IPL Literature Review
45
[Type the company address] 2012 Review of optical devices and their potential to be used to treat both medical and cosmetic conditions, including skin rejuvenation, tendinopathy and chronic wounds. This review was conducted as part of a summer placement with the regenerative medicine group at the Institute of Life Sciences of Swansea University. Rhys Alun Luckwell
-
Upload
rhys-alun-luckwell -
Category
Documents
-
view
79 -
download
0
Transcript of IPL Literature Review
Review of optical devices and their potential to be used to
treat both medical and cosmetic conditions, including skin
rejuvenation, tendinopathy and chronic wounds.
This review was conducted as part of a summer placement with the regenerative medicine group at the Institute of Life Sciences of
Swansea University.
Rhys Alun Luckwell
2012[Type the company address]
Rhys Luckwell July 2012
Rhys Luckwell
Review of optical devices and their potential to be used to treat both medical and cosmetic conditions, including skin rejuvenation, tendinopathy and chronic
wounds.
This review was conducted as part of a summer placement with the regenerative medicine group at the Institute of Life Sciences of Swansea University.
1
Rhys Luckwell July 2012
Contents
1) Abstract........................................................................................................3
2) Introduction....................................................................................................4
2.1) Connective tissue and associated extracellular matrix............................4
2.2) Physiology of the skin..............................................................................5
2.3) Physiology of tendons..............................................................................6
2.4) Wounds....................................................................................................7
3) Optical Devices............................................................................................10
3.1) Brief history of lasers and IPL.................................................................10
3.2) The reaction mechanism of photons......................................................10
3.3 Light-tissue interactions..........................................................................12
3.4) IPL devices.............................................................................................12
3.5) IPL Vs Lasers..........................................................................................12
4) Literature review.........................................................................................14
4.1) Skin rejuvenation................................................................................14
4.2) Tendinopathy.........................................................................................19
4.3) Chronic wounds......................................................................................23
5) Conclusion....................................................................................................27
6) References...................................................................................................28
1) Abstract
2
Rhys Luckwell July 2012
This literature review was conducted into how optical devices can be used in both
medicine and cosmetics. There is vast amount of literature and research on the effects of
optical devices and to cover it all in finite detail is not within the scope of this review.
Therefore, this review will focus on the effect of lasers,light emitting diodes (LED) and
concentrate mainly on intense pulsed light systems (IPL) devices on how they can
improve skin rejuvenation, chronic wounds and tendinopathy.
By looking at how such devices work on a cellular level and the effect they have In Vitro,
In Vivo and in clinical trials the potential benefits that optical devices can have will be
summarised. Such benefits include reducing the healing time of chronic wounds and
injured tendons, and allowing repair to restore the tissue to its former native biochemical
and biomechanical composition. In doing so, optical devices can help reduce the cost of
treatment allowing hospitals to save on expensive resources used to treat these cases
and limit the number of hospital beds being used at any given time
This review will also look at the benefits on IPL over traditional laser treatment. With IPL
devices being more mobile, cheaper and requiring less maintenance than lasers they
provide an attractive alternative to physicians and cosmetic retailers.
This review concludes that the use of optical devices in medicine and cosmetics has
tremendous potential and that IPL in particular has a big future role to play in the
treatment of skin rejuvenation, chronic wounds and tendinopathy.
3
Rhys Luckwell July 2012
2) Introduction
2.1) Connective tissue and associated extracellular matrix
Connective tissue is one of the four types of tissue of the body. Examples of connective
tissue include skin, bone, tendons, ligaments, adipose tissue and blood. For connective
tissue to carry out its structural role it must be supported by the extracellular matrix
(ECM). The ECM therefore is essential in providing a framework for tissue movement and
for the transmission of mechanical forces (Silver et al., 2003). However, the idea of the
ECM providing only ‘scaffolding’ for the tissue has been put to rest and it is now agreed
that the ECM is an important mediator of cellular events. It is thought that cell migration,
proliferation, survival, migration and differentiation are a result of ECM remodelling which
occurs through MMPs and their inhibitors. This process is coordinated by hormones and
growth factors (Nieto and Lutolf , 2011).
The ECM is composed of collagens, elastins, glycoproteins, proteoglycans and GAGs. It’s
the specific composition of these materials that give different connective tissues their
specific biochemical properties. These components are secreted by fibroblast cells.
Fibroblasts are spindle shaped cells that sit in the ECM that they have secreted and are
required for connective tissue homeostasis as well as being essential in the repair of
tissue. The most common protein found in ECM is collagen. Its fibrillar collagen (type I,
II,III and V) that provides the structural framework. These types of collagen can bare
great tensile forces. Another important collagen is FACIT collagen. FACIT collagen is
involved in transferring these tensile loads through connecting fibril collagen to other
parts of the ECM (Silver at al.,2003). The composition of ECM is in a dynamic equilibrium
of catabolism and anabolism. This equilibrium can change with age, thus affecting the
structure and strength of ECM. With age there is a decrease in proteoglycan content
(Suchuckett and Malemad, 1989), decrease in collagen type III (Mays et al.,1988),
fragmentation of elastin in skin and cardiac tissue and an unravelling of collagen in the
skin (Lavker et al., 1987).
4
Rhys Luckwell July 2012
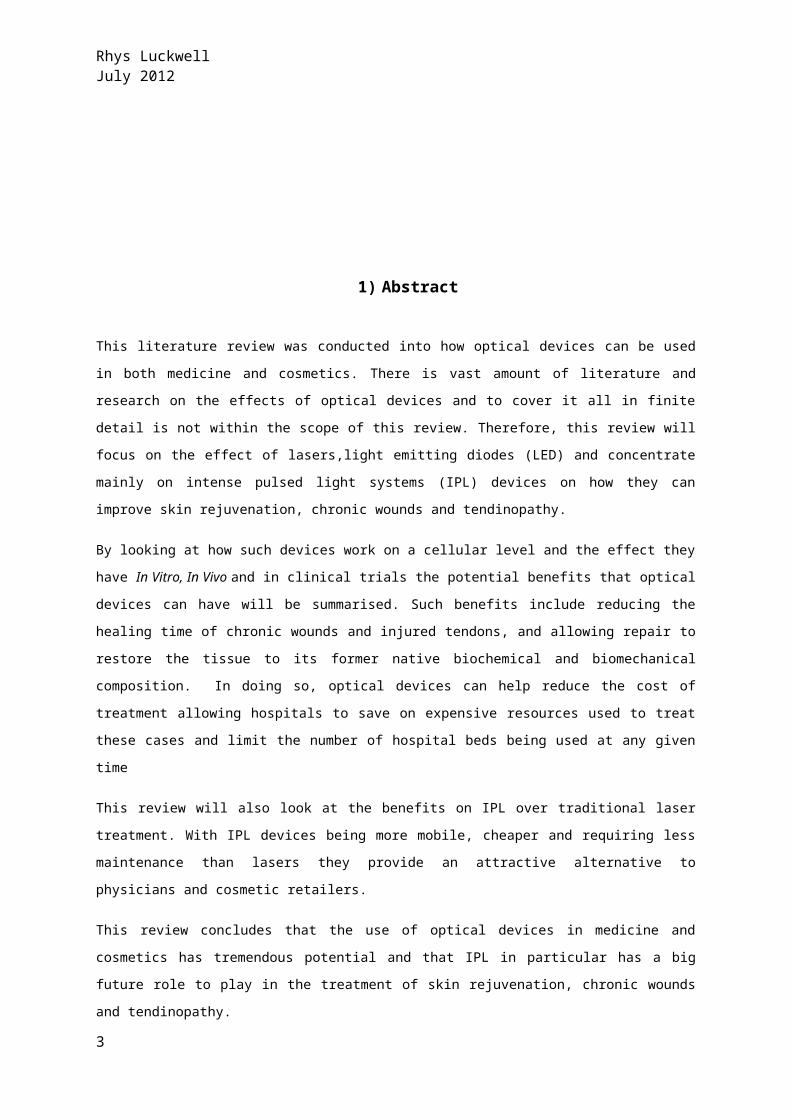
Figure 1) Scanning electron microscope image of a fibroblast interacting with the ECM that it has
secreted. The type I collagen can be clearly seen as a meshwork of intertwining fibres (Image
taken from Ree and Grinnell, 2008)
As mentioned, fibroblasts are essential in the repair of injured tissue. After an injury
fibroblasts undergo a phenotypic change that results in them being increasingly mobile
allowing them to migrate to the site of injury quicker (Raffetto et al., 2001). Factors such
as, U.V light, aging and diseased cells can disrupt the relationship between fibroblasts
and ECM environment in which they sit. This disruption can lead to the prolonged healing
of chronic wounds, wrinkles (Vedrenne et al., 2012) and a reduction in the diameter of
collagen fibrils in tendons which can cause a reduction in the mechanical strength of
tendons (Dressler et al., 2005).
The next part of this review will go look at the biochemical and physiological make up of
skin and tendons and provide and insight into the acute and chronic wound healing
processes.
2.2) Physiology of the skin
Firstly I will review the structure of skin and how it is related to its specific functions. I will also look at how the structure-function relationship is affected by factors such as age, smoking and U.V light.
2.2.1) Structure and Function of skin
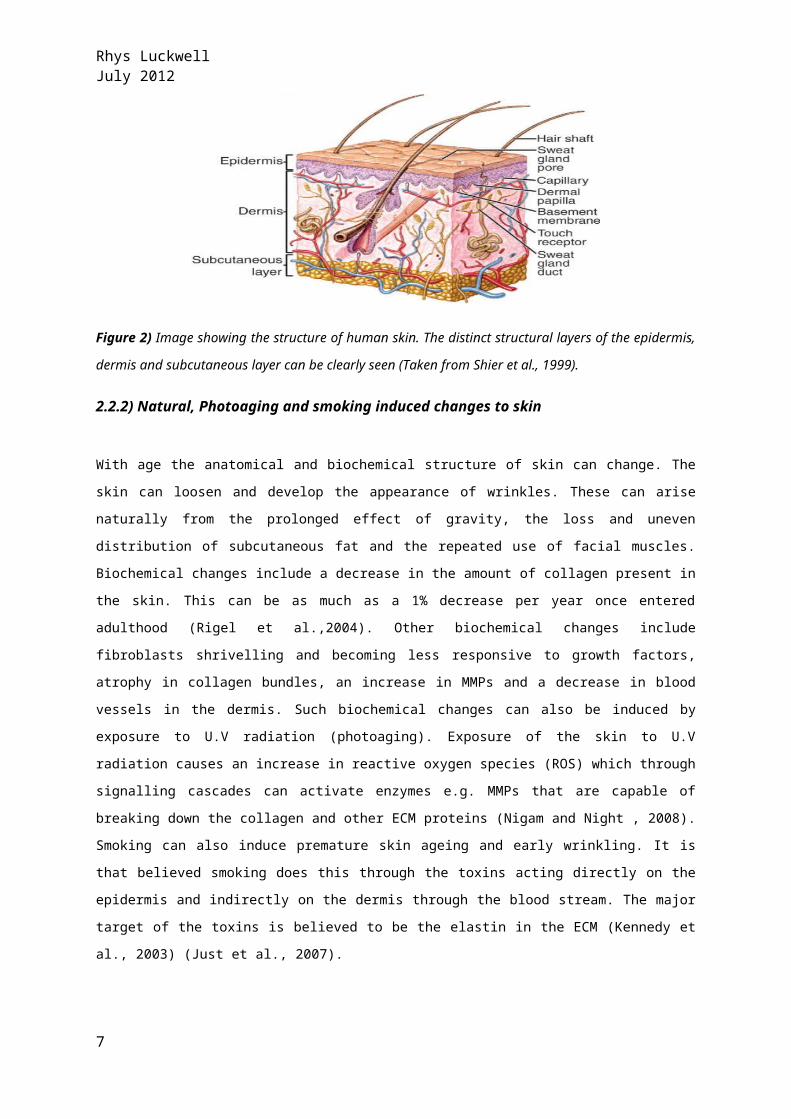
Skin has many functions. It provides protection, sensation, thermoregulation, metabolic
and immune functions. Skin is composed of 2 main layers, the epidermis and the dermis.
Below the dermis a layer of subcutaneous tissue (hyperdemis). Each layer is separated
by a basal membrane (Wysoki et al.,1999) (Prost-Squarcioni et al., 2008). The epidermis
is a protective layer made up of keratinised squamous tissue. This layer contains
keratinocytes, melanocytes, Langerhans cells and dendritic cells. The dermis is
composed of fibrous connective tissue which provides strength and elasticity through
collagen and elastin. Both fibrillar collagens (e.g. type I,III and V) and FACIT collagens
(e.g. type XI,IX) are found here (Prost-Squarcioni et al., 2008 ) . The dermis contains
fibroblasts, macrophages, mast cells, hair follicles and sweat glands. It also contains
blood vessels and nerves (Nigam and Night , 2008).
5
Rhys Luckwell July 2012
Figure 2) Image showing the structure of human skin. The distinct structural layers of
the epidermis, dermis and subcutaneous layer can be clearly seen (Taken from Shier et
al., 1999).
