“Introduction to AROC” A NATIONAL CLINICAL …€¦ · Establishing and Maintaining a National...
35
AROC Establishing and Maintaining a National Clinical Registry Frances Simmonds, AROC Director
Transcript of “Introduction to AROC” A NATIONAL CLINICAL …€¦ · Establishing and Maintaining a National...

AROC Establishing and Maintaining a National
Clinical Registry Frances Simmonds, AROC Director

A Australasian R Rehabilitation O Outcomes C Centre
A National Clinical Rehabilitation Registry

Rehabilitation population
• About 20% of Australians have a disability and 6% of the population has a profound or severe activity limitation.
• An increasing percentage of older people live alone - the ability to live in the community is often more dependent on functional independence than on medical factors

History of AROC - 1
• No specific way of classifying rehabilitation outside of acute system
• Diagnostic Related Groups (DRG’s) have 3 rehab codes; not specific
• Only one ICD-10 code for rehab, gives limited insight into rehabilitation

History of AROC - 2
• The Australian government commissioned study... • The Australian National Sub-Acute and Non-Acute
Case-mix Classification (AN-SNAP) developed by CHSD, University of Wollongong in 1997 – A bottom – up costing study – Identified the drivers in rehabilitation – Recorded RUG-ADL, Barthel, FIM – Recorded activity in 15 minute intervals

AN-SNAP classification study
• Involved 99 Australian and 5 NZ rehab units • Collected detailed clinical, service utilisation
and cost profile on over 30,000 sub-acute and non-acute episodes of care over a 3 month period – Sub-acute care - enhancement of quality of
life and/or functional status – Non-acute care - maintenance of current
health status if possible • v4 AN-SNAP in development
History of AROC - 3
• Rehabilitation doctors very involved in AN-SNAP project
• Wanted to use classification to begin to compare outcomes between different services
• Facilitated meeting of rehab sector stakeholders with objective of developing a national benchmarking system
• Outcome was business plan for development of AROC

AROC born in 2002 • AROC began as a joint initiative of the whole
Australian rehabilitation sector (providers, payers, regulators and consumers) with support from key New Zealand providers
• Established 1 July 2002 as a not-for-profit Centre • The Australasian Faculty of Rehabilitation Medicine
(AFRM) is the auspice body • The Australian Health Services Research Institute
(AHSRI) at the University of Wollongong is the data manager and responsible for AROC’s day to day operations

AROC Purpose
The purpose of AROC was established as, and continues to be:
• Develop a national benchmarking system to improve clinical rehabilitation outcomes for patients.
• Produce information on the efficacy of interventions through the systematic collection of outcomes information in both the inpatient and ambulatory settings.
• Provide annual reports that summarise the Australasian data.

AROC has 5 roles 1. Management of data - AROC is the national data
bureau that receives and manages data on rehabilitation services in Australia and New Zealand
2. National benchmarking centre providing for rehabilitation services
3. National certification for the Functional Independence Measure (FIM)
4. Education and training and research for the FIM and other rehabilitation outcome measures
5. Research and development - AROC develops research and development proposals and seeks external funding for its research agenda

AROC as sector advocate
• AROC well positioned to promote the importance of rehabilitation in the continuum of care
• When Rehabilitation is effectively provided it: – is the ‘glue’ that sticks together acute care and
community services – results in people with greater functional ability and more
independence – lowers the incidence of readmission back to acute care – minimises the requirement (and cost) of community
services required

AROC coverage – 232 rehabilitation services
NT 2
QLD 32
NSW 86
VIC 42
SA 8
WA 17
TAS 5
ACT 4
New Zealand 39
About 100,000 episodes per annum

AROC Funding
• Core funding – Annual funding – Subscription basis – Data submitting members - $ per bed – Non data submitting members – lump sum based
on historic calculation
• Ad-hoc funding for specific projects

AROC Governance
• Auspice body – AFRM (Australasian Faculty Rehabilitation Medicine)
• MAG – Management Advisory Committee • SCAC – Scientific and Clinical Advisory
Committee

