Intracranial and Spinal Ependymomas: Review of MR Images in … · 2009-07-07 · tramedullary...
10
Korean J Radiol 3(4), December 2002 219 Intracranial and Spinal Ependymomas: Review of MR Images in 61 Patients Objective: To compare the age distribution and characteristic MR imaging find- ings of ependymoma for each typical location within the neuraxis. Materials and Methods: During a recent eleven-year period, MR images of 61 patients with histologically proven ependymomas were obtained and retrospec- tively reviewed in terms of incidence, peak age, location, size, signal intensity, the presence or absence of cyst and hemorrhage, enhancement pattern, and other associated findings. Results: Among the 61 patients, tumor location was spinal in 35 (57%), infrar- tentorial in 19 (31%), and supratentorial in seven (12%). In four of these seven, the tumor was located in brain parenchyma, and in most cases developed between the third and fifth decade. Approximately half of the infratentorial tumors occurred during the first decade. The signal intensity of ependymomas was non- specific, regardless of their location. A cystic component was seen in 71% (5/7) of supratentorial, 74% (14/19) of infratentorial, and 14% (5/35) of spinal cord tumors. Forty- nine percent (17/35) of those in the spinal cord were associated with rostral and/or caudal reactive cysts. Intratumoral hemorrhage occurred in 57% (4/7) of supratentorial, 32% (6/19) of infratentorial, and 9% (3/35) of spinal cord tumors. In 17% (6/35) of spinal ependymomas, a curvilinear low T2 signal, suggesting marginal hemorrhage, was seen at the upper and/or lower margins of the tumors. Peritumoral edema occurred in 57% (4/7) of supratentorial, 16% (3/19) of infratentorial and 23% (8/35) of spinal cord tumors. Seventy-two percent (5/7) of supratentorial and 95% (18/19) of infratentorial tumors showed heteroge- neous enhancement, while in 50% (17/34) of spinal cord tumors, enhancement was homogeneous. Conclusion: Even though the MR imaging findings of ependymomas vary and are nonspecific, awareness of these findings, and of tumor distribution according to age, is helpful and increases the likelihood of correct preoperative clinical diagnosis. pendymomas are glial tumors derived from differentiated ependymal cells lining the ventricles of the brain and the central canal of the spinal cord (1). They are rare neoplasms of the central nervous system (CNS), accounting for approximately 2 9% of intracranial gliomas and 30 60% of in- tramedullary spinal tumors (2). A majority occur infratentorially, arising from the floor of the fourth ventricle (3), while most others arise from the outer wall of the lateral ventricles or within the spinal canal. These tumors have a variety of imaging characteristics, some of which are fairly spe- cific. Most previous reports of ependymomas have described their radiologic findings according to the site of origin, though a few have addressed the differences in MR imaging features, if any, found in a series of intracranial and spinal cord tumors ac- Ja-Young Choi, MD Kee-Hyun Chang, MD In Kyu Yu, MD Keon Ha Kim, MD Bae Joo Kwon, MD Moon Hee Han, MD In-One Kim, MD Index terms : Brain, ependymoma Brain, MR Spinal cord, ependymoma Spinal cord, MR Korean J Radiol 2002 ; 3: 219-228 Received March 20, 2002; accepted after revision August 22, 2002. Department of Radiology, Seoul National University College of Medicine; Institute of Radiation Medicine, SNUMRC; Clinical Research Institute, Seoul National University Hospital This study was supported in part by the 2001 BK21 Project for Medicine, Dentistry and Pharmacy. Address reprint requests to : Kee-Hyun Chang, MD, Department of Radiology, Seoul National University College of Medicine, 28 Yongon-dong, Chongno-gu, Seoul 110-744, Korea. Telephone: (822) 760-2584 Fax: (822) 743-6385 e-mail: [email protected] E
Transcript of Intracranial and Spinal Ependymomas: Review of MR Images in … · 2009-07-07 · tramedullary...

Korean J Radiol 3(4), December 2002 219
Intracranial and Spinal Ependymomas:Review of MR Images in 61 Patients
Objective: To compare the age distribution and characteristic MR imaging find-ings of ependymoma for each typical location within the neuraxis.
Materials and Methods: During a recent eleven-year period, MR images of 61patients with histologically proven ependymomas were obtained and retrospec-tively reviewed in terms of incidence, peak age, location, size, signal intensity, thepresence or absence of cyst and hemorrhage, enhancement pattern, and otherassociated findings.