2.2.2) Natural, Photoaging and smoking induced changes to skin
With age the anatomical and biochemical structure of skin can change. The skin can
loosen and develop the appearance of wrinkles. These can arise naturally from the
prolonged effect of gravity, the loss and uneven distribution of subcutaneous fat and the
repeated use of facial muscles. Biochemical changes include a decrease in the amount of
collagen present in the skin. This can be as much as a 1% decrease per year once
entered adulthood (Rigel et al.,2004). Other biochemical changes include fibroblasts
shrivelling and becoming less responsive to growth factors, atrophy in collagen bundles,
an increase in MMPs and a decrease in blood vessels in the dermis. Such biochemical
changes can also be induced by exposure to U.V radiation (photoaging). Exposure of the
skin to U.V radiation causes an increase in reactive oxygen species (ROS) which through
signalling cascades can activate enzymes e.g. MMPs that are capable of breaking down
the collagen and other ECM proteins (Nigam and Night , 2008). Smoking can also induce
premature skin ageing and early wrinkling. It is that believed smoking does this through
the toxins acting directly on the epidermis and indirectly on the dermis through the blood
stream. The major target of the toxins is believed to be the elastin in the ECM (Kennedy
et al., 2003) (Just et al., 2007).
2.3) Physiology of tendons
Tendons are fibrous connective tissue with a primary role of connecting muscle to bone.
Here they help transmit forces, change direction of pull and withstand compression and
sheer forces. Tendons are full of ECM that is secreted by specialised fibroblasts called
6
Rhys Luckwell July 2012
tenocytes which lie in the ECM between the collagen fibres. The main components of the
ECM are collagen type I, elastin and proteoglycans (Benjamin et al.,2008). Type I
collagen and elastin make up 65-80% and 2% of the dry mass of a collagen fibre
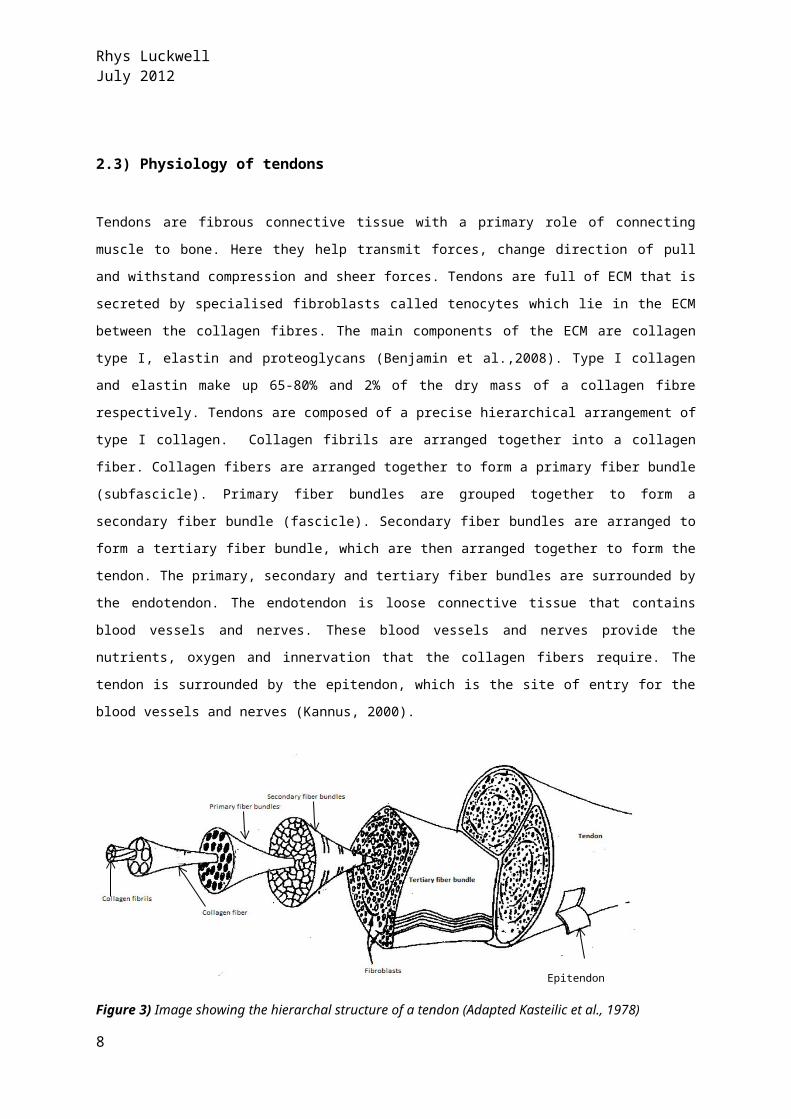
respectively. Tendons are composed of a precise hierarchical arrangement of type I
collagen. Collagen fibrils are arranged together into a collagen fiber. Collagen fibers are
arranged together to form a primary fiber bundle (subfascicle). Primary fiber bundles are
grouped together to form a secondary fiber bundle (fascicle). Secondary fiber bundles
are arranged to form a tertiary fiber bundle, which are then arranged together to form
the tendon. The primary, secondary and tertiary fiber bundles are surrounded by the
endotendon. The endotendon is loose connective tissue that contains blood vessels and
nerves. These blood vessels and nerves provide the nutrients, oxygen and innervation
that the collagen fibers require. The tendon is surrounded by the epitendon, which is the
site of entry for the blood vessels and nerves (Kannus, 2000).
Figure 3) Image showing the hierarchal structure of a tendon (Adapted Kasteilic et al.,
1978)
With respect to tendons, this review will focus on Achilles tendinopathy as the Achilles
tendon is the largest tendon in the human body (Benjamin et al.,2008) and is one of the
most commonly injured tendons taking weeks/months to heal. Tendinopathy is a
common case that can result from sports injury or when the tendon is subject to
unusually high loads (Cook et al.,2002). The Achilles tendon has a long repair time due to
it having a low blood supply, with the midpoint of the tendon being hypovascular and this
is the site most prone to injury (Doral et al., 2010). During this repair time, the tendon is
normally immobilised, thus preventing further change to the biochemistry of the tendon
(Oliveira et al., 2009). Other traditional treatments are also usually conservative, such as
eccentric training or electrotherapeutic modalities as part of physiotherapy programme
(Miners and Bougie, 2011). There are two forms of tendinopathy; inflammatory and
degenerative. The degenerative form is known as tendinosis. The inflammation is known
as tendinitis. Tendinitis can develop before any symptoms show. Symptoms of Achilles
7
Epitendon
Rhys Luckwell July 2012
tendinopathy typically occur at middle or insertion point of the tendon (Sussmilch-leitch
et al.,2012).
2.4) Wounds
The next part of the review will look at the process of acute wound healing and what leads to chronic wounds.
2.4.1) Acute Wound healing
A wound, as defined by Enoch and Price (2004) is a ‘break in the epithelial integrity of
the skin’ and heals normally through a dynamic cascade of events requiring coordination
of different cellular process. The cellular process involved in wound healing include;
mesenchymal cell differentiation, mitogenesis, angiogenesis, re- epithelialization,
collagen synthesis and alignment (Methieu et al.,2006).
There are four stages of acute wound healing; haemostasis, Inflammatory phase,
proliferation and remodelling (Enoch and Leaper, 2005).
2.4.1.1) HaemostasisHaemostasis is a dynamic process of when after injury blood vessels contract and the
coagulation cascade is initiated. This helps to minimize blood loss. Platelets adhere to the
exposed endothelial and aggregate to form the haemostatic plug (Ridel et al., 2007). This
haemostatic clot contains fibrin, fibronectin, von willebrand factor and provides the
primary meshwork for platelets aggregation. Platelets contain 3 types of secretory
granules; alpha granules, dense bodies and lysosomes (King and Reed, 2002). Alpha
granules and dense bodies in particular contain contents important in haemostasis. The
alpha granules contain growth factors such as IGF-1, EGF and TGF-β. These growth
factors initiate wound healing by activating fibroblasts, endothelial cells and
macrophages. Dense Bodies contain serotonin which increases the vascular permeability
of the vessels (Enoch and Price, 2004).
2.4.1.2) Inflammatory PhaseInflammation occurs with the activation of the complement cascade. The complement
proteins such as C5a attract neutrophils, macrophages and lymphocytes to the wound
(Campos et al.,2008). These phagocytes stick to the endothelial cells by a process of
margination and eventually move through the vessel wall by a process of diapedesis,
(Smith, 1993). Neutrophils engulf and destroy foreign bacteria through releasing reactive
oxygen species (ROS) thus helping to prevent wound infection (Guo and Dipetro, 2010).
8
Rhys Luckwell July 2012
Monocytes are attracted to the wound by chemoattractants such as complement
proteins, platelet factor V and TGF-B. On entering the wound monocytes become
macrophages and release cytokines and growth factors into the wound, playing a key
role in wound healing. These cytokines and growth factors attract fibroblasts,
keratinocytes and endothelial cells to then wound site where these cells stimulate tissue
repair (Mosser and Edwards et al., 2008). Decrease in macrophages numbers can lead
to poor wound healing as a result from slower rates of fibroblast proliferation and poor
angiogenesis.
2.4.1.3) ProliferationCharacterised by epithelial migration and proliferation and re-epithelialzation. Fibroblasts
migrate into the wound (as mentioned in response to such growth factors as TGF-B) and
begin to proliferate and make new ECM through secreting fibronectin, HA, collagen type I
and III and proteoglycans (PGs). Collagens play a structural role through providing
strength and integrity to the repair tissue (Guo and DiPetro, 2010).
2.4.1.4)Remodelling PhaseAs the new ECM continues to develop the fibronectin and the HA are slowly broken down
and the diameter of the collagen fibres increase, increasing the tensile strength of the
recovering wound.
During remodelling the collagen is in equilibrium of being broken down and synthesised.
Collagen is broken down by MMPs which are secreted by macrophages and fibroblasts.
As the remodelling process continues the numbers of MMPs decrease and the number of
TIMPs increase, thus promoting a net gain of ECM. This equilibrium is controlled by TGF-B
(Enoch and Price, 2004).
Collagen reorganisation is achieved by wound contraction. The contractile tissue
underneath the wound contracts bringing the wound margins together this is thought to
be controlled by myofibroblasts (Campos et al.,2008).
Macrophages and fibroblasts begin to decrease in number as a result of apoptosis which
is stimulated potentially due to a decrease in cytokines. Finally angiogenesis stops
resulting in an acellular and avascular scar (Enoch and Price, 2004).
2.4.2) Chronic Wound Healing
Chronic wounds occur as a result of malfunctions in this acute healing process described
above. A wound is defined as chronic if it has not managed to heal within 4 – 6 weeks
after injury and does not show signs of doing so (Banikol and Potzschke, 2012).
According to Banikol and Potzschke chronic wounds arise from many factors (poor
9
Rhys Luckwell July 2012
oxygenation, diabetes, nutrition). These factors can alter the cells metabolism, causing
the cell to become fixed in any of the 4 healing phases (Guo and Dipetro, 2010) this
disrupting the level of growth factors, cytokines and protease activity which play such a
crucial role in wound repair (Enoch and Price , 2004). The levels of MMP and serine
proteases such as neutrophil elastase have been found to increase in chronic wounds
compared to normal healing wounds (Yager et al., 1996). At the same time the level of
their specific inhibitors decreases which results in an increased degradation of the ECM
proteins. It’s the ECM proteins (Fibronectin, vitronectin and tenasin) that are responsible
for creating the ECM for collagen to be laid upon (Enoch and Price, 2004).
To summarise, disease cells associated with chronic wounds have distinctly different
biochemical and cellular features to acute wound;
i) Keratinocytes migrate less
ii) Change of fibroblast and keratinocyte phenotype
iii) Decrease in the amount of growth factors secreted
iv) Decreased response of fibroblasts to growth factors
v) Increase in MMP secretion by fibroblasts.
3) Optical Devices
3.1) Brief history of lasers and IPL
The first laser developed was the monochromatic light ruby laser which was developed in
1961 by Maiman (Raulin and Karsai 2011). This laser was a result of research through the
1950 that was based on Einstein’s principal of stimulating radiation (Greiges 2011). The
ruby laser was first used in dermatology in 1963 when Dr Leon Goldman used a ruby
laser to treat vascular lesions (Stier et al., 2008). In 1976 polychromatic light was used
by Muhlbauer to treat vascular lesions. This eventually led to IPL being launched for use
as a medical devices in 1994(Schoenwolf et al.,2011).
10
Rhys Luckwell July 2012
3.2) The reaction mechanism of photons
Optical devices can induce a biological effect by various reaction mechanisms. These
reactions include photochemical, photothermal (most commonly used in dermatology)
photoablation, plasma induced ablation and photomechanical. These different reactions
are achieved by changing the pulse duration and energy densities of the irradiance
(Weber et al., 2011). Here I will look at the most common three:
3.2.1) Photothermal
This reaction, through the principal of selective thermolyisis is often considered as the
principal reaction associated with IPL treatment. (Schoenewolf et al., 2011). Although
this is the reaction associated with use of IPL for hair removal and skin rejuvenation, the
other reactions are used in other IPL treatment.
Heat is produced in the targeted tissue as a result of photons being absorbed by
chromophores. This rise in temperature in the tissues results in damage to the living
tissue (Raulin and Karsai, 2011). The basis of photothermal reaction is photothermolysis.
Described by Anderson and Parish in 1983 where only the targeted tissue is destroyed
through heating (Raulin, 2003)(Anderson and Parish, 1983).
3.2.2) Photomechanical
This mechanism involves short periods of high intensity irradiance. The high energy
results in the breaking of intramolecular bonds. It’s a photomechanical reaction that is
used to remove tattoos (Thomson,1991) Jacques, 1992).
