Intracranial Aneurysm: Anatomic Factors That Predict ...ahaq/new/Intracranial aneurysm - anatomic...
5
Cohn P. Derdeyn, MD #{149} Christopher J. Moran, MD #{149} DeWitte T. Cross III, MD Eric W. Sherburn, MD #{149} Ralph G. Dacey, Jr, MD Intracranial Aneurysm: Anatomic Factors That Predict the Usefulness of Intraoperative Angiography’ Index terms: Aneurysm, intracranial, 17.73 #{149} Angiography, intraoperative, 17.73 1 From the Section of Neuroradiolog Mallinckrodt Institute of Radiology (C.P.D., C.J.M., D.T.C.); and the Department of Neurology and Neurosurgery (Neurological Surgery) (E.W.S., R.G.D.), Wash- ington University School of Medicine, 510 5 Kingshighway Blvd, St Louis, MO 63110 ;. Received April 23, 1997; revision requested June 13; revision received June 24; accepted July 8. Address reprint requests to C.P.D. C.P.D. supported by a grant from the RSNA/Siemens Medical Systems Research and Education Fund. C RSNA, 1997 335 PURPOSE: To correlate the size and location of intracranial aneurysm with the need to reposition the aneu- rysm clip after intraoperative angiog- raphy. MATERIALS AND METHODS: In 199 consecutive patients with 234 clipped intracranial aneurysms, 273 intraoperative angiographic studies were retrospectively reviewed. Aneu- rysm size and location, determined with preoperative angiographic and surgical reports, were correlated with the frequency of clip repositioning because of parent- or branch-vessel compromise or unexpected residual aneurysm. RESULTS: Findings from intraopera- live angiograms resulted in clip re- positioning in 46 of 273 (16.8%) stud- ies. Clip repositioning was statistically significantly less frequent with aneu- rysms of the posterior communicat- ing (three of 52 [5.7%] studies) and anterior choroidal (none of 12 stud- ies) arteries. High rates of clip repo- sitioning were found in aneurysms of the superior hypophyseal artery (seven of 18 [38.9%1 studies), supe- nor cerebellar artery (three of five [60.0%] studies), and bifurcation of the internal carotid artery (three of nine [33.3%] aneurysms). In 98 con- ventional follow-up angiographic studies, seven (7%) false-negative cases with unsuspected aneurysm neck remnant were found. CONCLUSION: The rate of clip re- positioning in aneurysms of the pos- tenor communicating or anterior choroidal arteries was less than that at other locations (P < .05). Intraop- erative angiography may not be nec- essary when aneurysms are at these two locations. I NTRAOPERATWE angiography after clipping of intracranial aneurysms is an established, useful procedure (1-4). The advantages of intraopera- tive angiography, compared with those of conventional postoperative studies, are all related to timing. De- spite limitations inherent in intraop- emative angiography, information gained with this technique can lead to modifications at initial surgery that prevent complications or obviate the need for a second operation. Modifi- cations may involve the adjustment of an aneurysm clip because of parent- or branch-vessel compromise or filling of residual aneurysm. The yield (ie, relative frequency of abnormal studies that lead to changes in the surgical approach) of intraop- erative angiography, however, is reba- tively low. In a recent report (4) of the largest series of which we are aware (100 intraoperative angiographic stud- ies after aneurysm clipping), a 12% frequency of clip repositioning or other changes in therapy due to an- giographic findings was reported. This rate of revision is similar to that reported in other series (1-3). The yield of intraopemative angiography could be improved if the technique were performed only in patients in whom an abnormal study was likely to be obtained. The purpose of this study was to determine if such a group of patients could be identified preoperativeby on the basis of aneurysm size and loca- tion. Radiology 1997; 205:335-339 MATERIALS AND METHODS After the clipping of 234 aneurysms in 199 patients between January 1994 