Interventional Treatment of Stroke · Interventional Treatment of Stroke Andrew F. Ducruet, MD...
83
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018
Transcript of Interventional Treatment of Stroke · Interventional Treatment of Stroke Andrew F. Ducruet, MD...
Interventional Treatment
of Stroke
Andrew F. Ducruet, MD Barrow Neurological Institute
2018 BNI Stroke Rehab Symposium
October 13, 2018

Disclosures
• Consultant: Medtronic, Penumbra,
Cerenovus

Lecture Overview
• Introduction
• Current State of Interventional
Stroke treatment
• Recent Clinical Studies
• Case Studies
• Future Directions

BNI Endovascular Stroke Volume
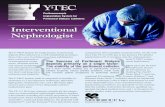
Mechanical Thrombectomy:
MERCI
Approved 2004
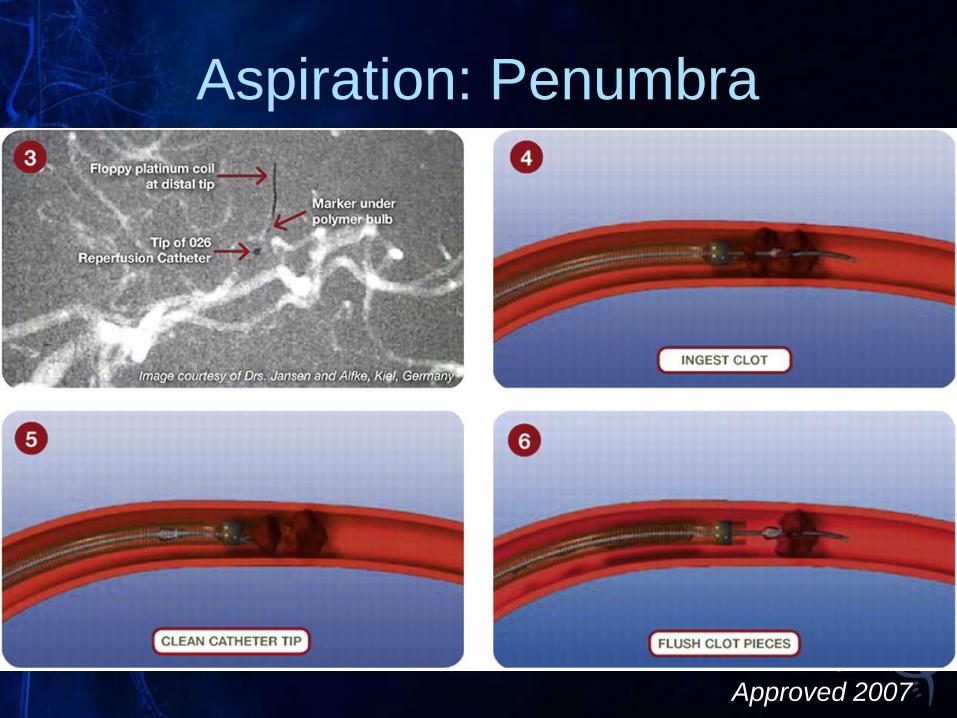
Aspiration: Penumbra
Approved 2007
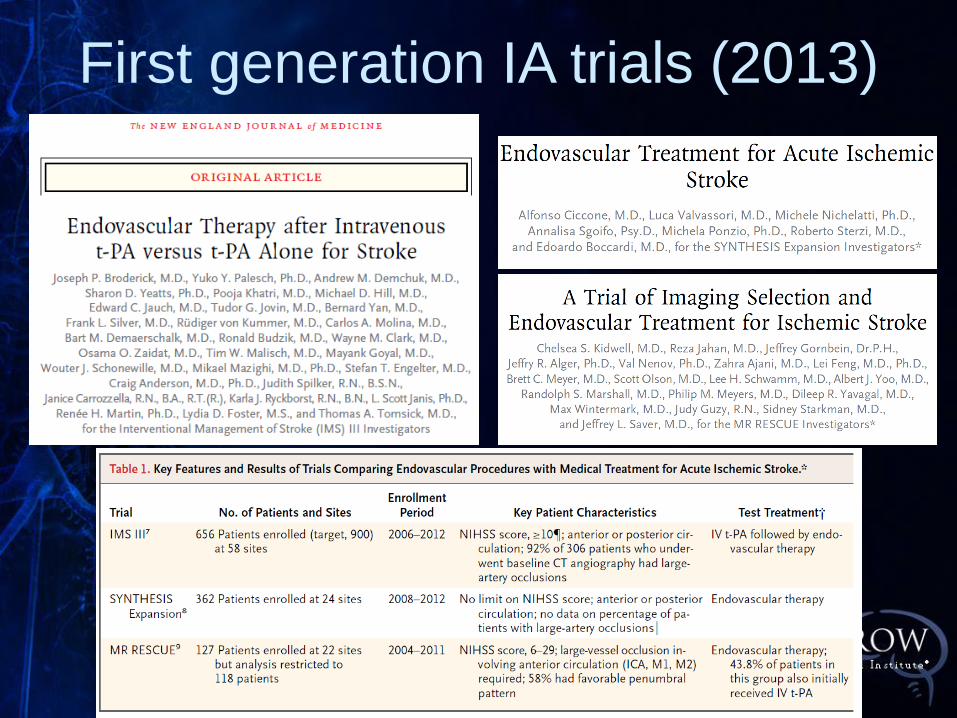
First generation IA trials (2013)

No difference in outcomes

Limits of 1st generation IA trials
• Improper patient selection
• Only 47% of patient had baseline CTA or
MRA documenting an occlusion
• Outdated devices incomplete
recanalization
• Only 27% TICI 2B/3
• Significant delays to reperfusion
• Mean 325 minutes in the endovascular cohort
with a strong time-treatment interaction • Every 30 minutes delay 10% worse outcomes

