
James C. McElnay School of Pharmacy The Queen’s University of Belfast Pharmaceutical care in...
46
James C. McElnay School of Pharmacy The Queen’s University of Belfast Pharmaceutical care in community pharma
-
Upload
roger-oconnor -
Category
Documents
-
view
216 -
download
1
Transcript of James C. McElnay School of Pharmacy The Queen’s University of Belfast Pharmaceutical care in...
James C. McElnaySchool of PharmacyThe Queen’s University of Belfast
Pharmaceutical care in community pharmacy

Pharmaceutical carePharmaceutical care
Three main components:
• ensure patient is receiving optimal drug therapy (minimise drug related
problems)
• patient education (illness, medication, healthy lifestyle, treatment goals,
need for compliance with medication regimens)
• monitoring patient outcomes
– self-monitoring plan
– monitoring of goal achievement

Outcomes of Pharmaceutical CareOutcomes of Pharmaceutical Care
cure of a disease (CAP)
elimination or reduction of a patient’s
symptomatology (asthma; diabetes, PUD)
arresting or slowing of a disease process (rheumatoid arthritis; diabetes; CHF;
COPD)
preventing a disease or symptomatology (smoking cessation)

H.PyloriH.Pylori eradication eradication
Brit. J. Clin. Pharmacol. (2002) 53,163-171.Brit. J. Clin. Pharmacol. (2002) 53,163-171.

MethodsMethods
• Study design • Prospective, randomised, controlled clinical trial
• Combination therapy used• Lansoprazole, amoxicillin and clarithromycin
• Patients• Endoscopy confirmed PUD with H. pylori• Intervention group (n = 38 )• Control group (n = 38)
• Pharmaceutical care intervention• Patient education (disease / need for compliance with treatment)• F/U telephone call midway through therapy

23.7
92.1
010
2030
4050
6070
8090
100
%
Control Intervention
Adherence rateAdherence rate

7273.7
94.7
50
60
70
80
90
100
Pre-study Control Intervention
Era
dica
ti r
ate
(%)
Eradication rateEradication rate

ConclusionsConclusions
• H pylori eradication rate and compliance rate were significantly
increased
• Significant difference between the routine clinical practice and
counselling enhanced treatment
• Involvement of pharmacist led to improved cost-effectiveness of
treatment

Question
• What percentage of community pharmacists provide robust advice to, and follow-up adherence checking of, patients who are receiving H. pylori eradication therapy?

Pharmaceutical care of asthma patients
J. Appl. Ther. (1997) 1, 145- 161 Pharmacotherapy (2001) 21, 1196-1203.

Comparison of inhaler scores in controls and in patients receiving education/monitoring intervention * p<0.05
* * *
40
50
6
750
8
90
10100
1 2 3 4 5 6
Assessment period: 1-3 baseline, 4-6 intervention
% I
nhal
er s
core
(±9
5% C
I)
Inhaler scores in control Inhaler scores in patients receiving education
J. Appl. Ther., 1, 145-161 (1997)
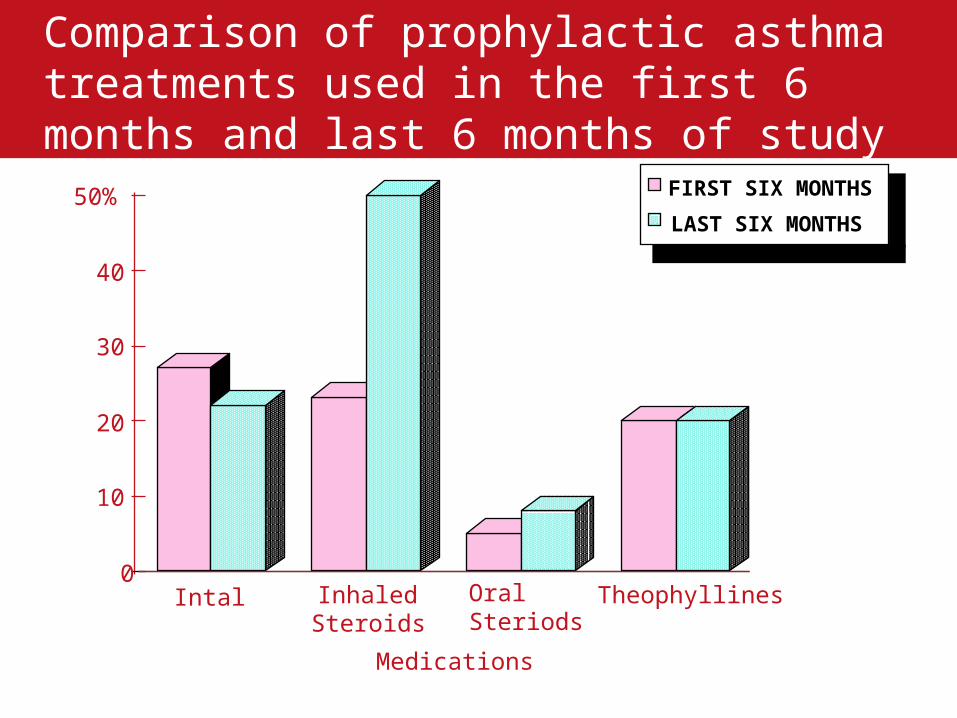
Comparison of prophylactic asthma treatments used in the first 6 months and last 6 months of study period
0
10
20
30
40
50%
Intal InhaledSteroids
Oral Steriods
Theophyllines
Medications
FIRST SIX MONTHS
LAST SIX MONTHS

