
InternatIonal lIver CanCer assoCIatIon 9 ILCA Annual ... · Chairs: Tania Roskams, MD (Belgium) and...
228
www.ilca2015.org INTERNATIONAL LIVER CANCER ASSOCIATION 4 6 September 2015 Paris Marriott Rive Gauche Hotel & Conference Center Paris, France FINAL PROGRAMME & BOOK OF ABSTRACTS 9 th ILCA Annual Conference
Transcript of InternatIonal lIver CanCer assoCIatIon 9 ILCA Annual ... · Chairs: Tania Roskams, MD (Belgium) and...

www.ilca2015.org
InternatIonal lIver CanCer assoCIatIon
4 6 september 2015Paris Marriott rive Gauche Hotel & Conference CenterParis, France
FInal ProGraMMe & BooK oF aBstraCts
9th ILCA Annual Conference


I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 3
Table of Contents
Letter of Welcome .......................................................................................... 5
Programme at a Glance ............................................................................. 6
ILCA 2015 Programme ............................................................................... 11
Thursday, 3 September 2015 ....................................... 12
Friday, 4 September 2015 .............................................. 18
Saturday, 5 September 2015 ........................................ 27
Sunday, 6 September 2015 ............................................ 37
Practicalities ....................................................................................................... 41
Exhibitors, Sponsors, Media and other Partners ................... 49
Speakers’ Portfolio ........................................................................................ 53
Book of Abstracts ............................................................................................ 71

I L C A A n n u A L C o n f e r e n C e , 2 0 1 54

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 5
Letter of Welcome
Dear ILCA members, colleagues and friends,
We are very pleased to welcome you to the 9th Annual Conference of the International Liver Cancer Association (ILCA), in the beautiful city of Paris.
Since its creation and inaugural conference in 2007, ILCA has grown steadily and successfully organised conferences in all parts of the world, with the sole aim of advancing liver cancer science and care worldwide.
For its 9th year running, ILCA is excited to offer liver cancer experts an international multidisciplinary forum to exchange the latest innovations in research and care.
The multidisciplinary programme of ILCA 2015 will feature:
•State-of-the-Art Lectures delivered by distinguished colleagues within the field
•Symposia focusing on cutting edge advancements on research and treatments
•General Sessions and e-Poster Viewing Tours focusing on the most innovative research
•Luncheon Workshops that will engage you in discussions with eminent professionals
•Plus! Pre-Conference Workshop on Immunopathogenesis and Immunotherapy in HCC
ILCA 2015 will also provide you with numerous opportunities to network and connect with colleagues and industry partners from all over the world during networking breaks, lunches and the welcome reception.
We look forward to welcoming you in Paris for our multidisciplinary event. We wish you many opportunities for learning, sharing, networking and advancing liver cancer science and care with us.
On behalf of the ILCA Governing Board
Peter R. Galle, MD, PhD Riccardo Lencioni, MD, PhDILCA President ILCA Executive Secretary
Riccardo Lencioni
Peter R. Galle

I L C A A n n u A L C o n f e r e n C e , 2 0 1 56
Thursday, 3 September 2015
ILCA Pre-Conference Workshop on Immunopathogenesis and Immunotherapy in HCC
12:00 – 13:00 Registration 13:00 – 13:10 Welcome & Opening 13:10 – 15:30 Pathophysiology of Tumoral Immune Response and Escape
Chairs: Tim Greten, MD (USA) and Martin F. Sprinzl, MD (Germany) • Legislation and Execution: How Adaptive Immune Cells Control NASH and NASH Driven HCC
Mathias Heikenwälder, MD, PhD (Germany) • Immune Phenotype of Hepatocellular Carcinoma and Clinical Outcome
Xin Wei Wang, PhD (USA) • The Immune Microenvironment of Hepatocellular Carcinoma: a Potential Target for Therapy
Valerie Chew, PhD (Singapore) • Immunosuppressive Mechanisms in NASH Induced HCC
Tim Greten, MD (USA) • Spontaneous Tumour-Directed T-cell Responses in Hepatocellular Carcinoma
Robert Thimme, MD (Germany) • Challenges in Immune Target Choice: Immune Effects of Tumour-Associated Antigens
Lisa Butterfield, PhD (USA) • Adaptive Immune Response to Sporadic and Virus-Induced Cancer
Gerald Willimsky, MD, PhD (Germany) 15:30 – 16:00 Coffee & Networking Break
16:00 - 18:40 Immune Therapeutic Approaches
Chairs: Peter R. Galle, MD, PhD (Germany) and Lisa Butterfield, PhD (USA) • Therapeutic Modulation of the Tumour Microenvironment
Martin F. Sprinzl, MD (Germany) • Oncolytic Immunotherapy Pexa-Vec in Hepatocellular Carcinoma
Caroline Breitbach, PhD (USA) • Glypican-3 as a Liver Cancer Target for Antibody-Based Therapies
Mitchell Ho, PhD (USA) • Immune Checkpoint Blockade for Cancer Immunotherapy
Ignacio Melero, MD, PhD (Spain) • Immune Therapy Using Immune Checkpoint Inhibitors in Hepatocelluar Carcinoma
Bruno Sangro, MD, PhD (Spain) • TCR-Redirected T-cells for T-cell Immunotherapy
Antonio Bertoletti, MD (Singapore) • Off-Target Immunotherapy Responses
Aurélien Marabelle, MD, PhD (France) • T-cell Therapy in Leukemia
Shannon Maude, MD, PhD (USA) 18:40 Closing Note
Programme at a Glance

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 7
Programme at a Glance
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
Friday, 4 September 2015
08:00 – 09:30 ILCA Symposium 1: Emerging Concepts for Understanding Liver Cancer Chairs: Tania Roskams, MD (Belgium) and Xin Wei Wang, PhD (USA)
• Integrated Molecular-Morphological Classification of HCC Michiie Sakamoto, MD, PhD (Japan)
• Cancer Mutanome Immunotherapy Ugur Sahin, MD (Germany)
• Significance of Mixed Hepatocellular – Cholangiocarcinoma Gregory J. Gores, MD (USA)
• Ectopic Lymphoid Structures as Microniches for Tumour Progenitor Cells Eli Pikarsky, MD, PhD (Israel)
09:30 – 10:30 State-of-the-Art Lecture 1: The Gut-Liver Axis: Microbiome and HCC
Chair: Peter R. Galle, MD, PhD (Germany) Speaker: Robert Schwabe, MD (USA)
10:30 – 11:00 Coffee & Networking Break 11:00 – 11:15 Welcome Address Peter R. Galle, MD, PhD (Germany) Riccardo Lencioni, MD, PhD (Italy) Morris Sherman, MD, PhD (Canada) 11:15 – 12:45 General Session 1: Molecular Pathogenesis of Liver Cancer I.
Chairs: Snorri Thorgeirsson, MD, PhD (USA) and Jessica Zucman-Rossi, MD, PhD (France) 12:45 – 13:00 Session Break 13:00 – 14:30 Bayer Lunch Symposium 14:30 – 14:45 Session Break 14:45 – 16:15 General Session 2: Molecular Pathogenesis of Liver Cancer II.
Chairs: Masatoshi Kudo, MD, PhD (Japan) and Ann-Lii Cheng, MD, PhD (Taiwan) 16:15 – 16:45 Coffee & Networking Break 16:45 – 18:15 ILCA Symposium 2: Controversies in Liver Cancer (Pros and Cons Session)
Chairs: Josep M. Llovet, MD (Spain/USA) and Kim Olthoff, MD (USA) • Liver Resection: Patients within/beyond the Guidelines
Norihiro Kokudo, MD, PhD (Japan) vs. Pietro E. Majno, MD (Switzerland) • BCLC is the Gold Standard: yes/no
Jordi Bruix, MD (Spain) vs. Ronnie Poon, MD, PhD (P. R. China) • Sorafenib Therapy in Child B
Jorge Marrero, MD (USA) vs. Luigi Bolondi, MD (Italy) 18:15 – 19:00 Welcome Reception

I L C A A n n u A L C o n f e r e n C e , 2 0 1 58
Programme at a Glance
Saturday, 5 September 2015
07:30 – 08:30 Celsion Symposium
08:30 – 10:00 General Session 3: Epidemiology, Staging and Prognosis Chairs: Kwang-Hyub Han, MD (Repulic of Korea) and Andrew Zhu, MD, PhD (USA)
10:00 – 11:00 e-Poster Viewing Tour & Networking Break 11:00 – 12:30 Plenary Session Chairs: Peter R. Galle, MD, PhD (Germany), Riccardo Lencioni, MD, PhD (Italy) and Morris Sherman, MD, PhD (Canada) 12:30 – 12:45 Session Break 12:45 – 14:00 ILCA Special Interest Groups (SIGs) Luncheon Workshops
12:45 – 14:00 Luncheon Workshop: Egypt Meets ILCA
Common Approaches and Regional Disparities Chairs: Peter R. Galle, MD, PhD (Germany) and Mahmoud El Meteini, MD (Egypt)
14:00 – 14:15 Session Break 14:15 – 15:45 General Session 4: Diagnosis and Curative Treatment Chairs: Sandrine Faivre, MD, PhD (France) and Myron Schwartz, MD (USA) 15:45 – 16:45 e-Poster Viewing Tour & Networking Break
SIG 1: Molecular Classification and Signalling Pathways Animal Models Relevant to Human Liver Cancer Chairs: Xin Wei Wang, PhD (USA) and Wen Xue, PhD (USA)
SIG 2: Surveillance, Biomarkers and Molecular Pathology HCC Early Detection Chairs: Amit Singal, MD (USA) and Massimo G. Colombo, MD (Italy)
SIG 3: Imaging and Loco-Regional Therapies Standardising TACE – Defining TACE Failure Chairs: Riad Salem, MD (USA) and Bruno Sangro, MD, PhD (Spain)
SIG 4: Target and Systemic Therapies Hepatocellular Carcinoma with Stem Cell Features: How Can We Define and Handle Them Chairs: Joong-Won Park, MD, PhD (Republic of Korea) and Tim Meyer, MD, PhD (United Kingdom)
SIG 5: Liver Surgery and Transplantation Surgery and Transplantation Chairs: Thomas Decaens, MD, PhD (France) and Katsuhiko Yanaga, MD, PhD (Japan)
SIG 6: Non-HCC Hepatic Malignancies Update Systemic Therapy Chairs: Shahid A. Khan, MD, PhD (United Kingdom) and Gregory J. Gores, MD (USA)

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 9
Programme at a Glance
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
Sunday, 6 September 2015
07:30 – 08:30 Bristol-Myers Squibb Symposium
08:30 – 09:15 ILCA General Assembly
09:15 – 09:45 Coffee & Networking Break
09:45 – 10:45 State-of-the-Art Lecture 2: Fibrolamellar Carcinoma Chair: Curtis C. Harris, MD (USA)
Speaker: Sanford M. Simon, PhD (USA)
10:45 – 12:15 General Session 5: From Drivers to Clinical Trials Chairs: Sheng-Long Ye, MD, PhD (P. R. China) and Morris Sherman, MD, PhD (Canada)
12:15 – 12:30 Closing Ceremony
16:45 – 18:30 ILCA Symposium 3: Advances in Transarterial Treatment of HCC Chairs: Peter R. Galle, MD, PhD (Germany) and Richard Finn, MD (USA)
• TACE for HCC: What We Know, and What We Need to Know after Three Decades of Experience Riccardo Lencioni, MD, PhD (Italy)
• Y90 Radioembolization for Hepatocellular Carcinoma: Demonstrating Efficacy through Data Riad Salem, MD (USA)
• Advances in Transarterial Tumour Therapy: Does Novel Technology Mean Better Outcomes? Thierry de Baere, MD (France)
• Targeting Glucose Metabolism: A New Class of Agents for Transarterial Treatment of HCC? Jean-François Geschwind, MD (USA)
18:30 – 19:30 Sirtex Symposium
ILCA is not responsible for topics and speakers selection of industry symposia, nor for the opinions and statements produced at the time of their celebration.

I L C A A n n u A L C o n f e r e n C e , 2 0 1 51 0
9 – 11 September 2016Vancouver, Canada
ILCA 2016The International Liver Cancer Association Announces its 10th Annual Conference
Conference Highlights:
State-of-the-Art Lectures
Cutting Edge Symposia
General Sessions
Interactive Luncheon Workshops
e-Poster Viewing Tours
Industry Exhibition
Networking Breaks and Reception
ilca2016.org Abstract submissions open in January 2016
The international multidisciplinary forum for liver cancer experts around the latest innovations in research and care

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 1 1
ILCA 2015 Programme

I L C A A n n u A L C o n f e r e n C e , 2 0 1 51 2
ILCA 2015 ProgrammeThursday, 3 September 2015
Thursday, 3 September 2015
12:00 – 13:00 Registration
13:00 – 13:10 Welcome & Opening
Peter R. Galle, MD, PhD (Germany)
13:10 – 15:30 Pathophysiology of Tumoral Immune Response and Escape
Chairs: Tim Greten, MD (USA) and Martin F. Sprinzl, MD (Germany)Forum Level -1
Legislation and Execution: How Adaptive Immune Cells Control NASH and NASH Driven HCCMathias Heikenwälder, MD, PhD (Germany)
Alterations in our lifestyle over the last decades including high caloric intake (e.g. through high fructose and high fat diet) combined with a sedentary lifestyle have augmented the worldwide incidence of overweight and metabolic syndrome, characterized by abdominal obesity, insulin resistance and Type-2 diabetes, hypertonia and dyslipidemia. This trend is not only observed in industrialized regions like the United States of America (USA) or Europe, but also now gradually in developed as well as developing countries. To date, it is believed that approximately 90 million Americans and 40 million Europeans suffer from a fatty liver (also called Non-alcoholic fatty liver disease (NAFLD)). By using a novel mouse model of NASH and NASH induced HCC, we were able to uncover cellular and molecular mechanisms that drive NASH and HCC. Here, I will describe our novel findings based on this model, paving a way to treat NASH and NASH induced HCC.
Immune Phenotype of Hepatocellular Carcinoma and Clinical OutcomeXin Wei Wang, PhD (USA)
Hepatocellular carcinoma (HCC) patients suffer from a poor survival rate and a high incidence of postoperative recurrence. It is thought that a deregulated microenvironment promotes tumorigenesis, since chronic inflammation and disruption of immune cell components and signaling events is associated with a high incidence of cancer. Indeed, HCC is considered a typical inflammation-associated cancer with approximately 80%-90% of cases arising from cirrhotic livers. While distinct molecular HCC tumour subgroups have been identified (Ye et al, Nat Med 9, 416-23, 2003; Roessler et al, Cancer Res 70, 10202–12, 2010), our laboratory and others have also demonstrated that liver microenvironment signatures are linked to HCC metastasis, recurrence and prognosis (Budhu et al, Cancer Cell 10, 99–111, 2006; Hoshida et al, Cancer Research 69, 7385-7392, 2009, Kim et al, PLoS Medicine, 11, 2014). More recently, we have investigated the contribution of stromal cell components to HCC outcome. In particular, we postulated that activated HSCs (A-HSCs), which play a key role in liver fibrosis and cirrhosis, may contribute directly to HCC recurrence, metastasis, and progression (Ji et al, Hepatology, 61, 2015). We identified and validated an A-HSC-specific gene expression signature associated with HCC recurrence and survival, and further showed that A-HSCs preferentially shift the gene expression patterns of monocyte populations from inflammatory to immunosuppressive signatures, which induce pro-tumorigenic and progressive features of HCC cells. Disrupting such interactions and signaling events between the inflammatory milieu and components of the microenvironment may be useful therapeutic strategies for preventing HCC tumour relapse and improving patient survival. Overall, these studies have underscored the significant contribution of the liver microenvironment to HCC recurrence, progression and outcome through reprogramming of the inflammatory milieu.
ILCA Pre-Conference Workshop on Immunopathogenesis and Immunotherapy in HCC

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 1 3
ILCA 2015 ProgrammeThursday, 3 September 2015
The Immune Microenvironment of Hepatocellular Carcinoma: a Potential Target for TherapyValerie Chew, PhD (Singapore)
Hepatocellular carcinoma (HCC) is an aggressive cancer that is linked to chronically dysregulated liver inflammation. However, appropriate immune responses can control HCC progression. We previously identified a 14 immune-gene signature that predicts patient survival in a total of 155 HCC patients from Singapore, Hong Kong and Zurich irrespective of patient ethnicity and disease aetiology. Importantly, it predicts the survival of patients with early disease (stages I and II), for whom classical clinical parameters provide limited information. This signature includes the chemokine genes CXCL10 and CCL5, markers of T helper 1 (Th1), CD8+ T and natural killer (NK) cells, inflammatory cytokines (tumour necrosis factor Alpha, interferon Gamma) and Toll-like receptor-3 (TL3).We further investigated the underlying mechanism TLR3 in HCC. TLR3 expression was also associated with longer survival in HCC patients (HR = 2.1, P = 0.002, n=172). TLR3 expression by both tumour parenchyma and tumour-infiltrating NK cells associates with patient survival. In-vitro, TLR3 activation increased cell death and enhanced chemokines (CXCL10 and CCL5) expression in TLR3+ SNU182 HCC cell line as well as promoted NK cell activation and its cytotoxicity against HCC cells. In vivo, using both a transplanted and spontaneous mouse models of liver tumour, treatment with TLR3 ligand increased intratumoral chemokines expression, T- and NK-cells activation and tumour infiltration as well as enhanced apoptosis and reduced proliferation of the tumour parenchyma cells.Hence, tumour immune microenvironment is critical for HCC progression and TLR3 is shown to be an important modulator of tumour progression and a potential target for immunotherapy.
Immunosuppressive Mechanisms in NASH Induced HCCTim Greten, MD (USA)
Non-alcoholic steatohepatitis (NASH) is an important risk factor for hepatocellular carcinoma (HCC). We studied T-cell responses in three different murine NASH/HCC models and observed a robust, selective loss of hepatic CD4 but not CD8 T-cells. Increased CD4+ T-cell death was detected in hepatic CD4 T-cells in NASH. Selective CD4 T-cell depletion further accelerated HCC development. Lipid-laden hepatocytes from mice on MCD diet induced selective CD4 but not CD8 T-cells death. Our results provide a new link between lipid metabolism dysfunction with impaired anti-tumour surveillance.
Spontaneous Tumour-Directed T-cell Responses in Hepatocellular CarcinomaRobert Thimme, MD (Germany)
Hepatocellular carcinoma (HCC) is one of the most common cancers worldwide. Despite its growing incidence, however, therapeutic options remain limited. Consequently, HCC patients suffer from a high mortality rate. New therapies for HCC are therefore urgently required. Immunotherapy is a promising approach for the treatment of HCC. The rationale for immunological intervention is based on the presence of high numbers of tumour-infiltrating T-cells in HCC tissue, the correlation between the density of lymphocytic infiltrates in HCC lesions and prognosis, and, most importantly, the finding that adoptive immunotherapy with interleukin (IL)−2/anti-CD3-stimulated autologous lymphocytes lowers postsurgical recurrence rates in humans. The central effectors in this scenario are CD8+ T-cells that recognize tumour-associated antigens (TAA) and kill tumour cells. TAA comprise a range of self-derived proteins rendered immunogenic in tumours either by mutation or aberrant expression. A variety of different TAA can spontaneously induce CD8+ T-cell responses in HCC patients; these include α-fetoprotein (AFP), glypican-3 (GPC-3), melanoma-associated gene-A1 (MAGE-A1), and New York-esophageal squamous cell carcinoma-1 (NY-ESO-1). In addition, TAA-specific responses can also be boosted in vivo in HCC patients by dendritic cell-based vaccination with tumour lysate. In our own previous work, we could show that naturally occurring TAA-specific CD8+ T-cell responses are present in patients with HCC and therefore constitute part of the normal T-cell repertoire. Moreover, the presence of these responses correlates with patient survival. However, the observation of impaired IFN-γ production suggests that the efficacy of such responses is functionally limited. These findings support the development of strategies that aim to enhance the total TAA-specific CD8+ T-cell response by therapeutic boosting and/or specificity diversification. However, further research will be required to help unlock the full potential of TAA-specific CD8+ T-cell responses.

I L C A A n n u A L C o n f e r e n C e , 2 0 1 51 4
ILCA 2015 ProgrammeThursday, 3 September 2015
Challenges in Immune Target Choice: Immune Effects of Tumour-Associated AntigensLisa Butterfield, PhD (USA)
Alpha Fetoprotein (AFP) is the most abundant serum protein in the fetus. It is transcriptionally repressed shortly after birth, and elevated AFP levels are associated with liver regeneration, chronic liver diseases and cancer. AFP represents an attractive antigen target for immunotherapy of HCC. We identified several MHC class I-restricted epitopes and observed that healthy donor and HCC patient CD8+ and CD4+ T-cells can recognize AFP. Three AFP-based clinical trials have been performed to test AFP peptides in adjuvant, on autologous DC and DNA/Adenovirus immunization of HCC patients. AFP is not simply an over-expressed passenger antigen produced in the majority of HCC tumours. We tested cord blood-derived normal AFP (nAFP) or HCC tumour-derived AFP (tAFP), and identified profound suppressive effects on dendritic cells (DC). Mechanistic studies revealed that the suppressive activity of tAFP is dependent on both the AFP protein and a low molecular weight species that co-purifies with tAFP. We also compared the ability of nAFP to tAFP to modulate human NK cell activity and longevity in vitro. These data show that nAFP and tAFP induce similar yet distinct changes in NK cell function and viability. Defining the impact of circulating AFP on NK cells and DC may be crucial to understand the immune deficits described in HCC patients. Therefore, novel therapeutic approaches that antagonize the regulatory properties of tAFP will be critical to enhance immunity and improve clinical outcomes.
Adaptive Immune Response to Sporadic and Virus-Induced CancerGerald Willimsky, MD, PhD (Germany)
Most cancers are recognized by the immune system and cancer-specific B and T-cells can be measured in mice and humans. Whether destructive or non-destructive CD8+ T-cell responses are induced is dependent on the inflammatory conditions in which the cancers develop. We have developed experimental models of physiological cancer development, which resemble the clinical situation as closely as possible. In these transgenic mice (LoxP-Tag) a dormant oncogene, SV40 T antigen (TAg), is either stochastically or spatio-temporally activated causing sporadic cancer. We found that TAg-specific CD8+ T-cells are initially amplified, but are rendered non-functional (i.e. anergic) during sporadic cancer development. Systemic TAg-specific tolerance was found to occur already during the premalignant stage of sporadic cancer development. In contrast to sporadic cancer, virus-induced hepatocellular carcinoma (HCC) that developed due to hepatocyte-specific, adenovirus-mediated activation of oncogenic TAg initially induced a destructive CD8+ T-cell response targeted against the virus and TAg, leading to clearance of the infected cells. Despite the presence of functional, antigen-specific memory CD8+ T-cells, a few virus-infected cells escaped immune clearance and progressed to HCC, that were not selected for low immunogenicity. Immune evasion occurred by poor T-cell infiltration and local inhibition by programmed cell death protein-1 (PD1) and its ligand PD-L1 in an antigen specific fashion.
15:30 – 16:00 Coffee & Networking Break
16:00 – 18:40 Immune Therapeutic Approaches
Forum Level -1
Chairs: Peter R. Galle, MD, PhD (Germany) and Lisa Butterfield, PhD (USA)
Therapeutic Modulation of the Tumour MicroenvironmentMartin F. Sprinzl, MD (Germany)
Therapy of hepatocellular carcinoma (HCC) still faces limited efficacy, which eventually leads to tumour progression and treatment failure. An important mechanism of therapeutic tumour resistance involves stromal cell populations, which promote compensatory neo-vascularization, accelerate tumour cell growth and induce tumour immune escape. Modulation of stromal cell function therefore represents an additional mode of action for cancer therapy. Particularly tumour-associated macrophages (TAM), myeloid-derived suppressor cells and regulatory T-cells are

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 1 5
promising therapeutic targets as they are regulators of HCC progression and local immunity. Current findings highlight this concept as some stromal cell populations respond to local ablative HCC therapy, which affects subsequent anti-tumoral immune responses. Moreso, tyrosine-kinase inhibition with Sorafenib promotes inflammatory macrophage function and tumour-directed innate immunity. However, hepatoma cell growth induction by TAM-like macrophages is suppressed by Sorafenib. Experimental approaches targeting NF-kappaB signalling were also introduced to change the local tumour milieu, leading to tumour regression in animal models. However, tailored approaches are mandatory to increase efficacy of therapeutic stromal modulation and reduce negative off-target effects. Therefore, the frontiers of stroma-directed tumour therapy include the selection of specific molecular targets, the improvement of direct stromal cell targeting and the identification of synergistic therapeutic modalities during HCC management.
Oncolytic Immunotherapy Pexa-Vec in Hepatocellular CarcinomaCaroline Breitbach, PhD (USA)
Pexa-Vec (pexastimogene devacirepvec; JX-594) is a cancer-targeted oncolytic and immunotherapeutic vaccinia virus engineered to selectively replicate and destroy cancer cells. Direct oncolysis plus granulocyte macrophage – colony stimulating factor (GM-CSF) expression also stimulates tumour vascular shutdown and anti-tumoral immunity, respectively. Over 300 patients with advanced cancers have been treated by intravenous (IV) and/or intratumoral (IT) injections to date. Treatment with Pexa-Vec has been generally well-tolerated to date, with acute, transient flu-like symptoms and transient hypotension being the most notable treatment-emergent adverse events. High-dose Pexa-Vec was associated with improved overall survival on a randomized Phase 2 study in patients with advanced hepatocellular carcinoma (HCC), as compared to a low-dose active control (14.1 mo vs 6.7 mo; HR 0.39; p=0.02), while a Phase 2b study in sorafenib-refractory HCC patients did not meet its primary endpoint of improvement in overall survival. A 600-patient global Phase 3 trial in primary liver cancer (hepatocellular carcinoma; HCC) is planned. First-line HCC patients will be enrolled; these patients have failed or are not eligible for locoregional treatments and have not received sorafenib. Patients will be randomized to receive Pexa-Vec followed by sorafenib versus sorafenib alone. The primary endpoint is overall survival; secondary endpoints include time to tumour progression, response rate and safety.
Glypican-3 as a Liver Cancer Target for Antibody-Based Therapies Mitchell Ho, PhD (USA)
Glypican-3 (GPC3) is highly expressed in hepatocellular carcinoma. Our lab has developed human monoclonal antibodies (HN3 and HS20) that recognize unique functional sites in GPC3 and inactivate Wnt/Yap signaling pathways known to be important for liver cancer pathogenesis. HN3 is a human heavy-chain antibody that recognizes the core protein of GPC3. The HS20 human antibody preferentially recognizes the heparan sulfate chains on glypicans. In addition, our lab is one of the first to validate GPC3 as a new target for antibody-toxin/drug conjugates. We have found that the HN3-based immunotoxin caused regression of liver cancer in mice. Its mechanism appears to involve both inhibition of cancer signaling (Wnt/Yap) and reduction in protein synthesis. Our work establishes GPC3 as a promising candidate for immunotoxin-based liver cancer therapy.
Immune Checkpoint Blockade for Cancer ImmunotherapyIgnacio Melero, MD, PhD (Spain)
Cancer immunotherapy chiefly relies on the ability of T-cells to specifically recognize mutated or overexpressed peptides associated to self-antigen presenting molecules. The ability of T-cells to be cytotoxic against cells infected with intracellular pathogens is a mechanism that can be exploited in cancer therapy, provided that cancer expresses mutated sequences, which can give rise to presented antigens. However, panoply of mechanisms exists to control and fine tune cytotoxicity. These mechanisms are mediated by cell surface receptors, soluble cytokines and other moieties that are susceptible of therapeutic intervention. Modulation of such mechanisms can be performed with monoclonal
ILCA 2015 ProgrammeThursday, 3 September 2015

I L C A A n n u A L C o n f e r e n C e , 2 0 1 51 6
ILCA 2015 ProgrammeThursday, 3 September 2015
antibodies acting as antagonists or as agonists of such immunomodulating molecules constituting what are termed immunostimulatory monoclonal antibodies.Up to date, the most successful of such agents have been antibodies tampering with the T-lymphocyte inhibitory receptors CTLA-4 and PD-1. Indeed, their potent unleashing of anti-tumor immune responses has been conducive to the approval of three new agents for the treatment of metastasic melanoma and one of them for metastatic non-small cell lung cancer. The mechanisms of action are contingent on a baseline immune response against sufficeintly antigenic cancer cells that is amplified by the new agents. Other inhibitory targets for such antibodies such as LAG-3, TIM-3, BTLA, TIGIT are being explored. Another subset of immunostimulatory monoclonal antibodies exerts their functions by acting agonistically on activatory receptors on immune system cells. These include antibodies directed to CD137, OX40, GITR, CD40, which are in phase I and II clinical trials, showing preclinical and clinical activity. Perhaps the most exciting feature of these novel immunotherapies is that they can be synergistically combined among themselves or with more conventional therapies of cancer.On advanced hepatocellular carcinoma, our group has reported clinical activity both with agents directed to CTLA-4 (Tremelimumab) and PD-1 (Nivolumab).
Immune Therapy Using Immune Checkpoint Inhibitors in Hepatocelluar CarcinomaBruno Sangro, MD, PhD (Spain)
Systemic treatment of hepatocellular carcinoma (HCC) is an unmet need. Evidence for the antigenicity of tumour cells the finding that immune check-point molecules play an essential role in tumour escape from the immune system and the outstanding results achieved by blocking these inhibitory receptors in the clinical arena are changing the scope of cancer immunotherapy. Immune checkpoint inhibitors including monoclonal antibodies that block the negative signals released by CTLA-4 or PD-1 receptors have produced appealing evidence of antitumor activity when given as monotherapy to patients with advanced HCC. Yet, if the multiplicity of immunosuppressive forces acting within the HCC microenvironment is considered, a combinatorial approach is advised. Locoregional therapies including thermal ablation, chemoembolization or radioembolization might elicit immunogenic tumour cell death and this in turn may enhance the antitumor efficacy of immune check-point inhibitors. In fact, immune cell infiltration and encouraging tumour remissions have been observed when the CTLA-4 blocking agent Tremelimumab is given in combination with subtotal chemoembolization or radiofrequency ablation. These strategies deserve further development in the next future.
TCR-Redirected T-cells for T-cell ImmunotherapyAntonio Bertoletti, MD (Singapore)
Cancer immunotherapy using a patient’s own T-cells redirected to recognize and kill tumour cells has achieved promising results in metastatic melanoma and leukemia. This technique involves harnessing a patient’s T-cells and then delivering a gene that encodes a new T-cell receptor (TCR) or a chimeric antigen receptor (CAR) that allow the cells to recognize specific cancer antigens. The potential for development of redirected T-cell therapy for persistent viral infections like HBV and their associated malignancies has started to be explored by different groups. We recently tested in a first-in-man clinical trial the ability of HBV-specific TCR redirected T-cells to target HBsAg-productive HCC, demonstrating that HBV-specific engineered T-cells recognize HCC cells with HBV-DNA integration (Qasim, et al. (2015).Journal of Hepatology, 62(2), 486–491). We will discuss the possibility to use hepatitis B viral antigens a tumour specific antigen in patients with HBV related HCC, and the new methods to produce to TCR redirected T-cells that can target virally infected or HBV related HCC cells.

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 1 7
Off-Target Immunotherapy ResponsesAurélien Marabelle, MD, PhD (France)
Cancer immunotherapies are not limited to systemic approaches. For more than a century, clinicians have also developed local therapies with immunostimulatory properties such as bacterial extracts, oncolytic viruses, cytokines, radiotherapy, etc. These local therapies have also been associated to some degree to distant effect on non-treated tumor lesions (so called “abscopal effect” in radiotherapy). Recent pre-clinical and clinical evidence suggest that these distant effects could be enhanced when used in combination with immune checkpoint targeted therapies. The tumor immune priming generated by local therapies could overcome the current issue of primary resistance to cancer immunotherapy.
T-cell Therapy in LeukemiaShannon Maude, MD, PhD (USA)
Adoptive transfer of T-cells engineered to express a chimeric antigen receptor (CAR) has emerged as a powerful, targeted immunotherapy with an innovative mechanism. By combining the specificity of a monoclonal antibody with the activation domains of T-cells, CARs deliver activated T-cells with potent cytotoxicity to antigen-expressing tumour cells. CD19-directed CAR-modified T-cell therapies for B cell malignancies are the best-studied and most advanced engineered T-cell therapy currently being tested. Dramatic clinical responses, with complete remission (CR) rates as high as 90%, have been reported in several clinical trials of CAR-modified T-cells with specificity to the B cell specific antigen CD19 in patients with relapsed and highly refractory acute lymphoblastic leukemia (ALL). Even more encouraging are sustained remissions observed in some patients without additional therapy. However, the most notable toxicity, cytokine release syndrome (CRS), can lead to life-threatening complications in a fraction of patients. Supraphysiologic T-cell proliferation, a hallmark of this therapy, contributes to both efficacy and CRS, posing a unique challenge for toxicity management. The current landscape of CD19 CAR T-cell therapy, CRS pathophysiology and management, and remaining challenges will be discussed.
18:40 Closing Note
Peter R. Galle, MD, PhD (Germany)
ILCA 2015 ProgrammeThursday, 3 September 2015

I L C A A n n u A L C o n f e r e n C e , 2 0 1 51 8
ILCA 2015 ProgrammeFriday, 4 September 2015
Friday, 4 September 2015
08:00 – 09:30 ILCA Symposium 1: Emerging Concepts for Understanding Liver Cancer
Scene AB RoomGround level
Chairs: Tania Roskams, MD (Belgium) and Xin Wei Wang, PhD (USA)
Integrated Molecular-Morphological Classification of HCC Michiie Sakamoto, MD, PhD (Japan)
Histopathological parameters and molecular markers are widely accepted as useful predictors of tumour aggressiveness in hepatocellular carcinoma. However, few studies have analyzed histopathological and molecular profiles comprehensively in one series, a fact that has resulted in fragmentation of information that could be applied in clinical practice. We conducted immunohistochemical expression analysis of biliary/stem cell markers, Wnt/β-catenin signaling-related molecules, p53, and cell proliferation markers in 162 hepatocellular carcinomas surgically resected from 142 patients and analyzed the results with respect to clinicopathological features. Immunohistochemical analysis broadly identified three groups: the biliary/stem cell marker-positive group, the Wnt/β-catenin signaling-related marker-positive group, and the biliary/stem cell marker- and Wnt/β-catenin signaling-related marker-negative group. p53 was frequently positive in the biliary/stem cell marker-positive group, but it was rarely positive in the Wnt/β-catenin signaling-related marker-positive group. The biliary/stem cell marker-positive group exhibited poor tumour differentiation, increased frequency of portal vein invasion and/or intrahepatic metastasis, and highly proliferative activity. In contrast, the biliary/stem cell marker- and Wnt/β-catenin signaling-related marker-negative group exhibited better tumour differentiation, a decreased frequency of portal vein invasion and/or intrahepatic metastasis, and less proliferative activity. The Wnt/β-catenin signaling-related marker-positive group showed neither tendency. The biliary/stem cell marker-positive group had the shortest time to recurrence among the three groups. In conclusion, immunohistochemical profiling of hepatocellular carcinoma reflects tumour aggressiveness and suggests the potential efficacy of immunohistochemistry-based subclassification of hepatocellular carcinoma.
Cancer Mutanome ImmunotherapyUgur Sahin, MD (Germany)
Mutations are regarded as ideal targets for cancer immunotherapy. As neo-epitopes with strict lack of expression in any healthy tissue, they are expected to be safe and could bypass the central tolerance mechanisms. The systematic use of mutations for vaccine approaches, however, is hampered by the uniqueness of the repertoire of mutations (“the mutanome”) in every patient’s tumour. We have recently proposed a personalized immunotherapy approach targeting the spectrum of individual mutations. Here we show in three independent murine tumour models that a considerable fraction of non-synonymous cancer mutations is immunogenic and that unexpectedly the immunogenic mutanome is pre-dominantly recognized by CD4+ T-cells (“the CD4+ immunome”). Vaccination with such CD4+ immunogenic mutations confers strong anti-tumour activity. Encouraged by these findings we set up a process comprising mutation detection by exome sequencing, selection of vaccine targets by solely bioinformatical prioritization of mutated epitopes predicted to be abundantly expressed and good MHC class II binders and rapid production of synthetic mRNA vaccines encoding multiple of these mutated epitopes. We show that vaccination with such poly-neo-epitopic mRNA vaccines induces potent tumour control and complete rejection of established aggressively growing tumours in miceMoreover, we demonstrate that CD4+ T-cell neo-epitope vaccination reshapes the tumour microenvironment and induces CTL responses against an independent immunodominant antigen in tumour bearing mice indicating orchestration of antigen spread. Analyses of corresponding human cancer types with the same bioinformatical algorithms showed the abundance of mutations predicted to bind to MHC class II in human cancers as well. In the meantime a first in human clinical study started demonstrating the clinical feasibility of the approach. Thus, the tailored immunotherapy approach introduced here may be regarded as a universally applicable blueprint for comprehensive exploitation of the huge neo-epitope target repertoire of cancers enabling targeting of every patient’s tumour with “just in time” produced vaccines.

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 1 9
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeFriday, 4 September 2015
Significance of Mixed Hepatocellular – CholangiocarcinomaGregory J. Gores, MD (USA)
Liver cancers may contain histological and molecular features of both HCC and iCCA; these malignancies are referred to as mixed HCC-iCCA using World Health Organization (WHO) criteria. In mixed tumours, the presence of cholangiocarcinoma histologic elements is often confirmed by positive cytokeratin 19 (CK19) staining. If one assumes that CK19 positivity defines a mixed tumour, then its incidence is approximately 11%. The WHO criteria and many authors have been reluctant to call CK19 positive HCC mixed tumours, preferring terms such as HCC with biliary/hepatic progenitor cell markers. However, one cannot infer cell lineage from morphology, as transformed mature hepatocytes are plastic and may assume a CCA phenotype. For example, NOTCH overexpression in hepatocytes will confer a malignant biliary phenotype. The definition of mixed HCC-iCCA lesions likely will continue to evolve. The identification of these lesions is important as they portend an adverse prognosis following liver resection or liver transplantation. Likely, they should also be stratified as an independent tumour subtype in clinical trials using systemic agents given their adverse prognosis. More attention is warranted regarding the diagnosis and management of this liver cancer subtype.
Ectopic Lymphoid Structures as Microniches for Tumour Progenitor Cells Eli Pikarsky, MD, PhD (Israel)
A central feature of tissue inflammation is the interaction between resident cells and immune cells. Cellular infiltration usually entails a diffuse influx of immune cells, scattered throughout the inflamed tissue. However, infiltrating leukocytes often form simple lymphoid aggregates or even more complex structures that histologically resemble lymphoid organs. Ectopic lymphoid-like structures (ELS) are often observed in cancer, yet their function is mostly obscure. We studied a mouse model of hepatocellular carcinoma (HCC), displaying abundant ELSs and found that they constitute immunopathological microniches wherein progenitor malignant hepatocytes first appear and thrive. These progenitors eventually gain self-sufficiency, egress their microniches and form tumours. The tumour promoting microniche milieu, depends on a competent adaptive immune system, and manifests a complex cellular and cytokine composition. HCC progenitor egression is associated with autocrine production of cytokines previously provided by the niche microenvironment. Our findings indicate that aberrant ELS formation, which in mice is induced by chronic NF-κB activation, can promote early stages of carcinogenesis by creating microniches within which cancer progenitors evolve. These specialized ELSs foster atypical hepatocytes that eventually acquire malignant properties. Identifying additional examples of immune-dependent spatially defined tumour microniches, their assembly principle, tumour progenitor support and egression mechanisms, may indicate effective ways to interfere with these processes. This could have important clinical implications, superior over non-discriminative immune stimulation or suppression, both of which may facilitate distinct phases of tumourigenesis.
09:30 – 10:30 State-of-the-Art Lecture 1: The Gut-Liver Axis: Microbiome and HCC
Scene AB Ground level
Chair: Peter R. Galle, MD, PhD (Germany) Speaker: Robert Schwabe, MD (USA)
Host and microbiota represent a complex supra-organism, in which the bacterial metagenome exceeds our own genome by a factor of 100. Accordingly, the bacterial microbiota carries out key metabolic functions and exerts an important role in the regulation of our immune system. This symbiotic relationship requires functional barriers that anatomically separate host and microbiota. When these multi-level barriers fail, the bacterial microbiota can trigger chronic inflammation and promote disease including cancer. Increased bacterial translocation, caused by increased intestinal permeability and dysbiosis, is characteristic for patients with chronic liver disease. Bacterial translocation not only leads to typical infectious complications of advanced liver disease – such as SBP and sepsis - but also contributes to hepatic inflammation, triggered by bacterial components termed pathogen-associated molecular patterns (PAMPs) such as LPS. PAMP-mediated activation of pattern recognition receptors such as Toll-like receptors (TLRs) mediates many of the disease-promoting effects of the bacterial microbiota. Studies

I L C A A n n u A L C o n f e r e n C e , 2 0 1 52 0
ILCA 2015 ProgrammeFriday, 4 September 2015
from our group have demonstrated a key contribution of the bacterial microbiota and TLR4, the receptors for LPS, in the promotion of hepatic fibrosis and hepatocellular carcinoma (HCC) in mice. Of note, treatment with non-absorbable antibiotics resulted in a significant reduction of fibrosis and HCC development. In addition to triggering inflammation, TLR4 also promotes cell survival, thereby enhancing carcinogenesis. Surprisingly, HCC prevention by antibiotics was most efficient when antibiotics where given in late stages of hepatocarcinogenesis, suggesting that for HCC prevention, antibiotics may be considered for patients with end-stage liver disease. Of note, the well-tolerated antibiotic Rifaximin, which is widely used in patients with chronic liver disease, was also able to prevent HCC in mice. Strategies to translate these findings into clinically applicable therapies will be discussed, focusing on different therapeutic approaches to inhibit the gut microbiota-TLR4 axis, and disease settings in which this could be applied.
10:30 – 11:00 Coffee & Networking BreakScene FoyerGround level
11:00 – 11:15 Welcome Address
Scene ABGround level
Peter R. Galle, MD, PhD (Germany), Riccardo Lencioni, MD, PhD (Italy) and Morris Sherman, MD, PhD (Canada)
11:15 – 12:45 General Session 1: Molecular Pathogenesis of Liver Cancer I.Scene ABGround level
Chairs: Snorri Thorgeirsson, MD, PhD (USA) and Jessica Zucman-Rossi, MD, PhD (France)
O-001 Identification of Co-Occurring Genetic Aberrations with Known Driver Mutation Directs Targeted Therapy in Cholangiocarcinoma
Chirag Nepal 1,*, Jesper B. Andersen 1
1BRIC, University of Copenhagen, Copenhagen, Denmark
O-002 The Thailand Initiative in Genomics and Expression Research for Liver Cancer (TIGER-LC): Defining Biological Subtypes of Hepatocellular Carcinoma and Cholangiocarcinoma by Integrated Genomics
Anuradha Budhu 1,*, Jittiporn Chaisaingmongkol 1 2, Hien Dang 1, So Mee Kwon 1, Siritida Rabibhadana 2, Benjarath Pupacdi 2, Marshonna Forgues 1, Vajarabhongsa Bhudhisawasdi 3, Nirush Lertprasertsuke 4, Anon Chotirosniramit 4, Chawalit Pairojkul 3, Chirayu U. Auewarakul 5, Thaniya Sricharunrat 5, Kannika Phornphutkul 6, Suleeporn Sangrajrang 7, Maggie Cam 8, Ping He 9, Stephen M. Hewitt 8, Xiaolin Wu 8, Snorri S. Thorgeirsson 8, Paul S. Meltzer 8, Christopher A. Loffredo 10, Robert H. Wiltrout 8, Curtis C. Harris 1, Chulabhorn Mahidol 2, Mathuros Ruchirawat 2, Xin W. Wang 1, and The TIGER-LC Consortium
1Laboratory of Human Carcinogenesis, National Institutes Of Health, Bethesda, United States, 2Chulabhorn Research Institute, Bangkok, 3Khon Kaen University, Khon Kaen, 4Chiang Mai University, Chiang Mai, 5Chulabhorn Hospital, Bangkok, 6Rajavej hospital and Lampang Cancer Center, Chiang Mai, 7National Cancer Institute, Bangkok, Thailand, 8National Institutes Of Health, 9Food and Drug Administration, Bethesda, 10Georgetown University Medical Center, Washington, DC, United States
O-003 Personalized Diagnostics in Hepatocellular Carcinoma: Unique Mutational Signatures with Potential to Guide Targeted Therapy
José P. Vaqué 1,*, Nuria García-Díaz 2, Susana Llerena 3, Soraya Curiel-Olmo 2, Laura Cereceda 2, Carmen Almaraz 2, Helena Pisonero 2, Carlos Rodriguez de Lope 3, Luis Martín 3, Carmen Cagigas 3, Federico Castillo 3, Roberto Fernandez 3, Ainara Azueta 3, Silvia Alvarez 3, Miguel Á. Piris 3, Javier Crespo 3
1Cell signaling, Universidad de Cantabria-IDIVAL-IBBTEC, 2IDIVAL, 3HUMV, Santander, Spain
O-004 Adeno-Associated Virus 2 (Aav2) Induces Recurrent Insertional Mutagenesis in Human Hepatocellular Carcinomas
Jean Charles Nault 1,*, Shalini Datta 1, Andrea Franconi 1, Sandrine Imbeaud 1, Maxime Mallet 1, Gabrielle Couchy 1, Eric Letouzé 1, Camilla Pilati 1, Benjamin Verret 1, Jean-Frédéric Blanc 2, Charles Balabaud 2, Julien Calderaro 3, Alexis Laurent 4, Mélanie Letexier 5, Paulette Bioulac-Sage 6, Fabien Calvo 7, Jessica Zucman-Rossi 1

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 2 1
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeFriday, 4 September 2015
1INSERM UMR1162, Paris, 2Service d’hépatologie, Bordeaux, 3Service d’anatomopathologie, Créteil, 4Service de chirurgie digestive, Creteil, 5Integragen, Paris, 6Service d’anatomopathologie, Bordeaux, 7INCA, Paris, France
O-005 Role of Lect2 in the Hepatic Immune Microenvironment during Liver Carcinogenesis Antoine L’Hermitte 1,*, Mathilde Cadoux 1, Gabrielle Couchy 2, Sandrine Pham 1, Marie Anson 1, Anne-Marie
Crain 1, Christine Perret 1, Jessica Zucman-Rossi 2, Chantal Desdouets 1, Jean-Pierre Couty 1
1Development Reproduction and Cancer, Institut Cochin INSERM U1016, 2Unité de génomique fonctionnelle des tumeurs solides, INSERM U1162, PARIS, France
O-006 Interrogation of Dnajb1-Prkaca Kinase Fusion as a Therapeutic Target in Fibrolamellar Hepatocellular Carcinoma
Stefanie Schalm 1*, Nicolas Stransky 1, Darshan Sappal 1, Erin Murphy 1, Adam Shutes 1, Joe Kim 1, Steve Wenglowsky 1, Kevin Wilson 1, Klaus Hoeflich 1, Christoph Lengauer 1, Andrew Garner 1
1Blueprint Medicines, Cambridge, United States
12:45 – 13:00 Session Break
Scene FoyerGround level
13:00 – 14:30 Bayer Lunch Symposium: Dogma and Dilemma in the Treatment of HCC Scene ABGround level
Welcome, Introduction and ObjectivesPeter R. Galle, MD, PhD (Germany)
Clinical Evidence vs. Clinical Experience in Daily Practice in the Treatment of HCCJordi Bruix, MD (Spain) and Richard Finn, MD (USA)
Why Target Therapies Fail in HCC: Drug Features or Study Designs?Josep M. Llovet, MD (Spain/USA) and Ann-Lii Cheng, MD, PhD (Taiwan)
How to Define if a Patient is Benefitting or no Longer Benefitting from a Treatment: Continuing vs. Switching a Treatment for HCC Based on Radiographical ExamMasatoshi Kudo, MD, PhD (Japan) and Jean-Luc Raoul, MD (France)
Concluding RemarksPeter R. Galle, MD, PhD (Germany)
14:30 – 14:45 Session Break
Scene ABGround level
14:45 – 16:15 General Session 2: Molecular Pathogenesis of Liver Cancer II.Scene ABGround level
Chairs: Masatoshi Kudo, MD, PhD (Japan) and Ann-Lii Cheng, MD, PhD (Taiwan)
O-007 Igf2 is an Oncogenic Driver in Hcc and Emerges as a Potential Target for Therapies Iris Martínez-Quetglas 1,*, Roser Pinyol 1, Daniel Dauch 2, Anna Portela 3, Judit Peix 1, Monica Higuera 1, Laia
Cabellos 1, Victoria Tovar 1, Clara Alsinet 1, Vicenzo Mazzaferro 4, Jessica Zucman-Rossi 5, Manel Esteller 3, Lars Zender 2, Josep M. Llovet 1 6 7
1Liver Cancer Translational Research Laboratory, Barcelona Clinic Liver Cancer Group (BCLC), Liver Unit, Hospital Clínic, IDIBAPS, CIBEREHD, University of Barcelona, Barcelona, Spain, 2Division of Translational Gastrointestinal Oncology, Department of Internal Medicine I, University of Tuebingen, Tuebingen, Germany, 3Cancer Epigenetics and Biology Programme, Bellvitge Biomedical Research Institute (IDIBELL), Barcelona, Spain, 4Fondazione IRCCS, Istituto Nazionale dei tumori (INT), Milan, Italy, 5Génomique fonctionnelle des tumeurs solides, Institut National de la Santé

I L C A A n n u A L C o n f e r e n C e , 2 0 1 52 2
ILCA 2015 ProgrammeFriday, 4 September 2015
et de la Recherche Médicale (INSERM), Paris, France, 6Institució Catalana de Recerca i Estudis Avançats (ICREA), Barcelona, Spain, 7Mount Sinai Liver Cancer Program, Division Liver Diseases, Icahn School of Medicine at Mount Sinai, New York, United States
O-008 Tumour Initiating Cells Are Mediators of Acquired Resistance to Sorafenib in Hepatocellular Carcinoma
Victoria Tovar 1,*, Helena Cornellà 1, Agrin Moeini 1, Samuel Vidal 2, Yujin Hoshida 3, Daniela Sia 3 4, Judit Peix 1, Clara Alsinet 1, Iris M. Quetglas 1, Manel Solé 1, Josep Domingo-Domenech 2, Augusto Villanueva 3 5, Josep M. Llovet 1 3 6
1Liver Cancer Translational Research Laboratory, BCLC Group, Liver Unit and Pathology Department, IDIBAPS, Hospital Clínic, CIBERehd, Universitat de Barcelona, Barcelona, Spain, 2Department of Pathology, Icahn School of Medicine at Mount Sinai, 3Liver Cancer Program, Division of Liver Diseases, Department of Medicine, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, United States, 4Gastrointestinal Surgery and Liver Transplantation Unit, National Cancer Institute, Milan, Italy, 5Division of Hematology and Medical Oncology, Icahn School of Medicine at Mount Sinai, New York, United States, 6Institució Catalana de Recerca i Estudis Avançats (ICREA), Barcelona, Spain
O-009 Stem-Cell Niche and Tumour-Associated Macrophages in Human Cholangiocarcinoma Chiara Raggi 1,*, Margherita Correnti 2, Luca Di Tommaso 3, Jesper B. Andersen 4, Domenico Alvaro 5, Massimo
Roncalli 6, Antonio Sica 7, Gianfranco Alpini 8, Pietro Invernizzi 1
1Liver Unit and Center for Autoimmune Liver Diseases, 2Humanitas Clinical and Research Center, 3Pathology Unit, Humanitas Research Hospital, Rozzano (MI), Italy, 4Biotech Research and Innovation Centre, University of Copenhagen, Copenhagen, Denmark, 5Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Rome, 6Pathology Unit, Humanitas Research Hospital, 7Laboratory of Molecular Immunology, Humanitas Clinical and Research Center, Rozzano (MI), Italy, 8Department of Research, Central Texas Veterans Health Care System, Temple, United States
O-010 Mixed Hepatocellular-Cholangiocarcinoma Tumours: Cholangiolocarcinomas and Stem-Cell Subtype Have Unique Molecular Traits
Agrin Moeini 1 2,*, Daniela Sia 1 2, Hui Dong 1, Zhongyang Zhang 3, Genis Camprecios 1, M Isabel Fiel 1, Oriana Miltiadous 1, Xiaochen Sun 1, Ke Hao 3, Yujin Hoshida 1, Swan N Thung 1, Augusto Villanueva 1, Myron E Schwartz 1, Josep M Llovet 1 2 4
1Mount Sinai Liver Cancer Program, Division of Liver Diseases, Department of Medicine, Department of Pathology, Recanati Miller Transplantation Institute, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, United States, 2Liver Cancer Translational Research Laboratory, Liver Unit, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Hospital Clínic, CIBERehd, Universitat de Barcelona, Barcelona, Spain, 3Icahn Institute for Genomics and Multiscale Biology, Icahn School of Medicine at Mount Sinai, New York, United States, 4Institució Catalana de Recerca i Estudis Avançats, Barcelona, Spain
O-011 Signatures of Known and New Mutational Processes Operative in Liver Cancers Eric Letouzé 1 2 3 4,*, Jayendra Shinde 1 2 3 4, Ludmil B. Alexandrov 5 6, Sandrine Imbeaud 1 2 3 4,
Kornelius Schulze 1 2 3 4, Julien Calderaro 1 2 3 4 7, Sandra Rebouissou 1 2 3 4, Gabrielle Couchy 1 2 3 4, Clément Meiller 1 2 3 4, Roser Pinyol 8, Laura Pelletier 1 2 3 4, Charles Balabaud 9 10, Alexis Laurent 11 12, Jean-Frederic Blanc 9 13, Vincenzo Mazzaferro 14, Fabien Calvo 1 2 3 4, Augusto Villanueva 8, Jean-Charles Nault 1 2 3 4 15, Paulette Bioulac-Sage 9 16, Michael R. Stratton 5, Josep M. Llovet 8 17 18, Jessica Zucman-Rossi 1 2 3 4 19
1UMR-1162, Génomique fonctionnelle des Tumeurs solides, IUH, INSERM, 2Labex Immuno-Oncology, Sorbonne Paris Cité, Faculté de Médecine, Université Paris Descartes, Paris, 3Sorbonne Paris Cité, UFR SMBH, F-93000, Université Paris 13, Bobigny, 4Université Paris Diderot, Paris, France, 5Cancer Genome Project, Wellcome Trust Sanger Institute, Hinxton, United Kingdom, 6Theoretical Division, Los Alamos National Laboratory, Los Alamos, United States, 7Department of Pathology, CHU Henri Mondor, Assistance Publique-Hôpitaux de Paris, Créteil, France, 8HCC Translational Research Laboratory, Barcelona-Clínic Liver Cancer Group, Institut d’Investigacions Biomèdiques August Pi i Sunyer, Liver Unit. CIBERehd, Hospital Clínic, Barcelona, Spain, 9UMR-1053, INSERM, 10Université de Bordeaux, Bordeaux, 11Department of Digestive and Hepatobiliary Surgery, CHU Henri Mondor, Assistance Publique-Hôpitaux de Paris, 12U955, INSERM, Créteil, 13CHU de Bordeaux, Department of Hepatology,

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 2 3
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeFriday, 4 September 2015
Hôpital Saint-André, Bordeaux, France, 14Department of Liver Surgery and Transplant, Fondazione Istituto Tumori, Milan, Italy, 15Hôpitaux Universitaires Paris – Seine Saint-Denis, Site Jean Verdier, Pôle d’Activité Cancérologique Spécialisée, Service d’Hépatologie, F-93143, Assistance Publique-Hôpitaux de Paris, Bondy, 16CHU de Bordeaux, Department of Pathology, Pellegrin Hospital, Bordeaux, France, 17Institució Catalana de Recerca i Estudis Avançats, Barcelona, Spain, 18Mount Sinai Liver Cancer Program (Division of Liver Diseases), Mount Sinai School of Medicine, New York, United States, 19Hôpital Europeen Georges Pompidou, F-75015, Assistance Publique-Hôpitaux de Paris, Paris, France
O-012 Activation of Stem-Like Cells in the Hepatic Microenvironment Is Associated with Prognostically Adverse Genomic Alterations in Hepatocellular Carcinoma
Darko Castven 1,*, Michael Fischer 1, Stefan Heinrich 2, Jesper B. Andersen 3, Matthias Matter 4, Martin Sprinzl 1, Stefanie Heilmann 5, Marcus Wörns 1, Snorri S. Thorgeirsson 6, Peter R. Galle 1, Hauke Lang 2, Jens U. Marquardt 1
1Department of Medicine I, 2Department of Surgery, University Hospital of Mainz, Mainz, Germany, 3BRIC, University of Copenhagen, Copenhagen, Denmark, 4Department of Pathology, University of Basel, Basel, Switzerland, 5Institute of Human Genetics, University of Bonn, Bonn, Germany, 6LEC, CCR/NCI/NIH, Bethesda, United States
16:15 – 16:45 Coffee & Networking Break
Scene FoyerGround level
16:45 – 18:15 ILCA Symposium 2: Controversies in Liver Cancer (Pros and Cons Session) Scene ABGround level
Chairs: Josep M. Llovet, MD (Spain/USA) and Kim Olthoff, MD (USA)
Liver Resection: Patients within/beyond the GuidelinesNorihiro Kokudo, MD, PhD (Japan) vs. Pietro E. Majno, MD (Switzerland)
Liver Resections for BCLC-C Patients with Vascular Invasion: A Japanese ExperienceNorihiro Kokudo, MD, PhD (Japan)
According to the BCLC guidelines endorsed by AASLD and EASL, the recommended treatment option is only sorafenib for patients with hepatocellular carcinoma (HCC) accompanied with vascular invasion. However, there is a subgroup of patients who can survive long after surgical treatment even at the very advanced stage of the disease. We have been applying surgical treatment for BCLC-C patients as long as they are operable. In this presentation we introduce our surgical strategies and patient outcome based on our database of 1,525 surgical resections for HCC (from Oct. 1994 to Dec. 2011).Portal Venous Tumour Thrombus (PVTT): Resectability for patients with macroscopic PVTT was judged based on liver function including ICG and the extent of liver resection required. Anatomic resection including hemihepatectomy or sectionectomy is required in most of the cases to remove possible micrometastases. To avoid too invasive procedures requiring portal vein resection and reconstruction, we have been applying so-called “peeling off technique (PO)” to preserve portal venous wall. HEPATIC VENOUS TUMOR THROMBUS (HVTT): patients with HVTT were classified as those with tumour thrombosis in a peripheral hepatic vein, including microscopic invasion (pHVTT, n=153), tumour thrombosis in a major hepatic vein (mHVTT, n=21), and tumour thrombosis of the inferior vena cava (IVCTT, n=13). Anatomic resections were applied when technically feasible. BILE DUCT TUMOR THROMBUS (BDTT): oqur surgical policy for HCC with BDTT is complete resection without removal of the extrahepatic bile duct. Preservation of bile duct using a “peeling off technique” is very important because ablation therapy or TACE for tumour recurrence, which should be very common in this setting, may cause severe cholangitis or liver abscess formation after bilio-enteric anastomoses. Indications, technical tips, and patient outcome for each subgroup of patients will be presented.Conclusion: Surgical treatment for BCLC-C patients is feasible in selected cases and provides chance for long-term survival.

I L C A A n n u A L C o n f e r e n C e , 2 0 1 52 4
ILCA 2015 ProgrammeFriday, 4 September 2015
Liver Resection for HCC within the Guidelines: Pleading for a Procrustean Bed? Pietro E. Majno, MD (Switzerland)
A procrustean solution is one that fits reality to an ideological scheme, from a Greek myth in which the rogue ironsmith Procrustes killed his guests cutting or stretching them to fit an iron bed. The BCLC guidelines have been often accused of representing such a bed.
A misunderstanding has to be cleared upfront. SIZE per se is NOT a contraindication to resection in the BCLC guidelines. Large solitary tumours of any size can be resected if the risks of liver failure can be avoided.
Portal hypertension: the contraindication relates to the poor long-term results of liver resection in these patients. Studies challenging the 10mmHg portal-venous gradient limit claim the low early mortality of surgery, but reproduce the same late mortality figures than in the published BCLC experience. The limit has to be interpreted as an incentive to seek for alternative (less invasive: percutaneous; or more radical: OLT) means of local control of the HCC.
Multiple tumours: the limit here is again be interpreted as an incentive to compare resection to more radical or less invasive means of local control of the HCC, as the probability of recurrence (under the form of hepatic metastases or de novo tumours) are much higher than for single tumours. Similar to portal hypertension, the literature on the results of resection for multiple tumours shows long-term recurrence and survival results equivalent to the BCLC experience. Exceptions are possible, and indeed should be pursued in specialized centres, and cases in which better local control of the disease is offered by resection do exist (e.g. peripheral lesions, large lesions).
Vascular invasion: signs a high probability of extrahepatic and intrahepatic multifocal disease in which alternatives for local control are less invasive (such as radioembolisation) or of systemic treatment (sorafenib) are more effective. However some patients with slowly progressive disease who are diagnosed at an advanced yet resectable stage benefit from this form of local control (preserved functional reserve, good general conditions). Such patients, often selected by a referral bias in specialized surgical centres, represent the most fertile field in which exceptions to the BCLC guidelines should be explored by cohort studies for tentative prognostic factors or direct comparison to alternatives (radioembolisation).
Extrahepatic spread: there are only very anecdotal cases of successful survival after resection. They should be taken as a memento that some patients do have an exceptional clinical course and part of our craft is to recognise them and adapt our treatment accordingly.
Overall the frame of the BCLC appears to be reasonable and useful. Deviation is of course possible, sometimes well justified, but as such it is important for it to be discussed in a multidisciplinary setting (where proponents of alternatives are well represented), explained to the patients, and documented. Respect of these rules will avoid drifting along the slopes that leads from ideal customized care to arbitrary decisions.
BCLC is the Gold Standard Jordi Bruix, MD (Spain) vs. Ronnie Poon, MD, PhD (P.R. China)
BCLC is the Gold Standard: yesJordi Bruix, MD (Spain)
The evaluation of patients diagnosed with hepatocellular carcinoma (HCC) includes their prognosis assessment and, optimally, a link to the first line option to be considered. For conventional practice it is key to include, in the treatment recommendation, those options that have been shown to be beneficial as per scientific strength. While prognosis is the first step, refined prediction of the expected outcome and treatment allocation requires a personalized approach taking into account aspects such as age, comorbidities and values. These will never be detailed in a general model, as all expert clinicians are aware of. Careful evaluation of patients will modulate treatment recommendation. In addition, despite higher or lower expected outcome, the treatment decision may not be modified, as the survival benefit of treatment may be higher than shifting to another option or even no treatment. In the research setting, the need for stratification is far more intense. Narrow definition of the target population and/

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 2 5
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeFriday, 4 September 2015
or stratification according to a given profile secure clean results and adequate balance between treatment arms. As any research proposal, the definition of the population and the stratification factor is an investigator decision. For general depiction of tumour stage and first line treatment to be considered, the model that has been widely adapted and validated is the BCLC model. It links staging with treatment and, within each stage and treatment, physicians are required to carefully decide among the available options. Clinical practice guidelines are there to expose the selection criteria and optimal profile for all available options in order to secure the best outcome for each patient. In that sense, it is worth stressing that liver function impairment is not accurately evaluated by the Child-Pugh classification. It is known that patients with Child-Pugh A may be decompensated and, among decompensated patients fitting into Child-Pugh B, specific parameters (spontaneous bacterial peritonitis, renal failure, episodes of encephalopathy) imply a poor outcome and should help to allocate patients to end-stage if not candidates to transplant. Such assessment is key in BCLC B stage, where the apparent heterogeneity is due to the wrong classification of single HCC > 5 cm as BCLC B and the dismissal of proper evaluation of liver function in Child-Pugh B cases and indication of TACE against the recommendation of BCLC and of all Western guidelines.
BCLC is the Gold Standard: noRonnie Poon, MD, PhD (P.R. China)
Sorafenib Therapy in Child BJorge Marrero, MD (USA) vs. Luigi Bolondi, MD (Italy)
Sorafenib Therapy in Child BJorge Marrero, MD (USA)
Sorafenib is the treatment of choice for patients with advanced hepatocellular carcinoma (HCC). However, the studies that lead to the approval of sorafenib did not include Child-Pugh B or C patients. Therefore, important question remains regarding the efficacy and safety of sorafenib in HCC patients that are classified as Child-Pugh B. The best data comes from the multicenter, multinational GIDEON study. This study showed that the safety profile of sorafenib was comparable between Child-Pugh groups. In both Child-Pugh A and Child-Pugh B patients, the greatest number of AEs occurred during the first 4 weeks of treatment. Interestingly, a large proportion of patients were able to continue sorafenib treatment beyond 28 weeks, including 21% of Child-Pugh B patients, suggesting that patients who are able to continue treatment beyond the initial period are able to continue for long periods and perhaps derive efficacy. In GIDEON, the majority of patients received an initial sorafenib dose of 800 mg, regardless of the Child-Pugh status. The median daily dose was comparable irrespective of Child-Pugh status, and the proportion of Child-Pugh A and Child-Pugh B patients receiving a sorafenib dose modification was broadly similar. The median overall survival was shorter in Child-Pugh B patients compared to Child-Pugh A, and the worsen survival in Child-Pugh B patients was most likely related to poorer liver function due to the natural progression of cirrhosis. Given the observational nature of the GIDEON study and lack of a control, the efficacy of sorafenib cannot be fully assessed.
Sorafenib Therapy in Child-Pugh B PatientsLuigi Bolondi, MD (Italy)
Child-Pugh B patients are of special interest in terms of sorafenib management, as the progression of their cirrhosis, rather than tumour progression, may result in the discontinuation of sorafenib. As a whole, the data available on the safety of sorafenib in Child-Pugh B patients suggest the feasibility of using this treatment in this population, taking into account that poorer clinical outcomes are to be expected due to worse liver function. In the GIDEON study, 61.5% of patients were classified as having Child-Pugh A status and 20.8% Child-Pugh B status. Overall, this non-interventional study showed that a greater proportion of Child-Pugh B than Child–Pugh A patients discontinued sorafenib because of AEs (40.1 versus 28.9%) or experienced Grade 3/4 AEs (14.1 versus 8.8%). Nonetheless, just

I L C A A n n u A L C o n f e r e n C e , 2 0 1 52 6
ILCA 2015 ProgrammeFriday, 4 September 2015
over a quarter of patients with Child-Pugh B cirrhosis (25.7%) were treated with sorafenib for over 24 weeks and TTP was comparable between the Child-Pugh A and B cohorts (4.7 vs 4.4 months, respectively). Not surprisingly, median survival in the Child-Pugh B cohort was shorter, by approximately 8 months (Table 2a). Similar findings were also observed in an Italian multicenter, open-label, phase II trial of sorafenib (800 mg/day), performed in 297 patients with Child-Pugh A (79%) and Child-Pugh B (21%) liver function (Pressiani et al. Ann. Oncol. 24(2), 406-411, 2013). Compared with their Child-Pugh A counterparts, patients with Child-Pugh B status had shorter PFS (2.1 vs 4.3 months); moderately shorter TTP (3.8 vs 4.2 months) and clearly reduced OS (3.8 vs 10.0 months). Again, the overall AE profile was similar in the two groups. However, more robust studies are necessary before confirming or disregarding the use of sorafenib in this subset of patients. The ongoing BOOST phase 3 study is aiming to address this question. This study will compare OS with sorafenib (800 mg/day) versus best supportive care in 320 patients with HCC and impaired liver function (Child-Pugh B; www.clinicaltrials.gov NCT01405573).
18:15 – 19:00 Welcome ReceptionScene FoyerGround level

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 2 7
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeSaturday, 5 September 2015
Saturday, 5 September 201507:30 – 08:30 Celsion Symposium: Intermediate HCC: Cure vs. Palliation
AuditoriumLevel -1 Chair: Riccardo Lencioni, MD, FSIR, EBIR (Italy)
Current Management of Intermediate HCC: Unmet Medical Needs Ronnie Poon, MBBS, MS, PhD (Hong Kong)
Intermediate HCC Treatment Paradigms and Lessons Learned Ghassan Abou-Alfa, MD (USA)
OPTIMA Phase III Clinical Trial: Study Design and Protocols Riccardo Lencioni, MD, FSIR, EBIR (Italy)
08:30 – 10:00 General Session 3: Epidemiology, Staging and Prognosis
Scene ABGround level
Chairs: Kwang-Hyub Han, MD (Republic of Korea) and Andrew Zhu, MD, PhD (USA)
O-013 Incidence of Hepatocellular Carcinoma in Alcoholic Compensated Cirrhosis, Preliminary Results of a Multicenter Prospective French and Belgian Cohort (Cirral)
Nathalie Ganne 1 2 3,*, Valerie Bourcier 1, Cendrine Chaffaut 4, Isabelle Archambaud 5, Frédéric Oberti 6, Jean-Marc Perarnau 7, Dominique Roulot 2 8, Alexandre Louvet 9, Christophe Moreno 10, Thong Dao 11, Romain Moirand 12, Odile Goria 13, Eric Nguyen-Khac 14, Jean Henrion 15, Stanislas Pol 16, Albert Tran 17, Victor de Ledinghen 18, Teresa Antonini 19, Nicolas Carbonell 20, Jean-Marie Peron 21, Violaine Ozenne 22, Xavier Amiot 23, Gabriel Perlemuter 24, Jean-Pierre Zarski 25, Sylvie Chevret 4
1APHP, Jean Verdier, Bondy, 2University Paris 13 Sorbonne Cité, Bobigny, 3INSERM UMR 1162, 4APHP, Saint-Louis, Paris, 5CHU, Nantes, 6CHU, Angers, 7CHU, Tours, 8APHP, Avicenne, Bobigny, 9CHU, Lille, France, 10CHU, Bruxelles, Belgium, 11CHU, Caen, 12CHU, Rennes, 13CHU, Rouen, 14CHU, Amiens, France, 15CHU, Jolimont, Belgium, 16APHP, Cochin, Paris, 17CHU, Nice, 18CHU, Bordeaux, 19APHP, Villejuif, 20APHP, Saint-Antoine, Paris, 21CHU, Toulouse, 22APHP, Lariboisière, 23APHP, Tenon, Paris, 24APHP, Antoine Béclère, Clamart, 25CHU, Grenoble, France
O-014 Hepatocellular Carcinoma (HCC) Scoring System for the Individualized Prediction of Liver Cancer in 1080 Hcv-Related Compensated Cirrhosis Included in the French Multicenter Prospective Cohort Anrs Co12 Cirvir
Valerie Bourcier 1, Nathalie Ganne 1,*, Richard Layese 2, Nabila Talmat 1, Petrov-Sanchez Ventzislava 3, Patrick Marcellin 4, Dominique Guyader 5, Stanislas Pol 6, Dominique Larrey 7, Victor De Lédinghen 8, Denis Ouzan 9, Fabien Zoulim 10, Jean-Claude Trinchet 1, Pierre Nahon 1, Françoise Roudot-Thoraval 2
1Hepatology, Jean Verdier hospital, BONDY, 2Henri Mondor hospital, CRETEIL, 3ANRS, Paris, 4Hepatology, Beaujon hospital, Clichy, 5Hepatology, Rennes hospital, Rennes, 6Hepatology, Cochin hospital, Paris, 7Hepatology, Montpellier hospital, Montpellier, 8Hepatology, Bordeaux hospital, Bordeaux, 9Hepatology, Institut A. Tzanck, Saint Laurent du Var, 10Hepatology, Hotel Dieu hospital, Lyon, France
O-015 Platelet Count Improves Prognostic Value of A-L-B-I Grade: Introducing a New P-A-L-B-I Score Sasan Roayaie 1,*, Ghalib Jibara 2, Sarah Berhane 3, Parissa Tabrizian 4, Joong-Won Park 5, Jijin Yang 6, Lunan
Yan 7, Guohong Han 8, Francesco Izzo 9, Mishan Chen 10, Jean-Frederic Blanc 11, Lewis Roberts 12, Masatoshi Kudo 13, Morris Sherman 14, Philip Johnson 3
1North Shore-LIJ Health System, Lenox Hill Hospital, New York, United States, 2Brookdale’s Medical Center, Brooklyn, 3University of Liverpool, Liverpool, United Kingdom, 4Mount Sinai Hospital, New York, United States, 5National Cancer Center, Seoul, Korea, Republic Of, 6Second Military Medical University, Shanghai, 7West China Hospital, Sichuan, 84th Military Medical University, Xian, China, 9National Cancer Institute of Naples, Naples, Italy, 10Sun Yat-sen University, Guangzhou, China, 11Hopital Saint Andre, Bordeaux, France, 12Mayo Clinic, Rochester, United States, 13Kinki University, Kyoto, Japan, 14University of Toronto, Toronto, Canada
I L C A A n n u A L C o n f e r e n C e , 2 0 1 52 8
ILCA 2015 ProgrammeSaturday, 5 September 2015
O-016 Diabetes, Hbv Infection and Smoking Are Independent Risk Factors for Developing Hepatocellular Carcinoma on Non-Fibrotic Liver in the Noflic French Multicenter Case-Control Study
Jean-Frédéric Blanc 1,*, Marie-Quitterie Picat 2, Aline Maillard 2, Caroline Bouyssou 1, Charlotte Costentin 3, Mariane Ziol 4, Olivier Rosmorduc 5, Laurence Chiche 6, Isabelle Rosa-Hezode 7, Luc Letenneur 2, Karen Leffondre 2, Adélaide Doussau 2, Jessica Zucman-Rossi 8
1Hepatology And Digestive Oncology, University Hospital of Bordeaux, 2ISPED, University of Bordeaux, Bordeaux, 3Hepatology, CHU Henri Mondor, Créteil, 4Pathology, CHU Jean Verdier, Bondy, 5Hepatology, CHU Saint-Antoine, Paris, 6Digestive Surgery, CHU Bordeaux, Bordeaux, 7Hepato-Gastroenterology, CHI Créteil, Creteil, 8INSERM, UMR 1162, Génomique Fonctionnelle des Tumeurs Solides, Institut Universitaire d’Hématologie, Paris, France
O-017 Patients with Alcohol Compared to Hcv-Related Hepatocellular Carcinoma (HCC) Have a Reduced Survival, Results of a Nationwide Study
Charlotte Costentin 1,*, Nathalie Goutte 2, Philippe Sogni 3, Noëlle Bendersky 4, Bruno Falissard 5, Olivier Farges 6
1Hepatology, Henri Mondor Hospital, Creteil, 2Hepato-biliary surgery, Beaujon Hospital - Paris VII University - INSERM U773, Clichy, 3Hepatology, Cochin Hospital - Paris Descartes University, Paris, 4Medical Informatics, Beaujon Hospital - Paris VII University, Clichy, 5Biostatistique, Paris-Sud University, INSERM U669, Paris, 6Hepatology – Hepato-biliary surgery, Beaujon Hospital - Paris VII University - INSERM U773, Clichy, France
O-018 Patient Knowledge and Barriers for Hepatocellular Carcinoma Surveillance among Patients with Cirrhosis
Amit G. Singal 1,*, Maleka Khambaty 1, Adam Yopp 1, Purva Gopal 1, Jasmin Tiro 1, Jorge Marrero 1
1UT Southwestern Medical Center, Dallas, United States
10:00 – 11:00 e-Poster Viewing Tour & Networking BreakScene FoyerGround level
Opened by Peter R. Galle, MD, PhD (Germany)
11:00 – 12:30 Plenary Session Scene ABGround level
Chairs: Peter R. Galle, MD, PhD (Germany), Riccardo Lencioni, MD, PhD (Italy) and Morris Sherman, MD, PhD (Canada)
O-019 Comprehensive and Integrative Genomic Characterization of Hepatocellular Carcinoma: the Tcga HCC Project
Lewis R. Roberts 1,*, David A. Wheeler 2
1Division of Gastroenterology and Hepatology, College of Medicine, Mayo Clinic and Mayo Clinic Cancer Center, Rochester, 2Baylor College of Medicine, Houston, United States
O-020 Prospective Assessment of Liver Cancer Occurrence in Compensated Hcv-Related Cirrhosis With Svr Using a Competing Risk Framework Reveals an Annual Incidence Below 1% and Specific Risk Factors (Anrs Co12 Prospective Cirvir Cohort)
Pierre Nahon 1,*, Valérie Bourcier 1, Richard Layese 2, Ventzi Petrov-Sanchez 3, Patrick Marcellin 4, Dominique Guyader 5, Stanislas Pol 6, Dominique Larrey 7, Fabien Zoulim 8, Dominique Roulot 9, Victor de Ledinghen 10, Jean-Pierre Zarski 11, Jean-Claude Trinchet 1, Françoise Roudot-Thoraval 2
1Hôpital Jean Verdier, Bondy, 2Hôpital Henri Mondor, Créteil, 3ANRS, Paris, 4Hôpital Beaujon, Clichy, 5Hôpital Potchaillou, Rennes, 6Hôpital Cochin, Paris, 7CHU Montpellier, Montpellier, 8CHU Lyon, Lyon, 9Hôpital Avicenne, Bobigny, 10CHU Pessac, Pessac, 11CHU Grenoble, Grenoble, France
President’s Note Peter R. Galle, MD, PhD (Germany) •NelsonFaustoAward •JuniorInvestigatorAward

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 2 9
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeSaturday, 5 September 2015
O-021 Objective Response by Mrecist Predicts Survival in Hepatocellular Carcinoma: a Multivariate, Time-Dependent Analysis from the Phase 3 Brisk-Ps Study*
Riccardo Lencioni 1,*, Joong-Won Park 2, Ferran Torres 3, Thomas Decaens 4, Eveline Boucher 5, Jean-Luc Raoul 6, Masatoshi Kudo 7, Charissa Chang 8, Valerie Boige 9, Eric Assenat 10, Yoon-Koo Kang 11, Ho-Yeong Lim 12, Ian Walters 13, Josep M. Llovet 8
1Diagnostic Imaging and Intervention, University of Pisa School of Medicine, Pisa, Italy, 2Center for Liver Cancer, National Cancer Center, Goyang, Korea, Republic Of, 3IDIBAPS, Hospital Clínic Barcelona, Barcelona, Spain, 4Service d’Hepato-Gastro-Enterologie, University of Paris-Est, Creteil, 5Service d’Oncologie Médicale, Central Eugene Marquis, Rennes, 6Service d’Oncologie Médicale, Institut Paoli Calmette, Marseille, France, 7Department of Gastroenterology and Hepatology, Kinki University School of Medicine, Osaka, Japan, 8Division of Liver Diseases, Mount Sinai School of Medicine, New York, United States, 9Service de Gastro-Enterologie, Institut Gustave Roussy, Villejuif, 10Service d’Hépato-Gastro-Entérologie, Hôpital Saint Eloi, Montpellier, France, 11Department of Oncology, Asan Medical Center, 12Division of Hematology-Oncology, Samsung Medical Center, Seoul, Korea, Republic Of, 13Bristol-Myers Squibb, Wallingford, United States
O-022 A Randomized Phase 2 Trial of Sorafenib Plus Intra-Arterial Cisplatin versus Sorafenib Alone for Advanced Hepatocellular Carcinoma
Manabu Morimoto 1*, Masafumi Ikeda 2, Satoshi Shimizu 2, Yoshitaka Inaba 3, Yasushi Kojima 4, Atsushi Hagihara 5, Masatoshi Kudo 6, Shoji Nakamori 7, Shuichi Kaneko 8, Rie Sugimoto 9, Toshiyuki Tahara 10, Takumi Ohmura 11, Kohichiroh Yasui 12, Keiko Sato 13, Hiroshi Ishii 14, Junji Furuse 15, Takuji Okusaka 16
1Department of Hepatobiliary and Pancreatic Medical Oncology, Kanagawa Cancer Center, Kanagawa, 2Department of Hepatobiliary and Pancreatic Oncology, National Cancer Center Hospital East, Kashiwa Chiba, 3Department of Diagnostic and Interventional Radiology, Aichi Cancer Center Hospital, Aichi, 4Department of Gastroenterology, National Center for Global health and Medicine Center Hospital, Tokyo, 5Department of Hepatology, Osaka City University Hospital, 6Department of Gastroenterology and Hepatology, Kinki University School of Medicine, 7Department of Hepatobiliary and Pancreatic Surgery, Osaka National Hospital, Osaka, 8Department of Gastroenterology, Kanazawa University Hospital, Kanazawa, 9Department of Hepato-Biliary-Pancreatology, National Hospital Organization Kyushu Cancer Center, Fukuoka, 10Department of Gastroenterology, Saiseikai Utsunomiya Hospital, Tochigi, 11Department of Gastroenterology, Sapporo Kosei General Hospital, Sapporo, 12Molecular Gastroenterology and Hepatology, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, 13Institute for Advancement of Clinical and Translational Science, Kyoto University Hospital, Kyoto, 14Clinical Research Center, Shikoku Cancer Center, Matsuyama, 15Department of Medical Oncology, Kyorin University, 16Department of Hepatobiliary and Pancreatic Oncology, National Cancer Center Hospital, Tokyo, Japan
12:30 – 12:45 Session BreakScene ABGround level
12:45 – 14:00 ILCA Special Interest Groups (SIGs) Luncheon Workshops
12:45 – 14:00 SIG 1: Molecular Classification and Signalling Pathways Animal Models Relevant to Human Liver Cancer
Scene ABGround Level
Chairs: Xin Wei Wang, PhD (USA) and Wen Xue, PhD (USA)
The cancer genome is highly complex, with hundreds of point mutations, translocations, and chromosome gains and losses per tumour. Likewise, the clinical presentation of hepatocellular carcinoma (HCC), a major type of primary liver cancer, is highly heterogeneous. Its diagnostic, prognostic and treatment assessment is often complicated by both tumour biology and compromised liver function due to underlying chronic inflammatory liver diseases such as fibrosis and cirrhosis. To understand the effects of various cancer genes, precise models that incorporate both genomic changes in tumour cells and appropriate hepatic microenvironmental milieu are needed. However, the presence of considerable genomic alterations constitutes a bottleneck and poses an enormous challenge to effectively rank, triage and evaluate these candidate driver genes as druggable targets. While mouse tumour models are powerful tools to study cancer biology and to facilitate bench-to-bedside research, mouse livers

I L C A A n n u A L C o n f e r e n C e , 2 0 1 53 0
ILCA 2015 ProgrammeSaturday, 5 September 2015
are highly sensitive to neoplastic transformation. Consequently, numerous genetically-modified mouse models for HCC are currently available. A critical question remains as to which mouse models are most relevant to human HCC. In this workshop, we will describe approaches to the construction and utility of various mouse models of human liver cancer, including germline, somatic and ex vivo models. The recent development of the CRISPR-Cas9 system, a powerful genome-editing tool for efficient and precise genome engineering, is transforming mouse-model generation. We will describe how CRISPR-Cas9 has been used to create mouse models of liver cancer with point mutations, deletions and complex chromosomal rearrangements. We will highlight the progress and challenges of such approaches, and how these models can be used to understand progression of liver tumours and to identify new strategies for cancer treatment. The generation of precision liver cancer mouse models will provide a rapid avenue for functional cancer genomics and pave the way for precision cancer medicine.
Topic outline1. The need for precision cancer models2. Traditional mouse model of liver cancer
- Chemical-induced- Germline mouse models: transgenic, knockout, etc.- Somatic mouse models: hydrodynamic system- Ex vivo: embryonic liver progenitor cell transplant
3. Generating mouse model through the CRISPR system- CRISPR mouse models- Engineering structural variations
4. Challenges
12:45 – 14:00 SIG 2: Surveillance, Biomarkers and Molecular Pathology HCC Early Detection
Forum ABLevel -1 Chairs: Amit Singal, MD (USA) and Massimo G. Colombo, MD (Italy)
Several societies, including the AASLD, EASL and APASL recommended HCC surveillance in patients with cirrhosis to improve early tumour detection and overall survival. Although a randomized trial in China demonstrated HCC surveillance significantly lowered annual mortality rates in patients with chronic HBV infection, there is no similar Level I evidence supporting HCC surveillance among patients with cirrhosis. Prior attempts to obtain randomized data failed due to poor patient enrollment, and the authors concluded a randomized trial in patients with cirrhosis might not be feasible. Data from HBV-infected patients cannot be extrapolated to those with cirrhosis due to lower sensitivity of ultrasound with a nodular liver, reduced eligibility for curative treatments such as resection, and higher competing risk of non-HCC mortality. HCC surveillance in patients with cirrhosis is supported by several cohort and case-control studies; however, two recent meta-analyses concluded higher quality data are needed given methodological limitations of current data including lead-time bias, length-time bias, and inadequate follow-up duration. Lack of high quality Level I data has led some providers to question the merits of HCC surveillance, contributing to underuse of HCC surveillance in clinical practice. In this luncheon workshop, Drs. Colombo and Singal will discuss current data evaluating HCC surveillance in patients with cirrhosis, areas of need for higher quality data, and the potential necessity/feasibility of obtaining Level I data.
12:45 – 14:00 SIG 3: Imaging and Loco-Regional Therapies Standardising TACE – Defining TACE Failure
Forum CLevel -1 Chairs: Riad Salem, MD (USA) and Bruno Sangro, MD, PhD (Spain)
Transarterial chemoembolization (TACE) is used for the treatment of hepatocellular carcinoma not amenable for resection or percutaneous ablation. TACE embraces different procedures that aim at inducing ischemic necrosis and increasing the exposure of tumour cells to cytotoxic agents. In conventional TACE this is accomplished by the sequential intra-arterial injection of chemotherapeutic agents mixed with Lipiodol and embolizing particles. Despite the efforts of scientific societies to standardize TACE procedures, there are

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 3 1
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeSaturday, 5 September 2015
worldwide variations of drug vehicles, cytotoxic agents and embolizing particles, angiographic endpoints and selectivity. Superselective catheterization and the use of calibrated particles (including cytotoxic drug-eluting beads) should be preferred. Repeating TACE ‘on demand’ depending on the observed response and not at fixed pre-planned intervals is recommended nowadays because of the lower toxicity associated with this approach.
Tumour response after conventional or DEB-TACE should be evaluated using EASL or modified RECIST criteria that take into account tumour shrinkage and tumour necrosis. In patients with no tumour, response to the first TACE sessions should be considered for treatment with radioembolization or the systemic agent Sorafenib. Decision algorithms based on scores that take into account changes in liver function, levels of transaminases and tumour response should be validated prospectively before they can be recommended for clinical use.
12:45 – 14:00 SIG 4: Target and Systemic Therapies Hepatocellular Carcinoma with Stem Cell Features: How Can We Define and Handle Them
Forum EFLevel -1
Chairs: Joong-Won Park, MD, PhD (Republic of Korea) and Tim Meyer, MD, PhD (United Kingdom)
Hepatocellular carcinoma (HCC) has proved relatively refractory to systemic therapy, which has been associated with a low response rate and marginal improvement in survival. The existence of hepatocellular cancer stem cells (CSC) has been proposed as one of the mechanisms of resistance and the identification and therapeutic targeting of this sub-population has been the subject of intense research. Current data suggest that the co-expression of markers such as EpCAM and AFP define a Hepatic CSC phenotype with the ability to self-renew, differentiate and initiate tumours. Key signalling pathways that are dysregulated include the Wnt/beta-catenin, AKT, TGF-β pathways but the challenge for therapeutic targeting is to differentiate Hepatic CSC from normal hepatic SC. A number of strategies based on inhibition of NF-kB, microRNAs and epigenetics have been proposed and clinical trials are ongoing.
Aim of the session is to address the following questions:1. Introduction – Cancer stem cells in HCC: theory, evidence, and definition2. Clinical meaning of primary liver cancer with CSC3. Clinical perspectives in diagnosis of HCC CSC: pathologic and radiologic views4. How can HCC CSC be targeted for therapy?5. Discussion and wrap-up
12:45 – 14:00 SIG 5: Liver Surgery and Transplantation Surgery and Transplantation
Forum GH Level -1 Chairs: Thomas Decaens, MD, PhD (France) and Katsuhiko Yanaga, MD, PhD (Japan)
Liver surgery (resection and transplantation) remains the best therapeutic option for hepatocellular carcinoma (HCC). Both treatment are associated with very good 5-year overall survival despite a huge difference in tumour recurrence rate.
European, American and Asian guidelines are restricting the use of liver resection and liver transplantation to some patients. However, recent studies are showing good results in extended criteria such as resection in portal hypertension patients, resection in case of portal invasion, liver transplantation with extended criteria, liver transplantation after down-staging.
During this luncheon, we will present these new data and discuss with the audience about perspectives.
12:45 – 14:00 SIG 6: Non-HCC Hepatic Malignancies Update Systemic Therapy
Forum IJLevel -1 Chairs: Shahid A. Khan, MD, PhD (United Kingdom) and Gregory J. Gores, MD (USA)
This workshop will begin with two short presentations, each of 15-20 minutes, followed by an open discussion and Q&A session.

I L C A A n n u A L C o n f e r e n C e , 2 0 1 53 2
ILCA 2015 ProgrammeSaturday, 5 September 2015
Professor Gores will explore recent advances in our understanding of the aetiopathogenesis of cholangiocarcinoma. He will cover risk factors (obesity, hepatitis C virus, primary sclerosing cholangitis); the diagnosis of CCA in patients with PSC; and oncogenic pathways such as IDH and FGFR fusions and their therapeutic indications.
Dr. Khan will then summarise the currently available non-surgical therapies for cholangiocarcinoma, including loco-regional treatments, and provide an update on systemic therapies. The focus will be on the therapeutic potential of targeting specific molecular pathways.
12:45 – 14:00 Luncheon Workshop: Egypt Meets ILCA Common Approaches and Regional Disparities
AuditoriumLevel -1 Chairs: Peter R. Galle, MD, PhD (Germany) and Mahmoud El Meteini, MD (Egypt)
HCC is the most deadly complication of chronic liver diseases and emerged into a substantial healthcare problem in both Western countries as well as Africa, including Egypt. A striking variation in epidemiological factors of HCC divides Egypt from the Western world, whereby complex etiological differences are mainly related to the prevalence of major associated risk factors. While HCV is the most important risk factor for the development of HCC in Egypt, alcohol intake and NASH are predominant in the western world. Over the recent years, stabilization of incidence rates were observed in the Western world. However, a continuous incline is documented in Egypt and predicted to peak within the next 10-20 years. Therefore, detailed characterization, collection of patient data as well as scientific analysis of common and distinct features of HCCs in the different regions are of utmost importance to foster global approaches for preventive, diagnostic and therapeutic strategies and to optimize patient management. The session will give an overview about common standards and distinct approaches between Egypt and Western countries. In particular, therapeutic approaches including surgery and loco-regional strategies will be discussed. In this context, the potential impact of new HCV treatment regimens for future HCC therapies will also be delineated. The overall goal is to define regions of common interest and to foster new collaborative clinical and scientific collaborations to overcome the current era of unmet therapeutic needs in HCC.
Epidemiology of HCC and Hepatitis C: Egyptian ExperienceMohamed Kamal Shaker, MD (Egypt)
TreatmentAshraf Omar, MD (Egypt)
Clinical TrialsMarcus-Alexander Wörns, MD (Germany)
ResearchJens U. Marquardt, MD (Germany)
14:00 – 14:15 Session BreakScene FoyerGround level
14:15 – 15:45 General Session 4: Diagnosis and Curative TreatmentScene ABGround level
Chairs: Sandrine Faivre, MD, PhD (France) and Myron Schwartz, MD (USA)
O-023 Comparisons of Outcomes after Liver Resection for Hepatocellular Carcinoma between the East and the West, a Propensity Score Matching Analysis
Tian Yang 1, Parissa Tabrizian 2,*, Jun-Hua Lu 1, Wan-Yee Lau 1, Kutaiba Alshebeeb 2, Sander Florman 2, Han Zhang 1, Meng-Chao Wu 1, Feng Shen 1, Myron E. Schwartz 2
1Hepatic Surgery, Eastern Hepatobiliary Surgery Hospital, Second Military Medical University, Shanghai, China, 2Transplant, Recanati/Miller Transplant Institute, New York, United States

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 3 3
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeSaturday, 5 September 2015
O-024 Liquid Biopsy to Detect and Characterise Circulating Tumour Cells in Patients with Hepatocellular Carcinoma Using High Resolution Imagestream Multichannel Fluorescent Microscopy
Helen L. Reeves 1 2, Laura F. Ogle 1,*, Deborah Stocken 3, Ruth Plummer 1 4, Nicola Curtin 1, David Jamieson 1
1Northern Institute for Cancer Research, Newcastle University, 2Liver Unit, Freeman Hospital, Newcastle upon Tyne Hospitals NHS Foundation Trust, 3Institute of Health and Society, Newcastle University, 4Northern Centre for Cancer Care, Freeman Hospital, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle-upon-Tyne, United Kingdom
O-025 Disentangling the Effects of Race/Ethnicity and Socioeconomic Factors on Liver Transplantation Rates for Hepatocellular Carcinoma
Umut Sarpel 1,*, Maria Suprun 2, Anastasia Sofianou 3, Yaniv Berger 1, Andreas Tedjasukmana 4, Zennur Sekendiz 5, Emilia Bagiella 2, Myron E. Schwartz 6
1Department of Surgery, Division of Surgical Oncology, 2Department of Population, Health Science and Policy, 3Department of Strategic Planning, 4Department of Neurosurgery, Mount Sinai Medical Center, New York, NY, United States, 5Ross University, Roseau, Dominica, 6The Recanati / Miller Transplantation Institute, Mount Sinai Medical Center, New York, NY, United States
O-026 Can Meloxicam, a Cox-2 Inhibitor, Prevent Hepatocellular Carcinoma Recurrence after Initial Curative Treatment? A Result of Randomised Controlled Trial
Yuko Takami 1,*, Masaki Tateishi 1, Tomoki Ryu 1, Kazuhiro Mikagi 1, Yoshiyuki Wada 1, Hideki Saitsu 1
1Department of Hepato-Billiary-Pancreatic Surgery, Kyushu medical center, Fukuoka, Japan
O-027 Prospective Pilot Study of Living Donor Liver Transplantation for Patients with HCC Exceeding Milan Criteria
Josep Maria Llovet 1,*, Mihai Pavel 2, Jordi Rimola 3, Maria Alba Diaz 4, Jordi Colmenero 5, Constantino Fondevila 6, Josep Fuster 7, Pere Ginès 5, Jordi Bruix 8, Juan Carlos Garcia-Valdecasas 6
1Barcelona-Clínic Liver Cancer Group (BCLC), Liver Unit, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), CIBEREHD, Universitat de Barcelona and Institució Catalana de Recerca i Estudis Avançats, 2Liver Transplant Unit, Digestive and Metabolic Diseases Institute, 3Liver Unit, Barcelona-Clínic Liver Cancer Group BCLC, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), CIBEREHD, Universitat de Barcelona, 4Pathology Department, Hospital Clínic, University of Barcelona, 5Liver Transplant Unit and Liver Unit, 6Liver Transplant Unit, Digestive and Metabolic Diseases Institute. Hospital Clínic, University of Barcelona, 7Liver Transplant Unit and Liver Unit, Barcelona-Clínic Liver Cancer Group (BCLC) Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), CIBEREHD, Universitat de Barcelona and Digestive and Metabolic Diseases Institute Hospital Clínic, University of Barcelona, 8Liver Unit, Barcelona-Clínic Liver Cancer Group (BCLC), Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), CIBEREHD, Universitat de Barcelona and Digestive and Metabolic Diseases Institute. Hospital Clínic, University of Barcelona, Barcelona, Spain
O-028 Liver Transplantation versus Resection for Small Intrahepatic Cholangiocarcinoma or Hepatocholangiocarcinoma on Cirrhosis
Eleonora De Martin 1 2 3, Michel Rayar 4 5 6, Damien Bergeat 7, Luis Carvalho 4, Maximiliano Gelli 1, René Adam 1 8 9, Denis Castaing 1, Daniel Cherqui 1 8 9, Antonio Sa Cunha 1 8 9, Didier Samuel 1, Emmanuel Boleslawski 10 11, Karim Boudjema 4 5 6, Eric Vibert 1 2 3,*
1Centre Hépato Biliaire, AP-HP Hopital Paul Brousse, 2UMR-S1193, Univ Paris-Sud, 3Unit 1193, Inserm, Villejuif, 4Service de Chirurgie Hépatobiliaire et Digestive, CHU de Rennes - Hopital Pontchaillou, 5Université de Rennes 1, 6UMR991, Inserm, 7Service de Chirurgie Digestive et Transplantations, CHU de Lille - Hopital Claude Huriez, Rennes, 8Univ Paris-Sud, 9Inserm, Villejuif, 10Service de Chirurgie Digestive et Transplantations, CHU de Lille - Hopital Claude Huriez, 11Univ Nord-de-France, Lille, France
15:45 – 16:45 e-Poster Viewing Tour & Networking Break
Scene FoyerGround level
Opened by Jessica Zucman-Rossi, MD, PhD (France)

I L C A A n n u A L C o n f e r e n C e , 2 0 1 53 4
ILCA 2015 ProgrammeSaturday, 5 September 2015
16:45 – 18:30 ILCA Symposium 3: Advances in Transarterial Treatment of HCCScene ABGround level
Chairs: Peter R. Galle, MD, PhD (Germany) and Richard Finn, MD (USA)
TACE for HCC: What We Know, and What We Need to Know after Three Decades of ExperienceRiccardo Lencioni, MD, PhD (Italy)
Transarterial chemoembolisation (TACE) is the most widely used treatment for hepatocellular carcinoma (HCC) worldwide. A meta-analysis of randomised trials has established TACE as the standard of care for patients classified as intermediate-stage according to the Barcelona Clinic for Liver Cancer (BCLC) staging system. The most popular TACE technique is the administration of an anticancer-in-oil emulsion followed by embolic agents. The key component of this procedure is Lipiodol, which is used both as a vehicle to carry and localise the chemotherapeutic agent inside the tumour and as a microembolic agent for tiny tumour vessels. Recently, the introduction of embolic, drug-eluting beads has provided an alternative to Lipiodol-based regimens. Clinical experiences have suggested that drug-eluting beads provide a combined ischemic and cytotoxic effect locally with low systemic toxic exposure. However, any TACE regimen, by interrupting blood flow to the tumour, may create conditions that permit or encourage angiogenesis. Surrogate markers of tissue hypoxia that increase after TACE include hypoxia-inducible factor 1 alpha and both plasma and hepatic vascular endothelial growth factor. Thus, inhibition of angiogenesis may be synergistic with TACE. The introduction of molecular targeted agents that inhibit tumour cell proliferation and angiogenesis to the therapeutic armamentarium for HCC has prompted the design of clinical trials aimed at investigating the synergies between loco-regional and systemic treatments. Encouraging safety and efficacy signals were captured by the phase II studies completed so far. However, further randomised controlled studies are required to understand the survival benefit associated with such combination regimens.
Y90 Radioembolization for Hepatocellular Carcinoma: Demonstrating Efficacy through DataRiad Salem, MD (USA)
Treatment options for liver tumours that cannot be resected are based on transarterial techniques. Y90 microspheres represent one of those transarterial options. During the past 15 years, numerous studies involving larger cohorts, comparative effectiveness and small randomized studies have provided evidence of the safety and efficacy of Y90 in HCC. The versatility of this therapy is also highlighted in with selective lobar/segmental infusion with the intent of preserving functional liver reserve, down-staging to resection, radio-frequency ablation or liver transplantation. Of recent significant interest are radiation segmentectomy and lobectomy, treatment options that challenge RFA and PVE in HCC. The role in portal vein thrombosis is also of significant clinical interest, given the limited outcomes with sorafenib in this scenario. This presentation will review the state of the science and present role of radioembolization in HCC, as well as provide an update on the ongoing randomized phase 3 trials.
Advances in Transarterial Tumour Therapy: Does Novel Technology Mean Better Outcomes? Thierry de Baere, MD (France)
Conventional TACE (c-TACE) using Lipiodol with doxorubicin or cisplatinum is established as a standard of care in intermediate stage HCC, due to positive results of randomized controlled trials published in 2002. Since this publication, no treatment has been demonstrated superior. However, many advances have been carried out by the medical community including: new compound to deliver intra-arterially, new technologies in image guidance, and refinement in patient selection. New compounds are new platforms to deliver doxorubicin in drug eluting beads (DEB), which today has failed to demonstrate superiority to c-TACE in 2 randomized studies with tumour response and OS as primary end points. Improvement in DEB technology is ongoing with loading of new agents such as sunitinib, or the development of resorbable beads that are expected to lower some of the side effects of DEB-TACE.

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 3 5
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeSaturday, 5 September 2015
Internal radiation therapy with Lipiodol I131 injected through the hepatic artery has demonstrated in the 90s to improve survival in HCC patients with portal vein thrombosis. Y90 loaded microsphere is an advancement in such a treatment that allows to target HCC patients with PVT and several randomized studies will soon be completed to validate this treatment approach.Image guidance and catheter navigation has evolved with the use of microcatheter and improvement in angiographic imaging, namely with cone beam CT-3D angiography (CBCT). Such CBCT angiography has been demonstrated to give additional information in ¾ of the procedures, and modify treatment in roughly 1/4 of the cases. Moreover, such imaging technologies allows for early detection of untreated targets and has been demonstrated on retrospective study to significantly technical success versus DSA and decrease local recurrence rates between grade A and B tumours (p \ 0.001). The 1-, 2-, and 3-year local recurrence rates in the DSA and CBCT groups from 48% to 30.6%, after 3 years.
Targeting Glucose Metabolism: A New Class of Agents for Transarterial Treatment of HCC?Jean-François Geschwind, MD (USA)
Hepatocellular carcinoma (HCC) is one of the most highly lethal malignancies in the world, making it the third most common cause of cancer related mortality worldwide. In the United States, the incidence of HCC is on the rise, secondary to a concomitant rise in hepatitis C viral (HCV) infection; in the past 2 decades the incidence of HCV-related HCC has tripled. Overall survival remains poor at less than 9 months and largely depends on the stage of the disease; patients with intermediate-stage disease have better 3-year survival expectancies than patients with advanced-stage disease (50% vs. 8%, respectively). In addition, the vast majority of patients are diagnosed at the advanced stage of the disease because of the asymptomatic nature of the disease, as well as because of the lack of an early-detection marker for HCC. Despite recent advances in therapeutic strategies, treating HCC remains a daunting task because of its aggressive nature — more specifically the risk of local invasion, metastatic spread, and the high rate of recurrence after curative therapies — as well as because HCC is largely refractory to systemic chemotherapy. Thus, an effective therapeutic strategy targeting HCC-specific or HCC-related pathway(s) is clearly needed. Furthermore, to make things even more challenging, because HCC typically occurs in the setting of underlying liver disease (cirrhosis), potential new drug candidates would have to also exhibit an extremely favorable toxicity profile.
Tumour metabolismOne of the most important phenotypes exhibited in cancer is the up-regulation of the major energy-producing pathway, glycolysis. This altered tumour-specific glycolytic phenotype, first discovered by the German scientist Otto Warburg decades ago, plays a crucial role in several biosynthetic processes that facilitate uninterrupted tumour growth and is an indispensible “metabolic event” critical for the sustained growth and invasion of tumours. Given the inefficiency of glycolysis compared with oxidative phosphorylation (2 ATP vs. 36 ATP molecules produced per glucose molecule, respectively), one could wonder why cancer cells prefer glycolysis. The main reason for this preference is that the cancer cells are able to generate ATP through glycolysis at a much faster rate than oxidative phosphorylation to meet the energy demands of aggressive malignant growth. Increased glucose metabolism via glycolysis provides cancer cells with essential substrates for rapid proliferation, ribose for nucleic acid synthesis and pyruvate for cell membrane assembly. Furthermore, an abundant supply of glucose also facilitates the metabolism of glucose via the pentose phosphate pathway (PPP), which is involved in several biosynthetic processes, as well as cellular defense (antioxidants) against reactive oxygen species (ROS). It is well known that HCC cells exhibit the high glycolytic rate of other aggressive malignant tumours through differential expression of enzymes involved in the first step of glucose metabolism. Indeed, whereas normal liver cells rely on glucokinase (type IV hexokinase) to catalyze the first step of glycolysis, HCC cells markedly up-regulate the expression of a different isoform, specifically type II HK (HK II), while substantially down-regulating glucokinase. Similarly, other glycolytic enzymes such as glyceraldehyde-3 phosphate dehydrogenase (GAPDH), LDH, and others are also up-regulated during the malignant transformation of HCC. The disparity in glycolytic rate between tumour cells and normal cells resulting in an increased demand for glucose by cancer cells has already been used diagnostically by positron emission tomography (PET) for tumour imaging with the glucose analog fluorodeoxyglucose (FDG) but has never been exploited as a potential therapeutic target. In fact, because this finding is so ubiquitous in cancer, it is considered a “biochemical signature” of tumour cells. This is why tumour metabolism has been aptly described as “cancer’s Achilles’ Heel,” suggesting it as a possible therapeutic target. Because malignant cells become addicted

I L C A A n n u A L C o n f e r e n C e , 2 0 1 53 6
ILCA 2015 ProgrammeSaturday, 5 September 2015
to glycolysis and dependent on this pathway to generate ATP, inhibition of glycolysis would severely abolish ATP generation in cancer cells and thus preferentially kill the malignant cells while sparing healthy surrounding cells. Targeting glycolysis for the treatment of cancer should, therefore, be a promising novel therapeutic strategy.
Targeting Tumour Metabolism: A New Class of Anticancer AgentsRenewed research interest on tumour metabolism combined with a growing understanding of the molecular mechanisms involved in the regulation of tumour glycolysis contributed to the development of agents targeting glycolysis. Although some of these agents were evaluated in preclinical tumour models for their therapeutic potential, most did not make it into the clinic because of a lack of efficacy and the presence of significant toxicities. Recently however, one such metabolic blocker, 3-bromopyruvate (3-BrPA), a halogenated analog of pyruvic acid, has gained considerable attention because of its significant antitumor effects and its low toxicity profile. The addition of the halogen bromine to the monocarboxylic acid, pyruvate, results in alkylating properties of the compound. As a result, 3-BrPA will bind to its target by forming an irreversible chemical bond. In vitro testing against human HCC cells demonstrated that 3-BrPA inhibits glycolysis and blocks ATP production, causing apoptosis in a dose-dependent manner. Further investigation with radiolabeled 3-BrPA identified the glycolytic enzyme, GAPDH, as the primary intracellular target of this agent. The binding of 3-BrPA to GAPDH caused inhibition of the enzyme activity and, therefore, glycolytic ATP production leading to apoptotic cell death. Image-guided procedures, especially intra-arterial therapies, play a key role in the treatment of patients with liver cancer. The advantage of locoregional approaches is that they provide not only access to the core but also to the edge of the tumour. In addition, much greater drug concentrations can be achieved within tumours while minimizing systemic exposure. As a result, intra-arterial delivery of 3-BrPA was tested in various animal models of liver cancer. Results were extremely encouraging as tumours were successfully eradicated, in most cases significantly prolonging survival in the process. Some animals were even cured despite the fact these tumours are extremely aggressive. Unlike other alkylating agents, 3-BrPA demonstrated tremendous specificity in molecular targeting, enforcing its antitumorigenic effects by promoting energy depletion, disruption of redox balance, and induction of intracellular stress in a concurrent fashion. Therefore, it appears that 3-BrPA is an extremely promising agent because of its tumour selectivity and ability to promote a multipronged antitumor effect. In summary, despite cancer’s extreme genetic heterogeneity, the reliance on glycolysis for energy needs and growth is a common pathway that most cancer cells share. As a result, targeting this pathway for therapeutic means is extremely attractive. A new agent 3-BrPA, which specifically inhibits this glycolytic pathway in tumours has already shown great promise in several animal models of liver cancer and could have a significant effect on the survival of patients with liver cancer. Clinical trials are to begin soon.
18:30 – 19:30 Sirtex Symposium: SIR-Spheres Y-90 Resin Microspheres – Developing a New Standard for Primary Liver CancersAuditorium
Level -1 Chairs: Jordi Bruix, MD (Spain) and Kai-Wen Huang, MD (Taiwan)
Welcome & Introduction Jordi Bruix, MD (Spain) and Kai-Wen Huang, MD (Taiwan)
Running HCC Phase III in Asia Pacific: SIRveNIB & Taiwan HCC guidelines Kai-Wen Huang, MD (Taipei, Taiwan)
Running HCC Phase III in Europe: SARAH and SORAMIC Jens Ricke, MD, PhD (Germany)
The Evidence to Support the Use of SIR-Spheres Y-90 Resin Microspheres in ICC Bruno Sangro, MD, PhD (Spain)
A New Study for SIR-Spheres Y-90 Resin Microspheres in ICC Jordi Bruix, MD (Spain)
Panel Discussion and Closing

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 3 7
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeSunday, 6 September 2015
Sunday, 6 September 2015
07:30 – 08:30 Bristol-Myers Squibb Symposium: Emerging Research in Immuno-Oncology: Hepatocellular Carcinoma
ForumLevel -1
Chair: Bruno Sangro, MD, PhD (Spain)
Welcome and Introduction Bruno Sangro, MD, PhD (Spain)
Rationale for Immuno-Oncology in HCC Bruno Sangro, MD, PhD (Spain)
Current and Emerging Immuno-Oncology Clinical Research in HCC Anthony El-Khoueiry, MD (USA)
What is the Future of HCC Treatment? US/EU Perspective Richard Finn, MD (USA)
What is the Future of HCC Treatment? Asia Perspective Ann-Lii Cheng, MD, PhD (Taiwan)
Q&A, Summary and Closing
08:30 – 09:15 ILCA General AssemblyScene ABGround level
09:15 – 09:45 Coffee & Networking BreakScene FoyerGround level
09:45 – 10:45 State-of-the-Art Lecture 2: Fibrolamellar Carcinoma
Scene ABGround level
Chair: Curtis C. Harris, MD (USA) Speaker: Sanford M. Simon, PhD (USA)
Fibrolamellar hepatocellular carcinoma (FLHCC) is a rare liver tumour that usually occurs in adolescents and young adults. Originally considered a variant of hepatocellular carcinoma (HCC), FLHCC is characterized by hepatocytes with deeply eosinophilic, granular cytoplasm interspersed with fibrous bands, without signs of cirrhosis as in HCC. We used genomic analysis to explore its molecular pathogenesis, comparing FLHCC paired with normal liver from the same patient.Our results demonstrated that the majority of the DNA is unremarkable with few recurrent mutations or structural variants such as amplifications or inversions. The major finding is a heterogeneous deletion of ~400 kB in chromosome 19, which produces a chimeric transcript and a fully functional protein, a fusion between the heat shock protein DNAJB1 and the catalytic subunit of protein kinase A (PRKACA). Our initial observation of this chimera in 15 out of 15 patients has now been expanded to 116 out of 116 patients. Differential expression analysis of RNA-seq revealed many changes in the gene expression in FLHCC as compared to its paired normal liver. These changes were highly consistent from patient to patient, suggesting a unifying pathogenesis. The RNA-seq from our FLHCC samples had little in common with HCC samples from the TCGA or published reports of other cancers. An analysis of protein expression correlated well with the RNA-seq results. Some observed changes can directly be linked to increased activity of PRKACA. Other changes involve pathways known to participate in the initiation and progression of other cancers, which, along with an increase of PRKACA activity, represent targets for therapeutic intervention. Several of these targets are now being explored in cellular models, genetic, and PDX mouse models, as well as clinical trials.

I L C A A n n u A L C o n f e r e n C e , 2 0 1 53 8
ILCA 2015 ProgrammeSunday, 6 September 2015
10:45 – 12:15 General Session 5: From Drivers to Clinical Trials Scene ABGround level
Chairs: Sheng-Long Ye, MD, PhD (P. R. China) and Morris Sherman, MD, PhD (Canada)
O-029 Tivantinib in Pretreated Hepatocellular Carcinoma (HCC): Tumour and Plasma Biomarker Analysis from the Randomized Controlled Phase 2 Trial (Rct)
Lorenza Rimassa 1,*, Giovanni Abbadessa 2, Nicola Personeni 1 3, Camillo Porta 4, Ivan Borbath 5, Bruno Daniele 6, Stefania Salvagni 7, Jean Luc Van Laethem 8, Hans Van Vlierberghe 9, Joerg Trojan 10, Enrico De Toni 11, Alan Weiss 12, Steven Miles 13, Antonio Gasbarrini 14, Monica Lencioni 15, Maria E. Lamar 16, Yunxia Wang 17, Reinhard Von Roemeling 18, Brian Schwartz 16, Armando Santoro 1
1Humanitas Cancer Center, Humanitas Clinical and Research Center, Rozzano, Italy, 2Clinical Development & Translational Medicine, ArQule, Burlington, MA, United States, 3Department of Medical Biotechnology and Translational Medicine, University of Milan, Milan, 4Oncologia Medica, Fondazione IRCCS Policlinico Universitario San Matteo, Pavia, Italy, 5Gastro-entérologie, Cliniques Universitaires Saint-Luc, Brussels, Belgium, 6Oncology, G. Rummo Hospital, Benevento, 7Oncologia Medica, Azienda Ospedaliera Parma, Parma, Italy, 8Gastro-entérologie, Erasme University Hospital, Brussels, 9Gastro-entérologie, Ghent University Hospital, Gent, Belgium, 10Internal Medicine, J. W. Goethe University Hospital, Frankfurt, 11Medicine II, Klinikum der Universitat Munchen-Groshadern, Munich, Germany, 12Gastroenterology, Vancouver General Hospital and British Columbia Cancer Clinic, Vancouver, Canada, 13Oncology, Cedar Sinai, Los Angeles, CA, United States, 14Patologia Speciale Medica e Semeiotica Medica, Policlinico Universitario Agostino Gemelli, Rome, 15Oncology, Azienda Ospedaliero-Universitaria di Pisa, Pisa, Italy, 16Clinical Development, 17Pharmacology, ArQule, Burlington, MA, 18Clinical Development, Daiichi-Sankyo, Edison, NJ, United States
O-030 Fgf19 Aberrations and Selective Targeting With Fgfr4 Inhibitors for Hepatocellular Carcinoma Klaus Hoeflich 1, Agrin Moeini 2, Margit Hagel 1, Chandra Miduturu 1, Daniela Sia 2, Roser Pinyol 3, Judit Peix 3,
Qiongfang Fong 1, Nicolas Stransky 1, Oleg Schmidt-Kittler 1, Josep Llovet 2, Christoph Lengauer 1, Ben Wolf *1
1Blueprint Medicines, Cambridge, 2Mount Sinai Liver Cancer Program, Icahn School of Medicine at Mount Sinai, New York, United States, 3Liver Cancer Translational Research Laboratory, BCLC group, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS)- Hospital Clínic, Liver Unit, Universitat de Barcelona, Barcelona, Spain
O-031 Preoperative Sorafenib-Induced Antitumor Activity in Patients with Resectable Hepatocellular Carcinoma (HCC): Results of the Bioshare Neoadjuvant Phase 2 Study from Gercor Irc
Mohamed Bouattour 1,*, Laetitia Fartoux 2, Olivier Rosmorduc 2, Eric Vibert 3, Charlotte Costentin 4, Olivier Soubrane 5, Maxime Ronot 6, Muriel Granier 7, Armand De Gramont 7, Jacques Belghiti 5, Valérie Paradis 8, Annemilaï Tijeras-Raballand 9, Alexandra Hadengue 10, David Brusquant 10, Benoist Chibaudel 10, Eric Raymond 7, Sandrine Faivre 7
1Hepatology, Beaujon University Hospital, Clichy, 2Hepatology, Saint-Antoine University Hospital, Paris, 3Hepato-Biliary Surgery, Paul-Brousse University Hospital, Villejuif, 4Hepatology, Henri-Mondor University Hospital, Creteil, 5Hepato-Biliary Surgery, 6Radiology, Beaujon University Hospital, Clichy, France, 7Medical Oncology, Centre Hospitalo-Universitaire Vaudois (CHUV), Lausanne, Switzerland, 8Pathology, Beaujon University Hospital, Clichy, 9AAREC FILIA RESEARCH, 10GERCOR, Paris, France
O-032 Randomized Phase Iib Study of Pexa-Vec (Pexastimogene Devacirepvec; Jx-594), an Oncolytic Immunotherapy Plus Best Supportive Care (Bsc) versus Bsc Alone in Patients with Hepatocellular Carcinoma (HCC) Who Failed Sorafenib Treatment (Traverse)
Markus Moehler 1,*, Han Chu Lee 2, Won Young Tak 3, Yee Chao 4, Seung Woon Paik 5, Ari Baron 6, Guy Ungerechts 7, Jean-Frederic Blanc 8, Mong Cho 9, Laura Findeiss 10, Francois Habersetzer 11, Derek Jonker 12, Philippe Merle 13, Leyo Ruo 14, Oliver Ebert 15, Tony Reid 16, Riccardo Lencioni 17, Adina Pelusio 18, Monika Lusky 19, Nicolas Stojkowitz 19, Marie Hennequi 19, David H. Kirn 18, Jean-Marc Limacher 19, Caroline J. Breitbach 18, Michel Homerin 19, James Burke 18, Jeong Heo 20
1Johannes Gutenberg-Universität Mainz, Mainz, Germany, 2Asan Medical Center, Seoul, 3Kyungpook National University Medical Center, Daegu, Korea, Republic Of, 4Taipei Veterans General Hospital, Taipei, Taiwan, 5Samsung Medical Center, Seoul, Korea, Republic Of, 6California Pacific Medical Center, San Francisco, United States, 7National Center for Tumour Diseases, DKFZ, Heidelberg, Germany, 8Centre Hospitalier Universitaire Hôpital Saint

I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 3 9
General Session Industry Symposium Symposium Workshop State-of-the-Art Lecture
ILCA 2015 ProgrammeSunday, 6 September 2015
André, Bordeaux, France, 9Pusan National University Yangsan Hospital, Yangsan, Korea, Republic Of, 10University of California Irvine Medical Center, Orange, United States, 11Hôpitaux Universitaires de Strasbourg - Hôpital Civil, Strasbourg, France, 12The Ottawa Hospital Regional Cancer Centre, Ottawa, Canada, 13Hôpital de la Croix Rousse, Lyon, France, 14Juravinski Hospital and Cancer Centre, Hamilton, Canada, 15Klinikum Rechts der Isar, Technische Universität München, München, Germany, 16University of California San Diego Moores Cancer Center, San Diego, United States, 17Pisa University School of Medicine, Pisa, Italy, 18SillaJen, San Francisco, United States, 19Transgene, Illkirch-Graffenstaden, France, 20Pusan National University Hospital, Busan, Korea, Republic Of
O-033 Ramucirumab (Ram) as Second-Line Treatment in Patients (Pts) with Advanced Hepatocellular Carcinoma (HCC): Japanese Subgroup Analysis of the Phase III Reach Trial
Etsuro Hatano 1,*, Masatoshi Kudo 2, Takuji Okusaka 3, Shinichi Ohkawa 4, Hirofumi Fujii 5, Akihide Masumoto 6, Junji Furuse 7, Yoshiyuki Wada 8, Hiroshi Ishii 9, Shuntaro Obi 10, Kuniaki Arai 11, Seiji Kawazoe 12, Osamu Yokosuka 13, Masafumi Ikeda 14, Katsuaki Ukai 15, Sojiro Morita 16, Hiroya Asou 17, Paolo B. Abada 18, Ling Yang 19, Andrew X. Zhu 20
1Kyoto University Hospital, Kyoto, 2Kinki University School of Medicine, Osaka, 3National Cancer Center Hospital, Tokyo, 4Kanagawa Cancer Center, Kanagawa, 5Jichi Medical University, Tochigi, 6Aso Corporation Iizuka Hospital, Fukuoka, 7Kyorin University Hospital, Tokyo, 8National Hospital Organization Kyushu Medical Center, Fukuoka, 9The Cancer Institute Hospital of Japanese Foundation for Cancer Research, 10Kyoundo Hospital, Sasaki Institute, Tokyo, 11Kanazawa University Hospital, Ishikawa, 12Saga-Ken Medical Centre, 13Chiba University Hospital, 14National Cancer Center Hospital East, Chiba, 15Sendai Medical Center, Miyagi, 16Kochi Health Sciences Center, Kochi, 17Eli Lilly and Company, Kobe, Japan, 18Eli Lilly and Company, Indianapolis, IN, 19Eli Lilly and Company, Bridgewater, NJ, 20Massachusetts General Hospital, Cancer Center, Harvard Medical School, Boston, United States
O-034 Results of a Proof-Of-Concept Phase 2 Trial of Tasquinimod in Patients with Advanced Hepatocellular Carcinoma Previously Treated With Sorafenib
Julien Edeline 1,*, Laetitia Fartoux 2, Hal Hirte 3, Christelle Descot 4, Nathalie Germann 4, Sandrine Faivre 5
1Département d’Oncologie Médicale, Centre Eugène Marquis, Rennes, 2Département d’Hépato-gastroentérologie, Hôpital Saint Antoine, Paris, France, 3Juravinski Cancer Centre, McMaster University, Hamilton, Canada, 4Ipsen Innovation, Les Ulis, 5Service de Cancérologie, Hôpital Beaujon, Clichy, France
12:15 – 12:30 Closing Ceremony
Scene ABGround level
Peter R. Galle, MD, PhD (Germany)

I L C A A n n u A L C o n f e r e n C e , 2 0 1 54 0

Practicalities
I L C A A N N U A L C O N F E R E N C E , 2 0 1 5 4 1
I L C A A n n u A L C o n f e r e n C e , 2 0 1 54 2
PracticalitiesAbout Paris
Synonymous with romance, glamour and gastronomy, Paris is constantly working to maintain its historic charm. The last few years have seen the dream destination of Paris add new tourist attractions to the breathtaking variety already on offer.
The fabulous choice of museums is continuously increasing. But Paris is, of course, much more than just a museum piece. Paris has a timeless familiarity for first-time and frequent visitors, with instantly recognisable architectural icons, along with exquisite cuisine, chic boutiques and priceless artistic treasures.
With over 180 museums and monuments to visit, there will always be something in Paris to interest you during your stay. This ranges from the world famous Eiffel Tower, to lesser known wonders such as the Moulin de la Charité.
Currency and Banking The official currency of France is the Euro. In Paris, you will come across a multitude of banks, many of which operate in French and other foreign languages. They are generally open from 09:00 to 17:00 or 18:00, from Monday to Friday. Some may be open on Saturdays. Certain branches may close at lunchtime, between 12:30 and 14:00.
Even though you may find some banks who will accept your currency in exchange for euros, you are more likely to come across exchange bureaux, which specialise in this type of transaction. Make sure you have some ID with you. In Paris, you will find numerous exchange bureaux in busy tourist areas and they are usually open on Sundays too.
Electricity The standard plug in Paris uses 230-240 Volts, with the two pin plug socket. For American electrical appliances, you may need a voltage transformer, as well as an adaptor for the plug. If your appliances are dual voltage, you do not need a transformer.
Emergency Phone NumberFor Police, Fire service or Medical service, call 112 (European Emergency Telephone Number).
Health and SafetyParis is generally considered a safe city, with a low risk of mugging and other serious offences compared to other major cities. However, if you wander around the Eiffel Tower, be careful as it is a known spot for pickpockets. If you need to contact the emergency services, ring 112.
Insurance and LiabilityILCA is insured only to meet claims arising from incidents caused
by the organisers and their equipment. Participants, exhibitors and visitors are strongly recommended to be properly insured against accidents they may suffer when travelling and during the conference.
Public TransportThe easiest and cheapest way to get around Paris is by using the extensive public transport available. This includes Metro, Bus, Noctilien (night bus service in Paris and its agglomeration) and RER (Réseau Express Régional – regional express network in Paris and its suburbs).
Taxis Taxis can be hard to find, especially at rush hour or early in the morning. The best way is to find a taxi rank (station de taxis, marked with a blue sign) on major roads, crossroads and at stations. A white light on a taxi’s roof indicates the car is free; an orange light means the cab is busy. There is a service charge of €2,10. The rates are then based on zone and time of day.
The following firms take phone bookings 24/7. Note that you will pay for the time it takes the taxi to reach you. If you wish to pay by credit card, mention it when you order.
Alpha +33 1 45 85 85 85, www.alphataxis.frG7 +33 1 47 39 47 39, www.taxisg7.comTaxis Bleus +33 8 91 70 10 10, www.taxis-bleus.com
RestaurantsParis is famous for having some of the finest restaurants in the world. In Paris, you will find a large range of international restaurants, but also traditional French cuisine to indulge yourself in some local culture. Champaign, bread, wine and French cheese will make your visit to Paris one to remember. Bread and cheese will usually be the main basic ingredients of your Parisian meal.
Taxes and TippingIn France, all prices shown include tax and service (the latter is around 15% of the total price). However, if the service has been particularly good, you may wish to leave a tip in order to show your appreciation. Generally, the amount is 5 to 10% of the total bill. If you receive remarkable service, don’t hesitate to leave 15%.
Time DifferenceParis is 1 hour ahead of GMT (GMT +1).
© P
aris
Tou
rist O
ffice
- P
hoto
grap
he :
Dani
el T
hier
ry
© P
aris
Tou
rist O
ffice
- P
hoto
grap
he :
Anne
mie
k Ve
ldm
an

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 4 3
PracticalitiesAbout the Conference
About ILCA The International Liver Cancer Association (ILCA) is the only international organisation devoted exclusively to liver cancer research for experts from all related disciplines.
ILCA aims at creating an international multidisciplinary forum to address the increasing incidence of liver cancer through the enhancement of the knowledge of clinical, translational and basic research, ultimately creating novel preventive, diagnostic and therapeutic strategies.
The purpose for which ILCA was established is the advancement of medical education, research and clinical care in the field of liver cancer.
Please come and visit us at the ILCA stand where the ILCA Team will be delighted to provide any information you may wish to have on ILCA activities, membership and future conferences. Information is also available at www.ilca-online.org.
AccreditationEACCME
The 9th ILCA Annual Conference is accredited by the European Accreditation Council for Continuing Medical Education (EACCME) to provide CME activity for medical specialists. The EACCME is an institution of the European Union of Medical Specialists (UEMS) – www.uems.net.
The 9th ILCA Annual Conference is designated for a maximum of 18 hours of European external CME credits.
Each medical specialist should claim only those hours of credit that he/she actually spent in the educational activity. The EACCME credit system is based on 1 ECMEC per hour with a maximum of 3 ECMECs for half a day and 6 ECMECs for a full-day event.
Through an agreement between the European Union of Medical Specialists and the American Medical Association, physicians may convert EACCME credits to an equivalent number of AMA PRA Category 1 Credits™. Information on the process to convert EACCME credit to AMA credit can be found at www.ama-assn.org/go/internationalcme.
BadgesFor security purposes, all participants will be issued with a conference badge onsite, which must be worn at all times during the conference and at any other officially related functions.
Certificate of AttendanceA certificate of attendance will be sent by email after the conference.
Conference Capture The main sessions of the conference will be recorded and made available to ILCA members and conference participants at www.ilca-online.org shortly after the event. You will be notified by email when the capture is available.
ILCA thanks its Diamond Partner, Bayer Healthcare, for making the Conference Capture possible through an unrestricted educational grant.
DisclaimerILCA and/or the conference organisers will not be liable for personal injury or safety of any participant, nor for any loss or damage of private property of registered participants during the conference.
e-Poster Viewing Tourse-Poster Viewing Tours will be held on Saturday, 5 September 2015 from 10:00 – 11:00 and from 15:45 – 16:45.
Both of the e-Poster Viewing Tours will be opened by ILCA prominent scientists – Prof. Peter R. Galle, ILCA President (in the morning from 10:00 – 11:00) and by Prof. Jessica Zucman-Rossi, ILCA Executive Secretary Elect (in the afternoon from 15:45 – 16:45) and will be partly dedicated to the 30 top scored abstracts displayed as paper board posters.
e-Posters
e-Posters will be displayed in the Scene Foyer, Ground level throughout the conference and e-Poster presenters will have the opportunity to introduce their research findings described in their e-Poster to the conference participants during the specific e-Poster Viewing Tours.
Paper board posters
Paper board poster presentations will take place at the beginning of each e-Poster Viewing Tour in the Poster of Excellence Area (Scene Foyer, Ground Level). Presenters will be invited to give a brief summary of their major findings described in the poster.
During the e-Poster Viewing Tours, all abstract authors must ensure that at least one author per poster is in attendance to present the research and answer any questions from visitors in attendance.

I L C A A n n u A L C o n f e r e n C e , 2 0 1 54 4
Please refer to the Book of Abstracts for details on poster locations during the e-Poster Viewing Tours.
General Sessions – Oral CommunicationsPresenters are allowed 10 minutes for each presentation, followed by 5 minutes for questions and answers. They must be present in the corresponding room at least 15 minutes before the session starts.
ILCA Pre-Conference Workshop on Immunopathogenesis and Immunotherapy in HCCThe main objective of this workshop is to understand the role of the immune system in hepatocarcinogenesis, define potential areas of immunotherapy in HCC and summarise current data on immunotherapy in HCC.
The members of the Workshop Organising Committee, Lisa H. Butterfield, Tim F. Greten and Martin F. Sprinzl, led by ILCA President, Peter R. Galle, will drive the content of the workshop and will subsequently work on producing the manuscript based on the contribution from the speakers and participants.
As a result of this workshop, another edition of ILCA Consensus Guidelines will be produced.
Industry ExhibitionThe Industry Exhibition will take place in the Scene Foyer (Ground Level). Opening hours are as follows:
Internet CaféThe Internet Café is available to all delegates in the Scene Foyer throughout the Industry Exhibition opening hours.
Junior Investigator AwardsILCA will recognise extraordinary achievements in liver cancer research across disciplines and support the professional development of four junior investigators in training. The awards will be given for novel and significant liver cancer research across the fields of basic cancer research; translational cancer research; cancer diagnosis; cancer prevention; or cancer patients treatment.
The investigators who submit the best clinical oral and best poster presentations and the best basic-translational oral and best poster presentations will be honoured on Saturday, 5 September 2015 during the Plenary Session of the 9th ILCA Annual Conference.
SIG Luncheon WorkshopsPre-registered luncheon workshop participants will receive a ticket with their badge, which will give them priority seating in the workshop room. Participants are allowed to take their lunch into workshop rooms.
Nelson Fausto Recognition AwardILCA will grant the Nelson Fausto Recognition Award at the 9th
ILCA Annual Conference to recognise a senior professional for outstanding contributions to liver cancer science.
Official LanguageThe official language of the conference is English. Simultaneous translation will not be provided.
Registration DeskThe registration desk is located in the Scene Foyer, on the Ground level and opens as follows:
Thursday, 3 September 2015: 12:00 – 19:00Friday, 4 September 2015: 07:00 – 19:00Saturday, 5 September 2015: 07:30 – 19:00Sunday, 6 September 2015: 07:30 – 12:00
PracticalitiesAbout the Conference
Friday, 4 September
10:30 – 11:00
12:45 – 14:45
Coffee break in exhibition areaSession breaks in the exhibition area and lunch in the plenary room
16:15 – 16:45
18:15 – 19:00
Coffee break in exhibition areaWelcome Reception in exhibition area
Saturday, 5 September
10:00 – 11:00 Coffee, Networking Break and e-Poster Viewing Tour
12:30 – 14:1515:45 – 16:45
Session break and lunchCoffee, networking break and e-Poster Viewing Tour
Sunday, 6 September
09:15 – 09:45 Coffee break in the exhibition area

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 4 5
PracticalitiesAbout the Conference
Speakers’ InformationThe Speakers’ ready room is located at the entrance of the conference area, on the Ground level, in the Studio Room, and is open at the same time as the registration desk.
Speakers are requested to submit their PowerPoint slides one day before the day of their presentation, and to be present in the corresponding room at least 15 minutes before the session starts.
VenueParis Marriott Rive Gauche Hotel & Conference Center17 Boulevard Saint JacquesParis 75014 FranceTel : +33 1 4078 7980Fax : +33 1 4588 4393
Welcome ReceptionOn Friday, 4 September 2015, all ILCA 2015 participants are cordially invited to join their colleagues and friends in the exhibition area for an informal networking experience from 18:15 onwards.
ILCA School of Liver Cancer 2016Hosted by the Barcelona Clinic Liver Cancer (BCLC), celebrating its 30th anniversary
Liver Cancer: Future Prospects in Management and Research
Learning objectives:
Incorporating epidemiology, molecular and clinical knowledge
Understanding the value and limitations of molecular profiling in providing robust clinical decision tools and identifying new treatment targets
Illustrating the challenges in personalised treatment decisions in the frame of evidence based medicine
Identifying the major basic and clinical research needs and how to face them through optimal study design and analysis.
7 – 8 March 2016Barcelona, Spain
Venue: Paranimf Hall | School of Medicine, University of Barcelona
A unique multidisciplinary and interactive educational platform for practitioners and investigators to learn about the principles and nuances of the diagnosis, management, and clinical investigation of liver cancer.
Supported by an educational grant from Bayer HealthCare
Pharmaceuticals Inc. ilca-online.orgStay tuned for more information

I L C A A n n u A L C o n f e r e n C e , 2 0 1 54 6
PracticalitiesAbout the Conference
Conference Area Floor Plan
Level -1
Forum
Pre-Conference workshop
Egypt Meets ILCA
SIG 2
SIG 4
SIG 5
SIG 6
SIG 3 B
A
C
EF
GH
IJ
Auditorium
Ground level
Scène
Registration desk
Speaker ready room
Conference Center
Entrance
Hotel Lobby
Exhibition area
Poster areae-Poster area
A
BCD
EF
Plenary room + SIG 1

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 4 7
Exhibition Area
PracticalitiesAbout the Conference
BMS
BayerCelsion
Humedics
Sirtex
Catering
Catering
Catering
e-posters
Scène F
Exhibition area
Entrance


4 9I L C A A N N U A L C O N F E R E N C E , 2 0 1 5
Exhibitors, Sponsors,Media and other Partners

I L C A A n n u A L C o n f e r e n C e , 2 0 1 55 0
Exhibitors, Sponsors, Media and other Partners
ILCA thanks all its partners and sponsors for their involvement in ILCA 2015.
Diamond Partner
Bayer is committed to delivering science for a better life by advancing a portfolio of innovative treatments. Bayer’s oncology franchise now includes three oncology products and several other compounds in various stages of clinical development. Together, these products reflect the company’s approach to research, which prioritises targets and pathways with the potential to impact the way that cancer is treated.
Gold Partners
Bristol-Myers Squibb is a global biopharmaceutical company whose mission is to discover, develop and deliver innovative medicines that help patients prevail over serious diseases.
For more information about Bristol-Myers Squibb, visit www.bms.com or follow us on Twitter.
Sirtex Medical is actively engaged in the field of liver-directed therapies for cancer patients.
Our innovative technology, SIR-Spheres® microspheres (Yttrium-90 resin beads), was approved in 2002 for use in the treatment of a variety of unresectable liver tumours a well as in hepatocellular carcinoma within the European Union under a CE Mark. SIR-Spheres® microspheres are presently used at more than 250 institutions in Europe.
®SIR-Spheres is a Registered Trademark of Sirtex SIR-Spheres Pty Ltd
Silver Partner
Celsion is a fully-integrated oncology company focused on developing a portfolio of innovative cancer treatments, including directed chemotherapies, immunotherapies and RNA- or DNA-based therapies. The Company’s lead program is ThermoDox®, a proprietary heat-activated liposomal encapsulation of doxorubicin, currently in Phase III development for the treatment of primary liver cancer and Phase II development for the treatment of recurrent chest wall breast cancer. The pipeline also includes GEN-1, a DNA-based immunotherapy for the localized treatment of ovarian and brain cancers. Celsion has three platform technologies for the development of novel nucleic acid-based immunotherapies and other anti-cancer DNA or RNA therapies, including TheraPlas™ and TheraSilence™.
For more information on Celsion, visit our website at www.celsion.com.
Bronze Partner
A phase 3, randomized, double-blind study of tivantinib (ARQ 197) in subjects with MET-High, Child-Pugh A, ECOG 0-1, inoperable, measurable hepatocellular carcinoma (HCC) who progressed or were intolerant to one prior systemic therapy including sorafenib.

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 5 1
Exhibitors, Sponsors, Media and other Partners
Sponsors & Exhibitors
Exhibitors
Humedics specializes in real-time liver function measurement. The Berlin based company has an innovative breath test, LiMAx, measuring liver function instantly at the bedside and identify underlying hepatic functional impairment. LiMAx provides doctors a better and safer basis in their decision making and has already successfully helped thousands of patients.
Coffee Break Partner
Media Partners ILCA thanks the following scientific publications for their support:

I L C A A n n u A L C o n f e r e n C e , 2 0 1 55 2
Exhibitors, Sponsors, Media and other Partners
Partner SocietiesILCA has established partnerships with several professional scientific societies and institutions that share the goal of advancing multidisciplinary research in liver cancer.
Related entities that have welcomed and/or supported ILCA since its foundation are: •American Association for Cancer Research (ACCR)
•American Association for the Study of Liver Diseases (AASLD)
•American Hepato-Pancreato-Biliary Association (AHPBA)
•Asian Pacific Association for the Study of the Liver (APASL)
•Cardiovascular and Interventional Radiology European Society (CIRSE)
•European Association for the Study of the Liver (EASL)
•European Liver and Intestine Transplant Association (ELITA)
•International Agency for Research on Cancer (IARC)
•Japanese Society of Hepatology (JSH)
•National Cancer Institute (NCI)
•World Gastroenterology Organisation (WGO)

Titre
5 3I L C A A N N U A L C O N F E R E N C E , 2 0 1 5
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 55 4
Speakers’ Portfolio
Antonio Bertoletti, MD (Singapore)
Antonio Bertoletti, MD is an expert in the field of viral hepatitis. He began working in viral hepatitis as a medical student at the University of Parma (Italy). During his MD specialization (1991) in infectious diseases, he spent two years at the Scripps Research Institute (La Jolla) characterizing for the first time in human the Hepatitis B virus (HBV) specific cytotoxic T-cells. He returned to the University of Parma, where he worked in the Department of Infectious Diseases as a Clinical Scientist continuing his study of human HBV specific T-cells (1991-1997), before joining The UCL Institute of Hepatology at the University College of London (UK) (1997).
In 2006, he moved to Singapore where he became the Director of Infection and Immunity Program at the Singapore Institute for Clinical Sciences (A*STAR) until 2013, before moving to the Emerging Viral Disease Program at Duke-NUS Medical School.
His current research focuses on understanding the impact of age in HBV infection/pathology and on the development of new immunological based therapies (TCR-redirected T-cells, HLA-peptide specific antibodies) for the treatment of HBV and Hepatocellularcarcinoma.
Luigi Bolondi, MD (Italy)
Luigi Bolondi is the president of the School of Medicine, University of Bologna, where he also serves as full professor of internal medicine and as Director of the postgraduate course in ultrasonology in internal medicine. He is the former Director of the PhD course in Medical Sciences for the University (2006-2012).
Prof. Bolondi has served as General Secretary (1981-1989) and President (1993-1995) of the Italian Society for Ultrasound in Medicine and Biology. He is a former President of the European Federation of Societies of Ultrasound in Medicine and Biology (1996-1999) and a former member of the board of the Italian Society for the Study of the Liver (1993-1996). He has served as the organizer of several medical meetings, including 4 national congresses of the Italian Society for Ultrasound in Medicine and Biology, a single-topic meeting in 2000 of the European Association for the Study of the Liver, the World Congress of Ultrasound in Medicine and Biology in 2000, and the 2006 European Congress for Ultrasound in Medicine and Biology, which was held in Bologna. He is an honorary member of the American Institute of Ultrasound in Medicine.
In addition to his extensive work in academia and scientific societies, Prof. Bolondi is a member of the editorial board of the Journal of Clinical Ultrasound, and a former member of the boards of Hepatology. Currently, he is the associate editor of the Journal of Hepatology. Prof. Bolondi is the author or co-author of 6 textbooks on hepatocellular carcinoma and diagnostic imaging, including 3 books published internationally. Additionally, he has written 55 textbook chapters and published more than 315 articles in leading international journals (H index = 54).
Caroline Breitbach, PhD (USA)
Caroline J. Breitbach is Vice President, Clinical & Translational Research at SillaJen Biotherapeutics (formerly Jennerex Biotherapeutics), focusing on the development of oncolytic immunotherapy for HCC. Caroline oversaw Phase 1 and Phase 2 clinical studies of Pexa-Vec, an oncolytic vaccinia virus, in patients with HCC. The program is now entering Phase 3 studies in sorafenib-naïve HCC patients; the Phase 3 protocol was finalized in collaboration with the FDA through the Special Protocol Assessment process.
Caroline received her undergraduate degree, Honours in Microbiology & Immunology, at McGill University in Montreal, Canada. She subsequently joined Dr. John Bell’s group at the University of Ottawa in Ottawa, Canada. Over the course of her PhD, she elucidated the mechanism by which oncolytic virus infection triggers a reduction in tumour perfusion and extensive cell death of uninfected tumour cells.

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 5 5
Jordi Bruix, MD (Spain)
Jordi Bruix is a Professor of Medicine at the University of Barcelona and director of the Barcelona Clinic Liver Cancer Group within the liver unit at the Hospital Clínic of Barcelona in Barcelona, Spain.
Dr. Bruix is a member of the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD). He founded the International Liver Cancer Association and was nominated President from 2006 to 2009. He has been the associate editor of the Journal of Hepatology, Liver Transplantation and Hepatology, and is currently the associate editor of Seminars in Liver Disease, while also being reviewer for several journals and official agencies in USA, Europe and Asia.
Dr. Bruix has been the principal investigator of studies and clinical trials that have changed the practice in the field of HCC, including the development of diagnostic criteria, prognostic models and the establishment of chemoembolization and sorafenib as conventional therapy. He has developed the BCLC staging and treatment strategy that has been endorsed by several international scientific associations to guide management of patients with HCC.
Dr. Bruix has authored more than 150 original investigations and led the Evidence-based Practice Guidelines for Hepatocellular Carcinoma at EASL, AASLD and WGO, as well as consensus statements to define endpoints in clinical trials that have paved the conduct and analysis of such investigations.
Lisa Butterfield, PhD (USA)
Lisa H. Butterfield, PhD, is a Professor of Medicine, Surgery and Immunology at the University of Pittsburgh and Director of the Immunologic Monitoring and Cellular Products Laboratory at the University of Pittsburgh Cancer Institute. She obtained her PhD in biology at UCLA, followed by postdoctoral fellowships in cellular immunology and cancer gene therapy.
Dr. Butterfield has investigated immunotherapy for HCC since 1997. She is a member of the Society of ImmunoTherapy of Cancer (SITC), serving on the Board of Directors, as Secretary-Treasurer, on the Immune Biomarkers Taskforce Steering Committee, and currently as society Vice President. She is Immune Biomarkers Section Editor for the Journal of Immunotherapy of Cancer (JITC).
She investigates cancer vaccines for hepatocellular cancer and for melanoma involving dendritic cells and adenoviruses and effector responses to tumour antigens. She is the IND Sponsor of a pilot HCC DNA Prime-Adenovirus Boost HCC vaccine and of the adenovirally-engineered dendritic cell vaccine for melanoma with John Kirkwood, MD, which is part of the University of Pittsburgh Skin SPORE.
Valerie Chew, PhD (Singapore)
Valerie Chew graduated from the National University of Singapore (NUS) in 2007, with a PhD in immunology. She joined the lab of Prof. Jean-Pierre Abastado in the Singapore Immunology Network (SIgN), Agency for Science, Technology and Research (A*STAR), for her postdoctoral research in tumour immunology. Her research interest is on tumour immune microenvironment, focusing primarily on Hepatocellular carcinoma (HCC).
Dr. Chew is the key researcher in a project that focuses on understanding the impact of tumour immune microenvironment on clinical outcomes in HCC patients. She discovered that a unique immune signature in HCC could accurately predict patient survival. Based on this discovery, the work is now being extended to testing one of the key immune modulators in preclinical HCC models.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 55 6
Dr. Chew’s work has gained recognition with awards such as the Young Research Collaborative Grant from A*STAR’s Joint Council (JCO) in 2012. Several of her research and collaborative works were published in high impact journals, including the Journal of the National Cancer Institute, Nature Genetics, Gut, and the Journal of Hepatology. Dr. Chew joined SingHealth Translational Immunology and Inflammation Centre (STIIC), Singapore, in January 2015 to advance her professional career in tumour immunology research.
Massimo G. Colombo, MD (Italy)
Massimo G. Colombo is a Professor of Gastroenterology at the University of Milan, Italy. His research studies interests include diagnosis and treatment of viral hepatitis and liver cancer. He is the chairman of the department of liver, kidney, lung and bone marrow units and organ transplant and of the division of gastroenterology and hepatology at the Policlinic University Hospital, Milan.
Prof. Colombo received a medical degree in medicine at the University of Milan, where he completed a residency in gastroenterology at the Policlinic Maggiore Hospital. He completed his fellowship in liver disease at the Mount Sinai Hospital in New York.
Prof. Colombo has been the editor-in-chief of the Journal of Hepatology from 2005 to 2009. He is affiliated with several professional associations and societies, including the American Association for the Study of Liver Diseases, the European Association for the Study of the Liver, and other professional bodies in Italy. He is an international lecturer and speaker, sits in the editorial board of many hepatology journals globally and has published more than 380 original manuscripts in peer-reviewed journals; 15,887 citations and H-index 52. In 2010, he received the EASL Recognition Award by the European Association for the Study of the Liver for outstanding medical and scientific contribution. In 2014, he received the Thannhauser Medal award from the German Gastroenterology Society for clinical and scientific contributions in the field of liver disease.
Thierry de Baere, MD (France)
Thierry de Baere graduated from Medical University of Paris XI. He is as full time interventional radiologist in Institut Gustave Roussy, which is the largest European cancer center since 20 years.
Dr. de Baere dedicated his clinical practice to liver cancer including radiofrequency ablation, hepatic intra-arterial chemotherapy, TACE and pre-operative portal vein embolization.
Dr. de Baere produced over 180 publications in peer reviewed journals. He is a member of Board of CIRSE and for the past four years, he served as Program Committee Chair and Vice-Chair of the European Course of Interventional Oncology.
Thomas Decaens, MD, PhD (France)
Thomas Decaens is an Associate Professor of Medecine at the University of Grenoble-Alpes. He focuses on teaching and research in hepatocellular carcinoma with focus on liver transplantation and targeted therapy. Dr. Decaens is member of the Institut Albert Bonniot (INSERM U823) directed by Professor Pierre Hainaut.
Dr. Decaens earned his medical degree in hepatology and gastroenterology in 2006 and his complementary medical degree in medical oncology in 2008. In addition, he graduated in molecular basis of oncogenesis from the University of Paris, earned a PhD in molecular carcinogenesis from the University of Paris in 2007, and got a post-doctoral position from the National Institutes of Health in Thorgeirsson lab (NCI, Bethesda, USA). He is now focusing his research on pre-clinical trials with rat cirrhotic models, nanoparticles and siRNA therapy. Dr. Decaens
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 5 7
is the coordinator of a large nationwide prospective study focused on the identification of new predictive factors of HCC recurrence after liver transplantation, and is implicated in numerous clinical trials of targeted therapy of HCC.
Dr. Decaens is a member of the scientific college of the Fédération Française de Cancérologie Digestive (FFCD) and member of the directory committee of the French network of liver tumour biobank. Dr. Decaens is reviewer for Hepatology, Journal of Hepatology, Liver International, Liver Transplantation and American Journal of Transplantation.
Jean-François Geschwind, MD (USA)
Jeff Geschwind is a Professor of Radiology, Surgery and Oncology and the Chairman of the Department of Radiology and Imaging Sciences at the Yale University School of Medicine and Yale New Haven Hospital. Dr. Geschwind began his early medical training at the University of Paris School of Medicine and completed his medical degree at Boston University School of Medicine, Boston, MA. He completed his residency training in diagnostic radiology at the University of California San Francisco.
At Johns Hopkins and now Yale, Dr. Geschwind has focused his clinical expertise on treating hepatic cancer and other malignancies, and created the Center of Oncologic Interventions.
As lead or co-investigator on more than 40 clinical trials, Dr. Geschwind’s research has been published in highly rated peer-reviewed journals, including the Journal of Clinical Oncology, Clinical Cancer Research, Radiology, and Annals of Surgery.
In 2008, Cambridge University Press published Dr. Geschwind’s book, Interventional Oncology Principles and Practice, which is considered the definitive texbook on interventional oncology.
Gregory J. Gores, MD (USA)
Gregory J. Gores is Reuben R. Eisenberg endowed Professor of Medicine and Physiology, is Executive Dean for Research at the Mayo Clinic College of Medicine, a distinguished investigator of the Mayo Foundation, and a past Chair of the Division of Gastroenterology and Hepatology. A native of North Dakota, he received his undergraduate (Phi Beta Kappa) and MD (Alpha Omega Alpha) degrees from the University of North Dakota. He received his training in internal medicine and gastroenterology at Mayo, Rochester, Minnesota. Dr. Gores is a member of the American Association for Clinical Investigation and the Association of American Physicians. He is also a past president of the American Association for the Study of Liver Diseases (AASLD) and the International Liver Cancer Association (ILCA). He has chaired the Hepatobiliary Pathobiology NIH Study Section and served as a member of the NIDDK Advisory Council. Currently, he is a member of the American Gastroenterological Association Governing Board. Due to his breadth and depth of interests, he has served as an associate editor for Hepatology on two separate terms and once for Gastroenterology.
He is the past recipient of a highly prestigious and competitive NIH MERIT Award, currently a principal investigator of three NIH R01 grants. He has co-authored more than 500 total publications, which have been cited over 25,000 times. His current h-index (number of papers with an identical number of citations) is 97. Well respected as a mentor, he has mentored over 70 post-doctoral research and clinical fellows. His clinical and research contributions include advances in our understanding of hepatobiliary malignancies, liver transplantation and mechanisms of liver cell injury. Dr. Gores was also listed amongst the top 400 highly influential biomedical investigators from 1996-2011 (Boyack KW. European Journal of Clinical Investigation, 43: 1339-1365, 2013).
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 55 8
Tim Greten, MD (USA)
Tim Greten received his clinical training in Gastroenterology, Hepatology and Medical Oncology at Hannover Medical School, Hannover, Germany, and his training in tumour immunology as a postdoctoral fellow in the laboratory of Dr. Pardoll at Johns Hopkins University, Baltimore, USA.
Since 2010, he is the Chief of the Gastrointestinal Malignancy Section at the Center for Cancer Research, National Cancer Institute, Bethesda, USA. As an expert in the field of tumour immunology and a physician scientist, he has studied tumour mediated immunosuppression in patients with HCC and how to overcome them. He is principal investigator of multiple clinical trials in HCC focusing on different immune-related aspects including but not limited to immunotherapy trials in this disease.
Dr. Greten has published more than 100 peer-reviewed publications, is member of the Editorial Board for Journal of Hepatology, Clinical Cancer Research, Associate Editor for United European Gastroenterology Journal and member of the American Association for Cancer Research, International Liver Cancer Association and European Association for the Study of the Liver.
Mathias Heikenwälder, MD, PhD (Germany)
Mathias Heikenwälder studied Genetics and Microbiology at the Max-Perutz laboratories and the Institute of Molecular Pathology (IMP) at the University of Vienna, Austria. After his Master-thesis at the Max-Delbrück Zentrum Munich (MDC), Berlin, Germany, in the laboratory of Prof. Martin Zenke, he moved to Zurich, Switzerland, to the Institute of Neuropathology at the ETH/University Hospital Zurich (USZ), to accomplish his Ph.D. on the role of the immune system and chronic inflammation on prion pathogenesis in the laboratory of Prof. Adriano Aguzzi. After one year of postdoc at the Insitute of Neuropathology (USZ), Mathias Heikenwälder became an independent staff scientist with his own funding and with the focus on chronic inflammation and tissue damage. In 2007, he was awarded the Prof. Max-Cloetta Professorship and started his own lab at the Department of Pathology (USZ). During this time, his laboratory described an inflammatory signature in the liver of chronic HBV and HCV patients that suffices to cause chronic liver inflammation and HCC (Haybaeck et al., Cancer Cell, 2009). In 2010, he moved to the Techische Universität München (TUM) to become Professor and to lead a laboratory on chronic inflammation, tissue damage and cancer. His laboratory established a mouse model of long-term NASH and NASH-induced HCC (Wolf et al. Cancer Cell 2014) as well as models to investigate tumour cell metastasis into the liver and the gastrointestinal tract (Wolf et al., 2012). Since July 2015, Mathias Heikenwälder is Department head of the Institute of Chronic inflammation and Cancer at the German Cancer Research Center (DKFZ), Heidelberg, Germany.
Mitchell Ho, PhD (USA)
Mitchell Ho is Chief of the Antibody Therapy Section, Laboratory of Molecular Biology, in the NCI. His research program focuses on antibody engineering technologies to generate therapeutic antibodies to heparan sulfate proteoglycans for cancer treatment. His lab has developed new antibodies and immunotoxins to glypican 3 that inactivate Wnt signaling and inhibit liver tumour growth.
Dr. Ho received his PhD from the University of Illinois at Urbana-Champaign. He was a postdoctoral fellow under Ira Pastan at the NCI. Dr. Ho is Chair of the NIH Antibody Interest Group, and serves on the Board of Distinguished Advisors for the Antibody Society. Dr. Ho regularly presents at various international symposia and is a member of the organizing committees for several major international conferences on therapeutic antibodies. He is also Chair of the Department of Biochemistry in the FAES Graduate School at the NIH.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 5 9
Shahid A. Khan, MD, PhD (United Kingdom)
Shahid Khan is a consultant hepatologist and adjunct reader at Imperial College London. He qualified from Guy’s Hospital Medical School in 1994 and underwent specialist training in the Northwest London. He was awarded a PhD for his studies on liver cancer from the University of London in 2003. Dr. Khan is the lead author on the British guidelines for cholangiocarcinoma and co-author for the ILCA guidelines. He has published extensively, including original research articles, reviews and book chapters. Dr. Khan is also director of clinical Studies at St Mary’s Hospital and admissions tutor panel for Imperial College London Medical School.
Norihiro Kokudo, MD, PhD (Japan)
Norihiro Kokudo is the Professor and Chairman at Hepato-Biliary-Pancreatic Surgery Division and Artificial Organ and Transplantation Division, Department of Surgery, University of Tokyo Hospital. He earned his MD in 1981, and then PhD in 1988 at University of Tokyo.
From 1989 to 1991, he stayed at the Department of Surgery of the University of Michigan as a visiting research investigator. After 6 years at the Cancer Institute Hospital, Tokyo, as a senior staff of GI surgery, he joined his current institution as an Associate Professor in 2001. He then rose to his current position in 2007. Dr. Kokudo has been conducting a number of research projects on surgical treatment of HCC, colorectal liver metastases, and living donor liver transplantation. As the chairman of the guideline committee, he compiled 3rd version of Japanese clinical practice guidelines for HCC in 2013.
Dr. Kokudo is currently the President of Japan Surgical Society. He is the President of the Asian-Pacific Hepato-Pancreato-Biliary Association (A-PHPBA), a member-at-large of International Hepato-Pancreato-Biliary Association (IHPBA), and a governing board member of ILCA. He is also a fellow of American College of Surgeons, and a member of International Society of Surgery and The Society of Surgical Oncology. He is an honorary regional editor for HPB, an associate editor of Liver Cancer, and on the editorial board of Annals of Surgery, World Journal of Surgery, Journal of HPB Science, Japanese Journal of Clinical Oncology, and Hepatogastroenterology.
Riccardo Lencioni, MD, PhD (Italy)
Riccardo Lencioni, MD, FSIR, EBIR, is board certified in radiology and gastroenterology. He is Professor and Director of Diagnostic Imaging and Intervention at Pisa University School of Medicine in Pisa, Italy.
Prof. Lencioni is one of the world’s foremost interventional oncology specialists, known especially for his highly influential work in liver cancer. He has been a leading member of several expert panels developing recommendations for research and clinical management of hepatocellular carcinoma. He has co-authored the white papers Design and Endpoints in Clinical Trials in Hepatocellular Carcinoma (2008), Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma (2010), and EASL-EORTC Clinical Practice Guidelines: Management of Hepatocellular Carcinoma (2012).
Prof. Lencioni is the Chairman of the World Conference on Interventional Oncology and Board Member of the European Conference on Interventional Oncology. He is a co-Founder of the International Liver Cancer Association, in which he currently acts as the Executive Secretary.
He is an associate editor of the journal Liver Cancer and serves as an editorial board member or reviewer for several other titles. Riccardo Lencioni has published 175 articles in peer-reviewed international journals indexed in PubMed and numerous chapters in textbooks of interventional radiology, gastroenterology, oncology and surgery. In addition, he has been the editor of seven books. According to the SCOPUS database, citations of his publications currently number in excess of 11,000 with an h index of 45. Riccardo Lencioni has been an invited or honorary lecturer at more than 450 international meetings or conferences.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 56 0
Pietro E. Majno, MD (Switzerland)
Pietro Edoardo Majno received his MD at the University of Milan in 1986 and is a fellow of the Royal College of Surgeons of England. He completed his basic surgical training in Great Britain and specialised in hepatobiliary surgery at the Henri Bismuth Hepatobiliary Institute in Villejuif, France, and in the Department of Surgery at the University Hospitals of Geneva.
Dr. Majno is the recipient of several awards, including the prize of the Swiss Society of Visceral Surgery in 2006 and the Swiss Transplantation Research Award in 2009. His main interests are in liver transplantation for hepatocellular carcinoma, segmental transplantations, and the treatment of colorectal liver metastases.
Dr. Majno’s work has been published in numerous peer-reviewed medical journals including The Lancet, Lancet Oncology, Hepatology, the Journal of Hepatology, Annals of Surgery, and the British Journal of Surgery.
Aurélien Marabelle, MD, PhD (France)
Aurélien Marabelle is the Clinical Director of the Cancer Immunotherapy Program at Gustave Roussy Cancer Center in Villejuif, France. He did his MSc and PhD in Oncology and Immunology at the Ecole Normale Supérieure de Lyon, France, the King’s College London, UK and the University of Lyon, France. He did his medical training at the University of Paris VI, France, and received his medical degree from the University of Clermont-Ferrand, France. He completed his residency training in between Clermont-Ferrand and Lyon, and his clinical fellowship in Léon Bérard Cancer Center in Lyon. After that, he did a 3-year post-doctoral research fellowship in Prof. Ronald Levy’s lab at Stanford University, California where he demonstrated the role of Treg depletion in the in vivo mechanism of action of anti-CTLA4 and anti-OX40. Dr. Marabelle’s clinical practice is dedicated to Early Phase Clinical trials in Cancer Immunotherapy and his translational research is focused on mechanisms of action of immune checkpoint monoclonal antibodies. He works as a Senior Medical Oncologist and an investigator in the Drug Development Department (DITEP) of Prof. Jean-Charles Soria. He is coordinating his translational research projects in the INSERM U1015 lab of Prof. Laurence Zitvogel. Dr. Marabelle is a member of ASCO and AACR.
Jorge Marrero, MD (USA)
Jorge Marrero is a liver transplant hepatologist with a focus in clinical research in hepatocellular carcinoma (HCC). He recently joined UT Southwestern as chief of clinical hepatology and medical director of liver transplantation.
His research focus covers early diagnosis, staging and novel therapies in the field of HCC. In terms of early diagnosis, his major contributions have been developing a strategy for validating biomarkers for early detection with the Early Detection Research Network of the National Cancer Institute (NCI); and he has performed several studies that lead to the development of osteopontin, des-gamma carboxyprothrombin, and human hepatocyte growth factor as potential novel serum markers for early detection. He currently is the principal investigator of an NCI-funded to prospectively validate these serum markers. With regards to the diagnosis of HCC, he developed the imaging characteristics for diagnosing HCC that are currently adopted by several international societies. With regards to staging of HCC, he performed the largest validation study of tumour staging using novel statistical analysis that led to the widespread adoption of tumour burden, liver function and performance status as measures of prognosis and staging. He has published several manuscripts on treatment, specifically on liver transplantation for early stage HCC and on novel therapies for advanced HCC. He was part of the study that led to the approval of sorafenib for advanced HCC. He also developed a novel model to measure the harm on patients listed for liver transplant when organs are used for unapproved indications.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 6 1
He is considered an expert in this topic and is part of several national and international committees. He is a founding member of the International Liver Cancer Association, a member of The American Association for the Study of Liver Disease and the American Gastroenterological Association (currently Chair of the Hepatobiliary Committee), and a member of the National Comprehensive Cancer Network’s Hepatobiliary Committee. Dr. Marrero has lectured globally and has written and reviewed numerous research articles and book chapters for publications such as the Gastroenterology, Hepatology and the Journal of Clinical Oncology.
Jens U. Marquardt, MD (Germany)
Jens U. Marquardt received his MD degree from the University of Heidelberg, Germany (Division of Toxicology and Cancer Risk Factors, German Cancer Research Center, Heidelberg, Germany). From 2008 to 2011, he performed a postdoctoral-fellowship at the Laboratory of Experimental Carcinogenesis (CCR/NCI/NIH), Bethesda under the mentorship of Dr. Snorri S. Thorgeirsson where his research focused on the functional and molecular characterization of hepatic cancer stem cells. In January 2011, Dr. Marquardt joined the Department of Medicine I, University of Mainz, Germany. His clinical focus is hepatobiliary malignancies.
His current research activities involve several aspects of translational hepatocarcinogenesis, hepatic cancer stem cells and systems hepatology.
Shannon Maude, MD, PhD (USA)
Shannon Maude, MD, PhD is an Attending Physician in the Division of Oncology at The Children’s Hospital of Philadelphia and an Assistant Professor of Pediatrics at the University Of Pennsylvania School Of Medicine. Dr. Maude received her MD and PhD degrees from the University Of Pennsylvania School Of Medicine as part of the Medical Scientist Training Program. She subsequently completed her Residency in Pediatrics and Fellowship in Pediatric Hematology/Oncology at The Children’s Hospital of Philadelphia. As a St. Baldrick’s Foundation Scholar, Dr. Maude has a special interest in novel therapies for acute lymphoblastic leukemia, particularly targeted therapy approaches and engineered T-cell therapy.
Ignacio Melero, MD, PhD (Spain)
Ignacio Melero MD, PhD, was trained in University of Navarra Medical School (Pamplona, Spain) and as a resident in Hospital Universitario de la Princesa (Madrid, Spain). Dr. Melero earned a doctor degree with extraordinary award in Medicine working on natural killer cell receptors under the supervision of Prof. Lopez-Botet (Universidad Autonoma de Madrid). Between 1994 and 1998, Dr. Melero worked at the Pharmaceutical Research Institute of Bristol Myers Squibb (Seattle, WA) on the costimulation of T-cell responses against tumours together with Lieping Chen and Karl E. Hellstrom.
In 1998 Dr. Melero returned to the University of Navarra, where he serves at the University Clinic, Center of Applied Medical Research (CIMA) and Medical school.
Dr. Melero was appointed full Professor of Immunology in 2004 and is currently the director of a multidisciplinary translational team working on immunotherapy of cancer.
Dr. Melero has published more than 150 research articles and received the BIAL award in Medicine (Portugal), Conde de Cartagena Award of the Royal Academy of Medicine and the Fundacion Lair Durantez Award.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 56 2
Tim Meyer, MD, PhD (United Kingdom)
Tim Meyer is a Professor of Experimental Cancer Medicine at UCL and Honorary Consultant in medical oncology at the Royal Free and ULCH Hospitals. He is cancer director of the NIHR/Wellcome UCH Clinical Research Facility and also director of the UCL Experimental Cancer Medicine Centre.
He was awarded his BSc in Physiology and his Medical Degree at UCL, and practised general medicine before specialising in medical oncology. He won a Clinical Research Training Fellowship from the Imperial Cancer Research Fund and was awarded his PhD in 1999. In 2002, he was appointed to his current post in which he specialises in the management of hepatocellular and neuroendocrine cancer. He leads a large portfolio of clinical trials and runs a translational research program in the UCL Cancer Institute.
Ashraf Omar, MD (Egypt)
Ashraf Omar is currently a Professor of Hepatology & Tropical Medicine at the Faculty of Medicine of the Cairo University in Egypt. He is Secretary General of the Egyptian Society of Liver Cancer (ESLC) and Director of the Multidisciplinary Liver Cancer Clinic in Cairo. He also serves as a member of Committee for Control of Viral Hepatitis at the Ministry of Health (NCCVH).
Professor Ashraf received the Cairo University Prize in Medicine in 2006 and he is a member of AASLD, EASL and ILCA.
Joong-Won Park, MD, PhD (Republic of Korea)
Joong-Won Park is a principal scientist of the National Cancer Center, Republic of Korea, and a professor of Graduate School of Cancer Science and Policy, NCC Korea. He was the Head of the Center for Liver Cancer, NCC, Korea from 2002 to 2010, and was the head of Translational and Clinical Research at the National Cancer Center Research Institute from 2008 to 2011.
Dr. Park completed his medical degree at Seoul National University in 1984, followed by a residency in internal medicine and a clinical fellowship in hepatology at Seoul National University Hospital. He completed a PhD in medicine at Seoul National University in 1996. He was an assistant and associate professor of Chung-Ang University Medical College from 1993 to 2002, and was a visiting scientist at the Center for Basic Research in Digestive Diseases, Mayo Clinic, Rochester, USA, from 1997 to 1999. Dr. Park has published extensively in both international and Korean journals and given many invited lectures on hepatitis and liver cancer. He serves as Chair of the Committee for the Hepatocellular Carcinoma Management Guidelines of the Korea Liver Cancer Study Group (KLCSG)-NCC Korea and is a member of the Korean Association for the Study of the Liver (KASL), the Asian-Pacific Association for the Study of the Liver (APASL), the American Association for the Study of Liver Diseases (AASLD), and the International Liver Cancer Association (ILCA). He served as Chair of the Scientific Committee for the APASL 2008 Seoul meeting, a Chair of the Scientific Committee of the KASL from 2003 to 2005, and as Chair of the Scientific Committee of the KLCSG from 2002 to 2004. Dr. Park’s research interests are the management of hepatocellular carcinoma, molecularly targeted therapy, and hepatocarcinogenesis.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 6 3
Eli Pikarsky, MD, PhD (Israel)
Eli Pikarsky currently serves as chairman of pathology at the Hadassah-Hebrew University Medical Center and is a member of the Lautenberg Center for Immunology and Cancer Research at the Hebrew University. He divides his time between research, teaching and clinical activity. He is the chairman of the research committee of the Israel Cancer Association and a member of the executive board of the EACR. Some of his major achievements were giving proof of the concept that inflammatory cytokines can modulate epithelial cell fate, rendering them more susceptible to malignant transformation; describing a new mode for liver regeneration based on hepatocyte hypertrophy; identifying an invasion suppression function of p53 in the gut and showing that tumour amplicons, which were thought solely to affect signaling processes in the malignant cells themselves, could also govern heterotypic intercellular communication. Thus, he identified a “microenvironmental tumour amplicon”, which shapes the microenvironment in a subset of hepatocellular carcinomas.
Ronnie Poon, MD, PhD (P.R. China)
Ronnie Poon is Suen Chi-Sun Professor in Surgery and Chair Professor of hepatobiliary and pancreatic surgery at the University of Hong Kong. He is currently the chief of the division of hepatobiliary and pancreatic surgery of Queen Mary Hospital. Professor Ronnie Poon is also ILCA Governing Board Member.
Prof. Poon’s main clinical and research interest is in liver cancer, ranging from surgical resection or ablation for early cancer to molecular targeted therapy for advanced disease. He also runs an active basic research program on tumour biology of liver cancer.
He is the author of over 300 full articles in international journals and 14 book chapters. He has contributed to the establishment of consensus guidelines on management and research on liver cancer by various international organisations, including Asian-Pacific Association for Study of the Liver and National Cancer Institute of the USA.
Prof. Poon has received several awards for his research accomplishment, including the Outstanding Researcher Award of the University of Hong Kong and James IV Traveling Fellowship. He has served as associate editor of the World Journal of Surgery and he also serves in the editorial board of several surgical, gastroenterology and oncology journals.
Ugur Sahin, MD (Germany)
Ugur Sahin, MD is a trained physician and Director of the Translational Cancer Institute TRON at the Johannes Gutenberg-University Mainz.
Prof. Sahin key interest is translating basic and applied science into innovation enabling individualized high-precision treatment of cancer patients. He has developed various cancer antigen discovery approaches such as SEREX, identified a multitude of novel pan-cancer immunotherapy targets for development of T-cell and antibody based therapies, developed novel synthetic RNA technologies and applications for cancer immunotherapy and pioneered the field of individualized cancer immunotherapy targeting individual cancer mutations identified by next generation sequencing.
Prof. Sahin is co-founder of the biotech companies Ganymed Pharmaceuticals and BioNTech group and founding director of the not-for-profit translational research institute TRON.
Prof. Sahin current research focuses on the development of individualized cancer immunotherapies.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 56 4
Michiie Sakamoto, MD, PhD (Japan)
Michiie Sakamoto is currently a Professor at the Department of Pathology since 2002, and a Vice-Dean of Keio University School of Medicine since 2009. Professor Sakamoto majored in pathology at Keio University Graduate School of Medicine and received a PhD degree in 1991. He was appointed as a research member in pathology division, National Cancer Center Research Institute in Tokyo in 1989, and nominated as a chief in the division in 1999.
Professor Sakamoto has conducted comprehensive analyses of gene expression correlating with multi-step development and histological subtypes of several types of cancers, and identified molecules applicable to individualized diagnosis and therapy.
Professor Sakamoto published over 200 international scientific papers in high quality English Journals. He is also serving as an editor-in-chief of Pathology International, an associate editor of Cancer Science and Hepatology Research.
His research interest is Molecular Pathology of Cancer (multistep-carcinogenesis, early cancer, invasion and metastasis) and Pathology Informatics.
Riad Salem, MD (USA)
Riad Salem, MD MBA is a Vice-Chair, image-guided therapy and chief, interventional radiology and oncology in the Department of Radiology at Northwestern University (Chicago). His areas of interest include the use of image-guided techniques for the treatment of malignancies. These include hemoembolisation, bland embolisation, radioembolisation, radiofrequency and cryo/alcohol ablation.
He is a graduate of McGill University in Montreal, Canada. He completed his radiology residency in Washington, DC. He has also completed a fellowship in interventional radiology (University of Pennsylvania), as well as a Master’s in Business Administration (Finance). He is a member of Alpha Omega Alpha medical honor society and a fellow of the Society of Interventional Radiology. He has lectured internationally and published extensively on the subject of image-guided interventions and interventional oncology.
Recently, he completed his term on the NCCN guidelines panel for hepatocellular carcinoma (2007-2010). His current research focus on hepatocellular carcinoma includes advances in minimally invasive therapies as well as imaging methodologies following locoregional treatment. He serves as co-PI of 2 international, randomised phase III trials involving locoregional therapy (radioembolisation) and sorafenib (STOP-HCC, YES-p).
Bruno Sangro, MD, PhD (Spain)
Bruno Sangro, MD, PhD, is Director of the Liver Unit at Clinica Universidad de Navarra, Aggregate Professor of Medicine at the University of Navarra School of Medicine, and senior researcher in the National Biomedical Research Network Center for Liver and Digestive Diseases (CIBERehd). He also serves in the Governing Board of the Division of Hepatology and Gene Therapy at the Center for Applied Biomedical Research (CIMA), in Pamplona, Spain, and is advisor for the Spanish and the European Agency for Medicinal Products.
His basic and clinical research has mainly focused on liver cancer, with a high priority on therapeutic innovation. The Liver Unit of Clinica Universidad de Navarra has pioneered several approaches to the treatment of liver cancer from expanded criteria for liver transplantation to locoregional vascular therapy including intraarterial infusion chemotherapy, transarterial embolization and radioembolization, and systemic advanced therapies including gene therapy or immunotherapy.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 6 5
Robert Schwabe, MD (USA)
Robert Schwabe studied medicine at the Universities of Heidelberg and Munich and completed a doctoral thesis in immunology at the Ludwig-Maximilians-University Munich. After his residency in internal medicine at the University of Heidelberg, and a postdoctoral fellowship in David Brenner’s laboratory at UNC Chapel Hill for a postdoctoral fellowship, Dr. Schwabe moved to Columbia University where he is currently an associate professor in medicine. Dr. Schwabe’s research investigates links between hepatic inflammation, fibrosis and liver cancer, with a particular focus on the role of the intestinal microbiota in the promotion of hepatocarcinogenesis. Dr. Schwabe serves as associate editor for Gastroenterology and is a member of the NIH HBPP study section.
Mohamed Kamal Shaker, MD (Egypt)
Mohamed Kamal El-Din Aly Fahmy Shaker is the Head of Tropical Medicine Department Faculty of Medicine Ain Shams University and Director of HCC Unit at Ain Shams University Hospitals. He is now President Elect of the African Association for the Study of Liver Diseases (AFASLD) and serves as Vice President of the Egyptian Society of Liver Cancer as well as President of the Committee of Treatment of Viral Hepatitis at Cairo branch Health Insurance Organization. Until 2012, he coordinated the Supreme Committee of the Liver in the Health Insurance Organization.
Dr. Shaker is a member of the American Association for the Study of Liver Diseases (AASLD), member of the National Committee for the Control of Viral Hepatitis and member of the Honorary Editorial Board of Journal of Hepatocellular Carcinoma. He is also one of the founders of the Arabic Society for the Study of Liver Diseases (ASSLD).
Dr. Shaker is often invited to give lectures about HCC in African region. He contributed to the meetings of the following distinguished societies: Libyan Society for Gastroenterology (2010), Syrian Society for Gastroenterology (2010), AASLD in San Francisco (2011), AASLD in Boston (2012), APASL in Istanbul (2015) and many more.
Sanford M. Simon, PhD (USA)
Sanford Simon graduated from Princeton University majoring in neuroscience. His graduate work, in physiology and biophysics, used electophysiology and computer modeling to study the release of transmitter from the presynaptic terminal. His post-doctoral studies were with Gunter Blobel at the Rockefeller University, on the mechanisms of protein translocation across membranes. This led to an independent faculty position at the Rockefeller University, in which he has studied the mechanisms of exocytosis and endocytosis, how pathogenic bacteria secrete toxins, has worked on developing a number of new imaging modalities with papers on microscopy as well as quantum dots. Half of his lab is currently examining the assembly of viruses and how nuclear pores operate. The other half of the lab studies pediatric cancers.
Amit Singal, MD (USA)
Amit Singal is currently an Associate Professor in the Division of Digestive and Liver Diseases and serves as Medical Director of the Liver Tumour Program at UT Southwestern Medical Center, Dallas Texas. Dr. Singal has completed several studies characterizing the efficacy and effectiveness of surveillance tests to detect hepatocellular carcinoma (HCC) at an early stage. In addition to highlighting the gap between the efficacy and effectiveness of HCC surveillance tools, he has demonstrated that HCC surveillance is underutilized, primarily due to providers failing to identify at-risk patients with cirrhosis as well as failing to order HCC surveillance among those with known cirrhosis. His current work focuses on evaluating intervention strategies to improve early detection of HCC. For his work to date, he was appointed as a Dedman Family Scholar of Clinical Care.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 56 6
Martin F. Sprinzl, MD (Germany)
Martin Sprinzl received his MD degree from the University of Heidelberg, Faculty of Medicine in 2001. Following his internship in internal medicine, he completed his gastro-enterology residency at the University Medical Center in Mainz, Germany, in 2012. Since his medical thesis, investigating experimental animal models of chronic hepatitis B, he dedicated his research interest to patho-mechanism of liver disease and followed translational approaches in clinical research. During a clinical leave, he joined the Institute of Virology at the Technical University/ Helmholtz Zentrum, Munich, where he focused on immunotherapy of hepatocellular carcinoma. In 2012 he was appointed senior registrar at the I. Medical Department, University Medical Center, Mainz heading the section of infectiology and the immunological laboratory.
Robert Thimme, MD (Germany)
Robert Thimme is the Director of the Department of Medicine II (Gastroenterology, Hepatology, Endocrinology and Infectious Diseases). His research focus lies on the immune responses in hepatitis B virus (HBV) and hepatitis C virus (HCV) infection as well as hepatocellular carcinoma (HCC). In recent years, he could show that tumour specific CD8 T-cell responses are detectable in the peripheral blood and in the liver of patients with HCC and that the strength of the tumour specific immune response correlates with the overall survival. The mechanisms of the failure of the tumour specific T-cell response to control the tumour long term is another focus of his research with a special emphasis on the expression of inhibitory receptors and the role of regulatory T-cells. His work is supported by grants from the DFG, BMBF, several foundations and the EU. He has published more than a hundred papers on the tissue of immunobiology of HBV, HCV and HCC and is or has been in the editorial boards of several journals, such as the Journal of Clinical Investigation, Gastroenterology, Journal of Hepatology and Journal of Infectous Diseases.
Xin Wei Wang, PhD (USA)
Xin Wei Wang is a Senior Investigator, Chief of the Liver Carcinogenesis Section, Deputy Chief of the Laboratory of Human Carcinogenesis, Center for Cancer Research at the National Cancer Institute (NCI). He received his PhD training from New York University School of Medicine and further research training from Roche Institute of Molecular Biology and the NCI. His major research interest over the past 15 years has been liver cancer, with a special focus on cancer functional genomics through several international collaborative initiatives on liver cancer genomics and clinical studies. Currently, he also serves on the ILCA Governing Board and Chair of the ILCA SIG on Molecular Classification and Signaling Pathways.
Gerald Willimsky, MD, PhD (Germany)
Gerald Willimsky obtained his diploma in Chemistry at the Technical University Berlin in 1990 and his PhD in Biochemistry and Microbiology at the Philipps-University Marburg in 1993. From 1993 – 1994 he underwent a postdoctoral fellowship at the Institut für genbiologische Forschung in Berlin and continued as postdoctoral scientist at Max-Delbrück Center for Molecular Medicine in Berlin till 2000.
Dr. Willimsky currently works as a research group leader with focus on primary mouse tumour models and translational medicine at the Institute of Immunology, Charité Campus Buch in Berlin.
Speakers’ Portfolio

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 6 7
Marcus-Alexander Wörns, MD (Germany)
Marcus-Alexander Wörns is Chief Senior Physician of the Department of Medicine I and head of the HCC outpatient department at the University Medical Centre of the Johannes Gutenberg-University in Mainz, Germany. He is working as a gastroenterologist with a clinical and scientific focus on hepatology and hepatobiliary oncology. He received his Venia legendi for Internal Medicine in 2014. He is a member of several national and international societies such as the German Association for Digestive Diseases (DGVS) and the European Association for the Study of the Liver (EASL), and serves as a reviewer for scientific journals such as the Journal of Hepatology and the American Journal of Gastroenterology.
Wen Xue, PhD (USA)
Wen Xue is currently an Assistant Professor at the RNA Therapeutics Institute at the University of Massachusetts Medical School. He was trained by Dr. Scott Lowe at Cold Spring Harbor Lab (2004-2009) and Dr. Tyler Jacks at MIT (2009-2014). He has a strong research background in the area of mouse models of liver cancer. His lab is using CRISPR genome editing to functionally dissect cancer mutations in liver cancer and to treat liver genetic disease. He has more than 20 original publications listed on PubMed. He has received a number of awards including an NCI-K99 Pathway to Independence Award, the Leukemia & Lymphoma Society Career Development Program Award and the American Association for Cancer Research (AACR) Pre-doctoral Fellowship.
Katsuhiko Yanaga, MD, PhD (Japan)
Katsuhiko Yanaga, MD, PhD, FACS, is a Professor and Division Chief of Digestive Surgery at the Jikei University School of Medicine, Tokyo, Japan. He graduated from Kyushu University, Japan in 1979 and underwent general surgical training in Japan and USA, while trained in liver transplantation at the University of Pittsburgh under Dr. Starzl during the vintage years (1986-1989).
Prof. Yanaga is the Governor-at-Large of the American College of Surgeons representing Japan, a board member of three Japanese surgical societies, and a Councilor of the Japan Society of Hepatology, Liver Cancer Study Group of Japan and Japanese Liver Transplantation Society.
Speakers’ Portfolio

GenesisLiver cancer is rapidly increasing worldwide, triggering widespread interest and strong focus surrounding all aspects of this disease. Given the naturally multidisciplinary nature of liver cancer, however, no single association has before the International Liver Cancer Association (ILCA) adopted a transversal approach to liver cancer by connecting expertise from interrelated fields, research and treatment levels. In response to this shortfall, ILCA was established in 2006 and is currently the only international organisation devoted exclusively to liver cancer across disciplines.
Our MissionILCA strives to advance research in the pathogenesis, prevention, and treatment of liver cancer, by promoting novel pathogenic, diagnostic and therapeutic interventions for liver cancer, and taking a transversal approach to research. Indeed, ILCA brings together scientists, physicians and allied professionals from all interrelated fields and countries, and strives to welcome and incorporate individuals involved in all the scientific disciplines devoted to basic, translational and clinical research in liver cancer as individual members. ILCA actively partners with other professional associations involved in any aspect related to liver cancer research, with the objective to join efforts for the benefit of science.
Joining Our CommunityWe invite you to discover more about ILCA on www.ilca-online.org, as well as to connect with our expanding group of interested physicians, scientists, and allied health professionals from various fields and from around the world.
Membership to ILCA not only provides you with exclusive benefits such as reduced registration rates to our Annual Conferences, exciting networking and educational opportunities and active involvement in association affairs; it also helps us to develop our activities and our reach to advance liver cancer research and care.
About ILCA
Contact usInternational Liver Cancer Association (ILCA)
Avenue de Tervueren 300B-1150 Brussels - Belgium
Tel: +32 2 789 2345Fax: +32 2 743 1550
Email: [email protected]
Executive CommitteePresident Peter R. Galle (Germany)Executive Secretary Riccardo Lencioni (Italy)Treasurer Morris Sherman (Canada)President Elect Richard Finn (USA)
CouncilAnn-Lii Cheng (Taiwan)
Norihiro Kokudo (Japan)
Ronnie Poon (P. R. China)
Peter Schirmacher (Germany)
Myron Schwartz (USA)
Xin Wei Wang* (USA)
Jessica Zucman-Rossi (France)
ILCA Governing Board
www.ilca-online.org
* Liaison in an advisory capacity

The International Liver Cancer AssociationPriming Knowledge in Liver Cancer across Disciplines
Share ILCA Mission •Advancing research in the pathogenesis, prevention
and treatment of liver cancer
•Promoting novel pathogenic, diagnostic and therapeutic interventions for liver cancer
• Bringing together scientists, physicians and allied professionals from all interrelated fields
Enjoy ILCA Membership •Exciting professional networking and educational opportunities
•Significant registration discounts to attend ILCA Annual Conferences and other educational events
• Access to the latest information on liver cancer related news and initiatives
• Active involvement in association affairs
•Opportunity to be involved in Special Interest Groups
•Opportunity to apply for the ILCA fellowship programme or to support one of your team members as a mentor through the fellowship application process
ILCA is the only international and multidisciplinary association devoted exclusively to liver cancer research, treatment and care
Join ILCA today !and participate in advancing liver cancer science worldwide
To learn more about ILCA, visit www.ilca-online.org

Notes

Contents
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5
Book of Abstracts
7 1

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s2
Book of Abstracts: Instructions for Useall abstracts listed in ILca’s 9th annual conference Book of abstracts have been assigned a prefix for the type of presentation, and a sequential abstract number. the authors whose names are in bold and followed by an asterisk are the presenting authors.
oral communication = o Poster = P
Oral Communications are listed by day and time of presentation. Posters and Top Scored PostersIn the Book of abstracts’ section, you will first find the top scored, then the Posters (e-Posters) listed by topics:
1. Molecular pathogenesis, molecular pathology, cell biology and translational research
2. epidemiology, staging and prognosis
3. Diagnosis, imaging and biomarkers
4. clinical trials and treatment research & Miscellaneous
e-Poster Viewing Tours30 top scored Posters will be presented in the form of paper board poster at the beginning of each e-Poster Viewing tour (15 paper poster presentations within each e-Poster Viewing tour) in the Poster of excellence area (scene foyer, Ground Level).Viewing of all e-Posters takes place in scene foyer, Ground Level room at the same time.
Top Scored poSTerS (paper posters):
• In the morning (as of 10:00) P-001, P-002, P-003, P-004, P-005, P-006, P-007, P-008, P-009, P-010, P-011, P-012, P-013, P-014, P-018
• In the afternoon (as of 15:45) P-015, P-016, P-017, P-019, P-020, P-021, P-022, P-023, P-024, P-025, P-026, P-027, P-028, P-029, P-030
Hanging and removal of paper board postersPoster boards will be marked with the final abstract numbers. Posters mounting time: Thursday, 3 September 2015, as of 14:00. Posters need to be mounted prior to thursday, 3 september 2015, 19:00. Posters removal time: Sunday, 6 September 2015, as of 10:00. Posters that have not been removed by 13:00 will be disposed of by the organisers.
top scored posters will also be available in the form of e-Posters on all e-Poster screens throughout the conference.
ALL poSTerS (e-posters):
During the e-Poster Viewing tours, posters can be viewed only on their dedicated screens in scene foyer, Ground level, as follows:
• Morning e-Poster Viewing Tour (10:00 - 11:00)screen 1: P-031, P-032, P-033, P-034, P-035screen 2: P-036, P-037, P-038, P-039screen 3: P-040, P-041, P-042, P-043, P-044screen 4: P-045, P-046, P-047, P-048screen 5: P-049, P-050, P-051, P-052screen 6: P-054, P-055, P-056, P-057screen 7: P-058, P-059, P-060, P-061screen 8: P-062, P-063, P-064, P-065, P-066screen 9: P-067, P-068, P-069, P-070screen 10: P-071, P-072, P-073, P-074, P-076screen 11: P-077, P-079, P-080screen 12: P-081, P-082, P-083, P-084screen 13: P-085, P-086, P-087, P-088screen 14: P-089, P-090, P-091, P-092screen 15: P-093, P-094, P-095, P-096screen 16: P-097, P-098, P-099, P-100screen 17: P-101, P-102, P-103, P-104screen 18: P-105, P-106, P-107, P-108, P-109screen 19: P-110, P-111, P-112, P-113, P-114screen 20: P-115, P-116, P-117, P-118, P-119
screen 21: P-120, P-121, P-122, P-123, P-124screen 22: P-125, P-126, P-127, P-128, P-129screen 23: P-130, P-131, P-132, P-133, P-134screen 24: P-135, P-136, P-137, P-138, P-139screen 25: P-140, P-141, P-142, P-143, P-144screen 26: P-145, P-146, P-147, P-148screen 27: P-149, P-150, P-151, P-152screen 28: P-153, P-154, P-155, P-156screen 29: P-157, P-158, P-159, P-160, P-161screen 30: P-162, P-163, P-164, P-165, P-166screen 31: P-167, P-168, P-169, P-170, P-171screen 32: P-172, P-173, P-174, P-175, P-176screen 33: P-177, P-179, P-180, P-181screen 34: P-182, P-183, P-184, P-185screen 35: P-186, P-187, P-188, P-189
• Afternoon e-Poster Viewing Tour (15:45 – 16:45)screen 1: P-190, P-191, P-192, P-193screen 2: P-194, P-195, P-196, P-197screen 3: P-198, P-199, P-200, P-201screen 4: P-203, P-204, P-205, P-206screen 5: P-207, P-208, P-209, P-210screen 6: P-212, P-213, P-214, P-215screen 7: P-216, P-217, P-218, P-219screen 8: P-220, P-221, P-222, P-223screen 9: P-224, P-225, P-226, P-227, P-228
screen 10: P-229, P-230, P-231, P-232, P-233screen 11: P-234, P-235, P-236, P-237, P-238screen 12: P-239, P-240, P-241, P-242screen 13: P-243, P-244, P-245, P-246, P-247screen 14: P-248, P-249, P-250, P-251screen 15: P-252, P-253, P-254, P-255, P-256screen 16: P-257, P-258, P-259, P-260screen 17: P-261, P-262, P-263, P-264, P-265screen 18: P-266, P-267, P-268, P-269screen 19: P-270, P-271, P-272, P-273, P-274screen 20: P-275, P-276, P-277, P-278screen 21: P-279, P-280, P-281, P-282, P-283screen 22: P-284, P-285, P-286, P-287screen 23: P-288, P-289, P-290, P-291, P-292screen 24: P-293, P-294, P-295, P-296screen 25: P-297, P-298, P-299, P-300, P-301screen 26: P-302, P-303, P-304, P-305screen 27: P-306, P-307, P-308, P-309, P-310screen 28: P-311, P-313, P-314, P-315screen 29: P-316, P-317, P-318, P-319, P-320screen 30: P-321, P-322, P-323, P-324screen 31: P-325, P-326, P-327, P-328, P-329screen 32: P-330, P-331, P-332, P-333, P-334screen 33: P-335, P-336, P-337, P-338screen 34: P-339, P-340, P-341, P-342, P-343screen 35: P-344, P-345, P-346, P-347, P-348
Index of Authorsthe Index of authors lists all abstract authors in alphabetical order. to locate the page of the abstract, first take note of the abstract number (example: P-002) and then locate the abstract, listed by type of presentation and in sequential order, in the table of contents, where you will find a reference for the page number.
Disclaimerthis Book of abstracts has been produced using author-supplied copies. editing has been restricted to minor spelling corrections where appropriate, otherwise every effort has been made to reproduce the abstracts as originally submitted. the organiser and publishers assume no responsibility for any injury and/or damage to persons or property as a matter of product liability, negligence or otherwise, or from any use or operation of any methods, products, instructions or ideas contained in the material herein. In view of rapid advances in medical sciences, independent verification of diagnoses and drug doses is recommended.

