January - March 2003 ewsletter
44
The word paradigm in present usage means the living model in our mind which we use to understand and explain the world. Our paradigm incorporates all of our basic assump- tions about the nature of reality. It is our worldview, it’s the lens through which we look at the world and it col- ors everything we see. This paradigm- lens is itself created and formed from the primal feelings living at the deepest levels of our heart and mind. Primal feelings are shared by all human beings, each of us having our own par- ticular mix depending on our individ- ual constitution and experience and on the culture in which we live. Most important in this inner mix of primal, basic feelings toward life and the world is whether love or fear rules. In ancient times the ruling paradigm was based on love for the world. Today our ruling scientific paradigm is based on fear of the world. At a deep uncon- scious level, but in medicine just below the surface, we live today in a fear- based paradigm. Because of this underlying fear, science and medicine assume that we must control, master and change nature in order to survive. The new paradigm now struggling to be born challenges us to develop the courage and selflessness to master and change ourselves in order to survive. The ruling paradigm of a cul- ture determines on what kind of knowledge governments are based, on what kind of knowledge the education of children and the pursuit of science are based, in short on what kind of knowledge enlightened civilization is based. If we could ask a well-educated citizen of ancient times what kind of knowledge should form the basis of an enlightened civilization, the answer most certainly would be “well, of course, knowledge of the gods and of their will.” The ruling paradigm shared by the peoples of the ancient world was God-centered and spirit- centered. But all that changed, because human consciousness is in constant evolution and the human heart and mind never stand still. Paradigms are like living things which grow, reach maturity and then become old, over- ripe and prone to illness and decay. The ancient spirit-centered ruling para- digm in Europe had become institu- tionalized in the church and by the 1500’s had grown old and corrupt, no longer able to keep up with changing evolving human consciousness. Then came a mighty paradigm shift as western science was brought to birth by Copernicus, Galileo and Newton. The human mind and senses had grad- ually been losing their capacity to experience spirit as a concrete reality. After Galileo, the physical matter of VRAN Newsletter January - March 2003 Page 1 January - March 2003 Editorial Edda West IS FEAR OF FEVER HURTING OUR CHILDREN ? As paradigms go in the world of disease management, there is none more deeply ingrained than the fear driven belief that without vaccinations we are doomed to attack from legions of killer dis- eases. It’s shadow partner, “fear of fever” compels us to suppress fever whenever it arises and insures our captivity to monop- oly, sickness oriented medicine. The medical/pharmaceutical empire flogs us with these tactics, imprinting fear in the collective psyche, the favourite tool with which they dominate the masses and usher us down the slippery slope of health breakdown and drug dependency. Vaccinations and fever suppres- sants, along with the overuse of antibiotics and exposure to multi- ple chemical contaminants in the INSIDE THIS ISSUE Page 12 - Measles in the Vaccination Age 13 - What’s Under the Hump? 15 - Letters 18 - Always Do Your Homework 20 - Shaken Baby Syndrome 21 - Who Let the Cat Out of the Bag 22 - News Clips Paradigm Shift cont. on page 4 Vaccination Risk Awareness Network Inc. Editorial cont. on page 6 THE PARADIGM SHIFT IN MEDICINE AND SCIENCE ewsletter Taken from a talk presented at the National Vaccine Information Center Conference, September, 2002 By Philip F. Incao, M.D. - February 10,2003
Transcript of January - March 2003 ewsletter

The word paradigm in present usagemeans the living model in our mindwhich we use to understand andexplain the world. Our paradigmincorporates all of our basic assump-tions about the nature of reality. It isour worldview, it’s the lens throughwhich we look at the world and it col-ors everything we see. This paradigm-lens is itself created and formed fromthe primal feelings living at the deepestlevels of our heart and mind. Primalfeelings are shared by all humanbeings, each of us having our own par-ticular mix depending on our individ-ual constitution and experience and onthe culture in which we live. Mostimportant in this inner mix of primal,basic feelings toward life and the worldis whether love or fear rules. Inancient times the ruling paradigm wasbased on love for the world. Todayour ruling scientific paradigm is basedon fear of the world. At a deep uncon-scious level, but in medicine just belowthe surface, we live today in a fear-based paradigm. Because of thisunderlying fear, science and medicineassume that we must control, masterand change nature in order to survive.The new paradigm now struggling tobe born challenges us to develop thecourage and selflessness to master andchange ourselves in order to survive.
The ruling paradigm of a cul-ture determines on what kind of
knowledge governments are based, onwhat kind of knowledge the educationof children and the pursuit of scienceare based, in short on what kind ofknowledge enlightened civilization isbased. If we could ask a well-educatedcitizen of ancient times what kind ofknowledge should form the basis of anenlightened civilization, the answermost certainly would be “well, ofcourse, knowledge of the gods and oftheir will.” The ruling paradigmshared by the peoples of the ancientworld was God-centered and spirit-centered.
But all that changed, becausehuman consciousness is in constantevolution and the human heart andmind never stand still. Paradigms arelike living things which grow, reachmaturity and then become old, over-ripe and prone to illness and decay.The ancient spirit-centered ruling para-digm in Europe had become institu-tionalized in the church and by the1500’s had grown old and corrupt, nolonger able to keep up with changingevolving human consciousness.
Then came a mighty paradigm shiftas western science was brought to birthby Copernicus, Galileo and Newton.The human mind and senses had grad-ually been losing their capacity toexperience spirit as a concrete reality.After Galileo, the physical matter of
VRAN Newsletter January - March 2003 Page 1
January - March 2003
EditorialEdda WestIS FEAR OF FEVER HURTINGOUR CHILDREN ?
As paradigms go in the worldof disease management, there isnone more deeply ingrained thanthe fear driven belief that withoutvaccinations we are doomed toattack from legions of killer dis-eases. It’s shadow partner, “fearof fever” compels us to suppressfever whenever it arises andinsures our captivity to monop-oly, sickness oriented medicine.The medical/pharmaceuticalempire flogs us with these tactics,imprinting fear in the collectivepsyche, the favourite tool withwhich they dominate the massesand usher us down the slipperyslope of health breakdown anddrug dependency.
Vaccinations and fever suppres-sants, along with the overuse ofantibiotics and exposure to multi-ple chemical contaminants in the
INSIDE THIS ISSUEPage
12 - Measles in the Vaccination Age
13 - What’s Under the Hump?
15 - Letters
18 - Always Do Your Homework
20 - Shaken Baby Syndrome
21 - Who Let the Cat Out of the Bag
22 - News Clips
Paradigm Shift cont. on page 4
V a c c i n a t i o n R i s k A w a r e n e s s N e t w o r k I n c .
Editorial cont. on page 6
THE PARADIGM SHIFT IN MEDICINEAND SCIENCE
ewsletterTaken from a talk presented at the National Vaccine InformationCenter Conference, September, 2002
By Philip F. Incao, M.D. - February 10,2003

Fundraising Help NeededDeep appreciation goes to those
VRAN members who have sentdonations to help with this year’sfundraising efforts. To date wehave received $4,025, which is onefifth of VRAN’s yearly operatingbudget of $20,000. Fundraising isan ongoing challenge and needs acommittee of dedicated people tomake this their special VRAN pro-ject. Please help us by donatingyour time, your ideas, and byorganizing fundraising efforts inyour area.
We are still offering Dr. SherriTenpenny’s dynamic vaccine videoas a bonus offer for your donationof $150 or more. We also thankthose members who have signedon with the Excel phone planwhich we hope will be a long termfundraiser for VRAN. Virtuallyeveryone uses long distance. Bytrying the Excel plan(s) you arehelping VRAN and getting low,competitive rates at the same time.Please call or email Edda for moredetails: 250-355-2525 [email protected] Edda and a fewhelpers will also continue to phoneVRAN members asking for yourhelp with this.
VRAN Memberships Due ForRenewal
Please remember that yourVRAN membership is renewedyearly in January. Membershiprenewals have been trickling in,but many remain outstanding.Membership donations is whatfunds the costs of newsletter print-ing and mailing and is still ourmain vehicle for vaccine risk edu-
cation. We are suggesting $35 forfamily membership and $75 forprofessional. Thank you for tak-ing the time to renew your mem-bership.
Annual General MeetingVRAN’s annual general meeting
will be held by telephone confer-ence from Winnipeg on Sunday,April 27. If you wish to partici-pate, please call Mary James at:204-895-9192
Total Health ConferenceWith special thanks to VRAN
members who so generously donat-ed their time at the recent TotalHealth Conference in Toronto.VRAN was given a spot at theconference book table. Dr. JasonWhittaker, Josephine Solomonsand Santo D’Agostino talked toconference attendees about vaccinerisk issues, handed out brochuresand sold some information pack-ages. Their commitment andenthusiasm is greatly appreciated.
BC REPORT, March, 2003By Susan Fletcher
I’ve caught the attention of twohigh-profile organizations. TheTroubadour Foundation was estab-lished by child entertainer Raffi topromote “honouring” of theworld’s children. I wrote a letterto Raffi, enclosed several vaccinearticles and expressed my wishthat we and others of like mindcould “form a synergistic partner-ship to work towards rescuing ourchildren’s health.” This packagewas delivered by hand and I soonreceived a warm reply fromTroubadour manager, CaterinaGeuer. She said they are aware of
Page 2 January - March 2003 VRAN Newsletter
VRAN NEWSLETTERVaccination Risk Awareness Network Inc.P.O. Box 169, Winlaw, B.C. V0G 2J0Coordinator and newsletter editor: Edda [email protected] 250-355-2525VRAN Board of Directors:Mary James, Leona Rew, Edda West, Frank LuschakVRAN Core Members:Edda West, Susan Fletcher, Lana Belvis, CatherineDiodati, Andreas Schuld, Rita Hoffman, Mary James
With thanks to Lisa Farr for the newsletter layout.
Statement of Purpose•VRAN was formed in October of 1992 in responseto growing parental concern regarding the safety ofcurrent vaccination programs in use in Canada.•VRAN continues the work of the Committee AgainstCompulsory Vaccination, who in 1982, challengedOntario’s compulsory “Immunization of School PupilsAct”, which resulted in amendment of the Act, andguarantees an exemption of conscience from any‘required’ vaccine.•VRAN forwards the belief that all people have theright to draw on a broad information base whendeciding on drugs offered themselves and/or theirchildren and in particular drugs associated withpotentially serious health risks, injury and death.VACCINES ARE SUCH DRUGS. •VRAN is committed to gathering and distributinginformation and resources that contribute to the creation of health and well being in our families andcommunities.
VRAN’s Mandate is:•To empower parents to make an informed decisionwhen considering vaccines for their children.•To educate and inform parents about the risks,adverse reactions, and contraindications of vaccinations. •To respect parental choice in deciding whether ornot to vaccinate their child.•To provide support to parents whose children havesuffered adverse reactions and health injuries as aresult of childhood vaccinations.•To promote a multi-disciplinary approach to childand family health utilizing the following modalities:herbalist, chiropractor, naturopath, homeopath,reflexologist, allopath (regular doctor), etc.•To empower women to reclaim their position as pri-mary healers in the family. •To maintain links with consumer groups similar toours around the world through an exchange of infor-mation, research and analysis, thereby enabling par-ents to reclaim health care choices for their families.•To support people in their fight for health freedomand to maintain and further the individual's freedomfrom enforced medication.
VRAN publishes a newsletter 4 times a year as ameans of distributing information to members andthe community. Suggested annual membership fees,including quarterly newsletter and your on-going support to the Vaccination Risk Awareness Network:$25.00—Individual $50.00—ProfessionalWe would like to share the personal stories of ourmembership. If you would like to submit yourstory, please contact Edda West by fax or e-mail,as indicated above.
VRAN website: www.vran.org
The contents of this publication reflect the opinion of the authors only. Theauthors are not licensed to practice medicine, nor are the opinions in any wayto be construed or intended as medical information. This publication is for infor-mational purposes only and should not be construed as medical advice. Theparticulars of any person’s concerns and circumstances should be discussedwith a medical doctor prior to making any decision which may affect the healthand welfare of that individual or anyone under his or her care.D
ISC
LAIM
ER
VRAN News cont. on page 3
VRAN NEWS

