Lesur O, Delorme N, Fromaget JM, Bernadac P, Polu JM. Computed tomography in the etiologic assessment of idiopathic spontaneous pneumothorax. Chest. 1990;98(2):341-7. http://dx.doi.org/10.1378/chest.98.2.341
5. Bense L, Lewander R, Eklund G, Hedenstierna G, Wiman LG. Nonsmoking, non-alpha 1-antitrypsin deficiency-induced emphysema in nonsmokers with healed spontaneous pneumothorax, identified by computed tomography of the lungs. Chest. 1993;103(2):433-8. http://dx.doi.org/10.1378/chest.103.2.433
6. Araki T, Nishino M, Zazueta OE, Gao W, Dupuis J, Okajima Y, et al. Paraseptal emphysema: Prevalence and distribution on CT
and association with interstitial lung abnormalities. Eur J Radiol. 2015;84(7):1413-8. http://dx.doi.org/10.1016/j.ejrad.2015.03.010
7. Miller WS. The Pleura. In: Miller WS, editor. The Lung. 2nd ed. Springfield, IL: Charles C. Thomas; 1947. p.145-58.
8. Reid L. Bullae. In: Reid L. The pathology of emphysema. London: Lloyd-Luke Medical Books; 1967. p.211-40.
9. Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246(3):697-722. http://dx.doi.org/10.1148/radiol.2462070712
10. Ohata M, Suzuki H. Pathogenesis of spontaneous pneumothorax. With special reference to the ultrastructure of emphysematous bullae. Chest. 1980;77(6):771-6. http://dx.doi.org/10.1378/chest.77.6.771
11. Oliveira MA, Alves FT, Silva MV, Croti UA, Godoy MF, Braile DM. Concepts of basic physics that every cardiovascular surgeon should know. Part 1-mechanics of fluids Rev Bras Cir Cardiovasc. 2010;25(1):1-10. http://dx.doi.org/10.1590/S0102-76382010000100006
12. Lichter I, Gwynne JF. Spontaneous pneumothorax in young subjects. A clinical and pathological study. Thorax. 1971;26(4):409-17. http://dx.doi.org/10.1136/thx.26.4.409
13. Vanderschueren RG. The role of thoracoscopy in the evaluation and management of pneumothorax. Lung. 1990;168 Suppl:1122-5. http://
A B
Figure 6. In A, schematic illustration of a cross-sectional CT scan used in the preoperative identification of emphysematous bullae. In B, the positioning of the required equipment for video-assisted thoracic surgery.
Figure 5. Lung specimen obtained by video-assisted surgery and showing bullae.
225J Bras Pneumol. 2016;42(3):222-226

Etiology of primary spontaneous pneumothorax
dx.doi.org/10.1007/BF02718252
14. Rivas de Andrés JJ, Torres Lanzas J. Thoracoscopy and spontaneous pneumothorax. Ann Thorac Surg. 1993;55(3):811. http://dx.doi.org/10.1016/0003-4975(93)90317-B
15. Sharma N, Justaniah AM, Kanne JP, Gurney JW, Mohammed TL. Vanishing lung syndrome (giant bullous emphysema): CT findings in 7 patients and a literature review. J Thorac Imaging. 2009;24(3):227-30. http://dx.doi.org/10.1097/RTI.0b013e31819b9f2a
16. Kim ES, Kang JY, Pyo CH, Jeon EY, Lee WB. 12-year experience
of spontaneous hemopneumothorax. Ann Thorac Cardiovasc Surg. 2008;14(3):149-53.
17. Chou SH, Li HP, Lee YL, Lee JY, Chiang HH, Tsai DL, et al. Video-assisted thoracoscopic surgery for postoperative recurrent primary spontaneous pneumothorax. J Thorac Dis. 2014;6(1):52-5.
18. Tsuboshima K, Nagata M, Wakahara T, Matoba Y, Matsumoto S, Maniwa Y. Relationship between postoperative bulla neogenesis at the staple line and the resected lung volume in primary spontaneous pneumothorax. Gen Thorac Cardiovasc Surg. 2015;63(10):572-5. http://dx.doi.org/10.1007/s11748-015-0568-1
226 J Bras Pneumol. 2016;42(3):222-226
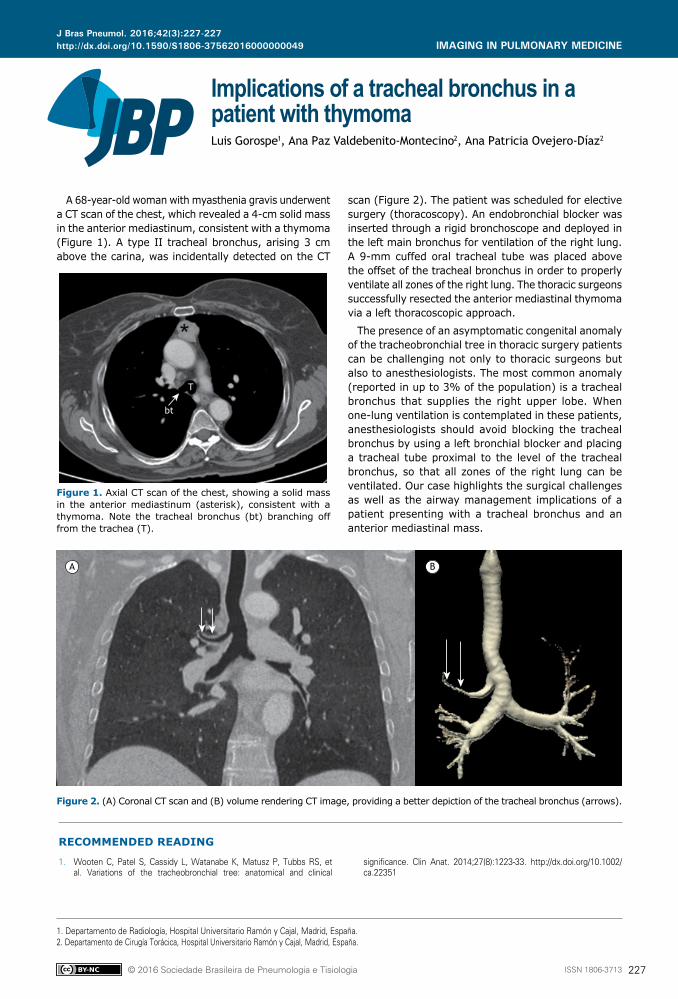
ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562016000000049
Implications of a tracheal bronchus in a patient with thymomaLuis Gorospe1, Ana Paz Valdebenito-Montecino2, Ana Patricia Ovejero-Díaz2
1. Departamento de Radiología, Hospital Universitario Ramón y Cajal, Madrid, España.2. Departamento de Cirugía Torácica, Hospital Universitario Ramón y Cajal, Madrid, España.
A 68-year-old woman with myasthenia gravis underwent a CT scan of the chest, which revealed a 4-cm solid mass in the anterior mediastinum, consistent with a thymoma (Figure 1). A type II tracheal bronchus, arising 3 cm above the carina, was incidentally detected on the CT
scan (Figure 2). The patient was scheduled for elective surgery (thoracoscopy). An endobronchial blocker was inserted through a rigid bronchoscope and deployed in the left main bronchus for ventilation of the right lung. A 9-mm cuffed oral tracheal tube was placed above the offset of the tracheal bronchus in order to properly ventilate all zones of the right lung. The thoracic surgeons successfully resected the anterior mediastinal thymoma via a left thoracoscopic approach.
The presence of an asymptomatic congenital anomaly of the tracheobronchial tree in thoracic surgery patients can be challenging not only to thoracic surgeons but also to anesthesiologists. The most common anomaly (reported in up to 3% of the population) is a tracheal bronchus that supplies the right upper lobe. When one-lung ventilation is contemplated in these patients, anesthesiologists should avoid blocking the tracheal bronchus by using a left bronchial blocker and placing a tracheal tube proximal to the level of the tracheal bronchus, so that all zones of the right lung can be ventilated. Our case highlights the surgical challenges as well as the airway management implications of a patient presenting with a tracheal bronchus and an anterior mediastinal mass.
Figure 1. Axial CT scan of the chest, showing a solid mass in the anterior mediastinum (asterisk), consistent with a thymoma. Note the tracheal bronchus (bt) branching off from the trachea (T).
Figure 2. (A) Coronal CT scan and (B) volume rendering CT image, providing a better depiction of the tracheal bronchus (arrows).
T
bt
A B
RECOMMENDED READING
1. Wooten C, Patel S, Cassidy L, Watanabe K, Matusz P, Tubbs RS, et al. Variations of the tracheobronchial tree: anatomical and clinical
significance. Clin Anat. 2014;27(8):1223-33. http://dx.doi.org/10.1002/ca.22351
J Bras Pneumol. 2016;42(3):227-227
227
IMAGING IN PULMONARY MEDICINE

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562016000000043
ABSTRACTPost-infectious bronchiolitis obliterans (PIBO) is a small airways disease characterized by fixed airflow limitation. Therefore, inhaled bronchodilators and corticosteroids are not recommended as maintenance therapy options. The management of PIBO currently consists only of close monitoring of affected patients, aimed at the prevention and early treatment of pulmonary infections. In recent years, there has been an increase in the incidence of PIBO in the pediatric population. Patients with PIBO are characterized by a progressive decline in lung function, accompanied by a decrease in overall functional capacity. Here, we report the case of a relatively young man diagnosed with PIBO and followed for three years. After short- and long-term therapy with an inhaled corticosteroid/long-acting β2 agonist combination, together with an inhaled long-acting antimuscarinic, the patient showed relevant improvement of airway obstruction that had been irreversible at the time of the bronchodilator test. The lung function of the patient worsened when he interrupted the triple inhaled therapy. In addition, a 3-week pulmonary rehabilitation program markedly improved his physical performance.
