Iso immune disease
143
-
Upload
santosh-kumari -
Category
Education
-
view
328 -
download
0
Transcript of Iso immune disease

ISO-IMMUNE DISEASE
PRESENTED BY
MS. SANTOSH KUMARI
TERMINOLOGY
• Iso - immune – means immune diseasein which the antibodies are produced asa result of antigens from another person.
• Autoimmune – in which the antigenscome from the same person.

Blood groups
•The differences in human blood are due to thepresence or absence of certain protein moleculescalled antigens and antibodies.
•The antigens are located on the surface of theRBCs and the antibodies are in the blood plasma.
•Individuals have different types andcombinations of these molecules.
•The blood group you belong to depends on whatyou have inherited from your parents.
DIFFERENT BLOOD GROUPS
• There are more than 20 genetically determinedblood group systems known today
Eg. ABO System,Rh-System, MNS System, KellSystem, Lewis System
•The AB0 and Rhesus (Rh) systems are the mostimportant ones used for blood transfusions.
•Not all blood groups are compatible with each other.Mixing incompatible blood groups leads to bloodclumping or agglutination, which is dangerous forindividuals.
Cont…

CLASSIFICATION OF BLOOD GROUPS
Major Blood Grouping System: ABO blood group system Rh blood group system because they cause major transfusion reaction.Minor Blood Grouping System: MNS blood group system p blood group system because they cause minor transfusion reaction.Familial Blood Grouping System: Kell, Daffy, Lutheran, Lewis, Deigo, and Many
more.

According to the ABO blood typing system there are four different kinds of blood types: A, B, AB or O (null).
ABO blood grouping system

Landsteiner Law• It was given by Karl Landsteiner in 1900.
• It states that ; If an agglutinogen ispresent on the RBC of an individual, thecorresponding agglutinin must be absentin the plasma of that individual and vice-versa.
• This law is only applicable to ABO bloodgrouping system.
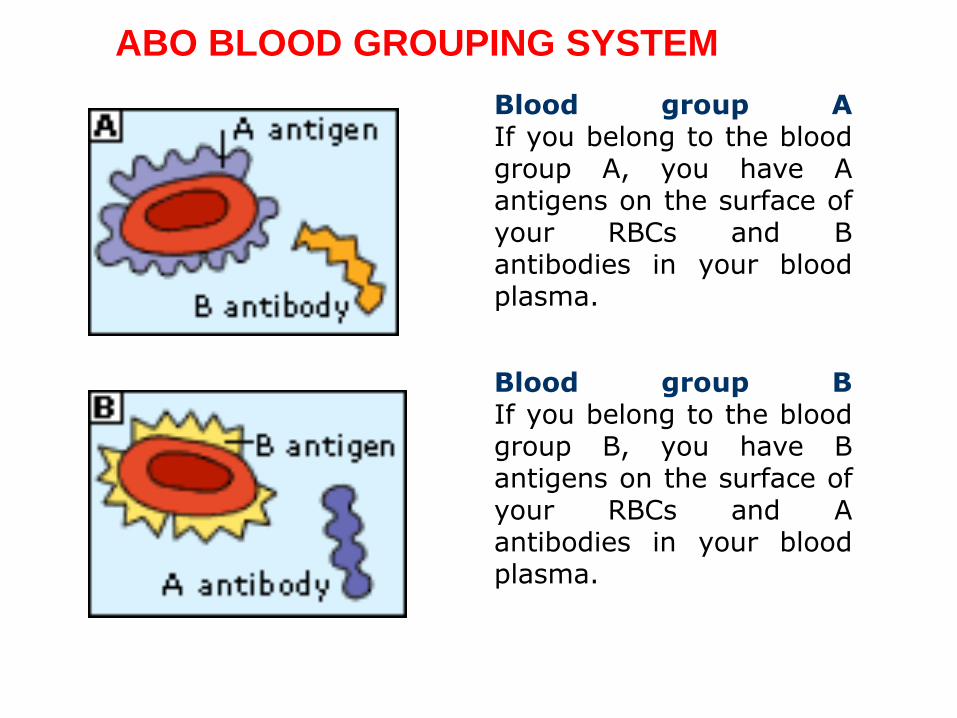
Blood group AIf you belong to the bloodgroup A, you have Aantigens on the surface ofyour RBCs and Bantibodies in your bloodplasma.
Blood group BIf you belong to the bloodgroup B, you have Bantigens on the surface ofyour RBCs and Aantibodies in your bloodplasma.
ABO BLOOD GROUPING SYSTEM

Blood group ABIf you belong to the blood groupAB, you have both A and Bantigens on the surface of yourRBCs and no A or B antibodiesat all in your blood plasma.
Blood group OIf you belong to the blood group O(null), you have neither A or Bantigens on the surface of your RBCsbut you have both A and B antibodiesin your blood plasma.

