International Rehabilitation Council for Torture Victims -...
43
SCIENTIFIC ARTICLE T ORTURE Volume 21, Number 2, 2011 98 Table of contents Introduction Background and history The complexity of rehabilitation: Some of the variables The challenges Designing outcome studies: study validity Programme definitions and examples Outcomes and indicators Research strategies Literature review Examples of instruments available Recommendations for the future Acronyms Website resources References Introduction The authors of this document intend to review the history of evaluation of torture treatment programmes, discuss the chal- lenges, and identify the research conducted to evaluate services. We outline research designs to measure outcome, including symptoms, level of function, and satisfac- tion. Research design, not data analysis, is the focus of this desk study. The outcomes research literature is summarized and cat- egorized. Finally, we discuss the advantages and limitations of the most commonly used assessment instruments, some of them cul- turally-appropriate, and recommend the best approaches to measure outcomes of treat- ment for torture survivors. This document intends not only to pro- vide the context in which outcome research has been conducted in the past, but how centres can move forward today despite limi- tations and obstacles. Background and history Since the 1970s, programmes for the reha- bilitation of politically-motivated torture sur- vivors around the world have been treating survivors of torture. However, the context in which rehabilitation occurs affects the perception of torture’s sequelae, diagnosis, treatment, and prognosis. Treatment of torture survivors occurs in their countries Evaluating the services of torture rehabilitation programmes: History and recommendations James M. Jaranson, M.D., M.A., M.P.H. & José Quiroga, M.D.
Transcript of International Rehabilitation Council for Torture Victims -...

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
198
Table of contentsIntroductionBackground and historyThe complexity of rehabilitation:Some of the variablesThe challengesDesigning outcome studies: study validityProgramme definitions and examplesOutcomes and indicatorsResearch strategiesLiterature reviewExamples of instruments availableRecommendations for the futureAcronymsWebsite resourcesReferences
IntroductionThe authors of this document intend to review the history of evaluation of torture treatment programmes, discuss the chal-lenges, and identify the research conducted to evaluate services. We outline research designs to measure outcome, including symptoms, level of function, and satisfac-tion. Research design, not data analysis, is the focus of this desk study. The outcomes research literature is summarized and cat-egorized. Finally, we discuss the advantages and limitations of the most commonly used assessment instruments, some of them cul-turally-appropriate, and recommend the best approaches to measure outcomes of treat-ment for torture survivors.
This document intends not only to pro-vide the context in which outcome research has been conducted in the past, but how centres can move forward today despite limi-tations and obstacles.
Background and historySince the 1970s, programmes for the reha-bilitation of politically-motivated torture sur-vivors around the world have been treating survivors of torture. However, the context in which rehabilitation occurs affects the perception of torture’s sequelae, diagnosis, treatment, and prognosis. Treatment of torture survivors occurs in their countries
Evaluating the services of torture rehabilitation programmes:
History and recommendations
James M. Jaranson, M.D., M.A., M.P.H. & José Quiroga, M.D.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
199
of origin, as well as in countries of both initial and final resettlement. Allodi (1991) defines two categories of treatment settings geographically: 1) “The North,” mostly countries of final resettlement, such as the industrialized nations in the continents of Europe, North America, and Australia, and 2) “The South,” mostly totalitarian “Third World” countries where torture is practiced. Allodi states that, in “The North,” torture was viewed as having the medical and psy-chological consequences of a traumatic stress, and treatment followed this model. In “The South,” on the other hand, torture was viewed as a component of the socio-politi-cal process, requiring preventive action and social change. It is important to remember that government-sanctioned torture uses the individual to repress and control the larger society and that both the individual and the society are affected.
The first programmes were in South America. In Chile, on September 11, 1973, the democratic government of Salvador Al-lende was overthrown by one of the more repressive dictatorships in the western hemi-sphere. A month later on October 19, 1973, the country’s first human rights organiza-tion, the Committee of Cooperation for Peace was created. The committee through the “Vicaria de la Solaridad” (Vicariate of Solidarity) gave legal, medical, economic, and spiritual assistance to victims of repres-sion. In 1975 the first torture rehabilitation programme under the name of “Founda-tion for Social Help of Christian Churches” (Fundacion de Ayuda Social de las Iglesias Cristianas or FASIC) was created (Reiter et al., 1986).
In Argentina the most repressive and bloody military dictatorship in Latin Amer-ica was in power from 1976 until 1983. It has been estimated that 30,000 people were “disappeared,” later tortured and killed.
The first human rights organization in Ar-gentina was the Mothers of the Plaza de Mayo, founded in April, 1977. The Mothers was an association of Argentinean mothers whose children disappeared during the Dirty War. In 1979, Dr. Diana Kordon started the “Group of Psychological Assistance to the Mothers of the Plaza de Mayo” (Grupo de Asistencia Psicologica de las Madres de la Plaza de Mayo) to psychologically help this group of women. This work continued until the creation in 1990 of the “Argentinian Team of Psychosocial Work” (Equipo Argen-tino de Trabajo e Investigacion Psicosocial or EATIP). In 1980 the “Center for Legal and Social Studies” (Centro de Estudios Legales y Sociales or CELS)) was founded to docu-ment and provide legal help to the victims and families of the repression (Reiter et al., 1986; Kersner D, 2002).
The democratic government of Uruguay was overthrown on June 27, 1973, and the military dictatorship and repression lasted until 1985. The “Service for Social Rehabili-tation” (Servicios de Rehabilitacion Social or SERSOC), founded in October of 1984, was the first rehabilitation center for survivors of torture in that country.
In the past two centuries, at least three major events paved the way in Europe for the development of the movement: 1) France, in 1789, adopted the first human rights declaration denouncing torture. Much of the rest of Europe adopted it soon after. 2) In 1863, swept along with the rising tide of humanism, the Red Cross became the first organization to treat wounded victims during war. 3) With the discovery of the atrocities in German and Japanese prisons and camps during World War II, public awareness of government-sanctioned torture grew and research on the long-term effects of concentration camp internment began (Jaranson, 1995). 4) In 1973, Amnesty In-

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1100
ternational officially recognized and first de-fined torture in its initial worldwide survey on torture. The universally accepted legal definition of torture was published in Article 1 of the Convention Against Torture in 1984 (Amnesty International, 1973).
A military coup overthrew the demo-cratic government of Greece in 1967 and a military junta seized power until 1975. Members of the opposition were subjected to severe repression and systematic torture. The first trial against a torturer since the Nuremberg trials began in Greece in August, 1975 (Amnesty, 1977a).
Elsewhere in Europe, a group of medi-cal doctors from Amnesty’s organization in Denmark published a report entitled “Evi-dence of Torture” (Amnesty International, 1977b) and subsequently, under the direc-tion of Dr. Inge Genefke, founded the Re-habilitation and Research Centre for Torture Victim (RCT) in 1982 and the International Rehabilitation Council for Torture Victims (IRCT) in 1985. At least 235 treatment programmes have been identified worldwide and 144 of them are currently members of the IRCT (Quiroga and Jaranson, 2005, and recent data of the IRCT).
In North America, the Canadian Centre for Victims of Torture (CCVT) in Toronto was informally organized in 1977 and be-gan assessing and treating torture victims in 1983. U.S. Amnesty International medical groups were founded in Los Angeles, San Francisco, Seattle, Washington and Boston in 1979-80. The Program for Torture Victims (PTV) in Los Angeles is the only survivor of these initial Amnesty groups. PTV began to document and treat Chilean survivors of tor-ture in 1980. The Center for Torture Victims (CVT) in Minneapolis was founded in 1985. Currently 26 groups are full members of the National Consortium of Torture Treatment Programmes (NCTTP).
The first descriptive study of victims of torture in the U.S. was presented at a symposium on “Research and practice in treatment and rehabilitation of survivors of torture, terrorism and hostage taking” at the 89th annual meeting of the American Psy-chological Association in Los Angeles, Au-gust, 1981. Later the results were published in a joint paper with Canada (Quiroga et al.,1981; Allodi et al.,1985).
Despite the long history of torture reha-bilitation throughout the world, only a small fraction of torture survivors actually receive treatment. Financial support for services never comes close to meeting the need. It is increasingly important for torture reha-bilitation centres to demonstrate that the resources are used most efficiently and effec-tively to help survivors. Otherwise, even the financial support available may be at risk.
The complexity of rehabilitation: Some of the variablesThe effects of torture on the individual have interacting social, political, cultural, economic, medical, psychological, and bio-logical dimensions. Nearly all clients have a major psychiatric disorder. Their course is chronic with exacerbations and remis-sions. They have multiple social problems: financial, housing, raising children, domestic strife, social isolation, etc. They may have multiple medical problems, some as a direct result of torture and others associated with severe stress, hypertension, and diabetes. The needs of survivors are multiple and, in response, the programmes have usually adopted a multidisciplinary approach. The components of these interventions vary sig-nificantly between centres as well as among the regions of the world.
The evidence that torture has psychiatric consequences is overwhelming but beyond the scope and intent of this review.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1101
Three overview studies will be cited here. In a meta-analysis, Steel et al. (2009) under-took a systematic review and meta-regression of the prevalence rates of PTSD and depres-sion in the refugee and post-conflict mental health field. Adjusting for methodological factors, reported torture emerged as the strongest factor associated with PTSD, fol-lowed by cumulative exposure to potentially traumatic events (PTEs), time since conflict, and assessed level of political terror. For de-pression, significant factors were number of PTEs, time since conflict-reported torture, and residency status. Johnson and Thomp-son (2008) provided a comprehensive and critical summary of the literature about the development and maintenance of post-traumatic stress disorder (PTSD) following civilian war trauma and torture. They found good evidence of a dose-response relation-ship between cumulative war trauma and torture and development and maintenance of PTSD, as well as some evidence that fe-male gender and older age are risk factors in development of PTSD. They also state that most epidemiologically sound studies found relatively low rates of PTSD. Some refugee variables could exacerbate symptoms of PTSD and contribute to their maintenance, while preparedness for torture, social and family support, and religious beliefs may all be protective against PTSD following war trauma and torture. Modvig and Jaranson (2004, Table 3.5) reviewed the percentage of traumatized persons with posttraumatic stress (PTS) diagnosis or significant symp-toms in population-based surveys or case-control studies (Ns > 100) and, in contrast to Johnson and Thompson, found rates as high as 43% current and 74% lifetime among 810 Bhutanese torture survivors in a refugee camp in Nepal (Van Ommeren et al., 2001).
In general, positive prognostic factors
include cultural, religious, political convic-tions, preparedness for torture (Basoglu, 1994) and effective coping strategies. Factors which negatively impact recovery include prior individual or family trauma or persecu-tion and dysfunctional personality traits. It is controversial whether the age at which the torture occurs makes a difference. Children and adolescents are potentially both more vulnerable and more resilient. Considerable work has attempted to identify what types of torture affect prognosis, but with limited success. The severity and protracted nature of torture do seem to negatively correlate with recovery (Mollica et al., 1998; Jaranson et al., 2004). However, after the torture has occurred, positive prognosis is associated with receiving treatment, achieving safety and security, such as a successful asylum claim, having stable life circumstances, and good social support. On the other hand, unstable life circumstances, discrimination, and allowing the perpetrators impunity are associated with negative outcome.
Because of the complexity of the sur-vivors and their circumstances and their individual prognostic factors, controlling for these factors is difficult if not impossible. Particularly in western countries, but also in the rest of the world, rehabilitation centres help survivors from many different coun-tries. To find large enough sample represent-ing a particular ethnic or cultural group is challenging.
The challengesStudies of the efficacy of different treat-ment approaches and of the indicators to measure successful outcomes have not been sufficiently or adequately completed. Few outcome studies exist, and all of them have limitations such as the lack of control groups, varying definitions of diagnostic cri-teria, poor or absent validation of assessment

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1102
instruments, small sample size, and other factors (Gurr and Quiroga, 2001).
Consequently, it is understandable that so little outcome research has been con-ducted, despite the long history of torture rehabilitation. Nonetheless, critics continue to voice their discontent with the status of outcome research in torture rehabilitation. One of the more vocal critics is Dr. Metin Basoglu, a psychiatrist, an experienced re-searcher in the field of trauma, and a zealous advocate of cognitive-behavioral therapy as the best treatment. His 2006 editorial in the British Medical Journal, “Little Outcome Evaluation Has Been Done in Torture Re-habilitation,” (Basoglu, 2006) generated dozens of responses from practitioners in the rehabilitation field, the vast majority ques-tioning his conclusion that, after 20 years of research, no progress has been demonstrated scientifically. This statement about the lack of outcome data potentially threatens the already limited funding available for serv-ices. Jaranson et al. (2007), for example, re-sponded to Basoglu’s editorial by stating:
1) Evidence-based treatments exist for symptom clusters but not for complex problems;
2) Rehabilitation of torture survivors is not equivalent to treating PTSD or depres-sion;
3) Rehabilitation centres for torture survi-vors offer multi-modal approaches to im-prove the lives of survivors in many ways; and
4) Clinicians avoid brief treatments, rec-ognizing the enormity of clients’ experi-ences and the consequences.
One might ask why, with all of these dif-ficulties, outcome studies should even be attempted. However, funders are increasing their requirements to demonstrate that serv-
ices at centres are effective and cost-efficient. Centres, of course, want to provide the best, most effective, and most efficient services possible.
Does Rehabilitation Work? We don’t know. Clinicians think so, but they have an investment in a positive outcome and are potentially biased. Clinicians see that their clients get better, but exactly why is unclear. If rehabilitation does work, what compo-nents are responsible? We don’t know what treatments are most effective.
Despite the prevalence of torture and its well-documented mental health conse-quences, until recently there has been rela-tively little scientific interest in the study of torture and its treatment. Nonetheless, the study of torture survivors may have impor-tant implications for human rights, theory, assessment, classification, treatment of trau-matic stress responses, and legal issues.
Why has so little priority been given to collecting outcome data? First of all, time and financial resources for research are scarce. Clinicians are often reluctant to pri-oritize research over direct clinical services, prevention and advocacy, may fear that ad-ditional questioning will re-traumatize cli-ents or breach their confidentiality, and have been reluctant to include untreated survivors in controlled trials, feeling a need to protect all survivors from re-traumatization (Ba-soglu et al., 2001). Other clinical issues for research include the importance of timing, trust, and sensitivity. Research can also af-fect treatment, whether it is integrated into the clinical programme or separated, and the research process can potentially re-trauma-tize the researchers themselves.
Studies of specific high risk groups among victims of organized violence, such as women, rape victims, children, orphans, family members, ex-soldiers, and others re-quire rigorous research methodology, often

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1103
costly research budgets, adequate sample sizes, academic expertise, and interdiscipli-nary collaboration.
Most torture rehabilitation programmes have neither the skilled research personnel nor the budget. Most donor organizations give funds only for the direct care of survi-vors and are not willing to finance necessary infrastructures for scientific research.
Studies conducted in refugee clinics and in other treatment settings rarely include control groups, generally have small samples, and are not designed to address the preva-lence of torture survival in communities.
Most of the information published on torture survival is descriptive. Few clini-cal outcome studies exist (Basoglu, 1998; Gurr and Quiroga, 2001). Estimates of the prevalence of torture have been unreliable and rarely attempted because epidemiologic studies are extremely difficult and often impossible to conduct. The sensitivity of the topic of torture makes it difficult to study, and refugees are challenging groups for re-search under any circumstances.
Some relatively recent publications help to elucidate and guide research in the field. Hollifield et al. (2002) reviewed the litera-ture measuring trauma and health status in refugees, analyzing 183 publications, concluding that most articles about refugee trauma or health are descriptive or include quantitative data from instruments with limited validity and reliability for refugees. Willis and Gonzalez (1998) reviewed the use of survey questionnaires to assess the health effects of torture. Spring et al. (2003) described an approach to gathering a sam-ple representative of refugee communities which are difficult to access. Sjolund et al. (2009) presented the results of a conference of experts, concluding that effect studies are urgently needed.
Designing outcome studies: study validityThe field of traumatic stress has experienced significant growth in the numbers of psy-chotherapy treatment studies conducted. The Conference on Innovations in Trauma Research Methods (CITRM), funded by NIMH in the mid-2000s, held a series of conferences to explore advances in the field of psychological trauma research. Several of the presenters published in the JTSS (Sonis et al., 2007; Schurr, 2007) and discussed ways to help both the readers of their work and psychotherapy researchers by reviewing key concepts in trial design that affect the internal validity of the research. The focus was on between-group randomized design and on outcome rather than process.
Outcome research in torture investigates possible cause-effect relationships between one or more groups of torture survivors re-ceiving a treatment compared with control groups not receiving treatment and requires strategies to control factors that influence the validity of inferences drawn from the findings. Torture outcome research has unique problems that create challenges in the design methods but it is still possible to conduct valid research.
Psychotherapy treatment outcome re-search should include features intended to control threats to internal validity, such as random assignment, fidelity to the manual, numbers of sessions, and well defined out-comes.
If it is not possible to use placebo control groups in outcome research, wait-list design may be used. This method controls for most internal validity threats.
A comparison design can be used where groups are assigned to usual care versus more complex care, usual care versus pro-longed exposure to care, or different type of psychotherapies. These designs permit infer-

