IORT - Accueilmeeting-com.ch/.../Senologie_septembre_2012/J.-M._Nogaret_-_IORT...• iort 1900 2012...
67
Jm.nogaret LAUSANNE 13.09.12 IORT screening minimalist treatments
Transcript of IORT - Accueilmeeting-com.ch/.../Senologie_septembre_2012/J.-M._Nogaret_-_IORT...• iort 1900 2012...

Jm.nogaret
LAUSANNE 13.09.12
IORT screening
minimalist treatments

MAXIMUM TOLERABLE TREATMENT
MINIMAL EFFICACE TREATMENT
SCREENING

SCREENING STAGE
D.C.I.S. 25 %
T < 2 cm 50 %
T > 2 cm 25 %

CONTROVERSIES
• Halsted
• Radiotherapy
• Modified mastectomy
• Adjuvant chemotherapy
• Conservative surgery
• Adjuvant hormonotherapy
• Sentinel node
• Neoadjuvant systemical treatment
• IORT
1900
2012

RADIATION AFTER CONSERVATIVE
SURGERY
• discussions none…
– local recurrences 10 years
– 25 - 30% without RT
– 6 -11% with RT
radiation is indispensable
n

TRUE LOCAL RECURRENCES
• 85% in the tumor bed Van Limbergen ’87, Fourquet ’80, Veronesi ‘2000…
• the % remaining tumor cells decrease from the area where the primary carcinoma exised
Holland ’85 et ‘90
IORT
very selective technique to intensify the local treatment:
a high single dose as exlusive or boost treatment

IORT in Europe
1905 first procedure
C. Comas
(1905, Barcelone)

PARTIAL BREAST RADIATION PBI
• INTRAOPERATIVE
IO(E)RT (NOVAC-7 MOBETRON) INTRABEAM (RX)
• POSTOPERATIVE
MAMMOSITE NEEDLES Ir 192 EXTERNAL RXT 3D OR IMRT

INTRA BEAM
RX 50 KV :
20 Gy contact
10 Gy 5 mm
5 Gy 10 mm
20-30 min

Raggi X 50 Kv
Xoft

Ir-192
! only 20-25 % patients
Pawlik et al. Cancer 2004; 100:490-8
MAMMOSITE
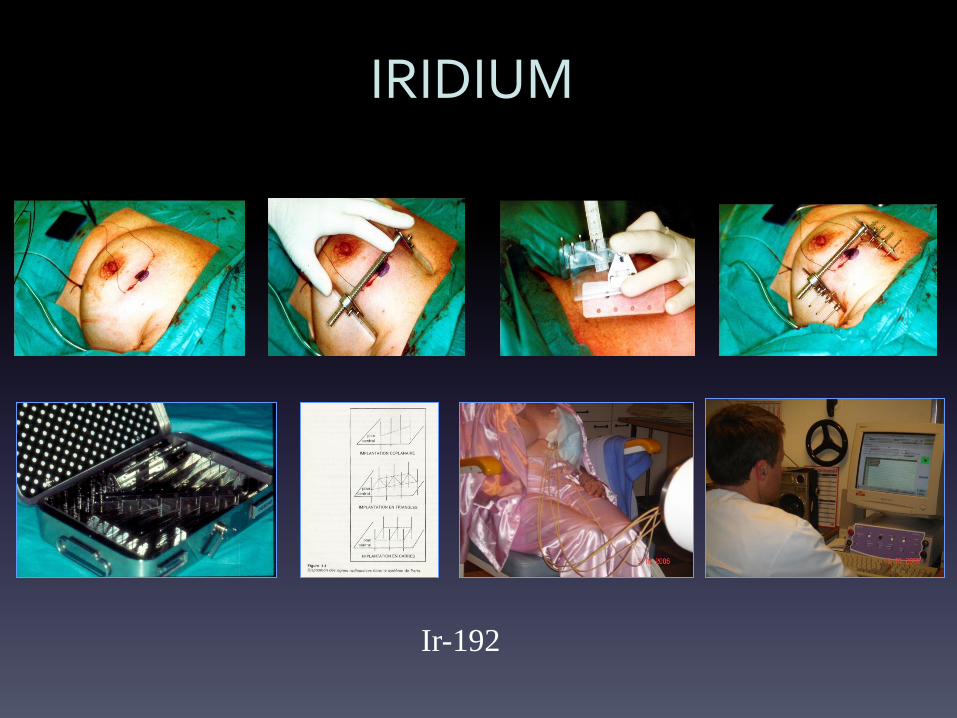
IRIDIUM
Ir-192

IOERT
mobile linear accelerator
can enter into the surgical theatre
Novac7, Hitesys Mobetron, Intraop

0
20
40
60
80
100
120
0 20 40 60
Depth (mm)
Rel
ativ
e d
ose
(%
)
X-ray source 50kVp (higher RBE)
DOSE DISTRIBUTION

QUESTIONS
• Local recurrences ?
• Side effects ?