3.2.3) Photochemical
There are two photochemical interactions described by Raulin and Karsai (2011);
biostimulation and photodynamic therapy (PDT). Biostimulation works on the basis that
when a chromophore absorbs a photon the energy of the photon causes a change in the
11
Rhys Luckwell July 2012
signalling pathways of the cell and thus changing the metabolism of the cell. The change
in metabolism can result in change of gene expression (Zungu et al., 2006).
Mitochondria are common targets. The effect of stimulating chromophores in
mitochondria can cause an increase in cellular respiration (Whelan et al., 2001). This
can result in:
i) Increased production of ROS
ii) Increased ATP synthesis
iii) Changes in the permeability of cell membranes
iv) Nitric oxide release
These effects can cause an increasing cell proliferation and ECM synthesis (Raulin and
Karsai, 2011).
Low-level laser therapy (LLLT) is an example of laser therapy that works by the
photochemical biostimulation mechanism. It works through this mechanism as the low
power emitted from LLLT is not significant to cause damage to the tissue through rising
the temperature.
The photodynamic mechanism involves 3 parts; i) light for activation ii) sensitizer iii)
molecular oxygen.
The sensitizers accumulate in the target tissue and then become exited on absorption of
photons. The energy from the exited sensitizer is then transferred to molecular oxygen.
This exiting the molecular oxygen, causing it to become a free radical, and destroying
the cell. Photodynamic therapy is used in tumour treatment and imaging as the
sensitizers are fluorescent (Raulin and Karsai, 2011).
3.3 Light-tissue interactions
Before these reactions can take place the photons must interact with the tissue and
become absorbed. Not all the photons will be instantly absorbed. Around 4-10% of
photons that are emitted onto tissue are reflected (Raulin and Karsai,2011). This
reflection is dependent on the angle of incidence, when the angle of incidence is 90
degrees the reflection is lowest. The other photons enter the tissue. Once in the tissue
the photons can become absorbed by chromophores or can become scattered changing
their direction. This scattering can be caused by structures within the tissue e.g. muscle
12
Rhys Luckwell July 2012
fibres. The extent of scattering is dependent on the wavelength of light, the spot size and
tissue particle size. Photons of the lager light wavelengths will penetrate deeper into the
tissue without being absorbed (Allemann and Kaufman, 2011).
3.4) IPL devices
IPL’s are flash lamps that emit pulsed polychromatic high intensity light (Babillis et al.,
2010) between wavelengths of 500-1,200 (Haedersdal et al., 2008). IPL devices have
great potential as there is great scope to alter the pulse duration, pulse frequency and
the fluence. Thus giving them the ability to be carefully manipulated to suit different skin
types and conditions. Due to the broad range of light emitted it is possible to activate
many chromophores with a single irradiance. Different target chromophores have
different maximum wavelength absorptions, e.g. Haemoglobin absorbs at 580 nm where
melanin absorbs between 400-750 nm. Therefore by selecting the correct parameters
IPL can selectively target the target tissue through specific reaction mechanisms (Raulin
et al.,2003).
The fact that the parameters of IPL devices are so flexible it demands expertise to ensure
the right parameters are selected so side effects can be avoided kept to the minimum.
Poor and careless use of IPL can cause hyperpigmentation (Babilas et al., 2010).
What is Hyperpigmentation and other side effects? Erythema?
3.5) IPL Vs Lasers
IPL technology is similar to lasers in the respect that energy from the laser/IPL device is
transferred to chromophores in the skin (Schoenewolf et al., 2011). The use of lasers,
although effective, does come with their limitations. Lasers have restrictions on the
range wavelength and beam of light emitted. The fact that lasers emit a narrow beam of
light limits the size of the target area that can be treated. LED and IPL devices emit
larger arrays of light allowing the treatment area to be larger. The other limitation with
lasers comes from the heat produced which can damage surrounding tissue and the
intensity of the beam can damage eyes (Whelan et al., 2001). Lasers are also less
mobile and need greater maintenance than IPL and LED devices (Fushimi et al., 2012).
13
Rhys Luckwell July 2012
4) Literature review
4.1) Skin rejuvenation
With regards to skin rejuvenation, treatment of chronic wound and tendinopathy the area
with greatest research on the effectiveness of IPL is skin rejuvenation. I will therefore
begin by reviewing the effectiveness of IPL in this field.
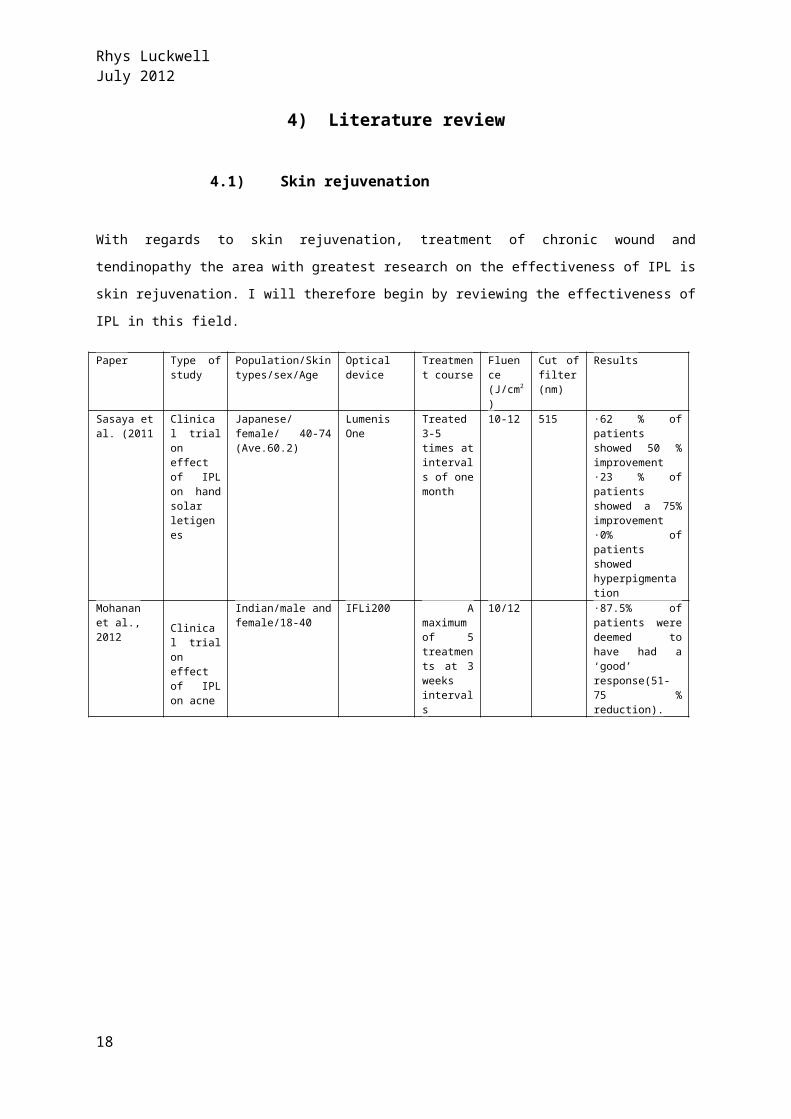
Paper Type of study
Population/Skin types/sex/Age
Optical device
Treatment course
Fluence (J/cm2)
Cut of filter (nm)
Results
Sasaya et al. (2011
Clinical trial on effect of IPL on hand solar letigenes
Japanese/female/ 40-74 (Ave.60.2)
Lumenis One
Treated 3-5 times at intervals of one month
10-12 515 ·62 % of patients showed 50 % improvement·23 % of patients showed a 75% improvement·0% of patients showed hyperpigmentation
Mohanan et al., 2012
Clinical trial on effect of IPL on acne
Indian/male and female/18-40
IFLi200 A maximum of 5 treatments at 3 weeks intervals
10/12 ·87.5% of patients were deemed to have had a ‘good’ response(51-75 % reduction).
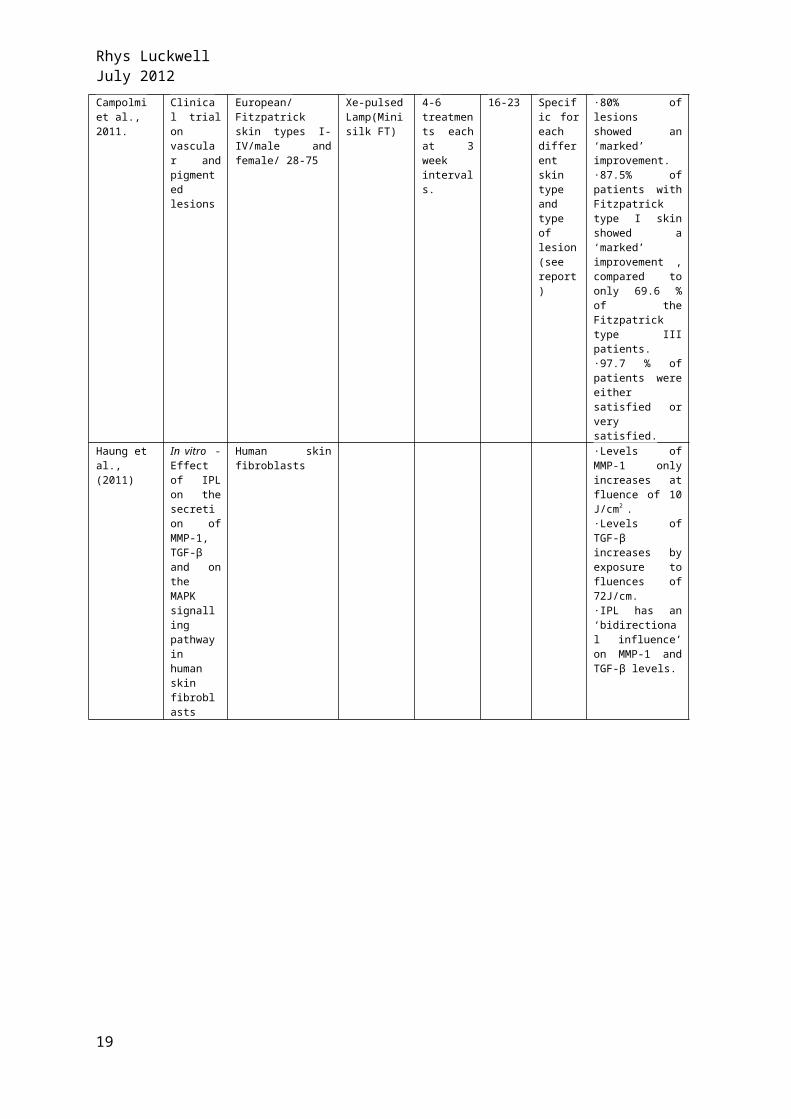
Campolmi et al., 2011.
Clinical trial on vascular and pigmented lesions
European/Fitzpatrick skin types I-IV/male and female/ 28-75
Xe-pulsed Lamp(Minisilk FT)
4-6 treatments each at 3 week intervals.
16-23 Specific for each different skin type and type of lesion (see report)
·80% of lesions showed an ‘marked’ improvement.·87.5% of patients with Fitzpatrick type I skin showed a ‘marked’ improvement , compared to only 69.6 % of the Fitzpatrick type III patients.·97.7 % of patients were either satisfied or very satisfied.
Haung et al.,(2011)
In vitro -Effect of IPL on the secretion of MMP-1, TGF-β and on the MAPK signalling pathway in human skin fibroblasts
Human skin fibroblasts
·Levels of MMP-1 only increases at fluence of 10 J/cm2 .·Levels of TGF-β increases by exposure to fluences of 72J/cm.·IPL has an ‘bidirectional influence’ on MMP-1 and TGF-β levels.
