
IUFD lecture - AWHONNWAawhonnwa.org/wp-content/uploads/2012/10/IUFD-lecture.pdf · • Increased...
14
6/3/16 1 Labor Induction Management: Caring for 2 nd and 3 rd Trimester Fetal Losses Rebecca Cypher, MSN, PNNP [email protected] Disclosure In the interest of full disclosure I wish to communicate that I have a professional relationship with PeriGen: Chief Nursing Officer Lucina Health: Clinical Advisor Professional Education Center: Speaker Objectives • Describe criteria of cervical ripening and labor induction techniques • Identify advantages, disadvantages and dosing recommendations of specific cervical ripening and labor induction techniques • Discuss risk management strategies to include informed consent, staffing resources, frequency of assessment and medical record documentation Diagnosis • Based on ultrasound • Absence of fetal cardiac activity • In person conversation • Empathetic and straight forward • Private area Six Key Phases of Fetal Loss Counseling 1. Timeof diagnosis 2. When making delivery plans 3. At delivery and immediately postpartum 4. During the weeks after discharge and postpartum visit 5. At a ”closure" meeting to review laboratory and pathology results 6. When the patient is considering another pregnancy Timing of Delivery • Patient acceptance of diagnosis is variable • NO rushed decisions about delivery • Absence of maternal co-morbidities • Severe pre- eclampsia • Timing and procedure discussed after patient acceptance • Interventions should be guided by maternal/parental desires • Potential long interval between fetal death and spontaneous labor • Limits cause of death information obtained on postmortem examination Chakhtoura NA , Reddy UM. Management of stillbirth delivery. S eminars in perinatology 2015;39:501 -5 04 ).
Transcript of IUFD lecture - AWHONNWAawhonnwa.org/wp-content/uploads/2012/10/IUFD-lecture.pdf · • Increased...

6/3/16
1
LaborInductionManagement:Caringfor2nd and3rd TrimesterFetalLosses
Rebecca Cypher, MSN, [email protected]
Disclosure
In the interest of full disclosure I wish to communicate that I have a professional relationship with
PeriGen: Chief Nursing OfficerLucina Health: Clinical AdvisorProfessional Education Center: Speaker
Objectives
• Describecriteriaofcervicalripeningandlaborinductiontechniques
• Identifyadvantages,disadvantagesanddosingrecommendationsofspecificcervicalripeningandlaborinductiontechniques
• Discussriskmanagementstrategiestoincludeinformedconsent,staffingresources,frequencyofassessmentandmedicalrecorddocumentation
Diagnosis
• Basedonultrasound• Absenceoffetal cardiacactivity
• Inpersonconversation• Empatheticandstraightforward
• Privatearea
SixKeyPhasesofFetalLossCounseling
1. Timeofdiagnosis2. Whenmakingdeliveryplans3. Atdeliveryandimmediatelypostpartum4. Duringtheweeksafter dischargeandpostpartumvisit5. Ata”closure"meetingtoreviewlaboratoryandpathologyresults6. Whenthepatientisconsideringanotherpregnancy
TimingofDelivery
• Patientacceptanceofdiagnosisisvariable• NOrusheddecisionsaboutdelivery
• Absenceofmaternal co-morbidities• Severe pre-eclampsia
• Timingandprocedurediscussedafterpatientacceptance• Interventionsshould beguidedbymaternal/parentaldesires
• Potentiallongintervalbetweenfetaldeathandspontaneouslabor• Limitscauseofdeath informationobtainedonpostmortemexamination
Chakhtoura NA, Reddy UM. Management of stillbirth delivery. Seminars in perinatology 2015;39:501 -5 04 ).

6/3/16
2
TimingandAnxiety
• Admittohospitalimmediately• Reasonableoption
• Alsoreasonableandsafetotaketimeindecidingnextsteps• Psychologicalcontroversy:
• Increasedriskoflifelonganxietyanddepression• induction>24hoursafterdiagnosis comparedto<6hours
Radestad I, Steineck G, Nordin C, Sjogren B. Psychological complications after stillbirth—influence of memories and immediate management: population based study. BMJ. 1996 Jun 15;312(7045 ): 15 05 -8.
CoagulationDisorders
• Etiology:• Releaseofthromboplastin fromfetal/placentacirculation tomaternalcirculation
• Thromblastin:• Stimulatesmaternalcoagulationsystemleading to intravascularconsumptionofclotting factorsandplatelets
• Increasedactivityoffibrinolyticpathway• Leadstobreakdownof fibrinogen to formfibrindegradationproductsandD-Dimers
• Leadstostillbirthretentionandcoagulopathy
TimingandRiskofCoagulationDisorders
• Spontaneouslaborusuallystarts1-2weeksafterfetaldeath• Avoids risks associatedwith induction
• Riskofcoagulationabnormalitiesincreaseswithwaiting• Pritchard:Notdetectedatless than5weeks
• Makecertainthefetusisdead.Frequentlyitwilltake3-4weekstoascertainthis”• Maslow: Detectedbeyond4week
• Increasedfrequencyinabruptionoruterineperforation
Mas low AD, Breen TW, Sarna MC, et a l . Prev alenc e of c oagulation abnormal i ties as s oc iated wi th in trauterine fe ta l death. Can J Anaes th 1996; 43:1237.P ri tch ard , Jack A. "Fetal d eath in u tero ."Ob stetrics & Gyn eco lo g y 1 4 .5 (1 9 5 9 ):5 7 3 -5 8 0 .
