Introduction Coagulation Disorders Hemostasis Management Extrinsic Pathway Intrinsic Pathway...
49
Introduction Coagulation Disorders Hemostasis Management Extrinsic Pathway Intrinsic Pathway Medications Labs Clinical Application Summary QUIZ Coagulation Disorders (Coagulopathy Presented by: Nardalyn Johnson, RN MSN Student Alverno College April 22, 2010 In collaboration with: Jim Molnar, APRN – Preceptor Jan Theis, APRN MSN 621 Instructors: Patricia Bowne Luanne Wielichowski
-
Upload
rachel-wilson -
Category
Documents
-
view
235 -
download
1
Transcript of Introduction Coagulation Disorders Hemostasis Management Extrinsic Pathway Intrinsic Pathway...

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Coagulation Disorders (Coagulopathy)
Presented by:Nardalyn Johnson, RN
MSN StudentAlverno College
April 22, 2010
In collaboration with:Jim Molnar, APRN – Preceptor
Jan Theis, APRN
MSN 621 Instructors:Patricia Bowne
Luanne Wielichowski

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
INTRODUCTION
The Interventional Radiology (IR) department multidisciplinary team works with patients who have various types of coagulation disorders.
Hemostasis management is complex due to the wide array of patient co-morbidities and demographics.
Coagulation Disorders
Malloy, P.C., Grassi, C. J., Kundy, S., Gervais, Miller, D. L., Osnis, R. B. et al. (2009). Consensus Guidelines for
Periprocedural Management of Coagulation Status and Hemostasis Risk in Percutaneous. Society of Interventional Radiology.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
• Objectives– Review importance of hemostasis management
in IR – Review coagulation disorders– Review the coagulation cascade (intrinsic and
extrinsic pathways)– Identify common lab tests– Identify common medications that can affect
hemostasis– Focus on clinical application of hemostasis in IR
Special Note:– Whenever you see an underlined word, move the
curser over the underlined word to view more information
Coagulation Disorders

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
A group of conditions that cause an individual to experience either:
Excessive bleeding
Excessive Clotting
Coagulation Disorders
Wellcome Images
Porth, C.M., 2005. Pathophysiology, 7th edition. Lippincott.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
A 49 yr old male Presents to IR for placement of a permCath to initiate dialysis. He returns to IR the following day due to excessive bleeding
during dialysis.
BP 159/75 HR 76 Temp 97.8Lab: INR 1.8 (0.9 – 1.3)
Case Study
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Why Does the IR multidisciplinary team need
to be concerned about patients with clotting or
bleeding disorders?
Hemostasis management
Coagulation Disorders
Click the diagram to reveal the answer