14

Rhys Luckwell July 2012
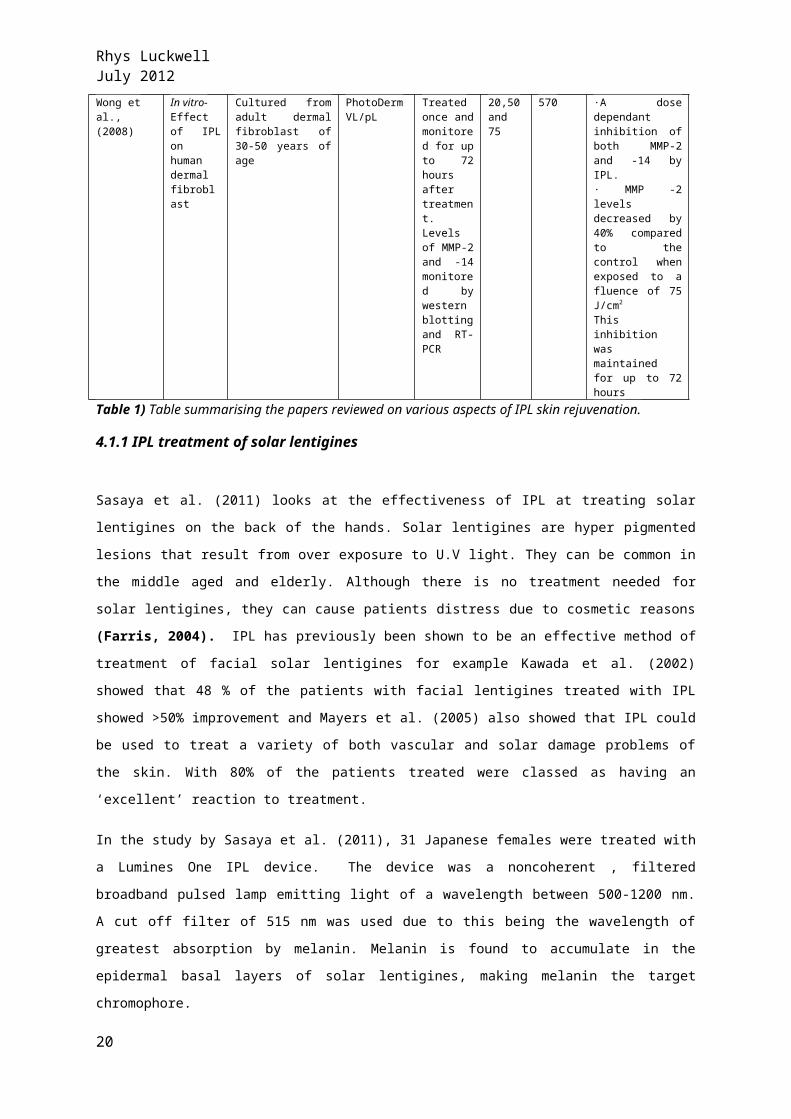
Wong et al.,(2008)
In vitro-Effect of IPL on human dermal fibroblast
Cultured from adult dermal fibroblast of 30-50 years of age
PhotoDerm VL/pL
Treated once and monitored for up to 72 hours after treatment. Levels of MMP-2 and -14 monitored by western blotting and RT-PCR
20,50 and 75
570 ·A dose dependant inhibition of both MMP-2 and -14 by IPL.· MMP -2 levels decreased by 40% compared to the control when exposed to a fluence of 75 J/cm2
This inhibition was maintained for up to 72 hours
Table 1) Table summarising the papers reviewed on various aspects of IPL skin rejuvenation.
4.1.1 IPL treatment of solar lentigines
Sasaya et al. (2011) looks at the effectiveness of IPL at treating solar lentigines on the
back of the hands. Solar lentigines are hyper pigmented lesions that result from over
exposure to U.V light. They can be common in the middle aged and elderly. Although
there is no treatment needed for solar lentigines, they can cause patients distress due to
cosmetic reasons (Farris, 2004). IPL has previously been shown to be an effective
method of treatment of facial solar lentigines for example Kawada et al. (2002) showed
that 48 % of the patients with facial lentigines treated with IPL showed >50%
improvement and Mayers et al. (2005) also showed that IPL could be used to treat a
variety of both vascular and solar damage problems of the skin. With 80% of the patients
treated were classed as having an ‘excellent’ reaction to treatment.
In the study by Sasaya et al. (2011), 31 Japanese females were treated with a Lumines
One IPL device. The device was a noncoherent , filtered broadband pulsed lamp emitting
light of a wavelength between 500-1200 nm. A cut off filter of 515 nm was used due to
this being the wavelength of greatest absorption by melanin. Melanin is found to
accumulate in the epidermal basal layers of solar lentigines, making melanin the target
chromophore.
Each patient received 3-5 treatments at 4-5 week intervals. The treatment consisted of a
fluence of 10-12 J/cm2 that was delivered at pulses of 4.0ms.
The results of the treatment suggest that IPL can be used as a potential method for
treatment of solar lentigines of the back of the hands. 52% of patients were rated by
physicians to have shown a moderate or marked improvement. Only 6% of the patients
showed no change and 0 patients showed side effects. With 94% of the patients
expressing some levels of satisfaction it indicates that IPL can be used as a tolerable and
attractive method of treating solar lentigines to the back of the hand.
15
Rhys Luckwell July 2012
4.1.2 IPL treatment of Acne
Acne is a chronic inflammatory disease which is mostly commonly found on sites such as
the face, shoulders and back. It is common for it to affect not only adolescents but also
young adults. It is caused by the abnormal breakdown of the follicular epithelium. This
results in the obstruction of the pilosebaceous canal which leads to the formation of
comedones (Bjerring and Christianse, 2011). The treatments of acne can be for both
medical and cosmetic purposes. Some cases require the treatment for serious
psychological issues compared to some patients who would like to have it treated merely
for vanity.
Mohanan and colleagues (2012) have investigated the effects of IPL on the Indian
population. There is vast amount of research on the effect of IPL on acne suffers of the
Western world but not on the Indian population. The Indian population may react
differently to IPL treatment due to the higher melanin content of the skin (Mohanan et
al., 2012) .
Mohanan and colleagues (2012) ran a 17 months study were they investigate the benefit
of IPL on Indians aged 18 – 40 that suffered from mild to moderate acne. Prior to
treatment with IPL the patients were asked for a period of 2 weeks to cleanse their skin
and to apply sun cream. They were also asked to stop any other on-going treatments e.g
antibiotic courses.
For the effect of IPL to be measured the total number of comedones, papules and
pustules were counted and photographs taken before each treatment of IPL.
The IPL device used was the IFL i200. The device emitted multiple pulses of light at an
average frequency of 0.25Hz at a fluence of 10-12 J/cm2.
All 8 patients that finished the trail were of Fitzpatrick skin type 3 or 4 and aged below
25. All showed a reduction in lesion count. The overall reduction ranged from 44% - 73%,
with 7 out of the 8 deemed to have showed a ‘good’ response. Greater reduction was
seen in the count of papules and pustules than comedones, but not a significant amount,
nor was there significant correlation between the different skin types.
The study showed minimal and impermanent side effects, therefore indicating that IPL
could prove effective at treating Indian acne sufferers, provided they also undertake
protection from the sun through sun creams (Mohanan et al., 2012).
16

Rhys Luckwell July 2012
4.1.3 IPL treatment on vascular and solar lesions
In a study by Campolmi et al. (2011) 85 patients with Fitzpatrick skin type’s I-IV between
the ages of 28 – 75 were treated with IPL and followed up for a period of 2 years. During
this time they received 4-6 treatments of IPL at 3 week intervals. The IPL device used
was Xe Pulsed Lamp. The pulse time was 3 – 8 ms with a double pulse, the pulse delay
was 10 ms. The fluence used was between 16 – 23 J/cm2 . Different cut off filters were
used for different lesions, this allowing different wavelengths to be emitted so different
lesions of different skin types could be specifically targeted. For vascular lesions a cut off
filter of 500 nm was used for skin types I and II, 520 nm was used for Fitzpatrick skin
types III and IV. Whereas for the pigmented lesions a cut off filter of 550 nm was used for
skin types I-III and 600 nm for IV.
The results of the study showed that all 85 patients showed improvements to their skin.
With 72 out of the 89 lesions that were strung across the 85 patients being deemed as
having a ‘marked’ improvement. The study found that 4 IPL treatments is needed for
improving the quality of pigmented lesions were as 6 IPL treatments were required for
vascular lesion. The results of the study by Campolmi et al.(2011) show that there is
difference in the efficiency of IPL with different skin types. 87.5 % of the Fitzpatrick skin
type I showed an marked improvement, whereas only 69.6 % of Fitzpatrick skin type III
shows a marked improvement. There was no significant correlation between the
efficiency of IPL with age. Best results were found when acting on Fitzpatrick skin
phototypes I-II with a wavelength of 500 – 520 nm and a pulse time of 8 ms.
Age % of age group that showed a ‘marked’
improvement
20-39 81.8
40-59 80.5
60-79 80.7
Table 2) Table showing the % of patients that showed a ‘marked’ improvement grouped
on age. No significant correlation was found.
The majority of the patients (55/85) showed no side effects and 97.7 said they were
either satisfied or very satisfied. Again this indicated that IPL is a safe and attractive
method for rejuvenating skin.
17
Rhys Luckwell July 2012
4.1.4 In Vitro analysis of IPL on levels of MMP-1 and TGF-β and the MAPK signalling cascade of human skin fibroblasts
Research by Huang et al. (2011) looked into the molecular biology behind the skin
rejuvenating actions of IPL. One way that IPL is thought to work is by effecting different
cytokines. It’s this specific action that causes the final out come to the targeted skin.
Haung et al. (2011) investigated the effect that IPL had on the levels of MMP-1 and TGF-
β1 that were secreted by human fibroblast cells. Haung and colleagues also looked at the
effect IPL had on the MAPK signalling cascade. Their results showed:
i) The level of MMP-1 secreted increased only when IPL was applied at a fluence
of 10 J/cm2 .
ii) TGF-β1 secretion was inhibited when IPL was applied at a fluence of below 36
J/cm2 .
iii) Levels of TGF-β1 increased when IPL was applied at a fluence of 72 J/cm2.
iv) MAPK signalling proteins decrease/become inhibited by IPL. This having a range
of effects;
- ) When ERK become inhibited MMP-1 secretion decreased but had no
significant effect on TGF-β1.
- ) Inhibition of JNK resulted in the increase of MMP-1 and decrease of TGF-β1
- ) P38 inhibition did not have a significant effect on MMP-1 levels but did
cause an increase in TGF-β1 secretion.
Huang et al. (2011) therefore suggests that it is this ‘bidirectional influence’ that IPL has
on MMP-1 and TGF-β1 that can cause skin rejuvenation. This coincides with other
research as it is known that TGF-β1 can induce angiogenesis, stimulate the production of
collagen I and III through activating fibroblasts, and cause the granulation of tissue
(Roberts et al., 1986).
4.1.5 In Vitro analysis of how IPL effects levels of MMP-2 and MMP-14 secreted by human dermal fibroblasts
A study by Wong et al. (2008) discusses the underlying effects that IPL has on biological
tissue by looking at how IPL affects human dermal fibroblasts. Wong and colleagues
cultured primary human dermal fibroblasts from a selection of adult skin dermis explants
that were between the ages of 30 -50 years old. Wong et al. were particularly interested
18
Rhys Luckwell July 2012
to see at how IPL effected the expression of MMPs and TIMPs, essential mediators that
maintain the firmness of skin.
The IPL device used was PhotoDerm VL/pL system. A cut off filter of 570 nm was used at
triple pulses of 7 ms at pulse intervals of 70 ms. Fluency’s of 20, 50 and 75 J/cm2 were
used. After irradiation the tissue was placed in DMEM/10% FBS and left for 74 hours. On
removal the fibroblast in lattices were taken for RNA isolation.
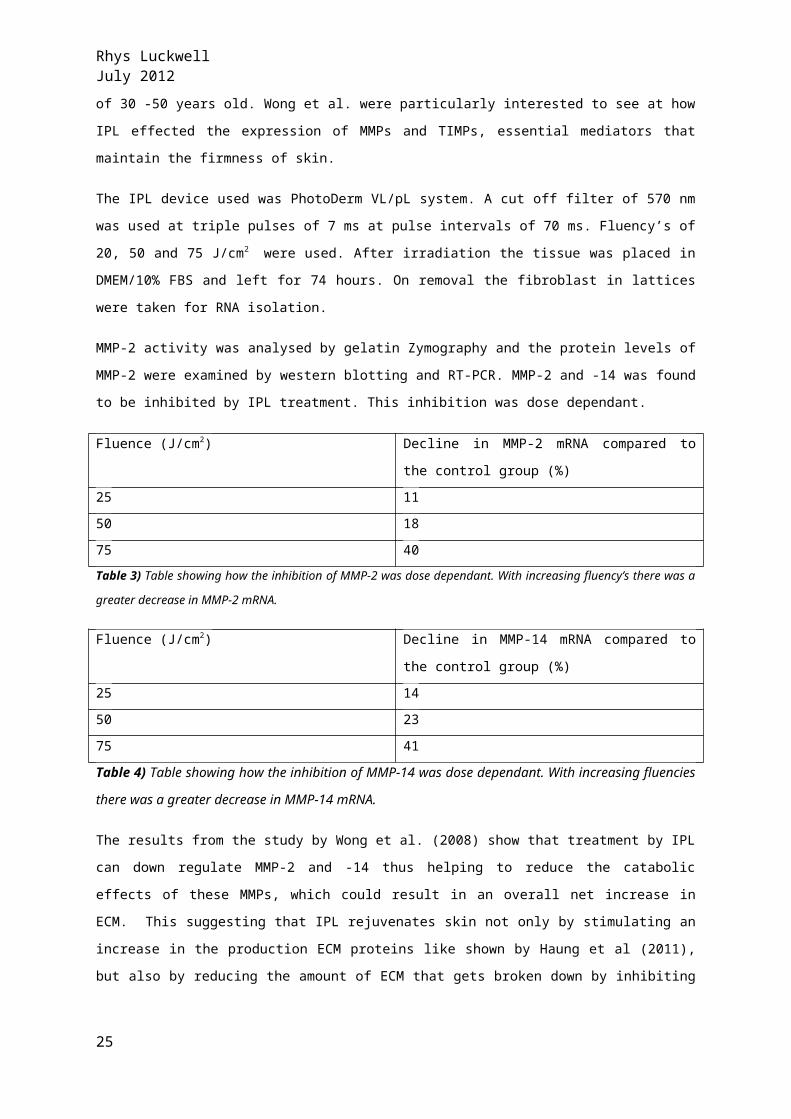
MMP-2 activity was analysed by gelatin Zymography and the protein levels of MMP-2
were examined by western blotting and RT-PCR. MMP-2 and -14 was found to be inhibited
by IPL treatment. This inhibition was dose dependant.