and December 1996, 273 consecutive intraop- erative angiograms were obtained. Two factors account for the difference between the number of aneurysms and the number of angiographic studies. First, repeated angiographic studies after clip reposition- ing were considered separately from the initial angiographic results during the same surgical procedure. Second, in pa- tients with multiple clipped aneurysms, each angiogmaphic examination of a treated aneurysm was considered a sepa- rate study. This series of patients did not include those who were treated for a dissecting aneurysm (n = 4) or those who underwent emergent intraoperative angiography in the operating room before craniotomy (n = 4). Also not included in this series were patients whose aneurysms were treated with surgical techniques (eg, trap- ping or proximal ligation) other than clip- ping of the aneurysm neck. One patient underwent surgical exploration without clipping. During the 3-year study period, six patients underwent craniotomy and surgical clipping without follow-up intra- operative angiography. A 5-F femoral sheath was placed during preoperative diagnostic angiography or while the patient was in the operating room (usually after the administration of anesthesia and before surgery). While not in use, the sheath was continuously flushed with hepaminized saline at arterial pressure. A radiolucent operating table (Skytron, Grand Rapids, Mich) and car- bon-fiber head holder (Mayfield radiolu- cent skull clamp; Ohio Medical, Cincin- nati) were used in all patients. The femoral
Transcript of Intracranial Aneurysm: Anatomic Factors That Predict ...ahaq/new/Intracranial aneurysm - anatomic...

Cohn P. Derdeyn, MD #{149}Christopher J. Moran, MD #{149}DeWitte T. Cross III, MDEric W. Sherburn, MD #{149}Ralph G. Dacey, Jr, MD
Intracranial Aneurysm: AnatomicFactors That Predict the Usefulnessof Intraoperative Angiography’
Index terms: Aneurysm, intracranial, 17.73 #{149}Angiography, intraoperative, 17.73
1 From the Section of Neuroradiolog� Mallinckrodt Institute of Radiology (C.P.D., C.J.M., D.T.C.);and the Department of Neurology and Neurosurgery (Neurological Surgery) (E.W.S., R.G.D.), Wash-ington University School of Medicine, 510 5 Kingshighway Blvd, St Louis, MO 63110 ;. ReceivedApril 23, 1997; revision requested June 13; revision received June 24; accepted July 8. Address reprintrequests to C.P.D. C.P.D. supported by a grant from the RSNA/Siemens Medical Systems Researchand Education Fund.
C RSNA, 1997
335
PURPOSE: To correlate the size andlocation of intracranial aneurysmwith the need to reposition the aneu-rysm clip after intraoperative angiog-raphy.
MATERIALS AND METHODS: In199 consecutive patients with 234clipped intracranial aneurysms, 273intraoperative angiographic studieswere retrospectively reviewed. Aneu-rysm size and location, determinedwith preoperative angiographic andsurgical reports, were correlated withthe frequency of clip repositioningbecause of parent- or branch-vesselcompromise or unexpected residualaneurysm.
RESULTS: Findings from intraopera-live angiograms resulted in clip re-positioning in 46 of 273 (16.8%) stud-ies. Clip repositioning was statistically
significantly less frequent with aneu-rysms of the posterior communicat-ing (three of 52 [5.7%] studies) andanterior choroidal (none of 12 stud-ies) arteries. High rates of clip repo-sitioning were found in aneurysmsof the superior hypophyseal artery(seven of 18 [38.9%1 studies), supe-nor cerebellar artery (three of five[60.0%] studies), and bifurcation ofthe internal carotid artery (three ofnine [33.3%] aneurysms). In 98 con-ventional follow-up angiographicstudies, seven (7%) false-negativecases with unsuspected aneurysmneck remnant were found.
CONCLUSION: The rate of clip re-positioning in aneurysms of the pos-tenor communicating or anteriorchoroidal arteries was less than thatat other locations (P < .05). Intraop-erative angiography may not be nec-essary when aneurysms are at thesetwo locations.