ExpectantManagement
• Weeklyprenatal visits• Homeassessment
• Temperature,presenceofabdominalpain, bleedingor labor
• Seriallabs• Minimaldataonbenefit• Consider baselinecoagulopathypanel
• Fibrinogen, platelets, PTT,aPTT• Recheckprior toneuraxial anesthesia
• Considerifdemise<4weeksChakhtoura NA, Reddy UM. Management of stillbirth delivery. Seminars in perinatology 2015;39:501 -5 04
Route
• Vaginaldelivery• Alwaysdesirable • Generally saferforwomanthancesareandelivery
• YES evenwithpriorLTCS
• Maternal requestforcesarean delivery• Avoidexperienceof laborandbirth• Informedconsent• Requires counselingonbenefitsandrisksofvaginalversuscesareandelivery
Essentials ofLaborManagement
6/3/16
3
Terminology
• CervicalRipening• Complexprocessof softeninganddistensibility• Consistency,position, effacementanddilation
• InductionofLabor• Useofpharmacologicaland/ormechanicalmethods to initiate labor• Includesunsuccessfulattemptsatinitiating labor, initiation oflabor followingspontaneous ruptureofmembraneswithout contractions
• Augmentation• Stimulationofuterinecontractionsusingpharmacologicmethodsorartificialruptureofmembranes toincreasecontractionfrequencyand/or strengthfollowing theonsetof spontaneous labororcontractionsfollowingspontaneous ruptureormembranes
“Indicationsforlaborinductionarenotabsolutebutshouldtakeintoaccountmaternalandfetalconditions,gestationalage,cervicalstatus,andotherfactors.”ACOG
• Abruptio Placentae• Chorioamnionitis
• FetalDemise• Prematureruptureofmembranes• Posttermpregnancy
• MaternalConditions• Hypertension• Diabetes• RenalDisease• Chronicpulmonarydisease• Antiphospholipid syndrome
• Fetalcompromise• Growth restriction• Isoimmunization• Oligohydramnios
AbsoluteContraindications
• Placentaorvasaprevia• Transverse fetallie• Umbilicalcordprolapse• Previousclassicalcesareandelivery• Myomectomy
• Enteredtheendometrial cavity
• Activegenitalherpes
StagesofLabor
• First Stage• Onset of labor until complete dilation• Two phases: latent and active
• Active transition: 8-10 cm• Second Stage
• Complete cervical dilation and effacement to delivery• Third Stage
• Placental Expulsion
FactorsAffectingBirthProcess:“P’s”
4“P’s”• Power:Contractions• Passage:Birthcanal
• Passenger:Fetus• Psyche:Emotions
5“P’s”• Power
• Passage• Passenger
• Position:Maternal• Psyche
PowerForcesrequiredtomovefetusthoughmaternalpelvis
• Primaryuterinepower• Myometriumadvancesfromquiettoactivewithlabor• Uterinemuscle:Composed of upperandlowersegments
• Uppersegment:activeandcontainspacemakerssites• Lowersegment:passivezone
• Physiologicretractionringbetweensegments• Facilitatesdescentanddilation

6/3/16
4
Power(continued)
• Effacement/shortening• Thinningofthe cervical canal• Reported inpercentage
• Dilation• Openingofcervical os• Allowspassage offetus
• Cervix• Position:posterior toanterior• Consistency: firmtosoft
Passage:Pelvis
• Bony boundaries • Shape and configuration that allows for delivery
• Conditions impacting passage• Musculoskeletal deformities/ diseases
• Contracted pelvis, dwarfism• Pelvic trauma• Cervical trauma or injury (DES, surgical procedures)
Passenger (Fetus/Placenta)
• Active participant in labor process• Descending, turning through pelvis
• Determined by• Fetal lie• Fetal attitude• Fetal presentation• Presenting part• Fetal position
Psyche• History
• Past/presentbirthexperience• Culturalconsiderations• Expectationsforbirthexperience
• Birthplanrealisticornot• Preparationforbirth• Supportsystem
• Psychosocialresponse• Emotionsduringphases oflabor
• Psychologicalreactionstolabor• Trainedsupportpersonatbedside
UterineActivity
• Importanttoknowuterinephysiology• Relationshiptofetaloxygenation• Doesitapplytofetallosses?NO
• CorrelationbetweenUAandacid-basestatus• Frequencyalonenotenoughfor
• “Passage”and“Passenger
UterineActivityTerminology• Frequency
– Beginning of contraction tobeginning of next one– Measured inminutes
• Duration– Length of contraction frombeginning toend (onsettooffset)– Measured inseconds
• Intensity– Strength of contraction– Assessed via palpation ormmHg (Montevideo units)
• Resting Tone– Intrauterine pressure when uterus isnotcontracting– Assessed via palpation ormmHg
– Relaxation Time– Time fromend of contraction tobeginning of next

6/3/16
5
MontevideoUnits
• 10minutetimeframe• Twomethods
• Measure peakintensity,oramplitude,inmmHgforeachcontractionandaddtogether
• Subtractbaselineuterinetonefrompeakcontractionpressureforeachcontractionandaddtogether
ShoulderDystocia• Obstetricemergency
• Mostlyunpredictableandunpreventable• Resultofsizediscrepancybetweenfetalshouldersandthepelvicinlet.
