Intravenous urography
56
I V U dr. rajendra prasad ray
Transcript of Intravenous urography

I V U dr. rajendra prasad
ray

• Once the principal investigation as imaging in urology.
• the term “IVP” commonly used in past.• Better terminology is “IVU”.• Also known as Excretory Urography

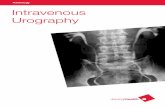
XRAY KUB
The standard plain radiographic imaging of theurinary tract is theKUB (kidneys, ureters and bladder), which
consists of I. a full length abdominal film and II. an upper abdominal (cross-kidney) film
• taken with the patient supine using a low voltage technique (60-65 kV) to maximise soft-tissue contrast.

1. The full length film o in inspirationo a 35 x 43 cm cassette o positioned with the lower border at the symphysis
pubis to ensure the urethra (particularly the prostatic urethra)
2. The cross-kidney film o in expirationo a 24 x 30 cm cassette o with the lower border 2.5 cm below the iliac crests
“The study typically includes that portion of the anatomy from the level of the diaphragm to the inferior pubic symphysis”

Fig. The KUB. (A) Full length and (B) cross kidney films

The outline of several anatomical structures can be seen on the KUB, o renal, o psoas and o bladder outlines, 1. the KUB is a relatively unreliable diagnostic tool 2. principal use is in the assessment of urinary tract
calculi.3. It is, however, extremely unreliable in the diagnosis
of ureteric calculi, with an accuracy of only around 50%.

The KUB is most usefully employed as part of an intravenous urogram (IVU) or to follow up a previously proven calculus.

As part of IVU:Patient positionAdequacy of bowel preparationAdequacy of the exposureDemonstration of urinary tract calcificationDetection of abnormalities of
Abdominal skeleton Intestinal gas pattern Soft tissues

calcification on the kubUrinary tract• Renal: calculi, renal cell carcinoma, tuberculosis, • Ureter: calculi, tuberculosis, schistosomiasis• Bladder: calculi, schistosomiasis, transitional cell carcinomaOutside the urinary tract• Musculoskeletal: costal cartilage calcification• Hepatobiliary: gallstones, hepatic granuloma• Pancreas: chronic pancreatitis• Adrenal: tuberculosis, Addison's disease• Spleen: granuloma• Aorta: atheroma, aneurysm• Venous: phlebolith• Uterine: fibroid• Lymphatic: calcified lymph nodes (presumed postinfective)

digital xray imaging
• Include CR and DR• Compturised radiology
o Photostimulable phosphors to capture the image o Read with a laser(red)o Computer software form a digital image

intravenous urography
• the classic routine investigation of uroradiology. • its role is now much diminished• its future is the subject of considerable debate• At this date, however, it is still widely used.

Currently the main indications are the1. Renal and ureteric calculi2. ureteric fistulas and strictures and complex
urinary tract infection (including tuberculosis).
3. persistent or frank haematuria,

preparation
1. the bowel purged with a strong laxative. Most patients will need only
clear liquids for 12 hours and an enema 1 hour before the procedure.
Patients with chronic constipation complete bowel prep with clear liquids for 12 to 24 hours and an enema 2 hours before the procedure.
Bowel preparation is now generally regarded as unhelpful and unpleasant for the patient
2. a period of 4 h starvation and fluid deprivation

• Traditionally fluid was restricted prior to the IVU to improve opacification on the collecting system.
• Dehydration is associated with an increased risk of nephrotoxicity, 1. diabetes mellitus, 2. myeloma, 3. hyperuricaemia, 4. sickle-cell disease and 5. pre-existing renal disease.
• The risk in healthy kidney i s very low. • Risk further can be reduced with avoidance of
dehydration.

Modern non-ionic contrast agents do not provoke an osmotic diuresis
the degree of opacification is unlikely to be significantly altered by dehydration.
Fluid restriction should therefore be avoided dehydration should be corrected first.

precautions
a routine inquiry about previous contrast exposure allergy Co morbidities and drug history
Serum creatinineEmergency drugs, oxygen and resuscitation equipment should also be readily available

procedure
The classical series of films 1. plain film (KUB)2. immediate, 3. 5 min4. 15 min,5. full length release and 6. Postmicturition
With some modifications. .