View Of Different Cells And Antibodies

Blood Group
Antigens Antibodies Can give blood to
Can receive
blood from
AB A and B None AB AB, A, B, O
A A B A and AB A and O
B B A B and AB B and O
O None A and B AB, A, B, O O

Blood group O is called "universal donor"because it has no antigens on RBC.
Blood group AB are called "universal receivers“ because it has no anti- bodies in the plasma.
The Rhesus (Rh) System

• The Rhesus factor gets its name fromexperiments conducted in 1937 by scientistsKarl Landsteiner and Alexander S. Weiner.
• Their experiments involved rabbits which,when injected with the Rhesus monkey's redblood cells, produced an antigen that ispresent in the red blood cells of manyhumans.
•The genotype is determined by the inheritance of 3pairs of closely linked allelic genes situated onchromosome 9 named as
D/d,
C/c,
E/e
……….. (Fisher- Race theory)

• A condition that occurs during pregnancy ifa blood and her
blood. Mother’s body create Rhantibodies against the baby’s blood.
• Also known as haemolytic disease of thefetus and newborn(HDFN).
Oct-15 18Rhesus Incompatibility
• First demonstrated in rhesus monkey
• Blood groups are classified as Rhpositive and Rh negative

• The Rh factor , Rh+ and Rh- usually refersspecifically to the presence or absence of antigen-D
•There are two alleles, or genetic variants , of thisantigen: D and d.
•A person who is Rh- has two recessive traits, dd.Anyone who has at least one D-DD or Dd-is Rh+

• A person's Rh type is generally most relevantwith respect to pregnancies
• If the pregnant woman and her husband areRh negative, there is no reason to worry aboutRh incompatibility

•If she is Rh negative and her husband is Rh positive,the baby will inherit the father's blood type ,creating incompatibility between mother and her fetus.
•If some of the fetal blood gets into mother's blood stream, her body will produce antibodies.
•These antibodies could pass back through the placenta and harm the developing baby's red blood cells, causing very mild to very serious anemia in the fetus.
Pathogenesis
Oct-15 Rhesus Incompatibility 23
1. Rh-ve mother carrying Rh+vefetus
2. Entry of fetus Rh+ve RBC into maternal circulation
3. Development of Rh antibodies by the mother
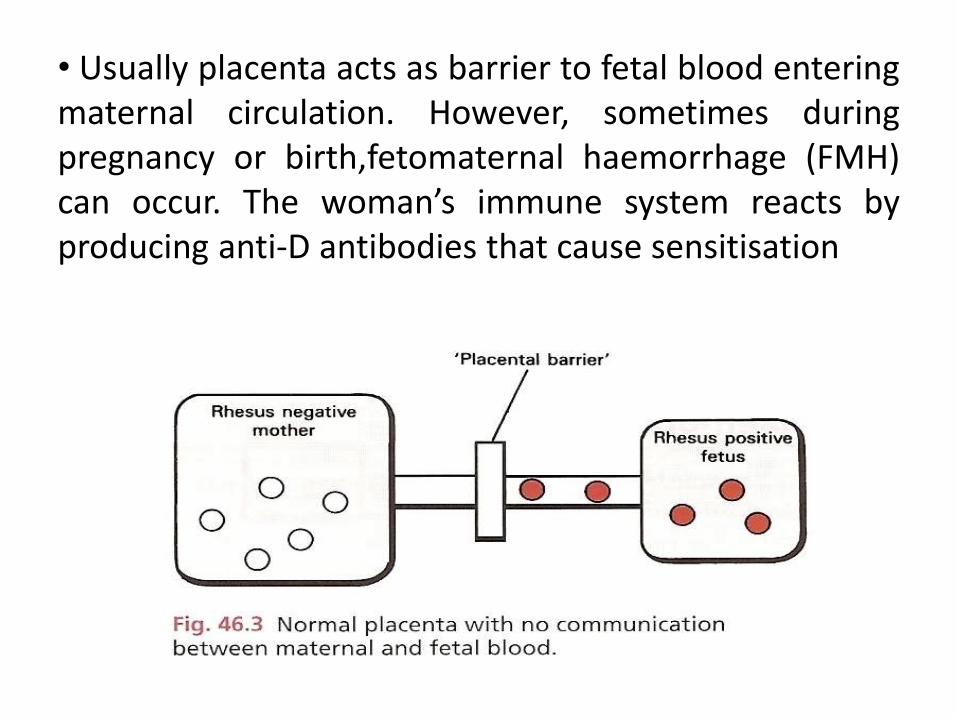
• Usually placenta acts as barrier to fetal blood enteringmaternal circulation. However, sometimes duringpregnancy or birth,fetomaternal haemorrhage (FMH)can occur. The woman’s immune system reacts byproducing anti-D antibodies that cause sensitisation