IORT, a single fraction of radiation, giving a high dose
as
Sole Treatment
Or Boost


IOERT boost
– 6 Institutions ISIORT-Europe – Oct ’98 till May ’05 – 1031 patients – Median FU : 52 months – LR : 5/1031
• DFS : 99.4%
Félix Sedlmayer, Strahlenther Onkol 2007; 183(2):32-34


IOERT boost
• Résults ( Salzburg ) – 378 patients stade I-II – 1996-2001 – Group 1 51-56 Gy + 12 Gy ( external boost )
Group 2 IORT 9 Gy ( boost ) + 51-56 Gy
R.Reitsamer,F.Sedlmayer et all. Int.J.Cancer 2006 jun 1; 118(11):2882-7)
Group 1 Group 2
local reccurences 5 y 4.3% 0%
Survival without recurrences 5y 90.9 % 95.8%

IORT boost
• Jules Bordet experience – 258 patients – 1988-2003 – FU 18 - 206 months – T0, T1, T2<3cm – 15 Gy 192 Ir + 50 Gy ERT
Philippson, Nogaret, Simon et al, Cancer Radiothérapie, 9 (2005) 501)
LR 3.5%

28 Institutions in 9 Countries
2,232 patients enrolled (started March 2000, closed May 2008 )
Age 45 years old or more, with IDC suitable for wide local excision
- IORT (20 Gy at the surface) vs conventional WBRT (40-56 Gy, w/w-out Boost)
- Each center could decide that patients randomized to IORT with
certain pathological finding (lobular, EIC+…) receive WBRT in
addition
Vaidya JS et al, Lancet, July 2010

TARGeted Intraoperative radioTherapy
(TARGIT)
Median age 63 years,
Tumor size < 1 cm in 36%,
50% between 1-2 cm
G3 tumors in 15%,
N+ in 17%
66% hormone therapy
12% chemotherapy
Vaidya JS et al, Lancet, July 2010

-No statistical difference in complication rate (11.5 in Targit arm vs 10.6% in EBRT arm)
TARGeted Intraoperative radioTherapy (TARGIT)

TARGeted Intraoperative radioTherapy (TARGIT)
At 4 years, 6 LR in the TARGIT group (1.2%), 5 in the EBRT group (0.95%)


Milan ELIOT out-trial on 1822 patients
Breast Cancer Res Treat, August 2010
< 1 cm: 613 patients (33.5%)

Milan ELIOT out-trial on 1822 patients
Breast Cancer Res Treat, August 2010
Negative node: 1301 patients (71.4%)

Milan ELIOT out-trial on 1822 patients
Breast Cancer Res Treat, August 2010
Grade 1: 467 patients (25.6%)

Milan ELIOT out-trial on 1822 patients
Breast Cancer Res Treat, August 2010
Absent: 1528 patients (83.9%)

Milan ELIOT out-trial on 1822 patients
Breast Cancer Res Treat, August 2010
Luminal A: 648 patients (35.6%)
Luminal B: 977 patients (53.6%)
Cerb +++ : 53 patients (2.9%)
Basal: 137 patients (7.5%)

Milan ELIOT out-trial on 1822 patients
Breast Cancer Res Treat, August 2010

Veronesi & Orecchia, Breast Cancer Res Treat, August 2010

Milan ELIOT out-trial on 1822 patients
Breast Cancer Res Treat, August 2010

ELIOT
1822 patients • Tumor < 25mm • Jan 2000-Dec 2008 • 21 Gy • médian FU : 36.1 mois
U.Veronesi et al Breast Cancer Res Treat (2010) 121: 141-151
LR 2.3%
Free survival 5 years
Free survival 10 years
97.4%
89.7%
severe fibrosis
mild fibrosis 0.1%
1.8%



ASTRO
suitable
ESTRO
low risk
ASTRO
cautionary
ESTRO
Intermediate
risk
ASTRO
unsuitable
ESTRO
contraindic
ation
Age ≥ 60 y > 50 y 50-59 y 40-50 y < 50 y ≤ 40 y
BRCA 1,2 mut Not present Present
Tumor size ≤ 2 cm ≤3 cm 2.1-3 cm > 3 cm
T stage T1 pT1-2 T2 T3-T4
Margins ≥ 2 mm ≥ 2 mm < 2 mm < 2 mm Positive Positive
Grade Any Any Any
LVSI No Not allowed Focal Not allowed Extensive Present
ER status Positive Any Negative Any
Multicentricity Unicentric only Pluricentric
Multifocality Clinically
unifocal ≤2cm
Clinically
unifocal 2.1-3cm
Multifocal >3cm
Histology Invasive ductal Invasive
ductal
Invasive
lobular
Invasive
lobular
Pure DCIS Not allowed Not allowed ≤3cm Allowed If > 3 cm
EIC Not allowed ≤3cm If > 3 cm
Associated LCIS Allowed Allowed Allowed
Nodal status pN0 (i-,i+) pN0 pN1mi, pN1a pN1, pN2, pN3 pNX, pN2a
Neoadj therapy Not allowed Not allowed Not allowed If used If used
Tableau 1

