Isolated scaphoid dislocation associated with axial carpal dissociation: An unusual injury report
7
Isolated Scaphoid Dislocation Associated With Axial Carpal Dissociation: An Unusual Injury Report Todd Horton, MD, San Diego, CA, Alexander Y. Shin, MD, William P. Cooney III, MD, Rochester, MN We present a report of a patient with an isolated scaphoid dislocation associated with a hyperex- tension and axial loading injury of the carpus required a careful and extensive clinical and radiographic evaluation leading to surgical intervention to reduce and stabilize the scaphoid and to reduce and hold internally the axial carpal injury. Knowledge of the anatomy and the potential injury patterns of the carpus will aid the hand surgeon with injury recognition and proper treatment. (J Hand Surg 2004;29A:1102–1108. Copyright © 2004 by the American Society for Surgery of the Hand.) Key words: Scaphoid dislocation, axial carpal dissociation, acute injury, diagnosis, treatment. Scaphoid dislocations have been described since 1930, usually as individual case reports and rarely as a series. 1–47 Scaphoid dislocations can be clas- sified as either isolated to the periscaphoid liga- ments or as an element of a more complex carpal injury. The dislocation can also be subdivided into subluxation, proximal dislocation, or total disloca- tion. Axial carpal injuries 31,48,49 involve typically mas- sive soft tissue trauma to the hand and present often as open injuries. The combination of an isolated scaphoid dislocation and axial carpal dissociation is exceedingly rare. We found only 11 cases report- ed. 5,9,15,16,26,29,31,37,40,42,46 Only 6 of those cases are in the English-language literature. 5,9,16,31,37,42 The non-English literature has described and discussed the injury pattern; however, the English literature is limited. The purpose of this case report is to describe this rare injury pattern and the associated injuries and to describe the surgical treatment of this injury. Case Report A 33-year-old man presented after sustaining an axial loading and hyperextension injury to his wrist. He reported immediate pain and deformity without neu- rovascular symptoms. He was evaluated initially clinically and radiographically and was diagnosed with a dislocation of the scaphoid (Fig. 1). The patient was treated with closed reduction un- der anesthesia (Fig. 2), was immobilized in a short arm splint, and was referred to us for definitive care 10 days after injury. After careful review and exam- ination of the radiographs we were concerned that From the Naval Medical Center San Diego, Department of Orthopaedic Surgery, San Diego, CA; and Department of Orthopedic Surgery, Hand Division, Mayo Clinic, Rochester, MN. Received for publication February 24, 2004; accepted in revised form June 18, 2004. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. Correspondence: Alexander Y. Shin, MD, Mayo Clinic, Division of Hand Surgery, 200 First St SW, Rochester, MN 55905. Copyright © 2004 by the American Society for Surgery of the Hand 0363-5023/04/29A06-0019$30.00/0 doi:10.1016/j.jhsa.2004.06.018 1102 The Journal of Hand Surgery
-
Upload
todd-horton -
Category
Documents
-
view
216 -
download
0
Transcript of Isolated scaphoid dislocation associated with axial carpal dissociation: An unusual injury report

S1asmist
sa
FSD
J
aa
H
1
Isolated Scaphoid DislocationAssociated With Axial Carpal
Dissociation: An Unusual InjuryReport
Todd Horton, MD, San Diego, CA, Alexander Y. Shin, MD,William P. Cooney III, MD, Rochester, MN
We present a report of a patient with an isolated scaphoid dislocation associated with a hyperex-tension and axial loading injury of the carpus required a careful and extensive clinical andradiographic evaluation leading to surgical intervention to reduce and stabilize the scaphoid andto reduce and hold internally the axial carpal injury. Knowledge of the anatomy and the potentialinjury patterns of the carpus will aid the hand surgeon with injury recognition and propertreatment. (J Hand Surg 2004;29A:1102–1108. Copyright © 2004 by the American Society forSurgery of the Hand.)
Key words: Scaphoid dislocation, axial carpal dissociation, acute injury, diagnosis, treatment.seeintl
rd
CAlrrcw
da1
caphoid dislocations have been described since930, usually as individual case reports and rarelys a series.1– 47 Scaphoid dislocations can be clas-ified as either isolated to the periscaphoid liga-ents or as an element of a more complex carpal
njury. The dislocation can also be subdivided intoubluxation, proximal dislocation, or total disloca-ion.