Fluence (J/cm2) Decline in MMP-2 mRNA compared to the
control group (%)
25 11
50 18
75 40
Table 3) Table showing how the inhibition of MMP-2 was dose dependant. With increasing
fluency’s there was a greater decrease in MMP-2 mRNA.
Fluence (J/cm2) Decline in MMP-14 mRNA compared to the
control group (%)
25 14
50 23
75 41
Table 4) Table showing how the inhibition of MMP-14 was dose dependant. With
increasing fluencies there was a greater decrease in MMP-14 mRNA.
The results from the study by Wong et al. (2008) show that treatment by IPL can down
regulate MMP-2 and -14 thus helping to reduce the catabolic effects of these MMPs,
which could result in an overall net increase in ECM. This suggesting that IPL rejuvenates
skin not only by stimulating an increase in the production ECM proteins like shown by
Haung et al (2011), but also by reducing the amount of ECM that gets broken down by
inhibiting MMPs. This helps to counter act the increase in MMPs that can occur from
exposure of skin to UVR (Wertz et al., 2004).
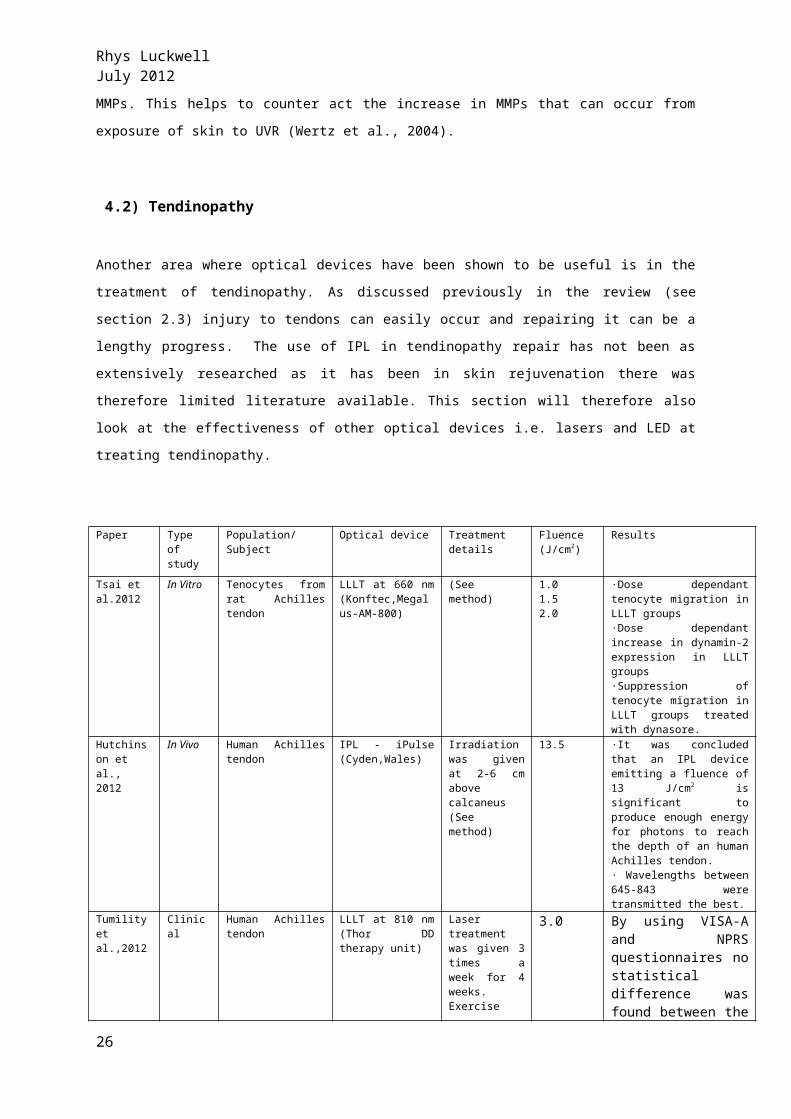
4.2) Tendinopathy
Another area where optical devices have been shown to be useful is in the treatment of
tendinopathy. As discussed previously in the review (see section 2.3) injury to tendons
19
Rhys Luckwell July 2012
can easily occur and repairing it can be a lengthy progress. The use of IPL in
tendinopathy repair has not been as extensively researched as it has been in skin
rejuvenation there was therefore limited literature available. This section will therefore
also look at the effectiveness of other optical devices i.e. lasers and LED at treating
tendinopathy.
Paper Type of study
Population/Subject
Optical device Treatment details
Fluence (J/cm2)
Results
Tsai et al.2012
In Vitro Tenocytes from rat Achilles tendon
LLLT at 660 nm (Konftec,Megalus-AM-800)
(See method) 1.01.52.0
·Dose dependant tenocyte migration in LLLT groups·Dose dependant increase in dynamin-2 expression in LLLT groups·Suppression of tenocyte migration in LLLT groups treated with dynasore.
Hutchinson et al., 2012
In Vivo Human Achilles tendon
IPL - iPulse (Cyden,Wales)
Irradiation was given at 2-6 cm above calcaneus (See method)
13.5 ·It was concluded that an IPL device emitting a fluence of 13 J/cm2 is significant to produce enough energy for photons to reach the depth of an human Achilles tendon.· Wavelengths between 645-843 were transmitted the best.
Tumility et al.,2012
Clinical Human Achilles tendon
LLLT at 810 nm (Thor DD therapy unit)
Laser treatment was given 3 times a week for 4 weeks.Exercise program consisted of heavy load eccentric movements twice a day every day of the week for a period of 12 weeks
3.0 By using VISA-A and NPRS questionnaires no statistical difference was found between the LLLT + exercise group and the Placebo + exercise group.
Stergirulas et al.,2008
Clinical Human Achilles tendon
LLLT at 820 nm (Biotherapy 2000)
Laser treatment was given twice a week between weeks 1-4 and once a week between weeks 5-8.Exercise program consisted of eccentric exercise 4 times a week for 8 weeks.
5.4 The LLLT + E.E group at week for showed similar results to the placebo + E.E group at week 12Suggesting that LLLT can decrease the repair time of tendinopathy
Bjordal et Clinical Human lateral LLLT – Various See paper for See paper LLLT at wavelength of
20
Rhys Luckwell July 2012
al., 2008 review elbow tendon treatments between wavelengths of 632 to 1094
individual methods
904 nm when applied directly to the lateral elbow tendon provided short term pain relief and increased mobility of joint. Dose dependant.
Table 5) Table summarising the papers reviewing the effect of optical devices to treat
tendinopathy
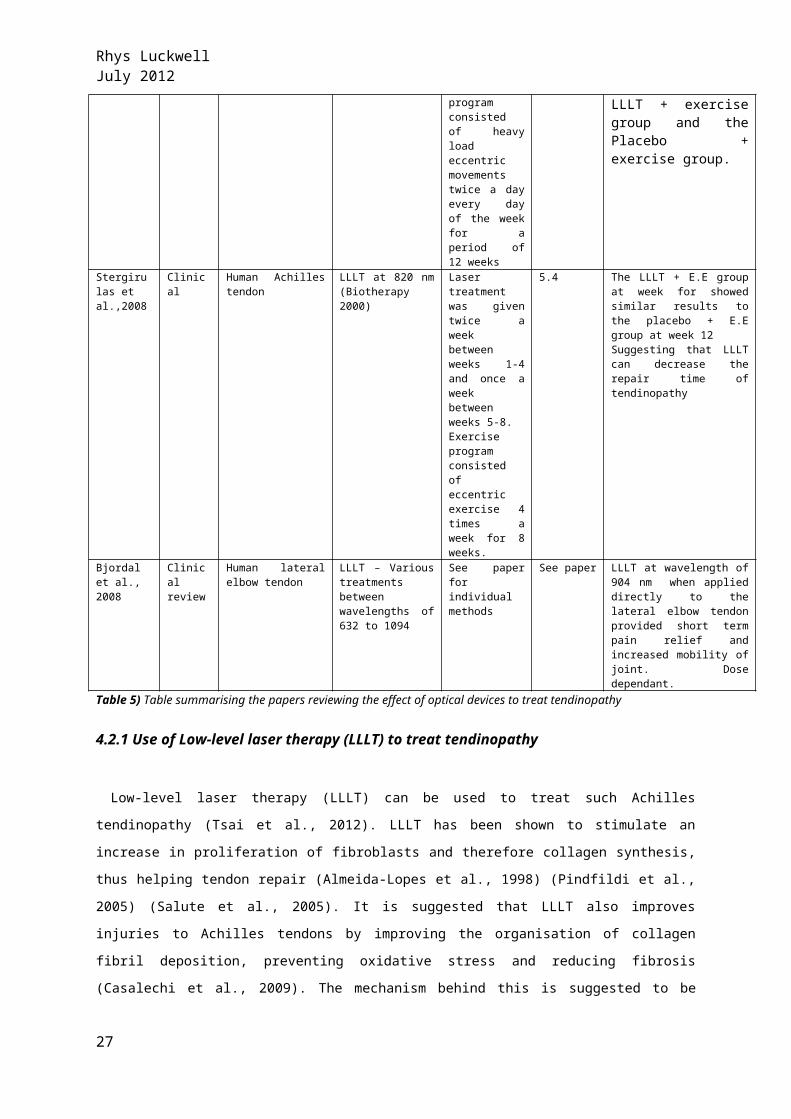
4.2.1 Use of Low-level laser therapy (LLLT) to treat tendinopathy
Low-level laser therapy (LLLT) can be used to treat such Achilles tendinopathy (Tsai et
al., 2012). LLLT has been shown to stimulate an increase in proliferation of fibroblasts
and therefore collagen synthesis, thus helping tendon repair (Almeida-Lopes et al., 1998)
(Pindfildi et al., 2005) (Salute et al., 2005). It is suggested that LLLT also improves
injuries to Achilles tendons by improving the organisation of collagen fibril deposition,
preventing oxidative stress and reducing fibrosis (Casalechi et al., 2009). The mechanism
behind this is suggested to be photochemical (see section 3.2.3) (Lane, 2006). LLLT has
also been shown to increase tenocyte proliferation and collagen I in pig tendons (Chen et
al., 2009).
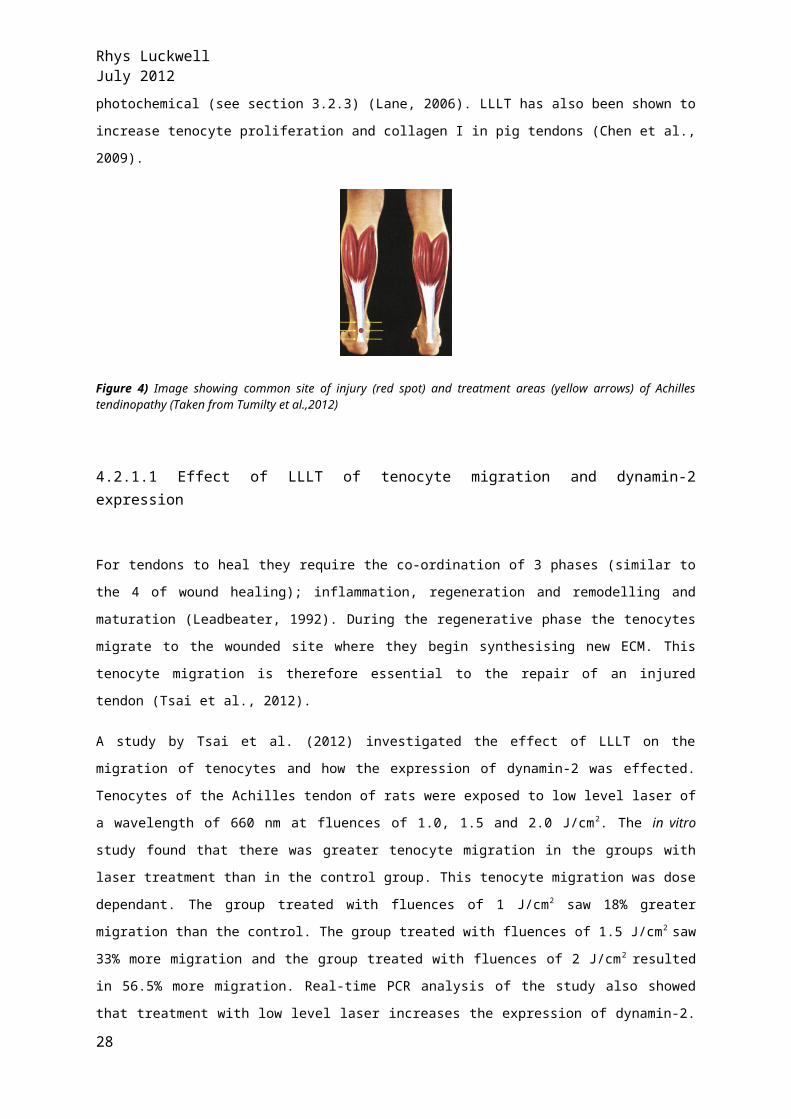
Figure 4) Image showing common site of injury (red spot) and treatment areas (yellow arrows) of Achilles tendinopathy (Taken from Tumilty et al.,2012)
4.2.1.1 Effect of LLLT of tenocyte migration and dynamin-2 expression
For tendons to heal they require the co-ordination of 3 phases (similar to the 4 of wound
healing); inflammation, regeneration and remodelling and maturation (Leadbeater,
1992). During the regenerative phase the tenocytes migrate to the wounded site where
they begin synthesising new ECM. This tenocyte migration is therefore essential to the
repair of an injured tendon (Tsai et al., 2012).