• Delivery offetalbodyispreventedbyimpaction• Fetalshoulderbehindsymphysispubis
• Delivery requiringmaneuversinadditiontogentledownwardtraction• Secondarydefinition
• Delivery withlongerthan60secondsbetweenheadandbody• Requiresuseofancillaryobstetricmaneuvers
PotentialRiskFactors
• Stronglyassociated• EFW>4500grams
• Some use>4000grams• Maternaldiabetes
• Pre-existingandGDM
• Historyofpriorshoulderdystocia• Maternal obesity• Increasedweightgain
• Multiparity• Posttermpregnancy• Disproportionatefetalgrowth
• Abdomen/chestcircumferencecomparedtoocciputofrontaldiameter
IntrapartumRiskFactors
• Laborinduction• Abnormallaborprogress• Prolongedsecondstage• Operativevaginalbirth
Chorioamnionitis:FeverPlusOneoftheFollowing
Clinical Parameters Suggestive of Chorioamnionitis
Maternal Fever T ≥ 100.4 °
Maternal Leukocytosis > 15, 000 cells/mm
Maternal Tachycardia > 100 bpm
Uterine/Fundal or Abdominal Tenderness
Tenderness or pain on palpation
Vaginal Discharge Foul smelling fluid or discharge
Adapted from: Tita AT, Andrews WW. Diagnos is and management of clinical chorioamnionitis . Clin Per inatol. 2010;37:339-354.Greenberg, Mara B., et al. "A firs t look at chorioamnionitis management practice variation among US obs tetricians ." Infectious diseases in obs tetr ics and gynecology 2012
ChorioamnionitisRISK FACTORS
Prolonged membrane rupture (≥ 12 hours )
Prolonged Labor
Meconium s tained fluid (heavy or particulate)
Nulliparity
↑ BMI
Regional anes thes ia (epidural fever)
Immunocompromised patients
Race/ethnic background (e.g. African American)
Urogenital Infections (Group B s trep, UTI, bacterial vaginos is )
Prior his tory of chorioamnionitis
Procedures (> 8 vaginal exams, amnioinfus ion, internal fetal monitoring)
Poor perineal hygiene (includes during labor)
Alcohol and tobacco use
Ad ap ted fro m: Tita AT, An d rews WW. Diag n o sis an d man ag emen t o f clin ical ch o rio amn io n itis. Clin Perin a to l. 2 0 1 0 ;3 7 :3 3 9 -3 5 4

6/3/16
6
Every hospital will need to customize the protocol—but the point is every hospital
needs one
CMQCC OB Hemorrhage Emergency Management Plan
!
!
Copyright California Department of Public Health, 2014; supported by Title V funds. Developed in partnership with California Maternal Quality Care Collaborative Hemorrhage Taskforce Visit: www.CMQCC.org for details
Obstetric Hemorrhage Emergency Management Plan: Table Chart Format version 2.0
Assessments Meds/Procedures Blood Bank Stage 0 Every woman in labor/giving birth
Stage 0 focuses on risk assessment and active management of the third stage.
• Assess every woman for risk factors for hemorrhage
• Measure cumulative quantitative blood loss on every birth
Active Management 3rd Stage:
• Oxytocin IV infusion or 10u IM
• Fundal Massage-vigorous, 15 seconds min.
• If Medium Risk: T & Scr • If High Risk: T&C 2 U • If Positive Antibody
Screen (prenatal or current, exclude low level anti-D from RhoGam):T&C 2 U
Stage 1 Blood loss: > 500ml vaginal or >1000 ml Cesarean, or VS changes (by >15% or HR ≥110, BP ≤85/45, O2 sat <95%)
Stage 1 is short: activate hemorrhage protocol, initiate preparations and give Methergine IM.
• Activate OB Hemorrhage Protocol and Checklist
• Notify Charge nurse, OB/CNM, Anesthesia
• VS, O2 Sat q5’ • Record cumulative
blood loss q5-15’ • Weigh bloody materials • Careful inspection with
good exposure of vaginal walls, cervix, uterine cavity, placenta
• IV Access: at least 18gauge • Increase IV fluid (LR) and
Oxytocin rate, and repeat fundal massage
• Methergine 0.2mg IM (if not hypertensive) May repeat if good response to first dose, BUT otherwise move on to 2nd level uterotonic drug (see below)
• Empty bladder: straight cath or place foley with urimeter
• T&C 2 Units PRBCs (if not already done)
Stage 2 Continued bleeding with total blood loss under 1500ml
Stage 2 is focused on sequentially advancing through medications and procedures, mobilizing help and Blood Bank support, and keeping ahead with volume and blood products.
OB back to bedside (if not already there) • Extra help: 2nd OB,
Rapid Response Team (per hospital), assign roles • VS & cumulative
blood loss q 5-10 min • Weigh bloody materials • Complete evaluation
of vaginal wall, cervix, placenta, uterine cavity • Send additional labs,
including DIC panel • If in Postpartum: Move
to L&D/OR • Evaluate for special
cases: -Uterine Inversion -Amn. Fluid Embolism
2nd Level Uterotonic Drugs: • Hemabate 250 mcg IM or • Misoprostol 800 mcg SL
2nd IV Access (at least 18gauge)
Bimanual massage Vaginal Birth: (typical order) • Move to OR • Repair any tears • D&C: r/o retained placenta • Place intrauterine balloon • Selective Embolization
(Interventional Radiology) Cesarean Birth: (still intra-op) (typical order) • Inspect broad lig, posterior
uterus and retained placenta
• B-Lynch Suture • Place intrauterine balloon
• Notify Blood Bank of OB Hemorrhage
• Bring 2 Units PRBCs to bedside, transfuse per clinical signs – do not wait for lab values
• Use blood warmer for transfusion
• Consider thawing 2 FFP (takes 35+min), use if transfusing > 2u PRBCs
• Determine availability of additional RBCs and other Coag products
Stage 3 Total blood loss over 1500ml, or >2 units PRBCs given or VS unstable or suspicion of DIC
Stage 3 is focused on the Massive Transfusion protocol and invasive surgical approaches for control of bleeding.
