Jackson Early Pilot Study Results 8.9 · Monovision Pinhole Treatments: Small Aperture Pinhole...
16
Early Pilot Study Results of Laser Scleral Microporation in Presbyopic Eyes • 1 Mitchell Jackson, MD • 2 AnnMarie Hipsley, DPT, PhD • 3 Sunil Shah, MD, FRCOphth • 4 Robert Ang, MD • 5 Luca Gualdi, MD • 6 Magda Rau, MD • 7 Eddie Hsiao, PhD Financial Interests: • Authors 1-7 Consultants, Ace Vision Group, Inc
Transcript of Jackson Early Pilot Study Results 8.9 · Monovision Pinhole Treatments: Small Aperture Pinhole...

Early Pilot Study Results of Laser Scleral Microporation in Presbyopic Eyes
• 1Mitchell Jackson, MD• 2AnnMarie Hipsley, DPT, PhD• 3Sunil Shah, MD, FRCOphth• 4Robert Ang, MD• 5Luca Gualdi, MD• 6Magda Rau, MD• 7Eddie Hsiao, PhD
Financial Interests:
• Authors 1-7 Consultants, Ace Vision Group, Inc

Lens Stiffness & Hardening is a well Known Cause for Loss of Accommodation
• The Stiff/Harden Lens imposes Resistance to the Ciliary Muscle contraction
• Ciliary Muscles Are Less Efficient• Less Force is Exerted on the Lens• This Impacts the Ability of the lens to change Shape • The Lens is Unable to adjust for various distances
Glasser A, Campbell MC. Biometric, optical and physical changes in the isolated human crystalline lens with age in relation to presbyopia. Vision Res. 1999 Jun;39(11):1991-2015.

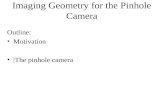
Presbyopia
Reduction of accommodative
capacity
52%
Reduction of binocular
interaction level
22%
Change of diaphragmatic
function of pupil
15%«Noise» in
light perception –
11%
Presbyopia formation
Rozanova O. Seeing presbyopia formation in depth. In: ISOP. Barcelona, Spain, 2015

Ocular Rigidity Has Been Correlated with Loss of Accommodation
• With increasing age, the connective tissues of the eye stiffen, largely due to the crosslinking that occurs with age.• Crosslinks are bonds between polymer chains, such as those in
synthetic biomaterials or the proteins in connective tissues.• In connective tissues, collagen and elastin can crosslink to
continuously form fibrils and microfibrils over time. • With increasing amounts of fibrils and microfibrils, the sclera stiffens,
undergoing a ‘sclerosclerosis’.• A stiff sclera may is less compliant to applied forces during
accommodation.

Comparison of Presbyopia Treatments: Pre-Cataract Patients
Confidential Materials Not for Distribution
Manipulating Corneal Optics: Multifocal CorneaBlended VisionMonovision
Pinhole Treatments: Small Aperture PinholePharmacological Pinhole
Biomechanical Accommodation Therapies: LSM/Scleral Implants/ Lens Softening DropsPresbyopia Surgical
Correction & Therapy Solutions
Measuring Results
FDA Endpoints
Effective Range of Focus (EROF)
Near Visual Acuity Lines of Vision
75% of patients with Distance Corrected Near Visual Acuity (DCNVA) of 20/40 or better at 12 months
Gain 2 lines of Uncorrected Near Visual Acuity (UNVA) in 70 % of patients at 6 months
Proportion of participants gaining 3 lines or more in binocular DCNVA at 1 month
5

Presbyopia Correction vs Presbyopia Therapy Procedures• All presbyopia correction procedures are compensatory procedures and not
restorative procedures. • Monovision whether it is laser induced or a contact lens application,
intentionally decreases binocularity and is not tolerated by the majority of presbyopes.
• Corneal presbyopic correction is an attempt to create multifocality or a bifocal cornea. All of these procedures have side effects of lost binocularity, stereopsis and distance vision.
• Accommodating IOL’s are only appropriate for cataract patients.• There is a gap for the emmetropic presbyope which produces a significant
opportunity to address the true problem of presbyopia without compromise.
An exception is the Laser Scleral Microporation Procedure

Animation

Setting: Single Arm Clinical Trial
Hyperopic EyesN=9
Myopic EyesN=1
Patient Population:
PresbyopesN=22 Eyes of 11 Patients
• Study Endpoints:– 75% of patients with Distance Corrected Near Visual Acuity (DCNVA) of 20/40
or better at 12 months

