Interproximal integrity of posterior partial-coverage ceramic
12
Restorative Dentistty Interproximal integrity of posterior partial-coverage ceramic restorations: Sequence of delivery and finishing William H, Liebenberg, BSc, BDS (Rand)* The coriservative, nonretentive cavity design of partial-coverage ceramic restorations provides a number of distinct advantages over traditional cast-metal options. However, unigue challenges are associated with precise delivery of the restoration and tbe cleanup of excess luting resin. Restorative success and long- term gingivai bealth are dependent on interproximal integrity at the restoration-tooth interface. This artide examines tbe variabies tbat affect tbis integrity and introduces a number of innovative techniques that assure meticulous delivery of posterior partial-coverage ceramic restorations. (Quintessence Int 1999-30- 807-818] Key words: adhesive technique, ceramic restoration, finishing, nonretentive cavity preparation, partiai- couerage restoration G old is an ideal restorative option for the moderate to extensive posterior lesion. It continues to be used with prudent operative diligence and success, Nevetiheless, the principles of retentive geometry and preventive coverage often result in the excessive sacri- fice of healthy tissue. Adhesive restorative dentistry offers noteworthy clinical potential for posterior appli- cations utilizing direct, semidirect, and indirect tech- niques with a wide array of materials. Single-appointment direct restorative options for the posterior dentition are ideally restricted to small to medium intracoronal lesions. Large multisurface defects in the posterior dentition are best restored with indirect, lahoratory-fabricated restorations when patients present with esthetic stipulations.' The physi- cal and mechanical properties of dental ceramic mate- rials, such as modulus of elasticity, hardness, and coef- ficient of thermal expansion, are closer to the properties of tooth enamel than are those of resin ma- terials.-'^ This fact, combined with the esthetic realism of ceramics,^"^ makes ceramic the material of choice when a tooth-colored restorative option is needed for conservative restoration of large, posterior, multisur- face defects in patients with esthetic needs,'"" •Private Practice, Nodh Vancouver, British Coiumbia, Canada Reprint requests: Dr William H. Liebenberg, Suite 201, 2609 Weslview Drive, North Vancouver, British Columbia, V7N 4M2 Canada. E-maii: ™iiebenb@direct,ca Presented at the Pacifio Dental Conference, Vanoouver, British Coiumbia, Canada, March 12-14, 1998. Esthetics is but one aspect of the restorative out- come. The objective of any restorative procedure in- cludes the establishment of a good long-term progno- sis for both the tooth and the restoration,'^ and the tooth takes precedence. The indirect adhesive prepa- ration is more conservative and is often chosen regardless of esthetic considerations. Adhesive, metal- free restorative options often result in less destruction of healthy tissue than the alternative partial gold restoration, are adhesive-reinforcing, and are less inva- sive of surrounding soft tissues,'^ All adhesive options arc technique sensitive, partic- ularly viith regard to the proximal portion of posterior teeth, where restricted access limits procedural dili- gence. This article discusses the delivery of partial- coverage ceramic restorations and the subsequent cleanup of excess luting resin and introduces innova- tive solutions to the procedural challenges. A CHANGE IN PREPARATION DESIGN Traditional cast-gold preparation design reflects the geometric necessity of adequate resistance, retentive features, and a tenuous cement bond. Because of con- cerns about occlusal forces and fracture resistance, the "safe" option of complete coverage is often selected. The ability to bond tooth-colored restorative mate- rials to tooth enamel reduces the need for extensive tooth preparation such as is necessary for complete coverage. Simonsen,''' in an editorial, questioned the profession's proclivity for complete coverage and labeled it a disservice in those cases when the same 807
Transcript of Interproximal integrity of posterior partial-coverage ceramic

Restorative Dentistty
Interproximal integrity of posteriorpartial-coverage ceramic restorations:Sequence of delivery and finishingWilliam H, Liebenberg, BSc, BDS (Rand)*
The coriservative, nonretentive cavity design of partial-coverage ceramic restorations provides a numberof distinct advantages over traditional cast-metal options. However, unigue challenges are associated withprecise delivery of the restoration and tbe cleanup of excess luting resin. Restorative success and long-term gingivai bealth are dependent on interproximal integrity at the restoration-tooth interface. This artideexamines tbe variabies tbat affect tbis integrity and introduces a number of innovative techniques thatassure meticulous delivery of posterior partial-coverage ceramic restorations. (Quintessence Int 1999-30-807-818]
Key words: adhesive technique, ceramic restoration, finishing, nonretentive cavity preparation, partiai-couerage restoration
Gold is an ideal restorative option for the moderateto extensive posterior lesion. It continues to be
used with prudent operative diligence and success,Nevetiheless, the principles of retentive geometry andpreventive coverage often result in the excessive sacri-fice of healthy tissue. Adhesive restorative dentistryoffers noteworthy clinical potential for posterior appli-cations utilizing direct, semidirect, and indirect tech-niques with a wide array of materials.
