Intro and Background (1) - Rowan Universityusers.rowan.edu/~farrell/Courses/Controlled...
25
1 Controlled Release Introduction and Background
Transcript of Intro and Background (1) - Rowan Universityusers.rowan.edu/~farrell/Courses/Controlled...
1
Controlled Release
Introduction and Background

2
Topics
n Definitionsn Classifications of CR Systemsq Rate control, physical form
n Design considerationsn Routes of administrationn Review of mass transfer

3
Definition of Controlled Release
n A system that:q Delivers an agent at a controlled rate for an
extended timeq Might localize drug action by spatial placement
near where it is neededq Might target drug action by using techniques to
deliver drug to a particular cell type
4
Controlled Release Agents
n In nature (?)q Oxygenation of bloodq Transport of nutrients
and waste through cell membranes
q Transport and evaporation of water (sweat) to control body temperature
n Engineered systems (?)q Drugsq Biocidesq Fragrances

5
Controlled Release vs. Sustained Release
n Controlled drug deliveryq Well-characterized and reproducible dosage formq Controls entry to the body according to the
specifications of the required drug delivery profilen rate and duration of delivery are designed to achieve
desired concentration
n Sustained Releaseq Release of drug is extended in timeq Rate and duration are not designed to achieve a
particular profile.
6
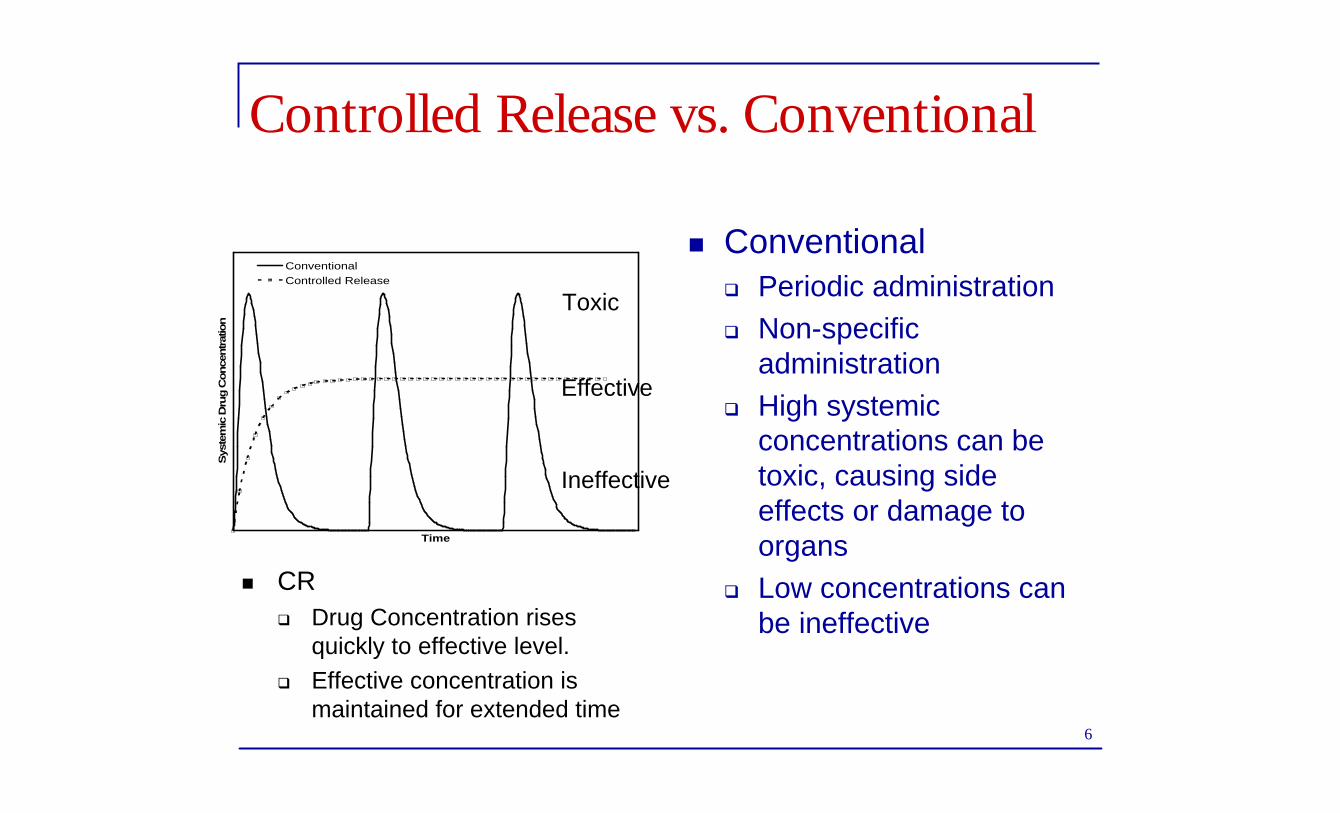
Controlled Release vs. Conventional
n Conventionalq Periodic administrationq Non-specific
administrationq High systemic
concentrations can be toxic, causing side effects or damage to organs
q Low concentrations can be ineffective
Time
Sys
tem
ic D
rug C
once
ntrat
ion
ConventionalControlled Release
Effective
Ineffective
Toxic
n CR q Drug Concentration rises
quickly to effective level. q Effective concentration is
maintained for extended time
7
Disadvantages of Conventional Delivery
n Inconvenientn Difficult to monitorn Careful calculation necessary to prevent
overdosingn Large amounts of drug can be “lost” when
they don’t get to the target organn Drug goes to non-target cells and can cause
damagen Expensive (using more drug than necessary)
(Brainstorm)