A preliminary postmicturition plain film (KUB) check exposure factors, centring and obvious pathology, particularly urinary tract
calcification.
Intravenous contrast is given relatively rapidly by hand. The standard dose is 50 ml of 350-370 strength
water-soluble contrast.

A cross-kidney film immediately after and 5 min after the injectionAbdominal compression is applied as soon as the 5 min film has been taken to inhibit ureteric drainage promote distension of the pelvicalyceal systems,
optimising their visualisation.
A further cross-kidney film is taken at 12-15 min to demonstrate this.

the compression is removeda full length film is taken immediately to offer the best opportunity of demonstrating the
ureters.
The patient is then asked to empty the bladdera further full length film is taken drainage of the upper tract and the postmicturition bladder volume.



Post contrast IVU films. • (A) Immediate, • (B) 5 min, • (C) 15 min film with
compression producing calyceal distension;
• (D) full length release; • (E) full length post
micturition.

AdditionallyDelayed film, oblique film , prone film

eventsintravenous injection.
12-20 s
contrast to reach the renal arteriesconcentration is maximal in the vascular compartment;
1st minute kidneys show diffuse enhancement. This is referred to as the NEPHROGRAM.
the first half minute, • contrast in the vascular compartment dominates and therefore the cortex is more enhanced than the
medullaIn the second half minute, • contrast in the tubules increases and enhancement of the kidneys is more diffuse.
the renal size and outlines are best seen

around 1 minContrast begins to appear in the calyces .contrast may also be visible in the collecting ducts as fine linear opacities running along the medullary pyramids towards the calyces. This may be referred to as pyelotubular stasis or, when less defined, as the medullary or pyramidal blush,.
After that
Contrast drains into the pelvis and ureter this phase may be referred to as the pyelogram.

compression (5min)impedes ureteric drainage distends the pelvicalyceal system, optimal visualisation of the pelvicalyceal system around 12-15 min.
compression released (after 15 min)
there is a transient increase in flow down the ureters release film offers the best chance of demonstrating the ureters.
The normal ureters exhibit continual peristalsis and on a single film it is Uncommon todemonstrate the entire length of both (oreven either) ureters. In most situations partial visualisation of a non-obstructed but otherwisenormal ureter is acceptable.

Compression is avoided in childrenaortic aneurysm. recent abdominal surgeryacute painful abdomen eg, renal colicUrinary tract obstructionIn any pt. stoma & IVC filterRenal failureMyeloma

modificationsThree circumstances
1.When there is significant acute obstruction• usually due to calculi, • there is delay in opacification of the collecting system. • The delay may be considerable, up to 24 h or more. • It is then necessary to perform the minimum number of additional films. • The time interval between films is approximately doubled, with films
taken at 0.5, 1, 2, 4, 16 and 24 h, as necessary.
in order to minimise the radiation exposure, if there is no opacification of an acutely obstructed kidney at 30 min it is
usually unhelpful to perform the next film before around 4 h after contrast injection.

2.Patients with proven or suspected ureteric calculus • may require one or more follow-up IVUs. • These should have the minimum number of films required to
answer the specific question, – example a full length plain and 15 min post contrast film may be
sufficient.
3.Pregnant Patient. the radiation exposure should be minimised.
1. a single full length preliminary film and 2. a delayed solitary full length film around 30-45 min may well be
enough.The collecting systems in pregnancy are capacious and the ureters
exhibit poor peristalsis.




HIGH DOSE UROGRAPHY• Not used now a days• Done in presence of mild renal failure• There must be no dehydration• A double dose(600 mg iodine/kg) of non-ionic
contrast medium used

ONE-SHOT IVUPlain film followed by a full length abdominal
radiograph 15 mins after injection of contrast.Uses - to demonstrate ureteric anatomy prior to
surgery where there may be risk of ureteric injury in renal trauma requiring exploration.

TOMOGRAMS ( NEPHROTOMOGRAMS )• Are well focused focal area films• Uses technique of collimation• Immediately following the injection of contrast material a
series of 3 nephrotomograms is made at 1 cm interval with the patient in supine position
Nephrotomography employs a wider angle of swing ( 25-40 0), producing relatively thin slices in sharp focus.
Allows excellent visualization of renal contours becoz shadows that may obscure the kidneys are blurred with the tomographic technique.

examples
• IVU showing left renal agenesis with bowel gas within the left renal bed.
• The large right kidney shows a bifid renal pelvis, the mildest form of renal duplication.

