
Jaffe PTL ALCL Afula - hematology.org.il … · JCO 2008;26:4124-4130 ©2008 by American Society of...
31
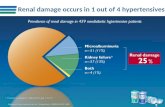
Page 1 Peripheral T-cell Lymphomas Anaplastic Large Cell Lymphoma Elaine S Jaffe, M.D. . JCO 2008;26:4124-4130 ©2008 by American Society of Clinical Oncology International T-cell Lymphoma Study: Frequency of Subtypes Study limited to adults Vose et al. JCO 2008 Peripheral T-cell Lymphoma, NOS • A diagnosis of exclusion, by definition a heterogeneous category • Characterized by a broad morphologic spectrum – New approaches include segregation of tumors of TFH origin (follicular variant) – Gene expression profiling recognizes tumors of TH1 and TH2 origin • The “diffuse large B-cell lymphoma” of the PTLs Lymphoepithelioid variant Peripheral T-cell lymphomas, not otherwise specified
Transcript of Jaffe PTL ALCL Afula - hematology.org.il … · JCO 2008;26:4124-4130 ©2008 by American Society of...

Page 1
Peripheral T-cell Lymphomas
Anaplastic Large Cell Lymphoma
Elaine S Jaffe, M.D.
.
JCO 2008;26:4124-4130
©2008 by American Society of Clinical Oncology
International T-cell Lymphoma Study: Frequency of SubtypesStudy limited to adults
Vose et al. JCO 2008
Peripheral T-cell Lymphoma, NOS
• A diagnosis of exclusion, by definition a heterogeneous category
• Characterized by a broad morphologic spectrum– New approaches include segregation of tumors of TFH
origin (follicular variant) – Gene expression profiling recognizes tumors of TH1
and TH2 origin
• The “diffuse large B-cell lymphoma” of the PTLs
Lymphoepithelioid variant
Peripheral T-cell lymphomas, not otherwise specified

Page 2
CD 3
Subclassification of PTCL, NOS by gene expression
TBX21 / TBET (Th1) Unclassifiable GATA3 (Th2)
Subclassification of PTCL, NOS: GATA3 & TBX21
GATA3Unclassifiable
TBX21 /TBET
0.91.412.08
Median OS (yrs)
TBX21/TBET (Th1 cells) - GATA3 (Th2 cells)

Page 3
Angioimmunoblastic T-cell Lymphoma
• Initially thought to be an abnormal reactive process, a disorder of immune regulation
– Later defined as a form of peripheral T-cell lymphoma
• The clinical syndrome is a nearly universal part of the disease definition
• One would be hesitant to make the diagnosis in the absence of the characteristic clinical picture
Angioimmunoblastic T-Cell Lymphoma
Clinical Features:
• Older adults, generalized lymphadenopathy
• Hepatosplenomegaly
• Skin rash, effusions, fever,
• Polyclonal hypergammaglobulinemia, hemolytic anemia
• Diverse constitutional signs & symptoms
• Aggressive clinical course, high risk of infectious complications with treatment
Angioimmunoblastic T-Cell Lymphoma
Pathologic Features:
• Arborizing vasculature
• Atypical T-lymphocytes with clear cytoplasm
• Scattered B-immunoblasts
• Plasmacytosis, eosinophils
• Regressed or absent follicles in most cases
• Some cases have follicular hyperplasia
B-cell areas compressed at periphery of the lymph node – far cortex
CD20

Page 4
Clear cells
BasophilicImmunoblasts
Angioimmunoblastic T-cell Lymphoma
is a disease of germinal center derived T-cells (TFH cell)
PD-1/CD279Normal tonsil
Angioimmunoblastic T-Cell LymphomaImmunophenotypic & Genotypic features
• CD4+, CD10+, PD-1+, BCL-6- T-cells (TFH)
• Expression of CXCL 13
• Extensive FDC CD21+ meshwork surrounding high endothelial venules (HEV)
• Scattered large B-cell blasts, often EBV+
• Polyclonal/ rarely monoclonal plasma cells
• > 90% TCR clonally rearranged
• 10-30% IG clonally rearranged
CXCL13 and Germinal Center TFH cells
• CXCL 13 causes induction and proliferation of
follicular dendritic cells
• CXCL 13 is involved in B-cell recruitment to
LN’s and activation of B-cells
• CXCL13 is required for the adhesion and arrest
of B-cells on HEV’s