Single-appointment direct restorative options forthe posterior dentition are ideally restricted to smallto medium intracoronal lesions. Large multisurfacedefects in the posterior dentition are best restoredwith indirect, lahoratory-fabricated restorations whenpatients present with esthetic stipulations.' The physi-cal and mechanical properties of dental ceramic mate-rials, such as modulus of elasticity, hardness, and coef-ficient of thermal expansion, are closer to theproperties of tooth enamel than are those of resin ma-terials.-'^ This fact, combined with the esthetic realismof ceramics,̂ "^ makes ceramic the material of choicewhen a tooth-colored restorative option is needed forconservative restoration of large, posterior, multisur-face defects in patients with esthetic needs,'""
•Private Practice, Nodh Vancouver, British Coiumbia, Canada
Reprint requests: Dr William H. Liebenberg, Suite 201, 2609 WeslviewDrive, North Vancouver, British Columbia, V7N 4M2 Canada. E-maii:™iiebenb@direct,ca
Presented at the Pacifio Dental Conference, Vanoouver, British Coiumbia,Canada, March 12-14, 1998.
Esthetics is but one aspect of the restorative out-come. The objective of any restorative procedure in-cludes the establishment of a good long-term progno-sis for both the tooth and the restoration,'^ and thetooth takes precedence. The indirect adhesive prepa-ration is more conservative and is often chosenregardless of esthetic considerations. Adhesive, metal-free restorative options often result in less destructionof healthy tissue than the alternative partial goldrestoration, are adhesive-reinforcing, and are less inva-sive of surrounding soft tissues,'^
All adhesive options arc technique sensitive, partic-ularly viith regard to the proximal portion of posteriorteeth, where restricted access limits procedural dili-gence. This article discusses the delivery of partial-coverage ceramic restorations and the subsequentcleanup of excess luting resin and introduces innova-tive solutions to the procedural challenges.
A CHANGE IN PREPARATION DESIGN
Traditional cast-gold preparation design reflects thegeometric necessity of adequate resistance, retentivefeatures, and a tenuous cement bond. Because of con-cerns about occlusal forces and fracture resistance, the"safe" option of complete coverage is often selected.
The ability to bond tooth-colored restorative mate-rials to tooth enamel reduces the need for extensivetooth preparation such as is necessary for completecoverage. Simonsen,''' in an editorial, questioned theprofession's proclivity for complete coverage andlabeled it a disservice in those cases when the same
807

• Liebenberg
result can be achieved through the tnore conservativeoption of partial coverage. Complete coverage can, inmany insfances, he regarded as overtreatment.
Preparation parameters
The potential for achieving esthetics is a fundamentalrationale for selecfion of a tooth-colored partial-cover-age restoration over the time-honored cast-goldrestoration. Esthetics is, however, of secondary impor-tance when the posterior dentition is restored. Boththe morphology and the original mechanical resis-tance of the tooth tnust be restored and both externaland internal adaptation must enhance the restorativeseal to prevent reeurrent caries, pulpal injury, anddentin sensitivity.'^
Some clinicians assume that the recognized rulesand principles of precision prosthodontics no longerapply to ceramic partial coverage restorations.'^ Thisfeeling derives, in part, from the ititmediate esthetic re-sult, whieh is relatively easily and consistently at-tained, regardless of the qitality of the primarily im-portant marginal fit. Ceramic restorations are estheticto the point of being virtually indistinguishable fromnatural teeth, and it is tempting to accept the primary(before bonding} tnarginal accuracy as "secondary" tothe overall treatment objective." The assumption thatthe resin excess will "fill in the marginal imperfec-tions" has not heen validated through research andmust be tested over time.'^ For now, it should be as-sutned that a precise primary fit of the ceramicrestoration is essential to the longevity of this treat-ment option.
The actual technical procedure is the single mostimportant factor in the fabrication of precise, durableceramic restorations. Tbe aecuracy of the fit and themarginal ceramic morphology is related to the ahilitiesof the dental technician rather than to the materialsused.'* Nevertheless, it remains incumhent on the clini-cian to provide preparations that enable the laboratoryto construct precise all-ceramic restorations efficientlyand to ensure the predictable stabilization of the toothduring the provisional and definitive restorativeprocess. Several textbooks'""^^ provide a comprehen-sive description of preparation principles as they relateto tooth-co)ored restorations in general.