• Mobilize team -Advanced GYN surgeon -2nd Anesthesia Provider -OR staff -Adult Intensivist • Repeat labs including
coags and ABG’s • Central line • Social Worker/ family
support
• Activate Massive Hemorrhage Protocol • Laparotomy: -B-Lynch Suture -Uterine Artery Ligation -Hysterectomy • Patient support -Fluid warmer -Upper body warming device -Sequential compression stockings
Transfuse Aggressively Massive Hemorrhage Pack • Near 1:1 PRBC:FFP • 1 PLT apheresis pack per 4-6 units PRBCs
Unresponsive Coagulopathy: After 8-10 units PRBCs and full coagulation factor replacement: may consult re rFactor VIIa risk/benefit
Blood Loss:1000-1500 ml
Stage 2Sequentially
Advance throughMedications &
Procedures
Pre-Admission
Time of admission
Identify patients with special consideration:Placenta previa/accreta, Bleeding disorder, or those who decline blood products
Follow appropriate workups, planning, preparing of resources, counseling and notification
Screen All Admissions for hemorrhage risk:Low Risk, Medium Risk and High Risk
Low Risk: Draw blood and hold specimenMedium Risk: Type & Screen, Review Hemorrhage ProtocolHigh Risk: Type & Crossmatch 2 Units PRBCs; Review Hemorrhage Protocol
All women receive active management of 3rd stageOxytocin IV infusion or 10 Units IM, 10-40 U infusion
Standard Postpartum Management
Fundal Massage
Vaginal Birth:Bimanual Fundal MassageRetained POC: Dilation and CurettageLower segment/Implantation site/Atony: Intrauterine BalloonLaceration/Hematoma: Packing, Repair as RequiredConsider IR (if available & adequate experience)
Cesarean Birth:Continued Atony: B-Lynch Suture/Intrauterine BalloonContinued Hemorrhage: Uterine Artery Ligation
To OR (if not there); Activate Massive Hemorrhage Protocol
Mobilize Massive Hemorrhage Team TRANSFUSE AGGRESSIVELY RBC:FFP:Plts Æ 6:4:1 or 4:4:1
IncreasedPostpartum Surveillance
Definitive SurgeryHysterectomy
Conservative SurgeryB-Lynch Suture/Intrauterine BalloonUterine Artery LigationHypogastric Ligation (experienced surgeon only)Consider IR (if available & adequate experience)
Fertility Strongly Desired
Consider ICUCare; Increased
Postpartum Surveillance
Verify Type & Screen on prenatal record;
if positive antibody screen on prenatal or current labs (except low level anti-D from Rhogam), Type & Crossmatch 2
Units PBRCs
CALL FOR EXTRA HELPGive Meds: Hemabate 250 mcg IM -or-
Misoprostol 600-800 SL or PO
Cumulative Blood Loss>500 ml Vag; >1000 ml CS>15% Vital Sign change -or-
HR ≥110, BP ≤85/45 O2 Sat <95%, Clinical Sx
Ongoing Evaluation:
Quantification of blood loss and
vital signs
Unresponsive Coagulopathy:After 10 Units PBRCs and full
coagulation factor replacement,may consider rFactor VIIa
HEMORRHAGE CONTINUES
Blood Loss:>1500 ml
Stage 3
Activate Massive
Hemorrhage Protocol
Blood Loss: >500 ml Vaginal
>1000 ml CSStage 1Activate
Hemorrhage Protocol
NO
Stage 0All Births
Transfuse 2 Units PRBCs per clinical signs
Do not wait for lab valuesConsider thawing 2 Units FFP
YES
YES NO
Ong
oing
Cum
ulat
ive
Blo
od L
oss
Eva
luat
ion
Cumulative Blood Loss>1500 ml, 2 Units Given,
Vital Signs Unstable
YESIncrease IV Oxytocin RateMethergine 0.2 mg IM (if not hypertensive)Vigorous Fundal massage; Empty Bladder; Keep WarmAdminister O2 to maintain Sat >95%Rule out retained POC, laceration or hematomaOrder Type & Crossmatch 2 Units PRBCs if not already done
Activate Hemorrhage ProtocolCALL FOR EXTRA HELP
Continued heavy bleeding
Increased Postpartum Surveillance
NO
NO
CONTROLLED
INCREASED BLEEDING
California Maternal Quality Care Collaborative (CMQCC), Hemorrhage Taskforce (2009) visit: www.CMQCC.org for detailsThis project was supported by funds received from the State of California Department of Public Health, Center for Family Health; Maternal, Child and Adolescent Health Division
Obstetric Emergency Management Plan: Flow Chart Format Release 2.0 7/9/2014
The Importance of IV Gauge
Gauge Gravity Flow Flow with Rapid Infuser
20 65 mL/min
18 140 mL/min 250 mL/min
16 190 mL/min 350 mL/min
14 300 mL/min 500 mL/min
Get 2nd Line In Before Vasoconstriction Develops!
ClotTube• 5ml in red top tube
• No anticoagulant• No clot activator
• 10 minutes• Failure to clot or dissolution of initial clot
• Coagulopathy present
MethodsofLaborInductionNon-Pharmacologic Surgical Pharmacologic
Complementary orAlternative Medicine
Dilation&Evacuation Prostaglandins
MechanicalDilators Hysterotomy Misoprostol
MembraneStripping Hysterectomy Oxytocin
Amniotomy
Complementary/AlternativeMedicineLackofsafetyandefficacydata
Nospecificrecommendationsinfetaldemise• Herbalsupplements
• Redraspberryleaf ,• Blueandblack cohosh• Evening primroseoil
• Breast stimulation• Sexualrelations• Acupuncture• TranscutaneousNerveStimulation
MechanicalDilators
• Hygroscopic/osmoticdilators• Laminaria
• Balloondevices• Foleycatheters• Doubleballoondevices• Extraamnioticsaline infusion
• Membranestripping/sweeping• Amniotomy

6/3/16
7
MechanicalDilators
Advantages• Cost• Stableatroomtemperature• Easystorage• Fewer sideeffects
Disadvantages• Ruptureofmembranes• Infection• Bleeding• Maternal discomfort
Hygroscopic/OsmoticDilators
• “Laminaria”ortypeofseaweed• Technique
• Placedduringspeculumexamination• Progressiveplacement• Sterilegauzepad• Recordnumberofdilators
BalloonDevices
• Foleycatheters/double balloons• Technique
• Speculum orblind placement• Inf lation of balloon
• 30-60ccoff luid• Gently retract and secure
• Traction• Extra-amniotic infusion (EASI)
• 18Ffoley catheter• Inf late balloonwith 30cc• Secure withtraction• NS infusion30drops/min (90cc/hr)• Maximum volume 2liters
MembraneStripping/Sweeping• Digitaldilatationofthecervix• Releasesprostaglandin• Technique
• Vaginalexamination• Membranesseparated frominternalos• Movinginacirculardirection
Amniotomy
• Pressureofpresentingpartoncervix• Bestwithfavorablecervix• Inconjunctionwithlowdoseoxytocin
• Shorten intervals frominduction todelivery
• Commitmenttodelivery
PharmacologicMethods
• Prostaglandins• Prostaglandin E1(PGE1)
• Misoprostol• Prostaglandin E2(PGE2)
• Gel: 0.5mgdinoprostone• Vaginal insert:10mgdinoprostone
• Oxytocin
AWHONN Webinar Series ©2009 42

6/3/16
8
SecondTrimesterManagement
• Optimalmethodsnotestablished• Inductionversussurgical
• IOLusedmoreoftenthandilationandevacuation• Maybegestational agerelated• Requires skilledclinicians inperformingD&E• Clinically importanttoobtain intactfetus• Allows forprocessof labor tooccur• Patientpreference
• BUT D&Econsideredsafer13to22-24weeks• Lowercomplication ratesthan IOL
Bry ant AG, Grimes DA, Garrett J M, Stuart GS. Sec ond-trimes ter abortion for fe ta l anomal ies or fe ta l death: labor induc tion c ompared wi th d i la tion and ev ac uation. Obs tetric s & Gy nec ology . 2011;117(4):788-92.