Page 5
CD21 CD21
CD10 CD3
Angioimmunoblastic T-cells Express CD10 CD10
Perifollicular Localization of AITL T-cells
PD1-CD279
What is the utility of PD-1 immunostaining in differential diagnosis of AITL vs Reactive
Hyperplasia ?
Exercise caution – Intensity is key !
PD-1+ T-cells are invariably present in reactive paracortical hyperplasia

Page 6
Reactive paracortical hyperplasia – 18 yo drug hypersensitivity
Strong PD-1 + cells in germinal centerWeak PD-1 in reactive paracortical T-cells
Nodal Peripheral T-cell Lymphomas of TFH Origin
NODALPTCL,NOS
Follicular
Variant
AITL
TFH
• Gene expression profiling and mutation analysis has helped to clarify the interrelationship among nodal T-cell lymphomas of TFH origin
Relative Level of Expression (x median value)
AITL ALK- NKALK+ TATL PTCL-NOS
Gene expression profiling allowed reclassification of 14% of PTCL, NOS as AITL
Gene expression signatures of PTCL; Iqbal et al. Blood 2014
Genomic Findings in AITL and TFH derived lymphomas
• 20-45% in IDH2, DNMT3A and TET2 in AITL
– Genes involved in pathogenesis of gliomas, AML
• TET2 mutations also seen in other PTCL of TFH origin (up to 60%)
• RHOA mutations in 60% of AITL and some PTCL, NOS, all with TET2
• IDH2 most specific for AITL
Lemonnier 2012, Cairns 2012; Couronne 2012, Sakata-Yanagimoto 2014, Palomero 2014
Nodal Peripheral T-cell Lymphomas (2008)
PTCL, NOS
T-zone variant
Lymphoepithelioid cell variant
Follicular variant
Angioimmunoblastic T-cell lymphoma

Page 7
Nodal Peripheral T-cell Lymphomas (2016)
PTCL, NOS
T-zone variant
Lymphoepithelioid cell variant
Follicular T-cell lymphoma
AngioimmunblasticT-cell lymphoma
Nodal peripheral T-cell lymphoma with TFH
phenotype
Follicular Variant of PTCLde Leval AJSP 2001
• Intrafollicular T-cell lymphomas derived from TFHcells
• Usually CD4+, BCL-6+, CD10+/-
• PD-1/CD279+
• Clusters of clear cells within GCs
• May simulate follicular lymphoma
• Lack typical clinical findings of AITL
• Will be grouped with AITL in revised WHO classsification
CD3BCL6
Peripheral T-cell lymphoma, T-zone variant
Perifollicular growth pattern
Plasmacytosis, Capsular fibrosis
CD4 phenotype
May have a better prognosis than other PTCL
More often localized LN presentation
REF: Rudiger et al., Am J Surg Pathol, 2000Warnke et al., Am J Clin Pathol, 2007
Peripheral T-cell lymphoma, T-zone variant

Page 8
CD4 CD8 CD5
CD3
Biphasic pattern for CD5
CD5
B-cell proliferations in AITL & PTCL
• EBV-positive– Variable numbers of EBV+ blasts, may be dominant
picture
– Hodgkin/Reed-Sternberg like cells
• EBV-negative– B-immunoblasts
– Polyclonal plasma cells
– Monotypic/ Monoclonal plasma calls
– Hodgkin/Reed-Sternberg like cells
EBER
CD20
CD20 + B-immunoblasts
EBV neg B-cell proliferations in Angioimmunoblastic T-cell lymphoma
Plasma cells
Often Abundant
May be monoclonal &atypical
Balague et al. Am J Surg Path 2007
Huppmann et al JCO 2012
T
T
T

Page 9
CD3
CD279/ PD-1
CD138
κ λ
TCR
IGH FR2
IGH FR3
Huppmann et al JCO 2012
Peripheral T-cell lymphoma with EBV+ HRS cellsQuintanilla-Martinez et al. Am J Surg Pathol 1999
CD30EBER
CD15
T-cell population clonal, Cytologically atypical Usually has a TFH phenotype“HRS-cells” are “B-lineage”
PTCL with HRS-like cells – An Update (57 cases)Nicolae et al AJSP 2013
• PTCL classified as AITL, PTCL, often with TFH markers
• Intimate relationship between the HRS-like cells & neoplastic T-cells
• HRS-like cells
–EBV-positive (52 cases)
–EBV-negative (5 cases)
• Progression to classical Hodgkin’s lymphoma not observed
CD15 CD30
CD3 CD10

