It has now been established that T2DM is an independent risk factor for osteoporotic fractures. 1 It...
25
-
Upload
marilyn-stevenson -
Category
Documents
-
view
218 -
download
0
Transcript of It has now been established that T2DM is an independent risk factor for osteoporotic fractures. 1 It...


It has now been established that T2DM is an independent
risk factor for osteoporotic fractures.1
1. Rubin MR, et al. Osteoporosis Risk in Type 2 Diabetes patients. Expert Rev Endocrinol Metab. 2013;8(5):423–5. 2. Giangregorio LM, et al. FRAX underestimates fracture risk in patients with diabetes. J Bone Miner Res. 2012;27(2):301–8. 3. Brown SA, et al. Osteoporosis: An Under-appreciated Complication of Diabetes. Clin Diabetes. 2004;22. 4. Abdulameer SA, et al. Osteoporosis and type 2 diabetes mellitus: what do we know, and what we can do? Patient Prefer Adherence 2012;6:435–48.
OSTEOPOROSIS AND TYPE 2 DIABETES – THE LINK
Introduction
Type 2 diabetes mellitus (T2DM) is one of the common chronic metabolic disorders across the world having a significant impact on an individual's health1
It has been estimated that T2DM affects over 366 million adults worldwide and the number is expected to rise up to 552 million by 20301
Osteoporosis is a condition where the bones become less dense and are susceptible to fractures.2,3 Osteoporosis can result in deformity, disability, pain and even death4

1. Brown SA, Sharpless JL. Osteoporosis: An Under-appreciated Complication of Diabetes. Clin Diabetes. 2004;22. 2. Hofbauer LC, et al. Osteoporosis in patients withdiabetes mellitus. J Bone Miner Res. 2007;22(9):1317–28. 3. Osteoporosis – Is There A Link With Diabetes? [Internet]. [cited 2015 Sep 3]. Available from: http://iddt.org/related-health-issues/osteoporosisis-there-a-link-with-diabetes 4. Xia J, et al. The relationship between insulin resistance and osteoporosis in elderly male type 2 diabetes mellitus and diabetic nephropathy. Ann Endocrinol (Paris). 2012;73(6):546–51.
OSTEOPOROSIS AND TYPE 2 DIABETES – THE LINK
Prevalence
The third National Health and Nutrition Examination Survey (NHANES III) estimated that about 13–18% women over 50 years of age in United States (U.S.) have osteoporosis with 37–50% having additional risk of low bone mass at the hip1
This disease alone causes more than 350,000 hip fractures each year in the U.S. and the annual number of fractures is expected to double by 20251
The Iowa Women’s Health Study involving 32,089 postmenopausal women revealed that women with type 1 diabetes mellitus (T1DM) were 12 times more likely to report hip fractures as compared to women without T1DM. Whereas, in case of T2DM the risk was 1.7-fold higher as compared to women without T2DM.2
A review of 16 studies found 140,000 hip fractures among 800,000 patients with type 1 diabetes and review of 12 studies revealed people with T2DM have 70% more risk of hip fracture3
A recent study by Xia et al. showed that elderly men with diabetes were more likely to have lowered bone mineral density and this is likely to be caused by insulin insufficiencies, decreased insulin sensitivity, and diabetic nephropathy in patients living4

Brown SA, Sharpless JL. Osteoporosis: An Under-appreciated Complication of Diabetes. Clin Diabetes. 2004;22. Available from: http://clinical.diabetesjournals.org/content/22/1/10.short?rss=1&ssource=mfc
OSTEOPOROSIS AND TYPE 2 DIABETES – THE LINK
Risk factors particular to patients with diabetes are included in Table 1

Type 1 diabetes is linked to low bone density. Patients with type 1 diabetes are insulin deficient, which may be required to promote bone growth and strength.2
Type 1 diabetes is typically developed at a young age when bone mass is still increasing. Bone mass is thought to reach its peak by the age of 30 years. Thus, young people with type 1 diabetes may never achieve a normal peak bone density and the maximum strength.2
Low peak bone mass may make an individual prone to develop osteoporosis in future life. People with type 1 diabetes are associated with celiac disease, which also reduces bone mass.2
Cytokines are thought to play a role in the development of both type 1 diabetes and osteoporosis2
Diabetes and osteoporosis are both frequent endocrine disorders. However, they seem to be
interconnected in several ways.1
1. Vestergaard P. Diabetes and Bone. J Diabetes Metab. 2011;S:1. doi:10.4172/2155-6156.S1-001. 2. What People With Diabetes Need to Know About Osteoporosis [Internet]. [cited 2015 Sep 3]. Available from: http://www.niams.nih.gov/Health_Info/Bone/Osteoporosis/Conditions_Behaviors/diabetes.asp
OSTEOPOROSIS AND TYPE 2 DIABETES – THE LINK
The Diabetes-osteoporosis Association