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Hemostasis
Definition: Hemostasis is the process of stopping blood loss.
This process occurs via the hemostatic mechanism known as blood coagulation
It is regulated by “activators” and “inhibitors”.
If Normal
If Abnormal
Seals blood vessels and prevents blood loss and
hemorrhage
Causes inappropriate bloodclotting or excessive bleeding
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
• Prevents cancellation of IR procedures due to appropriate pre-op procedure not done
• Prevents excessive bleeding pre, intra, or post procedure
• Decreased risk for post-procedural thrombosis
• Achieves hemostasis pre, intra, and prior to discharge
• Helps with healing
• Provide appropriate patient education
• Identify new protocols for patients with coagulation disorders
• Early identification of at risk patients pre-procedure
Why is Hemostasis Management Important?
http://www.vascularsolutions.com/company-info/contact
Nursing Outcomes
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Coagulation Disorders
Hemostasis management for patients undergoing percutaneous image-guided procedures can be complex due to the wide range of procedures and equally wide range of patient demographics and co-morbidities.
Some patients are on special medications that increase their risk for bleeding or have internal stents or other devices that predispose them to forming clots.
Microsoft clipart
Microsoft clipart
Malloy, P.C., Grassi, C. J., Kundy, S., Gervais, Miller, D. L., Osnis, R. B. et al. (2009). Consensus Guidelines for
Periprocedural Management of Coagulation Status and Hemostasis Risk in Percutaneous. Society of Interventional Radiology.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Five Stages for Achieving HemostasisClick each box along the pathway to reveal the steps
Move the curser over the underlined word to view more information
A Closer Look at “Hemostasis process”
Vessel spasm
Formation of platelet plug, platelet adhesion, & aggregation
Formation of fibrin clot and activationof intrinsic or extrinsic coagulation cascade
Clot retraction
Clot dissolution
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Clot retraction normally occurs within ____time
after a clot is formed
Coagulation Disorders
5 to 10 minutes 8 to 10 hours
2 to 4 hours 20 – 60 minutes
Clot retraction: is when the blood clot becomes smaller, squeezing serum from the clot and joining the edges of the broken vessel
Incorrect… This is abnormal and
could be due to low platelet
count
CORRECT!This is key
for hemostasis
NO…….This is not enough time and you are at risk for bleeding
TRY AGAIN…….It begins shortly after formation
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
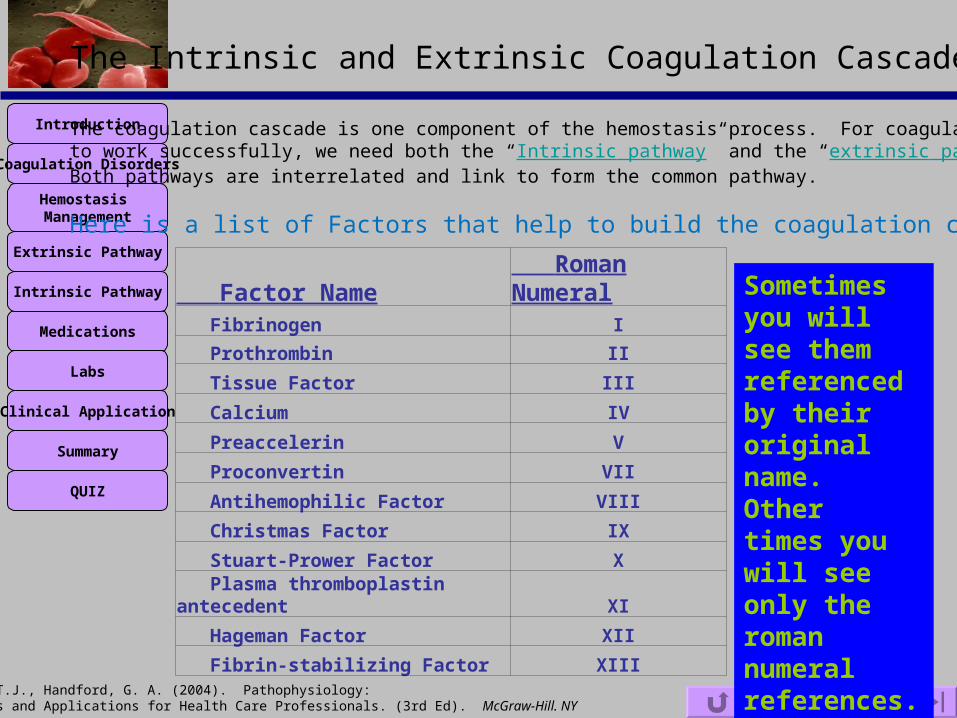
Factor Name Roman Numeral Fibrinogen I
Prothrombin II
Tissue Factor III
Calcium IV
Preaccelerin V
Proconvertin VII
Antihemophilic Factor VIII
Christmas Factor IX
Stuart-Prower Factor X
Plasma thromboplastin antecedent XI
Hageman Factor XII
Fibrin-stabilizing Factor XIII
The Intrinsic and Extrinsic Coagulation Cascade
The coagulation cascade is one component of the hemostasis process. For coagulationto work successfully, we need both the “Intrinsic pathway” and the “extrinsic pathway.” Both pathways are interrelated and link to form the common pathway.
Here is a list of Factors that help to build the coagulation cascade
Sometimes you will see them referenced by their original name. Othertimes you will see only the roman numeral references.
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
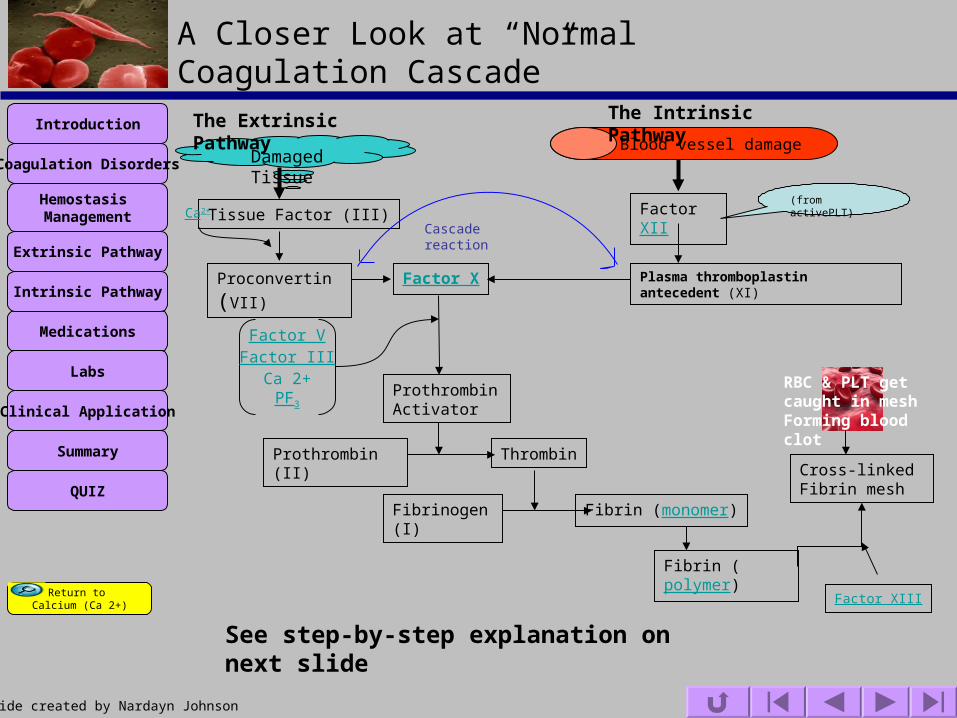
Damaged Tissue Blood vessel damage
The Extrinsic Pathway The Intrinsic Pathway
Tissue Factor (III)
Proconvertin(VII)
Ca2+
Factor X
ProthrombinActivator
Thrombin
Fibrinogen (I) Fibrin (monomer)
Fibrin (polymer)
A Closer Look at “Normal Coagulation Cascade”
Factor XII(from activePLT)
Plasma thromboplastin antecedent (XI)
Cascade reaction
Factor VFactor III
Ca 2+PF3
Prothrombin (II)Cross-linked Fibrin mesh
Factor XIII
RBC & PLT get caught in meshForming blood clot
See step-by-step explanation on next slide
Return to Calcium (Ca 2+)
Slide created by Nardayn Johnson
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
The extrinsic pathway gets initiated when there is damage to blood vessels or surrounding tissue (usually a fast process).
Factor III is released in response to damaged tissue which then
activates Factor VII with the help of calcium ions.
The intrinsic pathway (a slower process) is then activated when factor XI gets activated by Factor XII from active platelets.