the problems I raised and, like us,are concerned. She told us about anew group, the ‘CanadianPartnership for Children’s Healthand the Environment’. Edda hashad a positive exchange with con-tact, Tonya Surman, who told hershe would take her message to thegroup’s first meeting March 5th.We will contact them again.
The second group I tackled wasRotary. A four page spread in aJanuary newspaper said Rotary’smain purpose is “to encouragehigh ethical standards” and thatthe 4 clubs on the ‘Coast’ (popula-tion under 30,000) were set toraise US$12,000 during March tohelp in “Fulfilling our Promise toEradicate Polio” and “immunizemore than 2 billion children.”
I decided another campaign wasin order, wrote ‘The Ethics ofPolio Eradication’ and Edda sent itout on VRANWEB and to othersincluding the head of ‘Polio Plus’.The latter sent articles on AIDS,BSE and the defunct NIH SV40review, all of which I critiqued.My husband and I hand delivered320 copies of ‘The Ethics…’ tolocal businesses; most people, evena couple of Rotarians, thanked us.To the campaign coordinator,Heather, I delivered thirty articlesand a letter pointing out thatAlbert Sabin had publicly dispar-aged vaccines in 1985, the sameyear ‘Polio Plus’ began and hebecame Rotary’s advisor. Heathersaid she would read all. In hernext email she fingered WHO andUNICEF.
Things were quiet in Marchexcept for two ads asking for vol-unteers to work for a “Polio-FreeWorld”….could it be that some ofthe troops rebelled?
Several people, on seeing my dis-play at our Health Festival,remarked “Haven’t they got ityet?!!” Well, some have, ie thepeople who watched the Tenpennyvideo I’ve been showing. Theythanked me for helping them “get
it”. As for the rest of Canada…step up all of you willing to helpwith a Canadian Tenpenny speak-ing tour!
If you wish to receive a copy of“Ethics of Polio Eradication”please contact Edda West at:[email protected] or call 250-355-2525
Manitoba NewsBy Mary James
On January 13, 2003, the CBC-National News camera crew alongwith producer Grazyna Krupa andhealth reporter Maureen Taylorwere in Winnipeg, filming a minidocumentary entitled, “Kickingthe Sacred Cow of Vaccination.”
The producers at CBC -Nationalwere aware that a growing numberof parents are very worried aboutthe severe adverse reactions toroutine childhood immunizationsthat increasing numbers of chil-dren have experienced. Theydecided to investigate.
Twelve members of TheAssociation for Vaccine DamagedChildren were present for a twohour filming session. We wereencouraged to voice our concernswith the present vaccination pro-gram and to share our children’sstories of how they reacted totheir childhood vaccinations. Theinterviewer encouraged us to sharethe reception we received from ourfamily doctors and pediatriciansonce our child suffered a severereaction to his or her vaccination.Every parent present had experi-enced the same total denial fromtheir doctors that there was anyconnection, despite the fact thatin some cases the child reacted byseizuring within hours of the vac-cination..
Gloria and Lawrence Dignaziowere interviewed earlier in the dayregarding their daughter Sara’sreaction to her vaccination eightand one half years ago. Sara wasdiagnosed with a form of autismfollowing her 18 month DPT-Polio
VRAN Newsletter January - March 2003 Page 3
VRAN News cont. from page 2
VRAN News cont. on page 4
DID YOU KNOW ?There is no law that can force you
to vaccinate your children. The onlylaws relating to vaccination governschool pupils, not infants, and thesecan be waived through availableexemptions. If your child has exhibit-ed any of the following adverse reac-tions or conditions, you may wish todefer from continuing the course ofvaccinations.• If your child is ill or running a
fever.• If the child collapses or goes into a
shock-like state following a vac-cine.
• If the child has high pitchedscreaming for several hours; andcannot be comforted
• If the child has a temperature of38° C or higher after vaccination.
• If the child develops pain, redness,swelling, lump at the needle site
• If the child develops severe diarrheaand/or vomiting
• If the child has one or more con-vulsions or has a family history ofconvulsive disorders (eg. epilepsy);if the child has an evolving neuro-logical condition.
• If there is a family history of severeallergies and/or history of vaccinereactions.
• If the child has signs of brain injurysuch as a bulge in the soft spots ofthe head or a severe change of con-sciousness.
• If the child is receiving treatmentsthat suppress the immune system
• If the child has a widespread aller-gic reaction, rashes, hives, wheez-ing, trouble breathing.
• If the child develops swollenjoints/arthritis like symptoms
• If the child has an irregular heartbeatwithin several hours after vaccination.
• If the child is excessively sleepy fol-lowing vaccination.
• If the child has an episode of sleepapnoea (stops breathing duringsleep)

vaccination.We were informed that the docu-
mentary would air sometime inFebruary, unless the war in Iraqstarted, in which case the producerdid not know when it would bebroadcast. At any rate, we wouldbe notified of the date well inadvance. The producer asked usfor pictures of our vaccine injuredor deceased children, as shethought they would be incorporat-ed into the documentary.
Much to our surprise and dis-may, CBC Newsworld broadcastthe Dignazio family portion of thedocumentary a few weeks ago onHealth Matters, without notifyinganyone. The Dignazio familyfound out about it when Sara’saide at school phoned to informthem that she had just seen thefamily interviewed on a healthshow linking vaccines with autism.
When the Dignazio familydemanded an explanation as towhy they were never informed ofthe broadcast, they were told bythe producer, Grazyna Krupa thatit was mistakenly aired as part ofa feature on vaccines and autismfor Health Matters. She assuredthem that the CBC-National hadnot yet broadcast the documen-tary. She informed us that thedocumentary would be a muchshorter version than originallyplanned, and that it would not beas comprehensive as she hadhoped it would be.
In fact, the documentary wouldfocus only on Sara Dignazio andanother family in Britain whosechild also experienced autisticsymptoms following her vaccina-tion. Assurances were given to thefamily that they would receiveadvance notice when the documen-tary would be broadcast on CBCNational News.
We still have not heard when itwill be aired but will informeveryone on the VRAN email listas soon as we hear of the date. Wealso encourage you to write CBC
@ PO. Box 500, Station A,Toronto M5W 1E6 , AttentionGrazyna Krupa or email @ [email protected] demandingthat CBC-National show the fulldocumentary to Canadians.
On March 6, 2003, Mary Jamesspoke to a University of Winnipegclass, in a course entitled, Health,Healing and Spirituality on therisks and adverse reactions of rou-tine childhood vaccination. TheVRAN newsletter and web-sitewas shared with the participants.The class was filmed and broad-cast on Shaw cable televisionlocally.
On March 16, 2003, Leona Rewand Mary James spoke in Selkirk,Manitoba to a group of parentsabout the vaccination controversyin an informal session. Therewere many questions and a greatdiscussion followed. Specialthanks to Terry Morriseau forarranging the meeting and for thegroup donation of $100.00 forVRAN.
Alternatives to SARSLong time VRAN member and
naturopathic physician, Dr. VernaHunt has compiled a SARSPrevention Program, listing dietaryrecommendations, botanical medi-cine, supplements, essential oilsand homeopathic remedies. Youmay obtain her recommendationsvia email: [email protected], or senda stamped, self addressed envelopeto VRAN – P.O. Box 169, Winlaw,B.C. V0G 2JO.
Our Appreciation toVaccination Liberation forproducing their excellent SmallpoxAlert which we’ve included as asupplement to this edition of theVRAN newsletter. We’ve had toreduce the size of the VRANnewsletter in order to accommo-date the extra mailing weight ofthis supplement. You can alsoaccess the complete text ofSmallpox Alert via the Vaclib web-site at: www.vaclib.org
the universe assumed ever-growingimportance for the mind, and for sci-ence. To understand the deep innerreality of matter became the quest ofscience, eventually leading to theunsettling conclusion by modernphysics that the basis of all matter wasafter all non-material: energy. Thingswere coming full circle, as our para-digm, having shifted from spirit-basedto matter-based, then shifted to energy-based in the 20th century.
The birth of western sciencewas also the birth of a freer and moreindividualized human thinking. Galileowas a pioneer fighting for the freedomto think about reality in a way thatrespected no outer authority butrespected only the truth as he saw it.He stood for the inviolable right of thescientist to follow ones own con-science, free from outside pressure.This fresh, young scientific paradigmrepresented by Galileo became matureover the next couple of centuries. Itbecame well-established and institu-tionalized, and now has becomeentrenched and very powerful. Nowthe free spirits in science are again hav-ing a hard time. Their freedom to callit as they see it is again being curtailed;their academic freedom is threatened.And of course, today it’s not thechurch which threatens freedom ofthought in science, it is the system thatinstitutionalized science has becomewhich stifles individual freedom andcreativity. Most Americans todaybelieve that a scientist is free to pursuethe truth as she or he sees it, free fromany influence whatsoever. This is sadlynot the case.
History is repeating itself. The cor-ruption, immorality and tyranny of thechurch that fueled the Reformation inthe 16th century are now happening ininstitutionalized and commercializedscience and medicine. These are symp-toms of a terminal illness in a para-digm that has already made its greatest
Page 4 January - March 2003 VRAN Newsletter
VRAN News cont. from page 3 Paradigm Shift cont. from page 1
Paradigm Shift cont. on page 5

contributions to the evolution ofhumanity, and is now too old andinflexible to adapt to the changing con-sciousness of the 21st century.
It is human nature to resist changeand to fear loss of control and a loss ofsecurity. But a paradigm that mustlimit human freedom of thought inorder to preserve its power is nothealthy, and in fact is dying, and needsto be honored and to be laid to rest. Ifchange is to occur from the top down,then the day must come when it is therule, rather than the exception thatleading scientists love truth, and theirfreedom to pursue the truth, more thanthey fear the loss of their position andtheir material security.
When a paradigm dies, all of its giftswhich have stood the test of time arehonored, taken up and given fresh newlife by the infant paradigm which suc-ceeds it, just as in successive generationsof human beings. Paradigm shifts aredeaths and births unfolding a greaterevolution.
We are at a crossroads, and the forcesof change are moving in two opposingand irreconcilable directions. We havea choice between actively working forthe birth of a more human-centeredparadigm, or standing by while the pre-sent dying paradigm in biology andmedicine further expands its world
domination. Today’s institutionalizedand commercialized biology and medi-cine will apply its knowledge of theunderlying mechanisms of physical real-ity to create a mega-technology withever increasing power over the forces ofnature, both in the environment and inthe human being.
Science will develop the 200 or sovaccines now in the pipeline, and willalso increasingly develop and applygenetic engineering, gene therapy,cloning and a host of other things. It’soften said that you can’t stop progress,you can’t put the Genie back in the bot-tle. That’s true, it would be going back-wards in human evolution to try to putthe Genie back in the bottle. But thereal point is, we need to have the awak-ened moral discernment to reexamineour concept of progress and to under-stand just what kind of Genie we aredealing with, and we need to learn tomaster that Genie and not be its slave.We’ll never learn that until we developthe courage to stop fearing the worldand to change our paradigm.
Change is inevitable, but the kind ofchange, the kind of progress that comesabout can also happen from the bottomup. We, ordinary citizens can makechange happen if we have the valuesand the vision, and if we have thecourage to be activists for that visionand those values. A new more human-
centered paradigm in biology and medi-cine will be based on an ecological con-sciousness, affirming that we humansare intimately interconnected with andinter-dependent with all of creation. Inthe new paradigm, the freedom ofthought of the individual scientist, theindividual physician, and the individualclient/patient will be held sacred andwill be honored.
The basic assumption and attitude ofthe new paradigm will no longer be thatwe must control and dominate Naturein order to survive, but instead, that wemust, with great humility, learn aboutand respect Nature’s ways in order tolive in harmony with her – in order forthe human spirit to survive.
I am reminded of some lines by thepoet-playwright Christopher Fry, fromhis play A Sleep of Prisoners – the titlealone describes our modern conscious-ness very well :
“Thank God our time is now whenwrong comes up to face us everywhere,never to leave us until we take thelongest stride of soul we ever took.”
If humanity is to evolve in the direc-tion of greater health and freedom, andif we are to avoid destroying ourselvesand the world, then our new paradigmmust be one that puts the human spiritat the center of medicine and of science.
VRAN Newsletter January - March 2003 Page 5
Paradigm Shift cont. from page 4
About the author: Dr. Philip Incao is an Anthroposophic physician with a family practice in Denver, Colorado and haswritten many articles on children’s health from a wholistic perspective. He is a contributing author to a new book, TheVaccination Dilemma written by doctors, nurses and knowledgeable authorities on the vaccination debate. The bookreveals an alternative health care system that removes much of the fear from childhood disease. The book helps parents tounderstand how illness serves a unique need for every child and embraces health creating philosophies like homeopathy,anthroposophy and encourages parents to trust themselves and their children’s innate wisdom. Published by Lantern Books:www.lanternbooks.com, the book inspires trust in Nature’s wisdom.
Medical Science Present Paradigm - Matter-based
✦ Consciousness is a product of the physical body, andit plays no role in physical illness.
✦ Illness and healing are processes that follow physicallaws.
✦ Vaccines most likely strengthen the immune system.
New Paradigm - Energy-based
✦ Consciousness is not a product of the physical body,and it plays a role in all illness.
✦ Illness and healing have a spiritual dimension to themwhich strongly influences the underlying physical processes.
✦ Most vaccines change the immune system to decreasethe expression of acute inflammation and increase theexpression of chronic inflammation.

environment, are at the root of thedecline in children’s health and vitality,manifesting at large in the disablementof immune function, neurological func-tion, and upsurge of chronic diseasesin large segments of society today.Children in particular have been hithard as they are the most vulnerablemembers of society. New evidence isnow emerging that fever suppressantdrugs may be another contributing fac-tor to the explosive epidemic of neu-rodevelopmental disorders like autism.
As loving and caring parents, wenaturally want to help our children feelbetter when the inevitable fevers, flus,colds and various illnesses arise inchildhood. Many will reach for popu-lar over-the-counter remedies to sup-press fever and alleviate symptoms inthe belief that these products are reli-able, effective, and safe. But how safeare they really? And what are the riskswhen fever is suppressed and symp-toms masked? Does fever have a criti-cal function in fighting sickness thatwe have lost sight of?
There is plenty of scientific evidencevalidating the benefits of fever in fight-ing viral/bacterial inflammations andit’s important role in the healingprocess. Fever increases survival rateduring infectious diseases - basic infor-mation that has yet to reach the major-ity of people who remain misinformedand misled by pharmaceutical andmedical propaganda which still shame-lessly advocates the use of antipyreticdrugs at the first sign of fever. Themyth that untreated fevers will lead toseizures and brain damage is perpetu-ated ad nauseam. Fever is maligned,misunderstood and seen as an enemyto be feared rather than an ally thatsignals the immune system gearing upfor action.
Aspirin was once commonly used tosuppress fever until it was linked toReye’s syndrome when given to chil-dren with viral infections like influenzaand chickenpox. Reye’s syndrome is
an often fatal disease affecting thebrain and liver, a primary reason doc-tors switched to acetaminophen, whichwe now know to be the major cause ofliver failure. One disaster after anoth-er!
Acetaminophen is such a commoningredient used in both over-the-counter and prescription medications,people may be unaware of its presencein the many popular brands of fever,pain, colds and flu medications. HealthCanada recently issued an alert cau-tioning that the overuse of these over-the-counter remedies can lead to seri-ous liver toxicity and death.
“Parents should be especially cau-tious when giving children any prod-ucts containing acetaminophen. Forexample, the parent of a child with aflu-like illness may use one product totreat the child's fever and another totreat a runny nose, without realizingthat both products contain the sameingredients. A recently published arti-cle identified acetaminophen overdoseas the number one cause of acute liverfailure in the US, and most of theseoverdoses were unintentional. Often,several preparations of the same brand(e.g. Tylenol Pain and Tylenol Sinus) orseveral medications for the same symp-toms (e.g. Tylenol Cold, Neo-Citranand Sinutab) are found in the samehousehold and, when used together,can result in an overdose.” (1)
It is important to understand thatfever is not a disease, but rather asymptom of an illness. Controversiessurrounding the management of fevercause enormous anxiety in parents,often resulting in a knee-jerk, fearbased reaction to kill the fever withdrugs. As long as we remain captive tothe medical myth that nature made amistake in causing fever to arise duringillness, our children will be put at risk.There is an urgency for us to re-exam-ine our basic assumptions about thenature of fever and its evolutionaryrole in the survival of the species.
High fevers in some diseases like
measles and roseola are needed inorder to discharge the virus. In a clini-cal study of 56 children during ameasles epidemic in Ghana, Africa in1967, it was standard practice to treatevery case of measles with sedatives,antipyretics like aspirin and tylenol,cough suppressants, and also as neededwith antibiotics. In the first half of theepidemic, 35% of the children died.But the treating doctors also observedthat the children who survived wereusually the ones who had higher feversand more severe rashes than the oneswho died. Although the ones who diedseemed less sick than the survivors atthe beginning of the illness, they thenlater got pneumonia and died.
At a vaccine risk conference in 2000,Dr. Philip Incao cited this study as anexample of the vital role of fever. “Thedoctors began to think that the higherfevers and rash helped clear themeasles virus from the body andenhanced survival. And so half waythrough this measles epidemic, thedoctors revised their treatment andgave no sedatives, no aspirin ortylenol, nor cough suppressants, butstill gave antibiotics, antimalarials andblood transfusions if needed. In thisgroup, also of 56 children, only 7%died compared to 35% in the firstgroup. This is a dramatic demonstra-tion, and there are many others, of thevitally important basic principle that itis dangerous to suppress an inflamma-tory discharge.”
“Hippocrates recognized this overtwo thousand years ago. In anyinflammatory infectious disease, whatis discharged out of the body can befrightening to look at, but that’s notwhat kills us. What can kill us comesfrom the toxic effects of what’s leftinside the body and what’s not beingdischarged.”
“What I read in this study twentyyears ago confirmed what I experi-enced in my own practice, that thechildren who produced higher fevers
Page 6 January - March 2003 VRAN Newsletter
Editorial cont. from page 1
Editorial cont. on page 7