Contents
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 3
OrAl COmmUnICAtIOns
Friday, 4 september 2015
General session 1: molecular Pathogenesis of liver Cancer I....................... 10o-001 IDentIfIcatIon of co-occurrInG GenetIc aBerratIons WIth knoWn DrIVer
MutatIon DIrects tarGeteD theraPy In choLanGIocarcInoMa ........................10
o-002 the thaILanD InItIatIVe In GenoMIcs anD exPressIon research for LIVer
cancer (tIGer-Lc): DefInInG BIoLoGIcaL suBtyPes of hePatoceLLuLar
carcInoMa anD choLanGIocarcInoMa By InteGrateD GenoMIcs .....................10
o-003 PersonaLIzeD DIaGnostIcs In hePatoceLLuLar carcInoMa: unIque
MutatIonaL sIGnatures WIth PotentIaL to GuIDe tarGeteD theraPy ...............10
o-004 aDeno-assocIateD VIrus 2 (aaV2) InDuces recurrent InsertIonaL
MutaGenesIs In huMan hePatoceLLuLar carcInoMas .......................................11
o-005 roLe of Lect2 In the hePatIc IMMune MIcroenVIronMent DurInG
LIVer carcInoGenesIs ...........................................................................................11
o-006 InterroGatIon of DnajB1-Prkaca kInase fusIon as a theraPeutIc
tarGet In fIBroLaMeLLar hePatoceLLuLar carcInoMa .....................................11
General session 2: molecular Pathogenesis of liver Cancer II ..................... 12o-007 IGf2 Is an oncoGenIc DrIVer In hcc anD eMerGes as a PotentIaL
tarGet for theraPIes ...........................................................................................12
o-008 tuMor InItIatInG ceLLs are MeDIators of acquIreD resIstance
to sorafenIB In hePatoceLLuLar carcInoMa ....................................................12
o-009 steM-ceLL nIche anD tuMor-assocIateD MacroPhaGes In huMan
choLanGIocarcInoMa ..........................................................................................13
o-010 MIxeD hePatoceLLuLar-choLanGIocarcInoMa tuMors:
choLanGIoLocarcInoMas anD steM-ceLL suBtyPe haVe
unIque MoLecuLar traIts ....................................................................................13
o-011 sIGnatures of knoWn anD neW MutatIonaL Processes
oPeratIVe In LIVer cancers ..................................................................................13
o-012 actIVatIon of steM-LIke ceLLs In the hePatIc MIcroenVIronMent Is
assocIateD WIth ProGnostIcaLLy aDVerse GenoMIc aLteratIons In
hePatoceLLuLar carcInoMa ...............................................................................14
OrAl COmmUnICAtIOns
saturday, 5 september 2015
General session 3: Epidemiology, staging and Prognosis .............................. 15o-013 IncIDence of hePatoceLLuLar carcInoMa In aLcohoLIc coMPensateD
cIrrhosIs. PreLIMInary resuLts of a MuLtIcenter ProsPectIVe french
anD BeLGan cohort (cIrraL) ................................................................................15
o-014 hePatoceLLuLar carcInoMa (hcc) scorInG systeM for the InDIVIDuaLIzeD
PreDIctIon of LIVer cancer In 1080 hcV-reLateD coMPensateD
cIrrhosIs IncLuDeD In the french MuLtIcenter ProsPectIVe
cohort anrs co12 cIrVIr .....................................................................................15
o-015 PLateLet count IMProVes ProGnostIc VaLue of a-L-B-I GraDe:
IntroDucInG a neW P-a-L-B-I score ....................................................................16
o-016 DIaBetes, hBV InfectIon anD sMokInG are InDePenDent rIsk factors
for DeVeLoPInG hePatoceLLuLar carcInoMa on non-fIBrotIc LIVer
In the nofLIc french MuLtIcenter case-controL stuDy ..................................16
o-017 PatIents WIth aLcohoL coMPareD to hcV-reLateD hePatoceLLuLar
carcInoMa (hcc) haVe a reDuceD surVIVaL. resuLts
of a natIonWIDe stuDy .........................................................................................17
o-018 PatIent knoWLeDGe anD BarrIers for hePatoceLLuLar carcInoMa
surVeILLance aMonG PatIents WIth cIrrhosIs ...................................................17
Plenary session ................................................................................................. 17o-019 coMPrehensIVe anD InteGratIVe GenoMIc characterIzatIon of
hePatoceLLuLar carcInoMa: the tcGa hcc Project .........................................17
o-020 ProsPectIVe assessMent of LIVer cancer occurrence In coMPensateD
hcV-reLateD cIrrhosIs WIth sVr usInG a coMPetInG rIsk fraMeWork
reVeaLs an annuaL IncIDence BeLoW 1% anD sPecIfIc rIsk factors (anrs
co12 ProsPectIVe cIrVIr cohort) .......................................................................18
o-021 oBjectIVe resPonse By MrecIst PreDIcts surVIVaL In hePatoceLLuLar
carcInoMa: a MuLtIVarIate, tIMe-DePenDent anaLysIs froM the Phase 3
BrIsk-Ps stuDy * ...................................................................................................18
o-022 a ranDoMIzeD Phase 2 trIaL of sorafenIB PLus Intra-arterIaL cIsPLatIn
Versus sorafenIB aLone for aDVanceD hePatoceLLuLar carcInoMa .............19
General session 4: Diagnosis and Curative treatment ................................... 19o-023 coMParIsons of outcoMes after LIVer resectIon for hePatoceLLuLar
carcInoMa BetWeen the east anD the West a ProPensIty
score MatchInG anaLysIs ....................................................................................19
o-024 LIquID BIoPsy to Detect anD characterIse cIrcuLatInG tuMour ceLLs
In PatIents WIth hePatoceLLuLar carcInoMa usInG hIGh resoLutIon
IMaGestreaM MuLtIchanneL fLuorescent MIcroscoPy....................................20
o-025 DIsentanGLInG the effects of race/ethnIcIty anD socIoeconoMIc
factors on LIVer transPLantatIon rates for hePatoceLLuLar
carcInoMa ............................................................................................................21
o-026 can MeLoxIcaM, a cox-2 InhIBItor, PreVent hePatoceLLuLar carcInoMa
recurrence after InItIaL curatIVe treatMent?
a resuLt of ranDoMIseD controLLeD trIaL .......................................................21
o-027 ProsPectIVe PILot stuDy of LIVInG Donor LIVer transPLantatIon
for PatIents WIth hcc exceeDInG MILan crIterIa .............................................21
o-028 LIVer transPLantatIon Versus resectIon for sMaLL IntrahePatIc
choLanGIocarcInoMa or hePatochoLanGIocarcInoMa on cIrrhosIs ............22
OrAl COmmUnICAtIOns
sunday, 6 september 2015
General session 5: From Drivers to Clinical trials ......................................... 23o-029 tIVantInIB In PretreateD hePatoceLLuLar carcInoMa (hcc): tuMor anD
PLasMa BIoMarker anaLysIs froM the ranDoMIzeD controLLeD Phase
2 trIaL (rct) ..........................................................................................................23
o-030 fGf19 aBerratIons anD seLectIVe tarGetInG WIth fGfr4 InhIBItors for
hePatoceLLuLar carcInoMa ................................................................................23
o-031 PreoPeratIVe sorafenIB-InDuceD antItuMor actIVIty In PatIents WIth
resectaBLe hePatoceLLuLar carcInoMa (hcc): resuLts of the BIoshare
neoaDjuVant Phase 2 stuDy froM Gercor Irc ..................................................23
o-032 ranDoMIzeD Phase IIB stuDy of Pexa-Vec (PexastIMoGene DeVacIrePVec;
jx-594), an oncoLytIc IMMunotheraPy PLus Best suPPortIVe care (Bsc)
Versus Bsc aLone In PatIents WIth hePatoceLLuLar carcInoMa (hcc) Who
faILeD sorafenIB treatMent (traVerse) .............................................................24
o-033 raMucIruMaB (raM) as seconD-LIne treatMent In PatIents (Pts) WIth
aDVanceD hePatoceLLuLar carcInoMa (hcc): jaPanese suBGrouP
anaLysIs of the Phase III reach trIaL ..................................................................24
o-034 resuLts of a Proof-of-concePt Phase 2 trIaL of tasquInIMoD
In PatIents WIth aDVanceD hePatoceLLuLar carcInoMa PreVIousLy
treateD WIth sorafenIB .......................................................................................25
tOP sCOrED POstErs
P-001 MetforMIn use reDuceD MortaLIty anD DIsease ProGressIon after curatIVe
hePatIc resectIon In Very earLy-staGe hePatoceLLuLar carcInoMa: a
natIonWIDe PoPuLatIon-BaseD stuDy .................................................................26
P-002 ethnIcIty IMPacts aGGressIVeness of hcc DetecteD DurInG surVeILLance of
coMPensateD VIraL cIrrhosIs (anrs co12 cIrVIr ProsPectIVe cohort) ..........26
P-003 tM6sf2-t anD PnPLa3-G VarIants co-MoDuLate the rIsk of hePatoceLLuLar
carcInoMa In caucasIan PatIents WIth aLcohoLIc cIrrhosIs. Inter-cohort
VaLIDatIon In 1068 PatIents .................................................................................27
P-004 Phase I/IIa stuDy of aDjuVant IMMunotheraPy WIth tuMor antIGen-PuLseD
DenDrItIc ceLLs In PatIents WIth hePatoceLLuLar carcInoMa ........................27
P-005 Myc oncoGenIc actIVIty Is serPInB3-DePenDent throuGh yaP
InterPLay In hePatoceLLuLar carcInoMa ...........................................................27
P-006 sox9 reGuLates steM ceLL-LIke PhenotyPes anD MetastasIs In
hePatoceLLuLar carcInoMa throuGh Wnt/Beta-catenIn sIGnaLInG ................28
P-007 transcrIPtIonaL DereGuLatIon In hePatoBLastoMa PatIents PoInts
to neW oncoGenIc MechanIsMs..........................................................................28
P-008 LeVeL of ss-catenIn actIVatIon In ctnnB1-MutateD hePatoceLLuLar
aDenoMa anD carcInoMa Is reLateD to MutatIon tyPe anD Increases DurInG
tuMor ProGressIon .............................................................................................28
P-009 a neW score BaseD on exPLant PathoLoGy aLLoWs an InDIVIDuaLIzeD
PreDIctIon of hcc-recurrence after LIVer transPLantatIon .........................29
P-010 next-GeneratIon Des-r-carBoxy ProthroMBIn PreDIcts
VascuLar InVasIon In hcc ....................................................................................29

Contents
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s4
P-011 oxIDatIVe stress acceLerates the transforMatIon of ProLIferatInG
huMan hePatocytes WIth constItutIVe GP130 actIVatIon In contrast to
LIGanD-MeDIateD InterLeukIn 6 PathWay actIVatIon .........................................30
P-012 hIGh-throuGhPut MIrna-InhIBItors screenInG IDentIfIeD seLecteD MIrnas
InVoLVeD In the MoDuLatIon of DruG resPonse In choLanGIocarcInoMa ......30
P-013 MoDeL to PreDIct recurrence after LIVInG Donor LIVer
transPLantatIon for hePatoceLLuLar carcInoMa BeyonD
the MILan crIterIa ................................................................................................30
P-014 the use of Beta-BLockers Is assocIateD WIth a LoWer rIsk of DeVeLoPInG
hePatoceLLuLar carcInoMa In PatIents WIth cIrrhosIs ...................................31
P-015 VaLIDatIon of the “aB InItIo” LIVer transPLantatIon PoLIcy In
hePatoceLLuLar carcInoMa uPon DetectIon of rIsk factors
for recurrence after surGIcaL resectIon .......................................................31
P-016 hIV InfectIon Does not Worsen ProGnosIs of LIVer transPLantatIon In
hePatoceLLuLar carcInoMa ................................................................................31
P-017 aDherence to easL-eortc cLInIcaL GuIDeLInes for the ManaGeMent of
hePatoceLLuLar carcInoMa In fIeLD PractIce: resuLts froM
the Ita.LI.ca DataBase ..........................................................................................32
P-018 a noVeL choLanGIocarcInoMa PatIent DerIVeD xenoGraft enDoGenousLy
exPressInG an fGfr2-ccDc6 fusIon ProteIn shoWs DIfferentIaL sensItIVIty
to fGfr InhIBItors ................................................................................................32
P-019 hIGh-throuGhPut sMaLL MoLecuLe screenInG IDentIfIeD sMaLL DruGs
PotentIaLLy actIVe In choLanGIocarcInoMa ......................................................33
P-020 acquIsItIon of steM ceLL ProPertIes In tuMor-DerIVeD hePatocyte-LIke
ceLLs LeaDs to MetaBoLIc reProGraMMInG anD cheMoresIstance ................33
P-021 korean VaLIDatIon anD coMParIson of ProGnostIc scores for
transarterIaL cheMoeMBoLIzatIon: art, aBcr, haP, anD MoDIfIeD haP ...........33
P-022 DeLeterIous PassenGer MutatIons as a Marker for ProGressIon
toWarDs LIVer cancer .........................................................................................34
P-023 PreDIctIon MoDeL for the DeVeLoPMent of hePatoceLLuLar carcInoMa In
PatIents WIth chronIc hePatItIs B receIVInG antIVIraL treatMent ..................34
P-024 the VaLIDatIon of a neW MoDIfIeD chILD-turcotte-PuGh score usInG
InsuLIn-GroWth factor-1 as a ProGnostIc MoDeL for hePatoceLLuLar
carcInoMa ............................................................................................................34
P-025 cIrcuLatInG neutroPhILs anD the systeMMIc IMMune-InfLaMMatIon
InDex as ProGnostIc tooLs for PatIents WIth hePatoceLLuLar
carcInoMa ............................................................................................................34
P-026 extrahePatIc MetastasectoMy for hePatoceLLuLar carcInoMa:
PreDIctors of LonG terM surVIVaL ....................................................................35
P-027 LocoreGIonaL theraPIes IMProVe surVIVaL In PatIents WIth aDVanceD
hePatoceLLuLar carcInoMa treateD WIth sorafenIB .......................................36
P-028 nanoPartIcLe-DeLIVereD sMaLL InterferInG rna for astrocyte eLeVateD
Gene-1 anD aLL-trans retInoIc acID: a coMBInatorIaL theraPy for
hePatoceLLuLar carcInoMa ................................................................................36
P-029 a 3-ProteIn sIGnature to IMProVe cLInIcaL stratIfIcatIon
of chILDhooD LIVer cancer .................................................................................36
P-030 In PatIents WIth hePatoceLLuLar carcInoMa (hcc) anD MacroVascuLar
InVasIon (MVI) aMenaBLe to surGIcaL resectIon, a surVIVaL sIMILar to that
oBserVeD on sorafenIB can Be achIeVeD ..........................................................37
POstErs
molecular Pathogenesis, molecular Pathology, Cell Biology and translational research......................................................... 38P-031 the aaa+ atPase ruVB1 Is a Potent reGuLator of LIVer GLucose
MetaBoLIsM: IMPLIcatIons for hcc ProGressIon In conDItIonaL
knock-out MIce ....................................................................................................38
P-032 choLIne aDDIctIon In Beta-catenIn-MutateD hePatoceLLuLar carcInoMa .....38
P-033 reGuLatIon of GLyPIcan-3 By neW MIcrornas anD IMPLIcatIon In
hePatoceLLuLar carcInoMa ................................................................................38
P-034 a DIet-InDuceD Mouse MoDeL of steatohePatItIc hePatoceLLuLar
carcInoMa WIth a trascrIPtoMIc sIGnature that recaPItuLates huMan
DIsease ..................................................................................................................39
P-035 IncreaseD steMness of resIDuaL VIaBLe hePatoceLLuLar carcInoMa In
hyPoxIc MIcroenVIronMents InDuceD By transarterIaL
cheMoeMBoLIzatIon .............................................................................................39
P-036 IncreaseD MItochonDrIaL fIssIon ProMotes ceLL surVIVaL throuGh
ros-MeDIateD coorDInateD reGuLatIon of nf-ΚB anD P53 PathWays In
hePatoceLLuLar carcInoMa ................................................................................39
P-037 reGuLatIon of Beta-catenIn By MIcrornas In hePatoBLastoMa,
a rare PaeDIatrIc LIVer cancer ..........................................................................40
P-038 BIoLoGIc anD transLatIonaL sIGnIfIcance of MorPho-PhenotyPIc chanGes
occurrInG In huMan hePatocarcInoGenesIs .....................................................40
P-039 IMMunotoxIn tarGetInG GLyPIcan-3 reGresses LIVer cancer VIa DuaL
InhIBItIon of Wnt sIGnaLLInG anD ProteIn synthesIs ........................................41
P-040 transLatIonaL controL By nuP155 MoDuLates P53 tarGet Gene
exPressIon In LIVer cancer .................................................................................41
P-041 eVoLutIonary cancer faVoreD enGIneereD VaccInIa VIrus attenuates
MetastatIc hePatoceLLuLar carcInoMa ............................................................41
P-042 anaLysIs of exoMe sequencIes of choLanGIocarcInoMa saMPLes:
IDentIfIcatIon of DeLeterIous MutatIons anD Its PreVaLence screenInG In
BrazILIan PatIents ................................................................................................41
P-043 the actIVatIon of an ePItheLIaL to MesenchyMaL transItIon ProGraM By
InsuLIn/InsuLIn-LIke GroWth factor-1 recePtors Is InVoLVeD In
the acquIreD resIstance to antI-eGfr theraPy of huMan
choLanGIocarcInoMa ceLLs ................................................................................42
P-044 seruM MIr-10B* as a PotentIaL PreDIctIVe BIoMarker for sorafenIB
treatMents of aDVanceD hcc PatIents .............................................................42
P-045 hoxa13 exPressIon PreDIcts Worst ProGnosIs In hcc anD IMPacts on
sorafenIB resPonse.............................................................................................42
P-046 hePatoceLLuLar carcInoMa rePLIcatInG hePatItIs B VIrus .............................43
P-047 free ePIsoMaL anD InteGrateD hBV Dna In hBsaG-neGatIVe PatIents WIth
IntrahePatIc choLanGIocarcInoMa ....................................................................43
P-048 Why hcc runs a hIGh LocaL InVasIon anD recurrence rate But rareLy
systeMIc MetastasIs ............................................................................................44
P-049 MoLecuLar BIoMarkers for cheMoPreVentIon of hePatoceLLuLar
carcInoMa By acycLIc retInoID ..........................................................................44
P-050 exoMe sequencInG In earLy-staGe hePatoceLLuLar carcInoMa IDentIfIes
PtPn13 as a tuMour suPPressor ........................................................................44
P-051 zIc2 ProMotes ceLL ProLIferatIon anD MIGratIon In hePatoceLLuLar
carcInoMa By transcrIPtIonaLLy uPreGuLatInG Pak4 ......................................44
P-052 hIGher PhosPho-rB exPressIon assocIateD WIth Better actIVIty
of cycLIn DePenDent kInase 4/6 InhIBItor aBeMacIcLIB
on hePatoceLLuLar carcInoMa ..........................................................................45
P-054 recoMBInant aDenoVIrus encoDInG fat10 sMaLL InterferInG rna
InhIBIts hcc GroWth In VItro anD In VIVo ...........................................................45
P-055 PathoPhysIoLoGy of hePatItIs c VIrus (hcV)-reLateD hePatoceLLuLar
carcInoMa: hcV ProteIn exPressIon InDuces the actIVatIon of the akt1
IsoforM In hePatocytes throuGh an Mtorc2 DePenDent PathWay ................45
P-056 Dna DaMaGe causeD By DIetary InDuceD steatohePatItIs correLates WIth
hePatoceLLuLar carcInoMa DeVeLoPMent anD ProGressIon ..........................46
P-057 cataLase actIVIty InhIBItIon By hePatItIs c VIrus (hcV) In hcV-InDuceD
oxIDatIVe stress, a trIGGer of hePatIc carcInoGenesIs ...................................46
P-058 aLPha-santaLoL InhIBIts tuMor anD InDuces aPoPtosIs
In hePatoceLLuLar carcInoMas In VItro anD In VIVo .........................................46
P-059 noVeL GenoMIc Marker for PreDIctInG ProGnosIs In PatIents WIth
hePatoceLLuLar carcInoMa DetecteD By InteGratIon anaLysIs
of coPy nuMBer aLteratIons anD Gene exPressIon ProfILe:
resuLts froM LonG terM foLLoW-uP .................................................................47
P-060 Loss of e-caDherIn In PortaL VeIn tuMor throMBosIs of hePatoceLLuLar
carcInoMa can Be reVerseD By c-Met InhIBItor ...............................................47
P-061 treatMent of hcc ceLLs WIth sorafenIB InDuceD VarIatIons
In the ProfILe of the ceLL MethyLoMe ..............................................................47
P-062 axL exPressIon stratIfIes PatIents WIth Poor ProGressIon for
hePatoceLLuLar carcInoMa ................................................................................48
P-063 tert ProMoter MutatIon Pattern In MuLtIsteP
hePatocarcInoGenesIs: a stuDy of 7 PatIents ..................................................48
P-064 near InfrareD PhotoDynaMIc theraPy usInG InDocyanIne Green InhIBIts
tuMor GroWth of huMan hePatoceLLuLar carcInoMa ...................................49
P-065 coPy nuMBer VarIatIons characterIze PrIMary IntrahePatIc
choLanGIocarcInoMas anD theIr LyMPh noDe Metastases .............................49

Contents
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 5
P-066 MIcrorna-23B anD 193a as BIoMarkers anD theraPeutIc tooLs of
hePatocarcInoMa In coMBInatIon WIth sorafenIB ...........................................50
P-067 ePIGenetIc reGuLatIon of cIrcaDIan Gene exPressIon By tuMor
suPPressor sIrtuIn 6 ...........................................................................................50
P-068 effIcacy of PerIfosIne aLone In coMBInatIon WIth sorafenIB In a
transGenIc Mouse MoDeL of hePatoceLLuLar carcInoMa ..............................50
P-069 oxIDatIVe stress ProMotes PathoLoGIc PoLyPLoIDIzatIon In
nonaLcohoLIc fatty LIVer DIsease......................................................................51
P-070 hIGh exPressIon of MIr-135a In hcc Is assocIateD WIth earLy
recurrence after resectIon PotentIaLLy VIa DeVeLoPMent of
IntrahePatIc MIcro-Metastases .........................................................................51
P-071 LysoPhosPhatIDIc acID ProMotes hePatoceLLuLar carcInoMa InVasIon
By auGMentInG eGfr transactIVatIon, cytokeratIn 19 exPressIon
anD nf-ΚB actIVatIon...........................................................................................51
P-072 t ceLLuLar IMMune Defect of hePatoceLLuLar carcInoMa .............................51
P-073 hePatoceLLuLar aDenoMa can DeVeLoP on cIrrhotIc LIVer ............................52
P-074 the MIr-23B DoWnMoDuLatIon In hcc Is MeDIateD By Dna MethyLatIon .........52
P-076 LkB1: a key reGuLator of hePatocytes ProLIferatIon anD
GenoMe InteGrIty .................................................................................................52
P-077 oVerexPressIon of PerIostIn Is reLateD to Poor ProGnosIs of
hePatoceLLuLar carcInoMa ................................................................................53
P-079 oVerexPressIon of chaPeronIn contaInInG tcP1, suBunIt 3 In nucLeus of
cancerous ceLLs In hePatoceLLuLar carcInoMa Is a Marker for Poor
ProGnosIs .............................................................................................................53
P-080 LasP1-oVerexPressIon reVeaLs VIMentIn as Its neW MoLecuLar Partner
In huMan hePatoceLLuLar carcInoMa ceLLs .....................................................53
P-081 the hePatItIs B VIrus x ProteIn InDuces the PhenotyPe of ePItheLIaL-
MesenchyMaL transItIon throuGh controL cD44 In hcc ceLL LInes ..............54
P-082 MutatIons In the hcV-3a core Gene assocIateD WIth DeVeLoPMent to hcc ...54
P-083 effIcacy of PerIfosIne aLone anD In coMBInatIon WIth sorafenIB In a
transGenIc Mouse MoDeL of hePatoceLLuLar carcInoMa ..............................54
P-084 sorafenIB anD ceLecoxIB synerGIstIcaLLy InDuce ceLL Death of
hePatoceLLuLar carcInoMa throuGh er stress MeDIateD aPoPtosIs ...........55
P-085 f t y 720 (fInGoLIMoD) sensItIzes hePatoceLLuLar carcInoMa ceLLs to
sorafenIB-MeDIateD cytotoxIcIty ......................................................................55
P-086 VeGf-c936t anD VeGf-a1154G PoLyMorPhIsMs are not assocIateD WIth
cIrrhosIs anD chc ................................................................................................55
P-087 ProGnostIc VaLue of IMMunohIstocheMIcaL DetectIon of ProGenItor
ceLL, choLanGIocyte anD hePatocyte Markers In surGIcaLLy reMoVeD
hePatoceLLuLar carcInoMa ................................................................................55
P-088 MoDeLInG huMan hePatItIs B VIrus InfectIon WIth PLurIPotent
steM ceLL-DerIVeD hePatocytes .........................................................................56
P-089 Ber Gene (hoGG1,xrcc1) PoLyMorPhIsMs In hcc PatIents ................................56
P-090 MIcrorna exPressIon LeVeLs In hcc PatIents....................................................56
P-091 eMoDIn InhIBIt GroWth anD InDuceD aPoPtosIs In an ectoPIc
hePatoceLLuLar carcInoMa MoDeL By enhanceMent of ParP1 cLeaVaGe .....56
P-092 PhosPhoLIPase D1 contrIButes to huMan hePatoceLLuLar carcInoMa .........57
P-093 MetaBoLIc raDIotheraPy WIth IoDIne-131: effects In a huMan
choLanGIocarcInoMa ceLL LIne .........................................................................57
P-094 IoDIne-131: an oPtIon for the choLanGIocarcInoMa treatMent? ..................57
P-095 GLyPIcan-3 anD Beta-catenIn Gene exPressIon In PatIents WIth
hePatoceLLuLar carcInoMa, hePatItIs c or cIrrhosIs .....................................58
P-096 Den-InDuceD hePatocarcInoGenesIs In c57BL/6 MIce;
IMPact of tarGeteD theraPIes ............................................................................58
P-097 ocoxIn-VIusID® sLoWs DoWn tuMor ProGressIon of coLorrectaL
cancer MetastasIs DeVeLoPMent to the LIVer In a MurIne MoDeL .................58
P-098 effects of BorIc acID anD Borax theraPy on Dna DaMaGe,
LIPID PeroxIDatIon anD antIoxIDant systeM at Benzo(a)Pyrene anD
3-MethyLchoLanthrene aDMInIstereD rats ......................................................59
P-099 InVestIGate By tuneL MethoD of the effect of LInuM usItatIssIMuM
extract In the PreVentIon of exPerIMentaLLy afLatoxIn-InDuceD
LIVer anD kIDney LesIons In rats .........................................................................59
P-100 LIGase chaIn reactIon as a MoDaLIty for the DetectIon of PoInt
MutatIon In the Precore reGIon of hBV reLateD hcc cases:
a stuDy froM northern InDIa .............................................................................59
P-101 the effect of Borax on totaL antI oxIDatIVe- oxIDatIVe status
In DIfferent tIssues of rats aPPLIeD Benzo(a)Pyrene ......................................59
P-102 effect of huMan BILe on VIaBILIty anD MIGratIon of hePG2 ceLLs
hePatoceLLuLar carcInoMa ...............................................................................60
P-103 the caucasIan's orIGIn BacterIoPhaGe neW ProBaBLe tarGet aGent
In the treatMent for Inf treateD hcV assocIateD hcc ....................................60
P-104 InfLuence aDeMethIonIne on the MeLatonIn secretIon In PatIents
WIth not PreVIousLy treateD anD treateD-reLaPseD hePatItIs c ...................60
Epidemiology, staging and Prognosis ............................................................. 61P-105 the externaL VaLIDatIon of honG konG LIVer cancer cLassIfIcatIon for
PreDIctIon of surVIVaL In PatIents WIth hePatoceLLuLar carcInoMa: DIrect
coMParIson WIth BarceLona cLInIc LIVer cancer cLassIfIcatIon ...................61
P-106 DeVeLoPMent of a MoDeL PreDIctInG surVIVaL for recurrent
or ProGressIVe hePatoceLLuLar carcInoMa ....................................................61
P-107 MoDIfIcatIon of the cancer of the LIVer ItaLIan ProGraM score WIth
oBjectIVeLy assesseD LIVer reserVe IMProVes ProGnosIs PreDIctIon
for aDVanceD hePatoceLLuLar carcInoMa .......................................................61
P-108 oPtIMaL suBstaGInG of InterMeDIate staGe hePatoceLLuLar carcInoMa ......62
P-109 surVIVaL of PatIents WIth aDVanceD hePatoceLLuLar carcInoMa on
sorafenIB: an anaLysIs of seer-MeDIcare DataBase .........................................62
P-110 the costs of carInG for hePatoceLLuLar carcInoMa .....................................63
P-111 effect of WaItInG tIMe on tuMor PathoLoGy anD outcoMe In PatIents
WIth hePatoceLLuLar carcInoMa treateD WIth LIVer transPLantatIon .........63
P-112 coMBInatIon of MoDIfIeD resPonse eVaLuatIon crIterIa In soLID
tuMors anD hanD-foot-skIn reactIon: a neW ProGnostIc eVaLuatIon
for hePatoceLLuLar carcInoMa PatIents treateD WIth sorafenIB anD
transarterIaL cheMoeMBoLIzatIon ...................................................................64
P-113 LIVer stIffness MeasureMent (fIBroscan°r) DeterMInes the rIsk
of recurrence after raDIofrequency for earLy staGeD
hePatoceLLuLar carcInoMa ................................................................................64
P-114 utILIty of "art-score" In the sequentIaL cheMoeMBoLIzatIon for
hePatoceLLuLar carcInoMa treatMent .............................................................64
P-115 sorafenIB use In eLDerLy PatIents WIth aDVanceD hePatoceLLuLar
carcInoMa In the unIteD states: an anaLysIs of the
seer-MeDIcare DataBase .....................................................................................65
P-116 the art score couLD not PreDIct oVeraLL surVIVaL for rePeateD
transarterIaL cheMoeMBoLIzatIon In thaI PatIents WIth
hePatoceLLuLar carcInoMa ...............................................................................65
P-117 the haP score Is ProGnostIc In PatIents WIth aDVanceD
hePatoceLLuLar carcInoMa treateD By sorafenIB ..........................................66
P-118 BaseLIne PreDIctors of outcoMe for PatIents treateD By
sorafenIB for hePatoceLLuLar carcInoMa (hcc) .............................................66
P-119 PreDIctIon of cLInIcaL outcoMe after raDIoeMBoLIzatIon In hcc PatIents:
roLe of 18f-fDG Pet-ct ........................................................................................67
P-120 ProGnostIc sIGnIfIcance of InfLaMMatIon BaseD scores for
PatIents WIth hePatoceLLuLar carcInoMa treateD
WIth sorafenIB In a Western coLLectIVe ...........................................................67
P-121 outcoMes of resectIon for soLItary ≤ 5 cM IntrahePatIc
choLanGIocarcInoMa .........................................................................................67
P-122 IMPact of PreoPeratIVe renaL InsuffIcIency on short
outcoMe after hePatIc resectIon of hePatoceLLuLar carcInoMa ................68
P-123 WIDe resectIon MarGIn IMProVes surVIVaL In PatIents WIth earLy
IntrahePatIc choLanGIocarcInoMa ....................................................................68
P-124 hePatoceLLuLar carcInoMa In the aBsence of cIrrhosIs:
an etIoLoGy-BaseD cLInIcoPathoLoGIcaL stuDy ................................................68
P-125 aLBI score PreDIcts surVIVaL In PatIents WIth BcLc 0/a staGe
hePatoceLLuLar carcInoMa (hcc) InDePenDentLy of chILD
PuGh (cP) score anD treatMent aLLocatIon ......................................................69
P-126 aLBI score PreDIcts surVIVaL InDePenDentLy of hePatIc Venous
Pressure GraDIent (hVPG) anD InDocyanIne Green (IcG) cLearance
In hcc PatIents unDerGoInG resectIon ..............................................................69
P-127 coMParIson of staGInG systeMs for the PreDIctIon of ProGnosIs In
PatIents WIth hePatoceLLuLar carcInoMa unDerGoInG
transcatheter arterIaL cheMoeMBoLIzatIon ...................................................69

Contents
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s6
P-128 InfLuence of hePatItIs B VIrus Dna eLeVatIon on recurrence of
hePatoceLLuLar carcInoMa after surGIcaL resectIon anD the PreVentIVe
roLe of antIVIraL theraPy ...................................................................................69
P-129 unDetecteD asyMPtoMatIc aLcohoLIc cIrrhosIs unDerLIes the
DIaGnosIs of hcc out of surVeILLance ProGraMs In sPaIn. anaLysIs
of 750 cases In 74 centers .................................................................................70
P-130 sInGLe center anaLysIs of the resuLts after resectIon/transPLantatIon
In PatIents WIth coMBIneD hePatoceLLuLar carcInoMa anD
choLanGIocarcInoMa ..........................................................................................70
P-131 cLInIcaL characterIstIcs anD ProGnosIs In non-B non-c hePatoceLLuLar
carcInoMa PatIents WIth MoDest aLcohoL consuMPtIon ...............................71
P-132 assocIatIon BetWeen hePatItIs B VIrus Dna LeVeL & antIVIraL theraPy
on the recurrence of PatIents after LIVer resectIon for hePatItIs B
VIrus-reLateD hePatoceLLuLar carcInoMa .......................................................71
P-133 PerI-transPLant chanGe In afP LeVeL Is a usefuL PreDIctor of
hePatoceLLuLar carcInoMa recurrence foLLoWInG LIVer
transPLantatIon ..................................................................................................71
P-134 utILIzatIon rate of hePatoceLLuLar carcInoMa (hcc) surVeILLance
ProGraM anD factors assocIateD WIth surVeILLance In a LarGe referraL
center, thaILanD .................................................................................................72
P-135 IncIDentaL hePatoceLLuLar carcInoMa In LIVer transPLantatIon:
PreoPeratIVe fInDInGs anD PostoPeratIVe outcoMes ......................................72
P-136 GenotyPe anaLysIs of hePatoceLLuLar aDenoMa In jaPan ...............................72
P-137 cLInIcaL sIGnIfIcance of coMPLete anD coMPact LIPIoDoL uPtake of the
LesIon accoMPanIeD WIth reDuctIon of seruM VascuLar enDotheLIaL
GroWth factor LeVeLs at 1 Month after transcatheter arterIaL
cheMoeMBoLIzatIon for hePatoceLLuLar carcInoMa .....................................73
P-138 ePIDeMIoLoGy, DIaGnosIs, treatMent anD outcoMe of PatIents WIth LIVer
cancer at a GerMan thIrD LeVeL MeDIcaL center BetWeen 2008 anD 2012 ....73
P-139 PreDIctors of surVIVaL anD aDherence to PractIce GuIDeLInes
In a sInGLe center hcc cohort – a 12 year exPerIence ....................................73
P-140 sarcoPenIa Is assocIateD WIth an IncreaseD MortaLIty In
PatIents receIVInG reGIonaL theraPy for hePatoceLLuLar carcInoMa
as a BrIDGe to transPLantatIon .........................................................................74
P-141 asPects of aDVanceD staGe hcc anD PrIorItIes to treat In 796
BcLc-c eGyPtIan PatIents ....................................................................................74
P-142 characterIzatIon of hePatoceLLuLar carcInoMa In eGyPt:
rIsk factors, PresentatIon anD ProGnosIs ......................................................74
P-143 antI-hBe PosItIVIty Is ProtectIVe for hcc DeVeLoPMent In naïVe
hePatItIs B VIraL cIrrhotIc PatIents treateD WIth LonG-terM entecaVIr
MonotheraPy .......................................................................................................75
P-144 effIcacy of sorafenIB for oLIGoMetastatIc hePatoceLLuLar carcInoMa .....75
P-145 cLInIcaL features anD treatMent MoDaLItIes of LonG-terM surVIVors WIth
aDVanceD hePatoceLLuLar carcInoMa: a sInGLe InstItutIon cohort stuDy ..75
P-146 treatMent of hePatoceLLuLar carcInoMa In the eLDerLy ...............................75
P-147 hePatectoMy for hePatoceLLuLar carcInoMa LarGer than 10 cM:
PreoPeratIVe rIsk stratIfIcatIon to PreVent futILe surGery .........................76
P-148 LocoreGIonaL theraPy In PatIents WaItLIsteD for LIVer transPLant
IMProVes surVIVaL after transPLantatIon: an oBserVatIonaL stuDy ............76
P-149 hePatectoMy for hePatoceLLuLar carcInoMa: ...............................................76
IMPact of PostoPeratIVe MorBIDIty on LonG-terM outcoMe ........................76
P-150 cLInIcaL ParaMeters PreDIctIVe of outcoMes In sorafenIB-treateD
PatIents WIth aDVanceD hePatoceLLuLar carcInoMa ......................................77
P-151 fIBrosIs InDex anD fIBrosIs 4 score In PreDIctIon of hePatoceLLuLar
carcInoMa In chronIc hePatItIs c eGyPtIan PatIents .......................................77
P-152 cLInIcaL sIGnIfIcance of occuLt hePatItIs B InfectIon In PatIents WIth
non-hePatItIs B/non-hePatItIs c-reLateD hePatoceLLuLar carcInoMa
In a hePatItIs B enDeMIc area ..............................................................................77
P-153 factors assocIateD WIth hePatoceLLuLar carcInoMa surVeILLance
rates aMonG PatIents WIth cIrrhosIs In a PoPuLatIon-BaseD InteGrateD
heaLthcare DeLIVery systeM ...............................................................................78
P-154 effIcacy anD safety of sorafenIB In PatIents WIth aDVanceD
hePatoceLLuLar carcInoMa: aGInG Is not a ProBLeM.......................................78
P-155 PreDIctIon MoDeL for the DeVeLoPMent of hePatoceLLuLar carcInoMa
In PatIents WIth chronIc hePatItIs B receIVInG antIVIraL treatMent ..............78
P-156 WIDe resectIon MarGIn IMProVes surVIVaL In PatIents WIth earLy
IntrahePatIc choLanGIocarcInoMa ....................................................................79
Diagnosis, Imaging and Biomarkers ................................................................ 79P-157 outreach InVItatIons IMProVe hePatoceLLuLar carcInoMa
surVeILLance rates: resuLts of a ranDoMIzeD controLLeD trIaL
In a safety net heaLth systeM ............................................................................79
P-158 surface of the WhoLe aBDoMInaL MuscLes Better PreDIct oVeraLL
anD DIsease-free surVIVaL than surface of Psoas MuscLes ..........................79
P-159 hIGht VaLue of contrast enhanceD uLtrasounD (ceus) In DefInInG
a raPID DIaGnostIc anD theraPeutIc Work-uP for noDuLes <2 cM In
cIrrhotIc PatIents DurInG surVeILLance ...........................................................80
P-160 Pre-treatMent reD ceLL DIstrIButIon WIDth (rDW) to stratIfy
surVIVaL of PatIents WIth aDVanceD hePatoceLLuLar carcInoMa
unDerGoInG sorafenIB treatMent .....................................................................80
P-161 LIVer IMaGInG rePortInG anD Data systeM cateGorIzatIon of
hePatoceLLuLar carcInoMa usInG GaDoxetIc acID-enhanceD MrI:
coMParIson WIth MDct ........................................................................................81
P-162 hIGh exPressIon of yaP anD GLI1 reLateD to ePItheLIaL-MesenchyMaL
transItIon anD Poor ProGnosIs of hePatoceLLuLar carcInoMa after
surGery .................................................................................................................81
P-163 cIrcuLatInG tuMor ceLL DetectIon In PerIPheraL anD hePatIc VeIns In
PatIents WIth PotentIaLLy resectaBLe hePatoceLLuLar carcInoMa ..............81
P-164 earLy DerMatoLoGIcaL aDVerse eVents anD coMPLete raDIoLoGIcaL
resPonse In hcc PatIents treateD WIth sorafenIB. the LInk to
treatMent effIcacy .............................................................................................82
P-165 IMPact of fIBroBLast GroWth factor-2 anD Its recePtor Gene
PoLyMorPhIsMs on tuMor ProGressIon anD PatIent surVIVaL In PatIents
WIth hePatItIs B VIrus-assocIateD hePatoceLLuLar carcInoMa ......................82
P-166 VaLIDIty of BarceLona cLInIc LIVer cancer staGe a: assocIatIon of tuMor
sIze anD oVeraLL surVIVaL In a sInGLe hePatoceLLuLar carcInoMa ................82
P-167 GLutaMInase score serVes as the BIoMarker for PathoLoGIc
DIaGnosIs anD ProGnosIs of hePatoceLLuLar carcInoMa ...............................83
P-168 seruM anGIoPoIetIn LeVeLs correLate WIth seVerIty of PortaL
hyPertensIon But Do not PreDIct the Presence of hePatoceLLuLar
carcInoMa In cIrrhosIs .......................................................................................83
P-169 the autoPhaGy-reLateD Marker P62 Is usefuL for DIaGnosIs In huMan
hePatoceLLuLar carcInoMa ................................................................................84
P-170 IDentIfIcatIon of IMaGInG PreDIctor DIscrIMInatInG hIGh rIsk GrouP
for IntrahePatIc choLanGIocarcInoMa or coMBIneD hePatoceLLuLar-
choLanGIocarcInoMa In PatIents WIth chronIc LIVer DIsease on GaDoxetIc
acID-enhanceD MrI: cLassIfIcatIon tree anaLysIs .............................................84
P-171 aPPLIcatIon of contrast-enhanceD IntraoPeratIVe uLtrasounD usInG
PerfLuButane to hePatIc resectIon for LIVer cancer .....................................84
P-172 MIcrorna-452 ProMotes tuMor-InItIatInG ceLLs of hePatoceLLuLar
carcInoMa By actIVatInG Wnt/Beta-catenIn sIGnaLInG PathWay .....................85
P-173 effect of surGIcaL MarGIn status on tuMor recurrence after resectIon
for hePatoceLLuLar carcInoMa BaseD on PreoPeratIVe cIrcuLatInG
tuMor ceLLs LeVeL ...............................................................................................85
P-174 hePatoceLLuLar carcInoMa surVeILLance Is assocIateD WIth sIGnIfIcant
PotentIaL harMs In PatIents WIth cIrrhosIs .....................................................85
P-175 functIonaL nonInVasIVe IMaGInG of kuPffer ceLLs status usInG
raDIoLaBeLLeD MannosyLateD aLBuMIn .............................................................86
P-176 coMPLIcatIons after Percutaneous raDIofrequency aBLatIon (rfa)
of hePatoceLLuLar carcInoMa (hcc) In cIrrhosIs: 20 years
exPerIence In a sInGLe center .............................................................................86
P-177 coMPuter assIsteD surGery for GIant LIVer tuMors usInG a noVeL LIVer
seGMentatIon aPPLIcatIon ...................................................................................87
P-179 hIstoLoGIcaL exPressIon of MethIonIne aDenosyLtransferase (Mat) I
anD Mat II as Post-surGIcaL ProGnostIc surroGates In PatIents WIth
hePatItIs B VIrus-reLateD hePatoceLLuLar carcInoMa ....................................87
P-180 aLPha fetoProteIn (afP) resPonse couLD PreDIct the ProGnosIs of PatIents
receIVInG sorafenIB after stratIfIcatIon By IMaGInG eVaLuatIon ...................87
P-181 teLoMere DysfunctIon Is a rIsk factor for hePatoceLLuLar
carcInoMa In chronIc hePatItIs c ......................................................................87
P-182 What Is the roLe of surGery In the treatMent of recurrence of
hePatoceLLuLar carcInoMa after LIVer transPLantatIon? ............................88

Contents
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 7
P-183 outcoMes foLLoWInG yttrIuM-90 transarterIaL raDIoeMBoLIzatIon
for hePatoceLLuLar carcInoMa In PatIents WIth an eLeVateD
Pre-treatMent aLPha-fetoProteIn ....................................................................88
P-184 IntratuMoraL orGanIc catIon transPorter 1 exPressIon In
hePatoceLLuLar carcInoMa as a BIoMarker for sorafenIB treatMent
resPonse - a PILot stuDy .....................................................................................88
P-185 rIsk PreDIctIon MoDeL of hePatoceLLuLar carcInoMa In hosPItaL-BaseD
PoPuLatIon WIth hePatItIs B VIrus InfectIon......................................................89
P-186 DIaGnostIc PerforMance of contrast IMaGInG technIques In sMaLL
hePatoceLLuLar carcInoMa MeasurInG Less than 2 cM ..................................89
P-187 contrast-InDuceD DysPnea DurInG GD-eoB-DtPa enhanceD LIVer MrI:
anaLysIs of resPIratory GraPhs DurInG Breath-hoLD .....................................89
P-188 hIGh cIrcuLatInG MIcrorna-122 exPressIon Is a Poor ProGnostIc
Marker In PatIents WIth hePatItIs B VIrus-reLateD hePatoceLLuLar
carcInoMa Who unDerGo raDIofrequency aBLatIon .......................................90
P-189 annexIn a2 as a noVeL DIaGnostIc Marker f hePatoceLLuLar
carcInoMa In eGyPtIan PatIents .........................................................................90
P-190 ceus fInDInGs after IrreVersIBLe eLectroPoratIon aBLatIon:
can sIze of aBLatIon zone Be PreDIcteD earLIer ..............................................90
P-191 utILIty of MIcroVesIcLes as PLasMa BIoMarkers In PatIents
WIth hePatoceLLuLar carcInoMa .......................................................................91
P-192 IncreaseD seruM huMan ePIDIDyMIs ProteIn 4 (he4) In PatIents WIth
hePatoceLLuLar carcInoMa: a PotentIaL tuMor Marker ................................91
P-193 cIrcuLatInG scca-IGM coMPLex Is a usefuL BIoMarker to PreDIct the
outcoMe of theraPy In hcc PatIents .................................................................91
P-194 the roLe of the Mhc cLass I PoLyPePtIDe-reLateD chaIn a (MIca)
In the tertIary PreVentIon of hePatoceLLuLar carcInoMa In chronIc
hePatItIs c PatIents ..............................................................................................92
P-195 MuLtI-anaLyte anaLysIs of seruM cytokInes to PreDIct treatMent outcoMe
In PatIents WIth hePatoceLLuLar carcInoMa treateD WIth raDIotheraPy.....92
P-196 reGuLatIon of cD13 By hDac1 ProMotes nf-kB sIGnaLInG to enhance
hePatoceLLuLar carcInoMa ProGressIon .........................................................92
P-197 cIrcuLatInG MIrna-122 as a BIoMarker for hcV-InDuceD
hePatoceLLuLar carcInoMa ...............................................................................92
P-198 18fDG PosItron eMIssIon toMoGraPhy/coMPuteD toMoGraPhy (Pet-ct),
eLastoGraPhy anD contrast enhanceD uLtrasonoGraPhy to eVaLuate
DIaGnosIs, staGInG anD theraPy In nash-reLateD hcc .....................................93
P-199 DuaL-tracer 18f-fLuorochoLIne (fch) anD 18f-fLuoroDeoxyGLucose (fDG)
Pet/ct for the DIaGnosIs of tuMoraL PortaL VeIn throMBosIs In PatIents
WIth hePatoceLLuLar carcInoMa (hcc) ..............................................................93
P-200 a coMParIson of uLtrasounD, coMPuterIseD toMoGraPhy anD MaGnetIc
resonance IMaGInG fInDInGs BetWeen 38 cases of sIMPLe hePatIc
cysts anD 13 cases of MucInous cystIc neoPLasMs of the LIVer ..................93
P-201 usefuLness of aLPha-fetoProteIn for the DetectIon of hePatoceLLuLar
carcInoMa In PatIents WIth chronIc hePatItIs B VIrus InfectIon ....................93
P-203 cLInIcaL eVaLuatIon of content-BaseD IMaGe-retrIeVaL systeM In ct
DIaGnosIs for LIVer tuMors ................................................................................94
P-204 nonInVasIVe DIaGnosIs of MaLIGnant LIVer tuMors usInG shear WaVe
uLtrasounD eLastoGraPhy .................................................................................94
P-205 the effect of reDucInG Prostate VoLuMe on tuMor VoLuMes of PatIents
WIth hePatoceLLuLar carcInoMa treateD WIth sorafenIB ..............................94
P-206 hsa-MIr-15B anD VeGf Gene exPressIon assocIateD In LIVer cIrrhosIs anD
hePatoceLLuLar carcInoMa ................................................................................95
P-207 hcc DIfferentIatIon: quantItatIVe MrI stuDy of tuMor enhanceMent
on GD-BoPta enhanceD hePatoBILIary Phase ....................................................95
P-208 eVaLuatIon of treatMent resPonse of raDIotheraPy for hcc
usInG Pre- anD Post-treatMent MaGnetIc resonance IMaGInG ......................95
P-209 hIstoPathoLoGIcaL Pattern of hePatoceLLuLar carcInoMa
anD outcoMe of raDIofrequency aBLatIon ......................................................95
P-210 VaLIDatIon of the neW BcLc suBcLassIfIcatIon In a roManIan tertIary
GastroenteroLoGIcaL anD surGIcaL center.....................................................96
P-212 PreVaLence of hcc Was hIGher In PatIents WIth LoWer controLLeD
attenuatIon ParaMeter (caP) VaLue In non-VIraL chronIc hePatItIs ...............96
P-213 hsa-MIr-874 assocIatIon WIth VeGf Gene exPressIon In hePatoceLLuLar
carcInoMa anD cIrrhotIc LIVer ..........................................................................96
P-214 eVaLuatIon of DetectIon rate of LIVer tuMor exIstInG DeeP LocatIon
froM the surface usInG seconD GeneratIon aGent, sonazoID ........................97
P-215 quIck anD easy DetectIon MethoD of LIVer tuMor WIth neW
technoLoGy for us ..............................................................................................97
P-216 screenInG anD IDentIfyInG a noVeL ssDna aPtaMer aGaInst aLPha-
fetoProteIn usInG ce-seLex ................................................................................97
P-217 the MeanInG of afP, afP-L3 anD PIVka-II for eVaLuatInG recurrence
In PatIents WIth hePatoceLLuLar carcInoMa Who unDerWent
LIVer resectIon.....................................................................................................97
P-218 effIcacy of Loco-reGIonaL treatMent for hePatoceLLuLar carcInoMa
PrIor to LIVInG Donor LIVer transPLantatIon ...................................................98
P-219 sequentIaL seruM MetaBoLoMIc ProfILInG after raDIofrequency aBLatIon
of hePatoceLLuLar carcInoMa reVeaLs DIfferent resPonse Patterns
accorDInG to aetIoLoGy ......................................................................................98
P-220 hIGh accuracy of soLuBLe axL In the DIfferentIaL DIaGnosIs of
chronIc LIVer DIseases anD hePatoceLLuLar carcInoMa ................................98
P-221 the effect of BorIc acID on totaL antI oxIDatIVe- oxIDatIVe status In
DIfferent tIssues of rats aPPLIeD 3–MethyLchoLanthrene ...........................99
P-222 Percutaneous ManaGeMent of PostoPeratIVe stenosIs of the
BILIojejunaL anastoMosIs In hePatIc or PancreatIc cancer PatIents ...........99
P-223 hePatoBILIary carcInoMa WIth osteocLast-LIke GIant ceLLs:
fIrst case rePort ................................................................................................99
Clinical trials and treatment research & miscellaneous .............................100P-224 unresectaBLe hePatoceLLuLar carcInoMa > 5 cM: effIcacy anD
surVIVaL of MuLtIBIPoLar raDIofrequency aBLatIon ......................................100
P-225 hoW reLeVant Is InDocyanIne Green retentIon rate at 15 MInutes (IcG15)
assessMent Before an eLectIVe hePatectoMy In Western country? ...........100
P-226 MuLtIcentrIc stuDy of LIVer transPLantatIon In PatIents WIth
hePatoceLLuLar carcInoMa In BrazIL- PreLIMInary Data of 913 PatIents .....100
P-227 coMParIson BetWeen MIcroWaVe aBLatIon anD raDIofrequency
aBLatIon In the treatMent of hePatoceLLuLar carcInoMa ...........................101
P-228 coMParatIVe stuDy BetWeen raDIoeMBoLIzatIon anD cheMoeMBoLIzatIon
WIth DruG eLutInG BeaD In PatIents WIth hePatoceLLuLar carcInoMa ........101
P-229 raDIoeMBoLIzatIon Is a safe anD effectIVe treatMent for
hePatoceLLuLar carcInoMa WIth PortaL VeIn throMBosIs ...........................102
P-230 the oPtIMaL staGInG of the sInGLe LarGe hePatoceLLuLar carcInoMa .......102
P-231 an InternatIonaL oBserVatIonaL stuDy to assess the use of sorafenIB
after transarterIaL cheMoeMBoLIzatIon (tace) In PatIents WIth
hePatoceLLuLar carcInoMa (hcc): oPtIMIs InterIM anaLysIs .........................102
P-232 no touch MuLtIBIPoLar raDIofrequency aBLatIon for the treatMent of
hePatoceLLuLar carcInoMa WIthIn MILan crIterIa: LonG terM resuLts .......103
P-233 LIVer reGeneratIon after Major hePatectoMy Decreases
tuMoraL GroWth ...............................................................................................103
P-234 surVIVaL BenefIt of LocoreGIonaL theraPy for hePatoceLLuLar carcInoMa
WIth chILD-PuGh c LIVer functIon: a MuLtIcenter natIon-WIDe stuDy ..........103
P-235 eVaLuatIon of the LIVer carcInoGenesIs factors In jaPanese chronIc
hePatItIs B PatIents treateD WIth entecaVIr: MuLtIcenter trIaL ..................104
P-236 conVersIon theraPy WIth hePatIc arterIaL InfusIon cheMotheraPy
for LonG-terM ProGnosIs In PatIents WIth aDVanceD hePatoceLLuLar
carcInoMa InVoLVInG VascuLar InVasIon .........................................................104
P-237 effect of oraL antIVIraL treatMent on LonG-terM outcoMes of
raDIofrequency aBLatIon theraPy for hePatItIs B VIrus-reLateD
hePatoceLLuLar carcInoMa ..............................................................................105
P-238 coMParIson of transarterIaL cheMoeMBoLIzatIon anD hePatIc
resectIon for LarGe soLItary hePatoceLLuLar carcInoMa: a ProPensIty
score anaLysIs ...................................................................................................105
P-239 coMBInInG transarterIaL cheMoeMBoLIzatIon WIth raDIofrequency aBLatIon
Versus hePatIc resectIon By usInG ProPensIty score
MatchInG In hePatoceLLuLar carcInoMa .........................................................105
P-240 VascuLar recanaLIzatIon anD PartIcLe excLusIon after transcatheter
arterIaL eMBoLIzatIon WIth PoLyVInyL aLcohoL PartIcLe In hccs:
an hIstoPathoLoGIcaL eVIDence ........................................................................105
P-241 uk exPerIence of sorafenIB In PatIents WIth aDVanceD hePatoceLLuLar
carcInoMa .........................................................................................................106
P-242 hePatoceLLuLar carcInoMa In eLDerLy PatIents: fInaL resuLts
of the ItaLIan cohort of GIDeon stuDy ...........................................................106

Contents
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s8
P-243 sInGLe aGent actIVIty of the seconD-GeneratIon hyPoMethyLatInG aGent, sGI-110, In PatIents WIth hePatoceLLuLar carcInoMa (hcc) after ProGressIon on sorafenIB .....................................................................107
P-244 socIoeconoMIc DIsParItIes In access to sorafenIB .......................................107P-245 a LIVer-seLectIVe, aLLosterIc InhIBItor of acetyL-coa carBoxyLase
eLIcIts tuMor necrosIs anD IMProVes surVIVaL In cIrrhotIc rats WIth hePatoceLLuLar carcInoMa ..............................................................................108
P-246 effectIVeness of coMBIneD raDIofrequency aBLatIon/tace Versus tace/raDIofrequency aBLatIon on LocaL hcc recurrence anD DIsease controL .........................................................................................108
P-247 aLPha-fetoProteIn LeVeLs In chronIc hePatItIs c PatIents are assocIateD WIth systeMIc InsuLIn sensItIVIty anD can Be DecreaseD By LIfestyLe InterVentIon .......................................................................................108
P-248 sorafenIB treatMent In eLDerLy PatIents WIth hePatoceLLuLar carcInoMa ..........................................................................................................109
P-249 neutroPhIL-to-LyMPhocyte ratIo (nLr) Is PreDIctIVe factor for surVIVaL In PatIents WIth aDVanceD hcc treateD By sorafenIB ....................109
P-250 entecaVIr anD tenofoVIr More effectIVeLy reDuce the recurrence of hePatItIs B VIrus-reLateD hePatoceLLuLar carcInoMa after curatIVe treatMent than LoW-Potent antIVIraLs ..........................................................109
P-251 LonG terM outcoMe after resectIon of InterMeDIate (BcLc B) hePatoceLLuLar carcInoMa: coMParIson to transarterIaL cheMoeMBoLIzatIon ...........................................................................................109
P-252 LaMIVuDIne Vs. entecaVIr for the neWLy DIaGnoseD hePatItIs B-VIrus reLateD hePatoceLLuLar carcInoMa .................................................110
P-253 the effect of raDIotheraPy In LIVer-confIneD But non-resectaBLe BcLc staGe c hePatoceLLuLar carcInoMa: ProPensIty-MatcheD anaLysIs BaseD on natIonWIDe MuLtIcenter hcc cohort ..............................................110
P-254 the ProGnostIc factors of recurrence after coMPLete resPonse InDuceD By transarterIaL cheMoeMBoLIzatIon In hePatoceLLuLar carcInoMa ........110
P-255 DeVeLoPMent of transGenIc t-ceLLs as IMMunotheraPeutIcs anD ceLL carrIers of oncoLytIc VIrus for synerGIstIc treatMent of hePatoceLLuLar carcInoMa .........................................................................110
P-256 fInaL resuLts of the GIDeon stuDy accorDInG to PatIent etIoLoGy: the ItaLIan exPerIence .......................................................................................111
P-257 safety anD effIcacy of sorafenIB In steLLa stuDy, a MuLtIcenter, oBserVatIonaL, Phase IV stuDy In ItaLIan centers ..........................................111
P-258 retrosPectIVe PooLeD anaLysIs of aDVanceD hcc PatIents In sharP anD aP ranDoMIzeD cLInIcaL trIaLs ...................................................112
P-259 aDjuVant tace IMProVes outcoMes of PatIents WIth hePatoceLLuLar carcInoMa WIth MIcroVascuLar InVasIon .......................................................112
P-260 LaParoscoPIc Vs. oPen LIVer resectIon for hePatoceLLuLar carcInoMa of cIrrhotIc LIVer: a case–controL stuDy ..................................113
P-261 In PatIents WIth hcc anD MacroVascuLar InVasIon treateD WIth sorafenIB, afP VaLue≤1000 uI/L at BaseLIne anD VascuLar InVasIon not IncLuDInG 1st orDer Branches or MaIn trunk (VP1/2) are assocIateD WIth ProLonGeD surVIVaL .......................................................113
P-262 factors of PostoPeratIVe MortaLIty In seLecteD PatIents WIth reMnant LIVer VoLuMe to BoDy WeIGht ratIo exceeDInG 0.5% .......................................113
P-263 IMPact of Post-ProGressIon surVIVaL In sorafenIB-faILeD PatIents WIth aDVanceD hePatoceLLuLar carcInoMa....................................................114
P-264 effIcacy of sorafenIB for InterMeDIate-staGe hcc PatIents Who PreVIousLy unDerWent tace ..............................................................................114
P-265 InDIcatIon anD usefuLness of LIVer hanGInG ManeuVer for Major hePatectoMy of LIVer tuMor ............................................................................114
P-266 sarcoPenIa Is an InDePenDent ProGnostIc factor for aDVanceD hePatoceLLuLar carcInoMa ..............................................................................115
P-267 us-us fusIon IMaGInG In raDIofrequency aBLatIon theraPy for hePatoceLLuLar carcInoMa ..............................................................................115
P-268 a neW forMuLa for caLcuLatInG stanDarD LIVer VoLuMe WIthout usInG BoDy WeIGht ..............................................................................115
P-269 effIcacy of contInuous sorafenIB treatMent after raDIoLoGIcaL confIrMatIon of DIsease ProGressIon In PatIents WIth aDVanceD hePatoceLLuLar carcInoMa ..............................................................................116
P-270 neoaDjuVant theraPy for IntrahePatIc tuMors Before sorafenIB aDMInIstratIon ProLonGs surVIVaL tIMe of hePatoceLLuLar carcInoMa WIth extrahePatIc MetastasIs.......................................................116
P-271 aLteratIon of cIrcuLatInG MIcrorna In hePatoceLLuLar carcInoMa
PatIents treateD WIth transarterIaL cheMoeMBoLIzatIon ..........................116
P-272 coMParIson of the cLInIcaL outcoMes BetWeen stereotactIc
BoDy raDIatIon theraPy anD hyPofractIonateD raDIatIon theraPy for
InoPeraBLe hePatoceLLuLar carcInoMa ..........................................................117
P-273 coMBInatIon of sorafenIB anD conVentIonaL transarterIaL
cheMoeMBoLIzatIon In aDVanceD staGe hePatoceLLuLar carcInoMa ...........117
P-274 earLy eVaLuatIon of aLPha-fetoProteIn resPonse for PreDIctInG
outcoMes In sorafenIB treateD PatIents May Be MIsLeaDInG .......................117
P-275 aDVanceD BcLc-c hePatoceLLuLar carcInoMa (hcc): reaL LIfe
resuLts froM the Ita.LI.ca. MuLtIcentre DataBase .........................................118
P-276 enos PoLyMorPhIsMs In reLatIon to outcoMe In aDVanceD
hcc PatIents receIVInG sorafenIB ....................................................................118
P-277 a coMParIson of surVIVaL of PatIents WIth hePatoceLLuLar carcInoMa anD
PortaL VeIn InVasIon treateD By raDIoeMBoLIzatIon or sorafenIB .............118
P-278 surVIVaL BenefIt froM co-aDMInIstereD Beta BLocker anD cox-2
InhIBItor In PatIents WIth aDVanceD hePatoceLLuLar carcInoMa (hcc):
a ProsPectIVe cLInIcaL trIaL .............................................................................119
P-279 roBot-assIsteD LaParoscoPIc hePatectoMy for hePatoceLLuLar
carcInoMa: the henrI-MonDor exPerIence ......................................................119
P-280 hePatoceLLuLar carcInoMa anD occuPatIonaL enVIronMentaL
heaVy MetaLs exPosure Is there a reLatIon? .................................................119
P-281 a neW theraPeutIc assessMent score for aDVanceD hePatoceLLuLar
carcInoMa PatIents receIVInG hePatIc arterIaL InfusIon cheMotheraPy
ProPosaL of acth (assessMent for contInuous treatMent
WIth haIc) score .................................................................................................119
P-282 treatMent strateGy for hePatoceLLuLar carcInoMa accoMPanIeD
By seVere PortaL InVasIon .................................................................................120
P-283 LocoreGIonaL theraPy Versus transcatheter arterIaL cheMoeMBoLIzatIon
for InterMeDIate staGe hePatoceLLuLar carcInoMa PatIents ......................120
P-284 IscheMIc PreconDItIonInG WIth contInuous cLaMPInG DurInG LIVer
resectIon Is coMParaBLe WIth InterMIttent cLaMPInG of the
hePatoDuoDenaL LIGaMent for teMPorary InfLoW oBstructIon .................120
P-285 hePatIc resectIon for hePatoceLLuLar carcInoMa In PatIents
WIth renaL DysfunctIon ....................................................................................121
P-286 shouLD PatIents WIth hePatoceLLuLar carcInoMa BarceLona cLInIc
for LIVer cancer staGe c Be treateD WIth transarterIaL
cheMoeMBoLIsatIon? .........................................................................................121
P-287 are Pre-treatMent cLInIcaL ParaMeters usefuL In PreDIctInG
the outcoMes of hePatoceLLuLar carcInoMa PatIents treateD WIth
sorafenIB? a sInGLe centre, fIeLD-PractIce stuDy .........................................121
P-288 transarterIaL cheMoeMBoLIsatIon In the treatMent of
InterMeDIate-staGe hePatoceLLuLar carcInoMa; stuDy of factors
PreDIctIVe of surVIVaL. cLInIcaL exPerIence In a sInGLe centre In sPaIn ......122
P-289 treMeLIMuMaB – a MonocLonaL antIBoDy aGaInst ctLa-4 – In
coMBInatIon WIth LocaL tuMor aBLatIon (tace or rfa) In PatIents
WIth hePatoceLLuLar carcInoMa .....................................................................122
P-290 a ranDoMIzeD, DouBLe-BLInD, PLaceBo-controLLeD Phase 3 stuDy of
raMucIruMaB Versus PLaceBo as seconD-LIne treatMent In PatIents WIth
hePatoceLLuLar carcInoMa anD eLeVateD BaseLIne aLPha-fetoProteIn
foLLoWInG fIrst-LIne sorafenIB (reach-2) .......................................................122
P-291 PLace of sorafenIB In the ManaGeMent of untreataBLe recurrent
hePatoceLLuLar carcInoMa foLLoWInG LIVer transPLantatIon ...................123
P-292 tuMor recurrence after LIVer transPLantatIon for hePatoceLLuLar
carcInoMa: a systeMatIc reVIeW of VersatILe ManaGeMents .......................123
P-293 Percutaneous treatMents of InfILtratIVe hePatoceLLuLar carcInoMa
DeVeLoPeD on cIrrhosIs usInG MuLtIPoLar raDIofrequency aBLatIon
or Intra-arterIaL ethanoL InjectIon ...............................................................123
P-294 conVentIonaL cheMoeMBoLIzatIon Versus DruG eLutInG BeaDs In treatMent
of eGyPtIan PatIents WIth unresectaBLe hePatoceLLuLar carcInoMa:
three years surVIVaL .........................................................................................124
P-295 PretreatMent seruM soDIuM LeVeL as a ProGnostIc Marker for PatIents
WIth hePatoceLLuLar carcInoMa treateD WIth sorafenIB ............................124
P-296 eVaLuatIon of raDIotheraPy for PatIents WIth unresectaBLe
aDVanceD hePatoceLLuLar carcInoMa ............................................................124
Contents
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 9
P-297 oPtIMaL InterVaL BetWeen on-DeManD transarterIaL cheMoeMBoLIzatIon
In PatIents WIth unresectaBLe hePatoceLLuLar carcInoMa .........................124
P-298 coMParInG treatMent outcoMes BetWeen raDIoeMBoLIzatIon usInG
yttrIuM-90 MIcrosPheres anD concurrent cheMoraDIatIon theraPy for
LocaLLy aDVanceD for hePatoceLLuLar carcInoMa .......................................125
P-299 surVIVaL anD ProGnostIc factors In PatIents WIth InterMeDIate staGe
hePatoceLLuLar carcInoMa Who Were treateD WIth rePeateD
transarterIaL cheMoeMBoLIzatIon .................................................................125
P-300 coMBInatIon treatMent of trans-arterIaL cheMoeMoBoLIzatIon
foLLoWeD By raDIotheraPy WIth hyPertherMIa (cert) In hePatoceLLuLar
carcInoMa WIth PortaL VeIn tuMor throMBosIs: InterIM anaLysIs of
ProsPectIVe Phase II trIaL .................................................................................125
P-301 Percutaneous transhePatIc stent PLaceMent In 993 PatIents WIth
MaLIGnant BILIary oBstuctIon ..........................................................................126
P-302 safety anD effectIVeness of sorafenIB for the treatMent of
hePatoceLLuLar carcInoMa In PatIents WIth DIaBetes ..................................126
P-303 coMParatIVe effIcacy of MetronoMIc caPecItaBIne Versus Best suPPortIVe
care In recurrent hePatoceLLuLar carcInoMa after LIVer
trasPLantatIon. a case-controL stuDy ..........................................................126
P-304 the Post-sIr-sPheres surGery stuDy (P4s): LIVer surGery can Be safeLy
PerforMeD In PatIents WIth hePatoceLLuLar carcInoMa (hcc)
PreVIousLy treateD WIth seLectIVe InternaL raDIatIon theraPy (sIrt)
usInG y-90 resIn MIcrosPheres .........................................................................127
P-305 GeMcItaBIne anD oxaLIPLatIn for the treatMent of PeDIatrIc
PatIents WIth hePatoceLLuLar carcInoMa ......................................................127
P-306 transarterIaL cheMeoMBoLIzatIon WIth or WIthout sorafenIB for
InterMeDIate staGe hePatoceLLuLar carcInoMa ............................................127
P-307 hyaLuronIc acID Is a usefuL PreDIctor of LarGe aMount of ascItes after
LIVer resectIon for PatIents WIth hePatoceLLuLar carcInoMa ...................128
P-308 aDjuVant sorafenIB after r0 resectIon for PatIents WIth LocaLLy
aDVanceD hePatoceLLuLar carcInoMa (BcLc-staGe c): a case-MatcheD
coMParatIVe stuDy ............................................................................................128
P-309 assessMent of heaLth reLateD quaLIty of LIfe after hcc ManaGeMent
By raDIofrequency aBLatIon or tace In a sInGLe eGyPtIan stuDy ................128
P-310 Percutaneous raDIofrequency aBLatIon In eGyPtIan PatIents WIth
hePatoceLLuLar carcInoMa: aPPLIcaBILIty anD ProGnosIs ............................129
P-311 hePatIc arterIaL InfusIon cheMotheraPy (haIc) In transcatheter arterIaL
cheMoeMBoLIzatIon (tace)-refractory or IntoLerant hePatoceLLuLar
cancer (hcc) PatIents WIth Poor hePatIc functIon ........................................129
P-313 aPPLIcatIon of MetronoMIc cheMotheraPy for the PatIent WIth aDVanceD
hePatoceLLuLar carcInoMa WIth PortaL VeIn tuMor throMBosIs ...............129
P-314 sorafenIB Versus cytotoxIc cheMotheraPy for PatIents WIth recurrent
hePatoceLLuLar carcInoMa after LIVer transPLantatIon ............................130
P-315 rePeateD stereotactIc BoDy raDIotheraPy for recurrent
hePatoceLLuLar carcInoMa ..............................................................................130
P-316 treatMent of aDVanceD hePatoceLLuLar carcInoMa (hcc): a sInGLe
centre cost anaLysIs of yttrIuM 90 trans-arterIaL raDIo-eMBoLIzatIon
(tare) Versus sorafenIB ....................................................................................130
P-317 outcoMe of hePatIc resectIon for hePatoceLLuLar carcInoMa
In PatIents WIthout cIrrhosIs ...........................................................................131
P-318 effIcacy of sorafenIB In PatIents WIth InterMeDIate-staGe
hePatoceLLuLar carcInoMa: resuLts froM the Ita.LI.ca. DataBase ..............131
P-319 the effect of cx-4945, a ck2 InhIBItor, on choLanGIocarcInoMa (cca):
In VItro Data .......................................................................................................131
P-320 ProsPectIVe, MuLtIcenter, reGIstry stuDy of oxaLIPLatIn (eLoxatIn®)/5-
fLuorouracIL BaseD reGIMen for chInese LocaL aDVanceD or
MetastatIc hePatoceLLuLar carcInoMa PatIents IneLIGIBLe for curatIVe
resectIon anD LocaL treatMent ......................................................................131
P-321 effIcacy of coMBInatIon theraPy of hePatIc arterIaL InjectIon
cheMotheraPy WIth raDIotheraPy for unresectaBLe aDVanceD
hePatoceLLuLar carcInoMa coMPLIcateD By Major VascuLar tuMor
throMBosIs: anaLysIs of 26 cases ...................................................................132
P-322 cLInIcaL IMPact of aDDItIonaL Interferon aDMInIstratIon on
sorafenIB-treateD PatIents WIth recurrent aDVanceD hePatItIs
c- reLateD hePatoceLLuLar carcInoMa ...........................................................132
P-323 PreVaLence anD sIGnIfIcance of occuLt hePatItIs B VIrus InfectIon In
chronIc hePatItIs c In south korea .................................................................132
P-324 PILot stuDy of coMBInatIon theraPy of sorafenIB anD cytotoxIc
cheMotheraPeutIc aGent In PatIents WIth aDVanceD hePatoceLLuLar
carcInoMa refractory to sorafenIB MonotheraPy .....................................133
P-325 effectIVeness of MeLD, MeLDna, aPrI, anD fIB-4 as PreDIctors of
MortaLIty anD DeVeLoPMent of hcc In PatIents WIth cIrrhosIs – 5-year
foLLoW-uP stuDy ................................................................................................133
P-326 MetIV-hcc: a Phase 3 PLaceBo-controLLeD trIaL WIth tIVantInIB (arq 197),
In PatIents WIth seconD-LIne, Met-hIGh, InoPeraBLe hePatoceLLuLar
carcInoMa (hcc) .................................................................................................133
P-327 thyroID DysfunctIons In eGyPtIan PatIents WIth hePatoceLLuLar
carcInoMa after treatMent By transarterIaL cheMoeMBoLIzatIon ...........133
P-328 hePatIc arterIaL InfusIon cheMotheraPy for sorafenIB faILure
on aDVanceD hcc................................................................................................134
P-329 eMerGency enDoscoPIc VarIceaL LIGatIon foLLoWInG VarIceaL
ruPture In PatIents WIth aDVanceD hePatoceLLuLar carcInoMa
anD PortaL VeIn tuMor throMBosIs .................................................................134
P-330 outcoMe of resectIon for PuLMonary Metastases froM
hePatoceLLuLar carcInoMa: sInGLe-center exPerIence ................................134
P-331 the oPtIMaL treatMent MoDaLIty In PatIents WIth hePatoceLLuLar
carcInoMa anD PortaL hyPertensIon ..............................................................134
P-332 raDIoeMBoLIzatIon for the treatMent of IntrahePatIc
choLanGIocarcInoMa .......................................................................................135
P-333 PreVaLence of PortaL VeIn throMBosIs In eGyPtIan PatIents WIth
hePatoceLLuLar carcInoMa ..............................................................................135
P-334 effIcacy anD safety of transarterIaL cheMoeMBoLIzatIon usInG DruG
eLutInG BeaDs for hePatoceLLuLar carcInoMa .............................................135
P-335 transarterIaL cheMoeMBoLIzatIon contrIButeD surVIVaL
GaIn foLLoWInG coMBIneD cheMoraDIatIon theraPy for aDVanceD
hePatoceLLuLar carcInoMa ..............................................................................136
P-336 assessMent of Percutaneous raDIofrequency aBLatIon treatMent WIth
soLoIst anD LeVeen neeDLes for hePatoceLLuLar carcInoMa PatIents In
Bach MaI hosPItaL, hanoI ...................................................................................136
P-337 effects of MetforMIn on cLInIcaL outcoMe In aDVanceD hcc PatIents
receIVInG sorafenIB ...........................................................................................136
P-338 LIVer resectIon of LocaL recurrence InItIaLLy treateD By
raDIofrequency aBLatIon for coLorectaL LIVer MetastasIs Is More
extensIVe than PrIMary resectIon ...................................................................136
P-339 PreoPeratIVe Percutaneous transhePatIc PortaL VeIn eMBoLIzatIon ..........137
P-340 effIcacy anD safety of coMBIneD sequentIaL treatMent WIth
raDIofrequency aBLatIon anD sorafenIB In PatIents WIth hePatoceLLuLar
carcInoMa In InterMeDIate staGe IneLIGIBLe for tace: a ProsPectIVe
ranDoMIzeD oPen stuDy ....................................................................................137
P-341 DeVeLoPMent of a noVeL WeB-BaseD consuLtatIon serVIce for
a PaeDIatrIc rare tuMor: the sIoPeL cLInIcIan onLIne
consuLtatIon serVIce.........................................................................................138
P-342 Phase 3 ranDoMIzeD, DouBLe-BLInD, controLLeD stuDy of caBozantInIB
(xL184) Vs PLaceBo In suBjects WIth hePatoceLLuLar carcInoMa
Who haVe receIVeD PrIor sorafenIB (ceLestIaL): trIaL In ProGress ..............138
P-343 choLanGIocarcInoMa: neW theraPeutIc ProceDures anD the roLe of
Percutaneous BILIary DraInaGe. PoInt of VIeW of an InterVentIonaL
raDIoLoGIst ........................................................................................................138
P-344 sorafenIB after recurrence of treatMent WIth tace
In InterMeDIate hcc PatIents ...........................................................................139
P-345 the effort to IDentIfy the roLe of c-reactIVe ProteIn (crP)
In aDVanceD LIVer MaLIGnancIes treateD WIth transarterIaL
cheMoeMBoLIzatIon (tace) anD raDIofrequency aBLatIon (rfa) ...................139
P-346 foLLoW-uP resuLts of PatIents WIth MassIVe tuMor necrosIs after
transarterIaL cheMoeMBoLIzatIon .................................................................139
P-347 the MeanInG of afP, afP-L3 anD PIVka-II for eVaLuatInG recurrence In
PatIents WIth hePatoceLLuLar carcInoMa Who unDerWent
LIVer resectIon...................................................................................................139
P-348 h3B6527, an uLtra-seLectIVe anD Potent fGfr4 InhIBItor
for fGf19 DrIVen hePatoceLLuLar carcInoMa ................................................140

Oral Communications
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 0
Friday, 4 September 2015
General Session 1: Molecular Pathogenesis of Liver Cancer I.
O-001 IDenTIfICATIOn Of CO-OCCurrInG GeneTIC AberrATIOnS WITh KnOWn DrIVer MuTATIOn DIreCTS TArGeTeD TherAPy In ChOLAnGIOCArCInOMA
Chirag nepal* 1, jesper B. andersen1
1BrIc, university of copenhagen, copenhagen, Denmark
Introduction: cholangiocarcinoma (cca) is a treatment-refractory malignancy with heterogeneous pathobiology and dismal prognosis. several disease-causing mutations, e.g., IDh1r132G and krasG12D, have been shown to “drive” development of this malignancy. however, a complex issue remains as to account for the heterogeneous pool of “backseat” aberrations, which in chromosomal proximity to the causative variant likely are to influence drug response. this emphasizes the urgency for understanding the molecular heterogeneity of the disease to prompt patient stratification and advance therapeutic options.
Methods: to comprehensively characterize the genomic landscape in intrahepatic cca, we analyzed whole-exome sequencing (Wes) on a total of 142 patients. We performed a high-coverage (>150x) discovery screen on paired tumor and surrounding liver tissues from 15 icca patients, enriched for driver mutations in IDh1 and kras. the genetic variation (snVs, InDels, copy number (cn) and chromosomal rearrangements) was determined by three independent tools to identify high-confidence recurring variants. these aberrations were validated in a compiled training set of 127 iccas to determine recurrent co-occurring variants unique to each driver mutation (16 IDh1 and 25 kras).
results: In the pursuit of novel treatment options, we report a comprehensive annotation of the somatic landscape in icca. We identified in range 20-170 somatic deleterious mutations per patient, validated the prevalent hotspot mutations (kras(G12D) and IDh1(r132G)) and identified novel aberrations in genes e.g., cDc27, PaBPc3, BcLaf1, kIr2DL3, Potef, frG1 and ccr5, with no prior association to cca. new hotspot reoccurring mutations were found in BcLaf1(n627s), frG1(k258r), kIr2DL3(c270s). next, we performed unsupervised clustering on patients with mutations in krasG12D
and IDh1r132G and identified a unique prevalence (~70% in total) of mutated genes specific to each driver, suggesting that this set of unique “passenger genes” distinguish subsets of patients. observations from our Wes analysis were further confirmed in a public validation set of 127 iccas. next, we performed a prevalence screen of 48 cancer-related genes on additional 155 icca patients and confirmed the deregulation of multiple potential causal pathways, including fGfr2, PI3k/mtor, tP53, cDkn2a and notch1, which were all determined in our discovery screen.
Conclusion: our results suggest that association of “passenger” genes with a known disease-causing alteration may reveal unique patient subsets and multiple putative novel target genes, highlighting the potency of genomics-based directions for novel therapeutics.
Disclosure of Interest: none Declared
O-002 The ThAILAnD InITIATIVe In GenOMICS AnD exPreSSIOn reSeArCh fOr LIVer CAnCer (TIGer-LC): DefInInG bIOLOGICAL SubTyPeS Of hePATOCeLLuLAr CArCInOMA AnD ChOLAnGIOCArCInOMA by InTeGrATeD GenOMICS
Anuradha budhu* 1, jittiporn chaisaingmongkol1, 2, hien Dang1, so Mee kwon1, siritida rabibhadana2, Benjarath Pupacdi2, Marshonna forgues1, Vajarabhongsa Bhudhisawasdi3, nirush Lertprasertsuke4, anon chotirosniramit4, chawalit Pairojkul3, chirayu u. auewarakul5, thaniya sricharunrat5, kannika Phornphutkul6, suleeporn sangrajrang7, Maggie cam8, Ping he9, stephen M. hewitt8, xiaolin Wu8, snorri s. thorgeirsson8, Paul s. Meltzer8, christopher a. Loffredo10, robert h. Wiltrout8, curtis c. harris1, chulabhorn Mahidol2, Mathuros ruchirawat2, xin W. Wang1 and the tIGer-Lc consortium
1Laboratory of human carcinogenesis, national Institutes of health, Bethesda, united states, 2chulabhorn research Institute, Bangkok, 3khon kaen university, khon kaen, 4chiang Mai university, chiang Mai, 5chulabhorn hospital, Bangkok, 6rajavej hospital and Lampang cancer center, chiang Mai, 7national cancer Institute, Bangkok, thailand, 8national Institutes of health, 9food and Drug administration, Bethesda, 10Georgetown university Medical center, Washington, Dc, united states
Introduction: hepatocellular carcinoma (hcc) and cholangiocarcinoma (cca) represent two major histological cancer subtypes confined within the liver. they are clinically and biologically heterogeneous and are highly resistant to treatment, making liver cancer the second most lethal malignancy in the world. In thailand, liver cancer represents the primary cause of cancer-related death and is a major health problem. While hBV and hcV are major etiological factors for hcc globally, liver fluke infection (O. viverrini) is a major etiological factor for cca in thailand, especially in north-eastern thailand where O. viverrini is endemic and approximately 70% of liver cancers are cca. these unique risk factor patterns provide an opportunity to study cancer heterogeneity and unique liver tumor biology. the thailand Initiative in Genomics and expression research for Liver cancer (tIGer-Lc) consortium was established to identify genomic and expression factors that may modify hcc and cca susceptibility and progression. In a Phase I study, we determined molecular
subtypes and features of hcc and cca through systems integration of genomic, transcriptomic and metabolic profiles.
Methods: We performed genomic profiling of 398 surgical specimens derived from 199 liver cancer patients. We employed the affymetrix human transcriptome array 2.0 to examine transcriptome profiles, the affymetrix Genome-Wide human snP array 6.0 to determine somatic copy number alterations (scna) and Metabolon's DiscoveryhD4 platform to identify cancer metabolic profiles. unsupervised consensus clustering (ccluster), subclass Mapping (sM), Gene set enrichment analysis (Gsea), class comparison, loss of heterozygosity and minimum segmentation, Pearson and rank correlation algorithms were used to analyze omics data. the results were validated in 247 asian hcc cases.
results: transcriptomic analyses revealed that thai hcc mainly consisted of 3 stable subgroups (c1-c3), while thai cca contained 4 stable subgroups (c1-c4). Interestingly, hcc-c1 and cca-c1 subtypes shared a similar gene expression matrix, as did hcc-c2 and cca-c2 representing a separate pattern, which correlated with patient survival. these prognostic subtypes were validated in an independent asian hcc cohort. Gsea revealed that among 17 significantly altered canonical pathways in the c1 subtype, 8 are related to mitotic checkpoint signaling. In contrast, the main signaling pathways associated with the c2 subtype were related to cytokine and chemokine signaling. We found that the c1 subtype encompassed highly activated mitotic checkpoint genes and scna when compared to the c2 subtype, suggesting an association with a genomic instability phenotype. systems integration of the cancer transcriptome, scna and metabolome revealed key oncogenic drivers linked to the c1 subtype.
Conclusion: cca and hcc from asian populations consist of common molecular tumor subgroups with similar prognostic impacts and unique tumor biology. the molecularly classified c1 subtype in particular, may be sensitive to mitotic checkpoint blockage. our ability to rigorously classify and validate both hcc and cca using integrated systems biology tools may represent a new avenue for tumor subclassification and the development of targeted therapeutic interventions.
Disclosure of Interest: none Declared
O-003 PerSOnALIzeD DIAGnOSTICS In hePATOCeLLuLAr CArCInOMA: unIque MuTATIOnAL SIGnATureS WITh POTenTIAL TO GuIDe TArGeTeD TherAPy
José P. Vaqué* 1, nuria García-Díaz2, susana Llerena3, soraya curiel-olmo2, Laura cereceda2, carmen almaraz2, helena Pisonero2, carlos rodriguez de Lope3, Luis Martín3, carmen cagigas3, federico castillo3, roberto fernandez3, ainara azueta3, silvia alvarez3, Miguel Á. Piris3, javier crespo3
1cell signaling, universidad de cantabria-IDIVaL-IBBtec, 2IDIVaL, 3huMV, santander, spain
Introduction: hepatocellular carcinoma (hcc) is the 5 most prevalent cancer and the 2 most frequent cause of cancer-related death worldwide (746k deaths in 2012). from a genetic perspective, hcc is a very heterogeneous disease possibly reflecting its multiple etiological causes and being responsible for the failure of the pharmacological therapies already tested. the molecular characterization of individual cases of human cancer using next Generation sequencing (nGs) approaches can allow the detection of somatic mutations affecting a specific selection of genes in hcc lesions. these mutations can serve to improve our ability to diagnose, predict response and serve as basis to develop personalized therapies targeting specific mechanisms of disease.
Methods: 1. We designed a hcc specific library enrichment kit (112 genes) for nGs analysis (hepatoexome hereon) using the data from 34 human hcc lesions and 7 cell lines [1-3] focussing on: 1) Importance in hcc; 2) Mutated in hcc, independently of the frequency and 3) Potential to guide therapy. We analysed paired genomic Dna from ff samples: a) normal (blood); B) non-tumoral (cirrhotic) and tumoral (hcc). Dna is processed, sequenced, analysed and validated using an independent nGs approach. 2. hcc cell lines: hePG2 and snu-449 (atcc, us) and huh-7 (jcrB, japan). cells were characterized and treated with specific inhibitors as guided by individual molecular signatures. 3. We tested the effects of individualized therapies biologically (cell growth, Dna synthesis, cytotoxicity) and biochemically (WB)
results: -In Silico: to challenge the potential of the hepatoexome at characterizing hcc lesions, we first tested in silico its ability to detect somatic mutations. We performed a direct comparison of our selection of 112 genes with the mutational data recently described for 331 human hcc lesions from multiple etiologies [4, 5]. We detected somatic mutations in up to 68% of the lesions. Moreover using a total of 365 human hcc lesions and 7 cell lines we could classify our hits in 11 functional categories (fig 1) which perhaps resembles the molecular heterogeneity that we now know can be an important feature with critical implications in the pathobiology of hcc. -Ex vivo: We characterized paired samples from 23 hcc prospective patients with different etiologies. We did this in a timely compatible manner with the clinic (15 days) and could detect somatic mutations in 70% of the samples. Interestingly each patient had a unique mutational profile and in up to 50% of the cases we could associate this profile with the use of a specific therapy. -In vitro: We incubated hcc cell lines each with the appropriate therapy consisting in one or multiple combinations of inhibitors as guided by their individual mutational profile. We tested the biological and biochemical effects of each therapy and found that targeting multiple signalling pathways simultaneously can specifically improve the effects over cell growth and cytotoxicity.

Oral Communications
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 1
Friday, 4 September 2015
Image:
Conclusion: a. using the hepatoexome, we can detect somatic mutations with potential to guide therapy in hcc patients. B. hcc patients display unique mutational signatures, which can reflect the high degree of genetic heterogeneity of this disorder. c. Genetically-defined therapies can target case-specific disease mechanisms that promote hcc.
references: 1. Guichard, c., et al., nat Genet, 2012. 44(6): p. 694-8. 2.huang, j., et al., nat Genet, 2012. 44(10): p. 1117-21. 3. Broad, I., ccLe. http://www.broadinstitute.org. 4. kan, z., et al., Genome res, 2013. 23(9): p. 1422-33. 5. schulze, k., et al., nat Genet, 2015. 47(5): p. 505-11.
Disclosure of Interest: none Declared
O-004 ADenO-ASSOCIATeD VIruS 2 (AAV2) InDuCeS reCurrenT InSerTIOnAL MuTAGeneSIS In huMAn hePATOCeLLuLAr CArCInOMAS
Jean Charles nault* 1, shalini Datta1, andrea franconi1, sandrine Imbeaud1, Maxime Mallet1, Gabrielle couchy1, eric Letouzé1, camilla Pilati1, Benjamin Verret1, jean-frédéric Blanc2, charles Balabaud2, julien calderaro3, alexis Laurent4, Mélanie Letexier5, Paulette Bioulac-sage6, fabien calvo7, jessica zucman-rossi1
1InserM uMr1162, Paris, 2service d'hépatologie, Bordeaux, 3service d'anatomopathologie, créteil, 4service de chirurgie digestive, creteil, 5Integragen, Paris, 6service d'anatomopathologie, Bordeaux, 7Inca, Paris, france
Introduction: hepatocellular carcinomas (hcc) are related to various etiologies including hepatitis B and hepatitis c virus infection, alcohol intake, obesity, hemochromatosis. additional risk factors remain to be identified particularly in hcc developed on non-fibrotic liver. We identified a fragment of adeno-associated Virus type 2 (aaV2, a defective Dna virus considered as non-pathogenic and used as a vector for gene therapy) inserted in an hcc genome and this result prompted us to screen a large series of hcc samples.
Methods: We screened 150 hcc and matched non-tumor liver samples for aaV2 sequences using Pcr and next generation sequencing. expression of the genes targeted by viral integration was quantified and the functional consequences of aaV2 integration within TERT promoter was analyzed in 3 hcc cell lines using luciferase assay.
results: among the 150 tumors, we identified 7 cases (5%) with a clonal aaV2 insertion whereas no clonal insertion was found in the corresponding non-tumor liver tissues. In the first hcc tumor, we identified a 208 base pairs insertion of an aaV2 fragment within the TERT (coding for the telomerase reverse transcriptase) promoter. In hcc cell lines, we demonstrated that this aaV2 insertion resulted in an increased TERT promoter activity. Moreover, we showed that TERT was overexpressed in this tumor compared to the non-tumor liver and normal livers. We next identified 6 additional clonal somatic integrations of aaV2, all occurred within known cancer driver genes, CCNA2 (4 cases), CCNE1 or TNFSF10 leading to over-expression of the targeted gene without generating chimeric viral-endogenous functional fusion transcripts. In CCNA2 (coding for cyclin a2), the four integration sites were identified within intron 2 and aaV2 insertion ranged from 219 to 1,975bp occurring in both orientations. In CCNE1 (coding for cyclin e1), we identified a 368bp aaV2 integration within intron 4. In the remaining case, aaV2 integration occurred in the 3’ utr of TNSFS10 (coding for the receptor traIL), 244 bp after the stop codon. In 6 out of the 7 tumors, the inserted aaV2 included the 3’inverse tandem region. strikingly, almost all the tumors were developed on non-fibrotic liver (6 out of 7 cases, p<0.05) without known risk factor (5 out of 7, p<0.05), thus suggesting a particular pathogenic role of aaV2 in this subset of patients.
Conclusion: aaV2 is a new oncogenic virus involved in the pathogenesis of human hcc developed on normal liver by recurrent somatic integration in cancer driver genes as TERT, CCNA2, CCNE1 and
TNFS10. It challenges its safety as a vector for gene therapy in human.
Disclosure of Interest: none Declared
O-005 rOLe Of LeCT2 In The hePATIC IMMune MICrOenVIrOnMenT DurInG LIVer CArCInOGeneSIS
Antoine L'hermitte* 1, Mathilde cadoux1, Gabrielle couchy2, sandrine Pham1, Marie anson1, anne-Marie crain1, christine Perret1, jessica zucman-rossi2, chantal Desdouets1, jean-Pierre couty1
1Development reproduction and cancer, Institut cochin InserM u1016, 2unité de génomique fonctionnelle des tumeurs solides, InserM u1162, ParIs, france
Introduction: hepatocellular carcinoma (hcc) is the 3rd cause of cancer-related death worldwide. the tumour microenvironment (tMe) is recognized as a key actor during carcinogenesis and its role is particularly relevant in liver cancer since >80% of hcc emerge from a disrupted microenvironment. using relevant hcc liver tumor mouse models, we identified 2 critical interconnected effectors of the tMe controlling liver tumorigenesis: the invariant natural killer t cells (inkt) and Lect2. their specific deletion leads to the emergence of highly invasive hcc associated with lung metastasis (1).
our aim is to address functionally the regulatory role of Lect2 in the inflammatory response driven by hcc tumor development.
Methods: Preneoplastic (apc-/-) and tumoral (Lpk-myc) models (Wt and Lect2-deficient) that recapitulate human beta-catenin-dependent hcc are used. Immune liver content is analysed by flow cytometry, cell sorting and immunohistochemistry. the expression of Lect2 is analysed from a large cohort of human hcc samples by taqMan qPcr.
results: In order to understand the role of Lect2, we analyzed its expression in liver samples from a large and well-documented cohort of patients. We found a significant decrease in its expression in hcc samples that correlates both with the presence of vascular invasion and edmondson-steiner histological grades. these data strongly parallel our observations made from hcc mice models in which the absence of Lect2 severely aggravates liver tumorigenesis. Indeed, we found an arising of undifferentiated structures that constantly associate with lung metastasis. transcriptomic analysis of undifferentiated structures evidenced an eMt and metastasis molecular signatures confirmed by qPcr and immunohistochemical stainings. Interestingly, we found that downregulation of Lect2 expression associates significantly with the presence of inflammatory infiltrates in human hcc, strengthening the implication of Lect2 in the hepatic immune microenvironment. In hcc mice models, we found a strong accumulation of myeloid cells (cD11c- cD11b+ f4/80+ Ly6chi Ly6G-) in hcc livers and impressively more in hcc tumors arising in Lect2-deficient context. these cells were found to express Lect2 receptor cD209a and exhibit immature phenotype evidenced by low level of Mhc class II and cD1d that associated with a substantial increase in their ability to produce IL-10. these data suggest that Lect2 regulates the inflammatory response during hcc through a major targeting of myeloid cell functions. to fully determine the impact of myeloid cells on tumor aggressiveness, depletion strategies are currently ongoing. Moreover, as we identified that inkt cells were strong players controlling liver tumorigenesis interconnected with Lect2, we studied in more details their phenotype and cytokine secretion potential in hcc-Lect2-deficient context. Interestingly, we found that the cD4-negative inkt cells, known to retain strong anti-tumoral capacities produced substantially less Ifn-γ associated with a strong upregulation of PD1 suppressive marker. however, as these cells do not express cD209a-Lect2 receptor, this suggests an indirect role of Lect2 on anti-tumoral activities of inkt cells. finally, since myeloid and inkt cells interact actively, we hypothesize that Lect2 could affect myeloid cells that in turn impact on inkt cell functions.
Conclusion: altogether, these data suggest that Lect2 behaves during liver tumorigenesis as a strong inflammatory regulator of the liver microenvironment through a major targeting on liver myeloid and inkt cells.
references: (1) anson M et al., jcI 2012; 122(2):586–599.
Disclosure of Interest: none Declared
O-006 InTerrOGATIOn Of DnAJb1-PrKACA KInASe fuSIOn AS A TherAPeuTIC TArGeT In fIbrOLAMeLLAr hePATOCeLLuLAr CArCInOMA
Stefanie Schalm1*, nicolas stransky1, Darshan sappal1, erin Murphy1, adam shutes1, joe kim1, steve Wenglowsky1, kevin Wilson1, klaus hoeflich1, christoph Lengauer1, andrew Garner1
1Blueprint Medicines, cambridge, united states
Introduction: the molecular annotation of cancer frequently identified recurrent and characteristic genomic aberrations that deregulate key biological pathways. Protein kinase fusions have proved particularly fruitful for cancer drug discovery, since they often confer oncogenic dependency and thus provide a druggable node. fibrolamellar hepatocellular carcinoma (fL-hcc) is a rare, malignant and understudied tumor that arises in the otherwise normal liver of young adults. If diagnosed early

Oral Communications
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 2
Friday, 4 September 2015
enough, fL-hcc is treated by surgical resection. If unresectable, fL-hcc is usually fatal since it is largely resistant to therapy, thus there is an urgent need to identify effective treatment options. consequently, we sought to gain a deeper understanding of the molecular mechanisms underlying fL-hcc initiation and progression, with the hope that it would facilitate the development of improved diagnosis and treatment strategies.
Methods: We developed a computational genomics pipeline to specifically detect kinase fusions in rna-seq data and searched all the available tcGa liver cancer samples. the function of any candidate kinase fusion identified was assessed via gain of function/ loss of function experiments in liver cells, and in biochemical enzyme assays.
results: using our computational genomic pipeline, we identified a recurrent DnajB1-Prkaca fusion in three rna-seq liver cancer datasets, two of which were annotated as fL-hcc. In contrast, no other recurrent kinase fusions were identified in other forms of hepatocellular carcinoma. DnajB1-Prkaca consists of the first exon of DnajB1 that encodes the j domain, fused in-frame to exon two of the catalytic subunit of protein kinase a. expression of the fusion gene is placed under the control of the DnajB1 promoter, leading to elevated expression. Importantly, no other driver mutations were found in these samples, suggesting DnajB1-Prkaca as a likely driver of fL-hcc. to evaluate this hypothesis, we stably overexpressed DnajB1-Prkaca in hepG2 liver cancer cells and observed significant increases in Prkaca signaling as evidenced by elevated creB phosphorylation compared to vector control. furthermore, expression of DnajB1-Prkaca increased colony formation, which is a hallmark of cell transformation. to investigate how DnajB1-Prkaca enhanced Pka signaling, we carefully characterized the properties of DnajB1-Prkaca in biochemical kinase assays. DnajB1-Prkaca possessed comparable kinase activity to wild-type Prkaca and was similarly sensitive to inhibition by r subunits and a collection of proprietary small molecule kinase inhibitors.
Conclusion: our kinase fusion heuristic identified recurrent DnajB1-Prkaca fusions in fL-hcc, thus supporting the recently published literature. the mutational landscape, altered pathways and structural variants that characterized found in fL-hcc were distinct from hcc, further defining it as a distinct carcinoma. expression of DnajB1-Prkaca stimulated Pka signaling and further transformed liver cancer cells. the lack of a second-hit mutation in the genomic landscape of fL-hcc, combined with its ability to transform cells signifies that DnajB1-Prkaca is the primary driver of fL-hcc Interestingly, DnajB1-Prkaca appears subject to the same regulatory mechanisms as wild-type Prkaca. this suggests that elevated expression of DnajB1-Prkaca may perturb the delicate balance with inhibitory r subunits, consequently stimulating Pka signaling and driving carcinogenesis. Inhibition of DnajB1-Prkaca therefore offers a unique opportunity for targeted therapy drug discovery in fL-hcc.
Disclosure of Interest: s. schalm stocks of: Blueprint Medicines stockholder, n. stransky stocks of: Blueprint Medicines stockholder, D. sappal stocks of: Blueprint Medicines stockholder, e. Murphy stocks of: Blueprint Medicines stockholder, a. shutes stocks of: Blueprint Medicines stockholder, j. kim stocks of: Blueprint Medicines stockholder, s. Wenglowsky stocks of: Blueprint Medicines stockholder, k. Wilson stocks of: Blueprint Medicines stockholder, k. hoeflich stocks of: Blueprint Medicines stockholder, c. Lengauer stocks of: Blueprint Medicines stockholder, a. Garner stocks of: Blueprint Medicines stockholder
General Session 2: Molecular Pathogenesis of Liver Cancer II.
O-007 IGf2 IS An OnCOGenIC DrIVer In hCC AnD eMerGeS AS A POTenTIAL TArGeT fOr TherAPIeS
Iris Martínez-quetglas* 1, roser Pinyol1, Daniel Dauch2, anna Portela3, judit Peix1, Monica higuera1, Laia cabellos1, Victoria tovar1, clara alsinet1, Vicenzo Mazzaferro4, jessica zucman-rossi5, Manel esteller3, Lars zender2, josep M. Llovet1, 6, 7
1Liver cancer translational research Laboratory, Barcelona clinic Liver cancer Group (BcLc), Liver unit, hospital clínic, IDIBaPs, cIBerehD, university of Barcelona, Barcelona, spain, 2Division of translational Gastrointestinal oncology, Department of Internal Medicine I, university of tuebingen, tuebingen, Germany, 3cancer epigenetics and Biology Programme, Bellvitge Biomedical research Institute (IDIBeLL), Barcelona, spain, 4fondazione Irccs, Istituto nazionale dei tumori (Int), Milan, Italy, 5Génomique fonctionnelle des tumeurs solides, Institut national de la santé et de la recherche Médicale (InserM), Paris, france, 6Institució catalana de recerca i estudis avançats (Icrea), Barcelona, spain, 7Mount sinai Liver cancer Program, Division Liver Diseases, Icahn school of Medicine at Mount sinai, new york, united states
Introduction: hepatocellular carcinoma (hcc) is the 16th absolute cause of death world-wide and accounts for 90% of all liver cancers. IGf signaling has a relevant role in hcc pathogenesis and elucidation of its key molecular drivers is important to overcome the poor therapeutic results obtained so far by inhibiting this pathway. since IGf2 ligand have been shown to be overexpressed in hcc, we aimed 1) to elucidate the mechanism of IGf2 overexpression in hcc, 2) to explore the oncogenic potential of IGf2 in hcc cell lines and genetically modified animal models (GeMM), and 3) to determine the antitumoral efficacy of molecular therapies against this target in vitro and in vivo.
Methods: IGf2 signaling was analyzed by gene expression profiling, exomic mutations, Dna copy number variations and methylation status in a cohort of 228 hccs. activation of IGf2 promoters and their methylation status were assessed by qrt-Pcr and bisulfite sequencing. a murine hcc model was generated by administrating Den/ccl4 and IGf2 expression was evaluated. a GeMM overexpressing IGf2 in the liver was generated by hydrodynamic tail vein injection, and oncogenic potential of IGf2 was assessed. therapeutic potential of the anti IGf1/2 ligand monoclonal antibody BI836845 (Boerhinger Ingelheim), was tested in hcc cell lines performing cell viability and proliferation assays. Pathway activation was assessed by western blot. an hcc cell line showing low basal levels of IGf2 was stable transfected with an IGf2-plasmid (snu449-pIGf2) or an empty plasmid (snu449-pempty) and then treated with BI836845. a subcutaneous hcc xenograft model was generated to evaluate the antitumoral effect of BI836845 in vivo. Mice were randomized to receive placebo (n=10), sorafenib (n=10), BI836845 (n=10) or the combination sorafenib+BI836845 (n=10). tumor growth, toxicity and survival were set as endpoints.
results: In humans, 15% (31/207) of patients in our cohort showed IGf2 overexpression (fc>2), being hypomethylation of fetal promoters the main cause in 87% of cases (21/54 vs 7/171, p<0.0001). Patients with high levels of IGf2 showed significant association with stem-cell signatures (fDr<0.05). In a murine hcc model able to reproduce the sequential injury-fibrosis-malignancy cycle described in humans, 27% (9/33) of mice spontaneously overexpressed IGf2 in tumors, while none of the control mice showed altered expression. GeMM mice overexpressing IGf2 exclusively in the liver showed increased number/size of tumors and reduced survival (p=0.02) compared to control mice. selective IGf-ligands blockade with BI836845 significantly reduced cell viability and proliferation (30%, p=0.002) of cell lines with increased levels of IGf2. BI836845 also inhibited IGf-Insulin pathway activation, without interfering with insulin metabolic effects. In snu449 ectopic expression of IGf2 induced a 30% increase of proliferation rate compared to Wt snu449 and sensitized cells to BI836845. In a xenograft model the combination of sorafenib and BI836845 was well tolerated in a pilot study. We are currently evaluating the efficacy of sorafenib, BI836845 and their combination in vivo.
Conclusion: Preclinical evidence reveals that overexpression of IGf2 could be a key driver in the process of hepatocarcinogenesis in a subgroup of hcc patients. effective IGf2 blockage provides the rationale to test therapies based on monoclonal antibodies against IGf ligands.
Disclosure of Interest: none Declared
O-008 TuMOr InITIATInG CeLLS Are MeDIATOrS Of ACquIreD reSISTAnCe TO SOrAfenIb In hePATOCeLLuLAr CArCInOMA
Victoria Tovar* 1, helena cornellà1, agrin Moeini1, samuel Vidal2, yujin hoshida3, Daniela sia3, 4, judit Peix1, clara alsinet1, Iris M. quetglas1, Manel solé1, josep Domingo-Domenech2, augusto Villanueva3, 5, josep M. Llovet1, 3, 6
1Liver cancer translational research Laboratory, BcLc Group, Liver unit and Pathology Department, IDIBaPs, hospital clínic, cIBerehd, universitat de Barcelona, Barcelona, spain, 2Department of Pathology, Icahn school of Medicine at Mount sinai, 3Liver cancer Program, Division of Liver Diseases, Department of Medicine, tisch cancer Institute, Icahn school of Medicine at Mount sinai, new york, united states, 4Gastrointestinal surgery and Liver transplantation unit, national cancer Institute, Milan, Italy, 5Division of hematology and Medical oncology, Icahn school of Medicine at Mount sinai, new york, united states, 6Institució catalana de recerca i estudis avançats (Icrea), Barcelona, spain
Introduction: the multi-target tyrosine kinase inhibitor sorafenib is the unique fDa-approved therapy for patients with advance hcc. however, despite favorable initial response most patients develop disease progression. the precise molecular mechanisms underlying acquired resistance relevant for planning second line therapies are complex and not clearly elucidated. herein, we explore the role of tumour-initiating cells (t-Ics)- cancer stem cells- in the acquisition of resistance to sorafenib and the signalling pathways involved in this adaptative response of tumors.
Methods: hcc xenograft mice treated with sorafenib (n=26) were explored for long-term sensitivity (n=5) and development of acquired resistance (n=17, median= 42 days). to underscore the mechanism of acquired resistance we assess: 1) the role of t-Ics by in vitro sphere formation assays, and in vivo tumorigenesis assays using noD/scID mice, 2) activation of alternative signaling pathways and 3) the efficacy of anti-fGf and anti-IGf drugs in experimental models of hcc. Gene expression profiling (microarray, qrt-Pcr) and protein analysis (immunohistochemistry) were conducted. Gene pattern modules were used to generate a gene signature of acquired resistance to sorafenib and tested in 2 independent cohorts of hcc patients (n=442).
results: acquired resistance to sorafenib developed after a median of 42 days in 65% of mice (p<0.05). Long-term exposure to treatment resulted in hcc tumors with enrichment of progenitor cell features. We confirmed a significant enrichment of t-Ics in sorafenib-acquired resistant tumours (164 cells needed to create a tumour) vs. sorafenib-sensitive tumours (13400 cells needed) and vs. non-treated tumours (1292 cells needed), p<0.001. tumours with sorafenib-acquired resistance were enriched with IGf and fGf signaling activation cascades and gene sets of resistance to antitumoral therapies (fDr<0.05). In vitro, spheres derived from sorafenib-acquired resistant tumors were responsive to fGf or IGf inhibition with small molecules. furthermore, mice showing acquired

Oral Communications
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 3
Friday, 4 September 2015
resistance treated with an fGf-inhibitor (brivanib) vs. sorafenib showed delayed tumor growth, improved survival, and inhibition of fGfr1 activity and downstream signaling. We further generated a sorafenib-resistance 175-gene signature that was enriched with progenitor-cell features and predicted poor survival in two independent cohorts of hcc patients (n=223 and n=219, respectively), p<0.05.
Conclusion: sorafenib-induced acquired resistance is mainly driven by t-Ics with enrichment of progenitor markers and activation of IGf and fGf signaling. Inhibition of these pathways would benefit a subset of patients after sorafenib progression.
Disclosure of Interest: V. tovar: none Declared, h. cornellà: none Declared, a. Moeini: none Declared, s. Vidal: none Declared, y. hoshida: none Declared, D. sia: none Declared, j. Peix: none Declared, c. alsinet: none Declared, I. quetglas: none Declared, M. solé: none Declared, j. Domingo-Domenech: none Declared, a. Villanueva: none Declared, j. Llovet Grant support from: Bristol-Myers squibb partially supported the study with a research grant, advisory Board of: Prof. josep M. Llovet has been an advisory board member of Bristol-Myers squibb., consulting of: Prof. josep M. Llovet has been a consultant of Bristol-Myers squibb.
O-009 STeM-CeLL nIChe AnD TuMOr-ASSOCIATeD MACrOPhAGeS In huMAn ChOLAnGIOCArCInOMA
Chiara raggi* 1, Margherita correnti2, Luca Di tommaso3, jesper B. andersen4, Domenico alvaro5, Massimo roncalli6, antonio sica7, Gianfranco alpini8, Pietro Invernizzi1
1Liver unit and center for autoimmune Liver Diseases, 2humanitas clinical and research center, 3Pathology unit, humanitas research hospital, rozzano (MI), Italy, 4Biotech research and Innovation centre, university of copenhagen, copenhagen, Denmark, 5Department of Medico-surgical sciences and Biotechnologies, sapienza university of rome, rome, 6Pathology unit, humanitas research hospital, 7Laboratory of Molecular Immunology, humanitas clinical and research center, rozzano (MI), Italy, 8Department of research, central texas Veterans health care system, temple, united states
Introduction: cholangiocarcinoma (cca) is a dismal malignancy unresponsive to conventional therapies. cancer stem cells (cscs) are highly drug-resistant but molecular basis controlling their tumorigenic phenotype remain largely unknown. tumor-associated macrophages (taMs) exert several pro-tumoral functions including promotion of drug-resistance. Goal of this study is to identify new strategies for cca therapy by exploring crosstalk between taMs and cscs.
Methods: to select and enrich for stem-like compartment, 3 established intrahepatic cca-derived cell lines (sG231, hucct1, ccLP1) were cultured in 3D non-adherent condition in serum-free media to generate spheres (sph). thus, extensive analysis of gene expression, drug-responsiveness and in vivo tumorigenicity of cca-sph into nsG mice was performed. soluble mediators released by cca-sph were profiled to investigate the possible involvement in monocyte (cD14+) recruitment and/or macrophage (MØ) differentiation/activation by eLIsa of conditioned medium (cM). accordantly, monocyte differentiation and was investigated by facs analysis and rt-Pcr.
results: only malignant cholangiocytes retained sphere forming potential as compared to normal counterpart (h69, hiBecs). consistently, extensive molecular characterization of cca-sph showed over-expression of key genes associated to csc-like features (sG231 (78/84), hucct1 (68/84), ccLP1 (69/84)), epithelial-mesenchymal transition program (sG231 (78/84), hucct1 (68/84), ccLP1 (69/84)) and liver oncogenic pathways (sG231 (78/84), hucct1 (68/84), ccLP1 (69/84)), compared to cca cell grown as monolayer (mon), as control. In addition, cells dissociated from cca-sph possessed higher tumorigenicity upon subcutaneous (s.c.) transplantation into nsG mice (1,000 cells) as well as high resistance to common anti-cca drugs (e.g. cisplatin, 5-fluorouracil, oxaliplatin) by proliferation Mtt assay as compared to cca-mon. to investigate the effect of the stem-like component on monocytes, cD14+ were cultured in presence of cca-sph for 6 days. facs analysis revealed that in presence of cca sph-cM, cD14+ cells acquired expression of specific MØ-markers (cD68, cD115, hLa-Dr). Differentiation towards granulocytes and dendritic was excluded by cD66b and cD1a staining indicating that cca sph-cM was a strong MØ activator. cca-sph activated MØ (sph-MØ) retained peculiar taM-like features and high invasion capacity as shown by in vitro matrigel coated transwells. among soluble mediators released by cca-sph, only IL13, IL34 and osteoactivin were specifically present in all 3 cell lines as compared to mon-cM. combination of this 3 molecule in vitro were responsible of MØ differentiation, invasion and adhesion ability. notably presence of sph-MØ promoted and sustained cca-sph long-term self-renewal potential as compared to mon- MØ.Presence of MØ in human cca specimens (n=25) was evaluated by cD68+ immunostaining. the largest proportion of cD68+ cell was located in tumor-front. additionally, isolated mononuclear-subset from fresh resected cca samples revealed a peculiar phenotype of cca-associated MØ confirming our in vitro data.
Conclusion: our results suggested a prominent interplay between cca-cscs and MØ. these findings may provide a new venue for alternative therapeutic strategy in cca patients by targeting this synergistic interplay between cca-csc and MØ.
references: raggi c, Mousa h, correnti M, sica a. Invernizzi P. Oncogene 2015raggi c, Invernizzi P, andersen jB. J HEPATOL 2014raggi c, factor VM, seo D, Gillen Mc, holczbauer a, Marquardt ju, thorgeirsson ss. Hepatology, 2014
Disclosure of Interest: none Declared
O-010 MIxeD hePATOCeLLuLAr-ChOLAnGIOCArCInOMA TuMOrS: ChOLAnGIOLOCArCInOMAS AnD STeM-CeLL SubTyPe hAVe unIque MOLeCuLAr TrAITS
Agrin Moeini* 1, 2, Daniela sia1, 2, hui Dong2, zhongyang zhang3, Genis camprecios2, M Isabel fiel2, oriana Miltiadous2, xiaochen sun2, ke hao3, yujin hoshida2, swan n thung2, augusto Villanueva2, Myron e schwartz2, josep M Llovet1, 2, 4
12. Liver cancer translational research Laboratory, Liver unit, Institut d’Investigacions Biomèdiques august Pi i sunyer (IDIBaPs), hospital clínic, cIBerehd, universitat de Barcelona, Barcelona, spain, 2Mount sinai Liver cancer Program, Division of Liver Diseases, Department of Medicine, Department of Pathology, recanati Miller transplantation Institute, tisch cancer Institute, 33. Icahn Institute for Genomics and Multiscale Biology, Icahn school of Medicine at Mount sinai, new york, united states, 44. Institució catalana de recerca i estudis avançats, Barcelona, spain
Introduction: Mixed hepatocellular-cholangiocarcinoma tumors (hcc-icca) account for less than 1% of all primary liver cancers. Whether these tumors represent a unique clinical and molecular entity remains poorly understood. We aimed to conduct a comprehensive analysis of hcc-icca by integrating histological and molecular data.
Methods: a total of 19 patients with mixed hcc-icca were identified following the Who criteria. samples were classified based on histological features and immunohistochemistry (Ihc) for specific hepatocyte (heP1, GPc3), biliary (ck7, ck19) and stem-cell markers (epcaM, ncaM, saLL4). Whole-genome gene-expression (DasL assay, Illumina) and Dna copy number alterations (cna) analysis (humancyto snP12 array, Illumina) were performed. association with signaling pathways and gene expression signatures was evaluated with Gene set enrichment analysis (Gsea) and nearest template Prediction (ntP) method. Prevalent oncogenic mutations in hcc or icca (ctnnB1, fGfr2-fusions, IDh1, kras, Braf) were screened.
results: following Who criteria, hcc-icca samples were classified as classical (n=4), stem-cell feature (n=9) and cholangiolocellular carcinoma (cLc) (n=6). from the pathological standpoint, classical hcc-icca types were mainly epcaM positive (3/4, 75%) with expression of hepatocyte and biliary markers in the hcc-like and icca-like components, respectively. the stem-cell feature subtypes characteristically showed saLL4 positive staining (7/9 vs 0/10 others, p<0.001). In contrast, all cLc cases were negative for hepatocyte markers and positive for ck7, ck19, epcaM and particularly ncaM (6/6 for cLc vs 2/13 others, p<0.01). Gene expression analysis defined the stem-cell subtype as enriched with signatures of poor prognosis (p<0.01) -including signatures of stem cell phenotype (ePcaM, human ck19, liver stem cell, p<0.05)- and activated notch signaling. conversely cLc tumors showed significant up-regulation of cholangiocyte markers (KRT7, KRT19, ITGB4) and icca inflammation subclass (p<0.05), along with significant association with late tGf-beta gene signature and s1 class of hcc (p<0.01). copy number variation analysis revealed higher chromosomal instability -defined as total number of broad chromosomal arm alterations- in the stem-cell feature and classical subtypes compared to cLc (mean score 9.8-10.5 vs 2, p<0.01). non-cLc tumors had chromosomal aberrations recapitulating hcc and icca (e.g. gains in 1q and 8q, losses in 4q, 8p, 9q, and 16q). conversely, cLc show few aberrations and 4/6 of them had no detectable broad chromosomal alterations. Prevalent oncogenic mutations in hcc and icca were almost absent in hcc-icca tumors with only 3 mutations (fGfr2-BIcc1 fusion, Braf, IDh1) discovered in 1/19 cases (5%) each.
Conclusion: Mixed hcc-icca tumors represent a heterogeneous group of primary liver cancers. cholangiolocarcinoma subtype has a unique profile with low chromosomal instability, enrichment of tGf-beta signaling and biliary cell lineage markers. stem-cell feature subtype is defined by early progenitor markers (saLL4) and shares common molecular traits with more aggressive hcc and icca.
Disclosure of Interest: none Declared
O-011 SIGnATureS Of KnOWn AnD neW MuTATIOnAL PrOCeSSeS OPerATIVe In LIVer CAnCerS
eric Letouzé* 1, 2, 3, 4, jayendra shinde1, 2, 3, 4, Ludmil B. alexandrov5, 6, sandrine Imbeaud1, 2, 3, 4, kornelius schulze1, 2, 3, 4, julien calderaro1, 2, 3, 4, 7, sandra rebouissou1, 2, 3, 4, Gabrielle couchy1, 2, 3,
4, clément Meiller1, 2, 3, 4, roser Pinyol8, Laura Pelletier1, 2, 3, 4, charles Balabaud9, 10, alexis Laurent11,
12, jean-frederic Blanc9, 13, Vincenzo Mazzaferro14, fabien calvo1, 2, 3, 4, augusto Villanueva8, jean-charles nault1, 2, 3, 4, 15, Paulette Bioulac-sage9, 16, Michael r. stratton6, josep M. Llovet8, 17, 18, jessica zucman-rossi1, 2, 3, 4, 19
1uMr-1162, Génomique fonctionnelle des tumeurs solides, Iuh, InserM, 2Labex Immuno-oncology, sorbonne Paris cité, faculté de Médecine, université Paris Descartes, Paris, 3sorbonne Paris cité, ufr sMBh, f-93000, université Paris 13, Bobigny, 4université Paris Diderot, Paris, france, 5theoretical Division, Los alamos national Laboratory, Los alamos, united states, 6cancer Genome Project, Wellcome trust sanger Institute, hinxton, united kingdom, 7Department of Pathology, chu henri Mondor, assistance Publique-hôpitaux de Paris, créteil, france, 8hcc translational research Laboratory, Barcelona-clínic Liver cancer Group, Institut d'Investigacions Biomèdiques august Pi i sunyer, Liver unit. cIBerehd, hospital clínic, Barcelona, spain, 9uMr-1053, InserM, 10université de Bordeaux, Bordeaux, 11Department of Digestive and hepatobiliary surgery, chu henri Mondor,

Oral Communications
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 4
Friday, 4 September 2015
assistance Publique-hôpitaux de Paris, 12u955, InserM, créteil, 13chu de Bordeaux, Department of hepatology, hôpital saint-andré, Bordeaux, france, 14Department of Liver surgery and transplant, fondazione Istituto tumori, Milan, Italy, 15hôpitaux universitaires Paris – seine saint-Denis, site jean Verdier, Pôle d’activité cancérologique spécialisée, service d’hépatologie, f-93143, assistance Publique-hôpitaux de Paris, Bondy, 16chu de Bordeaux, Department of Pathology, Pellegrin hospital, Bordeaux, france, 17Institució catalana de recerca i estudis avançats, Barcelona, spain, 18Mount sinai Liver cancer Program (Division of Liver Diseases), Mount sinai school of Medicine, new york, united states, 19hôpital europeen Georges Pompidou, f-75015, assistance Publique-hôpitaux de Paris, Paris, france
Introduction: the mutational burden of a tumor is the outcome of multiple mutagenic processes operative over the lifetime of the patient. Different tumor types thus carry different mutational signatures, characteristic of specific carcinogens and/or Dna repair defects. for example, lung cancers have a predominance of G>t mutations due to the binding of tobacco carcinogens specifically on guanine residues. With the advent of whole exome (Wes) and whole genome sequencing (WGs), it is now possible to explore in-depth the diversity of mutational signatures of human tumors, and identify new mutagenic processes or Dna repair defects.
Methods: We have analyzed the patterns of somatic substitutions in a large series of hepatocellular adenomas (hca) and carcinomas (hcc) of diverse stages and etiologies by Wes (n=300) and WGs (n=30), as well as liver cancer data from public repositories. using the Wellcome trust sanger Institute mutational signatures framework1, we extracted the mutational signatures operative in each sample, and we correlated the identified signatures with the clinical and molecular characteristics of the tumors.
results: We found 8 mutational signatures present at different strengths in our samples. six of these signatures had been previously described in liver cancer or in other tumor types2, whereas the two other signatures were new. of note, one of these signatures (signature 16), characterized by t>c mutations with a strong transcriptional strand bias, is found exclusively in liver cancers and was present in almost all our cases, irrespective of stage and etiology. one of the two new signatures (signature 23) was encountered in a single tumor with a hypermutator phenotype, developed in a patient without cirrhosis but with black mineral deposits in the liver, hence this signature likely corresponds to a new mutagenic process operative in rare hcc cases. the other signature (signature 24) was encountered exclusively in african cases, most of which were infected by hBV and carried the r249s TP53 mutation characteristic of aflatoxin B1 exposure. finally, we used WGs data to reconstruct the clonal architecture of our hcc cases and characterize the mutational processes operative early and late in tumor development (figure).
Image:
Conclusion: Liver tumors display characteristic patterns of somatic mutations. some signatures are ubiquitous and may represent traces of the liver metabolism. others are found only in subsets of samples, and correspond to known (aflatoxin B1) or new mutagenic processes (signature 23), which remain to be fully explained. Mutational signature analysis is a powerful approach to understand the origin of somatic alterations, and to identify new etiologies of liver cancer.
references: 1. alexandrov, L. B., nik-zainal, s., Wedge, D. c., campbell, P. j. & stratton, M. r. Deciphering signatures of mutational processes operative in human cancer. Cell Rep. 3, 246–259 (2013).2. alexandrov, L. B. et al. signatures of mutational processes in human cancer. Nature 500, 415–421 (2013).
Disclosure of Interest: none Declared
O-012 ACTIVATIOn Of STeM-LIKe CeLLS In The hePATIC MICrOenVIrOnMenT IS ASSOCIATeD WITh PrOGnOSTICALLy ADVerSe GenOMIC ALTerATIOnS In hePATOCeLLuLAr CArCInOMA
Darko Castven* 1, Michael fischer1, stefan heinrich2, jesper B. andersen3, Matthias Matter4, Martin sprinzl1, stefanie heilmann5, Marcus Wörns1, snorri s. thorgeirsson6, Peter r. Galle1, hauke Lang2, jens u. Marquardt1
1Department of Medicine I, 2Department of surgery, university hospital of Mainz, Mainz, Germany, 3BrIc, university of copenhagen, copenhagen, Denmark, 4Department of Pathology, university of Basel, Basel, switzerland, 5Institute of human Genetics, university of Bonn, Bonn, Germany, 6Lec, ccr/ncI/nIh, Bethesda, united states
Introduction: hccs commonly develop in chronically damaged liver tissues. the resulting regenerative and inflammatory processes create an adverse microenvironment that promotes tumor-initiation and progression. expansion of cancer stem cells is commonly observed during this process. this putative cancer stem cell origin provides a plausible explanation for the observed phenotypic heterogeneity of hepatocellular cancers. however, despite profound therapeutic implications the prognostic relevance of cscs and their cellular localization within the tumor formation remain controversial.
Methods: expression levels and localization of established csc markers were assessed in pre-neoplastic lesions and two independent cohorts of hcc patients using qrt-Pcr, imunohistochemistry and Western-Blotting. Integrative whole genome and transcriptome analyses of different tumor regions as well as tumor-surrounding liver (sL) were performed to identify associated molecular alterations and integrated with our existing hcc database.
results: While classical hcc markers were induced in tumor tissue activation of cscs was predominantly observed in sL and continuously decreased from pre-neoplastic lesions to hcc. consistently, genomic and transcriptomic profiles between sL and different tumor regions were quite distinct. Progressive increase in genetic alterations and activation of pathways related to proliferation as well as apoptosis was observed in the tumor tissue, while the invasive tumor margin (tM) was characterized by inflammatory and eMt-related gene sets as well as activation of pro-survival signaling such as erk and fos. further, integration of the different signatures with our database of 53 hcc revealed that the tM signature was associated with the survival of hcc patients.
Conclusion: the csc phenotype is predominantly determined by the permissive tumor microenvironment. however, pro-oncogenic properties might originate in the tM. the activation of key oncogenic features as well as immune-response signaling indicates that the cross-talk between tumor and microenvironment might be a promising therapeutic and/or preventive target.
Disclosure of Interest: none Declared

Oral Communications
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 5
Saturday, 5 September 2015
General Session 3: epidemiology, Staging and Prognosis
O-013 InCIDenCe Of hePATOCeLLuLAr CArCInOMA In ALCOhOLIC COMPenSATeD CIrrhOSIS. PreLIMInAry reSuLTS Of A MuLTICenTer PrOSPeCTIVe frenCh AnD beLGAn COhOrT (CIrrAL)
nathalie Ganne* 1, 2, 3, Valerie Bourcier1, cendrine chaffaut4, Isabelle archambaud5, frédéric oberti6, jean-Marc Perarnau7, Dominique roulot2, 8, alexandre Louvet9, christophe Moreno10, thong Dao11, romain Moirand12, odile Goria13, eric nguyen-khac14, jean henrion15, stanislas Pol16, albert tran17, Victor de Ledinghen18, teresa antonini19, nicolas carbonell 20, jean-Marie Peron21, Violaine ozenne22, xavier amiot23, Gabriel Perlemuter24, jean-Pierre zarski25, sylvie chevret4
1aPhP, jean Verdier, Bondy, 2university Paris 13 sorbonne cité, Bobigny, 3InserM uMr 1162, 4aPhP, saint-Louis, Paris, 5chu, nantes, 6chu, angers, 7chu, tours, 8aPhP, avicenne, Bobigny, 9chu, Lille, france, 10chu, Bruxelles, Belgium, 11chu, caen, 12chu, rennes, 13chu, rouen, 14chu, amiens, france, 15chu, jolimont, Belgium, 16aPhP, cochin, Paris, 17chu, nice, 18chu, Bordeaux, 19aPhP, Villejuif, 20aPhP, saint-antoine, Paris, 21chu, toulouse, 22aPhP, Lariboisière, 23aPhP, tenon, Paris, 24aPhP, antoine Béclère, clamart, 25chu, Grenoble, france
Introduction: the aim of this cohort was to assess the incidence and predictive factors of hepatocellular carcinoma (hcc) in alcoholic compensated cirrhosis.
Methods: Patients were recruited in 26 centres. Inclusion criteria were histologically proven child-Pugh a cirrhosis, excessive alcohol intake according to the Who criteria, absence of infection by hBV (aghBs -) or hcV (anti-hcV -), no previous history of hcc. Patients were prospectively screened for hcc every 6 months by liver ultrasonography according to international guidelines. at inclusion then every years for 3 years, serum biobanks were collected and ethanol concentration in breath was measured.
results: from october 2010 to april 2015, 601 eligible patients were consecutively included in 22 active centres (20 in france, 2 in Belgium) of whom 51 were excluded from the analysis because of absence of liver biopsy (n = 7), child-Pugh ≥ B7 (n = 26), hcc (n = 8), miscellaneous (n= 4), consent withdrawn (n =6). of the 548 patients analyzed [median age 58.6 yrs (Iqr 51.3-64.2), males 67.3%, seniority of the cirrhosis estimated by median deadline since the biopsy of liver: 27.8 months (9.3-76.4), previous decompensation 65%, 358 (69.5%) were completely abstinent (median duration of alcohol withdrawn : 28.4 months) and 86 (16.7%) had still a mild consumption < 7 glasses/ week (absence of ethanol in breath for 346/428 patients at enrolment, 81.3 %). Most patients were smokers (past-history of tobacco 34.5%, active smokers 39.5%) and regular consumption of coffee (77.5%; median: 2 cups/ day; ≥ 3 cups/ days in 136/351 ie 38.7%). Metabolic syndrome defined according to International Diabetes federation (atP III criteria revised in 2005) was present in 91 patients (20.2%). at enrolment, 24 patients (4%) had a liver nodule (hemangioma n = 4, biliary cyst n = 9, regenerative nodule n = 2, miscellaneous/ aspecific n = 9) that was not anymore described during follow-up in 11 cases. Based on a median follow-up of 17 [5.9-26.2] months: i) liver nodule(s) occurred in 73 patients (60 without and 13 with nodule at baseline) (1-yr incidence: 10.7%); ii) hcc was diagnosed in 18 out of 73 cases with nodules (25%; 1-yr incidence 1.6%) without any statistically difference according to alcohol consumption or the presence of metabolic syndrome; these hcc were mainly within Milan criteria (n=15, 88%) and 7 underwent curative treatment (radiofrequency ablation); iii) 41 deaths occurred and were directly attributable to the liver disease in 36.6 % cases.
Conclusion: early results of this prospective cohort of patients with compensated alcoholic cirrhosis show that: a) only 25% of detected liver nodules are primary liver cancer; b) the minimal annual incidence of hcc is 1.6% during the first year of follow-up suggesting that surveillance of alcoholic cirrhosis is cost-effective; c) liver-related mortality already explains a third of deaths. additional enrolments are ongoing. this multicenter cohort constitutes the backbone permitting precise study of hcc and other complications of alcoholic cirrhosis, particularly through subsequent follow-up and nested studies exploiting high quality clinical data and biobank.
Disclosure of Interest: none Declared
O-014 hePATOCeLLuLAr CArCInOMA (hCC) SCOrInG SySTeM fOr The InDIVIDuALIzeD PreDICTIOn Of LIVer CAnCer In 1080 hCV-reLATeD COMPenSATeD CIrrhOSIS InCLuDeD In The frenCh MuLTICenTer PrOSPeCTIVe COhOrT AnrS CO12 CIrVIr
Valerie Bourcier1, nathalie Ganne* 1, richard Layese2, nabila talmat1, Petrov-sanchez Ventzislava3, Patrick Marcellin4, Dominique Guyader5, stanislas Pol6, Dominique Larrey7, Victor De Lédinghen8, Denis ouzan9, fabien zoulim10, jean-claude trinchet1, Pierre nahon1, françoise roudot-thoraval2
1hepatology, jean Verdier hospital, BonDy, 2henri Mondor hospital, creteIL, 3anrs, Paris, 4hepatology, Beaujon hospital, clichy, 5hepatology, rennes hospital, rennes, 6hepatology, cochin hospital, Paris, 7hepatology, Montpellier hospital, Montpellier, 8hepatology, Bordeaux hospital, Bordeaux, 9hepatology, Institut a. tzanck, saint Laurent du Var, 10hepatology, hotel Dieu hospital, Lyon, france
Introduction: this study aimed to develop and validate a simple scoring system to refine individualized prediction of hcc risk in patients with hcV-related compensated cirrhosis included in the french prospective multicentre anrs co12 cirVir cohort (1).
Methods: among 1323 patients with hcV-cirrhosis enrolled in the anrs co12 cirVir, 720 and 360 patients were randomly assigned to the training and validation sets, respectively. cox multivariate proportional hazards model was used to predict hcc occurrence in the population, then nomograms were computed to assess individualized risk.
results: During a mean follow-up of 51 months, 103 (14%) and 39 (11%) patients developed hcc, respectively in the training and validation cohorts. according to cox regression analysis, 5 variables were independently associated with the occurrence of hcc in the training cohort:
Factors Coefficient HR 95% HR CI P-value Score
Age >50 years 0.661 1.94 [1.15 ; 3.25] 0.012 2
Past exces. alcohol intake 0.443 1.56 [1.02 ; 2.38] 0.04 1
Plat. Count (x 109/ mm3) < 100 [100 ; 150]
0.937 0.575
2.55 1.78
1.53 ; 4.26]
[1.05 ; 3.02]
< 0.001 < 0.001
0.034
3 2
GGT (UI/l) > ULN 0.638 1.89 [1.07 ; 3.35] 0.028 2
Positive HCV RNA at end of follow-up
1.548 4.70 [2.61 ; 8.48] < 0.001 5
a 13-point risk score was derived in the training cohort using these 5 variables, the score of each variable being obtained by linear transformation of the coefficients and rounding. the population was stratified according to this scoring system into four groups, with hcc occurrence gradually increasing from 0% to 20% at 3 years, and 0% to 37% at 5 years, for patients with the lowest (score ≤ 2) and highest (score ≥ 11) hcc risk, respectively (figure 1a) and validated. the auc for the 1- and 3-year prediction were 0.75 [0.64; 0.85] and 0.75 [0.71;0.80] respectively. Derived from this score, a nomogram was also built, enabling individualized prediction of hcc occurrence at 1, 3 or 5 years.
Image:
Conclusion: an hcc score constructed using 4 baseline variables (age, past excessive alcohol consumption, platelets count, GGt serum level) and qualitative hcV rna at end-point is accurate to predict hcc at the individual level in french patients with hcV-cirrhosis, with or without sVr. external validation in non-french populations is warranted.
references: (1) trinchet et al. complications and competing risks of death in compensated viral cirrhosis (anrs co12 cirVir prospective cohort). hepatology. 2015 feb 11. doi: 10.1002/hep.27743.
Disclosure of Interest: none Declared

Oral Communications
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 6
Saturday, 5 September 2015
O-015 PLATeLeT COunT IMPrOVeS PrOGnOSTIC VALue Of A-L-b-I GrADe: InTrODuCInG A neW P-A-L-b-I SCOre
Sasan roayaie* 1, Ghalib jibara2, sarah Berhane3, Parissa tabrizian4, joong-Won Park5, jijin yang6, Lunan yan7, Guohong han8, francesco Izzo9, Mishan chen10, jean-frederic Blanc11, Lewis roberts12, Masatoshi kudo13, Morris sherman14, Philip johnson3
1north shore-LIj health system, Lenox hill hospital, new york, united states, 2Brookdale's Medical center, Brooklyn, -, 3university of Liverpool, Liverpool, united kingdom, 4Mount sinai hospital, new york, united states, 5national cancer center, seoul, korea, republic of, 6second Military Medical university, shanghai, 7West china hospital, sichuan, 84th Military Medical university, xian, china, 9national cancer Institute of naples, naples, Italy, 10sun yat-sen university, Guangzhou, china, 11hopital saint andre, Bordeaux, france, 12Mayo clinic, rochester, united states, 13kinki university, kyoto, japan, 14university of toronto, toronto, canada
Introduction: aLBI grade, based on albumin and log10 bilirubin, has been shown to be less subjective and more granular than child-Pugh class in its correlation with survival of patients with hepatocellular cancer (hcc)(ref). however, aLBI does not incorporate portal hypertension. We sought to determine if the addition of platelet count, an objective and widely used surrogate for portal hypertension, could improve the prognostic ability of aLBI.
Methods: Patients from BrIDGe, a multiregional longitudinal cohort study including hcc patients newly diagnosed between jan 1, 2005 and june 30, 2011, were randomly divided into separate training and validation cohorts. aLBI grade (1,2 or 3) was calculated based on albumin and log10 of total bilirubin as previously described (ref). Log10 of platelet (x1,000/μL) was used to create the new model as it provided a normal distribution. a cut-off of 2.1 was selected based on the median value. Multivariate analysis was conducted to determine if log10 platelet independently correlated with survival and to determine the hazard ratio. PaLBI score was constructed based on the results and tested in the validation cohort.
Multivariate analysis in the training cohort revealed that Log10 platelet with cut-off of 2.1 was independently associated with survival (table 1). Based on the observation that the hazard ratio for log10 Platelet (1.142) was roughly equivalent to the increase in hazard ratio for each aLBI grade, an additional point was added to the aLBI score if log10 Platelet was <2.1. no additional point was added if log10 platelet was >2.1. Multivariate analysis revealed that the new PaBLI was independently associated with survival in the validation cohort (table 1). PaLBI was also able to stratify child’s a patients from the validation cohort into 4 distinct groups with significantly different outcomes (p<0.001)(figure 1).
training cohort (n=3986) Validation cohort (n=3998)
hr P hr p
age >70y 1.340 0.002 1.266 0.002
Macrovascular Inv extrahepatic disease
1.275 1.758
0.005 <0.001
1.600 1.737
<0.001 <0.001
Who Ps>1 2.226 <0.001 2.672 <0.001
afP>400ng/ml tumor size >3cm
1.544
2.101
<0.001
<0.001
1.500
1.815
<0.001
<0.001
aLBI 1 2 3
ref 1.405 1.953
<0.001 <0.001
Log10 Platelet <2.1 1.142 .032
PaLBI 1 2 3 4
ref 1.506 2.123 3.764
0.003 <0.001 <0.001
Image:
Conclusion: the addition of platelet count did indeed improve the prognostic ability of the aLBI grade. the new PaLBI score, based on platelet count, albumin, and bilirubin, was able to accurately and independently stratify hcc patients with regards to survival in an independent validation cohort. PaLBI incorporates aspects of both liver function and portal hypertension. PaLBI is completely objective and more granular than child’s class.
references: johnson Pj, Berhane s, kagebayashi c, et al. assessment of Liver function in Patients with hepatocellular carcinoma: a new evidence-Based approach- the aLBI Grade. j clin oncol 2015. epub ahead of print.
Disclosure of Interest: none Declared
O-016 DIAbeTeS, hbV InfeCTIOn AnD SMOKInG Are InDePenDenT rISK fACTOrS fOr DeVeLOPInG hePATOCeLLuLAr CArCInOMA On nOn-fIbrOTIC LIVer In The nOfLIC frenCh MuLTICenTer CASe-COnTrOL STuDy
Jean-frédéric blanc* 1, Marie-quitterie Picat2, aline Maillard2, caroline Bouyssou1, charlotte costentin3, Mariane ziol4, olivier rosmorduc5, Laurence chiche6, Isabelle rosa-hezode7, Luc Letenneur2, karen Leffondre2, adélaide Doussau2, jessica zucman-rossi8
1hepatology and Digestive oncology, unIVersIty hosPItaL of BorDeaux, 2IsPeD, university of Bordeaux, Bordeaux, 3hepatology, chu henri Mondor, créteil, 4Pathology, chu jean Verdier, Bondy, 5hepatology, chu saint-antoine, Paris, 6Digestive surgery, chu Bordeaux, Bordeaux, 7hepato-Gastroenterology, chI créteil, creteil, 8InserM, uMr 1162, Génomique fonctionnelle des tumeurs solides, Institut universitaire d'hématologie, Paris, france
Introduction: the occurrence of hcc in non-fibrotic liver (nfhcc) is a rare event (5% of hcc patients) and factors contributing to their onset remain poorly understood. the aim of the case-control exploratory study nofLIc was to identify factors involved in hepatocarcinogenesis in non-fibrotic liver.
Methods: nofLIc is a french multicenter case-control study that included consecutive patients who developed hcc in a non-fibrotic liver, f0 or f1, proven by histological analysis. controls were matched for age and gender, they were recruited in people with gastro-intestinal screening and normal endoscopy, or in rheumatology and orthopedic departments. clinical data were collected including the parameters of the metabolic syndrome defined according to the nceP-atP3 criteria, viral serology, quantification of alcohol and tobacco use. Data were taken from the patient's medical record, the results of blood test performed for this study and a specific detailed epidemiologic survey. Logistic regressions adjusted for age, sex and geographical origin, were performed to determine the association of each of the risk factors with the status of the patient (case / control). a multivariate analysis was performed to study the effect of significant risk factors.
results: a total of 109 nfhcc (cases) and 163 controls were included in 12 hospitals between 2010 and 2013. Mean age of the nfhcc patients was 64.4 years, with 68.8% male. active hBV infection was detected in 6 cases (or 11.4, 95% 1.18-110.84, p=0.035). history of alcohol abuse was more frequent in nfhcc (or 2.13, 95% 1.09-4.16 p=0.026). a metabolic syndrome was identified in 28% of the patients developing nfhcc (or 3.3; 95% cI 1.62-6.82 p=0.001). among the components of metabolic syndrome, treated diabetes or fasting glucose ≥ 6.1mmol/l was significantly associated with nfhcc occurrence (or 3.08; 95% cI 1.67-5.69 p=0.0002), while there was no significant association with BMI, hypertension and dyslipidemia. smoking (defined by at least 100 smoked cigarettes and at least with a weekly smoking habit) was also associated with nfhcc (or 2.18 adjusted for age and sex; 95% cI 1.23-3.83 p = 0.0067). In multivariate analysis, hBV infection

Oral Communications
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 7
Saturday, 5 September 2015
(p=0.024), metabolic syndrome (P=0.0023) and tobacco use (p=0.0062) were independent risk factors for developing nfhcc.
Conclusion: nofLIc is the first case-control study specifically dedicated to the study of factors associated with the occurrence of hcc in non-fibrotic liver (f0/f1). the first analysis shows a significant association between metabolic syndrome, diabetes, hBV infection and smoking with the occurrence of hcc in non-fibrotic liver suggesting an important role of these factors in liver carcinogenesis.
Disclosure of Interest: none Declared
O-017 PATIenTS WITh ALCOhOL COMPAreD TO hCV-reLATeD hePATOCeLLuLAr CArCInOMA (hCC) hAVe A reDuCeD SurVIVAL. reSuLTS Of A nATIOnWIDe STuDy
Charlotte Costentin* 1, nathalie Goutte2, Philippe sogni3, noëlle Bendersky4, Bruno falissard5, olivier farges6
1hepatology, henri Mondor hospital, creteil, 2hepato-biliary surgery, Beaujon hospital - Paris VII university - InserM u773, clichy, 3hepatology, cochin hospital - Paris Descartes university, Paris, 4Medical Informatics, Beaujon hospital - Paris VII university, clichy, 5biostatistique, Paris-sud university, InserM u669, Paris, 6hepatology – hepato-biliary surgery, Beaujon hospital - Paris VII university - InserM u773, clichy, france
Introduction: Data on alcohol-related hcc are scarce. the aim of this study was to describe the incidence, management and prognosis of alcohol compared to hcV-related hcc, at a national level.
Methods: french healthcare databases (recording all hospital admissions) were screened to identify all adult patients who were hospitalized between 2007 and 2012 with a diagnosis of hcc. Incident cases of hcc were selected by defining the entry point as a first admission in 2009. Demographic data, associated conditions, underlying liver disease and etiology, as well as the type (teaching, general, private, charitable), location (within the 22 mainland regions), and annual hcc-caseload of the hospitals where patients were first managed (1st tertile <25, 2nd tertile 25-45; 3rd tertile >45), were retrieved. treatments were divided into curative (liver transplantation, resection, radiofrequency) or not. survival of incident-cases was computed from the time of diagnosis and adjusted for potential confounding variables. for the purpose of this study, patients with unknown etiology of liver disease, mixed etiologies or hBV were excluded, in order to compare two homogeneous populations of alcohol and hcV-related hcc.
results: Between 2009 and 2012, the study population included 13,942 (83.4%) incident-cases of alcohol and 2,774 (16.6%) hcV-related hcc. the incidence of alcohol- and hcV-related hcc varied up to 2 fold from one mainland region to another, and in some regions, alcohol accounted for up to 96% of hcc. alcohol- compared to hcV-related hcc occurred more often in men (89.2% vs 63.7% p<0.001), in patients with co-morbidities (55.9% vs 48.5%; p<0.001), underlying cirrhosis (95.4 vs 83.4%; p<0.001), decompensated cirrhosis (37.6 vs 20.3; p<0.001) and extra-hepatic spread (14.5 vs 12.9%, p=0.032). During follow-up, the optimal treatment was less frequently curative (20.2% vs 36.5%; p<0.001) and crude survival was significantly shorter (9.6 months [9.1-10.1] vs 20.1 months [18.6-22.3]; p<0.0001) in alcohol-related compared to hcV-related hcc. this difference remained significant when considering adjusted survival (11.4 [11.0-12.1] vs 14.1 [12.5-15.2] months; p=0.0008). In multivariate analysis, survival was significantly influenced by etiology, age, gender, underlying cirrhosis, liver decompensation at diagnosis, presence of extra-hepatic spread, co-morbidities and optimal treatment. It was also influenced by the type, annual hcc-caseload and regional location of the hospitals were the index admission occurred.
Conclusion: alcohol-related hcc have a reduced survival compared to hcV-related hcc after adjustment on confounders. the specific role of alcohol or the lack of optimal management including screening have to be evaluated in this population
Disclosure of Interest: none Declared
O-018 PATIenT KnOWLeDGe AnD bArrIerS fOr hePATOCeLLuLAr CArCInOMA SurVeILLAnCe AMOnG PATIenTS WITh CIrrhOSIS
Amit G. Singal* 1, Maleka khambaty1, adam yopp1, Purva Gopal1, jasmin tiro1, jorge Marrero1
1ut southwestern Medical center, Dallas, united states
Introduction: hepatocellular carcinoma (hcc) surveillance is recommended in patients wtih cirrhosis, but prior studies suggest fewer than 20% of at-risk patients undergo hcc surveillance. Patient attitudes and barriers to hcc surveillance are important to inform future intervention strategies but have not been studied to date. the aims of our study were to characterize patient-reported hcc surveillance rates, knowledge and potential barriers among a large cohort of patients with cirrhosis.
Methods: Patients with cirrhosis, confirmed by chart review, followed at an urban health system
were invited to complete a self-administered survey about hcc surveillance. We excluded patients with overt hepatic encephalopathy and those of low literacy who could not complete the survey. the survey was derived from validated surveys, pretested among patients before administration, and available in english and spanish. the survey assessed self-reported receipt of hcc surveillance, potential barriers to surveillance, and patient knowledge regarding hcc risk and surveillance. univariate and multivariate logistic regression analyses were used to identify correlates for receipt of hcc surveillance within 12 months, with significance defined as p<0.10 for univariate and p<0.05 for multivariate analyses.
results: the survey was administered to 409 patients, of whom 287 (70.2%) responded. Median age was 57 (range 22-85) years, and 157 (55.5%) were male. the cohort was socioeconomically disadvantaged, with 197 (71.1%) having an annual income below $10,000, and racially diverse, with 40.9% hispanics, 32.4% caucasians, and 24.0% Blacks. overall, 240 (83.6%) patients reported ultrasound-based hcc surveillance, with 189 (65.9%) reporting surveillance within 12 months. on univariate analysis, hcc surveillance within 12 months was associated with caucasian race, living alone, and concern about dying from hcc. on multivariate analysis, receipt of hcc surveillance was associated with caucasian race (or 2.08, 95%cI 1.17–3.70) and living alone (or 2.19, 95%cI 1.13–4.25). Most patients (87.3%) believed hcc surveillance is important, although surveillance rates did not differ by perception of importance (p=0.95). Most respondents recognized patients with cirrhosis are high risk for hcc (86.7%), ultrasound is recommended for surveillance (84.2%), surveillance should be done every 6-12 months (88.8%), and hcc can be cured if found at an early stage (78.5%). however, 46.2% of respondents believed a healthy diet could reduce hcc risk and preclude the need for hcc surveillance, 33.6% believed normal labs precluded the need for surveillance, and 28.7% believed hcc surveillance could be stopped after two normal ultrasound exams. the most common patient-reported barriers to completing hcc surveillance included scheduling delays for ultrasound appointments (34.6%), length of time for the scheduling process (27.1%), and co-pays for ultrasound exams (22.1%). few patients believed lack of trust in ultrasound quality (12.1%), pain (12.0%), fear of finding cancer (11.1%), or amount of time for ultrasound exams (11.1%) were important barriers to hcc surveillance.
Conclusion: over 1 in 3 patients with cirrhosis report not receiving hcc surveillance within one year. Patients have high levels of knowledge about hcc risk and surveillance; however misconceptions about diet and normal labs precluding the need for hcc surveillance may contribute to hcc surveillance underuse. Difficulty and delays with ultrasound scheduling are common barriers to completing hcc surveillance and serve as potential targets to increase surveillance rates.
Disclosure of Interest: none Declared
Plenary Session
O-019 COMPrehenSIVe AnD InTeGrATIVe GenOMIC ChArACTerIzATIOn Of hePATOCeLLuLAr CArCInOMA: The TCGA hCC PrOJeCT
Lewis r. roberts* 1, David a. Wheeler2
1Division of Gastroenterology and hepatology, college of Medicine, Mayo clinic and Mayo clinic cancer center, rochester, 2Baylor college of Medicine, houston, united states
Introduction: hepatocellular carcinomas (hccs) are heterogenous neoplasms of primary hepatocytes with pleomorphic histopathologic phenotypes. We present a comprehensive analysis of 192 hccs using multiple advanced genetic, genomic, transcriptomic and proteomic platforms from the cancer Genome atlas to provide a deeper understanding of the molecular features of this neoplasm, to classify them in a clinically-relevant manner, and to provide a public resource that identifies potential targets for emerging therapies.
Methods: hcc primary tumor samples were obtained from 192 patients with hcc who had undergone resection. Germline Dna from blood or non-malignant surrounding liver was used as a reference for detecting somatic alterations. We used Mut.sig.2cV to perform mutational analysis. six molecular platforms were analyzed: somatic copy number analysis, whole-exome sequencing, Dna methylation profiling, messenger rna sequencing, microrna (mirna) sequencing and reverse-phase protein array (rPPa).
results: Mutation analyses showed that tert promoter mutations was the most common somatic mutation and was present in 41% of hcc. further, the analysis revealed the first report of a germline mutation in the tert promoter in a 30 year old male who did not have other risk factors for hcc like viral hepatitis, possibly reflecting an inherited predisposition to hcc. other tumor suppressor genes recurrently inactivated by mutation included the cell cycle regulatory genes tP53 (32%), rB1 (8%), and Pten (3%), the Wnt/beta catenin pathway gene axIn1 (4%), and the chromatin remodeling genes arID1a (9%), BaP1 (6%), arID1B (4%), arID2 (4%), and PBrM1 (3%). Genes activated by oncogenic mutation included the beta catenin gene ctnnB1, which was mutated in 27% of hccs. Mutations were also found in the Mtor pathway genes, Mtor (4%), tsc2 (4%) and tsc1 (3%).
for molecular subtyping of hccs, initially unsupervised clustering was performed on 6 different

Oral Communications
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 8
Saturday, 5 September 2015
platforms to identify different molecular subtypes: mrna (n=5), methylation (hypomethylation n=3; hypermethylation n=4), copy number alteration (n=4), microrna (n=4) and protein array (n=2) When combined, integrated clustering using icluster resulted in a grouping of hccs into three superclusters, characterized as follows: icluster 1 had a low frequency of cDkn2a silencing, ctnnB1 mutation, a normal like methylation pattern, and overexpression of proliferation marker genes; iclusters 2 and 3 had a high frequency of cDkn2a silencing, ctnnB1 mutation, and overexpression of oxidative response genes; icluster 3 tumors had a higher degree of chromosomal instability, high frequency of 17p loss, and a highly altered methylation profile.
Conclusion: We present here a comprehensive co-mutational landscape of hcc and importantly, we identified a novel germline mutation in the tert promoter that may be associated with an inherited risk for hcc. Based on integrated analysis of genome, transcriptome, methylome and proteome, we showed that hccs naturally separate into three distinct groups that are associated with molecular and clinical characteristics.
Disclosure of Interest: none Declared
O-020 PrOSPeCTIVe ASSeSSMenT Of LIVer CAnCer OCCurrenCe In COMPenSATeD hCV-reLATeD CIrrhOSIS WITh SVr uSInG A COMPeTInG rISK frAMeWOrK reVeALS An AnnuAL InCIDenCe beLOW 1% AnD SPeCIfIC rISK fACTOrS (AnrS CO12 PrOSPeCTIVe CIrVIr COhOrT)
Pierre nahon* 1, Valérie Bourcier1, richard Layese2, Ventzi Petrov-sanchez3, Patrick Marcellin4, Dominique Guyader5, stanislas Pol6, Dominique Larrey7, fabien zoulim8, Dominique roulot9, Victor de Ledinghen10, jean-Pierre zarski11, jean-claude trinchet1, françoise roudot-thoraval2
1hôpital jean Verdier, Bondy, 2hôpital henri Mondor, créteil, 3anrs, Paris, 4hôpital Beaujon, clichy, 5hôpital Potchaillou, rennes, 6hôpital cochin, Paris, 7chu Montpellier, Montpellier, 8chu Lyon, Lyon, 9hôpital avicenne, Bobigny, 10chu Pessac, Pessac, 11chu Grenoble, Grenoble, france
Introduction: the objective was to prospectively assess the benefits of sustained viral response (sVr) on the incidence of primary liver cancer (PLc) in french patients with compensated hcV cirrhosis included in the cirVir cohort1 using competing risk analyses.
Methods: Patients with the following inclusion criteria were enrolled in 35 french centres: a) biopsy-proven hcV cirrhosis; b) child-Pugh a; c) absence of previous liver complications. Patients were prospectively followed-up every 6 months. sustained virological response (sVr) was defined as undetectable hcV rna at the end of a 12-week untreated follow-up period. a given event was arbitrarily considered as occurring in a patient who achieved sVr if it was recorded at least one year after successful treatment completion.
results: a total of 1323 patients were enrolled between March 2006 and june 2012 [age 55, men 63.5%, Genotype 1: 66%, 2: 6 %, 3: 17%, 4: 10%, 5-6: 1%]. at end-point in january 2015 (median follow-up of 51 months), the number (rates) of hcV patients with a negative viral load was 653 (51%) corresponding to sVr in 491 patients (40%) while the remaining 162 hcV negative patients were still undergoing antiviral treatment (mostly based on second generation Daas). PLc was diagnosed in 168 (162 hepatocellular carcinoma (hcc) and 6 cholangiocarcinomas) among which 17 were developed in sVr patients (P<0.001). sVr was an independent factor associated with a decreased incidence of hcc (cumulative incidence, 5-yrs cumI: 3.3% vs 21.8%, hr=0.21 [0.13-0.36], P<0.001). sVr patients also had lower incidences of liver decompensation (hr=0.17 [0.10-0.27], P<0.001), bacterial infection (hr=0.22 [0.13-0.35], P<0.001) and cardiovascular disease (hr=0.31 [0.19-0.52], P<0.001). except for lower afP levels at diagnosis in sVr patients (median 4.0 vs 19.3 ng/mL and afP>200 ng/mL: 0 % vs. 14.8%, P<0.001), hcc characteristics and outcome after diagnosis did not differ according to sVr. Metabolic syndrome (Ms) was associated with higher risk of hcc in sVr patients (P=0.04) but not in viremic patients (figure). In multivariate analysis, lower Pt<80% (hr=6.27 [2.30-17.07], P<0.001) was the only independent hcc risk factor in sVr patients. In viremic patients hcc predictors were older age>50 yrs, past excessive alcohol intake, higher GGt levels and lower platelet count. overall survival was higher in sVr patients (5-yrs cumI: 97.1% vs 83.2%, hr=0.21 [0.12- 0.34], P<0.001). Liver-related death (comprising death from PLc progression and liver failure) was lower in sVr patients (5-yrs cumI: 1.6% vs 8.6%, hr=0.21 [0.19- 0.39], P<0.001).
Image:
Conclusion: a five-fold reduction in hcc incidence is observed in patients with hcV compensated cirrhosis achieving sVr, leading to an annual incidence lower than 1%. risk factors and prognosis of hcc developed in this population may differ from that of viremic patients.
references: 1. trinchet et al. complications and competing risks of death in compensated viral cirrhosis (anrs co12 cirVir prospective cohort). hepatology. 2015 feb 11. doi: 10.1002/hep.27743.
Disclosure of Interest: none Declared
O-021 ObJeCTIVe reSPOnSe by MreCIST PreDICTS SurVIVAL In hePATOCeLLuLAr CArCInOMA: A MuLTIVArIATe, TIMe-DePenDenT AnALySIS frOM The PhASe 3 brISK-PS STuDy *
riccardo Lencioni* 1, joong-Won Park2, ferran torres3, thomas Decaens4, eveline Boucher5, jean-Luc raoul6, Masatoshi kudo7, charissa chang8, Valerie Boige 9, eric assenat10, yoon-koo kang 11, ho-yeong Lim 12, Ian Walters13, josep M. Llovet8
1Diagnostic Imaging and Intervention, university of Pisa school of Medicine, Pisa, Italy, 2center for Liver cancer, national cancer center, Goyang, korea, republic of, 3IDIBaPs, hospital clínic Barcelona, Barcelona, spain, 4service d'hepato-Gastro-enterologie, university of Paris-est, creteil, 5service d'oncologie Médicale, central eugene Marquis, rennes, 6service d'oncologie Médicale, Institut Paoli calmette, Marseille, france, 7Department of Gastroenterology and hepatology, kinki university school of Medicine, osaka, japan, 8Division of Liver Diseases, Mount sinai school of Medicine, new york, united states, 9service de Gastro-enterologie, Institut Gustave roussy, Villejuif, 10service d'hépato-Gastro-entérologie, hôpital saint eloi, Montpellier, france, 11Department of oncology, asan Medical center, 12Division of hematology-oncology, samsung Medical center, seoul, korea, republic of, 13Bristol-Myers squibb, Wallingford, united states
Introduction: mrecIst (modified response evaluation criteria In solid tumors) was developed to overcome the limitations of standard recIst in hepatocellular carcinoma (hcc) response assessment. retrospective studies have correlated objective response (or) by mrecIst with overall survival (os) in patients treated by loco-regional therapies. We investigated whether or by mrecIst predicted os using data from a double-blind, placebo-controlled, randomized phase III trial.
Methods: In the BrIsk-Ps study, 395 patients with advanced hcc who progressed on/after or were intolerant to sorafenib were randomly assigned (2:1) to receive brivanib plus best supportive care (Bsc) or placebo plus Bsc. tumor assessments were performed every 6 weeks by contrast-enhanced computed tomography or magnetic resonance imaging. assessment of response was done by central radiological review using mrecIst. statistically significant variables associated with os from univariate cox analysis, were included in the multivariate models. all statistics involving evolutionary events were done by means of time-dependent covariate analysis (sPss 18 and sas 9.2).
results: 210/226 (93%) patients in the brivanib arm and 101/108 (94%) in the placebo arm, who had baseline and on-study scans available for central blinded review, were evaluable according to mrecIst. 26/210 patients on brivanib and 2/101 on placebo achieved partial response (p<0.01). at the end of follow up, 284 patients had died, the median os for the brivanib arm being 9.4 months.

Oral Communications
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 9
Saturday, 5 September 2015
as per mrecIst response assessment, median os was 16.4 months (n=26; 95% cI, 15.7 – na) for brivanib responders and 8.3 months (n=237; 95% cI, 7.2 – 9.7) for brivanib non-responders (hazard ratio, 0.28; 95% cI, 0.14 – 0.55, p<0.01). Independent predictors of os at multivariate time-dependent analysis were or by mrecIst, vascular invasion/extrahepatic spread, afP > 200 ng/mL and bilirubin > 1.5 mg/dl.
Conclusion: or by mrecIst is an independent predictor of os in hcc patients receiving a systemic multikinase inhibitor, brivanib. mrecIst response is a marker of antitumor activity and warrants further evaluation in prospective clinical trials exploring novel agents in hcc patients.
references: * Llovet jM, Decaens t, raoul jL, et al. Brivanib in patients with advanced hepatocellular carcinoma who were intolerant to sorafenib or for whom sorafenib failed: results from the randomized phase III BrIsk-Ps study. j clin oncol 2013;31:3509-16
Disclosure of Interest: none Declared
O-022 A rAnDOMIzeD PhASe 2 TrIAL Of SOrAfenIb PLuS InTrA-ArTerIAL CISPLATIn VerSuS SOrAfenIb ALOne fOr ADVAnCeD hePATOCeLLuLAr CArCInOMA
Manabu Morimoto*1, Masafumi Ikeda2, satoshi shimizu2, yoshitaka Inaba3, yasushi kojima4, atsushi hagihara5, Masatoshi kudo6, shoji nakamori7, shuichi kaneko8, rie sugimoto9, toshiyuki tahara10, takumi ohmura11, kohichiroh yasui12, keiko sato13, hiroshi Ishii14, junji furuse15, takuji okusaka16
1Department of hepatobiliary and Pancreatic Medical oncology, kanagawa cancer center, kanagawa, 2Department of hepatobiliary and Pancreatic oncology, national cancer center hospital east, kashiwa chiba, 3Department of Diagnostic and Interventional radiology, aichi cancer center hospital, aichi, 4Department of Gastroenterology, national center for Global health and Medicine center hospital, tokyo, 5Department of hepatology, osaka city university hospital, 6Department of Gastroenterology and hepatology, kinki university school of Medicine, 7Department of hepatobiliary and Pancreatic surgery, osaka national hospital, osaka, 8Department of Gastroenterology, kanazawa university hospital, kanazawa, 9Department of hepato-Biliary-Pancreatology, national hospital organization kyushu cancer center, fukuoka, 10Department of Gastroenterology, saiseikai utsunomiya hospital, tochigi, 11Department of Gastroenterology, sapporo kosei General hospital, sapporo, 12Molecular Gastroenterology and hepatology, Graduate school of Medical science, kyoto Prefectural university of Medicine, 13Institute for advancement of clinical and translational science, kyoto university hospital, kyoto, 14clinical research center, shikoku cancer center, Matsuyama, 15Department of Medical oncology, kyorin university, 16Department of hepatobiliary and Pancreatic oncology, national cancer center hospital, tokyo, japan
Introduction: sorafenib has been acknowledged as a standard therapy for advanced hepatocellular carcinoma (hcc), and is available worldwide. hepatic arterial infusion chemotherapy (haIc) with cisplatin is still often performed in japan, because a favorable tumor-shrinking effect and long-term survival of the patients are sometimes observed in even patients with highly advanced hcc. Because no randomized controlled trials have demonstrated any survival advantage of haIc, no consensus has been reached as to the standard treatment for advanced hcc. the aim of this trial was to evaluate the efficacy and safety of sorafenib plus haIc with cisplatin (sP) vs. sorafenib alone (s) for advanced hcc.
Methods: In this multicenter open-labeled randomized phase II trial, advanced hcc patients with no prior chemotherapy and child Pugh a or B7 were randomly assigned 2:1 to receive sP (sorafenib: 800 mg, twice daily; haIc with cisplatin: 65 mg/m2, day 1, every 4 to 6 weeks up to a maximum of 6 cycles) or s (800 mg, twice daily) with portal vein tumor thrombosis and extrahepatic metastasis as dynamic allocation factors. the primary endpoint was overall survival, and secondary endpoints were time to progression, response rate by modified recIst, adverse events and serious adverse events. If the median survival of s is assumed as 7.0 months and that of sP as 9.5 months, the hazard ratio (hr) is 0.74. sP would be judged as favorable if hr is 0.74 or lower. a total of 105 patients was needed to estimate the 1-year survival rate with an accuracy of ±10%.
results: from june 2011 to December 2013, 108 patients were randomized (sP, n=66; s, n=42) and followed up to December 2014. In the full analysis set of 106 patients, the patient characteristics were well-balanced, except for portal vein tumor thrombosis and hepatitis c viral infection. the median survivals in the sP and the s arms were 10.6 and 8.7 months, respectively (crude hr [95% cI], 0.68 [0.44-1.04], p=0.073; and stratified hr by the allocation factors [95% cI], 0.60 [0.38-0.96], p=0.031). In the prespecified subgroup analysis of overall survival, patients with α-fetoprotein <400 ng/mL were significantly better survival in the sP arm (median, 14.8 month) than in the s arm (median, 8.7 month) (p=0.042). the median time to progression was 3.1 and 2.8 months in the sP and s arms (hr [95% cI], 0.78 [0.52-1.16], p=0.212; stratified hr [95% cI], 0.78 [0.59-1.21]). the response rate by central review (95% cI) was 21.7% (12.1-34.1%) in the sP arm and 7.3% (1.5-19.9%) in the s arm (p=0.009). the following adverse events were more frequent in the sP arm than in the s arm, (percentage in the sP/s arms): neutropenia, 60.0/43.9; leukocytopenia, 75.4/43.9; hemoglobin, 89.2/73.2; thrombocytopenia, 89.2/80.5; hyponatremia, 81.5/53.7; nausea, 41.4/19.5; and hiccups, 9.2/0.0, respectively. however, there were no differences on the frequencies of serious adverse events between two arms (sP, 16.9%; s, 24.4%).
Conclusion: according to the prespecified hr of 0.74, sP yielded favorable overall survival as
compared to s in patients with advanced hcc. a further phase III trial is warranted to confirm these results.
Disclosure of Interest: M. Morimoto research/education support from: Bayer yakuhin, yakult, shionogi, eli Lilly, kyowa-hakko-kirin, kowa, honoraria support from: Dainippon sumitomo, eisai, nippon kayaku, M. Ikeda research/education support from: Bayer yakuhin, novartis Pharma, Merck serono, kyowa hakko kirin, yakult, Dainippon sumitomo, taiho Pharmaceutical, eli Lilly japan, otsuka Pharmaceutical, chugai Pharmaceutical, oncotherapy science, Boehringer Ingelheim, kowa,, honoraria support from: novartis Pharma, Dainippon sumitomo, Bayer yakuhin, Bristol Myers, abbott japan, takeda Bio Development center, Merck serono, kyowa hakko kirin, yakult, Guerbet japan, advisory Board of: Bayer yakuhin, eisai, consulting of: nano carrier, s. shimizu honoraria support from: yakult, oLyMPus, y. Inaba advisory Board of: eisai, taiho, y. kojima research/education support from: Bayer yakuhin, kyowa-hakko-kirin, honoraria support from: taiho, chugai, stocks of: chugai Pharmaceutical, takeda, a. hagihara honoraria support from: Bayer yakuhin, Dainippon sumitomo, otsuka, chugai, MsD, M. kudo research/education support from: taiho, Bayer, BMs, kyowa hakko kirin, kowa, novartis, eli Lilly, honoraria support from: Ge healthcare japan, MsD, ajinomoto, eisai, otsuka, kyowa hakko kirin, Gsk, Guerbet japan, kowa, Daiichi sankyo, taisho toyama, Dainippon sumitomo, tiho, Mitsubishi tanabe, chugai, eli Lilly, nippon kayaku, nippon Boehringer Ingelheim, novartis, Bayer, BMs, janssen, Wako, advisory Board of: novartis, Bayer, consulting of: kowa,taiho, s. nakamori: none Declared, s. kaneko research/education support from: takeda Pharmaceutical, Daiichi sankyo, eisai, astellas Pharma, Bayer japan, taiho Phamaceutical, otsuka Pharmaceutical, Pfizer, Bristol-Myers squibb, MsD, toray Industries, eli Lilly japan, nippon Boehringer Ingelheim, honoraria support from: takeda Pharmaceutical, Daiichi sankyo, eisai, astellas Pharma, Bayer japan, taiho Phamaceutical, otsuka Pharmaceutical, Pfizer, Bristol-Myers squibb, MsD, toray Industries, eli Lilly japan, nippon Boehringer Ingelheim, takeda Pharmaceutical, Daiichi sankyo, eisai, astellas Pharma, Bayer japan, taiho Phamaceutical, otsuka Pharmaceutical, Pfizer, Bristol-Myers squibb, MsD, toray Industries, eli Lilly japan, nippon Boehringer Ingelheim, r. sugimoto research/education support from: nippon Boehringer Ingelheim, kyowa hakko kirin, honoraria support from: astrazeneca,abbott japan,Diichisankyo, t. tahara: none Declared, t. ohmura honoraria support from: eisai,Daiichi sankyo, Bayer, Dainippon sumitomo, century Medical, japan Blood Products, Piolax, k. yasui: none Declared, k. sato honoraria support from: eli Lilly japan, consulting of: Pharma, sumitomo chemical, h. Ishii honoraria support from: taiho, Bayer, torii, ely Lilly, ono kyowa kirin, ohtsuka,, j. furuse research/education support from: ono, yakult, Gsk, taiho, takeda, chugai, eli Lilly, sanofy, Bayer, novartis, Merk serono, Daiichi sankyo, torii, nippon kayaku, BMs, honoraria support from: chugai, taiho, eli Lilly, Bayer, eisai, ono, yakult, takeda, astellas, Daiichi sankyo, sumitomo Dainippon, Bms, nippon kayaku, ajinomoto, Meiji seika, sanofy, hisamitsu, Mitsubishi tanabe, sandoz, shionogi, kyowa hakko kirin, Merk serono, advisory Board of: zeria, astrazeneca, yakult, Merck serono, Gsk, chugai, taiho, Bayer, kowa, astellas, janssen, consulting of: kyowa hakko kirin, zeria, yakult, taiho, eisai, fujifilm, Boehringer, otsuka, j-Pharma, t. okusaka research/education support from: chugai Pharmaceutical co., Ltd, eli Lilly japan k.k., eisai co., Ltd., novartis Pharma k.k, shizuoka Industry, takeda Bio Development center Limite, yakult honsha co., Ltd., oncotherapy science, Inc., otsuka Pharmaceuical co., Ltd., taiho Pharmaceutical co., Ltd., sceti Medical Labo k.k., nippon Boehringer Ingelheim co., Ltd., kowa company, LtD, kyowa hakko kirin co., Ltd., Merck serono co., Ltd., ono Pharmaceutical co., Ltd., Bayer yakuhin, Ltd., Pfizer japan Inc., astrazeneca k.k., Dainippon sumitomo Pharma co., Ltd., honoraria support from: chugai Pharmaceutical co., Ltd., Pfizer japan Inc., novartis Pharma k.k., taiho Pharmaceutical co., Ltd., Merck serono co., Ltd., eli Lilly japan k.k., Dainippon sumitomo Pharma co., Ltd., eisai co., Ltd., Bayer yakuhin, Ltd., advisory Board of: chugai Pharmaceutical co., Ltd., novartis Pharma k.k., Bayer yakuhin,Ltd., Merck seromo co., Ltd., consulting of: eli Lilly japan k.k., yakult honsha co., Ltd., amgen, Dainippon sumitomo Pharma co., Ltd., taiho Pharmaceutical co., Ltd.. onco therapy science, Inc., nobelpharma co., Ltd.. ono Pharmaceutical co., Ltd.. nippon Boehringer Ingelheim co., Ltd., nano carrier co., Ltd., chugai Pharmaceutical co., Ltd., novartis Pharma k.k., zeria Pharmaceutical co., Ltd.
General Session 4: Diagnosis and Curative Treatment
O-023 COMPArISOnS Of OuTCOMeS AfTer LIVer reSeCTIOn fOr hePATOCeLLuLAr CArCInOMA beTWeen The eAST AnD The WeST A PrOPenSITy SCOre MATChInG AnALySIS
tian yang1, Parissa Tabrizian* 2, jun-hua Lu1, Wan-yee Lau1, kutaiba alshebeeb2, sander florman2, han zhang1, Meng-chao Wu1, feng shen1, Myron e. schwartz2
1hepatic surgery, eastern hepatobiliary surgery hospital, second Military Medical university, shanghai, china, 2transplant, recanati/Miller transplant Institute, new york, united states
Introduction: Given the considerable heterogeneity of patient populations, surgical indications, and frequently-used techniques of liver resection for hcc between the east and the West, it is unclear whether differences exist in surgical safety and long-term efficacy. this study aimed to compare perioperative and long-term outcomes after liver resection for patients with hepatocellular carcinoma (hcc) between two high-volume hepatic surgical centers respectively from the east and the West.
Methods: Data were retrospectively collected for 1,497 ethnic chinese patients undergoing curative

Oral Communications
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s2 0
Saturday, 5 September 2015
liver resection of hcc in the eastern hepatobiliary surgery hospital of shanghai, china (the east group, n = 1,229) and the Mount sinai hospital of new york (the West group, n = 268) from jan 2000 to Dec 2011. Patients’ baseline characteristics, operative variables, perioperative and long-term overall survival (os), and time-to-recurrence (ttr) were compared between these two groups. Propensity score matching analysis was used to minimize the bias in patient selection. Independent prognostic factors influencing os and ttr were identified by multivariate cox-regression analyses in the propensity-matched cohort.
results: Patients in the east group had worse liver function and more advanced tumors than those in the West group, while the latter were older, had more comorbidities, and a higher rate of hcV infection. Propensity score matching analysis created 239 pairs of patients. the overall, major, and minor morbidity rates before or after propensity matching were comparable between the two groups (all P > 0.05). Before propensity matching, patients in the east group had significantly poorer os (hr: 0.581, 95% cI: 0.467-0.724, P < 0.001) and ttr (hr: 0.831, 95% cI: 0.697-0.991, P = 0.039) than patients in the West group. however, after propensity matching, the os (hr: 0.877, 95% cI: 0.646-1.189, P = 0.396) and ttr (hr: 0.997, 95% cI: 0.786-1.264, P = 0.979) were comparable between the east and West groups (Figure 1). on multivariate cox-regression analyses, performance status 1-2, preoperative afP level > 400 ug/L, maximum tumor size > 5 cm, gross and microscopic vascular invasion, and multiple tumors were independent predictors of both os and ttr after curative resection for patients with hcc.
Image:
Conclusion: although differences existed in patient characteristics and operative variables between the eastern and Western centers, surgical safety and long-term efficacy of resection for hcc were comparable.
references: Bruix j, sherman M. Management of hepatocellular carcinoma: an update. Hepatology 2011;53:1020-1022fong zV, tanabe kk. the clinical management of hepatocellular carcinoma in the united states, europe, and asia: a comprehensive and evidence-based comparison and review. Cancer 2014;120:2824-2838torzilli G, Belghiti j, Makuuchi M. Differences and similarities in the approach to hepatocellular carcinoma between eastern and Western institutions. Liver Transpl 2004;10:s1-2esnaola nf, Mirza n, Lauwers Gy, Ikai I, regimbeau jM, Belghiti j, yamaoka y, curley sa, ellis LM, nagorney DM, Vauthey jn. comparison of clinicopathologic characteristics and outcomes after resection in patients with hepatocellular carcinoma treated in the united states, france, and japan. Ann Surg 2003;238:711-719
Disclosure of Interest: none Declared
O-024 LIquID bIOPSy TO DeTeCT AnD ChArACTerISe CIrCuLATInG TuMOur CeLLS In PATIenTS WITh hePATOCeLLuLAr CArCInOMA uSInG hIGh reSOLuTIOn IMAGeSTreAM MuLTIChAnneL fLuOreSCenT MICrOSCOPy
helen L. reeves1, 2, Laura f. Ogle* 1, Deborah stocken3, ruth Plummer1, 4, nicola curtin1, David jamieson1
1northern Institute for cancer research, newcastle university, 2Liver unit, freeman hospital, newcastle upon tyne hospitals nhs foundation trust, 3Institute of health and society, newcastle university, 4northern centre for cancer care, freeman hospital, newcastle upon tyne hospitals nhs foundation trust, newcastle-upon-tyne, united kingdom
Introduction: although biopsy of hepatocellular carcinoma (hcc) can provide information on the histopathology grade and molecular characteristics, it is not essential for diagnosis and hard to justify in the absence of a direct impact on an individuals’ care owing to risks of bleeding and tumour seeding. alternative hcc biomarkers are required to predict prognosis and stratify or monitor response to treatment. Blood is an accessible sampling method, yet clinically implemented blood test biomarkers are limited [1]. circulating tumour cells (ctcs) are cells that have been shed from the primary tumour and circulate in the peripheral blood, contributing to metastatic and recurrent disease. Identifying and characterising ctcs may have prognostic and/or predictive value. furthermore, targeting these cells may impact survival. although ctc are rare, technological advances have led to the development of more sensitive detection platforms. We have evaluated the Imagestreamχ MkII (amnis®, eMD Millipore), which combines facs with high-resolution multi-channel microscopy.
Methods: Blood samples (4ml) were from 69 hcc patients (table 1), 5 cirrhotic controls and 15 healthy volunteers. red blood cells were lysed; cD45-positive white blood cells (WBcs) were depleted immunomagnetically and platelets removed, with the maintenance of >50% ctcs. the remaining cell suspension was stained with immunofluorescent antibodies for: afP Glypican-3, epcaM, ck, Dna-Pk, cD45 and DaPI and processed through the Imagestreamχ MkII using IDeas® software.
results: ctcs were identified on the basis of cell area compared to WBcs (mean 351µm2 vs 116µm2), cD45 negativity and positive biomarker expression. Between 1 and 1642 ctcs/4ml were detected in 45/69 (65%) of hcc patient samples. ctc number correlated significantly with tumour size (0.242, p=0.04); portal vein thrombosis (PVt, 0.353, p=0.007) and child Pugh score (cPs 0.384, p=0.001). survival at 9 months in ctcs positive patients was 43% compared to 76% in ctc negative (Log rank chi-square, p=0.012), with a median overall survival from the date of blood sampling of 21.6 months versus 6 months. the presence of ctcs in the post treatment subgroup (table 1) was associated with poorer survival in multivariate (tumour size, PVt, cPs) analyses (p=0.001). for specific biomarkers, cytokeratin was expressed in 29%, epcaM in 18%, afP in 20%, glypican-3 in 12.5% and Dna-Pk in 24%. the presence of ctc-like objects negative for the classical biomarkers was associated with neutrophil count (0.297, p=0.014) and PVt (0.353, p=0.007). additional observations included lymphocyte attachment to ctcs and larger cells typical in morphology to macrophages.
Image:

Oral Communications
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 2 1
Saturday, 5 September 2015
Conclusion: ctcs were detected in two thirds of patients with hcc. Both the presence and the number of cells had prognostic value. the presence of ctc-like objects negative for classical epithelial biomarkers may represent a mesenchymal phenotype associated with vascular invasion. Dna-Pk can be detected in ctc and may have value as a predictive biomarker [2]. the clinical significance of ctc-lymphocyte interaction and associated macrophages is unknown but suggestive of immune system interplay which can be studied using IsχMkII. In combination, these data indicate exciting potential for ctc detection and characterisation as a liquid biopsy tool that will impact the management of patients with hcc.
references: 1. sherman, M., Alphafetoprotein: an obituary. j hepatol, 2001. 2. cornell, L., DNA-PK-A Candidate Driver of Hepatocarcinogenesis and Tissue Biomarker That Predicts Response to Treatment and Survival. clin can res, 2015.
Disclosure of Interest: none Declared
O-025 DISenTAnGLInG The effeCTS Of rACe/eThnICITy AnD SOCIOeCOnOMIC fACTOrS On LIVer TrAnSPLAnTATIOn rATeS fOr hePATOCeLLuLAr CArCInOMA
umut Sarpel* 1, Maria suprun2, anastasia sofianou 3, yaniv Berger1, andreas tedjasukmana4, zennur sekendiz5, emilia Bagiella 2, Myron e. schwartz6
1Department of surgery, Division of surgical oncology, 2Department of Population, health science and Policy, 3Department of strategic Planning, 4Department of neurosurgery, Mount sinai Medical center, new york, ny, united states, 5ross university, roseau, Dominica, 6the recanati / Miller transplantation Institute, Mount sinai Medical center, new york, ny, united states
Introduction: Liver transplantation offers the highest survival rate for eligible patients with hepatocellular carcinoma (hcc) but is not equally accesses by all groups. the primary aim of this study was to explore transplantation rates at a large hcc treatment center with specific focus on the effects of race/ethnicity and socioeconomic factors while controlling for tumor stage and liver function. We also sought to identify at what specific time point these effects occurred. additional outcomes of interest were the characteristics of individuals who failed to progress past initial diagnosis or who were excluded from the transplant waiting list, and the effect of race on resection in transplant-eligible patients.
Methods: a query of the electronic medical records was performed to identify all patients with hcc diagnosed 2003-2013. eligibility for transplantation was defined as tumor stage within Milan criteria, age ≤70, and an absence of contraindicated comorbidities. Patient visits along the transplant pathway were identified as: initial diagnosis, transplant specialist visit, formal transplant evaluation, unos listing, and transplantation. analyses were performed to identify predictors of transplantation among eligible patients, excluding those who were resected, while controlling for liver function and tumor stage.
results: out of 3,078 patients with confirmed hcc, 754 (24%) individuals were considered eligible for liver transplantation and of these 289 (38%) were ultimately transplanted. Multivariate analysis, which adjusted for tumor stage and underlying liver disease, demonstrated that commercial insurance (or=1.99, 95% cI [1.42, 2.79]) was associated with significantly higher odds of transplantation, whereas the odds of transplantation were lower for black patients (or=0.55, 95% cI [0.33, 0.91]), asians (or=0.58, 95% cI [0.33, 1.03]) and older patients (or=0.98, 95% cI [0.96, 1.00]). no individual step in the transplantation pathway was identified as being the dominant hurdle (figure 1). Patients who did not progress after diagnosis were more likely to be nonwhite (p-value=0.06), older than 70 years of age, have government insurance, and have advanced stage disease (p-values<0.001). Patients excluded from the transplantation process for nonmedical reasons were also more likely to be nonwhite (p=0.05) and government-insured (p=0.02). asian patients were more likely to undergo resection than their non-asian counterparts with similarly-staged tumors and eligibility characteristics (or=7.57, 95%cI [4.80, 11.95]).
Image:
Conclusion: Patients who are black or asian, and those insured by Medicaid or Medicare only are significantly less likely to receive liver transplantation for hcc, even when rigorously controlling for tumor stage and liver function. these individuals are also more likely to fail to progress past initial diagnosis, and to be excluded from the transplantation process for nonmedical reasons. no specific step along the path to transplantation was identified as the dominant hurdle. asian patients have lower transplantation rates, above and beyond the effect of higher resectability rates. While the reasons for worse hcc survival among certain groups are multiple and complex, some of the observed disparity is due to decreased rates of transplantation by racial minorities and those who are covered by government insurance.
Disclosure of Interest: none Declared
O-026 CAn MeLOxICAM, A COx-2 InhIbITOr, PreVenT hePATOCeLLuLAr CArCInOMA reCurrenCe AfTer InITIAL CurATIVe TreATMenT?
A reSuLT Of rAnDOMISeD COnTrOLLeD TrIAL
yuko Takami* 1, Masaki tateishi1, tomoki ryu1, kazuhiro Mikagi1, yoshiyuki Wada1, hideki saitsu1
1Department of hepato-Billiary-Pancreatic surgery, kyushu medical center, fukuoka, japan
Introduction: the recurrence rate of hepatocellular carcinoma (hcc) is high, even after curative treatments such as hepatic resection and microwave ablation. so we need chemopreventions that can effectively suppress hcc recurrence. cyclooxygenase-2 (cox-2) was recently found to be overexpressed in hcc. therefore, cox-2 inhibitors may offer a chemopreventive therapy for hcc. In this randomised controlled trial (rct) study, we evaluate the potential for meloxicam, a clinically used cox-2 inhibitor, to prevent hcc recurrence after initial curative treatment.
Methods: 232 consecutive patients underwent hepatic resection and/or microwave ablation as initial therapy for hcc at our institute between july 2008 and april 2011. 8 patients were excluded because of poor renal function, history of non-steroidal anti-inflammatory drug-related ulceration, or multiple cancers. the remaining 224 patients were randomised to a control group (n=113) or a meloxicam group (n=111). to patients of meloxicam group, meloxicam was administered at 15 mg daily (5 mg three times a day) as long as possible. the overall survival (os) and disease-free survival (Dfs) rates were determined.
results: the 1-, 3-, and 5-year os rates of meloxicam group were 95.4%, 82.4%, and 70.1%. those of control group were 98.2%, 85.1%, and 71.5% (P=0.9549). the corresponding Dfs rates of meloxicam group were 89.2%, 53.9%, and 44.0% and those pf control group were 86.5%, 57.0%, and 43.4% (P=0.6722). In os and Dfs among in patient groups, including those with hepatitis B or c virus infection, we could not find significant differences between the meloxicam and control groups. But in the subgroup of analysis of hcc patients without virus hepatitis (nonB-nonc hcc), significant differences were observed in Dfs between meloxicam group (1-year Dfs, 92.3%; 3-year Dfs, 75.8%; 5-year Dfs, 70.4%) and control group (1-year os, 83.3%; 3-year os, 48.1%; 5-year os, not obtained) (P=0.0211).
Conclusion: administration of the cox-2 inhibitor meloxicam may suppress recurrence after initial curative treatments in patients with nonB-nonc hcc.
Disclosure of Interest: none Declared
O-027 PrOSPeCTIVe PILOT STuDy Of LIVInG DOnOr LIVer TrAnSPLAnTATIOn fOr PATIenTS WITh hCC exCeeDInG MILAn CrITerIA
Josep Maria Llovet* 1, Mihai Pavel2, jordi rimola3, Maria alba Diaz4, jordi colmenero5, constantino fondevila6, josep fuster7, Pere Ginès5, jordi Bruix8, juan carlos Garcia-Valdecasas6
1Barcelona-clínic Liver cancer Group (BcLc), Liver unit, Institut d'Investigacions Biomèdiques august Pi i sunyer (IDIBaPs), cIBerehD, universitat de Barcelona and Institució catalana de recerca i estudis avançats, 2Liver transplant unit, Digestive and Metabolic Diseases Institute, 3Liver unit, Barcelona-clínic Liver cancer Group (BcLc,Institut d'Investigacions Biomèdiques august Pi i sunyer (IDIBaPs), cIBerehD, universitat de Barcelona, 4Pathology Department, hospital clínic, university of Barcelona, 5Liver transplant unit and Liver unit, 6Liver transplant unit, Digestive and Metabolic Diseases Institute. hospital clínic, university of Barcelona, 7Liver transplant unit and Liver unit, Barcelona-clínic Liver cancer Group (BcLc) Institut d'Investigacions Biomèdiques august Pi i sunyer (IDIBaPs), cIBerehD, universitat de Barcelona and Digestive and Metabolic Diseases Institute hospital clínic, university of Barcelona, 8Liver unit, Barcelona-clínic Liver cancer Group (BcLc), Institut d'Investigacions Biomèdiques august Pi i sunyer (IDIBaPs), cIBerehD, universitat de Barcelona and Digestive and Metabolic Diseases Institute. hospital clínic, university of Barcelona, Barcelona, spain
Introduction: Liver transplantation is the standard of care for patients with hepatocellular carcinoma (hcc) within Milan criteria not suitable for resection. nonetheless, during the last 20 years it became apparent that a subset of patients beyond Milan criteria might obtain acceptable survival outcomes. In parallel, living donor liver transplantation has emerged as a feasible alternative to overcome the paucity of donors.