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1104
ences of the additional benefits related to usual care.
Change can also occur for factors other than effectiveness of the treatment, or con-founding. Contemporary factors not related to treatment can interfere with the results and several factors may introduce bias to the internal validity of a study. For example, the natural history of disease, e.g., torture is a chronic condition with ups and downs, or the granting of political asylum usually decreases symptoms (Gangsei and Jaranson, 1996), and other life events can confound the results and decrease the validity. Other variables include the length and number of sessions, individual vs. group therapy, or dif-ferences between therapists. Contemporary factors not related to treatment can interfere with the results. Assessment and control of confounding is discussed in detail by Kurth and Sonis (2007).
For quality control, use of a manual is useful in psychotherapy research to facilitate consistent treatment delivery and for repli-cation and dissemination (Borkovec,1993; Schnurr, 2007). Of course, training, supervi-sion, and monitoring are an important part of this process.
Internal and external validity are the most important objectives in the selection of a research design and research instruments. The experimental approach is the most pow-erful research design because it controls the most important variables in torture outcome research but at the same time is most restric-tive, requiring a control group.
Validity is defined by the degree that the instrument measures what it is supposed to measure. Internal validity gives us assurance that the differences observed in the study are due to the intervention or treatment under investigation. External validity gives as assur-ance that the results of the study are general-izable beyond the subjects in the study. The
instrument must also be reliable, i.e., free of measurement errors.
Torture is a chronic process with exac-erbations and remissions of the symptoms through the years. A reactivation increases symptoms, and symptoms decrease during a controlled period.
Over time, the torture survivor may grow wiser, stronger, more experienced and better able to participate in interviews or answer questionnaires. In some studies the instrumentation changes between the pre- and post-test measurements. The group that drops out from the study may be different from the group that remains in the study. Each of these factors or their interactions could influence the results of the study.
The most important bias to the external validity of a study is the process of selection of participants in the research. Therefore, the validity of the study is related to the design method and the representativeness of sam-ple. Some design methods are more valid than others. The ideal design for outcomes study should be the experimental design with a random assignment to experimental and control groups.
Unfortunately, there are factors that make the selection of an experimental de-sign difficult. Even though we do not have a definitive study that shows the effectiveness of the treatment of torture survivors, we do have the clinical impression that treatment helps victims obtain relief of their symptoms and improvement in their functioning. By consensus, most clinicians and researchers believe that a control group is impossible be-cause refusing treatment to torture survivors is unethical.
In addition, the populations of torture survivors treated by the majority of those torture rehabilitation centres receiving refugees and asylum seekers from other countries are neither representative of the

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1105
total universe of torture survivors in the country of origin nor in the host country. In addition, the distribution of countries or ethnic groups receiving care in a center or programme varies from one year to the next. The small numbers, e.g., by country, demo-graphically, diagnoses, etc., can influence validity. Other factors include inconsistency of the data or inability to achieve cultural equivalence for questions or items. Finally, the difficulty separating an individual treat-ment from the overall intervention makes identifying the effect of a particular part of rehabilitation a challenging methodological issue.
Programme definitions and examplesIssues of concern for centres and funders include access to care, quality of care and cost of care.
To improve the quality of care we need to investigate: 1) Treatment efficacy (or clinical impact), which is measured at either individual or group level; 2) Treatment ef-fectiveness (or economic impact) which includes outputs, benefits, and outcomes; 3) Efficiency (or cost/ benefit analysis of the programme), which includes the inputs and can identify waste. Clinicians usually focus on the first, while administrators and funders tend to focus on the latter two.
Example: CliniciansA task force of senior clinicians from the United States was organized by David Kin-zie of the Oregon Health Sciences University and met annually during the years 2004-2006. Funded by the Langeloth Foundation, the purpose was two-fold: 1) to develop quality assurance criteria for torture treat-ment centres and 2) to develop a research plan to collect treatment outcome data across willing torture treatment centres in the U.S. This task force recommended sev-
eral principles be used by torture rehabilita-tion centres:
1) Measuring outcomes should be an inte-gral part of the care.
2) Practically, assessment must be inte-grated into the daily routine of the pro-gramme, not as separate research.
3) Outcome measurement should be part of a process which includes analysis and reporting of the data and improving the quality of care through education and training of the providers.
Dr. Kinzie commented on the difficulties of doing outcome of clinical efficacy: “Out-come study of medical and psychological treatments are inherently difficult. This is even more so with traumatized patients as the trauma varies in quality and quantity, resilience and social supports are unique, and unknown genetic factors play a role. For refugees, the difficulties are compounded by low literacy rates, prolonged traumas, loss of country, property, and ongoing stress in the host country. The variables are overwhelm-ing.” (unpublished).
Examples: Funding SourcesThe European Union (EU) (2008) has de-fined efficiency, effectiveness, impact and sustainability, concepts used to evaluate selected torture rehabilitation centres which the EU funded. The EU provides a consider-able amount of general operating funding for centres in Europe and in the developing world. Definitions follow:
Efficiency – Quality and adequacy of man-agement, suitable indicators or other tools of efficiency, management flexibility.
Effectiveness – Number of victims benefiting directly and indirectly, number of persons

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1106
benefiting from prevention activities through training and public awareness. Exchange of experiences, information, and practices among centres, effectiveness of regional projects.
Sustainability – Both financial and outcome sustainability improved. Visible signs of gov-ernment increasing their active support of torture survivors.
Impact – Effect on legislative and govern-mental changes, on prevention of torture, using suitable indicators or reporting tools of impact assessment. Any changes in mental-ity, awareness, or interpretation of torture in the more difficult countries.
Obviously, impact assessment is quite dif-ferent from monitoring or evaluating the efficiency or effectiveness of a programme, but the following chart provides some com-parisons (see Table 1).
The U.S. Office of Refugee Resettlement (ORR), administrator of the domestic fund-ing from the Torture Victims Relief Act, has required funded centres in the U.S. to docu-ment 17 data points. The Act was passed in 1998, and current funding has remained at $10M USD annually for domestic centres, in addition to another $10M USD for centres in the developing world and $7M USD for the UN Voluntary Fund for Torture Victims.
Outcomes and indicatorsPossible outcomes include symptom reduc-tion, quality of life, level of function, coping and resilience, social support, and client satisfaction. The most frequently measured outcomes include medical and psychological symptoms, level of functioning or disability, quality of life, and client satisfaction.
The mission of torture rehabilitation programmes has generally been to treat every survivor who requests care. For ethi-cal reasons programmes are unwilling to allocate a random control group, in spite of the fact that no one has proven the efficacy of the interventions. Nonetheless, some pro-grammes do have waiting lists, which could potentially be used as controls – although this presents ethical issues, as well.
The problem now faced is how to de-sign acceptable, experimental studies in the absence of a control group. The objective of measuring survivor (consumer) outcomes in torture rehabilitation programmes is to study the efficacy of the intervention compared to the goals of the programme. The informa-tion garnered should be used to improve the quality of services and care. Additional gains from measuring consumer outcomes include professional development and empowerment for the survivors of torture.
To improve the quality of care we need to investigate treatment efficacy (clinical impact) and treatment effectiveness (eco-
Table 1. Impact assessment vs. monitoring & evaluatin (Rovhe C, 1999).
Assessment Monitoring Evaluation Impact
Timing Frequently Periodically Infrequently, usually at the end of a project
Analysis Descriptive: inputs, outputs, activities
More analytical; Examines processes
Mainly analytical; Concerned with Long Term outcomes
Specificity Very specific, comparing a plan to its results
Also looks at processes
Less specific and considers external influences and events

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1107
nomic impact).Treatment efficacy can be measured at the individual and at the group level. Treatment effectiveness is measured as cost benefit and cost effectiveness of the programme to guide the allocation of re-sources. This type of evaluation uses a differ-ent methodology that is beyond the scope of this paper.
Programmes for the rehabilitation of tor-ture victims vary enormously in the specific types of therapeutic interventions utilized, sizes of the target populations, duration of the rehabilitation process, clarity and specifi-cations of goals, economic resources, profes-sional and staff manpower, data collection capabilities, and communications skills of the staff (Amris and Arenas, 2003).
Consumer outcomes measure the “ef-fect on a patient’s health status attributable to an intervention done by health profes-sionals or health services”. In other words, they measure the anticipated benefits after the implementation of the programme (An-drews, 1994).
Donald et al. (2002) have three basic criteria for the development of outcomes. Outcomes should 1) be congruent with the evidence, 2) be relevant for the level of ac-tion and stated clearly and concisely, and 3) have face validity to stakeholders.
Ideally, a separate research staff would develop and monitor outcome evaluation for a given torture rehabilitation centre. However, this is not often practical. In most situations, measuring outcomes should be an integral part of the care. Practically, the assessment must be integrated into the daily routine care of clients in the programme, not as a separate evaluation research compo-nent. In addition, the measure of outcomes should be a part of a process that includes an analysis and reporting of the outcome data, as well as incorporating the informa-tion in order to improve the quality of the
care through education and training of the providers. This methodology routinely used in health care is called “Continuous Qual-ity Development” and has been adopted as a national policy for the Regional Office for Europe of the World Health Organization (World Health Organization, 1993).
The best approach to evaluating the efficacy of the programme is a multidi-mensional, multidisciplinary measure of individual outcome. Another important area of evaluation and research is the percep-tion that the participants in a programme have of the outcome of their interventions. Professionals (service providers) often have a different assessment than the survivors (consumers) in relation to parameters such as quality of life, symptoms, and social skills (Stedman et al., 1997; Amris and Arenas, 2003). Some possible outcome domains include symptom reduction, quality of life, level of function, coping and resilience, so-cial support, client satisfaction, and cognitive ability.
In evaluation research, outcome meas-ures may include the application of some known scales and instruments before and after intervention. There are many instru-ments that can be used in each of these ar-eas of interest (See Examples of instruments available page 128). Several authors have defined some of the criteria for selecting a measurement or indicator for consumer outcome (Donald et al., 2002; Ciarlo et al., 1986; Green and Graceli, 1987; Andrews et al., 1994). Donald et al. (2002) have iden-tified ten criteria to guide in the develop-ment of outcome indicators, which should be congruent with the evidence, relevant for the level of action, stated clearly and concisely, have face validity to stockhold-ers, and be sensitive to changes over time, measurable, affordable, unique, and com-prehensive.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1108
The Consumer Outcome Project Advi-sory Group of the in Department of Mental Health and Family Services of Australia was created to review existing measures of consumer outcome. The group concluded that disability and quality of life were the most important outcomes to be measured, followed by consumer satisfaction and symp-toms. The group recommended the further testing of six instruments as potentially use-ful for routine outcome measurements (An-drews et al., 1994): Consumer measures in-cluded BASIS 32 (Symptoms Identification Scales), MHI (Mental Health Inventory) and the SF-36 (Short Form Survey); Pro-vider measurements included the HoNOS (Health of the Nations Outcomes Study), LSP (Life Skills Profile), and RFS (Role Function Scales). This is an example of how the Commonwealth Department approached this problem.
The choice of measurement instruments should be based on the specific objectives, outcomes, type of intervention implemented, and information needed, all of which will be unique to each programme.
Monzani et al. (2008) used the approach of the Australian Commonwealth Depart-ment to evaluate the effectiveness of com-munity mental health departments in the Lombardy region of Italy. Twice a year they surveyed 4,712 patients treated in ten men-tal health departments using the HoNOS. Overall, the mental health departments were effective in reducing HoNOS scores, and the main predictor of improvement was treat-ment, although length of care, gender, and diagnosis were weaker predictors.
Many instruments that are both valid and reliable can be used in different circum-stances.
There are also several publications that have analyzed the validity and reliability of each instrument and can be used for
reference in the selection of an instrument (Bowling, 1996; Bowling, 1997; Donald, 2002). Obviously, any outcome measure needs to be accepted by the professional staff and clients of the programme.
Instruments selected should be valid, reliable, standardized, translated and back-translated, and culturally equivalent. How-ever, these criteria are rarely met and, as a result, centres find themselves compromising the ideal scientific standards.
After a measure has been selected and implemented for a defined period of time, it should be evaluated to decide if it fulfills the goals of the research evaluation. Some programmes implement outcome measure-ments but do not systematically analyze the data.
Research strategiesWe have chosen to categorize the types of studies according to the classic text by Cook and Campbell (1979), as follows: Descriptive, Experimental, Quasi-Experimental Pretest-Posttest (One Group--including retrospec-tive chart reviews; More than One Group Randomized; More than One Group Non-Randomized; Qualitative (Phenomenology; Ethnography; Grounded Theory).
Descriptive StudiesThe purpose of a descriptive study is to delineate the facts and characteristics of a cohort of torture survivors. The study col-lects detailed factual information oriented to identify problems.
Most of the currently published torture literature is descriptive. A typical example is the study of Rasmussen on the medical aspects of torture. He describes, in the Dan-ish Medical Bulletin (Rasmussen, 1990), the torture methods and their relationship to symptoms and lesions in 200 victims of torture.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1109
In outcome descriptive studies the au-thor gives the details of the design of the programme and the indicators that will be used to measure the efficacy of the services given to torture survivors. An example is the Impact Assessment Study by Amris, but only two components of the five- part study were done and published (Amris and Are-nas, 2003; Amris and Arenas, 2005a, 2005b; Pedersen, 2005).
Experimental Design The experimental design is the gold standard model to measure the efficacy of an interven-tion because the researcher is able to control most of the confounding variables that affect the internal validity of an outcome study. The typical experimental design requires a random assignment of the torture survivors to experimental and control groups. Only the experimental group receives treatment. Treated torture survivors are compared with a control group of torture survivors who have not received treatment.
Random Selection Pretest Treatment Posttest
Experimental O1 X O2Control O1 O2
Torture rehabilitation programmes have generally concluded that is unethical to stop the treatment of a group of torture survivors to create a control group. Because of this limitation we have not found any papers in torture outcome literature that follow a true experimental design.
Quasi-Experimental DesignBecause an experimental design is not pos-sible for ethical reasons, the only alternatives are the quasi-experimental designs. The clas-sical study on quasi-experimental design is the book “Quasi Experimentation” by Tho-mas Cook and Donald Campbell (1979).
The quasi-experimental designs will always compromise the internal or external valid-ity of the research, and the researcher has to understand these limitations
One Group Pretest-Posttest DesignMost rehabilitation programmes have used a pre-post design in outcome studies of tor-ture survivors. Generally a group of torture survivors without a control group is evalu-ated with some measurement instruments before (pre-test) and after (post-test) a pe-riod of treatment.
Pretest Treatment Posttest
O1 X O2
Some studies have repeated the number of pre-test measurements as a way to use cli-ents as their own control; for example, using two pre- and one post-measures collected at three time points.
Pretest Treatment Posttest
O1 O2 X O3
More than One Group Pretest-Posttest: Either Randomized or Non-RandomizedAnother variation is dividing at random the torture population under study to different types of treatment or to a different intensity of treatment. One group receives a baseline care or usual care and the other (one or more groups) receives additional services. One avoids the ethical problem because all of them are treated. The researcher com-pares the outcomes among the groups.
Pretest Treatment Posttest
O1 X1 O2O1 X2 O2

