Antidiabetic E4orf1 protein prevents hepatic steatosis and ...

PATHOBIOLOGY
Interleukin 6 Alleviates Hepatic Steatosis andIschemia/Reperfusion Injury in Mice
With Fatty Liver DiseaseFeng Hong,1 Svetlana Radaeva,1 Hong-na Pan,1 Zhigang Tian,2 Richard Veech,3 and Bin Gao1
Fatty liver, formerly associated predominantly with excessive alcohol intake, is now alsorecognized as a complication of obesity and an important precursor state to more severeforms of liver pathology including ischemia/reperfusion injury. No standard protocol fortreating fatty liver exists at this time. We therefore examined the effects of 10 days ofinterleukin 6 (IL-6) injection in 3 murine models of fatty liver: leptin deficient ob/ob mice,ethanol-fed mice, and mice fed a high-fat diet. In all 3 models, IL-6 injection decreasedsteatosis and normalized serum aminotransferase. The beneficial effects of IL-6 treatment invivo resulted in part from an increase in mitochondrial � oxidation of fatty acid and anincrease in hepatic export of triglyceride and cholesterol. However, administration of IL-6 toisolated cultured steatotic hepatocytes failed to decrease lipid contents, suggesting that thebeneficial effects of IL-6 in vivo do not result from its effects on hepatocytes alone. IL-6treatment increased hepatic peroxisome proliferator-activated receptor (PPAR) � and de-creased liver and serum tumor necrosis factor (TNF) �. Finally, 10 days of treatment withIL-6 prevented the susceptibility of fatty livers to warm ischemia/reperfusion injury. Inconclusion, long-term IL-6 administration ameliorates fatty livers and protects against warmischemia/reperfusion fatty liver injury, suggesting the therapeutic potential of IL-6 in treat-ing human fatty liver disease. Supplementary material for this article can be found on theHepatology website (http://interscience.wiley.com/jpages/0270-9139/suppmat/index.html).(HEPATOLOGY 2004;40:933–941.)
The prevalence of fatty liver disease, primarilycaused by obesity and alcohol consumption, isapproximately 20% in the general population of
developed countries and is expected to increase further asa result of the alarming overall increase of obesity in the
general population.1 In the past, fatty liver disease wasconsidered a benign condition; however, mounting evi-dence indicates that fatty livers increase the risk of devel-oping progressive liver injury, such as nonalcoholicsteatohepatitis, fibrosis, and cirrhosis.1–4 Moreover, he-patic steatosis is also a frequent histopathological featureof chronic hepatitis C and accelerates the progression ofliver damage in these patients.5 Additionally, fatty liverstolerate poorly cold and warm ischemia/reperfusion in-jury and are associated with high mortality after majorsurgery and transplantation.6,7
Interleukin 6 (IL-6) is elevated in the plasma and pe-ripheral blood monocytes of patients with fatty diseases,including alcoholic liver disease and nonalcoholic steato-hepatitis, and elevation of IL-6 correlates with the pro-gression and severity of liver disease,8–11 suggesting thatIL-6 may be involved in the pathogenesis of fatty liverdisease. However, increasing evidence indicates that IL-6is an important hepatoprotective cytokine for promotingliver regeneration12–14 and protecting against liver injurycaused by various insults in lean animals.15–22 Althoughthe protective effect of IL-6 in lean livers has been well
Abbreviations: IL-6, interleukin 6; STAT, signal transducer and activator oftranscription factor; TNF, tumor necrosis factor; PPAR, peroxisome proliferator-activated receptor; SREBP, sterol regulatory element-binding protein; HE, hema-toxylin-eosin; alanine aminotransferase; RT-PCR, reverse-transcriptase polymerasechain reaction; bp, base pair; mRNA, messenger RNA; AST, aspartate aminotrans-ferase; MCD, methionine and choline-deficient; TUNEL, terminal deoxynucleoti-dyl transferase-mediated nick end labeling.
From the 1Section on Liver Biology, Laboratory of Physiologic Studies, NationalInstitute on Alcohol Abuse and Alcoholism, National Institutes of Health, Bethesda,MD; 2Institute of Immunology, School of Life Science, University of Science andTechnology of China, Hefei, Anhui, China; and 3Laboratory of Metabolism andMolecular Biology, National Institute on Alcohol Abuse and Alcoholism, NationalInstitutes of Health, Bethesda, MD.
Received February 10, 2004; accepted June 1, 2004.Address reprint request to: Bin Gao, M.D., Ph.D., Section on Liver Biology,
NIAAA/NIH, Park Bldg. Rm. 120, 12420 Parklawn Drive, MSC 8115, Be-thesda, MD 20892. E-mail: [email protected].
Copyright © 2004 by the American Association for the Study of Liver Diseases.Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/hep.20400
933

documented, the effects of IL-6 on fatty liver disease re-main unclear. Selzner and Clavien23 reported that treat-ment with IL-6 normalized proliferating-cell nuclearantigen expression in steatotic hepatocytes but failed toincrease DNA synthesis and mitosis in steatotic hepato-cytes in Zucker obese rats after partial hepatectomy, indi-cating that the mitogenic role of IL-6 is partiallyattenuated in Zucker rats. However, Torbenson et al.24
reported that activation of signal transducer and activatorof transcription factor 3 (STAT3), a downstream IL-6signal, was significantly higher in steatotic livers of ob/obmice after partial hepatectomy, suggesting that IL-6 sig-naling is highly induced in ob/ob murine fatty livers afterpartial hepatectomy. Previously, we showed that in vitroIL-6 treatment prevents mortality associated with fattyliver transplants in rats by protecting against endothelialcell necrapoptosis and consequent improvement in mi-crocirculation.25,26 In this study, we demonstrate thatlong-term—but not short-term—IL-6 treatment signifi-cantly alleviates steatosis and ischemia/reperfusion injuryin obesity- and ethanol-associated fatty livers. Further-more, we show that tumor necrosis factor (TNF)-�down-regulation and peroxisome proliferator-activatedreceptor (PPAR)-� up-regulation may be mechanismspartially contributing to the amelioration of fatty livers byIL-6.
