Interpretation of Laboratory Tests: A Case-Oriented Review of Clinical Laboratory Diagnosis (Part 2)...
72
Interpretation of Laboratory Tests: A Case-Oriented Review of Clinical Laboratory Diagnosis (Part 2) Roger L. Bertholf, Ph.D. Associate Professor of Pathology University of Florida Health Science Center/Jacksonville Mark A. Bowman, MT(ASCP), Ph.D. Associate Professor of Clinical Pathology Clinical Laboratory Sciences Program Director University of Iowa College of Medicine
-
Upload
zachary-lawerence -
Category
Documents
-
view
218 -
download
3
Transcript of Interpretation of Laboratory Tests: A Case-Oriented Review of Clinical Laboratory Diagnosis (Part 2)...

Interpretation of Laboratory Tests:A Case-Oriented Review of Clinical
Laboratory Diagnosis (Part 2)
Interpretation of Laboratory Tests:A Case-Oriented Review of Clinical
Laboratory Diagnosis (Part 2)
Roger L. Bertholf, Ph.D.Associate Professor of Pathology
University of Florida Health Science Center/Jacksonville
Mark A. Bowman, MT(ASCP), Ph.D.Associate Professor of Clinical Pathology
Clinical Laboratory Sciences Program Director
University of Iowa College of Medicine
Roger L. Bertholf, Ph.D.Associate Professor of Pathology
University of Florida Health Science Center/Jacksonville
Mark A. Bowman, MT(ASCP), Ph.D.Associate Professor of Clinical Pathology
Clinical Laboratory Sciences Program Director
University of Iowa College of Medicine

Case 1: Failure to ConceiveCase 1: Failure to Conceive

Case HistoryCase History
A couple visits their family doctor, complaining that the wife had been unable to become pregnant.
What questions should you ask?
A couple visits their family doctor, complaining that the wife had been unable to become pregnant.
What questions should you ask?

InfertilityInfertility
• Definition: One year of unprotected intercourse without pregnancy– 1°: No previous pregnancies
– 2°: Previous pregnancy (not necessarily live birth)
• Fecundability: Probability of achieving pregnancy within a menstrual cycle– 20-25% for normally fertile couples 90% of couples should conceive within one year
• 10-15% of couples experience infertility
• Definition: One year of unprotected intercourse without pregnancy– 1°: No previous pregnancies
– 2°: Previous pregnancy (not necessarily live birth)
• Fecundability: Probability of achieving pregnancy within a menstrual cycle– 20-25% for normally fertile couples 90% of couples should conceive within one year
• 10-15% of couples experience infertility

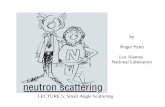
Probabilities of failure to conceiveProbabilities of failure to conceive
10
100
0 2 4 6 8 10 12
Months of unprotected intercourse
Per
cent
fai
led
Nulliparous
Parous
5 months
2.7 months
50

Requirements for conceptionRequirements for conception• Male must produce adequate numbers of normal, motile
spermatozoa• Male must be capable of ejaculating the sperm through a
patent ductal system• The sperm must be able to traverse an unobstructed
female reproductive tract• The female must ovulate and release an ovum• The sperm must be able to fertilize the ovum• The fertilized ovum must be capable of developing and
implanting in appropriately prepared endometrium
• Male must produce adequate numbers of normal, motile spermatozoa
• Male must be capable of ejaculating the sperm through a patent ductal system
• The sperm must be able to traverse an unobstructed female reproductive tract
• The female must ovulate and release an ovum• The sperm must be able to fertilize the ovum• The fertilized ovum must be capable of developing and
implanting in appropriately prepared endometrium

Sperm MorphologySperm Morphology
• % normal spermatozoa
• Head, acrosomal region
• Vacuoles
• Midpiece abnormalities
• Tail defects
• % normal spermatozoa
• Head, acrosomal region
• Vacuoles
• Midpiece abnormalities
• Tail defects