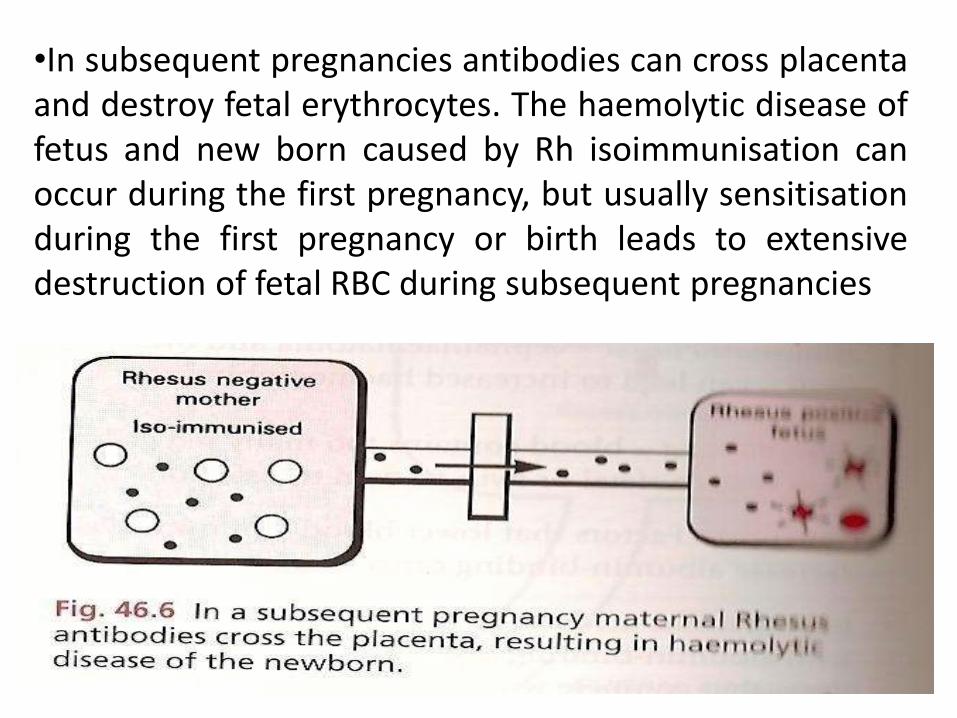
•In subsequent pregnancies antibodies can cross placentaand destroy fetal erythrocytes. The haemolytic disease offetus and new born caused by Rh isoimmunisation canoccur during the first pregnancy, but usually sensitisationduring the first pregnancy or birth leads to extensivedestruction of fetal RBC during subsequent pregnancies
Conditions which affects 1st pregnancy are:
• Miscarriage
• Abortion
• Feto-maternal haemorrage

Sign &symptom of Rh incompatibility:
• Rh incompatibility can cause symptoms rangingfrom very mild to fatal.
• Mildest form- Rh incompatibility:
1-Hemolysis (Destruction of the red blood cells)with the release of free hemoglobin into theinfant's circulation.
2- Jaundice (Hemoglobin is converted into,bilirubinwhich causes an infant to become yellow.

Fetal- hemolysis

Jaundice

Severe form- Rhincompatibility
1- Hydrops fetalis (Massive fetal red blood cell destruction).
2- It causes Severe anemiaFetal heartfailure Death of the infant shortly after delivery.

2- Total body swelling.
3- Respiratory distress (if the infant has been delivered)
4- Circulatory collapse.
5- Kernicterus. (Neurological syndrome in extremely jaundiced infants)
6- It occurs several days after delivery and is characterized initially by...
A) Loss of the Moro reflex.B)Poor Feeding.C) Decreased activity

LATER
• At last it may lead to death of the child immediately after its birth

1-There are no any physical symptoms can be seenin rh incompatibility.
2-If the woman just found out she is pregnant,sheshould undergo blood-type test. This testdetermines her blood type and Rh factor.
3-Blood test that will determine whether she is Rhpositive or Rh negative
DETECTION OF Rh INCOMPATIBILITY:
Treatment
• Intrauterine transfusion
• Elect time of delivery
• Exchange transfusion after delivery
• Phototherapy after delivery
• Top-up transfusion
(Hb falls below 7g/dl, prophylactic :oral folate)
Oct-15 36Rhesus Incompatibility

Intrauterine transfusion
• The fetus can die in utero from severe anaemiaand hydrops before he can be delivered.
• An intrauterine transfusion can prolong the lifein utero of a fetus to a gestation where the risksof prematurity are estimated as being less thanthose of the Rh disease. This can be done by an:1. Intraperitoneal transfusion guided byultrasound.2. Umbilical vein transfusion guided byultrasound.
Oct-15 Rhesus Incompatibility 37

• Rh-negative blood is either transfusedunder ultrasound control. Repeat asnecessary, according to amniotic opticaldensity, or fetal haematocrit. Theintravenous route is becoming increasinglythe preferred method.

Choose time of induction and best
method of delivery
• Balance the risks of prematurity (too soon) withthat of worsening Rh disease (too late).
• Consider the risks of vaginal delivery and beprepared for a lower segment Caesarean section(LSCS).
• Usually done only after 34 weeks of gestation.
• The paediatric team should be in close and asenior paediatrician present at the delivery
• fresh Rh-negative blood available.
Oct-15 Rhesus Incompatibility 39
Resuscitation and Exchange transfusion
• Good resuscitation is essential. In an anaemic.
premature infant, lung disease is common. It can be due to:
Surfactant deficiency at very early delivery.
Pulmonary oedema from anaemia and hypoproteinaemia.
Hypoplastic lungs secondary to pleural
effusions.
• In severe Rh haemolyticdisease of the newborn, an umbilical artery catheter should be inserted as soon as possible to assess and control PaO2 and pH.
• Central venous pressure should be measured.
Drain pleural effusions and ascites at resuscitation.
Oct-15 Rhesus Incompatibility 40
Indication for exchange
Transfusion:
1. Early: Decision mainly based on cord haemoglobin
(in addition consider history of previously affected babies).
• Cord haemoglobin <12g/dl.
• Strongly positive Coombs’ test.
• Cord bilirubin >85mmol/l.
2. Late: Usually done for hyperbilirubinaemia.
• The aims:
Treat anaemia.
Washes out IgG antibodies.
Decreases degree of haemolysis.
Removes bilirubin.
Prevents kernicterus.
Oct-15 Rhesus Incompatibility 41
Resuscitation and Exchange transfusion