8
Advantages of Controlled Release
n Reproducible rate, prolonged deliveryn Less frequent administration
q Better patient complianceq Increased convenience
n Reduced side effects because effective C is maintained
n Targeting can eliminate damage to non-target organs
n Less drug usedn Re-patenting without new drug development
(Brainstorm)

9
Challenges to Controlled Release
n Cost of formulation – preparation and processing
n Fate of controlled release system if not biodegradable
n Biocompatibilityn Fate of polymer additives, e.g., plasticizers,
stabilizers, antioxidants, fillers
10
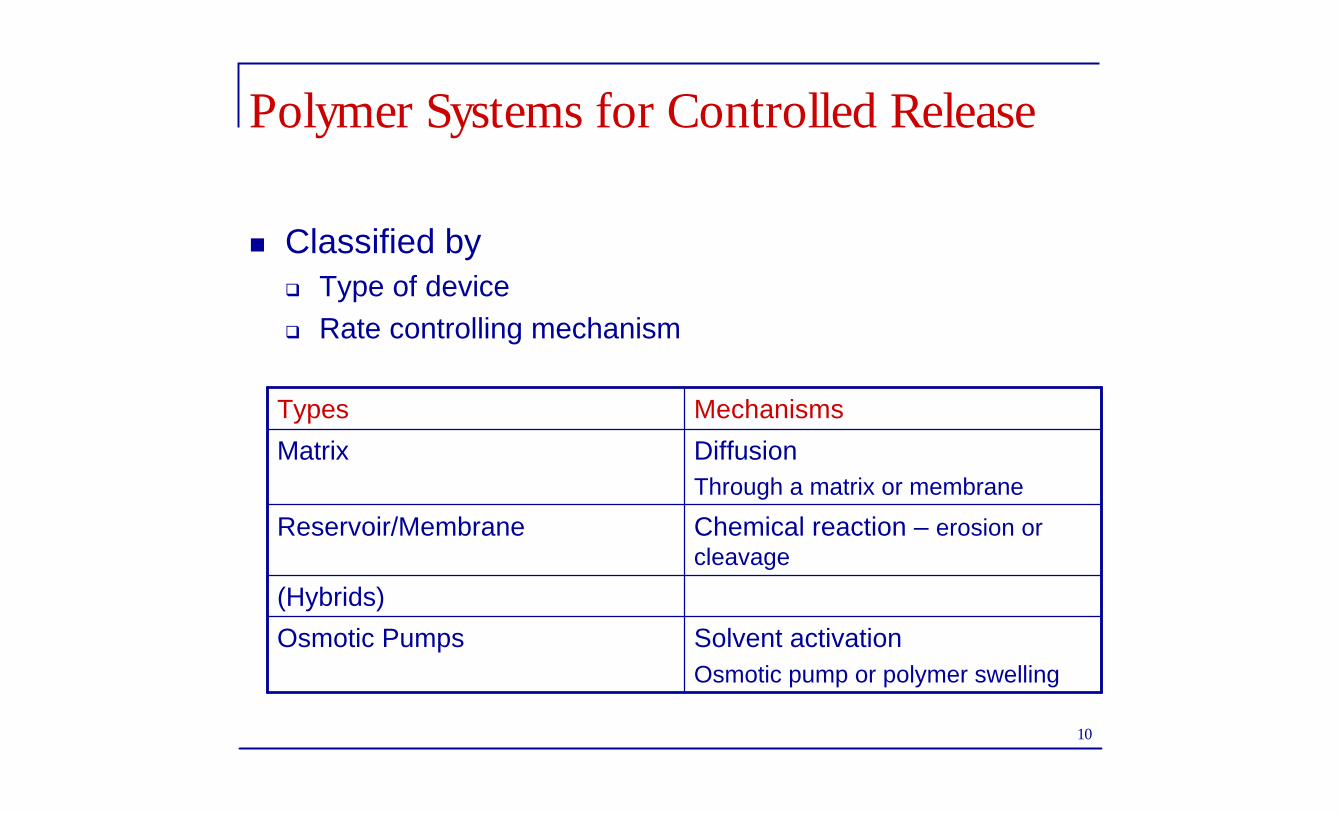
Polymer Systems for Controlled Release
n Classified byq Type of deviceq Rate controlling mechanism
Solvent activationOsmotic pump or polymer swelling
Osmotic Pumps
(Hybrids)
Chemical reaction – erosion or cleavage
Reservoir/Membrane
DiffusionThrough a matrix or membrane
Matrix
MechanismsTypes