Materials and Methods
Materials. Recombinant human IL-6 was producedby recombinant DNA technology as described previ-ously.25 Antibodies against STATs were obtained fromCell Signaling (Beverly, MA). Mcl-1, Bcl-2, and sterolregulatory element-binding protein (SREBP)-1 antibod-ies were purchased from Santa Cruz Biotechnology, Inc.(Santa Cruz, CA) and Bcl-xL antibody was obtained fromBD PharMingen (San Diego, CA). PPAR-� and PPAR-�antibodies were purchased from Research DiagnosticsInc. (Flanders, NJ).
Murine Models of Fatty Livers. Three murine mod-els of fatty livers were used: leptin-deficient ob/ob mice,ethanol-fed mice, and high fat-fed mice. Male ob/obmice, 8 to 10 weeks old, obtained from Jackson Labora-tory (Bar Harbor, ME) were obese with severe steatosis ofthe liver. For the high fat-induced fatty liver model, 8- to10-week old male C57BL/6 mice were fed a high-fat diet(Catalogue no. 88137; Harlan Teklad, Madison, WI) for10 weeks and developed severe steatosis of the liver. Forthe ethanol-induced fatty liver model, 7- to 8-week oldmale C57BL/6NCR mice (National Cancer Institute[NCI], National Institutes of Health [NIH], Bethesda,MD) were fed an ethanol-containing liquid Lieber-De-
Carli diet or control diet whereby ethanol was substitutedisocalorically with dextrin maltose (BioServ Inc., French-town, NJ) for 8 weeks. After 8 weeks of feeding, the micedeveloped significant steatosis of the liver.
Hepatic Triglyceride Secretion. The nonionic deter-gent Triton WR-1339 (Sigma, St. Louis, MO) was usedto measure hepatic triglyceride secretion as described pre-viously.27 Lipoproteins in the plasma are trapped by Tri-ton WR-1339, which allowed determination of thesecretion rate of hepatic triglyceride lipoproteins. Micewere injected with either IL-6 or saline and 12 mg TritonWR-1339 in 0.9% saline. One and 2 hours later, bloodwas collected, and levels of triglyceride were measured.
Hematoxylin-Eosin (HE) and Oil Red O Stainingof Liver Sections. Following fixation of the livers with10% formalin/phosphate-buffered saline, livers weresliced and stained with HE for histological examination.Liver steatosis was graded semiquantitatively based on thepercentage of hepatocytes according to the following cri-teria: grade 0, no hepatocytes involved; grade 1, 1% to25% of hepatocytes involved; grade 2, 26% to 50% ofhepatocytes involved; grade 3, 51% to 75% of hepato-cytes involved; and grade 4, 76% to 100% of hepatocytesinvolved. Hepatic lipid content was also determined bystaining with Oil Red O (Sigma).
Determination of Liver Injury. Liver injury causedby ischemia/reperfusion was quantified by measuringplasma enzyme activities of alanine aminotransferase(ALT) using a kit from DREW Scientific (Cumbria, UK),HE staining, and terminal deoxynucleotidyl transferase-mediated nick end labeling (TUNEL) assay. Hepatocel-lular necrosis was determined in HE-stained sectionsusing a semiquantitative scale by a point counting methodas previously described.16,28 An ordinal scale was used fordetermination of hepatocellular injury as follows: grade 0,minimal or no evidence of injury; grade 1, mild injuryconsisting of cytoplasmic vacuolation and focal nuclearpycknosis; grade 2, moderate to severe injury with exten-sive nuclear pycknosis, cytoplasmic hypereosinophilia,and loss of intercellular borders; and grade 3, severe ne-crosis with disintegration of hepatic cords, hemorrhage,and neutrophil infiltration. Thirty random sections wereexamined per slide to determine the percentage of ne-crotic cells. Apoptotic cells in sections were determined byTUNEL staining using ApopTag (Oncor, Gaithersburg,MD) as described previously.20
Biological Analysis of Hepatic Lipids. To measurehepatic lipids, livers were homogenized at 4°C in lysisbuffer containing 50 mmol/L Tris (pH 8.0), 150 mmol/LNaCl, 1% Triton X-100, and 0.5% Na DOC. Lipidsfrom the total liver homogenate were extracted using thechloroform/methanol method (2:1), evaporated, and dis-
934 HONG ET AL. HEPATOLOGY, October 2004

solved in 2-propanol. Amounts of triglyceride, total cho-lesterol, and phospholipids were assayed enzymaticallyusing kits obtained from Wako Pure Chemicals Co.(Richmond, VA).
Primary Mouse Hepatocyte Isolation and Culture.Hepatocytes were isolated and cultured as described pre-viously.29
Fatty Acid �-Oxidation Activity. Fresh livers werehomogenized in 4 volumes of 0.25 mol/L sucrose con-taining 1 mmol/L ethylenediaminetetraacetic acid in ahomogenizer using a tight-fitting Teflon pestle. Fatty acid�-oxidation activity was measured as described previ-ously30 and expressed as nmol/min/liver.
Reverse-Transcriptase Polymerase Chain Reaction(RT-PCR). RT-PCR was performed as described previ-ously.29 The primer sequences for TNF-� were forwardprimer, 5�CCA CAT CTC CCT CCA GAA AA-3� andreverse primer, 5�AGG GTC TGG GCC ATA GAA CT-3�. The expected PCR product was 258 base pair (bp).PCR using RNA without reverse transcription did notyield amplicons, indicating a lack of genomic DNA con-tamination. The PCR bands were scanned using StormPhosphoImager (Molecular Dynamics, Sunnyvale, CA).
Gel Mobility Shift Assay. Gel mobility shift assaywas performed as described previously.29 The double-stranded oligo containing the PPAR response ele-
ment 5�-GAACTAGGTCAAAGGTCATCCCCT-3�was used as the probe.