Asthma International Perspective
• Northern Ireland
• Netherlands
• Belgium
• Iceland
• Denmark
• Malta

Conclusion
Positive Impact on:• Health Related Quality of Life
• Inhaler Technique
• Peak Expiratory Flow
• Self-Reported Symptoms
• Pharmacist-patient Relationship
• Hospitalisation?

Question
• What percentage of community pharmacists provide good pharmaceutical care / medicines management to their asthma patients?
Care of elderly patientsCare of elderly patients
Pharmacotherapy (1999) 19,860-869
Pharm. World Sci. (2003) 25, 218-226
Pharmacoeconomics (2003) 21, 455-465
Clin Drug Invest (2003) 23, 119-128
Brit. J. Clin Pharmacol. (2005) 60, 183 - 193

Question
• What percentage of community pharmacists provide good pharmaceutical care / medicines management services to all their elderly patients?

Individualised smoking cessation programme (PAS)
Pharmacoeconomics (1998) 14,323-333
Addiction (2001) 96, 325-331.
Aim of smoking cessation study
The aim of the study was to examine, in a randomised controlled clinical trial, the success of the PAS model as a method of smoking cessation in the community pharmacy setting.

The PAS Smoking Cessation Model
STEP 1
STEP 4
STEP 3
STEP 2
To encourage and motivate clients using the pharmacy to stop smoking
To identify what type of help and support your client’s need to stop smoking
Gaining your client’s commitment to stop smoking
To support and monitor smokers wishing to stop smoking

Intervention subjects (PAS)
• Verbal advice and leaflets
• Client’s NRT needs and position on the cycle of change assessed
• Details of intervention recorded on individual patient file
• Return visit at established intervals

Control subjects
• Normal practice as usually performed in pharmacy (including use of NRT)
• Patient profile sheet completed
• Contact 3, 6 months and 1 year for feedback on smoking status

Outcome Measures
• Self reported smoking cessation at 3, 6 and 12 months
• Cotinine confirmed smoking cessation at 12 months
• Pharmacist views on the service (focus groups)

Results
• Intervention (PAS) (n=265)
– 14.34% smoking abstinence at 1 year (n=38)
• Control (ad hoc) (n=219)
– 2.74% smoking abstinence at 1 year (n=6)
• PAS significantly increases cessation
rates (P<0.01)

Sensitivity Analysis
Sensitivity analysis cost per life year saved per successful intervention*
Uptake rate (50% - 75%) £227.78 - £276.65Throughput rate (10 - 30 patients/yr) £318.09 - £262.97Success rate (5 - 25%) £553.14 - £110.75Natural cessation rate (0 - 2%) £213.20 - £364.04Relapse Rate (0 - 15%) £249.22 - £293.27Fixed costs (£40,000 - £70,000) £265.62 - £288.29Variable costs (£15 - £45 /patient) £159.26 - £394.65Discount rate (3 - 5%) £213.22 - £361.42
cost per life year saved per successful intervention based on a 45 year old male
Conclusions
• PAS model is much more cost-effective that a number of other disease prevention practices e.g. hyperlipidaemia treatment
• A clear case can be made for NHS remuneration of this pharmacy service

Question
• What percentage of community pharmacists provide robust smoking cessation programmes?
Integrated Medicines ManagementJournal of Evaluation in Clinical Practice (2007) 13, 781-788.

