

IRISH HIP FRACTURE DATABASE - s3-eu-west-1.amazonaws.com
172
IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 DRIVING IMPROVEMENT THROUGH TEAMWORK
Transcript of IRISH HIP FRACTURE DATABASE - s3-eu-west-1.amazonaws.com

IRISH HIP FRACTURE DATABASENATIONAL REPORT 2020
DRIVING IMPROVEMENT THROUGH TEAMWORK

REPORT PREPARED BY:
NATIONAL OFFICE OF CLINICAL AUDIT (NOCA)
The National Office of Clinical Audit (NOCA) was established in 2012 to create sustainable clinical audit programmes at national level. NOCA is funded by the Health Service Executive Office of the Chief Clinical Officer and operationally supported by the Royal College of Surgeons in Ireland. The National Clinical Effectiveness Committee (NCEC) defines national clinical audit as “a cyclical process that aims to improve patient care and outcomes by systematic, structured review and evaluation of clinical care against explicit clinical standards on a national basis” (NCEC, 2015, p. 2). NOCA supports hospitals to learn from their audit cycles.
Electronic copies of this report can be found at:https://www.noca.ie/publicationsBrief extracts from this publication may be reproduced provided the source is fully acknowledged
Citation for this report: National Office of Clinical Audit, (2021) Irish Hip Fracture Database National Report 2020. Dublin: National Office of Clinical Audit. ISSN 2565-537X (Print)ISSN 2565-5388 (Online)This report was published on 4th October 2021
National Office of Clinical Audit, 2nd Floor, Ardilaun House, Block B, 111 St Stephen’s Green, Dublin 2, D02 VN51
For more information about this report, contact
Tel: +353 (1) 402 8577 Email: [email protected]
DESIGNED BY
Dr Emer Ahern, Irish Hip Fracture Database Clinical Geriatrician Lead, Consultant Orthogeriatrician, Cork University Hospital
Louise Brent, Irish Hip Fracture Database and Major Trauma Audit Manager, National Office of Clinical Audit
Aisling Connolly, Communications and Events Lead, National Office of Clinical Audit
Dr Helena Ferris, Specialist in Public Health Medicine, Department of Public Health, Health Service Executive South
Prof. Tara Coughlan, Consultant Physician in Geriatric and Stroke Medicine, Tallaght University Hospital Brian Donovan, Head of Pricing, Healthcare Pricing Office Catherine Farrell and Ruth Kiely, Programme Managers, National Clinical Programme for Trauma and Orthopaedic Surgery, Royal College of Surgeons in Ireland Michelle Fitzgerald, Health and Social Care Professional Representative, member of the Irish Society of Chartered Physiotherapy, Physiotherapy Manager, Peamount Healthcare Dr Patrick Higgins, Consultant Anaesthetist, College of Anaesthesiologists of Ireland Ursula Kelleher, Irish Hip Fracture Database Audit Coordinator Representative, St Vincent’s University Hospital
WITH ASSISTANCE FROM THE IRISH HIP FRACTURE DATABASE GOVERNANCE COMMITTEE:
John Kelly, Deputy Chief Executive Officer, Tallaght University Hospital Mr Paddy Kenny, Consultant Orthopaedic Surgeon, Clinical Lead, National Clinical Programme for Trauma and Orthopaedic Surgery, RCSI
Prof. C Geraldine McMahon, Consultant in Emergency Medicine, St James’s Hospital
Lucy Nugent, Chief Executive Officer, Tallaght University Hospital
Dr Teresa O’Callaghan, National Quality Improvement Advisor, National Quality Improvement Team, Health Service Executive
Dr Mary Walsh, Health Research Board Postdoctoral Fellow, School of Public Health, Physiotherapy and Sports Science, University College Dublin
Prof. Conor Hurson, Irish Hip Fracture Database Clinical Orthopaedic Lead, Consultant Orthopaedic Surgeon, St Vincent’s University Hospital
Dr Fionnola Kelly, Head of Data Analytics & Research, National Office of Clinical Audit
Carlo Lodola, Senior Data Analyst, National Office of Clinical Audit
Bibiana Savin, Public and Patient Interest Representative, Sage Advocacy
Special thanks to Meabh McGirr, Data Analyst, National Office of Clinical Audit, for her assistance in preparing Chapter 10; and to John Hughes, SPHeRE Student, Royal College of Surgeons in Ireland, for support with the data analysis.
ACKNOWLEDGEMENTS
The Irish Gerontological Society (IGS) is an interdisciplinary professional organisation whose membership reflects the complexity and diversity of those interested in promoting the interests of older people and in how knowledge about ageing and later life can be enhanced and improved.
Its core purposes are education and research in the study of ageing and promoting a better understanding by the general public of ageing and related issues.
The Irish Institute for Trauma and Orthopaedic Surgery (IITOS) was established in 1999 as a charitable organisation. IITOS delivers higher surgical training in Ireland, under the governance of the Royal College of Surgeons in Ireland.
The Royal College of Surgeons in Ireland provides education and training in the fields of medicine and the health sciences at undergraduate and postgraduate level. The College has a strong international presence with Schools in Malaysia, Dubai and a University in Bahrain. RCSI also provides surgery and emergency medicine training in all recognised specialities and sub-specialities.

Irish Hip Fracture DatabaseNational Report 2020
Driving improvement through teamwork

NOCA NATIONAL OFFICE OF CLINICAL AUDIT4
CONTENTSNOCA ENDORSEMENT LETTER 8FOREWORD 9EXECUTIVE SUMMARY 10KEY FINDINGS 11KEY HIGHLIGHTS 2020 INFOGRAPHIC 12KEY RECOMMENDATIONS 14CAPTURING PATIENTS’ PERSPECTIVES 15Understanding hip fracture from the patient’s perspective 17Stay safe at home 17Be active at home 19
CHAPTER 1 INTRODUCTION 21
What are the aim and objectives of the IHFD and who is this report aimed at? 26Aim 26Objectives 26Who is this report aimed at? 26
CHAPTER 2 METHODOLOGY 27
Inclusion criteria 28Exclusion criteria 28COVID-19 definition 28Data collection 29Data analysis 29Hospitals included in the IHFD 30
CHAPTER 3 DATA QUALITY 33
Data quality statement 34Data coverage 35Data validation 35
CHAPTER 4 IRISH HIP FRACTURE STANDARDS & BEST PRACTICE TARIFF 37
IHFS 1 40IHFS 2 42IHFS 3 44IHFS 4 46IHFS 5 48IHFS 6 50IHFS 7 52Impact of the COVID-19 pandemic on activity and IHFS 54Best practice tariff 57BPT and coverage 58BPT payments by hospital 59BPT payments as a proportion of patient volume by hospital 61Golden hip award winner 2020 62Key findings from Chapter 4 66
CHAPTER 5 CASE MIX 67
1
5
3
2
4

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 5
CHAPTER 6 PATIENT PATHWAY 71
Mode of admission to hospital 72Reason for delay to surgery 73Cumulative time to surgery 74Type of anaesthesia 75Nutritional risk assessment 78Type of surgery 79Mobilisation: day of or day after surgery and mobilised by 82Key findings from Chapter 6 85
CHAPTER 7 OUTCOMES 87
Functional outcomes: Cumulative Ambulatory Score 88Destination on discharge 89Cumulative length of stay 90Reoperation within 30 days 91Key findings from Chapter 7 92
CHAPTER 8 QUALITY IMPROVEMENT 93
IHFD investment in QI 94Front-line ownership for QI 94National recognition for front-line IHFD QI projects 97Conclusion 102
CHAPTER 9 AUDIT UPDATE 103
Update on audit recommendations from 2019 104Research 106Publications 107Presentations 107
CHAPTER 10 ORGANISATIONAL SURVEY 109
CHAPTER 11 RECOMMENDATIONS 129
CHAPTER 12 CONCLUSION 137
REFERENCES 139
APPENDICES 143APPENDIX 1: IHFD DATASET 144APPENDIX 2: IHFD FREQUENTLY ASKED QUESTIONS 149APPENDIX 3: GLOSSARY OF TERMS AND DEFINITIONS 153APPENDIX 4: FREQUENCY TABLES 155APPENDIX 5: SPECIFICATIONS FOR COMPOSITE VARIABLES 166APPENDIX 6: ADDITIONAL INFORMATION 168APPENDIX 7: IHFD GOVERNANCE COMMITTEE MEETING ATTENDEES 2020 169
10
6
11
12
7
8
9

NOCA NATIONAL OFFICE OF CLINICAL AUDIT6
TABLES
TABLE 2.1 Data collection calendar 2020 29
TABLE 3.1 Overview of data quality for the IHFD 2020 34
TABLE 4.1 Irish hip fracture standards and best practice tariff measures 38
TABLE 4.2 Hip fracture patients with a diagnosis of COVID-19 56
TABLE 4.3 Total best practice tariff payments, by hospital and quarter, 2020 59
TABLE 4.4 Examples of items purchased using the BPT by hospital 60
TABLE 6.1 Reason for delay to surgery 73
TABLE 6.2 Type of surgery by fracture type (percentage) 80
TABLE 8.1 Hospital IHFD quality improvement projects and inititatives 95
TABLE 10.1 Hospital demographics and resources 111
TABLE 10.2 Policies and procedures 123
TABLE 10.3 Hospital hip fracture governance 124
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 7
FIGURES
FIGURE 1 Irish hip fracture standards 10
FIGURE 2 Anatomy of the hip 17
FIGURE 3 Home safety advice infographic 18
FIGURE 4 How to keep active at home 19
FIGURE 1.1 Timeline of COVID-19 pandemic in ireland 23
FIGURE 3.1 Coverage percentages per hospital, 2020 35
FIGURE 4.1Percentage of patients nationally who met each IHFS in 2018 (n=3751), 2019 (N=3701) and 2020 (N=3666)
39
FIGURE 4.2IHFS 1: percentage of patients admitted to an orthopaedic ward within 4 hours or admitted to theatre from ED within 4 hours, by individual hospital, 2019 (N=3701) and 2020 (N=3666)
41
FIGURE 4.3IHFS 2: percentage of patients receiving surgery within 48 hours (and within normal working hours), by individual hospital, 2019 (n=3536) and 2020 (n=3485)
43
FIGURE 4.4IHFS 3: percentage of patients who developed pressure ulcers following admission, by individual hospital, 2019 (n=3498) and 2020 (n=3481)
45
FIGURE 4.5IHFS 4: percentage of patients seen by a geriatrician or advanced nurse practitioner during admission, by individual hospital, 2019 (N=3701) and 2020 (N=3666)
47
FIGURE 4.6 IHFS 5: percentage of patients who received a bone health assessment in 2020 (n=3481) 48
FIGURE 4.6AIHFS 5: percentage of patients who received a bone health assessment, by individual hospital, 2019 (n=3498) and 2020 (n=3481)
49
FIGURE 4.7IHFS 6: percentage of patients who received a specialist falls assessment, by individual hospital, 2019 (n=3498) and 2020 (n=3481)
51
FIGURE 4.8:IHFS 7: percentage of patients mobilised by a physiotherapist on the day of or day after surgery 2020 (n=3485)
53
FIGURE 4.9: Hip fracture activity, by month, based on admission date (January 2019 - November 2020) 54
FIGURE 4.10:Percentage of hip fracture patients who met each of the seven Irish hip fracture standards, by month (January 2019 - December 2020)
55
FIGURE 4.11: Irish hip fracture database coverage, by year, 2013-2020 58
FIGURE 4.12 Proportion of hip fracture patients meeting best practice tariff standards, by hospital, 2020 61
FIGURE 6.1 Mode of admission to operating hospital, by hospital (N=3666) 72
FIGURE 6.2 Cumulative time to surgery (n=3485) 74
FIGURE 6.3 Percentage of patients by type of anaesthesia (n=3485) 75
FIGURE 6.3A Percentage of patients by type of anaesthesia, by hospital (n=3470) 76
FIGURE 6.4 Percentage of patients by nerve block usage, by hospital (n=3485) 77
FIGURE 6.5 Percentage of patients by nutritional risk assessment, by hospital (N=3666) 78
FIGURE 6.6 Percentage of patients by type of surgery (n=3485) 79
FIGURE 6.7 Percentage of patients with cemented or uncemented arthroplasties, by hospital (n=1815) 81
FIGURE 6.8Percentage of patients who were assessed by a physiotherapist on the day of or day after surgery, by hospital (n=3485)
83
FIGURE 6.8A Percentage of patients by mobilisation day of or day after surgery, by hospital (n=3467) 84
FIGURE 7.1 Percentage of patients by functional outcomes: CAS (n=2015) 88
FIGURE 7.2 Percentage of patients by destination on discharge (N=3666) 89
FIGURE 7.3 Percentage of patients by cumulative LOS (N=3666) 90
FIGURE 7.4 Percentage of patients by reoperation within 30 days (n=3485) 91
CONTENTS >

Dr Emer Ahern & Prof. Conor Hurson National Clinical Leads Irish Hip Fracture Database National Office of Clinical Audit 2nd Floor, Ardilaun House 111 St. Stephen’s Green,Dublin 2
20th September, 2021
Dear Dr Ahern/Prof. Hurson,
I wish to acknowledge the receipt of the Irish Hip Fracture Database National Report 2020.
Following review of this report by NOCA, I am delighted to endorse this report on behalf of the NOCA Governance Board.
I wish to congratulate you both and those involved, including Ms Louise Brent, for the continued efforts in developing and progressing this valuable quality improvement initiative. The IHFD audit continues to serve as an exemplar for quality improvement for all NOCA audits.
Please accept this as formal endorsement from the NOCA Governance Board of the Irish Hip Fracture National Report 2020.
Yours sincerely,
Dr Brian CreedonClinical DirectorNational Office of Clinical Audit
National Office of Clinical Audit2nd Floor
Ardilaun House, Block B111 St Stephen’s Green
Dublin 2, D02 VN51Tel: + (353) 1 402 8577
Email: [email protected]

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 9
FOREWORD
As Chief Clinical Officer in the HSE I welcome the latest “Irish Hip Fracture Database National Report 2020” report. In particular we would like thanks to be given to all of the healthcare staff involved in the care of hip fracture patients, including pre-hospital carers and the community discharge teams too. It has been an extraordinary year that has presented unprecedented challenges to Irish healthcare. This report is all about celebrating the efforts of our frontline staff involved in hip fracture care during such a challenging time. The focus has over the 18 months understandably been on COVID-19 but increased appreciation of secondary impacts on other conditions. All the more extraordinary that this audit demonstrates continued improvement in the quality and process of hip fracture care. Particular gains in the areas of bypass whereby 94% of patients are brought directly to the operating hospital, only a few short years after we were bringing patients directly to hospitals with no orthopaedic facility. I have to acknowledge the achievements in data collection at a time when there was so much disruption to healthcare. Since the introduction of the Best Practice Tariff in 2018 which was the vision of NCP Orthopaedics and Trauma, we now see year on year improvements in performance, with particular credit to Our Lady of Lourdes Hospital in Drogheda (OLOL) for their award.
I would like to thank the elective orthopaedic hospitals and private hospitals some of which took hip fracture and other trauma patients in the early phase of the pandemic to create capacity in the acute hospitals and facilitated the earlier discharge of patients with hip fractures. I would especially like to thank the Irish Hip Fracture Database (IHFD) clinical leads and hospital managers in each hospital for their commitment to the audit and in particular pay thanks to each and every one of the IHFD audit coordinators for their extraordinary efforts to collect this valuable data. Their commitment to this audit surpassed any expectation during such challenging times. Congratulations to all clinicians on this unique collaboration which exemplifies the value of multidisciplinary working for the welfare of patients.
Dr Colm HenryChief Clinical OfficerHealth Service Executive
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT10
EXECUTIVE SUMMARY
This is the eighth national report from the Irish Hip Fracture Database (IHFD). To date, the audit has captured data on more than 25,000 patients. The Irish Hip Fracture Database National Report 2020 includes data from 3,666 cases. Our data provide detailed information about the care, processes and outcomes of patients and allow each hospital to benchmark itself against comparable hospitals in Ireland and internationally. In an unprecedented year for the health system due to the impact from coronavirus disease 2019 (COVID-19), the audit has maintained a strong focus on the Irish Hip Fracture Standards (IHFS) detailed in Figure 1, and on the care and outcomes of hip fracture patients. Despite the COVID-19 pandemic disruption to the health service, this report shows the ongoing commitment of staff to high-quality patient care, clinical audit and quality improvement, with 99% of all eligible data being collected again by the dedicated audit coordinators in the participating hospitals.
Each hospital’s hip fracture governance committee is encouraged to use the quarterly and national reports for continuous quality improvement. Without the constant leadership provided by our hospital clinical leads and the dedication and hard work of our audit coordinators, this audit would not be possible. The National Office of Clinical Audit Executive Team and the IHFD Governance Committee wish to thank the clinical leads, audit coordinators and hospitals for their continued commitment to and engagement with this audit.
IRISH HIP FRACTURE STANDARDS (IHFS)
IHFS 1:
Be admitted to an orthopaedic ward within 4 hours
IHFS 3: Not develop a pressure ulcer
IHFS 2:
Receive surgery within 48 hours
IHFS 4:
Be seen by a geriatrician or advanced nurse practitioner
4 48
IHFS 5: Receive a bone health assessment
IHFS 6: Receive a specialist falls assessment
IHFS 7: Be mobilised by day after surgery by a physiotherapist
Pressure Ulcers to Zero
FIGURE 1: IRISH HIP FRACTURE STANDARDS
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 11
KEY FINDINGS
> In 2020, 99% of hip fracture data were captured by the Irish Hip Fracture Database (IHFD).
>One-third of patients nationally were admitted to an orthopaedic ward or to the operating theatre from the emergency department (ED) within 4 hours (Irish Hip Fracture Standard (IHFS) 1), compared with only one-quarter of patients in 2019.
> Compliance with IHFS 2, 3 and 4 have all remained largely unchanged since 2019.
> In 2020, a bone health assessment (IHFS 5) was carried out on 91% of patients nationally, compared with 94% in 2019.
> Eighty-five percent of patients nationally had a specialist falls assessment (IHFS 6) prior to discharge in 2020.
>The total money paid out as a result of the Best Practice Tariff (BPT) for 2020 was €710,000, with 20% of all hip fracture patients nationally meeting the IHFS and the BPT . This represents an improvement of five percentage points from 2019.
> Our Lady of Lourdes Hospital Drogheda had the highest proportion of patients meeting the BPT for 2020, with 43% of their patients receiving this level of care.
>Sixty-nine percent of patients received a nerve block pre-operatively in 2020, which is an increase of nine percentage points from 2019. The use of pre-operative nerve blocks ranged from 13% to 99% at hospital level.
> Forty-four percent of patients did not receive a documented nutritional risk assessment.
>Seventy-four percent of arthroplasties reported in 2020 were cemented, which was a slight decrease from 2019. However, there is a large variation in the use of bone cement at hospital level.
>Eighty-five percent of patients were mobilised on the day of or the day after surgery, of which 78% were mobilised by a physiotherapist and 91% of patients were assessed by a physiotherapist on the day of or the day after surgery. These variables have increased by two and four percentage points, respectively, from 2019.
> Twenty-eight percent of patients were discharged directly home from hospital, which represents an improvement of four percentage points from 2019.
>The mean length of stay (LOS) for hip fracture patients was 17.1 days and the median LOS was 11 days. This reduction equated to a savings of almost 10,000 acute hospital bed days in 2020 compared to 2019.
> Twenty-nine percent of patients were discharged from the acute hospital within 1 week, an improvement of four percentage points from 2019.
KEY FINDIN
GS
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT12
KEY HIGHLIGHTS 2020
IHFS 2: 75% of patients
received surgery within 48 hours
IHFS 3: 3% of patients developed
a pressure ulcer after admission
56% of patients received a
nutritional risk assessment
Data coverage of 99%
99%
75%
3%
56%
IHFS 1: 33% of patients were admitted to
an orthopaedic ward or went to theatre within four hours
33%69% of patients
received a pre-operative
nerve block for pain
69%
85% of patients admitted
from home
85%
94% of patients are brought direct to
operating hospital
94%
4
48
Pressure Ulcers to Zero
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 13
IHFS 4: 82% of patients were seen by a geriatrician
82%
IHFS 5: 91% of patients received a bone health assessment
91% 28% of patients were discharged directly home
28%
62,684 acute hospital bed days for hip fracture patients
62,684
IHFD 7: 78% of patients were mobilised by a physiotherapist on the day of or day after surgery
78%Median length of stay: 11 days
11
IHFS 6: 85% of patients received a specialist falls assessment
85%
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT14
KEY RECOMMENDATIONS
RECOMMENDATIONS FOR THE NATIONAL OFFICE OF CLINICAL AUDIT
• The National Office of Clinical Audit (NOCA) will continue to implement the new Irish Hip Fracture Standard (IHFS) 7 for early mobilisation, with a plan to add it to the Best Practice Tariff (BPT) in 2022.
• Through research, NOCA will progress the development of longer-term outcome measures for hip fracture.
RECOMMENDATIONS FOR THE HEALTH SERVICE EXECUTIVE
• The Health Service Executive (HSE), through the National Clinical Programme for Trauma and Orthopaedic Surgery, will:– promote and develop bundles of care in conjunction with the Irish Hip Fracture
Database (IHFD), e.g. pre-hospital, emergency department (ED), orthogeriatrics, anaesthetics, orthopaedics and rehabilitation
– advocate that no patient should be fasted repeatedly – promote the practice of performing a nutrition and delirium screen for all hip fracture
patients– promote community pathways in order to enable early supported discharges.
RECOMMENDATIONS FOR HOSPITAL MANAGERS, CLINICIANS AND AUDIT COORDINATORS
• The hip fracture governance committees (HFGCs) should continue to meet regularly in order to review the data and engage in quality improvement using the data.
• Focus on increasing compliance with the IHFS in order to attain the BPT, which includes the new IHFS 7 for early mobilisation from 1 January 2022.
• Evaluate local processes/protocols for pre-operative fasting, delirium screening and nutrition screening.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 15
CAPTURING PATIENT PERSPECTIVES
Ongoing public health concerns during the coronavirus disease 2019 (COVID-19) pandemic made 2020 a year like no other. Being a hip fracture patient is difficult at the best of times, and even more so during the period of multiple restrictions imposed by the ongoing COVID-19 public health emergency and the widely publicised prospect of a healthcare system unable to cope with the surge in cases requiring intensive care.
For many months during 2020, the public focus was on the figures emerging daily from healthcare settings in Ireland and abroad. The general public discourse indicated that times were changing and that the trajectory of change was unknown; staff members in the health and social care sector were redeployed, volunteers stepped up to help those who were cocooning, visiting restrictions and lockdown regulations were imposed, and people were advised to stay at home and avoid unnecessary admissions to hospital. The fear of the unknown, the speed of developments and the rate of change at organisational level were counteracted by the resilience, determination and great skill displayed by those working in the hospitals, whose mission was to look after their patients during this time of unprecedented challenges.
Undoubtedly, the environment has a considerable impact on patients’ experience in care settings and can influence patients’ outcomes post-discharge from hospital. The data presented in this report – demonstrating consistent excellent coverage (99%) – show that patients with hip fractures admitted to hospital continued to receive good care during 2020:
• The length of stay in hospital decreased.• More patients were admitted to an orthopaedic ward within 4 hours in 2020, 8 percentage
points more than in the previous year. • Almost the same percentage of patients (75%) received surgery within 48 hours in 2020 as
in 2019.• The incidence of pressure ulcers has remained stable (3%) over the last few years.• The same percentage of patients were seen by a geriatrician (82%) over the last 2 years.• The percentage of patients receiving a bone health assessment decreased slightly (by three
percentage points) in 2020 in comparison with 2019.• More patients received a specialist falls assessment than in 2019; this figure has improved
each year, from 47% in 2017 to 85% in 2020.• The new Irish Hip Fracture Standard shows that 78% patients were mobilised on the day of
or the day after their surgery.
COVID-19 does not appear to have had a hugely detrimental effect on the standards of care in acute hospitals in Ireland. However, more hip fracture patients were admitted to acute hospitals from the long-term care sector, and the percentage of new admissions to nursing homes remained at 4% in 2020. For patients, the transfer between the hospital and nursing home, along with their experience as inpatients and post-discharge, most certainly posed additional challenges during the pandemic, including new visiting restrictions, lack of direct interaction with family and friends, lack of accompaniment during transfer, limited supports in order to facilitate rehabilitation, strange interactions with others through personal protective equipment, adjusting to new protocols, and unprecedented generalised isolation.
On admission to hospital, some patients face rapid functional decline, loss of confidence in themselves, and a fear of falling again while walking. Some fear losing their dignity and independence and dread the prospect of not being able to return home. During their hospital stay amid the COVID-19 pandemic, difficult conversations with relatives, friends and carers happened indirectly via phone or video call, sometimes with no privacy if patients relied entirely
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT16
on staff to facilitate conversations; patients were also asked to isolate or restrict their movements and interactions with others during their time in hospital and upon discharge from hospital. The lack of informal supports usually provided to patients by their visitors was surely felt by all throughout the pandemic.
Although more patients returned home in 2020, they all faced further challenges post-discharge from hospital following hip surgery. The imposed isolation, lack of supports and fear of getting sick or dying, against the general backdrop of public health restrictions and advice to remain at home, have been part of the public discourse since March 2020. The wider impact of the pandemic on patients and the general public is yet to be determined. Nevertheless, the professionalism and dedication of the personnel in the acute hospitals across Ireland who are committed to providing a high standard of care to patients was evident, even during the exceptional circumstances of the pandemic.
The message “we are in this together” was heard and acted on time and time again during 2020. The teams in hospitals, the patients and the visitors all had to adapt quickly to a new reality, new ways of working, new regulations, and new ways of communicating and supporting each other. Resilience, a determination to succeed and open-mindedness proved to be valuable skills which kept people going. The learning from these difficult times will undoubtedly represent an important resource for future quality improvement initiatives at national level.
Bibiana Savin, Sage Advocacy
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 17
UNDERSTANDING HIP FRACTURE FROM THE PATIENT’S PERSPECTIVEWHAT IS A HIP FRACTURE?‘Hip fracture’ is a term used to describe a break or fracture in the upper portion of the thigh bone (femur) where the bone meets the pelvis. It is also commonly referred to as a ‘broken hip’, a ‘fractured neck of femur’ or a ‘proximal femur fracture’.
The hip joint is a ball and socket joint. The ball (head of the femur) is located on top of the thigh bone and the socket sits within the pelvis. The joint is contained within a fibrous capsule and much of the ball receives its blood supply through blood vessels in the capsule.
FIGURE 2: ANATOMY OF THE HIP
IntracapsularPelvis
Socket
Trochanteric
Subtrochanteric
Ball
Thigh bone(femur)
Extracapsular
STAY SAFE AT HOMEFalls most commonly occur in the home, and many things can be done to prevent these falls and make the home a much safer environment. During the pandemic, many older adults in Ireland effectively became housebound overnight. Older adults reported less physical activity and less social connections with family and friends, both of which are fundamental for health and well-being. Figure 3 shows some safety advice for the home in order to prevent people having falls and sustaining injuries like hip fractures. Figure 4 shows some key messages on how to keep active at home while also keeping safe.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT18
FIGURE 3: HOME SAFETY ADVICE
KITCHEN: Mop up spills straight away. Do not climb on chairs to reach high cupboards.
GARDEN AREAS: Make sure that paths are even and free of moss. Keep paths free of garden tools.
PETS: Be aware of where your pets are.
LIGHTING: Ensure adequate lighting in all rooms, steps and stairs. Use night lights inside and sensor lights outside.
BEDROOM: If you feel off balance or have difficulty dressing yourself, sit on the bed and get dressed there.
BATHROOM: Install grab rails. Use a non-slip mat. Be careful on wet floors.
REMOVE CLUTTER
STAIRS AND STEPS: Mark edges of steps clearly. Use slip- resistant strips. Install handrails the full length of the stairs/steps.
CORDS AND CABLES: Remove cords and cables from walkways.
FLOORS: Secure rugs (or remove them). Have non-slip floors.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 19
FIGURE 4: HOW TO KEEP ACTIVE AT HOME
Adapted from the work of Vanda Cummins, Primary Care Physiotherapist, HSE
STEP 1Break up periods of sitting by standing up from your chair at least once an hour. Regular movement helps to keep your mind and body feeling well
STEP 3Keep your bones and muscles strong with activities that require a bit of effort such as pushing, pulling, lifting or lowering activities. Climbing the stairs and doing housework also help keep you strong
STEP 2Include stretches in your daily routine to help improve posture and mobility
BE ACTIVE BE ACTIVE AT HOMEAT HOME
CONTENTS >


IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 21
CHAPTER 1INTRODUCTION
Irish Hip Fracture Database National Report 2013
1
IRISH HIP FRACTURE DATABASENATIONAL REPORT 2013Better, safer care
IrIsh hIp Fracture DatabaseNatioNal RepoRt 2015
Better, safer care
IRISH HIP FRACTURE DATABASENATIONAL REPORT 2017Better, safer care
FROM BROKEN BONETO WALKING HOME
irish Hip Fracture DatabaseNational Report 2014Better, safer care
IrIsh hIp Fracture DatabaseNatioNal RepoRt 2016Better, safer care
IRISH HIP FRACTURE DATABASENATIONAL REPORT 2018
RIGHT CARE, RIGHT PLACE,
RIGHT TIME, RIGHT TEAM.

NOCA NATIONAL OFFICE OF CLINICAL AUDIT22
CHAPTER 1: INTRODUCTIONIn December 2019, a novel strain of coronavirus – known as coronavirus disease 2019 (COVID-19) – was identified in the city of Wuhan in the Hubei province of China. This virus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has spread globally and continues to cause huge disruptions and strain on healthcare services, social life and economies all over the world. The first confirmed case in Ireland was identified on 29 February 2020. Although containment measures were put in place initially, a number of other cases were diagnosed in early March, with the first fatality recorded on 11 March 2020. On 27 March 2020 the Taoiseach, Leo Varadkar, announced a national stay-at-home order and ‘cocooning’ for older adults. This followed the announcement by the World Health Organization on the previous day that the outbreak was officially considered a pandemic.
The stay-at-home and cocooning orders were extended on 10 April until 5 May 2020. By 1 May 2020, there had been 20,833 cases and 1,265 deaths, leading the Taoiseach to announce a further extension of restrictions until 18 May 2020. On 15 May 2020, the Government of Ireland confirmed that phase one of easing the COVID-19 restrictions would begin on 18 May.
During this period of extreme societal and economic disruption, the Irish healthcare system was under huge stress and turbulence in preparation for a surge of sick patients with COVID-19. Measures to prepare for the surge were taken quickly to create capacity in the acute hospitals – particularly in the intensive care units – around Ireland in order to prevent the health service from becoming overwhelmed as had been seen in other countries, such as Italy and Spain.
During this time, patients with other illnesses and injuries continued to present to hospitals, including individuals with hip fractures. This presented a huge challenge to the well-established pathways of care for these patients. Emergency departments (EDs) were split into COVID-19 and non-COVID-19 EDs. Patients were screened for COVID-19 and isolated if they were admitted from a care facility such as a nursing home. Operating theatres developed processes to manage the additional infection risk between cases, reducing theatre throughput.
CHAPTER 1
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 23
FIGURE 1.1: TIMELINE OF THE COVID-19 PANDEMIC IN IRELAND
JAN 2020
DEC 2020
JAN 2021
AUG 2020
OCT 2020
JUN 2020
MAR2020
NOV 2020
JUL 2020
APR 2020
SEP 2020
MAY 2020
FEB2020
CHAPTER 1
27 January 2020 NPHET created
5 February 2020 Coronavirus Expert Advisory Group met
29 February 2020 First COVID-19 case identified in Ireland
11 March 2020 First fatality recorded from COVID-19
12 March 2020 Taoiseach announces school closures
18 May 2020 Easing of lockdown
June and July 2020 Daily cases and deaths reduced
August 2020 3 week lockdown imposed in 3 counties
September 2020 Cases and deaths begin to rise
September 2020 Second wave of COVID confirmed
27 March 2020 Taoiseach announces first lockdown
21 October 2020 Country moves to full lockdown for six weeks
1 December 2020 Lockdown eased to Level 3
30 December 2020 Full lockdown imposed. Third wave confirmed.
FIRS
T W
AVE
SECO
ND
WAV
ETH
IRD
W
AVE
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT24
CHAPTER 1
HIP FRACTURES
Hip fracture continues to be one of the most serious and costly injuries suffered by older adults globally. Hip fracture care takes the patient through a complex clinical pathway involving a wide range of specialties. It is a surrogate marker for the care of older adults in our acute hospitals and indicates how well the trauma service is functioning. In Ireland, it is estimated that acute hospital management of older adults with hip fractures alone costs €45 million annually (National Office of Clinical Audit, 2019). As life expectancy continues to increase, the annual number of hip fractures will also increase (Kelly et al., 2018), along with the need for hospital, rehabilitation and community services.
The Irish Hip Fracture Database (IHFD) is a clinically led, web-based audit that was established in 2013 under the governance of the National Office of Clinical Audit (NOCA). The overarching aim of the audit is to use data to improve the care provided to older adults who have a hip fracture. Data are collected through the Hospital In-Patient Enquiry (HIPE) IHFD Portal, which is supported by the Healthcare Pricing Office (HPO). The IHFD data are merged with the HIPE data and each episode of care is only completed upon discharge. International evidence has shown that the synergy of care standards, audit and feedback drives measurable improvements in hip fracture outcomes for patients (Neuburger et al., 2015). Seven standards of care, known as the Irish Hip Fracture Standards (IHFS), are audited in the IHFD (Figure 1).
This national report, based on IHFD data, describes how care was delivered to hip fracture patients during a very challenging period for our health service.
Ireland’s trauma system is undergoing a transformative process to develop two trauma networks in line with A Trauma System for Ireland: Report of the Trauma Steering Group (Department of Health, 2018). Two trauma networks have been established: the Central Trauma Network, with a Major Trauma Centre (MTC) to be situated in the Mater Misericordiae University Hospital; and the Southern Trauma Network, with an MTC located in Cork University Hospital. Each network will have a number of supporting trauma units (TUs). What this means for hip fracture patients is that they will be brought to a designated MTC or TU that will have the capacity and infrastructure to provide multidisciplinary hip fracture care and recovery.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 25
CHAPTER 1
Several recommendations were made in A Trauma System for Ireland: Report of the Trauma Steering Group (Department of Health, 2018) related to the importance of clinical audit and the processes of developing the new trauma system. The IHFD has already contributed several years’ worth of data to assist the National Office for Trauma Services, Health Service Executive (HSE) in its decision-making process and its evaluation of what changes are to be made to the national trauma care system and how. Several recommendations in the report also echoed many of the IHFD recommendations made in previous years; for example, the need for orthogeriatric services, fracture prevention, falls prevention, rehabilitation services and high-quality data. Therefore, the IHFD is appropriately positioned to monitor the impact that these changes to the trauma system will have on the care and outcomes of patients.
Internationally, clinical audits focusing on hip fracture care continue to deliver demonstrable improvements in care outcomes, most importantly in the reduction in mortality (Neuburger et al., 2015). The IHFD continues to collaborate internationally with many other established hip fracture registers in order to enhance learning and bring synergy to the standards of care measured across all audits – and, in recent months, in order to share learning from the pandemic.
In 2020, the IHFD made many strides forward, with sustained high levels of data coverage, as well as improvements in some of the IHFS and in compliance with Best Practice Tariff (BPT) standards. Data were used for research by publications such as “Trends in hip fracture care in the Republic of Ireland from 2013 to 2018: results from the Irish Hip Fracture Database” (Walsh et al., 2020), and in December 2020, COVID-19 report 1.0: Service impact from COVID-19: Analysis based on Irish Hip Fracture Database June 2019-May 2020 (NOCA, 2020) was published as a rapid learning report to be used by the healthcare system during the evolving pandemic. A subsequent report was then published in April 2021 entitled COVID-19 report 2.0: Service impact from COVID-19: Analysis based on Irish Hip Fracture Database June 2019-August 2020 (NOCA, 2021). Data were also published in healthcare magazines, such as the Healthcare Professional News and Irish Pharmacy News.
Internationally, a great deal of work was achieved through the International Multicentre Project Auditing COVID-19 in Trauma & Orthopaedics (IMPACT) global study, with publications such as Hall et al. (2021) capturing the effect of the COVID-19 pandemic on trauma and orthopaedic services. Work was also progressed through the development of the world-first Hip Fracture Registry (HFR) Toolbox by the Asia Pacific Fragility Fracture Alliance (APFFA) Hip Fracture Registry Working Group, in collaboration with the Fragility Fracture Network (FFN) Hip Fracture Audit Special Interest Group (2021). This resource features key information from existing hip fracture audits in order to help other countries and regions set up similar databases.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT26
CHAPTER 1
WHAT ARE THE AIM AND OBJECTIVES OF THE IHFD AND WHO IS THIS REPORT AIMED AT?
AIMTo maintain a prospective database of all patients in Ireland aged 60 years and over with a hip fracture in order to drive continuous quality improvement for better, safer care.
OBJECTIVES
u Improve and support the collection of high-quality clinical audit data on all hip fracture patients in Ireland for local and national reporting.
u Continue updating the dataset in order to ensure that the information in the audit remains relevant to the Irish healthcare system and patients.
u Share timely outputs and reports from the data and report any data or performance concerns back to the relevant stakeholders.
u Support/promote the use of IHFD data for quality improvement at local and national levels.
u Benchmark hip fracture care and outcomes nationally and internationally.
u Support the provision of high-quality data for research.
u Collect longer-term outcome data (e.g. quality of life and survival).
u Support the BPT (a tariff-based payment structure for hip fracture) and act as the primary data source for hip fracture key performance indicators (KPIs).
u Capture the patient voice/experience and disseminate audit findings to patients and the public in an accessible manner.
WHO IS THIS REPORT AIMED AT?
National report Summary report Hospital report
Healthcare professionals Patients and carers Healthcare professionals
Hospital managers Patient organisations Hospital managers
Hospital Groups Healthcare professionals
Patients and carers
Patient organisations
CONTENTS >