Keywords: Bronchiolitis obliterans/therapy; Infection/complications; Adrenergic beta-2 receptor antagonists/therapeutic use; Administration, inhalation; Anti-inflammatory agents/therapeutic use; Muscarinic antagonists/therapeutic use; Lung diseases/rehabilitation.
Impact of long-term treatment with inhaled corticosteroids and bronchodilators on lung function in a patient with post-infectious bronchiolitis obliteransCecilia Calabrese1, Nadia Corcione1, Gaetano Rea2, Francesco Stefanelli3, Ilernando Meoli3, Alessandro Vatrella4
Corresponding author:Cecilia Calabrese. Dipartimento di Scienze Cardio-Toraciche e Respiratorie, Seconda Università degli Studi di Napoli, Via Posillipo 276, 80123, Napoli, Italia.Tel.: 39 3473 675572. Fax: 39 0817 062365. E-mail: [email protected] support: None.
INTRODUCTION
Post-infectious bronchiolitis obliterans (PIBO) is currently recognized as an acquired disorder that is usually consequent to severe bronchiolitis occurring during infancy. (1,2) The incidence of PIBO in the pediatric population has increased over the last few years, and some cases are also incidentally diagnosed in adulthood. (3-8) PIBO is characterized by small-airway obstruction that is generally unresponsive or poorly responsive to bronchodilators.(9) We report the case of a relatively young man diagnosed with PIBO, whose airway obstruction improved after long-term treatment with inhaled bronchodilators and corticosteroids. In addition, a short-term pulmonary rehabilitation program resulted in better physical performance.
CASE REPORT
A 36-year-old man, exhibiting apparent good health, was referred to our outpatient clinic for pulmonary function testing before undergoing a surgical procedure (vocal cord polypectomy). The flow-volume curve showed moderate airflow limitation that was irreversible after inhalation of 400 µg of albuterol. In particular, the FEV1 was 2.36 L (58% of the predicted value); the FVC was 3.15 L (65% of the predicted value); the FEV1/FVC ratio was 69.6%; and the post-bronchodilator FEV1
was 2.4 L (2% increase). The patient history was then carefully collected. The patient reported no respiratory symptoms or previous lung disease, with the exception of intermittent allergic rhinitis and an episode of bronchiolitis (requiring hospitalization) during the first months of life. He categorized himself as a nonsmoker and reported no occupational exposure to toxic substances. On physical examination, crackles were heard at both lung bases. Therefore, whole-body plethysmography was performed. The plethysmography showed static lung hyperinflation characterized by an increased RV (3.05 L, 161% of the predicted value), although the TLC was normal (6.89 L, 99% of the predicted value). The DLCO was within the normal range. Arterial blood gas analysis demonstrated mild hypoxemia and a normal acid-base balance (PaO2: 72.2 mmHg; PaCO2: 40.6 mmHg; pH: 7.41; and HCO3
−: 25.6 mmol/L). The patient underwent HRCT, scans being obtained at the end of inspiration, as well as during the so-called “expiratory hold” respiratory maneuver (Figures 1A and 1B). The HRCT scans showed heterogeneous lung tissue density, characterized by areas of reduced attenuation in the absence of tissue destruction, located in the middle lobe, lingula, and lower lobes, which featured a “patchy distribution” pattern suggestive of small airways disease, accompanied by air trapping. In the areas of lowest density, a significant reduction in both the number and size of pulmonary vessels was
1. Dipartimento di Scienze Cardio-Toraciche e Respiratorie, Seconda Università degli Studi di Napoli, Italia.
2. Dipartimento di Radiologia, A. O. dei Colli, Ospedale Monaldi, Napoli, Italia.
3. Divisione di Pneumologia, A. O. dei Colli, Ospedale Monaldi, Napoli, Italia.
4. Dipartimento di Medicina e Chirurgia, Sezione di Malattie Respiratorie, Università degli Studi di Salerno, Italia.
Submitted: 11 February 2016. Accepted: 9 May 2016.
Study carried out at the A. O. dei Colli, Ospedale Monaldi di Napoli, Italia.
J Bras Pneumol. 2016;42(3):228-231
228
CASE REPORT
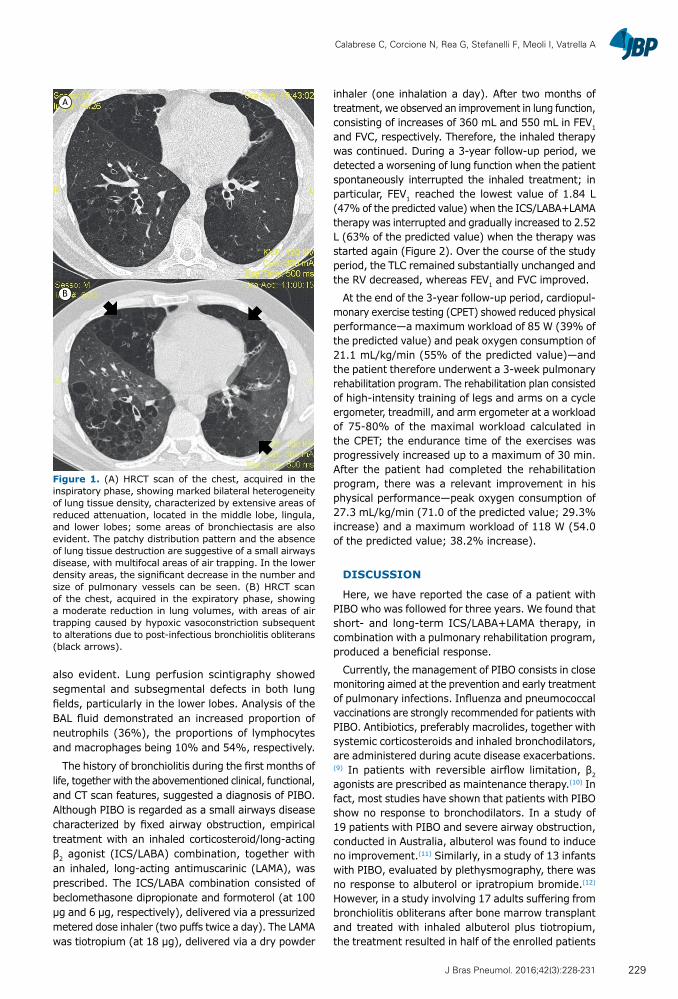
Calabrese C, Corcione N, Rea G, Stefanelli F, Meoli I, Vatrella A
also evident. Lung perfusion scintigraphy showed segmental and subsegmental defects in both lung fields, particularly in the lower lobes. Analysis of the BAL fluid demonstrated an increased proportion of neutrophils (36%), the proportions of lymphocytes and macrophages being 10% and 54%, respectively.
The history of bronchiolitis during the first months of life, together with the abovementioned clinical, functional, and CT scan features, suggested a diagnosis of PIBO. Although PIBO is regarded as a small airways disease characterized by fixed airway obstruction, empirical treatment with an inhaled corticosteroid/long-acting β2 agonist (ICS/LABA) combination, together with an inhaled, long-acting antimuscarinic (LAMA), was prescribed. The ICS/LABA combination consisted of beclomethasone dipropionate and formoterol (at 100 µg and 6 µg, respectively), delivered via a pressurized metered dose inhaler (two puffs twice a day). The LAMA was tiotropium (at 18 µg), delivered via a dry powder
inhaler (one inhalation a day). After two months of treatment, we observed an improvement in lung function, consisting of increases of 360 mL and 550 mL in FEV1
and FVC, respectively. Therefore, the inhaled therapy was continued. During a 3-year follow-up period, we detected a worsening of lung function when the patient spontaneously interrupted the inhaled treatment; in particular, FEV1 reached the lowest value of 1.84 L (47% of the predicted value) when the ICS/LABA+LAMA therapy was interrupted and gradually increased to 2.52 L (63% of the predicted value) when the therapy was started again (Figure 2). Over the course of the study period, the TLC remained substantially unchanged and the RV decreased, whereas FEV1 and FVC improved.
At the end of the 3-year follow-up period, cardiopul-monary exercise testing (CPET) showed reduced physical performance—a maximum workload of 85 W (39% of the predicted value) and peak oxygen consumption of 21.1 mL/kg/min (55% of the predicted value)—and the patient therefore underwent a 3-week pulmonary rehabilitation program. The rehabilitation plan consisted of high-intensity training of legs and arms on a cycle ergometer, treadmill, and arm ergometer at a workload of 75-80% of the maximal workload calculated in the CPET; the endurance time of the exercises was progressively increased up to a maximum of 30 min. After the patient had completed the rehabilitation program, there was a relevant improvement in his physical performance—peak oxygen consumption of 27.3 mL/kg/min (71.0 of the predicted value; 29.3% increase) and a maximum workload of 118 W (54.0 of the predicted value; 38.2% increase).