Results: Among the 61 patients, tumor location was spinal in 35 (57%), infrar-tentorial in 19 (31%), and supratentorial in seven (12%). In four of these seven,the tumor was located in brain parenchyma, and in most cases developedbetween the third and fifth decade. Approximately half of the infratentorial tumorsoccurred during the first decade. The signal intensity of ependymomas was non-specific, regardless of their location. A cystic component was seen in 71% (5/7) ofsupratentorial, 74% (14/19) of infratentorial, and 14% (5/35) of spinal cordtumors. Forty- nine percent (17/35) of those in the spinal cord were associatedwith rostral and/or caudal reactive cysts. Intratumoral hemorrhage occurred in57% (4/7) of supratentorial, 32% (6/19) of infratentorial, and 9% (3/35) of spinalcord tumors. In 17% (6/35) of spinal ependymomas, a curvilinear low T2 signal,suggesting marginal hemorrhage, was seen at the upper and/or lower margins ofthe tumors. Peritumoral edema occurred in 57% (4/7) of supratentorial, 16%(3/19) of infratentorial and 23% (8/35) of spinal cord tumors. Seventy-two percent(5/7) of supratentorial and 95% (18/19) of infratentorial tumors showed heteroge-neous enhancement, while in 50% (17/34) of spinal cord tumors, enhancementwas homogeneous.
Conclusion: Even though the MR imaging findings of ependymomas vary andare nonspecific, awareness of these findings, and of tumor distribution according toage, is helpful and increases the likelihood of correct preoperative clinical diagnosis.
pendymomas are glial tumors derived from differentiated ependymalcells lining the ventricles of the brain and the central canal of the spinalcord (1). They are rare neoplasms of the central nervous system (CNS),
accounting for approximately 2 9% of intracranial gliomas and 30 60% of in-tramedullary spinal tumors (2). A majority occur infratentorially, arising from the floorof the fourth ventricle (3), while most others arise from the outer wall of the lateralventricles or within the spinal canal.
These tumors have a variety of imaging characteristics, some of which are fairly spe-cific. Most previous reports of ependymomas have described their radiologic findingsaccording to the site of origin, though a few have addressed the differences in MRimaging features, if any, found in a series of intracranial and spinal cord tumors ac-
Ja-Young Choi, MDKee-Hyun Chang, MDIn Kyu Yu, MDKeon Ha Kim, MDBae Joo Kwon, MDMoon Hee Han, MDIn-One Kim, MD
Index terms:Brain, ependymomaBrain, MRSpinal cord, ependymomaSpinal cord, MR
Korean J Radiol 2002;3:219-228Received March 20, 2002; accepted after revision August 22, 2002.
Department of Radiology, Seoul NationalUniversity College of Medicine; Instituteof Radiation Medicine, SNUMRC; ClinicalResearch Institute, Seoul NationalUniversity Hospital
This study was supported in part by the2001 BK21 Project for Medicine,Dentistry and Pharmacy.
Address reprint requests to:Kee-Hyun Chang, MD, Department ofRadiology, Seoul National UniversityCollege of Medicine, 28 Yongon-dong,Chongno-gu, Seoul 110-744, Korea.Telephone: (822) 760-2584Fax: (822) 743-6385e-mail: [email protected]
E

cording to location (4). The purpose of this study is to re-view the overall MR imaging findings of ependymomasfound in various locations within the neuraxis, and foreach typical location, to compare the age distribution andcharacteristic features.
MATERIALS AND METHODS
We retrospectively reviewed the initial MR images, ob-tained at our institution between January 1990 and
January 2001, of 61 patients [M:F=39:22; age at presenta-tion, 1 70 (mean, 29.1) years] with proven primaryependymoma. For MR examinations, 0.5 , 1.0 , or 1.5-Tunits, produced by various manufacturers, were employed.Images were usually obtained using axial T2-weighted con-ventional or fast spin-echo sequences (TR/TE=4000/98)and sagittal T1-weighted sequences (TR/TE=450/10). Sixtypatients underwent enhanced spin-echo T1-weighted imag-ing in the axial and sagittal planes after the injection of 0.1mmol/kg gadopentetate dimeglumine (Magnevist;
Choi et al.
220 Korean J Radiol 3(4), December 2002
Fig. 1. A 21-year-old man with supraten-torial intraparenchymal ependymoma.A. Axial T2-weighted spin-echo (SE) im-age (4500/96) depicts a large tumor withan extensive cystic component (asterisk)in the left frontal lobe. The lesion focallyabuts the adjacent frontal horn of the lat-eral ventricle (open arrow), and there ismild peritumoral edema (arrowheads).B. Axial T1-weighted SE image (500/12)demonstrates an area of focal hyperin-tensity within the tumor (arrow),respre-senting intratumoral hemorrhage. Due,presumably, to its high protein content,the cystic component appears isointenseto gray matter.C, D. Axial (C) and sagittal (D) contrast-enhanced T1-weighted SE images(500/12) show heterogeneous enhance-ment and a well-defined tumor margin.The cystic portion is multi-septated andenhanced (arrowheads).
