
Introduction to regulation of medicines and health technologies: Global context of drug regulation...
35
Introduction to regulation of medicines and health technologies: Global context of drug regulation Dr Lembit Rägo Coordinator Quality Assurance and Safety: Medicines Essential Medicines and Health Products World Health Organization E-mail: [email protected]
-
Upload
sammy-costin -
Category
Documents
-
view
223 -
download
0
Transcript of Introduction to regulation of medicines and health technologies: Global context of drug regulation...

Introduction to regulation of medicines and health technologies:
Global context of drug regulation
Dr Lembit RägoCoordinatorQuality Assurance and Safety: MedicinesEssential Medicines and Health ProductsWorld Health OrganizationE-mail: [email protected]

2 |
ContentContent
Setting the scene. What products we have? What is the situation with medicines quality and regulatory affairs Globally?
– 3 case studies• Africa - antimalarial medicines quality survey and
falsified antimalrials• Pakistan – two "killer" medicines cases• Case study from NIS – a biosimilar case
Who is WHO? WHO activities to medicines quality assurance and regulation What is WHO doing to strengthen national regulatory authorities? Local production of Essential Medicines and its constraints Concluding remarks

3 |
What type of regulated products we have?What type of regulated products we have?
Regulated health products– Medicines, including biological products:
• Medicines – originator and "generic" products• Biological medicines
– Vaccines– Other biologicals: Monoclonal antibodies,
Interferons etc.– Blood products– Similar biotherapeutic products (biosimilars)
• Traditional/herbal medicines (complimentary medicines)
– Medical devices – in vitro diagnostics (IVDs)

4 |
Medicines: originator vs generic medicinesMedicines: originator vs generic medicines
New medicines or originator products– Need to prove safety, efficacy and quality
Multisourcse (generic) medicines– Focus on quality, safety and efficacy referred to originator– Safety and efficacy – bridging through bioequivalence studies– Interchangeability
• Pharmaceutical• Therapeutic
5 |
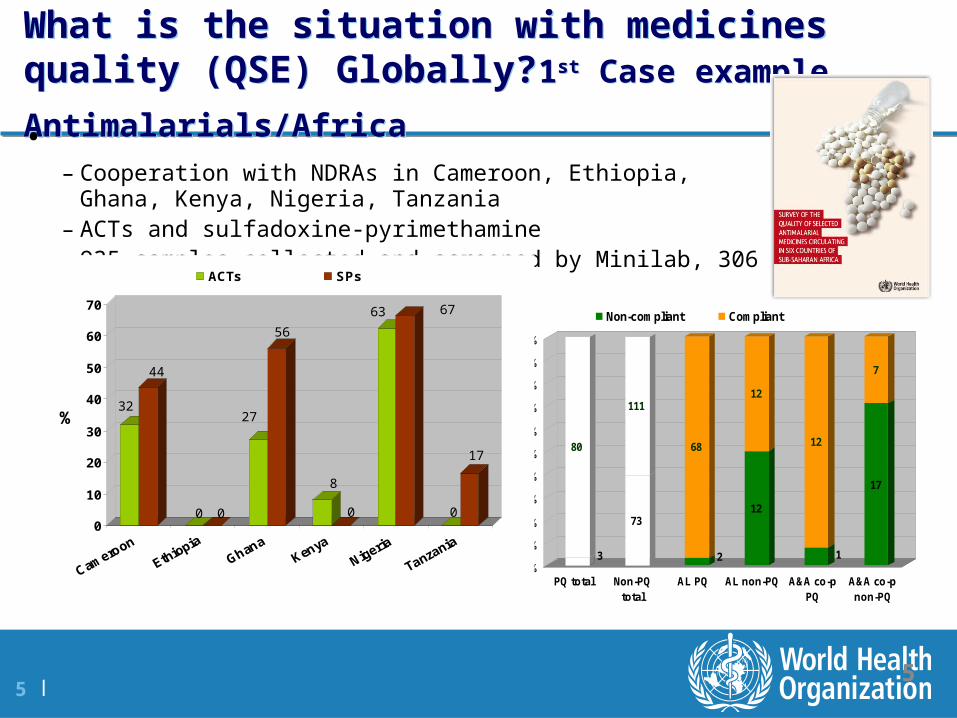
What is the situation with medicines quality (QSE)
Globally? 1st Case example. Antimalarials/Africa What is the situation with medicines quality (QSE)
Globally? 1st Case example. Antimalarials/Africa
5
3
80
73
111
2
68
12
12
1
12
17
7
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PQ total Non-PQtotal
AL PQ AL non-PQ A&A co-pPQ
A&A co-pnon-PQ
Non-compliant Compliant
• – Cooperation with NDRAs in Cameroon, Ethiopia, Ghana, Kenya, Nigeria, Tanzania– ACTs and sulfadoxine-pyrimethamine– 935 samples collected and screened by Minilab, 306 tested in laboratory
32
44
0 0
27
56
8
0
63 67
0
17
0
10
20
30
40
50
60
70
%
ACTs SPs