Axial carpal injuries31,48,49 involve typically mas-ive soft tissue trauma to the hand and present oftens open injuries. The combination of an isolated
rom the Naval Medical Center San Diego, Department of Orthopaedicurgery, San Diego, CA; and Department of Orthopedic Surgery, Handivision, Mayo Clinic, Rochester, MN.Received for publication February 24, 2004; accepted in revised form
une 18, 2004.No benefits in any form have been received or will be received fromcommercial party related directly or indirectly to the subject of this
rticle.Correspondence: Alexander Y. Shin, MD, Mayo Clinic, Division of
and Surgery, 200 First St SW, Rochester, MN 55905.Copyright © 2004 by the American Society for Surgery of the Hand0363-5023/04/29A06-0019$30.00/0
idoi:10.1016/j.jhsa.2004.06.018
102 The Journal of Hand Surgery
caphoid dislocation and axial carpal dissociation isxceedingly rare. We found only 11 cases report-d.5,9,15,16,26,29,31,37,40,42,46 Only 6 of those cases aren the English-language literature.5,9,16,31,37,42 Theon-English literature has described and discussedhe injury pattern; however, the English literature isimited.
The purpose of this case report is to describe thisare injury pattern and the associated injuries and toescribe the surgical treatment of this injury.
ase Report33-year-old man presented after sustaining an axial
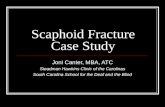
oading and hyperextension injury to his wrist. Heeported immediate pain and deformity without neu-ovascular symptoms. He was evaluated initiallylinically and radiographically and was diagnosedith a dislocation of the scaphoid (Fig. 1).The patient was treated with closed reduction un-
er anesthesia (Fig. 2), was immobilized in a shortrm splint, and was referred to us for definitive care0 days after injury. After careful review and exam-
nation of the radiographs we were concerned that
sw(ctrTlutswts
flps
naat
td
dlpTvj
edfissdfi
a4r
w(flwwd
Fe
Horton, Shin, and Cooney / Scaphoid Dislocation With Axial Carpal Dissociation 1103
ignificant ligamentous injury had occurred to therist. We obtained a magnetic resonance image
MRI) that showed complete disruption of the inter-arpal capitohamate and scapholunate ligaments andhe extrinsic dorsal radiocarpal, dorsal intercarpal,adioscaphocapitate, and long radiolunate ligaments.here was also a partial tear of the short radiolunate
igament and laxity of the palmar and dorsal radio-lnar ligaments. The MRI also showed edema withinhe radial styloid, diastasis of the capitohamate andcapholunate joints, and diffuse edema about therist. The triangular fibrocartilage complex was in-
act and there was no evidence of osteonecrosis of thecaphoid (Fig. 3).
The patient was examined under anesthesia withuoroscopy and wrist arthroscopy. The presurgicallan included repair of the scapholunate ligament andtabilization of the capitohamate diastasis.
Examination with fluoroscopy showed scapholu-ate diastasis with radial and ulnar deviation. Withxial loading there was a capitohamate diastasisnd middle- and ring-finger metacarpal base dias-asis.
Radiocarpal and midcarpal arthroscopy confirmedhe scapholunate, radioscaphocapitate, and long ra-
igure 1. (A,B) Anteroposterior and lateral radiographs showvidenced by the capitohamate incongruity.
iolunate ligament injuries and showed a complete p
isruption (Geissler grade IV) of the scapholunateigament. The short radiolunate ligament was tornartially and the lunotriquetral ligaments were stable.he radioscaphocapitate ligament could be reducedolarly with resultant reduction of the scaphocapitateoint.
Based on the clinical imaging and arthroscopicvaluations we decided to stabilize the capitohamateisruption with a capitohamate arthrodesis (K-wirexation with distal radius bone graft), reduce thecaphoid and repair the scapholunate ligament viauture anchors, and supplement the repair with aorsal capsulodesis of the dorsal intercarpal ligamentxed to the dorsal lunate (Fig. 4).After surgery the wrist was immobilized in a long
rm splint for 2 weeks and then in a short arm cast forweeks. The K-wires were removed at 6 weeks and
ange of motion therapy commenced.At the 6-month follow-up evaluation the patient
as re-examined clinically and radiographicallyFig. 5). Measurements of the wrist showed wristexion and extension of 55° and 65°, respectively,ith symmetric grip strength. The patient is liftingeights, doing push-ups, and playing rugby withoutifficulty. Radiographs show maintenance of the car-
ation of the scaphoid with an associated axial carpal injury
dislocal alignment.