Page 10
CD15 PAX5 EBER
CD10PD1
EBV-negative HRS like cells are also rosetted by neoplastic TFH cells
Angioimmunoblastic T-cell LymphomaTake Home Points & Remaining Questions
• AITL is characterized by proliferation and sometimes clonal expansion of B-cells, as well as neoplastic TFH-cells
• If B-cells are passively expanded secondary to function of TFH cells, why do they appear so atypical, or evolve to a clonal proliferation in some cases?
– Might they harbor some of the same mutations as the
neoplastic T-cells?
– Are PD-1 positive cells providing immunoprotection?
Adult T-Cell Leukemia/Lymphoma
• Endemic in Japan, Caribbean, associated with HTLV-I in endemic and ‘sporadic’ cases
• Medium-sized to large cells with pronounced nuclear pleomorphism, often polylobated cells in PB
• Reed-Sternberg-like cells may be present
• CD3+, CD4+, CD7-, CD25++, FoxP3 +/-
• Clonally integrated HTLV-I, rearranged TCR genes
Prevalence of HTLV-1 Worldwide

Page 11
Hodgkin’s-like picture in early ATLL - RS-like cells are EBV+ B-cells
Clinical Features ATLL
• Leukemia (more common in Japan)– Often without bone marrow infiltration
• Skin lesions > 60%• Hypercalcemia• Lytic bone lesions, 30%
• Lymphadenopathy
• Hepatosplenomegaly
• Stage IV, nearly 100%
ATLL Sezary

Page 12
ATLL Skin LesionsCutaneous Involvement ATLL
CD3
Immunophenotype of ATLL
• CD3+, CD4+, CD25++, FOXP3 +\-
• Negative for CD7
• CD30 variable
Cells phenotypically and functionally are Treg cells, function as suppressors of immune function
Correlates with immunodeficiency characteristic of ATLL
ATLL:Opportunistic infections in the absence of therapy or granulocytopenia
• Pneumocystis carinii pneumonia
• Cryptococcal meningitis
• Cytomegalovirus infections
• Candida
• Strongyloides
• Mycobacterial infections
Adult T-cell Lymphoma/Leukemiafrom Yamaguchi et al., Kawano et al.
Smoldering ATLL Chronic ATLLNormal WBC Increased WBCATL cells <3% ATL cells >10%No lymphadenopathy Mild lymphadenopathyNo hepatosplenomegaly Slight hepatosplenomegalySkin rash Skin rash variable
erythema, papulesNormal LDH, Ca++ LDH slightly inc, Ca++ nl.Survival > 2 yrs. Survival usually > 2 yrs.

Page 13
CD 3 CD25
Smoldering ATLL - Skin Biopsy
OS according to the clinical subtypes.
Hiroo Katsuya et al. Blood 2015;126:2570-2577©2015 by American Society of Hematology
Lymphomas of the Innate Immune System
T-cells, NK-like T-cells, NK-cells
• Often cutaneous, mucosal, spleen & BM
• Cytotoxic • Activated cells show
frequent apoptosis, necrosis
• Includes most pediatric T/NK neoplasms
Hepatosplenic T-cell lymphoma• Most common in young males
• May be seen with chronic immune suppression– Crohn’s disease, late occuring PTLD
• Hepatosplenomegaly, cytopenias, systemic symptoms; lack LN and PB involvement
• Aggressive behavior and dismal prognosis (<2y survival)
• Differential Dx: T-LGL in bone marrow, spleen

Page 14
CD3+, CD4-/CD8-, CD5-, CD56+, TCRγδ+
Nonactivated cytotoxic profile: TIA-1+, GZB-, Perforin-
Rare cases αβ, similar clinicopathologic and molecular features
Cytogenetics Isochromosome 7q, +8, -Y
Derive from functionally immature cytotoxic γδ T-cells with Vδ1 usage
Immunophenotype
CD5
TCRγ
CD56
TIA-1
Liver TCRγ
TCRγ CD56
BM