1. Initial adolescent accumulation of bone is diminished
2. Therefore, reaching a lower plateau with continued loss associated with hypercalciuria in early adult life
3. Followed by later onset and retardation of age-related bone loss
Krakauer JC, McKenna MJ, Buderer NF, et al. Bone loss and bone turnover in diabetes. Diabetes. 1995;44(7):775–82.
OSTEOPOROSIS AND TYPE 2 DIABETES – THE LINK
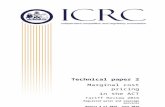
Figure 1 shows the effects of diabetes on BMD at different times of life

OSTEOPOROSIS AND TYPE 2 DIABETES – THE LINK
Depending on the age of onset, stages could overlap
Type 1 diabetes is associated with hypoglycaemia or low blood sugar reactions, vision problems and nerve damage which contributes to an increased risk of falls and related fractures
Type 2 diabetes was previously believed to provide bone protection. An increased bone mineral density (BMD) and weight in patients with type 2 diabetes prevented osteoporosis in such patients.
However, as with type 1 diabetes, people with type 2 diabetes too have an increased risk of falling because of peripheral neuropathy, possible hypoglycaemia, nocturia, and visual impairment. Because many type 2diabetic patients are obese and sedentary, this interferes with bone health.
What People With Diabetes Need to Know About Osteoporosis [Internet]. [cited 2015 Sep 3]. Available from: http://www.niams.nih.gov/Health_Info/Bone/Osteoporosis/Conditions_Behaviors/diabetes.asp

POSSIBLE MECHANISM OF DIABETES-INDUCED OSTEOPOROSIS
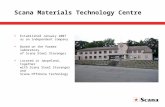
Although, exact underlying mechanism of pathogenesis is still unclear. It has been established that hyperglycaemia is a significant factor that contributes to the direct and indirect deleterious effects on osteoblast function and bone formation (Figure 2).
Diabetes mellitus (DM) promotes osteoclast function but suppress osteoblast function, thereby leading to accelerated bone loss, osteopenia and osteoporosis
DM/hyperglycemia induces production of macrophage colony stimulating factor (MCSF), tumour necrosis factor (TNF)-α and receptor activator of nuclear factor-κB ligand (RANKL), all of which are osteoblast-derived activators of osteoclast proliferation and differentiation
Moreover, DM/hyperglycaemia suppresses osteoblast proliferation and function, in part, by decreasing runt-related transcription factor (Runx)-2, osteocalcin and osteopontin expressions
Wongdee K, Charoenphandhu N. Osteoporosis in diabetes mellitus: Possible cellular and molecular mechanisms. World J Diabetes. 2011;2(3):41–8.

POSSIBLE MECHANISM OF DIABETES-INDUCED OSTEOPOROSIS
Adipogenic differentiation of mesenchymal stem cells is increased as indicated by the overexpression of adipocyte differentiation markers, including peroxisome proliferatoractivated receptor (PPAR)-γ, adipocyte fatty acid binding protein (aP2), adipsin and resistin
A decrease in neovascularization may further aggravate bone loss
Bone quality is also reduced as a result of advanced glycation end products (AGEs) production, which may eventually result in low impact or fragility fractures
Wongdee K, Charoenphandhu N. Osteoporosis in diabetes mellitus: Possible cellular and molecular mechanisms. World J Diabetes. 2011;2(3):41–8.

POSSIBLE MECHANISM OF DIABETES-INDUCED OSTEOPOROSIS
Wongdee K, Charoenphandhu N. Osteoporosis in diabetes mellitus: Possible cellular and molecular mechanisms. World J Diabetes. 2011;2(3):41–8.

T2D ASSOCIATED NON-ENZYMATIC GLYCATION INDUCED SKELETAL FRAGILITY
Although high bone mineral density (BMD) and high body mass index (BMI) can be seen in T2DM patients, they are associated with higher risk of fracture. Several studies have estimated that T2DM patients are at a 2–3 fold increased risk of hip fracture. These patients are prone to fall owing to a deficiency in bone microarchitecture and poor bone quality.
Thus, diabetic skeletal fragility is attributed to altered bone microarchitecture and/or poor bone quality. Accumulation of AGEs on collagen of bone extracellular matrix is thought to be the underlying mechanism for diabetes associated skeletal fragility.
AGEs can form covalent crosslinks throughout collagen fibrils differentially affecting collagen stability and mechanical properties of collagen
Karim L, Bouxsein ML. Effect of type 2 diabetes-related non-enzymatic glycation on bone biomechanical properties. Bone. 2015. pii: S8756-3282(15)00302-6.