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1110
More than One group Prettest-Posttest: Non-Randomized Control GroupIn this situation you compare two groups that are as similar as possible and you treat only one of them. An example should be to compare a group of survivors treated in a center with a similar ethnic group in the population that has not been treated.
Pretest Treatment Posttest
O1 X O2O1 O2
Qualitative StudiesQualitative Research seeks understanding of data that are complex and can be ap-proached only in context. The methods used in qualitative studies are in the areas of Phe-nomenology, Ethnography and Grounded Theory.
Phenomenology is a descriptive, reflex-ive, interpretative mode of inquiry on the personal experience lived by a participant. The information is gathered with interviews or in-depth conversations that are audio-taped for further analysis.
Ethnography provides means for explor-ing cultural or smaller sub-cultural units. The information is gathered through par-ticipant observation, field notes, interviews, videotapes or secondary documents, such as records, documents. The focus group is another option.
Grounded Theory develops theories or a theoretical framework grounded in data. Questions are about changing experiences over time. The researcher uses audiotaped interviews, participant and non-participant observations, conversations, and field notes as sources of information.
Literature review Nickerson et al. (2011) reviewed studies using two approaches to psychological treat-
ment of refugees: trauma-focused therapy (N= 10 with control group, N= 5 without control group) and multimodal interventions (N=4 without control group). Limitations included absence of or use of non-equivalent controls, small sample sizes, absence of post-treatment or long-term follow-up assess-ment, lack of blind assessment, restrictive in-clusion criteria, and lack of clear delineation of treatment components. They concluded that additional rigorous research into the ef-fectiveness of both modalities is needed in order to draw a firm conclusion. Crumlish and O’Rourke (2010) reviewed treatments evaluated with randomized, controlled meth-ology (N=10, total sample = 528) and found support for using narrative exposure therapy (NET) and cognitive behavioural therapy (CBT), although no treatment has a solid evidence base. Limitations included small sample size, variable trial quality (as rated with the Moncrieff scale,) rare use of power analysis, questionable minimization of bias, and infrequent use of culturally-validated outcome measures. Quiroga and Jaranson (2005), as part of a desk study reviewing the literature on torture rehabilitation from 1998 through 2004, initially reviewed 25 treatment outcome studies and were disap-pointed with the quality of most research. Dymi (2002), in a study at the University of Copenhagen and the IRCT intended to identify and compare methods of study suitable for analyzing treatment outcomes for rehabilitation of torture survivors, had previously reviewed outcome and related studies and reached a similar conclusion. He recommended that “the assessment of out-comes of rehabilitation treatment of torture survivors ought to make use of a combina-tion of qualitative and quantitative studies designed in accordance with the pattern of actual services offered by the respective centres.” (p. iv, abstract). Gurr and Quiroga

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1111
(2001), in the first desk study of torture re-habilitation literature until 1998, concluded that the effectiveness of available treatment programmes remained unproven. Measures differed across settings and changes could not be attributed to any single factor, includ-ing the intervention. Achievement of goals agreed upon by client and therapist was the best measure. Measurement of outcome was done by the service system, including man-agement, supervisor, as well as individual therapists, and the client, family, and cul-tural group. Better scoring of severity would be helpful in detecting changes over time.
In this desk study, we have not only in-cluded the 25 studies in Quiroga and Jaran-son (2005) but added more than 45 ad-ditional and more recent studies for a total of more than 70. Other ways of categorizing are important, such as whether the sample is entirely torture survivors or traumatized ref-ugees (which may include survivors), clinical or non-clinical, and U.S. or worldwide. The studies can be longitudinal or cross-sectional and can either demonstrate improvement or no improvement.
The organization of these studies in this desk study is first by torture survivors vs. traumatized refugees (which may also include torture survivors). Secondly, the studies are organized by research design in clinical samples. Within each subsection, the studies are arranged alphabetically by the primary author. Finally, fifteen studies which assess symptomatology in untreated popula-tions are summarized.
Torture survivorst
DescriptiveAlexander et al. (2007) described symptoms of anxiety, depression and PTSD among Bosnian (n=17) and Colombian (n=17) tor-ture survivors served by the Florida Center for Survivors of Torture, a programme of
Gulf Coast Jewish Family Services, Inc. Information from clients enrolled in the programme for six months or more was col-lated over a 14-month period in order to better prioritize and design services for the two distinct populations. On average, the Bosnians in this sample experienced tor-ture approximately 14 years ago, six years ago for the Colombians. Types of torture experienced by clients were documented using HURIDOCS and the number of fam-ily and friends affected by extreme trauma were counted. Employment and education levels were also identified. Findings showed that 100% of Bosnians were symptomatic for depression and over half experienced symptoms of PTSD compared to 35% of Colombians for depression and 18% for PTSD, despite the differences in years since the trauma occurred. High incidences of torture experienced by Bosnian clients and high numbers of family and friends affected support the high rates of symptoms. For the Colombian clients, high rates of employment and years of education, as well as earlier intervention, may contribute to their lower rates of symptoms. The two client groups are distinguished by the unique circumstances experienced by each, including punctuated wartime versus a prolonged insurgency, as well as the refugee versus asylum seeker ex-perience. This exploratory project informs the torture treatment model while recogniz-ing the importance of ethnic, political and cultural perspectives affecting the healing process.
Amris and Arenas (2003):The first phase of the Impact Assessment Study con-ducted by the International Rehabilitation Council for Torture Victims (IRCT) was an exploratory study of four centres to find the perception of torture and rehabilitation in different cultural settings by health profes-sionals and by clients. The results of the first

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1112
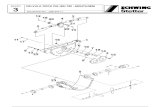
phase showed that all programmes used a multidisciplinary approach in the assessment and treatment of the clients, but the clinical practice and priorities varied, reflecting the professional profile and composition of staff across centres. The programmes used a broad spectrum of theories, methods, and treatment approaches. The clients had very concrete expectations of treatment such as pain relief, improved physical function, improved rela-tions with their families and interpersonal relationships within the community, and the capacity to return to work and provide for the family. Across centres the clients expressed satisfaction with the support, treatment, and rehabilitation they were provided. Only the first of five planned phases of the Impact As-sessment Study was completed. Figure 1 on the opposide page shows the overall plan.
The U.S. Office for Refugee Resettle-ment (ORR) has required the 27 torture treatment programmes that it funds to col-lect 17 descriptive data points, as follows:
17 Data points collected at intake as required by the U.S. Office for Refugee Resettlement (ORR)
Data Point 1. Client’s self-reported age when first sub-
jected to torture 2. Type of torture suffered 3. Primary complaint/presenting problem 4. Client’s sex 5. Immigration status at intake 6. Age at intake 7. Employment status at intake 8. Date of arrival in the U.S. 9. Country of origin10. Ethnicity11. Religion12. Housing status at intake 13. Total number of clients14. Number of clients by service category
(medical, mental health, social, legal)
15. Number of community trainings held16. Number of people trained by profession17. Number of hours contributed by pro
bono service
Eventually, ORR hopes to assess outcomes but is using this basic data collection as a first step.
Quasi-experimental: One group pretest-posttest Agger et al. (2009) tested the testimonial method, which represents a brief cross-cul-tural psychosocial approach to trauma, rela-tively easy to master in developing countries where torture is perpetrated and there are few resources for the provision of therapeu-tic assistance to the survivors. The method was first described in Chile by Cienfuegos and Monelli (1983) and has since been used in many variations in different cultural contexts. In this project the method was supplemented by culture-specific coping strategies (meditation and a ceremony). A pilot training project was undertaken be-tween Rehabilitation and Research Centre for Torture victims (RCT) in Copenhagen, Denmark, and People’s Vigilance Commit-tee for Human Rights (PVCHR) in Varanasi, India, to investigate the usefulness of the testimonial method. The project involved the development of a community-based testi-monial method, training of twelve PVCHR community workers, the development of a manual, and a monitoring and evaluation system comparing results of measures before the intervention and two to three months after the intervention. Twenty-three victims gave their testimonies under supervision. In the two first sessions the testimony was written and in the third session survivors participated in a delivery ceremony. Hu-man rights activists and community workers interviewed the survivors about how they

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1113
Phase I Interviews(clients, health prof.) Questionnaires
Explorative study
Drop-out „Experts„
Large scale multi-site study(quantitative-qualitative methodology)
Preliminary validation study
Prosessing data from study I and II
Adjustment of instrument
Prospective, baseline outcome study including 1-year follow-up applying the developed instrument
Clients Staff
Expert’sClients Staff
RelativesPhase II
Phase III
Phase IV
Phase V
Knowledge about the perception of torture and rehabilitation in different cultural settings from clients and health professionals
Knowledge about the perception of torture and rehabilitation in different socio-cultural settings from clients, health professionals and other significant persons
Indentifications of outcome indicators and development of a multidimentional assessment instrument for rehabilitation services
Effectiveness information on rehabilitation services provided to torture victims in different socoi-cultural settings
Figure 1. Five Phases og the impact of assessment stydy.
felt after the intervention. After testimonial therapy, almost all survivors demonstrated significant improvements in overall WHO-five Well-being Index (WHO-5) score. Four out of the five individual items improved by
at least 40%. Items from the International Classification of Functioning, Disability and Health (ICF) showed less significant change, possibly because the questionnaire had not been well understood by the community

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1114
workers, or due to poor wording, formula-tion and/or validation of the questions. All survivors expressed satisfaction with the process, especially the public delivery cer-emony, which apparently became a turning point in the healing process. Seemingly, the ceremonial element represented the neces-sary social recognition, re-connected the survivors with their community, and ensured that their private truth became part of social memory. Although this small pilot study without control groups or prior validation of the questionnaire did not provide high-ranking quantitative evidence or statistically significant results for the effectiveness of this version of the testimonial method, we did find it likely that it helps improve well-be-ing in survivors of torture in this particular context. A more extensive study is needed to verify these results, and better measures of ICF activities and participation functions should be used. Interviews with human rights activists revealed that it is easier for survivors who have gone through testimonial therapy to give coherent legal testimony.
Birck (2001) used standardized instru-ments and interviews to assess symptom change after two years of psychotherapy with 30 former patients at the Treatment Centre for Torture Victims (BZFO) in Berlin, Ger-many. Although intrusive PTSD symptoms had decreased, former patients were still highly symptomatic. Birck attributes this high symptom level to the phasic course of PTSD, which can be exacerbated by post-treatment stressful events.
Boehnlein et al. (1985) characterized the symptoms of PTSD one year after the first clinic visit, when the diagnosis was made for Cambodian concentration camp survivors at the Indochinese Refugee Clinic (now the Intercultural Psychiatric Clinic) in Portland, Oregon. Patients received pharmacologic and supportive therapy. At one year, two of
the 12 patients dropped out of treatment. Using the DIS, five of the 12 no longer met criteria for PTSD and three had improved symptoms (including one dropout), three were unchanged, and one had become worse (the other dropout). Improvement was es-pecially noted in the intrusive symptoms of PTSD.
Carlsson (2005) studied changes in symptoms of PTSD, depression, anxiety and quality of life over time and identified factors associated with mental health and health-related quality of life (QOL) of survi-vors treated at Rehabilitation and Research Centre (RCT) in Copenhagen, Denmark. (Carlsson JM, et al., 2006a; Carlsson JM, et al., 2005; Carlsson J, et al., 2006b). A concurrent cohort study interviewed 86 refugees attending a pre-treatment assess-ment at RCT in 2001-02, and 68 of them at 9 month follow-up (t9). The historical cohort study in 2002-03 included 151 of the 232 refugees attending a pre-treatment as-sessment at RCT in 1991-94. In both stud-ies, mental health sequelae and poor QOL persisted even many years after exposure to torture. High emotional distress was associ-ated with low QOL. No changes were found between the initial and the 9 month follow-up for the concurrent cohort, although the historical cohort (10 year follow-up) showed a slight decrease in psychiatric symptoms. High emotional distress was associated with low quality of life. Factors associated with emotional distress and low QOL were a large number of torture methods, lack of current occupation, and minimal social contacts. The concurrent cohort was also followed up at 23 months (t23) (Carlsson, 2008). There was an improvement in mental symptoms from t9-t23 (except for HSCL-depression). Still high levels of mental health problems persisted and no improvement in quality of life from t9-t23 was demonstrated.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1115
No consistent findings of predictors of changes in psychiatric symptoms and quality of life were found.
Cienfuegos and Monelli (1983), in per-haps the earliest attempt to study outcome of torture survivors, studied 39 tortured Chilean ex-prisoners and others from Chile who suffered trauma but not torture. The best results were found in those who were tortured (12 of 15 improved).
Curling (2005) explored the effectiveness of the use of an empowerment workshop, called Free to Grow1 (FTG), in the treat-ment of a group of torture survivors who had shown great reluctance to enter into psychotherapeutic interventions. Research into the effectiveness of the method was assessed using a series of tests measuring changes in empowerment, depression, anxi-ety and multiple operational definitions of health. Participants were also asked for feed-back using an unstructured self-report upon completion of the workshop. In addition, an exit interview was conducted after fol-low-up, five months after the first workshop session. Certain trends were detected despite the small numbers of participants (N=11) and incomplete questionnaires. According to most of the measures used, the intervention proved to have a positive sustained impact. At the exit interview all of the participants acknowledged experiencing increased levels of introspection and self-awareness, as well as a degree of growth and positive change. As a result, many participants were able to enter more mainstream psychotherapeutic interventions to deal with their remaining psychological and interpersonal problems.
Elsass (1998) interviewed 20 torture sur-vivors from the Middle East and their thera-pists from the Rehabilitation and Research Centre for Torture Victims (RCT) in Copen-hagen, Denmark. Although this study was much more complicated than reported here,
quantitative and qualitative outcome three months after the end of treatment found that 17 of 20 survivors evaluated treatment results as extremely positive.
Gangsei, Jaranson, et al. (1996, unpub-lished) at Survivors of Torture-International, San Diego, interviewed 26 asylum-seekers (12 women, 14 men) newly-admitted to San Diego center under a project funded by the California Endowment to improve access to medical services for torture survivors. Average age was 32 years with a range of 18 to 68. Participants received an average of 16 different services. Clients identified the number and severity of psychological and physical health problems and the difficulties these caused in work, daily activities, out-side activities, and relationships with others. After receiving services, clients again rated themselves on the same scales. Significant improvement in psychological and physical function and reduction in level of disability was found. Overall satisfaction was ex-tremely high (3.8 of 4.0). Half of the sample was granted asylum and showed far greater post-test improvement, despite starting with more problems.
Halvorsen and Stenmark (2010) pre-sented data on 16 torture survivors receiving 10 sessions of narrative exposure therapy (NET). Symptoms of PTSD and depres-sion, assessed by Clinician-Administered PTSD Scale (CAPS) and Hamilton Rating Scale for Depression (HRSD), decreased significantly from pre-treatment to 6-month follow-up, with Cohen’s d effect sizes of 1.16 and 0.84, respectively. Although treatment gains were moderate, further research on evidence-based treatments for PTSD and depression in refugee torture survivors is warranted.
Jaranson et al. (1995, unpublished) reviewed the charts of 220 clients at the Center for Victims of Torture (CVT) in