Activated factor XI and factor VII cause a cascade reaction which leads to the activation of factor X.
Activated Factor X with the help of calcium ions, Factor III, Factor V, and PF3 activates prothrombin activator which then converts prothrombin to thrombin.
Next, thrombin converts fibrinogen to fibrin which forms a loose mesh.
Fibrin along with factor III forms a denser network of mesh fibers which can trap RBC & PLT forming a successful clot.
The Coagulation Cascade Explained(See previous slide)
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Blood coagulation requires systematic activation of coagulation factors controlled by activators and inhibitors.
It is vital to promoting healing after a patient undergoes any percutaneous imaging procedure.
The Intrinsic and Extrinsic Coagulation Cascade
Microsoft clipart
Porth, C.M., 2005. Pathophysiology, 7th edition. Lippincott.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
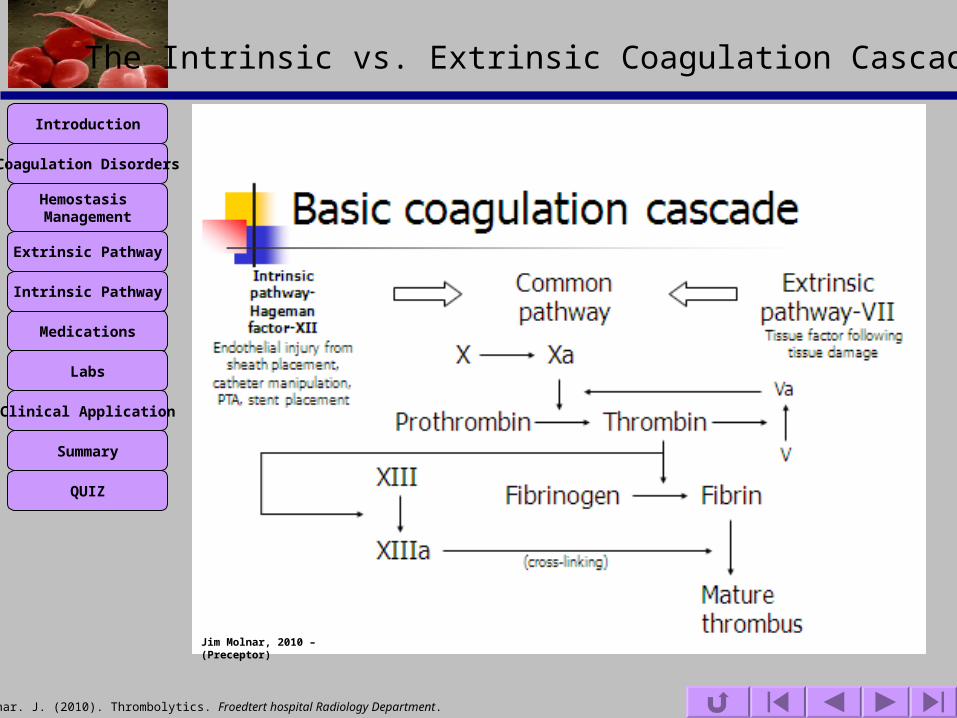
The Intrinsic pathway
A slow ProcessBegins in the blood itself
The Extrinsic pathway
A faster ProcessBegins with damage to blood vessel or surrounding tissue
The Intrinsic vs. Extrinsic Coagulation Cascade
Need both for Hemostasis
The activation of one procoagulation factor/enzyme leads to the activation of the next factor, similar to a domino effect.
“Most of the inactive procoagulation factors are present in the blood all the time.” (Porth, 2005)
Damage to tissue
Extrinsic pathwayGets activated
Small amount of Thrombin formed
Stimulus to Intrinsicpathway
Formation of moreThrombin
Produce large Amount of Fibrin
CoagulationSuccessful
+
Return to Protein C
Porth, C.M., 2005. Pathophysiology, 7th edition. Lippincott.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
CASE STUDY:
Recall the 49 yr old male who presented to IR for placement of a permCath to initiate dialysis.
He returned to IR the following day due to excessive bleeding problems during dialysis.
A defect in which pathway would cause bleeding problems?
Extrinsic Pathway
Try Again. This is not be most correct response
Intrinsic PathwayTry Again
There’s a better answerThink about the procedure performed
The Intrinsic vs. Extrinsic Coagulation Cascade
Both
Correct!
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
The Intrinsic vs. Extrinsic Coagulation Cascade
Jim Molnar, 2010 – (Preceptor)
Molnar. J. (2010). Thrombolytics. Froedtert hospital Radiology Department.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Abnormality in the clotting process can result if there is a problem with one or more factors (Porth, 2005).
This can lead to inappropriate activation at any point along the pathway depending on the factor(s)causing the problem (Nowak, 2004).
The Intrinsic vs. Extrinsic Coagulation Cascade
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY
Porth, C.M., 2005. Pathophysiology, 7th edition. Lippincott.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
• Calcium plays a key role in the coagulation cascade. It is “required in all but the first two steps of the clotting process.” (Porth, 2005)
• 3 types of calcium (calcium salts, protein bound, and ionized calcium)• **ionized calcium** aid in coagulation cascade
• Calcium = Factor IV
• Only need a small amount so patients with calcium deficiency will not necessarily exhibit any significant effect on coagulation cascade.
• If calcium gets inactivated when it is removed from the body, then blood will not clot.Think about the EDTA tubes that you use to collect blood. They contain chelating agent thatinactivates Ca++ that prevents the blood from clotting.
Ca2+
Calcium (ionized)
View coagulation pathway
Why are Ca 2+, Vitamin K, Protein C, and Platelets Important?
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
VITAMIN K
FUNCTION OF VITAMIN K: Needed by liver to produce clotting factors Needed to produce clotting Factors such as VII, IX, X and to synthesize Protein C Helps to regulate calcium…keeping it in your bones and out of your blood
Watch patients who are taking warfarin as it can decrease clotting by interfering with vitamin K and increase risk for excesses bleeding after a procedure You do not need much—just enough to prevent you from bleeding to death Older patients will need more vitamin K
Is a fat soluble vitamin andwithout it your blood will not clot
Why are Ca 2+, Vitamin K, Protein C, and Platelets Important?
http://www.hemophilia.org/NHFWeb/MainPgs/MainNHF.aspx?menuid=176&contentid=378&rptname=bleeding