CHAPTER 2METHODOLOGY
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT28
The IHFD collects data on hip fracture patients (aged 18 years and over) through a portal on the HIPE system in collaboration with the HPO. The reference population for the national report is limited to patients aged 60 years and over. Data from the HIPE system, such as age, gender, admission source, etc., are merged with additional IHFD data. The inclusion and exclusion criteria for this report are detailed below.
INCLUSION CRITERIAAnalysis is based on IHFD records as captured on the HIPE IHFD Portal software. It includes cases that were:
(i) discharged between 1 January 2020 and 31 December 2020, inclusive (the HIPE data file used was 2020_V14, extracted on 13 May 2021); this extraction date was later than anticipated due to disruption caused by the COVID-19 pandemic and the additional workload placed on hospital coding departments.
(ii) diagnosed on HIPE with either a hip fracture due to injury or with a specified type of fracture, other than periprosthetic, on IHFD add-on screens.
(iii) aged 60 years and over.
EXCLUSION CRITERIA(i) patients aged 59 years or under
(ii) patients who died as an inpatient are excluded from comparative analysis of IHFS 3, 5 and 6 but are included in the rest of the report.
For the purpose of this analysis, we define the pre-COVID-19 period as before 29 February 2020 and the COVID-19 pandemic period from 1 March 2020 onwards.
COVID-19 DEFINITIONHip fracture cases were defined as having a positive COVID-19 status if they had a secondary International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM) code recorded as:
U07.1: Coronavirus identified, confirmed by laboratory testing
OR
U07.2: Emergency use of U07.2 (COVID-19, virus not identified) is to be assigned when COVID-19 has been documented as clinically diagnosed COVID-19, including evidence supported by radiological imaging (i.e. where a clinical determination of COVID-19 is made but laboratory testing is inconclusive, not available or unspecified)
AND
B34.2: Coronavirus infection, unspecified site
OR
B97.2: Coronavirus as the cause of diseases classified to other chapters to identify the infectious agent.
HIPE
HIPE
CHAPTER 2: METHODOLOGY
CHAPTER 2
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 29
CHAPTER 2
DATA ANALYSISNOCA received the data extract on 15 May 2021. This was later than anticipated due to the COVID-19 pandemic. In 2020, data validation reports (DVRs) were distributed to the hospitals along with each quarterly report. Analysis for the national report was completed by the NOCA data analytics team following data checks with the HPO. The analysis was conducted using Statistical Package for the Social Sciences (SPSS) V25.
Data collection period Data collection target Data reporting date
01/01/2020–31/03/2020 30/06/2020 11/07/2020
01/04/2020–30/06/2020 30/09/2020 18/10/2020
01/07/2020–30/09/2020 31/12/2020 30/01/2021
01/10/2020–31/12/2020 30/04/2021* 18/05/2021
TABLE 2.1: DATA COLLECTION CALENDAR 2020
*The target date was extended by 4 weeks due to the COVID-19 pandemic.
DATA COLLECTIONThe data are collected in the local hospitals by audit coordinators who enter the data retrospectively from patient medical records. Each hospital has an audit coordinator and a clinical lead, and should have a hip fracture governance committee. A list of cases eligible for inclusion is identified by running a HIPE Discharge Report in the IHFD Portal. The data are entered through the HIPE IHFD Portal and linked with a hospital admission episode. The audit coordinator and clinical lead can generate local reports. The HPO issues monthly coverage reports to the IHFD Audit Manager, as well as extracts of data on a quarterly basis to NOCA for analysis. These data are analysed and quarterly reports are issued to hospitals and Hospital Groups. Most data are entered retrospectively and in accordance with the data collection targets (Table 2.1).
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT30
NOTE: Dublin Hospitals have been displayed collectively by hospital group
SAOLTA UNIVERSITY HEALTH CARE GROUPLetterkenny University HospitalMayo University HospitalSligo University HospitalUniversity Hospital Galway
RCSI HOSPITALSBeaumont HospitalConnolly HospitalOur Lady of Lourdes Hospital, Drogheda
DUBLIN MIDLANDS HOSPITAL GROUPMidland Regional Hospital, TullamoreSt James’s HospitalTallaght University Hospital
IRELAND EAST HOSPITAL GROUPMater Misericordiae University HospitalSt Vincent’s University Hospital
UL HOSPITAL GROUPUniversity Hospital Limerick
SOUTH/SOUTH WEST HOSPITAL GROUPCork University HospitalUniversity Hospital KerryUniversity Hospital Waterford
HOSPITALS AND PEOPLE WE WORK WITH
LETTERKENNY UNIVERSITY HOSPITAL
IHFD AUDIT COORDINATOR: Bruce MacGregor
IHFD CLINICAL LEAD: Mr Tony Shaju
UNIVERSITY HOSPITAL KERRY
IHFD AUDIT COORDINATOR: Esther O’Mahony
IHFD CLINICAL LEAD: Mr John Rice
MAYO UNIVERSITY HOSPITAL
IHFD AUDIT COORDINATOR: Suzanne O’Donnell
IHFD AUDIT COORDINATOR: Sinead Corley
IHFD CLINICAL LEAD: Mr Derek Bennett
UNIVERSITY HOSPITAL WATERFORD
IHFD AUDIT COORDINATOR: Lorraine Smith
IHFD AUDIT COORDINATOR: Gavin Egan
IHFD CLINICAL LEAD: Mr Terence Murphy
IHFD CLINICAL LEAD: Dr Niamh O’Regan
SLIGO UNIVERSITY HOSPITAL
IHFD AUDIT COORDINATOR: Ann Marie Mullen
IHFD CLINICAL LEAD: Mr William Gaine
CORK UNIVERSITY HOSPITAL
IHFD AUDIT COORDINATOR: Toni O’Keeffe
IHFD CLINICAL LEAD: Dr Emer Ahern
IHFD CLINICAL LEAD: Mr Shane Guerin
UNIVERSITY HOSPITAL GALWAY
IHFD AUDIT COORDINATOR: Louise Brennan
IHFD AUDIT COORDINATOR: Aoife Dempsey
IHFD CLINICAL LEAD: Mr Colin Murphy
UNIVERSITY HOSPITAL LIMERICK
IHFD AUDIT COORDINATOR: Pamela Hickey
IHFD CLINICAL LEAD: Dr Jude Ryan
IHFD CLINICAL LEAD: Mr Finbarr Condon
CHAPTER 2
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 31
ST VINCENT’S UNIVERSITY HOSPITAL
IHFD AUDIT COORDINATOR: Ursula Kelleher
IHFD CLINICAL LEAD: Prof. Conor Hurson
IHFD CLINICAL LEAD: Dr Rachael Doyle
IHFD AUDIT COORDINATOR: Philomena Gallagher
IHFD AUDIT COORDINATOR: Mary Mullen
IHFD AUDIT COORDINATOR: Karen Fitzpatrick
IHFD CLINICAL LEAD: Mr James Cashman
IHFD CLINICAL LEAD: Prof Joe Duggan
MATER MISERICORDIAE UNIVERSITY HOSPITAL
CONNOLLY HOSPITAL
IHFD AUDIT COORDINATOR: Jacinta Shields
IHFD CLINICAL LEAD: Mr Paddy Kenny
BEAUMONT HOSPITAL
IHFD AUDIT COORDINATOR: Anthony O’Loughlin
IHFD AUDIT COORDINATOR: Andrea Ormond
IHFD AUDIT COORDINATOR: Ruth Kavanagh
IHFD CLINICAL LEAD: Dr Linda Brewer
IHFD AUDIT COORDINATOR: Pheadra Monahan
IHFD CLINICAL LEAD: Mr Aaron Glynn
IHFD CLINICAL LEAD: Dr Helen O’Brien
OUR LADY OF LOURDES HOSPITAL, DROGHEDA
TALLAGHT UNIVERSITY HOSPITAL
IHFD AUDIT COORDINATOR: Pauline Harrison
IHFD CLINICAL LEAD: Prof. Tara Coughlan
IHFD CLINICAL LEAD: Mr Brendan O’Daly
CHAPTER 2
*We would also like to acknowledge Rosemary Masterson, Dr Conor Skerrit, Dr Siobhan Forman for collecting hip fracture data in 2020 in National Orthopaedic Hospital Cappagh
CONTENTS >
IHFD AUDIT COORDINATOR: Breda Conlon
IHFD CLINICAL LEAD: Ms Dorothy Niall
MIDLANDS REGIONAL HOSPITAL, TULLAMORE
ST JAMES’S HOSPITAL
IHFD AUDIT COORDINATOR: Ricardo Paco
IHFD CLINICAL LEAD: Mr Tom McCarthy
IHFD CLINICAL LEAD: Prof C. Geraldine McMahon


IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 33
CHAPTER 3DATA
QUALITYRelevance
Accessibility and clarity
Timeliness and punctuality
Coherence and comparability
Accuracy and reliability
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT34
DATA QUALITY STATEMENTDimensions of data quality
Assessment of dimension (IHFD)
RELEVANCE The IHFD updated the dataset for 2020 at the final IHFD Governance Committee meeting held in 2019. New variables implemented from 1 January 2020 included ‘is pre-fracture mobility documented’, ‘assessed by candidate/advanced nurse practitioner gerontology/orthopaedics’ and ‘reason why patients were not mobilised on the day after surgery’. New data fields were implemented through the monthly audit coordinator teleconferences and supporting documents. In 2020, four research requests were received. The quarterly reports have continued to evolve.
ACCURACY AND RELIABILITY
The accuracy of data refers to how closely the data correctly describe what they were designed to measure. Reliability refers to whether those data consistently measure, over time, the reality of the metrics that they were designed to represent. The reference population for the national report is limited to patients aged 60 years and over. The coverage for the reference population is part of the BPT, and the standard per reporting quarter is 90%. All hospitals achieved this standard for 2020. The overall national data coverage for the Irish Hip Fracture Database National Report 2020 is 99%. The DVRs are completed alongside the IHFD quarterly reports. Since the introduction of the DVRs, the data quality has continued to improve.
TIMELINESS AND PUNCTUALITY
NOCA issues data collection targets for each hospital to collect a minimum of 90% of its data per reporting quarter; a data collection calendar is used to assist in this process. The submission timeliness per quarter (i.e. the proportion of eligible cases on HIPE with IHFD data added) for 2020 was as follows: Quarter 1: 98%; Quarter 2: 98%; Quarter 3: 97%; and Quarter 4: 99%. The cumulative total at the end of the reporting period was 99%. The closing date for data entry for 2020 was revised to 30 April 2021, which is 4 weeks later than normal, due to disruption caused by the COVID-19 pandemic.
COHERENCE AND COMPARABILITY
Data are collected using national and international classifications, e.g. the International Classification of Diseases. The IHFS are evidence-based clinical standards of care adopted from the international literature and are comparable with many international hip fracture registers (Johansen et al., 2017). In 2020, data from multiple hip fracture registers were used and continue to be used in order to understand the impact of the COVID-19 pandemic on care for hip fracture patients.
ACCESSIBILITY AND CLARITY
The data for the audit are reported online via www.noca.ie. They are reported at hospital level. Infographics and summary reports ensure that the data are clear and easy to understand.
CHAPTER 3: DATA QUALITYThe purpose of the data quality statement is to highlight the assessment of the quality of the IHFD 2020 data using dimensions of data quality as laid out in Guidance on a data quality framework for health and social care (Health Information and Quality Authority, 2018) (Table 3.1) .
TABLE 3.1: OVERVIEW OF DATA QUALITY FOR THE IHFD 2020
CHAPTER 3
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 35
DATA COVERAGEThe final dataset used for this report includes 3,666 cases from 16 participating hospitals, with the number of cases ranging from 127 to 461 per hospital. Coverage is defined as the number of hip fracture cases with appropriate hip fracture diagnosis codes on HIPE which have additional IHFD data added to them and which meet the inclusion criteria detailed in Chapter 2. The coverage for 2020 is representative of all HIPE hip fracture cases coded with additional IHFD data for the 16 participating hospitals for the reference population highlighted in Chapter 2; this was calculated at 99%. Individual hospital coverage ranges from 97% to 100%.
DATA VALIDATIONIn 2020, the data were validated quarterly in line with the IHFD quarterly reports using the DVRs.
FIGURE 3.1: COVERAGE PERCENTAGES PER HOSPITAL, 2020
FIGURE 3.1 COVERAGE PERCENTAGES PER HOSPITAL 2020
110000%%
110000%%
110000%%
110000%%
110000%%
110000%%
110000%%
110000%%
110000%%
9999%%
9988%%
9988%%
9988%%
9988%%
9988%%
9977%%
9999%%
00%% 2200%% 4400%% 6600%% 8800%% 110000%%
BBeeaauummoonntt
CCoonnnnoollllyy
CCoorrkk
DDrroogghheeddaa
SStt VViinncceenntt’’ss
KKeerrrryy
LLeetttteerrkkeennnnyy
TTuullllaammoorree
MMaatteerr
WWaatteerrffoorrdd
LLiimmeerriicckk
TTaallllaagghhtt
MMaayyoo
GGaallwwaayy
SSlliiggoo
SStt JJaammeess’’ss
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
CHAPTER 3
CONTENTS >


IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 37
CHAPTER 4IRISH HIP FRACTURE
STANDARDS AND BEST PRACTICE TARIFF
IHFS 1: Time to orthopaedic
ward <4hours
IHFS 2:
Time to surgery <48 hours
IHFS 4:
Review by geriatrician
IHFS 6: Specialist falls
assessment
IHFS 3: Pressure ulcers
IHFS 7: Mobilised by
physiotherapist
4 48
Pressure Ulcers to Zero
IHFS 5: Bone health assessment
IRISH HIP FRACTURE
STANDARDS
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT38
CHAPTER 4: IRISH HIP FRACTURE STANDARDS AND BEST PRACTICE TARIFF This chapter focuses on the individual hospitals’ performance across the seven IHFS for clinical care. Each IHFS includes a figure showing the hospitals’ performance for 2019 and 2020 with the exception of IHFS 7 which was only introduced in 2020. This information is intended to allow hospitals to benchmark their individual performance against their previous performance and against other hospitals’ performance. There were improvements from 2019 to 2020 in IHFS 1 and IHFS 6. Despite the impact that COVID-19 had on the health service as a whole, there was only a slight decline in IHFS 2 and 5, with IHFS 3 and 4 remaining at the same level as 2019. Table 4.1 shows the definitions of the IHFS and Best Practice Tariff Measures.
CHAPTER 4
TABLE 4.1: IRISH HIP FRACTURE STANDARDS AND BEST PRACTICE TARIFF MEASURES
IRISH HIP FRACTURE STANDARDS BEST PRACTICE TARIFF MEASURES
IHFS 1: Patients with hip fracture should be admitted to an acute orthopaedic ward within four hours of presentation or brought directly to the theatre from the emergency department (ED) within four hours.
If patients are admitted to an orthopaedic ward within four hours of presentation, or if they go straight from the ED to the theatre within four hours, they meet IHFS 1.
IHFS 2: Patients with hip fracture should have surgery within 48 hours of admission, and during normal working hours (Monday to Sunday, 08.00–17.59).
If patients receive surgery within 48 hours and during normal working hours, they meet IHFS 2.
IHFS 3: Patients with hip fracture should be assessed and cared for with a view to minimising their risk of developing a pressure ulcer.
If patients do not develop a new Grade 2 or higher pressure ulcer during admission, they meet IHFS 3.
IHFS 4: Patients with a hip fracture should be reviewed routinely by a geriatrician or advanced nurse practitioner during their admission.
If patients are reviewed by a geriatrician or advanced nurse practitioner they meet IHFS 4
IHFS 5: Patients with hip fracture should have their bone health assessed to determine their need for therapy to prevent future osteoporotic fractures.
If patients receive a bone health assessment, they meet IHFS 5.
IHFS 6: Hip fracture patients should receive a specialist falls assessment and intervention to prevent further falls.
If patients receive a specialist falls assessment, they meet IHFS 6.
IHFS 7: Patients with a hip fracture should be mobilised on the day of or after surgery by a physiotherapist.
If patients are mobilised on the day of or day after surgery by a physiotherapist, they meet IHFS 7.
Minimum quarterly data coverage of 90% is required by individual hospitals.
Evidence of a local HFGC must be present in each hospital.
4
48
Pressure Ulcers to Zero
90%
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 39
CHAPTER 4
Figure 4.1 shows the national compliance with the IHFS from 2017 to 2020.
FIGURE 4.1: PERCENTAGE OF PATIENTS NATIONALLY WHO MET EACH IRISH HIP FRACTURE STANDARD IN 2017 (N=3497), 2018 (N=3751), 2019 (N=3701) AND 2020 (N=3666)
FIGURE 4.1 PERCENTAGE OF PATIENTS NATIONALLY WHO MET EACH IHFS IN 2017 (N=3497), 2018 (N=3751), 2019 (N
IIHHFFSS 11 IIHHFFSS 22 IIHHFFSS 33 IIHHFFSS 44 IIHHFFSS 55 IIHHFFSS 66 IIHHFFSS 77
22001177 1111%% 6699%% 33%% 5500%% 7733%% 4477%% 7733%%
22001188 1177%% 7722%% 33%% 6699%% 8844%% 7700%% 7744%%
22001199 2255%% 7766%% 33%% 8822%% 9944%% 8833%% 7777%%
22002200 3333%% 7755%% 33%% 8822%% 9911%% 8855%% 7788%%
00%%
1100%%
2200%%
3300%%
4400%%
5500%%
6600%%
7700%%
8800%%
9900%%
110000%%
PPEERR
CCEENN
TTAAGG
EE
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT40
IHFS 1IHFS 1: PERCENTAGE OF PATIENTS ADMITTED TO AN ORTHOPAEDIC WARD WITHIN 4 HOURS OF FIRST PRESENTATION OR OR ADMITTED TO THEATRE FROM THE EMERGENCY DEPARTMENT WITHIN 4 HOURS
In 2020, 92% (n=3389) of hip fracture patients were admitted to an orthopaedic ward during their hospital admission, and 33% (n=1225) were admitted to an orthopaedic ward or were admitted to the operating theatre from the emergency department (ED) within 4 hours (Figure 4.2). The median time to admission to an orthopaedic ward in 2020 was 5.1 hours, an improvement from 6.6 hours in 2019. In 2020, the proportion of patients who met this standard at the individual hospital level ranged from 15% to 71%.
Although compliance with this standard is improving, there is an opportunity to learn more from the hospitals that are achieving greater levels of compliance with this standard. Of note, the trajectory of improvement in this IHFS was very notable following the start of the COVID-19 pandemic and continues to improve each quarter. It is worth examining what has changed about the ED processing and management of patients throughout the duration of the pandemic. Twelve of the participating hospitals made improvements in 2020. A combination of the National Ambulance Service (NAS) and Dublin Fire Brigade (DFB) pre-alerting hospitals of a suspected hip fracture, the use of messaging apps to alert the trauma service about new patients (e.g. the Siilo app) and new pathways for COVID-19- and non-COVID-19-related admissions seems to be having a very positive impact on IHFS 1.
4
CHAPTER 4
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 41
CHAPTER 4
FIGURE 4.2: IRISH HIP FRACTURE STANDARD 1: PERCENTAGE OF PATIENTS ADMITTED TO AN ORTHOPAEDIC WARD WITHIN 4 HOURS OR ADMITTED TO THEATRE FROM EMERGENCY DEPARTMENT WITHIN 4 HOURS, BY INDIVIDUAL HOSPITAL, 2019 (N=3701) AND 2020 (N=3666)
FIGURE 4.2 IHFS 1: PERCENTAGE OF PATIENTS ADMITTED TO AN ORTHOPAEDIC WARD WITHIN 4 HOURS OR ADMITT
1166%%
77%%
22%%
44%%
3333%%
1122%%
2233%%
2277%%
1177%%
3388%%
2277%%
1100%%
2255%%
5544%%
3399%%
5566%%
2255%%
1155%%
1166%%
2222%%
2244%%
2244%%
2266%%
2299%%
3300%%
3300%%
3311%%
3333%%
3333%%
3377%%
4444%%
4499%%
7711%%
3333%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%% 7700%% 8800%%
GGaallwwaayy
WWaatteerrffoorrdd
KKeerrrryy
TTaallllaagghhtt
MMaayyoo
BBeeaauummoonntt
LLeetttteerrkkeennnnyy
TTuullllaammoorree
MMaatteerr
SSlliiggoo
SStt VViinncceenntt’’ss
SStt JJaammeess’’ss
CCoonnnnoollllyy
LLiimmeerriicckk
CCoorrkk
DDrroogghheeddaa
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
22002200 22001199
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT42
CHAPTER 4
48IHFS 2IHFS 2: PERCENTAGE OF PATIENTS RECEIVING SURGERY WITHIN 48 HOURS OF FIRST PRESENTATION (AND WITHIN NORMAL WORKING HOURS)
In 2020, surgery was carried out on 95% (n=3485) of hip fracture patients. Analysis indicates that 75% (n=2598) of those surgeries were conducted within 48 hours and during working hours (Monday to Sunday, 8.00am–5.59pm) (Figure 4.3); this represents a slight decrease from 2019. The median time to surgery was 25.6 hours, similar to what was recorded in 2019. The proportion of patients who met this standard at the individual hospital level ranged from 60% to 93%. The variance in individual hospital performance remains a concern, as surgery is the single most important intervention for hip fracture care and recovery.
In 2020, 59% (n=2049) of surgeries were carried out by a consultant orthopaedic surgeon and 25% (n=872) were carried out by a specialist registrar (see Appendix 6).
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 43
CHAPTER 4
1 165 patients did not have surgery in 2019 and 181 patients did not have surgery in 2020.
FIGURE 4.3: IRISH HIP FRACTURE STANDARD 2: PERCENTAGE OF PATIENTS RECEIVING SURGERY WITHIN 48 HOURS (AND WITHIN NORMAL WORKING HOURS), BY INDIVIDUAL HOSPITAL, 2019 (n=3536) AND 2020 (n=3485)1
FIGURE 4.3 IHFS 2: PERCENTAGE OF PATIENTS RECEIVING SURGERY WITHIN 48 HOURS (AND WITHIN NORMAL WO
6677%%
6600%%
6677%%
6688%%
6600%%
7744%%
7755%%
8822%%
7744%%
8800%%
8888%%
8866%%
8877%%
8855%%
8877%%
9966%%
7766%%
6600%%
6666%%
6666%%
6666%%
6677%%
7711%%
7766%%
7777%%
7799%%
8833%%
8833%%
8844%%
8844%%
8855%%
8855%%
9933%%
7755%%
00%% 2200%% 4400%% 6600%% 8800%% 110000%%
CCoorrkk
DDrroogghheeddaa
LLiimmeerriicckk
KKeerrrryy
WWaatteerrffoorrdd
TTuullllaammoorree
BBeeaauummoonntt
LLeetttteerrkkeennnnyy
SStt JJaammeess’’ss
GGaallwwaayy
TTaallllaagghhtt
MMaayyoo
SSlliiggoo
MMaatteerr
CCoonnnnoollllyy
SStt VViinncceenntt’’ss
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
22002200 22001199
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT44
CHAPTER 4
IHFS 3IHFS 3: PERCENTAGE OF PATIENTS DEVELOPING A PRESSURE ULCER FOLLOWING ADMISSION
Of those patients who were discharged in 2020, 3% (n=102) developed a pressure ulcer following admission (Figure 4.4). The proportion of patients at the individual hospital level who had a pressure ulcer ranged from 1% to 9% in 2020. It is reassuring to see that compliance with IHFS 3 was unchanged during the COVID-19 pandemic; this is a testament to the excellent multidisciplinary care provided to hip fracture patients during a very challenging period for the health service. A multidisciplinary approach to pressure ulcer care includes participation in the HSE’s Pressure Ulcer to Zero (PUTZ) initiative, which includes, early and regular assessment of pressure areas, early surgery, early mobilisation, and nutritional assessment. For the purposes of this report, pressure ulcers Grade 2 or higher that developed after admission (but no later than 120 days after admission) are included.
Pressure Ulcers to Zero
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 45
CHAPTER 4
2 203 patients died in 2019 and 185 patients died in 2020. These patients have been excluded from the analysis.
FIGURE 4.4: IRISH HIP FRACTURE STANDARD 3: PERCENTAGE OF PATIENTS WHO DEVELOPED PRESSURE ULCERS FOLLOWING ADMISSION, BY INDIVIDUAL HOSPITAL, 2019 (n=3498) AND 2020 (n=3481)2
FIGURE 4.4 IHFS 3: PERCENTAGE OF PATIENTS WHO DEVELOPED PRESSURE ULCERS FOLLOWING ADMISSION, BY IN
22%%
44%%
55%%
1133%%
00%%
22%%
44%%
22%%
33%%
55%%
66%%
11%%
11%%
22%%
22%%
33%%
33%%
99%%
66%%
55%%
55%%
44%%
44%%
44%%
33%%
33%%
33%%
33%%
22%%
11%%
11%%
11%%
11%%
33%%
00%% 22%% 44%% 66%% 88%% 1100%% 1122%% 1144%%
MMaatteerr
SSlliiggoo
BBeeaauummoonntt
SStt JJaammeess’’ss
LLeetttteerrkkeennnnyy
GGaallwwaayy
TTuullllaammoorree
DDrroogghheeddaa
TTaallllaagghhtt
MMaayyoo
KKeerrrryy
WWaatteerrffoorrdd
CCoonnnnoollllyy
CCoorrkk
SStt VViinncceenntt’’ss
LLiimmeerriicckk
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
22002200 22001199
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT46
CHAPTER 4
IHFS 4IHFS 4: PERCENTAGE OF PATIENTS REVIEWED BY A GERIATRICIAN OR ADVANCED NURSE PRACTITIONER AT ANY POINT DURING ADMISSION
Figure 4.5 shows that, nationally, 82% (n=3017) of patients were reviewed by a geriatrician or by an advanced nurse practitioner (ANP) at some point during their acute stay in 2020. In addition, 39% (n=1444) of patients were seen pre-operatively by a geriatrician. Sixty-three percent (n=1855) of those reviewed by a geriatrician (n=2935) had their review carried out by a consultant geriatrician.
During 2020, it was deemed acceptable that a patient who was reviewed by an ANP specialising in orthogeriatrics/gerontology or other relevant specialty met IHFS 4. ANPs reviewed 11% (n=420) of all patients. Due to the growth of orthogeriatric services in many of the IHFD participant hospitals, work is now underway to further develop a consensus for a model of orthogeriatric care for Ireland.
The proportion of patients who met IHFS 4 at the individual hospital level in 2020 ranged from 27% to 100%. During the early part of the COVID-19 pandemic, many of the geriatricians and ANPs involved in the care of hip fracture patients were redeployed locally to support the efforts to deal with COVID-19 patients. However, this redeployment was relatively short-lived, and best practice for optimal hip fracture care (combining orthopaedics and geriatrics) resumed quite quickly. Thanks to the extraordinary efforts of the multidisciplinary teams supporting the orthogeriatric services, there was no reduction in compliance with IHFS 4 in 2020 compared to 2019.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 47
CHAPTER 4
FIGURE 4.5: IRISH HIP FRACTURE STANDARD 4: PERCENTAGE OF PATIENTS SEEN BY A GERIATRICIAN OR ADVANCED NURSE PRACTITIONER DURING ADMISSION, BY INDIVIDUAL HOSPITAL, 2019 (N=3701) AND 2020 (N=3666)
FIGURE 4.5 IHFS 4: PERCENTAGE OF PATIENTS SEEN BY A GERIATRICIAN DURING ADMISSION, BY INDIVIDUAL HOSP
6699%%
2244%%
4433%%
8811%%
8822%%
9900%%
7722%%
8822%%
9911%%
9988%%
9911%%
9955%%
9966%%
9988%%
9955%%
7755%%
8822%%
2277%%
4455%%
6644%%
7711%%
7733%%
7733%%
7744%%
8822%%
8866%%
8877%%
9911%%
9944%%
9955%%
9955%%
9977%%
110000%%
8822%%
00%% 2200%% 4400%% 6600%% 8800%% 110000%%
LLeetttteerrkkeennnnyy
KKeerrrryy
CCoonnnnoollllyy
LLiimmeerriicckk
SSlliiggoo
MMaayyoo
TTaallllaagghhtt
TTuullllaammoorree
MMaatteerr
DDrroogghheeddaa
WWaatteerrffoorrdd
SStt JJaammeess’’ss
GGaallwwaayy
SStt VViinncceenntt’’ss
BBeeaauummoonntt
CCoorrkk
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
22002200 22001199
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT48
CHAPTER 4
3 185 patients died in 2020. These patients have been excluded from the analysis.4 Percentages may not sum to 100% due to rounding.
IHFS 5IHFS 5: PERCENTAGE OF PATIENTS RECEIVING A BONE HEALTH ASSESSMENT
In 2020, a bone health assessment was carried out on 91% (n=3180) of patients (Figure 4.6). Thirty-five percent (n=1267) of patients were recorded as having a previous fragility fracture (Appendix 6). This increase in recording of previous fragility fractures is likely a reflection of a more detailed past medical history being recorded in the patient’s medical notes due to the input from geriatricians and ANPs and is more in line with international evidence of previous fragility fractures. Ninety-five percent (n=3485) of all hip fractures in 2020 resulted from low-energy trauma (Appendix 6).
FIGURE 4.6: IRISH HIP FRACTURE STANDARD 5: PERCENTAGE OF PATIENTS WHO RECEIVED A BONE HEALTH ASSESSMENT IN 2020 (n=3481)3,4
FIGURE 4.6 IHFS 5: PERCENTAGE OF PATIENTS WHO RECEIVED A BONE HEALTH ASSESSMENT IN 2020 (n=3481)
99%%
99%%
66%%
55%%
1133%%
5599%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%% 7700%%
AAwwaaiittss oouuttppaattiieenntt aasssseessssmmeenntt
NNoo aasssseessssmmeenntt
AAsssseesssseedd –– nnoo bboonnee pprrootteeccttiioonn mmeeddiiccaattiioonn
AAwwaaiittss dduuaall--eenneerrggyy XX--rraayyaabbssoorrppttiioommeettrryy ssccaann
CCoonnttiinnuueedd ffrroomm pprree--aaddmmiissssiioonn
SSttaarrtteedd oonn tthhiiss aaddmmiissssiioonn
PPEERRCCEENNTTAAGGEE
BBOO
NNEE
HHEEAA
LLTTHH
AASSSS
EESSSSMM
EENNTT
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 49
CHAPTER 4
5 203 patients died in 2019 and 185 patients died in 2020. These patients have been excluded from the analysis.
Figure 4.6A shows that 10 of the participating hospitals achieved at least 90% compliance with this standard in 2020. The proportion of patients who had a bone health assessment at the individual hospital level ranged from 62% to 100% in 2020.
FIGURE 4.6A: IRISH HIP FRACTURE STANDARD 5: PERCENTAGE OF PATIENTS WHO RECEIVED A BONE HEALTH ASSESSMENT, BY INDIVIDUAL HOSPITAL, 2019 (n=3498) AND 2020 (n=3481)5
FIGURE 4.6A IHFS 5: PERCENTAGE OF PATIENTS WHO RECEIVED A BONE HEALTH ASSESSMENT, BY INDIVIDUAL HO
7722%%
7788%%
9977%%
9911%%
9988%%
9900%%
9944%%
9922%%
110000%%
9977%%
9966%%
9988%%
9977%%
9999%%
9977%%
9988%%
9944%%
6622%%
8833%%
8844%%
8866%%
8877%%
8899%%
9911%%
9922%%
9922%%
9955%%
9966%%
9966%%
9977%%
9988%%
110000%%
110000%%
9911%%
00%% 2200%% 4400%% 6600%% 8800%% 110000%%
CCoonnnnoollllyy
KKeerrrryy
LLiimmeerriicckk
SSlliiggoo
DDrroogghheeddaa
MMaayyoo
MMaatteerr
WWaatteerrffoorrdd
LLeetttteerrkkeennnnyy
SStt JJaammeess’’ss
TTuullllaammoorree
GGaallwwaayy
BBeeaauummoonntt
SStt VViinncceenntt’’ss
CCoorrkk
TTaallllaagghhtt
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
22002200 22001199
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT50
CHAPTER 4
IHFS 6IHFS 6: PERCENTAGE OF PATIENTS RECEIVING A SPECIALIST FALLS ASSESSMENT
Eighty-five percent (n=2946) of hip fracture patients had a specialist falls assessment during their admission in 2020 (Figure 4.7). This represents a two-percentage-point improvement from 2019. There continues to be variance in the level of compliance across the 16 participating hospitals, ranging from 49% to 100% in 2020. A specialist falls assessment should include a falls history (noting previous falls), cause of index fall (including medication review), and risk factors for falling and injury (including fracture). From this information, a plan of action to prevent further falls should be formulated.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 51
CHAPTER 4
6 203 patients died in 2019 and 185 patients died in 2020. These patients have been excluded from the analysis.
FIGURE 4.7: IRISH HIP FRACTURE STANDARD 6: PERCENTAGE OF PATIENTS WHO RECEIVED A SPECIALIST FALLS ASSESSMENT, BY INDIVIDUAL HOSPITAL, 2019 (n=3498) AND 2020 (n=3481)6
FIGURE 4.7 IHFS 6: PERCENTAGE OF PATIENTS WHO RECEIVED A SPECIALIST FALLS ASSESSMENT, BY INDIVIDUAL H
2277%%
4433%%
9966%%
8822%%
8844%%
8899%%
7700%%
8822%%
9988%%
8888%%
9966%%
9977%%
9977%%
9988%%
9999%%
7744%%
8833%%
4499%%
4499%%
7722%%
7744%%
7744%%
7744%%
7777%%
8833%%
8877%%
9911%%
9911%%
9944%%
9977%%
9988%%
9988%%
110000%%
8855%%
00%% 2200%% 4400%% 6600%% 8800%% 110000%%
KKeerrrryy
CCoonnnnoollllyy
LLeetttteerrkkeennnnyy
LLiimmeerriicckk
SSlliiggoo
MMaayyoo
TTaallllaagghhtt
TTuullllaammoorree
DDrroogghheeddaa
WWaatteerrffoorrdd
MMaatteerr
SStt JJaammeess’’ss
BBeeaauummoonntt
GGaallwwaayy
SStt VViinncceenntt’’ss
CCoorrkk
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
22002200 22001199
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT52
CHAPTER 4
IHFS 7IHFS 7: PERCENTAGE OF PATIENTS MOBILISED BY A PHYSIOTHERAPIST ON THE DAY OF OR DAY AFTER SURGERY
In 2020, IHFS 7 was introduced as a new standard with the plan to include it in the Best Practice Tariff (BPT) from 2022 onwards. Early mobilisation has been shown to reduce the risk of in-hospital mortality following hip fracture (Ferris et al., 2020) and to increase the likelihood of discharge home from hospital (Ferris et al., 2021). In 2020, 78% (n=2705) of patients achieved IHFS 7 (Figure 4.8). The IHFD has been reporting on early mobilisation since 2018 and it is considered one of the most influential modifiable factors for improving patient outcomes. The proportion of patients who met IHFS 7 at the individual hospital level ranged from 61% to 93% in 2020. The term mobilisation in this instance refers to the patient being stood out of bed at a minimum.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 53
CHAPTER 4
FIGURE 4.8: IRISH HIP FRACTURE STANDARD 7: PERCENTAGE OF PATIENTS MOBILISED BY A PHYSIOTHERAPIST ON THE DAY OF OR DAY AFTER SURGERY, BY INDIVIDUAL HOSPITAL, 2020 (N=3485)7
FIGURE 4.8: PERCENTAGE OF PATIENTS MOBILISED BY A PHYSIOTHERAPIST ON THE DAY OF OR DAY AFTER SURGERY
6611%%
6644%%
6655%%
7722%%
7733%%
7777%%
7799%%
7799%%
7799%%
8800%%
8811%%
9900%%
9911%%
9911%%
9933%%
9933%%
7788%%
00%% 2200%% 4400%% 6600%% 8800%% 110000%%
TTaallllaagghhtt
SStt VViinncceenntt’’ss
WWaatteerrffoorrdd
CCoorrkk
SSlliiggoo
BBeeaauummoonntt
TTuullllaammoorree
MMaayyoo
KKeerrrryy
DDrroogghheeddaa
CCoonnnnoollllyy
MMaatteerr
SStt JJaammeess’’ss
LLeetttteerrkkeennnnyy
LLiimmeerriicckk
GGaallwwaayy
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
7 181 patients did not have surgery in 2020
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT54
CHAPTER 4
During 2020, the COVID-19 pandemic had a huge impact on the Irish health service. The IHFD was able to produce two rapid learning reports during this period. These reports helped to inform the healthcare system how COVID-19 affected hip fracture patients in terms of activity, case mix, compliance with the IHFS, and outcomes. Case mix was largely the same, with slightly more patients being admitted from long-term care and with lower pre-fracture mobility.
Figure 4.9 shows admissions activity by month from January 2019 to November 2020. From the end of February 2020 onwards, there was a slight decrease in the number of admissions compared to the pre-COVID-19 period, but there may be some cases missing. Overall, hip fracture admissions remained at a high level despite the pandemic. In the initial weeks of the pandemic, acute hospitals created a lot of bed capacity in order to prepare for a potential surge in COVID-19 admissions; as such, many patient groups – including hip fracture patients – were diverted to other facilities. Some patients were operated on in the elective orthopaedic hospitals, such as National Orthopaedic Hospital Cappagh, and some were brought to private hospitals. Although we are confident that these numbers are small, there will be ongoing research done for this period and data from non-HSE hospitals will be sought. Data from National Orthopaedic Hospital Cappagh are included in this report, as that hospital had access to the IHFD Portal through HIPE.
FIGURE 4.9: MONTHLY HIP FRACTURE ACTIVITY BY MONTH BASED ON ADMISSION DATE (JANUARY 2019- NOVEMBE
MMeeaann
00
5500
110000
115500
220000
225500
330000
335500
440000
JJaann--
1199
FFeebb
--1199
MMaarr
--1199
AApprr
--1199
MMaayy
--1199
JJuunn--
1199
JJuull--
1199
AAuugg
--1199
SSeepp--
1199
OOcctt
--1199
NNoovv
--1199
DDeecc
--1199
JJaann--
2200
FFeebb
--2200
MMaarr
--2200
AApprr
--2200
MMaayy
--2200
JJuunn--
2200
JJuull--
2200
AAuugg
--2200
SSeepp--
2200
OOcctt
--2200
NNoovv
--2200
NNUU
MMBB
EERR OO
FF AA
DDMM
IISSSSII
OONN
SS
DDAATTEE
FIGURE 4.9: HIP FRACTURE ACTIVITY, BY MONTH, BASED ON ADMISSION DATE (JANUARY 2019–NOVEMBER 2020)
IMPACT OF THE COVID-19 PANDEMIC ON ACTIVITY AND IHFS
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 55
CHAPTER 4
One of the main focal points during the pandemic was the impact that it had on IHFS compliance. Figure 4.10 shows the compliance with each standard by month for the year leading up to the pandemic and until the end of 2020. There is a very noticeable drop in compliance with several IHFS in March and April 2020, when the first surge in hospitalisations from COVID-19 was expected. Findings from the hospital services survey conducted as part of the International Multicentre Project Auditing COVID-19 in Trauma & Orthopaedics (IMPACT) global study during this time showed that there was a lot of service restructuring, including the development of separate COVID-19 and non-COVID-19 ED admission pathways; staff redeployment, particularly health and social care professionals (HSCPs), geriatricians and nursing staff; and the reconfiguration of many of the orthopaedic wards in order to take other patients, just to name a few of the service changes. The full details can be found in the COVID-19 report 1.0: Service impact from COVID-19: Analysis based on Irish Hip Fracture Database June 2019-May 2020 (NOCA, 2020),and these were echoed in the recent publication by Hall et al. (2021) to which the IHFD contributed. Encouragingly, towards the end of 2020, compliance with many of the IHFS began to return to usual levels, and the level of staff redeployment was greatly reduced as the pandemic continued. Ultimately, as shown in this chapter, overall IHFS compliance remained at a very high level, which is directly attributable to the multidisciplinary teams in the hospitals working together during a very difficult time.
FIGURE 4.10: PERCENTAGE OF HIP FRACTURE PATIENTS WHO MET EACH OF THE SEVEN STANDARDS BY MONTH (January 2019-December 2020)
00%%
2200%%
4400%%
6600%%
8800%%
110000%%
JJaann--
1199
FFeebb
--1199
MMaarr
--1199
AApprr
--1199
MMaayy
--1199
JJuunn--
1199
JJuull--
1199
AAuugg
--1199
SSeepp--
1199
OOcctt
--1199
NNoovv
--1199
DDeecc
--1199
JJaann--
2200
FFeebb
--2200
MMaarr
--2200
AApprr
--2200
MMaayy
--2200
JJuunn--
2200
JJuull--
2200
AAuugg
--2200
SSeepp--
2200
OOcctt
--2200
NNoovv
--2200
DDeecc
--2200
PPEERR
CCEENN
TTAAGG
EE
DDAATTEE
IIHHFFSS 11:: AAddmmiitttteedd ttoo oorrtthhooppaaeeddiicc wwaarrdd wwiitthhiinn 44 hhoouurrss IIHHFFSS 22:: HHaadd ssuurrggeerryy wwiitthhiinn 4488 hhoouurrss
IIHHFFSS 33:: DDeevveellooppeedd aa pprreessssuurree uullcceerr IIHHFFSS 44:: SSeeeenn bbyy aa ggeerriiaattrriicciiaann
IIHHFFSS 55:: RReecceeiivveedd bboonnee hheeaalltthh aasssseessssmmeenntt IIHHFFSS 77:: MMoobbiilliisseedd bbyy pphhyyssiiootthheerraappiisstt
IIHHFFSS 66:: RReecceeiivveedd aa ssppeecciiaalliisstt ffaallllss aasssseessssmmeenntt
FIGURE 4.10: PERCENTAGE OF HIP FRACTURE PATIENTS WHO MET EACH OF THE SEVEN IRISH HIP FRACTURE STANDARDS, BY MONTH (JANUARY 2019–DECEMBER 2020)
From the end of February 2020 onwards, there was a slight decrease in the number of admissions compared to the pre-COVID-19 period, but there may be some cases missing. Overall, hip fracture admissions remained at a high level despite the pandemic.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT56
CHAPTER 4
TABLE 4.2: HIP FRACTURE PATIENTS WITH A DIAGNOSIS OF COVID-19
OUTCOMES2019 IHFD PATIENTS (N=3701)
2020 IHFD PATIENTS WITH COVID-19 (n=74)
Admitted to orthopaedic ward within 4 hours
25% 26% (n=19/74)
Received surgery within 48 hours*
76% 71% (n=20/68)
Developed a pressure ulcer**
3% ~
Reviewed by a geriatrician
82% 78% (n=58/74)
Received a bone health assessment**
94% 83% (n=44/53)
Received a specialist falls assessment**
83% 85% (n=45/53)
Mobilised by a physiotherapist*
78% 72% (n=49/68)
Inpatient mortality*** 5% 28% (n=21/74)
Mean LOS 20 days 33 days
Median LOS 12 days 25 days
* Includes only patients who had surgery** Includes only alive patients*** Cause of death is unknown ~ Denotes 10 cases or fewer
4
48
Pressure Ulcers to Zero
Table 4.2 compares the patients who had a hip fracture and a diagnosis of COVID-19 with all hip fracture patients from 2019. For 2020, 74 patients with IHFD data had a diagnosis of COVID-19. This group showed a lower level of compliance with the IHFS and had significantly increased mean and median length of stay (LOS) in hospital. Most noticeably, inpatient mortality increased from 5% in 2019 to 28% for this group in 2020. This is a small cohort of patients, so the data should be interpreted with caution; there will be further analysis conducted as more data become available for patients with both hip fracture and COVID-19.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 57
CHAPTER 4
BEST PRACTICE TARIFF
In 2018, the IHFD supported the introduction of the BPT. This process involved collaboration between the Healthcare Pricing Office, National Clinical Advisor and Group, the HSE, the National Clinical Programme for Trauma and Orthopaedic Surgery, and NOCA.
The BPT is a payment for hospitals operating on hip fracture patients (aged 60 years and over) which achieve eight standards of care for individual patients: the IHFS and two additional standards focusing on data quality and governance. The BPT is a performance incentive linked to quality care that is mandated by the IHFS and data quality standards (Table 4.1). Each hospital will receive €1,000 for every case that meets the BPT, and this money is to be used by the hospital to improve patient care within its trauma service. The BPT payment is structured so that 30% of the payment goes to hospital management and 70% to the trauma service. The BPT is reported quarterly to the IHFD participant hospitals, and the clinical lead for the local hip fracture governance committee (HFGC) links directly with the hospital finance manager to access the funds for the trauma service as designated by the HFGC. IHFS 7 will be included in the BPT payment in 2022.
Tariff-based incentives have been used in other healthcare systems internationally and may be associated with improved outcomes such as reduced mortality, reduced readmission rates and improved quality of care overall (Metcalfe et al., 2019); however, the potential unintended consequences of a tariff-based model need to be considered. The IHFD Research Group will evaluate the impact of the BPT and publish these findings.
This report shows that, despite the impact of the COVID-19 pandemic, data quality has continued to improve since 2019, with increased data coverage and clinical performance in 2020 that may or may not be entirely attributed to the introduction of the BPT since 2018. This level of improvement has been sustained and furthered from 2019.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT58
CHAPTER 4
BPT AND COVERAGEDuring the implementation of the BPT, the collection of sufficient data was ensured with the creation of an additional requirement for submitting 90% of data per reporting quarter and annually by each of the participating hospitals. In 2020, all eligible hospitals met this standard, and the level of coverage for the audit remained exceptionally high at 99%. Figure 4.11 shows the steady improvement in coverage each year since national reporting began for the IHFD.
FIGURE 4.11: IRISH HIP FRACTURE DATABASE COVERAGE, BY YEAR, 2013–2020
FIGURE 4.11 IHFD COVERAGE BY YEAR, 2013–2020
7788%%8844%% 8811%%
8866%%
9955%%9999%% 9999%% 9999%%
00%%
1100%%
2200%%
3300%%
4400%%
5500%%
6600%%
7700%%
8800%%
9900%%
110000%%
22001133 22001144 22001155 22001166 22001177 22001188 22001199 22002200
PPEERR
CCEENN
TTAAGG
EE
YYEEAARR
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 59
CHAPTER 4
BPT PAYMENTS BY HOSPITALIn 2018, the first financial payments of the BPT were issued to the IHFD participant hospitals. The payment increased from €278,000 in year one (2018) to €548,000 in year two (2019) and to €710,000 in year three (2020). That there is a clear correspondence between care standards and an incentivised payment has been borne out in data from the United Kingdom (UK) (Griffin et al., 2021).
A substantial amount of money has been paid out, and this has been shown to have had a positive effect on the trauma system overall, highlighting that 20% of patients with a hip fracture received the best practice standard of care in 2020, which represents a further improvement of five percentage points from 2019. The total payments that each hospital received for each quarter in 2020 are presented in Table 4.3.
Hospital Q1 2020 Q2 2020 Q3 2020 Q4 2020 Total
Midland Regional Hospital Tullamore €10 000 €13 000 €15 000 €3000 €41 000
St James’s Hospital €21 000 €5000 €12 000 €5000 €43 000
Tallaght University Hospital €12 000 €1000 €8000 €15 000 €36 000
Mater Misericordiae University Hospital €7000 €0 €0 €13 000 €20 000
St Vincent’s University Hospital €26 000 €24 000 €28 000 €17 000 €95 000
Connolly Hospital €15 000 €1000 €13 000 €10 000 €39 000
Our Lady of Lourdes Hospital Drogheda €33 000 €8000 €27 000 €22 000 €90 000
Beaumont Hospital €4000 €5000 €19 000 €20 000 €48 000
Letterkenny University Hospital €9000 €2000 €0 €3000 €14 000
Sligo University Hospital €12 000 €10 000 €4000 €3000 €29 000
University Hospital Galway €3000 €5000 €0 €8000 €16 000
Mayo University Hospital €6000 €3000 €3000 €0 €12 000
University Hospital Waterford €12 000 €18 000 €6000 €4000 €40 000
Cork University Hospital €37 000 €35 000 €31 000 €27 000 €130 000
University Hospital Kerry €0 €0 €0 €0 €0
University Hospital Limerick €33 000 €20 000 €0 €4000 €57 000
Total €240 000 €150 000 €166 000 €154 000 €710 000
TABLE 4.3: TOTAL BEST PRACTICE TARIFF PAYMENTS, BY QUARTER AND HOSPITAL, 2020
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT60
The money from the BPT was used at hospital level for the support of care in the trauma services; details of some of the purchases made using the money are shown by hospital in Table 4.4 Money was also allocated for quality improvement projects and for training and education of staff, including supporting staff to attend conferences and training and to carry out research.
Hospital Items purchased using BPT payments
Beaumont Hospital Electric beds; perching chairs; orientation clocks; lock slide sheets; Sara Steady one-person-use hoist; foot stools
Connolly Hospital Sara Steady standing hoist; return and bariatric return; theatre equipment; funding for ED training on fascia iliaca blocks
Cork University Hospital Thomas splints; bladder scanner; blocks education and equipment; operating theatre equipment; ward and office renovations; computers
Our Lady of Lourdes Hospital Drogheda
Plans to fund the IV Zoledronic Acid pathway; specialist seating; physiotherapy stairs; education; research
University Hospital Galway Bladder scanner for trauma ward
University Hospital Kerry N/A
Letterkenny University Hospital
Profiling bed for orthopaedic ward; cameras for orthopaedic theatre; ultrasound machine for ED orthopaedic library for ED continuous passive motion machine for orthopaedic ward
University Hospital Limerick
Additional physiotherapy and occupational therapy for accelerated discharge pathway directly home
Information booklet design and printing
Mater Misericordiae University Hospital
Orientation clocks, orthopaedic chairs, wheelchairs, bathroom aids, dynamaps, healthcare award application and conference fees for staff
Mayo University Hospital Had not yet been decided
Sligo University Hospital Hoist on ward; bladder scanner; portable ultrasound scanner; patient comfort chairs; underbody warming blanket in theatre; surgical research; orthopaedic theatre table; ED patient trolley with weighing facility (on order)
St James’s Hospital Scanning electron microscope scanner, arjo bed, barkby bariatric chairs, addons bed, oakham high back chair
St Vincent’s University Hospital
Osteoporosis & Metabolic conference Oxford; physiotherapy equipment; Musculoskeletal casting and splinting certificate; chairs and sofa; osteoporosis and metabolic bone research society training course; supply and fit PVC fr biosafe roller blinds; support for internal meetings
Tallaght University Hospital Orthopaedic chairs
Midland Regional Hospital Tullamore
Sara Steady standing aid; ReTurn and Belt; kitchen extension for trauma ward; Topro Taurus; photocopier for trauma ward; Lento Chair; TAC phoneVisual board; shelving for room in ward; computer for room in ward; library books; extra-wide chair; frames; parallel bars; gloves; Motomed Trainer; DopplerElectrocardiogram (ECG) machine; camera
University Hospital Waterford
Hip fracture Bleep; hip fracture trolley in ED; patient information leaflets from physiotherapists and occupational therapists traction attachment for beds; positioning cushion for radiology in order to facilitate lateral X-rays
TABLE 4.4: EXAMPLES OF ITEMS PURCHASED USING THE BEST PRACTICE TARIFF, BY HOSPITAL
CHAPTER 4
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 61
CHAPTER 4
BPT PAYMENTS AS A PROPORTION OF PATIENT VOLUME BY HOSPITALEach of the 16 hospitals participating in the IHFD had a different number of hip fracture patients in 2020, ranging from 127 to 461. Figure 4.12 shows what percentage of each hospital’s overall volume of hip fracture patients met the BPT. Figure 4.12 shows that 20% of all patients with a hip fracture received the best practice standard of care in 2020; this represents an improvement of five percentage points from 2019. Table 4.4 shows the amount of money paid to each hospital from the BPT.
FIGURE 4.12: PROPORTION OF HIP FRACTURE PATIENTS MEETING BEST PRACTICE TARIFF STANDARDS, BY HOSPITAL, 2020
FIGURE 4.12 PROPORTION OF PATIENTS MEETING BPT STANDARDS, BY HOSPITAL
00%%
77%%
99%%
1100%%
1100%%
1144%%
1177%%
1188%%
1199%%
1199%%
2211%%
2233%%
2255%%
2299%%
3300%%
4433%%
2200%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%%
KKeerrrryy
GGaallwwaayy
LLeetttteerrkkeennnnyy
WWaatteerrffoorrdd
MMaayyoo
MMaatteerr
LLiimmeerriicckk
TTaallllaagghhtt
CCoonnnnoollllyy
TTuullllaammoorree
BBeeaauummoonntt
SSlliiggoo
SStt JJaammeess''ss
CCoorrkk
SStt VViinncceenntt''ss
DDrroogghheeddaa
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT62
CHAPTER 4
GOLDEN HIP AWARD WINNER 2020Since 2017, the IHFD has been awarding the Golden Hip Award to the hospital with the greatest proportion of patients meeting the IHFS and BPT. In 2020, this award was given to Our Lady of Lourdes (OLOL) Hospital Drogheda, who also won the award in 2019. This year has seen OLOL Hospital Drogheda improve from 32% of patients meeting the IHFS and BPT in 2019 to 43% in 2020. The team in OLOL Hospital Drogheda describes below how they managed to achieve and sustain their improvements.
OUR LADY OF LOURDES HOSPITAL DROGHEDA
LEFT TO RIGHT: Lorraine Reynolds, Assitant Director of Nursing Emergency Department; Dr Helen O’Brien, Consultant Orthogeriatrician (Hip Fracture Committee Co-Chair); Thelma Halpin, Clinical Nurse Manager 2 Orthopaedics; Michelle Mc Court, Senior Orthopaedic Physiotherapist; Orla Cooney, Clinical Nurse Manager 1 Orthopaedic Theatre; Aiofe Mc Feeley, Orthogeriatric Registrar; Dr Matreja Prakash, Consultant Anaesthetist; Iffat Shoail, Occupational Therapist; Dr Farrah Mustafa, Consultant Emergency Department; Dr Niall O’Conor, Consultant Clinical Lead, Emergency Department; Mr Alan Walsh, Orthopaedic Consultant, Hip Fracture Committee Chair; Pheadra Monahan, CNM2 Orthopaedic Trauma Coordinator.
Colleagues in absentia: Bernadette Conlon, ANP Fragility Fractures; Ciaran Conlon, ADON Emergency Department; Danielle Carolan, Clinical Facilitator, CNM2; Eleanor Campbell, Senior Radiographer, Emergency Department; Eithne Dunnill, Unscheduled care, ADON; Shirley Timmons, Head of Bed Management; Dr Conor Kelly, Consult Emergency Department; Charlie Gordon, CNM2, Orthopaedic Theatre; Aine Davern, ADON, Orthopaedics and Surgery; Patricia Byrne, CNM1, Orthopaedics; Diane Britton, CNM1, Orthopaedics; Jennifer Keenan, CNM3, Orthopaedics and Surgery; Prof. Sherif El Masery, Surgical Clinical Director; Fiona Brady, General Manager; Sarah Mc Shane, Senior Physiotherapist; Annemarie Grogan, Dietician; Deirdre Bradley, SALT; Eilis Hand, Physiotherapist; Brendan Flemming, Physiotherapist; Elaine Mc Cabe, Physiotherapist; Sean Mc Entaggart, Physiotherapist; Janet Griffin, Physiotherapy Assistant; Rosie Taylor, Physiotherapy Assistant; Dr Patrick Doyle, Orthogeriatric Registrar; Dr Aidan Stankard, Orthogeriatric Registrar; Dr Naomi Davey, Orthogeriatric Reg; Dr Sarah Coveney, Orthogeriatric Reg; Mr Aaron Glynn, Orthopaedic Consultant; Mr Nasir Awan, Orthopaedic Consultant; Mr Amir Siddique, Orthopaedic Consultant; Mr Paul Harrington, Orthopaedic Consultant; Mr Muraili Sayana, Orthopaedic Consultant; Mr Khalid Khan, Orthopaedic Consultant; Mr Anant Mahapatra, Orthopaedic Consultant; Mr Mansoor Chaudhry, Orthopaedic Consultant; and the nurses and healthcare assistants involved in the care of our hip fracture patients.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 63
CHAPTER 4
Undoubtedly, the year 2020 will be forever etched in all of our minds, beginning with the rumblings of a new virus in the city of Wuhan, China surfacing in January. As COVID-19 reached our shores, the challenges continued to mount and by the end of the first quarter of 2020, our beloved orthopaedic ward had started to become the second high-intensity COVID-19 ward due to its individual rooms. This meant that all orthopaedic patients began to be redirected to an alternative surgical ward, losing the specialist skill set of the excellent Orthopaedic nursing and Multidisciplinary Team (MDT), who were required to stay on the ward. This team adapted well to managing acutely unwell COVID-19 patients, with their experience in managing perioperative medical complications being extremely beneficial. They upskilled in the management of patients on continuous positive airway pressure (CPAP) and bilevel positive airway pressure (BiPAP) on the ward and demonstrated how a true team works. The Trauma Coordinator Clinical Nurse Manager and the Fracture Liaison Service Advanced Nurse Practitioner (ANP) were redeployed to the acute ward and contact tracing, important roles at the beginning of the pandemic. The Orthogeriatrician and orthogeriatric team were redeployed to Acute Medicine at the end of the first quarter of 2020, and unfortunately, due to clinical commitments in Acute Medicine, it was no longer possible to deliver a proactive comprehensive geriatric assessment (CGA), falls and bone health assessment, or a management plan for all hip fracture and fragility fracture patients on admission. A reactive consult service was provided once aware of hip fracture patients and fragility fracture patients in the hospital. COVID-19 was everywhere and, as you are surely aware, hospital staff took a risk just turning up to work.
By the end of the second quarter of 2020, the orthopaedic ward, having weathered the first wave, was gradually returning to its original function. Hip fracture patients began to be admitted directly to the ward, once again benefitting from the orthopaedic nursing, orthopaedic team and MDT skill set. The orthogeriatric team was reinstated at this time, a move that was supported by NOCA’s position on the preservation of services for orthopaedic patients. As wave two of COVID-19 hit, there
was clear evidence that, as infection rates were high in the community and in residential care settings, orthopaedic patients were not only being admitted with fractures, but COVID-19 was becoming a precipitating factor in their falls.
Huge challenges faced the team and patients alike. Following on from 2019, in the first quarter of 2020, 56% of hip fracture patients in OLOL Hospital Drogheda met all of the IHFS and BPT standards. However, as the orthopaedic ward became a COVID-19 ward and specialist services were redeployed, only 18% of hip fracture patients met all of the IHFS and BPT standards in the second quarter of 2020. This further highlights the need for a dedicated orthopaedic ward at all times and a dedicated orthogeriatric service. The third quarter of 2020 saw improvements once normal services were resumed, with 47% of all hip fracture patients achieving all IHFS and BPT standards; this was maintained into the fourth quarter, with 45% of all hip fracture patients achieving all IHFS and BPT standards. When all orthopaedic services were preserved, almost one-half of hip fracture patients in OLOL Hospital Drogheda in 2020 achieved all national IHFS and BPT standards, which is an improvement from about one-third of hip fracture patients in 2019. This amounted to €90,000 in BPT revenue for hip fracture patients and orthopaedic patients in OLOL Hospital Drogheda in 2020.
As a team, we have maintained and improved upon the number of patients meeting all of the IHFS and BPT standards in OLOL Hospital Drogheda from 2019 to 2020. This is largely due to the continued efforts of a committed and motivated team, including the orthopaedic nursing team, the orthopaedic team, the orthogeriatric team, the Trauma Coordinator, the Fracture Liaison Service ANP, the ED team, the radiography team, the healthcare assistants, the bed management and unscheduled care team, the Surgical Assistant Director of Nursing, the General Manager and Senior Management Team, and, last but certainly not least, the extremely important and dedicated MDT of physiotherapists, occupational therapists, dieteticians, speech and language therapists, and medical social work. Maintaining IHFS 1, the percentage of patients admitted to the orthopaedic ward within 4 hours, is essential to
GOLDEN HIP AWARD STORY TWO: THE SEQUEL
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT64
CHAPTER 4
success in the IHFS and BPT standards and we managed to consistently achieve this for between 72% and 79% of hip fracture patients when services were intact. This was achieved through the ongoing use of our streamlined hip fracture pathway, buy-in from every member of the Hip Fracture Pathway Subgroup, education on IHFS at Orthopaedic Induction meeting, continuous audit by the Trauma Coordinator of IHFS 1, and regular meetings to address any patients not meeting this standard.
IHFS 1 (time to the ward) has a direct impact on the other IHFS, particularly IHFS 2 (time to surgery <48 hours) and IHFS 3 (pressure ulcers). The sooner the patient is on the orthopaedic ward, the sooner they are placed on a pressure-relieving mattress and receive proactive care from the orthopaedic nurses and MDT; it is therefore important to comprehensively address IHFS 1. This standard also impacts on when the orthogeriatric team can review the patient – which ideally is pre-operatively – in order to provide a prompt CGA, complete a medications review, rationalise polypharmacy, coordinate which medications need to be held perioperatively, and medically optimise the patient for theatre. Furthermore, early review by a geriatrician assists our anaesthetic colleagues in assessing patients’ fitness for theatre. Ongoing orthogeriatric review throughout the patient’s admission allows for an individualised bone protection plan, a collaborative multidisciplinary falls assessment with a focus on syncope overlap, and the prompt management of perioperative medical complications. The MDT is key to ensuring prompt rehabilitation with the aim of home discharge and identifying patients for off-site rehabilitation. A weekly MDT meeting guides rehabilitation goals and is patient-centred, adopting the ethos of “what matters to me”. The new IHFS 7 (mobilised on the day of or day after surgery by a physiotherapist) will also continue to focus the team on the importance of early mobilisation associated with reduced risk of delirium and mortality.
When comparing local IHFS compliance in OLOL Hospital Drogheda with national figures, ongoing challenges and goals for the future are highlighted. Compliance with IHFS 1 (time to the ward) in OLOL Hospital Drogheda stands at 71%, compared with the national average of 33%. The reasons for our ability to maintain
this have been outlined above. Conversely, IHFS 2 (time to surgery <48 hours) is clearly an ongoing challenge in OLOL Hospital Drogheda and remains at 66%, below the national average of 75%. Reasons for this are multifactorial: the second trauma theatre remains unopened, with “not enough time” often quoted as the principal reason for cancellation; the provision of paediatric orthopaedic surgery; the lack of protected hip fracture patient theatre slots; and day-to-day continuity challenges. Interestingly, compliance with the time to theatre standard increased to 75% in Quarter 3, on par with the national average, which indicates that theatre access improved following the cancellation of elective surgeries during COVID-19. Delays to theatre for frail, older hip fracture patients directly impacts on their mortality risk, complication risk, length of stay (LOS) and ability to mobilise on the day of or day after surgery. The Senior Management Team has recently set up a new working group to address IHFS 2 compliance, with the goal of improving our times to theatre. IHFS 3 (the rate of pressure ulcers) in OLOL Hospital Drogheda was 3% in 2020, the same as the national average. This is a concern for our site and has been reviewed, as we noted a rise in the pressure ulcer rate in the second half of 2020. This was the result of a lag effect from orthopaedic patients not being admitted to the specialist orthopaedic ward and services being redeployed in the second quarter of 2020. It was further compounded by the loss of our dedicated orthopaedic ward dietician in these quarters due to COVID-19; this individual has only recently been reinstated. IHFS 4, 5 and 6 in OLOL Hospital Drogheda all stand at 87%, compared with the national averages of 82%, 91% and 85%, respectively. This is likely due to the majority of orthogeriatric services across the country being redeployed to provide acute medical cover during COVID-19. IHFS 7 (mobilised on the day of or day after surgery by a physiotherapist) was consistently above the national average in each quarter, standing at 80% compared with 78%. The physiotherapy department is currently auditing IHFS 7 for 2021, looking at reasons why patients are not mobilised on the day of or day after surgery. This will include whether these patients were complaining of pain, had adequate analgesia prescribed, were delirious, were medically unwell, had a delay to theatre longer than 48 hours, or had a nerve block in the ED on admission. We will continue to strive to achieve the IHFS and BPT
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 65
CHAPTER 4
standards for all of our patients, as we know that this results in improved care across the board for all orthopaedic patients.
Maintaining the IHFS and striving for improvements in care for hip fracture patients has always been at the forefront of the team’s shared vision for OLOL Hospital Drogheda for 2020. As a team, individuals from all disciplines are members of the HFGC and attend the committee meetings. At these meetings, good performance is rewarded through approval to purchase items from each discipline’s equipment “wish list”. Following on from the team’s success in 2019, we used the BPT money awarded to purchase a bladder scanner for the ward, low-low beds for patients with a high risk of falls or with delirium, dementia-friendly clocks for patient rooms, and orthopaedic equipment for operating theatre. Excellent nursing leadership and ongoing motivation to undertake higher education and training qualifications has led to the upskilling of all healthcare workers on the ward in delirium recognition. Proactive identification of patients at high risk of falls is routine on the ward.
An additional ongoing challenge facing OLOL Hospital Drogheda is the large catchment area and the difficulty in gaining access to appropriate rehabilitation not only for our hip fracture patients, but for all orthopaedic patients. One positive outcome of the COVID-19 pandemic was the development of five dedicated orthogeriatric rehabilitation beds in Louth County Hospital (LCH) in June 2020. Although this led to improvements in LOS over the course of the year, LOS was still above the national average by 1 day in the fourth quarter of 2020. Unfortunately, a COVID-19 outbreak in the rehabilitation unit in December 2020 led to rehabilitation once again being interrupted and curtailed. At present, there is no MDT in LCH able to provide orthogeriatric rehabilitation due to resource issues. We are delighted to hear that orthogeriatric rehabilitation will recommence with appropriate physiotherapy, occupational therapy, and medical social work cover at the end of August 2021, and are grateful to the Senior Management Team for supporting this initiative. We greatly appreciate the ongoing support from the Monaghan Rehabilitation Unit for patients from this catchment area. We hope to develop stronger links with other rehabilitation units outside our Hospital Group in order to improve on pathways to rehabilitation for
patients from this geographical catchment area. It is important that these patients’ rehabilitation needs are met.
An exciting development over the last year has been the expansion of the Fracture Liaison Service (FLS) and OLOL Hospital Drogheda’s participation in the FLS pilot database. The Orthopaedic Clinical Lead assisted in ensuring that OLOL Hospital Drogheda was included as a pilot site. We are very fortunate to have an FLS ANP who has led the further development of the Intravenous Zoledronic acid day ward service, the coordination of bone protection treatment plans, the bone protection database, and the education of patients on their individualised treatment. The FLS ANP has set up virtual adherence and follow-up clinics at 4 months and 1 year following hip fracture and other fragility fractures as required. There are also two FLS clinics run in collaboration with the FLS ANP, with the Orthogeriatrician seeing all patients aged over 65 years and the Endocrinologist seeing those aged under 65 years with fragility fractures at true osteoporotic sites. Other patients admitted with fragility fractures at non-classical osteoporotic sites are seen routinely in a proactive consultation by the orthogeriatric team and the FLS ANP as the patients are admitted to the orthopaedic ward.
Other exciting new projects underway include the development of an analgesic pathway for use in orthopaedic patients aged both over and under 65 years. This has been completed in collaboration with the pain team, clinical pharmacy, the FLS ANP and the Orthogeriatrician. The ED is also undertaking a quality improvement project to improve the number of hip fracture patients receiving fascia iliaca nerve blocks on arrival in ED. Furthermore, the Cottage Day Hospital has opened and rolled out an FLS clinic as well. We are also very fortunate to have a senior specialist physiotherapist leading a new falls prevention class, with input from our Senior Day Hospital Dietician with an interest in sarcopenia and frailty, and from our Senior Day Hospital Occupational Therapist regarding fall safety strategies. Continued support from the General Manager and the Senior Management Team will allow our service to develop further, with improved times to theatre and access to rehabilitation for all of our patients. We are extremely grateful for their support of the orthopaedic service so that we can continue to deliver the right care, in the right place, at the right time, with the right team.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT66
KEY FINDINGS FROM CHAPTER 4
• In 2020, 92% of patients were admitted to an orthopaedic ward, compared with 95% in 2019.
• One-third of patients were admitted to an orthopaedic ward or to the operating theatre from the ED within 4 hours, compared with only one-quarter of patients in 2019.
• In 2020, 75% of surgeries were conducted within 48 hours and within normal working hours. This has remained almost the same since 2019, while the median time to surgery has decreased slightly to 25.6 hours.
• A geriatrician or an ANP reviewed 82% of patients at some point during their acute stay in 2020.
• In 2020, a bone health assessment was carried out on 91% of patients nationally (compared with 94% in 2019).
• Prior to discharge, 85% of patients nationally had a specialist falls assessment in 2020.
• The total money paid out as a result of the BPT for 2020 was €710,000, with 20% of all hip fracture patients nationally meeting the IHFS and achieving the BPT. This represents an improvement of five percentage points from 2019.
• Our Lady of Lourdes Hospital Drogheda had the highest proportion of patients meeting the BPT, with 43% of their patients receiving this level of care.
CHAPTER 4
CONTENTS >

CHAPTER 5CASE MIX
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT68
CHAPTER 5: CASE MIX
CHAPTER 5
GENDER AND AGE
8 An AMT score was recorded for 718 patients only.
33% 67%AGED 60-69
15%
AGED 90+
11% 11%
AGED 80-89
41%41%
AGED 70-79
33%
12%
13% 43%29% 16%
SOURCE OF ADMISSION
ABBREVIATED MENTAL TEST (AMT)8
4AT (RAPID CLINICAL TEST FOR DELIRIUM)
of hip fracturepatients were
admitted from home
85%of patients were transferred from another hospital
4%were admitted from a nursing home or other
long-stay facility
11%
AGE 79 (MEAN)
AGE 81 (MEAN)
31% OF PATIENTS HAVE COGNITIVE IMPAIRMENT
69% OF PATIENTS HAVE NORMAL COGNITION
33%
44% had a 4AT recorded on Day 1
26% had a 4AT recorded on Day 3
36% had a 4AT
recorded on day of discharge
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 69
CHAPTER 5
9 333 patients did not have an ASA grade recorded and have been excluded from the analysis.10 Only patients with scores for all three types of mobility are included in this analysis; 311 patients did not have an NMS recorded for either indoor
walking, outdoor walking, or shopping.
PRE-FRACTURE MOBILITY, NEW MOBILITY SCORE10
AMERICAN SOCIETY OF ANESTHESIOLOGISTS (ASA) PHYSICAL STATUS CLASSIFICATION (DRIPPS, 1963)9
FRACTURE TYPE
LOW FUNCTIONAL ABILITYHIGH FUNCTIONAL ABILITY
47% 53%
INTRACAPSULAR UNDISPLACED
8%
SUBTROCHANTERIC
6%
INTERTROCHANTERIC
37%
INTRACAPSULAR DISPLACED
40%
GRADE
1GRADE
3GRADE
2GRADE
4GRADE
5Healthy person
Severe systemic disease
Mild systemic disease
Severe systemic disease that is a constant threat to life
A moribund person who is not expected to survive without
the operation
1% 55%36% 8% 0%
CONTENTS >