AROC Dataset
• De-identified dataset … part of routine clinical data collection
• Bank of data items • Six possible pathways, each requiring a subset
of data items • Core data items + impairment specific items • Linkage key • Integrates collection of rehab ACHS clinical
indicators

Data Submission
• AROC Online Services (AOS) – Web based data entry – Access to reports – Extract own data
• Upload data to AOS – Data collected in own system – Incorporated in PMS (eg Synaptix, NSW publics;
Meditech, Ramsay) – Uploaded online via specific formatted text file extract

AROC Outputs • Routine periodic benchmarking reports • Annual AROC Report: the state of the rehabilitation
nation • National LOS and FIM Change benchmarks • Facilitate development of impairment specific outcome
targets (workshops) • Jurisdictional benchmarking workshops/quality forums • Data/data analysis access available for bona fide
research • Process support/ help desk (resources, verbal advice) • Training – dataset, FIM, process


Benchmarks by impairment

Benchmarks by AN-SNAP class

Preparation to Collect AROC Data • AROC Membership Form •FIM training/credentialing •AROC dataset training
Data Collection Form • Start with AROC proforma
•Modify to suit Unit’s processes •Submit to Forms Committee for Approval
•Include in Medical Record
Data Collection Process 1 • Rehab team discussion
•Allocate responsibility for each data item (eg. demographic items – admin staff impairment code – rehab physician clinical items – allied health team)
Data Collection Process 2 Use case conference to facilitate data collection directly onto data collection form in medical record, (especially clinical data items like suspension days, co-morbidities,
complications, leave days, relevant dates, FIM scores, etc)
Establish AROC Resource Folder •Keep in location easily accessible by rehab team
members. Include in it: •AROC Impairment Codes and the associated Coding Guidelines, •Suspensions Explained, • the AROC dataset and data dictionary •copies of relevant dataset training slides
Data Entry •Use AROC dataset compliant software
(ie SNAPshot, Synaptix (NSW) HBCIS (Qld) •Provide training for data entry person
•DO NOT require data entry person to make clinical decisions
Data Submission •Submit AROC Online Services (AOS) user name/
password request •Allocate responsibility to extract and submit
AROC data (usually data entry person)
1
2
3 7
6
5
4
Formal Multi-Disciplinary Rehab Plan Document •Part of medical record
•Use to document rehab plan, goals, and progress against these during the episode
FIM Credentialing •Allocate FIM champion
•Key FIM contact for AROC •Responsible to ensure unit staff maintain training and
credentialing status
Benchmarking Reports •Allocate responsibility to distribute
(widely) •Use as part of quality plan
•Use in team planning days (process review and optimisation; patient and/or unit level outcome target
setting)
Recommended AROC Data Collection Process

Benchmarking Reports • AROC provides analysis of each individual
member’s data, and also compares that data to: – themselves over time – analysis of peer providers – the national data – industry developed impairment specific target
outcomes

AROC Reports
• Analysis of all impairments, presenting the facilities data and comparing that to the either all public or all private data and the national data – six monthly
Core Reports
• Graphical representation of each facility against each relevant outcome target, and how the facility compares to peers – six monthly
Outcome Target Reports
• For stroke, brain injury, spinal cord injury, amputations, etc. provide greater analysis at an impairment level, and present facilities data and compare that to the national data - annually
Impairment Specific Reports

Benchmarking reports
AROC Benchmarking Reports are available to facility members electronically twice yearly

Anywhere Hospital
AROC Outcome Targets Report Inpatient – Pathway 3
July 2012 – June 2013
Australasian Faculty
of Rehabilitation
Medicine

