Interventional Radiology Guide SPD v3.qxd:Best Practice · interventional radiology published by...
56
NHS NHS Improvement Diagnostics HEART LUNG CANCER DIAGNOSTICS STROKE Towards best practice in interventional radiology NHS Improvement - Diagnostics June 2012 British Society of Interventional Radiology
Transcript of Interventional Radiology Guide SPD v3.qxd:Best Practice · interventional radiology published by...

NHSNHS Improvement
Diagnostics
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE
Towards best practice ininterventional radiology
NHS Improvement - Diagnostics
June 2012
British Society ofInterventional
Radiology

This document sets out case studies using servicedelivery models that provide benefits for patientsand staff. The clinical teams have shared theirlearning so that their experiences may be a stimulusto others to improve local interventional radiology(IR) services.

Executive summary
Key messages
Patient foreword
Glossary of terms
Abbreviations
Introduction
Networking
Funding issues
Facilities
Staffing and team working
Patient and public engagement and experience
Leadership
Low volume procedures
Case studies
Appendix A. NetworkingAppendix B. FundingAppendix C. Staffing and MDT workingAppendix D. Patient engagement and experienceAppendix E. Leadership
Bibliography and suggested further reading
Contacts
Acknowledgements
Contents
Towards best practice in interventional radiology
4
5
6
7
8
10
12
14
15
16
18
20
22
2432344551
52
53
54
3

Executive summary4
Towards Best Practice in Interventional Radiology draws together the major
findings that came out of the visits to interventional radiology (IR) services
at the proposed major Major Trauma Centres during 2011/12. Examples of
best practice to provide benefits for patients and staff are described.
The work by the NHS Improvement team to review IR services across
England confirms that further improvements in IR are necessary to ensure
equitable access to IR services for patients. The clinical teams at these
centres shared their learning so their experiences may be a stimulus to
others.
We urge you to read this report and to review the IR services you provide
for those in your care. This report will support you to improve local IR
services.
Professor Erika Denton* Professor Keith Willett*National Clinical Director for Imaging National Clinical Director for
Trauma Care
Executive summary
The views of Professor Erika Denton and Professor Keith Willett are given in aclinical capacity and as national experts in the field. They do not in themselvesimpose any mandatory requirements on NHS organisations althoughcommissioners are expected to take them into account.
Professor Erika DentonNational Clinical Directorfor Imaging
Professor Keith WillettNational Clinical Directorfor Trauma Care
*

5Key messages
Key messages
• High quality IR services are essential for safe and effective patient care.
• There is variation in provision of IR throughout England, particularly for potentially lifesaving emergency and out-of-hours procedures.
• Despite this there are already many examples of good practice and service delivery across the country.
• Networking will be essential to improve access to IR. There are challenges in developing effective operationaldelivery networks but there are already good examples ofthese in the UK.
• A good well resourced IR service can contribute to significant savings (both financial and non-financial) along care pathways in both planned and emergency care.
• The opportunity exists to use improvement techniques of standard work and visual management to create agreed standard operating procedures. This can support a network approach to providing on-call across a number of organisations.

Patient foreword6
Provision of IR services enhancesbetter outcomes for patientsreceiving elective and non electivecare for many conditions. Bothcommissioners and providers,including the medical profession andspecialist IR staff need to recognisethat patients and their carers needmore information and knowledgeabout IR services. Communicatingthe value of IR is vital to address thedifferences of providing acute care,such as when the patient arrivesunconscious and elective care whichrequires the patient’s consent for abooked procedure.
Importantly, patients and theirrepresentatives want to be assuredthat best practice in IR is provided toall service users on an equality ofaccess basis across the country. This isan aspirational objective whileservices are being improved andevidence gathered. The challenge forcommissioners and providers ofhealth care will be to ensure thatgood health care outcomes requiringIR are equally available wherever onelives.
Patient foreword
To be perceived as a world classservice, providers have to recognisethat patients’ groups are frustratedthat examples of best practice fromwithin and outside of the UK, be it inpatient management, practitionertraining or in communicating thevalue of IR are often overlooked‘because our organisation isdifferent.’ This is wasteful andarrogant. IR has the capacity totransform patient management, butthe benefits appear, to date, mostlyonly recognised by a small group ofhighly committed, specialist andpersonally motivated practitioners.Confusion about who performs IRpersists - surgery, or radiology? Itdoes not help the patient that thisdebate has persisted unresolved forover twenty years.
Patients’ representatives have to be ina position to challengecommissioners and providers on thetrue role of IR including a patientjourney based on examples of bestpractice, including adequate accessto out-patient clinics, admissionrights and support staff.
From a patient’s perspective IR offersthe opportunity for a better patientoverall experience including reducedlength of stay and improved clinicaloutcome.
Pat KellyLay MemberRoyal College of Radiologists Clinical Radiology Patient'sLiaison Group
Clive BoothFormer Chairman Royal College of Radiologists Clinical Radiology Patient'sLiaison Group

7Glossary of terms
A&E Accident and Emergency
AAA Abdominal Aortic Aneurysm
BSIR British Society of Interventional Radiology
CCG Clinical Commissioning Group
CEO Chief Executive Officer
CPX Cardiopulmonary Exercise Testing
CT Computed Tomography
CIP Cost Improvement Programme
DCC Direct Clinical Care
DGH District General Hospital
DOQI Disease Outcome Quality Initiative
ED Emergency Department
eEVAR Emergency Endovascular Aneurysm Repair
EPR Electronic Patient Record
EVAR Endovascular Aneurysm Repair
EWTD European Working time directive
HDU High Dependency Unit
HPB Hepato-biliary
HR Human Resources
HRG Healthcare Resource Group
IR Interventional Radiology
IT Information Technology
ITU Intensive Therapy Unit
IV Intravenous
IVC Inferior Vena Cava
MHRA Medicines and Healthcare Products Regulatory Agency
Glossary of terms
MR/MRI Magnetic Resonance Imaging
MDT Multidisciplinary Team
MTC Major Trauma Centre
NICE National Institute for Clinical Excellence
NVD National Vascular Society Database
OC On Call
OP Outpatient
PACS Picture Archiving Communication System
PbR Payment by Results
PCI Percutaneous Coronary Intervention
PICC Peripherally Inserted Central Catheter
PPM Planned Preventative Maintenance
QA Quality Assurance
QIP Quality Improvement Programme
RCR Royal College of Radiologists
RETA Registry of Endovascular Treatment of Aneurysms
RIS Radiology Information Systems
SLR Service Line Reporting
SVS Society for Vascular Surgery
TACE Transcatheter arterial chemoembolisation
TEVAR Thoracic Endovascular Aneurysm Repair
TIPS Transjugular intrahepatic portal systemic shunt
UAE/UFE Uterine Artery (or Fibroid) Embolisation
US Ultrasound

Procedure descriptor8
Embolisation
EVAR
Fistulogram
Hepatobiliary
Nephrostomy
TACE
TEVAR
TIPS or TIPPS
Procedure descriptor
A minimally invasive procedure which involves the selective occlusion ofblood vessels to prevent haemorrhage.
Endovascular repair used to treat an abdominal aortic aneurysm A graft isplaced in the aorta via the femoral arteries, without an abdominal incision,using X-rays to guide the graft into place. When this procedure is performedin an emergency setting it is called an Emergency Endovascular AneurysmRepair (eEVAR)
An X-ray taken of a fistula after a contrast medium has been injected.
A term used to describe the liver, gallbladder and bile ducts.
An artificial opening created between the kidney and the skin used to drainurine from the kidney to a bag outside the body.
A minimally invasive procedure to restrict the blood supply to a tumour.
A minimally invasive approach to repair a thoracic aortic aneurysm. A graftis placed in the aorta via the femoral arteries, using X-rays to guide the graftinto place.
A procedure where a metal tube is passed across the liver


Introduction10
Introduction
The White Paper, Equity andExcellence: Liberating the NHS1 andthe Health and Social Care Act 20122
details how the improvement ofhealthcare outcomes will bemeasured using outcomes achievedfor patients rather than the processesby which they are achieved.
Building on this aim, one of themajor purposes of The NHSOutcomes Framework 2011/123 was‘to act as a catalyst for driving qualityimprovement and outcomemeasurement throughout the NHS byencouraging a change in culture andbehaviour, including a stronger focuson tackling health inequalities.’
The NHS Outcomes Framework isstructured around five domains. Eachof the five domains will be supportedby a suite of NICE quality standardswhich will provide authoritativedefinitions of what high-quality carelooks like for a particular pathway ofcare. These quality standards arecurrently being prepared.
Towards Best Practice inInterventional Radiology sets out casestudies using service delivery modelsthat provide benefits for patients andstaff. They are set around seven keythemes:
• Networking• Funding• Facilities• Staffing/MDT working• Patient experience • Leadership • Low volume procedures,
and align the case studies to the fivedomains (table 1)
Domain 1
Domain 2
Domain 3
Domain 4
Domain 5
Preventing people from dying prematurely
Enhancing quality of life for people with long term conditions
Helping people to recover from episodes of ill health orfollowing injury
Ensuring that people have a positive experience of care
Treating and caring for people in a safe environment andprotecting them from avoidable harm
Table 1
1www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_117353 2www.legislation.gov.uk/ukpga/2012/7/contents/enacted/data.htm 3www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_122944

11Introduction
The site visits and this report wereinspired by the two reports oninterventional radiology published bythe Department of Health in 2009and 20104,5. The 2010 reportInterventional radiology: guidance forservice delivery discussed how theNHS can improve quality, safety andproductivity while deliveringcomparable or better outcomes forpatients with shorter hospital staysand fewer major complications. Itsuggests and describes how IRservices can help to ensure patientsafety whilst delivering the highestquality care.
A further driver was the 2010 reportby the NHS Clinical Advisory GroupRegional Networks for Major Trauma6
stated that ‘the delivery of effectiveongoing trauma care andmanagement relies upon appropriateavailability of imaging techniques.’
The key themes section within thedocument identifies ‘AcuteIntervention including...interventional radiology,’ and laid outa key recommendation:
At Major Trauma Centresinterventional radiologycapability will attend within 60minutes 24 hours a day.Interventional suites should beideally co-located with operatingrooms and/or resuscitation areas.
Interventional radiology was felt tobe a significant challenge by many ofthe proposed Major Trauma Centres(MTCs) and a series of site visits wereundertaken.
appendix to the document and alsoon the NHS Improvement website at(www.improvement.nhs.uk).Additional case studies will be addedon the website as they becomeavailable and new examples of bestpractice are identified.
Towards Best Practice inInterventional Radiology builds on thework done in 2011/12 to visit all ofthe agreed and proposed MajorTrauma Centres in England. It drawstogether the major findings thatcame out of the visits and citesexamples of best practice. Theseexamples are provided as an
4www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_109130 5www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_1219046www.excellence.eastmidlands.nhs.uk/welcome/improving-care/emergencyurgent-care/major-trauma
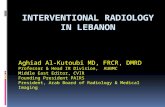
24/7 network coordinatorin ambulance service
On call medicalconsultant
On scene triage Enhancedcare team
Directtransfer(<45 mins)
Indirecttransfer(geography, timecritical intervention)
MAJOR TRAUMA CENTRE
Consultant led trauma teamImmediate operating theatre
All specialtiesImmediate CT scan
Interventional radiologySpecialist critical care
TRAUMA UNIT
Trauma teamImmediate CT scan
Resus, assess and ? transfer
?
Preferred acute patient pathway

Networking12
The recent Vascular Societypublication, The provision of servicesfor patients with vascular diseases20127 emphasises the importance ofgood clinical operational deliverynetworks. Whilst this documentlargely refers to vascular surgery andinterventional radiology (IR) related tovascular surgery the same principlesapply to all forms of IR.
In many UK hospitals there aredifficulties in providing interventionalprocedures required to support thefull range of clinical activity takingplace within that centre. This hasbeen confirmed by a recent detailedsurvey that shows variable andpatchy provision of IR throughoutEngland8. For example, manyhospitals admit acute medical andsurgical emergencies but have noprovision for emergency embolisationfor haemorrhage.
The areas of greatest difficulty arecomplex, low volume procedures andthe provision of emergency out-of-hours IR in general. This particularlyapplies to smaller acute hospitalswhere there will never be sufficientnumbers of specialised staff to createa stand-alone on call rota. It is likelythat effective networking betweencentres is the only means ofachieving a sustainable solution thatwill enable equitable access to IRservices across the country.
Networking
Setting up a operational deliverynetwork can be challenging withdifficulties that may include:
• historically poor communication between sites;
• possible threats to income flows;• reluctance of staff to work on new
and unfamiliar sites;• risks of transferring critically ill
patients;• bed availability if patients need to
be transferred between sites;• staff shortages;• differing practices and skill sets on
different sites; and• standardising equipment and
pathways across sites.
As with any service improvement,where these issues have beenovercome there has beenengagement and goodcommunication between cliniciansand managers on all involvedlocations. Examples of successfuloperational delivery networks indifferent geographical environmentsare given below.
Examples of good practice1.Networked on call IR servicesbetween several major centresaround Glasgow with radiologistsand nurses travelling to the patient’slocation. To overcome the issue ofavailability of specialist consumablesthe travelling staff carry a large boxof IR equipment such as wires,catheters and embolisation coils. Thisgood practice example is described inmore detail in the Appendix A.
2.Networked on call IR servicesbetween a large hospital in Coventrywith four interventional radiologistsand a smaller hospital in a nearby city(Nuneaton) with two interventionalradiologists. The emergency on callservice is based in Coventry. In orderto overcome the issues of differentskill sets, experience and workingpractices and the challenge ofworking in an unfamiliar environmentthe Nuneaton radiologists haveregular elective IR lists in Coventry.This good practice example isdescribed in more detail in theAppendix A.
DOMAIN
1DOMAIN
3DOMAIN
4DOMAIN
5
7Vascular Society of Great Britain and Ireland. The Provision of Services for Patients with Vascular Disease. London 2012. www.vascularsociety.org.uk/library/vascular-society-publications.html
8www.improvement.nhs.uk/diagnostics/InterventionalRadiology/IRServiceProvisionMap/tabid/114/Default.aspx Interventional Radiology Service Provision Mapping 2011

13Networking
3.Networked on call IR servicesbetween two similar sized hospitals ina rural setting (Exeter and Torbay),each with three interventionalradiologists. Week days and eveningsare covered locally with theradiologists on a 1:3 rota Monday toThursday on each site. Overweekends there is one interventionalradiologist on call for both sites,resulting in an acceptable 1:6weekend rota. The radiologist usuallytravels to the patient’s hospital andthere are interventional nurses andradiographers on call on both sites toenable this. This good practiceexample is described in more detail inthe Appendix A.
4.Agreed pathways between centresfor low volume/specialist servicessuch as hepatobiliary or thoracicaortic intervention.
5.Implementation of radiologynursing cross site rotation. Thesystem supports safe practice,increased knowledge base andnursing job satisfaction, plus aidsrecruitment. Cost savings can bemade by reducing two on call rotasto one. This good practice example isdescribed in more detail in theAppendix A.