A study by Tsai et al. (2012) investigated the effect of LLLT on the migration of tenocytes
and how the expression of dynamin-2 was effected. Tenocytes of the Achilles tendon of
rats were exposed to low level laser of a wavelength of 660 nm at fluences of 1.0, 1.5
21
Rhys Luckwell July 2012
and 2.0 J/cm2. The in vitro study found that there was greater tenocyte migration in the
groups with laser treatment than in the control group. This tenocyte migration was dose
dependant. The group treated with fluences of 1 J/cm2 saw 18% greater migration than
the control. The group treated with fluences of 1.5 J/cm2 saw 33% more migration and the
group treated with fluences of 2 J/cm2 resulted in 56.5% more migration. Real-time PCR
analysis of the study also showed that treatment with low level laser increases the
expression of dynamin-2. With a 14% and 35% increase in groups treated by 1.5 J/cm2
and 2.0 J/cm2 compared to the control group.
Dynamin-2 is a GTPase involved in cell migration through its role in expanding the
membrane lip through actin polymerisation (Kruchten, 2006). Therefore by up regulating
dynamin it enables tenocytes to migrate to the site of injury. The study also showed that
when the tendon samples were treated with dynasore, a non-competitive inhibitor of
dynamin (Macia et al., 2006), the migration of tenocytes that was induced by LLLT was
inhibited. This further shows that dynamin plays a role in cell migration. Therefore it
suggests that optical devices such as LLLT can be useful in the treatment of
tendinopathy by inducing gene expression of dynamin through stimulating the required
signalling pathway.
4.2.1.2 Effectiveness of LLLT at treating Achilles tendinopathy when combined with traditional eccentric exercise
Research by Tamility et al. (2012) looks at the possible benefits to Achilles tendinopathy
when combining LLLT with a traditional eccentric exercise programme. 40 patients
entered the trail and were divided into 2 groups, 20 LLLT and 20 placebo. The LLLT group
were subject to laser treatment and an eccentric exercise program whereas the placebo
group were subject to a placebo laser and the eccentric exercise programme. The laser
treatment consisted of 3 treatments a week for the first 4 weeks at a fluence of 3J/cm2.
The laser used was Thor DD laser therapy unit at a wavelength of 810nm. The exercise
protocol involved heavy load eccentric movements twice a day every day of the week for
the first 12 weeks of the trail with the first 4 weeks being supervised by a
physiotherapist. Through using a VISA-A and NPRS questionnaires the pain of the
patients was recorded at week 0, 4, 12 and 52. Out of the 33 patients (17 LLLT group, 16
placebo group) that finished the 52 week assessment there was found to be no
significant difference between them. This trial therefore suggests that there is no benefit
of combing LLLT with traditional Achilles tendinopathy treatment methods.
4.2.1.3 Effectiveness of LLLT combined with eccentric exercise at treating chronic Achilles tendinopathy in humans
22

Rhys Luckwell July 2012
A similar study to above was carried out by Stergiralas et al.(2008). Again this study
examines the potential of improving on traditional eccentric exercise therapy, which can
take a while to show progressive results, by combing it with LLLT. 52 patients were
randomly divided into 2 groups; LLLT + eccentric exercise or placebo + eccentric
exercise. Patients were included in the trail if they had been suffering from Achilles
tendinopathy for 6 months or more and had pain between 2-6 cm proximal to insertion
on the os calcaneus. The LLLT consisted of 12 treatments, with 2 treatments a week for
the weeks 1- 4 weeks then 1 treatment a week between weeks 5-8. The laser device
used was an infrared laser at a wavelength of 820 nm (Biotherapy 2000). The eccentric
exercise program involved 4 sessions a week for the 8 weeks. Weeks 9-12 were free of
treatment and used for follow up purposes.
The results of the study showed that at week 4 the LLLT group showed similar results to
the placebo group at week 12. This suggested that LLLT can be used alongside eccentric
exercise programmes to improve recovery of Achilles tendinopathy and potentially be
used instead of Nonsteroidal Antiflamatory drugs (NSAID) which can cause adverse side
effects such as gastrointestinal ulcers or cardiovascular problems (Marcos et al.2011).
4.4.1.4 Effectiveness of LLLT at treating lateral elbow tendinopathy
Another common tendon disorder that can result from sport injury or from day to day life
is lateral elbow tendinopathy (LET) also known as tennis elbow. Traditional treatments for
LET are similar to those discussed above for treatment of Achilles tendinopathy. Such as
steroid injections, NSAIDs and eccentric exercise (Bjordal et al.,2008)
A study by Bjordal et al., (2008) looks at the use of LLLT to treat LET. The study showed
that by emitting light of wavelength of 904 nm directly to the lateral elbow tendon it
could provide short term pain relief and greater mobility.
4.2. 2 Efficiency of IPL treatment on human Achilles tendinopathy
As discussed IPL has been proven to work on skin to reduce the appearance of vascular
lesions e.g. Rosacea and Pigmented lesions e.g. solar lentigines (section 4.1.3). One
problem with IPL however is that it is not yet known how the efficiency of IPL treatment is
effected as the depth of the target tissue increases (Hutchinson et al.,2012). If IPL can be
shown to reach such structures as Achilles tendons it could be used to treat
tendinopathy.
A study by Hutchinson et al. (2012) aimed to find if IPL transmission would reach a
human Achilles tendon when emitted on the surface of the skin. If their study showed
that IPL could be used to transmit light through tissue to that depth it’s possible that IPL
23
Rhys Luckwell July 2012
has potential in the treatment of Achilles tendinopathy. The study also set out to find the
amount of light that would be attenuated within the tendon.
Hutchinson and colleagues (2012) used 3 human Achilles tendons that were irradiated 2-
6 cm above the insertion into the calcaneus. The IPL device used was an model iPulse
(Cyden Ltd, Wales, UK). A single pulse of 25ms was used between wavelengths of 530-
1110 nm. The fluence used was 13 J/cm2. To analyse the transmission of light radiation a
standard SLR digital camera, spectrometer and an external energy meter were used. All
three devices found the IPL device to have emitted light radiation through the 3 samples.
4 – 8.1% of the fluence was found to have been transmitted through the sample by the
energy meter. The spectrometer showed that the longer wavelengths of light of between
645-843 nm were transmitted through the tissue the best. The percentage of light
radiation that was attenuated with the tendon was between 10.7-17.32 %.
Hutchison et al. (2012) concludes that the study suggests that an IPL device emitting a
fluence of 13 J/cm2 onto the surface of the skin produces significant light radiation that is
capable of penetrating to the depth of a human Achilles tendon. Therefore IPL could
provide beneficial to sufferers of Achilles Tendinopathy.
4.3) Chronic wounds
The last field that shall be reviewed is how optical devices can help in the repair of
chronic wounds. Chronic wounds are a strain on the worlds health care system. It is
estimated that chronic wounds cost the U.S health system between $6-$15 billion dollars
every year (Markova et al.,2012) and that 0.3% of the general population suffers from
chronic ulcers.. The most common ulcers are venous leg ulcers and diabetic foot ulcers
(Markova et al.,2012) (Costin et al.,2012). Chronic venous leg ulcers account for 70 –
90% of lower limb ulcers and may never heal (Kalkurni et al., 2007). Treatment of chronic
ulcers was described as inadequate by McMullin (2001) and over the last 10 years there
been no improvements in their treatment (Jones, 2009). Currently the best way to treat
chronic ulcers is through compression bandage which acts by decreasing venous
hypertension and improves blood flow through veins (O’Meara, 2009). It is therefore
these chronic wounds that will be the focus of this section.
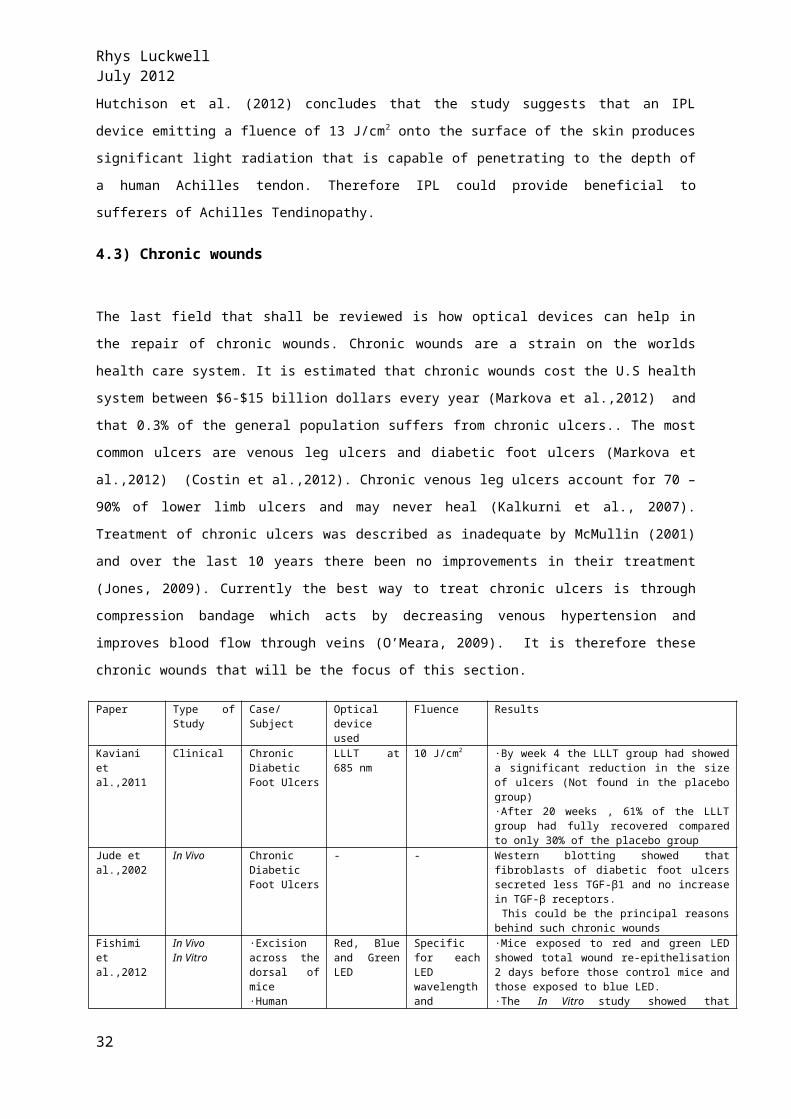
Paper Type of Study
Case/Subject Optical device used
Fluence Results
Kaviani et al.,2011
Clinical Chronic Diabetic Foot Ulcers
LLLT at 685 nm
10 J/cm2 ·By week 4 the LLLT group had showed a significant reduction in the size of ulcers (Not found in the placebo group)·After 20 weeks , 61% of the LLLT group had fully recovered compared to only 30% of the placebo group
Jude et al.,2002
In Vivo Chronic Diabetic Foot Ulcers
- - Western blotting showed that fibroblasts of diabetic foot ulcers secreted less TGF-β1 and no increase in TGF-β receptors. This could be the principal reasons behind such chronic wounds
24
Rhys Luckwell July 2012
Fishimi et al.,2012
In VivoIn Vitro
·Excision across the dorsal of mice·Human dermal fibroblasts
Red, Blue and Green LED
Specific for each LED wavelength and subject (See method)
·Mice exposed to red and green LED showed total wound re-epithelisation 2 days before those control mice and those exposed to blue LED.·The In Vitro study showed that fibroblasts exposed to green LED secreted a increased amount of cytokines.·In Vitro study also showed that keratinocyte migration increased when exposed to red and green LED.
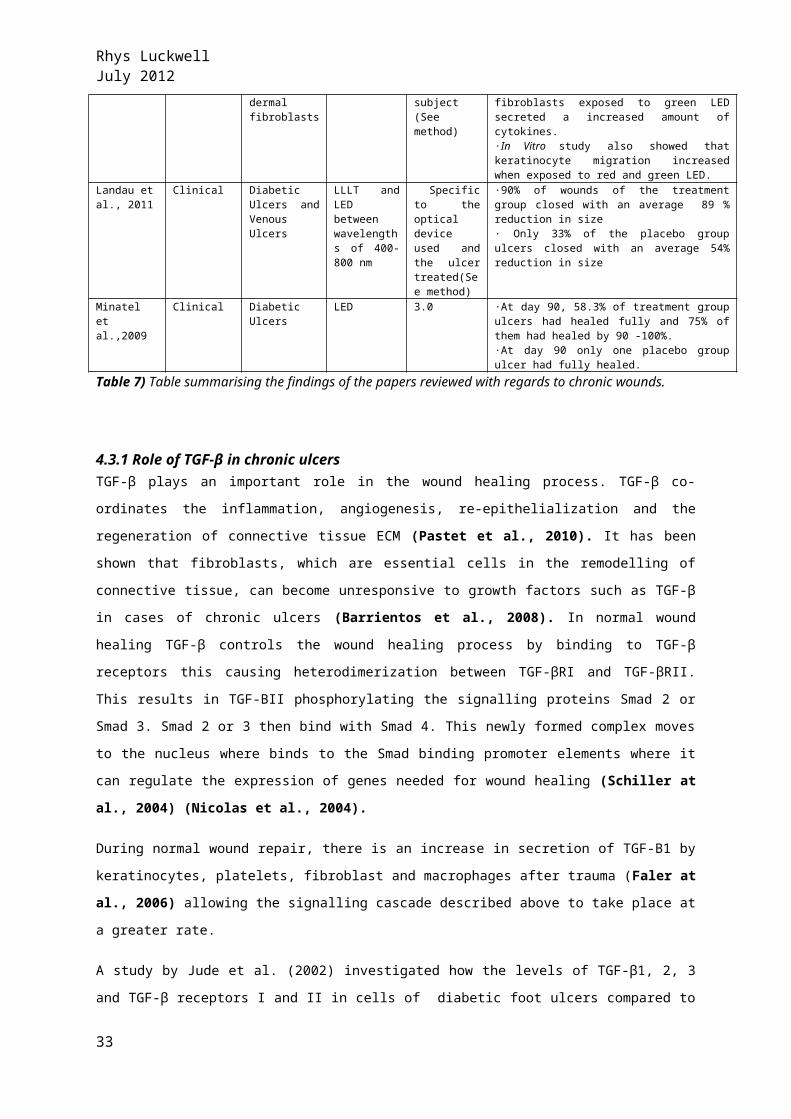
Landau et al., 2011
Clinical Diabetic Ulcers and Venous Ulcers
LLLT and LED between wavelengths of 400-800 nm
Specific to the optical device used and the ulcer treated(See method)
·90% of wounds of the treatment group closed with an average 89 % reduction in size· Only 33% of the placebo group ulcers closed with an average 54% reduction in size
Minatel et al.,2009
Clinical Diabetic Ulcers
LED 3.0 ·At day 90, 58.3% of treatment group ulcers had healed fully and 75% of them had healed by 90 -100%.·At day 90 only one placebo group ulcer had fully healed.