T2D ASSOCIATED NON-ENZYMATIC GLYCATION INDUCED SKELETAL FRAGILITY
AGEs are the post-translational modifications of collagen resulting from a spontaneous reaction between free floating sugars and amino acid residues on collagen fibers. However, data on AGEs is scarce and inconsistent. Therefore, a study was conducted to shed light on these areas.
o Authors conducted a literature search in the PubMed database using keywords or its combination such as “advanced glycation end-products”, “bone”, “collagen”, “diabetes”, “fracture”, “fracture risk”, “non-enzymatic glycation”, “skeletal fragility”, etc.
o About 100 relevant articles were reviewed to evaluate an association between AGEs in bone and bone’s biomechanical properties
o The results of in vitro experiments to simulate a diabetic state were examined and compared to ex vivo studies conducted in normal and diabetic human bone and diabetic animal models
Karim L, Bouxsein ML. Effect of type 2 diabetes-related non-enzymatic glycation on bone biomechanical properties. Bone. 2015. pii: S8756-3282(15)00302-6.

T2D ASSOCIATED NON-ENZYMATIC GLYCATION INDUCED SKELETAL FRAGILITY
Findings
Following are the well-known findings regarding nonenzymatic glycation in bone:
Increase in AGEs was associated with increase in age within a range of ∼20–100 years
In vitro studies have suggested that AGEs is associated with decreased osteoblast activity and altered osteoclast behaviour
AGEs content remain unchanged with a standard clinical dose of bisphosphonate however, it increases with increase in the bisphosphonate doses and decreases with parathyroid hormone treatment
Several studies have noted changes in bone biomechanical properties with in vitro AGEs. AGEs are also found to have an influence on the type and extent of microdamage formed.
AGE inhibitors can decrease AGE accumulation and restore biomechanical properties in animal models
Higher AGE content was seen in bone from diabetic rodent as compared to non-diabetic controls with corresponding changes in mechanical properties
Karim L, Bouxsein ML. Effect of type 2 diabetes-related non-enzymatic glycation on bone biomechanical properties. Bone. 2015. pii: S8756-3282(15)00302-6.

T2D ASSOCIATED NON-ENZYMATIC GLYCATION INDUCED SKELETAL FRAGILITY
Recommendations
However, several inconsistent result and unknown points which needs to be investigated are:
Reasons for drastic differences in levels of AGEs across the various published studies
Whether there are differences in glycation content between cancellous and cortical bone as the conflicting results were obtained with two studies
Effect of chemically-induced versus naturally produced AGEs on bone cell behaviour
Whether AGE levels modulation can be treated with anabolic or anti-resorptive treatment
Karim L, Bouxsein ML. Effect of type 2 diabetes-related non-enzymatic glycation on bone biomechanical properties. Bone. 2015. pii: S8756-3282(15)00302-6.

T2D ASSOCIATED NON-ENZYMATIC GLYCATION INDUCED SKELETAL FRAGILITY
Whether AGE inhibitors/breakers can modulate bone biomechanics in animal models and/or in human bone.
AGE levels in bones of patients with T2DM and how AGE levels are influenced by severity and duration of T2DM
Conclusion
The literature review linked diabetic skeletal fragility to altered bone quality. Further studies among bone tissue from patients with T2DM and assessment of the biomechanical consequences of accumulation of levels of AGEs are needed to support this association.
Karim L, Bouxsein ML. Effect of type 2 diabetes-related non-enzymatic glycation on bone biomechanical properties. Bone. 2015. pii: S8756-3282(15)00302-6.

IMPROVING INSULIN RESISTANCE ANDREDUCTION IN BONE LOSS
It is sufficiently evident from studies that there is an increased risk of fractures due to presence of diabetic vascular complications, advanced glycation of bone collagen, deranged bone turnover, and possibly certain types of anti-diabetic medications. Thus, a comprehensive management that includes vitamin D and calcium along with a tight metabolic control is most useful in diabetic patients with osteoporosis.1
It has been strongly emphasized by evidences that patients with type 1 as well as type 2 diabetes have an elevated risk of certain types of osteoporotic fractures. Therefore, it has been recommended that in diabetic patients regular bone health assessment should be conducted. In order to prevent fractures, improving bone density can be beneficial in such subjects.2
In diabetic patients suffering from osteoporosis, the treatment is similar as compared to patients without diabetes except for those with nephropathy or gastrointestinal complaints2
1. Okazaki R. Management of osteoporosis in diabetes mellitus – Japanese article. Nihon Rinsho. 2009;67(5):1003–10. 2. Brown SA, Sharpless JL. Osteoporosis: An Under-appreciated Complication of Diabetes. Clin Diabetes. 2004;22. Available from: http://clinical.diabetesjournals.org/content/22/1/10.short?rss=1&ssource=mfc