Oral Communications
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s2 2
Saturday, 5 September 2015
Methods: In 2002, we proposed for LDLt in child a-B patients with hcc a set of criteria that substantially expanded the conventional indications of transplantation (1 tumor up to 7cm, 5 tumors of < 3cm, 3 tumors < 5cm, or downstaging to Milan lasting 6 mo after loco-regional therapies) (Bruix& Llovet, hepatology 2002).
results: We herein present a prospective cohort of 22 patients with hcc fulfilling these criteria that were treated with LDLt between 2002 and 2014. Median age was 57 yrs, 20 men, hcV related 14, child-Pugh a:16, B:6, afP <100ng/mL: 21. Median time between pre-operative ct/MrI and transplant was of 2 mo; 12 patients received loco-regional therapies. at the time of LDLt, 10 cases presented downstaging and 12 were beyond Milan criteria. Pathological report showed that 12 patients (54%) exceeded our selection of expanded criteria. Perioperative mortality was 0%. after a median follow up of 78 mo, 7 patients have died, the 1-, 3-, 5- and 10-year survival was 95%, 84%, 77% and 69%, respectively. overall, 4 patients recurred (range 9-108 mo), the 5-y and 10-yr actuarial recurrence rate was of 13% and 25%. Perioperative complications occurred in 15 cases (13 with biliary leaks).
Conclusion: In conclusion, a proper selection of candidates for extended indications for LDLt of hcc patients provides long-term outcomes comparable to those obtained within Milan criteria. these criteria can be adopted by transplant units in the setting of research programs prior to be incorporated into guidelines once the results are confirmed.
Disclosure of Interest: none Declared
O-028 LIVer TrAnSPLAnTATIOn VerSuS reSeCTIOn fOr SMALL InTrAhePATIC ChOLAnGIOCArCInOMA Or hePATOChOLAnGIOCArCInOMA On CIrrhOSIS
eleonora De Martin1, 2, 3, Michel rayar4, 5, 6, Damien Bergeat7, Luis carvalho4, Maximiliano Gelli1, rené adam1, 8, 9, Denis castaing1, Daniel cherqui1, 8, 9, antonio sa cunha1, 8, 9, Didier samuel1, emmanuel Boleslawski10, 11, karim Boudjema4, 5, 6, eric Vibert *1, 2, 3
1centre hépato Biliaire, aP-hP hopital Paul Brousse, 2uMr-s1193, univ Paris-sud, 3unit 1193, Inserm, VILLejuIf, 4service de chirurgie hépatobiliaire et Digestive, chu de rennes - hopital Pontchaillou, 5université de rennes 1, 6uMr991, Inserm, 7service de chirurgie Digestive et transplantations, chu de Lille - hopital claude huriez, rennes, 8univ Paris-sud, 9Inserm, VILLejuIf, 10service de chirurgie Digestive et transplantations, chu de Lille - hopital claude huriez, 11univ nord-de-france, Lille, france
Introduction: Liver transplantation for small intrahepatic cholangiocarcinoma (icca) and/or hepatocholangiocarcinoma (hca) on cirrhosis is still debated. this multicentric study aimed to evaluate the long-term outcome of cirrhotic patients transplanted or resected with icca or hca discovered on the specimen.
Methods: Between 2002 and 2014, all cirrhotic patients transplanted for incidental icca or hca were identified in 3 french tertiary hPB centers. clinical, biological, histological data and long term outcome were analyzed and compared with cirrhotic patients who were resected for small icca or hca inferior to 5 cm. uni- and multivariate analysis were performed to identify prognostic factors of survival.
results: overall, 60 cirrhotic patients were identified with icca (n=44-73%) or hca (n=16-27%). the tumor was either resected (rs)(n=22-36%) or incidentally discovered in the explant after Lt (n=38-63%). Patients’ characteristics are summarized in table 1. there was no significant difference according to patient’s age, sex, BMI, etiology of cirrhosis, histological type of the tumor (icca versus hca), presence of a single or multiple nodules and afP level between Lt and rs patients. MeLD score was significantly higher in Lt patients. number of nodules was higher in Lt patients (2 [1-11] versus 1 [1-9] p=.0001), diameter of the biggest lesion was larger in rs patients (31 [15-50] versus 19 [5-40] p=.0001). Median follow-up was similar in both groups, (37 [5-126] months vs. 26 [2-122] months for Lt and rs patients, respectively (p=.238). the 3 months post-operative mortality was nil after Lt or after resection. overall patient survival at 1, 3 and 5 years was significantly better after Lt as compared to rs (92%, 79% and 75% versus 89%, 59% and 34% respectively, p=.030). recurrence at 1, 3 and 5 years was significantly lower in Lt compared to rs (11%, 15% and 20% versus 31%, 58% and 66%, respectively p=.001). In the multivariate analysis, Lt was the only independent predictive factor of better overall survival and lower recurrence rate.
Image:
Conclusion: Good long-term survival and low recurrence rate after Lt comparatively to liver resection confirm that small nodule of intrahepatic cholangiocarcinoma or hepatocholangiocarcinoma on cirrhosis should become a validate indication of Lt.
Disclosure of Interest: none Declared

Oral Communications
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 2 3
Sunday, 6 September 2015
General Session 5: from Drivers to Clinical Trials
O-029 TIVAnTInIb In PreTreATeD hePATOCeLLuLAr CArCInOMA (hCC): TuMOr AnD PLASMA bIOMArKer AnALySIS frOM The rAnDOMIzeD COnTrOLLeD PhASe 2 TrIAL (rCT)
Lorenza rimassa* 1, Giovanni abbadessa2, nicola Personeni1, 3, camillo Porta4, Ivan Borbath5, Bruno Daniele6, stefania salvagni7, jean Luc Van Laethem8, hans Van Vlierberghe9, joerg trojan10, enrico De toni11, alan Weiss12, steven Miles13, antonio Gasbarrini14, Monica Lencioni15, Maria e. Lamar16, yunxia Wang17, reinhard Von roemeling18, Brian schwartz16, armando santoro1
1humanitas cancer center, humanitas clinical and research center, rozzano, Italy, 2clinical Development & translational Medicine, arqule, Burlington, Ma, united states, 3Department of Medical Biotechnology and translational Medicine, university of Milan, Milan, 4oncologia Medica, fondazione Irccs Policlinico universitario san Matteo, Pavia, Italy, 5Gastro-entérologie, cliniques universitaires saint-Luc, Brussels, Belgium, 6oncology, G. rummo hospital, Benevento, 7oncologia Medica, azienda ospedaliera Parma, Parma, Italy, 8Gastro-entérologie, erasme university hospital, Brussels, 9Gastro-entérologie, Ghent university hospital, Gent, Belgium, 10Internal Medicine, j. W. Goethe university hospital, frankfurt, 11Medicine II, klinikum der universitat Munchen-Groshadern, Munich, Germany, 12Gastroenterology, Vancouver General hospital and British columbia cancer clinic, Vancouver, canada, 13oncology, cedar sinai, Los angeles, ca, united states, 14Patologia speciale Medica e semeiotica Medica, Policlinico universitario agostino Gemelli, rome, 15oncology, azienda ospedaliero-universitaria di Pisa, Pisa, Italy, 16clinical Development, 17Pharmacology, arqule, Burlington, Ma, 18clinical Development, Daiichi-sankyo, edison, nj, united states
Introduction: tivantinib is an oral inhibitor of Met, the tyrosine kinase receptor for hepatocyte growth factor. tivantinib has shown activity in Met-high patients in randomized, placebo controlled studies in hcc, nscLc, crc, and prostate cancer. arq 197-215 was a multi-center rct which enrolled 107 second-line hcc patients randomized 2:1 to oral tivantinib capsules or placebo. the primary endpoint of time to progression (ttP) in the intent-to-treat (Itt) population and the pre-determined secondary efficacy endpoints defined by Met status were reached, Met was also found to be a strong independent prognostic factor (1).
Methods: Met tumor status was determined with strict immunohistochemistry criteria (Met ≥2+ in ≥50% of tumor cells) using the Ventana sP-44 antibody. circulating Met, hGf, and afP were tested in plasma, and median values were used as cut-offs to determine high or Low status except for afP, where 75th percentile was used.
results: the interaction test between treatment and tumor Met levels in os was positive (p=0.0385). Median immunohistochemistry score (h-score) was 175 for Met-high, 40 for Met-Low patients, and 62% of evaluable samples were from biopsies taken before treatment with sorafenib. Met was found to be highly expressed in 40% of biopsies taken before and in 82% of biopsies taken after sorafenib. circulating baseline Met was prognostic (os: 4.57 vs 8.90 months in high vs Low, hr=0.61, p=0.026) and trended towards predicting tivantinib’s activity. circulating baseline hGf was prognostic (os: 4.96 vs 9.00 months in high vs Low, hr=0.6, p=0.02) and changes over time correlated with tumor response. afP was prognostic (os: 3.04 vs 7.66 months in high vs Low, hr=0.36, p<0.0001). no biomarker except for tumor Met was predictive of response to tivantinib.
Conclusion: tumor Met was highly prognostic and predictive of response to tivantinib. the ongoing MetIV-hcc phase 3 study will elucidate further the role of tivantinib, of Met, as well as tumor biology in this patient population.
references: 1. santoro a, rimassa L, Borbath I, et al. Lancet oncol 2013;14:55-63
Disclosure of Interest: L. rimassa: none Declared, G. abbadessa stocks of: arqule employee, n. Personeni: none Declared, c. Porta: none Declared, I. Borbath: none Declared, B. Daniele consulting of: Bayer, s. salvagni: none Declared, j. L. Van Laethem: none Declared, h. Van Vlierberghe: none Declared, j. trojan advisory Board of: Bayer, Lilly, BMs, e. De toni: none Declared, a. Weiss: none Declared, s. Miles: none Declared, a. Gasbarrini: none Declared, M. Lencioni: none Declared, M. Lamar stocks of: arqule employee, y. Wang stocks of: arqule employee, r. Von roemeling stocks of: Daiichi-sankyo employee, B. schwartz stocks of: arqule employee, a. santoro consulting of: BMs, Gsk, arqule, takeda, roche
O-030 fGf19 AberrATIOnS AnD SeLeCTIVe TArGeTInG WITh fGfr4 InhIbITOrS fOr hePATOCeLLuLAr CArCInOMA
klaus hoeflich* 1, agrin Moeini2, Margit hagel1, chandra Miduturu1, Daniela sia2, roser Pinyol3, judit Peix3, qiongfang fong1, nicolas stransky1, oleg schmidt-kittler1, josep Llovet2, christoph Lengauer1, ben Wolf *1
1Blueprint Medicines, cambridge, 2Mount sinai Liver cancer Program, Icahn school of Medicine at Mount sinai, new york, united states, 3Liver cancer translational research Laboratory, BcLc group, Institut d'Investigacions Biomèdiques august Pi i sunyer (IDIBaPs)- hospital clínic, Liver unit, universitat de Barcelona, Barcelona, spain
Introduction: Limited treatment options are available for patients with advanced hepatocellular carcinoma (hcc), and the multi-kinase inhibitor sorafenib remains the only approved standard of care. however, molecularly stratified treatment schemes are being developed for hcc and hold promise to benefit patients. for instance, fibroblast growth factor 19 (fGf19), the ligand for fibroblast growth factor receptor 4 (fGfr4), has been linked to hcc tumorigenesis in vivo. We aimed to establish the prevalence of fGf19 aberrations in hcc patients and to evaluate the efficacy of a novel selective fGfr4 inhibitor in hcc xenograft and PDx models with activated fGf19/fGfr4 signaling.
Methods: a cohort of 143 hcc samples collected in the setting of the hcc genomic consortium (hePtroMIc dataset) was analyzed for expression and copy number alterations of fGf19/fGfr4 pathway components using microarray data. real-time Pcr (qPcr and qrt-Pcr) was performed to validate fGf19, kLB and fGfr4 copy number and expression. fGf19 amplification was further confirmed by fIsh analysis. Gene set enrichment analysis (Gsea) and nearest template prediction (ntP) algorithms were used to further characterize the molecular profile of tumors with aberrant fGf19 expression. structure-based design principles were used to develop a potent and selective fGfr4 inhibitor. Its efficacy was then evaluated in vitro and in vivo using fGfr-driven hcc cell lines and mouse xenografts.
results: overall, 23% of hcc cases (33/143) overexpressed FGF19 (fold change≥4) when compared to adjacent non-tumoral tissue. focal high level amplification (hLa) of FGF19 was detected in 11 cases (11/143, 8%), and 9 of them showed significant overexpression of fGf19 compared to patients without amplification (median fold change 114 vs. 14, p<0.01). fIsh analysis further confirmed the presence of FGF19 amplification and was significantly correlated with fGf19 mrna levels (spearman rho: 0.675, p<0.01). In addition, patients with FGF19 amplification were significantly associated with molecular signatures of aggressive hcc (proliferation, s1 and s2 subclasses). Patients with fGf19 overexpression showed enrichment of activated fGfr downstream signaling and downregulation of bile acid synthesis gene sets (p<0.05, fDr<0.05). taken together, this suggests that fGfr4 inhibition might be an effective treatment strategy in hcc patients whose tumors have an active fGf19/fGfr4 signaling axis. notably, we have recently developed a potent, irreversible and exquisitely selective small molecule inhibitor of fGfr4, BLu9931. hcc cell lines with an activated fGfr4 signaling pathway displayed apoptosis and decreased proliferation following treatment with BLu9931. In vivo, fGfr4 inhibition resulted in dose-dependent tumor growth inhibition in a hcc xenograft model, and a subset of tumor-bearing mice experienced complete remission for 30 days after cessation of treatment. Moreover, BLu9931 resulted in tumor growth inhibition exceeding that of sorafenib in a fGfr4-dependent, patient-derived hcc xenograft model.
Conclusion: our findings suggest that 23% of hcc patients present aberrant expression of fGf19, and may respond to specific fGfr4 inhibition. BLu9931, a potent selective inhibitor of fGfr4 demonstrated efficacy in vitro and in vivo. the first-in-human study of BLu-554, a clinical candidate derived from BLu9931, is anticipated to begin this year in molecularly stratified hcc patients.
Disclosure of Interest: k. hoeflich stocks of: Blueprint Medicines, a. Moeini: none Declared, M. hagel stocks of: Blueprint Medicines, c. Miduturu stocks of: Blueprint Medicines, D. sia: none Declared, r. Pinyol: none Declared, j. Peix: none Declared, q. fong stocks of: Blueprint Medicines, n. stransky stocks of: Blueprint Medicines, o. schmidt-kittler stocks of: Blueprint Medicines, j. Llovet consulting of: Blueprint Medicines, c. Lengauer stocks of: Blueprint Medicines
O-031 PreOPerATIVe SOrAfenIb-InDuCeD AnTITuMOr ACTIVITy In PATIenTS WITh reSeCTAbLe hePATOCeLLuLAr CArCInOMA (hCC): reSuLTS Of The bIOShAre neOADJuVAnT PhASe 2 STuDy frOM GerCOr IrC
Mohamed bouattour* 1, Laetitia fartoux2, olivier rosmorduc2, eric Vibert3, charlotte costentin4, olivier soubrane5, Maxime ronot6, Muriel Granier7, armand De Gramont7, jacques Belghiti5, Valérie Paradis8, annemilaï tijeras-raballand9, alexandra hadengue10, David Brusquant10, Benoist chibaudel10, eric raymond7, sandrine faivre7
1hepatology, Beaujon university hospital, clichy, 2hepatology, saint-antoine university hospital, Paris, 3hepato-Biliary surgery, Paul-Brousse university hospital, Villejuif, 4hepatology, henri-Mondor university hospital, creteil, 5hepato-Biliary surgery, 6radiology, Beaujon university hospital, clichy, france, 7Medical oncology, centre hospitalo-universitaire Vaudois (chuV), Lausanne, switzerland, 8Pathology, Beaujon university hospital, clichy, 9aarec fILIa research, 10Gercor, Paris, france
Introduction: neoadjuvant therapy offers the opportunity of investigating new agents in early stage and allows direct access to tumor biology. this open-label, multicenter, phase II study aimed at investigating the activity of sorafenib including radiological, pathological and molecular changes in tumor from patients with resectable hcc.
Methods: a preoperative treatment consisting of 400 mg bid orally sorafenib was administered for 4 consecutive weeks followed by surgery 1 week after sorafenib discontinuation. Primary endpoints were antitumor activity and histological changes between paired biopsies and plasma biomarkers, from baseline and post sorafenib treatment. secondary endpoints were safety profile, r0 surgery along with post-surgical complications. residual disease characteristics were analyzed on surgical specimens.
results: among 30 patients enrolled, 29 were included (1 screen failure), 1 patient decided to stop

Oral Communications
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s2 4
Sunday, 6 September 2015
study after the first treatment dose, and 28 were evaluable for safety. neoadjuvant sorafenib was not feasible in 3 patients who presented limiting toxicities: grade 3 hand food syndrome (2 patients at day 10 and 12) and grade 3 hypertension (1 patient at day 14). twenty five patients (21 men; median age: 61.5 years) were evaluable for the primary endpoints. all evaluable patients were child Pugh a, 14 (56%) with chronic liver disease, 9 (36%) with cirrhosis and 2 patient (8%) with no underlying liver disease. the baseline median tumor size was 37 mm (17-220 mm) and 21 patients (84%) had a single lesion. the median duration and dosing of sorafenib for evaluable patients were 28 days (21-35d) and 793 mg/day (477 – 843 mg/day) respectively. overall, the safety profile of preoperative sorafenib was good. according to recIst criteria, all evaluable patients showed stable disease after 4 weeks of sorafenib. among 14 patients evaluated according to mrecIst and choi criteria, objective responses were observed for 4 (29%) and 7 (50%) patients respectively. all evaluable patients went on liver resection; median hospitalization duration was 8 days (4-59d) and no unexpected postoperative complication was observed (4 patients experienced post-operative ascites). r0 tumor resection was achieved in 22 patients (88%). surgical specimen showed macrovascular and microvascular invasion as well as satellite nodules in 12%, 48%, and 36% respectively. Intratumor necrosis was observed in 13 patients of 20 evaluable patients. Biomarkers from pre- and post-treatment tissue (Vimentin, ck19, e-cadherin, n-cadherin, ck7, MIB1, cD31, VeGf, cD133, ca9, p-s6, c-Met, cxcr4) and plasma (VeGf-c, ang2, PlGf, c-kIt, sDf-1, hGf, tGfb1) are currently assessed and will be presented during the meeting.
Conclusion: Preoperative BIoshare trial showed appropriate safety regarding both tolerance to sorafenib and surgical procedures. short term neoadjuvant treatment with sorafenib showed promising efficacy in terms of tumor response (mrecIst and choi) and will allow detailed evaluation of molecular changes in patient tumor tissues.
Disclosure of Interest: M. Bouattour honoraria support from: Bayer healthcare Pharmaceuticals, advisory Board of: Bayer healthcare Pharmaceuticals, L. fartoux: none Declared, o. rosmorduc: none Declared, e. Vibert: none Declared, c. costentin: none Declared, o. soubrane: none Declared, M. ronot: none Declared, M. Granier: none Declared, a. De Gramont: none Declared, j. Belghiti: none Declared, V. Paradis: none Declared, a. tijeras-raballand: none Declared, a. hadengue: none Declared, D. Brusquant: none Declared, B. chibaudel: none Declared, e. raymond: none Declared, s. faivre: none Declared
O-032 rAnDOMIzeD PhASe IIb STuDy Of PexA-VeC (PexASTIMOGene DeVACIrePVeC; Jx-594), An OnCOLyTIC IMMunOTherAPy PLuS beST SuPPOrTIVe CAre (bSC) VerSuS bSC ALOne In PATIenTS WITh hePATOCeLLuLAr CArCInOMA (hCC) WhO fAILeD SOrAfenIb TreATMenT (TrAVerSe)
Markus Moehler* 1, han chu Lee2, Won young tak3, yee chao4, seung Woon Paik5, ari Baron6, Guy ungerechts7, jean-frederic Blanc8, Mong cho9, Laura findeiss10, francois habersetzer11, Derek jonker12, Philippe Merle13, Leyo ruo14, oliver ebert15, tony reid16, riccardo Lencioni17, adina Pelusio18, Monika Lusky19, nicolas stojkowitz19, Marie hennequi19, David h. kirn18, jean-Marc Limacher19, caroline j. Breitbach18, Michel homerin19, james Burke18, jeong heo20
1johannes Gutenberg-universität Mainz, Mainz, Germany, 2asan Medical center, seoul, 3kyungpook national university Medical center, Daegu, korea, republic of, 4taipei Veterans General hospital, taipei, taiwan, 5samsung Medical center, seoul, korea, republic of, 6california Pacific Medical center, san francisco, united states, 7national center for tumor Diseases, Dkfz, heidelberg, Germany, 8centre hospitalier universitaire hôpital saint andré, Bordeaux, france, 9Pusan national university yangsan hospital, yangsan, korea, republic of, 10university of california Irvine Medical center, orange, united states, 11hôpitaux universitaires de strasbourg- hôpital civil, strasbourg, france, 12the ottawa hospital regional cancer centre, ottawa, canada, 13hôpital de la croix rousse, Lyon, france, 14juravinski hospital and cancer centre, hamilton, canada, 15klinikum rechts der Isar, technische universität München, München, Germany, 16university of california san Diego Moores cancer center, san Diego, united states, 17Pisa university school of Medicine, Pisa, Italy, 18sillajen, san francisco, united states, 19transgene, Illkirch-Graffenstaden, france, 20Pusan national university hospital, Busan, korea, republic of
Introduction: Pexa-Vec is an oncolytic immunotherapy based on a vaccinia virus attenuated by thymidine kinase inactivation and engineered to express granulocyte-macrophage colony stimulating factor (GM-csf). oncolysis plus GM-csf expression stimulates tumor vascular disruption and anti-tumor immunity. Pexa-Vec was well-tolerated in Phase I trials and was shown to replicate in metastatic tumors following intratumoral (It) or intravenous (IV) administration. a randomized dose ranging (108 plaque forming unites [pfu] vs 109 pfu) Phase II trial in 30 patients with primarily sorafenib-naïve hcc demonstrated prolonged survival in the high-dose Pexa-Vec arm (median overall survival (os) 14.1 vs 6.7 mo; hr 0.39, p=0.02).
Methods: traVerse was a prospective, multinational randomized Phase IIb study in patients with hcc who had failed sorafenib treatment. Patients were randomized 2:1 to Pexa-Vec plus Bsc versus Bsc. Patients randomized to Pexa-Vec received a dose of 109 pfu IV on Day 1 followed by up to 5 It treatments (109 pfu) between Day 8 and Week 18. the primary objective was to determine os. secondary objectives included time-to-tumor progression (ttP) based on modified recIst for hcc, disease control rate and safety & tolerability. Main inclusion criteria were advanced hcc having failed sorafenib (intolerance or radiographic progression), child-Pugh a-B7 (no ascites), and adequate organ function.
results: a total of 129 caucasian and asian patients (86/43 arm a/B) were randomized between oct 2011 and jun 2013. In arm a, 11 of 86 randomized patients (13%) received all 6 planned treatments; and 49% received at least 3 It treatments (1 IV plus 3 It) as administered in previous Pexa-Vec hcc trials. Median os for arm a was 4.2 months vs 4.4 months for arm B (p=0.426, hr=1.19; 95% cI: 0.78-1.80). ttP based on mrecIst criteria was 1.8 months vs 2.8 months for Pexa-Vec vs Bsc, respectively (p=0.478; hr 1.33; 95% cI: 0.61-2.90). however, due to a high and unbalanced censoring rate for analyses of ttP in arm a and arm B (44 vs 79%, respectively) these results should be interpreted with caution. the overall disease control rate was 13 vs 19% for arm a vs arm B, respectively. the most frequent adverse events (≥25%) in arm a vs arm B were pyrexia (80 vs 12%), chills (52 vs 4%), abdominal pain (38 vs 32%), decreased appetite (37 vs 12%), nausea (36 vs 16%), hypotension (29vs 12%), pustular rash (29vs 0%), anemia (26 vs 16%), fatigue (26 vs 8%) and ascites (25 vs 32%).
Conclusion: treatment with Pexa-Vec was generally well-tolerated and the ae profile in this study is generally consistent with previous trials. Pexa-Vec did not improve os or other efficacy measures vs Bsc in patients with 2nd line advanced hcc. several factors may have contributed to the study results including the limited number of patients completing treatment on arm a, the high percentage of radiographically non-evaluable patients, and the relatively more advanced hcc patient population on this study as suggested by the significantly shorter median os (4.2 vs 4.4 months on arms a and B, respectively) observed here vs what has been reported in other studies in second line hcc (~7-9 mos). as has been the experience with other immunotherapies, the traVerse results suggest that less advanced patients may be more likely to benefit from an oncolytic immunotherapy, as reported in our Phase 2 trial in predominantly sorafenib naïve patients. further development of Pexa-Vec will be pursued in 1st line hcc, for which a Phase III trial will be initiated.
Disclosure of Interest: M. Moehler: none Declared, h. c. Lee: none Declared, W. y. tak: none Declared, y. chao: none Declared, s. W. Paik: none Declared, a. Baron: none Declared, G. ungerechts: none Declared, j.-f. Blanc: none Declared, M. cho: none Declared, L. findeiss: none Declared, f. habersetzer: none Declared, D. jonker: none Declared, P. Merle: none Declared, L. ruo: none Declared, o. ebert: none Declared, t. reid: none Declared, r. Lencioni: none Declared, a. Pelusio stocks of: employee, M. Lusky: none Declared, n. stojkowitz stocks of: employee, M. hennequi stocks of: employee, D. kirn stocks of: stock holder, j.-M. Limacher stocks of: employee, c. Breitbach stocks of: employee, M. homerin stocks of: employee, j. Burke stocks of: employee, j. heo: none Declared
O-033 rAMuCIruMAb (rAM) AS SeCOnD-LIne TreATMenT In PATIenTS (PTS) WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA (hCC): JAPAneSe SubGrOuP AnALySIS Of The PhASe III reACh TrIAL
etsuro hatano* 1, Masatoshi kudo2, takuji okusaka3, shinichi ohkawa4, hirofumi fujii5, akihide Masumoto6, junji furuse7, yoshiyuki Wada8, hiroshi Ishii9, shuntaro obi10, kuniaki arai11, seiji kawazoe12, osamu yokosuka13, Masafumi Ikeda14, katsuaki ukai15, sojiro Morita16, hiroya asou17, Paolo B. abada18, Ling yang19, andrew x. zhu20
1kyoto university hospital, kyoto, 2kinki university school of Medicine, osaka, 3national cancer center hospital, tokyo, 4kanagawa cancer center, kanagawa, 5jichi Medical university, tochigi, 6aso corporation Iizuka hospital, fukuoka, 7kyorin university hospital, tokyo, 8national hospital organization kyushu Medical center, fukuoka, 9the cancer Institute hospital of japanese foundation for cancer research, 10kyoundo hospital, sasaki Institute, tokyo, 11kanazawa university hospital, Ishikawa, 12saga-ken Medical centre, 13chiba university hospital, 14national cancer center hospital east, chiba, 15sendai Medical center, Miyagi, 16kochi health sciences center, kochi, 17eli Lilly and company, kobe, japan, 18eli Lilly and company, Indianapolis, In, 19eli Lilly and company, Bridgewater, nj, 20Massachusetts General hospital, cancer center, harvard Medical school, Boston, united states
Introduction: the reach trial did not demonstrate a statistically significant improvement of overall survival (os) in the second-line treatment of pts with advanced hcc in the intent-to-treat (Itt) population (n=565). In pts with elevated (≥400 ng/mL) baseline alpha-fetoprotein (afP), a significant os improvement in the raM arm was demonstrated (1). results from a japanese subgroup analysis are presented.
Methods: os and progression-free survival (Pfs) were evaluated by kaplan-Meier method and hazard ratios (hrs) calculated using a cox regression model. Log-rank test was used to compare treatment arms. objective response rates (orrs) were compared using the cochran-Mantel-haenszel test. clinicaltrials.gov number nct01140347.
results: In the 93 Itt japanese pts, baseline pt characteristics were generally balanced between treatment arms, and most prognostic factors were similar to those of the Itt population. Median os was 12.9 months for the raM arm (n=45) and 8.0 months for the placebo (PBo) arm (n=48) (delta: 4.9 months, hr: 0.621, 95% cI: 0.391-0.986, p=0.0416). Median Pfs was 4.1 months for the raM arm and 1.7 months for the PBo arm (delta: 2.4 months, hr: 0.449, 95% cI: 0.285-0.706, p=0.0004). orrs were 11% (95% cI: 4.8-23.5) for the raM arm and 2% (95% cI: 0.4-10.9) for the PBo arm (p=0.0817). of japanese pts who received at least one dose of treatment (n=91), grade ≥3 treatment-emergent adverse events occurring in >5% of pts with a higher incidence for raM (n=44) than PBo (n=47) were ascites (3 [7%] vs. 1 [2%]), hypertension (3 [7%] vs. 1 [2%]), and cholangitis (3 [7%] vs. 0). In japanese pts with baseline afP ≥400 ng/mL, median os was 12.9

Oral Communications
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 2 5
Sunday, 6 September 2015
months for the raM arm (n=20) and 4.3 months for the PBo arm (n=22) (delta: 8.6 months, hr: 0.464, 95% cI: 0.232-0.926, p=0.0263).
Conclusion: In the japanese pts of the reach trial, raM improved os, Pfs, and orr, and demonstrated an acceptable safety profile. In japanese pts treated with raM with baseline afP ≥400 ng/mL, the results suggest an even greater os benefit. further evaluation of raM in japanese pts is warranted.
references: 1. zhu et al. j clin oncol 33, 2015, suppl 3; abstr 232.
Disclosure of Interest: e. hatano: none Declared, M. kudo: none Declared, t. okusaka research/education support from: chugai Pharmaceutical co., Ltd., eli Lilly japan k.k., eisai co., Ltd., novartis Pharma k.k., shizuoka Indusgtry, takeda Bio Development center Limited, yakult honsha co., Ltd., onco theapy science, Inc., otsuka Pharmaceuical co., Ltd., taiho Pharmaceutical co., Ltd., sceti Medical Labo k.k., nippon Boehringer Ingelheim co., Ltd., kowa company, LtD, kyowa hakko kirin co., Ltd., Merck serono co., Ltd., ono Pharmaceutical co., Ltd., Bayer, Ltd., Pfizer japan Inc., astrazeneca k.k., Dainippon sumitomo Pharma co., Ltd., honoraria support from: chugai Pharmaceutical co., Ltd., Pfizer japan Inc., novartis Pharma k.k., taiho Pharmaceutical co., Ltd., Merck serono co., Ltd., eli Lilly japan k.k., Dainippon sumitomo Pharma co., Ltd., eisai co., Ltd., Bayer, Ltd., fujI fILM co., Ltd., yakult honsya co., Ltd., consulting of: eli Lilly japan k.k., yakult honsha co., Ltd., amgen, Dainippon sumitomo Pharma co., Ltd., taiho Pharmaceutical co., Ltd., onco theapy science, Inc., nobelpharma co., Ltd., ono Pharmaceutical co., Ltd., nippon Boehringer Ingelheim co., Ltd., nano carrier co., Ltd., chugai Pharmaceutical co., Ltd., novartis Pharma k.k., zeria Pharmaceutical co., Ltd., s. ohkawa honoraria support from: eli Lilly and company, h. fujii: none Declared, a. Masumoto: none Declared, j. furuse research/education support from: ono Pharmaceutical, yakult, Glaxosmithkline, taiho Pharmaceutical, takeda, eli Lilly and company, sanofi, Bayer, Pfizer, Daiichi sankyo, torii Pharmaceutical, nippon kayaku, chugai japan, Merck co., Inc., novartis healthcare a/s, oncotherapy science, Inc., honoraria support from: taiho Pharmaceutical, eli Lilly and company, Bayer, eisai, ono Pharmaceutical, yakult, takeda, astellas Pharma, Daiichi sankyo, sumitomo Group, Dainippon sumitomo Pharma, Bristol-Myers squibb, nippon kayaku, ajinomoto, sanofi, Mitsubishi tanabe Pharma, hisamitsu Pharmaceutical, kyowa hakko kirin, Merck serono, chugai japan, sandoz Biopharmaceuticals, Meiji seika Pharma, novartis healthcare a/s, shionogi Ltd, consulting of: kyowa hakko kirin, zeria Pharmaceutical, Merck serono, Glaxosmithkline, taiho Pharmaceutical, Bayer, eisai, yakult, fujifilm, kowa, astellas Pharma, otsuka, janssen, nobelpharma, j-Pharma, Boehringer Ingelheim, chugai japan, oncotherapy science, Inc., astrazeneca, y. Wada: none Declared, h. Ishii: none Declared, s. obi: none Declared, k. arai: none Declared, s. kawazoe: none Declared, o. yokosuka research/education support from: Bayer, Merck, M. Ikeda research/education support from: Bayer, taiho, Boehringer-ingelheim, kowa, kirin, Merkserono, ono, oncotherapy, eisai, yakult,astrazeneca, Pfizer, Glaxosmithkline, Lilly, zeria, chugai, Dainippon-sumitomo, honoraria support from: Bayer, abbott, Bristol, yakult, novartis, Guerbet, takeda, krin, consulting of: Merkserono, eisai, Bayer, fujifilm, nanocarrier, seti medical labo., k. ukai: none Declared, s. Morita: none Declared, h. asou: none Declared, P. abada: none Declared, L. yang research/education support from: eli Lilly and company, stocks of: eli Lilly and company, a. zhu research/education support from: Bayer, onyx, consulting of: sanofi-aventis, amgen, exelixis
O-034 reSuLTS Of A PrOOf-Of-COnCePT PhASe 2 TrIAL Of TASquInIMOD In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA PreVIOuSLy TreATeD WITh SOrAfenIb
Julien edeline* 1, Laetitia fartoux2, hal hirte3, christelle Descot4, nathalie Germann4, sandrine faivre5
1Département d'oncologie Médicale, centre eugène Marquis, rennes, 2Département d’hépato-gastroentérologie, hôpital saint antoine, Paris, france, 3juravinski cancer centre, McMaster university, hamilton, canada, 4Ipsen Innovation, Les ulis, 5service de cancérologie, hôpital Beaujon, clichy, france
Introduction: no effective treatment options exist for advanced hcc following sorafenib failure. tasquinimod is a novel oral immunotherapy targeting the tumour microenvironment with immunomodulatory, anti-angiogenic and anti-metastatic properties that may provide benefit after sorafenib. hcc was one of four tumour types evaluated in this proof-of-concept study (tasq004; nct01743469) in addition to advanced ovarian, renal cell and gastric carcinomas.1
Methods: Patients (pts) aged ≥18 years with BcLc stage B or c hcc and child-Pugh class a and who have been previously treated with sorafenib received a daily dose of tasquinimod (starting dose 0.5mg/day orally, titrated to 1mg as tolerated). treatment was given continuously until radiological progressive disease, toxicity or patient withdrawal. ct/MrI were performed every 8 weeks. Primary endpoint was progression free survival (Pfs) rate at 16 weeks (recIst 1.1 criteria). secondary endpoints were Pfs rate at 16 weeks (choi criteria), response rate, Pfs, ttP (recIst 1.1 and choi), clinical benefit rate, overall survival (os), safety, pharmacokinetics (Pk) and biomarkers.
results: results for ovarian, renal and gastric cohorts have been presented previously.2,3 In the hcc cohort, 53 pts from 4 european countries and canada were enrolled from january 2012 to august 2014. Median age was 68 years (range: 23–83). ecoG performance status was 0 and 1 in 28
(53%) and 25 (47%) pts, respectively. at study entry, the majority of pts had BcLc staging c (87%); 30 pts (57%) had extrahepatic disease, 8 pts (15%) had portal vein thrombosis and 23 pts (43%) had alfa-fetoprotein ≥200 mg/L. hcc aetiology was alcoholic liver disease (28%) and hepatitis B/c (17%/9%). Median duration of tasquinimod treatment was 9.43 weeks (range: 0.7–56.3). target dose of 1mg was reached by 41 pts (77.4%). efficacy results according to recIst 1.1 and choi criteria (centrally reviewed) are summarized below (table). Median os was 6.7 months (95% cI: [5.7–8.9]). the most frequent treatment-emergent adverse events (all grades; incidence >15%, regardless of relationship) were fatigue (60%), decreased appetite (43%), nausea (40%), vomiting (36%), abdominal pain (30%), peripheral oedema (30%), constipation (28%), diarrhoea (26%), decreased weight (24%), dyspnoea (19%), back pain (17%), asthenia (17%), headache (17%) and insomnia (17%). Pk and biomarker analyses are ongoing.
Pfs at 16 wks [95% cI]
Pr* n (%)
sD* n (%)
clinical benefit (Pr+sD ≥12 wks) n (%)
Median Pfs (wks) [95% cI]
Median ttP (wks) [95% cI]
recIst 1.1 (n=53)
26.4% [15.3–40.3]
1 (1.9%) 29 (54.7%) 14 (26.4%) 15.86 [8.00–23.14]
15.86 [8.00–24.00]
choi criteria (n=53)
20.8% [10.8–34.1]
11 (20.8%) 17 (32.1%) not done 15.71 [8.00–16.43]
15.86 [8.00–16.43]
*Best overall response. Pr = partial response; sD = stable disease.
Conclusion: In pts with advanced hcc who had been treated with sorafenib, clinical activity of single agent tasquinimod observed in this study was modest. the favourable safety profile of tasquinimod in this population of hcc patients was consistent with previous studies.
references: 1. escudier B, et al. J Clin Oncol 2013;31(suppl): abstract tPs2622. 2. oza aM, et al. Ann Oncol 2014;25 (suppl 4): iv160–iv161: Poster 480P. 3. faivre s, et al. abstract and poster at the 8th ILca meeting, 5–7 september 2014, kyoto, japan: P-171.
Disclosure of Interest: none Declared

Top Scored Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s2 6
P-001 MeTfOrMIn uSe reDuCeD MOrTALITy AnD DISeASe PrOGreSSIOn AfTer CurATIVe hePATIC reSeCTIOn In Very eArLy-STAGe hePATOCeLLuLAr CArCInOMA: A nATIOnWIDe POPuLATIOn-bASeD STuDy
young-Seok Seo* 1, Mi-sook kim1, Won-Il jang1, Min-jung ko2
1radiation oncology, korea Institute of radiological & Medical sciences, 2economy evaluation, national evidence-based healthcare collaborating agency, seoul, korea, republic of
Introduction: Metformin is one of the most frequently prescribed antihyperglycemic drugs and is used as first-line therapy for type 2 diabetes mellitus (t2DM). Metformin use has been shown to reduce the incidence and mortality of some solid tumors in t2DM patients in the large population studies. although many studies had shown metformin use reduces incidence of hepatocellular carcinoma (hcc), there has been few studies into the survival benefit to the use of metformin in hcc. the purpose of this study is to investigate whether metformin used after hepatic resection reduce the risk of mortality and recurrence in a cohort of patients with very early-stage hcc.
Methods: a cohort of 5,494 patients with newly diagnosed early-stage hcc were identified from 2005 to 2011 from the korea central cancer registry (a population-based nationwide cancer registry in korea). this cohort was linked to the health Insurance review and assessment (hIra) service, which provided prescription records (the hIra database covered over 99.9% of all medical claims in south korea), and to mortality data from the korea national statistics to identify cancer-specific deaths. cox regression models were used to calculate hazard ratios (hr) for mortality and 95% cIs by metformin use and to adjust these hrs for potential confounders. Medication possession ratio (MPr) of metfromin was defined as the sum of days of metformin prescription duration divided by the total anti-diabetics prescription duration.
results: total 533 diabetic patients treated with metformin, 218 diabetic patients without metformin, and 4743non-diabetic patients were analyzed. overall, metformin use improved cancer-specific survival (css) and recurrence-free survival (rfs) in diabetic patients (css: fully adjusted hr, 0.40; 95% cI, 0.31-0.51; rfs: fully adjusted hr, 0.43; 95% cI, 0.35-0.53). a dose-response association was apparent; for example, a more marked reduction was apparent in hcc patients with MPr of metformin over 80% (css: fully adjusted hr, 0.49; 95% cI, 0.34-0.72; rfs: fully adjusted hr, 0.76; 95% cI, 0.55-1.07).
no. of patients relative risk
Metforminn=533
non-metformin
n=218
univariate multivariate
overall death
195 (37%) 124 (57%) 0.4146 (0.3303, 0.5205)
<.0001 0.4054 (0.3227, 0.5092)
<.0001
cancer specific death
169 (32%) 111 (51%) 0.4039 (0.3172, 0.5144)
<.0001 0.3968 (0.3114, 0.5057)
<.0001
recurrence 235 (44%) 151 (69%) 0.4342 (0.3532, 0.5339)
<.0001 0.4318 (0.351, 0.5313)
<.0001
Conclusion: In this large population-based cohort, metformin use after hepatic resection in very early-stage hcc was associated with longer rates of css and rfs. however, randomized study would be required.
Disclosure of Interest: none Declared
P-002 eThnICITy IMPACTS AGGreSSIVeneSS Of hCC DeTeCTeD DurInG SurVeILLAnCe Of COMPenSATeD VIrAL CIrrhOSIS (AnrS CO12 CIrVIr PrOSPeCTIVe COhOrT)
Pierre nahon* 1, eric Letouzé2, angela sutton3, Valérie Bourcier1, richard Layese4, Ventzi Petrov-sanchez5, nathalie charnaux3, jean-claude trinchet1, jessica zucman-rossi2, françoise roudot-thoraval6
1hôpital jean Verdier, Bondy, 2InserM u1162, Paris, 3InserM u1148, Bobigny, 4hôpital henri Mondor, créteil, 5anrs, Paris, 6hôpital heni Mondor, créteil, france
Introduction: racial differences have been reported as modifyers of hcc risk using healthcare databases but with major biases due to differences in access to care according to ethnicity. the objective of the cirVir cohort1 was to prospectively assess the incidence and characteristics of primary liver cancer (PLc) in french patients with compensated viral cirrhosis in a competing risk framework.
Methods: Patients with the following inclusion criteria were enrolled in 35 french centres: a) biopsy-proven hBV or hcV cirrhosis; b) child-Pugh a; c) absence of previous liver complications. Patients were prospectively followed-up every 6 months. ethnicity was defined by a predictive panel of 26 single nucleotide polymorphisms (snPs) assessed on peripheral Dna. samples were classified as europeans, africans or asians based on the closest 1000 Genomes population in a principal component analysis.
results: a total of 1671 patients were enrolled between March 2006 and june 2012 [age 55, men 67.2%, hcV 1323, hBV 317, hcV-hBV 31]. Patients were classified as europeans [eur, 1181 (84.4%)], africans [afr, 154 (11%)] or asians [as, 65 (4.6%)] (missing data 271). eur patients were older and had higher rates of comorbidities, in particular past excessive alcohol [28.4% vs. 14% (as) vs. 18.9% (afr), P=0.004] and tobacco consumption [24.4% vs. 19% (as) vs. 18.2% (afr), P<0.0001]. During a median follow-up of 51 months, PLc was diagnosed in 196 [187 hepatocellular carcinoma (hcc) and 9 cholangiocarcinomas). hcc risk gradually increased according to ethnicity with 5-yr cumulative incidence (cumI) ranging from 4.8% (as) vs. 10.4% (afr) vs. 13.4% (eur) (P=0.05). Liver decompensation (ascites, digestive haemorrhage, encephalopathy) also gradually increased according to the same pattern [5-yr cumI 1.6% (as) vs. 10.5% (afr) vs. 15.2%, (eur) P=0.007]. eur also had the highest 5-yr cumI of bacterial infection (P=0.04), extra-hepatic cancers (P=0.02), cardiovascular events (along with as, P=0.022), and had the lowest probability of overall survival [5-yr cumI 96.3% (as) vs. 95.3% (afr) vs. 89.7%, (eur) P=0.01]. In multivariate analysis, older age, lower platelet count and albuminemia, higher GGt level, past excessive alcohol consumption and lack of virological eradication or control at endpoint were independent risk factors of hcc occurrence. 31/187 hcc (16.6%) were diagnosed outside Milan criteria. In multivariate analysis, a periodicity>7 months between the 2 last imaging findings (or=2.54, P=0.039) and afr ethnicity (or=3.86, P=0.026) were independent predictors of hcc aggressiveness. 82/154 (53.2%) afr patients were born in africa, a feature that did not differ according to hcc development or severity.
Image:
Conclusion: When excluding biases due to differences in access to care, individuals with compensated viral cirrhosis of european descent seem to have a higher risk of hcc while those of african ancestry may develop more aggressive tumors. the identification of complex determinants explaining these differences, whether environmental or genetic, warrant further exploration.
references: 1. trinchet et al. complications and competing risks of death in compensated viral cirrhosis (anrs co12 cirVir prospective cohort). hepatology. 2015 feb 11. doi: 10.1002/hep.27743.
Disclosure of Interest: none Declared

Top Scored Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 2 7
P-003 TM6Sf2-T AnD PnPLA3-G VArIAnTS CO-MODuLATe The rISK Of hePATOCeLLuLAr CArCInOMA In CAuCASIAn PATIenTS WITh ALCOhOLIC CIrrhOSIS. InTer-COhOrT VALIDATIOn In 1068 PATIenTS
Pierre nahon* 1, qian cao2, erwan Guyot3, angela sutton3, nathalie Ganne-carrié1, eric quertimont4, christophe Moreno4, Denis franchimont4, jessica zucman-rossi2, eric trépo4
1hôpital jean Verdier, Bondy, 2InserM u1162, Paris, 3InserM u1148, Bobigny, france, 4université Libre de Bruxelles, Bruxelles, Belgium
Introduction: a genetic variant, tM6sf2 (rs58542926) c>t, involved in lipid metabolism, has been recently linked to liver damage in patients with nafLD. the aims of this study were 1) to assess the potential impact of tM6sf2 (rs58542926) c>t on alcoholic carcinogenesis, and 2) to evaluate its contribution to hcc risk stratification in combination with PnPLa3 (rs738409) c>G.
Methods: three distinct cohorts were genotyped for both snPs. the first one (Belgium, cohort 1/aLD) was a case-control cohort including alcoholic cirrhotics without (n=484) and with hcc (n=71). the second cohort (france, cohort 2/aLD) was a prospective cohort of alcoholic cirrhotics (n=249), enrolled between 1997 and 2007, currently followed-up and screened for hcc (incident cases during 68 months follow-up, n=51, 21%). the third cohort (france, cohort 3/hcV) was similar to the previous one and included 267 patients with hcV-related cirrhosis in whom 84 (31%) hcc were detected during 102 months of follow-up.
results: In the case-control cohort 1/aLD, patients with hcc were highly enriched in tM6sf2-t risk allele [20 (28.2%) vs. 70 (14.5%), P=0.0006). using a multivariable model (including age, gender, BMI and diabetes), this variant was independently associated with the presence of hcc [or = 2.5 (1.4-4.3), P=0.002]. In multivariable analysis, the risk for hcc increased in carriers of more than one PnPLa3-G and / or tM6sf2-t risk allele compare to those without (or=2.8 [1.3-5.7], P=0.007). In the prospective cohort 2/aLD, patients with the tM6sf2-t allele had a higher risk of hcc occurrence (hr = 2.49 [1.5-4.5], P=0.003). When the population was stratified into three groups according to the presence of none (n=179), at least one (n=64) or two (n=6) PnPLa3- G and/or tM6sf2-t risk alleles, the number of hcc cases gradually increased [27 (15.1%) vs. 19 (29.7%) vs. 5 (83.3%) respectively, P<0.0001]. this genotypic combination was an independent risk factor associated with hcc onset (hr=2.31 [1.5-3.4], P<0.0001). conversely, in the prospective cohort 3/hcV, tM6sf2-t allele was not significantly associated with hcc.
Image:
Conclusion: tM6sf2 (rs58542926) c>t is associated with hcc occurrence in patients with alcoholic cirrhosis but not with hcV infection. the risk of hcc increases in parallel with the number of PnPLa3-G and/or tM6sf2-t mutant alleles.
Disclosure of Interest: none Declared
P-004 PhASe I/IIA STuDy Of ADJuVAnT IMMunOTherAPy WITh TuMOr AnTIGen-PuLSeD DenDrITIC CeLLS In PATIenTS WITh hePATOCeLLuLAr CArCInOMA
Jeong-hoon Lee* 1, yoon Lee2, Min kyu heo2, jae-sung song2, ki-hwan kim2, hyunah Lee3, nam-joon yi4, kwang-Woong Lee4, kyung-suk suh4, yong-soo Bae2, 5, yoon jun kim1
1Department of Internal Medicine and Liver research Institute, seoul national university college of Medicine, seoul, 2jW creaGene research Institute, jW creaGene Inc., seongnam-si, 3samsung Medical center, school of Medicine, sungkyunkwan university, 4Department of surgery, seoul national university college of Medicine, seoul, 5Department of Biological science, sungkyunkwan university, suwon, korea, republic of
Introduction: to date, no adjuvant treatment has been shown to have a clear benefit in patients with hepatocellular carcinoma (hcc). In this prospective phase I/IIa study, we evaluated the safety and efficacy of adjuvant dendritic cell (Dc) therapy in hcc patients who received primary treatment for hcc.
Methods: twelve hcc patients who had no viable tumor after primary treatments were included. Dc vaccines pulsed with cytoplasmic transduction peptide (ctP)-attached alpha-fetoprotein (afP), glypican-3 (GPc-3) and melanoma-associated antigen 1 (MaGe-1) recombinant fusion proteins were injected subcutaneously. adverse effects, time to progression (ttP), and associated immune responses were evaluated after Dc vaccination. their ttP was compared with the historical controls matched according to treatment modality and tumor stage.
results: nine of 12 patients had no tumor recurrence up to 24 weeks after Dc vaccination. among a total of 144 adverse events, 129 events (89.6%) were regarded as adverse drug reactions (aDrs), all of which were grade 1 or 2. the majority of patients showed enhanced anti-tumor immune responses after Dc vaccination. recurrence-free patients exhibited relatively stronger anti-tumor immune responses after Dc vaccination in lymphocyte proliferation and Ifn-γ eLIsPot assays than patients who developed recurrence after Dc vaccination. the median time of ttP was 36.6 months in the Dc-vaccination group and 11.8 months in the control group (hazard ratio, 0.41; 95% confidence interval [cI], 0.18-0.95; P=.0031 by log-rank test).
Conclusion: adjuvant Dc vaccine was safe and well-tolerated in phase I/IIa study. Preliminary efficacy data warrant further clinical study in patients with hcc after primary treatments.
Disclosure of Interest: none Declared
P-005 MyC OnCOGenIC ACTIVITy IS SerPInb3-DePenDenT ThrOuGh yAP InTerPLAy In hePATOCeLLuLAr CArCInOMA
Cristian Turato* 1, stefania cannito2, Davide simonato1, Gianmarco Villano1, elisabetta Morello2, Liliana terrin1, santina quarta1, alessandra Biasiolo1, Mariagrazia ruvoletto1, silvano fasolato3, Giacomo zanus3, umberto cillo3, angelo Gatta1, Maurizio Parola4, Patrizia Pontisso1
1Department of Medicine, university of Padova, Padova, 2clinical and Biological sciences, university of turin, turin, 3unit of hepatobiliary surgery and Liver transplantation, university of Padova, Padova, 4clinical and Biological sciences, university of Padova, turin, Italy
Introduction: serpinB3 has been recently described as an early marker of liver carcinogenesis, but the potential mechanistic role of this serpin in tumour development is still poorly understood. Myc is one of the most important oncogenes in human cancer. somatic amplification and overexpression of Myc often correlate with more advanced and aggressive tumour forms, supporting its involvement in carcinogenesis. yes-associated protein (yap), the main effector of the hippo pathway, is a central regulator of proliferation and self-renewal of normal and cancer stem cells. this molecule, found up-regulated in hepatocellular carcinom (hcc), has been described also to increase Myc expression.
the present study has been designed in order to investigate whether serpinB3 may functionally modulate Myc in different experimental models and in human hcc specimens.
Methods: expression of Myc, yap and its target genes was evaluated in relation to serpinB3 expression in hcc specimens from 67 patients obtained at the time of surgical resection, in c57BL/6 mice transgenic for human serpinB3. In addition, mrna quantification and Western Blot analysis was performed in hepG2 and huh7 cells stably transfected with plasmid vectors carrying the serpinB3 gene. Moreover the inhibitory effect of serpinB3 on calpain was assessed by means of the calpain activity assay.
results: a positive correlation between Myc and serpinB3 expression was observed at transcription and protein level in hcc specimens, where Myc oncogene was found predominantly in the nucleus of cancer cells overexpressing serpinB3. Myc expression was significantly and mechanistically up-regulated by serpinB3 through calpain and hippo-dependent molecular mechanisms. recombinant serpinB3 protein was indeed capable to inhibit the activity of calpain in vitro, likely reducing its ability to cleave Myc in its non-oncogenic Myc-nick cytoplasmic form. furthermore, serpinB3 indirectly increased the transcription of Myc through the induction of yap pathway, as documented by a remarkable yap nuclear translocation and up-regulation of yap target genes in transgenic mice and in hepatoma cells overexpressing human serpinB3.

Top Scored Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s2 8
Conclusion: Data from the present study provide evidence that serpinB3 can improve the production of Myc oncogene through direct and indirect mechanisms that include the inhibition of generation of its cytoplasmic form and the activation of yap pathway.
Disclosure of Interest: none Declared
P-006 SOx9 reGuLATeS STeM CeLL-LIKe PhenOTyPeS AnD MeTASTASIS In hePATOCeLLuLAr CArCInOMA ThrOuGh WnT/beTA-CATenIn SIGnALInG
regina Lo* 1, 2, carmen Leung2, Winger Mak2, terence Lee1, 2, Irene ng1, 2
1state key Laboratory for Liver research, 2PathoLoGy, the unIVersIty of honG konG, honG konG, hong kong
Introduction: sry-related hMG-box gene 9 (sox9) is a member of the sex-determining region y (sry)-related high-mobility-group box transcription factors. sox proteins are crucial in human developmental process and regulate lineage restriction, cell differentiation and stem cell properties. Physiologically, sox9 promotes testis differentiation and drives cartilage formation. In the liver, sox9 is a marker for the progenitor/precursor cells and expressed during embryogenesis in intrahepatic bile ducts. sox9+ precursor cells are activated to facilitate hepatocyte regeneration during liver injury. In addition, sox9 was found over-expressed in human prostate, lung and colon cancers, and over-expression was associated with more aggressive clinicopathological features. these observations were further investigated by in vitro/in vivo experiments. to date, the functional roles and signaling pathway of sox9 with specific reference to its potential stemness properties in hepatocellular carcinoma (hcc) have not yet been elucidated.
Methods: the expression of sox9 in 46 clinical hcc samples was examined by real-time quantitative Pcr (qPcr) and immunohistochemistry (Ihc). to investigate the functional role of sox9 in hcc, we employed lentiviral-based knockdown approach to suppress sox9 in hcc cell line huh7. cell proliferation assay, migration and invasion transwell assays were performed. specifically to study the stemness features of sox9, non-adherent sphere formation assay, chemoresistance apoptosis assay using flow cytometry and subcutaneous inoculation in noD/scID mice were used. activity of Wnt/b-catenin pathway was measured by toP/foPflash reporter assay.
results: sox9 transcript level in hcc tumor tissues was significantly up-regulated as compared with the corresponding non-tumoral liver counterparts (p=0.004). twenty-eight cases (60.8%) showed up-regulation of sox9. the over-expression was confirmed by Ihc. By statistical correlation with various clinicopathological parameters, up-regulation of sox9 in hcc was associated with poorer tumor cell differentiation (p=0.006). With both Ihc and immunofluorescent stainings, we observed co-expression of sox9 and cytokeratin 19 (a hepatic progenitor cell marker) among hcc cells in clinical samples. sox9 was expressed in various hcc cell lines, but was undetectable in immortalized liver cell line Lo2. silencing of sox9 significantly inhibited hcc cell proliferation, migration and invasion. epithelial-mesenchymal transition was suppressed as demonstrated by up-regulation of e-cadherin and down-regulation of vimentin upon stable knockdown of sox9. Besides, there was significant down-regulation of multiple stemness-associated and chemoresistance-related genes in stable sox9-knockdown clones compared with non-target control. the number and size of tumorspheres were lower in the sox9-knockdown clones compared with control. the cells with stably knockdown of sox9 were more chemosensitive to both doxorubicin and cisplatin treatment. knockdown of sox9 suppressed tumorigenicity and self-renewal ability at limited dilution manner by subcutaneous inoculation in noD/scID mice. Prolonged tumor latency period was also observed. on signaling pathway, silencing of sox9 down-regulated the expression of phosphorylated (ser9)-Gsk3b, b-catenin, axin2, and c-myc, accompanied by a decrease in Wnt/b-catenin pathway activation by toP/foPflash reporter assay.
Conclusion: In summary, sox9 modulates stem cell-like phenotypes and metastasis in hcc through regulation of Wnt/b-catenin pathway.
Disclosure of Interest: none Declared
P-007 TrAnSCrIPTIOnAL DereGuLATIOn In hePATObLASTOMA PATIenTS POInTS TO neW OnCOGenIC MeChAnISMS
Katarzyna b. hooks* 1, 2, jérôme audoux3, 4, sarah Lesjean1, 2, anne-aurélie raymond1, 2, tony ernault5, 6, Laurence Brugières7, sophie Branchereau8, Monique fabre9, Marie-annick Buendia5, 6,
thérèse commes3, 4, christophe Grosset1, 2
1université de Bordeaux, 2InserM u1053, Bordeaux, 3université de Montpellier, 4InserM u1040, Montpellier, 5InserM uMr1193, 6centre hépatobiliaire, hôpital universitaire Paul Brousse, 7Gustave roussy Institute, Villejuif, 8hôpital Bicêtre, Le kremlin-Bicêtre, 9hôpital necker-enfants Malades, Paris, france
Introduction: Liver cancers are rare in children but the incidence of the most common form – hepatoblastoma (hB) – steadily increases and now is around 1.5 cases/million/year [1]. Due to international collaboration and establishing specialized centres, we observed a remarkable improvement in patients’ outcome. however, the pre- and post- surgical chemotherapies provide
very limited benefits for patients with high-grade tumour and result in significant hearing loss in more than 50% of cases.
to develop new prognostic tools and therapeutic targets with lower toxicity and efficiency we focused on pinpointing transcriptional changes associated with the tumorigenesis in hB.
Methods: We performed next generation sequencing of rna extracted from 25 matched hBL samples and normal livers. We constructed both polya+ and microrna libraries and sequenced them on an Illumina hiseq 2500. for polya+ we used 125 nt paired-end reads and for small rna library 50 nt single reads. the reads were mapped to human genome (crac [2] and tophat) and novel splice sites, chimeric transcripts and indels were extracted. for first two patients we performed differential expression analysis using Deseq2. We mapped differentially expressed genes to canonical and novel pathways using Ingenuity (qiagen) and we plan to predict genes affected by the deregulated micrornas using targetscan and Miranda.
results: so far the data for two patients, one with poor prognosis and one with good prognosis, were analysed. We found a clear activation of Wnt/β-catenin associated with either skipping of β-catenin exon 3 or overexpression of β-catenin [3]. src/ras pathway was also activated in both patients. We found a group of genes highly overexpressed in the tumoral tissues, including known oncogene GPc3 and multiple genes of either unknown function or not yet described to have involvement in hB. additionally we found many noncoding rnas deregulated, with some of them only expressed in high-grade tumour. We noticed that the perturbation of many antisense non-coding rnas correlates with that of their sense genes.
Conclusion: When completed our data will be the first comprehensive description of transcriptional landscape in hBL, including alteration of splice variants, chimeric transcripts and non-coding rnas. We will establish new prognostic biomarkers by defining a broad panel of rnas specifically deregulated in hB tissues, and more particularly in high-risk tumours. We will also perform network analysis to pinpoint new interactions between genes and non-coding transcriptome.
references: 1. czauderna P et al. hepatoblastoma state of the art: pathology, genetics, risk stratification, and chemotherapy. curr opin Pediatr. 2014 feb; 26(1):19-28.2. Philippe n et al., crac: an integrated approach to the analysis of rna-seq reads. Genome Biol. 2013 Mar 28; 14(3):r30.3. cairo s et al., hepatic stem-like phenotype and interplay of Wnt/beta-catenin and Myc signalling in aggressive childhood liver cancer. cancer cell. 2008 Dec 9; 14(6):471-84.
Disclosure of Interest: none Declared
P-008 LeVeL Of SS-CATenIn ACTIVATIOn In CTnnb1-MuTATeD hePATOCeLLuLAr ADenOMA AnD CArCInOMA IS reLATeD TO MuTATIOn TyPe AnD InCreASeS DurInG TuMOr PrOGreSSIOn
Sandra rebouissou* 1, 2, 3, 4, andrea franconi1, 2, 3, 4, julien calderaro1, 2, 3, 4, 5, Gabrielle couchy1, 2,
3, 4, eric Letouzé1, 2, 3, 4, sandrine Imbeaud1, 2, 3, 4, jean-charles nault1, 2, 3, 4, 6, charles Balabaud7, 8, Paulette Bioulac-sage7, 9, jessica zucman-rossi1, 2, 3, 4, 10
1uMr-1162, Génomique fonctionnelle des tumeurs solides, Iuh, InserM, 2Labex Immuno-oncology, sorbonne Paris cité, faculté de Médecine, université Paris Descartes, 3université Paris Diderot, Paris, 4sorbonne Paris cité, ufr sMBh, f-93000, université Paris 13, Bobigny, 5Department of Pathology, chu henri Mondor, assistance Publique-hôpitaux de Paris, créteil, 6hôpitaux universitaires Paris – seine saint-Denis, site jean Verdier, Pôle d’activité cancérologique spécialisée, service d’hépatologie, f-93143, assistance Publique-hôpitaux de Paris, Bondy, 7uMr-1053, InserM, 8université de Bordeaux, Bordeaux, 9chu de Bordeaux, Department of hepatology, hôpital saint-andré, Bordeaux, 10hôpital europeen Georges Pompidou, f-75015, assistance Publique-hôpitaux de Paris, Paris, france
Introduction: activating mutations in ß-catenin, encoded by the CTNNB1 gene, are one of the most frequent genetic alterations identified in hepatocellular carcinoma (hcc) and have been found in a subgroup of hepatocellular adenoma (hca) associated with high risk of malignant transformation. the aim of this study was to better understand the relationship between CTNNB1 mutation type, tumor phenotype and level of ß-catenin activation by analyzing a large series of benign and malignant hepatocellular tumors.
Methods: among a series of 571 hepatocellular tumors, we identified 209 CTNNB1 mutations in 139 hcc, 55 hca and 10 borderline hca/hcc lesions. Level of ß-catenin activation in tumors was assessed by measuring expression of target genes using quantitative rt-Pcr and immunohistochemistry. aberrations at chromosome 3p harboring CTNNB1, such as Dna copy number variation and copy-neutral loss of heterozygosity (Loh) were studied by cGh-snP array and whole-exome sequencing.
results: We identified 64 different CTNNB1 somatic mutations in the whole series of hepatocellular tumors analyzed. Point mutations were identified in 90% of the tumors while large in-frame deletions removing exon 3 of CTNNB1 were found in only 10% of the cases. Point mutations were distributed in five main hotspot regions. the first one was restricted to the ß-trcP binding domain, between

Top Scored Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 2 9
amino acid residues D32 and s37, whereas, the four other hotspots occurred at specific amino acid residues: t41, s45, k335 and n387. strikingly, mutational patterns of CTNNB1 were very different according to the tumor types: point mutations in the ß-trcP binding domain were frequent in hccs (50%) and were only found in rare cases of hcas (9%), large in-frame deletions were over-represented in borderline lesions while mutations at k335 and n387 were frequent and occurred quasi exclusively in hcas (40%). CTNNB1 mutations were also associated with different levels of ß-catenin activation. Large in-frame deletions and point mutations located within the ß-trcP binding site were related to a strong activation of ß-catenin while other mutations (t41, s45, k335 and n387) activate ß-catenin at a lower level. surprisingly, s45 mutants faintly activate ß-catenin in hcas while the same mutants showed significant higher activity in most of the hccs. In this group of hccs harboring a s45 ß-catenin mutant, we identified a second hit (chromosome gain or copy-neutral Loh) at the CTNNB1 locus leading to the selective duplication of the mutant allele in a subset of tumors. this finding suggests that a double dose of the mutated gene product may confer a selective advantage during tumor progression through hyperactivation of ß-catenin.
Conclusion: this study has highlighted new findings regarding to the role of ß-catenin mutations during hepatocarcinogenesis. ß-catenin mutation types are closely associated to ß-catenin activity with a preferential accumulation of weakly activating mutations in benign tumors and a selection of hyperactivating mutations in malignant tumors. these results suggest that high level of β-catenin activation may be required for tumor progression.
Disclosure of Interest: none Declared
P-009 A neW SCOre bASeD On exPLAnT PAThOLOGy ALLOWS An InDIVIDuALIzeD PreDICTIOn Of hCC-reCurrenCe AfTer LIVer TrAnSPLAnTATIOn
Charlotte Costentin* 1, Giuliana amaddeo1, christophe Duvoux1, julien calderaro2, alain Luciani3, alexis Laurent4, françoise roudot-thoraval5
1hepatology, 2Pathology, 3radiology, 4Digestive surgery, 5Public health, henri Mondor hospital, creteil, france
Introduction: after liver transplantation (Lt) for hepatocellular carcinoma (hcc), a standardized prediction of recurrence based on explant pathology would highly valuable in order to define patients who might benefit from post Lt adjuvant therapy or early changes in immunosuppressive regimens. We recently compared the accuracy of 4 explant-based models for prediction of recurrence (easL 2015 P0039). In this study, the “up to seven model”, using 2 variables (size of largest nodule and number of nodules) appeared to be the best tool to predict patients with a high risk of recurrence at 5 years post Lt (54.5±4.5% risk if score >7 ). the aim of this study was to design a new explant-based model including vascular invasion and tumor differentiation as predictors of recurrence and to test its accuracy against the “up to seven” model.
Methods: following uni- and multi-variate analysis of pathological predictors of recurrence in a series of 372 liver explants of patients transplanted for hcc between 2003 and 2005 and followed prospectively for 5 years, we built 2 predictive models. new score 1 included all independent pathological predictors (number of nodules, size of the largest, tumor differentiation, micro/macrovascular invasion, tumor burden (uni or bilobar)) and ranged from 0 to 9 points. new score 2 included all above mentioned variables except tumor differentiation (a variable that is not available when tumor is totally inactivated after bridging therapy) and ranged from 0 to 11 points. the accuracy of these 2 scores and the “up to seven” model without vascular invasion to predict 5 year-hcc recurrence was assessed by comparison of aucs of roc curves which were subsequently compared using the hanley&Mcneil method.
results: the “up to seven model” identified two distinct risk groups for 5 year-recurrence of hcc. new scores 1 and 2 identified 4 groups of patients with different levels of risks of recurrence ranging from 10 to >70% at 5 years. aucs were 0.7915 [0.73394 - 0.84907] for the “up to seven “ model, 0.7881 [0.73135 - 0.8448] for new score 1 and 0.7889 [0.7352 - 0.8427] for new score 2 (p=0.743). tumor differentiation did not improve accuracy to predict 5 year-hcc recurrence (new score 1 vs new score 2, p=0.49). using new score 2, a nomogram was built, giving the probability of recurrence at 1, 3 and 5 years post transplantation, according to the score value (fig)
Image:
Conclusion: a new score based on explant pathology, using number of nodules, size of the largest, vascular invasion and tumor burden has similar accuracy compared to the “up to seven” model to predict 5 year-hcc recurrence but allows a more individualized prediction of recurrence based on patients’ profile of explant findings
Disclosure of Interest: none Declared
P-010 nexT-GenerATIOn DeS-r-CArbOxy PrOThrOMbIn PreDICTS VASCuLAr InVASIOn In hCC
Shintaro yamazaki* 1, tomoharu kurokawa1, 1, tadatoshi takayama1
1nIhon unIVersIty schooL of MeDIcIne, tokyo, japan
Introduction: In hepatocellular carcinoma (hcc), des-r-carboxy prothrombin (DcP) more accurately reflects the malignant potential than alpha-fetoprotein (afP). next-generation DcP (nx-DcP) was created to overcome some of the limitations of conventional DcP. the aim of this study was to assess the predictive value of nx-DcP for the vascular invasion in hcc.
Methods: this prospective study included 82 consecutive patients scheduled to undergo resection for hcc. the patients were divided into two groups, those with or without pathological vascular invasion. the predictive power of the vascular invasion using afP, conventional DcP and nx-DcP were compared by a roc curve analysis and the correlation between tumor markers and the presence of vascular invasion was assessed.
results: there were 61 patients without pathological vascular invasion (the negative group) and 21 patients with vascular invasion (the positive group). the nx-DcP value [510.0 (10-98,450) mau/mL vs. 34.0 mau/mL (12-541), p<0.0001] was significantly higher in the positive group than that in the negative group while the afP value did not differ significantly between the two groups [9.7 ng/mL (1.6-43,960.0) vs. 11.0 ng/mL 1.6-1,650.0), p=0.49]. the area under the curve (auc) of nx-DcP (auc=0.813, sensitivity=71.4%, 1-specificity=13.1%) demonstrated a good sensitivity in the detection of the vascular invasion while the auc of afP was 0.550, (sensitivity=28.6%, 1-specificity=1.60%). the suitable cut-off value for determining the pathological vascular invasion of hcc was 33 mm (auc: 0.783, sensitivity=71.43%, 1-specificity=11.48%).

Top Scored Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s3 0
Conclusion: the value of nx-DcP is thus considered to be capable of predicting the presence of vascular invasion in hcc.
references: tameda M, shiraki k, sugimoto k, ogura s, Inagaki y, yamamoto n, Ikejiri M, takei y, Ito M, nobori t. Des-γ-carboxy prothrombin ratio measured by P-11 and P-16 antibodies is a novel biomarker for hepatocellular carcinoma. cancer sci. 2013;104:725-31- toyoda h, kumada t, osaki y, tada t, kaneoka y, Maeda a. novel method to measure serum levels of des-gamma-carboxy prothrombin for hepatocellular carcinoma in patients taking warfarin: a preliminary report. cancer sci. 2012;103:921-5.- takeji s, hirooka M, koizumi y, tokumoto y, abe M, Ikeda y, nadano s, hiasa y, onji M. Des-gamma-carboxy prothrombin identified by P-11 and P-16 antibodies reflects prognosis for patients with hepatocellular carcinoma. j Gastroenterol hepatol. 2013 ;28:671-7
Disclosure of Interest: none Declared
P-011 OxIDATIVe STreSS ACCeLerATeS The TrAnSfOrMATIOn Of PrOLIferATInG huMAn hePATOCyTeS WITh COnSTITuTIVe GP130 ACTIVATIOn In COnTrAST TO LIGAnD-MeDIATeD InTerLeuKIn 6 PAThWAy ACTIVATIOn
Ines Gil-Ibanez* 1, Denise heim1, johannes herden1, ann christin Parplys2, kerstin Borgmann2, Dirk schmidt-arras3, ansgar W. Lohse1, stefan rose-john3, henning Wege1
1Department of Gastroenterology and hepatology, 2Laboratory of radiobiology and experimental radiooncology, university Medical center hamburg-eppendorf, hamburg, 3Institute of Biochemistry, christian-albrechts-universität zu kiel, kiel, Germany
Introduction: In the context of chronic liver injury, pro-inflammatory signaling pathways and reactive oxygen species (ros) promote hepatocyte transformation. recently, interleukin 6 (IL-6) signaling has been established as an independent risk factor for hcc in patients with chronic hepatitis c. In addition, somatic gain-of-function mutations in the IL-6 signal transducer glycoprotein 130 (gp130) were found in 60% of inflammatory hepatocellular adenomas, benign liver lesions with high risk for transformation. however, the detailed mechanistic interactions between IL-6 signaling and oncogenic oxidative stress as driver for downstream transformation events are still unidentified. to elucidate these mechanisms, we activated gp130 in untransformed htert-immortalized human fetal hepatocytes (fh-htert) and challenged the cells with ros. additionally, we activated IL-6 trans-signaling with the designer cytokine hyper-IL-6 to compare ligand-independent with ligand-dependent IL-6 signaling.
Methods: fh-htert clones were generated via stable expression of a ligand-independent constitutively active gp130 construct (L-gp130). after phenotype characterization, we treated fh-htert L-gp130 clones with h2o2 after glutathione depletion and measured ros levels. expression levels of Dna-damage and antioxidant response genes were assessed by qPcr and Dna-double strand breaks (DsB) were determined by immunfluorescent staining for γ-h2ax and rad51. to examine DsB-induced cell cycle control mechanisms in our L-gp130 clones, p21 expression was assessed by qPcr and s-phase fractions were captured by Brdu incorporation. colony formation in soft agar was scored to investigate anchorage-independent growth, and finally, to compare ligand-independent signaling via L-gp130 activation with ligand-dependent IL-6 activation, we activated endogenous gp130 in fh-htert with hyper-IL-6 and recapitulated the experiments.
results: Ligand-independent IL-6 activation via L-gp130 was not sufficient to induce a fully transformed phenotype in our clones. however, challenge with oxidative stress accelerated the transformation process observed in long-term expansion culture and L-gp130 clones developed colony growth capabilities in soft agar with a frequency of up to 20 colonies per 5,000 seeded cells. as driving mechanism in our L-gp130 clones, we detected a decreased expression of antioxidant genes, in particular GPx3 and aPoe, causing 2- to 3-fold higher ros levels, and up to 6-fold more DsB in comparison to ros-treated control cells. Despite these higher ros levels and more DsB, fh-htert L-gp130 clones displayed similar p21 expression and an enhanced proliferation compared to fh-htert control (ros-induced s-phase reduction was completely abolished). In contrast to fh-htert L-gp130 clones, ligand-induced activation of IL-6 signaling via the designer cytokine hyper-IL-6 did not alter ros levels and cell cycle control in fh-htert after challenge with oxidative stress.
Conclusion: In contrast to ligand-dependent IL-6 pathway activation by hyper-IL-6, ligand-independent constitutive activation of gp130 resulted in increased levels of ros with significantly more DsB, possibly via an altered gp130-mediated oxidative stress response. an enhanced cell cycle turnover in gp130-active cells may therefore result in the accumulation of unrepaired DsB and finally to cellular transformation. In summary, we conclude that these mutation-associated gp130-induced mechanisms constitute a crucial step in the transition from hepatocellular adenoma or other pre-malignant lesions to hcc.
Disclosure of Interest: none Declared
P-012 hIGh-ThrOuGhPuT MIrnA-InhIbITOrS SCreenInG IDenTIfIeD SeLeCTeD MIrnAS InVOLVeD In The MODuLATIOn Of DruG reSPOnSe In ChOLAnGIOCArCInOMA
Io hong Cheong* 1, Michele Ghidini2, Matteo fassan3, caterina Vicentini4, Michele simbolo4, andrea Lampis2, jens hahne2, George Vlachogiannis2, francesco trevisani2, Luke Boulter5, rachel Guest6, stuart forbes6, Giulia ferrari1, Guido torzilli7, alessandro zerbi7, Massimo rugge3, aldo scarpa4, Lorenza rimassa7, armando santoro7, Massimo roncalli7, nicola Valeri2, Paul Workman1, chiara Braconi1
1Division of cancer therapeutics, 2Division of Molecular Pathology, Institute of cancer research, London, united kingdom, 3Dpt of Medicine, university of Padua, Padua, 4Dpt of Pathology, university of Verona, Verona, Italy, 5Mrc human Genetics unit Mrc IGMM, 6Mrc centre for regenerative Medicine, university of edinburgh, edinburgh, united kingdom, 7humanitas cancer center, humanitas clinical and research center, rozzano (MI), Italy
Introduction: cca are treated with cisplatin (c) and Gemcitabine (G). mirnas modulate drug response. however, the functional effect of microrna-inhibitors as sensitizers of chemotherapy has never been explored in cca. objective of this study is to define micrornas that mediate resistance to chemotherapy and may be exploited as targets of novel therapeutics.
Methods: high-throughput-screen (hst) of 1000 Lna-microrna-inhibitors (mircury-Lna™ Library, exiqon) was performed in triplicate for each cell line [Intrahepatic (ICC): sW1, snu-1079, ccLP; Extrahepatic (ECC) tfk, eGI, snu-1196). Library included 15x96-well plates with negative and Positive ctrLs per plate. cells were reverse-transfected for 48 hrs (50nM) and then treated with cG for 72 hrs. hits significant (ttest p<0.05) across 3 replicates were considered. mirna expression was assessed by taqman assay.
results: Ic50 for c and G was calculated and hst performed at Ic20-to-30 to enable identification of potential sensitizers. Inhibition of mir-21 sensitized cells to cG in 2/3 Icc cell lines; inhibition of mir-148a and let-7b increased resistance in Icc. these data are in line with published literature and confirm validity of our hst. an average of 49 mirnas per cell line enhanced cG activity by >20%. twelve mirna-inhibitors acted as sensitizers in all Icc cells, while 7 in ecc cells (p<0.05). Inhibitors of mir-1249, mir-133b, mir-1247 and mir-1228 decreased cell viability across all cell lines. mir-1249 expression was increased in a rat model of cca as well as in 36% of human resected cca tissues (n:30), compared to their matched adjacent tissues. When mir-1249 tumour expression was considered as binary predictor, kaplan Meyer analyses showed correlation with rfs (p:0.05). In this series adjuvant chemotherapy increased rfs over surgery only (hr 4.3 p:0.002). mir-1249 expression maintained correlation with rfs also in the two subgroups (surgery alone: p:0.003; adjuvant chemotherapy: p:0.05). Validation of hst data was carried out for mir-1249 by using MirVana anti-mir-1249 in ccLP, eGI, sW1, snu-478 and tfk cells. Inhibition of mir-1249 (25nM) did not alter cell viability in untreated cells or cells treated with DMso, while increased chemotherapy effect (by 0.88 in eGI, 0.58 in ccLP, 0.38 in sW1, and 0.46 in snu-478 cells). When c or G were kept at fixed doses with the other drug administered at scalar concentrations, we noticed a progressive increase in the enhancement of chemotherapy effect by mir-1249-inhibition as the c dose was progressively increased, suggesting that the effect of mir-1249-inhibition is dependent on c. mir-1249 basal expression inversely correlated with c Ic50 (r2:0.98). In line with these data we observed a significant correlation between low mir-1249 expression in pre-treatment bioptic tissues of cca patients (n:25) and reduced benefit from first line chemotherapy (Progression-free-survival: hr 0.47, p0.03; overall survival hr 0.32, p 0.004). We also noticed an inverse correlation between the basal expression of mir-1249 and the cell killing induced by anti-mir-1249 compared to anti-mir-ctrL in cG treated cca cells (r2:0.93). all together these data suggest that cells with low mir-1249 are more resistant to chemotherapy, and this effect is rescued by mir-1249 inhibition, likely related to an effect of platinum on mir-1249 expression.
Conclusion: We provided evidence that mirna-inhibition can sensitize cca cells to cG chemotherapy. mir-1249 inhibition seems to be a promising tool to enhance response to chemotherapy in cca. further studies are warranted to elucidate the mechanisms beyond these findings.
Disclosure of Interest: none Declared
P-013 MODeL TO PreDICT reCurrenCe AfTer LIVInG DOnOr LIVer TrAnSPLAnTATIOn fOr hePATOCeLLuLAr CArCInOMA beyOnD The MILAn CrITerIA
yuri Cho* 1, jeong-hoon Lee1, Dong hyeon Lee1, su jong yu1, nam-joon yi2, kwang-Woong Lee2, seoung hoon kim3, jong Man kim4, jae-Won joh4, yoon jun kim1, kyung-suk suh2, jung-hwan yoon1
1Department of Internal Medicine and Liver research Institute, 2Department of surgery, seoul national university college of Medicine, seoul, 3center for Liver cancer, national cancer center, Goyang-si, Gyeonggi-Do, 4Department of surgery, samsung Medical center, sungkyunkwan university school of Medicine, seoul, korea, republic of
Introduction: some subgroups of hepatocellular carcinoma (hcc) exceeding the Milan criteria

Top Scored Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 3 1
(Mc) experience substantial benefit from living donor liver transplantation (LDLt). this study aimed to develop and validate a model to predict tumor recurrence after LDLt (MoraL) for hcc beyond the Mc.
Methods: this multicenter study included a total of 566 consecutive patients who underwent LDLt in korea: the beyond-Mc cohort (n=205, the derivation [n=92] and validation [n=113] sets) and the within-Mc cohort (n=361).
results: using multivariate cox proportional hazard model, we derived the MoraL score (11x√protein induced by vitamin k absecence-II + 2x√alpha-fetoprotein), which provided a good discriminant function on time-to-recurrence (c-index=0.88). c-index was maintained similarly on both internal and external validations (mean 0.87 and 0.84, respectively). at cut-off of 314.8 (75th percentile value), a low MoraL score (≤314.8) was associated with significantly longer recurrence-free (vs. >314.8, hazard ratio [hr]=5.29, p<0.001) and overall survivals (hr=2.59, p=0.001) in the beyond-Mc cohort. the 5-year recurrence-free and overall survival rates of beyond-Mc patients with a low MoraL score were as high as 66.3% and 82.6%, respectively. the within-Mc patients with a high MoraL score showed a higher risk of recurrence than the beyond-Mc patients with a low MoraL score (hr=2.56, p=0.035). Patients who experienced decreasing MoraL score with prior treatment before LDLt (from high [>314.8] to low [≤314.8] MoraL score; n=6) showed longer time-to-recurrence after LDLt compared to those who had persistent high MoraL score (n=23) (p=0.062). Moreover, the MoraL score was significantly correlated with post-transplant histologic findings including edmondson-steiner nuclear grade of hcc, the presence of microvascular invasion, bile duct invasion, perineural invasion, and serosal invasion.
Conclusion: this new model to predict tumor recurrence of hcc beyond the Mc after LDLt provides refined prognostication. among beyond-Mc hcc patients those with a MoraL score ≤314.8 and no extrahepatic metastasis might be potential candidates for LDLt.
Disclosure of Interest: none Declared
P-014 The uSe Of beTA-bLOCKerS IS ASSOCIATeD WITh A LOWer rISK Of DeVeLOPInG hePATOCeLLuLAr CArCInOMA In PATIenTS WITh CIrrhOSIS
Iván herrera 1, 2, Sonia Pascual * 1, 2, Pedro zapater2, 3, 4, fernando carnicer1, 2, Pablo Bellot1, 2, jose such2, 4, jose María Palazón1, 2
1Liver unit, 2cIBerehd, 3clinic Pharmacology unit, hospital General universitario alicante, 4university Miguel hernández, alicante, spain
Introduction: a less incidence of hepatocellular carcinoma (hcc) in cirrhotic patients treated with beta-blockers (BB) for 5 years (4% vs 21% among untreated) has been described in a previous retrospective study (nkontchou, cancer Prev res 2012). other observational studies have reported an association between propranolol therapy and lower incidence of tumors such as malignant melanoma or breast cancer.aIM: the objective of the present study has been to analyze the incidence of hcc according BB treatment in cirrhotic patients followed prospectively in a surveillance program.
Methods: we included in the study all cirrhotic patients attended in the program for early detection of hcc between january 2006 and july 2007. end of follow up was in october 2014. Demographic, clinical and analytical data, treatments received and the occurrence of hcc was prospectively registered, including transplantation and /or death. Patients were classified as chronically taken or not BB. Differences between variables were analyzed with the student t test and the chi-square test as appropriate. the proportion of patients who remained free of tumor from diagnosis of cirrhosis and until the end of follow according to BB treatment or not were compared using f kaplan-Meier analysis and Breslow test. P value <0.05 was considered significant.
results: a total of 173 patients (73 treated and 100 untreated BB) were followed. the median time from diagnosis of cirrhosis until the end of follow-up was 11 years. at inclusion in the program there were no significant differences between patients untreated and treated with BB: age (61 ± 12 vs. 59 ± 11 years old; p = 0.29), percentage of males (73% vs. 70%; p = 0.65), child-Pugh (cP) (a: 50% vs. 55%; B: 35% vs. 32%; c: 15% vs. 13%; p = 0.41) and etiology of cirrhosis, hepatitis c virus (35% vs . 37%; p = 0.8). those treated with BB showed lower recount of platelets (121x103 ± 73x103 vs. 89x103 ± 52x103; p = 0.01) and quick index (73% ± 16 vs. 65%± 16; p = 0.02) and a greater proportion have had a previous episode of bleeding esophageal varices (11% vs. 45%; p = 0.001). overall, 28 patients developed hcc in follow up, 20 not treated with BB (20%) vs. 8 patients among treated with BB (11%). the annual incidence of hcc was 2.2%. the mean survival time of patients without hcc was 84 months vs 45 months in patients who developed hcc (p= 0.026). In 54% of cases the tumor was unique (mean diameter 28 mm) and a curative treatment was performed in 45% of all patients with hcc (surgery, liver transplant or percutaneo ablation). the survival analysis showed some differences in the cumulative proportion of cases of hcc between untreated and treated with BB at 5 years of diagnosis of cirrhosis of 6 and 3%, at 10 years of 19 and 6%, the 15 years of 24 and 16% and 20 years of 24 and 21%, respectively (p = 0.048). there were no significant differences in the incidence of hcc by the degree of basal cP, presence of diabetes mellitus or etiology of liver disease. the number of death was similar in both groups (58% vs. 63%; p = 0.506).
Conclusion: cirrhotic patients treated with beta-blockers have a lower cumulative probability of developing hcc, especially in the 10 years after diagnosis of cirrhosis
Disclosure of Interest: none Declared
P-015 VALIDATIOn Of The “Ab InITIO” LIVer TrAnSPLAnTATIOn POLICy In hePATOCeLLuLAr CArCInOMA uPOn DeTeCTIOn Of rISK fACTOrS fOr reCurrenCe AfTer SurGICAL reSeCTIOn
Joana ferrer* 1, alejandro forner2, 3, alexandre Liccioni2, Victor Molina1, Miquel navasa4, constantino fondevila1, juan carlos García-Valdecasas1, jordi Bruix2, 3, josep fuster1, 2
1hepatoBilioPancreatic surgery and transplant unit. Department of surgery. IcMDiM, 2Barcelona clinic Liver cancer (BcLc) group, Liver unit . august Pi i sunyer Biomedical research Institute (IDIBaPs), university of Barcelona, 3network for Biomedical research in hepatic and Digestive Diseases (cIBerehd), 4Liver unit.Liver transplantation unit. IcMDiM, hospital clinic Barcelona, Barcelona, spain
Introduction: surgical resection (sr) is the main treatment option in those patients with solitary hepatocellular carcinoma (hcc) and preserved liver function. regrettably, long-term outcome is impaired by hcc recurrence. Microvascular invasion and satellites identified in the specimen are pejorative markers of high risk of recurrence. although salvage liver transplantation (Lt) has been considered upon the detection of tumor recurrence, in some instances the recurrence is multifocal, exceeding the Lt criteria. a decade ago and based in a small number of patients, we proposed to enlist resected patients upon the detection of pejorative histological markers before the occurrence of recurrence (ab initio indication). the aim of this study is to evaluate the outcome of this treatment approach.
Methods: from 1995 to 2012, 164 patients with hcc underwent sr and were followed until March 2015. eighty-five patients were potential candidates to Lt (baseline hcc within Milan criteria (Mc) and younger than 68y) and were considered for Lt if the pathology showed microvascular invasion, satellites or additional nodule(s). those patients with no pejorative histological markers were followed-up and salvage Lt was considered upon the development of tumor recurrence/liver function impairment.
results: according to pathology, 37 patients (43.5%) were at high-risk and 48 (56.5%) at low-risk of recurrence. after a median follow-up of 61 months, 30 patients died and the median survival was 127 months and was different according to the pathology analysis (high- vs. low-risk: 140 vs. 123 months, p=0.039). seventeen out of 37 high-risk patients were transplanted, 2 are still on waiting list, 1 patient was lost, 5 presented recurrence beyond Mc during evaluation (median time from sr: 3.3 months, range 1.6-7.3), 5 patients were dropped out during waiting time (median time from sr: 21.9 month, range 4.3-29.2), 3 patients rejected to be enlisted and in 4 patients, Lt was contraindicated because of medical reasons. In those finally transplanted (n=17), the median time to Lt was 13 months, 7 patients developed tumor recurrence prior to Lt and in additional 3 patients, hcc foci were identified on the explant. after a median post-Lt follow-up of 55 months, two patients experienced tumor recurrence, 5 patients died, and the 5-year patient survival was 77.8%. regarding the 48 low-risk patients, 26 patients experienced tumor recurrence after a median follow-up of 72.8 months; eleven patients were transplanted, 1 is still on waiting list, 2 refused to be enlisted, 3 were excluded because of advanced age, 2 were excluded for medical reasons and in 5 cases, the recurrence was beyond Mc. In 2 patients with excellent liver function, re-resection was applied. after a median post-Lt follow-up of 59 months, two patients developed tumor recurrence at 59.9 months and 38 months, and 5 died. no significant differences in survival were observed between the transplanted vs. non-transplanted low-risk patients (median os 139 vs. 127 months, respectively, p=0.909).
Conclusion: enlistment of patients at high-risk of recurrence after resection before recurrence development seems a valid strategy and is associated with excellent long-term outcome. since we identified a proportion of patients with early (< 6 months), aggressive recurrence during the pre-Lt evaluation, we propose to wait at least 6 months before enlistment but once included, due the high risk of tumor recurrence, exception points should be assigned for being transplanted before recurrence appearance.
Disclosure of Interest: none Declared
P-016 hIV InfeCTIOn DOeS nOT WOrSen PrOGnOSIS Of LIVer TrAnSPLAnTATIOn In hePATOCeLLuLAr CArCInOMA
Alejandro forner* 1, fernando agüero2, christian Manzardo2, andrés Valdivieso3, Mariano Blanes4, rafael Barcena5, antoni rafecas6, Lluis castells7, antoni rimola8, jose María Miró2
1BcLc group Liver unit. IDIBaPs. cIBerehd., 2Infecious Disease Department, hospital clinic, Barcelona, 3surgery Department, hospital universitario de cruces, Bilbao, 4hospital universitario La fe, Valencia, 5hospital universitario ramón y cajal, Madrid, Madrid, 6hospital de Bellvitge. IDIBeLL, universidad de Barcelona., 7Internal Medicine. hepatology Department, hospital universitari Vall d‘hebrón, 8Liver unit, hospital clinic Barcelona. cIBerehd. IDIBaPs, Barcelona, spain

I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s3 2
top scored Posters
Introduction: the widespread use of combined antiretroviral therapy (cart) has dramatically reduced the hIV-related mortality. More prolonged survival allowed chronic liver disease, particularly those related to hcV infection, to become more clinically relevant. the incidence of hepatocellular carcinoma (hcc) has progressively increased among individuals with hIV infection over the past decades and up to 40% of liver-related mortality in patients with hIV infection is due to the development of hcc. Liver transplantation (Lt) is an effective procedure and the hIV infection is not considered a contraindication for this treatment option. Previous studies including a limited number of patients and/or short follow-up offer conflicting data regarding the impact of hIV on survival in patients hcc after Lt. the aim of this prospective multicenter study was to evaluate the influence of hIV infection in tumor recurrence and post-Lt survival in hcc patients treated by Lt.
Methods: Prospective cohort study including hIV infected patients undergoing Lt for hcc in 22 spanish hospitals (cohort fIPse) and transplanted hIV (-) patients matched for age, gender, year of Lt, hcV, hBV and hcc in a ratio 1: 3. Incidental hcc patients were excluded. enrollment began in january 2002 and the end of follow-up was in july 2014.
results: 74 patients hIV (+) patients and 222 hIV (-) underwent Lt for hcc during the study period. Most were men (86%) and had hcV co-infection (92%). hIV (+) patients were younger (47 vs. 51 years, p <0.001) and had genotype non-1 with higher frequency (55 vs. 25%) and less frequent hcV replication at the time of Lt (80% vs 90%) compared to hIV (-) patients. at the time of Lt, median [interquartile range] cD4/mm3 were 347 [238-523] and the majority of hIV (+) patients (96%) were on antiretroviral therapy. the hIV viral load was <50 copies/ml in 93%. there were no differences in waiting time until the Lt (4.5 vs. 5.4 months, p = 0.35), in baseline hcc characteristics at the moment of waiting list inclusion and on explant histological parameters between both groups. after a median follow-up of 46 [25-72] months, 25 (34%) hIV (+) patients and 64 (29%) hIV (-) patients died (p=0.421). causes of death in the two cohorts did not significantly differ. survival at 1, 3 and 5 years for hIV (+) patients compared to hIV patients (-) were 87%, 78% and 69% vs. 89%, 78% and 73% (p = 0.905). hcV infection (hr, 8.85 95% cI, 1.23 to 63.64) and the presence of satellite nodules (hr, 1.92; 95% cI, 1.13 to 3.24) were the only variables independently associated with mortality. at the end of follow-up, 12 (16%) hIV (+) patients and 32 (14%) hIV (-) patients had tumor recurrence. the probability of recurrence at 1, 3, and 5 years in hIV (+) and hIV (-) was 7%, 17% and 20% vs. 5%, 11% and 19%, respectively (p=0.876). analyzing jointly hIV patients (+) and hIV (-), microscopic vascular invasion (hr, 3.79; 95% cI, 1.67 to 8.57) was the only factor independently associated with hcc recurrence.
Conclusion: hIV infection has no impact on hcc recurrence or survival after Lt. these results support the indication of Lt in hIV-infected patients with hcc
Disclosure of Interest: none Declared
P-017 ADherenCe TO eASL-eOrTC CLInICAL GuIDeLIneS fOr The MAnAGeMenT Of hePATOCeLLuLAr CArCInOMA In fIeLD PrACTICe: reSuLTS frOM The ITA.LI.CA DATAbASe
rodolfo Sacco* 1, Valeria Mismas1, Luca Giacomelli1, sara Marceglia1, antonio romano1, Marco Bertini1, Michele Bertoni1, Graziana federici1, salvatore Metrangolo1, Giuseppe Parisi1, emanuele tumino1, Giampolo Bresci1
1Gastroenterology, cisanello Pisa university hospital Pisa - Italy, Pisa, Italy
Introduction: Data on adherence to joint guidelines for the management of hepatocellular carcinoma (hcc) published in 2012 by the european association for the study of the Liver (easL) and the european organization for research and treatment of cancer (eortc) are lacking. We retrospectively evaluated the adherence to easL-eortc guidelines in field-practice, using data from hcc patients registered in the nation-wide Italian database Ita.LI.ca. and diagnosed from 2012.
Methods: the Ita.LI.ca. database contains data of 5428 hcc patients treated at 18 Italian centers. Patients were stratified according to child-Pugh (cP) and and the Barcelona clinic Liver cancer (BcLc) classifications. We investigated the adherence to surveillance, diagnosis, and first-line treatment recommendations.
results: In Ita.LI.ca, 600 patients were diagnosed of hcc since 2012 (466 males; mean±sD age 67.4±10.9 years; 277(46.2%) cP-a and 163(27.2%) cP-B; 44(8%) BcLc-0, 193(35.1%) BcLc-a, 93(16.9%) BcLc-B, 172(31.3%) BcLc-c, 48(8.7%) BcLc-D). overall, 317(55.2%) were diagnosed during a surveillance program. of them, 231(57.9%) were cirrhotic (median surveillance duration: 6 months). four-hundred-ninety-six (85.3%, 449 cirrhotic) patients were diagnosed applying a radiological, 80(13.7%) a histological, and 6(1%) a cytological criterion. five (9.7%) patients in BcLc stage 0 with cP a, and single nodules underwent tumour resection; 3(1.4%) patients in BcLc-a received liver transplantation, and 83(43.1%) received radiofrequency ablation or Percutaneous ethanol Injection. Intermediate hcc-stage patients (BcLc-B) receiving tace were 45(47.9%), and advanced-stage patients (BcLc-c) receiving sorafenib were 38(21.9%). Palliative care was provided to terminal stage patients (BcLc-D) in 31(64.3%) cases.
Conclusion: the overall adherence in a “real-world” practice to easL-eortc guidelines was low, particularly in patients with early stage hcc. Difficulties inpatients staging and the high prevalence of older patients with relevant co-morbidities may partially explain these findings. strategies to help
improve adherence to international guidelines for hcc in field-practice and new scoring criteria are required.
Disclosure of Interest: none Declared
P-018 A nOVeL ChOLAnGIOCArCInOMA PATIenT DerIVeD xenOGrAfT enDOGenOuSLy exPreSSInG An fGfr2-CCDC6 fuSIOn PrOTeIn ShOWS DIfferenTIAL SenSITIVITy TO fGfr InhIbITOrS
yu Wang1, 2, hassan M. shaleh1, xiwei Ding1, 3, shaoqing Wang1, 4, kais zakharia1, Loretta k. allotey1, essa a. Mohamed1, catherine D. Moser1, roongruedee chaiteerakij1, 5, joseph M. Gozgit6, Mitesh j. Borad7, Lewis r. roberts * 1
1Division of Gastroenterology and hepatology, Mayo clinic, rochester, united states, 2Department of hepatobiliary surgery, nanfang hospital, southern Medical university, Guangzhou, 3Department of Gastroenterology, Drum tower hospital, affiliated to Medical school of nanjing university, nanjing, 4Department of Pathology, qiqihar Medical university, qiqihar, china, 5Department of Medicine, faculty of Medicine, chulalongkorn university and king chulalongkorn Memorial hospital, thai red cross society, Bangkok, thailand, 6arIaD Pharmaceuticals, Inc., cambridge, 7Division of hematology and Medical oncology, Mayo clinic, Phoenix, united states
Introduction: cholangiocarcinoma (cca) is a highly lethal cancer with limited therapeutic options and a poor prognosis. there is therefore a pressing need to develop novel therapies against this cancer. recent genomic analysis of cca tumors has revealed the presence of fGfr2 fusion proteins in up to 13% of intrahepatic ccas. the fGfr fusion proteins appear to play a key role in cancer progression. tumors harboring fGfr fusions have demonstrated enhanced sensitivity to fGfr inhibitors, suggesting that cca patients with fGfr2 fusions may benefit from targeted fGfr2 kinase inhibition. establishment of this primary cca patient derived xenograft (PDx) tumor model provides a powerful tool for exploring the mechanism of cca development and will be especially useful for screening potential effective fGfr inhibitors for efficacy in cca.the role of the fGfr kinase inhibitors ponatinib (aP24534), dovitinib (tkI-258) and BGj398 have not been evaluated in cca, particularly ccas bearing fGfr fusions. We aimed to establish a novel cca PDx mouse model bearing an fGfr2-ccDc6 fusion protein and assess the relative sensitivity of this PDx model to different fGfr inhibitors.
Methods: LIV31 is a PDx model derived in nsG scID mice from a metastatic lung nodule resected from a patient with stage IV intrahepatic cca. subsequent passage of the PDx tumor into nude mice was successful. Detailed genetic and genomic characterization using rna sequencing, array comparative genomic hybridization and break apart fIsh confirmed that LIV31 harbors a transcript encoding an fGfr2-ccDc6 fusion protein. this fusion protein has been shown in vitro to dimerize in the absence of ligand and increase cell proliferation. LIV31 cells were implanted subcutaneously into the flanks of nude mice. When tumor volumes reached 150-250 mm3 the mice were randomized into four groups: vehicle, ponatinib 25 mg/kg, dovitinib 30 mg/kg, or BGj398 15 mg/kg. the drugs were administered daily by oral gavage at doses previously shown to be tolerated by mice. tumor volume and mouse weight were measured once a week. tumor growth curves were compared. after a maximum of 63 days treatment, the animals were euthanized and xenografts were examined by histology, Ihc and Western blot for fGfr2 and the fGfr pathway downstream mediators pfrs2, pakt, and perk.
results: all three fGfr inhibitors significantly inhibited the growth of the fGfr2-ccDc6 fusion mouse xenograft tumors when compared with vehicle (P<0.0001), but none of the inhibitors completely eradicated the tumors. at the administered doses, BGj398 and dovitinib were more potent than ponatinib (P<0.0001) and BGj398 was superior to dovitinib (P<0.0003). histology showed that treated tumors were more well-differentiated than control tumors. all three tkIs strongly inhibited expression of well-established downstream markers of fGfr signaling phospho-fGfr, p-frs2, p-akt and p-erk1/2.
Image:

Top Scored Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 3 3
Conclusion: Ponatinib, dovitinib and BGj398 all significantly inhibited the growth of patient-derived cca xenografts bearing an oncogenic fGfr2-ccDc6 fusion gene. treatment efficacy from most to least effective was BGj398 > dovitinib > ponatinib. additional studies exploring the potential mechanisms underlying differences in response to particular fGfr inhibitors and the effects of combinations of other therapeutic agents with small molecule fGfr inhibitors are needed.
Disclosure of Interest: none Declared
P-019 hIGh-ThrOuGhPuT SMALL MOLeCuLe SCreenInG IDenTIfIeD SMALL DruGS POTenTIALLy ACTIVe In ChOLAnGIOCArCInOMA
Io hong Cheong* 1, rosemary Burke1, Paul clarke1, Matteo fassan2, Michele simbolo3, Giulia ferrari1, aldo scarpa3, Mark stubbs1, swee sharp1, rob van Montfort1, nicola Valeri4, Paul Workman1, chiara Braconi1
1Division of cancer therapeutics, the Institue of cancer research, London, united kingdom, 2Dpt of Medicine, university of Padua, Padua, 3Dpt of Pathology, university of Verona, Verona, Italy, 4Division of Molecular Pathology, the Institue of cancer research, London, united kingdom
Introduction: cholangiocarcinomas (cca) are chemo-resistant tumours, for which only the combination of cisplatin and gemcitabine (cG) prolongs overall survival. In addition, level a evidence is lacking for recommendation of cG in Intrahepatic cca. novel therapies are urgently needed to improve outcome of cca patients. In this study we aim to identify novel small molecule drugs that can be active against cca growth.
Methods: Intrahepatic (Icc) [sW1, snu-1079, ccLP-1], and extrahepatic (ecc) [snu-1196,tfk, eGI] cca cell lines were used. next-Generation-sequencing analysis using a 64-gene panel that included the most frequent mutated genes in human cca1 was performed. high-throughput screening technologies (hsts) were applied to screen 484 small molecules (at 3 concentrations: 80nM, 200nM, 800nM) against all 6 cca cell lines in triplicate. cell viability was normalized vs DMso, and t-test analysis applied for each single dose.
results: cells were confirmed to recapitulate the genetic background of human cca (mutations in tP53, BaP1, PBrM1, sMaD4, kras and IDh1 were detected). a number of drugs (median 68 per cell line) were significantly (p<0.05) active at all the concentrations. Gemcitabine and Polo-Like-kinase (PLk) inhibitors reduced cell viability in all our cell lines confirming the validity of the screening. We searched for enrichment of drugs in the same class to increase the confidence that the effect was dependent on the inhibition of a specific pathway. We noticed enrichment for microtubule associated drugs and mtor inhibitors in all cell lines. clinical trials are ongoing for microtubule-associated compounds (such as epothilone), and for mtor inhibitors in cca. an enrichment of histone-Deacetylases (hDac) Inhibitors was observed in snu-1079 cells which harbour mutations in IDh1 and PBrM1 chromatin remodelling genes. enrichment for eGfr inhibitors (including erlotinib) was observed in sW1, snu-1196 and tfk cells, suggesting that eGfr inhibition may be pursued in selected cases after identification of biomarkers of response (and may explain failure of recent phase III trials2). cediranib, a VeGfr inhibitor, which has not improved clinical outcome in phase II trial3, failed to reduce cell viability in our hst. aurora kinase (ak), and hsP90 inhibitors were effective in all cell lines. tozasertib (ak inhibitor) was commonly active across Icc cells, while barasertib and sns-314-Mesylate (ak inhibitors) were active across ecc cells. Danusertib, which is an ak inhibitor with activity also on the fGfr was significantly effective across the doses in ccLP, sW1 and tfk. Ponatinib, a multi-target inhibitor (including fGfr1) was effective in ccLP, sW1 and tfk. other fGfr inhibitors were not consistently effective. auy922 (hsP90 inhibitor) activity was confirmed in a larger panel of cca cell lines. Ic50 was as follows: eGI 23nM, tfk 31nM, snu-1196 40nM, snu-245 500nM, snu-869 61nM, snu-478 40nM, Witt 33nM, sW1 50nM, ccLP 6nM. cells with higher nqo1 mrna expression had lower Ic50 to auy922.
Conclusion: We applied hst to test the activity of a range of small molecules in cca cells. Drugs which failed to show improved outcome in clinical trials have not shown any activity in our screening. We identified candidate drugs, such as hsP90 and ak inhibitors, that may be exploited for the treatment of cca. our data suggest that pre-clinical evidence on the activity of small drugs may better guide the design of clinical trials in human cca.
references: 1simbolo oncotarget. 2014 15;5(9):2839.2Lee Lancet oncol. 20123(2):181.Valle jclinoncol 32:2014
Disclosure of Interest: none Declared
P-020 ACquISITIOn Of STeM CeLL PrOPerTIeS In TuMOr-DerIVeD hePATOCyTe-LIKe CeLLS LeADS TO MeTAbOLIC rePrOGrAMMInG AnD CheMOreSISTAnCe
Karim fekir* 1, 2, hélène Dubois-Pot-schneider1, 2, florian cabillic1, 2, Denise Glaise1, 2, claudine rauch1, 2, Bernard fromenty1, 2, fabrice Morel1, 2, anne corlu1, 2
1InserM uMr991, 2université de rennes, rennes, france
Introduction: human hepatocellular carcinoma (hcc) heterogeneity promotes recurrence and
resistance against therapies. recent studies reported that hcc can derive from adult hepatocytes, hepatoblasts but also hepatic stem/progenitors. Moreover, the presence of cancer stem cells (cscs) in tumors derived from all these cell types suggests that any cell of the hepatic lineage could acquire stem cell properties upon acquired oncogenic transformation. recently, we have shown by that inflammatory environment promoted the retrodifferentiation of tumor-derived hepatocyte-like cells into stem/progenitor cells confirming that microenvironment greatly influences the cell fate. one of the main difficulties to characterize hepatic progenitor/csc is the lack of experimental models representative of these cells. the native heparG cells, isolated from a differentiated hcV derived tumor, retain the capacity to differentiate into hepatocytes- and biliary-like cells and therefore could be considered as human hepatic progenitors. In addition, under specific conditions, the hepatocytes-heparG are able to retrodifferentiate into hepatic stem/progenitor cells that can give rise to both hepatocyte- and biliary-like cells. In this study, using heparG cells, we identified molecular effectors involved in the acquisition and maintenance of stem cell features.
Methods: heparG stem cells (side population or sP) were isolated and anchorage-independent cultures from heparG progenitors were performed. transcriptional analysis allowed us to identify profound changes in the gene profiles of both sP and sphere-forming cells. shrna or specific inhibitors were used to analyze the involvement of signaling pathways.
results: hierarchical clustering of the differentially expressed genes showed that sP and sphere-forming cells were closer to h9 embryonic stem cells than to heparG progenitors and differentiating heparG cells. acquisition of stem cells features was correlated with increased expression of cytokines IL-6, IL-11, tGfβ, involved in the hepatocyte retrodifferentiation process, and anGPtL4 produced in both tumor and peritumoral liver tissues. In addition, reduced mitochondria activity and higher glycolytic pathway were detected in sP and sphere-forming cells. We demonstrated that anGPtL4 regulated cell invasion, expression of the anti-inflammatory cytokine, IL-11 and pyruvate dehydrogenase kinase 4 (PDk4), which inhibits the mitochondrial enzyme pyruvate dehydrogenase. the anGPtL4 downstream effector erk was involved in these processes, while PI3k/akt pathway was crucial for cell survival. Interestingly, sphere-forming cells were resistant to sorafenib and among heparG differentiating cell population, viable cells after sorafenib treatment displayed stem cells features and expressed anGPtL4 and PDk4. We showed that inhibition of anGPtL4 increased the sensitivity of sphere-forming cells to sorafenib. Moreover, the inhibition of PDk4 activity by sodium dichloroacetic acid (Dca) induced sphere-forming cell death and its association with chemotherapy increased cell toxicity in differentiating cell population.
Conclusion: our data demonstrated that csc developed mechanisms that modulate inflammatory response, energy homeostasis and specific metabolic abilities that contribute to chemoresistance. reestablishment of mitochondria activity by Dca or targeting anGPtL4, in combination with chemotherapy could open new therapeutic opportunities for hcc.
Disclosure of Interest: none Declared
P-021 KOreAn VALIDATIOn AnD COMPArISOn Of PrOGnOSTIC SCOreS fOr TrAnSArTerIAL CheMOeMbOLIzATIOn: ArT, AbCr, hAP, AnD MODIfIeD hAP
hae Lim Lee* 1, si hyun Bae1, jung suk oh2, ho jong chun2, jeong Won jang1, jong young choi1, seung kew yoon1
1Devision of hepatology, Department of Internal Medicine, catholic Liver research center, the catholic university of korea, 2Department of radiology, seoul st. Mary's hospital, the catholic university of korea, seoul, korea, republic of
Introduction: transarterial chemoembolization (tace) is one of the treatment options for unresectable hepatocellular carcinoma (hcc). Because various clinical stages of hcc were treated with tace, their prognosis varies. there are four prognostic scores for tace: art, aBcr, haP and modified haP (mhaP). however, there is lack of validation of these scores, especially in korea. the aim of this study is to validate and compare these scores.
Methods: from october 2008 to february 2014, total of 1211 patients with hcc were treated with tace in seoul saint Mary’s hospital. among them, 800 patients underwent at least two sessions of tace within 90 days. 549 patients were excluded due to prior treatment from other hospitals, post-tace liver transplantation, combined treatment with tace, child pugh class c, or end stage renal disease. finally, total of 251 patients were analyzed.
the validation in art, aBcr, haP, and mhaP score was performed. the overall survival (os) was calculated using the kaplan-Meier method and these scores were compared using the auroc curve.
results: Mean age was 59.2(±10.6) and hepatitis B related hcc was 70.9%. Median follow up period was 24.2 months (1.9-77.0) and median cycles of tace was four. from these scores, os of each group was calculated: art (63.7, 37.7 months in 0-1.5, ≥2, P=0.142), aBcr (57.6, 18.1, 7.9 in ≤0, 1-3, ≥4, P<0.001), haP (60.2, 52.2, 20.8, 10.8 in 0, 1, 2, >2, P<0.001), mhaP (58.7, 48.7, 16.6, 7.9 in 0, 1, 2, >2, P<0.001). and the auroc of survival was calculated(0.508, 0.709, 0.662, 0.652 in 1 year and 0.498, 0.679, 0.654, 0.650 in 2 years, in art, aBcr, haP, mhaP, respectively).
Conclusion: In our study, aBcr, haP and mhaP were well applied for differentiation in os in

Top Scored Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s3 4
patients treated with tace. however, art was not applicable. according to the comparison of these scores, aBcr was best predictable prognostic score for tace.
Disclosure of Interest: none Declared
P-022 DeLeTerIOuS PASSenGer MuTATIOnS AS A MArKer fOr PrOGreSSIOn TOWArDS LIVer CAnCer
Magdalena A. budzinska* 1, 2, thomas tu1, fabio Luciani2, nicholas shackel1, 3
1centenary Institute, 2school of Medical sciences, the university of new south Wales, 3australian national Liver transplantation unit, royal Prince alfred hospital, sydney, australia
Introduction: hepatocellular carcinoma (hcc) is associated with alterations in a small set (~5) of driver genes, though none have been shown to be necessary or sufficient for tumourigenesis. the vast majority of mutations unique to the patients (known as passenger mutations) have so far been ignored. some passenger mutations are deleterious and may act as markers for cancer progression. a previous study has shown that deleterious passenger mutations (DPMs) occur more frequently in tumour tissue compared to surrounding non-tumour tissue. the accumulation of DPMs was hypothesised to be due to: 1) that DPMs occur more frequently than driver mutations; and 2) that the build-up of DPM eventually offsets the survival advantage conferred by driver mutations. therefore, we aim to detect DPMs in liver disease progression and hypothesise that DPMs accumulate in hepatocytes in precancerous conditions leading up to hcc.
Methods: We have performed whole exome sequencing of pre-cancerous liver tissues: 12 patients with limited level of liver injury and 6 hcV-positive patients with liver cirrhosis. We have also analysed publically available paired hcc and surrounding non-tumour datasets. to compare different data we only analysed mutations that occurred in protein-coding genes and filtered out probable germline mutations. Poly-Phen2 was employed to predict impact of variants on protein function.
results: consistent with prior studies, hcc genomes contained significantly more DPMs compared to paired non-tumour tissue (p<0.001 by paired two-tailed t-test). comparison with non-cirrhotic and cirrhotic tissues showed significantly lower proportion of DPMs to tumour and non-tumour tissues. Moreover, we observed a significantly more DPMs in non-tumour tissue as the numbers of damaging mutations in putative driver genes increase. DPMs were evenly distributed across the genome and the majority were unique for each patient, suggesting they are truly passenger mutations.
Conclusion: this study has 2 main findings. firstly, non-tumour tissue is not normal and likely contains pre-cancerous mutations. this is consistent with our previous studies showing significant clonal expansion of hepatocytes in chronic hepatitis virus infection. We are currently sequencing liver Dna from hcV-positive patients with liver cirrhosis and/or hcc, and non-infected normal controls to determine when. secondly, DPMs accumulate in tumour vs. non-tumour liver tissue regardless of the aetiology of hcc. this suggests that DPM load may be used in future as a marker of hcc risk, omitting the need to detect often heterogeneous and rare driver mutations.
Disclosure of Interest: none Declared
P-023 PreDICTIOn MODeL fOr The DeVeLOPMenT Of hePATOCeLLuLAr CArCInOMA In PATIenTS WITh ChrOnIC hePATITIS b reCeIVInG AnTIVIrAL TreATMenT
Jem-Ma Ahn* 1, yeon seok seo1, tae hyung kim1, sun young yim1, young kul jung1, ji hoon kim1, hyunggin an2, hyung joon yim1, hong eun yeon1, kwan soo Byun1, soon ho um1
1Division of Gastroenterology, Department of Medicine, 2Department of Biostatistics, korea university, seoul, korea, republic of
Introduction: although several models predicting development of hepatocellular carcinoma (hcc) in patients with chronic hepatitis B (chB) have been already published, a new prediction model is required for the patients who receive long-term antiviral therapy with sustained suppression of viral replication. thus this study was performed to establish and validate a new model for predicting development of hcc in chB patients with anti-viral treatment, based on histological data.
Methods: consecutive patients with chB who received antiviral therapy with liver biopsy between 2001 and 2013 were enrolled in a training set, and those who received antiviral therapy without liver biopsy were included in a validation set, respectively. cox-regression analysis was performed to identify independent factors and to establish a new prediction model for hcc development. the predictive efficacy of the new model was compared with risk estimation for hcc in chB (reach-B) model.
results: training and validation sets were consisted of 478 and 553 patients. In the training set, their mean age was 39.9 ± 12.1 years and 333 patients (69.7%) were male. fibrosis stage on liver biopsy was as following: f01 in 98 (20.5%) patients, f2 in 160 (33.5%) patients, f3 in 165 (34.5%) patients, and f4 in 55 (11.5%) patients. During the follow-up of 63.8 ± 43.2 months, hcc developed in 18 patients. In multivariate analysis, age, BMI, heavy alcohol consumption, platelet count, and
hBeag were independent factors for predicting hcc development. With these independent variables and their beta coefficients, a hcc prediction model was established. aucs of our model for predicting hcc within 5 and 10 years were 0.910 and 0.892, respectively. In the validation set, aucs were 0.849 and 0.907, respectively. In training and validation sets, aucs of our model were significantly higher than those of reach-B model.
Conclusion: there was significant difference in the predictive factors for hcc development between patients who were treated with long-term antiviral therapy and those without antiviral therapy. our new prediction model was very accurate and useful for predicting hcc development in patients with chB receiving antiviral therapy.
references: 1. arends P, sonneveld Mj, zoutendijk r, et al. entecavir treatment does not eliminate the risk of hepatocellular carcinoma in chronic hepatitis B: limited role for risk scores in caucasians. Gut 2014.2. yang hI, yuen Mf, chan hL, et al. risk estimation for hepatocellular carcinoma in chronic hepatitis B (reach-B): development and validation of a predictive score. The Lancet Oncology 2011; 12(6): 568-74.3. yuen Mf, tanaka y, fong Dy, et al. Independent risk factors and predictive score for the development of hepatocellular carcinoma in chronic hepatitis B. Journal of hepatology 2009; 50(1): 80-8.4. Wong VW, chan sL, Mo f, et al. clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers. journal of clinical oncology: official journal of the American Society of Clinical Oncology 2010; 28(10): 1660-5.
Disclosure of Interest: none Declared
P-024 The VALIDATIOn Of A neW MODIfIeD ChILD-TurCOTTe-PuGh SCOre uSInG InSuLIn-GrOWTh fACTOr-1 AS A PrOGnOSTIC MODeL fOr hePATOCeLLuLAr CArCInOMA
Dong hyeon Lee* 1, jeong-hoon Lee1, yuri cho1, jung-ju yoo1, Minjong Lee1, young youn cho1, eun ju cho1, su jong yu1, yoon jun kim1, jung-hwan yoon1
1Department of Internal Medicine and Liver research Institute, seoul national university college of Medicine, seoul national university hospital, seoul, korea, republic of
Introduction: the child-turcotte-Pugh (ctP) score is widely used to determine prognosis in patients with liver disease. however, the ctP score has some limitations, such as subjective interpretation of parameters and limited discriminatory ability. on this account, by replacing both ascites and encephalopathy grades with plasma insulin-growth factor (IGf)-1 level, a modified ctP (IGf-ctP) scoring system had been proposed. this study aimed to validate IGf-ctP score model as a prognostic maker for hepatocellular carcinoma (hcc) in hepatitis B virus endemic area.
Methods: this was a post-hoc analysis of a prospective cohort study conducted at seoul national university hospital (seoul, korea). cox regression model and log rank test were used to assess the relationships between overall survival (os) and both ctP and IGf-ctP scoring systems. harrell’s c-index and u-statistics were used to compare the prognostic performance of both scores.
results: a total of 393 patients were included. During the follow-up period (median follow-up duration, 59.1 months), 55 patients died. according to ctP model, 334, 57, and 2 patients were classified as class a, B, and c, respectively. according to IGf-ctP model, 318, 57, and 18 were classified as class a, B, and c. IGf-ctP score was able to predict death more accurately (c-index=0.604, 95% confidence interval [cI]=0.539-0.668) than ctP score (c-index=0.558, 95% cI=0.501-0.614) (P=0.011 by u-statistics). In multivariate analysis, IGf-ctP score was still remained as an independent predictor of overall survival (P=0.001), whereas ctP score was lost its discriminatory ability (P=0.106) after adjustment for the presence of cirrhosis, serum alpha-fetoprotein level, tumor size, and lymph node spread. In addition, patients classified as class a by ctP but class B by IGf-ctP had significantly worse os than those classified as class a by both IGf-ctP and ctP (hr=2.85, 95% cI=1.20-6.78, P=0.018).
Conclusion: IGf-ctP score demonstrates better discriminatory function in hcc patients than ctP score. for more accurate prognostication for hcc patients, it could be better to replace ctP score with ctP-IGf score.
Disclosure of Interest: none Declared
P-025 CIrCuLATInG neuTrOPhILS AnD The SySTeMMIC IMMune-InfLAMMATIOn InDex AS PrOGnOSTIC TOOLS fOr PATIenTS WITh hePATOCeLLuLAr CArCInOMA
helen L. reeves1, 2, Laura f. Ogle* 1, Ghazanfar a. anwar2, Deborah stocken3, David jamieson1
1northern Institute for cancer research, newcastle university, 2Liver unit, freeman hospital, newcastle upon tyne hospitals nhs foundation trust, 3Institute of health and society, newcastle university, newcastle-upon-tyne, united kingdom
Introduction: In patients with hepatocellular carcinoma (hcc), it is estimated that 90% cases

Top Scored Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 3 5
develop on a background of inflammation. furthermore, inflammatory cells central to both innate and adaptive immune responses are key determinants of tumour progression. recent reports suggest that numbers of circulating neutrophils, lymphocytes and platelets have prognostic value in patients undergoing resection [1]. We have explored these candidate biomarkers in a broader cohort of patients with hcc.
Methods: Blood count data from 632 consecutive patients presenting to the newcastle-upon-tyne foundation trust between 2000 and 2010 [2] was interpreted alongside demographic data and disease characteristics. the systemic immune-inflammation index (sII) (neutrophils/lymphocytes x platelet count) was calculated [1]. associations with tumour stage, liver function, performance status (Pst) and survival were explored.
results: the neutrophil, lymphocyte, neutrophil/lymphocyte ratio, platelet counts and sII each correlated significantly in a stepwise fashion with BcLc stage (table 1). notably, neutrophil count was associated with tumour grade (tnM, table 1), a falling lymphocyte count was associated with childs Pugh (cP) stage, while both were significantly associated with ecoG Pst, the final component of BcLc. Data are shown as median values. statistics was using kruskal Wallis test across categories within defined stages of BcLc a-D, cP a-c, tnM 1-4 and Pst 0-4. ns-not significant, **p<0.001; ***p<0.0001. neutrophil count was significantly associated with survival, as was the combination sII score. Median survival was significantly different between three patient groups defined by the sII (figure 1) – with survival of 21.2, 7.7 and 2.4 months respectively (p<0.0001; hr 1.45 and 2.5; Multivariate cox regression). the association was independent of BcLc stage as well as treatment received.
Grade BcLca BcLcB BcLcc BcLcD cPa cPB cPc
neutrophilsLymphocytesPlatelets
3.481.57135
3.821.61164
4.411.43178
5.15***1.14***184***
4.161.52191
3.971.15147
4.23ns
1.11***127***
nLr 2.27 2.43 2.83 4.24** 2.73 2.81 3.96***
sII 306 394 614 789*** 506 482 532ns
grade tnM1 tnM2 tnM3 tnM4 Pst0 Pst1 Pst2 Pst4
neutrophilsLymphocytesPlatelets
3.881.38161
3.361.53132
4.761.34191
5.41***1.36ns
259***
3.711.54145
4.051.37172
5.031.27184
7.06***0.93**197***
nLr 2.60 2.29 3.29 3.35*** 2.39 2.75 3.38 7.59**
sII 433 333 709 991*** 353 546 732 1657***
Image:
Conclusion: these data support the emerging role of neutrophil-driven inflammation as a driver of hcc progression. In addition, numbers of circulating inflammatory cells have prognostic value, with neutrophils positively associated with advanced tumour grade, reduced lymphocyte associated with poorer liver function, and combination scores associated with tumour and liver disease parameters. notably, the sII had independent prognostic value, performing well across all aetiologies, stages of disease and treatment groups.
references: 1. hu, B. et al, Systemic immune-inflammation index predicts prognosis of patients after curative resection for HCC. clin can res, 2014. 20:6212-22. 2. Dyson, j. et al, HCC: The impact of obesity, type 2 diabetes and a multidisciplinary team. j hepatol, 2014. 60:110-7
Disclosure of Interest: none Declared
P-026 exTrAhePATIC MeTASTASeCTOMy fOr hePATOCeLLuLAr CArCInOMA: PreDICTOrS Of LOnG TerM SurVIVAL
yaniv Berger1, Marina heskel1, samantha n. aycart1, john h. spivack2, Daniel M. Labow1, umut Sarpel* 1
1Department of surgery, Division of surgical oncology, 2Department of Population health science and Policy, Mount sinai Medical center, new york, ny, united states
Introduction: While the resection of isolated metastatic disease has a survival benefit for certain malignancies, the role of extrahepatic metastasectomy (eM) for hepatocellular carcinoma (hcc) is not well established. We report our institutional experience with eM in a cohort of hcc patients with focus on predictors of long term survival.
Methods: all patients diagnosed with metastatic hcc at the Mount sinai hospital 2001-2014 were retrospectively reviewed to identify those who underwent eM with therapeutic intent. cases of pathologically negative eM, incomplete macroscopic resection, or diagnostic/palliative eM were excluded from our cohort. survival probabilities (measured from the date of metastasectomy) were calculated using the kaplan-Meier method; associations among multiple clinicopathological variables and survival were analyzed by the log rank test. Information criteria based approach was used for multivariate cox regression model building.
results: out of 440 metastatic hcc cases, we identified 85 patients (mean age 58.8±11.7 years, 81.2% male) who underwent 104 eM procedures. eM sites included lung (n=36), peritoneum (n=22), abdominal / mediastinal lymph nodes (n=19), musculoskeletal sites (n=18) and adrenal (n=9). Most patients underwent metachronous eM following primary liver resection (n=44) or transplantation (n=25); in 13 patients, synchronous hepatectomy + eM was performed as the initial procedure. at the time of eM, 49 patients (57.6%) had no intrahepatic hcc.the median time from initial hcc diagnosis to metastasis (pre-eM metastasis free interval) was 18.1 months. the median number and mean largest size of metastases resected was 1 (range 1-12) and 3.6±2.9 cm, respectively. Postoperatively, the median length of hospital stay was 4 days (range 0-32) and there were 2 cases of in-hospital mortality, which both occurred in patients who underwent concurrent hepatectomy and eM.the median follow up period was 20.9 months, during which 55 patients (64.7%) died. the 1-year, 2-year and 5-year survival rates for eM patients were 77.4%, 53.1% and 25.1%, respectively. the median extrahepatic and intrahepatic progression-free survival periods were 7.7 and 16.2 months, respectively. at last follow up, 5 patients were alive and disease free >2 years (range: 2.4-10.0 years) after eM.eM patients had superior median overall survival (os) when compared to a cohort of metastatic hcc patients treated with sorafenib (27.2 vs. 7.4 months, respectively, p<0.001) but also had more favorable baseline characteristics in terms of tumor burden (p<0.001), liver function (p<0.001) and number of metastatic sites (p=0.01).on univariate analysis, factors found to correlate with favorable os within the eM group Included lung resection (figure 1a), pre-eM metastasis-free interval≥3 months (p=0.04), preoperative alpha fetoprotein level≤100 ng/ml (p=0.02), child-Pugh score=5 (p=0.03), largest metastasis resected≤3cm (p=0.006) and number of metastases resected≤2 (figure 1b). on multivariate analysis, number of metastases resected>2 was found to be an independent predictor of poor survival (p=0.0099, hr=2.058), whereas child-Pugh score>5 and short pre-eM metastasis-free interval approached statistical significance.
Image:

Top Scored Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s3 6
Conclusion: although cure remains elusive following metastases from hcc, long term survival may be achieved in highly selected patients. the presence of greater than 2 extrahepatic lesions, poor liver function, and short pre-eM metastasis free interval are unfavorable prognostic factors that may help guide surgical decision-making.
Disclosure of Interest: none Declared
P-027 LOCOreGIOnAL TherAPIeS IMPrOVe SurVIVAL In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA TreATeD WITh SOrAfenIb
umut Sarpel* 1, yaniv Berger1, 1, john h. spivack2, Marina heskel1, samantha n. aycart1, robert e. sweeney3, Martin P. edwards4, Myron e. schwartz5, edward kim4
1Department of surgery, Division of surgical oncology, 2Department of Population health science and Policy, 3Department of surgery, 4Department of radiology, 5the recanati / Miller transplantation Institute, Mount sinai Medical center, new york, ny, united states
Introduction: In patients with advanced hepatocellular carcinoma (hcc), sorafenib is the standard of care and the only treatment with a proven survival benefit. Liver-directed locoregional therapies (Lrtx) are often employed in this population although it is unknown whether their addition improves prognosis over sorafenib alone.
Methods: a query of the medical records was performed to identify all hcc patients from 2006-2014 with extrahepatic metastasis and/or gross vascular invasion (GVI) who had received sorafenib during their treatment. any duration/dose of sorafenib therapy was considered sufficient for inclusion. Lrtx types were transarterial chemoembolization (tace), yttrium-90 radioembolization (y90), and external beam radiation therapy (eBrt). Patients were excluded from analysis if they were not candidates for Lrtx due to child-Pugh c cirrhosis, or because of adequate control of the primary tumor (e.g. history of resection or complete response to prior Lrtx). Patients with a history of Lrtx before the date of metastasis were allowed. eligible patients were then divided into two groups: sorafenib vs. sorafenib plus Lrtx, based on intention to treat as determined by chart review. Propensity score matching was used to balance both groups in terms of age, gender, major comorbidities, performance status, liver disease, liver function, vascular invasion, hepatic tumor burden, and number of metastatic sites. the sensitivity of results to changes in the propensity score model was assessed by weight trimming. Guarantee time bias was ruled out using the conditional landmark method at cutpoints of 30, 60 and 90 days. kaplan-Meier curves in the reweighted treatment arms were created to assess the survival difference associated with intended treatment status.
results: a total of 337 eligible patients were identified with extrahepatic metastasis and/or GVI who had received sorafenib during their treatment (mean age 61.2±10.4 years; males 81%; hepatitis c 46%; ecoG score 0-1 88%, score 2-3 12%; child-Pugh grade a 63%, grade B 37%; GVI 64.9%; extrahepatic metastasis 51.6%; median afP 314 ng/mL). Lrtx was intended in 247 of these patients, with 90 patients in the sorafenib only arm. Lrtx was actually delivered in 199 patients, with 138 patients receiving only sorafenib. Lrtx type was tace (73.9%), y90 (18%) or eBrt (7%); with more than one type/session used in 106 patients during the study period. the median time from diagnosis of advanced stage disease to Lrtx was 27 days. Median survival in the sorafenib arm was 123 days (95% cI: 90-157) vs. 272 days (95% cI: 228-313) in the sorafenib plus intention to treat Lrtx arm (figure 1). a propensity score weighted proportional hazards model using intention to treat as a single predictor of survival demonstrated benefit to Lrtx (hr=0.552, 95% cI: 0.452-0.672). an as-treated analysis also revealed benefit to treatment with Lrtx (hr=0.468, 95% cI: 0.383-0.572).
Image:
Conclusion: our cohort of patients with advanced hcc had poor prognostic features including
worse liver function and performance status that limited overall survival despite treatment with sorafenib. a survival benefit was seen with the addition of Lrtx to sorafenib, based on the use of propensity score matching and an intention to treat analysis. these results suggest that liver-directed locoregional therapies should be considered in addition to the standard of care treatment with sorafenib in eligible patients with extrahepatic metastasis and/or GVI.
Disclosure of Interest: none Declared
P-028 nAnOPArTICLe-DeLIVereD SMALL InTerferInG rnA fOr ASTrOCyTe eLeVATeD Gene-1 AnD ALL-TrAnS reTInOIC ACID: A COMbInATOrIAL TherAPy fOr hePATOCeLLuLAr CArCInOMA
Devanand Sarkar* 1, Devaraja rajasekaran1, jyoti srivastava1, kareem ebeid2, rachel Gredler1, Maaged akiel1, nidhi jariwala1, chadia robertson1, xue-ning shen1, ayesha siddiq1, Paul B. fisher1, aliasger salem2
1human and Molecular Genetics, Virginia commonwealth university, richmond, 2Pharmaceutical sciences and experimental therapeutics, university of Iowa, Iowa city, united states
Introduction: there is virtually no effective treatment for advanced hcc mandating development and evaluation of novel therapy for this fatal malady. here we propose a combination of nanoparticle-delivered sirna for aeG-1 and atra as a potential therapy for hcc. the rationale behind this combination is: (1) Previous studies have firmly established the important regulatory role of aeG-1 in hepatocarcinogenesis thereby identifying aeG-1 as a bona fide target for hcc treatment. (2) since aeG-1 is a scaffold protein a small molecule inhibitor of aeG-1 may not be possible to develop. considering the fact that i.v. injection of payload is efficiently delivered to the liver, rnai therapy might be quite effective for hcc. Indeed, clinical trials using nanoparticle-delivered sirna for other oncogenes have demonstrated significant therapeutic efficacy for hcc. thus nanoparticle-delivered aeG-1 sirna might be an effective way to counteract hcc. (3) aeG-1 interacts with retinoid x receptor (rxr) and thus inhibits retinoic acid (ra)-induced cytotoxicity. analogs of retinoic acid have been evaluated for hcc in previous clinical trials without producing effective results which might be due to blockade of ra action by overexpressed aeG-1 in hcc patients. Indeed, we demonstrated that ex vivo treatment of human hcc cells with a lentivirus expressing aeG-1 shrna along with i.p. injection of atra resulted in synergistic and marked inhibition of subcutaneous xenografts in nude mice.
Methods: Liver-targeted nanoplexes were developed by conjugating poly(amidoamine) (PaMaM) dendrimers with polyethylene glycol (PeG) and lactobionic acid (Gal) (PaMaM-PeG-Gal) which were complexed with aeG-1 sirna (PaMaM-aeG-1si). the polymer conjugate was characterized by 1h-nMr, MaLDI and mass spectrometry, and optimal nanoplex formulations were characterized for surface charge, size and morphology. orthotopic xenografts of human hcc cell qGy-7703 expressing luciferase (qGy-luc) were established in the livers of athymic nude mice and tumor development was monitored by bioluminescence imaging (BLI). tumor-bearing mice were treated with PaMaM-sicon, PaMaM-sicon+atra, PaMaM-aeG-1si and PaMaM-aeG-1si+atra. atra was administered i.p. at a dose of 10 mg/kg and 500 mg of sirna, conjugated with PaMaM-PeG-Gal at a ratio of 5:1, was administered i.v. per injection. a total of 8 injections were administered twice a week and the mice were sacrificed 2 weeks after the last injection.
results: In the control group the tumor developed aggressively. atra showed little effect due to high aeG-1 levels in qGy-luc cells. PaMaM-aeG-1si showed significant reduction in tumor growth and the combination of PaMaM-aeG-1si+atra showed profound and synergistic inhibition so that the tumors were almost undetectable by BLI. a marked decrease in aeG-1 level was observed in tumor samples treated with PaMaM-aeG-1si. the group treated with PaMaM-aeG-1si+atra nanoplexes showed increased necrosis, inhibition of proliferation and increased apoptosis when compared to other groups.
Conclusion: Liver is an ideal organ for rnai therapy and atra is an approved anti-cancer agent. our exciting observations suggest that the combinatorial approach might be an effective way to combat hcc and should be evaluated in more stringent animal models to accrue baseline information for a potential clinical trial.
Disclosure of Interest: none Declared
P-029 A 3-PrOTeIn SIGnATure TO IMPrOVe CLInICAL STrATIfICATIOn Of ChILDhOOD LIVer CAnCer
Marina Simon* 1, 2, Mikel azkargorta3, Laura Guerra4, Lara nonell5, Manuel Lopez-santamaria6, Marta Garrido7, Diego Plaza8, francisco hernandez6, Marta Mendiola4, Marie annick Buendia9, felix elortza3, Isabel ojanguren10, ramon Planas2, 10, Maria-rosa sarrias2, 11, Margarita sala1, 2, 10, carolina armengol1, 2
1childhood Liver oncology Group (c-LoG), health sciences research Institute Germans trias i Pujol (IGtP), 2cIBerehd, Badalona, Barcelona, 3Proteomics Platform, Proteored-IscIII, cIc bioGune, Derio, Bizkaya, 4Pathology Department, universitary hospital La Paz, Madrid, 5Microarray analysis service,

Top Scored Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 3 7
Mar Institute of Medical research (IMIM), Barcelona, 6Pediatric surgery Department, universitary hospital La Paz, Madrid, 7Pathology Department, universitary hospital Vall d'hebron, Barcelona, 8Pediatric oncology Department, universitary hospital La Paz, Madrid, spain, 9centre hepatobiliaire Paul Brousse, Villejuif, france, 10Gastroenterology Department, universitary hospital Germans trias i Pujol (hGtiP), 11Innate Immunity Group, IGtP, Badalona, Barcelona, spain
Introduction: hepatoblastoma (hB) and hepatocellular carcinoma (hcc) are the predominant malignant liver tumors in childhood. the etiology of hB is unknown, but it differs from hcc by the absence of hepatitis virus infection or cirrhosis. In contrast to hcc, curative treatment for hB patients is possible by combining chemotherapy and surgery. nevertheless, 20% of hB patients do not survive cancer. Moreover, survivors can be affected by serious side effects related to chemotherapy, such as irreversible hearing loss and cardiomyopathies. current clinical stratification relies only on clinical and pathological parameters such as pre-treatment tumor extension, age, afP levels, multifocality, distant metastases and small cell undifferentiated (scu) histology. the aim of the present study was to identify new molecular biomarkers to help to a better patient stratification and consequently, improve the outcome of childhood liver cancer.
Methods: a total of 94 childhood liver cancer patients (mean age 5 years, sera afP range: 150-7.627.330 ng/ml, 21 with metastasis, mean follow-up: 46 months, 18 deaths) were included in the study. sixteen of them, classified according to the previously described c1 (n=11) and c2 (n=5) prognostic subclasses, together with 8 normal liver (nL) were selected for proteomic analysis. Protein extracts were analyzed by two complementary techniques, 2D Difference Gel electrophoresis (2D-DIGe) and Label-free (Lf) nLc Ms/Ms. Prognostic biomarkers were identified by supervised analysis comparing the proteomic profiling of c1 vs c2 hB subtypes. further selection included comparison with nL. Biomarker validation was performed by western blot of total liver protein extracts and immunohistochemistry in an independent series of 78 patients, including 4 childhood hcc.
results: eight biomarkers were selected (fc±2, p-value<0.01) among total differently expressed proteins obtained by supervised analysis and then, analyzed by western blotting in the discovery set. three of them (37.5%), namely a tumor suppressor, an immune system related protein and a cytoskeleton protein, were further validated immunohistochemistry. the expression changes (overexpression or underexpression) of these 3 biomarkers showed a strong association with patient event free survival (efs) (log rank<0.05). Moreover, the combination of these 3 biomarkers was able to improve the efs prediction of the current clinical stratification (log rank=0.013), mainly for the intermediate and poor prognostic stratums.
Conclusion: We have defined a 3-protein prognostic signature by performing a proteomic study. this signature could be easily applied at the clinical practice by performing an immunohistochemistry using normal liver as a reference. our results suggest that this 3–protein signature could be a powerful tool to improve current clinical stratification, and consequently the outcome of pediatric patients with liver cancer.
Disclosure of Interest: none Declared
P-030 In PATIenTS WITh hePATOCeLLuLAr CArCInOMA (hCC) AnD MACrOVASCuLAr InVASIOn (MVI) AMenAbLe TO SurGICAL reSeCTIOn, A SurVIVAL SIMILAr TO ThAT ObSerVeD On SOrAfenIb CAn be AChIeVeD
Charlotte Costentin* 1, eric Vibert2, françoise roudot-thoraval3, thomas Decaens4, nathalie Ganne5, Bernard Paule6, christian Letoublon7, Melanie chiaradia8, julien calderaro9, rene adam2, Ivan Bricault10, Giuliana amaddeo1, Daniel cherqui11, olivier seror12, Didier samuel6, christophe Duvoux1, alexis Laurent13
1hepatology, henri Mondor hospital, creteil, 2hepato-biliary surgery, Paul Brousse hospital, Villejuif, 3Public health, henri Mondor hospital, creteil, 4Gastroenterology and hepatology, chu Grenoble, Grenoble, 5hepatology, jean Verdier hospital, Bondy, 6hepatology, Paul Brousse hospital, Villejuif, 7Digestive surgery, chu Grenoble, Grenoble, 8radiology, 9Pathology, henri Mondor hospital, creteil, 10radiology, chu Grenoble, Grenoble, 11hepato-biliary surgery, Paul Brousse hospital, creteil, 12radiology, jean Verdier hospital, Bondy, 13Digestive surgery, henri Mondor hopital, creteil, france
Introduction: a median survival of 8 months has been reported in the sharP trial in hcc with macrovascular invasion treated with sorafenib. In contrast, several surgical retrospective studies report overall survivals ranging from 12 to 20 month in this setting. the aim of this study was to describe characteristics and overall survival in hcc patients with macrovascular invasion (MVI) treated with surgery or sorafenib as the first treatment step.
Methods: 142 patients with hcc and macro-vascular invasion, without extra-hepatic spread, treated either with surgical resection (group 1; n=75) or sorafenib (group 2; n=67) in 4 french centers as first-line treatment after diagnosis of MVI were retrospectively reviewed. Patient characteristics are listed in table 1.
results: In group1, post-operative death (<3 months) was 14.7% (n=11) while 7.5% of the patients (n=5) in group 2 died within 3 months post sorafenib initiation (p=0.196). In group 1, 29 patients (45%) had additional therapy during follow-up either adjuvant or for recurrence (including tace, chemotherapy (ct), sorafenib, thermo-ablation, or additional resection procedures), and one patient
was transplanted. In group 2, median treatment duration was 6.4 months and 20 (30%) patients had additional therapy either in addition to sorafenib or as second line (including tace, ct, radiotherapy or radioembolization). no patient was transplanted or resected after sorafenib initiation. Median overall survival (os) was 12.0 months (Ic95%:5.5-18.5) in group 1 and 12.9 months (Ic95%: 8.3-17.5) in group 2 (p=0.61). at year 3, 7 patients were alive in group 1 vs 2 in group 2. taking into account the imbalance in baseline characteristics, a propensity analysis was performed, identifying 57 patients with similar characteristics. Median overall survival in this population was 7.2 months (Ic95%: 3.7-10.6) in group 1 and 12.6 months (Ic95%: 7.1-18.0) in group 2 (p=0.89). In multivariate analysis, prognostic factors associated with survival in the whole population (resection + sorafenib) were Pt time <60% (hr=2.40, p=0.016), size of larger nodule>50 mm hr=1.69, p=0.046), macrovascular invasion involving 1st order branch or main trunk (hr=1.948, p=0.042) and additionnal therapy (hr=0.500, p=0.024). Median os in the resection+additional therapy group of patients (n=29) was 25.2 [8.8-41.6] months and 24.3 [15.9-32.7] months in the sorafenib+additional therapy (n=20), (p=0.82).
Image:
Conclusion: 1- In patients with hcc and MVI amenable to surgical resection, a survival similar to that observed on standard of care, sorafenib, can be achieved. Palliative surgery may therefore be a valuable alternative in this setting, especially in patients intolerant to sorafenib. 2- In our study a multimodal treatment strategy was associated with remarkable prolonged survival, a finding which deserves further investigations.
Disclosure of Interest: none Declared

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s3 8
Molecular Pathogenesis, Molecular Pathology, Cell biology and Translational research
P-031 The AAA+ ATPASe ruVb1 IS A POTenT reGuLATOr Of LIVer GLuCOSe MeTAbOLISM: IMPLICATIOnS fOr hCC PrOGreSSIOn In COnDITIOnAL KnOCK-OuT MICe
Tommaso Mello* 1, 2, francesca zanieri1, oxana Bereshchenko3, elisabetta ceni1, Mirko tarocchi1, Giada Marroncini1, simone Polvani1, sara tempesti1, stefano Milani1, 2, andrea Galli1, 2
1Dept. of Biomedical experimental and clinical sciences, university of florence, 2soD Gastroenterologia 1, careggi university hospital, florence, 3univerity of Perugia, Perugia, Italy
Introduction: the aaa+ atPase ruvbl1 is overexpressed in several human cancers, including hepatocellular carcinoma (hcc), in which high ruvbl1 expression correlates with a poor prognosis. a growing body of data from in vitro models supports the concept that deregulation of ruvbl1 expression occurs in cancer to promote its growth and progression, making this protein an attractive target for anti-cancer therapies. however, whether ruvbl1 participate in the oncogenic transformation and cancer progression in vivo remains speculative. to challenge this question we realized a hepatocyte-conditional ruvbl1 hemizygous mouse and evaluated the tumor onset and progression up to one year after Den injection.
Methods: ruvbl1 hemizygous mice were obtained by crossing ruvbl1-floxed with albumin-cre deleter mice. the male offspring were subjected to a single i.p. injection of Den (5mg/kg) to induce liver cancer, and were monitored at 3, 6, 9 and 12months after cancer induction. Gene expression analysis was performed by qPcr, western blot and immunohistochemistry. Proteomic profiling of ruvbl1-silenced hepa1-6 cells was performed by 2D-DIGe.
results: ruvbl1 protein expression was reduced by a 45% in total liver extracts of hemizygous mice. conditional liver-hemizygous mice showed no obvious phenotype with respect to liver size, viability and liver function (ast-aLt), however their body weight was 15% higher than ruvbl1-floxed mice and they had significant alteration of glucose, triglycerides and cholesterol serum levels.Despite an initial delay in the onset of liver cancer at 6 months of age, Den injected ruvbl1+/- mice eventually developed significantly larger tumors than control mice 9 and 12 months after cancer induction. Most importantly, ruvbl1 was overexpressed in all tumors regardless of the mouse genetic background, strongly suggesting that its over-expression actively drives hcc progression. We found that hepatocyte-conditional ruvbl1+/- mice had reduced hepatocyte turnover, reduced liver glycogen storage, developed insulin resistance and showed increased tissue oxidative stress. expression of mtor and its downstream targets was reduced in ruvbl1+/- mice. the down-regulation of mtor pathway was further confirmed in vitro by ruvbl1 silencing in hcc cell lines. Moreover, proteomic profiling and gene ontology analysis of ruvbl1-silenced hepatoma cells revealed altered carboxylic acid metabolism and reduced expression of key enzymes of the glycolysis pathway.
Conclusion: this is the first report highlighting a role of ruvbl1 as a major regulator of glucose hepatic metabolism. contrary to our expectations, we found that although in hepatocyte-conditional ruvbl1+/- mice the onset of hcc is initially delayed, its progression is accelerated. the reduced hepatocyte turnover observed in ruvbl1+/- mice likely causes the initial delay in the appearance of liver cancer, while the onset of insulin-resistance and hyperglycemia fuel the growth of ruvbl1-overexpressing cancer cells. the underlying molecular mechanisms involve the impairment of the mtor pathway and glycolitic flux. ruvbl1 is considered an attractive target for novel anticancer therapies, nevertheless this report highlights the potential risks of prolonged ruvbl1 inhibition in a intact mammalian organism.
Acknowledgement: this research is founded by the Italian Ministry of health through grant Gr-2009-1600315.
Disclosure of Interest: none Declared
P-032 ChOLIne ADDICTIOn In beTA-CATenIn-MuTATeD hePATOCeLLuLAr CArCInOMA
Chiara Sartor* 1, angélique Gougelet1, nadia senni1, Pascale Bossard1, Marie Lequoy2, Laetitia fartoux2, Dominique Wendum2, olivier rosmorduc2, sabine colnot1
1Inserm u1016 Institut cochin, 2hôpital saint antoine, Paris, france
Introduction: In hepatocellular carcinoma (hcc), frequent mutations occur in the CTNNB1 gene, encoding the β-catenin, and this represents 15 to 40% of hcc1. hccs mutated for β-catenin are so considered as well-differentiated, cholestatic and of relative better prognosis2. that’s why distinct therapeutic strategies should be employed according to the mutational status of β-catenin in liver tumors. among which we recently proposed a targeting of the microrna mir-34a3. the non-invasive and early molecular diagnosis of hcc is therefore a current issue. Different methodologies are actually used, like serum markers or histological examination, but the most promising and less invasive ones are imaging methods: in particular computed tomography/positron emission tomography (ct/Pet). the most common used tracer is the 18fluorodeoxiglucose (18fDG), even if
18flurocholine is now emerging. It is already used routinely in detecting prostate cancer, and we recently demonstrated a medical interest in using 18flurocholine Pet/ct in detecting a part of hcc, not visible with 18fDG Pet/ct4. Moreover choline pathway has been shown increased in different cancer tissues, due to its involvement in producing phospholipids and methyl-groups5.
Methods: the mutant mouse used mimics human hccs with ctnnB1 mutations. It consists in a hepatospecific and tamoxifen-inducible knock-out of apc, the major brake of β-catenin pathway. Depending on the dose of tamoxifen injected, apc knock-out can be obtained in all hepatocytes, or in single cells to let cancer develop after months. cancer development was assessed by micro-ultrasonography, afterwards Pet/ct were performed. Primary hepatocytes cultures were also performed on apc total knock-outs, to analyze flows of radiolabelled choline. Pet/ct analysis was performed in human patients in st.antoine hospital (Paris): after surgery removal, tumors were both frozen and included in paraffin.
results: hccs from apc-mutant mice (n=8) were negative for 18fDG Pet/ct, and positive for 18flurocholine Pet/ct. similarly, we got preliminary data with 4 human hccs mutated in ctnnB1: they were positive for 18flurocholine Pet/ct, whereas the 4 hccs non mutated in ctnnB1 gene were negative for 18flurocholine Pet/ct. In both the murine and human cohort of beta-catenin-activated tumors, cePt1 and chka, two key enzymes of choline metabolism were found increased at mrna and protein (Ihc) levels. In apc total knock-out livers, a metabolomic analysis showed an accumulation in choline-derived phospholipids. In vitro, apc-ko hepatocytes (compared to apc-wt hepatocytes) increased their incorporation of 14c radiolabelled choline into very low density lipoproteins (VLDLs) and phospholipids, but also into Dna. In apc-ko tumor samples also, we found an increase of radiolabelled choline in Dna after 2h of incubation. Interestingly, we found that in apc-ko tumors/livers, Dna is hypermethylated in cpG islands.
Conclusion: 18flurocholine Pet/ct analysis could be done to diagnose ctnnB1-mutated hccs. But, it can be postulated to be a therapeutic target: it could participate to liver tumorigenesis, as the addiction of hccs to choline is involved in Dna hypermethylation, and in the metabolism of VLDL and phospholipids constituting the cell membrane.
references: 1. De La coste, a. et al. Proc. Natl. Acad. Sci. U. S. A. 95, 8847–8851 (1998).2. audard, V. et al. J. Pathol. 212, 345–352 (2007).3. Gougelet, a. et al. Gut (2015). doi:10.1136/gutjnl-2014-3089694. fartoux L, et al. nucl Med commun (2012) 33(7):757-65.5. Glunde, k., et al. Nat. Rev. Cancer 11, 835–848 (2011).
Disclosure of Interest: none Declared
P-033 reGuLATIOn Of GLyPICAn-3 by neW MICrOrnAS AnD IMPLICATIOn In hePATOCeLLuLAr CArCInOMA
flora Cartier* 1, sarah Lesjean1, jessica zucman-rossi2, katarzyna hooks1, francis sagliocco1, christophe Grosset1
1university of Bordeaux, InserM u1053, Bordeaux, 2university of Paris 7, InserM u674, Paris, france
Introduction: Glypican-3 (GPc3) is a membrane-anchored protein overexpressed in two types of liver cancer: hepatocellular carcinoma (hcc) and hepatoblastoma. GPc3 controls key signalling pathways such as Wnt/beta-catenin pathway, which is involved in liver development and carcinogenesis. this oncogenic protein is also used as a diagnosis and prognosis marker and constitutes a therapeutic target in liver cancers. In order to inhibit the expression of GPc3 and prevent its oncogenic effect, our studies focused on the post-transcriptional regulation of GPC3 by micrornas (mirnas) in liver tissue. We previously identified five mirnas as well as the endoribonuclease Ire1-alpha as GPC3 regulators (1-2).
Methods: to identify new GPC3-regulating mirnas in hcc cells, we used a functional screening system named Dual-fluorescence funreG (1). huh7 cells co-expressing the tomato and the GfP transgenes with either 3’utr and/or 5’utr of GPC3 were transfected by each mirna from a library (mirBase V17.0; 1712 mirnas; qiagen). the mirnas inducing a significant variation of the GfP/tomato ratio compared to the control rna were selected as candidates. subsequently we evaluated the role of these mirnas on GPC3 expression and in liver carcinogenesis using classical molecular and cellular approaches in hcc cells.
results: the screening allowed us to identify 16 new mirnas controlling GPC3 through the 3’utr, 5’utr or both. the effect of these mirnas on endogenous-GPc3 protein expression was studied in tumoural huh7 cells by flow cytometry and Western blotting. among 16 mirnas, ten can regulate the endogenous expression of GPc3 protein. the relative and absolute expression of those ten mirnas was evaluated by rt-qPcr and showed that five mirnas are under-expressed in hcc patients. We tested the effect of these five mirnas on the phenotype of huh7 cells in vitro. they significantly inhibit cell proliferation and block the cell cycle at the G0/G1 stage in vitro. three of the mirnas are more efficient in inducing growth arrest than a sirna against GPc3. additionally, mir-a can induce cell apoptosis in several tumoural liver cell lines in vitro. Mirna target prediction programs show that mir-a has a non-conventional predicted target site in 3’utr of GPc3 mrna. Moreover, in silico analyses suggest that mir-a could regulate several other oncogenic genes involved in hepatocellular carcinogenesis. We are currently testing additional oncogenic targets.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 3 9
Conclusion: We identified ten new mirnas controlling GPc3 protein expression in hcc cells using a functional screening. among these mirnas five are significantly decreased in hcc and could participate in GPc3 overexpression in liver carcinogenesis. these five mirnas can block tumoural cell growth and mir-a can induce tumoural cell apoptosis in vitro. Mir-a, B, c, D and e might act as tumour suppressors in hcc and constitute new potential therapeutic agents. the anti-tumoural effect of our best candidate mir-a is currently being tested in vivo in chorioallantoic chicken membrane model (caM) and will be soon investigated in mice.
references: 1- Maurel M. et al, hepatology, 20132- Maurel M. et al, rna, 2013
Disclosure of Interest: none Declared
P-034 A DIeT-InDuCeD MOuSe MODeL Of STeATOhePATITIC hePATOCeLLuLAr CArCInOMA WITh A TrASCrIPTOMIC SIGnATure ThAT reCAPITuLATeS huMAn DISeASe
Amon Asgharpour* 1, sophie cazanave1, Pierre Bedossa2, yujin hoshida3, robert Vincent1, faridoddin Mirshahi1, Mulugeta seneshaw1, kalyani Daita1, Puneet Puri 1, arun sanyal1
1Internal Medicine, Division of Gastroenterology, hepatology, and nutrition, Virginia commonwealth university, richmond, united states, 2Pathology, hospital Beaujon, university Paris-Diderot, Paris, france, 3Division of Liver Diseases, Department of Medicine, Liver cancer Program, tisch cancer Institute, Icahn school of Medicine at Mount sinai, new york, united states
Introduction: nonalcoholic fatty liver disease (nafLD) is the most common cause of chronic liver disease. It is an important risk factor for hepatocellular cancer (hcc) which can develop even in the absence of cirrhosis. hcc developing in the background of nafLD has some distinct features including a predominantly s1 subclass molecular transcriptome. this steatohepatitic subclass of hcc is becoming the leading indication for liver transplantation secondary to hcc. there is no established method for the prevention and specific treatment of hcc in nafLD due to a lack of a viable preclinical model that recapitulates the phases of human nafLD and hcc. We here described a diet-induced model of nafLD in a stable isogenic mouse that progresses from fatty liver to steatohepatitis and then advanced fibrosis and hcc without the need for any chemical carcinogens or gene manipulation.
Methods: an isogenic mouse strain derived from a c57Bl/6j and 129sl/svImj background was created and maintained with inbreeding. Mice were fed either a chow diet (cD, harlan tD.7012) or a high-fat high-cholesterol diet (WD, harlan tD.88137) with either normal tap water (nW) or high fructose-glucose solution (sW, 23.1g/l d-fructose + 18.9 g/l d-glucose) for 8,16 and 52 wks.histology was assessed by h&e and sirius red. histologic scoring was performed using the nafLD activity score (nas) and fibrosis scoring was done at early and late time points. Biochemical parameters were measured in mouse serum and mrna was isolated from liver tissue. transcriptome analysis using the Illumina mouse WG6 expression Beadchip kits (Illumina) was performed on the following groups: (1) cD+nW x 8 wks, (2) WD+sW x 8 wks, (3) cD+nW x 52 wks, (4) WD+sW x 52 wks, (5) hcc from mice on WD+sW x 52 wks. Mouse hcc gene expression was compared to a human molecular hcc gene dataset (186 gene signature for cirrhosis and hcc).
results: compared to cD+nW, mice fed WD+sW gained gross body weight (p<0.01), liver weight (p<0.01) and became insulin resistant (p<0.05) over 52 wks. after 8 wks of WD+sW, mice developed extensive steatosis (p<0.05) and hepatocyte ballooning (p<0.05) compared to cD+nW. By 16 wks early fibrosis with steatohepatitis was seen in mice receiving WD + sW while neither were seen with cD+nW (p<0.05). By week 36-52, there was increasing fibrosis with some bridging fibrosis with tumor formation. 89%(8/9) of mice on a WD+sW developed hcc at 52 wks, whereas no mice (0/15) fed cD+nW developed hcc (p< 0.01). additionally, 40% (6/15) of mice fed with a WD+nW developed well-differentiated (WD) hcc. Males were more susceptible to hcc on the WD+sW compared to females as evident by tumor burden. In mice fed a WD +sW that developed tumors, 100% had WD hcc (8/8), 37.5% (3/8) had poorly-differentiated (PD) hcc and 25% (2/8) had adenomas. Interestingly, foci of hcc were seen within adenomas. additionally, the transcriptomic signature of the hcc tumors in WD+sW fed mice were similar to aggressive human hcc of the s1 and s2 subclasses (nes and fDr: 1.46 and 0.01, and 1.42 and 0.01 respectively). Gene set enrichment analysis in WD+sW fed mice revealed upregulation in Wnt and tGf-β signaling as a top ranking changes, based on statistical significance, as early as 8 weeks of diet. upregulation in Wnt signaling is a hallmark of s1 hcc, the steatohepatitic hcc variant.
Conclusion: this simple model of nash and hcc that resembles human disease in terms of its triggers, serology, phenotype, histology, transcriptome and outcomes can facilitate preclinical development for these conditions.
Disclosure of Interest: none Declared
P-035 InCreASeD STeMneSS Of reSIDuAL VIAbLe hePATOCeLLuLAr CArCInOMA In hyPOxIC MICrOenVIrOnMenTS InDuCeD by TrAnSArTerIAL CheMOeMbOLIzATIOn
hyungjin rhee* 1, ji hae nahm1, haeryoung kim2, Gi hong Gi hong3, jeong eun yoo1, Myoung ju koh1, hye sun Lee4, young nyun Park1
1Department of Pathology, Brain korea 21 PLus Project for Medical science, Integrated Genomic research center for Metabolic regulation, yonsei university college of Medicine, seoul, 2Department of Pathology, seoul national university Bundang hospital, seongnam, 3Department of surgery, 4Biostatistics collaboration unit, Department of research affairs, yonsei university college of Medicine, seoul, korea, republic of
Introduction: the biological behavior of hepatocellular carcinoma (hcc) is influenced by hypoxic microenvironments; however the clinicopathological characteristics of residual viable hcc after transarterial chemoembolization (tace) remain unclear.
Methods: the expression of hypoxia- (carbonic anhydrase-Ix [caIx], hIf1α), stemness- (k19, epcaM, oct3/4, nanog), and epithelial-mesenchymal transition (eMt)-related markers (snail, twist) were investigated by immunohistochemistry or real-time rt-Pcr in three hcc cohorts. clinicopathologic features and outcomes were compared between non-necrotic hccs and hccs with spontaneous or tace-induced necrosis.
results: In cohort 1 (n=339, resected hccs without tace), caIx(+) hccs exhibited higher k19 and epcaM protein expression, as well as more invasive pathological features. caIx expression and tnM stage were independent predictors of extrahepatic recurrence, and the addition of caIx to tnM stage significantly increased the time-dependent integrative area under the curves (iauc). In cohort 2 (n=100, resected hccs with or without tace), hccs expressing high levels of caIx mrna more frequently showed greater levels of hIf1α, stemness-, and eMt-related marker mrna and more invasive pathological features than hccs expressing low levels of caIx mrna. the mrna levels of hypoxia-, stemness-, and eMt-related markers were well correlated each other. In cohort 3 (n=85, explanted hccs with or without tace), the expressions of caIx, k19, and epcaM increased with a greater number of tace sessions. caIx expression was shown to be an independent factor for survival, and combination of caIx with serum afP, microvascular invasion, or Milan criteria significantly increased iauc values for survival.
Conclusion: the expressions of hypoxia-, stemness-, and eMt-related markers were well correlated and increased in necrotic hccs under hypoxia, especially with higher numbers of tace sessions. caIx may be a valuable predictor of outcomes after hepatic resection/transplantation.
Disclosure of Interest: none Declared
P-036 InCreASeD MITOChOnDrIAL fISSIOn PrOMOTeS CeLL SurVIVAL ThrOuGh rOS-MeDIATeD COOrDInATeD reGuLATIOn Of nf-Κb AnD P53 PAThWAyS In hePATOCeLLuLAr CArCInOMA
Jinliang xing* 1
1state key Laboratory of cancer Biology and experimental teaching center of Basic Medicine, fourth Military Medical university, xi’an, china
Introduction: Mitochondrial morphology is dynamically remodeled by fusion and fission in cells, and dysregulation of this process is closely implicated in tumorigenesis. however, the mechanism by which mitochondrial dynamics influence cancer cell survival is greatly less clear, especially in hepatocellular carcinoma (hcc) (1). In most mammalian cells, mitochondria are a major source of ros (reactive oxygen species), which are generally elevated in cancer cells and functionally act as essential signaling molecules in the regulation of the tumor development and progression (2). Moreover, mounting evidences have demonstrated that ros mainly mediate the activation of akt signaling pathway in kinds of tumors, including hcc. the transcription factors p53 and nf-κB determine cellular survival and are involved in the pathogenesis of most-if not all-cancers. the crosstalk between these transcription factors becomes increasingly appreciated as an important mechanism operative during all stages of tumorigenesis(3). our study facilitates our understanding of the pathological roles played by mitochondrial dynamics and provides a strong evidence for novel strategy targeting proteins of mitochondrial fission machinery in hcc treatment.
Methods: In this study, we systematically investigated the alteration of mitochondrial dynamics and its functional role in the regulation of hcc cell survival. furthermore, the underlying molecular mechanisms and therapeutic application were deeply explored.
results: Mitochondrial fission was frequently upregulated in hcc tissues mainly due to an elevated expression ratio of Drp1/Mfn1, which significantly contributed to poor prognosis of hcc patients. Increased mitochondrial fission by Drp1 forced expression promoted the survival and growth of hcc cells both in vitro and in vivo mainly by inhibiting mitochondria-dependent apoptosis and facilitating cell proliferation. alternatively, inhibition of apoptosis by increased mitochondrial fission was regulated by the activation of autophagy. We further demonstrated that the survival-promoting role

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s4 0
of increased mitochondrial fission was mediated via the elevated ros production and subsequent activation of akt, which facilitated the MDM2-mediated p53 degradation and IκB kinase (Ikk)-mediated transcriptional activity of nf-κB in hcc cells. also, a crosstalk between p53 and nf-κB pathways was found to be involved in the regulation of mitochondrial fission-mediated cell survival. Moreover, treatment with mitochondrial division inhibitor-1 significantly suppressed tumor growth in in vivo xenograft nude mice model.
Image:
Conclusion: our findings demonstrate that increased mitochondrial fission plays a critical role in regulation of hcc cell survival, which provides a strong evidence for this process as drug target in hcc treatment.
references: 1. Westermann B. Mitochondrial fusion and fission in cell life and death. nat rev Mol cell Biol. 2010;11:872-84.2. clerkin js, naughton r, quiney c, cotter tG. Mechanisms of ros modulated cell survival during carcinogenesis. cancer Lett. 2008;266:30-6.3. Webster Ga, Perkins nD. transcriptional cross talk between nf-kappaB and p53. Mol cell Biol. 1999;19:3485-95.
Disclosure of Interest: none Declared
P-037 reGuLATIOn Of beTA-CATenIn by MICrOrnAS In hePATObLASTOMA, A rAre PAeDIATrIC LIVer CAnCer
emilie Indersie* 1, 2, sarah Lesjean1, 2, francis sagliocco1, 2, tony ernault3, 4, katarzyna hooks1, 2, Monique fabre5, Laurence Brugières6, sophie taque7, sophie Branchereau8, catherine Guettier8, Michael Grotzer9, Marie-annick Buendia3, 4, christophe Grosset1, 2
1InserM u1053, 2université de Bordeaux, Bordeaux, 3InserM uMr1193, 4centre hépatobiliaire – chu Paul Brousse, Villejuif, 5hopital necker, Paris, 6Institut Gustave roussy, Villejuif, 7chu rennes, rennes, 8hopital Bicêtre, Le kremlin-Bicêtre, france, 9the sIoPeL Liver tumor and tissue Banking Program, university children's hospital, zürich, switzerland
Introduction: hepatoblastoma (hB) is the most common paediatric liver cancer. It is characterized by activating mutations in b-catenin gene and abnormal activation of Wnt signalling pathway that lead to overexpression of b-catenin, a multifunctional protein that drives cell transformation and tumour growth. b-catenin is therefore a key therapeutic target in hB. encouraged by the recent entry of mir-34a in a phase-I clinical trial for the treatment of adult patients with unresectable primary liver cancer or hepatic metastases, we decided to identify micrornas (mirnas) that target b-catenin and consequently inhibit hB cells proliferation in vitro and block hB-derived tumour growth in vivo.
Methods: We screened a library of 1712 mirnas using a robust dual-fluorescence reporter screening system (Df-funreG (1)) and selected candidates mirnas that potentially down-regulate b-catenin expression through its 5’ or 3’ untranslated regions (utr) in huh6 cell line derived from
hB. then, we confirmed the inhibitory effect of the candidate mirnas on endogenous b-catenin mrna and protein levels. We measured the expression of the most relevant canditates mirnas in a collection of patient' tissues including 37 tumour samples and 30 normal livers. finally, we analysed the effect of mirnas down-regulated in tumours on oncogenic features as cell proliferation, cell cycle, apoptosis and senescence.
results: using Df-funreG method we selected 26 mirnas candidates as b-catenin-regulating mirnas. nine out of 26 micrornas significantly decreased endogenous b-catenin expression in huh6 cell line, while known b-catenin-regulating micrornas mir-34a-5p and mir-200a-3p had no detectable effect. By measuring expression of these nine micrornas in patients’ tissues we found five mirnas significantly down-regulated in tumour samples compared to normal livers. similar results were obtained in 22 matched pairs of tumour/normal liver samples. all five mirnas decreased hB cell proliferation in vitro by arresting cells in G01/G1 phase and preventing s phase progression. Moreover, three mirnas were particularly effective and inhibited hB cell proliferation by more than 70%. surprisingly, none of these mirnas induced apoptosis and one only slightly increased number of cells undergoing senescence. those results suggest mirnas induce hB cell quiescence and could confer cancer cell dormancy. We are currently studying the therapeutic benefit of combining these micrornas with cisplatin (standard chemotherapeutic drug in hB treatment) with the aim of increasing the sensitivity of hB cells to the chemotherapy.
Conclusion: We identified five b-catenin-regulating mirnas that are promising candidates for mirna-based therapy in hB patients and we began patenting process. the anticancer activity of these mirnas on hB tumour growth will be soon studied in vivo using chick embryo chorioallantoic membrane model. If the use of b-catenin-regulating mirnas in preclinical studies proves to achieve inhibition of hB progression with lower doses of cisplatin, it could lead to novel treatment option with fewer side effects for hB patients. as b-catenin is a potent driver oncogene in many cancers, our study might also find relevant applications in other adult and paediatric malignancies.
references: 1. M. Maurel, s. jalvy et al. Hepatology 57, 195-204 (2013)
Disclosure of Interest: none Declared
P-038 bIOLOGIC AnD TrAnSLATIOnAL SIGnIfICAnCe Of MOrPhO-PhenOTyPIC ChAnGeS OCCurrInG In huMAn hePATOCArCInOGeneSIS
Amedeo Sciarra* 1, Luca Di tommaso1, Masayuki nakano2, annarita Destro1, Guido torzilli1, Matteo Donadon1, Marco Maggioni3, Massimo roncalli1
1Pathology and surgery, humanitas research hospital and university of Milan, Milan, Italy, 2Pathology, shonan fujisawa tokushukai hospital, fujisawa, japan, 3Pathology, Policlinico of Milan hospital, Milan, Italy
Introduction: human hepatocarcinogenesis in cirrhosis is thought to be multistep and characterized by a spectrum of nodular lesions, ranging from high grade dysplastic nodule (hGDn) to early (e-hcc) to progressed hcc (p-hcc). aim of this study was to investigate the morpho-phenotypical changes of this sequence and to evaluate their translational significance.
Methods: the vascular profile, the ductular reaction/stromal invasion and the overexpression of 5 biomarkers (GPc3, hsP70, Gs, chc, and ezh2) was assessed by immunocytochemistry and semiquantitatively scored in a east-West series of 60 resected small hepatocellular nodules (9 hGDn, 26 e-hcc and 25 small p-hcc).
results: the proposed score nicely separated the 3 groups of nodules as individual entities (p<0.01). In the sequence, biomarkers overexpression progressively increased with parallel decrease of the ductular reaction; the vascular remodeling started very early (hGDn) but did not further develop in a proportion of hcc. e-hcc was the most heterogeneous entity, with only marginal overlap with hGDn and p-hcc. a subclass of e-hcc (9/26) without evidence of stromal invasion was also identified, suggesting a “preinvasive stage” of the disease. for diagnosis, the application of 4 and 5 biomarkers (rather than the usual 3) improved the sensitivity of the immunocytochemical assay for the detection of e-hcc (77% and 96% vs. 50%); furthermore the use of biomarkers in alternative combinations was also able to increase the sensitivity of the test (Gs+chc+ezh2: 81%; Gs+chc+ezh2+hsP70: 92%).
Conclusion:this study supports the multistep nature of human hepatocarcinogenesis and suggests that e-hcc is more heterogeneous than previously thought; it also provides information of potential translational significance into the clinical practice.
references: 1. the International consensus Group for hepatocellular neoplasia. Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. hepatology 2009;49:658-64.2. Di tommaso L, et al. advanced precancerous lesions in the liver, Best Pract res clin Gastroenterol 2013;2: 269-84.3. tremosini s, et al. Prospective validation of an immunohistochemical panel (glypican 3, heat shock protein 70 and glutamine synthetase) in liver biopsies for diagnosis of very early hepatocellular carcinoma. Gut 2012;6:1481-7.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 4 1
4. cai My, et al. ezh2 protein: a promising immunomarker for the detection of hepatocellular carcinomas in liver needle biopsies. Gut 2011;60:967-76.
Disclosure of Interest: none Declared
P-039 IMMunOTOxIn TArGeTInG GLyPICAn-3 reGreSSeS LIVer CAnCer VIA DuAL InhIbITIOn Of WnT SIGnALLInG AnD PrOTeIn SynTheSIS
Wei Gao1, yifan zhang1, Mingqian feng1, Dimiter Dimitrov2, Mitchell ho* 1
1Laboratory of Molecular Biology, national cancer Institute, Bethesda, 2Laboratory of experimental Immunology, national cancer Institute, frederick, united states
Introduction: Glypican-3 (GPc3) is a cell surface heparan sulfate proteoglycan that associates with Wnt and other growth factors in liver cancer.
Methods: We develop two monoclonal antibodies targeting GPc3. the first antibody (hn3) recognizes a functional epitope and inhibits Wnt signaling, whereas the second antibody (yP7) recognizes a c-terminal epitope but does not inhibit Wnt signaling. Both are fused to a fragment of Pseudomonas exotoxin a (Pe38) to create immunotoxins.
results: Interestingly, the immunotoxin based on hn3 (hn3-Pe38) has superior anti-tumor activity as compared to yP7 (yP7-Pe38) both in vitro and in vivo. Intravenous administration of hn3-Pe38 alone, or in combination with chemotherapy, induces regression of hep3B and hepG2 liver tumor xenografts in mice. this study establishes GPc3 as a promising candidate for immunotoxin-based liver cancer therapy. our results demonstrate immunotoxin-induced tumor regression via dual mechanisms: inactivation of cancer signaling via the antibody and inhibition of protein synthesis via the toxin.
Conclusion: We have developed a human monoclonal antibody (hn3) that recognizes a unique functional site in GPc3 and inactivates Wnt/yap signaling pathways known to be important for liver cancer pathogenesis. We have validated GPc3 as a target for antibody-toxin/drug conjugates and generated an immunotoxin based on hn3. along with our collaborators, we are pursuing clinical development of the anti-GPc3 immunotoxin targeting liver cancer.
references: 1: Gao W, tang z, zhang yf, feng M, qian M, Dimitrov Ds, ho M. Immunotoxin targeting glypican-3 regresses liver cancer via dual inhibition of Wnt signalling and protein synthesis. Nat Commun. 2015 Mar 11;6:6536. doi: 10.1038/ncomms7536.2: Gao W, kim h, feng M, Phung y, xavier cP, rubin js, ho M. Inactivation of Wnt signaling by a human antibody that recognizes the heparan sulfate chains of glypican-3 for liver cancer therapy. Hepatology. 2014 aug;60(2):576-87. doi:10.1002/hep.26996. epub 2014 jun 18. 3: feng M, Gao W, Wang r, chen W, Man yG, figg WD, Wang xW, Dimitrov Ds, ho M. therapeutically targeting glypican-3 via a conformation-specific single-domain antibody in hepatocellular carcinoma. Proc Natl Acad Sci U S A. 2013 Mar 19;110(12):e1083-91. doi: 10.1073/pnas.1217868110. epub 2013 Mar 5. 4: ho M, kim h. Glypican-3: a new target for cancer immunotherapy. Eur J Cancer. 2011 feb;47(3):333-8. doi: 10.1016/j.ejca.2010.10.024. epub 2010 nov 26. review.
Disclosure of Interest: none Declared
P-040 TrAnSLATIOnAL COnTrOL by nuP155 MODuLATeS P53 TArGeT Gene exPreSSIOn In LIVer CAnCer
Kerstin holzer* 1, alessandro ori2, juliane Winkler1, amy cooke3, amparo andres-Pons2, eva eiteneuer1, Peter schirmacher1, Martin Beck2, stephan singer1
1Institute of Pathology, university hospital heidelberg, 2structural and computational Biology, 3Director's research, european Molecular Biology Laboratory, heidelberg, Germany
Introduction: almost all signaling cascades of (liver-)cancer relevant pathways have to pass the nuclear pore complex (nPc) as the only gate between the cytoplasm and the nucleus. the nPc is embedded in the nuclear envelope and consists of multiple copies of ~30 different nucleoporins (nups). emerging evidence indicates that besides their role in transport some nups can also modulate cancer-relevant pathways on additional levels. In this context we could recently show that nup98 stabilizes the mrna of a subset of p53 target genes such as p21 and thereby shapes the p53-response1. a previously performed rnai screen revealed that also other nups can be linked to the p53 pathway. In this study we aim to analyze the requirement of nup155 for p53 target gene induction and the underlying regulatory mechanism.
Methods: using targeted and discovery proteomics as well as conventional immunoblotting the impact of sirna-mediated nup155 knockdown on the global proteome and on p53 targets was investigated in different cell lines. subsequent mechanistic analyses involved protein half-life experiments as well as subcellular and polysome fractionation combined with qrt-Pcr. to identify potential mediators of nup155-dependent p53 target gene regulation an rnai screen was performed followed by appropriate validation experiments.
results: knockdown of nup155 in hepG2 cells (p53 wild-type) by rnai followed by nutlin- and camptothecin-treatment resulted in reduced p21 protein accumulation while the induction of other p53 targets (e.g. bax and 14-3-3 sigma) remained unaffected. similar phenotypic changes occurred after nup155 depletion in hep3B-4Bv cells and in a cell line expressing p21 from a tet-sensitive cDna construct (“tet off”). Interestingly, p21 mrna induction was not significantly affected in these cell lines. cycloheximide chase experiments did not point towards a role of nup155 in p21 protein stability, neither was the p21 mrna export altered. hypothesizing that nup155 may regulate p21 mrna translation we performed polysome fractionation experiments. consistent with this hypothesis we observed an increased subpolysome/polysome p21 mrna-ratio in the absence of nup155. the depletion of “Putative ribosomal rna methyltransferase 1 (ftsj1)”, which emerged from the above mentioned discovery proteomic approach and rnai screen, recapitulated the same effects on p21 protein without affecting its mrna level. finally, exogenously expressed ftsj1 was sufficient to rescue decreased p21 protein after nup155 knockdown.
Conclusion: our data suggest that nup155 regulates p21 mrna translation through ftsj1 demonstrating a previously unrecognized level of p53 target gene regulation by nPc components.
references: 1. singer, s., zhao, r. et al. Mol cell (2012)
Disclosure of Interest: none Declared
P-041 eVOLuTIOnAry CAnCer fAVOreD enGIneereD VACCInIA VIruS ATTenuATeS MeTASTATIC hePATOCeLLuLAr CArCInOMA
So young yoo* 1, seo young Bang1, su-nam jeong1, hyun young Woo2, ki tae yoon2, Mong cho2, Dae hwan kang2, tae ho hwang3, jeong heo2
1BIo-It foundry technology Institute, Pusan national university, 2Department of Internal Medicine, college of Medicine, Pusan national university and Medical research Institute, 3Department of Pharmacology, Pusan national university school of Medicine, Busan, korea, republic of
Introduction: Despite many anti-cancer drugs were developed for cancer treatment over the past 30 years, the majority of solid tumors remain incurable once they are metastatic. recently, engineered vaccinia virus based therapy showed the promising results in advanced hcc patients, however its efficacy on the metastatic liver cancer has not been well assessed yet. here, we developed an evolutionary cancer favored engineered vaccinia virus (cVV), named “496GfP”, made by repeated selective replication in cancerous tissues and then deleted viral thymidine kinase genes, and investigated its therapeutic effects on metastatic liver cancer model.
Methods: four liver cancer cell lines, hepG2, snu354, snu449 and sk-hep-1 were tested to establish metastatic liver cancer model. Migration assay and tumorigenicity was examined. cancer stem cell markers cD133 and cD44 expression and metastatic marker cMet expression were examined. their sensitivity to cVV or anticancer drug sorafenib and cisplatin was investigated in vitro and in vivo. the highest metastatic and tumorigenic sk-hep-1 were selected and injected directly onto the liver tissue to develop liver-to-colon metastasis. Metastasis was confirmed after 2weeks. animal were divided as groups and sorafenib, cVV or sorafenib+cVV were treated and examined the metastatic regions in each group.
results: It was found that cancer stem cell markers cD44 expressions seems to correlate with their metastatic characteristics. cellular migration and liver tumorigenicity was in accordance with cD44 expression. our cVV showed higher cytotoxicity on all the liver cells regardless of cD44 expression whereas anti-liver cancer agents, sorafenib and cisplatin didn’t show the dose dependent sensitivity in cD133 or cD44 expressing cancer cells (snu354, snu449 and sk-hep-1). When cells were directly injected onto liver tissues, metastasis to colon regions were found in only three cells (snu354, snu449 and sk-hep-1) and their metastatic rates were exactly in accordance with cD44 expression rates. sorafenib, cVV or sorafenib with cVV were treated in animal model via oral, peritoneal or ora/peritoneal routes. Interestingly, mestastatic regions were rarely found in cVV treated groups (cVV or sorafenib with cVV) whereas metastatic regions were still found in sorafenib treated regions.
Conclusion: taken together, it is concluded that our cVV works in eradicating metastatic cD44 expressing cells, providing our cVV may be the promising therapeutic reagent targeting metastatic liver cancer cells.
Disclosure of Interest: none Declared
P-042 AnALySIS Of exOMe SequenCIeS Of ChOLAnGIOCArCInOMA SAMPLeS: IDenTIfICATIOn Of DeLeTerIOuS MuTATIOnS AnD ITS PreVALenCe SCreenInG In brAzILIAn PATIenTS
Débora C. Moraes* 1, Vivian resende1, eitan friedman2, Luiz de Marco1, Luciana Bastos-rodrigues 3
1Department of surgery, universidade federal de Minas Gerais, Belo horizonte, Brazil, 2the susanne Levy Gertner oncogenetics unit, chaim sheba Medical center, tel-hashomer, Israel, 3Department of Basic sciences, universidade federal de juiz de fora, Governador Valadares, Brazil

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s4 2
Introduction: cholangiocarcinoma (cca) is a malignant tumor with treatment limitations and exceptionally poor prognosis. although cca is relatively rare, its overall incidence is increasing worldwide. futhermore, cholangiocarcinoma is the second cause of primary malignant tumor of the liver, accounting for 10–20% of deaths from hepatobiliary cancers. over the past years, several studies have yielded new insights into the molecular mechanisms of cholangiocarcinoma tumorigenesis and it is possible to notice singular prevalent mutations according to cca etiology and, in addition, the geographical origin of the patients. exome studies also contributed to the detection of new therapeutic target genes specific to cca treatment of particular populations. therapies targeting PTPN3 gene, for example, can be more indicated to north americans and chineses patients as a result of the specific presence of mutations affecting these populations. hence, the distinct mutational patterns identified in exome studies of ccas suggest the need to expanding studies in more cholangiocarcinoma patients. thus, the present study aimed to search and analyze point mutations in Brazilian intra and extrahepatic cholangiocarcinoma samples.
Methods: tissue from 30 Brazilian patients who had been surgically treated for cholangiocarcinoma were investigated. two (klatskin cca) of the samples were randomly selected for exome sequencing using the Illumina hiseq 2500 platform. files containing captured sequences were analyzed in Variant analysis program using two different filters: one, to identify the common point mutations between the two extrahepatic Brazilian cholangiocarcinoma samples; and the other filter to verify the common point mutations between these klatskin samples and the point mutations previously published. We used sequence homology-based tools to predict the potential impact of all nonsynonymous mutations and their pathways and interaction information were collected in appropriate databases. Deleterious or possible deleterious nonsynonymous mutations are being validated by conventional sanger sequencing.
results: In the present study we identified 214 point mutations in 55 genes in common to the two extrahepatic cholangiocarcinomas. We found seven missense mutations (in seven different genes) likely to be deleterious and, among them, only one has already been reported in cca exome studies. Pathways of these seven mutated genes are associated with regulation of another transcription genes, activation of protein kinases, mitosis progress control, Dna replication, apoptosis regulation, and hepatic duct malformation. concerning the data between Brazilian samples and the previously published point mutations in ccas, we recognized common 321 point mutations, consisting of 189 missense mutations. Initial results of deleterious potential of the missense mutations (in six different genes) are expected to modify the structure or function of the proteins encoded by these genes. the six mutated genes have a key role in histone methylation activity, inhibition of G-protein, and intracellular signaling.
Conclusion: our preliminary study provides comprehensive catalogue of genetic alterations in Brazilian cholangiocarcinoma patients and allows for a better understanding of the impact of new or previously described genetic alterations in Brazilian patients.
Disclosure of Interest: none Declared
P-043 The ACTIVATIOn Of An ePITheLIAL TO MeSenChyMAL TrAnSITIOn PrOGrAM by InSuLIn/InSuLIn-LIKe GrOWTh fACTOr-1 reCePTOrS IS InVOLVeD In The ACquIreD reSISTAnCe TO AnTI-eGfr TherAPy Of huMAn ChOLAnGIOCArCInOMA CeLLS
Javier Vaquero* 1, 2, audrey clapéron1, 2, Martine Mergey1, 2, cindy Lobe1, 2, christèle Desbois-Mouthon1, 2, françoise Praz1, 2, Laura fouassier1, 2
1InserM, uMr_s 938, centre de recherche saint-antoine, f-75012, 2sorbonne universités, uPMc univ Paris 06, uMr_s 938, centre de recherche saint-antoine f-75012, Paris, france
Introduction: cholangiocarcinoma (cca) is a highly fatal tumor that arises from biliary epithelial cells. cca has a very poor prognosis due to its late clinical presentation and the lack of effective non-surgical therapies. epidermal Growth factor receptor (eGfr), a tyrosine kinase receptor, is overexpressed in cca tumors and plays a major role in cca progression. thus, eGfr has been envisaged as molecular target for cca therapy. however, clinical trials using anti-eGfr, such as the small-molecule tyrosine kinase inhibitor (tkI) erlotinib, did not provide a therapeutic benefit in patients with cca, suggesting resistance to tyrosine kinase inhibitors (i.e. erlotinib). In the present study, we intend to unravel the underlying cellular and molecular mechanisms involved in acquired resistance to erlotinib in cca.
Methods: cell pools resistant to erlotinib were obtained by treating four human cca cell lines (hucct1, eGI-1, sk-cha-1 and Mz-cha-1) with increasing concentrations of erlotinib (0-20 μM) for a long period of time (6-9 months). cell viability was determined by Mtt assay after exposure to erlotinib for 72 h. expression of epithelial and mesenchymal markers was investigated by rt-qPcr, western blot and immunofluorescence. signaling pathways were analyzed by phosphoprotein arrays, immunoprecipitation and western blot. a dual tkI, BMs-536924, was used to inhibit the insulin/insulin-like growth factor-1 receptors (Ir/IGf1r).
results: as expected, the four erlotinib resistant cca cell pools showed reduced sensitivity to erlotinib toxicity compared to their parental counterparts. In contrast to parental cells, resistant cell
pools displayed a scattered phenotype, which was accompanied by a disruption of the adherens junctions as attested by the internalization and/or decreased expression of e-cadherin, as well as dephosphorylation and nuclear translocation of β-catenin. In pools with acquired resistance to erlotinib, the expression of epithelial to Mesenchymal transition (eMt)-transcription factors (snaIL, sLuG and zeB-1) was induced. additionally, the expression of cancer stem cell (csc) markers (i.e. aLDh, cD61, cD117, cD133 and aBcG2) was also up-regulated in erlotinib-resistant cells. all members belonging to the erBB family (erBB1/eGfr, erBB2, erBB3 and erBB4) were inhibited, whereas Ir and IGf1r were activated and IGf2, a ligand for Ir/IGf1r, was overexpressed in resistant cells compared to untreated cells. treatment of resistant pools with BMs-536924 reduced the expression of snaIL, sLuG and zeB-1 in the four cell lines. Moreover, co-treatment of cca cells with erlotinib plus BMs-536924 was able to sensitize the resistant pools to erlotinib toxicity.
Conclusion: the activation of the IGf signaling axis could contribute to the resistance of cca cells to erlotinib through the establishment of an eMt program.
Disclosure of Interest: none Declared
P-044 SeruM MIr-10b* AS A POTenTIAL PreDICTIVe bIOMArKer fOr SOrAfenIb TreATMenTS Of ADVAnCeD hCC PATIenTS
Da-Liang Ou* 1, yu-yun shao1, chih-hung hsu1, 2, zi-rui feng2, Bin-shyun Lee2, ann-Lii cheng1, 2, chiun hsu1, 2
1Graduate Institute of oncology, college of Medicine, national taiwan university, 2Department of oncology, national taiwan university hospital, taipei, taiwan
Introduction: Micrornas have been found to play important roles in hepatocarcinogenesis and may also help to regulate the drug responses of hepatocellular carcinoma (hcc) cells. We previously found that mir-10b* was significantly suppressed in sorafenib-resistant hcc cell lines. the present study sought to explore the predictive value of mir-10b* expression for sorafenib treatments of advanced hcc patients.
Methods: mir-10b* levels in sera from healthy volunteers or advanced hcc patients who received sorafenib as first-line therapy, which were collected after informed consent, were measured using quantitative rt-Pcr. the levels of mir-10b* was presented as 2^−∆ct (cycle threshold), normalized with mammalian u6 rna levels. sorafenib-sensitive (huh-7 and hepG2, Ic50 5-6 μM) and resistant (huh-7r and hepG2r, Ic50 14-15 μM) hcc cell lines were tested for cell growth and apoptosis after sorafenib treatment and modulation of mir-10b* expression (by pre-mir-10b* or anti-mir-10b*, ambion) using Mtt assay and flow cytometry.
results: among the hcc patients (n=45, median age 59.2 years), hcc etiology was hepatitis B virus and hepatitis c virus in 69% and 20% of patients, respectively. almost 90% of patients had Barcelona clinic Liver cancer stage c disease and child a liver reserve. serum levels of mir-10b* were higher in hcc patients than in healthy volunteers (n=6) (mean ± sD, 0.5226 ± 0.1128 vs. 0.0778 ± 0.0089). the 3rd quartile (q3) of serum mir-10b* levels in the healthy volunteers (0.1015) was used to classify hcc patients with high (≥ 0.1015, n = 27) and low (< 0.1015, n = 18) mir-10b* levels. Patients with high mir-10b levels had significantly longer os (median, 13.9 vs. 3.5 months, p = 0.021). secretion of mir10b* into medium after sorafenib treatment correlated with sorafenib sensitivity of the hcc cell lines tested. sorafenib-induced apoptosis in hcc cells was significantly enhanced by over-expression of mir10b* and partially abrogated by knock-down of mir10b*.
Conclusion: high serum mir10b* levels were associated with longer os in hcc patients who received sorafenib treatment. the potential mechanisms by which mir10b* regulated sorafenib-induced apoptosis in hcc cells warrant further exploration.
Disclosure of Interest: D.-L. ou: none Declared, y.-y. shao: none Declared, c.-h. hsu: none Declared, z.-r. feng: none Declared, B.-s. Lee: none Declared, a.-L. cheng research/education support from: Bayer-schering Pharma, consulting of: Bayer-schering Pharma, c. hsu research/education support from: Bayer-schering Pharma
P-045 hOxA13 exPreSSIOn PreDICTS WOrST PrOGnOSIS In hCC AnD IMPACTS On SOrAfenIb reSPOnSe
Luca quagliata* 1, cristina quintavalle1, Valeria Perrina1, Matthias Matter1, Massimo roncalli2, clemente cillo3, Luigi terracciano1
1Institute of Pathology, university hospital Basel, Basel, switzerland, 2Pathology Department, humanitas research hospital, Milan, 3university of naples federico II, naples, Italy
Introduction: although significant advances in hcc diagnosis and management have been made, for advanced stages no therapeutic options exist beside sorafenib. recently, we showed that hoxa13 expression in hcc liver biopsies correlates with poor survival and metastasis incidence. furthermore, we showed that hoxa13 expression increases hcc cells proliferation in vitro. With this confirmed our previous data on a larger cohort of samples and to investigated hoxa13 impact on cells’ sorafenib response.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 4 3
Methods: a liver tMa (tissue microarray) comprises a total of n=305 specimens, n=82 normal liver tissues, n=108 cirrhotic patients and n=115 hccs, has been stained for hoxa13, ck-7, ck-19, e-cad. Protein levels have been correlated with patients’clinical data. In vitro experiments to stably modulate hoxa13 expression (gain and loss of function) have been performed using the hcc derived cell lines: hep-G2, snu449 and PLc5. subsequently, cells have been treated with sorafenib and cell cycle analysis, proliferation, migration and drug response have been tested. finally, hoxa13 expression has been analyzed in a cohort of sorafenib treated patients.
results: hoxa13 is altered in 41% of hcc resected analyzed samples, thus confirming our previous results obtained using liver biopsies. high hoxa13 levels are associated with poorer outcome and higher grading (edmondson and BcLc). Increased hoxa13 expression is associated to stem progenitor markers expression, such as ck-7 and ck19. furthermore, high hoxa13 expression is coupled with diminished levels of e-cad, providing a molecular basis for its association with metastasis in hcc. In addition, in vitro experiments show that hoxa13 overexpression results in higher resistance to sorafenib exposure. conversely, hoxa13 down regulation sensitize hcc cells to sorafenib. finally, sorafenib-treated hoxa13 expressing patients show worste survival compared to hoxa13 negative patients.
Conclusion: here we show that hoxa13 Ihc-based protein levels analysis can predict hcc outcome and correlates as well with a number of tumor features (e.g. grade). Given further investigations, we propose that hoxa13 could be used as a marker for hcc aggressiveness. In addition, our in vitro and in vivo preliminary data concerning hoxa13 and sorafenib response suggest that hoxa13 might influence therapy outcome.
Disclosure of Interest: none Declared
P-046 hePATOCeLLuLAr CArCInOMA rePLICATInG hePATITIS b VIruS
Boris halgand1, Lise rivière2, Guillaume fallot3, christophe Desterke4, Mylene sebagh3, julien calderaro3, Paulette Bioulac-sage5, Didier samuel3, christine neuveut2, Cyrille feray* 1
1InserM 955, creteil, 2cnrs 3015, Paris, 3InserM 785, 4InserM 972, Villejuif, 5InserM 1053, Bordeaux, france
Introduction: chronic infection with hepatitis B virus (hBV) is a major cause of hepatocellular carcinoma (hcc). In the nucleus of infected hepatocytes, the covalently closed circular (ccc) Dna is the template for viral replication and transcription. Both integrated hBV Dna 1 and hBV cccDna might be present in tumour tissues 2, 3 4. We have investigated whether hBV-replicating hcc may have clinical, virological or transcriptomic characteristics. We focused in the hBx protein which is involved in hcc.
Methods: ninety nine hBsag-positive patients were studied: 72% had a cirrhosis and 94% were treated by antiviral drugs. hBV Dna, hBV cccDna and hBV rna were quantified in hcc and in the non tumoral liver (nt). the x region from non-integrated hBV Dna was sequenced. transcriptomic studies hcc and nt were analyzed through agilent. hBx sequences were cloned in lentiviral vector and analyzed for colony forming assay and for transactivation.
results: 1) hBV Dna was detected in hcc and in (nt) in 83 and 91 cases. hBV cccDna was detected more frequently in the nt (66/99 vs. 39/99; p=0.001). absence of microvascular invasion (MI) was strongly correlated to higher levels of hBV Dna, hBV cccDna and hBV rna in both hcc. the presence of hBV cccDna in hcc was predictive for the 2-year survival (65 % vs. 40 %; p =0.02) after resection.2) Primers amplifying the full-length hBV Dna showed differences in genotype between hcc and nt in 11/63 patients. this indicated mutations in the replicative (non integrated) form of hBV. nine amino acid positions between hcc and nt were mutated in at least three subjects. hcc hBx was less cytotoxic than nt hBx in 5/7 patients.3) transcriptional analysis (Pca and Gsea) showed separated subgroups according to the presence of MI and to the detection of hBV cccDna in tumours. nctP, the cellular receptor for hBV, was down-regulated in hcc with MI. In hBV cccDna-positive hcc, down-regulated genes belonged to pathways involved in mitosis confirming the antagonism between hBV replication and mitosis.
Image:
Conclusion: under antiviral therapy, hcc can express hBV rna and replicate hBV Dna. replication of hBV in hcc was demonstrated by the tumoral comportmentalization of hBV genotypes and was linked to a low incidence of microvascular invasion and to transcriptional signatures. Moreover, some hBV-replicating hccs harboured recurrent mutations in hBx, leading to change in function with weak transactivation and low cytotoxicity. this particular type of hcc appears to be weakly invasive, well differentiated and infected by specific intra-tumour hBV variants with modified activities.
references: 1. sung Wk, zheng h, Li s, et al. Genome-wide survey of recurrent hBV integration in hepatocellular carcinoma. nat Genet 2012;44:765-9.2. Pollicino t, squadrito G, cerenzia G, et al. hepatitis B virus maintains its pro-oncogenic properties in the case of occult hBV infection. Gastroenterology 2004;126:102-10.3. Wong Dk, yuen Mf, Poon rt, et al. quantification of hepatitis B virus covalently closed circular Dna in patients with hepatocellular carcinoma. j hepatol 2006;45:553-9.4. faria Lc, Gigou M, roque-afonso aM, et al. hepatocellular carcinoma is associated with an increased risk of hepatitis B virus recurrence after liver transplantation. Gastroenterology 2008;134:1890-9; quiz 2155.
Disclosure of Interest: none Declared
P-047 free ePISOMAL AnD InTeGrATeD hbV DnA In hbSAG-neGATIVe PATIenTS WITh InTrAhePATIC ChOLAnGIOCArCInOMA
Teresa Pollicino* 1, cristina Musolino2, Gianluca tripodi2, Marika Lanza2, Giuseppina raffa2, carlo saitta2, salvatore Benfatto1, concetta Beninati1, Giuseppe navarra3, Pietro Invernizzi4, Domenico alvaro5, Giovanni raimondo2
1Pediatric, Gynecological, Microbiological, and Biomedical sciences, 2clinical and experimental Medicine, 3human Pathology, university hospital of Messina - Italy, Messina, 4autoimmune Liver Diseases, humanitas clinical and research center, Milan, 5Medico-surgical sciences and Biotechnologies, Polo Pontino, La sapienza university, rome, Italy
Introduction: Intrahepatic cholangiocarcinoma (Icc) is a fatal primary liver cancer with very poor prognosis. Genome-wide studies have made major advances in understanding the molecular basis of this disease, although most aspects remain unclear. accumulating evidence indicates that chronic hBV infection is associated with an increased risk of Icc development and suggests an etiological role of hBV in the development of this tumor. aims of the study were to investigate the prevalence of occult hBV infection (oBI) in cases with Icc and to characterize the molecular status of hBV in oBI-positive Icc specimens.
Methods: frozen paired tumor and non-tumor tissue specimens from 40 hBsag-negative patients with Icc, who underwent surgical resection were tested for oBI by 4 different hBV-specific nested Pcr. to reveal hBV cccDna, Dna extracts were digested with a plasmid-safe atP-dependent Dnase and amplified by nested Pcr with cccDna-specific primers. finally, for the detection of hBV Dna integrations the alu-Pcr technique was coupled to deep-sequence analysis.
results: hBV genomic sequences were detected in tumor and/or non-tumor specimens from 28 of the 40 (70%) Icc patients analysed. In particular, 20/40 (50%) tumors and 13/23 (56.5%) non-tumor tissues were hBV Dna positive. hBV cccDna was detected in tissue specimens from 10/28 oBI-positive patients (36%) (both in tumor and non-tumor specimens in 3 patients; only in tumor tissues in 4 patients; only in non-tumor tissues in 3 patients). hBV integrants were detected in 3 of 10 cases examined so far, and included portions of the hBx gene sequence (including the Basic core Promoter/enhancer II) in 2 cases and part of the core gene sequence in one case. the analysis

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s4 4
of the integration sites revealed that the hBx sequences were located 3,374 nucleotides upstream the sequence encoding the cat eye syndrome critical region protein 5 isoform and within the coding sequence of the thromboxane a synthase 1, respectively, and that the core gene sequence was located within the cystinosin isoform 1 precursor coding sequence.
Conclusion: occult hBV infection is highly prevalent in patients with Icc. Both free viral genomes and integrated hBV Dna can be detected in these cases. these results suggest an involvement of hBV in the carcinogenic process leading to Icc development even in cases with occult infection.
Disclosure of Interest: none Declared
P-048 Why hCC runS A hIGh LOCAL InVASIOn AnD reCurrenCe rATe buT rAreLy SySTeMIC MeTASTASIS
Sen-yung hsieh* 1, jei-Ming Peng1, chih-yung chiou1
1Liver research unit, chang Gung Memorial hospital, taoyuan, taiwan
Introduction: hcc tends to intrahepatic spreading and recurrence, but rarely systemic dissemination, suggesting that hcc cells are potentially invasive but are restricted to metastasis by unidentified mechanisms. We set forth to identify the molecular basis that drives hcc cells to be highly invasive but locally restrained.
Methods: We performed a loss-of-function screening for genes/pathways related to hcc invasion by using a lentivirus-base human kinome/phosphatome rna interference screening. We also conducted a retrospective cohort study by using cox proportional regression modeling to search for clinical factors related to hcc extrahepatic metastasis in a total of 3105 hcc cases with up to 5 yr follow-up.
results: a novel tumor invasion suppressor gene (tIs) was identified via an rnai screening on human kinome/phosphatome in human hcc cells. Mechanistic studies revealed that tIs is a novel actin binding protein that suppresses actin filament (f-actin) formation, including filopodia, lamellipodia and invadopodia. silencing of tIs leads to conversion of epithelial cancer cells to mesenchymal traits (epithelial-mesenchymal transition, eMt) with filopodia and lamellipodia formation, while ectopic expression reverts the mesenchymal traits back to epithelial characteristics (Met). Moreover, the eMt induced by tIs silencing is dependent on actin cytoskeleton remodeling via the activation of notch signaling. clinically, tIs was frequently downregulated in many human cancers including hcc. It was further downregulated in hcc in metastatic sites. Downregulation of tIs is associated with vascular invasion and higher recurrence of hcc. cox regression analysis revealed that platelets play a pivotal role in orchestrating hcc extrahepatic dissemination. high platelet count (> 212x10^6/mL) predicts an extrahepatic metastasis of early hcc (hr = 2.08; P < 0.001), while low platelet count (< 118 x10^6/mL) is significantly associated with lower extrahepatic metastasis incidence (hr = 0.54; P < 0.001) following initial curative treatment of hcc. however, low platelet counts predict a lower overall survival of patients with hcc.
Conclusion: hcc can be highly invasive. tIs, a novel actin cytoskeleton regulator, orchestrates the transition between epithelial and mesenchymal traits for hcc to invasion and colonization. the novel tIs-notch signalling can serve as therapeutic targets to prevent and treat hcc metastasis. relative rare extrahepatic metastasis of hcc is attributable to cirrhotic thrombocytopenia. Pretreatment platelet count is a reliable and readily available marker to identify subgroups of early hcc patients with high risk of metastasis during the following-up, who might benefit from adjuvant therapies to prevent recurrence and metastasis. Low platelet count is associated with low survival of patients with hcc, suggestive of the roles of platelets in liver regeneration and its reflection of the underlying severity of liver cirrhosis. Platelet is a double-edge sword in hcc progression and prognosis.
Disclosure of Interest: none Declared
P-049 MOLeCuLAr bIOMArKerS fOr CheMOPreVenTIOn Of hePATOCeLLuLAr CArCInOMA by ACyCLIC reTInOID
xian-yang qin* 1, harukazu suzuki1, Masao honda2, keita kanki3, Goshi shiota3, naoto Ishibashi4, Masahito shimizu5, hisataka Moriwaki5, soichi kojima1
1rIken center for Life science technologies, Wako, 2Graduate school of Medical sciences, kanazawa university, kanazawa, 3Graduate school of Medicine, tottori university, yonago, 4Pharmaceutical Division, koWa company, tokyo, 5Department of Gastroenterology, Gifu university, Gifu, japan
Introduction: the poor prognosis of hepatocellular carcinoma (hcc) is partly due to its high rate of recurrence after the initial treatment. acyclic retinoid (acr) is currently under phase III clinical trials in japan to prevent the recurrence and development of hcc in patients after surgical removal of the primary tumors1,2. Previous in vitro experiments showed that acr selectively suppresses the growth of human hcc cells (jhh7, huh7, and hepG2) but not normal human hepatic cells (hc)3. In the present study, the genome-wide transcriptome analysis was performed to identify novel biomarkers for treatment of hcc with acr having cancer-selective growth suppression effect.
Methods: Gene expression profiles of jhh7 and hc cells treated with acr were measured
using next-generation sequencing-based cap analysis Gene expression (caGe) analysis. Genes differentially expressed after acr treatment in jhh7 cells but not in hc cells were selected. Inhibitory effect of acr on Mycn expression was confirmed using real-time Pcr in culture cells, animal models and liver biopsy samples of hcc patients administered with acr (n = 6). Mycn-dependent signaling pathways underlying the growth suppression activity of acr were investigated using knowledge-based ingenuity pathway analysis (IPa), rna interference technology, chemical inhibitors and luciferase assays. relationship between Mycn expression and tumor recurrence in hcc patients (n = 102) was evaluated using the log-rank test. correlations between Mycn and liver cancer stem cell (csc) markers were determined using Pearson correlation coefficients based on microarray database or immunostaining of hcc cells.
results: Mycn was expressed in jhh7 cells but not in hc cells, while acr inhibited Mycn expression in hcc cells and mouse models. In contrast, the ethyl analogues of acr, which showed no growth suppression activity, did not inhibit Mycn expression in hcc cells. acr also selectively suppressed the growth of Mycn-amplified neuroblastoma cells, but not that without Mycn amplification. furthermore, four out of 6 liver biopsies of hcc patients (66.7%) who had received 8 weeks of acr treatment (600 mg/day) after definitive treatment showed decreased Mycn expression (< 0.5-fold). Pathway analysis using IPa suggested an sp1/Mycn/caspase-8 signaling pathway underlying the anticancer effect of acr. upon knockdown of Mycn, hcc cells showed suppressed cell growth and increased caspase-8 activity. an sp1 inhibitor suppressed Mycn expression, whereas a caspase-8 inhibitor restored acr-induced growth suppression in hcc cells. finally, clinical analysis indicated that Mycn expression in hcc tumors was significantly correlated with csc markers afP, epcaM and cD133 but not cD90, and negatively associated with recurrence of early-stage hcc.
Conclusion: Mycn is a new biomarker of eligibility for acr treatment that correlates with liver csc with progenitor features and poor prognosis of hcc. acr suppressed hcc cell growth through an sp1/Mycn/caspase-8 dependent signaling pathway.
references: 1. Muto, y. et al. n engl j Med., 334:1561-1267 (1996); 2. okita, k. et al. j Gastroenterol., DoI: 10.1007/s00535-014-0996-1 (2014); 3. tatsukawa, h. et al. Mol cancer, 10:4 (2011)
Disclosure of Interest: none Declared
P-050 exOMe SequenCInG In eArLy-STAGe hePATOCeLLuLAr CArCInOMA IDenTIfIeS PTPn13 AS A TuMOur SuPPreSSOr
zhan hao* 1, jiang jiahao1, hu zhiqiang1, Luo chubin1
1Liver cancer Institute, zhongshan hospital, fudan university, shanghai, china
Introduction: hepatocellular carcinoma (hcc) is the second leading cause of cancer mortality and carries a dismal prognosis. the present study aimed to identify early mutations implicated in hcc tumourigenesis and progression.
Methods: We sequenced the exomes of 5 hBV-related early-stage hcc (ehcc) and paired peripheral blood samples and performed gene ontological analysis of the single-nucleotide variants. of the frequent mutations identified, we tested the effects of PTPN13 in vitro. additionally, its clinical relevance was evaluated in a tissue microarray analysis of samples from 282 hcc patients.
results: We identified a mutational signature of dominant t:a>a:t transversion and significantly enriched pathways that included ecM-receptor interaction, focal adhesion and axon guidance. a total of 8 genes (PTPN13, MUC16, USH2A, TENM4, UNC79, DNAH17, PCLO and PDE1C) were frequently mutated in hcc. the protein tyrosine phosphatase (PtP) PtPn13 was further evaluated for its clinical relevance in hcc. Various hcc cell lines expressed very low PtPn13 protein levels. In vitro, PtPn13 overexpression significantly inhibited hcc cell progression, possibly by inhibiting epithelial-mesenchymal transition through inactivation of the eGfr signalling pathway. tissue microarray analysis revealed that high PtPn13 expression was correlated with a favourable prognosis in postoperative hcc patients.
Conclusion: our findings elucidated the mutation profile of hBV-related ehcc and identified the tumour suppressor PtPn13 as an alternative therapeutic target for hcc.
Disclosure of Interest: none Declared
P-051 zIC2 PrOMOTeS CeLL PrOLIferATIOn AnD MIGrATIOn In hePATOCeLLuLAr CArCInOMA by TrAnSCrIPTIOnALLy uPreGuLATInG PAK4
jing-Ping yun1, chris zhiyi zhang1, Shi-xun Lu* 1, Li-Li Liu1
1Department of Pathology, sun yat-sen university cancer center, Guangzhou, china
Introduction: zic2 has been demonstrated crucial to the progression of human cancers. our study aims to investigate the clinical significance of zic2 and its role in hepatocellular carcinoma (hcc).