IVU demonstrating a horseshoe kidney.
“Flower vase appearance “

Duplex ureters onIVU: complete
bilateral

Duplex ureter partialleft-sided

• a non-opacified partly obstructing ureterocele surrounded by opacified urine in the bladder
• A later full length film shows opacification of the distended upper moiety ureter running down to the opacified ureterocele

• IVU demonstrating the characteristic stretching of calyces by cysts in polycystic kidneys.
• Spider leg appearance

Left megaureter on IVU showing dilatation of the entire length of the ureter with secondary pelvi calyectasis

Intravascular radiologic Contrast Media
• Iodine is the most common element (atomic no 127)• carriers of the iodine elements, increasing solubility and
reducing toxicity. • Four basic types
1. ionic monomer, 2. nonionic monomer, 3. ionic dimer, and 4. nonionic dimer.
• All are derived from a 2,4,6 tri-iodinated benzene ring compound
• Approximately 90% will be eliminated by the kidneys within 12 hours of administration


Physiological effects:• HOCM have an osmolality that is 5 times greater than
physiologic osmolality of body cells.1.The hyperosmolar agents are associated with • erythrocyte damage, • endothelial damage, • v asodilation, • hypervolemia, • interruption of the blood-brain barrier, and • cardiac depression. 2.Chemotoxic reactions
• cardiac, vascular, neurologic, and renal toxicity.

Adverse drug reactions (ADR)
idiosyncratic anaphylactoid (IA) nonidiosyncratic (NI) reactions
idiosyncratic anaphylactoid (IA) • The exact mechanism of IA reactions is not known • thought to be a combination of systemic effects. • Not result from a true IgE antibody immunologic reaction to the
contrast media • IA reactions are not dose dependent.
Severe reactions have been reported after only 1 mL injected at the beginning of the procedure and
Can occurr after completion of a full dose despite no reaction to the initial test dose

nonidiosyncratic (NI) reactions • dose dependent • related to the
1. osmolality, 2. concentration, 3. volume, and 4. injection rate of the IRCM.

Incidence:ADRs are more common with HOCM (12%) compared with LOCM (3%)
Risk factor:Previous adverse reaction to IRCM history of asthma history of known allergy to iodine, severe cardiac disease, renal insufficiency, dehydration, sickle cell anemia, anxiety, apprehension, hyperthyroidism, and presence of adrenal pheochromocytoma.

Minor and intermediate reactions do not require treatment.
severe contrast reactions requires prompt o resuscitationo rapid administration of epinephrine is the treatment
of choice o Current guidelines recommend immediate delivery
of 0.01 mg/kg of body weight to a maximum of 0.5 mg of 1 : 1000 concentration of epinephrine, injected IM in the lateral thigh as first-line treatmen .

Premedication Strategies• No known premedication strategy eliminate
the risk of a severe adverse reaction• use of corticosteroids, antihistamines, H1 and
H2 antagonists, and ephedrine.

Contrast-Induced Nephropathy
CIN is defined as 1. a rise in serum creatinine 25% above baseline, or
more than 0.5 mg/dL 2. within 3 days following exposure to contrast
media, 3. in the absence of an alternative cause.
• combination of tubular injury and renal ischemiaRisk factors:• Patient related• Non patient related

patient-related risk factors 1. chronic kidney disease (creatinine clearance <60
mL/min), 2. diabetes mellitus, 3. dehydration, 4. congestive heart failure, 5. age, 6. hypertension, 7. low hematocrit, and 8. ventricular ejection fraction less than 40%.

Non–patient-related risk factors1. high-osmolar contrast agents, 2. ionic contrast, 3. increased contrast viscosity, and 4. large-contrast volume infusion
cutoff value for serum creatinine • varied widely among radiology practices. • 35% used 1.5 mg/dL, • 27% used 1.7 mg/ dL, and • 31% used 2.0 mg/dL

the prevention of CIN • hydration, • bicarbonate, • iso- or low-osmolar contrast media, and • N-acetylcysteine. Furosemide was found to increase the risk of
developing CIN

...thank you