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1116
Minneapolis, Minnesota. Using independent clinician evaluators, overall 64% showed im-proved function, 35% were unchanged, and 3% declined. Of those who completed treat-ment, 86% showed improvement, while only 39% of those who left treatment prematurely showed improvement within the five-year study period (1991-95).
McColl et al. (2010) have presented the results of the IRCT’s (International Rehabilitation Council for Torture Victims) Global Health Project. This project part-nered five IRCT network rehabilitation centres (in Gaza, Egypt, Mexico, Honduras, and South Africa) working in very differ-ent contexts. The project provided local and regional training, facilitated knowledge exchange between centres, implemented psychotherapeutic treatment, and collected data to evaluate the interventions. In 2008, data from 306 patients and/or their records was collected, but 48% dropped out before the three month assessment and an ad-ditional 20% before the six month assess-ment, leaving 97 (32%) torture survivors to complete all three assessments. A high level of traumatic events was experienced (e.g. 64% with head trauma, 24% with ongoing torture injury problems), resulting in high prevalence of anxiety, depressive, PTSD, and somatic symptoms. Results indicated a mod-est drop in symptoms over the six months of the study.
Musisi et al. (2000) conducted a three-year (1996-99) retrospective study of 310 patients attending the Centre for Treat-ment and Rehabilitation of Torture Victims (ACTV) in Kampala. Treatment included psychotherapy, physiotherapy, and minimal pharmacotherapy. There was a significant re-duction in symptoms with treatment in most cases, but minimal improvement in some.
Reeler and Mbape (1998) found in a pilot study at Amani Foundation in Zim-
babwe that 12 adults torture survivors who completed brief psychotherapy showed im-provement, using the Clinician Administered PTSD Scale (CAPS).
Samsøe et al. (2007) monitored an ex-tended, personally designed, multidiscipli-nary treatment of 21 torture victims, earlier exposed to both physical and psychological torture, over nine months with assessment of outcome. The physiotherapy comprised elements such as massage, exercise on land, balance training and stimulation of proprio-ception, all aiming at regaining body aware-ness. The effect of treatment was measured using the fibrositis index. Non-parametric statistics using the Wilcoxon test was ap-plied. Prior to treatment the median score of the fibrositis index was 15 points (range 2-34). After nine months of multidisciplinary treatment the median score of the fibrositis index was 2 points (range 0-15). This de-crease in experienced muscle pain was statis-tically significant (p<.0001). Following nine months of treatment, only one torture victim in the study could be classified as suffering from fibromyalgia when applying the fibro-sitis index.
Quasi-experimental: More than one group pretest-posttest non-randomizedNeuner et al. (2010) evaluated whether stressors caused by the asylum procedure and psychological consequences of torture contribute to the maintenance of PTSD symptoms and interfere with treatment. In a pilot randomized controlled trial, the authors examined the efficacy of trauma-fo-cused treatment in 32 asylum-seekers with PTSD resulting from state-sponsored vio-lence and other traumatic events. Narrative exposure therapy (NET) was compared with treatment as usual (TAU), with a focus on stabilization and psychoactive medication. Six months after treatment, a significant

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1117
reduction of posttraumatic stress symptoms was found in the NET participants but not in the TAU group. Although treatment gains were moderate, these results indicate that NET is a promising approach for the treat-ment of PTSD in asylum-seekers living in unstable conditions.
Tol et al. (2009) examined the effective-ness of brief multi-disciplinary treatment for low-income torture survivors in Nepal using a naturalistic comparative design with help-seeking torture survivors and internally displaced persons assigned to a treatment and a comparison group respectively ( N = 192; treatment group N = 111, comparison group N = 81). Baseline measurements on psychiatric symptomatology, disability, and functioning and a five-month follow-up (N = 107; treatment group N = 62; comparison group N = 45), were employed. Interven-tion consisted of brief psychosocial services, minimal medical services and/or legal as-sistance. Study groups were generally com-parable and non-completers did not signifi-cantly differ from completers. The treatment group improved more than the comparison group on somatic symptoms, subjective well-being, disability and functioning, with mostly moderate effect sizes. Treatment was therefore moderately effective, reducing the nonspecific mental health consequences of torture, but disability scores remained high. For clients presenting with more severe mental health problems, other treatments in the resource-poor Nepali context need to be sought.
QualitativeMoio (2008) conducted a qualitative ap-proach to examine the consequences of state sponsored torture as experienced and made meaningful by women refugee survivors. In-depth interviews explored how women felt about life after torture: the meaning of the
experience over time, the personal, psycho-logical, and social effects, what was helpful to healing, and their outlook on the future. Findings indicated that the overwhelm-ing majority of participants demonstrated resiliency in response to external forces that challenged their internal coherence, systems of belief, and their re-adjustment in the aftermath of torture and forced migra-tion experiences. Results also showed that women were capable of resiliency by using pro-active problem solving, making deci-sions, and carrying out plans while still suf-fering distress. None of the women initially conceptualized their suffering as illness. Approximately half of the participants em-braced their diagnoses of PTSD and depres-sion after exposure to therapy. The other half remained skeptical of medicalizing their distress and took an instrumental approach for the purposes of managing symptoms. Most women found the therapeutic relation-ship helpful to healing because it provided a trustworthy, skilled individual who encour-aged and believed in their testimony and taught them practical skills. Participants overwhelmingly preferred working exclu-sively with women, whether in individual or group settings. Those participating in wom-en’s group therapy reconstituted the clinical environment into a social space promot-ing community for sharing gender-specific knowledge and mutual support. Implications for social work with survivors are discussed; contributions to the controversy over the validity and efficacy of PTSD for survivors of state sponsored torture are also discussed (http://gradworks.umi.com/33/46/3346914.html Retrieved 8/28/2010).
Traumatized refugeesDescriptive Grodin et al. (2008) seek to explore the po-tential value of Qigong and T’ai Chi practice

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1118
as a therapeutic intervention to aid in the treatment of survivors of torture and refugee trauma. The common effects of torture and refugee trauma are surveyed with a focus on post-traumatic stress disorder. An alternative theoretical framework for conceptualizing and healing trauma is presented. Evidence is reviewed from the scientific literature that describes how Qigong and T’ai Chi have been used in studies of the general popu-lation to alleviate symptoms that are also expressed in torture survivors. Observations are presented from a combined, simplified Qigong and T’ai Chi intervention with a convenience sample of four refugee survivors of torture. Preliminary observations from four cases and a review of the literature sup-port the potential efficacy of incorporating Qigong and T’ai Chi into the treatment of survivors of torture and refugee trauma.
Mueller et al. (2010) studied the mental health of failed asylum seekers (N = 40) and a matched sample of asylum seekers (N = 40). Asylum seekers and refugees often suf-fer from severe psychopathology in the form of post-traumatic stress disorder (PTSD). Since PTSD impacts memory functions, and because asylum applications rely on personal accounts, asylum seekers with PTSD are at greater risk of rejection than refugees. Participants were administered structured interviews on sociodemographics, flight, and exile as well as standardized questionnaires on PTSD, anxiety, depression and pain. Both samples were severely affected: >80% exhibited at least one clinically significant condition. Given the great vulnerability of these individuals, the long and unsettling asylum processes as practised in western host countries appears problematic, as does the withdrawal of health and social welfare benefits. Finally, high rates of psychopathol-ogy amongst failed asylum seekers indicates that refugee and humanitarian decision-
making procedures may be failing to identify those most in need of protection.
Pantic (1998) discussed integrative ge-stalt group therapy for Bosnian children and their families, helping them to overcome their problems, avoid long-term sequelae, and reach acceptance of their experiences in a search for meaning and identity.
Sehwail and Rasras (2002) of Palestine conducted a cognitive behavior group prima-rily of survivors of torture in Israeli prisons or otherwise traumatized by Israelis. A psy-chotherapist and co-therapist conducted the group. The authors comment that their pa-tients were more likely to accept education or counseling than to focus on the trauma, but many members disclosed their traumatic histories. Of the twelve group members, eight reported benefit and four were partially improved.
Quasi-experimental: one group pretest-posttest Abdalla and Elklit (2001) of the Danish Red Cross developed a psycho-educational project for 490 Kosovar refugee children. Intrusive memories and hypervigilance decreased, while self-satisfaction increased significantly.
Boehnlein et al. (2004) assessed treat-ment outcome by chart review in 23 Cam-bodian refugee patients with PTSD, all of whom had been treated continuously for at least ten years at the Intercultural Psychi-atric Program in Portland, Oregon. Using symptom, disability, and quality of life in-struments, thirteen were improved, but the remaining ten were still impaired.
Brune et al. (2002) reviewed 141 charts of consecutively treated refugees in Hamburg, Germany, finding that a firm belief system was an important predictor for better therapy outcome. Psychotherapy ranged from 3 months to 6 years with a mean of 2 years.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1119
Ekblad and Roth (1997) tested the as-sessment of PTSD and associated symptoms for immigrants and refugees at a psychiatric outpatient clinic in Sweden. Thirty-three were assessed at baseline, 22 at follow-up in one year using the SCID, HTQ, and HSCL-25. No changes were found in PTSD or depression.
Farrag et al. (2007) aimed to evaluate the effectiveness of the psychosocial reha-bilitation approach in helping clients with their mental health problems. The study compared the scores on tests for anxiety, de-pression and post-traumatic stress disorder obtained by a sample of 38 torture survivors before and after receiving services.
Folkes (2002) evaluated 31 refugee and immigrant clients’ retreatment, then again after 30 days. A significant decrease in all symptom subgroupings of PTSD was found.
Goodkind (2002) studied the effect of building upon Hmong refugee strengths, experiences, and interests, finding that this was effective in increasing quality of life and English proficiency, while decreasing distress levels.
Goodkind (2005) assessed the effective-ness of a community-based advocacy and learning intervention for Hmong refugees using a comprehensive, multi-method strat-egy, which included a within-group lon-gitudinal design with four data collection points and in-depth qualitative recruitment and post-intervention interviews. The inter-vention’s impact on five aspects of refugee well-being was examined: participants’ psy-chological well-being, quality of life, access to resources, English proficiency, and knowl-edge for the U.S. citizenship exam. Twenty eight Hmong adults and 27 undergraduate students participated together in the inter-vention, which had two major components: (1) Learning Circles, which involved cul-tural exchange and one-on-one learning
opportunities for Hmong adults, and (2) an advocacy component that involved under-graduates advocating for and transferring advocacy skills to Hmong families to in-crease their access to resources in their com-munities. Undergraduate paraprofessionals and Hmong participants worked together for six to eight hours per week for six months. Growth trajectory analysis revealed promis-ing quantitative findings. Participants’ qual-ity of life, satisfaction with resources, English proficiency, and knowledge for the U.S. citi-zenship test increased and their levels of dis-tress decreased over the course of the inter-vention. Mediating analyses suggested that participants’ increased quality of life could be explained by their improved satisfaction with resources. Qualitative data helped to support and explain the quantitative data, as well as providing insight into other outcomes and processes of the intervention. Policy, practice, and research implications are dis-cussed.
Goodkind (2006) studied refugees who resettle in a new country and face numerous struggles, including overcoming past trau-mas and coping with post-migration stres-sors, such as lack of meaningful social roles, poverty, discrimination, lack of environ-mental mastery, and social isolation. Thus, in addition to needing to learn concrete language skills and gain access to resources and employment, it is important for refugees to become a part of settings where their experiences, knowledge, and identity are val-ued and validated. The Refugee Well-Being Project (RWBP) was developed to promote the well-being of Hmong refugees by creat-ing settings for mutual learning to occur between Hmong adults and undergraduate students. The RWBP had two major compo-nents: (1) Learning Circles, which involved cultural exchange and one-on-one learning opportunities, and (2) an advocacy compo-

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1120
nent, which involved undergraduates advo-cating for and transferring advocacy skills to Hmong families to increase their access to resources in their communities. The project was evaluated using a mixed quantitative and qualitative approach. This article dis-cusses data from qualitative interviews with participants, during which the importance of reciprocal helping relationships and mutual learning emerged as significant themes.
Halcón et al. (1995; 2010, in press) found that groups of Somali and Oromo (Ethiopian) women responded positively to the health realization model of intervention. The health realization model is a commu-nity-oriented, psycho-educational interven-tion that shows promising results in a variety of settings and populations including high risk and traumatized individuals and groups. Based on a resiliency framework, this in-tervention assists people to put intrusive thoughts into a manageable perspective and improve their daily functioning through learning a process of thought recognition. (Related publication: Halcón et al., 1997).
Hermansson et al. (1996; 2002) inves-tigated mental health over time in exile and explored variables related to mental health in war-wounded male refugees admitted for somatic care in Sweden for greater than four weeks. Measures included a well-being scale, HSCL-25, and PTSS-10. At baseline N=61 and follow-up N=54 and N=44, no improvement was found in well-being, but prevalence of PTSD was estimated at 50%.
Hinton et al. (2006) described for Vi-etnamese refugees (a) how headache- and orthostasis-focused panic attacks are gener-ated, (b) a culturally sensitive treatment for PTSD with comorbid headache- and or-thostasis-focused panic attacks, and (c) the outcome of a treatment series. In a multi-ple-baseline, across-subjects design (N = 3), all patients demonstrated treatment-related
improvement of headache- and orthostasis-associated panic attacks and in the repeated-measures, within-subjects design, all patients greatly improved across treatment on meas-ures of psychopathology.
Jorgensen et al. (2010) used the In-ternational Classification of Functioning, Disability and Health (ICF) to develop an interdisciplinary instrument consisting of a Core Set, a number of codes selected from ICF, to describe the overall health condi-tion of traumatized refugees. The authors intended to test 1) whether this tool could prove suitable for an overall description of the functional abilities of traumatized refu-gees before, during, and after the interven-tion, and 2) whether the Core Set could be used to trace a significant change in the functional abilities of the traumatized refu-gees by comparing measurements before and after the intervention. In 2007, eight rehabilitation centres for traumatized refu-gees in Denmark agreed on a joint project to develop a tool for interdisciplinary docu-mentation and monitoring, including physi-cal, mental and social aspects of the person’s health condition. Seven centers completed the project. The project selected a Compre-hensive Core Set of 106 codes among 1,464 possible codes used by an interdisciplinary group of international and national experts in rehabilitation of traumatized refugees. The Comprehensive Core Set was furthermore reduced to a Brief Core Set of 32 codes. Six clients who fulfilled the inclusion criteria were randomly selected from each center. All were scored within a four week period after the start, before any intervention was initiated, and up to a month after the first scoring. The results from this project led to the conclusion that it is possible to develop an instrument based on the ICF classifica-tion. The instrument is useful for a general description of the total health conditions