11
Matrix Systems
n Drug is physically blended with the polymerq Dissolved or dispersed
n This is the simplest and cheapest device
At t=0
Polymer matrix contains uniformly dissolved or dispersed drug
At time t
Drug is being released by some rate-controlling mechanism

12
Reservoir Systems
n With or without a rate-controlling membranen Geometric Formq Microbead – thin polymer coating around
particles or dropletsq Microtube – polymeric hollow fiber
Microbeads Microtube

13
The Osmotic Pump
Rigid semipermeablemembrane
Osmotic agent
Flexible impermeable wall
Reservoircontainingdrug
14
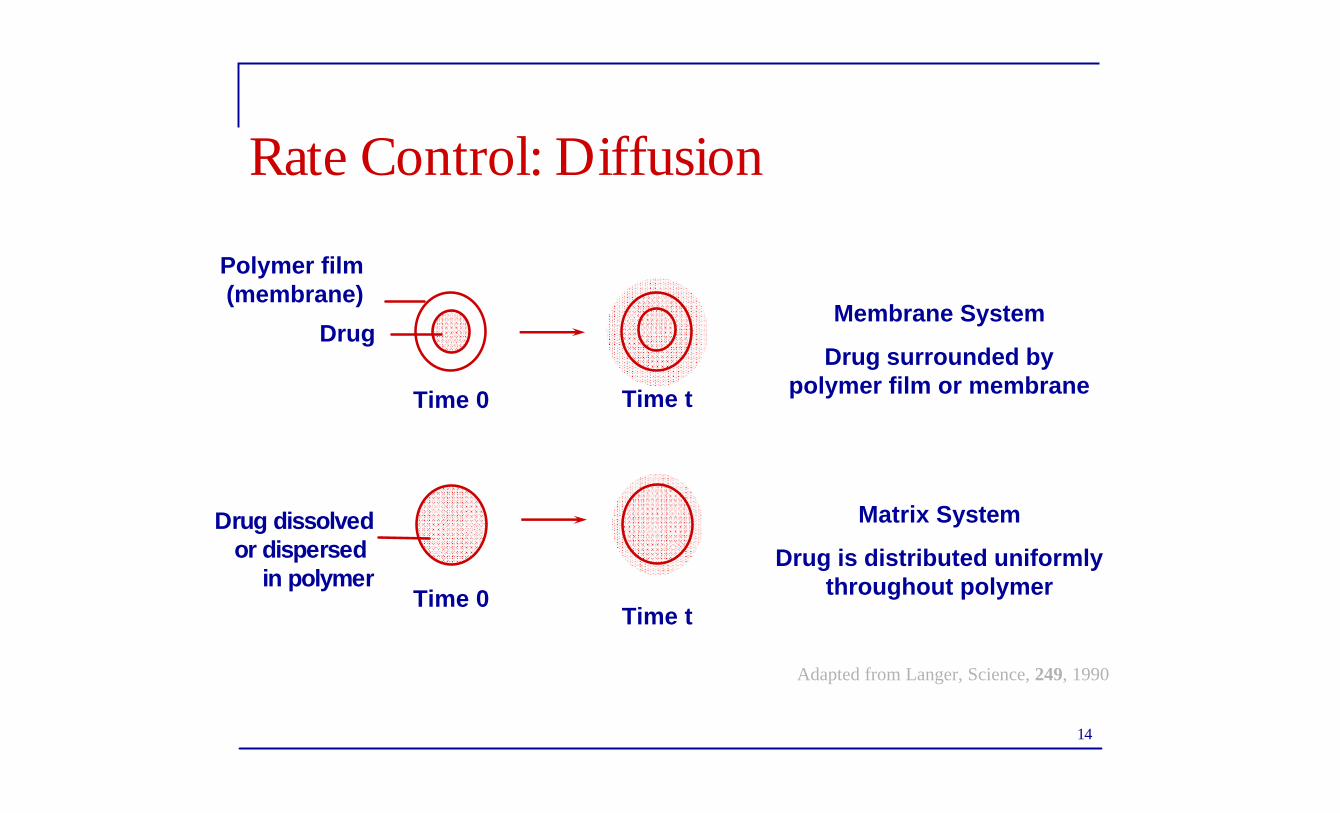
Rate Control: Diffusion
Drug dissolvedor dispersed
in polymer
Adapted from Langer, Science, 249, 1990
Polymer film (membrane)
Drug
Time 0 Time t
Time 0Time t
Membrane System
Drug surrounded by polymer film or membrane
Matrix System
Drug is distributed uniformly throughout polymer