Page 15
Recurrent Mutations in HSTCL
• HSTCL STAT5B (33%); STAT3 (10%)
SETD2 (71%)
• T-LGL STAT3 (40%); STAT5B (2%)
• T-ALL JAK1, JAK3, STAT5B (subset)
• T-PLL STAT5B (36%)
Clinical Spectrum of Cutaneous T-cell lymphomas
Activated Cytotoxic Immunophenotype
Primarily Dermal T-cell lymphoma Cutaneous TCL - “panniculitis-like”

Page 16
Cutaneous Gamma Delta T-cell lymphoma – may involve mucosal sitesStomach Subcutaneous
Non-hepatosplenic T-cell lymphomasMainly cutaneous, but also involving other extranodal
sites Garcia-Herrera et al. AJSP 2011
• Skin / subcutaneous tissue 31%
• Skin + other (GI, LN) 19%
• Small bowel 19%
• Tongue 6%
• Orbit 6%
• Lung 6%
• LN 12%
50%
Subcutaneous Panniculitis-Like T-cell Lymphoma
CLINICAL FEATURES:
Broad age range (1 yr to 57 yrs) Median age - 30
Males = Females
Deep subcutaneous nodules
primarily affecting extremities, trunk
Overall survival > 80% 5 years
Low risk of nodal involvement
Subcutaneous Panniculitis-Like T-cell Lymphoma
MORPHOLOGY:
Usually confined to subcutis
Absence of dermal, epidermal involvement
Necrosis and karyorrhexis prominent
May show vascular invasion
Primarily lobular distribution

Page 17
CCD8 TIA-1
Subcutaneous Panniculitis-like T-cell Lymphoma
Immunophenotype & Genotype
Activated T-cytotoxic phenotype
• CD3+, CD8+
• TIA-1+, Granzyme B+, Perforin +
• CD56 negative - in contrast to • EBV-negative
• TCR genes rearranged
Differential Diagnosis of SPTCLLupus erythematosus profundus
• Mixture of T-cells, B-cells, plasma cells
• Lobular pattern with preserved septa
• Fibrinoid change in connective tissue
• Interstitial infiltration, but infrequent rimming of fat spaces
• Mixture of CD4+/CD8+ cells
• Scattered gamma-delta T-cells
• Increased PDC’s (CD123+)
CD3 CD4 CD8

Page 18
TCR gamma CD123 Subcutaneous Panniculitis-like TCL & Lupus
Willemze et al. Blood 2008
• 19% of patients with SPTCL (αβ) had history of autoimmune disorder
– SLE, RA, ITP
Pincus et al. Am J Derm 2009
• 5 patients with established SLE and “SPTCL”– 3/5 had clonal TCR genes
– Variable numbers of B-cells in all cases
– 1 patient had progressive disease (HPS)
– 3 in CR (prednisone, Vorinostat)
Subcutaneous Panniculitis-like TCLvs. Lupus profundus – Not always easy
• Oligoclonal T-cell populations can be seen in some
patients with lupus, inclusive of the cutaneous
lesions
• Correlate clinical, histological, and genetic features
• One should be cautious about making the diagnosis
of SPTCL in a patient with lupus
Primary cutaneous CD8 positive aggressive epidermotropic cytotoxic T-cell lymphoma (Provisional)
Primary cutaneous CD4 positive small/medium T-cell LPD (revised term 2016)

Page 19
Primary cutaneous CD4 positive small/medium T-cell LPD
Primary cutaneous CD4+ small/ medium“T-cell LPD” (2016)
• Usually localized, often involving head and scalp
• Distinction with atypical hyperplasia often difficult
• Lesions sometimes contain numerous B-cells
• Good prognosis if single lesion, most < 3 cm – Infrequent recurrences, no deaths
– Patients with bulky or advanced disease (very few) had aggressive course
CD3 CD4
PD-1
TFH phenotypePD-1+ but usually CD10-Clonal by PCR
Enteropathy Associated T-cell Lymphoma (EATL)
• Broad morphological spectrum Adjacent mucosa shows villous atrophy
• CD3+, CD103+, Cytotoxic markers, TCR often double negative for CD4/CD8
Often presents with intestinal perforationaggressive clinical course with poor prognosis
Enteropathy-associated T-Cell Lymphoma[Classical form or Type I]
• Associated with celiac disease
–95% of patients have HLA-DQ2 and HLA-DQ8
–Autoantibodies against tissue transglutaminase
–Antibodies against gliadin
–Gluten-free diet may reduce risk of lymphoma
Ireland Italy Netherlands Sweden USA
Overall
Diagnosed
Celiac Disease IcebergsF.A. Hamilton, NIDDK
1% of White population in the U.S. has “laboratory celiac disease”