A B
C D

Schering, Berlin, Germany).Three observers reviewed all MR images, reaching a con-
sensus. Tumor location was categorized as supratentorial,infratentorial, or spinal, the last of these being subcatego-rized as cervical, thoracic, or filar. If a tumor extendedacross two or more regions, it was classified according tothe site of its greatest mass. At each location, the positionof a tumor was determined. Supratentorial ependymomaswere classed as transependymal if they arose within theventricular system but breached the ependymal lining toinvade surrounding parenchyma, or as intraventricular or
MR Imaging of Intracranial and Spinal Ependymomas
Korean J Radiol 3(4), December 2002 221
Table 1. Age Distribution of Ependymomas for Each Loc-ation
Age Supratentorial Infratentorial Spinal cord
10 1 10 0211 20 0 01 0521 30 3 03 1031 40 2 01 0541 50 1 01 0751 60 0 03 0361 70 0 00 03
Total 7 19 35
Fig. 2. A 34-year-old man with supraten-torial transependymal ependymoma.A. Axial T2-weighted SE image (5000/99) depicts a slightly hyperintense, largetumor located within the frontal horns ofboth lateral ventricles (open arrow),which are dilated.B. Axial T1-weighted SE image (600/12)shows that the tumor is slightly hy-pointense and has a lobulated margin.C, D. Axial (C) and coronal (D) contrast-enhanced T1-weighted SE images(500/12) depict parenchymal invasionadjacent to the left frontal horn (arrow-heads), with heterogeneous enhance-ment.
A B
C D
intraparenchynal. Infratentorial tumors were either intra-ventricular, or were associated with extension from thefourth ventricle through the foramen of Magendie orLuschka. A spinal tumor was considered central if axialimaging showed that no more than 60% of its cross-sec-tional area was located to one side of the midline, or eccen-tric if this was not the case (5). The size of an intracraniallesion was determined according to its longest diameter,and for a spinal location, according to the number of spinalsegments involved.
For each imaging sequences, the signal intensity of an in-
tracranial and a spinal tumor was compared, respectively,with that of gray matter and spinal cord.
A tumor was considered to have a cystic component if acyst associated with it contained an enhanced nodule orhad an enhanced wall. Especially in spinal cord ependymo-mas, this type of tumor is in contradistinction to the nonen-hanced, non-neoplastic rostral and caudal reactive cysts of-ten associated with spinal cord tumors. The distinction be-tween rostral /caudal cysts and reactive dilatation of thecentral canal can be difficult, and secondary reactive dilata-tion of this kind was classified as a cyst (6). If areas of high
Choi et al.
222 Korean J Radiol 3(4), December 2002
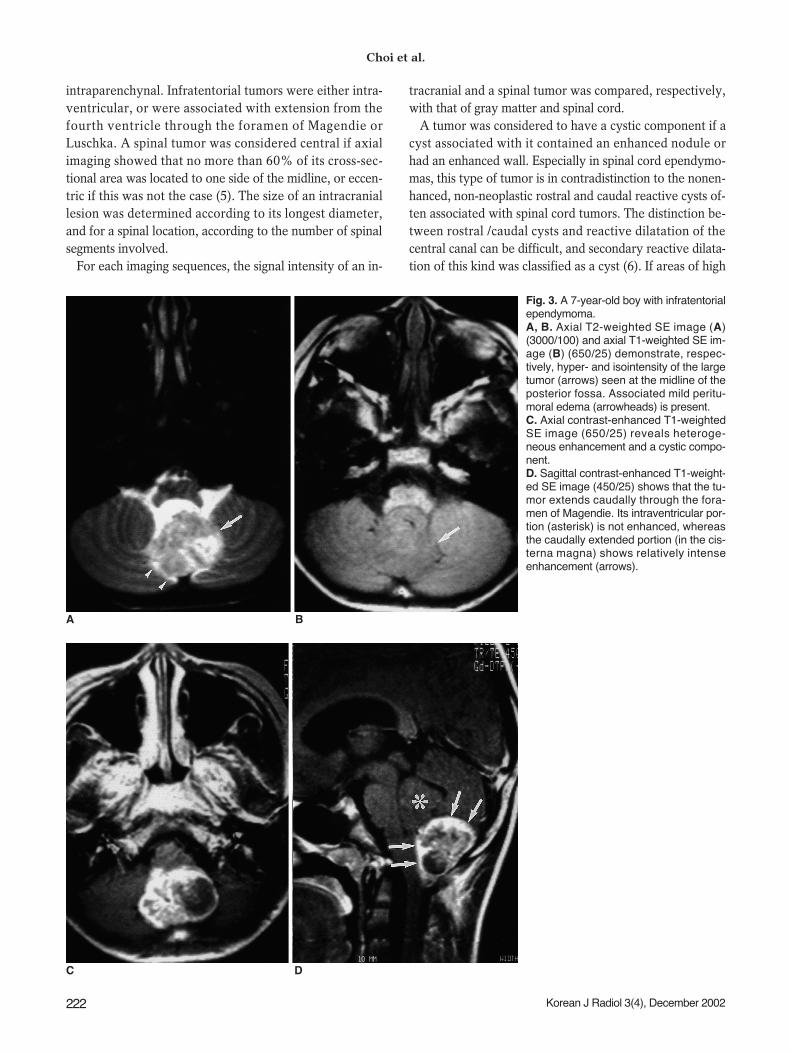
Fig. 3. A 7-year-old boy with infratentorialependymoma.A, B. Axial T2-weighted SE image (A)(3000/100) and axial T1-weighted SE im-age (B) (650/25) demonstrate, respec-tively, hyper- and isointensity of the largetumor (arrows) seen at the midline of theposterior fossa. Associated mild peritu-moral edema (arrowheads) is present.C. Axial contrast-enhanced T1-weightedSE image (650/25) reveals heteroge-neous enhancement and a cystic compo-nent.D. Sagittal contrast-enhanced T1-weight-ed SE image (450/25) shows that the tu-mor extends caudally through the fora-men of Magendie. Its intraventricular por-tion (asterisk) is not enhanced, whereasthe caudally extended portion (in the cis-terna magna) shows relatively intenseenhancement (arrows).