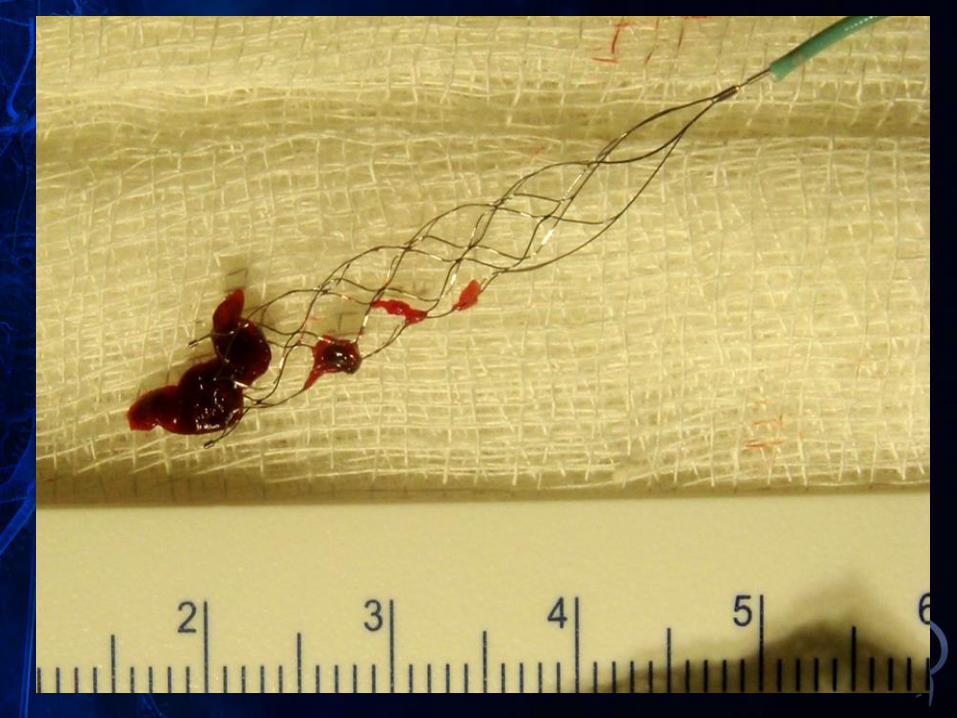
Stentrievers: 2012


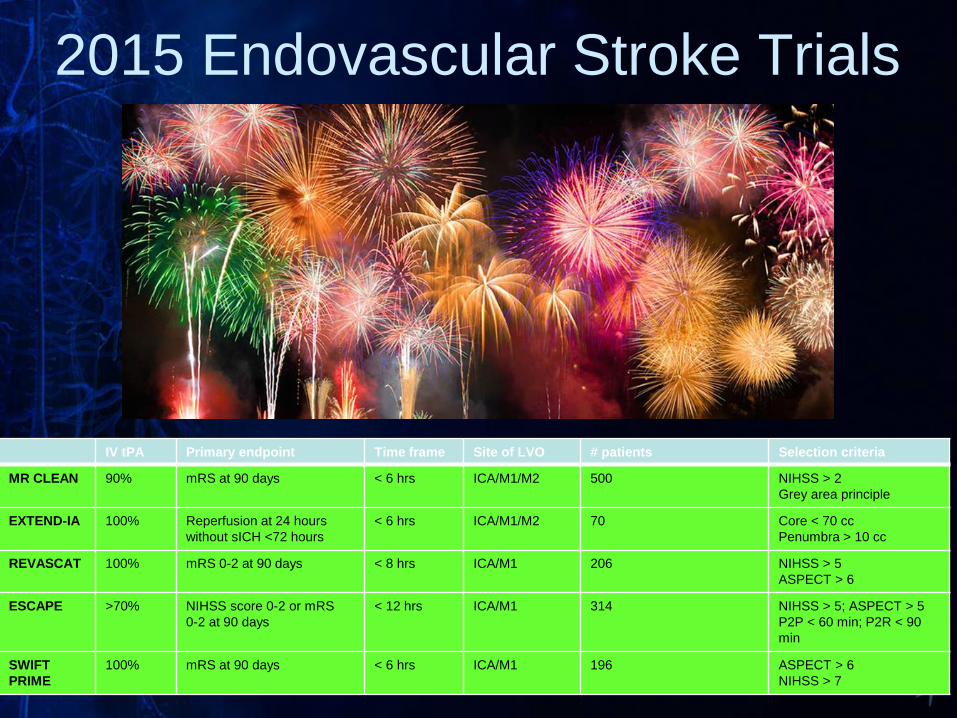
IV tPA Primary endpoint Time frame Site of LVO # patients Selection criteria
MR CLEAN 90% mRS at 90 days
< 6 hrs ICA/M1/M2 500 NIHSS > 2
Grey area principle
EXTEND-IA 100%
Reperfusion at 24 hours
without sICH <72 hours
< 6 hrs
ICA/M1/M2
70 Core < 70 cc
Penumbra > 10 cc
REVASCAT 100% mRS 0-2 at 90 days < 8 hrs ICA/M1 206 NIHSS > 5
ASPECT > 6
ESCAPE >70% NIHSS score 0-2 or mRS
0-2 at 90 days
< 12 hrs ICA/M1 314 NIHSS > 5; ASPECT > 5
P2P < 60 min; P2R < 90
min
SWIFT
PRIME
100% mRS at 90 days < 6 hrs ICA/M1 196 ASPECT > 6
NIHSS > 7
2015 Endovascular Stroke Trials

MR CLEAN trial (Netherlands)
– ASPECTS 8-10:
75%
(Berkhemer et al NEJM 2015)
mRS 0-2 at 90d:
- 32.6% vs. 19.1%
- absolute diff: 13.5%
- NNT = 7
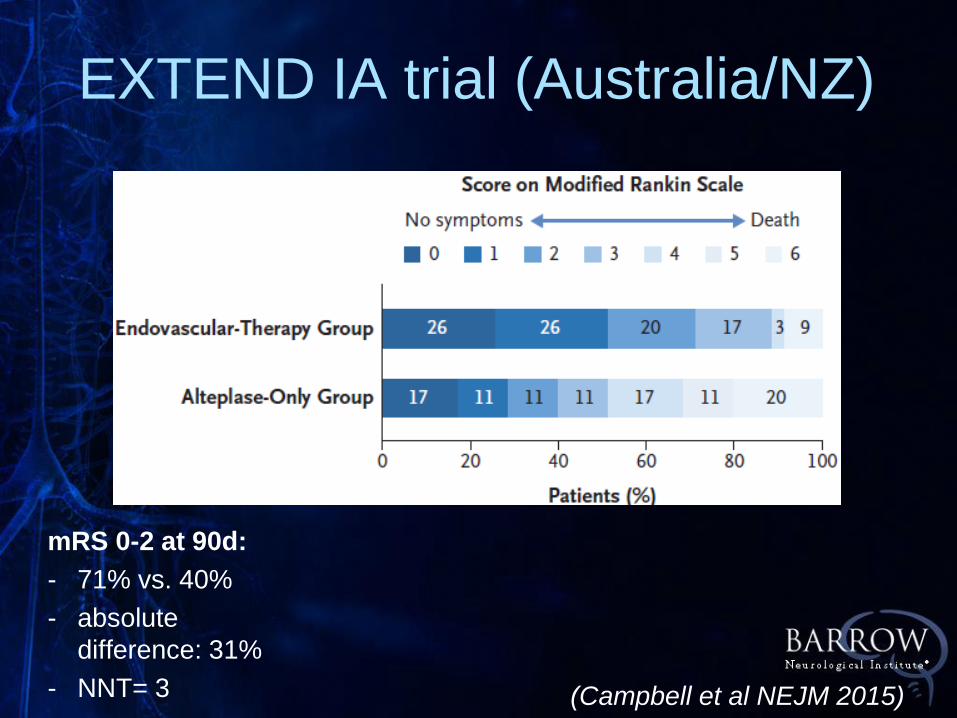
EXTEND IA trial (Australia/NZ)
(Campbell et al NEJM 2015)
mRS 0-2 at 90d:
- 71% vs. 40%
- absolute
difference: 31%
- NNT= 3
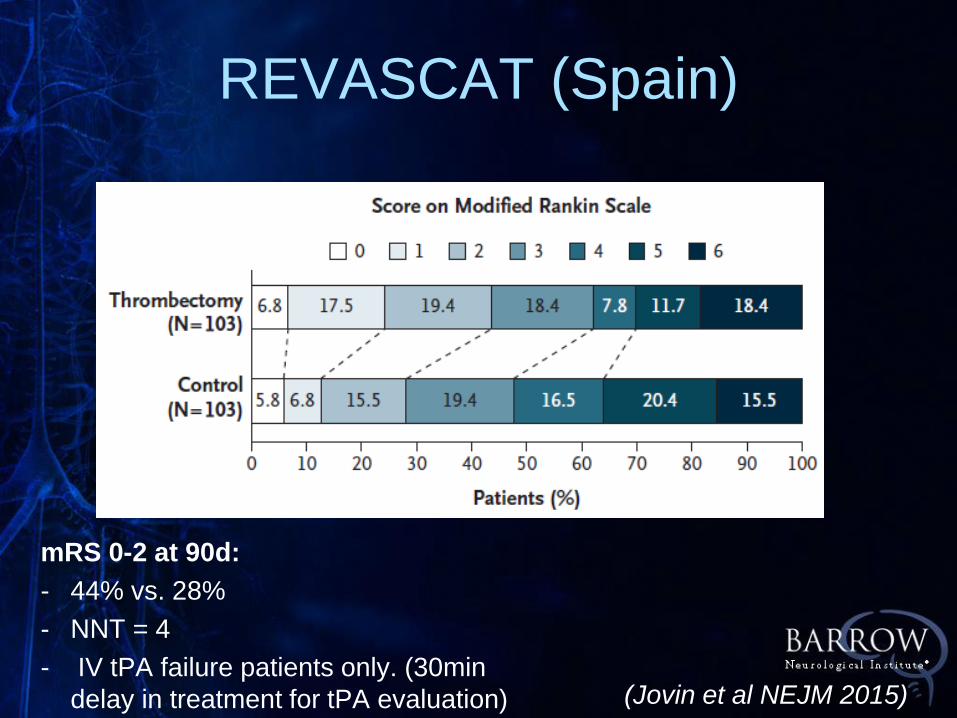
REVASCAT (Spain)
(Jovin et al NEJM 2015)
mRS 0-2 at 90d:
- 44% vs. 28%
- NNT = 4
- IV tPA failure patients only. (30min
delay in treatment for tPA evaluation)