and strong rashes, and good dischargesof mucous and pus, were healthier andmore robust and had stronger immunesystems than the children who pro-duced a low intensity of these symp-toms. These robust children in mypractice, who vigorously externalizedand healed their infections sponta-neously, often without antibiotics, hadhad little or no antibiotics, orantipyretics, or vaccinations in theirlives. And the other children who hadhad all their vaccinations, and lots ofantipyretics, and antibiotics – who hadhad a lot of suppressive, internalizingmedical treatments, these childrennever got high fevers. And these chil-dren were the ones who were morelikely to have allergies and autoim-mune problems.” (2)
The pervasive belief that fever isdangerous and must be suppressed dis-regards the scientific evidence demon-strating its beneficial role in inflamma-tory diseases. The immune systemdepends on the essential role of feverto accomplish myriad tasks when gear-ing up to fight infections. NewZealand researcher Hilary Butler hasassembled an impressive list of cita-tions from medical literature to provethis point. We are grateful for herwork, and include these excerpts as anaddendum to this article.
“Doctors do a great disservice toyou and your child when they pre-scribe drugs to reduce fever” says Dr.Robert Mendelsohn, pediatrician andauthor of How To Raise A HealthyChild in Spite of Your Doctor. “Feverphobia is a disease of pediatricians, notparents, and to the extent that parentsare victimized by it, doctors are atfault.” Parents are left to fear thattheir child’s temperature will keep ris-ing unless measures are taken to con-trol it . “They don’t tell you thatreducing his temperature will do noth-ing to make the patient well or thatour bodies have a built-in mechanism,not fully explained, that will prevent
an infection-induced temperature fromreaching 106 degrees F (41 degrees C)(3)
Mendelsohn emphasizes that, “Onlyin the case of heatstroke, poisoning, orother externally caused fevers is thisbodily mechanism overwhelmed andinoperative.” This would also includedrug reactions and overdose.
Fever: Your Body’s Defense AgainstDisease is the title of chapter 7 in Dr.Mendeloshn’s book, and undoubtedlyone of the best guidelines ever writtenfor parents seeking a balanced andaccurate perspective of the beneficialand defensive role of fevers in child-hood. He condemns the useless anddangerous practice of fever suppressionthrough drugs. “If your child con-tracts an infection, the fever thataccompanies it is a blessing, not acurse. The spontaneous release ofpyrogens cause the body temperatureto rise, a natural defense mechanismneeded to fight disease. The presenceof fever tells you that the repair mech-anisms of the body have gone intohigh gear. It is something to rejoiceover, not to fear.”(3)
He counters the myth that high fevercauses seizures. “Many parents arefearful of fevers because they have wit-nessed a convulsive seizure and believethat their child may experience one ifhis temperature is allowed to rise toohigh. High fevers do not cause convul-sions. They result when the tempera-ture rises at an extremely rapid rateand are relatively uncommon. It is esti-mated that only 4 percent of childrenwith high fever experience fever relatedconvulsions. There is no evidence thatthose who do have them suffer anyserious aftereffects as a result.” (3)
“Fevers produced by viral or bacteri-al infections will not cause brain dam-age or permanent physical harm.Fevers are a common symptom in chil-dren and are not an indication of seri-ous illness unless associated withmajor changes in appearance andbehavior or other additional symptoms
such as respiratory difficulty, extremelistlessness or loss of consciousness.The height of a fever is not a measureof the severity of an illness.” (3)
Numerous studies have shown thatfever enhances the immune response byincreasing mobility and activity ofwhite cells called leucocytes which dis-able bacteria and viruses and removedamaged tissue from the body. A com-plex sequence of immune activities isactivated by fever. Antiviral andantibacterial properties of interferonare also increased with fever. With arise in temperature, iron is removedfrom the blood and stored in the liver,further disabling the rate at which bac-teria can multiply. Studies of artificiallyinduced fevers in laboratory animalsinfected with disease have shown thatelevated temperatures enhancesurvival, while lowered temperaturesincrease the death rate. (4)
There is an exception however.When fever arises in a newborn babyin the first few weeks of life, there is aheightened level of caution.“Newborn babies may suffer frominfections related to obstetrical inter-ventions during delivery, prenatal orhereditary conditions, aspiration pneu-monia from amniotic fluid forced intothe lungs because of overmedication ofthe mother during delivery…and expo-sure to the legion of germs thatabound in the hospital itself”, writesDr. Mendelsohn who advises parentsto seek medical help if a baby runs afever in the first two months of life.Breastfeeding plays a critical role inpreventing infections in infants.Breastfed babies are superbly protectedfrom a vast range of pathogens andhave a lesser risk of developing feversin the newborn phase of life.
It is known that the blood-brain bar-rier is not intact until at least 6 weeksof life. This is why fever in very younginfants, raises a big caution flagbecause of the ease with whichpathogens, viruses/bacteria can gainaccess to the baby's brain/nervous sys-
Editorial cont. on page 8
VRAN Newsletter January - March Page 7
Editorial cont. from page 6

tem creating a higher risk for meningi-tis. When medical help is sought for afeverish infant under 6 weeks of age, itmay lead to invasive procedures likespinal taps, antibiotics, steroids andfever suppressants, which are also notwithout risk. If a parent disagrees withthe course of treatment, they are likelyto encounter hostility from the medicalstaff, as recently happened to a Boisearea mother who lost custody of her 5week old baby when she took her tothe local ER for a check up.
The baby had been fussy and fever-ish all day, and the mother wanted tomake sure everything was alright. Sheconsented to blood tests, urinalysis, x-ray and I.V., but declined the spinaltap and wanted to wait for what thetest results might show. She calculatedthat there was about a 95% chanceher baby did not have meningitis andlikely had the same cold the family hadjust gotten over. Her decision to forgothe spinal tap and antibiotics prompt-ed the hospital to call Child ProtectiveServices and the baby was taken fromher. The doctor felt the child’s life wasin danger because the mother refused“life-saving treatment”, despite the factthat the baby had improved signifi-cantly after some hours on I.V..
It would seem prudent to protectnewborn infants during this early, vul-nerable time from exposure to any sit-uation, or procedures that would putthem at risk of developing fevers. Yet,the majority of newborns and younginfants are vaccinated in the first 6-8weeks of life. Doctors know full wellthat the injection of vaccine cocktailscontaining a brew of viral/bacterialparticles, foreign proteins, adjuvantsand chemical preservatives will likelyprecipitate a feverish reaction in alarge number of babies. They evenanticipate this, and often advise par-ents to dose the child with “babytylenol” prior to going in for theshot(s). And in the aftermath of vacci-nation, the standard reassurance given
to worried parents calling the doctor’soffice with a fussy, feverish newly vac-cinated baby, is “It’s perfectly normal –nothing to worry about. Just give thebaby some tylenol.”
In their determination to initiate vac-cine agendas as soon as possible, thereis a curious and willful blindnessamongst doctors in the vaccine estab-lishment. Why is there no concernabout the impact of vaccine inducedfevers in infants during this criticalearly period of life? Why is it that if aspontaneous fever arises in the new-born, it is viewed as a potential med-ical emergency, but if the fever is vac-cine induced, it is brushed off as “nor-mal” and parents are advised to sup-press it with antipyretics?
The medical mindset that imposesvaccine schedules in early infancy vio-lates a fundamental precautionaryprinciple which disregards the fragilityof the baby and the vulnerability of theimmature brain/nervoussystem/immune system. Just look at thedouble standard operative here. Onthe one hand parents are cautioned toseek immediate medical help if feverdevelops in the newborn, yet are heav-ily pressured to submit their babies tomultiple vaccines without regard forthe fact that these injections are theprimary cause of fever in younginfants. Fever is knowingly inducedduring these early weeks of life, whenall common sense and instinct shouldprevail to protect the infant from thisoutcome.
It is not only the vaccine inducedfevers which raise a caution. Whilethe fever signals the infant’s immuneresponse to the artificially implantedviral/bacterial and chemical agentshe/she is forced to cope with, the big-ger question is - what deeper affect dothese toxic substances have, now thatthey have access to the blood stream,vital organs and the immaturebrain/nervous system? And what addi-tional insult to injury occurs when theresulting fever is then manipulated
with antipyretic drugs preventing thenormal mobilization of the immunesystem?
A new theory regarding a potentialcause of autism is currently beingexplored by Dr. Anthony R. Torres,M.D., Senior Scientist and Director ofthe BioMedical Lab at Utah StateUniversity. His hypothesis questionswhether fever suppression is involvedin the etiology of autism and neurode-velopmental disorders.
Dr. Torres is investigating evidencesuggesting that the etiology of autisminvolves infections of the pregnantmother or of a young child. “Mostinfections result in fever that is rou-tinely controlled with antipyretics suchas acetaminophen. The blocking offever inhibits processes that evolvedover millions of years to protectagainst microbial attack. Immunemechanisms in the central nervous sys-tem are part of this protectiveprocess.” (4)
“Pathological infections, includingvaccinations, commonly result in fever.For example, 50-60% of young chil-dren develop fever after receivingMMR vaccine”, and are routinelytreated with fever suppressants. Manyparents report their children slippedinto autism following MMR shots. Dr.Torres has also found that “43% ofmothers with an autistic child experi-enced upper respiratory tract, influen-za-like, urinary or vaginal infectionsduring pregnancy compared to only26% of control mothers”, suggestingthat in some cases autism may belinked to the “sequella of pathogenicinfections, especially those of viral ori-gin.”(4)
Suppressing fever during pregnancyand labour may effect the fetus asresearch has shown that aceta-minophen “significantly decreasedmaternal and fetal serum IL-6”, animmune factor the infant is incapableof producing at birth and depends onfrom the mother.(4) A press release
Page 8 January - March 2003 VRAN Newsletter
Editorial cont. from page 7
Editorial cont. on page 9

(Oct./02) from the British ThoracicSociety cautions that a recent studylinks paracetamol, an acetaminophenbased drug similar to tylenol to child-hood asthma when used by the motherin late pregnancy.(5)
The central nervous system andscores of factors in the immune systemwork synergistically to achieve opti-mum immune function. What affectsone affects the other. Dr. Torres pointsto evidence that acetaminophen is animmunosuppresive agent. In highlytechnical language, he describes thecomplex activities launched by theimmune system and the many signalsrelayed to control centres in the brainwhen the body is fighting pathogenicorganisms. The activation of pyrogensstimulates the rise of fever and “pro-duction of various cytokines (immunecells) from organs in the viscera (gut)”– the gut being the primary and largestimmune organ of the body. Key sig-nals carried along the vagus nervewhich connects the gut/brain immunepathways, and which are normallymediated by prostaglandins, can beblocked by antipyretics like aceta-minophen, thereby derailing the com-plex sequences of immune signals thatflow between the gut and the brain. (4)
Dr. Torres postulates that the block-age of fever with antipyretics, whetherinduced by infections or vaccinations,interferes with normal immunologicaldevelopment in the brain, leading toneurodevelopmental disorders in cer-tain genetically and immunologicallydisposed individuals. The effects mayoccur in utero or at a very young agewhen the immune system is rapidlydeveloping. (4)
Kathy Blanco, President of CHILD-SCREEN www.childscreen.org, herselfa mother of autistic children, predictsthat these findings will not be popularwith mainstream medicine and are“potentially a public relations timebomb”. Searching for advice on feversand vaccine reactions on the internet,
Blanco found that the majority advise,‘If your child has a fever during a reac-tion to a vaccine, give them aceta-minophen’.
“This all too common advice mayactually cause autism. However, if Dr.Torres’ groundbreaking theory provestrue, it could be the means of savingthousands of children from becomingautistic.”
Currently, a tremendous amount offear is being whipped up over the out-break of SARS (severe acute respirato-ry syndrome) in this country. Healthofficials are in an uproar, even hintingthat this may be the “Big One” - thepandemic they’ve been anticipating foryears, even though it’s not influenza.Draconian quarantine measures arebeing implemented, and some sourcesare speculating whether this is a train-ing exercise to test the population’swillingness to submit to quarantine inpreparation for biowarfare attack. Todate there has been no definitive iden-tification of the pathogen, althoughthere is speculation that it is a form ofcorona virus, the family of virusesfound in the common cold. At onepoint it was thought it might be relat-ed to the paramyxo virus which isrelated to measles and canine distem-per –there’s even speculation thatchlamydia could be involved. Themeasles virus has been mutating andits footprint identified in some nastycases of encephalitis and respiratoryinfections in Asia in recent years.Already plans are rolling to start vac-cine development which is surprisingsince the virus or viral combination isyet to be identified.
Early reports described SARS asbeginning with a dry cough that keepsgetting worse, and that some peopleget headache, body ache, a “skyrocket-ing fever or blotchy rash on their bod-ies”, and as illnesses go, this one seemsfairly “vicious”. Treatment? Peopleare given a “battery of drugs – cock-tails of antibiotics and antiviral med-ications”.(6) They’re probably getting
strong doses of fever suppressants aswell……which has left me wonderingwhether antipyretics diminished theimmune capabilities of those who havedied from SARS. Is this one of thosediseases that needs a high fever to rallythe immune system to optimal output?Are the aggressive medical treatmentsactually creating a higher risk ofdeath?
Homeopathic and Naturopathichealing modalities have a long andtrusted history in the prevention andtreatment of epidemic diseases. One ofthe greatest antivirals known is vita-min C, which has been used with stu-pendous success in both the preventionand treatment of infectious diseases.Highly effective treatment protocolshave been developed by administeringascorbates of vitamin C intravenouslyin critical situations and are document-ed in medical literature and accessiblethrough Dr. Robert Cathcart’s websitewith links to Dr. Klenner, and LinusPauling. (7) Intravenous vitamin Cshould be available for every patientfacing acute and critical illnesses, butthe current medical monopoly blocksaccess to this simple and highly effec-tive treatment.
Writes health activist CroftWoodruff, “In the spring of 2000 Ireferred a young relative, who was suf-fering from an acute case of mononu-cleosis, to a medical doctor whoadministered four separate intravenousinjections of vitamin C as sodiumascorbate over as many days. Theresults were quite dramatic. Thepatient recovered completely, albeitwith a newly acquired respect for thepower of vitamin C as a healingagent.”
Our mistrust of natural processes,and reliance on drug oriented medicinehas obscured our understanding of theimportance of childhood illnesses andthe necessity of fever as a vital aspectof the maturation of the immune sys-tem enabling a strong & resilient foun-
Editorial cont. on page 10
VRAN Newsletter January - March 2003 Page 9
Editorial cont. from page 8