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Protein C
A special anticoagulant protein. Activated Protein C functions as an anticoagulant, limiting clot formation (down regulates the coagulation cascade). Resistance to activated Protein C prevents Protein C from cleaving to Factor V and/or VIII.
You need the help of vitamin K to help build Protein C.
Do not confuse this with “C-reactive protein.” This is produced in the liver and is a
bi-product of inflammation.
Why are Ca 2+, Vitamin K, Protein C, and Platelets Important?
View Positive feedback
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
You found out during testing that JT has a Protein C deficiency.
This deficiency predisposes him to __________?
Venous Thrombosis
Click here
Why are Ca 2+, Vitamin K, Protein C, and Platelets Important?

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Why are Platelets important for Hemostasis?
Platelets are very important in hemostasis management
You need enough to prevent excessive bleeding, but too many can be problematic because they cause hypercoagulation
Some patients may have internal stents or other devices that predispose them to forming clots
Cancer patients who have decreased platelet count are at increased risk for bleeding
Wellcome Images
King, K. W. (2010). Platelet Activation and von Willebrand Factor (vWF). IU School of Medicine.
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Why are Platelets important for Hemostasis?
CASE STUDY
KLS presents to IR for permCath evaluation due to poor blood flow. This is his third visit to IR in one mouth.
KLS requests a new catheter because he believes something is wrong with the current catheter.
Lab tests prior to procedure reveal:INR=1.0 (0.9-1.3), Plt = 654 (150-350), PTT 24 (25-33)
You change the catheter, but two weeks later he is back again. It makes no sense to keep changing the catheter. It appears his bodyis forming thrombi around the catheter causing decreased blood flow.
Medical Decision: In addition to performing a catheter stripping procedure, he is started on Aspirin 325 mg by mouth MWF to help decrease platelet aggregation. Aspirin would help to decrease platelet aggregation.
Microsoft clipart
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
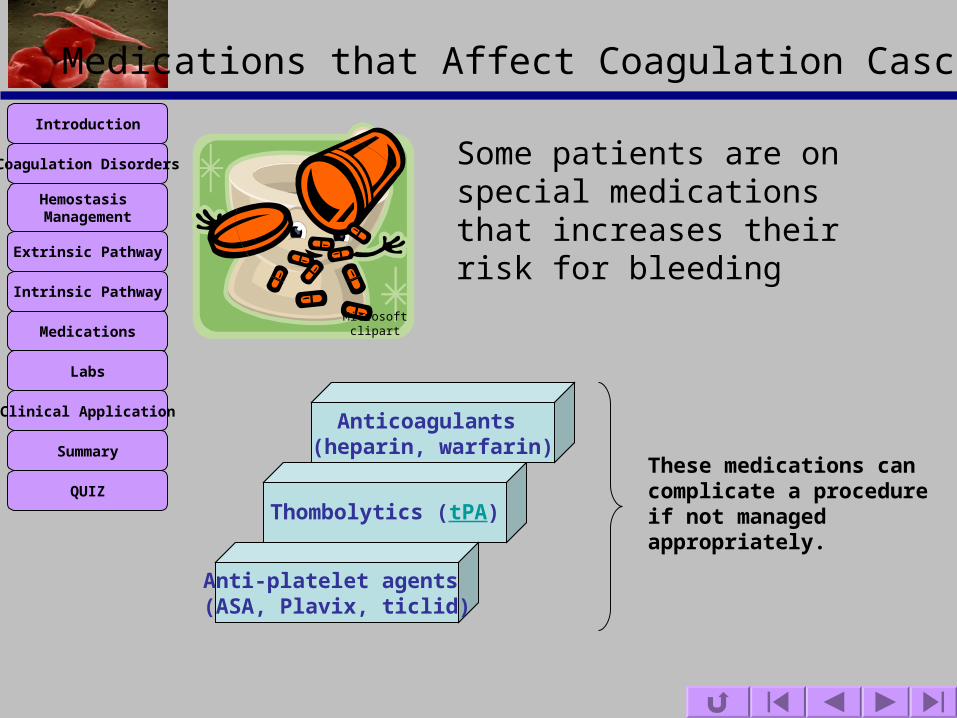
Medications that Affect Coagulation Cascade
Some patients are on special medications that increases their risk for bleeding
Thombolytics (tPA)
Anticoagulants (heparin, warfarin)
Anti-platelet agents (ASA, Plavix, ticlid)
These medications can complicate a procedure if not managed appropriately.
Microsoft clipart

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Anticoagulants
Medications that Affect Coagulation Cascade
Two commonly used drugs in the US are:
Warfarin (Coumadin) Heparin
Vitamin K antagonist
Decrease production ofFactors II, VII, IX, X
Prevent thrombosis
Activate anti-thrombin III
Blocks thrombin
Warfarin: is “prescribed to ~2 million newpatients per Year in US” (USA Today, 2010).Therefore, your chance of having a patient on this medication is high.
E.g. prescribed to patients with history ofDVT, PE, prosthetic heart valve etc. Anticoagulants help with hemostasisby preventing inappropriate blood clotting in vessels.
They chip away at clot making it smaller
Prevents thrombosis in veins
Close hemostasis management is important pre, intra, and post procedure to prevent excessive bleeding complications.
Remember labs: INR, PT
Heparin - released from tissue basophils and inactivates thrombin.
Sternberg, S. (2010). Gene test cuts complications from blood thinner warfarin. USA Today.
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
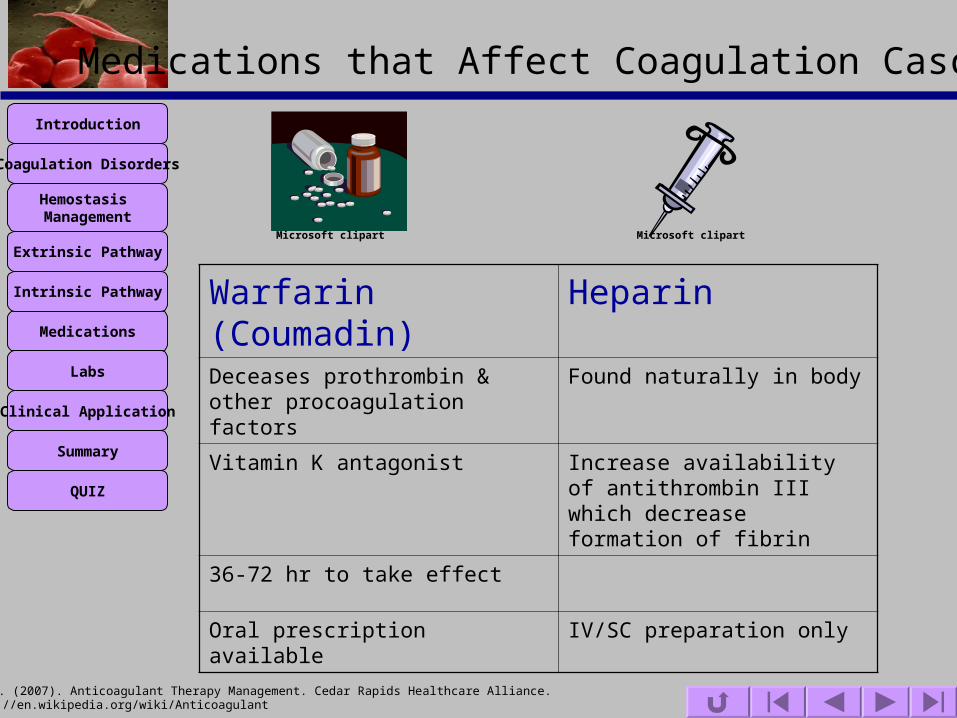
Medications that Affect Coagulation Cascade
Warfarin (Coumadin) HeparinDeceases prothrombin & other procoagulation factors
Found naturally in body
Vitamin K antagonist Increase availability of antithrombin III which decrease formation of fibrin
36-72 hr to take effect
Oral prescription available IV/SC preparation only
Microsoft clipart Microsoft clipart
Huber, C. (2007). Anticoagulant Therapy Management. Cedar Rapids Healthcare Alliance.http://en.wikipedia.org/wiki/Anticoagulant