DISCUSSION
Here, we have reported the case of a patient with PIBO who was followed for three years. We found that short- and long-term ICS/LABA+LAMA therapy, in combination with a pulmonary rehabilitation program, produced a beneficial response.
Currently, the management of PIBO consists in close monitoring aimed at the prevention and early treatment of pulmonary infections. Influenza and pneumococcal vaccinations are strongly recommended for patients with PIBO. Antibiotics, preferably macrolides, together with systemic corticosteroids and inhaled bronchodilators, are administered during acute disease exacerbations.(9) In patients with reversible airflow limitation, β2 agonists are prescribed as maintenance therapy.(10) In fact, most studies have shown that patients with PIBO show no response to bronchodilators. In a study of 19 patients with PIBO and severe airway obstruction, conducted in Australia, albuterol was found to induce no improvement.(11) Similarly, in a study of 13 infants with PIBO, evaluated by plethysmography, there was no response to albuterol or ipratropium bromide.(12) However, in a study involving 17 adults suffering from bronchiolitis obliterans after bone marrow transplant and treated with inhaled albuterol plus tiotropium, the treatment resulted in half of the enrolled patients
A
B
Figure 1. (A) HRCT scan of the chest, acquired in the inspiratory phase, showing marked bilateral heterogeneity of lung tissue density, characterized by extensive areas of reduced attenuation, located in the middle lobe, lingula, and lower lobes; some areas of bronchiectasis are also evident. The patchy distribution pattern and the absence of lung tissue destruction are suggestive of a small airways disease, with multifocal areas of air trapping. In the lower density areas, the significant decrease in the number and size of pulmonary vessels can be seen. (B) HRCT scan of the chest, acquired in the expiratory phase, showing a moderate reduction in lung volumes, with areas of air trapping caused by hypoxic vasoconstriction subsequent to alterations due to post-infectious bronchiolitis obliterans (black arrows).
229J Bras Pneumol. 2016;42(3):228-231
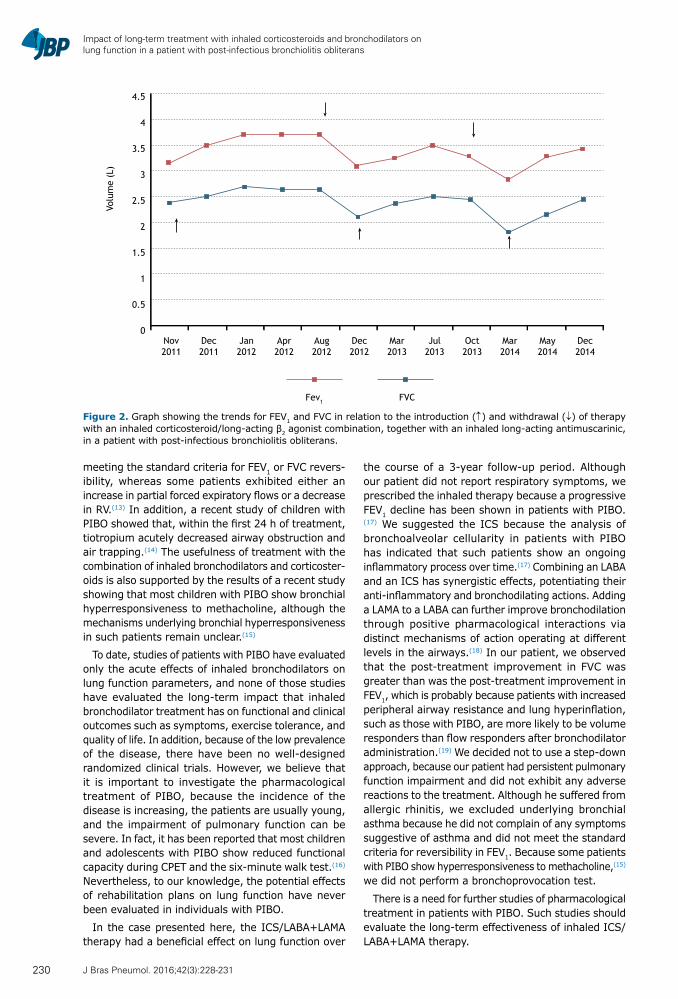
Impact of long-term treatment with inhaled corticosteroids and bronchodilators on lung function in a patient with post-infectious bronchiolitis obliterans
meeting the standard criteria for FEV1 or FVC revers-ibility, whereas some patients exhibited either an increase in partial forced expiratory flows or a decrease in RV.(13) In addition, a recent study of children with PIBO showed that, within the first 24 h of treatment, tiotropium acutely decreased airway obstruction and air trapping.(14) The usefulness of treatment with the combination of inhaled bronchodilators and corticoster-oids is also supported by the results of a recent study showing that most children with PIBO show bronchial hyperresponsiveness to methacholine, although the mechanisms underlying bronchial hyperresponsiveness in such patients remain unclear.(15)
To date, studies of patients with PIBO have evaluated only the acute effects of inhaled bronchodilators on lung function parameters, and none of those studies have evaluated the long-term impact that inhaled bronchodilator treatment has on functional and clinical outcomes such as symptoms, exercise tolerance, and quality of life. In addition, because of the low prevalence of the disease, there have been no well-designed randomized clinical trials. However, we believe that it is important to investigate the pharmacological treatment of PIBO, because the incidence of the disease is increasing, the patients are usually young, and the impairment of pulmonary function can be severe. In fact, it has been reported that most children and adolescents with PIBO show reduced functional capacity during CPET and the six-minute walk test.(16) Nevertheless, to our knowledge, the potential effects of rehabilitation plans on lung function have never been evaluated in individuals with PIBO.
In the case presented here, the ICS/LABA+LAMA therapy had a beneficial effect on lung function over
the course of a 3-year follow-up period. Although our patient did not report respiratory symptoms, we prescribed the inhaled therapy because a progressive FEV1 decline has been shown in patients with PIBO.(17) We suggested the ICS because the analysis of bronchoalveolar cellularity in patients with PIBO has indicated that such patients show an ongoing inflammatory process over time.(17) Combining an LABA and an ICS has synergistic effects, potentiating their anti-inflammatory and bronchodilating actions. Adding a LAMA to a LABA can further improve bronchodilation through positive pharmacological interactions via distinct mechanisms of action operating at different levels in the airways.(18) In our patient, we observed that the post-treatment improvement in FVC was greater than was the post-treatment improvement in FEV1, which is probably because patients with increased peripheral airway resistance and lung hyperinflation, such as those with PIBO, are more likely to be volume responders than flow responders after bronchodilator administration.(19) We decided not to use a step-down approach, because our patient had persistent pulmonary function impairment and did not exhibit any adverse reactions to the treatment. Although he suffered from allergic rhinitis, we excluded underlying bronchial asthma because he did not complain of any symptoms suggestive of asthma and did not meet the standard criteria for reversibility in FEV1. Because some patients with PIBO show hyperresponsiveness to methacholine,(15) we did not perform a bronchoprovocation test.
There is a need for further studies of pharmacological treatment in patients with PIBO. Such studies should evaluate the long-term effectiveness of inhaled ICS/LABA+LAMA therapy.
Figure 2. Graph showing the trends for FEV1 and FVC in relation to the introduction (↑) and withdrawal (↓) of therapy with an inhaled corticosteroid/long-acting β2 agonist combination, together with an inhaled long-acting antimuscarinic, in a patient with post-infectious bronchiolitis obliterans.
4.5
4
3.5
3
2.5
2
1.5
1
0.5
0
Volu
me
(L)
Nov2011
Dec2011
Jan2012
Apr2012
Aug2012
Dec2012
Mar2013
Jul2013
Oct2013
Mar2014
May2014
Dec2014
Fev1 FVC
230 J Bras Pneumol. 2016;42(3):228-231

Calabrese C, Corcione N, Rea G, Stefanelli F, Meoli I, Vatrella A
REFERENCES1. Swyer PR, James GC. A case of unilateral pulmonary emphysema.
Thorax 1953;8(2):133-6. http://dx.doi.org/10.1136/thx.8.2.1332. Moore AD, Godwin JD, Dietrich PA, Verschakelen JA, Henderson
WR Jr. Swyer-James syndrome: CT findings in eight patients. AJR Am J Roentgenol 1992;158(6):1211-5. http://dx.doi.org/10.2214/ajr.158.6.1590109
3. Boyacı N, Karakaş Ö, Yalçin F, Yildiz S, Çeçe H. A case of Swyer-James-MacLeod syndrome diagnosed in adulthood. Tuberk Toraks. 2013;61(4):355-6. http://dx.doi.org/10.5578/tt.6131
4. Capela C, Gouveia P, Sousa M, Regadas MJ. Adult diagnosis of Swyer-James-MacLeod syndrome: a case report. J Med Case Rep. 2011;5:2. http://dx.doi.org/10.1186/1752-1947-5-2
5. Desai NR, Palomino J, Hayek H, Shames J, Simeone F. A 63-year-old man with recurrent pulmonary infections: a case of Swyer-James Macleod syndrome. J La State Med Soc. 2010;162(6):346-9.