I NTRAOPERATWE angiography afterclipping of intracranial aneurysms
is an established, useful procedure
(1-4). The advantages of intraopera-tive angiography, compared withthose of conventional postoperativestudies, are all related to timing. De-spite limitations inherent in intraop-
emative angiography, informationgained with this technique can lead tomodifications at initial surgery thatprevent complications or obviate theneed for a second operation. Modifi-cations may involve the adjustment of
an aneurysm clip because of parent-or branch-vessel compromise or fillingof residual aneurysm.
The yield (ie, relative frequency ofabnormal studies that lead to changesin the surgical approach) of intraop-erative angiography, however, is reba-tively low. In a recent report (4) of thelargest series of which we are aware(100 intraoperative angiographic stud-ies after aneurysm clipping), a 12%frequency of clip repositioning or
other changes in therapy due to an-giographic findings was reported.This rate of revision is similar to thatreported in other series (1-3). Theyield of intraopemative angiography
could be improved if the techniquewere performed only in patients inwhom an abnormal study was likelyto be obtained.
The purpose of this study was todetermine if such a group of patientscould be identified preoperativeby onthe basis of aneurysm size and loca-tion.
Radiology 1997; 205:335-339
MATERIALS AND METHODS
After the clipping of 234 aneurysms in
199 patients between January 1994 andDecember 1996, 273 consecutive intraop-erative angiograms were obtained. Twofactors account for the difference betweenthe number of aneurysms and the numberof angiographic studies. First, repeatedangiographic studies after clip reposition-ing were considered separately from theinitial angiographic results during thesame surgical procedure. Second, in pa-tients with multiple clipped aneurysms,each angiogmaphic examination of atreated aneurysm was considered a sepa-rate study.
This series of patients did not includethose who were treated for a dissectinganeurysm (n = 4) or those who underwentemergent intraoperative angiography inthe operating room before craniotomy(n = 4). Also not included in this serieswere patients whose aneurysms weretreated with surgical techniques (eg, trap-ping or proximal ligation) other than clip-ping of the aneurysm neck. One patientunderwent surgical exploration withoutclipping. During the 3-year study period,six patients underwent craniotomy andsurgical clipping without follow-up intra-operative angiography.
A 5-F femoral sheath was placed duringpreoperative diagnostic angiography orwhile the patient was in the operatingroom (usually after the administration ofanesthesia and before surgery). While notin use, the sheath was continuouslyflushed with hepaminized saline at arterialpressure. A radiolucent operating table(Skytron, Grand Rapids, Mich) and car-bon-fiber head holder (Mayfield radiolu-cent skull clamp; Ohio Medical, Cincin-nati) were used in all patients. The femoral

Table IRevision of Oip Placement according to Aneurysm Location
Frequency of Frequency ofNo. of No. of Revisions No. of No. of Revisions
Arterial Location Studies Revisions (%)* Aneurysms Revisions (%)*
All sites 273 46 16.8 (±4.5) 234 30 12.8 (±4.2)Middle cerebral 60 14 23.3 (±10.6) 49 8 16.3 (±10.3)Anterior communi-
caring 52 8 15.4 (±9.8) 45 5 11.1 (±9.2)Posterior commu-
nicating 52 3 5.7 (±6.3)t 50 3 6.0 (±6.6)Ophthalmic 23 3 13.0 (±13.7) 20 2 10.0 (± 13.1)Superior hypophy-
seal 18 7 38.9 (±22.8)t 3 27.3 (±26.5)tPericallosal 14 3 21.4 (±22.8) 11 2 18.2 (±22.8)Basilar tip 14 1 7.7 (±13.4) 13 1 7.7 (±14.5)Anterior choroidal 12 0 0.0 (±25.0) 12 0 0.0 (±27.3)Bifurcation of
internal carotidartery
Superior cerebellar
125
33
25.0 (±24.5)60.0 (±42.9)
93
32
33.3 (±30.7)t66.6 (±53.3)t
Posterior inferiorcerebellar 4 0 0.0 (±75.0) 4 0 0.0 (±75.0)
Posterior cerebral 3 1 33.3 (±53.3) 3 1 33.3 (±53.3)Anterior cerebral
(Al segment) 2 0 0.0 2 0 0.0 (±0.0)Vertebrobasilar
junction 1 0 0.0 1 0 0.0 (±0.0)Anterior inferior
cerebellar I 0 0.0 1 0 0.0 (±0.0)
* Numbers in parentheses are 95% confidence leveL
t Rate of revision was statically significantly different than the overall rate (P < .05).
