3494 Case Report Type 1 narcolepsy without cataplexy and ...

Henry Ford Hospital Medical Journal Henry Ford Hospital Medical Journal
Volume 36 Number 1 Article 7
12-1988
Isolated Cataplexy: A Familial Study Isolated Cataplexy: A Familial Study
Kristyna M. Hartse
Frank J. Zorick
Jeanne M. Sicklesteel
Thomas Roth
Follow this and additional works at: https://scholarlycommons.henryford.com/hfhmedjournal
Part of the Life Sciences Commons, Medical Specialties Commons, and the Public Health Commons
Recommended Citation Recommended Citation Hartse, Kristyna M.; Zorick, Frank J.; Sicklesteel, Jeanne M.; and Roth, Thomas (1988) "Isolated Cataplexy: A Familial Study," Henry Ford Hospital Medical Journal : Vol. 36 : No. 1 , 24-27. Available at: https://scholarlycommons.henryford.com/hfhmedjournal/vol36/iss1/7
This Article is brought to you for free and open access by Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in Henry Ford Hospital Medical Journal by an authorized editor of Henry Ford Health System Scholarly Commons.

Isolated Cataplexy: A Familial Study
Kristyna M. Hartse, PhD,* Frank J. Zorick, MD,̂ Jeanne M. Sicklesteel, BA,t and Thomas Roth, PhD+
Four members of a family, a mother, her two sons, and the mother's second cousin, presented with a history of isolated cataplexy withoul excessive daytime sleepiness or other symptoms typical of narcolepsy. They were polygraphically monitored during one night followed by a day of multiple nap tests. No subjecl manifested objective daytime sleepiness as measured by .short latencies to sleep onset during daytime naps, and no subjecl exhibited periods of sleep onset rapid eye movement sleep in either the night or nap recordings. The incidence of isolated cataplexy in this family was traced by history through six generations. We conclude lhal isolated cataplexy in this family is a genetically transmilted dominant trait with incomplete penetrance which occurs independently of daytime sleepiness and the full-blown narcolepsy syndrome. (Henry Ford Hosp Med J 1988:36:24-7)
N arcolepsy is a disorder of excessive daytime sleepiness (EDS) which may be associated with symptoms of cata
plexy, sleep paralysis, and hypnagogic hallucinations (1). Al though sleep paralysis and hypnagogic hallucinations can occur as benign events in normal subjects (2), cataplexy, the complete or partial loss of skeletal muscle tone occurring in response to strong emotional stimuli during waking, is a symptom unique to narcolepsy. Polysomnographic recordings, however, are essential for the unequivocal diagnosis of narcolepsy. The distinctive electrophysiological feature of narcolepsy is the presence of sleep onset rapid eye movement (SOREM) periods (3). SOREM periods, like the rapid eye movement (REM) periods that occur at regular intervals throughout the night, are characterized by rapid eye movements, chin muscle atonia, and a low-amplitude EEG similar to that of wakefulness. In contrast to normal subjects who have 90 to 100 minutes of non-REM sleep prior to the first REM period of the night, the narcoleptic typically wi l l make the transition between wakefulness and REM sleep with less than 15 minutes of intervening non-REM sleep. In comparison to normal subjects, daytime nap recordings of narcoleptic patients reveal the presence not only of rapid latencies to sleep onset but also of SOREM periods in daytime naps (1,4,5).
The appearance of isolated cataplexy in the absence of typical narcolepsy symptoms, particularly EDS, is extremely rare. Gelardi and Brown (6) and Vela Bueno et al (7) have presented evidence for isolated cataplexy in several members of two different families. Roth (8) has also observed two cases of isolated cataplexy. None of these individuals complained of EDS. A single night of polysomnographic recording failed to reveal the presence of SOREM in individuals affected only with isolated cataplexy. However, in none of these studies was daytime somnolence evaluated with multiple nap tests. The conclusion that narcolepsy was absent in these individuals cannot be confidently made solely on the basis of this single recording. Only 44% to 49% of narcoleptic patients reportedly have SOREM at night (9-11). Thus, a strong possibility exists that a subject who may in
fact have narcolepsy wil l not have SOREM at night. A more rigorous test to determine that individuals with isolated cataplexy do not have undetected narcolepsy would be the demonstration that polygraphically defined EDS and SOREM periods during daytime naps are absent.