6. Garg R, Aga P, Saheer S, Jabeed P, Singh A, Hassan G, et al. Swyer-James-MacLeod syndrome with ipsilateral herniation of hyperinflated hyperlucent lung. BMJ Case Rep. 2011;2011. pii: bcr0520114191. http://dx.doi.org/10.1136/bcr.05.2011.4191
7. Metin B, Özkan E, Sariçam M, Ariba OK. Swyer-James-MacLeod syndrome with renal ectopy misdiagnosed as pneumothorax and chest tube drained: Case study. J Thorac Cardiovasc Surg. 2013;145(5):e44-7. http://dx.doi.org/10.1016/j.jtcvs.2013.01.035
8. Sen HS, Taylan M, Abakay O, Sezgi C, Cetincakmak MG. Adult diagnosis of Swyer-James-Macleod syndrome: retrospective analysis of four cases. Respir Care. 2014;59(4):e51-4. http://dx.doi.org/10.4187/respcare.02552
9. Lino CA, Batista AK, Soares MA, de Freitas AE, Gomes LC, M Filho JH, et al. Bronchiolitis obliterans: clinical and radiological profile of children followed-up in a reference outpatient clinic. Rev Paul Pediatr. 2013;31(1):10-6. http://dx.doi.org/10.1590/S0103-05822013000100003
10. Champs NS, Lasmar LM, Camargos PA, Marguet C, Fischer GB, Mocelin HT. Post-infectious bronchiolitis obliterans in children. J Pediatr (Rio J). 2011;87(3):187-98. http://dx.doi.org/10.2223/jped.2083
11. Chang AB, Masel JP, Masters B. Post-infectious bronchiolitis
obliterans: clinical, radiological and pulmonary function sequelae. Pediatr Radiol. 1998;28(1):23-9. http://dx.doi.org/10.1007/s002470050286
12. Teper AM, Kofman CD, Maffey AF, Vidaurreta SM. Lung function in infants with chronic pulmonary disease after severe adenoviral illness. J Pediatr. 1999;134(6):730-3. http://dx.doi.org/10.1016/S0022-3476(99)70289-1
13. Barisione G, Bacigalupo A, Crimi E, Brusasco V. Acute bronchodilator responsiveness in bronchiolitis obliterans syndrome following hematopoietic stem cell transplantation. Chest. 2011;139(3):633-9. http://dx.doi.org/10.1378/chest.10-1442
14. Teixeira MF, Rodrigues JC, Leone C, Adde FV. Acute bronchodilator responsiveness to tiotropium in postinfectious bronchiolitis obliterans in children. Chest. 2013;144(3):974-80. http://dx.doi.org/10.1378/chest.12-2280
15. Yoo Y, Yu J, Kim DK, Choi SH, Kim CK, Koh YY. Methacholine and adenosine 5’-monophosphate challenges in children with post-infectious bronchiolitis obliterans. Eur Respir J. 2006;27(1):36-41. http://dx.doi.org/10.1183/09031936.06.00019605
16. Mattiello R, Sarria EE, Stein R, Fischer GB, Mocelin HT, Barreto SS, et al. Functional capacity assessment in children and adolescents with post-infectious bronchiolitis obliterans. J Pediatr (Rio J). 2008;84(4):337-43. http://dx.doi.org/10.2223/jped.1807
17. Cazzato S, Poletti V, Bernardi F, Loroni L, Bertelli L, Colonna S, et al. Airway inflammation and lung function decline in childhood post-infectious bronchiolitis obliterans. Pediatr Pulmonol. 2008;43(4):381-90. http://dx.doi.org/10.1002/ppul.20784
18. Pelaia G, Vatrella A, Busceti MT, Gallelli L, Calabrese C, Terracciano R, et al. Pharmacologic rationale underlying the therapeutic effects of tiotropium/olodaterol in COPD. Ther Clin Risk Manag. 2015;11:1563-72. http://dx.doi.org/10.2147/TCRM.S84151
19. Pisi R, Aiello M, Zanini A, Tzani P, Paleari D, Marangio E, et al. Small airway dysfunction and flow and volume bronchodilator responsiveness in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10:1191-7. http://dx.doi.org/10.1183/13993003.congress-2015.pa3357
231J Bras Pneumol. 2016;42(3):228-231

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562016000000119
Reversed halo sign in invasive fungal infectionsEdson Marchiori1, Bruno Hochhegger1, Gláucia Zanetti1
1. Departamento de Radiologia, Universidade Federal do Rio de Janeiro, Rio de Janeiro (RJ) Brasil.
TO THE EDITOR:
Recent studies conducted in Brazil(1-3) have stressed the importance of the reversed halo sign (RHS) in the diagnosis of lung diseases in immunocompetent patients. However, the RHS in immunocompromised patients has not received the same emphasis. Here, we report the case of a 51-year-old female patient who presented with a 10-day history of generalized ecchymosis and weakness. A complete blood count revealed a hemoglobin concentration of 9.0 g/dL, a white blood cell count of 60 × 109/L, a neutrophil count of 1 × 109/L (peripheral blasts, 20%), and a platelet count of 80 × 109/L. A diagnosis of acute leukemia was suspected. A bone marrow biopsy was performed and confirmed a diagnosis of acute myeloid leukemia. Treatment was started with cytarabine and daunorubicin. The patient experienced dry cough and right-sided pleuritic pain during the treatment period. A CT scan of the chest showed a right upper lobe mass with the characteristics of an RHS (Figure 1). Bronchoscopy revealed no abnormalities. Aspergillus fumigatus was isolated by cultures from an open lung biopsy sample. The patient was started on oral voriconazole and responded well to treatment, with symptom improvement and resolution of the pulmonary lesion.
The RHS is a chest CT finding defined as a focal, rounded area of ground-glass opacity surrounded by a nearly complete ring of consolidation. The RHS has been reported in a wide spectrum of diseases, including noninfectious diseases and infectious diseases such as invasive fungal infections (IFIs).(4,5) Because of this broad differential diagnosis, the RHS is considered a nonspecific sign. However, certain morphological characteristics of the RHS can aid in establishing a diagnosis. In immunocompromised patients, a reticular pattern within the halo and a thick rim of consolidation are highly suggestive of IFI.(4,5)
With regard to the reticular RHS, information regarding the immunological status of the patient is fundamental for the differential diagnosis. In immunocompetent patients, the reticular RHS corresponds, as a rule, to pulmonary infarction, usually secondary to thromboembolic disease. Suspicion of infarction from thromboembolic disease requires immediate confirmation by D-dimer testing and CT angiography. In severely immunocompromised patients (e.g., stem cell transplant recipients and patients with hematological malignancy), the reticular RHS is taken to indicate the presence of IFI (in particular, pulmonary zygomycosis or angioinvasive pulmonary aspergillosis), which is treated as such without culture or histological confirmation. Although the final diagnosis should be based on the clinical manifestations, a lung biopsy is required in some cases.(4,5)
IFIs are associated with high morbidity and mortality. Therefore, patients with IFI should be treated immediately, given that early administration of high-dose antifungal therapy has been associated with improved outcomes. (4,5) Diagnosis can be challenging, especially for general radiologists encountering patients outside the context of transplantation centers, and any delay in treatment can significantly increase mortality. In conclusion, a reticular pattern within the RHS and a thick rim of consolidation in an immunocompromised patient are highly suggestive of IFI.
Figure 1. Axial CT image (mediastinal window setting) showing two right upper lobe masses, one of which has the characteristics of the reversed halo sign. The posterior lesion has irregular thickened walls, and a reticular pattern is visible within the reversed halo.
REFERENCES
1. Souza Jr AS, Souza AS, Soares-Souza L, Zanetti G, Marchiori E. Reversed halo sign in acute schistosomiasis. J Bras Pneumol. 2015;41(3):286-8. http://dx.doi.org/10.1590/S1806-37132015000004444
2. Marchiori E, Zanetti G, Hochhegger B. Reversed halo sign. J Bras Pneumol. 2015;41(6):564. http://dx.doi.org/10.1590/S1806-37562015000000235
3. Queiroz RM, Gomes MP, Valentin MV. Pulmonary paracoccidioidomycosis showing reversed halo sign with nodular/coarse contour. Radiol Bras. 2016;49(1):59-60. http://dx.doi.org/10.1590/0100-
3984.2015.00714. Marchiori E, Marom EM, Zanetti G, Hochhegger B, Irion KL, Godoy
MC. Reversed halo sign in invasive fungal infections: criteria for differentiation from organizing pneumonia. Chest. 2012;142(6):1469-73. http://dx.doi.org/10.1378/chest.12-0114
5. Godoy MC, Viswanathan C, Marchiori E, Truong MT, Benveniste MF, Rossi S, et al. The reversed halo sign: update and differential diagnosis. Brit J Radiol. 2012;85(1017):1226-35. http://dx.doi.org/10.1259/bjr/54532316
J Bras Pneumol. 2016;42(3):232-232
232
LETTER TO THE EDITOR
ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562016000000025
An old risk factor for COPD: rest in peace, 15%Paulo César Rodrigues Pinto Corrêa1,2
1. Departamento de Clinica Médica, Universidade Federal de Ouro Preto – UFOP – Ouro Preto (MG) Brasil.2. Centro Universitário de Belo Horizonte – UNI-BH – Belo Horizonte (MG) Brasil.