CHAPTER 6PATIENT
PATHWAY
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT72
CHAPTER 6
CHAPTER 6: PATIENT PATHWAY
MODE OF ADMISSION TO HOSPITAL
Figure 6.1 shows that 94% (n=3455) of hip fracture patients in 2020 presented directly to an ED in an operating hospital; this has increased slightly since 2019 and is a direct result of the IHFD data being used by the National Clinical Programme for Trauma and Orthopaedic Surgery, the National Ambulance Service (NAS), the Dublin Fire Brigade (DFB) and the HSE to introduce a national bypass for hip fracture. This work is still ongoing and is currently being reviewed by the HSE National Office for Trauma Services. A further 5% (n=195) of patients were transferred from an ED in a non-operating hospital to a ward in an operating hospital and were seen by an orthopaedic team. Figure 6.1 also displays this information at hospital level; the percentage of patients presenting directly to an ED in an operating hospital ranged from 82% to 99% in 2020.
11 Please note percentages may not sum to 100% due to rounding.
FIGURE 6.1: MODE OF ADMISSION TO OPERATING HOSPITAL, BY HOSPITAL (N=3666)11
FIGURE 6.1 MODE OF ADMISSION TO OPERATING HOSPITAL, BY HOSPITAL (N=3666)
8822%%
8877%%
9922%%
9922%%
9933%%
9955%%
9966%%
9966%%
9966%%
9977%%
9988%%
9988%%
9988%%
9988%%
9988%%
9999%%
9944%%
1188%%
1133%%
66%%
88%%
66%%
33%%
33%%
33%%
44%%
11%%
22%%
22%%
22%%
22%%
11%%
11%%
55%%
22%%
11%%
22%%
11%%
22%%
11%%
00%% 2200%% 4400%% 6600%% 8800%% 110000%%
WWaatteerrffoorrdd
CCoonnnnoollllyy
MMaatteerr
SStt JJaammeess’’ss
GGaallwwaayy
MMaayyoo
SStt VViinncceenntt’’ss
TTaallllaagghhtt
LLiimmeerriicckk
BBeeaauummoonntt
LLeetttteerrkkeennnnyy
CCoorrkk
KKeerrrryy
SSlliiggoo
DDrroogghheeddaa
TTuullllaammoorree
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
DDiirreeccttllyy ttoo EEDD iinn aann ooppeerraattiinngg hhoossppiittaall SSeeeenn bbyy aann oorrtthhooppaaeeddiicc tteeaamm UUnnkknnoowwnn
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 73
CHAPTER 6
REASON FOR DELAY TO SURGERY
One-quarter (25%; n=887) of patients received surgery more than 48 hours after their admission to hospital in 2020. For 10% (n=87), no reason was given for their delay to surgery. Completion of this data field has improved significantly following the introduction of the new data validation process. For the 800 patients who had a recorded reason for delay, ‘Awaiting medical review, investigation or stabilisation’ (57%; n=454) was the most common reason provided. This was followed by ‘Awaiting space on theatre list’ (16%; n=124) (Table 6.1).
TABLE 6.1: REASON FOR DELAY TO SURGERY
Reason for delay to surgery (if >48 hours) n %
Awaiting orthopaedic diagnosis or investigation 32 4%
Awaiting medical review, investigation or stabilisation 454 57%
Awaiting inpatient or high-dependency bed 7 1%
Awaiting space on theatre list 124 16%
Problem with theatre/equipment 6 1%
Problem with theatre/surgical/anaesthetic staff cover 10 1%
Cancelled due to list over-run 60 8%
Other 55 7%
Not known 52 7%
Total 800 100%
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT74
CHAPTER 6
12 181 patients did not have surgery in 2020.
CUMULATIVE TIME TO SURGERY
Figure 6.2 shows that 42% (n=1472) of patients received their surgery within 24 hours, 59% (n=2044) within 36 hours, and 76% (n=2638) within 48 hours of presentation to hospital, although some of these patients received their surgery outside of normal working hours (n=28). This is similar to the 2019 data. In 2021, the percentage of patients who received their surgery within 24, 36 and 48 hours will continue to be reported quarterly.
FIGURE 6.2: CUMULATIVE TIME TO SURGERY (n=3485)12
FIGURE 6.2 CUMULATIVE TIME TO SURGERY (n=3485)
4422%%
5599%%
7766%%
00%%
1100%%
2200%%
3300%%
4400%%
5500%%
6600%%
7700%%
8800%%
9900%%
110000%%
<<1122 <<2244 <<3366 <<4488 <<6600 <<7722 <<8844 <<9966 <<110088 <<112200 >>112200
PPEERR
CCEENN
TTAAGG
EE
HHOOUURRSS
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 75
CHAPTER 6
TYPE OF ANAESTHESIA
Spinal anaesthetic (SA) only continues to be the predominant type of anaesthesia used (55%; n=1931) (Figure 6.3). It is also used in combination with general anaesthetic (GA) (3%; n=92) or, increasingly, with a nerve block (21%; n=716). Figure 6.3A displays this information at hospital level. There appears to be a large variation in the type of anaesthesia used in individual hospitals; however, most hospitals predominantly used SA on their patients. This is the second year that the percentage of patients receiving a nerve block pre-operatively is being reported at hospital level (Figure 6.4). The percentage of patients receiving a nerve block pre-operatively has increased by nine percentage points, from 60% in 2019 to 69% in 2020. This pain management intervention reduces the need for opioid analgesia and has been associated with better pain management in the perioperative and postoperative period (Ritcey et al., 2016). There appears to be a large variation in pre-operative nerve block use in hospitals, with figures ranging from 13% to 99%. Further improvements in the level of reporting for this variable are expected over time.
FIGURE 6.3: PERCENTAGE OF PATIENTS BY TYPE OF ANAESTHESIA (n=3485)13,14,15
FIGURE 6.3 PERCENTAGE OF PATIENTS BY TYPE OF ANAESTHESIA (n=3485)
5555%%
2211%%
1133%%
88%%
33%%
11%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%%
SSAA oonnllyy
SSAA aanndd nneerrvvee bblloocckk
GGAA oonnllyy
GGAA aanndd nneerrvvee bblloocckk
GGAA aanndd SSAA
OOtthheerr
PPEERRCCEENNTTAAGGEE
TTYYPP
EE OO
FF AA
NNAA
EESSTTHH
EESSIIAA
13 181 patients did not have surgery and have been excluded from analysis.14 Please note percentages may not sum to 100% due to rounding.15 Less than five cases had an SA and a combined spinal-epidural and have been combined with the ‘other’ category in
Figure 6.3.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT76
CHAPTER 6
16 181 patients did not have surgery and 15 patients were not categorised as receiving either GA or SA. They have been excluded from the analysis.
17 Please note percentages may not sum to 100% due to rounding.
FIGURE 6.3A PERCENTAGE OF PATIENTS BY TYPE OF ANAESTHESIA, BY HOSPITAL (n=3470)
4488%%
4422%%
2233%%
4400%%
3366%%
3311%%
3300%%
3311%%
3300%%
1188%%
1199%%
1122%%
55%%
44%%
55%%
22%%
2211%%
5500%%
5566%%
5577%%
6600%%
6633%%
6666%%
6677%%
6677%%
7700%%
8800%%
8800%%
8877%%
9933%%
9933%%
9955%%
9988%%
7766%%
11%%
22%%
2200%%
11%%
44%%
33%%
22%%
22%%
11%%
11%%
33%%
33%%
33%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%% 7700%% 8800%% 9900%% 110000%%
SStt JJaammeess’’ss
SStt VViinncceenntt’’ss
CCoonnnnoollllyy
MMaatteerr
TTuullllaammoorree
GGaallwwaayy
BBeeaauummoonntt
TTaallllaagghhtt
MMaayyoo
DDrroogghheeddaa
SSlliiggoo
LLeetttteerrkkeennnnyy
CCoorrkk
KKeerrrryy
LLiimmeerriicckk
WWaatteerrffoorrdd
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
GGAA SSAA BBootthh
FIGURE 6.3A: PERCENTAGE OF PATIENTS BY TYPE OF ANAESTHESIA, BY HOSPITAL (n=3470) 16, 17
CONTENTS >
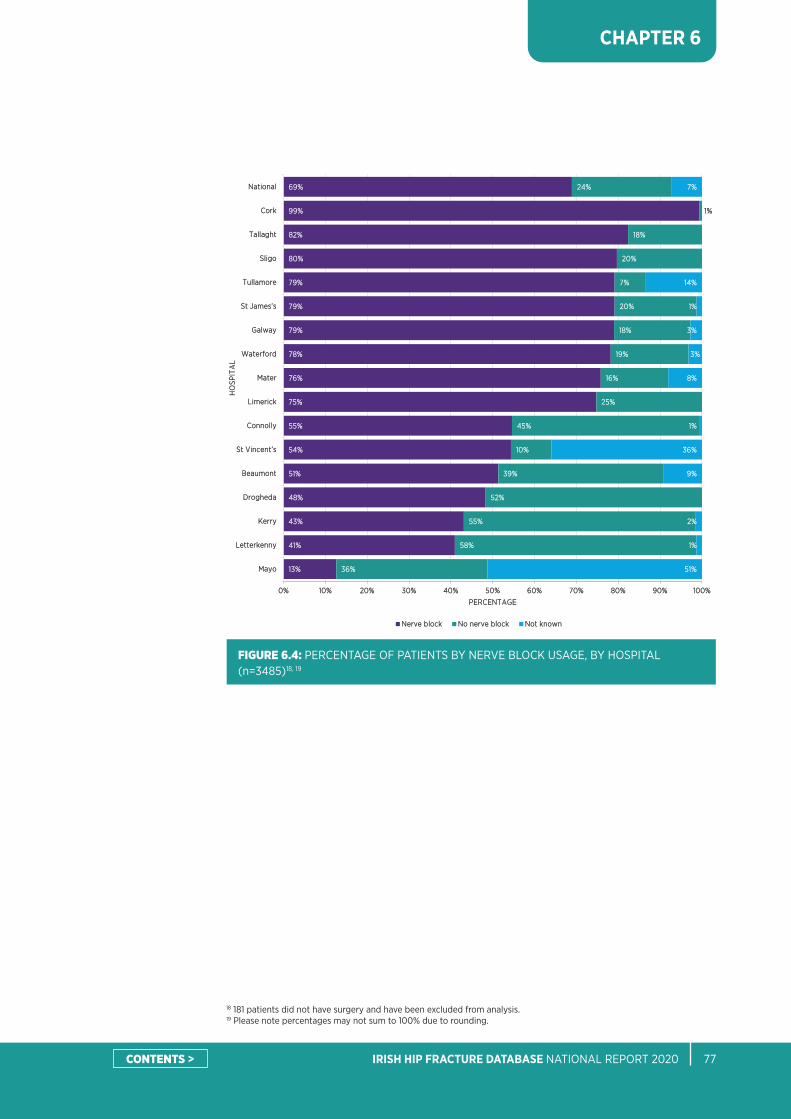
IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 77
CHAPTER 6
18 181 patients did not have surgery and have been excluded from analysis.19 Please note percentages may not sum to 100% due to rounding.
FIGURE 6.4: PERCENTAGE OF PATIENTS BY NERVE BLOCK USAGE, BY HOSPITAL (n=3485)18, 19
FIGURE 6.4 PERCENTAGE OF PATIENTS BY NERVE BLOCK USAGE (n=3485)
1133%%
4411%%
4433%%
4488%%
5511%%
5544%%
5555%%
7755%%
7766%%
7788%%
7799%%
7799%%
7799%%
8800%%
8822%%
9999%%
6699%%
3366%%
5588%%
5555%%
5522%%
3399%%
1100%%
4455%%
2255%%
1166%%
1199%%
1188%%
2200%%
77%%
2200%%
1188%%
11%%
2244%%
5511%%
11%%
22%%
99%%
3366%%
11%%
88%%
33%%
33%%
11%%
1144%%
77%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%% 7700%% 8800%% 9900%% 110000%%
MMaayyoo
LLeetttteerrkkeennnnyy
KKeerrrryy
DDrroogghheeddaa
BBeeaauummoonntt
SStt VViinncceenntt’’ss
CCoonnnnoollllyy
LLiimmeerriicckk
MMaatteerr
WWaatteerrffoorrdd
GGaallwwaayy
SStt JJaammeess’’ss
TTuullllaammoorree
SSlliiggoo
TTaallllaagghhtt
CCoorrkk
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
NNeerrvvee bblloocckk NNoo nneerrvvee bblloocckk NNoott kknnoowwnn
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT78
CHAPTER 6
NUTRITIONAL RISK ASSESSMENT
Nutritional risk assessment was introduced to the IHFD dataset in 2018. The purpose of this variable is to determine the percentage of patients who have had a nutritional risk assessment during admission and to ascertain the nutritional status of those patients. Evidence shows that nutrition is a key modifiable risk factor for survival following hip fracture, with poor nutrition contributing to the risk of death after hip fracture (Johansen et al., 2017; Duncan et al., 2006). Malnutrition can play a key role in determining a patient’s recovery and outcomes following hip fracture and reflects the multidisciplinary nature of hip fracture patients’ care. Nutritional care is a priority for the HSE, with the publication of the Food, Nutrition and Hydration Policy for Adult Patients in Acute Hospitals and subsequent publication by the Department of Health of National Clinical Guideline No. 22: Nutrition screening and use of oral nutrition support for adults in the acute care setting (Department of Health, 2020).
Figure 6.5 shows that just under one-half of hip fracture patients did not have a nutritional risk assessment during their admission in 2020. Forty-one percent (n=1505) of hip fracture patients were within normal limits, 13% (n=470) were at risk of malnourishment and 2% (n=63) were categorised as malnourished. Although these are still early data, there is large variation in the proportion of assessments that were performed at hospital level. The IHFD will continue to record this variable, and in time these data will provide valuable insights into the nutritional status of hip fracture patients.
20 Please note percentages may not sum to 100% due to rounding.
FIGURE 6.5: PERCENTAGE OF PATIENTS BY NUTRITIONAL RISK ASSESSMENT, BY HOSPITAL (N=3666)20
FIGURE 6.5 PERCENTAGE OF PATIENTS BY NUTRITIONAL RISK ASSESSMENT (N=3666)
110000%%
9966%%
9933%%
9900%%
5555%%
4488%%
3344%%
3333%%
2277%%
2211%%
1166%%
66%%
55%%
44%%
11%%
4444%%
11%%
11%%
11%%
55%%
1199%%
11%%
11%%
44%%
11%%
11%%
22%%
22%%
22%%
22%%
33%%
44%%
99%%
2288%%
22%%
3399%%
33%%
1166%%
66%%
1199%%
2277%%
1177%%
3366%%
1133%%
11%%
44%%
77%%
4400%%
3399%%
1199%%
6655%%
3333%%
7755%%
6688%%
8855%%
7755%%
6688%%
8811%%
6644%%
4411%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%% 7700%% 8800%% 9900%% 110000%%
TTuullllaammoorree
LLiimmeerriicckk
GGaallwwaayy
WWaatteerrffoorrdd
DDrroogghheeddaa
SStt VViinncceenntt’’ss
MMaatteerr
TTaallllaagghhtt
LLeetttteerrkkeennnnyy
CCoonnnnoollllyy
BBeeaauummoonntt
MMaayyoo
SStt JJaammeess’’ss
KKeerrrryy
SSlliiggoo
CCoorrkk
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
NNoo aasssseessssmmeenntt ppeerrffoorrmmeedd IInnddiiccaatteess mmaallnnoouurriisshheedd IInnddiiccaatteess rriisskk ooff mmaallnnuuttrriittiioonn IInnddiiccaatteess nnoorrmmaall
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 79
CHAPTER 6
TYPE OF SURGERY
Thirty-six percent (n=1243) of patients underwent a cemented hemiarthroplasty and 18% (n=629) underwent an internal fixation by intramedullary (IM) nail (short) in 2020 (Figure 6.6). Table 6.2 details the fixation of fractures by fracture type. Ninety-four percent (n=1371) of patients with an intracapsular fracture (displaced) underwent either a hemiarthroplasty or a total hip replacement (THR), whereas 82% (n=221) of patients with an intracapsular fracture (undisplaced) underwent either a hemiarthroplasty or a THR. Ninety-three percent (n=1226) of patients with an intertrochanteric fracture underwent internal fixation, whereas 94% (n=206) of patients with a subtrochanteric fracture underwent internal fixation.
21 181 patients did not have surgery and have been excluded from analysis.
FIGURE 6.6: PERCENTAGE OF PATIENTS BY TYPE OF SURGERY (N=3485)21
FIGURE 6.6 PERCENTAGE OF PATIENTS BY TYPE OF SURGERY (n=3485)
3366%%
1188%%
1144%%
1122%%
1122%%
33%%
22%%
11%%
22%%
00%% 55%% 1100%% 1155%% 2200%% 2255%% 3300%% 3355%% 4400%%
AArrtthhrrooppllaassttyy hheemmii cceemmeenntteedd
IInntteerrnnaall ffiixxaattiioonn IIMM nnaaiill ((sshhoorrtt))
IInntteerrnnaall ffiixxaattiioonn IIMM nnaaiill ((lloonngg))
IInntteerrnnaall ffiixxaattiioonn ddyynnaammiicc hhiipp ssccrreeww
AArrtthhrrooppllaassttyy hheemmii uunncceemmeenntteedd
AArrtthhrrooppllaassttyy TTHHRR cceemmeenntteedd
AArrtthhrrooppllaassttyy TTHHRR uunncceemmeenntteedd
IInntteerrnnaall ffiixxaattiioonn ssccrreewwss
OOtthheerr
PPEERRCCEENNTTAAGGEE
OOPP
EERRAA
TTIIOO
NN
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT80
CHAPTER 6
Seventy-four percent of arthroplasties reported in 2020 were cemented (n=1339), which was a slight decrease from 2019 (Figure 6.7). However, a large proportion of patients received uncemented implants in a number of hospitals.
The use of cemented prostheses is supported by the National Institute for Health and Care Excellence (NICE) in its clinical guideline, Hip fracture: management (NICE, 2011). It concludes that cement use has a statistically significant benefit in terms of mobility and pain (although the scale of this benefit may not be clinically significant). Since this guidance was published in 2011, there have been significant improvements in uncemented implant technology, and small clinical trials suggest greatly improved outcomes with contemporary uncemented implants, without the risks that come from using bone cement. In 2015, in response to concerns relating to adverse cardiovascular events associated with cemented hemiarthroplasty (referred to as bone cement implantation syndrome (BCIS)), NICE added further guidance to the safety guideline on reducing the risk from cemented hemiarthroplasty for hip fracture, which was drawn from a collaborative multidisciplinary working group document produced by the Association of Anaesthetists of Great Britain and Ireland (AAGBI), the British Orthopaedic Association (BOA) and the British Geriatric Society (BGS) (Griffiths et al., 2015).
National hip fracture registries and ongoing trials will be very helpful in this context, and are also likely to provide further valuable information regarding the use of cemented compared with uncemented hemiarthroplasty. Due to the observational rather than randomised nature of the data, it will be vital to remove potential reporting biases and to collect sufficient information to allow for case mix adjustment.
The IHFD pilot for a new and more detailed list of implant options was not progressed during 2020 due to the impact from the COVID-19 pandemic, but this will continue in 2021.
TABLE 6.2: PERCENTAGE OF SURGERY TYPE, BY FRACTURE TYPE (n=3485)
Type of fracture
Type of Operation Intracapsular (displaced)
Intracapsular (undisplaced)
Intertrochanteric Subtrochanteric
Internal fixation dynamic hip screw (DHS) 3% 9% 25% 4%
Internal fixation screws 1% 5% 2% 1%
Internal fixation IM nail (long) 1% 2% 23% 73%
Internal fixation IM nail (short) 1% 2% 43% 16%
Arthroplasty hemi cemented 63% 60% 5% 1%
Arthroplasty hemi uncemented 24% 15% 1% 1%
Arthroplasty THR cemented 4% 4% 0% 1%
Arthroplasty THR uncemented 3% 3% 1% 1%
Other 0% 0% 1% 2%
Total 100% 100% 100% 100%
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 81
CHAPTER 6
FIGURE 6.7: PERCENTAGE OF PATIENTS WITH CEMENTED OR UNCEMENTED ARTHROPLASTIES, BY HOSPITAL (n=1815)22
FIGURE 6.7 PERCENTAGE OF PATIENTS WITH CEMENTED OR UNCEMENTED ARTHROPLASTIES, BY HOSPITAL (n=1815)
1111%%
1122%%
1166%%
7722%%
7755%%
7755%%
8877%%
9911%%
9933%%
9966%%
9966%%
9977%%
9988%%
9988%%
9999%%
110000%%
7744%%
8899%%
8888%%
8844%%
2288%%
2255%%
2255%%
1133%%
99%%
77%%
44%%
44%%
33%%
22%%
22%%
11%%
2266%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%% 7700%% 8800%% 9900%% 110000%%
SStt VViinncceenntt’’ss
TTuullllaammoorree
GGaallwwaayy
WWaatteerrffoorrdd
SSlliiggoo
MMaayyoo
TTaallllaagghhtt
DDrroogghheeddaa
SStt JJaammeess’’ss
CCoorrkk
KKeerrrryy
LLiimmeerriicckk
BBeeaauummoonntt
MMaatteerr
LLeetttteerrkkeennnnyy
CCoonnnnoollllyy
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
CCeemmeenntteedd UUnncceemmeenntteedd
22 Percentages may not sum to 100% due to rounding.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT82
CHAPTER 6
MOBILISATION: DAY OF OR DAY AFTER SURGERY AND MOBILISED BY
Early mobilisation of hip fracture patients is a key measure of the standard of care and is directly linked to better outcomes (Dubljanin-Raspopović et al., 2013; Hirose et al., 2010). Recent evidence from Ferris et al. (2020) indicated that the risk of in-hospital mortality for hip fracture patients was reduced for those mobilised on the day of or the day after surgery. Based on the strength of this evidence and the current international consensus on early mobilsation reflected in other hip fracture registries and guidelines (e.g. Australian & New Zealand Hip Fracture Registry (2020); NICE, 2011; Waddell, 2011; Scottish Intercollegiate Guidelines Network, 2009), the IHFD Governance Committee introduced a new IHFS (IHFS 7) in 2020.
The new IHFS measures the percentage of patients mobilised by a physiotherapist on the day of or the day after surgery, and was published in the quarterly reports in 2020; it is also scheduled to become part of the Best Practice Tariff (BPT) from 1 January 2022. It was originally intended for addition to the BPT in 2021, but due to the ongoing disruptions from both COVID-19 and the May 2021 cyberattack on the HSE, opportunities to hold workshops and communicate with the hospitals were limited.
The percentage of patients assessed by a physiotherapist on the day of or day after surgery has increased by four percentage points from 2019, to 91% nationally (Figure 6.8). This ranged from 74% to 100% depending on the individual hospital.
Figure 6.8A shows that 85% of patients were mobilised on the day of or day after surgery, representing an improvement of two percentage points compared to 2019. For the purposes of this standard, the term ‘mobilised’ means that the patient has stood up at a minimum as agreed by the IHFD Governance Committee. Patients who are mobilised by a physiotherapist on the day of or day after surgery will be considered to have met IHFS 7, provided the patient’s function (Cumulative Ambulatory Score) on the first postoperative day is also recorded. The reason why mobilisation was not possible in those patients who were not suitable to mobilise (e.g. if medically unfit to mobilise) must be recorded in the newly created data field, ‘reason for not mobilising’.
In 2020, 78% (n=2705) of hip fracture patients were mobilised on the day of or day after surgery by a physiotherapist and 7% (n=232) were mobilised by somebody else (‘other’). Levels of mobilisation on the first postoperative day are also captured by the Cumulative Ambulatory Score, which was added to the dataset in 2016 and provides a more objective description of function (Chapter 7). Our ability to examine functional outcomes will increase when data quality for the Cumulative Ambulatory Score improves.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 83
CHAPTER 6
FIGURE 6.8: PERCENTAGE OF PATIENTS WHO WERE ASSESSED BY A PHYSIOTHERAPIST ON THE DAY OF OR DAY AFTER SURGERY, BY HOSPITAL (n=3485)23
FIGURE 6.8A PERCENTAGE OF PATIENTS WHO WERE ASSESSED BY A PHYSIOTHERAPIST ON THE DAY OF OR DAY AFTER SURGERY, BY HOSPITAL (n=3485)
7744%%
8800%%
8855%%
8855%%
8877%%
9933%%
9955%%
9966%%
9966%%
9977%%
9977%%
9988%%
9988%%
9988%%
9988%%
110000%%
9911%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%% 7700%% 8800%% 9900%% 110000%%
WWaatteerrffoorrdd
CCoorrkk
KKeerrrryy
SSlliiggoo
BBeeaauummoonntt
MMaatteerr
TTuullllaammoorree
MMaayyoo
LLeetttteerrkkeennnnyy
SStt JJaammeess’’ss
SStt VViinncceenntt’’ss
GGaallwwaayy
TTaallllaagghhtt
DDrroogghheeddaa
CCoonnnnoollllyy
LLiimmeerriicckk
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
23 181 patients did not have surgery and have been excluded from analysis.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT84
CHAPTER 6
24 181 patients did not have surgery and 26 patients had ‘not known’ recorded. These patients have been excluded from analysis.25 Please note percentages may not sum to 100% due to rounding.
FIGURE 6.8A: PERCENTAGE OF PATIENTS BY MOBILISATION ON THE DAY OF OR DAY AFTER SURGERY, BY HOSPITAL (n=3467)24,25
FIGURE 6.8 PERCENTAGE OF PATIENTS BY MOBILISATION DAY OF OR DAY AFTER SURGERY, BY HOSPITAL (n=3467)
6611%%
6644%%
6655%%
7722%%
7733%%
7788%%
7799%%
7799%%
8800%%
8800%%
8811%%
9900%%
9933%%
9933%%
9933%%
9944%%
7788%%
3311%%
1122%%
1144%%
77%%
44%%
11%%
88%%
11%%
77%%
3399%%
3366%%
33%%
1166%%
1133%%
1155%%
2211%%
1177%%
2200%%
2200%%
1111%%
1100%%
77%%
66%%
77%%
55%%
1155%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%% 7700%% 8800%% 9900%% 110000%%
TTaallllaagghhtt
SStt VViinncceenntt’’ss
WWaatteerrffoorrdd
CCoorrkk
SSlliiggoo
BBeeaauummoonntt
MMaayyoo
TTuullllaammoorree
KKeerrrryy
DDrroogghheeddaa
CCoonnnnoollllyy
MMaatteerr
LLiimmeerriicckk
GGaallwwaayy
SStt JJaammeess’’ss
LLeetttteerrkkeennnnyy
NNaattiioonnaall
PPEERRCCEENNTTAAGGEE
HHOO
SSPPIITT
AALL
YYeess ((bbyy pphhyyssiiootthheerraappiisstt)) YYeess ((bbyy ootthheerr)) NNoott mmoobbiilliisseedd
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 85
CHAPTER 6
KEY FINDINGS FROM CHAPTER 6
• Ninety-four percent (n=3455) of patients presented directly to an ED in an operating hospital.
• Seventy-six percent (n=2638) of patients received their surgery within 48 hours. This is similar to the percentage reported in 2019.
• Sixty-nine percent of patients received a nerve block pre-operatively in 2020, which is an increase of nine percentage points from 2019. The use of pre-operative nerve blocks ranged from 13% to 99% at hospital level.
• Forty-four percent of patients had no documented nutritional risk assessment in 2020.
• Seventy-four percent of arthroplasties reported in 2020 were cemented (n=1339), which was a slight decrease from 2019. However, there was a high degree of variation in the use of bone cement at hospital level.
• Eighty-five percent (n=2937) of patients were mobilised on the day of or the day after surgery, and 91% of patients were assessed by a physiotherapist on the day of or the day after surgery. These variables have increased by two and four percentage points, respectively, from 2019.
CONTENTS >


CHAPTER 7OUTCOMES
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT88
CHAPTER 7
CHAPTER 7: OUTCOMES
FUNCTIONAL OUTCOMES: CUMULATIVE AMBULATORY SCORE Functional outcomes, measured by the Cumulative Ambulatory Score (CAS), act as indicators of postoperative outcomes. This measure was introduced to the IHFD in 2016 as a validated measure for hip fracture patients (Kristensen et al., 2012; Kristensen et al., 2009). The main aim of hip fracture management is for the patient to return to their previous function, and the CAS aims to capture that.
Although data completeness has improved for this data field, there continues to be a high proportion of missing or incomplete data entry in this report (n=994, 27%) missing for day after surgery; (n=1553, 42%) missing for day of discharge). A significant improvement in data quality is required in order to provide objective information regarding patient functional outcomes and to guide rehabilitation planning. The day 1 CAS must be documented in order for an episode of care to be eligible for the BPT for IHFS 7 from 1 January 2022. The Health and Social Care Professional (HSCP) Lead for the IHFD will coordinate a workshop with physiotherapists in the participating hospitals in advance of this, and the IHFD Audit Manager will communicate the details of this IHFS to the hospitals.
For Figure 7.1, only patients with a valid CAS recorded for their first postoperative day and for their day of discharge were included (n=2015). Figure 7.1 shows that 23% (n=471) of patients with CAS data recorded achieved independent mobility (a CAS of 6) by the day on which they were discharged from the acute hospital. This was the same percentage as that recorded in 2019.
FIGURE 7.1: PERCENTAGE OF PATIENTS BY FUNCTIONAL OUTCOMES: CUMULATIVE AMBULATORY SCORE (n=2015)
FIGURE 7.1 PERCENTAGE OF PATIENTS BY FUNCTIONAL OUTCOMES: CAS (n=2015)
88%%
66%%
1155%%
6633%%
55%%
22%%
11%%
44%%
33%%
55%%
4455%%
99%%
1111%%
2233%%
00%% 1100%% 2200%% 3300%% 4400%% 5500%% 6600%% 7700%%
00
11
22
33
44
55
66
PPEERRCCEENNTTAAGGEE
CCUU
MMUU
LLAATTII
VVEE
AAMM
BBUU
LLAATTOO
RRYY
SSCC
OORR
EE
DDaayy ooff ddiisscchhaarrggee DDaayy aafftteerr ssuurrggeerryy
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 89
CHAPTER 7
DESTINATION ON DISCHARGE
Figure 7.2 shows that 28% (n=1026) of patients were discharged directly home from hospital, which represents an improvement of four percentage points from 2019; a further 28% (n=1009) required rehabilitation at an off-site facility. There was no change in the percentage of patients recorded as new admissions to a nursing home or long-stay care facility compared to 2019.
FIGURE 7.2: PERCENTAGE OF PATIENTS BY DESTINATION ON DISCHARGE (N=3666)
FIGURE 7.2 PERCENTAGE OF PATIENTS BY DESTINATION ON DISCHARGE (N=3666)
2288%%
2288%%
1155%%
88%%
88%%
55%%
44%%
33%%
22%%
0% 5% 10% 15% 20% 25% 30%
Home
Off-site rehabilitation unit
Return admission to nursing home or long-staycare
Convalescent care
Other
Died
New admission to nursing home or long-stay care
On-site rehabilitation unit
Not known
PPEERRCCEENNTTAAGGEE
DDIISS
CCHH
AARR
GGEE
DDEESS
TTIINN
AATTII
OONN
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT90
CHAPTER 7
CUMULATIVE LENGTH OF STAY
In 2020, the number of acute hospital bed days occupied by hip fracture patients was 62,684 days; this represents a 13% decrease from the 72,314 days reported in 2019 and a savings of almost 10,000 bed days. Cumulative length of stay (LOS) is measured on the HIPE system as the number of calendar days from the date the patient is admitted to a ward in the operating hospital to the date the patient is discharged from the operating hospital. Figure 7.3 shows the cumulative percentages for the LOS of all patients; 29% of patients were discharged within 1 week and 64% were discharged within a fortnight. This is a four-percentage-point improvement at both 7 days and 14 days compared to 2019. The mean LOS for hip fracture patients was 17.1 days, which is a decrease of almost 2.5 days from the 19.5 days reported in 2019. The median LOS decreased by 1 day (to 11 days) over the same period.
As seen in the COVID-19 report 1.0: Service impact from COVID-19: Analysis based on Irish Hip Fracture Database June 2019-May 2020 (NOCA, 2020), there was a steep decline in LOS in the first few months of the COVID-19 pandemic that ultimately resulted in a 1-day overall reduction in the median LOS for 2020. Feedback from the hospitals found that this steep decline in the early part of the pandemic was a result of a number of new processes, including an increase in internal rehabilitation beds; a reduction in external rehabilitation beds (and thus more involvement with the community intervention teams and early supported discharge teams to discharge patients directly home); the patients themselves wanting to go directly home in more cases; greater family involvement; and the use of a new pathway: transfers to off-site facilities, including private hospitals and standalone orthopaedic hospitals.
FIGURE 7.3: PERCENTAGE OF PATIENTS BY CUMULATIVE LENGTH OF STAY (N=3666)
FIGURE 7.3 PERCENTAGE OF PATIENTS BY CUMULATIVE LOS (N=3666)
11%%
2299%%
6644%%
8888%%9977%% 9988%% 9999%%
00%%
1100%%
2200%%
3300%%
4400%%
5500%%
6600%%
7700%%
8800%%
9900%%
110000%%
≤11 ≤77 ≤1144 ≤3300 ≤6600 ≤9900 ≤112200
PPEERR
CCEENN
TTAAGG
EE
CCUUMMUULLAATTIIVVEE LLOOSS ((ddaayyss))
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 91
RE-OPERATION WITHIN 30 DAYS
Reoperation acts as a marker of quality of care. Figure 7.4 shows that 88% (n=3081) of patients were not reoperated on within 30 days of their initial surgery. However, data were missing or not documented for this field in 10% (n=346) of cases.
NOCA is working with IHFD data collectors to improve the coding of this question and towards collecting longer-term outcome measures. NOCA is also collaborating on the Health Research Board (HRB)-funded Hip Fracture Outcome and Geographic Equality (HipFORGE) research project, which will explore methods for collecting longer-term data in this patient group. In 2021, the IHFD follow-up data portal will be updated in order to allow for the collection of information on residential status, New Mobility Score, pain, readmission details, reoperation, bone protection status, and quality of life (EQ-5D-5L) at 30, 120 and 365 days.
CHAPTER 7
FIGURE 7.4: PERCENTAGE OF PATIENTS BY REOPERATION WITHIN 30 DAYS (n=3485)
FIGURE 7.4 PERCENTAGE OF PATIENTS BY REOPERATION WITHIN 30 DAYS (n=3485)
8888%%
22%%1100%%
NNoo YYeess NNoott kknnoowwnn
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT92
CHAPTER 7
KEY FINDINGS FROM CHAPTER 7
• Twenty-three percent (n=471) of patients achieved the maximum CAS of 6, thus indicating independent mobility, on discharge from the acute hospital. This is the same as the percentage recorded in 2019.
• Twenty-eight percent (n=1026) of patients were discharged directly home from hospital, which represents an improvement of four percentage points from 2019.
• The mean LOS for hip fracture patients was 17.1 days and the median LOS was 11 days. This reduction equated to a savings of almost 10,000 acute hospital bed days in 2020 compared to the number used in 2019.
• Twenty-nine percent of patients were discharged from the acute hospital within 1 week, an improvement of four percentage points from 2019.
CONTENTS >

