Introducing the cranial approach in osteopathy and the treatment of infants and mothers
5
Introducing the cranial approach in osteopathy and the treatment of infants and mothers Christian Sullivan Osteopathy is one of the most commonly known treatments for lower back pain. However, media coverage is increasingly recognizing the potential of osteopathic care for a wide range of conditions across all age groups. In this article the role of osteopathic care in the treatment of pregnant mothers, the newborn and infants is considered. The aim of this paper is to stimulate further investigation by health care professionals into the potential benefits of osteopathic care for a range of clients. I have avoided lengthy technical aspects, hoping rather to expand on the thinking behind the approach, and welcome correspondence on any aspect of this paper. Unfortunately, there is a lack of good research evidence to date to support many of the claims and assertions made by osteopathy. However, with recent accreditation of the first Osteopathic MSc, a significant accumulation of such data over the next decade is anticipated. Christian Sullivan DO, MRO, Registered Osteopath, 6 Market Street, Bradford on Avon, Wiltshire BAI S I LN, UK (Requests for offprints to CS) BACKGROUND TO CRANIAL OSTEOPATHY In 1899 an osteopathic student William Sutherland observed the detail of the suture bevelling on the edge of the sphenoid bone. He was struck by their similarity to the gills of a fish, and, although he had been taught that the bones of the adult skull were fused, here seemed evidence of a very definite design for motion. He decided to investigate the possibility of inter- cranial bone mobility and spent the next decade try- ing to disprove what he had found. His anatomical studies led him to discover an intricately interrelated system of articulations between the 27 bones of the skull. Motion was indeed present and appeared to have very definite roles. Further exploration uncovered an apparently reciprocal movement of the sacrum between the ilia. Suthertand postulated that the firm attachment of the dura of the central nervous system, firstly at the fora- men magnum and CI-2 cervical vertebrae, then again at the $2 level within the canal of the sacrum, was responsible for this. Over time he described in minute detail the cranial bone sutures and how the course of exiting cranial nerves could be influenced by disturbance in the motion mechanism he had observed. He devised and implemented a series of experiments to discover if these observations were accurate and found that by strapping his own skull to embarrass motion of specific bones he could re-create symptom pictures he was seeing in some of his patients. Sutherland postulated that the central nervous system had an inherent mobility, and that embarrass- ment of this movement by bony restriction would lead to disease states (this is by no means a represen- tation of the totality of Sutherland's concept and is simplified here). In time Sutherland devised diagnostic and treat- ment modalities for the evaluation and treatment of presenting patients. Though initially ridiculed for his ideas, 50 years of further study and investigation have validated many aspects of his work. Under- graduate courses in Sutherland's work are now a standard part of osteopathic training in the UK. HISTORY Whilst osteopathy has recently celebrated the centenary of the establishment of the first college, ComplementaryTherapiesin Nursing & Midwifery (I 997) 3, 72-76 1997PearsonProfessionalLtd
-
Upload
christian-sullivan -
Category
Documents
-
view
213 -
download
1
Transcript of Introducing the cranial approach in osteopathy and the treatment of infants and mothers

Introducing the cranial approach in osteopathy and the treatment of infants and mothers Christian Sullivan
Osteopathy is one of the most commonly known treatments for lower back pain. However, media coverage is increasingly recognizing the potential of osteopathic care for a wide range of conditions across all age groups. In this article the role of osteopathic care in the treatment of pregnant mothers, the newborn and infants is considered.
The aim of this paper is to stimulate further investigation by health care professionals into the potential benefits of osteopathic care for a range of clients. I have avoided lengthy technical aspects, hoping rather to expand on the thinking behind the approach, and welcome correspondence on any aspect of this paper. Unfortunately, there is a lack of good research evidence to date to support many of the claims and assertions made by osteopathy. However, with recent accreditation of the first Osteopathic MSc, a significant accumulation of such data over the next decade is anticipated.
Christian Sullivan DO, MRO, Registered Osteopath, 6 Market Street, Bradford on Avon, Wiltshire BAI S I LN, UK
(Requests for offprints to CS)
B A C K G R O U N D T O C R A N I A L O S T E O P A T H Y
In 1899 an osteopathic student William Sutherland observed the detail of the suture bevelling on the edge of the sphenoid bone. He was struck by their similarity to the gills of a fish, and, although he had been taught that the bones of the adult skull were fused, here seemed evidence of a very definite design for motion.