Funding issues14
Almost without exception during thesite visits to the MTCs, funding issuesand concerns were raised by all ofthe teams visited. The issues felllargely into five categories.
Getting income for referrals fromother hospitalsThis was a significant cost pressurefor many departments. There werefew examples of agreed referralpathways and funding streams.Where a referral protocol was inplace it was mostly between clinicalspecialties and the first IR knew ofthe origin of the patient was whenthey received the request.
This was reported as a much moresignificant problem where DGHsprovided an in hours or simple IRservice but did not undertakecomplex procedures or provide anout of hour’s service.
TariffsDespite significant progress centrallymany sites reported that the tariff didnot adequately reflect the actual costof delivering the service. This wasparticularly apparent in centresoffering a tertiary level of care wherethey were asked to undertake themost complex cases and often theout of hours work for surroundingDGHs.
Funding issues
Clinical codingInterventional radiology cases oftenproceed or change once the patientis ‘on the table’ and this is not alwaysreflected accurately in the notes oron the Radiology Information System(RIS). This makes accurate clinicalcoding impossible. Clinical coding ismost usually done by a team ofadmin staff remote from radiology. Insome centres there was littlerecognition of why it is important toaccurately reflect the procedurecodes and in others frustrations thatthey felt powerless to influence theprocess.
Internal re-chargingSeveral sites had set up a system ofinternal charging. Setting up thesystem had proved to be a lot ofinitial work but where it was workingwell was felt to be hugely beneficial.
The two primary reasons cited were;• to influence decisions that affect
the service by showing how much ‘income’ the service could generate; and
• to reflect back to referrers the true costs of an IR intervention.
Service line reporting (SLR)SLR measures profitability of itsservices by monitoring cost, income,activity and use of resources. It canenable a trust to increase itsproductivity by providing financialinformation to make informed
decisions, prioritise new servicedevelopments or plan new clinicalinvestments. However where aservice costs more to deliver than theincome it receives for delivering theservice it takes a team with foresightto recognise the non financialincentives of delivering this service.
Examples of good practice 1.Accuracy of coding for IRprocedures is vital to reflect workloadand ensures maximum income for IRdepartments. This ensures thatresources follow clinical activity. Thisgood practice example is described inmore detail in the Appendix B.
2.Internal recharging was seenworking well in several of the sitesvisited. At least two sitesdemonstrated that it was possible toreduce unit costs.
3.Sites delivering an OP service orpost procedure telephone follow upwere working with their clinicalcoding teams to secure the tariff forimaging services.
DOMAIN
1DOMAIN
2DOMAIN
3DOMAIN
5

15Facilities
Equipment and siteTheatre design should ensure that allconsumable equipment (cathetersstents, embolic material etc) is in asuitable equipment storage areaimmediately accessible from the IRtheatre. Consumable equipmentshould include a full range ofequipment suitable for embolisationto control haemorrhage, stents andstent grafts suitable for major andminor vessel repair and a ‘bail outbox’ with everything needed forcomplications.
Major Trauma Centres should be ableto provide Thoracic EndovascularAneurysm Repair (TEVAR) forappropriate cases and facilities,pathways and workforce should be inplace to support this activity.
At present, there is variation in theprovision of emergency EndovascularAneurysm Repair (eEVAR) forruptured abdominal aneurysms. Trialdata on open surgical versusendovascular repair will report in thenear future and are likely to informfuture practice. Where the service isprovided, the InterventionalRadiology facilities should preferablybe of theatre standard ventilation andif being used for endovascular repairshould comply with the relevantMHRA (Medicines and Healthcareproducts Regulatory Agency)
Facilities
guidance – Delivering an EVARService (2010)9. It should be ofsufficient size to permit fullanaesthetic facilities, including pipedgases, drugs and anaestheticequipment.
The theatre environment should havea staffed recovery area to allowreception and onward transfer ofpatients to other environments.
The theatre should be located asclose as possible to the emergencyCT scanner and care taken to ensurea rehearsed rapid transfer facility.
IT linksAccess to Picture Archiving &Communication Systems (PACS)workstations and RIS systems shouldbe available within the IR theatre.Teleradiology links are vital andaccess to a robust and rapid transferof imaging scans from hospitalsthroughout the local traumaoperational delivery network isessential. If image exchange portalsare required these must be testedregularly and robustly to ensure thereare no delays in image transfer andshould be available 24/7 at bothsending and receiving hospitals.
Examples of good practice1.Monthly QA checks on dose andimage quality are recorded on adatabase and displayed graphically.This allows trends to be quicklyidentified and in one site hadsupported a dose reduction ofapproximately 30%.
2.Having procedure trolleys made upand ready for quick access whenrequired in an emergency was inplace at several of the sites visited.
3.IT resilience for CT scanners thatmay be required for major trauma,had been achieved by hardwiring aPC for each scanner separate fromPACS within the CT control room.
DOMAIN
4DOMAIN
5
9Joint Working Group to produce guidance on delivering an Endovascular Aneurysm Repair (EVAR) Service. (2010) www.mhra.gov.uk/home/groups/clin/documents/news/con103000.pdf

Staffing and team working16
The provision of an IR service requiresteamwork both within radiology andwith other specialities. Planningservice provision will relate to demandwhich in turn will vary depending onclinical commitments locally and use ofother resources (see networkingabove). Staffing levels will reflect thisand will need to be tailored forindividual departments. The IR teamusually comprises radiologists, IRnurses, IR radiographers, clinicalassistants and support staff includingclerical staff, porters and managerialsupport.
24/7 availability of IR nursing staff andradiographers with experience of IRtheatre is essential. All day, every dayavailability of an InterventionalRadiologist with experience inembolisation for haemorrhage controland treatment of vascular injuries withstent and stent grafts is essential.
There are different issues relating toeach of the groups involved in theclinical care of IR patients.
RadiologistsInterventional radiologists’ portfoliosand workload vary enormously andthere are many different IR servicemodels across the NHS.
IR as part of a vascular service. At least two NHS trusts now provide IRservices under the umbrella of vascularservices, separated from the ImagingDepartment. Advantages:• integrated working with vascular
surgery;
Staffing and team working
• easier separation/identification offunding;
• protection of demands from non-IRradiology;
• autonomy for service provision; andeasier access to outpatient facilities.
Disadvantages: • IR radiologists will usually drop other
radiology skills. Although this maymean greater individual experience,the workload will need to be greaterto provide the elective work andtherefore justify enough IRradiologists to maintain an on-callrota;
• maintaining a non-vascular IR serviceand on call rota; and
• vascular surgery contributes avariable proportion, often less than50%, of the IR vascular workload.
IR as part of the radiology service. Advantages:• IR radiologists with other
subspecialty skills can be employed.This can justify a greater number ofIR radiologists and aid provision ofon-call IR.
Disadvantages:• maintaining competency with non IR
demands a fixed time commitment;• identification of funding and
funding streams.
IR as part of a operational deliverynetwork service. Please see ‘networking’ section.
Interventional radiographersAll IR units will have radiographers oncall for IR procedures. In larger unitsthe radiographers will all be trained inIR and probably assisting in elective IR
procedures for most of their time atwork. However, even in larger unitsthe number of trained IR radiographersmay be small and the on call maytherefore be onerous. Combining theon call with radiographers from e.g.CT, Cardiac Labs and Neuro-intervention could have the advantageof creating a larger pool ofradiographers; however, careful localplanning is required as PercutaneousCoronary Intervention (PCI) and neuro-intervention can use up a lot ofradiographer time. Maintainingcompetency across these differentsubspecialties would then be required.
Interventional nursesThe RCR document Guidelines forNursing Care in InterventionalRadiology (2006)10 emphasized theimportance of nurses in IRdepartments. Effectively all radiologydepartments that undertake IRprocedures now have their ownnurses. However, the job descriptionvaries widely between trusts. Almostall units with significant IR demand willalso provide an on-call IR nurse service.Some larger institutions even providetwo nurses on call. Pooling nursesfrom other departments has beenintroduced to facilitate this and mayinvolve cross covering of neuro-intervention and cardiac theatres.
Extended role of IR nurses has beensuccessfully introduced in a number ofinstitutions and includes amongstothers:• involvement in an IR out-patient
clinic;• pre-assessment of patients;
DOMAIN
4
10www.rcr.ac.uk/docs/radiology/pdf/GuidelinesforNursing

17Staffing and team working
• insertion of central lines;• undertaking arterial punctures;• ascites drainages; and• nurse led pain control.
The role of an IR nurse in the patientpathway is variable. There is potentialfor involvement in the pre-operative,pre-procedural, procedural andrecovery components. Many hospitalshave recovery areas managed outsidethe radiology department. One of theadvantages to this arrangementincludes the flexibility in staffing alarger unit. Having recovery ‘in-house’has the advantage of protected bedsand specialised skills.
Examples of good practice1.Radiology matrons were in place at
several of the sites visited. This rolegave the service opportunities ofsupport and input at a seniornursing level that was found to beinvaluable.
2.A cascade system has beenestablished to ensure that the IRresponse in an emergency situationof a ruptured aortic aneurysm isefficient and timely and that eachmember of the team is aware oftheir role. This good practiceexample is described in more detailin the Appendix C.
3.Many IR departments find additionalpressure on a Friday afternoon andMonday morning IR lists due tobottlenecks of in-patient demand.
Friday afternoon lists over run withprocedures that could wait until thefollowing day but not over a wholeweekend. One site has instigatedregular weekend daytime IR lists toovercome this issue. This has helpedto relieve pressure on beds andreduced length of stay. This goodpractice example is described inmore detail in the Appendix C.
4.Historically, surgical placement oflines required an in-patient stay,theatre time and a surgeon /anaesthetist. This service wasidentified as ideal for advancedpractice and several sites havemoved to the placement of lines byradiology nurses or radiographers.This good practice example isdescribed in more detail in theAppendix C.
5. Where the IR out of hours workloadis insufficient to warrant a shiftsystem a ‘light duties’ rota can beintroduced. At one site each IRperforms a week on call and fullweek-end cover. During this weekno routine lists are booked for theon call IR. The diagnostic and nonclinical components of aninterventional radiologist’s job canstill be covered during this week,but at hours that are more flexibleto allow sufficient rest after anonerous night on call. This goodpractice example is described inmore detail in the Appendix C.
6.Patients treated by EVAR requiresurveillance scans at one month, 6months, 12 months and annuallythereafter to monitor aneurysm sacsize and check for the presence ofendoleaks as per Society for VascularSurgery (SVS) guidelines. Patientscan be lost to follow up. One sitehas developed a robust system toensure that patients are invited fortheir surveillance scans in a timelymanner. This good practice exampleis described in more detail in theAppendix C.
7.Patient selection and prioritisation ofelective patients requiring EVAR ledone site to develop a database witha scoring system to aid the decisionmaking process. The database trackselective patients through their workup for EVAR and subsequent post-procedural surveillance. Additionally,the database allows prospective datacollection on aneurysm morphology,device performance and unitmortality, morbidity and therequirement for secondaryintervention. This good practiceexample is described in more detailin the Appendix C.
8.Extending the role of theradiographer has been developed inan IR department, underpinned byprotocols approved by the Trustprotocols group. This good practiceexample is described in more detailin the Appendix C.

The Government has shown anongoing commitment to involvepeople in their own healthcare and inthe planning, review and delivery ofhealth care. Equity and Excellence –Liberating the NHS¹ states ‘Too often,patients are expected to fit aroundservices, rather than services aroundpatients….’ Patient and publicengagement and experience hasbecome a statutory requirement of allNHS organisations. It ensures thatservice providers have theopportunity to listen, understand andrespond to service user needs,perceptions and expectations. Thiscan then be used to informcontinuous improvement and servicetransformation.
Stakeholder engagement includingpatient representation will berequired in development of carepathways. The Regional TraumaNetwork Engagement Project11, usinga multi strand engagement approach,appeared to ensure that sufficientbreadth and depth of contributionswere achieved. The combination ofactivities facilitated both quick andeasy responses from a high volume ofself selecting respondents as well assupporting in-depth and consideredcontributions from a carefullyselected mix of stakeholdersincluding patients exploring theirexperiences and makingrecommendations. Although anumber of patients were not able to
comment those that did were able todescribe the reassurance that clinicalstaff provided. On reflection,patients were able to identify anumber of weaknesses through theirtrauma pathway including:• the need for better pre-hospital
assessment to ensure people aretransferred to a hospital bestequipped to treat their injuries;
• a number of hospitals which theywere taken to were not equippedto deal with their needs;
• in some instances ambulancescaused great discomfort and werenot adequately equipped totransport them;
• sometimes care was perceived tobe sub standard by professionalswho did not have the expertise todeal with their injuries and in someinstances wrong treatmentresulting in prolonged and multipletreatments and delayed recovery;and
• a complete lack of co-ordinationand support once people aredischarged from acute hospitalcare.
This is the type of structured processwhich is required to further developservices in ways which ensurespatient confidence in service delivery.
Most of the sites visited recognisedthe value of engaging with patientsand service users in a variety of ways.
• Evidence suggests a strong linkbetween good communication andpatient satisfaction and many ofthe sites visited invested time indirect communication between theIR team and the service user.
• Almost all undertake regularpatient audit review of services,however it must be recognised thatthe gathering of feedback to makechanges or improvements toservices, is of little use if sites thenfail to act upon the feedbackwithin the organisation.
• All sites used a variety ofinformation leaflets, both nationaland local however it must be keptin mind that studies12 show thathealth information for patients andthe public is written at an aboveaverage reading ability, making itdifficult for some service users tounderstand.
• The British Society of InterventionalRadiology (BSIR) have developed anumber of patient literature leafletsthese have been developed toprovide standard and consistentmessaging for patients and reducethe need for local IR teams tospend time developing their own.
Patient and public engagement and experience (PPEE)18
Patient and public engagement and experience (PPEE)
DOMAIN
4
11Department of Health. Regional Trauma Networks. Engagement Strands Report (2010) London12Coulter A and Ellins J. (2006) The quality enhancing interventions project: patient focused interventions. London: The Health Foundation.