Integrated Medicines Management (IMM)
Healthcare organisations face major challenges including:
• Suboptimal prescribing
• Poor patient adherence to prescribed medication regimens
• Adverse drug reactions and interactions
• Medication administration errors
• Inadequate communication across the primary/secondary interface

IMM readmission statistics
Time to readmission (days)
4003002001000
Cum
pro
port
ion
of r
eadm
issi
ons
.5
.4
.3
.2
.1
0.0
Normal care
IMM

Influence of medicines management on patient knowledge of medicines
0
20
40
60
80
100
120
1st Major 1st Minor 2nd Major 2nd Minor
Poor product Knowledge
Poor purpose knowledge
Poor dosage knowledge
Poor instruction knowledge

Prescription queries
0
10
20
30
40
50
60
70
Major 1st Minor 1st Major 2nd Minor 2nd
Query Item
Query Condition
Product Discrepancies
Direction Discrepancies
Query Directions
Inadequate Directions
Query Formulation
Query Combination
Prescription queries

Medication storage seen during home visits
0
5
10
15
20
25
30
35
40
45
50
Major 1st Minor 1st Major 2nd Minor 2nd
Inappropriate Containers
Inappropriate Location
Damaged Container
Obsolete Products
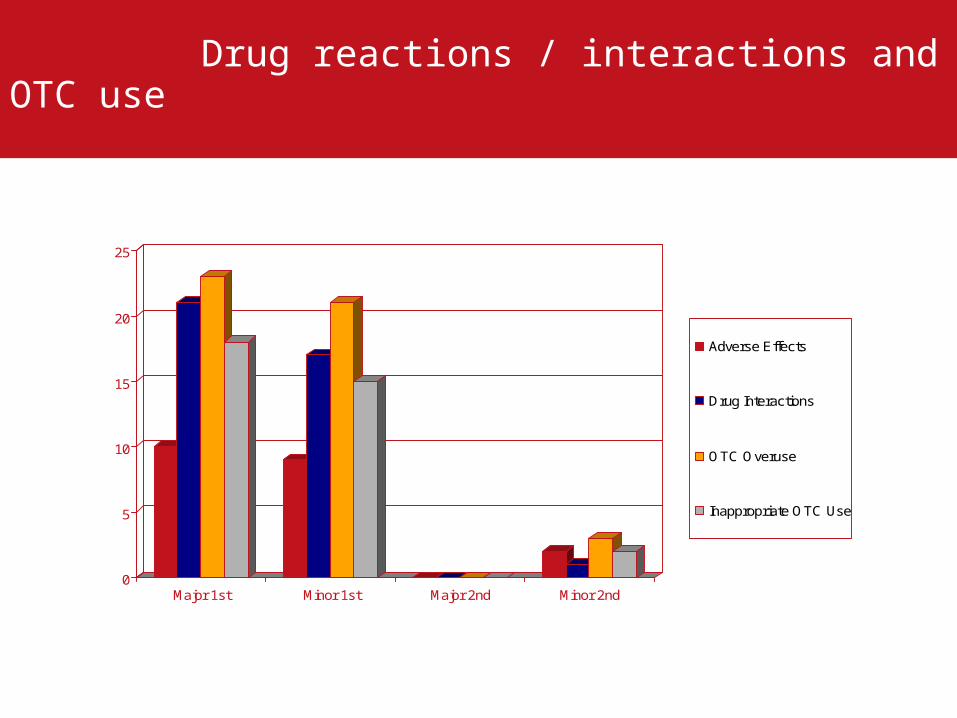
Drug reactions / interactions and OTC use
0
5
10
15
20
25
Major 1st Minor 1st Major 2nd Minor 2nd
Adverse Effects
Drug Interactions
OTC Overuse
Inappropriate OTC Use