SurgicalProcedure:
• Cervicalripening• Laminariaormisoprostol• Ultrasoundguidedprocedure• Removaloffetusandplacenta
• Cannulaandspecial forceps
• Awarenessbyentireteam ofprocedureresults
SurgicalProcedure:D&E• Medication
• Doxycycline100mgpo1hrprior toprocedureand200mgafterprocedure• ORpostoperativemetronidozole500mgorally twicex5days
• Cervical ripening• Misoprostol 200mgin theposterior fornix4hoursprior toprocedure• OR laminariax12-24hours
• Dilationandevacuationunderultrasoundguidance• Cannulaandspecial forceps
• Dischargeafteranesthesia wornoffandvaginalbleeding isminimal• Administer Rhoghamifpatient isRhnegative• Schedulefollow-up visit in1-2weeks• PrescribeNSAIDs
Bry ant AG, Grimes DA, Garrett J M, Stuart GS. Sec ond-trimes ter abortion for fe ta l anomal ies or fe ta l death: labor induc tion c ompared wi th d i lation and ev ac uation. Obs tetric s & Gy nec ology . 2011 Apr 1 ;117(4):788-92.
Bry ant AG, Grimes DA, Garrett J M, Stuart GS. Sec ond-trimes ter abortion for fe ta l anomal ies or fe ta l death: labor induc tion c ompared wi th d i lation and ev ac uation. Obs tetric s & Gy nec ology . 2011 Apr 1 ;117(4):788-92.
PGE2VaginalSuppositories
• 20mgsuppositoryq4hours• Redoseuntilcontractionscausecervicalchange• <28weeks• Sideeffects
• Fever,nausea,vomitinganddiarrhea• Pretreatmentmedications

6/3/16
9
SecondTrimesterManagement
• Drugofchoice• Misoprostol forlate2ndtrimester (≥22weeks)• Optimumregimennotestablished
• Suggested Dose• 200to400mcgvaginally• Repeating doseevery3hours• Maximumcumulativedose=1400mcgin24hours
• Meandeliverytime• 10to11hours
Gomez Ponce de Leon R, Wing D, Fiala C. Misoprostol for intrauterine fetal death. Int J GynaecolObstet 2007; 99 Suppl 2:S190.
Literature
• Systematicreview of14RCT’s• Dosing: 100 to400mcg(butsometimesmore….)• Routes:oral, vaginal, sublingual, buccal• Frequenciesofadministration: q3to12hours
• Vaginaldosingjustaseffectiveasoraldosingwithin48hours• 100% delivery rate
• Vaginaldosingalonecomparedtovaginaldosingandoxytocinlesseffective indelivery<24hours
• Nodifferencein<48hours
Gómez PD, Wing DA. Misoprostol for termination of pregnancy with intrauterine fetal demise in the second and third trimester of pregnancy-a systematic review. Contraception . 2009 Apr;79(4):259 .
Alternatives• Misoprostol100mcgvaginally
• Repeat q6to12hoursforamaximumof4doses• Pregnanciesat18to26weeks
• Seconddosecanbedoubledto200mcg• Maximumcumulativedoseis800mcgin24hours
● Misoprostol 100mcgor200mcgvaginally•q4hours• Mifepristone(RU486)Misoprostolregimen(<20weeks but>20weeks???)
• Mifepristone200mgor600mg• Followedbymisoprostol200or400mcg24to48hourslater
Gomez Ponce de Leon R, Wing D, Fiala C. Misoprostol for intrauterine fetal death. Int J GynaecolObstet 2007; 99 Suppl 2:S190.
Mifepristone
• Antiprogestin• Increasesuterinesensitivitytoprostaglandins
• Allows for lowerdoses• Fewerside effects
• Alternative optionGemeprost• Notavailable inUnitedStates
MifepristoneandMisoprostolReferences
• Chaudhuri P, DattaS.Mifepristone andmisoprostol compared withmisoprostol alone for induction of labor in intrauterine fetaldeath:Arandomized trial. JObstet Gynaecol Res 2015;41:1884.
• Panda S, JhaV, Singh S.Role ofCombination OFMifepristone andMisoprostol Verses Misoprostol alone in Induction ofLabour in LateIntrauterin FetalDeath:AProspective Study.JFamilyReprodHealth 2013;7:177.
• Wagaarachchi PT, Ashok PW, Narvekar NN,etal. Medical management oflate intrauterine death using acombination ofmifepristone andmisoprostol. BJOG 2002;109:443.