19Patient and public engagement and experience (PPEE)
• Patients must be made aware ofthe risks and benefits of IR whencompared to more conventionalsurgical or medical procedures. Thisis not always possible when urgentintervention is required in traumasituations. Patients can be assuredby good clinical governance thatrisk is minimised and managed byrobust clinical protocols based onbest evidence and constant reviewof critical incidents.
Examples of good practice
1.Several sites have set up new andfollow up patient clinics in imagingor out-patient (OP) departments forinterventional radiologists to see,counsel and consent new patientsand to see follow up patients. Anincrease in patient satisfaction hasbeen demonstrated. These goodpractice examples are described inmore detail in the Appendix D.
2.Other sites follow up their patientspost procedure by telephone. Thisattracts a tariff.
3.Patient feedback followingfistuloplasty revealed that patientsfound the procedure extremelypainful and traumatic and alsosuggested that some patients mayrefuse further interventions. Thispoor quality experience needed tobe addressed and a nurse led painmanagement service using anopiate analgesia was introduced.This has had a major impact oneffective pain management. Resultsfrom a pain audit tool showed thata large percentage of patientssubsequently reported a pain scoreof less than five and patients werehappier to return for furtherprocedures. This good practiceexample is described in more detailin the Appendix D.
4.Several sites have introduceddedicated written care pathways toensure consistency of care inpatient needing either elective oremergency intervention.
5.An IR patient satisfaction surveyhas been undertaken to gainfeedback about the quality of theservice. The aim was to determinethe patient experience andhighlighted any potential areas forimprovement. This good practiceexample is described in more detailin the Appendix D.

A good IR service requires close teamwork and cross discipline co-operation to ensure correct patientand procedure selection and timelyservice delivery, particularly in thesetting of acute trauma. Skilful andinspirational leadership at all levels inthe team maintains morale underworking conditions that are often athigh stress levels. Developing IRteams into effective components of amajor trauma team needs strongexecutive leadership, particularly withthe forthcoming challenges ofvascular reconfiguration adding tothe pressure for services.
Executive leadership has been seen tohave an important role in thedevelopment and function of IRteams. Where good leadership wasseen the importance of IR wasrecognised and the teams were morelikely to be supported by adequateresource in terms of equipment andmanpower, and to figure in thestrategic plans of the Trust. Wherethis was not evident IR teams aremore likely to be understaffed andworking with substandard oroutdated facilities, struggling toidentify the way forward.
Financial solvency is clearly a keycomponent of the ability of the Trustto achieve success in this field as IR isan expensive modality, although IRmay be (and usually is) considerablycheaper than other treatmentoptions13. Good financial leadershipat executive level however will realisethe potential of IR to generateincome by appropriate operationaldelivery network arrangements, andby ensuring that activity is correctlycaptured and charged.
Within IR teams we have seenexamples of good leadership fromclinicians, radiographers and nursingstaff. Conversely we have seenexamples where elements of theteam are dispirited by a sense of lackof involvement and integration eitherowing to lack of leadership by theirprofessional peers or of the widerteam. Good leadership supports allmembers of the team to make themfeel useful and valued, and alsoprovides the possibility of professionaldevelopment of team memberswithin their own sphere.Co-operative working acrosstraditional boundaries can lead to agreater sense of teamwork andenhance the robustness of theservice. An example of this would benon consultant led services such asline insertion developed by nursingand/or radiographic staff with thenecessary support from consultantcolleagues. Patients and clinicianshave benefited considerably wherethis has been achieved.
Clinical and strategic leadership isvital in developing links withneighbouring Trusts both in terms ofestablishing appropriate referralpathways and protocols and increating effective clinical operationaldelivery networks. This might assistwith managing demand and ensuringthat appropriate patients are referredon to IR centres.
Leadership and support from ITservices is also important to ensurethat communications are maintained24 hours 7 days a week, particularlyin relation to image transfer, and wehave seen several examples whereteams have struggled to provideoptimum patient care becauseimages cannot be transferred to thetertiary centre in a timely manner.
Across the country the effectivenessof leadership is very variable, notablyat executive level. Sites exhibitinggood leadership are often hardpressed but cope with enormouspressures, whereas demoralisationand stress are the hallmark of siteswhere some elements of this effectiveleadership are missing.
Leadership20
Leadership
DOMAIN
3DOMAIN
4DOMAIN
5

21Leadership
Examples of good practice1.The introduction of a ‘radiologist of
the day’ to whom all queries aredirected allows other IR staff to geton with work without interruption.This system has improvedproductivity and made managingthe workload simpler. All work isclearly displayed on a white boardand this is constantly updated. Itcontains a list of pending cases sothe team are aware of outstandingcases, priority can easily be re-ordered or if an opportunitypresents the appropriate case caneasily be added. The interventionalradiologists cross cover for eachother, vet and add cases to eachother’s lists.
2.A monthly diary meeting attendedby all IR consultants wherecommitments are discussed inadvance so that the team knowwho to approach on any givensession to discuss or performemergency interventions. Wherepossible absences are covered butlists are not booked if a sessioncannot be covered. This preventspatients having to have theirprocedures cancelled. This goodpractice example is described inmore detail in the Appendix E.

Some clinical scenarios andprocedures occur sufficientlyinfrequently that it may be difficult tomaintain clinical and technical skills.Given the complexity and differencesof this across organisations an exactdefinition of what constitutes a lowvolume procedure is not possible. Ithas been suggested that, as a rule ofthumb, a procedure should beconsidered to be of low volume if,typically, an operator is exposed to aclinical scenario at a frequency of lessthan once every three months. In thecontext of trauma, this threshold maybe reached for procedures such asthoracic stent grafting for aortictrauma. More generally evencommon presentations may becomelow volume for an individual if he/sheis not exposed in day to day practicebecause others have a specialinterest. In reality, IR practitioners willknow when skills and experience arebeing eroded through lack ofexposure and must be expected totake steps to maintain skills especiallywhere these skills are likely to berequired in the emergency setting.
Analysing the problems posed by lowvolume procedures, and thinkingabout solutions, is best done byconsidering the initial clinicalpresentation, the technical skillsrequired and the post operative carethat will give the patient the bestchance of survival.
Patient selectionSelecting the right patient for aparticular treatment pathway requiresexperience. Even if the technical skillsare well honed poor patient selectioncan have disastrous consequences.Practitioners are encouraged to:• have a low threshold for calling
and discussing cases withexperienced colleagues, bothlocally and at other centres ofexcellence. Teleradiology and datatransfer can play a major role here.All IR radiologists providingemergency IR cover should be ableto access images at home;
• where possible develop writtenreferral criteria and appropriatetreatment algorithms for all clinicalscenarios particularly those whichmight be considered low volumefor everyone in the department.These should be updated throughdirect experience and newliterature;
• set up regular morbidity andmortality meetings both withindepartments and within regions toshare experience. Such meetingsmust be recognised in job plans;and
• remember that informed consentneeds to include the information tothe patient that the clinical scenariois unusual and experience is limitedand that there is an alternativeoutside of IR.
ProceduralAll members of an IR team need tomaintain technical and clinical skills.This applies equally to radiologists,radiographers and nurses. Howeverwithin a team at any one time theremay be different levels of experience.For example a radiologist of limitedexperience of bronchial embolisationsmight be working with a nurse orradiographer who has experience ofmany bronchial embolisations. Goodteamwork is key to successfuloutcomes in all clinical environmentsbut perhaps more so when dealingwith low volume procedures. Equallyanaesthetic support is vital and allowsthe IR team to concentrate onprocedural technical skills.
Optimise the chances of a successfuloutcome by: • good honest pre-procedural team
briefing that MUST include all whowill be involved;
• having written procedureguidelines to use as a refresher;
• maintaining competency in allprocedures that might happen asan emergency out of hours.Remember that many technicalskills are transferable e.g. UAEprovides perfect high volume skillsets that can be transferred to theoccasionally performedembolisation for post partumhaemorrhage. Emergency TEVARwill be more familiar to thosecarrying out many abdominal aorticEVARs;
Low volume procedures22
Low volumeprocedures
DOMAIN
1DOMAIN
2DOMAIN
3DOMAIN
4DOMAIN
5

23Low volume procedures
• maintaining competencies bydoubling up i.e two radiologistsworking together during elective orday time emergency procedures.Again it is important that theabsolute need for this is recognisedby hospital management and thatit is built into job plans and costingof procedures;
• considering external training wherefeasible;
• using simulation techniques whereavailable to maintain familiaritywith devices and clinical decision.Such facilities exist and will becomemore widely available in the future;
• signing up to a ‘maintenance ofcompetency agreement’ and clarifywhat procedures the IR team ishappy to undertake, both in anelective and in an emergencysetting. Stick to the agreementand review it regularly; and
• recognising where there arescenarios where skills cannot bemaintained, formal pathways mustbe available to other hospitalclinicians, preferably published onthe hospitals trust intranet. Formalagreements must be made with thereferral hospitals andcommissioners involved in suchdecisions and pathways. Anexample of a procedure that mightrequire such action would be TIPSfor uncontrollable bleeding.
Despite the above it is recognisedthat in the emergency setting it maybe in the patient’s best interest toattempt a life saving procedure evenif inexperienced in that technique.With use of the measures discussedabove it may be possible to mitigateagainst any potential adverseoutcomes should this scenario occur.
There are ways in which clinical andtechnical skills can be maintained tocover all clinical scenarios. Patientsafety demands that every effort ismade to do this on the part ofindividuals and teams. Managementmust play their part in providing anenvironment that patients can haveconfidence in. All IR teams will comeacross clinical scenarios which willpresent them with new challenges.The recognition by all involved oftheir limitations in such situations,seeking advice and help acutely butthinking ahead electively willultimately provide the best possibleoutcomes.
Examples of good practice1.In Nottingham the radiologists
double up for low volume casessuch as TEVAR and TIPS and theykeep a record of who has donewhat, making sure that they allmaintain sufficient numbers ofcases.

24
SummarySince October 2011, a full out ofhours interventional radiology servicehas been provided at the UniversityHospital Coventry and WarwickshireNHS Trust (UHCW) site on a 1:6basis. This has involved fourconsultants from UHCW with agreedcontractual support from two furtherconsultant interventional radiologistsfrom a neighbouring Trust (GeorgeEliot Hospital, Nuneaton). UHCW isa large 1200 bed modern teachinghospital which now has majortrauma centre status. George EliotHospital is a smaller district generalhospital. The two sites are around10 miles apart.
Context and background UHCW is set up to be a MajorTrauma Centre. Vascular services forthe three acute Warwickshire Trustshad previously been reconfiguredsuccessfully with six vascularsurgeons participating in acentralised on-call service at theUHCW site. A fourth consultantinterventional radiologist wasappointed in September 2010. Thisallowed the move to a full cover outof hours IR rota for vascular andtrauma services. The Trust has allmajor medial and surgical subspecialities on site with theexception of specialist paediatricsurgery.
How was the change made? Informal clinical level discussionsbetween consultants from the twohospitals with subsequent discussionat clinical director level. Once broadprinciples were agreed, managementmeetings took place to agree preciseoperation and clinical governancestructures.
The realignment of the diagnosticimaging rotas demanded asignificant change for all UHCWconsultant radiologists (bodyimaging 1:7, neuroimaging 1:9 andintervention 1:6). The number ofspecialist registrars assigned to thedepartment was increased enablinga 1:7 out of hours compliantregistrar rota to support thediagnostic service.
The George Eliot consultants arepaid an agreed number of DCCs tocover their daytime and out of hoursIR cover.
ResultsOverall impact The changes have been verypositively received by our clinicalcolleagues. Provision of the rotaenabled UHCW to achieve full MajorTrauma Centre status. This has beena major advance in delivery ofspecialist care to the patients ofCoventry and Warwickshire andprovides an excellent base for furtherdevelopment of IR services in thefuture. In the first few months ofoperation, numerous patients havebenefited from prompt percutaneousintervention and avoided opensurgery.
How was the change measured? A log of out of hours interventionalprocedures has been kept along withan hours monitoring exercise for theconsultants involved. In addition,the impact on nursing andradiography staff has been loggedover the initial months in order toassess the service impact andrequirements for the future.
The two George Eliot consultantsoperate on a 1:6 rolling general on-call rota at the George Eliot site andperform a dual on-call beingavailable concurrently for the UHCWIR rota. The UHCW general andneuro rotas were reconfigured torelease Intervention consultants forthe IR rota who in turn dovetail withthe George Eliot rota.
It was agreed that UHCW would payfor one weekly in hours direct clinicalcare (DCC) of intervention activityfor the two George Eliot Radiologiston the UHCW site for basic servicedelivery and so that they could play acentral role in the Trust’s IR activity.These sessions started three monthsin advance of the on-call rota toenable familiarisation with localstaff, rooms and equipment.
A clinical lead for IR was appointedand a specialist group formed. Theclinical lead co-ordinated all thearrangements and madepresentations to relevant clinicalcolleagues (Emergency Department,Anaesthesia, General Surgery andOrthopaedics).
What resources/ investmentwere needed?A sterile ultrasound (US) needleguide was purchased to enable USguided intervention for consultantswho required it. A documentdetailing the agreed clinical servicewas developed following thetemplate provided by the RoyalCollege of Radiologists. With thisinformation, a review of on the shelfstents and embolisation coils wasundertaken to cover the emergencyworkload; essentially the stock wasdoubled.
Delivering an out of hours IR service utilisingconsultants from a neighbouring hospitalUniversity Hospital Coventry and Warwickshire NHS Trust
A: Networking