TO THE EDITOR:
A frequent subject of consideration in textbooks and articles in Pulmonology is the information that only 10-15% of patients who smoke are likely to develop COPD.(1,2) This information is also mentioned in the first and second COPD consensus guidelines established by the Sociedade Brasileira de Pneumologia e Tisiologia (SBPT, Brazilian Thoracic Association), with the rates being 15% and 12%, respectively.(3,4) Although there was a review of the epidemiology of COPD in the SBPT consensus document released in 2006,(5) the main epidemiological focus of that review was the important study known as PLATINO—Projeto Latino-Americano de Investigação em Obstrução Pulmonar (Latin American Project for the Investigation of Obstructive Lung Disease); however, it failed to challenge the aforementioned concept.(5) The text itself provided grounds for such a challenge, when it pointed out that the PLATINO study—despite its cross-sectional nature—found that the prevalence of COPD in the > 60-year age group was 25.7%.(5)
The figure of 15% gained prominence in the medical literature in 1977, when Fletcher & Peto published an article in the British Medical Journal,(6) summarizing a book released in the previous year.(7) At least two different points in the publication, the authors state that susceptibility is probably not an all-or-nothing attribute; in fact, there is probably a susceptibility spectrum.(7)
Because of the limited length of this communication, it is impossible to provide an in-depth, detailed analysis of the methodological issues of the aforementioned book. In brief, the study conclusions were drawn on the basis of short-term (8-year) follow-up (1961-1969) of 792 patients, of whom at least 17 had a clinical diagnosis of asthma (without continuous treatment).(7) Surveys were conducted in the summer of 1961, followed by others every six months until the summer of 1969 (except in the winters of 1966 and 1967). The age groups formed in the first survey in 1961 included individuals aged 30-34 years, 35-39 years, and so on, and the oldest age group consisted of individuals aged 55-59 years. At each survey, FEV1 was measured three times, and this variable was measured in 16 surveys.(7) The mean FEV1 (in liters) of the sample in the initial survey in 1961 was 3.22 ± 0.72 L, and 4.3% of the individuals had an FEV1 < 2.0 L.(7) FVC was measured twice in seven surveys, after FEV1 was measured.(7)
In their book, Fletcher & Peto showed the decline in FEV1 by smoking status (103 nonsmokers, 122 former smokers who had quit smoking before 1962, 387 smokers of up to 15 cigarettes per day, and 180 smokers who
smoked more than 15 cigarettes per day on average) in men with and without airflow obstruction by spirometry.(7) The men considered as having airflow obstruction were those with an FEV1 < 2.5 L (individuals with a height of 1.71 m), which corresponds to an FEV1 between 50% and 80% of predicted, which is classified by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria as GOLD II (moderate COPD)!. A total of 13% of the 792 patients showed airflow obstruction: therefore, the famous figure of 15% is a rounding up from 13%!(7,8) Those 13% represent the smokers who were susceptible enough to become very ill because of reduced pulmonary function.
Therefore, there are at least four methodological issues in the study by Fletcher & Peto: 1) eligibility criteria, which allowed the inclusion of asthma patients; 2) spirometry criteria for obstruction: as per the current criteria, a greater number of smokers would have been classified as having COPD and would therefore be called susceptible; 3) the study follow-up period of only 8 years: the classic FEV1 decline curve is an extrapolation based on a short period of observation, a fact that was acknowledged by the authors themselves; and 4) a bias was introduced in 1968 by the authors, who felt obliged to advise smokers with obstruction and with the steepest slope of the FEV1 curve to quit smoking.(7)
Several cohorts with long-term follow-up(9-11) have estimated the risk of smokers developing COPD by using the simplest and most widely used measure in epidemiology: the incidence rate. The number of smokers who continue to smoke and develop airway obstruction has been increasing in various cohorts because a fraction of the patients followed fail to die from competing risks (e.g., cardiovascular risk) at earlier ages.
The Copenhagen City Heart Study (CCHS) is a pro-spective, population-based study with a random sample of 19,329 white men and women aged 20-93 years and randomly drawn from the Copenhagen Population Registry, Denmark, on January 1, 1976.(9) As part of the CCHS, 8,045 men and women aged 30-60 years and having normal pulmonary function at baseline were followed for 25 years.(10) Spirometry tests were performed in 1981-1983, 1991-1994, and 2001-2003. Four pulmonary function tests were obtained in 2,022 people; the smoking status of those individuals was determined at the fourth test: 581 were never-smokers; 371 were former smokers, and 1,070 were smokers. Among the smokers, there were 614 continuing smokers.(10) The 25-year cumulative incidence of COPD was 35.5% in the continuing smokers, and COPD was classified as
J Bras Pneumol. 2016;42(3):233-234
233
LETTER TO THE EDITOR

An old risk factor for COPD: rest in peace, 15%
clinically significant in 24.3% of those individuals.(10) In contrast, the 25-year cumulative incidence of COPD was only 7.8% in the never-smokers.(10)
The Obstructive Lung Disease in Northern Sweden Studies (Olin) have been collecting cross-sectional and longitudinal data on respiratory diseases, including pulmonary function, in various groups drawn from the general population, at different time points since 1985. The first Olin cohort was recruited in December of 1985, consisting of 6,610 individuals born in 1919-1920, 1934-1935, and 1949-1950.(11) In 1996, the third survey of that cohort was carried out, and responses were obtained from 5,189 individuals. The objective was to measure the prevalence of COPD, as defined by the GOLD criteria, in the cohort. A random sample of 1,500 individuals were invited to undergo a structured interview and pulmonary function tests in 1996 and 1997, and 1,237 completed spirometry with a satisfactory technique.(11) In 1996-1997, the prevalence of smoking was 23.6% in men and 25.6%
in women. Those born in 1919-1920, 1934-1935, and 1949-1950 were 46-47 years old, 61-62 years old, and 76-77 years old, respectively, at the time. The study data show that, in the 76- to 77-year age group, continuing to smoke made 50% of the individuals develop COPD, as defined by the GOLD criteria.(11) Age and smoking have a multiplicative effect, and the odds ratio for COPD in the individuals who were in the 76- to 77-year age group and smoked was 33.66 (95% CI: 10.53-107.58).(11)
In conclusion, a more careful analysis of the classic book by Fletcher & Peto(7) and the long-term follow-up of several cohorts allow us to reject the still widely quoted idea that “only 15% of smokers are susceptible to COPD”. We have the responsibility of correctly informing the new generation of pulmonologists and of making it widely known to our patients and the general population that up to 50% of smokers will develop COPD if they smoke long enough and do not die earlier from competing risks. Rest in peace, 15%!
REFERENCES
1. Ouellette DR. The answer is fifteen percent: what Is the question? Chest. 2004;125(1);3-5. http://dx.doi.org/10.1378/chest.125.1.3
2. Ito I, Nagai S, Hoshino Y, Muro S, Hirai T, Tsukino M, et al. Risk and severity of COPD is associated with the group-specific component of serum globulin 1F allele. Chest. 2004;125(1):63-70. http://dx.doi.org/10.1378/chest.125.1.63
3. Sociedade Brasileira de Pneumologia e Tisiologia. I Consenso Brasileiro de Doença Pulmonar Obstrutiva Crônica (DPOC). J Pneumol. 2000;26(Suppl 1):S1-S52.
4. Sociedade Brasileira de Pneumologia e Tisiologia. II Consenso Brasileiro sobre Doença Pulmonar Obstrutiva Crônica – DPOC. J Bras Pneumol. 2004;30(Suppl 5):S1-S42.
5. Sociedade Brasileira de Pneumologia e Tisiologia [homepage on the Internet]. Brasília: Sociedade Brasileira de Pneumologia e Tisiologia; c2008 [updated 2008 Jun 20; cited 2016 Apr 1]. Consenso brasileiro sobre doença pulmonar obstrutiva crônica – DPOC - Sociedade Brasileira de Pneumologia e Tisiologia – SBPT - revisão de alguns aspectos de epidemiologia e tratamento da doença estável - 2006. [Adobe Acrobat document, 24p.] Available from: http://www.sbpt.org.br/downloads/arquivos/Consenso_DPOC_SBPT_2006.pdf
6. Fletcher C, Peto R. The natural history of chronic airflow obstruction. Br Med J. 1977;1(6077):1645-8. http://dx.doi.org/10.1136/bmj.1.6077.1645
7. Fletcher C, Peto R, Tinker C, Speizer F. The natural history of chronic bronchitis and emphysema. New York: Oxford University Press; 1976.
8. Rennard SI, Vestbo J. Natural histories of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(9):878-83. http://dx.doi.org/10.1513/pats.200804-035QC
9. Schnohr P, Jensen G, Lange P, Scharling H, Appleyard M. The Copenhagen City Heart Study. Tables with data from the third examination 1991-1994. Eur Heart J. 2001;3(suppl H):H1-H83.
10. Løkke A, Lange P, Scharling H, Fabricius P, Vestbo J. Developing COPD: a 25 year follow up study of the general population. Thorax. 2006;61(11):935-9. http://dx.doi.org/10.1136/thx.2006.062802
11. Lundbäck B, Lindberg A, Lindström M, Rönmark E, Jonsson AC, Jönsson E, et al. Not 15 but 50% of smokers develop COPD?--Report from the Obstructive Lung Disease in Northern Sweden Studies. Respir Med. 2003;97(2):115-22. http://dx.doi.org/10.1053/rmed.2003.1446
234 J Bras Pneumol. 2016;42(3):233-234

ISSN 1806-3713© 2016 Sociedade Brasileira de Pneumologia e Tisiologia
http://dx.doi.org/10.1590/S1806-37562016000000070
Inhalation therapy in mechanical ventilationÂngelo Roncalli Miranda Rocha1,2,3, Caio Henrique Veloso da Costa1
1. UTI Geral, Hospital Geral do Estado Professor Osvaldo Brandão Vilela, Maceió (AL) Brasil. 2. UTI, Hospital Escola Dr. Hélvio Auto, Universidade Estadual de Ciências da Saúde de Alagoas, Maceió (AL) Brasil. 3. Centro de Estudos Superiores de Maceió, Maceió (AL) Brasil.