Adherence issues
0
20
40
60
80
100
120
Major 1st Minor 1st Major 2nd Minor 2nd
Need More Help?
Omitted Dose
Extra Dose
Poor Inhaler Tech
Forgetful
Problem Opening Meds
Problem with Label
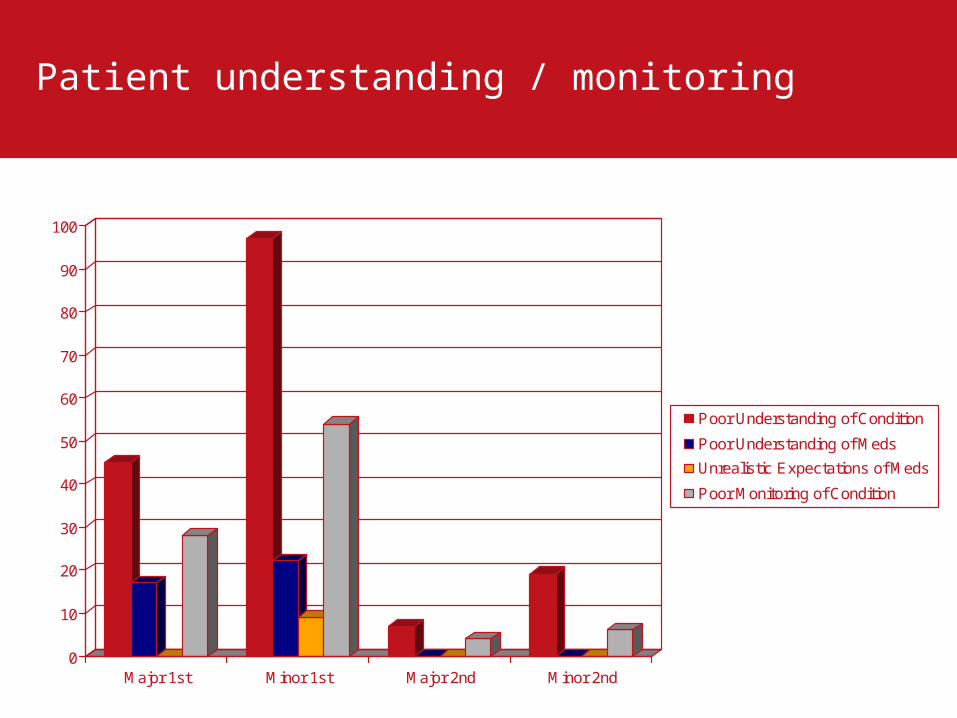
Patient understanding / monitoring
0
10
20
30
40
50
60
70
80
90
100
Major 1st Minor 1st Major 2nd Minor 2nd
Poor Understanding of Condition
Poor Understanding of Meds
Unrealistic Expectations of Meds
Poor Monitoring of Condition

Question
• What percentage of community pharmacists provide robust integrated medicines management services to patients?

Behavioural Pharmaceutical Care Scale (BPCS)
N. Ireland 1996 vs 2006
AJHP (1998) 55, 2009-2013.

BPCS Scores 1996 vs. 2006
Respondents’ Scores
1996 2006
Dimension and Domain No. Max Mean + SD Mean + SD
Direct Patient Care Activities 17 85 33.5 14.2 30.6 13.9
Documentation 6 30 10.2 6.2 9.3 5.9
Patient Assessment 6 30 9.3 7.2 6.6 6.4
Therapeutic Plans 2 10 3.4 3.1 3.3 3.2
Record Screening 1 5 4.1 1.5 4.5 1.2
Patient Consultation 1 5 3.4 1.6 3.5 1.5
Verification of Patient
Understanding 1 5 3.6 1.7 3.7 1.7

BPS Scores 1996 vs. 2006
Respondents’ Scores
1996 2006
Dimension and Domain No. Max Mean + SD Mean + SD
Referral and Consultation
Activities
8 40 18.3 5.2 19.8 5.5

BPS Scores 1996 vs. 2006
Respondents’ Scores
1996 2006
Dimension and Domain No. Max Mean + SD Mean + SD
Instrumental Activities 7 35 23.0 3.8 23.8 3.7
Counselling Location 1 5 3.7 0.9 3.8 1.0
Filled prescription validation 1 5 4.7 0.8 4.9 0.4
Informational Support 1 5 3.6 1.2 3.6 1.1
Evaluation of patient satisfaction 1 5 2.0 1.0 1.9 0.9
Competency Improvement 1 5 3.2 0.9 3.6 0.9
Performance Evaluation 1 5 2.1 1.1 2.2 1.0
Provision of Medical Information 1 5 3.8 0.9 3.9 0.8
BPCS
Response Rate
1996 45.5 (n=230)
2006 41.4% (n=213)
Mean Scores
1996 74.7 + 19.3 [46.7% of achievable score]
2006 74.1 + 19.2 [46.3% of achievable score]
(maximum possible score = 160)

Translation of Research
Bench → Bedside
Clinical Trials → Policy and Routine PracticeTranslation
Translation

Community Pharmacy - untapped healthcare resource
• Community pharmacists trusted by patients
• Highly trained healthcare professionals available without appointment in the
High Street
• We have run a number of successful initiatives (in collaboration with GPs) via
community pharmacies
– Care of asthma patients
– Repeat dispensing
– Smoking cessation
– OTC drug abuse
– Care of elderly patients
– Medicines management
– Treatment of URTIs (minor ailment scheme)

Questions
• Does the responsibility of researchers end when trials are completed and published?
• Who is responsible for translating research results into policy and routine practice?
• Why is policy often not evidence based, e.g. emergency hormonal contraception and pharmacist prescribing in the UK introduced ahead of robust research?
• Do researchers keep pharmacy services negotiators fully informed of research outcomes and is this evidence used in negotiations with payers?



