The interproximai challenge
Restrictive anatomic features limit access and provide aunique therapeutic challenge in the interdental area.The achievement of interdental integrity with ceramicpaiiial-coverage restorations requires excellence in thepreparation, impression, provisionalization, lahoratoryfahrication, and definitive resin luting procedures. This
article restricts itself to the delivery sequence and theunique challenges associated with the removal of excessresin luting cement in restrictive interpcuximal areas.
INTERPROXIMAL CLEANUP
Light-activated resin cements with dtial chemical-curing components are now routinely used to ensureuniform bonding, even in deep interproximai prepara-tions.̂ ^^•' As the ceramic restoration is seated to thepreparation substrate, excess luting resin is squeezedout at the periphery. The excess luting resin on allaccessihle cavosurfaces is removed with a fine brushmoistened witb bonding (unfilled) resin, as recom-mended by Tay et al." This technique relies on visualaccess, because the tactile proprioception afforded bya fine brush is essentially insignificant. Interproximaicleanup requires a more arduous procedure to ensureinterproximai integrity.
The placement sequence is a factor of draw, whichis largely determined by the interpreparation flare(parallelism hetween adjacent preparations). Withbigbly divergent preparations, it is not uneommon fortecbnicians to indicate the preferred placement se-quence, so that particular restorations are "cemented"first to accommodate placement of the adjacent units.Consequently, with botb simultaneous and individualapproaches, it is the ensuing laboratory-fabricatedinterproximai configuration that dictates the place-ment sequence.
The simultaneous "rapid-seating" approach is oftenfavored because of its perceived efficiency; however,interproxima! integrity is consistently compromised.Individual seating is the preferred option heeause itfaeilitates direct access to the proximal gingival mar-gins. Often factors other than the laboratory prescrip-tion help determine the placement sequence. Thesefactors relate to the competency of the interproximairesin cleanup.
CONCAVE GINGIVAL MARGINS
The objective of interproximai eleanup is to remove allexcess resin from the embrasure area, because inter-proximai integrity is one of the most influential factorsin tbe patient's ability to keep the area free of plaque.This is traditionally done with the interproximai pas-sage of tufted floss, but this teehnique is only efticientin those embrasure areas wbere the proximal form isconvex or flat in outline.
The mesial developmental depression of maxillaryfirst premolars is a distinctive concavity in toothmorphology. There are many similar eoneavities
aer f2, 1999

• Liebenberg •
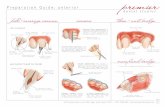
Fig l a The geomettic divergen! embrasure lorm (outline) revealsttie challenge of interproximal resin cleanup subsequent to äehra-tive bonding of indirect ceramic restorations. Abrasive finishingstrips cannot approximate concave gingival margins.
Fig 1b Concurrent bonding of adjacent restorations facilitatescomplete sealing as verified at (tie try-in procedure. Hcweve',cleanup ot excess inter próxima I luting resin is at best impreciselyexecuted in the concavities revealed in Fig la, necessitating prox-imal finishing with abrasive strips
within the cer\'ical architecture of posterior teeth. Thefloss, during interproximal passage, will only reachconvex or flat surfaces; thus efficient "cleaning" is lim-ited to these intimate contact areas. The difficulty ofintcrproxitTial resin cleanup in concave areas must besolved. Figures la and lh show the challenge ofcleanup after concurrent honding of adjacent restora-tions with opposing concave surfaces.
PROTECTING PROXIMAL SURPACES ATCAVITY PREPARATION
Protection of the uninvolved adjacent surface begins atthe cavity preparation phase, when proximal intactaxial surfaces are protected from iatrogenic damageduring rotary instrumentation. The InterGuard (NyKongevej) is an innovative gadget, in that tbe curvatureafforded hy the coiled ends of the metal matrixfacilitate clear access to tbe axial margins for the cavitypreparation effort (Fig 2a). Alternatively, any sectionalmetai matrix can he utilized, Pre-preparation toothseparation with wedges or a BiTine Ring (Darway) or aG-Ring of the Composi-tight matrix system (GarrisonDental Solutions) improves procedural acuity and re-duces the chance of nicking adjacent sound surfaces.
PROTECTING PROXIMAL SURFACESFROM ETCHANT
It is easier to remove resin frotn an unetched surfacethan from an etched surface, so it is prudent to limitetching to the restored tooth and to shieid ail adjacentsurfaces that are not involved in the restorative effort.
This vigilance applies to both the etchant procedure atthe initial sealing phase ¡preparation appointment)and the etchant for definitive bonding at the deliveryappointment. Although the use of a gel-deliverymediutTt allows selective application, tbe procedure istitiie consuming, and it is often impossible to appiy theetchant gingerly and stay within tbe generally recom-mended 15-second application time on tbe entirepreparation substrate.