336 Radiology November 1997
sheath was draped to allow access duringangiography. Care was taken to avoid
placement of radiopaque materials overthe patient’s head, neck, and chest. The oper-ating room table was positioned to allowspace for the bedside angiographic unit.
Selective catheter placement of the de-
sired vessel was performed in standardfashion with the 5-F arterial sheath imme-diately before angiography. Manual injec-tions were performed. Three views of eachlesion were routinely obtained, includinganterior, lateral, and oblique projections,and attempts were made to duplicate use-fiil preoperative views. In many patients, theneurosurgical head-holding device preventedpredse duplication ofstandard views.
A bedside digital subtraction unit (OECDiasonics, Salt Lake City Utah) that con-sisted of a C-arm fluoroscope, a digital im-age processor and storage unit, and avideo monitor was used in all cases. Thisunit allows performance of routine fluo-roscopy and real-time digital subtractionangiography. The recorded images couldbe reviewed at different speeds and frame-by-frame. Permanent hard-copy imageswere made for the radiologic file with aphotographic unit. The preoperative diag-
nostic studies were available in the operat-ing room for comparison in all cases. Allstudies were interpreted by the attendingneuroradiobogist (C.P.D., C.J.M., D.T.C.),and results were discussed with the neuro-surgeon (R.G.D.). The femorab sheath wasremoved in either the recovery room or theintensive care unit, which allowed routineobservation by the nursing staff of thepuncture site and lower extremity.
The medical records, including surgicaland radiographic reports, were reviewedin all patients. Information gathered in-cluded (a) information about the intraop-erative or postoperative complicationspossibly attributable to angiography orsurgery, (b) the recorded findings of theintraoperative studies, and (c) the sun-geon’s notes about intraoperative decisionsmade on the basis of the angiographic results.
Preoperative and intraoperative angiograms
and surgical reports were reviewed to deter-mine aneurysm size and location. Measureddiameters of aneurysms of the anterior circu-lation were corrected for magnification withthe method described by Zubillaga and co-workers (5). With this method, the actual di-
ameter ofthe internal carotid artery proximal
to the bifurcation is assumed to be 3.4 mm. Aproximal basilar artery diameter of 3.3mmwas used in cases of aneurysm of the poste-
nor circulation (5). Aneurysm size wasgraded as follows: small (diameter < 10
mm), large (diameter, 10-25 mm), and gi-
ant (diameter > 25 mm). Statistical anaby-
sis was performed with the x2 test, withstatistically significant differences inferredat the P < .05 level. Aneurysm location
was categorized by using established con-ventions. Internal carotid artery aneu-rysms were named for the nearest branchvessel of origin (eg, superior hypophyseal
artery aneurysms) even if the vessel was
not visible on angiograms.At our institution, postoperative angiog-
raphy is generally reserved for patients
who do not respond to medical treatmentfor vasospasm and who are candidates forendovascular treatment. These postopera-tive studies were reviewed, and findingswere correlated with those from the intra-operative study to assess accuracy withintraoperative angiograms.
RESULTS
Aneurysm clips were repositioned
on the basis of intraoperative angio-graphic findings from 46 of 273 (16.8% ±4.5 [mean ± 95% confidence level])studies of 234 aneurysms (Table 1).
The repositioning rate per aneurysmwas lower (30 of 234 [12.8% ± 4.2]
aneurysms) than the 16.8% rate per an-giographic study. The 46 intraoperativeangiograms with findings that bed torevision of clip placement were pen-
formed in 30 cases of aneurysm. Two
on more revisions were necessary in 10
of these 30 aneurysms. Findings from
an initial study that bed to clip reposi-
tioning were, therefore, associated with astatistically significantly higher nate ofsubsequent revision of clip placement(10 of 30 [33.3% ± 16.9] aneurysms).