DScldwdWrs
slaot
tic
iGdbhc
rbtcpgdjl
bp
Fta
1104 The Journal of Hand Surgery / Vol. 29A No. 6 November 2004
iscussioncaphoid dislocations are uncommon, with only 60ases reported,1–47,50,51 usually as case reports or asimited case series. The combined injury of scaphoidislocation with axial carpal instability is rare andas first described in 1934 by Buzby.7 Nearly aecade later this injury pattern was reintroduced byoodd-Walker45 and Russell,33 who described case
eports of scaphoid subluxations and dislocations as-ociated with other carpal and radius fractures.
In 1973 Nigst52 elaborated on Bindi’s6 1964 clas-ification of isolated scaphoid dislocations and sub-uxations as purely palmar or dorsal or radial palmarnd radial dorsal. He also described the mechanismf axial disruption of the distal carpal row that allowshe capitate to collapse into the scaphoid fossa.
In 1993 Richards et al31 categorized injury pat-erns as simple (isolated to the scaphoid with anntact distal carpal row) or complex (scaphoid dislo-
igure 2. (A,B) Anteroposterior lateral and oblique radiographhe capitohamate joints were reduced; however, the wrist rlignment.
ation with axial carpal dislocation). The complex w
njury classification of Richards was similar to that ofarcia-Elias et al,48,53 who classified axial carpalislocation into an axial-ulnar, axial-radial, or com-ined axial-radial-ulnar injury pattern. Garcia-Elias,owever, did not include scaphoid dislocations in hislassification.
Connell and Dyson9 and McNamara and Corley23
eported on scaphoid dislocations before Richards31
ut did not recognize formally the association be-ween their reported scaphoid dislocations and theoncomitant axial dissociation. Connell, however,roposed a mechanism of injury, describing a diver-ent force that traveled proximally between the mid-le and ring metacarpals splitting the capitohamateoint and dislocating the scaphoid from the radius andunate.
Sakada et al34 in 1998 described a case of com-ined scaphoid and hamate dislocations withoutroximal migration of the capitate, which can be seen
n after closed reduction under anesthesia. The scaphoid anded unstable despite the near anatomic restoration of carpal
s takeemain
ith axial carpal capitohamate dissociation and

sp
pctdstdstmsca
ppbaHt
tveathstmad
s
4Fpilisddwamddcc
Horton, Shin, and Cooney / Scaphoid Dislocation With Axial Carpal Dissociation 1105
caphoid dislocation. No mechanism of injury wasroposed.Leung et al20 in 1998 described simple and com-
lex injury patterns associated with scaphoid dislo-ation and added primary versus secondary and par-ial versus total to the classifications. Primaryislocations result directly from the injury whereasecondary dislocations are persistent dislocations af-er closed reduction of the proximal carpus. Simpleislocations involve only the radioscaphoid andcapholunate articulations whereas complex disloca-ions involve also the capitohamate and middle-ringetacarpal articulations. Partial dislocations retain
ome soft tissue attachments (usually distal) andomplete dislocations have loss of all soft tissuettachments.