MisoprostolSideEffects
• Nauseaandvomiting• Diarrhea
• Associatedmostwithhigherdoses
• Noninfectiousfever• Combinedmethods
• Higher ratescomparedtomisoprostol only
Perritt JB, Burke A, Edelman AB. Interruption of nonviable pregnancies of 24–28 weeks ' gestation us ingmedical methods .Contraception. 2013 Sep 30;88(3):341-9.

6/3/16
10
Whyis28weeksacut-off
• Uterus lesssensitivetooxytocin• Prostaglandinsandmechanicaldilatorsmayberequired
• Prostaglandin side-effects
• “Keepinmindthatalthoughsideeffects(uterinetachysystole,nausea,vomiting,diarrhea)andsafetyremainimportantconsiderationsforthepatientinthesecircumstances,thefetalwellbeingisnolongeranissue”(Gabbe)
HighDoseOxytocin
• Effective especiallyifotheroptionsnotavailable• Dosing
• 6mU/min• Increaseby6mU/minat45minuteintervalsuntilcontractionsare effective
• Donotexceed40mU/min
Abed iasl Z, Sheikh M ,P oo ran sari P , Farahan i Z, K alan i F. Vagin al misop ro sto l versu s in travenou s o xyto cin fo r th emanagemen t o f second -trimester p regnan cieswith in trau terin e fetal d eath : A randomized cl in ical trial . Jo u rnal o fOb stetrics and Gynaeco lo gy Research . 2 0 1 5 Jan 1 .
Yapar EG,Senö z S, Ürkü tü r M ,Batio glu S, Gökmen O.Second trimester p regnan cy termination in clud in g fetal d eath : comparison o f five d i fferen t method s.Eu ropean Jou rnal o fOb stetrics &Gyneco lo gy and Rep rodu ctive B io lo gy.1 9 9 6 Nov3 0 ;6 9 (2 ):9 7 -1 0 2 .
AlternativeHighDoseOxytocin
Winkler C L, Gray SE, Hau th JC , Owen J, TUCK ER J. M id -second -trimester l ab o r in du ctio n :co n cen trated o xyto cin compared wi th p ro stagland in E2 vagin al su ppo si to ries. Ob stetri cs &Gyneco lo gy. 1 9 9 1 Feb 1 ;7 7 (2 ):2 9 7 -3 0 0 .
Owen J, Hau th JC , Win klerC L, Gray SE. M id trimester p regn an cy termin atio n : a randomized trial o fp ro stagland in E 2 versu s co ncen trated o xyto cin . American jo u rn al o fo b stetri cs an d gyn eco lo gy. 1 9 9 2 Oct3 1 ;1 6 7 (4 ):1 1 1 2 -6 .
WaterIntoxication• Oxytocinisananti-diuretic
• Highdoses lead tohyponatremia(~40mU/min)• Prostaglandin usehasdecreasedneedforprolongedoxytocin
• Hyponatremiaetiology• Attributed tohemodilution with IVfluids• Increasedexcretionofsodium in theurine• Shiftof sodiumfromextracellular tointracellular fluid
• Relationbetweensymptomsandplasmasodiumconcentration• Critical range:120-125mmol(mEq)/l
Ahmad AJ, Clark EH, Jacobs HS. Water intoxication associated with oxytocin infusion. Postgraduate medical journal. 1975 Apr 1;51(594):2 49 -5 2.
WaterIntoxication• Quantityofinfusedfluidismoreimportantthanoxytocinconcentration
• Lowdose (2-5mU/min)actasantidiuretic• Demonstratedwithin 10-15minutes
• Oxytocin-inducedhyponatremia• Receivedmore than3.5litersof fluid (fluidswithD5)
• Symptoms• Headache,anorexia,nausea,vomiting, tachycardia,abdominalpain, lethargy,drowsiness, unconsciousness, grandmalseizures, andLossofconsciousness orGrandmalseizures “AlteredLOCaredifficult totospot inlaborbuthavebeen retrospectivelynoted in somepatients”
• Differentialdiagnosis: Eclampsia• “Normotensive,noproteinuriawithedema”• Confirmedbyserumelectrolytes
• Potentially irreversible neurologic injury\
Feeney J G. Water in tox ic ation and ox y toc in . Br Med J (Cl in Res Ed). 1982 J u l 24;285(6337):243-Ahmad AJ, C lark EH, Jacob s HS. Water In to xication asso ciation with o xyto cin in fu sion .. Ob stetrical &Gyneco lo gical Su rvey. 1 9 7 6 Mar1 ;3 1 (3 ):1 9 6 -7 ..