6 |
Falsified/Counterfeit antimalarials also common (1st Case example. Cont).
Falsified/Counterfeit antimalarials also common (1st Case example. Cont).
Several notifications about falsified antimalarials – no active ingredient or … containing paracetamol
WHO issues also public Drug Alerts
http://www.who.int/medicines/publications/drugalerts/drugalertindex/en/index.html

7 |
What is the situation with medicines quality (QSE) Globally? 2nd Case example – Pakistan 1.
What is the situation with medicines quality (QSE) Globally? 2nd Case example – Pakistan 1.
More than 107 death case and 450 severe ADRs with isosorbide mononitrate manufactured in Pakistan
Clinically resembled Dengue fever
Passed quality control testing
… forensic investigation – contained pyrimethamine in toxic quantities
Reason – totally ignoring GMP and negligence
8 |
What is the situation with medicines quality (QSE) Globally? 2nd Case example – Pakistan 2.
What is the situation with medicines quality (QSE) Globally? 2nd Case example – Pakistan 2.
Dextromethorphan killing more than 20 people
All death cases seemed to be linked to drug addiction
… forensic analysis revealed that the medicine contained also high percentage of levomthorphan (potent opiate)
API manufacturing quality failure
Site in India closed

9 |
What is the situation with medicines quality
(QSE) Globally? 3rd Case example – NIS biosimilar
What is the situation with medicines quality
(QSE) Globally? 3rd Case example – NIS biosimilar
A biosimilar approved in a NIS country several years ago
Patient complaints, MPs involved …
Approval based on … regulations about chemical generic medicines!
Company profile – not very credible
Question why it was authorized remains open.

10 |
What these case stories are telling?What these case stories are telling?
Quality of medicines is still an issue in many jurisdictions
Many countries do not have functional regulatory systems in place for product approval (MA, registration)
– Dossier assessment weak or absent– Inspectorates do not function properly
Many de facto do not control their markets nor do they control the supply chain
– No effective control of imports– No effective licensing of all the activities - manufacturing, retail- and whole
sale, hospital pharmacies– No traceability of products at any point of supply chain
Lack of capacity doing all the necessary and no system in place to rely on those who have the capacity

11 |
WHO activities in the field of health products regulation (medicines incl. biologicals, medical
devices)
WHO activities in the field of health products regulation (medicines incl. biologicals, medical
devices)
Setting policies, norms and standards – for access, rational use, quality, safety and efficacy
Assessment of national regulatory systems, regulatory support and capacity building
Promoting regulatory harmonization and information exchange – safety, quality, best practices etc.
Assuring safety and quality of selected products for United Nations family through prequalification programme (medicines, vaccines, diagnostics)

12 |
WHO is mandated to “develop, establish and promote international standards with respect to food, biological, pharmaceutical and similar products” (Article 2, WHO Constitution);
WHO Expert Committee on Specifications for Pharmaceutical Preparations
WHO Expert Committee on Biological Standardization Both complimentary to ICH activities
Joint FAO/WHO Expert Committee on Food Additives
Standards and WHOStandards and WHO

13 |
http://www.who.int/medicines/areas/quality_safety/regulation_legislation/assesment/en/index.html

14 |
International Conferences of Drug Regulatory Authorities (ICDRA)
International Conferences of Drug Regulatory Authorities (ICDRA)
Biennial Global meetings bringing together regulators from around 100 nations
Promoting information and best practices exchange, cooperation, harmonization and convergence
Several initiatives started in ICDRA environment– ICH initial discussions– AMRH initiative initial discussions– Reports from various harmonization initiatives