Comparison of CriteriaComparison of Criteria
WHO (1987)
WHO (1992)
Strict (1986)
% Normal 50 30 14
Head length (m) 3.0-5.0 4.0-5.5 5.0-6.0
Head width (m) 2.0-3.0 2.5-3.5 2.5-3.5
W/L 1.5-2.0 1.5-1.75 1.0-1.67

Evaluation of semenEvaluation of semen
• 2-3 days abstinence prior to collection
• Gelation/liquefaction (macroscopic)
• Color/volume/consistency/pH
• 2-3 days abstinence prior to collection
• Gelation/liquefaction (macroscopic)
• Color/volume/consistency/pH

Sperm morphologySperm morphology

Sperm motilitySperm motility

The Endocrine SystemThe Endocrine System
Hypothalamus/Pituitary/Pineal
Thyroid/Parathyroid
ThymusAdrenalPancreas
Kidney
Testis
Ovary

Evaluation of male infertilityEvaluation of male infertility
H&P
Follow-upSemen analysis
PCTAntisperm antibodies
Sperm mucuous penetration
Repeat
LH, FSH, Testosterone
N A
N
N
A
A

Male Hypothalamic-Pituitary-Gonadal Axis
Male Hypothalamic-Pituitary-Gonadal Axis
GnRH
LH, FSH
TestosteroneInhibin
FSH acts on Sertoli cellsLH acts on Leydig cells

Male reproductive endocrinologyMale reproductive endocrinology
LH FSH Testosterone Diagnosis
Hypothalamic or pituitary failure
Gonadal failure
N N Germinal compartment failure
N N or Androgen resistence
N N N Idiopathic

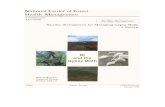
Causes of female infertilityCauses of female infertility
Pelvic factors50%
Immunologic factors
5%
Other15%
Ovulatory disorders
30%
Pelvic factors50%
Immunologic factors
5%
Other15%
Ovulatory disorders
30%

Female Hypothalamic-Pituitary-Gonadal Axis
Female Hypothalamic-Pituitary-Gonadal Axis
GnRH
LH, FSHEstradiol
Progesterone
FSH stimulates follicular growthLH stimulates ovulation

Cyclical changes in female reproductive hormones
Cyclical changes in female reproductive hormones
1 4 8 12 16 20 24 28
Days since onset of menses
FSH LH Estradiol Progesterone
1 4 8 12 16 20 24 28
Days since onset of menses
FSH LH Estradiol Progesterone
Ovulation

Evaluation of amenorrheaEvaluation of amenorrhea
• Vaginal• Uterine• Ovarian• Adrenal disorders• Thyroid disorders• Pituitary/hypothalamic
disorders
• Vaginal• Uterine• Ovarian• Adrenal disorders• Thyroid disorders• Pituitary/hypothalamic
disorders
• Pregnancy/lactation• Uterine• Ovarian• Adrenal disorders• Thyroid disorders• Pituitary disorders• Hypothalamic disorders• Iatrogenic
• Pregnancy/lactation• Uterine• Ovarian• Adrenal disorders• Thyroid disorders• Pituitary disorders• Hypothalamic disorders• Iatrogenic
Primary causes Secondary causes

Primary amenorrheaPrimary amenorrhea
• 40% due to Turner’s syndrome or pure gonadal dysgenesis– Turner’s syndrome: 45X karyotype– Pure GD: 46XX or XY karyotype
• Müllerian duct agenesis or dysgenesis
• Testicular feminization– Androgen receptor deficiency in XY karyotype
• 40% due to Turner’s syndrome or pure gonadal dysgenesis– Turner’s syndrome: 45X karyotype– Pure GD: 46XX or XY karyotype
• Müllerian duct agenesis or dysgenesis
• Testicular feminization– Androgen receptor deficiency in XY karyotype

Secondary amenorrheaSecondary amenorrhea
• Pregnancy is the most common cause
• Prolactin elevation– Tumor– Iatrogenic
• Thyroid disease– Effects on the metabolism of estrogens and
androgens
• Pregnancy is the most common cause
• Prolactin elevation– Tumor– Iatrogenic
• Thyroid disease– Effects on the metabolism of estrogens and
androgens

