
Internal Medicine Specialty Leader Update Navy ACP 2014 Daniel Seidensticker, MD, FACP, FACC CDR,...
41
Internal Medicine Specialty Leader Update Navy ACP 2014 Daniel Seidensticker, MD, FACP, FACC CDR, MC, USN
-
Upload
destin-girdler -
Category
Documents
-
view
293 -
download
2
Transcript of Internal Medicine Specialty Leader Update Navy ACP 2014 Daniel Seidensticker, MD, FACP, FACC CDR,...

Internal Medicine Specialty Leader Update
Navy ACP 2014
Daniel Seidensticker, MD, FACP, FACCCDR, MC, USN

Navy Medicine
• Mission– We enable readiness,
wellness, and health care to Sailors, Marines, their families, and all others entrusted to us worldwide – be it on land or at sea
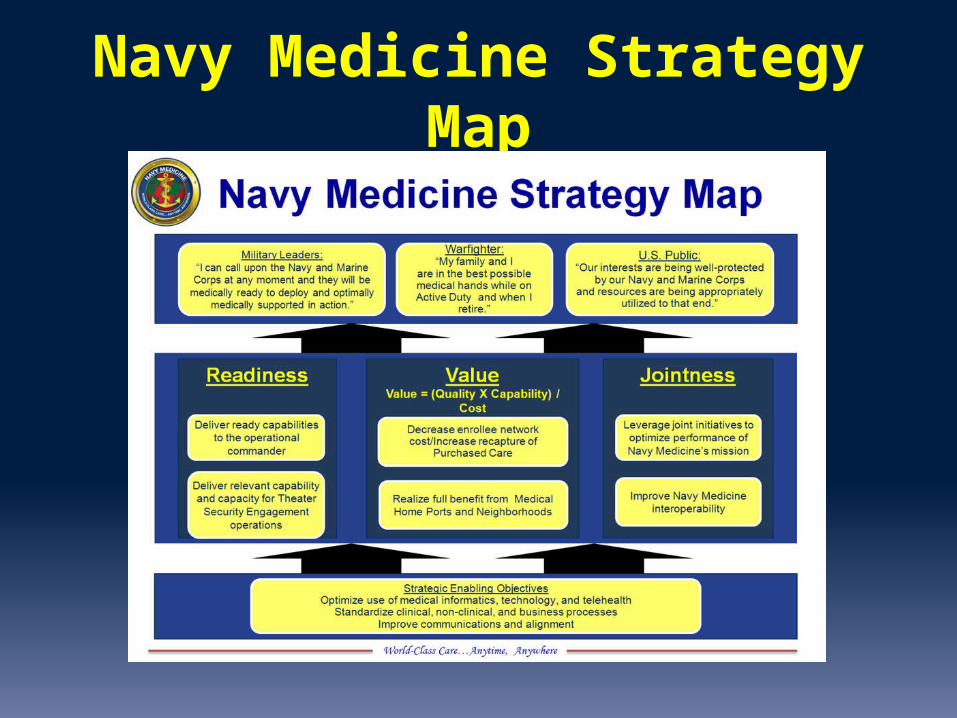
Navy Medicine Strategy Map

Internal Medicine Leads the Way
RADM Colin ChinnCommand Surgeon, US PaCom
RADM Brian MonahanThe Attending Physician for US
Congress and US Supreme Court
CAPT Chris CulpPacific Fleet Surgeon
CAPT Mark Turner5th Fleet surgeon
RDML Brian PechaMedical officer of Marine Corps
CAPT John SandersCO, Naval Medical Research Center

CAPT Kyle PetersenCO, NAMRU-6 Lima
CAPT John GilstadCO, NAMRU 3-Cairo
CAPT Jeff TimbyDeputy Medical Officer of USMC
FMF Specialty Leader
EXECUTIVE OFFICERS:CAPT Michael McGinnis NH GuamCAPT Adam Armstrong NAMRU-6 LimaCAPT Fred Yeo Naval Submarine Medical Research Laboratory

Internal Medicine Leads the Way
• Who is your mentor?
• Whom are you mentoring?
• How should a mentor help you?