In this study we used nighttime recordings and daytime nap tests to evaluate four members of a family—a mother, her two sons, and the mother's second cousin—who are affected with isolated cataplexy and who did not present with any other known symptom of narcolepsy. The high familial incidence of this unusual phenomenon, which is known in the family as "kinking," has been extensively documented by family members, thus allowing the history of "kinking" to be traced through several generations.
Methods Subjects
The mother, a healthy, white, 27-year-old, has had recurring episodes of bodily muscle weakness lasting approximately 5 to 30 seconds since age 8 months. As a baby, the episodes were induced by tickling; as a child and teenager, they were always precipitated by laughter. Fear, anger, excitement, or surprise have never precipitated an attack. She describes herself during these attacks as being awake and aware of her sum^undings but "floating" and unable to move. The ease with which cataplexy can be induced has decreased with age such that laughter-induced cataplexy now occurs only when she is fatigued. She has
Submitted for publication: October 20. 1987. Accepted for publication: April 14, 1988. * Fomierly Sleep Disorders Center Henry Ford Hospital. Currently Sleep Disorders Cen
ter, St Louis University Hospitals. St Louis. MO. tSleep Disorders Center. Henry Ford Hospital. Address correspcmdence to Dr Hartse, Sleep Disorders Center St Louis University Hos
pitals, 1221 S Grand, St Louis, MO 63104,
24 Henry Ford Hosp Med J—Vol 36, No 1, 1988 Isolated Cataplexy—Hartse et al

no history of daytime sleepiness, disturbed nocturnal sleep, sleep apnea, hypnagogic hallucinations, or sleep paralysis.
Both children, aged 5 Vi and 2 Vi, exhibit brief cataplectic episodes with laughter or tickling. The older child first experienced cataplexy at age 3 months, and the younger child manifested cataplectic attacks at age 8 months. Like their mother, cataplexy is induced only by laughter or tickling. Both children are normal in their physical, intellectual, and emotional development. Neither child is considered excessively sleepy during the day.
In addition to these subjects, a second cousin of the mother on her father's side, who resides in Los Angeles, CA, agreed to participate in the study. This 27-year-old woman has experienced episodes of cataplexy since age 2 or 3; her cataplexy is also induced only by laughter. The episodes last for 10 to 15 seconds, end spontaneously, have decreased in frequency with age, and occur now only when she is fatigued. She also has no history of daytime sleepiness, disturbed nocturnal sleep, sleep apnea, sleep paralysis, or hypnagogic hallucinations.
Polysomnographic recording The mother and her youngest son were monitored for one
night using standard techniques for continuous recording of the central and occipital EEG, chin muscle activity, and eye movements. The mother's cousin was monitored at the Holy Cross Hospital Sleep Disorders Center in Mission Hills, CA, using identical procedures. On the day following the all-night recording, the Multiple Sleep Latency Test (MSLT) was conducted in all three subjects using an identical protocol. At 10 AM, 12 PM, 2 PM, and 4 PM, the subjects were instmcted to lie down in a quiet, dark room and to try and fall asleep. If sleep did not occur within 30 minutes, the nap was terminated. If stage I or REM sleep occurred within the 30-minute period, the nap was terminated 15 minutes after the first epoch of either stage. The maximum length of time in bed per nap was 45 minutes. Subjects were cautioned to remain awake between naps and were observed by technicians to assure that sleep did not occur.
The older son did not have a nighttime polysomnographic recording performed, but the daytime MSLT was performed at a later date. His mother reported that his nighttime sleep at home before the MSLT was the same as usual. She remained with her son during the day of nap testing.