The frequency of clip repositioningwas statistically significantly higher
than average for aneurysms in the
superior hypophyseal and superior
cemebelbar arteries. The frequency of
clip repositioning was statistically sig-
nificantly higher for aneurysms at thebifurcation of the internal carotid am-
temy compared with the frequency forall clipped aneurysms, but not whenthe number of studies performed wasconsidered. High rates of clip reposi-honing that did not reach statisticalsignificance were also seen for aneu-
mysms in the middle cerebral artery
and pericallosal artery. The rate of cliprepositioning was also statisticallysignificantly more frequent for large
aneurysms (Table 2).
The mate of clip repositioning wasstatistically significantly lower than
average for aneurysms in the poste-non communicating artery and in theanterior choroidal artery. If these twosimilar and adjacent locations alongthe posterior wall of the supraclinoidinternal carotid artery proximal to thebifurcation are considered together,
the revision rate was even smaller(three of 64 [4.7% ± 5.1%] angiograms
and three of 60 [4.8% ± 5.3%] aneu-rysms) and achieved statistical signifi-cance for all aneurysms, as well as fortotal studies.
The reasons for clip repositioningcould be grouped into two categories:
(a) parent- or branch-vessel compro-mise and (b) residual aneurysm. The
category of residual aneurysm encom-passed three situations: persistent fill-
ing of the sac, filling of a neck rem-nant, or filling of an uncipped adjacent
lobe or of a second aneurysm. The rela-tive frequency of these two findings

Table 2
Revision of Clip Placement according to Aneurysm Size
No. of No. of Frequency of No. of No. of Frequency ofSize Studies Revisions Revisions (%)* Aneurysms Revisions Revisions (%)*
All sizes 273 46 16.8 (±4.5) 234 30 12.8 (±4.2)Small 240 37 15.4 (±4.6) 215 24 11.2 (±4.2)Large 22 8 36.4 (±20.1)t 19 5 26.3 (±19.8)tGiant 6 1 16.7 (±29.8) 5 1 20.0 (±35.1)
* Numbers in parentheses are 95% confidence level.t Rate of revision was statistically significantly different than the overall rate (P < .05).
Table 3Reasons for Revision of Clip Placement according to Aneurysm Location
Vessel Residual Vessel ResidualNo. of Compromise Aneurysm No. of Compromise Aneurysm
Arterial Location Studies (%) (%) Aneurysms (%) (%)
Allsites 273 17 29 234 11 19Middlecerebral 60 11 3 49 6 2Anterior communi-
cating 52 0 8 45 0 5Posterior communi-
cating 52 0 3 50 0 3Ophthalmic 23 0 3 20 0 2Superior hypophyseal 18 0 7 11 0 3Pericallosal 14 3 0 11 2 0Superior cerebellar 5 0 3 5 0 2Basilartip 14 1 0 13 1 0
Bifurcation of theinternal carotid 12 2 1 9 2 1
Posterior cerebral 3 0 1 3 0 1
p
.4�
a.
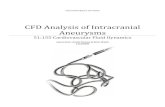
Figure 1. Unexpected filling of residual aneurysm at the superior hypophyseal artery after
initial clip placement. (a) Oblique lateral intraoperative angiogram demonstrates residual fill-
ing of the aneurysm sac (arrow). On the basis of this information, the jaws of the aneurysm clipwe’re opened, and the clip was extended anteriorly. A subtraction artifact (arrowhead) of the
fenestrated aneurysm clip overlies the supraclinoid carotid artery. (b) Same view from the re-
peated intraoperative angiogram demonstrates no filling of the aneurysm and no compromise
of internal carotid artery flow. Arrowhead = subtraction artifact due to the presence of the clip.
b.