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Medications that Affect Coagulation Cascade
Why Give Heparin by IV or SC preparation Versus taking it by mouth?
Answer
It is unable to cross membrane of GI Tract

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Medications that Affect Coagulation Cascade
A patient scheduled for central line placement in IR with a recent history of Pulmonary Emboli (PE)
Anticoagulant medication: Warfarin 4 mg by mouth dailyRecent lab: INR 2.1 (0.9-1.3)
Which of the following instructions should be given to the patient?
a) Hold Warfarin 3 days before procedure Initiate Lovenox therapy Hold AM dose of Lovenox prior to procedure Recheck INR prior to procedure
b) Hold Warfarin 7 days before procedure Initiate Lovenox therapy Hold AM and PM dose of Lovenox prior to procedure Recheck INR prior to procedure
c) Hold Warfarin 5 days prior to procedure
X NoOnly need 3 days
X Try Again
Correct Due to different half live of preformed clotting factors
Click on the correct response:

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Medications that Affect Coagulation Cascade
Article Published by USA Today 3/16/2010 Title: Gene Test Cuts Complication from Blood Thinner
Warfarin
Points from article:
It takes time for a doctor to settle on a safe and effective dose when prescribing warfarin.
“Roughly 1 in 5 patients are hospitalized for bleeding within six months of starting the drug. Others develop a life-threatening blood clot.”
“Warfarin is the second-greatest cause of hospitalization due to drug complication.”
“Warfarin is prescribed to 2 million new patients in the USA each year.”
Genetic tests can be used to personalize warfarin treatment and decrease the rate of hospitalization.
See full article at: http://www.usatoday.com/news/health/2010-03-16-warfarin-gene_N.htm
Sternberg, S. (2010). Gene test cuts complications from blood thinner warfarin. USA Today.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Thombolytics (tPA)
Medications that Affect Coagulation Cascade
TB reported to IR for tunneled catheter evaluation with a report from the dialysis center of poor blood flow.
Medical decision: tPA catheterPost evaluation: Catheter flush & aspirate w/o difficulty
A protein that breaks down blood clot
CatalysesPlasminogen
Plasmin
FibrinDegradation
A clot-busting medication
Important for cell migration and tissue healing
Increase activity = increase bleeding
Decreased activity = thrombosis
tPA
FMLH Radiology
Thrombolytic drug. Retrieved March 19, 2010 from http://en.wikipedia.org/wiki/Thrombolytic_drug