dation of health to evolve. When wediscard the old fears and lift the veil ofignorance, we are then empowered tosee with our innate intelligence, thereal picture unfolding in front of us -and recognize that the artificial manip-ulation of children’s immune systems,via mass vaccination programs, indis-criminate use of antipyretics andantibiotics, rather than protecting, isthreatening their health – their future.
The encouraging and wise words ofDr. Incao may help us shed old fearsand embrace a new relationship toNature – “Every childhood inflamma-tion, every cold, sore throat, earache,fever and rash is a healing crisis and acleansing process, a strong effort bythe human spirit to remodel the body,to make it a more suitable dwelling.Anthroposophic and homeopathicremedies aid and promote this cleans-ing process and help the illness towork its way out of the body so thathealing can occur.”(8) In a personalconversation recently, Dr. Incaoreminded me that – “ It takes a whileto free our mind from the imprison-ment, and our need to adhere to politi-cal correctness for fear of being judgedradical. Illness is part of life. It is notalien or abnormal and has to beaccepted as a part of life. Every break-down is a spiritual growth opportuni-ty. We need to learn how to deal withand work through it – this is part ofthe new paradigm.”
References: 1. Health Canada Advisory, Feb. 13/2003: .2. Philip Incao, M.D. – excerpt from a talk given at
NVIC conference 20003. Robert Mendelsohn, M.D. How To Raise a Healthy
Child in Spite of Your Docotor.4. Anthony R. Torres, M.D.-Is Fever Suppression
Involved In The Etiology Of Autism AndNeurodevelopmental Disorders?” .
5. Press Release, British Thoracic Society (BTS),28/10/2002 http://www.brit-thoracic.org.uk/admin/action.lasso?-database=btsnews&-layout=cgi&-
response=news_detail.html&-op=eq&id=209&-search6. The Globe & Mail, Mar.17/03 –Cause of Deadly
Pneumonia Still Eludes Scientists7 Dr. Robert Cathcart MD: at: /
8 Philip Incao, M.D. Chapter on How To TreatChildhood Illnesses, pge. 61; The VaccinationDilemma, and personal communication, April, 2003.
Sources of Complimentary andAlternative Healing Modalities:
Fever in children: A Blessing in Disguise,by Linda B White, M.D. and Sunny Mavor,Mothering Magazine, Issue 95,July/August, 1999, available on line at:www.mothering.com
Sheri Nakken website – great links tohomeopathic sources of information:http//www.nccn.net/~wwithin/vaccine.htm
Alternatives & Antidotes to InfectiousDiseases – Year end VRAN Newsletter,2001, lists many alternative healing modal-ities – available electronically at:[email protected]
EXTRACTS FROM MEDICAL LITERA-TURE: TYLENOL, PARACETAMOL,IBUPROFEN etc.Compiled by Hilary Butler
Could the increase in all forms ofmeningitis and other infectious diseasecomplications and deaths be becausefor the last 40+ years, the first thingparents do at the slightest sign of tem-perature is push paracetamol? Ibelieve so, because what you weren’ttold was this:
"Not all fevers need to be treatedbut many physicians do so to relieveparental concern." (Eur J Ped 1994Jun; 153 (6): 394-402)
"An elevation in temperature fol-lowing bacterial infection results in asignificant increase in host survival"(Science 1975 Apr 11; 188 (4184):166-8)
"Many components of the nonspe-cific host defence response to infectionsuch as leukocyte mobility, lymphocytetransformation, and the effects ofinterferon, appear to be enhanced byelevations in temperature that simulatemoderate fevers. In addition, some evi-dence indicates that a fever in conjunc-
tion with the changes in plasma ironlevels known to occur during infec-tions is a synergistic host defenceresponse." (Pediatrics 1980, No: 66 (5): 720 - 723)
"Parental fever phobia and its corre-lates...surprising, higher socioeconomicstatus was not associated with a lesserdegree of fever phobia...undue fear andoverly aggressive treatment of fever areepidemic among parents of infants andyoung children, even among the highlyeducated and well-to-do. considerableeffort will be required on the part ofpediatricians and other child healthworkers to reeducate parents about thedefinition, consequences and appropri-ate treatment of fever." (Pediatrics1985 June;75 (6) 1110-1113)
"There is no convincing evidencethat naturally occuring fevers areharmful. In contrast, animal studieshave shown that fever helps animals tosurvive and infection whereasantipyretic increases mortality.Moreover there is considerable in vitroevidence that a variety of humanimmunological defences function betterat febrile temperatures than at normalone." (The Lancet, Volume 337,March 9, 1991)
"Many cytokines are endogenousmediators of fever including inter-leukin (IL) -, 1 beta, IL-6 and others.Tumor necrosis factor-alpha may beboth an endogenous pyrogen and anendogenous antipyretic or cryogen."(Neuroimmunomodulation 1995 Jul-Aug; 2 (4):216-223)
"There is overwhelming evidence infavor of fever being an adaptive hostresponse to infection... as such, it isprobable that the use ofantipyretic/anti-inflammatory/analgesicdrugs, when they lead to suppressionof the fever, result in increased morbid-ity and mortality during most infec-tions; this morbidity and mortality
Page 10 January - March 2003 VRAN Newsletter
Editorial cont. from page 9
Editorial cont. on page 11
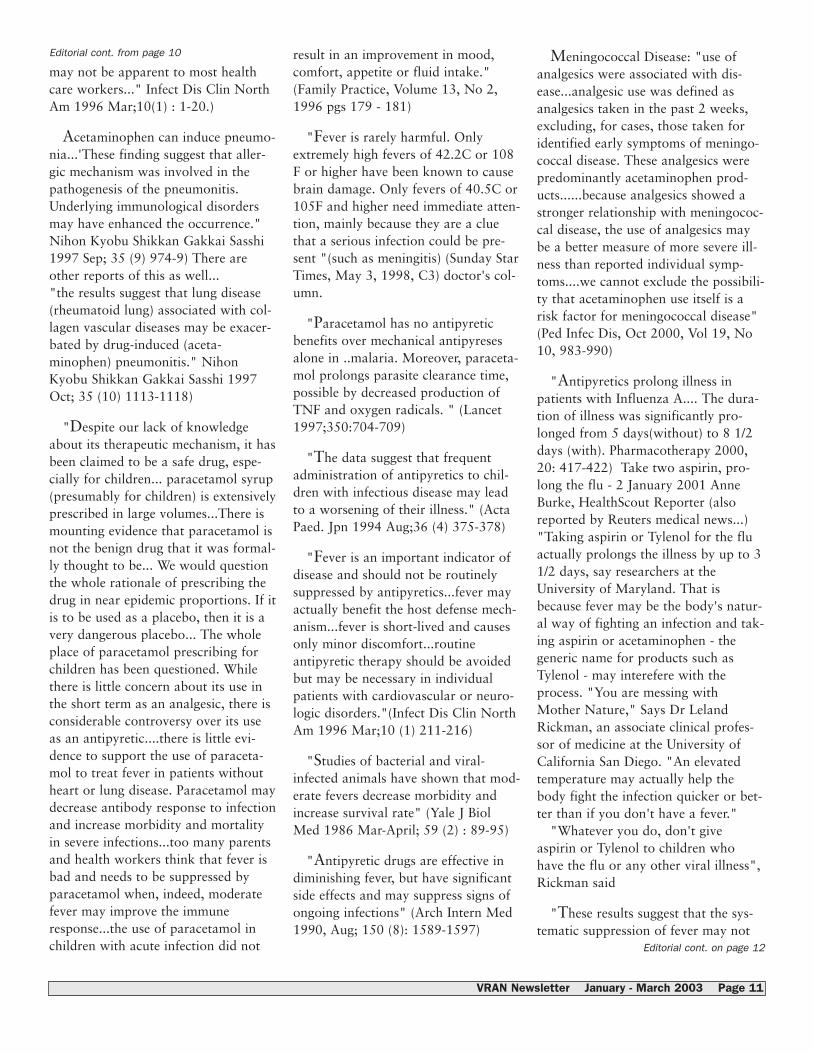
may not be apparent to most healthcare workers..." Infect Dis Clin NorthAm 1996 Mar;10(1) : 1-20.)
Acetaminophen can induce pneumo-nia...'These finding suggest that aller-gic mechanism was involved in thepathogenesis of the pneumonitis.Underlying immunological disordersmay have enhanced the occurrence."Nihon Kyobu Shikkan Gakkai Sasshi1997 Sep; 35 (9) 974-9) There areother reports of this as well..."the results suggest that lung disease(rheumatoid lung) associated with col-lagen vascular diseases may be exacer-bated by drug-induced (aceta-minophen) pneumonitis." NihonKyobu Shikkan Gakkai Sasshi 1997Oct; 35 (10) 1113-1118)
"Despite our lack of knowledgeabout its therapeutic mechanism, it hasbeen claimed to be a safe drug, espe-cially for children... paracetamol syrup(presumably for children) is extensivelyprescribed in large volumes...There ismounting evidence that paracetamol isnot the benign drug that it was formal-ly thought to be... We would questionthe whole rationale of prescribing thedrug in near epidemic proportions. If itis to be used as a placebo, then it is avery dangerous placebo... The wholeplace of paracetamol prescribing forchildren has been questioned. Whilethere is little concern about its use inthe short term as an analgesic, there isconsiderable controversy over its useas an antipyretic....there is little evi-dence to support the use of paraceta-mol to treat fever in patients withoutheart or lung disease. Paracetamol maydecrease antibody response to infectionand increase morbidity and mortalityin severe infections...too many parentsand health workers think that fever isbad and needs to be suppressed byparacetamol when, indeed, moderatefever may improve the immuneresponse...the use of paracetamol inchildren with acute infection did not
result in an improvement in mood,comfort, appetite or fluid intake."(Family Practice, Volume 13, No 2,1996 pgs 179 - 181)
"Fever is rarely harmful. Onlyextremely high fevers of 42.2C or 108F or higher have been known to causebrain damage. Only fevers of 40.5C or105F and higher need immediate atten-tion, mainly because they are a cluethat a serious infection could be pre-sent "(such as meningitis) (Sunday StarTimes, May 3, 1998, C3) doctor's col-umn.
"Paracetamol has no antipyreticbenefits over mechanical antipyresesalone in ..malaria. Moreover, paraceta-mol prolongs parasite clearance time,possible by decreased production ofTNF and oxygen radicals. " (Lancet1997;350:704-709)
"The data suggest that frequentadministration of antipyretics to chil-dren with infectious disease may leadto a worsening of their illness." (ActaPaed. Jpn 1994 Aug;36 (4) 375-378)
"Fever is an important indicator ofdisease and should not be routinelysuppressed by antipyretics...fever mayactually benefit the host defense mech-anism...fever is short-lived and causesonly minor discomfort...routineantipyretic therapy should be avoidedbut may be necessary in individualpatients with cardiovascular or neuro-logic disorders."(Infect Dis Clin NorthAm 1996 Mar;10 (1) 211-216)
"Studies of bacterial and viral-infected animals have shown that mod-erate fevers decrease morbidity andincrease survival rate" (Yale J BiolMed 1986 Mar-April; 59 (2) : 89-95)
"Antipyretic drugs are effective indiminishing fever, but have significantside effects and may suppress signs ofongoing infections" (Arch Intern Med1990, Aug; 150 (8): 1589-1597)
Meningococcal Disease: "use ofanalgesics were associated with dis-ease...analgesic use was defined asanalgesics taken in the past 2 weeks,excluding, for cases, those taken foridentified early symptoms of meningo-coccal disease. These analgesics werepredominantly acetaminophen prod-ucts......because analgesics showed astronger relationship with meningococ-cal disease, the use of analgesics maybe a better measure of more severe ill-ness than reported individual symp-toms....we cannot exclude the possibili-ty that acetaminophen use itself is arisk factor for meningococcal disease"(Ped Infec Dis, Oct 2000, Vol 19, No10, 983-990)
"Antipyretics prolong illness inpatients with Influenza A.... The dura-tion of illness was significantly pro-longed from 5 days(without) to 8 1/2days (with). Pharmacotherapy 2000,20: 417-422) Take two aspirin, pro-long the flu - 2 January 2001 AnneBurke, HealthScout Reporter (alsoreported by Reuters medical news...)"Taking aspirin or Tylenol for the fluactually prolongs the illness by up to 31/2 days, say researchers at theUniversity of Maryland. That isbecause fever may be the body's natur-al way of fighting an infection and tak-ing aspirin or acetaminophen - thegeneric name for products such asTylenol - may interefere with theprocess. "You are messing withMother Nature," Says Dr LelandRickman, an associate clinical profes-sor of medicine at the University ofCalifornia San Diego. "An elevatedtemperature may actually help thebody fight the infection quicker or bet-ter than if you don't have a fever."
"Whatever you do, don't giveaspirin or Tylenol to children whohave the flu or any other viral illness",Rickman said
"These results suggest that the sys-tematic suppression of fever may not
Editorial cont. on page 12
VRAN Newsletter January - March 2003 Page 11
Editorial cont. from page 10

