Introduction to streptococci species

of 18
Transcript of Introduction to streptococci species
-
8/14/2019 Introduction to streptococci species
1/18
-
8/14/2019 Introduction to streptococci species
2/18
INTRODUCTION
The streptococci are gram-positive sphericalbacteria that characteristically form pairs orchains during growth. They are widely distributedin nature. Some are members of the normalhuman flora; others are associated with importanthuman diseases attributable in part to infection bystreptococci, in part to sensitization to them.
Streptococci elaborate a variety of extracellularsubstances and enzymes.
The streptococci are a large and heterogeneousgroup of bacteria and no one system suffices toclassify them. Yet, understanding the classificationis key to understanding their medical importance.
-
8/14/2019 Introduction to streptococci species
3/18
CLASSIFICATION
The classification of streptococci into majorcategories has been based on a series ofobservations over many years: (1) colonymorphology and hemolytic reactions on bloodagar; (2) serologic specificity of the cell wallgroup-specific substance and other cell wall orcapsular antigens; (3) biochemical reactions and
resistance to physical and chemical factors; and(4) ecologic features. Molecular genetics have alsobeen used to study the streptococci. Combinationsof the above methods have permitted theclassification of streptococci for purposes ofclinical and epidemiologic convenience, but as theknowledge evolved, new methods have been
introduced with the result that severalclassification systems have been described. Insome cases, different species names have beenused to describe the same organisms; in otherinstances, some members of the same specieshave been included in another species orclassified separately.
Streptococcus pyogenes
Most streptococci that contain the group A
antigen are S pyogenes. It is a prototypical
-
8/14/2019 Introduction to streptococci species
4/18
human pathogen. It is used here to illustrate
general characteristics of streptococci and
specific characteristics of the species. Spyogenes is the main human pathogen
associated with local or systemic invasion and
post streptococcal immunologic disorders. S
pyogenes typically produces large (1 cm in
diameter) zones of haemolysis around colonies
greater than 0.5 mm in diameter. They are PYR-positive (hydrolysis of L-pyrrolidonyl-2-
naphthylamide) and usually are susceptible to
bacitracin.
Diseases Attributable to Local Infection with Spyogenes and Their By-Products
Streptococcal Sore ThroatThe most common infection due to -hemolytic Spyogenes is streptococcal sore throat orpharyngitis. S pyogenes adhere to thepharyngeal epithelium by means of lipoteichoicacid-covered surface pili. The glycoproteinfibronectin (MW 440,000) on epithelial cells
probably serves as lipoteichoic acid ligand. Ininfants and small children, the sore throat occursas a sub acute nasopharyngitis with a thin serousdischarge and little fever but with a tendency ofthe infection to extend to the middle ear and themastoid. The cervical lymph nodes are usuallyenlarged. The illness may persist for weeks. In
-
8/14/2019 Introduction to streptococci species
5/18
older children and adults, the disease is moreacute and is characterized by intense
nasopharyngitis, tonsillitis, and intense rednessand edema of the mucous membranes, withpurulent exudate, enlarged, tender cervicallymph nodes, and (usually) a high fever. Twentypercent of infections are asymptomatic. A similarclinical picture can occur with infectiousmononucleosis, diphtheria, gonococcal infection,and adenovirus infection.
S pyogenes infection of the upper respiratorytract does not usually involve the lungs.Pneumonia, when it does occur, is rapidlyprogressive and severe and is most commonly asequela to viral infections, eg, influenza ormeasles, which seem to enhance susceptibility
greatly.Streptococcal Pyoderma
Local infection of superficial layers of skin,especially in children, is called impetigo. Itconsists of superficial vesicles that break downand eroded areas whose denuded surface iscovered with pus and later is encrusted. It
spreads by continuity and is highlycommunicable, especially in hot, humid climates.More widespread infection occurs in eczematousor wounded skin or in burns and may progress tocellulitis. Group A streptococcal skin infectionsare often attributable to M types 49, 57, and 59
-
8/14/2019 Introduction to streptococci species
6/18
61 and may precede glomerulonephritis but donot often lead to rheumatic fever.