He decided to investigate the possibility of inter- cranial bone mobility and spent the next decade try- ing to disprove what he had found. His anatomical studies led him to discover an intricately interrelated system of articulations between the 27 bones of the skull. Motion was indeed present and appeared to have very definite roles.
Further exploration uncovered an apparently reciprocal movement of the sacrum between the ilia. Suthertand postulated that the firm attachment of the dura of the central nervous system, firstly at the fora- men magnum and C I - 2 cervical vertebrae, then again at the $2 level within the canal of the sacrum, was responsible for this.
Over time he described in minute detail the cranial bone sutures and how the course of exiting
cranial nerves could be influenced by disturbance in the motion mechanism he had observed. He devised and implemented a series of experiments to discover if these observations were accurate and found that by strapping his own skull to embarrass motion of specific bones he could re-create symptom pictures he was seeing in some of his patients.
Sutherland postulated that the central nervous system had an inherent mobility, and that embarrass- ment of this movement by bony restriction would lead to disease states (this is by no means a represen- tation of the totality of Sutherland's concept and is simplified here).
In time Sutherland devised diagnostic and treat- ment modalities for the evaluation and treatment of presenting patients. Though initially ridiculed for his ideas, 50 years of further study and investigation have validated many aspects of his work. Under- graduate courses in Sutherland's work are now a standard part of osteopathic training in the UK.
H I S T O R Y
Whilst osteopathy has recently celebrated the centenary of the establishment of the first college,
Complementary Therapies in Nursing & Midwifery (I 997) 3, 72-76 �9 1997 Pearson Professional Ltd

The cranial approach in osteopathy 73
A central principle of osteopathic care focuses upon the concept of compensation; that is, structural adaption for an event or previous injury.
the origins of this therapy go back some 35 years. Dr A T Still, a laypreacher and country doctor, devel- oped a system of structural analysis and correction based on the premise that, since man was made in God's image, he was structurally perfect. It was argued that deviation from that structural perfection would lead to disease and ill health.
Still designed a framework in the form of three principles on which to base osteopathic education. These may be familiar now, but need to be consid- ered in the light of emerging 'scientific' health care models of a century ago:
�9 The body is an integral unit. Its structure and function are interdependent.
�9 The body has inherent healing abilities in that body systems have built-in self-regulating and self-healing processes.
�9 The circulatory system, along with the nervous system, provides the integrative function in these relationships.
Still maintained that compromise in the control of circulatory and drainage function of the body was the root cause of the disease state and that structural anomalies and dysfunctions would probably be iden- tifiable as the maintaining factor of ill health, The cause could be remote from the symptomatic site and thus a need for a holistic evaluation of the patient. Structure and function are interdependent, both at the gross level of the entire organism and at specific anatomical/physiological levels.
OSTEOPATHY TODAY
Osteopathic training consists of 4years ' full-time study. Education includes in-depth study of patho- logy, differential diagnostic clinical methodology, endocrinology and individual body systems. The use of X-ray and other diagnostic tools is examined alongside the development of palpatory skills which are progressively refined over the 4 years. Courses are integrated within the out-patient units attached to each college, in which students must spend some 2000 hours prior to graduation.
Modern anatomy and physiology continue to confirm the pathways by which the treatment regimes effect results. However, people are also per- ceived as unique and subject to the myriad pressures and burdens of life, thus a need for total 'holistic' evaluation of our patients remains paramount.
An osteopathic case history will comprise symp- tom evaluation; extensive clinical review (health care screening past and present, medication usage, etc.); and consideration of social, family and occu- pational factors. It may result in additional tests being ordered or referral to the patient's GP for fur- ther consideration.
When evaluating patients' posture, mechanical structure and movement, emphasis is placed on the need for total integration, and structural as mechani-
cal function is assessed in the patient. Treatment may begin at a site remote from the area of present- ing symptom or pain if it is determined that this is where the greatest effect can be made in relieving stresses on the whole of the person's body.
A central principle of osteopathic care focuses upon the concept of compensation; that is, structural adaption for an event or previous injury. This can lead to a decrease in the overall amount of adaptabil- ity remaining available in that person or system with which to cope with additional stresses. This, if left untended, could lead to further illness.
