Intraosseous correction of misdirected cannulated screws and fracture malalignment using a bent tip...
5
1 3 Arch Orthop Trauma Surg (2013) 133:883–887 DOI 10.1007/s00402-013-1740-7 ORTHOPAEDIC SURGERY Intraosseous correction of misdirected cannulated screws and fracture malalignment using a bent tip 2.0 mm guidewire: technique and indications John A. Scolaro · Milton Lee (Chip) Routt Received: 22 February 2013 / Published online: 16 April 2013 © Springer-Verlag Berlin Heidelberg 2013 is prepared. Injuries to the surrounding neurovascular structures can occur when instrumentation such as sharp pins, drills, or screws exit the defined pelvic OFPs’ cortical limits [2]. Stereotactic navigation and/or advanced multidimen- sional imaging have been advocated to improve percuta- neous pelvic screw insertion accuracy and safety [3–5]. Several authors have evaluated intra-operative somatosen- sory evoked potential (SSEP) monitoring during pelvic and acetabular surgery to reduce the risk of local neuro- logical injury [6–8]. These ancillary measures underscore the importance of proper surgical pre-operative planning, intraoperative technique and knowledge of pelvic osseous anatomy. Numerous challenges frustrate the placement of percu- taneous pelvic screws. One is the inability to make “mid- technique” directional changes of a poorly positioned guidewire or drill once an initial pathway has been estab- lished. This initial “misdirection” error results in a screw that has a good starting point, but a misdirected path and therefore inaccurate, final location and/or length. Another challenge is placing a screw when the defined pelvic OFPs is altered by fracture comminution and fracture displace- ment that distort the normal alignment of the OFP to the point that the drill or guidewire passage is not routinely possible. We present a reliable and effective simple technique that allows for “mid-technique” correction of a misguided or poorly located cannulated drill within any of the pelvic OFPs. This technique also allows medullary manipulation and reduction of a poorly aligned pelvic OFP for subsequent screw insertion. This technique does not substitute for poor technique in any circumstance. We describe its use to opti- mize the position of screws within the pelvic OFPs for opti- mal fixation stability. Abstract Percutaneous pelvic screw placement is a technically demanding procedure. A precise intraosseous pathway must be prepared before screw placement into any osseous fixation pathway of the pelvis. Adjustments to a drill or guidewire become increasingly difficult as the instrument is advanced within the pelvis. We present a reli- able and reproducible technique using a 2.0 mm guidewire that allows for correction of an initially misdirected drill within the pelvis. This technique also allows for manipula- tion and reduction of certain malaligned pelvic fractures prior to percutaneous cannulated screw placement. This technique does not substitute for poor surgical technique but is used to optimize the position of percutaneously placed pelvic screws. Keywords Pelvis · Percutaneous · Cannulated screws · Intraosseous fixation pathway Introduction Percutaneous pelvic screw placement is a technically demanding procedure requiring the surgeon to have a thor- ough understanding of the pelvic osseous fixation pathways (OFPs) and their fluoroscopic imaging [1]. The most com- monly used pelvic OFPs are iliosacral, anterior column, and pelvic brim. Pelvic fixation screws are inserted safely within the OFPs only after an accurate and precise pathway J. A. Scolaro (*) · M. L. Routt Department of Orthopaedics and Sports Medicine, Harborview Medical Center, University of Washington, 325 9th Avenue, Seattle, WA 98104, USA e-mail: [email protected]
-
Upload
milton-lee -
Category
Documents
-
view
212 -
download
0
Transcript of Intraosseous correction of misdirected cannulated screws and fracture malalignment using a bent tip...

1 3
Arch Orthop Trauma Surg (2013) 133:883–887DOI 10.1007/s00402-013-1740-7
ORTHOPAEDIC SURGERY
Intraosseous correction of misdirected cannulated screws and fracture malalignment using a bent tip 2.0 mm guidewire: technique and indications
John A. Scolaro · Milton Lee (Chip) Routt
Received: 22 February 2013 / Published online: 16 April 2013 © Springer-Verlag Berlin Heidelberg 2013
is prepared. Injuries to the surrounding neurovascular structures can occur when instrumentation such as sharp pins, drills, or screws exit the defined pelvic OFPs’ cortical limits [2].