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1121
(physical and mental functional ability as well environmental impact) of traumatized refugees. The tool helps to describe changes in the functional abilities used in connection with the preparation of the plan of action. The ICF Core Set for traumatized refugees has not yet been validated.
Kivling-Boden and Sundbom (2001, 2002) investigated the self-rated post-traumatic symptom levels compared with baseline and the subjects’ life situations, emphasizing the relationship between the labor market, social contacts, and knowl-edge of Swedish. Subjects were traumatized refugees from the former Yugoslavia seen as outpatients at a psychiatric unit in Sweden for a minimum of a month. Twenty-seven of the initial 52 were followed-up at three years and completed the HTQ at baseline and follow-up, and a clinical interview for PTSD at baseline. No difference in PTSD symptom scores or diagnosis of PTSD were found, but unemployment, social isolation, and dependence upon social welfare were as-sociated with PTSD symptoms at follow-up. On follow-up, social welfare dependence was high and unemployment at 32% was six fold the mainstream Swedish labor force. Posi-tive factors were housing and a reasonable knowledge of the Swedish language.
Mollica et al. (1990) evaluated changes in symptoms and perceived distress of 21 Cambodian, 13 Hmong/Laotian, and 18 Vi-etnamese patients in Boston before and after a 6-month treatment period. Most patients improved significantly, with Cambodians having the greatest and Hmong/Laotians the least reductions in depressive symptoms. Although psychological symptoms improved, many somatic symptoms worsened.
Onyut et al. (2005) created and evalu-ated the efficacy of KIDNET, a child-friendly version of Narrative Exposure Ther-apy (NET), as a short-term treatment for
children. Six Somali children suffering from PTSD aged 12–17 years resident in a refu-gee settlement in Uganda were treated with four to six individual sessions of KIDNET by expert clinicians. Symptoms of PTSD and depression were assessed pre-treatment, post-treatment and at nine months follow-up using the CIDI Sections K and E. Important symptom reduction was evident immediately after treatment and treatment outcomes were sustained at the 9-month follow-up. All patients completed therapy, reported func-tioning gains and were helped to reconstruct their traumatic experiences into a narrative with the use of illustrative material. NET may be safe and effective to treat children with war related PTSD in the setting of refugee settlement in developing countries.
Stepakoff et al. (2006) described, for Liberian and Sierra Leonean survivors of torture and war living in the refugee camps of Guinea, a psychosocial programme (1999-2005) with three main goals: (a) to provide mental health care, (b) to train local refugee counselors, and (c) to raise commu-nity awareness about war trauma and mental health. Utilizing paraprofessional counselors under the close, on-site supervision of ex-patriate clinicians, the treatment model blended elements of western and indigenous healing. The core component consisted of relationship-based supportive group coun-seling. Clinical interventions were guided by a three stage model of trauma recovery (safety, mourning, reconnection), which was adapted to the realities of the refugee camp setting. Over 4,000 clients were provided with counseling and an additional 15,000 were provided with other supportive serv-ices. Results from follow-up assessments indicated significant reductions in trauma symptoms and increases in measures of daily functioning and social support during and after participation in groups.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1122
Weine et al. (1998) studied 20 Bosnian refugees in Chicago before and after receiv-ing testimony psychotherapy, and at two and six months. The authors found significant decreases in PTSD diagnosis and symptom severity, depressive symptoms, and increased Global Assessment of Function (GAF) scores at post-treatment, with additional ef-fect on follow-ups. This is the first known study to use standardized instruments to evaluate the efficacy of a psychological treat-ment for a group of refugees with PTSD.
Quasi experimental:more than one group pretest-posttest randomizedBolton et al. (2007) assessed, from May-December, 2005, the effect of locally feasible interventions on depression, anxiety, and conduct problems among 314 adolescents, ages 14-17, who had survived war and displacement. In two camps for internally displaced persons in northern Uganda, lo-cally developed screening tools assessed the effectiveness of interventions in reducing symptoms of depression and anxiety, amel-iorating conduct problems, and improving function among those who met study criteria and were randomly allocated (N = 105, psy-chotherapy-based intervention [group inter-personal psychotherapy]; N = 105, activity-based intervention [creative play]; N = 104 wait-control group [individuals wait-listed to receive treatment at the study’s end]). Intervention groups met weekly for 16 weeks. Participants and controls were reas-sessed at the end of study. Primary outcome measure was a decrease in score (denoting improvement) on a depression symptom scale. Secondary measures were improve-ments in scores on anxiety, conduct problem symptoms, and function scales. Depression, anxiety, and conduct problems were assessed using the Acholi Psychosocial Assessment Instrument with a minimum score of 32
as the lower limit for clinically significant symptoms (maximum scale score, 105). Differences in change of the adjusted mean score for depression symptoms between group interpersonal psychotherapy and con-trol groups was 9.79 points (95% confidence interval [CI], 1.66-17.93). Girls receiving group interpersonal psychotherapy showed substantial and significant improvement in depression symptoms compared with con-trols (12.61 points; 95% CI, 2.09-23.14). Improvement among boys was not statisti-cally significant (5.72 points; 95% CI, –1.86 to 13.30). Creative play showed no effect on depression severity (–2.51 points; 95% CI, –11.42 to 6.39). There were no statistically different improvements in anxiety in either intervention group. Neither intervention im-proved conduct problems or function scores.
Dybdahl (2001) studied 42 mother-child dyads internally displaced in Bosnia-Herze-govina randomly assigned to psychosocial support with basic medical care compared with 45 dyads receiving only medical care. The treatment group showed positive effects on mothers’ mental health, children’s weight gain, and measures of children’s psychoso-cial functioning and mental health.
Drozdek (1997) studied a sample of 120 male concentration camp survivors from Bosnia-Herzegovina in Dutch asylum centres given early outpatient treatment for PTSD for six months. Three treatment groups (group therapy, medications, combi-nation group therapy and medications) and two control groups (refused treatment, did not meet PTSD diagnosis). Fifty randomly chosen subjects from the initial 120 were re-tested at the end of treatment and at three years. No differences were found among the treatment groups. The author concluded that treatment was effective in the short-term, less so in the long-term.
Neuner et al. (2004) studied the use of

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1123
narrative exposure therapy (NET), a short-term approach based on cognitive-behavioral and testimony therapy, and evaluated the efficacy of NET in a randomized controlled trial. Sudanese refugees living in a Ugandan refugee settlement (N = 43) and diagnosed as suffering from posttraumatic stress disor-der (PTSD) received either four sessions of NET, four sessions of supportive counseling (SC), or psychoeducation (PE) completed in one session. One year after treatment, only 29 percent of the NET participants but 79 percent of the SC group and 80 percent of the PE group still fulfilled PTSD criteria. These results indicate that NET is a promis-ing approach for the treatment of PTSD for refugees living in unsafe conditions.
Neuner et al. (2008) examined whether trained lay counselors could carry out ef-fective treatment of posttraumatic stress disorder (PTSD) in refugee settlement. In a randomized controlled dissemination trial in Uganda with 277 Rwandan and Somal-ian refugees diagnosed with PTSD, the authors investigated the effectiveness of psy-chotherapy administered by lay counselors. Strictly manualized narrative exposure therapy (NET) was compared with more flexible trauma counseling (TC) and a no-treatment monitoring group (MG). Fewer participants (4%) dropped out of NET treatment than TC (21%). Both active treat-ment groups were statistically and clinically superior to MG on PTSD symptoms and physical health but did not differ from each other. At follow-up, a PTSD diagnosis could not be established anymore in 70% of NET and 65% TC participants, whereas only 37% in MG no longer met PTSD criteria. Short-term psychotherapy carried out by lay counselors with limited training can be ef-fective to treat war-related PTSD in refugee settlement.
Paunovic and Ost (2001) conducted the
first known randomized psychological treat-ment outcome study with a refugee sample. Six out of 20 were torture survivors. Both treatments showed large improvements on measures of PTSD, anxiety, depression, quality of life and cognitive schemas before and after treatment, and at six month follow-up. No difference between CBT and expo-sure therapy was found.
Quasi experimental: more than one group pretest-posttest non-randomizedArcel et al. (2003) studied two groups of internally displaced Bosnia torture survivors at the Centre for Torture Victims, Sarajevo. The first group (N = 65) was assessed from 1997-99, or two to four years after the end of the war in December 1995. The second group (N = 26) was assessed in 2000-01 or five to six years after the end of the war. Group 1 (N = 65), (three months pre to post assessment) was assessed two to four years after the war and Group 2 (N = 26), five to six years after the war. Both groups received intensive short-term treatment, Group 1 for three months, Group 2 for six months. Group 1 showed post-test improve-ment on almost all psychological symptoms, but Group 2, with longer treatment, had even more improvement except for depres-sive symptoms. Improvement in adaptive coping mechanisms occurred even with the shorter treatment.
Fox et al. (1998) evaluated home visits conducted with follow-up at 10, 20, and 33 weeks by school nurses and bilingual teach-ers to Southeast Asian refugee women in the U.S. For comparison, women who did not receive the home visits were twice evaluated for mental health status ten weeks apart. Home visits reduced depression for subjects compared with controls.
Hinton et al. (2004) examined the feasi-

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1124
bility, acceptability, and therapeutic efficacy of a culturally adapted cognitive-behavior therapy (CBT) for twelve Vietnamese refu-gees with treatment-resistant PTSD and panic attacks. These patients were treated in two separate cohorts of six with staggered onset of treatment. Repeated measures, Group X Time ANOVAs and between-group comparisons, indicated significant improve-ments with large effect sizes (Cohen’s d) for all outcome measures: Harvard Trauma Questionnaire (HTQ; d = 2.5); Anxiety Sensitivity Index (ASI: d = 4.3); Hopkins Symptom Checklist-25 (HSCL-25), anxiety subscale (d = 2.2); and Hopkins Symptom Checklist-25, depression subscale (d = 2.0) scores. The severity of culturally related headache-and orthostasis-cued panic attacks improved significantly across treatment.
Hinton et al. (2005) examined the therapeutic efficacy of a culturally adapted cognitive-behavior therapy for Cambodian refugees with treatment-resistant posttrau-matic stress disorder (PTSD) and comordid panic attacks using a cross-over design, with 20 patients in the initial treatment (IT) con-dition and 20 in delayed treatment (DT). Repeated measures indicated significantly greater improvement in the IT condition, with large effect sizes (Cohen’s d) for all outcome measures: Anxiety Sensitivity Index (d = 3.78), Clinician-Administered PTSD Scale (d = 2.17), and Symptom Checklist 90-R subscales (d = 2.77). Likewise, the severity of culturally-related neck-focused and orthostasis-cued panic attacks, including flashbacks associated with these subtypes, improved across treatment.
Igreja et al. (2004) examined the ef-fectiveness and feasibility of a testimony method to ameliorate post-traumatic stress symptoms. Participants (n=206) belonged to former war zones in Mozambique. They were divided into a case (n=137) and a
non-case group (n=69). The case group was randomly divided into an intervention (n=66) and a control group (n=71). Symp-toms were measured during baseline assess-ment, post-intervention and at an 11-month follow-up. Post-intervention measurements demonstrated significant symptom reduc-tion in both the intervention and the control group. No significant differences were found between the intervention and the control group. Follow-up measurements showed sustained lower levels of symptoms in both groups, and some indications of a positive intervention effect in women. A remarkable drop in symptoms could not be linked di-rectly to the intervention. Feasibility of the intervention was good, but controlling the intervention in a small rural community ap-peared to be a difficult task.
Kinzie and Leung (1989) described the results of clonidine-imipramine therapy for PTSD in 12 Cambodian refugees diagnosed with PTSD at the Indochinese Psychiatric Clinic (now the Intercultural Psychiatric Program) in Portland, Oregon. Imipramine was prescribed initially and, if symptoms persisted after one to two months, clonidine was added. Nine patients were followed-up using HDRS, PTSD, and a depression checklist adapted from the DSM-III-R. The majority no longer met criteria for depres-sion with decreases in Hamilton scores, while PTSD global symptoms improved in six patients, but only in two to the extent that DSM-III-R diagnoses were not met.
Knezevic and Opacic (2004) studied changes in PTSD and co-morbid symptoma-tology in 123 clients from CRTV IAN Bel-grade after three months of psychotherapy. The quality and intensity of symptomatology was measured in two time points, before treatment and after 12 psychotherapeutic sessions (three months) using self-report by clients as well as a structured clinical inter-

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1125
view by independent evaluators who did not take part in the psychotherapeutic process. The authors found a statistically significant reduction both in the intensity of PTSD symptomatology and the co-morbid symp-tomatology. These results were compared with the results of follow-up of the changes in identical symptomatology of internally displaced persons over a two-year period. The results from this quasi-control group reduced the possibility of attributing the re-duction in psychopathological indicators of the treated group to spontaneous recovery or to the effect of other beneficial influences outside of treatment.
Smajkic et al. (2001) studied 32 Bosnian refugees at a mental health clinic receiving open trials of Sertraline (N=15), Paroxetine (N=12), or Venlafaxine (N=5). Sertraline and Parexetine showed significant improve-ment at six weeks in PTSD symptom sever-ity, depression, and Global Assessment of Function (GAF), while Venlafaxine did not improve depression and had high side effect rates. All 32 still had PTSD diagnoses at six weeks.
Salo et al. (2008) examined the role of individual and group treatment and self and other representations in predicting post-traumatic symptoms and growth among 115 former Palestinian political prisoners. Twenty participated in individual therapy and 19 in group therapy; 76 belonged to the control group. The results showed that post-traumatic symptoms decreased only in the individual therapy, whereas no decrease was found in group therapy or control groups across 1 year. Somatic symptoms decreased generally, whereas no general or treatment-related change was found in posttraumatic growth. As hypothesized, representations characterized by positive contents (benevo-lent, ambitious, and not punitive) predicted decrease in symptoms and increase in post-
traumatic growth. Furthermore, positive content and mature, differentiated, and not ambivalent structure of representations pre-dicted decrease in posttraumatic symptoms and increase in posttraumatic growth in group therapy, but not in individual therapy. The role of cognitive-emotional reworking of interpersonal representations in trauma therapies is discussed.
Westermeyer (1988) studied a com-munity sample of matched pairs of Hmong refugees who had major depression, 15 treated and 15 without treatment. The pa-tient group had higher symptom levels prior to treatment and at follow-up reported fewer depressive symptoms than controls.
Symptom prevalence without intervention measured at >1 time The importance of the following studies is to emphasize the long-term implications of failure to provide treatment for torture survivors and traumatized refugees. These include assessing depression and other men-tal health symptoms as well as general health in community samples, PTSD, depression, disability in refugees living in camps, psy-chological and social needs for asylum seek-ers and refugees, and PTSD in war refugees living in reception centres. These 15 studies measured symptom prevalence at more than one time period when no intervention was provided. These studies provide a view of the natural history of selected populations which did not receive treatment.
Beiser et al. (1993) and Beiser and Hou (2001) examined the risk-reducing effect of unemployment and the protective effect of language facility in a community sample of Southeast Asian refugees recently arrived in Canada. Three time frames (1993 study: two to four years; 2001 study: 10 years) were used. At the time of the first follow-up, comparing 319 Canadians at the first fol-

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1126
low-up with the sample, 608 of whom com-pleted all three measurements (sample sizes 1,346, 1,169, and 647). Using the Canadian Refugee Resettlement Project symptoms inventory, prevalence of depression declined from 6.48% to 2.27%, unemployment rates declined, and English language proficiency increased over ten years.
Ekblad et al. (2000, 2002) charted psy-chological and social needs and constructed a model for care and support of newly-ar-rived asylum seekers and refugees. The au-thors studied 218 refugees from Kosovo in the Humanitarian Evacuation Programme a few months after their arrival in Sweden. At three months, 131 were assessed and 91 at six months using the HTQ, HSCL-25, GHQ, SOC-12, and AQ-RSV. Estimated levels of PTSD were similar at baseline and follow-up in this untreated population. De-pression, anxiety and aggression (PTSD) were common in these post-migratory Ko-sovars.
Hauff and Vaglum (1995) studied the prevalence and course of mental disorders among Vietnamese refugees using a model including variables from different research traditions. A consecutive community cohort of 145 Vietnamese boat refugees aged 15 and older were personally interviewed upon their arrival in Norway and three years later. Unexpectedly, no decline in self-rated psy-chological distress (SCL-90-R) was found and almost 25% suffered from psychiat-ric disorder and 17.7% from depression (Present State Examination). Female gender, extreme traumatic stress in Vietnam, nega-tive life events in Norway, lack of a close confidant, and chronic family separation were identified as predictors of psychopa-thology. The effects of war and persecution were long-lasting and compounded by ad-versity factors in exile. A uniform course of improvement in mental health after resettle-
ment cannot be expected in all contexts. The affected refugees need systematic rehabilita-tion. (See also Vaage et al., 2010)
Hinton et al. (1997) examined the im-pact of pre-migratory traumatic experiences and socio-demographic characteristics on fu-ture depression and compared the social pat-terning of depression in two ethnic groups. They used a stratified consecutive sample of Vietnamese and Chinese refugees from Vietnam (N=196) and followed up 114 be-tween 12 and 18 months using the depres-sion subscale of the HSCL-25. No change in depression scores was found, but older Vietnamese, single status, and pre-migratory veteran status at follow-up, and less profi-ciency in English at baseline were associated with depression.
Lie (2002) studied the changes in psy-chological symptoms and general health over three years as well as the impact of risk factors such as torture, trauma, and demo-graphic status on distress and social func-tion in 462 newly settled refugees, mainly Bosnians, in Norway. Using the HSCL-25, HTQ, PTSS-16, and GAF, 240 refugees showed unchanged symptoms of emotional distress, anxiety, depression, and psycho-logical function, but an increase in PTSD. Pre-migratory life-threatening trauma and post-migratory unemployment, unresolved family reunion, and reduced social contact increased risk for elevated mental symptoms and lower levels of psychological function at follow-up. Analyses for predictors of changes in mental health over time were only signifi-cant for traumatic events in Norway.
Mollica et al. (2001) studied 1) associa-tions between PTSD, depression, disability, baseline risk factors, and status at follow-up; 2) chronicity of psychiatric disorders and disability, and 3) the association between psychiatric disorders, disability, mortality, and emigration. Of a baseline sample of