Clear Mylar strips have traditionally hccn used toshield tbe adjacent tootb. Aitbough acceptable, thetechnique is somewhat ciimhersome hecause the stripsare easily dislodged. This author prefers to use aiength of plumber's Teflon tape (purcbased from alocal hardware store) to shield adjacent teeth duringthe etching procedure. Figure 2h shows how theplumber's tape bas heen wrapped around the mesialportion of the third molar, thereby shielding that toothduring the sealing procedure at the preparation phase.Close examination of the distogingival margin of thesealed preparation substrate (Fig 2c) reveals tbe chal-lenge of applying the etcbant to the second molarwithout contacting the adjacent proximal surfaces.
At the definitive bonding appointment, the adjacentteeth are once again shielded during the etchingprocess and, more impottantly, tbe resin cleanup. Thetraditional means of protecting the approximal sur-faces from excess resin attachment is to place a Mylarstrip in the interproximal space, thereby limiting theoverflow of luting resin in tbat area. The Mylar stripcan tben be used as a "matrix," hecause it fences offtbe inaccessible interproximal gingival margin.However, this matrix assemblage precludes perfectseating of the ceramic restoration because of the thick-ness of the Mylar substance. Cotnpensatory space.
809

Licbenbe'g
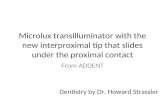
Fig 2a Provision oí interproximai integrity in the finai restorationis dependent on adequate protection ot the unrestored adjacentproximai surfaces during cavity preparation
Fig 2b A iength of Tetion piumber's (ape is used to shieid Ihe ad-jacent proximai surface Ircm the etchant during the adhesive seai-ing procedure prior to the finai impression
Fig 2c Sealing has been completed at the preparation appoint-ment Note the almost completely convex form of the proximai gin-givai margin, indicative of intimate and lavorable contact betweencleaning (tufted fioss) and finishing (abrasive strips) instruments.
%
Fig 2d The unrestored proximai surfaces are shielded withplumber's tape at the definitive bonding appointment. In this way,excess resin is not bonded to the adjacent proximal surfaces andIS easiiy removed.
which is generated by distending the interproximalspace with wedges, is often a h¡t-or-miss process; direconsequences arise if the proximal contact between atooth with a bonded restoration and its neighbor isfound to be wanting. If wooden wedges are needed,they will require some manipulafion, either reshapingor redirection.
The author previously introduced a customizedMylar strip technique in which a trapezoidal troughallows full seating at the contact while the matrix"isthmus"' covers the gingival margin and limits theresin overflow to an accessible area, where it is re-moved with a fine sable brush moistened with bond-ing (unfilled) resin.'' This technique, however, relieson the stability of the Mylar strip, and the author nowprefers to use the plumber's tape at the definitivebonding appointment. Figure 2d reveals how thepltimber's tape is used bofh mesially and distally to
shield not only the adjacent intact proximal tooth sur-face but also the recently placed adjacent direct resincomposite restorations.
The dual-CLtre resin cement on the mesio-occlusalportion of the restoration is then partially activatedwith a 5-second exposure from the visible light unit.The unfinished interproximal gingival contact area,with its excess of resin cement, is not ready for com-piete activation, because the excess cement wouldconstitute an area for plaque accumulation. A lengthof tufted Superfloss [Oral B) is threaded through theinterproximal space. The spongy section of theSuperfloss is loaded with a drop of unfilled resin andthen seesawed across the resin composite luting agentand gingival ceramic margin.'' Final bonding activa-tion is completed with 60-second applications at sev-eral exposure sites. This interproximal polymerizationis done with the Superfloss in situ.
810 Sber 12, 1999

• Liebenberg •
The floss is then forced upward out of the contactarea. This movement invariahly unseats the flange ofthe excess bonding agent, whieh often impedes theocclusal passage of floss. This outward passage of flossmay have to he repeated several times to release un-yielding interproximal resin.
Minimal polishing of the contact areas with resincomposite finishing strips is required once the bondingis completed. It is imperative that the interproximalflnishing procedure not degenerate into a recontour-ing session with the overzealous use of altiminumoxide and diamond-coated interdental strips. Thesestrips have the potential to eompromise the integrityof the interdental eontact area.
The rubber dam is removed, and ocelusal adjust-ments are made. Only essential trimming is done atthis cementation appointment to allow undisturbedcompletion of the dual-cure polymerization process.The flnal polishing and occlusal adjustments are donewhen the patient returns in an unanesthetized condi-tion. One of the chief advantages of a ceramic restora-tion is its close color match with tooth structure,which makes the interproximal extension undetec-table. Similarly, the fine interproximal resin flash iseasily overlooked in the clinical situation.