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 4 5
Methods: qrt-Pcr, western blot and immunohistochemistry were performed to examine the expression of zic2 in hcc. the in vitro and in vivo effects of zic2 on hcc cell growth were determined. Luciferase and chIP assays were conducted to confirm the association of zic2 with Pak4 and mir-1271.
results: our data showed that zic2 expression was noticeably increased in hcc tissues. zic2 overexpression remarkably promoted cell proliferation and migration. Gene microarray indicated Pak4 as a potential target of zic2. the knockdown of zic2 decreased, whereas zic2 re-expression increased the expression of Pak4, at both mrna and protein levels, resulting in the alteration of raf/Mek/erk pathway. chIP and luciferase assays indicated that zic2 directly bound to Pak4 promoter and modulated its activity. Pak4 silence attenuated zic2-mediated cell growth. In a cohort of 615 patients with hcc, zic2 was positively correlated with Pak4, and significantly associated with overall and disease-free survival. Multivariate analyses revealed that both proteins were independent indicators of poor outcome in hcc. In addition, zic2 mrna was found reversely connected with the expression of mir-1271. further study showed that zic2 expression was inhibited by mir-1271. re-introduction of mir-1271 markedly abolished zic2-promoted cell proliferation and migration.
Conclusion: our findings suggest that zic2 is a valuable biomarker for hcc prognosis and the mir-1271/zic2/Pak4 regulatory network plays an important role in hcc progression.
references: 1. chan DW, Liu VW, Leung Ly, yao kM, chan kk, cheung an, ngan hy. zic2 synergistically enhances hedgehog signalling through nuclear retention of Gli1 in cervical cancer cells. j Pathol 2011;225:525-34.2. Pfister s, schlaeger c, Mendrzyk f, Wittmann a, Benner a, kulozik a, scheurlen W, radlwimmer B, Lichter P. array-based profiling of reference-independent methylation status (aPrIMes) identifies frequent promoter methylation and consecutive downregulation of zIc2 in pediatric medulloblastoma. nucleic acids res 2007;35:e51.3. Marchini s, Poynor e, Barakat rr, clivio L, cinquini M, fruscio r, Porcu L, Bussani c, D'Incalci M, erba e, romano M, cattoretti G, katsaros D, koff a, Luzzatto L. the zinc finger gene zIc2 has features of an oncogene and its overexpression correlates strongly with the clinical course of epithelial ovarian cancer. clin cancer res 2012;18:4313-24.4. siu Mk, chan hy, kong Ds, Wong es, Wong oG, ngan hy, tam kf, zhang h, Li z, chan qk, tsao sW, stromblad s, cheung an. p21-activated kinase 4 regulates ovarian cancer cell proliferation, migration, and invasion and contributes to poor prognosis in patients. Proc natl acad sci u s a 2010;107:18622-7.
Disclosure of Interest: none Declared
P-052 hIGher PhOSPhO-rb exPreSSIOn ASSOCIATeD WITh beTTer ACTIVITy Of CyCLIn DePenDenT KInASe 4/6 InhIbITOr AbeMACICLIb On hePATOCeLLuLAr CArCInOMA
yu-yun Shao* 1, hang Lin1, han-yu Wang1, yong-shi Li1, ann-Lii cheng1, chih-hung hsu1
1national taiwan university hospital, taipei city, taiwan
Introduction: treatment options for advanced hepatocellular carcinoma (hcc) are limited. novel treatment is warranted for advanced hcc. We explored the antitumor activity of abemaciclib, an inhibitor for cyclin dependent kinases (cDk) 4 and 6, on hcc cells.
Methods: In a panel of hcc cell lines including huh7, hepG2, hep3B, PLc5, hLe, sk-hep1, snu387, snu398, snu423, snu449, and snu475, abemaciclib was examined for its effect on cell viability, cell cycle distribution, and apoptosis induction. the expressions of cDk 4/6 and its associated proteins including phospho- (p-) rb, cyclin D1, and p16 were evaluated to see whether they were associated with the antiproliferative effect of abemaciclib.
results: abemaciclib showed various anti-proliferative activities in hcc cell lines. the Ic50s to abemaciclib by the 6-day Mtt assay was 53 nM for huh7, 112 nM for hepG2, and 172 nM for sk-hep1. By contrast, abemaciclib up to 750 nM showed little antiproliferative effect on hep3B, hLe, and snu423. a high expression of p-rb was strongly associated with a lower Ic50 in cell lines (r = −0.727). rb expression was very low in hep3B and hLe. the expression of cDk4 (r = −0.526) or cDk6 (r = −0.558) was moderately associated with the Ic50s, but that of cyclin D1 (r = −0.235) or p16 (r = −0.338) had little correlation. after 72 hours of abemaciclib treatment, huh7 cells showed G1 arrest in a dose-dependent manner. apoptosis assays including annexin V/propidium iodide staining, cleaved ParP-1, and cleaved caspase 3 confirmed the occurrence of apoptosis in huh7 cells treated with abemaciclib. abemaciclib at the concentration near the Ic50 inhibited the phosphorylation of rb.
Conclusion: abemaciclib appears to be preferentially active against hcc cells with high p-rb expression. further studies are warranted.
Disclosure of Interest: none Declared
P-054 reCOMbInAnT ADenOVIruS enCODInG fAT10 SMALL InTerferInG rnA InhIbITS hCC GrOWTh In VITrO AnD In VIVO
Chen Ping* 1
1Department of hepatobiliary surgery, Daping hospital, third Military Medical university, chongqing, china
Introduction: hepatocellular carcinoma is an aggressive and rapidly fatal malignancy representing the common cancer worldwide. the ubiquitin-like modifier fat10, recently reported to be overexpressed in 90% of hepatocellular carcinoma carcinomas. however, the exact function of fat10 in hepatocellular carcinoma is not clear. In the present study, we utilized adenovirus-mediated rna interference to knock down fat10 expression in hepatocellular carcinoma cells and observed its effects on hepatocellular carcinoma cell growth in vitro and in vivo.
Methods: 1. Inhibitory effect of ad-sirna/fat10 to hcc cell growth in vitrocell proliferation was measured by a colorimetric assay using Mtt; for colony forming assay, cells were seeded into 10cm culture dishes and were treated with ad-sirna/fat10 or controls for 18 days, cell colonies were fixed with glutaraldehyde, and stained with crystal violet and visible colonies were manually counted; standard fluorescence-activated cell sorter analysis was used to determine the distribution of cells in cell cycle and apoptosis rate of the cells.2. tumor challenge assay in vivo.nude mice were challenged with subcutaneous injection of hep3B cells into the left flank to induce primary tumors. two weeks after tumor cell inoculation, mice were divided randomly into three groups (ten mice per group) and were received an intratumor injection of of ad-sirna/fat10 or ad-sirna/Lacz . the control mice received 100μL PBs. tumor volume and mean lifespan of the mice were observed. tumor volume was measured in two dimensions and calculated as follows: length/2×width2.
results: the results demonstrated that interference of fat10 could inhibit cell proliferation by inhibiting the cell cycle s-phase entry and inducing cell apoptosis. In addition, in vivo experiments showed that adenovirus ad-sirna/fat10 significantly suppressed tumor growth and prolonged the lifespan of tumor bearing mice.
Conclusion: the results suggest that knockdownof fat10 by adenovirus-delivered sirna may be a promising therapeutical strategy for treatment of hepatocellular carcinoma.
Disclosure of Interest: none Declared
P-055 PAThOPhySIOLOGy Of hePATITIS C VIruS (hCV)-reLATeD hePATOCeLLuLAr CArCInOMA: hCV PrOTeIn exPreSSIOn InDuCeS The ACTIVATIOn Of The AKT1 ISOfOrM In hePATOCyTeS ThrOuGh An MTOrC2 DePenDenT PAThWAy
Mohamed r. Imache* 1, jacqueline Polyte1, jean-Michel Pawlotsky1, herve Lerat2
1equipe 18, Inserm u955, 2equipe 18, university of Paris-est / Inserm u955, creteil, france
Introduction: the Pi3k-akt pathway is a critical intracellular node regulating cell survival and proliferation. activation of the akt pathway has been reported in many cancers, including hepatocellular carcinoma (hcc). We previously showed that c-Myc is overexpressed through an akt-dependent mechanism in the livers of hcV-infected patients and transgenic mice (fL-n/35) expressing the entire repertoire of hcV proteins (Higgs et al., Oncogene 2013).
Methods: the present study aimed at unraveling the molecular mechanisms of hepatocyte akt activation during hcV infection using human liver biopsies and transgenic mice.
results: We observed a significant hyperphosphorylation of akt-ser473 in non-tumoral hepatic tissues from hcV-infected patients with hcc as compared to hBV-infected or non-infected alcoholic patients. hyperphosphorylation of akt-ser473 was also observed in 3 months-old hcV transgenic mouse livers as compared to wild-type mice, which persisted after eGf treatment. the akt1 isoform (not akt2) was the activated form. We observed an increase in the phosphorylation of mtor-ser2448 within the mtorc2 complex and a concomitant increased kinase activity of this complex, associated with reduced phosphorylation of p70s6k-thr389 and PDk1-ser241. Within the mtorc2 complex, rictor P70s6k-dependent phosphorylation (at thr1135) induces an inhibition of mtorc2 kinase activity. In keeping with the lower phosphorylation of p70s6k, we observed a lower phosphorylation of thr1135-rictor in the hepatocytes from fL-n/35 mice.
Conclusion: our results suggest that hcV protein expression modulates the negative feedback loop that controls akt phosphorylation, thus leading to its hyperactivation, which potentially plays a role in subsequent carcinogenetic events. numerous molecules targeting the PI3k/akt pathway have been used in other cancers than hcc. our results suggest these approaches could be valuable to prevent or treat hcV-associated hcc.
references: M.r. higgs, h Lerat, and j-M Pawlotsky. hepatitis c virus-induced activation of

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s4 6
β-catenin promotes c-Myc expression and a cascade of pro-carcinogenetic events. oncogene (2013) 32:4683-93
Disclosure of Interest: none Declared
P-056 DnA DAMAGe CAuSeD by DIeTAry InDuCeD STeATOhePATITIS COrreLATeS WITh hePATOCeLLuLAr CArCInOMA DeVeLOPMenT AnD PrOGreSSIOn
helen L. reeves1, 2, Ahmed Mahdi* 1, quentin anstee2, 3, Dina tiniakos3, john Lunec1
1northern Institute for cancer research, newcastle university, 2Liver unit, freeman hospital, newcastle upon tyne hospitals nhs foundation trust, 3Institute of cellular Medicine, newcastle university, newcastle-upon-tyne, united kingdom
Introduction: hepatocellular carcinoma (hcc) complicates chronic liver disease. the prevalence of non-alcoholic fatty liver disease (nafLD) is rising markedly and in parts of the western world is now the commonest hcc predisposing factor. oxidative stress induced cellular and Dna damage reportedly play a central role in the progression of simple fatty liver to steatohepatitis, fibrosis and hcc. In a dietary model of nafLD and hcc, Dna damage has been assessed, as has the impact of supplementation with the antioxidant bucillamine.
Methods: c3h/he mice with impaired glucose tolerance, fed the american lifestyle (aLIos) diet, develop nash, fibrosis and hcc at 1 year. tissues from control (n=24) and aLIos (n=23) diets were compared, including grading of nafLD and hcc on h&e sections. Immunohistochemical quantification of γh2ax foci and ki67 assessed Dna damage and proliferative responses. slides were scanned and analysed using aperio Imagescope, scoring positively stained nuclei as percentage of total nuclei in 30 periportal, intermediate and perivenular zones.
results: nafLD grade and hcc burden were more severe in aLIos fed mice (table 1). fat accumulation was most prominent in portal tract zones, in association with a dramatic increase in nuclei with γh2ax foci. numbers of tumours was associated with body weight, steatosis, microvesicular steatosis, Mallory denk bodies, lipogranulomas, lobular inflammation, fibrosis stage, ki67 and γh2ax positive nuclei. In multivariate analyses, microvesicular steatosis (p=0.001) and γh2ax positive nuclei (p=0.002) were significantly associated with tumour number. In a similar analysis, lobular inflammation, fibrosis stage and ki67 were significantly associated with tumour size. Bucillamine treatment dramatically reduced the number of γh2ax positive nuclei in both control and aLIos diet animals (0.16±0.02 and 0.43±0.07 respectively, compared to data in table 1), in association with a trend to reduced tumour size (mm) compared to aLIos fed animals at 48 weeks (4.8±1.4 vs 7.65±1.63).
Image:
Conclusion: c3h/he mice fed the aLIos develop more severe liver injury in association with a marked increase in periportal Dna damage. the combination contributes to a significant increase in numbers and size of hcc. this model will be useful for further study of mechanisms underlying initiation and progression of hcc in nafLD.
Disclosure of Interest: none Declared
P-057 CATALASe ACTIVITy InhIbITIOn by hePATITIS C VIruS (hCV) In hCV-InDuCeD OxIDATIVe STreSS, A TrIGGer Of hePATIC CArCInOGeneSIS
Philippe Chouteau* 1, ségolène Brichler1, Patrice Bruscella1, alexandre florimond1, jean-Michel Pawlotsky1
1national reference center for Viral hepatitis B, c, and Delta, Department of Virology, and InserM u955, créteil, france
Introduction: hepatitis c virus (hcV) infection is a major risk factor for the onset and progression of hepatocellular carcinoma (hcc). chronic hcV infection induces the accumulation of reactive oxygen species (ros) in infected livers leading to oxidative stress. Little is known about alterations of intracellular antioxidant defense pathways involved in hcV-related oxidative stress. cellular catalase is an enzyme that detoxifies hydrogen peroxide (h2o2), a ros known to control cell proliferation, thus playing a major role in the cellular antioxidant defense mechanism.
the aim of this study was to characterize the expression and activity of cellular catalase, using different in vitro and in vivo models of hcV replication or hcV protein expression.
Methods: the expression and activities of cellular catalase was explored in hcV-infected human liver samples, in the fL-n/35 transgenic mouse model, expressing the whole hcV orf (genotype 1b) exclusively within the hepatocytes and in huh7.5 cells infected with the jfh1 viral clone (genotype 2a).
results: cirrhotic liver samples from hcV-infected patients exhibited a significant decrease of their intracellular catalase activity when compared to alcoholic and hBV-infected cirrhotic liver samples. however, the intrahepatic catalase protein levels were not different between these three groups of patients. In order to explore the impact of hcV protein expression in vivo in the absence of local inflammation and immune response, the transgenic (tg) mouse model expressing the full-length hcV orf (fL-n/35 mice) was used. tg mouse livers display high levels of oxidative stress. We observed a significantly higher oxidative nuclear Dna damage, together with an increase in the amount of advanced oxidation protein products, in tg livers compared to their wild type (wt) littermates. Like in human samples, the level of h2o2 detoxification in tg mice livers was weak. Primary hepatocytes isolated from tg mice displayed a dramatic, up to 80%, reduction of catalase activity when compared to wt mice. remarkably, catalase expression (mrna and protein levels) was similar in tg and wt liver samples and isolated primary hepatocytes. the jfh1-based cell-culture system was used to assess catalase expression and activity in a fully replicating system. Like in the other models, a dramatic increase in the intracellular oxidative stress level was observed in hcV-infected cells, concomitant to a significant decrease of catalase activity without alteration of catalase expression.
Conclusion: hcV infection is responsible for a default in intracellular catalase activity. this alteration is not related to the protein expression. this phenotype is observed as a result of the sole hcV protein expression, in the absence of local inflammation, and is independent of the hcV genotype. this mechanism could, at least in part, contribute to the hcV-induced intracellular oxidative stress, a major trigger of hcc.
Disclosure of Interest: none Declared
P-058 ALPhA-SAnTALOL InhIbITS TuMOr AnD InDuCeS APOPTOSIS In hePATOCeLLuLAr CArCInOMAS In VITrO AnD In VIVO
Sarita Saraswati* 1, a. a. alhaider1
1Pharmacology, king saud university, riyadh, saudi arabia
Introduction: hepatocellular carcinomas (hcc) are highly malignant and aggressive tumors lack of effective therapeutic drugs. Preliminary reports suggest that alpha-santalol (as) possesses anti-tumor activity. however, its effect on hepatocellular carcinoma is still unknown. therefore, we investigated the chemopreventive potential of as in vitro and in vivo.
Methods: We studied the antiangiogenic activity of as using huVecs and hcc in vitro and rat aortic assay ex vivo, matrigel plug assay in vivo. cell cycle arrest and apoptosis were analyzed by flow cytometry. Immunohistochemical staining and tuneL expression were studied in tumor samples of hepG2-xenografted nude mice.
results: as significantly inhibited VeGf-stimulated proliferation, migration, invasion and tube formation of endothelial cells. as also inhibited VeGf-induced microvessel sprouting in rat aortic assay and inhibited angiogenesis in matrigel plug assay with significantly decreased area of infiltrating cD31-positive endothelial cells. as (2-20 μmol/L) inhibited the proliferation of the cells in dose- and time-dependent manners with an Ic50 value of nearly 7.5 μmol/L at 48 h. as suppressed VeGf-induced phosphorylation of VeGfr2 in huVecs and also suppressed the constitutive activation of akt/mammalian target of rapamycin (mtor) signal transduction pathway in huVecs as well as in hcc cells. Moreover, as decreased the expression of hsp90 and suppressed akt phosphorylation and nf-κB expression in hepG2 cells. as decreased the expression of cyclin a, cyclin B, cyclin D1, cyclin e and Bcl-2 with activation of caspase-3 and increased expression of Bax. as showed

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 4 7
significant inhibition of tumor growth in a dose-dependent manner in mouse xenograft model. In the xenograft mice, as administration decreased the tumor growth by 60%, and markedly increased the expression of Bax, cleaved caspase-3 and tuneL and decreased the expression of cyclin D,VeGf, cD31 and ki-67 in tumor tissues.
Conclusion: our data demonstrate the antiangiogenic effects of as on hcc cells via akt/mtor signaling pathway and suggest that as may be a potential therapeutic agent for the treatment of hcc patients.
Disclosure of Interest: none Declared
P-059 nOVeL GenOMIC MArKer fOr PreDICTInG PrOGnOSIS In PATIenTS WITh hePATOCeLLuLAr CArCInOMA DeTeCTeD by InTeGrATIOn AnALySIS Of COPy nuMber ALTerATIOnS AnD Gene exPreSSIOn PrOfILe: reSuLTS frOM LOnG TerM fOLLOW-uP
hyo Jung Cho* 1, soon sun kim1, joo han Park1, choong kyun noh1, sung Won cho1, jae youn cheong1
1Department of Gastroenterology, ajou university school of Medicine, suwon, korea, republic of
Introduction: Genomic marker for predicting the prognosis of hepatocellular carcinoma (hcc) is not identified. the aim of this study was to explore the novel genomic biomarker predicting hcc prognosis by integration analysis of Dna copy number alterations (cna) and gene expression profile.
Methods: a total of 50 tumor samples obtained from hcc patients who underwent hepatic resection were analyzed. array comparative genomic hybridization (cGh) and expression array were performed on 45 and 31 hcc tissue samples, respectively. overall survival (os) and tumor recurrence were investigated using long term follow-up (> 9 years) data. concordant results of Dna copy number and expression were retrieved by integrative analysis.
results: cox proportional hazard model indicated that the cna in 310 genomic regions, including 4p15, 4p16, 9p11, 9p12, 9p13, were significantly associated with os (P <0.05). In addition, 42 amplified regions and 176 deleted regions were also associated with os. among genes with concordant results between cna and expression profile, overexpression of tLe4 (P = 0.033), nuDt2 (P = 0.041) and xPa (P = 0.026) were identified as predictor of longer os. In the analysis of tumor recurrence, 592 genomic regions with cna were associated with tumor recurrence. Integration analysis revealed that the overexpression of 8 genes [MrPL50 (P = 0.013), frMPD1 (P = 0.012), nr4a3 (P = 0.021), sPaG8 (P = 0.048), unc13B (P = 0.024), Loc389207 (P = 0.019), MaPkaP1 (P = 0.019) and Whsc1 (P = 0.035)] was significantly associated with less tumor recurrence. Gene enrichment and functional annotation analysis demonstrated that the clinicopathologic characteristics of tumor (tumor size, stage, vascular invasion, differentiation) were associated with genes related to the regulation of cell proliferation and cell cycle, apoptosis and cell signaling pathway.
Conclusion: the integration analysis of Dna copy number alteration and expression profile correlated with long term follow-up data identified the potential prognostic markers predicting survival and tumor recurrence in patients with hcc who underwent surgical resection.
Disclosure of Interest: none Declared
P-060 LOSS Of e-CADherIn In POrTAL VeIn TuMOr ThrOMbOSIS Of hePATOCeLLuLAr CArCInOMA CAn be reVerSeD by C-MeT InhIbITOr
Takashi Kokudo* 1, yoshinori Inagaki1, kiyoshi hasegawa1, chikara shirata1, junichi kaneko1, nobuhisa akamatsu1, junichi arita 1, yoshihiro sakamoto1, norihiro kokudo1
1hepato-Biliary-Pancreatic surgery Division and artificial organ and transplantation Division, Department of surgery, Graduate school of Medicine, the university of tokyo, tokyo, japan
Introduction: Portal vein tumor thrombosis (PVtt) is related to poor prognosis in patients with hepatocellular carcinoma (hcc). however, little is known about the mechanism of PVtt formation and effective treatment for hcc patients with PVtt. c-met inhibitor has recently been reported to be a promising treatment for hcc.1 We here investigated the molecular characteristics of PVtt and the effect of c-met inhibitor.
Methods: surgical specimens of 20 hcc patients with PVtt were analyzed. human hcc cell lines huh-7 and skhep-1 were used for experimental study. subcutaneously transplanted xenograft model was used for in vivo study. c-met inhibitor su11274 was used both in vitro and in vivo analysis. the e-cadherin expression was analyzed through immunohistochemistry and Western blot analysis.
results: Immunohistochemistry revealed significant decrease of e-cadherin positive cells in PVtt compared to the original main tumor. this result was confirmed through protein analysis (fig. a). In vitro, sk-hep1 cells showed sheet formation after c-met inhibitor administration (fig. B), and the
expression level of e-cadherin was elevated (fig. c). this result was also confirmed in huh-7 cells. this sheet formation through c-met inhibitor attenuated migration of sk-hep-1 cells (fig. D). In vivo, after administration of c-met inhibitor, skhep-1 xenograft showed elevated expression of e-cadherin.
Image:
Conclusion: Loss of e-cadherin correlates with formation of PVtt and c-met inhibitor increased the expression of e-cadherin both in vitro and in vivo. c-met inhibitor may be a promising treatment for preventing PVtt formation.
references: 1.santoro a, rimassa L, Borbath I, et al. tivantinib for second-line treatment of advanced hepatocellular carcinoma: a randomised, placebo-controlled phase 2 study. Lancet oncol 2013 jan;14:55-63.
Disclosure of Interest: none Declared
P-061 TreATMenT Of hCC CeLLS WITh SOrAfenIb InDuCeD VArIATIOnS In The PrOfILe Of The CeLL MeThyLOMe
edoardo abeni1, alessandro salvi1, Michele traversa1, Bruna arici1, Giuseppina De Petro* 1
1Dept of Molecular and translational Medicine, Division of Biology and Genetics, university of Brescia, Brescia, Italy
Introduction: sorafenib (sf) is currently the standard treatment for advanced (unresectable or metastatic) hepatocellular carcinoma (hcc). sharP and aP (1,2) clinical trials confirmed the effectiveness of sf compared to placebo, with median survival of nearly 3 months longer for patients treated with sf than for those given placebo. Moreover sf has severe side effects and patients develop resistance quickly (3). although there are a lot of studies directed at clarifying the role of sf in hcc, a clear mechanism of action that explains its anti-tumor activity has not fully elucidated. epigenetic alterations, such as Dna methylation, play a decisive role in the development and progression of hcc. to our knowledge, there are no studies on the Dna methylation changes in hcc cells treated with sf on global level. therefore, the present study was designed to determine the effects of sf on the methylome of human hcc cells to better understand its mechanism of action and to find new molecular targets that can improve its effectiveness.
Methods: hcc ha22t/VGh cells were treated with sf for 24 hours. the Dna methylation changes between sf-treated and untreated-cells were evaluated using methylated Dna immunoprecipitation (MeDIP) combined with affymetrix human Promoter 1.0r chips. the raw data were imported into Partek Genomics suite and differentially methylated regions (dmr) were obtained using anoVa combined with Mat algorithm. the associated genes were subjected to functional enrichment analysis using DaVID and WebGestalt. the microarray results were validated by coBra and direct bisulfite sequencing. the correlation between Dna methylation level and mrna expression was tested by qPcr.
results: We found 1230 genes differentially methylated in ha22t/VGh cells treated with sf compared to untreated cells (fig.1). the functional enrichment analysis displayed enriched several Go terms and different signaling pathways related to tumorigenesis and cancer progression. Moreover the Dna methylation levels of several cancer-associated non-coding genes were changed. In general, we found a trend where oncogenes were hypermethylated and tumor suppressor genes were hypomethylated after sorafenib treatment. finally, the Dna methylation variation of 5 selected genes was experimentally tested and validated and the correlation between Dna methylation level and mrna expression was confirmed for 3 out of 5 selected genes.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s4 8
Image:
Conclusion: this is the first study that evaluated the effects of sf on Dna methylation profile in hcc cells. our results suggest that sf treatment in hcc cells could affect the Dna methylation level of different genes associated with apoptosis, invasion and angiogenesis. Moreover we found Dna methylation changes in genes belonging to signaling pathways known to be related to mechanism of action of sf. In conclusion these results identified novel sf targets genes and confirmed previous results found by other groups at Dna methylation level, increasing knowledge of sf mechanism of action. the genes found differentially methylated could be targets in a new design of multi-target and combined therapies and to better understand the emergence of resistance in hcc.
references: 1.Llovet jM, ricci s, Mazzaferro V, hilgard P, Gane e, Blanc jf, et al. n engl j Med 2008;359:378–90. 2. cheng aL, kang yk, chen z, tsao cj, qin s, kim js, et al. Lancet oncol 2009;10:25–34. 3. Llovet jM, hernandez-Gea V. clin cancer res. 2014 apr 15;20(8):2072-9.
Disclosure of Interest: none Declared
P-062 AxL exPreSSIOn STrATIfIeS PATIenTS WITh POOr PrOGreSSIOn fOr hePATOCeLLuLAr CArCInOMA
Kui Wang* 1, jian Liu2
1Department of hepatic surgery, 2the eastern hepatobiliary surgery hospital, shanghai, china
Introduction: axl is a receptor tyrosine kinase which is important in multiple human malignancies. In this study we investigated its primary function and prognostic role in hepatocellular carcinoma (hcc).
Methods: the axl expression was examined in several hcc cell lines and paired tumor or nontumorous samples. then, we examined cell growth curve, cell apoptosis through annexin V-staining and cell migration through transwell assay and wound healing assay in sMMc-7721 cells with axl over-expressed or depleted through transfected with wild-type of axl (axl-Wt) or sirna against axl (si-axl), respectively. finally, the prognostic role of axl was investigated in a prospective cohort of 246 consecutive hcc patients underwent liver resection.
results: We found axl was positive in 22% of tumor tissues of hcc samples and all four cell lines. over-expressing axl in sMMc-7721 cells accelerated cell growth, promoted wound recovery and cell migration into the bottom chamber and inhibited cell apoptosis, while knock-down of axl exerted opposite effect in these aspects. Intratumoral axl expression was significantly associated with serum afP (P = 0.003), multiple tumors (P<0.001), absence of encapsulation (P=0.003), microvascular invasion (P=0.004), and later tnM stage (P <0.001). Patients with positive axl staining had higher 5-year recurrence rate (92% vs. 71%, P<0.001) and lower 5-year survival rate (9% vs. 48%, P<0.001) than those with negative axl staining. the multivariate analyses showed that axl expression was an independent factor affecting tumor recurrence (hr: 1.725; 95% cI: 1.219-2.441) and survival (1.847; 1.291-2.642).
Image:
Conclusion: tumoral axl expression suggests more aggressive tumor invasiveness and predicts worse prognosis for hcc patients underwent resection.
references: 1. jemal a, siegel r, Ward e, et al. cancer statistics, 2009. ca cancer j clin 2009; 59: 225-249.2. Llovet jM, Beaugrand M. hepatocellular carcinoma: present status and future prospects. j hepatol 2003;38 suppl 1:s136-149.3. Llovet jM, fuster j, Bruix j. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection Versus transplantation. hepatology 1999; 30:1434-1440.4. arii s, yamaoka y, futagawa s, et al. results of surgical and nonsurgical treatment for small-sized hepatocellular carcinomas: a retrospective and nationwide survey in japan. hepatology 2000; 32:1224-1229.5. Minagawa M, Makuuchi M, takayama t, et al. selection criteria for repeat hepatectomy in patients with recurrent hepatocellular carcinoma. ann surg 2003; 238:703-710.
Disclosure of Interest: none Declared
P-063 TerT PrOMOTer MuTATIOn PATTern In MuLTISTeP hePATOCArCInOGeneSIS: A STuDy Of 7 PATIenTS
Luca Di Tommaso* 1, jean charles nault2, julien calderaro2, annarita Destro1, Marco Maggioni3, amedeo sciarra1, Gabrielle couchy2, jessica zucman-rossi2, Massimo roncalli1
1Irccs IstItuto cLInIco huManItas, rozzano, Italy, 2InserM, uMr-1162, Paris, france, 3Policlinico of Milan, Milano, Italy
Introduction: tert promoter mutation has been shown as the earliest genetic alteration of human hepatocarcinogenesis, being reported in 16% low grade dysplastic nodules (LGDn), 19% high grade dysplastic nodules (hGDn), 61% early hepatocellular carcinoma (ehcc) and 42% small and progressed hepatocellular carcinoma (phcc).
We investigated tert promoter mutation in multiple hepatocellular nodules (hn) including hcc detected in 7 patients, to elucidate the pattern of occurrence of this molecular change in human hepatocarcinogenesis.
Methods: the series included 7 patients (5M, 2f; mean age 61.7 years, range 46-74 years; 4 hcV, 1 hBV, 1 nash and 1 unknown) harboring 32 hn (7 cirrhotic nodules; 7 LGDn; 4 hGDn; 5 ehcc one with features of nodule in nodule n/n; 9 phcc) with a mean of 4,5 hn/patient (range 4-7). four patients received liver transplantation and three surgical resection.
results: tert promoter mutation was seen in 6/7 patients (85.6%) and in 9/32 (28%) hn: 0/7 cirrhotic nodules, 0/7 LGDn, 1/4 (25%) hGDn, 3/5 (60%) ehcc and 5/9 (55%) phcc. the mutational hot spot was always located at -124 base pairs before the atG start of tert (G>a substitution). In 3 patients (cases 2, 3 and 4) the mutation was detected in phcc but not earlier; in other 3 patients (cases 5, 6 and 7) it was seen in precursors (including e-hcc) but not later in 2 of them. result are illustrated in figure 1.
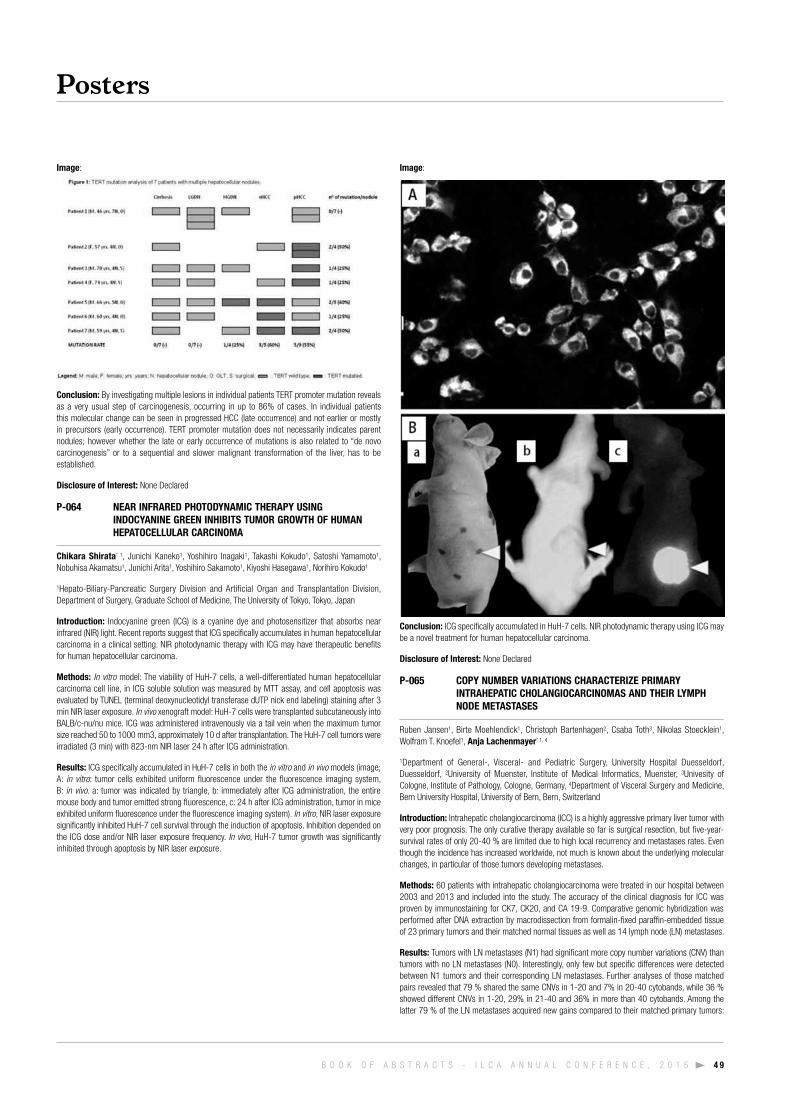
Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 4 9
Image:
Conclusion: By investigating multiple lesions in individual patients tert promoter mutation reveals as a very usual step of carcinogenesis, occurring in up to 86% of cases. In individual patients this molecular change can be seen in progressed hcc (late occurrence) and not earlier or mostly in precursors (early occurrence). tert promoter mutation does not necessarily indicates parent nodules; however whether the late or early occurrence of mutations is also related to “de novo carcinogenesis” or to a sequential and slower malignant transformation of the liver, has to be established.
Disclosure of Interest: none Declared
P-064 neAr InfrAreD PhOTODynAMIC TherAPy uSInG InDOCyAnIne Green InhIbITS TuMOr GrOWTh Of huMAn hePATOCeLLuLAr CArCInOMA
Chikara Shirata* 1, junichi kaneko1, yoshihiro Inagaki1, takashi kokudo1, satoshi yamamoto1, nobuhisa akamatsu1, junichi arita1, yoshihiro sakamoto1, kiyoshi hasegawa1, norihiro kokudo1
1hepato-Biliary-Pancreatic surgery Division and artificial organ and transplantation Division, Department of surgery, Graduate school of Medicine, the university of tokyo, tokyo, japan
Introduction: Indocyanine green (IcG) is a cyanine dye and photosensitizer that absorbs near infrared (nIr) light. recent reports suggest that IcG specifically accumulates in human hepatocellular carcinoma in a clinical setting. nIr photodynamic therapy with IcG may have therapeutic benefits for human hepatocellular carcinoma.
Methods: In vitro model: the viability of huh-7 cells, a well-differentiated human hepatocellular carcinoma cell line, in IcG soluble solution was measured by Mtt assay, and cell apoptosis was evaluated by tuneL (terminal deoxynucleotidyl transferase dutP nick end labeling) staining after 3 min nIr laser exposure. In vivo xenograft model: huh-7 cells were transplanted subcutaneously into BaLB/c-nu/nu mice. IcG was administered intravenously via a tail vein when the maximum tumor size reached 50 to 1000 mm3, approximately 10 d after transplantation. the huh-7 cell tumors were irradiated (3 min) with 823-nm nIr laser 24 h after IcG administration.
results: IcG specifically accumulated in huh-7 cells in both the in vitro and in vivo models (image; a: in vitro: tumor cells exhibited uniform fluorescence under the fluorescence imaging system, B: in vivo. a: tumor was indicated by triangle, b: immediately after IcG administration, the entire mouse body and tumor emitted strong fluorescence, c: 24 h after IcG administration, tumor in mice exhibited uniform fluorescence under the fluorescence imaging system). In vitro, nIr laser exposure significantly inhibited huh-7 cell survival through the induction of apoptosis. Inhibition depended on the IcG dose and/or nIr laser exposure frequency. In vivo, huh-7 tumor growth was significantly inhibited through apoptosis by nIr laser exposure.
Image:
Conclusion: IcG specifically accumulated in huh-7 cells. nIr photodynamic therapy using IcG may be a novel treatment for human hepatocellular carcinoma.
Disclosure of Interest: none Declared
P-065 COPy nuMber VArIATIOnS ChArACTerIze PrIMAry InTrAhePATIC ChOLAnGIOCArCInOMAS AnD TheIr LyMPh nODe MeTASTASeS
ruben jansen1, Birte Moehlendick1, christoph Bartenhagen2, csaba toth3, nikolas stoecklein1, Wolfram t. knoefel1, Anja Lachenmayer* 1, 4
1Department of General-, Visceral- and Pediatric surgery, university hospital Duesseldorf, Duesseldorf, 2university of Muenster, Institute of Medical Informatics, Muenster, 3univesity of cologne, Institute of Pathology, cologne, Germany, 4Department of Visceral surgery and Medicine, Bern university hospital, university of Bern, Bern, switzerland
Introduction: Intrahepatic cholangiocarcinoma (Icc) is a highly aggressive primary liver tumor with very poor prognosis. the only curative therapy available so far is surgical resection, but five-year-survival rates of only 20-40 % are limited due to high local recurrency and metastases rates. even though the incidence has increased worldwide, not much is known about the underlying molecular changes, in particular of those tumors developing metastases.
Methods: 60 patients with intrahepatic cholangiocarcinoma were treated in our hospital between 2003 and 2013 and included into the study. the accuracy of the clinical diagnosis for Icc was proven by immunostaining for ck7, ck20, and ca 19-9. comparative genomic hybridization was performed after Dna extraction by macrodissection from formalin-fixed paraffin-embedded tissue of 23 primary tumors and their matched normal tissues as well as 14 lymph node (Ln) metastases.
results: tumors with Ln metastases (n1) had significant more copy number variations (cnV) than tumors with no Ln metastases (n0). Interestingly, only few but specific differences were detected between n1 tumors and their corresponding Ln metastases. further analyses of those matched pairs revealed that 79 % shared the same cnVs in 1-20 and 7% in 20-40 cytobands, while 36 % showed different cnVs in 1-20, 29% in 21-40 and 36% in more than 40 cytobands. among the latter 79 % of the Ln metastases acquired new gains compared to their matched primary tumors:

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s5 0
36 % showed isolated gains on chromosome 12q14 and more than 20% displayed isolated gains on chromosome 1p13, 2p23, 7p22, 7q11, 11q12 and 14q12. additional mutational analyses were performed for kras and tP53, but showed no specific results. heterogeneity scores were higher in n0 tumors (3,15) compared to n1 tumors (1,64). correlations with clinical data showed significant worse survival rates for patients with n1 tumors compared to patients with n0 tumors (p = 0.044), while gender, tumor size and distant metastases had no significant input.
Conclusion: Patients with nodal positive Iccs show significant worse survival rates and significant more cnVs than those without Ln metastases. specific gains and losses characterize the different stages and lymph node metastases of intrahepatic cholangiocarcinoma and are currently further analyzed to detect key genes responsible for the metastatic process.
Disclosure of Interest: none Declared
P-066 MICrOrnA-23b AnD 193A AS bIOMArKerS AnD TherAPeuTIC TOOLS Of hePATOCArCInOMA In COMbInATIOn WITh SOrAfenIb
alessandro salvi1, edoardo abeni1, Ilaria Grossi1, Lia ferrari1, Bruna arici1, rita Gardella1, sergio ferraboli1, nazario Portolani2, Giuseppina De Petro* 1
1Dept of Molecular and translational Medicine, Division of Biology and Genetics, 2Dept. of clinical and experimental Medicine, surgical clinic, university of Brescia, Brescia, Italy
Introduction: human hepatocellular carcinoma (hcc) presents many challenges. It is the sixth most common cancer and the third most common cause of cancer-related mortality worldwide. Most patients will develop an advanced stage of the disease. Most patients with hcc have underlying cirrhosis which would have an adverse impact on their survival. Much effort is needed to identify molecular risk factors for putative hcc patients, to know molecular mechanisms underlying the development and progression of hcc to develop novel therapeutic options. Micrornas are short non coding rnas involved in several physiological and pathological conditions. for hcc, increasing evidence describes mirs as prognostic markers and good tools for molecular targeted therapies. In our studies, after identifying uPa and c-met overexpression as unfavourable prognostic factors of hcc (1-2) we focused our attention on mirna-mediated downregulation of uPa and c-met.
Methods: Bioinformatic prediction of mirs targeting uPa and c-met 3’utr was performed by Pictar and other algorithms. Mir-23b was validated as negative co-regulator of uPa and c-met, mir-193a was validated as negative regulator of uPa in hcc cell lines by transient transfections of mir and anti-mir molecules, consequent expression analysis of uPa and c-met gene targets by Western blotting and real time rt-Pcr and by consequent biological effects study on cell migration, proliferation and apoptosis. the molecular interactions between mir-23b and uPa and c-met 3’utr mrnas and between mir193a and 3’utr uPa mrna were verified by luciferase reporter assay. the mir23b and 193a expression levels were evaluated by stem-loop real time Pcr in tumoral and peritumoral tissues from 50 hcc patients. the hcc cells were co-treated with sorafenib and mir-193a and the effects on cellular proliferation and apoptosis were tested (3-4).
results: the mir-23b resulted a negative co-regulator of uPa and c-met in the hcc cells tested and the mir-193a as a negative regulator of uPa. We found the expression of both mirnas dysregulated in hcc, downregulated in hcc respect to peritumoral tissues and more in the cirrhotic hccs than in non-cirrhotic ones. transfection of hcc cells with mir-23b decreased proliferation and migration, transfection of hcc cells with mir193a decreased proliferation and increased apoptosis and combined treatment with sorafenib led to further proliferation inhibition and to further apoptosis increase.
Conclusion: our results present new advances in the post-transcriptional mir-mediated mechanisms of uPa and c-met, they suggest a new strategy to impair the aggressive behaviour of hcc cells with novel designs of pre-clinical approaches for multitarget and multi-agents therapies of the hcc. further our results outline the differential expression of mir-23b and 193a in cirrhotic and non-cirrhotic hccs, thereby contributing to advances for novel molecular biomarkers of hcc progression.
references: 1. De Petro G et al cancer res. 1998, 58, 22342. tavian D et al Int j cancer 2000, 87,6443. salvi a et al feBs j 2009,276,29664. salvi a et al Molecular cancer 2013, 12, 162
Disclosure of Interest: none Declared
P-067 ePIGeneTIC reGuLATIOn Of CIrCADIAn Gene exPreSSIOn by TuMOr SuPPreSSOr SIrTuIn 6
Katharina Wolf* 1, kerstin selak1, Martin Ganas1, Peter r. Galle1, susanne strand1
1first Department of Internal Medicine, university Medical center, johannes Gutenberg university, Mainz, Germany
Introduction: Disruption of circadian rhythms can increase the risk of obesity, metabolic syndrome,
and cancer in both human night-shift workers and animal disease models.1 sirtuin 6 (sIrt6) is a naD-dependent deacetylase and aDP ribosyl transferase that influences cell metabolism, Dna repair and telomere maintenance, inflammation and cancer development.2 however, the whole spectrum of sIrt6-dependent processes and their detailed mechanisms are not yet fully understood. In our studies, we take a closer look on the effect of a systemic sIrt6 deficiency in liver disease with a focus on the circadian genes which regulate about 10% of all genes in the genome.3
Methods: Mouse liver tissue was sampled at different zeitgeber times (zt) for rt-Pcr and Western Blot to study the expression of the core clock and clock-controlled genes (ccGs). furthermore, the histone modifications of the retinoic acid receptor-related orphan receptor response element (rore), located in the promoter region of several ccGs, was investigated via chromatin immunoprecipitation (chIP). finally, we performed reporter gene assays to determine the activation of rore.
results: We found a significant deregulation in the transcriptional expression of the ccGs cry1, BMaL1 and rev-erbα in the liver of sIrt6 deficient mice. chIP analysis of rore revealed a different pattern of activating and silencing histone modifications as well as an altered binding of the transcription factor rorα. these findings correlate with the changed transcriptional activity of rore in the reporter gene assay.
Conclusion: In addition to the interplay of sIrt6 and cLock:BMaL found in liver-specific sIrt6 knockout mice,4 our experiments revealed a severe chronodisruption in the liver of the mice with a loss of sIrt6. the altered histone modification pattern suggests that the deacetylase sIrt6 influences the ccG expression. Because chronodisruption is closely linked to cancer development,3
the results presented here support an oncogenic role for the loss of sIrt6 which may be associated with poor clinical outcome in hcc patients.5
references: 1turek et al., Obesity and metabolic syndrome in circadian clock mutant mice, science 2005.2kugel et al., Chromatin and beyond: the multitasking roles for SIRT6, tIBs 2014.3Masri et al., Circadian clocks, epigenetics, and cancer, current opinion in oncology 2015.4Masri et al., Partitioning Circadian Transcription by SIRT6 Leads to Segregated Control of Cellular Metabolism, cell 2014.5Marquardt et al., Sirtuin-6-dependent genetic and epigenetic alterations are associated with poor clinical outcome in hepatocellular carcinoma patients, hepatology 2013.
Disclosure of Interest: none Declared
P-068 effICACy Of PerIfOSIne ALOne In COMbInATIOn WITh SOrAfenIb In A TrAnSGenIC MOuSe MODeL Of hePATOCeLLuLAr CArCInOMA
Mi na Kim* 1, 2, Do young kim1, kwang-hyub han1
1Department of Internal Medicine, yonsei university college of Medicine, 2Department of Internal Medicine, cha Gangnam center, cha university, seoul, korea, republic of
Introduction: for patients with advanced hepatocellular carcinoma (hcc), sorafenib is the only systemic drug to show survival benefit. however, considering that the response rate of sorafenib is relatively low, novel therapeutic strategies are needed to improve survival in patients with hcc. Perifosine has shown antitumor activity by inhibition of akt phosphorylation in many advanced solid tumors. this study investigated the effect of perifosine alone and in combination with sorafenib in an hrasG12V plus short-hairpin rna downregulating p53 (shp53) transgenic mouse model of hcc.
Methods: the mouse model of hcc was generated by hydrodynamic injection of transgenes hrasG12V/shp53, and the mice were treated with perifosine alone and in combination with sorafenib to evaluate effects of drugs on tumor growth and survival. tumor cell proliferation and tumor angiogenesis were evaluated by immunohistochemical analysis of ki-67 and cD31, respectively. tumor cell apoptosis was detected by using the terminal deoxynucleotidyl transferase-mediated dutP nick end labeling (tuneL) assay. Levels of key enzymes in the PI3k/akt, ras/raf/MaPk, and caspase pathways were evaluated by western blot analysis, and levels of vascular endothelial growth factor (VeGf) were determined by immunohistochemistry and western blot analysis.
results: treatment with perifosine for 5 weeks alone and in combination with sorafenib, strongly inhibited tumor growth and increased survival. Perifosine inhibited hcc cell proliferation, induced apoptosis, and decreased tumor angiogenesis. furthermore, its combination with sorafenib enhanced these effects. In addition, akt phosphorylation was decreased by perifosine and further decreased by combination treatment. although perifosine alone did not appear to activate the caspase pathway, combination treatment increased the cleavage of caspase-3, caspase-9, and poly (aDP-ribose) polymerase (ParP). Perifosine did not affect VeGf levels, as assessed by immunohistochemistry and western blot analysis.
Conclusion: Perifosine alone and in combination with sorafenib showed antitumor effects in an hrasG12V plus shp53 transgenic mouse model of hcc. the preclinical effect of current study represents a strong rationale for clinical trials using perifosine alone and in combination with sorafenib in the treatment of hcc patients.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 5 1
Disclosure of Interest: none Declared
P-069 OxIDATIVe STreSS PrOMOTeS PAThOLOGIC POLyPLOIDIzATIOn In nOnALCOhOLIC fATTy LIVer DISeASe
Geraldine Gentric1, Vanessa Maillet1, Valérie Paradis2, Ganna Panasyuk3, Bernard fromenty4, séverine celton-Morizur1, Chantal Desdouets* 5
1Institut cochin, Paris, 2Pathology Department, Beaujon hospital, assistance Publique–hôpitaux de Paris, clichy, 3InserM u1151/cnrs uMr 8253, necker enfants Malades Institute, Paris, 4InserM, u991, université de rennes 1, rennes, 5Inserm u1016 Institut cochin, Paris, france
Introduction: Polyploidization is one of the most dramatic changes that can occur in the genome. In the liver, physiological polyploidization events occur during both liver development and throughout adult life. We showed previously that insulin signaling controls the genesis of polyploid hepatocytes during liver development through the PI3k/akt pathway by regulating the late stages of mitosis (1, 2). the close connection between liver physiology and insulin signaling prompted us to investigate whether polyploidy is modified in nonalcoholic fatty liver disease (nafLD), a widespread hepatic metabolic disorder that is believed to be a risk factor for hepatocellular carcinoma (hcc).
Methods: We used both mouse models and patients suffering from nafLD to demonstrate that the molecular and cellular mechanisms controlling liver polyploidization are altered profoundly during the course of this metabolic disease.
results: In murine models of nafLD, the parenchyma of fatty livers displayed alterations of the polyploidization process, including the presence of a large proportion of highly polyploid mononuclear cells, which are rarely observed in normal hepatic parenchyma. Biopsies from patients with nonalcoholic steatohepatitis (nash) revealed the presence of alterations in hepatocyte ploidy compared with tissue from control individuals. hepatocytes from nafLD mice revealed that progression through the s/G2 phases of the cell cycle was inefficient. this alteration was associated with activation of a G2/M Dna damage checkpoint, which prevented activation of the cyclin B1/cDk1 complex. furthermore, we determined that oxidative stress promotes the appearance of highly polyploid cells, and antioxidant-treated nafLD hepatocytes resumed normal cell division and returned to a physiological state of polyploidy.
Conclusion: collectively, these findings indicate that oxidative stress promotes pathological polyploidization and suggest that this is an early event in nafLD that may contribute to hcc development (3).
references: 1. celton-Morizur, s., et al. j clin Invest. 2009; 119: 1880-7.2. Gentric, G. and c. Desdouets. am j Pathol. 2014; 184: 322-31.3. Gentric, G., et al. j clin Invest. 2015; 125: 981-92.
Disclosure of Interest: none Declared
P-070 hIGh exPreSSIOn Of MIr-135A In hCC IS ASSOCIATeD WITh eArLy reCurrenCe AfTer reSeCTIOn POTenTIALLy VIA DeVeLOPMenT Of InTrAhePATIC MICrO-MeTASTASeS
Johann Von felden* 1, Denise heim1, kornelius schulze1, 2, florian ewald3, Björn nashan3, ansgar W. Lohse1, henning Wege1
1I. Department for Internal Medicine, university Medical center hamburg-eppendorf, hamburg, Germany, 2Génomique fonctionnelle des tumeurs solides, université Paris Descartes, Paris, france, 3Department for hepatobiliary and transplant surgery, university Medical center hamburg-eppendorf, hamburg, Germany
Introduction: hcc has a dismal prognosis with recurrence rates of up to 70% following liver resection (Lr) (1). In most cases, early recurrence (<12 months) is driven by intrahepatic micro-metastases at the time of Lr. to this regard, current histological parameters (e.g. microscopic vascular invasion) have only limited predictive power and molecular mechanisms are poorly understood (2-4). the aim of this study is to analyze the expression of different micro-rnas (mirnas) in the resected hcc and the surrounding liver to detect patients at high risk for early recurrence.
Methods: In 62 patients, who underwent Lr for hcc between 2011 and 2014, liver and tumor tissue was collected during surgery. 40 patients with recurrence <12 months (r+) or with absence of recurrence for >24 months after Lr (r-) were compared for grading, t, L, V, and r status. If tissue quality permitted, the expression of various mirnas was measured in the resected hcc and the surrounding liver by quantitative Pcr. Liver tissue of patients with benign liver tumors served as control. expression levels were dichotomously evaluated and the mean expression in the surrounding liver was used as calibrator.
results: 11 women and 29 men with 64.0±10.2 years of age, including 15 with liver cirrhosis, were analyzed. r+ was diagnosed 6.2±4.5 months after Lr according to recIst criteria (n=29). surveillance of r- was 26.2±5.2 months (n=11). Increased expression of mir-135a (n=16) and t3 status (n=10) were significantly associated with r+ (p<0.05), while grading, L, V status, and
the expression of mir-21, mir-122 and mir-125a showed no correlation with r+. all t3 tumors had a high expression of mir-135a (p<0.01). In addition, 4 out of 6 patients with high expression of mir-135a in t1/2 status were r+.
Conclusion: We confirmed the high rate of early recurrence of t3 hcc after Lr. early recurrence was also associated with an increased expression of mir-135a, regardless of tumor size. In a recent study, mir-135a has been associated with vascular invasion and metastases via activation of metastasis suppressor 1 (Mtss-1) (5); and therefore, could represent a molecular mechanism for early recurrence and a putative marker for risk stratification of patients undergoing Lr.
references: 1. ferlay j et al. International journal of cancer, 2010. 2. Imamura h et al. journal of hepatology, 2003. 3. Llovet jM et al. seminars in Liver Disease, 2005. 4. hoshida y et al. new england journal of Medicine, 2008. 5. Liu s et al. journal of hepatology, 2011.
Disclosure of Interest: none Declared
P-071 LySOPhOSPhATIDIC ACID PrOMOTeS hePATOCeLLuLAr CArCInOMA InVASIOn by AuGMenTInG eGfr TrAnSACTIVATIOn, CyTOKerATIn 19 exPreSSIOn AnD nf-Κb ACTIVATIOn
yun bin Lee* 1, jung-hwan yoon2, Dong hyeon Lee2, yuri cho2, su jong yu2, jeong-hoon Lee2, yoon jun kim2, chung yong kim2, hyo-suk Lee2
1Department of Internal Medicine, cha Bundang Medical center, cha university, seongnam-si, 2Department of Internal Medicine and Liver research Institute, seoul national university college of Medicine, seoul, korea, republic of
Introduction: Lysophosphatidic acid (LPa) is a lipid mediator that has diverse biological activities associated with cell proliferation, migration and survival. LPa has been implicated in the etiology of cancer due to its involvement in tumor growth, invasion and metastasis. the aim of this study was to investigate if LPa promotes invasion of hepatocellular carcinoma (hcc) cells and to elucidate which signaling pathway is modulated by LPa under hypoxic condition.
Methods: We performed in vitro experiments using human hcc cell line (snu761). Invasion of cells was assessed using invasion assay kit and the phenotypic changes after LPa treatment were examined using immunoblot analysis. the expression of cytokeratin (ck) 19 was specifically suppressed by sirna transfection. the cells were treated with aG 1478 and guggulsterone, which are inhibitors of epidermal growth factor receptor (eGfr) and nuclear factor kappa B (nf-κB) activation, respectively.
results: treatment of LPa significantly augmented ck 19 expression leading to acceleration of hcc cell invasion under hypoxic condition (1% o2, 5% co2, 94% n2). knockdown of ck 19 by sirna under hypoxia attenuated LPa-stimulated invasion of hcc cells. aG 1478 reduced LPa-stimulated invasion of hcc cells and attenuated the increased ck 19 expression induced by LPa. aG 1478 and guggulsterone showed additive effect on attenuating LPa-stimulated invasion of hcc cells.
Conclusion: collectively, these results suggest that LPa promotes invasiveness of hcc cells by augmenting eGfr transactivation, ck 19 expression and nf-κB activation under hypoxic condition. therefore, selective blockade of LPa receptor may have therapeutic potential in ck 19-positive hccs, particularly in the tumors exposed to hypoxic environments.
Disclosure of Interest: none Declared
P-072 T CeLLuLAr IMMune DefeCT Of hePATOCeLLuLAr CArCInOMA
Wanyu Li* 1, jinglan jin1, yue qi1, fengjiao Wang1, junqi niu1
1the first hospital of jilin university, changchun, china
Introduction: Background and aims hepatitis B virus (hBV) and hepatitis c virus(hcV) are leading causes of liver cirrhosis and hepatocellular carcinoma. the outcome of hcc is largely determined by the host immune response, with virus-specific cytotoxic t-cells being able to mediate immunity.hepatocellular carcinoma (hcc) has high mortality and no adequate treatment. our aim was to study the phenotypes of peripheral blood lymphocyte subsets (t, nk, B and regulatory t cells) and th cytokine secretion in hcc patients.
Methods: Phenotypes of peripheral blood lymphocyte subsets (t, nk, B and regulatory t cells) were performed by flowcytometry(facs).serum th cytokines (Ifn-γ, tnf-alpha, IL-10, IL-6, IL-4, IL-2) were measured by cytometric bead array (cBa) in 22 hcc patients and 21 healthy donors.there was no correlation between hepatic inflammation,hBeag status ,hBVDna and the percentage lymphocyte subsets,the level of cytokines.
results: In our study,hcc patients had a lower proportion of cD3+cD8+t cells, while the proportion

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s5 2
of cD3+cD4+t cells and the ratio of cD4 to cD8 t cells were higher than those of healthy controls. these findings show that there is no difference of the frequencies of nk,B ,treg (p>0.05)and the levels of th cytokine between the hcc groups and healthy donors(p>0.05).there was no signifcant difference of the ratio of naive (cD27-) B cells to memory (cD27+) B cells (p>0.05) there was no correlation between hepatic inflammation,hBeag status ,hBVDna and the percentage lymphocyte subsets,the level of cytokines (p>0.05).
Image:
Conclusion: We concluded that cD8+t cells are depleted and the ratio of cD4 t cells to cD8+t cells is imbalanced in hcc predicting a cellular immune defect. the loss of cD8+t cells may contribute to carcinoma.
Disclosure of Interest: none Declared
P-073 hePATOCeLLuLAr ADenOMA CAn DeVeLOP On CIrrhOTIC LIVer
Julien Calderaro* 1, 2, jean charles nault3, 4, charles Balabaud5, Gabrielle couchy4, Marie-christine saint-Paul6, Daniel azoulay7, elie-serge zafrani1, Dalila Mehdaoui1, Paulette Bioulac-sage5, jessica zucman-rossi4, 8
1Pathology, henri Mondor university hospital, 2université Paris est créteil, créteil, 3hepatology, hopital jean Verdier, Bondy, 4Inserm, uMr-1162, Génomique fonctionnelle des tumeurs solides, equipe Labellisée Ligue contre le cancer, Paris, 5Inserm,uMr-1053, université Bordeaux segalen, Bordeaux, 6Pathology, centre hospitalier universitaire de nice, nice, 7surgery, henri Mondor university hospital, créteil, 8université Paris Descartes, Labex Immuno-oncology, Paris, france
Introduction: hepatocellular adenoma (hca) is a rare and benign neoplasm that typically occurs in young women with a history of long-term use of oral contraceptive drugs (1,2). recent molecular studies have unravelled that it is a heterogeneous entity and a molecular classification comprising four molecular subgroups characterised by pathological and molecular features is now widely accepted (1,2). the most frequent hca subtype, namely inflammatory hca (Ihca), harbour somatic activating mutations of genes involved in the interleukin 6 pathway that lead to high crP and saa expression (1). If hca are considered to occur virtually always in non-fibrotic, non-cirrhotic parenchyma, macronodules with strong saa expression arising in the setting of alcoholic cirrhosis have recently been reported (3,4). the aim of our study was to analyse a series of hepatocellular benign nodules developed on cirrhotic livers that share pathological and molecular features with Ihca.
Methods: We performed a clinical, pathological and molecular study of 10 benign hepatocellular neoplasms developed in 3 patients with cirrhosis. all cases were referred to our laboratory for diagnostic expertise, and were reviewed by pathologists specialised in liver diseases. Markers allowing hca classification (LfaBP, Glutamine synthetase, c reactive Protein and serum amyloid a expression) were assessed by quantitative real-time Pcr and immunohistochemical experiments. samples were systematically sequenced for CTNNB1 (exons 2, 3, 4, 6, 7, and 8), HNF1A (exons 1–10), IL6ST (exon 6), GNAS (exon 8), STAT3 (exons 2, 5, 16, and 20) and TERT (promoter).
results: Patients were 51, 54 and 37 years old; two were male and one female. all had chronic liver disease related to metabolic syndrome and/or alcohol intake. alpha foeto protein serum levels were within normal adult ranges. two patients had a single tumor, while the third developed more than 30 lesions, eight of which were investigated. Microscopic examination showed well-differentiated neoplasms composed of hepatocytes arranged in thin trabeculae without significant atypia. hallmark
histological features of Ihca (inflammatory infiltrates, dystrophic vessels) were identified in 9/10 cases. high crP and saa protein and mrna levels were observed in all cases. sequencing experiments revealed IL6ST (n=8), STAT3 (n=1) and GNAS (n=1) somatic activating mutations. no mutations in the TERT promoter were found.
Conclusion: these 10 hepatocellular benign neoplasms developed in patients with established cirrhosis displayed both pathological and molecular features of inflammatory hca. these findings strongly support the existence of true Ihca developed in the setting chronic liver disease and cirrhosis.
references: 1. nault jc, Bioulac-sage P, zucman-rossi j. hepatocellular benign tumors-from molecular classification to personalized clinical care. Gastroenterology. 2013 2. Bioulac-sage P, rebouissou s, thomas c, Blanc jf, saric j, sa cunha a, et al. hepatocellular adenoma subtype classification using molecular markers and immunohistochemistry. hepatology. 20073. sasaki M, yoneda n, kitamura s, sato y, nakanuma y. a serum amyloid a-positive hepatocellular neoplasm arising in alcoholic cirrhosis: a previously unrecognized type of inflammatory hepatocellular tumor. Mod Pathol. 2012 4. sasaki M, yoneda n, sawai y, Imai y, kondo f, fukusato t, et al. clinicopathological characteristics of serum amyloid a-positive hepatocellular neoplasms/nodules arising in alcoholic cirrhosis. histopathology. 2014
Disclosure of Interest: none Declared
P-074 The MIr-23b DOWnMODuLATIOn In hCC IS MeDIATeD by DnA MeThyLATIOn
Ilaria Grossi1, alessandro salvi1, Bruna arici1, nazario Portolani2, Giuseppina De Petro* 1
1Dept of Molecular and translational Medicine, Division of Biology and Genetics, 2Dept. of clinical and experimental Medicine, surgical clinic, university of Brescia, Brescia, Italy
Introduction: hepatocellular carcinoma (hcc) is one of the most common human malignancy with an extremely poor prognosis. micrornas are small non-coding rnas that negatively regulate gene expression. mirs dysregulation frequently occurs in cancer, also in hcc, and the inactivation of some mirs is mediated by aberrant Dna methylation. In recent years, we have experimentally validated mir-23b as negative coregulator of uPa (uk) and c-met (a tkr) and mir-193a as negative regulator of uPa; the expression of these two mirs resulted down-regulated in hcc respect to peritumoral tissues (Pt). since in silico analysis has revealed the presence of cpG island near the sequences coding these mirs, the purpose of this study was to investigate the methylation status of mir-23b and mir-193a in hcc.
Methods: hcc cell lines were treated with the demethylating agent 5-aza-2’-deoxycytidine (5-aza-dc). the effects on mirs expression were evaluated by stem-loop qPcr and the effects on uPa and c-met expression were analyzed by qPcr and western blotting. We profiled the expression of mir-23b and mir-193a by stem-loop qPcr in hcc and Pt tissues from 59 and 67 hcc patients respectively and we verified Dna methylation status in a subset of 24 hcc cases by methylation-specific Pcr (MsP) .
results: to determine whether the down-regulation of mir-23b and mir-193a in hcc is mediated by Dna methylation, we first studied the effects of 5-aza-dc treatment in hcc cell lines at low expression levels of mir-23b and mir-193a. 5-aza-dc treatment increased the expression of both mirs in hepG2 cells and caused the modulation of their targets uPa and c-met. next, we correlated the expression levels of mir-23b and mir-193a with the Dna methylation status of their relative cpG island in hcc and Pt tissues. In the cohort examined, we confirmed the down-regulation of mir-23b and mir-193a in hcc respect to Pt tissues. mir-23b methylation level was significantly higher in hcc than Pt tissues (p=0.05), suggesting that mir-23b is partially silenced by iper-methylation. Instead mir-193a resulted generally hypomethylated in hcc tissues.
Conclusion: our results outline new advances in the epigenetic regulation of mirs that regulate hcc unfavourable prognostic markers (i.e. uPa and c-met) and suggest the use of hypomethylating agent in combination with/or without mir mimics to recover mirs expression in hcc cell lines and in animal experimental models of hcc development.
references: 1. salvi a et al feBs j 2009,276,29664. salvi a et al Molecular cancer 2013, 12, 162
Disclosure of Interest: none Declared
P-076 LKb1: A Key reGuLATOr Of hePATOCyTeS PrOLIferATIOn AnD GenOMe InTeGrITy
Vanessa Maillet1, mathieu Diribarne1, Véronique fauveau1, antoine L'hermitte1, thomas Guilbert1, séverine celton-Morizur1, christine Perret1, Chantal Desdouets* 1
1Institut cochin, Paris, france

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 5 3
Introduction: Liver kinase B1 or LkB1 (also called serine threonine kinase 11) is an evolutionarily conserved protein kinase which is involved in a diverse array of cellular processes, including energy homeostasis, cell polarity, apoptosis and cell growth. all these processes play a role in cancer initiation and progression. their relative contribution to LkB1-mediated tumor suppression remains unclear. Interestingly, previous results have demonstrated that haploinsufficiency of LkB1 in the liver leads to the development of hepatocellular carcinomas. In the current study, we evaluate the potential effect of LkB1 deletion on hepatocyte proliferation.
Methods: We use hepatocyte specific LkB1 knockout mice to dissect the role of LkB1 in hepatocyte proliferation. We study the kinetics of liver regeneration after partial hepatectomy (Ph). Livers (control and ko) are dissected at different time points after Ph in order to analyze Dna replication, division completion and various signaling pathways involved in hepatocytes proliferation.
results: We first observe that following partial hepatectomy, LkB1 (-/-) hepatocytes exhibit early entry into s phase and prolonged proliferation leading to hepatomegaly. the priming events, lipid droplet accumulation protein anabolic responses and energetic balance appear to be intact in LkB1 ko livers. however, deletion of LkB1 impacts specifically on G1/s transition by regulating the expression of key players involved in the initiation of s phase such as cyclin e1, a2, and the kinase inhibitor p21. Interrestingly, loss of LkB1 in hepatocytes also alters genomic integrity. LkB1 (-/-) hepatocytes present a block in metaphase/anaphase transition, associated with the increase of mitotic errors. a recent transcriptomic analysis highlighted the activation of different markers of the spindle assembly checkpoint, such as Mad2 and Bubr1. In line with these results, we observe that LkB1 deficient hepatocytes present an alteration of ploidy profile at the end of the regenerative process.
Conclusion: collectively, these findings emphasize the key role of LkB1 in the regulation of hepatocyte proliferation and particularly on the maintenance of Dna and ploidy integrity.
Disclosure of Interest: none Declared
P-077 OVerexPreSSIOn Of PerIOSTIn IS reLATeD TO POOr PrOGnOSIS Of hePATOCeLLuLAr CArCInOMA
Se young Jang* 1, yu rim Lee1, sun kyung jang 1, suhyun Lee1, soo young Park1, Won young tak1, young oh kweon1
1Department of Internal Medicine, kyungpook national university hospital, Daegu, korea, republic of
Introduction: Periostin is an extracellular matrix protein and known to be related to the metastatic potential and prognosis of human cancers in recent studies. however, few studies showed the expression level of periostin and its association with prognosis of hepatocellular carcinoma. We analyzed periostin overexpression and its implication for prognosis of hepatocellular carcinoma.
Methods: a total of 149 patients who underwent surgical resection in kyungpook national university hospital between 2006 and 2010 were selected and retrospectively reviewed. all tissue specimens were formalin-fixed and paraffin-embedded for immunohistochemistry staining. a tissue microarray (tMa) containing tissue from hcc (n=149), adjacent non-tumor tissues of hcc patients was constructed and immunohistochemistry was performed on 4mm sections.
results: expression of periostin was associated with microvascular invasion (or=3.383; p=0.001), multiple tumors (or=2.631; p=0.020), and higher modified uIcc stage (or=2.945, p=0.004). the cumulative overall survival rates at 1-, 3-, and 5-year were 97.8%, 82.2%, and 74.9%, respectively. the recurrence free survival rates at 1-, 3-, and 5-year were 91.1%, 62.9%, and 49.2%, respectively. the patients with positive periostin expression have significantly poor overall survival (p=0.021) and recurrence free survival (p=0.032). By cox hazard regression model, effect of microvascular invasion on survival is significantly different according to the expression of periostin (negative: hr=3.876, p=0.004; positive: hr=1.059, p=0.895).
Image:
Conclusion: In our study, overexpression of periostin is related to poor survival and periostin is not significant risk factor for prognosis under microvascular invasion is controlled. effect of microvascular invasion on survival is significantly different according to the expression of periostin. there is possibility of existence of modifying effect of periostin expression on microvascular invasion.
references: 1. Lv y, Wang W, jia WD, et al. high-level expression of periostin is closely related to metastatic potential and poor prognosis of hepatocellular carcinoma. Med oncol 2013;30:385.2. Wang W, sun qk, he yf, et al. overexpression of periostin is significantly correlated to the tumor angiogenesis and poor prognosis in patients with esophageal squamous cell carcinoma. Int j clin exp Pathol 2014;7:593-601.3. hu f, Wang W, zhou hc, et al. high expression of periostin is dramatically associated with metastatic potential and poor prognosis of patients with osteosarcoma. World j surg oncol 2014;12:287.
Disclosure of Interest: none Declared
P-079 OVerexPreSSIOn Of ChAPerOnIn COnTAInInG TCP1, SubunIT 3 In nuCLeuS Of CAnCerOuS CeLLS In hePATOCeLLuLAr CArCInOMA IS A MArKer fOr POOr PrOGnOSIS
xiao Cui* 1, zhao Li1, ye j. zhu1
1Department of hepatobiliary surgery, Peking university People's hospital, Beijing, china
Introduction: chaperonin containing tcP1, subunit 3 (cct3), a critical subunit of the chaperonin containing tcP-1 (cct or tric) which is essential for folding certain proteins into their native structure for biological function. this report analyzed the involvement of cct3 in tumor progression and prognosis of hepatocellular carcinoma, and explored the possible mechanisms.
Methods: cct3 expression levels were examined in hcc specimens, adjacent non-cancerous tissues and normal liver tissues of human by quantitative real-time Pcr(qrt-Pcr), Western blotting and immunohistochmeistry (Ihc). the correlations between clinicopathological characteristics and prognosis were analyzed. the molecular mechanisms of cct3 expression on cell cycle progression and invasion were also explored by 3-[4,5-dimethylthiazol-2-yl]-2,5 diphenyl tetrazolium bromide (Mtt) assay, cell counting experiment, cell cycle assay, colony formation assay, apoptosis assay, invasion assay, immunocytochemistry (Icc).
results: expression of cct3 in mrna and protein levels were up-regulated in cancerous tissues compared to adjacent non-cancerous tissues and normal liver tissues. cct3 accumulating in nucleus of cancer cells was associated with poor prognosis in hcc patients. knock-down cct3 expression could not only significantly suppress cell proliferation, but also obviously inhibit cell invasion in vitro. Mechanistic analyses showed that signal transducer and activator of transcription 3 (stat3) activation was decreased after knocking down cct3 in hepG2 cell line.
Conclusion: overexpression of cct3 in nuclei of cancerous cells is associated with hcc progression. cct3 could be an important target for affecting activation of stat3 in hcc.
Disclosure of Interest: none Declared
P-080 LASP1-OVerexPreSSIOn reVeALS VIMenTIn AS ITS neW MOLeCuLAr PArTner In huMAn hePATOCeLLuLAr CArCInOMA CeLLS
alessandro salvi1, Italia Bongarzone2, Lia ferrari1, edoardo abeni1, Bruna arici1, Maida De Bortoli3, sabrina scuri1, Daniela Bonini1, Ilaria Grossi1, anna Benetti4, Gianluca Baiocchi4, nazario Portolani4, Giuseppina De Petro* 1
1Dept of Molecular and translational Medicine, university of Brescia, Brescia, 2Laboratory of Proteomics, Irccs Istituto nazionale dei tumori, Milano, 3Laboratory of Proteomics, Irccs Istituto nazionale dei tumori, 4Dept of clinical and experimental Medicine, university of Brescia, Brescia, Italy
Introduction: hepatocellular carcinoma is the third most common cause of cancer-related mortality worldwide. We have previously reported that LasP-1 is a downstream protein of the urokinase type plasminogen activator (uPa) and its mediator in the migration of hcc cells. LasP-1 is overexpressed in some human malignancies and it is involved in tumor development and metastases, but its role in hcc is poorly understood. In the present study we investigated the biological role of LasP-1 in hcc by a molecular and biological characterization of LasP-1 expression in human hcc specimens and in cultured hcc cells. We have ascertained the expression level of LasP-1 mrna in hcc with different hepatic background disease and we have biologically characterized the ectopic LasP-1 overexpression in hcc cells.
Methods: the expression levels of LasP-1 mrna were evaluated by qrt-Pcr in tissues from biopsies of 55 hcc patients with different hepatic background disease. the molecular interactors of LasP-1 were identified by the proteomic analysis of the co-immunoprecipitated fractions using MaLDI-tof mass spectrometer. the co-localization of the LasP-1 and its putative partner vimentin, was examined by confocal immunofluorescence analysis.
results: We identified 3 groups of patients with high, equal or low LasP-1 mrna levels in hcc tissues compared to their correspondent adjacent peritumoral (Pt) tissues. In particular we found that i) the hccs displayed a higher LasP-1 mrna level in hcc compared to Pt tissues; ii) the expression levels of LasP-1 mrna in female hccs were significantly higher compared to male hccs; iii) the

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s5 4
cirrhotic hccs displayed a higher LasP-1 mrna. further, the biological characterization of the ectopic LasP-1 overexpression in hcc cells, using MaLDI-tof mass spectrometer on the LasP-1 co-immunoprecipitated fractions, displayed vimentin as a novel putative partner of LasP-1.
Conclusion: our results suggest that LasP-1 mrna overexpression may be mainly implicated in female hccs and cirrhotic hccs; and that LasP1 may play its role with vimentin in hcc cells. the identification of groups of hcc patients with shared molecular and clinical characteristics is important to set up the follow-up of the patients and to study better therapies. the finding that LasP-1 can collaborate with VIM and uPa in aggressive hcc cells may be of help in future studies of innovative therapies targeting these molecules alone or in combination.
references: 1.salvi a, neoplasia, 2009, 11, 2072.salvi a, Int j oncol, 2015, 48,1901
Disclosure of Interest: none Declared
P-081 The hePATITIS b VIruS x PrOTeIn InDuCeS The PhenOTyPe Of ePITheLIAL-MeSenChyMAL TrAnSITIOn ThrOuGh COnTrOL CD44 In hCC CeLL LIneS
na ri Park1, jung hoon cha1, hye Lim kim1, Won hee hur1, jeong Won jang1, hae Lim Lee1, soon kyu Lee1, Si hyun bae* 1, jong young choi1, seung kew yoon1
1the catholic university Liver research center, Department of Internal Medicine, seoul st. Mary’s hospital, the catholic university, seoul, korea, republic of
Introduction: the hepatitis B virus x protein (hBx) can induce hepatocarcinogenesis and may also be involved in epithelial-mesenchymal transition (eMt). the character of metastatic cells is strongly correlated to eMt and cell adhesion molecules such as cadherin and cD44. Moreover, cD44 has been identified in cancer stem cells (csc) of many tumors. cD44 is also strongly correlated to eMt and poor prognosis of hcc. this study aimed to determine whether hBx increases eMt phenotype with high expression of cD44 in hcc.
Methods: hBx mrna expression were confirmed by rt-Pcr in four hcc cell lines(snu-354, snu-368, huh7, PLc/Prf5). to identify a liver cancer stem cell (Lcsc) population, we determined expression of several putative Lcsc markers, including cD44, cD90, cD133 and epcaM through fluorescence-activated cell sorter (facs). In tGf-β treat cells, cD44-/+ sorted cells and snu-354, 368/hBx-sirna cells, morphological changes were evaluated using microscopy. also, expression of eMt-related proteins detected by western blot analysis. the PLc/Prf5 cell was used to establish an hBx overexpression model.
results: at the facs analysis, the cD44 was expressed in high purity in hBx-expressing cell lines snu-354 (69.37±4.96%) and snu-368 (82.09±3.15%) cell lines. Whereas Lcsc markers including cD90, cD133 and epcaM remained in low purity of below 1%. the tGf-β treat cells and cD44+ cells showed morphological changes from an epithelial to a spindle-like mesenchymal morphology and accompanied by loss of e-cadherin expression and gain of n-cadherin and β-catenin expression. In addition, the down-regulated expression of n-cadherin and β-catenin expression and the upregulated expression of e-cadherin were more obvious in hBx-sirna cells compared with control cells. overexpression of hBx increased cD44 expression.
Conclusion: hBx increases the expression of eMt-related proteins in cD44+ hcc cells. Interestingly, hBx was knocked down using hBx-sirna induce loss of cD44. furthermore, transfected hBx significantly increased cD44 expression . therefore, hBx promotes the eMt of hcc cell lines through cD44 expression.
Disclosure of Interest: none Declared
P-082 MuTATIOnS In The hCV-3A COre Gene ASSOCIATeD WITh DeVeLOPMenT TO hCC
João P. Moreira* 1, fernanda M. Malta1, Livia B. Lima1, Denise Paranaguá-Vezzozo1, Luciana kikuchi1, aline chagas 1, regiane s. s. M. alencar1, claudia tani1, nairo M. sumita2, Venâncio a. f. alves 2, joão renato r. Pinho1, flair j. carrilho1
1Gastroenterology, 2Patology, school of Medicine, university of são Paulo, são Paulo, Brazil
Introduction: hepatitis c virus (hcV) infection is a major etiology of hepatocellular carcinoma (hcc) around the world. carcinogenesis may result indirectly from longstanding hepatic inflammation and fibrosis. carcinogenesis may result indirectly from longstanding hepatic inflammation and fibrosis. It also may arise directly from viral proteins and their interaction with the host intracellular machinery. clinical studies have revealed that amino acid (aa) substitutions at position 70 and 91 of genotype 1b hcV (core region) are associated with hcc. understand the mechanisms of carcinogenesis by hcV are important for designing future means of diagnosis, treatment, and prevention of hcc.
Methods: In the present study, we analyzed the viral genotypes and the presence of mutations in the core region of hcV, from patients with hcc andpatients without cirrhosis. Most of patients had
early stage detection of hcc. Direct sequence derived from sanger's method was used to generate sequences. Demographic, biochemical and serological characteristics have been also evaluated.
results: a total of 115 patients were enrolled in this study (61 with hcc and 54 with cirrhosis). the average age of patients with hcc was significantly higher than in patients without hcc (63 vs. 59.5 years, P<0.02). a major proportion of male was observed in the hcc group (63.91% vs. 50%). hcc group had significantly higher alpha-fetoprotein (P<0.007) and significantly lower serum albumin values than the group without hcc (P<0.007). the most frequent genotype is 1b in both groups but other genotypes were found. Mutations r70q and L/c91M were mainly found in hcc patients infected by hcV-1b. Interesting, patients infected by hcV-3a from hcc group, showed significant mutations in six positions and were statistically different compared to the cirrhosis patients.
Conclusion: We can predict that these mutations may result from adaptations required for hcV to survive in cells damaged by years of chronic infection. Longitudinal studies are needed to determine whether the mutations are the cause or the consequence of disease-related changes in the liver.
references: 1. Miura, M., et al., Deep-sequencing analysis of the association between the quasispecies . nature of the hepatitis c virus core region and disease progression. j Virol, 2013.2. Who, hepatitis c global prevalence. Weekly epidemiological record, 1999. 3. Who, World health organization: hepatitis c. 2014. 4. kikuchi, L., et al., clinical and epidemiological aspects of hepatocellular carcinoma in Brazil. antivir ther, 2013.5. Venook, a.P., et al., the incidence and epidemiology of hepatocellular carcinoma: a global and regional perspective. oncologist, 2010.6. raimondi, s., et al., hepatitis c virus genotype 1b as a risk factor for hepatocellular carcinoma development: a meta-analysis. j hepatol, 2009.7. khan, a., et al., epidemic spread of hepatitis c virus genotype 3a . and relation to high incidence of hepatocellular carcinoma in . Pakistan. j Med Virol, 2009.8. kim, s., et al., Development of hepatitis c virus genotype 3a cell culture system. hepatology, 2014.
Disclosure of Interest: none Declared
P-083 effICACy Of PerIfOSIne ALOne AnD In COMbInATIOn WITh SOrAfenIb In A TrAnSGenIC MOuSe MODeL Of hePATOCeLLuLAr CArCInOMA
Mi na Kim* 1, 2, Do young kim1, simon W. ro3, kwang-hyub han1
1Department of Internal Medicine, yonsei university college of Medicine, 2Department of Internal Medicine, cha Gangnam center, cha unicersity, 3Institute of Gastroenterology, yonsei university college of Medicine, seoul, korea, republic of
Introduction: for patients with advanced hepatocellular carcinoma (hcc), sorafenib is the only systemic drug to show survival benefit. however, considering that the response rate of sorafenib is relatively low, novel therapeutic strategies are needed to improve survival in patients with hcc. Perifosine has shown antitumor activity by inhibition of akt phosphorylation in many advanced solid tumors. this study investigated the effect of perifosine alone and in combination with sorafenib in an hrasG12V plus short-hairpin rna downregulating p53 (shp53) transgenic mouse model of hcc.
Methods: the mouse model of hcc was generated by hydrodynamic injection of transgenes hrasG12V/shp53, and the mice were treated with perifosine alone and in combination with sorafenib to evaluate effects of drugs on tumor growth and survival. tumor cell proliferation and tumor angiogenesis were evaluated by immunohistochemical analysis of ki-67 and cD31, respectively. tumor cell apoptosis was detected by using the terminal deoxynucleotidyl transferase-mediated dutP nick end labeling (tuneL) assay. Levels of key enzymes in the PI3k/akt, ras/raf/MaPk, and caspase pathways were evaluated by western blot analysis, and levels of vascular endothelial growth factor (VeGf) were determined by immunohistochemistry and western blot analysis.
results: treatment with perifosine for 5 weeks alone and in combination with sorafenib, strongly inhibited tumor growth and increased survival. Perifosine inhibited hcc cell proliferation, induced apoptosis, and decreased tumor angiogenesis. furthermore, its combination with sorafenib enhanced these effects. In addition, akt phosphorylation was decreased by perifosine and further decreased by combination treatment. although perifosine alone did not appear to activate the caspase pathway, combination treatment increased the cleavage of caspase-3, caspase-9, and poly (aDP-ribose) polymerase (ParP). Perifosine did not affect VeGf levels, as assessed by immunohistochemistry and western blot analysis.
Conclusion: Perifosine alone and in combination with sorafenib showed antitumor effects in an hrasG12V plus shp53 transgenic mouse model of hcc. the preclinical effect of current study represents a strong rationale for clinical trials using perifosine alone and in combination with sorafenib in the treatment of hcc patients.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 5 5
P-084 SOrAfenIb AnD CeLeCOxIb SynerGISTICALLy InDuCe CeLL DeATh Of hePATOCeLLuLAr CArCInOMA ThrOuGh er STreSS MeDIATeD APOPTOSIS
sera yang1, yong-han Paik* 1, 2, so hee kang1, su hyun Park2, jonghwa kim1
1Department of Medicine, samsung Medical center, sungkyunkwan university school of Medicine, 2Department of health science and technology, samsung advanced Institute for health science and technology, sungkyunkwan university, seoul, korea, republic of
Introduction: sorafenib, a multi-kinase inhibitor, is currently recommended for the treatment of advanced hepatocellular carcinoma (hcc). however, the response rate of sorafenib in advanced hcc treatment are not satisfactory and there is a rationale for investigating its use in combination with other agents. celecoxib is known as a selective cyclooxygenase-2 (cox-2) inhibitor and has been known to exhibit anti-tumor effects in hcc cells but the mechanism is still largely unknown. the aim of this study was to investigate the synergistic effect of celecoxib on the anti-tumor activity of sorafenib in hcc and to determine the underlying molecular mechanism.
Methods: hcc cell line PLc/Prf/5 were treated with sorafenib and/or celecoxib, and then proliferation was analyzed by Mts assay. cell death was evaluated by annexin staining and facs analysis. Western blot was also used to study the mechanism of the induced cell death.
results: Mts assay revealed that each of sorafenib and celecoxib marginally inhibited hcc cell proliferation. however, the combination of sorafenib and celecoxib showed a synergistic effect at 48h of incubation, while the effect was less strongly observed with 2,5-dimethyl-celecoxib (DMc, a derivative of celecoxib that lacks cox2-inhibitory function). using flow cytometry, we found that the combined treatment synergistically increased the population of annexin+/PI+ at 48h, indicating the increased apoptosis. the increased cleavage of caspase-8 and ParP was also demonstrated in Western blot. In addition, we also found that er stress marker proteins, such as GrP78/Bip, choP, and spliced xBP-1, were dramatically increased in the combined treatment of sorafenib and celecoxib. these data indicated that the apoptosis induced by combined treatment of sorafenib and celecoxib resulted from er-stress.
Conclusion: combined treatment of sorafenib and celecoxib synergistically inhibit the growth of hcc cells via inducing er-stress mediated apoptosis. this finding raises the possibility of the combined treatment using sorafenib and celecoxib for the augmentation of anticancer effect of sorafenib in hcc.
Disclosure of Interest: none Declared
P-085 f T y 720 (fInGOLIMOD) SenSITIzeS hePATOCeLLuLAr CArCInOMA CeLLS TO SOrAfenIb-MeDIATeD CyTOTOxICITy
Dilruba Ahmed* 1, Petra j. de Verdier1, charlotta ryk2, oscar Lunqe1, Per stål3, jenny flygare1
1Laboratory Medicine, karolinska Institutet, huddinge, 2Department of urology, karolinska Institutet, stockholm, 3Medicine, karolinska Institutet, huddinge, sweden
Introduction: the multi-tyrosine kinase inhibitor sorafenib is used in the therapy of advanced hepatocellular carcinoma. however, limited effects encourage combination treatments aiming at improved survival. the sphingosine analogue fty720 (fingolimod), which is approved for treatment of multiple sclerosis, has shown tumor suppressive effects in cell lines and animal models of hepatocellular carcinoma. here we combined sorafenib with fty720 in order to sensitize the hepatocellular carcinoma cell line huh7 to sorafenib treatment.
Methods: Viability, cytotoxicity, cell cycle progression and cell death were investigated using the xtt assay, flow cytometry analysis of cells labeled with PI or annexin-V and PI and DaPI-staining of isolated nuclei. apoptosis and autophagy were analyzed by western blotting of ParP, cytochrome c, aIf, p62 and Lc3II in whole cell lysates or cell fractions.
results: We show that fty720, at non-cytotoxic doses, sensitized huh7 to effects on viability induced by treatment with increasing doses of sorafenib in a time-dependent manner. Moreover, studies of the mechanisms behind the cytotoxicity revealed significantly increased G1 arrest and cell death following combined treatment. caspase-dependent and -independent apoptosis were observed and features of autophagy blockage were detected.
Conclusion: our results suggest that fty720 sensitizes hepatocellular carcinoma cells to cytotoxic effects and disrupts cytoprotective autophagy induced by treatment with sorafenib alone. these findings warrant further investigations of combined treatment with sorafenib and fty720 in vivo in order to develop more effective treatment of hepatocellular carcinoma.
Disclosure of Interest: none Declared
P-086 VeGf-C936T AnD VeGf-A1154G POLyMOrPhISMS Are nOT ASSOCIATeD WITh CIrrhOSIS AnD ChC
Maria eduarda L. Baitello1, rafael f. ferreira1, renato f. D. Silva* 2, 2, 2, Doroteia r. s. souza1, Graciele D. tenani1, Ilka D. f. s. f. Boin3, Margarida abrantes4, Marcela a. D. s. Pinhel1, rita de cássia M. a. Da silva2
1Molecular Biology, faMerP, 2Liver transplantation unit, hospital de Base de são josé do rio Preto, sao jose do rio Pretro, 3surgery, universidade estadual de campinas, campinas, Brazil, 4Biofísica, universidade de coimbra, coimbra, Portugal
Introduction: hepatocellular carcinoma (hcc) is the most aggressive form of liver cancer, accounting for 80-90% of cases of primary liver cancer. risk factors for hcc include hepatitis c virus (hcV) and B (hBV), alcoholic cirrhosis, prolonged exposure to aflatoxin, inherited metabolic diseases, and genetic changes that can affect various cellular pathways, acting in the carcinogenic process. VeGf-a gene belongs to the family of vascular endothelial growth factor and is responsible for the activation of signaling pathways that promote endothelial cell growth, migration, differentiation and control of vascular permeability. objectives: to evaluate the association of the polymorphisms c936t and a1154G of the gene to vascular endothelial growth factor (VeGf-a) with cirrhosis and hepatocellular carcinoma (hcc) and progression to hepatic transplantation and death, besides to identify risk factor to the disease.
Methods: Were selected 102 patients with histopathological clinical diagnosis of primary hcc (G1), 117 patients with isolated histopathological clinical diagnosis of cirrhosis (G2) and 127 control individuos (G3). the polymorphisms of VeGf-a were genotyped by Pcr/rfLP (polymerase chain reaction/restriction fragments lenght polymorphism). clinical data were collected from questionnaires and medical records. significance level was assumed for P value < 0.05.
results: Prevailed the homozigous wild to VeGf-c936t (c/c) and VeGf-a1154G (G/G) in G1 (71% and 60%, respectively) G2 (72% and 51%, respectively) and G3 (71% and 60%, respectively), with no differences between the groups (P>0,05). In G1, evolved to hepatic transplant 30 (29%) and to death 23 (23%), with no relationship with the genetic profile (P>0,05). In VeGf-c936t, c/c genotype showed global survival of 56,2±10,9% in 36 months, while in c/t was 49,5±13,8%. In VeGf-a1154G, the global survival in 36 meses in G/G was 60,8±11,3%, while in _/a was 48,3±12,1%. no significant difference was observed in both cases (P=0,582 and P=0,186, respectively). cirrhosis prevailed in G1 (84%), followed c hepatitis (50%) and B hepatitis (21%), while c hepatitis stood out in G2 (49%), followed B hepatitis (10%). Drinking habit prevailed in G1 (56%) and G2 (50%), versus G3 (13%, P<0,0001, to both) and smoking habit in G1 (50%) compared to G3 (21%, P<0,0001).
Conclusion: the VeGf-c936t and VeGf-a1154G polymorphisms are not associated with cirrhosis and chc, which should be confirmed in larger studies, and prospective character. however, smoking and drinking habits have emerged as independent risk factors for the disease.
Disclosure of Interest: none Declared
P-087 PrOGnOSTIC VALue Of IMMunOhISTOCheMICAL DeTeCTIOn Of PrOGenITOr CeLL, ChOLAnGIOCyTe AnD hePATOCyTe MArKerS In SurGICALLy reMOVeD hePATOCeLLuLAr CArCInOMA
Cecilia A. escanhoela*1, Paulo a. odorissi2, elaine c. ataide1, jose Vassalo2, fernando a. soares3, Paulo Latuf filho2, Ilka f. Boin1
1unit of Liver transplantation, 2Pathology, state university of campinas, campinas, 3Pathology, hospital do cancer, sao Paulo, Brazil
Introduction: hepatocellular carcinoma (hcc) commonly originate from premalignant hepatocellular lesions in cirrhotic livers. recent studies detecting immunohistochemical markers of more undifferentiated hepatocytes and cholangiocytes have suggested that some hcc may originate from these cells, with a controvertible prognostic difference. the purpose of our study was to identify any prognostic potential related to progenitor cell, cholangiocyte and hepatocyte markers, studied immunohistochemically.
Methods: twenty-seven cases of surgical hcc were studied, with a follow-up period of up to 161 months. We used the tissue Microarray technique with evaluation of hepPar1, ck7, ck19, oV-6, cD117 and cD133 antibodies.
results: 67% were histologically classified as edmondson-steiner Grade I and II, versus 33% grade III. only ck7 positivity showed correlation with survival (p=0.046), maintaining this tendency by cox regression for all the associated factors (p=0.053). cases positive for the highest number of antibodies (without hepPar1) had the lowest survival rate, increasing by 2.5-fold the relative risk for each positive antibody (p=0.033). the case with the lowest survival rate was the only one with dual ck7/ck19 positivity.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s5 6
Image:
Conclusion: hcc cases that were positive for ck7 had a worse prognosis, with increased risk of death and metastases among cases with cumulative positivity for progenitor cell and cholangiocyte markers.
references: 1. robrechts c, De Vos r, Van den heuvel M, Van cutsem e, Van Damme B, Desmet VPrimary liver tumour of intermediate (hepatocyte-bile duct cell) phenotype: a progenitor cell tumour? 2. kim h, Park c, han kh, choi j, kim yB, kim jk 3. Durnez a, Verslype c, nevens f, fevery j, aerts r, Pirenne jhistopathology4. Walther z, jain D
Disclosure of Interest: none Declared
P-088 MODeLInG huMAn hePATITIS b VIruS InfeCTIOn WITh PLurIPOTenT STeM CeLL-DerIVeD hePATOCyTeS
Srikumar Sengupta* 1, johan a. den Boon2, Brian e. McIntosh1, james a. thomson1, Paul ahlquist2
1regenerative Biology, 2Virology, Morgridge Institute for research, Madison, united states
Introduction: human hepatitis B virus (hBV) is the major cause of hepatocellular carcinoma worldwide. studying hBV, however, has been hampered by the lack of a suitable in vitro system, as the only normal cell type that supports productive hBV infection, primary human hepatocytes (Phhs), have limited availability and between donors vary tremendously in their susceptibility to hBV. Importantly, Phhs are refractory to long-term culture, de-differentiating rapidly ex-vivo, giving them a very short useful life in vitro.
Methods: human pluripotent stem cell (Psc)-derived hepatocytes are stable in culture making them ideal for longer-term studies of viral life cycle. We infected Psc-derived hepatocytes with infectious hBV particles.
results: We show that Psc-derived hepatocytes are susceptible to hBV infection that is abrogated by blocking the hBV receptor. these cells produce intermediate viral replication products and generate infectious particles that are able to re-infect fresh hepatocytes in culture.
Conclusion: thus, Psc-derived hepatocytes support productive hBV infection and present an in vitro model for studies of virus-host interactions and the role of host genetics in virus susceptibility, screens for antiviral compounds and other important applications.
references: aggregate culture of human embryonic stem cell-derived hepatocytes in suspension are an improved in vitro model for drug metabolism and toxicity testing.sengupta s, johnson BP, swanson sa, stewart r, Bradfield ca, thomson ja.toxicol sci. 2014 jul;140(1):236-45. doi: 10.1093/toxsci/kfu069. epub 2014 apr 20.PMID:24752503
Disclosure of Interest: none Declared
P-089 ber Gene (hOGG1,xrCC1) POLyMOrPhISMS In hCC PATIenTS
Wojciech Malecki* 1, jolanta Bialkowska1, Maciej s. jablkowski1, janusz szemraj2
1Department of infectious and Liver Diseases, 2Medical Biochemistry Department, Medical university, Lodz, Poland
Introduction: It is known that an increased oxidative Dna damage, as well as mutations and deletions in genes, which encode antioxidant and Dna repair proteins, are associated with the development of primary hepatocellular carcinoma. Dna base-excision repair genes, hoGG1 and xrcc1, play an important role in preserving genetic stability in mammalian cells against any damage, caused by different factors. however, it is unclear whether an altered expression and function of these Dna repair genes could support susceptibility to hepatocellular carcinoma (hcc)
. In our study, associations were determined between the polymorphisms of the genes, encoding two key proteins of Dna base excision repair (hoGG1 ser326cys and xrcc1 arg 280his), as well as hcc risk was estimated. the data from the current study demonstrated some associations of the two Dna repair gene polymorphisms with hcc risk.
Methods: Dna was isolated for genotyping from 100 hcc patients and processed into 100 histologically unchanged liver paraffin blocks. the polymorphisms of Dna base-excision repair genes, hoGG1 and xrcc1, was identified by the high resolution Melting (hrM) technique in the presence of LcGreen Plus dye (Idaho) or by the sequencing method.
results: the obtained data showed that the xrcc1 280his polymorphism was associated with hBV infection and hcc family history to increase hcc risk, the same as the hoGG1 326cys genotype.
Conclusion: the data from the current study demonstrated associations of the two Dna repair gene polymorphisms with hcc risk.
the study was supported by Grant no. uMo-2012/05/B/nz5/01852 from the national center of science
Disclosure of Interest: none Declared
P-090 MICrOrnA exPreSSIOn LeVeLS In hCC PATIenTS
Maciej S. Jablkowski* 1, jolanta Bialkowska1, Wojciech Malecki1, janusz szemraj2
1Department of infectious and Liver Diseases, 2Medical Biochemistry Deapartment, Medical university, Lodz, Poland
Introduction: hepatocellular carcinoma (hcc) is one of the most common malignancies with major features including chronic inflammation and cytokine effects on fibrosis development and liver cell proliferation. the understanding of hcc pathogenesis is important to develop effective prevention and treatment measures of this highly malignant cancer. an early identification of changes at the epigenetic level may thus be fairly beneficial. a group of small noncoding functional rnas (micrornas) is one of the factors which control changes in cell phenotype at the epigenetic level the aim of the study was to identify micrornas as prognostic molecular markers, useful in the early identification of liver tumour differentiation and progression, the panel including 12 microrna genes (miR-21, miR-224, miR-34a, miR221, miR-222, miR-106, miR-303; miR26a/b, let-7g, miR-122, miR-422b, miR-145, miR-199)
Methods: the expression levels of 12 microrna genes (miR-21, miR-224, miR-34a, miR221, miR-222, miR-106, miR-303; miR26a/b, let-7g, miR-122, miR-422b, miR-145, miR-199) were estimated by the rq-Pcr method in paraffin specimens from 100 normal and 100 hcc patients. the Microrna expression profile was evaluated by the taqMan microrna array assay
results: the highest expression levels were observed in mir 21, 224 (triple) mir 9 and 222 (double), as compared to the controls but the expression level of mir 145, 214 was 1.5 times lower.
Conclusion: the observed changes in the expression profiles of the examined micrornas may trigger studies on bigger groups of patients and allow for identification and precise determination of liver tumor type and progression.this work was supported by Grant no. uMo-2012/05/B/nz5/01852 from the national center of science
Disclosure of Interest: none Declared
P-091 eMODIn InhIbIT GrOWTh AnD InDuCeD APOPTOSIS In An eCTOPIC hePATOCeLLuLAr CArCInOMA MODeL by enhAnCeMenT Of PArP1 CLeAVAGe
jung Woo Im1, Sang youn hwang*1, Gwang Mo yang1, seon-Mi Lee1, ki jeong jeon1
1Dongnam Institute of radiological & Medical sciences, Busan, korea, republic of
Introduction: the application of radiotherapy of hepatocellular carcinoma (hcc) is limited due to radioresistance in tumor and radiotoxicity in nontumorous liver. therefore, study for radioresistance mechanism and improvement of killing effect of irradiation by therapeutic insult such as radiosensitizer etc. emodin (1,3,8-trihydroxy-6-methylanthraquinone), a family of plant derived polyphenol has been proven to have anticancer properities. there is limited data about role of emodin as radiosensitizer in vivo study. In this study, we examined the followings: (i) whether emodin attenuated radioresitance of hcc in xenograft mouse model, (ii) what was the mechanism of radiosensitization.
Methods: one human hepatoma cell line (hepG2) was implanted in BaLB/c nude mice. these bearing ectopic (right flank) xenografts were treated with four different manners; none (control) irradiation (10Gy, one fraction), emodin (5 mg/kg), and irradiation combined with emodin. emodin was administered eight times for four weeks intraperitoneally. tumor volume was measured by veriner caliper and tumor was harvested within three days after final injection of emodin. Immunoblot anaylsis were performed using harvested tumor lysate.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 5 7
results: the growth of tumor was significantly suppressed as following order: combination group > irradiation only > emodin only (fig.1). combination of irradiation and emodin maximally enhanced ParP1 cleavage (fig.2). Interestingly, emodin was not aggravated radiation induced hepatitis.
Image:
Conclusion: emodin enhances the activity of irradiation in tumor growth suppression in vivo via enhancement of ParP cleavage. therefore, our findings may provide new insights into understanding the pharamacological mechanism of emodin as radiosensitizer in hcc and may aid in the design of new therapeutic strategies for the radioresistant hcc.
Disclosure of Interest: none Declared
P-092 PhOSPhOLIPASe D1 COnTrIbuTeS TO huMAn hePATOCeLLuLAr CArCInOMA
fei Wang* 1, junjie xiao1
1tongji university, shanghai, china
Introduction: hepatocellular carcinoma (hcc) represents the third leading cause of death related to cancer. Phospholipase D (PLD) has critically been involved in cell proliferation, migration, differentiation and survival. however, the role of PLD in the pathogenesis of hcc remains unclear. here we showed that PLD1 but not PLD2 was overexpressed in hcc cells (hePG2 and Bel-7402) compared to human normal L-02 hepatocytes. PLD1 was required for the proliferation, migration and invasion of hcc cells without affecting apoptosis and necrosis while forced expression of PLD1 was sufficient to promote the proliferation, migration and invasion of hcc cells.
Methods: By using hcc xenograft models, we demonstrated that PLD1 inhibition attenuated tumor growth, epithelial mesenchymal transition (eMt), angiogenesis, and metastasis of hcc in mice. Interestingly, PLD1 was highly expressed in tumor tissues of hcc patients. mtor and akt were identified as critical pathways responsible for the role of PLD1 in the control of proliferation, migration and invasion of hcc cells.
results: Interestingly, PLD1 was highly expressed in tumor tissues of hcc patients. mtor and akt were identified as critical pathways responsible for the role of PLD1 in the control of proliferation, migration and invasion of hcc cells.
Conclusion: taken together, this study indicates that PLD1 contributes to human hcc via controling proliferation, migration, invasion, angiogenesis, and eMt of hcc cells. PLD1 inhibition represents a novel attractive therapeutic target for hcc.
Disclosure of Interest: none Declared
P-093 MeTAbOLIC rADIOTherAPy WITh IODIne-131: effeCTS In A huMAn ChOLAnGIOCArCInOMA CeLL LIne
Margarida abrantes1, ana filipa M. D. Brito1, renato f. D. Silva* 2, ana c. ribeiro1, rafael f. ferreira3, Ilka D. f. s. f. Boin4, alexandra I. fernandes1, rita de cássia M. a. Da silva2, Doroteia r. s. souza3, Maria filomena r. Botelho1, josé Guilherme L. r. tralhão1
1Biofísica, universidade de coimbra, coimbra, Portugal, 2Liver transplantation unit, hospital de Base de são josé do rio Preto, 3Molecular Biology, faMerP, sao jose do rio Pretro, 4surgery, universidade estadual de campinas, campinas, Brazil
Introduction: cholangiocarcinoma (cc) is a tumour with poor prognosis and limited therapeutic options. recently, it was shown that cc has increased expression of sodium-iodide symporter (nIs), a molecule that mediates the iodine uptake. It is already known that nIs is a key component in the successful metabolic radiotherapy, using iodine-131 (131I), in the treatment of thyroid tumours, being also under investigation for the treatment of extrathyroidal tumours. thus, the aim of this study was to evaluate the therapeutic efficacy of metabolic radiotherapy with 131I in a human cc cell line.
Methods: the human cc cell line used was tfk-1. the cells were subjected to irradiation with increasing doses of 131I (1 Gy to 60 Gy), in order to evaluate and characterize the effects of metabolic radiotherapy. forty-eight hours after irradiation, it was used flow cytometry in order to evaluate the effect on cell viability and the type of induced cell death, as well as Bax, BcL-2 and cytochrome c expression, mitochondrial membrane potential, cell cycle changes, intracellular peroxides, superoxide anion, and glutathione production. superoxide dismutase activity was also evaluated. ros and antioxidants production were also evaluated 2 hours after irradiation.
results: It was observed that the treatment with 131I induced a decrease in cell viability in a dose dependent manner. the predominant type of cell death was apoptosis, followed by an increase in the Bax/BcL-2 ratio. In agreement with these results, there was also the release of cytochrome c, and mitochondrial membrane depolarization. concerning cell cycle, were not detected differences between the conditions and control cells. two hours after the irradiation, it was observed an increase in intracellular peroxides production, but there were no differences in superoxide anion production. forty-eight hours after the irradiation were not detected differences in both intracellular peroxides and superoxide anion production. It were observed differences in superoxide dismutase production, both 2 and 48 hours after irradiation. concerning glutathione, it was observed a decreased production only 48 hours after irradiation, and for the higher doses.
Conclusion: the treatment with 131I induces a decrease on cell viability and cell death mainly by apoptosis in tfk-1 cell line, as everything indicates, through mitochondrial pathway. Intracellular peroxides seem to be involved in this process. thus, metabolic radiotherapy with 131I may be a promising option for the treatment of cc.
Disclosure of Interest: none Declared
P-094 IODIne-131: An OPTIOn fOr The ChOLAnGIOCArCInOMA TreATMenT?
ana filipa M. D. Brito1, Margarida abrantes1, renato f. D. Silva* 2, ana c. ribeiro1, rafael f. ferreira3, Ilka D. f. s. f. Boin4, alexandra I. fernandes1, rita de cássia M. a. Da silva2, Doroteia r. s. souza3, josé Guilherme L. r. tralhão1, Maria filomena r. Botelho1
1Biofísica, universidade de coimbra, coimbra, Portugal, 2Liver transplantation unit, hospital de Base de são josé do rio Preto, 3Molecular Biology, faMerP, sao jose do rio Pretro, 4surgery, universidade estadual de campinas, campinas, Brazil
Introduction: cholangiocarcinoma (cc) is a malignancy with poor prognosis and a reduced survival rate, becoming crucial to investigate new therapeutic options for this highly aggressive type of tumour. recently, it was shown that cc, like other extrathyroidal tumours, has increased sodium-iodide symporter (nIs) expression . this molecule is responsible for cellular iodine uptake and is a key molecule in the metabolic radiotherapy with iodine-131 (131I) used for the treatment of thyroid tumours, opening the possibility of a new therapeutic approach for cc. thus, the aim of this study was to evaluate the therapeutic efficacy of metabolic radiotherapy with 131I in a human cc cell line, and in a human cholangiocytes cell line (1,2)
Methods: two human cell lines were used, one of cc (tfk-1) and another of normal cholangiocytes (h69). It was evaluated the nIs expression in both cell lines, by immunofluorescence. then, it were performed 131I influx and efflux studies in tfk-1 cells. subsequently, the cells were irradiated with increasing doses of 131I (0,35 to 60 Gy), in order to evaluate and characterize the effects of metabolic radiotherapy. the effect on cell survival was assessed by clonogenic assay in both cell lines. to determine the possible Dna damages caused in tfk-1 cells, it was performed the comet assay.
results: It was found that the two cell lines expresses nIs, both at the cytoplasm and cell membrane. Interestingly, preliminary data suggest that after irradiation with 20 Gy of 131I, tfk-1 membranar nIs expression increase but in h69 cells decrease. through influx and efflux studies it was observed that tfk-1 cells capture and retain 131I . It was noted that the treatment with 131I induced a decrease on cell survival of tfk-1 cells, on a dose dependent manner. concerning h69

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s5 8
cell line, irradiation with 131I doesn’t affect cell survival. It was verified that 131I induce Dna breaks in tfk-1 cells in a dose dependent manner.
Conclusion: according to these results, tfk-1 cells expresses nIs, which allows 131I uptake. consequently, irradiation with 131I induced severe Dna damage and caused a decrease in tfk-1 cells survival. In contrast h69 cell line also express nIs, but irradiation with 131I does not affect h69 cells survival. thus, metabolic radiotherapy with 131I could be a promising option for cc treatment.
references: 1. Gatto M, alvaro D. new insights on cholangiocarcinoma. World j Gastrointest oncol. 2010 Mar 15;2(3):136-45. doi: 10.4251/wjgo.v2.i3.136.2. razumilava n1, Gores Gj. classification, diagnosis, and management of cholangiocarcinoma. clin Gastroenterol hepatol. 2013 jan;11(1):13-21.e1; quiz e3-4. doi: 10.1016/j.cgh.2012.09.009. epub 2012 sep 13.
Disclosure of Interest: none Declared
P-095 GLyPICAn-3 AnD beTA-CATenIn Gene exPreSSIOn In PATIenTS WITh hePATOCeLLuLAr CArCInOMA, hePATITIS C Or CIrrhOSIS
rafael f. ferreira1, rita de cássia M. a. Da silva2, Doroteia r. s. souza1, Graciele D. tenani1, Maria eduarda L. Baitello1, Ilka D. f. s. f. Boin3, Margarida abrantes4, Marcela a. D. s. Pinhel1, renato f. D. Silva* 2
1Molecular Biology, faMerP, 2Liver transplantation unit, hospital de Base de são josé do rio Preto, sao jose do rio Pretro, 3surgery, universidade estadual de campinas, campinas, Brazil, 4Biofísica, universidade de coimbra, coimbra, Portugal
Introduction: hepatocellular carcinoma (hcc) is the most common type of liver cancer and its risk factors includes hepatitis c (hcV) and B (hBV), alcoholic cirrhosis, and genetics changes. In this context, there is the glypican-3 (GPc3) associated to angiogenesis and other pathways related with carcinogenesis (1).
Methods: hepatic fragment of fifty patients were studied, divided in four groups: G1 = 15 with hcc; G2 = 17 with cirrhosis of any etiology; G3 = 06 with hcV without cirrhosis; G4 = 12 controls. GPC3 and CTNNB1 were analyzed using reverse transcriptase and real time polymerase chain reaction (rt-Pcr). statistical analysis comprised anoVa and kruskal-Wallis test (P<0.05). the transcription levels were normalized for GaPDh and β-actin genes. the relative expression of the genes of interest was determined by the comparative method ∆∆ct.
results: Gene expression for GPc3 was similar between groups (P> 0.145). however, the highlight was the expression of that gene in patients with hcc (G1 = 2.90 ± 3.36) compared to patients with cirrhosis (G2 = 0.76 ± 1.04) or hcV (G3 = 1.20 ± 1.64). Gene expression for CTNNB1 apresentou diferenças entre os grupos. notou-se aumento da expressão em pacientes com cirrose (G2 = 1,87±1,86) em relação a pacientes com chc ou Vhc (G1 = 0,53±0,61; G3 = 0,15±0,15; P=0,031).
Conclusion: changes in GPc3 expression cannot be involved in the carcinogenesis process in patients with hcc, cirrhosis or hepatitis c, however, it is necessary the extension of this study. Increased gene expression of β-catenin in patients with cirrhosis may suggest relationship with fibrotic liver disease present in this regeneration, given that overexpression of this protein leads to the activation of the Wnt pathway, responsible for growth, proliferation and differentiation. therefore, the β-catenin may present as a potential marker of cirrhosis, but larger studies are necessary to confirm the results.
references: 1- yang sL, fang x, huang zz, Liu xj, xiong zf, Liu P, yao hy, Li ch. can serum glypican-3 be a biomarker for effective diagnosis of hepatocellular carcinoma? a meta-analysis of the literature. Dis Markers. 2014; 2014:127831. doi: 10.1155/2014/127831. epub 2014 oct 14.
Disclosure of Interest: none Declared
P-096 Den-InDuCeD hePATOCArCInOGeneSIS In C57bL/6 MICe; IMPACT Of TArGeTeD TherAPIeS
Alexandros Giakoustidis* 1, Paola andreani1, theophilos Poutachidis2, katerina angelopoulou3, argyrios sklavos3, Paschalis Gavriilidis3, thomas Goulopoulos3, thanasis Gargavanis3, nikolaos antoniadis3, argyro zacharioudaki4, Vasilios Papadopoulos2, antonios Michalopoulos2, Vasilios Papalois4, Vasilios Papanikolaou3, Dimitrios Giakoustidis3, Daniel azoulay1
1service de chirurgie Digestive et hépatobiliaire, hôpital henri Mondor, assistance Publique-hôpitaux de Paris-université Paris-est, Paris, france, 2aristotle university of thessaloniki, thessaloniki, Greece, 3Division of transplant surgery, Department of surgery, aristotle university of thessaloniki, thessaloniki, 4elpen research centre, athens, Greece
Introduction: hepatocellular carcinoma (hcc) is one of the most common liver cancers especially in countries where hepatitis is endemic. We describe the successful Den-induced hepatocarcinogenesis in c57BL/6 mice and investigate the impact of 2 different waiting periods (10 and 12 months), and two targeted therapies including aurora kinases inhibitor and toPk inhibitor.
Methods: In 40 male mice c57BL/6 Den-induced hepatocarcinogenesis was achieved. Den, 5mg/kg bw, was administered intraperitoneally on their 15th day of life. We divided the 40 mice in two major categories according to the post hepatocarcinogenesis waiting periods (10 and 12 months). We then allocated 4 groups with 10 experimental subjects. Group a (10 months) control hcc group, group B (10 months) with administration of anti-aurora (Pha-739358, DanusertIB), group c (12 months) control hcc, and group D (12 months) with administration of anti-toPk (hI-toPk-32). another 10 mice, group e, served as normal control group with no intervention. all animals were sacrificed on the 10th or 12th month of their life according to the protocol. Liver, lungs and serum were retrieved for analyses.
results: histopathology analysis showed achievement of hcc genesis in the Den group when compared to the normal control group. after 12 months (group c) hepatocarcinogenesis was marked as increased when compared to the 10 months (group a). administration of targeted therapies resulted in improvement of the morphology of the liver with a decrease in the number and size of liver lesions when compared to untreated groups. additionally targeted therapies intervened in the hcc signal transduction via downregulating the expression of different molecules.
Conclusion: Den-induced hepatocarcinogenesis proved to develop hcc successfully in mice. targeted therapies for hcc demonstrated an inhibitory effect in the development of hcc and intervened in the hcc development cell signaling.
Disclosure of Interest: none Declared
P-097 OCOxIn-VIuSID® SLOWS DOWn TuMOr PrOGreSSIOn Of COLOrreCTAL CAnCer MeTASTASIS DeVeLOPMenT TO The LIVer In A MurIne MODeL
Joana Marquez* 1, jorge Mena1, Iera hernandez1, eduardo Vilar2, aitor benedicto1, Beatriz arteta1, eduardo sanz2, elvira olaso1
1university of the baque country, basque country, 2catalysis s.l, Madrid, spain
Introduction: colorrectal cancer (crc) is the third most common disease worldwide and the second leading cause of death from cancer in Western countries. the prognosis and survival of this disease are clearly determined by its metastasis to the liver and not by the primary lesion. now it is widely accepted that reactive oxygen species, (ros) and reactive nitrogen species (rns), induced by soluble factors produced within the tumor-bearing tissue, cause oxidative damage and plays a crucial role in regulating expression of genes associated with cancer cell growth and survival, angiogenesis, invasion and, finally, metastasis. these insights are fostering new approaches including the introduction of nutritional supplements, as ocoxin-Viusid® (catalysis s.L) as a complement to the traditional antitumoral therapies, not only to treat cancer but also as a way to improve life-quality of cancer patients. since this nutritional supplement has recognized anti-inflammatory and anti-oxidative properties, we aimed to analyzed their effect on tumor progression of colorectal cancer to the liver.
Methods: first, the effect of the administration pattern of 100 ul ocoxin-Viusid® in the metastatic development to the liver was analyzed. to do so, murine c26 colon carcinoma cell were intra splenically inoculated and, liver metastatic area was quantified histologically. then, an additional dose of 50 ul ocoxin-Viusid® was tested. additionally, the expression of caspase 3 and ki67 was quantified by immunohistochemistry by using specific antibodies. also, rna expression level for inflammatory factors in total liver was carried out by quantitative rt-Pcr.
results: histological analysis shows a significant decrease in liver area occupied by the tumor in livers collected from 100 ul doses ocoxin- Viusid® treated mice, when treatment started after 7 days of tumor cell inoculation, comparing to those collected from control mice, or under different administration approaches or doses. Moreover, an increase in apoptosis and a decrease in proliferation was observed in tumor foci from those mice highlighted by caspase-3 and ki67 expression respectively. additionally, an increase in rna expression for the inflammatory cytokines IL10, IL-6 and tnf-α and a decreased expression for IL1-β was detected.
Conclusion: here we show that ocoxin- Viusid® reduced the progression of metastatic development of crc to the liver. this was correlated to an increase in apoptosis of tumor cells, and to a decrease in their proliferation. this might be mediated, at least in part, by the modulation in the repertoire of inflammatory cytokines. thus; these results point out ocoxin- Viusid® as a potential co-adyuvant treatment to increase the efficiency of traditional drugs and the life-quality of patients suffering from this disease.
references: 1. Vilar Gomez e, sanchez rodriguez y, torres Gonzalez a, et al. Viusid, a nutritional supplement, increases survival and reduces disease progression in hcV-related decompensated cirrhosis: a randomised and controlled trial. BMj open. 2011 jan 1;1(2):e000140. 2. Landskron G, De la fuente M, thuwajit P et al . chronic Inflammation and cytokines in the tumor Microenvironment Volume 2014, article ID 149185.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 5 9
P-098 effeCTS Of bOrIC ACID AnD bOrAx TherAPy On DnA DAMAGe, LIPID PerOxIDATIOn AnD AnTIOxIDAnT SySTeM AT benzO(A)Pyrene AnD 3-MeThyLChOLAnThrene ADMInISTereD rATS
Gokhan Oto* 1, serkan yildirim2, semiha Dede3, hulya ozdemir1, zabit yener2, ayse usta4, Mehmet taspinar5
1Pharmacology, yuzuncu yil university, Medical faculty, 2Pathology, 3Biochemistry, yuzuncu yil university, Veterinary faculty, 4Biochemistry, yuzuncu yil university, faculty of science, 5Medical Biology, yuzuncu yil university, Medical faculty, Van, turkey
Introduction: Polycyclic aromatic hydrocarbons are immunotoxic and carcinogenic chemicals that are widely distributed in the environment. the most toxic and the best studied are benzo[a]pyrene (B(a)P) and 3-methylcholanthrene (3-Mc). In this study cytoprotective effects of boric acid (Ba) and borax (Bx) therapy on 3-methylcholanthrene (3-Mc) and benzo(a)pyrene (B(a)P) administered rats were studied.
Methods: rats were divided into 9 groups including 12 animals in each group. 1st group was set as control. total doses of 100mg/kg of B(a)P to 2nd group and 3-Mc to 3rd group was intraperitoneally administered twice a week and it was given at 4 equal doses in total. 4th group received only 300 mg/L of boric acid (Ba) and 5th group were administered with only 300 mg/L of borax (Bx) via drinking water. B(a)P + Ba to 6th group; 3-Mc + Ba to 7th group, B(a)P + Bx to 8th group and 3-Mc + Bx to 9th group was administered respectively and study was terminated at 150th day.
results: In histopathological analyses hydropic degeneration in liver in only B(a)P administered group; interstitial pneumonia in lung in B(a)P + Ba administered group and both hydropic degeneration in liver and interstitial pneumonia in lung was observed in B(a)P + Bx administered group. fibrosarcoma was developed in all of the 3-Mc administered groups. excluding fibrosarcoma, diffuse hepatocellular carcinoma was developed only in 3-Mc administered group. therapy of Ba and Bx showed recovery in only pathological aspect compared to B(a)p and 3-Mc administered groups. this recovery was more prominent in Ba therapy applied groups. 8-ohdG level was elevated in all groups compared to control group. MDa level increased only at B(a)P or 3-Mc administered groups compared to control whereas it decreased in B(a)P + Ba administered group. soD and GPx activities increased in B(a)P + Bx and 3-Mc + Bx groups compared to other groups.
Conclusion: results of this study show that degree of cytotoxic impact of B(a)P or tumor formations caused by 3-Mc may be attenuated with Ba and Bx therapy.
references: 1. skupinska, k., Misiewicz, I., kasprzycka-Guttman, t., 2004. Polycyclic aromatic hydrocarbons: physicochemical properties, environmental appearance and impact on living organisms. acta Pol. Pharm. 61 (3), 233–240.2. chen, G., White, P.a., 2004. the mutagenic hazards of aquatic sediments: a review. Mutat. res. 567 (2–3), 151–225.3. Davila, D.r., Davis, D.a.P., campbell, k., cambier, j.c., zigmond, L.a., Burchiel, s.W., 1995. role of alterations in ca2+-associated signaling pathways in the immunotoxicity of polycyclic aromatic hydrocarbons. j. toxicol. environ. health 45, 101–126.4. yu, h., 2002. environmental carcinogenic polycyclic aromatic hydrocarbons: photochemistry and phototoxicity. j. environ. sci. health c environ. carcinog. ecotoxicol. rev. 20 (2), 149–183.
Disclosure of Interest: none Declared
P-099 InVeSTIGATe by TuneL MeThOD Of The effeCT Of LInuM uSITATISSIMuM exTrACT In The PreVenTIOn Of exPerIMenTALLy AfLATOxIn-InDuCeD LIVer AnD KIDney LeSIOnS In rATS
serkan yildirim1, Gokhan Oto* 2, ahmet c. oner3
1Pathology, yuzuncu yil univesity, Veterinary faculty, 2Pharmacology, yuzuncu yil university, Medical faculty, 3Pharmacology - toxicology, yuzuncu yil univesity, Veterinary faculty, Van, turkey
Introduction: aflatoxicosis is a mycotoxicosis developing acute or chronic, caused by aflatoxins in animals and humans. Liver is the main organ affected by aflatoxins and necrosis, fibrosis and hepatocarcinogenesis are absorved histopatologically. aflatoxins are known especially with their hepatotoxic and hepatocarcinogenic effects. according to studies it’s known that Linum usitatissimum extract (Lue) has many pharmacologic effects including antioxidant, immunomodulatory and anticancerogenic. In this study, the effects of Lue on prevention of aflatoxin-induced liver and kidney lesions in rats in terms of biochemical and histopathological were investingated.
Methods: for this purpose; a total of 40 rats were alloted into 4 groups which have 10 rats in each group. experimental groups; Group a (control group ) was given normal rat food, Group B (afB1) 2 mg/kg af, Group c (Lue) 2 mg /rat/day and Group D (afB1 + Lue) 2 mg/kg af +2 mg /rat/day were given Lue added food. at the end of 3 months of experiment period, the rats were sacrificed, tissue samples were taken from rats applied necropsis for histopathologic. Processed for immunohistochemical staining, in situ tuneL method.
results: according to immonohistochemical findings; Many apoptotic cells were detected in the livers an kidney of af groups, whereas there were few apoptotic cells in afB1 + Lue groups.
Conclusion: results of this study show that Lue has preventive effects on aflatoxin-induced liver and kidney lesions in rats with aflatoxicosis
references: 1. ahmed, M.a.e., ravikanth, k., rekhe, D.s., Maini, s. 2009. histopathological alterations in aflatoxicity and its amelioration with herbomineral toxin binder in broilers. Veterinary World, 2(10): 390-3922. oguz, h., 1997. the Preventive efficacy of Polyvinylpolypyrrolidone (PVPP) alone and its combination with the other adsorbents into Broiler feeds against aflatoxicosis. Ph.D. thesis. university of selcuk, Institute of health sciences, konya.3. Özen, h., karaman, M., Çigremis, y., tuzcu, M., Özcan, k., erdag. D., 2009. effectiveness of melatonin on aflatoxicosis in chicks. Res Vet Sci, 86, 485-489,4. Preetha, s.P., kanniappan, M., selvakumar, e., nagaraj, M., Varalakshmi, P., 2006. Lupeol ameliorates aflatoxin B1-induced peroxidative hepatic damage in rats. comparative Biochemistry and Physiology c toxicology and Pharmacology 143, 333–339.
Disclosure of Interest: none Declared
P-100 LIGASe ChAIn reACTIOn AS A MODALITy fOr The DeTeCTIOn Of POInT MuTATIOn In The PreCOre reGIOn Of hbV reLATeD hCC CASeS: A STuDy frOM nOrThern InDIA
Abdul Malik* 1
1Maulana azad Medical college, uttar Pradesh, India
Introduction: Mutant hepatitis B with precore stop codon has been reported to be associated with severe liver damage in hBeag negative patients with hepatocellular carcinoma. clinically, the biological importance of pre-core G1896a mutation is not well established. the purpose of the present study was to determine hepatitis B virus genotypes and also to elucidate the association of G1896a mutation of precore gene and the severity of liver damage in hBV related hcc cases.
Methods: Detection of hBV Dna sequences was carried out by polymerase chain reaction (Pcr) using primers derived from the precore region of hBV genome. Ligase chain reaction (Lcr) assay was performed to screen the presence or absence of G1896a mutation. Direct nucleotide sequencing was done to confirm the results of Lcr. a total of 116 hBV related cases who attended the medical out Patients Department and wards of Lok nayak hospital, new Delhi, India were screened over the period of 3 years.Patients having super-infection with hDV/hcV/hIV and past history of interferon therapy were excluded.
results: sequence analysis of viral Dna established that the G1896a mutation was observed in 32 cases in hcc cases. Phylogenetic analysis revealed 60% isolates belonged to genotype a, while 20% belonged to genotype D and 20% belonged to genotype e.
Conclusion: the present data suggests that precore G1896a mutations is responsible for 27.2% of the patients of asian Indian origin suffering from hBV related hcc cases and these cases are more symptomatic and aggressive in patients with the mutant form of the virus as compared with the wild form.
Disclosure of Interest: none Declared
P-101 The effeCT Of bOrAx On TOTAL AnTI OxIDATIVe- OxIDATIVe STATuS In DIfferenT TISSueS Of rATS APPLIeD benzO(A)Pyrene
Bahat comba1, Gokhan Oto* 2, arzu comba3, siddik keskin4
1Physiology, yuzuncu yil university, Veterinary faculty, 2Pharmacology, 3urology, 4Biostatistics, yuzuncu yil university, Medical faculty, Van, turkey
Introduction: Benzo(a)pyrene (B(a)P) - a type of Pah - is a potent tobacco carcinogen has been used in previous studies to understand molecular insights of cancer. coal-processing waste products, petroleum sludge, asphalt, creosote, and tobacco smoke, all contain high levels of B(a)P. aim of this study was to evaluate effects of Borax (Bx) on total anti oxidative (tas)-oxidative status (tos) and oxidative stress index (osI) in liver, lung, kidney and brain tissues of rats applied B(a)P.
Methods: In this study, rats were divided into 4 groups and each group were containing 6 rats. 1st group was separated as control group. 100 mg/kg total dosage of B(a)P was applied to the 2nd group 2 times a week total in 4 equal dosage with i.p. way. only Bx 300 mg/L was applied to 3rd group in drinking water. B(a)P+Bx was applied to 4th group. the study was completed at 150th day. tissues of the rats were homogenized in ice-cold saline phosphat buffer (PBs), 1:10 w/v in ph 7.4. after centrifugation at 10000g for 15 min at 4 °c, the supernatant was extracted and analyzed tas-tos by spectrophotometric kits. osI was calculated from the formula.
results: the liver tissue tas and tos in other groups were higher than control group. tas level

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s6 0
was the highest; tos and osI were the lowest in the lung tissue of 4. group. tos and osI were the highest of 3. group; the lowest of 4. group in kidney tissue. Brain tas was higher in the 3. and 4. groups than others group.
Conclusion: as a result, Bx supplementation in drinking water can demonstrate different effects on tas-tos-osI in different tissues of rats applied B(a)P. In case of exposure to B(a)P, Bx may shown antioksidan effect to the reduction of oxidative stress in lung, kidney and brain tissues.
references: 1 Pfeifer GP, Denissenko Mf, olivier M, et al (2002). tobacco smoke carcinogens, Dna damage and p53 mutations in smoking-associated cancers. oncogene, 21, 7435-51.2 Verma n1, Pink M, rettenmeier aW, schmitz-spanke s. (2012). review on proteomic analyses of benzo[a]pyrene toxicity. Proteomics, 12 (11), 1731-55.
Disclosure of Interest: none Declared
P-102 effeCT Of huMAn bILe On VIAbILITy AnD MIGrATIOn Of hePG2 CeLLS hePATOCeLLuLAr CArCInOMA
renato f. D. Silva* 1, Débora a. P. D. c. zuccari2, jucimara colombo2, rita de cassia M. a. da silva3, Livia c. ferreira2, Ilka f. f. s. Boin4, thaiz f. Borin2
1surgery, Liver transplantation unit, hospital de Base de são josé do rio Preto, 2Molecular Biology, faMerP, 3Liver transplantation unit, hospital de Base de são josé do rio Preto, sao jose do rio Pretro, 4surgery, unIcaMP, campinas, Brazil
Introduction: hepatocellular carcinoma (hcc) is the sixth most common cancer worldwide. the invasion of the bile duct system is a rare condition (1,7%) and the resulting impact on the disease prognosis is not well known. some studies indicate that the bile may exhibit anti-proliferative and pro-apoptotic action on tumor cells. the aim of this study was to analyze the viability of hepatocellular carcinoma hepG2 cells after treatment with human bile.
Methods: Bile was extracted from one male patient after cholecystectomy under sterile conditions and stored at -20° c. hepG2 cells were cultured at 37° c and 5% co2 in DMeM - low glucose with 10% fetal bovine serum and 1% penicillin/streptomycin solution. cell viability was measured by counting in neubauer chamber after trypan blue staining. the averages of viable cells were compared in different groups, using the anoVa test, followed by Bonferroni test. all values were the expressed as the average ± standard Deviation (sD). the value of P<0.05 was considered statistically significant. all analyzes Were Performed using GraphPad PrIsM4 software.
results: the results showed dose-dependent reduction in cell viability (P<0.05) after treatment with bile at concentration of 12.5, 25 and 50% diluted in DMeM – low glucose for 24 h (fig I), while the concentration of 6.25% did not affect cell viability (P> 0.05).
Image:
Conclusion: these data suggest that bile has anti-proliferative role in liver cancer cells by mechanisms that must be investigated.
references: Meng, k.W.; Dong, M.; zhang, W.G.; huang, q.x. clinical characteristics and surgical prognosis of hepatocellular carcinoma with bile duct invasion. Gastroenterol res Pract, v.2014, 2014. doi: 10.1155/2014/604971.Moon, D.B.; hwang, s.; Wang, h.j.; yun, s.s.; kim, k.s.; Lee, y.j.; kim, k.h.; Park, y.k.; xu, W.; kim, B.W.; Lee, D.s.; Lee, D.h.; kim, h.j.; Lim, j.h.; choi, j.s.; Park, y.h.; Lee, s.G. surgical outcomes of hepatocellular carcinoma with bile duct tumor thrombus: a korean multicenter study. World j surg, v.37, p.443-451, 2013.zhao, j.y.; chen, z.h.; Lin, W.; zhog, x.y.; chen, x.; Pen, j.; hong, z.f. Bear bile powder induces apoptosis of human hepatocellular carcinoma cells via mitochondrion-dependent pathway. chin j Integr Med, v.20, p.123-129, 2014a.zhao, j.y.; Liu, L.W.; shen, a.L.; Lin, W.; cao, z.y.; zhuang, q.c.; hong, z.f. effect of bear bile powder on stat3 pathway in hepatocellular carcinoma xenograft. zhongguo zhong xi yi jie he za zhi, v.34, p.976-981, 2014b.
Disclosure of Interest: none Declared
P-103 The CAuCASIAn'S OrIGIn bACTerIOPhAGe neW PrObAbLe TArGeT AGenT In The TreATMenT fOr Inf TreATeD hCV ASSOCIATeD hCC
Alexandre Tavartkiladze* 1, teimuraz t. sordia2
1Medical oncologist, Internist and Molecular Medicine specialist, 2Georgian cancer and Internal Medicine research center, tbilisi, Georgia
Introduction: Liver cancer is one of the major lethal malignancies worldwide. the main histological subtype is hepatocelular carcinoma, wich is derived from hepatocytes, the predominant epithelial cell type in the liver, and often retains biochemical and morphological markers of hepatocyte differenciation. Bacteriophages can be used effectively to cure bacterial infections. they can also switch the tumor microenvironment to one advantageous for anticancer treatment. In this review, results of the influence of bacteriophages on cancer processes are presented which have implications for the perspective application of phage therapy in patients with primary liver cancer – helatocellular carcinoma (hcc) with hcV infection.
Methods: this type of bacteriophage were isolated from water of the lake named “chinchao Lake” which is located in the caucasus region, mountains of Georgia, approximately 2400 meters above sea level. a total of 14 patients cell cultures (aged from 35 to 54 years) with locally advanced hcc associated hcV Inf treated patients were studied. control group was represented by 12 healthy persons hepatocytes cultures (aged from 34 to 62 years). Incubation all the cell culture were in co2
incubator at 12 days, medium for the cell culture were used plasma for own each patients. We have studied in all the cells cultures for each separately before and after incubation with “chinchao Lake Bacteriophage” some genes expression include in the cell cycle (table #1 and table #2). Monitoring was conducted on the cells proliferative activity by others biological methods (atP-tca, Western-Blot, Prc/rt-Pcr and fluorescent Microscopy).
results: our results showed that expression of oncogenes and tumor suppressor genes was very decreased after influence the specific “chinchao Lake Bacteriophage”. this result indicate that bacteriophage is include while some unknown pathways that need a additional researches, which we have planned already and is in the study phase. the statistical results is presented the diagram #1. It’s also one very interesting occasion, that Gene 5-Lipoxigenase (5-Lox) was normal before bacteriophage influence and his expression will increased after bacteriophage influence. Protein 5-Lox is important enzyme in inflammatory and cancer aetiopathogenese and 5-Lox coding gene is pineal hormone – MeLatonIn bounding site. It’s known that Melatonin is very lower in oncology patients especially hcc (in own research also).
Image:
Conclusion: this research is very important about natural treatment of cancer. In the nature exist natural anti-cancer agent as: “cat & mouse”, “wolf & rabbit”, “Bacteria & antibiotic Produced mushroom” etc. this research declare very interesting and biological very important role this phage in the cancer treatment. We now that it’s necessary to continue many of the research in this direction.
Disclosure of Interest: none Declared
P-104 InfLuenCe ADeMeThIOnIne On The MeLATOnIn SeCreTIOn In PATIenTS WITh nOT PreVIOuSLy TreATeD AnD TreATeD-reLAPSeD hePATITIS C
Alexandre Tavartkiladze* 1
1Medical oncologist, Internist and Molecular Medicine specialist, Georgian cancer and Internal Medicine research center, tbilisi, Georgia
Introduction: a number of experimental studies showed that melatonin, the main hormone of the pineal gland, exhibits chronobiological, anticancer and immunomodulation effects. It has been also known that In the patient with hepatitis c have disturbed the chronobiological melatonin secretion and decreased the plasma level of Melatonin. the study was aimed to estimate melatonin secretion and their serum levels in patients with not previously treated and in parallel treatment by Inf of hepatitis c and plasma levels Inf-alpha and gamma-Inf in the both group.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 6 1
Methods: a total of 18 patients (aged from 24 to 57 years) with not previously treated hepatitis c were studied. control group was represented by 16 patients (aged from 23 to 61 years) with hepatitis c treatment period by Inf. Plasma levels of melatonin and Inf (alpha and gamma) were estimated by liquid chromatography.
results: our results showed that plasma melatonin levels in patients with not previously treated hepatitis c was almost 20 times lower (0.11 ± 0.06 pcg/ml) than in control group (2.3 ± 0,38 pcg/ml, p<0,01). Liver function tests will be noticeable amelioration in control group, also endogenous Inf-alpha and gamma-Inf was 8.7 times high in control group.
Conclusion: Melatonin plasma levels and serum concentration of Inf-alpha and gamma-Inf significantly increase in patients with hepatitis c in parallel treatment by Inf + ademethionine. taking into consideration that both melatonin and Inf-alpha and gamma-Inf are chronobiologically active substances, we suggest that disturbances in circadian rhythm might contribute to the pathogenesis of hepatitis c and ademethionine participate in the methylation reaction in the biosynthesis of Melatonin (by methylation of enzyme hIoMt).
Disclosure of Interest: none Declared
epidemiology, Staging and Prognosis
P-105 The exTernAL VALIDATIOn Of hOnG KOnG LIVer CAnCer CLASSIfICATIOn fOr PreDICTIOn Of SurVIVAL In PATIenTS WITh hePATOCeLLuLAr CArCInOMA: DIreCT COMPArISOn WITh bArCeLOnA CLInIC LIVer CAnCer CLASSIfICATIOn
young-Sun Lee* 1, ji hoon kim1, seong hee kang1, tae suk kim1, yang jae yoo1, sang jun suh1, young kul jung1, yeon seok seo1, hyung joon yim1, jong eun yeon1, kwan soo Byun1
1Department of Internal Medicine, korea university college of Medicine, seoul, korea, republic of
Introduction: the aim of this study is to validate hong kong Liver cancer (hkLc) system comparing with Barcelona clinic Liver cancer (BcLc) system for prediction of survival in hepatocellular carcinoma (hcc) patients.
Methods: from 2004 to 2009, the medical records of 2293 hcc patients were retrospectively reviewed. Performance status, child-Pugh score, tumor characteristics, treatment modality and survival were collected. each patient was classified following both of hkLc and BcLc staging.
results: fifty percent of patients died during study period and median overall survival (os) was 15 (0-181) months. the median overall survival was 39, 25, 21, 10.5, 6, 4, 2, 9, and 1 months in hkLc stage I, IIa, IIb, IIIa, IIIb, Iva, IVb, Va and Vb, respectively. Both hkLc and BcLc well differentiated the survival (p<0.001). however, hkLc significantly well predicted 1 and 2 year of survival than BcLc (auroc; 0.817 vs 0.793, p=0.0002; 0.806 versus 0.78 in 2 year, p=0.0001). In the patients in BcLc B and hkLc II, the curative therapy group recommended by hkLc showed better survival compared to tace which recommended by BcLc (69 vs. 29 months, p=0.002). In BcLc B, the patients who treated according to hkLc showed better survival than who treated by BcLc (54 vs. 28 months, p<0.001). In the patients in BcLc c and hkLc II, the curative therapy group recommended by hkLc showed better survival compared to systemic therapy which recommended by BcLc (28 vs. 4 months, p<0.001). In BcLc c and hkLc III, the tace group recommended by hkLc showed better survival compared to systemic therapy which recommended by BcLc (8 vs. 4 months, p=0.026). In BcLc c, the patients who treated according to hkLc showed better survival than who treated by BcLc (6 vs. 3 months, p<0.001).
Conclusion: In our population, the hkLc system showed better survival compared to BcLc system. the more curative and individualized therapy could be considered by hkLc for management of hcc patients resulting in improvement of prognosis compared to BcLc, especially early stage of hcc.
references: 1. Llovet jM, Bru c, Bruix j. Prognosis of hepatocellular carcinoma: the BcLc staging classification. semin Liver Dis. 1999;19(3):329-38.2. yau t, tang Vy, yao tj, fan st, Lo cM, Poon rt. Development of hong kong Liver cancer staging system with treatment stratification for patients with hepatocellular carcinoma. Gastroenterology. 2014;146(7):1691-700.
Disclosure of Interest: none Declared
P-106 DeVeLOPMenT Of A MODeL PreDICTInG SurVIVAL fOr reCurrenT Or PrOGreSSIVe hePATOCeLLuLAr CArCInOMA
Sang Il Choi* 1, ami yu2, Bo hyun kim1, eun jeong ko1, sun seob Park1, Byung ho nam2, joong-Won Park1
1center for Liver cancer, 2Biometric research Branch, national cancer center, Goyang-si, korea, republic of
Introduction: Most prognostic models developed for hepatocellular carcinoma (hcc) are based on data collected at the time of diagnosis. however, the patient’s tumor burden, underlying liver function, and performance status are certain to change over time, subsequently affecting the prognosis of the patient. therefore, we aimed to develop a risk score model to predict the survival of patients receiving subsequent treatment for recurrent or progressive hcc.
Methods: of 1972 patients in a cohort who were newly diagnosed with hcc at the national cancer center, korea, between january 2004 and December 2009, 1301 who had progressive or recurrent disease after the initial treatment were enrolled. they were randomly classified into the development cohort (75%, n = 976) and the validation cohort (25%, n = 325). With the development cohort, a survival prediction model for recurrent or progressive hcc patients was established using the multivariate cox proportional hazards model. the performance of the model was evaluated using the c-statistic and hosmer-Lemeshow χ2 statistic on the validation cohort.
results: according to the multivariate analysis, age, albumin, Model for end-stage Liver Disease (MeLD) score, tumor factors (such as number of nodules, size of the largest nodule, vascular invasion, and extrahepatic metastasis), serum alpha-fetoprotein (afP) level, presence of ascites, first line treatment modality, and the best response after the initial treatment, were independent prognostic factors for overall survival. using these variables, a survival prediction model was developed and tested on the development cohort and the predefined validation cohort. the respective c-statistics and χ2 statistics of this novel model for the validation cohort were 0.836 (95% confidence interval [cI] 0.806-0.865) and 6.339; 0.808 (95% cI 0.781-0.834) and 4.408; and 0.803 (95% cI 0.777-0.829) and 10.960, for 1-, 3-, and 5-year survival, respectively.
Conclusion: a survival prediction model for patients with recurrent or progressive hcc was developed and validated. this model predicted survival successfully using variables at the time of recurrence or progression and may be of further prognostic value for these patients.
Disclosure of Interest: none Declared
P-107 MODIfICATIOn Of The CAnCer Of The LIVer ITALIAn PrOGrAM SCOre WITh ObJeCTIVeLy ASSeSSeD LIVer reSerVe IMPrOVeS PrOGnOSIS PreDICTIOn fOr ADVAnCeD hePATOCeLLuLAr CArCInOMA
yu-yun Shao* 1, tsung-hao Liu1, chih-hung hsu1, ann-Lii cheng1
1national taiwan university hospital, taipei city, taiwan
Introduction: the cancer of the Liver Italian Program (cLIP) is a commonly used staging system of hepatocellular carcinoma (hcc) and also useful in predicting prognosis of advanced hcc. the cLIP scoring criteria incorporate the child-turcotte-Pugh (ctP) score, which involves subjective and objective measurements to assess liver reserve. recently 2 new scoring systems that evaluate liver reserve with only objective findings, the insulin-like growth factor (IGf)-ctP score (kaseb etl al. j natl cancer Inst 2014) and the albumin-bilirubin (aLBI) grade (johnson et al. j clin oncol 2015), were proposed. We hypothesized that the modification of cLIP by replacing the ctP score with the IGf-ctP score or aLBI grade could improve its prognosis prediction of advanced hcc.
Methods: We included all patients who received first-line antiangiogenic therapy for advanced hcc from May 2005 to june 2013 at national taiwan university hospital, taipei, taiwan and consented to have their peripheral blood collected. Liver reserve was assessed by the criteria of ctP, IGf-ctP, and aLBI. We calculated the cLIP scores with traditional ctP, IGf-ctP (IGfctP-cLIP) or aLBI (aLBI-cLIP) according to the table. We used a cox’ proportional hazard model to evaluate the accuracy of every scoring system in predicting overall survival (os). We also put all scoring systems together in a cox’s model involving a stepwise variable selection procedure to see which exceled. finally, concordance (c) indexes for os prediction were calculated for every scoring system.
results: a total of 142 patients were included; 74% had hepatitis B virus etiology and 18% had hepatitis c virus etiology. Most (92%) patients had Barcelona-clinic Liver cancer c stage. By the ctP criteria, 137 patients were classified as ctP class a, and 5 as class B. among patients with ctP a liver reserve, IGf-ctP could further divide them into class a (n = 99) and class B (n = 38) with significantly different prognosis (p = 0.028). aLBI could also divide them into grade 1 (n = 99) and grade 2 (n = 38) with significantly different prognosis (p = 0.001). the highest cLIP, IGfctP-cLIP, and aLBI-cLIP score was 4 (n = 33), 5 (n = 12), and 5 (n = 12), respectively. cLIP, IGfctP-cLIP and aLBI-cLIP could all differentiate prognosis among various scoring groups (all p < 0.001). however, both IGfctP-cLIP and aLBI-cLIP, compared to cLIP, had higher r2 (0.240 vs. 0.249 vs. 0.216) and lower aIc (996.8 vs. 995.0 vs. 1001.1), indicating them to be superior in prognosis prediction. In

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s6 2
the cox’s model allowing variable selection, aLBI-cLIP exceled as an independent predictor for os, whether or not adjusted for hepatitis etiology, treatment, and performance status. aLBI-cLIP had higher c indexes than both cLIP and IGfctP-cLIP (0.724 vs. 0.703 vs. 0.702).
scoring system Variables 0 1 2
all tumor morphology
uninodular & extension ≤ 50%
Multinodular & extension ≤ 50%
Massive or extension > 50%
α-fetoprotein (ng/mL)
< 400 ≥ 400 ---
Portal vein thrombosis
no yes ---
cLIP ctP a B c
IGfctP-cLIP IGf-ctP a B c
aLBI-cLIP aLBI grade 1 2 3
Conclusion: Modification of cLIP scoring with objectively assessed liver reserve improves its prognosis prediction.
Disclosure of Interest: none Declared
P-108 OPTIMAL SubSTAGInG Of InTerMeDIATe STAGe hePATOCeLLuLAr CArCInOMA
Jae Min Lee* 1, yeon seok seo1, tae hyung kim1, jem Ma ahn1, sun young yim1, young kul jung1, ji hoon kim1, hyunggin an2, hyung joon yim1, jong eun yeon1, kwan soo Byun1, soon ho um1, ho sang ryu1
1Department of Internal Medicine, 2Department of Biostatistics, korea university college of Medicine, seoul, korea, republic of
Introduction: Because the intermediate stage hepatocellular carcinoma (hcc) in the Barcelona clinic Liver cancer system is composed of a heterogeneous population, prognosis of patients in this stage is also very heterogeneous1,2. therefore, substaging of these patients are needed for predicting their prediction and deciding appropriate treatment option. this study was performed to establish substaging system for these patients.
Methods: Patients with newly diagnosed as intermediate stage hcc were enrolled. cox-regression analysis was performed to evaluate prognostic factors and establish the prediction model.
results: a total of 444 patients with intermediate stage hcc were enrolled in this study. age was 60.2±11.7 years and 375 (84.5%) were men. child-Pugh score was 5.9±1.2 and 341 (76.8%) and 103 (23.2%) patients were classified as child-Pugh grades a and B, respectively. number of nodules was 1, 2 or 3, and >4 in 133 (30.0%), 142 (32.0%), and 169 (38.1%) patients, respectively, and size of the largest nodule was ≤3 cm, >3 cm and ≤10 cm, and >10 cm in 59 (13.3%), 325 (73.2%), and 60 (13.5%) patients, respectively. type of treatment was resection, radiofrequency ablation ± transarterial chemoembolization (tace), tace alone, and supportive care in 68 (15.3%), 90 (20.3%), 234 (52.7%), and 52 (11.7%), respectively. In a multivariate cox-regression analysis, number of nodules, size of the largest nodule, and child-Pugh score were independent predictive factors for survival (adjusted by type of treatment). using these parameters and their hazard ratios, new substaging system, the cns (child-Pugh score, number of nodules, and size of the largest nodule) score, was established. survival differed significantly according to the cns scores. When patients were classified into 4 substages according to the cns score, median survival times were 64.9, 38.3, 21.5, and 5.3 months, respectively.
Conclusion: a new substaging system was useful for predicting prognosis of patients with intermediate stage hcc.
references: [1] Bolondi L, et al. heterogeneity of patients with intermediate (BcLc B) hepatocellular carcinoma: proposal for a subclassification to facilitate treatment decisions. semin Liver Dis. 2012 nov;32(4):348-59. [2] ha y, et al. clinical appraisal of the recently proposed Barcelona clinic Liver cancer stage B subclassification by survival analysis. j Gastroenterol hepatol. 2014 apr;29(4):787-93.
Disclosure of Interest: none Declared
P-109 SurVIVAL Of PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA On SOrAfenIb: An AnALySIS Of Seer-MeDICAre DATAbASe
neehar D. Parikh* 1, Vincent Marshall2, rajesh Balkrishnan2, Vahakn shahinian3
1Gastroenterology, 2college of Pharmacy, 3kidney epidemiology and cost center, university of Michigan, ann arbor, united states
Introduction: sorafenib, a multikinase inhibitor, is the only chemotherapeutic approved for use in the us for the treatment of advanced hcc. We aimed to examine the outcomes of elderly patients with advanced hcc in the us. We performed a secondary analysis of continuously enrolled Medicare beneficiaries with hcc diagnoses from 2007-2009, based on seer diagnosis codes. our primary aim was to determine survival in patients treated with sorafenib and predictors of survival.
Methods: We compared advanced stage patients with hcc (stage III/IV) who received only sorafenib within 6 months of diagnosis to advanced stage patients with hcc who received no therapy (control.) We also analyzed sorafenib related outcomes in patients for prevalent hcc (any stage, but with diagnosis greater than 6 months from sorafenib use.) We calculated the charlson comorbidity index 12 months prior to diagnosis and an aggregate variable for decompensated cirrhosis (presence of esophageal varices or variceal banding, ascites or paracentesis, hepatic encephalopathy or use of neomycin, lactulose, or rifaximin.) We performed univariate (kaplan Meier with log rank test) and multivariate (cox regression) analyses for predictors of survival.
results: the baseline characteristics of the patient are shown in table 1. the kaplan Meier survival curves for the incident versus control group are shown in figure 1 (p<0.001). the median survival benefit for patients on sorafenib was 88 days. In the multivariate analysis, significant predictors of improved survival in incident hcc were treatment with sorafenib (hr: 0.66; 95% cI: 0.57-0.78), and being seen at a transplant center (hr: 0.76; 95% cI: 0.64-0.91.) Predictors of worse survival included stage IV disease (hr: 1.41; 95%cI: 1.25-1.59), decompensated cirrhosis (hr: 1.43; 95%cI: 1.26-1.63,) and residing in an urban setting (hr: 1.46; 95% cI: 1.22-1.75.) In a subanalysis of patients with decompensated cirrhosis, sorafenib use did show a survival benefit (hr: 0.63, 95% cI: 0.49-0.81) with a median survival benefit of 31 days.
Incident (n=228) control (n=870)
age (median; range) 69.4±9.4 72.9±9.7
sex (M; %) 168 (73.7) 642 (73.8)
Decompensated cirrhosis (%) 86 (37.7) 356 (40.9)
urban (%) 158 (69.3) 597 (68.6)
rural (%) 14 (6.1) 54 (6.2)
teaching hospital (%) 129 (56.6) 416 (47.8)
survival from Diagnosis (Days) 217±222 148±198
Image:
Conclusion: We have shown that sorafenib is associated with improved survival in patients with advanced hcc, however the survival benefit is modest, especially in patients with any decompensation. treating center, cancer stage, and severity of cirrhosis impact survival in these patients and may be useful in deciding who may experience the greatest benefit from sorafenib therapy.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 6 3
P-110 The COSTS Of CArInG fOr hePATOCeLLuLAr CArCInOMA
raxitkumar jinjuvadia1, augustine salami1, suthat Liangpunsakul2, reena Salgia* 1
1henry ford hospital, Detroit, 2Indiana university, Bloomington, united states
Introduction: hepatocellular carcinoma (hcc) accounts for significant morbidity, mortality and financial burden. the aim of this study is to evaluate temporal trends of hospitalizations from hcc and evaluate its financial impact in the united states.
Methods: the national Inpatient sample (nIs) databases (from 2002 to 2011) which are collected as part of the healthcare cost and utilization Project by agency for healthcare research and quality were utilized for this study. Individuals with age ≥ 18 years were included in this study. the hospitalizations with a diagnosis of hcc were captured by IcD-9 code. the national estimates of hospitalization were derived using sample weights provided by nIs. the change in total average charges per each hospitalization over the years was calculated after taking inflation into account. sas 9.3 was utilized for the statistical analysis.
results: hcc-related hospitalizations have increased significantly from 24,925 in the year 2002 to 52,568 by the year 2011. hcc represented the primary diagnosis in 11,182–16,981 of these hospitalizations and a secondary diagnosis in 13,743-35,586 hospitalizations. Most of the hcc-related hospitalizations were for white males (male: 70%; white: 55%). among patients with a secondary hospitalization diagnosis of hcc, hepatic encephalopathy (4%), sepsis (4%) and acute renal failure (2.5%) were noted to be the most common admitting diagnoses. notably, there was a significant decrease in inpatient mortality among these patients from year 2002 (13.5%) to 2011 (9.9%) (p<0.001). During this same time period, there was also a significant decrease in length of stay per hcc-related hospitalization from 6.5 days to 5.6 days (p<0.001). after adjusting for inflation, the cost per hospitalization increased by 46.8% ($15,153) in 2011 compared to 2002 (table 1). Medicare was the most common expected primary payer for these hcc-related hospitalizations (45%).
Image:
Conclusion: over the past decade, there has been an increase in hcc-related hospitalizations in the united states, and an associated increase in financial burden related to these hospitalizations. however, inpatient mortality and the length of stay of these hospitalizations has decreased.
Disclosure of Interest: none Declared
P-111 effeCT Of WAITInG TIMe On TuMOr PAThOLOGy AnD OuTCOMe In PATIenTS WITh hePATOCeLLuLAr CArCInOMA TreATeD WITh LIVer TrAnSPLAnTATIOn
Maarouf A. hoteit* 1, 2, Vandana khungar1, 2, kim olthoff2, 3, abraham shaked2, 3
1Gastroenterology and hepatology, 2Penn transplant Institute, 3transplant surgery, university of Pennsylvania, Philadelphia, united states
Introduction: Liver transplantation (oLt) is the preferred treatment for patients with unresectable hepatocellular carcinoma (hcc) meeting Milan (t2) criteria. the allocation system in the united states allows increased priority for hcc meeting t2 criteria with exception points upgraded every 3 months. a prolonged waiting time on the list could be associated with worse explant hcc pathology due to tumor progression, and impact long term outcomes. our goal is to evaluate the effect of waiting time on explant pathology findings and the outcome of hcc treated with oLt.
Methods: We reviewed our institutional oLt database for patients with hcc transplanted between january 2003 and june 2014. Patients meeting t2 MeLD exception point criteria were included. Patients with incidental hcc, regional review board-approved non-standard exceptions, no hcc exception points granted, and living donor recipients were excluded. Waiting time was defined as the time starting the date of exception point allocation to the date of transplant. end of follow up was 3/31/2015.
results: a total of 337 patients met study criteria. Most were men (79.2%) and had hcV (76.0%). the mean age at transplant was 58.2 ± 7.8 years. the median waiting time was 8 months (Iqr 4.6-13.0 months). Most (80.8%) had neoadjuvant liver-directed therapy prior to transplant. the median post oLt follow up was 3.7 years (Iqr 1.7-6.5 years). the hcc recurrence rate was 11.3 %, and 26.7 % died during follow up. When stratified by explant pathology, there was no difference in waiting time between tumors exceeding Milan criteria and those within Milan criteria (234 [127-400] vs 244 [139-380] days, p=0.74), but tumors exceeding ucsf criteria on explant had a trend for a shorter waiting time (199 [114-354] vs 251 [141-396] days, p=0.06). additionally, there was no difference in waiting time between tumors with or without microvascular invasion (230 [120-384] vs 243 [152-190] days, p=0.2), or between tumors with or without poor differentiation (239 [145-390] vs 244 [98-393] days, p=0.27). there was a trend for patients with recurrence to have a shorter waiting time (212 [134-307] vs 251 [137-396], p=0.1). Patients with a waiting time < 9 months had significantly increased 3-year probability of post oLt recurrence of hcc compared to patients with a longer waiting time (13.7% [9.2-20.1] vs 6.6 % [3.3-12.8], P=0.03). there was a non-significant trend for patients with ≥ 9 months waiting time to have improved 3-year post oLt survival (86.3% [78.9-91.2] vs 77.2% [70.2-82.8], P=0.3), especially in hcV-negative patients (93.7% [76.8-96.4] vs 78.0% [61.7-88.0], p=0.18).
Image:
Conclusion: Prolonged pretransplant waiting time is not associated with worsening hcc explant pathology, or post transplant outcomes. In fact, the probability of post transplant hcc recurrence was increased in patients transplanted with less than 9 months of waiting time. this effect is likely due to improved patient selection as a result of longitudinal observation of tumor behavior under the current exception point allocation rules. this observation may help guide future policies regarding exception point allocation in patients with hcc awaiting liver transplant.
Disclosure of Interest: none Declared

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s6 4
P-112 COMbInATIOn Of MODIfIeD reSPOnSe eVALuATIOn CrITerIA In SOLID TuMOrS AnD hAnD-fOOT-SKIn reACTIOn: A neW PrOGnOSTIC eVALuATIOn fOr hePATOCeLLuLAr CArCInOMA PATIenTS TreATeD WITh SOrAfenIb AnD TrAnSArTerIAL CheMOeMbOLIzATIOn
Wenjun Wang1, Wei Bai1, yan zhao1, Lei Liu1, Man yang1, enxin Wang1, Dongdong xia1, jie yuan1, ruiting Duan1, jing niu1, zhanxin yin1, jielai xia2, Guohong han* 1
1Department of Liver Disease and Digestive Interventional radiology, xijing hospital of Digestive Diseases, fourth Military Medical university, 2Department of Medical statistics, fourth Military Medical university, xi’an, china
Introduction: the modified response evaluation criteria in solid tumors (mrecIst) plays a pivotal role in assessing hepatocellular carcinoma (hcc) response to transarterial chemoembolization (tace) or sorafenib therapy. In addition, growing evidences reveal that the hand-foot-skin reaction (hfsr) can predict a positive response to sorafenib treatment. here, we aimed to combine the mrecIst and hfsr to establish a new prognostic evaluation for hcc patients undergoing sorafenib and tace and compared its prognostic value with mrecIst and hfsr criteria, respectively.
Methods: Between january 2009 and December 2013, 176 intermediate-advanced hcc patients with preserved liver function and eastern cooperative oncology Group (ecoG) score0/1 treated with combination therapy were consecutively enrolled. the therapeutic responses were assessed by mrecIst and hfsr criteria at 1, 2 and 3 months, respectively. uni/multivariate cox regressions were used to investigate the earliest time when treatment responses could be accurately assessed. then according to the mrecIst and hfsr assessed at that time, sMart (sorafenib with Modified recIst assessment plus hand-foot-skin reaction in tace) prognostic evaluation was developed: sMart a, responders on both assessments; sMart B, responders on either of assessment and sMart c, non-responders on both assessments. furthermore, we explore the prognostic value of sMart for predicting os in comparison with mrecIst and hfsr in relation to likelihood ratio, akaike information criterion (aIc) and c-index.
results: the earliest time at which the responses of mrecIst and hfsr correlated with the survival was 2 months after therapy. the sMart identified three groups with different prognosis: the sMart a had the longest os, followed by sMart B and sMart c (30.5, 17.4, and 8.3 months, respectively; P<0.001, figure 1). compared mrecIst and hfsr, the sMart had the highest likelihood ratio and c-index, and lowest aIc, demonstrating that the sMart had a better performance in predicting the survival (table 1).
table 1. comparison of sMart with mrecIst and hfsr criteria
Prognostic criteria Likelihood ratio aIc c-index
sMart 32.1395 923.403 0.64535
mrecIst 15.8826 939.660 0.59339
hfsr 15.4143 940.129 0.59323
Image:
Conclusion: the sMart prognostic evaluation, based on combining the mrecIst and hfsr, is clinical useful to predict survival of hcc patients at an early time point after combination therapy.
Disclosure of Interest: none Declared
P-113 LIVer STIffneSS MeASureMenT (fIbrOSCAn°r) DeTerMIneS The rISK Of reCurrenCe AfTer rADIOfrequenCy fOr eArLy STAGeD hePATOCeLLuLAr CArCInOMA
Soo young Park* 1, Won young tak1, young oh kweon1, se young jang1, yu rim Lee1, sun kyung jang1, soo hyun Lee1
1hepatology, kyungpook national university hospital, Daegu, korea, republic of
Introduction: advanced fibrosis is one of strong risk factors for recurrence of hepatocellular carcinoma (hcc) after curative therapy. recently, Liver stiffness measurement (LsM) using transient elastography showed role of risk stratification after surgical resection for hcc as well as noninvasive diagnosis of cirrhosis. We aimed to investigate the predictive value of LsM in patients undergone radiofrequency ablation (rfa) for hcc.
Methods: Between jan. 2013 and Dec. 2014, we prospectively measured the LsM of patients who achieved complete remission of early staged hcc after rfa for hcc. rfa was performed percutaneously and LsM was measured using fibroscanr before or after procedure when confounding factors were adjusted. Variables were analyzed for prediction of recurrence in serial imaging studies.
results: a total of 133 patients were evaluated for LsM and followed-up for 33 months (5-134). the mean age was 61.7 years (41-82) with 101 male patients. one hundred twelve patients (84.2%) had single hcc while 21 patients (15.8%) had multiple tumors. Mean size of tumor was 2.0 cm. hcc was recurred in 46 patients (34.6%). thirty seven cases of recurrence were observed with 25 intrahepatic distant recurrence (18.8%), 11 local recurrence (8.3%) and one extrahepatic recurrence (0.8%). LsM was the only significant different variable between patients with recurrence and remission (24.8 kPa vs 15.2 kPa, P=0.001). In multivariate analysis, LsM was the only independent predictor for recurrence (hr 1.044, 95% confidence interval 1.016-1.072, P=0.002). LsM cutoff value (12.5 kPa) best stratify the study population with 74.4 % sensitivity and 52.9 % specificity from receiver operating curves (area under the receiver operating characteristic curve = 0.637). Patients with LsM > 12.5 kPa showed higher risk of recurrence with hazard ratio of 3.273 ( 95% confidence interval 1.461-7.332, P=0.004)
Image:
Conclusion: LsM can be useful in identifying hcc patients at greater risk of recurrence after rfa
Disclosure of Interest: none Declared
P-114 uTILITy Of "ArT-SCOre" In The SequenTIAL CheMOeMbOLIzATIOn fOr hePATOCeLLuLAr CArCInOMA TreATMenT
Iván herrera Marante* 1, 2, sonia Pascual1, 2, Pedro zapater2, 3, 4, javier Irurzun5, cristina Peña1, fernando carnicer1, 2, Pablo Bellot1, 2, María rodríguez1, 2, fernando sánchez5, Pedro de la Iglesia5, santiago Gil5, josé María Palazón1
1Liver unit. Department of Gastroenterology, 2ciberehd, 3clinic Pharmacology unit, hospital General universitario alicante, 4university Miguel hernández, 5unit of Vascular and Interventional radiology, hospital General universitario alicante, alicante, spain
Introduction: transarterial chemoembolization (tace) is the treatment of choice in patients with

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 6 5
hepatocellular carcinoma (hcc) in intermediate stage. recently, a new scoring system for decision-making in the re-treatment with tace has been proposed: the art score (sieghart, hepatology 2013), so that ≥2.5 points after the 1st session of tace would select those patients who will not be benefit from a 2nd session.aIM: the purpose of this study has been to validate the usefulness of art score in our series of patients treated with tace sequentially.
Methods: patients with hcc treated with tace between january 1996 and December 2009 (follow up to December 2012) were included. as in sieghart study, patients in which tace was performed before liver transplantation and those who received only one tace session were excluded. the sequence of treatment was: initial tace session, 2nd session at 3 months and every 6-12 months depending on response and liver function, evaluated after each treatment session. after the 1st session, all patients were evaluated including: blood test, child-Pugh (cP) calculation, adverse events registration and response to treatment (performed with ct / MrI as appropriate) according to the easL-recIstm criteria. sessions were discontinued in case of: decompensated liver disease or worsening of liver function, severe adverse effects, intractable progression or complete response. the variables collected were: stage and etiology of liver disease, characteristics of the tumor, BcLc stage, response to treatment and survival. the value of art-score was calculated after the first tace session (0-1.5 points and ≥2.5 points). the cumulative survival (from the date of the 2nd session until death, last alive contact or end of study) was calculated using the kaplan-Meier and differences between survivals were compared using log-rank test.
results: 156 patients were treated with tace (117 conventional tace and 39 tace Dc-BeaDs). as in the study referred, 72 patients in whom only one session was performed were excluded. the survival of these patients was 12.13 months (95% cI 10.73-13.53). the other 84 patients were included (25 tace Dc-beads, mean age 69.6 ± sD 8.8, 63% male). cP stage: a 80%, B 20%. BcLc stage: a 40%, B 60%. etiology: 30% alcohol, 48% hcV and 11% alcohol and virus. uninodular tumor 49% (mean diameter 71.2 mm ± sD 29.1), multinodular 51%. response after the first session: 30% complete response, 52% partial response and 18% non response. overall survival: 27.9 months (95% cI 22.07-33.72). survival art 0-1.5 score: 27.56 months (95% cI 14.76-40.36), art score ≥2.5: 27.9 months (95% cI 16.98-38.81), p = 0.241.
Conclusion: in our series, survival after the second session of tace was not related to the score obtained by calculating art score, probably because the population on which we decided to perform the second tace is already selected properly with clinical and laboratory criteria. therefore, in our experience, this new scoring system does not improved the previously established criteria for clinical decision making.
Disclosure of Interest: none Declared
P-115 SOrAfenIb uSe In eLDerLy PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA In The unITeD STATeS: An AnALySIS Of The Seer-MeDICAre DATAbASe
neehar D. Parikh* 1, Vincent D. Marshall2, Vahakn shahinian3, rajesh Balkrishnan2
1Gastroenterology, 2college of Pharmacy, 3kidney epidemiology and cost center, university of Michigan, ann arbor, united states
Introduction: sorafenib was approved for the treatment of advanced hcc in the us in 2007. the seer-Medicare database is a linked database that contains information on cancer diagnoses, outcomes, and claims data in Medicare beneficiaries. We aimed to examine the uptake of sorafenib use in the us and predictors of sorafenib use in patients with advanced hcc.
Methods: We performed a secondary analysis of the seer-Medicare database from continuously enrolled Medicare beneficiaries with hcc diagnoses from 2007-2009, based on seer diagnosis codes. using Part D data, we examined the trend in number of script filled after the introduction of sorafenib on the market for incident (stage III/IV hcc with sorafenib use within 6 months of diagnosis) and prevalent hcc (any stage, but with diagnosis greater than 6 months from sorafenib use and after receipt of an additional mode of therapy.) for the predictors of use we compared advanced stage patients with hcc (stage III/IV) who received only sorafenib within 6 months of diagnosis to advanced stage patients with hcc who received no therapy (control.) We calculated the charlson comorbidity index 12 months prior to diagnosis and an aggregate variable for decompensated cirrhosis (presence of esophageal varices or variceal banding, ascites or paracentesis, hepatic encephalopathy or use of neomycin, lactulose, or rifaximin.) We performed univariate and multivariate analyses for predictors of use versus non-use.
results: the baseline characteristics of the cohorts are shown in table 1. overall 20.9 % of patients incident advanced hcc were treated with sorafenib and this increased by 3.9% per year over the treatment period studied. the uptake of sorafenib, measured by number of active prescriptions, is shown in figure 1. there were no differences in sorafenib uptake when stratified by seer region or facility type. Predictors of sorafenib use or non-use included if the treating facility was a teaching hospital (or: 1.79; 95% cI: 1.14-2.82), non-white or non-black race (or: 1.62; 95% cI: 1.06-2.48), each year of patient age (or: 0.96; 95% cI: 0.94-0.98), and charlson comorbidity index (or: 0.81; 95% cI: 0.72-0.91.)
Incident (n=228) control (n=870) Prevalent (n=364)
age (median; range) 69.5±9.4 72.9±9.7 67.9±8.6
sex (M; %) 168 (73.7) 642 (73.8) 261 (71.7)
charlson Index 0.8±1.3 1.3±1.7 1.3±1.6
Decompensated cirrhosis (%)
86 (37.7) 356 (40.9) 178 (48.9)
teaching hospital (%) 129 (56.6) 416 (47.8) 263 (72.3)
number of prescriptions 2.9±3.7 4.7±5.4
Duration of therapy (days) 85.8±111.1 140.5±161.4
Image:
Conclusion: We have shown that there was a steady uptake and dissemination of sorafenib usage across the united states soon after it’s introduction to the market in 2007, however, only a minority of patients were treated. Being treated at a teaching facility and being a member of a non-black or non-white racial group was a significant predictor of use, while advanced age and more comorbidities were predictors of non-use. elderly patients with advanced stage hcc experience significant variations in care.
Disclosure of Interest: none Declared
P-116 The ArT SCOre COuLD nOT PreDICT OVerALL SurVIVAL fOr rePeATeD TrAnSArTerIAL CheMOeMbOLIzATIOn In ThAI PATIenTS WITh hePATOCeLLuLAr CArCInOMA
Kessarin Thanapirom* 1, nopavut Geratikornsupuk2, roonhgruedee chaiteerakij1, nutcha Pinjaroen3, sombat treeprasertsuk1, Piyawat komolmit1
1Medicine, chulalongkorn university, Bangkok, 2Medicine, queen savang Vadhana Memorial hospital, chonburi, 3radiology, chulalongkorn university, Bangkok, thailand
Introduction: recently, the assessment for retreatment with transarterial chemoembolization (tace) or art score was developed to identify patients who are suitable for repeated tace. We aimed to validate the art score in thai hepatocellular carcinoma (hcc) cohort and to predict the overall survival (os) in patients with intermediate stage hcc re-treated with tace.
Methods: from 2005 to 2014, there were 445 patients with hcc treated with at least 3 tace sessions in king chulalongkorn Memorial hospital, thailand. of these, 74 patients (16.6%) who had intermediated stage of BcLc system were included. tumor response was assessed according to mrecIst criteria. the art score prior the 3rd tace was evaluated in comparison to the tace naïve liver.
results: of 74 patients, 51 patients (68.9%) had an art score of 0-1.5 and the remaining of 23 patients (31.1%) had art of ≥2.5. the mean overall survival (os) was 21.6 months with 1-, 3- and 5-year survival of 69.0%, 22.6%, 7.8%, respectively. the mean os was not different between patients with art score ≥ 2.5 and those with art score of 0-1.5 (28.2 months vs.37.7 months, p=0.34; figure1). Patients with art score of 0-1.5 had significantly higher 1- year survival rate than those with art score ≥ 2.5 (77% vs. 52%, p=0.034). In contrast to previous study (hucke f, et al, j hepatol. 2014), our study showed some different baseline characteristics as shown in table 1. the art score prior the 3rd tace of our patients could not predict the os (figure 1). By using multivariate analysis, only multifocal of tumor number remained a significant predictor of worse one year survival rate (hr=4.34, 95%cI=1.13-16.62, p=0.032).
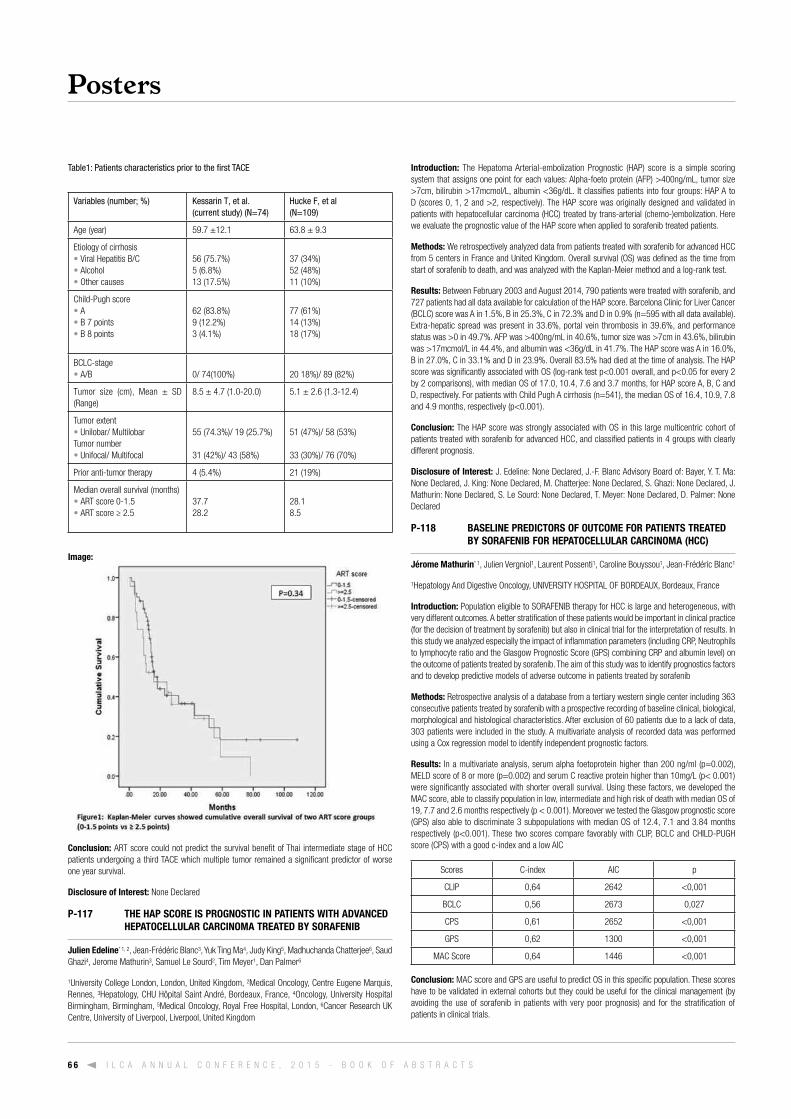
Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s6 6
Table1: Patients characteristics prior to the first TACE
Variables (number; %) Kessarin T, et al. (current study) (N=74)
Hucke F, et al (N=109)
age (year) 59.7 ±12.1 63.8 ± 9.3
etiology of cirrhosis• Viral hepatitis B/c• alcohol• other causes
56 (75.7%)5 (6.8%)13 (17.5%)
37 (34%)52 (48%)11 (10%)
child-Pugh score• a• B 7 points• B 8 points
62 (83.8%)9 (12.2%)3 (4.1%)
77 (61%)14 (13%)18 (17%)
BcLc-stage• a/B
0/ 74(100%)
20 18%)/ 89 (82%)
tumor size (cm), Mean ± sD (range)
8.5 ± 4.7 (1.0-20.0) 5.1 ± 2.6 (1.3-12.4)
tumor extent• unilobar/ Multilobartumor number• unifocal/ Multifocal
55 (74.3%)/ 19 (25.7%) 31 (42%)/ 43 (58%)
51 (47%)/ 58 (53%) 33 (30%)/ 76 (70%)
Prior anti-tumor therapy 4 (5.4%) 21 (19%)
Median overall survival (months)• art score 0-1.5• art score ≥ 2.5
37.728.2
28.18.5
Image:
Conclusion: art score could not predict the survival benefit of thai intermediate stage of hcc patients undergoing a third tace which multiple tumor remained a significant predictor of worse one year survival.
Disclosure of Interest: none Declared
P-117 The hAP SCOre IS PrOGnOSTIC In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA TreATeD by SOrAfenIb
Julien edeline* 1, 2, jean-frédéric Blanc3, yuk ting Ma4, judy king5, Madhuchanda chatterjee6, saud Ghazi4, jerome Mathurin3, samuel Le sourd2, tim Meyer1, Dan Palmer6
1university college London, London, united kingdom, 2Medical oncology, centre eugene Marquis, rennes, 3hepatology, chu hôpital saint andré, Bordeaux, france, 4oncology, university hospital Birmingham, Birmingham, 5Medical oncology, royal free hospital, London, 6cancer research uk centre, university of Liverpool, Liverpool, united kingdom
Introduction: the hepatoma arterial-embolization Prognostic (haP) score is a simple scoring system that assigns one point for each values: alpha-foeto protein (afP) >400ng/mL, tumor size >7cm, bilirubin >17mcmol/L, albumin <36g/dL. It classifies patients into four groups: haP a to D (scores 0, 1, 2 and >2, respectively). the haP score was originally designed and validated in patients with hepatocellular carcinoma (hcc) treated by trans-arterial (chemo-)embolization. here we evaluate the prognostic value of the haP score when applied to sorafenib treated patients.
Methods: We retrospectively analyzed data from patients treated with sorafenib for advanced hcc from 5 centers in france and united kingdom. overall survival (os) was defined as the time from start of sorafenib to death, and was analyzed with the kaplan-Meier method and a log-rank test.
results: Between february 2003 and august 2014, 790 patients were treated with sorafenib, and 727 patients had all data available for calculation of the haP score. Barcelona clinic for Liver cancer (BcLc) score was a in 1.5%, B in 25.3%, c in 72.3% and D in 0.9% (n=595 with all data available). extra-hepatic spread was present in 33.6%, portal vein thrombosis in 39.6%, and performance status was >0 in 49.7%. afP was >400ng/mL in 40.6%, tumor size was >7cm in 43.6%, bilirubin was >17mcmol/L in 44.4%, and albumin was <36g/dL in 41.7%. the haP score was a in 16.0%, B in 27.0%, c in 33.1% and D in 23.9%. overall 83.5% had died at the time of analysis. the haP score was significantly associated with os (log-rank test p<0.001 overall, and p<0.05 for every 2 by 2 comparisons), with median os of 17.0, 10.4, 7.6 and 3.7 months, for haP score a, B, c and D, respectively. for patients with child Pugh a cirrhosis (n=541), the median os of 16.4, 10.9, 7.8 and 4.9 months, respectively (p<0.001).
Conclusion: the haP score was strongly associated with os in this large multicentric cohort of patients treated with sorafenib for advanced hcc, and classified patients in 4 groups with clearly different prognosis.
Disclosure of Interest: j. edeline: none Declared, j.-f. Blanc advisory Board of: Bayer, y. t. Ma: none Declared, j. king: none Declared, M. chatterjee: none Declared, s. Ghazi: none Declared, j. Mathurin: none Declared, s. Le sourd: none Declared, t. Meyer: none Declared, D. Palmer: none Declared
P-118 bASeLIne PreDICTOrS Of OuTCOMe fOr PATIenTS TreATeD by SOrAfenIb fOr hePATOCeLLuLAr CArCInOMA (hCC)
Jérome Mathurin* 1, julien Vergniol1, Laurent Possenti1, caroline Bouyssou1, jean-frédéric Blanc1
1hepatology and Digestive oncology, unIVersIty hosPItaL of BorDeaux, Bordeaux, france
Introduction: Population eligible to sorafenIB therapy for hcc is large and heterogeneous, with very different outcomes. a better stratification of these patients would be important in clinical practice (for the decision of treatment by sorafenib) but also in clinical trial for the interpretation of results. In this study we analyzed especially the impact of inflammation parameters (including crP, neutrophils to lymphocyte ratio and the Glasgow Prognostic score (GPs) combining crP and albumin level) on the outcome of patients treated by sorafenib. the aim of this study was to identify prognostics factors and to develop predictive models of adverse outcome in patients treated by sorafenib
Methods: retrospective analysis of a database from a tertiary western single center including 363 consecutive patients treated by sorafenib with a prospective recording of baseline clinical, biological, morphological and histological characteristics. after exclusion of 60 patients due to a lack of data, 303 patients were included in the study. a multivariate analysis of recorded data was performed using a cox regression model to identify independent prognostic factors.
results: In a multivariate analysis, serum alpha foetoprotein higher than 200 ng/ml (p=0.002), MeLD score of 8 or more (p=0.002) and serum c reactive protein higher than 10mg/L (p< 0.001) were significantly associated with shorter overall survival. using these factors, we developed the Mac score, able to classify population in low, intermediate and high risk of death with median os of 19, 7.7 and 2.6 months respectively (p < 0.001). Moreover we tested the Glasgow prognostic score (GPs) also able to discriminate 3 subpopulations with median os of 12.4, 7.1 and 3.84 months respectively (p<0.001). these two scores compare favorably with cLIP, BcLc and chILD-PuGh score (cPs) with a good c-index and a low aIc
scores c-index aIc p
cLIP 0,64 2642 <0,001
BcLc 0,56 2673 0,027
cPs 0,61 2652 <0,001
GPs 0,62 1300 <0,001
Mac score 0,64 1446 <0,001
Conclusion: Mac score and GPs are useful to predict os in this specific population. these scores have to be validated in external cohorts but they could be useful for the clinical management (by avoiding the use of sorafenib in patients with very poor prognosis) and for the stratification of patients in clinical trials.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 6 7
Disclosure of Interest: j. Mathurin: none Declared, j. Vergniol: none Declared, L. Possenti: none Declared, c. Bouyssou: none Declared, j.-f. Blanc advisory Board of: BayersP, Lilly oncology
P-119 PreDICTIOn Of CLInICAL OuTCOMe AfTer rADIOeMbOLIzATIOn In hCC PATIenTS: rOLe Of 18f-fDG PeT-CT
Wonseok Kang* 1, Mijin yun2, jin-young choi3, jong yun Won3, seung up kim1, kwang-hyub han1, Do young kim1
1Internal Medicine, 2nuclear Medicine, 3radiology, yonsei university college of Medicine, seoul, korea, republic of
Introduction: yttrium-90 radioembolization (y-90 re) has emerged as a valuable therapeutic option for nonsurgical treatment of hepatocellular carcinoma (hcc). We aimed to investigate the prognostic value of 18f-fluorodeoxyglucose (fDG) positron emission tomography-computed tomography (Pet-ct) in predicting progression-free survival (Pfs) after y-90 re in patients with hcc.
Methods: Between 2009 and 2013, a total of 40 patients with hcc were treated with y-90 re. 18f-fDG Pet-ct was performed before treatment and maximum standardized uptake value (suVmax) was obtained in each patient. tumor response was evaluated in accordance with modified recIst criteria every 3 months after y-90 re. chi square tests, kaplan-Meier method and cox proportional hazards model were used for statistical analysis.
results: the median age was 56.5 years, and 29 (72.5%) were males; 36 (90.0%) patients were in child-Pugh class a. Patients with low suVmax (<6.1) had a higher disease control rate than those with high suVmax (≥6.1) (55.6% vs. 23.1%, respectively; P = 0.05). Median Pfs was significantly longer in patients with low suVmax than those with high suVmax (22.1 vs. 6.5 months, respectively; P = 0.03). In addition, a longer Pfs was observed in patients with BcLc stage a or B than those with BcLc stage c (P = 0.01). In multivariate analyses, low suVmax was found to be a significant prognostic factor for a lower risk of disease progression (adjusted hazard ratio [hr] 0.40, 95% confidence interval [cI] 0.17 – 0.95; P = 0.04), along with BcLc stage a or B (adjusted hr 0.27, 95% cI 0.10 - 0.76; P = 0.01).
Conclusion: a high suVmax based on 18f-fDG Pet-ct performed before treatment and BcLc stage were independent prognostic factors for Pfs after y-90 re in hcc patients.
Disclosure of Interest: none Declared
P-120 PrOGnOSTIC SIGnIfICAnCe Of InfLAMMATIOn bASeD SCOreS fOr PATIenTS WITh hePATOCeLLuLAr CArCInOMA TreATeD WITh SOrAfenIb In A WeSTern COLLeCTIVe
Arndt Weinmann* 1, 2, 3, sandra koch1, 2, Martin sprinzl1, 2, 3, Peter Galle2, 3, Marcus Wörns2, 3
1clinical registry unit (cru), 2Department of Internal Medicine I, 3center for cirrhosis Mainz (ccM), unIVersIty MeDIcaL center MaInz, Mainz, Germany
Introduction: Inflammation based scores like the neutrophil-to-lymphcyte ratio (nLr), the Glasgow Prognostic score (GPs), the modified GPs (mGPs), platelet/lymphocyte ratio (PLr), the prognostic index (PnI) and crP/albumin ratio have a prognostic value in patients with hepatocellular carcinoma (hcc) undergoing surgery or treatment with sorafenib.
Methods: We retrospectively analyzed all consecutive patients with confirmed hcc treated with sorafenib between 2007 and 2013. end of followup was December 31th, 2014. nLr, GPs, PnI were calculated for each patient at the beginning of sorafenib treatment, if adequate data was available.survival depending on the inflammation scores was calculated using the kaplan-Meier-method. Prognostic markers for survival were calculated by multivariate analysis.
results: scores could be calculated for 148 from 168 patients. etiology of underlying liver disease was mainly alcohol (30.8%), followed by chronic hepatitis c (20.5%) and chronic hepatitis B (19.2%). a significant survival difference was found for the nLr (cut-off 3, p<0.01), GPs (p<0.001), mGPs (p=0. 0012) and crP/albumin ratio (p<0.001) but not for the PLr (p=0.126). Multivariate analysis demonstrated the PnI and nLr and portal vein thrombosis to be independently associated with survival in sorafenib treated patients, while child stadium, crP/albumin ratio, mGPs, GPs and PLr did not reach statistical significance.
Conclusion: the inflammation based scores PnI and nLr demonstrated a prognostic value in hcc patients treated with sorafenib in a western collective. Inflammation based scores have the potential of clinical utility to identify patients who are likely not to derive significant benefit from a systemic therapy.
Disclosure of Interest: none Declared
P-121 OuTCOMeS Of reSeCTIOn fOr SOLITAry ≤ 5 CM InTrAhePATIC ChOLAnGIOCArCInOMA
Paola Tarchi* 1, Parissa tabrizian2, jake Prigoff2, Myron e. schwartz2
1surgery, university hospital of trieste, trieste, Italy, 2transplant, recanati/Miller transplantation Institute, new york, united states
Introduction: resection remains the treatment of choice for intrahepatic cholangiocarcinoma (Icc) achieving 5 year survival rates of 22-40%. the outcome of early stage Icc remains unclear. the aim of this analysis was to examine the outcomes of patients with solitary ≤ 5 cm Icc.
Methods: a retrospective chart review was performed on all patients undergoing resection for primary Icc from 1995-2015. Group 1 included patients with early stage Icc defined as asymptomatic, solitary ≤ 5 cm lesions. clinical data were abstracted and differences between the groups (Group1: early stage vs. Group 2: late stage) were analyzed. statistical analysis was performed to identify variables associated with poor outcome.
results: 123 patients underwent liver resection for primary Icc. early Icc was found in 33 (27 %) patients. Patients in Group 1 had a higher rate of underlying liver disease (50% vs. 19.3%, p < 0.001), cirrhosis (14.7% vs. 2.3%, p = 0.019), minor resection (38.2% vs. 12.5%, p = 0.001), favorable pathologic features including decreased rate of perineural invasion (18.2% vs. 36.8%, p = 0.05), vascular invasion (micro/macro) (18.2% vs. 36.8%, p = 0.05), lymph node involvement (25.4% vs. 44.1%, p = 0.05), and satellite nodules (17.6% vs. 32.2%, p < 0.05). factors associated with overall poor outcome in the entire cohort were patients in Group 2 (p = 0.025), positive margin (p = 0.04), presence of satellite nodules (p = 0.008), and multinodularity (p = 0.058). factors associated with recurrence in Group 1 were presence of satellite nodules (p = 0.004), and tumor size ≥ 4 cm (p = 0.031). recurrence in Group 1 were intrahepatic in 67% and occurred within the first 2 years after resection in 78%. factors associated with decreased survival in Group 1 was transfusion requirement (p = 0.018). Median follow up was 30 months. the 1, 3 and 5 year recurrence rates were lower in Group 1 vs. Group 2 (21.4% vs. 36%), (28.6% vs. 62.7%), and (39.3% vs. 66.7%) respectively (p = 0.004) (figure 1a). the 1, 3 and 5 year survival rates were higher in Group 1 vs. Group 2 (92.9% vs. 86.7%), (71.4% vs. 65.3%), and (71.4%vs. 53.3%) respectively (p = 0.111) (figure 1b).
Image:

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s6 8
Conclusion: resection of Icc within Milan criteria can achieve 5 year survival rates up to 71%. results were comparable to patients undergoing transplantation for hepatocellular cancer. future well designed clinical studies are needed to validate our findings and justify transplantation in patients with early Icc.
Disclosure of Interest: none Declared
P-122 IMPACT Of PreOPerATIVe renAL InSuffICIenCy On ShOrT OuTCOMe AfTer hePATIC reSeCTIOn Of hePATOCeLLuLAr CArCInOMA
Azoulay Daniel* 1, Lim chetana1, compagnon Philippe1, Laurent alexis1, salloum chady1
1hPB surgery and liver transplantation, hopital henri Mondor, aPhP, creteil, france
Introduction: renal insufficiency adversely affects operative outcomes after hepatectomy. however, the impact of preoperative renal insufficiency on short-term outcome after hepatectomy for hepatocellular carcinoma is not well known.
Methods: all patients who underwent hepatectomy at henri Mondor hospital between 1989 and 2015 were identified from a prospective maintained database. renal function was analyzed by preoperative serum creatinine (scr) level. Primary outcomes were any complications, major morbidity (clavien-Dindo ≥ Grade III complications) and in-hospital mortality.
results: four hundred and four patients had preoperative scr levels available. Preoperative renal insufficiency was defined as scr ≥ 111 µmol/L, 1 standard deviation higher than the mean value (87 ± 24 µmol/L) for the cohort. forty- five patients (11.1%) had scr ≥ 111 µmol/L. overall, complications occurred in 159 patients, major complications in 54 patients, and in-hospital mortality rate was 8.2%. Patients with preoperative renal insufficiency experienced more postoperative liver failure (15.6% vs. 4.2%; p = 0.0015) than those without. In-hospital mortality rate was significantly higher in patients with preoperative renal insufficiency (17.8% vs. 7%, p = 0.0125). on multivariate analysis, 2 preoperative and 1 intraopertive independent predictors of mortality were identified: scr ≥ 111 µmol/L (P = 0.0027; or = 4.2; cI = 1.6 - 10.6); platelet count < 150.000 (P = 0.0043; or = 3.2: cI = 1.4 - 7); and associated procedures (P < 0.0001; or = 6.8; cI = 3.1 - 15.2).
Conclusion: Patients with preoperative serum creatinine ≥ 111 µmol/L are associated with an increased risk of postoperative liver failure and mortality. Liver resection should be considered with caution in patients with preoperative renal insufficiency when aggressive surgical procedures are indicated
Disclosure of Interest: none Declared
P-123 WIDe reSeCTIOn MArGIn IMPrOVeS SurVIVAL In PATIenTS WITh eArLy InTrAhePATIC ChOLAnGIOCArCInOMA
Ma Ka Wing* 1, she Wong hoi1, Poon t. P. ronnie1, 2, Lo chung Mau1, 2, chueung tan to1
1surgery, queen Mary hospital, 2the university of hong kong, hong kong, china
Introduction: Intrahepatic cholangiocarcinoma (Icc) is known for its lethal disease nature and there were studies focusing on factors that might affect disease survival; among these factors, resection margin status remains one of the few modifiable factors that a surgeon could possibly manipulate to alter the disease outcome. however, the significance of clear margin and margin width continue to be a topic of debate. this study serves to share our opinion on this issue.
Methods: a retrospective review of a prospectively maintained database was performed in Department of surgery, queen Mary hospital, university of hong kong. consecutive patients diagnosed to have Icc and with surgical resection performed in curative intent were retrieved, while patients with cholangiohepatocellular carcinoma, klaskin tumour, tumour of extrahepatic bile duct and uncertain tumour pathology were excluded. clinico-pathological data were analysed statistically.
results: from 1991 to 2013, there were 107 patients underwent hepatectomy for Icc. Gender predilection was not observed with 59 males and 48 females, median age of the patients was 61. the median tumour size was 6cm (1-17cm) and most of them (43%) were moderately differentiated adenocarcinoma. clear resection margin were achieved in 95 patients (88.8%) and the median margin width was 0.5cm (0-4cm). the hospital length of stay and operative mortality were eleven days and 2.8% respectively. the disease free survival and overall survival were 17.5 months (0.5-276.3) and 25.1 months (0.2-276.3) respectively. Multivariate analysis showed that margin width was an independent factor associated with disease free survival (P= 0.015, 95% c.I. 0.4-0.9). subgroup analyses showed that the increase resection margin to 0.84 cm was associated with improved overall survival in patients with solitary tumour (P=0.029) and node negative disease (P=0.017). Discriminant analysis showed that the overall survival increased from 42 months to 185 months when margin width was greater than 0.84cm (p=0.015) in patients with both solitary tumour and node negative disease.
Image:
Conclusion: aggressive resection to achieve wide margin maximize chance of cure in patient with early Icc.
Disclosure of Interest: none Declared
P-124 hePATOCeLLuLAr CArCInOMA In The AbSenCe Of CIrrhOSIS: An eTIOLOGy-bASeD CLInICOPAThOLOGICAL STuDy
Chang Woo Shim* 1, joong-Won Park1, Bo hyun kim1, chang-Min kim1, eun kyung hong1
1center for Liver cancer, national cancer center, korea, Goyang, korea, republic of
Introduction: although hepatocellular carcinoma (hcc) usually develops in cirrhotic liver, a proportion also develops in the absence of cirrhosis. our objective was to identify the etiology-based clinicopathological features of underlying cirrhosis in korean patients with hcc.
Methods: of a cohort of 2876 patients first diagnosed and treated at the national cancer center, korea, between 2000 and 2009, 710 surgically treated patients were enrolled. these patients were collected prospectively, and relevant clinical data and pathologic characteristics of surgical specimens were reviewed retrospectively. cirrhosis was diagnosed by pathology.
results: of 710 patients, 178 (25%) did not have cirrhosis (nLc group); 81% had modified International union against cancer stage I or II disease and 94% had child-Pugh class a liver function. the median age was 54 years, and males comprised 83% of the population (M:f = 590:120). the median overall survival (os) was 90.3 months (95% confidence interval [cI]: 87.1-93.5); there was no statistically significant difference in os between the nLc and cirrhosis groups. the main cause of hcc was hepatitis B virus (hBV) infection (77.2%), followed by cryptogenic disease (11.0%), alcoholic disease (6.2%), and hepatitis c virus (hcV) infection (5.6%). according to etiology, hcc patients with hBV infection, hcV infection, alcoholic disease, and cryptogenic disease did not have underlying cirrhosis in 19.2%, 32.5%, 50.0%, and 48.7% of cases, respectively. compared to the cirrhosis group, the nLc group was significantly more likely to be younger, and have a larger tumor size, lower alpha-fetoprotein level, and more non-hBV etiologies. In the nLc group, 73 patients (41.0%) were hBV negative, but 61 of 73 (83%) were positive for hepatitis B core IgG antibody (anti-hBc ab). In the cirrhosis group, 89 patients (16.7%) were hBV negative, but 70 of 89 (78.6%) were positive for anti-hBc ab. cirrhosis was observed in 73% (390/532) by imaging studies. Pathology review for fibrosis grading is currently underway.
Conclusion: a considerable proportion of hcV infection, alcoholic disease, and cryptogenic disease associated hcc cases had anti-hBc antibody and did not involve cirrhosis in this korean cohort.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 6 9
P-125 ALbI SCOre PreDICTS SurVIVAL In PATIenTS WITh bCLC 0/A STAGe hePATOCeLLuLAr CArCInOMA (hCC) InDePenDenTLy Of ChILD PuGh (CP) SCOre AnD TreATMenT ALLOCATIOn
Simona Onali* 1, aileen Marshall1, Dinesh sharma1, Pam o' Donoghue1, emily Dannhorn1, Philip johnson2, james o' Beirne1
1sheila sherlock Liver centre, royal free hospital, London, 2Department of Molecular and clinical cancer Medicine, university of Liverpool, Liverpool, united kingdom
Introduction: BcLc 0/a stage hcc patients are considered candidates for curative treatments. Within the BcLc classification, liver function is assessed by cP score despite this score not being derived from patients with hcc. aLBI is a novel evidence based score derived from a large cohort of hcc patients and has been shown to define different prognostic groups even within cP a 1. We studied the performance of aLBI score in a well characterised cohort of patients with BcLc 0/a stage hcc to determine if aLBI score impacted on prognosis.
Methods: consecutive patients with BcLc 0/a hcc, evaluated between 2010-2014 at the royal free hospital were included. all patients had a performance score of 0 and were undergoing evaluation for potential resection. Patients were considered resectable if they had hVPG≤10mmhg or hVPG≥10mmhg with good liver function as assessed by IcG clearance. aLBI score was calculated at the time of hVPG and IcG clearance measurement and divided into 3 grades as per published cutoffs. kaplan Meier and cox regression analysis were used to assess the impact of aLBI on survival.
results: 67 patients were included: 64 (95.5%) were cP a, 3 (4.5%) were cP B. 60 (89%) had uninodular tumour and 7 (10.4%) multifocal (≤3 tumours ≤30mm). 46 (69%) underwent resection, 4 (6%) rfa, 9 (14%) tae, 3 (5%) oLt, 3(5%) either no treatment or undergoing evaluation. Median follow up was 9 months (13-54). 10 (15%) patients died during follow up. cause of death was hcc-related n= 4, liver failure n=4, non-liver related n=2. In kaplan Meier analysis cP score was not associated with difference in survival. cox regression analysis revealed aLBI score as the only significant factor related to survival and was independent of cP score and treatment allocation(p=0.002, or=15, 95%cI=3-80). of patients with aLBI grade 1, 44 (83%)were considered suitable and underwent resection vs only 2 (14%) with aLBI 2. one-year survival was 88% in patients with aLBI grade 1 and 43% in patients with aLBI grade 2 (p=0.002).
Conclusion: In patients with BcLc 0/a stage hcc aLBI score clearly defines patients with different prognosis regardless of child Pugh score and treatment allocation. aLBI grade 2 patients are very rarely suitable candidates for resection. aLBI score is more informative than child Pugh score in patients with early stage hcc and may be useful in determining treatment allocation.
references: 1. johnson Pj et al. assessment of Liver function in Patients With hepatocellular carcinoma: a new evidence-Based approach-the aLBI Grade. j clin oncol. 2015 feb 20;33(6):550-8
Disclosure of Interest: none Declared
P-126 ALbI SCOre PreDICTS SurVIVAL InDePenDenTLy Of hePATIC VenOuS PreSSure GrADIenT (hVPG) AnD InDOCyAnIne Green (ICG) CLeArAnCe In hCC PATIenTS unDerGOInG reSeCTIOn
aileen Marshall1, Simona Onali* 1, Dinesh sharma1, Pam o' Donoghue1, emily Dannhorn1, Philip johnson2, james o' Beirne1
1sheila sherlock Liver centre, royal free hospital, London, 2Department of Molecular and clinical cancer Medicine, university of Liverpool, Liverpool, united kingdom
Introduction: a new evidence based model, the albumin-Bilirubin (aLBI) grade†, has been recently proposed for assessing liver function in patients with hepatocellular carcinoma(hcc). We aimed to evaluate the impact of aLBI in predicting decompensation and survival after liver resection(Lr) for hcc.
Methods: consecutive patients undergoing resection for hcc between 2011-2014 at the royal free hospital were evaluated. Demographic, clinical data and histopathological features of resected tumour were collected. Patients underwent hVPG and IcG clearance measurement to evaluate potential resectability. aLBI score was calculated pre and post-operatively. Patients were divided into 3 categories (aLBI 1,2,3) according to published aLBI score cut-offs. cox regression was used to identify predictors of decompensation and survival post Lr.
results: 48 patients were included with a median post Lr follow up 17 months (1-54): male 42(87.5%), mean age 63 years (28-83). Median hVPG 6 mmhg(2-15), median IcG PDr 18.2 (6.1-29.4), median IcG r15 6.5 (1.2-19.2). all patients had a child Pugh score a5.46 (96%) had a pre-Lr aLBI grade 1 and 2 (4%) had an aLBI grade 2. clinically significant portal hypertension (hVPG≥10mmhg) was found in 11 (23%) patients. eight (19%) patients had an IcG PDr <15, while three (6%) had IcG r15>15. thirty (62,5%) patients underwent an anatomical resection, while 18 (37,5%) had a wedge resection. Post-Lr decompensation was observed in 5(10%) patients: ascites n=4, encephalopathy n=1 at a median of 10 days post-Lr.
12(25%) patients had hcc recurrence after a mean time of 11 months (5-28). 7 (15%) died after a mean follow up of 15 months (1-40), 3 of them due to tumour recurrence. Patients with 1 hcc <30 mm had 100% survival (mean follow up 20 months, range 9-32). 2 patients with pre-Lr aLBI grade 2 died after 7 and 11 months due to hcc recurrence and decompensated cirrhosis, respectively.cox regression analysis of pre Lr variables (hVPG, IcG, cPs, aLBI, hcc size) showed that the only factor associated with survival was pre-Lr aLBI score (p=0.019).
Conclusion: aLBI, an evidence based prognostic score specific to hcc, provides significant information regarding Lr outcome in patients with hcc, independently of hVPG, IcG clearance and child Pugh score.
references: † johnson Pj et al. assessment of Liver function in Patients With hepatocellular carcinoma: a new evidence-Based approach-the aLBI Grade. j clin oncol. 2015 feb 20;33(6):550-8
Disclosure of Interest: none Declared
P-127 COMPArISOn Of STAGInG SySTeMS fOr The PreDICTIOn Of PrOGnOSIS In PATIenTS WITh hePATOCeLLuLAr CArCInOMA unDerGOInG TrAnSCATheTer ArTerIAL CheMOeMbOLIzATIOn
Sung Won Lee* 1, nam Ik han1, hyun yang1, hae Lim Lee1, hee chul nam1, jeong Won jang1, si hyun Bae1, jong young choi1, seung kew yoon1
1Division of hepatology, Department of internal medicine, the catholic university of korea, seoul, korea, republic of
Introduction: the Barcelona clinic Liver cancer (BcLc) staging system recommends patients with intermediate stage hepatocellular carcinoma (hcc) to receive transcatheter arterial chemoembolization (tace). however, in real clinical practice, patients diagnosed at early stage or advanced stage also receive tace due to various reasons. several staging systems and prognostic scores for hcc have been suggested but inconsistent results have been reported so far on which system is the most reliable. the prediction of prognosis becomes more difficult for patients who receive tace due to the heterogeneous patient characteristics. therefore, we compared BcLc staging system, japan Integrated staging (jIs) score and the recently introduced hongkong liver cancer staging system for predicting prognosis and survival in patients undergoing tace.
Methods: a consecutive cohort study was performed with 485 hcc patients who received tace as the first line therapy at seoul st. Mary's hospital between 2005 and 2010. all patients were classified by BcLc, jIs and hongkong staging systems. We analyzed the predictive factors for survival, prognostic performance of each system and their discriminatory ability for death at 1,3 and 5 years.
results: Median overall survival was 24.6 months with a median follow up of 19.1 months. Multivariate analysis for the predictive factors of survival showed child-pugh class a, afP ≤ 200ng/ml, tumor size ≤ 5cm, no portal vein tumor thrombosis and no extrahepatic metastasis as the favorable factors for survival. Median survival ranged from 49 to 7 months for BcLc, 51.9 to 6.2 months for jIs and 53.2 to 3.4 months for hongkong staging system. all three systems successfully differentiated survival according to stages (p<0.0001). In the cox regression model, hongkong staging system showed better performance compared to jIs and BcLc. Discriminatory ability for death, evaluated by roc curve area analysis, was slightly higher for hongkong staging system at one, three and five years (p>0.05).
Conclusion: In patients undergoing tace, hongkong liver cancer staging system showed superior tendency in predicting prognosis and survival. further evaluation in a larger number of patients is necessary.
Disclosure of Interest: none Declared
P-128 InfLuenCe Of hePATITIS b VIruS DnA eLeVATIOn On reCurrenCe Of hePATOCeLLuLAr CArCInOMA AfTer SurGICAL reSeCTIOn AnD The PreVenTIVe rOLe Of AnTIVIrAL TherAPy
yang Jae yoo* 1, ji hoon kim1, sung hee kang1, young sun Lee1, tae suk kim1, sang jun suh2, young kul jung2, yeon seok seo3, hyung joon yim2, jong eun yeon1, kwan soo Byun1
1Department of Internal Medicine, korea university Medical college Guro hospital, 2Department of Internal Medicine, korea university Medical college ansan hospital, 3Department of Internal Medicine, korea university Medical college anam hospital, seoul, korea, republic of
Introduction: surgical resection is the treatment of choice for early stage hepatocellular carcinoma (hcc). Previous studies revealed that reactivation of hepatitis B virus is associated with the recurrence of hepatitis B virus (hBV) related hcc after surgical resection. We aimed to investigate the influence of hBV Dna elevation on hcc recurrence and the preventive role of antiviral therapy.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s7 0
Methods: one hundred eleven patients who had BcLc stage 0 or a and received surgical resection as primary therapy were enrolled. hBV Dna elevation was defined as reactivation (increase >1log10 Iu/ml or re-emergence of hBV Dna) in patients without preoperative antiviral therapy or virologic breakthrough in patients with preoperative antiviral therapy (n=62).
results: Mean age was 54.1±9.4 years and male consisted 76.6% (n=85). all patients belonged in child class a. BcLc 0 consisted 29.7% (n=33) and 30.6% (n=34) had hepatitis B envelope antigen positivity and 42.3% (n= 47) had hBV Dna level ≥ 2000 Iu/mL at the time of surgery. overall 1 year, 3 year, 5 year recurrence was 17.3%, 36.4%, 40%.In multivariate analysis for risk factors of recurrence, multiple tumor, hBV Dna elevation, aLt ≥ 30 Iu/L, were independently associated with hcc recurrence.In subgroup analysis, patients with preoperative antiviral therapy showed similar hcc recurrence rate with patients who start antiviral therapy after resection and significantly higher recurrence rate than patients with no antivirals during follow up.In multivariate analysis for risk factors of hBV Dna elevation, age < 50 years, no preoperative antiviral therapy, hBV Dna ≥ 2000 remained as risk factors.to rule out the antiviral effect, we investigated risk factors for hcc recurrence in each group with or without preoperative antiviral therapy.In patients with preoperative antiviral therapy, multiple tumor was the only risk factor for hcc recurrence.In patients without preoperative antiviral therapy, male sex and hBV Dna elevation were independent risk factors for hcc recurrence.risk factors for hBV Dna elevation were further analyzed in patients without preoperative antiviral therapy. age < 50 years and hBV Dna ≥ 2000 Iu/mL were independent risk factors for hBV Dna elevation.
Conclusion: hBV Dna elevation after resection increases the risk of hcc recurrence irrespective of preoperative antiviral therapy. however, hBV Dna elevation is an independent risk factor for recurrence in patients without preoperative antiviral therapy. therefore, perioperative antiviral therapy should be considered to prevent hBV Dna elevation and recurrence, especially in patients with age < 50 years and/or hBV Dna ≥ 2000 Iu/mL.
references: Influence of hepatitis B virus reactivation on the recurrence of hBV-related hepatocellular carcinoma after curative resection in patients with low viral loadLee jI, kim jk, chang hy et al. Impact of postoperative hepatitis B virus reactivation in hepatocellular carcinoma patients who formerly had naturally suppressed virus. j Gastroenterol hepatol 2014; 29(5): 1019–1027
Disclosure of Interest: none Declared
P-129 unDeTeCTeD ASyMPTOMATIC ALCOhOLIC CIrrhOSIS unDerLIeS The DIAGnOSIS Of hCC OuT Of SurVeILLAnCe PrOGrAMS In SPAIn. AnALySIS Of 750 CASeS In 74 CenTerS
Carlos rodriguez-Lope* 1, ana Matilla2, Maria teresa ferrer3, Maria rosa rota4, Beatriz Minguez5, javier fernandez-castroagudín6, Inmaculada ortiz7, sonia Pascual8, jose Luis Lledo9, adolfo Gallego10, juan arenas11, javier fuentes12, carlos aracil13, Montserrat forne14, carolina Muñoz15, fernando Pons16, Margarita sala17, Mercedes Iñarrairaegui18, Marta Martin-Llahi19, Victoria andreu20, carmen Garre21, Paloma rendon22, javier crespo1, Manuel rodríguez23, jordi Bruix24, Maria Varela23
1Department of Gastroenterology and hepatology, hospital universitario Marqués de Valdecilla. IDIVaL, santander, 2Department of Gastroenterology and hepatology, hospital General universitario Gregorio Marañon, Madrid, 3Department of Gastroenterology and hepatology, hospital Virgen del rocío, sevilla, 4Department of Gastroenterology and hepatology, hospital universitario de Bellvitge, hospitalet de Llobregat, 5Department of hepatology, hospital unversitario Vall d'hebron, Barcelona, 6Department of Gastroenterology and hepatology, hospital clinico universitario de santiago, santiago de compostela, 7Department of Gastroenterology and hepatology, hospital universitario Doctor Peset, Valencia, 8Department of Gastroenterology and hepatology, hospital General universitario de alicante, alicante, 9Department of Gastroenterology and hepatology, hospital universitario ramón y cajal, Madrid, 10Department of Gastroenterology and hepatology, hospital de la santa creu i sant Pau, Barcelona, 11Department of hepatology, hospital Donostia, Donostia, 12Department of hepatology, hospital universitario Miguel servet, zaragoza, 13Department of Gastroenterology and hepatology, hospital universitario arnau de Vilanova, Lleida, 14Department of Gastroenterology and hepatology, hospital universitario Mutua de terrassa, terrassa, 15Department of Gastroenterology and hepatology, hospital universitario 12 de octubre, 16Department of Gastroenterology and hepatology, hospital universitario Puerta de hierro, Madrid, 17Department of hepatology, hospital universitario Germans trias i Pujol, Badalona, 18Department of hepatology, clinica universitaria de navarra, Pamplona, 19Department of Gastroenterology, hospital Moises Broggi, sant joan Despi, 20Department of Gastroenterology and hepatology, hospital de Viladecans, Barcelona, 21Department of Gastroenterology and hepatology, hospital universitario Virgen dela arrixaca, Murcia, 22Department of Gastroenterology and hepatology, hospital Puerta del Mar, cadiz, 23Liver unit, hospital universitario central de asturias, oviedo, 24BcLc group. Liver unit, hospital clinic. IDIBaPs. university of Barcelona. cIBerehd., Barcelona, spain
Introduction: Between october 2008 and january 2009 we have performed a national survey of incident hepatocellular carcinoma (hcc) with 705 cases registered in 62 centers in spain [1].
the main conclusion of that study was that 53% of patients were diagnosed beyond surveillance programs with more advanced disease and less likely to receive radical therapies. We have performed a similar study with the aim of analyze the reasons behind the high proportion of hcc diagnosed without previous surveillance.
Methods: We invited 103 centers (email to previous participants plus notification via spanish association for the study of the Liver [aeeh] website). Investigators prospectively registered demographic, clinical and tumor characteristics, first treatment choice and eligibility for liver transplantation (oLt). a specific informed consent was obtained from all patients included in the study.
results: Between october 2014 and january 2015, 74 centers throughout spain registered 750 incident cases of primary liver cancer: hcc (n= 712), intrahepatic cholangiocarcinoma (Icc) (n=33), mixed hcc-Icc (n= 2), adenocarcinoma (n=1), carcinoma (n=1), neuroendocrine (n=1). the main characteristics of hcc patients were: men 81%; age 67 years (27 – 94); cirrhosis 87%; chronic liver disease 9% and healthy liver 4%. Main etiologies were alcohol 35%, hcV 30%, hcV + alcohol 15%, nafLD 6% (previously 2.4%) and hBV 4%; mean child-Pugh class score 6 (5-13); mean number of nodules 1 (range 1-20); diffuse distribution or uncountable nodules 5%; vascular invasion 18%; extrahepatic disease 8%. Most patients were ecoG Performance status 0 (58%) and staging according to BcLc system was as follows BcLc-0: 11%, BcLc-a: 43%, BcLc-B: 19%, BcLc-c: 16% and BcLc-D: 11%. Main treatments applied were percutaneous ablation (22.2%), tace (21.6%), resection (11%) and sorafenib (10.1%). ten percent (n=71) of patients were evaluated for oLt.
fifty-two percent (n=365) of the patients were diagnosed outside surveillance programs: 278 (77%) by chance or at the same time that the underlying liver disease; 63 (17%) were not adherent to surveillance and 21 (6%) had chronic liver disease but were not included into surveillance because diagnosis of end-stage of liver cirrhosis had not been clearly established. Patients diagnosed out of surveillance had more advanced BcLc stage (p<0.001), vascular invasion (28% vs 6%, p<0.001), extrahepatic disease (13% vs 3%, p<0.001), larger nodules (54 vs 29 mm; p < 0.001), received less radical therapies (35% vs 58%, p<0.001), and were less frequently evaluated for liver transplantation (8% vs 13%, p = 0.032). these patients were mainly male (p<0.001), with alcohol chronic liver disease (p<0.001) and active alcohol drinkers (p<0.001). no differences were detected according to ethnicity (p = 0.773), or between hospitals reporting above or below 15 cases (p = 0.254).
Conclusion: compared to the previous survey, the proportion of hcc detected out of surveillance program has not decreased. the main cause is the absence of prior diagnosis of liver disease. these patients are more frequently male with active alcohol use. Detection of chronic liver disease in asymptomatic population and improvement of the adherence to surveillance especially in patients with alcoholic liver disease are the main factors to progress in the early detection of hcc.
references: 1 - Varela M et al Med clin (Barc). 2010; 134(13): 569-76.
Disclosure of Interest: none Declared
P-130 SInGLe CenTer AnALySIS Of The reSuLTS AfTer reSeCTIOn/TrAnSPLAnTATIOn In PATIenTS WITh COMbIneD hePATOCeLLuLAr CArCInOMA AnD ChOLAnGIOCArCInOMA
josep Marti1, elisa sefora Pierobon1, Paola tarchi1, Isabel fiel2, Ganesh Gunasekaran* 1, sander florman1, Marcelo facciuto1, swan thung2, Myron schwartz1
1recanati/Miller transplant Institute, 2Department of Pathology, Icahn school of Medicine at Mount sinai, new york, united states
Introduction: combined hepatocellular carcinoma and cholangiocarcinoma (hcc-cc) is a rare subtype of primary liver carcinoma and its best treatment is still unknown. the aim of our study was to analyze the outcomes of patients with hcc-cc undergoing resection and liver transplantation (Lt).
Methods: retrospective results analysis of patients with pathologically proven hcc-cc treated with resection or Lt in our center from 1993 to 2014.
results: sixty-seven patients underwent resection for hcc-cc and 29 patients underwent Lt. the majority of the patients were men (77.1%) and median age was 56.8 years (16–82). Lt patients had higher bilirubin and Inr but lower platelets than resection patients. at pathological analysis, resection patients had fewer tumor nodules and more frequently unilateral than Lt patients but with similar size. overall survival after surgical treatment of hcc-cc was 42.6% at 5 years and overall disease-free survival was 56% at 2 years. there were no differences between resection and Lt groups in patient survival or recurrence. Patients with nodules larger than 5cm had similar recurrence but worse survival than those with smaller nodules but this survival difference was only significant for patients undergoing Lt when stratified by type of surgical treatment. there were no overall differences in recurrence or survival by histological subtypes but cholangiolocellular carcinoma had a trend for higher recurrence compared to the rest of progenitor cell hcc-cc.
Conclusion: Patients who undergo Lt for hcc-cc have poorer liver function and higher tumor burden than those undergoing resection but both groups show similar recurrence and survival. these results show that hcc-cc should not be a contraindication for Lt although resection should still be preferred whenever feasible because of the scarcity of available organs for Lt.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 7 1
Disclosure of Interest: none Declared
P-131 CLInICAL ChArACTerISTICS AnD PrOGnOSIS In nOn-b nOn-C hePATOCeLLuLAr CArCInOMA PATIenTS WITh MODeST ALCOhOL COnSuMPTIOn
Takahiro yamasaki* 1, 2, yohei urata2, Issei saeki2, shuji Iwai3, Masaaki kitahara Masaaki kitahara4, yoshiyuki sawai5, kazunari tanaka6, tomoko aoki7, 8, shouta Iwadou9, naoki fujita naoki fujita10, yasuhiro nakayama11, tatsuji Maeshiro12, taro takami2, Isao sakaida2
1Department of oncology and Laboratory Medicine, 2Department of Gastroenterology and hepatology, yamaguchi university Graduate school of Medicine, yamaguchi, 3Department of hepatology, osaka city university Graduate school of Medicine, osaka, 4Department of Gastroenterology, Graduate school of Medicine, kanazawa university, kanazawa, 5Department of Gastroenterology, Ikeda Municipal hospital, osaka, 6center for Gastroenterology, teine keijinkai hospital, sapporo, 7Division of hepatobiliary and Pancreatic Diseases Department of Internal Medicine, 8ultrasound Imaging center, hyogo college of Medicine, hyogo, 9Department of Internal Medicine, hiroshima city hiroshima citizens hospital, hiroshima, 10Department of Gastroenterology and hepatology, Mie university school of Medicine, Mie, 11first Department of Internal Medicine, faculty of Medicine, university of yamanashi, yamanashi, 12first Department of Internal Medicine, faculty of Medicine, university of the ryukyus, okinawa, japan
Introduction: the hepatocellular carcinoma (hcc) type categorized as negative for hepatitis B surface antigen and antibody to hepatitis c virus (nBnc-hcc) has become more common in japan. alcoholic hcc (aLD-hcc) accounts for the majority of nBnc-hcc cases. although alcohol is a potent carcinogen, there have been few reports on the influence of modest alcohol consumption in nBnc-hcc. this study aimed to investigate the clinical characteristics and prognosis of nBnc-hcc in patients with modest alcohol consumption.
Methods: from 2007 to 2010, 2,283 hcc patients were evaluated at 10 hospitals. We collected detailed etiology data of 588 nBnc-hcc patients and compared the clinical characteristics and prognosis between aLD-hcc and modest alcohol-hcc patients. We stratified hcc patients with alcohol consumption of more than 20 but less than 60 g/day to the modest alcohol-hcc group, whereas the aLD-hcc group included those with an alcohol intake of ≥60 g/day.
results: there were 69 hcc patients with modest alcohol consumption, accounting for 3% of all hcc patients evaluated. this patient group had significantly more women (10.1%) and higher prevalence of child-Pugh class a (89.9%), hypertension (55.1%), and advanced disease stage (stage IV, 27.5%), and were diagnosed with hcc at an older age (mean, 71.4 years) than the aLD-hcc group (266 patients). additionally, among the modest alcohol-hcc patients, diabetes was significantly more common in the anti-hBc negative subgroup (57.6%) than in the anti-hBc positive subgroup (27.8%). the 1-, 3-, 5-, and 7-year cumulative survival rates in the modest alcohol-hcc group were 78.6%, 71.3%, 42.0%, and 25.2%, respectively. on the other hand, the 1-, 3-, 5-, and 7-year cumulative survival rates in the aLD-hcc group were 83.1%, 61.2%, 47.2%, and 35.5%, respectively. no significant difference in survival was observed between the two patient groups regardless of significant differences in tumor staging. alcohol consumption and metabolic factors were not significant independent predictors of survival.
Conclusion: the clinical characteristics of modest alcohol-hcc included advanced staging, favorable liver reserve capacity, and older age at diagnosis. hcc development in patients with modest alcohol consumption might relate to metabolic factors. although about 30% of the evaluated hcc cases were in advanced stages, the prognosis of nBnc-hcc patients with modest alcohol consumption was relatively favorable.
Disclosure of Interest: none Declared
P-132 ASSOCIATIOn beTWeen hePATITIS b VIruS DnA LeVeL & AnTIVIrAL TherAPy On The reCurrenCe Of PATIenTS AfTer LIVer reSeCTIOn fOr hePATITIS b VIruS-reLATeD hePATOCeLLuLAr CArCInOMA
Tae yoo* 1, 1, kyung-suk suh2, kwang-Woong Lee2, nam-joon yi2
1surgery, hallym university Dongtan sacred heart hospital, hwaseong-si, 2surgery, seoul national university college of Medicine, seoul, korea, republic of
Introduction: hepatitis B virus (hBV) levels correlate with the development of hepatocellular carcinoma (hcc), but the role of viral load and treatment in hcc recurrence after tumor resection remains unclear. herein we aimed to investigate the significance of hBV Dna levels & antiviral agent for predicting recurrence in hcc patients who underwent curative liver resection.
Methods: from 2005 to 2010, 341 hBV-related hcc patients who underwent tumor resection in snuh were enrolled. hBV Dna levels (pre-, postop. period) & antiviral treatment were analyzed for association with hcc recurrence, together with other clinical variables.
results: of the 294 patients, patients(n=164) with low postop. hBV Dna (1x103 Iu) had better
outcome than those(n=130) with high load in recurrence (5yr-recurrence free survival(rfs)=43.2 vs. 22.2%, p<0.001). In terms of antiviral agents, untreatment group(n=136) had worse outcome than treatment group(n=158) in recurrence (5yr-rfs=28.3 vs 56.3%, p<0.001). In subgroup analysis, if the treatment group had high hBV viremia postoperatively, they had good rfs as group with low viremia (5yr-rfs=54.1 vs. 58.3%). But, even if untreated patients had low viremia, they had poor outcomes as untreatment group with high viremia (5-yr rfs=37.1 vs. 11.9%). Moreover, whether it is advanced stage(3) or not, low postop. hBV load showed the better recurrence outcome but, antiviral treatment did not present difference in advanced stage. finally, postop afP levels as well as well as postop hBV Dna antiviral therapy, tumor size, microvascular invasion were independent risk factors for rfs in multivariated analysis.
Conclusion: Low hBV Dna load and antiviral therapy may be important factors after the curative treatment of hBV-related hcc in terms of tumour recurrence. therefore, to maintain the low level of hBV viremia, antiviral therapy should be considered after curative treatment of hcc.
references: jaw-ching Wu et al. risk factor for early and late recurrence in hepatitis B-related hepatocellular carcinoma. journal of hepatology 51 (2009) 890-897
Disclosure of Interest: none Declared
P-133 PerI-TrAnSPLAnT ChAnGe In AfP LeVeL IS A uSefuL PreDICTOr Of hePATOCeLLuLAr CArCInOMA reCurrenCe fOLLOWInG LIVer TrAnSPLAnTATIOn
Tae yoo* 1, kwang-Woong Lee2, nam-joon yi2, kyung-suk suh2
1surgery, hallym university Dongtan sacred heart hospital, hwaseong-si, 2surgery, seoul national university college of Medicine, seoul, korea, republic of
Introduction: Pretransplant alpha-fetoprotein (afP) is a useful tumor marker predicting recurrence of hcc. Little is known, however, about the relationship between changes in afP concentration and prognosis. this study investigated the clinical significance of change in peri-transplant afP level as a predictor of hcc recurrence.
Methods: Data from 125 hcc patients with elevated pretransplant afP level who underwent Lt between february 2000 and December 2010 were retrospectively reviewed.
results: Patients with afP normalization within 1 month after Lt were classified into the rapid normalization group (n=97), with all other patients classified into the non-rapid normalization group (n=28). tumor recurrence was observed in 17 of the 25 patients (17.5%) with rapid normalization; of these, 11 had high and six had normal afP levels at recurrence. In contrast, tumor recurrence was observed in 24 of the 28 patients (85.7%) without rapid normalization, with all 24 having high afP levels at recurrence. Multivariate analysis showed that non-rapid normalization (hr=4.41, p<0.001), sex (hr=3.26, p=0.03), tumor size (hr=1.15, p=0.001), and microvascular invasion (hr=2.65, p=0.005) were independent risk factors for recurrence-free survival.
Image:
Conclusion: rapid normalization of post-Lt afP level at 1 month is a useful clinical marker for hcc recurrence. special strategies are needed for patients who do not show rapid normalization.
references: 1. Debruyne en, Delanghe jr. Diagnosing and monitoring hepatocellular carcinoma with alpha-fetoprotein: new aspects and applications. clinica chimica acta; international journal of clinical chemistry. 2008;395(1-2):19-26.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s7 2
2. trevisani f, D'Intino Pe, Morselli-Labate aM, Mazzella G, accogli e, caraceni P, et al. serum alpha-fetoprotein for diagnosis of hepatocellular carcinoma in patients with chronic liver disease: influence of hBsag and anti-hcV status. journal of hepatology. 2001;34(4):570-5.3. yao fy, ferrell L, Bass nM, Watson jj, Bacchetti P, Venook a, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. hepatology. 2001;33(6):1394-403.4. zou WL, zang yj, chen xG, shen zy. risk factors for fatal recurrence of hepatocellular carcinoma and their role in selecting candidates for liver transplantation. hepatobiliary & pancreatic diseases international : hBPD Int. 2008;7(2):145-51.5. Wang zx, song sh, teng f, Wang Gh, Guo Wy, shi xM, et al. a single-center retrospective analysis of liver transplantation on 255 patients with hepatocellular carcinoma. clinical transplantation. 2010;24(6):752-7.
Disclosure of Interest: none Declared
P-134 uTILIzATIOn rATe Of hePATOCeLLuLAr CArCInOMA (hCC) SurVeILLAnCe PrOGrAM AnD fACTOrS ASSOCIATeD WITh SurVeILLAnCe In A LArGe referrAL CenTer, ThAILAnD
Piyanat chattieng1, nopavut Geratikornsupuk1, jonggi choi2, sombat treeprasertsuk1, Piyawat komolmit1, roongruedee Chaiteerakij* 1, 2
1Medicine, chulalongkorn university, Bangkok, thailand, 2Gastroenterology and hepatology, Mayo clinic, rochester, united states
Introduction: several guidelines have recommended hcc surveillance program in patients with cirrhosis. although surveillance has been shown to be associated with early stage at diagnosis and an increased likelihood of receiving potentially curative treatment, the reported surveillance rates remain low in several countries, i.e. 20% in the us and europe and 41% in korea1. the rate of hcc surveillance has never been studied in thailand, where liver cancer is the most common cause of cancer death2. We therefore aimed to 1) determine the rate of hcc surveillance in cirrhotic patients diagnosed with hcc in a major referral center in Bangkok, thailand; 2) determine factors associated with surveillance; and 3) determine outcome of patients diagnosed with hcc through surveillance.
Methods: Patient and tumor characteristics, surveillance, treatment and survival of 340 consecutive patients with cirrhosis who was diagnosed with hcc between 2010 and 2013 were retrospectively reviewed. surveillance was defined as having repeated abdominal ultrasonography within 1 year prior to the hcc diagnosis. factors associated with surveillance were analyzed using the Logistic regression. survivals of patients with and without surveillance were estimated using the kaplan-Meier method and compared using the Log-rank test.
results: of the 340 patients, 79% were male with a mean age of 60 years. hepatitis B (49%), hepatitis c (22%), alcohol (12%) and non-alcoholic fatty liver disease (12%) were the most common etiologies of cirrhosis. sixty seven (20%) were diagnosed with hcc through surveillance. cirrhosis caused by chronic viral hepatitis B or c infection was the only factor associated with an increased chance of receiving surveillance (adjusted odds ratio 3.7, 95% cI 1.8-8.4, p=0.0003). age, gender, child-Pugh classification, the Model for end-stage Liver Disease (MeLD) score, and the year of hcc diagnosis were not associated with surveillance. the surveillance group had a higher proportion of patients diagnosed with the Barcelona-clinic Liver cancer (BcLc) stage a (76% vs. 33%, P<0.0001), and of patients eligible for potentially curative treatment (74% vs. 36%, P<0.0001), which in turn, had a longer median survival (37 vs. 11 weeks, P<0.0001). after accounting for the lead-time bias, the surveillance group had a better median survival if the assumed tumor volume doubling time was less than 90 days (P=0.047).
Conclusion: this study highlights the underutilization of hcc surveillance in thailand. even at a major referral center, the rate of hcc surveillance remains low at only 20%. Patients with viral hepatitis B or c-induced cirrhosis had a higher chance of being on surveillance. Patients undergoing surveillance had a significantly better survival than those not receiving surveillance. Given the potential survival benefit of surveillance, increasing the surveillance rate in patients at risk for hcc is needed. further study to better understand potential barriers of surveillance including physician and patient factors is warranted.
references: 1. http://www.index.go.kr/potal/main/eachDtlPageDetail.do?idx_cd=14402. http://bps.moph.go.th/sites/default/files/cancer_0.pdf
Disclosure of Interest: none Declared
P-135 InCIDenTAL hePATOCeLLuLAr CArCInOMA In LIVer TrAnSPLAnTATIOn: PreOPerATIVe fInDInGS AnD POSTOPerATIVe OuTCOMeS
Maarouf hoteit* 1, 2, Vandana khungar1, 2, kim olthoff2, 3, abraham shaked2, 3
1Gastroenterology and hepatology, 2Penn transplant Institute, 3Division of transplant surgery, university of Pennsylvania, Philadelphia, united states
Introduction: Patients with decompensated cirrhosis listed for liver transplantation (oLt) undergo protocol surveillance imaging for hepatocellular carcinoma (hcc) aiming to detect early stage hcc that would require increased priority for transplantation. Despite close surveillance, however, some patients have hcc detected incidentally at the time of explant pathological analysis. We aim to examine preoperative findings and related postoperative outcomes in patients with incidental hcc.
Methods: We reviewed our institutional oLt database for patients with hcc transplanted between january 1997 and December 2014. We included all patients who had evidence of hcc on explant pathology with no known diagnosis of hcc preoperatively.
results: a total of 2,072 liver transplants were performed during the study period, of whom 498 had a known hcc prior to oLt and 75 had incidental hcc (4.8%). Most patients with incidental hcc were men (84.0%) and had hcV (57.3%). the mean age at transplant was 56.7 ± 7.1 years. the median waiting time prior to transplant was 238 days (Iqr 57-787 days). the median follow up was 5.2 years (Iqr 2.5 – 8.7 years). the hcc recurrence rate was 10.7 % (8/75). the majority of incidental tumors (39/75, 52.0%) consisted of a single small lesion (<3cm) on explant. none of these patients had a recurrence of hcc after transplantation. the recurrence rate of larger incidental tumors was 8/36 (22.2%). focal indeterminate liver lesion(s) were noted on preoperative imaging in 5/39 (12.8%) of patients with single small incidental tumors, which was not statistically different from patients with larger tumors 7/36 (19.4%), P=0.51. Patients with larger incidental tumors had higher peak pre-transplant afP (14.1 [Iqr 7.0-24.9] vs 6.7 [Iqr 3.1 – 10.8], P=0.003).
Conclusion: While incidental tumors with high risk pathological features may be difficult to detect prior to transplantation even in retrospect, they tend to be associated with higher afP values which should be cause for vigilant evaluation in potential transplant recipients. In our experience, transplanting a patient with high risk incidental hcc was an uncommon event, representing 2.3% of the total transplants for indications other than hcc.
Disclosure of Interest: none Declared
P-136 GenOTyPe AnALySIS Of hePATOCeLLuLAr ADenOMA In JAPAn
Masahiko Sugitani* 1, asami Izu1, noriko kinukawa1, Masahiro ogawa2, shintaro yamazaki3, tadatoshi takayama3, hiroshi hano4, takashi yao5, naoya nakamura6, yukio Morishita7, hiroaki kanda8, koshi Matsumoto9, seisyu hayashi10, syun-ichi ariizumi11, Msakazu yamamoto11, Masayuki nakano12
1Pathology, 2Internal Medicine, 3Digestive surgery, nihon university school of Medicine, 4jikei Medical university, 5juntendo university, tokyo, 6tokai university, Isehara, 7tokyo Medical university, Ibaragi, 8japanese foundation for cancer research, tokyo, 9ebina General hospital, ebina, 10komagome hospital, 11tokyo Wemen's Medical university, tokyo, 12syonan fujisawa tokusyukai hospital, fujisawa, japan
Introduction: hepatocellular adenoma (hca) is low prevalent in japan rather than europe and usa and hca genotype in japanese patients is only a few reported. We analyzed hca genotype in several areas of japan.
Methods: resected liver specimens with nodular lesion were collected among japanese patients with under diagnosis of almost definitive or suspicious of hca from hospitals, totally 23, in kanto, tokai and kinki regions of japan. In order to confirm diagnosis as hca and to analyze hca genotypes, immunohistochemical examination was performed using autoimmunostaining instrument (Discovery, Ventana/roche). antibodies used were as follows: liver fatty acid binding protein (abcam), glutamine synthetase (Millipore), Beta-catenin (Dako), serum amyloid a (abcam), crP (abcam).
results: forty-one cases were found to be as for hca. number of cases of male/female was 21/20. Distribution of age decades of 2nd, 3rd, 4th, 5th, 6th, 7th and 8th were 3, 8, 6, 6, 6, 5 and 7 (from 15 to 79, mean 47.1 years old). six cases were with glucose storage disease (type Ia), and 4 cases had past history of administration of pill, steroids or related drugs. three and one cases were positive for hBsag and anti-hcV, respectively. five and six cases were social drinkers and moderate drinkers of alcohol, respectively. five cases were pointed out as diabetes mellitus and/or hyperlipidemia. two cases were obesity. thirteen cases had multiple nodular lesions. size of nodule was distributed from 1 to 14 cm in diameter. four cases were cirrhotic in non-tumor area. In hca genotypes, hnf1-alpha inactivated hca, beta-catenin activated hca, inflammatory hca and unclassified hca were 17 (41.5%), 2 (4.9%), 19 (46.3%) and 3 (7.3%) cases, respectively. one case coexisted with hca and hepatocellular carcinoma (hcc) at the operation, and in one case, hcc occurred after 23 years later of hca detection. hca genotype of the former case was beta-catenin activated hca, and that of the latter was unclassified hca. Background of the former was diabetes mellitus, and that of the latter was glucose storage disease (type Ia). Both were without cirrhosis.
Conclusion: Prevalence of 4 genotypes of hca was considered to be similar tendency between that of japan and Western countries.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 7 3
P-137 CLInICAL SIGnIfICAnCe Of COMPLeTe AnD COMPACT LIPIODOL uPTAKe Of The LeSIOn ACCOMPAnIeD WITh reDuCTIOn Of SeruM VASCuLAr enDOTheLIAL GrOWTh fACTOr LeVeLS AT 1 MOnTh AfTer TrAnSCATheTer ArTerIAL CheMOeMbOLIzATIOn fOr hePATOCeLLuLAr CArCInOMA
Soo hyung ryu* 1, soo yeon jo1, Won jae yoon1, jin nam kim1, jeong seop Moon1
1Department of Internal Medicine, seoul Paik hospital, Inje university college of Medicine, seoul, korea, republic of
Introduction: the complete and compact lipiodol uptake of the lesion after transcatheter arterial chemoembolizaion (tace) for hepatocellular carcinoma (hcc) has been considered as an indicator of a successful procedure. Vascular endothelial growth factor (VeGf) has known to be up-regulated in hcc. We intended to evaluate the usefulness of the compact lipiodol uptake at 1 month after tace in predicting recurrence and its association with change of serum VeGf levels.
Methods: a total of 60 hcc patients who underwent tace were subjected (male:female=47:13; age: 64 ± 8 years; 39 hBV, 21 hcV, 40 child-Pugh class a, 20 B, 3 BcLc stage 0, 25 a, 17 B, 15 c). the size of hcc < 3cm and ≥ 3 cm was noted in 35 and 25 cases, respectively. no cases showed extra-hepatic metastasis at tace. Paired blood samples before and 1 month after tace were obtained from all patients to analyze the changes of serum VeGf levels using an enzyme-linked immunosorbent assay (eLIsa). abdominal ct was done at 1 month after tace and every 3 months thereafter.
results: the complete and compact lipiodol uptake was frequently noted in the smaller tumor size less than 3 cm (P=0.004) and lower Barcelona clinic Liver cancer (BcLc) stage (P=0.000) and lower child-Pugh class (P=0.085). In addition, the compact lipiodol uptake was associated with the reduction of serum VeGf level after tace. In 25 compact uptake group, 11 have a decrease of VeGf level, 5 of 25 with incomplete uptake revealed the reduction (P=0.064). the reduction of serum alpha fetoprotein (afP) was also frequently noted in compact uptake group (P=0.006). of 48 cases which have a 3 month follow-up ct after tace, 7 of 28 with compact lipiodol uptake, 4 of 10 with incomplete uptake without marginal viable tumor, and all of 4 with incomplete uptake and suspected marginal viable hcc after 1 month showed recurrence of hcc at 3 months after tace (P=0.013).
Conclusion: the complete and compact lipiodol uptake of the hcc lesion was associated with a decrease of VeGf level at 1 month compared with that of pre-tace and can predict recurrence of hcc at 3 month follow-up ct after tace.
Disclosure of Interest: none Declared
P-138 ePIDeMIOLOGy, DIAGnOSIS, TreATMenT AnD OuTCOMe Of PATIenTS WITh LIVer CAnCer AT A GerMAn ThIrD LeVeL MeDICAL CenTer beTWeen 2008 AnD 2012
Tobias Werner* 1, Britt hinrichs1, adib Moharram-zadeh1, jennifer sauer1, kristin schmidt1, kornelius schulze1, harald Ittrich2, Gerhard adam2, Martina sterneck1, eike-Gert achilles3, Björn nashan3, ansgar W. Lohse1, henning Wege1
1I. Medical Departement, 2Department of Diagnostic and Interventional radiology, 3Department of hepatobiliary and transplant surgery, university Medical center hamburg eppendorf, hamburg, Germany
Introduction: hcc is one of the most common malignant diseases worldwide with rising incidence rates in the Western world. here we describe our real-life experience regarding the diagnosis, treatment, and outcome for patients with hcc at a tertiary German liver center.
Methods: We screened our patient database and extracted all patients with IcD code c22.0 treated at the university Medical center hamburg-eppendorf between 2008 and 2012. We retrospectively collected epidemiologic, diagnostic, treatment-related and outcome data from the electronic patient charts. outcome analysis was only performed for patients with the initial diagnosis of hcc during the 5-year study period. to increase follow-up data, we also contacted general practitioners to obtain current survival information.
results: Within the study period (60 months), we identified 607 patients treated with hcc at our tertiary liver center (male/female 494/113, median age 67 years, range 23-93 years). Liver cirrhosis was present in 82.5%. etiology of the underlying liver disease was (multiple selections possible) alcohol in 44.8%, hcV in 25.4%, hBV in 16.0%, nash in 6.9%, and other in 18.9% (not known in 25.4%). hcc was initially suspected in 34.6% because of symptoms, in 21.8% during surveillance, and in 16.0% as an incidental finding (not known in 27.7%). the diagnosis was confirmed through ct/MrI-criteria in 48.1% and via histology in 47.3% (not known in 4.6%). staging according to BcLc at initial diagnosis was early stage (a) in 30.0%, intermediate stage (B) in 39.5%, advanced stage (c) in 25.0%, and end stage (D) in 5.1%. outcome analysis was performed for 504 patients with initial diagnosis in the 5-year study period. follow-up data was accessible for 398 patients.
Median (mean) survival as extracted for the initial tumor stage was 53.0 (39.6) months for BcLc a, 18.5 (26.0) months for BcLc B, 5.0 (9.2) months for BcLc c, and 1.0 (6.1) months for BcLc D. additionally, we evaluated the outcome based on whether the first treatment was as recommended in the current easL-eortc practice guideline (BcLa a: resection, ablation, transplantation; BcLc B: tace; BcLc c: sorafenib; BcLc D: Bsc). the median (mean) survival for BcLc B patients with initial therapy according to easL-eortc (63%) was 16.7 (24.5) months versus 27.1 (28.7) months for patients receiving an alternative therapy. the median (mean) survival for BcLc c patients with initial therapy according to easL-eortc (32%) was 5.9 (9.0) months versus 3.8 (9.0) months for patients receiving an alternative therapy.
Conclusion: our patient cohort represents the real-life setting in a tertiary liver center in Germany. With less than 25%, the rate of patients diagnosed during surveillance was unexpectedly low, however comparable to current data from the usa. outcome analysis based on the initial therapy demonstrated a better survival for patients in BcLc B not treated with tace. this finding is explained by the application of resection and/or transplantation in this group. furthermore, the rather limited survival in BcLc c patients is associated to the high number of patients not suitable for systemic therapy (almost 70%), mostly due to insufficient liver function parameters.
Disclosure of Interest: none Declared
P-139 PreDICTOrS Of SurVIVAL AnD ADherenCe TO PrACTICe GuIDeLIneS In A SInGLe CenTer hCC COhOrT – A 12 yeAr exPerIenCe
Peeraphatdit B. thoetchai1, eric Dieperink2, astrid knott2, Paul thuras2, Christine Pocha* 3
1Medicine, university of Minnesota, 2Psychiatry, Vha, uMn, Minneapolis, united states, 3hepatology, university of Berne, Berne, switzerland
Introduction: factors predicting survival of hcc patients are still being investigated. stage based treatment should lead to optimal outcome however real world data have shown that adherence to guidelines is low especially in patients with intermediate tumors. easL guidelines (2001) distinguished between early and intermediate-advanced hcc. In 2005, aasLD guidelines incorporated the BcLc algorithm.
Methods: a retrospective chart review of patients diagnosed with hcc (IcD-9: 155.0) between 2000 and 2011 was performed. Demographic, patient-, tumor-, and treatment-related factors were correlated with survival. chi-square and logistic regression were used to determine factors associated with mortality. kaplan-Meier curves were constructed to estimate survival.
results: of the 238 patients (99% male, mean age 63 years), 82% were caucasian and 52% had chronic hepatitis c. cirrhosis was evident in 195 (83%), with decompensation in 78 (33%) patients. all-cause mortality was 84% with mean follow-up of 17 mos. co-morbidities were common: alcohol abuse (54%), hypertension (47%), diabetes (36%), depression (29%), cardiac disease (27%), and substance use disorders (22%). hypertension (p<0.038) and alcoholic liver disease (p<0.045) were associated with non-survivor status, whereas cirrhosis, ctP score, MeLD score and number of lesions were not. afP > 400ng/mL did not predict mortality. More than 50% of patients presented with advanced hcc (BcLc stage c [119, 50%] or D [49, 21%]). as expected, more advanced BcLc stage was associated with poor survival (p<0.001). of the 120 (70%) of all patients receiving some treatment, half received first line treatment with curative intent. receiving any kind of treatment was associated with improved survival (p<0.001) with no difference in survival related to receiving curative, palliative or both curative and palliative treatment. the proportion of patients not receiving any treatment remained stable over time. from 11/2005-2011, only 33% (48/144) patients received recommended stage based hcc treatment mainly affecting stage 0-B. for BcLc stage D supportive care is recommend; however 13/49 patients received curative (6) or palliative therapy (7), respectively. Despite only moderate guideline adherence survival was significantly better from 2006 on; median 16 vs. 7 mos (p=0.006) however did not differ between patients receiving BcLc recommended first line treatment or not.
Conclusion: all-cause mortality for hcc remains high. optimizing co-morbid conditions, i.e., hypertension and alcohol abuse, may improve outcomes. the predictive value of afP is still uncertain. our results confirm that adherence to hcc management guidelines is low affecting largely BcLc stage B patients due to the variability and heterogeneity in tumor burden and ctP scores among these patients. In contrary, non-adherence seen in patients with early stage hcc is something new. stage was not the only driver of treatment decisions and hence the prognosis and treatment allocation of hcc depends on more than just BcLc stage demanding further investigation.
Disclosure of Interest: none Declared

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s7 4
P-140 SArCOPenIA IS ASSOCIATeD WITh An InCreASeD MOrTALITy In PATIenTS reCeIVInG reGIOnAL TherAPy fOr hePATOCeLLuLAr CArCInOMA AS A brIDGe TO TrAnSPLAnTATIOn
Jean-Sébastien Pelletier* 1, Michelle zaldana2, Didier chalhoub3, Dirk van der Windt2, David t. fetzer4, andrey sinelnikov5, Michael a. Dunn6, alessandro furlan5, allan tsung2
1surgery, McGill university, Montréal, canada, 2surgery, 3epidemiology, university of Pittsburgh Medical center, Pittsburgh, 4radiology, university of texas southwestern Medical centre, Dallas, 5radiology, 6Gastroenterology, university of Pittsburgh Medical center, Pittsburgh, united states
Introduction: sarcopenia, low muscle mass, has been implicated as an important prognostic factor for both malignant1,2 as well as non-malignant conditions.3-5 It is commonly found in patients with cancer and it is the most frequent complication in patients with cirrhosis.6 therefore, patients treated for hepatocellular carcinoma (hcc) are at high risk to develop this condition. the aim of this retrospective review was to assess if sarcopenia negatively impact prognosis in patients receiving regional liver therapy for hcc as a bridge to liver transplantation (oLt).
Methods: from january 1st 2006 to December 31st 2010, patients with hcc undergoing initial regional liver therapy as a bridge to transplantation were studied. Included patients qualified as transplantation candidates by Milan criteria. Body composition was measured on a single axial pre-treatment ct image at the L3 level. clinical records were reviewed for the number of treatments ultimately received, the response to treatment based on resIst criteria, time to disease progression, time to receipt of liver transplantation, and overall survival.
results: a total of 59 patients were included. sarcopenic patients were more likely to be male, have a history of alcohol abuse and encephalopathy and were less likely to suffer from dyslipidemia. there was not a significant difference in the number of treatments received, response to treatment, time to disease progression or time to receipt of liver transplant. on multivariate analysis, sarcopenic patients had a significantly higher mortality (hr=2.80).
Conclusion: In spite of similar treatment characteristics, sarcopenic patients undergoing regional hepatic therapy for hcc have a significantly higher mortality as compared to non-sarcopenic patients. further research is needed on the feasibility and the benefit of the treatment of sarcopenia for this patient population.
references: 1. Prado cMM, Lieffers jr, Mccargar Lj, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 2008;9(7):629–635. doi:10.1016/s1470-2045(08)70153-0.2. Prado cMM, Baracos Ve, Mccargar Lj, et al. Body composition as an independent determinant of 5-fluorouracil-based chemotherapy toxicity. Clin Cancer Res. 2007;13(11):3264–3268. doi:10.1158/1078-0432.ccr-06-3067.3. cosquéric G, sebag a, Ducolombier c, thomas c, Piette f, Weill-engerer s. sarcopenia is predictive of nosocomial infection in care of the elderly. Br J Nutr. 2006;96(5):895–901.4. Park sW, Goodpaster Bh, strotmeyer es, et al. accelerated Loss of skeletal Muscle strength in older adults With type 2 Diabetes: the health, aging, and Body composition study. Diabetes Care. 2007;30(6):1507–1512. doi:10.2337/dc06-2537.5. Montano-Loza aj, junco jM, Prado cMM, et al. Muscle Wasting Is associated With Mortality in Patients With cirrhosis. Clin Gastroenterol Hepatol. 2012;10(2):166–173. doi:10.1016/j.cgh.2011.08.028.6. tsien c, shah sn, Mccullough aj, Dasarathy s. reversal of sarcopenia predicts survival after a transjugular intrahepatic portosystemic stent. Eur J Gastroenterol Hepatol. 2013;25(1):85–93. doi:10.1097/MeG.0b013e328359a759.
Disclosure of Interest: none Declared
P-141 ASPeCTS Of ADVAnCeD STAGe hCC AnD PrIOrITIeS TO TreAT In 796 bCLC-C eGyPTIAn PATIenTS
Amr el fouly* 1, ahmed el Dorry2, Mohamed salah3, neveen el fouly4, Mahmoud el Meteini5, Mohamed k. shaker3 and hepatoma Group ain shams university
1radioisotpe Department, eaea, 2Intervention radiology, 3tropical Medicine, ain shams university, 4health radiation research, eaea, 5Liver tranplant surgery, ain shams university, cairo, egypt
Introduction: hepatitis c virus (hcV) is the main cause of liver cirrhosis in 12-15% of egyptian population. a statistical model predicts to reach the peak of hcc related mortality by year 2040. hcc ranked the 2nd common malignancy in males. BcLc staging is the standard validated approach used worldwide for treatment of hcc. sorafenib is the only standard line of care for advanced stages BcLc stage "c". But there is shortage of medical insurance that cover the medical expenses and treatments for all patients over the country. the aim was to focus on different aspects of advanced hcc when different staging integrated with BcLc approach in order to rearrange the indications and priorities to compensate the demands.
Methods: During the past three years 2063 new hcc patients had been presented in hcc-
clinic in ain shams university hospital. advanced hccs were observed in 796(40%) at time of diagnosis. they were classified by different criteria such as: Performance status (Pst), child-Pugh classification, and tnM-classification ajcc 6th edition. also further analysis of serum afP, tumor size, uni- or bi-lobar hcc and extrahepatic Disease (ehD) were evaluated.
results: hcV was the major cause of liver cirrhosis in 93% of advanced hcc, while hBsag was positive in 16%. Males had 6 folds higher than females; hcc was more relevant in rural areas. Mean age of 59.8 yrs (+8.3), mean hcc size in PVt patients of 7.5cm(+3), and median serum afP in PVt was 467ng/dl. Good Pst-0 was associated in 199(25%); child a liver cirrhosis in 362(45%); Milan's criteria was fulfilled in 118(15%); unilobar hcc in 548(69%) and vascular invasion excited in 454(57%). In further subgroup analysis: single hcc with PVt was associated in 74(9%); Bilobar hcc with PVt in 308(40%); hcc with lymph-node(Ln) metastasis in 32(4%); PVt with Ln-metastasis in 43(6%); and distant-ehs in 57(7%). the egyptian ministry of health provided sorafenib free of charge for advanced hccs with good Pst (0-1); child a, serum albumin >3mg/dl, serum bilirubin <3mg/dl and platelets >100,000/mm3. In respect to this, the total number of the indicated patients for sorafenib had been reduced to 262/796(33%) in our center.
Conclusion: for socio-economic reasons, treatment of advanced stage hcc with sorafenib is still challenging in egypt. unfortunately this is due to high number of advanced hccs at time presentation, and shortage of uniform standard health insurance. thus, integrative analysis between different hcc staging criteria could help for better patients selection and provide the priority for patients to treat. on the other hand, strong hcc screening program is essential to provide early hcc diagnosis.
Disclosure of Interest: none Declared
P-142 ChArACTerIzATIOn Of hePATOCeLLuLAr CArCInOMA In eGyPT: rISK fACTOrS, PreSenTATIOn AnD PrOGnOSIS
Alaa Awad Taha* 1, ahmad el-ray1, Maged el-Ghannam1, ahmad helmy2, emad esmat2, nevin yilmaz3
1hepatogastroenterology, 2General surgery, theodor Bilharz research Institute, cairo, egypt, 3hepatogastroenterology, Mugla university, Mugla, turkey
Introduction: hepatocellular carcinoma (hcc) is a major malignancy in egypt with a significantly rising incidence over the last two decades. Identification of risk factors, different patterns of clinical presentation and prognostic factors is of great importance in disease control strategy building.
Methods: Demographic, clinical, laboratory and imaging data of 2387 patients with hcc attending outpatient clinic during the period from january 2005 to December 2013 were statistically analyzed together with data of their follow up schedule.
results: Mean age at presentation was 56.2 y, male to female ratio was 5.3 : 1 and 75.32% of patients (1798/2387) were living in rural areas. of those patients from urban areas, 65% (383/589) were living in areas with poor health services and low level of sanitary supplies. hcV was the recognized etiologic agent in 70.1% of patients (1673), hBV in 9% (215) and dual viral infection in 20.9% (499). Liver cirrhosis could be detected at presentation in 98.7% of patients (2356). history of schistosomiasis was detected in 61.96% of patients (14797) and 57.4% of patients (1371) were cigarette smokers. of the whole number of patients, 645 (27%) were diagnosed incidentally during investigations for other conditions, 430 (18%) detected on regular surveillance program for patients with chronic hepatitis and 1312 (55%) were symptomatizing. the main presenting symptoms were; abdominal pain (42%), ascites (28.7%), upper gastrointestinal bleeding (22.9%), fatigue (3.4%) and hepatic encephalopathy (3%). Levels of serum alfa fetoprotein (afP) were above 300 ng/ml in 811 patients (33.98%), while triphasic ct study of abdomen was diagnostic in 2192 patients (91.8%). MrI was required in only 7% of patients while needle biopsy was performed only in 150 patients (6.3%). at presentation 66% of patients were at late stages not eligible for specific treatment. 20.2% were candidates for transarterial chemoembolization (tace) and only 13.8% were candidates for curative therapy, either resection (1%), radiofrequency ablation (rfa) (9%) and percutaneous ethanol injection (PeI) (3.8%). surgery related mortality was present in 4% of patients underwent resection while no procedure related mortality was detected in patients underwent rfa, PeI or tace. recurrence within one year was detected in 20.8% of patients following resection, 28.8% following rfa, and 32.97% following PeI. three year survival was 66.67% after resection, 72.55% after rfa, 71.43% after PeI and 30.29% after tace. Presence of ascites and/or portal vein tumor thrombosis at presentation were recognized as independent factors associated with poor survival in patients not eligible for specific treatment.
Conclusion: hcV is the leading cause of hcc in egypt. other risk factors include male gender, living in rural areas, liver cirrhosis, hBV infection, history of schistosomiasis and cigarette smoking. triphasic ct is still the main diagnostic tool, while serum level of afP has relatively low sensitivity in diagnosis of hcc. role of biopsy is limited to minor sector of patients. Most of the patients in egypt present at late stages and are not candidate for specific therapy. ascites and/or portal vein tumor thrombosis are the major factors associated with poor survival.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 7 5
P-143 AnTI-hbe POSITIVITy IS PrOTeCTIVe fOr hCC DeVeLOPMenT In nAïVe hePATITIS b VIrAL CIrrhOTIC PATIenTS TreATeD WITh LOnG-TerM enTeCAVIr MOnOTherAPy
eun Sun Jang* 1, jong ho Lee1, seong Min chung1, junhyeon cho1, jin-Wook kim1, sook-hyang jeong1
1Internal Medicine, seoul national university Bundang hospital, seongnam, korea, republic of
Introduction: hepatitis B virus (hBV) Dna suppression by antiviral agent can reduce fibrosis progression or cancer developement in patients with chronic hBV infection. although hBeag serostatus is a strong risk factor for hepatocellular carcinoma (hcc), it is not yet known clearly whether anti-hBe status is independently associated with hcc in hBV-related cirrhotic patients under long-term etV treatment.
Methods: We performed a retrospective analysis of data from 303 naïve hBV-related cirrhosis patients who were treated with 0.5 mg etV monotherapy for at least 1 year between March 2007 and august 2013 in seoul national university Bundang hospital (seongnam, republic of korea). subjects were categorized into 4 group according to hBeag and anti-hBe status: group a (hBeag positive, anti-hBe negative), B (hBeag positive, anti-hBe positive), c (hBeag negative, anti-hBe negative), D (hBeag negative, anti-hBe positive).
results: Mean age of enrolled patients was 50.3 (sD 9.9) years old and 193 (63.7%) were males. the number of subjects in the subgroup categorized by hBeag/anti-hBe status were 113 (37.9%, group a), 17 (5.7%, group B), 23 (7.7%, group c), and 145 (48.7%, group D), respectively. During the follow-up period of 37.1 (sD 16.7) months, 2 patients (0.7%) died, 2 (0.7%) received a liver transplant, and 25 (8.3%) developed hcc. cumulative hcc incidences in group a, B, c, and D were 3.5%, 0%, 10%, and 1.7% at 3-year, 4.7%, 0%, 14.8%, and 2.5% at 5-year, respectively (p=0.029). the multivariate analysis showed that anti-hBe positivity (hr 0.133, 95% cI 0.034-0.524; p= 0.015) and achievement of undetectable hBV Dna level (hr 0.95, 95% cI 0.014-0.635; p=0.015) were independent protective factors for developing hcc after adjustment for age and gender in hBeag negative cirrhotic patients receiving long-term etV treatment.
Conclusion: surveillance for hcc development should be performed strictly in naïve hepatitis B related cirrhotic patients who show incomplete virologic response and those without anti-hBe.
Disclosure of Interest: none Declared
P-144 effICACy Of SOrAfenIb fOr OLIGOMeTASTATIC hePATOCeLLuLAr CArCInOMA
Kiruthikah Thillai* 1, 2, Dimitris ziogas1, 2, ruhe chowdhury1, 2, Dionysis Papadatos-Pastos1, thubeena Manickavadagar1, abid suddle1, nigel heaton1, john o'Grady1, Paul ross1, 2, Debashis sarker1, 2
1Institute of Liver studies, king's college hospital, 2Medical oncology, Guy's and st thomas' nhs trust, London, united kingdom
Introduction: hepatocellular carcinoma (hcc) is the second leading cause of cancer related mortality worldwide. standard treatment for advanced disease is sorafenib, which is associated with modest survival benefits. We hypothesized that patients with oligometastatic disease treated with sorafenib have improved outcomes over those with extensive metastases
Methods: a retrospective analysis of all patients with advanced hcc treated with sorafenib at a large hcc centre. 190 patients were identified (177 patients with sorafenib alone, 13 patients treated with combined sorafenib and erlotinib/placebo as part of the search trial). Disease distribution was defined as intra-hepatic, oligometastatic (3 ≤extra-hepatic metastases) and extensive (> 3 metastases) at the time of starting sorafenib. overall survival (os), progression free survival (Pfs) and toxicities were recorded.
results: the median age for all patients was 66 years (26-87), 157 male and 33 female. underlying liver disease included hepatitis B (n=39, 20.4%,) hepatitis c (n=38, 19.9%), alcoholic liver disease (n=38, 19.9%), non-alcoholic fatty liver disease (n=27, 14.1%), unknown aetiology (n=42, 21.9%) and other (n=7, 3.6%). 157 patients had child-Pugh a status, 33 had child-Pugh B. 113 patients had intra-hepatic disease, 45 = extensive disease and 32=oligometastatic disease. Median os for all patients treated with sorafenib was 7.6months(m) and Pfs was 4.3m. for patients with oligometastatic disease, os was significantly longer than the extensive group (10.4m vs. 6.3m p=0.034) as was Pfs (5.9m vs. 2.8m p=0.028). the aLBI prognostic model was calculated for all patients with oligometastatic disease (aLBI 1 [n=18], aLBI 2 [n=12], aLBI 3[n=2]). os in the aLBI 1 group was significantly longer compared with aLBI 2 (11.97m vs. 2.9m [p=0.042]).toxicities were comparable within the oligometastatic and extensive cohorts.
Conclusion: this study suggests that patients with oligometastatic disease have improved survival outcomes compared with patients with extensive disease. Within the oligometastatic group, patients with aLBI score 1 lived longer compared with aLBI score 2, providing validation of this prognostic model in this group of patients. further prospective research is needed to confirm these findings.
Disclosure of Interest: none Declared
P-145 CLInICAL feATureS AnD TreATMenT MODALITIeS Of LOnG-TerM SurVIVOrS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA: A SInGLe InSTITuTIOn COhOrT STuDy
kyung hee kim 1, Joong-Won Park*1, 2, bo hyun Kim*1, chang-Min kim1, Byung ho nam2
1center for Liver cancer, 2Department of cancer control and Policy, Graduate school of cancer science and Policy, national cancer center, Goyangsi, korea, Democratic People's republic of
Introduction: the prognosis of patients with advanced hepatocellular carcinoma (hcc) is poor despite systemic or local treatments. We analyzed the characteristics of long-term survivors (Lts) with advanced hcc to determine the prognostic and treatment factors responsible for long-term survival.
Methods: Between january 2001 and December 2009, 582 patients were diagnosed as having modified International union against cancer (muIcc) stage IV hcc, with child-Pugh (cP) class a liver function at the national cancer center, korea. among them, we compared clinical features and treatment modalities of the Lts group (survival > 2 years; n = 60) with those of the control (c) group (survival < 1 year; n = 438).
results: for 498 patients, the median overall survival (os) was 4.6 months (95% cI: 4.2-5.0): 37.3 months (95% cI: 33.1-41.5) in the Lts group and 4.1 months (95% cI: 3.7-4.4) in the c group. compared to the c group, Lts group patients were significantly more likely to be older and to have non-hepatitis B virus etiology, lower tumor numbers, smaller tumor size, nodular-type tumors, absence of portal vein invasion, and better liver function. Ill-defined tumors, portal vein invasion, alpha-fetoprotein (afP) ≥ 400 ng/ml, and cP a6 proved to be independent prognostic variables. transarterial chemoembolization (tace) was most commonly performed in 58.4% of all patients of both groups, followed by systemic chemotherapy (20.7%), supportive care (14.9%), radiotherapy (3.8%), and surgical resection (2.0%). In the Lts group, none received supportive care, and treatment with resection, tace, and radiotherapy showed favorable outcomes in univariate analysis. however, multivariate analysis failed to show any significant association between treatment modalities and long-term survival.
Image:
Conclusion: tumor type, portal vein invasion, afP level, and cP score were significantly associated with long-term survival of patients with advanced hcc. treatment modalities did not statistically affect survival outcome in this cohort.
Disclosure of Interest: none Declared
P-146 TreATMenT Of hePATOCeLLuLAr CArCInOMA In The eLDerLy
Mazen el atrache1, khalid George1, Mona hassan1, rami abboud1, amir Prushani1, syed-Mohammed jafri1, reena Salgia* 1
1henry ford hospital, Detroit, united states
Introduction: the incidene of hepatocellular carcinoma (hcc) in the elderly (>70 years of age) has been on the rise. In most instances, this population does not qualify for liver transplantation. the aim of this study is to evaluate the outcomes of treatment modalities in elderly patients diagnosed with hcc.
Methods: a retrospective chart review was performed for patients diagnosed with hcc over the age of 70, from 2006 to 2013, at a large tertiary care center. Baseline characteristics including age, gender, race and etiology of hcc were obtained. MeLD score, child Pugh class, BcLc staging, tumor size and number and the presence of vascular invasion were noted. Pertinent laboratory data was obtained. treatment complications, hcc recurrence, and mortality were noted. Patients were classified according to treatment modality. Differences were tested using kruskal-Wallis test and fisher’s exact test. cox regression analysis was performed. survival analysis models were tested using kaplan-Meier survival estimates.
results: 165 patients were included in this study. Mean age was 75.3 ± 5.1 years. the etiology of hcc was cryptogenic cirrhosis in 40%,hepatitis c in 30%, alcoholic cirrhosis in 20%, nash

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s7 6
cirrhosis in 6% and hepatitis B in 3% of patients. the average MeLD at the time of hcc diagnosis was 10.6 ± 4.0. 43% of patients were within Milan and 46% were within ucsf criteria at the time of initial diagnosis. Macro-vascular invasion was present in 30% of patients. Initial treatment for hcc included observation (12%), radiofrequency ablation (32%), trans-arterial chemoembolization (38%), surgical resection (9%), and sorafenib alone (10%). the rfa and tace patients had significantly smaller tumor size (p<0.0001), and more patients were child Pugh class a liver function and within Milan and ucsf criteria (p<0.0001) at the time of diagnosis. Patients in these two groups less frequently were found to have vascular invasion (p<0.0001). Patients who received rfa or sorafenib had a higher post-treatment creatinine (p=0.011). Patients who received rfa and tace had lower post-treatment platelet count (p=0.004), lower total bilirubin after 4 weeks (p=0.02 and p=0.04, respectively). the rates of anemia, infections and length of post-procedure hospital stay were significantly higher in the resection group (p=0.02). recurrence of hcc was significantly lower in the resection group (p=0.02). Patients who underwent surgical resection had a lower rate of hcc recurrence (p=0.02) and a longer disease-free survival period (p<0.0001).
Conclusion: rfa and tace are the most common initial hcc treatments for elderly patients diagnosed with hcc. surgical resection has a lower rate of hcc recurrence compared to rfa or tace, but has more immediate post-procedure complications in this population. there is no difference in mortatily among these subgroups. treatment of the elderly should be individualized and focused on quality of life.
Disclosure of Interest: none Declared
P-147 hePATeCTOMy fOr hePATOCeLLuLAr CArCInOMA LArGer ThAn 10 CM:
PreOPerATIVe rISK STrATIfICATIOn TO PreVenT fuTILe SurGery
Azoulay Daniel* 1, compagnon Philippe1, salloum chady1, Laurent alexis1, Lim chetana1
1hPB surgery and liver transplantation, hopital henri Mondor, aPhP, creteil, france
Introduction: Patient selection is important to achieve good outcomes and to obviate futile surgery in patients with huge (≥10 cm) hepatocellular carcinoma (hcc). the aim of this study was to identify independent predictors of futile outcomes, defined as death within 3 months from surgery or within 1 year from early recurrence following hepatectomy for huge hcc.
Methods: the outcomes of 149 patients with huge hccs that were resected from 1995 to 2012 were analyzed. Multivariate logistic regression analysis was performed to identify preoperative independent predictors of futility.
results: the independent predictors of 3-month mortality (18.1%) were as follows: total bilirubin levels > 34 µmol/L (p = 0.0443; or = 16.470), a platelet count < 150,000/mL (p = 0.0098; or = 5.039), and the presence of portal vein tumor thrombosis (p = 0.0041; or = 5.138). the presence of portal vein tumor thrombosis was the sole independent predictor of 1-year recurrence-related mortality (17.2%). the 3-month and 1-year recurrence-related mortality rates were 6.3% and 7.1% for patients with Barcelona clinic Liver cancer (BcLc) stage a; 12.5% and 14% for patients with BcLc stage B; and 37.8% (p = 0.0002) and 75% (p = 0.0002) for patients with BcLc stage c.
Conclusion: according to our data, among patients undergoing hepatectomy for huge hcc, those with high bilirubin level, low platelet count, and portal vein thrombosis have a higher risk to undergo futile surgery. the presence of portal vein tumor thrombosis should be regarded as a relative contraindication to surgery.
Disclosure of Interest: none Declared
P-148 LOCOreGIOnAL TherAPy In PATIenTS WAITLISTeD fOr LIVer TrAnSPLAnT IMPrOVeS SurVIVAL AfTer TrAnSPLAnTATIOn: An ObSerVATIOnAL STuDy
sushrut trakroo1, kamran qureshi2, sirish sanaka2, Scott McLafferty*3, ryan Bonshock3, abdullah al-osaimi2, antonio Di carlo1, andreas karachristos1, Lee Peng2, Mohammed eyad y. alsabbagh 2, Vishal Patel4, Gary cohen 3
1Division abdominal organ transplant, Department of surgery, 2Division of hepatology, 3Department of radiology, temple university hospital, 4Division of hepatology, hahnemann university hospital, Philadelphia, united states
Introduction: With the continual shortage of organs, the median time to liver transplant (Lt) for wait-listed (WL) adult patients has been continually rising (1). for patients with hepatocellular carcinoma (hcc), waitlist time of over 6-12 months is a risk factor for tumor progression beyond Milan’s criteria for transplantation. Locoregional therapies (Lrt) including transarterial chemoembolization (tace), microwave ablation (MW) and yttrium-90 radioembolization (y-90) are used to delay hcc progression and decrease dropout rates (2). however, there is no conclusive data on the overall survival (os) and recurrence free survival (rfs) in these patients after Lt due to lack of prospective multicenter studies (3). We aim to study the impact of Lrt on mortality, os and rfs in WL patients who underwent Lt.
Methods: of a total of 88 patients, 77 consecutive patients (Mean age 60 ± 6.5 years, M/f=61:16) from our prospectively compiled database listed for Lt from january 2009 to august 2014 were included. eleven were excluded as they had their care transferred to other centers or were lost to follow up. survival was estimated using kaplan-Meyer analysis and a p-value of <0.05 was considered significant.
results: forty of the 53 patients who underwent Lt had Lrt. of the 13 who had no Lrt pre-Lt, 4 had hcc diagnosed at explant and 9 were transplanted within 6 weeks of diagnosing hcc as their lab MeLD was significantly higher than patients who received Lrt(p< 0.001). of the 24 remaining patients, all of whom received Lrt, 14 were delisted: 8 because of hcc progression and 6 due to multiple comorbidities. ten patients are currently on the waitlist for Lt. the overall and hcc related mortality in patients who had Lrt before Lt were 22.5% (9/40) and 5% (2/40) respectively. this was lower than in non-Lrt transplanted patients who showed an overall and hcc related mortality of 46.1% (6/13) and 15.4% (2/13) respectively. this difference was not statistically significant. the median os of the 77 patients listed for Lt was 5.3 years. the 1 and 3 year os (fig. 1a) of patients who did not receive Lrt prior to Lt was significantly lower (76% and 52%) than in patients who received pre-transplant Lrt (100% and 81%).
the 1 and 3 year os in patients who received Lrt but were not transplanted was significantly lower (70% and 42.5%) than in patients who received Lt after Lrt (95% and 75%). on analyzing the rfs, 4 of 13 (30.8%) patients who did not receive Lrt prior to Lt had recurrence as compared to only 2 out of 40 (5%) who received Lrt pre-transplant. the 1 and 3 year rfs (fig. 1b) in non-Lrt patients were significantly lower (89% and 62%) than in patients who received Lrt prior to Lt (100% and 90%).
Image:
Conclusion: significantly improved 1 and 3 year overall survival and recurrence free survival were observed in patients who received Lrt prior to Lt as compared to patients who did not receive Lrt prior to transplant. randomized prospective multicenter trials are warranted.
references: 1. http://srtr.transplant.hrsa.gov/annual_reports/2012/pdf/03_liver_13.pdf 2. frangakis, c, et al. chemoembolization decreases drop-off risk of hepatocellular carcinoma patients on the liver transplant list. cardiovasc Intervent radiol 2011; 34(6): 1254-1261.3. Lesurtel M, et al. transarterial chemoembolization as a bridge to liver transplantation for hepatocellular carcinoma: an evidence-based analysis. am j transplant 2006; 6: 2644-2650.
Disclosure of Interest: none Declared
P-149 hePATeCTOMy fOr hePATOCeLLuLAr CArCInOMA: IMPACT Of POSTOPerATIVe MOrbIDITy On LOnG-TerM
OuTCOMe
Azoulay Daniel* 1, Lim chetana1, compagnon Philippe1, Laurent alexis1, salloum chady1
1hPB surgery and liver transplantation, hopital henri Mondor, aPhP, creteil, france
Introduction: the negative impact of postoperative complications on long term outcome is well documented for several cancer surgeries. the impact of postoperative morbidity on long-term survival after hepatectomy for hepatocellular carcinoma remains inconclusive with scarce studies demonstrating conflicting results. the aim of this study was to determine the impact of complications following liver resection for hcc upon long-term survival.
Methods: all patients who underwent hepatectomy for hepatocellular carcinoma between 1989 and 2015 were studied. Patients with postoperative complication were compared with those without complication. after excluding in-hospital mortality, multivariate analysis was performed to determine the specific influence of postoperative complications after surgery upon long-term survival.
results: from a prospective database of 456 consecutive patients who underwent hepatic resection for hepatocellular carcinoma, 41 (9%) patients who died within the hospital stay were excluded. the overall morbidity rate was 34.2% (n=141 patients). the median follow-up was 26.5 months. at

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 7 7
multivariate analysis, the occurrence of postoperative complication was independently associated with poor survival (hr = 1.5; cI = 1.1-2.0; P = 0.015).
Conclusion: the present study demonstrates that the occurrence of postoperative complication adversely impacts long-term prognosis following hepatectomy for hepatocellular carcinoma. complications should be prevented and the surgical Improvement Project might be adapted to the specific situation of liver resection for hepatocellular carcinoma.
Disclosure of Interest: none Declared
P-150 CLInICAL PArAMeTerS PreDICTIVe Of OuTCOMeS In SOrAfenIb-TreATeD PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA
regiane Alencar* 1, Luciana o. o. kikuchi2, cláudia M. tani2, aline L. chagas2, cinira c. camargo2, túlio e. f. Pfiffer3, flair j. carrilho2
1Division of Gastroenterology and hepatology, Department of Gastroenterology, university of são Paulo school of Medicine, hospital das clínicas, Instituto do cancer do estado de são Paulo, 2Division of Gastroenterology and hepatology, Department of Gastroenterology, university of são Paulo school of Medicine, hospital das clínicas, 3oncology, Instituto do câncer do estado de são Paulo, são Paulo, Brazil
Introduction: sorafenib is an orally active multikinase inhibitor approved for the treatment of advanced hepatocellular carcinoma (hcc) and is the only systemic treatment associated with a survival benefit in advanced stage. the aims of this study were to evaluate the tolerance and survival of sorafenib-treated patients, and to identify potential prognostic factors of survival.
Methods: a total of 88 hcc patients treated with sorafenib from june 2010 to january 2014 were retrospectively reviewed. overall survival was the primary endpoint for the analysis. Various clinical parameters including tumour stage and adverse effects to sorafenib were analysed. univariate and multivariate analysis were carried out to identify clinical parameters predictive of the effect of sorafenib.
results: there were 64 (73%) males and 24 (27%) females included in this study, with a median age of 61 years. 80 (91%) patients had child-Pugh class a cirrhosis. Most patients were classified as BcLc c (82%). hepatitis c virus was the predominant cause of hcc (68%). sorafenib was the initial treatment modality in 43%. the presence of dermatologic adverse event predicted a better overall survival in the multivariate analysis. Better survival was also observed in patients with afP level < 1000 ng/ml in the last visit (p = 0.003). according to duration of sorafenib therapy, patients were divided in 2 groups: (a) < 10 months (n = 65), and (B) ≥ 10 months (n = 23). Median time of sorafenib therapy was 3.7 months in group a and 20.2 months in group B. overall survival was 16.7 and 36.7 months, in group a and B, respectively [or 3.8; 95% cI 1.8-7.7; p<0.001].
Conclusion: advanced hcc patients treated with sorafenib who experienced dermatologic adverse event and afP level < 1000 ng/ml showed better overall survival. as expected, longer sorafenib therapy (≥ 10 months) was associated to better survival.
Disclosure of Interest: none Declared
P-151 fIbrOSIS InDex AnD fIbrOSIS 4 SCOre In PreDICTIOn Of hePATOCeLLuLAr CArCInOMA In ChrOnIC hePATITIS C eGyPTIAn PATIenTS
hany r. Shabana* 1, Marwa s. askar2, Mohamed M. elrakhawy3, Mohammad a.- harrass4
1Internal medicine ,hepatology and gastroenterology unit, Mansoura universityt.specialized Medical hospital., Mansoura, 2Blood Bank, aga hospital,Ministry of health, aga,Dakahlia, 3Diagnostic and Interventional radiology, 4clinical Pathology Department, Mansoura university, Mansoura, egypt
Introduction: hepatocellular carcinoma (hcc) is one of the most serious causes of cancer mortality in egypt due to the burden of chronic hepatitis c (chc)(1).the degree of liver fibrosis is the strongest indicator of the risk of hcc development in these patients(2). We aimed at determining the usefulness of both fibrosis 4 (fIB4) score and fibrosis index (fI) as predictors of the risk of hcc development in these patients.
Methods: the study included 111 patients with chc and hcc (group I) and 222 patients with chc without hcc (group II). chc was diagnosed by eLIsa for hcV antibody and serum hcV rna .hcc diagnosis was based on easL criteria i.e. focal hepatic lesion with arterial phase enhancement and washout in portal and delayed phases, obtained by contrast enhanced abdominal ct and or MrI.Liver fibrosis assessment was carried out for all patients using fIB4 score and fI.fIB4 score was calculated using the following formula:( age x ast ) / ( Platelets x ( sqr ( aLt ) ) (3).fI was calculated using the following formula:8.28 - [(0.01 x Platelets (10^9/L) - [1.08 * (10 * serum albumin (g/L))]] (4).We computed roc curve for both fIB4 score and fI concerning the prediction of hcc. ssLr was calculated as the proportion of diseased subjects with a test result in a given range divided by the
proportion of non diseased subjects with a test result in the same range (5).
results: Both fIB4 and fI were significantly higher in group I.fIB4 score was 7.16±5.79 in group I versus 3.43±3.15 in group II (P ≤000). fI was 3.56±1.06 in group I versus 2.41±1.07 in group II (P≤000).the cut off value of fIB4 score above which there was a high risk of hcc was ≥2.32.the area under the curve (auc) was 77.7%, sensitivity was 91.2%, specificity was 56%,positive predictive value(PPV) of 49.5%,negative predictive value (nPV) of 93.1%,accuracy of 67.3% and positive likelihood ratio (Lr) of 2.07. as regards fI,the cut off value above which there was a high risk of hcc was ≥3.13.the auc was 78.1%, sensitivity was 70.4 %, specificity was 78.4 % , PPV of 64.4%,nPV of 82.6%,accuracy of 75.5 % and positive Lr of 3.26 (curve).the ssLr for hcc presence by fIB4 score was 0.07 in score< 2, 1.22 in score 2 to 4 and 2.43 in score >4. the ssLr by fI was 0.22 in score < 2, 1.02 in score 2 to 4 and 5.05 in score >4.
Image:
Conclusion: fI and fIB4 score could be used as predictors of the risk of hcc development in patients with chc. however,fI is better than fIB4 and patients expressing fI >4 have ssLr for hcc presence of 5.05 and are in need for closer follow up.
references: (1) anwar Wa, khaled hM, amra ha, et al. changing pattern of hepatocellular carcinoma (hcc) and its risk factors in egypt: Possibilities for prevention.(2) Masuzaki r, tateishi r, yoshida h,et al .risk assessment of hepatocellular carcinoma in chronic hepatitis c Patients by transient elastography. J Clin Gastroenterol 2008; 42(7): 839-843(3) Martínez sM1, crespo G, navasa M, et al.non invasive assessment of liver fibrosis. hepatology. 2011 jan;53(1):325-35.(4) ohta t, sakaguchi k, fujiwara a, et al.simple surrogate index of the fibrosis stage in chronic hepatitis c patients using platelet count and serum albumin level. acta Med okayama. 2006 apr;60(2):77-84.(5)Beck jr. Likelihood ratios.another enhancement of sensitivity and specificity. Arch Pathol Lab Med 1986; 110: 685–686
Disclosure of Interest: none Declared
P-152 CLInICAL SIGnIfICAnCe Of OCCuLT hePATITIS b InfeCTIOn In PATIenTS WITh nOn-hePATITIS b/nOn-hePATITIS C-reLATeD hePATOCeLLuLAr CArCInOMA In A hePATITIS b enDeMIC AreA
bo hyun Kim* 1, joong-Won Park1, sang-hyun hwang2, chang-Min kim1
1center for Liver cancer, 2center for Diagnostic oncology, national cancer center, Goyang, korea, republic of
Introduction: occult hepatitis B virus (hBV) infection has been suggested as a potential factor for progression of liver disease or development of hepatocellular carcinoma (hcc). the aim of this study was to identify a role of occult hBV infection in non-hepatitis B/non-hepatitis c-related hcc
Methods: Data of 1,967 patients newly diagnosed with hcc at a single institute between 2004 and 2009 were reviewed. of 313 patients negative for hBsag and anti-hcV, 86 with available sample were tested for hBV Dna using a real time Pcr assay (abbott realtime hBV assay). those who were positive for hBV Dna Pcr (n=6) were compared with those negative (n=80).

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s7 8
results: the median age of 86 patients was 65 years, and 73 (84.5%) were male. of 6 patients positive for hBV Dna, 4 had a level of less than 100 Iu/mL and 2 had a level of more than 100 Iu/mL. Liver function was classified as child-Pugh a in 90.7%. according to the modified uIcc stage, 7.0%, 50.0%, 20.9%, 15.1%, and 7.0% had stage I, II, III, IVa, and IVb disease, respectively. Baseline characteristics were comparable between patients negative and positive for hBV Dna. Median transplantation-free survival was better in the Dna-negative group (75.9 months vs. 15.9 months; P=0.0821). univariate analysis indicated that ecoG performance status 1 or greater (P=0.0004), modified uIcc stage (P<0.0001), serum afP level of ≥ 200 ng/mL (P=0.0069), child-Pugh class a (P=0.0168), BMI of 25 or more (P=0.083) and hBV Dna positivity (P=0.0821) were predictors for transplantation-free survival. according to the multivariate analysis modified uIcc stage IVb (hazard ratio 6.35, 95% confidence interval 1.01-39.91) and hBV Dna positivity (hazard ratio 4.06; 95% confidence interval 1.29-13.33) were independent prognostic factors for transplantation-free survival.
Conclusion: Patients who were positive for hBV Dna tended to show poorer survival than those who were negative, although tumor characteristics were comparable. advanced tumor stage and hBV Dna positivity were independent prognostic factors for transplantation-free survival in non-hepatitis B/non-hepatitis c-related hcc.
Disclosure of Interest: none Declared
P-153 fACTOrS ASSOCIATeD WITh hePATOCeLLuLAr CArCInOMA SurVeILLAnCe rATeS AMOnG PATIenTS WITh CIrrhOSIS In A POPuLATIOn-bASeD InTeGrATeD heALThCAre DeLIVery SySTeM
Amit Singal* 1, jasmin tiro1, xilong Li1, Beverley adams-huet1, jessica chubak2
1ut southwestern Medical center, Dallas, 24Group health research Institute, seattle, united states
Introduction: fewer than 1 in 5 patients receive hepatocellular carcinoma (hcc) surveillance; however, most studies were performed in select patient populations, such as acadmic or Veterans affairs medical centers, which may not be informative of practice patterns in population-based community practices. the aims of our study were to characterize guideline-concordant hcc surveillance rates and patient-level factors associated with surveillance among a population-based cohort of patients with cirrhosis.
Methods: We retrospectively characterized hcc surveillance among patients with cirrhosis followed between january 2010 and December 2012 at Group health, an integrated health care system in Washington state of the united states. consistent surveillance was defined as an ultrasound every 6 months, and inconsistent surveillance was defined as ≥1 ultrasound during the two-year period. univariate and multivariate analyses were conducted to identify correlates of hcc surveillance receipt.
results: of 1137 patients with cirrhosis, 28 (2.5%) underwent consistent surveillance, 365 (32.1%) had inconsistent surveillance, and 744 (65.4%) received no surveillance. Inconsistent surveillance rates were 27.4% among the 84 patients followed for 6 – <12 months, 27.6% among the 58 patients followed for 12 – <18 months, 33.6% among the 995 patients followed for 18-24 months. correlates of hcc surveillance receipt in multivariate analysis included hepatology subspecialty care (or 1.88, 95%cI 1.44 – 2.46), child Pugh B/c cirrhosis (or 1.61, 95%cI 1.07 – 2.43), elevated ast (or 1.63, 95%cI 1.13 – 2.35), and etiology of liver disease. compared to hcV-infected patients, those with alcohol-related cirrhosis (or 0.63, 95%cI 0.42 – 0.93) and nonalcoholic steatohepatitis (or 0.39, 95%cI 0.28 – 0.56) were less likely to undergo surveillance. these risk factors demonstrated acceptable discrimination between the presence and absence of inconsistent surveillance (c-statistic of 0.69).
Conclusion: only 1 in 3 patients undergo inconsistent hcc surveillance, and less than 3% of patients receive guideline-concordant hcc surveillance. high-quality data evaluating benefits and harms of hcc surveillance in patients with cirrhosis are needed to increase adoption of hcc surveillance in clinical practice.
Disclosure of Interest: none Declared
P-154 effICACy AnD SAfeTy Of SOrAfenIb In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA: AGInG IS nOT A PrObLeM
Dimitrios ziogas* 1, Dionysis Papadatos-Pastos 1, kiruthikah thillai1, ruhe chowdhury1, thubeena Manickavadagar1, abid suddle1, john o'Grady1, nigel heaton1, Paul j. ross1, Debashis sarker1
1Department of oncology, king’s college hospital, London, united kingdom
Introduction: sorafenib is the standard of care for patients with advanced hepatocellular carcinoma (hcc). Data regarding the use of sorafenib in the elderly are insufficient as these patients are often under-represented in large registration trials. In the present study, we assessed the efficacy and safety of sorafenib in the elderly.
Methods: Data from consecutive patients who received sorafenib in our institution since its licensing
were included in the analysis. In order to recognize any impact of age in the prognosis of hcc under sorafenib treatment, patients were divided into two groups: (a) those that were ≤75 years old prior to starting sorafenib and (B) those that were >75 years old. the primary endpoints were overall survival (os) and time to disease progression or treatment discontinuation (ttP/ttD); while as secondary endpoints, safety profile and dose modifications were also evaluated. kaplan-Meier analysis using a log-rank test was performed to determine the difference between groups. through a univariate and a multivariate analysis, we examined in parallel the prognostic effect of certain clinical variables at the beginning of sorafenib in os and ttP/ttD.
results: Data from 190 patients, M:f (157:33), median age 66 years (range, 26-87) were studied (group a:151 and group B:39 patients). older hcc patients of group B were more frequently affected by more than 2 comorbidities compared to the younger group a (43.59% versus 20.53%, p=0.006). the most common underlying liver disease was hepatitis (B or c) and non-alcoholic fatty liver disease for patients in arm a and B respectively. Between patients in two age groups (a versus B), no significant differences were found in os (median, 95%cI): 7.1 (5.5-8.7) months versus 10.4 (6.5-14.3) months, p=0.360 and in ttP/ttD (median, 95%cI): 4.2 (2.3-6.2) months versus 5.6 (3.1-8.1) months, p=0.356. In terms of safety there was no significant difference in the frequency of grade 1-2 and grade 3-4 toxicities between the two groups. the rate of dose reductions was also comparable in the two groups (a:34.44% and B:35.90%, p=0.853). on the other hand, patients with a child-Pugh B at baseline, had a shorter os (adjusted hr=2.17, 95%cI:1.24-3.79, P=0.007) and a shorter ttP/ttD (adjusted hr=4.64, 95%cI:2.55-8.42, p=0.001) compared to patients with a child-Pugh a (log-rank, p=0.004 and p=0.001, respectively).
Conclusion: this analysis suggests that elderly patients with advanced hcc do not have a worse clinical outcome when compared to their younger counterparts when treated with sorafenib and tolerate it well. age alone should not be a discriminating factor for the management of patients with advanced hcc.
Disclosure of Interest: none Declared
P-155 PreDICTIOn MODeL fOr The DeVeLOPMenT Of hePATOCeLLuLAr CArCInOMA In PATIenTS WITh ChrOnIC hePATITIS b reCeIVInG AnTIVIrAL TreATMenT
Jem Ma Ahn* 1, yeon seok seo1, tae hyung kim1, sun young yim1, young kul jung1, ji hoon kim1, hyunggin an 2, hyung joon yim1, hong eun yeon 1, kwan soo Byun1, soon ho um1
1Division of Gastroenterology, Department of Medicine, 2Department of Biostatistics, korea university, seoul, korea, seoul, korea, republic of
Introduction: although several models predicting development of hepatocellular carcinoma (hcc) in patients with chronic hepatitis B (chB) have been already published, a new prediction model is required for the patients who receive long-term antiviral therapy with sustained suppression of viral replication. thus this study was performed to establish and validate a new model for predicting development of hcc in chB patients with anti-viral treatment, based on histological data.
Methods: consecutive patients with chB who received antiviral therapy with liver biopsy between 2001 and 2013 were enrolled in a training set, and those who received antiviral therapy without liver biopsy were included in a validation set, respectively. cox-regression analysis was performed to identify independent factors and to establish a new prediction model for hcc development. the predictive efficacy of a new model was compared with risk estimation for hcc in chB (reach-B) model.
results: training and validation sets were consisted of 478 and 553 patients. In the training set, their mean age was 39.9 ± 12.1 years and 333 patients (69.7%) were male. fibrosis stage on liver biopsy was as following: f01 in 98 (20.5%) patients, f2 in 160 (33.5%) patients, f3 in 165 (34.5%) patients, and f4 in 55 (11.5%) patients. During the follow-up of 63.8 ± 43.2 months, hcc developed in 18 patients. In multivariate analysis, age, BMI, heavy alcohol consumption, platelet count, and hBeag were independent factors for predicting hcc development. With these independent variables and their beta coefficients, a hcc prediction model was established. aucs of our model for predicting hcc within 5 and 10 years were 0.910 and 0.892, respectively. In the validation set, aucs were 0.849 and 0.907, respectively. In training and validation sets, aucs of our model were significantly higher than those of reach-B model.
Conclusion: there was significant difference in the predictive factors for hcc development between patients who were treated with long-term antiviral therapy and those without antiviral therapy. our new prediction model was very accurate and useful for predicting hcc development in patients with chB receiving antiviral therapy.
references: 1. arends P, sonneveld Mj, zoutendijk r, carey I, Brown a, fasano M, et al. entecavir treatment does not eliminate the risk of hepatocellular carcinoma in chronic hepatitis B: limited role for risk scores in caucasians. Gut 2014.2. yang hI, yuen Mf, chan hL, han kh, chen Pj, kim Dy, et al. risk estimation for hepatocellular carcinoma in chronic hepatitis B (reach-B): development and validation of a predictive score. Lancet oncol 2011;12:568-574.3. yuen Mf, tanaka y, fong Dy, fung j, Wong Dk, yuen jc, et al. Independent risk factors and

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 7 9
predictive score for the development of hepatocellular carcinoma in chronic hepatitis B. j hepatol 2009;50:80-88.4. Wong VW, chan sL, Mo f, chan tc, Loong hh, Wong GL, et al. clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers. j clin oncol 2010;28:1660-1665.
Disclosure of Interest: none Declared
P-156 WIDe reSeCTIOn MArGIn IMPrOVeS SurVIVAL In PATIenTS WITh eArLy InTrAhePATIC ChOLAnGIOCArCInOMA
Ma Ka Wing* 1, she Wong hoi1, Poon t. P. ronnie1, 2, Lo chung Mau1, 2, cheung tan to1
1surgery, queen Mary hospital, 2the university of hong kong, hong kong, china
Introduction: Intrahepatic cholangiocarcinoma (Icc) is known for its lethal disease nature and there were studies focusing on factors that might affect disease survival; among these factors, resection margin status remains one of the few modifiable factors that a surgeon could possibly manipulate to alter the disease outcome. however, the significance of clear margin and margin width continue to be a topic of debate. this study serves to share our opinion on this issue.
Methods: a retrospective review of a prospectively maintained database was performed in Department of surgery, queen Mary hospital, university of hong kong. consecutive patients diagnosed to have Icc and with surgical resection performed in curative intent were retrieved, while patients with cholangiohepatocellular carcinoma, klaskin tumour, tumour of extrahepatic bile duct and uncertain tumour pathology were excluded. clinico-pathological data were analysed statistically.
results: from 1991 to 2013, there were 107 patients underwent hepatectomy for Icc. Gender predilection was not observed with 59 males and 48 females, median age of the patients was 61. the median tumour size was 6cm (1-17cm) and most of them (43%) were moderately differentiated adenocarcinoma. clear resection margin were achieved in 95 patients (88.8%) and the median margin width was 0.5cm (0-4cm). the hospital length of stay and operative mortality were eleven days and 2.8% respectively. the disease free survival and overall survival were 17.5 months (0.5-276.3) and 25.1 months (0.2-276.3) respectively. Multivariate analysis showed that margin width was an independent factor associated with disease free survival (P= 0.015, 95% c.I. 0.4-0.9). subgroup analyses showed that the increase resection margin to 0.84 cm was associated with improved overall survival in patients with solitary tumour (P=0.029) and node negative disease (P=0.017). Discriminant analysis showed that the overall survival increased from 42 months to 185 months when margin width was greater than 0.84cm (p=0.015) in patients with both solitary tumour and node negative disease.
Image:
Conclusion: aggressive resection to achieve wide margin maximize chance of cure in patient with early Icc.
Disclosure of Interest: none Declared
Diagnosis, Imaging and biomarkers
P-157 OuTreACh InVITATIOnS IMPrOVe hePATOCeLLuLAr CArCInOMA SurVeILLAnCe rATeS: reSuLTS Of A rAnDOMIzeD COnTrOLLeD TrIAL In A SAfeTy neT heALTh SySTeM
Amit Singal* 1, jasmin tiro1, katharine Mccallister1, caroline Mejias1, Lei xuan1, jorge Marrero1, ethan halm1
1ut southwestern Medical center, Dallas, united states
Introduction: hepatocellular carcinoma (hcc) surveillance is associated with early tumor detection and improved survival, but its effectiveness is limited by underuse, particularly among underserved populations. there are no randomized trials evaluating interventions to improve hcc surveillance rates to date. the aim of our study was to compare clinical effectiveness of mailed outreach and patient navigation strategies to increase surveillance rates in a racially diverse and socioeconomically disadvantaged cohort of patients.
Methods: Patients with documented or suspected cirrhosis at a large urban safety-net health system in the united states were randomized to receive mailed outreach invitations for surveillance ultrasonography, mailed outreach plus patient navigation, or usual care with opportunistic, visit-based screening. Documented cirrhosis was defined using IcD-9 codes for cirrhosis or cirrhosis-related complications, and suspected cirrhosis was defined as an ast to platelet ratio index (aPrI) ≥ 1.5 in the presence of underlying liver disease. We excluded patients with child c cirrhosis who were not transplant candidates and those with significant comorbid conditions given limited benefit of hcc surveillance. Patients who did not respond to outreach invitations within 2 weeks received up to 3 follow-up reminder telephone calls. the primary study outcome was completion of an abdominal ultrasound for surveillance purposes within 6 months of randomization. We used an intent- to-screen principle for analyses. We are randomizing a total of 1800 patients in groups of 300 (i.e. 100 patients per arm), with results of the first two groups (n=600 patients) presented herein.
results: Baseline patient characteristics (n=600) across the three groups were similar. Mean age was 55 (range 22 – 87) years and 60% were men. the cohort was racially/ethnically diverse with 36% Black, 35% hispanic, and 28% White. Most patients (79%) patients had documented cirrhosis, with 21.0% having suspected cirrhosis. cirrhosis was due to hcV in 54%, alcohol in 19%, nash in 15%, and hBV in 4%. rates of scheduled surveillance ultrasounds were significantly higher in the outreach/patient navigation arm (34.0%) and outreach alone arm (26.5%) than usual care (11.5%; p<0.001 for both comparisons). Because of the back-log for getting ultrasounds completed in our safety net health system, the proportion of ultrasounds completed in the first 2 months of the trial have lagged and are not yet different among the 3 arms (9.5% for usual care, 12.5% for outreach alone, and 13.5% for outreach/patient navigation; p=0.44). an additional 8.0%, 9.0%, and 7.0% of patients in the three arms, respectively, had a diagnostic ultrasound or contrast-enhanced ct/MrI imaging scheduled, so surveillance ultrasound was not required. ultrasound scheduling was a direct result of outreach efforts in 32.8% (21 of 61) of outreach alone patients and 52.6% (40 of 76) of outreach/patient navigation patients. Patients with documented cirrhosis were significantly more likely to complete or schedule an ultrasound than those with suspected cirrhosis (30% vs. 18%, p=0.005).
Conclusion: outreach strategies and patient navigation can significantly increase hcc surveillance rates. further follow-up data to compare the effectiveness of hcc surveillance outreach and patient navigation for promoting surveillance ultrasound completion will be available for the meeting in september.
Disclosure of Interest: none Declared
P-158 SurfACe Of The WhOLe AbDOMInAL MuSCLeS beTTer PreDICT OVerALL AnD DISeASe-free SurVIVAL ThAn SurfACe Of PSOAS MuSCLeS
Thibault Voron* 1, Lambros tselikas2, Daniel Pietrasz1, frederic Pigneur2, chady salloum1, Philippe compagnon1, alexis Laurent1, alain Luciani2, Daniel azoulay1
1Department of Digestive and hepatobiliary surgery, 2Department of radiology, henri-Mondor hospital, créteil, france
Introduction: Liver resection for hepatocellular carcinoma (hcc) leads to long-term survival in selected patients. however, in clinical setting, preoperative prognosis assessment and selection of treatment are mainly based on one of the following tumor staging classifications: tnM, cancer of the Liver Italian Program (cLIP), Barcelona clinic Liver cancer (BcLc), or japan Integrated staging (jIs). these tumor-staging classifications include tumor characteristics (tumor size, number of nodules, tumor markers) and underlying liver function but rarely patient characteristics although general condition of hcc patients has been described as an independent prognostic factor. recently low muscle mass (named sarcopenia) estimated by ct scan imaging has been shown to be an independent prognostic factor for overall and disease-free survival. however, based on various studies, sarcopenia was evaluated by the surface of the whole abdominal muscles (abdosarco) or the surface of the psoas only (Psoassarco).

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s8 0
the purposes of this study were to evaluate the prevalence of sarcopenia among european patients with resectable hcc according to the measurement strategy used and to assess the best definition of sarcopenia to predict overall and disease-free survival.
Methods: all consecutive patients who underwent liver resection for hcc in our institution, between february 2006 and september 2012, were included. Data were extracted from our prospectively collected database and analysed retrospectively. a univariate and multivariate analysis evaluating prognostic factor of postoperative mortality was performed, including preoperative, surgical and histopathological factors.
results: among 198 patients who underwent hepatectomy for hcc, 109 patients had an available ct scan and represent the study cohort. although there is a strong correlation between the surface of the whole abdominal muscles and the surface of the psoas (Pearson correlation coefficient: r=0.735; p<0.001), the prevalence of sarcopenia differed between the two measurement strategies. fifty-nine patients (54%) were considered sarcopenic according with surface of whole abdominal muscles (abdosarco) whereas 64 patients (58.7%) were considered sarcopenic when surface of psoas have been uses (Psoassarco). Patients in abdosarco group had significantly shorter mean overall survival (38,4 months vs 55,8 months,p=0.015) and shorter mean disease-free survival (20 months vs 52 months, p<0.0001) than non-abdosarco patients. In multivariate analysis, abdosarco was found to be an independent predictor of poor overall survival (hr=3.19;p=0.013) and disease-free survival (hr=2.60;p=0.001). on the contrary, although patients in Psoassarco group had significantly shorter mean disease-free survival (38 months vs 61 months; p=0.005) and was found to be an independent predictor of poor disease-free survival (hr=2.65; p=0.001), sarcopenia assessed by surface of the psoas only was not predictive of overall survival in univariate or multivariate analysis.
Conclusion: sarcopenia assessed by the surface of whole abdominal muscles in ct scan imaging was found to be a strong and independent prognostic factor for mortality and recurrence after hepatectomy for chc in european patients. even if the assessment of sarcopenia by measurement of the surface of psoas is simpler and faster, this method overestimates the prevalence of sarcopenia and does not predict overall survival as well as the surface of the whole abdominal muscles.
Disclosure of Interest: none Declared
P-159 hIGhT VALue Of COnTrAST enhAnCeD uLTrASOunD (CeuS) In DefInInG A rAPID DIAGnOSTIC AnD TherAPeuTIC WOrK-uP fOr nODuLeS <2 CM In CIrrhOTIC PATIenTS DurInG SurVeILLAnCe
Antonio Giorgio* 1, Luca Montesarchio1, umberto scognamiglio1, Pietro Gatti2, carmine coppola3, Valentina Giorgio4, Paolo Matteucci5
1Internal medicine, tortorella clinical Institute, salerno, 2Internal medicine, fasano hospital, fasano, 3Internal medicine, gragnano hospital, gragnano, 4gastroenterology, policlinico gemelli, 5radiology, campus biomedico, roma, Italy
Introduction: the disappearence of portal blood flow and the arterial vascularization is the hallmark of hepatocarcinogenesis, leading from benign regenerating nodules to well differentiated hcc. therefore the capability of a dynamic imaging modality, used soon after the conventional sonographic recognition during surveillance of cirrhotics, such as ceus, to detect the arterial hypervascurarization of small nodules arising in a cirrhotic liver, is crucial,in order to to promote a rapid diagnostic and therapeutic work-up, avoiding a late diagnosis, inabling an early treatment and improving survival. the aim of the study was to evaluate the capability of ceus to detect arterial vascularization of single, small ≤ 2 cm hcc nodules arising in cirrhotics during surveillance in order to short the diagnostic and therapeutic work-up of hcc patients.
Methods: from october 2009 to september 2014, out of 1757 cirrhotics consecutively referred for surveillance of development of hcc, 243 new, single, clearly visible nodules, 7-20 mm in diameter, were detected. 229 out of 243 nodules had a conclusive hystologic diagnosis and composed the study group. 137 were males, median age 61(range 51-86 years); cirrhosis was related to hcV in 145 patients ,to hBV in 39, to alchol abuse in 12 and mixed etiology in 33. 189 and 30 patients had chid a child B cirrhosis, respectively.on us 27 nodules were hyperechoic, 171 hypoechoic and 31 isoechoic. after conventional us all patients underwent ceus and contrast-enhanced MrI.after ceus and ce-MrI all patients underwent percutaneous us guided needle biopsy of the nodule with a 18 G cutting needle in all cases.hystologic diagnosis of hcc diagnosis was made by a 20 years expert liver pathologist according to the hystological criteria of the International Working Party. the result of percutaneous biopsy was used as gold standard for hcc diagnosis in all cases. ceus was performed using 2,4 ml of sonoVue, using last generation, high definition, commercially available machines . Mr imaging was performed using a 1.5-t system machine .for contrast-enhanced dynamic Mr imaging, 0.1 mmol/kg of body weight dose of gadobenatedimeglumine was used.
results: on hystology, 199 of 229 nodules were hcc and 30 were benign lesions . ceus showed arterial hypervascularity in 190 nodules (94.5%) and all these arterial-hyperhenanced nodules were hcc [sensitivity: 95,5%, specificity: 100%, PPV: 100%; nPV: 76,9%]. of the 39 ceus arterial-unenhanced nodules, 30 were benign and 9 were well-differentiated hcc. of note, 17 out of 21 (81%) hyperechoic angioma like-lesions wich as a final diagnoses of hcc, showed arterial
hypervascularity and all of these were hystologically hcc. ceMrI showed arterial hypervascularity in 199 nodules (86,9%). of these, only 193 (97%) were hystologically hccs while 6 were benign. [sensitivity: 97%; specificity: 80%; PPV: 97%; nPV: 80%]. of the 30 MrI arterial-unenhanced nodules (17%), 24 were benign and 6 were well-differentiated hcc. the concordance between ceus and ceMrI versus the gold standard, i.e liver biopsy, was 0,96 and 0,95, respectively. cohen’s kappa was 0,85 for the ceus and 0,78 for the MrI. the concordance between ceus and MrI was 0.98.
Conclusion: ceus has a great capability in demonstrating the main specific finding of hcc as arterial hypervascularity in hcc nodules < 2 cm discovered during us surveillance. Because only 4,5% of new nodules escape the demonstration of arterial hyervascularity, ceus must be performed immediately after conventional us to contrast the malignant fate of small lesions arising in cirrhotics.
Disclosure of Interest: none Declared
P-160 Pre-TreATMenT reD CeLL DISTrIbuTIOn WIDTh (rDW) TO STrATIfy SurVIVAL Of PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA unDerGOInG SOrAfenIb TreATMenT
carlotta ferrari1, David j. Pinato2, antonello Gibbin1, ramya ramaswami2, Giulia Guaschino1, Michela e. Burlone1, james Black2, Laura sellers2, rohini sharma2, Mario Pirisi*1
1università del Piemonte orientale, novara, Italy, 2Imperial college London - hammersmith hospital, London, united kingdom
Introduction: the red cell distribution width (rDW), an inflammation-driven variation in erythrocyte volume, is an objective, inexpensive and widely available biomarker of early mortality across various disease states, including hepatocellular carcinoma (hcc).[1] Given that inflammation is both pathogenic and prognostic in hcc, we investigated whether the rDW may help phenotyping the heterogeneity of advanced hcc to identify those patients in whom treatment with sorafenib might be futile.
Methods: a multicenter dataset of 86 patients with advanced hcc was generated from two retrospectively collected cohorts of consecutive patients from Italy (novara, n=40, 47%) and uk (London, n=46, 53%): 67/86 (78%) were male; mean age was 67 years; 55/86 (64%) belonged to child-Pugh-turcotte (cPt) class a. sorafenib was dispensed according to the Italian and British national health system guidelines. the pre-treatment rDW was analyzed in relationship to overall survival, powered on a 73% event rate at the end of follow-up. Log-rank test and multivariate cox regression analysis of survival outcomes were conducted using stata 13.1 (statacorp LP, 4905 Lakeway Drive, college station, tx).
results: Median os was 8.3 months, whilst median treatment duration was 4 months. the median rDW value was 15.2% (interquartile range, 14.2-17.1). the table presents median os with corresponding 95% cI in the studied population, stratified according to rDW quintiles (p <0.004 at the logrank test for trend).
rDW quintile Median os, days 95% cI for median os
1 (≤14.0%) 466 189-678
2 (14.1-14.9%) 351 199-591
3 (15.0-15.8%) 265 144-473
4 (15.9-17.1%) 170 129-457
5 (≥17.2%) 130 68-305
Multivariate analysis revealed the rDW as the only independent predictor of os (regression coefficient = 0.2319, hazard ratio = 1.25, 95%cI 1.12-1.42; p<0.001) following adjustment for cPt score, age, gender and center dispensing treatment. the Image presents the observed os (continuous lines) vs. the predicted survival (dotted lines) based on the model. Patients are dichotomized into those belonging to rDW quintiles 1 to 4 (blue and green symbols) and those belonging to the 5th rDW quintile (red and orange symbols).

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 8 1
Image:
Conclusion: Pre-treatment rDW is a promising stratifying biomarker in advanced hcc, capable of identifying patient subgroups with progressively worse survival probabilities. for patients with advanced hcc and an elevated rDW, best supportive care may be appropriate, given their dim prognosis despite sorafenib.
references: 1. smirne c et al. evaluation of the red cell distribution width as a biomarker of early mortality in hepatocellular carcinoma. Dig Liver Dis (2015, in press).
Disclosure of Interest: none Declared
P-161 LIVer IMAGInG rePOrTInG AnD DATA SySTeM CATeGOrIzATIOn Of hePATOCeLLuLAr CArCInOMA uSInG GADOxeTIC ACID-enhAnCeD MrI: COMPArISOn WITh MDCT
Ijin Joo* 1, jeong Min Lee1, Dong ho Lee1, su joa ahn1, joon koo han1
1radiology, seoul national university hospital, seoul, korea, republic of
Introduction: the Liver Imaging reporting and Data system (LI-raDs) is a system for standardized interpretation and reporting of ct and MrI in patients at risk for hepatocellular carcinoma (hcc). Different from previous ones, the current version of LI-raDs (v2014) incorporates the use of hepatobiliary contrast agents into the diagnostic algorithm. In this study, we applied gadoxetic acid-enhanced MrI for the LI-raDs categorization of hccs and compared the categorization with that of contrast-enhanced MDct.
Methods: this retrospective study included 146 consecutive patients with 158 pathologically confirmed hccs who underwent both gadoxetic acid-enhanced MrI and dynamic contrast-enhanced MDct. according to LI-raDs v 2014, two radiologists independently assigned LI-raDs categories (Lr1 to Lr5) on gadoxetic acid-enhanced MrI and MDct, respectively. sensitivities of Lr5 (definitely hcc) in the diagnosis of hccs were compared between two imaging modalities, and inter-observer agreements in the assignment of Lr5 were calculated using kappa statistics.
results: In pathologically confirmed hccs (n=158), frequencies of Lr5, Lr4, and Lr3 or less on gadoxetic acid-enhanced MrI were 82.9%, 16.5%, and 0.6% in reviewer 1; and 75.3%, 24.7%, and 0% in reviewer 2, respectively. MDct results showed 78.5%, 17.7%, and 3.8% of Lr5, Lr4, and Lr3 or less in reviewer 1; and 81.0%, 17.1%, and 1.9% in reviewer 2, respectively. there were no statistically significant difference in the sensitivities of Lr5 by gadoxetic acid-enhanced MrI and MDct in both reviewers (P=0.396 and 0.276, respectively). Both gadoxetic acid-enhanced MrI and MDct showed fair inter-observer agreement of kappa values of 0.430 and 0.452, respectively.
Conclusion: the LI-raDs v2014 categorization using gadoxetic acid-enhanced MrI showed comparable sensitivity and inter-observer agreement with that of contrast-enhanced MDct in the diagnosis of hcc.
Disclosure of Interest: none Declared
P-162 hIGh exPreSSIOn Of yAP AnD GLI1 reLATeD TO ePITheLIAL-MeSenChyMAL TrAnSITIOn AnD POOr PrOGnOSIS Of hePATOCeLLuLAr CArCInOMA AfTer SurGery
Chao Sun* 1, Bo hu1, yang xu1, WeiGuo tang1, qiMan sun1, Liqi xie2
1Liver cancer Institute & zhong shan hospital, fudan university, 2Institutes of Biomedical sciences, fudan university, shanghai, china
Introduction: hippo pathway plays important role in regulating cell migration and proliferation, which are essential for the induction of metastasis in hepatocellular carcinoma (hcc). yes-associated Protein (yaP), which is a major effector of hippo pathway, serves as a transcriptional co-activator for a wide range of genes that govern cell growth and division.
Methods: yaP expression was measured in stepwise metastatic hcc cell lines, tumor, peritumoral tissues, and normal liver tissues by quantitative real-time Pcr and Western blot. the role of yaP in hcc was investigated by yaP depletion using small interfering rna. We investigated yaP’s role in the regulation of cell migration and proliferation in hcc cells, and then assessed its clinical significance in 254 hcc patients who underwent curative surgical resection during feb 15. 2004 to Dec 15. 2005. Prognostic significance was assessed using kaplan–Meier survival estimates and log-rank tests.
results: We confirmed that hyperactive yaP promoted the epithelial-to-mesenchymal transition (eMt) in hcc cells and significantly increased their invasiveness. overexpression of yaP in tumor samples is associated to both tumor recurrence and poor prognosis of hcc patients after surgery. furthermore, the up-regulation of yaP was also shown to activate the expression of Gli1, which is the key factor of hedgehog pathway. Gli1 knockdown suppressed yaP’s impact on eMt and inhibited the migration of hcc cells.
Conclusion: our study offers the first experimental evidence that Gli1 acts as a mediator for yaP-dependent regulation of eMt and hcc cell proliferation, suggesting the diagnostic and prognostic value of yaP, Gli1, and the eMt biomarkers such as e-cadherin, n-cadherin and Vimentin for hcc patients.
Disclosure of Interest: none Declared
P-163 CIrCuLATInG TuMOr CeLL DeTeCTIOn In PerIPherAL AnD hePATIC VeInS In PATIenTS WITh POTenTIALLy reSeCTAbLe hePATOCeLLuLAr CArCInOMA
Julien edeline* 1, 2, simona onali3, tuVinh Luong4, sachuda Veerasamy5, Leah ensell1, helen Lowe1, john hartley1, james oBeirne3, tim Meyer6
1university college London, London, united kingdom, 2Medical oncology, centre eugene Marquis, rennes, france, 3hepatology, 4Pathology, 5royal free hospital, 6Medical oncology, university college London, London, united kingdom
Introduction: using the cellsearch system, the prognostic value of circulating tumor cells (ctc) has been shown in various epithelial cancers, both in advanced and early stage disease. the cellsearch system detects ctcs based on epcaM expression which is variable in hcc and linked to a stem cell phenotype with adverse prognosis. few data exist regarding ctc detection in the peripheral blood in hepatocellular carcinoma (hcc), and no previous study has analyzed blood samples from the hepatic vein.
Methods: Patients were recruited to this study if they were planned to undergo hepatic wedge pressure gradient measurement as part of a pre-operative assessment for hepatic resection of hcc. hcc was diagnosed by radiological or pathological criteria. During the procedure, 7.5mls blood was taken concurrently from the peripheral and hepatic vein and ctcs were enumerated using the cellsearch system. correlations with clinical and pathological data were assessed using a fisher’s exact test for proportions, and using a student’s t test for continuous variables.
results: In total, 21 patients were included; 20 had paired hepatic vein and peripheral samples and 1 had only hepatic vein sample. all patients were cirrhotic; 11 due to hepatitis c virus, 3 due to alcohol, 3 due to non-alcoholic steato-hepatitis, 4 due to others or mixed etiologies. one patient had a radiological thrombosis of the left portal vein, 5 had more than 1 lesion. BcLc stage was 0 in 3 patients, a in 12, B in 4 and c in 2. Median radiological size was 25 mm (range 6-90), median alpha-feto protein (afP) was 20 ng/mL (range 3-22,637). at the time of analysis, 11 patients had undergone surgery (10 resections and 1 liver transplantation): tumor was well, moderately and poorly differentiated in 1, 9 and 1 cases respectively, and microscopic vascular invasion was present in 5 cases. overall, ctc positivity in the peripheral blood was found in only 1 of 20 (5%) patients. ctc positivity in the hepatic vein blood was found in 4 of 21 (19%) patients (1 cell/7.5mL in 3, 3 cells/7.5mL in 1) all of whom were negative in peripheral blood. every patient positive for ctc in the hepatic vein had a solitary lesion, while the patient positive for ctc in the peripheral blood had 2 lesions. Median radiological size of the greatest lesion was 30 mm in case of ctc positivity in the hepatic vein vs 22 mm in case of ctc negativity (p=0.25), while median afP was 124 vs 16 ng/
Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s8 2
mL, respectively (p=0.31). regarding the 11 patients with pathologic data, among the 5 patients with microscopic vascular invasion, 3 (60%) were ctc positive in hepatic vein, while no patient without microscopic vascular invasion were ctc positive. however, the small numbers precluded statistical significance (fisher’s exact test p=0.061). In the 11 patients with pathologic data, epcaM expression was found by immunohistochemistry in 2 patients, including one ctc positive in hepatic vein; 2 other ctc positive patients were epcaM negative in the resected tumor.
Conclusion: epcaM positive-ctc were rarely detected in patients with early-stage hcc undergoing work-up before surgery. however, ctc were more frequently found in the hepatic vein sample and this may be associated with vascular invasion.
Disclosure of Interest: none Declared
P-164 eArLy DerMATOLOGICAL ADVerSe eVenTS AnD COMPLeTe rADIOLOGICAL reSPOnSe In hCC PATIenTS TreATeD WITh SOrAfenIb. The LInK TO TreATMenT effICACy
Álvaro Díaz* 1, jordi rimola2, reig Maria1, anna Darnell2, María Varela 3, fernando Pons4, Manuel hernandez-Guerra5, Manuel Delgado6, javier castroagudin7, ana Matilla 8, carmen ayuso2, jordi Bruix1
1Barcelona clinic Liver cancer (BcLc) Group. Liver unit, 2Barcelona clinic Liver cancer (BcLc) Group, radiology Department, hospital clínic Barcelona, IDIBaPs, cIBerehd, university of Barcelona, Barcelona, 3Liver unit, hospital universitario central de asturias, oviedo, 4servicio de Digestivo, hospitaluniversitario Puerta de hierro, Madrid, 5Liver unit, university hospital of the canary Islands, canary Islands, 6servicio de Digestivo, hospital universitario, La coruña, 7Liver unit, hospital clínico universitario de santiago, santiago de compostela, 8servicio de Digestivo, hospital General universitario Gregorio Marañón, Madrid, spain
Introduction: sorafenib improves the overall survival (os) of patients with advanced hepatocellular carcinoma (hcc) and delays the radiologic tumor progression (tP). however, the benefit of sorafenib is downturned due to the absence of complete response (cr) in the sharP trial. there are few reports of hcc patients with cr under sorafenib treatment but the criteria to define cr are heterogeneous (mrecIst in retrospective analysis, recIst v1.0 and choi criteria).
aim: to analyze the profile of the patients who achieve cr with the same response criteria as used in the sharP trial and the rate of cr in hcc patients under sorafenib
Methods: We conducted a nationwide survey among 17 spanish centers which treated hcc with sorafenib and retrospectively collected all cases with registered cr. Baseline characteristics, the presence of dermatological adverse events within the first 60 days (Dae60) after starting sorafenib and the cause of treatment discontinuation were annotated. their radiological images at 4 time points (pre-sorafenib, at the time of cr and at least 1 month after cr to confirm it), were centrally reviewed by 2 independent radiologists applying the sharP modifications for recIst v1.0 disregarding contrast uptake pattern.
results: 1027 hcc patients were treated with sorafenib between 2007 to March 2014, 20 out of them were initially registered locally as cr, but 8 were excluded after central reading due to absence of baseline target lesion (3), target lesion treated simultaneously with radiofrequency or resection (2) and non-confirmed cr at central radiology review (3).finally, we report 12 hcc patients who achieved cr under sorafenib [58% hcV+, median age 59.7 years [49.8-77.9], 83% child-Pugh (cP) a, Ps 0 92 %, BcLc-B 33 y BcLc-c 67]. all but 1 started at full dose (800 mg/day). the daily dose at the time of cr was: 800mg in 4 patients, 600 mg in 1, 400mg in 3, 200 mg in 1. three patients had discontinued sorafenib prior to registering cr due to adverse events. the median follow-up, treatment duration, treatment duration until cr and mean os were 58, 28, 13 and 75 months, respectively. all but 1 patient had developed Dae60. six patients had discontinued sorafenib at the end of follow-up (3 for vascular events, 2 for patient decision and 1 due to liver decompensation). two patients developed tumor recurrence after discontinuing sorafenib.
Conclusion: complete response under sorafenib is an uncommon event (around1%), but it may occur. Dae60 are registered in almost all cases with such positive evolution and thus, this association supports the relationship between a specific immune/inflammatory patient profile and improved response to sorafenib. accordingly, assessment of the genetic make-up and the inflammatory/immunologic profile of the patients may help understand the mechanism of action of sorafenib and move to a predictive medicine with refined response prediction to therapy.
Disclosure of Interest: Á. Díaz : none Declared, j. rimola advisory Board of: Bioclinica and robarts clinical trials, r. Maria advisory Board of: Bayer, a. Darnell: none Declared, M. Varela advisory Board of: Bayer, f. Pons: none Declared, M. hernandez-Guerra: none Declared, M. Delgado advisory Board of: Bayer, j. castroagudin advisory Board of: Bayer, a. Matilla : none Declared, c. ayuso: none Declared, j. Bruix Grant support from: Bayer, Daichi, arqule, advisory Board of: Bayer, Biocompatibles, novartis, consulting of: Bayer, Daichi, arqule, BMs, Glaxo, kowa, Lilly, novartis, roche
P-165 IMPACT Of fIbrObLAST GrOWTh fACTOr-2 AnD ITS reCePTOr Gene POLyMOrPhISMS On TuMOr PrOGreSSIOn AnD PATIenT SurVIVAL In PATIenTS WITh hePATITIS b VIruS-ASSOCIATeD hePATOCeLLuLAr CArCInOMA
hyo Jung Cho* 1, choong kyun noh1, soon sun kim1, sung Won cho1, jae youn cheong1
1Gastroenterology, ajou university school of Medicine, suwon, korea, republic of
Introduction: the fibroblast growth factor (fGf), vascular endothelial growth factor and hepatocyte growth factor play a critical role in hepatocellular carcinoma (hcc). We determined the association of single nucleotide polymorphisms (snPs) of growth factor signaling related genes with the development and progression of tumor and overall survival in patients with hepatitis B virus (hBV)-associated hcc.
Methods: We assessed 9 snPs of fGf1, fGf2, fGf receptor (fGfr)-2, flt-1 and c-Met gene in 245 patients with hcc and 483 chronic hBV carriers without hcc.
results: none of all tested snPs was associated with the risk of hcc in chronic hBV carriers. fGf2 rs308379 a allele was significantly associated with small tumor size, early tumor stage and less vascular invasion. flt-1 rs4771249 c allele was associated with low alpha-fetoprotein level. In kaplan-Meier analysis, the patients with fGf2 rs308447 tt genotype showed decreased survival than the patients with cc or ct genotype (P = 0.016) and fGf2 rs308379 a allele carrier had a shorter survival than tt genotype (P = 0.020). In addition, fGfr2 rs1219648 cc genotype was significantly associated with increased survival (P = 0.047). Multivariate cox proportional analysis revealed that fGf2 rs308379 aa genotype [hazard ratio (hr) = 0.635, P = 0.033] and advanced tumor stage (hr = 2.819) were independent prognostic factors for overall survival in patients with hcc.
Conclusion: these observations suggest that the snP of fGf2 and fGfr2 gene can be a potential indicator of the tumor progression and the survival in patients with hBV-associated hcc.
Disclosure of Interest: none Declared
P-166 VALIDITy Of bArCeLOnA CLInIC LIVer CAnCer STAGe A: ASSOCIATIOn Of TuMOr SIze AnD OVerALL SurVIVAL In A SInGLe hePATOCeLLuLAr CArCInOMA
yeonjung ha* 1, ju hyun shim1, kang Mo kim1, young-suk Lim1, han chu Lee1
1asan Medical center, university of ulsan college of Medicine, seoul, korea, republic of
Introduction: Barcelona clinic Liver cancer (BcLc) staging system allocates patients based on multifactorial parameters, including tumor size and number. according to BcLc policy, patients with a single hepatocellular carcinoma (hcc) and preserved liver function belong to stage a, regardless of tumor size. however, in the treatment perspective, sorting out patients with potentially unresectable disease is needed in order to predict survival more accurately and to prevent unnecessary surgery.
Methods: We analyzed the asan Liver center database from 2004 to 2007 on 297 patients, who were initially diagnosed with single BcLc a hcc but treated with transarterial chemoembolization. We fit cox regression model to evaluate the prognostic factors, and receiver operating characteristics (roc) curve was used to identify the optimal cut-off of tumor size. survival analysis using kaplan-Meier curve with log-rank test was done to see whether the cut-off dichotomized patients’ survival.
results: the mean tumor size was 5.5 ± 3.7 cm in all patients. on univariate and multivariate analyses, infiltrative tumor type (odds ratio [or] 2.64 (1.68-4.15), P<0.001), tumor size (or, 1.10 (1.06-1.14), P<0.001), age (1.02 (1.00-1.04), P=0.023), and alpha-fetoprotein level (1.00 (1.00-1.00), P=0.006) were significantly associated with overall survival (multivariate data shown), whereas child-Pugh class and Model for end-stage Liver Disease score were not. the optimal tumor size to predict the overall survival was 4.05 cm on roc analysis. compared with individuals with > 4.0 cm tumor, those with smaller lesion were more likely to survive (median survival 64.2 [40.2-88.2] months vs 32.9 [28.6-37.1] months, P<0.001).
Conclusion: In patients with a single BcLc a hcc, tumor size of > 4.0 cm predicts the overall survival; thus this cut-off may be considered when stratifying patients. additional studies to compare the survival outcome with subjects undergoing surgical resection of large (> 4.0 cm) tumor are needed in future.
references: 1. Llovet jM, Bru c, Bruix j. Prognosis of hepatocellular carcinoma: the BcLc staging classification. seminars in liver disease. 1999;19(3):329-38.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 8 3
P-167 GLuTAMInASe SCOre SerVeS AS The bIOMArKer fOr PAThOLOGIC DIAGnOSIS AnD PrOGnOSIS Of hePATOCeLLuLAr CArCInOMA
xianbiao shi1, 2, chen yan2, 3, Gang Meng2, jun chen4, jiwu Wei2, 5, yong jiang2, 6, yitao Ding1, 2,
Decai yu* 1, 2
1Department of hepatobiliary surgery, the affiliated Drum tower hospital, school of Medicine, nanjing university, 2jiangsu key Laboratory of Molecular Medicine, Medical school of nanjing university, nanjing, 3Department of hepatobiliary surgery, the third affiliated hospital of soochow university, changzhou, 4Department of Pathology surgery, the affiliated Drum tower hospital, school of Medicine, nanjing university, 5nanjing university hightech Institute at suzhou, nanjing, 6Department of Pathology surgery, the third affiliated hospital of soochow university, changzhou, china
Introduction: Glypican-3 (GPc3), glutamine synthetase (Gs), and alpha fetoprotein (afP) etc. have been used as the hepatocellular carcinoma (hcc) biomarkers, but the sensitivity and specificity in the pathological diagnosis and prognosis for hcc is not high[1]. as we know, glutaminolysis plays a huge role in the process of tumor proliferation and metabolism. Mitochondrial glutaminase is the major limiting enzyme that converts glutamine to glutamate in glutaminolysis[2]. our previous study showed that high expression of GLs1 and low expression of GLs2 in hcc correlated with survival time of hcc patients, and expression of GLs1 and GLs2 were independent indexes for survival time[3]. so it is assumed that GLs score, combined with expression of GLs1 and GLs2 protein, were correlated with the pathological diagnosis or prognosis of hcc.
Methods: We investigated the expression and distribution of GLs1, GLs2, GPc3, Gs, and afP in a large set of clinical samples including hcc, normal liver, and other liver diseases obtained from the affiliated Drum tower hospital, Medical school of nanjing university. the first group of tissues (group 1) were paired tumor and adjacent non-tumor tissues from 112 patients with hepatocellular carcinoma (hcc) undergoing partial hepatectomy. the second group of tissues (group 2) included 5 hepatocellular adenomas (hca), 10 dysplastic nodules (Dn), 12 focal nodular hyperplasias (fnh), 44 fibrotic liver (fL), and 22 normal liver (nL) samples from living donors or donations after cardiac death of donors. the third group of tissues on a commercially available microarray (shanghai Biochip company Ltd, shanghai, china, hLiv-hcc180sur-01), which included 90 paired tt and nt of hcc, was used to analyze the relationship between GLs1 expression and the biological behaviors of hcc patients. GLs1 was scored according to the intensity: 2 for strongly positive, 1 for weakly positive, and 0 for negative, while GLs2 was scored: 0 for strongly positive, 1 for weakly positive, and 2 for negative.
results: GLs score was higher in hcc than adjacent non-tumor tissue, and se and sP of GLs score for hcc was 96% and 86. 41% respectively, when the threshold for GLs score was set at grade 3 (fig. a and B). and GLs score is not associated with clinical features of the patients with hcc, the expression of GPc3, and some tumor characteristics (table 1), while GLs score were independent indexes for survival time (fig. c).
Image:
Conclusion: this investigation of a large number of human hcc specimens confirms that GLs score is a potential biomarker for hcc pathological diagnosis and prognosis.
references: 1. tremosini s, forner a, Boix L, Vilana r, Bianchi L, reig M, rimola j, rodriguez-Lope
c, ayuso c, sole M et al: Prospective validation of an immunohistochemical panel (glypican 3, heat shock protein 70 and glutamine synthetase) in liver biopsies for diagnosis of very early hepatocellular carcinoma. Gut 2012, 61(10):1481-1487.2. DeBerardinis rj, cheng t: q's next: the diverse functions of glutamine in metabolism, cell biology and cancer. Oncogene 2010, 29(3):313-324.3. yu D, shi x, Meng G, chen j, yan c, jiang y, Wei j, Ding y: kidney-type glutaminase (GLs1) is a biomarker for pathologic diagnosis and prognosis of hepatocellular carcinoma. Oncotarget 2015.
Disclosure of Interest: none Declared
P-168 SeruM AnGIOPOIeTIn LeVeLS COrreLATe WITh SeVerITy Of POrTAL hyPerTenSIOn buT DO nOT PreDICT The PreSenCe Of hePATOCeLLuLAr CArCInOMA In CIrrhOSIS
brian J. hogan* 1, Ioanna Parisi1, tim Meyer2, james P. o'Beirne1
1Institute for Liver and Digestive health, 2ucL cancer Institute, ucL, London, united kingdom
Introduction: hepatocellular carcinoma (hcc) is one of the most devastating complications of chronic liver disease and outcome is improved by early detection. hcc is a highly vascular tumour and tumour angiogenesis plays a key role in progression. recent reports demonstrate that the angiogenic cytokine angiopoietin-2 (anG-2) is prognostic in hcc, although its role in hcc pathogenesis has not been defined [1,2]. to further understand anG-2 in the context of hcc, we have measured serum levels in patients with cirrhosis with and without hcc.
Methods: We assessed serum levels of angiopoietin-1 (anG-1) and anG-2 in patients having hepatic venous pressure gradient (hVPG) measurements performed at our centre. anG-1 and anG-2 levels were measured in serum using commercially available eLIsa kits (quantikine® human Immunoassays, r&D systems Inc., Minneapolis, usa) according to the manufacturers instructions. all participants gave informed consent and the national health service research and ethics service approved the study.
results: 48 patients with cirrhosis were assessed, of which 13 had hcc. the aetiology of their liver disease was alcohol in 44%, viral hepatitis in 25%, non-alcohol related fatty liver disease in 13%, autoimmune in 8%, cryptogenic in 6%, a combination of alcohol and non-alcohol related fatty liver in one patient (2%) and alpha-1 anti-trypsin disease in one patient (2%). there was a trend towards a higher hVPG and MeLD in the ‘no hcc’ group and this increased severity of liver disease may account for the higher absolute values of anG-2 and lower anG-1 in this group.
In all cases the anG-2/anG-1 ratio strongly correlated with the hVPG with a correlation co-efficient of 0.632 (p<0.001) by spearman’s rho. [see figure 1].
all
(n=48)hcc
(n=13)no hcc(n=35)
hcc v no hcc
anG-1 (pg/mL) 19990(10090 - 32290)
24850(12790 - 35105)
19690(9663 - 28765)
p=0.366
anG-2 (pg/mL) 5468(2681 – 9765)
3752(2485 – 6146)
6238(3485 - 10745)
p=0.199
anG-2/anG-1 ratio
0.28(0.17 – 0.65)
0.20(0.07 – 0.49)
0.31(0.17 – 0.77)
p=0.131
afP (kunits/L) 4.8(3.0 – 12.4)
17.3(5.8 – 663.7)
4.1(2.7 – 4.8)
p<0.001
hVPG (mmhg) 13.0(8.0 – 16.0)
12.0(6.5 – 15.5)
13.0(8.0 – 17.0)
p=0.453
MeLD 12(8 – 23)
11(8-17)
13(9 – 24)
p=0.389
table 1 – Median (interquartile range) anG-1, anG-2, anG-2/anG-1 ratio, afP, hVPG and MeLD in patients with cirrhosis with and without hcc.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s8 4
Image:
Conclusion: there was no significant difference in the circulating angiopoietin levels in cirrhotic patients with or without hcc. however, the anG-2/anG-1 ratio correlated strongly with hVPG suggesting that the increased levels of pro-angiogenic cytokines previously reported in hcc, may be secondary to the severity of fibrosis and/or portal hypertension rather than the presence hcc.
references: 1. Bupathi M, kaseb a, janku f. angiopoietin 2 as a therapeutic target in hepatocellular carcinoma treatment: current perspectives. onco targets ther 2014;7:1927-1932.2. Llovet jM, Pena ce, Lathia cD, shan M, Meinhardt G, Bruix j, Group sIs. Plasma biomarkers as predictors of outcome in patients with advanced hepatocellular carcinoma. clin cancer res 2012;18:2290-2300.
Disclosure of Interest: none Declared
P-169 The AuTOPhAGy-reLATeD MArKer P62 IS uSefuL fOr DIAGnOSIS In huMAn hePATOCeLLuLAr CArCInOMA
Chang Jae hur* 1, jung Min Lee1, jeong Min kim1, hye Min Park1, kyung ho yang1, yu na kang2, koo jeong kang3, Woo jin chung1, jae seok hwang1, Byoung kuk jang1
1Department of Internal Medicine, 2Department of Pathology, 3Department of surgery, keimyung university school of Medicine, Daegu, korea, republic of
Introduction: several studies showed that accumulation of p62 by impaired autophagy was related with tumorigenesis including hcc. recent study reported that p62 immunohistochemical (Ihc) staining can be helpful in the diagnosis of hcc. therefore, we studied in order to verify the usefulness of p62 Ihc staining for pathologic diagnosis of hcc.
Methods: We retrospectively analyzed 186 patients with hcc that was confirmed histologically after complete surgical resection at keimyung university Dongsan hospital in Daegu, korea, from 2001 to 2011. the expression of p62 was analyzed by Ihc on hcc and surrounding non-tumor tissues. Ihc stainings including Glutamine synthetase(Gs), Glypican 3(GPc3) and heat shock protein 70(hsP70) were also analyzed to compare with p62. statistical values and correlations with clinical features were evaluated using the chi-square test and Mcnemar analysis.
results: P62 Ihc analysis of hcc and surrounding non-tumor tissue showed 97.8% of sensitivity, 83.3% of specificity, 90.6% of accuracy, 85.4% of PPV and 97.5% of nPV. sensitivities of Gs, GPc3 and hsP70 were 53.8%, 39.2% and 32.3%, respectively. specificities were 94.1%, 97.8% and 98.4%. accuracies were 73.9%, 68.5% and 65.3%. PPVs were 90.1%, 94.8% and 95.2%. nPVs were 67.0%, 61.7% and 59.2%. combinations of p62 and other markers showed no statistical benefit. P62 expression was correlated with edmonson-steiner Grades (p=0.024), however, it was not correlated with tnM stage, BcLc stage, child-Pugh class, time to recurrence. GPc3 was correlated with edmonson-steiner Grades (p=0.034). none of the four markers was correlated with overall survival period.
Conclusion: P62 showed higher sensitivity, accuracy and nPV than Gs, GPc3 and hsP70. these results suggest that the p62 Ihc staining can be useful marker for hcc diagnosis.
Disclosure of Interest: none Declared
P-170 IDenTIfICATIOn Of IMAGInG PreDICTOr DISCrIMInATInG hIGh rISK GrOuP fOr InTrAhePATIC ChOLAnGIOCArCInOMA Or COMbIneD hePATOCeLLuLAr-ChOLAnGIOCArCInOMA In PATIenTS WITh ChrOnIC LIVer DISeASe On GADOxeTIC ACID-enhAnCeD MrI: CLASSIfICATIOn Tree AnALySIS
hyun Jeong Park* 1, kyung Mi jang2, tae Wook kang2, kyoung Doo song2, young kon kim2, seong hyun kim2, joung youn kim3, juna Goo3, Min jung Park4
1radiology, chung-ang university hospital, 2radiology, 3Biostatistics and clinical epidemiology center, samsung medical center, seoul, 4radiology, ajou university school of medicine, suwon, korea, republic of
Introduction: accurate diagnosis of hepatocellular carcinoma (hcc) from intrahepatic cholangiocarcinoma (Ihcc) and combined hepatocellular-cholangiocarcinoma (chc) is important because of different treatment option and disease prognosis. occasionally, hccs and Ihccs could show atypical enhancement and similar enhancement patterns on gadoxetic acid-enhanced Mr imaging and chcs can also reveal overlapping features with classic hccs or Ihccs. therefore, it would be important that identify the imaging determinants discriminating the high risk group of Ihcc and chc for liver cancer in patients with chronic liver disease on gadoxetic acid-enhanced MrI
Methods: Pathologically proven 40 Ihccs, 24 chcs and 91 hccs satisfying Milan criteria in patients with chronic liver disease were enrolled in this study. Mr imaging variables including morphologic features, signal intensity and enhancement pattern of the tumors were used to identify the high risk group for Ihcc and chc in patients with chronic liver disease.
results: on the classification tree analysis, arterial rim enhancement and non-globular shape were the first and second variables discriminating the subgroups for risk of Ihcc and chc. of 45 tumor showed arterial rim enhancement and non-globular shape on MrI, 41(91%) tumors were 29 Ihccs and 12 chcs.
Conclusion: arterial rim enhancement and non-globular shape of the tumor on MrI were the important determinants related with probability of Ihcc and chc in patients with chronic liver disease.
references: Bruix j, sherman M, american association for the study of Liver D. Management of hepatocellular carcinoma: an update. hepatology 2011;53(3):1020-1022.Lee Ws, Lee kW, heo js, et al. comparison of combined hepatocellular and cholangiocarcinoma with hepatocellular carcinoma and intrahepatic cholangiocarcinoma. surg today 2006;36(10):892-897.Park hj, kim yk, Park Mj, Lee Wj. small intrahepatic mass-forming cholangiocarcinoma: target sign on diffusion-weighted imaging for differentiation from hepatocellular carcinoma. abdom Imaging 2013;38(4):793-801.an c, kim DW, Park yn, chung ye, rhee h, kim Mj. single hepatocellular carcinoma: Preoperative Mr Imaging to Predict early recurrence after curative resection. radiology 2015:142394.kawamura y, Ikeda k, hirakawa M, et al. new classification of dynamic computed tomography images predictive of malignant characteristics of hepatocellular carcinoma. hepatol res 2010;40(10):1006-1014.asayama y, nishie a, Ishigami k, et al. Distinguishing intrahepatic cholangiocarcinoma from poorly differentiated hepatocellular carcinoma using precontrast and gadoxetic acid-enhanced MrI. Diagn Interv radiol 2015;21(2):96-104.Mitchell DG, Bruix j, sherman M, sirlin cB. LI-raDs (Liver Imaging reporting and Data system): summary, discussion, and consensus of the LI-raDs Management Working Group and future directions. hepatology 2015;61(3):1056-1065.
Disclosure of Interest: none Declared
P-171 APPLICATIOn Of COnTrAST-enhAnCeD InTrAOPerATIVe uLTrASOunD uSInG PerfLubuTAne TO hePATIC reSeCTIOn fOr LIVer CAnCer
Junichi Arita* 1, akinori Miyata1, satoshi yamamoto1, nobuhisa akamatsu1, junichi kaneko1, yoshihiro sakamoto1, kiyoshi hasegawa1, norihiro kokudo1
1hepatobiliary-Pancreatic surgery Division, university of tokyo, tokyo, japan
Introduction: contrast-enhanced intraoperative ultrasound (ce-Ious) using perflubutane has been developed as a novel tool for liver surgery. Perflubutane has a peculiarity of accumulating in the kupffer cells of the liver, thus enabling stable contrast effect on ultrasound in a dedicated mode. the aim of this study is to assess the utility of this technique.
Methods: consecutive 192 patients with 10 or less hcc tumors were enrolled. a focal liver nodule is tentatively diagnosed as hcc if it is hypervascular in the vascular phase and/or hypoechoic in the kupffer phase. newly found nodules during conventional Ious and newly found during ce-Ious were assessed. consecutive 100 patients with 12 or less crLM tumors were enrolled. all of Gd-eoB-enhanced MrI, contrast-enhanced ct, contrast-enhanced ultrasound were performed preoperatively, and Ious and ce-Ious were performed intraoperatively. anatomical hepatic resection was performed in a novel method using both ce-Ious and indocyanine green. additionally, hepatic parenchymal

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 8 5
transection was performed with intermittent ce-Ious guidance in the patients undergoing.
results: In hcc study, 79 new nodules including 17 hcc tumors were identified using Ious, and differential diagnosis using ce-Ious resulted in 65% of sensitivity, 94% of specificity, and 87% of accuracy. additional 21 nodules were identified during the kupffer phase of ce-Ious and 14 of them in 11 patients were finally diagnosed as hcc. In crLM study, 25 new nodules including 21 crLM tumors were identified using Ious, and ce-Ious correctly differentiated all of them besides one benign nodule. additional 22 nodules were identified using ce-Ious, and 17 nodules in 16 patients were histologically diagnosed as crLM. anatomical hepatic resections were successfully done using the novel method; an injection of contrast agent in a portal tributary and parenchymal filling with contrast agent was clearly confirmed using ce-Ious, the intrahepatic boundary of the hepatic volume fed by the aimed portal tributary was clearly demonstrated using ce-Ious, and the boundary on the liver surface was clearly demonstrated using near infrared monitor because of indocyanine green accumulation. In intermittent ce-Ious reference during hepatic resection, the tumor margin was better demonstrated and the relationship among tumors, intrahepatic vasculatures, and liver transection plane was obtained more clearly than in conventional Ious.
Conclusion: ce-Ious is essential in liver surgery for liver cancer.
Disclosure of Interest: none Declared
P-172 MICrOrnA-452 PrOMOTeS TuMOr-InITIATInG CeLLS Of hePATOCeLLuLAr CArCInOMA by ACTIVATInG WnT/beTA-CATenIn SIGnALInG PAThWAy
zhiyun zheng* 1, Lin zhou1, zhe yang1, haiyang xie1, Liming Wu1, chunyang xing1, Bingyi Lin1, tianchi chen1, shusen zheng1
1Department of hepatobiliary and Pancreatic surgery, first affiliated hospital, zhejiang university school of Medicine, hangzhou, china
Introduction: Micrornas (mirnas) play important roles in tumor differentiation and oncogenesis. tumor-initiating cells (t-Ics) is thought to be the key reason for the recurrence and metastasis of hepatocellular carcinoma(hcc). however, the role of microrna-452(mir-452) in hcc remains ambiguous.
Methods: We enriched t-Ic population which showed stem-like traits of self-renewal and tumor initiation by serial passages of hepatospheres with chemotherapeutic agents including doxorubicin and sorafenib. the expression of mir-452 was measured in hcc cell lines using real-time Pcr and tissues using in-situ hybridization(Ish). hcc cell lines were transduced with lentiviruses that stably expressed mir-452 or shrna-mir-452. Western blotting, co-immunoprecipitation, immunofluorescence, and luciferase reporter assays were used to measure expression and activity of sox7, beta-catenin ,tcf4.
results: In the drug-resistant spheres, mir-452 was found to be increased comparing with differentiated progenies. the mir-452 was significantly overexpressed in tumor tissue than that in adjacent normal tissue(P<0.001). Its expression level was proportional to tnM stage(P<0.001) and patients overall survival(P<0.001). overexpression of mir-452 promoted t-Ics related properties such as selfrenewal, tumor intiation and tumor metastasis, whereas mir-452 depletion reduced these traits. Moreover, western blotting showed that nuclear beta-catenin and tcf4 were upregulated when overexpressing mir-452, while these were downregulated when deleting mir-452 expression. then, with the target prediction tool(targetscan), sox7 was predicted to be a potential target of mir-452, which were proved by luciferase reporter assay and western blotting. rescue experiment showed that overexpressing sox7 with lenti-sox7 orf could significantly reverse the phenotype of mir-452 overexpression. futher, Luciferase reporter assay of the Wnt signaling reporter (toPflash and foPflash) indicated that sox7 could inhibit the activity of Wnt signaling pathway in hek293t cell. Immunofluorescent assays showed that sox7 was co-localizaed with either β-catenin or tcf4 protein in nucleus. then, co-immunopreciptation analyses proved that sox7 could interact with β-catenin and tcf4 proteins. rescue experiment of sox7 could significantly decrease the nuclear beta-catenin and tcf4 proteins expression.
Conclusion: up regulation of mir-452 in hcc might be involved in the regulation of t-Ics and tumor oncogenesis and may be an potential therapeutic target for hcc therapy.
Disclosure of Interest: none Declared
P-173 effeCT Of SurGICAL MArGIn STATuS On TuMOr reCurrenCe AfTer reSeCTIOn fOr hePATOCeLLuLAr CArCInOMA bASeD On PreOPerATIVe CIrCuLATInG TuMOr CeLLS LeVeL
xin-rong yang* 1, yun-fan sun1, jian zhou1, jia fan1
1Liver surgery Department, Liver cancer Institute & zhong shan hospital, shanghai, china
Introduction: how to balance the relationship between complete removal of tumor and maximum
preservation of liver function is the key for hepatocellular carcinoma (hcc) patients undergoing hepatic resection. Inadequate surgical margins may result in high local recurrence due to microvascular invasion (mVI) by tumor cells, while excessively resections may cause more functional liver parenchyma lost and result in hepatic failure. our previous study indicated that a preoperative circulating tumor cells (ctc) ≥2 was an independent prognosticator for early recurrence in hcc after surgery, and recurrent foci developed were mostly observed near the surgical margin of remnant liver. however, there is no data on what constitutes an adequate surgical margin in those patients. herein, we investigated the correlation between preoperative ctc load and features of mVI and the optimum surgical margin threshold for hcc patients based on preoperative ctc level.
Methods: We prospectively enrolled 26 hcc patients to evaluate the relationship between ctc counts and features of mVI and another cohort of 179 hcc patients to examine the optimal surgical margin. ctcs were detected by cellsearch system. the numbers of mVI and its distance from the tumor were recorded based on histological analysis. the width of resection margin was defined as closest distance from tumor edge to the transection plane of the liver parenchyma.
results: In 26 patients, 20 patients had mVI detected. the proportions of patients with farthest mVI distance of 0.5cm, 1cm, 2cm, 3cm and >3cm were 19.2%, 19.2%,15.4%, 11.5% and 11.5% respectively. of all microvessels invaded, 45.6% distributed ≤0.5cm from tumor edge, 18.4% within >0.5 to ≤1cm, 20.4% within >1 to ≤2cm, 12.2% within >2 to≤3cm and 3.4% >3cm. the number of ctc was positively correlated with the farthest distance of mVI from the tumor edge (r=0.697, P<0.001) and the number of microvessels invaded (r=0.656, P<0.001). In 12 patients who had ≥2ctc detected, the mean distance of mVI from tumor was significantly farther than those with ctc<2 (2.29±0.41 vs. 0.64±0.19, P<0.001), and the number of microvessels invaded was significantly higher than those with ctc<2 (9.50±1.04 vs. 2.36±2.23, P=0.006). In 179 patients, 73 had ctc of ≥2 preoperatively. among them, 55.6% had resection margin width of ≤0.5cm, 18.9% within>0.5 to ≤1cm, 17.8% within>1 to ≤2cm and 7.7% within >2 to ≤3cm. compared with a margin of >1 to ≤2cm, patients with margin width of ≤0.5cm (81.6% vs. 38.5%, P=0.003) and of >0.5 to ≤1cm (81.6% vs. 38.5%, P=0.048) were associated with a significantly higher risk of postoperative recurrence. however, when a >1 to ≤2 cm margin was compared with a margin of >2 to ≤3cm (38.5% vs. 33.3%, P=0.924), no significant difference in the risk of recurrence was observed. Patients with a margin of >1 cm had reduced rates of recurrence (35.3% vs. 78.5%) and shorter time to recurrence (P=0.002) compared with those with a ≤1cm margin. In 106 patients with ctc<2, there was no significant difference in recurrence risk between a margin of >1cm and ≤1cm (31.2% vs. 34.5%, P=0.709), as well as a ≤0.5cm margin and a margin of >0.5 to ≤1cm (31.6% vs. 20%, P=0.338).
Conclusion: the load of ctc before surgery positively correlated with the number and distance of mVI. In patient with ≥2 ctc detected, a threshold of 1cm is the optimal width of surgical margin, which might have a similar impact as a larger margin do and facilitate the preservation of functional liver parenchyma. In patients with <2 ctc, a width ≤0.5cm will be enough for hepatic resection.
Disclosure of Interest: none Declared
P-174 hePATOCeLLuLAr CArCInOMA SurVeILLAnCe IS ASSOCIATeD WITh SIGnIfICAnT POTenTIAL hArMS In PATIenTS WITh CIrrhOSIS
Amit Singal* 1, omair atiq1, Purva Gopal1, adam yopp1, sanjeeva kalva1, jorge Marrero1
1ut southwestern Medical center, Dallas, united states
Introduction: hepatocellular carcinoma (hcc) surveillance tools have minimal direct harms; however, there are potential downstream harms from follow-up diagnostic tests. an assessment of screening-related harms is crucial given many primary care providers question the benefits of hcc surveillance. In fact, two recent systematic reviews concluded an assessment of hcc surveillance harms was a high priority area for future research. the aim of our study was to quantify and characterize potential harms of hcc surveillance among a large cohort of patients with cirrhosis.
Methods: We conducted a retrospective cohort study among patients with cirrhosis followed at a safety-net health system. We recorded surveillance abdominal imaging and/or alpha fetoprotein (afP) testing between january 2010 and December 2013. We defined a false positive surveillance test as a suspicious liver mass on ultrasound or afP >20 ng/mL, with no hcc diagnosis during follow-up evaluation. We defined indeterminate tests as an ultrasound with a subcentimeter masses or coarse echotexture or afP 11-19 ng/mL. We recorded potential harms of hcc surveillance including ct or MrI scans, biopsies, or any procedures performed as a direct result of surveillance testing, as determined by the recorded indication in the medical record. Predictors of harm were identified using univariate and multivariate logistic regression, with statistical significance defined as p≤0.05.
results: We identified 603 patients with cirrhosis, with median follow-up of 2.8 years. Median age was 53 years, and 67% were male. the most common liver diseases were 50% hepatitis c, 30% alcohol-induced, and 12% nonalcoholic steatohepatitis. nearly half (47%) of patients were receiving hepatology specialty care. hcc surveillance was performed in 463 with ≥1 surveillance ultrasound and 457 with ≥1 afP level. of 32 incident hcc, 8 tumors were found incidentally and 24 (75%) were detected by surveillance - 13 by surveillance ultrasound, 6 by surveillance afP, and

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s8 6
5 by surveillance ultrasound and afP. over the same time period, false positive surveillance tests led to diagnostic cross sectional imaging in 123 (22.3%) patients, of whom 49 (8.9%) had multiple ct and/or MrI studies. two (0.4%) patients underwent biopsy after 8 ct/MrI negative scans and 1 (0.2%) patient underwent angiogram after 7 negative ct/MrI studies. false positive surveillance tests - hepatic mass >1 cm on ultrasound (38%) and false positive afP (25%) – were the trigger for the majority of surveillance harms. however, patients also underwent unnecessary diagnostic testing for indeterminate tests - coarse hepatic echotexture (25%) and/or subcentimeter masses on surveillance ultrasound (12%). on multivariate analysis, surveillance harms were associated with viral liver disease (or 1.60, 95%cI 1.04-2.46), receipt of hepatology care (or 2.32, 95%cI 1.52-3.59), and enrollment in the county healthcare subsidy plan that did not have a deductible (or 2.21, 95%cI 1.45 – 3.40).
Conclusion: over 1 in 5 patients experience harm from hcc surveillance, with nearly 10% having multiple diagnostic exams. ultrasound results in more hcc surveillance harms than afP in clinical practice given high rates of diagnostic testing for indeterminate lesions. Better hcc surveillance tools, with higher specificity, are urgently needed.
Disclosure of Interest: none Declared
P-175 funCTIOnAL nOnInVASIVe IMAGInG Of KuPffer CeLLS STATuS uSInG rADIOLAbeLLeD MAnnOSyLATeD ALbuMIn
Vineet Mahajan* 1, robert comley2, siddesh hartimath1, klaas Poelstra3, catharina reker-smit3, jan kamps4, jurgen sijbesma1, janine Doorduin1, Michel koole1, rudi Dierckx1, erik D. Vries1
1nuclear Medicine and Molecular Imaging, university Medical center Groningen, Groningen, netherlands, 2f. hoffmann La roche, Basel, switzerland, 3Pharmacokinetics and toxicology, university of Groningen, 4Medical biology, university Medical center Groningen, Groningen, netherlands
Introduction: kupffer cells (kc), specialized macrophages, constitutes ~ 15% of the total liver cell population, are responsible for maintaining liver homeostasis and have a vital role in innate immune responses, host defence, immune tolerance, chronic hepatotoxicity and many liver diseases. currently, there is no accepted method to monitor kupffer cell status in vivo. this method is beneficial for our understanding of the early phases of liver toxicity, the progression of various liver diseases and mechanisms of liver regeneration. It will also provide a novel way to monitor the efficacy of treatment and transplant survival. Positron emission tomography (Pet) is a non-invasive imaging technique that allows quantification and visualization of biochemical processes by monitoring the distribution of molecules labelled with positron emitting isotopes. the aim of this project is to develop a novel Pet imaging method to assess kupffer cell activity/number and validate it in animal models mimicking liver toxicity.
Methods: our strategy focused on radiolabeled mannosylated human serum albumin (mhsa) derivatives that target kupffer cells via the mannose receptor (cD206). hsa was mannosylated by conjugation with p-aminophenyl mannose that was activated with thiophosgene. three modified proteins with variable mannose loading (18-mhsa, 10-mhsa, and 5-mhsa) were synthesized and labelled by conjugation with n-succinimidyl 4-[18f]fluorobenzoate (sfB). the pharmacological properties of, 18-mhsa and 10-mhsa, were investigated in vivo (ex vivo biodistribution and in vivo Pet in healthy rats and rat models that mimick liver toxicity). Biodistribution studies were performed in male Wistar rats to evaluate the distribution of the tracer in healthy animals. In addition, dynamic Pet images of liver, were acquired for 30 and 60mins, immediately after the injection of 5–15 MBq of [18f]sfB-mhsa.
results: ex–vivo biodistribution and kinetic studies demonstrated [18f] sfB-18-mhsa was stable plasma, and displays saturable binding to the cD206 receptors in liver. In vivo, dynamic Pet data was acquired for 30 and 60 minutes after injection of 5-15 MBq of [18f]sfB-18-mhsa in rats (n=5). radioactivity in blood gradually decreased over time from the first time point (10 seconds) onward. hepatic uptake at 30 and 60 min was high (suV 11.3±2.4 at 30 min; suV 8.9±3.3 at 60 min; p<0.03), as was accumulation in the kidney (suV 24±7), due to metabolism in liver and rapid clearance of radioactivity from the blood pool via renal–urinary route. Blocking of the receptor by using fully saturating doses (20 fold excess) of the unlabelled 18-mhsa, decrease in uptake in target regions (organs with immune-related function (bone-marrow, spleen and liver; liver suV 0.819±1.1at 30 min; suV 4.5±0.7 at 60 min; p<0.03), is observed. In contrast, blocking studies with [18f] sfB-5-mhsa as a tracer and unlabelled 5-mhsa as a blocker showed an increase in suV values, indicating nonspecific uptake of the 5-mhsa analogue. Pet data was analysed by both Logan and Patlak graphical analysis using the metabolite-corrected plasma curve as input function. the data was well described by the Logan model, but not by the Patlak model, indicating reversible binding kinetics. Initial results from acute liver toxicity models suggests reduction in tracer uptake
Image:
Conclusion: [18f]sfB-18-mhsa is readily labelled, stable in plasma and shows specific binding in liver, and likely reflects the binding of the tracer to cD206 receptors in kupffer cells. [18f]sfB-18-mhsa provide a tool to asses kupffer cell activity, although further validation is in progress.
Disclosure of Interest: none Declared
P-176 COMPLICATIOnS AfTer PerCuTAneOuS rADIOfrequenCy AbLATIOn (rfA) Of hePATOCeLLuLAr CArCInOMA (hCC) In CIrrhOSIS: 20 yeArS exPerIenCe In A SInGLe CenTer
Antonio Giorgio* 1, valentina giorgio2, luca montesarchio3, paolo matteucci4, umberto scognamiglio5, carmine coppola6, pietro gatti7
1Internal medicine, tortorella clinical Institute, salerno, Italy, salerno, 2gastroenterology, Policlinico gemelli, roma, 3tortorella clinical Institute, salerno, Italy, salerno, 4radiology, campus biomedico, roma, 5radiology, tortorella clinical Institute, salerno, Italy, salerno, 6Internal medicine, grano hospital, gragnano, 7fasano hospital, brindisi, Italy
Introduction: aIM:to report 20 years experience on complications after rfa of hcc in cirrhotics with special emphasis on change of child class, haemorragic events and deaths.
Methods: from april 1994 to March 2014, 1787 rfa procedures were performed percutaneously under ultrasound guidance in 1162 consecutive cirrhotics (57-85 years; mean 68; 882 males ; 852 child a, 310 child B ). Diameter of hcc nodules ranged from 1.2 to 6.8 cm. Protrombintime (Pt) and platelet count were > 50% and 50.000 mm3, respectively; total bilirubin ranged from 0,80 and 3.4 mg/dl (mean 1.6 ).three rfa devices were employed: hooks elecrtrode-needle ( 170 cases ), perfused electrode-needle (1041 cases ) and cold electrode- needle ( 476 cases). 67 cirrhotics underwent rfa on both intraparenchymal hcc nodule and tumor thrombus in the main portal vein (PVtt) .
results: Mortality: 4 patients (0,4%) died after rfa : 2 for haemoperineum, 1 for haemotorax, 1 for liver failure. no patient treated for both intraparenchimal hcc and PVtt died.Morbidity: changes in child class of cirrhosis were observed in 19 patients (1.6%): 8 child a cirrhotics had development of liver decompesation (ascites and /or jaundice and /decreased Pt) changing from child a to child B class in 7 and from child a to child c in 1 case, respectively. 11 child B patients changed to child c class. 6 patients had haemoperitneum with no death. abscess formation was observed in 2 patients. one patient had intraepatic haematoma resolved spontaneously.Conclusion: rfa of hcc in cirrhotic patients can be considered safe, even in case of advanced disease, such as invasion of portal venous system. care must be made in the evaluation and surveillance of functional liver reserve. haemorragic adverse events remain the leading cause of mortality.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 8 7
P-177 COMPuTer ASSISTeD SurGery fOr GIAnT LIVer TuMOrS uSInG A nOVeL LIVer SeGMenTATIOn APPLICATIOn
Apollon zygomalas* 1, Dionissios karavias1, Dimitrios koutsouris2, Ioannis Maroulis1, Dimitrios karavias1, konstantinos Giokas2, Vasileios Megalooikonomou1
1university of Patras, Patras, 2national technical university of athens, athens, Greece
Introduction: anatomical liver resection is the preferred treatment for several types of liver tumors. however, giant liver tumors (>10cm in diameter) pose technical difficulties during the preoperative planning regarding liver volumetry, future liver remnant (fLr) calculation, tumor association with hepatic vascular tree or other adjacent anatomical structures, and definition of the resection plane. We developed a preoperative planning and intraoperative image guidance application which implements a novel semiautomatic liver segmentation algorithm. the aim of this study was to evaluate our application for cases of giant liver tumors.
Methods: from june 2013 to December 2014 all patients at the hepatobiliary unit of our hospital with giant liver tumors undergoing elective hepatectomies were enrolled in this prospective study. the liver imaging studies were independently performed for each patient at various radiological centers including our hospital, using different imaging protocols. We developed a semiautomatic liver segmentation algorithm and a preoperative planning application in MatLaB® (the MathWorks, Inc., natick, Massachusetts, u.s.a) optimized for use by surgeons. quantitative and qualitative (preoperative vs intraoperive) evaluation was performed. the liver segmentation results were evaluated against manual traced liver segmentations which were considered as ground truth. the accuracy of liver segmentation was assessed using; 1) the Dice similarity index (sI, %), 2) the Volumetric overlap error (Voe, %), 3) the relative Volume Difference (rVD, %) and 4) the symmetric Mean absolute surface Distance (sMaD, mm).
results: seven patients were included in this study. the mean age was 57 years (range 30-77). the mean tumor diameter was 12.4cm (range 10-17cm). the overall liver volume parenchyma segmentation time (computation time and interaction time) ranged from 5min to 9min with an average of 7.4min(sD±1.5). the average computer analysis (segmentation, volumetry, virtual hepatic resection planning and visualization) time was 38min/dataset (sD±3.9). the correlation coefficient (cc) between traced liver segmentations and the semiautomatic segmentations was 0.99 (95% cI, 0.97-0.99; p<0.0001). the average standardized fLr calculated by ProMytheIa was 62% and that calculated using manual boundary tracing was 63.1% (p=0.28) with a cc of 0.99 (95% cI, 0.98-0.99; p<0.0001). Mean sI was 95.62% (sD±1.55) with an average Voe of 8.36% (sD±2.83) and an average rVD of -3.9% (sD±3.33). Mean sMaD was 1.6mm (sD±0.79). the 3D liver models and the virtual liver resections had a qualitative acceptable correlation with the real intraoperative findings and the final liver resections.
Conclusion: the patient specific 3D models produced using our semiautomatic segmentation algorithm proved to be accurate for the preoperative planning of giant liver tumors surgery and effectively enhanced the intraoperative medical image guidance.
Disclosure of Interest: a. zygomalas Grant support from: for PhD studies by the onassis foundation, D. karavias : none Declared, D. koutsouris : none Declared, I. Maroulis : none Declared, D. karavias: none Declared, k. Giokas: none Declared, V. Megalooikonomou: none Declared
P-179 hISTOLOGICAL exPreSSIOn Of MeThIOnIne ADenOSyLTrAnSferASe (MAT) I AnD MAT II AS POST-SurGICAL PrOGnOSTIC SurrOGATeS In PATIenTS WITh hePATITIS b VIruS-reLATeD hePATOCeLLuLAr CArCInOMA
Mijung Jun* 1, ju hyun shim1, joo ho Lee2, Gi-Won song3, yangsoon Park4, eunsil yu4, sung-gyu Lee3, jihyun an1, Danbi Lee1, kang Mo kim1, young-suk Lim1, han chu Lee1, young-hwa chung1, yung sang Lee1
1Gastroenterology, asan medical center, 2Gastroenterology, cha university of Medicine and science, 3surgery, 4Pathology, asan medical center, seoul, korea, republic of
Introduction: It has been found that methionine adenosyltransferase 1a (Mat1a) gene, encoding isoenzymes Mat I/III, is dysregulated in hepatocellular carcinoma (hcc), and reduced Mat1a expression correlates with worse hcc prognosis. the x protein of hepatitis B virus (hBV) inhibits apoptosis in hcc cells through enhancing the expression of Mat2a gene, encoding Mat II. Ma1a/Mat2a switch has been severally demonstrated to be involved in hepatocarcinogenesis. We aimed to investigate prognostic implication of Mat I and Mat II protein expression in hBV-infected patients undergoing hepatic resection for hcc.
Methods: In this study, we used a tissue microarray constructed from archival surgical specimens of 166 patients with hBV-related hcc who underwent curative hepatectomy at asan Medical center. the tumor tissue microarray was immunohistochemically stained with primary antibodies against Mat I and Mat II. We examined pre- and post-surgical clinical factors related to Mat 1 and Mat II, using logistic regression analysis, and predictive effect of the two proteins on post-surgical recurrence and survival, using cox proportional hazards model.
results: of the 166 patients, 74.1% were male with a mean age of 52.8 ± 8.7 years, 94% were child-Pugh class a disease, and 55.4% had liver cirrhosis. In terms of histological factors, most patients had solitary tumor (93.4%) and tumors of 5cm or less (74.7%). Microvascular invasion and edmondson grade III/IV tumors were observed in 30.7% and 66.9%, respectively of the patients. During a median follow-up of 39 months (range 5-81 months), 12 deaths and 63 recurrences had been found, where 52 recurrences occurred early within 2 years after resection. Mat I and Mat II were positively expressed in 83.7% and 87.3%, respectively of the 166 tumor tissues. Mat I expression was independently associated with male and tumors of 5 cm or less (adjusted P<0.05 for both). expression of Mat II had a significant relationship with only serum afP >200 ng/mL (adjusted P<0.05). Multivariate cox regression analyses showed that Mat II expression was significantly correlated with shorter times to overall and early recurrences (hazard ratios 9.97 and 8.26, respectively; adjusted P<0.05 for both), as was not positive Mat I (hazard ratio 1.13; P=0.730). Immunopositivity for two proteins did not influence overall survival (P>0.05 for both). Mat I : Mat II activity ratio below 1.0 was observed in 12.7% of the patients, and not significantly associated with post-surgical recurrence and survival outcomes.
Conclusion: Immunohistological expression of Mat II in tumor may be helpful in predicting and monitoring tumor recurrence, especially in the early phase after hepatic resection, in patients with hBV-related hcc.
Disclosure of Interest: none Declared
P-180 ALPhA feTOPrOTeIn (AfP) reSPOnSe COuLD PreDICT The PrOGnOSIS Of PATIenTS reCeIVInG SOrAfenIb AfTer STrATIfICATIOn by IMAGInG eVALuATIOn
hitomi Takda* 1, yutaka yasui1
1Gastroenterology and hepatology, Musashino red cross hospital, Musashino-shi, tokyo, japan
Introduction: the aim of this study was to determine the usefulness of the combination of afP measurement and imaging evaluation for the prediction of patient prognosis after sorafenib treatment.
Methods: We retrospectively analyzed 173 patients treated with sorafenib between july 2009 and january 2015. contrast-enhanced computed tomography (ct) or magnetic resonance imaging (MrI) and blood test such as afP measurement were performed at baseline and at week 4 after treatment initiation. after that, serum afP level was measured every 4 weeks and ct or MrI was performed every 4 12 weeks; imaging was evaluated using modified recIst criteria. afP responders were defined as patients whose serum afP level decreased >20% from baseline within 8 weeks of initiating sorafenib treatment.
results: out of the 173 patients, 132 were males and 41 were females, with and the mean patient age was 70 years (26 90). the median survival was 512 days (26 2054), and the median duration of sorafenib treatment was 130 days (5 2054). among patients with stable disease (sD) at week 4, those with a >20% increase in serum afP level had a significantly higher rate of developing progressive disease (PD) at week 8s than those without an increase in serum afP level (38% vs. 13%, p = 0.001). among patients without PD at week 8, afP responders demonstrated significantly longer survival than non-responders (median survival 532 days vs. 349 days, p = 0.0001). among afP responders, additional treatment other than sorafenib after PD did not significantly improve overall survival (os) compared with those who received no additional treatment (p = 0.098). however, among afP non-responders, additional treatment other than sorafenib after PD significantly improved os compared with those who received no additional treatment (p < 0.0001)
Conclusion: afP response to sorafenib was useful in predicting patient prognosis after stratification using imaging evaluation. among patients with sD, an increase in serum afP level (>20%) within 4 weeks was indicative of developing PD at week 8. afP response among patients without PD at week 8 could be a sign of better survival. additional treatment other than sorafenib after PD increased the survival rate in afP non-responders but not in afP responders.
Disclosure of Interest: none Declared
P-181 TeLOMere DySfunCTIOn IS A rISK fACTOr fOr hePATOCeLLuLAr CArCInOMA In ChrOnIC hePATITIS C
Andreza C. Teixeira* 1, natalia f. scatena1, Barbara a. santana-Lemos1, alice chagas1, Guilherme V. rosa2, Ênio D. Mente2, jorge elias-junior1, Valdair f. Muglia1, rodrigo t. calado1, ana L. Martinelli1
1Internal Medicine, 2surgery and anatomy, school of Medicine of ribeirão Preto-usP, ribeirão Preto, Brazil
Introduction: telomeres consist of repetitive Dna sequences (ttaGGG) associated with a specialized protein complex (shelterin) at the ends of linear chromosomes that erode with mitotic cell division. cells with high proliferative capacity express telomerase, composed by a reverse transcriptase (tert), a rna template (terc), and associated proteins, which maintains telomere lengths. When they are too short, telomeres signal the arrest of cell proliferation, senescence, and apoptosis. short telomeres have been implicated in several diseases, such as aplastic anemia, acute leukemia, cirrhosis and cancer.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s8 8
Methods: We evaluated the telomere length in chronic hepatitis c patients, in three different groups: a) mild or moderate fibrosis (n=87), b) cirrhosis (n=58), and c) hepatocellular carcinoma (hcc) (n=69). a hundred healthy subjects from the same geographical area were enrolled as control. telomerase mutations (TERT and TERC) were evaluated in 43 hcc patients. the telomere length was determined in peripheral blood leukocytes by real-time Pcr, and values were expressed as relative telomere/single-copy gene (t/s) ratio. the telomerase mutations (TERT and TERC) were screened by sanger sequencing, using ABI Prism BigDye Terminator v3.1 kit (applied Biosystems, california, usa).
results: the median age of patients at the time of hcc diagnosis was 57 years, with 85.5% being males. telomere lengths were significantly shorter in hcc patients (t/s=0.6195±0.19) compared to cirrhosis (t/s=0.7539±0.26) (P=0.0009), mild or moderate fibrosis (t/s=0.7818±0.0.32) (P=0.0041), and healthy controls (t/s=0.8227±0.30) (P<0.0001). no significant difference in telomere length was found between mild or moderate hepatitis c and cirrhosis (P=0.7915). a novel tert a243V mutation was found in one patient with hcc (1/43), with severe disease (BcLc D).
Conclusion: these results suggest that telomere erosion is a risk factor for the development of hcc in patients with chronic hepatitis c. the role of telomere dysfunction and telomerase mutations needs more investigation.
references: calado rt, young ns. telomere diseases. n engl j Med. 2009 Dec 10;361(24):2353-65. carulli L, anzivino c. telomere and telomerase in chronic liver disease and hepatocarcinoma, World j Gastroenterol. 2014 May 28;20(20):6287-92.
Disclosure of Interest: none Declared
P-182 WhAT IS The rOLe Of SurGery In The TreATMenT Of reCurrenCe Of hePATOCeLLuLAr CArCInOMA AfTer LIVer TrAnSPLAnTATIOn?
Jasmijn Selten* 1, 2, Marc-antoine allard3, john herrera kok4, carlos castro Benitez3, katsunori Imai4, oriana ciacio3, Gabriela Pittau3, eric Vibert3, antonio sa cunha3, Daniel cherqui3, Denis castaing3, jan Ijzermans1, rene adam3
1transplantation surgery, erasmus Mc, rotterdam, netherlands, 2centre hepatobiliaire, Paul Brousse hopital, 3centre hepatobiliaire, 4centre hepatobilaire, hopital Paul Brousse, Villejuif, france
Introduction: the treatment of recurrence of hepatocellular carcinoma (hcc) after liver transplantation (Lt) is still a matter of debate. the purpose of this study is to identify the prognostic factors for survival post-transplantation for hcc in a retrospective analysis
Methods: all patients between 1991 and 2013 transplanted for hcc in a single center were included for analysis. a surgical treatment was realized in case of local recurrence in selected patients. clinical, biological and histological characteristics pre- and post-transplantation were compared between resected and non-resected patients.
results: 73 patients had a recurrence after a median disease-free interval of 15.9 months. the median overall survival was 19 months, with a 3-year survival of 23%. there was a unifocal recurrence in 38 patients (53%), intrahepatic in 13 (19%), intra- and extrahepatic in 6 (6%) and extrahepatic in 51 (73%). 33 patients (47%) were eligible for resection of recurrence. the overall survival for resected patients after transplantation was 32% after 3 years, versus 14% for non-resected patients (p= 0.008). In univariate analysis, an elevated alpha-foetoproteine (afP) at recurrence > 100ng/ml, macrovascular invasion pre-transplantation and, multifocal recurrence were other significant factors of survival. In multivariate analysis an afP level > 100ng/ml, macrovascular invasion pre-transplantation and surgical resection remained independent variables.
Conclusion: recurrence of hcc after liver transplantation is associated with a negative prognostic. the resection of the recurrent disease in selected patients significantly improves the survival independently of other prognostic factors and has to be considered methodically.
references: kim, h. r. et al. treatment of recurrent hepatocellular carcinoma after liver transplantation. Asia. Pac. J. Clin. Oncol. 7, 258–69 (2011).regalia, e. et al. Pattern and management of recurrent hepatocellular carcinoma after liver transplantation. J. Hepatobiliary. Pancreat. Surg. 5, 29–34 (1998).yoon, y. c., hong, t. h., you, y. k. & kim, D. G. clinical analysis of recurrent hepatocellular carcinoma after living donor liver transplantation. Clin. Transplant. 27, e192–8 (2013).16. Duvoux, c. et al. Liver transplantation for hepatocellular carcinoma: a model including α-fetoprotein improves the performance of Milan criteria. Gastroenterology 143, 986–94.e3; quiz e14–5 (2012).escartin, a et al. recurrence of hepatocellular carcinoma after liver transplantation. Transplant. Proc. 39, 2308–10 (2007).hirokawa, f. et al. surgical treatment of extrahepatic recurrence of hepatocellular carcinoma. Langenbecks. Arch. Surg. (2014). doi:10.1007/s00423-014-1230-6roayaie, s. et al. recurrence of hepatocellular carcinoma after liver transplant: patterns and prognosis. Liver Transpl. 10, 534–40 (2004).regalia, e. et al. Pattern and management of recurrent hepatocellular carcinoma after liver transplantation. J. Hepatobiliary. Pancreat. Surg. 5, 29–34 (1998).
roayaie, s. et al. recurrence of hepatocellular carcinoma after liver transplant: patterns and prognosis. Liver Transplant. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transplant. Soc. 10, 534–540 (2004).
Disclosure of Interest: none Declared
P-183 OuTCOMeS fOLLOWInG yTTrIuM-90 TrAnSArTerIAL rADIOeMbOLIzATIOn fOr hePATOCeLLuLAr CArCInOMA In PATIenTS WITh An eLeVATeD Pre-TreATMenT ALPhA-feTOPrOTeIn
joseph titano1, Derek Biederman1, amitha kamath1, Myron schwartz2, sander florman2, aaron fischman1, rahul Patel1, francis s. nowakowski1, robert Lookstein1, edward Kim* 1
1radiology, 2recanati-Miller transplantation Institute, Icahn school of Medicine at Mount sinai, new york, united states
Introduction: yttrium-90 transarterial radioembolization (tare) is a locoregional therapy used in the treatment of hepatocellular carcinoma (hcc). alpha-fetoprotein (afP) is a protein produced by the majority of hepatocellular carcinomas and is used to track disease progression and response to treatment. In this study, we evaluate the post-treatment outcomes of tare in patients with unresectable hcc and a pre-treatment alpha-fetoprotein (afP) > 400 ng/mL.
Methods: We retrospectively reviewed 747 patients treated with tare from 1/2008- 1/2015. of this total, 107 patients [65.2 (58.6 – 72.4) years, male: 87, female: 20] underwent tare for unresectable hcc with an afP > 400 ng/mL [median afP: 3312 (970-15930) ng/mL] within 90 days prior to treatment. Patients were stratified according to etiology of hcc, sorafenib therapy (receiving at the time of tare: 56), prior treatment (naïve: 44, ablation: 12, chemoembolization: 45, resection: 20, transplantation: 5), child-Pugh class (a: 70, B: 36, c: 1), ecoG performance status (Ps0: 47, Ps1: 31, Ps2: 12), tumor characteristics (solitary: 40, multifocal: 67), lobar distribution (unilobar: 63, bilobar: 44), vascular invasion (present: 43, absent: 64), and BcLc stage (a: 10, B: 24, c: 72, D: 1). the primary outcome variable was overall survival. secondary outcome variables included clinical and laboratory toxicities at 90 days (ctcae v4), imaging response (mrecIst), time-to-progression, and afP response (afP decrease ≥ 50% within 90 days post-tare).
results: a total of 117 tare treatments were administered. eight patients were lost to follow up. clinical toxicities included grade 1/2 fatigue (25%), abdominal pain (20%), nausea (12%), and ascites (2%). Laboratory toxicities included grade 1/2 bilirubin (44%), ast (69%), and aLt (39%) and grade 3/4 bilirubin (16%), ast (8%), and aLt (1%). the 30- and 90-day mortality rates were 1% and 19% respectively. the objective response rate was 39% (complete: 18%, partial: 21%) and the disease control rate was 54%. the median (95% cI) time to progression was 4.5 (3.6 – 5.4) months. seventeen patients had an afP response. the median (95% cI) overall survival was 8.6 (5.6 - 11.2) months. Patients with an afP response survived a median of 16.4 (11.2 – 20.3) months while afP non-responders had a median survival of 5.4 (4.1 – 8.6) months. univariate analysis (log-rank) demonstrated the following variables to correlate with improved overall survival: ecoG < 1 [p = 0.01, hr: 1.9 (1.1 to 3.1)] and afP response [p < 0.001, hr: 3.1 (1.7 – 5.5)].
Conclusion: In our cohort, patients with an afP response had a median survival of 16.4 months while afP non-responders had a median survival of 5.4 months. Performance status (ecoG < 1) was also associated with improved post-tare survival.
Disclosure of Interest: j. titano: none Declared, D. Biederman: none Declared, a. kamath: none Declared, M. schwartz consulting of: Gilead sciences Inc, Inova Diagnostics Inc, s. florman advisory Board of: abbVie Inc, Bristol-Myers squibb, Gilead sciences Inc, a. fischman consulting of: surefire Medical Inc, terumo corp, r. Patel consulting of: sirtex, arstasis Inc, f. nowakowski: none Declared, r. Lookstein consulting of: Bayer aG, johnson & johnson, Boston scientific corp, e. kim advisory Board of: onyx Pharmaceuticals, consulting of: koninklijke Philips electronics, BtG International Inc
P-184 InTrATuMOrAL OrGAnIC CATIOn TrAnSPOrTer 1 exPreSSIOn In hePATOCeLLuLAr CArCInOMA AS A bIOMArKer fOr SOrAfenIb TreATMenT reSPOnSe - A PILOT STuDy
Daniel Grimm* 1, jonas Lieb1, Veronika Weyer2, johanna knapstein1, felix Darstein1, anja Lautem3, Maria hoppe-Lotichius3, sandra koch1, arno schad4, joern M. schattenberg1, Marcus a. Wörns1, arndt Weinmann1, Peter r. Galle1, tim zimmermann1
1I. Dept. of Medicine, 2Institute of Medical Biostatistics, epidemiology and Informatics, 3Department of General-, Visceral- and transplantation surgery, 4Department of Pathology, university Medical center Mainz, Mainz, Germany
Introduction: the definition of novel prognostic and predictive biomarkes is crucial in hepatocellular carcinoma (hcc). Drug transporters are essential in controlling the absorption and disposition of pharmaceutics, thereby playing a key role in efficacy and safety of drugs. It is known that the polyspecific organ cation transporter 1 (oct1) is one the most important active influx pumps for