Murine Model of Partial Ischemia/ReperfusionLiver Injury. Adult male mice were anesthetized byisoflurane inhalation, followed by a midline laparotomy.All structures in the portal triad to the left and medianliver lobes were occluded with a vascular clamp to inducepartial ischemia (70%). After 50 minutes, the vascularclamp was removed; animals were sacrificed 6 hours later,and the serum was collected to measure ALT levels.
Murine Model of Total Liver Ischemia/Reperfu-sion. To examine the effects of IL-6 treatment on thesurvival after ischemia/reperfusion, the murine modelof total hepatic ischemia was used as described pre-viously.31 Briefly, after the midline laparotomy, a partial(30%) hepatectomy was performed with resection of thecaudate, right lateral, and quadrate lobes, and papillaryprocess. Total hepatic ischemia was then achieved by plac-ing the vascular microclamps across the pedicles of themedian and left lateral lobes at the level of the hilum. After60 minutes of ischemia, the clip was removed, and theabdominal cavity was closed. Mice were then observeddaily until postsurgical day 7 to determine survival.
Western Blot Analysis. Western blot analysis wasperformed as described previously.29
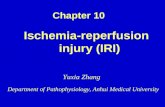
Fig. 1. IL-6 treatment reduces liver weight without affecting bodyweight. Eight-week-old ob/ob mice were treated daily with subcutaneousinjection of 1 �g/g of IL-6 (n � 10) or saline (n � 10) for 10 days. (A)Mice were weighed daily. (B) On day 11, mice were sacrificed, liverweight was measured, and liver/body weight ratios were calculated. (C)The ratios of epididymal (Ep) or subcutaneous (Sub, fat pad-to-bodyweight were also calculated. (D) A representative picture of saline andIL-6 treated ob/ob mouse livers is shown. Note the pale appearance ofsteatotic livers of saline-treated ob/ob mice and the red appearance ofIL-6-treated ob/ob mouse livers. *P � .05 in comparison with ob/obgroup with saline.
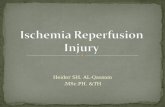
Fig. 2. IL-6 treatment ameliorates fatty livers, improves liver histology,and normalizes serum aminotransferase activity in ob/ob mice. (A)Eight-week-old ob/ob mice were administered IL-6 (1 �g/g, subcuta-neous) daily for various numbers of days (upper panel) or with variousdoses (lower panel) of IL-6 daily for 5 days. Mice were then sacrificed,(A) their livers were stained with HE, and (B) hepatic steatosis wasscored. (C-E) Eight-week-old ob/ob mice were administered IL-6 (1�g/g, subcutaneous) daily for 10 days. The mice were then killed, (C)their livers were stained with Oil Red O, (D) hepatic triglyceride levelswere measured, and (E) serum ALT levels were measured. Values shownin panels B, D, and E represent means � SEM from 5 to 10 mice in eachgroup. **P � .01. ***P � .001 in comparison with ob/ob grouptreated with saline.
HEPATOLOGY, Vol. 40, No. 4, 2004 HONG ET AL. 935

Statistical Analysis. For comparing values obtainedin 3 or more groups, 1-way ANOVA was used, followedby post hoc Tukey test. Statistical significance was taken atthe P less than .05 level.
Results
Long-Term IL-6 Treatment Ameliorates Fatty Liv-ers in Ob/Ob Mice. Subcutaneous injection of IL-6 for10 days did not significantly reduce body weight (Fig. 1A)or food intake (data not shown). In contrast, liver weightand liver-to-body weight ratios were reduced in the IL-6–treated group compared to the saline treatment group(P � .05; Fig. 1B), whereas the epididymal and subcuta-neous fat pad-to-body weight ratios remained unchanged(Fig. 1C). Initially, the livers of ob/ob mice were pale inappearance, but they became a homogenous red afterlong-term IL-6 treatment, indicating that steatosis wasalleviated in IL-6-treated ob/ob mice (Fig. 1D).
Histological analysis of the livers with HE stainingshowed that steatosis was significantly improved 5 daysafter treatment with IL-6 (1 �g/g) and almost completelyrecovered 10 days and 20 days after treatment. As shownin Fig. 2A, lipid droplets accumulated in nearly 100% ofhepatocytes in both periportal and pericentral areas inuntreated ob/ob mice. In comparison, lipid droplet accu-mulations in hepatocytes were significantly decreased af-ter 5 days of IL-6 injections, particularly in the periportalareas. After longer treatment with IL-6 (10-20 days), lipiddroplets were diminished in both periportal and perive-nular areas (Figs. 2A and B). Treatment with higher dosesof IL-6 (2-5 �g/g) for 5 days also significantly alleviatedsteatosis in the livers of ob/ob mice (Fig. 2A), but thesedoses caused significant reductions in food intake andbody weight gain (data not shown). As added confirma-tion, Oil Red O staining showed that large lipid dropletsobserved in the livers of ob/ob mice were markedly dimin-ished in the 10-day IL-6 treatment group (Fig. 2C), andquantitation of lipid contents revealed that IL-6 treat-ment reduced the levels of hepatic triglyceride (Fig. 2D).Finally, treatment of ob/ob mice with IL-6 for 10 daysreduced the serum levels of ALT (Fig. 2E).
Long-Term IL-6 Treatment Reverses Fatty Liversin Mice Fed a High Fat Diet and Ethanol-Fed Mice.Next, we examined whether IL-6 treatment also alleviatedsteatosis in mice fed a high-fat diet and ethanol-fed mice.Mice fed a high-fat diet for 10 weeks developed severesteatosis in the liver, which was significantly attenuatedafter long-term IL-6 treatment, as demonstrated by OilRed O staining. As shown in Supplementary Fig. 1A, OilRed O staining showed that large lipid droplets in thelivers of mice fed a high-fat diet were diminished after 10
days of IL-6 treatment. Quantitation of the lipid contentsrevealed that IL-6 treatment significantly reduced hepaticlevels of triglyceride in mice fed a high-fat diet (Supple-mentary Fig. 1B). Similarly, mice fed a liquid diet con-taining 5% ethanol for 8 weeks developed significantsteatosis, which was significantly improved after 5 days ofIL-6 treatment, as demonstrated by Oil Red O staining(Supplementary Fig. 1C) and quantitation of hepatic lev-els of triglyceride (Supplementary Fig. 1D).