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1127
534 Bosnian refugees initially interviewed in Croatian camps, the 376 followed-up at three years were administered the HTQ, HSCL-25, SF-20, and the WHO functional disability scale. The prevalence of PTSD, depression, and disability was still high, with 43% meeting DSM-IV criteria for depres-sion, alone or co-morbid with PTSD, and 16% who were asymptomatic at baseline were symptomatic for psychiatric disorder on follow-up. Mortality was associated with male gender, older age, and social isolation.
Nygard et al. (1995) studied the preva-lence and course of PTSD among 150 Bosnian war refugees living in Norwegian reception centres. Of the 150 administered a PTSD checklist at baseline, 134 completed follow up at six months and one year. The number of participants with PTSD in-creased from baseline for first follow-up and then stayed high.
Sondergaard et al. (2001) investigated the perception of life events/conditions in relationship to the health of 86 Iraqi refu-gees recently resettled in Sweden. Question-naires of life events and on-going difficulties, the SCID, CAPS, GHQ-28, HTQ, and IES were administered to 74 at baseline, 67 at three months, 57 at six months, and 53 at nine months. Positive mental health (GHQ-28) was associated with positive events outside Sweden, while negative health (GHQ-28) was associated with negative events within Sweden. Family reunion had a significant positive effect on self-rated health for those with PTSD.
Vaage et al. (2010) found that there is no long-term prospective study (>20 years) of the mental health of any refugee group. To investigate the long-term course and predictors of psychological distress among Vietnamese refugees in Norway, eighty Vi-etnamese, 57% of an original cohort inter-viewed in 1982 (T1)) and 1985 (T2), com-
pleted a self-report questionnaire prior to a semi-structured interview. Mental health was measured using the Symptom Checklist-90-Revised (SCL-90-R). The SCL-90-R mean Global Severity Index (GSI) decreased sig-nificantly from T1 to T3 (2005–6), but there was no significant change in the percent-age reaching threshold scores (GSI =1.00). Trauma-related mental disorder on arrival and the trajectory of symptoms over the first three years of resettlement predicted mental health after 23 years. Although the self-reported psychological distress decreased significantly over time, a substantially higher proportion of the refugee group still reached threshold scores after 23 years of resettlement compared with the Norwegian population. The data suggest that refugees reaching threshold scores on measures such as the SCL-90-R soon after arrival warrant comprehensive clinical assessment. (See also Hauff and Vaglum,1995).
Westermeyer et al. (1984, 1989, 1990, 1997) studied 97 of 102 Hmong refugees in Minnesota older than 16 years in 1977 and approximately 89 on follow-up at two and five to seven years using the Zung Depres-sion Scale and the SCL-90. Zung depres-sion scores decreased a first follow-up, then increased. SCL-90 scores increased in those with normal or borderline scores at baseline, but decreased for those with elevated scores at baseline. The largest change occurred at first follow-up, no change at second follow-up, but overall trend in SCL-90 subscale scores was improvement.
These studies evaluated: multidiscipli-nary and short-term multidisciplinary treat-ment; psychotherapy; psychiatric treatment – outpatient, pharmacology; psychotherapy versus medication; selective serotinergic re-uptake inhibitor (SSRI) treatment; out-patient psychopharmacology treatment for refugees; outpatient PTSD treatment;

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1128
culturally sensitive treatment for PTSD; cognitive-emotional reworking of interper-sonal representations; psycho-educational treatment; testimony: method/therapy/ psychotherapy; brief psychotherapy; nar-rative exposure therapy; integrative gestalt treatment; Qigong and T’ai Chi practice; Cognitive Behavioral Therapy (CBT) and CBT groups; culturally adapted CBT; belief systems model; psychosocial rehabilitation/treatment; thought field treatment; commu-nity intervention; health realization; somatic care; physiotherapy; home visit interventions; and empowerment workshops.
Examples Of Instruments AvailableThe selection of instruments to use is com-plicated. Dymi (2002) identified 88 potential instruments in domains of outcome (Appen-dix 7, pp. 49-50) selected from the text by McDowell and Newell (1996).
Fabiansen (2001), in research done at IRCT to identify instruments for use in a quantitative impact assessment, recom-mended the Harvard Trauma Questionnaire (HTQ) to measure PTSD in combination
with the Short Form-36 Health Survey (SF-36) to measure quality of life.
Unfortunately, cross-cultural validation is rare. Scales and questionnaires are sometimes translated and back-translated into additional languages but there is no current compendium of the change in sta-tus. Since most can be accessed by typing the name of the questionnaire or scale us-ing a search engine for the worldwide web, this may be the best way to get the latest information.
The following are examples of instru-ments which have been selected for use in research.
Symptom Checklists– Hopkins SCL-25 (anxiety and depres-
sion)—translated into more than 30 lan-guages with good psychometric proper-ties
– SCL-90– SCL-110– Health Symptom Checklist (HSC)– Symptoms Identification Scales (BASIS
32)
NOTE: Self-rating scales are problematic because of high illiteracy rates and lack of data from clinical observation.
PTSD Structured1) Clinician-Administered PTSD Scale
(CAPS) is the most frequently used by mental health professionals to evalu-ate development of PTSD and complex PTSD symptoms even after repeated events.
2) Watson PTSD Interview
NOTE: Clinician-administered scales are labor intensive and difficult to do in busy clinics.
Table 2. Number of outcome studies by research design
Torture Survivors
Traumatized Refugees
Descriptive 2 4
Experimental 0 0
Quasi-Experimental Pretest-Posttest
1 Group 16 21
> 1 Group Randomized
0 6
> 1 Group Non-Randomized
2 10
Qualitative
Ethnography 1 0

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1129
PTSD Rating scales1) Harvard Trauma Questionnaire (HTQ)
includes exposure to events, brain trauma, general posttraumatic symp-toms, and associated symptoms (complex PTSD) and has cut-off score for DSM criteria, translated into more than 30 lan-guages with good psychometric proper-ties.
2) Impact of Events Scale (IES)3) Mississippi Combat Scale4) Posttraumatic Stress Checklist-Civilian
Version (PCL-C) is a self-report Likert scale with 17 items and has shown high internal consistency and reliability as well as a strong correlation with PTSD diag-nosis using the CAPS
5) Many Others
NOTE potential problems: Cut-off scores vary by ethnic and patient group; Scoring for DSM-IV criteria (X symptoms from symp-tom group Y must be present – this might result in a negative or distorted finding, e.g., if avoidance is predominant, intrusion cri-teria might only be fulfilled later when the survivor is confronted with triggers; cultural and linguistic factors make a difference).
Anxiety Rating Scales1) Hopkins Symptom Checklist, Anxiety
Scale (HSCL-25) is short, well-validated, and translated into many languages.
2) Spielberger’s State-trait Anxiety Inven-tory
3) Hospital Anxiety and Depression Scale (HADS)
4) Anxiety disorder module of the Struc-tured Clinical Interview for DSM-IV (SCID)
Screening Scales For Use In Primary Care Settings1) Index of Psychological Distress of Santé
Québec (IDPESQ)
2) Prime-MD3) Self-Report Questionnaire (SRQ-20)
Depression Rating Scales1) Hopkins Symptom Checklist, Depression
Scale (HSCL-25) is short, well-validated, translated into many languages, and is the best documented in torture survivors
2) Zung Self-Rating Depression Scale3) Hamilton Depression Scale (HDS)4) Beck Depression Inventory (BDI)5) Hospital Anxiety and Depression Scale
(HADS)
NOTE: For the above scales, a distortion of results by items based on somatic symptoms is possible and could reflect physical injury sequelae (e.g., BDI), but less prominent in the HADS. Overlap is high with brain trauma and posttraumatic stress symptoms.6) Mood disorder module of the SCID
Depression Screening Scales1) Index of Psychological Distress of Santé
Québec (IDPESQ) is useful screening2) Prime-MD did not adequately distinguish
affective disorders when compared with the gold standard of clinician diagnosis.
3) Vietnamese Depression Scale (VDS) – Kinzie et al.
Cognitive Testing– Mini Mental Status Exam (MMSE) is a
very western ethnocentric 30-point scale. Attempts have been made to develop a shorter scale that is more culture-free. Westermeyer, Jaranson et al. developed a 13-point scale that is relatively culture-free but is neither validated nor trans-lated into languages other than English.
Quality of Life1) World Health Organization Quality of
Life (WHOQOL-Bref, 26-Item Measure)

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1130
2) Quality of Life Inventory (QOLI-B) Oc-cupation/work (level of function)
Coping/resilience– Minnesota International Coping Scale
(MICS)—Developed by Johnson et al., Refugee Population Study, University of Minnesota
Social Support– Duke-UNC Social Support
Client Satisfaction1) Client Satisfaction Questionnaire (CSQ-
8)2) Sheehan Treatment Experiences and Ex-
pectancies (2-Item Measure)3) Client Access to Services Questionnaire
(CAS-Q)
Family Function1) Sheehan2) “Families in Transition” questionnaire
developed by Robertson et al. of the Ref-ugee Population Study at the University of Minnesota
DiagnosisStructured and Semi-Structured Clinical In-terviews offer a reproducible standard with good test-retest reliability. The following have been validated in many languages and are seen as “gold standards” for diagnosis, including PTSD.
1) Structured Clinical Interview for DSM-IV (SCID), for use by experienced raters.
2) Composite International Diagnostic In-terview (CIDI) uses ICD-10 and DSM-IV classification systems--administered by non-professional raters.
3) Schedules for Clinical Assessment in Neuropsychiatry (SCAN), based on the Present State Exam (PSE) using ICD-10
and DSM-IV classification systems-ad-ministered only by trained clinicians.
NOTE: There are still problems with diag-nostic assessment tools, as has been shown in minor changes leading to major variations in prevalence shown by epidemiological surveys. This has important implications for assessing services needs.
Trauma History1) Harvard Trauma Questionnaire (HTQ)2) Trauma Symptom Inventory (TSI)
Occupation/work (Level Of Function)1) Short Form (SF-36, SF-12)2) Functional Impairment Scale – Medical
(FIS-M), to assess the extent to which major medical conditions interfere with functioning
3) Functional Impairment Scale – Psychiat-ric (FIS-P), to assess the extent to which PTSD symptoms interfere with function-ing
NOTE: The FIS scales were developed by Johnson et al. of the Refugee Population Study at the University of Minnesota
4) Life Skills Profile (LSP)5) Role Function Scales (RFS)6) Global Assessment of Function (GAF)7) Sheehan Disability Scale8) International Classification of Func-
tioning, Disability and Health (ICF), (complementary with the ICD diagnostic system). This important instrument is discussed in some detail below:
The ICF is a classification, developed by WHO, which describes health and associated condi-tions in terms of functioning instead of symp-toms or diagnosis. Therefore, the ICF can be applied to either healthy or disabled persons.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1131
The application of the ICF at the indi-vidual level can help assess a person’s level of function, plan interventions to maximize his/her functioning, evaluate the outcomes of an intervention, and self-evaluate capacity for mobility or communication. At the insti-tutional level, the ICF can help in education and training, for resource planning and de-velopment, for quality improvement, and for management and outcome evaluation. At the social level, the ICF can help document eligi-bility criteria for state or social benefits, affect social policy development such as legislation, regulations, guidelines, or needs assessments, or, in environmental assessment, changes in social policy, economic analysis, and research.
The ICF uses a bio-psycho-social model where the bodily functions, activities and participation of an individual are related to his/her health conditions, personal, and envi-ronmental factors.
Of the multiple body functions described in ICF, the most important for the study of torture victims are the mental functions.
ICF defines activity as the execution of a task by an individual and participation as the involvement in a life situation. Both activity and participation have limitations. Activity limitations are the difficulties an individual may have in executing activities and partici-pant restrictions are the problems that an individual may experience in his/her involve-ment in life situations.
The activities and participation are meas-ured in a qualifiers scale of five grades: In Grade 1 the person is normal without any limitations, in Grade 2 the person has mild, Grade 3 moderate, Grade 4 severe limita-tions, and Grade 5 complete limitation or dis-ability (World Health Organization, 2001).
Instruments Used By CentresAlthough now dated, Dymi (2002, p. 51)) catalogued the instruments used by IRCT
centres in Table 3 next page (minor cop-yedits by JMJ):
To assess anxiety and depression we rec-ommend the Hopkins Symptom Checklist 25 (HSCL-25), which has been translated into more than thirty languages, has good psycho-metric properties, and is relatively simple to administer. Very few instruments can claim this widespread use, and consequently the re-sults can be compared with other studies. The Harvard Trauma Scale (HTQ) has similar claims for the assessment of PTSD. Another useful PTSD rating scale is the Posttraumatic Stress Checklist-Civilian Version (PCL-C), which has 17 items based upon the DSM cri-teria for PTSD, and has shown high internal consistency and reliability. These instruments can be used for the client to self-report, but are sometimes administered by clinicians for survivors who are illiterate or when the scales are not translated into their languages.
For scales that must be used by the clini-cian rather than self-administered, we rec-ommend the Clinician-Administered PTSD Scale (CAPS), which is highly correlated with the self-administered PCL-C.
For cognitive testing, the Mini Mental Status Exam (MMSE) is about the only instrument available, but it has severe limita-tions when used cross-culturally.
For quality of life, the short version of the World Health Organization Quality of Life (WHOQOL-Bref) inventory has 26 items and has been used in many countries.
For programmes that do not wish to develop their own client satisfaction surveys, we recommend an 8-item instrument, the Client Satisfaction Questionnaire (CSQ-8).
For trauma history, the HTQ is recom-mended.
To assess level of function, we recom-mend the Short Form 12-item (SF-12) or the SF-36, the Global Assessment of Function (GAF), or the more complicated

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1132
Table 3. Health Measuring Instruments and databases actually being used by various Centres for Rehabili-tation of Torture Victims (incomplete data from a workshop in CPH 26 October 2001)
Names of Instrument Acronym What it is used for Centre/Country
1. The Self-Reporting Questionnaire SRQ-20 Measure physical, psychological and psychiatric status/symptoms and depression
Calabar, West Africa
2. The PTSD Questionnaire for Adults (Watson 1991) (ref. From Libby T. Arcel’s book)
DSM-III-R Measure of PTSD Eastern Europe
3. Harvard trauma questionnaire (ver-sion both in Chinese and in Eng-lish), developed by the Indochinese Psychiatry Clinic, Brighton Marine Public Health Center and the Har-vard Program in Refugee Trauma and Management, Lotus Founda-tion c 1991 Richard F Mollica MD
HTQ Measure of PTSD Chinese speak-ing refugee groups
4. (Simple data tables ... Instrument used?)
RESTART Center Tripoli Lebanon
5. Medical Assessment Sheet Used for refugees by UNHCR?
Measure physical, psychological and psychiatric status/symptoms and depression
Amman?
6. P.A.T. Client Registration/Referral Form
Measure physical, psychological and psychiatric status/symptoms and depression
Kampuchea
7. Rehabilitation (Types of torture documented in CVICT in 2000) Data on torture survivors provided services, in Nepal
Measure physical, psychological and psychiatric status/symptoms and depression
CVICT Nepal
8. Confidential Card for Client monitoring programme at CVICT in Nepal
Measure physical, psychological and psychiatric status/symptoms and depression
CVICT Nepal
9. The Self-Reporting Questionnaire (developed by WHO) Available in Arabic, French, Hindi, Portuguese, Somali and Spanish.
SRQ Measure general psychological Distress
?
10. The Self-Reporting Questionnaire English and Ndebele version
SRQ-8 ?
11. Hamilton Depression Scale (Hamil-ton 1960)
DSM-III Measure depression ?
12. Impact of Events Scale 8 Item Child/adolescent Scale (IES-8)
IES Measure of PTSD Measure of stress response syndromes, PTSD
?
13. Impact of Events Scale (15 ques-tions – Michael O’Sullivan)
IES Measure progress with private clients
?
14. The Social Adjustment Scale –Self-Report
SAS-SR