It has been demonstrated that improvement in glycaemic control may have protective effect on patients with non-
insulin dependent diabetes mellitus (NIDDM/type 2 diabetes mellitus).2
IMPROVING INSULIN RESISTANCE ANDREDUCTION IN BONE LOSS
1. Abdulameer SA, Sulaiman SA, Hassali MA, et al. Osteoporosis and type 2 diabetes mellitus: what do we know, and what we can do? Patient Prefer Adherence. 2012;6:435–48. 2.Okazaki R, Totsuka Y, Hamano K, et al. Metabolic improvement of poorly controlled noninsulin-dependent diabetes mellitus decreases bone turnover. J Clin Endocrinol Metab. 1997;82(9):2915–20.
Studies have demonstrated that glycaemic control can protect T2DM patients from bone loss while insulin levels have an important effect on low BMD1
The long-term net balance between bone resorption and bone formation is considered as bone loss. Hence, even if the bone turnover is affected by poor glycaemic control, it may not show if the duration of poor control is short or if the bone mass is measured when there is a stable glycaemic control for some time.2
Many studies have exhibited that serum osteocalcin (OC), a marker of bone turnover is in fact decreased in patients with NIDDM. In diabetic patients, OC may not present correctly as the synthesis and secretion of OC from osteoblasts is regulated by the ambient glucose levels. So, for assessing bone turnover, the sensitivity and specificity of each biochemical marker must be considered.2

IMPROVING INSULIN RESISTANCE ANDREDUCTION IN BONE LOSS
Addressing this subject, Okazaki and colleagues conducted a study to examine the effect of glycaemic control on bone turnover using several specific bone markers. A rigid management program was given to the poorly controlled NIDDM subjects. Before and 3 weeks after treatment, the bone markers were evaluated.
The bone resorption markers used were urinary deoxypyridinoline (Dpd) and type I collagen carboxyterminal telopeptide (CTx) while serum bone type alkaline phosphatase (BALP) and OC were used as the bone formation markers
The study enrolled all the NIDDM patients who had a HbA1c level of >8% at the Department of Metabolism and Endocrinology, Kanto Teishin Hospital. Fasting blood glucose was obtained on the second day after admission and on the day before discharge. Pyrilinks-D kit after acid hydrolysis was used to assay urine total Dpd while urine CTx was assayed using Cross-Laps kit. The samples before and after glycaemic control were used to measure the metabolic bone markers, intact parathyroid hormone (PTH)and 1,25(OH)2D.
Okazaki R, Totsuka Y, Hamano K, et al. Metabolic improvement of poorly controlled noninsulin-dependent diabetes mellitus decreases bone turnover. J Clin Endocrinol Metab. 1997;82(9):2915–20.

IMPROVING INSULIN RESISTANCE ANDREDUCTION IN BONE LOSS
Results
After treatment, serum calcium (Ca) levels remain unaffected while serum phosphate (Pi) levels significantly increased. Glycaemic control was found to significantly decrease the urinary excretion of Ca and Pi. It was also associated with the decrease in the fractional excretion of Pi (P<0.0001).
The mean serum 1,25(OH)2D which were in the normal range before treatment decreased significantly after treatment. There was no effect of the type of treatment (insulin or noninsulin) on any change in the markers, except for urinary calcium excretion.
Improvement in glycaemic control led to a significant reduction the resorption markers
There was also a significant decrease in the levels of serum BALP and total ALP after metabolic improvement. On the other hand, serum OC which was low before treatment, showed a significant increase
Okazaki R, Totsuka Y, Hamano K, et al. Metabolic improvement of poorly controlled noninsulin-dependent diabetes mellitus decreases bone turnover. J Clin Endocrinol Metab. 1997;82(9):2915–20.

IMPROVING INSULIN RESISTANCE ANDREDUCTION IN BONE LOSS
There was a significant correlation between the changes in Dpd and CTx and all the indices of glycaemic control such as HbA1c, mean blood glucose (MBG), and urinary sugar (US), urinary Ca and serum 1,25(OH)2D
A correlation also existed between serum BALP and changes in glycaemic indices and urinary Ca (Table 2)
Okazaki R, Totsuka Y, Hamano K, et al. Metabolic improvement of poorly controlled noninsulin-dependent diabetes mellitus decreases bone turnover. J Clin Endocrinol Metab. 1997;82(9):2915–20.