15 |
Prequalification programme – powerful engine for facilitating quality manufacture
http://apps.who.int/prequal/
Prequalification programme – powerful engine for facilitating quality manufacture
http://apps.who.int/prequal/

16 |
16
Prequalification of Medicines ProgrammePrequalification of Medicines Programme
Since 2001 the UN Prequalification Programme managed by WHO is ensuring that medicines procured with international funds are of assessed and inspected for quality, efficacy and safety, involves
Prequalification programme for medicines (finished dosage forms)
Prequalification of active pharmaceutical ingredients (APIs)
Prequalification of quality control (QC) laboratories
The Prequalification Programme is an action plan for expanding access to priority essential medicines in the following four areas:
- HIV/AIDS - Tuberculosis- Malaria- Reproductive Health- Selected individual products for other diseases (Flu, Zinc
sulphate)
17 |
17
Extensive collaboration: working with regulators … for
regulators • Not duplicating work done be stringent regulatory
authorities– SRA approval of new and generic products – abridged
procedure– US FDA tentative approvals – based on confidentiality
agreement including in the PQ products list– European Medicines Agency (EMA) – Art 58 … and beyond – Collaboration with EDQM, in particular in the area of APIs
(confidentiality agreements with US FDA, EDQM, EMA …)
• Active participation and involvement of – Regulatory authority experts from well resourced and less
resourced settings

18 |
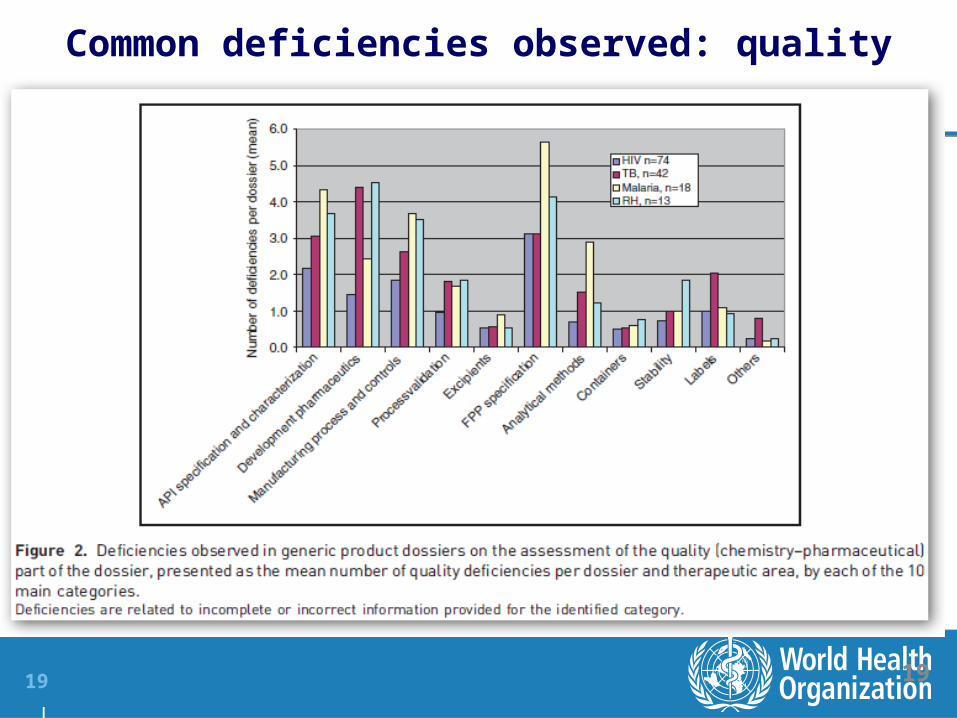
Common deficiencies for dossiers
19 |
Common deficiencies observed: quality
19

20 |
Key achievements
Contribution to increased access to quality medicines, for example:
– in 2012, 8 million people living with HIV and in need of treatment were receiving treatment, around 6.5 million of whom were taking WHO-prequalified antiretrovirals (ARVs);
– and sales of WHO-prequalified artemisinin-based combination antimalarials exceeded 180 million individual treatment courses in 2010)
UNAIDS. World AIDS Day Report 2012. Geneva, UNAIDS, 2012.
WHO. World Malaria Report, 2011. Geneva, World Health Organization, 2011.
20