“Suitable”
1.5% at 5-y
R. Orecchia, Genève, sept 2011

“Good”
1.9% at 5-y
R. Orecchia, Genève, sept 2011

MOBETRON OUR STUDY

INCLUSION CRITERIA
More than 40 years old
Ductal invasive carcinoma (preoperative biopsy)
pT less than 20 mm (peroperative analysis)
Free margins (peroperative analysis)
Unicentric (MRI)
Unifocal (MRI)
All HR
All grade
pN0 (peroperative analysis)
No EIC or LVI (preop biopsy)

MOBETRON
Mobile linear accelerator self
shielded and ‘light’ (1,2 T)
Operate with 9 GHz instead of 3
Accelerated electrons beam
of 4, 6, 9 and 12 MeV
Dose rate: 10 Gy/min

Mobetron
Aluminium applicators of
3 to 10 cm diameter
Flat or beveled (15° et 30°)
boluses of 5 or 10 mm for every applicator

SURGICAL TECHNIC
tumor resection till the muscle detachment of the gland shield positioning on the muscle
suture of the tumor bed applicator positionning

muscle pectoral
face Profil

cône en place-protection de la peau
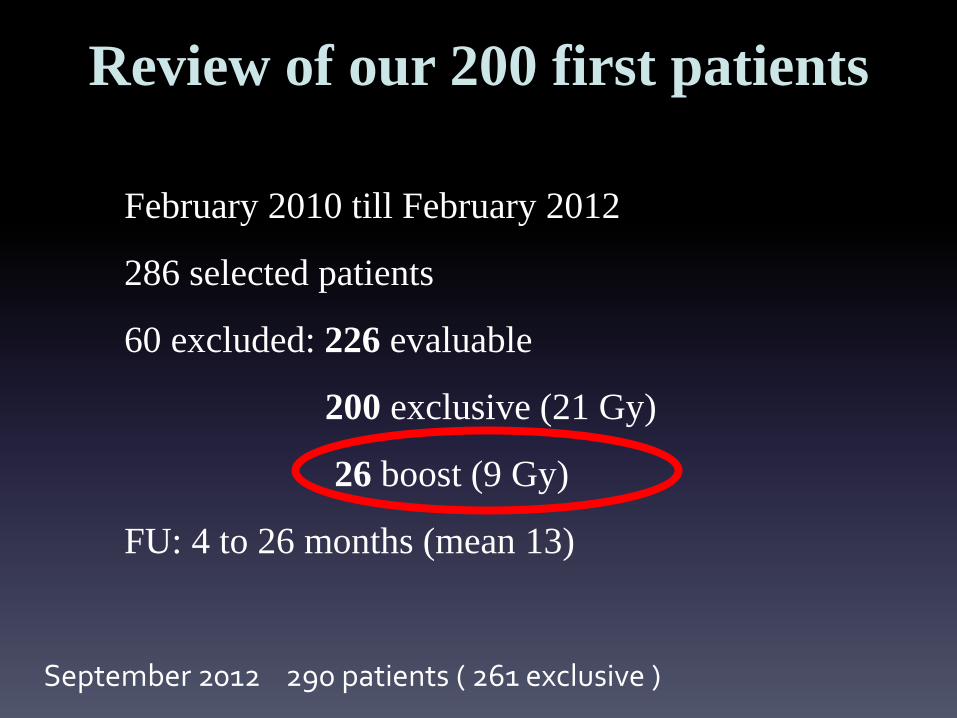
February 2010 till February 2012
286 selected patients
60 excluded: 226 evaluable
200 exclusive (21 Gy)
26 boost (9 Gy)
FU: 4 to 26 months (mean 13)
Review of our 200 first patients
September 2012 290 patients ( 261 exclusive )

AGE
Review of our 200 first patients
Age distribution for treated patients
9%
37%54%
40-49
50-60
>60

STAGE
Review of our 200 first patients
T1a T1b T1c Total
Nb 3 81 120 204
% 1.5 39.7 58.8 100