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 8 9
pharmaceuticals, including antitumor drugs like the kinase inhibitor sorafenib. the aim of this pilot study was to define the role of intratumoral oct1 expression as a biomarker for systemic treatment with sorafenib in hcc patients.
Methods: oct1 mrna expression levels were determined in 60 well characterized primary human hepatocellular carcinoma samples acquired at the university Medical center Mainz. Patients were divided into two groups by median according to oct1 expression levels. the data was retrospectively correlated with clinical parameters.
results: Intratumoral oct1 expression is a significant prognostic factor for patients treated with sorafenib according to cox regression analysis (hr 0.653 ; 95% cI 0.430-0.992; p=0.046). In a sensitivity analysis, a decent survival benefit could be shown using the lower quartile of intratumoral oct1 expression as a cutoff. Importantly, neither baseline afP levels (p=0.062) nor treatment-induced afP response (p=0.191) were associated with intratumoral oct1 mrna expression levels.
Conclusion: this pilot study indicates a promising role for intratumoral oct1 expression as a biomarker in hcc therapy. however, further prospective studies are warranted on this topic.
Disclosure of Interest: none Declared
P-185 rISK PreDICTIOn MODeL Of hePATOCeLLuLAr CArCInOMA In hOSPITAL-bASeD POPuLATIOn WITh hePATITIS b VIruS InfeCTIOn
young kwang choo1, hyun Deok shin1, suk Bae kim1, Il han Song* 1
1Department of Internal Medicine, Dankook university college of Medicine, cheonan, korea, republic of
Introduction: hepatitis B virus (hBV) infection is a main cause of hepatocellular carcinoma (hcc) in hBV-endemic region. risk prediction of hcc is necessary for providing adequate screening/surveillance strategies to the high-risk individuals. We aimed to develop a risk prediction model of hcc in korean patients with chronic hBV infection.
Methods: We selectively recruited 1,871 patients with chronic hBV infection from Dankook university hospital, and established independent risk factors for hcc through cox regression model. each regression coefficient was converted into integer risk score. hcc risks were estimated from flamingham study risk score functions. receiver operating characteristic (roc) curves were used to assess predictive accuracy of this model.
results: the following independenct risk factors for hcc were established: age, gender, liver cirrhosis, serum alanine aminotransferase, bilirubin, albumin, platelet, and hBV Dna level, hBeag serostatus. hcc risk rate was ranged from 0.03% to 79.84% at 3-years, 0.09% to 98.89% at 5-years, 0.12% to 99.83% at 7-years, and 0.35% to 100% at 10-years, with total cumulative risk score ranging from 0 to 27 points. cumulative risk score of 15 was proposed as a significant cut-off value with 90% specificity for hcc development, with the area under roc of 0.910 (95% cI, 0.892-0.928). hcc development rates of 3-, 5-, 7-, and 10-years at risk score 15 were 3.6%, 9.7%, 13.5%, and 32.7%, respectively.
Conclusion: We developed a risk prediction model of hcc based on routine clinical parameters in hospital-based individuals with chronic hBV infection. this model needs to be confirmed by external validation for reproducibility of model characteristics.
Disclosure of Interest: none Declared
P-186 DIAGnOSTIC PerfOrMAnCe Of COnTrAST IMAGInG TeChnIqueS In SMALL hePATOCeLLuLAr CArCInOMA MeASurInG LeSS ThAn 2 CM
Seong hee Kang* 1, jong eun yeon1, young sun Lee1, tae suk kim1, yang jae yoo1, sang jun suh1, young kul jung1, yang shin Park2, chang hee Lee2, yeon seok seo1, ji hoon kim1, hyung joon yim1, kwan soo Byun1
1Department of Internal Medicine, Division of Gastroenterology and hepatology, 2Department of radiology, korea university college of Medicine, seoul, korea, Guro-gu, seoul, korea, republic of
Introduction: recent guidelines recommend ultrasound follow-up for nodules (< 1 cm) discovered via ultrasonography surveillance (us) in liver cirrhosis patients. nodules larger than 1cm should be followed the recall policy with either dynamic contrast 4-phase ct scan or contrast enhanced MrI. there is no specified recall policy of nodule less than 1 cm found on us. We evaluated ct and MrI efficacy in hepatocellular carcinoma (hcc) diagnosis in nodules lesser than 1cm and 1~2 cm.
Methods: We retrospectively analyzed 130 us-detected liver nodules in lesser than 2 cm, which were all confirmed histologically either by percutaneous biopsy or surgical specimen. Image studies were examined by 2 radiologists experienced in imaging of the liver, who were unaware of the results of the biopsy. the diagnostic performance of the two imaging work-up strategies were single imaging
scan only (ct or MrI), and two imaging scans (combining 2 contrast enhanced imaging scans).
results: histologically, hcc was confirmed in 110 of 130 (84.6%) nodules. of the 36 nodules of <1 cm size, 29 were histologically confirmed as hcc (80.5%). Imaging characterized 24 of 29 hccs (< 1 cm) with the typical hcc vasculature (82.7%; single image positive: 4; two image positive: 20). Imaging revealed false-negatives in 14%, (5/36) nodules of < 1 cm. In nodules (< 1 cm), sensitivity, positive predictive value (PPV), and diagnostic accuracy were 80.0%, 66.6%, and 66.6% for single, and 83.3%, 95.2%, and 81.4%, for two images, respectively. of 81 hcc nodules measuring 1-2 cm, 79 possessed the typical hcc vasculature (97.5%; single image: 24; two images: 55). In (1-2 cm) hcc nodules, sensitivity, PPV, and diagnostic accuracy were 96.0%, 92.3%, and 90.3% for single, and 98.2%, 94.8%, and 93.6%, for two images, respectively.
Conclusion: In hccs (< 1 cm), our study suggests that two imaging modalities provided limited diagnostic efficacy; invasive percutaneous biopsy may be needed. In hccs (1-2 cm), single or two imaging modalities produced similar diagnostic efficacy. further studies are needed, with long term follow-up in a larger cohort of (< 1 cm) hcc patients.
references: 1) Leoni s, Piscaglia f, Golfieri r, camaggi V, Vidili G, Pini P, Bolondi L. the impact of vascular and nonvascular findings on the noninvasive diagnosis of small hepatocellular carcinoma based on the easL and aasLD criteria. am j Gastroenterol 2010;105:599-6092) forner a, Vilana r, ayuso c, Bianchi L, sole M, ayuso jr, Boix L, et al. Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: Prospective validation of the noninvasive diagnostic criteria for hepatocellular carcinoma. hepatology 2008;47:97-1043) Park Mj, kim ys, Lee Wj, Lim hk, rhim h, Lee j. outcomes of follow-up ct for small (5-10-mm) arterially enhancing nodules in the liver and risk factors for developing hepatocellular carcinoma in a surveillance population. eur radiol 2010;20:2397-2404
Disclosure of Interest: none Declared
P-187 COnTrAST-InDuCeD DySPneA DurInG GD-eOb-DTPA enhAnCeD LIVer MrI: AnALySIS Of reSPIrATOry GrAPhS DurInG breATh-hOLD
yang Shin Park* 1, chang hee Lee1
1korea university Guro hospital, seoul, korea, republic of
Introduction: Gd-eoB-DtPa, hepatocyte-specific Mr contrast agent, is widely used in liver imaging for detection and characterization of focal liver lesions. however, contrast-related dyspnea is emerging as a major cause of degraded hepatic arterial phase in Gd-eoB-DtPa enhanced MrI, resulting in difficulty in radiologic diagnosis. therefore, we objectively evaluate respiratory graphs during breath-hold and determine incidence of contrast-related dyspnea in Gd-eoB-DtPa enhanced liver MrI.
Methods: 154 patients underwent Gd-eoB-DtPa enhanced liver MrI. During acquisition of precontrast and hepatic arterial phase, respiratory graphs were obtained and and graded on a 4-point scale, with the highest grade indicating poor breath hold. to evaluate the effect of Gd-eoB-DtPa on breath hold, respiratory graphs obtained during precontrast and hepatic arterial phase for each patient were compared. contrast-induced dyspnea was defined as a difference in standard deviation values between precontrast and hepatic arterial phase was greater than 200. then, hepatic arterial phase images were evaluated using a 5-point scale, with the highest score indicating poor image quality. finally, we evaluated the difference of image quality for hepatic arterial phase between patients with and without gadoxetic acid-related dyspnea using student t test.
results: Based on the analysis of respiratory graphs, the incidence of breath-holding difficulty during hepatic arterial phase was 23.4% (33/154) and the incidence of contrast-induced dyspnea was 6.5% (10/154). In comparison of image qualities between patients with and without contrast-induced dyspnea, patients with contrast-induced dyspnea showed poorer image quality for hepatic arterial phase than patients without gadoxetic acid-related dyspnea (3.75 ± 0.35 vs 1.57 ± 0.60; P < 0.001).
Conclusion: During Gd-eoB-DtPa enhanced liver MrI, the incidence of contrast-induced dyspnea was 6.5%. objective analysis of respiratory graphs is useful for evaluation of contrast-induced dyspnea and image quality in Gd-eoB-DtPa enhanced liver MrI.
references: 1. Davenport Ms, caoili eM, kaza rk, hussain hk. Matched within-patient cohort study of transient arterial phase respiratory motion-related artifact in Mr imaging of the liver: gadoxetate disodium versus gadobenate dimeglumine. radiology. 2014;272(1):123-31.2. Davenport Ms, Viglianti BL, al-hawary MM, et al. comparison of acute transient dyspnea after intravenous administration of gadoxetate disodium and gadobenate dimeglumine: effect on arterial phase image quality. radiology. 2013;266(2):452-61.3. Pietryga ja, Burke LM, Marin D, jaffe ta, Bashir Mr. respiratory motion artifact affecting hepatic arterial phase imaging with gadoxetate disodium: examination recovery with a multiple arterial phase acquisition. radiology. 2014;271(2):426-34.4. Davenport Ms, Bashir Mr, Pietryga ja, Weber jt, khalatbari s, hussain hk. Dose-toxicity relationship of gadoxetate disodium and transient severe respiratory motion artifact. ajr am j roentgenol. 2014;203(4):796-802.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s9 0
5. Bashir Mr, castelli P, Davenport Ms, et al. respiratory motion artifact affecting hepatic arterial phase Mr imaging with gadoxetate disodium is more common in patients with a prior episode of arterial phase motion associated with gadoxetate disodium. radiology. 2015;274(1):141-8.
Disclosure of Interest: none Declared
P-188 hIGh CIrCuLATInG MICrOrnA-122 exPreSSIOn IS A POOr PrOGnOSTIC MArKer In PATIenTS WITh hePATITIS b VIruS-reLATeD hePATOCeLLuLAr CArCInOMA WhO unDerGO rADIOfrequenCy AbLATIOn
hyo Jung Cho* 1, soon sun kim1, choong kyun noh1, joo han Park1, sung Won cho1, jae youn cheong1
1Department of Gastroenterology, ajou university school of Medicine, suwon, korea, republic of
Introduction: We investigated the prognostic potential of plasma mir-122 levels in patients with hepatitis B virus (hBV)-related hcc after hepatic resection or radiofrequency ablation (rfa).
Methods: a total of 120 patients with hBV-related hcc who underwent hepatic resection (n = 63) or rfa (n = 57) were included. the pretreatment plasma mir-122 level was assessed using quantitative real time polymerase chain reaction, and the correlation between mir-122 expression and various clinical parameters was investigated.
results: Multivariate cox regression analysis demonstrated that, in all patients, a low platelet count (<100 × 109/L), low albumin level (≤3.5 g/L), and advanced tumor stage (modified union for International cancer control stage III/IV) were independent prognostic factors for disease-free survival, while a low albumin level and advanced tumor stage were independent prognostic factors for overall survival (os). In a subgroup analysis of patients who underwent rfa, the patients with high mir-122 expression (>100) had significantly lower os on kaplan-Meier analysis (P = 0.042) (figure 1a). furthermore, high mir-122 expression (hazard ratio [hr] = 2.27; 95% confidence interval [cI] = 1.12–6.35; P = 0.025) and advanced tumor stage (hr = 2.27; 95% cI = 1.23–4.18; P = 0.009) were independent risk factors for poor os in patients treated with rfa. the combination of mir-122 and tumor stage resulted in an area under the curve of 0.818 for predicting 1-year os in patients who underwent rfa.
Image:
Conclusion: high plasma mir-122 expression was associated with poor os in patients with hBV-related hcc who underwent rfa.
Disclosure of Interest: none Declared
P-189 AnnexIn A2 AS A nOVeL DIAGnOSTIC MArKer f hePATOCeLLuLAr CArCInOMA In eGyPTIAn PATIenTS
Mohamed k. shaker1, Ghada sabbour1, hanzada abdel fattah1, Iman Montasser* 1, ahmed el Dorry2
1ain shams university hcc clinic, 2ain shams university hcc clinic, cairo, egypt
Introduction: hepatocellular carcinoma (hcc) is the fifth most common malignancy in the world. In egypt, hcc was reported to account for about 4.7% of chronic liver disease (cLD) patients. about 30% of hcc cases with normal serum afP levels are hardly diagnosed before clinical manifestations appear, and this highlights the need for new biomarkers for hcc. annexins are a family of proteins that bind anionic phospholipids in a calcium-dependent manner .annexin a2 is almost undetectable in normal liver and chronic hepatitis tissues, while highly positively detected in hcc, also serum levels of annexin a2 are elevated in early stage hcc patients which are afP-negativeaIM: the aim of the study was to investigate the clinical utility of annexin a2 serum level as novel diagnostic marker of hepatocellular carcinoma (hcc) and to correlate its level with alpha fetoprotein.
Methods: this study was carried out in hcc clinic (hepatoma group), ain shams university, cairo; egypt and included two patient groups and one control group Group 1: fifty patients with early stage hepatocellular carcinoma diagnosed according to the BcLc (BcLc a); Group 2:twenty five patients with chronic liver disease diagnosed based on clinical, laboratory, and ultrasonographic investigations; control Group: fifteen healthy, age and sex-matched subjects who were seronegative for hepatitis viral markers and have normal liver function tests. all groups were subjected to thorough history taking, full clinical examination, and laboratory investigations including liver functions, viral markers, and afP and annexin a2 estimation using eLIsa technique.
results: this study revealed a highly significant difference between patients with hcc, cLD, and controls regarding serum annexin a2 levels (130, Iqr15-240 ;15, Iqr15-17 and 17 Iqr 15-30 ng/ml, respectively). annexin a2 level was persistently elevated in patients with hcc with normal afP levels representing its useful role in early detection and follow-up of patients treated for hcc. the area under the curve (auc) of annexin a2 was 0.865; the cut-off value was established at 30 ng/ml with sensitivity of 70% and specificity of 97.5%); while the sensitivity and specificity of afP at cutoff value 200 ng/dl were 20% and 100% respectively. the difference between auc of annexin a2 and that of afP was 0.21which mounted statistical significance.
Conclusion: annexin a2 could represent a useful tool as a marker for detection of hcc.annexin a2 could represent a useful tool as a marker for detection of hcc.
Disclosure of Interest: none Declared
P-190 CeuS fInDInGS AfTer IrreVerSIbLe eLeCTrOPOrATIOn AbLATIOn: CAn SIze Of AbLATIOn zOne be PreDICTeD eArLIer
Manxia Lin* 1, xiaoyan xie1, Ming kuang2
1Institute of Diagnostic and Interventional ultrasound, 2Department of hepatobiliary surgery, sun yat-sen university, Guangzhou, china
Introduction: ablation is considered an important method of treatment for liver cancer and thermal ablation is the most widely used worldwide. Irreversible electroporation (Ire) ablation emerged as a new ablative modality, the principles of which are very different from other ablation methods. early assessment of ablation zone for Ire ablation is crucial. however, imaging findings of Ire ablation zone is dynamic and also change over time, which is totally different from other ablation modality. thorough comprehension to the dynamic imaging findings after Ire ablation is required, in order to conduct Ire ablation and to know when and how to assess efficacy of Ire ablation. there are studies reported about the dynamic evolution of the baseline ultrasound (Bus) findings within 2h after Ire ablation, and considered the best time to assess efficacy of Ire ablation is 90-120 minutes after Ire ablation. contrast-enhanced ultrasound (ceus) is considered to have a more superior capability than Bus in detection, diagnosis and monitoring the treatment efficacy. this study is intended to describe the Bus and ceus performance within 2h after Ire ablation, and to evaluate whether ceus can predict the size of ablation zone after Ire ablation, if so, when is the best time.
Methods: the institutional animal care and use committee approved the use of the animal model in this study. six Ire ablations were performed in vivo in two miniature pigs liver under ultrasound guidance. Bus and ceus assessment was performed at four time interval within 2 hours (phaseI, II, III and IV) after Ire ablation. the boundary of ablation zone on ultrasound (us) was defined by consensus of two radiologists and the size of ablation zone was measured in length and width. animals were sacrificed 2-3 hours after last Ire ablation. size of ablation zone at gross pathologic assessment was measured and was defined as reference standard. the sizes measured on us were compared to reference standard using paired two-tailed student t tests, and the deviation between them was calculated.
results: the us imaging of Ire ablation zone evolved overtime and was different from each other at different time interval after Ire ablation. the ablation zone displayed as a non-enhancement and a hypo-enhanced area at phaseI and phase II, respectively. a hyper-enhanced rim appeared in the peripheral of ablation zone at phase III and phase IV. the size of ablation zone at gross pathologic assessment was 3.4 cm±0.2 in length (range:3.1-3.7cm) and 2.3 cm±0.2 (range:2.0-2.6cm) in width. Greatest accuracy and correlation with reference standard were seen in portal phase on ceus assessment at phase I when the ablation zone was defined as non-enhanced area. the deviation was 0.05cm±0.08 in length (P=0.202) and -0.05cm±0.08 in width (P=0.203) and the correlation was 0.943 (P=0.005) and 0.917 (P=0.010) in length and width, respectively. Measurement obtained on Bus assessment at phase III also showed great accuracy, and the correlation was 0.799 (P=0.056) in length and 0.970 (P=0.001) in width, respectively. the sizes of ablation zone measured on Bus assessment at phase I and II and that measured on ceus assessment at phase II, III and IV were all significantly smaller than reference standard (all P<0.05).
Conclusion: Bus and ceus imaging with 2h after Ire ablation are dynamic and evolve. non-enhancement area in the portal phase on ceus assessment with 10min after Ire ablation can best predict the size of Ire ablation zone. size of ablation zone can be predicted earlier using ceus assessment.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 9 1
P-191 uTILITy Of MICrOVeSICLeS AS PLASMA bIOMArKerS In PATIenTS WITh hePATOCeLLuLAr CArCInOMA
robert Cheng* 1, 2, thomas tu2, susan McLennan2, nicholas shackel1, 2
1aW Morrow Gastroenterology and Liver centre, royal Prince alfred hospital, camperdown, 2Liver Injury and cancer, centenary Institute, sydney, australia
Introduction: hepatocellular carcinoma (hcc) is a hypervascular neoplasm with high levels of apoptosis and necrosis. to date there has been a paucity of early diagnostic plasma biomarkers for hcc. Microvesicles (MV) are sub-micron vesicles secreted from cell plasma membrane in both physiological and pathological states. We investigated the utility of MV as a diagnostic and prognostic biomarker for hcc.
Methods: fresh blood samples were collected from patients attending the hepatology clinic at royal Prince alfred hospital, sydney, australia. these include patients with hepatocellular carcinoma (n=12), patients with hepatic cirrhosis (n=11), and normal healthy volunteers (n=6). Blood was processed immediately by centrifuging at 200g for 10 minutes followed by 10,000g for 20 minutes to derive platelet-free plasma, which was then centrifuged for 100,000g for 90 minutes to pellet MVs. the MV pellets were resuspended in 0.1 micron-filtered Phosphate Buffered saline (PBs) and diluted (1:50) prior to being analysed on the nanosight LM10-hsBft nanoparticle characterisation system.Biochemical and clinical data of these patients were also recorded, including liver function tests, full blood counts, coagulation studies, afP, tumour activity on imaging, creatinine, child-Pugh and MeLD scores, and disease aetiology. significance testing was performed using unpaired t-tests between groups.
results: Microvesicle secretion into plasma of hcc patients is elevated 3.4 fold compared with normal human plasma (mean particle concentration: 518.4 ± 81 x 106 vs. 154.1 ± 31 x 106 / mL, p<0.001) and 2.5 fold compared with cirrhotic patients’ plasma (518.4 ± 81 x 106 vs. 205.0 ± 29 x 106 / mL, p<0.003); there is no difference between normal and cirrhotic patient plasma MV concentration (154.1 ± 31 x 106 vs. 205.0 ± 29 x 106 / mL, p=0.25). there is no significant variation between the MV sizes of the three groups. analysis of MV in hcc and liver cirrhosis patients were further stratified by MeLD score (> 15 or < 15); in hcc patients, plasma MV concentration was increased by 2.4 fold in the MeLD < 15 group compared with MeLD > 15 (607.1 ± 268 x 106 vs. 252.6 ± 47 x 106 / mL, p=0.05), whereas in the cirrhosis group stratifying by MeLD did not show a difference between plasma MV concentration (251.5 ± 77 x 106 vs. 187.6 ± 103 x 106 / mL, p<0.003). subgroup analyses were performed by stratifying plasma MV concentration by tumour activity as diagnosed by imaging and by afP levels, and neither was significant.
Image:
Conclusion: Plasma MV secretion is significantly increased in hcc patients compared to cirrhosis and normal plasma. When stratified by MeLD score, hcc patients with low MeLD score (<15) had significant elevation of plasma MV concentration compared with patients with high MeLD score (>15). there is no such trend in the plasma MV concentration of the cirrhosis group. therefore, plasma MV concentration may be useful as a diagnostic biomarker for hcc in patients with low MeLD scores.
Disclosure of Interest: none Declared
P-192 InCreASeD SeruM huMAn ePIDIDyMIS PrOTeIn 4 (he4) In PATIenTS WITh hePATOCeLLuLAr CArCInOMA: A POTenTIAL TuMOr MArKer
zhen zeng* 1, Liyan hao1, Guanghua rong1, yongping yang1
1center of therapeutic research for Liver cancer, the 302 hospital, BeIjInG, china
Introduction: human epididymis protein 4 (he4), also known as whey acidic protein (WaP) type four disulphide(WfDc2), has been proved to be a promising tumor marker in epithelial ovarian cancer and several other cancers, while its potential clinical utilities as either tumor marker or prognostic indicator in hepatocellular carcinoma(hcc) have not been evaluated .
Methods: serum he4 level in 50 patients with hepatitis B virus (hBV) related hcc and 30 age and gender matched healthy controls (hc) were assayed by enzyme-linked immunosorbent assay (eLIsa, fujirebio Diagnostics, sweden). serum α-fetoprotein (afP) in all subjects was assayed by electrochemiluminescence immunoassay (roche, switzerland).
results: serum he4 levels in patients with hcc were significantly increased compared to that of hcs (96.6±45.4 pg/ml vs. 51.6±14.7 pg/ml, P =0.001). By setting an optimal cut-off value of 74.1 pg/ml, the sensitivity and specificity of serum he4 for diagnosing hcc were 76.0 % and 90.0%, respectively. In addition, serum he4 level in afP negative hcc patients (< 20 ng/ml, n=14) was also significantly increased (110.1±59.7 pg/ml) and showed no differences to that of afP positive hcc patients (91.4±39.3 pg/ml, n=36, p=0.194).
Image:
Conclusion: serum he4 level increased in patients with hcc and could be a potential tumor marker for hcc.
references: karlsen ns, karlsen Ma, høgdall ck, høgdall eV. he4 tissue expression and serum he4 Levels in healthy Individuals and Patients with Benign or Malignant tumors: a systematic review. (2014) cancer epidemiol Biomarkers Prev 23:2285-2295.
Disclosure of Interest: none Declared
P-193 CIrCuLATInG SCCA-IGM COMPLex IS A uSefuL bIOMArKer TO PreDICT The OuTCOMe Of TherAPy In hCC PATIenTS
filomena Morisco1, Maria Guarino1, Giovanni G. Di Costanzo* 2, andrea Gallotta3, silvia camera1, Giorgio fassina3, raffaella tortora1, francesco auriemma1, concetta tuccillo4, nicola caporaso1
1Department of clinical Medicine and surgery, Gastroenterology unit, university of naples "federico II", 2Liver unit, aorn “a.cardarelli”, naples, 3xeptagen spa, Marghera, Venice, 4Department of clinical and experimental Medicine "f. Magrassi and a. Lanzara", Gastroenterology unit, second university of naples, naples, Italy
Introduction: every year hepatocellular carcinoma (hcc) develops in about 3–4% of cirrhotic patients. the squamous cell carcinoma antigen (scca) has been found elevated in liver cancer specimens by immunohistochemistry, and detected in complex with IgM (scca-IgM) in serum of patients with hcc. the aim of this study was to evaluate the ability of serological scca-IgM levels to predict the efficacy of hcc therapy.
Methods: from april 2012 to april 2014, 216 patients with a new diagnosis of hcc were enrolled in a prospective study. the diagnosis of hcc was made according to the aasLD 2010 guidelines. the patients were staged and treated according to BcLc staging system; in particular, BcLc stage a and B were treated with loco-regional therapy, and BcLc stage c were treated with sorafenib. response to therapy was evaluated with imaging techniques, according to the mrecIst criteria. serum scca-IgM levels were determined by the elisa hepa-Ic kit (xeptagen spa, Venezia, Italy) at basal time (t0) and after one month of treatment (t1). the quantization of the complex scca-IgM was expressed in arbitrary units (au/mL).
results: at the time of diagnosis, scca-IgM was reactive in 168/216 patients (78%), mean±sD: 274.4±263.2 au/mL. at baseline and one month into therapy, scca-IgM levels were significantly lower in the patients that responded positively to therapy, compared to those who had a negative response (median values at t0: 125.9 au/mL [c.I. 50-187.9] vs. 165.1 au/mL [c.I. 117.3-209.9]; median values at t1: 113.4 au/mL [c.I 50-195] vs. 170.6 au/mL [c.I. 111.7-344.2]) (Mann Whitney u test p < 0.05). also, the difference in the marker serum levels between t1 and t0 (t1-t0)(Dscca-IgM) was significantly different between positive and negative responders (Mann Whitney u test p < 0.05).
Conclusion: these results suggest that the determination of scca-IgM complex may be helpful in predicting the response to therapy in patients with hcc.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s9 2
references: fransvea e, trerotoli P, sacco r, et al. scca-Ic serum levels are predictive of clinical response in hcV chronic hepatitis to antiviral therapy: a multicentric prospective study. journal of Viral hepatitis 2012, 19, 704-10Giannini eG, Basso M, Bazzica M, contini P, Marenco s, savarino V, Picciotto a. successful antiviral therapy determines a significant decrease in squamous cell carcinoma antigen-associated (scca) variants’ serum levels in anti-hcV positive cirrhotic patients. j Viral hepatitis 2010; 17:563-8Pontisso P, quarta s, caberlotto c, Beneduce L, Marino M, Bernardinello e, et al. Progressive increase of scca–IgM immune complexes in cirrhotic patients is associated with development of hepatocellular carcinoma. Int j cancer 2006;119:735–40.
Disclosure of Interest: none Declared
P-194 The rOLe Of The MhC CLASS I POLyPePTIDe-reLATeD ChAIn A (MICA) In The TerTIAry PreVenTIOn Of hePATOCeLLuLAr CArCInOMA In ChrOnIC hePATITIS C PATIenTS
Jee-fu huang* 1, chung-feng huang1, Wan-Long chuang1, Ming-Lung yu1
1kaohsiung Medical university hospital, kaohsiung city, taiwan
Introduction: antiviral therapy has a positive effect in the secondary prevention of hepatocellular carcinoma (hcc) in chronic hepatitis c (chc) patients. the current study aimed to assess its efficacy in the tertiary prevention and to validate the performance of the Mhc class I polypeptide-related chain a (MIca) level in the prediction of hcc recurrence.
Methods: a multi-centre study enrolling 105 consecutive hcc patients post curative therapies were prospectively recruited. the primary outcome measurement was recurrence of hcc.
results: the mean observational period was 52.7 months (range= 3.9-121.5 months). 56 (53.3%) patients achieved sustained virological response (sVr). after completion of treatment, 43 (41.0%) patients developed hcc recurrence, and 24 (55.8%) of them had their recurrence within 6 months after completion of therapy. thirty-three (89.2%) of the patients with hcc recurrence were of de novo pattern. those responders tended to have a lower cumulative incidence of recurrence than those non-responders (43.2 vs 84.8/ 100 person month, P= 0.13). those non-responders with a high MIca level (> 100 pg/mL) carried the lowest cancer-free survival than those non-responders with a low MIca level and those responders (P= 0.002). cox regression hazard analysis showed a high baseline MIca level (odds ratio [or]= 4.8, 95% confidence interval [cI]= 1.1-20.8, P= 0.04) and a low platelet count (<100,000/mm3) (or= 5.4, 95% cI= 1.1-27.0, P= 0.04) predicted hcc recurrence.
Conclusion: antiviral therapy carried a limited effect in the tertiary prevention of hcc. a high MIca level predicted hcc recurrence, particularly among those non-responders.
Disclosure of Interest: none Declared
P-195 MuLTI-AnALyTe AnALySIS Of SeruM CyTOKIneS TO PreDICT TreATMenT OuTCOMe In PATIenTS WITh hePATOCeLLuLAr CArCInOMA TreATeD WITh rADIOTherAPy
hyejung Cha* 1, eun jung Lee1, jinsil seong2
1Department of radiation oncology, 2radiation oncology, yonsei university college of Medicine, seoul, korea, republic of
Introduction: cytokine, which is involved in chronic inflammation and also related with tumor aggressiveness and resistance to treatment in many cancers. however, the significance of cytokines has been investigated limitedly about in tumor response of radiotherapy (rt). the aim of this study was to analyze the serum cytokine levels and identify the significance of the serum cytokines on treatment outcome in patients with hepatocellular carcinoma (hcc) treated with rt.
Methods: In this prospective study, patients with hcc who treated with rt were eligible. Blood samples were collected before and after completion of whole rt course. serum cytokine levels measured using cytokine Bead array kits were analyzed with patients’ clinical profiles and treatment responses.
results: Between september 2008 and october 2009, 51 patients were included in analysis. Median follow-up duration was 12.3 months (range, 0.5-62.3). forty-seven patients were diagnosed as modified uIcc stage III or IV at timing of rt. Baseline serum IL-8 level increased as stage increased and IL-6 level was high in patients with pre-rt treatment history (treatment-non-naïve). higher baseline serum IL-6 level was observed in patients with treatment failure including overall, infield, and outfield failure than those without treatment failure. In subgroup analysis, the significant difference of serum IL-6 level was observed only in treatment-non-naïve comparing to treatment-naïve patients. Median overall survival and progression-free survival (Pfs) were 13.9 and 7.7 months, respectively. elevated serum IL-6 level was significantly associated with Pfs for infield failure (hr 1.011, p<0.0001).
Conclusion: the current findings suggest that the assessment of baseline serum IL-6 level may be helpful to predict treatment outcome after rt for hcc, especially in patients who had treatment history before rt.
Disclosure of Interest: none Declared
P-196 reGuLATIOn Of CD13 by hDAC1 PrOMOTeS nf-Kb SIGnALInG TO enhAnCe hePATOCeLLuLAr CArCInOMA PrOGreSSIOn
bo hu* 1, chao sun1, Wei-Guo tang1, yang xu1
1zhongshan hospital, shanghai, china, shanghai, china
Introduction: aminopeptidase-n (aPn/cD13), a cancer stem cell marker, plays an important role in tumor neoangiogenic process and the development of metastases. however, its protein regulation and molecular function in hepatocellular carcinoma (hcc) remains obscure.
Methods: the expression levels of cD13 and hDac1 were investigated by q-Pcr, western blot and immunostaining in a variety of hcc cell lines and tissues. clinical significance of cD13 expression was analyzed in 253 patients sample with clinico-pathological characteristics and follow-up information. role of cD13 in complex with hDac1 in hcc progression was monitored through patient derived xenografts, Microarray assay and co-immunoprecipitation were used for mechanism analysis.
results: We reported that elevated expression of cD13 (11.9%, 30/253) in human hcc predicted poor survival and disease recurrence after surgery. Multivariate analysis identified cD13 expression as an independent predictor for postoperative recurrence and overall survival. cD13 combined with hDac1 as a compound to promote hcc cell proliferation, invasion and tumor formation in vitro and in vivo. Mechanistically, cD13 and hDac1 could physically associate as a complex, which lead to activation of nf-kB/p65 signaling targets via hDac1 deacetylase activity. clinically, down-regulation of cD13 and hDac1 enhanced the sensitivity of sorafenib-resistant cells upon sorafenib treatment.
Conclusion: cD13 and hDac1 physically associate as a complex regulating hcc progression via nf-kB/p65 signaling. cD13 may serve as a novel prognostic marker and therapy target for hepatocellular carcinoma.
Disclosure of Interest: none Declared
P-197 CIrCuLATInG MIrnA-122 AS A bIOMArKer fOr hCV-InDuCeD hePATOCeLLuLAr CArCInOMA
Lobna Mourad* 1, eman el-ahwany2, Mona zoheiry2, hoda abu-taleb3, faten nagy2, Maged el-Ghanam4, Moataz hassan4, suher zada5
1Biotechnology, the american university in cairo, 2Immunology, 3environmental, 4hepato-Gastroenterology, theodor Bilharz research Institute, 5Biology, the american university in cairo, cairo, egypt
Introduction: Infection with hepatitis c virus (hcV) persists in most infected individuals and can lead to the development of chronic hepatitis, cirrhosis and hepatocellular carcinoma (hcc). recent studies revealed the crucial role micrornas (mirnas) play in various liver diseases, especially in hcc. Micrornas are small non-coding rna molecules, which have an important function in regulating rna stability and gene expression. recently, it has been reported that serum and other body fluids contain sufficiently stable microrna signatures. thus, the profiles of circulating micrornas have been explored in a variety of studies aiming at the identification of novel non-invasive biomarkers. the aim of the study is to develop a non-invasive diagnostic tool based on measuring the serum levels of different mirnas in order to detect hcV-induced hcc at the early stages of the disease.
Methods: In this study, five main mirnas (mirna-122a, mirna-125a, mirna-139, mirna-145 and mirna-199a) were selected according to previous studies that demonstrated their noticeable expression pattern during the development of hcc. the materials of the current study included the sera of 42 cases of chronic hepatitis c (chc) without cirrhosis, 45 cases of chc with cirrhosis (Lc), 38 cases of hcc with hcV and 40 normal healthy cases served as control. the five mirnas were measured using real-time reverse transcription-polymerase chain reaction. the conventional hcc markers α-fetoprotein (afP), lens culinaris agglutinin-reactive afP (afP-L3%), and des-γ-carboxyprothrombin (DcP) were measured with commercial kits.
results: serum levels of mirna-122a, mirna-125a, mirna-139, mirna-145 and mirna-199a were significantly decreasing (P< 0.01) in hcc than in both chc and Lc groups. as a single marker, mirna-122a had the highest sensitivity for hcc, followed by mirna-125a, mirna-145, mirna-139 and mirna-199a.
Conclusion: these findings indicate that measurement of serum levels of mirna-122a, mirna-125a, mirna-139, mirna-145 and mirna-199a can help to differentiate hcc from chc and Lc. our results suggest that serum mir-122 might serve as a novel and potential noninvasive biomarker for hcV-induced hcc.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 9 3
P-198 18fDG POSITrOn eMISSIOn TOMOGrAPhy/COMPuTeD TOMOGrAPhy (PeT-CT), eLASTOGrAPhy AnD COnTrAST enhAnCeD uLTrASOnOGrAPhy TO eVALuATe DIAGnOSIS, STAGInG AnD TherAPy In nASh-reLATeD hCC
fernando G. Barros costa1, jose tadeu stefano1, caio s. Levy1, Mariana M. torres1, camila Maria L. Machado2, carlos alberto Buchpiguel3, Marcelo t. sapienza3, Bruno cogliati4, roger chammas2, Maria cristina chammas5, flair j. carrilho1, Claudia P. Oliveira* 1
1Gastroenterology (LIM-07), 2Laboratório de oncologia experimental (LIM-24), Departamento de radiologia e oncologia, 3Laboratório de Investigação Médica radioisótopos (LIM-43), Departamento de radiologia e oncologia, unIVersIty of sao PauLo schooL of MeDIcIne, 4Department of Pathology,, school of Veterinary Medicine and animal science, university of são Paulo, são Paulo, 5Department of radiology, unIVersIty of sao PauLo schooL of MeDIcIne, sao PauLo, Brazil
Introduction: non-alcoholic steatohepatitis (nash) has been associated with hepatocellular carcinoma (hcc) often arising in histologically advanced disease. We developed an experimental model of nash-related hcc and differentiated benign from malignant lesions and the stage of tumor development using B-mode and Doppler ultrasonography and 18fDG positron emission tomography/computed tomography (Pet-ct)
Methods: nash-related hcc were induced in 20 adult sprague-Dawley rats, weighing 250-300g by the combination of high fat diet deficient in choline (Dhc) [35 % of total fat, enriched with 54 % trans fatty acids (rhoster Ltda, Brazil)] and diethylnitrosamine (Den) (sigma chemical IuPac nitrosodiethylamine, Missouri, usa ) at a dose of 100 mg/ L in drinking water water for 16 weeks. B-mode and Doppler ultrasonography was performed weekly in these animals. the animals were assessed twice (8 and 16 weeks) in micro-sPect/Pet/ct equipment model LabPet4 (trifoil imaging). Before the ct basal acquisition a tail venous access were performed for contrast media administration (150mg/kg of rat weight of an iodinated contrast media). all cts were acquired with 80kvp, 512x512 matrix and 0,17mm pixel size. a baseline and 3 fast-post (≤1min between than) contrast images were acquired followed by 18f - fluorodeoxyglucose. the 18fDG images were acquired after an interval of 60 minutes post intrapenian injection (55.5 MBq). the ct studies were reconstructed by filtered background projection. Both images were exported as DIcoM to amide software.
results: Lesions with vascularization were considered indicative of malignancy, (sensitivity of 29% before and 71% after ceus and specificity of 71% before and 96% after contrast injection). elastograms of positive lesions showed areas of high stiffness, indicative of malignancy. this malignancy was confirmed by the histologic evaluation (sensitivity of 90% and a specificity of 60%). after ceus analysis, 4 nodules that were not observed on Bmode ultrasonography were identified. early wash-in was significantly associated with malignancy (sensitivity of 88% and specificity of 67%). ct showed low-attenuation lesions with early contrast enhancement. In Pet analyses, some of these lesions have increased 18fDG uptake, suggesting a high glycolytic metabolic rate.
Conclusion: this animal model replicates the major stages of nash including cirrhosis and hcc and micro-sPect/Pet/ct equipment model LabPet4 could be used in diagnosis and to evaluate novel therapeutic approaches.
Disclosure of Interest: none Declared
P-199 DuAL-TrACer 18f-fLuOrOChOLIne (fCh) AnD 18f-fLuOrODeOxyGLuCOSe (fDG) PeT/CT fOr The DIAGnOSIS Of TuMOrAL POrTAL VeIn ThrOMbOSIS In PATIenTS WITh hePATOCeLLuLAr CArCInOMA (hCC)
Julia Chalaye* 1, Laurence Baranes2, charlotte costentin3, chetana Lim4, edouard herin2, julien calderaro5, alain rahmouni2, Daniel azoulay4, emmanuel Itti1, alain Luciani2
1nuclear Medicine, 2radiology, chu henri Mondor, 3hepatology, 4hBP surgery and Liver transplant unit, hopital henri Mondor, aPhP, 5Pathology, chu henri Mondor, creteIL, france
Introduction: to evaluate the performances of dual-tracer fch and fDG Pet/ct imaging to diagnose tumoral portal vein thrombosis
Methods: eighty-five consecutive patients with hcc and referred for staging with dual-tracer Pet/ct were included. Pet/ct were analyzed by a nuclearist being unaware of the results of other imaging techniques. a tumoral thrombus was defined on Pet/ct as a linear area of abnormal uptake in correspondence of a vessel, either an increased or decreased uptake on fch scan, or an increased uptake on fDG scan. considered as the standard of reference the ct or MrI (performed less than one month around Pet/ct) were analized separately by a single radiologist. the presence of tumoral thrombus was determined on usual diagnostic criteria. the tumoral origin of the thrombus when doubtful was assessed on the follow up, ceus or pathological analysis.
results: eighteen portal tumoral thromboses were found. fDG Pet/ ct was positive or doubtful in 17/18 tumoral thromboses, while dual-tracer Pet/ct increased the diagnostic confidence by
excluding one false positive and identifying one additional true positive. overall, the sensitivity, specificity and accuracy were respectively 94.4%, 98.5% and 97.6% for fDG Pet/ct, and 100%, 100% and 100% for dual-tracer Pet/ct.
Conclusion: In patients with hcc, dual-tracer Pet/ct enables an accurate diagnosis of tumoral portal vein thrombosis, which has an essential prognostic value. the joint reading of morphological images and metabolic images provides good confidence for portal tumor thrombosis diagnosis.
Disclosure of Interest: none Declared
P-200 A COMPArISOn Of uLTrASOunD, COMPuTerISeD TOMOGrAPhy AnD MAGneTIC reSOnAnCe IMAGInG fInDInGS beTWeen 38 CASeS Of SIMPLe hePATIC CySTS AnD 13 CASeS Of MuCInOuS CySTIC neOPLASMS Of The LIVer
Peter L. z. Labib* 1, zan Bajwa2, thomas Luff2, David stell1, christopher Briggs1
1hPB surgery, 2radiology, Derriford hospital, Plymouth, united kingdom
Introduction: Mucinous cystic neoplasms (Mcn) of the liver are rare neoplasms with malignant potential that warrant complete surgical excision. however, imaging is often not accurate enough to differentiate between simple hepatic cysts (sc) and Mcn, making the decision between surgical and conservative management a challenge. Previous literature has focused on the ability of computerised tomography (ct) to distinguish between sc and Mcn, but there is less information available on the role of Magnetic resonance Imaging (MrI) in pre-operative diagnosis of this condition. We aimed to see if ultrasound scan (uss), ct or MrI could distinguish between sc and Mcn.
Methods: Between january 2006 and october 2014, 51 patients underwent 60 radiologically-guided or surgical interventions for symptomatic or radiologically suspicious liver cysts. Pre-intervention imaging reports were reviewed to look for reporting of septations, increased echogenicity, wall thickening, wall irregularity, wall calcification, biliary or vascular deviation or the presence of daughter cysts. the eventual histological diagnoses were compared with both the radiological features seen on the pre-intervention imaging and the Multidisciplinary team (MDt) outcomes for whether or not the cysts looked simple or complex in nature.
results: there were 38 cases of sc and 13 cases of Mcn. thirty patients with sc had a pre-intervention uss (78.9%), 30 had a ct (78.9%) and 12 underwent MrI (26.7%). In contrast, 10 patients with Mcn underwent pre-intervention uss (76.9%), 11 had a ct (86.7%) and 8 underwent MrI (61.5%). there was no significant difference in average cyst size between sc and Mcn (p=0.47). neither was there any significant difference in the presence of any individual radiological characteristic on uss, ct or MrI. Mcn was more likely if only a single cyst was present on the imaging (p=0.0157). an MDt outcome stating that a cyst was complex in nature was the most significant predictor for Mcn (p=0.0008).
Conclusion: Individual radiological characteristics seen on uss, ct or MrI are unable to differentiate between sc and Mcn. the presence of a single cyst on pre-intervention imaging and an MDt outcome of a cyst being complex were more likely to predict the presence of Mcn of the liver.
Disclosure of Interest: none Declared
P-201 uSefuLneSS Of ALPhA-feTOPrOTeIn fOr The DeTeCTIOn Of hePATOCeLLuLAr CArCInOMA In PATIenTS WITh ChrOnIC hePATITIS b VIruS InfeCTIOn
Sun young yim* 1, yeon seok seo1, tae hyung kim1, jemma ahn1, hyonggin an2, soon ho um1, ho sang ryu1
1Internal medicine, 2Biostatistics, korea university college of Medicine, seoul, korea, republic of
Introduction: serum alpha-fetoprotein (afP) is widely used as a screening test for the detection of hepatocellular carcinoma (hcc) in patients with high-risk. however, many studies suggested that diagnostic accuracy of afP for hcc is not sufficient. Poor diagnostic accuracy of afP can be explained by the fact that serum afP level can elevate without hcc in some conditions, such as severe necroinflammation or hepatic regeneration. this study was performed to evaluate the role of afP as screening marker for detecting hcc in chronic hepatitis B (chB) patients with different alanine aminotransferase (aLt) levels.
Methods: Patients with positive hepatitis B surface antigen for more than 6 months were enrolled in this retrospective study. serum afP levels at baseline, during aLt elevation, after normalization, 3, 6, 9, 12 months thereafter, and at the time of hcc diagnosis were collected. Persistently normal aLt (PnaLt) was defined as normal aLt levels that is maintained for more than 12 months. the usefulness of serum afP level was evaluated using an area under the receiver operating characteristic curve (auroc) analysis.
results: a total of 846 chB patients were enrolled. hcc was initially diagnosed in 110 patients (13%) with a mean serum afP level of 61,749.9±271,694.6 ng/mL. the area under the receiver

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s9 4
operating characteristic curve (auroc) for detection of hcc at baseline using afP was 0.839 among all patients and 0.904 among only those with a normal aLt level. to clarify the relationship between the aLt and afP levels, the dependence of the afP level on the aLt level was analyzed in patients without hcc at baseline. the afP levels during aLt elevation, at normalization, and 3, 6, 9, and 12 months thereafter were 91.1±17.3, 10.3±0.9, 5±0.3, 3.8±0.1, 3.5±0.1, and 3.3±0.1 ng/mL, respectively. among the 631 patients without hcc at baseline, the incidence of hcc within 5 and 10 years was 3.3% and 11%, respectively. the afP level was significantly higher concomitant with hcc diagnosis (34.3±47.1 ng/mL) than with persistently normal aLt (PnaLt; 4.0±2.0 ng/mL, P =0.001). the auroc for detecting hcc was 0.919, and a cutoff level of 17.5 ng/mL yielded specificity and positive predictive value of 100%.
Conclusion: serum afP level above 17.5 ng/mL concomitant with PnaLt indicates the presence of hcc and warrants further evaluation. Diagnosis of hcc using this cutoff value should be validated in a larger sample size.
references: harada t, shigeta k, noda k, fukumoto y, nishimura h, Mizuta M, et al. clinical implications of alpha-fetoprotein in liver cirrhosis: five-year follow-up study. hepatogastroenterology 1980;27:169-175.takikawa y, suzuki k. Is afP a new reliable marker of liver regeneration in acute hepatic failure? j Gastroenterol 2002;37:681-682.oka h, tamori a, kuroki t, kobayashi k, yamamoto s. Prospective study of alpha-fetoprotein in cirrhotic patients monitored for development of hepatocellular carcinoma. hepatology 1994;19:61-66.
Disclosure of Interest: none Declared
P-203 CLInICAL eVALuATIOn Of COnTenT-bASeD IMAGe-reTrIeVAL SySTeM In CT DIAGnOSIS fOr LIVer TuMOrS
Masahiro endo* 1, takeshi aramaki2, emima Bekku2, rui sato2, koiku asakura1
1Division of Diagnostic radiology, 2Division of Interventional radiology, shizuoka cancer center, shizuoka, japan
Introduction: now, vast amounts of image diagnostic data files are retained in Pacs, which are not effectively utilized for routine clinical practice. It is considered that reference of past similar cases is valuable for radiologists same as texts or papers in ct diagnosis. synapse case Match (content-based Image-retrieval system, fujifilm corporation, jaPan) has released as an only system which is able to support radiologists to diagnose hepatic ct by presenting similar ct image with confirmed pathological and/or clinical diagnosis from image database in japan. the purpose of this study is to describe the outline of this system and assess diagnostic efficacy in ct diagnosis for liver tumors in routine clinical setting.
Methods: With the approval of the institutional review board of shizuoka cancer center, we built an original database that contained ct images, diagnostic report and confirmed diagnosis of about 300 patients with liver tumors including hepatocellular carcinomas, cholangiocarcinomas, metastatic tumors, hemangiomas, simple cysts and other hepatic originated tumors.With this database, we evaluated this system that combines image processing with Pacs.the outline of this system is as follows:1) Marking of abnormal tumorous lesion: at first, a user identifies an abnormal tumorous lesion in liver on abdominal ct images of a new patient and draws a diameter of the lesion using a mouse. through the use of machine-learning techniques, the system automatically marks the border of the lesion.2) searching similar images: once the tumorous lesion is confirmed, the image-analysis program automatically calculates feature indices of the lesion when the user clicks a search button. and the system continuously compares the marked feature indices for the new case and those of stocked cases in the database.3) Displaying results: finally, the thumbnail of similar ct series in the database is displayed in the order from the acquired degree of similarity on the Pacs monitor. the number of retrieved cases by the system was set to top 10 in clinical setting.for evaluation of clinical efficacy for this system, five observers implemented the three grading evaluations to review whether this system could retrieve visually similar cases and the actual cases match the assumed diagnosis by using consequent 20 cases (8 cases of hepatocellular carcinoma, 7 cases of metastatic tumor, 3 cases of hemangioma, and a case of cyst and cholangiocarcinoma, respectively).
results: It was judged as to be similar in 7.5±4.9 cases on average and standard deviation in each retrieved top 10 cases. furthermore, it was found out that they are matched to the actual diagnosis in 7.0±4.9 cases. no difference in each tumor was observed.
Conclusion: this content-based Image-retrieval system is able to search images visually and diagnostically similar to the actual case based on only image analysis. and it is expected that the past diagnostic data files will be utilized as reference information for diagnosis of next patients with liver tumors by using this system. furthermore, it is considered that this system would be the first step for automatic ct diagnostic system in liver tumors, and take a role of a search engine for imaging biobanks in future.
references: endo M. et al.,content-based image-retrieval system in chest computed tomography for a solitary pulmonary nodule: method and preliminary experiments. Int j comput assist radiol surg. 2012; 7:331-8.
Disclosure of Interest: none Declared
P-204 nOnInVASIVe DIAGnOSIS Of MALIGnAnT LIVer TuMOrS uSInG SheAr WAVe uLTrASOunD eLASTOGrAPhy
hiroko Iijima* 1, 2, takashi nishimura1, 2, chikage nakano1, 2, chizu shiomi1, 2, tomoko aoki1, 2, kazunori yoh2, akio Ishii2, tomoyuki takashima2, yoshiyuki sakai2, nobuhiro aizawa2, hiroki nishikawa2, naoto Ikeda2, yoshinori Iwata2, hirayuki enomoto2, seiichi hirota3, jiro fujimoto4, shuhei nishiguchi2
1ultrasound Imaging center, 2Division of hepatobiliary and Pancreatic Disease, Department of Internal Medicine, 3Department of surgical Pathology, 4Department of hepato-Biliary-Pancreatic surgery, hyogo college of Medicine, nishinomiya, japan
Introduction: In recent years, the evaluation of liver fibrosis using ultrasound elastography to estimate liver stiffness has become an important alternative to liver biopsy. our institution was an early adopter of shear wave ultrasound elastography, a widely-used, noninvasive method of assessing liver fibrosis. In addition to liver fibrosis, we also have been using shear wave ultrasound elastography for differentiating between various malignancy liver tumors. In this study, we assessed the utility of shear wave ultrasound elastography in differenciating between malignant liver tumors (hepatocellular carcinoma, hcc; metastatic liver cancer, Met’s; intrahepatic cholangiocarcinoma, Icc; and cholangiolocellular carcinoma, cocc).
Methods: We evaluated 219 cases (male, 155; female, 64; average age, 68.5±9.84.; hcc, 137; Met’s, 55; Icc 9; cocc, 3) diagnosed by imaging or histological studies at our institution from october 2008 to february 2015. shear wave ultrasound elastography was performed using Virtual touch quantification (Vtq) by siemens acuson s2000/s3000. shear wave velocities (Vs value m/s) were measured 3 to 5 times at a similar depth roI for tumoral and nontumoral regions with mean values recorded. this study was approved by the hospital ethics committee at our institution.
results: tumor diameters (mm, mean ± sD) were as follows: hcc, 35.7 ± 26.1; Met’s, 27.9 ± 14.7; Icc, 63.8 ± 57.7; and cocc, 66.3 ± 50.0. Vs values from B-mode findings were as follows: hyperechoic hcc, 1.66 ± 0.43; hypoechoic hcc, 1.63 ± 0.81; and mosaic hcc, 1.86 ± 0.74. regarding the degree of tumoral differentiation, well-differentiated hcc was 1.56 ± 0.43, moderately differentiated was 1.78 ± 0.78, and poorly differentiated was 1.68 ± 0.85. Vs values from B-mode findings with or without marginal low area of hcc is 1.65 ± 0.57 and 1.89 ± 0.87 respectively. no significant difference in Vs values, an indicator of tumoral density, were observed in any cases. tumoral and nontumoral Vs values according to tumor type were as follows: hcc, 1.77± 0.74 and 1.89 ± 0.68; Met’s, 2.66 ± 1.04 and 1.26 ± 0.34; Icc, 2.35 ± 0.80 and 1.49 ± 0.46; cocc, 3.17 ± 0.56 and 1.88 ± 1.26. these data which demonstrate Vs values for hcc were significantly lower than those for Met’s and cocc (P < 0.001). In cases of Met’s, tumoral Vs values were greater than nontumoral Vs values (P < 0.001). In the primary sites of Met’s, to investigate stomach, pancreas, large intestine, kidney and lung Vs values were determined as 3.09± 1.02, 1.84± 0.94, 2.41 ± 0.63, 2.80±1.07 and 2.99±1.75 respectively. no significant difference was observed in Vs values according to primary tumor sites.
Conclusion: the measurement of Vs values of malignant liver tumor using shear wave ultrasound elastography may be useful in the noninvasive differential diagnosis of hcc and Met’s or cocc.
Disclosure of Interest: none Declared
P-205 The effeCT Of reDuCInG PrOSTATe VOLuMe On TuMOr VOLuMeS Of PATIenTS WITh hePATOCeLLuLAr CArCInOMA TreATeD WITh SOrAfenIb
Taiga Otsuka* 1, kaori Gotanda1, yoshihito kubotsu1, norimasa araki1, kenichiro Murayama1, saori kamachi1, hiroshi Isoda1, futa koga1, shunya nakashita1, Iwata ozaki1, yuichiro eguchi1
1hepatology, saga university hospital, saga, japan
Introduction: Molecular targeted agents are widely used to treat cancer; however, these agents influence hormone-sensitive tissues. recently, there is a report that a reduction in prostate volume and an improvement in urinary symptoms were observed in patients treated with sunitinib for advanced renal cell carcinoma. We assessed the correlation between prostate volume change and treatment outcomes in patients treated with sorafenib for hepatocellular carcinoma (hcc).
Methods: We reviewed consecutive male patients who administered sorafenib for hcc until 2013 in our institution. Patients who performed plain and enhanced ct prior to sorafenib treatment and 4 week after initiation of sorafenib were included. We evaluated prostate volume and tumor volume of hcc using the advanced Workstation Volume share 5 (Ge healthcare, japan).
results: sixteen male patients were included in this study. Prostate volume was significantly

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 9 5
decreased after initiation of sorafenib therapy (P < 0.01). Median prostate volume at pretreatment and 4 week after treatment were 27.5mL and 22.2mL, respectively. the changes in volume, which ranged from +2.2% to −36.3%, did not correlate with decrease in tumor volume (r = −0.14). the median percentage decrease of prostate was −18%, we classified patients into groups with < −18% and ≥ −18% prostate change in volume, respectively. Baseline characteristics were not statistically different between groups. according to recIst version 1.1, the objective response and disease control rates were not significantly different between groups (P = 0.12 and P = 0.46, respectively). the median percentages of target tumor volume change were +11.8% and +20.2% in the < −18% and ≥ −18% groups, respectively (P = 0.83).
Conclusion: In patients with hcc treated with sorafenib, prostate volume was reduced to the same extent as in patients with renal cell carcinoma treated with sunitinib. however, there was no correlation between prostate volume reduction and the antitumor effect of sorafenib against hcc.
Disclosure of Interest: none Declared
P-206 hSA-MIr-15b AnD VeGf Gene exPreSSIOn ASSOCIATeD In LIVer CIrrhOSIS AnD hePATOCeLLuLAr CArCInOMA
andre r. c. P. oliveira1, Marcia M. u. castanhole1, camila agren1, erika c. Pavarino1, rita D. c. M. a. silva1, eny M. Goloni-Bertollo1, renato f. D. Silva* 1, 2
1faMerP, sao jose do rio Pretro, Brazil, 2surgery, faMerP, sao jose do rio Pretro, Brazil
Introduction: Liver cirrhosis (Lc) is the main risk factor for hepatocellular carcinoma (hcc), and its formation is related to altered gene expression and angiogenesis. VEGF gene is translated to Vascular endothelial Growth factor secreted by injured tissues and is related to angiogenic processes. this gene has its regulation performed by micrornas (mirna, mir), that are single stranded molecules with approximately 22 nucleotides; its functions are related to inhibition of mrna translation in cells. objective: the aim of this study was to assess VEGF gene and mir-15b expression (predicted regulator) in Lc and hcc.
Methods: 13 samples of hcc, 17 samples of Lc and 10 samples of healthy liver tissue were collected, rna and proteins were extracted and expression was assessed by rt-qPcr. statistical analyzes were performed by t test, Wilcoxon test and Mann-Whitney test.
results: results showed that mir-15b expression was significantly increased in hcc (median 1.078 and p=0.0002), whereas VEGF gene expression was decreased (median 0.432 and p=0.0001). however mir-15b expression was significantly decreased in Lc (median 0.6867 and p<0.0001) and VEGF gene expression was increased (median 4.65 and p=0.0177). these results showed that mir-15b expression may be related to VEGF gene expression.
Conclusion: further performances will test mirna interaction with studied gene in cell lines. this comparison may produce new data and knowledge about this gene and its possible interaction with the assessed mirna.
references: Biselli-chicote PM, oliveira arcP, Pavarino ec et al. VeGf gene alternative splicing: pro- and anti-angiogenic isoforms in cancer. j cancer res clin oncol, 2012;138(3):363-70.fattovich G, stroffolini t, zagni I et al. hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology 2004;127:535-50.kohlhapp fj, Mitra ak, Lengyel e, Peter Me .Micrornas as mediators and communicators between cancer cells and the tumor microenvironment. oncogene, 2015. doi: 10.1038/onc.2015.89.
financial support: caPes, cnPq, faPesP.
support: faMerP, funfarMe.
Disclosure of Interest: none Declared
P-207 hCC DIfferenTIATIOn: quAnTITATIVe MrI STuDy Of TuMOr enhAnCeMenT On GD-bOPTA enhAnCeD hePATObILIAry PhASe
françois Legou* 1, Melanie chiaradia1, chetana Lim2, frederic Pigneur1, Laurence Baranes1, Marjane Djabbari1, hicham kobeiter1, julien calderaro3, ariane Mallat4, alexis Laurent2, Daniel azoulay2, alain rahmouni1, alain Luciani1
1radiology, chu henri Mondor, 2hBP surgery and Liver transplant unit, hopital henri Mondor, aPhP, 3Pathology, chu henri Mondor, 4hepatology, hopital henri Mondor, aPhP, creteIL, france
Introduction: to asses the added value of Gd-BoPta-enhanced hepatobiliary phase imaging to distinguish hepatocellular carcinomas according to their pathological differentiation.
Methods: this prospective study was IrB approved and the requirement for informed consent was waived. twenty five patients with 26 resectable hcc BcLc a (8 well differentiated, 13 moderatly differentiated and 5 poorly differentiated) naïve of any treatment, and who underwent orthotopic liver transplantation or hepatectomy were included. all patients underwent a preoperative liver MrI
after Gd-BoPta injection included delayed hepatobiliary phase acquisitions. two readers reviewed all images in terms of signal intensity (sI) features on unenhanced, and hepatobiliary phase images to establish the Lesion-to-Liver contrast enhancement ratio (LLcer). the LLcer was correlated to pathological differentiation (Mann Whitney, roc).
results: the LLcer of well differentiated hcc (mean 14.2% ± 14.2) was significantly higher than that of moderately to poorly differentiated hcc (mean -6.26% ± 7.1) (p<0.0002). using a cut-off value of +4.6% yielded a 94% specificity and 100% sensitivity for discriminating well differentiated from moderate to poorly differentiated hcc.
Conclusion: LLcer at the hepatobiliary phase after Gd-BoPta injection allows the differentiation of well-differentiated from moderately to poorly differentiated hcc.
references: seale Mk, catalano oa, saini s, hahn Pf, sahani DV (2009) hepatobiliary-specific Mr contrast agents: role in imaging the liver and biliary tree. radiographics 29:1725-1748reimer P, schneider G, schima W (2004) hepatobiliary contrast agents for contrast-enhanced MrI of the liver: properties, clinical development and applications. eur radiol 14:559-578
Disclosure of Interest: none Declared
P-208 eVALuATIOn Of TreATMenT reSPOnSe Of rADIOTherAPy fOr hCC uSInG Pre- AnD POST-TreATMenT MAGneTIC reSOnAnCe IMAGInG
Woo Kyoung Jeong* 1, jung hee kim2, sohee song1, young kon kim1, Dongil choi1, hee chul Park3, jeong Il yu3, joon-hyeok Lee2
1radiology, 2Medicine, 3radiation oncology, samsung Medical center, seouL, korea, republic of
Introduction: evaluation of treatment response following radiotherapy for hcc is challenging because irradiated liver shows changed signal intensity due to increased arterial hyperemia and delayed clearance of contrast agent in the index tumor area. the purpose of study us to explore whether change of Mr imaging features after radiotherapy, especially changes in post-treatment imaging, could help evaluate viability of hepatocellular carcinoma (hcc).
Methods: fourty-three patients (mean age, 62.6 years; M:f=37:6) who underwent planning MrI before radiotherapy for hcc and followed by post-treatment MrI within 3 months were enrolled. two radiologists reviewed pre- and post-treatment MrI including dynamic enhancement and diffusion weighted imaging. Imaging features evaluated by two radiologists were index tumor size, index viable tumor size, arterial enhancement, hypointensity on portal venous and equilibrium phases, hyperintensity on diffusion weighted imaging. the reviewers also investigated interval change of imaging feature such as disappearance of arterial enhancement with washout pattern. Imaging observation was performed for 6 months to evaluate remaining viable tumors in the index area. Pearson’s chi-square tests were performed for contingency table analyses.
results: except one patient who expired within the observation period, 15 patients (15/42; 36%) shows progression of the disease, and they were confirmed by surgical excision (n=2) and additional tace (n=8). Mean diameters of the index tumor and size of viable tumor were respectively 3.9±2.3 cm and 2.9±1.9 cm, and changed to 3.1±2.1 cm and 1.9±1.6 cm, respectively. arterial enhancement with washout on post-treatment MrI and disappearance of arterial enhancement with washout features were significantly related to 6-month remaining viability (all p<0.001), and interval decrease in the size of viable tumor and disappearance of hyperintensity on diffusion weighted imaging seemed to have a trend of relationship (p=0.077 and 0.053, respectively).
Conclusion: change of imaging features suggesting viable hcc including arterial hypervascularity with washout would be a strong feature for treatment response after radiotherapy of hcc.
Disclosure of Interest: none Declared
P-209 hISTOPAThOLOGICAL PATTern Of hePATOCeLLuLAr CArCInOMA AnD OuTCOMe Of rADIOfrequenCy AbLATIOn
shaimaa el-Mahdy1, asmaa Gomaa1, nermine ehsan2, Mohamed elwaraky3, Imam Waked*1
1hepatology, 2Pathology, 3radiology, national Liver Institute, shebeen elkom, Menoufiya, egypt
Introduction: histological differentiation is a main prognostic factor for hepatocellular carcinoma (hcc), however, few studies assessed the relation between histological grade of hcc and prognosis using different treatment modalities. Whether the histopathologic characteristics of hcc and the grade of differentiation can predict recurrence after radiofrequency ablation (rfa) was assessed in this series.
Methods: twenty patients with nodular hcc were treated with rfa in a tertiary referral center in egypt during 2014. all patients underwent sonography-guided percutaneous tumor biopsy and were classified as edmondson-steiner grade I hcc (n = 9) grade II hcc (n = 4), or grade III hcc (n = 7). all patients underwent contrast-enhanced triphasic helical ct examination before and one and
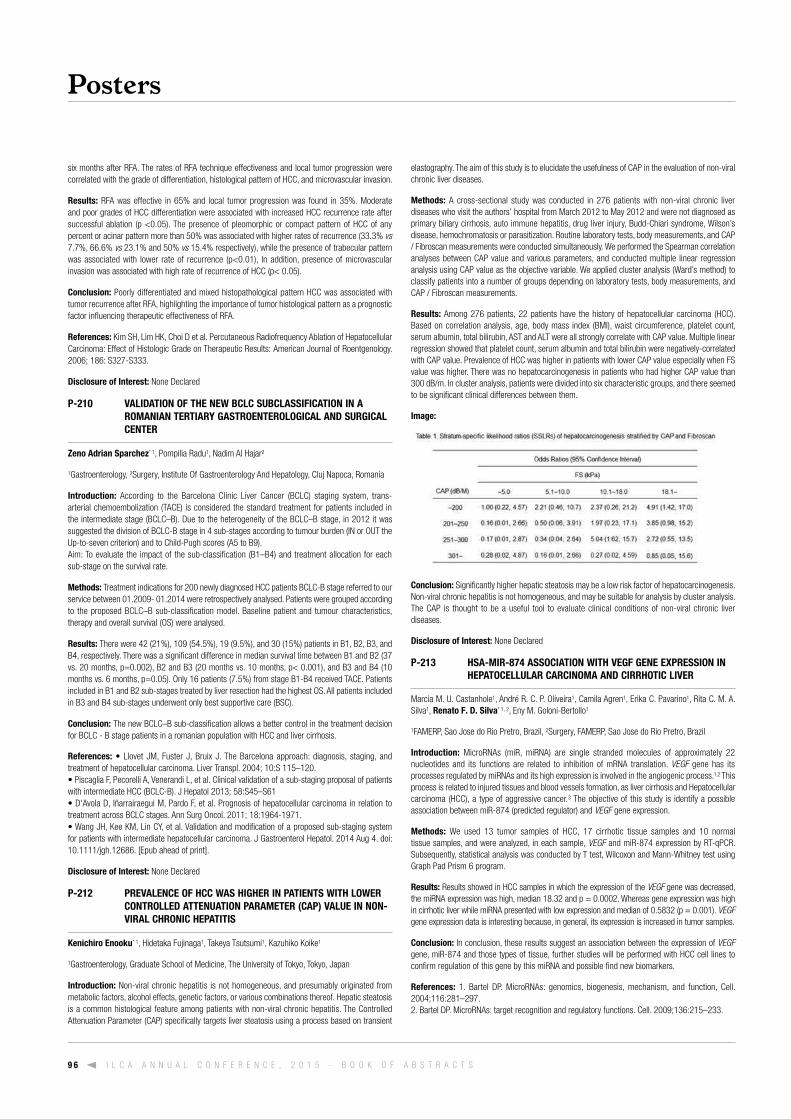
Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s9 6
six months after rfa. the rates of rfa technique effectiveness and local tumor progression were correlated with the grade of differentiation, histological pattern of hcc, and microvascular invasion.
results: rfa was effective in 65% and local tumor progression was found in 35%. Moderate and poor grades of hcc differentiation were associated with increased hcc recurrence rate after successful ablation (p <0.05). the presence of pleomorphic or compact pattern of hcc of any percent or acinar pattern more than 50% was associated with higher rates of recurrence (33.3% vs 7.7%, 66.6% vs 23.1% and 50% vs 15.4% respectively), while the presence of trabecular pattern was associated with lower rate of recurrence (p<0.01), In addition, presence of microvascular invasion was associated with high rate of recurrence of hcc (p< 0.05).
Conclusion: Poorly differentiated and mixed histopathological pattern hcc was associated with tumor recurrence after rfa, highlighting the importance of tumor histological pattern as a prognostic factor influencing therapeutic effectiveness of rfa.
references: kim sh, Lim hk, choi D et al. Percutaneous radiofrequency ablation of hepatocellular carcinoma: effect of histologic Grade on therapeutic results: american journal of roentgenology. 2006; 186: s327-s333.
Disclosure of Interest: none Declared
P-210 VALIDATIOn Of The neW bCLC SubCLASSIfICATIOn In A rOMAnIAn TerTIAry GASTrOenTerOLOGICAL AnD SurGICAL CenTer
zeno Adrian Sparchez* 1, Pompilia radu1, nadim al hajar2
1Gastroenterology, 2surgery, Institute of Gastroenterology and hepatology, cluj napoca, romania
Introduction: according to the Barcelona clinic Liver cancer (BcLc) staging system, trans-arterial chemoembolization (tace) is considered the standard treatment for patients included in the intermediate stage (BcLc–B). Due to the heterogeneity of the BcLc–B stage, in 2012 it was suggested the division of BcLc-B stage in 4 sub-stages according to tumour burden (In or out the up-to-seven criterion) and to child-Pugh scores (a5 to B9). aim: to evaluate the impact of the sub-classification (B1–B4) and treatment allocation for each sub-stage on the survival rate.
Methods: treatment indications for 200 newly diagnosed hcc patients BcLc-B stage referred to our service between 01.2009- 01.2014 were retrospectively analysed. Patients were grouped according to the proposed BcLc–B sub-classification model. Baseline patient and tumour characteristics, therapy and overall survival (os) were analysed.
results: there were 42 (21%), 109 (54.5%), 19 (9.5%), and 30 (15%) patients in B1, B2, B3, and B4, respectively. there was a significant difference in median survival time between B1 and B2 (37 vs. 20 months, p=0.002), B2 and B3 (20 months vs. 10 months, p< 0.001), and B3 and B4 (10 months vs. 6 months, p=0.05). only 16 patients (7.5%) from stage B1-B4 received tace. Patients included in B1 and B2 sub-stages treated by liver resection had the highest os. all patients included in B3 and B4 sub-stages underwent only best supportive care (Bsc).
Conclusion: the new BcLc–B sub-classification allows a better control in the treatment decision for BcLc - B stage patients in a romanian population with hcc and liver cirrhosis.
references: • Llovet JM, Fuster J, Bruix J. The Barcelona approach: diagnosis, staging, and treatment of hepatocellular carcinoma. Liver transpl. 2004; 10:s 115–120.• Piscaglia F, Pecorelli A, Venerandi L, et al. Clinical validation of a sub-staging proposal of patients with intermediate hcc (BcLc-B). j hepatol 2013; 58:s45–s61• D'Avola D, Iñarrairaegui M, Pardo F, et al. Prognosis of hepatocellular carcinoma in relation to treatment across BcLc stages. ann surg oncol. 2011; 18:1964-1971. • Wang JH, Kee KM, Lin CY, et al. Validation and modification of a proposed sub-staging system for patients with intermediate hepatocellular carcinoma. j Gastroenterol hepatol. 2014 aug 4. doi: 10.1111/jgh.12686. [epub ahead of print].
Disclosure of Interest: none Declared
P-212 PreVALenCe Of hCC WAS hIGher In PATIenTS WITh LOWer COnTrOLLeD ATTenuATIOn PArAMeTer (CAP) VALue In nOn-VIrAL ChrOnIC hePATITIS
Kenichiro enooku* 1, hidetaka fujinaga1, takeya tsutsumi1, kazuhiko koike1
1Gastroenterology, Graduate school of Medicine, the university of tokyo, tokyo, japan
Introduction: non-viral chronic hepatitis is not homogeneous, and presumably originated from metabolic factors, alcohol effects, genetic factors, or various combinations thereof. hepatic steatosis is a common histological feature among patients with non-viral chronic hepatitis. the controlled attenuation Parameter (caP) specifically targets liver steatosis using a process based on transient
elastography. the aim of this study is to elucidate the usefulness of caP in the evaluation of non-viral chronic liver diseases.
Methods: a cross-sectional study was conducted in 276 patients with non-viral chronic liver diseases who visit the authors’ hospital from March 2012 to May 2012 and were not diagnosed as primary biliary cirrhosis, auto immune hepatitis, drug liver injury, Budd-chiari syndrome, Wilson’s disease, hemochromatosis or parasitization. routine laboratory tests, body measurements, and caP / fibroscan measurements were conducted simultaneously. We performed the spearman correlation analyses between caP value and various parameters, and conducted multiple linear regression analysis using caP value as the objective variable. We applied cluster analysis (Ward’s method) to classify patients into a number of groups depending on laboratory tests, body measurements, and caP / fibroscan measurements.
results: among 276 patients, 22 patients have the history of hepatocellular carcinoma (hcc). Based on correlation analysis, age, body mass index (BMI), waist circumference, platelet count, serum albumin, total bilirubin, ast and aLt were all strongly correlate with caP value. Multiple linear regression showed that platelet count, serum albumin and total bilirubin were negatively-correlated with caP value. Prevalence of hcc was higher in patients with lower caP value especially when fs value was higher. there was no hepatocarcinogenesis in patients who had higher caP value than 300 dB/m. In cluster analysis, patients were divided into six characteristic groups, and there seemed to be significant clinical differences between them.
Image:
Conclusion: significantly higher hepatic steatosis may be a low risk factor of hepatocarcinogenesis. non-viral chronic hepatitis is not homogeneous, and may be suitable for analysis by cluster analysis. the caP is thought to be a useful tool to evaluate clinical conditions of non-viral chronic liver diseases.
Disclosure of Interest: none Declared
P-213 hSA-MIr-874 ASSOCIATIOn WITh VeGf Gene exPreSSIOn In hePATOCeLLuLAr CArCInOMA AnD CIrrhOTIC LIVer
Marcia M. u. castanhole1, andré r. c. P. oliveira1, camila agren1, erika c. Pavarino1, rita c. M. a. silva1, renato f. D. Silva* 1, 2, eny M. Goloni-Bertollo1
1faMerP, sao jose do rio Pretro, Brazil, 2surgery, faMerP, sao jose do rio Pretro, Brazil
Introduction: Micrornas (mir, mirna) are single stranded molecules of approximately 22 nucleotides and its functions are related to inhibition of mrna translation. VEGF gene has its processes regulated by mirnas and its high expression is involved in the angiogenic process.1,2 this process is related to injured tissues and blood vessels formation, as liver cirrhosis and hepatocellular carcinoma (hcc), a type of aggressive cancer.3 the objective of this study is identify a possible association between mir-874 (predicted regulator) and VEGF gene expression.
Methods: We used 13 tumor samples of hcc, 17 cirrhotic tissue samples and 10 normal tissue samples, and were analyzed, in each sample, VEGF and mir-874 expression by rt-qPcr. subsequently, statistical analysis was conducted by t test, Wilcoxon and Mann-Whitney test using Graph Pad Prism 6 program.
results: results showed in hcc samples in which the expression of the VEGF gene was decreased, the mirna expression was high, median 18.32 and p = 0.0002. Whereas gene expression was high in cirrhotic liver while mirna presented with low expression and median of 0.5832 (p = 0.001). VEGF gene expression data is interesting because, in general, its expression is increased in tumor samples.
Conclusion: In conclusion, these results suggest an association between the expression of VEGF gene, mir-874 and those types of tissue, further studies will be performed with hcc cell lines to confirm regulation of this gene by this mirna and possible find new biomarkers.
references: 1. Bartel DP. Micrornas: genomics, biogenesis, mechanism, and function, cell. 2004;116:281–297. 2. Bartel DP. Micrornas: target recognition and regulatory functions. cell. 2009;136:215–233.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 9 7
3. tao zh, Wan jL, zeng Ly, et al. mir-612 suppresses the invasive-metastatic cascade in hepatocellular carcinoma. j exp Med. 2013;8;210(4):789-803.
financial support: caPes; faPesP Process number 2012/10321-6, cnPq.
support: faMerP/funfarMe
Disclosure of Interest: none Declared
P-214 eVALuATIOn Of DeTeCTIOn rATe Of LIVer TuMOr exISTInG DeeP LOCATIOn frOM The SurfACe uSInG SeCOnD GenerATIOn AGenT, SOnAzOID
Masako Izuta* 1, chikara ogawa1, Mitsushige shibatoge1, Masatoshi kudo2
1Gastroenterology and hepatology, takamatsu red cross hospital, takamatsu city, 2Gastroenterology and hepatology, kinki university, osakasayama city, japan
Introduction: In japan, to diagnose the liver tumor using the second generation contrast-enhanced agent, sonazoid is a common method and very useful. But sometimes it is difficult to diagnose liver tumors located over 10cm from the surface.In this study we evaluated the detection rate of liver tumors existing in deep location from the surface using sonazoid.
Methods: from august 1, 2010 to March 31, 2014, a total of 1503 nodules were examined using sonazoid at takamatsu red cross hospital. 310 nodules were over 8cm below the surface, and we evaluated the detection rate of those nodules for each 1 cm over 8cm below.equIPMentthe ultrsound machines used in this study were LoGIq e9 (Ge healthcare), ascendus (hItachI aLoka Medial), aPLIo 500 and xario xG (toshiba Medical systems).
results: the average size of the liver tumors located more than 8cm below the surface was 31.1mm (2-160mm). the detection rate for tumors located more than 8cm but less than 9 was 87.9% (94/107). for tumors located more than 9cm, but less than 10cm, the rate goes down to 80.0% (37/46). for over 10cm deep tumors, the rate is 78% (72/92), for 11cm it’s 72.7% (24/33), for over 12cm, it’s 72.7% (16/22) and for over 13cm, it falls to 60% (3/5). the detection rate decreased the farther the tumors were located below the surface.DIscussIonthey say that it is difficult to detect liver tumors existed in more than 10cm depth. If we define detection of liver tumors as detecting that in vascular phase or post vascular phase, as the depth of liver tumors is deeper than 10cm, the detection rate falls worse.although the depth of liver tumorr is upwards 11cm and less than 13cm, the detection rate is 72.7%.We infer that is because we tend to experience excluding the case who has thick subcutaneous fat ans deep attenuation and changing more right enhance mode.Ge : corded phase inversion(cPI) and amplitude modulation(aM)toshiba :phase modulation(PM) and amplitude modulation(aM)
Conclusion: though the detection rate falls the deeper the tumor is located, sonazoid is still a very useful method for detecting nodules up to 10cm below the surface.
Disclosure of Interest: none Declared
P-215 quICK AnD eASy DeTeCTIOn MeThOD Of LIVer TuMOr WITh neW TeChnOLOGy fOr uS
Chikara Ogawa* 1, 2
1gastroenterology and hepatology, kinki university faculty of Medicine, osakasayama,, 2gastroenterology and hepatology, takamatsu red cross hospital, takamatsu, japan
Introduction: sometimes it is difficult to detect small liver tumor for us and to image positional relationship between the tumor and vessels, especially subcostal view. In this study, we evaluated the usefulness of a new technology, virtual us imaging device as a tool to assist novice sonographers.
Methods: a prospective blinded pilot study was conducted involving patients with liver lesions. two sonographers and two medical doctors with less than 5 years of experience performed us examinations. Detecting time on us and the success rate for detecting liver lesions with/without using the virtual us imaging device, synaPse VIncent (fujifilm Medical co.), before us examination was evaluated.
results: 32 patients with the following 42 liver lesions were included: liver cyst (n = 24), hemangioma (n = 8), hepatocellular carcinoma (n = 6), liver metastasis (n = 4). the maximal diameter of these lesions ranged from 0.3 to 1.5 cm (mean ± sD, 0.8 ± 0.4 cm).the average time for detecting liver lesions on us was 47.8 seconds (range: 7-113) with VIncent and 112.9 seconds (range: 14-313) without VIncent before us examination. there were significant differences in the duration of us examination with/without VIncent (p = 0.0002, student’s t-test). the rates for accurately detecting liver lesions were 100% and 76.2% (16/21) in us beginner with/without VIncent respectively. significantly higher detection rates in the us beginners were compared to without VIncent (p = 0.047, fisher’s exact test).
Conclusion: Before us examination, a reference with VIncent could contribute to the successful detection of liver lesions, even with 1cm, and time-saving for us beginners. and this technology has led to success in taking clear imaging for ceus and performing safe rfa therapy.
references: ohshima s: Volume analyzer synaPse VIncent for liver analysis. j hepatobiliary Pancreat sci 20 4;2 :235--238. ohshima s: Volume analyzer synaPse VIncent for liver analysis. j hepatobiliary Pancreat sci 20 4;2 :235--238.
Disclosure of Interest: none Declared
P-216 SCreenInG AnD IDenTIfyInG A nOVeL SSDnA APTAMer AGAInST ALPhA-feTOPrOTeIn uSInG Ce-SeLex
Wei-zhong Wu* 1, Li-Li Dong1, qi-Wen tan2, Wei ye3, Dong-Li Liu1, hai-feng chen3, yang Liu1, jing-Wu kang4, jia fan1, Wei Guo2
1Liver cancer Institute, 2Department of Laboratory Medicine, zhongshan hospital, 3school of Life sciences and Biotechnology, shanghai jiao tong university, 4shanghai Institute of organic chemistry, chinese academy of sciences, shanghai, china
Introduction: alpha-fetoprotein (afP) is a liver cancer associated protein and has long been utilized as a serum tumor biomarker of disease progression. afP is usually detected in hcc patients by an antibody based system. recently, however, aptamers generated from systematic evolution of ligands by exponential enrichment (seLex) were reported to have an alternative potential in targeted imaging, diagnosis and therapy.
Methods: afP-bound ssDna aptamers were screened and identified using capillary electrophoresis (ce) seLex, and then sequentially clonied, sequenced and motif analyzed.
results: four aptamers, aP206, aP244, aP250 and aP273, were found with higher combining power to afP, while the remaining had not. these positive aptamers showed similar binding affinity to afP within a micromole range. among them, aP273 had the highest affinity (kd = 0.5 μM), which was much stronger than the second one aP244 (kd = 4.8 μM).after transfected with aP273 at the final concentration of 100 nM, cell migration and invasion of both afP expressed hcc cells were significantly suppressed compared with a mock aptamer aP211. on the other hand, no obvious changes occurred in a549 cells.the tertiary structures of aP273 displayed much more helix and formed a tight structure than that of aP211. and even more, the well-helical structure may be important in the protein recognition.
Conclusion: our results indicate that ce-seLex technology is an efficient method to screen specific protein-bound ssDna, and aP273 could be used as an agent in afP-based staining, diagnosis and therapy, although more works are still needed.
Disclosure of Interest: W.-z. Wu Grant support from: national science foundation of china (81272437, 81472675), L.-L. Dong: none Declared, q.-W. tan: none Declared, W. ye: none Declared, D.-L. Liu: none Declared, h.-f. chen: none Declared, y. Liu: none Declared, j.-W. kang: none Declared, j. fan: none Declared, W. Guo: none Declared
P-217 The MeAnInG Of AfP, AfP-L3 AnD PIVKA-II fOr eVALuATInG reCurrenCe In PATIenTS WITh hePATOCeLLuLAr CArCInOMA WhO unDerWenT LIVer reSeCTIOn
sung hoon kim1, Sang hyun Ahn* 1, Moon young kim2, soon koo Baik2
1Department of surgery, 2Department of Internal Medicine, yonsei university Wonju college of Medicine, Wonju, korea, republic of
Introduction: alpha-fetoprotein (afP) and prothrombin time induced by vitamin k absence-II (PIcka-II) have been used a diagnostic and surveillance marker for hepatocellular carcinoma (hcc). however, many patients showed less level than optimal level that previously reported in many studies.
We investigated the meaning of the afP and PIVka-II, additionally lens culinaris agglutinin-reactive fraction of afP (afP-L3) for evaluating recurrence of hcc.
Methods: We retrospectively reviewed the medical records of patients who underwent liver resection. We investigated the recurrence and association with preoperative and postoperative level of afP, afP-L3 and PIVka-II.
results: Median afP, afP-L3 and PIVka-II were 8.5 ng/dL, <0.5% and 24 mau/mL, respectively.Median tumor size was 2.4cm. six patients (8.6%) had grossly portal vein invasion (PVI). Microscopic PVI was found in 8 patients (11.4%). During median 17month follow-up period, 19 patients had recurrence. a univariate analysis revealed that delta afP-L3, tumor size, gross PVI, satellite nodule, microscopic PVI, bile duct invasion and microvessel invasion were significant prognostic factors of recurrence. however, multivariate analysis revealed that only delta afP-L3 less than 50% was significant prognostic factors.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s9 8
Conclusion: as the surveillance program has been generalized in patients with high risk of hcc, identification of early and resectable hcc has been increased. however, many patients showed normal level of tumor marker and surgical resection showed still high recurrence rate. although more large-scaled study will be needed, we may predict the recurrence risk according to the change of afP-L3.
Disclosure of Interest: none Declared
P-218 effICACy Of LOCO-reGIOnAL TreATMenT fOr hePATOCeLLuLAr CArCInOMA PrIOr TO LIVInG DOnOr LIVer TrAnSPLAnTATIOn
Mohamed k. shaker1, Mahmoud el Meteini1, Iman Montasser* 1, Mohamed el Gharib1, hany dabbous1, ahmed el Dorry1
1ain shams university hcc clinic, cairo, egypt
Introduction: BackGrounD: hepatocellular carcinoma (hcc) is the fifth most common malignancy in the world. liver transplantation is the best available option for early hepatocellular carcinoma (hcc) its application is limited by stringent selection criteria .Milan criteria have remained the paradigm for the selection of the best candidates for Lt in the past 10 years Down-staging of hcc is an attractive alternative to simply expanding the tumor size limits to meet Milan criteria. Loco-regional therapies used for down staging, laparoscopic radiofrequency ablation (rfa) and transcatheter arterial chemoembolization (tace)aim: the aim of this study was to evaluate the outcome of hcc patient after liver transplantation who received pre-transplant loco-regional treatment.
Methods: Data was retrieved from the files of patients with (hcc) who underwent liver transplantation and received pre-transplant loco-regional treatment during the period from December 2011till December 2013. (a) Pre-treatment assessment including full personal history taking and thorough clinical examination, alpha fetoprotein (afP) level, child Pugh score, MeLD score, waiting time for liver transplantation., abdominal ultrasound and duplex, triphasic spiral ct or MrI abdomen before and after loco-regional therapy B) histopathological evaluation of the explants: including :number of hcc nodules, size. Grade based on the edmondson and steiner criteria, presence of viable malignant cells and microvascular or capsular invasion.
results: the mean age for the enrolled patients was 52±7.04, 93.1% were males, mean MeLD was 8.23±1.89, 41.38% were child B, and 10 patients were child c. Mean waiting time from the last intervention to transplantation was 8.48±6.83 months, mean afP before locoregional therapy was 308±1240 ng/dl while after locoregional therapy it became 47.41±112.15 ng/dl (p=0.013). twenty two patients were within the Milan criteria and 7 patients were beyond Milan criteria. eighty focal lesions (range 0.6-6cm; mean: 2±1.09cm) were subjected to locoregional therapy; 10 patients underwent rfa, 11 patients had tace, one patient underwent microwave ablation and 7 patients had several sessions of rfa and tace. the histopathological findings of the explanted livers showed complete necrosis in 28 lesions, partial necrosis in 3 lesions and 21 lesions turned to be macro degenerative and dysplastic nodules. there was statistical significant discrepancy in total focal lesions size between the results of the last triphasic ct before transplantation and the histopathological findings (p=0.01) ;also ,there was statistical significant differences between both as regards the interpretation of well ablated lesions (complete necrosis) (p=0.001).however, there was no statistical significant difference between the imaging modality and histopathology regarding the number of focal lesions(p=0.14)
Conclusion: Locoregional therapies provide good option for patients on waiting list for liver transplantation, and patients not fulfilling Milan criteria as test of time to assess the biological behavior of the tumor. however, Liver transplantation is the therapy of cure even for those with apparently successful locoregional therapy.
Disclosure of Interest: none Declared
P-219 SequenTIAL SeruM MeTAbOLOMIC PrOfILInG AfTer rADIOfrequenCy AbLATIOn Of hePATOCeLLuLAr CArCInOMA reVeALS DIfferenT reSPOnSe PATTernS ACCOrDInG TO AeTIOLOGy
corentine Goossens1, Pierre nahon2,3, Laurence Le Moyec4, Mohamed nawfal triba1, nadia Bouchemal1, roland amathieu1,5, nathalie Ganne-carrié2,3, Marianne ziol6,7, jean-claude trinchet2,3,7, nicolas sellier8, abou Diallo9, olivier seror3,8, Philippe Savarin* 1
1université Paris 13, sorbonne Paris cité, csPBat, uMr 7244, cnrs, Bobigny, france, 2Groupe hospitalier Paris seine-saint-Denis, pôle d’activités cancérologiques spécialisées, aPhP, hôpital jean Verdier, Bondy et université Paris 13, sorbonne Paris cité, ufr sMBh, Bobigny, france, 3InserM u1162, Génomique fonctionnelle des tumeurs solides, université Paris 5, Paris, france, 4université d’evry Val d’essonne, uBIae, InserM u902, evry, france, 5service d’anesthésie-réanimation, Ghu PssD, hôpital jean Verdier, Bondy et université Paris 13, sorbonne Paris cité, ufr sMBh, Bobigny, france, 6aPhP, service d’anatomie Pathologique, hôpital jean Verdier, Bondy et université Paris 13, sorbonne Paris cité, ufr sMBh, Bobigny, france, 7BB-0033-00027. centre de ressources
Biologiques Maladies du foie, Groupe hospitalier Paris-seine-saint-Denis, Bondy, france, 8aPhP, service de radiologie, hôpital jean Verdier, Bondy, france, 9service d’Information Médicale, Ghu PssD, hôpital jean Verdier, Bondy, france
Introduction: radiofrequency ablation (rfa) is commonly performed as a curative approach in patients with hepatocellular carcinoma (hcc). however, the risk of tumor recurrence is difficult to predict due to a lack of reliable clinical and biological markers. Metabolomics appears to be a promising technique leading to the identification and characterization of new biomarkers. the objectives of the present study were to explore preoperatively and at various time points post-rfa the metabolic profile of serum samples from hcc patients and to detect the different adaptations to rfa.
Methods: sequential sera obtained before and after rfa procedures in 120 patients with hcc developed in cirrhosis were investigated using nuclear Magnetic resonance (nMr) metabolomics. a multilevel orthogonal Projection to Latent structure (oPLs) analysis was used in order to discriminate the metabolic intra-individual changes caused by the rfa.
results: It appeared that the recurrence-free survival time differed according to the cause of the underlying cirrhosis. two distinct serum metabolomic profiles of hcc patients could be determined according to the viral and non-viral aetiology of the liver disease, this distinction being further observed with specific and distinct metabolic responses after rfa procedure.
Conclusion: Likewise observed for timing of recurrence, biochemical adaptations as demonstrated by nMr metabolomics depend on the aetiology. this discovery suggests that investigations in hcc and its response to treatment should further be pursued more closely with the biochemical point of view to implement new personalized therapeutic management.
Disclosure of Interest: none Declared
P-220 hIGh ACCurACy Of SOLubLe AxL In The DIfferenTIAL DIAGnOSIS Of ChrOnIC LIVer DISeASeS AnD hePATOCeLLuLAr CArCInOMA
Mirko Dengler1, katharina staufer2, Patrick reichl1, Patrick starlinger2, christine Brostjan2, thomas Gruenberger2, thomas Weiss3, christian Müller4, Michael trauner4, heidemarie huber1, Wolfgang Mikulits* 1
1Department of Medicine I, Div.: Institute of cancer research, 2Department of surgery, Medical university of Vienna, Vienna, austria, 3Department of Pediatrics and juvenile Medicine, center for Liver cell research, university hospital regensburg, regensburg, Germany, 4Division of Gastroenterology and hepatology, Department of Internal Medicine III, Medical university of Vienna, Vienna, austria
Introduction: Diagnosis of hepatocellular carcinoma (hcc) at early stages allows curative therapies, whereas treatment options at later stages are very limited. state-of-the-art diagnosis of hcc by ultrasonography and determination of serum α-fetoprotein (afP) levels shows moderate sensitivity and limited specificity, thus highlighting the need for more accurate biomarkers in the diagnosis of early stage hcc. In this multicenter study we assessed the potential of soluble axl (saxl) as a diagnostic biomarker of early hcc and cholangiocellular carcinoma (ccc) as well as examined the value of saxl in the differential diagnosis between chronic liver diseases (cLDs) and hcc.
Methods: Levels of saxl, a cleavage product of the receptor tyrosine kinase axl, were analyzed by enzyme-linked immunosorbent assay in 814 serum samples from centers in europe and china.
results: analysis of saxl showed significantly increased levels in hcc as compared to healthy controls. receiver operating characteristics (roc) curve analysis revealed high sensitivity and specificity of saxl in very early stage hcc (BLcL 0) and early hcc (BcLc a) compared to afP. hcc patients negative for afP displayed significant saxl serum levels and combination of saxl and afP improved diagnostic accuracy in very early hcc patients. Differential diagnosis revealed high levels of saxl in hcc versus cLDs derived from non-alcoholic fatty liver disease (nafLD/nash), autoimmune hepatitis (aIh), primary sclerosing cholangitis (Psc) and primary biliary cirrhosis (PBc). these cLDs were further categorized by fibrosis and cirrhosis scoring and roc curve analyses showed accurate values of saxl in the differential diagnosis between fibrosis/cirrhosis and hcc. noteworthy, saxl failed to be elevated in ccc and in secondary hepatic malignancies derived from colorectal carcinoma. furthermore, independent stress testing revealed long-term storage and temperature stability which corroborates the potential of saxl as valuable biomarker in clinical diagnostics.
Conclusion: saxl is a stable biomarker showing enhanced levels in hcc but not in ccc or secondary liver malignancies. assessment of saxl levels in blood samples allows accurate differential diagnosis of very early hcc versus fibrosis and cirrhosis, suggesting that saxl is a promising diagnostic biomarker for routine clinical use.
Disclosure of Interest: M. Dengler: none Declared, k. staufer Grant support from: k.s. received travel grants from roche, MsD and novartis, honoraria support from: k.s. received speaker honorarium from roche and Biotest., P. reichl: none Declared, P. starlinger: none Declared, c. Brostjan: none Declared, t. Gruenberger: none Declared, t. Weiss: none Declared, c. Müller: none Declared, M. trauner: none Declared, h. huber: none Declared, W. Mikulits: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 9 9
P-221 The effeCT Of bOrIC ACID On TOTAL AnTI OxIDATIVe- OxIDATIVe STATuS In DIfferenT TISSueS Of rATS APPLIeD 3–MeThyLChOLAnThrene
Gokhan Oto* 1, Bahat comba2, hulya ozdemir1, arzu comba3
1Pharmacology, yuzuncu yil university, Medical faculty, 2Physiology, yuzuncu yil university, Veterinary faculty, 3urology, yuzuncu yil university, Medical faculty, Van, turkey
Introduction: Polycyclic aromatic hydrocarbons (Pahs) are the most common contaminants in the environment. 3-Methylcholanthrene (3-Mc) is a polycyclic aromatic hydrocarbon (Pah) common in polluted urban air and is a potent carcinogenic agent often used in experimental cancer studies. the influence of Pahs on the antioxidant system in mammalian systems has received only limited attention. aim of this study was to evaluate effects of boric acid (Ba) on total anti oxidative (tas)-total oxidative status (tos) and oxidative stress index (osI) in liver, lung, kidney and brain tissues of rats applied 3-Mc.
Methods: In this study, rats were divided into 4 groups and each group were containing 6 rats. 1st
group was separated as control group. 100 mg/kg total dosage of 3-Mc was applied to the 2nd group 2 times a week total in 4 equal dosage with i.p. way. only Ba 300 mg/L was applied to 3rd group in drinking water. 3-Mc + Ba was applied to 4th group. the study was completed at 150th day. tissues of the rats were homogenized in ice-cold saline phosphat buffer (PBs), 1:10 w/v in ph 7.4. after centrifugation at 10000g for 15 min at 4 °c, the supernatant was extracted and analyzed tas-tos by spectrophotometric kits. osI was calculated from the formula.
results: tas, tos and osI in the liver tissue of 4th group was the highest. the lung tas level was the highest in the 2nd group; the lowest in 4th group. the kidney tas was the highest in group 4th; the lowest in 2nd group. tos and osI in the brain tissue of the 4th group were higher than other groups.
Conclusion: as a result, Ba supplementation in drinking water can demonstrate different effects on tas-tos-osI in different tissues of rats applied 3-Mc. In case of exposure to 3-Mc, Ba may shown antioksidan effect to the reduction of oxidative stres in kidney tissue.
references: 1 Gressani kM, kabler sL, o’sullivan MG et al (1999). strain-dependent lung tumor formation in mice transplacentally exposed to 3-methylcholanthrene and post-natally exposed to butylated hydroxytoluene. carcinogenesis 20: 2159–165.2 jin y, Miao W, Lin x, Pan x, ye y, xu M and fu z (2014). acute exposure to 3-methylcholanthrene induces hepatic oxidative stress via activation of the nrf2/are signaling pathway in mice. Environmental Toxicology, 29 (12), 1399–1408.
Disclosure of Interest: none Declared
P-222 PerCuTAneOuS MAnAGeMenT Of POSTOPerATIVe STenOSIS Of The bILIOJeJunAL AnASTOMOSIS In hePATIC Or PAnCreATIC CAnCer PATIenTS
Paris Pappas* 1, Polytimi Leonardou1, chrysovalantis Vergadis1
1radiology, LaIkon hospital, athens, Greece, Penteli, Greece
Introduction: Benign stenosis of the bilioenteric anastomoses has been well studied in the international literature (1,2).the aim of our study is to evaluate the percutaneous restoration of a stenosed bilioenteric anastomosis, created during resection of malignant tumor of the liver or pancreas.
Methods: We evaluated 93 patients who were referred to our department over the last 10 years (2005-2014) presenting with signs of extrahepatic biliary stricture.Percutaneous biliary drainage performed in all patients.In 68 of 93 (73%) bile culture demonstrated microbes in the sample.In 9 of 93 patients (9.6%) we didn’t succeed to pass our materials through the stenosis-occlusion.among those 9 patients,3 were treated surgically,while the other six remained with external drainage lifelong,due to contra-indications of surgical treatment and reduced life expectancy.of the 84 patients where we succeeded to access the intestine, the 18 (21.5%) carrying multiple bilio- or hepatico-jejunal anastomoses.
results: among those 84 patients,4 had only a dilatation (balloon diameter 6-8 mm and length 4cm), since it was estimated that the stenosis was of purely benign etiology-one patient even twice with an interval of three years.these 4 patients had been operated with partial pancreatectomy and all had already exceeded five years survival(3).to the 80 remaining patients, 117 metal stents were placed in total, self or balloon expandable, with diameters of 4-10 mm and lengths of 15-60mm.(4,5).re-intervention was needed in 9 of the 80 patients (11%) after 3 to 18 months. During a follow up period of 3 months to 8.5 years, 27 of our 93 patients are still alive. complications:none of the 93 patients showed signs of bleeding or choloria or pancreatitis following intervention.cholangiitis appeared in 23 of the 93 patients (25%), which were treated conservatively.Deaths within 30 days occurred in 6 patients (6.5%),however no death considered as a complication of the procedure.
Conclusion: Percutaneous access of the stenosis of a bilio-enteric anastomosis on the ground of a hepatic or pancreatic malignancy appears to be the only way, and only on failure surgery is justified.
references: (1).j Minim access surg. 2012 jul;8(3):99-101. doi: 10.4103/0972-9941.97599.transhepatic metallic stenting for hepaticojejunostomy stricture following laparoscopic cholecystectomy biliary injury: a case of successful 20 years follow-up.Donatelli G1, Mutter D, Dhumane P, callari c, Marescaux j(2). hepatogastroenterology. 2009 jan-feb;56(89):43-6. an experience of treatment of postoperative biliary stricture at a single japanese institute.nanashima a1, abo t, sumida y, nonaka t, tanaka k, hidaka s, sawai t, yasutake t, nagayasu t.(3). j Gastrointest surg. 2007 Dec;11(12):1704-11. epub 2007 oct 11.Long-term anastomotic complications after pancreaticoduodenectomy for benign diseases.reid-Lombardo kM1, ramos-De la Medina a, thomsen k, harmsen Ws, farnell MB.(4). abdom Imaging. 2003 sep-oct;28(5):678-83Percutaneous insertion of metallic endoprostheses in the biliary tree in 66 patients: relief of the obstruction.Pappas P1, Leonardou P, kurkuni a, alexopoulos t, tzortzis G.(5).Langenbecks arch chir suppl kongressbd. 1996;113:762-6.[Palliative therapy of inoperable malignant occlusive jaundice--stent implantation or biliodigestive anastomosis].truong s1, conze j, Willis s, kasperk r, schumpelick V.
Disclosure of Interest: none Declared
P-223 hePATObILIAry CArCInOMA WITh OSTeOCLAST-LIKe GIAnT CeLLS: fIrST CASe rePOrT
ruana rocha1, jose Vassallo1, Miriam trevisan1, francisco callejas neto2, jose c. Pareja2, Cecilia escanhoela* 1
1Pathology, 2Digestive surgery, unicamp, campinas, Brazil
Introduction: osteoclast-like giant cells (oGc) component in carcinomas are reported in a wide variety of organs including breast, thyroid, pancreas, gallbladder and stomach. the nature of the oGc of such tumors has been extensively debated. several authors have believed on reactive nature of these cells, especially when oGc were seen inside of a conventional carcinoma. hepatic neoplasms with oGc are quite uncommon. few cases of hepatocellular carcinoma with oGc have been described previously.
Methods: We report the first case of hepatobiliary carcinoma with an abundant component of oGc in a non-cirrotic liver. a liver tumor was found on ct scan in an asymptomatic 47-year-old woman.
results: a needle biopsy was performed and showed a dense lymphohistiocytic infiltrate rich in Langhans-like giant cells, mature and immature fibroblasts and neoformed vessels with extensive necrosis area associated. some isolated atypical cells with broad cytoplasm and pleomorphic and hyperchromatic nuclei were observed. Immunohistochemistry showed that the atypical cells were hep Par-1 positive, suggesting a diagnosis of hepatocellular carcinoma. a right hepatectomy was performed. In an examination of the surgical specimens the tumor, 5,7 x 4,5 x 3,6 cm in size, was demarcated and lobulated. histologically the tumor consisted of a malignant epithelial neoplasia with solid and trabecular pattern of polygonal cells with broad cytoplasm and vesicular nuclei, with a moderate pleomorfism, and some areas with irregular tubular structures of varying size with necrosis associated. It is observed an intense and diffuse inflammatory response with dense lymphohistiocytic infiltrate and numerous large multinucleated giant cells, the so-called oGc. Immunohistochemical study showed that the oGc component were cD68 positive (fig. 1), but cytokeratin negative, while the rest of neoplasia expressed strongly and diffusely ae1ae3 and ck7; hep Par-1 was widely positive, especially in areas with a rich lymphohistiocytic infiltrate. the areas with biliary differentiation had been highlighting by ck7 and ca19-9´s positivity. carcinomatous metastasis were detected in nine lymph nodes.
Image:

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 0 0
Conclusion: Based on its aggressive clinical course and poor prognosis, the recognition of this entity is indispensable.
references: 1) tanahashi c, nagae h, nukaya t, hasegawa M, yatabe y. combined hepatocellular carcinoma and osteoclast-like giant cell tumor of the liver: possible clue to histogenesis. Pathol Int 2009;59:813-816.2) Ikeda t, seki s, Maki M, noguchi n, kawamura t, arii s, et al. hepatocellular carcinoma with osteoclast-like giant cells: possibility of osteoclastogenesis by hepatocyte-derived cells. Pathol Int. 2003;53:450–456.3) Dioscoridi L, Bisogni D, freschi G.hepatocellular carcinoma with osteoclast-like giant cells: report of the seventh case in the literature. case rep surg. 2015: 836105. doi: 10.1155/2015/836105. epub 2015 feb 22.4) ahaouche M, cazals-hatemD, sommacale D, cadranel jf, Belghiti j, Degott c.a Malignant hepatic tumour with osteoclast-like giant cells.histopathology. 2005; 46(5):590-2.5) rudloff u, Gao zq, fields s, Gecelter Gr. osteoclast-like giant cell tumor of the liver: a rare neoplasm with an aggressive clinical course. j Gastrointest surg.2005;9(2):207-14.
Disclosure of Interest: none Declared
Clinical Trials and Treatment research & Miscellaneous
P-224 unreSeCTAbLe hePATOCeLLuLAr CArCInOMA > 5 CM: effICACy AnD SurVIVAL Of MuLTIbIPOLAr rADIOfrequenCy AbLATIOn
Gisele nkontchou* 1, olivier sutter2, Valerie Bourcier1, jean-charles nault1, Pierre nahon1, nathalie Ganne carrie1, hayette amerane2, fatna Bouhaf2, abou a. Diallo3, nicolas sellier2, olivier seror2
1Liver unit jean verdier hospital, 2radiology unit jean Verdier hospital, 3Medical Information Department jean Verdier hospital, bondy, france
Introduction: Liver resection when feasible can offer long survival in patients with large hcc (> 5 cm) and sometime advanced stages (BcLc-c) of hepatocellular carcinoma (hcc). unfortunately, only patients without or with very well compensated cirrhosis are amenable to resection. for non resectable patients palliative treatments mainly trans-arterial chemoembolization are often considered. Multibipolar rfa (Mbprfa) which can ablate large liver tumors far beyond 5cm diameter could be therefore considered as alternative curative option in these patients
Methods: this study reports the efficacy (response, survival) of Mbprfa in hcc > 5cm diameter including intrasegmental infiltrative forms and segmental portal invasion in patients with cirrhosis not amenable to resection. 83 consecutive patients (69 years, 67 male, BcLc a/B/c: 48/19/7, 74 naïve) with up to three hcc, the largest nodule > 5cm in diameter (median: 6.2cm, 5.1-9cm, 22 infiltrative, 12 with segmental portal invasion) underwent Mbprfa. complete ablation rate, and for the naïve patients recurrence free survival (rfs) and overall survival (os) were assessed. Multivariate cox proportional hazards regression assessed the factors associated with survival
results: complete ablation rate, and for the naïve patients recurrence free survival (rfs) and overall survival (os) were assessed. Multivariate cox proportional hazards regression assessed the factors associated with survival. complete ablation was observed in 78/83 (94%) patients. three (3.6%) severe complications occurred: one (1.2%) death due to sepsis, one abscess requiring drainage, one tract seeding. after a median follow-up of 26.1 months [1-112 months], the cumulative 3 and 5-years os in naïve patients was 54 % [41-65] and 36 % [24-48] respectively. In univariate analysis risk factors of survival were child pugh B class, vascular invasion and infiltrative form.
Infiltrative form (p=0.0041) was the only independent predictors of overall survival. In non-infiltrative naïve patients (n= 56) the 1-3 years rfs were 64 % [50%>75%] and 27 % [16%>39%] respectively.
Conclusion: Mbprfa provides long survivals in inoperable patients with large hcc especially for patients with non-infiltrative form. other approachs are needed for infiltrative form.
Disclosure of Interest: none Declared
P-225 hOW reLeVAnT IS InDOCyAnIne Green reTenTIOn rATe AT 15 MInuTeS (ICG15) ASSeSSMenT befOre An eLeCTIVe hePATeCTOMy In WeSTern COunTry?
eric Vibert* 1, Bertrand Le roy2, cyril cosse3, Badr serji1, emilie Gregoire4, nicolas Golse5, jean-yves Mabrut5, yves Patrice Le treut4, Denis castaing1, antonio sa cunha1, rené adam1, Daniel cherqui2
1centre hépato Biliaire, hopital Paul Brousse - aPhP, 2centre hépato Biliaire, hopital Paul Brousse, VILLejuIf, 3service de chirurgie Digestive amiens, chu amiens, amiens, 4service de chirurgie hépatique, hopital de la timone, Marseille, 5service de chirurgie hépatique, hopital de la croix rousse - hcL, Lyon, france
Introduction: objectives. Identify the interest of IcGr15 before liver resections.Background data. IcGr15 is largely used in asia to evaluate the functional liver reserve and determine the extent of hepatectomy, especially in f3/f4 patients. IcGr15 is rarely used in Western country where the functional reserve is mainly evaluated with the MeLD score and/or platelet count. the relevancy of IcGr15 in such conditions is unknown.
Methods: this prospectively-designed study included consecutive adult-patients undergoing elective-hepatectomy in 3 hPB-centers for primary liver tumors. Primary outcome was 3-months postoperative ascites and secondary outcome was 90-days mortality and severe morbidity (Dindo-clavien grade>II). explanatory variables were only preoperative (including age, gender, BMI, comorbidities, cirrhosis, major hepatectomy, MeLD and platelet rate) collected prospectively on a dedicated-website. Due to no homogenous liver function repartition, patients with portal vein embolization were excluded. Mean MeLD score and platelet rate was 8±2 and 206±98G/L. Multivariable-regression models were used to identify independent preoperative data predictors of 3-months outcomes. to improve the robustness of our data, bootstrap simulations (n = 1000) were performed.
results: Between December-2012 and june-2013, 163 patients (63 major hepatectomies including 32 right hepatectomy and 100 minor hepatectomies) were included. at the 3-months, in f0/f2 patient (n=70) and f3/f4 (n=93), the rate of 1/ postoperative ascites were 2.9% and 9.7% (p<0.001); 2/ mortality was 7% and 1% (p<0.03) and severe morbidity was 20% and 19.4% (p=0.92) respectively. In all the population, no preoperative factor was retrieved as correlated to 3-months outcomes. In f3/f4 patient, no preoperative factor of mortality and severe morbidity could be identified but diabete (p=0.03), IcGr15 (p=0.05) and platelet rate (p=0.08) were predictive of 3-months postoperative ascites. roc identified a cutoff of 15% as being associated with increased 3-months postoperative ascites with good accuracy (auroc 0.71, cI95% 0.52-0.90, p=0.94) for IcGr15. the identified platelet cutoff (140G/L) had insufficient accuracy (auroc 0.66, cI95% 0.50-0.83) to be used. among f3/f4 patients with preoperative IcGr15 > 15% (n=28/93), the global rate of 3 month postoperative ascites was 25% without significant difference according to the extent of hepatectomy.
Conclusion: In population of f3/f4 patients selected with MeLD score and platelet rate, the IcGr15 is the best method to predict 3 months postoperative ascites when is superior to 15%.
Disclosure of Interest: none Declared
P-226 MuLTICenTrIC STuDy Of LIVer TrAnSPLAnTATIOn In PATIenTS WITh hePATOCeLLuLAr CArCInOMA In brAzIL- PreLIMInAry DATA Of 913 PATIenTS
Aline Chagas* 1, 2, Luciana o. o. kikuchi1, 2, Guilherme felga3, angelo a. Mattos4, renato f. silva5, rita de cassia M. a. silva5, fernanda Branco6, Márcio D. almeida3, Ilka f. Boin7, josé h. P. Garcia8, Luiz c. D’albuquerque2, 9, flair j. carrilho1, 2, Brazilian hcc study Group10
1Division of Gastroenterology and hepatology, Department of Gastroenterology, university of sao Paulo school of Medicine, 2sao Paulo clinicas Liver cancer Group, 3Liver transplant, hospital Israelita albert einstein, sao Paulo, 4Department of Gastroenterology, fundação universidade federal de ciências da saúde de Porto alegre, Porto alegre, 5serviço de Gastroenterologia e unidade de transplante de fígado, hospital de Base - funfarMe, faculdade de Medicina de são josé do rio Preto, são josé do rio Preto, 6Department of Gastroenterology, santa casa de Misericórdia de Porto alegre, Porto alegre, 7Digestive surgery Department, state university of campinas, campinas, 8centro de transplante de fígado do ceará, Department of surgery and Liver transplantation, federal university of ceará, fortaleza, 9Department of Gastroenterology, university of sao Paulo school of Medicine, 10Brazilian hcc study Group, sao Paulo, Brazil
Introduction: Liver transplantation (Lt) is the treatment of choice for patients with cirrhosis and unresectable early hepatocellular carcinoma (hcc). the aim of this multicentric study was to analyze the demographic characteristics, clinical features and outcomes of patients submitted to liver transplantation with hcc in Brazil.
Methods: We conducted a national multicentric retrospective study to analyze the results of liver transplantation in patients with hepatocellular carcinoma (hcc). Medical records of 913 transplanted patients with hepatocellular carcinoma, between 2006 -2014, from 10 transplant centers in Brazil, were retrospectively analyzed. Patient and tumor characteristics, pathologic data and rate of tumor recurrence were collected.
results: of the 913 hcc transplanted patients, median age was 57 years and 81% were male. etiology of cirrhosis was hcV in 60%. at diagnosis, most patients had uninodular hcc (57%) and median tumor burden was 30mm. During the waiting list period, hcc treatment was performed in 63%. chemoembolization (tace), ablation therapy (PeI/rf), surgery and combined therapy were used in 80%, 13%, 6% and 1% patients, respectively. In explant analysis, tumor was uninodular in 45% and moderately differentiated in the majority of cases (66%). Median hcc size was 28mm. Vascular invasion and satellite nodules were observed in 24.5% and 25% of patients, respectively. In 818 patients that survived beyond the immediate post-transplant period, mean follow-up was 27,7 months (±23,8), an overall survival was 70% in 5 years. recurrence occurred in 8/818 (8%) cases, at a mean time of 15months (1.5-76m). sites of recurrence were 40% in liver, extrahepatic in 46%

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 0 1
and both hepatic and extrahepatic in 14%. Vascular invasion and alpha-fetoprotein (afP) level before liver transplantation were risk factors for tumor recurrence. the presence of hcc recurrence was directly related to poor survival. female gender, need for re-transplantation, vascular invasion and explant outside the Milan criteria were also predictors of poor survival.
Conclusion: Liver transplantation for hepatocellular carcinoma in Brazil was associated with an overall survival of 70% in 5 years. hcc recurrence ocurred in 8% of patients. the presence of vascular invasion and afP before liver transplantation were associated with increased risk of tumor recurrence. female, vascular invasion, explant outside the Milan criteria and hcc recurrence were related to poor survival. an lang=en-us style='mso-ansi-language:en-us'>In explant analysis, tumor was uninodular in 45% and moderately differentiated in the majority of cases (66%). Median hcc size was 28mm. Vascular invasion and satellite nodules were observed in 24.5% and 25% of patients, respectively. In 818 patients that survived beyond the immediate post-transplant period, mean follow-up was 27,7 months (±23,8), an overall survival was 70% in 5 years. recurrence occurred in 8/818 (8%) cases, at a mean time of 15months (1.5-76m). sites of recurrence were 40% in liver, extrahepatic in 46% and both hepatic and extrahepatic in 14%. Vascular invasion and alpha-fetoprotein (afP) level before liver transplantation were risk factors for tumor recurrence. the presence of hcc recurrence was directly related to poor survival. female gender, need for re-transplantation, vascular invasion and explant outside the Milan criteria were also predictors of poor survival.
Disclosure of Interest: none Declared
P-227 COMPArISOn beTWeen MICrOWAVe AbLATIOn AnD rADIOfrequenCy AbLATIOn In The TreATMenT Of hePATOCeLLuLAr CArCInOMA
ahmad eldorry1, Mahmoud elmeteini2, Mostafa hamed3, heba abdella3, Ahmad A. e. Madkour* 3, Mohamed shaker3
1radiodiagnosis and Interventional radiology, 2General surgery, 3tropical medicine, ain shams university, cairo, egypt
Introduction: Liver cancer is the sixth most common cancer and the third cause of cancer-related death and accounts for 7% of all cancers. hcc represents more than 90% of primary liver cancers and is a major global health problem. Local ablation competes with surgery for hepatocellular carcinoma<3 cm and may be considered as first-line treatment depending on age,associated comorbidities and location of the tumor
Methods: this study was a prospective interventional comparative study.40 patients with hcc, all were BcLc a with a single lesion less than 5cm, were randomized into two groups through systemic randomization. Group I include 20 patients who underwent PMc and group II include 20 patients who underwent rfa and both groups were followed up at 1,4,7,10,13 months through clinical examination ,liver function tests and triphasic spiral ct with calculation of child score ,Pst, BcLc if active tumor tissue and fulfillment of Milan criteria.the collected data were coded, tabulated, and statistically analyzed using IBM sPss statistics (statistical Package for social sciences) (V. 22.0) software version 22.0, IBM corp., chicago, usa, 2013
results: complete tumor ablation was achieved in 100% of both groups by single session. no local recurrences were detected along the follow-up period. Distal intrahepatic recurrence was seen in 11 patients (55%) in rfa group and 7 patients (35%) in PMc group which was statistically insignificant. no distal extra hepatic recurrence along the study.
first recurrence among study groups:
PMc rfa PP/r
total number of recurrences 7 (35.0%) 11 (55.0%) 0.204
time of 1st recurrence (months)
fu1 3 (42.9%) 3 (27.3%) 0.506
fu2 0 (0.0%) 3 (27.3%)
fu3 0 (0.0%) 2 (18.2%)
fu4 1 (14.3%) 1 (9.1%)
fu5 3 (42.9%) 2 (18.2%)
survival and disease-free survival were 95% and 65% in PMc group, while in rfa group they were 90% and 45% by the end of the study.
no procedure-related mortality or major complications occurred.
Image:
Conclusion: PMc and rfa are safe procedures with low complication rate for the treatment of hcc. Both are effective models of treatment with no significant differences between them
Disclosure of Interest: none Declared
P-228 COMPArATIVe STuDy beTWeen rADIOeMbOLIzATIOn AnD CheMOeMbOLIzATIOn WITh DruG eLuTInG beAD In PATIenTS WITh hePATOCeLLuLAr CArCInOMA
Myeong Jun Song* 1, si hyun Bae1, jong young choi1, seung kew yoon1
1Internal Medicine, college of Medicine, the catholic university, seoul, korea, republic of
Introduction: chemoembolization is one of several standards of care treatment for unresectable hepatocellular carcinoma (hcc). chemoembolization with drug-eluting bead and radioembolization with yttrium-90 microspheres are novel, transarterial approach to locoregional therapy. We performed a comparative effectiveness analysis of these therapies in patients with unresectable hcc.
Methods: We collected data from 320 patients, who were treated with transarterial locoregional therapies (chemoembolization with drug eluting bead or radioembolization) between july, 2009 and May, 2013. We excluded patients who were not appropriate for comparison and analyzed data from 104 (68 who received chemoembolization and 36 who received radioembolization). Patients were followed for signs of toxicity; overall survival was the primary outcome measure. secondary outcomes included safety, response rate, and time-to-progression.
results: abdominal pain and increased transaminases were more frequent following chemoembolization (P<0.05). overall survival was similar between groups that received chemoembolization (41.3 months) and radioembolization (37.3 months, P=0.117). among patients with intermediate stage disease, there was a trend that patients treated with chemoembolization had a higher response rate than with radioembolization (72% vs. 61.9%, respectively, P=0.203). although time-to-progression was longer following radioembolization than chemoembolization (14.9 months vs. 8.1 months, respectively, P=0.024), median survival times were not statistically different (42.2 months vs. 50.1 months, respectively, P=0.769).
Conclusion: Patients with hcc treated by chemoembolization with drug eluting bead or radioembolization with yttrium-90 microspheres had similar survival times. radioembolization resulted in longer time-to-progression and less toxicity than chemoembolization in intermediate stage.
Disclosure of Interest: none Declared

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 0 2
P-229 rADIOeMbOLIzATIOn IS A SAfe AnD effeCTIVe TreATMenT fOr hePATOCeLLuLAr CArCInOMA WITh POrTAL VeIn ThrOMbOSIS
young young cho1, yun hwan kim2, Geum-youn Gwak3, si hyun Bae4, Do young kim5, jeong heo6, yoon Jun Kim* 1
1Department of Internal Medicine and Liver research Institute, seoul national university college of Medicine, 2Department of radiology, college of Medicine, korea university, anam hospital, 3Department of Medicine, samsung Medical center, sungkyunkwan university school of Medicine, 4Department of Internal Medicine, kangnam st. Mary's hospital, the catholic university of korea college of Medicine, 5Department of Internal Medicine, yonsei university college of Medicine, seoul, 6Internal Medicine, Pusan national university college of Medicine, Pusan, korea, republic of
Introduction: hepatocellular carcinoma (hcc) patients with portal vein thrombosis (PVt) have limited treatment options, and sorafenib is the current treatment of choice. radioembolization using yttrium-90 microsphere (y90) is a new treatment modality for hcc and is emerging as a treatment strategy for hcc with PVt.
Methods: In a multicenter prospective cohort the total number of 154 patients was treated with y90 in 6 tertiary referral hospitals in korea. among them, 47 patients had PVt. Patients undergoing sorafenib treatment with PVt were selected as control, and 77 patients were selected. treatment response was analyzed according to modified response evaluation criteria in solid tumors. time to progression (ttP) and overall survival (os) were analyzed. to adjust for the between-group differences in baseline characteristics, inverse probability weighting (IPW) using propensity scores was used.
results: Median os and ttP between y90 group and sorafenib group were significantly better at y90 group (13.0 months and 6.0 months; P<0.01, 6.0 months and 3.0 months; P<0.01), respectively. after balancing population with IPW, there were still significant difference in os (P<0.01) and ttP (P=0.03). Multivariate analysis showed only extent of PVt predicted survival, main PVt had worse survival compared to segmental PVt ((hazard ratio [hr], 3.16; 95% confidence interval [cI], 1.41-7.04; P<0.01). there were more severe adverse effects (over Grade 3) in sorafenib group (P=0.03).
Conclusion: In hcc patients with PVt, y90 showed superior response rates compared to sorafenib even after balancing the population with IPW, and has favorable adverse effects. y90 can be considered as a new treatment option in this population.
Disclosure of Interest: none Declared
P-230 The OPTIMAL STAGInG Of The SInGLe LArGe hePATOCeLLuLAr CArCInOMA
young Kul Jung* 1, yeon seok seo1, chang ho jung1, jI hoon kIM1, tae hyung kim1, yang jae yoo1, seong hee kang1, sun young yim1, sang jun suh1, hyunggin an2, hyung joon yim1, jong eun yeon1, kwan soo Byun1, soon ho um1
1Internal Medicine, 2Department of Biostatistics, korea university college of Medicine, seoul, korea, seoul, korea, republic of
Introduction: optimal staging for hepatocellular carcinoma (hcc) is very important for predicting prognosis and decision of treatment option. although the BcLc staging system is properly classify patients into 5 groups and provides predicted survival and optimal treatment option, staging and optimal treatment for single large hcc (sLhcc) is still controversial. this study was performed to evaluate the optimal staging for these patients.
Methods: among patients with newly diagnosed hcc of BcLc stages a or B were included in this study. Patients were classified into three groups according to the tumor burden: group 1, patients with single nodule >2 cm and £5 cm in diameter; group 2, patients with single nodule >5 cm in diameter; and group 3, patients with 2 or 3 nodules >3 cm diameter or those with >3 nodules. survival analysis was performed according to the tumor stage group, the type of treatment, and child-Pugh grade.
results: a total of 1,005 patients were enrolled. the age was 59.3±10.6 years and 788 patients (78.4%) were male. Most common cause of liver disease was chronic hepatitis B virus infection (66.0%). according to the tumor stage group, 613 (61.0%), 124 (12.3%), and 268 (26.7%) patients were classified into the groups 1, 2, and 3, respectively. In the groups 1, 2, and 3, 464 (75.7%), 108 (87.1%), and 209 (78.0%) patients, respectively, were child-Pugh grade a. two-hundred two (20.1%), 311 (30.9%), and 492 (49.0%) patients were treated with surgical resection, rfa±tace, and tace, respectively. on the multivariate analysis, survival patients in the group 2 was significantly lower than the group 1, while it did not differ from survival of group 3. In addition, in the subgroup analysis, survival of patients in the group 2 did not differ between surgical resection and rfa±tace, while survival of patients with surgical resection or rfa±tace were significantly better than survival of patients with tace. this pattern was also found in patients of group 3, while it was not in patients of group 1: in group 1, survival was superior both to rfa±tace and tace alone.
Conclusion: Prognosis of patients with sLhcc was lower than those with sLhcc-excepted BcLc a and similar with those with BcLc B. survival in patients with sLhcc was comparable between after surgical resection and after rfa±tace. our results suggest that the optimal stage of sLhcc was BcLc stage B rather than BcLc stage a. In addition, rfa±tace could be optimal treatment option for these patients.
Disclosure of Interest: none Declared
P-231 An InTernATIOnAL ObSerVATIOnAL STuDy TO ASSeSS The uSe Of SOrAfenIb AfTer TrAnSArTerIAL CheMOeMbOLIzATIOn (TACe) In PATIenTS WITh hePATOCeLLuLAr CArCInOMA (hCC): OPTIMIS InTerIM AnALySIS
Markus Peck-radosavljevic* 1, jean-Luc raoul2, han chu Lee3, Masatoshi kudo4, keiko nakajima5, ann-Lii cheng6 and on behalf of the oPtIMIs Investigators
1Medical university of Vienna, Vienna, austria, 2Institut Paoli-calmettes, Marseille, france, 3asian Medical center, seoul, korea, Democratic People's republic of, 4kinki university school of Medicine, osaka, japan, 5Bayer healthcare Pharmaceuticals, Whippany, nj, united states, 6national taiwan university hospital, taipei, taiwan
Introduction: transcatheter arterial embolization (tace) is currently recommended for the treatment of patients (pts) with intermediate-stage hepatocellular carcinoma ([hcc] Barcelona clinic Liver cancer [BcLc] stage B). however, it remains unclear which pts are to benefit from tace, or when tace should be switched to alternative treatments.
Methods: oPtIMIs is an observational study of patients who are treated with tace followed by sorafenib or without sorafenib after tace. the study will enroll 1650 pts with hcc who are classified as BcLc stage B or higher and for whom a decision to treat with tace is made at time of study entry. We performed an interim analysis after 500 (pts) were observed for > 6 months. this analysis describes patient characteristics, tace eligibility at the time of tace initiation, tace procedures including types, frequency, and selectivity, and other treatments for hcc.
results: of 489 eligible pts, 475 received tace and were included in this analysis from the following regions: europe/canada n=156, asia (excluding japan/china) n=148, japan n=91, and china n=80. the majority of the pts are asian (68.4%). at baseline, 339 (71.4%) pts were BcLc B and 111(23.4%) were BcLc c. further patient characteristics are provided in the table. Mean time from initial diagnosis to study entry was 4.9 months (range 0-172). Mean time from tace treatment to initiation of non-tace treatment was 4.6 mos (range 0.09-13.1). at time of the first tace, the percentage of pts not indicated for tace according to international guideline/consensus was high (55% overall, 86% china, 52% europe and asia, and 35% japan ). conditions not indicated for tace in greater than 10% of pts included the presence of ecoG Ps >1 29.5%), BcLc c or D (23.8%), child Pugh B/c (20.6%), and vascular invasion (10.1%). Prior to the first tace, 29 (6.1%) pts already had extra hepatic spread. selectivity of tace varied across regions; proportions of whole liver/lobular ranged from 27.5% to 77.6% and sub-segmental tace range from 18.8 to 64.8%, indicating a significant difference in tace procedures. the interval between 1st and 2nd tace varied region to region; from 4 to 627 days. the median time to tace ineligibility according to the protocol definition was 92 days in (n=62) pts who were eligible for tace. analyses are ongoing and further data will be presented

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 0 3
Image:
EUROPE
N=148(100%)
ASIA (Excl. China/JPN)
N=156 (100%)
JAPAN N=91 (100%)
CHINA N=80 (100%)
Total N=475 (100%)
Number Enrolled Pts, N (%) 156 (100.0%) 162 (100.0%) 91 (100.0%) 80 (100.0%) 489 (100.0%) Number TACE Pts, N (%) 148 ( 94.9%) 156 ( 96.3%) 91 (100.0%) 80 (100.0%) 475 ( 97.1%) Number Pts Treated with sorafenib, N (%) 30 ( 19.2%) 45 ( 27.8%) 12 ( 13.2%) 32 ( 40.0%) 119 ( 24.3%)
Age, Years, Mean (SD) Range
65.9 (11.0) 22-90
63.7 (9.9) 32-86
72.9 (9.2) 50-95
57.9 (11.7) 18-77
64.3 (12.1) 18-95
Sex, Male N (%) 120 (81.1) 117 (75.0) 68 (74.7) 70 (87.5) 375 (78.9) Race, Asian N (%) 1 (0.7)* 153 (98.1) 91 (100) 80 (100) 325 (68.4) Number of target lesions at initial TACE, N (%) 0 0 1 ( 0.6%) 2 ( 2.2%) 0 3 ( 0.6%) 1 37 ( 25.0%) 51 ( 32.7%) 22 ( 24.2%) 24 ( 30.0%) 134 ( 28.2%) 2 39 ( 26.4%) 48 ( 30.8%) 17 ( 18.7%) 22 ( 27.5%) 126 ( 26.5%) 3 27 ( 18.2%) 22 ( 14.1%) 9 ( 9.9%) 11 ( 13.8%) 69 ( 14.5%) >3 39 (26.5) 32 (20.4) 38 (41.8) 23 (28.9) 135 (27.6) Longest Diameter (mm) Median (Range) 45 (11-163) 52 (10-158) 27 (10-180) 59 (13-159) 45 (10-180) BCLC Stage, N (%) B 111 ( 75.0%) 115 ( 73.7%) 86 ( 94.5%) 27 ( 33.8%) 339 ( 71.4%) C 21 ( 14.2%) 34 ( 21.8%) 4 ( 4.4%) 52 ( 65.0%) 111 ( 23.4%) D 1 ( 0.7%) 2 ( 1.3%) 0 1 ( 1.3%) 4 ( 0.8%) Child-Pugh Score, N (%) A (5-6 points) 12 ( 26.1%) 9 ( 36.0%) 22 ( 56.4%) 3 ( 33.3%) 46 ( 38.7%) B (7-9 points) 1 ( 2.2%) 0 1 ( 2.6%) 0 2 ( 1.7%) Etiology, N (%) Hepatitis B 13 ( 8.8%) 68 ( 43.6%) 11 ( 12.1%) 56 ( 70.0%) 148 ( 31.2%) Hepatitis C 44 ( 29.7%) 51 ( 32.7%) 50 ( 54.9%) 1 ( 1.3%) 146 ( 30.7%) Alcohol 70 ( 47.3%) 34 ( 21.8%) 20 ( 22.0%) 8 ( 10.0%) 132 ( 27.8%)
TACE Location, N (%)
Whole liver 16 ( 10.8%) 25 ( 16.0%) 8 ( 8.8%) 10 ( 12.5%) 59 ( 12.4%)
Right 71 ( 48.0%) 63 ( 40.4%) 14 ( 15.4%) 45 ( 56.3%) 193 ( 40.6%)
Left 23 ( 15.5%) 18 ( 11.5%) 3 ( 3.3%) 7 ( 8.8%) 51 ( 10.7%)
Segmental TACE 17 (11.5%) 33 (21.1%) 23 (25.3%) 23 (28.8%) 96 (20.2%)
Subsegmental TACE 48 (32.4%) 70 (44.9%) 59 (64.8%) 15 (18.8%) 194 (40.8%) Condition not indicated for TACE at initial TACE, N (%) Overall 77 ( 52.0%) 81 ( 51.9%) 32 ( 35.2%) 69 ( 86.3%) 259 ( 54.5%) ECOG PS >=1 34 ( 23.0%) 57 ( 36.5%) 11 ( 12.1%) 38 ( 47.5%) 140 ( 29.5%) BCLC C or D 20 ( 13.5%) 36 ( 23.1%) 4 ( 4.4%) 53 ( 66.3%) 113 ( 23.8%) Advanced Liver Disease (Child Pugh B/C) 32 ( 21.6%) 31 ( 19.9%) 22 ( 24.2%) 13 ( 16.3%) 98 ( 20.6%)
Vascular Invasion 7 ( 4.7%) 12 ( 7.7%) 2 ( 2.2%) 27 ( 33.8%) 48 ( 10.1%) Extrahepatic Spread, Present 3 ( 2.0%) 11 ( 7.1%) 0 15 ( 18.8%) 29 ( 6.1%) Vascular Invasion, Specification N (%) Portal Vein Thrombosis 5 ( 3.4%) 9 ( 5.8%) 1 ( 1.1%) 25 ( 31.3%) 40 ( 8.4%) Hepatic Vein Invasion 3 ( 2.0%) 3 ( 1.9%) 1 ( 1.1%) 2 ( 2.5%) 9 ( 1.9%) Embolization Agent, N (%) Lipiodol 73 ( 49.3%) 124 ( 79.5%) 79 ( 86.8%) 73 ( 91.3%) 349 (73.5%) DC-Beads 51 ( 34.5%) 13 ( 8.3%) 17 ( 18.7%) 0 81 ( 17.1%)
Univariate OS Pooled Analysisa With Major Prognostic Factors
Conclusion: this study shows significant regional differences in tace treatment and patient selection for tace. these data also indicate the real life practice with tace deviates from current guidelines, indicating educational needs and standardization of procedures/indications for tace It is important to evaluate outcomes of patients from various practices with tace and other treatments.
Disclosure of Interest: M. Peck-radosavljevic Grant support from: arqle, honoraria support from: arqle, j.-L. raoul Grant support from: Bayer healthcare, honoraria support from: Bayer healthcare, BMs, BtG, and taiho, h. c. Lee Grant support from: Bayer healthcare, Bioclinica, Bristol-Myers squibb, Dong-a, and novartis, honoraria support from: Bayer healthcare, M. kudo: none Declared, k. nakajima conflict with: employee of Bayer healthcare Pharmaceuticals, a.-L. cheng: none Declared
P-232 nO TOuCh MuLTIbIPOLAr rADIOfrequenCy AbLATIOn fOr The TreATMenT Of hePATOCeLLuLAr CArCInOMA WIThIn MILAn CrITerIA: LOnG TerM reSuLTS
Seror Olivier* 1, Gisele nkontchou2, jean charles nault2, Pierre nahon2, nathalie Ganne-carrié2, Véronique Grando2, norah zentar3, Michel Beaugrand2, jean-claude trinchet2, abou Diallo4, nicolas sellier3
1radiology unit, jean Verdier hospital, 2Liver unit jean verdier hospital, 3radiology unit jean verdier hospital, 4Medical Information departement jean Verdier hospital j, Bondy, france
Introduction: this study was aimed to assess the effectiveness of no-touch multibipolar radiofrequency ablation (ntmbprfa) of hepatocellular carcinoma (hcc) meeting Milan-criteria.
Methods: Informed consent from patient was waived. 132 hcc (diameter 10-45mm; 39 ≥30mm) in 108 consecutive patients meeting Milan criteria (median age: 65 years) all apart two with cirrhosis were treated with ntmbprfa, consisting of activating, in bipolar mode, three to four electrodes inserted just outside the tumor. follow-up was assessed every three months by computed tomography or magnetic resonance imaging. survivals probabilities were computed using kaplan-Meyer method. Predictive factors of tumor-progression and overall-survival were assessed using hazard-cox-proportional model.
results: complete ablation was achieved for the 132 nodules. three major complications occurred (2.7%): hemothorax in one patient, and liver failure in two, with major portal-systemic shunts. one patient died (0.9%) and one was transplanted. Minor complications occurred in 20 patients (18.5%). after a median 40.3-month [2-84 months] of follow-up, 3- and 5-year local and overall tumor-progression-free survival were 96%,94%, 49%and 35%, respectively. neither tumor diameter (>30mm) nor location abutting a large vessel were associated with local tumor-progression. tumor
diameter (>30mm) was the only parameter predictive of overall tumor-progression (P=0.0036). Independent factors associated with shorter overall survival were child-Pugh class B, age >65-years and platelet count <150G/L (P<0.003).
Conclusion: ntmbprfa of hcc up to 45 mm provides very high local tumor-progression free survival.
Disclosure of Interest: none Declared
P-233 LIVer reGenerATIOn AfTer MAJOr hePATeCTOMy DeCreASeS TuMOrAL GrOWTh
Lilian Schwarz* 1, Lionel nicol2, Paul Mulder3, céline savoye-collet4, Michel scotté1, eric Vibert5
1Digestive oncology unit, 2chu rouen, 3InserM u1073, aDen - rouen university, 4Department of Digestive Imaging, chu rouen, rouen, 5centre hépato Biliaire, hopital Paul Brousse, VILLejuIf, france
Introduction: surgical treatment of bilobar liver metastases could imply two steps hepatectomy with a first stage of right portal vein occlusion (PVo) associated with minor hepatic resection (left liver) and major hepatic resection (right hepatectomy) during the second step. this strategy is supported by the dogma of tumor growth during liver regeneration following major hepatectomy, especially in the contralateral liver. for this reason, current practice are to perform first, a minor hepatectomy in the future remnant liver that decreased its volume associated to a PVo to perform during a second step a major hepatectomy. this experimental study aims to evaluate in relevant model of bilateral tumors, the impact of liver regeneration after 1/ major hepatectomy, 2/ portal vein ligation and 3/ minor hepatectomy on the tumor growth to validate or not this concept of two-step hepatectomy.
Methods: Bilobar colorectal liver metastases were induced in 40 BDIx rats (7w, 250g) by injection of DhDk12 syngenic colon cancer cells. 1 million of DhDk12 were injected beneath liver capsule of the left liver lobe to induce a macroscopic unique metastases, and 1,5 millions were injected through the portal vein after clamping just above the portal bifurcation to induce multiple micrometastasis of the right liver lobe and caudate lobe. 7 days after the tumor cells injection, on the side of macroscopic unique tumor, animals underwent minor hepactomy (30%Phx, n=10), major hepatectomy (70%Phx, n=10), portal vein ligation (PVo, n=10) or only a laparotomy (sham, n=10). Mr imaging (4.7 tesla) of the liver was used for in vivo analysis of tumor implantation and growth at post-operative day (PoD) 10, 17 and 24 from tumor cells injection. tumor volumes on the side of microscopic tumors were measured by semi-automatic method, using Myrian® expert software (Intrasense, france). Pathological analysis of surgical specimen was also analyzed.
results: Mortality rate after surgery was 5%. the tumors were moderately hypointense on Mr t1-weighted and hyperintense on t2-weighted. at day 10, micrometastases of the caudate and right lobes are detectable as multiple nodules sub millimetric subcapsular of a mean volume of 0.109 ± 0.08 cm3, without difference between groups. tumor volumes were significantly increased after PVo, comparing to other groups, at PoD 17 (0.90±0.16 vs 0.67±0.13 cm3; p=0.015) and at PoD 24 (3.2±0.62 vs 2.1±0.55 cm3 ; p=0.035). after both 30%Phx and sham, tumor volumes (0.70±0.12 vs 0.67±0.13cm3 at day 17 and 2.3±0.58 vs 2.4±0.74cm3 at day 24) and tumor growth rates (548±117 vs 518±117% at day 17 and 228±77 vs 254±53% at day 24) were not different. Interestingly, lower tumor volumes were significantly observed after 70%Phx comparing to PVo group at day 17 (0.63±0.14cm3, p=0.008) and to the 3 others groups at day 24 (1.8±0.44cm3,
p<0.04). Pathological results are on-going and will be reported during the ILca meeting.
Conclusion: contrary to PVo, a major hepatectomy decreases the growth of tumor in the remnant liver as compared to a laparotomy and minor hepatectomy. the positive impact of major hepatectomy on tumor growth that have been yet described in hcc (yokoyama, Br j cancer 2000) justified to reconsidered the strategy of two-hepactomy and/or to develop innovative method as portal flow modulation to avoid PVe before major hepatectomy for liver metastases.
Disclosure of Interest: none Declared
P-234 SurVIVAL benefIT Of LOCOreGIOnAL TherAPy fOr hePATOCeLLuLAr CArCInOMA WITh ChILD-PuGh C LIVer funCTIOn: A MuLTICenTer nATIOn-WIDe STuDy
Masatoshi Kudo* 1, satoshi kitai1, naoshi nishida1, namiki Izumi2, Michiie sakamoto3, yutaka Matsuyama4, takafumi Ichida5, osamu nakashima6, osamu Matsui7, yonson ku8, norihiro kokudo9, Masatoshi Makuuchi10, for the Liver cancer study Group of japan11
1Department of Gastroenterology and hepatology, kinki university school of Medicine, osaka-sayama, 2Department of Gastroenterology and hepatology, Musashino red cross hospital, Musashino, 3Department of Pathology, keio university school of Medicine, 4Department of Biostatistics, school of Public health, university of tokyo, tokyo, 5shonan-east General hospital, kanagawa, 6Department of clinical Laboratory Medicine, kurume university hospital, kurume, 7Department of radiology, kanazawa university Graduate school of Medical science, kanazawa, 8Department of surgery, kobe university Graduate school of Medicine, kobe, 9hepato-Biliary-Pancreatic surgery Division, artificial organ and transplantation Division, Department of surgery, Graduate school of Medicine, university

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 0 4
of tokyo, 10Department of surgery, japanese red cross Medical center, tokyo, 11for the Liver cancer study Group of japan, osaka-sayama, japan
Introduction: hepatocellular carcinoma (hcc) with decompensated liver cirrhosis (Lc) is a life-threatening condition; liver transplantation (Lt) is the standard first-line treatment. however, application of Lt can be limited due to a shortage of donated livers. this study aimed to clarify the effect of non-Lt therapy on the survival of hcc patients with decompensated Lc.
Methods: of the 58,886 hcc patients registered in the nationwide survey of the Liver cancer study Group of japan (january 2000–December 2005), we included 1,344 patients with primary hcc and child-Pugh (c-P) grade c for analysis in this retrospective cohort study. among the included patients, 108 underwent Lt, 273 were treated by local ablation therapy (Lat), 370 were treated by transarterial chemoembolization (tace), and 593 received best supportive care (Bsc). the effect of Lt, Lat, and tace on overall survival (os) was analyzed using multivariate and propensity score analyses.
results: Patient characteristics did not differ significantly between each treatment group and the Bsc group, after propensity score matching. Lat (hr = 0.568; 95% cI, 0.40-0.80) and tace (hr = 0.691; 95% cI, 0.50-0.96) were identified as significant contributors to os if the c-P score was less than 11 and tumor conditions met the Milan criteria.
figure legend. (a) a comparison of overall survival between the Bsc and Lat groups with child-Pugh scores of 10 or 11, after matching patient backgrounds using propensity score analysis. (B) a comparison of overall survival between the Bsc and tace groups with child-Pugh scores of 10 or 11, after matching patient backgrounds using propensity score analysis. (c) a comparison of overall survival between the Bsc and Lat groups with child-Pugh scores of 12-15, after matching patient backgrounds using propensity score analysis. (D) a comparison of overall survival between the Bsc and tace groups with child-Pugh scores of 12-15, after matching patient backgrounds using propensity score analysis.
Image:
Conclusion: for patients with hcc within the Milan criteria and a c-P score of 10 or 11, locoregional treatment showed a potential benefit on survival.
Disclosure of Interest: none Declared
P-235 eVALuATIOn Of The LIVer CArCInOGeneSIS fACTOrS In JAPAneSe ChrOnIC hePATITIS b PATIenTS TreATeD WITh enTeCAVIr: MuLTICenTer TrIAL
Koichi Takaguchi* 1, takashi kumada2, noritomo shimada3, hidenori toyota2, nobutaka Baba1, akemi tsutsui1, atsushi hiraoka4, toru Ishikawa5, kunihiko tsuji6
1hepatology, kagawa Prefectural central hospital, takamatsu, 2Gastroenterology, ogaki Municipital hospital, ogaki, 3Gastroenterology, otakanomori hospital, Matsudo, 4Gastroenterology, ehime Prefectural central hospital, Matsuyama, 5Gastroenterology, saiseikai niigata second hospital, niigata, 6Gastroenterology, teine keijinnkai hospital, sapporo, japan
Introduction: the prognosis of chronic hepatitis B(chB) patients was significantly improved by an appearance of nucleside analogue (na). however, liver carcinogenesis was rarely appeared in the patients with na administrated chB patients, we evaluated risk factor for liver carcinogenesis in such cases.
Methods: We investigated 555 chB patients treated with entecavir. (excluded hcc patients). (median age, 54 (16-92). male/female 335/225 Genotype (a/B/c/D/n.d.) 15/65/343/1/79, hBV-Dna (log copies/ml) 6.2 (2.1-9.9), hBsag (log Iu/ml) 3.3 (1.5-7.4), hBeag (+/-/n.d.) 211/337/12, ast (Iu/l) 47 (13-1434), aLt (Iu/l) 53 (8-2170), t-Bil (mg/dl) 0.8 (0.1-14.0), alb (g/dl) 4.1 (2.0-5.0), platelet (/µl) 15.2 (3.2-38.8) fIB4-index 2.2(0.4-39.9) afP (ng/ml) 5.0 (0.8-514.9), duration of entecavir (year) 4.3 (0.1-10.9), Ifn +/- 46/509. We investigated host factors (age, gender, liver fibrosis), virus factors (virus genotype, quantity), treatment factors (treatmen period, Ifn use), and fib-4 index which reflects liver fibrosis between development of hcc patients and non hcc patients.
results: of the 555 patients, 49 (8.8%) patients developed hcc during entecavir treatment. the rates of liver carcinogenesis of three years, five years and seven years were 4.7%, 9.7%, 15.0% each. the risk factor which was significantly different between development to hcc patients and non-development patients was man (p <0.001), fibrosis degree (p <0.001), genotype c (p=0.009), platelet counts (p <0.001), fIB-4 index high levels (p <0.001), afP high levels (p=0.001). there were no differences (P=0.922) between 46 cases with a history of the Ifn therapy before the etV treatment and no Ifn therapy patients. In patients with fiB-4 index below 2.0, three, five, seven years hcc development rate was 2.7%, 4.7%, 12.9%. Whereas in fib-4 index up to 2.0 patients they showed 6.0%, 12.9%, 19.7%. there was significant difference (P=0002) at hcc development rates between fib-4 index below 2.0 and up to 2.0 group. fib-4 index decline rate at one year after entecavir treatment 11.8% in patients with development to hcc was significantly (p=0.027) lower than that of 22.2% in patients without hcc development.
Conclusion: In patients with entecavir treated chB patients, sequential fib-4 index mesurement was useful marker of development to hcc.
Disclosure of Interest: none Declared
P-236 COnVerSIOn TherAPy WITh hePATIC ArTerIAL InfuSIOn CheMOTherAPy fOr LOnG-TerM PrOGnOSIS In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA InVOLVInG VASCuLAr InVASIOn
hiroaki nagamatsu* 1, takashi niizeki2, takuji torimura3
1Division of Gastroenterology, yame general hospital, yame, 2Division of internal medicine, 3Division of Gastroenterology, kurume university school of Medicine, kurume, japan
Introduction: sorafenib is recognized as a standard treatment for advanced unresectable hepatocellular carcinoma (hcc) with vascular invasion worldwide. however, the therapeutic efficacy is limited. We retrospectively evaluated the effectiveness of conversion therapy with hepatic arterial infusion chemotherapy (haIc) targeting to improve long-term prognosis.
Methods: from january 2004 to December 2014, among 270 patients who received the treatment with cisplatin (cDDP) and 5-fluorouracil (5-fu) via the reservoir system at our institution and affiliated kurume university hospital, 189 with inoperable hepatocellular carcinoma involving vascular invasion without extrahepatic metastasis were enrolled in the study (mean age, 68.9 years; child-Pugh class a/B/c, 114/66/9 cases; portal vein tumor thrombosis in 2nd branch/1st branch/trunk, 80/66/43 cases ).all 189 patients received haIc via the reservoir system. after chemolipiodolization, the patients were treated with cDDP 50 mg followed by 5-fu 1,250 mg via a balloon pump for 5 days (nfP therapy1)). In patients who achieved partial response (Pr) after nfP and in whom conversion therapy was feasible, hepatectomy (hr), trancecatheter arterial chemoembolization (tace), or radiotherapy (rt) was performed to achieve cancer-free outcome. tumor response, in terms of best overall response, by nfP was evaluated with m-recIst. cumulative overall survival (os) after nfP was estimated using kaplan-Meier survival curves, and multivariate analysis was performed to identify prognostic factors affecting os using cox proportional hazards models. for factors with significant difference in the multivariate analysis, os was compared using log-rank test.
results: a total of 136 patients (72%) responded to nfP therapy, of which 58 patients achieved cancer-free outcome (31%; nfP only, 17 patients; nfP +hr, 18 patients; nfP +tace, 18 patients, nfP +rt, 5 patients). Median os (Mst) after haIc in all patients was 18 months. significant factors for os included cancer-free outcome (hazard ratio, 0.184; P=0.001) and addition of hr (hazard ratio, 0.105; P=0.003). Mst in patients who responded was 29 months, and in patients who achieved cancer-free outcome, it was extended to 57 months.three - and five-year survival rates were 78% and 21% in patients treated with nfP only, 87% and 71% in nfP+hr, 47% and 16% in nfP+tace, and 67% and 33% in nfP+rt patients (P=0.028), respectively.
Conclusion: nfP therapy demonstrated favorable tumor response in patients with advanced hepatocellular carcinoma with vascular invasion. addition of conversion therapy, specifically, hr, targeting cancer-free outcome made possible long-term survival.
references: 1) nagamatsu h, hiraki M, torimura t, et al : Intra-arterial therapy with cisplatin suspension in lipiodol and 5-fluorouracil for hepatocellular carcinoma with portal vein thrombosis. aP & t 2010 ; 32 : 543-550.
Disclosure of Interest: none Declared

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 0 5
P-237 effeCT Of OrAL AnTIVIrAL TreATMenT On LOnG-TerM OuTCOMeS Of rADIOfrequenCy AbLATIOn TherAPy fOr hePATITIS b VIruS-reLATeD hePATOCeLLuLAr CArCInOMA
Won Sohn* 1, tae Wook kang2, ju yeon cho3, Min Woo Lee Lee2, hyo keun Lim2, Dong hyun sinn2, Geum-youn Gwak2, Moon seok choi2, joon hyeok Lee2, kwang cheol koh2, seung Woon Paik2, Byung chul yoo2, hyunchul rhim2, yong-han Paik2
1Bundang jesaeng hospital, sungnam, 2samsung Medical center, sungkyunkwan university school of Medicine, seoul, 3chosun university hospital, Gwang-ju, korea, republic of
Introduction: this study was aimed to investigate the effect of oral antiviral treatment on the prognosis of hepatitis B virus (hBV)-related hepatocellular carcinoma (hcc) after radiofrequency (rf) ablation therapy.
Methods: Between january 2003 and December 2010, 228 patients without history of antiviral treatment were treated with rf ablation for a single hBV-related hcc. We divided the patients into two groups, patients with antiviral treatment (n=125) or patients without (n=103), based on whether oral antiviral treatment was administered after rf ablation. recurrence-free survival and overall survival were compared between both groups in the full cohort and the propensity score-matched cohort. We also assessed risk factors for hcc recurrence and overall survival after rf ablation.
results: In the matched cohort, the probability of recurrence-free survival at 5 year were 14.7% for non-antiviral treatment group and 43.8% for antiviral treatment group, respectively (p<0.001). the probability of overall survival at 5 year were 77.2% for non-antiviral treatment group and 93.5% for antiviral treatment group, respectively (p=0.002). a multivariable analysis showed that risk factors for hcc recurrence were larger tumor size (hazard ratio (hr)=1.30, p=0.022), higher level of serum hBV Dna (hr=1.11, p=0.005), and serum afP level ≥20 ng/mL (hr=1.66, p=0.005). overall survival was associated with larger tumor size (hr=1.86, p=0.001) and child-Pugh class B (hr=2.13, p=0.019). oral antiviral treatment after rf ablation was significantly associated with a lower risk of tumor recurrence and death (hr=0.33, p<0.001, and hr=0.44, p=0.004).
Conclusion: use of oral antiviral treatment was associated with a favorable outcome in terms of tumor recurrence and overall survival in patients with hBV-related hcc after rf ablation.
Disclosure of Interest: none Declared
P-238 COMPArISOn Of TrAnSArTerIAL CheMOeMbOLIzATIOn AnD hePATIC reSeCTIOn fOr LArGe SOLITAry hePATOCeLLuLAr CArCInOMA: A PrOPenSITy SCOre AnALySIS
yun bin Lee* 1, Dong hyeon Lee2, yuri cho2, su jong yu2, jeong-hoon Lee2, jung-hwan yoon2, hyo-suk Lee2, hyo-cheol kim3, nam-joon yi4, kwang-Woong Lee4, kyung-suk suh4, jin Wook chung3, yoon jun kim2
1Department of Internal Medicine, cha Bundang Medical center, cha university, seongnam-si, 2Department of Internal Medicine and Liver research Institute, 3Department of radiology, 4Department of surgery, seoul national university college of Medicine, seoul, korea, republic of
Introduction: the optimal treatment strategy for large solitary hepatocellular carcinoma (hcc) is still controversial. this study compared long-term survival following hepatic resection and transarterial chemoembolization (tace) of large solitary hcc.
Methods: a total of 91 and 68 consecutive patients with large (≥5 cm) solitary hccs who underwent hepatic resection and tace, respectively, were analyzed. overall survival and time to progression (ttP) were estimated using the kaplan–Meier method and compared using the cox proportional hazards model. to control for treatment-selection bias, matched groups of patients were selected using a propensity score matching method, and survival analysis was repeated.
results: During the follow-up period (median 60.7, range 0.5–122.2 months), 42 (46%) patients in the hepatic resection group and 35 (51%) patients in the tace group died. the 1-, 3-, and 5-year overall survival rates of the hepatic resection and tace groups were 91.1%, 80.0%, 66.4% and 89.8%, 72.8%, 49.6%, respectively (P=0.023). ttP was significantly longer in resected patients (P<0.001). hBsag positivity and the absence of portal hypertension were independent predictors for favorable overall survival. for patients with platelet counts ≤100,000/mm3, child-Pugh score 6, smaller hccs (≤7 cm), or portal hypertension, hepatic resection and tace yielded similar overall survival rates. after propensity score matching, tace was comparable to hepatic resection in overall survival (P=0.293), whereas ttP remained longer in resected patients (P=0.001).
Conclusion: tace can lead to results comparable to those of hepatic resection in the treatment of large solitary hcc, particularly in patients with clinically presumed portal hypertension.
Disclosure of Interest: none Declared
P-239 COMbInInG TrAnSArTerIAL CheMOeMbOLIzATIOn WITh rADIOfrequenCy AbLATIOn VerSuS hePATIC reSeCTIOn by uSInG PrOPenSITy SCOre MATChInG In hePATOCeLLuLAr CArCInOMA
young Kul Jung* 1, sang jun suh1, hyung joon yim1, ji hoon kim2, yeon seok seo3, soon ho um3, jong eun yeon3, kwan soo Byun4, oh sang kwon5, yun soo kim5, ju hyun kim5
1Internal Medicine, korea university ansan hospital, Gyenggi-do, 2korea university Guro hospital, 3Internal Medicine, korea university anam hospital, 4Internal Medicine, korea university Guro hospital, seoul, 5Internal Medicine, Gachon univ Gil hospital, Incheon, korea, republic of
Introduction: there is still no consensus whether radiofrequency ablation (rfa) or hepatic resection (hr) is the better treatment for early hepatocellular carcinoma (hcc) patient. In this study, the efficacy and safety of combined tranarterial chemoembolization (tace) and rfa with that of hr in patients with hcc.
Methods: Patients with early hcc (BcLc o/a) (n=648) of 4 tertiary hospitals were enrolled in this retrospective study. Primary end points of this study were cumulative overall survival (os) and disease free survival (Dfs) after propensity score matching. Propensity scores were computed by modeling a logistic regression with the dependent variable as the odds of undergoing tace with rfa, and the independent variables as age, sex, child-Pugh score, location of tumor and number of tumors. for statistical analysis, the independent t-test or Mann-Whitney u-test for continuous variables, chi-square test or fisher’s exact test for categorical variables were performed. Disease-free survival and overall survival were estimated and compared by the kaplan-Meier method and log-rank test. the paired t-test, cochran-Mantel-haenszel test and stratified log-rank test were also used in the matched analysis. statistical significance was set at P<0.05. sPss version 20(sPss, chicago, Illinois, usa)
results: as an initial treatment, 265 patients were undergone tace with rfa and 383 patients underwent hr. the 1 year, 2 year, and 5 year Dfs of tace and rfa group were 75.9 %, 54.7%, and 24.1%, respectively and those of hr group were 78.1%, 65.1% and 40%, respectively. the median Dfs of tace with rfa was 42.4 months and that of hr was 25.1 months (p< 0.001). the 1 year, 2 year, and 5 year overall survival of tace and rfa group were 99.3%, 96.8% and 91.5% and those of hr group were 90.7%, 74.1%, 74.1% (P=0.819). after propensity score matching, the 1 year, 2 year, and 5 year Dfs of tace and rfa group were 80.1%, 56.8% and 26.6% and those of hr group were 74.0%, 60.6%, 31.2% (p=0.925). on subgroup analysis for single tumor and maximal size of tumor ≤ 2 cm, cumulative Dfs during follow-up were 43.8% in tace and rfa vs. 53.1% in hr (p=0.895). on size ≤ 3 cm, cumulative Dfs were 42.4% in tace and rfa vs. 52.5% in hr (p=0.677). on 3cm < size ≤ 5cm, cumulative Dfs were 29.6% in tace and rfa vs. 40.7% in hr (p=0.513). Most common complication on both group was elevation of ast/aLt (grade 2), most severe complication were happened 3 cases of hr group. one is severely elevated bilirubin without encephalopathy; the others were death due to renal failure or sepsis. In tace with rfa group, liver segmental infarction were happened in 2 cases.
Conclusion: combined tace and rfa could be alternative choice of initial treatment in early hcc patients.
Disclosure of Interest: none Declared
P-240 VASCuLAr reCAnALIzATIOn AnD PArTICLe exCLuSIOn AfTer TrAnSCATheTer ArTerIAL eMbOLIzATIOn WITh POLyVInyL ALCOhOL PArTICLe In hCCS: An hISTOPAThOLOGICAL eVIDenCe
Tu Vinh Luong* 1, roberta Manuguerra2, Damiano arciuolo3
1cellular Pathology, royal free hospital, London, united kingdom, 2cellular Pathology, university hospital of Parma, Parma, 3cellular Pathology, universita’ cattolica del sacro cuore, rome, Italy
Introduction: transarterial embolisation (tae) is a locoregional therapy used in pre-orthotopic liver transplantation and pre-resection in order to “downstage” hepatocellular carcinoma (hcc). one of the embolising agents in use is polyvinyl alcohol (PVa). PVa is not biodegradable and thus is considered by many to be a “permanent” embolic agent.histologic vascular consequences of PVa embolization in hccs have received little attention and little literature is available.In this study we rebut the current belief that PVa-induced vascular occlusion is permanent.
Methods: We reviewed 33 patients who underwent tae with PVa (45-150 microns) for hcc, followed by liver transplantation (79%) or surgical resection (21%).the histopathologic features of the resected hccs were described with the emphasis on the anatomic localisation of embolic material (intra-luminal, within the arterial wall, outside the arterial wall).

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 0 6
results: the interval period between tae and surgery was variable, ranging from 20 to 348 days with a median interval of 109 days. the histopathological examination of 5 patients (15%) who underwent surgery within a month from tae showed PVa particles mainly localised within the vessel lumina and only occasionally within the arterial wall; whilst the remaining 28 patients (85%) who had surgery after a month showed PVa particles in all three defined anatomical locations. 7 cases (20%) showed partial tumour necrosis (<50%) and were associated with higher numbers of PVa transvascular migration. the picture shows refractile foreign particles surrounded by foreign body giant cells embedded in thickened vessel walls, and partially migrating outside the vessel wall with partial luminal recanalisation.
Image:
Conclusion: the present study showed that PVa-induced vascular occlusion in hccs was not permanent: the transvascular migration of PVa particles defined as the presence of embolic material within the media-adventitia or outside the vessel wall was observed in all cases. Within the first month from tae, PVa particles started to migrate within the media-adventitia with partial luminal recanalisation. after a month from tae the embolic material was observed outside the vessels with complete luminal recanalisation.
It is important for clinicians and surgeons to be are aware of this phenomenon in order to better plan the time of surgery after tae, as the efficacy of tae depends on the long-term evolution of embolised vessels.
references: 1. Ming-yuan Lee, Vincent P. chuang, chao-jung Wei, tsung-yen cheng, Ming-tsu cherng. “histopathologic correlation of hepatocellular carcinoma after transcatheter arterial chemoembolization with polyvinyl alcohol particle of various sizes”. european journal of radiology 81 (2012) 1976–1979.2. alexandre Laurent, Michel Wassef, julien namur, jacques Martal, Denis Labarre and jean-Pierre Pelage. “recanalization and particle exclusion after embolization of uterine arteries in sheep: a long-term study”. fertility and sterility. Vol. 91, no. 3, March 2009.
Disclosure of Interest: none Declared
P-241 uK exPerIenCe Of SOrAfenIb In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA
judy king1, Daniel Palmer2, 3, Philip johnson2, 3, Paul ross4, richard hubner5, janine Graham6, suzanne Darby7, chiara Braconi8, chinenye Iwuji9, Dan swinson10, Peter collins11, kinnari Patel12, jenny nobes13, Iqtedar Muazzam14, claire Blesing15, amy kirkwood16, stephen nash16, Tim Meyer*1
1royal free London nhs foundation trust, London, 2university of Liverpool, Liverpool, 3university of Birmingham, Birmingham, 4king’s college hospital, London, 5christie nhs foundation trust, Manchester, 6the newcastle upon tyne nhs foundation trust, newcastle, 7sheffield teaching hospitals nhs foundation trust, sheffield, 8university of Glasgow, Beatson West of scotland cancer centre, Glasgow, 9Leicester royal Infirmary, Leicester, 10Leeds teaching hospitals nhs trust, Leeds, 11university hospitals Bristol nhs foundation trust, Bristol, 12oxford university hospitals nhs trust, oxford, 13norfolk and norwich university hospitals nhs foundation trust, norfolk, 14hull and east yorkshire hospitals nhs trust, hull, 15Great Western hospital nhs trust, swindon, 16ucL cancer trials centre, London, united kingdom
Introduction: sorafenib is standard treatment for advanced hepatocellular carcinoma (hcc), based on two placebo controlled randomised trials(1, 2). We performed a retrospective national audit of hcc patients treated with sorafenib in the uk and compared the outcomes for those with child Pugh (cP) a vs B, and albumin-bilirubin (aLBI (3): a recently published model for assessment of liver dysfunction in hcc) grade 1 vs 2.
Methods: sorafenib-treated (st) patients were identified via the cancer Drugs fund. Data was collected retrospectively from medical and pharmacy records. the primary outcome was overall survival (os), estimated by kaplan-Meier
results: Data was obtained for 448 st patients from 15 hospitals. the median age was 68y (range 17-89), 38% had extra-hepatic disease and 75% had a performance status of ≤1. at baseline, 77% were cP a, 16.1% were cP B, 37.5% were aLBI grade 1 and 47.5% were aLBI grade 2. Median time on sorafenib was 3.6 months with an average daily dose of 590mg. the most common adverse events (ae) leading to a dose reduction or treatment interruption were fatigue (45.4%), reduced performance status (33%), diarrhoea (32.6%), skin reaction (24.1%) and liver dysfunction (22.3%). the main difference in ae between cP a and B patients receiving sorafenib was the incidence of liver dysfunction: 18.2% vs 39.5% for cP a vs B, respectively. the main reasons for stopping sorafenib were radiological progression (29%), toxicity (25%) or clinical progression/death (38.3%). In the multivariate analysis of the st population, the independent predictors of mortality were previous local therapy, bilirubin, albumin and afP (table 1). Median os for 448 evaluable st patients (342 events) was 8.5 months. for cP a (n=343) vs B (n=72) median survival was 9.5 vs 4.6 months; hr:1.53 (95% cI 1.16-2.03), p=0.003. for patients with an aLBI grade of 1 (n=168) vs 2 (n=214) median survival was 12.9 vs 5.9 months; hr 1.92 (95% cI 1.51-2.44) p<0.001
table 1
Variable Multivariable
hr (95% cI) p value
Previous local therapy no -
yes 0.74 (0.58-0.96) 0.023
Bilirubin <17 -
≥17 1.68 (1.30-2.16) <0.001
albumin <36 -
≥36 0.74 (0.56-0.96) 0.025
afP <400 -
≥400 1.41 (1.09-1.82) 0.008
Conclusion: the overall survival for patients with cP a disease is in line with previously published data and we confirm the poor outcome for those with cP B disease (4, 5). In addition, we demonstrate that the recently published aLBI grading system separates the sorafenib-treated population into two main sub-groups which are numerically distinct from cP stage and consequently have different clinical outcomes
references: 1) Llovet, j.M., et al. 2008. N.Engl.J.Med., 359, (4) 378-390; 2) cheng, a.L., et al. 2009. Lancet Oncol., 10, (4) 25-34; 3) johnson, P.j., et al. 2015. J.Clin.Oncol., 33, 4) 550-558;Iavarone, M., et al. 2011. Hepatology, 54, (6) 2055-2063; 5) Lencioni, r., et al. 2013. Int.J.Clin.Pract. PM:24283303;
Disclosure of Interest: none Declared
P-242 hePATOCeLLuLAr CArCInOMA In eLDerLy PATIenTS: fInAL reSuLTS Of The ITALIAn COhOrT Of GIDeOn STuDy
Teresa zolfino* 1, Vito Lorusso2, salvatore D'angelo3, Domenico sansonno4, Lydia Giannitrapani5, antonio Benedetti6, Vincenzo Montesarchio7, adolfo francesco attili8, angela Buonadonna9, sandro Barni10, antonio Gasbarrini11, Mario Pirisi12, umberto cillo13, antonino Picciotto14, erica Villa15, Petros Giovanis16, Graziella Pinotti17, carlo saitta18, claudia erminero19, Massimo De Giorgio20, Bruno Daniele21
1ao G. Brotzu, cagliari, 2Irccs ospedale di Bari, Bari, 3ao san Giuseppe Moscati, avellino, 4aou Policlinico consorziale di Bari G. Bacelli, Bari, 5aouP Paolo Giaccone, cagliari, 6aou ospedali riuniti, Po umberto I, torrette di ancona, ancona, 7aorn ao dei colli Monaldi-cotugno cto, napoli, 8azienda Policlinico umberto I, roma, 9centro di riferimento oncologico cro, aviano, 10ao ospedale treviglio-caravaggio, treviglio, 11Policlinico universitario a. Gemelli - ucsc, roma, 12aou Maggiore della carità, novara, 13aou di Padova, Padova, 14Irccs auo s.Martino Ist, Genova, 15aou Policlinico, Modena, 16azienda u.L.s.s. n. 9 di treviso, treviso, 17ospedale di circolo e fondazione Macchi, Varese, 18aou Policlinico G. Martino, Messina, 19Bayer spa, Milano, 20ao Papa Giovanni xxIII, Bergamo, 21ao Gaetano rummo, Benevento, Italy
Introduction: GIDeon (Global Investigational of therapeutic Decisions in hcc and of its treatment with sorafenib) is a global, prospective, non-interventional study in unresectable hcc (uhcc) patients (pts) receiving sorafenib. over 3200 pts were enrolled worldwide. the aim was to evaluate safety and efficacy of sorafenib in real life clinical practice1,2. elderly pts are often underrepresented in clinical trials and thus related data are limited. the aim of this analysis was to evaluate the tolerability and efficacy of sorafenib in pts 70 years of age or older in the Italian cohort of the GIDeon study.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 0 7
Methods: Patients with uhcc candidates for systemic therapy in whom a decision to treat with sorafenib was taken, were eligible for enrollment. Patient and tumor characteristics, safety and efficacy were analyzed by age. the median age of 70 years was also chosen as the cut-off to define the elderly patient subgroup. as an observational study, all results are descriptive in nature.
results: In Italy, 278 pts were enrolled overall, of which 271 were valid for safety and 274 valid for efficacy analysis. Median age was 70 (44-90) years. of the total of 274 pts, 141 were ≥ 70 years. Performance status (ecoG Ps 0,1,2) were 65/26/9% respectively for the younger age subgroup and 58/35/6% respectively for the elderly subgroup. stage of disease (according to BcLc) was 11/24/62/2% (a,B,c,D) for the younger subgroup and 14/39/42/1% for the elderly subgroup. Macroscopic vascular invasion and extrahepatic spread were 33% and 29% respectively in the younger age group and 19% each in the elderly. child-Pugh a was present in 73% in the younger subgroup and 83% in the elderly subgroup.Median os was 10 (8-18) months in the younger age subgroup and 20 (12-23) months in the elderly pts. the median ttP was also longer in the elderly group than in the younger subgroup, 7.6 and 5 months respectively.the median duration of treatment was similar in both subgroup: 4.2 and 3.5 months respectively. the standard starting dose (400 mg bid) was administered in 89% of the younger pts and 85% of the elderly pts.the type and incidence of adverse events (ae) (serious and non-serious) were similar in the younger and the elderly subgroups and in line with the known sorafenib safety profile. the most frequent aes were gastrointestinal (diarrhea), dermatologic (hand-foot skin reaction/rash) and fatigue.
Image:
Conclusion: In the Italian cohort of the GIDeon study sorafenib showed to be well-tolerated and an effective treatment option in both younger pts and elderly pts. elderly pts had longer os than younger pts possibly because of more advanced disease in the younger subgroup. however due to the limitation and potential bias of an observational non-randomized study it is not possible to attribute this difference to a different treatment effect.
references: 1. Lencioni r, kudo M, ye sL, et al. Int j clin Pract. 2014 May;68(5):609-17. 2. Marrero ja, Lencioni r, ye sL et al. j clin oncol 31, 2013 (suppl; abstr 4126).
Disclosure of Interest: t. zolfino: none Declared, V. Lorusso: none Declared, s. D'angelo research/education support from: none, Grant support from: none, honoraria support from: none, stocks of: none, advisory Board of: none, consulting of: none, conflict with: none, D. sansonno: none Declared, L. Giannitrapani: none Declared, a. Benedetti: none Declared, V. Montesarchio: none Declared, a. f. attili: none Declared, a. Buonadonna: none Declared, s. Barni: none Declared, a. Gasbarrini: none Declared, M. Pirisi: none Declared, u. cillo: none Declared, a. Picciotto: none Declared, e. Villa: none Declared, P. Giovanis: none Declared, G. Pinotti: none Declared, c. saitta: none Declared, c. erminero conflict with: Bayer spa, M. De Giorgio: none Declared, B. Daniele honoraria support from: Bayer, advisory Board of: Bayer
P-243 SInGLe AGenT ACTIVITy Of The SeCOnD-GenerATIOn hyPOMeThyLATInG AGenT, SGI-110, In PATIenTS WITh hePATOCeLLuLAr CArCInOMA (hCC) AfTer PrOGreSSIOn On SOrAfenIb
Anthony el-Khoueiry* 1, Mary Mulcahy2, tanios Bekaii-saab3, richard kim4, crystal s. Denlinger5, rakesh Goel6, shweta Gupta7, simone jueliger8, richa Dua7, aram oganesian7, harold keer7, john nemunaitis9
1usc norris comprehensive cancer center, Los angeles, 2northwestern university, robert h. Lurie comprehensive cancer center, chicago, 3the ohio state university comprehensive cancer center, columbus, 4h. Lee Moffitt cancer center and research Institute, tampa, 5fox chase cancer center, Philadelphia, united states, 6the ottawa hospital cancer centre, ottawa, canada, 7astex Pharmaceuticals, Inc., Pleasanton, united states, 8astex Pharmaceuticals, cambridge, united kingdom, 9Mary crowley Medical research center, Dallas, united states
Introduction: sorafenib treatment improves survival in advanced hcc, but no therapy has demonstrated significant activity after progression on sorafenib. Increased methylation of genes implicated in tumorigenesis has been described in hcc and has been associated with outcome and
etiology. We investigated sGI-110, a subcutaneous (sc) next generation hypomethylating agent in advanced hcc patients after sorafenib failure.
Methods: adults with histologically confirmed, advanced-stage hcc who had documented radiological progression on sorafenib or verified intolerance to sorafenib despite dose reductions were enrolled. Prior locoregional therapy was allowed. other eligibility criteria included: ecoG Ps 0-1, child Pugh a or B with a score of ≤ 7, no recent hepatic encephalopathy or ascites not manageable with medical therapy. sGI-110 (sc) was given on D1-5 of a 28-day cycle (Dailyx5). Blood samples were taken for Pk/PD analysis. tumor biopsy was performed prior to initiation of study therapy and on cycle 1 day 8 or cycle 2 day 8. Patients were imaged every 8 weeks and allowed to continue treatment after radiologic but not clinical progression. end points include disease control rate (Dcr) at 16 weeks, overall response rate, progression-free survival, and overall survival.
results: 50 hcc patients (43M/7f; median age 60 years [range 32-82]; ecoG Ps 0/1: 21/29; child Pugh a/B: 42/8; prior systemic treatments median 2[range 1-8]) were enrolled. the initial dose of sGI-110 was 60 mg/m2 Dailyx5 (4 patients treated), but the dose was decreased to 45 mg/m2 /day for subsequent patients due to grade 4 neutropenia. there were 17 subjects with grade 4 neutropenia (only one with fever). Grade 3 related events occurring in 10% or more patients include myelosuppression (neutropenia-36%, leukopenia-28% ) and increased ast (10%). complete Pk data were available from 16 patients (3f/13M). the Pk profile for sGI-110 after 45 mg/ m2 showed protracted conversion to deliver active metabolite decitabine with exposure window lasting beyond 8-hr with mean(sD) decitabine auc exposures of 94(22) ng*hr/mL . of 43 evaluable patients, disease control at 16 weeks was observed in 26% of evaluable subjects (duration of mean 168 days, median 162 days). 34% of subjects had sD, and one subject demonstrated a Pr. Potent Dna demethylation was achieved as measured by LIne-1 assay reaching an average demethylation in blood of -34.5% ±12.06. Paired tumor biopsies were obtained from 32 subjects. LIne-1 demethylation in tumor Dna was observed in 22 subjects (68.7%) with an average of -14.24% demethylation. additionally, MzB1 (tumor suppressor gene) demethylation was observed 17 subjects (68%) with an average demethylation of -34%. six out of seven patients with Dcr (and evaluable tissue) had potent MzB1-specific demethylation (-24.6% ± 5.7; range: 10.2-47.1). Pfs and os will be presented at the meeting.
Conclusion: sGI-110 was well tolerated at a dose of 45 mg/m2 administered sc on D1-5 of a 28-day cycle in patients with advanced hcc. Pk profile was consistent with that seen in previous studies and provided more persistent decitabine exposures compared to IV infusion. Disease control for 16 weeks was seen in 26% of patients. evidence of biologic activity was manifested by LIne-1 and MzB-1 demethylation in the tumor. the tolerability of single-agent sGI-110 at doses producing pharmacodynamics effects in tumor tissue in combination with preliminary evidence of modest activity suggests the value of future trials of sGI-110 in combination with other agents in hcc.
Disclosure of Interest: a. el-khoueiry research/education support from: astex Pharmaceuticals, Inc., Grant support from: astex Pharmaceuticals, Inc., M. Mulcahy: none Declared, t. Bekaii-saab: none Declared, r. kim: none Declared, c. Denlinger research/education support from: astex Pharmaceuticals, Inc., Grant support from: astex Pharmaceuticals, Inc., r. Goel: none Declared, s. Gupta conflict with: astex Pharmaceuticals, Inc., s. jueliger conflict with: astex Pharmaceuticals, Inc., r. Dua conflict with: astex Pharmaceuticals, Inc., a. oganesian conflict with: astex Pharmaceuticals, Inc., h. keer conflict with: astex Pharmaceuticals, Inc., j. nemunaitis: none Declared
P-244 SOCIOeCOnOMIC DISPArITIeS In ACCeSS TO SOrAfenIb
Marina heskel1, john spivack2, celina ang3, francesca Gany4, umut Sarpel* 1
1surgery, 2Population health science and Policy, 3hematology-oncology, Mount sinai Medical center, 4Immigrant health and cancer Disparities service, Memorial sloan kettering cancer center, new york, united states
Introduction: Minorities and groups with low socioeconomic status have higher rates of hepatocellular carcinoma (hcc) and tend to present with higher disease stage. currently, the only treatment shown to prolong survival in advanced hcc is oral sorafenib. the retail cost of sorafenib is high and insurance coverage of sorafenib varies considerably, with out of pocket costs reaching over one thousand dollars per month for some patients. Given that high cost of treatment has been shown to impede access to care, we sought to determine whether access to sorafenib was associated with certain socioeconomic and demographic factors.
Methods: a search of the electronic medical records was used to identify all cases of hcc at our institution from 2004-2013 and a manual review was performed to confirm diagnosis and stage. a query for “sorafenib” was used to identify patients who had been prescribed this treatment. our cohort consisted of a case sample of 352 patients with advanced hcc who were prescribed sorafenib, and a background sample of 959 patients with non-advanced hcc. the ‘case-Background’ method was used for analysis; wherein the distribution of sociodemographic factors in the advanced population was approximated by the distribution of these factors in the non-advanced population. race/ethnicity, insurance status, and distance from the hospital were abstracted from the medical records. the patient’s zip code of residence was used to determine median income and percentage of bachelor’s degree holders for the region, based on u.s. census data. candidates for sorafenib use consisted of patients with distant metastases, gross vascular invasion, or tumors that had progressed despite maximal loco-regional therapies. additionally, candidates were required to meet laboratory criteria demonstrating normal hepatic and renal function and coagulation parameters.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 0 8
results: the rate of sorafenib prescription among candidate patients was 46.7%. there was a strong association between rate of sorafenib prescription and residence in a zip code with higher socioeconomic status (ses), defined as a factor of median income and education level (or=2.05, p<0.01). this finding was unchanged by inclusion or exclusion of other variables including race/ethnicity, insurance status, or distance from the hospital. according to our model, a patient who was under 65 years of age, white, covered by commercial insurance, and of high ses would have a 47% relative increase in the rate of sorafenib prescription than a similar patient of low socioeconomic status.
Conclusion: our results show that residence in an area with higher socioeconomic status – defined as a combination of income and education level – was associated with approximately twice the odds of being prescribed sorafenib than those in low ses areas, even when controlling for tumor stage and liver function. this finding is concerning because sorafenib remains the only approved and evidence-based treatment for patients with advanced hepatocellular carcinoma. Differential access by socioeconomic status contributes to cancer disparities, therefore future efforts to improve access to care should include a targeted intervention of groups with less than median income and education levels.
Disclosure of Interest: none Declared
P-245 A LIVer-SeLeCTIVe, ALLOSTerIC InhIbITOr Of ACeTyL-COA CArbOxyLASe eLICITS TuMOr neCrOSIS AnD IMPrOVeS SurVIVAL In CIrrhOTIC rATS WITh hePATOCeLLuLAr CArCInOMA
bryan C. fuchs* 1, Danielle k. DePeralta1, omeed Moaven1, Lan Wei1, jeremy Greenwood2, sathesh Bhat2, William f. Westlin3, h. j. harwood3, rosana kapeller3, kenneth k. tanabe1, Geraldine harriman3
1surgery, Massachusetts General hospital, Boston, 2schrodinger, new york, 3nimbus therapeutics, cambridge, united states
Introduction: hepatocellular carcinoma (hcc) is increasing in incidence worldwide. current treatment options for hcc are limited, and as such, prognosis is extremely poor with a 5-year survival less than 12%. therefore, there is an urgent medical need for new therapeutic strategies. Metabolic attenuation is a promising approach to cancer therapy, and rate-limiting steps in key biosynthetic pathways are particularly attractive targets. acetyl-coa carboxylase (acc) occupies a unique position in fatty acid (fa) metabolism, responsible for both increased fa synthesis and reduced fa oxidation. using state-of-the-art structure-based drug design and crystal structures of the human acc2 biotin carboxylase domain, we identified nD-654, a hepatoselective (~3000:1 liver to muscle exposure), allosteric acc inhibitor that binds to the acc subunit dimerization site and inhibits the enzymatic activity of both acc1 (Ic50 = 3 nM) and acc2 (Ic50 = 8 nM), and inhibits fa synthesis in rats (eD50 = 0.3 mg/kg). here, we test the hypothesis that nD-654 can prevent hcc growth and improve survival time in a rat model of cirrhosis and hcc.
Methods: Male Wistar rats were treated weekly with 50 mg/kg diethylnitrosamine (Den) to induce sequential development of fibrosis, cirrhosis and hcc. at the first signs of hcc development (14 wks), rats were treated daily by oral gavage with vehicle containing either 0 or 10 mg/kg nD-654. at the end of the study (18 wks), tumor nodules were counted and liver and tumor tissue was analyzed to assess the effects of nD-654 on disease progression. In a follow-up study, Den-injured rats were treated daily by oral gavage with vehicle containing either 0, 10 or 30 mg/kg nD-654 beginning at 14 weeks and were followed for survival.
results: When measured four hours after the final dose, nD-654 showed preferential liver exposure, with steady state levels reaching 3.7±1.8 µM in cirrhotic tissue and 2.2±1.8 μM in tumor tissue. nD-654 did not alter body weight or food consumption, but reduced serum triglyceride levels by 35%. Importantly, nD-654 significantly (p < 0.01) inhibited hcc development in Den-injured livers from an average of 15.8 tumors nodules in controls to an average of 7.1 tumor nodules in nD-654-treated rats. analysis of tumor tissue revealed that nD-654 decreased tumor cell proliferation as assessed by Pcna staining. In addition, compared to vehicle control, nD-654 induced massive tumor necrosis, as assessed by h&e staining, but minimal apoptosis, as assessed by caspase-3 staining. In the follow-up study, inhibition of acc significantly improved median survival time in this lethal model of cirrhosis and hcc from 114 days in vehicle control animals to 126 (p = 0.02) and 129 days (p = 0.009) in animals treated with either 10 or 30 mg/kg nD-654. finally, nD-654 produced a dose-dependent decrease in fibrosis as assessed by the collagen proportional area (cPa) of sirius red stained histological sections.
Image:
Conclusion: these results provide further evidence that de novo lipogenesis is an important mediator of hepatic fibrosis and carcinogenesis and that selective inhibition of hepatic acc is a viable cancer metabolism therapeutic strategy for treating hcc and liver fibrosis/cirrhosis.
Disclosure of Interest: B. fuchs Grant support from: nimbus therapeutics, D. DePeralta: none Declared, o. Moaven: none Declared, L. Wei: none Declared, j. Greenwood conflict with: schrodinger, s. Bhat conflict with: schrodinger, W. Westlin conflict with: nimbus therapeutics, h. harwood conflict with: nimbus therapeutics, r. kapeller conflict with: nimbus therapeutics, k. tanabe: none Declared, G. harriman conflict with: nimbus therapeutics
P-246 effeCTIVeneSS Of COMbIneD rADIOfrequenCy AbLATIOn/TACe VerSuS TACe/rADIOfrequenCy AbLATIOn On LOCAL hCC reCurrenCe AnD DISeASe COnTrOL
ahmed el Dorry1, nevien el fouly*2, amr el fouly3, runia el folly4, ahmed M. hussein1, Mohamed el Garib1, Mohamed k. shaker4 and hepatoma Group ain shams university
1Intervention radiology, ain shams university, 2health radiation research, 3radioisotpe Department, eaea, 4tropical Medicine, ain shams university, cairo, egypt
Introduction: hepatocellular carcinoma (hcc) is the third cancer related mortality worldwide. In intermediate stage hcc patients, tace is the standard line of care according to BcLc therapeutic algorithm as palliative treatment. combined therapies for hcc, heat ablation (rfa) and trans-arterial chemoembolization (tace) in selected patients could achieve better response and disease control when compared with tace alone as monotherapy. aim: is to compare the effectiveness of combined heat ablation followed by tace and vice versa on overall survival (os), time to recurrence (ttr), disease free survival (Dfs) and objective response.
Methods: this study was conducted in ain shams university hospital, during time period between feb. 2011 and aug. 2014. In sixty eight hcc patients, 56(82%) males and 12(18%) females, mean age 59 yrs(+7.2), divided into two cohorts: the first cohort included 34 patients treated with tace followed by rfa with mean time between procedures of 48.8 days (±19), while the second cohort included 34 patients treated with rfa followed by tace with mean time between procedures of 2.2 days (±1.7). comparative analysis between both techniques regarding clinical toxicities, radiological response, overall survival and time to recurrence.
results: child a liver cirrhosis was represented in 86% and 100% in patients treated with rfa/tace and tace/rfa respectively, while child B was represented in 14% and 0% respectively. tumor stages at baseline was represented as BcLc-a in 14% and 41%, while BcLc-B was 86% and 59% among rfa/tace and tace/rfa patients respectively. Mean tumor size was 5.2cm (+0.8) in rfa/tace group versus 4.7cm (+1.1) in tace/rfa group. the objective radiological response was 91% versus 82% in hcc patients after treatment with rfa/tace and tace/rfa, respectively. successful down-staging within Milan was more achieved after rfa/tace, P= 0.03. Median time to recurrence ttr was 30.1 months (95cI: 17.1-43.0) after (rfa/tace); compared to 19.6 months (95cI: 14.9-24.3) after tace/rfa; P= 0.37. the 1yr ttLr after was (5% and 16%) after rfa/tace and tace/rfa respectively, and 2yr- ttLr was (19% and 49%) respectively with (P=0.03). overall 1yr- and 2yr- survival was (100% and 74%) respectively after rfa/tace versus (85% and 65%) after tace/rfa with P=0.37. Median Disease free survival was 23.2 months (95cI:18.1-28.2) in (rfa/tace) and was 17.1 months (95% cI: 12.2-22.0) in (tace/rfa) with P= 0.27.
Conclusion: combined treatment with rfa/tace for hepatocellular carinoma showed trends for better local tumor control and downstaging in proper selected patients when compared to tace/rfa.
Disclosure of Interest: none Declared
P-247 ALPhA-feTOPrOTeIn LeVeLS In ChrOnIC hePATITIS C PATIenTS Are ASSOCIATeD WITh SySTeMIC InSuLIn SenSITIVITy AnD CAn be DeCreASeD by LIfeSTyLe InTerVenTIOn
Taro Shibuki* 1, yasunori kawaguchi2, shinji Iwane3, toshihiko Mizuta1
1internal medicine, Imari-arita kyoritu hospital, arita town, nishimatuura county, 2hepatobiliary and Pancreatology Division, saga-ken Medical centre koseikan, 3hepatology, saga university hospital, saga city, japan
Introduction: It is known that higher serum alpha-fetoprotein (afP) levels in hcV-infected patients correlate with higher occurrence of hepatocellular carcinoma (hcc). Meanwhile, many studies have shown that insulin resistance (Ir) also can affect hepatocarcinogenesis in patients with chronic hepatitis c (chc). first, we examined the association between serum afP levels and Ir in patients with chc. second, a prospective study was conducted to examine whether lifestyle intervention could decrease serum afP levels or not.
Methods: first, we retrospectively investigated 300 hcV-infected patients without hcc. Patients who underwent liver biopsy and oral glucose tolerance test were included in this analysis and patients taking medications for diabetes mellitus were excluded. In 265 patients who met these criteria (137 men,

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 0 9
128 women, median age 57 years, range 24-75 years), we analyzed factors associated with elevated afP levels (≥10 ng/mL). next, we prospectively introduced a dietary and exercise intervention to 26 patients showing whole-body insulin sensitivity index (WBIsI) <5 (15 men, 11 women, median age 60 years, range 37-71 years), and evaluated the change of data. the target of this intervention was weight loss ≥ 5% of initial body weight. WBIsI was calculated as 10,000 /√[fasting glucose × fasting insulin × mean glucose (0–120) × mean insulin (0–120)]. Visceral fat area (Vfa cm2) at the umbilical level was measured by abdominal computed tomography.
results: the prevalence of afP elevation was 22.3% (59/265). univariate analysis revealed that BMI, platelet counts, albumin, ast, aLt, γ-Gt, glucose intolerance, WBIsI, hepatic inflammation and fibrosis were associated with elevated afP values. Multivariate analysis revealed that platelet count ≥15×104 /μL (or: 2.7, 95% cI: 1.3–5.9, P=0.01), ast ≥50 Iu/L (or: 3.4, 95% cI: 1.2–9.5, P=0.02), γ-Gt ≥35 Iu/L (or: 2.5, 95% cI: 1.1–5.9, P=0.04), WBIsI <5.0 (or: 3.6, 95% cI: 1.5–8.3, P<0.01) and stage 3/4 fibrosis (or: 3.6, 95% cI: 1.4–9.5, P<0.01) were independently associated with afP elevation. the Baysian network analysis revealed that ast, hepatic fibrosis and WBIsI were directly associated with elevated afP levels. In 26 patients taking a lifestyle intervention, BMI, γ-Gt, total cholesterol, triglyceride, Vfa and afP (pre vs. post: 12.9 ± 12.4 vs. 9.2 ± 5.9 ng/mL, P=0.045) decreased, and WBIsI (pre vs. post: 3.2 ± 1.2 vs. 4.3 ± 2.1, P=0.0007) increased significantly.
Conclusion: a systemic Ir leads to serum afP elevation in hcV-infected patients. Lifestyle modification to chc patients with Ir might reduce the risk of hcc occurrence.
Disclosure of Interest: none Declared
P-248 SOrAfenIb TreATMenT In eLDerLy PATIenTS WITh hePATOCeLLuLAr CArCInOMA
Teppei Sakamoto* 1, joji tani1
1Department of Gastroenterology and neurology, kagawa university faculty of Medicine, Miki-cho, japan
Introduction: sorafenib is the standard treatment for advanced hepatocellular carcinoma (hcc). recently, hcc patients around 80 years increase. We aimed to evaluate safety and efficacy of sorafenib in the elderly population.
Methods: We retrospectively reviewed data from patients treated with sorafenib for hcc at our group. We compared safety and efficacy data across different age groups.
results: since 2009, 254 patients were treated, 192 patients (75.6%) were <80 years old and 62 patients (24.4%) were ≥80 years old. the frequency of a response rate (13.0% vs. 16.7%) and a tumor control rate (48.8% vs. 64.5%) was similar between the two groups. the frequency of dose reduction (64.5% vs. 47.6%) was similar between the two groups. the frequency of toxicities was similar between the two groups: liver dysfunction (15.1% vs. 22.6%), bleeding (11.0% vs. 8.1%), hand-foot skin reaction (55.2% vs. 53.2%), diarrhea (16.1% vs. 12.9%) and hypertension (20.8% vs. 24.2%). the frequency of interruption of treatment and definitive discontinuation of treatment due to toxicity reduction was similar between the two groups. there was a trend toward less frequent of treatment after sorafenib in the elderly group (33.9% vs. 22.4%) and significantly less frequent of local treatment with sorafenib in the elderly group (25.0% vs. 8.1%)(P=0.0043). Median progression-free survival was 3.9 months in the younger age and 3.1 months in the the elderly group (P=0.0202), while median overall survival was 9.7 months in the younger age and 8.7 months in the elderly group.
Conclusion: sorafenib showed similar results in terms of safety and efficacy in the elderly and younger hcc populations. sorafenib treatment is a reasonable option in fit elderly patients presenting with advanced hcc.
Disclosure of Interest: none Declared
P-249 neuTrOPhIL-TO-LyMPhOCyTe rATIO (nLr) IS PreDICTIVe fACTOr fOr SurVIVAL In PATIenTS WITh ADVAnCeD hCC TreATeD by SOrAfenIb
Shuntaro Obi* 1, sinpei sato1, takahisa sato1, toshuhiro kawai1, Miho kanda1
1Gastroenterology and hepatology, kyoundo hospital of the sasaki institute, tokyo, japan
Introduction: Inflammation plays a critical role in the development and progression of various cancers1).Inflammation-related markers, such as neutrophil to lymphocyte ratio (nLr), have been linked to clinical outcomes in patients with various malignances.sorafenib is now considered the first-line treatment for patients with advanced stage hepatocellular carcinoma (hcc) with good liver function worldwide. however, predictive factor of sorafenib is not clear. the aim of this study was to investigate the prognostic significance of the blood neutrophil-to-lymphocyte ratio (nLr) in patients with advanced hcc treated by sorafenib.
Methods: a total of one handled nineteen patients with advanced hcc, not eligible for locoregional
therapy, treated with sorafenib were enrolled. the overall survival (os) of patients with high nLr (>5) was compared with patients with low nLr (≤ 5). clinical prognostic factors such as liver function, tumoral characteristics, and nLr were analyzed.
results: Median os was 8.9 months. the mean nLr at baseline was 2.76 (range, 0.96-9.38). the median os of patients with a high nLr was 5.8 months compared with 9.0 months for patients with a low nLr (P = 0.018). BcLc stage B, afP-L3>36%, Portal vein invasion, and nLr>5 were all predictors of poorer overall survival. Multivariate analysis showed that only nLr>5 was independent predictors of poorer overall survival.
Conclusion: high baseline nLr (nLr>5) was associated with worse os for patients with advanced hcc treated with sorafenib.
references: 1. Mantovani a, allavena P, sica a, Balkwill f: cancer-related inflammation. nature 2008;454:436–444.
Disclosure of Interest: none Declared
P-250 enTeCAVIr AnD TenOfOVIr MOre effeCTIVeLy reDuCe The reCurrenCe Of hePATITIS b VIruS-reLATeD hePATOCeLLuLAr CArCInOMA AfTer CurATIVe TreATMenT ThAn LOW-POTenT AnTIVIrALS
hongkeun Ahn* 1, jeong-hoon Lee1, hyeki cho1, young youn cho1, Minjong Lee1, jeong-ju yoo1, yuri cho1, Dong hyeon Lee1, eun ju cho1, su jong yu1, yoon jun kim1, jung-hwan yoon1, hyo-suk Lee1
1Department of Internal Medicine and Liver research Institute, seoul national university college of Medicine, seoul, korea, seoul, korea, republic of
Introduction: the effect of antiviral potency of nucleos(t)ide analogues (nas) on the recurrence of hepatocellular carcinoma (hcc) in chronic hepatitis B (chB) patients has not been well investigated. this study aimed to evaluate the association of the potency of antivirals and the risk of hepatitis B virus (hBV)-related hcc recurrence after potentially curative treatment.
Methods: We performed a retrospective analysis of data from 473 consecutive hepatitis B virus (hBV)-related hcc patients treated with radio-frequency ablation (rfa, n=261) or resection (n=212). according to the potency of antiviral treatments, total population was divided into three groups: group a (no antiviral treatment, n=224), group B (low-potent na: telbivudine, adefovir, clevudine, and lamivudine; n=76), group c (high-potent na: entecavir [etV] and tenofovir disoproxil fumarate [tDf]; n=173). recurrence-free survival (rfs) in three groups were analyzed by kaplan-Meier curve analysis and cox proportional hazards model.
results: the median follow-up duration was 56.9 months. the median rfs was 38.3, 43.6, and 92.9 months in group a, group B, and group c, respectively (P=0.012 by log-rank test). In multivariate analysis, group c had significantly prolonged rfs (hazard ratio [hr]=0.55, 95% confidence interval [cI]=0.42–0.74; P<0.001) after adjustment for hBeag status, tumor numbers, and serum levels of albumin and alanine aminotransferase. In subgroup analyses, patients with baseline high hBV Dna titers (≥2,000 Iu/mL), group c showed significantly longer rfs as compared to those treated with other nas (hr=0.40, 95% cI=0.24–0.65; P<0.001). however, in patients with baseline low hBV Dna titers (<2,000 Iu/mL), there were not significant effect on rfs between groups B and c (hr=1.17, 95% cI=0.63–2.18; P=0.620).
Conclusion: high-potent antiviral agents (etV or tDf) reduce the risk of hcc recurrence compared to low-potent antivirals as well as no antivirals, especially in patients with high viral titer.
Disclosure of Interest: none Declared
P-251 LOnG TerM OuTCOMe AfTer reSeCTIOn Of InTerMeDIATe (bCLC b) hePATOCeLLuLAr CArCInOMA: COMPArISOn TO TrAnSArTerIAL CheMOeMbOLIzATIOn
Jun young Kim* 1, Dong hyun sinn1, Gyu-seong choi2, jong Man kim2, choon hyuck David kwon2, jae-Won joh2, sung Wook shin3, sung ki cho3, Geum-youn Gwak1, Moon seok choi1, joon hyeok Lee1, kwang cheol koh1, Byung chul yoo1, seung Woon Paik1
1Medicine, 2surgery, 3radiology, samsung Medical center, sungkyunkwan university school of Medicine, seoul, korea, republic of
Introduction: transarterial chemoembolization (tace) is the first-line recommended therapy for patients with intermediate hepatocellular carcinoma (hcc) in the BcLc staging system. however, in clinical practice, some patients receive hepatectomy. We compared long-term outcome in these patients.
Methods: a total of 277 patients with intermediate stage hcc who were treated with either hepatectomy or tace were analyzed.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 1 0
results: the median survival was significantly better for resection than tace (5.3 vs. 2.6 years, p = 0.002), however, when adjusted for age, child-Pugh class, maximal tumor size, tumor number, uni- or bi-lobal involvement, and afP levels, there was no significant survival difference by treatment modality [hazard ratio (hr): 1.42, 95% cI (0.91-2.22), p = 0.11]. In sub-group analysis, resection showed better survival than tace in child-Pugh score 5, maximal tumor size ≤ 5cm or > 10cm, and tumor number ≤ 3, however, there was no survival difference in patients with child-Pugh score ≥ 6, tumor size between 5-10cm, and tumor number ≥ 4. When patients were sub-grouped according to the child-Pugh class, tumor number and size, resection (n = 26) provided survival benefit over tace (n = 58) for those with child-Pugh class 5, less than 3 tumors, and tumor size ≤ 5cm or > 10cm [adjusted hr: 0.41 (95% cI: 0.20-0.84), p = 0.015], but not the rest of patients [adjusted hr for resection (n = 26) vs. tace (n = 167): 0.73 (95% cI: 0.44-1.21), p = 0.22].
Conclusion: resection can be first-line treatment option for intermediate stage hcc when certain criteria are met. In this study, child-Pugh score 5, tumor number ≤ 3, and tumor size ≤ 5 or > 10 cm were the criteria.
Disclosure of Interest: none Declared
P-252 LAMIVuDIne VS. enTeCAVIr fOr The neWLy DIAGnOSeD hePATITIS b-VIruS reLATeD hePATOCeLLuLAr CArCInOMA
Jung hee Kim* 1, Dong hyun sinn1, kyunga kim2
1internal medicine, 2Biostatistics and clinical epidemiology center, samsung medical center, seoul, korea, republic of
Introduction: antiviral therapy is a key element in the management of hepatitis B virus (hBV)-related hepatocellelular carcinoma (hcc) patients. however, little is known whether entecavir (etV) is more effective than a less potent drug, lamivudine (LaM), in reducing the risk of death, hepatic decompensation and recurrence in hBV-related hcc.
Methods: a retrospective cohort of 451 newly-diagnosed, hBV-related hcc patients without antiviral therapy at diagnosis, and started antiviral therapy with either etV (n = 249) or LaM (n=202) were enrolled. Mortality, new-onset hepatic decompensation (ascites, variceal bleeding, hepatic encephalopathy), and recurrence after curative therapy were compared.
results: the overall survival rate was better in etV than LaM (50.2% vs. 40.1% at 3-years, p = 0.003). LaM was independent factor for overall mortality [hazard ratio (hr), 1.28; 95 % confidence interval (cI), 1.01-1.64, p = 0.040]. among 318 patients without previous hepatic decompensation, decompensation-free survival rate was better in etV than LaM (71.6% vs. 54.6% at 3-years, p < 0.001). LaM was independent risk factor for new-onset hepatic decompensation (hr, 1.62; 95% cI, 1.10-2.38, p = 0.013). among 177 patients who had curative therapy, recurrence-free survival rate was better in etV than LaM (52.3% vs. 32.6% at 3-years, p < 0.001). LaM was independent risk factor for recurrence after curative therapy (hr, 1.73; 95% cI, 1.18-2.51, p = 0.004).
Conclusion: etV showed better overall survival, decompensation free survival, and recurrence free survival than LaM treated newly-diagnosed hBV-related hcc patients, which suggests potent antiviral drug should be used over less potent drug for these patients.
Disclosure of Interest: none Declared
P-253 The effeCT Of rADIOTherAPy In LIVer-COnfIneD buT nOn-reSeCTAbLe bCLC STAGe C hePATOCeLLuLAr CArCInOMA: PrOPenSITy-MATCheD AnALySIS bASeD On nATIOnWIDe MuLTICenTer hCC COhOrT
hong In yoon1, Inkyung jung2, Mi sun kim1, kwang-hyub han3, 4, Jinsil Seong* 1, 4
1radiation oncology, 2Biostatistics & Medical Informatics, 3Internal Medicine, yonsei university college of Medicine, 4korean Liver cancer study Group, seoul, korea, republic of
Introduction: the aim of this study is to validate the efficacy of radiotherapy (rt) compared to other treatments and to identify the clinical features which showed survival benefit by rt in liver-confined but Barcelona clinic Liver cancer (BcLc) stage c non-resectable hepatocellular carcinoma (hcc).
Methods: hcc data from the korea central cancer registry were used to perform the systemic randomized sampling. the database, collected from 47 institutions in korea, included information about age, gender, performance status (Ps), smoking history, pack years, tumor size, α-fetoprotein (afP), child-pugh class or score, number of tumor mass, nodal metastasis, portal vein (PV), hepatic vein, bile duct, hepatic artery invasion, the etiology of hcc and survival. a total number of patients were 4596. among them, we excluded patients according to the exclusion criteria as follows: 1) BcLc a, B, and D; 2) distant metastasis; 3) patients who underwent surgery as the first treatment or no treatment; 4) missing information for clinical factors. In this study, a total of 593 patients were included. sixty-seven patients were treated with rt and defined as rt group. the others were sorted as non-rt group. among rt group, 52 patients underwent treatments that combined rt and other treatment within 4 weeks after the first treatment and were defined as combination rt group. the
rest who received only rt was defined as rt only group. We performed propensity score matching (PsM) of 1 to 1 ratio to compare rt or combination rt group with non-rt group, respectively. PsM was also performed for subgroup with tumor size ≥ 10 cm. the endpoint was overall survival (os). all statistical analyses were 2-sided with P ≤ 0.05 and conducted using sas, version 9.2.
results: Median follow-up time for surviving patients was 48 months (range, 36.6-72.5). Before PsM, non-rt group (n=526) showed significantly longer os than rt group (n=67, median survival time (Mst) 12.3 vs. 8.4 months, P = 0.001), and there was significant difference in Ps, PV invasion, age, tumor size, and afP between two groups. after PsM between rt and non-rt groups (n=67), all clinical factors were evenly distributed between two groups. In survival analysis, os of rt group was not significantly different from that of non-rt group (hazard ratio (hr) 1.34, 95% confidence interval (cI) 0.94-1.91, P = 0.11). In rt group, combination rt group improved significantly os compared to rt only group (10.2 vs. 4.6 months, P = 0.01). to verify the effect of rt combining other treatment, we also performed PsM to compare combination rt group (n=52) with non-rt group. after PsM, the os of combination rt and non-rt group was not statistically different, although combination rt group had longer Mst (10.7 vs. 6.9 months, hr 1.01, 95% cI 0.65-1.55, P = 0.98). thereafter, we conducted PsM between combination rt and non-rt groups in subgroup with tumor size ≥ 10 cm (n=31). We observed that there was significant difference of Mst between two groups (10.1 vs. 5.4 months, bootstrap 95% cI of difference in Mst, 0.2-11.8), and combination rt group achieved better os despite no statistical significance (hr 0.69, 95% cI 0.4-1.19, P = 0.17).
Conclusion: this nationwide retrospective cohort study demonstrates that the survival outcome of rt combining other therapy was comparable to those of other treatments. radiotherapy as a combined modality can be one of the options for this liver confined but non-resectable BcLc c hcc patients.
Disclosure of Interest: none Declared
P-254 The PrOGnOSTIC fACTOrS Of reCurrenCe AfTer COMPLeTe reSPOnSe InDuCeD by TrAnSArTerIAL CheMOeMbOLIzATIOn In hePATOCeLLuLAr CArCInOMA
shin ok jeong1, eui Bae kim1, Soung Won Jeong* 1, jae young jang1, sae hwan Lee1, sang Gyune kim1, sang-Woo cha1, young seok kim1, young Deok cho1, hong soo kim1, Boo sung kim1, yong jae kim1, suyeon Park1
1soonchunhyang university hospital, seoul, korea, republic of
Introduction: transarterial chemoembolization (tace) is the most widely used treatment modality in patients with unresectable hepatocellular carcinoma (hcc). overall survival mainly depends on tumor response and some patients show long term complete remission (cr) after tace. however, the predictive factors for recurrence after tace induced cr has not been clarified yet. the aim of the study is to investigate the predictive factors of recurrence after tace induced cr in patients with hcc.
Methods: among 852 newly diagnosed hcc patients, 395 patients were treated with tace as a first therapy. among these, 123 consecutive patients who achieved cr after tace were evaluated. We analyzed the factors to recurrence including age, gender, viral markers, model for end stage liver disease (MeLD) score, child-Pugh score, size of tumors, number of tumors, tumor stage, serum alpha-fetoprotein (afP) and lipiodol uptake.
results: of the 123 patients with initial cr, recurrent hcc was detected in 59 patients during a median period of 34 months. overall recurrence rate of patients with tace induced cr was 47% and the overall 1-, 2-, and 3-year cumulative recurrence rates were 23%, 40%, and 43%, respectively. survival rates of 395 patients treated with tace were 67%, 52%, and 39% after 1-, 2-, 3-year, respectively. the cumulative survival rates in patients without cr versus with cr were as these : 56% vs 92% after 1-year, 39% vs 81% after 2-year, 28% vs 64% after 3-year (P<0.001). In multivariate analyses, the significant factors that affected recurrence were advanced tumor stage (stage III, IV) (hazard ratio (hr) 7.198, P<0.001) and high serum afP level (>400ng/mL) (hr 1.944, P=0.034).
Conclusion: advanced tumor stage (stage III, IV) and high serum afP level (>400ng/mL) were the risk factors of the recurrence after tace induced cr in patients with hcc.
Disclosure of Interest: none Declared
P-255 DeVeLOPMenT Of TrAnSGenIC T-CeLLS AS IMMunOTherAPeuTICS AnD CeLL CArrIerS Of OnCOLyTIC VIruS fOr SynerGISTIC TreATMenT Of hePATOCeLLuLAr CArCInOMA
Lisa zeitlinger*1, David Grunert1, sabine Mall2, jennifer altomonte1, angela M. krackhardt2, oliver ebert 1
1II. Medizinische klinik, 2III. Medizinische klinik, klinikum rechts der Isar, technische universität München, Muenchen, Germany