Gilula54 described 3 radiographic arcs of the car-us. The first arc is along the proximal border of theroximal carpal row, the second along the distalorder of the proximal carpal row, and the thirdlong the proximal border of the distal carpal row.e suggested that if these arcs are disrupted ligamen-
ous injury of the carpus must be investigated.Andre et al2 proposed that with hyperdorsiflexion
he proximal pole of the scaphoid slides down theolar slope of the radius and is ejected volarly. If thenergy of injury is not dissipated the capitate thenbuts the radial dorsal rim and is forced to fall intohe scaphoid fossa. The lunate, triquetrum, andamate maintain their ligamentous integrity and thehearing force between the capitate and hamate isransmitted distally between the middle and ringetacarpals. Polveche et al29 reported a case in 1995
nd also supported this injury mechanism in theiriscussion and literature review.The mechanisms of injury attributed to both
caphoid dislocations and axial carpal dislocation
™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™igure 3. (A,B) Anteroposterior and axial MRI show com-lete disruption of the intercarpal capitohamate (gray arrowsn A show edema in the capitate and hamate where theigament had been avulsed and white arrow in B showsncongruity of capitate and hamate articulation) andcapholunate ligaments (A, white arrow) and the extrinsicorsal radiocarpal, dorsal intercarpal (C, white arrow), ra-ioscaphocapitate, and long radiolunate ligaments. (C) Thereas also a partial tear of the short radiolunate ligament (gray
rrow) and laxity of the palmar and dorsal radioulnar liga-ents. The MRI also shows edema within the radial styloid,iastasis of the capitohamate and scapholunate joints, andiffuse edema about the wrist. The triangular fibrocartilageomplex was intact and there was no evidence of osteone-
rosis of the scaphoid.
Fsc
Fc
1
igure 4. After capitohamate arthrodesis with distal radius bone graft and K-wire fixation and reduction of the scaphoid withcapholunate ligament repair and dorsal capsulodesis, the anteroposterior and lateral radiographs show realignment of the
arpus and reduction of the axial carpal instability.igure 5. Follow-up radiographs obtained 6 months after surgery. The anteroposterior and lateral radiographs show adequate
arpal alignment and maintenance of the scapholunate interval with fusion of the capitohamate joint.106

itcaoitba
dcl
mtnArolo
apasicwnpddarssv
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
Horton, Shin, and Cooney / Scaphoid Dislocation With Axial Carpal Dissociation 1107
nclude hyperextension injury with axial loading ofhe wrist. Initial diagnostic evaluation must in-lude standard anteroposterior, lateral, oblique,nd radioulnar deviation radiographs. Arthrogramr MRI can be used to assess the ligamentousntegrity of the intercarpal joints if gross subluxa-ion is not obvious. Arthroscopy may be used asoth a diagnostic and therapeutic modality if im-ging modalities are nondiagnostic.
Treatment has ranged historically from closed re-uction and casting to percutaneous fixation afterlosed or open reduction and to open reduction andigament reconstruction with internal fixation.
In almost all reported cases, after proper treat-ent the patients have returned to their prior ac-
ivities with only moderate limitations. There is aearly universal loss of range of wrist motion.vascular injury to the scaphoid has not been
eported with this injury pattern, possibly becausef the frequent retention of the distal scaphoidigamentous structures and possible preservationf some of the vascular supply.In the present case the patient sustained a fall withhyperextension and axial load injury. The injury
attern followed loosely Richards’s,31 Leung’s,20
nd Garcia-Elias’s48,53 primary complex axial-radialcaphoid dislocation with axial carpal instability. Thenjury involved a disruption of the distal carpus at theapitohamate joint and then extended proximallyith disruption of the radioscaphocapitate, scapholu-ate, and long radiolunate ligaments allowing theroximal scaphoid dislocation. There was also dorsalisruption of the dorsal radiocarpal ligament andorsal intercarpal ligament when the carpus dividedxially. After open reduction, scapholunate ligamentepair, and capsulodesis and capitohamate arthrode-is the patient has returned to prior activity withlight loss of motion and by his own report is “doingery well.”
eferences1. Amamilo SC, Uppal R, Samuel AW. Isolated dislocation of
carpal scaphoid. J Hand Surg 1985;10B:385–388.2. Andre S, Feuilhade de Chauvin P, Candau B, Tomeno B.
Luxation radio-dorsale du scaphoide. A propos d’un cas.[Posterior dislocation of the scaphoid: report of one case.]Rev Chir Orthop Reparatrice Appar Mot 1981;67(5):577–580.
3. Andrews FT. A dislocation of the carpal bones. The scaph-oid and semilunar: report of a case. J Michigan State MedSoc 1932;31:269.
4. Antuna SA, Antuna-Zapico JM. Open dislocation of the carpalscaphoid: a case report. J Hand Surg 1997;22A:86–88.
5. Baulot E, Perez A, Hallonet D, Grammont PM. La luxation 2
palmaire et divergente scapho-lunaire. A propos d’un cas.[Scaphoid and lunate palmar divergent dislocation: a reportof a case.] Rev Chir Orthop Reparatrice Appar Mot1997;83(3):265–269.