Page 20
CD30
Enteropathy Associated T-cell Lymphoma, Types I & II are distinct
EATL IUsually αβ
Celiac diseaseN European
EATL IUsually αβ
Celiac diseaseN European
EATL IUsually αβ
Celiac diseaseN European
EATL IIUsually γδ
EpitheliotropicAsian, Hispanic
γδ
Monomorphic epitheliotropic intestinal T-cell lymphoma
(EATL II)
• Medium sized cells with
clear cytoplasm
• CD56 +, CD8+, CD4-
• Usually gamma delta +
• MAT kinase +

Page 21
Recurrent Mutations in Intestinal T-cell Lymphomas
Authors
Nairismagi 2016
• EATL II αβ and γδ
Roberti 2016
• EATL II
Nicolae 2016
•EATL Type II > I
– αβ and γδ and TCR silent
Mutations
• 63% STAT5B
• 35% JAK3, 24% GNAI2
• 93% SETD2
• 60% STAT5B, 46% JAK3
• 67 % JAK/STAT pathway
STAT5B/ JAK3/ STAT3
• 24% RAS pathway
KRAS/ NRAS/ BRAF
JAK/STAT Pathway is an attractive target for therapyof Cytotoxic T-cell Lymphomas and Leukemias
T-cell & NK cell Lymphomas of Gastrointestinal Tract
Extranodal NK/TEBV+ NK or T Mainly Asian
MEITL
γδ > αβ
EATL“Classical”
αβ > γδ
All clinically aggressiveAll cytotoxic
EBV+ T/NK cell lesions – WHO update (2016) Y-H Ko, L Quintanilla Martinez, H Kimura, ES Jaffe
• EBV-associated HLH (non-neoplastic)
• Cutaneous CAEBV
– Hydroa Vacciniforme LPD (T/NK)
– Severe Mosquito Bite Allergy (NK)
• Systemic CAEBV, T-cell or NK-cell
• Systemic EBV+ T-cell lymphoma of childhood
• Aggressive NK-cell leukemia
• Extranodal NK/T-cell lymphoma, nasal type
Marked variation in clinical behavior from indolent to highly aggressive
• Hydroa-vacciniforme-like LPD• Asian or Hispanic children• Lesions in sun exposed areas• Chronic course but may progress to
acute phase with systemic disease
EBER
Cells of T-cell or less often NK cellorigin
Systemic CAEBV
Most often Asian or Hispanic children
T-cell or NK-cell origin
Symptoms for > 3mos. after acute EBV infection
Involves BM, liver, spleen
May be accompanied by HLH

Page 22
Asian or Hispanic children
Acute systemic illness with hemophagocytic syndrome
Usually an acute presentation
EBV+ T-cells are clonal
May follow chronic active EBV infection (CAEBV)
Overlaps with what has been termed severe CAEBV
Systemic EBV+ T-cell Lymphoma 2 yo Hispanic M
Double Label CD8/ EBER
Let’s switch gears …….
Anaplastic Large Cell Lymphoma
• Paradigm for process used to define disease entities (REAL)
• First recognized based on
–Morphology - sinusoidal growth
–Antigenic phenotype - CD30+• Studies of molecular pathogenesis led to new
diagnostic tools
–RT-PCR and ALK-1 monoclonal antibody• New diagnostic tools define the borderlands of
the disease
Anaplastic Large Cell Lymphoma
• The ultimate histologic spectrum of ALCL is both broader and narrower than the original concept
• Small cell and lymphohistiocytic variants included
• Most Hodgkin’s-like and highly pleomorphic CD30+ lymphomas excluded
• New diagnostic tools enhance our diagnostic acumen on routine H&E (e.g. “Hallmark cells”)
• Importantly, what we recognize as ALCL has clinical and prognostic significance

Page 23
CD30
ALK CD30Anaplastic Large Cell Lymphoma
Clinical Features
• Presents most commonly in lymph nodes
• Cutaneous & extranodal involvement may be seen
• Most common in children, young adults
• Frequent presence of systemic symptoms
• Aggressive natural history but good response to chemotherapy