A clinically identical infection can be caused by Saureus and sometimes both S pyogenes and Saureus are present.
Invasive Group A Streptococcal Infections,Streptococcal Toxic Shock Syndrome, and ScarletFever
Fulminant, invasive S pyogenes infections with
streptococcal toxic shock syndrome arecharacterized by shock, bacteremia, respiratoryfailure, and multiorgan failure. Death occurs inabout 30% of patients. The infections tend tofollow minor trauma in otherwise healthy personswith several presentations of soft tissueinfection. These include necrotizing fasciitis,
myositis, and infections at other soft tissue sites;bacteremia occurs frequently. In some patients,particularly those infected with group Astreptococci of M types 1 or 3, the diseasepresents with focal soft tissue infectionaccompanied by fever and rapidly progressiveshock with multiorgan failure. Erythema and
desquamation may occur. The S pyogenes of theM types 1 and 3 (and types 12 and 28) that makepyrogenic exotoxin A or B are associated withthe severe infections.
Pyrogenic exotoxins AC also cause scarlet feverin association with S pyogenes pharyngitis or
-
8/14/2019 Introduction to streptococci species
7/18
with skin or soft tissue infection. The pharyngitismay be severe. The rash appears on the trunk
after 24 hours of illness and spreads to involvethe extremities. Streptococcal toxic shocksyndrome and scarlet fever are clinicallyoverlapping diseases.
EPIDEMIOLOGY, PREVENTION AND CONTROL
humans can be asymptomatic nasopharyngeal orperineal carriers of S pyogenes, the organismshould be considered abnormal if it is detectedby culture or other means. The ultimate sourceof group A streptococci is a person harboringthese organisms. The individual may have aclinical or subclinical infection or may be acarrier distributing streptococci directly to otherpersons via droplets from the respiratory tract orskin. The nasal discharges of a person harboringS pyogenes are the most dangerous source forspread of these organisms.
Many other streptococci (viridans streptococci,enterococci, etc) are members of the normalflora of the human body. They produce diseaseonly when established in parts of the body wherethey do not normally occur (eg, heart valves). Toprevent such accidents, particularly in the courseof surgical procedures on the respiratory,gastrointestinal, and urinary tracts that result in
-
8/14/2019 Introduction to streptococci species
8/18
temporary bacteremia, antimicrobial agents areoften administered prophylactically to persons
with known heart valve deformity and to thosewith prosthetic valves or joints.
Control procedures are directed mainly at thehuman source:
(1) Detection and early antimicrobial therapy ofrespiratory and skin infections with group Astreptococci. Prompt eradication of streptococcifrom early infections can effectively prevent thedevelopment of poststreptococcal disease. Thisrequires maintenance of adequate penicillinlevels in tissues for 10 days (eg, benzathinepenicillin G given once intramuscularly).Erythromycin is an alternative drug, althoughsome S pyogenes are resistant.
(2) Antistreptococcal chemoprophylaxis inpersons who have suffered an attack ofrheumatic fever. This involves giving oneinjection of benzathine penicillin Gintramuscularly, every 34 weeks, or daily oralpenicillin or oral sulfonamide. The first attack ofrheumatic fever infrequently causes major heartdamage; however, such persons are particularlysusceptible to reinfections with streptococci thatprecipitate relapses of rheumatic activity andgive rise to cardiac damage. Chemoprophylaxisin such individuals, especially children, must becontinued for years. Chemoprophylaxis is not
-
8/14/2019 Introduction to streptococci species
9/18
used in glomerulonephritis because of the smallnumber of nephritogenic types of streptococci.
An exception may be family groups with a highrate of poststreptococcal nephritis.