Table 7) Table summarising the findings of the papers reviewed with regards to chronic
wounds.
4.3.1 Role of TGF-β in chronic ulcersTGF-β plays an important role in the wound healing process. TGF-β co-ordinates the
inflammation, angiogenesis, re-epithelialization and the regeneration of connective tissue
ECM (Pastet et al., 2010). It has been shown that fibroblasts, which are essential cells
in the remodelling of connective tissue, can become unresponsive to growth factors such
as TGF-β in cases of chronic ulcers (Barrientos et al., 2008). In normal wound healing
TGF-β controls the wound healing process by binding to TGF-β receptors this causing
heterodimerization between TGF-βRI and TGF-βRII. This results in TGF-BII
phosphorylating the signalling proteins Smad 2 or Smad 3. Smad 2 or 3 then bind with
Smad 4. This newly formed complex moves to the nucleus where binds to the Smad
binding promoter elements where it can regulate the expression of genes needed for
wound healing (Schiller at al., 2004) (Nicolas et al., 2004).
During normal wound repair, there is an increase in secretion of TGF-B1 by keratinocytes,
platelets, fibroblast and macrophages after trauma (Faler at al., 2006) allowing the
signalling cascade described above to take place at a greater rate.
A study by Jude et al. (2002) investigated how the levels of TGF-β1, 2, 3 and TGF-β
receptors I and II in cells of diabetic foot ulcers compared to normal cells. By using
western blotting to determine the protein levels of TGF-β Jude et al. found that fibroblasts
associated with diabetic ulcers secreted reduced levels of TGF-β1 compared to normal
cells nor is there the increase in TGF-βRII which is associated with normal healing cells. In
theory by stimulating TGF-β release the wound healing process of such chronic wounds
could be improved and thus reducing the healing time.
25
Rhys Luckwell July 2012
4.3.2 Treatment of Chronic Ulcers with optical devices
Chronic wounds can be treated through laser treatment. As Laser and LED treatment are
non-invasive treatments they are of particular use in patients who are at increased risk of
infection from surgical treatment, for example diabetic sufferers whose poor immunity
puts them at the risk of opportunistic infections (Kalani et al., 2003).
4.3.2.1 LLLT for chronic diabetic foot ulcers
A study by Kaviani et al. (2011) looked into the benefit of low level laser therapy on
chronic diabetic foot ulcers. In this study, 23 patients were followed for 20 weeks. With
13 being treated with LLLT and 10 with a placebo treatment. The LLLT given was at a
wavelength of 685 nm at a fluence of 10 J/cm2. The study found that after week 4 there
had been a significant reduction in the size of the ulcers in the LLLT patients. This was
not found in the placebo group. After the 20 week follow up period, 8 out of the 13
patients who had been treated with LLLT had fully recovered compared to only 3 out of
the 10 in the placebo group. This suggested that LLLT could decrease the healing time of
chronic diabetic ulcers.
4.3.2.2 LED and LLLT for treatment of chronic diabetic ulcers and venous ulcers
A study by Landau et al. (2011) conducted research on a small group of both diabetic
and venous ulcer patients. The study investigates the effect of wavelengths between
400-800 nm had on these wounds. The participant were divided into either placebo or
treatment groups. The treatment group consisted of 10 patients with a total of 19 ulcers.
The placebo group consisted of 6 patients with a total of 6 ulcers. The laser treatment
involved treatment of 180mw/cm twice a day.
The results of the study showed that 90% of the treatment group ulcers closed with an
89% reduction in size, whereas only 33% of the placebo group ulcers closed with a 54%
reduction in size. Although these results come from a small pool of patients they
significantly show that treatment with low level lasers can improve chronic ulcers
26
Rhys Luckwell July 2012
4.3.2.2 LED treatment of chronic wounds
The other optical device which has been shown to improve the rate of chronic wound
healing is LED. Fushimi et al. (2012) investigated the effects of LED on both In vivo and In
vitro by analysing wound repair in 8 week old male mice and in human dermal fibroblast
respectively.
The In vivo study involved each mouse having an 8mm excision made across its dorsal
side and were divided into 4 groups; control (no LED exposure), red LED (638 nm, 0.3
J/cm2), blue LED (456 nm, 0.3 J/cm2) and green LED (518 nm, 0.3 J/cm2). The 3 LED
groups were exposed to 20 minutes of irradiation every other day from a distance of 10
cm. The wound size was measured before each irradiation period. By day 11 the groups
exposed to the red and green LED showed complete epitheliazation of the wound. The
blue LED and control group showed total epitheliazation on day 13. Therefore form the
study it can be suggested that exposure to red or green LED can decrease the healing
time of wounds. In In vitro studies also used 4 groups; red LED (638 nm,0.6 J/cm2 ), blue
LED (456 nm, 0.3 J/cm2 ), green LED (518 nm,0.2 J/cm2 ). By measuring the mRNA and
protein levels by using RT-PCR and an ELISA assay respectively and also keratinocyte
migration, by using a migration assay the results showed that exposure to green LED
caused an increase in cytokine(HGF,KGF, Leptin ,IL-8 and VEGF) secretion by fibroblast
cells. The results from the study also showed that migration of keratinocyte also
increased on exposure to both red and green LED. The study by Fushimi et al. (2012)
therefore suggests that green LED can improve wound healing by increasing
keratinocyte migration and by increasing the levels of cytokines secreted by fibroblasts.
The secretion of cytokines and keratinocyte migration to wound site are essential aspects
to the repair of wounds, as discussed previously.
4.3.2.3 Effectiveness of LED on chronic diabetic ulcers
A study by Minatel et al. (2009) carried out research on the effect of LED on chronic
diabetic leg ulcers that have failed to respond to other treatments. The study comprised
of a treatment and placebo group with 14 patients in both. The patients in the treatment
group were subject to two treatment of LED a week at a fluence of 3 J/cm2 for 90 weeks.
The ulcers were analysed at days 15, 30, 45, 60, 75 and 90. The results suggested that
LED treatment could improve the healing of diabetic ulcers. At day 90 58% of the
27
Rhys Luckwell July 2012
treatment group ulcers had fully healed and 75% had recovered by between 90-100%.
Compared to the placebo group, which at day 90, only one ulcer showed complete
healing and no other ulcer from that group healed by 90% +.
There has been plenty of research and literature supporting the beneficial effect of lasers
and LED therapy on chronic wounds, such as diabetic and chronic venous ulcers.
However, these methods of treatment do have their negatives. Lasers and LED as well as
being expensive are fixed at one wavelength. Although there is no doubt over the
potential strength of a laser some research groups question whether the output from a
LLLT or LED is really strong enough to stimulate an effect in the tissue (Posten et al.,
2005). A potential optical device that could also benefit the treatment of chronic wound
are IPL devices. As reviewed IPL has been proven to help rejuvenate the skin and possess
potential in wound healing.
28
Rhys Luckwell July 2012
5) Conclusion
Optical devices, such as IPL have great promise in a number of medical and cosmetic
applications. It had been shown that through different biochemical reactions that photons
emitted from optical devices can rejuvenate skin, improve the healing of chronic wound
and help in treatment of tendinopathy. It has been shown that the molecular basis
behind these actions is through stimulating fibroblast proliferation, increasing the
synthesis and organised attachment of collagen, greater production of other ECM
components (proteoglycans, glycoproteins, elastin) increase in growth factor and
cytokine production (KGF, HGF, VGEF, TGF-B),stimulate angiogenesis, epithelialization of
wounds, decrease numbers of MMPs and induce the stimulation of macrophage and
neutrophils.
Although there is not as extensive research on the beneficial effects of IPL on wound
healing and tendinopathy as there is on its use in skin rejuvenation and for hair removal
it is fair to say that there is enough potential benefits and theory on why IPL could be
used to help improve these problems to warrant further research. For example,
decreasing the healing time of chronic wounds has many benefits such as reducing the
use of compression bandages thus saving costs and can also free up hospital beds
reducing the burden on health care resources. IPL also possess practical benefits over
lasers and LED, such as price, greater flexibility in terms of selection of parameters and
are more mobile.
To conclude, optical devices have many uses in both medicine and cosmetics. Further
research into the use of IPL to treat chronic wounds and tendinopathy is needed as there
is potential for IPL treatment to reduce costs and resources needed to treat these
diseases.
29
Rhys Luckwell July 2012
6) References
1) Almeida-Lopes, L., Rigau, J., Za˜ngaro, R.A., Guidugli-Neto, J. and Jaeger M.M.M. 2001.Comparison of the low level laser therapy effects on cultured human gingival fibrobalts proliferationusing different irradiance and same fluence. Lasers in Surgical Medicicne 29:179–184.
2) Anderson, R.R. and Parrish. R.R. 1983. Selective photothermolysis: Precise microsurgery by selective absorption of pulsed radiation Science 220:524–527.
3) Babilas, P., Schreml, S., Szeimies, R.M. and Landthaler, M.2010. Intense pulsed light (IPL): a review. Lasers in Surgical Medicine 42:93-104.
4) Barnikol, W.K. and Pötzschke, H.2012. A novel, non-invasive diagnostic clinical procedure for the determination of an oxygenation status ofchronic lower leg ulcers using peri-ulceral transcutaneous oxygen partial pressure measurements: Results of its application in chronic
venous insufficiency (CVI). German Medical Sciences [On Line] 10. Available at:
http://www.egms.de/static/en/journals/gms/2012-10/000162.shtml5) Barrientos, S., Stojadinovic, O., Golinko, M.S., Brem, H. and Tomic-Canic, M. 2008. Growth
factors and cytokines in wound healing. Wound Repair and Regeneration 16:585-601.6) Benjamin, M., Kaiser, E. and Milz, S. 2008. Structure-function relationships in tendons: a
review. Journal of Anatomy 212:211-28.7) Bjordal JM, Lopes-Martins RA, Joensen J, Couppe C, Ljunggren AE, Stergioulas A, Johnson MI.
2008. A systematic review with procedural assessments and meta-analysis of low level laser therapy in lateral elbow tendinopathy (tennis elbow). BMC Muscoskeletal Disorders 9:75
8) Bogdan-Allemann , I., Kaufman, J., Geiges, M.L. I. and Goldberg, D.J.2011. Basics in Dermatological Laser Applications. Current Problems in Dermatology 42: 7–23
9) Brem, H. and Tomic-Canic, M. 2007. Cellular and molecular basis of wound healing in
diabetes. Journal of Clinical Investigation 117: 1219–1222.10) Campolmi, P., Bonan, P., Cannarozzo, G., Bruscino, N., Troiano, M., Prignano, F. and Lotti,
T.2011. Intense pulsed light in the treatment of non-aesthetic facial and neck vascular lesions: report of 85 cases. Journal of the European Academy of Dermatology and Venereology 25:68-73.
11) Campos, A.C., Groth, A.K and Branco AB.2008. Assessment and nutritional aspects of wound healing. Current Opinion in Clinical Nutrition and Metabolic Care 11:281-8.
12) Costin GE, Birlea SA, Norris DA. 2012. Trends in wound repair: cellular and molecular basis of regenerative therapy using electromagnetic fields. Current Molecular Medicine 12:14-15
13) Doral, M.N., Alam, M., Bozkurt, M., Turhan, E., Atay, O.A., Dönmez, G. and Maffulli, N.2010. Functional anatomy of the Achilles tendon. Knee Surgery, Sports Traumatology, Arthroscopy 18:638-43.
14) Dressler, M.R., Butler, D.L., Wenstrup, R., Awad, H.A., Smith, F. and Boivin, G.P.2002. A potential mechanism for age-related declines in patellar tendon biomechanics. Journal of Orthopaedic Research 20:1315-22.