IL-6 Does Not Alleviate Steatosis in Cultured Stea-totic Hepatocytes. To understand the molecular mecha-nism underlying the effects of IL-6 treatment on fattyliver in vivo, we examined the effects of IL-6 on steatosisin cultured steatotic hepatocytes. Oil Red O staining re-vealed that lipid droplets in steatotic hepatocytes were notaffected in the absence or presence of IL-6 (500 ng/mL)after 5 days in culture (Supplementary Fig. 2A). Quanti-tation of lipid contents revealed that triglyceride levels inhepatocytes were not reduced after IL-6 treatment (Sup-plementary Fig. 2B), and the levels of triglyceride in thesupernatant were similar in both IL-6–treated and -un-treated cells (Supplementary Fig. 2C). We also tested theeffects of various concentrations of IL-6 (50-2,000 ng/mL) on hepatic steatosis in cultured hepatocytes, and nosignificant effects were observed (data not shown).
IL-6 Treatment Stimulates Hepatic TriglycerideSecretion and Hepatic Fatty Acid � Oxidation. Theeffects of IL-6 treatment on serum lipids were examined.As shown in Fig. 3, IL-6 administration caused rapid el-evations in serum triglyceride and cholesterol levels inboth ob/ob mice and lean C57BL/6 mice with peak effectat 12 hours (Figs. 3A and B). Serum triglyceride andcholesterol levels were also elevated after long-term IL-6treatment (Fig. 3C). We next determined whether theIL-6–induced elevation in serum lipid contents was dueto stimulation of hepatic lipoprotein secretion. Hepaticsecretion of lipoproteins was determined using the Triton1339 technique. As shown in Fig. 3D, triglyceride secre-tion increased 2.1-fold in IL-6–treated animals comparedto saline-treated mice (P � .01). Finally, long-termIL-6 treatment slightly—but significantly—stimulatedpalmitic acid � oxidation in the liver mitochondria (Fig.3E; P � .05). The same treatment did not affect peroxi-somal oxidation of lignoceric acid (Fig. 3E).
IL-6 Down-regulates Hepatic and Serum Levels ofTNF-�. TNF-� has been implicated in the developmentof fatty livers,32,33 and IL-6 treatment has been shown todown-regulate TNF-� in several models of liver in-jury.16,34 Therefore, we sought to examine whether IL-6amelioration of fatty livers was mediated by down-regu-lation of TNF-�. As shown in Fig. 4A, TNF-� messengerRNA (mRNA) expression was significantly greater in the
936 HONG ET AL. HEPATOLOGY, October 2004

livers of ob/ob mice compared to wild type C57BL/6mice. Long-term IL-6 treatment, however, decreasedTNF-� mRNA expression in the livers of ob/ob mice(P � .001; Fig. 4A). Moreover, treatment with IL-6 for10 days down-regulated serum TNF-� levels in ob/obmice and mice fed a high-fat diet (Fig. 4B).
Long-Term IL-6 Treatment Up-regulates PPAR-�Protein Expression and DNA Binding Activity ofPPAR. To further understand the molecular mecha-nisms underlying IL-6 amelioration of fatty liver, expres-sion of PPAR, which increases fatty-acid oxidation,35–37
and protein expression of SREBP, which increases fattyacid and cholesterol synthesis, were examined. As shownin Fig. 5A, expression of PPAR-� protein was elevated inthe livers of IL-6–treated ob/ob mice, whereas expression
of PPAR-� and SREBP-1 was not affected by IL-6 treat-ment. Furthermore, results of the gel mobility shift assayshowed that DNA binding of the PPAR/PXR het-erodimer in hepatic nuclear extracts from IL-6–treatedob/ob mice was significantly higher than that from non-treated ob/ob mice (Fig. 5B). Incubation with PPAR-�antibody significantly reduced DNA binding of PPAR/PXR in hepatic nuclear extracts from IL-6–treated ob/obmice, suggesting that IL-6 treatment enhances the DNAbinding of PPAR-�/PXR. Conversely, treatment of cul-tured hepatocytes with various concentrations of IL-6(100-500 ng/mL) did not affect the expression and DNAbinding of PPAR-� protein (data not shown). Taken to-gether, our findings indicate that in vivo treatment withIL-6 for 10 days increases the expression and DNA bind-ing of PPAR-� in the liver.
Long-Term, but Not Short-Term IL-6 TreatmentProtects Steatotic Livers From Warm Ischemia/Reper-fusion Injury. Camargo et al.16 previously reported thatIL-6 protected against warm ischemia/reperfusion injury
Fig. 3. IL-6 treatment stimulates hepatic triglyceride secretion andhepatic fatty acid � oxidation. (A and B) C57BL/6 mice or ob/ob micewere administered a single dose of IL-6 (1 �g/g, subcutaneous). Aftervarious time periods, mice were sacrificed, and serum levels of (A)triglyceride and (B) cholesterol were measured. (C) Ob/ob mice wereadministered IL-6 (1 �g/g, subcutaneous) daily for 10 days. Mice werethen sacrificed, and hepatic lipid contents were measured. (D) Ob/obmice were treated with saline or IL-6 (1 �g/g) and Triton WR-1339 (12mg). One and 2 hours later, blood was collected and levels of triglyceridewere determined. The difference (� triglyceride) in serum triglyceridelevels between 1 and 2 hours is equivalent to the rate of secretion oftriglyceride-containing lipoproteins. (E) Ob/ob mice were administeredIL-6 (1 �g/g, subcutaneous) daily for 10 days. Mice were then sacri-ficed, and livers were collected for determination of lignoceric acidoxidation or palmitic acid oxidation. Values shown represent means �SEM from 3 mice (A and B), 10 mice (C), 4 mice (D), and 10 mice (E)in each group. *P � .05. **P � .01 in comparison with saline-treatedgroup.