All recordings were scored for sleep stages according to standard criteria (12). Stage 1 sleep onset latency in daytime naps was determined by the disappearance of waking alpha activity for greater than 50% of the 30-second epoch. Videotape recordings were made in conjunction with simultaneous polygraphic monitoring during cataplectic attacks in both children.
Family history The cataplexy which these four subjects experience also oc
curs in many other members of their family. Through correspondence with older family members, the mother has traced "kinking" through several generations of her family tree.
Results The nighttime polysomnographic recordings showed no evi
dence for SOREM periods in the mother, her younger son, or her
Table Summary of Daytime Nap Recordings
Naps* Latency to
Stage 1 (min) Latency to
Stage 2 (min)t Latency to
REM (min)t
Nap 1 A 26.5 35,0 — B no sleep no sleep no sleep C 3.0 6,5 — D 11.0 — Mean latency 17.6 ± 1 1 . 1 22,4 ± 11,1 —
Nap 2 A no sleep no sleep no sleep B 21.0 26.0 C 10.0 — D 20.5 26.0 Mean latency 20.4 ± 7.1 28.0 ± 2.0 —
Nap 3 A 23.0 32.0 H no sleep no sleep no sleep C 10.5 11.0 D 18.5 26.0 Mean latency 20.5 ± 7.1 24.8 ± 8.2 —
Nap 4 A 7.0 — B no sleep no sleep no sleep C 14.0 — D 21.0 Mean latency 18.0 ± 8.5 — —
Grand Mean 19.1 ± 8.7 27.0 ± 7.3
*A = the mother. B second cousin.
= the older son, C = the younger son. and D - the mother s
' The dash indicates that this sleep stage did not occur Note; If the subject did not reach stage 1 or 2. the latency to either stage was assigned
the value ofthe numberof minutes in bed in calculating the mean.
cousin. The latencies to REM sleep at night were 182.5 minutes, 250.5 minutes, and 59.5 minutes in each subject, respectively. In fact, with the exception of the cousin, these REM latencies were somewhat increased compared to normal subjects (13). Although the cousin's latency was somewhat decreased compared to normal subjects, it was not within the range of that reported in narcoleptics. No subject exhibited evidence prior to the first REM period for stage 7 sleep (14), which has been described as the displacement of REM sleep variables, such as rapid eye movements or chin muscle atonia, into the non-REM sleep stages. In summary, no polygraphic evidence in the nighttime recordings suggested the presence of SOREM or a diagnosis of narcolepsy.
The daytime nap recordings confirmed the absence of SOREM periods as well as the absence of sleepiness in all four subjects (Table). Inspection of the recordings revealed no evidence for stage 7 sleep in the mother's or her cousin's naps. However, the 10 AM nap of the younger son showed five periods lasting 3 to 6 seconds in which eye movements were associated with decreased, but not absent, chin muscle tonus and K-com-plexes typical of stage 2 sleep. These brief, REM-like episodes meet the criteria for stage 7 sleep. The shortest latencies to stages 1 and 2 also occurred in this nap. No evidence for stage 7 sleep was present in any other nap of the younger son. Two 10- to 15-second episodes occurred in the older child's 12 PM nap which were interpreted as possible stage 7 sleep. However,
Henry Ford Hosp Med J—Vol 36. No 1, 1988 Isolated Cataplexy—Hartse el ai 25

I T t L n mn
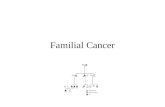
Figure—The family tree: o = unaffected females: O fw/?/! numbers) = number of unaffected females: • = females affected with isolated cataplexy; o = unaffected males; o (with numbers) = number of unaffected males; ^ = tnales affected with isolated cataplexy; O (with number) = number of persons of unknown sex or history; large hatched circle = the mother in this report; large hatched squares = her two sons; and the arrow indicates the mother's cousin.
no stage 7 sleep or clear SOREM occurred in any other nap of this subject.