WHAT TO EXPECT
Treatment from an osteopath trained in these tech- niques is very gentle. There is no gross manual manipulation or 'cracking' of joints. As such, this treatment modality is very well suited to the care of acute problems across the age range from infants to the very elderly. However, whilst many patients benefit from this approach, it is for the treatment of young infants that 'cranial' osteopathy is probably best known at present.
Common problems treated by cranial osteopathy
Osteopaths trained in cranial techniques commonly treat infants and the newborn for conditions such as poor feeding/suckling, feeding patterns where the child pulls away distressed after a few moments, or feeding patterns with regular sickness (often at a similar time interval after feeding). Treatment is directed towards the normalization of tissue tension in the cranial base area and frequently affords relief to the suffering child.
Distortion of the jugular foramen may initiate embarrassment of venous return from the skull by a few per cent. Infants with red or tight shiny scalps may fit well into this group and often present with marked irritability, needing constant attention and distraction to suppress crying. They are often dis- tressed if placed supine and prefer to sit up. These children may respond extremely well to gentle cranial release procedures.
Treatment consists of careful palpatory evalua- tion of the cranial base area to detect the strain pattern and muscular guarding which accompanies such types of sub-acute lesion patterns. Gentle manipulative attention eases and balances tension in the area. No significant external force is applied as the natural expansive agencies which 'reinflate' all babies' heads after the birth compression are avail- able to the child to effect the necessary changes once tensions have been normalized.
Infants and young children with recurrent mid- dle ear infections are a common presentation in 'cranial ' osteopathic practice. As described earlier, the petrous portion of the temporal bone interposes

74 Complementary Therapies in Nursing & Midwifery
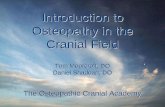
9,10,and and internal jugular vein exit here
Mandible Basi sphenoid
\ / Hard palate
Cq~ dt~Ylaar ~
-'Hypoglossal (12th) canal
11 th cranial nerves/ I t Stylomastoid foramen (7th Cr nerve)
Foramen magnum
Figure Newborn cranial base (inferior view).
Mothers are commonly treated for acute episodes of low back pain during pregnancy.
itself between the occiput and sphenoid bones (Fig.). This leaves it vulnerable to influence from any distortion in the relationship of, or the mobility available in, adjacent cranial base bones. Two pri- mary factors may influence the scope for the eustachia tube, the source of pressure equilibrium and drainage from the middle ear, to function prop- erly. Firstly, if the mobility of the bone itself is impaired, the drainage mechanism may be deprived of the natural rhythmical motion acting in a 'pump' type manner on the cartilaginous portion of the tube. Secondly, aberrant tensions in the muscles of the soft palate, which take their origin from the car- tilaginous portion of the tube, may distort the tube and impair drainage.
Again, careful osteopathic evaluation and gentle corrective treatment of any structural abnormality may secure relief from this potentially very serious condition, without the need to resort to invasive surgery.
OSTEOPATHY IN PREGNANCY A N D LABOUR
The mechanical burdens placed upon the mother's structure by the expanding fetus and uterus can have profound effects, Adaption is important as the mother may develop either a posteriorly rotated pelvis and 'sway back', or an anterior rotation and hyperlordosis with a magnificent bump. Many osteopaths offer to evaluate women planning preg- nancy for areas of poor function within the pelvis and spine in order to help prevent the misery of back pain in later months of pregnancy. Women who are planning a pregnancy and who have a known history of back problems would be well advised to seek such attention. Those with a history of traumatic injury (perhaps a significant fall, car crash or other
trauma) might well have sustained injuries long since adapted to, which will present as their compen- sation is put under the stress of pregnancy,
Mothers are commonly treated for acute episodes of low back pain during pregnancy. They respond extremely well as a rule, and a therapeutic bond can be formed between mother and practitioner which will allow a further avenue for enquiry for the new mother as she negotiates the development of her child.
Though no recorded case of miscarriage exists, treatment before 12 and at 16weeks is generally avoided to negate any chance of precipitating mis- carriage at these more sensitive periods of the pregnancy.