Stereotactic navigation and/or advanced multidimen-sional imaging have been advocated to improve percuta-neous pelvic screw insertion accuracy and safety [3–5]. Several authors have evaluated intra-operative somatosen-sory evoked potential (SSEP) monitoring during pelvic and acetabular surgery to reduce the risk of local neuro-logical injury [6–8]. These ancillary measures underscore the importance of proper surgical pre-operative planning, intraoperative technique and knowledge of pelvic osseous anatomy.
Numerous challenges frustrate the placement of percu-taneous pelvic screws. One is the inability to make “mid-technique” directional changes of a poorly positioned guidewire or drill once an initial pathway has been estab-lished. This initial “misdirection” error results in a screw that has a good starting point, but a misdirected path and therefore inaccurate, final location and/or length. Another challenge is placing a screw when the defined pelvic OFPs is altered by fracture comminution and fracture displace-ment that distort the normal alignment of the OFP to the point that the drill or guidewire passage is not routinely possible.
We present a reliable and effective simple technique that allows for “mid-technique” correction of a misguided or poorly located cannulated drill within any of the pelvic OFPs. This technique also allows medullary manipulation and reduction of a poorly aligned pelvic OFP for subsequent screw insertion. This technique does not substitute for poor technique in any circumstance. We describe its use to opti-mize the position of screws within the pelvic OFPs for opti-mal fixation stability.
Abstract Percutaneous pelvic screw placement is a technically demanding procedure. A precise intraosseous pathway must be prepared before screw placement into any osseous fixation pathway of the pelvis. Adjustments to a drill or guidewire become increasingly difficult as the instrument is advanced within the pelvis. We present a reli-able and reproducible technique using a 2.0 mm guidewire that allows for correction of an initially misdirected drill within the pelvis. This technique also allows for manipula-tion and reduction of certain malaligned pelvic fractures prior to percutaneous cannulated screw placement. This technique does not substitute for poor surgical technique but is used to optimize the position of percutaneously placed pelvic screws.
Keywords Pelvis · Percutaneous · Cannulated screws · Intraosseous fixation pathway
Introduction
Percutaneous pelvic screw placement is a technically demanding procedure requiring the surgeon to have a thor-ough understanding of the pelvic osseous fixation pathways (OFPs) and their fluoroscopic imaging [1]. The most com-monly used pelvic OFPs are iliosacral, anterior column, and pelvic brim. Pelvic fixation screws are inserted safely within the OFPs only after an accurate and precise pathway
J. A. Scolaro (*) · M. L. Routt Department of Orthopaedics and Sports Medicine, Harborview Medical Center, University of Washington, 325 9th Avenue, Seattle, WA 98104, USAe-mail: [email protected]

884 Arch Orthop Trauma Surg (2013) 133:883–887
1 3
Technique
Correction of misdirected cannulated screw
This technique can be performed within any of the available OFPs of the pelvis [1]. The first step is recognition that a wayward initial pathway has been created (Fig. 1a, b). The misdirected guidewire or drill is removed from the pelvis. The blunt end of a 2.0 mm guidewire is then manually bent using pliers approximately 0.75 cm from the tip of the wire approximately 15–20°. A more acute bend will prohibit the modified guidewire from entering the cortical entrance hole or prevent the bent guidewire from following the initial path of the drill until the point of correction. A more acute bend in the guidewire can also prevent its removal after place-ment of the cannulated screw.