25
How has good practice beensustained?All six consultants continue theirnormal update, clinical governanceand appraisal processes. Inparticular, the IR group has formed aquarterly meeting for business andclinical case review/presentation. Afuture specialist IR MDT andmorbidity/mortality meeting isplanned. All consultants nowsubmit their personal data at theBSIR national registries for bothvascular and non vascular indexprocedures.
Lessons learntThe collaboration between the twohospitals has resulted in an excellentworking arrangement for theprovision of a specialist IR service tothe local population. Theconsultants had the vision to seehow future service configurationsmight be shaped and have beencommendably flexible in assisting alarger organisation to make thenecessary advances. Patients fromCoventry and Nuneaton includingthe whole catchment area for theMajor Trauma Centre will benefit asa result of this.
The concept of the two George Eliotconsultants being on call for bothdiagnostic and interventionalradiology appears sustainable todate.
Future plansThe rota provides an excellentplatform for further developmentsincluding acute EVAR/TEVAR andexpansion into acute colorectalstenting. A business case for uterinefibroid embolisation (UFE) is at anadvanced stage and once theseelective patients have begun toattend the department, anappropriately provided service foracute post partum haemorrhage willbe enabled.
We plan to develop a local specialistIR MDT with a morbidity/mortalitycomponent to the meeting.
From this established base, we planto build a service which can expandand adapt to the future andchanging needs of our localpopulation adopting new techniquesand technologies as they becomeavailable.
ContactDr James Harding, Consultant RadiologistEmail: [email protected]

26
SummaryRadiology nursing cross site rotationwas implemented in Newcastle uponTyne Hospitals NHS Foundation Trust(NuTH), in order to provide a singlenurse on call rota, to support theinterventional radiologists. Itprovides registered nursing cover foremergency out of hours radiologicalintervention. Registered nursesbelow band 7 are rostered to workin the radiology departments at theRoyal Victoria Infirmary and FreemanHospitals. Each radiologydepartment performs differentinterventional procedures, althoughthere is some overlap. This waschallenging in terms of skills andexperience and required careful andcomprehensive planning. This systemaims to provide safe practice,increased knowledge base andnursing job satisfaction, plus aidrecruitment. Cost savings were alsomade by reducing two on call rotas,to one.
Context and background The interventional radiologists at theRoyal Victoria Infirmary (RVI) and theFreeman Hospital (FH) implementeda single radiologist on call rotaspecifically aimed at providing out ofhours cover for emergencyinterventional radiologicalprocedures across both sites inOctober 2009.
Following this, there was a review ofradiology nursing and it was decidedthat the registered nurses could mirrortheir system. The idea was to provideexperienced nurses who would beknowledgeable, safe and proficient inassisting with all types of interventionundertaken on each site. They wouldalso have good geographicalknowledge of both sites and knowwhere equipment was stored.
Although this system of working hadbeen informally discussed with thenursing staff in previous years, aformal meeting was arranged out ofhours in order to avoid anyinterruptions. Both registered nursesand health care assistants wereinvited and an agreement was madeto give staff who attended, timeback in lieu. A matron chaired themeeting and most staff attended.
At that time there were both positiveand negative comments made aboutthe introduction of this system. Thesenior sisters compiled a written staff survey that was completedanonymously. The results showedthat some staff were reluctant tomake the change in practice whilstothers looked forward to thechallenge and variety of work.
A nursing rota was developed toinclude cross site rotation of qualifiednurses below band 7, between bothhospital radiology departments. Thiscommenced in June 2010.
The two band 7 senior sisterspermanently remain on theirindividual sites as managers,although work closely together andfrequently visit the opposite site.One of them previously worked onthe opposite site and therefore had a good overview of the service onboth sites. This helped inunderstanding how staff needed to be allocated on each site.
In October 2010, the mostexperienced radiology nurses beganto participate in a single nurse oncall rota that covered the RVI andFH. The less experienced joined therota at a later date when they weredeemed competent.
We believed that the nursing andmedical staff would provide a moreefficient service when workingtogether on a regular basis, therebygetting to know each other well. Wefelt this to be an important part ofproviding a high standard, out ofhours interventional radiologyservice, when the RVI became a level1 Major Trauma Centre in April 2012.
The aim was also to create a flexibleservice as the registered nurses wouldbe able to cover their colleagues oneither site during holidays, sicknessand leave due to the Europeanworking time directive. Theexperience gained would enable safepractice to occur when working oncall without the presence and supportof other radiology nursing colleagues.
There was also a financial incentive,as savings would be made byreducing two on call nursing rotas,to one. As only one on call rota wasnow required, changes to the skillmix of staff nurses and health careassistants could be made, resultingin further cost savings for theradiology directorate.
This system would reduce theamount of on call undertaken by thenurses from 1:5 to 1:10, therebyimproving their work life balance. Incontrast however, it would reducethe amount of on call undertaken,thereby reducing the amount ofovertime paid to staff.
How was the change made? Firstly, discussions between thesenior sisters, matron and medicalstaff were made and it was agreedthat it could be advantageous toimplement cross site working forqualified nurses below band 7.
Implementation of radiology nursing cross site rotationNewcastle upon Tyne Hospitals NHS Foundation Trust
A: Networking

27
What resources/ investmentwere needed?Initially savings were limited asexperienced staff (including band 7senior sisters) provided on call coverfor the less experienced, until theywere deemed competent toundertake solo on call. In effect, thisreverted back to having two nurseson call together, but for shorterperiods of time.
Ultimately money was saved on thenursing staff budget by reducing thenurses on call from two to one asonly one standby payment neededto be made. Also, the band 7 seniorsisters withdrew from the on callrota, thereby reducing the costscreated through more expensiveovertime payments.
Time investment was required to:• undertake extra training for staff
who were assessed by the seniorsisters on an individual basis;
• set up quarterly cross site meetingsthat alternate across site. Initiallythese were arranged out of hours,but recently, with the cooperationof the medical staff, they havebeen arranged for early in themorning to avoid minimaldisruption to the work load;
• compile new rotas, holiday and offduty requests spreadsheets;
• improve and update equipmentlists on both sites as a learningtool and aid during call outs; and
• create a medical devicecompetency list to include medicaldevices used across site, and use itas a training guide for staff.
The senior sisters invested a lot oftime with staff as they explainedregularly, the need for cross siterotation to occur and its advantages
for the directorate and Trust. Therewas some well-established staff whowere reluctant to change. We dealtwith this by encouraging staffinvolvement and asking them todiscuss how they felt the rotationshould be implemented. Thisallowed staff to feel more involved inthe process.
ResultsOverall impact Cross site rotation has given theregistered radiology nursing staffconfidence to participate inproviding a single nurse on call rotathat covers two hospital radiologydepartments. It provides a safesystem of working and continuity forthe radiologists on call. Staffrelationships have developed furtherduring cross site rotation. Patientsbenefit by receiving safe care fromwell trained, knowledgeable andexperienced staff.
How was the change measured? Quarterly cross site staff meetingswere set up and minutes taken toprovide an update for those whocould not attend.
The staff survey was repeated after12 months. The results were fairlysimilar to the results of the initialsurvey
How has good practice beensustained?All new radiology nursing jobs areadvertised to work across both sites.
Cross site rotation has continued,although the frequency of rotationdepends on staff experience andtraining required, therefore isorganised on an individual basis.
A list of medical devicecompetencies was compiled, traininggiven and sign off when staff werecompetent. The competencies areundertaken on an annual basis.
Band 7 sisters continue to shadowstaff on call when necessary.
Lessons learntAlthough the possibilities of crosssite rotation had been discussedoccasionally during the previous fewyears, the staff still did not seemprepared for the change in practice.
In hindsight we feel that formal staffdiscussions could have been startedearlier in an effort to allow staffmore time to come to terms with thechanges.
Newly appointed staff who wereemployed on the basis of workingacross site, were very positive inwhat they could gain from workingin two separate environments andwere excited by the learningopportunities presented. Currentlythey are happy and feel as thoughtheir working practice is wellbalanced.
After 18 months of cross siterotation, the established nurses havesettled down well and the wholegroup are sharing knowledge andbest practice across site.
Future plansContinue with the rotation.
ContactDr Ralph Jackson, Consultant RadiologistEmail: [email protected]

28
SummaryTwo neighbouring DGHs, 25 milesapart in a rural location each havethree interventional radiologists. Inorder to provide formal on call IRservices 24/7 they have developed anetworked solution.
Context and background Royal Devon and Exeter has acatchment population ofapproximately 370,000 and Torbay’scatchment resident population isapproximately 280,000. There aresignificant increases in transientpopulation during holiday seasons.
At each site there are threeinterventional radiologists.Emergency out-of-hours IR had beenprovided on an ‘ad hoc’ basis. Withincreasing frequency of cases therewas significant risk of being unableto find a willing or available staffmember (radiologist, radiologynurse, interventional radiographer)and staff were becoming unhappyabout being called in when not oncall.
The two Torbay and three Exetervascular surgeons have been runninga successful cross-site emergency oncall vascular surgical service forseveral years. For this service theusual approach is for the emergencypatient to be transferred byambulance to the on call site ifrequired. The interventionalradiologists initially favoured asimilar model for an IR on callservice, feeling unenthusiastic abouthaving to do urgent cases in anunfamiliar environment.
What resources/ investmentwere needed?There was a relatively small increasein pay costs, for the changes in jobplans and on call frequency for theradiologists and for the formal oncall for the nurses andradiographers. (In Torbay thisequated to approximately anadditional £66,000 per annum andhad been built into the businesscases for recent general radiologistappointments.)
ResultsOverall impact There is always interventionalradiology emergency cover at bothsites, 24/7, providing a safe andsecure service. This is extremely well-received by the other clinicianswithin the hospitals. Increasedawareness of the service has led to asignificant increase in out-of-hourscases compared to the previous ad-hoc arrangements. However, all ofthese cases are felt to be appropriateand the frequency of call-outs is stillrelatively low. In order to maintain adegree of control and to ensureappropriateness of referrals the oncall interventional radiologists willonly take calls from consultants.
How was the change measured? Diaries of activity are kept and theservice audited.
How was the change made? The Torbay radiologists started theirown in-house on call service whilstdiscussions were ongoing in Exeter.This was on a 1:3 rota, clearly notsustainable in the long term. In thefirst year of this service the caseswere audited and it was felt by thereferring clinicians and intensive careteams that a significant minority ofpatients would not have beensuitable for transfer if Exeter hadbeen on call.
The planned model was thereforechanged with the default positionbeing that the on call radiologisttravels to the site of the patient. Theradiologists visited each other’sdepartments to get to know thelayout and staff. Consumables suchas wires and catheters were similarin each department but allradiologists satisfied themselves thattheir preferred kit was available onboth sites.
On both sites the discussion andplanning included radiologydepartment managers, medicaldirectors and senior executives, theradiology nurses and interventionalradiographers, and the generalradiologists.
On weekday evenings and nightseach site covers its own emergencywork. From Friday evening toMonday morning and on bankholidays there is one interventionalradiologist on call, covering bothsites. The radiologists’ rota istherefore 1:3 week days, 1:6weekends. For every night andweekend there are radiology nursesand interventional radiographers oncall at both sites. This service hasbeen running for 20 months.
Networked on call interventional radiology across two sitesSouth Devon Healthcare NHS Foundation Trust and Royal Devon and Exeter NHS Foundation Trust
A: Networking

29
How has good practice beensustained?The radiologists from both sites meetto discuss the service and casesperformed. Now that both thevascular surgeons and theinterventional radiologists havecross-site rotas this has encouragedfurther development of formal cross-site MDT working.
Lessons learntAs in many radiology departmentsthere was reluctance from thegeneral radiologists regarding thesechanges as the interventionalradiologists would come off thegeneral on call rota. To some extentthis was ameliorated by linking thesechanges with expansion in overallradiologist numbers in response togrowing workload. Now that theservice is well-established themajority of non-interventionalradiologists are very happy with it;they no longer have the difficulty ofbeing asked to arrange an urgentinterventional case at the weekend,either feeling forced to dosomething they are uncomfortablewith or having to phone around tofind a colleague who is not on call.
As an unexpected consequence fortwo DGHs, on a few occasions atweekends we have received patientstransferred from another hospitalbecause the clinicians there areaware that we have the only formalIR on call service in the region.
The agreed portfolio of workcovered on both sites on callincludes nephrostomy, abscessdrainage, peripheral vascularintervention and embolisation forhaemorrhage. Renal access work isonly done at Exeter and thereforefistula salvage was not included.Only one of the six radiologistsperforms TIPSS and two of theTorbay radiologists do not performPTCs. These procedures are thereforeonly provided on an ad hoc basis,depending on which radiologist is oncall or contactable. We thought thatwe had thought of everything butdid not realise that the Exetersurgeons ask for urgent colonicstenting for obstruction whereas thisis not done at Torbay. This is the oneprocedure that was requested at theweekend by an Exeter surgeon butcould not be performed as the oncall radiologist was from Torbay.
Future plansThe service is working well andappears sustainable. We continue tostrengthen the links between the IRand vascular surgical units at bothsites.
ContactDr R Seymour, Consultant RadiologistEmail: [email protected]

30
SummaryA case for change to workcollaboratively across several Truststo deliver a 24/7 IR service topatients every day of the year.
Context and background There was increasing recognition ofthe importance of IR in patientpathways particularly forhaemorrhage control with variationin access to out of hoursinterventional radiology across thelocal areas. There was no formal IRon call rota and the informal rotawas placing stress on specific pointsof the IR team.
There were nine trainedinterventional radiologists across thearea however on-call was part of thegeneral diagnostic rota. There wasno formal nurse on-call rota at thetime of inception. Equipment andequipment levels across the areaparticularly of consumables wasvaried.
How was the change made? The clinical case for change wasestablished with the clinical teamincluding nurses and radiographersin a series of facilitated meetings.The managerial support wasexcellent after the case for changewas established and resourcesupport was agreed. We did notfocus only on OOH services andaccepted that we would have tochange in hours services as well.
ResultsOverall impact • The change has provided a 24
hour IR on call service on every dayof the year with improved equityof access to IR services.
• There has been direct positivefeedback for the IR team. Havingdeveloped the case for changethey recognised the impact theywere making in acute care.
• Reduced referral time for out ofhours work received very positivefeedback from all clinical staff andenhanced the profile of IR servicesacross the area.
• Consolidation of consumablesacross sites was very valuable inservice provision and has resultedin a cost saving.
• Using the separate projects ofprocurement etc did develop asense of identity among the units.
• The IR manual was very valuable,particularly in the initial stages forboth external and internal groups.
How was the change measured? We have published audits of ourservice against the RCR guidance for24/7 IR services. We have a research/audit interest in outcomes for IRtechniques and have submitted forpublication a paper on 30 dayoutcomes after OOH intervention.
How has good practice beensustained?The on call service requires aconsistent focus and evolves asclinical requirements change. Wehave established an InterventionalForum that meets regularly todiscuss all aspects of the service. Theforum contains representation fromradiographers, nurses andmanagerial structures.
The agreement for new posts wasestablished within an overallframework that included improvingcross-cover and working in hoursbetween adjacent units and mergingequipment and procurement to bothreduce costs and improve cross-siteworking.
An IR on-call manual was developed.It included both processes andprocedures. This allowed the clinicalgroups to debate the detail of serviceprovision prior to service introduction.
What resources/ investmentwere needed?• Additional staff funding was
required. This was not seen solelyto support out of hours but wasframed to improve serviceprovision and equality of accessboth in and out of hours.
• Medical staff required changes tojob plans - this impacted on thediagnostic on-call rota. Furtherredesign of diagnostic rotaoccurred.
• Medical staff had to accommodatechanges that meant cross-siteworking both in and out of hours.
• Nursing staff required significantnegotiation to terms andconditions - this took aconsiderable time to workthrough. For a period reducednumbers of nursing staffparticipated and this placedpressure on this group. Nursingstaff also had to adapt to cross-siteworking across several hospitals.
• Most sites already had dedicatedradiographic staff, however therewas concern about undertakingunfamiliar procedures.
Development of cross-site 24/7/365 interventionalon-call service covering nine individual hospital unitsNHS Greater Glasgow & Clyde
A: Networking