TRH
TSH
T4(T3)
T3
(rT3)
Regulation of thyroid hormonesRegulation of thyroid hormones

Thyroid disease and infertilityThyroid disease and infertility
• Hypothyroidism– Pre-pubertal
• Delayed sexual maturation, or rarely, precocious puberty
– Post-pubertal• TSH may have leuteotropic effect
• Hyperthyroidism– Amenorrhea
• Hypothyroidism– Pre-pubertal
• Delayed sexual maturation, or rarely, precocious puberty
– Post-pubertal• TSH may have leuteotropic effect
• Hyperthyroidism– Amenorrhea

EndometriosisEndometriosis
• Appearance of endometrial tissue elsewhere in the pelvic cavity.– Origin is uncertain
• One of the most common diseases of menstruating women
• Involved in 20-50% of infertility cases
• Appearance of endometrial tissue elsewhere in the pelvic cavity.– Origin is uncertain
• One of the most common diseases of menstruating women
• Involved in 20-50% of infertility cases

Causes of infertilityCauses of infertility
Endometriosis5%
Seminal Defect25%
Tubal Defect22%
Other4%
Ovulation Defect27%
Unexplained17%
Endometriosis5%
Seminal Defect25%
Tubal Defect22%
Other4%
Ovulation Defect27%
Unexplained17%

Unexplained infertilityUnexplained infertility
• Exclusionary diagnosis, after all diagnostic tests are normal
• Most studies report a 15-25% incidence• Conservative protocol:
– Semen analysis, mid-luteal phase progesterone, tubal patency
• Liberal protocol:– Above, plus cervical mucous evaluation,
endometrial maturation, immunology studies
• Exclusionary diagnosis, after all diagnostic tests are normal
• Most studies report a 15-25% incidence• Conservative protocol:
– Semen analysis, mid-luteal phase progesterone, tubal patency
• Liberal protocol:– Above, plus cervical mucous evaluation,
endometrial maturation, immunology studies

Immunological causes of infertilityImmunological causes of infertility
• Male or female?
• Source– Vaginal fluid (IgA, IgE)– Fallopian tubes (IgA)
• Variations throughout cycle
• Experimental induction of infertility– Baskin, 1932– Animal studies
• Male or female?
• Source– Vaginal fluid (IgA, IgE)– Fallopian tubes (IgA)
• Variations throughout cycle
• Experimental induction of infertility– Baskin, 1932– Animal studies

Anti-sperm autoantibodiesAnti-sperm autoantibodies
• 1955: Rumke and Hellinga demonstrate association between humoral autoantibodies to sperm and unexplained infertility– Results were controversial, and hampered by
inadequate analytical techniques– Humoral antibodies do not effect fertility
unless they exist in the reproductive tract
• Antibodies must be demonstrated on the sperm surface
• 1955: Rumke and Hellinga demonstrate association between humoral autoantibodies to sperm and unexplained infertility– Results were controversial, and hampered by
inadequate analytical techniques– Humoral antibodies do not effect fertility
unless they exist in the reproductive tract
• Antibodies must be demonstrated on the sperm surface

Effect of sperm autoantibodiesEffect of sperm autoantibodies
• Spontantous agglutination• Motility/penetration
– Binding to tail
• Disruption– IgG mediated complement fixation (tail)– Seminal fluid contains complement inhibitors,
so membrane attack occurs in the female reproductive tract
• Spontantous agglutination• Motility/penetration
– Binding to tail
• Disruption– IgG mediated complement fixation (tail)– Seminal fluid contains complement inhibitors,
so membrane attack occurs in the female reproductive tract

Anti-sperm antibodies in the femaleAnti-sperm antibodies in the female
• Clinically significant only in high titers (in serum)
• Anti-sperm antibodies may exist in vaginal secretions or cervical mucus even when humoral antibodies are not detected
• Clinically significant only in high titers (in serum)
• Anti-sperm antibodies may exist in vaginal secretions or cervical mucus even when humoral antibodies are not detected