(Goyal et al NEJM 2015)
mRS 0-2 at 90d:
- 53.0%, vs. 29.3%
- absolute diff: 24%
- NNT = 4
ESCAPE trial (international)
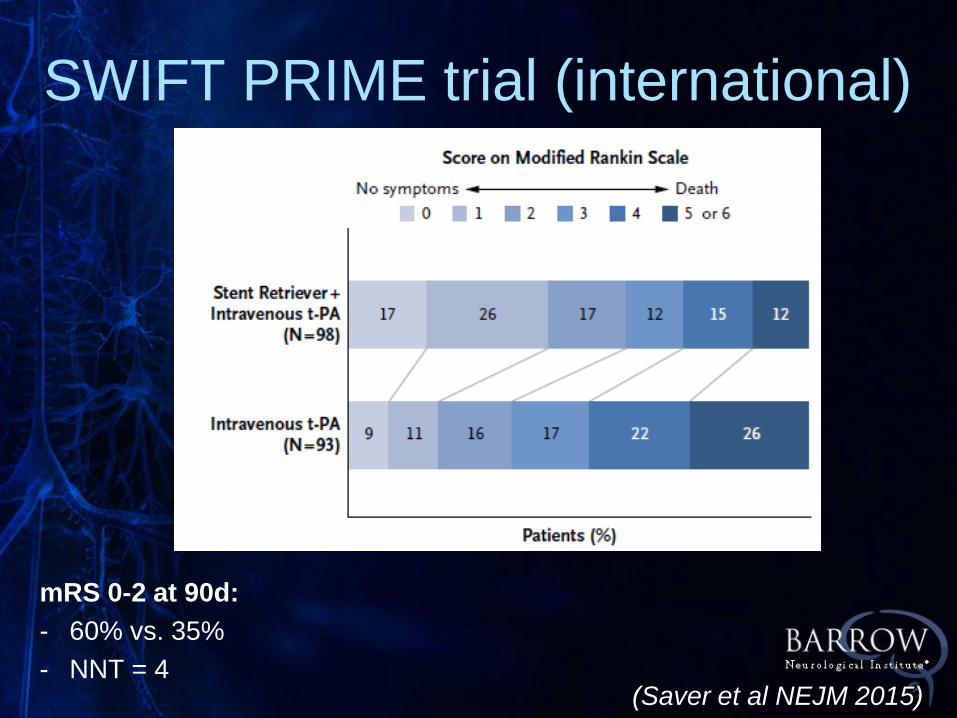
SWIFT PRIME trial (international)
(Saver et al NEJM 2015)
mRS 0-2 at 90d:
- 60% vs. 35%
- NNT = 4

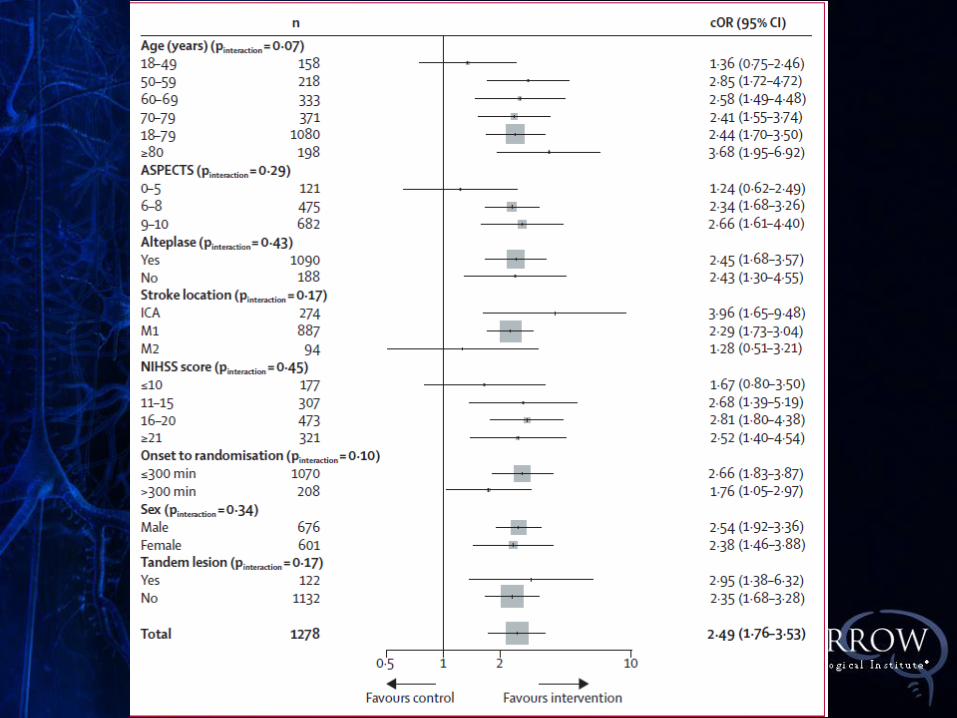
(Goyal et al Lancet 2016)


BNI Vascular Neurology

BESTU: October 2017

Wall Street Journal. 2/6/18
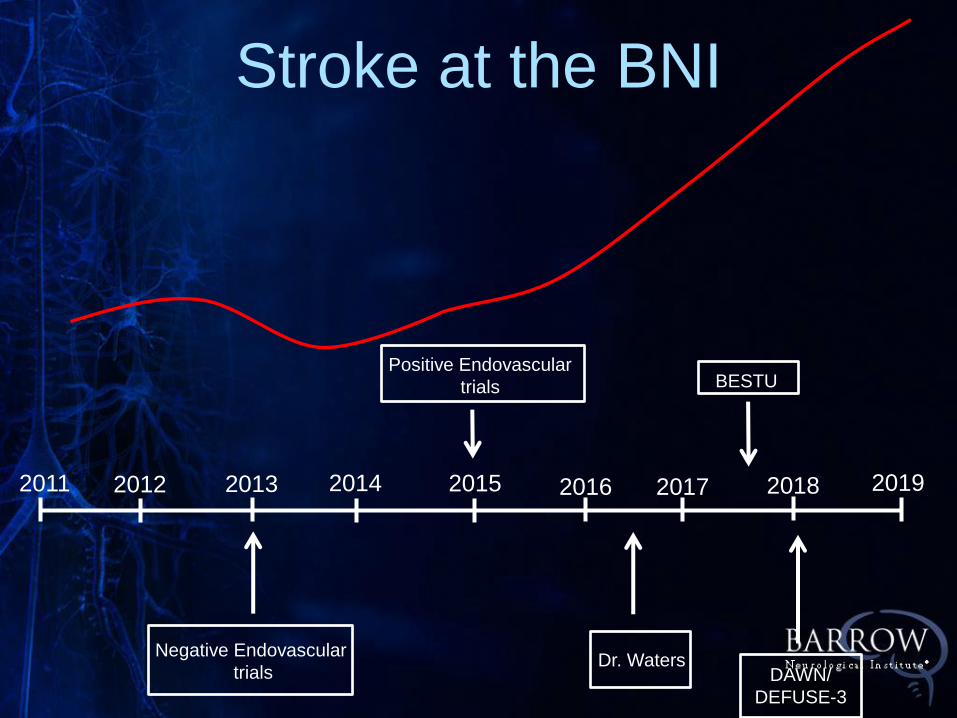
Stroke at the BNI
Positive Endovascular
trials
2011 2015 2014 2013 2012 2017 2016 2019
Negative Endovascular
trials
2018
BESTU
DAWN/
DEFUSE-3
Dr. Waters
Endovascular Stroke
Treatment in 2018:
Techniques