Margins are evaluated under magnification with asharp explorer in the method traditionally used for goldmargins and are polished accordingly. Interproximalperfection, although elusive, is optimized when accurateimpressions are made, appropriate ceramic technique isfollowed, and the restoration is carefully bonded.
SEQUENCE OF DELIVERY
Effect on interproximai integrity
From a laboratory technician's view, the placementsequence is again a factor of draw, largely determinedby the interpreparation flare. For highly divergentpreparations, technicians will often indicate a pre-ferred placement sequence.
The advent of the nonretentive, defect-related cavityform has, however, introduced a new parameter in theplacement sequence equation. The 3 partial-coverageceramic restorations shown in Fig 3a reflect thedilemma of selecting the appropriate delivery se-quence. Onee the primary (try-in before bonding) fit ofthe restorations has been verifled, the next step is tochoose the appropriate placement sequence. This se-quence must account for not only insertion and re-trieval but also considerations of interproximalcleanup. Concave proximal surfaces take precedence,because direct access is crucial in facilitating thoroughresin cleanup. Figure 3b reveals the favorable circum-
ferential convex form of all 3 teeth; therefore, theplacement sequenee could, in this instance, be dictatedby retentive-seating priorities.
In keeping with recent adhesive, defect-related eav-ity forms, no allowance was made for retention in thepreparation design (Fig 3c); henee, variation in theplacement sequence was a real possibility. In suchcases it is best to fit the least retentive restoration last,because its positional seating will be guided by thealready seated proximal restoration.
In this instance, the author mistakenly bonded thepremolar with a slight distal displacement, which ne-cessitated adjustment to facilitate complete seating ofthe adjacent ceramic restoration. Finishing procedureswere protracted because displacement affected the en-tire restoration-tooth interface (Fig 3d). It would havebeen prudent to have placed the retentive and self-aligning restorations on the molars flrst, in which in-stance the proximal surface of the first molar wouldhave guided and facilitated complete seating of thenonretentive, minimal premolar restoration.
With more traditional retentive cavity forms (Fig4a), there is indexed seating and very little chance ofaskew alignment during delivery. In these cases, thetry-in procedure not only verifies the primary fit of theceramic restorations but also allows an evaluation ofthe selected seating sequence (Fig 4b). The slightlyconcave mesial gingival margin of the flrst molar isbest cleaned while direct access is accommodatedfrom the mesial aspect, before delivery of the premo-lar restoration. Once cleaned, the mesial margin isdraped with a length of plumber's tape to shield thealready flnished ceramic-tooth interface from attach-ment of exeess resin during delivery of the second pre-molar (Fig 4c),
In spite of these precautions, excess resin may bepresent at the interproximal line angles even aftercleanup of the premolar with tufted floss and mini-appHcator and brush (Fig 4d). It is imperative that thetechnique sensitivity of bonded ceramic restorationsbe acknowledged, thereby ensuring that the quest forinterproximal integrity surpasses the quest for the easilyobtainable esthetic outcome.
Errors in sequence
It is fairly common to deliver adjacent, dissimilar indi-reet restorations at the same appointment. Partial-coverage ceramic restorations are invariably bondedbefore adjacent porcelain-fused-to-metal (PFM)restorations to accommodate rotary adjustments toproximal surfaces. It is far less risky to adjust {andpolish) the proximal surface of a FFM restoration thanthe proximal surface of an unbonded (somewhat frag-ile) ceramic restoration.
811

• Liebenberg
Fig 3a These three par ti al-coverage ceramic restorations reveaithe diiemma ot seiecting the appropriate delivery sequence Thissequence must account tor not only insertion and retrievai butaiso interproximal cieanup.
Fig 3b Concave proximai surfaces take precedence, becausedirect access is crucial in taciiitating thorough cieanup ot resin. All3 ct these teeth have tavorabie, circumlerentiai, convex form. Thedelivery sequenoe can, therefore. De dictateü by retentive inser-tion faotors.
Fig 3c (lefi) A minimai. Class ii, defect-re i ate d cavity preparationIS present in tiie second premoiar. No ailowance has been madetor retention (right) Tiie restoration iias been bonded witti a siightdistai displacement, wtiich necessitates additionai adjustrrtent totaciiitate compiete seating ct the adjacent restoration.
Fig 3d Finishing procedures are protracted because dispiace-ment aftects the entire resto rat i on-toot h interface, it the retentiveand self-aiigning restorations had been piaced on ttie moiars first,the proximal surface ot the first melar vjould have taciiitated com-plete seating ot ttie nonretentive premoiar restoration
In addition, bonding the partial-coverage restora-tion ahead of the complete-coverage PFM allows strictisolation for the exacting bonding procedure. Oncebonding is completed, the conventional rubber datnisolation is then easily changed to general field isola-tion (slit-dam isolation) to facilitate access to thegingival margin which, in a PFM restoration, usuallyclosely approximates the gingival sulcus.