LABOUR
During labour the sacrum, within the pelvis, will be obliged to first counter-nutate (tip backwards) to open the pelvic inlet, and then, in second stage, to nutate to open the birth canal and help get the coc- cyx out of the way. These will be extremes of range, unused in everyday activity. Potential exists here for the joint to become subluxed and fixated at this extreme of range. In particular, if the mother is supine during her labour, or spends time in the lithotomy position, the scope for disruption to the sacro-iliac joint is exaggerated. Fixing the sacrum against the bed limits movement and relative flex- ion of the lumbar spine with the lifting of the pelvis, can initiate a range of potential injuries. Chronic low back pain may then be the con- sequence due to the strained ligaments. Such pain is commonly perceived as 'normal ' after labour. Many female patients directly link childbirth to the onset of low back pain which persists into later decades, which, on examination, shows signs of

The cranial approach in osteopathy 75
An important therapeutic relationship is often fostered between the osteopath, the new mother and the baby.
exaggerated sacral nutation and chronic ligamen- tous distress.
Sutherland proposed a link between the sacrum and membranes of the cranium via the dura mater, This continuity extends to the dural membranes which line and transect the cranial cavity, the falx cerebri and the tentorium cerebelli. The tentorium separates the cerebellum from the mid and fore brain. It continues forward and blends with the membranous sheet which forms the roof of the pitu- itary fossa where it is anchored firmly. Sutherland proposed that all of this membranous system acted as a mechanism to absorb distortions within the cra- nium, and referred to this as the 'Reciprocal Tension Membranous System'. He postulated that this entire mechanism could be influenced by tension any- where in it.
Thus, should the sacrum (the lower pole of the whole mechanism) become fixed in an extreme of motion, it could create a potential tension through- out the whole membranous system. Additionally, Sutherland suggested that an extreme case of fixa- tion of the sacrum which could potentially affect the function of the pituitary gland. Whilst this notion may seem curious, new mothers have reported a 'lifting cloud' or 'clearing' of emotional fluctuations once treatment has been applied to release a jammed sacro-iliac joint after a difficult labour.
Additionally, some infant feeding positions can lead to thoracic vertebral, rib cage and muscle strains. These can respond well to gentle osteopathic techniques and additional advice to complement that of the midwife, health visitor or GP on modified feeding positions.
C RAN IAL ANATOMY AN D CHILDBIRTH
Osteopaths who choose to study 'cranial' osteopathy refine their knowledge of the relevant anatomy in considerable detail. This is complemented by sensi- tive palpatory skills, facilitating the detection of other minute and apparently tmobservable tensions within a structure.
This is particularly significant when considering the anatomical region of the infant cranial base. The stout structure of the occiput is ossified from a carti- laginous model in the fetus. However, it remains in four parts at term. These are not fully fused until around 6 years of age. Anterior to the occiput, and articulating via a cartilaginous 'disc ' , is the sphe- noid bone which will make up the majority of the posterior orbit wall and, interposing almost as wedges, are the two petrous portions of the tempo- ral bones (Fig. 1). These various foramina allow the passage of several important structures which include the brain stem, the carotid arteries, the inter- nal jugular veins, the 9th (glossopharyngeal), lOth (vagus), l l th (accessory), 12th (hypoglossal) cra-
nial nerves and, more anteriorly, the 7th (facial) cra-
nial nerve. This area is subject to considerable compression
and torsion forces. The uterus pushes down on the body of the fetus with the cranial vault and the top of the neck on to the cranial base taking the brunt of the pressure. Next there is a twisting rotation as the fetal head descends within the birth canal. Should some form of distortion occur and be retained in this area, an embarrassment of these nerves might lead to associated entrapment phenomena. For example, embarrassment of the hypoglossal nerve, as it exits anterior to the condyle, could occur and lead to diffi- culties in control of the tongue, suckling and possi-
bly speech development. Similarly, if distortion influences the 9th, 10th
and 1 lth cranial nerve bundles in the jugular fora- men, there may be disturbances to swallowing reflexes from the 9th, increased sensitivity of the stomach and upper two-thirds of the digestive tract from the vagus nerve, and possible problems with tonicity in the sterno-mastoid and trapezius muscles
from the 1 lth.
JUST THE HEAD?