Devices that produce aerosol particles of < 2 µm in mass median aerodynamic diameter are more efficient during mechanical ventilation than are those that produce larger particles. Other factors influencing aerosol drug delivery to mechanically ventilated patients include the aerosol-generating device, the condition of the ventilator circuit, the artificial airway, and the ventilator settings. Next-generation nebulizers known as vibrating membrane nebulizers or vibrating mesh nebulizers have recently been developed, their aerosol delivery efficiency having been estimated to be twice to three times as high as that of jet nebulizers.
Ari et al.(1) conducted an experimental study comparing jet nebulizers and vibrating membrane nebulizers in terms of their efficacy in simulated pediatric and adult lung models during mechanical ventilation. The authors found that drug (albuterol sulfate) delivery was 2- to
4-fold greater with a vibrating mesh nebulizer than with a jet nebulizer (p = 0.001). It is of note that active humidification was used in that study.
Given the wide range of variables that can influence inhaled drug delivery to patients on mechanical ventilation, we read with great interest the review article by Maccari et al.(2) However, we found it surprising that the authors did not include vibrating membrane nebulizers among the nebulizers for use in mechanically ventilated patients. In addition, Figure 1 in the aforementioned study(2) shows a heat and moisture exchanger. The authors reported that the use of humidifying devices reduces aerosol deposition and the number of deposited particles by as much as 40%. An update of the American Association for Respiratory Care guidelines recommends that filtered heat and moisture exchangers be removed during nebulization. (3) This can be confusing and misleading to the reader.
REFERENCES
1. Ari A, Atalay OT, Harwood R, Sheard MM, Aljamhan EA, Fink JB. Influence of nebulizer type, position, and bias flow on aerosol drug delivery in simulated pediatric and adult lung models during mechanical ventilation. Respir Care. 2010;55(7):845-51.
2. Maccari JG, Teixeira C, Gazzana MB, Savi A, Dexheimer-Neto FL, Knorst MM. Inhalation therapy in mechanical ventilation. J Bras
Pneumol. 2015;41(5):467-72. http://dx.doi.org/10.1590/S1806-37132015000000035
3. American Association for Respiratory Care, Restrepo RD, Walsh BK. Humidification during invasive and noninvasive mechanical ventilation: 2012. Respir Care. 2012;57(5):782-8. http://dx.doi.org/10.4187/respcare.01766
J Bras Pneumol. 2016;42(3):235-236
235
CORRESPONDENCE

Inhalation therapy in mechanical ventilation
AUTHORS’ REPLY
Juçara Gasparetto Maccari1,2, Cassiano Teixeira1,2,3
We thank you for your interest in and criticisms of our review article.
Indeed, recent improvements in nebulizer treatment have led to the development of vibrating membrane nebulizers (also known as vibrating mesh nebulizers), which generate aerosol particles that are more suitable for lung deposition, as demonstrated in in vitro studies. Therefore, vibrating membrane nebulizers are more efficient than jet nebulizers and can deliver higher doses of aerosolized drugs to the distal airways. (1) However, given that there have been few clinical studies evaluating the use of this new technology in patients on mechanical ventilation, questions remain regarding the use of vibrating membrane nebulizers in clinical practice, including questions regarding the
optimal dose of medication for use with vibrating membrane nebulizers. Other factors limiting the use of vibrating membrane nebulizers include their high cost and the difficulty in cleaning them.(2) In addition, vibrating membrane nebulizers are not widely used in Brazil. Given that the primary objective of our review article was to aid in daily clinical practice, we addressed issues related to inhalers that are available in most ICUs in Brazil.
Humidification is indeed associated with increased particle impaction in the ventilator circuit and can reduce aerosol deposition in the distal airways by as much as 40%.(2) However, the recommendation to remove the heat and moisture exchanger (shown in Figure 1 in our study) during nebulization is controversial, given that heating and humidification are aimed at preventing hypothermia, endotracheal tube obstruction, atelectasis, bronchospasm, and respiratory infection.(2)
1. CTI-Adulto, Hospital Moinhos de Vento, Porto Alegre (RS) Brasil. 2. CTI-Central, Complexo Hospitalar da Santa Casa de Porto Alegre, Porto Alegre (RS) Brasil. 3. Universidade Federal de Ciências da Saúde de Porto Alegre – UFSCPA – Porto Alegre (RS) Brasil.
REFERENCES
1. Ari A. Jet, ultrasonic, and mesh nebulizers: an evaluation of nebulizers for better clinical outcomes. Eurasian J Pulmonol. 2014;16:1-7. http://dx.doi.org/10.5152/ejp.2014.00087
2. Dhand R, Guntur VP. How best to deliver aerosol medications to mechanically ventilated patients. Clin Chest Med. 2008;29(2):277-96. http://dx.doi.org/10.1016/j.ccm.2008.02.003
236 J Bras Pneumol. 2016;42(3):235-236

The Jornal Brasileiro de Pneumologia (J Bras Pneumol, Brazilian Journal of Pulmonology) ISSN-1806-3713, published once every two months, is the official organ of the Sociedade Brasileira de Pneumologia e Tisiologia (Brazilian Thoracic Society) for the publi-cation of scientific papers regarding Pulmonology and related areas.
After being approved by the Editorial Board, all articles will be evaluated by qualified reviewers, and anonymity will be preserved throughout the review process.
Articles that fail to present merit, have significant errors in methodology or are not in accordance with the editorial policy of the journal will be directly rejected by the Editorial Board, with no recourse. Articles may be written in Portuguese, Spanish or English. In the online version of the Journal (www.jornaldepneumologia.com.br, ISSN-1806-3756), all articles will be made available in Spanish or Portuguese, as well as in English. Authors may submit color figures. However, the cost of printing figures in color, as well as any related costs, will be borne by the authors.
For further clarification, please contact the Journal Secretary by e-mail or by telephone.
The Jornal Brasileiro de Pneumologia upholds the World Health Organization (WHO) and International Committee of Medical Journal Editors (ICMJE) policies regarding the registration of clinical trials, recognizing the importance of these initiatives for the registra-tion and international, open-access dissemination of information on clinical trials. Therefore, as of 2007, the Journal only accepts clinical trials that have been given an identification number by one of the clinical trials registries meeting the criteria established by the WHO and the ICMJE. This identification number must be included at the end of the abstract.
Within this context, the Jornal Brasileiro de Pneumologia adheres to the definition of a clinical trial as described by the WHO, which can be summa-rized as “any study that prospectively assigns human beings to be submitted to one or more interventions with the objective of evaluation the effects that those interventions have on health-related outcomes. Such interventions include the administration of drugs, cells and other biological products, as well as surgical proce-dures, radiological techniques, the use of devices, behavioral therapy, changes in treatment processes, preventive care, etc
Authorship criteria
An individual may be considered an author of an article submitted for publication only if having made a significant intellectual contribution to its execution. It is implicit that the author has participated in at least one of the following phases: 1) conception and planning of the study, as well as the interpretation of the findings; 2) writing or revision of all preliminary drafts, or both, as well as the final revision; and 3) approval of the final version.
Simple data collection or cataloging does not consti-tute authorship. Likewise, authorship should not be conferred upon technicians performing routine tasks, referring physicians, doctors who interpret routine exams or department heads who are not directly involved in the research. The contributions made by such individ-uals may be recognized in the acknowledgements.
The accuracy of all concepts presented in the manu-script is the exclusive responsibility of the authors. The number of authors should be limited to eight, although exceptions will be made for manuscripts that are consid-ered exceptionally complex. For manuscripts with more than six authors, a letter should be sent to the Journal describing the participation of each.
Presentation and submission of manuscripts
All manuscripts must be submitted online from the home-page of the journal. The instructions for submis-sion are available at: www.jornaldepneumologia.com.br/sgp. Although all manuscripts are submitted online, they must be accompanied by a Copyright Transfer Statement and Conflict of Interest Statement signed by all the authors based on the models available at: www.jornaldepneumologia.com.br.
It is requested that the authors strictly follow the editorial guidelines of the journal, particularly those regarding the maximum number of words, tables and figures permitted, as well as the rules for producing the bibliography. Failure to comply with the author instruc-tions will result in the manuscript being returned to the authors so that the pertinent corrections can be made before it is submitted to the reviewers.
Special instructions apply to the preparation of Special Supplements and Guidelines, and authors should consult the instructions in advance by visiting the homepage of the journal.
The journal reserves the right to make stylistic, grammatical and other alterations to the manuscript.
With the exception of units of measure, abbrevia-tions should be used sparingly and should be limited only to those that are widely accepted. These terms are defined in the List of Abbreviations and Acronyms accepted without definition in the Journal. Click here (List of Abbreviations and Acronyms). All other abbrevi-ations should be defined at their first use. For example, use “C-reactive protein (CRP)”, and use “CRP” there-after. After the definition of an abbreviation, the full term should not appear again. Other than those accepted without definition, abbreviations should not be used in titles, and their use in the abstracts of manuscripts should be avoided if possible.