Fig. 4. IL-6 down-regulates hepatic and serum levels of TNF-�. (A)Ob/ob mice were administered IL-6 (1 �g/g, subcutaneous) or salinedaily for 10 days. Total liver RNA from IL-6–treated ob/ob mice, saline-treated mice, or C57BL/6 mice were subjected to RT-PCR analysis ofTNF-� and �-actin. (A) Relative density of TNF-� to �-actin was quan-titated. (B) Ob/ob mice or mice fed a high-fat diet were administeredIL-6 (1 �g/g, subcutaneous) or saline daily for 10 days. Serum TNF-�levels were measured. Values shown are means � SEM from 4 mice (A)and 10 mice (B) in each group. *P � .05. ***P � .001 in comparisonwith saline-treated ob/ob group.
HEPATOLOGY, Vol. 40, No. 4, 2004 HONG ET AL. 937

in lean animals. However, the effects of IL-6 on warmischemia/reperfusion injury in fatty livers remain unclear.As shown in Fig. 6A, ischemia for 50 minutes and reper-fusion for 6 hours caused only a slight elevation in serumaspartate aminotransferase (AST) levels in lean animals,whereas the same treatment caused a dramatic elevation inserum AST levels in ob/ob mice. Pretreatment with IL-6for 10 days but not 1 day protected fatty livers from warmischemia/reperfusion injury in ob/ob mice (7,736 � 1851U/L in IL-6–treated ob/ob mice vs. 24,493 � 3033 U/Lin ob/ob mice; P � .001). Additionally, treatment withIL-6 for 10 days also protected fatty livers from ischemia/reperfusion injury in mice fed high-fat diets (Fig. 6B).
Next, apoptotic and necrotic cell death were examinedin IL-6–treated and -untreated ob/ob mouse livers. Asshown in Fig. 6C, less than 10% of necrotic cells and lessthan 5% TUNEL-positive hepatocytes were detected inthe livers of lean control mice after 50 minutes ischemia/6hours reperfusion, while the same treatment caused ne-crosis and apoptosis of 80% and 5%, respectively, ofhepatocytes in the livers of ob/ob mice. Both necrosis andapoptosis were reduced in the livers of ob/ob mice treatedwith IL-6 for 10 days but not in those treated for 1 day.
The effects of IL-6 treatment on ob/ob mouse survivalafter ischemia/reperfusion were also studied by using amodel of total hepatic ischemia as described previously.31
As shown in Fig. 6E, all wild type C57BL/6 mice survived60 minutes of total ischemia, but 9 of 10 ob/ob mice diedwithin 2 days after 60 minutes total ischemia. Conversely,9 of 10 IL-6–treated ob/ob mice survived 60 minutes oftotal ischemia.
IL-6 Induces Weaker Hepatic STAT3 Activation inOb/Ob Mice Compared to Lean Mice. IL-6 activationof antiapoptotic signals and genes have been well docu-mented in lean animals15–22; these signals and genes ap-pear to play important roles in the protective effects ofIL-6 in various forms of liver injury. In the present study,we examined IL-6 activation of antiapoptotic STAT3 sig-nals in fatty livers. As shown in Supplementary Fig. 3A,IL-6 injection induced STAT3 phosphorylation in thelivers of ob/ob mice and lean C57BL/B6 mice, with peakeffect at 1 hour and returning to basal levels at 8 hoursafter injection. IL-6 activation of hepatic STAT3 in ob/obmice was lower than in lean C57BL/6 mice (Supplemen-tary Fig. 3A). Western blot analysis showed that levels of
Fig. 5. IL-6 treatment up-regulates PPAR-� protein expression and DNA binding activity of PPAR/PXR. Ob/ob mice were administered IL-6 (1 �g/g,subcutaneous) or saline daily for 10 days. On day 11, mice were sacrificed and protein extracts were prepared for (A) Western blot analysis of PPAR-�,PPAR-�, or SREBP-1 or (B) gel mobility shift analysis of DNA binding of PPAR. (B) Anti–PPAR-� antibody (Ab) was included in the left-most lane forsupershift analysis. Relative density of (A) PPAR-� to �-actin and (B) fold induction of PPAR/PXR binding in panel B were quantified and shown (left).The PPAR binding in the first lane (sample 1) was defined as 1. Values shown represent means � SEM from 6 mice in each group. **P � .01 incomparison with saline-treated ob/ob group.
938 HONG ET AL. HEPATOLOGY, October 2004

Bcl-2 and Bcl-xL were elevated in the livers of IL-6–treated ob/ob mice compared to saline-treated ob/ob mice(Supplementary Fig. 3B).
DiscussionIn the present study, we demonstrate that in addition
to its well-documented antiapoptotic functions in theliver, IL-6 also ameliorates fatty liver disease. This ame-lioration is not due to reduced food intake and bodyweight, since subcutaneous injection of IL-6 (1 �g/g) for10 days reduced liver weight and liver-to-body weightratios but did not affect food intake, body fat pads, andbody weight (Fig. 1). In contrast, chronic intracerebro-ventricular injection of IL-6 was shown to decrease bodyweight and body fat pads but did not affect liver weight.38
Taken together, these findings suggest that IL-6 amelio-ration of fatty livers is mediated by a peripheral effect,likely through stimulation of hepatic triglyceride secre-tion and hepatic fatty acid � oxidation (Fig. 3). In Fig. 3,we clearly show that long-term and short-term IL-6 treat-ments elevate serum levels of triglyceride and cholesterolin both lean and ob/ob mice; this is likely due to IL-6stimulation of hepatic triglyceride secretion (Fig. 3D). Atpresent, the molecular mechanisms for IL-6 stimulationof triglyceride secretion remain unclear. Similarly, stimu-lation in rats of hepatic triglyceride secretion by IL-6 wasfound to be independent of endogenous cat-echolamines.27 Treatment with IL-6 does not stimulatetriglyceride secretion in cultured steatotic hepatocytes(Supplementary Fig. 2), suggesting that the stimulatoryeffect of IL-6 on hepatic triglyceride in vivo is mediated byan indirect mechanism.