A B
C D

signal intensity were obscured at non-enhanced T1-weight-ed imaging, intratumoral hemorrhage was thought to bepresent. In ependymomas of the spinal cord, the presenceor absence of a low signal intensity rim at the boundariesof the tumor at T2-weighted imaging, which suggestedmarginal hemorrhaging, was also evaluated.
Peritumoral edema was scored as absent, mild (affectingan area less than half that of the tumor), moderate (affect-ing an area greater than half that of tumor, but not greaterthan that of the tumor itself), or marked (affecting an area
greater than that of the tumor).The presence and pattern of tumor enhancement and the
definition of enhanced borders were assessed. The en-hancement pattern was qualitatively evaluated as eitherhomo- or heterogeneous, and enhanced margins as eithersharply or poorly defined.
RESULTS
Of 61 ependymomas, seven (12%) were supratentorial,
MR Imaging of Intracranial and Spinal Ependymomas
Korean J Radiol 3(4), December 2002 223
Fig. 4. A 3-year-old boy with infratentorialependymoma.A. Axial T2-weighted SE image (4500/96) depicts a large slightly hyperintensemass in the fourth ventricle. The massextends to the right cerebellopontine an-gle and prepontine cistern through bothlateral recesses and the foramen ofLuschka (arrowheads), encasing a linearsignal void (arrow) thought to be a vascu-lar structure.B. T1-weighted SE image (500/12) re-veals the presence of a small area of fo-cal high signal intensity (open arrow)within the mass, suggesting intratumoralhemorrhage.C, D. Axial (C) and sagittal (D) contrast-enhanced T1-weighted SE images(500/12) show heterogeneous enhance-ment, with multiple cystic componentsand associated peripheral rim enhance-ment. The mass extends to the cerebel-lopontine angle bilaterally, and to the lev-el of the upper cervical cord caudally (ar-rows).A B
C D

19 (31%) were infratentorial, and 35 tumors (57%) werespinal.
Age and Gender Distribution for Each LocationMost supratentorial ependymomas (in six of seven pa-
tients) occurred in adults between their third and fifthdecade. Ten infratentorial tumors (53%), on the otherhand, developed during the first decade. Spinal cord tu-mors were found among all age groups, with two-thirds oc-curring in these between their third and fifth decade. Thefindings appear in Table 1.
The overall male to female ratio was 1.8:1 (39:22). Four(57%) of seven patients with supratentorial tumors, 12(63%) of 19 with infratentorial tumors, and 23 (66%) of35 with spinal cord tumors were male.
Tumor LocationOf seven supratentorial ependymomas, one was entirely
intraventricular, four were entirely intraparenchymal (Fig.1), and two were transependymal (Fig. 2). Of 19 infraten-torial tumors, only one was confined within the fourth ven-tricle. Sixteen (84%) extended caudally via the foramen of
Choi et al.
224 Korean J Radiol 3(4), December 2002
Fig. 5. A 30-year-old woman with spinal ependymoma of the cervical cord.A, B. Sagittal T2-weighted SE image (A) (4000/120) shows that the mass at the level of C-5 to C-6 (arrows) is heterogeneously hyperin-tense, while T1-weighted image (B) (671/12) shows hypointensity. Associated rostral and caudal cysts are also visible.C. Sagittal contrast-enhanced T1-weighted SE image (671/12) shows homogeneous enhancement and a well-defined, enhanced border(arrows). Extensive associated rostral and caudal cysts (asterisks) extend from the level of the foramen magnum to T-3.