Medical Corps Manning
Type Manning Billets
Staff 2864 2471
GME 1009 1054
Total 3873 3524
• Overall manning is 110% of billeted end strength
• Increased retention– Normal attrition 10%/year– Currently 8%/year
Source: Worldbook october 2013
Total MC billets in 2013: 3740
Total staff billets in 2013: 2706

Medical Corps Manning
Specialty Manning
AEROSPACE MEDICINE 63%
ANESTHESIA 136%
AVIATION MEDICINE 98%
DERMATOLOGY 109%
DIAGNOSTIC RAD 136%
EMERGENCY MED 119%
FAMILY PRACTICE 93%
GENERAL MEDICINE 106%
INTERNAL MED 111%NEURO SURG 120%
NEUROLOGY 96%
NUCLEAR MEDICINE 200%
OB/GYN 107%
Specialty Manning
OCC MED 102%
OPHTHAMOLOGY 111%
ORTHOPEDIC SURG 113%
OTOLARYNGOLOGY 113%
PATHOLOGY 98%
PEDIATRICS 111%
PHYS MED & REHAB 200%
PREV MED 100%
PSYCHIATRY 92%
RADIATION ONC 90%
SURGERY 88%
UNDERSEA MED 84%
UROLOGY 103%
By Specialty

Internal Medicine by Specialty
Specialty Manning Billets % Manning
General IM 100 69+17 116ID 34 31 110Pulm/CCM 33 46 72GI 24 20 120Heme/Onc 13 12 108Endo 9 8 113Nephro 10 9 111Rheum 7 5 140Allergy 8 6 133Card 36 29 124
Source: Worldbook Sep 2014

Is IM really overmanned?
• Probably close to being right sized• The billet structure is not current with hospital
needs– NH Camp Pendleton: 1 GIM billet, 5 IM staff– NH Beaufort: 1 GIM billet, 3 IM staff
• Several other Specialties have same issues
From the OOMC
• RADM Raquel Bono– Chief of the Medical Corps
• CAPT Mae Pouget– Deputy Chief of the MC
• October 21 FACEBOOK TOWNHALL meeting with RADM Bono– 21 October 1200-1300– https://www.facebook.com/USNavymedicine

From the OOMC• No change in special pays
– Static since 2010
• HPSP has met recruiting goal (FY08-14)

From the OOMC
• MEDHOME– Empanelment targets 1100-1300
Navy A
verag
e
NMC Portsmouth
FHCC Grea
t Lak
es
NH Beaufort
NH Camp Le
jeune
NH Jacks
onville
NH Pensac
ola
NHC Annapolis
NHC Charlest
on
NHC Cherry P
oint
NHC Corpus C
hristi
NHC New En
gland
NHC Patuxe
nt Rive
r
NHC Quan
tico
USNH Guan
tanam
o Bay
USNH Nap
les
USNH Rota
USNH Si
gonell
a
NMC San Dieg
o
NH Bremert
on
NH Camp Pen
dleton
NH Lemoore
NH Oak
Harbor
NH Twen
tynine P
alms
NHC Hawaii
USNH Guam
USNH O
kinaw
a
USNH Yo
kosu
ka0
200400600800
1,0001,2001,4001,6001,800
MedHome and the Neighborhood
• MGMA Standards based on 2012 report– 40% of nationwide average for each specialty
• Intentionally low to account for deployments, clinical inefficiencies