No evidence was present in any subject for pathological daytime sleepiness as demonstrated by rapid sleep onset latencies in daytime naps. The mean latency to stage I sleep across all subjects ranged between 17.6 ±11.1 minutes (nap 1) to 20.5 ± 7.1 minutes (nap 3). Only in the first nap of the younger son and in the last nap of his mother did the latency to stage 1 approach latencies of 5 minutes or less previously reported in narcoleptic patients (4,5,15). In the younger son, three of four stage I latencies were 10 minutes or longer; in the older son, no sleep occurred in three of four naps; in the mother, three of four stage 1 latencies were 10 minutes or longer; and in the mother's cousin, four of four stage 1 latencies were longer than 10 minutes. The grand mean to stage 1 sleep onset across all subjects and all naps was 19.1 ± 8.7 minutes. Thus, no convincing evidence was present in the MSLT for either the presence of SOREM periods or EDS in any of the four subjects.
In both children, cataplectic attacks were induced by their mother tickling them. The attacks lasted from 1 or 2 to 20 seconds and were characterized by brief drooping of the head in the shortest attacks to complete flacidity of the entire body during the longest attacks. Spontaneous recovery of muscle tonus was rapid and took from less than 1 to about 5 seconds. Polygraphic recordings confirmed the absence of muscle tonus during the attacks. Excessive movement artifact, however, obscured the EEG. Neither child appeared to experience any discomfort or anxiety as the result of the episodes. Although the younger child was crying and fearful upon first arriving in the Sleep Disorders Center, he did not experience any muscle weakness characteristic of cataplexy.
The incidence of cataplexy in this family is shown in the Figure. In the direct line of descent of the children and their mother, it is not certain whether the mother's great-great-grandfather (generation I) experienced "kinking." However, the brother of her great-great-grandfather had cataplexy which was present in his succeeding generations, indicating that one parent of generation I probably had cataplexy. The familial history of other members of generation I is unknown. Both the mother's great-grandmother (generation II) and grandmother (generation III) were affected. Neither our subject's father (generation IV) nor
her sisters (generation V) are affected. Our subject's cousin is also the only sibling in her family who is affected, but her mother is affected. Both males and females in the family are affected, although females are more often affected than males. Of generarion I's offspring, 42% (24/57) of females and 27% (14/52) of males are affected; 35% (38/109) ofall descendants are affected, suggesting that isolated cataplexy in this family is a dominant trait with incomplete penetrance. In every family that has an affected male or female parent, at least one offspring is affected. The two exceptions are an affected female in generation IV and an affected male in generation III who produced no affected male or female offspring. Conversely, it is apparently not necessary for a parent to be affected in order to produce affected offspring. In the direct line of descent of the mother and her two sons, neither her father or his brother are affected, yet each of these men has a single affected female offspring who in tum produced affected offspring. Although not entirely reliable by history, no reports document any symptoms of EDS in this family.
Discussion The major conclusions of this study are that isolated cataplexy
can occur independently of EDS or the other symptoms of narcolepsy and can be genetically transmitted through successive generations. Several lines of evidence support these conclusions. First, the onset of cataplectic attacks began in all four of our subjects earlier than age 3. Very early age of onset is atypical of narcolepsy. The peak onset age of daytime somnolence and cataplectic attacks in surveys of large narcoleptic populations has been reported to range from about 12 to 20 years (16-19). All the subjects in our study showed signs of cataplexy at a much younger age. Similarly, the family with isolated cataplexy described by Vela Bueno et al (7) exhibited an onset age of 3 months. In a second study of isolated familial cataplexy, the age of onset was somewhat later, between 5 to 10 years (6), but this is still younger than the typical age reported for narcoleptics. Second, none of our subjects showed SOREM characteristic of narcolepsy. Although both children exhibited some brief, ambiguous periods which may be interpreted as stage 7 sleep, this finding does not support a diagnosis of narcolepsy. Both Maron et al (20) and Karacan et al (21) have observed REM
26 Henry Ford Hosp Med J—Vol 36. No 1, 1988 Isolated Cataplexy—Hart.sc et al

sleep in the daytime naps of some normal subjects. We also have found that some normal subjects exhibit REM onsets during MSLT moming naps (9). It is important to reemphasize that neither child exhibited full-blown SOREM periods characteristic of the narcoleptic. Third, none of our subjects showed evidence of pathological sleepiness as measured by an increased tendency to fall asleep during daytime naps. Although the younger child was the only subject to fall asleep in every nap and had the shortest sleep latencies, he still was not as sleepy as narcoleptic patients.