(3) Eradication ofS pyogenes from carriers. Thisis especially important when carriers are in areassuch as obstetric delivery rooms, operatingrooms, classrooms, or nurseries. Unfortunately,it is often difficult to eradicate -hemolytic
streptococci from permanent carriers, andindividuals may occasionally have to be shiftedaway from "sensitive" areas for some time.
TREATMENT
All S pyogenesare susceptible to penicillin G, andmost are susceptible to erythromycin. Some areresistant to tetracyclines. Antimicrobial drugs
have no effect on established glomerulonephritisand rheumatic fever. In acute streptococcalinfections, however, every effort must be madeto rapidly eradicate streptococci from thepatient, eliminate the antigenic stimulus (beforeday 8), and thus prevent poststreptococcaldisease. Doses of penicillin or erythromycin that
-
8/14/2019 Introduction to streptococci species
10/18
result in effective tissue levels for 10 daysusually accomplish this. Antimicrobial drugs are
also very useful in preventing reinfection with -hemolytic group A streptococci in rheumaticfever patients.
Streptococcus agalactiae
These are the group B streptococci. Theytypically are -hemolytic and produce zones of
-
8/14/2019 Introduction to streptococci species
11/18
hemolysis that are only slightly larger than thecolonies (12 mm in diameter). The group B
streptococci hydrolyze sodium hippurate andgive a positive response in the so-called CAMPtest (Christie, Atkins, Munch-Peterson).
Group B streptococci are part of the normalvaginal flora in 525% of women. Group Bstreptococcal infection during the first month oflife may present as fulminant sepsis, meningitis,
or respiratory distress syndrome. Intravenousampicillin given to mothers, who carry group Bstreptococci and are in labor, preventscolonization of their infants and group Bstreptococcal disease.
-
8/14/2019 Introduction to streptococci species
12/18
Viridans Streptococci
The viridans streptococci include S mitis, Smutans, S salivarius, S sanguis, and others.Typically they are -hemolytic, but they may benonhemolytic. Their growth is not inhibited byOptochin, and colonies are not soluble in bile(deoxycholate). The viridans streptococci are themost prevalent members of the normal flora of
the upper respiratory tract and are important forthe healthy state of the mucous membranesthere. They may reach the bloodstream as aresult of trauma and are a principal cause ofendocarditis on abnormal heart valves. Someviridans streptococci (eg, S mutans) synthesizelarge polysaccharides such as dextrans or levansfrom sucrose and contribute importantly to thegenesis of dental caries.
In the course of bacteraemia, viridansstreptococci, pneumococci, or enterococci maysettle on normal or previously deformed heartvalves, producing acute endocarditis. Rapiddestruction of the valves frequently leads to fatal
cardiac failure in days or weeks unless aprosthesis can be inserted during antimicrobialtherapy.
Sub acute endocarditis often involves abnormalvalves (congenital deformities and rheumatic oratherosclerotic lesions). Although any organismreaching the bloodstream may establish itself on
-
8/14/2019 Introduction to streptococci species
13/18
thrombotic lesions that develop on endotheliuminjured as a result of circulatory stresses, sub
acute endocarditis is most frequently due tomembers of the normal flora of the respiratory orintestinal tract that have accidentally reachedthe blood. After dental extraction, at least 30% ofpatients have viridans streptococcalbacteraemia. These streptococci, ordinarily themost prevalent members of the upperrespiratory flora, are also the most frequentcause of sub acute bacterial endocarditis. Thegroup D streptococci (enterococci and S bovis)also are common causes of sub acuteendocarditis. About 510% of cases are due toenterococci originating in the gut or urinary tract.
The lesion is slowly progressive, and a certainamount of healing accompanies the activeinflammation; vegetations consist of fibrin,platelets, blood cells, and bacteria adherent tothe valve leaflets. The clinical course is gradual,but the disease is invariably fatal in untreatedcases. The typical clinical picture includes fever,anemia, weakness, a heart murmur, embolicphenomena, an enlarged spleen, and renal
lesions.
-Hemolytic streptococci and enterococci vary in
their susceptibility to antimicrobial agents.