Conference Travel
– Google “bumed travel policy”
– “Mission critical” to attend conferences (board review ‘courses’ already approved)
– ALL attendees MUST be named with conference submission package.
– EACH ATTENDEE must be mission critical reason– Commands are referring to submitted lists
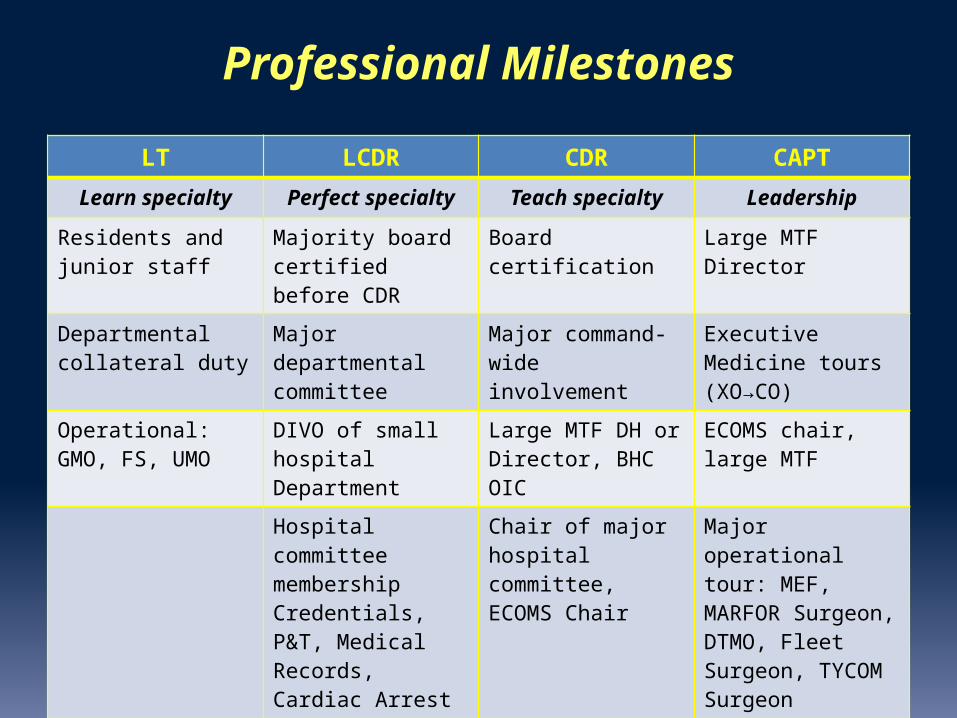
Professional Milestones
LT LCDR CDR CAPTLearn specialty Perfect specialty Teach specialty Leadership
Residents and junior staff
Majority board certified before CDR
Board certification Large MTF Director
Departmental collateral duty
Major departmental committee
Major command-wide involvement
Executive Medicine tours (XO→CO)
Operational: GMO, FS, UMO
DIVO of small hospital Department
Large MTF DH or Director, BHC OIC
ECOMS chair, large MTF
Hospital committee membershipCredentials, P&T, Medical Records, Cardiac Arrest
Chair of major hospital committee,ECOMS Chair
Major operational tour: MEF, MARFOR Surgeon, DTMO, Fleet Surgeon, TYCOM Surgeon
Operational: Regimental Surgeon, FS, UMO
Operational: MLG, DIV, Wing Surgeon, CATF Surgeon, SMO
Major BUMED, BUPERS, TMA, TRO tours
BUMED, BUPERS tour Senior Clinician
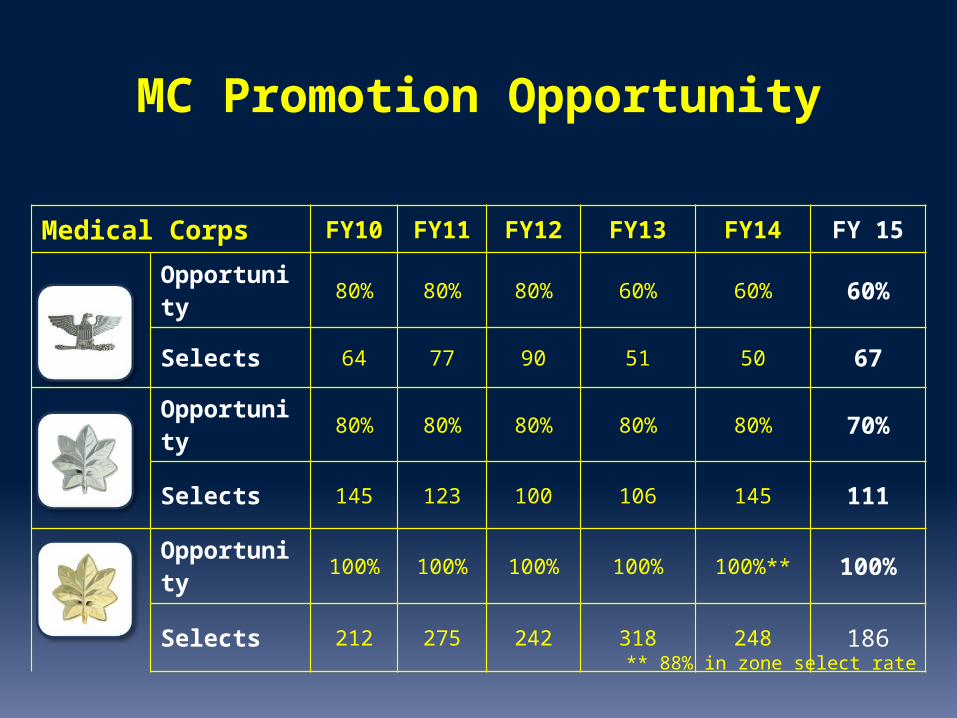
MC Promotion Opportunity
Medical Corps FY10 FY11 FY12 FY13 FY14 FY 15
Opportunity 80% 80% 80% 60% 60% 60%
Selects 64 77 90 51 50 67
Opportunity 80% 80% 80% 80% 80% 70%
Selects 145 123 100 106 145 111
Opportunity 100% 100% 100% 100% 100%** 100%
Selects 212 275 242 318 248 186
** 88% in zone select rate