A B C
Table 2. Summary of MR Imaging Findings of Ependymomas
Supratentorial (n=7) Infratentorial (n=19) Spinal (n=35)
Signal intensity low iso high low iso high low iso highT2WI 0 (0%)0 1 (14%) 6 (86%) 0 (0%)0 02 (11%) 17 (89%) 00 (0%)0 02 (6%)0 33 (94%)T1WI 3 (43%) 3 (43%) 1 (14%) 8 (42%) 11 (58%) 00 (0%)0 11 (31%) 22 (63%) 02 (6%)0
Cystic component 5 (71%) 14 (74%) 05 (14%)Intratumoral hemorrhage 4 (57%) 06 (32%) 03 (9%)0Hemosiderin cap 0 (57%) 00(57%) 06 (17%)Peritumoral edema 4 (57%) 03 (16%) 08 (23%)Enhancement pattern
Homogeneous 1 (14%) 01 (5%)0 17 (50%)Heterogeneous 5 (72%) 18 (95%) 14 (41%)Non-enhancement 1 (14%) 00 (0%)0 03 (9%)0
Note. T2WI = T2-weighted imaging, T1WI= T1-weighted imaging, In one patient with a spinal tumor, contrast-enhanced scanning was not performed.

Magendie (Fig. 3), and 12 (63%) into the cerebellopontineangle through the lateral recesses and the foramen ofLuschka. Ten extended both caudally and laterally viaboth the foramina of Magendie and Luschka (Fig. 4). Of 35spinal cord tumors, 14 (40%) were cervical, 10 (29%)were thoracic, and 11 (31%) were filar in location.Transaxial images showed that the epicenters of 32 (91%)of these 35 tumors corresponded to the center of the spinalcord.
Tumor SizeThe longest diameter of supratentorial tumors ranged
from 2.5 to 6.0 (mean, 4.5) cm; for intraparenchymal andintraventricular tumors, respectively, this measurement
was 5.0 and 3.8 cm. Infratentorial tumors ranged in sizefrom 3.0 to 7.0 (mean, 4.9) cm, and the extent of spinalcord tumors, measured along their neuraxis, was 1 13(mean, 3.1) vertebral segments.
Signal Intensity At TI-weighted imaging, three (43%) of seven supraten-
torial tumors were isointense relative to gray matter, andthree others (43%) were hypointense (Fig. 2B); 11 (58%)of 19 infratentorial tumors and 22 (63%) of 35 spinal cordtumors were isointense. At T2-weighted imaging, six(96%) of seven supratentorial, 17 (89%) of 19 infratentori-al and 33 (94%) of 35 spinal cord tumors were hyperin-tense relative to the signal intensity of gray matter. The
MR Imaging of Intracranial and Spinal Ependymomas
Korean J Radiol 3(4), December 2002 225
Fig. 6. A 50-year-old woman with spinalependymoma at the thoracic level.A. Sagittal T2-weighted SE image(3500/108) depicts an extensive hetero-geneous lesion of mixed signal intensityin almost the entire spinal cord. Rostraland caudal cysts with inner multifocal flu-id fluid levels (arrowheads) are exten-sive, and after previous hemorrhage, he-mosiderin has been deposited. In addi-tion, a dark line suggesting hemosiderindeposition (open arrow) is noted alongthe cord and the bottom of the caudalcyst. Asterisk indicates the T-5 level ofthe small enhancing tumor seen in B.B. Sagittal contrast-enhanced T1-weight-ed SE image (500/14) depicts a smallarea of slightly heterogeneous enhance-ment at the T-5 level of the spinal cord(asterisk).
A B
Table 3. Summary of MR Imaging Findings of Spinal Cord Ependymomas
Cervical (n=14) Thoracic (n=10) Filar (n=11)
Signal intensity low iso high low iso high low iso highT2WI 0 (0%)0 1 (7%)0 13 (93%) 0 (0%)0 1 (10%) 9 (90%) 0 (0%)0 0 (0%)0 11 (100%)T1WI 6 (43%) 8 (57%) 00 (0%)0 3 (30%) 5 (50%) 2 (20%) 2 (18%) 9 (82%) 00 (0%)00
Cystic component 3 (21%) 1 (10%) 1 (9%)0Reactive cyst 9 (64%) 6 (60%) 2 (18%)Intratumoral hemorrhage 1 (7%)0 1 (10%) 1 (9%)0Hemosiderin cap 4 (29%) 1 (10%) 1 (9%)0Peritumoral edema 4 (29%) 3 (30%) 1 (9%)0Enhancement pattern
Homogeneous 9 (64%) 4 (40%) 5 (45%)Heterogeneous 5 (36%) 4 (40%) 4 (36%)Non-enhancement 0 (0%)0 2 (20%) 1 (9%)0
Note. T2WI = T2-weighted imaging, T1WI= T1-weighted imaging

others were isointense.