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Anti-platelet agents
Medications that Affect Coagulation Cascade
Suppress platelet aggregation
Prevent thrombosis in arteries whileanticoagulants (Warfarin & heparin,
Prevent thrombosis in veins
Inhibit COX enzyme
Decrease Platelet Synthesis of TXA2
Decrease Pathway in platelet activation
Two commonly used drugs in the US are:
Aspirin (ASA) Ticlid
Blocks ADP receptor on platelet
surface
Prevent Thrombusformation
Antiplatelet. Retrieved March 19, 2010 from http://en.wikipedia.org/wiki/Antiplatelet_drug
King, K. W. (2010). Platelet Activation and von Willebrand Factor (vWF). IU School of Medicine.
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
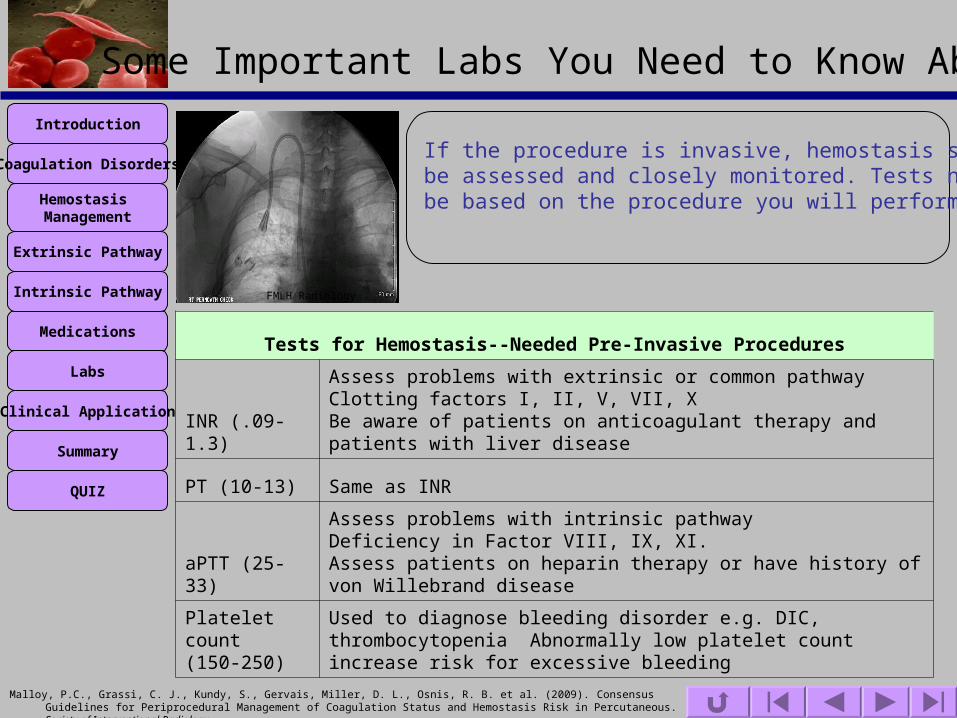
Some Important Labs You Need to Know About
If the procedure is invasive, hemostasis status should be assessed and closely monitored. Tests needed will be based on the procedure you will perform.
Tests for Hemostasis--Needed Pre-Invasive Procedures
INR (.09-1.3)
Assess problems with extrinsic or common pathwayClotting factors I, II, V, VII, X Be aware of patients on anticoagulant therapy and patients with liver disease
PT (10-13) Same as INR
aPTT (25-33)
Assess problems with intrinsic pathway Deficiency in Factor VIII, IX, XI. Assess patients on heparin therapy or have history of von Willebrand disease
Platelet count (150-250)
Used to diagnose bleeding disorder e.g. DIC, thrombocytopenia Abnormally low platelet count increase risk for excessive bleeding
FMLH Radiology
Malloy, P.C., Grassi, C. J., Kundy, S., Gervais, Miller, D. L., Osnis, R. B. et al. (2009). Consensus Guidelines for Periprocedural Management of Coagulation Status and Hemostasis Risk in Percutaneous. Society of Interventional Radiology.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Functions of the Liver
Most clotting Factors are produced in the liver
Factor Name Roman Numeral Source Fibrinogen I Liver
Prothrombin II Liver * * Tissue Factor III Damages cells
Calcium IV Gut and bone
Preaccelerin V Liver and platelet
Proconvertin VII Liver * *
Antihemophilic Factor VIII Platelets and endothelium
Christmas Factor IX Liver * *
Stuart-Prower Factor X Liver * *
Plasma thromboplastin antecedent XI Liver
Hageman Factor XII Liver
Fibrin-stabilizing Factor XIII Liver
* * Dependent on vitamin K for synthesis in liver
Microsoft clipart
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
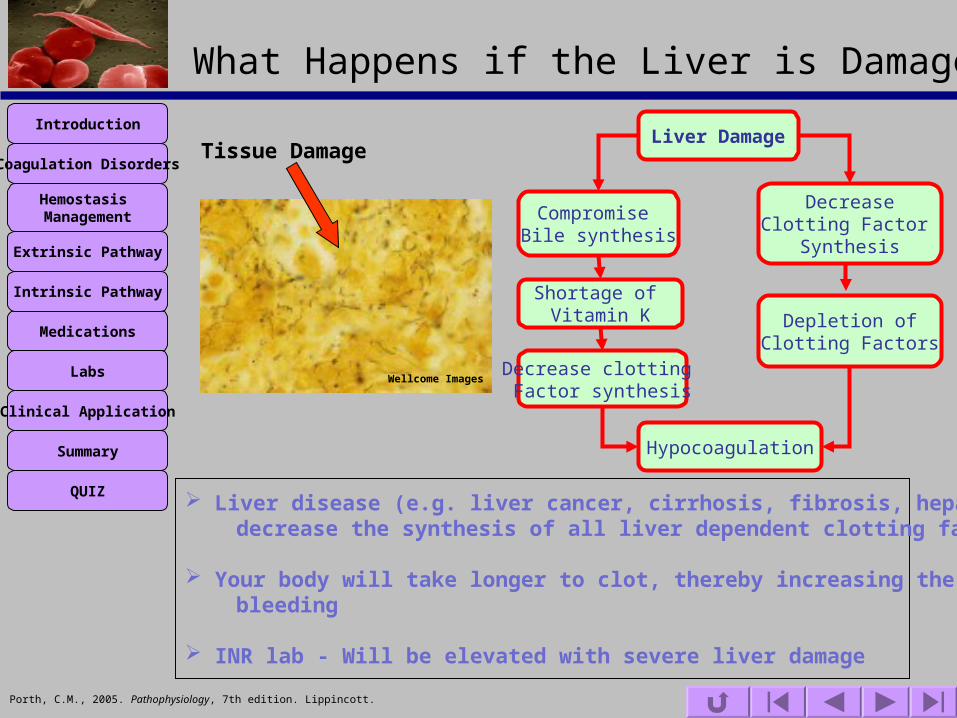
What Happens if the Liver is Damaged?
Tissue DamageLiver Damage
DecreaseClotting Factor
Synthesis
Depletion ofClotting Factors
Hypocoagulation
Compromise Bile synthesis
Shortage of Vitamin K
Decrease clotting Factor synthesis
Liver disease (e.g. liver cancer, cirrhosis, fibrosis, hepatitis) will decrease the synthesis of all liver dependent clotting factor
Your body will take longer to clot, thereby increasing the risk for bleeding
INR lab - Will be elevated with severe liver damage
Wellcome Images
Porth, C.M., 2005. Pathophysiology, 7th edition. Lippincott.
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Case Study
Patient with increased liver function test present to IR for liver biopsy
History of ESRD, kidney transplant, on immunosuppression,basal cell carcinoma, fatty liver
Lab: Liver fn panel, Plt 99 (150-350) Hgb 7.2 Stat type & cross
IR medical team decision: 2 units packed RBC ordered, 1 unit infused prior to
procedure
What happens if the Liver is Damaged?