15
Diffusion Systems
Contac® 12 Hour Cold Capsules
Nocoderm® Patch
Ocusert®
(Pilocarpine for Glaucoma)
16
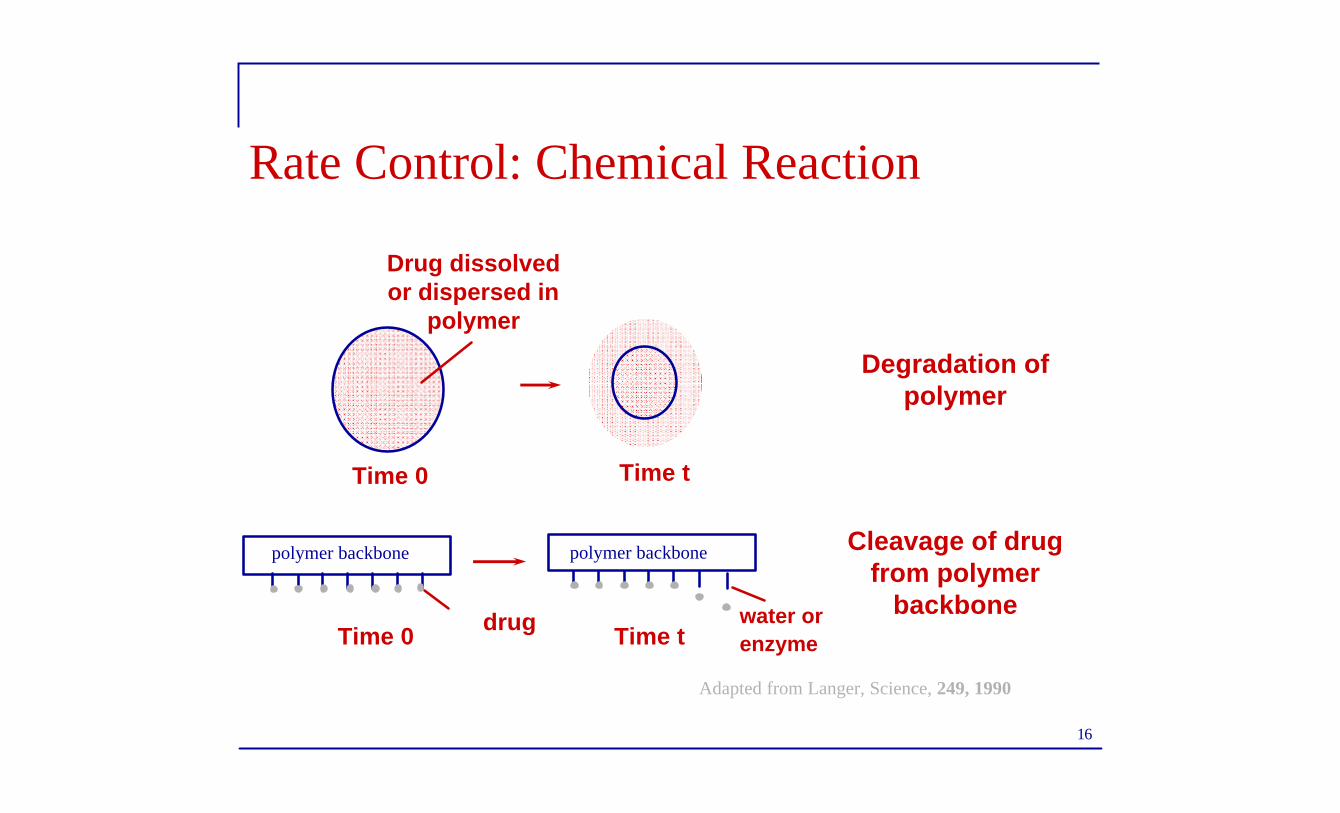
Rate Control: Chemical Reaction
water or enzyme
Cleavage of drugfrom polymer
backbone
Adapted from Langer, Science, 249, 1990
Time tTime 0 drug
polymer backbone polymer backbone
Degradation of polymer
Drug dissolved or dispersed in
polymer
Time 0 Time t
17
Biodegradable Systems
n Implants for release of anticancer drugsn Lupron Depot®
q Injectable microspheresq Once per month injectonq Prostrate cancer, fertility treatment, early puberty
n Malaria vaccine