Diagnosis of immune-related infertility
Diagnosis of immune-related infertility
• Post-coital test– Evaluates sperm viability in the cervical mucus
• Humoral antibodies– Not diagnostic
• Demonstration of antibodies on the sperm surface
• Post-coital test– Evaluates sperm viability in the cervical mucus
• Humoral antibodies– Not diagnostic
• Demonstration of antibodies on the sperm surface

Case 3: Unexplained Weight LossCase 3: Unexplained Weight Loss

Case HistoryCase History
A 62 year old man visited his family doctor because of weight loss from 185 lbs. to 163 lbs. The patient was not obese prior to his weight loss, and he described his appetite as “normal.” He had occasional indigestion. The patient was afebrile, and vital signs were normal. The patient had normal bowel movements.
What other questions would you ask this patient?
A 62 year old man visited his family doctor because of weight loss from 185 lbs. to 163 lbs. The patient was not obese prior to his weight loss, and he described his appetite as “normal.” He had occasional indigestion. The patient was afebrile, and vital signs were normal. The patient had normal bowel movements.
What other questions would you ask this patient?

Pre-testPre-test
• What are “tumor markers”?
• What are desirable characteristics of a tumor marker?
• In what ways are tumor markers used?
• What are “tumor markers”?
• What are desirable characteristics of a tumor marker?
• In what ways are tumor markers used?

Leading causes of death in the United States
Total Deaths Percent of total
All causes 2.391,399 100
Cardiovascular disease 725,192 30.3
Cancer 539,838 23.0
Cerebrovascular 167,366 7.0
COPD 124,181 5.2
Accidents 97,860 4.1
Source: National Vital Statistics Report (1999 data)

Types of tumor markersTypes of tumor markers
• Enzymes and isoenzymes
• Hormones
• Oncofetal antigens
• Carbohydrate antigens
• Receptors
• Oncogene products
• Genetic markers
• Enzymes and isoenzymes
• Hormones
• Oncofetal antigens
• Carbohydrate antigens
• Receptors
• Oncogene products
• Genetic markers

Desirable characteristics of tumor markers
Desirable characteristics of tumor markers
• Easy to measure
• Specific for tumor
• Always present with tumor
• Easy to measure
• Specific for tumor
• Always present with tumor

Sensitivity vs. SpecificitySensitivity vs. Specificity
• Sensitivity and specificity are inversely related.

Mar
ker
con
cen
trat
ion
- +Disease

Sensitivity vs. SpecificitySensitivity vs. Specificity
• Sensitivity and specificity are inversely related.
• How do we determine the best compromise between sensitivity and specificity?

Receiver Operating Characteristic
Receiver Operating Characteristic
Tru
e p
osi
tive
rat
e(s
ensi
tivi
ty)
False positive rate1-specificity

Evaluating the clinical performance of laboratory tests
Evaluating the clinical performance of laboratory tests
• The sensitivity of a test indicates the likelihood that it will be positive when disease is present
• The specificity of a test indicates the likelihood that it will be negative when disease is absent
• The predictive value of a test indicates the probability that the test result, positive or negative, correctly classifies a patient

Predictive ValuePredictive Value
The predictive value of a clinical laboratory test takes into account the prevalence of a certain disease, to quantify the probability that a positive test is associated with the disease in a randomly-selected individual, or alternatively, that a negative test is associated with health.

IllustrationIllustration• Suppose you have a new marker for liver
cancer
• The test correctly identified 98 of 100 patients with confirmed liver cancer (What is the sensitivity?)
• The test was positive in 15 of 100 patients with no evidence of liver cancer (What is the specificity?)

Test performanceTest performance
• The sensitivity is 98.0%
• The specificity is 85%
• Liver cancer has an incidence of 1.5:100,000
• What happens if we screen 1 million people?