Phototherapy
• Placing newborn baby under a halogen orfluorescent lamp with their eyes covered.
• Lowers the bilirubin levels in the baby’s bloodthrough photo-oxidation.
• During phototherapy, intravenous hydration isrequired.
Oct-15 Rhesus Incompatibility 42
Phototherapy of neonatal jaundice

Prevention and Prophylaxis
• Anti-D immunoglobulin to all Rh-negative womenat 28 and 34 weeks routinely-RAADP Or give anti-D immunoglobulin
if she has a:
Therapeutic abortion.
Spontaneous abortion/ectopic pregnancy.
Amniocentesis.
Any bleeding in pregnancy/threatened miscarriage.
External Cephalic Version.
After delivery at any gestation within 72Hours.
Oct-15 44Rhesus Incompatibility

NURSING MANAGEMENTDIAGNOSIS
Risk for injury from breaking down products of RBCs in greater numbers than normal and functional immaturity of the liver.
Goals
• Will receive appropriate therapy to accelerate bilirubin excretion.
• Will experience no complications from phototherapy.
• Will experience no complications from exchange transfusin.

• Interrupted family process R/T infant with potentially adverse physiologic response.
• Family will receive emotional support.
• Family will be prepared for home care of the neonate.

• NURSING CARE for Rh incompatibility DURING PHOTOTHERAPY
1. Remove clothing to proper skin exposure.2.Turn infant frequently to expose all skin area.3. Record and report jaundice and blood levels of bilirubin.4. Record and report if any change in body temperature

5. Cover and check eyes with eye patches to prevent eye injury.
-Be sure the eyes close before applying eye patch to prevent corneal irritation.
-Should be loose enough to avoid pressure.
-Eye patches should be changed every 8houly and eye care given.
6.Nurse should expect the infant’s stools to be green and the urine dark because of photo degradation products.

7. Serum bilirubin and hematocrit should be monitored during therapy and for 24 hours following therapy.
8.In case of breast milk jaundice stop breast feeding temporarily.
9. Maintain feeding intervals to prevent dehydration.

Summary:



Oct-15 Rhesus Incompatibility 53

IUFD
Introduction• In addition to cases in which a fetus dies during
delivery as a result of asphyxia (oxygendeprivation if the umbilical cord becomestwisted) or difficult labor.
• Others can die in utero before labor starts.followed by expulsion of the fetus from theuterus within a few days.
• However, in rare instances the dead fetus is notexpelled from the uterus at once, but is retainedfor several weeks.

• Fetal death refers to the spontaneous death ofa fetus at any time during pregnancy, althoughthe term is often used interchangeably with‘stillbirth’.
• A stillbirth is a death that occurs after 20weeks of gestation.
Definition of IUFD
Intrauterine fetal death: is the clinical term forthe death of a baby in the uterus, duringpregnancy and before birth. The term isusually used for pregnancy losses thathappen after the 20th week of gestation.
Epidemiology
•In the present investigation the epidemiologicalfactors responsible for intrauterine fetal deathsafter 20 week of gestation were studied.
•A retrospective study of 16882 pregnanciesregistered and managed in the Department ofObstetrics and Gynecology, in united state

Continue…..
One hundred and three cases of intrauterinefetal deaths were registered and treatedexpectantly out of 16882 total pregnanciesregistered during the four year study period.The stillbirth rate was 6.1 per 1000 total births.

EtiologyPregnancy complications:- Pre-eclamptic toxemia- Antepartum haemorrhage : placenta previa,
abruptio placentaePre- existing medical disease and acute
illness:- Chronic hypertension- Chronic nephritis- Diabetes- Severe anemia- Hyperpyrexia- Syphilis, Hepatitis, toxoplasmosis etc.
Hyperpyrexia

Cont..
• Fetal
- Congenital malformation
- Rh-incompatibility
- Post maturity
• External version
• Idiopathic 20 –30%
Cont…
• Maternal Complications
• Decreased platelets
• Decreased fibrinogen
• Increased PT/PTT (Clotting times)
• Clinical bleeding / oozing from all sites
RX involves DELIVERY, pRBC’s, FFP, PLATELETS,Supportive Management
Cont….• Depression, Anxiety, Psychosocial
• Anxiety with future pregnancies
• May have repeat losses (depending on causes)
• Bleeding ---> can lead to DIC but may onlyrequire blood product replacement
• Pain, Infection (similar to any other delivery)
Risk factors•Multiple pregnancy•Advanced maternal age•History of fetal demise (IUFD)•Maternal infertility•Maternal haemoconcentration•Maternal colonization with certain pathogens•Small for gestational age infant•Obesity•Paternal age•African American race

Clinical features
• Absence of fetal movement
• Vaginal bleeding
• Abdominal pain
• Small uterus than the duration of pregnancy
• Sometimes secretion of colostrum occur few days after death of fetus in uterus.