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1133
International Classification of Functioning, Disability and Health (ICF).
Recommendations For The FutureNickerson et al. (2011) emphasize the neces-sity of developing an evidence base using a multi-stage evaluation process which estab-lishes the efficacy of an intervention, then its impact, and finally develops implementation models. These authors warn that failing to systematically evaluate programs will result in “the stagnation of knowledge and en-trenchment of practices, some of which may be without demonstrated efficacy.”
Outcome research in torture is challeng-ing, but it is still possible to conduct valid research. When torture treatment centres conclude that is not possible to use random control groups, then the only option is to use quasi-experimental designs.
The few published studies have most frequently used a pre-post evaluation with one or more groups to measure the efficacy of the therapeutic intervention. For those studies with comparison groups, few are randomly selected, most are non-random. These latter designs permit inferences of the benefits of the study groups.
Several studies have shown that there is significant variation among centers located in the countries where torture is practiced compared with host country centres that receive refugees and asylum seekers. In the host countries, the treated population is usually much more heterogeneous than in those countries where torture occurs. The chosen therapeutic intervention can threaten the internal validity of a research design. It is very important in the design of a pre-post outcome study to include features intended to control threats to internal validity. In host countries, those of final resettlement, the ef-fect of receiving asylum is perhaps the most important confounding factor.
Before selecting the best instrument and research design, each center should analyze the population receiving care in their pro-gramme, the types of treatment delivered, and the outcomes they want to measure.
Perhaps most importantly, centres must start collecting data. Even if only descriptive or demographic data is available, this data should be collected. Eventually programme evaluation can develop into outcome of treatment efficacy and, finally, the impact of the programme.
How can we possibly do research that is scientifically excellent? When developing an outcome study, it is important to remember a caveat by Voltaire: “The best is the enemy of the good.” Even if you can’t do an evalu-ation that meets all of the scientific criteria for perfection, please start doing something.
AcronymsNCTTP National Consortium of Torture
Treatment ProgramsNPCT National Partnership for Community
TrainingNCB National Capacity Building ProjectIRCT International Rehabilitation Council
for Torture VictimsISHHR International Society for Health and
Human RightsORR Office of Refugee ResettlementEU European UnionWHO World Health OrganizationICD International Classification of Diseases
(by WHO)DSM Diagnostic and Statistical Manual (by
the American Psychiatric Association)
Website resourcesNational Capacity Building Project (NCB), Center for Victims of Torture (CVT)www.cvt.org, a technical resource funded by ORR conducts trainings on develop-ment, use, and interpretation of outcome

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1134
performance measurements and indicators and has developed a Performance Meas-urement Evaluation toolkit (http://www.healtorture.org). On this website there are four archived webinars on technical aspects of performance measurement and other re-lated resources for programmes for torture survivors. The NCB has created and reor-ganized the Organizational Self-Assessment Matrix with 28 capacity-building dimensions in seven major categories. Completing this matrix is required, along with a technical assistance plan, for the sub-grants offered to support the capacity-building activities of programmes. Training institutes are also provided each year and educational webinars are offered monthly. Other activities and re-sources can be found on the websites.
The National Partnership for Community Training (NPCT) www.acf.hhs.gov, funded by ORR, is oper-ated by Gulf Coast Jewish Family Services and its partners, the Majorie Kovler Center for the Treatment of Survivors of Torture, and the Harvard Program in Refugee Trauma. They surveyed federally-funded treatment programmes and member pro-grammes of the NCTTP to document the best, promising, and emerging practices and evaluation methods. Nineteen respondents started the online survey and 12 completed it, providing contact information for follow-up interviews. The partnership identified the following types of studies to assess torture rehabilitation services:
Anecdotal – An assessment using observa-tions and accounts from program staff, sur-vivors and providers;
Pre-Service Assessment – A means of assessing existing conditions before or during engage-ment in programme activities;
Pre/Post-Service Assessment – A means of as-sessing conditions prior to and immediately following engaging in programmeactivities;
Qualitative Documentation – A standard as-sessment using standardized methodology through narratives, quotes, statements etc.;
Quantitative Documentation – A standard as-sessment using numbers and quantities;
Randomized Control Trial – A study design in which patients/clients with similar de-mographic characteristics are randomly assigned to either a treatment group or a control group. Both groups receive the same baseline services, but the patients/clients in the treatment group receive an additional service and the control group does not re-ceive this additional service. This additional service is being studied.
Key themes in the narratives included multi-disciplinary approaches, culturally appropri-ate and competent services, holistic, inte-grated services, and strength-based services. Respondents reported providing 38 services or practices each with 66% evaluated. Pre-post service assessments were the most com-mon and case management and community training were the frequently evaluated. No RCTs were conducted.
The project has finished a compilation of the evidence-based literature about best, promising and merging practices in the torture treatment field with the goal of in-creasing the capacity for centres to provide effective treatment to survivors of torture. This document, entitled “Best, promising, and emerging practices: a compendium for providers working with survivors of torture”, has been published as a thematic issue of the Torture Journal.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1135
The National Consortium for Torture Treatment Programs (NCTTP) www.ncttp.org has collected five or six de-mographic data points since 2004. Recently, this group has increased its efforts to make it possible for all 34 centres members of the NCTTP to contribute to this effort and has expanded the scope to collect approximately 20 data points. At this stage, the effort is descriptive but the goal is to move towards multi-center outcome research.
Amnesty International ([email protected]) publishes an online Bulletin Report, Amnesty International News for Health Professionals, sent gratis to those who request it. This Report includes Am-nesty reports, statements and news articles not only on Torture but also on Children, the Death Penalty, Health Workers, Mental Health, Prisons and Detention Centres, Sexual Violence, Transmissible Diseases, and Water and Sanitation. Relevant conferences/courses and publications are cited. Send an email to [email protected] in order to be provided with contact details.
The International Society for Health and Human Rights (www.ishhr.com ) is an as-sociation for health workers who help those affected by human rights violations that aims to gather knowledge about the effects of hu-man rights violations, exchange experiences and information about treatment methods, and contribute to the development of psy-chosocial interventions on the individual and community levels. Members live in almost 50 countries. The website is a valu-able resource for papers, video presentations, training materials for health workers, as well as materials aimed at assisting victims of hu-man rights violations and dealing with com-munity reconstruction and disaster relief.
The International Rehabilitation Coun-cil (IRCT) (www.irct.org ), an umbrella for more than 140 independent torture treat-
ment organizations in over 70 countries, has an on-line newsletter, links to other organi-zations with similar interests, and other rele-vant information. Issues of the Torture Jour-nal, published by the IRCT, are available for review or articles can be downloaded.
References– Abdalla K, Elklit A (2001). A nation-wide screen-
ing survey of refugee children from Kosovo. Tor-ture 2001;11(2):45-9.
– Agger I, Raghuvanshi L, Khan SS et al (2009). Testimonial therapy: a pilot project to improve psychological wellbeing among survivors of tor-ture in India. Torture 2009;19:204-17.
– Alexander A, Blake S, Bernstein M (2007). The staying power of pain: a comparison of torture survivors from Bosnia and Columbia and their rates of anxiety, depression and PTSD. Torture 2007;17:1-10.
– Allodi F (1991). Terrorism and torture. In: Gha-dirian A-M, Lehmann HE, eds. Environment and psychopathology. New York: Springer Publishing Company, 1991:141-57.
– Allodi F, Randall G, Lutz E et al (1985). Physi-cal and psychiatric effects of torture: two medical studies. In: Stover E, Nightingale E, eds. The breaking of bodies and minds: torture, psychiat-ric abuses and the health professionals. New York: WH Freeman, 1985:58-78.
– Amris S, Arenas J (2003). The IRCT Impact assessment study (I-V). Outcome of torture reha-bilitation at specialised centres from the clients’ and health professionals’ perspective. Torture 2003;13(Suppl 1).
– Amris S, Arenas J (2005a). Impact assessment in rehabilitation of torture survivors. A long term research programme based in a global multi-center study design. Theoretical considerations. In: Berliner P, Arenas J, Haagensen JO, eds. Torture and organized violence. Contributions to a professional human rights response. Dansk psykologisk Forlag, 2005:124-54.
– Amris S, Arenas J (2005b). Impact assessment in rehabilitation of torture survivors. A long term research programme based in a global multi-center study design. Part II. An exploratory study of outcome of torture rehabilitation at specialized centers from clients’ and health professionals’ perspectives. In: Berliner P, Arenas J, Haagensen JO, eds. Torture and organized violence. Contri-butions to a professional human rights response, Dansk psykologisk Forlag, 2005:155-205.

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1136
– Amnesty International (1973). Report on torture. New York: AI U.S.A., 1973.
– Amnesty International (1977a). Torture in Greece. The first torture trial 1975. New York: Amnesty International U.S.A., 1977.
– Amnesty International (1977b). Evidence of tor-ture. London: Amnesty International Secretariat, 1977.
– Andrews G, Peters L, Teeson M (1994). Meas-urement of consumer outcome in mental health: a report to the National Mental Health Informa-tion Strategy Committee. Sydney: Clinical Re-search Unit for Anxiety Disorder, 1994.
– Arcel LT, Popovic S, Kucukalic A et al (2003). The impact of short-term treatment on torture survivors. The change in PTSD, other psycho-logical symptoms and coping mechanisms after treatment. ln: Arcel LT, Popovic S, Kucukalic A et al, eds. Treatment of torture and trauma sur-vivors in a post-war society. Sarajevo: Association for rehabilitation of torture victims - Centre for torture victims, 2003:135-57.
– Beiser M, Hou F (2001). Language acquisition, unemployment and depressive disorder among Southeast Asian refugees: a 10-year study. Soc Sci Med 2001;53:1321-34.
– Beiser M, Johnson PJ, Turner RJ (1993). Un-employment, underemployment and depressive affect among Southeast Asian refugees. Psychol Med 1993;23:731-43.
– Basoglu M (1998). Behavioural and cognitive treatment of survivors of torture. In: Jaranson JM, Popkin MK, eds. Caring for victims of torture. Washington DC: American Psychiatric Press, 1998.
– Basoglu M (2006). Little outcome evaluation has been done in torture rehabilitation. BMJ 2006;333:1230-1.
– Basoglu M et al (1994). Psychological effects of torture: a comparison of tortured with non tor-tured political activists in Turkey. Am J Psychiatry 1994;151:76-81.
– Basoglu M, Jaranson JM et al (2001). Torture and mental health: a research overview. In: Ger-rity E, Keane TM, Tuma F, eds. The mental health consequences of torture. New York: Klu-wer Academic/Plenum Publishers, 2001:35-62.
– Birck A (2001). Torture victims after psy-chotherapy – a two-year follow-up. Torture 2001;11(2):55-8.
– Boehnlein JK, Kinzie JD, Ben R et al (1985). One-year follow-up study of posttraumatic stress disorder among survivors of Cambodian concen-tration camps. Am J Psychiatry 1985;142:956-9.
– Boehnlein JK, Kinzie JD, Sekiya U et al (2004).
A ten year outcome study of traumatized Cam-bodian refugees. J Nerv Ment Dis 2004;192:658-63.
– Bolton P, Bass J, Betancourt T et al (2007). Interventions for depression symptoms among adolescent survivors of war and displacement in northern Uganda: a randomized controlled trial. JAMA 2007;298:519-27.
– Borkovec TD (1993). Between groups therapy outcome research: design and methodology. NIDA Research Monographs 1993;137:249-89.
– Bowling A (1996). Measuring disease. Philadel-phia: Open University Press, 1996.
– Bowling A (1997). Measuring health, a review of quality of life measurement scales. Philadelphia: Open University Press, 1997.
– Brune M, Haasen C, Krausz M et al (2002). Belief systems as coping factors for traumatized refugees: a pilot study. European Psychiatry 2002;17:451-8.
– Carlsson JM (2005). Mental health and health-related quality of life in tortured refugees (PhD thesis). University of Copenhagen, Denmark, 2005.
– Carlsson J (2008). Mental health changes in tortured refugees admitted to multidisciplinary treatment. Presented at the World Psychiatric Association Congress, Prague, Czech Republic, September 25, 2008.
– Carlsson JM, Mortensen EL, Kastrup M (2005). A follow-up study of mental health and health-related quality of life in tortured refugees in multidisciplinary treatment. J Nerv Ment Dis 193:651-7.
– Carlsson JM, Mortensen EL, Kastrup M (2006a). Predictors of mental health and quality of life in male torture refugees. Nord J Psychiatry 2006;60:51-7.
– Carlsson J, Olsen DR, Mortensen EL et al (2006b). Mental health and health-related quality of life. A 10 year follow up in tortured refugees. J Nerv Ment Dis 2006;194:725-31.
– Ciarlo JA, Edwards DW, Kiresuk TJ et al (1986). The assessment of client/patient outcome tech-niques for use in mental health programmes (Contract No 278-80-005) Washington, D.C.: National Institute of Mental Health, 1986.
– Cienfuegos J, Monelli C (1983). The testimony of political repression as a therapeutic instru-ment. Am J Orthopsychiatry 1983;53:43-51.
– Cook T, Campbell D (1979). Quasi experimenta-tion. Design and analysis for field settings. Bos-ton: Houghton Mifflin Company, 1979.
– Crumlish N, O’Rourke K (2010). A systematic

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1137
review of treatments of post-traumatic stress dis-order among refugees and asylum-seekers. J Nerv Ment Dis 2010;198:237-51.
– Curling P (2005). The effectiveness of empower-ment workshops with torture survivors. Torture 2005;15(1):9-15.
– Donald M, Dower J, Woodward R et al (2002). Outcome and indicators, measurements tools and databases. Australia: University of Queensland. Commonwealth Department of Health and Age-ing, 2002.
– Drozdek B (1997). Follow-up study of con-centration camp survivors from Bosnia-Herze-govina: Three years later. J Nerv Ment Dis 1997;185:690-4.
– Dybdahl R (2001). Children and mothers in war: an outcome study of a psychosocial intervention programme. Child Dev 2001;72:1214-30.
– Dymi K (2002). Methodological issues in assess-ing the outcome of health rehabilitation treat-ment of torture survivors. Copenhagen: IRCT, 2002.
– Ekblad S (2000). A survey of somatic, psycho-logical and social needs of mass displaced refu-gees from the Kosova province while in Sweden. Stress Research Reports, 293. Stockholm, 2000.
– Ekblad S, Roth G (1997). Diagnosing posttrau-matic stress disorder in multicultural patients in a Stockholm psychiatric clinic. J Nerv Ment Dis 1997;185:102-7.
– Ekblad S, Prochazka H, Roth G (2002). Psycho-logical impact of torture: a 3-month follow-up of mass-evacuated Kosovan adults in Sweden. Les-sons learnt for prevention. Acta Psychiatr Scand 2002;106 (Suppl 412):30-6.
– Elsass P (1998). The existence of a torture syn-drome: a quantitative and qualitative study of 20 torture survivors and their therapists. Torture 1998;8(2):58-64.
– European Union (2008). Evaluation on support to prevention of torture and torture rehabilitation centres. 2008.
– Fabiansen C (2001). Assessing the health impact of torture victims’ rehabilitation: a review of rel-evant available instruments. IRCT/DOCU docu-ment, 2001 (unpublished).
– Farrag M, Abdulkhaleq H, Abdelkarim G et al (2007). The psychosocial rehabilitation approach in treating torture survivors. Ethnicity and Dis-ease 2007;17(Suppl 2):85-7.
– Folkes CE (2002). Thought field therapy and trauma recovery. International Journal of Emer-gency Mental Health 2002;4(2):99-103.
– Fox PG, Cowell JM, Montgomery AC et al (1998). Southeast Asian refugee women and de-
pression: a nursing intervention. Int J of Psychiatr Nurs Res 1998;5:423-32.
– Gangsei, Jaranson et al (1996). Multidisciplinary treatment model: survivors of Torture Interna-tional. San Diego, 1996 (unpublished).
– Goodkind JR (2002). Promoting refugee well-be-ing: A community-based advocacy and learning intervention. Ann Arbor: Michigan State Univer-sity, Hmong Center, Multicultural Resources and Education, 2002.
– Goodkind JR (2005). Effectiveness of a commu-nity-based advocacy and learning programme for Hmong refugees. American Journal of Commu-nity Psychology 2005;36:77-93.
– Goodkind JR (2006). Promoting Hmong refu-gees’ well-being through mutual learning: valuing knowledge, culture, and experience. American Journal of Community Psychology 2006;37:387-408.
– Green RS, Gracely EJ (1987). Selecting a rat-ing scale for evaluating services to the chroni-cally mentally ill. Community Ment Health J 1987;23:91-102.
– Grodin M, Piwowarczyk L, Fulker D et al (2008). Treating survivors of torture and refugee trauma: a preliminary case series using Qigong and Tai Chi. J Altern Complement Med 2008;14:801-6.
– Gurr R, Quiroga J (2001). Approaches to torture rehabilitation. A desk study covering effects, cost-effectiveness, participation and sustainability. Torture 2001;11(Suppl 1):1-35.
– Halcón L, Robertson C, Jaranson J (1995). Inno-vative refugee stress & coping intervention: pilot study. University of Minnesota, School of Nurs-ing, 1995.
– Halcón L, Robertson C, Monson K et al (2007). A Theoretical Framework for using Health Reali-zation to Reduce Stress and Coping in Refugee Communities. Journal of Advanced Holistic Nursing 2007;25:186-94.
– Halcón L, Robertson C, Monsen K. Evaluat-ing health realization for coping among refugee women. J Loss Trauma (in press).
– Halvorsen JØ, Stenmark H (2010). Narrative ex-posure therapy for posttraumatic stress disorder in tortured refugees: a preliminary uncontrolled trial. Scand J Psychol 2010;51:495-502.
– Hauff E, Vaglum P (1995). Organised violence and the stress of exile. Predictors of mental health in a community cohort of Vietnamese refugees three years after resettlement. Br J Psy-chiatry 1995;166:360-7.
– Hermansson AC, Thyberg M, Timpka T (1996). War-wounded refugees: the types of injury and