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 1 1
Introduction: Due to obvious limitations of conventional cancer therapies, oncolytic viruses have emerged as novel alternative agents to specifically target and cause cytolysis of cancer cells. In particular, we have demonstrated that oncolytic vesicular stomatitis virus (VsV), applied via hepatic arterial infusion, results in significant tumor necrosis and survival prolongation in immune-competent rats bearing multifocal, orthotopic hcc. nevertheless, the systemic delivery of virus faces limited efficacy due to rapid clearance from circulation. the use of cell carriers represent an ideal approach to overcome this challenge, by offering the possibility to shield oncolytic viruses against neutralizing components of the blood and non-specific uptake by circulating immune cells, while simultaneously providing a delivery mechanism through specific homing of the carrier cells to the tumor. In particular, the use of t-cell receptor (tcr) transgenic t-cells to deliver oncolytic viruses to tumors expressing the target antigen is an appealing strategy, as it not only provides tumor specificity in virus delivery and transfer, but the carrier cells themselves possess a direct antitumor effector function, allowing additive or potentially synergistic therapeutic effects with viral therapy.
Methods: t-cells were enriched from PBMcs isolated from whole human blood, and tcr transgenic cells were generated by retroviral transduction. cells were characterized in vitro for activation, function, and infectibility by facs analysis and eLIsa assay, and VsV replication kinetics were monitored by tissue culture infectious dose 50 (tcID50) assay. the ability of t-cells to shield VsV from inactivation from neutralizing antibodies was evaluated by incubation with serum obtained from VsV-immunized rats. In addition, co-culture experiments were performed with tumor cells to determine the ability of t-cells to transfer virus to the targeted cells and to characterize the effects of VsV on both cell types and to determine a potential synergy of cytotoxic t-cells with oncolytic viral therapy.
results: In vitro infections demonstrated that VsV is able to infect up to 15 - 30 % of t-cells in a dose- and time-responsive manner, and viral progeny were able to infect and replicate in target tumor cells to titers several logs higher than those achieved in t-cells alone. Moreover, VsV-infected t-cells maintained their ability to become activated upon stimulation with target tumor cells, as evidenced by cD25 expression and interferon-gamma production, as well as their cytolytic effector function, which resulted in increasing tumor cell lysis with increased effector-to-target cell ratios. In addition, incubation of infected t-cells with virus-neutralizing serum demonstrated a substantial shielding effect of the virus, with similar intracellular titers achieved as those observed in cells incubated with control serum or PBs.
Conclusion: taken together, these results indicate that the use of tcr transgenic t-cells as carriers of oncolytic VsV could provide a potent combination therapy for hcc, by enriching the viral load at the tumor site to optimize the direct oncolytic effect of the virus and simultaneously delivering a powerful immune therapy to target the remaining tumor cells which evade viral infection. further in vivo investigations to demonstrate homing of VsV-loaded t-cells to the tumor and the potential for additive or synergistic therapeutic effects are warranted.
Disclosure of Interest: none Declared
P-256 fInAL reSuLTS Of The GIDeOn STuDy ACCOrDInG TO PATIenT eTIOLOGy: The ITALIAn exPerIenCe
salvatore D'angelo1, Domenico Germano2, Teresa zolfino* 3, Domenico sansonno4, Giuseppe Montalto5, antonio Benedetti6, Vincenzo Montesarchio7, adolfo francesco attili8, angela Buonadonna9, sandro Barni10, antonio Gasbarrini11, Mario Pirisi12, umberto cillo13, simona Marenco14, erica Villa15, Petros Giovanis16, Graziella Pinotti17, carlo saitta18, claudia erminero19, Massimo De Giorgio20, Vito Lorusso21
1aorn Moscati, avellino, 2ao G. rummo, Benevento, 3ao G. Brotzu, cagliari, 4aou Policlinico consorziale di Bari G. Bacelli, Bari, 5aouP Paolo Giaccone, Palermo, 6aou ospedali riuniti, Po umberto I, torrette di ancona, ancona, 7aorn ao dei colli Monaldi-cotugno cto, napoli, 8azienda Policlinico umberto I, roma, 9centro di riferimento oncologico cro, aviano, 10ao ospedale treviglio-caravaggio, treviglio, 11Policlinico universitario a. Gemelli - ucsc, roma, 12aou Maggiore della carità, novara, 13aou di Padova, Padova, 14Irccs auo s.Martino Ist, Genova, 15aou Policlinico, Modena, 16azienda u.L.s.s. n. 9 di treviso, treviso, 17ospedale di circolo e fondazione Macchi, Varese, 18aou Policlinico G. Martino, Messina, 19Bayer spa, Milano, 20ao Papa Giovanni xxIII, Bergamo, 21Irccs ospedale di Bari, Bari, Italy
Introduction: sorafenib is the only targeted agent indicated for the treatment of hepatocellular carcinoma (hcc). the global, prospective, non-interventional GIDeon (Global Investigational of therapeutic Decisions in hcc and of its treatment with sorafenib) study enrolled over 3200 patients (pts) with unresectable hcc (uhcc) treated with sorafenib in real-life clinical practice conditions. the primary objective of the study was to evaluate the safety of sorafenib in hcc patients in clinical practice. secondary objective was efficacy1,2. We report the final analysis of the Italian subgroup of patients according to etiology.
Methods: Patients with uhcc for whom the decision to administer sorafenib was taken were eligible for enrollment. Disease and patients characteristics were assessed at baseline. sorafenib dose, adverse events (aes) and disease assessments were reported at follow-up.
results: of 278 pts enrolled in Italy, 274 were evaluable for efficacy and 271 for safety analysis. the median age was 70 years (range: 44-90), 227 pts (83%) were male, 266 pts (97%) caucasian and disease stage was BcLc-B in 87(32%) and BcLc-c in 142(52%) pts. the etiology of the underlying liver disease was recorded as hepatitis B (hep-B) in 58(21%) pts, hep B only in 39(14%) pts, hepatitis
c (hep-c) in 157(57%), hep-c only in 119(43%) pts, alcohol use in 112(41%) pts and nonalcoholic steatohepatitis (nash) in 7(2.6%) pts. overall adverse events were slightly more frequent in pts with hep-B (88%) than those with hep-c (75%) or alcohol use (75%). the type and incidence of aes were consistent among all subgroups, the most frequent being gastrointestinal (diarrhea/ascites), dermatologic (hand-foot skin reaction/rash) and fatigue. there were no new unexpected aes.Median os in days (months) in pts with hep-B, hep-c, alcohol use, nash, hep-B only and hep-c only were 351(11.5), 617(20.5), 402(13.1), 211(6.9), 351(11.5) and 633(20.7) respectively.
Image:
Conclusion: the most frequent etiology was hep-c followed by alcohol use and hep-B. safety was consistent with the known profile of sorafenib3. overall survival was longer in the subgroup of hep-c pts than in the other etiology subgroups. this has also been reported in previous analyses4.
references: 1. Lencioni r, kudo M, ye sL, et al. Int j clin Pract. 2014 May;68(5):609-17. 2. Marrero ja, Lencioni r, ye sL et al. j clin oncol 31, 2013 (suppl; abstr 4126). 3. Llovet jM, ricci s, Mazzaferro V, et al. n engl j Med 2008; 359: 378–390. 4. Bruix j, raoul jL, sherman M, et al. j hepatol. 2012 oct;57(4):821-9.
Disclosure of Interest: s. D'angelo research/education support from: none, Grant support from: none, honoraria support from: none, stocks of: none, advisory Board of: none, consulting of: none, conflict with: none, D. Germano: none Declared, t. zolfino: none Declared, D. sansonno: none Declared, G. Montalto: none Declared, a. Benedetti: none Declared, V. Montesarchio: none Declared, a. f. attili: none Declared, a. Buonadonna: none Declared, s. Barni: none Declared, a. Gasbarrini: none Declared, M. Pirisi: none Declared, u. cillo: none Declared, s. Marenco: none Declared, e. Villa: none Declared, P. Giovanis: none Declared, G. Pinotti: none Declared, c. saitta: none Declared, c. erminero conflict with: Bayer spa, M. De Giorgio: none Declared, V. Lorusso: none Declared
P-257 SAfeTy AnD effICACy Of SOrAfenIb In STeLLA STuDy, A MuLTICenTer, ObSerVATIOnAL, PhASe IV STuDy In ITALIAn CenTerS
Giovan Giuseppe Di Costanzo* 1, rodolfo sacco2, Giorgio de stefano3, Vincenzo Montesarchio3, Giuseppe cabibbo4, teresa zolfino5, Patrizia carucci6, salvatore Pisconti7, ferdinando De Vita8, Petros Giovanis9, adolfo francesco attili10, claudia erminero11, tommaso fontana12, Bruno Daniele13
1cardarelli, napoli, 2ospedale cisanello, Pisa, 3aorn dei colli ospedali Monaldi-cotugno-cto, napoli, 4Policlinico Giaccone, Palermo, 5ao G. Brotzu, cagliari, 6ospedale Molinette, torino, 7ospedale Moscati, taranto, 8seconda università di napoli, napoli, 9azienda u.L.s.s. n. 9 di treviso, treviso, 10azienda Policlinico umberto I, roma, 11Bayer spa, Milano, 12ospedale civile di Bisceglie, Bisceglie, 13ao G. rummo, Benevento, Italy
Introduction: sorafenib, a multikinase inhibitor, is the only systemic treatment approved for hepatocellular carcinoma (hcc). It prolonged overall survival in two randomized placebo controlled trials in non-resectable hcc patients (pts)1,2. Data collected on sorafenib in routine clinical practice provides valuable information on patient characteristics, etiology, pattern of disease and treatment modalities in a specific geographical area. this helps to better understand the use of sorafenib in order to maximize its safety and efficacy.
Methods: steLLa (sorafenib treatment modalities for hepatoceLLular carcinoma patients in ltaly) is a phase IV, prospective, non-interventional, multi-center study conducted in Italian centers, aiming to evaluate the efficacy and safety of sorafenib (standard approved dose of 400 mg/bid) in terms of overall survival rate at 12 months (primary endpoint) in patients with hcc under daily-life treatment conditions. additional objectives were safety and overall survival. Patients with hcc, candidates for systemic therapy and in whom a decision to treat with sorafenib has been made, were enrolled. the observation period for each patient is the time from the start of therapy with sorafenib to withdrawal of consent, death, or the last visit.
results: a total of 234 pts were enrolled. of these 224 received sorafenib and were valid for the intention-to-treat (Itt) analysis and 214 pts were valid for safety analysis. Patient and disease characteristics were: male 79%, median age 70 years, hepatitis c virus infection was the predominant etiology in 115(51%) pts, followed by alcohol abuse in 58(26%) pts and hepatitis B virus infection in 42(19%) pts; ecoG performance status 0/1/2 was present in 143(64%), 69(31%) and 11(5%) respectively; child-Pugh class a/B/c was present in 179(80%), 34(15%) and 2(1%) respectively. sorafenib was administered in intermediate stage hcc (BcLc B) in nearly 1/3 of the overall study population. the distribution per BcLc stage was BcLc a/B/c: 10(4.5%), 67(30%) and 146(65%) respectively.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 1 2
the overall survival rate at 12 months was 54% [90% cI: 48-60%]. adverse events (all grades) occurred in 176(82%) pts whereas drug-related adverse events (all grades) occurred in 151(71%), most of which were grade 1 or 2 (11% and 29% respectively). the most frequent drug-related aes were gastrointestinal (33%), dermatologic (30%), fatigue (27%) and anorexia (13%). Drug-related aes resulting in permanent discontinuation of study drug occurred in 31% of patients.
Conclusion: the steLLa study provides additional insight on the use of sorafenib in Italian centers in routine clinical practice. the overall survival rate at 12 months compares favourably with that observed in the phase III sharP study. this may be explained by a lower percentage of BcLc c pts than in sharP (65% and 82% respectively).the safety profile was comparable in nature and frequency to that seen in other studies under real-life conditions, with no new safety signals observed.
references: 1. Llovet jM, et al. n engl j Med 2008; 359: 378–390.2. cheng aL, et al. Lancet oncol 2009; 10: 25–34.
Disclosure of Interest: G. G. Di costanzo: none Declared, r. sacco: none Declared, G. de stefano: none Declared, V. Montesarchio: none Declared, G. cabibbo: none Declared, t. zolfino: none Declared, P. carucci: none Declared, s. Pisconti: none Declared, f. De Vita: none Declared, P. Giovanis: none Declared, a. f. attili: none Declared, c. erminero conflict with: Bayer spa, t. fontana: none Declared, B. Daniele honoraria support from: Bayer, advisory Board of: Bayer
P-258 reTrOSPeCTIVe POOLeD AnALySIS Of ADVAnCeD hCC PATIenTS In ShArP AnD AP rAnDOMIzeD CLInICAL TrIALS
Jordi bruix* 1, ann-Lii cheng2, Gerold Meinhardt3, keiko nakajima3, yoriko Desanctis3, josep Llovet4
1Liver unit. hospital clínic, university of Barcelona, Barcelona, spain, 2national taiwan university hospital, taipei, taiwan, 3Bayer healthcare Pharmaceuticals, Whippany, nj, 4Mount sinai Liver cancer Program, Icahn school of Medicine at Mount sinai, new york, ny, united states
Introduction: the current investigation is aimed at assessing prognostic factors and predictors of survival to sorafenib through an exploratory pooled analysis of patients with advanced hcc randomized into the sorafenib phase 3 trials, sharP (n=602) and asia-Pacific (aP; n=226).
Methods: Both sharP and aP trials showed a significant overall survival (os) benefit of sorafenib over placebo. to identify prognostic factors for os, exploratory univariate and multivariate analyses were performed using the cox proportional hazard regression model. Both tumor and non-tumor related baseline variables were assessed (see table). hazard ratios (hr) and median os were evaluated across the pooled subgroups in a similar manner. to assess consistency of sorafenib benefit, the interaction term between the treatment and each subgroup was evaluated using cox proportional hazard model. this exploratory analysis should be interpreted cautiously as it may be influenced by small sample size and low event count across subgroups. no adjustment was performed for multiplicity.
results: overall, 827 patients (448 sor; 379 PBo) were included. at baseline aP compared to sharP patients had more advanced disease, a higher prevalence of extrahepatic disease (ehs), ecoG Ps 1-2, and a lower percentage of hcV (12% vs 73%) vs hBV (30% vs 8%). Prognostic factors for os were BcLc stage, tumor burden, tumor size, ecoG Ps, bilirubin and albumin in both arms. a sorafenib benefit for os was consistently observed across all subgroups, with numerically lower hrs observed for patients without ehs, tumor burden, and with hcV. sorafenib showed consistent survival benefit regardless of race and hBV status. Both patients with or without hBV or alcohol (etoh) intake observed hr’s suggesting benefit (with hBV hr= 0.78; etoh hr= 0.82) and patients without these risk factors had numerically lower hrs (w/o hBV hr= 0.69; etoh hr= 0.67). a longer survival time for patients with hcV was observed on sorafenib compared with placebo (hr 0.47; p interaction, p=0.035) vs patients without hcV (hr 0.81). In addition to hcV, a treatment by subgroup interaction was observed at the 10% significance level for ehs, tumor burden, and number of target lesions at baseline. all these interactions had similar direction in sorafenib treatment effect with only some differences observed in magnitude.
Image:
Baseline covariates N
(PBO;SOR*) Events
Median OS(mos) HR (SOR/PBO)
[95% CI]
Treatment Interaction P-valueb PBO SOR
Tumor related variables ECOG PS
0.465 ( 1 vs 0)
0 373 (183;190) 224 9.8 13.0 0.71 [0.54-0.92] 1 and 2 454 (196;258) 323 4.8 7.4 0.67 [0.54-0.84]
BCLC stage 0.431
(C vs B) Stage B 113 ( 55;58) 58 13.4 15.1 0.78 [0.46-1.32] Stage C 714 (324;390) 489 6.0 8.5 0.69 [0.57-0.82]
Tumor burden 0.081
(Present vs Absent) Absent 229 (107;122) 112 10.6 15.7 0.53 [0.37-0.78] Present 598 (272;326) 435 5.6 7.3 0.77 [0.64-0.93]
MVI 0.947
(Yes vs No) No 515 (230;285) 294 10.0 12.7 0.70 [0.56-0.88] Yes 310 (148;162) 252 4.5 6.0 0.69 [0.53-0.89]
EHS 0.015
(Yes vs No) No 365 (178;187) 218 7.2 13.8 0.55 [0.42-0.72] Yes 462 (201;261) 329 7.0 7.3 0.84 [0.67-1.05]
MVI without EHS 0.283
(Yes vs No) No 689 (307;382) 440 8.5 9.5 0.74 [0.62-0.90] Yes 136 (71;65) 106 4.5 6.8 0.53 [0.35-0.80]
Number of target lesions
0.078 (0, 1, 2, 3, >3)
1 208 (99;109) 130 7.0 8.8 0.73 [0.51-1.05] 2 165 (79;86) 99 9.3 11.8 0.59 [0.40-0.89] 3 147 (70;77) 91 5.5 11.5 0.49 [0.32-0.75]
> 3 295 (130;165) 218 6.4 7.3 0.85 [0.65-1.12] Hepatitis B No 540 (266;674) 349 7.4 9.9 0.69 [0.55-0.85] 0.516 Yes 236 (90;146) 172 4.8 6.5 0.78 [0.57-1.06] (Yes vs No) Hepatitis C No 568 (265;303) 398 6.8 7.6 0.81 [0.66-0.99] 0.035 Yes 199 (88;111) 120 7.9 14.0 0.47 [0.32-0.69] (Yes vs No) Alcohol Use No 636 (287;349) 419 6.5 9.4 0.67 [0.55-0.81] 0.361 Yes 191 (92;99) 128 8.5 9.5 0.82 [0.58-1.17] (Yes vs No) Non-tumor related variables Albumin (median=3.96 g/dL)
median 355 (143;212) 277 4.1 6.6 0.64 [0.50-0.82] 0.943 > median 472 (236;236) 270 9.8 13.6 0.63 [0.49-0.80] (> median vs median)
Total bilirubin (median=0.77 mg/dL) median 473 (214;259) 287 9.2 10.7 0.70 [0.56-0.89] 0.934
> median 354 (165;189) 260 4.9 6.7 0.72 [0.56-0.93] (> median vs median)
Race Asian 274 (100;174) 203 4.8 6.7 0.78 [0.59-1.04] 0.3664 Non-Asian 553 (279;274) 344 7.9 11.4 0.67 [0.54-0.82] (Non-Asian vs Asian)
*SOR group one subject with BCLC stage D was excluded; aITT population; bWald test for individual effects (p-value)
Univariate OS Pooled Analysisa With Major Prognostic Factors
Conclusion: the sorafenib benefit was generally consistent irrespective of patient’s baseline characteristics and prognostic factors for survival, suggesting all subgroups evaluated, including race, had benefit. etiology did not emerge as independent predictor of outcome. Patients with lower tumor burden and hcV may have a potentially greater magnitude of benefit from sorafenib. these findings should be taken into consideration for the design of future clinical trials in hcc patients.
Disclosure of Interest: j. Bruix research/education support from: Daichi, arquile, Bayer, honoraria support from: Bayer, Biocompatibles, BMs, novartis, consulting of: Daichi, arquile, Bayer, Biocompatibles, BMs, novartis, and roche, a.-L. cheng: none Declared, G. Meinhardt conflict with: employee of Bayer healthcare Pharmaceuticals, k. nakajima conflict with: employee of Bayer healthcare Pharmaceuticals, y. Desanctis conflict with: employee of Bayer healthcare Pharmaceuticals, j. Llovet research/education support from: Bayer healthcare, Boehringer Ingelheim, honoraria support from: Bayer healthcare, BMs, Lilly, nanostring, consulting of: Bayer healthcare, BMs, Lilly, Gsk, nanostring, Biosphere Medical, and Boehringer Ingelheim
P-259 ADJuVAnT TACe IMPrOVeS OuTCOMeS Of PATIenTS WITh hePATOCeLLuLAr CArCInOMA WITh MICrOVASCuLAr InVASIOn
Shuqun Cheng* 1
1the eastern hepatobiliary surgery hospital, shanghai, china
Introduction: Microvascular invasion (MiVI) is a major risk factor of survival outcomes following curative resection inpatients with hepatocellular carcinoma (hcc).randomizedcontrolled trials (rct) showed postoperative adjuvant transcatheter arterial chemoembolization(Ph-tace) to be beneficial topatients with advanced hcc, but the data on its impact on patients with hcc with MiVI are scarce. We aimed to investigate the impact of Ph-tace on such patients.
Methods: from january 2004 to june 2013, all patients with hcc with MiVI who underwent partial hepatectomy (Ph) in our team were studied retrospectively. after exclusion, the patients with hcc with MiVI were divided into two groups, the Ph group and the Ph-tace group. In the Ph-tace group, adjuvant tace was given 4 weeks after Ph. univariate and multivariate analyses were used to identify the prognostic significance of Ph-tace.
results: of 1934 patients with hcc with MiVI, after exclusion using pre-defined exclusion criteria, 185 patients entered into the Ph group and 137 patients into the Ph-tace group. the 1-, 2-, 3- and 5-year recurrence-free survival (rfs) rates were 69.4%,55.6%, 46.9%,34.9% and 47.0%,

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 1 3
36.3%, 34.1%, 30.4.% for the Ph-tace group and the Ph group, respectively (log-rank, Χ2=6.309, p=0.012). the 1-, 2-, 3- and 5-year overall survival (os) rates were94.1%, 78.6%, 71.3%,53.7% and 79.1%, 62.3%, 54.3%, 43.5% for the Ph-tace group and the Ph group, respectively((log-rank, Χ2 =7.537, p = 0.006). Multivariate cox proportional hazards regression analysis revealed Ph-tace to be an independent risk factor of postoperative rfs and os (p=0.003; hazard ratio (hr): 0.641; 95% cI: 0.478-0.861 and p=0.001; hr: 0.602; 95% cI: 0.440–0.822 for rfs and os,respectively).
Conclusion: Ph-tace provided better rfs and os for patients with MiVI hcc than patients who underwent Ph alone. adjuvant tace was beneficial to patients with hcc with MiVI after r0 liver resection
Disclosure of Interest: none Declared
P-260 LAPArOSCOPIC VS. OPen LIVer reSeCTIOn fOr hePATOCeLLuLAr CArCInOMA Of CIrrhOTIC LIVer: A CASe–COnTrOL STuDy
Azoulay Daniel* 1, Memeo ricardo1, salloum chady1, Laurent alexis1, compagnon Philippe1, De angelis nicola1
1hPB surgery and liver transplantation, hopital henri Mondor, aPhP, creteil, france
Introduction: Laparoscopic liver resection is considered a safe and feasible alternative to open surgery for malignant liver lesions. however, laparoscopic surgery in cirrhotic patients remains challenging. the aim of this retrospective case–control study was to compare morbidity, mortality, and long-term patient survival between laparoscopic liver resections (LLr) and open liver resections (oLr) for hepatocellular carcinoma (hcc) in patients with histologically proven cirrhosis.
Methods: a total of 45 patients treated with LLr were matched by cause of cirrhosis, child-Pugh score, type of surgical resection (subsegmentectomy, segmentectomy, and bisegmentectomy), tumor number, tumor size, and alpha-fetoprotein value with 45 patients treated with oLr. Pre-, intra-, and post-operative variables were compared between groups.
results: compared with oLr, the LLr group displayed a significantly shorter operative time (140 vs. 180 min; p = 0.02), shorter hospital stay (7 vs. 12 days; p < 0.0001), and lower morbidity rate (20 vs. 45 % of patients; p = 0.01). a higher rate of r0 resection was observed in the LLr group than in the oLr group (95 vs. 85 %; p = 0.03). Postoperative ascites was more frequently observed in the oLr group (18 vs. 2 %; p = 0.01). Mortality, patient, and disease-free survival rates were similar between groups. the 1-, 5-, and 10-year survival rates were 88, 59, and 12 %, respectively, in the LLr group and 63, 44, and 22 % in the oLr group (p = 0.27).
Conclusion: significantly shorter operative times, better resection margins, lower postoperative complications, and shorter hospital stay were observed in the LLr group compared with the oLr group. LLr and oLr have similar overall and disease-free survival rates in cirrhotic hcc patients.
Disclosure of Interest: none Declared
P-261 In PATIenTS WITh hCC AnD MACrOVASCuLAr InVASIOn TreATeD WITh SOrAfenIb, AfP VALue≤1000 uI/L AT bASeLIne AnD VASCuLAr InVASIOn nOT InCLuDInG 1ST OrDer brAnCheS Or MAIn TrunK (VP1/2) Are ASSOCIATeD WITh PrOLOnGeD SurVIVAL
Charlotte Costentin* 1, françoise roudot-thoraval2, thomas Decaens3, nathalie Ganne4, Bernard Paule5, eric Vibert6, Melanie chiaradia7, christian Letoublon8, julien calderaro9, Giuliana amaddeo1, olivier seror10, Ivan Bricault11, Didier samuel5, alexis Laurent12, christophe Duvoux1
1hepatology, 2Public health, henri Mondor hospital, creteil, 3Gastroenterology and hepatology, chu Grenoble, Grenoble, 4hepatology, jean Verdier hospital, Bondy, 5hepatology, 6hepato-biliary surgery, Paul Brousse hospital, Villejuif, 7radiology, henri Mondor hospital, creteil, 8Digestive surgery, chu Grenoble, Grenoble, 9Pathology, henri Mondor hospital, creteil, 10radiology, jean Verdier hospital, Bondy, 11radiology, chu Grenoble, Grenoble, 12Digestive surgery, henri Mondor hopital, creteil, france
Introduction: according to easL-oertc guidelines, sorafenib is the standard of care for advanced hepatocellular carcinoma (hcc) BcLc-c although in the sharP trial, macrovascular invasion (MVI) was associated with a poor prognosis. however, in patients with MVI, survival had been assessed for patients with MVI with or without extrahepatic spread (ehs) (8 months) but not in the group of patients with MVI but no ehs. the aim of this study was therefore to describe outcome and predictors of survival in patients with hcc and MVI but no extra-hepatic spread treated with sorafenib.
Methods: 67 patients with hcc and macro-vascular invasion but no extra-hepatic spread treated with sorafenib were identified in the database of 4 french centers (Bondy, créteil, Grenoble,Villejuif) and retrospectively studied.
results: Patients were mostly males (88.1%), mean age 65.5±9.6 with underlying cirrhosis (89.4%). etiology of liver disease was alcohol ±nash (38.8%), viral hepatitis (35.8%), nash without
alcohol (14.9%), other (10.4%). child-Pugh score was a and B in 59 (86.4%) and 8 (13.6%) patients, respectively. hcc was uni-nodular in 17 patients (25.4%), infiltrative in 32 patients (47.8%), bilobar in 22 patients (33.3%). Median size of the larger nodule was 70 [50-100] mm. Macro-vascular invasion distribution was: Vp1+2 (invasion of or distal to the second order branches of the portal vein (PV)) in 8 patients (12.0%), Vp3 (invasion of 1st order branches of the PV) in 20 patients (30%), Vp4 (invasion of the main trunk of the PV and/or contra-lateral portal vein branch) in 32 patients (47.5%) and hepatic vein±Vp in 7 patients (10.5%). Median afP level at baseline was 408 [32-2695] ng/ml. Median follow up was 6.7 [4.0-15.1] months. Median treatment duration on sorafenib was 6.4 months, and 20 (30%) patients had additional therapies during follow up, either during sorafenib therapy or as second line (including tace, ct, radiotherapy or radioembolization). no patient was transplanted or resected after sorafenib intiation. Median overall survival was 12.6 months (Ic95%: 8.4-16.7). In univariate analysis, afP>1000 uI/L and 1st order branches/troncular portal vascular invasion (Vp3-Vp4) were negatively associated with survival (p=0.049 and 0.031 respectively). In multivariate analysis, both parameters were independently associated with death: afP>1000 (hr 2.188 [1.09-4.41], p=0.029), Vp3-Vp4 (hr 2.874[1.19-6.94], p=0.019). Median overall survival in patients with these 2 prognostic factors was 8.4 [4.2-12.5] months vs 16.9 [11.6-22.2] months in patients with one or none of these prognostic factors (p <0.001) (fig).
Image:
Conclusion: In hcc patients stage BcLc c related to macro-vascular invasion without extra-hepatic spread, afP>1000 uI/L and Vp3-Vp4 macro-vascular invasion are independent predictors of reduced survival. Long-term survival (median 16 months) was observed in patients with one or none of these 2 prognostic factors.
Disclosure of Interest: none Declared
P-262 fACTOrS Of POSTOPerATIVe MOrTALITy In SeLeCTeD PATIenTS WITh reMnAnT LIVer VOLuMe TO bODy WeIGhT rATIO exCeeDInG 0.5%
Lena M'ba Assonzock* 1, Badr serji2, olivier farges3, yves Patrice Le treut4, jean-Marc regimbeau5, stéphanie truant1, françois-rené Pruvot1, eric Vibert2, emmanuel Boleslawski1 and achBt french hepatectomy study Group
1chirurgie Digestive et transplantations, chru de Lille-hopital huriez, Lille, 2centre hépato-Biliaire, hôpital Paul Brousse, aPhP, Villejuif, 3chirurgie Digestive et hépato-bilio-pancréatique, hôpital Beaujon, aPhP, clichy, 4chirurgie Générale et transplantation hépatique, chu La timone, Marseille, 5chirurgie Digestive, chu amiens-Picardie, amiens, france
Introduction: Patient-selection on remnant-liver-volume-to-body-weight-ratio (rLVBWr) ≥0.5% for major liver resection has gained increasing popularity. the aim of this study was to determine predictors of postoperative mortality and liver failure when liver resection is performed using this criteria.
Methods: all consecutive patients undergoing liver-resection in 5 hPB-centres were enrolled and patients at high-risk of postoperative-liver-failure (PLf) underwent preoperative ct-scan measurement of remnant-liver-volume and were included. Portal vein embolization (PVe) was used

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 1 4
whenever remnant-liver was estimated to be insufficient. Primary outcome was 90-day mortality. PLf was defined by the 50-50 criteria. Multivariable-regression models were used to identify independent predictors of mortality and PLf in patients with rLVBWr ≥0.5%.
results: from December 2012 to july 2014, 303 patients (sex-ratio 0.57, median age 52 years) undergoing liver volume assessment were included. there were 274 major hepatectomies and 36 re-hepatectomies. underlying liver was healthy in 115 patients. chemotherapy-induced liver disease, chronic liver disease (f3-f4), cholestatic liver disease and steatosis >30% was observed in 89, 55, 27 and 17 patients respectively. PVe was used in 80 patients, of whom 43% had an initial rLVBWr<0.5%. the median rLVBWr at the time of liver-resection was 0.89%(Iqr 0.42; range: 0.35-2.89) in the entire cohort and 0.86% (Iqr 0.41; range 0.44-2.89) in patients with underlying liver disease. only 6 patients still had a rLVBWr<0.5% at the time of liver-resection. In the 297 patients with rLVBWr≥0.5%, independent predictors of 90-day mortality (7.7%) were age >60 yrs (or=4.47, 95%cI=1.23-16.2, p=0.023) and blood loss >1000 cc (or=5.02, 95%cI=1.82-13.8, p=0.002). In the 185 patients with rLBWr≥0.5% and underlying liver disease, these were diabetes mellitus (or=4.42, 95%cI=1.14-17.1, p=0.032), duration of surgery >420 min (or=4.08, 95%cI=1.08-15.4, p=0.039) and blood loss >1000 cc (or=7.82, 95%cI=1.93-31.7, p=0.004). In patients with rLVBWr ≥0.5%, rLVBWr was not predictive of 90-day mortality (rLVBWr=0.80% vs. 0.90%; p=0.49), including in the group with underlying liver disease (rLVBWr=0.84% vs. 0.87%; p=0.91), and rLVBWr was also not different in the 11 patients with PLf (0.80 vs. 0.86; p=0.94).
Image:
Conclusion: rLVBWr≥0.5% could be safely used to select patients undergoing liver-resection, even in the presence of underlying liver disease. no other remnant-liver-volume cut-off was identified in this study to better predict postoperative outcome.
Disclosure of Interest: none Declared
P-263 IMPACT Of POST-PrOGreSSIOn SurVIVAL In SOrAfenIb-fAILeD PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA
Sadahisa Ogasawara* 1, tetsuhiro chiba1, yoshihiko ooka1, naoya kanogawa1, tomoko saito1, tenyu Motoyama1, eiichiro suzuki1, akinobu tawada1, osamu yokosuka1
1Department of Gastroenterology and nephrology, Graduate school of Medicine, chiba university, chiba, japan
Introduction: there are few reports of progress variations and prognostic factors after progression in sorafenib-failed patients with advanced hepatocellular carcinoma (hcc).
Methods: this was a prospective study on child-Pugh a and B patients with advanced hcc who were treated with sorafenib at chiba university hospital. We analyzed 1) the correlation of patient characteristics between baseline and at the time of progression and 2) the prognostic factors for survival from the date of sorafenib failure (post-progression survival, PPs).
results: of the 89 enrolled patients, 70 were diagnosed to have disease progression according to the response evaluation criteria in solid tumors criteria version 1.1. of the 36 patients with child–Pugh a5, 13 progressed to child–Pugh a6 at the baseline, whereas 2 progressed to child–Pugh B at the time of progression. of the 11 patients with child-Pugh a6, 3 progressed to child-Pugh B at the time of progression. at the baseline, 30 patients were without macrovascular invasion (MVI) and extrahepatic metastasis (ehM), 7 patients were with MVI (without ehM), 22 patients were with ehM (without MVI), and 11 patients were with MVI and ehM. twenty-six of 30 patients (87%) without MVI and ehM had no MVI and ehM at the time of progression. Multivariate cox’s regression analysis
revealed that child–Pugh score ≥7, MVI, alpha fetoprotein (afP) >400 ng/dL, and new extraheptic lesion at the time of progression were significant predictive factors for PPs.
Conclusion: clinical factors, such as child–Pugh score ≥7, MVI, afP >400 ng/dL, and new extrahepatic lesion at the time of progression predicted poor overall survival in sorafenib-failed patients. these factors may be considered for the stratification of second-line trial.
Disclosure of Interest: s. ogasawara: none Declared, t. chiba: none Declared, y. ooka: none Declared, n. kanogawa: none Declared, t. saito: none Declared, t. Motoyama: none Declared, e. suzuki: none Declared, a. tawada: none Declared, o. yokosuka Grant support from: Bayer yakuhin, Ltd
P-264 effICACy Of SOrAfenIb fOr InTerMeDIATe-STAGe hCC PATIenTS WhO PreVIOuSLy unDerWenT TACe
yutaka yasui* 1, kaoru tsuchiya1, Masayuki kurosaki1, hitomi takada1, Mayu higuchi1, natsuko nakakuki1, nobuharu tamaki1, shoko suzuki1, hiroyuki nakanishi1, jun Itakura1, namiki Izumi1
1Department of Gastroenterology and hepatology, Musashino red cross hospital, Musashino-city, japan
Introduction: survival benefits have been clearly shown with sorafenib treatment in patients with advanced-stage nonresectable hepatocellular carcinoma (hcc). on the other hand, the efficacy of sorafenib in patients with intermediate-stage hcc whose tumors could not be controlled with repeated transcatheter arterial chemoembolization (tace) has not been elucidated. currently, such patients have been categorized as “tace refractory”. the aim of the present study was to clarify the efficacy of sorafenib in patients who have a past treatment history of tace.
Methods: In total, 173 patients who underwent sorafenib therapy at our hospital were retrospectively analyzed. In particular, we evaluated 81 patients whose last treatment was tace prior to sorafenib treatment and recorded the time to progression (ttP), overall survival (os), and treatments undertaken after sorafenib failure. the modified recIst criteria were used to evaluate the imaging response of sorafenib.
results: In total, the median ttP was 130 days and the median os was 512 days. of the 81 patients whose last treatment was tace prior to sorafenib, 10 had major vascular invasion (MVI), 12 had extrahepatic spread (ehs), and 1 had both MVI and ehs. of those without MVI, the serum albumin level was significantly lower in patients with a history of tace than in those without it (mean albumin level was 3.4 g/dl and 3.7 g/dl, respectively, p = 0.01). of the 58 patients who had previously been treated with tace and had no MVI or ehs, the median ttP was 131 days and the median os was 489 days. of those patients, 31 received other treatments after sorafenib failure, including 18 with re-tace, 6 with hepatic arterial infusion chemotherapy, and 7 with systemic chemotherapy. there were no significant differences in survival after PD between the 18 patients who underwent re-tace and those with other therapies after sorafenib PD (median survival time was 587 days and 387 days, respectively, p = 0.34).
Conclusion: for patients with recurrent intrahepatic hcc that could not be controlled with tace, sorafenib showed a median os of 16 months. In such patients, the serum albumin level declined compared with the patients who had no previous tace history. although evaluated as tace refractory at the initiation of sorafenib, re-tace after sorafenib PD could be a treatment of choice. however, the clinical features of patients who could benefit from re-tace remain unclear and need further study.
Disclosure of Interest: none Declared
P-265 InDICATIOn AnD uSefuLneSS Of LIVer hAnGInG MAneuVer fOr MAJOr hePATeCTOMy Of LIVer TuMOr
Masaru Inagaki* 1, koji kitada1, hiroki kajioaka1, naoyuki tokunaga1, hiromi Iwagaki1
1Department of surgery, national organization fukuyama Medical center, fukuyama, japan
Introduction: Liver hanging maneuver is a useful technique in anterior approach of major hepatectomy. however, the impact and application have not been fully investigated. We herein analyzed the indication and usefulness of liver hanging maneuver for major hepatctomy.
Methods: 331 hepatectomy were performed in our institution from March 2003 to september 2014. 45 patients with liver tumor (hepatocellular carcinoma in 18, intrahepatic cholangiocarcinoma in 11, metastatic liver tumor in 5, and the others in 11) considered for major hepatectomy using liver hanging maneuver. the patients were divided into a group with conventional approach(group1), a group with conventional approach with hanging maneuver(group2), and a group with anterior approach with hanging maneuver(group3). Group 2 included relative indication of hanging maneuver for major hepatectomy with or without caudate lobe resection. Group 3 included absolute indication of liver hanging maneuver, such as huge liver tumor with difficulty of mobilization, tumor thrombosis in inferior vena cava and tumor invasion into diaphragm.
results: We introduced liver hanging maneuver from March 2003. Group 1 included 42 caes (5 right hepatectomy, 4 extended right hepatectomy,, 6 right trisegmentectomy 11 left hepatectomy

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 1 5
15 extended left hepatectomy, and left 1 trisegmentectomy). Group 2 included 34 cases (10 right hepatectomy, 5 extended right hepatectomy,, 1 left hepatectomy, 15 extended left hepatectomy, 2 trisegmentectomy and 1 sectionectomy). Group 3 included 11 cases (4 right hepatectomy, 3 extended right hepatectomy,, 2 left hepatectomy, 1 extended left hepatectomy,right and 1 trisegmentectomy). Indications of Group 3 were huge liver tumor with difficulty of mobilization in 9, tumor thrombosis in inferior vena cava in one and tumor invasion into diaphragm in 3. operative Blood loss in group 2 was significantly fewer than in group 3 (group2: 954.8±716.0, group3:1770.9±1084.2, p=0.038). operative Blood loss of right hepatectomy in group 2 was fewer than in group 1 (p=0.10). operation time of left hepatectomy in goup 2 were longer than group 1 (p=0.14).
Conclusion: Liver hanging maneuver facilitates anterior approach of major hepatectomyfor liver tumor. In conventional right hepatectomy, operative blood loss can be decreased using liver hanging maneuver. In left hepatectomy, liver hanging maneuver is useful in cases with simultaneous caudate lobectomy, without increasing blood loss.
Disclosure of Interest: none Declared
P-266 SArCOPenIA IS An InDePenDenT PrOGnOSTIC fACTOr fOr ADVAnCeD hePATOCeLLuLAr CArCInOMA
Saori Kamachi* 1, taiga otsuka1, kaori Gotanda1, akihito kubotsu1, norimasa araki1, kenichiro Murayama1, hiroshi Isoda1, futa koga1, shunya nakashita1, Iwata ozaki1, yuichiro eguchi1, keizo anzai1
1Division of hepatology, Diabetes, Metabolism and endcrinology, saga university hospital, saga, japan
Introduction: sarcopenia, defined as low level skeletal muscle mass, is often observed in patients with liver cirrhosis. sarcopenia was recently reported to related to poor prognosis in patients with hepatocellular carcinoma (hcc) after curative treatment. this study investigated the correlation between sarcopenia and prognosis in patients with advanced hcc ineligible to curative surgery or locoregional therapy.
Methods: this study included consecutive patients with advanced hcc who were treated with sorafenib or hepatic arterial infusion chemotherapy (haIc) between april 2004 and May 2013. skeletal muscle index at the third lumbar vertebrae (L3 sMI) was determined on computed tomography scans. sarcopenia was defined by using sex-specific cut-off (L3 sMI <40.0 cm2/m2 for women; <45.0 cm2/m2 for men).
results: thirty-six patients were included in this study, including 24 treated with sorafenib and 12 with haIc. twenty-eight patients (78%) were men, and median age was 65 years (range 32-81 years). Median L3 sMI was 45.9 cm2/m2 (range 25.8-68.9 cm2/m2). sarcopenia was observed in 13 patients, 8 men (32%) and 4 women (50%). the median survival times were 8.3 months in sarcopenic patients and 19.4 months in non-sarcopenic patients (P = 0.04). the 1- and 3-year survival rates were 33% and 0%, respectively, in sarcopenic patients and 69% and 35%, respectively in non-sarcopenic patients. univariate cox regression analysis showed that sarcopenia (hazard ratio [hr], 2.67; 95% confidence interval [cI], 1.07-6.65; P = 0.04) and child-Pugh class B (hr, 2.53; 95% cI, 0.93-6.85; P = 0.05) were correlated with survival. Multivariate cox regression analysis showed that sarcopenia was independently prognostic factor for survival in patients with advanced hcc (hr, 2.83; 95%cI, 1.13-7.09; P = 0.03).
Image:
Conclusion: sarcopenia is an independent prognostic indicator of survival for patients with advanced hcc treated with sorafenib or haIc.
Disclosure of Interest: none Declared
P-267 uS-uS fuSIOn IMAGInG In rADIOfrequenCy AbLATIOn TherAPy fOr hePATOCeLLuLAr CArCInOMA
yasunori Minami* 1, tomohiro Minami1, Masatoshi kudo1
1Gastroenterolgy and hepatology, kinki university faculty of Medicine, osaka-sayama, japan
Introduction: It is often difficult to assess the ablation margin of radiofrequency ablation (rfa) therapy on ultrasonography (us). therefore, contrast-enhanced ct or MrI is widely performed a few days after rfa for early treatment response assessment in japan. In contrast, us-us fusion imaging can display the synchronous images of before/after rfa side-by-side according to the us probe action, and ablation margin of rfa might be evaluated three-dimensionally immediately after rfa. this study investigated the effectiveness of us-us fusion imaging in rfa for hcc.
Methods: Between july 2014 and february 2015, 27 patients (19 men, 8 women) with 31 hypervascular hccs were enrolled. Before ablation, three dimensional volume data of us were obtained by sweep scanning, and we traced the edge of hcc for coloring the entire tumor on the data. after ablation, a hyperechoic area was seen on B-mode us. us-us fusion imaging showed the synchronous images of before/after rfa side-by-side after images registration. Moreover, an overlay of us images before/after rfa could reveal an ablation margin three-dimensionally by showing the colored tumor inside hyperechoic area.
results: the maximal diameters of all tumors ranged from 0.7 to 1.8 cm (mean, 1.3 cm) on us. complete tumor necrosis was achieved by a single session of rf ablation in all patients. We did not encounter local tumor progression and severe complication during the observation period.
Conclusion: us-us fusion imaging in rfa is an efficient approach for hccs, and have potential to cancel early ct/MrI assessment of treatment response if ablation margin could be accurately evaluated by us-us fusion imaging immediately after rfa.
Disclosure of Interest: none Declared
P-268 A neW fOrMuLA fOr CALCuLATInG STAnDArD LIVer VOLuMe WIThOuT uSInG bODy WeIGhT
Takashi Kokudo* 1, kiyoshi hasegawa1, emilie uldry2, junichi kaneko1, nobuhisa akamatsu1, yoshihiro sakamoto 1, nicolas Demartines2, norihiro kokudo1, nermin halkic2
1hepato-Biliary-Pancreatic surgery Division and artificial organ and transplantation Division, Department of surgery, Graduate school of Medicine, the university of tokyo, tokyo, japan, 2Department of surgery, university hospital chuV, Lausanne, switzerland
Introduction: the standard liver volume (sLV) is widely used in liver surgery, especially for living donor liver transplantation (LDLt). all the reported formulas for sLV use body surface area or body weight, which can be influenced strongly by the general condition of the patient.1
Methods: We analyzed the liver volumes of 180 japanese donor candidates and 160 swiss patients with normal livers to develop a new formula. the dataset was randomly divided into two subsets, the test and validation sample, stratified by race. the new formula was validated using 50 LDLt recipients.
results: Without using body weight-related variables, age, thoracic width measured using computed tomography (figure), and race independently predicted the total liver volume (tLV). a new formula: 203.3 - (3.61 × age) + (58.7 × thoracic width) - (463.7 × race [1 = asian, 0 = caucasian]), most accurately predicted the tLV in the validation dataset as compared with any other formulas. the graft volume for LDLt was correlated with the postoperative prothrombin time, and the graft volume/sLV ratio calculated using the new formula was significantly better correlated with the postoperative prothrombin time than the graft volume/sLV ratio calculated using the other formulas or the graft volume/body weight ratio.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 1 6
Image:
Conclusion: the new formula derived using the age, thoracic width and race predicted both the tLV in the healthy patient group and the sLV in LDLt recipients more accurately than any other previously reported formulas.
references: 1. Pomposelli jj, tongyoo a, Wald c, Pomfret ea. Variability of standard liver volume estimation versus software-assisted total liver volume measurement. Liver transpl 2012;18:1083-1092.
Disclosure of Interest: none Declared
P-269 effICACy Of COnTInuOuS SOrAfenIb TreATMenT AfTer rADIOLOGICAL COnfIrMATIOn Of DISeASe PrOGreSSIOn In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA
yoshiyuki Wada* 1, 2, yuko takami1, 2, Masaki tateishi1, 2, tomoki ryu1, 2, kazuhiro Mikagi1, 2, hideki saitsu1, 2
1Department of hepato-Biliary Pancreatic surgery, 2clinical research Institute, national hospital organization kyushu Medical center, fukuoka, japan
Introduction: the survival benefits of sorafenib treatment for advanced hepatocellular carcinoma (hcc) have already been established. sorafenib improves the overall survival of hcc patients in the absence of an objective response. the cytostatic characteristics of sorafenib may be different from those of cytotoxic anticancer agents that cause tumor shrinkage. In the sharP and asia–Pacific trials, the sorafenib treatment was permitted until symptomatic disease progression. In addition, the sorafenib treatment until symptomatic disease progression (PD) revealed statistically significant survival improvement. We hypothesized that radiological PD may not be recognized as a criterion for discontinuing the sorafenib treatment. the purpose of this study was to clarify the effectiveness of continuous sorafenib treatment after radiologically confirmed PD.
Methods: from june 2009 to December 2013, a retrospective study investigated the effectiveness of continuous sorafenib treatment in 90 patients with advanced hcc after the confirmation of radiological PD using the modified response evaluation criteria in solid tumors. the overall survival and progression-free survival was assessed. furthermore, subgroups were analyzed to determine clinical factors relevant to survival benefits for continuous sorafenib treatment after radiologically confirmed PD.
results: of the 90 patients with radiologically confirmed PD, 50 patients continued to receive the sorafenib treatment, whereas 40 patients discontinued the treatment. all patients with continuous sorafenib treatment were treated with the same dosage of sorafenib after radiologically confirmed PD. the mean survival time post-initial PD in the former group (13.0 months) was longer than that in the latter group (4.4 months; p = 0.008). In the continuous sorafenib treatment group, time to progression (ttP) post-initial PD was 2.4 months. ttP post-initial PD of the patients with initial ttP of >4 months was superior compared with that of the patients with an initial ttP of <4 months (4.2 months and 2.1 months, respectively, p < 0.001). furthermore, the subgroup analysis showed
a statistically significant survival benefit for continued sorafenib treatment post-radiological PD in the following groups: eastern cooperative oncology Group (ecoG) performance status (Ps) 0 or 1 at confirmation of disease progression (p = 0.048), extrahepatic spread (p = 0.02), and no macrovascular invasion (p = 0.02).
Conclusion: continued sorafenib treatment upon radiologically confirmed PD improved the survival of patients with advanced hcc, particularly those with an initial ttP of >4 months. therefore, continued sorafenib treatment should be considered for patients with ecoG Ps 0 or 1, those with extrahepatic spread, and/or those without macrovascular invasion.
Disclosure of Interest: none Declared
P-270 neOADJuVAnT TherAPy fOr InTrAhePATIC TuMOrS befOre SOrAfenIb ADMInISTrATIOn PrOLOnGS SurVIVAL TIMe Of hePATOCeLLuLAr CArCInOMA WITh exTrAhePATIC MeTASTASIS
yohei Kooka* 1, hiroaki nagamatsu1, masaru Morita1, Masahito nakano2, takuji torimura2
1Department of Gastroenterology and hepatology, yame General hospital, yame, 2Division of Gastroenterology, kurume university school of Medicine, kurume, japan
Introduction: sorafenib is recognized as a standard treatment for hepatocellular carcinoma (hcc) with extrahepatic metastasis. We retrospectively evaluated the efficacy of treatment for intrahepatic tumors before administration of sorafenib in hcc patients with extrahepatic metastasis.
Methods: from january 2010 to December 2014, one hundred one patients who received the treatment with sorafenib forhcc with extrahepatic metastasis at kurume Liver cancer study Group (kLcsG) were enrolled in the study (mean age, 69.3 years; child-Pugh class a / B, 76 / 25 cases; t3a / t3b ,58 / 43 cases; lung metastasis / other metastases,67 / 34cases). We classified 101 patients to group a and B. Group a patients(n=69) were treated for intrahepatic tumors before administration of sorafenib, group B patients(n=32) were treated with sorafenib solely for hcc with extrahepatic metastasis including intrahepatic tumor stage,t3a or t3b. comparison between the two groups was estimated using Mann-Whitney u test . tumor response by sorfaenib was evaluated with m-recIst. cumulative overall survival (os) after diagnosis of extrahepatic metastasis was estimated using kaplan–Meier survival curves, and os of group a and B was compared using log-rank test.
results: of the 101 patients treated with sorafenib 5, 46 and 50 patients had a Pr, sD and PD, respectively (response rate was 5 %, and disease control rate was 50%.). the 6, 12, 18 and 24 month survival rates were 65%, 41%, 31% and 16%, respectively. the median survival time (Mst) of these patients was 10.6 months. there were no significant differences between group a and group B for age, child-Pugh score, tumor size, tumor stage, metastatic sites, afP and DcP levels and dose of sorafenib. Mst in group a and B was 12.1 months, and 5.5 months, respectively (P<0.001).
Conclusion: neoadjuvant therapy for intrahepatic tumors before administration of sorafenib in hcc patients with extrahepatic metastasis including intrahepatic tumor stage,t3a or t3b was effective.
references: yoo j, Lee sh, Lee M, Lee Dh, cho y, et al. comparison of the effects of transarterial chemoembolization for advanced hepatocellular carcinoma between patients with and without extrahepatic metastases. PLoS One 9(11): e113926. doi: 10.1371/journal.pone.0113926. PMID:25427152hu h, Duan z, Long x, hertzanu y, tong x, xu x, shi h, Liu s, yang z. comparison of treatment safety and patient survival in elderly versus nonelderly patients with advanced hepatocellular carcinoma receiving sorafenib combined with transarterial chemoembolization: a propensity score matching study. PLoS One 10(2): e0117168. doi: 10.1371/journal.pone.0117168. PMID: 25689846
Disclosure of Interest: none Declared
P-271 ALTerATIOn Of CIrCuLATInG MICrOrnA In hePATOCeLLuLAr CArCInOMA PATIenTS TreATeD WITh TrAnSArTerIAL CheMOeMbOLIzATIOn
Seong hee Kang* 1, 1, jong eun yeon1, eun jung ko1, young sun Lee1, tae suk kim1, yang jae yoo1, ji hoon kim1, kwan soo Byun1
1Department of Internal Medicine, Division of Gastroenterology and hepatology, korea university college of Medicine, seoul, korea, Guro-gu, seoul, korea, republic of
Introduction: recently, the role of serum microrna (mir) as diagnostic marker for hepatocellular carcinoma (hcc) is suggested by some authors. In hcc, elevation of many mir including 122, 221, 224 compared with Lc were reported. also, reduction of serum mir 21 was shown in hcV related hcc after surgical resection. although, there were few studies focus on changing circulating mir level after the hcc treatment, for hcc, alteration of serum mir in hcc patients treated with tace which are the most common treatment modality for hcc are sparse. the present study is aimed to investigate the change of serum mirna level after tace and its role in as predictor for treatment response.

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 1 7
Methods: 116 serum samples were used for analysis. Before and after the tace, 76 serum samples from 38 patients with hcc were collected and 40 serum samples from 20 patients with chronic hepatitis B and/or liver cirrhosis without hcc were used as a control. three mirs (mir-221, 224 and 18a) which showed significant changes in previous study were selected. the exosomes in serum samples before and after tace from hcc patients and liver cirrhosis patient without hcc were isolated and total rna was purified from the exosomes. the expression levels of the three target mirnas were analyzed by quantitative real-time polymerase chain reaction. treatment response was determined by mrecIst.
results: according to mrecIst, treatment response after tace were follow as; no response (6, 15.8%), partial response (14, 36.8%) and complete response (18, 47.4%). In hcc group, serum mir after the tace compared with baseline were significantly reduced for mir-224 (0.62 vs. 1 fold, P=0.002) and 18a (0.69 vs. 1 fold, P<0.001). the serum mir-221 was tended to be reduced after tace although it has no statistical significance (0.76 vs. 1 fold, P=0.089). In contrast, the fold change in expression of serum mir-221 (P=0.501), mir-224 (P=0.223) and 18a (P=0.491) were not significantly changed in control group (P=ns). changes of serum mirs tend to be correlated in predicting the tace response, although it has not statistical significance.
Conclusion: serum mirs including 224 and 18a had diagnostic significance in hcc patients. also, the serum mir was significantly decreased after tace in hcc patients. therefore, circulating mirs might be the promising marker for hcc treatment, although it has no statistical significance in predicting treatment response.
references: 1) Borel f, konstantinova P, jansen PL. Diagnostic and therapeutic potential of mirna signatures in patients with hepatocellular carcinoma. j hepatol 2012;56:1371-832) Meng f, henson r, Wehbe-janek h, et al. Microrna-21 regulates expression of the Pten tumor suppressor gene in human hepatocellular cancer. Gastroenterology 2007;133:647-583) Wang y, Lee at, Ma jz, et al. Profiling microrna expression in hepatocellular carcinoma reveals microrna-224 up-regulation and apoptosis inhibitor-5 as a microrna-224-specific target. j Biol chem 2008;283:13205-15
Disclosure of Interest: none Declared
P-272 COMPArISOn Of The CLInICAL OuTCOMeS beTWeen STereOTACTIC bODy rADIATIOn TherAPy AnD hyPOfrACTIOnATeD rADIATIOn TherAPy fOr InOPerAbLe hePATOCeLLuLAr CArCInOMA
Seung heon Lee* 1, kyu chan Lee1, seok ho Lee1, kihoon sung1
1Department of radiation oncology, Gachon university Gil Medical center, Incheon, korea, republic of
Introduction: the objective of this study was to compare the clinical outcomes between stereotactic body radiation therapy (sBrt) and moderate hypofractionated (fraction size of 3-5 Gy) radiation therapy (rt) for inoperable hepatocellular carcinoma.
Methods: Between january, 2010 and august, 2014, 42 intrahepatic lesions in 40 hepatocellular carcinoma patients were treated. at first, sBrt treatment planning was performed in all patients adopting the constraint that at least 700 mL of normal liver should not receive a total dose > 17 Gy for patients with child-Pugh score of 5 and > 15 Gy with child-Pugh score of 6 or more. If the dosimetric result of the sBrt plan did not meet the constraint or tumor was located far too close to stomach, duodenum, small bowel, or heart, moderate hypofractionated schedules were used. the constraint in hypofractionated rt group was that mean liver dose was kept less than 28 Gy. twenty-six lesions were treated with sBrt scheme of 45-60 Gy in 4-6 fractions and 16 lesions were treated with hypofractionated rt scheme of 51-60 Gy in 12-20 fractions.
results: the median follow-up duration was 19.2 months. the response rates for sBrt group and hypofractionated rt group were 100% and 62.5%, respectively. the two-year local control rates for sBrt group and hypofractionated rt group were 96.2% and 44.7% (p=0.0001), and the overall survival rates were 89.5% and 40.1% (p= 0.0001), respectively. the two-year regional progression free survival rates for two groups were 50.8% and 24.3% (p=0.2026), respectively. Multivariate analysis showed that sBrt (p= 0.003), local control (p= 0.014), regional control (p= 0.018), tumor volume (p= 0.023), tumor diameter (p= 0.034), and response (p= 0.040) were independent predictors of overall survival and sBrt (p= 0.029) was the only independent predictor of local control.
Conclusion: We confirmed efficacy of sBrt for inoperable hepatocellular carcinoma. the significant correlation between local control and sBrt and between overall survival and local control supports the clinical value of sBrt in these patients
references: 1. seo ys, kim Ms, yoo sy, cho ck, choi cW, kim jh, et al. Preliminary result of stereotactic body radiotherapy as a local salvage treatment for inoperable hepatocellular carcinoma. j surg oncol. 2010;102(3):209-14.2. son sh, choi Bo, ryu Mr, kang yn, jang js, Bae sh, et al. stereotactic body radiotherapy for patients with unresectable primary hepatocellular carcinoma: dose-volumetric parameters
predicting the hepatic complication. International journal of radiation oncology, biology, physics. 2010;78(4):1073-80.3. andolino DL, johnson cs, Maluccio M, kwo P, tector aj, zook j, et al. stereotactic body radiotherapy for primary hepatocellular carcinoma. International journal of radiation oncology, biology, physics. 2011;81(4):e447-53.4. kim jy, yoo ej, jang jW, kwon jh, kim kj, kay cs. hypofractionated radiotheapy using helical tomotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. radiation oncology. 2013;8:15.5. scorsetti M, comito t, cozzi L, clerici e, tozzi a, franzese c, et al. the challenge of inoperable hepatocellular carcinoma (hcc): results of a single-institutional experience on stereotactic body radiation therapy (sBrt). j cancer res clin oncol. 2015.
Disclosure of Interest: none Declared
P-273 COMbInATIOn Of SOrAfenIb AnD COnVenTIOnAL TrAnSArTerIAL CheMOeMbOLIzATIOn In ADVAnCeD STAGe hePATOCeLLuLAr CArCInOMA
Joerg Trojan* 1, Markus Göller2, eckart schott3, oliver Waidmann1, Martin Welker1, k fischer4, L schmidt4, P Paprottka4, s zangos1, t Vogl1, W Bechstein1, s zeuzem1, frank kolligs4
1universitätsklinikum frankfurt, frankfurt, 2universitätsklinikum erlangen, erlangen, 3universitätsmedizin Berlin, Berlin, 4klinikum der universität München, München, Germany
Introduction: sorafenib is the standard of care in patients with advanced Barcelona Clinic Liver Cancer (BcLc) stage c. although prospective, randomized results on the use of selective, lipiodol-based, conventional transarterial chemoembolization (ctace) either alone or in combination with sorafenib in BcLc stage c are lacking, ctace has been reported to allow a better local tumor control in selected patients. the aim of this study was to analyze efficacy and tolerability of the use of sorafenib and tace either alone or in combination in a cohort of BcLc-c patients at three large German liver centers in clinical routine.
Methods: retrospective cohort-study of patients with advanced hcc treated with sorafenib and ctace, or sorafenib or tace alone between january 2007 and november 2012. this cohort analysis was performed to compare these three treatment options with respect to efficacy and safety. the study was approved by the local ethical committees
results: a total of 201 patients with advanced hcc were included in this retrospective analysis. Patients have been treated with the combination of sorafenib and ctace (group a; n=54), sorafenib (group B; n=82) or ctace (group c; n=65) according to the choice of the treating liver center. the median age of patients was 64, 66 and 67 years, and 87%, 88% and 82% of patients were male, respectively. In group a, B and c PVI was present in 33%, 33% and 38% of the patients and ehs was present in 41%, 46% and 34%. the median cLIP score was equal between patient cohorts. Median time-to-progression was 7.0 months (95% cI: 4.3-9.7), 4.1 months (95% cI: 3.6-4.7) and 5.0 months (95% cI: 2.9-7.1) in groups a, B and c. Median overall survival was 16.5 months (95% cI: 15.0-18.1), 8.4 months (95% cI: 6.0-10.8) and 10.5 months (95% cI: 7.5-13.6), respectively. the incidence of toxicity was not increased by the combination of ctace and sorafenib. the most common sorafenib-associated aes were diarrhea, hand-foot-skin reactions, and fatigue with no significant increase in group a compared to group B. the most common ctace-related aes were abdominal pain, nausea, fevers, ascites, and fatigue.
Conclusion: ctace is frequently used as additional locoregional treatment in selected patients. the combination of ctace and sorafenib resulted in a substantial overall survival benefit in selected patients in in clinical routine with no unexpected side effects.
Disclosure of Interest: j. trojan honoraria support from: Bayer, advisory Board of: Bayer, M. Göller: none Declared, e. schott advisory Board of: Bayer, o. Waidmann: none Declared, M. Welker: none Declared, k. fischer: none Declared, L. schmidt: none Declared, P. Paprottka: none Declared, s. zangos: none Declared, t. Vogl: none Declared, W. Bechstein: none Declared, s. zeuzem: none Declared, f. kolligs advisory Board of: Bayer
P-274 eArLy eVALuATIOn Of ALPhA-feTOPrOTeIn reSPOnSe fOr PreDICTInG OuTCOMeS In SOrAfenIb TreATeD PATIenTS MAy be MISLeADInG
Giovan Giuseppe Di Costanzo* 1, raffaella tortora1, filomena Morisco2, filippo Lampasi1, alfonso Galeota Lanza1, Massimo De Luca1, Luigi addario1, Gabriella cordone1, Maria Guarino2, Luigia falco1, Maria teresa tartaglione1, Ioana Grigore1, francesco Paolo Picciotto1, nicola caporaso2
1Department of transplantation - Liver unit, cardarelli hospital, 2clinical Medicine and surgery - Gastroenterology unit, university of naples "federico II", naples, Italy
Introduction: Previous studies have shown that alpha-fetoprotein response (afP-r) can be useful for predicting outcomes in sorafenib treated patients with hepatocellular carcinoma (hcc). however, at what time-point afP-r should be evaluated is not clearly defined. the aim of this study was to compare the performances of afP-r evaluation at 4 and 12 weeks of sorafenib treatment.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 1 8
Methods: from a prospectively maintained database, data of 100 child-Pugh a cirrhotic patients treated with sorafenib for hcc and with a pre-treatment value of afP ≥ 20ng/mL were retrospectively examined. afP-r was defined as the percent change in afP concentration according to the formula (4 or 12 weeks afP – baseline afP)/baseline afP *100. Patients were categorized as either responders or nonresponders on the basis of a decrease in afP concentration >20%. survival was visualized using kaplan–Meier curves and compared by the log-rank test.
results: Median overall survival (os) and time-to-progression were 11 (95%cI, 8.7-13.2) and 10 months (95%cI, 3.0-16.9), respectively. at 12 weeks, radiological response (rr) according mrecIst was observed in 72.5% of cases: 3 complete response, 26 partial response, and 37 stable disease. at 4 weeks, 39 patients had positive afP-r; of these, 14 (35.9%) were nonresponders at week 12. among 66 nonresponders at week 4, 9 (14.7%) patients were responders at week 12. at this time-point, 34 patients were responders. afP-r at 4 weeks was unrelated both to os (12 vs 9 months, p=.132) and ttP (10 vs 11 months, p=.748). at 12 weeks, afP-r predicted both os (15 vs 9 months, p=.009) and ttP (18 vs 6 months, p=.006). When afP-r was tested in predicting rr, the sensibility and specificity were 42.4% and 96%, predictive positive and negative values were 96.5% and 38.7%, respectively. only 1 among 29 afP responders showed negative rr.
Conclusion: In evaluating afP-r, treatment week 4 is an inadequate time-point. at 12 weeks, afP-r predicted both os and ttP. furthermore, positive afP-r at week 12 has a very high specificity in predicting a good rr.
Disclosure of Interest: none Declared
P-275 ADVAnCeD bCLC-C hePATOCeLLuLAr CArCInOMA (hCC): reAL LIfe reSuLTS frOM The ITA.LI.CA. MuLTICenTre DATAbASe
fabio farinati* 1, Veronica Vanin1 on behalf of Ita.LI.ca., caterina Pozzan1, alessia Gazzola1, francesca Murer1, alessandro Vitale1 on behalf of Ita.LI.ca., umberto cillo1 on behalf of Ita.LI.ca., franco trevisani2 on behalf of Ita.LI.ca.
1Padua university, Padua, 2Bologna university, Bologna, Italy
Introduction: as intermediate stage hcc, also advanced stage hcc (BcLc-c) may include patients with different clinical features and different prognosis. sorafenib is the standard of care in BcLc-c hcc but, due to the heterogeneity of the disease, baseline patients’ characteristics can lead to different therapeutic choices that affect patients’ survival. We aimed at assessing survival in BcLc-c hcc, whether treatments alternative to best supportive care (up to 2008) or sorafenib (from 2008) are used, which are the features of the patients who are treated more aggressively and which are the respective survivals.
Methods: from a series of 5382 patients from the Ita.LI.ca. database, observed from 1986 to 2014, we selected 580 patients with advanced hcc according to the BcLc staging system. In these patients we assessed the main demographic, clinical, and oncological determinants of survival and analysed the reasons beyond the different treatment choices. the patients were subgrouped in 4 time cohorts, the last of which dates from the introduction of sorafenib in the clinical practice (2008).
results: tumor burden, portal thrombosis, child-Pugh class, ascites, ecoG status, afP levels and treatment exerted a significant impact on survival. at cox regression burden, ecoG status, afP and treatment were selected as independent predictors of survival. the best survival results were achieved with radical treatments (surgical resection and percutaneous ablation, 10%) (median survival 11 months, I.c. 5-17, then with palliative therapies such as tace/tae (16%, 10 months, I.c. 6-14) or sorafenib. the drug was administered to 69 patients, 27% overall of the last cohort, with median survival of 8 months, I.c. 6-10, but in the cohort eligible patients were in fact 136 and only 50% were treated with sorafenib. In the group of patients treated with more radical treatments, the baseline characteristics that influenced the treatment choice and os were tumor burden, with more frequent monofocal lesions in patients treated more aggressively (p<0.001), and bilirubin levels (p=0.033). on the other hand, with respect to patients treated with Bcs, worse clinical features, such as child-Pugh class B (p=0.001), Ps 2 score (p<0.001), presence of ascites (p<0.001), bilirubin levels (p= 0.001) and again tumour burden (p<0.001) were significantly more frequent.
Conclusion: some BcLc-c patients, on the basis of their clinical features, can be aggressively treated and this leads to an improved survival. sorafenib is used in a lower than expected proportion of patients. however, if patients’ clinical features are permissive, sorafenib is useful and confers a significant gain in terms of survival when compared to Bsc.
Disclosure of Interest: none Declared
P-276 enOS POLyMOrPhISMS In reLATIOn TO OuTCOMe In ADVAnCeD hCC PATIenTS reCeIVInG SOrAfenIb
Andrea Casadei Gardini* 1, Giorgia Marisi1, Luca faloppi2, Mario scartozzi3, Paola ulivi1, francesco Giuseppe foschi4, stefano tamberi5, Giovanni Luca frassineti1
1Irst-Irccs, forli, 2universita di ancona, ancona, 3universita cagliari, cagliari, 4Medicina interna, 5oncologia, faenza, Italy
Introduction: cancer cells adapt to hypoxic microenvironment through the activation of many molecules, including endothelial nitric oxide synthase (enos). sorafenib, by blocking the vascular endothelial growth factor receptors (VeGfrs), inducesan inhibition of enos activity with a consequent decrease of the production of nitric oxide (no). no is associated with an increase of tumor angiogenesis, tumor invasion and metastasis formation. In our study we analysed the role ofenos polymorphisms in relation to clinical outcome in patients with hepatocellular carcinoma treated with sorafenib.
Methods: from a database of 257 patients diagnosed with hepatocellular carcinoma from 2004 to 2014. Peripheral blood samples or ffPe tumor tissues were available for Dna extraction and genotyping analysis. three enos polymorphisms(enos +894 G/t, enos Vntr 27bp 4a/b, enos -786 c/t) were analyzed by direct sequencing or real time Pcr method.We analyzed 68 patients for -786 c/t polymorphism. all the candidate genotypes were evaluated to identify a potential correlation with progression free survival (Pfs) and overall survival (os)
results: With regard enos-786 the presence of the t allele both in homozygosity (tt) and in heterozygosity(tc) was associated with a statistically significant longer Pfs with respect to patients with cc genotype (6.0 versus 2.6 months,respectively, p < 0.0001). no correlations were observed in relation to os (p = 0.368).
Conclusion: enos -786 could represent prognostic markers in patients with advanced hepatocellular carcinoma treated with sorafenib.
Disclosure of Interest: none Declared
P-277 A COMPArISOn Of SurVIVAL Of PATIenTS WITh hePATOCeLLuLAr CArCInOMA AnD POrTAL VeIn InVASIOn TreATeD by rADIOeMbOLIzATIOn Or SOrAfenIb
Manuel de la Torre* 1, juan Buades-Mateu1, Pedro de la rosa2, alberto Lué3, javier Bustamante4, M trinidad serrano3, Milagros testillano4, sara Lorente3, alexandra Gomez5, juan I. arenas5, Mercedes Iñarrairaegui6, Bruno sangro6
1clínica universidad de navarra, 2complejo hospitalario de navarra, Pamplona, 3hospital universitario Lozano Blesa, zaragoza, 4hospital universitario de cruces, Bilbao, 5hospital universitario Donostia, san sebastián, 6clinica universidad de navarra and cIBerehD, Pamplona, spain
Introduction: Based on the results of randomized controlled trials, Western scientific guidelines recommend sorafenib (sor) as the treatment for hepatocellular carcinoma (hcc) with portal vein invasion (PVI). In phase 2 trials, radioembolization (re) using yttrium-90 microspheres has shown high response rates and prolonged survival. re is thus used in some centers as first line treatment for PVI patients, with sor initiated upon progression. our main aim was to compare the survival of hcc patients with PVI treated by re or sor in a cohort in which treatment allocation depended basically on the treating hospital.
Methods: all hcc patients with PVI treated in 4 spanish hospitals between 2005 and 2013 with re or sor were retrospectively analyzed. re is only performed in 1 hospital in which it was considered first option for these patients. survival curves were calculated from the initiation of sor or the date of re using kM method and compared using logrank test. a multivariate prognostic model including those variables identified in the univariate analysis was generated using cox regression analysis and it was adjusted by a propensity score based on those factors identified as determinants of the probability of exposure to re again by cox regression analysis.
results: 73 patients were studied (26 treated by re and 47 by sor). Both groups were only different in the presence of diffuse tumors or with uncountable nodules (re: 38%; sor: 8%; p=0.008) and in the maximal diameter of the main lesion (average: re: 106 mm; sor: 65 mm; p=0.005). components of the propensity score were tumor size, extrahepatic disease, diffuse tumor, bilirubin > 2 mg/dL and nLr. In the re group, 14 patients received sor after a median of 4.9 months (Iqr: 1.9-9.6) after re. Global median overall survival was 6.7 months (95%cI 5.2-8.1). survival was significantly better in the re group when the patients in the re were censored at the time of starting sor [re: 22.8 months (95%cI 3.1-42.5) vs. sor: 5.4 months (95%cI 2.7-8.1); p=0.007] or not [re: 8.8 months (95%cI 1.8-15.8) vs. sor: 5.4 months (95%cI 2.7-8.1); p=0.04]. the multivariate model adjusted by propensity score identified the following variables as having independent prognostic power: re [hr: 0.42 (0.23-0.0.77); p=0.005], ecoG=2 [hr: 3.25 (1.57-6.72); p=0.001] and bilirubin > 2 mg/dL [hr: 2.66 (1.33-5.32); p=0.006].
Conclusion: In a cohort of patients with hcc and PVI, first line treatment with re was associated with a more prolonged survival compared to sor. this finding warrants randomized clinical trials in the same patient population.
Disclosure of Interest: M. de la torre: none Declared, j. Buades-Mateu: none Declared, P. de la rosa: none Declared, a. Lué: none Declared, j. Bustamante: none Declared, M. t. serrano: none Declared, M. testillano: none Declared, s. Lorente: none Declared, a. Gomez: none Declared, j. arenas: none Declared, M. Iñarrairaegui honoraria support from: Bayer healthcare and sirtex Medical, B. sangro honoraria support from: Bayer healthcare and sirtex Medical, advisory Board of: Bayer healthcare and sirtex Medical

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 1 9
P-278 SurVIVAL benefIT frOM CO-ADMInISTereD beTA bLOCKer AnD COx-2 InhIbITOr In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA (hCC): A PrOSPeCTIVe CLInICAL TrIAL
Gouri Shankar bhattacharyya* 1, shailesh a. Bondarde2, Ghanashyam Biswas3, Govind Babu4, Debasis Datta5, newell Bascomb6, hemant Malhotra7
1Medical oncology, fortis hospital, kolkata, 2Medical oncology, shatabdi super specialty ospital, nashik, 3Medical oncology, sparsh hospital and critical care, Bhubaneshwar, 4Medical oncology, kidwai Memorial Institute of oncology, Bangalore, 5fortis hospital, kolkata, India, 6Vicus therapeutics, Morristown, united states, 7Medical oncology, sMs Medical college hospital, jaipur, India
Introduction: Preclinical and clinical reports in various solid tumors report an improvement in overall survival when patients are taking beta blockers and/or selective nsaIDs (cox-2 inhibitors). Data reported previously on the use of the beta blocker propranolol (P) and the partially selective cox-2 inhibitor etodolac (e) administered with sorafenib (s) in advanced hepatocellular carcinoma patients showed a significant improvement in survival and a reduction in inflammatory related side effects. the co-administration of P and e is thought to target the regulation of the neuro-immune systems activated in cancer that induce changes in tumor microenvironment, immune system balance, and hPa axis leading to tumor promotion and immune tolerance. the current study evaluates the impact of the co-administration of P and e on the clinical outcome in advanced hcc patients compared to patients receiving s as standard of care first line therapy.
Methods: Patients with advanced hcc were eligible for this investigator initiated study. Patients who were not able to receive or tolerate sorafenib received Pe by mouth daily. the timing of Pe administration was designed to maximize the therapeutic benefit and minimize side effects such as sleep disturbance and alteration of the diurnal melatonin cycle. the primary endpoint was survival. twenty-three patients were randomized to either sorafenib alone (Group s, n=12) or propranolol and etodolac (Group Pe, n=11). the median age was 54.6 and 54.9 years for s and Pe, respectively. the patients were predominantly hepatitis B virus positive and cirrhotic status child-Pugh B. c-reactive protein (crP) was 71.6 in Group s and 72.6 in Group Pe. the population was well-balanced between arms.
results: twelve month survival was 18.2% (2/11) for Group s and 36.4% (4/11) for Group Pe. Median survival for patients in Group s was 9.6 months and 11.0 month for patients in Group Pe. hand foot skin reaction, a major dose-limiting toxicity for sorafenib, was present at grade 2 or 3 in 72.7% of Group s and none in Group Pe. the Pe treatment was well-tolerated with no unexpected adverse events.
Conclusion: administration of Pe increased 12 month survival and median overall survival compared to patients receiving sorafenib without any safety concerns. no unexpected adverse reactions were seen. additional studies on the use of this combination in patients with hcc is warranted.
Disclosure of Interest: G. s. Bhattacharyya: none Declared, s. Bondarde: none Declared, G. Biswas: none Declared, G. Babu: none Declared, D. Datta: none Declared, n. Bascomb conflict with: Vicus therapeutics, h. Malhotra: none Declared
P-279 rObOT-ASSISTeD LAPArOSCOPIC hePATeCTOMy fOr hePATOCeLLuLAr CArCInOMA: The henrI-MOnDOr exPerIenCe
Chady Salloum* 1, alexis Laurent1, chetana Lim1, compagnon Philippe1, Gérard Pascal1, Daniel azoulay1
194010, hôpital henri Mondor, service de chirurgie hépato-Bilio-Pancréatique et transplantation hépatique. créteil, france., créteil, france
Introduction: Laparoscopic hepatectomy remains technically challenging specially on cirrhosis. the recent introduction of robotic surgical systems has revolutionized the field of minimally invasive surgery in many different surgical specialties in regards to 3-dimensional images and better instrumentations.
Methods: Between july 2011 and november 2014, we performed 15 hepatic resections for hepatocellular carcinoma by robot-assisted laparoscopic approach (left lateral sectionectomy n=5, atypical resection segment 2 n= 2, atypical resection segment 3 n= 3, atypical resection segment 4 n=1, atypical resection segment 5 n=1, atypical resection segment 6 n=3). cirrhosis child Pugh a was present in 14 patients and one patient had a normal liver parenchyma. a Da Vinci robotic surgical system (Intuitive surgical, Mountain View, ca, usa) with three arms was used and two additional laparoscopic ports for the assistant surgeons were added. no Pringle maneuver was used. the dissection was carried out with the bipolar forceps and the harmonic curved shears. In case of left lateral sectionectomy, the division of the vascular pedicles for segments 2 and 3 was performed with endoGIa staplers. Prospectively collected data was analysed retrospectively.
results: overall mean operative time was 170.1 ± 70.5 minutes (range :60-290). overall mean intraoperative blood loss was 208 ± 240 ml (range :20-900). two open conversion (13.3%) were needed due to bleeding. one patients (6.6%) had postoperative complications (biliary fistula treated conservatively). there was no mortality and no reoperations. Mean hospital stay was 5.6 ± 2 days
(range :3-10). all patients had r0 resection with a mean margin of 13.3 ± 16mm (range: 1-65 mm). four patients had resection as a bridge to liver transplantation and were transplanted safely with minimal adhesions at the time of transplantation.
Conclusion: robot-assisted laparoscopic hepatectomy for hepatocellular carcinoma is feasible and safe. further evaluation with clinical trials is required to assess for improvement in outcomes and to validate its real benefits. Long-term oncologic outcomes are still pending.
Disclosure of Interest: none Declared
P-280 hePATOCeLLuLAr CArCInOMA AnD OCCuPATIOnAL enVIrOnMenTAL heAVy MeTALS exPOSure IS There A reLATIOn?
Amal T. A. Ahmed* 1, elsayed elokda2, Mostafaa hamed1, Mohamed shaker1
1tropical medicine, 2community, occupational health and enviromenta medicine, ain shams university, cairo, egypt
Introduction: hepatitis c and B were considered the unique risk factors encountered for hcc however epidemiological studies indicate that human liver is susceptible also to environmental carcinogens including heavy metals. lead and cadmium are two heavy metals widely distributed in the egyptian community especially in rural community. Variety of pesticides, fertilizers in addition to drinking water contamination together with smoking were considered sources of different chemicals especially those two heavy metals. objectives: to determine the possible relation between blood lead and cadmium and hepatocellular carcinoma (hcc).
Methods: Methodology: three groups were included 50 hcc, 50 chronic hepatitis were compared to 50 matched control group. all subjects were asked to fill an interview questionnaire that covers detailed socio-demographic, occupational and environmental risk factors. Gas chromatography was used for measurement of blood heavy metals in whole blood sample
results: Blood cadmium level was higher among hcc group compared to chronic hepatitis group and controls (1.6±0.4, 1.2±0.3 and 1±0.4) respectively with statistically significant difference in between (p0.01). no statistically significant difference between the studied groups as regard blood lead level (14.8±5, 12.5±3.4 and 12±4.7) respectively (p =0.21). cadmium level inversely correlated versus albumin level r=-0.30 and p=0.02. cadmium is positively correlated versus age r=0.32 and p=0.02. on the other hand no statistically significant correlation could be detected between cadmium versus. Lead was positively correlated versus age r=-0.29 and p=0.04. on the other hand no statistically significant correlation could be detected between lead versus other variables p>0.05. no statistically significant difference between males and females as regard lead and cadmium.
Conclusion: cadmium may present an environmental carcinogenic effect on the liver. smoking represents the main environmental source of cadmium among hcc patients.
Disclosure of Interest: none Declared
P-281 A neW TherAPeuTIC ASSeSSMenT SCOre fOr ADVAnCeD hePATOCeLLuLAr CArCInOMA PATIenTS reCeIVInG hePATIC ArTerIAL InfuSIOn CheMOTherAPy PrOPOSAL Of ACTh (ASSeSSMenT fOr COnTInuOuS TreATMenT WITh hAIC) SCOre
Issei Saeki* 1, takahiro yamasaki2, norikazu tanabe1, takuya Iwamoto3, toshihiko Matsumoto1, Isao hidaka1, tsuyoshi Ishikawa3, taro takami1, naoki yamamoto1, Isao sakaida1
1Department of Gastroenterology and hepatology, 2Department of oncology and Laboratory Medicine, 3yamaguchi university Graduate school of Medicine, ube, japan
Introduction: hepatic arterial infusion chemotherapy (haIc) and sorafenib are recommended treatment options for advanced hepatocellular carcinoma (hcc) in japan. We previously reported that the median survival time was significantly shorter in haIc non-responders than in haIc responders (7.2 vs. 17.8 months). Because of the poor prognosis of haIc non-responders, it is important to identify patients who may benefit from continuous haIc treatment. although hcc staging can predict patient prognosis, there are currently no assessment scores to aid decision-making with regard to continuous haIc treatment. therefore, we aimed to establish a new therapeutic assessment score for such patients.
Methods: our institutional review board approved this study. We retrospectively analyzed 90 advanced hcc patients with elevated baseline alpha-fetoprotein (afP, ≥20 ng/mL) and/or des-gamma-carboxy prothrombin (DcP, ≥40 mau/mL) levels (child-Pugh a/B, 75/15; tumor stage II–III/IV according to the Liver cancer study Group of japan criteria, 28/62). Patients received haIc with low-dose cisplatin and 5-fluorouracil. afP and DcP levels were assessed at the end of a half course of haIc (2 weeks), and response was defined as a reduction ≥ 20% from baseline. We analyzed 13 factors (11 pre-treatment factors [age, gender, etiology, child-Pugh class, extrahepatic spread,

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 2 0
tumor stage, pre-treatment, portal vein tumor thrombosis, inferior vena cava invasion, afP level, and DcP level] and 2 factors related to changes between pre-treatment and the end of a half-course of haIc [afP and DcP responses]) as predictors of survival, using the cox proportional hazards model.
results: In multivariate analysis, child-Pugh class a (hazard ratio [hr] 1.99, P = 0.018), afP response (hr 2.17, P = 0.007), and DcP response (hr 1.90, P = 0.030) were independent prognostic predictors. considering the child-Pugh class, afP response, and DcP response, we developed an assessment for continuous treatment with haIc (acth) score, ranging from 0 to 3. Patients stratified into 2 groups according to their acth score showed significantly different prognoses (≤ 1 vs. ≥ 2 points: median survival time, 15.1 vs. 8.7 months; P = 0.003). for patients with a score ≥ 2 after a half course of haIc, switching to a new and more effective treatment may be considered.
Conclusion: the acth score, which considers 3 simple factors, may help in therapeutic assessment for hcc patients receiving haIc, and could make it possible to use a new treatment earlier for non-responders.
Disclosure of Interest: none Declared
P-282 TreATMenT STrATeGy fOr hePATOCeLLuLAr CArCInOMA ACCOMPAnIeD by SeVere POrTAL InVASIOn
hisashi nakayama* 1, tadatoshi takayama1, tokio higaki1, Masamichi Moriguchi1
1Department of Digestive surgery, nihon university school of Medicine, tokyo, japan
Introduction: to investigate the treatment strategy for hepatocellular carcinoma (hcc) accompanied by severe portal invasion.
Methods: sever portal invasions were classified into two groups: Vp3 [invasion of first order branches of the portal vein detected] and Vp4 [invasion of the main trunk of the portal vein and/or contralateral portal vein branch to the primary involved lobe detected]. of 1,318 patients treated between 1990 and 2013, 95 with Vp3-4 hcc underwent surgery (n=22), transcatheter arterial chemoembolization (tace) (n=50) or hepatic arterial infusion (haI) (n=23). surgery was performed for resectable Vp3-4 liver cancer and no residual cancer was left macroscopically. tace was performed in all cases of Vp3 liver cancer using a protocol of 50-100 mg/body Ia-call (or epirubicin) + lipiodol + Gelfoam. haI was used for Vp4 liver cancer based on administration of 5fu at 500 mg/day from a subcutaneously embedded reservoir for 5 days, followed by withdrawal for 11 days; or administration of 50-100 mg/body Ia-call. overall survival and response rates were compared between tumor thrombus stages and among treatment methods.
results: (1) treatment outcomes: the 1-, 3-, and 5-year survival rates of Vp3 cases (n=16) after surgery were 80%, 55%, and 55%, respectively, and those of Vp4 cases (n=6) were 17%, 17%, and 0%, respectively. the median blood loss in all 22 patients was 842 mL (range 120-4,491 mL), the complication rate was 22%, the operative mortality was 0%, and 3 patients survived without recurrence (duration of follow-up: 4-52 months). the tumor recurred in the liver in 14 patients, as a distant metastasis in 5, and as a bile duct tumor thrombus in 1. In patients treated with tace, the response rate was 15% and the disease control rate was 56% (cr/Pr/sD: 1/7/21). In patients treated with haI, the response rate was 21% and the disease control rate was 65% (cr/Pr/sD: 2/3/10). (2) comparison between stages: the mean survival times after surgery in Vp3 and Vp4 cases were 1,913 and 198 days, respectively, but the difference was not significant (p=0.08). the mean survival times of Vp3 and Vp4 cases after non-surgical therapy were 164 and 254 days, respectively, and the outcome of Vp4 cases treated with haI was more favorable than that of Vp3 cases treated with tace. (3) comparison among treatment methods: the outcome of surgery was significantly more favorable than that of tace in Vp3 cases, but there was no significant difference in outcome between surgery and haI in Vp4 cases. the tumor marker level at one month after therapy was evaluated in 35 patients treated with tace, and was reduced by ≥20% in 24 of these patients. similarly, the tumor marker level was evaluated in 17 patients treated with haI, and was reduced by ≥20% in 8 of these patients. the mean survival times of patients with and without this reduction in tumor markers were 281 and 103 days, respectively, after tace (p=0.0012), and 773 and 203 days, respectively, after haI (p=0.0013), showing that the outcomes of the two therapies were more favorable in patients with tumor marker reduction. hepatic arterial chemotherapy was administered as adjuvant therapy after surgery in 8 patients, but had no significant effect on survival compared to surgical patients treated without adjuvant therapy.
Conclusion: these results suggest that the first-line treatment for hcc with portal invasion should be surgery for Vp3 cases and hepatic arterial infusion for Vp4 cases. If tumor markers do not decrease rapidly, another treatment should be considered. the effect of postoperative adjuvant therapy was unclear.
Disclosure of Interest: none Declared
P-283 LOCOreGIOnAL TherAPy VerSuS TrAnSCATheTer ArTerIAL CheMOeMbOLIzATIOn fOr InTerMeDIATe STAGe hePATOCeLLuLAr CArCInOMA PATIenTS
Chika nishioka* 1, takumi akiyama1, yasunori kawaguchi1, Wataru yoshioka1, shunya nakashita1, seiji kawazoe1
1saga japan, saga-ken medical centre koseikan, saga, japan
Introduction: according to the Barcelona clinic Liver cancer (BcLc) staging system, chemoembolization is the first-line treatment for BcLc stage B hepatocellular carcinoma (hcc). It remains unclear whether locoregional therapy such as resection or radiofrequency ablation (rfa) is effective for intermediate stage hcc. therefore, this study was designed to evaluate the effectiveness of locoregional treatment in BcLc stage B hcc.
Methods: We retrospectively investigated 134 consecutive patients who were diagnosed with BcLc stage B hcc from january 2001 to December 2013. twenty-four patients were excluded, because five patients were treated with first-line chemotherapy, 15 lacked data, and four dropped out immediately after treatment. one hundred and ten patients were included in this study. forty-six patients were treated with transcatheter arterial chemoembolization (tace), and the remaining 64 patients were treated with the locoregional therapy: 13 with rfa;27 with rfa+tace;16 with resection;and four each with resection+rfa or resection+tace (Loco group). continuous variables were expressed as median (range). Progression-free survival (Pfs) and overall survival (os) were expressed as median and 95% confidence interval and compared between the two groups.
results: the following baseline characteristics did not differ significantly between the Loco and tace groups: male sex, 82 vs. 78%; α-fetoprotein (afP), 21 (2–706,300 ng/mL) vs. 43 (2–29,851 ng/mL); des-gamma carboxyprothrombin (DcP), 181 (10–50,159 mau/mL) vs. 780 (16–68,300 mau/mL); and tumor diameter, 42 (12–120 mm) vs. 44 (13–158 mm). however, significant differences existed for: age, 72 (26–87 y) vs. 76 (57–85 y) (p<0.05); total bilirubin, 0.8 (0.3–2.0 mg/dL) vs. 0.9 (0.2–2.8 mg/dL) (p<0.01); child–Pugh class (a/B), 61/3 vs. 33/13 (p<0.01); tumor number, 2 (1–11) vs. 4 (1–50) (p<0.01); and tumor distribution(hemi/bilobar), 46/18 vs. 11/35 (p<0.01). Pfs and os between the Loco and tace groups were 13.2 (8.1–18.1) vs. 4.2 (2.6–6.8) (p<0.01), and 45.8 (37.5–54.1) vs. 24.6 (16.0–33.2) (p=0.01), respectively. Predictive factors for Pfs were treatment [locoregional treatment, hazard ratio (hr) 0.55, p<0.05] and DcP values (>320 mau/mL, hr 1.62, p<0.05), and for os, DcP (>320 mau/mL, hr 1.74, p<0.05) and afP (>31 ng/ml, hr 2.09, p<0.01). treatment was not a significant prognostic factor by multivariate analysis (hr 0.70, p=0.25).
Conclusion: Locoregional therapy such as resection or rfa delayed tumor progression, but did not improve os of patients with BcLc stage B hcc.
Disclosure of Interest: none Declared
P-284 ISCheMIC PreCOnDITIOnInG WITh COnTInuOuS CLAMPInG DurInG LIVer reSeCTIOn IS COMPArAbLe WITh InTerMITTenT CLAMPInG Of The hePATODuODenAL LIGAMenT fOr TeMPOrAry InfLOW ObSTruCTIOn
Lileswar Kaman* 1, amritanshu sharma1, arunanshu Behera1, rajinder singh1
1General surgery, PGIMer< chandigarh, India, chandigarh, India
Introduction: surgical resection is the primary modality for treatment of liver cancer. the prime concern in liver resection is to minimize blood loss and to avoid transfusions during surgery. Inflow obstruction by clamping the portal triad can reduce bleeding during parenchymal transection of liver resection. But this maneuver may cause ischemic and reperfusion injury. Intermittent clamping of portal triad (Pringles maneuver) is an established protective strategy against prolonged ischemic injury. Ischemic preconditioning with continuous clamping is also advocated against prolonged ischemic injury during liver resection. But the present knowledge is not sufficient to make a definite decision. this study was done to compare these two techniques in term of blood loss, transfusion requirement, and postoperative liver function tests and outcome in liver resection.
Methods: a total 20 patients scheduled for major liver resection (more than 3 segments of liver) were enrolled. Patients were divided in to two groups group a – (Ischemic preconditioning with continuous clamping) and group B – (Intermittent clamping- Pringles maneuver) by randomization. all patients underwent surgery and resection was done using either of the one technique during parenchymal transection according to the randomization. Intra operative and postoperative variables (immediately after surgery, 3rd, 7th and 10th postoperative day) were compared for the two groups.
results: Demographics and disease profile were comparable in the two groups. all the preoperative parameters were comparable in the two groups. Blood loss during surgery in group a was 605 ml (sD-528.33 ml) and in group- B, was 485 ml (sD-604.63 ml, p 0.251). the liver function tests in the two groups were comparable. the ast and aLt levels were comparable in the post operative day (p 0.134 and p 0.107). the aLP levels were also similar in the two groups (p 0.64). the coagulation profile (prothrombin time) was also comparable in the two groups (p 0.52). the albumin levels were also

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 2 1
similar in the two groups (0.292). the post operative morbidity was similar in the two groups (p 0.56). there was no mortality. the length of post operative hospital stay was not different in the two groups.
Conclusion: this study shows similar results for both these clamping techniques during liver resection.
Disclosure of Interest: none Declared
P-285 hePATIC reSeCTIOn fOr hePATOCeLLuLAr CArCInOMA In PATIenTS WITh renAL DySfunCTIOn
Chikara Shirata* 1, kiyoshi hasegawa1, takashi kokudo1, suguru yamashita1, satoshi yamamoto1, junichi arita1, nobuhisa akamatsu1, junichi kaneko1, yoshihiro sakamoto1, norihiro kokudo1
1hepato-Biliary-Pancreatic surgery Division and artificial organ and transplantation Division, Department of surgery, Graduate school of Medicine, the university of tokyo, tokyo, japan
Introduction: It is well known that preoperative renal dysfunction (rD) is a risk factor for increased morbidity and mortality in patients undergoing vascular and cardiac surgery. as a result of recent advantages in surgical techniques and perioperative management, liver resection has become a safe. however, the effect of preoperative rD on outcomes after hepatectomy for hepatocellular carcinoma (hcc) is unknown. this study aimed to clarify the validity of hepatectomy for hcc in rD patients.
Methods: In this study, we defined preoperative estimated Glomerular filtration rate < 40 mL/min/1.73m2Bsa as rD. In the tokyo university hospital, we performed the first surgical resection for hcc in 713 patients between october 2002 and july 2014. among them, 47 cases (6.6%) were included to this study as the rD group. Median age of the patients in the rD group was 70 years. Patients in the rD group had high frequency of pre-existing diabetes mellitus (68%), cardiovascular disease (38%), and preoperative anemia defined as hemoglobin < 12.0 g/dl (70%). 13 rD patients (28%) had liver cirrhosis, and 16 patients (34%) received preoperative hemodialysis. We analyzed the short- and long-term outcomes in the rD group.
results: In the rD group, the median operative time was 359 (interquartile range [Iqr] 280-453) minutes, and the median blood loss was 900 (Iqr 400-1575) ml. 14 patients (30%) require intraoperative red blood cell transfusion. Incidence of postoperative major complication (clavien grade 3 to 5) was 21%. 2 patients (4.3%) required newly initiated hemodialysis postoperatively. Median hospital stay was 15 (Iqr 12-19) days and mortality within 90 days was observed in 3 cases (6.4%), in which the cause of mortality was cancer in two and liver insufficiency in one. the 5-year survival rate was 47.1% in the rD group, which seemed to be low comparing to the previous outcomes after resection of hcc (53.4-56%) 1-2. rD patients with child-Pugh class a had relatively good 5 year survival rate (58.3%).
Conclusion: although presence of preoperative rD is likely to adversely affects long-term outcomes, hepatic resection for hcc can be safely done even in patients with rD and provide acceptable prognosis, especially in the presence of good liver function.
references: 1. torzilli G, et al. ann surg 2013;257:929-2. Ikai I, et al. hepatol res 2007;37:676-
Disclosure of Interest: none Declared
P-286 ShOuLD PATIenTS WITh hePATOCeLLuLAr CArCInOMA bArCeLOnA CLInIC fOr LIVer CAnCer STAGe C be TreATeD WITh TrAnSArTerIAL CheMOeMbOLISATIOn?
helen L. reeves1, 2, Ghazanfar A. Anwar* 3, Littler Peter2, Laura f. ogle1, Deborah stocken4, kate sumpter2
1northern Institute for cancer research, newcastle university, 2hepatopancreatobiliary Multidisciplinary team, 3Liver unit, freeman hospital newcastle upon tyne nhs foundation trust, 4Institute for health and society, newcastle university, newcastle-upon-tyne, united kingdom
Introduction: the prognosis of patients with hepatocellular carcinoma (hcc) undergoing transarterial chemoembolization (tace) is variable. We have explored the BcLc algorithm and the recently introduced haP score, which awards a point for each of the factors afP >400ng/ml, tumour size >7cm, serum albumin < 36 g/l, total bilirubin > 17, and their prognostic value in discriminating overall survival.
Methods: Prognostic scores were studied retrospectively in 140 consecutive patients with hcc presenting to our unit between 2004 and 2010. hcc was diagnosed according to easL guidelines and all patients received selective tace (doxorubicin lipiodol and polyvinyl alcohol particles) as their 1st line therapy. statistical analyses was using univariate and multivariate cox regression studying overall survival (os).
results: the median age of the study population was 70 years, reflecting metabolic risk factors and alcohol excess as the major predisposing factors, rather than viral hepatitis (no evidence cLD n=20,
alcohol related liver disease n=39, non-alcoholic fatty liver disease n=38, hcV n=11, hBV n=7, haemochromatosis n=9, cryptogenic n=7, aIh, n=2, PBc n=6, a1at n=1). 113 were men and 27 were women. the cohort included BcLc-a (n= 22), BcLc-B (n=45) and BcLc-c (n=73) patients. although the combination haP score discriminated months survival (table 1), the component parts were not each independent predictors by univariate analysis, particularly when considered as categorical rather than continuous variables as used in the score. taking all cases, the strongest predictors of survival, with a p value <0.0001, included afP, tumour size and albumin, as well as tumour number and performance status. In comparison, the component parts of the BcLc grade (number, size, childs Pugh score, Pst) were each independently and significantly associated with survival in the cohort, and this score had better survival discrimantion between grades (table 1). selecting only BcLc a/B cases, the haP score was not a significant discrimator of survival. Within this selected sub-group, tumour number and size were the strongest predictors of survival, with no significant contribution from either afP or bilirubin. Within the BcLc – c patients, the median survival was 8.3 months in those with haP score 0. We explored awarding points for BcLc grade, scoring 0, 1 or 2 points for successive grades, but adding a point for tumour size > 7cm or tumour number >5. this revised ‘newcastle’ score had significant discriminatory capacity for the entire cohort (table 1, p<0.001), as well as for the BcLc a/B (p = 0.015) and BcLc-c (p=0.001) subgroups. Despite enhanced discrimination between subgroups, however, ‘best’ median survival in the BcLc-c subgroup was 8.7 months.
Image:
Conclusion: BcLc is a better predictor of survival than the haP score in our patients. Within BcLc a/B patients, an algorithm incorporating the contribution of tumour size and number beyond the parameters defined within BcLc grade, rather than afP or bilirubin, performs well but may have little additional clinical utility. similarly, these factors enhance discriminatory capacity in BcLc-c patients, but fail to identify any subgroup with a median survival above 8.7 months. tace should not be considered in BcLc-c patients unless all other prognostic factors are favourable and medical therapy is either unavailable or contraindicated.
Disclosure of Interest: none Declared
P-287 Are Pre-TreATMenT CLInICAL PArAMeTerS uSefuL In PreDICTInG The OuTCOMeS Of hePATOCeLLuLAr CArCInOMA PATIenTS TreATeD WITh SOrAfenIb? A SInGLe CenTre, fIeLD-PrACTICe STuDy
Giovan Giuseppe Di Costanzo* 1, raffaella tortora1, filippo Lampasi1, alfonso Galeota Lanza1, filomena Morisco2, Luigi addario1, Massimo De Luca1, Maria Guarino2, Gabriella cordone1, Maria teresa tartaglione1, francesco Paolo Picciotto1, Luigia falco1, Ioana Grigore1, nicola caporaso2
1Department of transplantation - Liver unit, cardarelli hospital, 2Department of clinical Medicine and surgery - Gastroenterology unit, university of naples "federico II", naples, Italy
Introduction: sorafenib is the only drug approved for the treatment of hepatocellular carcinoma (hcc). however, clinical and biochemical parameters predictive of effectiveness are still undefined. the aim of this study was to search for pre-treatment factors predicting tumor response to sorafenib.
Methods: Between october 2009 and october 2014, 362 patients with unresectable hcc were consecutively treated with sorafenib at Liver unit of cardarelli hospital. among these, 313 patients (74% males, median age 68, 88% child-Pugh a, 77% BcLc c, 50% portal thrombosis, 33% extrahepatic metastasis) with sufficient clinical data were analysed. overall survival (os) and time to tumor progression (ttP) were considered to evaluate tumor response. kaplan-Meier method, univariate and multivariate cox proportional hazards were used. P <.05 was used to indicate statistical significance. all variables with P <.1 were considered for multivariate analysis.
results: the median os and ttP were 9 months. the median treatment duration was 3 (1-56) months. Median daily dose was 629mg and ≥ 400mg in 278/313 (89%) patients. clinical or radiological progression was observed in 44% of patients. according to mrecIst criteria, 3-month radiological response was evaluated in 196 patients: complete response in 6 (3%) patients, partial response in 51 (26%) and stable disease in 90 (46%) was observed. at univariate analysis, male
Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 2 2
gender (P=.013), alpha-fetoprotein (afP) >20ng/mL (P=.026), ascites (0.025), and absence of diabetes (P=.031) were associated with a shorter ttP. at multivariate analysis, only male gender (hr 1.80; 95%cI 1.15-2.83; P=.010) and alpha-fetoprotein >20ng/mL (hr 1.49; 95%cI 1.01-2.22; P=.046) resulted independently predictive of disease progression. the variables related to poor os at univariate analysis were: male gender (P=.020), afP >20ng/mL (P=.000), ascites (P=.005), WBc <5.3*109/L (P=.019), alkaline phosphatase >x1.5 upper limit of normal range (uLn) (P=.009), aLt >x1.5 uLn (P=.000), bilirubin >1mg/dL (P=.001), albumin <3.5g/dL (P=.045), and cLIP score >3 (P=.040). at multivariate analysis, afP >20ng/mL (hr 1.91; 95%cI, 1.37-2.64; P=.000), aLt >x1.5 uLn (hr 1.68; 95%cI 1.24-2.29; P=.001), ascites (hr 1.67; 95%cI 1.14-2.43; P=.008), and bilirubin >1mg/dL (hr 1.34; 95%cI 1.00-1.79; P=.048) were independently related to poor os. Patients with all four of these unfavourable factors had a shorter survival as compared to patients without these factors (6 vs 35 months; P=.000).
Conclusion: sorafenib is effective in the treatment of hcc: in 30% of patients a complete and partial tumor response was observed. ttP was shorter in males with increased afP. ascites, and higher values of afP, bilirubin and aLt predicted a poor os. Pre-treatment variables may be of some help in predicting the prognosis of hcc patients treated with sorafenib.
Disclosure of Interest: none Declared
P-288 TrAnSArTerIAL CheMOeMbOLISATIOn In The TreATMenT Of InTerMeDIATe-STAGe hePATOCeLLuLAr CArCInOMA; STuDy Of fACTOrS PreDICTIVe Of SurVIVAL. CLInICAL exPerIenCe In A SInGLe CenTre In SPAIn
Inmaculada Ortiz* 1, adolfo del Val1, jose María tenías2, elena Lonjedo3, fructuoso Delgado3, Victor j Morales1, eduardo Moreno-osset1
1Digestive Diseases, hospital Dr. Peset, 2family and community Medicine teaching unit., eVes, 3radiology, hospital Dr. Peset, Valencia, spain
Introduction: transarterial chemoembolisation (tace) is currently the treatment of choice for hepatocellular carcinoma (hcc) in the Barcelona-clinic Liver cancer (BcLc) classification intermediate stage. although it is the most widely used therapy, many aspects remain to be clarified, primary among them being identifying the best candidates within the broad and heterogeneous group of patients the intermediate stage covers. the aim of this study was to determine overall survival after tace and identify the factors predictive of survival.
Methods: from May 2002 to june 2010, all patients diagnosed with intermediate-stage hcc were included prospectively to receive treatment with conventional tace plus adriamycin and lipiodol. further treatment sessions were given if persistence of the tumour was detected on radiological follow-up with dynamic imaging tests (“on-demand strategy”). In each case, tace was indicated after assessment by a multidisciplinary committee. the treatment was discontinued if tumour progression, vascular invasion, extrahepatic spread or worsening of liver function were observed during follow-up. clinical, analytical and radiological variables were obtained for all cases. survival was estimated using the kaplan Meyer method and prognostic factors analysed using the cox regression model.
results: a total of 123 patients were included. Mean age was 70.58 years. objective response was obtained in 35.7% of the cases. the most common complication was post-embolisation syndrome (33.3%). treatment-related mortality was 3.3%. Median overall survival was 29.2 months. In the multivariate analysis using the cox regression model, age over 65 (p = 0.02), functional status 0 (p < 0.001), tumour size less than 5 cm (p = 0.016), objective response (p = 0.003) and re-embolisation (p = 0.001) were significant independent prognostic factors associated with longer survival. the actuarial survival at 1, 2, 3 and 4 years was 81%, 59%, 42% and 26% respectively.
Prognostic factors HR (IC95%) p
age 0,963 (0,933 – 0,994) 0,020
functional status 2,24 (1,45 – 3,44) <0.001
tumour size 1,76 (1,11 – 2,79) 0,016
objective response 2,18 (1,30 – 3,64) 0,003
re-embolisation 0,51 (0,33 – 0,77) 0,001
Conclusion: the patients surviving longest were aged over 65, with good performance status and hcc less than 5 cm in diameter, who had radiological objective response after therapy and underwent at least two sessions of tace through the “on-demand” strategy. the results of this study may help improve selection of the patients with intermediate-stage hcc who will obtain greater benefit in terms of survival.
Disclosure of Interest: none Declared
P-289 TreMeLIMuMAb – A MOnOCLOnAL AnTIbODy AGAInST CTLA-4 – In COMbInATIOn WITh LOCAL TuMOr AbLATIOn (TACe Or rfA) In PATIenTS WITh hePATOCeLLuLAr CArCInOMA
Tim f. Greten* 1, austin Duffy1, oxana rusher1, sid kerkar1, David kleiner1, William figg1, seth steinberg1, nadine abi-jouedeh1, elliot Levy1, Bradford Wood1
1ncI, Bethesda, united states
Introduction: tremelimumab is a fully human monoclonal antibody that binds to ctLa-4 expressed on the surface of activated t lymphocytes and results in inhibition of B7-ctLa-4-mediated downregulation of t-cell activation. Both transcatheter arterial chemoembolization (tace) and radiofrequency ablation (rfa) have been shown to induce a peripheral immune response which may enhance the effect of anti-ctLa4 treatment in patients with advanced hcc.
Methods: Patients with hcc [childs Pugh a/B7; Barcelona clinic Liver cancer stage B/c; ecoG 0/1; sorafenib refractory/intolerant (BcLc stage c only)] were enrolled in a pilot study of tremelimumab at 2 dose levels (DL1 and DL2) until PD (irrecIst). subtotal tace or rfa was performed during study week 6 with DLt evaluation period encompassing first 8 weeks of study. tumor biopsy at baseline and at time of rf/tace. Immune monitoring on peripheral blood cells
results: 20 pts were enrolled with n=18 evaluable for primary endpoint. Baseline characteristics: M:f 15:3; Median age = 54(range 42-76); cirrhosis present in 13pts; BcLc stage B/c: 4/14; hepatitis B/c/neg: 4/10/4. 8 pts received tace, 10 underwent rfa during week 6 of tremelimumab therapy. no DLt encountered. Most common toxicity was pruritus. one patient developed pulmonitis and was taken off study but remains disease-free at 16months. of n=12 pts evaluable for response outside of tace/rfa-treated lesion 4 (33%) achieved confirmed partial responses. 8 of 9 pts with quantifiable hcV experienced a marked reduction in viral load. 4 of 4 hBV patients experienced a reduction in quantative hepBsag. 6-week tumor biopsies showed immune cell infiltration on all evaluable patients. analysis of immune cell phenotype is ongoing. Median ttP for the study population (n=18) was 7.4months.
Conclusion: tremelimumab in combination with subtotal tace or rfa in patients with advanced hcc is safe and feasible. obtaining tumor biopsies at baseline and at the time of rfa/tace is safe. evidence of immune cell infiltration was seen on evaluable patients. encouraging clinical activity has been seen with objective confirmed responses, ttP 7.4m and possibly surrogate reductions in hcV viral load and hBsag.
Disclosure of Interest: none Declared
P-290 A rAnDOMIzeD, DOubLe-bLInD, PLACebO-COnTrOLLeD PhASe 3 STuDy Of rAMuCIruMAb VerSuS PLACebO AS SeCOnD-LIne TreATMenT In PATIenTS WITh hePATOCeLLuLAr CArCInOMA AnD eLeVATeD bASeLIne ALPhA-feTOPrOTeIn fOLLOWInG fIrST-LIne SOrAfenIb (reACh-2)
Andrew x. zhu* 1, Peter r. Galle2, Masatoshi kudo3, richard s. finn4, Ling yang5, Paolo abada6, shao-chun chang6, josep M. Llovet7
1Dana farber cancer Institute, harvard Medical school, Boston, united states, 2universitatsmedizin, Mainz, Germany, 3kinki university school of Medicine, osaka, japan, 4university of california, Los angeles, 5eli Lilly and company, Bridgewater, 6eli Lilly and company, Indianapolis, 7Icahn school of Medicine at Mount sinai, new york, united states
Introduction: ramucirumab is a human IgG1 monoclonal antibody that inhibits ligand activation of the vascular endothelial growth factor receptor 2 (VeGfr2), a key mediator of angiogenesis. the reach study was a global, randomized, double-blind, placebo-controlled Phase 3 study that assessed ramucirumab (ram) in the treatment of patients with advanced hepatocellular carcinoma (hcc) after prior sorafenib. While significant improvement in overall survival (os) in the overall population (n=565) was not achieved (hazard ratio [hr]=0.866; 95% cI 0.717–1.046; p=0.1391), a clinically meaningful improvement in os was observed in the pre-specified subgroup of patients with elevated baseline alpha-fetoprotein (afP) level ≥400 ng/mL (n=250)(hr=0.674; 95% cI 0.508–0.895; p=0.0059). the safety profile of ram in hcc patients was considered manageable. confirmation of the survival benefit from ram treatment in patients with a baseline afP level ≥400 ng/mL will be assessed in the current reach-2 trial.
Methods: reach-2 is a randomized, double-blind, placebo-controlled phase III study of ram and best supportive care (Bsc) versus placebo and Bsc as second-line treatment in patients with hcc and elevated baseline afP following first-line therapy with sorafenib. eligible patients will be randomized 2:1 to receive ram (8mg/kg) or placebo as an intravenous infusion on Day 1 of each 14-day cycle until radiographic or clinical disease progression or until criterion for discontinuation are met.
eligible patients are required to have a diagnosis of hcc based on (1) histopathologic or cytologic findings or (2) in the absence of histologic confirmation, a diagnosis of cirrhosis and hcc with

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 2 3
classical imaging characteristics. Patients must have received prior sorafenib as the only systemic therapeutic intervention for advanced hcc; duration of prior sorafenib treatment ≥14 days, and discontinued sorafenib ≥14 days prior to randomization. additional requirements include child-Pugh score <7 (child-Pugh class a only); Barcelona clinic Liver cancer (BcLc) stage c disease or BcLc stage B disease not amenable or refractory to locoregional therapy, afP ≥400 ng/mL, and eastern cooperative oncology Group performance status of 0 or 1. eligible patients are ≥18 years of age or of an age acceptable according to local regulations, whichever is older. Patients with previous or current hepatic encephalopathy or clinically meaningful ascites, recent hepatorenal syndrome, prior liver transplant, or hepatic locoregional therapy after sorafenib are not eligible.
results: the primary objective of this study is to assess the os for patients treated with ram versus placebo. assuming an hr of 0.7 and 2:1 randomization, 318 events are required to achieve 85% statistical power with the use of a log-rank test at 2 sided type I error of 0.05. the primary analysis will be performed after approximately 318 deaths have been observed, and study target enrollment of approximately 399 patients (assuming 20% censoring rate). secondary objectives include progression free survival, time to radiographic progression, objective response rate, safety, and patient reported outcome measures. additional objectives include assessment of biomarkers relevant to ram, angiogenesis, and hcc.
Conclusion: In the reach study, a survival benefit from ramucirumab treatment was observed in the pre-specified subgroup of hcc patients with baseline afP ≥400 ng/mL. the potential os benefit in this subgroup warrants confirmation, and supports the current design of the reach-2 trial.
Disclosure of Interest: a. x. zhu research/education support from: Bayer, eli Lilly and company, novartis, advisory Board of: sanofi-aventis, eisai, BMs, celgene, Bluprint, P. r. Galle advisory Board of: eli Lilly and company, Bayer, BMs Blueprint, jennerex, Daiichi, M. kudo: none Declared, r. s. finn: none Declared, L. yang conflict with: eli Lilly and company, P. abada conflict with: eli Lilly and company, s.-c. chang conflict with: eli Lilly and company, j. M. Llovet Grant support from: Bayer health Pharmaceuticals, Bristol-Meyers squibb, Boehringer Ingelheim, Blueprint, honoraria support from: eli Lilly and company, advisory Board of: Bayer healthcare Pharmaceuticals, Bristol-Meyers squibb, eli Lilly and company, Blueprint, celsion, Glaxosmithkline, Boehringer Ingelheim, novartis, consulting of: eli Lilly and company
P-291 PLACe Of SOrAfenIb In The MAnAGeMenT Of unTreATAbLe reCurrenT hePATOCeLLuLAr CArCInOMA fOLLOWInG LIVer TrAnSPLAnTATIOn
Azoulay Daniel* 1, De angelis nicola1, Lim chetana1, salloum chady1, compagnon Philippe1, Laurent alexis1, feray cyrille1
1hPB surgery and liver transplantation, hopital henri Mondor, aPhP, creteil, france
Introduction: Management of hepatocellular carcinoma (hcc) recurrence after liver transplantation (Lt) remains highly challenging. curative-intent treatments should be attempted whenever feasible, whereas palliative therapies are administered in case of untreatable progression or presentation of hcc recurrence (up-hcc). sorafenib has been recently proposed as systemic therapy to manage hcc recurrence in Lt patients. the aim of the present study was to compare survival rates of Lt patients receiving sorafenib or best supportive care (Bsc) for hcc recurrence not amenable to curative-intent treatments (up-hcc).
Methods: two cohorts of Lt patients with up-hcc recurrence receiving sorafenib (n=15) or Bsc (n=18) were compared for demographic, operative, and follow-up variables by univariate and cox regression analyses.
results: Introduction: Management of hepatocellular carcinoma (hcc) recurrence after liver transplantation (Lt) no group difference was observed for demographic and clinical characteristics at the time of Lt and hcc recurrence diagnosis. the 81.2% of patients were classified within the Milano criteria and 53.1% with micro-vascular invasion. hcc recurrence was diagnosed 17.8 months (sD: 14.5) after Lt, with 17 patients (53.1%) presenting with early hcc recurrence (< 12 months). one-year survival rate from up-hcc recurrence was 23.9% for Bsc and 60% for sorafenib group (p=0.002). the type of treatment (Bsc vs. sorafenib) was found to be an independent predictor of survival (hazard ratio: 3.46 [95%cI: 1.34-8.9]; p=0.01). Due to adverse effects, 8 patients (53.3%) and 2 patients (13.3%) required respectively dose reduction and drug withdrawal in the sorafenib group.
Conclusion: sorafenib positively impacts on patient’s survival and is superior to Bsc in case of up-hcc recurrence in Lt patients.
Disclosure of Interest: none Declared
P-292 TuMOr reCurrenCe AfTer LIVer TrAnSPLAnTATIOn fOr hePATOCeLLuLAr CArCInOMA: A SySTeMATIC reVIeW Of VerSATILe MAnAGeMenTS
Azoulay Daniel* 1, De angelis nicola1
1hPB surgery and liver transplantation, hopital henri Mondor, aPhP, creteil, france
Introduction: hepatocellular carcinoma (hcc) recurrence after liver transplantation (Lt) drastically affects patient survival. Management of hcc recurrence involves a wide range of local and systemic treatment modalities that lack established guidelines. We performed a systematic literature review to investigate the efficacy (survival) and safety of hcc recurrence treatments in Lt patients.
Methods: Literature search was performed on various online databases without a time limit until november 2014. all clinical studies (including case reports) describing survival after hcc recurrence in Lt patients were retrieved for a full-text evaluation. a total of 59 studies were included: 14 case reports, 35 retrospective case series, 8 retrospective case-control studies, 1 prospective cohort study, and 1 prospective case-control study.
results: Based on all included studies, the mean hcc recurrence rate was 16% of all Lts for hcc. a total of 838 Lt patients presented with hcc recurrence. the median time from Lt to hcc recurrence was 12 months (range 2-132 months). the majority of patient cases (65%) were hcc extra-hepatic recurrences, involving lung, bone, adrenal gland, peritoneal lymph nodes, and rarely the brain. survival for all treatment modalities pooled together was 15.8 months after initiation of treatment. surgical resection of localized hcc recurrence and sorafenib for controlling systemic spread of hcc recurrence were associated with higher survival (32.5 and 14.8 months, respectively). however, sorafenib, especially when combined with mtor, was frequently associated with severe side effects that required dose reduction or discontinuation.
Conclusion: hcc recurrence management in Lt patients is challenging and associated with poor prognosis independent of the type of treatment.
Disclosure of Interest: none Declared
P-293 PerCuTAneOuS TreATMenTS Of InfILTrATIVe hePATOCeLLuLAr CArCInOMA DeVeLOPeD On CIrrhOSIS uSInG MuLTIPOLAr rADIOfrequenCy AbLATIOn Or InTrA-ArTerIAL eThAnOL InJeCTIOn
Jean Charles nault* 1, Gisèle nkontchou1, Pierre nahon1, Véronique Grando1, Valérie Bourcier1, Marianne ziol2, sandrine Barge1, nicolas sellier3, nathalie Ganne-carrie1, olivier seror4
1Liver unit, jean Verdier hospital, 2Department of pathology, 3Department of radiology, 4Department of radiology, jean Verdier hospital, Bondy, france
Introduction: Infiltrative hepatocellular carcinoma (hcc) is a subset of hcc characterized by a difficult diagnosis, a dismal prognosis and limited therapeutic options as systemic therapies are usually only considered. We aim to describe the outcomes of infiltrative hcc treated by percutaneous treatment including multipolar radiofrequency ablation (mrfa) and percutaneous intra-arterial ethanol injection (PIaeI).
Methods: all cirrhotic patients with infiltrative hcc and treated by mrfa or PIaeI in our institution between 2002 and 2013 were included. We assessed radiological response using mrecIst criteria and afP level one month after treatment. survival was analyzed using kaplan Meier method, log rank test and cox univariate then multivariate analyses.
results: fifty-one patients were considered eligible for mrfa or PIaeI (median age : 65 years (range: 48-81), males: 90%). cirrhosis etiologies were alcohol abuse (34, 67%), hepatitis c virus (17, 33%), hepatitis B virus (8, 16%) and/or nash (8, 16%). Patients were child-Pugh a and B in 90% and 10% respectively. hccs were multinodular in 31%, the median size of the main tumor was 60 mm (30-200), Macrovascular invasion was observed in 59%. hccs were classified as BcLc stage a, B and c in 24%, 18% and 59% respectively. the median serum level of afP was 125 ng/ml (2-215000). 20 patients were treated using mrfa and 31 by PIaeI. tumor burden and portal obstruction rates were lower in patients treated by mrfa as compared to patients treated by PIaeI. treatment-related adverse events occurred in 58%, mainly post-ablation syndrome (31%), and one death (2%). at the end of follow-up, 40 patients (83%) experienced tumour progression and 40 patients died (78%). Median progression-free survival was 7.46 months and actuarial rates of progression free-survival at 1, 2, 3 and 4 years were 35%, 9%, 4% and 2%, respectively. Median os for the entire population was 18.3 months, and actuarial rates of survival at 1, 2, 3 and 4 years were 63%, 35%, 20% and 12%, respectively. Macrovascular invasion, BcLc stage or types of treatment were not associated with overall survival and tumor progression. In contrast, baseline serum bilirubin>normal (hr: 2.98 (95%cI: 1.38-6.50), P=0.0057) and the sum of the diameter of the nodules (hr: 1.02 (95%cI: 1.003-1.04) P=0.0221)) were significantly associated with poor overall survival in multivariate analysis. Patients with a sum of the size of all nodules < 70 mm and with a normal bilirubin level had the longest os (median os 29.9 months) compared to patients bearing only one of these factors (median os 15.9 months) or those who combined a sum of size

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 2 4
of all nodules > 70 mm anD higher total bilirubin level (median os 5.7 months, P < 0.0001). the radiological response using mrecIst criteria and an alphafetoprotein decrease 1 month post-procedure was associated with increased overall survival (P=0.0002 and P=0.024, respectively).
Conclusion: Despite an overall poor prognosis, infiltrative hcc can be safely treated using percutaneous approaches with unexpected benefits on survival of these difficult-to-treat patients. Patients with both a high bilirubin level (> 1.2 mg/dl) and a tumor burden of more than 70 mm have a very poor prognosis and are not good candidates for percutaneous treatment.
Disclosure of Interest: none Declared
P-294 COnVenTIOnAL CheMOeMbOLIzATIOn VerSuS DruG eLuTInG beADS In TreATMenT Of eGyPTIAn PATIenTS WITh unreSeCTAbLe hePATOCeLLuLAr CArCInOMA: Three yeArS SurVIVAL
ahmed k. eldorry1, Mahmoud elmeteini2, nadia a. abdelkader3, Mohamed a. abuelmaaty1, Maha M. elgafary4, heba I. aly3, Mohamed S. Khalaf* 3, Mohamed k. shaker3
1Department of diagnostic radiology, 2Department of surgery, 3tropical medicine, 4commmunity medicine and statistics, ain shams university, cairo, egypt
Introduction: transarterial chemoembolization (tace) is a commonly used primary treatment for unresectable hepatocellular carcinoma (hcc); however improving its tolerability and survival results is an important issue. Drug eluting beads is a drug embolization system for loading with chemotheraputic agents in the treatment of malignant hypervascularized tumors. Being non resorpable, beads prolong local drug delivery time and decrease systemic toxicity. this study was held to compare between conventional tace (ctace) and drug eluting beads (DeB) in treatment of egyptian patients with unresectable hepatocellular carcinoma.
Methods: this prospective controlled clinical trial was held in ain shams univerisity hospitals during the period from april 2011 till october 2014. fifty hcc proven patients (25 underwent conventional tace and 25 underwent tace using drug eluting beads) were enrolled in this study. Patients were followed up for signs of toxicity, tumour response and survival. repeated tace performed on demand according to the allocated line of treatment. Primary end point was overall survival while response rate and time to progression were considered as secondary end points.
results: fifty patients with hcc (5 BcLc a and 45 BcLc B) underwent total of 77 sessions (37 DeB tace and 40 ctace). DeB tace was associated with lower incidence of hepatotoxicity (p< 0.001) and thrombocytopenia (p=0.01). overall median time to progression was seven months in both groups. overall median survival time in conventional and drug eluting beads was 15 and 24 months respectively. three years survival was 14% in conventional tace and 33% in drug eluting beads (p =0.068).
Conclusion: chemoembolization using drug eluting beads was associated with less hepatotoxicity and myelosuppression. Median time to progression was similar in both groups. Despite being statistically insignificant, DeB tace was associated with better survival trend.
Disclosure of Interest: none Declared
P-295 PreTreATMenT SeruM SODIuM LeVeL AS A PrOGnOSTIC MArKer fOr PATIenTS WITh hePATOCeLLuLAr CArCInOMA TreATeD WITh SOrAfenIb
Kenichiro Murayama* 1, shunya nakashita2, taiga otsuka1, seiji kawazoe2, kimihiko yanagita3, yasushi Ide4, takao Ide5, keisuke ario6, yuichiro eguchi7, toshihiko Mizuta8
1hepatology Division, saga university hospital, 2hepatobiliary and Pancreatology Division,, saga-ken Medical centre koseikan, saga, 3Department of Internal Medicine, saiseikai karatsu hospital, 4Department of Internal Medicine, karatsu red cross hospital, karatsu, 5Department of surgery, saga university hospital, saga, 6Gastroenterology Division, nho ureshino Medical center, ureshino, 7Liver center, saga university, saga, 8Department of Internal Medicine, Imari arita kyoritsu hospital, imari, japan
Introduction: sorafenib is commonly used to treat patients with advanced hepatocellular carcinoma (hcc). however, we lack readily available prognostic markers. hyponatremia is associated with poor prognosis for certain malignancies. therefore, we assessed the prognostic value of serum sodium level in patients with hcc treated with sorafenib.
Methods: We reviewed 147 consecutive patients with advanced hcc who were administered sorafenib from 2008 to 2013. We included patients with child–Pugh class a liver disease and excluded those treated with diuretics. hyponatremia was defined here as serum sodium ≤140 meq/L before sorafenib therapy.
results: seventy-eight patients were included and classified as normonatremic (n = 29) or hyponatremic (n = 49). Baseline characteristics were similar between the two groups. seventeen
and twenty-seven patients with Barcelona clinic Liver cancer stage c were normonatremic (58.6%) or hyponatremic (55.1%), respectively. the median survival times of patients with hyponatremia or normonatremia were 9.0 and 17.0 months, respectively, (P = 0.04). cox proportional hazards model analysis revealed that hyponatremia was a significant prognostic factor (hazard ratio, 1.88; 95% confidence interval, 1.02–3.46; P = 0.04) as well as α-fetoprotein and des-γ-carboxy-prothrombin levels. the objective response and disease control rates were 14.8 and 7.3% in normonatremic and 55.6 and 46.3% in hyponatremic patients, respectively.
Conclusion: serum sodium levels before treatment with sorafenib may serve as a simple prognostic factor for patients with hcc.
Disclosure of Interest: none Declared
P-296 eVALuATIOn Of rADIOTherAPy fOr PATIenTS WITh unreSeCTAbLe ADVAnCeD hePATOCeLLuLAr CArCInOMA
Tsubasa Tsutsumi* 1, hiroaki nagamatsu1, naohisa Mizukami2, takuji torimura3
1Department of Gastroenterology and hepatology, 2Department of radiology, yame General hospital, yame, 3Division of Gastroenterology, kurume university school of Medicine, kurume, japan
Introduction: We retrospectively evaluated the therapeutic efficacy of radiotherapy in patients with unresectable advanced hepatocellular carcinoma (hcc) showing simple nodular type with extranodular growth or confluent multinodular type, or hcc which was refractory or intolerant to trancecatheter arterial chemoembolization (tace).
Methods: among 100 patients (macroscopic vascular invasion, 20 cases; extrahepatic metastasis, 21 cases) who were treated with radiotherapy for hcc between january, 2011 and December, 2014 at yame republic hospital, fifty nine patients who had simple nodular type hcc with extranodular growth or confluent multinodular type hcc, or with hcc showing refractory or intolerant to tace were enrolled in the study (mean age, 76.1 years; child-Pugh class a/B, 46/13 cases; single/multiple tumors, 37/22 cases; stereotactic body radiotherapy(sBrt)/conventional radiotherapy(crt), 47/12; refractory to tace/tace intolerance/hcc with simple nodular type with extranodular growth or confluent multinodular type, 23/3/33 cases). the mean tumor size was 36 mm (range, 20–100 mm). radiotherapy was performed in patients with hcc refractory to tace within 3 months after treatment with tace, and in hcc patients with simple nodular type with extranodular growth or confluent multinodular type within 7 days after tace. radiotherapy was performed solely in patients who showed intolerant to tace. sBrt or crt was determined according to the location of hcc. Mean dose of sBrt was 48.7Gy (range, 40–60 Gy), and that of crt was 58.4Gy (range, 50–66 Gy). Local disease control was evaluated based on the presence of local recurrence. We estimated progression-free survival (Pfs) and overall survival (os) using kaplan-Meier curves. os with or without local and intrahepatic recurrence was compared using log-rank test. We also evaluated adverse events.
results: adverse events included decline of child-Pugh score by 2 or more points in 3 patients, and pleural effusion or ascites in 9 patients. Local recurrence occurred in 4 patients. Disease control rate was 93.2%. 1-year Pfs was 90.4%. Median os(Mst) after radiotherapy was 16.5 months. Mst in patients with or without local recurrence was 10.3 and 18.3 months, respectively (P=0.601). Mst in patients with or without intrahepatic recurrence was 16.1 and 42.9 months, respectively ( P=0.016).
Conclusion: radiotherapy for hcc showed favorable tolerability in hcc showing refractory or intolerance to tace or showing simple nodular type with extranodular growth or confluent multinodular type Intrahepatic recurrence was a factor of poor prognosis.
references: alexis Bujold, christine a.Massey, john j.kim, et al. ;sequential Phase 1 and II trials of stereotactic Body radiotherapy for Locally advanced hepatocellular carcinoma. : j clin oncol 31.april 1,2013Gi-ae kim, ju hyun shim, sang Min yoon, et al. ; comparison of chemoembolization with and without radiation therapy and sorafenib for advanced hepatocellular carcinoma with Portal Vein tumor thrombosis: a Propensity score analysis. : j Vasc Intrv radiol 2015
Disclosure of Interest: none Declared
P-297 OPTIMAL InTerVAL beTWeen On-DeMAnD TrAnSArTerIAL CheMOeMbOLIzATIOn In PATIenTS WITh unreSeCTAbLe hePATOCeLLuLAr CArCInOMA
Kang Mo Kim* 1, hyung-Don kim1, jihyun an1, Dong Il Gwon2, ji hoon shin2, Gi-young ko2, hyun-ki yoon2, kyu-Bo sung2, han chu Lee1
1Department of Gastroenterology, asan Liver center, 2Department of radiology, asan Medical center, university of ulsan college of Medicine, seoul, korea, republic of
Introduction: We evaluated clinical impact of different interval between multiple transarterial chemoembolization (tace) sessions in patients with unresectable hepatocellular carcinoma (hcc).

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 2 5
Methods: retrospective historical cohort study was performed. Between 2006 and 2012, a total of 305 consecutive hcc patients received multiple sessions of on-demand tace by two independent physicians with different management policy in terms of tace interval at asan medical center. of these patients, 180 had interval less than 60 days (shortened interval group) between 1st and 2nd
tace (conventional interval group) and the other 125 had tace interval of 60 days or longer.
results: Patients in shortened interval group had larger hcc nodules, more portal vein invasion, lower portion of favorable response to the tace and more portion of child-Pugh class a. shortened interval group underwent more sessions of tace (6.6 vs. 5.5 sessions, P=0.011) while total number of admission (7.8 vs. 8.7, P=0.066) and total hospital stay (54.5 vs. 55.6 days, P=0.767) were similar compared to conventional interval group. overall survival (os) between two groups were similar by kaplan-Meier analysis in both the full cohort and propensity score matched cohort (P=0.121 and P=0.998, respectively). While os was comparable between two groups in patients with child-Pugh class a (P=0.403), shortened interval group showed inferior survival in those with child-Pugh class B (P=0.005).
Conclusion: on-demand tace with interval less than 60 days could be considered for patients with child-Pugh class a, whereas wider tace interval would be more appropriate for patients with child-Pugh class B.
Disclosure of Interest: none Declared
P-298 COMPArInG TreATMenT OuTCOMeS beTWeen rADIOeMbOLIzATIOn uSInG yTTrIuM-90 MICrOSPhereS AnD COnCurrenT CheMOrADIATIOn TherAPy fOr LOCALLy ADVAnCeD fOr hePATOCeLLuLAr CArCInOMA
Kyu Sik Jung* 1, Do young kim1, Mi yeun kim1, jinsil seong2, jong yun Won3, Beom kyung kim1, seung up kim1, jun yong Park1, sang hoon ahn1, kwang-hyub han1
1Department of Internal Medicine, 2Department of radiation oncology, 3Department of radiology, yonsei university college of Medicine, seoul, korea, republic of
Introduction: Previous studies revealed that both of radioembolization with yttrium-90(90y) and concurrent chemoradiation therapy (ccrt) showed comparably good treatment outcome in the intermediate and advanced stages of hcc. the aim of this study is to comparing treatment outcome between radioembolization and ccrt in the intermediate and advanced stages of hcc.
Methods: In this retrospective study, 170 treatment-naive patients with BcLc stage B (n=48) or c (n=122), who were treated by ccrt (n=104) or radioembolization with 90y (n=66), were analyzed. overall survival (os), progression free survival (Pfs), tumor response at 1 month after treatment, and complication rate were compared between ccrt group (n=104) and radioembolization group (n=66).
results: os (12.5 month for ccrt group vs. 14.0 months for radioembolization group, P=0.753) and Pfs (4.5 month for ccrt vs. 5.6 month for radioembolization group, P=0.176) was comparable between two groups. at tumor response at 1 month after treatment, objective response rate (complete response or partial response) was significantly higher in ccrt group than radioembolization group (45.2% vs. 15.2%, P<0.001), but disease control rate (complete response, partial response or, stable disease) was higher in radioembolization group than ccrt group (89.4% vs. 75.0%, P=0.021). complication related treatment was lower in radioembolization group with marginal statistical significance (15.4% vs. 4.5%, P=0.043), but the proportion of patients, who underwent curative treatment (surgery or liver transplantation) according to downstaging of hcc, tend to be higher in ccrt group (17.3% vs. 7.6%, P=0.071).
Conclusion: Both ccrt and radioembolization revealed comparable response rate and survival in the intermediate and advanced stages. Despite similar os and Pfs, it is important to select proper candidate for each treatment modality considering patients tumor burden and liver functions.
Disclosure of Interest: none Declared
P-299 SurVIVAL AnD PrOGnOSTIC fACTOrS In PATIenTS WITh InTerMeDIATe STAGe hePATOCeLLuLAr CArCInOMA WhO Were TreATeD WITh rePeATeD TrAnSArTerIAL CheMOeMbOLIzATIOn
Jung hee Kim* 1, Woo kyoung jeong2, Won sohn3, yong-han Paik1, sung Wook sin2, sung Gi jo2
1internal medicine, 2radiology, samsung Medical center, seoul, 3Medicine, Bundang jesaeng General hospital, seong-nam si, korea, republic of
Introduction: there have been several efforts to define transarterial chemoembolization (tace) refractoriness. however, repeated tace is commonly performed even in patients with hepatocellular carcinoma (hcc) who meet tace refractoriness criteria in the real clinical practice. In this study, we analyzed of the clinical outcomes according to disease progression pattern in BLcL-B hcc patients who received repeated tace.
Methods: Between january 2009 to December 2011, a total of 173 patients with intermediate stage (BcLc-B) hcc underwent repeated tace. We analyzed the outcomes according to disease progression pattern and evaluated the prognostic factors for overall survival.
results: among 173 patients, 155 (92.3%) were male, and mean age was 58.8 years old. Median follow up duration was 35.2 (range 1.7-83.8) months, and median number of repeated tace was five (range 2-16) times. Disease progression was observed in 155 patients (89.6%), and the patterns of disease progression were intrahepatic recurrence (n=64, 41.3%), macrovascular invasion (n= 34, 21.9 %), and extrahepatic spread (n=57, 36.8%). the patients who showed disease progression were treated as follows; repeated tace (n=27), tace plus additional locoregional therapy (n= 41), sorafenib (n= 29), radiation therapy (n=8), sorafenib combined with radiation therapy (n=11), palliative surgery(n=5) and supportive care (n=34). the median duration of overall survival was 35.0 (range 1.7-83.8) months. the overall survival was longer in intrahepatic recurrence group than macrovascular invasion or extrahepatic spread group. (median duration: 41.2 months vs. 35.9 months vs. 22.5 months, p ≤ 0.001) Multivariable analysis showed that overall survival was associated with initial -fetoprotein over 200ng/mg[hazard ratio (hr) 1.79; 95 % confidence interval (cI), 0.08-2.96, p = 0.023], capability of advancement of tace catheter tip into the feeding artery (selective tace) [hr 0.32, cI 0.20-0.53, p <0.001] in the last tace procedure. among 64 patients with intrahepatic recurrence, the overall survival was better in a group of repeated tace than those who changed therapy to alternative treatments. (median duration: 48.7 months vs. 25.6 months, p≤ 0.001) Multivariable analysis in this subgroup showed that overall survival was associated with repeated tace [hr 0.14 cI 0.04-05, p = 0.002] and capability of advancement of tace catheter tip into the feeding artery (selective tace) [hr 0.44, cI 0.20-0.98, p =0.046].
Conclusion: selective tace was independent prognostic factor for overall survival in in BLcL-B hcc patients who received repeated tace. among the patients with intrahepatic recurrence, the patients who could receive repeated tace had better survival than those who changed therapy to alternative treatments.
Disclosure of Interest: none Declared
P-300 COMbInATIOn TreATMenT Of TrAnS-ArTerIAL CheMOeMObOLIzATIOn fOLLOWeD by rADIOTherAPy WITh hyPerTherMIA (CerT) In hePATOCeLLuLAr CArCInOMA WITh POrTAL VeIn TuMOr ThrOMbOSIS: InTerIM AnALySIS Of PrOSPeCTIVe PhASe II TrIAL
Jeong Il yu* 1, hee chul Park1, Dongryul oh2, jae Myoung noh2, sang hoon jung2, hye young kim1, Byung chul yoo2, Geum-youn Gwak2, yong han Paik2, Moon seok choi2, joon hyeok Lee2, kwang cheol koh2, seung Woon Paik2, Dong hyun sinn2, sung Wook shin2, sung ki cho2
1radiation oncology, 2samsung Medical center, seoul, korea, republic of
Introduction: the purpose of the present study is to evaluate the objective response and toxicity of the trans-catheter arterial chemoembolization (tace) followed by radiotherapy (rt) and hyperthermia (cert) in hepatocellular carcinoma (hcc) patients with portal vein tumor thrombosis (PVtt).
Methods: this study is designed as a single-center, non-randomized prospective phase II trial subjective of hcc with PVtt. the patient was first treated with tace, and after one week the four-dimensional computed tomography simulation and first session of hyperthermia were conducted. the respiration gated rt planned as ten fractions started after another one week. six sessions of hyperthermia according to the energy escalation protocol was delivered twice a week. response evaluation was planned at one month after rt completion using modified response evaluation criteria in solid tumors, and toxicity was checked by using the common terminology criteria for adverse events Version 4.0.
results: this interim analysis was conducted with the patients enrolled from october 2013 to november 2014. During the study period, 56 patients were screened and 51 of them consented to participate in this trial. and finally 46 patients (90.2%) who received at least one session of hyperthermia were eligible and enrolled. six sessions of hyperthermia were completed in 33 patients (64.7%). the median follow-up was 6.7 months (range, 2.0 to 15.0 months). overall, complete response was observed in 10 (21.7%), partial response in 27 (47.8%), and stable disease in 5 (10.9%) patients. Most of the toxicities were grade I or II. there was one death related with severe pneumonia of unknown cause in contralateral lung which was developed one month after treatment. and one patient could not complete planned treatment because of continuous elevation of bilirubin after tace. as a late toxicity, no classic radiation induced liver disease was developed and 13 (28.3%) asymptomatic gastroduodenal toxicities were noticed in routine esophagogastroduodenoscopy. the local progression-free survival, progression-free survival, and overall survival rates were 75.1%, 29.8%, and 78.9% at one year, respectively.
Conclusion: Despite the sample size and follow-up period are not enough to draw concrete conclusion at present, cert showed promising response rate with acceptable toxicities in hcc patients with PVtt.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 2 6
references: yu jI, Park hc, Lim do h, et al. scheduled interval trans-catheter arterial chemoembolization followed by radiation therapy in patients with unresectable hepatocellular carcinoma. j korean Med sci 2012;27:736-43.
Disclosure of Interest: none Declared
P-301 PerCuTAneOuS TrAnShePATIC STenT PLACeMenT In 993 PATIenTS WITh MALIGnAnT bILIAry ObSTuCTIOn
Paris Pappas* 1, Polytimi Leonardou1
1radiology, LaIkon hospital, athens, Greece, Penteli, Greece
Introduction: Percutaneous biliary drainage is a method that reliefs patients from the symptoms of biliary obstruction and allows administration of antineoplastic agents, which are excreted or metabolized via liver, in patients with malignancy[1]. the purpose of our study was to evaluate the efficacy of percutaneous transhepatic biliary drainage and percutaneous implantation of biliary stents in malignant biliary obstruction.
Methods: 993 patients underwent percutaneous transhepatic catheterization in our department, suffered from malignant biliary obstruction (MBo). 186 of MBo patients had developed postoperative stricture of bilioenteric anastomosis, caused either by connective tissue development or by recurrence of malignancy. the rest of MBo patients suffered from unresectable malignancies that were obstructing the biliary tract. 108 of MBo patients received only external percutaneous biliary drainage, either because they were about to be operated (73) or due to inability of crossing the obstruction (35-3,5%). the rest 885 patients underwent percutaneous implantation of biliary stents; 296 patients were managed with drainage of both (left and right) main hepatic ducts (174 in t configuration placement of stents through one biliary duct and 120 with y configuration placement of stents through the two biliary ducts) and in 589 patients stents were placed at the common bile duct or at one of the main hepatic ducts. Biliary drainage was performed with conscious sedation, under flouroscopic guidance. the obstructed region was dilated with a baloon and afterwards a self-expanding matallic stent was placed[2]. a second stent was placed if the length of the obstructed region required so. at the end of the procedure we inserted an external drainage tube that remained closed for about 2 days, for hemostasis and for conserving the access pathway[2].
results: the method has been successful and effective in decreasing the levels of total bilirubin and relieving the jaundice-related symptoms in 897/993 (90.3%) of the patients. Post-procedure imaging revealed complete deletion of bile duct dilatation on these patients. In 12/993 (1,2%) patients hemorrhage was induced that has been successfully managed with embolization of hepatic artery branch. the procedure provided palliation from pruritus in terminal patients without the morbidity and mortality of the operative procedures.[3]
Conclusion: Percutaneous biliary drainage and stent implantation is a well tolerated and safe method and also a palliative and effective way to improve quality of life, especially in a group of patients with short life expectancy.In patients with longer life expectancy, stent placement may be appropriate if they understand that additional intervention is likely[4,5].
references: 1) anne M.covey, karen t. Brown, Palliative percutaneous drainage in malignant biliary obstruction. j of supportive oncology Volume 4, number 7 july/ august 2) Pappas P, Leonardou P, et al.abdom Imaging. 2003 sep-oct;28(5):678-83.PMID: 14628875 [PubMed - indexed for MeDLIne] 20063) M e clouse, D evans, et al. Percutaneous transhepatic biliary drainage. complications due to multiple duct obstructions. ann surg 1983 july;198(1): 25-294) Lee Bh, choe Dh, et al. Metallic stents in malignant biliary obstruction: prospective long-term clinical results. am j roentgenol 1997;168:741-745.Mathieson jr, McLoughlin rf, et al. Malignant obstruction of the common bile duct: long-term results of Gianturco-rosch metal stents used as initial treatment. radiology 1994;192:663-667
Disclosure of Interest: none Declared
P-302 SAfeTy AnD effeCTIVeneSS Of SOrAfenIb fOr The TreATMenT Of hePATOCeLLuLAr CArCInOMA In PATIenTS WITh DIAbeTeS
Giovan Giuseppe Di Costanzo* 1, raffaella tortora1, filomena Morisco2, Massimo De Luca1, Luigi addario1, Maria Guarino2, Gabriella cordone1, Luigia falco1, Ioana Grigore1, nicola caporaso2
1Department of transplantation - Liver unit, cardarelli hospital, 2clinical Medicine and surgery - Gastroenterology unit, university of naples "federico II", naples, Italy
Introduction: Diabetes may increase the risk of side effects in patients treated with systemic therapies for cancer and may influence changes in the metabolism of drugs. furthermore, diabetes may worsen the outcomes of patients with cirrhosis and hepatocellular carcinoma (hcc). however, tyrosine kinase inhibitors can affect the insulin signaling pathway and improve glycemic control in diabetics. studies evaluating sorafenib treatment in diabetics with hepatocellular carcinoma (hcc) are lacking. the aim of this study was to retrospectively evaluate safety and effectiveness
of sorafenib treatment in patients according to the presence (DIaB) or absence (nDIaB) of diabetes.
Methods: from a prospectively maintained database, 313 patients (82 DIaB and 231 nDIaB) with unresectable hcc treated with sorafenib at Liver unit of cardarelli hospital were evaluated. chi-square test, kaplan-Meier method, and multivariate cox proportional hazards model were used. P <.05 was used to indicate statistical significance.
results: no differences in demographics, liver function, and cancer stage between DIaB and nDIaB groups were observed. all DIaB patients were affected by type 2 diabetes and the majority were treated with administration of exogenous insulin. the median duration of sorafenib treatment was 4 (range 1-41) months in DIaB and 3 (1-56) months in nDIaB. Main adverse events (fatigue, skin toxicity, diarrhea, hypertension) occurred with comparable frequency in both groups. the median overall survival was similar among groups (10 months in DIaB and 9 months in nDIaB). the median time to clinical or radiological progression (ttP) was 19 months in DIaB and 9 months in nDIaB groups (P=.024).
Image:
Conclusion: this is the first study that evaluated the interaction between diabetes and sorafenib treatment for hcc. sorafenib therapy in diabetic patients was safe. overall survival was comparable between DIaB and nDIaB groups. unexpectedly, a longer ttP in DIaB as compared to nDIaB group was observed. this finding needs to be evaluated in prospective studies.
Disclosure of Interest: none Declared
P-303 COMPArATIVe effICACy Of MeTrOnOMIC CAPeCITAbIne VerSuS beST SuPPOrTIVe CAre In reCurrenT hePATOCeLLuLAr CArCInOMA AfTer LIVer TrASPLAnTATIOn. A CASe-COnTrOL STuDy
Giovanni brandi* 1, Maria aurelia Barbera1, flavia neri1, Giorgio frega1, andrea Palloni1, stefania De Lorenzo1, Matteo cescon1, Giorgio ercolani1, antonio Daniele Pinna1, Matteo ravaioli1
1Policlinico s.orsola Malpighi, Bologna, Italy
Introduction: hepatocellular carcinoma (hcc) is one of the major indications to liver transplantation (Lt); the tumour recurrence occurs in about 10-30% cases. the management of the recurrence includes surgical, locoregional treatments or systemic treatment. a recent study reported a survival benefit of pts treated with sorafenib in this setting. In advanced hcc, metronomic capecitabine (Mc) showed an overall survival benefit in phase II (controlled) study. this case-control study evaluated the efficacy of metronomic capecitabine compared to best supportive care (Bsc) after hcc recurrence.
Methods: We retrospectively analysed data from a prospectively collected database. the pts treated with liver transplantation were included in the analysis at the moment of hcc recurrence. all patients were divided into two groups according to different treatment, when hcc recurrence was deemed untreatable with surgical or locoregional treatment: control arm with Bsc and treatment arm with metronomic capecitabine (500 mg b.i.d.). overall survival from recurrence was chosen as primary disease outcome.
results: of a total of 37 patients, 20 received Bsc (group 1) and 17 metronomic capecitabine (group 2). the two groups were well matched at baseline for: age; gender; etiology; pre-Lt treatment; pre-Lt tumor stage at imaging; MeLD, chILD and pathology stage at Lt; immunosuppression treatment; time to recurrence; pattern and site of recurrence; and afP, chILD, MeLD at recurrence. only microvascular invasion (p=0.013) and the tumor stage at the recurrence without Milan criteria

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 2 7
(p = 0.02) was prevalent in groups 1. Median time to recurrence was similar for all patients (13-14 months). overall survival in the metronomic capecitabine group was significantly improved (median survival: 22 vs 7 months, p=0.036). at a multivariate analysis the independent variables associated to an improved survival were: absence of episodes of acute rejection after transplantation (p=0.03), recurrence within Milan criteria (p=0.02) and treatment with metronomic capecitabine after untreatable progression (p=0.008). no G3-G4 side effects were reported in capecitabine group.
Conclusion: Metronomic capecitabine is associated with a survival benefit, with acceptable safety profile in pts with hcc recurrence after Lt.
references: ravaioli M, ercolani G, cescon M, Vetrone G, Voci c, Grigioni Wf, D'errico a, Ballardini G, cavallari a, Grazi GL. Liver transplantation for hepatocellular carcinoma: further considerations on selection criteria. Liver transpl. 2004 sep;10(9):1195-202.Welker MW, Bechstein Wo, zeuzem s, trojan j. recurrent hepatocellular carcinoma after liver transplantation–an emerging clinical challenge. transpl Int. 2012; 26(2):109-118sposito c, Mariani L, Germini a, reyes Mf, Bongini M, Grossi G, Bhoori s, Mazzaferro V. comparative efficacy of sorafenib versus best supportive care in recurrent hepatocellular carcinoma after liver transplantation: a case-control study. j of hepatol 2013; 59: 59-66Brandi G, de rosa f, agostini V, Di Girolamo s, andreone P, Bolondi L, serra c, sama c, Golfieri r, Gramenzi a, cucchetti a, Pinna aD, trevisani f, Biasco G. Metronomic capecitabine in advanced hepatocellular carcinoma Patients:aPhase II study. the oncologist 2013;18:1256-1257
Disclosure of Interest: none Declared
P-304 The POST-SIr-SPhereS SurGery STuDy (P4S): LIVer SurGery CAn be SAfeLy PerfOrMeD In PATIenTS WITh hePATOCeLLuLAr CArCInOMA (hCC) PreVIOuSLy TreATeD WITh SeLeCTIVe InTernAL rADIATIOn TherAPy (SIrT) uSInG y-90 reSIn MICrOSPhereS
bruno Sangro* 1, Michael schon2, rheun-chuan Lee3, Derek Manas4, rohan jeyarajah5, Georgios katsanos6, Geert Maleux7, antonio Pinna8, Lourens Bester9, David L. Morris10, David Iannitti11, Pierce chow12, richard stubbs13, Paul Gow14, Irene Bargellini15, kevin fisher16, Wan-yee Lau17, konstantinos kouladouros2, Vincent Donckier18, Georgio ercolani8, fernando Pardo19
1Liver unit, clinica universidad de navarra and cIBerehD, Pamplona, spain, 2klinikum karlsruhe, karlsruhe, Germany, 3taipei Veterans General hospital and national yang-Ming university school of Medicine, taipei, taiwan, 4university of newcastle upon tyne, newcastle nhs trust, newcastle upon tyne, united kingdom, 5Methodist Dallas Medical center, Dallas, united states, 6hôpital erasme, université Libre de Bruxelles, Brussels, 7university hospitals Leuven, Leuven, Belgium, 8university of Bologna, s. orsola-Malpighi, Bologna, Italy, 9st. Vincent’s hospital, sydney, 10st George hospital, university of new south Wales, kogarah, australia, 11carolinas Medical center, charlotte, united states, 12national cancer center, singapore, singapore, 13Wakefield clinic, Wellington, new zealand, 14austin hospital, heidelberg, australia, 15Pisa university hospital, Pisa, Italy, 16saint francis hospital, tulsa, united states, 17the chinese university of hong kong, hong kong, hong kong, 18hôpital erasme & Institut jules Bordet, Brussels, Belgium, 19clinica universidad de navarra, Pamplona, spain
Introduction: sIrt (or radioembolization) is increasingly used for the treatment of patients with hcc. It has been postulated that by inducing perihepatic or peritumoral fibrosis, causing or worsening portal hypertension, and/or by inducing subclinical lung damage, sIrt could make liver surgery more hazardous. the aim of this study was to evaluate the safety of liver surgery after sIrt.
Methods: P4s is an international, multicentre retrospective analysis of outcomes associated with liver resection (Lr) or transplantation (Lt) following sIrt using y-90 resin microspheres (sIr-spheres, sirtex Medical). Primary endpoints were peri-operative and 90-day post-operative morbidity (clavien-Dindo scale) and mortality. analysis used standard statistical methods. Data were captured on sIrt, surgery (between august 1998 and May 2014) and follow-up.
results: the outcomes of 49 patients with hcc treated by Lr (n=23) or Lt (n=26) were analyzed. Patients were mainly cirrhotics (Lr 61%; Lt 92%). nearly one-fourth (24%) had been previously submitted to other procedures including tace (18%), resection (4%) or ablation (2%), 9% had chemotherapy pre- or post-sIrt, and 8% had portal vein thrombosis or occlusion. regarding sIrt, 18% of patients received ≥2 sessions and 27% received sIrt to whole liver. Before surgery, 20% had total bilirubin ctc grade ≥2, 74% had comorbidities (mostly diabetes, hypertension and cardiopathy). Median asa score was 3 (asa ≥3: Lr 61%; Lt 81%). Lr included minor (35%), major not extended (48%) and extended resections (17%); 8% of Lt patients had living-related donor Lt. Median time from last sIrt to surgery was 8.0 (Lr) and 7.4 (Lt) months, respectively. Median post-operative stay [Iqr] was 8.0 [4.0] (Lr) and 11.0 [8.0] (Lt) days, respectively. the incidence of complications grade ≥3 was 4% (Lr) and 15% (Lt). Pulmonary-specific complications occurred only in 1 patient (grade 2) in the Lt group and was not potentially related to prior sIrt. any grade liver failure was observed in 0% (Lr) and 3.8% (Lt; 1 grade 2). 90-day readmission rates were 4% (Lr) and 27% (Lt) while no 90-day all-cause mortality was observed in either group. Median survival from the time of surgery has not been reached in any group with median post-surgery follow up of 28.5 (Lr) and 23.7 (Lt) months, respectively.
Conclusion: sIrt using y-90 resin microspheres does not increase morbidity or mortality after liver resection or transplantation. a beneficial effect of sIrt as an adjunct tool for liver resection and transplantation of hcc warrants further research
Disclosure of Interest: none Declared
P-305 GeMCITAbIne AnD OxALIPLATIn fOr The TreATMenT Of PeDIATrIC PATIenTS WITh hePATOCeLLuLAr CArCInOMA
allison f. o'neill1, Marcio h. Malogolowkin2, Laurence Brugieres3, Michela casanova4, james I. Geller5, Irene schmid6, rajkumar Venkatramani7, Patrick thompson8, jim feusner9, Arun A. rangaswami* 10
1Pediatric oncology, Dana-farber cancer Institute, Boston, 2Department of Pediatrics, university of california, Davis, Davis, united states, 3Department of Pediatrics, Institut Gustave roussy, Villejuif, france, 4Department of Pediatrics, Irccs fondazione Istituto nazionale tumori, Milano, Italy, 5uc Department of Pediatrics, unniversity of cincinnati, cincinnati, united states, 6Department of Pediatrics, Dr. von hauner childrens hospital, Munich, Germany, 7Department of Pediatrics, children’s hospital of Los angeles, Los angeles, 8Department of Pediatrics, university of north carolina, chapel hill, 9Department of Pediatrics, children’s hospital oakland research Institute, oakland, 10Department of Pediatrics, stanford university, Palo alto, united states
Introduction: Pediatric patients with hepatocellular carcinoma (hcc) are often treated with hepatoblastoma-directed therapy despite distinct histologies and natural histories. Patients with unresectable or metastatic disease fare poorly with less than 20% overall survival indicating a need for new therapeutic approaches. adult studies have demonstrated hcc responses to Gemcitabine and oxaliplatin (Gemox) as either frontline or retrieval therapy. We compiled data from pediatric oncologists regarding their experiences treating pediatric hcc patients with Gemox.
Methods: an international working group comprised of children’s oncology Group (coG), société Internationale d’oncologie Pédiatrique (sIoP), and the japanese study Group for Pediatric Liver tumors (jPLt) members met in tübingen Germany in March 2014 to discuss prospective treatment strategies for pediatric patients with hcc. We designed a secure electronic survey to collect de-identified patient information regarding disease histology, age, dose, response, and toxicity.
results: of 50 physicians polled, 20 responded. eight physicians treated 24 patients (10 conventional, 14 fibrolamellar, fL) with Gemox. Patient age ranged from 4-24 years. all patients received Gemcitabine 1000mg/m2 and oxaliplatin 100mg/m2 with the majority receiving q2 week dosing. Gemox was given first-line once and second-line ~60% of the time. using recIst criteria, seven patients (29%) achieved an upfront partial response (Pr) and seven patients (29%) achieved stable disease with a duration ranging from 3-16 months (all fL). Pr was sustained for 4-5 cycles; no patients became resectable. ten patients progressed. eleven patients experienced toxicities including grade 3-4 cytopenias, grade 3 nausea/vomiting and fever/neutropenia, and hepatopathy, neuropathy, or allergic reaction.
Conclusion: this is the most comprehensive report to date of Gemox use in pediatric patients with hcc. In the retrieval setting, response rates are more promising than those reported for adults (18%). these results support the potential trial of Gemox as first line therapy in pediatric hcc.
references: 1. ries LaG sM, Gurney jG, Linet M, tamra t, young jL, Bunin Gr (eds). seer Program 1975-1995 ncI, seer Program. nIh, Pub. no. 99-4649. Bethesda M, 1999.2. czauderna P, Mackinlay G, Perilongo G, et al. hepatocellular carcinoma in children: results of the first prospective study of the International society of Pediatric oncology group. j clin oncol 2002;20:2798-804.3. katzenstein hM, krailo MD, Malogolowkin Mh, et al. hepatocellular carcinoma in children and adolescents: results from the Pediatric oncology Group and the children's cancer Group intergroup study. j clin oncol 2002;20:2789-97.4. Louafi s, Boige V, Ducreux M, et al. Gemcitabine plus oxaliplatin (GeMox) in patients with advanced hepatocellular carcinoma (hcc): results of a phase II study. cancer 2007;109:1384-90.5. Mir o, coriat r, Boudou-rouquette P, et al. Gemcitabine and oxaliplatin as second-line treatment in patients with hepatocellular carcinoma pre-treated with sorafenib. Med oncol 2012;29:2793-9.6. zaanan a, Williet n, hebbar M, et al. Gemcitabine plus oxaliplatin in advanced hepatocellular carcinoma: a large multicenter aGeo study. j hepatol 2013;58:81-8.
Disclosure of Interest: none Declared
P-306 TrAnSArTerIAL CheMeOMbOLIzATIOn WITh Or WIThOuT SOrAfenIb fOr InTerMeDIATe STAGe hePATOCeLLuLAr CArCInOMA
yan zhao1, 2, hailiang Li3, Wei Bai4, jueshi Liu5, Weifu Lv6, sonia sahu7, sheng Guan8, xiao qin9, Wenhui Wang10, Weixin ren11, Wei Mu12, Weidong Guo13, shanzhi Gu14, yilong Ma15, jielai xia16, rafael Duran17, Daiming fan4, Guohong han* 4
1Department of Liver Disease and Digestive Interventional radiology, xijing hospital of Digestive Diseases, fourth Military Medical university, 2Department of Gastroenterology, first affiliated hospital

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 2 8
of the Medical college, xi’an jiaotong university, xi'an, 3henan cancer hospital, the affiliated cancer hospital of zhengzhou university, zhengzhou, 4xijing hospital of Digestive Diseases, fourth Military Medical university, xi'an, 5hunan Provincial People’s hospital, changsha, 6anhui Provincial hospital, hefei, china, 7Brigham and Women's hospital, harvard Medical school, Boston, united states, 8the first affiliated hospital of zhengzhou university, zhengzhou, 9the first affiliated hospital of Guangxi Medical university, nanning, 10the first affiliated hospital of Lanzhou university, Lanzhou, 11the first affiliated hospital of xinjiang Medical university, ulumuqi, 12the south west hospital, third Military Medical university, chongqing, 13Baogang hospital of Inner Mongolia, Baotou, 14hunan cancer hospital of central south university, changsha, 15tumor hospital of Guangxi Medical university, nanning, 16Department of Medical statistics, fourth Military Medical university, xi'an, china, 17centre hospitalier universitaire Vaudois, university of Lausanne, Lausanne, switzerland
Introduction: the proof of the survival benefit of sorafenib combined with transarterial chemoembolization (tace) over tace alone for intermediate-stage hepatocellular carcinoma (hcc) is lacking. the aim of this study is to evaluate the efficacy of combination therapy compared to tace monotherapy.
Methods: In this multicenter retrospective cohort study, 606 consecutive hcc patients with intermediate-stage and child-Pugh class a-B (≤7) were included. of them 202 received combination therapy and 404 received tace monotherapy. In the combination therapy group, patients with ≥ grade 2 dermatologic adverse events (aes) within the first two months of sorafenib initiation were defined as responders to combination therapy; whereas those with < grade 2 were defined as nonresponders. the primary endpoint was overall survival (os). Propensity score analysis was used to balance the baseline characteristic differences.
results: the difference in os between the two groups in entire cohort was not significant (22.3 vs. 17.9 months, P=0.343) although the trend of longer survival towards combination therapy. of note, in the combination therapy group, a prolonged median os was observed in 83 responders than that in 119 nonresponders (28.9 vs. 16.8 months, P=0.004). Multivariate analysis showed nonresponders were associated with increased risk of death compared with responders (hr=1.85; 95% cI 1.27-2.68, P=0.001). furthermore, the responders in the combination group had a significantly longer survival than patients treated with tace monotherapy (27.9 vs.18.3 months, P=0.046). the multivariate analysis showed that the hazard ratios of tace monotherapy for os was 1.692 (95%cI 1.163-2.463; P=0.006).
Conclusion: combination therapy in responders results in longer overall survival than tace monotherapy. the future randomized controlled study related to sorafenib should focus on the responders who are evaluated by dermatologic aes.
Disclosure of Interest: none Declared
P-307 hyALurOnIC ACID IS A uSefuL PreDICTOr Of LArGe AMOunT Of ASCITeS AfTer LIVer reSeCTIOn fOr PATIenTS WITh hePATOCeLLuLAr CArCInOMA
Takayuki Shimizu* 1, Mitsuru Ishizuka1, shozo Mori1, yukihiro Iso1, Masato kato1, Mitsugi shimoda1, taku aoki1, keiichi kubota1
1second Department of surgery, Dokkyo Medical university, Mibu, japan
Introduction: Large amount of ascites is one of the severe complications after liver resection for patients with hepatocellular carcinoma (hcc). Because postoperative large amount of ascites (PLa) provokes liver failure, predicting PLa is important to undergo safe liver resection for such patients.
Methods: four hundred hcc patients who had undergone liver resection were divided into two groups as follows: Group a, patients without PLa; Group B, patients with PLa. PLa was defined as follows: exceeding 10ml/kg/day ascites after liver resection. uni- and multivariate analyses were used to assess the clinical features associated with PLa. kaplan-Meier analysis and log rank test were used to compare the survival curves between groups a and B.
results: the median of PLa was 110 mL/day in Group a and 650 mL/day in Group B, respectively. among 17 clinical features significantly associated with PLa in univariate analysis, the result of multivariate analysis revealed that body mass index (BMI) (>22 vs. <22, kg/m2), albumin (>3.5 vs. <3.5g/dL), hyaluronic acid (ha) (<200 vs. >200, ng/mL), bleeding volume (<620 vs. >620, mL) and total intraoperative in-out balance (<5.0 vs. >5.0, mL/kg/hr) were significantly associated with PLa. especially, ha (<200 vs. >200, ng/mL) (or, 3.518; 95% cI, 1.637–7.742; P = 0.001) was the most useful predictor of PLa, because the area under the receiver operating characteristic (roc) curve of ha was the highest among these 5 features. relapse–free, cancer–specific and overall survival rates were significantly poorer in Group B than those in Group a.
Conclusion: PLa was closely associated with a poor prognosis of patients with hcc. especially, elevated ha (>200 ng/mL) can predict PLa of such patients.
Disclosure of Interest: none Declared
P-308 ADJuVAnT SOrAfenIb AfTer r0 reSeCTIOn fOr PATIenTS WITh LOCALLy ADVAnCeD hePATOCeLLuLAr CArCInOMA (bCLC-STAGe C): A CASe-MATCheD COMPArATIVe STuDy
feng xia* 1, Wan-yee Lau2, Lili Wu1, hongbo huan1, kuansheng Ma1
1Institute of hepatobiliary surgery, southwest hospital, third military medical university, chongqing, 2faculty of Medicine, the chinese university of hong kong, hong kong, china
Introduction: Liver resection for advanced hcc patients remains controversial, although some reports showed survival benefit in patients with more advanced hcc. however, early tumor recurrence is common after resection for hcc with macrovascular invasion, multinodular or large hcc. there is still no universally accepted adjuvant therapy for hcc after radical surgery and tumor recurrence is still the main cause of death for these patients. It has been reported that sorafenib can be used as an adjuvant therapy to decrease the risk of recurrence after potentially curative treatment in animal research and in clinical pilot studies.
Methods: thirty four hcc patients who were classified as BcLc-stage c received adjuvant sorafenib for high-risk of tumor recurrence after curative liver resection at a tertiary care university hospital. these patients were compared with a case-matched control group of 68 patients who received curative liver resection for hcc during the study period in a 1:2 ratio.
results: the tumor recurrence rate was significantly lower in the sorafenib group (15/34, 44.1%) than the control group (51/68, 75%, P = 0.002). the median disease-free survival was 12 months in the sorafenib group, and 10 months in the control group. univariate analysis showed tumor number more than 3, macrovascular invasion, hilar lymph nodes metastasis, and treatment with sorafenib were significant factors of disease-free survival. Multivariate analysis showed tumor number more than 3, and treatment with sorafenib were significant risk factors of disease-free survival in the cox proportional hazards model. the disease-free survival and cumulative overall survival in the sorafenib group were significantly better than the control group (P = 0.034, and 0.016, respectively).
Conclusion: this study demonstrated the potential benefit and safety of adjuvant sorafenib in reducing hcc recurrence and in extending disease-free and overall survivals for patients with hcc BcLc stage c after curative resection.
references: 1. Bruix j, sherman M, american association for the study of Liver Diseases. Management of hepatocellular carcinoma: an update. hepatology 2011; 53: 1020–1022.2. torzilli G, Belghiti j, kokudo n, takayama t, capussotti L, nuzzo G, et al. a snapshot of the effective indications and results of surgery for hepatocellular carcinoma in tertiary referral centers: is it adherent to the easL/aasLD recommendations?: an observational study of the hcc east-West study group. ann surg. 2013;257(5):929-9373. saab s, Mctigue M, finn rs, Busuttil rW. sorafenib as adjuvant therapy for high-risk hepatocellular carcinoma in liver transplant recipients: feasibility and efficacy. exp clin transplant. 2010 Dec;8(4):307-313.4. Wang sn, chuang sc, Lee kt. efficacy of sorafenib as adjuvant therapy to prevent early recurrence of hepatocellular carcinoma after curative surgery: a pilot study. hepatol res. 2014;44(5):523-531.5. Ishizawa t, hasegawa k, aoki t, takahashi M, Inoue y, sano k, et al. neither multiple tumors nor portal hypertension are surgical contraindications for hepatocellular carcinoma. Gastroenterology. 2008;134(7):1908-1916.
Disclosure of Interest: none Declared
P-309 ASSeSSMenT Of heALTh reLATeD quALITy Of LIfe AfTer hCC MAnAGeMenT by rADIOfrequenCy AbLATIOn Or TACe In A SInGLe eGyPTIAn STuDy
hassan hamdy1, eman Barakat1, hazem eL-hariri2, nevien eL-fouly3, runia eL-folly* 4, amr Mahmmoud5
1tropical Medicine, Professor, 2community Department, assisstant Lecturer, 3tropical Medicine, Lecturer, 4tropical Medicine, assisstant Professor, nasr city, egypt, 5Department of radiology, faculty of Medicine, ain-shams university, egypt
Introduction: standardized assessment of hrqoL may potentially provide physicians with valuable information before treatment decision. among patients with chronic liver disease and hepatocellular carcinoma (hcc); as one of the major squeal of chronic liver diseases, impairment in hrqoL has been reported. for that purpose, the relationship between subjective hrqoL scores and hcc stage according to BcLc staging system should be further analyzed. according to BcLc therapeutic algorithm; hcc patients in early stage, rfa is one of curative treatment modality, however hcc patients in intermediate stage, tace is the standard line of care as palliative treatment.
Methods: eighty hcc patients on top of chronic liver disease, 58 (72.5%) males and 22 (27.5%) females, mean age (51.8± 6.2), were categorized into 2 groups according to the different treatment modality. Group I: 40 hcc patients treated with radiofrequency ablation (rfa), Group II: 40 hcc patients treated with trans-arterial chemoembolization (tace). control Group: 40 cLD patients without hcc. hepatocellular carcinoma was diagnosed according to guidelines of american

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 2 9
association for the study of liver diseases. the sf-36 questionnaires will be fulfilled before and one month after the intervention.
results: the parameters of health-related quality of life (hrqoL) in control group were significantly better than hcc groups before intervention. While after intervention, assessment of hrqoL in control group was significantly better than those after tace but nearly equal to those after rfa. all parameters of (hrqoL) were evaluated before and after intervention in each group. In group I, all parameters of hrqoL were improved post-rfa with statistically significant difference (P<0.05). however in group II, all items of (hrqoL) were improved post-tace but without statistically significant difference (P>0.05). regarding the response after intervention in the two groups, hrqoL was better in those with complete response (70% in group I and 55% in group II) than those with incomplete response (30% in group I and 40% in group II) with statistically significant difference post-rfa (P<0.05).
Conclusion: Patients with hcc have worse hrqoL than patients with chronic liver disease without hcc. Improvements in overall hrqoL in hcc patients were achieved after intervention especially after rfa. the patients with complete response after intervention had better parameters of hrqoL than those with incomplete response.
Disclosure of Interest: none Declared
P-310 PerCuTAneOuS rADIOfrequenCy AbLATIOn In eGyPTIAn PATIenTS WITh hePATOCeLLuLAr CArCInOMA: APPLICAbILITy AnD PrOGnOSIS
Alaa Awad Taha* 1, ahmad el-ray1, Maged el-Ghannam1, nevin yilmaz2
1hepatogastroenterology, theodor Bilharz research Institute, cairo, egypt, 2hepatogastroenterology, Mugla university, Mugla, turkey
Introduction: hepatocellular carcinoma (hcc) is a significant health problem in egypt and is one of the major malignancies particularly in males. Incidence of hcc is increasing drastically in egypt over the previous two decades. ablative procedures, and in particular, percutaneous radiofrequency ablation (rfa) are important therapeutic modalities for this disease. the aim of this work is to study the percentage of egyptian patients with hcc who are candidates for this procedure, its efficacy and prognosis in terms of recurrence and survival.
Methods: Patients attended outpatient clinic, from january 2005 to December 2010, were thoroughly examined and fully investigated. hcc was diagnosed by detection of hepatic nodule(s) on abdominal ultrasound examination and typical findings on triphasic ct scanning of abdomen. serum alfa fetoprotein (afP) was determined in all patients. criteria of inclusion for treatment by rfa include patients with solitary hcc lesion < 5 cm, or multiple (up to 3) lesions < 3 cm each, with compensated liver cell function, absence of evidence of macrovascular invasion and absence of distant metastatic lesions. Patients were treated with rfa and followed up at 3 months interval for a total period of 4 years. follow up program included abdominal ultrasonography, triphasic ct scanning of abdomen and assessment of serum afP level. efficacy was considered when achieving complete necrosis of the lesion(s) with no detectable viable tumorous tissue. recurrence was considered when typical features of lesion enhancement at arterial phase and rapid washout at delayed phase were detected on triphasic abdominal ct scanning with or without elevated serum afP levels. Mortalities due to other causes than hcc recurrence were excluded from the study.
results: only 171 patients from a total of 1897 patients with hcc (9%) were candidates for treatment with rfa. complete necrosis of the lesion(s) could be achieved in 167 patients (97.7%). recurrence of hcc within 1 year following rfa was recognized in 49 patients (28.7%). cumulative rates of recurrence after 2, 3 and 4 years were 38.6%, 57.3% and 89.5% respectively. recurrence was recognized within the same ablated lesion(s) in 78 patients (51% from patients with recurrence) while patients who developed new hepatic lesions were 71 (46.4%). extrahepatic recurrence was detected in 4 patients only (2.6%) and the main sites for this pattern of recurrence were flat bones (hip bone, vertebrae and scapula). Patients who were candidate for re-ablation by rfa were 60 (40.3% of patients with intrahepatic recurrence).
Conclusion: rfa is eligible for a small sector of egyptian patients with hcc and it is has a very high efficacy. rfa is associated with a significant rate of recurrence, and this rate is increasing over the years following treatment. Many patients with intrahepatic recurrence are candidates for re-ablation.
Disclosure of Interest: none Declared
P-311 hePATIC ArTerIAL InfuSIOn CheMOTherAPy (hAIC) In TrAnSCATheTer ArTerIAL CheMOeMbOLIzATIOn (TACe)-refrACTOry Or InTOLerAnT hePATOCeLLuLAr CAnCer (hCC) PATIenTS WITh POOr hePATIC funCTIOn
Takeshi Aramaki* 1, emima Bekku1, rui sato1, Michihisa Mariguchi1, Masahiro endo2
1Div.of Interventional radiology, 2Division of Diagnostic radiology, shizuoka cancer center, shizuoka, japan
Introduction: sorafenib is currently the only treatment option for hepatocellular cancer (hcc) patients who prove refractory to or intolerant of transcatheter arterial chemoembolization (tace)[1][2]. sorafenib is indicated in patients with child-Pugh a, but no standard therapy is available for patients with child-Pugh B or c, or poor hepatic function. the present study retrospectively assessed the safety and efficacy of hepatic arterial infusion chemotherapy (haIc) in tace-refractory or intolerant hcc patients with child-Pugh B or c.
Methods: of the 128 patients who underwent haIc at our hospital between september 2002 and December 2013 using a percutaneously implantable port catheter system, we assessed safety and efficacy in those with child-Pugh B or c and no extrahepatic lesions. among the patients, we targeted the 38 with child-Pugh B or c and no extrahepatic lesions.
results: We evaluated 38 patients; 6 women, 32 men; mean age, 64.5 years; hepatitis virus history, B/c/B+c/non=14/19/1/4; vascular invasion y/n=32/6. the chemotherapy regimen consisted of 5-fluorouracil (5-fu)/interferon in 15 patients and cisplatin/5-fu in 23 patients. response rate was 31.6% and overall survival was 168 days. no serious adverse events were observed. reasons for treatment discontinuation/termination were disease progression (n=30), hepatic artery occlusion (n=3), other adverse events (n=3), refusal of treatment by the patient (n=1) and complete remission (n=1).
Image:
Conclusion: haIc can be performed safely in tace-refractory or intolerant hcc patients with child-Pugh B or c. a randomized controlled trial is now needed to assess whether this therapy contributes to improved survival.
references: 1) Llovet jM, ricci s, Mazzaferro V, hilgard P, Gane e, Blanc jf, de oliveira ac, et al: sorafenib in advanced hepatocellular carcinoma. n engl j Med 2008;359:378–390.2)cheng aL, kang yk, chen z, tsao cj, qin s, kim js, Luo r, et al: efficacy and safety of sorafenib in patients in the asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomized, double-blind, placebo-controlled trial. Lancet oncol 2009;10:25–34.
Disclosure of Interest: none Declared
P-313 APPLICATIOn Of MeTrOnOMIC CheMOTherAPy fOr The PATIenT WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA WITh POrTAL VeIn TuMOr ThrOMbOSIS
Soonkyu Lee* 1, hyun yang2, hae Lim Lee2, seung kew yoon2, ho jong chun3, jung suk oh3, angelo B. Lozada2, jong young choi2, si hyun Bae2, ji Won han2
1Department of Internal Medicine, 2Department of Internal Medicine, 3Department of radiology, college of Medicine, the catholic university of korea, seoul, korea, seoul, korea, republic of
Introduction: Metronomic chemotherapy (Met) is frequent administration of comparatively low doses of chemotherapeutic agent without extended break. In some advanced cancer, the paradigm of chemotherapy is shifted from maximum tolerated dose (MtD) chemotherapy to Met.the aim of this study is to evaluate the efficacy and safety of Met comparing with conventional transcatheter arterial chemoembolization (tace) for the patients with advanced hcc with PVtt.
Methods: total 65 patients with advanced hcc with PVtt who had undergone Met were analyzed between june, 2005 and august, 2013. epirubicin 35 mg/body surface area (Bsa) was administrated every 4 weeks, and cisplatin 15 mg/Bsa and 5-fluorouracil 50 mg/Bsa were administrated weekly for 3 weeks through hepatic arterial chemoport accompanying with 1 week break. and, total 55 patients who had undergone conventional tace were analyzed as control group.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 3 0
results: the median cycle of Met was 2 (1-15). overall survival of Met group and tace group were 158 days (100-216) and 95 days (68-122), respectively (P=0.001). the cox proportional-hazard model showed that a higher risk of death was correlated with extrahepatic metastasis (hr=1.668, P=0.048), higher child-pugh score (hr=1.326, P=0.019), and larger tumor size (hr=1.086, P=0.001). and Met showed better survival outcome than conventional tace (hr=0.275, P<0.001).
Conclusion: Met showed favorable outcome in terms of overall survival than conventional tace in patients with advanced hcc with poor liver function. therefore, in patients with advanced hcc with PVtt, especially in cases of poor liver function, extrahepatic metastasis or large tumor size, Met may be considered as a treatment option.
Disclosure of Interest: none Declared
P-314 SOrAfenIb VerSuS CyTOTOxIC CheMOTherAPy fOr PATIenTS WITh reCurrenT hePATOCeLLuLAr CArCInOMA AfTer LIVer TrAnSPLAnTATIOn
eun Jeong Ko* 1, Bo hyun kim1, sang Myung Woo1, seung Duk Lee1, seong hoon kim1, Woo jin Lee1, eun kyung hong1, chang-Min kim1
1center for liver cancer, national cancer center, korea, Gyeonggi-do, korea, republic of
Introduction: as hepatocellular carcinoma (hcc) has become a major indication for liver transplantation (Lt), post-Lt hcc recurrence is also increasing. however, chemotherapy has been scarcely studied. the aim of this study was to evaluate the outcomes and prognostic factors of systemic chemotherapy in patients with post-Lt hcc recurrence.
Methods: a total of 394 patients with hcc who underwent Lt between jan 2005 and seP 2013 were enrolled. Data of patients given palliative chemotherapy for recurrent hcc after Lt were reviewed. Patients receiving sorafenib as a first-line systemic agent were compared with those receiving cytotoxic chemotherapy (cisplatin-based regimen) in the pre-sorafenib era.
results: hcc has recurred in 83 out of 394 patients who underwent Lt. forty-five patients (median age 54, range [37-73]; male 81.1%) received palliative chemotherapy. histological examination of the explanted liver showed macro- and microvascular invasion in 35.6% and 76.8%, respectively. a total of 85.4% had a pathological stage t3/t4 by the modified uIcc system. Median time to recurrence was 8.4 months (95% confidential interval [cI], 5.5-11.3). as a first-line systemic therapy, sorafenib (arm s, n=33) or cytotoxic chemotherapy (arm c, n=12) was given. Median overall survival (os) was 7.5 months (95% cI, 5.1-9.9) and 18.0 months (95% cI: 7.9-28.1) in arm s and arm c, respectively (P=0.03); the corresponding median time to progression (ttP) was 4.4 months (95% cI, 2.8-5.9) and 3.8months (95% cI, 2.4-5.2), respectively (P=0.75). at the initiation of chemotherapy, 42.4% of arm s and 50.0% of arm c had extrahepatic spread only (P=0.74). arm s had more portal vein invasion (12.1 % vs. 0.0%; P=0.67) and a serum alpha-fetoprotein (afP) level of ≥ 400 ng/mL (42.4% vs. 33.3%; P=0.73); however, they were less frequently given additional therapies after progression (45.5% vs. 75.5%; P=0.10) compared to arm c. the grade 3/4 hematological toxicity was more common in arm c (15.2% vs. 25.0%; P=0.66), and so was grade 3/4 hepatic toxicity in arm s (33.3% vs. 8.3%; P=0.136).Multivariate analysis indicated that pathological type of tumor (massive/infiltrative type) at the time of transplantation (hr 2.83; 95% cI, 1.43-5.56), the multiple intrahepatic lesions (≥3) at the time of chemotherapy (hr 2.39; 95% cI, 0.09-0.43), the treatment with sirolimus (hr 0.335; 95% cI, 0.140-0.808), and the subsequent treatment after initial chemotherapy (hr 0.190; 95% cI, 0.062-0.547) were independent prognostic factors associated with the os.
Conclusion: Patients receiving cytotoxic agents as a first-line systemic therapy seemed to have better os, but similar ttP when compared with those receiving sorafenib. the type of tumor (massive/infiltrative type) at the time of transplantation, multiple intrahepatic tumors at the time of chemotherapy, sirolimus use and the subsequent treatment after initial chemotherapy were independent prognostic factors associated with the os of patients with recurrent hcc after Lt.
Disclosure of Interest: none Declared
P-315 rePeATeD STereOTACTIC bODy rADIOTherAPy fOr reCurrenT hePATOCeLLuLAr CArCInOMA
Won Il Jang* 1, Mi-sook kim1, chul koo cho1, young seok seo1, chul ju han2, jin kim2, su cheol Park2, sang Bum kim3, eung-ho cho3
1radiation oncology, 2Internal Medicine, 3surgery, korea Institute of radiological & Medical sciences, seoul, korea, republic of
Introduction: Intrahepatic recurrence is the most common pattern of failure after curative treatment in the patients with hepatocellular carcinoma (hcc). In regard to primary hcc, the treatment strategy for recurrent intrahepatic hcc is determined by the function of the liver and the macroscopic tumor features. the purpose of this study is to determine the feasibility and efficacy of repeated stereotactic body radiotherapy (sBrt) for inoperable recurrent hcc.
Methods: We retrospectively reviewed 28 recurrent hcc patients who were treated with the repeated sBrt at korea cancer center hospital between january 2004 and May 2014. all patients were unsuitable for surgery or local ablation and had incomplete response to transarterial chemoembolization. twenty-seven patients (96%) underwent the repeated sBrt for intrahepatic recurrence other than the lesion with the 1st sBrt, and only one patient underwent re-irradiation for the same lesion with the 1st sBrt. twenty-seven patients (96%) had child-turcotte-Pugh (ctP) class a (a5 in 23 and a6 in 4, respectively). the median dose was 51 Gy (range, 30-60 Gy in 3–5 fractions) and 44 Gy (range, 30–60 Gy in 3-4 fractions) in the 1st and the repeated sBrt, respectively.
results: the median follow-up duration was 11 months (range, 2–56 months). the median interval between the first and the repeated sBrt was 11 months (range, 2–48 months). the 2-year local failure-free and overall survival rates were 77% and 42%, respectively. three patients (11%) experienced deteriorating of ctP score by greater than or equal to 2 within 3 months of sBrt without disease progression. the total mean normal liver dose was the most significant predictor for hepatic deterioration after the repeated sBrt.
Image:
Conclusion: this study showed that the repeated sBrt can be safely and effectively administered to the patients with inoperable recurrent hcc, and these results suggest that this technique might be considered a salvage treatment. We suggest that patients with the repeated sBrt should be treated using the total mean normal liver dose constraint of 32 Gy3 or less. a further well-controlled large-scale study and longer follow-up are needed to determine the optimal dose-volume constraints and characterize late complications.
Disclosure of Interest: none Declared
P-316 TreATMenT Of ADVAnCeD hePATOCeLLuLAr CArCInOMA (hCC): A SInGLe CenTre COST AnALySIS Of yTTrIuM 90 TrAnS-ArTerIAL rADIO-eMbOLIzATIOn (TAre) VerSuS SOrAfenIb
Maria Grazia Luca* 1, Massimo De Giorgio1, Giulia Magini1, anna Baldan1, francesca Mangiola2, Giorgio Virotta3, roberto nani4, roberto agazzi4, alessandro Vitale5, stefano fagiuoli1
1gastroenetrology, hPGxxIII, bergamo, 2Internal Medicine and Gastroenterology, Policlinico a. Gemelli, roma, 3medicina nucleare, 4radiologia, hPGxxIII, Bergamo, 5chirurgia epatobiliare a trapianto epatico, azienda ospedaliera universitaria, Padova, Italy
Introduction: In a selected population of advanced hcc patients tare seems to give promising results. We aimed to compare a single centre costs for sorafenib and tare
Methods: 166 consecutive advanced hcc patients (M 86%, median age 67 yrs) treated with sorafenib between june 2009 and june 2014 (Group sor) and 19 (M 84%, median age 64 yrs, BcLc B 31,5%) treated with tare between june 2011 and june 2014 (Group tare) were compared. Patients were grouped for treatment time (Group sor 1: < 2 months of treatment; Group sor 2: > 2 months of treatment). Group sor 1 drug expenses were not further considered according with the agreed "pay for result policy". In group sor 2, 24 pts (group sor 3) presented monolobar disease and no methastasis (BcLc B 54%) so as to be potentially treated with tare. sorafenib cost was calculated according with the total effective caps intake for each patients (28,7 euro/caps).tare costs included yttrium-90 and hospitalization expense (17.761 euro/patient).
results: Median time of treatment in Group sor 3 was 272 days (154-994) with a median intake of 2,8 tablets/day. all the patients in the group tare were treated with a single treatment session. Median follow up time was respectively 476 days (154-1518) for the Group sor 3 and 266 days (47-867) for the Group tare. survivals at 12, 18, 24 and 36 months were respectively 66,7%, 37,5%,

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 3 1
24,3% and 19.4% for the Group sor 3 and 64.1%, 64.1%, 64.1% and 32% for the Group tare (Log rank p=0.446). the GLoBaL treatment costs for Group sor 3 and for Group tare were € 671.809,6 and € 337.459,00 respectively (median € 27992/pt in sor3 vs € 17761/pt in tare; p =0.028).
Conclusion: In comparison to sorafenib, tare seems lead to a lower expense in a single centre treatmen strategies for advanced hcc
Disclosure of Interest: none Declared
P-317 OuTCOMe Of hePATIC reSeCTIOn fOr hePATOCeLLuLAr CArCInOMA In PATIenTS WIThOuT CIrrhOSIS
Anupama nookala* 1, andrew henn2, nabiha shamsi1, Marsha finkelstein2, coleman smith1, 2, srinevas reddy2, Michael Min2, Paola ricci1
1Division of Gastroenterology, hepatology, and nutrition, university of Minnesota, 2Virginia Piper cancer Institute, abbott northwestern hospital, Minneapolis, united states
Introduction: hepatocellular carcinoma (hcc) survival after resection has improved in the past 20 years.1 In patients with hcc in a non-cirrhotic liver, 1-, 3-, and 5-year survival rates were 75.4%, 54.7%, and 38.9% respectively.2 In another study, 54 patients developed recurrence at a median interval of 30.96 months. of these, 31.5% and 24.1% occurred during 1 and 5 years, respectively.3 We studied survival and tumor recurrence following surgical resection of hcc in a community hospital with long standing surgical oncology expertise. the primary outcome was overall patient survival at 1-, 3-, and 5 years. the secondary outcomes were hcc recurrence rates, time to hcc recurrence, and predictors of survival and recurrence.
Methods: a retrospective review of all subjects who underwent hepatic resection for hcc at abbott northwestern hospital in Minneapolis, Minnesota, usa, in years 2004 to 2014. 37 of 42 total patients were non-cirrhotics and included in the study. recurrence data was available on 35 of 37 patients. recurrence was defined as image documented lesion consistent with hcc (i.e. ct, MrI), any time post resection. time to recurrence was measured in months. kaplan-Meier method curves were obtained for recurrence and overall survival. cox regression analysis was used to explore co-factors of recurrence and survival. factors tested for risk of recurrence included preoperative risk factors of chronic liver disease and alpha-fetoprotein (afP); recurrence was added to these factors to predict death. tumor-specific features and non-tumoral liver histology were collected.
results: Median time to last patient contact was 33 months. Mean age was 60.0 (sD: 13.5), range: 31-84, 19 (51.4 %) female. age of males and females were similar, mean (sD) of 58.1 (12.4) and 61.9 (14.6) respectively (p=0.395, two-sided t-test). tumor specific features were collected: median tumor size 7.5 cm (range 2.2-22.5cm), unifocal tumor (89.2%), tumors with satellite lesions (10.8%), angiolymphatic invasion (45.9%), non-tumoral steatosis (32.4%), and non-tumoral fibrosis (2.7%). overall and recurrence free survival at 1-, 3-, and 5 years was 87.9%>69.2%>44.4% and 80%>52.2%>31.6% respectively, of observable patients. sex (male vs. female) was the only factor that was significantly related to survival, log-rank=0.041, by kaplan-Meier method. Mean (se) survival estimate was 50.4 (8.9) months for males, and 70.2 (5.3) months for females. 7/19 (36.8%) females and 6/16 (37.5%) males had recurrence. Median time to recurrence was 8.8 months (range: 2.3-45.6 months) based on 6 recurrences for males, and 30.2 months (range: 1.7-36.7 months) based on 7 recurrences for females. cox regression analysis identified that along with sex, recurrence (p-value=0.021) impacted survival. afP and preoperative risk factors of chronic liver disease did not predict recurrence.
Conclusion: non-cirrhotic hcc occurred in an even larger proportion of females when compared to published data. females lived significantly longer than males after resection of non-cirrhotic hcc. hcc recurrence rate was similar in females and males, however time to recurrence was longer in females although not statistically significant. Differently from other studies, afP was not predictive of recurrence. overall and recurrence-free survival analysis were comparable to recent studies.
references: 1. fan st, et al. ann surgery,2011;253:745-75. 2. faber W, et al. surgery,2013;153(4):510-7. 3. chiche L, et al. World j surg,2013;37(10):2410-8.
Disclosure of Interest: none Declared
P-318 effICACy Of SOrAfenIb In PATIenTS WITh InTerMeDIATe-STAGe hePATOCeLLuLAr CArCInOMA: reSuLTS frOM The ITA.LI.CA. DATAbASe
rodolfo Sacco* 1, Valeria Mismas1, Luca Giacomelli1, sara Marceglia1, antonio romano1, Marco Bertini1, Michele Bertoni1, Graziana federici1, salvatore Metrangolo1, Giuseppe Parisi1, emanuele tumino1, Giampolo Bresci1
1Gastroenterology, cisanello Pisa university hospital Pisa - Italy, Pisa, Italy
Introduction: sorafenib represents the elective treatment for patients affected from advanced-stage (BcLc-c according to the Barcelona clinic of Liver cancer classification) hcc; this molecule is also recommended in patients with intermediate-stage (BcLc-B) disease who have failed or are
not eligible to transareterial chemoembolization (tace). however, further information on the use of sorafenib in patients with BcLc-c hcc is warranted. this study analyses the efficacy of sorafenib in patients with BcLc-B hcc, with respect to those with BcLc-c disease, in the nation-wide Italian database Ita.LI.ca.
Methods: the Ita.LI.ca. database contains data of 5428 hcc patients treated at 18 Italian centers. all patients with either BcLc stage B or c and who received sorafenib were considered. overall survival (os), time to progression (ttP), and disease control rate (Dcr) were evaluated. safety considerations were also performed.
results: a total of 243 patients were included. of these, 61 were in BcLc-B stage (29 received ≥1 tace prior to sorafenib) and 182 in BcLc-c. In the overall population, median ttP was 8 months (95%cI 6-9), median os was 13 months (95%cI 10-15.5), and Dcr was 28.3% (complete response, cr=1.6%; partial response, Pr=8.9%; stable disease, sD=17.8%). Patients in BcLc-B stage had a median ttP of 10 months (95%cI 6-14), a median os of 19 months (95%cI 12.5-26.5), and a Dcr of 39.1% (cr=2.4%; Pr=9.8%; sD=26.8%), whereas patients in BcLc-c stage had a median ttP of 7 months (95%cI 6-8), a median os of 11 months (95%cI 10-15.5), and a Dcr of 25.3% (cr=1.3%; Pr=8.7%; sD=15.3%). the safety profile of sorafenib was similar in the two sub-populations.
Conclusion: these “field-practice” findings suggest that the administration of sorafenib in BcLc-B patients with hcc may be effective and is not associated with any new safety warning
Disclosure of Interest: none Declared
P-319 The effeCT Of Cx-4945, A CK2 InhIbITOr, On ChOLAnGIOCArCInOMA (CCA): In VITrO DATA
kais zakharia1, catherine D. Moser1, Mitesh j. Borad2, Lewis r. roberts* 1
1Division of Gastroenterology & hepatology, Mayo clinic, rochester, 2Division of hematology/oncology, Mayo clinic, arizona, united states
Introduction: there is a need to develop effective therapies for cca due to the suboptimal outcomes with the current standard gemcitabine (Gem) and cisplatin (cis) therapy. casein kinase II (ck2) is a serine/threonine selective protein kinase that has been implicated in cancer progression making it an attractive target for anticancer treatment. cx-4945 is a first in class, orally available and highly selective inhibitor of ck2 protein kinase. cx-4945 has shown antitumor activity in other human cancers. In this study we investigated the anti-neoplastic effect of cx-4945 on 3 different cca cells.
Methods: cck8 and colony formation assays were used to assess cell viability in cultures of hucct1, eGI-1, and the new primary patient derived cca cell line LIV27 after treatment with cx-4945 alone or in combination with Gem, cis or both. the half maximal inhibitory concentrations (Ic50) were calculated using the chou-talalay technique. Western immunoblotting was used to assess the effect of cx-4945 on akt pathway in cca cells.
results: cx-4945 significantly decreased cell viability of hucct1, eGI-1 and LIV27 in a time dependent and a dose dependent manner (with Ic50 of 7.3, 9.5, and 9.4 μM respectively at 72 hours). cx-4945 inhibited colony formation in hucct1 and eGI-1 with Ic50 of 3.8 and 1.6 μM respectively. cx-4945 inhibited akt phosphorylation at two different phosphorylation sites (serine473 and serine129) suggesting that it acts through the akt pathway. cx-4945 had a synergistic (if higher doses used) or additive effect (if lower doses used) when combined with either cis or Gem on hucct1, eGI-1 and LIV27 cells. addition of cx-4945 to both Gem and cis together (1/4 Ic50s, ½ Ic50s, ¾ Ic50s and Ic50s) further decreased viability of hucct1 cells.
Conclusion: cx-4945 has an anti-proliferative effect on cca cell cultures. the anti-proliferative effect of cx-4945 correlates with effects on akt cell signaling. cx-4945 enhanced the anti-proliferative effect of both cis and Gem in vitro. additional studies are needed to validate and extend these findings.
Disclosure of Interest: none Declared
P-320 PrOSPeCTIVe, MuLTICenTer, reGISTry STuDy Of OxALIPLATIn (eLOxATIn®)/5-fLuOrOurACIL bASeD reGIMen fOr ChIneSe LOCAL ADVAnCeD Or MeTASTATIC hePATOCeLLuLAr CArCInOMA PATIenTS IneLIGIbLe fOr CurATIVe reSeCTIOn AnD LOCAL TreATMenT
Shukui qin* 1, jun Liang2, jianming xu3, ying cheng4, jia he5
1People’s Liberation army cancer center, Bayi hospital, nanjing, 2Department of Medical oncology, the affiliated hospital of Medical college qingdao university, qingdao, 3the affiliated hospital of academy of Military Medical sciences, Beijing, 4Department of Medical oncology, jilin Province cancer hospital, changchun, 5Department of health statistics, second Military Medical university, shanghai, china