be useful in patients without severecranial trauma or significant hypox-emia. Letting fever take its naturalcourse does not seem to harm patientswith systemic inflammatory responsesyndrome, or influence the discomfortlevel AND MAY SAVE COSTS."(wow!!!) (Arch Intern Med 2001, Jan8; 161 (1) 121-123)
Chickenpox treated withTylenol/Ibuprofen provokes bacterialskin infections into fulminant necrotis-ing fasciitis (Pediatr I(Pediatrics Vol103, No 4, April 1999, 783-784 and785-790) (Infect Med1999 16 (5):307)Just two of many references forantipyretic induced complications ofchickenpox. (In MMWR - May 15,1998, Vol 47 No 18. All cases ofVaricella related deaths were treatedwith antipyretics. No causal associa-tion was investigated or ascribed. The"solution" to the problem was consid-ered to be mandatory vaccination.)
Hilary Butler – “What you do as aparent, is your choice. Make sure thatit is an "informed" choice. Get thearticles referenced, do a med-linesearch - retrieve any others. READ thewhole articles. Give them to your doc-tor to read, and discuss them withhim/her. Most importantly, if you feelyour child has an immunodeficiency,get your child tested so that you knowwhat you are dealing with. How achild handles any infectious disease isdependant upon the immune systeminherited, nutritional status, life-style,environment and resultant stresses andhow the child reacts to them. Thechoice is yours.”
With appreciation to Hilary Butlerand The Immunization AwarenessSociety, New Zealand for their per-mission to reprint this review, pub-lished in WAVES – Vol. 14, No. 4,2002
One of the statistics that is bandiedabout these days is that 1-3 out of1000 die of measles in developedcountries like the United States.
If that is the case, however, it begsthe question, “Why?” Because, in thepast, at least in the United States, thedeath rate from measles was consider-ably lower.
The Washington Post and othershave reported that measles has becomemore deadly because the epidemiologyhas shifted to infants and adults, forwhom the disease is more serious. As Istated in my 1993 testimony to theInstitute of Medicine:
“We also cannot ignore the impactof vaccines on changing epidemiologywhen considering their risks and bene-fits. For instance, measles may havebeen made a more serious diseasebecause of measles vaccination. Priorto widespread vaccination, once a pop-ulation had been exposed to measles,few adults or infants contracted it,adults due to lifelong immunity andinfants due to maternal antibodies.(Full text at website below) Now,adults AND infants are getting themeasles, with serious consequences. Iwould like to include reference to arecent Washington Post article entitled:
“Measles Still Menace to Infants:Vaccinated Moms Pass Less Immunityto Babies’. In this article it was notedthat although in 1976 3% of measlescases occurred in children less thanone, today more than 25% do. Theauthor also indicated that prior to vac-cination, 3 to 4 million measles casesoccurred with around 500 deaths. Thiswould make the case-fatality ratio forthat period between 1 to 2 per 10,000.In the years 1989, 1990 and 1991combined, however, it was reportedthat around 55,000 people got themeasles and 166 died, making the
case-fatality ratio dramatically higherat 3 out of 1,000. At this rate, fewerthan 175,000 cases per year would benecessary to result in the same numberof deaths which used to occur whenthere were millions of cases.”
While as reported by ElisabethRosenthal, in the New York Times in1991, “Officials at the Centers forDisease Control note that the deathrates may be somewhat inflatedbecause mild cases of measles areprobably not being reported.
Such underreporting would makedeath rates artificially high. Atkinson(of the CDC) said there may be twiceas many cases nationally as have beenreported.”
She went on to write: “But manydoctors still believe the trend is realand alarming. ‘The death rates areclearly much higher this time around,and the hospitalization rate is extraor-dinary.’ said Dr. Samuel Katz, profes-sor of pediatrics at Duke UniversityMedical School who is a measlesexpert.”
And as I wrote in an open letter tothe producers and sponsors of NBC’s“ER”, which garnered many hundredsof signatures:
“An example of an unexamined‘fact’ you presented to your viewerswas the statement that 1 out of 500measles cases die. Perhaps your sourcesdid not explain this to you, but theU.S. measles death rate used to be farlower prior to vaccination. So if thisstatistic is correct, one should askwhat is the likely reason for thisincreased measles death rate. Theprobable cause is that adults andinfants, for whom measles can be quiteserious, now get the measles, ratherthan children, for whom it is generallybenign. (Please bear in mind that the
Page 12 January - March 2003 VRAN Newsletter
Editorial cont. from page 11
Measles cont. on page 13
MEASLES IN THE VACCINATION AGE:IS IT NOW DEADLIER ?By Sandy Mintz - September 13,2002

greater risk for adults and infants isnot our opinion, but the opinion ofmany, including Dr. Sam Katz, one ofthe developers of the measles vaccine.In a chapter on measles vaccine in theThird Edition of ‘Vaccines’, he writeswith two others: ‘The risk of seriouscomplications and death is increased ininfants and adults.’ And later, ‘Thehighest risk of death was in childrenyounger than 1 year and adults.’)*
*It is interesting to note that in a1990 article on measles vaccine, writ-ten by Drs. Walter Orenstein, Directorof the National Immunization Programat the CDC, and Lauri Markowitz, oneof the co-authors of both the 1990article and the Katz article and former-ly of the CDC, it was stated: ‘>From1950 to 1959, an annual average ofmore than 500,000 cases and 500deaths were reported. However, thetrue number of infections was estimat-ed to be 10 times as high.’ In otherwords, if only reported cases are con-sidered, the death rate appears to be1/1000. If you factor in the number ofunreported cases, quite high during theera when measles was common, thedeath rate drops to 1/10,000. In themore recent Katz ‘Vaccines’ article, co-written with Redd and Markowitz, itsays that the death rate is 1 to 3 in1000 cases (pg.223), even though laterin the article they say that there usedto be, ‘in the prevaccine era’ (pg. 229),around 500 deaths among 4,000,000cases (actually 1.25/10,000 cases).Either they are exaggerating the cur-rent death rate, or it has gone up. Wesubmit that if the death rate has risen,measles vaccine is the cause, havingchanged measles epidemiology so thathigh-risk groups now more often getthe measles. “
Thus it would appear that themeasles death rate post-vaccination hasindeed become higher.
Are we to take the fact that measlesappears to have become more deadlyto mean a higher death rate is a benefit
of vaccination? Or are we to acknowl-edge it as a risk?
If measles vaccine fails to controlmeasles over time, i.e., the vaccinewanes and revaccination does notwork, and at the same time the diseasefails to be eradicated, is our future tobe filled with large outbreaks and highdeath rates because measles vaccinehas changed the epidemiology ofmeasles in such a way that increasedincidence among infants and adults isthe result?
Wouldn’t it be a good idea for ustake our heads out of the sand andthoroughly investigate the benefits andrisks of vaccination without presuppo-sitions, preconditions, or the influenceof those who seek to gain financiallyfrom their use?
About the Author:Sandy Mintz, is a mother, healthresearcher and veteran vaccine riskeducator. She has been widelyacclaimed for her weekly “Scandals”column, a series of well researched andhard hitting articles that shed light onthe far reaching health impact of massvaccination policies.For a broader perspective of the con-cerns raised in this article, you mayaccess all supportive articles and back-ground research by going to:http://www.vaccinationnews.com/Scandals/Sept_13_02/Scandal33.htm
Sandy Mintz home site at VaccinationNews:http://www.vaccinationnews.com
Mandated vaccinations, or vaccina-tions administered without the recipi-ent's knowledge of risks, or fullyinformed consent, begs what is per-haps the most fundamental of all ques-tions: Who owns our bodies? Webelieve that we are in control of ourlives and, therefore, “own” ourselves.But, if someone outside of ourself hasthe authority to subject us to medicalexperimentation without our knowl-edge or fully informed consent, thenwe cannot logically argue ownership ofourselves any more convincingly thana laboratory animal, can we?
An article entitled “The ComplicatedTask of Monitoring Vaccine Safety”appeared in the Public Health Reportsof January/February 1997. This is apublication of the U.S. Department ofHealth and Human Services. Theauthors were Susan Ellenberg andRobert Chen. Below is an excerpt fromtheir rather revealing synopsis:
“Vaccines, like all other pharmaceu-tical products, are not entirely risk-free; while most known side effectsare minor and self-limited, some vac-cines have been associated with veryrare but serious adverse effects.Because such rare effects are oftennot evident until vaccines come intowidespread use, the Federal govern-ment maintains ongoing surveillanceprograms to monitor vaccine safety.The interpretation of data from suchprograms is complex and associatedwith substantial uncertainty. A con-tinual effort to monitor these dataeffectively and to develop more pre-cise ways of assessing risks of vac-cines is necessary to ensure publicconfidence in immunization programs.”
VRAN Newsletter January - March 2003 Page 13
Measles cont. from page 12
Under the Hump cont. on page 14
WHAT’S UNDERTHE HUMP ?Public Health Service admits“substantial uncertainty”regarding vaccine safetyBy Michael P. Wright

The writers admit that the clinicaltrials of vaccines are not sufficient toidentify and measure the risk levelsassociated with adverse events. Ineffect, the vaccinated population itselfbecomes an experimental group. Theyalso admit that there is “substantialuncertainty” associated with interpre-tation of data from surveillance pro-grams.
Further, the writers do not see anyneed to assess the belief that vaccinesare effective and good for publichealth. They accept this view as a pos-tulate. They see the questioning of vac-cination programs by some members ofthe public as a problem, and the onlychallenge for them is to defeat the
skepticism. For those who remain skeptical, con-
sideration of problems of vaccine safe-ty should take place with the commonstatistical concept of the normal distri-bution (bell-shaped curve) in mind. Anold statistics book from my collegedays provides a good starting point forthe argument:
...it is interesting to note that a verylarge number of random variablesobserved in nature possess a frequen-cy distribution which is approxi-mately bell-shaped or, as the statisti-cian would say, is approximately anormal probability distribution.~William Mendenhall(Introduction to Statistics, p. 116)
In nature we have all kinds of mea-surable events and phenomena. Somehumans are tall, some are short, butmost are of medium height. Regardingadverse events to vaccines, some arevery mild, and some are very serious.We can expect the normal adverseevent to be somewhere in between. Ifall adverse events were known andscored by severity level, the resultsexpressed as a graph most likely wouldform a bell-shaped curve. At one endof the curve would be the “rare” cata-strophic adverse effects and at theother end the mild effects such as tem-porary redness and swelling withoutother problems. The big question is:What do we have under the hump ofthe curve?
Page 14 January - March 2003 VRAN Newsletter
Under the Hump cont. from page 13
The writers for Public HealthReports use the phrase “known sideeffects,” and assure us that most are“minor and self-limited.” Are thereunknown adverse effects which devel-op later in childhood or adult life and
which have not been recognized asconsequences of vaccination?
From what we know about normaldistributions we would expect that inthe middle would be the most commontypes of adverse events -- those less
serious than the rare catastrophesnoted contemporaneously with vacci-nations but still serious enough to befigured into the process of weighingrisks versus benefits (if there are any)of vaccination.