Stentrievers
Trevo Solitaire
Embotrap
3D
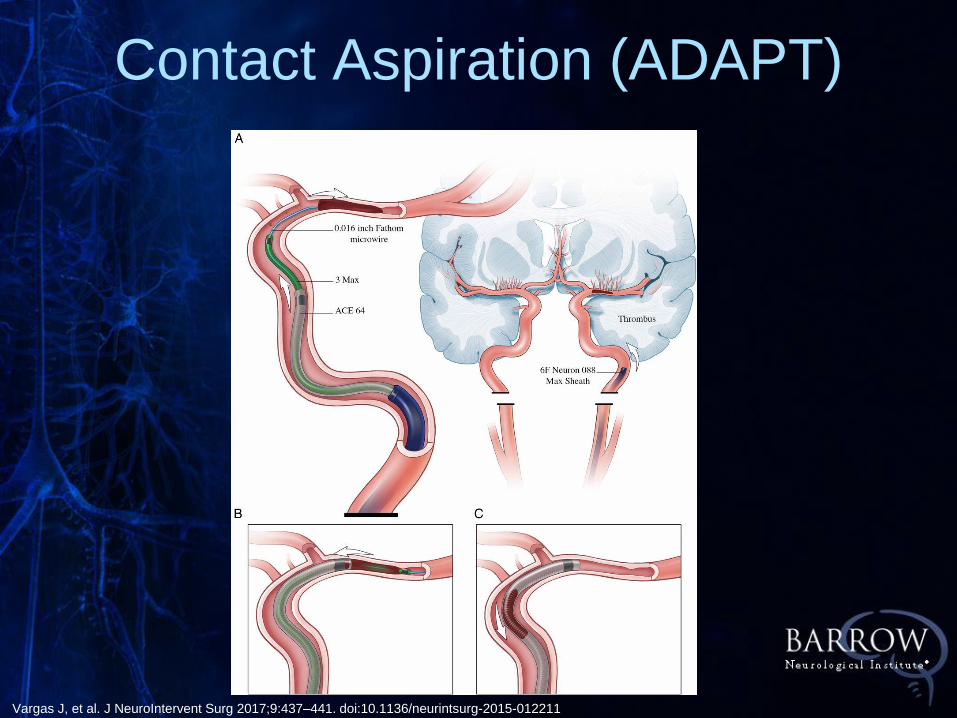
Contact Aspiration (ADAPT)
Vargas J, et al. J NeuroIntervent Surg 2017;9:437–441. doi:10.1136/neurintsurg-2015-012211
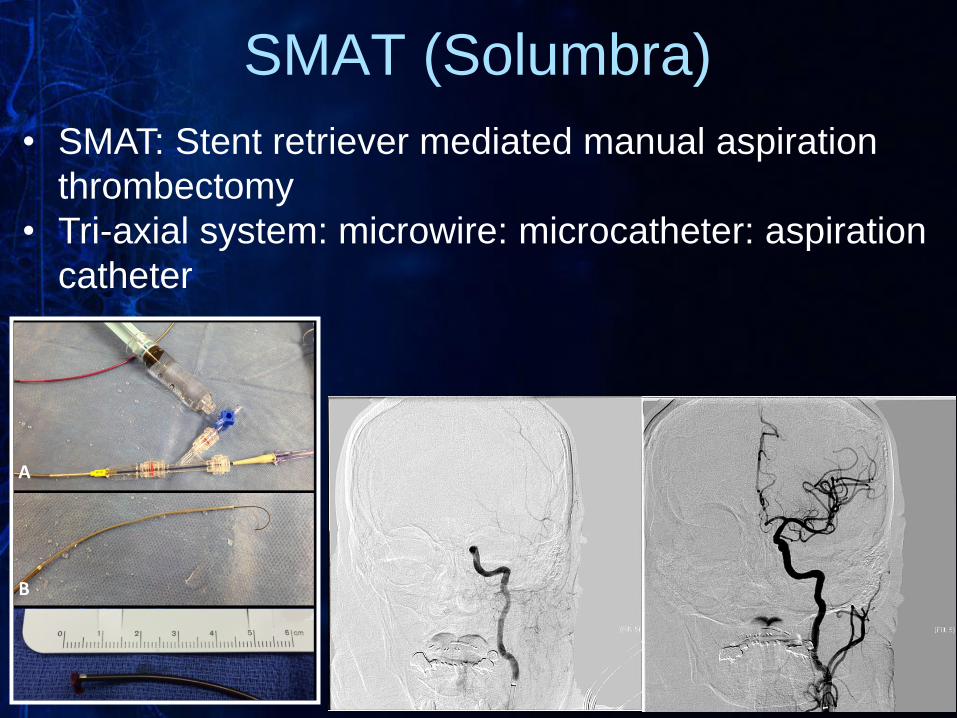
• SMAT: Stent retriever mediated manual aspiration
thrombectomy
• Tri-axial system: microwire: microcatheter: aspiration
catheter
SMAT (Solumbra)


Recent Endovascular Stroke
Clinical Trials

DAWN Trial
N Engl J Med. 2018 Jan 4;378(1):11-21.

• 500 patients (pivotal); 50 sites
• 6-24 hours
• NIHSS > 9
• ICA or M1 occlusion
• Medical therapy vs. thrombectomy (Trevo)
DAWN Trial
N Engl J Med. 2018 Jan 4;378(1):11-21.

• Clinical Imaging Mismatch (CIM)
• Core defined on DWI or rCBF maps
(RAPID)
• 0-20 cc core & NIHSS >= 10 (≥ 80yr)
• 0-30 cc core & NIHSS >= 10 (< 80yr)
• 31-50 cc core & NIHSS ≥ 20 (< 80yr)
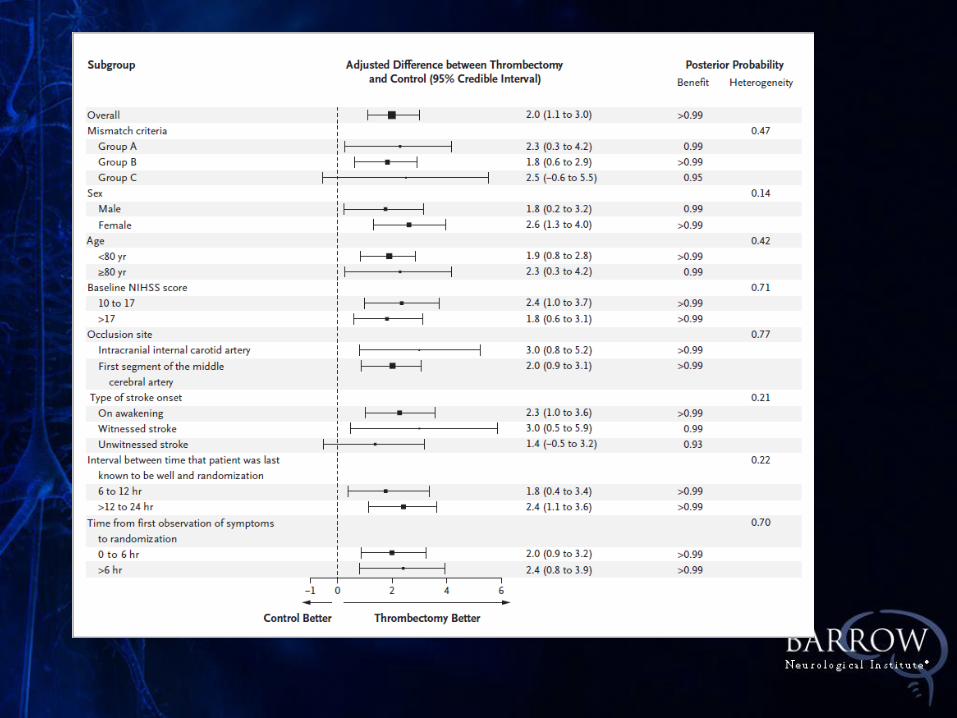
DAWN Trial
N Engl J Med. 2018 Jan 4;378(1):11-21.
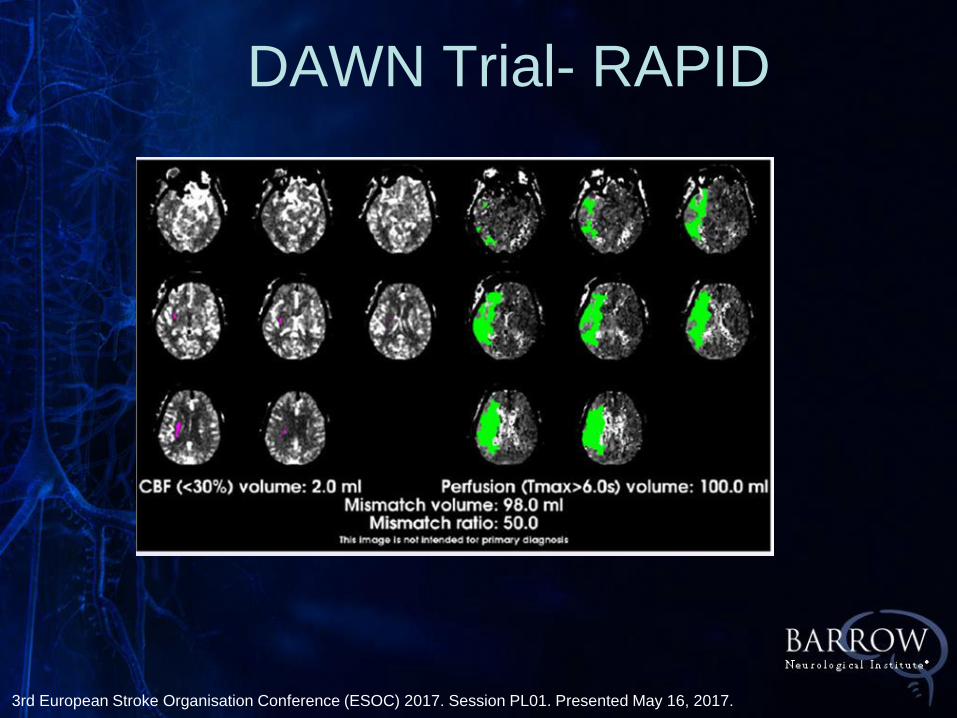
3rd European Stroke Organisation Conference (ESOC) 2017. Session PL01. Presented May 16, 2017.
DAWN Trial- RAPID
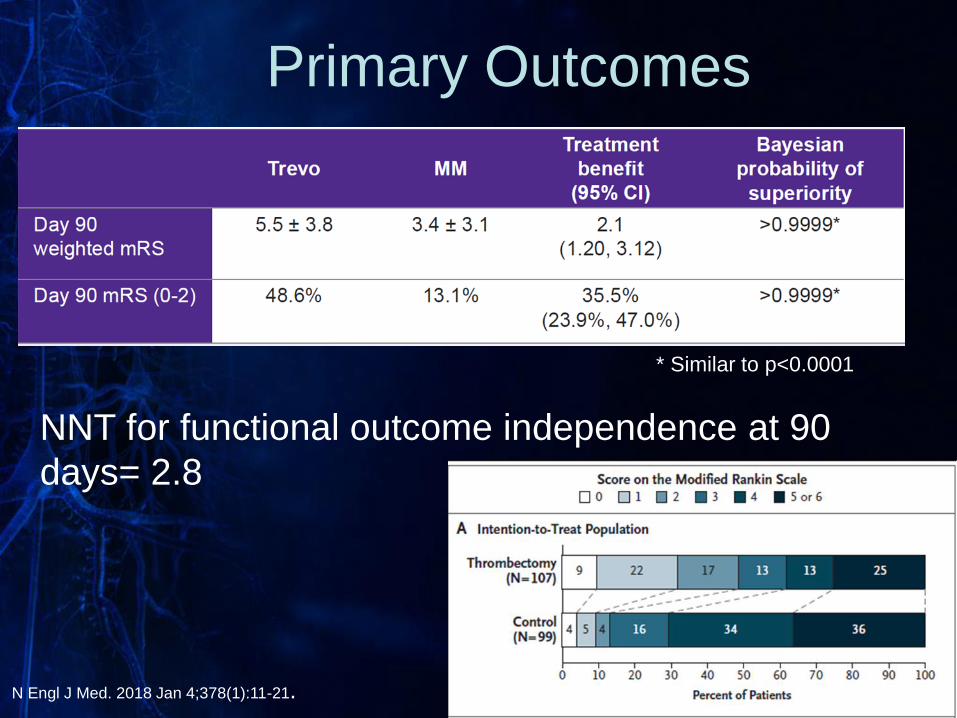
Primary Outcomes
NNT for functional outcome independence at 90
days= 2.8
* Similar to p<0.0001
N Engl J Med. 2018 Jan 4;378(1):11-21.
DAWN Trial Conclusions
• Thrombectomy associated with higher
functional independence compared to
medical therapy
• Treatment effect size in DAWN is highest
of any stroke trial
• Thrombectomy in patients > 6h showed
comparable safety profile to thrombectomy
performed < 6h
DEFUSE-3
N Engl J Med. 2018 Feb 22;378(8):708-718.