6/3/16
11
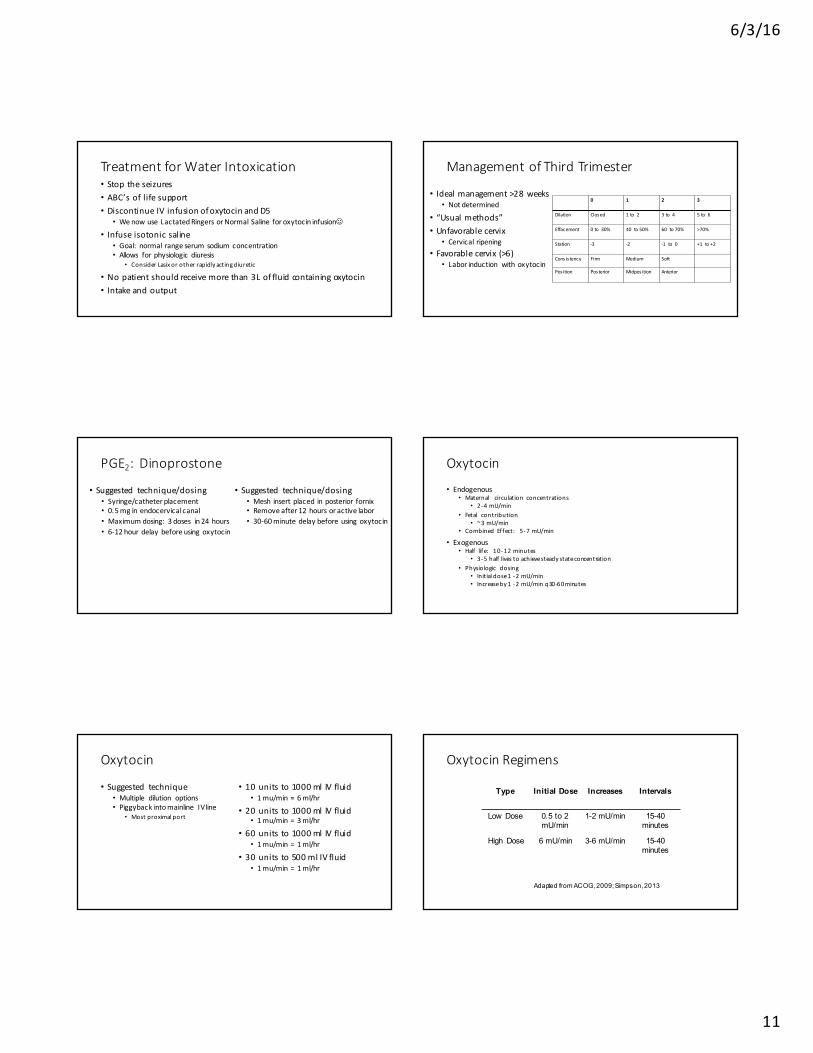
TreatmentforWaterIntoxication• Stoptheseizures• ABC’soflifesupport• DiscontinueIVinfusionofoxytocinandD5
• WenowuseLactatedRingersorNormalSaline foroxytocininfusionJ
• Infuseisotonicsaline• Goal:normal rangeserumsodiumconcentration• Allows forphysiologicdiuresis
• ConsiderLasixorotherrapidlyactingdiuretic
• Nopatientshouldreceivemorethan3Loffluidcontainingoxytocin• Intakeandoutput
ManagementofThirdTrimester
• Idealmanagement>28weeks• Notdetermined
• “Usualmethods”• Unfavorablecervix
• Cervical ripening• Favorablecervix(>6)
• Laborinduction withoxytocin
0 1 2 3
Dilation Closed 1to 2 3to 4 5to 6
Effacement 0to 30% 40 to50% 60 to70% >70%
Station -3 -2 -1 to 0 +1 to+2
Cons is tency Firm Medium Soft
Pos ition Posterior Midpos ition Anterior
PGE2:Dinoprostone
• Suggested technique/dosing• Syringe/catheterplacement• 0.5mginendocervicalcanal• Maximumdosing:3doses in24hours• 6-12hourdelaybeforeusingoxytocin
• Suggested technique/dosing• Mesh insertplaced inposterior fornix• Removeafter12hoursoractivelabor• 30-60minutedelaybeforeusingoxytocin
Oxytocin
• Endogenous• Maternal circulation concentrations
• 2-4mU/min• Fetal contribution
• ~3mU/min• Combined Effect: 5-7mU/min
• Exogenous• Half life: 10-12minutes
• 3-5half livestoachievesteadystateconcentration• Physiologic dosing
• Initialdose1-2mU/min• Increaseby1-2mU/minq30-60minutes
Oxytocin
• Suggested technique• Multiple dilution options• Piggybackintomainline IVline
• Mostproximalport
• 10unitsto1000mlIVfluid• 1mu/min=6ml/hr
• 20unitsto1000mlIVfluid• 1mu/min=3ml/hr
• 60unitsto1000mlIVfluid• 1mu/min=1ml/hr
• 30unitsto500mlIVfluid• 1mu/min=1ml/hr
OxytocinRegimens
Type Initial Dose Increases Intervals
Low Dose 0.5 to 2 mU/min
1-2 mU/min 15-40 minutes
High Dose 6 mU/min 3-6 mU/min 15-40 minutes
Adapted from ACOG, 2009; Simpson, 2013

6/3/16
12
Misoprostol
• Well studied in 2nd trimester demises• Insuff icient evidence in 3rd trimester
• 25 to50mcgvaginally• Repeat q4hours ifless than2contractions in 10minutes
• Second dose canbedoubled to50 to100mcg• Maximum of6doses
• Maximum cumulative dose =600mcgin 24hours• Oxytocin
• Initiated 4hours afteradministration of the last dose• Augmentation of labor
LaborInductioninThirdTrimesterStillbirthsGawron&Kiley,2013
• Objective• Managementof3rd trimester stillbirths 28weeks
• Academichospital• Chartreview: 74deliveries
• Demographics• History• Inductionmethodanddeliveryinterval• Adverseoutcome
• Results• ”Safedeliverywithin 24hours” regardlessofmethod
Gawron LM, Ki ley J W. Labor induc tion outc omes in th i rd-trimes ter s ti l lb i rths . In ternational J ournal o f Gy nec ology & Obs tetric s . 2013 Dec 31;123(3):203-6.
Gawron LM, Ki ley J W. Labor induc tion outc omes in th i rd-trimes ter s ti l lb i rths . In ternational J ournal o f Gy nec ology & Obs tetric s . 2013 Dec 31;123(3):203-6.
Gawron LM ,K i ley JW.Labo r in du ction ou tcomes in th i rd -trimester sti l lb i rth s. In tern ational Jou rnal o fGyneco lo gy &Ob stetrics. 2 0 1 3 Dec3 1 ;1 2 3 (3 ):2 0 3 -6 .