Additional experiments suggest that at least 2 mecha-nisms may be involved in IL-6 amelioration of fatty liverdisease. First, chronic IL-6 treatment down-regulates he-patic TNF-� expression and serum TNF-� levels. In-creasing evidence suggests that TNF-� plays a critical rolein the development of steatosis in obesity- and ethanol-induced fatty liver.32,33 For example, blocking TNF-�signaling with a probiotic (modifying the intestinal flora)or anti–TNF-� antibodies alleviates fatty livers in ob/obmice,32 and deletion of the TNF-� gene abolishes devel-opment of ethanol-induced fatty livers.33 In the presentstudy, we show that treatment with IL-6 for 10 daysdown-regulates expression of hepatic TNF-� mRNA andserum TNF-� levels in ob/ob mice (Fig. 4). The inhibi-tory effect of IL-6 on TNF-� and soluble TNF receptorp55 production also has been reported in various modelsof liver injury.16,34,39 Taken together, IL-6 treatment invivo alleviates hepatic steatosis, at least in part, by inhibi-tion of TNF-� activity. The second potential mechanismby which IL-6 ameliorates fatty liver may be through up-regulation of PPAR-�. The inhibitory effect of PPAR-�in the development and progression of fatty liver is welldocumented. Mice deficient in PPAR-� develop severehepatic steatosis after fasting or feeding on a high-fat dietor a methionine and choline-deficient (MCD) diet,35–37
but activation of PPAR-� by the agonist Wy14,643 ame-liorated alcoholic fatty liver30 and MCD-induced steato-hepatitis.37,40 The critical role of PPAR-� in amelioratingsteatosis is mediated through regulation of a wide varietyof genes involved in peroxisomal, mitochondrial, and mi-crosomal fatty acid oxidation systems in the liver.41
In this study, we demonstrate that treatment of ob/obmice with IL-6 for 10 days enhances PPAR-� proteinexpression and DNA binding activity of PPAR-�/PXR inthe liver (Fig. 5), and increases palmitic acid oxidation in
Fig. 6. Long-term, but not short-term IL-6 treatment protects steatoticlivers from warm ischemia/reperfusion injury. (A) Ob/ob mice weretreated with IL-6 (1 �g/g, subcutaneous) or saline for 1 day or daily for10 days. (B) Mice fed a high-fat diet were administered IL-6 (1 �g/g,subcutaneous) or saline daily for 10 days. (A and B) Mice were subjectedto a 50-minute ischemia/6-hour reperfusion treatment as described inMaterials and Methods. Serum AST levels were measured. (C and D)After a 50-minute ischemia/6-hour reperfusion treatment, mouse liversfrom panel A were subjected to (C) HE staining for determination ofnecrosis (only grade 3 injury was counted as necrosis) or (D) to TUNELstaining for determination of apoptosis (A-D) Values shown representmeans � SEM from 7 mice in each group. *P � .05; **P � .01; ***P� .001; in comparison with the corresponding saline-treated group(white bar). (E) Effect of IL-6 treatment on survival after 30% partialhepatectomy plus 60 minutes of ischemia. Survival for 7 days was100%, 10%, and 90% for lean male C57BL/6 mice, male ob/ob mice,and IL-6–treated male ob/ob mice, respectively.
HEPATOLOGY, Vol. 40, No. 4, 2004 HONG ET AL. 939

the liver, suggesting that up-regulation of PPAR-� may bean important mechanism in the IL-6 amelioration of he-patic steatosis.
Another important finding is that IL-6 treatment pro-tects steatotic livers from ischemia/reperfusion injury.High mortality (14%) is associated with fatty livers aftermajor surgery compared to 2% in normal livers6,7 andthere is currently no known treatment to reduce such highmortality. In rodents, fatty livers are more susceptible towarm or cold ischemia/reperfusion injury6,42,43; it wasalso shown in the present study that warm ischemia/reperfusion induced much higher levels of ALT and mor-tality in ob/ob mice compared to lean control mice (Fig.6). Moreover, we demonstrate that necrosis is the majorform of cell death in the livers of ob/ob mice after isch-emia/reperfusion (Fig. 6); this is consistent with previousstudies.42–45 Long-term IL-6 treatment markedly pre-vents ischemia/reperfusion-induced liver injury in ob/obmice and mice fed high-fat diets (Fig. 6). This hepatopro-tective effect likely results from a decrease of hepatic ste-atosis and TNF-� and activation of the antiapoptoticSTAT3 signal after IL-6 treatment. First, steatosis hasbeen recognized as an important risk factor for hepaticsurgery and ischemia/reperfusion injury.6,43,45 Thus, a de-crease of hepatic lipid content after long-term IL-6 treat-ment could be an important mechanism in IL-6protection against hepatic ischemia/reperfusion injury inob/ob mice. Second, TNF-� has been shown to be anessential mediator not only for the development of he-patic ischemia/reperfusion injury but also for the hepato-protective effects of ischemic preconditioning.46–49
Down-regulation of TNF-� has been implicated in thehepatoprotective effect of IL-6 in hepatic ischemia/reper-fusion injury in lean animals.16 Therefore, it is plausiblethat inhibition of TNF-� also contributes partly to IL-6amelioration of hepatic ischemia/reperfusion in ob/obmice in addition to IL-6 alleviation of hepatic steatosis.Finally, the hepatoprotective role of STAT3 has been welldocumented in a variety of models of liver injury bymeans of activation of antiapoptotic proteins (such asBcl-2 and Bcl-xL),15–22 and lean transgenic mice overex-pressing Bcl-2 are resistant to hepatic ischemia and reper-fusion.50 In the present study, we showed that IL-6treatment also activated STAT3, Bcl-2, and Bcl-xL in thesteatotic livers of ob/ob mice (Supplementary Fig. 3), sug-gesting that activation of these antiapoptotic signals couldbe an important mechanism in the hepatoprotective effectof IL-6 in ischemia/reperfusion injury of steatotic livers.