Impairment Specific Outcome Targets
• Benchmarking workshop & development of impairment specific outcome targets driven by desire to: – evolve benchmarking beyond comparison of actual to
aspiration for an (evidence based) target
– focus benchmarking at the impairment level
– identify and collect impairment specific data items … which may include additional outcome measures especially relevant to a given impairment
Page 27
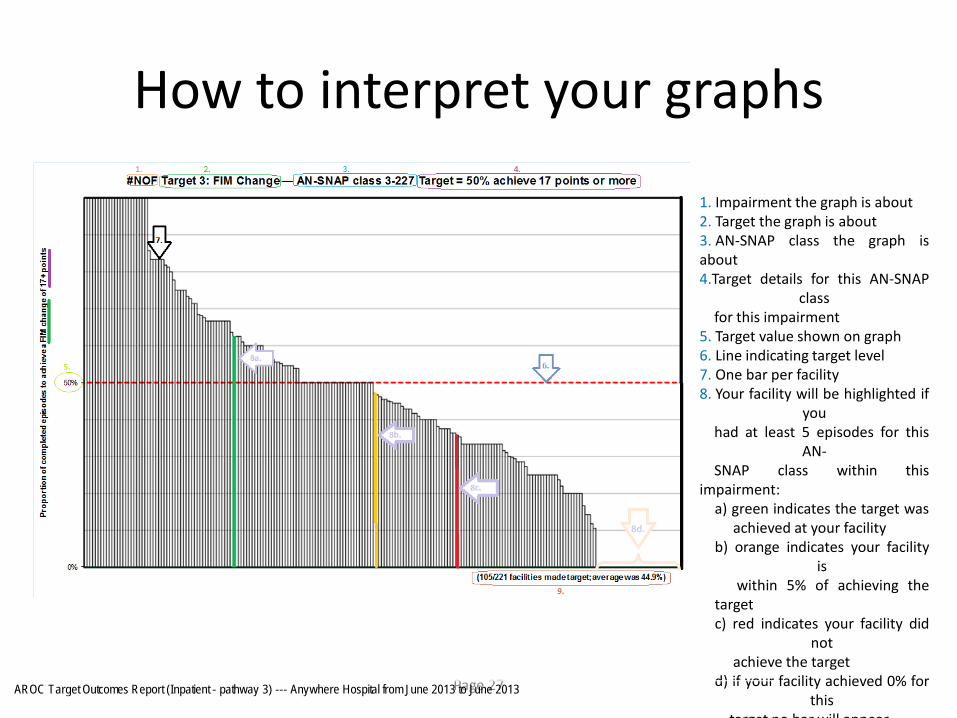
How to interpret your graphs
1. Impairment the graph is about 2. Target the graph is about 3. AN-SNAP class the graph is about 4.Target details for this AN-SNAP
class for this impairment 5. Target value shown on graph 6. Line indicating target level 7. One bar per facility 8. Your facility will be highlighted if
you had at least 5 episodes for this
AN- SNAP class within this impairment:
a) green indicates the target was achieved at your facility b) orange indicates your facility
is within 5% of achieving the target c) red indicates your facility did
not achieve the target d) if your facility achieved 0% for
this target no bar will appear
8d.
AROC Target Outcomes Report (Inpatient - pathway 3) --- Anywhere Hospital from June 2013 to June 2013

AROC Impairment Specific Report Inpatient – Pathway 3
ORTHOPAEDIC FRACTURES
January 2012 – December 2012
Australasian Faculty
of Rehabilitation
Medicine
Anywhere Hospital

Case mix adjustment

Casemix Adjustment
• AROC uses the AN-SNAP classification to statistically control for differences in the types of patients attending different hospitals
• Once we control for differences in the mix of patients, remaining differences in rehabilitation service performance start to reflect real differences between providers
• Facility LOS and FIM change adjusted for casemix to compare with sector data

CARMI – Facility LOS (Expected, Actual, Difference)
31

CARMI – Facility FIM Motor change (Expected, Actual, Difference)
32

Conclusion • Casemix information is now routine in Australia • Due to AROC, measuring rehabilitation patient
outcomes is also now routine • AROC data used in day to day clinical decision
making as well as benchmarking/ review/ reflection • Data collection integrated into standard
rehabilitation processes • Continue to learn how to use data to drive
improvements in both efficiency and patient outcomes

EVIDENCE

AROC Contact Details
Australasian Rehabilitation Outcomes Centre Australian Health Services Research Institute
iC Enterprise 1, Innovation Campus University of Wollongong NSW 2522
Phone: 02-4221-4411 Email: [email protected]
Web: ahsri.uow.edu.au/aroc