CHAPTER 8QUALITY
IMPROVEMENT
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT94
CHAPTER 8
CHAPTER 8: QUALITY IMPROVEMENTThis chapter will focus on the national approach to quality improvement (QI) by the IHFD audit. This includes training, dissemination of this training, and front-line ownership for QI. Although there has always been some focus on QI since the beginning of the audit, there has been a much more structured effort made to incorporate it into the audit since 2017. The timeline below details the progress of QI in the IHFD.
IHFD INVESTMENT IN QI
FRONT-LINE OWNERSHIP FOR QI
The IHFD and Major Trauma Audit (MTA) Audit Manager, Louise Brent, completed the Diploma in Quality and Leadership, which was led by the Royal College of Physicians of Ireland and funded by the HSE, along with Aisling Connolly, Communications and Events Lead, NOCA, and Dr Rachael Doyle, Consultant Geriatrician, St Vincent’s University Hospital.
In May 2019, a co-design workshop was held in the RCSI with the HSE QIT and the IHFD audit coordinators and clinical leads to develop a meaningful programme of QI education that would support the hospitals and the audit.
In the Irish Hip Fracture Database National Report 2017 (NOCA, 2018), six hospitals that were performing the best in each IHFS were invited to share a story about how their local QI work led to such success in that particular standard. In addition, a summary table of other QI work and areas identified for improvement from each of the 16 participating hospitals was included in Chapter 9.
In September and October 2019, a 2-day Foundation Programme for QI (based on the co-design workshop) was held in the RCSI with a team of three invited from each of the IHFD participating hospitals. The goal of this work was to equip the team from each hospital with a good knowledge of QI methodologies and tools to bring back to their hospital’s hip fracture governance committee (HFGC) in order to further support local QI projects.
At the seventh Irish Hip Fracture Meeting held in the Royal College of Surgeons in Ireland (RCSI), each of the 16 hospitals participating in the audit were invited to present a local QI project using a structured template. Following that meeting, Dr Philip Crowley, National Director of the HSE Quality Improvement Team (QIT), encouraged the IHFD to liaise with the HSE QIT in order to progress the QI work.
In 2020, a detailed organisational survey was conducted, much of which is presented in Chapter 10; one of the components of the survey was to list QI projects currently underway in each of the hospitals. These QI projects will be listed in this chapter in Table 8.1.
2017
2019
2018
2020
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 95
CHAPTER 8
TABLE 8.1: HOSPITAL IHFD QUALITY IMPROVEMENT PROJECTS AND INITITATIVES
Hospital Improvements made Areas for Improvement
Beaumont Hospital 1. Creation of admissions booklet/ hip fracture pathway
2. Hip alert introduced through ED triage
3. Orthogeriatric registrar appointment
1. Breach of IHFS 1 (internal processes)2. Weekend physiotherapy service3. Reduce pressure ulcer rates
Connolly Hospital 1. Femoral nerve block2. ANP led follow-up clinic
1. IHFS
Cork University Hospital
1. Revised hip fracture pathway introduced
2. Orthopaedic passport introduced3. Pain protocol and fasting protocol
developed4. Revised discharge pathway and
transfer letter developed
1. No escalation policy2. No protocol for patients on
anticoagulants in theatre
Our Lady of Lourdes Hospital Drogheda
1. Standard 1 fast track pathway 2. New theatre suite February 2020 3. Improvement in all standards except
standard 2
1. Standard 2 2. Access to second orthopaedic
theatre with dedicated hip fracture slots
University Hospital Kerry
1. Appointment of candidate Advanced Nurse Practitioner – bone health medication is being prescribed
2. Hip Fracture Group formed and regular meetings held; also communicated with heads of various departments to implement standards to improve patient care
3. Finalising the formation of the HFGC
1. Difficulty recruiting key stakeholders involved in hip fracture care to the HFGC
2. No money received from BPT
NB: In 2021, the University Hospital Kerry HFGC was established and the first meeting was held.
Letterkenny University Hospital
1. Purchased an ultrasound for ED to assist with femoral blocks
1. Lack of orthogeriatric service due to loss of staff
University Hospital Limerick
1. Accelerated Community Discharge Care plan (ACDC) (QI project described in the next section)
2. Delirium screening tool introduced3. Falls prevention strategy developed
1. Improve ED time to ward (IHFS 1)2. Nutrition screening too to be
introduced3. Catheter care improvement
Mater Misericordiae University Hospital
1. Dedicated hip bed in orthopaedic ward introduced
2. Implementation of communication alert to trauma team for hip fracture patients
3. Weekend physiotherapy service introduced
1. Achieving the 4-hour target for IHFS 1
2. Reducing hospital length of stay3. Review of patients that will never
meet theatre key performance indicator (KPI), as they are medically unfit
Mayo University Hospital
1. Organising HFGC meetings to be held quarterly (all stakeholders contacted)
2. Improvement in data quality
1. Orthopaedic ward has mix of medical and surgical pts on the ward (as it was a COVID-19 ward during the crisis)
2. Need to improve IHFS 1 compliance
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT96
Sligo University Hospital
1. Hoist with weighing option introduced
2. Increased use of femoral block for pain relief for hip fracture patients
3. Acute pain service/frailty service introduced
1. Lack of ANPs and Clinical Nurse Specialists for orthopaedics
2. Orthogeriatrician hours needs to be increased and resourced
3. Lack of space on ward/theatre
St James’s Hospital 1. Reduction of rate of pressure ulcers 2. Increase in number of patients
admitted to specialised ward within 4 hours (IHFS 1)
3. Fascia illiaca block on arrival improved
4. Early support and discharge improvement
1. Timely surgery and delays due to anticoagulation needs improvement
2. Theatre and staff availability needs to be increased
3. 0.2 whole time equivalent (WTE) for orthogeriatrician support for hip fractures; no dedicated registrar in geriatrics currently
St Vincent’s University Hospital
1. Intentional rounding introduced2. Improved communication with staff
through WhatsApp group3. Dementia/delirium-friendly ward
(ongoing)4. Pilot of an integrated care pathway
(began before the COVID-19 pandemic)
1. Rehabilitation during the COVID-19 pandemic era
2. Delays to surgery during the COVID-19 pandemic era
Tallaght University Hospital
1. IHFS 1 improved2. IHFS 5 improved
1. Orthogeriatric service needs further resourcing
2. Clinical nurse specialist, trauma post required
3. Rehabilitation facilities
Midland Regional Hospital Tullamore
1. Fast-track pathway in ED introduced2. Protected bed on the trauma ward
for hip fracture patient3. Weekend physiotherapy service to
include day 1 assessment and review on day 2 if not mobile on day 1
1. Fracture liaison service needed2. Dual-energy X-ray absorptiometry
(DXA) service limited3. Lack of rehabilitation options upon
discharge
University Hospital Galway
1. All patients receiving a comprehensive geriatric assessment from a geriatrician, including bone health assessment, falls review and medication review2. Improvement from anaesthetics in using general anaesthetic where possible instead of waiting for
2–3 days for patients on anticoagulant drugs
1. Lack of formal identification of hip fracture bed at ward level, no agreement at management level to establish protected bed status2. System failure to process hip fracture patients within a 4-hour period (IHFS 1)3. Failure to progress retention/ recruitment of staff on a
consistent basis
University Hospital Waterford
1. Hip bypass introduced2. Hip fracture Bleep introduced3. One protected bed for hip fracture
created
1. Management of anti-coagulants needs improvement
2. More protected beds required3. Delirium management needs
improvement
CHAPTER 8
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 97
CHAPTER 8
NATIONAL RECOGNITION FOR FRONT-LINE IHFD QI PROJECTS In 2021, two QI projects from the IHFD were shortlisted for the NOCA Quality Improvement Champion Award at the NOCA Annual Conference, one of which won the overall NOCA Quality Improvement Champion Award. Below are the details of these two exceptional projects and the team from University Hospital Limerick (the winner of the NOCA Quality Improvement Champion Award), and the staff at the Mater Misericordiae University Hospital who were highly commended.
UNIVERSITY HOSPITAL LIMERICK
QI PROJECT TITLE: Accelerated Community Discharge Care plan (ACDC)
PROJECT LEADS: Nur Atikah Mohd Asri, Pamela Hickey, Stephen White
PROJECT TEAM: Orthogeriatric and Orthopaedic Team; Trauma Ward
Left to right: Hannah Murphy Staff Grade Occupational Therapist; Pamela Hickey Clinical Nurse Specialist Orthopaedics; Cathryn Ryan ADPHN/CIT service manager; Declan Mc Namara Director of nursing; Stephen White Senior Physiotherapist; Dr Jude Ryan Consultant ortho-geritrican
BACKGROUND AND AIMSHip fractures are associated with high 1-year mortality rates and poor functional outcomes. Rehabilitation is often required; however, high demand for rehabilitation services often caused significant discharge delays in our institution. Guided by the Sláintecare vision of integrated care model, University Hospital Limerick established the ACDC in December 2019 with the aim of facilitating the early and safe transition of orthogeriatric patients’ direct discharge home via continuous multidisciplinary team (MDT) support of early community-based rehabilitation. Secondary outcomes included decreasing inpatient LOS, reducing demand for inpatient rehabilitation, and improving IHFS compliance.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT98
CHAPTER 8
METHODA retrospective cohort study was performed with IHFD data collected between January and June 2019 (n=76), which was compared with data collected from a similar cohort in 2020 (n=65). Further sub-analysis was performed by stratifying the data into three groups: group 1 (n=32) was enrolled in the ACDC, group 2 (n=76) was the 2019 cohort who met the ACDC criteria and group 3 (n=33) met the ACDC criteria but lived outside catchment area. Patients admitted to UHL between 23 March and 11 May 2020 were excluded in order to minimise the impact of COVID-19 as a confounding factor. The criteria for acceptance to the ACDC programme include:
1. having a home address within 20 miles of University Hospital Limerick2. having independent pre-morbid baseline or sufficient community support3. having no significant cognitive impairment4. having no substance abuse issues5. being motivated to engage in the ACDC programme6. being medically fit for discharge7. having the potential to achieve agreed goals within 2 weeks of starting the ACDC programme
Outcome measures observed were: 1. LOS2. IHFS compliance, 3. 30-day readmission4. 30-day mortality rate
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS).
RESULTSDemographic information was comparable to the national figures for the 6-month period studied. Of the 2020 cohort, 50.7% fit the ACDC criteria but lived outside the catchment area; 78.1% of the 2020 cohort were discharged directly home compared to 24.2% in 2019 (p=0.001). Mean LOS was significantly shorter (p=0.001) for the 2020 cohort (21.84 days, ±8.3 days) compared to the 2019 cohort (37.24 days, ±6.7 days). Significant improvements were observed (p=0.001) in four out of the six IHFS. The 30-day readmission rates and 30-day mortality rates were comparable between the 2019 and 2020 cohorts. Analysis of the three groups revealed a significant reduction in LOS in group 1 (9.3 days, ±6.9 days) compared to group 2 (11.39 days, ±12.2 days) and group 3 (12.4 days, ±11.1 days), as well as a higher rate of direct discharge home in group 1 (78.1%) compared to group 2 (25.0%) and group 3 (24.2%). Compared to standard care, ACDC allowed average savings of 2 acute inpatient bed days, 6 rehabilitation bed days and 3 weeks of transitional funding for bed days. This represented an average total savings of €5,526 per patient enrolled in the programme, which up to June 2020 totalled an overall savings of €176,832. Projected potential savings for all the patients who met the ACDC inclusion criteria within the 6-month study period was €359,190, with the annual savings projection for 2020 being €713,380.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 99
CHAPTER 8
QUALITY IMPROVEMENT PLANFollowing the ‘hip fracture quality improvement collaborative’ arranged by NOCA and the HSE QIT in December 2019, a trio comprising an orthopaedic Clinical Nurse Manager, an orthogeriatric registrar and a physiotherapist (PT) devised the concept of the ACDC. The community MDT was initially engaged in the process, and the activity-based funding that was secured for the new programme was utilised to hire an additional occupational therapist (OT) and PT during the trial period; however, as the ACDC was a pilot programme, community MDT supports were only available for patients living within a 20-mile radius of Limerick city. With the goal of educating patients and providing reference material for their continuing treatment and daily home exercises, a hip fracture booklet (HFB) was created and supplied to all patients in the ACDC programme.
Clear patient selection criteria were established in order to ensure that only suitable candidates were selected, thus preventing potential risky or failed discharges. Clear communication lines were established between acute and community services, with a back-up plan for urgent review in the orthopaedic clinic made available for any patients in difficulty.
STAKEHOLDER ENGAGEMENTACDC’s success can be attributed to the stakeholders’ enthusiasm: the project’s multidisciplinary nature makes every stakeholder feel a sense of ownership in the programme’s success. However, this project’s greatest success factor was the patients’ participation and confidence in the programme. This was strengthened by the creation of the HFB, and by allowing easy access to a safety net if required.
Patients’ ACDC journey begins the moment they arrive in the hospital, where they receive full medical, PT and OT input, both pre- and postoperatively, in order to optimise care. The dedication of the PTs and OTs ensures that postoperative patients are ready as soon as possible through intensive 20-minute PT and OT sessions twice daily. Patients and family members were heavily involved in education and daily exercise, with the treatment plan being clearly documented in the HFB. This booklet is utilised by all MDT members from acute to community care, and also provides a continuation and a reference point for patients.
The community MDT is instrumental because without their buy-in and dedication, the ACDC programme would not have taken off so successfully. Effective communication and weekly meetings helped to iron out the issues that were identified during the trial period. Through the ACDC, the patient is provided daily access to HCA and receives two PT and OT sessions per week at home. Any issues are communicated to acute services and addressed immediately. This improved stakeholders’ confidence in the programme and minimised complications to the patient.
SUSTAINING THE IMPROVEMENTClear communication lines and the availability of fail-safe referral pathways were integral to ACDC’s success. The HFB provides a central reference point for all stakeholders: it is used as an educational tool by MDT in acute services, as a reference tool and diary for the patient, as a follow-up tool by community MDT, and as a reference point and visual aid during the patient’s follow-up in the virtual orthopaedic clinic. Because of the pilot programme’s success, ACDC has been extended beyond the 20-mile limit, with new hubs rolled out in counties Clare and Tipperary by the end of January 2021.
The ACDC programme has continued to grow, with more than 120 patients enrolled to date. We have seen a reduction in our acute LOS from 17 days in 2019 to 12 days in 2020 and to date in 2021. We have also seen an increase in patients going directly home, from 20% in 2019 to 50% in 2020 and 2021.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT100
CHAPTER 8
MATER MISERICORDIAE UNIVERSITY HOSPITAL
QI PROJECT TITLE: Improving IHFS 1
PROJECT LEADS:
Mary Mullen, ANP, Orthogeriatrics; Dr Sandra O’Malley, Orthopaedic Senior House Officer (SHO); Mr Keith Synnott, Consultant Orthopaedic Surgeon; Dr Vinny Raminah, Consultant ED Physician; Prof. Joe Duggan, Consultant Geriatrician; Dr Liz Callaly, Consultant Geriatrician; Ruth Buckley, Quality Manager; Karen Fitzpatrick, Data Co-Ordination Lead.
PROJECT TEAM: Mater Misericordiae University Hospital Hip Fracture Governance Committee
Left to right: Mary Mullen, Advanced Nurse Practitioner in Orthogeriatrics, Dr Sandra O’Malley, Orthopaedic Senior House Officer
BACKGROUND AND AIMSHip fractures are a common injury associated with increased morbidity/mortality in older adults. They also contribute to the spiralling costs of an already overburdened health system. The IHFD is a web-based clinical audit that measures hip fracture care, initiates secondary prevention, and ultimately helps MDT to improve patient outcomes. This is achieved through benchmarking six clinical KPIs and two non-clinical KPIs (NOCA, 2020). Our IHFD clinical audit data in 2018 showed that only 1% of patients within the Mater Misericordiae University Hospital (MMUH) achieved IHFS 1.
The local HFGC set a target of admitting patients to the orthopaedic ward/direct to theatre within 4 hours of initial registration at the hospital. Our first objective was to interrogate the data for accuracy and explore potential gaps and areas for improvement across the hip fracture patient pathway. The second objective was to secure and maintain a protected hip fracture bed. Finally, our third objective was to assess how we communicated as a team.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 101
CHAPTER 8
We also identified the need to evaluate our performance as a team across the patient pathway. The hip fracture pathway is dependent on five specialties: ED, orthopaedic surgery, theatre, orthogeriatrics and physiotherapy. Effective communication within this stakeholder group is paramount in order to ensure the safe, timely transfer of patients to the ward. Proactive discussions and cross-examination of our audit data continued during local HFGC meetings, where we also explored what changes could be made in order to achieve greater and sustained improvement.
METHODWe created a process for collecting real-time data on the hip fracture pathway. Using Dendrite Intellect software, we developed a new audit tool for auditing hip fracture patients, enabling greater data analysis and measurement of improvements in real time.
Next, we migrated from the traditional referral/communication method via phone/bleep to a more robust phone messaging application called Siilo. This was employed as the means to improve communication and enhance team performance. We created a hip fracture pathway group on Siilo with all key MDT stakeholders and specialties involved. This provided us with a secure, live communication hub that was accessible to stakeholders via their mobile phone.
RESULTSSiilo allowed us to create a sense of urgency pertaining to the hip fracture pathway and over time we started to see improvements and results, and we began to function better as a team. Siilo has increased efficiency within the hip fracture pathway with better, faster decision-making through direct knowledge exchange, engaging the entire team simultaneously.
At the most recent HFGC meeting, live data courtesy of the Dendrite Intellect software outlined how we had made significant progress in admitting patients to the orthopaedic ward within 4 hours. Compliance with IHFS 1, improved from 17% in July to 83% in September.
QUALITY IMPROVEMENT PLANBased on the Plan Do Study Act (PDSA) cycle, our approach was twofold. Initially we reviewed the way data were collected within MMUH throughout 2019 and for the first 6 months of 2020. On completion of this review, we recognised that live data were paramount to the success of the hip fracture patient pathway; as a result, a Dendrite Intellect software programme was designed and launched by the hospital’s Data Co-ordination Lead which allowed us to view live data on a daily/weekly basis. This software was instrumental within the hip fracture pathway as it provided live audit data which allowed us to see how the hospital was performing at any one time while facilitating ongoing changes to enhance the patient’s journey and experience.
Using Siilo as a team, we developed a communication platform among the healthcare professionals involved in the care of hip fracture patients beginning with the patients’ initial presentation with a hip fracture in the ED. Siilo-based messaging is a catalyst for stakeholder collaboration and has facilitated greater dialogue within the hip fracture group on Siilo. The Siilo messenger app is a secure method for exchanging information, is General Data Protection Regulation compliant, and is healthcare specific.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT102
CHAPTER 8
STAKEHOLDER ENGAGEMENTThe orthopaedic team pioneered and championed the shift towards this messaging app and it is now being rolled out to other teams within the MMUH: to date, 1,100 MMUH staff members have downloaded and are registered on the app. With each radiologically confirmed hip fracture patient that presents in ED, an alert notifies all stakeholders within the hip fracture group on Siilo that there is a new hip fracture patient in ED. Our ED colleagues create a case record which outlines past medical history, medications, etc. and includes diagnostic imaging. This informs all stakeholders and enables faster decision-making and identification of the requirement for a theatre slot and inpatient bed. The current hip fracture group on Siilo consists of MDT members, with various administrators appointed from different disciplines and teams taking responsibility for granting and amending access to the group. This application acts as a patient management tool, with current stakeholders including ED medics, the orthopaedic team, theatre staff, anaesthetics, Patient Flow coordinator, St Agnes Ward staff, the Orthogeriatrics ANP/Registrar and physiotherapist.
As a means of ongoing audit within the Siilo messaging application and with the objective of improving patient outcomes, the site nurse managers were included, as they can negotiate access to the orthopaedic bed outside of normal working hours, ensuring that this is accessible 24 hours per day. In addition, we are in discussion with the app developers to determine whether further changes to the app could be made for the hip fracture group on Siilo; for example, implementing a ticking clock counting down the time from initial presentation until transfer to bed or theatre.
SUSTAINING THE IMPROVEMENT Launching the Dendrite Intellect software programme has allowed us to capture and explore live data, highlighting gaps in the hip fracture patient pathway and opportunities for improvement.
The implementation of the Siilo messaging app has enhanced our communication across specialties. The simultaneous delivery of real-time messaging to all stakeholders has driven this necessary change and allowed us to achieve our aim of hip fracture patients accessing a bed on the orthopaedic ward within 4 hours of initial presentation to ED. Siilo has acted as a secure communication tool, coordinating care of hip fracture patients among appropriate stakeholders while accelerating decision-making. A cohesive team dynamic has been established that ensures timely management of this patient cohort and enhanced patient care.
Siilo supports and echoes both NOCA’s and Sláintecare’s goals, with the right care, in the right place, at the right time, and with the right team all being involved in this pathway.
CONCLUSIONThe IHFD will continue to build upon and support the great QI work being done at the front line by all of the hospitals involved in the audit in order to improve standards of care and innovate locally to meet patient needs.
CONTENTS >

CHAPTER 9AUDIT UPDATE
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT104
CHAPTER 9
CHAPTER 9: AUDIT UPDATE
UPDATE ON AUDIT RECOMMENDATIONS FROM 2019
Recommendations for the HSE Update
The Health Service Executive (HSE) National Office for Trauma Services, in collaboration with the National Clinical Programme for Trauma and Orthopaedic Surgery, will:
Improvements made for the recommendations from 2019
• continue to prioritise and operationalise a national hip fracture bypass for all hospitals
• In 2020, there was further improvement in the percentage of hip fracture patients being brought directly to the operating hospital (94%)
• improve pathways of care for hip fracture through the trauma system, i.e. ED, operating theatre and rehabilitation
• The percentage of patients being admitted through the ED has also continued to improve throughout 2020, although time to surgery has remained largely unchanged as COVID-19 created more challenges due to requirements to screen patients pre-operatively, allow extra time between cases and conduct additional cleaning in the operating theatre.
• Community supports to enable early supported discharges
• More patients were discharged directly home (28%) and the LOS declined by 2.5 days in 2020 compared to 2019. Feedback from the hospitals was that they had much more engagement with the community teams during the pandemic, which helped to facilitate earlier discharges.
Recommendations for hospital managers, clinicians and audit coordinators
Update
Hospital hip fracture governance committees should follow NOCA’s guidance for governance committees and meet quarterly to discuss and prioritise IHFD areas for attention.
Despite the pandemic, HFGCs continued to meet less often throughout the pandemic.
Focus on increasing compliance with the IHFS to attain the BPT.
More hospitals met the BPT in 2020, with the resulting money paid out totalling €710,000. The percentage of patients who met the BPT standards increased to 20% in 2020 from 15% in 2019.
Develop and resource a multidisciplinary orthogeriatric service.
In Chapter 10, details of the orthogeriatric services are described for each of the IHFD participating hospitals; work is ongoing to develop a consensus on a model for orthogeriatric care for Ireland.
This chapter highlights the progress made on last year’s recommendations, as well as key achievements in research, publications and presentations.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 105
CHAPTER 9
Comply with the new IHFS for early mobilisation, which will measure the percentage of patients mobilised by a physiotherapist on the day of or the day after surgery.
Each hospital’s compliance with the new IHFS was reported to them quarterly throughout 2020 and 2021. IHFS 7 will become part of the BPT in 2022.
Prioritise the discharge of patients directly home from hospital where possible.
In 2020, more patients were discharged directly home (28%) than in 2019 (24%).
HFGCs should follow NOCA’s guidance for governance committees and meet quarterly to discuss and prioritise IHFD areas for attention.
All hospitals have a HFGC which, despite COVID-19, managed to maintain a strong focus on the IHFS and audit.
Focus on increasing compliance with the IHFS to attain the BPT.
More hospitals met the BPT in 2020, with the resulting money paid out totalling €710,000.
Recommendations for NOCA Update
Support hospitals to attain high levels of data coverage and quality until at least 2022, as they recover from the effects of the COVID-19 pandemic.
Hospitals achieved 99% data coverage in 2020, with all hospitals achieving more than 90% data coverage.
Introduce a new IHFS for early mobilisation – measuring the percentage of patients mobilised by a physiotherapist on the day of or the day after surgery – to quarterly reports in 2020.
IHFS 7 was added to the IHFD quarterly reports in 2020 and communicated back to the hospitals.
Develop workshops to create a learning culture for quality improvement with the clinical leads and audit coordinators of the IHFD.
Due to the COVID-19 pandemic, the IHFD workshop was postponed; however, regular contact with the audit coordinators was maintained throughout the year and resources were shared virtually.
Implement processes for the introduction of long-term outcome measures in the IHFD.
NOCA is collaborating on the Health Research Board (HRB)-funded 3-year Hip Fracture Outcome and Geographic Equality (HipFORGE) project which will explore methods for and make recommendations on collecting long-term outcomes in this patient population in Ireland. This project commenced in June 2021.
Develop a research group for the IHFD, including Public and Patient Interest (PPI) representatives.
The IHFD research group was set up and ethical approval was received to conduct secondary analysis of the IHFD data. Several publications were submitted and published throughout 2020 and 2021.
Conduct an organisational audit to look at resources, governance and quality improvement at hospital level in 2020.
An organisational survey was conducted during 2020, the details of which are provided in Chapter 10.
Increase engagement with PPI representatives to:• raise awareness of topics such as falls prevention
and frailty• create information resources for patients about
what to expect while in hospital, on discharge, and for rehabilitation
• create opportunities for multistakeholder engagement around key issues faced by patients.
Throughout 2020, PPI activity was reduced due to COVID-19, although this activity will be resumed in 2021.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT106
CHAPTER 9
RESEARCH
HRB Grant awarded
The HipFORGE project is being led by Dr Mary Walsh (University College Dublin) and funded by the HRB.
Hip fracture is a serious event in the lives of older people, with around one in five individuals dying in the first year after their injury and many more losing their independence. In Ireland, little is currently known about how people recover in the longer term after hip fracture and many do not receive follow-up. For several years, the IHFD has had a stated goal to facilitate the collection of longer-term hip fracture outcomes as part of routine audit. These outcomes would include survival, mobility and quality of life up to 1 year after the injury. Hospitals need to be supported to conduct this follow-up through education about methods that are acceptable to people with hip fracture and that have been successful in Ireland and internationally. Through the HipFORGE project, advice will be developed for local audit coordinators with regard to long-term outcome data collection in Ireland. This will be based on existing literature and input from patients, family members, health professionals and researchers. The HipFORGE project also aims to identify the best-evidence based tools to facilitate hip fracture care comparisons between hospitals in the Irish setting by accounting for the types of patients that they treat. Finally, it will explore whether people who live in different areas of the country are receiving equal standards of care after hip fracture, regardless of what hospital they attend.
HipFORGE is being funded by a 3-year fellowship through the HRB Applying Research into Policy and Practice postdoctoral scheme and is based at the School of Public Health, Physiotherapy and Sports Science in University College Dublin. It involves a collaboration with NOCA as well as with clinical and academic professionals from around Ireland and from Oxford University in the UK. The project commenced in June 2021.
European Health Data and Evidence Network (EHDEN)
In 2021, the IHFD, along with many other hip fracture registries, submitted an application to EHDEN led by Professor Xavier Griffin in Oxford University. The application was successful and will explore how these registries can link and use the data collaboratively in order to answer research questions on an international scale.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 107
CHAPTER 9
PUBLICATIONS
Recent publications from the IHFD include:
Ferris, H., Brent, L., Sorensen, J., Ahern, E. and Coughlan, T., 2021. Discharge destination after hip fracture: findings from the Irish hip fracture database. European geriatric medicine, pp.1-10.
Hall, A.J., Clement, N.D., MacLullich, A.M.J., Ojeda-Thies, C., Hoefer, C., Brent, L., White, T.O. and Duckworth, A.D. (2021) IMPACT of COVID-19 on hip fracture services: A global survey by the International Multicentre Project Auditing COVID-19 in Trauma & Orthopaedics. Surgeon, S1479-666X(21), pp. 00092-00095.
Walsh, M.E., Ferris, H., Coughlan, T., Hurson, C., Ahern, E., Sorensen, J. and Brent, L. (2020) Trends in hip fracture care in the Republic of Ireland from 2013 to 2018: results from the Irish Hip Fracture Database. Osteoporosis International, 32(4), pp. 727-736.
PRESENTATIONS
Throughout 2020, many major conferences were cancelled or changed to virtual events. The IHFD presented at the following in 2020 and 2021:
• Irish Orthopaedic Association Conference 2020
• Irish Hip Fracture Meeting 2020
• EBPOM Anaesthesia Conference 2020
• British Geriatric Society Conference 2021
• HSE ‘Older Persons Impacted by COVID – Time to Get Moving Again’ Webinar 2021
• IIPOSI Citizens assembly 2021
• ISQUA conference 2021.
CONTENTS >