Cyst and HemorrhageFive (71%) of seven supratentorial, 14 (74%) of 19 in-
fratentorial, and five (14%) of 35 spinal cord ependymo-mas had an intratumoral cystic component (Fig. 4). Four ofthe five supratentorial tumors with this component wereintraparenchymal (Fig. 1), and in 17 (49%) of 35 spinalcord tumors, rostral (n=16) and/or caudal (n=14) reactivecysts were present. Among the 14 cervical cord tumors,cyst type was rostral (n=9), caudal (n=10), or both (n=9)(Fig. 5), while the ten thoracic cord tumors contained ei-ther rostral (n=5), caudal (n=3), or both types of cyst (n=3).The cysts associated with the 11 filar tumors were eitherrostral (n=2), caudal (n=1) or of both types (n=1).
Intratumoral hemorrhage occurred in 13 (21%) of the 61ependymomas [in four (57%) of seven supratentorial, six(32%) of 19 infratentorial, and three (9%) of 35 spinalcord tumors] (Figs. 1 and 4). At T2-weighted imaging,rim(s) of low signal intensity, suggesting marginal hemor-rhage between normal and tumor tissue, were seen at theupper or lower margins of six (17%) of 35 spinal cordependymomas; four of the six were cervical (Fig. 7), onewas thoracic (Fig. 6), and one was filar.
Peritumoral EdemaPeritumoral edema occurred in four (57%) of seven
supratentorial, three (16%) of 19 infratentorial, and eight(23%) of 35 spinal cord tumors. Among supratentorial tu-
mors the edema was mild in two cases (Fig. 1), moderate inone, and severe in one, three (75%) of four intraparenchy-mal supratentorial tumors showed no or mild edema. In allthree infratentorial tumors the edema was mild, andamong spinal cord tumors it was mild in six and moderatein two (Fig. 7).
Enhancement PatternAmong the 60 patients who underwent contrast-en-
hanced scanning, tumor enhancement was demonstrated in56 patients (93%); in 53 (95%) of these (five of six supra-tentorial, 18 of 19 infratentorial, 30 of 31 spinal cord tu-mors), the enhanced margins were sharply defined.Enhancement was heterogeneous in five (71%) of sevensupratentorial tumors and 18 (95%) of 19 infratentorial tu-mors (Fig. 2C), while among 34 spinal cord tumors, the ob-served pattern was homogeneous in 17 cases (50%) (Fig.5) and heterogeneous in 14 (41%) (Fig. 6). In three cases(9%) there was no enhancement.
The MR imaging findings of ependymomas for each loca-tion and spinal tumors for each subtype are summarized inTables 2 and 3, respectively.
DISCUSSION
Ependymomas develop most often in children, adoles-cents and young adults, but may also occur in older agegroups (3). In our series, most supratentorial ependymo-mas developed during the third to fifth decade, while ap-
Choi et al.
226 Korean J Radiol 3(4), December 2002
Fig. 7. A 27-year-old man with ependy-moma of the cervical cord.A. Sagittal T2-weighted SE image(3500/120) shows that in the upper cervi-cal cord, a heterogeneously intensemass with a low signal intensity rim (ar-rows) at its upper and lower margins ispresent. Associated peritumoral edema(arrowheads) is also apparent.B. Sagittal contrast-enhanced T1-weight-ed SE image (500/15) of the tumor de-picts heterogeneous mild enhancement.
A B

proximately 50% of infratentorial ependymomas occurredduring the first decade. Spinal cord tumors occurred be-tween the first and seventh decade, with approximatelytwo-thirds developing between the third and fifth.Although no significant difference in the frequency ofependymomas between the two genders has been reported(7), in our series they occurred 1.8 times more frequentlyin males than in females.
Although ependymomas are classically considered to oc-cur most frequently in the fourth ventricle - infratentorialregion (8), the most common location in our series was thespinal cord (57% of 60 lesions), followed by infratentorialand then supratentorial. Of all intracranial ependymomas,approximately 60% are infratentorial and 40% are supra-tentorial (9), though in our series, the ratio was approxi-mately 7:3. Whereas supratentorial tumors tend to beparenchymal, infratentorial tumors are usually intra-ventricular (10), and we observed similar findings. The ex-traventricular location of most supratentorial ependymo-mas has been attributed to their origin in extraventricularependymal cell rests (11), which are reported to occurmainly in regions where subependymal neural glia extendinto adjacent white matter, e.g. at the angled margins ofthe ventricles (12). All four supratentorial intraparenchy-mal tumors in our series were large (average diameter, 5.0cm), and focally abutted the adjacent ventricle. Thus, theseimaging features may help differentiate between ependy-moma and other supratentorial tumors.