31
Lessons learnt• Clinical leadership within each of
the groups was essential and thiswas enhanced by the projects andan understanding of the case forchange.
• The process was at times difficultand required real persistence - thismay not have happened withoutthe above.
• Defining the scope of services isessential - the IR team involvedwould not have signed up to anopen ended agreement. Inaddition, we had to accept thatthe important targets to coverwere the common life threateningemergencies initially haemorrhage.We have since adopted a widerrange of procedures.
• We were merging units that didnot previously have a closeworking relationship. We used thedevelopment of the discreteprojects; procurement ofconsumable equipment, facilitatedmeetings and development of IRmanual to help form a morecohesive unit.
• There were initial challenges fromdiagnostic colleagues due to theimpact on their rota. We couldhave perhaps involved them moreclosely in the development of thecase for change.
• Achieving a sustainable nursingon-call has required on goingwork. The nursing group have verymuch supported this initiativehowever negotiation of terms andconditions is time consuming.
• We rationalised equipment acrossthe sites to facilitate cross-siteworking for all staff groups. Wealso developed embolisation bags- this is a portable completeconsumable kit which includescontrast catheters embolic agents.This is stored at two sites acrossthe area and is transported tocases outside the main units.
ContactDr Iain Robertson, Consultant RadiologistEmail:[email protected]

32
SummaryThe introduction of Payment byResults (PbR) meant that it was vitalto accurately record and code IRprocedures in order for the correcttariff to be applied. This project has: • improved the accuracy and
visibility of IR procedures withinclinical notes following regularcase review meetings with clinicalcoding department andcommissioning manager;
• lead to the implementation ofclinical recognition within PAS andthe electronic patient record (EPR)(currently in phased replacementof PAS) for clinic episodes; and
• established IR Consultant waitinglists for key IR procedures.
Context and background IR has expanded rapidly in the lastdecade to offer a wide-range ofminimally-invasive treatments acrossmany different specialties includingtrauma, vascular surgery, oncology,gynaecology and gastroenterology.
The introduction of PbR rewardedincreased clinical activity withincreased income based on the tarifffor a patient “spell”. This systemwas based on a model of a “spell”being defined as a referral to ahospital clinic with furtherinvestigations or treatmentsthereafter. Traditionally, radiologyhas been regarded as a supportservice with locally negotiated globalbudgets and in most cases has takenreferrals from other hospitalspecialities and therefore the tarifffor a treatment has been assigned tothe “clinical” specialty. Interventionalradiologists are increasinglyrecognising the need to take onclinical care of patients.
A list of key procedural codes wasidentified for IR procedures anddistributed to the IR suites (based ontwo sites) and also an abbreviatedlist to ultrasound and CT whereimage-guided biopsies or drains areperformed.
A policy was introduced that allinterventional procedures should berecorded on an operation sheet, anda red sticker with “interventionalprocedure” placed in the clinicalnotes to highlight the procedure toclinical coding. Radiologists wereencouraged to avoid abbreviations,clearly state the procedure and addthe procedure code. If there wereany major co-morbidities then theseshould also be stated. One particularexample identified was for colonicstent insertion where specificallystating “bowel obstructionsecondary to colonic carcinoma”rather than “bowel obstruction”would significantly alter the tariff toreflect the co-morbidity of thepatient.
The majority of angioplasty or stentprocedures for peripheral vasculardisease are currently performed asday-case procedures withinradiology. Following referral fromvascular surgery there is a radiologypre-assessment clinic to assesssuitability for a day-case procedure.A member of the clerical departmentwho had undertaken PAS trainingidentified these clinic episodes werenot being recognised and thatpatients were being admitted undervascular surgery for their day-caseprocedure, even though care for thisepisode was completely under IR.
There are examples where this isvital, for instance uterine arteryembolisation where patients expecta consultation with theinterventional radiologist in an out-patient setting prior to and after theprocedure and for the radiologist totake on their care during theirhospital spell.
There are barriers to development ofIR services including lack of out-patient clinics, lack of junior medicalstaff, lack of in-patient beds,shortages in radiology nurses andpoor provision of 24-hour covernationally. There is poor awarenessof the scope of IR among the publicand to some extent referring GPs.
There is a national trend towardscentralisation of vascular surgicalunits and Major Trauma Centres.Although these changes are led byvascular surgery and trauma, IR isoften key in delivering services.Traditional funding arrangementscan limit investment in radiologyinfrastructure.
How was the change made? Coders currently use clinical notes toidentify procedures and patient co-morbidities that map to the finaltariff healthcare resource group(HRG). Radiology procedures arecurrently reported on a radiologyinformation system (RIS). Thisgenerates a paper report. Thecoders will only pick this up if thishas been filed and is visible, or ifthere is a clinical entry to flag themto look on RIS. Regular case reviewmeetings were arranged with theclinical coding manager and thecommissioning manager forcompleted patient spells.
Ensuring accuracy of coding for interventional radiology (IR)procedures to reflect workload and maximise income to IRdepartments and so ensure resources follow clinical activityOxford University Hospitals NHS Trust
B: Funding

33
Changes were agreed to recognisethe clinic episode for the pre-assessment and to establish thepatient onto an IR consultant waitinglist so the tariff would pass to the IRday-unit. This puts the unit onto arealistic funding stream as workloadis set to expand rapidly due tocentralisation of vascular surgery inour region.
The importance of clinic episodesand IR consultant waiting lists wasalso identified in relation to fibroidembolisation. Patients were beingadmitted to the gynaecology wardas emergency admissions undergynaecology. Involvement of thecommissioning manager and IRclerical staff established the pre-procedure MRI and consultation as aPAS clinic episode with placement ofthe patient onto an IR consultantwaiting list. This enabled thegynaecology ward staff to admit thepatient as an elective procedureunder the IR consultant for theirhospital spell. A similar model hasbeen applied to patients withvascular malformations.
What resources/ investmentwere needed?Time to meet, engagement withcoding manager, commissioningmanager, clerical staff withinradiology.
ResultsOverall impact • Better understanding of process
and importance.• Accurate recording of information.• Positive effect on team morale
both in IR and clinical coding.• New set of useful information for
IR team to use when negotiatingfor additional resources.
How was the change measured? Subjective improvement in visibilityof IR procedures within coding,positive feedback from codingmanager.
Increase in radiology income difficultto measure as no separate budgetline for IR income within overallradiology budget. However increasein income has been incorporatedinto Cost Improvement Programme(CIP).
Recently implementation of EPRacross the Trust has had teethingproblems with booking day-casepatients, this has been immediatelyidentified as a loss of income.
How has good practice beensustained?Less frequent but ongoing meetingsbetween clinical coders and IR
Lessons learntWorth investing the time which isalways at a premium
Future plansCurrent clinic episodes are carriedout ad-hoc in ultrasound/MRI/day-case/office settings. The next stageof this plan is to create dedicatedsession in out-patients. The aim is toincorporate this into consultant jobplans. The clinic would be used forvascular pre-assessment, fibroidembolisation consultations, vascularmalformations referrals and in futureextended, for example, to reviewpatients with who have had inferiorvena cava (IVC) filter placement.Patients could potentially be referreddirectly from GP for some of theseprocedures.
There are further plans to take onjunior doctors (F2) doctors to enablegreater clinical engagement on thewards following procedures for in-patients.
Plans to improve profile of IR in thelocal health system, i.e. GP studydays, information campaigns,involvement of local media andpatient support groups.
Separate work is underway toestablish service level agreements(SLA) between radiology and clinicalspecialities.
ContactDr Mark Bratby, Consultant RadiologistEmail: [email protected]

34
SummaryA cascade system is in place toensure that the IR response to aruptured aortic aneurysm is efficientand timely. Each member of theteam is aware of their role in thecascade.
The vascular surgeon on-call informsthe IR radiologist on-call when apatient with a ruptured/dissectedaorta is either in ED or is anexpected transfer. The CT imagesare reviewed by the IR radiologistand the vascular surgeon and if thedecision is made that anendovascular repair is appropriatethe following cascade system isused.
What resources/ investmentwere needed?Time to agree guideline.
ResultsOverall impact Improvement to patient journey.Reduced stress levels for staff.
How has good practice beensustained?Guideline passed on to all new staff.
ContactDr Claire Cousins, Consultant RadiologistEmail:[email protected]
Context and background The vascular surgeons andinterventional radiologists at CUHhave been providing an EVAR servicefor ruptured abdominal aorticaneursyms (AAA) since 2005. Sincethen there have been 15-20 casesper year. A guideline has been putin place; • to identify radiological and
radiographic personnel required toprovide IR support duringemergency EVAR or TEVAR;
• to establish a pathway ofcommunication from vascularsurgeon to interventionalradiologist to radiographer(s) thatis efficient; and
• to identify equipment required.
A cascade system for emergency IRCambridge University Hospital NHS Foundation Trust
C: Staffing and MDT working
Ruptured/dissected aorta- endovascular repair
appropriate
IR radiologist informsIR radiographer
Is repair to take place in IRtheatre or angio suire?IR theatre Angio suite
IR radiographer informs emergencydepartment radiographer who goes
to theatre to prepare the x-rayequipment.
IR radiographer goes to theatre toprepare contrast and injector.
IR radiographer informs IR nurse. Both proceed to
the angio suite andprepare equipment.

35
SummaryDue to increased demand forservices pressure was put on Fridayafternoon and Monday morning IRlists. Friday afternoon lists regularlyover ran with procedures that couldwait until the following day but notover a whole weekend.
Context and background Pressure on Friday afternoon andMonday morning IR lists due tobottlenecks of in-patient demand.Regularly over-running Fridayafternoon lists and requests for IRprocedures on call that could havewaited until the following morningbut could not have waited over awhole weekend.
How was the change made? Instigated regular weekend daytimeIR lists (running 10 -2) in addition tothe already extended working dayduring the week (2.5 sessions ofscheduled room activity)
What resources/ investmentwere needed?• Negotiated consultant job plans to
allow time off in lieu elsewhere inthe week (requires adequateconsultant staffing).
• Tie the initiative in with Trustobjectives on reducing length ofstay and In-patient keyperformance indicators.
• Ensure adequate staffing forradiographers and nurses.
Future plansThe initiative has been verysuccessful to date and now needs tobe extended to cover both daysevery weekend. New staff(consultants, nurses, radiographers)joining the Trust are appointed withthe expectation of doing someweekend work.
ContactDr Paul Crowe, Consultant RadiologistEmail:[email protected]
ResultsOverall impact • More even distribution of work
throughout the week without theFriday afternoon and Mondaymorning peaks in demand.
• More flexibility in schedulinginpatient work.
• Less demand for weekend on-callactivity with urgent in-patientwork accommodated on weekendlists.
How was the change measured? Data collection.
How has good practice beensustained?The consultants working weekendschose to do so and are happy withtheir new working arrangementsand weekday time off in lieu(consultants work one day alternateweekends on a rolling fortnightlyrota)
Lessons learntOnce set up, in the future werecommend cover arrangements areagreed for periods of absence, studyleave and annual leave to retaincontinuity of service. At present theweekend working is only one list perweekend, alternating betweenSaturday and Sunday. The aim is tohave a list every Saturday andSunday, the main limitation being IRconsultant, radiographers andnursing numbers. Such provisionwould further improve the timelinessof service delivery, reduce length ofstay and reduce demand for IR oncall work at weekends.
Providing an extended IR serviceHeart of England NHS Foundation Trust
C: Staffing and MDT working

36
SummaryManchester Royal Infirmary is atertiary centre for renal andhaematology services. Demand fortunnelled line insertion isapproximately 350-400 per year.Historically lines were placedsurgically but this service is nowprovided by a nurse / radiographerteam. This has reduced waiting timesand increased efficiency.
Context and background Historically placing tunnelled linessurgically required an in-patient stay,theatre time and a surgeon /anaesthetist. Waiting times were longand renal patients often requiredtemporary dialysis access whilstwaiting. Failure rate due to poorpositioning was approximately 50%.The move to placement of tunnelledlines in radiology led to a sharpincrease in workload. This service wasidentified as ideal for advancedpractice. A renal nurse practitionerand subsequently the lead radiologynurse and senior radiographers weretrained in tunnelled line placement.
How was the change made? A protocol for placement oftunnelled central venous linesperformed by nurses was drawn upand approved by the Trust RiskManagement Committee. Thenurses were trained by a consultantradiologist. Following training thenurses undertook uncomplicatedinternal jugular Hickman and Tesiotunnelled line placements. Auditdemonstrated that the skills forsuccessful line placement could berapidly acquired. Two dedicated listsper week were established and therenal specialist nurse provided liaisonbetween radiology and service users.
ResultsOverall impact • The changes have been very
positively received by service users.Patients have expressed animproved experience because ofstaff continuity.
• Dedicated lists on a Tuesday andThursday mornings mean thatthere is more availability andregular lists have improved patientpreparation.
• Audit demonstrated an averagewait of 1.9 days compared to theprevious several days to weekswhen undertaken by surgery.
• This move to “‘right access at theright time’ means that lesstemporary lines are inserted withthe associated reduction ininfection rates.
• Staff continuity and ownership ofthe service has meantstandardisation of practice anddocumentation.
• Nurses recognise the proceduralinformation in the notes and havenamed contacts.
• Costs are reduced. The cost perprocedure is halved whenundertaken by two radiographerscompared with a consultant andscrub nurse.
• Theatre time is not required. • Length of stay is reduced. The
procedure can be undertaken onan out-patient basis.
• Increased job satisfaction for thoseundertaking the role.
A radiographer joined the team andfollowing staff changes anotherradiographer was trained. The teamconsists of three staff members,which allow for the service tocontinue during annual leave /sickness. The team assumes fullresponsibility for the serviceincluding planning the lists, patientinformation and preparation,documentation and troubleshooting. A specific patientinformation leaflet has beenproduced.
Experience has resulted inprogression of the service to includedifficult access / line exchange and asuccessful registrar trainingprogramme is also being delivered
The consultant renal nursedeveloped a tool for managing lineinfections. This “MR VICTOR” tool isnow widely used.
What resources/ investmentwere needed?The extra lists required investment inradiographic staffing. The list waspart of a general expansion in IRwhich resulted in the appointmentof a full time senior radiographer.
Consultant time was required fortraining/audit/advice.
The job description of the consultantrenal nurse was required to beavailable for line insertion lists. 50%of time is dedicated to the accessservice.
Nurse/radiographer led tunnelled line insertionCentral Manchester University Hospitals NHS Foundation Trust
C: Staffing and MDT working