DEFUSE-3 Design
• Age 18-90 years
• ICA or M1 occlusion
• Treatment between 6-16 hours last known
well
• NIHSS ≥6
• Perfusion imaging required
• Initial infarct volume <70cc • Ratio of ischemic tissue to infarct of >1.8
• Absolute value of penumbra of >15cc
• Any FDA-approved thrombectomy device
N Engl J Med. 2018 Feb 22;378(8):708-718.
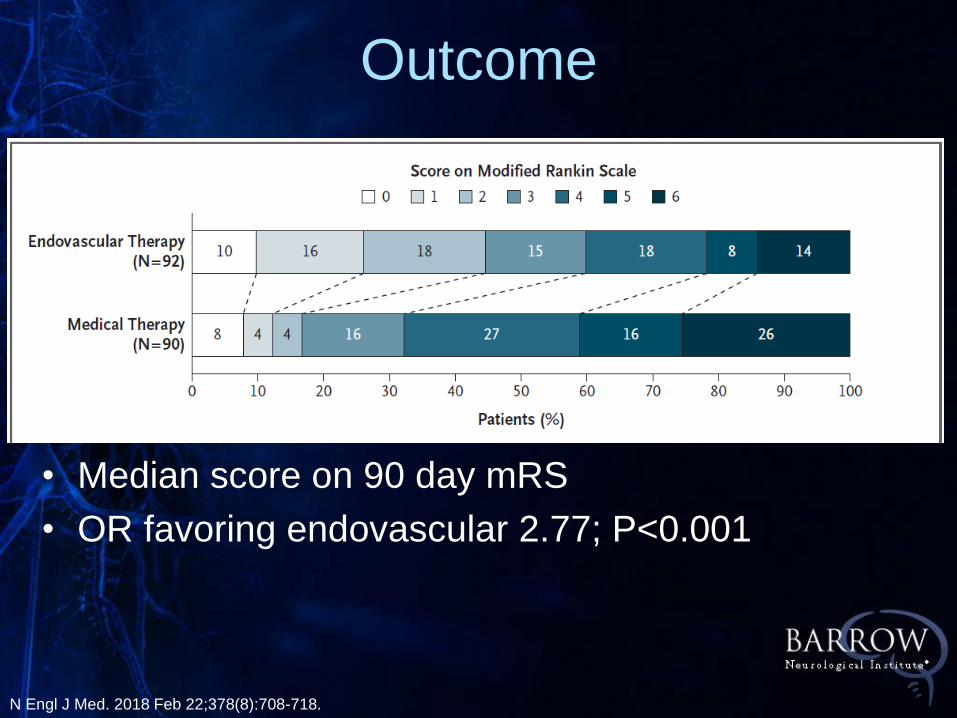
• Median score on 90 day mRS
• OR favoring endovascular 2.77; P<0.001
Outcome
N Engl J Med. 2018 Feb 22;378(8):708-718.

DEFUSE-3 Findings
• More inclusive than DAWN
• 40% of DEFUSE patients would not
qualify for DAWN
• Larger Core infarcts than DAWN
(70 vs. 50)
• Milder Symptoms (NIHSS ≥ 6)

2018 Guidelines Update

Aspiration vs. Stentriever
• Contact aspiration vs. stentriever
• Randomized, open-label, blinded endpoint trial at 8
centers in France (10/15-10/16)
• 192 randomized to aspiration vs. 189 to
stentriever
• Primary outcome: TICI 2B/3 revascularization • 85.4% in aspiration arm vs. 83.1% in stentriever (p=0.53)
• Secondary outcomes: change in NIHSS at 24h,
mRS at 90 days
• No significant differences
ASTER Trial
• Data presented at 2018 ISC
• 134 patients in aspiration arm, 136 patients in
stentriever arm, 15 centers
• Primary endpoint : mRS = 0-2 at 90 Days
• Secondary endpoints : mRS shift, TICI 2c or 3 within
45 min of groin puncture, time from groin puncture to
TICI 2b/3
• Aspiration was non-inferior • 49% in stentriever vs. 52% in aspiration (P=0.0014)
• 20% in aspiration required stentriever
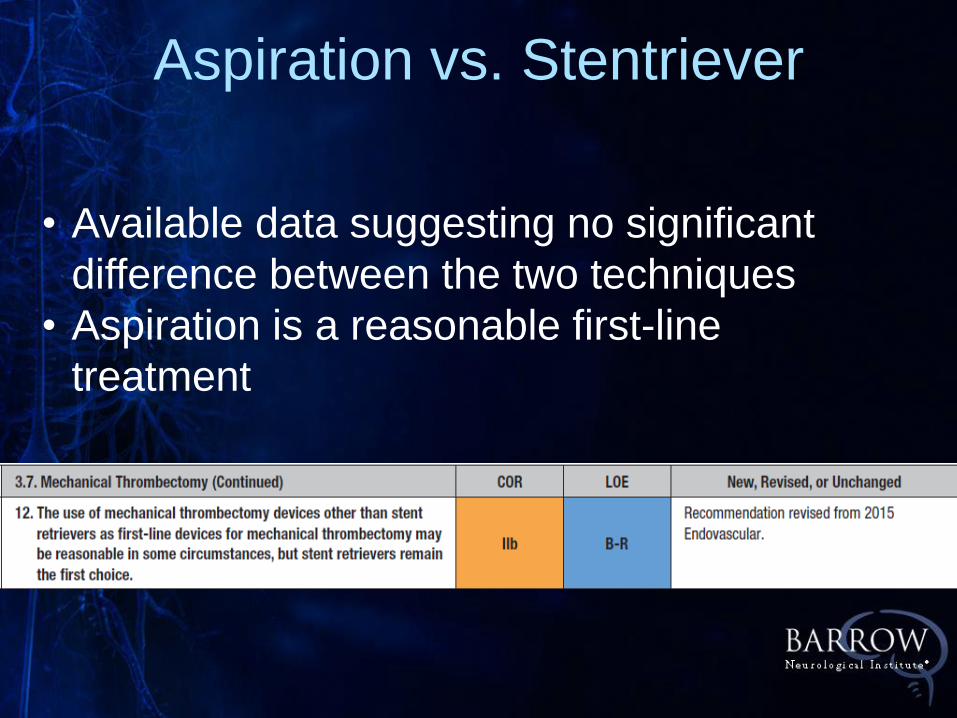
Aspiration vs. Stentriever
• Available data suggesting no significant
difference between the two techniques
• Aspiration is a reasonable first-line
treatment