6. Bindi R. The dislocation of the carpal scaphoid. Bol TrabSoc Argent. Orthop Traumatol 1969;29:194–201.
7. Buzby BF. Isolated radial dislocation of carpal scaphoid.Ann Surg 1934;100:533–555.
8. Cherif MR, Ben Ghozlen R, Chehimi A, Annabi H, TrabelsiM, Mbarek M, Ben Hassine H. Luxation isolée du scaphoïdecarpien. A propos d’un cas avec revue de la littérature.[Isolated dislocation of the carpal scaphoid: a case reportwith review of the literature.] Chir Main 2002;21(5):305–308.
9. Connell MC, Dyson RP. Dislocation of the carpal scaphoid:report of a case. J Bone Joint Surg 1955;37B:252–253.
0. Crespi M, Peretti L. A case of isolated dislocation of thecarpal scaphoid. Chir Organi Mov 1979;65(5):631–635.
1. Deburge A, Pidhorz L. The subluxation anterior-posterior ofthe carpal scaphoid. Ann Chir 1969;23:163–167.
2. Engkvist O, Ekenstam F. Closed dislocation of the scaphoid:a case report and review of the literature. Scand J PlastReconstr Surg 1986;20:239–242.
3. Fishman MC, Dalinka MK, Osterman L. Case report 309.Diagnosis: complete volar subluxation of the right scaphoidbone and fracture of the right capitate bone. Skeletal Radiol1985;13:245–247.
4. Geonczeol T, Assefa A, Tari G. A scaphoideum fedett,izolalt ficama. [Isolated closed dislocation of the scaphoidbone.] Magy Traumatol Orthop Helyreallito Seb 1984;27(1):67–69.
5. Haas HG. Traumatische Kahnbeinfehlstellungen an derHand. [Traumatic scaphoid bone mispositioning of thehand.] Monatsschr Unfallheilkd Versicher Versorg Ver-kehrsmed 1973;76(1):14–19.
6. Higgs SL. Two cases of dislocation of carpal scaphoid. ProcR Soc Med 1930;23(2):1337–1339.
7. Hokan R, Bryce GM, Cobb NJ. Dislocation of scaphoid andfractured capitate in a child. Injury 1993;24(7):496–497.
8. Inoue G, Maeda N. Isolated dorsal dislocation of the scaph-oid. J Hand Surg 1990;15B:368–369.
9. Kuth JR. Isolated dislocation of the carpal navicular: a casereport. J Bone Joint Surg 1939;21A:479–483.
0. Leung YF, Wai YL, Kam WL, Ip PS. Solitary dislocation ofthe scaphoid: from case report to literature review. J HandSurg 1998;23B:88–92.
1. Machan FG. Die traumatische Kahnbeinfehlstellung an derHand. [Traumatic scaphoid bone malposition of the hand.]Zentralbl Chir 1985;110(10):626–627.
2. Maki NJ, Chuinard RG, D’Ambrosia R. Isolated, completeradial dislocation of the scaphoid: a case report and reviewof the literature. J Bone Joint Surg 1982;64A:615–616.
3. McNamara MG, Corley FG. Dislocation of the carpalscaphoid: an 8-year follow-up. J Hand Surg 1992;17A:496–498.
4. Milankov M, Somer T, Jovanovic A, Brankov M. Isolateddislocation of the carpal scaphoid: two case reports.J Trauma 1994;36:752–754.
5. Murakami Y. Dislocation of the carpal scaphoid. Hand 1977;9:79–81.
6. Nusselt S. Radiale Kahnbeinverrenkung am handgelenk.

2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
1108 The Journal of Hand Surgery / Vol. 29A No. 6 November 2004
[Radial scaphoid bone dislocation in wrist joint: report on anunusual injury.] Chirurg 1977;48(7):431–433.
7. Pai CH, Wei DC, Hu ST, Hou SP, Hsu MN. Carpal bonedislocations: review of 20 cases. J Formos Med Assoc 1990;89(8):696–703.