In summary, our results show that treatment with IL-6has beneficial effects on fatty livers, including the allevia-tion of steatosis, improvement of liver history, normaliza-tion of serum aminotransferase activity, and prevention of
ischemia/reperfusion injury. In addition to the previouslyidentified therapeutic potential of IL-6 in preventing fattyliver transplant failure25,26 and ischemia/reperfusion in-jury of lean livers,15,16 these findings suggest another clin-ical application of IL-6 in protecting fatty livers fromwarm ischemia/reperfusion injury and ameliorating fattyliver disease.
References1. Falck-Ytter Y, Younossi ZM, Marchesini G, McCullough AJ. Clinical
features and natural history of nonalcoholic steatosis syndromes. SeminLiver Dis 2001;21:17–26.
2. McCullough AJ. Update on nonalcoholic fatty liver disease. J Clin Gas-troenterol 2002;34:255–262.
3. Sanyal AJ. AGA technical review on nonalcoholic fatty liver disease. Gas-troenterology 2002;123:1705–1725.
4. Mulhall BP, Ong JP, Younossi ZM. Non-alcoholic fatty liver disease: anoverview. J Gastroenterol Hepatol 2002;17:1136–1143.
5. Adinolfi LE, Gambardella M, Andreana A, Tripodi MF, Utili R, RuggieroG. Steatosis accelerates the progression of liver damage of chronic hepatitisC patients and correlates with specific HCV genotype and visceral obesity.HEPATOLOGY 2001;33:1358–1364.
6. Selzner M, Clavien PA. Fatty liver in liver transplantation and surgery.Semin Liver Dis 2001;21:105–113.
7. Belghiti J, Hiramatsu K, Benoist S, Massault P, Sauvanet A, Farges O.Seven hundred forty-seven hepatectomies in the 1990s: an update to eval-uate the actual risk of liver resection. J Am Coll Surg 2000;191:38–46.
8. Hill DB, Marsano L, Cohen D, Allen J, Shedlofsky S, McClain CJ. In-creased plasma interleukin-6 concentrations in alcoholic hepatitis. J LabClin Med 1992;119:547–552.
9. McClain CJ, Barve S, Deaciuc I, Kugelmas M, Hill D. Cytokines inalcoholic liver disease. Semin Liver Dis 1999;19:205–219.
10. Hill DB, Barve S, Joshi-Barve S, McClain C. Increased monocyte nuclearfactorkappaB activation and tumor necrosis factor production in alcoholichepatitis. J Lab Clin Med 2000;135:387–395.
11. Kugelmas M, Hill DB, Vivian B, Marsano L, McClain CJ. Cytokines andNASH: a pilot study of the effects of lifestyle modification and vitamin E.HEPATOLOGY 2003;38:413–419.
12. Cressman DE, Greenbaum LE, DeAngelis RA, Ciliberto G, Furth EE, PoliV, et al. Liver failure and defective hepatocyte regeneration in interleukin-6-deficient mice. Science 1996;274:1379–1383.
13. Zimmers TA, McKillop IH, Pierce RH, Yoo JY, Koniaris LG. Massiveliver growth in mice induced by systemic interleukin 6 administration.HEPATOLOGY 2003;38:326–334.
14. Peters M, Blinn G, Jostock T, Schirmacher P, Meyer zum BuschenfeldeKH, Galle PR, et al. Combined interleukin 6 and soluble interleukin 6receptor accelerates murine liver regeneration. Gastroenterology2000;119:1663–1671.
15. Selzner M, Camargo CA, Clavien PA. Ischemia impairs liver regenerationafter major tissue loss in rodents: protective effects of interleukin-6. HEPA-TOLOGY 1999;30:469–475.
16. Camargo CA Jr, Madden JF, Gao W, Selvan RS, Clavien PA. Interleukin-6protects liver against warm ischemia/reperfusion injury and promotes he-patocyte proliferation in the rodent. HEPATOLOGY 1997;26:1513–1520.
17. Kovalovich K, Li W, DeAngelis R, Greenbaum LE, Ciliberto G, Taub R.Interleukin-6 protects against Fas-mediated death by establishing a criticallevel of anti-apoptotic hepatic proteins FLIP, Bcl-2, and Bcl-xL. J BiolChem 2001;276:26605–26613.
18. Streetz KL, Tacke F, Leifeld L, Wustefeld T, Graw A, Klein C, et al.Interleukin 6/gp130-dependent pathways are protective during chronicliver diseases. HEPATOLOGY 2003;38:218–229.
19. Blindenbacher A, Wang X, Langer I, Savino R, Terracciano L, Heim MH.Interleukin 6 is important for survival after partial hepatectomy in mice.HEPATOLOGY 2003;38:674–682.
940 HONG ET AL. HEPATOLOGY, October 2004

20. Hong F, Kim WH, Tian Z, Jaruga B, Ishac E, Shen X, et al. Elevatedinterleukin-6 during ethanol consumption acts as a potential endogenousprotective cytokine against ethanol-induced apoptosis in the liver: involve-ment of induction of Bcl-2 and Bcl-x(L) proteins. Oncogene 2002;21:32–43.
21. Hong F, Jaruga B, Kim WH, Radaeva S, El-Assal ON, Tian Z, et al.Opposing roles of STAT1 and STAT3 in T cell-mediated hepatitis: regu-lation by SOCS. J Clin Invest 2002;110:1503–1513.
22. Streetz KL, Wustefeld T, Klein C, Kallen KJ, Tronche F, Betz UA, et al.Lack of gp130 expression in hepatocytes promotes liver injury. Gastroen-terology 2003;125:532–543.
23. Selzner M, Clavien PA. Failure of regeneration of the steatotic rat liver:disruption at two different levels in the regeneration pathway. HEPATOL-OGY 2000;31:35–42.
24. Torbenson M, Yang SQ, Liu HZ, Huang J, Gage W, Diehl AM. STAT-3overexpression and p21 up-regulation accompany impaired regenerationof fatty livers. Am J Pathol 2002;161:155–161.