21 |
PQP achievements 2009‒2012:
21
In addition:– prequalification of 28 active pharmaceutical ingredients (APIs), all of
which can be used for manufacturer of UNITAID priority products– prequalification of 19 medicines quality control laboratories (QCLs),
so that prequalified QCLs can now be found in all six WHO regions

22 |
Capacity building provided a core value of the programme. Participants in various capacity building workshops organized or co-
organized by PQP during 2007‒2012
22

23 |
Access to essential medicines remains a problem*Access to essential medicines remains a problem*
In spite of progress, especially with communicable diseases (HIV/AIDS, malaria and TB), the access to essential medicines remains a huge problem
Chronic diseases—mainly cardiovascular disease, cancer, chronic respiratory diseases, and diabetes—were estimated to cause more than 60% (35 million) of all deaths in 2005; more than 80% of these deaths occurred in low-income and middle-income countries.
NCDs have negative impact on individuals, and family economic production and wellbeing. For example, estimated loss in national income from heart diseases, stroke and diabetes in 2005 were $18 billions in China, $11 billion in the Russian Federation, $9 billion in India and $43 billion in Brazil.
Access to medicines for mental disorders remains poor – up 70% may not get treatment in low-income countries
24 |
Concept of local production*: Specific to local production WHO activities
Concept of local production*: Specific to local production WHO activities
Project: Improving access to medicines in developing countries through technology transfer related to medical products and local production.
Implemented by the Department of Public Health Innovation and Intellectual Property of the World Health Organization (PHI/HIS/WHO) in partnership with the United Nations Conference on Trade and Development (UNCTAD) and the International Centre for Trade and Sustainable Development (ICTSD) with funding from the European Union (EU).
Objective of the project: To increase access – especially for the poor in developing and least developed countries – to medicines, vaccines and diagnostics.
25 |
Special web site http://www.who.int/phi/publications/local_production/en/index.html
Special web site http://www.who.int/phi/publications/local_production/en/index.html

26 |
Relevant publications Relevant publications
Local production for access to medical products: Developing a framework to improve public health, 2011
Local production for access to medical products: Developing a framework to improve public health, 2011
Trends in local production of medicines and related technology transfer, 2011
Pharmaceutical production and related technology transfer: Landscape report, 2011
Pharmaceutical production and related technology transfer: Landscape report, 2011
….

27 |
Chances for Developing Countries and Least Developed Countries*
Chances for Developing Countries and Least Developed Countries*
Old concepts do not hold – three "power centres" for pharmaceutical manufacturing with different logic and interest but – convergence on going
New emerging
economise (BRICS)
Lower-middle income and low
income countries
(including African countries)
Old industrialised
countries (EU, US, Japan,
Canada etc.)

28 |
Industrialised countriesIndustrialised countries
Substantial industrial capacity Not much dependent on local manufacture, less generic markets Base for research based industries - consolidating into few giants with
new functions – marketing powerhouses, contracting a lot out Generic industries merging and going Global Machinery/lab equipment monopoly shifting away – China producing
production and lab equipment Increasing Globalization and work sharing
– 80 % APIs from India and China, also a lot of excipients and packing materials
– Contract manufacturing for FPPs (India)
– R&D – more and more in "developing world" – clinical trials, basic research slowly following