The Future
• Larger Core infarcts
• Low NIHSS
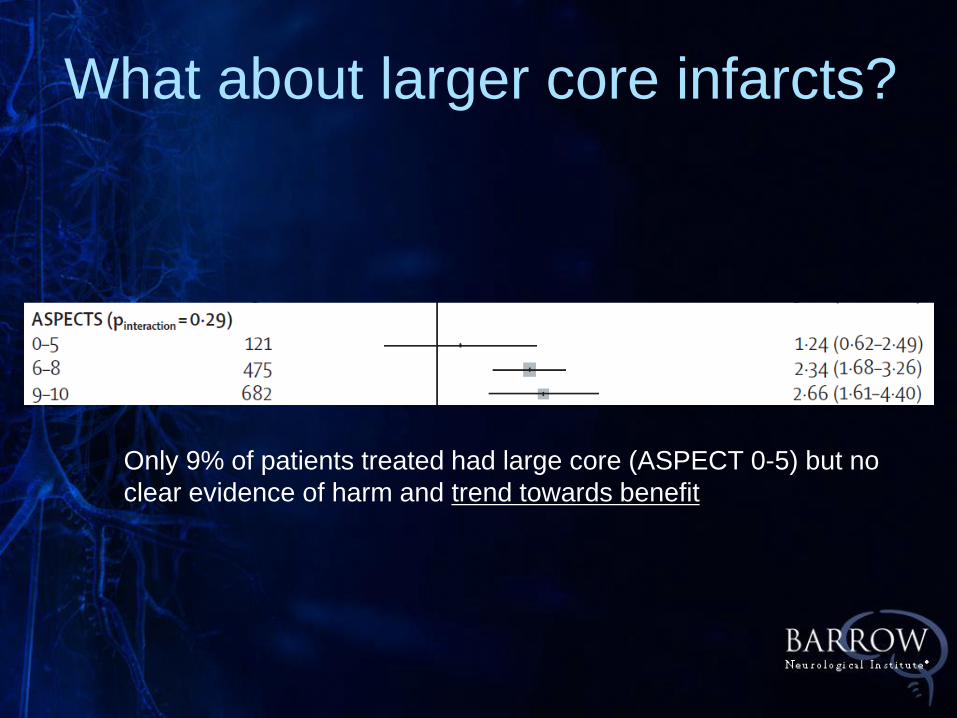
What about larger core infarcts?
Only 9% of patients treated had large core (ASPECT 0-5) but no
clear evidence of harm and trend towards benefit

Stroke size and cost: Each additional 1cc of infarct increased hospitalization cost by $122.35
Streib et al (submitted)
Case 1: Large Core Infarct
• 37 year old male last known well 14-16
hours prior to admission, with history of
altercation at a party
• Awoke with right MCA syndrome
• NIHSS = 19
• CTA shows tandem occlusion right
MCA/ICA