8. Parkes JC, Stovell PB. Dislocation of the carpal scaphoid: areport of two cases. J Trauma 1973;13:384–388.
9. Polveche G, Cordonier D, Thery D, Desrousseaux JF. A rarevariety of dislocation of the carpus. External verticaldislocation: a case report and review of the literature. AnnChir Main 1995;14(3):159–166.
0. Reid JM. Isolated dislocation of the carpal scaphoid. Aus-tralas Radiol 1969;13:376–379.
1. Richards RS, Bennett JD, Roth JH. Scaphoid dislocationwith radial-axial carpal disruption. Am J Roentgenol 1993;160:1075–1076.
2. Ritchie DA, Gibson PH. Isolated dislocation of the scaphoid.Injury 1988;19(6):405–406.
3. Russell TB. Intercarpal dislocation and fracture dislocations.J Bone Joint Surg Br 1949;31:524–531.
4. Sakada T, Ninomiya S, Ohmori M. Simultaneous dislocationof the scaphoid and hamate bones. J Hand Surg 1998;23B:93–95.
5. Sandstrom B. Luxation av os naviculare carpi. [Dislocationof the scaphoid bone.] Nord Med 1967;77(4):117.
6. Schlossbach T. Dislocation of the carpal navicular bone notassociated with fracture. J Med Soc New Jersey 1954;51:533–534.
7. Sides D, Laorr A, Greenspan A. Carpal scaphoid: radio-graphic pattern of dislocation. Radiology 1995;195:215–216.
8. Stambough JL, Mandel RJ, Duda JR. Volar dislocation ofthe carpal scaphoid: a case report and review of the litera-ture. Orthopedics 1986;9:565–570.
9. Szabo RM, Newland CC, Johnson PG, Steinberg DR,Tortosa R. Spectrum of injury and treatment options forisolated dislocation of the scaphoid. A report of three cases.J Bone Joint Surg 1995;77A:608–615.
0. Szanto E, Rupnik J. Az os scaphoideum izolalt ficama.
[Isolated dislocation of the scaphoid bone.] Magy TraumatolOrthop Helyreallito Seb 1984;27(3):205–208.
1. Takami H, Takahashi S, Ando M. Dislocation of the carpalscaphoid associated with median nerve compression: casereport. J Trauma 1992;33:921–923.
2. Taylor AR. Dislocation of the scaphoid. Postgrad Med J1969;45(521):186–189.
3. Thomas HO. Isolated dislocation of the carpal scaphoid.Acta Orthop Scand 1977;48:369–372.
4. Thompson TC, Campbell RD, Arnold WD. Primary andsecondary dislocation of the scaphoid bone. J Bone JointSurg 1964;46B:73–82.
5. Woodd-Walker GB. Dislocation of the carpal scaphoid re-duced by open operation. Brit J Surg 1943;30:380–381.
6. Yammine K, Lecorre N, Montagliari C. Interscapholunatecarpal axial dislocation: a case report. Rev Chir OrthopReparatrice Appar Mot 2000 86(2):193–6.
7. Yasuda T. Isolated dislocation of the carpal scaphoid: a casereport. Nippon Geka Hokan 1997;66(2):59–65.
8. Garcia-Elias M, Dobyns JH, Cooney WP III, Linscheid RL.Traumatic axial dislocations of the carpus. J Hand Surg1989;14A:446–457.
9. Shin AY, Glowacki KA, Bishop AT. Dynamic carpalinstability: a case report. J Hand Surg 1999;24A:781–785.
0. Drewniany JJ, Palmer AK. Isolated, complete radial dislo-cation of the scaphoid. J Bone Joint Surg 1983;65A:871–872.
1. Habernek H, Orthner E. Zur Luxation des Handkahnbeins.[Dislocation of the scaphoid bone of the hand.] Unfallchi-rurgie 1989;15(6):285–288.
2. Nigst H. Luxations et subluxations du scaphoide. [Disloca-tions and subluxations of the scaphoid.] Ann Chir 1973;27C:519–525.
3. Garcia-Elias M, Bishop AT, Dobyns JH, Cooney WP III,Linscheid RL. Transcarpal carpometacarpal dislocations, ex-cluding the thumb. J Hand Surg 1990;15A:531–540.
4. Gilula LA. Carpal injuries: analytic approach and case ex-
ercises. Am J Radiol 1979;133:503–517.