AnalysisAnalysis
• In 1 million people, there will be 15 cases of liver cancer.
• Our test will (most likely) identify all of these cases (TP)
• Of the 999,985 healthy subjects, the test will be positive in 15%, or about 150,000 (FP).

Predictive value of the positive test
Predictive value of the positive test
The predictive value is the % of all positives that are true positives:
%01.0
100000,15015
15
100
FPTP
TPPV

What about the negative predictive value?
What about the negative predictive value?
• TN = 849,985
• FN = 0
%100
1000985,849
985,849
100
FNTN
TNPV

Summary of predictive valueSummary of predictive value
Predictive value describes the usefulness of a clinical laboratory test in the real world.
Or does it?

Lessons about predictive valueLessons about predictive value
• Even when you have a very good test, it is generally not cost effective to screen for diseases which have low incidence in the general population. Exception?
• The higher the clinical suspicion, the better the predictive value of the test. Why?

Use of tumor markersUse of tumor markers
• Screen for disease
• Diagnosis of symptomatic patients
• Staging
• Prognostic indicators
• Detect recurrence of disease
• Monitoring response to therapy
• Radioimmunolocalization
• Screen for disease
• Diagnosis of symptomatic patients
• Staging
• Prognostic indicators
• Detect recurrence of disease
• Monitoring response to therapy
• Radioimmunolocalization

Prostate-specific antigenProstate-specific antigen
• A serine protease in the kallikrein family– Produced exclusively by epithelial cells in the
prostate
• Forms complexes with 1-antichymotrypisin (ACT) and 2-macroglobulin– Most immunoassays measure both free PSA and
PSA-ACT, but not PSA-AMG
• A serine protease in the kallikrein family– Produced exclusively by epithelial cells in the
prostate
• Forms complexes with 1-antichymotrypisin (ACT) and 2-macroglobulin– Most immunoassays measure both free PSA and
PSA-ACT, but not PSA-AMG

Prostate cancerProstate cancer
• 2nd most common cancer (19%), and 2nd leading cause of cancer death, in men
• Sensitivity of PSA (at 4.0 g/L) is 78%; specificity is approximately 33%.
• PSA concentration correlates with clinical stage of cancer
• PSA is used to monitor therapy
• 2nd most common cancer (19%), and 2nd leading cause of cancer death, in men
• Sensitivity of PSA (at 4.0 g/L) is 78%; specificity is approximately 33%.
• PSA concentration correlates with clinical stage of cancer
• PSA is used to monitor therapy

Free PSAFree PSA
• Measurement of uncomplexed (free) PSA can improve the specificity– Reported as %fPSA
• Prostate cancer is associated with higher concentrations of PSA-ACT
• BPH is associated with higher free PSA concentrations
• Measurement of uncomplexed (free) PSA can improve the specificity– Reported as %fPSA
• Prostate cancer is associated with higher concentrations of PSA-ACT
• BPH is associated with higher free PSA concentrations

hCGhCG
• Glycoprotein secreted by the syncytiotropoblastic cells of the placenta subunit is shared with LH, FSH, TSH subunit is specific to hCG
• Assays can measure intact (sandwich) or both intact and subunit– Cancer patients produce both intact hCG and
subunit
• Glycoprotein secreted by the syncytiotropoblastic cells of the placenta subunit is shared with LH, FSH, TSH subunit is specific to hCG
• Assays can measure intact (sandwich) or both intact and subunit– Cancer patients produce both intact hCG and
subunit

Use of hCGUse of hCG
• Pregnancy
• Elevated with virtually all trophoblastic tumors– C/P Hyatidiform mole ()– Choriocarcinoma
• Elevated in 70% of nonseminomatous testicular tumors
• Pregnancy
• Elevated with virtually all trophoblastic tumors– C/P Hyatidiform mole ()– Choriocarcinoma
• Elevated in 70% of nonseminomatous testicular tumors