37
• The success of the original renaland haematology service has ledto this becoming a Trust wideservice. Lines are now placedregularly for ITU, gastroenterology,gynaecology and cardiology. Therenal access service is also offeredto neighbouring Trusts.
• New starter nurses fromhaematology and renal servicesattend lists.
• Approximately eight hours perweek of consultant radiologisttime is now available for otherprocedures.
How was the change measured? • Audit of waiting times and
infection rates. • All completion images sent to
consultant radiologist forassessment of position
• Complication rates compared toDOQI standards.
How has good practice beensustained?• Recording and review of
complications by consultantradiologist.
• Audit of waiting times. • Training of further staff to ensure
numbers of trained staff aremaintained.
• Involvement in all Trust initiativese.g. Trust wide central venouscatheter (CVC) audit and‘Matching Michigan – theManchester Experience,’ tomaintain knowledge and profile.
• Close liaison with service users,e.g. meetings to ensure the servicemeets their requirements.
Lessons learnt• The collaboration between the
renal consultant nurse andradiology has enabled this serviceto flourish.
• Initial problems with patientpreparation which led to somecomplications have been resolvedby the design and publishing of achecklist to ensure patients arecorrectly prepared. This checklist isavailable on the hospital intranetand is completed for all lineinsertions.
Future plans• This provides an excellent platform
for further developments includingradiographer /nurse ledfistulogram procedures andperipherally inserted centralcatheter (PICC) line insertion.
• The service continues to expandand further lists may be required inthe future to maintain the waitingtimes. Provision of emergency slotsin each working day would beideal.
• Patient booklet to be produced forHickman lines.
ContactDr. Nick Chalmers, Consultant RadiologistEmail:[email protected]

38
SummaryTo introduce a 24/7 on call rotaadhering to ‘European Working timeDirective’ (EWTD) and rationalisingadditional cost to the Trust requiredadditional IR posts and a freeing upof IR and other diagnostic workloadduring the working week.Each IR performs a week on call. Oncall starts at 5pm on week days andfinishes at 8am the followingmorning. Full week-end coverprovided.
During the week no routine lists willbe booked for the on call IR.Protocol CT and MRI lists cancontinue and MDTs and non clinicalactivities can also be maintained.
Context and background Out of hours IR continues to increasein frequency, and although stilluncommon this often requires IRinvolvement during the night. Therewas little or no flexibility to cancelbooked IR lists for the followingmorning. A shift system was theobvious answer, but since the IRswould not be fully employed duringthe night a ‘light duties’ rota wasintroduced.The diagnostic and non clinicalcomponents of an IR’s job can still becovered during this week, but athours that are more flexible to allowsufficient rest after an onerous nighton call.
How was the change made? • Detailed e-job planning with
directorate/ divisional and Trust HRsupport was required.
• Each IR’s normal week dayworking was examined. Crosscover for lost IR lists was providedwhere possible, but where not wasallocated to one or other of twonew IR consultant post planned.
How was the change measured? 1.The biggest impact was in the
number of out of hours CT guideddrains performed. These numberswere easy to record and plannedchanges are being made to relocate these into a five day a weekin hours drain service. This has inturn led to reduced delays indrainage and improved patientrecovery and earlier discharge.
2.Availability for core IR proceduresincluding emergency embolisationand nephrostomy has been closeto 100%.
3.There has been no change in theCT or MRI reporting delays.
How has good practice beensustained?With good team work, trust supportand enthusiasm.
Lessons learntThe ‘light duties’ model works well,although added to booked leave itmeans that each IR is away from theIR suite for many weeks a year.Afternoon IR clinics, audit andmandatory training can also beperformed during these ‘light’weeks.
Future plansThe fifthIR post has been advertised.The sixth post is well on its way. We will be looking to a group e-jobplan to ensure not only 24/7 cover,but 52 week cover for booked leave.
ContactDr Nigel Hacking, Consultant RadiologistEmail: [email protected]
• Assurances were given that plainfilm reporting, CT and MRI workload should be unaffected.
• Overall worked hours wereplanned to balance out as closelyas possible. An estimate of out ofhours work performed in theevenings, nights and week-endswere balanced by hours availablefor rest at home.
• The on call IR comes in at 5pm.They are then available to performCT guided drains on five days aweek and perform urgent IR onany urgent cases booked duringthe day, such as nephrostomy. Ifthere is no IR activity then the IRuses the period between 5-7pm toreport scans etc.
The on call rota commenced inSeptember 2010. Consultantshortages have limited this cover tofive or occasionally four of the one insix slots provided. Shortfalls weremade up by overtime payments foradditional slots covered until newappointments were made in2011-2012.
What resources/ investmentwere needed?Two new consultant IR posts, alocum consultant initially followed byplanned substantive posts.
ResultsOverall impact Since September 2010 we have hadan almost continuous IR on call rotacovering all on call IR procedures,including abscess drainage, butexcluding e-EVAR/ e-TVAR and TIPS.
‘Light duties’ on call IR rotaUniversity Hospitals Southampton NHS Foundation Trust
C: Staffing and MDT working

39
Improving patient follow-up pathway postendovascular aneurysm repair (EVAR)Central Manchester University Hospitals NHS Foundation Trust
C: Staffing and MDT working
SummaryEVAR patients need regular imagingfollow-up. The radiographers haveestablished and maintained adatabase to ensure that CT scans arecarried out at appropriate intervals.
The vascular lab technicians haveconducted an audit to compareultrasound with CT for follow-up.Ultrasound has been shown to be areliable method following asatisfactory CT scan at one year. Thisreduces radiation and contrastmedium exposure. Theradiographers and vascular lab havedeveloped liaison to ensure thatfollow-up is transferred from CT toUS appropriately. The vascular labtechnicians have redeployed staff toaccommodate the new workload.
Context and background The majority of aortic aneurysms arenow treated by EVAR rather thanopen surgery. At this centre 102EVAR were performed in 2009compared with 23 in 2004. Eachpatient requires CT surveillance scansat one month, six months, 12months and annually thereafter tomonitor aneurysm sac size andcheck for the presence of endoleaksas per Society of Vascular Surgeonsguidelines. In 2007 it becameapparent that patients were beinglost to follow up and therefore theinterventional radiographersdeveloped a robust system to ensurethat patients were invited for theirsurveillance scans in a timelymanner. A database is maintainedcontaining the records of all EVARpatients and the dates of theirsurveillance scans.
In recent years, many centres haveadopted US rather than CT forfollow-up. If it is reliable, it saves onexposure to radiation and contrastmedia. The switch from CT to USfollow-up has implications forworkload in the vascular lab.
How was the change made? EVAR databaseInitially patients who had undergoneEVAR after 2004 were identified,recorded on the database and thosewho had been lost to follow up wereinvited for a CT surveillance scan.All patients subsequentlyundergoing EVAR were placed onthe database and referred for a CTscan one month post-op. Thedatabase allowed the radiographerto record CT scan attendance datesand identify when further referralsneeded to be requested. All referralsto CT were made by theradiographer using the clinical workstation (CWS). This extended rolewas agreed by the consultantvascular radiologists and the CTsuperintendent.
US auditCT and US appointments werecoordinated in order to carry out aprospective audit of the reliability ofUS to detect significant findings suchas endoleak. This was coordinatedby the radiographers. The CT and USwere reported independently of eachother and reports were compared.
Transfer to US follow-upA business case was prepared by theVascular Lab and presented tomanagement. Liaison wasestablished between the vascularradiographers and the vascular lab totransfer follow-up from CT to USafter a satisfactory one year scan.
What resources/ investmentwere needed?Allocated time was given to theradiographer to keep the databaseup to date. Vascular lab technicianswere redeployed by rationalisation ofother commitments. The vascular labservice will ultimately provide 500scans annually. This equates to a 0.5WTE technician.
ResultsOverall impact All patients who have undergoneEVAR are invited for their necessarysurveillance scans on schedule. Thisensures that any endoleaks aredetected and treated if required. Thetransfer to US will result in a saferimaging modality for patients and areduction in the burden on theoverstretched CT service by up to500 cases per year.
How was the change measured? All surveillance scans requested andperformed are recorded on thedatabase allowing for audit.
A study to determine the sensitivityand specificity of colour duplexultrasonography (CDU) compared toCT in this centre was undertakenusing patients enrolled on oursurveillance plan. This found 81%accuracy in detecting endoleaks. Ofthe remaining 19%, 8% were un-diagnostic due to patient bodyhabitus.

40
How has good practice beensustained?All radiographers take theresponsibility of adding the cases theyare involved with to the database andrequesting the first follow up scan atthe appropriate time.
Initially one member of theinterventional team was involved inmaintaining the database andreferring patients for scans, nowthere are two radiographers toensure efficient practice.
Maintaining the liaison betweenvascular lab and vascularradiographers. We were awarded‘highly commended’ in theinnovation and efficiency section ofthe Trust ‘We are proud of youawards’ this year.
Lessons learntLiaison between disciplines wascrucial to success.
Future plansTo continue to attempt to secure theresources for vascular lab to allowthe continuing increase in workload.
To maintain close liaison betweenthe vascular lab and the vascularradiographers to ensure patientsreceive timely and appropriate followup.
To continue to identify suitable casesto transfer to ultrasound at the 12month scan.
To ensure that follow up ismaintained once the patient movesto vascular lab. It is harder for theradiographers to track patients asthe IT system is different.
Audit to ensure vascular labaccuracy.
ContactDr. Nick Chalmers, Consultant RadiologistEmail:[email protected]

41
EVAR database with scoring system which helpssimplify the decision making process for selectionand prioritising of patientsThe Leeds Teaching Hospitals NHS Trust
C: Staffing and MDT working
SummaryThis database is designed to aid thetracking of elective patients withabdominal and thoracic aortic- andiliac- aneurysms through their workup for EVAR and subsequent post-procedural surveillance.
Additionally, the database allows theprospective collection of data onaneurysm morphology, deviceperformance and unit mortality,morbidity and the requirement forsecondary intervention which willallow subsequent audit of practiceand devices performance.
Context and background The framework for improving theresults of elective AAA repair; TheVascular Society (2011) suggestedthe following: • all patients should undergo
standard preoperative assessmentand risk scoring, including cardiac,respiratory, renal, diabeticassessment, assessment ofperipheral vascular disease andanatomical AAA assessment withCT angiography to determine theirsuitability for EVAR (1);
• each hospital should have definedpathways for the correction ofsignificant medical risks(cardiology/renal/respiratory)before intervention;
• all patients should be seen in pre-assessment by an anaesthetistwith experience in elective vascularanaesthesia. At this stage,medication should be reviewedand optimised for the intervention(2); and
• all elective procedures should bereviewed preoperatively in an MDTthat includes surgeon(s) andradiologist(s) as a minimum.
Ideally, a vascular anaesthetistshould also be involved to considerfitness issues that may affectwhether open repair or EVAR isoffered. Facility to offer bothprocedures should be availableeither in house, or by referralthrough an agreed pathway.
Figure 1: The ideal AAA patientpathway - adapted from the AAA QIP (quality improvementprogramme) website.
The Leeds EVAR database consists ofa single ‘flat’ table ‘main table’ withother linked tables for drop-downmenu options. The database is aconvenient method for surgeons andradiologists to track elective EVARpatients’ progress from initialconsultation to MDT, procedure,imaging and 30 day, one year andfive year follow up.
The database is made up of variousforms which interact as informationis entered establishing acomprehensive and easy to usedataset and scoring system. It isaccessed via any trust PC runningMicrosoft Access via a trust widedrive. Security is provided by thetrust PC and network accesssoftware (Novell). The database isonly made available to those peoplewith good reason to access it.
Figure 2: Home form
This form has 12 buttons, eachcorresponding to a different task,and arranged in vertical columns bythe general task area, work up,procedure, sizing etc. In general,buttons lower down the pagecorrespond to steps later in thepatient pathway.
A button is chosen corresponding tothe task to be performed. Eachbutton opens a new form wheredata entry is facilitated.
The exit button closes the databaseand quits Microsoft Access
Figure 3: New Patient Data page
Patient data and clinical work-upneeded is entered by the surgeonusually in clinic. There is also a linkbutton to enter AAA QIP clinicaldata (figure 4). From this the AAAQIP clinical traffic-light code isautomatically generated.