“Desmoplastic development” is the term used to de-scribe the way in which infratentorial ependymomas ex-tend through the outlet foramina of the fourth ventricle in-to the subarachnoid space of the posterior cranial fossa.The prevalence of desmoplastic development through theforamen of Magendie and/or Luschka in our study wassimilar to that previously reported (13).
The signal intensity of ependymomas is nonspecific. Inour study, regardless of their location within the neuraxis,they were hypo- to isointense to gray matter at non-en-hanced T1-weighted imaging, and hyperintense at T2-weighted imaging, findings which were similar to those ofother CNS tumors (14, 15).
Supratentorial ependymomas are commonly cystic (be-tween 40 and 85%) (10 12, 16), and in our series, 71%(5/7), including all that were supratentorial, had cysticcomponents. Our results confirm the observation of Furieand Provenzale (17), who reported that supratentorial ex-traventricular ependymomas are typically large cysticmasses. As for infratentorial ependymomas, Tortori-Donatiet al. (13) reported that MR imaging depicted cystic changein 65% of such cases; in our series, 74% (14/19) had cysticcomponents. In contrast to intracranial ependymomas,
these of the spinal cord are not usually cystic (between 4and 50%) (5, 18); in our series, only 14% (5/35) had an in-tratumoral cystic component. Rostral and/or caudal cystsare frequently associated with intramedullary tumors of allhistologic types (19). These cysts are important becausethey reflect a reactive process within the spinal cord, donot contain neoplastic cells, and do not need to be resected(19). However, the prevalence of associated reactive cystsdoes not serve as a distinguishing feature of ependymomas:Epstein et al. (20) reported that about 30% of tumors wereassociated with a rostral or caudal cyst similar to that notedin spinal cord astrocytoma cases. The frequency of associ-ated cysts in our series (49%) was slightly higher.
Intratumoral hemorrhage occurs infrequently in ependy-momas, with a prevalence of 0 to 13% in three reportedseries (5, 10, 21). In ours, the figure was slightly higher(21%), with regional variation (highest in supratentorial tu-mors, 57%; lowest in spinal cord tumors, 9%). At T2imaging, the presence of a low-signal rim along the rostralor caudal margin of a spinal cord tumor is a fairly specificindicator of ependymoma, and was found in 20% and64% of cases in the series investigated, respectively, byFine et al. (5) and Nemoto et al. (22). The rim is due to thepresence of hemosiderin at the margin of the tumor, aris-ing, presumably, from prior subclinical tumoral hemor-rhage, and is often referred to as a ‘hemosiderin cap’. Inour series, the ‘cap’ occurred slightly less frequently, in17% of cases. It was more frequently observed in cervicaltumors (29%), a finding similar to that of Fine et al. (5),and one which may support the idea that motional differ-ences in neural tissues that occur at the relatively sharp in-terface between a tumor and the spinal cord partly accountfor the higher prevalence of marginal hemorrhage in thecervical region (22).
Where there is parenchymal involvement, peritumoraledema is usually mild. In our series, all infratentorialependymomas, 94% of spinal cord ependymomas, and71% of supratentorial ependymomas showed no or mildperitumoral edema. We believe that the relative lack ofperitumoral edema in infratentorial and spinal tumors re-sults from the space limitation imposed by their intra-ventricular or intraspinal location.
Most ependymomas in our series (93%) showed contrastenhancement, though the pattern of this varied. It was het-erogeneous in 71% of supratentorial and 95% of infraten-torial ependymomas, but homogeneous in 50% of spinalcord tumors. Parizel et al. (23) stated that spinal cordependymomas generally show intense, homogeneous en-hancement, while Fine et al. (5), on the other hand, report-ed heterogeneous enhancement in 65% (15/23) of suchcases. In our study, five of 16 infratentorial ependymomas
MR Imaging of Intracranial and Spinal Ependymomas
Korean J Radiol 3(4), December 2002 227

with caudal extension through the foramen of Magendiehad an unenhanced intraventricular portion, whereas thecaudally extended portion showed relatively intense en-hancement. The margin of the enhanced area was sharplydefined in 95% (53/56) of our cases. Fine et al. (5) statedthat this finding is a characteristic feature of spinal cordependymoma and is analogous to the surgical andhistopathologic observation of a generally well-defined in-terface between ependymomas and adjacent spinal cord.Johnson et al. (24), however, emphasized that in intracra-nial tumors, isolated tumor-cell infiltration may exist out-side the margin of contrast enhancement.