The modified bent tip guidewire is inserted and advanced within the wayward pathway of the OFP until it has reached the point at which the desired correction needs to be made. At this point, the guidewire is then rotated under biplanar fluoroscopic guidance until the bent tip is pointed in the direction of the intended correction. A mallet is then used to gently advance the bent tip of the guidewire so that it engages into its improved intended bone pathway. The advancement of the bent tip guidewire must be checked on biplanar fluoroscopic views to ensure progression is in the desired direction and location (Fig. 2a, b). The appropriate cannulated drill for the planned screw is then advanced over the straight portion of the guidewire creating the improved and intended pathway. We routinely use a standard 4.5 mm cannulated drill (DePuy Synthes, West Chester, PA, USA) over the 2.0 mm bent tip guidewire. The drill follows the
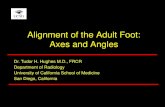
Fig. 1 Intraoperative fluoroscopic pelvic a inlet and b outlet images during placement of a transiliac–transsacral screw showing initially misdirected cannulated drill in a posterior to anterior and in b cranial to caudal direction
Fig. 2 Fluoroscopic pelvic a inlet and b outlet images showing placement of a modified 2.0 mm guidewire positioned to make in a posterior and in b cranial correction

885Arch Orthop Trauma Surg (2013) 133:883–887
1 3
guidewire until the new path has been established. This new path is confirmed on two fluoroscopic views as the drill is advanced (Fig. 3a, b). The drilling must be halted at a point before the bend in the guidewire to avoid: (1) binding of the drill on the guidewire, (2) notching or amputation of the bent guidewire tip by the drill, or (3) advancement of the guidewire in an unwanted direction or location. The can-nulated drill is then removed from the bone, followed by removal of the bent tip guidewire.
If a solid cortical screw is to be used within the OFP, the appropriate sized calibrated drill bit is placed within the new path. Correct placement is confirmed on orthogo-nal fluoroscopic views and the drill is advanced until the desired depth has been reached. The length of the screw is confirmed using the calibrated drill with a protective drill sleeve of known length or using an identical drill bit and
placing it alongside the inserted calibrated drill and measur-ing the exposed length. The drill is removed and an appro-priate length screw is placed, ensuring again on biplanar fluoroscopy that the new path has been followed.
If a cannulated screw is selected, a straight guidewire is re-inserted into the new redirected osseous path that has been created. Biplanar fluoroscopic views confirm placement within the new corrected path. The wire is then advanced to the desired length and measured using a cannulated system depth gauge or guidewire of identical length, as described previously. A cannulated screw of measured length is then inserted.
Correction of fracture malalignment
This technique can also be utilized when the fracture dis-placement disrupts the alignment of the OFP. The guidewire or drill is removed from the bone when it cannot maintain its intraosseous path or navigate an area of displacement. The blunt end of a 2 mm guidewire is modified in the same fash-ion as described above, and placed within the drilled osse-ous tunnel. The bent tip guidewire is rotated under biplanar fluoroscopy until the tip is positioned to successfully advance within the malaligned OFP (Fig. 4a, b). A mallet is used to advance the wire slowly past the fracture or deformity. Spe-cific rotations of the bent tip guidewire often improve the fracture reduction to realign the fragments. The successful advancement of the wire to the final desired position of the screw is confirmed on biplanar fluoroscopy. The screw length is measured using an unmodified 2 mm guidewire placed alongside the modified guidewire and measuring the wire’s extraosseous length. A cannulated screw of desired size and length is then inserted over the modified guidewire (Fig. 5a, b). Advancement of the screw past the zone of malalignment should be checked with biplanar fluoroscopy to ensure that the screw follows the guidewire’s intraosseous path of the guidewire. The guidewire is removed beyond the tip of the screw before the final position of the screw is achieved. If the guidewire is not removed, it can be bent, broken or trapped by the tip of the cannulated screw. In order to avoid unwanted binding of the bent tip guidewire on the cannulated screw end, the surgeon may opt for a cannulated screw with a wider internal diameter. We use the 2 mm guidepin with a larger inner diameter cannulated screw (Zimmer, Warsaw, IN, USA) to avoid guidepin binding on the screw end. Final biplanar fluoroscopic views confirm final position and length of the screw as well as alignment of the OFP.
Discussion
Percutaneous screw fixation has the ability to provide reliable stability to various sites of pelvic ring instability
Fig. 3 Fluoroscopic pelvic a inlet and b outlet images showing a cannulated drill being advanced over the modified guidewire with successful correction of the initial misdirection

886 Arch Orthop Trauma Surg (2013) 133:883–887
1 3
following trauma [9]. Once the insertion site is prepared, the surgeon usually performs small adjustments during pathway preparation to ensure that a safe and correct pathway for the screw is created. Adjustments are easily made before the ini-tial entry path has been created. These adjustments become increasingly more difficult once the drill (or guidewire) is within the pelvis. We present a technique which allows for “mid-technique” corrections of the screw pathway, once a trajectory has been established and cannot be corrected by changes to drill aim.