I propose that the adverse effectsinclude neurological damage fromrepeated doses of mercury and otherfactors in vaccines and that these prob-lems manifest at a later stage of child-hood development in the form ofbehavioral disorders and learning dis-ability in many of our youth. This kindof adverse event has not been recog-nized by the vaccine-pushers in govern-ment and industry. It needs to beresearched and the risk levels need tobe measured.
American public health agencies notinterested
Unfortunately, I learned at the 1996CDC conference that the advancedmedical diagnostic system I haddesigned to assess risk of HIV infec-tions (which may also be applied tohepatitis B and chlamydia) did nothave a chance of being implemented byAmerican public health agencies. Otherliterature at the conference indicatedthat the big push was on for indiscrim-inate universal vaccination of infantsfor hepatitis B. Since the hep B virus isblood-borne and contracted by behav-iors and risk situations that usuallydon't emerge until adolescence oradulthood, I think this practice is bothwasteful and hazardous from thestandpoint of adverse effects from vac-cination. At the conference I noticedmany booths of pharmaceutical com-panies.
British vaccine-pusher calls me“Hopelessly wrong”
In particular I remember one meet-ing in which there was a discussionabout vaccine safety. During the ques-tion and comment period I made thestatement that the decision to vaccinatefor a particular disease should bebased upon the comparison of tworisks:
1. the risk of contracting a seriousillness if not vaccinated; and 2. the risk of a serious adverse eventif vaccinated. I recall that two CDC officials
expressed stern disagreement with mystatement. I was also told by an arro-gant British doctor that I was “hope-lessly wrong.” Vaccine safety advocateDr. Kristine Severyn identified him tome as being on the payroll of a phar-maceutical company. She is with theOhio Parents for Vaccine Safety. Thiswas a disillusioning experience.
There is much to criticize about theflaws in American medical culture. Weare over-medicalized, over-diagnosed,over-drugged and over-vaccinated. Agood argument was made along theselines by Richard D. Lamm, formergovernor of Colorado. It is entitled“The Ethics of Excess,” and is inPublic Health Reports, May/June1996. No. 3.
About the Author:Michael Wright is the inventor of aninnovative medical diagnostic systemdesigned to anonymously assess risk ofHIV infections. It can also be appliedto chlamydia and hepatitis B. It is astate-of-the-art system for use by com-puters for medical diagnostic decisionsupport (MDDS). He was the first inthe medical press to report using a sys-tem of this nature. His project reportwas published in the 1996 CDC con-ference abstracts.
Michael Phillip Wright AIDS dissentwebsite readers can link to governmentwebsites confirming his grant historyand publication record:http://members.aol.com/mpwright9/aids10.htmlhttp://members.aol.com/mpwright9/aids.html
Story excerpted from the IdahoObserver, - January 15, 2003. For thefull story – go to:http://proliberty.com/observ-er/20030104.htm
Ameeta Mathur,Hepatitis B Vaccination ProgramDirector, Toronto, Publich Health DepartmentOctober 1, 2002
Dear Ameeta,
In October of 1999, my son Markwas a student at JB Tyrrell SeniorPublic School. We received notificationthat all grade 7 students would beimmunized against Hepatitis B. therewere mild side effects outlined in theliterature provided. Unfortunately weassumed that the information had beenwell researched.
Mark received his first dose onOctober 23. Within days he developednausea, fatigue, a croup like coughwhich required Emergency room inter-vention, headache and general malaise.These sympotoms persisted on and offover the next two months. We wereassured that although they began soonafter the Hepatitis B immunization,there was no possibility that the twowere related. Countless times we weretold, “This is the safest vaccine on themarket.” The pharmaceutical compa-nies have obviously been very effectiveat conveying their message.
By January, Mark was healthy again,attending school, playing competitivehockey. We were advised to get thesecond shot in the series, at a clinic atthe Scarborough Board of Education.Within 12 hours of the second immu-nization, Mark developed severe nau-sea, fatigue, headache, photophobiaand muscle pain. The croup likecough returned and he was treatedtwice in ER for severe respiratory dis-tress. He developed dizziness and thenan odd pattern of nausea and gaggingthat would last for several hours at atime. He was admitted to North YorkGeneral Hospital and invetigated byan Infectious Disease Specialist. We
Under the Hump cont. from page 14
Letters cont. on page 16
VRAN Newsletter January - March 2003 Page 15
LETTERS

were assured that he had contracted avirus. Despite exhausitve viral studies,no virus was identified. Mark wasbedridden and did not return to schoolfor 3 months.
I spoke to several nurses at theToronto Public Health Department. Iwas told that they were not familiarwith this type of adverse reaction.They had no information about med-ical support for this type of situation.They advised me to see my family doc-tor and made no attempt to followMark’s progress.
Over the next three years, Markmissed countless days of school. Hesuffered from nausea, fatigue, arthral-gia so severe he could barely walk tothe bathroom, dizziness, headache,flushing, repeated bouts of gaggingand multiple episodes of croup andasthma. Even in grade 9, two yearsafter the initial immunizatin, he con-tinued to suffer from the same oddpattern of symptoms and was absentfor a total of 89 school days.
After being assessed by a number ofphysicians at The Hospital for SickChildren, he was finally diagnosedwith Chronic Fatigue ImmuneDeficiency syndrome. What we hadsuspected all along was finallyacknowledged. There have been severeand debilitating side effects from theHepatitis B vaccine. In the medical lit-erature, this phenomenon has beenwell documented. This was not an iso-lated incident.
In retrospect, as a mother with abaccalaureate degree in nursing, I real-ize how naïve it was to assume that thepotential side effects had been ade-quately communicated. In theCompendium of Pharmaceuticals andSpecialties, every medication has acomplete listing, symtom by symptom,of side effects that have been identi-fied, regardless of how rare. Howcould a genetically engineered proteinmixed with Thimerosal, a mercurybased preservative, injected intramus-
cularly, have no significant side effectsor risks? Why aren’t physicians suspi-cious when an unusual and unex-plained illnes follows vaccine adminis-tration? Why are these incidents notreported?
Since Mark became ill, I have done agreat deal of research. I would hopethat the Toronto Public HealthDepartment takes responsibility forensuring informed consent, communi-cating parents’ rights to forgo immu-nization for reasons of conscience orreligion, and for monitoring childrenwhere an advers reaction is suspected.
All the potential risks of this vaccineshould be clearly communicated. Howmany parents know what Thimerosalis? How do you expect them to knowif their child has an allergy to this mer-cury based preservative? Given all theinformation available about its toxiceffects, why is the Toronto PublicHealth Department allowing a vaccine,which still contains it, to be adminis-tered?
As a parent, I have watched mychild suffer immeasureably. In light ofincreasing evidence that vaccines maybe linked to a wide spectrum of neuro-logic and autoimmune disorders, I urgeyou to take your responsibility veryseriously so that other children are notdamaged by this vaccine. Be sure thatchildren like Mark don’t fall throughthe cracks.
Sincerely, Maureen Dragasevich
Note: We thank VRAN member,Maureen D. for forwarding us the let-ter she wrote to Toronto PublicHealth, to which she has received noacknowledgement of any kind.
* * * * * * * * * * * * * * * * *CBC T.V’s Marketplace Expose onMedical Ghostwriting (Intro to thesegment)
March 25, 2003 -“Medical ghost-writing. It's a world that could makeyour doctor prescribe the wrong
drug….. People with scientific back-grounds are paid to stay in the shad-ows and crank out favourable reportsfor drug companies. Then, drug com-panies get doctors to put their nameson the studies - for money, prestige, orperks.”http://www.cbc.ca/consumers/indepth/medical/index.html
Susan Fletcher responds
“It is tragic that what used to be anoble and humanitarian pursuit, iepure science, is being systematicallytrashed by the contemptible trickery ofghostwriters, the medical professionalswho endorse their reports and, ofcourse most of all, the pharmaceuticalindustry. With such a dragnet of decep-tion how are we to trust even the"raw" data from research? How med-ical professionals and "scientists" cancontinue to mouth their reverence forthe "god of science" while corruptingit to gain personal wealth and power isbeyond me.
No greater deception has occurredthan that of the vaccine industry wherenewborns are offered up as sacrificiallambs, their guardians brainwashedinto thinking they are doing the rightthing for their child and society.Neither they nor most of the medicalprofession who do the brainwashing,having themselves been brainwashed inmedical school, have a clue that thesechildren are participating in the real"safety study".
The whole of the world’s populationis gradually becoming increasinglyimmune crippled through vaccine-induced loss of natural and passiveimmunity and endangered by thethreat of vaccine-induced pathogenicmutants. WE SHOULD ALL BE UPON OUR FEET IN OUTRAGE!
Susan’s response – Posted March 28,2002 on Marketplace messageboardhttp://interact.cbc.ca/cgi-bin/WebX?8@@.ee8a9dc.773a90fe
Letters cont. on page 17
Page 16 January - March 2003 VRAN Newsletter
Letters cont. from page 15

Scott and Sheri Hunter share Kirk’sStory - 3 years later
It's been a three year epic story of abattle-weary family perseveringthrough difficult heart-ripping painand medical ridicule against all odds.
It amazes me how time has screamedby. Many of you in similar circum-stances can relate I'm sure. Watchingyour child every hour of every dayconcerned that they might yet beripped from your steadfast grip.Sleeping when you can, waking hun-dreds of times through the night tosubtle changes in breathing patterns,suffering through toxic drug therapyyour infant child won't take unless dis-guised in a meal, drugs designed tohelp that often can cause more troublethan the disease. Then realizing herefuses to eat because the food tastelike drugs and still refusing to eat evenwhen they are removed because of theassociation.
The emergency staff know you byname, you fight daily a host of healthprofessionals, pediatricians, neurolo-gists, that deny vaccine injury. Youfight for occupational therapy, speechlanguage pathology, physio, andunderstanding. All the while research-ing on your own the drugs, their sideeffects, alternative therapy, treatmentoptions, traveling to city after citypicking large professional brains toostrained to really help. Trying to keepemployed as the bills mount, losingincome while a spouse becomes a fulltime caregiver…..$'s for the Mayoclinic…..$'s for non-recovered drugsand remedy costs, countless $'s on gasand hotels, unrecovered respite care,special therapy devices, diet scales,processors, special organic food anddrink....and don't even talk about dia-pers! $$$$!
Exhaustively meeting and e-mailinghealth administrators, policy makers,politicians, pharmaceuticals, mediaand governments...all the while work-ing through depression, Paxil with-
drawal side effects and still trying tomake time to be a "normal" family forthe sake of our first son who is mostlyleft to fend for himself. Watching hisparents struggle while his brother laps-es into yet another intractable grandmal seizure, turns blue and the EMT'sarrive for the second time in twomonths with oxygen. Only the hearti-est of old friends still call. Family isscared to death to be within miles ofthe demilitarized Hunter house buteagerly offer unqualified help.
What a truly tragic story...it's surre-al, beyond belief and it's happening tous. It's been three years and we'recompletely and thoroughly rung out.
The story is incomplete however.The rest has yet to be written as Sheriand I do all we can to influence theauthor…..we're writing a story of tri-umph and faith. Despite the odds ourneurologist and statistics gave Kirk, heis making incredible progress. Not thekind you see as a casual observer butmonolithic advances to the initiated.
After 16 months of 10 seizures a day(lasting10-20min each), on daily drugtherapy that included maximum dosesof tegretol (carbamazepine) andclobozam (frisium) as well as a 4:1ketogenic diet, we now have a 3 yearold son that walks, runs, climbs stairs,laughs, eats regular food (gluten-lac-tose free) and causes his brother trou-ble. He is gaining weight and growinglike a weed and mostimportantly…..drug free! He is notcompletely without seizures and does-n't yet talk but is developing despitethe professionals’ insistence it was acongenital condition possibly triggeredby vaccine. They said he would ceaseto develop beyond the onset of seizuresat 6 months. They were wrong!
His seizures were not congenital,they were a product of his own brokenimmune system hopelessly thrown intochaos by the vaccine. The reason Iknow this is a direct result of his suc-cessful therapy. Over two years ago webegan seeing a homeopath in Winnipeg
by pure chance. While on an Ottawabound flight in February 2000, myfather spoke by accident with awoman who worked for the ManitobaMinister of Health. After hearing ofour story she referred him to a coura-geous woman she had met attemptingto change the way government seeshomeopathic care... enter Dr. LeelamaNielsen. We decided to visit her as anafter thought while attending mybrothers wedding the followingSeptember 2000.
As Kirk's condition was aggravatedby the stress of travel he was having15 seizures a day several minutes longwhen we walked into the clinic. Wewere taken by surprise when Dr.Nielsen looked Kirk over and withinminutes declared without tests he hada urinary tract infection. With equalhaste she began shoving unmeasureddrops of Colubrina (a remedy) in hismouth, and when we began toprotest.…ours too. We were skepticaland afraid because previous attemptsto help Kirk homeopathically were metwith even more seizures. We left forSaskatoon the following day on ahomeopathic regimen and Kirk wentwithout a seizure for three weeks andhad one seizure a month total for thenext EIGHT following our visit ! Hehad previously not enjoyed a seizurefree day since the vaccine injury inDecember1999. We began to eliminatetegretol by Christmas, and by the fol-lowing April he was off all drugs. Weslowly weaned him off the ketogenicdiet until completely by January 2002.
Today he has small seizures that arepurposefully aggravated by remediesand has the occasional "bad day" aswe continue to right the immunologi-cal ship. Dr. Nielsen's clinic nowenjoys another 100 or so clients madeup of friends, family and other injuredchildren who have witnessed Kirk'sprogress. It's hasn't been easy as westill are strapped in every fashion. Wecan't yet imagine where the strength
Letters cont. on page 18
VRAN Newsletter January - March 2003 Page 17
Letters cont. from page 16

and money will come from each andevery day, but there are good days andweeks, and that for now is enough.
It is important to Sheri and I to tellothers our story of hope knowing thereis precious little out there. In no mea-sure do we profess others might see thesame results, but truly feel we mustshare the seeming miracle God and thiswoman have performed thus far. Wecannot know what's ahead and it'svery much two steps forward - oneback. We can only pray things willcontinue to improve. We encouragethose who would like to know more tocontact us through Edda West atVRAN. For Kirk's original story,Collateral Damage, visitwww.vran.org
Lupus is a devastating autoimmunedisease that no one should have to dealwith, let alone a teenager with the restof her life ahead of her. My name isPriscilla and I am currently 22 yearsold and have been coping with this lifealtering disease for the past five years.
As a teenager, I was active, energeticand healthy with no major health con-cerns other than the odd cold. I wentto school, played the piano, worked apart-time job, and was a member ofthe Royal Canadian Sea Cadets attend-ing and teaching various summer train-ing programs. I was a happy girlenjoying my life and looking forwardto new experiences. I was not expect-ing the subsequent events that changedmy life after receiving the hepatitis Bvaccination.
In grade eleven, my high school wasrunning a mandatory hepatitis B vacci-nation clinic. We were all obligated toreceive the vaccine. The school hadprovided us with an information pack-age about the vaccine, which led mymother and I to believe that the vac-cine was safe and that by taking it, itcould only help. Nowhere amongstthe two pages were listed any of theside affects associated with the vacci-nation. My mother signed the consentform and I received a series of threeshots, the last was in April of 1997.Shortly after, I began to notice changesin my health.
In the summer of 1997, I was seven-teen years old and attending a summertraining course in Kingston, Ontariofor 8 weeks. It was additional trainingoffered by the Sea Cadet programwhich required a high amount of phys-ical exercise. I was rather excited andup to the task; however, throughoutthe duration of the 8 weeks, I began tonotice that I would bruise fairly easily,and most bruises, I was unable toexplain what had caused them. I
began to notice that my nose wouldbleed frequently. Some episodes wouldlast up to one hour. Weeks passed andI returned home to begin anotherschool year. It was in the fall of thatyear that I was called into the emer-gency department because my nosewould not stop bleeding. My familydoctor had found a low platelet countin one of my blood tests from bloodwork to determine why I was bruising.At that point, I was diagnosed withITP. I was first injected with platelets,which did not help, then later I wastreated with high dose oral steroids,intravenous steroids and another formof treatment, which seemed to workwell was IVIG (gamma-globulin). Iwent through several of the IVIG treat-ments, which seemed to improve myplatelets and bring them from a dan-gerously low 2,000 up to an acceptable50,000 (normal range from 150,000 to400,000). I was taking a regular doseof oral steroids called Prednisone tokeep my immune system under controlso that my platelets would remain sta-ble. This treatment seemed to workfor a while; however, prednisone is ananti-inflammatory drug that suppressesthe immune system. Soon after, I camedown with a cold which caused anoth-er steep drop in my platelets and;therefore, I had to endure more aggres-sive treatment. At this point, myOncologist had tested me for Lupus;the results had read that I was on theborderline of Lupus. The doctor hadtold me that Lupus was an autoim-mune disorder and that I need notworry since I was only borderline. Ilistened to him and tried to move onwith my life.
After hurdling over this first obstaclewith my health, my mother and I hadbegun researching about my condition.Upon digging through various reports,we discovered one that linked thehepatitis B vaccination with various
Letters cont. from page 17
Page 18 January - March 2003 VRAN Newsletter
Do Your Homework cont. on page 19
ALWAYS DO YOUR HOMEWORKBy Priscilla Pajda