Volume 205 #{149}Number 2 Radiology #{149}337
for each aneurysm location is shown
in Table 3. For internal carotid artery
aneurysms above the dunal ring butproximal to the bifurcation, all reposi-tionings were undertaken because of
residual aneurysm. At the superior
hypophyseal location, three of 11 an-
eurysms continued to fill after initial
clipping (Fig 1). In two of these three
aneurysms, multiple surgical adjust-
ments were needed to exclude the an-
eurysm from the circulation. All ante-nor communicating artery aneurysmsthat needed clip revision were for me-
sidual aneurysm, as well. At the tn-
furcation of the middle cerebral artery,most revisions were necessary to im-prove parent-or branch-vessel flow
(abnormal findings from 11 of 14 in-
traopenative angiogmams led to reposi-
tioning) (Fig 2).
Conventional angiography was pen-
formed in 98 of the 234 cases of clippedaneurysms. Unexpected residual aneu-rysm was noted in seven (7% false-nega-tive rate) cases. One of the seven false-
negative studies is shown in Figure 3.
No unexpected parent- or branch-vessel
compromise was seen. No complicationswere observed after intraoperative angi-ography.
DISCUSSION
The goal of surgery in cases of an-
eurysm is to exclude the aneurysmfrom the circulatory system without
compromising flow through parent orbranch vessels. The frequency of in-
complete aneurysm obliteration is notknown. Feuerberg et al (6) found me-
sidual aneurysm in one of 27 (4%)
treated intracranial aneurysms. Clipped
aneurysms with small (1-2 mm inlength) neck remnants have been
shown to enlarge and bleed (6-8).Branch-vessel occlusion caused by an
aneurysm clip may also complicatesurgery. After the clipping of 78 con-
secutive aneurysms, MacDonald et al(9) reported nine unexpected major-
vessel occlusions on postoperative
angiognams obtained urgently or rou-
tinely. Six of these occlusions resulted
in disability due to infarct. In addi-
tion, residual aneurysm was seen insix patients. Three of these six patients
with residual aneurysm underwentrepeated surgery. The frequency ofthese undesired events was 19.2% (15of 78 aneurysms)and was similar to
the rate of clip repositioning observedin our large series and to that reported
by other investigators (1-4).
The data from our investigationsuggest that certain aneurysm boca-
tions and sizes are associated with
particular rates of clip replacement
after intraopenative angiognaphy. A
low rate of clip repositioning after in-
tnaopenative angiography was ob-
served with aneurysms at the rela-
lively easily exposed and well-visualizedsupraclinoid segment of the internal
carotid artery. A change in clip place-
ment was not necessary in any of the
12 aneurysms of the anterior choroi-
dal artery. Revision of clip placementwas necessary in only three of the 50aneurysms of the posterior communi-cating artery. These findings contrast
with those of Alexander et al (4). In
their study of 100 craniotomies, cliprepositioning was necessary in five of27 aneurysms of the posterior commu-
nicating artery. Not all patients in
their series, however, underwent in-tmaoperative angiography; among pa-tients who did not undergo intraop-
erative angiognaphy were six patients

r
b.
,.
I... -
a.
�,1
I4
C.
338 Radiology November 1997
with aneurysms of the posterior com-
municating artery.
High frequencies of unexpected re-
sidual aneurysm that necessitated clipmanipulation were observed at the
superior hypophyseal artery, at the
bifurcation of the internal carotid an-
tery, and at the superior cerebellar ar-
tery. Aneurysms arising from the su-perior hypophyseal artery can be
difficult to �risualize; these aneurysms
are close to the cavernous sinus and
the relatively fixed position of the in-
ternal carotid artery at the durab ring,
which makes exposure of the aneu-rysm neck challenging. All revisions of
clip placement in aneurysms of the
superior hypophyseal artery were per-
formed for residual filling of the aneu-
rysm sac (Fig 1). Adequate exposure ofaneurysms of the superior cerebellan
artery and of the bifurcation of the
internal carotid artery may also be dif-
ficult. Parent- or branch-vessel com-
promise was a frequent finding after
clipping of aneurysms of the middle
cerebral artery. Aneurysms at this lo-
cation often involve origins of branch
vessels, and complete obliteration of
the aneurysm may be difficult without
compromising parent- on branch-yes-
sel flow.