In summary, slightly more than half of the 61 ependymo-mas occurred in the spinal cord. Approxi-mately half theinfratentorial ependymomas occurred during the firstdecade of age. Supratentorial ependymomas developedmore frequently in brain parenchyma than in the ventricle.The signal intensity of an ependymoma is not specific, re-gardless of its location. The incidence of a cystic compo-nent was significantly higher in intracranial than in spinalependymomas. The rate of focal intratumoral hemorrhagewas higher in intracranial than in spinal tumors. A‘hemosiderin cap’ was seen in 17% (6/35) of spinalependymomas, most commonly in cervical tumors (4/6).Most ependymomas were accompanied by no or mild peri-tumoral edema, irrespective of their location. The ob-served pattern of contrast enhancement was more fre-quently heterogeneous in intracranial than in spinalependymomas.
References1. Russel DS, Rubenstein LJ. Pathology of tumors of the nervous
system, 5th ed. Baltimore: Williams & Wilkins, 1989:192-2192. Rezai AR, Woo HH, Lee M, Cohen H, Zagzag D, Epstein FJ.
Disseminated ependymomas of the central nervous system. JNeurosurg 1996;85:618-624
3. Fokes EC, Earle KM. Ependymomas: clinical and pathologicalaspects. J Neurosurg 1969;30:585-594
4. Lefton DR, Pinto RS, Martin SW. MRI features of intracranialand spinal ependymomas. Pediatr Neurosurg 1998;28:97-105
5. Fine MJ, Kricheff II, Freed D, Epstein FJ. Spinal cord ependy-momas: MR imaging features. Radiology 1995;197:655-658
6. Kahan H, Sklar EM, Post MJ, Bruce JH. MR characteristics of
histopathologic subtypes of spinal ependymoma. AJNR Am JNeuroradiol 1996;17:143-150
7. Greenfield JG. Greenfield’s Neuropathology, 6th ed. New York:Oxford University Press, 1992:636-644
8. Barone BM, Elvidge AR. Ependymoma: a clinical survey. JNeurosurg 1970;33:428-438
9. Kernhan JW, Sayre GP. Tumors of the central nervous system:Atlas of tumor pathology Section X, Fascicle 35. Washington:Armed Forces Institute of Pathology, 1952
10. Armington WG, Osborn AG, Cubberley DA, et al. Supratento-rial ependymoma: CT appearance. Radiology 1985;157:367-372
11. Swartz JD, Zimmerman RA, Bilaniuk LT. Computed tomogra-phy of intracranial ependymomas. Radiology 1982;143:97-101
12. Svien HJ, Mabon RF, Kernohan JW, Craig W. Ependymoma ofthe brain: pathologic aspects. Neurology 1953;3:1-15
13. Tortori-Donati P, Fondelli MP, Cama A, Garre ML, Rossi A,Andreussi L. Ependymomas of the posterior cranial fossa: CTand MRI findings. Neuroradiology 1995;37(3):238-243
14. Lee BCP, Kneeland JB, Cahill PT, Deck MDF. MR recognitionof supratentorial tumors. AJNR Am J Neuroradiol 1985;62:508-512
15. Komiyama M, Yagura H, Baba M, et al. MR imaging: possibilityof tissue characterization of brain tumors using T1 and T2 val-ues. AJNR Am J Neuroradiol 1987;8:65-70
16. Coulon RA, Till K. Intracranial ependymomas in children: a re-view of 43 cases. Child’s Brain 1977;3:154-168
17. Furie DM, Provenzale JM. Supratentorial ependymomas andsubependymomas: CT and MR appearance. J Comput AssistTomogr 1995;19:518-526
18. Li MH, Holtas S. MR imaging of spinal intramedullary tumors.Acta Radiol 1991;32:505-513
19. Goy AMC, Pinto RS, Raghavendra BN, Epstein FJ, Kricheff II.Intramedullary spinal cord tumors: MR imaging, with emphasison associated cysts. Radiology 1986;161:381-386
20. Epstein FJ, Farmer JP, Freed D. Adult intramedullary spinalcord ependymomas: the result of surgery in 38 patients. JNeurosurg 1993;79:204-209
21. Naidich TP, Zimmerman RA. Primary brain tumors in children.Semin Roentgenol 1984;19:100-114
22. Nemoto Y, Inoue Y, Tashiro T, et al. Intramedullary spinal cordtumors: significance of associated hemorrhage at MR imaging.Radiology 1992;182:793-796
23. Parizel PM, Bakeriaux D, Rodesch G, et al. Gd-DTPA-enhancedMR imaging of spinal tumors. AJNR Am J Neuroradiol1989;10:249-258
24. Johnson PC, Hunt SJ, Drayer BP. Human cerebral gliomas: cor-relation of postmortem MR imaging and neuropathologic find-ings. Radiology 1989:1713-1771
Choi et al.
228 Korean J Radiol 3(4), December 2002