Page 24
Anaplastic Large Cell LymphomaExtranodal Sites of Involvement (Falini, Blood 1999)
Site %Skin 22%Soft tissue 22%Bone 22%Bone marrow 15%Lung 15%Liver 10%Other sites <10%
PB, pleura, muscle, CNS, gut, testicle, parotid gland
May be the sole manifestation of diseaseOschlies et al. Haematologica 2013
ALCL
Bone marrowInvolvement
Scatteredsingle cells inbiopsy & smear
Anaplastic Large Cell LymphomaImmunophenotype
• CD30+, EMA+, ALK+, clusterin +, CD 15-, LCA +
• T-cell antigen expression variable:
CD 2+, CD5+, CD4+/-, CD 8-/+, CD3 often negative
• Activated cytotoxic ag expression:
TIA-1 +, perforin +, granzyme B+, CD25+
ALK
CD30 EMA
Granzyme B
ALK

Page 25
Nucleophosmin Anaplastic Lymphoma Kinase
t(2;5) cytoplasmic/nuclear/
nucleolar
ALKNPM
t(1;2)
Tropomyosin 3
cytoplasmicALKTPM3
t(2;17)
Clathrin heavy chain cytoplasmic
granularALKCLTC
Inv2 ALKATICATIC (Pur H gene)
cytoplasmic
t(2;3) ALKTFGTrk Fusion Gene
cytoplasmic
Translocations and fusion proteins involving ALK
Frequency
70-80%
10-20%
2-5%
2-5%
2-5%
1-2%t(2;19) /others ?ALK?
Staining Histological Spectrum of ALCL, ALK+
• Anaplastic large cell lymphoma– Common– Lymphohistiocytic – Small cell
• Other common histological patterns– Sarcomatoid appearance with myxoid stroma– Hypocellular with edematous background
Histologic Variants of ALCLLymphohistiocytic or Histiocyte-Rich
(Pileri et al., Histopathology, 1990)
• Common in children and young adults
• Abundant histiocytes with pink cytoplasm mask minor population of tumor cells
• May be mistaken for infectious or reactive process - delay in diagnosis is common
• Recurrent biopsies contain fewer histiocytes, more tumor cells
Lymphohistiocytic variant of ALCL CD30
CD30
Histologic Variants of ALCLSmall Cell Variant (Kinney et al., AJSP, 1993)
• Common in children and young adults
• Usually presents in lymph nodes
• Most tumor cells are small, with clear cytoplasm, irregular nuclei
• Minor population of classical ALCL cells, often around blood vessels
• May be mistaken for PTL, NOS, but neoplastic cells are often CD 3 negative
• ALK +, but small cells may show variable staining

Page 26
PC
ALCL
Small Cell Variant of ALCL CD 30
Time to treatment failure curve according to the presence of a small-cell (SC) and/or lymphohistiocytic (LH) component (n = 361 patients).
Lamant L et al. JCO 2011;29:4669-4676
©2011 by American Society of Clinical Oncology
Other Histological Patterns in ALCLSarcomatoid or Hypocellular
• Myxoid stroma with prominent fibroblasts
• Edematous, often hypocellular infiltrate
• Differential diagnosis includes ALK+
myofibroblastic tumors - also children
• ALCL may present as soft tissue or bone lesion,
differential diagnosis with sarcoma
Sarcomatoid variant of ALCL

Page 27
ALCL resembling NS CHL Vassalo et al AJSP 2006 CD30 ALK
Hodgkin’s Like ALCL is NOT ALCL “Hodgkins Like ALCL”
• Originally proposed as a variant of ALCL, but most cases are aggressive variants of CHL or “grey zone” lymphomas
• Common in young males with med masses
• Capsular thickening, nodular fibrosis
• Sheeting out of Reed-Sternberg-like cells– May contain eosinophils, neutrophils
• ALK- negative
but usually CD30+, CD15 -/+, CD20 -/+, PAX5+
OCT-2, Bob.1 usually +
ALK-negative ALCL Should have very similar morphology and phenotype as ALK + ALCL
Note Hallmark Cells
Required: Cohesive growth pattern with hallmark-like cellsStrong and uniform CD30 expressionDesirable but not essential: EMA+, Cytotoxic +, Sinusoidal growth, Loss of “T-cell ag”