Diagnosis of IUFD• In most patients, the only symptom is decreased
fetal movement. An inability to obtain fetal hearttones upon examination suggests fetal demise;however, this is not diagnostic and death must beconfirmed by diagnostic tests .
• Labor should be induced as soon as possible afterdiagnosis. Patient responses vary in regard to thisrecommendation; some wish to begin inductionimmediately, while others wish to delay inductionfor a period of hours or days until they areemotionally prepared.

Cont…
• Blood test because it comes negative within a week after the death of the fetus.
• The secretion of estriol it is a type of estrogen produced by an active placenta in the mother’s urine falls sharply.

Treatment & management
• Explain the problem to the woman and herfamily. Discuss with them the options ofexpectant or active management.
• Medical induction of labor: Medicine is usedto start labor and fetus delivered naturally.

Pain management• Pain management in patients undergoing
induction of labor for fetal death is usually easierto manage than in patients with live fetuses.
• Higher doses of narcotics are available to thepatient and often a morphine is sufficient forsuccessful pain control. Should a patient desiresuperior pain control to intravenous narcotics,epidural anesthesia should be offered.


NURSING MANAGEMENTDiagnosis
Anticipatory grieving related to fetal loss
Intervention
• To give the patient time to gather support from her family and to fathom the reality of the situation.
• Provide psychological support.
• Provide counseling to the mother as well as family.
Nursing health care guidelines at home
• Teach the patient to be aware of the signs andsymptoms that could indicate postpartumcomplications:
• Pain in the calf of the leg; increase in vaginalbleeding; foul odor of vaginal discharge; fever;burning with urination; persistent mood charge;or a hard, reddened area on the breast.

• Explain that the patient should not haveintercourse or drive a car until after thepostpartum check.
• Encourage participation in a bereavementsupport group, even if the patient andsignificant other seem to be coping with theloss.
• They may be able to help other couples cope.

IUGR


SGA IUGR
NORMAL FOETAL GROWTH
• Cellular hyperplasia
• Hyperplasia and hypertrophy
• Hypertrophy
STAGES
• Stage I (Hyperplasia)
- 4 to 20 weeks
- Rapid mitosis
- Increase of DNA content

Cont…
• Stage II (Hyperplasia & Hypertrophy)
- 20 to 28 weeks
- Declining mitosis.
- Increase in cell size.

Cont…
• Stage III ( Hypertrophy)- 28 to 40 weeks- Rapid increase in cell size.- Rapid accumulation of fat, muscle and
connective tissue.
• 95% of fetal weight gain occurs during last 20 weeks of gestations.

CAUSES OF IUGR
• Maternal factors
• Fetal factors
• Placental factors
• Environmental factors
MATERNAL FACTORS
•Medical disease
•Malnutrition BMI < 19 twice the risk of
IUGR
•Multiple pregnancy
• Smoking (460 gm < then none smoker)
Cont…
•Alcohol 12-fold increase risk of IUGR
•Drugs Beta- Blockers(Atenolol in
second trimster, Anticoagulants,
Anticonvulsants( phenytoin)
•Hypoxemia
• Infections UTI, Malaria, TB, Genital
Infections

Cont …
• Small stature/ low pre-pregnancy weight
• Teen pregnancy
• Primi gravida
• Grand multiparity

FETAL FACTORS• A Chromosome Defect-
In second trimester 20% SGA fetuseshave chromosomal abnormality
Triploid is most common under 26 wks.
Trisomy-18 is common after 26 wks .
Other are 21(Down’s syndrome), 16, 13,xo (turner’s syndrome).
Cont….
• Exposure to an infection-
• German measles (rubella), cytomegalovirus, herpes simplex, tuberculosis, syphilis, or toxoplasmosis, TB, Malaria, Parvo virus

Cont…
• birth defects
• (cardiovascular, renal, anencephally, limb defect, etc).
• A primary disorder of bone or cartilage.
• A chronic lack of oxygen during development (hypoxia
• Placenta or umbilical cord defects.

PLACENTAL FACTORS
• Uteroplacental Insufficiency Resulting From -.
– Improper / inadequate trophoblastic invasion and placentation in the first trimester.
– Lateral insertion of placenta.
–Reduced maternal blood flow to the placental bed.