Whenever the authors mention any substance or uncommon piece of equipment they must include the catalogue model/number, name of manufacturer, city and country of origin. For example:
“. . . ergometric treadmill (model ESD-01; FUNBEC, São Paulo, Brazil) . . .”
In the case of products from the USA or Canada, the name of the state or province should also be cited. For example:
“. . . guinea pig liver tTg (T5398; Sigma, St. Louis, MO, USA) . . .”
Manuscript preparation
Title Page: The title page should include the title (in Portuguese and in English); the full names, highest academic degrees and institutional affiliations of all authors; complete address, including telephone number, fax number and e-mail address, of the principal author; and a declaration of any and all sources of funding.
Abstract: The abstract should present the informa-tion in such a way that the reader can easily understand without referring to the main text. Abstracts should not exceed 250 words. Abstracts should be structured as follows: Objective, Methods, Results and Conclusion. Abstracts for review articles and case reports may be unstructured.
Abstracts for brief communications should not exceed 100 words.
Summary: An abstract in English, corresponding in content to the abstract in Portuguese, should be included.
Keywords: Three to six keywords in Portuguese defining the subject of the study should be included as well as the corresponding keywords in English. Keywords in Portuguese must be based on the Descritores em Ciência da Saúde (DeCS, Health and Science Keywords), published by Bireme and available at: http://decs.bvs.br, whereas keywords in English should be based on the
INSTRUCTIONS FOR AUTHORS
National Library of Medicine Medical Subject Headings (MeSH), available at: http://www.nlm.nih.gov/mesh/MBrowser.html.Text:
Original articles: For original articles, the text (excluding the title page, abstracts, refer-ences, tables, figures and figure legends) should consist of 2000 to 3000 words. Tables and figures should be limited to a total of five. The number of references should not exceed 30. Original articles should be divided into the following sections: Introduction, Methods, Results, Discussion, Acknowledgments, and References. The Methods section should include a statement attesting to the fact the study has been approved by the ethics in human research committee or the ethics in animal research committee of the governing institution. There should also be a section describing the statistical analysis employed, with the respective references. In the Methods and Results sections, subheadings may be used, provided that they are limited to a reason-able number. Subheadings may not be used in the Introduction or Discussion.
Review and Update articles: Review and Update articles are written at the request of the Editorial Board, which may occasionally accept unso-licited manuscripts that are deemed to be of great interest. The text should not exceed 5000 words, excluding references and illustrations (figures or tables). The total number of illustrations should not exceed eight. The number of references should not exceed 60.
Pictorial essays: Pictorial essays are also submitted only at the request of the Editors or after the authors have consulted and been granted permis-sion by the Editorial Board. The text accompanying such essays should not exceed 3000 words, excluding the references and tables. No more than 12 illus-trations (figures and tables) may be used, and the number of references may not exceed 30.
Case Reports: Case Reports should not exceed 1500 words, excluding title page, abstract, refer-ences and illustrations. The text should be composed of: Introduction, Case Report, Discussion and References. It is recommended that any and all infor-mation that might identify the patient be withheld, and that only those laboratory exams that are impor-tant for the diagnosis and discussion be presented. The total number of illustrations (figures or tables) should not exceed three, and the number of refer-ences should be limited to 20. When the number of cases presented exceeds three, the manuscript will be classified as a Case Series, and the same rules applicable to an original article will be applied.
Brief Communications: Brief communications should not exceed 1500 words, excluding references and tables. The total number of tables and figures should not exceed two, and the references should be limited to 20. The text should be unstructured.
Letters to the Editor: Letters to the Editor should be succinct original contributions, not exceeding 800 words and containing a maximum of 6 references. Comments and suggestions related to previously published materials or to any medical theme of interest will be considered for publication.
Correspondence: Authors may submit comments and suggestions related to material previ-ously published in our journal. Such submissions should not exceed 500 words.
Imaging in Pulmonary Medicine: Submissions should not exceed 200 words, including the title, text, and references (no more than three). Authors may include up to three figures, bearing in mind that the entire content will be published on a single page.
Tables and Figures: All tables and figures should be in black and white, on separate pages, with legends and captions appearing at the foot of each. All tables and figures should be submitted as files in their original format. Tables should be submitted as Microsoft Word files, whereas figures should be submitted as Microsoft Excel, TIFF or JPG files. Photographs depicting surgical procedures, as well as those showing the results of exams or biopsies, in which staining and special techniques were used will be considered for publi-cation in color, at no additional cost to the authors. Dimensions, units and symbols should be based on the corresponding guidelines set forth by the Associação
Brasileira de Normas Técnicas (ABNT, Brazilian Association for the Establishment of Technical Norms), available at: http://www.abnt.org.br.
Legends: Legends should accompany the respec-tive figures (graphs, photographs and illustrations) and tables. Each legend should be numbered with an Arabic numeral corresponding to its citation in the text. In addition, all abbreviations, acronyms, and symbols should be defined below each table or figure in which they appear.
References: References should be listed in order of their appearance in the text and should be numbered consecutively with Arabic numerals. The presenta-tion should follow the Vancouver style, updated in October of 2004, according to the examples below. The titles of the journals listed should be abbrevi-ated according to the style presented by the List of Journals Indexed in the Index Medicus of the National Library of Medicine, available at: http://www.ncbi.nlm.nih.gov/entrez/journals/loftext.noprov.html. A total of six authors may be listed. For works with more than six authors, list the first six, followed by ‘et al.’Examples: Journal Articles1. Neder JA, Nery LE, Castelo A, Andreoni S, Lerario
MC, Sachs AC et al. Prediction of metabolic and cardiopulmonary responses to maximum cycle ergometry: a randomized study. Eur Respir J. 1999;14(6):1204-13.
Abstracts2. Singer M, Lefort J, Lapa e Silva JR, Vargaftig BB.
Failure of granulocyte depletion to suppress mucin production in a murine model of allergy [abstract]. Am J Respir Crit Care Med. 2000;161:A863.
Chapter in a Book3. Queluz T, Andres G. Goodpasture’s syndrome.
In: Roitt IM, Delves PJ, editors. Encyclopedia of Immunology. 1st ed. London: Academic Press; 1992. p. 621-3.
Official Publications4. World Health Organization. Guidelines for
surveillance of drug resistance in tuberculosis. WHO/Tb, 1994;178:1-24.
Theses5. Martinez TY. Impacto da dispnéia e parâmetros
funcionais respiratórios em medidas de qualidade de vida relacionada a saúde de pacientes com fibrose pulmonar idiopática [thesis]. São Paulo: Universidade Federal de São Paulo; 1998.
Electronic publications6. Abood S. Quality improvement initiative in nursing
homes: the ANA acts in an advisory role. Am J Nurs [serial on the Internet]. 2002 Jun [cited 2002 Aug 12]; 102(6): [about 3 p.]. Available from: http://www.nursingworld.org/AJN/2002/june/Wawatch.htm
Homepages/URLs7. Cancer-Pain.org [homepage on the Internet]. New
York: Association of Cancer Online Resources, Inc.; c2000-01 [updated 2002 May 16; cited 2002 Jul 9]. Available from: http://www.cancer--pain.org/
Other situations:In other situations not mentioned in these author
instructions, authors should follow the recommenda-tions given by the International Committee of Medical Journal Editors. Uniform requirements for manu-scripts submitted to biomedical journals. Updated October 2004. Available at http://www.icmje.org/.