CT Head admission
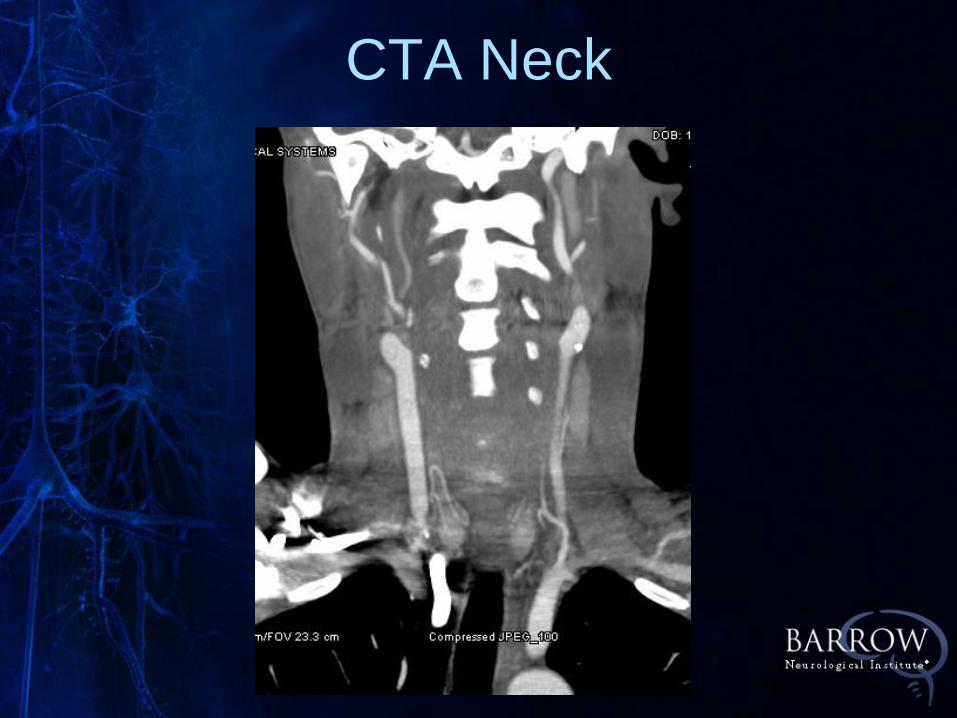
CTA Neck

CTA Head

CT Perfusion
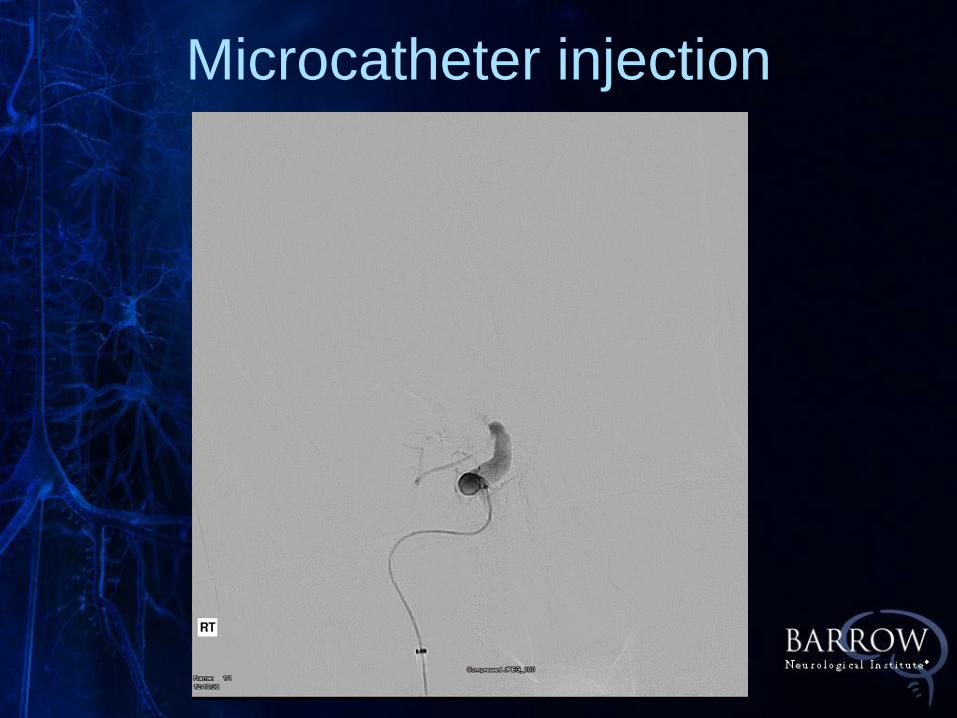
Microcatheter injection

Post-thrombectomy
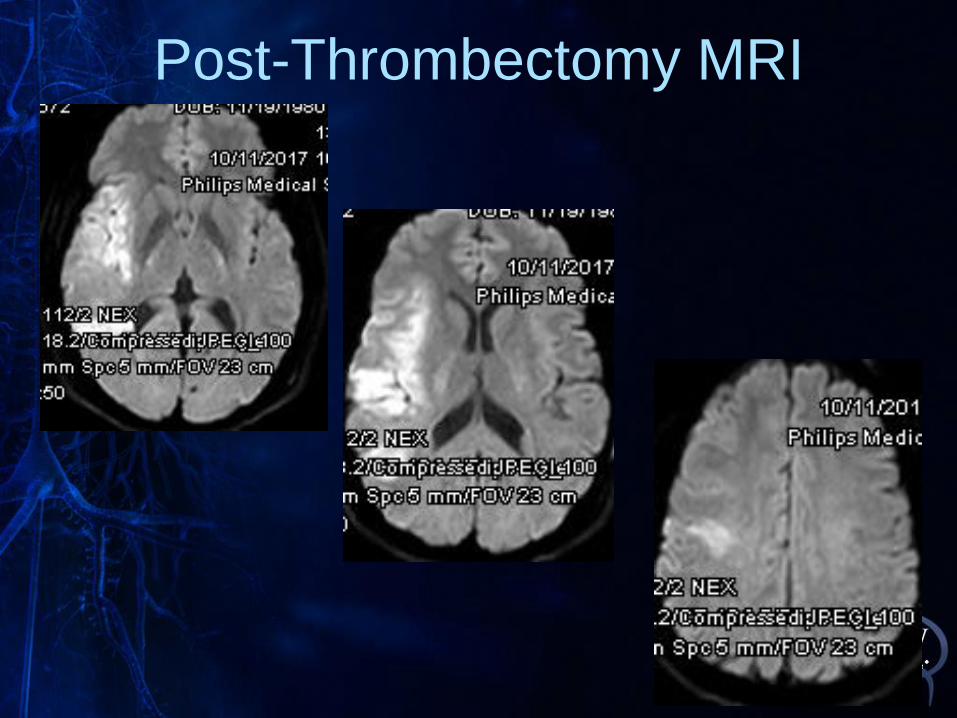
Post-Thrombectomy MRI

• Showed rapid improvement over next
several days
• Discharged on day 5 intact except
4+/5 in left hand
• Lost to follow-up
Case #1
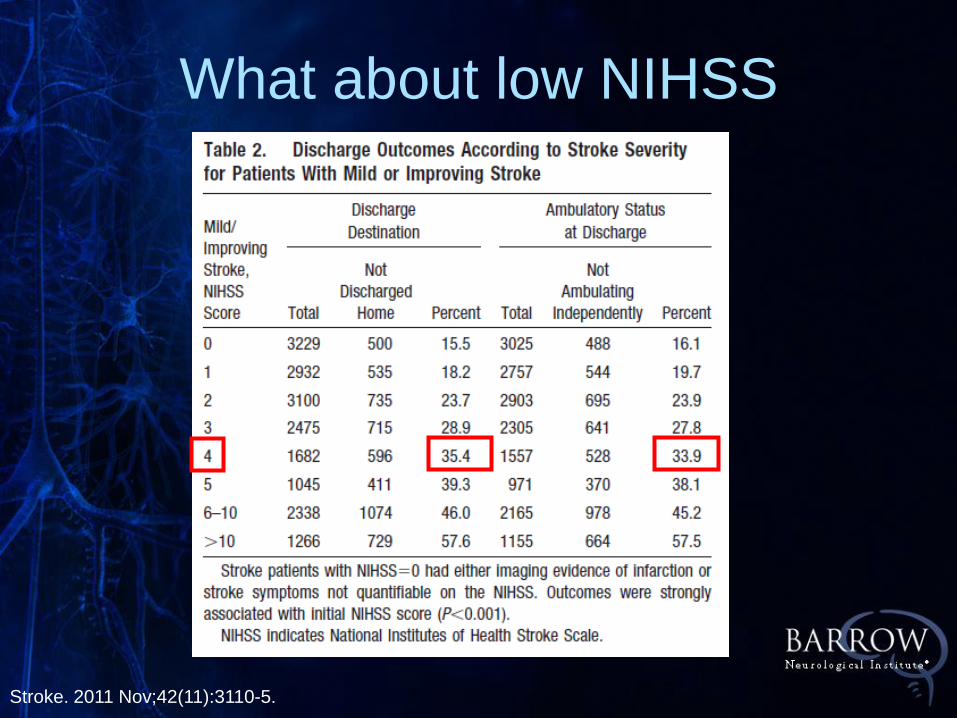
What about low NIHSS
Stroke. 2011 Nov;42(11):3110-5.

J Neurointerv Surg. 2016 Sep 2 Epub
• NIHSS ≤5
• LVO
• mRS 0-2

• 52 yo male with hypertension
• Onset of facial droop, slurred speech
mild left sided drift at work
• Urgicare ER
• 9.5 hours post-onset
• NIHSS = 4
Case #2: Low NIHSS
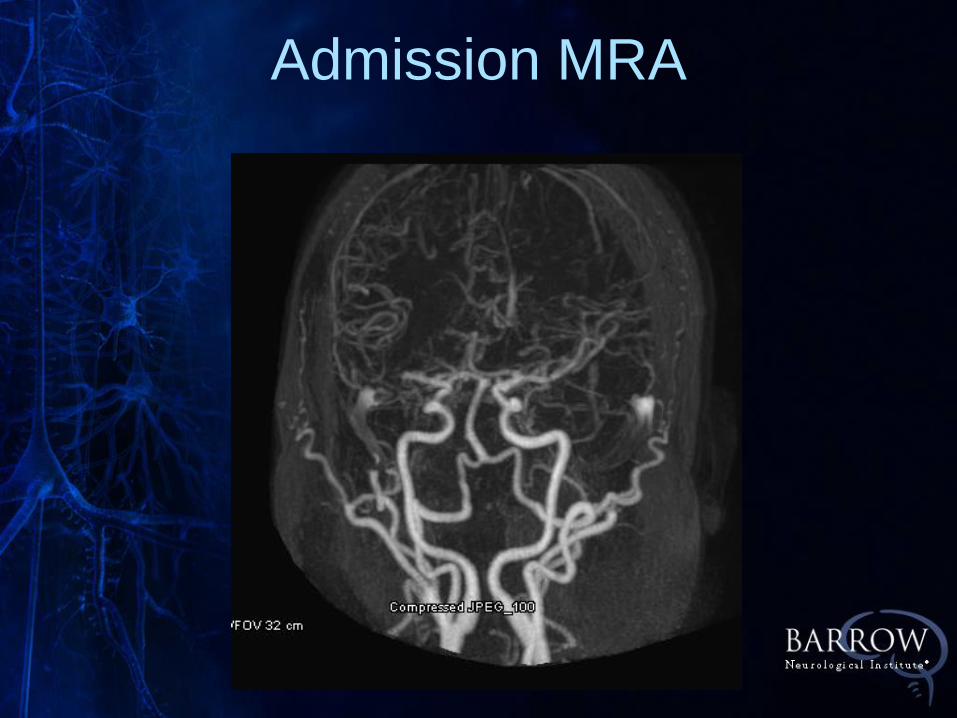
Admission MRA
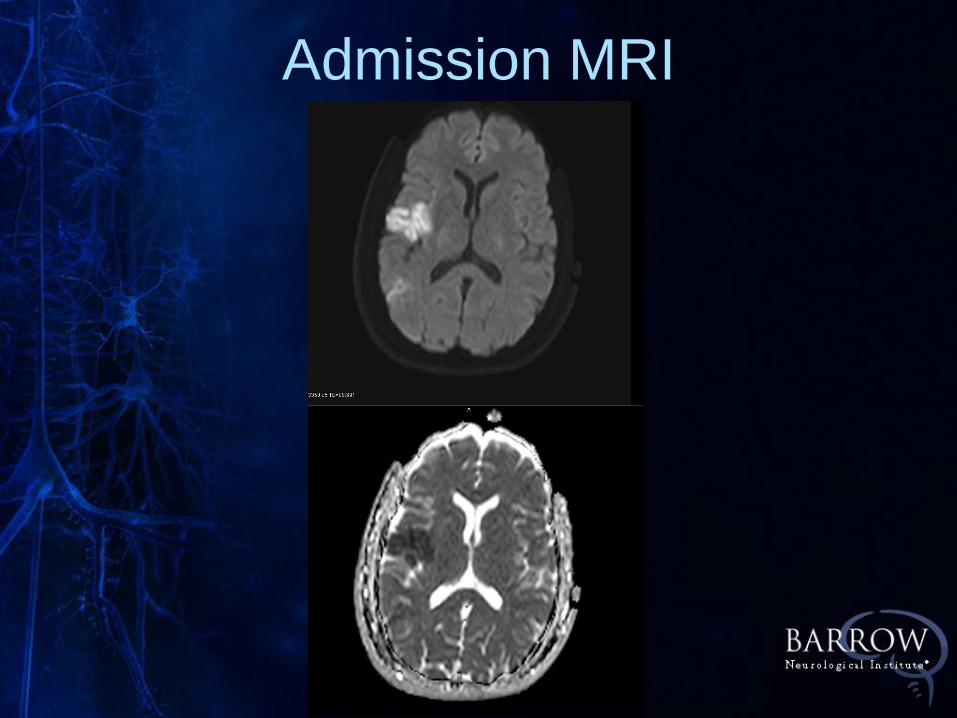
Admission MRI