Cont…
• Fetoplacetal Insufficiency Due To-.
–Vascular anomalies of placenta and cord.
–Decreased placental functioning mass-.
• Small placenta, abruptio placenta,
placenta previa, post term pregnancy

Normal & IUGR Newborn babies

Normal & IUGR Placentas
Environmental Causes of IUGR
• High altitude - lower environmental oxygen saturation
• Toxins
Types of IUGR
• Symmetric IUGR
(33 % of IUGR Infants)
• Asymmetric IUGR
(55 % of IUGR)
• Combined type IUGR
(12 % of IUGR)

SYMMETRICAL
• Height, weight, head circ proportional
• Early pregnancy insult:
• Commonly due to congenital infection, geneticdisorder, or intrinsic factors
• Reduced no of cells in fetus
• Normal ponderal index
• Low risk of perinatal asphyxia
• Low risk of hypoglycemia

PONDERAL INDEX
• The ponderal index is used determine thoseinfants whose soft tissue mass is belownormal for their stage of skeletaldevelopment.
Ponderal Index = birth weight x 100crown-heel length

Cont…
• Typical values are 20 to 25.
• Those who have a ponderal index below the 10th % can be classified as SGA
• PI is normal in symmetric IUGR.
• PI is low in asymmetric IUGR
ASSYMETRICAL
• Later in pregnancy:
• Commonly due to utero placental insufficiency, maternal malnutrition, hypoxia, or extrinsic factors
• Low ponderal index
• Cell number remains same but size is small
• Increased risk of asphyxia
• Increased risk of hypoglycemia

• Growth restriction in the stage of hypertrophy
• Brain sparing effect
• Head growth remains normal but abdominal girth slows down


Newer Classification
1. Normal Small Fetuses-
• Have no structural abnormality, normal
umbilical artery & liquor but wt., is less.
• They are not at risk and do not need any special
care.

Abnormal Small Fetuses- have chromosomal
anomalies or structural malformations. They
are lost cases and deserve termination as
nothing can be done.
Growth Restricted Fetuses- are due to impaired
placental function. Appropriate & timely
treatment or termination can improve
prospects.

CLINICAL FEATURES
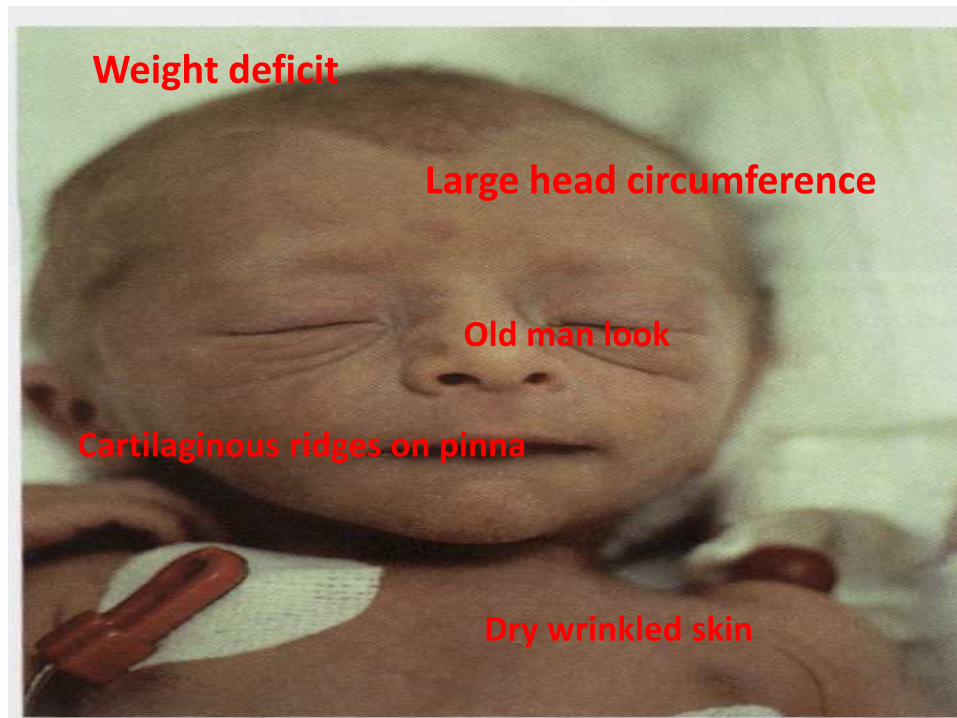
Weight deficit
Dry wrinkled skin
Large head circumference
Old man look
Cartilaginous ridges on pinna

Length remain unaffected
Open eyes
Thin umbilical cord
Well defined creases
Normal reflexesAlert and active
Normal cry

• Scaphoid abdomen
• Signs of recent wasting- soft tissue wasting- diminished skin fold thickness- decrease breast tissue- reduced thigh circumference
• Signs of long term growth failure- Widened skull sutures, large fontanelles- shortened crown – heel length- delayed development of epiphyses