CHAPTER 10ORGANISATIONAL
SURVEY
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT110
CHAPTER 10: ORGANISATIONAL SURVEY
CHAPTER 10
The IHFD conducted the first facilities survey in 2016, and in 2017 it conducted a survey of the governance structure related to the audit in local hospitals. In 2020, these surveys were repeated. This chapter will help to add more granularity to the data provided in the earlier data chapters and demonstrate how the investment in resources at a hospital level has led to the successes and improvements achieved within this audit in recent years.
Comparison between the previous surveys shows that:
• All hospitals are very engaged in the IHFD audit
• There has been an increase in the number of trauma beds, with some hospitals protecting a bed specifically for hip fracture patients
• Most hospitals now have an orthogeriatric service
• ANP roles focused on the care of hip fracture patients are being developed
• Work is still needed in order to improve operating theatre access and health and social care professional (HSCP) input at weekends
• There has been an increase in the pre-operative use of nerve blocks
• Ambulance pre-alerts to ED are increasing
• More protocols are being used for pain assessment, delirium, nutrition and pre-operative fasting, but more are still needed
• All hospitals have a HFGC
• HFGCs are more robust than they were in the first survey in terms of the number of meetings held, the content of the meetings, and attendees are from a more broad representation of the multidisciplinary team involved in hip fracture care.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 111
CHAPTER 10
Hospital name Beaumont Connolly Cork Drogheda
Number of hip fracture cases per year (aged ≥60 years) 234 203 455 207
% completeness of data entry for 2020 100% 100% 100% 100%
Trauma service description Direct and indirect Direct Direct Direct
Number of trauma beds35 32 (orthopaedics/
urology) 40 31
Number of ring-fenced trauma beds 1 1 40 31
Is there a dedicated hip fracture bed on the trauma ward? Yes Yes Yes Yes
Can hip fracture patients be brought straight to theatre from ED? Yes Yes No
Acute admission to Orthopaedic ward/surgical ward
Orthopaedic ward Orthopaedic ward Orthopaedic ward
Hours of designated trauma list per week
168 40 scheduled + out of hours
63 70
Is there a dedicated trauma theatre at weekends? Yes No Yes Yes
Are hip fractures prioritised on the theatre list? Yes Yes Yes Yes
Number of whole-time equivalent (WTE) orthopaedic doctors
3 orthopaedic consultants (+5 part-time) 6 specialist registrars (SpRs)/registrars 3 SHOs 4 interns
5 orthopaedic consultants2 SpRs 4 registrars3 SHO3 Interns
6 orthopaedic consultants +4.5 ) 11 SpRs/registrars 3 SHOs 3 interns
8 orthopaedic consultants 8 SpRs/registrars 6 SHOs 3 interns
Number of hours per week of orthogeriatric input
6 geriatric consultant 1 WTE SpR/registrar 0 SHO 0 intern
1 orthogeriatric registrar assigned to see hip fracture patients but no set amount of hours
39 WTE geriatric consultant 1 WTE SpR/registrar 1 WTE SHO 0 intern
39 geriatric consultant 39 SpR/registrar 39 SHO 39 intern
Year the orthogeriatric service commenced 2010 2015 2018
Composition/model of orthogeriatric service
Daily round by registrar Weekly consultant-led ward round
orthogeriatric registrar reviews hip fracture patients
Daily ward round by consultant
Proactive orthogeriatric service MDT-led weekly meetings
Is there a dedicated social worker for the orthopaedic service? Yes Yes No Yes
Number of cANPs/ANPs, clinical nurse specialists specialising in fragility fracture inpatients
1 cANP 1 cANP1 CNS
1 trauma CNS 1 Fracture Liaison Service (FLS) ANP 1 trauma CNS
Number of WTE fracture liaison nurses 0 0 0 0
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT112
CHAPTER 10
Hospital name Galway Kerry Letterkenny Limerick
Number of hip fracture cases per year (aged ≥60 years) 219 128 154 328
% completeness of data entry for 2020 98% 100% 100% 98%
Trauma service description Direct and indirect Direct Indirect Direct
Number of trauma beds36 37 29
Number of ring-fenced trauma beds 28 0 29
Is there a dedicated hip fracture bed on the trauma ward? Yes (when available) No No Yes
Can hip fracture patients be brought straight to theatre from ED? Yes No Yes Yes
Acute admission to Orthopaedic ward Any ward Orthopaedic ward Orthopaedic ward
Hours of designated trauma list per week
Trauma theatre 7 days per week
Two lists – 8 hours No trauma list, hip fracture patients operated on emergency list
48
Is there a dedicated trauma theatre at weekends? Yes No No Yes (not Saturday)
Are hip fractures prioritised on the theatre list? Yes No No Yes
Number of whole-time equivalent (WTE) orthopaedic doctors
11 orthopaedic consultants 11 SpRs/registrars 11 SHOs 5 interns
3 orthopaedic consultants 5 SpRs/registrars 5 SHOs 0 interns
4 orthopaedic consultants 4 SpRs/registrars 6 SHOs 0 interns
6 orthopaedic consultants 10 SpRs/registrars 9 SHOs 4 interns
Number of hours per week of orthogeriatric input
8–10 geriatric consultant 25–30 SpR/ registrar 0 SHO 0 intern
1 geriatric consultant 1 SpR/registrar 0 SHO 0 intern
0 geriatric consultant 0 SpR/registrar 0 SHO 0 intern
2 geriatric consultant 39 SpR/registrar 0 SHO 0 intern
Year the orthogeriatric service commenced 2018 2020 2017 2014
Composition/model of orthogeriatric service
Daily round by the SpR/registrar and a consultant geriatrician with input from the trauma CNS Twice-weekly MDT
ANP-led service discussed with geriatric consultant
ANP review referrals sent to on-call medical team, attended to by geriatrician if on call
Consult-based service Twice-weekly MDT ward rounds
Is there a dedicated social worker for the orthopaedic service? Yes No No Yes
Number of cANPs/ANPs, clinical nurse specialists specialising in fragility fracture inpatients
1 trauma CNS 1 cANP 1 ANP 1 orthopaedic CNS 1 ANP
Number of WTE fracture liaison nurses 0 0 1 0
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 113
CHAPTER 10
Hospital name Mater Mayo Sligo St James’s
Number of hip fracture cases per year (aged ≥60 years) 138 123 127 169
% completeness of data entry for 2020 100% 98% 98% 97%
Trauma service description Direct and indirect Direct Direct Direct
Number of trauma beds30 31 (trauma/
elective) 18 62
Number of ring-fenced trauma beds 15 9 12–14 0
Is there a dedicated hip fracture bed on the trauma ward? Yes No No No
Can hip fracture patients be brought straight to theatre from ED? Yes Yes No Yes
Acute admission to Orthopaedic ward Orthopaedic ward Orthopaedic ward Orthopaedic ward
Hours of designated trauma list per week
Emergency list (which includes trauma list)
Daily trauma list (at end of elective list)
20 45
Is there a dedicated trauma theatre at weekends? Yes Yes No Yes
Are hip fractures prioritised on the theatre list? Yes No Yes Yes
Number of whole-time equivalent (WTE) orthopaedic doctors
8 orthopaedic consultants 5 SpRs/registrars 5 SHOs 3 interns
4 orthopaedic consultants 7 SpRs/registrars 7 SHOs 0 interns
5 orthopaedic consultants 5 SpRs/registrars 6 SHOs 0 interns
4.2 orthopaedic consultants 5 SpRs/registrars 1 SHO 4 interns
Number of hours per week of orthogeriatric input
3 geriatric consultant 20 SpR/registrar 0 SHO 0 intern (39 ANP)
2 geriatric consultant 0 SpR/registrar 0 SHO 0 intern (10 ANP)
3 geriatric consultant 0 SpR/registrar 0 SHO 0 intern
6 geriatric consultant 6 SpRs/Registrars 0 SHO 0 intern
Year the orthogeriatric service commenced 2002 2018 2016 2013
Composition/model of orthogeriatric service
Integrated Orthogeriatric Model
Reviewed by ANP older person and then weekly MDTs with geriatrican
Geriatric consult service
Liaison consultants service
Is there a dedicated social worker for the orthopaedic service? Yes No Yes No
Number of cANPs/ANPs, clinical nurse specialists specialising in fragility fracture inpatients
1 ANP 1 ANP older person 1 frailty nurse (cANP)
Number of WTE fracture liaison nurses 0 0 1
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT114
CHAPTER 10
Hospital name St Vincent’s Tallaght Tullamore Waterford
Number of hip fracture cases per year (aged ≥60 years) 321 203 213 388
% completeness of data entry for 2020 100% 98% 100% 99%
Trauma service description Direct Direct and indirect Direct and indirect Direct and indirect
Number of trauma beds40 31 58
Number of ring-fenced trauma beds 0 6 1 1
Is there a dedicated hip fracture bed on the trauma ward? No Yes Yes Yes (when available)
Can hip fracture patients be brought straight to theatre from ED? Yes Yes Yes Yes
Acute admission to Orthopaedic ward/surgical ward
Orthopaedic ward Orthopaedic ward Orthopaedic ward
Hours of designated trauma list per week
60.5 90 168 56
Is there a dedicated trauma theatre at weekends? Yes Yes Yes Yes
Are hip fractures prioritised on the theatre list? Yes Yes Yes Yes
Number of whole-time equivalent (WTE) orthopaedic doctors
7 orthopaedic consultants 5 SpRs/registrars 4 SHOs 3 interns
5.86 orthopaedic consultants 15 SpRs/registrars 5 SHOs 4 interns
6 orthopaedic consultants 6 SpRs/registrars 4 SHOs 3 interns
9.5 orthopaedic consultants 7 SpRs/registrars 10 SHOs 4 interns
Number of hours per week of orthogeriatric input
24 geriatric consultant 32 SpRs/Registrars 0 SHO 0 intern
39 geriatric consultant
3–5 geriatric consultant 5 SpRs/Registrars 0 SHO 0 intern
39 geriatric c onsultant 39 SpRs/Registrars 0 SHO 0 intern
Year the orthogeriatric service commenced 2005 2020 2013 2019
Composition/model of orthogeriatric service
Consultant-led rounds, daily rounds, registrar based on ward MDT weekly Virtual clinic at 1 year
Ward rounds 2–3 times per week, weekly MDT
Integrated orthogeriatric service (6–10 hours per week)
Consult liaison Registrar assesses within 24–72 hours of admission. Twice-weekly rounds thereafter.
Is there a dedicated social worker for the orthopaedic service? Yes Yes No No
Number of cANPs/ANPs, clinical nurse specialists specialising in fragility fracture inpatients
1 orthopaedic CNS 1 CNS FLS x 1 0 1 trauma CNS 1 ANP
Number of WTE fracture liaison nurses 0.5 1 0 1
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 115
CHAPTER 10
Hospital name Beaumont Connolly Cork Drogheda
Number of WTE nursing staff in the orthopaedic department
ANP/cANP: 1 CNS: 0 CNM3: 1 CNM2: 1 CNM1: 2 Staff nurse: 23
ANP/cANP: 1CNS: 1CNM 3: 0CNM 2: 1CNM 1: 2Staff nurse: 23
ANP/cANP: 0 CNS: 0 CNM3: 0 CNM2: 2 CNM1: 2 Staff nurse: 60
ANP/cANP: 1 CNS: 1 CNM3: 1 CNM2: 1 CNM1: 2 Staff nurse: 29
Nursing staff:patient ratio in the orthopaedic department in the am/pm and on night duty
AM: 5:6 PM: 5:6Night: 4
AM: 7PM: 7Night: 4
AM: 1:7 PM: 1:7 Night: 1:5/1:7/1:12
AM: 7 PM: 7 Night: 4
How many staff in the department have higher education in orthopaedics?
2 6 4 6
Number of HCAs in the am/pm and on night duty
AM: 2–3 PM: 3 Night: 0
AM: 2PM: 2Night: 1
AM: 1 PM: 1 Night: 0.5
AM: 2 PM: 2 Night: 2
Are hip fracture patients mobilised on day 1 routinely?
Yes By physiotherapist or nurse
Yes By physiotherapist
Yes By physiotherapist
Yes By physiotherapist
Is pain management given prior to mobilisation routinely? Yes Yes Yes Yes
Monday–Friday WTE for Physiotherapist (PT) and Physiotherapist Assistant (PTA)
PT: 2 PTA: 1
PT: 1PTA: 0
PT: 2 PTA: 0
PT: 3.5 PTA: 0.9
Saturday WTE for PT and PTA PT: 1 PTA: 0
PT: 1PTA: 0
0 PT: 1 PTA: 0
Sunday WTE for PT and PTA 0 PT: 1PTA: 0
0 PT: 1 PTA: 0
Year that weekend physiotherapy commenced 2017 1990's 2008
Monday–Friday WTE for Occupational Therapist (OT) and Occupational Therapist Assistant (OTA)
OT: 0.9 OTA: 0.2
OT:1OTA: 1
OT: 1 OTA: 0
OT: 1 OTA: 1 (but not designated orthopaedic)
Weekend OT 0 0 0 0
Does PT service at weekends see day 1 hip fracture patients?
Saturday: Yes Sunday: No
Saturday: YesSunday: Yes
Saturday: No Sunday: No
Saturday: Yes Sunday: Yes
Does PT see non-day 1 hip fracture patients on weekends? Yes Yes No Yes
Rehabilitation sites – on-site or off-site? Off-site Off-site Off-site Off-site
Name of rehabilitation hospitals that hip fracture patients are discharged to from the acute hospital
Clontarf Orthopaedic Hospital St Joseph’s Hospital Raheny
Cappagh National Orthopaedic HospitalClontarf Orthopaedic Hospital
South Infirmary Victoria University Hospital
Louth County Hospital rehabilitation (from May 2020) Monaghan rehabilitation CIRROS Navan (from May 2020)
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT116
CHAPTER 10
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
Hospital name Galway Kerry Letterkenny Limerick
Number of WTE nursing staff in the orthopaedic department
ANP/cANP: 0 CNS: 1 CNM3: 0 CNM2: 1 CNM1: 1 Staff nurse: 23
ANP/cANP: 1 CNS: 0 CNM3: 0 CNM2: 1 CNM1: 1 Staff nurse: 19.7
1 ANP/cANP: 0 CNS: 1 CNM3: 0 CNM2: 2 CNM1: 0 Staff nurse: 28
ANP/cANP: 1 CNS: 1 CNM3: 0 CNM2: 1 CNM1: 2 Staff nurse: 24
Nursing staff:patient ratio in the orthopaedic department in the am/pm and on night duty
AM: 8 PM: 8 Night: 8
AM: 1:6 PM: 1:8 Night: 1:8
AM: 3 PM: 2 Night: 2
AM: 6 PM: 4 Night: 4
How many staff in the department have higher education in orthopaedics?
5 1 3 8
Number of HCAs in the am/pm and on night duty
AM: 3 PM: 3 Night: 1
AM: 1 PM: 1 Night: 0
AM: 6 PM: 4 Night: 2
AM: 2 PM: 2 Night: 1
Are hip fracture patients mobilised on day 1 routinely?
Yes By physiotherapist
Yes By physiotherapist
Yes By physiotherapist
Yes By physiotherapist
Is pain management given prior to mobilisation routinely? Yes Yes Yes No
Monday–Friday WTE for Physiotherapist (PT) and Physiotherapist Assistant (PTA)
PT: 2.5 PTA: 1
PT: 1 PTA: 1
PT: 1.5 PTA: 1
PT: 2 PTA: 0.5
Saturday WTE for PT and PTA
PT: 2 (on call) PTA: 0
0 PT: (on call) PTA: (on call)
PT: 1 (on call) PTA: 0
Sunday WTE for PT and PTA
PT: 2 (on call) PTA: 0
0 PT: (on call) PTA: (on call)
PT: 1 (on call) PTA: 0
Year that weekend physiotherapy commenced
2006 N/A 2001
Monday–Friday WTE for Occupational Therapist (OT) and Occupational Therapist Assistant (OTA)
OT: 1.5 OTA: 0
OT: 1 OTA: 0
OT: 1 OTA: 0.5
OT: 1 OTA: 0
Weekend OT 0 0 0 0
Does PT service at weekends see day 1 hip fracture patients?
Saturday: Yes Sunday: Yes
Saturday: No Sunday: No
Saturday: Yes Sunday: Yes
Saturday: Yes Sunday: Yes
Does PT see non-day 1 hip fracture patients on weekends? No No No
Rehabilitation sites – on-site or off-site? On-site On-site Off-site
Name of rehabilitation hospitals that hip fracture patients are discharged to from the acute hospital
Unit 4 and Hospital Ground Merlin Park University Hospital (with access to community nursing units with identified AHP support)
Killarney Community Hospital Kenmare Community Hospital Listowel Community Hospital
St Camillisus Community Hospital St Ita’s Community Hospital Hospital of Assumption Thurles St Joseph’s Hospital Ennis St Patrick’s Hospital Cashel
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 117
CHAPTER 10
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
Hospital name Mater Mayo Sligo St James’s
Number of WTE nursing staff in the orthopaedic department
ANP/cANP: 1 CNS: 0 CNM3: 1 CNM2: 1 CNM1: 1 Staff nurse: 26.12
ANP/cANP: 1 CNS: 0 CNM3: 0 CNM2: 1 CNM1: 1 Staff nurse: 29
ANP/cANP: 0 CNS: 0 CNM3: 0 CNM2: 1.5 CNM1: 0 Staff nurse: 18
ANP/cANP: 0 CNS: 1 CNM3: 1 CNM2: 1 CNM1: 1 Staff nurse: 19
Nursing staff:patient ratio in the orthopaedic department in the am/pm and on night duty
AM: 6 PM: 6 Night: 4
AM: 5 PM: 5 Night: 3
AM: 7 PM: 4:5 Night: 3
AM: 5 PM: 5 Night: 3
How many staff in the department have higher education in orthopaedics?
0 12 13 0
Number of HCAs in the am/pm and on night duty
AM: 2–3 PM: 2–3 Night: 1
AM: 2 PM: 2 Night: 1
AM: 2 PM: 1 Night: 1
AM: 3–4 PM: 3 Night: 2
Are hip fracture patients mobilised on day 1 routinely?
Yes By physiotherapist
Yes By physiotherapist
Yes By physiotherapist or nurse
Yes By physiotherapist
Is pain management given prior to mobilisation routinely? Yes Yes Yes Yes
Monday–Friday WTE for Physiotherapist (PT) and Physiotherapist Assistant (PTA)
PT: 2.5 PTA: 0.5
PT: 1.3 PTA: 1
PT: 1 PTA: 0
PT: 2.5 PTA: 1
Saturday WTE for PT and PTA PT: (cover for day 1 hips only) PTA: 0
PT: 0.5 PTA: 0
PT: 1 (as necessary) PTA: 0
PT: 1 PTA: 0
Sunday WTE for PT and PTA PT: (cover for day 1 hips only) PTA: 0
PT: 0.5 PTA: 0
PT: 1 (as necessary) PTA: 0
PT: 1 PTA: 0
Year that weekend physiotherapy commenced
2016 Pre-2000 2019 2009
Monday–Friday WTE for Occupational Therapist (OT) and Occupational Therapist Assistant (OTA)
OT: 2 OTA: 0
OT: 1 OTA: 0
OT: 1.5 OTA: 0
OT: 1 OTA: 0
Weekend OT 0 0 0 0
Does PT service at weekends see day 1 hip fracture patients?
Saturday: Yes Sunday: Yes
Saturday: Yes Sunday: Yes
Saturday: Yes Sunday: Yes
Saturday: Yes Sunday: Yes
Does PT see non-day 1 hip fracture patients on weekends? No No No Yes
Rehabilitation sites – on-site or off-site? Off-site Off-site Off-site On-site and
Off-site
Name of rehabilitation hospitals that hip fracture patients are discharged to from the acute hospital
Clontarf Hospital National Orthopaedic Hospital Cappagh Clements Unit
Sacred Heart Hospital, Castlebar
St John’s Hospital Sligo St Patrick’s Hospital Carrick-on-Shannon Leitrim
Clontarf Orthopaedic Hospital MISA rehabilitation Home rehabilitation
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT118
CHAPTER 10
Hospital name St Vincent’s Tallaght Tullamore Waterford
Number of WTE nursing staff in the orthopaedic department
ANP/cANP: 0 CNS: 1 CNM3: 1 CNM2: 2 CNM1: 2 Staff nurse: 21
ANP/cANP: 0 CNS: 0 CNM3: 0 CNM2: 1 CNM1: 1.2 Staff nurse: 28
ANP/cANP: 0 CNS: 2 CNM3: 1 CNM2: 2 CNM1: 1 Staff nurse: 31
ANP/cANP: 1 CNS: 1 CNM3: 0.3 CNM2: 2 CNM1: 4 Staff nurse: 39.6
Nursing staff:patient ratio in the orthopaedic department in the am/pm and on night duty
AM: 4:5 PM: 4:5 Night: 4
AM: 6 PM: 6 Night: 4
AM: 5:25 PM: 5:25 Night: 3:25
AM: 5 PM: 4 Night: 3 (per ward)
How many staff in the department have higher education in orthopaedics?
9 10 13 11
Number of HCAs in the am/pm and on night duty
AM: 4 PM: 4 Night: 3
AM: 1 PM: 1 Night: 1
AM: 2 PM: 2 Night: 1
AM: 2 PM: 2 Night: 1
Are hip fracture patients mobilised on day 1 routinely?
Yes By physiotherapist or nurse
Yes By physiotherapist
Yes By physiotherapist
Yes By physiotherapist or nurse
Is pain management given prior to mobilisation routinely? Yes Yes Yes Yes
Monday–Friday WTE for Physiotherapist (PT) and Physiotherapist Assistant (PTA)
PT: 2 PTA: 2
PT: 2.7 PTA: 0.5
PT: 1.5 PTA: 0.5–1.0
PT: 1 PTA: 1
Saturday WTE for PT and PTA
PT: 1.5 PTA: 0
Cover on as-needed basis
PT: 0.5 PTA: 0
0
Sunday WTE for PT and PTA
PT: 1.5 PTA: 0
Cover on as- needed basis
PT: 0.5 PTA: 0
0
Year that weekend physiotherapy commenced
2015 for day 2 2019 for day 1
1998 2019
Monday–Friday WTE for Occupational Therapist (OT) and Occupational Therapist Assistant (OTA)
OT: 1 OTA: 0
OT: 1 OTA: 0
OT: 1 OTA: 0
OT: 1 OTA: 0
Weekend OT 0 0 0 0
Does PT service at weekends see day 1 hip fracture patients?
Saturday: Yes Sunday: Yes
Saturday: Yes Sunday: Yes
Saturday: Yes Sunday: Yes
Saturday: No Sunday: No
Does PT see non-day 1 hip fracture patients on weekends? No No Yes No
Rehabilitation sites – on-site or off-site? Off-site Off-site None Off-site
Name of rehabilitation hospitals that hip fracture patients are discharged to from the acute hospital
Royal Hospital Donnybrook St. Colmcille’s Hospital, Leopardstown Park Hospital, Clontarf
Peamount, Clontarf No rehabilitation hospital
St Patrick’s Waterford Dungarvan St Patrick’s Cashel Hospital of the Assumption Thurles St Colombus Thomastown St Johns Wexford Sacred Heart Carlow
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 119
CHAPTER 10
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
Hospital name Beaumont Connolly Cork Drogheda
Do hip fracture patients receive a nerve block pre-operatively? Yes Yes Yes Yes
Who performs the nerve block?ED team ED team ED team ED team
Is pain routinely assessed and scored in the ED? Yes Yes No Yes
Is pain score recorded at rest and during movement on the ward? Yes Yes Yes Yes
Do you assess patients for delirium in the ED? Yes No No No
Do you assess patients for delirium regularly on the ward? Yes Yes Yes Yes
Do you have routine or consult-based dietetic support within the department?
Routine Consult Consult Routine
Do you provide clear fluids up to 2 hours prior to surgery to fasting patients?
No No Yes No
Do you have a falls clinic?Yes No No No
Who carries out specialist falls assessments?
Geriatrician and MDT
Orthogeriatric registrar
Orthogeriatrician Orthogeriatrician
Are the hip fracture patients followed up in OutPatients Department If so, by whom and when?
Yes Yes- at 6 weeks by Orthopaedic ANP
Yes – at 6 weeks Yes – at 6 weeks (except for hemiarthroplasty patients)
Who prescribes bone protection medication?
Orthogeriatrician Orthogeriatric registrar
Orthogeriatrician Orthogeriatrician
Is Dual-energy X-ray absorptiometry (DXA) on-site? Yes No Yes No
Who collects the data for the IHFD?
Audit Coordinator for IHFD
CNM2 orthopaedics
Trauma Coordinator
Trauma Coordinator
How much WTE (in hours) is protected for the collection of the IHFD data?
7 0 0 3
Does the data coordinator have an office to collect the data in? Yes Yes Yes Yes
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT120
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
Hospital name Galway Kerry Letterkenny Limerick
Do hip fracture patients receive a nerve block pre-operatively? Yes Yes Yes Yes
Who performs the nerve block?ED team ED team ED team ED team
Is pain routinely assessed and scored in the ED? Yes No Yes Yes
Is pain score recorded at rest and during movement on the ward? Yes Yes Yes Yes
Do you assess patients for delirium in the ED? Yes No No Yes
Do you assess patients for delirium regularly on the ward? Yes No No Yes
Do you have routine or consult-based dietetic support within the department?
Consult Consult Consult Consult
Do you provide clear fluids up to 2 hours prior to surgery to fasting patients?
No (up to 4 hours) No No Yes
Do you have a falls clinic?No Yes Yes
Who carries out specialist falls assessments?
Physiotherapist, geriatric ANP
Fraction liaison nurse
Orthogeriatric registrar
Are the hip fracture patients followed up in OutPatients Department If so, by whom and when?
Yes – at 6 weeks by operating consultant
Routine appointment at fracture clinic by registrar/consultant
Yes – at 6 weeks (consultant review in fracture clinic)
Yes – at 6 weeks (review with orthopaedic CNS)
Who prescribes bone protection medication?
Orthogeriatric team
GP GP Orthogeriatric team
Is Dual-energy X-ray absorptiometry (DXA) on-site? No Yes Yes Yes
Who collects the data for the IHFD?
Orthopaedic CNS Nurse Fracture Liaison Nurse
Orthopaedic CNS
How much WTE (in hours) is protected for the collection of the IHFD data?
0 26 0 0
Does the data coordinator have an office to collect the data in? Yes Yes Yes Yes
CHAPTER 10
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 121
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
Hospital name Mater Mayo Sligo St James’s
Do hip fracture patients receive a nerve block pre-operatively? Yes No Yes Yes
Who performs the nerve block?ED team ED doctors ED team or
anaesthesiologist ED team
Is pain routinely assessed and scored in the ED? Yes Yes Yes Yes
Is pain score recorded at rest and during movement on the ward? No Yes Yes Yes
Do you assess patients for delirium in the ED? Yes No Yes Yes
Do you assess patients for delirium regularly on the ward? Yes Yes Yes Yes
Do you have routine or consult-based dietetic support within the department?
Consult Consult Consult Consult
Do you provide clear fluids up to 2 hours prior to surgery to fasting patients?
No Yes No No
Do you have a falls clinic?No No No Yes
Who carries out specialist falls assessments?
Specialist geriatric team, ANP
ANP older person Orthogeriatrician Consultant geriatrician and MDT meetings
Are the hip fracture patients followed up in OutPatients Department If so, by whom and when?
Yes – followed up by orthogeriatric and orthopaedic services
Yes – by orthopaedic consultant
Hemiarthroplasty patients discharged to care of general practitioner (GP). Intertrochanteric fractures reviewed by orthopaedic team in OPD.
Yes (orthopaedic consultant/ registrar)
Who prescribes bone protection medication?
Orthogeriatric team and ANP
Consultant Orthogeriatrician Bone health team
Is Dual-energy X-ray absorptiometry (DXA) on-site? Yes No Yes Yes
Who collects the data for the IHFD?
Data Manager and ANP
Nurse Senior Theatre Nurse
Trauma Coordinator
How much WTE (in hours) is protected for the collection of the IHFD data?
Not defined 5 4 (on an ad hoc basis) 0.5
Does the data coordinator have an office to collect the data in? Yes No No Yes
CHAPTER 10
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT122
CHAPTER 10
TABLE 10.1: HOSPITAL DEMOGRAPHICS AND RESOURCES CONTINUED
Hospital name St Vincent’s Tallaght Tullamore Waterford
Do hip fracture patients receive a nerve block pre-operatively? Yes Yes Yes Yes
Who performs the nerve block?ED team ED team or
anaesthesiologist ED team ED team
Is pain routinely assessed and scored in the ED? Yes Yes Yes Yes
Is pain score recorded at rest and during movement on the ward? Yes Yes Yes No
Do you assess patients for delirium in the ED? No Yes No No
Do you assess patients for delirium regularly on the ward? Yes Yes Yes Yes
Do you have routine or consult-based dietetic support within the department?
Routine Consult Consult Consult
Do you provide clear fluids up to 2 hours prior to surgery to fasting patients?
No Yes No Yes
Do you have a falls clinic?No Yes Yes Yes
Who carries out specialist falls assessments?
Orthogeriatrics and physiotherapists
Age related Healthcare
Geriatrician Orthogeriatrician
Are the hip fracture patients followed up in OutPatients Department If so, by whom and when?
Yes – at 6 weeks in relevant consultant’s clinic (virtual orthogeriatric follow-up clinic held 1 year post-hip fracture by orthogeriatrician)
Yes (except for hemiarthroplasty patients)
Yes Yes – by orthopaedics
Who prescribes bone protection medication?
Orthogeriatrics/ orthopaedic team
CNS osteoporosis geriatrician
Geriatrician Orthogeriatrician
Is Dual-energy X-ray absorptiometry (DXA) on-site? Yes Yes Yes Yes
Who collects the data for the IHFD?
Orthopaedic CNS Orthopaedic Coordinator
CNM2 Orthopaedic OPD
Trauma Coordinator and admin
How much WTE (in hours) is protected for the collection of the IHFD data?
0 0 4 0
Does the data coordinator have an office to collect the data in? Yes Yes Yes No
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 123
CHAPTER 10
Pathways/policies/protocols Be
aum
ont
Conn
olly
Cork
Dro
ghed
a
Gal
way
Kerr
y
Lett
erke
nny
Lim
eric
k
Mat
er
May
o
Slig
o
St J
ames
’s
St V
ince
nt’s
Talla
ght
Tulla
mor
e
Wat
erfo
rd
Do you have a standardised pathway of care for hip fracture patients?
Yes No Yes No Yes No No Yes Yes No Yes Yes Yes No Yes Yes
Is there a protocol to fast-track hip fracture patients through ED?
Yes Yes Yes Yes Yes Yes No Yes Yes No Yes Yes Yes Yes Yes Yes
Is there a process to pre-alert ED when a suspected hip fracture patient is being brought in?
Yes Yes Yes No No No No No Yes No No Yes Yes Yes No Yes
Do you have a protocol on pain management for hip fracture patients?
Yes Yes Yes Yes Yes No Yes No Yes Yes Yes Yes Yes No Yes No
Do you have a protocol for nutritional assessment of hip fracture patients?
Yes Yes Yes Yes No No Yes No Yes Yes Yes Yes Yes No No No
Do you have a protocol for delirium management for hip fracture patients?
Yes Yes Yes Yes Yes No No Yes Yes No No No Yes No No No
Do you have a rehabilitation pathway for hip fracture patients?
Yes Yes Yes Yes Yes Yes Yes Yes Yes No Yes Yes Yes Yes No No
Do you have regular staff education sessions for the care of hip fracture patients?
Yes Yes Yes Yes No No Yes Yes Yes No No Yes No No Yes Yes
TABLE 10.2: POLICIES AND PROCEDURES
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT124
TABLE 10.3: HOSPITAL HIP FRACTURE GOVERNANCE
Hospital name Beaumont Connolly Cork Drogheda
Do you have a hospital HFGC?
Yes Yes Yes Yes
When was this established? 2016 2017 2017 2014
How often does the committee meet?
3 times per year Quarterly Monthly Bimonthly
Who is the chair of the committee?
Dr Linda Brewer Geriatrician
Mr Paddy Kenny, Orthopaedic Consultant
Mr Colm Taylor, Orthopaedic Consultant
Mr Alan Walsh, Orthopaedic Consultant
Is an agenda provided for each meeting?
Yes Yes Yes Yes
Are minutes taken for each meeting?
Yes Yes Yes Yes
Are members of the following specialties represented on the HFGC? Orthopaedics Geriatrics Anaesthetics Emergency medicine Radiology Ambulance HSCPs Nursing Social work Quality and safety Risk management Senior hospital management Rehabilitation Administration PPI Representative HIPE Other
Yes Yes Yes Yes Yes No No Yes Yes No No No Yes Yes Yes NoNo
YesYesYesYesYesYesYesYesYesNoYesYesNoYesNoNoNo
Yes Yes Yes Yes No Yes Yes Yes No No No Yes Yes Yes No No No
Yes Yes Yes Yes Yes No No Yes No No No Yes No No No No No
Which of the following topics are discussed at the HFGC meetings? IHFS Data quality BPT Quality improvement Patient safety Early mobility Inpatient falls Length of stay Mortality Delayed discharges Staffing Service needs Clinical incidents Complaints/compliments
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No
Yes Yes YesYesNoYesNoYesYesYesNoYesNoNo
Yes Yes Yes Yes Yes Yes Yes Yes Yes No Yes Yes Yes Yes
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No
CHAPTER 10
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 125
TABLE 10.3: HOSPITAL HIP FRACTURE GOVERNANCE CONTINUED
Hospital name Galway Kerry Letterkenny Limerick
Do you have a hospital HFGC?
Yes Yes Yes Yes
When was this established? 2018 2021 2018 2017
How often does the committee meet?
Monthly Monthly Quarterly Quarterly
Who is the chair of the committee?
Dr Michelle Canavan, Geriatrician
Ms Emer Conroy, Orthopaedic Consultant
Mr Tony Shaju, Orthopaedic Consultant
Mr Finbarr Condon, Orthopaedic Consultant
Is an agenda provided for each meeting?
Yes Yes Yes Yes
Are minutes taken for each meeting?
Yes Yes Yes Yes
Are members of the following specialties represented on the HFGC? Orthopaedics Geriatrics Anaesthetics Emergency medicine Radiology Ambulance HSCPs Nursing Social work Quality and safety Risk management Senior hospital management Rehabilitation Administration PPI Representative HIPE Other
Yes Yes Yes Yes No No No Yes Yes No No Yes Yes Yes No Yes NCHD N/A
Yes No No Yes No No Yes Yes No Yes No Yes No No No No No
Yes Yes Yes Yes No No Yes Yes No Yes No Yes No No No Yes No
Which of the following topics are discussed at the HFGC meetings? IHFS Data quality BPT Quality improvement Patient safety Early mobility Inpatient falls Length of stay Mortality Delayed discharges Staffing Service needs Clinical incidents Complaints/compliments
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No No N/A
Yes No Yes Yes Yes No No Yes Yes No Yes Yes Yes No
Yes Yes Yes Yes Yes Yes Yes Yes Yes No No Yes Yes Yes
CHAPTER 10
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT126
TABLE 10.3: HOSPITAL HIP FRACTURE GOVERNANCE CONTINUED
Hospital name Mater Mayo Sligo St James's
Do you have a hospital HFGC?
Yes Yes Yes Yes
When was this established? 2017 2018 2017 2018
How often does the committee meet?
Bimonthly Every 6 months 5–6 times per year Every 6 months
Who is the chair of the committee?
Prof. Joe Duggan, Geriatrician
Mr Derek Bennett, Orthopaedic Consultant
Ann Marie Mullen, IHFD Coordinator
Prof. Geraldine McMahon, Emergency Medicine Consultant Mr Joe Queally, Orthopaedic Consultant
Is an agenda provided for each meeting?
Yes No Yes Yes
Are minutes taken for each meeting?
Yes No Yes Yes
Are members of the following specialties represented on the HFGC? Orthopaedics Geriatrics Anaesthetics Emergency medicine Radiology Ambulance HSCPs Nursing Social work Quality and safety Risk management Senior hospital management Rehabilitation Administration PPI Representative HIPE Other
Yes Yes Yes Yes Yes No Yes Yes No Yes No Yes Yes Yes No Yes No
Yes Yes No No No No No Yes No No No Yes No No No No No
Yes Yes Yes Yes Yes No Yes Yes No No No Yes Yes Yes No Yes Bed manager
Yes Yes Yes Yes No No Yes Yes No Yes Yes Yes Yes Yes No No No
Which of the following topics are discussed at the HFGC meetings? IHFS Data quality BPT Quality improvement Patient safety Early mobility Inpatient falls Length of stay Mortality Delayed discharges Staffing Service needs Clinical incidents Complaints/compliments
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes N/ANo
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No
Yes Yes Yes Yes Yes Yes No No Yes Yes Yes Yes Yes No
Yes Yes Yes Yes Yes Yes Yes Yes Yes No No Yes No No
CHAPTER 10
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 127
TABLE 10.3: HOSPITAL HIP FRACTURE GOVERNANCE CONTINUED
Hospital name St Vincent's Tallaght Tullamore Waterford
Do you have a hospital HFGC?
Yes Yes Yes Yes
When was this established? 2013 2018 2016 2018
How often does the committee meet?
Monthly Every 6 weeks Quarterly Every 2–3 months
Who is the chair of the committee?
Prof. Conor Hurson, Orthopaedic Consultant
David Askin, Fracture Liaison Nurse
Ms Dorothy Niall, Orthopaedic Consultant
Mr Terence Murphy, Orthopaedic Consultant
Is an agenda provided for each meeting?
Yes Yes Yes Yes
Are minutes taken for each meeting?
Yes Yes Yes Yes
Are members of the following specialties represented on the HFGC? Orthopaedics Geriatrics Anaesthetics Emergency medicine Radiology Ambulance HSCPs Nursing Social work Quality and safety Risk management Senior hospital management Rehabilitation Administration PPI Representative HIPE Other
Yes Yes No Yes Yes No Yes Yes No Yes No Yes Yes Yes No Yes Community care
Yes Yes Yes Yes No No Yes Yes Yes No No Yes Yes No No No No
Yes Yes Yes Yes Yes No Yes Yes No Yes No Yes Yes No No No No
Yes Yes Yes Yes Yes Yes Yes Yes No Yes Yes Yes No No No No Theatre
Which of the following topics are discussed at the HFGC meetings? IHFS Data quality BPT Quality improvement Patient safety Early mobility Inpatient falls Length of stay Mortality Delayed discharges Staffing Service needs Clinical incidents Complaints/compliments
Yes Yes Yes Yes Yes Yes Yes Yes No No Yes Yes Yes Yes
Yes Yes Yes Yes Yes Yes Yes Yes Yes No Yes Yes Yes Yes
Yes Yes Yes Yes Yes Yes Yes No No No No Yes No No
Yes Yes Yes Yes Yes Yes No No No No Yes Yes No No
CHAPTER 10
CONTENTS >


IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 129
CHAPTER 11RECOMMENDATIONS
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT130
CHAPTER 11
CHAPTER 11: RECOMMENDATIONS
RECOMMENDATIONS FOR THE NATIONAL OFFICE OF CLINICAL AUDIT RECOMMENDATION 1The National Office of Clinical Audit (NOCA) will continue to implement the new Irish Hip Fracture Standard (IHFS) 7 for early mobilisation, with a plan to add it to the Best Practice Tariff (BPT) in 2022.
Rationale
• Research published in 2020 by Ferris et al. (2020) using IHFD data from 2013 to 2017 identified that early mobilisation was an independent predictor of inpatient mortality, and the only modifiable factor resulting from the research.
• Other hip fracture registers, including the UK’s National Hip Fracture Database (NHFD), the Scottish Hip Fracture Audit (SHFA), and the Australian & New Zealand Hip Fracture Registry (ANZHFR), have all introduced early mobilisation as a hip fracture standard in recent years.
• In 2020, the IHFD highlighted to hospitals that this new standard was being introduced, and compliance was reported back to the hospitals quarterly with the plan to include IHFS 7 in the BPT from 1 January 2022.
What action should be taken?
• NOCA will continue to communicate this implementation to the hospitals through the IHFD quarterly reports and with a workshop for HSCPs.
• The quarterly hospital reports will be amended for Q1 2022 onwards in order to take account of IHFS 7.
• Data collected for why a patient was not mobilised on the day of or the day after surgery will be evaluated by the IHFD Governance Committee and HSCP lead in 2021, with a plan to add IHFS 7 to the BPT from 1 January 2022.
Who will benefit from this action/recommendation?
• Hip fracture patients will receive more timely and appropriate treatment, leading to reduced inpatient mortality.
• Earlier mobilisation should lead to fewer postoperative complications, such as pressure injuries, chest infections and constipation, and more patients may be able to be discharged directly home.
• IHFS 7 should help to prioritise HSCP staffing and input into the care of hip fracture patients.
Who is responsible for implementing this action/recommendation?
• NOCA is responsible for informing the clinical leads, audit coordinators, hospitals and hospital managers about the new IHFS.
• The IHFD HSCP representative is responsible for informing all physiotherapists working in the 16 IHFD participant hospitals about the new IHFS.
When will this be implemented?
From 1 January 2022.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 131
CHAPTER 11
RECOMMENDATION 2Through research, NOCA will progress the development of longer-term outcome measures for hip fracture.
Rationale
• The IHFD only collects data during patients’ in-hospital acute episode of care.
• Long-term outcome measures can reveal how healthcare services and interventions have, over time, affected patients’ quality of life, daily functioning, symptom severity, survival, and residence, as well as the patients’ point of view, therefore informing healthcare services whether healthcare interventions actually make a difference to people’s lives (Williams et al., 2016).
• Research funding was secured by Dr Mary Walsh through the HRB to conduct a 3-year research study into the development of long-term outcome measures for hip fracture.
What action should be taken?
• The HRB-funded study (HipFORGE project) commenced in June 2021.
• The roll-out of the IHFD follow-on dataset will be continued as more hospital and rehabilitation sites show interest. The HIPE IHFD follow-on portal includes outcome measures linked to the best evidence available, including residential status, New Mobility Score, pain, reoperation and readmission details, bone protection status, and quality of life (EQ-5D-5L) at 30, 120 and 365 days after surgery.
Who will benefit from this action/recommendation?
• NOCA will be able to provide long-term outcome data for reporting.
• Clinicians and healthcare workers will better understand the impact of hip fracture care and outcomes in the longer term, and will be able to evaluate care pathways.
• Patients will be able to provide feedback and contribute to the audit.
Who is responsible for implementing this action/recommendation?
• NOCA will oversee the activation of the HIPE IHFD follow-on portal with the Healthcare Pricing Office (HPO).
• Dr Mary Walsh will lead the HipFORGE research project.
When will this be implemented?
The research commenced in June 2021.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT132
CHAPTER 11
RECOMMENDATIONS FOR THE HEALTH SERVICE EXECUTIVE RECOMMENDATION 3The Health Service Executive (HSE), through the National Clinical Programme for Trauma and Orthopaedic Surgery, will:1. promote and develop bundles of care in conjunction with the Irish Hip Fracture Database
(IHFD), e.g. pre-hospital, emergency department (ED), orthogeriatrics, anaesthetics, orthopaedics and rehabilitation
2. advocate that no patient should be fasted repeatedly 3. promote the practice of performing a nutrition and delirium screen for all hip fracture
patients4. promote community pathways in order to enable early supported discharges.
Rationale
• As Ireland’s trauma system continues to be reconfigured, it is imperative that the IHFD data are used to continually enhance the patient pathway of care.
• One-quarter of patients are not operated on within 48 hours, and the organisational survey (Chapter 10) shows that fasting protocols for hip fracture patients vary widely between hospitals.
• There continue to be gaps in the data, particularly for delirium screening and nutrition screening. The standardisation of care and assessment for all older trauma patients to include these assessments would have far-reaching benefits as part of the wider trauma system.
• The COVID-19 pandemic has helped to facilitate better communication between the acute hospitals and the community services, which has led to reduced length of stay (LOS) and more patients being discharged directly home.
What action should be taken?
• The HSE, through the National Clinical Programme for Trauma and Orthopaedic Surgery, should use the data from this report in order to inform improved pathways of care, care bundles, standardised protocols and community integration.
Who will benefit from this action/recommendation?
• Patients will benefit from a more streamlined, efficient and appropriate pathway of care, resulting in more timely interventions and better outcomes.
• The HSE will benefit from a more efficient use of resources, with patients being discharged directly home following fewer complications.
Who is responsible for implementing this action/recommendation?
• The HSE National Office for Trauma Services, in collaboration with the National Clinical Programme for Trauma and Orthopaedic Surgery, are responsible for using the findings from this report to inform the development of the trauma system.
When will this be implemented?
This will be implemented as part of the trauma system reconfiguration.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 133
CHAPTER 11
Rationale
• The BPT requires that each hospital has a HFGC that is invested in quality improvement.
What action should be taken?
• Chairs of the hospital HFGCs should aspire to meet the guidance criteria for governance issued by NOCA.
Who will benefit from this action/recommendation?
• Hospitals will strengthen their processes to use clinical audit data from the IHFD in order to improve care.
• NOCA will benefit from further compliance with the audit’s standards for data quality, care and governance.
• Patients will benefit from improved services, processes and resources.
Who is responsible for implementing this action/recommendation?
• Hospital managers and IHFD clinical leads should ensure that the hospital is compliant with the BPT standard for HFGCs.
When will this be implemented?
This action continues to be implemented during 2021.
RECOMMENDATIONS FOR HOSPITAL MANAGERS, CLINICIANS AND AUDIT COORDINATORSRECOMMENDATION 4The hip fracture governance committees (HFGCs) should continue to meet regularly in order to review the data and engage in quality improvement using the data..
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT134
RECOMMENDATION 5Focus on increasing compliance with the IHFS in order to attain the BPT, which includes the new IHFS 7 for early mobilisation from 1 January 2022.
Rationale
• In order to obtain the BPT, each hip fracture case must meet the seven IHFS as well as the data quality and governance standards.
• In the Irish Hip Fracture Database National Report 2020, only 20% of all hip fracture cases met the BPT, which consisted of six clinical standards at that time. Early mobilisation has been shown to be a key modifiable factor for improving hip fracture patient outcomes.
What action should be taken?
• Hospitals should prepare to include IHFS 7 as part of the BPT and should also review their physiotherapy services.
• Hospitals should review the data for hip fracture patients who are not mobilised on the day of or day after surgery in order to evaluate areas for improvement or additional resource requirements.
Who will benefit from this action/recommendation?
• Patients will have better outcomes if they receive the highest standard of care.
• Compliant hospitals will receive higher amounts of the BPT, which can be invested back into the services provided.
• Staff morale will improve if hard work is recognised and rewarded by this tariff.
Who is responsible for implementing this action/recommendation?
• Hospital managers and HFGCs are responsible for identifying opportunities for better compliance with the BPT.
When will this be implemented?
1 January 2022.
CHAPTER 11
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 135
CHAPTER 11
RECOMMENDATION 6Evaluate local processes/protocols for pre-operative fasting, delirium screening and nutrition screening.
Rationale
• The Irish Hip Fracture Database National Report 2020 shows that there are current deficits in pre-operative fasting, delirium screening and nutrition screening.
• Patients who are fasted repeatedly, are malnourished or have unmanaged delirium have a higher risk of poor outcomes.
What action should be taken?
• Hospitals should review local practice for pre-operative fasting, delirium screening and nutrition screening in order to determine whether there are protocols in place.
• New protocols should be created or existing protocols enhanced where deficits are identified.
Who will benefit from this action/recommendation?
• Patients will benefit from a reduction in complications and will have better outcomes.
• Hospitals will benefit from requiring fewer complex interventions and likely improved the LOS and discharged destination.
Who is responsible for implementing this action/recommendation?
• HFGCs should evaluate the pre-operative fasting, delirium screening and nutrition screening protocols locally.
When will this be implemented?
Throughout 2021.
CONTENTS >