42
Figure 4: AAA QIP clinicalinformation.
This is a series of questions mirroringthose from the AAA QIP programmedesigned to easily identify, fromeasily accessible clinical data, a crudeestimate of fitness for AAA repair,and assigning a traffic-light code(red, amber or green) according tothis fitness. The traffic light code isautomatically generated from thequestion answers.
Figure 5: Physiological data
All patients listed to undergo EVARfor AAA should undergo cardio-pulmonary exercise (CPX) testing.The CPX test results and otherphysiological and biochemical datacan be entered on this page. There isa box for free text entry about thepatient’s physiological fitness and asubjective score can be entered bythe anaesthetist, which categorisesthe patient into low, medium or highrisk for EVAR (and also assigned atraffic light colour). This score is notpart of AAA QIP recommendations.
Figure 7: Sizing form
Once a decision to perform EVAR ismade, sizing information can beentered. Any pre-EVAR proceduresrequired can be entered here, andthese cross-reference to the bookingform. The database also keeps alldevice details in one place so theyare easy to cross reference and trackwhen they arrive.
A procedural details form allowsentry of how the EVAR was done,how long it took, who was involvedand what the blood loss was. Thisdata can be ported across to apredictive model of EVAR outcome(Australasian College of Surgeonspredictive database of EVARoutcome). Procedural time andestimated blood loss are datarequired for the BSIR RETA andRETTaD registries, as well as theNVD.
30 day, one year and five yearoutcomes and secondaryintervention is also tracked using afilter on patients who haveundergone EVAR. This allows liveinterrogation (for example, we knowthat in Leeds, the 30 day mortalityfor new patient elective EVAR for2011 was zero percent)
The anatomy of the aneurysm is alsograded 1-5 based on its anatomicalsuitability for EVAR - this is derivedfrom the AAA QIP recommendedanatomy scoring scale.• Grade 1 - simple procedure, no
adverse features, anticipatedprocedure time less than twohours,
• Grade 3 - several adverse featuresrequiring adjunctive interventionor surgery, anticipated proceduretime >2 hours, or fenestrated case
• Grade 5 - anatomically unsuitablefor EVAR.
Figure 6: MDT print outs afterpatient’s data has been entered.
All this information is summarised ona print out which lists all patientscurrently being worked up orawaiting EVAR. The list is ordered byweeks from referral. The list isdiscussed patient by patient at aweekly MDT to ensure no-one is lostin the system. Some patients mayrequire little discussion and some areextensively discussed and a decisionto proceed or not is made. Patientsautomatically drop off the list if anactive decision is made not to treat.This is recorded elsewhere in thedatabase. The three sets of trafficlight codes are easily visible for eachpatient in boxes in the centre of theprintout.

43
What resources/ investmentwere needed?• Database design took many hours
work, and has evolved slowly froma simple register to the morecomplex design currentlyimplemented. This was done by asingle clinician in our unit
• IT input was needed to allowdeployment on a specific drive onthe hospital intranet, and to limitaccess.
ResultsOverall impact • Significantly reduced peaks and
troughs in EVAR servicethroughput. We now have asteady ‘drip’ of cases rather thannone and then several all at once.
• Much more nuanced discussion inMDT as all have anatomical andphysiological data immediately tohand to assess suitability, and ifsuitable how, where and when theprocedure will be undertaken.
• Subjective impression of overallreduction in work up time forEVAR patients (not formallyaudited as yet).
• Better communication withindepartment as to how manyEVARs there are to do and whowill be doing them.
• Instant access to data on EVARpatients, e.g. 30 day mortality, oneyear mortality, average necklength, average number of piecesinserted, requirement forsecondary interventions, etc. Someof this data is mirrored in the NVDbut we now have ownership ofour own.
How has good practice beensustained?• Constant encouragement of
clinicians and other team membersto use the database. Elective AAApatients are not discussed in theMDT unless they have beenentered onto the database.
• Issues with lack of access to PCshave been resolved withtemporary use of paper versions ofsizing and EVAR procedure forms,which are then transferred to thedatabase by hand.
Lessons learnt• Achieving engagement by all
disciplines required somepersistence with adoption of a“zero-tolerance” policy (i.e.patients would only be discussedat the MDT if the relevant datawere on the database [includingpatient demographics, imagingreports and physiologicalassessments].
• The database only tracks AAAsassessed for treatment/treatedwith EVAR. Open AAA repair is notincluded.
• Transposing the database to aweb-based system would allow itto run on any PC, even those notrunning MS Access. IT skills forthis are development are notcurrently available ‘in-house’.Whilst the database continues toevolve the flexibility to quicklymodify the database is useful; thiswould be lost with a web-basedsystem. Where trusts provide AAAservices in a hub and spoke orother networked system aweb-based system, with relevantpatient confidentiality safe-guards,may be the most pragmaticapproach in the future.
Future plans• Include some models of predicted
mortality with and without EVARbased on physiological dataentered. This may improvedecision making in the MDT.
• Allow date stamping of criticalsteps to allow delays in the workup of patients to be identified andresources allocated to improvethese.
• Possibly link to NVD so that datadoes not have to be entered twice– a big project, for relatively littlegain.
• Offer to other trusts. This hasalready happened to an extent viaAAA QIP programme, distributedunder the GNU public licence.
• Consider PPM/RIS integration.
ContactDr Simon McPherson, Consultant Radiologist and Clinical LeadEmail:[email protected]

44
SummaryAngiography, angioplasty andstenting being undertaken by aradiographer. Leading to further roleextension into venography,fistulography, venoplasty,fistuloplasty and vascular accessprocedures (line insertions).
Context and background A vacancy for consultantinterventional radiologist led to anincreasing workload for theremaining consultant and anincreasing waiting list.
How was the change made? Approval to implement the changewas given by the lead radiologistand imaging services manager. Wedrew up extended role protocolswhich were submitted andsubsequently approved by the TrustProtocols Group. Training wasdelivered in house until adequatecompetency was achieved.
What resources/ investmentwere needed?• Back fill for radiographer.• Funding for radiographer re-band
Overall impact • Reduced workload for radiologist.• Reduced waiting times.• Greater job satisfaction for the
post holder.
How was the change measured? By monitoring the reduction inwaiting times.
Future plansTraining of other radiographers.Role extension for otherinterventional procedures e.g. IVC filters.
ContactDavid BarkerInterventional RadiographerEmail: [email protected]
Radiographer extended role in the InterventionalRadiology DepartmentUniversity Hospitals Birmingham NHS Foundation Trust
C: Staffing and MDT working

45
SummaryRegular new and follow up patientclinics have been set up for fibroidembolisation patients in a dedicatedOP room. Formal thermal ablation,hepatobiliary and urology clinics areplanned for 2012.
A room has now opened with theradiology department for IRs to see,counsel and consent new patients inadvance and to see follow uppatients on a routine basis.
Nurse pre assessment is also possiblein this room.
Context and background Outpatient activity for planned IRprocedures is increasing. Fibroid andthermal ablation clinics have runinformally in consultants offices forthe last few years and have beencoded on the RIS (RadiologyInformation System) since 2010.
How was the change made? • A dedicated RIS code has been
applied to OP activity since 2010.• From 2011 a formal ‘Fibroid Clinic’
is booked through the hospitalcomputer management system(e-CAMIS).
• This formalised booking and datarecording allows IR OP activity tobe recorded for the first time forradiology.
• This formal OP activity attractsappropriate OP funding.
This activity could not be recorded inradiology before appropriate codeswere available and will still not beseen within the trust until formalapproval from the OP managerialteam is gained.
Joint clinics (e.g. with vascular orgynae surgeons) have a role, but thisusually generates activity for theother clinical specialty and notradiology and so must not be reliedupon to raise IRs profile within theorganisation.
Future plansWe will be opening formal HPB andthermal ablation clinics in 2012 withmore to follow.
Electronic and paper letters will besent out to referring clinicians andtheir GPs to raise the profile of IR asan independent clinical specialty.
ContactDr Nigel Hacking, Consultant RadiologistEmail: [email protected]
What resources/ investmentwere needed?Cooperation between radiology anddivisional managers as well as OPmanagers.
Freeing up IR time on tight job planshas only been possible withradiology/divisional support andincreasing IR numbers to ensure fullIR room utilisation.
ResultsOverall impact Patient satisfaction is improving andpatient information sheets andconsent in advance is becoming thenorm.
How was the change measured? Repeat consent audits are plannedfor 2012.
Annual figures for IR activity havebeen recorded on RIS for 2010-2011and e-CAMIS figures will be availablefor 2011-2012.
How has good practice beensustained?Our insistence that OP clinics are notan option. We must embrace andexpand these and allow changes inour working lives and job plans toreflect these changes.
Lessons learntInitial informal clinics held incramped consultant offices withmultiple interruptions lead to patientcomplaints.
Starting an interventional radiology clinic University Hospitals Southampton NHS Foundation Trust
D: Patient engagement and experience

46
SummaryA patient satisfaction survey wascompleted within interventionalradiology (IR) to gain feedback frompatients on the quality of the serviceprovided by the IR team in the Hulland East Yorkshire Hospitals NHSTrust. The aim of the survey was todetermine the patient experienceand highlight any potential areas forimprovement. We envisage thesurvey will ultimately provide anongoing audit of services to ensurecontinuous improvement of thepatient care experience.
• 82% of the patients surveyedfound the staff extremely friendlyand helpful giving an ‘excellent’scoring.
• 84% decided that the privacy anddignity they received was‘excellent’ and 14% felt it was‘very good.’
• 69% found the cleanliness to be‘excellent’ whilst 29% found it‘good.’
• 99% of patients said theinformation they receivedregarding their procedure waspositive.
Context and background Within interventional radiology arecent detailed patient satisfactionsurvey had not been completed. Asa unit we were continuously tryingto improve and felt this was an idealopportunity to find out andincorporate patient views andpreferences. The department hasjust opened a Radiology Day Unitand the survey preceded thisdevelopment. It is our intention torun the survey again to demonstrateif the unit has improved the patientcare experience.
• Regarding privacy and dignity -98% felt that they did haveenough privacy when discussingtheir treatment and 100% feltthey had enough privacy whilstbeing treated. 12% unfortunatelydid have to share a recovery areawith a member of the opposite sexand 17% felt the toilet facilitieswere at an inadequate distancefrom the recovery area.
• Regarding cleanliness - 58-60%felt the recovery area andprocedure room where clean and38-40% respectively felt they weresatisfactory. Most patients (95%)did notice the posters asking staffto wash their hands and themajority (98%) did see that handgel was available.
• The nursing staff had an excellentresult (100%) regardingconfidence from the patientshowever 10% did say the staffdiscussed other issues in theirpresence.
• Although 85% did receive a letterthat fully explained the procedureprior to admission the informationthey were given in the IRdepartment varied with theinformation they received prior totheir arrival, possibly from clinicetc.
How was the change measured? With the opening of the RadiologyDay Unit certain aspects from thesurvey have been addressed. Thereare two separate four bedded areaswhich allow for single sex postprocedure recovery. A patient is notseen in a theatre gown in any of therecovery areas and in addition thetoilets are now in very closeproximity to the recovery areas.The staff have been praised for their
How was the change made? A survey was developed with thehelp of the whole team. Onehundred surveys were handed topatients post intervention and askedif they would either leave it on theward before discharge or return it inthe post.
Sixty four completed surveys werereturned and the results analysed.
What resources/ investmentwere needed?The main resource needed was timeand a nurse coordinated the surveyin terms of delivery, return andanalysis. We were assisted by amember of the clinical audit team toprepare and approve the survey.
ResultsOverall impact The survey was an invaluable tool todemonstrate patients’ views on theircare. It brought to our attentionboth positives and negatives and hasallowed us to act on both.
• We found that the communicationfrom the staff in the departmentat all levels was excellent fromexplaining the risks, benefits,complications and what wouldhappen to the patient all comingout at 97% or higher and 96.5%said that if they asked an IR nursean important question they got ananswer that they couldunderstand.
• 100% of patients said there wasalways a member of staff availableto talk to about their worries orfears.
• 98.5% of the patients felt thatthey were involved in the decisionmaking about their treatment andpost procedure care was explainedto them.
Interventional Radiology Patient Satisfaction SurveyHull and East Yorkshire Hospitals NHS Trust
D: Patient engagement and experience

47
communication with the patients butit has also heightened awareness ofthe fact that patients feel they arespoken over in their presence whichis unprofessional.
Hand washing posters, and screensavers are still on display around thedepartment in addition to hand gels.There is now more space and staff torecover patients within the new dayunit and this has had a positiveeffect on cleanliness which will bemonitored over a period of time.
How has good practice beensustained?The issues raised from the surveyhave been taken on board duringplanning of care delivery in the newRadiology Day Unit.
Lessons learnt• We learnt that patient information
leaflets alone do not seem to givea complete picture of theprocedures that the patientundergoes.
• A pre assessment clinic for the dayunit has been started which wouldhelp in this regard.
• Issues related to privacy anddignity, location of patient toiletshave been solved by theintroduction of the Radiology DayUnit.
Future plansA similar audit will be conductedlater in 2012 to measure outcomesof the day unit on patient caredelivery / experience.
ContactAnita Echlin, Superintendent RadiographerEmail: [email protected]

48
SummaryIn some areas, inpatient procedureswere being cancelled at short noticeby patients who changed their mindsabout proceeding with treatments.This was usually because of poorunderstanding of what theintervention involved, creating naturalanxiety. However this led to poor useof an expensive interventional suite,wasted appointments and beds. Aradiology clinic was instituted toensure these women received theappropriate information beforeaccepting the procedure and formed arelationship with the IR who would beresponsible for their treatment.
Context and background Patients being referred for uterineembolisation for symptomatic fibroidsoften had unrealistic expectations.They also clearly expected to see thedoctor who would be performing theirtreatment before the day of thetreatment and to be followed up bythat doctor. With increasing numbersof referrals it was clear that a regularclinic was required to see new patientsand follow-up those who hadundergone treatment. This clinicwould also be suitable to discusspatients referred for other complexinterventions to ensure they weresuitable and understood the pros andcons of any proposed interventionbefore proceeding. Patients withvascular malformations are regularlyseen in this clinic, having been referredby either plastic or vascular surgery.
How was the change made? 1. Approaches were made to the
outpatients department but therewas either no space or desire toaccommodate a new clinic. Therewas also a lack of understandingwhy radiology required a clinicdespite repeated explanations.
How was the change measured? 1.The number of patients who do not
arrive for their appointment.2. The numbers of inpatient
procedures cancelled on the day.
How has good practice beensustained?At the moment I am the only IRconsultant who sees patients in a clinicand have successfully incorporated thisinto my job plan as an episode ofdirect clinical care, initially replacing anepisode of supporting clinical care.
Lessons learntIf the normal channels fail, look forunconventional alternatives. I spent alot of unproductive time trying to seemy patients within a vascular surgicalclinic where the staff had no time orunderstanding of the needs ofradiology. There is no reason why theclinic has to be run in a busyoutpatients department and thiswould have been set up much earlierif I had appreciated that fact. Very fewresources are required. The support ofradiology colleagues and an officespace followed by setting the clinic upon the hospital appointments systemand training of the secretarial staff inthe use of this system is all that wasneeded.
Future plansThis will be rolled out to my other IRcolleagues who see patients forintervention.
To incorporate such a clinic in the jobplans of new IR consultants.
ContactProfessor A-M Belli, Consultant RadiologistEmail: [email protected]
2. A small, suitable US room in themain radiology department wasidentified as being free at a timewhen I would be able to run a clinic.
3. The clinic was set up on the hospitalappointment system underDiagnostics (Prof Belli Clinic). Thissystem had a category for“diagnostics” already installed.
4. A clinic was established and mysecretary trained to run the clinicand enter patients. No nursingassistance is required. Patients aredirected to the waiting room by thestaff at the front desk of theradiology department.
What resources/ investment wereneeded?The room was available.My secretary trained. I incorporated the clinic into my jobplan.
ResultsOverall impact Whereas <50% of my patientsattended for follow-up before theclinic, now 99% attend as theyidentify me as their treating doctor.I receive direct referrals from GPs forpatients who wish to explore thepossibility of fibroid embolisation.I see patients with vascularmalformations and arrange theirtreatments.
I receive referrals from many cliniciansboth inside and outside my hospitalwho are unsure if an intervention isrequired and so send patients for myopinion.
Once patients decide to proceed withtreatment, it is very rare for them tocancel, usually only if there areextenuating circumstances, ratherthan a ‘change of mind’.
Introduction of radiology clinicSt George’s Healthcare NHS Trust
D: Patient engagement and experience