diseases such as multiple sclerosis,Lupus, ITP and the many more. Ifonly we had received this informationpackage before the vaccine, we wouldhave been better informed and wouldhave fought not to receive the vaccine.
For one year, my platelets were on aroller coaster ride, going up and downconstantly. My mother and I evenwent to see an ITP specialist atMcMaster University in London,Ontario. The doctor strongly suggest-ed that I have my spleen removed,because he felt that this would be thebest possible treatment. I decided,with the support of my mother that Iwould keep my spleen. I felt thatremoving my spleen would not be theanswer.
I continued treatment with pred-nisone and began to notice the undesir-able physical side affects of bloatingand weight gain. This continued overthe year and in the fall of 1998, Ibegan to notice severe joint pain,migraines, nausea, which I thoughtwere all symptoms of the flu. I soonrealized that it was something muchmore serious. When I started to noticethat my urine was turning red, that iswhen I visited my family doctor. Uponlooking at the urine sample, sheacknowledged that there was a prob-lem and the test confirmed that mykidneys were in distress. Upon furthertesting in the emergency department,my Oncologist re-diagnosed me withacute Lupus Nephritis and I was hospi-talized for the following four weeks.He later told me that the ITP was thebeginning of my disease with Lupus.He also told me that this was gradefour Lupus, the most aggressive formthat attacks the body itself, in my case,the kidneys. Not only did I now havelow platelets, but also my kidneys werenow on the verge of shutting down.
The doctors tried all sorts of treat-ment from high dose steroids, IVIGand even cyclophosphomide (a form ofchemotherapy). I had a bad allergic
reaction to the cyclophosphomide andI had to convince my doctors that Iwould not take any more of that drug.Over the next few weeks, my kidneyfunction began to improve, enough sothat I was able to be discharged fromthe hospital and go home. Due to theill effects of the cyclophosphomidetreatment and my medical condition,my muscle mass decreased as did mystrength. It was difficult to walk andclimb stairs. I was eventually rehabili-tated and after three months of thera-py and extra tutoring, I was able toreturn to school to complete my finalyear and graduate from high school.
Over the next couple of years, mydisease seemed to be well managed. Iwas able to complete one year of stud-ies at the University of Toronto; how-ever, in October of 2000, my lupusflared up and I was admitted to thehospital yet again. This time around,the kidneys were hit even harder. Iwas experiencing renal failure. Inorder to save them, and myself, mydoctors started me on kidney dialysis.In one week, I gained 50 pounds ofwater weight and ballooned out to thepoint where it felt like my skin wascracking. It was very difficult for meto walk and I was practically bed-rid-den until the dialysis machine was ableto remove a considerable amount ofwater from my body. To this day Ihave horrible stretch marks all over mybody that may fade with time, butnever go away. After spending threemonths in my hospital bed, I wascleared to go home; however, I wouldhave to return to the hospital 3 times aweek to be dialyzed for four hourseach time. Needless to say, I wasunable to complete my second year ofuniversity and I am still waiting to behealthy enough to resume my studies.
Although I am still being treatedwith prednisone, I have been taking acocktail of other drugs; some to sup-press my immune system, one to lowerblood pressure and another to lowermy heart rate. Some drugs I take are
to counter the effects of other drugs. Iwas concerned about the side effects Iwas experiencing from the variousmedications. I felt that the drugs alonewould not cure me. I researched alter-native methods to combine with mymedical treatment. Over the next fewyears, I went to see iridologists, home-opaths and even a doctor that practicesin environmental medicine. I changedmy diet, taken herbal supplements andvitamins, anything that could possiblyhelp. I even went to see a chiropractorand an acupuncturist to see if theycould help.
Furthermore, the dialysis was physi-cally and emotionally draining. I hadno strength or energy to do anything.I was constantly miserable. I evenchanged my acupuncturist to one thatused a different technique. Whilegoing to him for treatment, I alsochanged my diet. I avoided meat andanimal products and continued to doso over the next 6 weeks. After 8months of being dialysis dependant, Iwas able to stop dialysis. My doctorswere amazed that I did not need any-more dialysis since my blood tests wererelatively stable.
I know that my kidneys are severelyscarred and could never be repaired;however, I am grateful that for thetime being, I do not require dialysis. Iclosely monitor the status of my condi-tion and continue to take my medica-tion along with alternate forms oftreatment. To conclude, I regret takingthe Hepatitis B vaccination. I believethat if I refused the vaccine, I wouldcurrently be living a normal andhealthy life. To this day, none of myfamily members have taken theHepatitis B vaccination nor would theyeven consider it. After diligentlyresearching the side effects of variousvaccinations, they have chosen todecline the newly advocated Flu vac-cine. My advice to anyone who is con-sidering taking any sort of vaccina-tion…please do your homework!
VRAN Newsletter January - March 2003 Page 19
Do Your Homework cont. from page 18

The father of a two month oldCalgary boy, who suffered bleeding inthe brain and retinal hemorrhaging,faced a charge of aggravated assault inconnection with injuries discoveredafter the child was admitted to hospitalfor emergency care. The court wastold that the baby was in good healthat 7 a.m., then deteriorated later in theday and was rushed to hospital.Pediatric specialist in child abuse, Dr.Neil Cooper testified that the baby hadall the “typical injuries associated withhaving been violently shaken.”
Under cross-examination by thedefense lawyer Laurie Hnatiuk,Cooper said it is not uncommon forchildren to be shaken shortly afterbeing immunized. The baby had histwo-month shots five days prior –because they become irritable and“people lose it easier” in thoseinstances.(story reported in Calgary Herald,Nov.5/02) (1)
Child abuse “experts” in NorthAmerica, UK, Australia jump on anycase that involves brain swelling/bleedsand retinal bleeding as grounds for SBSprosecution. In their determination toprove child abuse, they refuse to con-sider evidence of vaccine complicity inbrain injuries. Shaken Baby Syndrome(SBS) remains an unproven theory, yetis increasingly used to prosecute inno-cent parents whose babies succumb tolife threatening vaccine injuries.
Writes Dr. Frederick H. Roy, M.D.in Ocular Differential Diagnosis,“increased intracranial pressure (fromany cause) are listed as possible causesof retinal hemorrhages, as well as theDPT, polio, and MMR vaccines.Retinal hemorrhages have been causedby occlusion of the central retinal veinfollowing a hepatitis B vaccine, andchildhood resuscitation followingevents other than trauma.” (4)
Dr.Patrick D. Barnes, M.D.,Pediatric Neuroradiolgist, cautionsabout jumping to conclusions whendiagnosing brain injuries - "To date,there is no scientific basis that indi-cates how much, or how little force isnecessary to produce traumatic injuryto the developing CNS, (central ner-vous system)…..The medical and imag-ing evidence, particularly where thereis only CNS injury, cannot accuratelydiagnose presumed intentional injury.”He goes on to say that there are manyclinical features that may mimic abuse,which include……”accidental injury,certain coagulopathies, vascular dis-eases, infectious or post-infectiousconditions (e.g. post vaccinal), meta-bolic disorders, neoplastic diseases,certain therapies, and some congenitaland dysplastic disorders.” (2)
Frighteningly, the Canadian JointStatement on Shaken Baby Syndrome,an official policy paper endorsed byHealth Canada and other agencies, isconstructed on erroneous, and scientif-ically unsubstantiated presumptionsthat promulgate the SBS myth andignores recent studies which disproveviolent shaking as the sole cause ofthese type of injuries.(3)(5)
Dr. Harold E. Buttram, M.D. has,for several years intensely studied thefield of SBS and followed the work ofveteran physicians and researcher inthis field. In his detailed rebuttal tothe Joint Statement on SBS he showsthat many of the premises and claimson which SBS accusations and convic-tions are being made are flawed anderroneous…“if a large portion of SBSaccusations are the result of misdiag-nosis, as many are coming to believe,then we are witnessing a rapidly grow-ing reign of terror against the familiesof English-speaking countries.” (4)
The tragic case of Alan Yurko,wrongfully sentenced to serve life + tenyears for the death of his baby boy as
a cover for vaccine induced injuriesand medical malpractice is familiar tomany. In the prevailing climate, thiscould happen to any one of us. Yurkois one of hundreds, possibly thousandsof innocent parents who have beenimprisoned for SBS which has replacedsudden infant death syndrome as acover for vaccine induced injuries.
Despite being born premature andhaving a multitude of health problemscontraindicating the administration ofvaccines, the baby Alan was injectedwith the most reactive lot of DTaP vac-cine, one of 810 vaccine “hot” lotsreported to the U.S.Vaccine AdverseEvent Reporting System (VAERS).Contributing to the baby’s death onadmittance to hospital for “cardiacarrest and apnea”, were excessivedoses of sodium bicarbonate and 8.8times the amount of heparin recom-mended for an infant, causing bleedingof the brain and all the symptomsleading to the misdiagnosis of SBS.
More than two dozen autopsy mis-takes have been identified whichinclude listing baby Alan as blackwhen he is white, a head circumference10 cms less than when he was born, adetailed exam of non existent heart tis-sue as baby Alan’s heart and internalorgans were “harvested” for trans-plants to other infants prior to autop-sy.
Last December, two Florida men’ssentences were commuted when it wasdiscovered an incompetent medicalexaminer incorrectly established thedeaths of the babies in their care to beshaken baby syndrome. Since therelease of those two men, local mediainterest in Yurko’s case has increaseddramatically and Yurko supporters allover the world have been writing let-ters, sending emails and faxes, andmaking phone calls to those who couldhave a say in reopening this case. If Yurko’s appeal is heard and won, orsentence is commuted, a convincingprecedent will have been set and other
Shaken Baby Syndrome cont. on page 21
Page 20 January - March 2003 VRAN Newsletter
SHAKEN BABY SYNDROMEA COVER FOR VACCINE INJURY