CHAPTER 12CONCLUSION
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT138
CHAPTER 12
CHAPTER 12: CONCLUSIONThis report has reaffirmed the extraordinary commitment of the multidisciplinary teams involved in hip fracture care in the 16 hospitals involved in this audit. The efforts made by the audit coordinators throughout the COVID-19 pandemic to continue collecting such a high level of data ensured that hip fracture patients remained a priority through a very difficult and challenging period for Ireland’s health service. Providing such high-quality and timely data allowed rapid learning reports to be created in order to help the health service understand and adapt as the pandemic continued. This report shows the importance of clinical audit and standards in ensuring that hip fracture patients receive a high standard of care.
The long-term effects of the COVID-19 pandemic remains to be seen, but thankfully, the IHFD will continue to contribute to the learning and research.
Most notable in this report is the progress and development of the orthogeriatric services, advanced nurse practitioner roles and HSCP input since 2018. The data from this audit can be used as a key driver not only for the best standard of care but as a catalyst for applying multidisciplinarity to many other patient groups. It is anticipated that there will be a big focus on research using the IHFD data in 2021 and 2022 in order to fully understand how the audit has contributed to improvements in clinical care, governance and outcomes.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 139
REFERENCES
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT140
REFERENCES
Asia Pacific Fragility Fracture Alliance (APFFA) Hip Fracture Registry Working Group, in collaboration with the Fragility Fracture Network (FFN) Hip Fracture Audit Special Interest Group (2021) The Hip Fracture Registry (HFR) Toolbox. Available from: https://apfracturealliance.org/hfr-toolbox/ [Accessed 10 August 2021]
Australian and New Zealand Hip Fracture Registry Annual Report of Hip Fracture Care 2020. Australian and New Zealand Hip Fracture Registry, August 2020; Sydney
Department of Health (2018) A Trauma System for Ireland: Report of the Trauma Steering Group[Internet]. Dublin: Department of Health. Available from: https://health.gov.ie/wp-content/uploads/2018/02/Report-of-the-Trauma-Steering-Group-A-Trauma-System-for-Ireland.pdf [Accessed 07 August 2021].
Department of Health (2020) Nutrition screening and use of oral nutrition support for adults in the acute care setting: National Clinical Guideline No. 22 [Internet]. Dublin: Department of Health. Available from: https://www.gov.ie/en/collection/bf15f5-nutrition-screening-and-use-of-oral-nutrition-support-for-adults-in-/ .
Dripps, R. (1963) New classification of physical status. Anesthesiology, 24, p. 111.
Dubljanin-Raspopović, E., Marković-Denić, L., Marinković, J., Nedeljković, U. and Bumbaširević, M. (2013) Does early functional outcome predict 1-year mortality in elderly patients with hip fracture? Clinical Orthopaedics and Related Research, 471(8), pp. 2703-2710.
Duncan, D.G., Beck, S.J., Hood, K. and Johansen, A. (2006) Using dietetic assistants to improve the outcome of hip fracture: a randomised controlled trial of nutritional support in an acute trauma ward. Age and Ageing, 35(2), pp. 148-153.
Ferris, H., Brent, L. and Coughlan, T. (2020) Early mobilisation reduces the risk of in-hospital mortality following hip fracture. European Geriatric Medicine, 11(4), pp. 527-533.
Ferris, H., Brent, L., Sorensen, J., Ahern, E. and Coughlan, T., 2021. Discharge destination after hip fracture: findings from the Irish hip fracture database. European geriatric medicine, pp.1-10.
Griffin, X.L., Achten, J., Parsons, N., Costa, M.L. and the WHiTE collaborators (2021) Does performance-based remuneration improve outcomes in the treatment of hip fracture? results from the WHiTE multicentre hip fracture cohort. The Bone & Joint Journal, 103-B(5), pp. 881-887.
Griffiths, R., White, S.M., Moppett, I.K., Parker, M.J., Chesser, T.J.S., Costa, M.L., Johansen, A., Wilson, H. and Timperley, A.J. (2015) Safety guideline: reducing the risk from cemented hemiarthroplasty for hip fracture 2015: Association of Anaesthetists of Great Britain and Ireland, British Orthopaedic Association, British Geriatric Society. Anaesthesia, 70(5), pp. 623-626.
Hall, A.J., Clement, N.D., MacLullich, A.M.J., Ojeda-Thies, C., Hoefer, C., Brent, L., White, T.O. and Duckworth, A.D. (2021) IMPACT of COVID-19 on hip fracture services: A global survey by the International Multicentre Project Auditing COVID-19 in Trauma & Orthopaedics. Surgeon, S1479-666X(21), pp. 00092-00095.
Health Information and Quality Authority (2018) Guidance on a data quality framework for health and social care. Dublin: Health Information and Quality Authority.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 141
Hirose, J., Ide, J., Yakushiji, T., Abe, Y., Nishida, K., Maeda, S., Anraku, Y., Usuku, K. and Mizuta, H. (2010) Prediction of postoperative ambulatory status 1 year after hip fracture surgery. Archives of Physical Medicine and Rehabilitation, 91(1), pp. 67-72.
Johansen, A., Golding, D., Brent, L., Close, J., Gjertsen, J.-E., Holt, G., Hommel, A., Pedersen, A.B., Röck, N.D. and Thorngren, K.-G. (2017) Using national hip fracture registries and audit databases to develop an international perspective. Injury, 48(10), pp. 2174-2179.
Kelly, M.A., McGowan, B., McKenna, M.J., Bennett, K., Carey, J.J., Whelan, B. and Silke, C. (2018) Emerging trends in hospitalisation for fragility fractures in Ireland. Irish Journal of Medical Science, 187(3), pp. 601-608.
Kristensen, M.T., Bandholm, T., Holm, B., Ekdahl, C. and Kehlet, H. (2009) Timed up & go test score in patients with hip fracture is related to the type of walking aid. Archives of Physical Medicine and Rehabilitation, 90(10), pp. 1760-1765.
Kristensen, M.T., Jakobsen, T.L., Nielsen, J.W., Jørgensen, L.M., Nienhuis, R.J. and Jønsson, L.R. (2012) Cumulated Ambulation Score to evaluate mobility is feasible in geriatric patients and in patients with hip fracture. Danish Medical Journal, 59(7), A4464.
Metcalfe, D., Zogg, C.K., Judge, A., Perry, D.C., Gabbe, B., Willett, K. and Costa, M.L. (2019) Pay for performance and hip fracture outcomes: an interrupted time series and difference-in-differences analysis in England and Scotland. The Bone & Joint Journal, 101-B(8), pp. 1015-1023.
National Institute for Health and Care Excellence (2011) Hip fracture: management [Internet]. [CG124]. London: National Institute for Health and Care Excellence. Available from: https://www.nice.org.uk/guidance/cg124 [Accessed 11 June 2021].
National Office of Clinical Audit (2019) Irish Hip Fracture Database National Report 2018. Dublin: National Office of Clinical Audit.
National Office of Clinical Audit, (2020) COVID-19 report 1.0: Service impact from COVID-19: Analysis based on Irish Hip Fracture Database June 2019-May 2020. Dublin: National Office of Clinical Audit.
National Office of Clinical Audit, (2021) COVID-19 report 2.0: Service impact from COVID-19: Analysis based on Irish Hip Fracture Database June 2019-August 2020. Dublin: National Office of Clinical Audit.
Neuburger, J., Currie, C., Wakeman, R., Tsang, C., Plant, F., De Stavola, B., Cromwell, D.A. and van der Meulen, J. (2015) The impact of a national clinician-led audit initiative on care and mortality after hip fracture in England: an external evaluation using time trends in non-audit data. Medical Care, 53(8), pp. 686-691.
O’Hare, J.A. (2008) Anatomy of the ward round. European Journal of Internal Medicine, 19(5), pp. 309-313.
Ritcey, B., Pageau, P., Woo, M.Y. and Perry, J.J. (2016) Regional nerve blocks for hip and femoral neck fractures in the emergency department: a systematic review. Canadian Journal of Emergency Medicine, 18(1), pp. 37-47.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT142
Scottish Intercollegiate Guidelines Network (2009) Management of hip fracture in older people: A national clinical guideline [Internet]. [111]. Edinburgh: Scottish Intercollegiate Guidelines Network. [Accessed 1 August 2021].
Walsh, M.E., Ferris, H., Coughlan, T., Hurson, C., Ahern, E., Sorensen, J. and Brent, L., 2020. Trends in hip fracture care in the Republic of Ireland from 2013 to 2018: results from the Irish Hip Fracture Database. Osteoporosis international, pp.1-10.
Waddell, J. (ed.) (2011) National Hip Fracture Toolkit [Internet]. Bone and Joint Canada. Available from: http://boneandjointcanada.com/wp-content/uploads/2014/05/National-hip- fracture-toolkit-June-2011.pdf [Accessed 1 August 2021].
Williams, K., Sansoni, J.E., Morris, D., Grootemaat, P.E. and Thompson, C.J. (2016) Patient-reported outcome measures: Literature review. Sydney: Australian Commission on Safety and Quality in Health Care.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 143
APPENDICES
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT144
APPENDIX 1: IHFD DATASET
HIPE Portal Data Entry/Hip Fracture Admission (V8.0.3) 7 February 2020
Question Options
1. Date of trauma causing hip fracture
1A. Time of trauma causing hip fracture
2. Type of trauma 1 High-energy trauma, 2 Low-energy trauma8 Unknown, 9 Not documented
3. Date of arrival at first presenting hospital
3A. Time of arrival at first presenting hospital
4. Admission via ED in operating hospitall 1 Yes, 2 No
4A. Date of arrival in ED of operating hospital
4B. Time of arrival in ED of operating hospital
4C. Date left ED in operating hospital
4D. Time left ED in operating hospital
4E. Did patient go directly to theatre from ED?
1 Yes, 2 No
4F. Date seen by orthopaedic team in operating hospital (if not admitted via ED)
4G. Time seen by orthopaedic team in operating hospital (if not admitted via ED)
4H. Did patient fall during an existing inpatient admission in operating hospital?
1 Yes, 2 No
5. Type of ward admitted to in operating hospital
1 Orthopaedic ward 2 Never admitted to orthopaedic ward 9 Not documented
5A. Date of admission to orthopaedic ward
5B. Time of admission to orthopaedic ward
6. Is pre-fracture mobility documented? 1 Yes, 2 No
6A. Pre-fracture indoor walking 0 Unable1 Assistance of one person2 With an aid3 Independent
6B. Pre-fracture outdoor walking 0 Unable 1 Assistance of one person 2 With an aid 3 Independent
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 145
APPENDIX 1: IHFD DATASET
HIPE Portal Data Entry/Hip Fracture Admission (V8.0.3) 7 February 2020
Question Options
6C. Pre-fracture shopping 0 Unable 1 Assistance of one person 2 With an aid 3 Independent
6D. Pre-fracture New Mobility Score (sum A+B+C)
7. AMT performed 1 Yes, 2 No 3 Patient refused, 9 Not documented
7A. AMTS 00–10
7B. Delirium assessment 4AT Day 1 1 Yes, 2 No
7B2. If yes, enter score 00–12
7C. Delirium assessment 4AT Day 3 1 Yes, 2 No
7C2. If yes, enter score 00–12
7D. Delirium assessment 4AT any other time 1 Yes, 2 No
7D2. If yes, enter score 00–12
8. Side of fracture 1 Left, 2 Right, 3 Both
8A. Type of fracture 1 Intracapsular – displaced 2 Intracapsular – undisplaced 3 Intertrochanteric 4 Subtrochanteric 5 Periprosthetic 8 Other 9 Not documented
8B. Type of fracture (Other, please specify)
8C. Type of fracture (right) See Q8A
8D. Type of fracture (right, other, please specify)
9. Pathological 1 Atypical, 2 Malignancy 3 No, 9 Not documented
10. History of previous fragility fracture(s) 1 Yes, 2 No, 9 Not documented
11. Pre-op medical assessment
1 Routine by geriatrician 2 Routine by medical physician 6 None 7 Geriatric review following request 8 Medical physician review following request 9 Not documented
CONTENTS >
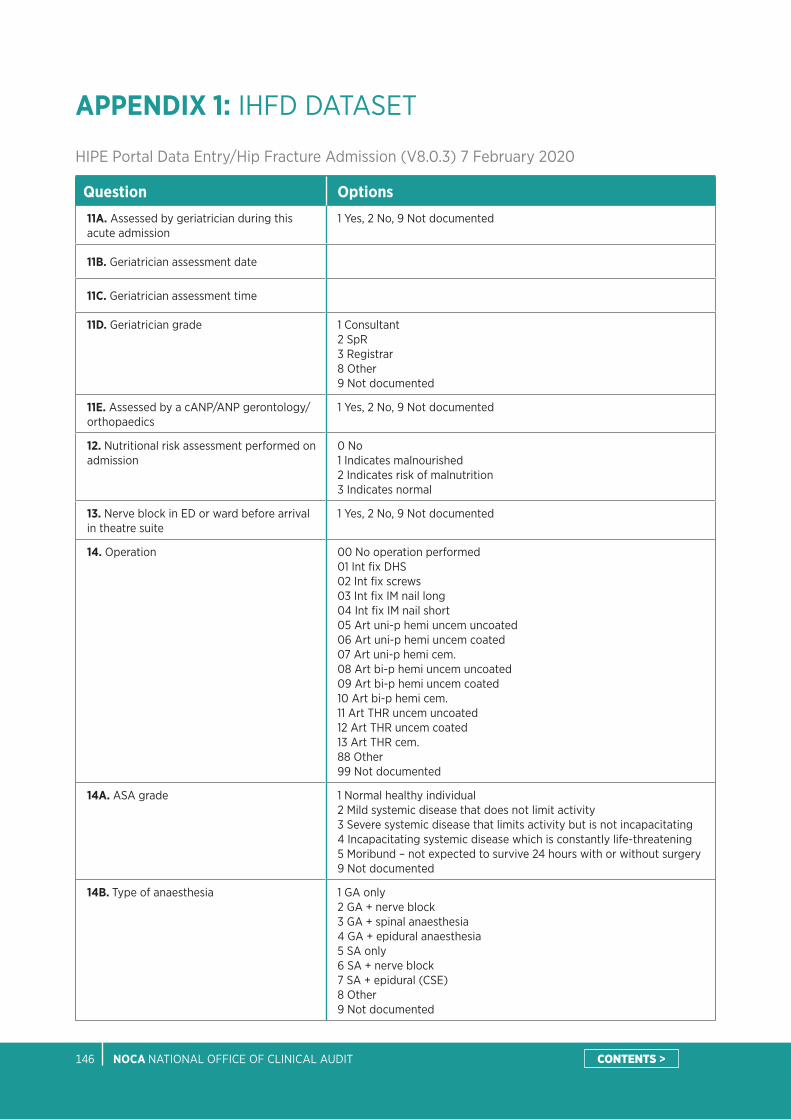
NOCA NATIONAL OFFICE OF CLINICAL AUDIT146
APPENDIX 1: IHFD DATASET
HIPE Portal Data Entry/Hip Fracture Admission (V8.0.3) 7 February 2020
Question Options11A. Assessed by geriatrician during this acute admission
1 Yes, 2 No, 9 Not documented
11B. Geriatrician assessment date
11C. Geriatrician assessment time
11D. Geriatrician grade 1 Consultant 2 SpR 3 Registrar 8 Other 9 Not documented
11E. Assessed by a cANP/ANP gerontology/orthopaedics
1 Yes, 2 No, 9 Not documented
12. Nutritional risk assessment performed on admission
0 No 1 Indicates malnourished 2 Indicates risk of malnutrition 3 Indicates normal
13. Nerve block in ED or ward before arrival in theatre suite
1 Yes, 2 No, 9 Not documented
14. Operation 00 No operation performed 01 Int fix DHS 02 Int fix screws 03 Int fix IM nail long 04 Int fix IM nail short 05 Art uni-p hemi uncem uncoated 06 Art uni-p hemi uncem coated 07 Art uni-p hemi cem. 08 Art bi-p hemi uncem uncoated 09 Art bi-p hemi uncem coated 10 Art bi-p hemi cem. 11 Art THR uncem uncoated 12 Art THR uncem coated 13 Art THR cem. 88 Other 99 Not documented
14A. ASA grade 1 Normal healthy individual 2 Mild systemic disease that does not limit activity 3 Severe systemic disease that limits activity but is not incapacitating 4 Incapacitating systemic disease which is constantly life-threatening 5 Moribund – not expected to survive 24 hours with or without surgery 9 Not documented
14B. Type of anaesthesia 1 GA only 2 GA + nerve block 3 GA + spinal anaesthesia 4 GA + epidural anaesthesia 5 SA only 6 SA + nerve block 7 SA + epidural (CSE) 8 Other 9 Not documented
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 147
APPENDIX 1: IHFD DATASET
HIPE Portal Data Entry/Hip Fracture Admission (V8.0.3) 7 February 2020
Question Options
14C. Surgeon grade 1 Consultant 2 SpR 3 Registrar 4 SHO 8 Other 9 Not documented
14C2. Was consultant orthopaedic surgeon present in the operating room?
1 Yes 2 No 9 Not documented
14D. Anaesthetist grade 1 Consultant 2 SpR 3 Registrar 4 SHO 8 Other 9 Not documented
14D2. Was consultant anaesthetist present in the operating room?
1 Yes 2 No 9 Not documented
14E. Date of primary surgery
14F. Time of primary surgery
14H. Reason if delay >48 hours 0 No delay – surgery <48 hours 1 Awaiting orthopaedic diagnosis or investigation 2 Awaiting medical review investigation or stabilisation 3 Awaiting inpatient or high-dependency bed 4 Awaiting space on theatre list 5 Problem with theatre/equipment 6 Problem with theatre/surgical/anaesthetic staff cover 7 Cancelled due to list over-run 8 Other 9 Not documented
14H2. Other reason if delay >48 hours
14J. Mobilised on day of or day after surgery1 Yes 2 No, 9 Not documented
14J2. Mobilised by1 Physiotherapist 8 Other, 9 Not documented
14J3. If no, reason why 1 Pain 2 Confusion/agitation/delirium 3 Patient declined 4 Medically not fit 5 Not mobile pre-fracture 6 Physiotherapy staffing issues 7 Other staffing issues 8 Other 9 Not documented
CONTENTS >
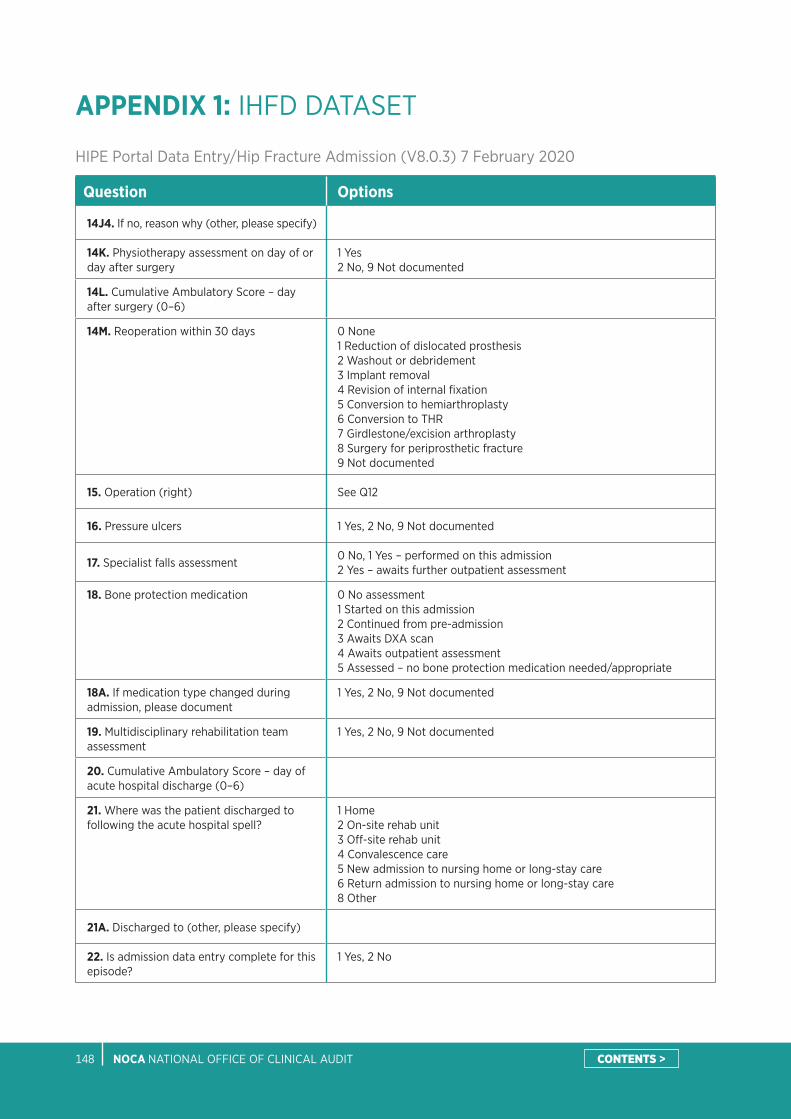
NOCA NATIONAL OFFICE OF CLINICAL AUDIT148
APPENDIX 1: IHFD DATASET
HIPE Portal Data Entry/Hip Fracture Admission (V8.0.3) 7 February 2020
Question Options
14J4. If no, reason why (other, please specify)
14K. Physiotherapy assessment on day of or day after surgery
1 Yes2 No, 9 Not documented
14L. Cumulative Ambulatory Score – day after surgery (0–6)
14M. Reoperation within 30 days 0 None 1 Reduction of dislocated prosthesis 2 Washout or debridement 3 Implant removal 4 Revision of internal fixation 5 Conversion to hemiarthroplasty 6 Conversion to THR 7 Girdlestone/excision arthroplasty 8 Surgery for periprosthetic fracture 9 Not documented
15. Operation (right) See Q12
16. Pressure ulcers 1 Yes, 2 No, 9 Not documented
17. Specialist falls assessment0 No, 1 Yes – performed on this admission 2 Yes – awaits further outpatient assessment
18. Bone protection medication 0 No assessment 1 Started on this admission 2 Continued from pre-admission 3 Awaits DXA scan 4 Awaits outpatient assessment 5 Assessed – no bone protection medication needed/appropriate
18A. If medication type changed during admission, please document
1 Yes, 2 No, 9 Not documented
19. Multidisciplinary rehabilitation team assessment
1 Yes, 2 No, 9 Not documented
20. Cumulative Ambulatory Score – day of acute hospital discharge (0–6)
21. Where was the patient discharged to following the acute hospital spell?
1 Home 2 On-site rehab unit 3 Off-site rehab unit 4 Convalescence care 5 New admission to nursing home or long-stay care 6 Return admission to nursing home or long-stay care 8 Other
21A. Discharged to (other, please specify)
22. Is admission data entry complete for this episode?
1 Yes, 2 No
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 149
APPENDIX 2: IHFD FREQUENTLY ASKED QUESTIONS
Question Answer
What does IHFD stand for? Irish Hip Fracture Database
How do I get access to the IHFD? Contact the Irish Hip Fracture Database and Major Trauma Audit Manager ([email protected]), who will then arrange access via the HPO.
What do I do if I forget my username and password?
Contact [email protected]
Can I view anyone else’s data? No; each hospital is registered separately and can only view its local data.
Can more than one person in a hospital be given access to the database for data entry?
Yes, as many as you wish; however, the request must come from the clinical lead.
How long will it take to enter data? Entering the data takes less than 15 minutes per patient entry, but time must be factored in for collection of the data (i.e. sourcing notes, access to IT systems, and administrative duties). There are two options for data entry, which will vary according to experience, but will usually consist of the following:
1. Pre-dischargea. Type in the Medical Record Number, e.g. 1234567.b. Click on ‘New Case’.c. Enter the hip fracture data.d. Click on ‘Store’.
Note: Only select the option ‘Store as Non-Admitted Episode’ if you are sure the patient was not admitted during this episode of care. If you choose to enter pre-discharge data, the system will automatically merge the hip fracture data and the HIPE data after the patient has been discharged.
2. Post-dischargea. Type in the Medical Record Number, e.g. 1234567.b. Click on the relevant discharge date.c. Enter the hip fracture data under the ‘Optional’ tab.d. Click on ‘Store’.
Once submitted, can I retrieve records to edit content?
Yes, at any time.
What if date of trauma is not documented?
If unknown, enter ‘99-99-9999’ for date and time fields only; otherwise, select the option ‘Not documented’. Where possible, do not leave any question unanswered.
What if the patient is transferred from another hospital?
Document the hospital the patient first presents at, for example if the patient presents at a hospital with no orthopaedic service and has to be transferred to an operating hospital. The clock starts ticking from the time of presentation at the first ED; or, if it is a transfer from within a hospital with no orthopaedic service to an operating hospital, enter the date and time the patient was seen by an orthopaedic team, as this was the most likely time the diagnosis was made. In most cases, the first presenting hospital will be the same as the operating hospital. This should still be documented.
If the patient is admitted from within hospital, how do I record this?
We recognise that some patients may sustain a hip fracture while already in hospital or may require acute medical management (i.e. they are not admitted primarily due to a fractured hip). In this case, complete Q4H.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT150
APPENDIX 2: IHFD FREQUENTLY ASKED QUESTIONS
Question Answer
What constitutes admission to orthopaedic ward?
Includes dedicated orthopaedic/trauma wards or dedicated geriatrician-staffed hip fracture wards.
Enter ‘orthopaedic ward’ if the patient was an inpatient on an orthopaedic ward at any time during the acute hip fracture spell.
What is the AMT Score (Abbreviated Mental Test Score)?
This 10-item version is a simple and robust screening tool for the acute patient. Full assessment for confused people (AMT Score less than 7) requires more detailed tools to screen for cognitive impairment (Mini-Mental State Examination) or presence of delirium (4AT).
What is the 4AT? The 4AT is a simple, quick (<2 minute) and effective bedside tool which helps practitioners to detect delirium in their day-to-day practice.
What fracture type is classed as intertrochanteric?
Basal and basicervical fractures are to be classed as intertrochanteric.
What fracture types are recorded in the IHFD?
Hip fracture cases either identified as a HIPE Injury Diagnosis Code S72.00 to S72.2 OR with a specified type of fracture (e.g. intracapsular – displaced, intracapsular – undisplaced, intertrochanteric, or subtrochanteric) are recorded in the IHFD.
What is arthroplasty? Any replacement of the upper femur, including unipolar and bipolar hemiarthroplasties and total hip replacements.
What is a pathological fracture? A broken bone, caused not by trauma alone, but so weakened by disease as to break with abnormal ease. Pathological fractures are characteristic of primary and metastatic malignant disease and myeloma. Answer ‘malignancy’ only if a primary or secondary malignancy is present at the fracture site.
What is an atypical fracture? Atypical fractures are transverse femoral fractures with an unusual cortical spike medially which occur in the subtrochanteric and shaft regions (you should only enter subtrochanteric fractures to the database). They follow low-trauma injuries and patients may report pre-injury pain.
What are normal working hours? The National Confidential Enquiry into Perioperative Deaths reports from 1997 and 2003 define ‘out of hours’ as any time outside of 8.00am to 5.59pm on weekdays, and any time on a Saturday or Sunday.
When is considered the time of primary surgery?
The time of primary surgery is taken from the time of induction of anaesthesia. The time is shown in hours to two decimal places, e.g. 1.25 = 1 hour 15 minutes, 3.50 = 3 hours 30 minutes, and 2.67 = 2 hours 40 minutes.
When does the clock start ticking? As soon as the patient arrives in an ED or is seen by the orthopaedic team in the operating hospital.
What is an ASA grade? The American Society of Anesthesiologists (ASA) devised a pre-operative risk grade based on the presence of comorbidities at the time of surgery. The ASA’s (Dripps, 1963) physical status classification is:
1. Healthy person.2. Mild systemic disease.3. Severe systemic disease.4. Severe systemic disease that is a constant threat to life.5. A moribund person who is not expected to survive with or without the
operation.
This grading does not take into account acute illness, hence a patient can be ASA 1 and ‘unfit’.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 151
APPENDIX 2: IHFD FREQUENTLY ASKED QUESTIONS
Question Answer
What is meant by ‘Routine by geriatrician’?
Review by a geriatrician at the registrar level or above.
What is meant by ‘Review by ANP’? A review by an advanced nurse practitioner (ANP) is considered the same as a review by a geriatrician.
What is meant by ‘Medical review following request’?
Review by a member of the medical team at the registrar level or above following a request from the orthopaedic service or ED.
Reasons for delay to surgery Please document only the main reason for delay. Options are:
• Medically unfit – awaiting orthopaedic diagnosis/investigation: this means waiting for an MRI scan or other confirmation of diagnosis.
• Medically unfit – awaiting medical review, investigation or stability: this means waiting for a medical review, as the patient remains medically unfit for surgery/anaesthetic. (If this option is selected, a free text box will appear on the database to be populated with a brief description of the medical issues.)
• Administrative/logistic – awaiting inpatient or high-dependency bed.
• Administrative/logistic – awaiting space on theatre list.
• Administrative/logistic – problem with theatre/equipment.
• Administrative/logistic – problem with theatre/surgical/anaesthetic staff cover.
• Cancelled due to theatre over-run: this option is to be used when the patient has been allocated a theatre slot, but for some reason the list has over-run.
• Other: any reason other than those given in the list above. If you select ‘Other’, an empty box will appear so you can populate it with the reason for delay.
• No operation performed.
What definition of pressure ulcer is used for the IHFD?
Did the patient acquire a new pressure ulcer (Grade 2 or above) during the acute admission?
• This should be answered as ‘yes’ only if the patient has developed a Grade 2 pressure ulcer or above during their acute orthopaedic admission.
• Ignore ulcers acquired during an acute stay but which were acquired more than 120 days after admission.
• If nothing is documented and the patient has left the hospital, ‘not documented’ must be recorded.
What is the definition of a ward round?
The ward round is a parade through the hospital of professionals where most decisions concerning patient care are made. The round provides an opportunity for the multidisciplinary team to listen to the patient’s narrative and jointly interpret their concerns. From this unfolds diagnosis, management plans, prognosis formation, and the opportunity to explore social, psychological, rehabilitation, and placement issues.
Physical examination of the patient at the bedside still remains important (O’Hare, 2008).
What is the definition of mobilised? Mobilised means that the patient has stood out of bed at a minimum. To meet IHFS 7 mobilisation must be done by a physiotherapist on the day of or after surgery.
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT152
APPENDIX 2: IHFD FREQUENTLY ASKED QUESTIONS
Question AnswerWhat is a specialist falls assessment?
A systematic assessment by a suitably trained person, e.g. a geriatrician or a specialist assessment trained nurse, which must cover the following domains:• falls history (noting previous falls)• cause of index fall (including medication review)• risk factors for falling and injury (including fracture)• medication review.From this information, the assessor must formulate and document a plan of action to prevent further falls.
What is the definition of multidisciplinary rehabilitation assessment team?
A group of people of different professions (and including as a minimum a physiotherapist, occupational therapist, nurse, and doctor) with job plan responsibilities for the assessment and treatment of hip fracture patients, and who convene (including face to face or via a virtual ward round) regularly (and at least weekly) to discuss patient treatment and care and to plan shared clinical care goals.
What drugs constitute bone protection therapy?
Not just calcium and vitamin D:
1. Bisphosphonates (oral, combined with calcium/ vitamin D, intravenously) • Etidronate• Alendronate• Risedronate• Ibandronate• Zoledronate• Pamidronate
4. Parathyroid hormone• PTH 1-34• PTH 1-84
2. Denosumab 5. Strontium• Strontium ranelate
3. HRT and SERMS • HRT (various)• Tibolone• Raloxifene
6. Calcium and vitamin D• Calcitriol • Calcium and vitamin D – various• Alpha-calcidol (or One alpha)
7. Calcitonin
What is the minimum age? We collect data on all patients aged 18 years and over, but to date, we only report on those aged 60 years and over in the national report.
What is the pre-fracture New Mobility Score?
This wa a new field for 2016, and there has been communication directly with physiotherapy departments regarding the collection of this score.If you do not have a score recorded for any of Q6A, Q6B and Q6C, then leave them blank.
How do I calculate Q6D if not all fields are answered?
Q6D will auto-calculate.
Does the CAS need to be recorded daily?
No, just on the day after surgery and again on the day of acute hospital discharge.
In relation to the CAS, what happens if the patient is discharged at the weekend and there are no physiotherapists on duty?
Retrospectively fill it in on the following Monday based on the nursing note on the day of discharge, or the last physiotherapist’s note if it was recent.
What is required for Q21 – Where was the patient discharged to following the acute hospital spell?
Fill in the option which represents the reason/intent for the patient’s initial care after being discharged to a location other than home.
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 153
APPENDIX 3: GLOSSARY OF TERMS AND DEFINITIONS
ACRONYM FULL TERM
4AT rapid clinical test for delirium
AAGBI Association of Anaesthetists of Great Britain and Ireland
AFFINITY National Falls and Bone Health Project (2018–2023)
AMT Abbreviated Mental Test
ANP/ cANP advanced nurse practitioner/ candidate advanced nurse practitioner
ANZHFR Australian & New Zealand Hip Fracture Registry
ASA American Society of Anesthesiologists
BCIS bone cement implantation syndrome
BGS British Geriatric Society
BIU Business Intelligence Unit
BOA British Orthopaedic Association
BPT Best Practice Tariff
CAS Cumulative Ambulatory Score
CNS clinical nurse manager
CNM clinical nurse specialist
COVID-19 coronavirus disease 2019
DFB Dublin Fire Brigade
DHS dynamic hip screw
DVR data validation report
DXA dual-energy X-ray absorptiometry
ED emergency department
FFN Fragility Fracture Network
FLS Fracture Liaison Service
GA general anaesthetic
HCA health care assistant
HFGC hip fracture governance committee
HIPE Hospital In-Patient Enquiry
HIQA Health Information and Quality Authority
HPO Healthcare Pricing Office
HSCP health and social care professional
HSE Health Service Executive
ICD-10-AM International Classification of Diseases, Tenth Revision, Australian Modification
IGS Irish Gerontological Society
IHFD Irish Hip Fracture Database
IHFS Irish Hip Fracture Standards
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT154
APPENDIX 3: GLOSSARY OF TERMS AND DEFINITIONS
ACRONYM FULL TERM
IITOS Irish Institute for Trauma and Orthopaedic Surgery
IM intramedullary
KPI key performance indicator
LOS length of stay
MDT multidisciplinary team
MTC Major Trauma Centre
NAS National Ambulance Service
NHFD National Hip Fracture Database (UK)
NICE National Institute for Health and Care Excellence
NMS New Mobility Score
NOCA National Office of Clinical Audit
NPHET National Public Health Emergency Team
OLOL Our Lady of Lourdes
PPI Public and Patient Interest
PUTZ Pressure Ulcer to Zero
QIT Quality Improvement Team
RCSI Royal College of Surgeons in Ireland
SA spinal anaesthetic
SARS-Co-2 severe acute respiratory syndrome coronavirus 2
SHFA Scottish Hip Fracture Audit
SHO Senior House Officer
SpR Specialist Registrar
SPSS Statistical Package for the Social Sciences
THR total hip replacement
TU trauma unit
UK United Kingdom
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 155
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 4.1: PERCENTAGE OF PATIENTS NATIONALLY WHO MET EACH IRISH HIP FRACTURE STANDARD IN 2017 (N=3497), 2018 (N=3751), 2019 (N=3701) AND 2020 (N=3666)
FIGURE 4.2: IRISH HIP FRACTURE STANDARD 1: PERCENTAGE OF PATIENTS ADMITTED TO AN ORTHOPAEDIC WARD WITHIN 4 HOURS OR ADMITTED TO THEATRE FROM EMERGENCY DEPARTMENT WITHIN 4 HOURS, BY INDIVIDUAL HOSPITAL, 2019 (N=3701) AND 2020 (N=3666)
2017 2018 2019 2020n N % n N % n N % n N %
IHFS 1 402 3497 11% 637 3751 17% 923 3701 25% 1225 3666 33%IHFS 2 2314 3336 69% 2561 3554 72% 2672 3536 76% 2598 3485 75%IHFS 3 85 3320 3% 101 3567 3% 108 3498 3% 102 3481 3%IHFS 4 1754 3497 50% 2589 3751 69% 3029 3701 82% 3017 3666 82%IHFS 5 2407 3320 73% 2992 3567 84% 3289 3498 94% 3180 3481 91%IHFS 6 1546 3320 47% 2483 3567 70% 2912 3498 83% 2946 3481 85%IHFS 7 2438 3336 73% 2617 3554 74% 2732 3536 77% 2705 3485 78%
HOSPITAL2019 2020
n N % n N %National 923 3701 25% 1225 3666 33%Beaumont Hospital 29 246 12% 60 235 26%Connolly Hospital 54 220 25% 79 211 37%Cork University Hospital 171 437 39% 228 461 49%Our Lady of Lourdes Hospital Drogheda 122 217 56% 155 218 71%University Hospital Galway 40 244 16% 35 227 15%University Hospital Kerry ~ 152 * 28 128 22%Letterkenny University Hospital 28 121 23% 46 161 29%University Hospital Limerick 150 278 54% 144 331 44%Mater Misericordiae University Hospital 26 157 17% 42 138 30%Mayo University Hospital 38 116 33% 31 127 24%Sligo University Hospital 54 141 38% 40 130 31%St James’s Hospital 19 190 10% 56 169 33%St Vincent’s University Hospital 88 321 27% 107 326 33%Tallaght University Hospital 7 200 4% 49 203 24%Midland Regional Hospital Tullamore 64 234 27% 64 213 30%University Hospital Waterford 30 427 7% 61 388 16%
~ Denotes 5 or fewer cases* Further suppression required to prevent disclosure of five cases or fewer
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT156
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 4.3: IRISH HIP FRACTURE STANDARD 2: PERCENTAGE OF PATIENTS RECEIVING SURGERY WITHIN 48 HOURS (AND WITHIN NORMAL WORKING HOURS), BY INDIVIDUAL HOSPITAL, 2019 (n=3536) AND 2020 (n=3485)
FIGURE 4.4: IRISH HIP FRACTURE STANDARD 3: PERCENTAGE OF PATIENTS WHO DEVELOPED PRESSURE ULCERS FOLLOWING ADMISSION, BY INDIVIDUAL HOSPITAL, 2019 (n=3498) AND 2020 (n=3481)
HOSPITAL2019 2020
n N % n N %National 2672 3536 76% 2598 3485 75%Beaumont Hospital 177 235 75% 171 226 76%Connolly Hospital 184 212 87% 166 196 85%Cork University Hospital 281 419 67% 269 450 60%Our Lady of Lourdes Hospital Drogheda 121 201 60% 136 205 66%University Hospital Galway 186 232 80% 181 219 83%University Hospital Kerry 97 142 68% 81 123 66%Letterkenny University Hospital 98 119 82% 115 149 77%University Hospital Limerick 181 269 67% 206 313 66%Mater Misericordiae University Hospital 123 145 85% 105 124 85%Mayo University Hospital 93 108 86% 100 119 84%Sligo University Hospital 117 135 87% 103 123 84%St James’s Hospital 134 182 74% 125 158 79%St Vincent’s University Hospital 301 312 96% 288 311 93%Tallaght University Hospital 168 192 88% 155 187 83%Midland Regional Hospital Tullamore 166 223 74% 146 206 71%University Hospital Waterford 245 410 60% 251 376 67%
HOSPITAL2019 2020
n N % n N %National 108 3498 3% 102 3481 3%Beaumont Hospital 11 233 5% 11 221 5%Connolly Hospital ~ 212 * ~ 204 *Cork University Hospital 10 410 2% 6 437 1%Our Lady of Lourdes Hospital Drogheda ~ 199 * 6 212 3%University Hospital Galway ~ 230 * 8 214 4%University Hospital Kerry 9 143 6% ~ 121 *Letterkenny University Hospital 0 118 0% 6 152 4%University Hospital Limerick 8 267 3% ~ 317 *Mater Misericordiae University Hospital ~ 143 * 12 129 9%Mayo University Hospital 6 110 5% ~ 121 *Sligo University Hospital ~ 138 * 8 127 6%St James’s Hospital 23 179 13% 7 155 5%St Vincent’s University Hospital ~ 300 * ~ 306 *Tallaght University Hospital 6 183 3% 6 191 3%Midland Regional Hospital Tullamore 8 228 4% 9 206 4%University Hospital Waterford ~ 405 * 6 368 2%
~ Denotes five cases or fewer* Further suppression required to prevent disclosure of five cases or fewer
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 157
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 4.5: IRISH HIP FRACTURE STANDARD 4: PERCENTAGE OF PATIENTS SEEN BY A GERIATRICIAN OR ADVANCED NURSE PRACTITIONER DURING ADMISSION, BY INDIVIDUAL HOSPITAL, 2019 (N=3701) AND 2020 (N=3666)
HOSPITAL2019 2020
n N % n N %National 3029 3701 82% 3017 3666 82%Beaumont Hospital 234 246 95% 227 235 97%Connolly Hospital 95 220 43% 135 211 64%Cork University Hospital 328 437 75% 459 461 100%Our Lady of Lourdes Hospital Drogheda 212 217 98% 190 218 87%University Hospital Galway 234 244 96% 216 227 95%University Hospital Kerry 36 152 24% 57 128 45%Letterkenny University Hospital 84 121 69% 43 161 27%University Hospital Limerick 226 278 81% 236 331 71%Mater Misericordiae University Hospital 143 157 91% 119 138 86%Mayo University Hospital 104 116 90% 93 127 73%Sligo University Hospital 115 141 82% 95 130 73%St James’s Hospital 181 190 95% 159 169 94%St Vincent’s University Hospital 314 321 98% 310 326 95%Tallaght University Hospital 143 200 72% 151 203 74%Midland Regional Hospital Tullamore 193 234 82% 174 213 82%University Hospital Waterford 387 427 91% 353 388 91%
FIGURE 4.6: IRISH HIP FRACTURE STANDARD 5: PERCENTAGE OF PATIENTS WHO RECEIVED A BONE HEALTH ASSESSMENT IN 2020 (n=3481)
BONE HEALTH ASSESSMENT n %Assessed – no bone protection medication 202 6%Awaits DXA scan 169 5%Awaits outpatient assessment 301 9%Continued from pre-admission 460 13%Started on this admission 2048 59%No assessment 301 9%Total 3481 100%
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT158
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 4.6A: IRISH HIP FRACTURE STANDARD 5: PERCENTAGE OF PATIENTS WHO RECEIVED A BONE HEALTH ASSESSMENT, BY INDIVIDUAL HOSPITAL, 2019 (n=3498) AND 2020 (n=3481)
FIGURE 4.7: IRISH HIP FRACTURE STANDARD 6: PERCENTAGE OF PATIENTS WHO RECEIVED A SPECIALIST FALLS ASSESSMENT, BY INDIVIDUAL HOSPITAL, 2019 (n=3498) AND 2020 (n=3481)
HOSPITAL2018 2019
n N % n N %National 3289 3498 94% 3180 3481 91%Beaumont Hospital 227 233 97% 215 221 97%Connolly Hospital 153 212 72% 126 204 62%Cork University Hospital 398 410 97% 437 437 100%Our Lady of Lourdes Hospital Drogheda 195 199 98% 184 212 87%University Hospital Galway 225 230 98% 205 214 96%University Hospital Kerry 112 143 78% 100 121 83%Letterkenny University Hospital 118 118 100% 140 152 92%University Hospital Limerick 260 267 97% 267 317 84%Mater Misericordiae University Hospital 135 143 94% 117 129 91%Mayo University Hospital 99 110 90% 108 121 89%Sligo University Hospital 125 138 91% 109 127 86%St James’s Hospital 173 179 97% 147 155 95%St Vincent’s University Hospital 298 300 99% 299 306 98%Tallaght University Hospital 179 183 98% 191 191 100%Midland Regional Hospital Tullamore 220 228 96% 197 206 96%University Hospital Waterford 372 405 92% 338 368 92%
HOSPITAL2018 2019
n N % n N %National 2912 3498 83% 2946 3481 85%Beaumont Hospital 227 233 97% 215 221 97%Connolly Hospital 92 212 43% 99 204 49%Cork University Hospital 305 410 74% 436 437 100%Our Lady of Lourdes Hospital Drogheda 195 199 98% 184 212 87%University Hospital Galway 225 230 98% 209 214 98%University Hospital Kerry 39 143 27% 59 121 49%Letterkenny University Hospital 113 118 96% 109 152 72%University Hospital Limerick 219 267 82% 234 317 74%Mater Misericordiae University Hospital 137 143 96% 118 129 91%Mayo University Hospital 98 110 89% 90 121 74%Sligo University Hospital 116 138 84% 94 127 74%St James’s Hospital 174 179 97% 145 155 94%St Vincent’s University Hospital 298 300 99% 300 306 98%Tallaght University Hospital 128 183 70% 147 191 77%Midland Regional Hospital Tullamore 188 228 82% 171 206 83%University Hospital Waterford 358 405 88% 336 368 91%
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 159
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 4.8: IRISH HIP FRACTURE STANDARD 7: PERCENTAGE OF PATIENTS MOBILISED BY A PHYSIOTHERAPIST ON THE DAY OF OR DAY AFTER SURGERY, BY INDIVIDUAL HOSPITAL, 2020 (n=3485)
HOSPITAL n N %National 2705 3485 78%Beaumont Hospital 173 226 77%Connolly Hospital 159 196 81%Cork University Hospital 324 450 72%Our Lady of Lourdes Hospital Drogheda 164 205 80%University Hospital Galway 203 219 93%University Hospital Kerry 97 123 79%Letterkenny University Hospital 136 149 91%University Hospital Limerick 291 313 93%Mater Misericordiae University Hospital 111 124 90%Mayo University Hospital 94 119 79%Sligo University Hospital 90 123 73%St James’s Hospital 143 158 91%St Vincent’s University Hospital 198 311 64%Tallaght University Hospital 114 187 61%Midland Regional Hospital Tullamore 163 206 79%University Hospital Waterford 245 376 65%
CONTENTS >
FIGURE 6.1: MODE OF ADMISSION TO OPERATING HOSPITAL, BY HOSPITAL (N=3666)
HOSPITAL
Directly to ED in an operating hospital
Seen by an orthopaedic team
Not known
n % n % n %National 3455 94% 195 5% 16 0%Beaumont Hospital 228 97% ~ * * *Connolly Hospital 184 87% 27 13% 0 0%Cork University Hospital 450 98% 11 2% 0 0%Our Lady of Lourdes Hospital Drogheda 213 98% ~ * * *University Hospital Galway 212 93% 13 6% * *University Hospital Kerry 125 98% ~ * 0 0%Letterkenny University Hospital 157 98% ~ * 0 0%University Hospital Limerick 318 96% 13 4% 0 0%Mater Misericordiae University Hospital 127 92% 8 6% * *Mayo University Hospital 121 95% ~ * * *Sligo University Hospital 127 98% ~ * 0 0%St James’s Hospital 156 92% 13 8% 0 0%St Vincent’s University Hospital 313 96% 11 3% * *Tallaght University Hospital 195 96% 7 3% * *Midland Regional Hospital Tullamore 211 99% ~ * 0 0%University Hospital Waterford 318 82% 70 18% 0 0%
~ Denotes five cases or fewer* Further suppression required to prevent disclosure of five cases or fewer
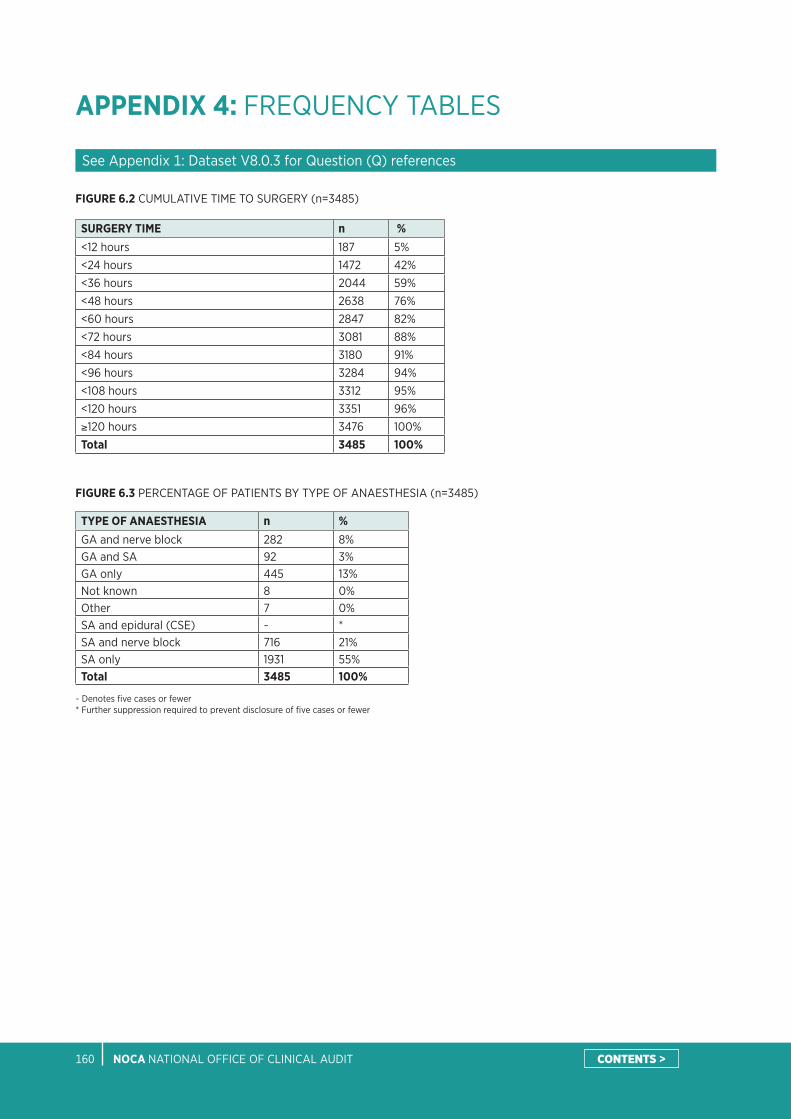
NOCA NATIONAL OFFICE OF CLINICAL AUDIT160
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 6.2 CUMULATIVE TIME TO SURGERY (n=3485)
SURGERY TIME n %<12 hours 187 5%<24 hours 1472 42%<36 hours 2044 59%<48 hours 2638 76%<60 hours 2847 82%<72 hours 3081 88%<84 hours 3180 91%<96 hours 3284 94%<108 hours 3312 95%<120 hours 3351 96%≥120 hours 3476 100%Total 3485 100%
CONTENTS >
FIGURE 6.3 PERCENTAGE OF PATIENTS BY TYPE OF ANAESTHESIA (n=3485)
TYPE OF ANAESTHESIA n %GA and nerve block 282 8%GA and SA 92 3%GA only 445 13%Not known 8 0%Other 7 0%SA and epidural (CSE) ~ *SA and nerve block 716 21%SA only 1931 55%Total 3485 100%
~ Denotes five cases or fewer* Further suppression required to prevent disclosure of five cases or fewer