15) Enoch, S. and Leaper, D. J. 2005. Basic science of wound healing. Surgery 23: 37–42.16) Faler, B.J., Macsata, R.A., Plummer, D., Mishra, L. and Sidawy, A.N.2006. Transforming
growth factor-beta and wound healing. Perspectives in Vascular Surgery and Endovascular Therapy 18:55-62.
30
Rhys Luckwell July 2012
17) Farris, P.K.2004. Combination therapy for solar lentigines. Journal of Drugs and Dermatology 3:23-6.
18) Fushimi, T., Inui, S., Nakajima, T., Ogasawara, M., Hosokawa, K. and Itami, S.2012. Green light emitting diodes accelerate wound healing: characterization of the effect and its molecular basis in vitro and in vivo. Wound Repair and Regeneration 20:226-35.
19) Guo, S. and Dipietro, L.A. 2010. Factors affecting wound healing. Journal of Dental Research 89:219-29.
20) Haedersdal, M., Togsverd-Bo, K. and Wulf, H.C.2008. Evidence-based review of lasers, light sources and photodynamic therapy in the treatment of acne vulgaris. Journal of the European Academy of Dermatology and Venereology 22:267-78.
21) Huang, J., Luo, X., Lu, J., Chen, J., Zuo, C., Xiang, Y., Yang, S., Tan, L., Kang, J. and Bi, Z. 2011. IPL irradiation rejuvenates skin collagen via the bidirectional regulation of MMP-1 and TGF-β1mediated by MAPKs in fibroblasts. Lasers in Medical Science 26:381-7.
22) Hutchison, A.M., Beard, D.J., Bishop, J., Pallister, I. and Davies, W. 2012. An investigation of the transmission and attenuation of intense pulsed light on samples of human Achilles tendon and surrounding tissue. Lasers in Surgical Medicine 44:397-405.
23) Jacques, S.L.1992. Laser-tissue interactions. Photochemical, photothermal, and photomechanical. Surgical Clinics of North America 72:531-58.
24) Jones, K.R. 2009. Why do chronic venous leg ulcers not heal? Journal of Nursing Care Quality 24:116-24.
25) Jude, E.B., Blakytny. R., Bulmer, J., Boulton, A.J. and Ferguson, M.W. 2002. Transforming growth factor-beta 1, 2, 3 and receptor type I and II in diabetic foot ulcers. Diabetic Medicine 19:440–7.
26) Just, M., Ribera, M., Monsó, E., Lorenzo, J.C. and Ferrándiz, C. 2007. Effect of smoking on skin elastic fibres: morphometric and immunohistochemical analysis. The British Journal of Dermatology. 156:85-91
27) Kalani, M., Apelqvist, J., Blombäck, M., Brismar, K., Eliasson, B., Eriksson, J.W, Fagrell, B., Hamsten, A., Torffvit, O and Jörneskog, G.2003. Effect of dalteparin on healing of chronic foot ulcers in diabetic patients with peripheral arterial occlusive disease: a prospective, randomized, double-blind, placebo-controlled study. Diabetes Care 26:2575-80.
28) Kastelic J, Galeski A, Baer E. 1978. The multicomposite structure of tendon. Connective Tissue Research 6:11-23
29) Kaviani, A., Djavid, G.E., Ataie-Fashtami, L., Fateh, M., Ghodsi, M., Salami, M., Zand, N., Kashef, N. and Larijani, B. 2011. A randomized clinical trial on the effect of low-level laser therapy on chronic diabetic foot wound healing: a preliminary report. Photomedicine and Laser Surgery 29:109-14.
30) Kawada, A., Shiraishi, H., Asai, M., Kameyam, H., Sangen, Y., Aragane, Y. and Tezuka, T. 2002. Clinical improvement of solar lentigines and ephelides with an intense pulsed light source. Dermatological Surgery 28:504-8.
31) Kannus, P. 2000. Structure of the tendon connective tissue. Scandinavian Journal of Medicine and Science in Sports 10:312-20
32) Kennedy C, Bastiaens MT, Bajdik CD, Willemze R, Westendorp RG, Bouwes Bavinck JN; Leiden Skin Cancer Study. 2003. Effect of smoking and sun on the aging skin. Journal of Investigative Dermatology 120:548-54
33) King, S.M. and Reed, G.L. 2002. Development of platelet secretory granules. Seminars in Cell & Developmental Biology 13:293-302.
34) Landau Z, Migdal M, Lipovsky A, Lubart R. 2011. Visible light-induced healing of diabetic or venous foot ulcers: a placebo-controlled double-blind study. Photomedicine and Laser Surgery 29:399-404
35) Mays, P.K., Bishop, J.E. and Laurent, G.J.1988. Age-related changes in the proportion of types I and III collagen. Mechanism of Ageing and Development 45:203-12.
36) Markova A and Mostow EN. 2012. US skin disease assessment: ulcer and wound care. Dermatological Clinics 30 :107-11
37) McMullin, G.M. 2001. Improving the treatment of leg ulcers. Medical Journal of Australia 175:375-8.
31
Rhys Luckwell July 2012
38) Miners, A.L. and Bougie, T.L. 2011. Chronic Achilles tendinopathy: a case study of treatment incorporating active and passive tissuewarm-up, Graston Technique, ART, eccentric exercise, and cryotherapy. Journal of the Canadian Chiropractic Association 55:269-79
39) Minatel DG, Frade MA, França SC, Enwemeka CS. 2009. Phototherapy promotes healing of chronic diabetic leg ulcers that failed to respond to other therapies. Lasers in Surgery and Medicine 41:433-41
40) Mohanan S, Parveen B, Annie Malathy P, Gomathi N. 2012. Use of intense pulse light for acne vulgaris in Indian skin--a case series. International Journal of Dermatology 51:473-6.
41) Mosser, D.M. and Edwards, J.P.2008. Exploring the full spectrum of macrophage activation. Nature Reviews Immunology 8:958-69.
42) Nicolás, F.J., De Bosscher, K., Schmierer, B. and Hill, C.S. 2004. Analysis of Smad nucleocytoplasmic shuttling in living cells. Journal of Cellular Science 117:4113-25.
43) Nieto, N. and Lutolf, M.P. 2011. Extracellular matrix bioengineering and systems biology approaches in liver disease. Systems and Synthetic Biology 5:11-20.
44) Nigam, Y. and Knight, J.2008. Exploring the anatomy and physiology of ageing. Part 11--The skin. Nursing Times 104:24-5.
45) Oliveira, F.S., Pinfildi, C.E., Parizoto, N.A., Liebano, R.E., Bossini, P.S., Garcia, E.B. and Ferreira LM.2009. Effect of low level laser therapy (830 nm) with different therapy regimes on the process of tissue repairin partial lesion calcaneous tendon. Lasers in Surgical Medicine 41:271-6.
46) Marcos RL, Leal Junior EC, Messias Fde M, de Carvalho MH, Pallotta RC, Frigo L, dos Santos RA, Ramos L, Teixeira S, Bjordal JM, Lopes-Martins RÁ.2011. Infrared (810 nm) low-level laser therapy in rat achilles tendinitis: a consistent alternative to drugs. Photochemistry and Photobiology 87:1447-52
47) O'Meara, S., Cullum, N.A. and Nelson, E.A.2009. Compression for venous leg ulcers.
Cochrane database of systematic reviews21.[On Line] Avaiable :
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000265.pub2/full48) Pastar, I., Stojadinovic, O., Krzyzanowska, A., Barrientos, S., Stuelten, C.,
Zimmerman, K., Blumenberg, M., Brem, H., Tomic-Canic, M. 2010. Attenuation of the transforming growth factor beta-signaling pathway in chronic venous ulcers. Molecular Medicene 16:92-101.
49) Posten, W., Wrone, D.A., Dover, J.S., Arndt, K.A., Silapunt, S. and Alam M.2005. Low-level laser therapy for wound healing: mechanism and efficacy. Dermatological Surgery 31:334-40.
50) Prost-Squarcioni, C., Fraitag, S., Heller, M., Boehm, N.2008. Functional histology of dermis. Ann Dermatol Venereol 135:5-20.
51) Raffetto, J.D., Mendez, M.V., Marien, B.J., Byers, H.R., Phillips, T.J., Park, H.Y. and Menzoian, J.O. 2001. Changes in cellular motility and cytoskeletal actin in fibroblasts from patients with chronic venous insufficiency and in neonatal fibroblasts in the presence of chronic wound fluid. Journal of Vascular Surgery 33(6):1233-41.
52) Raulin, C., Greve, B. and Grema, H.2003. IPL technology: a review. Lasers Surgical Medicine 32:78-87.
53) Rhee, S. and Grinnell, F.2008. Fibroblast Mechanics in 3D Collagen Matrices. Advances in Drug Delivery Research 59:1299-1305
54) Roberts, A.B., Sporn, M.B., Assoian, R.K., Smith, J.M,. Roche, N.S., Wakefield, L.M., Heine, U.I., Liotta, L.A., Falanga, V., Kehrl, J.H., et al.1986. Transforming growth factor type beta: rapid induction of fibrosis and angiogenesis in vivo and stimulation of collagen formation in vitro. Proceedings of the National Academy of Sciences 83:4167-71.
55) Sasaya, H., Kawada, A., Wada, T., Hirao, A. and Oiso, N. 2011. Clinical effectiveness of intense pulsed light therapy for solar lentigines of the hands. Dermatological Therapy 24:584-6.
56) Schiller M, Javelaud D, Mauviel A. 2004. TGF-beta-induced SMAD signaling and gene regulation: consequences for extracellular matrix remodeling and wound healing. Journal of Dermatological Sciences 35:83-92.
32
Rhys Luckwell July 2012
57) Schoenewolf, N.L., Barysch, M.J. and Dummer, R.2011. Intense pulsed light. Current Problems in Dermatology 42:166-72.
58) Sussmilch-Leitch SP, Collins NJ, Bialocerkowski AE, Warden SJ, Crossley KM. 2012. Physical therapies for Achilles tendinopathy: systematic review and meta-analysis. Journal of Foot and Ankle research 5 [On Line] Can be found at: http://www.jfootankleres.com/PhysicaltherapiesforAchillestendinopathy:systematicreviewandmeta-analysis
59) Silver, F.H., DeVore, D. and Siperko, L.M.2003. Invited Review: Role of mechanophysiology in aging of ECM: effects of changes inmechanochemical transduction. Journal of Applied Physiology 95:2134-41.
60) Shier, D.N., Butler, J.L. and Lewis R.1999. Hole's Essentials of Human Anatomy & Physiology (8th Edition)
61) Smith CW. 1993. Endothelial adhesion molecules and their role in inflammation. Canadian Journal of Physiology and Pharmacology 71:76-87.
62) Tsai WC, Hsu CC, Pang JH, Lin MS, Chen YH, Liang FC. 2012. Low-Level Laser Irradiation Stimulates Tenocyte Migration with Up-Regulation of Dynamin II Expression. PLoS One 7 [On Line].Can be found at:
http://www.ncbi.nlm.nih.gov/pubmed/226664963) Tumilty S, McDonough S, Hurley DA, Baxter GD. 2012. Clinical effectiveness of low-level
laser therapy as an adjunct to eccentric exercise for the treatment of Achilles' tendinopathy: a randomized controlled trial. Archive of Physical Medicine and Rehabilitation 5:733-9
64) Vedrenne, N., Coulomb, B., Danigo, A., Bonté, F. and Desmoulière A. 2012.The complex dialogue between (myo)fibroblasts and the extracellular matrix during skin repair processes and ageing. Pathological Biology 60:20-7.
65) Weber, R.J., Taylor, B.R., Engelman, D.E., Bogdan-Allemann, I. and Goldberg, D.J.2011. Basics in Dermatological Laser Current Problems in Dermatology 42:24–34
66) Wertz, K., Seifert, N., Hunziker, P.B., Riss, G., Wyss, A. and Lankin, C. 2004. Beta-carotene inhibits UVA-induced matrix metalloprotease 1 and 10 expression in keratinocytes by a singlet oxygen-dependent mechanism. Free Radical Biology and Medicine 37:654—70.
67) Whelan HT, Smits RL Jr, Buchman EV, Whelan NT, Turner SG, Margolis DA, Cevenini V, Stinson H, Ignatius R, Martin T, Cwiklinski J, Philippi AF, Graf WR,Hodgson B, Gould L, Kane M, Chen G, Caviness J.2001. Effect of NASA light-emitting diode irradiation on wound healing. Journal of Clinical Laser Medical Surgery 19:305-14.
68) Wong, W.R., Shyu, W.L., Tsai, J.W., Hsu, K.H., Lee, H.Y., Pang, J.H. 2008. Intense pulsed light modulates the expressions of MMP-2, MMP-14 and TIMP-2 in skin dermal fibroblasts cultured within contracted collagen lattices. Journal of Dermatological Sciences 51:70-3.
69) Wysocki, A.B.1999. Skin anatomy, physiology, and pathophysiol. The Nursing clinics of North America 34:777 -97.
70) Yager, D.R., Zhang, L.Y., Liang, H.X., Diegelmann, R.F. and Cohen, I.K.1996. Wound fluids from human pressure ulcers contain elevated matrix metalloproteinase levels and activity compared to surgical wound fluids. Journal of Investigative Dermatology 107:743-8.
71) Zungu, I.L., Hawkins- Evans, D. and Abrahamse, H.2009. Mitochondrial responses of normal and injured human skin fibroblasts following low level laser irradiation--an in vitro study. Photochemistry and Photobiology 85:987-96.
33