IMPROVING INSULIN RESISTANCE ANDREDUCTION IN BONE LOSS
Conclusion
It can be elucidated from this study that in poorly controlled NIDDM patients, improvement in glucose control is associated with a decrease in markers of bone resorption and formation except OC
Irrespective of treatment (diet, oral hypoglycaemic agents, insulin or combination), metabolic improvement has similar effects on the bone turnover
These observations laid stress on the fact that good diabetic control may not only prevent microvascular complications but also osteoporosis by reducing bone loss
Okazaki R, Totsuka Y, Hamano K, et al. Metabolic improvement of poorly controlled noninsulin-dependent diabetes mellitus decreases bone turnover. J Clin Endocrinol Metab. 1997;82(9):2915–20.

MANAGEMENT OF OSTEOPOROSIS WITHVITAMIN D IN DIABETES
A relatively consistent association between low vitamin D status and prevalence of T2DM is shown in a meta-analysis by Kulie et al. A low vitamin D level which is evident in T2DM is an established risk factor for osteoporosis.1 Thus, an important way of management in T2DM patients who are at the risk of developing osteoporosis is improving vitamin D level.
Low bone mass, decreased bone strength and an increased risk of low-energy fractures are the characteristic of osteoporosis2
The Rotterdam study, the largest study on BMD in T2DM, confirmed that the presence of treated T2DM carries an increased fracture risk3
1. Kulie T, Groff A et al. Vitamin D: an evidence-based review. J Am Board Fam Med. 2009;22(6):698–706. 2. Lupsa BC, Insogna K. Bone Health and Osteoporosis. Endocrinol Metab Clin North Am. 2015;44(3):517–30. 3. Hofbauer LC, Brueck CC, Singh SK, et al. Osteoporosis in patients with diabetes mellitus. J Bone Miner Res. 2007;22(9):1317–28.

MANAGEMENT OF OSTEOPOROSIS WITHVITAMIN D IN DIABETES
Four randomized, placebo-controlled clinical trials were carried out to evaluate role of vitamin D3 in the treatment of fractures (Table 3)
Vieth R. The role of vitamin D in the prevention of osteoporosis. Ann Med. 2005;37(4):278–85.

MANAGEMENT OF OSTEOPOROSIS WITHVITAMIN D IN DIABETES
All four the studies using approximately 20 μg/day of vitamin D3 showed a reduction in fracture risk. A vitamin D3 dose of 20 μg/day is the lowest dose which has shown fracture reduction in randomized clinical trials. This is the only nutrient with a demonstrable effect on fractures.1
A randomized, double-blind, controlled clinical trial was conducted for the duration of 1 year including 192 women, to determine if early changes in bone markers could predict long-term response in BMD after calcium and vitamin D supplementation in ambulatory elderly women with vitamin D deficiency (25(OH)D <12 ng/mL). They were randomized to receive either the supplementation (n=95) or a placebo (n=97). Supplementation significantly increased BMD and normalized 25(OH)D when compared to placebo.2
A strong improvement in lower extremity function based on walking speed and sit-to-stand speed and in serum 25(OH)D levels was seen in NHANES analysis. Thus, vitamin D supplements help in the management of fall prevention, which in turn may reduce osteoporotic fractures.3
1. Vieth R. The role of vitamin D in the prevention of osteoporosis. Ann Med. 2005;37(4):278–85. 2. Grados F, Brazier M, Kamel S et al. Prediction of Bone Mass Density Variation by Bone Remodeling Markers in Postmenopausal Women with Vitamin D Insufficiency Treated with Calcium and Vitamin D Supplementation. J Clin Endocrinol Metab. 2003;88(11):5175–9. 3. Nieves JW. Osteoporosis: The role of micronutrients. Am J ClinNutr. 2005;81(5):1232S–1239S

SUMMARY
Globally, T2DM affects over 366 million adults and the number is expected to rise up to 552 million by 2030.
T2DM is an independent risk factor for osteoporotic fractures as contributes to the direct and indirect deleterious effects on osteoblast function and bone formation.
Various studies have shown that vitamin D supplementation significantly increased BMD, reduced fracture risk and normalized 25(OH)D levels.
A comprehensive management that includes vitamin D and calcium along with a tight metabolic control is most useful in diabetes patients with osteoporosis.