Large aneurysms were associated
with higher rates of clip repositioning.
This finding is not surprising because
visualization of parent and branch
vessels can be more difficult with
larger aneurysms. Giant aneurysms
were not associated with high rates of
revision, but only six of these lesionswere included in this series. Alexander
et al (4) found a statistically signifi-
cantly higher frequency of clip reposi-
tioning in the 11 giant aneurysms they
studied.
No complications attributable to
intraoperative angiography were en-
countered in this retrospective review.
Derdeyn et ab (3) noted one possible
embolic complication in 87 transfemo-
ral catheter placements at intraopera-
tive angiography. Alexander et al (4)
reported one possible embolic compli-
cation in 100 transfemoral studies. The
working conditions in the operatingroom are different from those in the
angiography suite, and the apparentimprovement in the complication rate
of Alexander et al may reflect the ben-
efit of experience.The resolution on intraoperative
angiograms is not as high as that on
conventional angiograms. Small yes-sels such as the anterior choroidab an-tery and perforating vessels often are
not visualized on intraoperative an-
giograms. In addition, the head holder
can limit the angles at which angio-
Figure 2. Unexpected branch-vessel occlu-
sion after clipping of a complex aneurysm of
the middle cerebral artery. (a) Anteroposte-
nor preoperative angiogram of the right in-
ternal carotid artery shows a large, lobulated
aneurysm (arrow) at the trifurcation. An in-
tracerebral hematoma was present with mass
effect. Narrowing of the Ml and Al segments
of the proximal middle cerebral and anterior
cerebral arteries was consistent with vaso-
spasm. (b) Oblique anteroposterior initialintraoperative angiogram obtained after clip-
ping demonstrates no filling of the aneurysm
or of the previously visualized branches of
the middle cerebral artery. Arrow = subtrac-
tion artifact due to the presence of the aneu-
rysm clip. (c) Angiogram acquired after the
clip was repositioned shows restoration of
flow to the branch. Of necessity, the residual
aneurysm (arrow) was left in place.
graphic projections are obtained. Con-
yentional angiography in a dedicatedangiography suite offers biplane capa-
bility, which doubles the number of
views obtained with each injection
and provides higher resolution and
greaten flexibility with regard to pro-
jections. Despite the limitations of in-traoperative angiography, however,
diagnostic information regarding par-
ent- and branch-vessel patency and
the status of the clipped aneurysm is
usually obtained. The radiologist per-
forming these studies must be thor-
oughly familiar with the preoperative
cerebral angiogmam to ensure that in-
traoperative images will optimally
provide clinically relevant infonma-
tion.
An unexpected residual aneurysm
neck was identified on seven of the 98
(7()/()) postoperative angiognams in this
series; note that no vessel occlusions
were found. In general, the false-nega-
tive results obtained in cases of small
neck remnants were often attributableto limited resolution and limited
availability of angiographic projec-
tions with the current intraopenative
angiogmaphic equipment (Fig 3). The
actual rate of false-negative findingsfrom intraopemative angiography in
cases of an unsuspected residual an-
eurysm cannot be determined from
our data because only those patientssuspected of having vasospasm Un-
denwent conventional angiographyafter surgery. Our 7% nate is similar
to that found in other studies of this
technique. Martin et al (1) noted threefalse-negative intraopemative studiesin their series with angiognaphic fob-
low-up in 62 patients. Two residualaneurysm sacs were overlooked, and
a small residual nidus of an anteniove-nous malformation was overlooked in
a third case. In the series of Barrow etal (2), one residual aneurysm sac was
noted in 17 postoperative studies afteraneurysm clipping. With subsequent
angiography, Derdeyn et al (3) ob-
served two unexpected, small residual
aneurysms (false-negative studies) on
25 studies of aneurysms.While intraopenative angiogmaphy
cleanly offers several advantages in

a. b. C.
t_.