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 161
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 6.3A PERCENTAGE OF PATIENTS BY TYPE OF ANAESTHESIA, BY HOSPITAL (n=3470)
HOSPITALBoth GA SA Total
n % n % n % NNational 92 3% 727 21% 2651 76% 3470Beaumont Hospital 6 3% 68 30% 152 67% 226Connolly Hospital 40 20% 45 23% 111 57% 196Cork University Hospital 12 3% 21 5% 417 93% 450Our Lady of Lourdes Hospital Drogheda ~ * 36 18% 163 80% 204University Hospital Galway 8 4% 66 31% 141 66% 215University Hospital Kerry ~ * ~ * 111 93% 119Letterkenny University Hospital ~ * 18 12% 130 87% 149University Hospital Limerick ~ * 15 5% 294 95% 310Mater Misericordiae University Hospital 0 0% 49 40% 75 60% 124Mayo University Hospital 0 0% 36 30% 83 70% 119Sligo University Hospital ~ * 23 19% 99 80% 123St James’s Hospital ~ * 75 48% 78 50% 155St Vincent’s University Hospital 7 2% 131 42% 173 56% 311Tallaght University Hospital ~ * 58 31% 126 67% 187Midland Regional Hospital Tullamore ~ * 75 36% 129 63% 206University Hospital Waterford ~ * 6 2% 369 98% 376
~ Denotes five cases or fewer* Further suppression required to prevent disclosure of five cases or fewer
CONTENTS >
FIGURE 6.4 PERCENTAGE OF PATIENTS BY NERVE BLOCK USAGE, BY HOSPITAL (n=3485)
HOSPITALNerve block No nerve block Not known Total
n % n % n % NNational 2402 69% 826 24% 257 7% 3485Beaumont Hospital 116 51% 89 39% 21 9% 226Connolly Hospital 107 55% 88 45% ~ * 196Cork University Hospital 447 99% ~ * 0 0% 450Our Lady of Lourdes Hospital Drogheda 99 48% 106 52% 0 0% 205University Hospital Galway 173 79% 40 18% 6 3% 219University Hospital Kerry 53 43% 68 55% ~ * 123Letterkenny University Hospital 61 41% 86 58% ~ * 149University Hospital Limerick 234 75% 79 25% 0 0% 313Mater Misericordiae University Hospital 94 76% 20 16% 10 8% 124Mayo University Hospital 15 13% 43 36% 61 51% 119Sligo University Hospital 98 80% 25 20% 0 0% 123St James’s Hospital 125 79% 31 20% ~ * 158St Vincent’s University Hospital 169 54% 30 10% 112 36% 311Tallaght University Hospital 154 82% 33 18% 0 0% 187Midland Regional Hospital Tullamore 163 79% 15 7% 28 14% 206University Hospital Waterford 294 78% 70 19% 12 3% 376
~ Denotes five cases or fewer* Further suppression required to prevent disclosure of five cases or fewer

NOCA NATIONAL OFFICE OF CLINICAL AUDIT162
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 6.5 PERCENTAGE OF PATIENTS BY NUTRITIONAL RISK ASSESSMENT, BY HOSPITAL (N=3666)
HOSPITAL
Indicates malnourished
Indicates normal
Indicates risk of malnutrition
No assessment performed
Total
n % n % n % n % NNational 63 2% 1505 41% 470 13% 1628 44% 3666Beaumont Hospital 0 0% 160 68% 37 16% 38 16% 235Connolly Hospital ~ * 158 75% 6 3% 45 21% 211Cork University Hospital 0 0% 295 64% 166 36% 0 0% 461Our Lady of Lourdes Hospital Drogheda ~ * 88 40% 9 4% 120 55% 218University Hospital Galway ~ * 10 4% ~ * 211 93% 227University Hospital Kerry ~ * 87 68% 35 27% ~ * 128Letterkenny University Hospital ~ * 53 33% 63 39% 44 27% 161University Hospital Limerick ~ * ~ * ~ * 319 96% 331Mater Misericordiae University Hospital 26 19% 26 19% 39 28% 47 34% 138Mayo University Hospital ~ * 108 85% 7 6% 7 6% 127Sligo University Hospital ~ * 105 81% 22 17% ~ * 130St James’s Hospital ~ * 127 75% 32 19% 8 5% 169St Vincent’s University Hospital 15 5% 126 39% 28 9% 157 48% 326Tallaght University Hospital ~ * 131 65% ~ * 66 33% 203Midland Regional Hospital Tullamore 0 0% 0 0% ~ * 212 100% 213University Hospital Waterford ~ * 27 7% 11 3% 348 90% 388
~ Denotes five cases or fewer* Further suppression required to prevent disclosure of five cases or fewer
FIGURE 6.6 PERCENTAGE OF PATIENTS BY TYPE OF SURGERY (n=3485)
TYPE OF SURGERY n %Arthroplasty hemi cemented 1243 36%Arthroplasty hemi uncemented 410 12%Arthroplasty THR cemented 96 3%Arthroplasty THR uncemented 66 2%Internal fixation dynamic hip screw 429 12%Internal fixation IM nail (long) 497 14%Internal fixation IM nail (short) 629 18%Internal fixation screws 51 1%Other 64 2%Total 3485 100%
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 163
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 6.7: PERCENTAGE OF PATIENTS WITH CEMENTED OR UNCEMENTED ARTHROPLASTIES, BY HOSPITAL (n=1815)
HOSPITALCemented Uncemented Total
n % n % NNational 1339 74% 476 26% 1815Beaumont Hospital 107 98% ~ * 109Connolly Hospital 111 100% 0 0% 111Cork University Hospital 215 96% 9 4% 224Our Lady of Lourdes Hospital Drogheda 102 91% 10 9% 112University Hospital Galway 20 16% 104 84% 124University Hospital Kerry 55 96% ~ * 57Letterkenny University Hospital 67 99% ~ * 68University Hospital Limerick 161 97% ~ * 166Mater Misericordiae University Hospital 59 98% ~ * 60Mayo University Hospital 52 75% 17 25% 69Sligo University Hospital 47 75% 16 25% 63St James’s Hospital 65 93% ~ * 70St Vincent’s University Hospital 18 11% 145 89% 163Tallaght University Hospital 90 87% 14 13% 104Midland Regional Hospital Tullamore 12 12% 85 88% 97University Hospital Waterford 158 72% 60 28% 218
~ Denotes five cases or fewer* Further suppression required to prevent disclosure of five cases or fewer
CONTENTS >
FIGURE 6.8: PERCENTAGE OF PATIENTS WHO WERE ASSESSED BY A PHYSIOTHERAPIST ON THE DAY OF OR DAY AFTER SURGERY, BY HOSPITAL (n=3485)
HOSPITAL n N %National 3169 3485 91%University Hospital Limerick 312 313 100%Connolly Hospital 193 196 98%Our Lady of Lourdes Hospital Drogheda 201 205 98%Tallaght University Hospital 183 187 98%University Hospital Galway 214 219 98%St Vincent’s University Hospital 302 311 97%St James’s Hospital 153 158 97%Letterkenny University Hospital 143 149 96%Mayo University Hospital 114 119 96%Midland Regional Hospital Tullamore 196 206 95%Mater Misericordiae University Hospital 115 124 93%Beaumont Hospital 196 226 87%Sligo University Hospital 105 123 85%University Hospital Kerry 104 123 85%Cork University Hospital 359 450 80%University Hospital Waterford 279 376 74%

NOCA NATIONAL OFFICE OF CLINICAL AUDIT164
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
FIGURE 6.8A: PERCENTAGE OF PATIENTS BY MOBILISATION ON THE DAY OF OR DAY AFTER SURGERY, BY HOSPITAL (n=3467)
HOSPITAL
Not mobilised
Yes (by other)
Yes (by physiotherapist)
Total
n % n % n % NNational 530 15% 232 7% 2705 78% 3467Beaumont Hospital 34 15% 16 7% 173 78% 223Connolly Hospital 21 11% 16 8% 159 81% 196Cork University Hospital 72 16% 52 12% 324 72% 448Our Lady of Lourdes Hospital Drogheda 41 20% 0 0% 164 80% 205University Hospital Galway 14 6% ~ * 203 93% 218University Hospital Kerry 24 20% ~ * 97 80% 122Letterkenny University Hospital 7 5% ~ * 136 94% 144University Hospital Limerick 21 7% ~ * 291 93% 313Mater Misericordiae University Hospital 13 10% 0 0% 111 90% 124Mayo University Hospital 25 21% 0 0% 94 79% 119Sligo University Hospital 16 13% 17 14% 90 73% 123St James’s Hospital 10 7% 0 0% 143 93% 153St Vincent’s University Hospital 112 36% ~ * 198 64% 311Tallaght University Hospital 73 39% 0 0% 114 61% 187Midland Regional Hospital Tullamore 35 17% 8 4% 163 79% 206University Hospital Waterford 12 3% 118 31% 245 65% 375
~ Denotes five cases or fewer* Further suppression required to prevent disclosure of five cases or fewer
FIGURE 7.1: PERCENTAGE OF PATIENTS BY FUNCTIONAL OUTCOMES: CUMULATIVE AMBULATORY SCORE (n=2015)
Day after surgery Day of dischargeCUMULATIVE AMBULATORY SCORE n % n %6 23 1% 471 23%5 38 2% 230 11%4 98 5% 180 9%3 1272 63% 906 45%2 297 15% 103 5%1 128 6% 51 3%0 159 8% 74 4%
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 165
APPENDIX 4: FREQUENCY TABLES
See Appendix 1: Dataset V8.0.3 for Question (Q) references
DISCHARGE DESTINATION n %Home 1026 28%Off-site rehabilitation unit 1009 28%Return admission to nursing home or long-stay care 543 15%Convalescent care 311 8%Other 283 8%Died 185 5%New admission to nursing home or long-stay care 139 4%On-site rehabilitation unit 96 3%Not known 74 2%Total 3666 100%
FIGURE 7.2: PERCENTAGE OF PATIENTS BY DESTINATION ON DISCHARGE (N=3666)
FIGURE 7.3: PERCENTAGE OF PATIENTS BY CUMULATIVE LENGTH OF STAY (N=3666)
CUMULATIVE LOS (DAYS) n %≤1 43 1%≤7 1069 29%≤14 2341 64%≤30 3228 88%≤60 3540 97%≤90 3611 98%≤120 3638 99%Total 3666 100%
REOPERATION WITHIN 30 DAYS n %No 3081 88%Yes 58 2%Not known 346 10%Total 3485 100%
FIGURE 7.4: PERCENTAGE OF PATIENTS BY REOPERATION WITHIN 30 DAYS (n=3485)
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT166
APPENDIX 5: SPECIFICATIONS FOR COMPOSITE VARIABLES
FIGURE 4.2: ADMISSION TO ORTHOPAEDIC WARD OR THEATRE WITHIN 4 HOURS FROM ED
4.2.1. Composite variable based on Q3–Q4B, Q4F–Q4H and Q5–Q5B, as follows:
See Appendix 1: Dataset for question references.
* If patients go to theatre directly from ED, and within 4 hours of first presentation, they are included.
CATEGORY* SPECIFICATION
Admitted to orthopaedic ward If Q5=1
- Admitted within 4 hours If Q5=1 and time interval is calculated as within 4 hours
- Admitted after 4 hours If Q5=1 and time interval is calculated as more than 4 hours
- Time interval not known If Q5=1 and time interval is not known
Patient admitted directly to theatre within 4 hours If Q5=1 and time to surgery is calculated as within 4 hours
Never admitted to orthopaedic ward If Q5=2
Not known If Q5=9
CATEGORY SPECIFICATION
Within 4 hours If interval range is 0–240 minutes
After 4 hours If interval range is 241–525 600 minutes
Not known If relevant dates and times are missing; or the interval range is invalid, i.e. <0 minutes; or the interval is implausible, i.e. >525 600 minutes (1 year)
4.2.2. Time interval determination for patients admitted to orthopaedic ward (Q5=1):
(a) If admitted via ED (Q4=1), then the time interval is calculated from the date and time of arrival at the first presenting hospital (Q3–Q3A) or from the date and time of arrival at the ED of the operating hospital (Q4A–Q4B), whichever is earlier, to the date and time admitted to an orthopaedic ward (Q5A–Q5B).
(b) If not admitted via ED (Q4=2), then: (i) for inpatient fall cases (Q4H=1), the time interval is calculated from the date and time seen by an orthopaedic team in the operating hospital (Q4F–Q4G) to the date and time admitted to an orthopaedic ward (Q5A–Q5B); (ii) for other cases, the time interval is calculated from the date and time of arrival at either the first presenting hospital (Q3–Q3A) or from the date and time seen by an orthopaedic team (Q4F–Q4G), whichever is earlier, to the date and time admitted to an orthopaedic ward (Q5A–Q5B); and if the date and time of arrival at the first presenting hospital (Q3–Q3A) is not recorded, and the date and time seen by an orthopaedic team (Q4F–Q4G) postdates the date and time admitted to an orthopaedic ward (Q5A–Q5B), then the time interval is set at 0 minutes.
4.2.3. Determination of time interval categories
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 167
APPENDIX 5: SPECIFICATIONS FOR COMPOSITE VARIABLES
FIGURE 4.3 TIME TO SURGERY – 48 HOURS/WORKING HOURS
4.3.1. Composite variable based on Q3–Q4B, Q4F–Q4G, Q5–Q5B, Q14 and Q14E–Q14F, as follows:
See Appendix 1: Dataset for question references.
CATEGORY SPECIFICATION
Within 48 hours and working hours (Monday–Sunday, 8.00am–5.59pm)
If Q14=01–88, and time interval is calculated as within 48 hours, and time of surgery is within specified working hours
Within 48 hours but out of hours (Monday–Sunday, 6.00pm–7.59am)
If Q14=01–88, and time interval is calculated as within 48 hours, and time of surgery is within specified working hours
After 48 hours If Q14=01–88, and time interval is calculated as more than 48 hours
Not known If Q14=01–88, and time interval is not known
4.3.2. Time interval determination for patients who had surgery (Q14=1–88):
(a) If admitted via ED (Q4=1), then the time interval is calculated from the date and time of arrival at the first presenting hospital (Q3–Q3A), or from the date and time of arrival at the ED of the operating hospital (Q4A–Q4B), whichever is earlier, to the date and time of surgery (Q14E–Q14F). If Q3–Q3A and Q4A–Q4B are missing and the patient was admitted to an orthopaedic ward (Q5=1), then the time interval is estimated by using the date and time admitted to an orthopaedic ward (Q5A–Q5B) as its starting point.
(b) If not admitted via ED (Q4=2), then: (i) for inpatient fall cases (Q4H=1), the time interval is calculated from the date and time seen by an orthopaedic team in the operating hospital (Q4F–Q4G) to the date and time of surgery (Q14E–Q14F); (ii) for other cases, the time interval is calculated from the date and time of arrival at either the first presenting hospital (Q3–Q3A) or from the date and time seen by an orthopaedic team (Q4F–Q4G), whichever is earlier, to the date and time of surgery (Q14E–Q14F); (iii) if the date and time of arrival at the first presenting hospital (Q3–Q3A) is not recorded, and the date and time seen by an orthopaedic team (Q4F–Q4G) postdates the date and time admitted to an orthopaedic ward (Q5A–Q5B), then the time interval is calculated from the date and time of admission to an orthopaedic ward to the date and time of surgery (Q14E–Q14F); and (iv) if Q3–Q3A and Q4A–Q4B are missing and the patient was admitted to an orthopaedic ward (Q5=1), then the time interval is estimated by using the date and time admitted to an orthopaedic ward (Q5A–Q5B) as its starting point.
CATEGORY SPECIFICATION
Within 48 hours and working hours (Monday–Sunday, 8.00am–5.59pm)
If interval range is 0–2880 minutes; and time of surgery (Q14F) range is 8.00am–5.59pm
Within 48 hours but out of hours (Monday–Sunday, 6.00pm–7.59am)
If interval range is 0–2880 minutes; and time of surgery (Q14F) range is 6.00pm–7.59am
After 48 hours If interval range is 2881–525 600 minutes (1 year)
Not known If relevant dates and times are missing; or interval is invalid, i.e. <0 minutes; or interval is implausible, i.e. >525 600 minutes (1 year)
4.3.3. Determination of time interval and working hours categories:
FIGURE 4.5: PERCENTAGE OF PATIENTS REVIEWED BY A GERIATRICIAN AT ANY POINT DURING ADMISSION
4.5.1. Composite variable based on Q11A/Q11E:
CATEGORY SPECIFICATION
Assessed by a geriatrician during this acute admission If Q11A=1
Assessed by a cANP/ANP gerontology/orthopaedics If Q11E=1
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT168
APPENDIX 6: ADDITIONAL INFORMATION
* Only includes patients assessed by a geriatrician during their acute admission.** Only includes patients who received surgery during their acute admission.*** Excludes patients who died in hospital.
TYPE OF TRAUMA n %
High-energy trauma 85 2%
Low-energy trauma 3485 95%
Not known 96 3%
Total 3666 100%
PATHOLOGICAL n %
Atypical 37 1%
Malignancy 52 1%
No 3314 90%
Not known 263 7%
Total 3666 100%
PREVIOUS FRAGILITY FRACTURE n %
Yes 1267 35%
No 2150 59%
Not known 249 7%
Total 3666 100%
GERIATRICIAN GRADE* n %
Consultant 1855 63%
Specialist registrar (SpR) 549 19%
Registrar 237 8%
Other 85 3%
Not known 209 7%
Total 2935 100%
SURGEON GRADE** n %
Consultant 2049 59%
SpR 872 25%
Registrar 533 15%
Other 23 1%
Not known 8 0%
Total 3485 100%
ANAESTHETIST GRADE*** n %
Consultant 3226 93%
SpR 46 1%
Registrar 147 4%
Senior house officer (SHO) 46 1%
Not known 20 1%
Total 3485 100%
MULTIDISCIPLINARY REHABILITATION TEAM ASSESSMENT*** n %
Yes 3246 93%
No 220 6%
Not known 15 0%
Total 3481 100%
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 169
APPENDIX 7: IHFD GOVERNANCE COMMITTEE MEETING ATTENDEES 2020
3 = Attended7 = Did not attend
N/A = Not applicableP = Proxy attendedR = RetiredM = Maternity
Representative Name 24/01/20 25/05/20 24/08/20 19/10/20
IHFD Clinical Geriatrician Lead Dr Emer Ahern 3 CHAIR 3 7
IHFD and MTA Manager Louise Brent 3 3 3 3
Communications and Events Lead Aisling Connolly 3 M M M
Irish Gerontology Society Prof Tara Coughlan 3 3 3 3
Healthcare Pricing Office Brian Donovan 3 7 3
National Clinical Programme for Trauma and Orthopaedic Surgery Catherine Farrell 3 3 7 3
Specialist in Public Health Medicine Dr Helena Ferris N/A N/A 3 3
Health and Social Care Professional (HSCP) Representative Michelle Fitzgerald 3 3 3 3
Consultant Anaesthetist Dr Patrick Higgins 3 3 7 3
IHFD Clinical Orthopaedic Lead Prof. Conor Hurson CHAIR 7 CHAIR CHAIR
IHFD Audit Coordinators Representative Ursula Kelleher 3 3 7 3
Senior Healthcare Management Lucy Nugent/John Kelly 3 3 7 7
National Clinical Programme for Trauma and Orthopaedic Surgery; Irish Institute for Trauma and Orthopaedic Surgery
Mr Paddy Kenny 3 3 7 3
Emergency Medicine Representative Prof C Geraldine McMahon 3 7 3 7
Private Hospitals Association (by invite only) Mr Maurice Neligan 7 7 7 7
HSE National Quality Improvement Team Dr Teresa O’Callaghan 7 R N/A N/A
Public/Patient Involvement Representative Bibiana Savin 3 3 3 3
Research Representative Dr Mary Walsh 3 3 3 M
CONTENTS >

NOCA NATIONAL OFFICE OF CLINICAL AUDIT170
NOTES
CONTENTS >

IRISH HIP FRACTURE DATABASE NATIONAL REPORT 2020 171
NOTES
CONTENTS >


