CT Perfusion
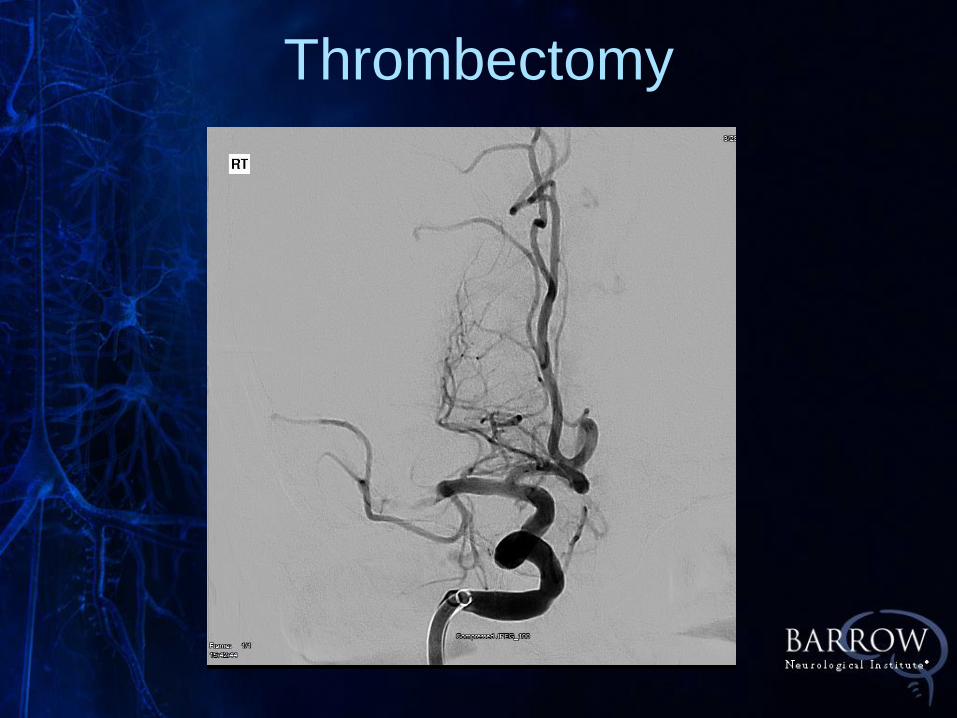
Thrombectomy

Thrombectomy

Post-Thrombectomy

• Immediate improvement of drift and
facial ,speech rapidly normalized
• Discharged home neurologically
intact following workup for AFib
Case #2

• 44 yo otherwise healthy male
• Onset of dizziness, dysphagia,
left facial numbness beginning
on 7/25 in the afternoon
• In the ER, CT head normal,
NIHSS 0.
Case #3:Low NIHSS, Basilar
• Admitted to MGMC due to
difficulty with balance
• MRA and CTA suggestive of
proximal basilar occlusion
Case #3:Low NIHSS, Basilar

• On admission to SJHMC, he has
severe vertigo when sitting up
accompanied by nausea /vomiting,
lateral gaze nystagmus
• NIHSS = 0
Case #3
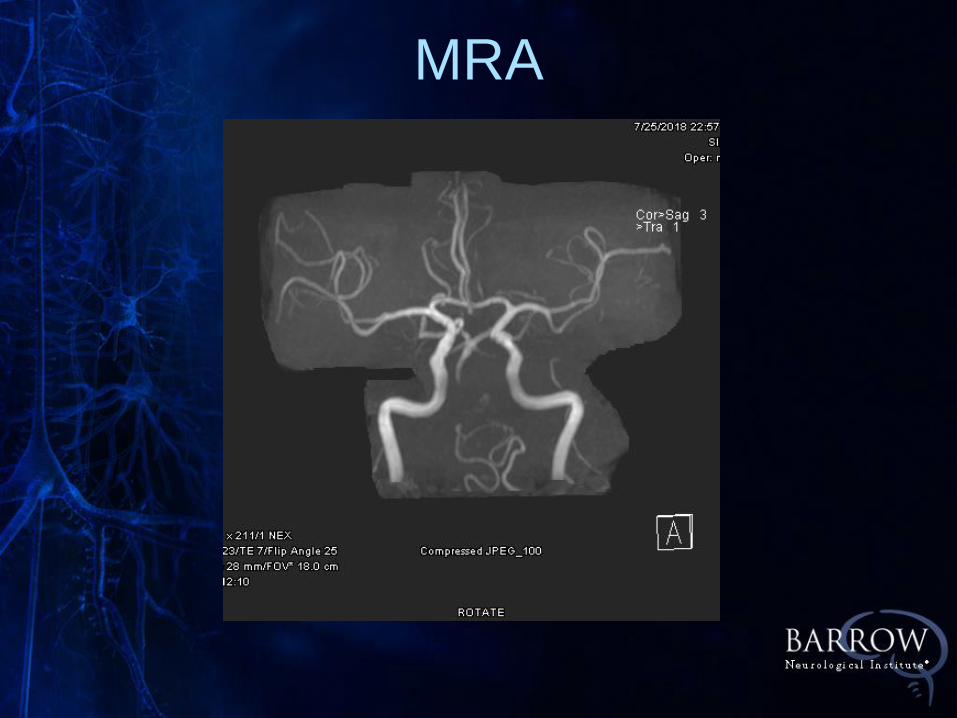
MRA

Right Subclavian

Right ICA

Left Vertebral
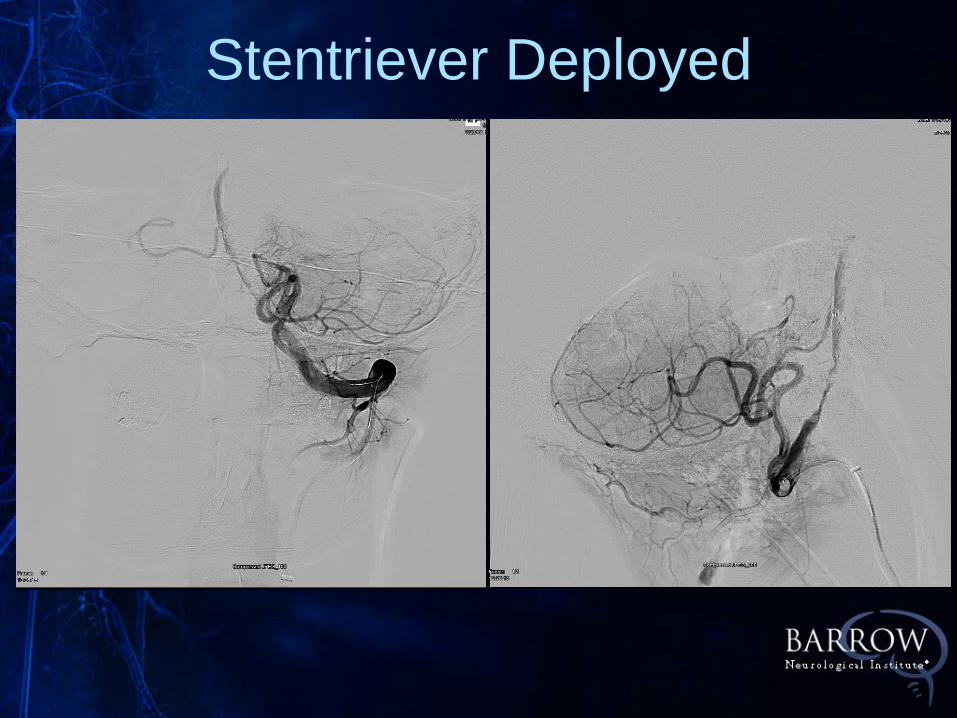
Stentriever Deployed

Left Vertebral post-Thrombectomy

• Symptoms immediately
resolved following
treatment
• MRI shows only
punctate infarcts left
occipital lobe
• Discharged home on
post-procedure day #2
Case #3

Future Directions
• IN EXTREMIS: Montpelier
• Clinically severe stroke and
ASPECTS 0-5
• Low NIHSS (<6) and M1 occlusion