Particularly in bacterial endocarditis, antibiotic
susceptibility tests are useful to determine which
-
8/14/2019 Introduction to streptococci species
14/18
drugs may be used for optimal therapy. Amino
glycosides often enhance the rate of bactericidal
action of penicillin on streptococci, particularlyenterococci.
Streptococcus pneumonia
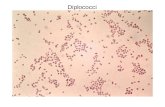
The pneumococci (S pneumoniae) are gram-positive diplococci, often lancet-shaped orarranged in chains, possessing a capsule ofpolysaccharide that permits typing with specificantisera. Pneumococci are readily lysed bysurface-active agents, which probably remove or
-
8/14/2019 Introduction to streptococci species
15/18
inactivate the inhibitors of cell wall autolysins.Pneumococci are normal inhabitants of the upper
respiratory tract of 540% of humans and cancause pneumonia, sinusitis, otitis, bronchitis,bacteraemia, meningitis, and other infectiousprocesses.
Epidemiology, Prevention, & Control
Pneumococcal pneumonia accounts for about
60% of all bacterial pneumonias. In thedevelopment of illness, predisposing factors aremore important than exposure to the infectiousagent, and the healthy carrier is more importantin disseminating pneumococci than the sickpatient.
It is possible to immunize individuals with type-specific polysaccharides. Such vaccines canprobably provide 90% protection againstbacteremic pneumonia. A polysaccharide vaccinecontaining 23 types is licensed in the UnitedStates. This vaccine is appropriate for elderly,debilitated, or immunosuppressed individuals. Apneumococcal conjugate vaccine contains
capsular polysaccharides conjugated todiphtheria CRM197 protein. This seven-valentvaccine is recommended for all children aged 223 months, to help prevent ear infections, andfor selected children aged 2459 months.
-
8/14/2019 Introduction to streptococci species
16/18
ENTEROCOCCI
The enterococci have the group D group-specificsubstance and were previously classified as
group D streptococci. Because the group D cellwall specific antigen is a teichoic acid, it is not anantigenically good marker; enterococci areusually identified by characteristics other thanimmunologic reaction with group-specificantisera. They are part of the normal entericflora. They are usually nonhemolytic, but
occasionally -hemolytic. Enterococci are PYR-positive. They grow in the presence of bile andhydrolyze esculin (bile esculin-positive). Theygrow in 6.5% NaCl. They grow well at between10 C and 45 C whereas streptococci generallygrow at a much narrower temperature range.
They are more resistant to penicillin G than the
streptococci, and rare isolates have plasmidsthat encode for -lactamase. Many isolates arevancomycin-resistant.
There are at least 12 species of enterococci.Enterococcus faecalis is the most common andcauses 8590% of enterococcal infections, whileEnterococcus faecium causes 510%. The
-
8/14/2019 Introduction to streptococci species
17/18
enterococci are among the most frequent causesof nosocomial infections, particularly in intensive
care units, and are selected by therapy withcephalosporins and other antibiotics to whichthey are resistant. Enterococci are transmittedfrom one patient to another primarily on thehands of hospital personnel, some of whom maycarry the enterococci in their gastrointestinaltracts. Enterococci occasionally are transmittedon medical devices.
BIBLIOGRAPHY
Bisno AL, Stephens DL: Streptococcus pyogenes.
In: Mandell, Douglas, and Bennett's Principles
and Practice of Infectious Diseases, 6th ed.
Mandell GL, Bennett JE, Dolin R (editors).Churchill Livingstone, 2005.
Ruoff KL, Whiley RA, Beighton D: Streptococcus.
In: Manual of Clinical Microbiology, 8th ed.
Murray PR et al (editors). ASM Press, 2003.
-
8/14/2019 Introduction to streptococci species
18/18
Jawetz, Melnick, & Adelberg's Medical
Microbiology, Twenty-Fourth Edition, The
McGraw-Hill Companies, 2007.