29 |
New emerging economiesNew emerging economies
Increasing industrial capacity in many areas with needs for new markets, still at large generic markets but with increasing share of originator products
Increasingly part of work sharing and taking over certain functions
– API, excipients, packaging materials, machinery production etc.
Participating in Global R&D– Clinical trials increasing, CROs developing, basic research
Developing its own original R&D for new productsGeneric industries developing and consolidating, going
Global reaching out to old industrialised country markets (India) and developing country markets (China)
30 |
Lower-middle income and low income countries(including African countries)
Lower-middle income and low income countries(including African countries)
Local manufacture may (?) be more important, mostly generic markets Bigger dependence on outside country/region resources (almost 100%
for APIs, excipients, packing materials machinery) Less part of Global R&D – less clinical trials, in many no CROs, no
participation in basic research Generic companies small and not reaching further than country or sub-
region Many have either no or only limited industrial capacity Relative lack qualified human resources and knowledge base Less business freedom and less attractive investment environment Local policies may disfavour local manufacturing More problems with good governance in pharmaceutical sector
31 |
Sustainable local production in Africa needs favourable environment and … collaboration between countries and
access to markets
Sustainable local production in Africa needs favourable environment and … collaboration between countries and
access to markets
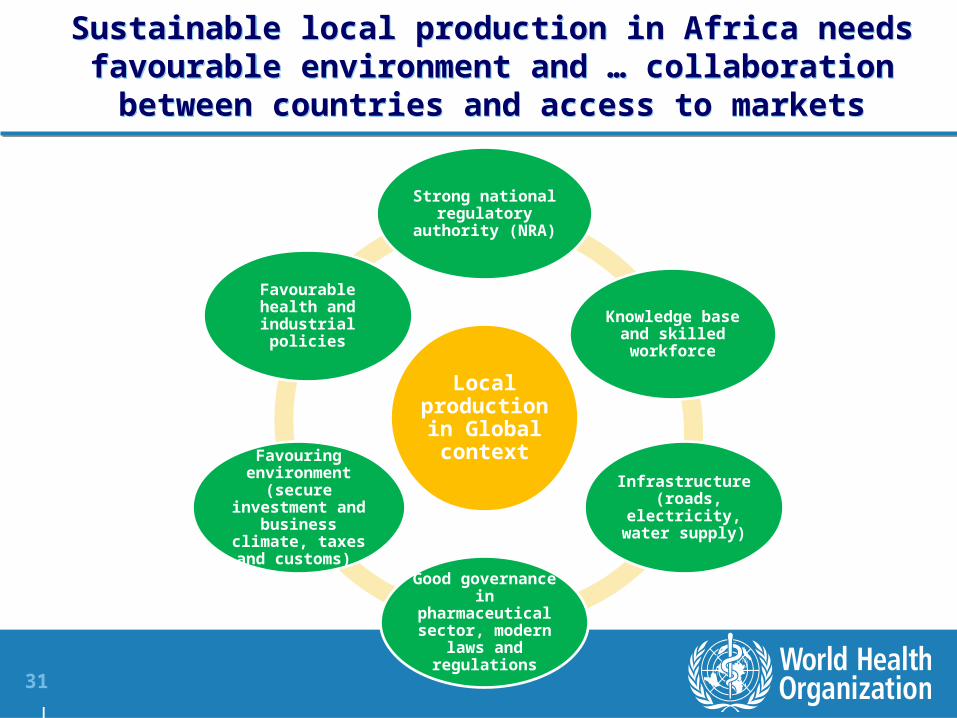
Local production in Global context
Strong national regulatory
authority (NRA)
Knowledge base and skilled workforce
Infrastructure (roads, electricity,
water supply)
Good governance in pharmaceutical
sector, modern laws and
regulations
Favouring environment
(secure investment and business
climate, taxes and customs)
Favourable health and industrial
policies
32 |
WHO position and experiences (particularly in the light of improved access to essential medicines)
WHO position and experiences (particularly in the light of improved access to essential medicines)
Local manufacturing may facilitate access but is not a goal in its own right
– Dramatic quality problems have occurred (e.g.Pakistan examples)
– Locally produced essential medicines may be of lower quality and higher price
– Health care providers and patients do not care where the medicines come from provided they are safe, of good quality and affordable
Some products likely more feasible for local production than others e.g. blood products, antivenom sera
Locally produced medicines must meet international standards for Quality, Safety and Efficacy
– Risk-based step-by-step approach possible, but no compromise on final goal
33 |
Concluding remarks (1) Concluding remarks (1)
Governments' commitment to create enabling environment for access to quality medicines in all of its complexity is important
– Good Governance principles implemented, especially in pharmaceutical sector, are one of the foundation
Efficient highly qualified national regulatory authority is a must
Sub-regional and regional collaboration between governments and regulators is vital to create a predictable harmonized "quality market for quality products"
34 |
Concluding remarks (2)Concluding remarks (2)
WHO has promoted regulatory capacity building, collaboration and harmonization long time and will continue to do so being open to new ideas
Making medicines is not any more a "local" business and the era of only locally operating regulators with different standards starts to end
Through its prequalification programme and other technical activities WHO has obtained unique experience and expertise about the problems existing.
WHO has also given substantial technical help to local manufacturers including API manufacturers in China and FPP manufacturers in several regions including Africa.
35 |
The time of poor quality medicines for poor people should be over Poor people also deserve good quality medicines
Regulators have important role to play to make it happen


