FY14 Promotions - LCDR
• Precept: 100% selection of IZ candidates• 186 x 1.0 = 186 = max # of selects• 4 (AZ) + 168 (IZ) + 14 (BZ) = 186
• IM: 0 AZ 16/17 IZ; 1 BZ selected
Zone Eligible Selected %
AZ 13 4 36IZ 186 168 90BZ 442 14 3
FY14 O-4 Selection Results
http://www.public.navy.mil/bupers-npc/boards/activedutyofficer/05staff/Documents/FY-14/FY14%20AO5S%20STATS.pdf

FY15 Promotions - CDR
• Precept: 70% selection of IZ candidates• 159x 0.7 = 111 = max # of selects• 78 (IZ) + 33(AZ) = 111• IM: 66% IZ (10/15) 8 AZ selected
Zone Eligible Selected %
AZ 92 33 36IZ 159 78 49BZ 373 0 0
FY15 O-5 Selection Results
http://www.public.navy.mil/bupers-npc/boards/activedutyofficer/05staff/Documents/FY-15/FY-15%20AO5S%20CONVENING%20ORDER.pdf
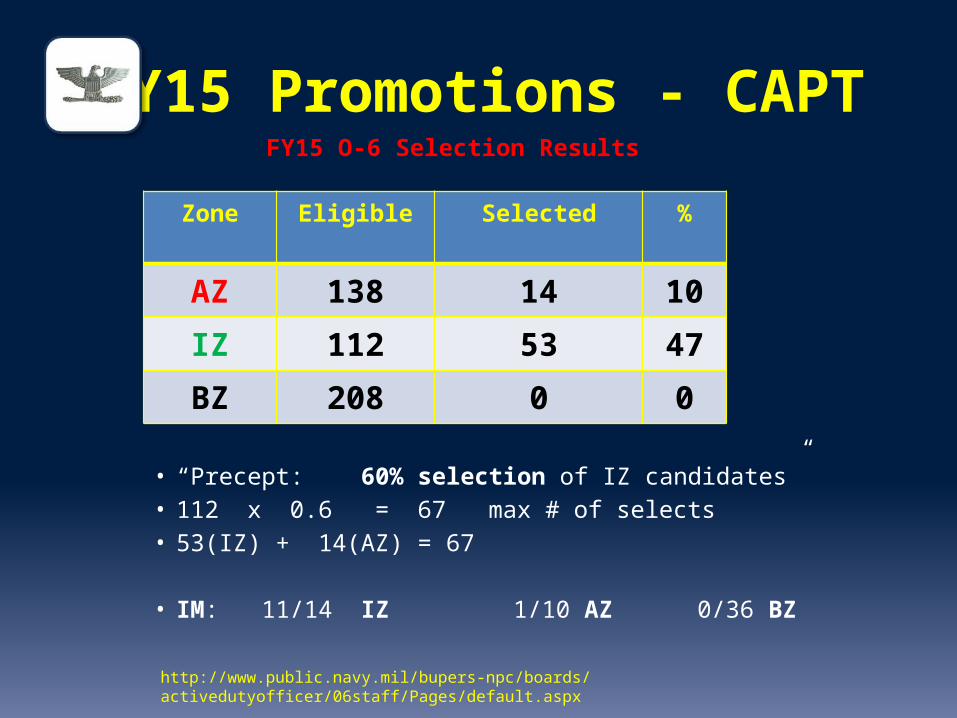
FY15 Promotions - CAPT
• “Precept: 60% selection of IZ candidates”• 112 x 0.6 = 67 max # of selects• 53(IZ) + 14(AZ) = 67
• IM: 11/14 IZ 1/10 AZ 0/36 BZ
Zone Eligible Selected %
AZ 138 14 10
IZ 112 53 47
BZ 208 0 0
FY15 O-6 Selection Results
http://www.public.navy.mil/bupers-npc/boards/activedutyofficer/06staff/Pages/default.aspx