Methods• Primary study targets:
• UNVA/UIVA/UDVA• Measurements made with:
• iTracey objective wavefront aberrometry• ETDRS precision vision customized charts
• Abbreviations used¹:• UNVA: Uncorrected near VA• UIVA: Uncorrected intermediate VA• UDVA: Uncorrected distance VA
• Criteria:• Age 48 +• UDVA 20/40 or better• DCNVA 20/50 or worse• MRSE : +/- 0.5D• Astigmatism: < 1D• Reading Ad < 1.5D
Note: Data was collected in Snellen and converted to logMAR notation¹Reprinted from Kohnen T. New Abbreviations for Visual Acuity Values. J Cataract Refract Surg. 2009;35(7):1145.
Image From: Consistency Between Visual Acuity Scores Obtained at Different Test Distances Theory vs Observations in Multiple Studies. Arch Ophthalmol. 2002;120(11):1523-1533. doi:10.1001/archopht.120.11.1523

Laser Scleral Microporation Procedure (LSM)
• Procedure:• Laser scleral microporation in
4 quadrants• Less than 8 secs a quadrant• 5mmx5mm matrix • ER:YAG laser• Five critical anatomic zones
• Mechanism of Action: • Uncrosslinking scleral
myofibrils• Restore mechanical
efficiency of the natural accommodative mechanism
• Improve biomechanical mobility to achieve accommodative power
Treatment laser beam creation of individual micropores
Scleral uncrosslinking

Five critical zones of anatomical and physiological significance1,2
• Zone 1) 0.0-1.3mm from anatomical limbus (AL); distance from the AL to the superior boundary of ciliary muscle/scleral spur;
• Zone 2) 1.3-2.8mm from AL; distance from the sclera spur to the inferior boundary of the circular muscle;
• Zone 3) 2.8-4.7mm from AL; distance from the inferior boundary of the circular muscle to the inferior boundary of the radial muscle;
• Zone 4) 4.7-6.6mm from AL; inferior boundary of the radial muscle to the superior boundary of the posterior vitreous zonule zone; and
• Zone 5) 6.6-7.3mm from AL; superior boundary of the posterior vitreous zonule zone to the superior boundary of the ora serrata.
LSM Treatment Zones
1. Croft MA, Nork TM, McDonald JP, Katz A, Lutjen-Drecoll E, Kaufman PL. Accommodative movements of the vitreous membrane, choroid, and sclera in young and presbyopic human and nonhuman primate eyes. Invest Ophthalmol Vis Sci. 2013;54(7):5049-5058.
2. Goldberg DB. Computer-animated model of accommodation and presbyopia. J Cataract Refract Surg. 2015;41(2):437-445.

Mircoporation Completed on One Eye

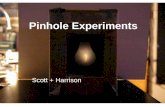
Presbyopia Patients – Binocular Visual Acuity
0% 0% 0% 0%
40%
60%
80%
100%
0%20%40%60%80%
100%
20/20 20/25 20/32 20/40
Perc
ent o
f Pat
ient
Eye
s
UNVA (20/x of better)
Gen I Preop Gen I Postop (1 Month)
Data from IRB Registered Pilot Clinical Trial; N=11 PatientsData collection is ongoing
P = 0. 0001; Improvement from Preop to 1 Month Postop

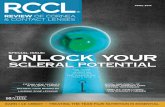
Presbyopia Patients: Intraocular Pressure (IOP)
Data from IRB Registered Pilot Clinical Trial; N=11 PatientsData collection is ongoing
16
12
0.0
5.0
10.0
15.0
20.0
Intr
aocu
lar P
ress
ure
(mm
Hg)
Pre-OP Post-OP
25% Improvement

Discussion1. Preliminary results suggest LSM performed using the Er:YAG laser to be a safe
and effective procedure for restoring visual performance in all ranges of vision including near, intermediate, and distance.
2. The mechanism of action of LSM is decreased biomechanical stiffness in rigid sclera by uncrosslinking scleral microfibrils to improve mobility rejuvenating areas over the ciliary muscles.
3. Preliminary results are compelling and studies are ongoing. 4. Patients gained a median of 4.5 lines of near and intermediate visual acuity
(range 2-8); mean gain of 7 lines of Jaeger.5. There were no complications in early cases.6. UDVA remained stable with no vision compromises.

Thank you!