innocent parents may be released fromprison. Your supportive letters willgreatly enhance Alan Yurko’s chancesfor a successful appeal.
Sample letters:http://www.vaclib.org/news/dyurkolet-ter.htm#lettersYurko website: Research, articles,appeal documents: www.freeyurko.bizland.com
Final Note: The Yurko Project is indesperate need of funds in order forthe upcoming appeal trial to have thesuccessful outcome we are anticipating. Donations can be made at: http://freeyurko.bizland.com/donate
References:1. Pediatrician tells court baby violently
shaken; Calgary Herald, Nov.5/022. Patrick D. Barnes, M.D. Ethical Issues in
Imaging Nonaccidental Injury: ChildAbuse; Topics in Magnetic ResonanceImaging Vol. 13 No. 2 :85-94, Nov.2002
3. Health Canada weblink to JointStatement on SBS: http://www.hc-sc.gc.ca/dca-dea/publications/jointstate-ment_web_e.html
4 Dr. Harold E. Buttram, M.D. A Rebuttalto the Joint Statement on Shaken BabySyndrome, Minister of Public Works andGovernment Services, Ottawa, 2001. –www.vran.org General Issues – ShakenBaby Syndrome
5 Brain Study Casts Doubt on ShakenBaby Deaths : The Telegraph 21/06/01reports new study lead by Dr. JennianGeddes, Journal Brain as reported in theNew Scientist June 13, 2001http://www.telegraph.co.uk/connected/main.jhtml?xml=/connected/2001/06/21/eenshak21.xml&secureRefresh=true&_requestid=150771
Editor’s note: With appreciation tolong time VRAN member RitaHoffman for sending us this admissionfrom allergist, Dr. Peter Vadas,Director of Allergy and ClinicalImmunology at St. Michael’s Hospitalin Toronto when he appeared onHealth on the Line – Discovery HealthChannel, 2002. Says Rita, “ Perhapswe are at least partly responsible forforcing these allergists to deal with theimmune system carnage that has beencaused by vaccination. It looks likethey can't deny it any longer!!
A. Haines: Welcome back. Joining usnow is Dr. Peter Vadas, Director ofAllergy and Clinical Immunology at St.Michael's Hospital in Toronto. Dr.Vadas has written numerous researcharticles about allergies. Thank you forbeing here.
P. Vadas: It's my pleasure.
A. Haines: I wanted to ask you firstoff, as an expert in this field, whetheror not we are seeing more peanut aller-gies or is it just that there is moreawareness?
P. Vadas: No, there is a combination ofboth factors. Generally speaking allallergies are on the rise in WesternIndustrialized nations and that includesfood allergies in particular and peanutallergies specifically.
A. Haines: Why is that?
P. Vadas: Well, there are a number offactors, it's a little bit technical, butthe easy answer is part of it has to dowith the amount of consumption.There is more exposure to peanuts atsusceptible ages and if you look at theamount of consumption then the pro-
portion of people with peanut allergyrises along with consumption but it'smore than that. There are factors to dowith how we vaccinate our kids veryearly on in life, how much drugs,antibiotics we give the kids early on inlife all of which tend to predisposemore towards allergy.
A. Haines: So do you think early vacci-nation is not a good thing?
P. Vadas: No, I think it's a wonderfulthing. It's an absolutely crucial thingfrom the standpoint of public health tominimize the likelihood of severe infec-tions, but on the other hand, one ofthe spin offs is that there are a certainproportion of the population that aregoing to be more prone to developingallergies as a consequence of that.
* * * * * * * * * * * * * * * *
Says Rita, “The sad part is the inter-viewer left it at that. Further on in theshow it showed that as many as600,000 Canadians may be affected byanaphylaxis. All that immune systemcarnage for the so called “good of all”.Between 1986 and 1990 there were 63deaths in Canada from anaphylaxis."A conservative estimate is that 2% ofthe population (approx. 600,000Canadians) may be affected by poten-tially life-threatening allergies". -Source Anaphylaxis Network ofCanada
VRAN Newsletter January - March 2003 Page 21
Shaken Baby Syndrome cont. from page 20
OOOPS -WHO LET THE CAT OUT OF THE BAG ?
Ontario Universal Flu Program a DudA retrospective study of 5 Ontario
hospitals published in the July, 2002issue of Canadian Journal ofEmergency Medicine found that “therewas no significant correlation betweeninfluenza rates and EmergencyDepartment volumes.” Data from 5hospitals showed that, “during influen-za season, acute respiratory diagnosesaccounted for only 4.4% of ED visitsand influenza for only 0.34% of visits.During the influenza season after theuniversal immunization campaign, EDvisits increased at all sites. The studyconcluded that, “a universal influenzaimmunization campaign is unlikely toaffect ED volume.” Since 2000,Ontario has spent over $100 millionon its “universal” flu vaccine program.http://www.caep.ca/004.cjem-
jcmu/004-00.cjem/vol-4.2002/v44-245.htm
Childhood Vaccines Linked to Autism,Heart Disease - March 27, 2003
A new study authored by Dr. MarkGeier, M.D., President of the GeneticCenters of America, appears to con-firm the link between thimerosal con-taining vaccines and the proliferationof neurodevelopment disorders such asautism, speech disorders, as well asheart disease. Over the last 20 years,and since the widespread use ofthimerosal in vaccines, autism rateshave increased by more than 800 per-cent, from one in about 2,500 childrenin the mid-1980s to one in about 300children in 1996. The findings of thestudy are published in the current issueof the Journal of American Physicians
and Surgeons For the complete articlego to: http://www.aapsonline.org
Health Canada states that mercurybased thimerosal, has been removedfrom 11 of the “routinely recommend-ed” pediatric vaccines currently in usein Canada, but that trace amounts stillremain in some from the manufactur-ing process. According to table 3 ofHealth Canada’s statement onthimerosal, “many licensed vaccinescontain thimerosal as a preservative”.Presumably these are for adult use. Forthe Statement on Thimerosal and vac-cine tables, please refer to:http://www.hc-sc.gc.ca/pphb-dgspsp/publicat/ccdr-rmtc/03vol29/acs-dcc-1/index.htmlThird death after smallpox shot,restrictions urged – Mar. 28/03
Page 22 January - March 2003 VRAN Newsletter
Currently Canada has no accessible vaccine reaction reporting system, and Health Canada’s unspoken policy seems to be toblock the search for records of vaccine adverse reactions – to make it so difficult that only the most persistent will succeedin obtaining these records. The following is from the U.S. Vaccine Adverse Events Reporting System (VAERS). Pleaseremember it represents between 1-10% of vaccine reactions that actually happen. The majority, 90% or more of vaccinereactions, injuries and deaths remain unreported and obscured. In Canada, death following vaccination is not counted inany official records that we are aware of, but hidden away and lumped into Sudden Infant Death statistics.
Adverse Reactions reported to VAERS from 1999-2002, age 0-6 years.Source: http://www.medalerts.org/vaersdb/DTaP - 16,544 adverse reactions reportedFlu - 419Hep - 13,363Hib - 22,463MMR - 18,680OPV - 22,915*VARC - 11,246 (1995-2002)
Hospitalizations reported to VAERS from 1999-2002, age 0-6 years.DTaP - 1,631 hospitalizations reportedFlu - 41Hep - 1,840Hib - 3,224MMR - 1,736OPV - 2,868*VARC - 576 (1995-2002)
VACCINE REACTION REPORTS
NEWSCLIPS
Deaths reported to VAERS from 1999-2002, age 0-6 yearsDTaP - 394 deaths reportedFlu - 11Hep - 642Hib - 843MMR - 110OPV - 866*VARC - 34 (1995-2002)
* VARC = Chickenpox vaccine

The Centers for Disease Control andPrevention's Advisory Committee onVaccine Practices (ACIP) held an emer-gency meeting to discuss two heartattack deaths, two incidents of heartinflammation, and three cases of chestpain in healthcare workers who hadrecently received the smallpox vaccine.The third death was a 55 year oldNational Guardsman who was foundto have “substantial” heart disease.The virus used in the vaccine, vacciniavirus, is known to cause inflammationof the heart muscle and lining, so thecases of inflammation were not sur-prising, said Melinda Wharton of theCDC's National ImmunizationProgram. Some experts speculate thatthe inflammatory reaction to the livevirus might be triggering heart attacksor other problems in people already atrisk. Excerpted from :http://www.reutershealth.com/en/index.html
EPA Children’s Health Report Altered Parents are questioning how a pur-
portedly comprehensive report releasedby the U.S. Environmental ProtectionAgency (EPA), that clearly acknowl-edges concerns about mercury damageto the neurological development offetuses, infants and children, can failto mention vaccines, a major source ofexposure to these vulnerable groups.They have accused the EnvironmentalProtection Agency (EPA) of alteringthe report and failing to include vac-cines as an important source of mer-cury exposure. Lyn Redwood, RN,President of SAFE MINDS and parentof a child who received 125 times hisEPA allowable exposure to mercuryfrom thimerosal containing vaccines,asks, "How can EPA caution pregnantwomen to avoid tuna that containsapproximately 17 mcg of mercury, butremain silent on the fact that someinfants were exposed to 237.5 mcg ofmercury from their vaccines?" Parentsare demanding the original EPA reportbe released immediately and thatmoney be allocated for unbiased inves-
tigations into thimerosal and adverseneurological outcomes.http://www.safeminds.org/
Vaccine Articles in Canadian MedicalAssociation Journal
The March, 2003 issue of theCanadian Medical Association Journalhas published several interesting vac-cine articles that offer a glimpse of theprevailing mindset and are available online at: http://www.cmaj.ca/cti/collec-tion/vaccination?page=1
Best of all is Susan Fletcher’s boldand feisty letter to the editor, whichthe CMAJ has also posted on its web-site, and titled “Why all the ChronicDiseases in Children? Canada NeedsRigorous Vaccine Studies” Followingis an excerpt from her letter:
“It is heartening to see that HealthCanada and public health authoritiesare now starting to show concernabout the dismal state of Canadians’health, especially young Canadians’,and actively promote lifestyle changes.But with all the autism, learning dis-abilities, asthma, diabetes, etc afflictingso many of our children today it isimperative that we go beyond that andfind and rout the environmental andother factors that are causing thischronic disease. Vaccine informationgroups such as the one to which Ibelong have for many years suggesteda connection between such disease andthe use of vaccines, especially multi-dose vaccines. To date we have notseen any NIH reviews or vaccine trialsthat have had the validity to conclu-sively show that such a connectiondoes not exist. In view of the tremen-dous amount of non-infectious diseasein our children, I propose that, ratherthan lobby the federal government foradditional universal vaccine programs,the CMAJ lobby the government tosponsor vaccine trials of unquestion-able rigour so that once and for all wecan determine whether or not vaccinesare a source of chronic ill health in ourchildren….. It’s my guess that, if thiswere done, it might lead to a different“Enlightenment”. To read Susan
Fletcher’s complete letter go to:http://www.cmaj.ca/cgi/elet-ters/168/5/533
Voices of Safety International (VOISI)A Voices of Safety International
report has concluded that “Childrenwho received all of the AAP recom-mended vaccinations were 14 timesmore likely to become learning dis-abled and 8 times more likely tobecome autistic compared with chil-dren who were never vaccinated.” Theresearch is based on the response fromparents of approximately 1400 chil-dren. The children were divided intothree groups: those who received"All", "Some" or "None" of routinelyrecommended vaccines. Report andresearch tables can be viewed at:http://www.voicesofsafety.com/t1-ph-v50-2-research-addendum.htm
VOISI is also working to set stan-dards for newborn screening forimmunologic fragility. In the first stan-dard for screening the strength of anewborn's immune system before giv-ing the Hep B shot, the results of arecent 1623 sample study showed thatapproximately 2 1/2% of newbornshave hyper IgE, a sign of immununeanomaly. V50.3A - Standard to DelayVaccinating Newbornshttp://www.voicesofsafety.com/tl-ph-v50-3a-standard.htm
National Immunization ConferenceVictoria, B.C. - December, 2002
A main conference theme was thedevelopment of a national immuniza-tion strategy which would co-ordinatevaccine agendas across Canada. On ahumorous note, health officials arelooking for chiropractors willing toforward the cause of vaccinations.There’s also a rather humorous pictureof the Queen waving a stick over Dr.Arlene King of the PlanningCommittee as if knighting her for vac-cination deeds well done:http;//www.hc-sc.gc.ca/pphb-dgspsp/cnic-ccni/2002/dn-pq-02/20021202_e.html#a
VRAN Newsletter January - March 2003 Page 23
Newsclips cont. from page 22

Page 24 January - March 2003 VRAN Newsletter
RESOURCE &INFORMATION LISTImmunization: History, Ethics,Law & Healthby Catherine Diodati. Best newbook about vaccines. Please orderfrom VRANCost: $35 + $5 postage
Immunization—The RealityBehind The Mythby Walene James.
What Every Parent Should KnowAbout Childhood Immunizationby Jamie Murphy
Vaccinations: Are They ReallySafe and Effective?by Neil Z. Miller
How To Raise a Healthy Child InSpite of Your Doctorby Robert Mendelsohn, M.D.
Universal Immunization —Medical Miracle or MasterfulMirage?by Dr. Raymond Obomsawinavailable from Health ActionNetwork(604) 435-0512
A Shot in The Darkby Dr. Harris L. Coulter &Barbara Loe Fisher
Vaccination, Social Violence,Criminality: The Medical Assaulton The American Brainby Dr. Harris L. Coulter
Vaccination—Medical Assault onthe Immune Systemby Viera Scheibner Ph.D.to order: ( 204) 895-9192
The Immune Trioby Dr. Harold ButtramTo order call 215-536-5168
Every Second Childby Dr. Archie Kalokerinos (204)895-9192
Vaccinations and Immunization:Dangers, Delusions and Alternativesby Dr. Leon Chaitow.
What About Immunizations?Exposing the Vaccine Philosophyby Cynthia Cournoyer Nelson’sBooks, Box 2302 Santa Cruz, CA,95063
Natural Alternatives to Vaccinationby Dr. Zoltan Rona, M.D.1-877-920-8887
Vaccinations—The Rest of the Storypublished by MotheringMagazine. P.O. Box 1690-SantaFe, N.M. 87504.
The Immunization Decision—AGuide for Parentsby Dr. Randal Neustaedter.
The Case Against Immunizationsby Richard Moscovitch M.D.available from American Instituteof Homeopathy, 1500Massachusetts Ave. N.W.Washington, D.C. 20005.
The Immunization Resource Guideby Diane Rozarioavailable from Vaccine PolicyInstitute(937) 435-4750
Vaccination—The Hidden TruthNew Video. Five medical doctorsspeak out about vaccine risks.Order from VRANCost—$40 + $5 postage
MANY OF THESE TITLESCAN BE ORDERED FROMPARENT BOOKS INTORONTO(416) 537-8334 √
To order information packages, books, videos, or to subscribe to the newsletter,
contact VRAN
P.O. BOX 169WINLAW, BC
VOG 2J0
or call 250-355-2525email: [email protected]
FOR DIRECT ACCESS TO TOP VACCINE AWARENESS SITES,PLEASE REFER TO VRAN’S NEW WEBSITE AT: www.vran.org

Newsclips cont. on page 26
VRAN Newsletter March - June 2002 Page 25
West Nile Virus cont. from page 24

Page 26 March - June 2002 VRAN Newsletter
Hepatitis A Vaccine cont. on page 27

VRAN Newsletter March - June 2002 Page 27
Hepatitis A Vaccine cont. from page 26

Page 28 March - June 2002 VRAN Newsletter
Pertussis Remedies cont. from page <None>

Newsclips cont. from page 28
Newsclips cont. on page 30
VRAN Newsletter March - June 2002 Page 29

VRAN Newsletter March - June 2002 Page 30
Newsclips cont. from page 29

VRAN Newsletter March - June 2002 Page 31
Autism, ADD/ADHD cont. on page 32

Page 32 March - June 2002 VRAN Newsletter
Autism, ADD/ADHD cont. from page 31

VRAN Newsletter March - June 2002 Page 33
CIPRO cont. from page 32
Smallpox cont. on page 34

Page 34 March - June 2002 VRAN Newsletter
Smallpox cont. from page 33
Newsclips cont. on page 35

VRAN Newsletter March - June 2002 Page 35
Newsclips cont. from page 34
Newsclips cont. on page 36

Page 36 March - June 2002 VRAN Newsletter
Newsclips cont. from page 35
Newsclips cont. on page 37

VRAN Newsletter March - June 2002 Page 37
Newsclips cont. from page 36

Page 38 March - June 2002 VRAN Newsletter
THE SUM OF ALL FEARSby Kathy Blanco
The Sum of All Fears cont. on page 39
VRAN Newsletter March - June 2002 Page 39
FETAL ALCOHOLEFFECTS ORIMMUNIZATIONEFFECTS?by Diane Fuller
The Sum of All Fears cont. from page 38

Page 40 March - June 2002 VRAN Newsletter
Fetal Alcohol cont. on page 41
Fetal Alcohol cont. from page 39

VRAN Newsletter March - June 2002 Page 41
Fetal Alcohol cont. from page 40

Page 42 March - June 2002 VRAN Newsletter

VRAN Newsletter March - June 2002 Page 43

Page 44 March - June 2002 VRAN Newsletter