PROMOTION BOARDS• Google “BUPERS “
– “about BUPERS – us navy” “boards” “active duty staff officer “ “05 staff”
• Timing of sub-specialty training must be considered for O-5/O-6
• Competitive FITREPs– Breaking out in COMPETETIVE peer group– “rightward progression” while in rank
• Increasing leadership role and positional responsibility!
• Ensure your photo is up to date, in current rank!• Document Board Certification
• Manage your online Officer record, OSR/PSR
• Document accomplishments during FTOS training– Publications, Research Presentations Class rankings

From the OOMC• MilSuite
– One place to organize key data to answer frequent questions or find points of contact
– Reduce reliance on email– More communication between the hospitals – We shouldn’t have to recreate the wheel

2014 Change…2015 uncertainty
• Ebola is an evolving problem
• ISIS -- Syria, Iraq?• How will transition in Afghanistan go?
• 2016 budget: what will it be, and how will it affect us?
• Another year into e MSM’s
• GMO Conversions ??

Unique Opportunities• CAPT Matthew Lim
– BUMED liaison, Global affairs,DHHS
• LCDR Jamie Peterson– BUMED Medical Student
Recruiting/Admin Fellow
• CAPT Utz– Health attache to VietNam
• MBA program – Navy PG School distance learning
program

Billets 2015• Currently
– NMCP– NMCSD– WRNMMC– NH Beaufort– NH Camp Lejeune– NH Jacksonville– NH 29 Palms– NH Guam– NH Okinawa– NH Guantanamo– NAMI (Pensacola)– FHCC (Great Lakes)– Bremerton
Billets 2014
• Priority will be given to Staff– Returning from OCONUS, arduous sea duty– Deployment– Rank
• GMESB is next milestone, results released Dec 2014
• Board certification required for MEDCEN billets• Residents will be slated in January
• Specialty leaders are working closely with BUPERS for best fit for each individual, Command and Navy
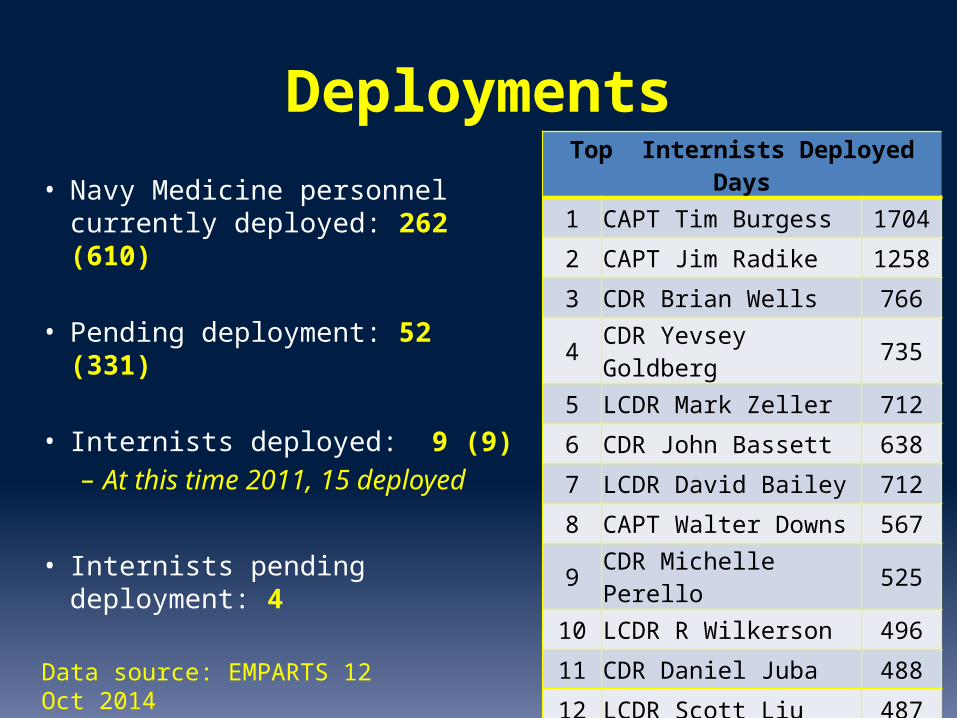
Deployments
• Navy Medicine personnel currently deployed: 262 (610)
• Pending deployment: 52 (331)
• Internists deployed: 9 (9)– At this time 2011, 15
deployed
• Internists pending deployment: 4
Top Internists Deployed Days
1 CAPT Tim Burgess 1704
2 CAPT Jim Radike 1258
3 CDR Brian Wells 766
4 CDR Yevsey Goldberg 735
5 LCDR Mark Zeller 712
6 CDR John Bassett 638
7 LCDR David Bailey 712
8 CAPT Walter Downs 567
9 CDR Michelle Perello 525
10 LCDR R Wilkerson 496
11 CDR Daniel Juba 488
12 LCDR Scott Liu 487
13 CAPT Kurt Henry 471Data source: EMPARTS 12 Oct 2014