The incidence of isolated cataplexy in several generations of this family is striking. Narcolepsy also has a familial incidence, which has been widely reported in the literature (18,22-25). The genetic model for transmission of isolated cataplexy has been suggested by Vela Bueno et al (7) to be one of autosomal dominant inheritance. Our findings support this conclusion, although the trait does not appear to be fully penetrant in this family. In dogs, genetic studies of inherited narcolepsy-cataplexy suggest that this disorder is perpetuated by an autosomal recessive mode of transmission (26). This docs not appear to be the case in the present family since affected individuals who married unrelated individuals from outside the family produced affected offspring.
Several recent studies on the human immune system have demonstrated that 100% of narcoleptic patients have a human leukocyte antigen (HLA) which is DR2 positive, whereas other groups of nonnarcoleptic, hypersomnolent patients do not show this high incidence of HLA-DR2 poshivity (27-30). All narcoleptic patients in these studies had EDS as well as cataplexy. It would be interesting to determine whether persons who do not complain of EDS but who manifest isolated auxiliary symptoms of narcolepsy such as familial cataplexy or familial sleep paralysis (31) also show HLA-DR2 positivity. With continuing studies in this area, the specific factors that contribute to the development of isolated cataplexy, nonnarcoleptic EDS syndromes, and narcolepsy will be more clearly understood.
Acknowledgment We thank the Sleep Disorders Center at Holy Cross Hospital
in Mission Hills, CA, for their assistance in this study.
References 1. Sleep Disorders Classification Committee. Diagnostic classification of
sleep and arousal disorders. Association of Sleep Disorders Centers and the Association for the Psychophysiological Study of Sleep. Sleep 1979;2; I-I37.
2. Fukuda K. Miyasita A, Inugami M, Ishihara K. High prevalence of isolated sleep paralysis: Kanashibari phenomenon in Japan. Sleep 1987;10:279-86.
3. Guilleminault C, Dement WC, Passouant P (eds). Narcolepsy. New York: Spectrum, 1976.
4. Mitler MM, Van Den Hoed J, Carskadon MA, et al. REM sleep episodes during the multiple sleep latency test in narcoleptic patients. Electroencephalogr Clin Neurophysiol 1979;46:479-81.
5. Richardson GS, Carskadon MA, Ragg W, Van Den Hoed J, Dement WC, Mitler MM. Excessive daytime sleepiness in man: Multiple sleep latency measurement in narcoleptic and control subjects. Electroencephalogr Clin Neurophysiol 1978;45:621-7.
6. Gelardi JM, Brown JW. Hereditary cataplexy. J Neurol Neurosurg Psychiatry 1967;30:455-7.
7. Vela Bueno A, Campos Castello J, Jimenez Baos R. Hereditary cataplexy: Is it primary cataplexy? Waking and Sleeping 1978;2:125-6.
8. Roth B. Narcolepsy and hypersomnia. In: Williams RL, Karacan I , eds. Sleep disorders: Diagnosis and treatment. New York: John Wiley, 1978:29-59.
9. Hartse KM, Roth T, Zorick F, Moyles T. REM sleep episodes during multiple naps of narcoleptic subjects (abstract). In: Chase MH, Kripke DF, Walter PL, eds. Sleep research, Los Angeles: University of Califomia, Brain Information Service, Brain Research Institute, 1980;9:203.
10. Montplaisir J. Disturbed nocturnal sleep. In: Guilleminault C, Dement wc , Passouant P, eds. Narcolepsy. New York: Spectrum, 1976:43-56.