All correspondence to the Jornal Brasileiro de Pneumologia should be addressed to:
Prof. Dr. Rogério Souza Editor-Chefe do Jornal Brasileiro de Pneumologia
SCS Quadra 01, Bloco K, Salas 203/204 - Ed. Denasa. CEP: 70.398-900 - Brasília - DF, Brazil
Telefones/Fax: 0xx61-3245-1030, 0xx61-3245-6218
Jornal Brasileiro de Pneumologia e-mail address:[email protected] (Assistente Editorial - Luana Campos)
Online submission of articles:www.jornaldepneumologia.com.br
ASSOCIAÇÃO ALAGOANA DE DOENÇAS DO TÓRAXPresidente: Tadeu Peixoto LopesSecretário: Artur Gomes NetoEndereço: Rua Professor José Silveira Camerino, nº 1085 - Sala 501, Pinheiro,CEP: 57057-250- Maceió – ALTelefone: (82)30321967 (82) | (82)996020949Email: [email protected] [email protected]
ASSOCIAÇÃO CATARINENSE DE PNEUMOLOGIA E TISIOLOGIA Presidente: Márcio Andrade MartinsSecretário: Antônio Cesar CavallazziEndereço: Rodovia SC, 401 Km 4 – 3854 - Saco GrandeCEP: 88.032 - 005 - Florianópolis – SCTelefone: (48)32310314 E-mail: [email protected] | site: www.acapti.org.br
ASSOCIAÇÃO DE PNEUMOLOGIA E CIRUGIA TORÁCICA DO ESTADO DO RIO GRANDE DO NORTE
Presidente: Paulo Roberto de AlbuquerqueSecretária: Suzianne Ruth Hosannah de Lima PintoEndereço: Av. Campos Sales, 762 - TirolCEP: 59.020-300 - Natal – RNTelefone: (84)32010367 – (84)99822853E-mail: [email protected]
ASSOCIAÇÃO MARANHENSE DE PNEUMOLOGIA E CIRURGIA TORÁCICAPresidente: Maria do Rosario da Silva Ramos CostaSecretária: Denise Maria Costa HaidarEndereço: Travessa do Pimenta, 46 - Olho D‘Água CEP: 65.065-340 - São Luís – MATelefone: (98)3226-4074 | Fax: (98)3231-1161 E-mail: [email protected]
ASSOCIAÇÃO PARAENSE DE PNEUMOLOGIA E TISIOLOGIAPresidente: Carlos Augusto Abreu AlbérioSecretária: Márcia Cristina Corrêa VasconcelosEndereço: Faculdade de Medicina - Praça Camilo Salga do - 1 - Umarizal CEP: 66050-060 - Belém – PATel: (91)8115-5048E-mail: [email protected]
SOCIEDADE AMAZONENSE DE PNEUMOLOGIA E CIRURGIA TORÁCICAPresidente: Evandro de Azevedo MartinsSecretária: Clio da Rocha Monteiro HeidrichEndereço: Av. Joaquim Nabuco, 1359 Centro HospitalBeneficentePortuguesa-SetorCirurgia Torácica CEP: 69020030- Manaus – AMTelefone: (92)3234-6334E-mail: [email protected]
SOCIEDADE BRASILIENSE DE DOENÇAS TORÁCICASPresidente: Bianca Rodrigues SilvaSecretário: Edgar Santos MaestroEndereço: Setor de Clubes Sul, Trecho 3, Conj. 6 CEP: 70.200-003 - Brasília – DFTel/fax: (61) 3245-8001 – (61)8406-8948E-mail: [email protected] | [email protected]
SOCIEDADE CEARENSE DE PNEUMOLOGIA E TISIOLOGIA Presidente: Mara Rúbia Fernandes de FigueiredoSecretária: Thiago de Oliveira MendonçaEndereço: Av. Dom Luis, 300, sala 1122, AldeotaCEP: 60160-230 - Fortaleza – CETelefone: (85) 3087-6261 - 3092-0401E-mail: [email protected] | site: www.scpt.org.br
SOCIEDADE DE PNEUMOLOGIA DA BAHIAPresidente: Guilherme Sóstenes Costa MontalSecretária: Dalva Virginia Oliveira Batista NevesEndereço: ABM - Rua Baependi,162. Sala 03 - Terreo - OndinaCEP: 40170-070 - Salvador – BATel/fax: (71) 33326844E-mail: [email protected] | [email protected]
SOCIEDADE DE PNEUMOLOGIA DO ESPÍRITO SANTOPresidente: Cilea Aparecida Victória MartinsSecretária: Karina Tavares Oliveira Endereço: Rua Eurico de Aguiar, 130, Sala 514 –Ed. Blue Chip. Praia do CampoCEP: 29.055-280 - Vitória – ESTelefone: (27)3345-0564 Fax: (27)3345-1948E-mail: [email protected]
SOCIEDADE DE PNEUMOLOGIA DO MATO GROSSOPresidente: Carlos Fernando Gossn Garcia Secretário: Paulo Cesar da Silva NevesEndereço: Av. Miguel Sutil, n 8000, Ed. Santa Rosa Tower, sala 1207. Bairro: Santa RosaCEP: 78040-400Cidade: Cuiaba - MTTelefone: (65) 3052-3002E-mail: [email protected]
SOCIEDADE DE PNEUMOLOGIA E TISIOLOGIA DO MATO GROSSO DO SULPresidente: Angela Maria Dias de QueirozSecretária: Lilian AndriesEndereço: Rua Dr. Arthur Jorge n° 2117 - 902, Bairro São Francisco CEP: 79010-210 - Campo Grande - MS Telefone: (67)33252955 / (67)99853782E-mail: [email protected]
SOCIEDADE DE PNEUMOLOGIA E TISIOLOGIA DO ESTADO DO RIO DE JANEIRO
Presidente: Gilmar Alves ZonzinSecretária: Mônica Flores RickEndereço: Rua da Lapa, 120 - 3° andar - salas 301/302 - Centro CEP: 20.021-180 - Rio de Janeiro – RJTel/fax: (21) 3852-3677E-mail: [email protected] | site: www.sopterj.com.br
SOCIEDADE DE PNEUMOLOGIA E TISIOLOGIA DO RIO GRANDE DO SULPresidente: Paulo Roberto GoldenfumVice: Adalberto Sperb RubinEndereço: Av. Ipiranga, 5.311, sala 403 CEP: 90.610-001 - Porto Alegre – RSTelefone: (51)3384-2889 Fax: (51)3339-2998E-mail: [email protected] | www.sptrs.org.br
SOCIEDADE GOIANA DE PNEUMOLOGIA E TISIOLOGIAPresidente: Maria Rosedália de MoraesSecretária: Roseliane de Souza AraújoEndereço: Galeria Pátio 22 - Rua 22 nº 69, Sala 17 Setor OesteCEP: 74.120-130 - Goiânia – GOTelefone: (62)3251-1202 / (62)3214-1010E-mail: [email protected]
SOCIEDADE MINEIRA DE PNEUMOLOGIA E CIRURGIA TORÁCICAPresidente: David Vogel Koza Secretária: Ana Cristina De Carvalho Fernandez FonsecaEndereço: Av. João Pinheiro, 161 - sala 203 - Centro CEP: 30.130-180 - Belo Horizonte – MGTel/fax: (31)3213-3197E-mail: [email protected]
SOCIEDADE PARAIBANA DE PNEUMOLOGIA E CIRURGIA TORÁCICA Presidente: José George Cunha Carneiro BragaSecretário: José Gerson GadelhaEndereço: Rua Maria Caetano Fernandes de Lima, 225 - TambauzinhoCEP: 58042-050 – João Pessoa - PBTelefone: (83)93020555 E-mail: [email protected]
SOCIEDADE PARANAENSE DE TISIOLOGIA E DOENÇAS TORÁCICAS Presidente: Lêda Maria RabeloSecretária Geral: Daniella Porfírio NunesEndereço: Av. Sete de Setembro, 5402 - Conj. 105, 10ª andar Batel CEP: 80240-000 - Curitiba – PRTel/fax: (41)3342-8889E-mail: [email protected] | www.pneumopr.org.br
SOCIEDADE PAULISTA DE PNEUMOLOGIA E TISIOLOGIA Presidente: Regina Maria de Carvalho PintoSecretária: Silvia Carla Sousa RodriguesEndereço: Rua Machado Bittencourt, 205, 8° andar, conj. 83 - Vila Clementino CEP: 04.044-000 São Paulo – SPTelefone: 0800 17 1618E-mail: [email protected] | www.sppt.org.br
SOCIEDADE PERNAMBUCANA DE PNEUMOLOGIA E TISIOLOGIAPresidente: Adriana Velozo GonçalvesSecretária: Ana Lúcia Pereira Lima Alves DiasEndereço: Rua João Eugênio de Lima , 235 - Boa Viagem CEP: 51030-360 - Recife – PETel/fax: (81)3326-7098E-mail: [email protected]
SOCIEDADE PIAUIENSE DE PNEUMOLOGIA E TISIOLOGIAPresidente: Cromwell Barbosa de Carvalho MeloSecretária: Tatiana Santos Malheiros NunesEndereço: Avenida Jose dos Santos e Silva, 1903 Nucleo de Cirurgia TorácicaCEP: 64001-300- Teresina – PITelefone: (86)32215068E-mail: [email protected]
SOCIEDADE SERGIPANA DE PNEUMOLOGIA E TISIOLOGIA Presidente: Anaelze Siqueira Tavares TojalSecretário: Ostílio Fonseca do ValeEndereço: Av. Gonçalo Prado Rollemberg, 211, Sala 11 Bairro São JoséCEP: 49050-370- Aracaju - SE Telefone: (79) 21071412E-mail: [email protected]
Estaduais da Sociedade Brasileira de Pneumologia e Tisiologia
EVENTS 2015/2016
NACIONAIS
Curso de Imersão em PneumologiaData: 17 a 18 de junho de 2016
Local: SERHS Natal Grand Hotel – Natal/RNInformações: [email protected]
Fone: 0800 61 6218
VII Curso Nacional de Ventilação Mecânica
IV Curso Nacional de SonoData: 18 a 20 de agosto de 2016
Local: São Paulo/SPInformações: [email protected]
Fone: 0800 61 6218
XXXVIII Congresso Brasileiro de Pneumologia e Tisiologia
XI Congresso Luso-Brasileiro de Pneumologia
XIV Congresso Brasileiro de Endoscopia Respiratória
Data: 11 a 15 de outubro de 2016Local: Rio de Janeiro - RJ
Informações: [email protected]: 0800 61 6218
INTERNACIONAIS
ATS 2016Data: 13 a 18 de maio de 2016Local: San Francisco/CA-USA
Informações: www.thoracic.org
SEPAR 2016Data: 10 a 13 de junho de 2016
Local: Granada/EspanhaInformações: www.separ.es
ALAT 2016Data: 06 a 09 de julho de 2016
Local: Centro de Convenções Casa Piedra, Santiago/Chile
Informações: https://www.congresosalat.org/
ERS 2016Data: 03 a 07 de setembro de 2016
Local: Londres, Reino UnidoInformações: www.ersnet.org




