Osteopathic care of infants extends to a full evalua- tion of the structure and integrity of function of the musculo-skeletal system. Particular care is taken to examine the respiratory mechanics of the child. Children with a tendency to chronic recurrent chest infection may also be victims of poor rib cage excur- sion and quite frequently seek osteopathic help when multiple courses of antibiotics have only held the sit-
uation at bay. Osteopathic examination and treatment of the
quality and range of thoracic excursion would be a primary consideration in treatment of the asthmatic child, with a view to aiding mechanical function and promoting healthy function of the sympathetic nerve
chain. Postural advice and exercise regimes are also
offered to growing children with early low back or thoracic pain. Evaluation after traumatic injury, fractures, etc. may help to catch early situations of abnormal or asymmetrical structural tension which could potentially influence healthy growth.
An important therapeutic relationship is often fostered between the osteopath, the new mother and the baby. An average consultation usually lasts at least 30 minutes and, as a result, the osteopath can become a valuable source of information and reas- surance to parents. Advice on general aspects of health and some of the options currently available in health care today can be discussed and considered. Indeed, the existence of this journal reflects the growing number of health visitors, midwives and practice nurses who are actively seeking information on these options as the rate of enquiry from patients
increases.

76 Complementary Therapies in Nursing & Midwifery
C O N C L U S I O N
This brief overview of aspects of the philosophy, rationale and approaches of osteopathic care of mothers and infants cannot do justice to the total extent of care offered by the growing group of osteopaths who are working in this field. The full depth and scope of this approach have not yet been fully explored.
Osteopathic practice is now governed by an Act of Parliament with protection of title, standards of training and regulation of practice similar to those of medicine. The recent introduction of an osteopathic MSc should soon begin to add substantially to the body of research-based evidence confirming the efficacy already acknowledged by the recipients of the 2 million or so osteopathic treatments given annually in the UK at present.
The application of Dr Sutherland's approach to the evaluation and treatment of the newborn and infants is the manifestation of a valuable primary health care tool. It is my fervent hope and belief
that in the near future osteopaths will feature rou- tinely on maternity units, checking all infants for possible unresolved birth strain and allowing each child to express their own unique potential to the
full.
FURTHER READING
Fryman V, Carney, Springall 1992 Effect of Osteopathic Medical Management on Neurologic Development in Children. Journal of American Osteopathic Association 92
Green J H, Silver P H S 1981 An Introduction to Human Anatomy. Oxford University Press, Oxford
Guyton A 1990 Textbook of Medical Physiology. Saunders, London
Magoun H 1976 Osteopathy in the Cranial Field. The Journal Printing Company, Kirksville, Missouri, USA
Sutherland W G 1967 Contributions of Thought. Sutherland Cranial Teaching Foundation, USA
Sutherland W G 1990 Teachings in the Science of Osteopathy. Sutherland Cranial Teaching Foundation, USA
Williams 1989 Gray's Anatomy, 37th Edn. Churchill Livingstone, London
Sudden Death: A Research Base for Practice Bob Wright
Churchill Livingstone, 1996, 2nd edn, 151 pages
When I was a young nurse 40 years ago, the bereaved was offered a cup of tea and, if their grief was very profound, a tot of brandy from a closely monitored supply. And that was that. If any of us queried the procedures, we were told bereavement was not an illness and that the sooner normality was restored the better for everyone.
However, times have changed and from the vantage point of the busy Accident and Emergency Department at Leeds General Infirmary, Bob Wright has much to share with us. He has obviously experi- enced a great deal, thought about it, shared his thoughts with colleagues, and made himself familiar with all the literature relating to the subject published over the past 50 years. This book contains some inter- esting facts, e.g. bereavements following suicide are
more devastating than any other form; and studies revealed that 68% of parents had not been approached about organ donation and 59% said that they wished they had. While the possible benefits of yoga, massage and aromatherapy are mentioned, the consolation of religion is studiously avoided.
The 5 pages on holistic care give the author's philosophy under the headings physical, emotional, intellectual, social and spiritual. Only one work of reference is cited (Herbert Otto's 1975 article Holistic therapy) in an otherwise copious bibliog- raphy of 109 different sources. More than once we are told there is no right or wrong response to sud- den death, neither is there any miraculous interven- tion or quick fix available. The book is, on the whole, user-friendly and well worth reading. The questionnaire for 'Teaching and Training to Care' is a masterpiece of self-analysis. I tried it out on myself.
Brian Plumb SRN, UK