The problem with this delivery sequence (partial-coverage ceramic restorations before PFM restorations)is that there is a potential for variance in the seating ofthe ceramic restoration when nonretentive cavitypreparation forms are involved. The author committedthis error while bonding a ceramic restoration to theflat, nonretentive cavity form of a mandibular second
molar (Figs 5a and 5b). The restorations were tried inbefore placement of the rubber dam to verify the preci-sion of both the fit and the proximal contacts. The damwas applied and the ceramic restoration was inadver-tently bonded with a slight distal cant. This may appearto be an easily observable error; however, It is easilydone given that the resin luting agent, the tooth, andthe restoration are al! "tooth colored,"
The rubber dam setup was changed to general fieldisolation to accommodate access to the intrasulcularcircumferential margin of the PFM crown on the firstmolar {Fig 5c). The previously verified contact be-tween the PFM restoration and the ceramic was nowopen because of the inadvertent distal displacement ofthe ceramic restoration during bonding. The open
812 Niimhm )2,

Liebenberg •
F¡g 4a Refeniiue cavity forms, in ifiis insfance a consequence ofpreexisiing ailoy resfOfafions, ailow more prediofable piacemenf ofíesforalions, even wnen fliey are piaced singly.
Fig 4b in addifion to verifying the primary fit of fhe ceramicrestorations, a try-in procedure aliows an evaluation of liie se-lected seating sequence. The patfi of Insertion can oflen be ham-pered by negieofiul laboratory fabricafion procedures.
Fig 4c Direct access aiiows fhorougii cleanup of ihe siigtitiymore concave proximai surface cf fhe first moiar. This resforcdsurface is fhen draped and shieided wilfi a length of piumber'sfape fo prevent excess iuting resin on fhe second resforafion frombonding to fhe ieading restoralion.
Fig 4d Close examinarían of the interproiimai iine angles reveáisthe presence of excess resin
contact reduced the restorative effort to a failure (Fig5d). An afternative delivery sequence, in which thePFM erown was used as a seating guide, could haveprevented this catastrophe.
Use of proximai restorations as a seating guide
For adjacent defect-related adhesive cavity prepara-tions in which no consideration has been given toantidisplacement retentive form, it is best to place theunbonded proximal ceramic restoration in position asa positioning and seating guide during the bonding ofthe first restoration. Because of its nonretentive form,the restoration will have to be stabilized in positionwhile it acts as a positioning guide. Figures 6a to 6p
introduce an innovative technique utilizing plumber'stape stabilized with cyanoacryiate.
1. Subsequent to try-in of the ceramic restorations,verification of the seating sequence, and adhesivepreparation of the substrate, a single ceramicrestoration is covered and secured in place with alength of plumber's tape.
2. Tbe ends of the tape are anchored to the rubberdam with cyanoacryiate, which bonds instanta-neously and provides positional stability to thedraped restoration.
3. The leading restoration is loaded with luting resinand spot bonded along the opposite occiusal cavo-surface margin.
813

Liebenberg
Fig 5a Isolation setup facilitating bonding of a oeramic restoia-tion to ttie flat, nonretentive cavity form of the mandibuiar secondmoiar.
Fig 5b Tfne alcchcl-matked black spot provides buocal and lin-gual crienfation; however, ttie nonrelentive substrate form permitsvarianoe in the mesiai and distai seating positions. The restorationshouid have been positioned mote mesially (arrow)
Fig 5c The dental dam is split to create general fieid isolation,allowing intracrevicular managernent of soft tissues and optimaicementation ol the PFM orown to the endodontioally treated firstmolar.
Fig 5d Although proximal coniaot was verified at ttie try-irprocedure, the contact is open because ot the inadvertent distadispiacement ot the ceramio restomtion on the seoond moiar. Araiternative deiivery sequenoe, in which the PFM orown wouid beused as a positional prop, oould have prevented this catastrophe.
Fig 6a No consideration has been given to antidisplacementretentive form in these defeot-related adhesive cavily prepara-tions, Tradilionai occiusai dovetaiis or interiocks fouî/Ziies; wouidfurther undermine the integrity of the aiready compromised teetn.
Fig Eb The mandatory try-in verifies the exactiluue nf the pri-mary (before bonding) fit of these 2 proximal ceramic restorationsand aliows an evaluation of the aptimai seating sequence
814 VolumeSQ.JiLimhsr \2. 1999

Li eben berg •
Rg 6c Careful examination of the buccai ceramic-tooth interlacereveals the attending margin of error (arrows). The ceramicrestoration can, without the guiding prcximal surlace of the adja-cent restoration, be unwittingly bonded beyond the preparationQuiline.