49
SummaryIntroduction of an opiate analgesiato relieve pain effectively duringfistuloplasty.
The nursing sister and charge nurseliaised with the vascular radiologistsand the renal specialists whoidentified Fentanyl as a safe andsuitable analgesia to trial.
The existing radiology nursing teamwere all trained and competent inthe administration and monitoring ofFentanyl. Nurses have begun to playa primary role in assessing pain,titrating analgesia under thedirection of a radiologist andmonitoring the cardiovascular statusof the patient.
Following the commencement ofFentanyl a further pain audit tool ledby the nursing team was utilised togain a representative sample.
Context and background The radiology department atManchester Royal Infirmary deliversa fistuloplasty service to regainpatency for clotted and stenosedfistulas. The department worksclosely with its own internal renalservices but also take referrals fromother Manchester NHS Hospitals.The department undertakesapproximately 250 fistuloplastyprocedures per annum.
Patient feedback revealed thatpatients found the procedureextremely painful and traumatic.Anecdotal information alsosuggested that some patients mayrefuse further interventions and optfor central lines for renal dialysisinstead. This is not the best optionfor long-term management. There isevidence that a fistula is thepreferred method and should bepreserved if at all possible14. Thispoor quality experience needed tobe addressed and a change proposalwas put into place.
How was the change made? A date for the commencement ofFentanyl as the analgesic of choice infistuloplasty patients was agreed at aradiology vascular meeting andcascaded down to staff. Doses of50mcg of Fentanyl should beincremented throughout theprocedure either via an IV cannulafor nurse administration for clottedfistula’s or via an access sheath bythe radiologists for stenosed fistulas.The pain assessment audit tool wasdevised to gain numerical painscoring post Fentanyl administration.The desired outcome was tomaintain a pain score of less thanfive throughout the procedure. All ofthe nursing staff were motivated toimplement the change. Otherstakeholders within the team weresupportive of the change
What resources/ investmentwere needed?Nursing staff with the required skillswere readily available and thenecessary equipment and fundingwas also in place.
However the availability of twonurses for fistuloplasty procedureshas been an issue with one for theexisting ‘scrub assistant role’ andone to be the ‘pain nurse.’ Theradiographers have shown a highlevel of flexibility in cross-coveringroles to ensure that a nurse isavailable to administer Fentanyl andmonitor the patient accordingly.
ResultsOverall impact The use of Fentanyl appears to havehad a major impact on effectivelymanaging pain. The patients aremore positive and happier to returnfor further procedures. Frequentattenders express much moresatisfaction with the level of painexperienced.
The results from data collection fromthe pain audit tool showed that alarge percentage of patients had apain score of less than five.
Nurse led effective pain management in fistuloplastyCentral Manchester University NHS Foundation Trust
D: Patient engagement and experience
14 The National Kidney Foundation Disease Outcomes Quality Initiativehttp://www.kidney.org/professionals/kdoqi/

50
How was the change measured? Via an audit tool incorporating anumerical pain assessment tool. Thechange was measured by collatingthe numerical pain scores perpatients. Pain was measured in 40patients at different stages of theprocedure The data was audited andanalysed by the lead nurse andnursing sister. During this time noadverse effects were experienced.An improvement in the managementof pain was clearly identifiable andreinforced the need to continue withthe implementation.
How has good practice beensustained?The positive audit findings havebeen presented to both the IR teamand radiology. This has reinforcedthe need for its continued practice.
The lead nurse has encouraged andpromoted the provision of nursingstaff for this role using the ongoingflexibility of other members of theteam.
Lessons learnt• The collaboration between the
teams has been extremelysuccessful in this instance and hasempowered individuals to identifymore potential improvements.
• The results show that the proposalwas successful and ongoingreviews should take place.
• The utilisation of a retrospectivepatient experience questionnairemay have been beneficial. Thiscould have identified furtherpatient perspective ideas forimprovements to the quality of thepatients pain experience.
Future plans• A business case for more nursing
support as the ad hoc system ofrelying on a radiographer to beavailable is not sustainable in thelong term – especially if this isrolled out to other procedures.
• Improvements to the painexperience for TIPPS procedures.Fentanyl is currently given in dosesfor this procedure however itseffectiveness is questionable andthe desired effect does notcurrently appear to be routinelyachieved.
ContactDr Nicholas Chalmers, Consultant RadiologistEmail: [email protected]

51
Monthly diary management meeting and cross cover provisionSt George’s Healthcare NHS Trust
E: Leadership
SummaryAs a Major Trauma Centre, it isessential that an IR consultant isavailable at all times in the hospitalduring normal working hours to dealwith emergencies and that if aconsultant is away for their list, theteam should know who to approachto discuss or perform emergencyinterventions. A weekly diary is setup and discussed months inadvance, to ensure all absences arecovered and ensuring that it is clearwhich consultant should beapproached.
Context and background IR Staff rarely but occasionallyplanned to be away at the same timeas there was no forum to discusswho should attend key meetings. Onbecoming a Major Trauma Centre, itwas clear that a formal arrangementwas required to ensure that at leastone IR consultant would be availablein the hospital at all times duringnormal working hours and to ensurethat there was a fair system in placeto help people attend a variety ofmeetings. In addition, radiographicand junior staff would not necessarilyknow who was available if thoseconsultants were doing diagnosticlists elsewhere in the hospital,leading to confusion and timewasting. Also, patients would bebooked for interventional procedureseven when the consultant covering alist had to cover two rooms or a listin another part of the hospital,leading to stress.
How was the change made? 1. Instituted a monthly diary meeting
on the first Tuesday of each monthattended by all IR consultants. Thebookings diary for eachinterventional room and theconsultants’ leave diary were alsobrought to this meeting. A weeklytemplate to reflect consultants’absences was created and a systemof named consultants providingeither full cover (in which caseelective procedures can be booked)or cross cover (when electiveprocedures are cancelled but thenamed consultant can becontacted for emergencies thatmay arise) was created. At the timeof diary setting, the lists arecancelled if appropriate. This isdone up to three months inadvance but refreshed each month.
2. This timetable is available in the IRsuite so that all staff know whoshould be contacted in case ofemergency.
3. All IR consultants have thesetimetable sent to themelectronically for checking andknow that they are individuallyresponsible for ensuring their list iscovered if they are away.
What resources/ investmentwere needed?None other than consultants time for30-40 minutes once a month.
ResultsOverall impact There is always a named IRconsultant attached to each IRsession in normal working hours so itis clear who needs to be contactedfor emergencies and urgent cases.
Lists are cancelled if nobody is ableto offer full cover for a room, so thattrainees are not left unsupervisedand patients’ treatments are notpostponed or cancelledunnecessarily.
How was the change measured? Review of weekly timetables sincethis was started shows ALL sessionscovered by a named consultant.
How has good practice beensustained?All IR consultants participate in theprocess and are supportive andattend the monthly meetings. Theyaccept responsibility for ensuringtheir list is covered if they are awayand in the rare situation of nobodybeing available, that they cannottake leave.
Lessons learntRegular monthly meetings at thesame time of the month, means thateveryone knows when the diarymeetings are held.
Shared responsibility for ensuringcover is arranged for all sessions butindividual responsibility for ensuringown list covered or leave cancelled. All timetables distributed to all IRconsultants each month.
Future plansTo continue to ensure IR coveralways available. This system hasbeen rolled out to other specialistareas of radiology e.g. paediatricradiology.
ContactProfessor A-M Belli, Consultant RadiologistEmail: [email protected]

Bibliography and suggested further reading52
Our thanks go to all the pilot sitesthat have tested andimplemented changes andproduced the case studies forothers to benefit from.
British Society of Interventional Radiologyhttp://www.bsir-qi.com/commissioners/bsir-rag-status-map/
Department of Health. Interventional Radiography: Guidance for Service Delivery (2010) London.http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_121904
Department of Health. Interventional radiology: improving quality and outcomes for patients. A report fromthe National Imaging Board. (2009) London.http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_109130
General Medical Council. Good Medical Practice (2006, updated 2009) London.http://www.gmc-uk.org/static/documents/content/GMP_0910.pdf
NHS Clinical Advisory Group. Regional Networks for Major Trauma Report (2010)http://www.excellence.eastmidlands.nhs.uk/welcome/improving-care/emergencyurgent-care/major-trauma/
The Royal College of Radiologists. Standards in Vascular Radiology (2011) London.http://rcr.ac.uk/docs/radiology/pdf/BFCR(11)6_vascular.pdf
The Royal College of Radiologists. Good practice guide for clinical radiologists, Second edition (2012) London http://www.rcr.ac.uk/docs/radiology/pdf/BFCR(12)1_Good%20Practice.pdf
NHS Improvementhttp://www.improvement.nhs.uk/diagnostics/InterventionalRadiology.aspx
The Vascular Society of Great Britain and Irelandhttp://www.vascularsociety.org.uk/
University of Birmingham A guide to capturing and using patient, public and service user feedback effectively(2009) NHS West Midlandshttps://www.gpc.eoe.nhs.uk/downloadFile.php?doc_url...gJdF_nhs/1314361922_gJdF_nhs_west_midlands.pdf
Bibliography and suggested further reading

53Contacts
Mrs Lesley Wright - Director, Diagnostics, NHS Improvement Email: [email protected]
Ms Carole Smee – National Improvement Lead, NHS ImprovementEmail: [email protected]
Mrs Victoria Brown – National Improvement Lead, NHS ImprovementEmail: [email protected]
Mr Ian Snelling – Senior Analyst, NHS Improvement Email: [email protected]
Mrs Glynis Wivell - National Associate, NHS Improvement Email: [email protected]
Dr Richard Seymour - National Clinical Lead, NHS Improvement Email: [email protected]
Dr Andy Beale – National Clinical Lead, NHS Improvement Email: [email protected]
Dr Graham Hoadley - National Clinical Advisor, NHS ImprovementEmail: [email protected]
Dr Tony Nicholson – Consultant RadiologistEmail: [email protected]
Dr Ian Robertson – Consultant Radiologist & President of British Society of Interventional Radiology Email: [email protected]
Contacts

Acknowledgements54
We would like to thank all those who gave freely of their time and energy to inform this report, most particularly the IR teams at all of the sites visited.
Aintree University Hospitals NHS Foundation Trust
Barts Health NHS Trust (Barts and The London Hospital)
Brighton and Sussex University Hospitals NHS Trust
Cambridge University Hospitals NHS Foundation Trust (Addenbrookes Hospital)
Central Manchester University Hospitals NHS Foundation Trust
Hull and East Yorkshire Hospitals NHS Trust (Hull Royal Infirmary)
Imperial College Healthcare NHS Trust
King’s College Hospital NHS Foundation Trust
Lancashire Teaching Hospitals NHS Foundation Trust
Leeds Teaching Hospital NHS Trust
Newcastle upon Tyne Hospitals NHS Foundation Trust
North Bristol NHS Trust (Southmead Hospital)
Nottingham University Hospitals NHS Trust
Oxford Radcliffe Hospitals NHS Trust
Plymouth Hospitals NHS Trust (Derriford)
Salford Royal NHS Foundation Trust
Sheffield Teaching Hospitals NHS Foundation Trust
South Tees Hospitals NHS Trust (Middlesbrough Hospital)
St George’s Healthcare NHS Trust
University Hospitals Birmingham NHS Foundation Trust (Queen Elizabeth Hospital)
University Hospital of North Staffordshire NHS Trust
University Hospital of South Manchester NHS Foundation Trust (Wythenshawe Hospital)
University Hospital Southampton NHS Foundation Trust
University Hospitals of Coventry and Warwickshire NHS Trust
Acknowledgements


HEART
LUNG
CANCER
DIAGNOSTICS
STROKE
NHSNHS Improvement
©N
HS
Impr
ovem
ent
2012
|A
ll Ri
ghts
Res
erve
d Pu
blic
atio
n Re
f: N
HSI
MP/
diag
nost
ics0
02 -
Jun
e 20
12
NHS ImprovementNHS Improvement’s strength and expertise lies in practical service improvement. It has over adecade of experience in clinical patient pathway redesign in cancer, diagnostics, heart, lungand stroke and demonstrates some of the most leading edge improvement work in Englandwhich supports improved patient experience and outcomes.
Working closely with the Department of Health, trusts, clinical networks, other health sector
partners, professional bodies and charities, over the past year it has tested, implemented,
sustained and spread quantifiable improvements with over 250 sites across the country as
well as providing an improvement tool to over 2,000 GP practices.
NHS Improvement
3rd Floor | St John’s House | East Street | Leicester | LE1 6NB
Telephone: 0116 222 5184 | Fax: 0116 222 5101
www.improvement.nhs.uk
Delivering tomorrow’simprovement agenda for the NHS