Review of our 200 first patients Collimator distribution for all patients
Collimator size (dia in mm) distribution for
PBI
45 mm
17,6%
50 mm
36,8%
55 mm
28,4%
60 mm
15,2%
40 mm
0,0%
35 mm
0,5%65 mm
1,5%

Review of our 200 first patients
ENERGY DISTRIBUTION for PBI
0% 9%
48%
43% 4 MeV6 MeV 9 MeV 12 MeV
Energy distribution

HISTOLOGY
Review of our 200 first patients
pN0 pN1mic pN1a Total
Nb 190 8 6 204
% 93.1 3.9 2.9 100
AP ductal lobular mixt mucinus Total
Nb 192 7 1 4 204
% 94.1 3.4 0.5 2.0 100
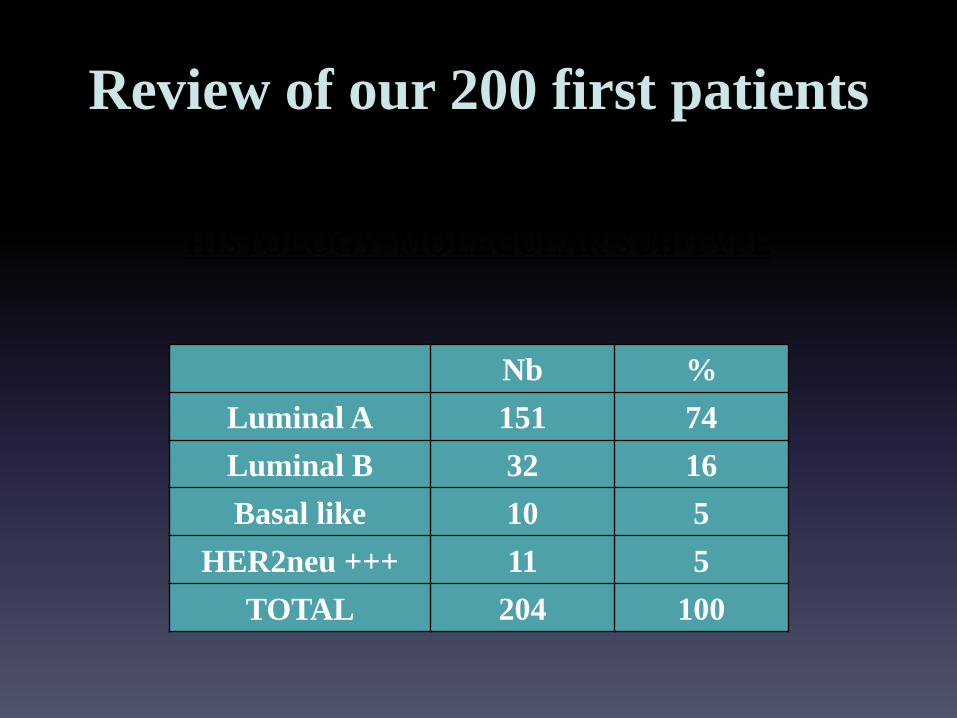
HISTOLOGY: MOLECULAR SUB-TYPE
Review of our 200 first patients
Nb %
Luminal A 151 74
Luminal B 32 16
Basal like 10 5
HER2neu +++ 11 5
TOTAL 204 100

COMPLICATIONS
Review of our 200 first patients
Nb %
None 194 95
Hematoma 3 1.5
Infection 3 1.5
Scar rupture 2 1
inflamation 1 0.5
Infection + scar rupture 1 0.5
TOTAL 204 100

COSMESIS
Review of our 200 first patients
59
32
9
00
10
20
30
40
50
60
%
Cosmesis for PBI Treatments
Very Good
Good
Fair
Bad
CONCLUSIONS (2)
Review of our 200 first patients
► Importance of preoperative diagnosis
► Follow-up to short in most of the studies and
the risk of local relapse continue after 5 years

CONCLUSIONS (3)
Review of our 200 first patients
► Complications rate very low
► Side effects moderated
► Maximal protection of the normal tissues
► Gain in quality of life

CONCLUSIONS

obvious progress
MORE EFFICINCY LESS MORBIDITY MORE COMFORT
IORT

YESTERDAY

TODAY
RT post Chimio néo adj+chir
Sein d, A.L, 3 mois
RT post op Co-60
Sein g, 6 mois
Rec bilat post RT bilat
pour multicentrique

TOMORROW
postoperative:
• 3 - 6 weeks
intraoperative:
1 day….
More effective !

RECURRENCES AND SURVIVAL
20% LR 5 years
5% mortality 15 years
EBCTCG, Lancet, 366-déc 2006

Toute vérité franchit trois étapes. D’abord elle est ridiculisée. Ensuite, elle subit un forte opposition. Puis, elle est considérée
comme ayant toujours été une évidence….
ARTHUR SCHOPENHAUER