PlacentaPrevia
• Earlypregnancy doesnotprecludevaginaldelivery• <24weeksincreasedEBL
• Noincrease in infection,hysterectomy,postoperative transfusion
• Nopublishedstudies• Impactofplacentapreviaat>24– 28weeks
• Probablyhigherbloodlossrates• Insufficientevidencetomakerecommendations
Thomas AG, Alv arez M, Friedman F, Brodman ML, Kim J , Loc k wood C. The effec t o f p lac enta prev ia on b lood loss in s ec ond trimes ter pregnanc y termination. Obs tet Gy nec ol 1994;84:58–60Perri tt JB ,Bu rkeA,Edelman AB . In terrup tion o fn onviab le p regnan cies o f2 4–2 8 weeks' gestation u sin g med ical method s. Con tracep tion . 2 0 1 3 Sep 3 0 ;8 8 (3 ):3 4 1 -9.
PriorCesareanSection:Liveborn
• ProbabilityforSuccessfulInductionhttps://mfmu.bsc.gwu.edu/PublicBSC/MFMU/VGBirthCalc/vagbirth.html
• LowRiskofUterineRupture(stillhigherthanunscarreduterus)• ~0.5– 1%(onepriorLTCS);3.7%for2priorLTCS
• UnfavorableCervix• Limiteddataonhowtoapproach
• Methods• MechanicalandPharmacologicMethods
ACOG, 2010; Cahill et al, 2010; Metx et al, 2012; Shanks & Cahill, 2011Hoffman MK, Sciscione A, Srinivasana M, Shackelford DP, Ekbladh L.Uterine rupture inpatients with a prior cesareandelivery: the impact ofcervical ripening. Obstetrical &gynecological survey. 2005 Jan 1;60(1):22-3.

6/3/16
13
VBACCalculatorhttps://mfmu.bsc.gwu.edu/PublicBSC/MFMU/VGBirthCalc/vagbirth.html
UterineRupture RatesFactors Rates
UnscarredUterus 1/5700 to1/20,000 pregnancies(RARE)0.0175%to0.005%
UnscarredUteruswithOxytocin Uncertain:3.6-43%ScarredUterus(all comers) 325per100,000womenundergoingTOL
0.325%Inductionoflaboratterm(37-40weeks) 1,500per100,000
1.5%Spontaneous labor 800per100,000
0.8%Inductionat>40weeks 3,200per100,000
3.2%Signore C, Spong CY. Vaginal birth after cesarean: new insights manuscripts from an NIH consensus development conference, March 8–10, 2010. In Seminars in perinatology 2010 Oct (Vol. 34, No. 5, p. 309).
BeAlert for Signs of Uterine Rupture• Maternal tachycardiaandhypotension
• Complete rupture=maternal shock
• Hematuria• Vaginalbleeding:May/maynotbepresent• Pain
• Shearing,tearing, subrapubic• Occurswithepidural• Continuesaftercontractions
• Recedingpresentingpart/fetalstationloss• Palpablefetalpartinabdomen
PriorCesareanSectionandMisoprostol• Contraindicatedintermlaborinductionwithlivefetus• SAFEforfirst- andsecond-trimesterdemises(upto28weeks)• Misoprostolonlyregimenindemisecases(Cayrac)
• Noreportedcasesofuterine rupture inwomenwith priorcesarean
• Mifepristone-misoprostolregimens• Uterine rupture:4.8%(Cayrac)
• Successoftheregimenandoverallmorbidity• Similar forwomenwithandwithoutprioruterine incision
Perritt JB, BurkeA,EdelmanAB.Interruption ofnonviablepregnancies of24–28weeks 'gestationus ingmedicalmethods .Contraception.2013Sep30;88(3):341-9.CayracM,FaillieJL,FlandrinA,BoulotP. Second-andthird-trimester managementofmedicaltermination ofpregnancyandfetaldeathinuteroafter prior caesareansection.EuropeanJournalofObstetrics &GynecologyandReproductiveBiology.2011Aug31;157(2):145-9.
MisoprostolinPriorCesareanSection
• Criteria• Priorcesareansection• Misoprostol use16-28weeks
• Initial agent
• 509patients• Uterine rupturerate
• Oneprior: 0.4%• Twoprior: 0%• Priorclassical: 50%
“UniqueGroup”
• Creasy &Resnik• Individualize; use oxytocin protocolsandcervical ripening withfoley
• Gabbe• Candidates forinductionof labor• Does notmention misoprostol inpriorLTCS
• Williams• Outcomes were atf irstdiscouraging butrecent evidence is less pessimistic
• Berghella,2009andGoyal,2009:28weeksorless• UptoDate
• If thecervix isunfavorable, we suggest cervical ripening using a mechanical methodrather thana prostaglandin
• Favorable cervix: oxytocin

6/3/16
14
LimitedData….
• Limiteddata• Priorclassicaluterine incision• Myomectomy
• Overalluterinerupturerate• 1-12% in thispopulation• Repeatcesareansection isappropriate
Chakhtoura NA, Reddy UM. Management of stillbirth delivery. Seminars in perinatology 2015;39:501 -5 04 ).
HowLongIsTooLong?
• Nopublishedstudiesonregimensafter24-48hours• Isolatedreportsofrefractorycasesafter 48hours
• Deliveryby72hours
• Considermedicationholiday• Changeregimens• Cesarean formaternalindications
• Arrestdisorders
Perritt JB, Burke A, Edelman AB. Interruption of nonviable pregnancies of 24–28 weeks ' gestation us ingmedicalmethods . Contraception. 2013 Sep30;88(3):341-9
RiskManagementStrategies• Informedconsent• Unitpolicyorprotocol
• Standardized institutionally based• Ripening,induction,augmentation
• Chainofcommand• Methodsanddosages• Complications• Interventions• Multidisciplinary input• Staffexpectations
• Staffing• PharmacologicCervicalRipening: 1:2• OxytocininLabor:1:1• Nothingaddressing fetal loss
• Patientacuity• Availability of supportpersonnel• Doula
• Medicalrecorddocumentation• Checklist???• Charting frequency• Evidenceofinformedconsent• Order set


