Alpha-FetoproteinAlpha-Fetoprotein• Major fetal protein (70 kd glycoprotein)
– Synthesized in the yolk sac, fetal liver, GI tract, kidney– Structurally related to albumin
• Used as a marker for neural tube defects• Moderate elevations in liver disease
(hepatitis/cirrhosis)• Concentrations >1000 g/L are associated with
hepatocellular carcinoma– Lower cutoff is used for screening
• Major fetal protein (70 kd glycoprotein)– Synthesized in the yolk sac, fetal liver, GI tract, kidney– Structurally related to albumin
• Used as a marker for neural tube defects• Moderate elevations in liver disease
(hepatitis/cirrhosis)• Concentrations >1000 g/L are associated with
hepatocellular carcinoma– Lower cutoff is used for screening

Combined AFP/hCGCombined AFP/hCG• Useful for differentiating germ cell tumors• Useful for differentiating germ cell tumors
AFP hCG
Yolk sac tumors nl
Choriocarcinoma nl Embryonal carcinoma Seminomas nl Teratoma nl nl
Nonseminomatous testicular tumor or

Carcinoembryonic antigenCarcinoembryonic antigen
• Family of up to 36 large, cell-surface glycoproteins
• Elevated in . . .– 70% of colorectal cancers
– 45% of lung cancers
– 50% of gastric cancers
– 40% of breast cancers
– 55% of pancreatic cancers
– 25% of ovarian cancers
– 40% of uterine cancers
• Family of up to 36 large, cell-surface glycoproteins
• Elevated in . . .– 70% of colorectal cancers
– 45% of lung cancers
– 50% of gastric cancers
– 40% of breast cancers
– 55% of pancreatic cancers
– 25% of ovarian cancers
– 40% of uterine cancers

Use of CEAUse of CEA
• Elevated in non-malignant conditions:– Cirrhosis, emphysema, rectal polyps, benign
breast disease, ulcerative colitis
• Most useful in staging and monitoring recurrence of disease
• Elevated in non-malignant conditions:– Cirrhosis, emphysema, rectal polyps, benign
breast disease, ulcerative colitis
• Most useful in staging and monitoring recurrence of disease

Carbohydrate AntigensCarbohydrate Antigens
• Glycoproteins expressed by tumor cells (surface or excretory)
• High molecular weight mucins (mucopolysaccaride protein)
• Glycoproteins expressed by tumor cells (surface or excretory)
• High molecular weight mucins (mucopolysaccaride protein)

Breast cancerBreast cancer
• Most common malignancy in U.S. women (7% of women develop breast cancer by age 70)
• Episialin is expressed by mammary epithelium
• CA 15-3, CA 549, and CA 27.29 are three distinct epitopes on episialin
• Most common malignancy in U.S. women (7% of women develop breast cancer by age 70)
• Episialin is expressed by mammary epithelium
• CA 15-3, CA 549, and CA 27.29 are three distinct epitopes on episialin

Specificity of episialin markersSpecificity of episialin markers
Sensitivity Specificity
CA 15-3 69% Pancreatic, lung, ovarian, colorectal, liver
CA 549 77% Ovarian, prostate, lung
CA 27.29 58% 98% (FDA –approved for monitoring recurrence)

CA 125CA 125
• High MW glycoprotein recognized by mAb OC125– Isolated from a serous ovarian tumor
• Elevated in 50% of stage I ovarian cancer• Elevated in 90%+ of stage II, III, and IV• Overall, sensitivity 95%; specificity 82%;
PPV 78%; NPV 91%.
• High MW glycoprotein recognized by mAb OC125– Isolated from a serous ovarian tumor
• Elevated in 50% of stage I ovarian cancer• Elevated in 90%+ of stage II, III, and IV• Overall, sensitivity 95%; specificity 82%;
PPV 78%; NPV 91%.

