Jane Davison Daisy Garland Ketogenic Dietitian Nottingham Children’s Hospital.
29
Jane Davison Daisy Garland Ketogenic Dietitian Nottingham Children’s Hospital
-
Upload
leslie-stephens -
Category
Documents
-
view
214 -
download
0
Transcript of Jane Davison Daisy Garland Ketogenic Dietitian Nottingham Children’s Hospital.

Jane Davison
Daisy Garland Ketogenic DietitianNottingham Children’s Hospital

What is the ketogenic diet?
• It is a high fat, low carbohydrate and adequate protein diet used in the treatment of intractable epilepsy
• It aims to decrease the number and severity of the patients’ seizures
• Therefore improving the quality of life and hopefully reducing medication use

Indications for use
• Intractable childhood epilepsy* *incomplete seizure control despite > 2 AED
• GLUT 1 deficiency syndrome• PDH deficiency • Consider as early treatment for myoclonic astatic epilepsy • Age not a barrier but works well in younger children, e.g. under 10years

Efficacy
• Randomised controlled trial at GOS 2008
• 150 patients
• After 3 months 38% had >50% seizure reduction compared with 6%
in the control phase
• 7% had >90% reduction in seizures

Efficacy
• Study also compared the Classical and MCT (Medium Chain
Triglyceride) diets
• Results showed no difference in efficacy or tolerability between
the 2 diets after 3,6, and 12 months
• Those on the MCT version had a little more nausea

Once selected
• Family agree to a 3 month commitment period on the diet as there is a huge investment of professional time
• 3 months is the best time scale to determine outcomes• Diet usually advised for up to 2 years• Expectations from medical team and families need to be
discussed to assist future monitoring

The dietetic aims
• To achieve ketosis by providing fat for metabolism• To ensure that growth is adequate• To ensure nutritional well being is not compromised• To implement a dietary regimen that is palatable and
possible to comply with

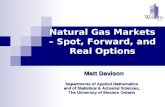
Normal diet
Energy distribution from a normal diet:
Protein
Fat
Carbohydrate

Ketogenic diet
Energy distribution from a classical ketogenic diet:
Protein
Fat
Carbohydrate

Types of Ketogenic Diet
• Classical 4:1 and 3:1 ratio i.e. Calorie controlled with 4 or 3 parts fat to 1 part protein and carbohydrate
combined• MCT diet (medium chain triglycerides) Calorie controlled 40-60% energy from MCT allows a little more flexibility but high
MCT intake can lead to nausea

Types of Ketogenic Diet• Modified Ketogenic diet 60% fat 30% protein 10% CHO The carbohydrate intake is limited to approximately 20g per day Less strict still needs good knowledge of foods to choose Energy intake monitored for weight control• Low Glycaemic Index (GI) diet Energy distribution as above but choice of foods with GI less than 50 typically high fibre foods Total carbohydrate load 40-60g per day

Protein
lean meats
small amount of lentils
fish
eggsCheddar cheese
small amount of nuts

Fatcream cheese
double cream
mayonnaise
oils(e.g. olive oil, sunflower oil)
avocadobutter or margarine
Liquigen
Calogen

Carbohydrate
carrots
swede
tomatoes
mushrooms
raspberries
strawberries
peaches
pear
broccoliceleriac
Preferred sources of carbohydrate

CarbohydrateSources of carbohydrate to avoid
bread
peaches
sweets
cake
rice
pasta
chocolate
biscuits
sugar

Example of Foods
• F

Examples of foods

Products for the Ketogenic diet
• KetoCal 4:1Multi fibre For enteral feeding• 200ml carton 300kcal 6.2gP 1.2gCarb 29.6gFat
• KetoCal 3:1 powder For enteral feeding Suitable from birth

Supplementation Products
• Calogen 50% LCT fat• CarbZero 20% LCT fat
• Liquigen 50% MCT fat• Betaquik 20% MCT fat
• Vitamin and Minerals e.g. Fruitivits Phlexy Vits

Monitoring
• Growth: weight, height, and well being
• Bloods, urine other tests e.g. ECG, renal USS
• Record of seizures • Record of ketosis -Blood use Abbott meter Freestyle Optium Neo (need lancets & ketone strips) aim 2-5mmol/l -Urine use Ketostix aim for (+2 to +4) or 8-16mmol/l

Short term problems
• Nausea• Vomiting• Hypoglycaemia• Acidosis• Sleepiness• Dehydration• Diet refusal

Long term problems
• Constipation • Renal stones• Abnormal lipid profile• Growth• Bone demineralization and fractures

Excess ketosis
• Rapid panting or breathing• Facial flushing, vomiting • Irritability and unexpected tiredness• Acidosis• Blood ketone reading 6mmol/l or “Hi” with symptoms Treat with 1-2 tablespoons of sweet drink If no improvement after 15
minutes repeat and contact Dr

Illness
• If IV fluids needed use 0.9% saline
• 4 hourly blood glucose
• Avoid sugar and carbohydrate containing drugs and IV
solutions

Other considerations
• Carnitine It is a protein which is necessary to carry fat into the mitochondria
to be broken down to energy (ATP) KD high in fat therefore ↑need KD low in lysine + methionine needed to synthesize carnitine ↑Excretion of acylcarnitine with ketosis

Nottingham experience
• Daisy Garland funding since 2009 initially 0.5WTE now service is 0.3WTE with 0.2WTE funded from Daisy Garland
• Over 30 patients have been put on the diet in 5 years
• November 2014 Current patients 13 paediatric patients plus 1 adult gastrostomy fed patient

Nottingham experience
• 3 metabolic patients• 6 gastrostomy fed patients experiencing >75% seizure reduction
and 1 with complete seizure freedom weaned off medication and is now weaning off diet gradually
• 4 on oral K.D. diet having >75% seizure reduction• 2 waiting to start

Websites
• www.thedaisygarland.org.uk• www.matthewsfriends.org.uk• www.charliefoundation.org

Keto santa’s!