Fig 6d Both tooth substrates are ccpiously covered with phos-phoric acid, thereby ensuring thorough and adequate condition-ing cf the critical gingivai approximating preparation margins.
Fig 6e The first moiar is draped and secured in piace withpiumbers tape. The ends ol the tape are anchored to the dentaldam with cyanoacrylate, which bonds instantly.
Fig 5Í The leading restoration (in this case, the second moiar) iswbrated into position; the excess iuting resin is cleaned from theaocessibie margins with a miniapplioator. The restoration is thenspot bended (attenuated poiymenzing light beam) occiusally
Fig 6g The piumbers tape is remoued, freeing the unbondedceramic restoration on the first molar: the restoration is then liftedoff the preparation base with a plastic-tipped instrument This se-quence mas rehearsed and verified at the try-in procedure.
Fig 6h (left) With the adjacent unbended ceramic restoration re-moved, direct access is now afforded to the spot-bonded leadingrestoration Cleanup of excess resin oan be diiigently executedwith a dry brush technique, (right) Precise sealing is yielded bythe presence of the guiding proximal surlace cf the unbonded ad-jacent restoration.
815

Liebenberg
Fig 6i The succeeding restoraiion is vibrated inlo place andheld in position with a bail burnishing instrument while the excesscemenl Is removed from the accessibie margins.
Fig 6j The restoraiion is spot-bonded in position lo provide sta-bility dunng the tufled fioss removai of the interproximai excessiuting resin.
Fig 6k The Superfloss is withdrawn from the embrasure space.A iengtii of thinner déniai fioss is then maneuvered through ttieocciusai contact and wrapped around the proximai iine angles toremove additionai resin fiange.
Fig 61 To prevent formation of an oxygen-inhibited surtaoe iayer,the entire restorative interface is flooded with giycerin. This appii-cation inciudes the criticai and inaccessible inlerproximai area.
Fig 6m Final iight poiymerization exposure is provided from vari-ous projecting sources, ensunng thorough initiation of the iight-cured component ol the duai-cured resin adhesive.
Fig 6n The smooth suriace ot the axiai iine angies is a tribute tothe successfui and metiouious seating and cieanup techniques.
816 ober 12, 1999

• Liebenberc
Fig 60 Regardless of the aforemeniioned smoothness, it isanticipated that the unfiiled bonding resin wouid have pooied to-ward the inverted rubber dam, and this cervical fiange is gingerlyremoved vjith an abrasive strip.
Fig 6p The immediateiy postoperative buccal view reveáis therestrictive anatomic proximities thai create a unique therapeuticchalienge.
4, The plumber's tape is removed, and the unbondedguiding restoration is gently removed from itspreparation base,
5, The proximal margin of the leading restoration ismeticulously cleaned of excess resin; direct accessis available from the mesial aspect.
6, Once light polymerisation is completed, thesucceeding ceramic restoration is bonded in posi-tion after the appropriate shielding of the alreadybonded restoration.
CONCLUSION
Although the anatomic proximities of the embrasurearea are restrictive, it is possible to deliver these chal-lenging restorations successfully, provided that theyare delivered with care. Technology will continue toprovide clinicians and technicians with novel materi-als and treatment modalities. To save time, clinicianswill continue to seek procedural shortcuts. Although itis tempting to place multiple units simultaneously, it isabundantly clear that interproximal cleanup is notsimply a matter of passing tufted floss between multi-ple units.
Individual placement of indirect restorations hasthe advantage of facilitating direct access to the proxi-mal surface of the leading restoration so that cleanupcan be diligently executed before final polymerizationis initiated. Adhesive, nonretentive cavity forms pro-vide an accompanying dilemma with the individualplacement approach, because there is a potential formispositioning of the leading restoration, which mayprevent full seating of the succeeding restoration. Thisarticle has described these influential variables and
introduced a number of innovative techniques, includ-ing one in which a proximal restoration is provision-ally stabilized in place while the leading restoration isspot bonded. The guiding restoration is then removedto facilitate proximal access and is bonded followingthe appropriate proxirnal cleanup.
Access to the proximal surface of the last restora-tion will be restricted, and this is why the sequence ofplacement is of vital importance. The ideal placementsequence must allow, when possible, direct access todifficuh concave proximal surfaces. The last proximalsurface to be cleaned should be convex or flat, therebyaccommodating complete removal of excess lutingresin with the interproximal passage of tufted floss.
Esthetics has been the drawing card for ceramicrestorations. Regardless of this distinction, it is pru-dent to acknowledge that esthetics is of secondaryimportance when restoring the posterior dentition.Chosen restorative materials and clinical techniquesmust optimally restore the original mechanical resis-tance and the physiologic morphology of the tooth sothat it may resume its function in the proper way,Interproximal integrity is a reflection of the attainmentof these parameters in the critical embrasure area andis deserving of restorative precision.