DU-PAN-2DU-PAN-2
• 100-500 kd mucin (80% carbohydrate)• Found mainly in pancreatic and biliary
epithelium– Also in breast, bronchi, salivary glands, stomach,
colon, intestine
• 60% sensitivity for pancreatic cancer• 45% sensitivity for biliary tract cancer• 44% sensitivity for hepatocellular carcinoma
• 100-500 kd mucin (80% carbohydrate)• Found mainly in pancreatic and biliary
epithelium– Also in breast, bronchi, salivary glands, stomach,
colon, intestine
• 60% sensitivity for pancreatic cancer• 45% sensitivity for biliary tract cancer• 44% sensitivity for hepatocellular carcinoma

Blood group antigensBlood group antigens
CA 19-9 Sensitivity 80% for pancreatic cancer;, 30% for colorectal cancer
CA 19-5 GI, pancreatic, ovarian cancer
CA 50Sensitivity 90% for pancreatic cancer; as high as 73% for Duke’s stage C or D colon cancer. Also elevated in esophageal, liver, gastric cancer
CA 72-4 Sensitivity 40% in GI cancer, 40% in lung cancer, 36% in ovarian cancer
CA 242 Sensitivity 75% for pancreatic cancer, 70% for colorectal cancer, 44% for gastric cancer

Other tumor markersOther tumor markers
• Oncogenes– ras, HER-2/neu, bcl-2, c-myc
• Suppressor genes– Retinoblastoma, p53, BRCA1 and 2
• Receptors– ER/PR
• Oncogenes– ras, HER-2/neu, bcl-2, c-myc
• Suppressor genes– Retinoblastoma, p53, BRCA1 and 2
• Receptors– ER/PR

Oncogene associationsOncogene associations
N-ras AML, neuroblastoma
K-ras Leukemia, lymphoma
c-mycB, T-cell lymphoma, small cell lung cancer
HER-2/neu Breast, ovarian, GI cancer
bcl-2 Leukemia, lymphoma

Pancreatic cancerPancreatic cancer
• Fourth most common cause of cancer deaths in men (fifth in women)– Incidence is increasing worldwide– 2:1 male preference
• Early diagnosis is unusual– Epigastric pain and significant weight loss are
the most common presenting signs
• 1 year survival is <10%; 5 year is 2%.
• Fourth most common cause of cancer deaths in men (fifth in women)– Incidence is increasing worldwide– 2:1 male preference
• Early diagnosis is unusual– Epigastric pain and significant weight loss are
the most common presenting signs
• 1 year survival is <10%; 5 year is 2%.

Cancer incidence and mortality in the United States (cases per 100,000)
Males Females
Site Incidence Deaths Incidence Deaths
Lung 91.5 (2) 57.7 (1) 52.0 (2) 41.0 (1)
Prostate 160.6 (1) 33.9 (2)
Breast 1.3 0.3 131.9 (1) 28.8 (2)
Colon/rectum 67.4 (3) 26.3 (3) 49.0 (3) 18.5 (3)
Pancreas 12.1 12.2 (4) 9.5 9.3 (4)
Source: Cancer 2002;94 (1999 data)

Incidence and mortality of GI/pancreatic tumors (1999 data)
Site New Cases (est.) Deaths (actual)
Colon/rectum 129,400 57,155
Pancreas 28,600 29,081
Stomach 21,900 12,711
Esophageal 12,500 11,917
Source: SEER Cancer Statistics Review 1973-1999

Laboratory values in pancreatic cancer
Laboratory values in pancreatic cancer
• Serum amylase is usually elevated, but only after significant progression of the disease– Does not distinguish between pancreatitis and carcinoma
• At least half of pancreatic adenocarcinomas are ductal and mucin-producing– CA19-9 is the best marker (80-90% sensitivity)
• 5% are endocrine (islet cells) and may be hormone secreting– Insulinoma (β-islet cells), glucagonoma (-islet cells),
somatostatin, calcitonin, ACTH
• Serum amylase is usually elevated, but only after significant progression of the disease– Does not distinguish between pancreatitis and carcinoma
• At least half of pancreatic adenocarcinomas are ductal and mucin-producing– CA19-9 is the best marker (80-90% sensitivity)
• 5% are endocrine (islet cells) and may be hormone secreting– Insulinoma (β-islet cells), glucagonoma (-islet cells),
somatostatin, calcitonin, ACTH