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 3 2
Introduction: hepatocellular carcinoma (hcc) is the fourth most common cancer and the second leading cause of cancer death in china. While oxaliplatin (eloxatin®) has been approved for systemic chemotherapy in chinese hcc patients in 2013, the regimens and dosages vary a lot between different hospitals and clinicians. therefore, it’s critical and urgent to collect evidence from daily clinical practice in order to help establish evidence-based guideline for oxaliplatin use in chinese hcc patients.
Methods: this is a prospective, multicenter, registry study designed to assess the safety and efficacy for systemic chemotherapy with eloxatin®/5-fu based regimen in locally advanced and metastatic hcc patients who are ineligible for curative resection and local treatment. Patients aged 18-70 years with histologically, cytologically or clinically diagnosed hcc will be recruited into this study if they are ineligible for or not willing to accept curative resection and local treatment and intended to receive eloxatin®/5-fu based systemic chemotherapy. Patient will be excluded from the study if he/she is receiving any other study treatments or experimental medical treatment within 30 days prior to screening visit, or documented allergy to platinum compound. Pregnant or lactating women or women of childbearing potential without proper contraceptive methods will also be excluded. In contrast to randomized controlled clinical trial, there is no imposed experimental intervention. the treatment is determined solely by the patient’s physician. Patients will be followed-up till death, or patient’s withdraw, or 12 months after the last eligible patients’ enrollment. the primary endpoint is to assess the frequency of drug-related grade 3/4 liver toxicity. the secondary endpoints include the frequency and severity of all other adverse events, treatment efficacy (i.e., overall survival, progression free survival, objective response rate, disease control rate), as well as treatment exposures (i.e., number of chemo-cycles, actual dose intensity, relative dose intensity). the exploratory endpoints are correlations between patient characteristics and treatment efficacy and safety. according to the results from each study which evaluated foLfox4 regimen (fluorouracil, leucovorin, and oxaliplatin) in advanced hcc patients in asia, the incidence of drug-related grade 3/4 liver toxicity was 10.0%. the sample size of this study is therefore calculated to be 417 patients, which produces a two-sided 95% confidence interval with a width equal to 6.0%. Given an approximate dropout rate of 15%, the study plans to enroll 500 patients in total.
results: this study is registered at International clinical trials registry Platform with the registration no. of chictr-oPc-15005865. It is now in the patient recruitment stage. the first patient was enrolled on sep 1st, 2014. the study is expected to last for 30 months, including enrollment for 18months plus follow up for 12 months after the last eligible patients’ enrollment. the final report of the study is planned in 2017.
Conclusion: the data captured and reported in this registry study will reflect a "real world" approach to the treatment of patients with locally advanced and metastatic hcc who are not applicable for resection and local treatment. the results from this study will definitely help to optimize the use of oxaliplatin (eloxatin®) for chinese hcc patients in the future.
Disclosure of Interest: none Declared
P-321 effICACy Of COMbInATIOn TherAPy Of hePATIC ArTerIAL InJeCTIOn CheMOTherAPy WITh rADIOTherAPy fOr unreSeCTAbLe ADVAnCeD hePATOCeLLuLAr CArCInOMA COMPLICATeD by MAJOr VASCuLAr TuMOr ThrOMbOSIS: AnALySIS Of 26 CASeS
Joji Tani* 1, hisaaki Miyoshi2, hirohiro yoneyama2, tsutomu Masaki2
1Department of Gastroenterology and neurology, 2faculty of Medicine, kagawa university, Mliki-cho, japan
Introduction: hepatocellular carcinoma (hcc) is the most common fatal malignant neoplasm of the liver and the third leading cause of cancer-related deaths worldwide. hcc complicated by vascular tumor thrombosis is associated with poor prognosis and has no established standard treatment. the aim of this study was to retrospectively evaluate the response rate, survival outcome, and adverse effects of hepatic artery infusion chemotherapy (haIc) for intrahepatic tumor combined with local radiotherapy in patients with advanced hcc complicated by vascular tumor thrombosis.
Methods: subjects were 26 patients with advanced hcc complicated by high-grade vascular invasion with sufficient residual hepatic function, regardless of the degree of disease progression. haIc consisted of cisplatin in lipiodol emulsion combined with 5-fluorouracil (5-fu). haIc was continued as long as liver function and other conditions permitted. radiotherapy was given at a total dose of 2 Gy on 25-28 occasions (total dose, 50-56 Gy). after treatment completion, response to treatment, outcome, and adverse reactions were prospectively analyzed.
results: the maximum responses to radiotherapy for vascular invasion as assessed by the m-recIst criteria were cr in 8 patients, Pr in 14, sD in 4, and PD in 0, giving a response rate of 84.6% and a tumor control rate of 100%. the maximum responses to the combination therapy for the entire tumor as assessed by the m-recIst criteria were cr in 1 patient, Pr in16, sD in 6, and PD in 3, for a response rate of 65.3% and a tumor control rate of 88.4%. the median survival time was 16.3 months for all 26 cases. Localization of the tumor in either lobe of the liver was identified as a significant independent predictor of prolonged survival. Grade 3 hepatic atrophy was observed
in 3 patients within 3 months of radiotherapy, but they could all continue with the study regimen.the combination therapy was well tolerated, with no serious adverse reactions, except for reactivation of hepatitis B in 1 patient.
Conclusion: combination therapy consisting of haIc using cisplatin in lipiodol emulsion combined with 5-fu and radiotherapy appears to be a safe and effective treatment option for patients with hcc complicated by unresectable hcc with vascular invasion.
Disclosure of Interest: none Declared
P-322 CLInICAL IMPACT Of ADDITIOnAL InTerferOn ADMInISTrATIOn On SOrAfenIb-TreATeD PATIenTS WITh reCurrenT ADVAnCeD hePATITIS C- reLATeD hePATOCeLLuLAr CArCInOMA
hisakazu Doi* 1
1Gastroenterology and hepatology, nagahama red cross hospital, nagahama, japan
Introduction: sorafenib has been considered the only effective treatment option for advanced hcc but the clinical benefit of sorafenib remains to be insufficient. the aim of this study was to investigate whether Ifn administration in combination with sorafenib could provide additional benefits on clinical outcomes in patients with recurrent advanced hepatitis c-related hcc.
Methods: this retrospective study included all consecutive 27 patients with recurrent advanced hepatitis c-related hcc who have failed at least one or more previous locoregional therapies between 2009-2015. We divided the patients into two groups; control group (n=14) received sorafenib alone (400mg, 800mg), treatment group; (n=13) received sorafenib (200mg, 400mg) plus Ifn (PeG Ifn 90μg, Ifnα 300Mu). survival rate, adverse events and factors related to treatment effects were analyzed. overall survival was calculated using kaplan Meier method.
results: treatment group was 13 patients (92% male, median age 73 yrs, child a/B/c: 10/3/0, previous treatment: tace/rfa/oPe/haIc/other; 7/9/1/4/1), and control group was14 patients (57% male, median age 77 yrs, child a/B/c: 10/4/0, previous treatments tace/rfa/oPe/haIc/other: 8/7/0/2/0). Backgrounds except for gender were not statistically different. the reasons for stopping previous therapies (e.g. impairment of liver function test, portal vein thrombosis/distant metastasis and/or multiple/huge hccs) were not statistically different between two groups (P=0.122, 0.248, 0.07, respectively). tumor control rate (cr, Pr or sD) in both groups were similar (treatment group: 13/10, 76.9% and control group: 9/14, 64.3%, P=0.2369). treatment group was observed significantly longer median overall survival than control group (37 months vs. 13.3 months, P=0.0026). In addition, patients who achieved Pr or sD in the treatment group revealed a significantly longer survival as compared with control group which also achieved Pr or sD (43 months vs. 20.5 months, P=0.001). especially among the patients <76 yrs old, treatment group was significantly longer survival than control group (P=0.0037), whereas among the patients 77 yrs old, there was no statistical difference between two groups (P=0.669). During the treatment periods, adverse events were mild in treatment group.
Conclusion: adding Ifn on sorafenib monotherapy had significant impact on the survival especially in patients <76 yrs old with recurrent advanced hepatitis c- related hcc. further studies are needed to confirm the additional role of Ifn on sorafenib monotherapy.
Disclosure of Interest: none Declared
P-323 PreVALenCe AnD SIGnIfICAnCe Of OCCuLT hePATITIS b VIruS InfeCTIOn In ChrOnIC hePATITIS C In SOuTh KOreA
Junhyeon Cho* 1, sang soo Lee2, joo yeong Baeg1, yun suk choi1, yejoo jeon1, jung Wha chung1, eun sun jang1, jin Wook kim1, sook-hyang jeong1
1Internal Medicine, seoul national university Bundang hospital, seongnam-si, 2Internal Medicine, Gyeongsang national university hospital, jinju-si, korea, republic of
Introduction: the presence of hepatitis B virus (hBV) Dna in hBV surface antigen (hBsag)-negative patients is defined as occult hBV infection (oBI). Whether oBI plays a role in development of cirrhosis or hepatocellular carcinoma (hcc) is unclear. this study aimed to investigate the prevalence and clinical significance of oBI in patients with chronic hepatitis c (hcV) infection.
Methods: using 182 plasma samples from hBsag negative, chronic hcV patients (chronic hepatitis, n=83; liver cirrhosis, n=47; hcc, n=52), hBV Dna was amplified by nested Pcr with 4 sets of primers in s, c, P and x orf of hBV genome. oBI positivity defined as hBV Dna amplification within at least two different regions of hBV genome, and clinical factors related to oBI positivity were analysed. In addition, sequence analysis of the entire s open reading frame (orf) (pre s1, pre s2, and s) for 5 oBI patients was performed.
results: the overall oBI prevalence in chronic hcV infection was 17.6 % (32/182) with 18.1%, 23.4%, and 11.5% in chronic hepatitis, cirrhosis and hcc, respectively (p=0.425). there was no

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 3 3
significant factor associated with oBI. During mean f/u of 36.3 mo, 24 patients showed disease progression, and the independent factors for disease progression were increasing age and decreasing platelet count. sequence analysis of the entire s orf (pre s1, pre s2, and s) showed that all of 5 hBV strains were genotype c2, and oBI unique mutations such as q10t/e in pre s1, L13V pre s2, and t64I and t190I in s were found in more than one oBI sample.
Conclusion: the prevalence of oBI in chronic hcV patients was less than 20% in korea. oBI was not associated with disease progression to cirrhosis or hcc. hBV in oBI positive patients were genotype c2 with reported oBI unique mutations in s orf.
Disclosure of Interest: none Declared
P-324 PILOT STuDy Of COMbInATIOn TherAPy Of SOrAfenIb AnD CyTOTOxIC CheMOTherAPeuTIC AGenT In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA refrACTOry TO SOrAfenIb MOnOTherAPy
seon-Mi Lee1, Sang youn hwang* 1, jung Woo Im1, ki jeong jeon1
1Dongnam Institute of radiological & Medical sciences, Busan, korea, republic of
Introduction: there is not proven effective therapy in patients with advanced hepatocellular carcinoma (hcc) refractory to sorafenib. We aimed to evaluate the efficacy and safety of using combination therapy of sorafenib and cytotoxic agent in patients with advanced hcc with disease progression on sorafenib monotherapy.
Methods: eligible advanced hcc patients with documented radiological evidence of disease progression with sorafenib treatment were recruited. all patients received doxorubicin at 60 mg/m2 every 3 weeks or tegafur/uracil 125mg/m2 twice daily with sorafenib for a maximum of 6 cycles. response assessments using both recIst and modified recIst criteria were performed after 2 or 3 cycles of therapy.
results: thirteen patients were enrolled in the study. the median age was 59 years (range, 43-71) and all patients were in ecoG performance status 1. Doxorubicin was used in 6 patients and tegafur/uracil was used in 7 patients. eleven patients (85%) were chronic hepatitis B and all patients had child a cirrhosis. the median overall survival was 11 months (range 4-26 months) and the median progression-free survival was 3 months (range 1-13 months). two patients (15.3%) achieved partial response, 7 patients (53.8%) had stable disease, and 4 (30.9%) patients had progression disease. four patients (67%) in doxorubicin group experienced febrile neutropenia, 2 patients (28.5%) in tegafur/uracil group experienced grade 3 diarrhea.
Conclusion: our study suggests that the combination of sorafenib and cytotoxic agent can be effective and safe strategy that achieves promising rates of local and systemic control in hcc patients refractory for sorafenib monotherapy. a further well controlled, large scaled study to prove survival benefit is recommended.
Disclosure of Interest: none Declared
P-325 effeCTIVeneSS Of MeLD, MeLDnA, APrI, AnD fIb-4 AS PreDICTOrS Of MOrTALITy AnD DeVeLOPMenT Of hCC In PATIenTS WITh CIrrhOSIS – 5-yeAr fOLLOW-uP STuDy
Ji Wan Kim* 1, jeong han kim1, soon yong ko1, Won hyeok choe1, so young kwon1
1Department of Internal Medicine konkuk university school of Medicine, Digestive Disease center, seoul, korea, republic of
Introduction: Liver cirrhosis increases the risk of mortality and development of hepatocellular carcinoma (hcc); therefore, determining the predictors associated with mortality and hcc development are of vital importance. several indices have been widely used to predict mortality and/or hcc development in patients with liver related diseases. the purpose of this study was to investigate the predictive value of proposed indices on mortality and hcc development in cirrhosis patients.
Methods: the medical records of 404 liver cirrhosis patients admitted to konkuk university hospital from 2005 to 2009 were retrospectively reviewed. excluding 60 patients who could not be followed, the data of 344 patients were analyzed.
results: During the follow-up, 55 patients developed hcc and 125 died. new hcc patients had significantly lower cP score, MeLD, and MeLDna levels than non-hcc patients. While no significance was found in aPrI and fIB-4, non-hcc patients had significantly shorter follow-up duration than hcc patients. those who died had significantly higher cP score, MeLD, MeLDna, aPrI and fIB-4 than living patients.among all patients, those with fIB-4 greater than the 4.50 cut point had significant risk (or=3.329, 95%cI=1.427-7.771) associated with new hcc. furthermore, fIB-4 greater than the 9.50 cut point was significantly associated with mortality (or=2.738, 95%cI=1.168-6.419).
Conclusion: fIB-4 was predictive of both new hcc and mortality. thus, fIB-4 may have more predictive value for death and hcc development in cirrhosis patients.
Disclosure of Interest: none Declared
P-326 MeTIV-hCC: A PhASe 3 PLACebO-COnTrOLLeD TrIAL WITh TIVAnTInIb (Arq 197), In PATIenTS WITh SeCOnD-LIne, MeT-hIGh, InOPerAbLe hePATOCeLLuLAr CArCInOMA (hCC)
armando santoro1, camillo Porta2, Lorenza rimassa* 3, Ivan Borbath4, Bruno Daniele5, richard finn6, jean Luc raoul7, aiwu ruth he8, joerg trojan9, Markus Peck-radosavljevic10, Giovanni abbadessa11, Maria Lamar12, terri Goldberg13, jordi Bruix14
1oncology hematology, humanitas cancer center, humanitas clinical and research center, rozzano, 2oncologia Medica, fondazione Irccs Policlinico universitario san Matteo, Pavia, 3oncologia ematologia, humanitas cancer center, humanitas clinical and research center, rozzano, Italy, 4Gastro-enterologie, cliniques universitaires saint-Luc, Brussels,, Belgium, 5oncology, G. rummo hospital, Benevento, Italy, 6oncology, ucLa jonsson comprehensive cancer center, Los angeles, united states, 7oncology, Institut Paoli - calmettes, Marseille, france, 8oncology, 8Georgetown university hospital, Lombardi comprehensive cancer center, Washington Dc, united states, 9Gastroenterology, j. W. Goethe university hospital, frankfurt, Germany, 10Gastroenterologie und hepatologie, Medizinische universitaet Wien, Vienna, austria, 11clinical Development, translational Medicine, 12clinical Development, arqule, Inc, Burlington, 13clinical Development, Daiichi-sankyo, edison, united states, 14Liver unit, BcLc Group, Liver unit, hospital clinic, university of Barcelona, IDIBaPs, cIBerehd, Barcelona, spain
Introduction: tivantinib is a selective, non-atP competitive, oral inhibitor of Met, the hepatocyte growth factor (hGf) receptor. no worsening of liver function in cirrhotic hcc patients (pts) taking tivantinib 360mg BID (capsules) was found in a phase 1b study (santoro et al, Br j cancer, 2013). Patients with Met-high, second line hcc benefited of tivantinib in a randomized, placebo-controlled phase 2 study (overall survival: 7.2 months on tivantinib, 3.8 months on placebo, hr: 0.38, p=0.01), at both 360mg BID and 240mg BID capsule doses (1).
Methods: enrollment for this phase 3 clinical trial (arq 197-a-u303, nct01755767) is ongoing. eligible pts must present with child Pugh a; ecoG performance score <1; inoperable recIst 1.1 measurable disease; adequate bone marrow, liver and kidney functions; no prior liver transplant. Patients must have had radiographic disease progression after one sorafenib containing systemic first line therapy or have be unable to tolerate sorafenib; their tumor samples must be deemed Met-high by Ihc at a central laboratory to be eligible. approximately 303 pts are randomized 2:1 to receive tivantinib 120mg BID (tablets) or placebo (120mg of tablets have shown similar exposures to 240mg of capsules). Pts are stratified by vascular invasion, metastases, and alphafetoprotein level, and they are evaluated by ct or MrI scan at 8-week intervals.
results: the primary endpoint is overall survival (os). secondary endpoints include progression-free survival and safety. treatment continues until confirmed disease progression or unacceptable toxicity. Participating centers are located in europe, australia, new zealand, and the americas.
Conclusion: this phase 3 trial in second-line hcc is expected to complete patient selection by end of 2015, and an interim analysis is planned when approximately 60% of os events are reached.
references: santoro a, rimassa L, Borbath I, et al. Lancet oncol 2013;14:55-63
Disclosure of Interest: a. santoro consulting of: BMs, Gsk, arqule, takeda, roche, c. Porta: none Declared, L. rimassa: none Declared, I. Borbath: none Declared, B. Daniele consulting of: Bayer, r. finn: none Declared, j. L. raoul: none Declared, a. r. he: none Declared, j. trojan: none Declared, M. Peck-radosavljevic: none Declared, G. abbadessa stocks of: arqule employee, M. Lamar stocks of: arqule employee, t. Goldberg stocks of: Daiichi-sankyo employee, j. Bruix consulting of: Bayer-schering, novartis, BMs, BtG-Biocompatibles, eisai, kowa, arqule, terumo, Gilead, Bio-alliance, roche, abbVie
P-327 ThyrOID DySfunCTIOnS In eGyPTIAn PATIenTS WITh hePATOCeLLuLAr CArCInOMA AfTer TreATMenT by TrAnSArTerIAL CheMOeMbOLIzATIOn
Amal T. A. Ahmed* 1, amany Maher2, ahmed a. elkhattib1
1tropical medicine, 2medical research center, molecular biology, ain shams university, cairo, egypt
Introduction: transarterial chemoembolization (tace) involves the application of iodide in the form of lipiodol mixed with a chemotherapeutic agent (1). although required for thyroid hormone synthesis, excess intra-thyroid iodide can paradoxically decrease the organification of iodide and subsequent hormone synthesis, a phenomenon termed the "acute Wolff-chaikoff effect" (2).
Aim of the work: evaluation of the thyroid dysfunctions after tace for patients with hepatocellular carcinoma.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 3 4
Methods: the study was approved by the local ethical committee. We included 30 patients with hepatocellular carcinoma who were eligible for tace according to Barcelona clinic for Liver cancer (BcLc) 2010. We excluded patients with history of antiviral therapy, thyroid diseases and residence in iodine deficiency areas. after written consent, all patients were subjected to history taking concerning thyroid disorders, clinical examinations and laboratory investigations (liver profile, renal functions tests,) and tsh, ft3, ft4 before tace, one weak and one month later.
results: there were 24 (80%) males and 6 (20%) females with mean age 54.9±5.17. after one week we had 4 patients (13.3%) had high tsh levels, one patient (3.3%) had low level, and 25 patients (83.3%) stay within normal level, after one month, 27 patients (90%) had normal level, and 3 patients (10%) had low level, while no patient (0%) had high level with statistically significant difference (p<0.05). also we found that ft4 levels after one week, 5 patients (16.7%) had high level, and 3 patients (10%) had low level, while 22 patients (73.3%) stay within normal level, after one month, 9 patients (30%) had high level, and no patient (0%) was found with low level while 21 patients (70%) had normal level with statistically significant difference (p<0.05). changes in ft3showed that after one week, 2 patients (6.7%)had high level, and 2 patients (6.7%) had low level, while 26 patients (86.7%)had normal level, after one month ,4 patients (13.3%) had high level, and one patient (3.3%)had low level, and 25 patients (83.3%)had normal level with statistically non-significant difference.
Conclusion: thyroid dysfunctions after tace presented in 16.7% of patients and could be hypo or hyper-thyroidism.
references: Miraglia r, Pietrosi G, Maruzzelli L,
Disclosure of Interest: none Declared
P-328 hePATIC ArTerIAL InfuSIOn CheMOTherAPy fOr SOrAfenIb fAILure On ADVAnCeD hCC
Shinpei Sato* 1, takahisa sato1, shuntaro obi1, toshihiro kawai1
1gastroenterology, kyoundo hospital, tokyo, japan
Introduction: sorafenib(sf) is the first choice as treatment for advanced hcc . however, the response rate is extremely low rate with less than 5%. In the case of a patient progresses after sf introduction, there are few reports that showed usefulness as the second treatment. We examined the effectiveness of the Ifn/5fu hepatic arterial infusion as the second treatment in the case of sf failure (progress disease, side effect ).
Methods: subcutaneously interferon injection and 5fu hepatic arterial infusion (Ifn/5fu) was treated for 26 cases from 2008 to 2012 in the cause of sf failure. 19 men, 7 woman, age 70 years old (24-79), tumor diameter 6.3cm (0-16), tumor number 10 (2-30),stage III 7 ,IVa 9, IVb 10 (38%). Portal vein tumor invasion positive was17patients (65%). child a was 21patients, B was 5 patients. the protocol assumed 1 course only Ifn for combination of Ifn and 5fu, latter half two weeks for two weeks in the first half for four weeks. the effect measurement performed an image evaluation once in tumor marker, at least two courses every course. the curative effect followed by recIst criteria.
results: the treatment effect was cr0, Pr5(19%), sD14(54%), PD7(27%), and the response rate was 19%. the disease control rate was 73%. the decrease of the L3 concentration did not obtained, but afP was significantly decreased with 1547 810, DcP6689 4667. as for 17 cases that decreased with both afP and DcP more than 20%, it was admitted to (66%). (P=0.03) where the case that afP decreased significantly accepted a convalescence improvement effect. however, We did not recognize the significant difference about the case that DcP decreased. Mst after the Ifn/5fu was 5.4 month. all survival Mst from initial treatment was 4.6 years. there were no side effects of Grade 3 and the falling off.
Conclusion: In sf failure, the tumor marker was decreased to 66%. It was a low value that the response rate was 19%. however, it was useful as the second treatment in achieving Mst 5.4months in case of stage IVb was 38%.
Disclosure of Interest: none Declared
P-329 eMerGenCy enDOSCOPIC VArICeAL LIGATIOn fOLLOWInG VArICeAL ruPTure In PATIenTS WITh ADVAnCeD hePATOCeLLuLAr CArCInOMA AnD POrTAL VeIn TuMOr ThrOMbOSIS
Toshihiro Kawai* 1, yoko yashima1, takafumi sugimoto1, takahisa sato1, Miho kanda1, shinpei sato1, shuntaro obi1
1Gatroenterology and hepatology, kyoundo hospital, tokyo, japan
Introduction: the outcome of ruptured varical treatment in patients with hepatocellular carcinoma (hcc) and portal vein tumor thrombus (PVtt) is unclear. We evaluated the outcomes defined as rebleeding, of patients with PVtt who underwent emergency treatment of potentially fatal variceal bleeding.
Methods: a total of 62 consecutive patients with PVtt and endoscopically proven esophageal or gastric variceal bleeding, who were admitted in our hospital between 2007 and 2012, were included. emergent endoscopy was performed within 24 hours after hemorrhage. the bleeding varices were ligated using a pneumatic eVL device. rescue therapies (i.e., sengstaken-Blakemore balloon tamponade) were applied when necessary.
results: Most of patients were decompensated cirrhosis with the liver function stages of the patients were child-Pugh B (56%) or c (36%). 58 patients (94%) had esophageal variceal bleeding and 4 (6%) patient had gastric variceal bleeding. 35 patients (56%) had portal vein tumor thrombosis of main trunk. except for one patient, the bleeding was managed using endoscopic variceal ligation (98%). 24 patients experienced rebleeding, and a median overall survival time of 36 days. absence of portal vein tumor thrombus in the main trunk was associated with rebleeding-free survival (hazard ratio 3.706, p=.0223), and α-fetoprotein-L3 < 37.4% (hazard ratio 0.464, p=.015) and child-Pugh class a/B (hazard ratio 0.398, p=.007) were related to over-all survival.
Conclusion: eVL is a safe and effective treatment of variceal ruptures, even in patients with hcc and PVtt. after successful hemostasis, alleviation of the underlying liver function impairment and tumor control are equally important for better prognosis.
Disclosure of Interest: none Declared
P-330 OuTCOMe Of reSeCTIOn fOr PuLMOnAry MeTASTASeS frOM hePATOCeLLuLAr CArCInOMA: SInGLe-CenTer exPerIenCe
young Mi hong* 1, ki tae yoon1, Mong cho1, Dae hwan kang1, hyung Wook kim1, cheol Woong choi1, su Bum Park1, jeong heo2, hyun young Woo2, Won Lim2
1Pusan national university yangsan hospital, yangsan, 2Pusan national university hospital, Busan, korea, republic of
Introduction: the Lung is one of the most common sites for extrahepatic metastasis from hepatocellular carcinoma (hcc). no effective treatment modality exists for pulmonary metastases from hcc and the outcome of pulmonary metastasectomy of hcc has not yet been thoroughly investigated. therefore, we aimed to evaluate the outcome of pulmonary metastasectomy due to hcc.
Methods: Between May 2010 and june 2012, 12 patients with pulmonary metastases from hcc underwent pulmonary resection. We retrospectively reviewed 12 patients who underwent pulmonary metastasectomy from hcc and analyzed the clinical outcomes by both the overall survival and cancer-specific survival after pulmonary resection.
results: eight patients were male and four were female (median age, 60 (range, 42-72) years). four patients had undergone liver transplantation for hcc before pulmonary metatasectomy. although one patient presented recurrence in the liver before pulmonary metastasectomy, hepatic recurrence did not affect an overall survival after pulmonary metastasectomy. of the 12 patients, 7 patients underwent a single session of pulmonary metastasectomy and 5 patients underwent more than 2 sessions. there were no surgery-related deaths or complications. the overall survival rate after the initial pulmonary metastasectomy was 92% and 61 % at 2 and 3 years, respectively. the cancer-specific survival rate was 91% and 80% at 2 and 3 years. no factors were associated with the survival after pulmonary metastasectomy.
Conclusion: although our study did not revealed prognostic factors, we showed good overall survival rates after the resection of pulmonary metastases from hcc. therefore, we suggest that pulmonary metastasectomy could conduct valuable role in the treatment of pulmonary metastases from hcc because it may provide a opportunity of long-term survival.
Disclosure of Interest: none Declared
P-331 The OPTIMAL TreATMenT MODALITy In PATIenTS WITh hePATOCeLLuLAr CArCInOMA AnD POrTAL hyPerTenSIOn
sung hoon kim1, hye-Jin Do* 2
1Department of surgery, 2Department of anesthesiology, yonsei university Wonju college of Medicine, Wonju, korea, republic of
Introduction: Portal hypertension (Pht) was introduced as an important prognostic factor in patients with hepatocellular carcinoma (hcc). Pht could be accurately determined by hepatic venous pressure gradient (hVPG) through hepatic vein catheterization.hVPG to determine Pht was not performed routinely because of invasiveness. We investigated the effect of elevated hVPG in patients with hepatocellular carcinoma who received different treatment modalities and evaluated which was optimal treatment modality in patients with hcc and Pht and compared hVPG with other markers of portal hypertension.
Methods: after hVPG measurement, 36 patients who received treatment for hcc were enrolled in this study. Measurement of hVPG was performed by a single intervention radiologist at our institution. Wedged hepatic venous pressure (WhVP) was measured by occlusion of the hepatic vein; free

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 3 5
hepatic venous pressure (fhVP) was the measured pressure of the non-occluded hepatic vein. hVPG was determined by the difference between WhVP and fhVP. an hVPG of more than 10 mmhg was defined as a significant Pht.We identified treatment outcomes according to the hVPG and analyzed correlation between hVPG and other markers. additionally, we investigated the prognostic factors for high grade complication in patients with elevated hVPG.
results: Median hVPG was 12mmhg (range 4-28). high grade complications were developed in patients underwent only radiofrequency ablation (rfa) or transcatheteric arterial embolization (tace). however, treatment modality and Pht were not associated with high grade complications. there was no survival difference in patients underwent liver resection (p=0.157) or rfa (p=0.578) according to hVPG. fibroscan® was most correlated with hVPG (ρ=0.797; p<0.001).
Conclusion: although our study has the limitation of a small number of cases, curative treatment modalities including liver resection and rfa may be safely applied to patients with portal hypertension. fibroscan® may be a reliable non-invasive method to determine Pht.
Disclosure of Interest: none Declared
P-332 rADIOeMbOLIzATIOn fOr The TreATMenT Of InTrAhePATIC ChOLAnGIOCArCInOMA
Mercedes Iñarrairaegui* 1, 2, 3, alzina alejandra1, ana chopitea4, jose Ignacio Bilbao3, 5, fernando rotellar3, 6, Macarena rodriguez3, 7, javier rodriguez3, 4, Delia D'avola1, 2, 3, Bruno sangro1, 2, 3
1Liver unit, clinica universitaria, 2cIBerehD, 3IDIsna, 4oncology, 5Interventional radiology, 6surgery, 7nuclear Medicine, clinica universitaria, Pamplona, spain
Introduction: the treatment of unresectable intrahepatic cholangiocarcinoma (Icc) is challenging due to the limited efficacy of systemic chemotherapy. although scarcely tested, liver radioembolization with yttrium 90 microspheres (re) has shown promising disease control rates and survival. our aim was to analyze the safety and long term outcome of patients with uIcc treated with re, with and without concomitant chemotherapy.
Methods: a retrospective analysis was performed of all Icc patients treated with re from 1/2006 to 12/2014 with a follow-up longer than two months. We collected patient characteristics, procedure data and incidence of re induced toxicity. time to progression was calculated from re date to progression or death, and global survival from re till death or last visit. concomitant chemotherapy was considered when patients received re during treatment with gemcitabine based chemotherapy.
results: six out of the 27 patients treated with re were excluded due to insufficient follow-up leaving 21 patients for analysis. three to 10 m after the first re, 4 patients received a second re to the treated area (n= 2) or the contralateral lobe (n=2). Median age was 65 years and half the patients were males. 61% had extrahepatic disease (mainly lymph nodes). nine patients received re as first-line treatment alone (n=5) or in combination with gemcitabine and oxaliplatin (n=4), and the remaining were treated as salvage therapy after progression to chemotherapy (n= 4) or as consolidation therapy following disease control with chemotherapy (n= 8). In 2 patients from this last group gemcitabine-based chemotherapy was not interrumpted after re. therefore, 6 patients received combined treatment with re and chemotherapy. re was bilobar (16%), extended lobar (24%), lobar (48%) or segmentary (12%). Median activity administered was 1.3 GBq. In 32% of cases, the prescribed dose could not administered due to pain or stasis. Median follow-up was 11 months (Iqr 8-26). Median survival was 16 months (95%cI 10-22). four patients underwent resection 2 to 9 months after re. censoring these patients at time of surgery, median survival was 11 months (95%cI 9-14). according to the type of treatment, median survival was 16 months for first line treatment, 17 months for consolidation and 17 months for salvage therapy. Median time to progression was 9 months without differences according to the type of treatment. no re-induced liver disease was observed. Billirrubine had no changes two months after re in patients treated with concomitant chemotherapy. two patients developed gastric ulcer secondary to re.
Conclusion: In this small and heterogeneous group of patients with Icc, re has shown a safety profile similar to that described in other tumors, both alone and in combination with concomitant chemotherapy. survival and time to progression are encouraging and justify controlled prospective trials in this indication.
Disclosure of Interest: none Declared
P-333 PreVALenCe Of POrTAL VeIn ThrOMbOSIS In eGyPTIAn PATIenTS WITh hePATOCeLLuLAr CArCInOMA
eman Barakat* 1, amal t. abdelmoez1, Mohammed G. abuelmaaty2, khaled M. abdelaziz3, Amr el fouly* 2
1tropical medicine, 2radiology medicine, 3community and enviromental and occuopational health, ain shams university, cairo, egypt
Introduction: Background: there is a growing incidence of hepatocellular carcinoma (hcc) in egypt. hepatocellular carcinoma is also associated with a reported incidence of portal vein thrombosis (PVt) 20%>65%.
aims: were to characterize the prevalence and risk factors for PVt in patients with hcc, and determine the overall impact of PVt on survival.
Methods: Patients and Methods the total number of patients was 1121. this study included two groups, group 1: all hcc patients without PVt (902) 80.5% of total number: formed of 622 cases from old records of hcc unit tropical Medicine Department ain shams university and 280 cases newly diagnosed their ages 56.44±8.78 and 733 (81.2%) males and 169 (18.8%) female . Group 2; all hcc patients with PVt (219) 19.5%: formed of 164 cases from old records of hcc unit and 55 cases newly diagnosed, their ages 55.79+ 9.47, 187 (85.4%) males and 32 (14.6%) females. Inclusions criteria: egyptian nationality, documented diagnosis of hcc according to Barcelona 2010 schedule for diagnosis, diagnosis of malignant PVt. We excluded patients with systemic illness that affects survival e.g. heart failure, renal failure, other malignancy. all patients were subjected to: full medical history: Laboratory investigations: complete Blood Picture, liver profile (alanine aminotransferase (aLt) aspartate aminotransferase (ast), serum albumin, total and direct serum bilirubin, and Inr. renal profile: blood urea nitrogen (Bun), creatinine, serum alpha-fetoprotein level. Imaging studies: abdominal ultrasound, triphasic spiral ct scan of the abdomen, Duplex for portal vein for assessment of patency. the child-Pugh score, okuda and BcLc staging and the MeLD score were determined for newly discovered PVt patients while child-Pugh was only calculated for patients from old records and newly diagnosed hcc patients without PVt. follow up and end points: follow up after one month and four months later from time of diagnosis of PV thrombosis. each follow up visit included the same as previous (clinical history taking full clinical examination, laboratory investigations and imaging studies. all the 55 hcc patients with PVt had their follow up till the end of the 4 months or till the patient die.
results: Both groups were matched as regards age and sex (p>0.05). Prevalence of PVt among egyptian patients with hepatocellular carcinoma is (19.5%). the highest predictor for the presence of portal vein thrombosis were jaundice, splenomegaly, ascites child class c and afP>100ng/ml. Deterioration of liver functions along follow up duration (p<0.05). higher survival among patients with okuda 1 compared to other patients (p<0.05). 23.6% of patients with PVt still alive at the end of 4 months follow up duration.
Conclusion: Prevalence of PVt among egyptian patients with hepatocellular carcinoma is 19.5%, predictors for the presence of portal vein thrombosis are jaundice, splenomegaly and ascites, child c and afP>100ng/ml.
Disclosure of Interest: none Declared
P-334 effICACy AnD SAfeTy Of TrAnSArTerIAL CheMOeMbOLIzATIOn uSInG DruG eLuTInG beADS fOr hePATOCeLLuLAr CArCInOMA
Akihiro Deguchi* 1, junichi kageyama2, tsutomu Masaki3
1Division of Gastorenterology, 2Division of radiology, kagawa rosai hospital, Marugame-shi, 3Department of Gastroenterology and neurology, kagawa university, school of Medicine, Miki-cho, japan
Introduction: transarterial chemoembolization (tace) using a drug-eluting bead (DeB-tace) for hepatocellular carcinoma (hcc) is a new treatment method in japan. In this study we evaluated the efficacy and safety of DeB-tace for the patients with unresectable hepatocellular carcinoma.
Methods: 24 patients (M: f=18:6, age (mean) 68, child a: B=18:6, stage II:III:IV=8:13:3) with unresectable hcc who underwent 44 DeB tace procedures in 10 months were studied. DeB tace procedures using hepasphere eluting cDDP in 27 sessions and Dc Bead eluting epirubicin in 17 sessions were performed. the objective radiological response was classified according to response evaluation criteria in solid tumors (recIst) v.1.1 by dynamic ct at one month after therapy. adverse events were evaluated using ncI ctcae v. 4.03.
results: the imaging response was assessed in each session as partial response (Pr), stable disease (sD) and progressive disease (PD) in 26 (59.1%), 10 (22.7%), and 8 (18.2%) respectively. In most effective case, huge hcc that was 96mm in tumor diameter became smaller as 45 mm and also in the tumor marker, afP decreased from 102.4 to 5.4 and PIVkaII decreased from 31400 to 34 after 3 session of DeB-tace. as the complication, grade 1 level of pyrexia, vomiting, and abdominal pain were observed in 17%, 6%, and 11% respectively. there was no case in which child-Pugh score got worse except for the case with PD.
Conclusion: DeB-tace is safe and effective in achieving local tumor control in patients with unresectable hcc.
references: Prajapati et al. survival, efficacy, and safety of small versus large doxorubicin drug-eluting beads tacechemoembolization in patients with unresectable hcc.ajr am j roentgenol. 2014 Dec;203(6):W706-14. doi: 10.2214/ajr.13.12308.
Disclosure of Interest: none Declared

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 3 6
P-335 TrAnSArTerIAL CheMOeMbOLIzATIOn COnTrIbuTeD SurVIVAL GAIn fOLLOWInG COMbIneD CheMOrADIATIOn TherAPy fOr ADVAnCeD hePATOCeLLuLAr CArCInOMA
Kwan Sik Lee* 1, ja kyung kim1, jung Il Lee1
1Dept. of Internal Medicine, yonsei university college of Medicine, seoul, korea, republic of
Introduction: combined chemoradiation therapy (ccrt) followed by intraarterial chemotherapy (Iac) has been reported to be beneficial for advanced hepatocellular carcinoma (hcc) with portal vein thrombosis (PVt). however, hepatic arterial chemoembolization (tace) was generally not accepted for this situation. the aim of this study is to evaluate the role of following intermitttent tace instead of Iac after ccrt.
Methods: thirty-seven patients were treated by ccrt as the initial treatment for hcc with PVt between 2009 and 2014. Iac through hepatic arterial chemoport and intermittent tace (Group a) followed in 18 patients and only Iac were repeated in 19 patients (Group B). We excluded the patients who had extra-hepatic metastasis, active peptic ulcer, and inadequate hepato-renal function. for ccrt, infusion of 5-fu (500 mg/day) via chemoport was given during the first and last five days of external radiation therapy (rtx) for 5 weeks. for Iac, infusion of cisplatin (70~100mg/m2 for one day) with 5-fu (750~1000mg for 3 days) was repeated monthly.
results: Mean age was 55 year; male to female was 32 to 5. underlying liver diseases were hepatitis B, hepatitis c and non-B/c in 26, 2 and 10 patients, respectively. Mean follow-up duration was 14 months (3-65 months). the objective response (cr+Pr) rates in tumor size after 1 month after ccrt were 45.9%. the mean level of αfP after 1 month after ccrt were decreased in 81% of patients. During follow up, complete response was noted in 3 patients. one patient underwent resection for cure. Median overall survival duration was 12.4 months. overall survival of group a was significantly better than that of group B (mean 42.5 vs. 12.2 months, p=0.001).
Conclusion: adding intermittent transarterial chemoembolization contributed survival gain following combined chemoradiation therapy for advanced hepatocellular carcinoma with portal vein thrombosis. further prospective study for the factors favoring tace after ccrt is warranted.
Disclosure of Interest: none Declared
P-336 ASSeSSMenT Of PerCuTAneOuS rADIOfrequenCy AbLATIOn TreATMenT WITh SOLOIST AnD LeVeen neeDLeS fOr hePATOCeLLuLAr CArCInOMA PATIenTS In bACh MAI hOSPITAL, hAnOI
hang V. Dao* 1, Dao Long1
1Gastroenterology department, Bach mai hospital, hanoi, Viet nam
Introduction: hepatocellular carcinoma (hcc) is a common disease in the world as well as in Vietnam. In Vietnam, according to Globocan 2012, hcc ranks the second for the prevalence and the first for the mortality. radiofrequency ablation (rfa) is a local therapy to destroy tumor tissue by heat.
Methods: an interventional longitudinal study on hcc patients having ≤ 3 tumors with each tumor size ≤ 3cm or one tumor ≤ 5 cm; child Pugh a or B. the study was conducted in Gastroenterology department of Bach Mai hospital from november 2011 to april 2015.
results: 127 patients were performed 368 times of rfa with the mean ablation times being 2.9±1.5 times. there were 81 patients treated only by rfa and 46 patients treated by rfa combined with tace.the mean age of patients was 58.1±10.3 and male/female ratio was 6:1. there were 31.5% of patients had no symptoms and the most prevalent symptoms were abdominal pain and fatigue. hBV was the prevalent cause of hcc with 67.7%. there were 70.1% of patients having 1 tumor, 23.6% having 2 tumors and only 6.3% of patients having 3 tumors. the mean size of tumor was 3.2±1.1 cm.the rfa procedure was safe with complication rate being 1.1% including hemothorax, ascites, pleural effusion and hypervagal reaction, responsed to the internal medicine. fever and abdominal pain occurred in 13.6% ablation times. after 1 months of the first rfa: 117 patients had complete and partial responses according to mrecIst criteria (92.1%), after 9 months: 105 patients had complete and partial responses (82.7%). 49 patients (38.6%) had better clinical response with gain weight and less fatigue. During following-up time (18,1±7,5 months), 5 patients died (3.9%), 22 patients had a new lesion (17.3%), 3 patients had portal vein thrombosis (2.3%), 1 patient had abdominal lympho node(0.8%), 1 patient had needle tract seeding (0.8%).
Conclusion: rfa with soloist and LeVeen needles is a safe technique and effective to improve the quality of life for hcc patients in Vietnam.
references: 1. GloBocan, 2012 http://www-dep.iarc.fr2. easL - eortc (2012). clincal Practice Guidelines: Management of hepatocellular carcinoma. journal of hepatology, 56: 908 - 433. forner a, eyuso c, Varela M (2009). evaluation of tumor response after locoregional therapies in hepatocellular carcinoma: are response evaluation criteria in solid tumors reliable? cancer, 115(3): 616 - 23.
Disclosure of Interest: none Declared
P-337 effeCTS Of MeTfOrMIn On CLInICAL OuTCOMe In ADVAnCeD hCC PATIenTS reCeIVInG SOrAfenIb
Andrea Casadei Gardini* 1, Luca scartozzi2, Luca faloppi3, Giorgia Marisi1, emanuela scarpi1, Giovanni Luca frassineti1
1Irst-Irccs, forli, 2universita cagliari, cagliari, 3universita ancona, ancona, Italy
Introduction: several studies reported an association between type 2 diabetes mellitus (DM2) andhepatocellular carcinoma (hcc). Data from several retrospective studies and meta-analysis have demonstrated a riskreduction of about 50% of developing hcc in cirrhotic patients treated with metformin for DM2. several in vitrostudieshave shown anti-tumor activity of metformin (M) in hcc. the aim of this study is to evaluate the different outcomesofpatients that have received or not metformin during treatment with sorafenib (s).
Methods: from 257 patients diagnosed with hcc from 2004 to 2014, 93 patients consecutively treated with sorafenib were analyzed. of these, 42 patients (45.2%) were diabetic and 31 (33.3%) of these have received M for DM2.Progression-free survival (Pfs), overall survival (os) and their 95% confidence Interval (95% cI) were estimated by kaplan-Meier method and compared with log-rank test.
results: the concomitant use of s and M was associated with a median Pfs of 2.6 months (95% cI 1.9-3.3) comparedto 5.0 months (95% cI 2.5-8.2) for patients who have not received M (p=0.029). the concomitant use of s and M was associated with a median os of 10.4 months (95% cI 3.9-14.4) compared to 15.1 months (95% cI 11.7-17.8) for patients who have not received M (p=0.014).
Conclusion: these findings could be explained by an increased tumor aggressiveness and resistance to s in patientstreated with M. M usually enhanced the activity of s, but probably molecular alterations in transporter genes ortranscription factors involved in M molecular action and pharmacokinetics could contribute to a different response tothese drugs combination. further studies are needed to confirm the data and to identify possible mechanisms ofresistance that may occur during treatment with s.
Disclosure of Interest: none Declared
P-338 LIVer reSeCTIOn Of LOCAL reCurrenCe InITIALLy TreATeD by rADIOfrequenCy AbLATIOn fOr COLOreCTAL LIVer MeTASTASIS IS MOre exTenSIVe ThAn PrIMAry reSeCTIOn
yoshikuni Kawaguchi* 1, kiyoshi hasegawa1, akio saiura2, rihito nagata1, Michiro takahashi1, junichi kaneko1, yoshihiro sakamoto3, norihiro kokudo1
1hepato-Biliary-Pancreatic surgery Division, Department of surgery, the university of tokyo, 2Department of Gastroenterological surgery, cancer Institute hospital, 3Department of hepato-Biliary-Pancreatic surgery, japanese red cross Medical center, tokyo, japan
Introduction: radiofrequency ablation (rfa) has been increasingly applied not only for the treatment of hepatocellular carcinoma but also for that of colorectal liver metastasis (cLM) which can be surgically removed. however, rfa for cLM has been shown to be associated with a high local recurrence rate, and no optimal treatment for rfa failure has yet to be established. the aim of this study is to evaluate the feasibility and outcome of liver resection for local recurrence after rfa.
Methods: a retrospective study of 17 patients, who underwent liver resection for local recurrence after rfa for resectable cLM, was carried out. In each case, the surgical procedures involved in the actual surgery were compared with those envisioned for the primary resection if rfa had not been selected to address invasiveness between actual and envisioned procedures. envisioned surgical procedures were determined by a hepatic surgery expert at a high-volume center in a blinded manner.
results: Liver resection for rfa-recurrence was more invasive than the envisioned surgical procedure in 10 cases (58%). Moreover, technically demanding procedures were more frequently required in patients who underwent liver resection for rfa-recurrence compared to the envisioned surgical procedures; major hepatectomy, 8 cases[47%] vs. 1 case[6%] (P<0.001); excision and/or reconstruction of the major hepatic veins, 3 cases[18%] vs. 0 case[0%] (P=0.035); excision of diaphragm: 3 cases[18%] vs. 0 case[0%] (P=0.035). operative time and estimated blood loss were 446 [111-842] min (median [range]) and 740 [90-2730] mL, respectively. surgical margin was positive in 2 (13%) of 16 patients undergoing liver resection. no mortality occurred while two patients (12 %) developed complications which were classified as Grade III or IV of clavien-Dindo classification. the 1-, 3-, and 5-year overall survival rates were 92%, 45%, and 45%, respectively, while the 1-, 3-, and 5-year recurrence-free survival rates were 60%, 28%, and 28%, respectively (figure 1).

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 3 7
Image:
Conclusion: Liver resection of local recurrence after rfa for cLM required more-invasive and technically demanding procedures, although it proved to be feasible and safe. the indication of rfa for cLM, thus, should be limited to unresectable cases, and patients with resectable cLM should be thoroughly advised not to undergo rfa, but liver resection which is an established curative treatment.
Disclosure of Interest: none Declared
P-339 PreOPerATIVe PerCuTAneOuS TrAnShePATIC POrTAL VeIn eMbOLIzATIOn
Paris Pappas* 1, Polytimi Leonardou1
1radiology, LaIkon hospital, athens, Greece, Penteli, Greece
Introduction: our aim was to define the effect of preoperative portal vein embolization for inducing selective hypertrophy of non diseased portion of liver[1],[2].
Methods: During a 5 years study period, transhepatic right portal vein embolization was performed in 38 patients with space occupying lesion in right liver lobe with the aid of surgical glue and metallic coils, in 33 of them trough an intercostal right lobe paracentesis and in 5 through a transabdominal left lobe. contraindication to the method were disorters of coagulation, portal vein hypertension, biliary duct dilatation and renal insufficiency[4]. selective catheterization was done with 4f catheters (“Vertebral” or “simmons” configuration), diameter of the coils was 0,035 intches. coils were placed in secondary portal branches[3]. surgical glue was also delivered through the catheter at the level of the right portal vein respectively.
results: no patient developed any major complication except post-embolic pain, vomiting or nausea in some cases. computed tomographic volumetry performed before and 1 to 5 months after right portal vein embolization showed left liver volume increase in 40-80%.
Conclusion: transhepatic ipsilateral or contralateral right portal vein embolization with use of surgical glue and coils is safe ,effective method for inducing contralateral hypertrophy before a right hepatectomy[5],[6].
references: 1) nagino M, et al. changes in hepatic lobe volume in biliary tract cancer patients after right portal vein embolization. hepatology. 1995;21:434–439. [2) Makuuchi M, et al. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. surgery. 1990;107:521–527.3) Makuuchi M, et al. Preoperative transcatheter embolization of the portal venous branch for patients receiving extended lobectomy due to the bile duct carcinoma. j jpn soc clin surg. 1984;45:14–20.4) De Baere t, et al. Preoperative portal vein embolization for extension of hepatectomy indications. hepatology. 1996;24:1386–1391. doi: 10.1002/hep.510240612.5) Imamura h, et al. Preoperative portal vein embolization: an audit of 84 patients. hepatology. 1999;29:1099–1105. doi: 10.1002/hep.510290415.6) Madoff Dc, et al. Portal vein embolization in preparation for major hepatic resection: evolution of a new standard of care. j Vasc Interv radiol. 2005;16:779–90.
Disclosure of Interest: none Declared
P-340 effICACy AnD SAfeTy Of COMbIneD SequenTIAL TreATMenT WITh rADIOfrequenCy AbLATIOn AnD SOrAfenIb In PATIenTS WITh hePATOCeLLuLAr CArCInOMA In InTerMeDIATe STAGe IneLIGIbLe fOr TACe: A PrOSPeCTIVe rAnDOMIzeD OPen STuDy
De Stefano Giorgio* 1, farella nunzia1, Iodice Valentina1, scognamiglio umberto1, signoriello Giuseppe2
1aorn ospedali Dei colli P.o.D. cotugno, 2Dipartimento salute Mentale, servizio statistica Medica, naples, Italy
Introduction: tace is considered the gold standard for patients (pts) with hepatocellular carcinoma in Intermediate stage (BcLc-B hcc). Pts with contraindications or ineligible for tace are candidates for sorafenib (s). aim of the present study is to verify efficacy and safety of a combined treatment radiofrequency ablation (rfa)and s in pts with BcLc-B hcc ineligible for tace. Primary endpoint: overall survival in both groups. secondary endpoints: validation of ceus for evaluation of rfa efficacy; safety and efficacy of combined rfa+s.
Methods: a prospective randomized open-label study is expected to enroll during 12 months 124 pts with BcLc-B hcc (3-5 hccs nodules ≥ 3cm≤ 5 cm), not eligible for tace or who refused tace. Pts will be randomized 1:1 into two arms: Group a: s 400 mg bid; Group B: combined sequential treatment rfa+s. In Group B s will be administered for 2 weeks; then s will be stopped from 15th to 19th day to perform rfa scheduled on day 17. ceus to assess the extent of necrosis and biochemical tests will be performed 24 hours after rfa. In case of complete necrosis, pts will re-take s 2 days after the rfa and will be followed-up . In case of incomplete necrosis, 2 days after rfa, pts will start again s at full dosage for 11 days, then drug will be stopped 2 days before the 2th rfa and resumed 2 days after procedure ( up to 3 sessions of rfa; up to 2 nodules or a single nodule up to 5 cm, for session). seven days after the last rfa therapeutic efficacy will be evaluated with ceus and three-phase contrast-enhanced (ce- ct). fig.1 shows the follow-up flow-chart .
results: from December 2014 up to March 2015, 18 pts for group were enrolled, all pts are alive. to date, statistical evaluation in terms of survival, safety and efficacy of treatment in the 2 group is impossible due to the too small sample size and the short time of observation.
Image:
Conclusion: to date, statistical evaluation in terms of survival, safety and efficacy of treatment in the 2 group is impossible due to the too small sample size and the short time of observation.
references: 1- evolving strategies for the management of intermediate-stage hepatocellular carcinoma: available evidence and expert opinion on the use of transarterial chemoembolization. raoul jL, sangro B, forner a, et al. cancer treat rev. 2011 May;37(3):212-20. 2- Management of hepatocellular carcinoma: an update. Bruix j, sherman M; american association for the study of Liver Diseases. hepatology. 2011 Mar;53(3):1020-2. 3- the intermediate hepatocellular carcinoma stage: should treatment be expanded?Piscaglia f, Bolondi L. Dig Liver Dis. 2010 jul;42 suppl 3:s258-63. 4- sorafenib in advanced hepatocellular carcinoma. Llovet jM, ricci s, Mazzaferro V, et al for the sharP Investigators study Group. n engl j Med. 2008 jul 24;359(4):378-90.
Disclosure of Interest: none Declared

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 3 8
P-341 DeVeLOPMenT Of A nOVeL Web-bASeD COnSuLTATIOn SerVICe fOr A PAeDIATrIC rAre TuMOr: The SIOPeL CLInICIAn OnLIne COnSuLTATIOn SerVICe
Arun rangaswami* 1, eugenia rinaldi2, allison o'neill3, Beate haeberle4, rudolf Maibach5, Derek roebuck6, alexander towbin7, Dolores Lopez-terrada8, eiso hiyama9, rebecka Meyers10, Piotr czauderna11
1Pediatrics / hematology-oncology, stanford university, Palo alto, united states, 2Information systems, cineca, Bologna, Italy, 3Pediatrics / hematology-oncology, harvard university, Boston, united states, 4Pediatric surgery, Medical university of Munich, Munich, Germany, 5trial affairs, IBcsG, Berne, switzerland, 6radiology, Great ormond street hospital for sick Vchildren, London, united kingdom, 7radiology, university of cincinnati, cincinnati, 8Pathology, Baylor college of Medeicine, houston, united states, 9Pediatric surgery, hiroshima university, hiroshima, japan, 10Pediatric surgery, university of utah, salt Lake city, united states, 11Pediatric surgery, Medical university of Gdansk, Gdansk, Poland
Introduction: Because liver tumors are very rare in children, individual clinician experience is often quite limited. yet the treatment decisions which must be made can be complex and diagnostic dilemmas are common. this is especially true with relapsed/refractory patients. optimal care requires coordination between surgeons, oncologists, radiologists, and pathologists. In an effort to improve care, clinicians representing the four major international trial groups, cooperated to develop a novel web-based consultation service
Methods: supported by a grant from encca (the european network for cancer research in children and adolescents), representatives from sIoPeL, GPoh, coG, and jPLt developed a web-based service accessed through the sIoPeL home-page. clinicians may submit a consultation request for assistance in diagnosis, radiographic or pathologic evauluation, and management of non-clinical-trial-eligible patients. the request is directed to a specific discipline or groups of disciplines (surgery, oncology, radiology, pathology) or can be directed to all disciplines. the request is reviewed by one of two moderators and then sent on to a panel of acknowledged experts in each of the four disciplines, and representing all cooperative groups. the panel provides evidence-based information regarding diagnosis and treatment options, with the website facilitating an opportunity for online discussion amongst the experts. these options are summarized and circulated back to the panelists and treating insitution. the treating institution must attest to possesion of ultimate responsibility for making management decisions in order to gain access to the site. total consultation time is seven days.
results: this consultation service is in final development and was launched in january, 2015. to date over six cases have been reviewed.
Conclusion: It represents an opportunity to enhance the care of children with rare tumors and facilitates education of clinicians caring for such challenging patients. such a consultation service may serve as a model for cooperative management of other paediatric rare malignancies.
references: the research leading to these results has received funding from the european union's seventh framework Programme (fP7/2007-2013) under the project encca, grant agreement n° 261474the authors have no financial interests to declare.
Disclosure of Interest: none Declared
P-342 PhASe 3 rAnDOMIzeD, DOubLe-bLInD, COnTrOLLeD STuDy Of CAbOzAnTInIb (xL184) VS PLACebO In SubJeCTS WITh hePATOCeLLuLAr CArCInOMA WhO hAVe reCeIVeD PrIOr SOrAfenIb (CeLeSTIAL): TrIAL In PrOGreSS
Ghassan K. Abou-Alfa* 1, ann-Lii cheng2, tim Meyer3, anthony B. el-khoueiry4, hoo G. chun5, jennifer j. knox6, anne Borgman hagey7, steven W. Milwee7, Milan Mangeshkar7, robin k. kelley8
1Medical oncology, Memorial sloan kettering cancer center and Weill cornell Medical college, new york, united states, 2Medical oncology, national taiwan university hospital, taipei, taiwan, 3Medical oncology, royal free hospital, London, united kingdom, 4Medical oncology, university of southern california keck school of Medicine, Los angeles, united states, 5Medical oncology, seoul saint Mary's hospital of korea, catholic university, seoul, korea, republic of, 6Medical oncology, Princess Margaret cancer center, toronto, canada, 7clinical Development, exelixis, 8Medical oncology, university of california, san francisco hellen Diller family comprehensive cancer center, san francisco, united states
Introduction: cabozantinib is an oral receptor tyrosine kinase inhibitor (tkI) with activity against tyrosine kinases including Met, ret and VeGfrs. Met and VeGfr signaling have been implicated in tumor neo-angiogenesis and invasion. Met is overexpressed in hcc compared with non-tumor liver tissue, with higher Met expression linked to poor prognosis.1,2 currently, there are no approved systemic therapies for patients with advanced hepatocellular carcinoma (hcc) who progress post sorafenib. cabozantinib prolonged survival in a Met-driven transgenic mouse model of hcc3 and has demonstrated clinical activity in multiple solid tumor types, including 41 patients with advanced hcc treated in a phase 2 randomized discontinuation study.4,5
Methods: this phase 3, randomized, double-blind study evaluates the efficacy and safety of cabozantinib compared with placebo in patients with advanced hcc previously treated with sorafenib and who have progressed following 1-2 prior systemic treatments for hcc. Patients must be ≥ 18 year old, have child-Pugh score of a and ecoG Ps ≤ 1. Patients are randomized 2:1 to receive either cabozantinib or placebo. stratification factors are etiology of disease, geographic region and the presence of extrahepatic spread of disease and/or macrovascular invasion. the primary endpoint is overall survival. secondary endpoints are progression-free survival and objective response rate by recIst 1.1. additional endpoints include safety, tolerability, assessment of circulating tumor cells, serum bone markers and plasma biomarkers, and effects on bony disease assessed by bone scan and health-related quality of life (hrqoL) using the euroqol health questionnaire (eq-5D-5L). enrollment was initiated in september 2013. target recruitment is 760 patients. a total of 621 events planned with up to 2 interim analyses (at 311 and 466 events) would provide 90% power to detect a 31.6% increase in overall survival (os) (hr=0.76).
results: trial enrollment in progress.
Conclusion: trial completion expected in 2017.
references: 1.kaposi-novak P, et al. j clin Invest. 2006; 116: 1582-1595.2. ueki t, et al. hepatology. 1997; 25: 619-623.3. Data courtesy of D. yang and j.M. Bishop, ucsf.4. cohn aL, et al. j clin oncol. 2012; 30 (4 suppl): abstract 261.5. Verslype c, et al. j clin oncol. 2012; 30 (15 suppl): abstract 4007.
Disclosure of Interest: G. abou-alfa research/education support from: exelixis, consulting of: exelixis, a.-L. cheng consulting of: exelixis, t. Meyer consulting of: exelixis, a. el-khoueiry honoraria support from: exelixis, consulting of: exelixis, h. chun research/education support from: exelixis, consulting of: exelixis, j. knox : none Declared, a. Borgman hagey stocks of: exelixis, conflict with: exelixis, s. Milwee stocks of: exelixis, conflict with: exelixis, M. Mangeshkar stocks of: exelixis, conflict with: exelixis, r. kelley research/education support from: exelixis, consulting of: exelixis
P-343 ChOLAnGIOCArCInOMA: neW TherAPeuTIC PrOCeDureS AnD The rOLe Of PerCuTAneOuS bILIAry DrAInAGe. POInT Of VIeW Of An InTerVenTIOnAL rADIOLOGIST
Paris Pappas* 1, Polytimi Leonardou1, chrysovalantis Vergadis1, George sotiropoulos2, evangelos felekouras2
1radiology, 2surgery, LaIkon hospital, athens, Greece, Penteli, Greece
Introduction: until resently surgical treatment of cholangiocarcinoma of the porta hepatis didn’t had any chance. these patients were considered inoperable, thus taking their treatment comforting with stenting (1). In this context, percutaneous biliary access was very common, since successful stenting in biliary obstruction at the level of the liver hilum with endoscopic access (ercP) is rare (2).today cholangiocarcinoma of the liver hilum considered potentially resectable (3,4) and this has created a new field of applications of percutaneous access.according to the literature, preoperative biliary decompression on cholangiocarcinoma of the liver hilum is necessary bilaterally, or at least for the lobe to be maintained (4) however, it can be sometimes decided during surgery . also there are conflicting opinions as to which is the best access - percutaneously or endoscopically. the fact is that percutaneous drainage has more chance of success (5).
Methods: During the last 8 years in our Institution preoperative percutaneous drainage applied regularly, usually bilaterally, by placing drains of internal - external type, which expire into the duodenum.the method has been applied with 100% technical and clinical success on 47 patients. another 3 patients had endoscopically placed biliary endoprostheses bilaterally, whereas 6 more patients had no biliary drainage at all.all these 56 patients were later on operated and all of them had a successful partial hepatectomy, with r0 or r1 surgical margins.
results: rarely (2 / 56, 3.5% in our study) is observed a bile collection in the hepatectomy region (biloma), which is commonly imputed to oozing of the surface of the hepatectomy, or leakage from bilioenteric anastomosis . the bilomas were drained percutaneously and, if the leakage was great, the bile could be diverted through percutaneous biliary drainage until it dries. In another 2 cases stenosis of the bilioenteric anastomosis developed early postoperatively (<30 days), that was also treated percutaneously. all these 4 cases of leakage or stenosis developed in patients with no preoperative biliary drainage, either percutaneously or endoscopically.
Conclusion: the progress of surgical treatment of cholangiocarcinoma has caused a change to the approach of the disease concerning the role of the interventional radiologist, with greater involvement nowadays than just the simple palliative treatment applied previously.
references: 1.alastair L. young et al.: evolution of the surgical management of perihilar cholangiocarcinoma in a Western centre etc., hPB 2011, 13, 483-4932. kloek jj et al: endoscopic and percutaneous preoperative biliary drainage in patients with

Posters
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 3 9
suspected hilar cholangiocarcinoma. j Gastrointest. surg 2010 jan,14(1): 119-25.3. Geng zhimin et al: advances in diagnosis and treatment of hilar cholangiocarcinoma - a review,Med sci Monit, 2013, 19:648-6564. kevin c. soares et al:hilar cholangiocarcinoma: diagnosis, treatment options, and management. hepatobiliary surg nutr 2014, 3(1) : 18-34 5. Management of hilar cholangiocarcinoma in the north of england: sD Mansfield et al; World j Gastrenterol, 2005)
Disclosure of Interest: none Declared
P-344 SOrAfenIb AfTer reCurrenCe Of TreATMenT WITh TACe In InTerMeDIATe hCC PATIenTS
Dimitrios Dimitroulopoulos* 1, Dimitrios kypreos1, apostolos Malahias1, Matina hatzinikolaou1, Loukas theodoropoulos1, nikolaos saribegioglou1, stavros stavrinidis1, klisthenis tsamakidis1, Dimitrios xinopoulos1
1Gastroenterology, agios savvas cancer hospital, athens, Greece
Introduction: the benefit of sorafenib administration to hepatocellular cancer (hcc) patients after recurrence to previous chemoembolization (tace) treatment is not yet adequate studied. the aim of the present study was to estimate the efficacy of sorafenib (nexavar) administration in hcc, intermediate stage, patients after recurrence to previous tace treatment.
Methods: retrospectively was estimated the efficacy of sorafenib, (overall survival [os] and time to disease progression [ttDP]) in 12 patients (Group a) with intermediate stage hcc after recurrence to treatment with tace (1-3 taces, median 2). the results were compared with these of an historical and similar to etiology, morphology, stage of cirrhosis and performance status, group of 15 hcc, intrmediate stage, patients treated only with tace (Group B).
results: there were not any significant differences in disease characteristics between the two studied groups. the index of disease control for group a was 62.2%, the mean ttDP was 4.2 months and the os was 21.2 months. for Group B the index of the disease control was 30.6% (P=0.001), the mean ttDP was 2.3 months (hazard ratio 0,44, P<0,01) and the os 13.4 months (hazard ratio 0,57, P<0,001). the multivariate analysis revealed that the addition of sorafenib was the most important factor for the os and the prolongation of the ttDP.
Conclusion: the administration of sorafenib seems to be an attractive therapeutic approach for intermediate stage hcc patients after recurrence to previous chemoembolization treatment.
Disclosure of Interest: none Declared
P-345 The effOrT TO IDenTIfy The rOLe Of C-reACTIVe PrOTeIn (CrP) In ADVAnCeD LIVer MALIGnAnCIeS TreATeD WITh TrAnSArTerIAL CheMOeMbOLIzATIOn (TACe) AnD rADIOfrequenCy AbLATIOn (rfA)
Andreas Tooulias* 1, antonios fantakis1, athanassios Piahas1, Dimitrios chatziisaak1, Georgios Marakis1, Georgios tsoulfas1
1surgery, aristotle university of thessaloniki, thessaloniki, Greece
Introduction: to evaluate the management of advanced hepatocellular carcinoma (hcc) and hepatic metastatic disease with a protocol of combined transarterial chemoembolization (tace) and percutaneous radiofrequency ablation (rfa) at a hepatobiliary center.
Methods: Patients who underwent conventional tace and/or rfa for unresectable liver malignancies between october 2010 and March 2015 were studied. Demographic data, etiology and staging, as well as survival and recIst criteria were examined. crP values were also measured prospectively.
results: thirty patients underwent a total of 39 conventional taces and 21 rfas. they included 23 men and 7 women, with a median age of 67.7 years (range 48-87 years). five patients died during this study period, and twenty five remained alive. overall survival rates at 6 months, 1 year and 3 years from the first procedure are 90%, 90% and 83.33% respectively. the overall responses to the procedures using response evaluation criteria in solid tumors (recIst) were; 5 (16,67%) complete responses (cr), 4 (13,33%) partial responses (Pr), 1 (3,33%) steady disease (sD), and 14 (46,67%) progressive diseases (PD). 6 of the patients could not be calculated at the moment. Mean serum crP levels preoperatively, immediately postoperatively and at 1-, 3-, 6-, 9- and 12-month periods are 2.82mg/dl, 6.58mg/dl, 3.12mg/dl, 2.15mg/dl, 1.29mg/dl, 0.82mg.dl and 2.04mg/dl respectively. from this data, we notice a trend of increasing values in a period of 1 year after the initial treatment session.
Conclusion: Patients with advanced liver malignancies may benefit greatly from the use of ctace and rfa in preserving liver function during the disease, as well as in extending the overall survival. additionally, both ctace and rfa can be used effectively in the management advanced liver malignancies, either primary or metastatic.
references: 1. zhiyun zheng, Lin zhou, sheng Gao, zhe yang, jia yao, shusen zheng, “Prognostic role of c-reactive Protein in hepatocellular carcinoma: a systematic review and Meta-analysis”, Int. j. Med. sci. 2013; 10(6):653-664. doi: 10.7150/ijms.6050.2. jun hj, ki hs, Lee kh, Park kj, Park sy, cho sB, Park ch, joo ye, kim hs, choi sk, rew js. “Impact of c-reactive protein level on the prognosis of patients with hepatocellular carcinoma undergoing tace”. cl Mol hepatol 2013;19:70-7.3. kunzli B, abitabile P, Maurer c. “radiofrequency ablation of liver tumors: actual limitations and potential solutions in the future”. World j hepatol 2011 jan 27;3(1):8-14.4. Barman PM, sharma P, krishnamurthy V, Willatt j, Mccurdy h, Moseley rh, su GL. “Predictors of Mortality in Patients with hepatocellular carcinoma undergoing transarterial chemoembolization”. Dig Dis sci 2014 nov, vol 59;11:2821-5.
Disclosure of Interest: none Declared
P-346 fOLLOW-uP reSuLTS Of PATIenTS WITh MASSIVe TuMOr neCrOSIS AfTer TrAnSArTerIAL CheMOeMbOLIzATIOn
Tae-Seok Seo* 1, Myung Gyu song1, chul Min Park1, chang hee Lee1, kyung ah kim1, jae Woong choi1, jongmee Lee1, yang shin Park1
1radiology, korea university Guro hospital, korea university college of Medicine, seoul, korea, republic of
Introduction: the purpose of this study was to evaluate clinical and radiologic findings in patients with massive tumor necrosis after transarterial chemoembolization (tace).
Methods: We retrospectively reviewed clinical and radiologic findings of 10 patients who had large hepatocellular carcinoma (hcc) with massive tumor necrosis after tace. the patients consisted of 9 males and 1 female ranging in age from 50 -74 years. We performed tace with adriamycin and embolic materials such as polyvinyl alchohol(PVa) and gelfoam. Liver dynamic ct scans were performed before and after tace. Mssive necrosis was defined to complete or near complete necrosis on follow-up ct scan obtained after tace in patients with hcc larger than 5cm in diameter. We evaluated clinical symptoms, laboratory findings, radiologic findings, and amount of adriamycin and embolic materials.
results: Mean maximum diameter of hcc on axial ct image was 10.3 cm (range: 7-18 cm). amounts of adriamycin were 50mg in 8 patients and 40mg in 2 patients. embolic materials were PVa in 2 patients, gelfoam in 6 patients, and PVa with gelfoam in 2 patients. Mean elevated aLt after tace was 529 Iu/L (range: 104-1226 Iu/L). Mean elevated ast after tace was 694 Iu/L (range: 138-1754 Iu/L). Mean elevated total bilirubin was 2.3 mg/dL (range: 0.6-7.5 mg/dL). Pleural effusion was noted in 4 patients after tace. newly developed ascites was noted in 4 patients. Pain of patients after tace was subsided after mean 3.8 days (range: 2-8 days). however pain was not subsided in 3 patients.
Conclusion: these clinical findings and radiologic findings were helpful for better understanding massive necrosis of hcc after tace.
P-347 The MeAnInG Of AfP, AfP-L3 AnD PIVKA-II fOr eVALuATInG reCurrenCe In PATIenTS WITh hePATOCeLLuLAr CArCInOMA WhO unDerWenT LIVer reSeCTIOn
sung hoon kim1, Sang hyun Ahn* 2, Moon young kim3, soon koo Baik4
1Department of surgery, yonsei university Wonju college of Medicine, Wonju severance christian hospital, 2Department of surgery, 3Department of Internal medicine, yonsei university Wonju college of Medicine, 4Department of Internal medicine, yonsei university Wonju college of Medicine, Wonju severance christian hospital, Wonju, korea, republic of
Introduction: alpha-fetoprotein (afP) and prothrombin time induced by vitamin k absence-II (PIcka-II) have been used a diagnostic and surveillance marker for hepatocellular carcinoma (hcc). however, many patients showed less level than optimal level that previously reported in many studies.We investigated the meaning of the afP and PIVka-II, additionally lens culinaris agglutinin-reactive fraction of afP (afP-L3) for evaluating recurrence of hcc.
Methods: We retrospectively reviewed the medical records of patients who underwent liver resection. We investigated the recurrence and association with preoperative and postoperative level of afP, afP-L3 and PIVka-II.
results: Median afP, afP-L3 and PIVka-II were 8.5 ng/dL, <0.5% and 24 mau/mL, respectively.Median tumor size was 2.4cm. six patients (8.6%) had grossly portal vein invasion (PVI). Microscopic PVI was found in 8 patients (11.4%). During median 17month follow-up period, 19 patients had recurrence. a univariate analysis revealed that delta afP-L3, tumor size, gross PVI, satellite nodule, microscopic PVI, bile duct invasion and microvessel invasion were significant prognostic factors of recurrence. however, multivariate analysis revealed that only delta afP-L3 less than 50% was significant prognostic factors.

Posters
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 4 0
Conclusion: as the surveillance program has been generalized in patients with high risk of hcc, identification of early and resectable hcc has been increased. however, many patients showed normal level of tumor marker and surgical resection showed still high recurrence rate. although more large-scaled study will be needed, we may predict the recurrence risk according to the change of afP-L3.
Disclosure of Interest: none Declared
P-348 h3b6527, An uLTrA-SeLeCTIVe AnD POTenT fGfr4 InhIbITOr fOr fGf19 DrIVen hePATOCeLLuLAr CArCInOMA
Anand Selvaraj*1, erik corcoran1, heather coffey1, sudeep Prajapati1, Ming-hong hao1, nicholas Larsen1, takashi satoh1, jeremy Wu1, suzanna Bailey1, kana Ichikawa1, sandeep akare2, George Lai2, Lihua yu1, Peter fekkes1, john Wang1, Markus Warmuth1, Peter smith1, Dominic reynolds1
1h3 Biomedicine, 300 technology sq, cambridge, Ma 02139, usa, 2eisai, 4 corporate Dr, andover, Ma 01810, usa.
Introduction: hepatocellular carcinoma (hcc) has limited treatment options and generally poor prognosis. recent genomic studies have identified fGf19 as a driver oncogene in hcc. fGf19 is a gut secreted hormone that acts in the liver through fGfr4 to regulate bile acid synthesis. consistent with the notion that fGf19 is a driver oncogene in hcc, transgenic mice overexpressing fGf19 form liver tumors and genetic ablation of fGfr4 prevented tumor formation. these data suggest targeting fGfr4 would have therapeutic benefit in hcc with altered fGf19 signaling. While a number of Pan-fGfr inhibitors are being clinically evaluated, their application to fGf19-driven hcc will be limited by their fGfr1-3 related dose limiting toxicities.
Methods: using structure guided design, we have generated a highly selective covalent fGfr4 inhibitor, h3B6527, and tested it in a variety of model systems including hcc cell lines, hcc cell line xenografts and hcc patient derived xenografts. Genomic data from tcGa guided the selection of these models that have aberrant fGf19 levels due to fGf19 amplification and fGf19 overexpression. additionally, we have conducted preliminary monkey studies to address potential bile acid related toxicities due to fGf19/fGfr4 inhibition.
results: Biochemical and cellular selectivity assays showed that h3B6527 is >300 fold selective towards fGfr4 compared to other fGfr isoforms. addition of h3B6527 to fGf19 amplified hcc cell lines lead to dose dependent inhibition of fGf19/fGfr4 signaling and concomitant reduction in the viability of cells. Importantly, these effects were only observed in fGf19 altered hcc cell line models. h3B6527 dosing in mice lead to PD modulation and tumor regression in fGf19 altered hcc cell line derived xenografts and hcc patient derived xenografts without displaying any fGfr1-3 related toxicities. Prior studies in monkeys, using an fGf19 neutralizing antibody, have pointed to potential bile acid related toxicities that could preclude the clinical development of agents blocking fGf19 function. here we show, unlike the fGf19 neutralizing antibody, h3B6527 did not elicit a spike in serum bile acid levels and associated diarrhea suggesting the small molecule mode of inhibition is a viable strategy for treating fGf19 driven hcc.
Conclusion: Patient stratification and highly selective drugs are critical factors for the successful clinical development of targeted anti-cancer agents. here we have shown that inhibiting fGfr4 using an exquisitely selective small molecule may provide therapeutic benefit to fGf19 altered hcc patients. our genomic analysis has pointed to approximately 30% of hcc patients with altered fGf19 signaling that could potentially benefit form h3B6527 treatment.
Disclosure of Interest: all authors are employees of h3 Biomedicine or eisai Pharmaceuticals.

Authors Index
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 4 1
Name Abstract Name Abstract
abada, Paolo ................................................................................................................... P-290abada, Paolo ...................................................................................................................o-033abbadessa, Giovanni .............................................................................................P-326, o-029abboud, rami .................................................................................................................. P-146abdel fattah, hanzada...................................................................................................... P-189abdelaziz, khaled ............................................................................................................. P-333abdelkader, nadia ............................................................................................................ P-294abdella , heba ................................................................................................................. P-227abdelmoez, amal ............................................................................................................. P-333abeni, edoardo ..........................................................................................P-080, P-066, P-061abi-jouedeh, nadine ........................................................................................................ P-289abou-alfa, Ghassan ......................................................................................................... P-342abrantes, Margarida ........................................................................P-095, P-093, P-094, P-086abuelmaaty, Mohamed ..................................................................................................... P-294abuelmaaty, Mohammed .................................................................................................. P-333abu-taleb, hoda .............................................................................................................. P-197achilles, eike-Gert ............................................................................................................ P-138adam, Gerhard ................................................................................................................ P-138adam, rene .......................................................................................................... P-182, P-030adam, rené ..........................................................................................................P-225, o-028adams-huet, Beverley ...................................................................................................... P-153addario, Luigi ...........................................................................................P-302, P-287, P-274agazzi, roberto ................................................................................................................ P-316agren, camila ....................................................................................................... P-206, P-213agüero, fernando ............................................................................................................ P-016ahlquist, Paul................................................................................................................... P-088ahmed, amal ........................................................................................................ P-327, P-280ahmed, Dilruba ................................................................................................................ P-085ahn, hongkeun ................................................................................................................ P-250ahn, jem Ma ........................................................................................................ P-155, P-108ahn, jemma .................................................................................................................... P-201ahn, jem-Ma ................................................................................................................... P-023ahn, sang hoon .............................................................................................................. P-298ahn, sang hyun .................................................................................................... P-217, P-347ahn, su joa ..................................................................................................................... P-161aizawa, nobuhiro ............................................................................................................. P-204akamatsu , nobuhisa .......................................................... P-060, P-268, P-064, P-285, P-171akare, sandeep .............................................................................................................. P-348akiel, Maaged .................................................................................................................. P-028akiyama, takumi .............................................................................................................. P-283al hajar, nadim ................................................................................................................ P-210alejandra, alzina .............................................................................................................. P-332alencar, regiane .............................................................................................................. P-150alencar, regiane ............................................................................................................. P-082alexandrov, Ludmil ...........................................................................................................o-011alexis, Laurent .................................................................... P-291, P-260, P-147, P-149, P-122alhaider, a a ................................................................................................................... P-058allard, Marc-antoine ........................................................................................................ P-182allotey, Loretta ................................................................................................................. P-018almaraz, carmen .............................................................................................................o-003almeida, Márcio ............................................................................................................... P-226al-osaimi, abdullah ......................................................................................................... P-148alpini, Gianfranco ............................................................................................................o-009alsabbagh , Mohammed eyad .......................................................................................... P-148alshebeeb, kutaiba .........................................................................................................o-023alsinet, clara ....................................................................................................... o-008, o-007altomonte, jennifer .......................................................................................................... P-255alvarez, silvia...................................................................................................................o-003alvaro, Domenico .................................................................................................o-009, P-047alves , Venâncio .............................................................................................................. P-082aly, heba ......................................................................................................................... P-294amaddeo, Giuliana .....................................................................................P-261, P-030, P-009amathieu, roland ............................................................................................................ P-219amerane, hayette ........................................................................................................... P-224amiot, xavier ...................................................................................................................o-013an, hyonggin .................................................................................................................. P-201an, hyunggin ..................................................................................P-023, P-155, P-230, P-108an, jihyun ............................................................................................................ P-179, P-297andersen, jesper ......................................................................................o-012, o-009, o-001andreani, Paola................................................................................................................ P-096andres-Pons, amparo ...................................................................................................... P-040andreu, Victoria ............................................................................................................... P-129ang, celina ...................................................................................................................... P-244angelopoulou, katerina .................................................................................................... P-096
anson, Marie ...................................................................................................................o-005anstee, quentin .............................................................................................................. P-056antoniadis, nikolaos ......................................................................................................... P-096antonini, teresa ...............................................................................................................o-013anwar, Ghazanfar .................................................................................................. P-025, P-286anzai, keizo ..................................................................................................................... P-266aoki, taku ........................................................................................................................ P-307aoki, tomoko ........................................................................................................ P-131, P-204aracil, carlos ................................................................................................................... P-129arai, kuniaki ....................................................................................................................o-033araki, norimasa .................................................................................................... P-266, P-205aramaki, takeshi ................................................................................................... P-203, P-311archambaud, Isabelle .......................................................................................................o-013arciuolo, Damiano ............................................................................................................ P-240arenas, juan ................................................................................................................... P-129arenas, juan ................................................................................................................... P-277arici, Bruna.....................................................................................P-080, P-074, P-066, P-061ariizumi, syun-Ichi .......................................................................................................... P-136ario, keisuke ................................................................................................................... P-295arita , junichi ................................................................................P-060, P-064, P-285, P-171armengol, carolina ........................................................................................................... P-029arteta, Beatriz .................................................................................................................. P-097asakura, koiku ................................................................................................................. P-203asgharpour, amon ............................................................................................................ P-034askar, Marwa ................................................................................................................... P-151asou, hiroya ....................................................................................................................o-033assenat, eric....................................................................................................................o-021ataide, elaine ................................................................................................................... P-087atiq, omair ...................................................................................................................... P-174attili, adolfo francesco ...............................................................................P-256, P-242, P-257audoux, jérôme ............................................................................................................... P-007auewarakul, chirayu .......................................................................................................o-002auriemma, francesco ...................................................................................................... P-193aycart, samantha .................................................................................................. P-026, P-027ayuso, carmen ................................................................................................................ P-164azkargorta, Mikel ............................................................................................................. P-029azoulay, Daniel......................................................... P-207, P-199, P-096, P-158, P-073, P-279azueta, ainara..................................................................................................................o-003Baba, nobutaka ............................................................................................................... P-235Babu, Govind ................................................................................................................... P-278Bae, si hyun ............................................................ P-228, P-229, P-021, P-313, P-081, P-127Bae, yong-soo ................................................................................................................. P-004Baeg, joo yeong .............................................................................................................. P-323Bagiella , emilia ...............................................................................................................o-025Bai, Wei ................................................................................................................ P-306, P-112Baik, soon koo ..................................................................................................... P-217, P-347Bailey, suzanna ............................................................................................................... P-348Baiocchi, Gianluca ............................................................................................................ P-080Baitello, Maria eduarda.......................................................................................... P-095, P-086Bajwa, zan ...................................................................................................................... P-200Balabaud, charles ............................................................................................................o-004Balabaud, charles ......................................................................................o-011, P-008, P-073Baldan, anna ................................................................................................................... P-316Balkrishnan, rajesh ............................................................................................... P-109, P-115Bang, seo young .............................................................................................................. P-041Barakat, eman ...................................................................................................... P-333, P-309Baranes, Laurence ................................................................................................ P-207, P-199Barbera, Maria aurelia ...................................................................................................... P-303Barcena, rafael ............................................................................................................... P-016Barge, sandrine .............................................................................................................. P-293Bargellini, Irene ................................................................................................................ P-304Barni, sandro ........................................................................................................ P-256, P-242Baron, ari .......................................................................................................................o-032Barros costa, fernando .................................................................................................... P-198Bartenhagen, christoph .................................................................................................... P-065Bascomb, newell ............................................................................................................. P-278Bastos-rodrigues , Luciana .............................................................................................. P-042Beaugrand, Michel ........................................................................................................... P-232Bechstein, W ................................................................................................................... P-273Beck, Martin .................................................................................................................... P-040Bedossa, Pierre ................................................................................................................ P-034Behera, arunanshu ........................................................................................................... P-284Bekaii-saab, tanios .......................................................................................................... P-243Bekku, emima....................................................................................................... P-203, P-311

Authors Index
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 4 2
Name Abstract Name Abstract
Belghiti, jacques ..............................................................................................................o-031Bellot, Pablo ......................................................................................................... P-014, P-114Bendersky, noëlle ............................................................................................................o-017Benedetti, antonio ................................................................................................. P-256, P-242Benedicto, aitor................................................................................................................ P-097Benetti, anna ................................................................................................................... P-080Benfatto, salvatore ........................................................................................................... P-047Beninati, concetta ............................................................................................................ P-047Bereshchenko, oxana....................................................................................................... P-031Bergeat, Damien ..............................................................................................................o-028Berger, yaniv ..............................................................................................P-026, P-027, o-025Berhane, sarah ................................................................................................................o-015Bertini, Marco ....................................................................................................... P-017, P-318Bertoni, Michele .................................................................................................... P-017, P-318Bester, Lourens ................................................................................................................ P-304Bhat, sathesh .................................................................................................................. P-245Bhattacharyya, Gouri shankar .......................................................................................... P-278Bhudhisawasdi, Vajarabhongsa ........................................................................................o-002Bialkowska, jolanta ............................................................................................... P-089, P-090Biasiolo, alessandra ......................................................................................................... P-005Biederman, Derek ............................................................................................................ P-183Bilbao, jose Ignacio ......................................................................................................... P-332Bioulac-sage, Paulette .....................................................................................................o-004Bioulac-sage, Paulette ................................................................... P-046, o-011, P-008, P-073Biswas, Ghanashyam ....................................................................................................... P-278Black, james ................................................................................................................... P-160Blanc, jean-frederic .................................................................................o-011, o-032, o-015Blanc, jean-frédéric .....................................................................o-004, P-117, P-118, o-016Blanes, Mariano ............................................................................................................... P-016Blesing, claire .................................................................................................................. P-241Boige , Valerie ..................................................................................................................o-021Boin, Ilka ........................................................................................P-095, P-093, P-094, P-086Boin, Ilka ......................................................................................................................... P-226Boin, Ilka ......................................................................................................................... P-102Boin, Ilka ......................................................................................................................... P-087Boleslawski, emmanuel .........................................................................................P-262, o-028Bondarde, shailesh .......................................................................................................... P-278Bongarzone, Italia............................................................................................................. P-080Bonini, Daniela ................................................................................................................. P-080Bonshock, ryan ............................................................................................................... P-148Borad, Mitesh ....................................................................................................... P-018, P-319Borbath, Ivan ........................................................................................................P-326, o-029Borgman hagey, anne ..................................................................................................... P-342Borgmann, kerstin ........................................................................................................... P-011Borin, thaiz...................................................................................................................... P-102Bossard, Pascale ............................................................................................................. P-032Botelho, Maria filomena ........................................................................................ P-093, P-094Bouattour, Mohamed ........................................................................................................o-031Bouchemal, nadia ........................................................................................................... P-219Boucher, eveline...............................................................................................................o-021Boudjema, karim .............................................................................................................o-028Bouhaf, fatna ................................................................................................................. P-224Boulter, Luke.................................................................................................................... P-012Bourcier, Valerie ........................................................................................ o-013, o-014, P-224Bourcier, Valérie ........................................................................................P-293, P-002, o-020Bouyssou, caroline ................................................................................................P-118, o-016Braconi, chiara ..........................................................................................P-012, P-019, P-241Branchereau, sophie ............................................................................................. P-037, P-007Branco, fernanda ............................................................................................................ P-226Brandi, Giovanni ............................................................................................................... P-303Breitbach, caroline ...........................................................................................................o-032Bresci, Giampolo ................................................................................................... P-017, P-318Bricault, Ivan ......................................................................................................... P-261, P-030Brichler, ségolène ............................................................................................................ P-057Briggs, christopher .......................................................................................................... P-200Brito, ana filipa ..................................................................................................... P-093, P-094Brostjan, christine ........................................................................................................... P-220Brugieres, Laurence ......................................................................................................... P-305Brugières, Laurence .............................................................................................. P-037, P-007Bruix, jordi ..............................................................o-027, P-258, P-326, P-164, P-015, P-129Bruscella, Patrice ............................................................................................................. P-057Brusquant, David..............................................................................................................o-031Buades-Mateu, juan ........................................................................................................ P-277Buchpiguel, carlos alberto ................................................................................................ P-198
Budhu, anuradha .............................................................................................................o-002Budzinska, Magdalena ..................................................................................................... P-022Buendia, Marie annick ...................................................................................................... P-029Buendia, Marie-annick .......................................................................................... P-037, P-007Buonadonna, angela ............................................................................................. P-256, P-242Burke, james .................................................................................................................o-032Burke, rosemary ............................................................................................................. P-019Burlone, Michela .............................................................................................................. P-160Bustamante, javier .......................................................................................................... P-277Byun, kwan soo .................... P-271, P-023, P-155, P-230, P-108, P-105, P-186, P-239, P-128cabellos, Laia ..................................................................................................................o-007cabibbo, Giuseppe ........................................................................................................... P-257cabillic, florian ................................................................................................................ P-020cadoux, Mathilde .............................................................................................................o-005cagigas, carmen .............................................................................................................o-003calado, rodrigo ............................................................................................................... P-181calderaro, julien .....................................................P-207, P-199, o-004, P-046, o-011, P-008, .......................................................................................... P-073, P-261, P-030, P-009, P-063callejas neto, francisco ................................................................................................... P-223calvo, fabien ...................................................................................................... o-004, o-011cam, Maggie ...................................................................................................................o-002camargo, cinira ............................................................................................................... P-150camera, silvia .................................................................................................................. P-193camprecios, Genis ...........................................................................................................o-010cannito, stefania .............................................................................................................. P-005cao, qian ........................................................................................................................ P-003caporaso, nicola .............................................................................P-193, P-302, P-287, P-274carbonell , nicolas ...........................................................................................................o-013carnicer, fernando ................................................................................................ P-014, P-114carrilho, flair ................................................................................................................... P-198carrilho, flair .............................................................................................P-082, P-150, P-226cartier, flora .................................................................................................................... P-033carucci, Patrizia ............................................................................................................... P-257carvalho, Luis ..................................................................................................................o-028casadei Gardini, andrea ........................................................................................ P-276, P-337casanova, Michela ........................................................................................................... P-305castaing, Denis ..........................................................................................P-182, P-225, o-028castanhole, Marcia ............................................................................................... P-206, P-213castells, Lluis .................................................................................................................. P-016castillo, federico..............................................................................................................o-003castro Benitez, carlos ...................................................................................................... P-182castroagudin, javier ......................................................................................................... P-164castven, Darko ................................................................................................................o-012cazanave, sophie ............................................................................................................. P-034celton-Morizur, séverine ........................................................................................ P-069, P-076ceni, elisabetta ................................................................................................................ P-031cereceda, Laura ..............................................................................................................o-003cescon, Matteo ................................................................................................................ P-303cha, hyejung ................................................................................................................... P-195cha, jung hoon .............................................................................................................. P-081cha, sang-Woo ............................................................................................................... P-254chady, salloum ................................................................... P-291, P-260, P-147, P-149, P-122chaffaut, cendrine ...........................................................................................................o-013chagas, alice ................................................................................................................... P-181chagas, aline ................................................................................................................... P-150chagas , aline ...................................................................................................... P-082, P-226chaisaingmongkol, jittiporn ..............................................................................................o-002chaiteerakij, roongruedee ..................................................................................... P-134, P-018chaiteerakij, roonhgruedee .............................................................................................. P-116chalaye, julia .................................................................................................................. P-199chalhoub, Didier .............................................................................................................. P-140chammas, Maria cristina ................................................................................................. P-198chammas, roger ............................................................................................................. P-198chang, charissa ..............................................................................................................o-021chang, shao-chun ........................................................................................................... P-290chao, yee .......................................................................................................................o-032charnaux, nathalie ........................................................................................................... P-002chatterjee, Madhuchanda ................................................................................................. P-117chattieng, Piyanat ............................................................................................................ P-134chatziisaak, Dimitrios ....................................................................................................... P-345chen, hai-feng ................................................................................................................ P-216chen, jun ........................................................................................................................ P-167chen, Mishan ..................................................................................................................o-015chen, tianchi ................................................................................................................... P-172
Authors Index
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 4 3
Name Abstract Name Abstract
cheng, ann-Lii ......................................................... P-107, P-044, P-052, P-342, P-258, P-231cheng, robert .................................................................................................................. P-191cheng, shuqun ................................................................................................................ P-259cheng, ying ..................................................................................................................... P-320cheong, Io hong ................................................................................................... P-012, P-019cheong , jae youn ....................................................................................P-188, P-165, P-059cherqui, Daniel .............................................................................. P-182, P-225, P-030, o-028chetana, Lim ..................................................................................P-291, P-147, P-149, P-122chevret, sylvie .................................................................................................................o-013chiaradia, Melanie .....................................................................................P-207, P-261, P-030chiba, tetsuhiro ............................................................................................................... P-263chibaudel, Benoist ...........................................................................................................o-031chiche, Laurence .............................................................................................................o-016chiou, chih-yung ............................................................................................................. P-048cho, chul koo .................................................................................................................. P-315cho, eun ju ......................................................................................................... P-024, P-250cho, eung-ho .................................................................................................................. P-315cho, hyeki ....................................................................................................................... P-250cho, hyo jung ...........................................................................................P-188, P-165, P-059cho, ju yeon ................................................................................................................... P-237cho, junhyeon ...................................................................................................... P-323, P-143cho, Mong ................................................................................................o-032, P-330, P-041cho, sung ki ........................................................................................................ P-251, P-300cho, sung Won .........................................................................................P-188, P-165, P-059cho, young Deok ............................................................................................................. P-254cho, young youn ................................................................................................... P-024, P-250cho, young young ............................................................................................................ P-229cho, yuri ............................................................................ P-071, P-238, P-013, P-024, P-250choe, Won hyeok ............................................................................................................. P-325choi, cheol Woong ........................................................................................................... P-330choi, Dongil ..................................................................................................................... P-208choi, Gyu-seong ............................................................................................................. P-251choi, jae Woong .............................................................................................................. P-346choi, jin-young................................................................................................................ P-119choi, jong young ................................................................ P-228, P-021, P-313, P-081, P-127choi, jonggi .................................................................................................................... P-134choi, Moon seok ........................................................................................P-237, P-251, P-300choi, sang Il .................................................................................................................... P-106choi, yun suk .................................................................................................................. P-323choo, young kwang ......................................................................................................... P-185chopitea, ana ................................................................................................................. P-332chotirosniramit, anon .......................................................................................................o-002chouteau, Philippe ........................................................................................................... P-057chow, Pierce ................................................................................................................... P-304chowdhury, ruhe .................................................................................................. P-154, P-144chuang, Wan-Long .......................................................................................................... P-194chubak, jessica ............................................................................................................... P-153chubin, Luo ..................................................................................................................... P-050chun, ho jong ...................................................................................................... P-021, P-313chun, hoo ....................................................................................................................... P-342chung, jin Wook ............................................................................................................. P-238chung, jung Wha ............................................................................................................ P-323chung, seong Min .......................................................................................................... P-143chung, Woo jin................................................................................................................ P-169chung, young-hwa ........................................................................................................... P-179chung Mau, Lo ..................................................................................................... P-123, P-156ciacio, oriana .................................................................................................................. P-182cillo, clemente................................................................................................................. P-045cillo, umberto .................................................................................P-275, P-005, P-256, P-242clapéron, audrey ............................................................................................................. P-043clarke, Paul ..................................................................................................................... P-019coffey, heather ............................................................................................................... P-348cogliati, Bruno ................................................................................................................. P-198cohen, Gary..................................................................................................................... P-148collins, Peter ................................................................................................................... P-241colmenero, jordi ..............................................................................................................o-027colnot, sabine ................................................................................................................. P-032colombo, jucimara ......................................................................................................... P-102comba, arzu ......................................................................................................... P-221, P-101comba, Bahat ....................................................................................................... P-221, P-101comley, robert ................................................................................................................ P-175commes, thérèse ............................................................................................................ P-007compagnon, Philippe ....................................................................................................... P-158cooke, amy ..................................................................................................................... P-040
coppola, carmine ................................................................................................. P-176, P-159corcoran, erik .................................................................................................................. P-348cordone, Gabriella .....................................................................................P-302, P-287, P-274corlu, anne ...................................................................................................................... P-020cornellà, helena ...............................................................................................................o-008correnti, Margherita .........................................................................................................o-009cosse, cyril ..................................................................................................................... P-225costentin, charlotte ......................................P-199, o-031, o-017, P-261, P-030, P-009, o-016couchy, Gabrielle ................................................... o-004, o-011, P-008, o-005, P-073, P-063couty, jean-Pierre ...........................................................................................................o-005crain, anne-Marie ............................................................................................................o-005crespo, javier .......................................................................................................P-129, o-003cui, xiao .......................................................................................................................... P-079curiel-olmo, soraya .........................................................................................................o-003curtin, nicola ...................................................................................................................o-024cyrille, feray .................................................................................................................... P-291czauderna, Piotr .............................................................................................................. P-341D’albuquerque, Luiz ........................................................................................................ P-226Da silva, rita De cassia ................................................................................................... P-102Da silva, rita De cássia ..................................................................P-095, P-093, P-094, P-086Dabbous, hany ................................................................................................................ P-218Daita, kalyani ................................................................................................................... P-034Dang, hien ......................................................................................................................o-002D'angelo, salvatore ............................................................................................... P-256, P-242Daniel, azoulay ........................................................ P-291, P-292, P-260, P-147, P-149, P-122Daniele, Bruno ............................................................................... P-326, o-029, P-242, P-257Dannhorn, emily .................................................................................................... P-125, P-126Dao, hang ....................................................................................................................... P-336Dao, thong ......................................................................................................................o-013Darby, suzanne ................................................................................................................ P-241Darnell, anna ................................................................................................................... P-164Darstein, felix .................................................................................................................. P-184Datta, Debasis ................................................................................................................. P-278Datta, shalini ...................................................................................................................o-004Dauch, Daniel ..................................................................................................................o-007D'avola, Delia .................................................................................................................. P-332De Bortoli, Maida ............................................................................................................. P-080De Giorgio, Massimo ..................................................................................P-316, P-256, P-242De Gramont, armand ........................................................................................................o-031De La Iglesia, Pedro ......................................................................................................... P-114De La rosa, Pedro ........................................................................................................... P-277De La torre, Manuel ......................................................................................................... P-277De Ledinghen, Victor ............................................................................................ o-013, o-020De Lédinghen, Victor ........................................................................................................o-014De Lorenzo, stefania ........................................................................................................ P-303De Luca, Massimo .....................................................................................P-302, P-287, P-274De Marco, Luiz ................................................................................................................. P-042De Martin, eleonora ..........................................................................................................o-028De Petro, Giuseppina .......................................................................P-080, P-074, P-066, P-061De stefano, Giorgio .......................................................................................................... P-257De toni, enrico .................................................................................................................o-029De Verdier, Petra .............................................................................................................. P-085De Vita, ferdinando .......................................................................................................... P-257Decaens, thomas ......................................................................................P-261, P-030, o-021Dede, semiha .................................................................................................................. P-098Deguchi, akihiro ............................................................................................................... P-334Del Val, adolfo .................................................................................................................. P-288Delgado, fructuoso .......................................................................................................... P-288Delgado, Manuel .............................................................................................................. P-164Demartines, nicolas ......................................................................................................... P-268Den Boon, johan ............................................................................................................. P-088Dengler, Mirko ................................................................................................................ P-220Denlinger, crystal ............................................................................................................ P-243Deperalta, Danielle ........................................................................................................... P-245Desanctis, yoriko .............................................................................................................. P-258Desbois-Mouthon, christèle ............................................................................................. P-043Descot, christelle .............................................................................................................o-034Desdouets, chantal ....................................................................................P-069, o-005, P-076Desterke, christophe ........................................................................................................ P-046Destro, annarita .................................................................................................... P-038, P-063Di carlo, antonio .............................................................................................................. P-148Di costanzo, Giovan Giuseppe ..........................................................P-302, P-287, P-274, P-257Di costanzo, Giovanni ....................................................................................................... P-193Di tommaso, Luca ......................................................................................o-009, P-038, P-063

Authors Index
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 4 4
Name Abstract Name Abstract
Diallo, abou .......................................................................................................... P-232, P-219Diallo, abou .................................................................................................................... P-224Diaz, Maria alba ...............................................................................................................o-027Díaz , Álvaro..................................................................................................................... P-164Dieperink, eric ................................................................................................................. P-139Dierckx, rudi ................................................................................................................... P-175Dimitroulopoulos, Dimitrios ............................................................................................... P-344Dimitrov, Dimiter .............................................................................................................. P-039Ding, xiwei ...................................................................................................................... P-018Ding, yitao ....................................................................................................................... P-167Diribarne, Mathieu ........................................................................................................... P-076Djabbari, Marjane ............................................................................................................. P-207Do, hye-jin...................................................................................................................... P-331Doi, hisakazu ................................................................................................................... P-322Domingo-Domenech, josep ..............................................................................................o-008Donadon, Matteo ............................................................................................................ P-038Donckier, Vincent ............................................................................................................. P-304Dong, hui ........................................................................................................................o-010Dong, Li-Li....................................................................................................................... P-216Doorduin, janine .............................................................................................................. P-175Doussau, adélaide ...........................................................................................................o-016Dua, richa ....................................................................................................................... P-243Duan, ruiting ................................................................................................................... P-112Dubois-Pot-schneider, hélène........................................................................................... P-020Duffy, austin .................................................................................................................... P-289Dunn, Michael ................................................................................................................. P-140Duran, rafael ................................................................................................................... P-306Duvoux, christophe ....................................................................................P-261, P-030, P-009ebeid, kareem ................................................................................................................. P-028ebert, oliver .........................................................................................................o-032, P-255edeline, julien ...........................................................................................o-034, P-163, P-117edwards, Martin ............................................................................................................... P-027eguchi, yuichiro .........................................................................................P-266, P-205, P-295ehsan, nermine ............................................................................................................... P-209eiteneuer, eva .................................................................................................................. P-040el atrache, Mazen ............................................................................................................ P-146el Dorry, ahmed ..............................................................................P-189, P-218, P-246, P-141el folly, runia .................................................................................................................. P-246el fouly, amr ..............................................................................................P-246, P-141, P-333el fouly, neveen ................................................................................................... P-246, P-141el Garib, Mohamed ........................................................................................................... P-246el Gharib, Mohamed ........................................................................................................ P-218el Meteini, Mahmoud ............................................................................................ P-218, P-141el-ahwany, eman ............................................................................................................. P-197eldorry, ahmad................................................................................................................. P-227eldorry, ahmed................................................................................................................. P-294el-folly, runia .................................................................................................................. P-309el-fouly, nevien ............................................................................................................... P-309elgafary, Maha ................................................................................................................. P-294el-Ghanam, Maged .......................................................................................................... P-197el-Ghannam, Maged ............................................................................................. P-142, P-310el-hariri, hazem ............................................................................................................... P-309elias-junior, jorge............................................................................................................ P-181elkhattib, ahmed .............................................................................................................. P-327el-khoueiry, anthony ........................................................................................................ P-243el-khoueiry, anthony ........................................................................................................ P-342el-Mahdy, shaimaa .......................................................................................................... P-209elmeteini, Mahmoud ............................................................................................. P-294, P-227elokda, elsayed ................................................................................................................ P-280elortza, felix .................................................................................................................... P-029elrakhawy, Mohamed ....................................................................................................... P-151el-ray, ahmad ...................................................................................................... P-142, P-310elwaraky, Mohamed ......................................................................................................... P-209endo, Masahiro ..................................................................................................... P-203, P-311enomoto, hirayuki ............................................................................................................ P-204enooku, kenichiro ............................................................................................................ P-212ensell, Leah ..................................................................................................................... P-163ercolani, Georgio .............................................................................................................. P-304ercolani, Giorgio ............................................................................................................... P-303erminero, claudia .......................................................................................P-256, P-242, P-257ernault, tony ......................................................................................................... P-037, P-007escanhoela, cecilia .......................................................................................................... P-223escanhoela, cecilia .......................................................................................................... P-087esmat, emad ................................................................................................................... P-142
esteller, Manel .................................................................................................................o-007ewald, florian .................................................................................................................. P-070fabre, Monique ..................................................................................................... P-037, P-007facciuto, Marcelo ............................................................................................................. P-130fagiuoli, stefano .............................................................................................................. P-316faivre, sandrine ................................................................................................... o-034, o-031falco, Luigia ..............................................................................................P-302, P-287, P-274falissard, Bruno ...............................................................................................................o-017fallot, Guillaume .............................................................................................................. P-046faloppi, Luca ........................................................................................................ P-276, P-337fan, Daiming ................................................................................................................... P-306fan, jia ................................................................................................................ P-216, P-173fantakis, antonios ............................................................................................................ P-345farges, olivier .......................................................................................................o-017, P-262farinati, fabio .................................................................................................................. P-275fartoux, Laetitia ....................................................................................... o-034, o-031, P-032fasolato, silvano .............................................................................................................. P-005fassan, Matteo ................................................................................................................ P-019fassan, Matteo ................................................................................................................ P-012fassina, Giorgio ............................................................................................................... P-193fauveau, Véronique .......................................................................................................... P-076federici, Graziana ................................................................................................. P-017, P-318fekir, karim ..................................................................................................................... P-020fekkes, Peter .................................................................................................................. P-348felekouras, evangelos ...................................................................................................... P-343felga, Guilherme .............................................................................................................. P-226feng, Mingqian ................................................................................................................ P-039feng, zi-rui ..................................................................................................................... P-044feray, cyrille .................................................................................................................... P-046fernandes, alexandra ............................................................................................ P-093, P-094fernandez, roberto .........................................................................................................o-003fernandez-castroagudín, javier ........................................................................................ P-129ferraboli, sergio ............................................................................................................... P-066ferrari, carlotta ................................................................................................................ P-160ferrari, Giulia ........................................................................................................ P-012, P-019ferrari, Lia ............................................................................................................ P-080, P-066ferreira, Livia ................................................................................................................... P-102ferreira, rafael ..............................................................................P-095, P-093, P-094, P-086ferrer, joana ................................................................................................................... P-015ferrer, Maria teresa ......................................................................................................... P-129fetzer, David .................................................................................................................... P-140feusner, jim .................................................................................................................... P-305fiel, Isabel ....................................................................................................................... P-130fiel, M Isabel ...................................................................................................................o-010figg, William .................................................................................................................... P-289findeiss, Laura ...............................................................................................................o-032finkelstein, Marsha .......................................................................................................... P-317finn, richard ................................................................................................................... P-326finn, richard s. ............................................................................................................... P-290fischer, k ........................................................................................................................ P-273fischer, Michael ...............................................................................................................o-012fischman, aaron .............................................................................................................. P-183fisher, kevin .................................................................................................................... P-304fisher, Paul ...................................................................................................................... P-028florimond, alexandre ........................................................................................................ P-057florman, sander ........................................................................................o-023, P-130, P-183flygare, jenny ................................................................................................................ P-085fondevila, constantino .........................................................................................o-027, P-015fong, qiongfang ..............................................................................................................o-030fontana, tommaso ........................................................................................................... P-257forbes, stuart .................................................................................................................. P-012forgues, Marshonna ........................................................................................................o-002forne, Montserrat ............................................................................................................ P-129forner, alejandro ................................................................................................... P-015, P-016foschi, francesco Giuseppe ............................................................................................. P-276fouassier, Laura ............................................................................................................... P-043franchimont, Denis .......................................................................................................... P-003franconi, andrea ..................................................................................................o-004, P-008frassineti, Giovanni Luca ....................................................................................... P-276, P-337frega, Giorgio .................................................................................................................. P-303friedman, eitan ................................................................................................................ P-042fromenty, Bernard................................................................................................. P-069, P-020fuchs, Bryan ................................................................................................................... P-245fuentes, javier ................................................................................................................ P-129
Authors Index
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 4 5
Name Abstract Name Abstract
fujii, hirofumi ..................................................................................................................o-033fujimoto, jiro ................................................................................................................... P-204fujinaga, hidetaka............................................................................................................ P-212furlan, alessandro ........................................................................................................... P-140furuse, junji ........................................................................................................ o-033, o-022fuster, josep .......................................................................................................o-027, P-015Galeota Lanza, alfonso .......................................................................................... P-287, P-274Galle, Peter ...................................................................................................................... P-120Galle, Peter ................................................................................................o-012, P-184, P-067Galle, Peter r. .................................................................................................................. P-290Gallego, adolfo ................................................................................................................. P-129Galli, andrea .................................................................................................................... P-031Gallotta, andrea ............................................................................................................... P-193Ganas, Martin .................................................................................................................. P-067Ganne, nathalie .............................................................................o-013, o-014, P-261, P-030Ganne carrie, nathalie .................................................................................................... P-224Ganne-carrie, nathalie .................................................................................................... P-293Ganne-carrié, nathalie .......................................................................................... P-003, P-219Ganne-carrié, nathalie .................................................................................................... P-232Gany, francesca .............................................................................................................. P-244Gao, Wei .......................................................................................................................... P-039Garcia, josé .................................................................................................................... P-226García-Díaz, nuria ...........................................................................................................o-003Garcia-Valdecasas, juan carlos ........................................................................................o-027García-Valdecasas, juan carlos ........................................................................................ P-015Gardella, rita ................................................................................................................... P-066Gargavanis, thanasis ....................................................................................................... P-096Garner, andrew ................................................................................................................o-006Garre, carmen ................................................................................................................. P-129Garrido, Marta ................................................................................................................. P-029Gasbarrini, antonio .....................................................................................o-029, P-256, P-242Gatta, angelo ................................................................................................................... P-005Gatti, Pietro .......................................................................................................... P-176, P-159Gavriilidis, Paschalis ......................................................................................................... P-096Gazzola, alessia ............................................................................................................... P-275Geller, james ................................................................................................................... P-305Gelli, Maximiliano .............................................................................................................o-028Gentric, Geraldine ............................................................................................................ P-069George, khalid ................................................................................................................. P-146Geratikornsupuk, nopavut ...................................................................................... P-116, P-134Germann, nathalie ...........................................................................................................o-034Germano, Domenico......................................................................................................... P-256Ghazi, saud ..................................................................................................................... P-117Ghidini, Michele ............................................................................................................... P-012Gi hong, Gi hong ............................................................................................................. P-035Giacomelli, Luca ................................................................................................... P-017, P-318Giakoustidis, alexandros ................................................................................................... P-096Giakoustidis, Dimitrios ...................................................................................................... P-096Giannitrapani, Lydia .......................................................................................................... P-242Gibbin, antonello .............................................................................................................. P-160Gil, santiago .................................................................................................................... P-114Gil-Ibanez, Ines ................................................................................................................ P-011Ginès, Pere .....................................................................................................................o-027Giokas, konstantinos ........................................................................................................ P-177Giorgio, antonio .................................................................................................... P-176, P-159Giorgio, De stefano .......................................................................................................... P-340Giorgio, Valentina .................................................................................................. P-176, P-159Giovanis, Petros .........................................................................................P-256, P-242, P-257Giuseppe, signoriello ........................................................................................................ P-340Glaise, Denise .................................................................................................................. P-020Goel, rakesh ................................................................................................................... P-243Goldberg, terri ................................................................................................................. P-326Göller, Markus .................................................................................................................. P-273Goloni-Bertollo, eny ............................................................................................... P-206, P-213Golse, nicolas .................................................................................................................. P-225Gomaa, asmaa ................................................................................................................ P-209Gomez, alexandra ............................................................................................................ P-277Goo, juna ........................................................................................................................ P-170Goossens, corentine ....................................................................................................... P-219Gopal, Purva .........................................................................................................P-174, o-018Goria, odile......................................................................................................................o-013Gotanda, kaori ...................................................................................................... P-266, P-205Gougelet, angélique ......................................................................................................... P-032Goulopoulos, thomas ....................................................................................................... P-096
Goutte, nathalie ...............................................................................................................o-017Gow, Paul ........................................................................................................................ P-304Gozgit, joseph ................................................................................................................. P-018Graham, janine ............................................................................................................... P-241Grando, Véronique ............................................................................................................ P-293Grando, Véronique ........................................................................................................... P-232Granier, Muriel ................................................................................................................o-031Gredler, rachel ................................................................................................................ P-028Greenwood, jeremy ......................................................................................................... P-245Gregoire, emilie ............................................................................................................... P-225Greten, tim ...................................................................................................................... P-289Grigore, Ioana ............................................................................................P-302, P-287, P-274Grimm, Daniel .................................................................................................................. P-184Grosset, christophe ....................................................................................P-037, P-007, P-033Grossi, Ilaria...............................................................................................P-080, P-074, P-066Grotzer, Michael ............................................................................................................... P-037Gruenberger, thomas ...................................................................................................... P-220Grunert, David.................................................................................................................. P-255Gu, shanzhi ..................................................................................................................... P-306Guan, sheng .................................................................................................................... P-306Guarino, Maria ................................................................................P-193, P-302, P-287, P-274Guaschino, Giulia ............................................................................................................. P-160Guerra, Laura .................................................................................................................. P-029Guest, rachel .................................................................................................................. P-012Guettier, catherine ........................................................................................................... P-037Guilbert, thomas .............................................................................................................. P-076Gunasekaran, Ganesh ...................................................................................................... P-130Guo, Wei.......................................................................................................................... P-216Guo, Weidong .................................................................................................................. P-306Gupta, shweta ................................................................................................................. P-243Guyader, Dominique ............................................................................................. o-014, o-020Guyot, erwan ................................................................................................................... P-003Gwak, Geum-youn ..........................................................................P-237, P-251, P-229, P-300Gwon, Dong Il .................................................................................................................. P-297ha, yeonjung .................................................................................................................... P-166habersetzer, francois ......................................................................................................o-032hadengue, alexandra ......................................................................................................o-031haeberle, Beate ............................................................................................................... P-341hagel, Margit ...................................................................................................................o-030hagihara, atsushi .............................................................................................................o-022hahne, jens .................................................................................................................... P-012halgand, Boris ................................................................................................................. P-046halkic, nermin ................................................................................................................. P-268halm, ethan ..................................................................................................................... P-157hamdy, hassan ............................................................................................................... P-309hamed, Mostafa ............................................................................................................. P-227hamed, Mostafaa ............................................................................................................. P-280han, chul ju .................................................................................................................... P-315han, Guohong ............................................................................................o-015, P-306, P-112han, ji Won ..................................................................................................................... P-313han, joon koo ................................................................................................................. P-161han, kwang-hyub ............................................................... P-119, P-298, P-068, P-083, P-253han, nam Ik .................................................................................................................... P-127hano, hiroshi ................................................................................................................... P-136hao, ke ...........................................................................................................................o-010hao, Liyan ....................................................................................................................... P-192hao, zhan ........................................................................................................................ P-050hao, Ming-hong .............................................................................................................. P-348harrass, Mohammad ........................................................................................................ P-151harriman, Geraldine ......................................................................................................... P-245harris, curtis....................................................................................................................o-002hartimath, siddesh ........................................................................................................... P-175hartley, john .................................................................................................................... P-163harwood, h. ..................................................................................................................... P-245hasegawa, kiyoshi ................................................... P-060, P-268, P-338, P-064, P-285, P-171hassan, Moataz .............................................................................................................. P-197hassan, Mona .................................................................................................................. P-146hatano, etsuro .................................................................................................................o-033hatzinikolaou, Matina ....................................................................................................... P-344hayashi, seisyu ................................................................................................................ P-136hcc study Group, Brazilian ............................................................................................... P-226he, aiwu ruth .................................................................................................................. P-326he, jia............................................................................................................................. P-320he, Ping ..........................................................................................................................o-002

Authors Index
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 4 6
Name Abstract Name Abstract
heaton, nigel ........................................................................................................ P-154, P-144heilmann, stefanie ...........................................................................................................o-012heim, Denise ........................................................................................................ P-070, P-011heinrich, stefan ...............................................................................................................o-012helmy, ahmad .................................................................................................................. P-142henn, andrew .................................................................................................................. P-317hennequi, Marie ..............................................................................................................o-032henrion, jean ..................................................................................................................o-013heo, jeong ................................................................................... o-032, P-229, P-330, P-041heo, Min kyu ................................................................................................................... P-004herden, johannes ............................................................................................................ P-011herin, edouard ................................................................................................................. P-199hernandez, francisco ....................................................................................................... P-029hernandez, Iera ................................................................................................................ P-097hernandez-Guerra, Manuel ............................................................................................... P-164herrera , Iván ................................................................................................................... P-014herrera kok, john ............................................................................................................ P-182herrera Marante, Iván ....................................................................................................... P-114heskel, Marina ...........................................................................................P-026, P-244, P-027hewitt, stephen ...............................................................................................................o-002hidaka, Isao ..................................................................................................................... P-281higaki, tokio .................................................................................................................... P-282higuchi, Mayu .................................................................................................................. P-264higuera, Monica ...............................................................................................................o-007hinrichs, Britt ................................................................................................................... P-138hiraoka, atsushi ............................................................................................................... P-235hirota, seiichi .................................................................................................................. P-204hirte, hal .........................................................................................................................o-034hiyama, eiso .................................................................................................................... P-341ho, Mitchell ..................................................................................................................... P-039hoeflich, klaus ..................................................................................................... o-030, o-006hogan, Brian .................................................................................................................... P-168holzer, kerstin .................................................................................................................. P-040homerin, Michel ..............................................................................................................o-032honda, Masao ................................................................................................................. P-049hong, eun kyung ................................................................................................. P-124, P-314hong, young Mi ................................................................................................................ P-330hooks, katarzyna .................................................................................................. P-037, P-033hooks, katarzyna ............................................................................................................. P-007hoppe-Lotichius, Maria .................................................................................................... P-184hoshida, yujin ........................................................................................... o-008, P-034, o-010hoteit, Maarouf ................................................................................................................ P-135hoteit, Maarouf ................................................................................................................ P-111hsieh, sen-yung .............................................................................................................. P-048hsu, chih-hung .........................................................................................P-107, P-044, P-052hsu, chiun ....................................................................................................................... P-044hu, Bo .................................................................................................................. P-162, P-196huan, hongbo .................................................................................................................. P-308huang, chung-feng ......................................................................................................... P-194huang, jee-fu ................................................................................................................. P-194huber, heidemarie ............................................................................................................ P-220hubner, richard ............................................................................................................... P-241hur, chang jae ................................................................................................................ P-169hur, Won hee .................................................................................................................. P-081hussein, ahmed ............................................................................................................... P-246hwang, jae seok ............................................................................................................. P-169hwang, sang youn ................................................................................................ P-324, P-091hwang, sang-hyun .......................................................................................................... P-152hwang, tae ho ................................................................................................................. P-041Iannitti, David ................................................................................................................... P-304Ichida, takafumi ............................................................................................................... P-234Ichikawa, kana................................................................................................................. P-348Ide, takao ........................................................................................................................ P-295Ide, yasushi .................................................................................................................... P-295Iijima, hiroko .................................................................................................................... P-204Ijzermans, jan ................................................................................................................. P-182Ikeda, Masafumi .................................................................................................. o-033, o-022Ikeda, naoto .................................................................................................................... P-204Im, jung Woo........................................................................................................ P-324, P-091Imache, Mohamed ........................................................................................................... P-055Imai, katsunori ................................................................................................................. P-182Imbeaud, sandrine ...........................................................................................................o-004Imbeaud, sandrine ................................................................................................o-011, P-008Inaba, yoshitaka ...............................................................................................................o-022
Inagaki, Masaru ............................................................................................................... P-265Inagaki, yoshihiro ............................................................................................................. P-064Inagaki, yoshinori ............................................................................................................. P-060Iñarrairaegui, Mercedes ..............................................................................P-332, P-277, P-129Indersie, emilie ................................................................................................................ P-037Invernizzi, Pietro ....................................................................................................o-009, P-047Irurzun, javier .................................................................................................................. P-114Ishibashi, naoto ............................................................................................................... P-049Ishii, akio ......................................................................................................................... P-204Ishii, hiroshi ......................................................................................................... o-033, o-022Ishikawa, toru .................................................................................................................. P-235Ishikawa, tsuyoshi ........................................................................................................... P-281Ishizuka, Mitsuru .............................................................................................................. P-307Iso, yukihiro ..................................................................................................................... P-307Isoda, hiroshi ........................................................................................................ P-266, P-205Itakura, jun ..................................................................................................................... P-264Itti, emmanuel .................................................................................................................. P-199Ittrich, harald ................................................................................................................... P-138Iwadou, shouta ............................................................................................................... P-131Iwagaki, hiromi ................................................................................................................ P-265Iwai, shuji ........................................................................................................................ P-131Iwamoto, takuya .............................................................................................................. P-281Iwane, shinji ................................................................................................................... P-247Iwata, yoshinori ............................................................................................................... P-204Iwuji, chinenye................................................................................................................. P-241Izu, asami ........................................................................................................................ P-136Izumi, namiki ........................................................................................................ P-234, P-264Izuta, Masako .................................................................................................................. P-214Izzo, francesco ................................................................................................................o-015jablkowski, Maciej ................................................................................................ P-089, P-090jafri, syed-Mohammed .................................................................................................... P-146jamieson, David ...................................................................................................o-024, P-025jang, jeong Won ............................................................................................................. P-228jang, Byoung kuk ............................................................................................................ P-169jang, eun sun ...................................................................................................... P-323, P-143jang, jae young .............................................................................................................. P-254jang, jeong Won .......................................................................................P-021, P-081, P-127jang, kyung Mi ................................................................................................................ P-170jang, se young ..................................................................................................... P-113, P-077jang, sun kyung ................................................................................................... P-113, P-077jang, Won Il ..................................................................................................................... P-315jang, Won-Il .................................................................................................................... P-001jansen, ruben ................................................................................................................. P-065jariwala, nidhi ................................................................................................................. P-028jeon, ki jeong ...................................................................................................... P-324, P-091jeon, yejoo ...................................................................................................................... P-323jeong, shin ok ............................................................................................................... P-254jeong, sook-hyang ............................................................................................... P-323, P-143jeong, soung Won ........................................................................................................... P-254jeong, su-nam ................................................................................................................ P-041jeong, Woo kyoung ............................................................................................... P-208, P-299jeyarajah, rohan ............................................................................................................. P-304jiahao, jiang ................................................................................................................... P-050jiang, yong ...................................................................................................................... P-167jibara, Ghalib ..................................................................................................................o-015jin, jinglan ...................................................................................................................... P-072jinjuvadia, raxitkumar ...................................................................................................... P-110jo, soo yeon .................................................................................................................... P-137jo, sung Gi ..................................................................................................................... P-299joh, jae-Won ...................................................................................................... P-013, P-251johnson, Philip .............................................................................. P-125, P-126, o-015, P-241jonker, Derek .................................................................................................................o-032joo, Ijin ........................................................................................................................... P-161jueliger, simone .............................................................................................................. P-243jun, Mijung ..................................................................................................................... P-179jung, chang ho ............................................................................................................... P-230jung, Inkyung .................................................................................................................. P-253jung, kyu sik ................................................................................................................... P-298jung, sang hoon ............................................................................................................. P-300jung, young kul ................................P-023, P-155, P-230, P-108, P-105, P-239, P-186, P-128ka Wing, Ma ......................................................................................................... P-123, P-156kageyama, junichi ........................................................................................................... P-334kajioaka, hiroki ................................................................................................................ P-265kalva, sanjeeva ................................................................................................................ P-174

Authors Index
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 4 7
Name Abstract Name Abstract
kamachi, saori...................................................................................................... P-266, P-205kaman, Lileswar .............................................................................................................. P-284kamath, amitha ............................................................................................................... P-183kamps, jan .................................................................................................................... P-175kanda, hiroaki ................................................................................................................. P-136kanda, Miho ......................................................................................................... P-329, P-249kaneko, junichi ...................................................... P-060, P-268, P-338, P-064, P-285, P-171kaneko, shuichi ...............................................................................................................o-022kang, Dae hwan ................................................................................................... P-330, P-041kang, jing-Wu ................................................................................................................. P-216kang, koo jeong .............................................................................................................. P-169kang, seong hee ............................................................................P-271, P-230, P-105, P-186kang, so hee ................................................................................................................... P-084kang, sung hee ............................................................................................................... P-128kang, tae Wook .................................................................................................... P-237, P-170kang, Wonseok ................................................................................................................ P-119kang, yu na ..................................................................................................................... P-169kang , yoon-koo .............................................................................................................o-021kanki, keita ..................................................................................................................... P-049kanogawa, naoya ............................................................................................................ P-263kapeller, rosana .............................................................................................................. P-245karachristos, andreas ...................................................................................................... P-148karavias, Dimitrios ........................................................................................................... P-177karavias , Dionissios......................................................................................................... P-177kato, Masato ................................................................................................................... P-307katsanos, Georgios .......................................................................................................... P-304kawaguchi, yasunori ............................................................................................. P-283, P-247kawaguchi, yoshikuni ....................................................................................................... P-338kawai, toshihiro .................................................................................................... P-329, P-328kawai, toshuhiro .............................................................................................................. P-249kawazoe, seiji ............................................................................................o-033, P-283, P-295keer, harold ..................................................................................................................... P-243kelley, robin .................................................................................................................... P-342kerkar, sid ....................................................................................................................... P-289keskin, siddik .................................................................................................................. P-101khalaf, Mohamed ............................................................................................................. P-294khambaty, Maleka ............................................................................................................o-018khungar, Vandana ................................................................................................ P-135, P-111kikuchi, Luciana .............................................................................................................. P-082kikuchi, Luciana ............................................................................................................... P-150kikuchi, Luciana .............................................................................................................. P-226kim, sang Bum ................................................................................................................ P-315kim, Beom kyung............................................................................................................. P-298kim, Bo hyun ...................................................................... P-152, P-145, P-106, P-124, P-314kim, Boo sung ................................................................................................................ P-254kim, chang-Min .............................................................................P-152, P-145, P-124, P-314kim, chung yong ............................................................................................................. P-071kim, Do young .................................................................... P-119, P-298, P-229, P-068, P-083kim, edward ......................................................................................................... P-183, P-027kim, eui Bae ................................................................................................................... P-254kim, haeryoung ............................................................................................................... P-035kim, hong soo ................................................................................................................ P-254kim, hye Lim .................................................................................................................. P-081kim, hye young ............................................................................................................... P-300kim, hyo-cheol ............................................................................................................... P-238kim, hyung Wook ............................................................................................................. P-330kim, hyung-Don ............................................................................................................... P-297kim, ja kyung.................................................................................................................. P-335kim, jeong han ............................................................................................................... P-325kim, jeong Min ................................................................................................................ P-169kim, ji hoon ......................... P-271, P-023, P-155, P-230, P-108, P-105, P-186, P-239, P-128kim, ji Wan ..................................................................................................................... P-325kim, jin ........................................................................................................................... P-315kim, jin nam ................................................................................................................... P-137kim, jin Wook .................................................................................................................. P-323kim, jin-Wook ................................................................................................................. P-143kim, joe ..........................................................................................................................o-006kim, jong Man ..................................................................................................... P-013, P-251kim, jonghwa .................................................................................................................. P-084kim, joung youn ............................................................................................................. P-170kim, ju hyun ................................................................................................................... P-239kim, jun young ................................................................................................................ P-251kim, jung hee ...........................................................................................P-252, P-208, P-299kim, kang Mo ............................................................................................P-179, P-166, P-297
kim, ki-hwan ................................................................................................................... P-004kim, kyung ah ................................................................................................................. P-346kim, kyung hee ............................................................................................................... P-145kim, kyunga .................................................................................................................... P-252kim, Mi na ........................................................................................................... P-068, P-083kim, Mi sun ..................................................................................................................... P-253kim, Mi yeun.................................................................................................................... P-298kim, Mi-sook ........................................................................................................ P-001, P-315kim, Moon young .................................................................................................. P-217, P-347kim, richard .................................................................................................................... P-243kim, sang Gyune ............................................................................................................ P-254kim, seong hoon ............................................................................................................ P-314kim, seong hyun ............................................................................................................ P-170kim, seoung hoon ........................................................................................................... P-013kim, seung up ...................................................................................................... P-119, P-298kim, soon sun ..........................................................................................P-188, P-165, P-059kim, suk Bae ................................................................................................................... P-185kim, sung hoon .........................................................................................P-217, P-331, P-347kim, tae hyung .................................................................. P-023, P-201, P-155, P-230, P-108kim, tae suk ..................................................................................P-271, P-105, P-186, P-128kim, yong jae ................................................................................................................. P-254kim, yoon jun ..............................................P-071, P-238, P-013, P-024, P-250, P-004, P-229kim, young kon ..................................................................................................... P-170, P-208kim, young seok ............................................................................................................. P-254kim, yun soo ................................................................................................................... P-239kim , yun hwan ................................................................................................................ P-229king, judy ............................................................................................................ P-117, P-241kinukawa, noriko ............................................................................................................. P-136kirkwood, amy ................................................................................................................. P-241kirn, David .......................................................................................................................o-032kitada, koji ...................................................................................................................... P-265kitai, satoshi .................................................................................................................... P-234kleiner, David ................................................................................................................... P-289knapstein, johanna .......................................................................................................... P-184knoefel, Wolfram .............................................................................................................. P-065knott, astrid ..................................................................................................................... P-139knox , jennifer ................................................................................................................. P-342ko, eun jeong ...................................................................................................... P-106, P-314ko, eun jung .................................................................................................................. P-271ko, Gi-young .................................................................................................................... P-297ko, Min-jung ................................................................................................................... P-001ko, soon yong .................................................................................................................. P-325kobeiter, hicham .............................................................................................................. P-207koch, sandra ........................................................................................................ P-184, P-120koga, futa ............................................................................................................ P-266, P-205koh, kwang cheol ......................................................................................P-237, P-251, P-300koh, Myoung ju ............................................................................................................... P-035koike, kazuhiko................................................................................................................ P-212kojima, soichi .................................................................................................................. P-049kojima, yasushi ................................................................................................................o-022kokudo, norihiro ...........................................P-060, P-234, P-268, P-338, P-064, P-285, P-171kokudo, takashi ..............................................................................P-060, P-268, P-064, P-285kolligs, frank ................................................................................................................... P-273komolmit, Piyawat ................................................................................................. P-116, P-134kooka, yohei .................................................................................................................... P-270koole, Michel ................................................................................................................... P-175kouladouros, konstantinos ................................................................................................ P-304koutsouris , Dimitrios ....................................................................................................... P-177krackhardt, angela ........................................................................................................... P-255ku, yonson....................................................................................................................... P-234kuang, Ming .................................................................................................................... P-190kubota, keiichi ................................................................................................................. P-307kubotsu, akihito ............................................................................................................... P-266kubotsu, yoshihito ............................................................................................................ P-205kudo, Masatoshi ................... P-267, P-234, o-033, P-231, P-290, P-214, o-015, o-022, o-021kumada, takashi .............................................................................................................. P-235kurokawa, tomoharu ........................................................................................................ P-010kurosaki, Masayuki .......................................................................................................... P-264kweon, young oh .................................................................................................. P-113, P-077kwon, choon hyuck David ............................................................................................... P-251kwon, oh sang ................................................................................................................ P-239kwon, so Mee .................................................................................................................o-002kwon, so young .............................................................................................................. P-325kypreos, Dimitrios ............................................................................................................ P-344

Authors Index
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 4 8
Name Abstract Name Abstract
Labib, Peter ..................................................................................................................... P-200Labow, Daniel .................................................................................................................. P-026Lachenmayer, anja ........................................................................................................... P-065Lai, George ..................................................................................................................... P-348Lamar, Maria ................................................................................................................... P-326Lamar, Maria ...................................................................................................................o-029Lampasi, filippo .................................................................................................... P-287, P-274Lampis, andrea ................................................................................................................ P-012Lang, hauke ....................................................................................................................o-012Lanza, Marika .................................................................................................................. P-047Larrey, Dominique ................................................................................................ o-014, o-020Larsen, nicholas ............................................................................................................. P-348Latuf filho, Paulo ............................................................................................................. P-087Lau, Wan-yee ............................................................................................o-023, P-304, P-308Laurent, alexis .................................. P-207, o-004, o-011, P-158, P-279, P-261, P-030, P-009Lautem, anja ................................................................................................................... P-184Layese, richard ....................................................................................... o-014, P-002, o-020Le Moyec, Laurence ........................................................................................................ P-219Le roy, Bertrand .............................................................................................................. P-225Le sourd, samuel............................................................................................................. P-117Le treut, yves Patrice ............................................................................................ P-225, P-262Lee, Bin-shyun ................................................................................................................ P-044Lee, chang hee .........................................................................................P-346, P-187, P-186Lee, Danbi ....................................................................................................................... P-179Lee, Dong ho ................................................................................................................... P-161Lee, Dong hyeon ................................................................ P-071, P-238, P-013, P-024, P-250Lee, eun jung .................................................................................................................. P-195Lee, hae Lim ..................................................................................P-021, P-313, P-081, P-127Lee, han chu ...................................................................... P-179, P-166, o-032, P-231, P-297Lee, hye sun ................................................................................................................... P-035Lee, hyo-suk ............................................................................................P-071, P-238, P-250Lee, hyunah .................................................................................................................... P-004Lee, jae Min .................................................................................................................... P-108Lee, jeong Min ................................................................................................................ P-161Lee, jeong-hoon .................................................... P-071, P-238, P-013, P-024, P-250, P-004Lee, jong ho .................................................................................................................. P-143Lee, jongmee .................................................................................................................. P-346Lee, joo ho ..................................................................................................................... P-179Lee, joon hyeok .......................................................................................P-237, P-251, P-300Lee, joon-hyeok .............................................................................................................. P-208Lee, jung Il ...................................................................................................................... P-335Lee, jung Min .................................................................................................................. P-169Lee, kwan sik .................................................................................................................. P-335Lee, kwang-Woong ............................................................. P-133, P-132, P-238, P-013, P-004Lee, kyu chan ................................................................................................................ P-272Lee, Min Woo Lee ............................................................................................................ P-237Lee, Minjong ......................................................................................................... P-024, P-250Lee, rheun-chuan ........................................................................................................... P-304Lee, sae hwan ................................................................................................................ P-254Lee, sang soo ................................................................................................................. P-323Lee, seok ho ................................................................................................................... P-272Lee, seon-Mi ........................................................................................................ P-324, P-091Lee, seung Duk ............................................................................................................... P-314Lee, seung heon.............................................................................................................. P-272Lee, soo hyun ................................................................................................................. P-113Lee, soon kyu .................................................................................................................. P-081Lee, soonkyu ................................................................................................................... P-313Lee, suhyun .................................................................................................................... P-077Lee, sung Won ................................................................................................................ P-127Lee, sung-Gyu ................................................................................................................. P-179Lee, terence .................................................................................................................... P-006Lee, Woo jin ................................................................................................................... P-314Lee, yoon ........................................................................................................................ P-004Lee, young sun .........................................................................................P-271, P-186, P-128Lee, young-sun................................................................................................................ P-105Lee, yu rim .......................................................................................................... P-113, P-077Lee, yun Bin ......................................................................................................... P-071, P-238Lee, yung sang ................................................................................................................ P-179Leffondre, karen ..............................................................................................................o-016Legou, françois ............................................................................................................... P-207Lencioni, Monica ..............................................................................................................o-029Lencioni, riccardo ............................................................................................... o-032, o-021Lengauer, christoph ............................................................................................. o-030, o-006Leonardou, Polytimi .........................................................................P-339, P-301, P-343, P-222
Lequoy, Marie .................................................................................................................. P-032Lerat, herve ..................................................................................................................... P-055Lertprasertsuke, nirush ....................................................................................................o-002Lesjean, sarah ...........................................................................................P-037, P-007, P-033Letenneur, Luc .................................................................................................................o-016Letexier, Mélanie .............................................................................................................o-004Letoublon, christian .............................................................................................. P-261, P-030Letouzé, eric .................................................................................o-004, o-011, P-008, P-002Leung, carmen ............................................................................................................... P-006Levy, caio ........................................................................................................................ P-198Levy, elliot ....................................................................................................................... P-289L'hermitte, antoine ...............................................................................................o-005, P-076Li, hailiang ...................................................................................................................... P-306Li, Wanyu ........................................................................................................................ P-072Li, xilong ......................................................................................................................... P-153Li, yong-shi ..................................................................................................................... P-052Li, zhao ........................................................................................................................... P-079Liang, jun ....................................................................................................................... P-320Liangpunsakul, suthat ...................................................................................................... P-110Liccioni, alexandre ........................................................................................................... P-015Lieb, jonas ...................................................................................................................... P-184Lim, chetana .............................................................................................P-207, P-199, P-279Lim, hyo keun ................................................................................................................ P-237Lim, Won ......................................................................................................................... P-330Lim, young-suk ..................................................................................................... P-179, P-166Lim , ho-yeong ...............................................................................................................o-021Lima, Livia ...................................................................................................................... P-082Limacher, jean-Marc ......................................................................................................o-032Lin, Bingyi ....................................................................................................................... P-172Lin, hang ......................................................................................................................... P-052Lin, Manxia ...................................................................................................................... P-190Liu, Dong-Li ..................................................................................................................... P-216Liu, jian .......................................................................................................................... P-062Liu, jueshi ....................................................................................................................... P-306Liu, Lei ............................................................................................................................ P-112Liu, Li-Li .......................................................................................................................... P-051Liu, tsung-hao ................................................................................................................ P-107Liu, yang ......................................................................................................................... P-216Liver cancer study Group of japan, for the ...................................................................... P-234Lledo, jose Luis ............................................................................................................... P-129Llerena, susana ...............................................................................................................o-003Llovet, josep ........................................................................................................o-030, P-258Llovet, josep ....................................................................................................... o-008, o-021Llovet, josep ....................................................................................................... o-007, o-011Llovet, josep M................................................................................................................o-010Llovet, josep M. ............................................................................................................... P-290Llovet, josep Maria ..........................................................................................................o-027Lo, regina ....................................................................................................................... P-006Lobe, cindy ..................................................................................................................... P-043Loffredo, christopher ........................................................................................................o-002Lohse, ansgar ............................................................................................P-070, P-011, P-138Long, Dao ........................................................................................................................ P-336Lonjedo, elena ................................................................................................................. P-288Lookstein, robert ............................................................................................................ P-183Lopez-santamaria, Manuel ............................................................................................... P-029Lopez-terrada, Dolores..................................................................................................... P-341Lorente, sara ................................................................................................................... P-277Lorusso, Vito ......................................................................................................... P-256, P-242Louvet, alexandre .............................................................................................................o-013Lowe, helen ..................................................................................................................... P-163Lozada, angelo ............................................................................................................... P-313Lu, jun-hua ....................................................................................................................o-023Lu, shi-xun ..................................................................................................................... P-051Luca', Maria Grazia .......................................................................................................... P-316Luciani, alain ..................................................................................P-207, P-199, P-158, P-009Luciani, fabio .................................................................................................................. P-022Lué, alberto ..................................................................................................................... P-277Luff, thomas.................................................................................................................... P-200Lunec, john ..................................................................................................................... P-056Lunqe, oscar ................................................................................................................... P-085Luong, tu Vinh ................................................................................................................. P-240Luong, tuvinh .................................................................................................................. P-163Lusky, Monika .................................................................................................................o-032Lv, Weifu ......................................................................................................................... P-306

Authors Index
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 4 9
Name Abstract Name Abstract
Ma, kuansheng ................................................................................................................ P-308Ma, yilong ....................................................................................................................... P-306Ma, yuk ting .................................................................................................................... P-117Mabrut, jean-yves ........................................................................................................... P-225Machado, camila Maria .................................................................................................... P-198Madkour, ahmad .............................................................................................................. P-227Maeshiro, tatsuji ............................................................................................................. P-131Maggioni, Marco ................................................................................................... P-038, P-063Magini, Giulia ................................................................................................................... P-316Mahajan, Vineet ............................................................................................................... P-175Mahdi, ahmed ................................................................................................................. P-056Maher, amany .................................................................................................................. P-327Mahidol, chulabhorn .......................................................................................................o-002Mahmmoud, amr ............................................................................................................ P-309Maibach, rudolf ............................................................................................................... P-341Maillard, aline ..................................................................................................................o-016Maillet, Vanessa .................................................................................................... P-069, P-076Mak, Winger .................................................................................................................... P-006Makuuchi, Masatoshi ....................................................................................................... P-234Malahias, apostolos ......................................................................................................... P-344Malecki, Wojciech ................................................................................................. P-089, P-090Maleux, Geert .................................................................................................................. P-304Malhotra, hemant ............................................................................................................ P-278Malik, abdul ..................................................................................................................... P-100Mall, sabine..................................................................................................................... P-255Mallat, ariane................................................................................................................... P-207Mallet, Maxime ................................................................................................................o-004Malogolowkin, Marcio ....................................................................................................... P-305Malta, fernanda ............................................................................................................... P-082Manas, Derek .................................................................................................................. P-304Mangeshkar, Milan ........................................................................................................... P-342Mangiola, francesca ........................................................................................................ P-316Manickavadagar, thubeena ................................................................................... P-154, P-144Manuguerra, roberta ....................................................................................................... P-240Manzardo, christian ......................................................................................................... P-016Marakis, Georgios ............................................................................................................ P-345Marceglia, sara ..................................................................................................... P-017, P-318Marcellin, Patrick ................................................................................................. o-014, o-020Marenco, simona ............................................................................................................. P-256Maria, reig ...................................................................................................................... P-164Mariguchi, Michihisa ........................................................................................................ P-311Marisi, Giorgia ...................................................................................................... P-276, P-337Maroulis , Ioannis ............................................................................................................. P-177Marquardt, jens ..............................................................................................................o-012Marquez, joana ............................................................................................................... P-097Marrero, jorge ...........................................................................................P-174, o-018, P-157Marroncini, Giada ............................................................................................................. P-031Marshall, aileen .................................................................................................... P-125, P-126Marshall, Vincent ............................................................................................................. P-109Marshall, Vincent ............................................................................................................. P-115Marti, josep .................................................................................................................... P-130Martín, Luis .....................................................................................................................o-003Martinelli, ana .................................................................................................................. P-181Martínez-quetglas, Iris .....................................................................................................o-007Martin-Llahi, Marta .......................................................................................................... P-129Masaaki kitahara, Masaaki kitahara .................................................................................. P-131Masaki, tsutomu ................................................................................................... P-334, P-321Masumoto, akihide ...........................................................................................................o-033Mathurin, jerome ............................................................................................................. P-117Mathurin, jérome ............................................................................................................. P-118Matilla , ana ......................................................................................................... P-164, P-129Matsui, osamu ................................................................................................................ P-234Matsumoto, koshi ............................................................................................................ P-136Matsumoto, toshihiko ....................................................................................................... P-281Matsuyama, yutaka .......................................................................................................... P-234Matter, Matthias ...................................................................................................P-045, o-012Matteucci, Paolo ................................................................................................... P-176, P-159Mattos, angelo ................................................................................................................. P-226Mazzaferro, Vicenzo .........................................................................................................o-007Mazzaferro, Vincenzo........................................................................................................o-011M'Ba assonzock, Lena ..................................................................................................... P-262Mccallister, katharine ....................................................................................................... P-157Mcintosh, Brian ................................................................................................................ P-088Mclafferty, scott ............................................................................................................... P-148
Mclennan, susan ............................................................................................................. P-191Megalooikonomou, Vasileios ............................................................................................. P-177Mehdaoui, Dalila .............................................................................................................. P-073Meiller, clément ...............................................................................................................o-011Meinhardt, Gerold ............................................................................................................ P-258Mejias, caroline ............................................................................................................... P-157Mello, tommaso ............................................................................................................... P-031Meltzer, Paul ....................................................................................................................o-002Mena, jorge .................................................................................................................... P-097Mendiola, Marta ............................................................................................................... P-029Meng, Gang .................................................................................................................... P-167Mente, Ênio ..................................................................................................................... P-181Mergey, Martine ............................................................................................................... P-043Merle, Philippe ................................................................................................................o-032Metrangolo, salvatore............................................................................................ P-017, P-318Meyer, tim .......................................................................... P-168, P-342, P-163, P-117, P-241Meyers, rebecka ............................................................................................................. P-341Michalopoulos, antonios ................................................................................................... P-096Miduturu, chandra ...........................................................................................................o-030Mikagi, kazuhiro ...................................................................................................o-026, P-269Mikulits, Wolfgang ............................................................................................................ P-220Milani, stefano ................................................................................................................. P-031Miles, steven ...................................................................................................................o-029Miltiadous, oriana ............................................................................................................o-010Milwee, steven ................................................................................................................ P-342Min, Michael ................................................................................................................... P-317Minami, tomohiro ............................................................................................................ P-267Minami, yasunori .............................................................................................................. P-267Minguez, Beatriz .............................................................................................................. P-129Miró, jose María .............................................................................................................. P-016Mirshahi, faridoddin ......................................................................................................... P-034Mismas, Valeria..................................................................................................... P-017, P-318Miyata, akinori ................................................................................................................. P-171Miyoshi, hisaaki ............................................................................................................... P-321Mizukami, naohisa ........................................................................................................... P-296Mizuta, toshihiko .................................................................................................. P-247, P-295Moaven, omeed ............................................................................................................... P-245Moehlendick, Birte .......................................................................................................... P-065Moehler, Markus ..............................................................................................................o-032Moeini, agrin ............................................................................................o-030, o-008, o-010Mohamed, essa ............................................................................................................... P-018Moharram-zadeh, adib..................................................................................................... P-138Moirand, romain ..............................................................................................................o-013Molina, Victor ................................................................................................................... P-015Montalto, Giuseppe .......................................................................................................... P-256Montasser, Iman ................................................................................................... P-189, P-218Montesarchio, Luca ............................................................................................... P-176, P-159Montesarchio, Vincenzo ..............................................................................P-256, P-242, P-257Moon, jeong seop ........................................................................................................... P-137Moraes, Débora ............................................................................................................... P-042Morales, Victor j .............................................................................................................. P-288Moreira, joão .................................................................................................................. P-082Morel, fabrice .................................................................................................................. P-020Morello, elisabetta ............................................................................................................ P-005Moreno, christophe ...............................................................................................o-013, P-003Moreno-osset, eduardo .................................................................................................... P-288Mori, shozo ..................................................................................................................... P-307Moriguchi, Masamichi ...................................................................................................... P-282Morimoto, Manabu ...........................................................................................................o-022Morisco, filomena ...........................................................................P-193, P-302, P-287, P-274Morishita, yukio................................................................................................................ P-136Morita, Masaru ................................................................................................................ P-270Morita, sojiro ...................................................................................................................o-033Moriwaki, hisataka ........................................................................................................... P-049Morris, David ................................................................................................................... P-304Moser, catherine ................................................................................................... P-018, P-319Motoyama, tenyu ............................................................................................................. P-263Mourad, Lobna ................................................................................................................ P-197Mu, Wei ........................................................................................................................... P-306Muazzam, Iqtedar ........................................................................................................... P-241Muglia, Valdair ................................................................................................................. P-181Mulcahy, Mary ................................................................................................................. P-243Mulder, Paul .................................................................................................................... P-233Müller, christian .............................................................................................................. P-220

Authors Index
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 5 0
Name Abstract Name Abstract
Muñoz, carolina ............................................................................................................... P-129Murayama, kenichiro .................................................................................P-266, P-205, P-295Murer, francesca ............................................................................................................. P-275Murphy, erin ....................................................................................................................o-006Musolino, cristina ............................................................................................................ P-047nagamatsu, hiroaki ....................................................................................P-236, P-270, P-296nagata, rihito .................................................................................................................. P-338nagy, faten ..................................................................................................................... P-197nahm, ji hae ................................................................................................................... P-035nahon, Pierre .............................................................................................P-293, P-224, P-219nahon, Pierre ......................................................................P-232, o-014, P-003, P-002, o-020nakajima, keiko .................................................................................................... P-258, P-231nakakuki, natsuko ........................................................................................................... P-264nakamori, shoji................................................................................................................o-022nakamura, naoya ............................................................................................................ P-136nakanishi, hiroyuki ........................................................................................................... P-264nakano, chikage .............................................................................................................. P-204nakano, Masahito ............................................................................................................ P-270nakano, Masayuki ................................................................................................. P-038, P-136nakashima, osamu .......................................................................................................... P-234nakashita, shunya ..........................................................................P-266, P-205, P-283, P-295nakayama, hisashi ........................................................................................................... P-282nakayama, yasuhiro ......................................................................................................... P-131nam, Byung ho ..................................................................................................... P-145, P-106nam, hee chul................................................................................................................. P-127nani, roberto ................................................................................................................... P-316naoki fujita, naoki fujita .................................................................................................. P-131nash, stephen ................................................................................................................. P-241nashan, Björn ....................................................................................................... P-070, P-138nault, jean charles .............................................................o-004, P-293, P-232, P-073, P-063nault, jean-charles ...................................................................................o-011, P-008, P-224navarra, Giuseppe ........................................................................................................... P-047navasa, Miquel ................................................................................................................ P-015nawfal triba, Mohamed ................................................................................................... P-219nemunaitis, john ............................................................................................................. P-243nepal, chirag ...................................................................................................................o-001neri, flavia ...................................................................................................................... P-303neuveut, christine ............................................................................................................ P-046ng, Irene ......................................................................................................................... P-006nguyen-khac, eric ...........................................................................................................o-013nicol, Lionel ..................................................................................................................... P-233nicola, De angelis ......................................................................................P-291, P-292, P-260niizeki, takashi ................................................................................................................ P-236nishida, naoshi ................................................................................................................ P-234nishiguchi, shuhei ........................................................................................................... P-204nishikawa, hiroki ............................................................................................................. P-204nishimura, takashi ........................................................................................................... P-204nishioka, chika ................................................................................................................ P-283niu, jing .......................................................................................................................... P-112niu, junqi ........................................................................................................................ P-072nkontchou, Gisele ................................................................................................. P-232, P-224nkontchou, Gisèle ........................................................................................................... P-293nobes, jenny ................................................................................................................... P-241noh, choong kyun ....................................................................................P-188, P-165, P-059noh, jae Myoung ............................................................................................................. P-300nonell, Lara ..................................................................................................................... P-029nookala, anupama ........................................................................................................... P-317nowakowski, francis ........................................................................................................ P-183nunzia, farella ................................................................................................................. P-340o' Beirne, james .................................................................................................. P-125, P-126o' Donoghue, Pam ................................................................................................ P-125, P-126obeirne, james ............................................................................................................... P-163o'Beirne, james .............................................................................................................. P-168oberti, frédéric ................................................................................................................o-013obi, shuntaro................................................................................. P-329, P-249, o-033, P-328odorissi, Paulo ................................................................................................................. P-087oganesian, aram ............................................................................................................. P-243ogasawara, sadahisa ....................................................................................................... P-263ogawa, chikara .................................................................................................... P-215, P-214ogawa, Masahiro ............................................................................................................. P-136ogle, Laura ................................................................................................o-024, P-025, P-286o'Grady, john ....................................................................................................... P-154, P-144oh, Dongryul ................................................................................................................... P-300oh, jung suk ........................................................................................................ P-021, P-313
ohkawa, shinichi .............................................................................................................o-033ohmura, takumi ...............................................................................................................o-022ojanguren, Isabel ............................................................................................................. P-029okusaka, takuji .................................................................................................... o-033, o-022olaso, elvira ..................................................................................................................... P-097oliveira, andre ................................................................................................................. P-206oliveira, andré ................................................................................................................. P-213oliveira, claudia ............................................................................................................... P-198olivier, seror .................................................................................................................... P-232olthoff, kim ......................................................................................................... P-135, P-111onali, simona ............................................................................................P-125, P-126, P-163o'neill, allison .................................................................................................................. P-341o'neill, allison .................................................................................................................. P-305oner, ahmet..................................................................................................................... P-099ooka, yoshihiko ................................................................................................................ P-263ori, alessandro ................................................................................................................ P-040ortiz, Inmaculada .................................................................................................. P-288, P-129oto, Gokhan ...................................................................................P-099, P-098, P-221, P-101otsuka, taiga .............................................................................................P-266, P-205, P-295ou, Da-Liang ................................................................................................................... P-044ouzan, Denis ...................................................................................................................o-014ozaki, Iwata .......................................................................................................... P-266, P-205ozdemir, hulya ...................................................................................................... P-098, P-221ozenne, Violaine ..............................................................................................................o-013Paik, seung Woon .......................................................................... P-237, P-251, o-032, P-300Paik, yong han ................................................................................................................. P-300Paik, yong-han ..........................................................................................P-237, P-299, P-084Pairojkul, chawalit ............................................................................................................o-002Palazón, jose María ........................................................................................................ P-014Palazón, josé María ......................................................................................................... P-114Palloni, andrea ................................................................................................................. P-303Palmer, Dan ..................................................................................................................... P-117Palmer, Daniel.................................................................................................................. P-241Panasyuk, Ganna ............................................................................................................. P-069Papadatos-Pastos , Dionysis .................................................................................. P-154, P-144Papadopoulos, Vasilios .................................................................................................... P-096Papalois, Vasilios .............................................................................................................. P-096Papanikolaou, Vasilios ...................................................................................................... P-096Pappas, Paris..................................................................................P-339, P-301, P-343, P-222Paprottka, P ..................................................................................................................... P-273Paradis, Valérie .....................................................................................................o-031, P-069Paranaguá-Vezzozo, Denise ............................................................................................. P-082Pardo, fernando .............................................................................................................. P-304Pareja, jose ..................................................................................................................... P-223Parikh, neehar ................................................................................................................. P-115Parikh, neehar ................................................................................................................. P-109Parisi, Giuseppe .................................................................................................... P-017, P-318Parisi, Ioanna .................................................................................................................. P-168Park, chul Min ................................................................................................................. P-346Park, hee chul ...................................................................................................... P-208, P-300Park, hye Min .................................................................................................................. P-169Park, hyun jeong ............................................................................................................. P-170Park, joo han ....................................................................................................... P-188, P-059Park, joong-Won .................................................... P-152, P-145, P-106, P-124, o-015, o-021Park, jun yong ................................................................................................................ P-298Park, Min jung ................................................................................................................ P-170Park, na ri ...................................................................................................................... P-081Park, soo young .................................................................................................... P-113, P-077Park, su Bum .................................................................................................................. P-330Park, su cheol ................................................................................................................. P-315Park, su hyun .................................................................................................................. P-084Park, sun seob ............................................................................................................... P-106Park, suyeon .................................................................................................................. P-254Park, yang shin ..........................................................................................P-346, P-187, P-186Park, yangsoon ................................................................................................................ P-179Park, young nyun ............................................................................................................. P-035Parola, Maurizio ............................................................................................................... P-005Parplys, ann christin ....................................................................................................... P-011Pascal, Gérard ................................................................................................................. P-279Pascual, sonia ...........................................................................................P-014, P-114, P-129Patel, kinnari ................................................................................................................... P-241Patel, rahul ..................................................................................................................... P-183Patel, Vishal ..................................................................................................................... P-148Paule, Bernard ...................................................................................................... P-261, P-030

Authors Index
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 5 1
Name Abstract Name Abstract
Pavarino, erika ...................................................................................................... P-206, P-213Pavel, Mihai ....................................................................................................................o-027Pawlotsky, jean-Michel ......................................................................................... P-055, P-057Peck-radosavljevic, Markus .................................................................................. P-231, P-326Peix, judit ................................................................................................o-030, o-008, o-007Pelletier, jean-sébastien .................................................................................................. P-140Pelletier, Laura .................................................................................................................o-011Pelusio, adina .................................................................................................................o-032Peña, cristina .................................................................................................................. P-114Peng, jei-Ming ................................................................................................................ P-048Peng, Lee ........................................................................................................................ P-148Perarnau, jean-Marc .......................................................................................................o-013Perlemuter, Gabriel ...........................................................................................................o-013Peron, jean-Marie ...........................................................................................................o-013Perret, christine ....................................................................................................o-005, P-076Perrina, Valeria ................................................................................................................ P-045Personeni, nicola .............................................................................................................o-029Peter, Littler ..................................................................................................................... P-286Petrov-sanchez, Ventzi ..........................................................................................P-002, o-020Pfiffer, túlio ...................................................................................................................... P-150Pham, sandrine ...............................................................................................................o-005Philippe, compagnon ............................................... P-291, P-260, P-147, P-149, P-122, P-279Phornphutkul, kannika......................................................................................................o-002Piahas, athanassios ......................................................................................................... P-345Picat, Marie-quitterie .......................................................................................................o-016Picciotto, antonino ........................................................................................................... P-242Picciotto, francesco Paolo ..................................................................................... P-287, P-274Pierobon, elisa sefora ...................................................................................................... P-130Pietrasz, Daniel ................................................................................................................ P-158Pigneur, frederic ................................................................................................... P-207, P-158Pilati, camilla ..................................................................................................................o-004Pinato, David ................................................................................................................... P-160Ping, chen ....................................................................................................................... P-054Pinhel, Marcela ..................................................................................................... P-095, P-086Pinho, joão renato .......................................................................................................... P-082Pinjaroen, nutcha ............................................................................................................. P-116Pinna, antonio.................................................................................................................. P-304Pinna, antonio Daniele ...................................................................................................... P-303Pinotti, Graziella .................................................................................................... P-256, P-242Pinyol, roser .............................................................................................o-030, o-007, o-011Piris, Miguel.....................................................................................................................o-003Pirisi, Mario ...............................................................................................P-160, P-256, P-242Pisconti, salvatore ............................................................................................................ P-257Pisonero, helena ..............................................................................................................o-003Pittau, Gabriela ................................................................................................................ P-182Planas, ramon ................................................................................................................. P-029Plaza, Diego..................................................................................................................... P-029Plummer, ruth .................................................................................................................o-024Pocha, christine ............................................................................................................... P-139Poelstra, klaas ................................................................................................................ P-175Pol, stanislas ............................................................................................o-013, o-014, o-020Pollicino, teresa ............................................................................................................... P-047Polvani, simone ............................................................................................................... P-031Polyte, jacqueline ............................................................................................................ P-055Pons, fernando ..................................................................................................... P-164, P-129Pontisso, Patrizia .............................................................................................................. P-005Porta, camillo .......................................................................................................P-326, o-029Portela, anna ...................................................................................................................o-007Portolani, nazario .......................................................................................P-080, P-074, P-066Possenti, Laurent ............................................................................................................. P-118Poutachidis, theophilos .................................................................................................... P-096Pozzan, caterina .............................................................................................................. P-275Prajapati, sudeep ............................................................................................................ P-348Praz, françoise ............................................................................................................... P-043Prigoff, jake .................................................................................................................... P-121Prushani, amir ................................................................................................................. P-146Pruvot, françois-rené ...................................................................................................... P-262Pupacdi, Benjarath ...........................................................................................................o-002Puri , Puneet ................................................................................................................... P-034qi, yue ............................................................................................................................ P-072qin, shukui ...................................................................................................................... P-320qin, xian-yang ................................................................................................................. P-049qin, xiao.......................................................................................................................... P-306quagliata, Luca ................................................................................................................ P-045
quarta, santina ................................................................................................................ P-005quertimont, eric ............................................................................................................... P-003quetglas, Iris ...................................................................................................................o-008quintavalle, cristina ......................................................................................................... P-045qureshi, kamran .............................................................................................................. P-148rabibhadana, siritida .......................................................................................................o-002radu, Pompilia ................................................................................................................. P-210rafecas, antoni ................................................................................................................ P-016raffa, Giuseppina ............................................................................................................. P-047raggi, chiara ...................................................................................................................o-009rahmouni, alain .................................................................................................... P-207, P-199raimondo, Giovanni ......................................................................................................... P-047rajasekaran, Devaraja ...................................................................................................... P-028ramaswami, ramya ......................................................................................................... P-160rangaswami, arun ........................................................................................................... P-341rangaswami, arun ........................................................................................................... P-305raoul, jean Luc ............................................................................................................... P-326raoul, jean-Luc ....................................................................................................P-231, o-021rauch, claudine ............................................................................................................... P-020ravaioli, Matteo ............................................................................................................... P-303rayar, Michel ...................................................................................................................o-028raymond, anne-aurélie .................................................................................................... P-007raymond, eric..................................................................................................................o-031rebouissou, sandra ..............................................................................................o-011, P-008reddy, srinevas ............................................................................................................... P-317reeves, helen ................................................................................ o-024, P-056, P-025, P-286regimbeau, jean-Marc .................................................................................................... P-262reichl, Patrick ................................................................................................................. P-220reid, tony .......................................................................................................................o-032reker-smit, catharina ...................................................................................................... P-175ren, Weixin...................................................................................................................... P-306rendon, Paloma ............................................................................................................... P-129resende, Vivian................................................................................................................ P-042reynolds, Dominic ........................................................................................................... P-348rhee, hyungjin ................................................................................................................. P-035rhim, hyunchul ................................................................................................................ P-237ribeiro, ana .......................................................................................................... P-093, P-094ricardo, Memeo ............................................................................................................... P-260ricci, Paola ...................................................................................................................... P-317rimassa, Lorenza .......................................................................................P-326, o-029, P-012rimola, antoni.................................................................................................................. P-016rimola, jordi ........................................................................................................o-027, P-164rinaldi, eugenia ............................................................................................................... P-341rivière, Lise ..................................................................................................................... P-046ro, simon ........................................................................................................................ P-083roayaie, sasan ................................................................................................................o-015roberts, Lewis .................................................................................................................o-015roberts, Lewis ...........................................................................................P-018, o-019, P-319robertson, chadia ............................................................................................................ P-028rocha, ruana .................................................................................................................. P-223rodriguez, javier ............................................................................................................. P-332rodriguez, Macarena ....................................................................................................... P-332rodríguez, Manuel ........................................................................................................... P-129rodríguez, María ............................................................................................................. P-114rodriguez De Lope, carlos ................................................................................................o-003rodriguez-Lope, carlos .................................................................................................... P-129roebuck, Derek ............................................................................................................... P-341romano, antonio ................................................................................................... P-017, P-318roncalli, Massimo ............................................................... P-045, o-009, P-038, P-012, P-063rong, Guanghua .............................................................................................................. P-192ronnie, Poon ........................................................................................................ P-123, P-156ronot, Maxime .................................................................................................................o-031rosa, Guilherme .............................................................................................................. P-181rosa-hezode, Isabelle ......................................................................................................o-016rose-john, stefan ........................................................................................................... P-011rosmorduc, olivier ................................................................................... o-031, P-032, o-016ross, Paul ............................................................................................................ P-144, P-241ross, Paul ....................................................................................................................... P-154rota, Maria rosa ............................................................................................................. P-129rotellar, fernando ............................................................................................................ P-332roudot-thoraval, françoise ..................................... o-014, P-002, o-020, P-261, P-030, P-009roulot, Dominique ................................................................................................ o-013, o-020ruchirawat, Mathuros ......................................................................................................o-002rugge, Massimo .............................................................................................................. P-012

Authors Index
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 5 2
Name Abstract Name Abstract
ruo, Leyo .......................................................................................................................o-032rusher, oxana ................................................................................................................. P-289ruvoletto, Mariagrazia ...................................................................................................... P-005ryk, charlotta .................................................................................................................. P-085ryu, ho sang ....................................................................................................... P-201, P-108ryu, soo hyung ............................................................................................................... P-137ryu, tomoki ..........................................................................................................o-026, P-269sa cunha, antonio......................................................................................P-182, P-225, o-028sabbour, Ghada .............................................................................................................. P-189sacco, rodolfo ...........................................................................................P-017, P-318, P-257saeki, Issei .......................................................................................................... P-131, P-281sagliocco, francis ................................................................................................. P-037, P-033sahu, sonia ..................................................................................................................... P-306saint-Paul, Marie-christine .............................................................................................. P-073saito, tomoko .................................................................................................................. P-263saitsu, hideki ........................................................................................................o-026, P-269saitta, carlo ...............................................................................................P-047, P-256, P-242saiura, akio ..................................................................................................................... P-338sakai, yoshiyuki .............................................................................................................. P-204sakaida, Isao ........................................................................................................ P-131, P-281sakamoto, Michiie ............................................................................................................ P-234sakamoto, teppei ............................................................................................................. P-248sakamoto , yoshihiro ................................................ P-060, P-268, P-338, P-064, P-285, P-171sala, Margarita ..................................................................................................... P-029, P-129salah, Mohamed .............................................................................................................. P-141salami, augustine ............................................................................................................ P-110salem, aliasger ................................................................................................................ P-028salgia, reena........................................................................................................ P-110, P-146salloum, chady ..................................................................................................... P-158, P-279salvagni, stefania ............................................................................................................o-029salvi, alessandro .............................................................................P-080, P-074, P-066, P-061samuel, Didier ............................................................................... P-046, P-261, P-030, o-028sanaka, sirish .................................................................................................................. P-148sánchez, fernando .......................................................................................................... P-114sangrajrang, suleeporn ....................................................................................................o-002sangro, Bruno ............................................................................................P-304, P-332, P-277sansonno, Domenico ............................................................................................ P-256, P-242santana-Lemos, Barbara .................................................................................................. P-181santoro, armando ......................................................................................P-326, o-029, P-012sanyal, arun .................................................................................................................... P-034sanz, eduardo.................................................................................................................. P-097sapienza, Marcelo ........................................................................................................... P-198sappal, Darshan ..............................................................................................................o-006saraswati, sarita .............................................................................................................. P-058saribegioglou, nikolaos .................................................................................................... P-344sarkar, Devanand ............................................................................................................. P-028sarker, Debashis ................................................................................................... P-154, P-144sarpel, umut .................................................................................. P-026, P-244, P-027, o-025sarrias, Maria-rosa ......................................................................................................... P-029sartor, chiara ................................................................................................................... P-032sato, keiko ......................................................................................................................o-022sato, rui .............................................................................................................. P-203, P-311sato, shinpei ........................................................................................................ P-329, P-328sato, sinpei ..................................................................................................................... P-249sato, takahisa............................................................................................P-329, P-249, P-328satoh, takashi ................................................................................................................ P-348sauer, jennifer ................................................................................................................. P-138savarin, Philippe .............................................................................................................. P-219savoye-collet, céline ........................................................................................................ P-233sawai, yoshiyuki .............................................................................................................. P-131scarpa, aldo ......................................................................................................... P-012, P-019scarpi, emanuela ............................................................................................................. P-337scartozzi, Luca................................................................................................................. P-337scartozzi, Mario ............................................................................................................... P-276scatena, natalia ............................................................................................................... P-181schad, arno ..................................................................................................................... P-184schalm, stefanie ..............................................................................................................o-006schattenberg, joern ........................................................................................................ P-184schirmacher, Peter ........................................................................................................... P-040schmid, Irene .................................................................................................................. P-305schmidt, kristin................................................................................................................ P-138schmidt, L ....................................................................................................................... P-273schmidt-arras, Dirk .......................................................................................................... P-011schmidt-kittler, oleg ........................................................................................................o-030
schon, Michael ................................................................................................................ P-304schott, eckart .................................................................................................................. P-273schulze, kornelius ......................................................................................P-070, P-138, o-011schwartz, Brian ...............................................................................................................o-029schwartz, Myron ................................................................................................... P-130, P-183schwartz, Myron ............................................................................o-023, P-121, P-027, o-025schwartz, Myron e ...........................................................................................................o-010schwarz, Lilian ................................................................................................................. P-233sciarra, amedeo ................................................................................................... P-038, P-063scognamiglio, umberto ......................................................................................... P-176, P-159scotté, Michel .................................................................................................................. P-233scuri , sabrina ................................................................................................................. P-080sebagh, Mylene ............................................................................................................... P-046sekendiz, zennur .............................................................................................................o-025selak, kerstin................................................................................................................... P-067sellers, Laura................................................................................................................... P-160sellier, nicolas ...............................................................................P-293, P-232, P-224, P-219selten, jasmijn ................................................................................................................ P-182selvaraj, anand ................................................................................................................ P-348seneshaw, Mulugeta ....................................................................................................... P-034sengupta, srikumar ......................................................................................................... P-088senni, nadia .................................................................................................................... P-032seo, tae-seok .................................................................................................................. P-346seo, yeon seok ..................... P-023, P-201, P-155, P-230, P-108, P-105, P-186, P-239, P-128seo, young seok .............................................................................................................. P-315seo, young-seok .............................................................................................................. P-001seong, jinsil .............................................................................................P-298, P-253, P-195serji, Badr ............................................................................................................ P-225, P-262seror, olivier ...................................................................... P-293, P-224, P-261, P-030, P-219serrano, M trinidad .......................................................................................................... P-277shabana, hany................................................................................................................. P-151shackel, nicholas .................................................................................................. P-022, P-191shahinian, Vahakn ................................................................................................. P-109, P-115shaked, abraham .................................................................................................. P-135, P-111shaker, Mohamed ................................................................................................. P-280, P-227shaker, Mohamed ................................................................................................. P-189, P-218shaker, Mohamed ................................................................................................. P-246, P-141shaker, Mohamed ............................................................................................................ P-294shaleh, hassan ................................................................................................................ P-018shamsi, nabiha ................................................................................................................ P-317shao, yu-yun .............................................................................................P-107, P-044, P-052sharma, amritanshu ......................................................................................................... P-284sharma, Dinesh .................................................................................................... P-125, P-126sharma, rohini ................................................................................................................ P-160sharp, swee .................................................................................................................... P-019shen, feng .....................................................................................................................o-023shen, xue-ning ................................................................................................................ P-028sherman, Morris ..............................................................................................................o-015shi, xianbiao .................................................................................................................... P-167shibatoge, Mitsushige ...................................................................................................... P-214shibuki, taro .................................................................................................................... P-247shim, chang Woo ............................................................................................................ P-124shim, ju hyun ...................................................................................................... P-179, P-166shimada, noritomo .......................................................................................................... P-235shimizu, Masahito ............................................................................................................ P-049shimizu, satoshi ..............................................................................................................o-022shimizu, takayuki ............................................................................................................. P-307shimoda, Mitsugi ............................................................................................................. P-307shin, hyun Deok .............................................................................................................. P-185shin, ji hoon ................................................................................................................... P-297shin, sung Wook .................................................................................................. P-251, P-300shinde, jayendra .............................................................................................................o-011shiomi, chizu ................................................................................................................... P-204shiota, Goshi ................................................................................................................... P-049shirata, chikara ........................................................................................P-060, P-064, P-285shutes, adam ..................................................................................................................o-006sia, Daniela ..............................................................................................o-030, o-008, o-010sica, antonio ...................................................................................................................o-009siddiq, ayesha ................................................................................................................. P-028sijbesma, jurgen ............................................................................................................. P-175silva, renato ................................................................................................................... P-226silva, renato .................................................P-206, P-213, P-095, P-093, P-094, P-102, P-086silva, rita ....................................................................................................................... P-213silva, rita ....................................................................................................................... P-206
Authors Index
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 5 3
Name Abstract Name Abstract
silva, rita De cassia......................................................................................................... P-226simbolo, Michele .................................................................................................. P-012, P-019simon, Marina ................................................................................................................. P-029simonato, Davide ............................................................................................................. P-005sin, sung Wook ............................................................................................................... P-299sinelnikov, andrey ............................................................................................................ P-140singal, amit ...............................................................................................P-174, P-153, P-157singal, amit .....................................................................................................................o-018singer, stephan................................................................................................................ P-040singh, rajinder ................................................................................................................ P-284sinn, Dong hyun ............................................................................P-237, P-251, P-252, P-300sklavos, argyrios .............................................................................................................. P-096smith, coleman ............................................................................................................... P-317smith, Peter .................................................................................................................... P-348soares, fernando ............................................................................................................ P-087sofianou , anastasia .........................................................................................................o-025sogni, Philippe .................................................................................................................o-017sohn, Won ............................................................................................................ P-237, P-299solé, Manel .....................................................................................................................o-008song, Gi-Won .................................................................................................................. P-179song, Il han ..................................................................................................................... P-185song, jae-sung ............................................................................................................... P-004song, kyoung Doo ........................................................................................................... P-170song, Myeong jun ........................................................................................................... P-228song, Myung Gyu ............................................................................................................. P-346song, sohee .................................................................................................................... P-208sordia, teimuraz .............................................................................................................. P-103sotiropoulos, George ........................................................................................................ P-343soubrane, olivier ..............................................................................................................o-031souza, Doroteia ...............................................................................P-095, P-093, P-094, P-086sparchez, zeno adrian ..................................................................................................... P-210spivack, john .................................................................................................................. P-244spivack, john ....................................................................................................... P-026, P-027sprinzl, Martin ......................................................................................................o-012, P-120sricharunrat, thaniya .......................................................................................................o-002srivastava, jyoti ............................................................................................................... P-028stål, Per .......................................................................................................................... P-085starlinger, Patrick ............................................................................................................. P-220staufer, katharina ............................................................................................................ P-220stavrinidis, stavros ........................................................................................................... P-344stefano, jose tadeu ......................................................................................................... P-198steinberg, seth ................................................................................................................ P-289stell, David ...................................................................................................................... P-200sterneck, Martina ............................................................................................................. P-138stocken, Deborah .....................................................................................o-024, P-025, P-286stoecklein, nikolas ........................................................................................................... P-065stojkowitz, nicolas ..........................................................................................................o-032strand, susanne .............................................................................................................. P-067stransky, nicolas .................................................................................................. o-030, o-006stratton, Michael ..............................................................................................................o-011stubbs, Mark ................................................................................................................... P-019stubbs, richard ............................................................................................................... P-304such, jose ...................................................................................................................... P-014suddle, abid ......................................................................................................... P-154, P-144sugimoto, rie ..................................................................................................................o-022sugimoto, takafumi .......................................................................................................... P-329sugitani, Masahiko ........................................................................................................... P-136suh, kyung-suk .................................................................. P-133, P-132, P-238, P-013, P-004suh, sang jun .................................................................... P-230, P-105, P-239, P-186, P-128sumita, nairo ................................................................................................................... P-082sumpter, kate .................................................................................................................. P-286sun, chao ............................................................................................................ P-162, P-196sun, qiman ..................................................................................................................... P-162sun, xiaochen ..................................................................................................................o-010sun, yun-fan ................................................................................................................... P-173sung, kihoon ................................................................................................................... P-272sung, kyu-Bo................................................................................................................... P-297suprun, Maria ..................................................................................................................o-025sutter, olivier ................................................................................................................... P-224sutton, angela ..................................................................................................... P-003, P-002suzuki, eiichiro ................................................................................................................ P-263suzuki, harukazu ............................................................................................................. P-049suzuki, shoko .................................................................................................................. P-264sweeney, robert .............................................................................................................. P-027
swinson, Dan .................................................................................................................. P-241szemraj, janusz .................................................................................................... P-089, P-090tabrizian, Parissa ...................................................................................... o-023, P-121, o-015taha, alaa awad .................................................................................................... P-142, P-310tahara, toshiyuki ..............................................................................................................o-022tak, Won young..........................................................................................P-113, o-032, P-077takada, hitomi ................................................................................................................. P-264takaguchi, koichi ............................................................................................................. P-235takahashi, Michiro ........................................................................................................... P-338takami, taro ......................................................................................................... P-131, P-281takami, yuko ........................................................................................................o-026, P-269takashima, tomoyuki ....................................................................................................... P-204takayama, tadatoshi ..................................................................................P-010, P-282, P-136takda, hitomi ................................................................................................................... P-180talmat, nabila ..................................................................................................................o-014tamaki, nobuharu ............................................................................................................ P-264tamberi, stefano .............................................................................................................. P-276tan, qi-Wen..................................................................................................................... P-216tan to, cheung ................................................................................................................ P-156tan to, chueung .............................................................................................................. P-123tanabe, kenneth .............................................................................................................. P-245tanabe, norikazu ............................................................................................................. P-281tanaka, kazunari ............................................................................................................. P-131tang, Weiguo ................................................................................................................... P-162tang, Wei-Guo ................................................................................................................. P-196tani, claudia .................................................................................................................... P-082tani, cláudia ................................................................................................................... P-150tani, joji ............................................................................................................... P-321, P-248taque, sophie .................................................................................................................. P-037tarchi, Paola ......................................................................................................... P-130, P-121tarocchi, Mirko ................................................................................................................ P-031tartaglione, Maria teresa ....................................................................................... P-287, P-274taspinar, Mehmet ............................................................................................................. P-098tateishi, Masaki ....................................................................................................o-026, P-269tavartkiladze, alexandre ........................................................................................ P-104, P-103tawada, akinobu .............................................................................................................. P-263tedjasukmana, andreas ....................................................................................................o-025teixeira, andreza .............................................................................................................. P-181tempesti, sara ................................................................................................................. P-031tenani, Graciele .................................................................................................... P-095, P-086tenías, jose María ........................................................................................................... P-288terracciano, Luigi ............................................................................................................. P-045terrin, Liliana ................................................................................................................... P-005testillano, Milagros........................................................................................................... P-277thanapirom, kessarin ....................................................................................................... P-116theodoropoulos, Loukas ................................................................................................... P-344thillai, kiruthikah ................................................................................................. P-154, P-144thoetchai, Peeraphatdit .................................................................................................... P-139thompson, Patrick ........................................................................................................... P-305thomson, james ............................................................................................................. P-088thorgeirsson, snorri ............................................................................................. o-012, o-002thung, swan ................................................................................................................... P-130thung, swan n ................................................................................................................o-010thuras, Paul .................................................................................................................... P-139tijeras-raballand, annemilaï ............................................................................................o-031tiniakos, Dina .................................................................................................................. P-056tiro, jasmin ...............................................................................................P-153, o-018, P-157titano, joseph ................................................................................................................. P-183tokunaga, naoyuki ........................................................................................................... P-265tooulias, andreas ............................................................................................................. P-345torimura, takuji ..........................................................................................P-236, P-270, P-296torres, ferran ..................................................................................................................o-021torres, Mariana ................................................................................................................ P-198tortora, raffaella .............................................................................P-193, P-302, P-287, P-274torzilli, Guido ........................................................................................................ P-038, P-012toth, csaba ..................................................................................................................... P-065tovar, Victoria....................................................................................................... o-008, o-007towbin, alexander ............................................................................................................ P-341toyota, hidenori ............................................................................................................... P-235trakroo, sushrut............................................................................................................... P-148tralhão, josé Guilherme ........................................................................................ P-093, P-094tran, albert ......................................................................................................................o-013trauner, Michael ............................................................................................................. P-220traversa, Michele ............................................................................................................. P-061

Authors Index
I L C A A n n u A L C o n f e r e n C e , 2 0 1 5 - B o o k o f A B s t r A C t s1 5 4
Name Abstract Name Abstract
treeprasertsuk, sombat ......................................................................................... P-116, P-134trépo, eric ....................................................................................................................... P-003trevisan, Miriam............................................................................................................... P-223trevisani, francesco ......................................................................................................... P-012trevisani, franco .............................................................................................................. P-275trinchet, jean-claude .........................................................o-014, P-232, P-002, o-020, P-219tripodi, Gianluca .............................................................................................................. P-047trojan, joerg ..............................................................................................P-326, o-029, P-273truant, stéphanie ............................................................................................................. P-262tsamakidis, klisthenis ...................................................................................................... P-344tselikas, Lambros ............................................................................................................ P-158tsoulfas, Georgios ........................................................................................................... P-345tsuchiya, kaoru ............................................................................................................... P-264tsuji, kunihiko ................................................................................................................. P-235tsung, allan ..................................................................................................................... P-140tsutsui, akemi ................................................................................................................. P-235tsutsumi, takeya ............................................................................................................. P-212tsutsumi, tsubasa ........................................................................................................... P-296tu, thomas .......................................................................................................... P-022, P-191tuccillo, concetta ............................................................................................................. P-193tumino, emanuele ................................................................................................. P-017, P-318turato, cristian................................................................................................................. P-005ukai, katsuaki ..................................................................................................................o-033uldry, emilie ..................................................................................................................... P-268ulivi, Paola ....................................................................................................................... P-276um, soon ho .......................................................... P-023, P-201, P-155, P-230, P-108, P-239umberto, scognamiglio .................................................................................................... P-340ungerechts, Guy .............................................................................................................o-032urata, yohei .................................................................................................................... P-131usta, ayse ....................................................................................................................... P-098Valdivieso, andrés ............................................................................................................ P-016Valentina, Iodice ............................................................................................................... P-340Valeri, nicola ......................................................................................................... P-012, P-019Van Der Windt, Dirk .......................................................................................................... P-140Van Laethem, jean Luc ...................................................................................................o-029Van Montfort, rob ............................................................................................................ P-019Van Vlierberghe, hans ......................................................................................................o-029Vanin, Veronica ................................................................................................................ P-275Vaqué, josé .....................................................................................................................o-003Vaquero, javier ................................................................................................................ P-043Varela, Maria ................................................................................................................... P-129Varela , María .................................................................................................................. P-164Vassallo, jose .................................................................................................................. P-223Vassalo, jose ................................................................................................................... P-087Veerasamy, sachuda ........................................................................................................ P-163Venkatramani, rajkumar ................................................................................................... P-305Ventzislava, Petrov-sanchez .............................................................................................o-014Vergadis, chrysovalantis ........................................................................................ P-343, P-222Vergniol, julien ................................................................................................................ P-118Verret, Benjamin ..............................................................................................................o-004Vibert, eric ........................................ P-233, o-031, P-182, P-225, P-261, P-030, P-262, o-028Vicentini, caterina ............................................................................................................ P-012Vidal, samuel ...................................................................................................................o-008Vilar, eduardo................................................................................................................... P-097Villa, erica ............................................................................................................ P-256, P-242Villano, Gianmarco ........................................................................................................... P-005Villanueva, augusto ...................................................................................o-008, o-011, o-010Vincent, robert ................................................................................................................ P-034Virotta, Giorgio ................................................................................................................. P-316Vitale, alessandro .................................................................................................. P-275, P-316Vlachogiannis, George ...................................................................................................... P-012Vogl, t ............................................................................................................................. P-273Von felden, johann .......................................................................................................... P-070Von roemeling, reinhard ..................................................................................................o-029Voron, thibault ................................................................................................................. P-158Vries, erik ........................................................................................................................ P-175Wada, yoshiyuki ........................................................................................ o-026, P-269, o-033Waidmann, oliver ............................................................................................................. P-273Waked, Imam .................................................................................................................. P-209Walters, Ian .....................................................................................................................o-021Wang, enxin .................................................................................................................... P-112Wang, fei ........................................................................................................................ P-092Wang, fengjiao ................................................................................................................ P-072Wang, han-yu .................................................................................................................. P-052
Wang, kui ........................................................................................................................ P-062Wang, shaoqing ............................................................................................................... P-018Wang, Wenhui ................................................................................................................. P-306Wang, Wenjun ................................................................................................................. P-112Wang, xin ........................................................................................................................o-002Wang, yu ......................................................................................................................... P-018Wang, yunxia ..................................................................................................................o-029Wang, john ..................................................................................................................... P-348Warmuth, Markus ........................................................................................................... P-348Wege, henning ..........................................................................................P-070, P-011, P-138Wei, jiwu ........................................................................................................................ P-167Wei, Lan .......................................................................................................................... P-245Weinmann, arndt .................................................................................................. P-184, P-120Weiss, alan ......................................................................................................................o-029Weiss, thomas ................................................................................................................ P-220Welker, Martin.................................................................................................................. P-273Wendum, Dominique ........................................................................................................ P-032Wenglowsky, steve ...........................................................................................................o-006Werner, tobias ................................................................................................................. P-138Westlin, William ............................................................................................................... P-245Weyer, Veronika ............................................................................................................... P-184Wheeler, David .................................................................................................................o-019Wilson, kevin ...................................................................................................................o-006Wiltrout, robert ................................................................................................................o-002Winkler, juliane................................................................................................................ P-040Wolf, Ben.........................................................................................................................o-030Wolf, katharina ................................................................................................................ P-067Won, jong yun ...................................................................................................... P-119, P-298Wong hoi, she ...................................................................................................... P-123, P-156Woo, hyun young .................................................................................................. P-330, P-041Woo, sang Myung ........................................................................................................... P-314Wood, Bradford ................................................................................................................ P-289Workman, Paul ..................................................................................................... P-012, P-019Wörns, Marcus .....................................................................................................o-012, P-120Wörns, Marcus ................................................................................................................ P-184Wu, Meng-chao ...............................................................................................................o-023Wu, Lili ........................................................................................................................... P-308Wu, Liming ...................................................................................................................... P-172Wu, Wei-zhong ................................................................................................................ P-216Wu, xiaolin ......................................................................................................................o-002Wu, jeremy ..................................................................................................................... P-348xia, Dongdong ................................................................................................................. P-112xia, feng ......................................................................................................................... P-308xia, jielai .............................................................................................................. P-306, P-112xiao, junjie ...................................................................................................................... P-092xie, haiyang..................................................................................................................... P-172xie, Liqi ........................................................................................................................... P-162xie, xiaoyan ..................................................................................................................... P-190xing, chunyang ................................................................................................................ P-172xing, jinliang ................................................................................................................... P-036xinopoulos, Dimitrios ........................................................................................................ P-344xu, jianming.................................................................................................................... P-320xu, yang ............................................................................................................... P-162, P-196xuan, Lei ......................................................................................................................... P-157yamamoto, Msakazu ........................................................................................................ P-136yamamoto, naoki ............................................................................................................. P-281yamamoto, satoshi ....................................................................................P-064, P-285, P-171yamasaki, takahiro ................................................................................................ P-131, P-281yamashita, suguru ........................................................................................................... P-285yamazaki, shintaro ................................................................................................ P-010, P-136yan, chen ........................................................................................................................ P-167yan, Lunan ......................................................................................................................o-015yanagita, kimihiko ............................................................................................................ P-295yang, Gwang Mo ............................................................................................................. P-091yang, hyun ........................................................................................................... P-313, P-127yang, jijin ........................................................................................................................o-015yang, kyung ho ................................................................................................................ P-169yang, Ling ............................................................................................................o-033, P-290yang, Man ....................................................................................................................... P-112yang, sera ....................................................................................................................... P-084yang, tian ........................................................................................................................o-023yang, xin-rong ................................................................................................................ P-173yang, yongping ................................................................................................................ P-192yang, zhe ........................................................................................................................ P-172

Authors Index
B o o k o f a B s t r a c t s - I L c a a n n u a L c o n f e r e n c e , 2 0 1 5 1 5 5
Name Abstract Name Abstract
yao, takashi ..................................................................................................................... P-136yashima, yoko .................................................................................................................. P-329yasui, kohichiroh ..............................................................................................................o-022yasui, yutaka ........................................................................................................ P-180, P-264ye, Wei ............................................................................................................................ P-216yener, zabit...................................................................................................................... P-098yeon, hong eun..................................................................................................... P-023, P-155yeon, jong eun ............................................P-271, P-230, P-108, P-105, P-186, P-239, P-128yi, nam-joon ...................................................................... P-133, P-132, P-238, P-013, P-004yildirim, serkan ..................................................................................................... P-099, P-098yilmaz, nevin ........................................................................................................ P-142, P-310yim, hyung joon ...............................P-023, P-155, P-230, P-108, P-105, P-239, P-186, P-128yim, sun young .................................................................. P-023, P-201, P-155, P-230, P-108yin, zhanxin ..................................................................................................................... P-112yoh, kazunori ................................................................................................................... P-204yokosuka, osamu .................................................................................................o-033, P-263yoneyama, hirohiro .......................................................................................................... P-321yoo, Byung chul .........................................................................................P-237, P-251, P-300yoo, jeong eun ................................................................................................................ P-035yoo, jeong-ju .................................................................................................................. P-250yoo, jung-ju ................................................................................................................... P-024yoo, so young .................................................................................................................. P-041yoo, tae ................................................................................................................ P-133, P-132yoo, yang jae .................................................................... P-271, P-230, P-105, P-186, P-128yoon, hong In .................................................................................................................. P-253yoon, hyun-ki ................................................................................................................. P-297yoon, jung-hwan ............................................................... P-071, P-238, P-013, P-024, P-250yoon, ki tae .......................................................................................................... P-330, P-041yoon, seung kew ................................................................ P-228, P-021, P-313, P-081, P-127yoon, Won jae ................................................................................................................. P-137yopp, adam ..........................................................................................................P-174, o-018yoshioka, Wataru ............................................................................................................. P-283yu, ami ............................................................................................................................ P-106yu, Decai ......................................................................................................................... P-167yu, eunsil ........................................................................................................................ P-179yu, jeong Il ........................................................................................................... P-208, P-300yu, Ming-Lung ................................................................................................................ P-194yu, su jong ....................................................................... P-071, P-238, P-013, P-024, P-250yu, Lihua ........................................................................................................................ P-348yuan, jie ......................................................................................................................... P-112yun, jing-Ping ................................................................................................................. P-051yun, Mijin ........................................................................................................................ P-119zacharioudaki, argyro ....................................................................................................... P-096zada, suher ..................................................................................................................... P-197zafrani, elie-serge ........................................................................................................... P-073zakharia, kais ....................................................................................................... P-018, P-319zaldana, Michelle ............................................................................................................. P-140zangos, s ........................................................................................................................ P-273zanieri, francesca ............................................................................................................ P-031zanus, Giacomo ............................................................................................................... P-005zapater, Pedro ...................................................................................................... P-014, P-114zarski, jean-Pierre ............................................................................................... o-013, o-020zeitlinger, Lisa ................................................................................................................. P-255zender, Lars ....................................................................................................................o-007zeng, zhen ...................................................................................................................... P-192zentar, norah .................................................................................................................. P-232zerbi, alessandro ............................................................................................................. P-012zeuzem, s ....................................................................................................................... P-273zhang, chris zhiyi ............................................................................................................ P-051zhang, han .....................................................................................................................o-023zhang, yifan .................................................................................................................... P-039zhang, zhongyang ...........................................................................................................o-010zhao, yan ............................................................................................................. P-306, P-112zheng, shusen................................................................................................................. P-172zheng, zhiyun .................................................................................................................. P-172zhiqiang, hu .................................................................................................................... P-050zhou, jian ....................................................................................................................... P-173zhou, Lin ......................................................................................................................... P-172zhu, andrew ....................................................................................................................o-033zhu, andrew x. ................................................................................................................ P-290zhu, ye ............................................................................................................................ P-079zimmermann, tim ............................................................................................................ P-184ziogas, Dimitrios .............................................................................................................. P-154ziogas, Dimitris ................................................................................................................ P-144
ziol, Mariane....................................................................................................................o-016ziol, Marianne ...................................................................................................... P-293, P-219zoheiry, Mona .................................................................................................................. P-197zolfino, teresa ...........................................................................................P-256, P-242, P-257zoulim, fabien ..................................................................................................... o-014, o-020zuccari, Débora ............................................................................................................... P-102zucman-rossi, jessica.....................................................................................................o-004zucman-rossi, jessica.......................................................o-007, o-011, P-008, o-005, P-033, .......................................................................................... P-003, P-002, P-073, P-063, o-016zygomalas, apollon .......................................................................................................... P-177


www.ilca2015.org
InternatIonal lIver CanCer assoCIatIon
4 6 september 2015Paris Marriott rive Gauche Hotel & Conference CenterParis, France
FInal ProGraMMe & BooK oF aBstraCts
9th ILCA Annual Conference


