18
Rate Control: Solvent Activation
Drug dissolved
in polymer
Time 0
Time t
Swollen Polymer from which drug has been released
Swelling allows drug to migrate more easily
Adapted from Langer, Science, 249, 1990
Time 0 Time t
Osmotic pressure causeswater to penetrate,forming pores and releasing drug
Pores permit release
Drug dispersed
in polymer
19
Design Considerations
n Basic componentsq Active agentq Polymer
n Polymer design considerations (?)q Physical propertiesn Glass transition temperaturen Diffusion characteristics
q Compatibility with activeq Stability – must not decompose in storageq Biocompatibility of polymer and degradation productsq Ease of formulation and fabricationq Mechanical properties are stable when drug is addedq Cost
20
Design considerations
n Agentq Physicochemical propertiesn Stabilityn Solubilityn Partitioningn Chargen Protein binding propensity
21
Design Considerations
n Route of deliveryn Target sites
q Desired site for efficacyq Sites to avoid to minimize side effects
n Type of therapy q Acute or chronic – rate and durationn e.g., 1 yr contraceptive implant vs. antibiotic for acute infection
n Patient conditionq Cognative ability and memoryq Physical condition – ambulatory, bedridden, etc.

22
Routes of Administration for CR
n Parenteral – outside GI tractq Usually refers to
injectablesn Subcutaneousn Intramuscularn Intraperitonealn Intravenous
n Advantagesq Bypasses some routes of
metabolic clearance
n Disadvantages (?)q Painfulq Inconvenient

23
Routes of Administration
n Oralq Most common routen Easy to formulate and manufacturen Patient compliance is generally goodn Inexpensive dosage form
q Tricky due to environment of GI tractn pH degradationn Enzymatic degradationn Intestinal motility – affects residence time
q Single patient and patient-to-patient variationsn Absorption limitations in stomach

24
Routes of Administration
n Buccal/ Sublingualq Thin mucous membraneq Rich blood supplyq Mild pH ~6.0
n Nasalq Easy administrationq Rapid absorptionq Bypasses certain
clearance routes
n Rectalq No pH or enzymatic
degradation as in oral (+)q More effective than
buccal or sublingual for some drugs (+)
q Limited absorption (-)
n Pulmonaryq Large S.A. for absorption

25
Routes of Administration
n Transdermalq Accessible organ, large surface areaq Avoid first pass metabolismq Avoid GI incompatibility of drugsq Good patient complianceq Transport across skin can be a challenge
n Ocularq Localized delivery for eye disordersq Good absorption for many drugsq Loss of drug in tears