This technique allows for minor but important direc-tional corrections within the OFPs of the pelvis. It is not a substitute for a poor starting point or insufficient knowl-edge of the pelvic osseous anatomy. The blunt end of the 2.0 mm guidewire should be less dangerous than a sharp ended or threaded guidewire, but could potentially harm
local structures. Finally, advancement of a cannulated screw or drill can potentially notch, bind, or cut the bent tip guidewire.
The use of a modified bent tip guidewire has obvious limitations. A cannulated screw must be used and the pre-operative plan must confirm that the patient’s OFP will accept such an implant. A solid cortical screw may not be successful with this technique unless the achieved medul-lary manipulative reduction is maintained when the guide-wire is removed. Fractures of the pelvic ring with significant displacement often do not allow for a modified guidewire to be used for reduction. Other reduction maneuvers such as manual manipulation, external fixation or an appropriate open exposure can be utilized to aid in fracture reduction, but are not always successful.
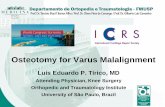
Fig. 4 Biplanar fluoroscopic images of the modified guidewire advanced past the zone of injury into the medial segment of the ramus
Fig. 5 Fluoroscopic a inlet and b combined outlet obturator oblique images confirming final position of screw within the superior pubic ramus

887Arch Orthop Trauma Surg (2013) 133:883–887
1 3
In conclusion, a modified bent tip 2.0 mm guidewire allows the surgeon to make minor yet important corrections to the initially misdirected path of percutaneously placed screws within the OFPs of the pelvis. It can also be used to correct certain fracture malalignment before percutaneous screw fixation.
References
1. Bishop JA, Routt ML Jr (2012) Osseous fixation pathways in pelvic and acetabular fracture surgery: osteology, radiology, and clinical applications. J Trauma Acute Care Surg 72(6):1502–1509
2. Routt ML Jr, Simonian PT, Mills WJ (1997) Iliosacral screw fixa-tion: early complications of the percutaneous technique. J Orthop Trauma 11(8):584–589
3. Tonetti J, Carrat L, Lavalleé S, Pittet L, Merloz P, Chirossel JP (1998) Percutaneous iliosacral screw placement using image guided techniques. Clin Orthop Relat Res 354:103–110
4. Blake-Toker AM, Hawkins L, Nadalo L, Howard D, Arazoza A, Koonsman M, Dunn E (2001) CT guided percutaneous fixation of sacroiliac fractures in trauma patients. J Trauma 51(6):1117–1121
5. Citak M, Hüfner T, Geerling J, Kfuri M Jr, Gänsslen A, Look V, Kendoff D, Krettek C (2006) Navigated percutaneous pelvic sac-roiliac screw fixation: experimental comparison of accuracy between fluoroscopy and Iso-C3D navigation. Comput Aided Surg 11(4):209–213
6. Moed BR, Ahmad BK, Craig JG, Jacobson GP, Anders MJ (1998) Intraoperative monitoring with stimulus-evoked electromyo-graphy during placement of iliosacral screws. An initial clinical study. J Bone Joint Surg Am 80(4):537–546
7. Helfet DL, Koval KJ, Hissa EA, Patterson S, DiPasquale T, Sand-ers R (1995) Intraoperative somatosensory evoked potential monitoring during acute pelvic fracture surgery. J Orthop Trauma 9(1):28–34
8. Vrahas M, Gordon RG, Mears DC, Krieger D, Sclabassi RJ (1992) Intraoperative somatosensory evoked potential monitoring of pelvic and acetabular fractures. J Orthop Trauma 6(1):50–58
9. Routt ML Jr, Nork SE, Mills WJ (2000) Percutaneous fixation of pelvic ring disruptions. Clin Orthop Relat Res 375:15–29