DIAGNOSIS OF IUGR
• History
• Risk factors
• Last menstrual period - most precise size of uterus
• Time of quickening (detection of fetal movements)
• Examination
• Maternal serum screening
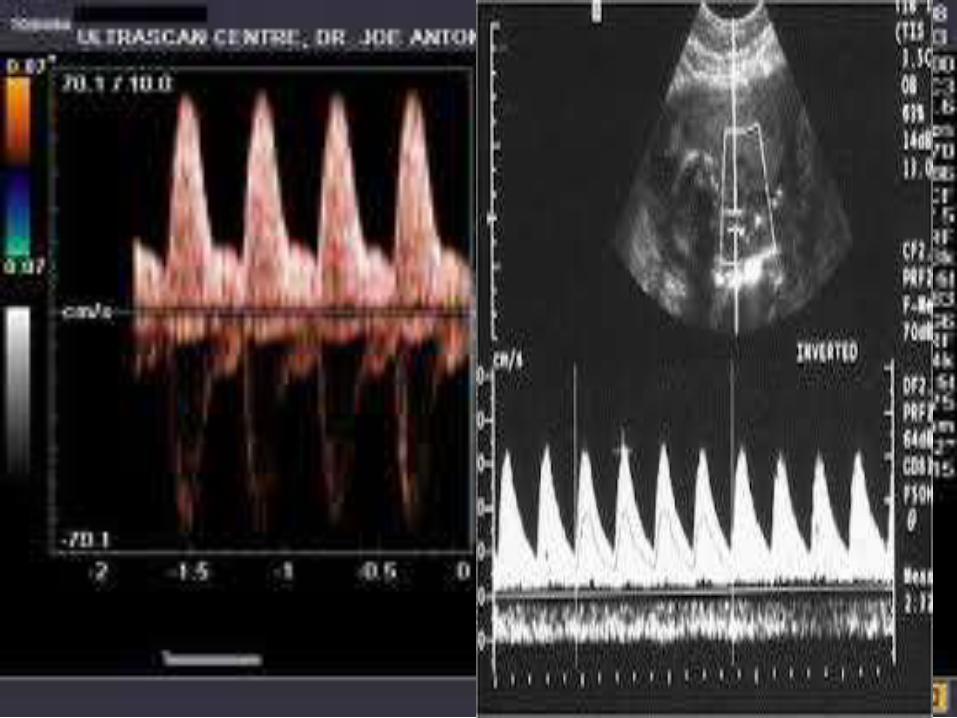
Uterine Artery Doppler Velocimetry
- Notching of the waveform /reduce EDF associated 3-fold increase in risk of FGR.
• Combination of un-explain elevated maternal AFPis powerful predictor of adverse perinataloutcome (FGR)
• Increase AFP combine with echogenic bowel isstrong predictor of FGR

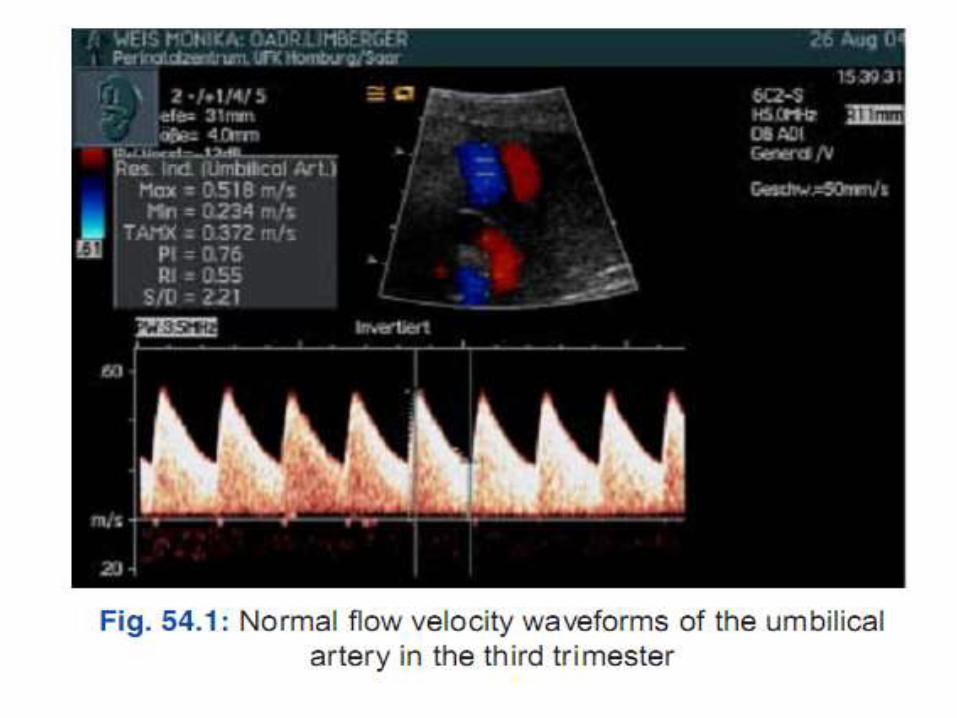
• DOPPLER OF THE UMBILICAL ARTERY
• Reduced end diastolic flow.
• Absent end diastolic flow
• Reversed end diastolic flow( severe cases)


Problems
• Hypoxia- Perinatal asphyxia
- Persistent pulmonary hypertension
- meconium aspiration
• Thermoregulation- Hypothermia due to diminished subcutaneous fat and elevated surface/volume ratio
Metabolic
- Hypoglycemia
- result from inadequate glycogen stores.
- diminished gluconeogenesis.
- increased BMR
- Hypocalcemia
- due to high serum glucagon level, which stimulate calcitonin excretion

• Hematologic - hyperviscosity and polycythemia due to increase erythropoietin level sec. to hypoxia
• Immunologic- IUGR have increased protein catabolism and decreased in protein, prealbumin and immunoglobulins, which decreased humoraland cellular immunity.
• Fetal distress,
• Hypoxia, Acidosis and Low Apgar Score at birth.Increased perinatal morbidity and mortality
• Grade 3-4 intraventricular haemorrhage
• Necrotizing enterocolitis
• BIOPHYSICAL
• HC:AC
• Brfore 32 wks more than 1
• 32—34 wks app 1
• FEMUR LENGTH
• FL:AC IS 22at all gest wks from 21 wks to term
• More than 23.5 indicate IUGR
• AFI
• <2 Suggest IUGR
• PI