11. Zorick F, Roehrs T, Wittig R. Lamphere J, Sicklesteel J, Roth T. Sleep-wake abnormalities in narcolepsy. Sleep 1986;9:189-93.
12. Rechtschaffen A, Kales A (eds). A manual of standardized terminology, techniques, and scoring system for sleep stages of human subjects. Bethesda: United States National Institute of Neurological Disease and Blindness. 1968.
13. Williams RL. Karacan 1. Hursch CJ (eds). Electroencephalography (EEG) of human sleep: Clinical applications. New York: John Wiley. 1974.
14. Raynal D. Polygraphic aspects of narcolepsy. In: Guilleminault C, Dement WC, Passouant P, eds. Narcolepsy. New York: Spectrum, 1976:671-84.
15. Hartse KM, Zorick FJ, Sicklesteel JM, Piccione PM, Roth T. Nap recordings in the diagnosis of daytime somnolence (abstract). In: Chase MH, Kripke DF, Walter PL. eds. Sleep research. Los Angeles: University of California, Brain Information Service, Brain Research Institute, 1979;8:190.
16. Honda Y, Asaka A, Tanimura M, Furusho T. A genetic study of narcolepsy and excessive daytime sleepiness in 308 families with a narcolepsy or hypersomnia proband. In: Guilleminault C, Lugaresi E, eds. Sleep wake disorders: Natural history, epidemiology, and long term evolution. New York: Raven Press, 1983:187-99.
17. Kessler S. Genetic factors in narcolepsy. In: Guilleminault C, Dement wc , Passouant P, eds. Narcolepsy New York: SpecUum, 1976:285-302.
18. Kessler S, Guilleminault C, Dement WC A family study of 50 REM narcoleptics. Acta Neurol Scand 1974;50:503-12.
19. Sours JA. Narcolepsy and other disturbances in the sleep-waking rhythm: A study of 115 cases with a review of the literature. J Nerv Ment Dis 1963;137:525-42.
20. Maron L, Rechtschaffen A, Wolpert EA. Sleep cycle during napping. Arch Gen Psychiatry 1964;11:503-8.
21. Karacan I , Finley WW, Williams RL, Hursch CJ. Changes in stage l-REM and stage 4 sleep during naps. Biol Psychiatry 1970;2:261-5.
22. Baraitser M, Parkes JD. Genetic study of narcoleptic syndrome. J Med Genet 1978;15:254-9.
23. Daly DD, Yoss RE. A family with narcolepsy. Mayo Clin Proc 1959;34:313-20.
24. Krabbe E. Magnussen G. On narcolepsy. 1. Familial narcolepsy. Acta Psychiatr Scand 1942;17:149-73.
25. Nevsimalova-Bruhova S, Roth B. Heredofamilial aspects of narcolepsy and hypersomnia. Archives Suisses de Neurologic, Neurochirurgie et de Psy-chiaU-ie 1972;110:45-54.
26. Baker TL, Foutz AS, McNemey V, Mitler MM, Dement WC. Canine model of narcolepsy: Genetic and developmental determinants. Exp Neurol 1982;75:729-42.
27. Billiard M, Seignalet J, Besset A, Cadilhac J. HLA-DR2 and narcolepsy. Sleep 1986;9:149-52.
28. Honda Y, Juji T, Matsuki K, et al. HLA-DR2 and Dw2 in narcolepsy and in other disorders of excessive somnolence without cataplexy. Sleep 1986;9; 133-42.
29. Langdon N, Lock C, Welsh K, et al. Immune factors in narcolepsy. Sleep 1986;9:143-8.
30. PoirierG, Montplaisir J, Decary F, Momege D, Lebrun A. HLA antigens in narcolepsy and idiopathic central nervous system hypersomnolence. Sleep 1986;9:153-8.
31. Lobzin VS. Sleep and wakening paralysis (cataplexy). Soviet Psychology and Psychiatry 1962;1:42-7.
Henry Ford Hosp Med J—Vol 36, No 1, 1988 Isolated Cataplexy—Hartse et al 27