I Jfr�.d. e.
Figure 3. False-negative intraoperative angiogram. (a) Preoperative angiogram shows a largeinternal carotid artery aneurysm at the ophthalmic level. (b) On the anteroposterior intraopera-
tive angiogram, no definite residual aneurysm filling is depicted, and the study was consid-
ered to he normal. (c) A similar view from the postoperative angiogram shows definite re-sidual lateral filling (arrow) of the aneurysm beneath the clips. (d) Findings on the lateralintraoperative angiogram are unremarkable and are similar those on (e) the postoperative lat-
eral angiogram.
Volume 205 #{149}Number 2 Radiology #{149}339
the surgical treatment of aneurysms,
this procedure also has some limita-
tions. First, intraoperative angiogra-
phy necessitates more operating-room
time (average of 45 minutes [3]) and
consequently increases cost. Second,intraoperative angiography is associ-
ated with a small risk of angiographiccomplications. Third, intraoperativeangiographic equipment does not pro-
�‘ide the resolution available with
equipment in modem angiography
suites. The magnitude of the rate of
false-negative intraopenative angio-
grams in cases of aneurysm neck rem-
nant and the subsequent effect of this
rate on outcome are unknown. Finally,
the information gained with intnaop-
enative angiognaphy may not result in
improved outcome. For example, de-
spite identification of an abnormality
such as branch-vessel occlusion andrapid surgical correction, an infarct
may still occur (3).
The data from this study demon-strate that different aneurysm diam-
eters and locations are associated withdifferent rates of clip repositioning
after intraoperative angiogmaphy. The
yield of intraoperative angiognaphy is
high in cases of large aneurysms and
of aneurysms of the superior hy-
pophyseal artery, superior cerebellan
artery, and bifurcation of the internal
carotid artery. The need for intraop-
enative angiography should be antici-pated in these situations. The rate ofclip repositioning in aneurysms of the
posterior communicating and anterior
choroidal arteries is low, and intraop-
enative angiognaphy may not be nec-
essary, in these cases. #{149}
� � ReferencesD � Martin NA, Bentson J, Vinucla F, et al. In-
traoperative digital subtraction angiographyand the surgical treatment of intracranialaneurysms and vascular malformations. J Ne’u-rosurg 1990; 73:526-533.
2. Barrow DL, Boyer KL, Joseph GJ. lntraop-
erative angiography in the management ofneurovascular disorders. Neurosurgery
�, 1992; 30:153-159../. 3. Derdeyn CP. Moran CJ, Cross DT, Grubb RL,
Dacey RG. lntraoperative digital subtractionangiography: a review of 112 consecutive cx-aminations. AJNR 1995; 16:307-308.
4. Alexander TD, Macdonald RL, Weir B, Kow-
alczuk A. Intraoperative angiography inaneurysm surgery: a prospective study of100 craniotomies. Neurosurgery 1996; 39:10-18.
5. Zubillaga AF, Guglielmi G, Vinuela F, Duck-wiler GR. Endovascular occlusion of intra-
cranial aneurysms with electrically detach-able coils: correlation of aneurysm neck size
and treatment results. AJNR 1994; 15:815-820.
6. Feuerberg I, Lindquist C, Lindqvist M,Steiner L. Natural history of postoperative
aneurysm rests. J Neurosurg 1987; 66:30-34.7. Drake CG, Vanderlinden RG. The late con-
sequences of incomplete surgical treatmentof cerebral aneurysms. J Neurosurg 1967;27:226-238.
8. Lin T, Fox AJ, Drake CG. Regrowth of an-eurysm sacs from residual neck followinganeurysm clipping. J Neurosurg 1989; 70:556-560.
9. MacDonald R, Wallace M, Kestle J. Role ofangiography following aneurysm surgery.Neurosurg 1993; 79:826-832.