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1138
influence of disability on well-being and social integration. Med Confl Surviv 1996;12:284-302.
– Hermansson AC, Timpka T, Thyberg M (2002). The mental health of war-wounded refugees: an 8-year follow-up. J Nerv Ment Dis 2002;190:374-80.
– Hinton WL, Tiet Q, Tran CG et al (1997). Pre-dictors of depression among refugees from
– Vietnam: a longitudinal study of new arrivals. J Nerv Ment Dis 1997;185:39-45.
– Hinton DE, Tran M, Safren S et al (2004). CBT for Vietnamese refugees with treatment-resistant PTSD and panic attacks: a pilot study. J Trauma Stress 2004;17:429-33.
– Hinton DE, Chhean D, Vuth P et al (2005). A randomized controlled trial of cognitive-behavior therapy for Cambodian refugees with treatment-resistant PTSD and panic attacks: A cross-over design. J Trauma Stress 2005;18:617-29.
– Hinton D, Safren S, Pollack M et al (2006). Cog-nitive-behavior therapy for Vietnamese refugees with PTSD and comorbid panic attacks. Cogn Behav Pract 2006;3:271-81.
– Hollifield M, Warner T, Lian N et al (2002). Measuring trauma and health status in refugees. JAMA 2002;288:611-21.
– Igreja V, Kleijn WC, Schreuder BJ et al (2004). Testimony method to ameliorate post-traumatic stress symptoms. Community-based intervention study with Mozambican civil war survivors. Br J Psychiatry 2004;184:251-7.
– Jaranson J (1995). Governmental torture: status of the rehabilitation movement. Transcultural Psychiatric Research Review 1995;32:253-86.
– Jaranson J, Hubbard J, Popkin M (1995). Survi-vors of government-sanctioned torture: a study of referral patterns, descriptive characteristics, and service utilization of clients at the Center for Victims of Torture, 1991-95. 1995 (unpublished).
– Jaranson JM, Butcher J, Halcon L et al (2004). Somali and Oromo refugees: correlate of tor-ture and trauma history. Am J Public Health 2004;94:591-8.
– Jaranson JM et al (2007). Standard therapy for all torture survivors?: rapid response to M. Ba-soglu. Rehabilitation of traumatised refugees and survivors of torture. BMJ 2006;333:1230-1. BMJ 30 January 2007.
– Johnson H, Thompson A (2008). The develop-ment and maintenance of post-traumatic stress disorder (PTSD) in civilian adult survivors of war trauma and torture: a review. Clin Psychol Rev 2008;28:36-47.
– Jorgensen U, Melchiorsen H, Gottlieb AG et al (2010). Using the International Classification
of Functioning, Disability and Health (ICF) to describe the functioning of traumatized refugees. Torture 2010;20:1-20.
– Kersner D (2002). Los derechos humanos en la Argentina hoy. In: Paisajes del dolor, senderos de Esperanza. Buenos Aires: EATIP, 2002:31-5.
– Kinzie JD, Leung P (1989). Clonidine in Cam-bodian patients with posttraumatic stress disor-der. J Nerv Ment Dis 1989;177:546-50.
– Kivling-Boden G, Sundbom E (2001). Life situ-ation and posttraumatic symptoms: a follow-up study of refugees from the former Yugoslavia liv-ing in Sweden. Nord J Psychiatry 2001; 55:401-8.
– Kivling-Boden G, Sundbom E (2002). The relationship between post-traumatic symptoms and life in exile in a clinical group of refugees from the former Yugoslavia. Acta Psychiatr Scand 2002;105:461-8.
– Knezevic G, Opacic G (2004). Changes in the intensity and frequency of psychiatric prob-lems related to traumatic experience after three months of treatment. In: Zeljko S, Goran K, Vladimir J et al, eds. Torture in war: conse-quences and rehabilitation of victims: Yugoslav experience. Belgrade: IAN Center for Rehabilita-tion of Torture Victims, 2004:221-32.
– Kurth T, Sonis J (2007). Assessment and control of confounding in trauma research. J Trauma Stress 2007;20:807-20.
– Lie B (2002). A 3-year follow-up study of psychosocial functioning and general symp-toms in settled refugees. Acta Psychiatr Scand 2002;106:415-25.
– McColl H, Higson-Smith C, Gjerding S et al (2010). Rehabilitation of torture survivors in five countries: common themes and challenges. Inter-national Journal of Mental Health Systems, June 18, 2010. www.ijmhs.com/content/4/1/16.
– McDowell I, Newell C (1996). Measuring health: a guide to rating scales and questionnaires. Ox-ford: Oxford University Press, 1996.
– Modvig J, Jaranson JM (2004). A global perspec-tive of torture, political violence and health. In: J Wilson, Drozdek B, eds. Broken spirits: the treat-ment of traumatized asylum seekers, refugees, war and torture victims. New York: Brunner-Routledge Press, 2004:33-52.
– Moio JA (2008). Resiliency and recovery: an exploration of meaning and personal agency for women survivors of state sponsored torture (dissertation for doctor of philosophy in social welfare). Los Angeles: University of California, 2008. http://gradworks.umi.com/33/46/3346914.html (28 Aug 2010).

S C I E N T I F I C A R T I C L E
TO
RT
UR
E Vo
lum
e 2
1, N
um
be
r 2, 2
01
1139
– Mollica RF, McInnes K, Pham T et al (1998). The dose-effect relationships between torture and psychiatric symptoms in Vietnamese ex-political detainees and a comparison group. J Nerv Ment Dis 1998;186:543-53.
– Mollica RF, Sarajlic N, Chernoff M et al (2001). Longitudinal study of psychiatric symptoms, dis-ability, mortality, and emigration among Bosnian refugees. JAMA 2001;286:546-54.
– Mollica RF, Wyshak G, Lavelle J et al (1990). Assessing symptom change in Southeast Asian refugee survivors of mass violence and torture. Am J Psychiatry 1990;147:83-8.
– Mueller J, Schmidt M, Staeheli A et al (2010). Mental health of failed asylum seekers as com-pared with pending and temporarily accepted asylum seekers. Eur J Public Health 2010;0:ckq016v1-ckq016 (epub ahead of print July 14, 2010).
– Musisi S, Kinyanda E, Liebling H et al (2000). Post-traumatic torture disorder in Uganda. Tor-ture 2000;10(3):81-7.
– Neuner F, Schauer M, Klaschik C et al (2004). A comparison of narrative exposure therapy, supportive counseling, and psychoeducation for treating posttraumatic stress disorder in an Af-rican refugee settlement. Journal of Consulting and Clinical Psychology 2004;72:579-87.
– Neuner F, Onyut PL, Ertl V et al (2008). Treat-ment of posttraumatic stress disorder by trained lay counselors in an African refugee settlement: a randomized controlled trial. Journal of Consult-ing and Clinical Psychology 2008;76:686-94.
– Neuner F, Kurreck S, Ruf M et al (2010). Can asylum-seekers with posttraumatic stress disorder be successfully treated?: a randomized controlled pilot study. Cogn Behav Ther 2010;39:81-91.
– Nickerson A, Bryant RA, Silove et al (2011). A critical review of psychological reatments of posttraumatic stress disorder in refugees. Clin Psychol Rev 2011;31:399-417.
– National Partnership for Community Training (2011). Best, promising and emerging practices: a compendium for providers working with survi-vors of torture. Torture 2011;21:1-66.
– Nygard M, Malterud K (1995). Enkel kartleggn-ing av posttraumatisk stressforstyrresle hos Bosniske krigsflyktninger i Norge. Tidssk Nor Laegeforen 1995;115:1971-4.
– Onyut LP, Neuner F, Schauer E et al (2005). Narrative Exposure Therapy as a treatment for child war survivors with posttraumatic stress disorder: two case reports and a pilot study in an African refugee settlement. BMC Psychiatry 2005;5:5-7.
– Opacic G, Knezevic G (2004). Changes in the intensity and frequency of psychiatric prob-lems related to traumatic experience after three months of treatment. In: Spiric Z, Knezevic G, Jovic V et al, eds. Torture in war: consequences and rehabilitation of victims – Yugoslav experi-ence. Belgrade: IAN, 2004:221-32.
– Pantic Z (1998). Integrative gestalt group therapy with refugee children. In: Arcel LT, ed. War victims, trauma and the coping process: armed conflict in Europe and survivor responses. Co-penhagen: International Rehabilitation Council for Torture Victims, 1998:351-9.
– Paunovic N, Ost L-G (2001). Cognitive-behav-ior therapy vs. exposure therapy in the treat-ment of PTSD in refugees. Behav Res Ther 2001;39:1183-97.
– Pedersen T (2005). Impact assessment in reha-bilitation of torture survivors. Part III. Anthropo-logical reflections and perspectives. In: Berliner P, Arenas J. Haagensen JO, eds. Torture and organ-ized violence. Contributions to a professional hu-man rights response. Dansk psykologisk Forlag, 2005:206-44.
– Quiroga J, Deutsch A, O’Grady K (1981). Medi-cal and psychological sequelae in Latin American survivors of torture: a preliminary report (pub-lished as joint paper with Canada, 1981).
– Quiroga J, Jaranson JM (2005). Politically-mo-tivated torture and its survivors: a desk study review of the literature. Torture 2005;15(2-3):1-111.
– Rasmussen OV (1990). Medical aspects of tor-ture. Torture types and their relation to symp-toms and lesions in 200 victims. Dan Med Bull 1990;37(suppl 1): 1-88.
– Reeler AP, Mbape PT (1998). A pilot study of a brief form of psychotherapy for survivors of tor-ture. Torture 1998;8(12):120-5.
– Reiter RB, Zunzunegui MV, Quiroga J (1986). Guidelines for field reporting of basic human rights violations. Human Rights Quarterly 1986;8:628-33.
– Roche C (1999). Impact assessment for develop-ment agencies: leaning to value change. Oxford: Oxfam, 1999.
– Salo J, Punamäki R-L, Qouta S et al (2008). In-dividual and group treatment and self and other representations predicting posttraumatic recovery among former political prisoners. Traumatology 2008;14:45-61.
– Samsøe B, Bartels EM, Genefke I (2007). Treat-ment of torture victims: a longitudinal clinical study. Torture 2007;17:11-7.
– Schnurr PP (2007). The role of hard places in

S C I E N T I F I C A R T I C L E
TO
RT
UR
E V
olu
me
21
, N
um
be
r 2
, 2
01
1140
psychotherapy outcome research. J Trauma Stress 2007;20:779-92.
– Sehwail M, Rasras K (2002). Group therapy for victims of torture and organized violence. Torture 2002;21(2):55-7.
– Sjolund BH, Kastrup M, Montgomery E et al (2009). Rehabilitating torure survivors. J Rehabil Med 2009;41:689-96.
– Smajkic A, Weine S, Djuric-Bijedic Z et al (2001). Sertraline, paroxetine, and venlafaxine in refugee posttraumatic stress disorder with depres-sion symptoms. J Trauma Stress 2001;14:445-52.
– Sondergaard HP, Ekblad S, Theorell T (2001). Self-reported life event patterns and their rela-tion to health among recently resettled lraqi and Kurdish refugees in Sweden. J Nerv Ment Dis 2001;189:838-45.
– Sonis J, King DW, King LA et al (2007). In-novations in trauma research methods, 2006. J Trauma Stress 2007;20:775-7.
– Spring M, Westermeyer J, Halcon L et al (2003). Sampling in difficult-to-access refugee and immigrant communities. J Nerv Ment Dis 2003;191:813-9.
– Stedman T, Yellowlees P, Mellsop G et al (1997). Measuring consumer outcome in mental health. Field testing of selected measures of consumer outcome in mental health. Canberra: ACT, De-partment of Health and Family Services, 1997.
– Steel Z, Chey T, Silove D et al (2009). Associa-tion of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and dis-placement: a systematic review and meta-analysis. JAMA 2009;302:537-49.
– Stepakoff S, Hubbard J, Katoh M et al (2006). Trauma healing in refugee camps in Guinea: a psychosocial programme for Liberian and Sierra Leonean survivors of torture and war. Am Psy-chol 2006;61:921-92.
– Tol WA, Komproe IH, Jordans MJD et al (2009). Brief multi-disciplinary treatment for torture sur-vivors in Nepal: a naturalistic comparative study. Int J Soc Psychiatry 2009;55:39-56.
– Vaage AB, Thomsen PH, Silove D et al (2010). Long-term mental health of Vietnamese refu-gees in the aftermath of trauma. Br J Psychiatry 2010;196:122-5. http://bjp.rcpsych.org/cgi/con-tent/abstract/196/2/122.
– van Ommeren M, Jong JT, Sharma B et al (2001). Psychiatric disorders among tortured Bhutanese refugees in Nepal. Arch Gen Psychia-try 2001;58:475–82.
– Weine SM, Kulenovic AD, Pavkovic I et al (1998). Testimony psychotherapy in Bos-
nian refugees: a pilot study. Am J Psychiatry 1998;155:1720-6.
– Westermeyer J (1988). A matched pairs study of depression among Hmong refugees with particular reference to predisposing factors and treatment outcome. Soc Psychiatry Psychiatr Epidemiol 1988;23:64-71.
– Westermeyer J, Neider J, Vang TF (1984). Ac-culturation and mental health: a study of Hmong refugees at 1.5 and 3.5 years postmigration. Soc Sci Med 1984:18:87-93.
– Westermeyer J, Neider J, Callies A (1989). Psy-chosocial adjustment of Hmong refugees during their first decade in the United States. A longitu-dinal study. J Nerv Ment Dis 1989;177:132-9.
– Westermeyer J, Callies A, Neider J (1990). Welfare status and psychosocial adjustment among 100 Hmong refugees. J Nerv Ment Dis 1990;178:300-6.
– Westermeyer J, Uecker J (1997). Predictors of hostility in a group of relocated refugees. Cult Divers Ment Health 1997;3:53-60.
– Willis GB, Gonzalez A (1998). Methodological issues in the use of survey questionnaires to as-sess the health effects of torture. J Nerv Ment Dis 1998;186:283-9.
– World Health Organization (1993). Continuous quality development: a proposed national policy. Copenhagen: WHO, Regional Office of Europe, 1993.
– World Health Organization (2001). International Classification of Functioning, Disability and Health (ICF). Geneva: WHO, 2001.