Deployments 2013
SURGERY
ANESTHESIA
EMERGENCY M
ED
INTERNAL M
ED
FAM
ILY PRACTICE
Ortho
PSYCHIATRY
Neurosu
rgery
OB/GYN
02468
10121416
Total number CURRENTLY deployed by specialty

Deployment
• 50 Internists with >300 days of deployment• 99 Internists with zero days of deployment
(includes trainees)
• Navy Medicine tracks deployed days via EMPARTS– Not a perfect database, requires manual data entry– Ensure your deployments are correctly reflected in
the systemData source: EMPARTS 12 Oct 2014

Deployment
• IM has/had habitual relationships for specific IAs– Pacific Partnership– Continuing Promise– EMF Kandahar (pulm/cc)– JTF GTMO (NE-2213)– EMF Djibouti (NE-2089)– Embedded Training Teams (NE-4255)– Forward Surgical Teams (NE-5326, NE-5254)

Deployment Forecast FY15
• Discussion with POMIs, nothing imminent
• Any Surprises in Afghanistan next spring?• Syria, ISIS, Ebola….• Fiscal Climate affecting Humanitarian Missions
• Our Primary Role Is to Support These Deployments. We all must be ready….

Deployments
• For IM, what does it mean to be “operationally ready” (currency)?
• How do we measure that?• What type of training would that require?
• What impact would that have?

IM Deployment Business Rules1. No position is too important to deploy (except CO).2. No one shall be recommended for deployment until everyone has
deployed a first time.3. Total deployed days taken in to account for deployment recommendation4. In order to facilitate consolidation of knowledge and board passage,
recently graduated fellows should be protected from deployment during their first post-GME year.
5. Prior overseas PCS moves will not count towards IAs.6. Deployer order may be modified based upon extenuating circumstances
and the needs of the Navy (i.e. a specific specialty is required or a particular institution is already heavily deployed).
7. Volunteers will always be solicited prior to assigning deployers.8. Volunteering for one assignment, does NOT move you higher on the list
for the next available assignment.9. Chain of Command (and subspecialty SL if applicable) will be engaged
prior to SL recommendation.10. Will avoid by name requests, if possible, to sourcing MTF.
THANK YOU!
• Thank you for your professionalism
• Thank you for your hard work and dedication to our patients
• Thank you for constantly striving to improve Navy Medicine
Points of Contact
• CDR Daniel Seidensticker IM Specialty [email protected]
• CDR Joel Schofer [email protected]
• CAPT Harry Ward Reserve IM [email protected]

Thank you for your service!
“Cogito ergo I.M.”
Supplemental slides

Also note, for a general internist each paRVU is worth $46.35 a Navy general internist to generate $88,899 in equivalent production.
2012 MGMA report (below),Navy MGMA 40% targets (right)

Promotion Guidance
• Timing of sub-specialty training must be considered if coming in to zone for O-5/O-6
• Ensure your photo is up to date, in current rank!
• Manage your online Officer record, OSR/PSR
• Document accomplishments during FTOS training– Publications, Research Presentations Class rankings
Professional Guidance

From the OOMC
• FITREPs are written for Promotion Board members
• Expectations– All MC Officers will complete residency – All MC Officers will achieve board certification
• O-6 board looks for demonstrated leadership– Clinical– Academic– Operational– Executive
• Pass PRT/BCA
Professional Guidance

Change is coming to Navy Medicine
• Enhanced Multiservice Markets (eMSM’s)– PUGET Sound, Hampton Roads– National Capital Region– San Antonio, National Capital, Colorado Springs,
Pearl Harbor– NMCSD, Camp Lejeune considered their own mini
markets– CO of that eMSM will have operational control of
all facilities


