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Role of Inflammation & Effects on Coagulation
• Inflammation is a biochemical and cellular process that occurs in vascularized tissues
• Inflammation in the liver will affect coagulation
Tissue
Damage
Liver Damage
DecreaseClotting Factor
Synthesis
Depletion ofClotting Factor
Hypocoagulation
Inflammation
Wellcome Images
Porth, C.M., 2005. Pathophysiology, 7th edition. Lippincott.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
chronic inflammatory process (outside the liver) can trigger the clotting cascade.
Clotting causes damage through lack of perfusion (ischemia) to vital organs, such as the liver, kidneys, heart which would then activates the clotting cascade which increase clotting.
Role of Inflammation & Effects on Coagulation
Decrease activity of natural anticoagulant mechanism
Hypercoagulation
Chronic Inflammation
Impairs Fibrinolytic system
Esmon, C. T. (2005). The interactions between inflammation and coagulation . British Journal of Haematology. 131(14) 417-430.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Which of these Factors is not synthesized in the liver?
a) Prothrombin (Factor II)
b) Antihemophilic Factor (Factor VIII)
c) Hageman Factor (Factor XII)
d) Stuart-Prower Factor (Factor X)
X Incorrect
X No
X Try Again
CorrectSource: Platelets and endothelium
Click on the correct response:
What happens if the Liver is Damaged?

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
•The stress response protects the individual from threats to homeostasis.• Trauma as a result of percutaneous image-guided procedures can induce the stress response
Stress Adaptation Response & Effects on Coagulation
Case Study
50 yr old Male presents to IR for treatment with drug eluting bead chemoembolization
Diagnosed with neuroendocrine cancer w/liver metastasisHad multiple hypertensive crises recently
BP 133/65 R=18 HR 72 wt=245#
The patient is at risk of a hypertensive crisisMed requested = Alpha blockade
Medication ordered = phentolamine (REGITINE) 5 mg
Reason: Phentolamine prevent stress response (hypertensive crisis) which may occur due to stress or due to a surgical procedure.
Hypertension damages the blood vessels thereby affecting the coagulation cascade
Microsoft clipart
Hehne, R. A. (2004). Pharmacology for Nursing Care. (5th Ed). Saunders. Missouri

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Role of Aging & Effects on Coagulation
Aging
**Defective VesselSupport Due to
Weakness in Connective Tissue
IncreaseBleeding Risk
Increased Vessel Fragility
Aging
Vitamin KDeficiency **
DecreasedClotting Factor
Synthesis by Liver
Hypocoagulation
** Older patients will need more vitamin K** With aging, the skin becomes thinner so tissues supporting underlying blood vessels are more fragile
Microsoft clipart
Toloza, E, (2005). Bruises. Department of Emergency Medicine, University of Texas at Houston School of Medicine.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Role of Genetics & Effects on Coagulation
Deficiencies in clotting factors may be due to genetics
Factor VIII/IX Deficiency Hemophilia
Factor V Deficiency Owren’s Disease
Factor X DeficiencyStuart-Prower Factor Deficiency
Microsoft clipart
Taylor, A.K. (1997). Venous Thrombosis and the Factor V (Leiden) Mutation. The Mountain States Genetics Foundation (14).
For all Bleeding and Clotting Disorders. Retrieved March 8, 2010 from http://www.hemophilia.org/NHFWeb/MainPgs/MainNHF.aspx?menuid=176&contentid=378&rptname=bleeding
Porth, C.M., 2005. Pathophysiology, 7th edition. Lippincott.

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
Video Links
1. http://www.hopkinsmedicine.org/hematology/Coagulation.swf
A review of the coagulation cascade can be found at the following link
Microsoft clipart

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
List The Five Stages for Achieving HemostasisClick each box to reveal the correct response
A Closer Look at the “Hemostasis Process”
Vessel spasm
Formation of platelet plug, platelet adhesion, & aggregation
Formation of fibrin clotActivate intrinsic or extrinsic coagulation cascade
Clot retraction
Clot dissolution
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
The Interventional Radiology (IR) department multidisciplinary team work with patients who have various types of coagulation disorders. Hemostasis management is complex due to the wide array of patient co-morbidities of patients undergoing percutaneous image-guided procedures in IR. This complexity is further complicated by the wide range of procedures and patient demographics.
Some patients are on special medications that increases their risk for bleeding or have internal stents or other devices that predispose them to forming clots.
The use of Thombolytics (tPA), anti-coagulants (heparin, warfarin), or anti-platelet agents (ASA, Plavix, ticlid) can complicate a procedure if notmanaged appropriately.
Medical interdisciplinary team understanding of the various coagulation disorders will assist in medical care to patients. This would include pre-op measures to prevent lengthy delays or costly cancellation of procedures.
Summary
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
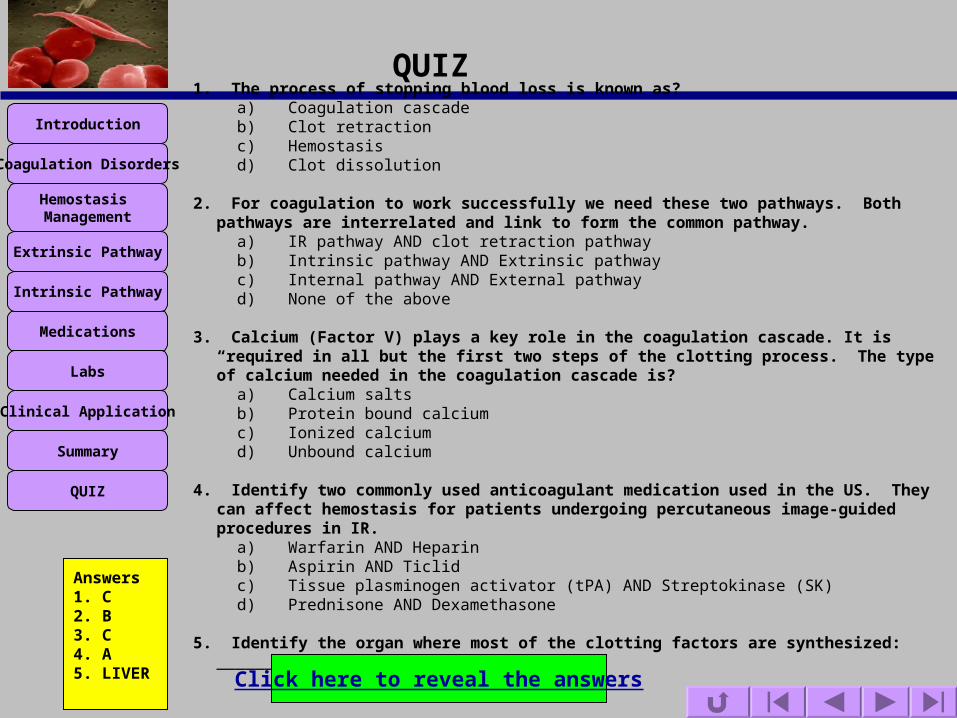
QUIZ
1. The process of stopping blood loss is known as?a) Coagulation cascadeb) Clot retractionc) Hemostasisd) Clot dissolution
2. For coagulation to work successfully we need these two pathways. Both pathways are interrelated and link to form the common pathway.
a) IR pathway AND clot retraction pathwayb) Intrinsic pathway AND Extrinsic pathwayc) Internal pathway AND External pathway d) None of the above
3. Calcium (Factor V) plays a key role in the coagulation cascade. It is “required in all but the first two steps of the clotting process. The type of calcium needed in the coagulation cascade is?
a) Calcium saltsb) Protein bound calciumc) Ionized calciumd) Unbound calcium
4. Identify two commonly used anticoagulant medication used in the US. They can affect hemostasis for patients undergoing percutaneous image-guided procedures in IR.
a) Warfarin AND Heparinb) Aspirin AND Ticlidc) Tissue plasminogen activator (tPA) AND Streptokinase (SK)d) Prednisone AND Dexamethasone
5. Identify the organ where most of the clotting factors are synthesized: ____________________
Click here to reveal the answers
Answers1. C 2. B3. C4. A5. LIVER

Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
References
Porth, C.M., 2005. Pathophysiology, 7th edition. Lippincott.
Nowak, T.J., Handford, G. A. (2004). Pathophysiology: Concepts and Applications for Health Care Professionals. (3rd Ed). McGraw-Hill. NY
Hehne, R. A. (2004). Pharmacology for Nursing Care. (5th Ed). Saunders. Missouri
Rayfield, S., Manning, L. (1998). Nursing made Insanely Easy. (2nd Ed). ICAN Louisiana
Sternberg, S. (2010). Gene test cuts complications from blood thinner warfarin. USA Today.
Huber, C. (2007). Anticoagulant Therapy Management. Cedar Rapids Healthcare Alliance.
Guyton, A.C., Hall, J.E. 2000. Medical Physiology. 10th edition. Saunders.
Malloy, P.C., Grassi, C. J., Kundy, S., Gervais, Miller, D. L., Osnis, R. B. et al. (2009). Consensus Guidelines for Periprocedural Management of Coagulation Status and Hemostasis Risk in Percutaneous. Society of Interventional Radiology.
Hemostasis. Retrieved March 24, 2010 from http://www.mhhe.com/biosci/esp/2002_general/Esp/folder_structure/tr/m1/s7/trm1s7_3.htm
Tissue Plasminogen Activator (tPA). Retrieved March 24, 2010 from http://www.americanheart.org/presenter.jhtml?identifier=4751
Symptoms of Coagulation Disorders. Retrieved March 24, 2010 from http://www.signsofbleeding.com/index.php?page=4
Tissue plasminogen activator. Retrieved March 19, 2010 from http://en.wikipedia.org/wiki/Tissue_plasminogen_activator
Coagulation Cascade. Retrieved March 12, 2010 from http://www.hopkinsmedicine.org/hematology/Coagulation.swf
Thrombophilia or Hypercoagulable States. Retrieved March 12, 2010 from http://www.peds.ufl.edu/residency/resources/hematology/th_states.pdf
Radiological Society of North America (2010). Radiology Info: the Radiology information for patients. Radiological Society of North America, Inc.
For all Bleeding and Clotting Disorders. Retrieved March 8, 2010 from http://www.hemophilia.org/NHFWeb/MainPgs/MainNHF.aspx?menuid=176&contentid=378&rptname=bleeding
Thrombolytic drug. Retrieved March 19, 2010 from http://en.wikipedia.org/wiki/Thrombolytic_drug
King, K. W. (2010). Platelet Activation and von Willebrand Factor (vWF). IU School of Medicine.
Molnar. J. (2010). Thrombolytics. Froedtert hospital Radiology Department.
Anticoagulants. Retrieved March 19, 2010 from http://en.wikipedia.org/wiki/Anticoagulant
Antiplatelet. Retrieved March 19, 2010 from http://en.wikipedia.org/wiki/Antiplatelet_drug
Ganda. K. (2005). The Clotting Pathway. TUFTSOPENCOURSEWARE ,Tufts University.
Toloza, E, (2005). Bruises. Department of Emergency Medicine, University of Texas at Houston School of Medicine.
Introduction
Coagulation Disorders
Hemostasis Management
Extrinsic Pathway
Intrinsic Pathway
Medications
Labs
Clinical Application
Summary
QUIZ
References
Taylor, A.K. (1997). Venous Thrombosis and the Factor V (Leiden) Mutation. The Mountain States Genetics Foundation (14).
mcGilvray,I. , Rotstein, O.D.(2001). Assessment of Coagulation in Surgical Critical Care Patients. Department of surgery, University of Toronto and Toronto General Hospital, Canada.
Esmon, C. T. (2005). The interactions between inflammation and coagulation . British Journal of Haematology. 131(14) 417-430.
Contact InformationNardalyn Johnson, [email protected]