PREVENTION OF HYPOTHERMIA
• MUMMIFICATION
• KMC
• NESTING
• DELAY BATH
• WARMER
MAINTAINING BREATHING
• VENTILATOR
• C PAP
• 02 SUPPLEMENTATION

NUTRITION FLUID AND FEEDING
• <30– IV FLUIDS, NG ,KATORI, BREAST FEEDS
• 30—34 NG ,KATORI, BREAST FEEDS
• >34 KATORI, BREAST FEEDS
Monitoring
• Vital signs
• Activity and behaviour.
• Color; Pink, pale, grey, blue, yellow.
• Tissue perfusion
• Fluids, electrolytes and ABG's.

COMPLICATION
Cont…

• Bronchopulmonary dysplasia
• Metabolic disturbances and hypoglycemia
• Polycytemia
• Hypothermia
• Impaired cognitive function and cerebral paresis

MEDICAL MANAGEMENT
• ASPIRIN THERAPY
• Other forms of treatment that have been studied are
• nutritional supplementation,
• zinc supplementation,
• fish oil,
• hormones and
• oxygen therapy

NURSING MANAGEMENT (During Pregnancy)
Diagnosis
• Impaired nutritional status less then body requirement related to malnutrition.
Intervention
• To correct malnutrition by providing balanced diet.
• To take extra calories from normal i.e. 300 calories extra.
• To provide nutritious foods, juices, fruits etc.

Diagnosis
• Decreased uteroplacental circulation related to reduced blood flow to maternal surface or placental cause.
Intervention
• Adequate bed red in left lateral position.
• Provide low dose of aspirin i.e. 50 mg daily.
• Prove o2 to mother at the rate of 2.5 L/min bynasal prong for short term for prolongation ofpregnancy.
Diagnosis
• Decreased knowledge status of motherrelated to IUGR, its complication to baby.
Intervention
• Provide knowledge to the mother.
• Provide health education to mother related toself care as well as related to diet.
• Provide detailed information about hercondition of baby as well as complication forbaby.
NURSING MANAGEMENT FOR BABYRisk for infection related to poor immunityGoalCare at neonatal intensive care unitIntervention• The NICU should be warm, free from excessive sound
smoothing light.• Protection from infection should be ensured by aseptic
measures and effective hand washing.• Rough handling and painful procedure should be
avoided.• Baby should be placed on soft comfortable, “nestled”
and cushioned bed.• Continuous monitoring of the baby’s clinical status are
vital aspects.

Decreased body temperature related to IUGRGoalMaintenance of stable body temperatureIntervention• Baby should be received in a pre warmed radiant
warmer or incubator. Environmental temperatureshould be maintained according to baby’s weightand age.
• Baby’s skin temperature should be maintained 36.5to 37.5 degree celcious.
• Baby birth weight of less than 1200gm should becared in the NICU incubator with 60 to 70 %humidity, oxygen and thermo nutral environmentfor better thermal control and prevent heat loss.

Decreased body weight of baby related to IUGR.GoalMaintenance of nutrition and hydrationIntervention• Caloric needs of non-growing LBW babies during first
week of life are 60 kcal/ kg/ day on 7th is to bestepped up gradually to 100 on 14th day and about120-150 on 21st day, to maintain satisfactorygrowth.
• Human milk is the first choice of nutrition for all LBWbabies. Colostrums, hind milk, foremilk, and pretermmilk help faster growth of baby.
• If breast milk is not available cows milk in proportionof 1:1 (milk: water) for 1st month and 2:1 duringsecond month is an alternative substitute.

CONCLUSION
AND
SUMMARY
RESEARCH ARTICLETITLE - Study of causes and complications of intra
uterine fetal death (IUFD)
OBJECTIVES - This study were to study the causes ofIntra Uterine Fetal Death (IUFD), associatedcomplications and to suggest preventive measures.
METHODS - Study design: retrospective observationalstudy. This study was carried out over a period of 3months (April 2014- June 2014) at a tertiary carehospital. Inclusion criteria was all IUFD >20 weeks of
gestation.

RESULTOut of 1850 total births during the study period80 IUFD occurred. Hence proportion of IUFDwas 4.3%. In this study, Still Birth Rate (SBR) asper WHO criteria (28 weeks) was 22.1 per 1000.Registered patients were 24 (30%) whereas 56(70%) were emergency admissions. Majority ofcases, 48 (60%) were multigravidae with pastobstetric history of abortion and IUFD in 13(16.2%) and 9 (11.2%) respectively. In 31(38.7%) no identifiable cause of IUFD was foundwhereas cause was identified in 49 (61.3%).

Conclusions
Anemia, PIH, accidental haemorrhage wereleading causes of IUFD. Majority of womenwho had IUFD were emergency admissionwho had not received adequate antenatalcare. A significant proportion of IUFD ispreventable by health education to patientsand community for regular antenatal care,about warning signs during antenatal period,hospital delivery and early referral.