ACKNOWLEDGMENTS
The author wouM like !o exiend his sincere graiitude to Mr Lee Culp.CDT, of Mosaic Studios, New York: Mr Bill Parkes, CDT, of SandersDentai Ceramics. Anchorage, Alaska; and Mr Jack Liem, RDT, andMr Andrew Cheung, RDT, of Neodent Dental Laboratories,Vancouver, for Ihe «ramie artiitry depicted in this article.
817

• Liebenberg
REFERENCES
1. Liebenberg WH. Partial coverage indirect toofh-eoloredrestorations: Steps fo clinical success. Am ) Dent 1999;12:201-209.
2. Pameijer CH, Grosstnan D, Adair P|. Physical properties ofa casfable ceramic dental resforative mafei'ial [abstract 827],J Denf Res 1980;59:474,
3. Derand T. Sfress analysis of cemented or resin-bondedloaded porcelain inlays. Dent Mater 1991;7:21-24.
4. Lopes LMP, Leifao JGM, Douglas WH. Effect of a newinlay/onlay resforafive material on cuspal reintorcemenf,Quinfessence Inf 1991;22:641-645.
5. Malcolm P|, Hood JAA. The effecf of cast resforations inreducing cusp flexibility in restored feetli [abstracf 67]. JDent Res 1977;56:D207.
6. Sorensen JA, Sulfan E, Condon |R. Tliree-body in vifro wearof enamel against dental ceramics [absfract 909). ] Dent Res1999;78:219.
7 Sorensen |A, Choi C, Fanusca Ml, Mifo WT. IPS Empresserown sysfem: Three-year clinical trial resulfs | Calif DentAssoc 1998;26(2]:130-136.
8. Chrisfensen G|. A look at fhe sfate-of-fhe-art toofh-coloredinlays and onlays. J Am Dent Assoc 1992;123:66-70.
9. Banks RG. Conservative posterior ceramic resforafions: Aliterafure review, ] Prosthef Dent 1990;63:619-626.
10. Liebenberg WH. Partial coverage and the incompletelycracked footh: Steps fo success using resin bonded ceramicrestorations. J Esfhet Dent 1995;7:155-166,
11. Liebenberg WH. Treating incomplete fractures in posteriorteeth with resin-bonded parfial-coverage ceramic restora-tions: A clinical reporf. Quintessence Int 1996;27:7J9-747.
12. Ott Klaus HR. Criteria for the selection of a resforative. In:Mormann WH (ed). CAD/CIM in Aesthefic Dentistry.Chicago: Quintessence, 1996:195-198.
13. Wagenberg BD. Exposing adequate tooth structure forresforafive dentistry, Int J Periodontics Restorative Dent1989:9:323-329.
14. Simonsen R|. Why crowns? [editorial|. Quintessence Int1995 ¡26:1.
15. Vale WA Cavity preparafion. Irish Dent Rev 1955;2:33-4I.16. Dietsehi D, Magne P, Holz J. An in vitro study of parame-
ters related to marginal and internal seal of bonded restora-tions. Quintessence !nt 1993;24:281-291.
17. Liebenberg WH. Variables which affect the marginal aecu-racy of the resin bonded posterior ceramie restoration: Apictorial essay, J Dent Assoc South Afr 1993;8:469-473.
18. Licbenberg WH. Achieving interdental integrity in resin-bonded posterior eeramic restorations. Pract PeriodontAesthet Dent I994;6(5):43-51.
19. Bergmann P, Noack M|, Roulet J-F. Marginal adaptationwifh glass-ceramic inlays adhesively luted with glycerine gel.Quintessence Int 1991;22:739-744.
20. Garbcr DA, Goldstein RE. Efched Porcelain Inlays andOnlays. Chicago: Quintessence. 1993
21. Roulet |-F, Herder S. Bonded Ceramic Inlays. Chicago;Quintessence, 1991.
22. Diefsehi D, Spreafieo R. Adhesive Mefal-Free Restorations:Currenf Concepfs for the Esthetie Treatment of PosteriorTeeth. Chicago: Quinfessence, 1997.
23. Mclnnes-Ledoux PM, Ledoux WR, Weinberg R, Kappold A.Luting casfable ceramic restorations-A bond strength siudy[abstract 802]. J Dent Res 1987;66:207
24. Jordan RF. Esthetic composite bonding. Philadelphia:Decker, 1987
25. Tay WM, Lynch E, Auger D. Effects of some finishing tech-niques on cervical margins of porcelain laminates.Quintessence Int 1987;18:599-602.
818 12, 1999