Page 28
Vose et al. JCO 2008
ALK+
ALK-
Activating mutations of JAK1 or STAT3 or both (20%)Crescenzo Cancer Cell 2015
Constitutive Activation of the JAK/STAT pathway in
Systemic and Cutaneous ALK-negative ALCL
0
10
20
30
40
50
60
70
80
90
100
0 24 48 72 96 120 144 168 192 216 240
Per
cent
Sur
viva
l
Months After ALCL Diagnosis
p<0.0001
Genetic correlates with survival in ALCL, ALK+/ ALK-Feldman et al. Blood 2014
DUSP22 (# 22)ALK+ (# 32) P63 (# 6)
ALK neg, no aberrations (#45)
Subset with DUSP22 RComparable to ALK+
DUSP22 translocations also seen in primary cutaneous CD30+ T LPD
• LYP with 6p25.3 (<5%) 11 pts with localized skin lesions (Karai 2013)
– Same translocation (DUSP 22 locus), as in systemic ALCL, ALK-
• Primary cutaneous ALCL with 6p25.3 – 3 patients, pagetoid reticulosis-like pattern (Onaindia
2015
– C-ALCL, intralymphatic localization, skin limited (Samols2014)
• Evidence for close relationship between some cases of systemic and cutaneous ALCL
Implant-associated anaplastic large cell lymphoma, ALK-negative
• Seen with a variety of breast implants, both saline and silicone
• Usually years after implant
• Symptoms related to accumulation of seroma fluid in cavity surrounding the implant
• Diagnosis best made by cytology
• Cells grow within cavity and on surface of cavity lining, usually without invasion
Location of ALCL Adjacent to Breast Implant
Breast
Implant
(Seroma)
Modified from Thompson PA et al Haematologica 2010

Page 29
CD30
Biological Features
• Clonal TCR reported in most but not all cases
• JAK1 & STAT3 mutations – Similar to ALK+/ALK- ALCL (Blombery 2016)
• Surprisingly indolent course, despite very atypical cytological features
• Therapy varies in literature
–Chemo, Radiation, Observation following removal
• Removal of implant is probably adequate therapy in most cases – if no invasion of capsule

Page 30
CD30 CD3 Ax LN
Breast implant–associated anaplastic large-cell lymphomaLong Term Follow up in 60 Patients
Miranda R N et al. JCO 2014;32:114-120
93% CR in patients with disease confined to the capsule72% CR in patients with a mass No difference in OS or PFS in patients who had chemorx
Recommended rx: Implant removal with capsulectomy
Histological Spectrum of ALCL
• Marked variation in cell size from case to case
–Hallmark cells are always present
• Distinctive architectural features
–Sinusoidal infiltration
–Perivascular rosetting
• Cellular density varies markedly
–Hypercellular to hypocellular
–Hypocellular cases may simulate an inflammatory process

Page 31
Pitfalls in the Diagnosis of ALCL
• CD30 is not specific for ALCL
+ in CHL, +/- in EBV+ B-cell lymphomas, other T-cell
lymphomas, embryonal carcinoma
• ALCL is not a wastebasket for pleomorphic or “anaplastic”
tumors. The term “ALCL” was based in part on the
sinusoidal growth and unusual cytologic features, not
resembling normal lymphs.
Many ALCL are not pleomorphic, but monomorphic
• Reed-Sternberg-like cells are uncommon in ALCL
HD PTCL
CD30+EMA+LCA+CD15-CD3 -/+
t(2;5)NPM;ALK
ImmunophenotypicStudies
Ki-1+Sinusoidallymphoma
MolecularPathogenesis
Definitionof Entity
Hallmark cellsALK+
MH
Initial Description
EVOLUTION OF ANAPLASTIC LARGE CELL LYMPHOMA
Fully integrated with the revised WHOClassification
Recently released












![4.Lu177 Treatment of GEP NETs - Human Health Campus...Kooij PP, et al. J Clin Oncol 2008;26:2124-2130. Title 4.Lu177 Treatment of GEP NETs [Compatibility Mode] Author paezd Created](https://static.fdocuments.us/doc/165x107/612f21af1ecc515869433f9b/4lu177-treatment-of-gep-nets-human-health-campus-kooij-pp-et-al-j-clin.jpg)