25. Sun Z, Klein AS, Radaeva S, Hong F, El-Assal O, Pan HN, et al. In vitrointerleukin-6 treatment prevents mortality associated with fatty liver trans-plants in rats. Gastroenterology 2003;125:202–215.
26. Selzner M, Graf R, Clavien PA. IL-6: a magic potion for liver transplanta-tion? Gastroenterology 2003;125:256–259.
27. Nonogaki K, Fuller GM, Fuentes NL, Moser AH, Staprans I, Grunfeld C,et al. Interleukin-6 stimulates hepatic triglyceride secretion in rats. Endo-crinology 1995;136:2143–2149.
28. Yadav SS, Sindram D, Perry DK, Clavien PA. Ischemic preconditioningprotects the mouse liver by inhibition of apoptosis through a caspase-dependent pathway. HEPATOLOGY 1999;30:1223–1231.
29. Radaeva S, Jaruga B, Hong F, Kim WH, Fan S, Cai H, et al. Interferon-alpha activates multiple STAT signals and down-regulates c- Met in pri-mary human hepatocytes. Gastroenterology 2002;122:1020–1034.
30. Fischer M, You M, Matsumoto M, Crabb DW. Peroxisome proliferator-activated receptor alpha (PPARalpha) agonist treatment reverses PPARal-pha dysfunction and abnormalities in hepatic lipid metabolism in ethanol-fed mice. J Biol Chem 2003;278:27997–28004.
31. Yadav SS, Gao W, Harland RC, Clavien PA. A new and simple techniqueof total hepatic ischemia in the mouse. Transplantation 1998;65:1433–1436.
32. Li Z, Yang S, Lin H, Huang J, Watkins PA, Moser AB, et al. Probiotics andantibodies to TNF inhibit inflammatory activity and improve nonalco-holic fatty liver disease. HEPATOLOGY 2003;37:343–350.
33. Yin M, Wheeler MD, Kono H, Bradford BU, Gallucci RM, Luster MI, etal. Essential role of tumor necrosis factor alpha in alcohol-induced liverinjury in mice. Gastroenterology 1999;117:942–952.
34. Mizuhara H, Uno M, Seki N, Yamashita M, Yamaoka M, Ogawa T, et al.Critical involvement of interferon gamma in the pathogenesis of T-cellactivation-associated hepatitis and regulatory mechanisms of interleukin-6for the manifestations of hepatitis. HEPATOLOGY 1996;23:1608–1615.
35. Kersten S, Seydoux J, Peters JM, Gonzalez FJ, Desvergne B, Wahli W.Peroxisome proliferator-activated receptor alpha mediates the adaptive re-sponse to fasting. J Clin Invest 1999;103:1489–1498.
36. Hashimoto T, Fujita T, Usuda N, Cook W, Qi C, Peters JM, et al.Peroxisomal and mitochondrial fatty acid beta-oxidation in mice nullizy-gous for both peroxisome proliferator-activated receptor alpha and perox-isomal fatty acyl-CoA oxidase. Genotype correlation with fatty liverphenotype. J Biol Chem 1999;274:19228–19236.
37. Ip E, Farrell GC, Robertson G, Hall P, Kirsch R, Leclercq I. Central role ofPPARalpha-dependent hepatic lipid turnover in dietary steatohepatitis inmice. HEPATOLOGY 2003;38:123–132.
38. Wallenius K, Wallenius V, Sunter D, Dickson SL, Jansson JO. Intracere-broventricular interleukin-6 treatment decreases body fat in rats. BiochemBiophys Res Commun 2002;293:560–565.
39. Tilg H, Trehu E, Atkins MB, Dinarello CA, Mier JW. Interleukin-6 (IL-6)as an anti-inflammatory cytokine: induction of circulating IL-1 receptorantagonist and soluble tumor necrosis factor receptor p55. Blood 1994;83:113–118.
40. Ip E, Farrell G, Hall P, Robertson G, Leclercq I. Administration of thepotent PPARalpha agonist, Wy-14,643, reverses nutritional fibrosis andsteatohepatitis in mice. HEPATOLOGY 2004;39:1286–1296.
41. Reddy JK. Nonalcoholic steatosis and steatohepatitis. III. Peroxisomal be-ta-oxidation, PPAR alpha, and steatohepatitis. Am J Physiol GastrointestLiver Physiol 2001;281:G1333–G1339.
42. Selzner M, Rudiger HA, Sindram D, Madden J, Clavien PA. Mechanismsof ischemic injury are different in the steatotic and normal rat liver. HEPA-TOLOGY 2000;32:1280–1288.
43. Selzner N, Selzner M, Jochum W, Clavien PA. Ischemic preconditioningprotects the steatotic mouse liver against reperfusion injury: an ATP de-pendent mechanism. J Hepatol 2003;39:55–61.
44. Jaeschke H, Lemasters JJ. Apoptosis versus oncotic necrosis in hepaticischemia/reperfusion injury. Gastroenterology 2003;125:1246–1257.
45. Serafin A, Rosello-Catafau J, Prats N, Xaus C, Gelpi E, Peralta C. Ischemicpreconditioning increases the tolerance of fatty liver to hepatic ischemia/reperfusion injury in the rat. Am J Pathol 2002;161:587–601.
46. Jaeschke H. Molecular mechanisms of hepatic ischemia-reperfusion injuryand preconditioning. Am J Physiol Gastrointest Liver Physiol 2003;284:G15–G26.
47. Rudiger HA, Clavien PA. Tumor necrosis factor alpha, but not Fas, me-diates hepatocellular apoptosis in the murine ischemic liver. Gastroenter-ology 2002;122:202–210.
48. Teoh N, Leclercq I, Pena AD, Farrell G. Low-dose TNF-alpha protectsagainst hepatic ischemia-reperfusion injury in mice: implications for pre-conditioning. HEPATOLOGY 2003;37:118–128.
49. Teoh N, Field J, Sutton J, Farrell G. Dual role of tumor necrosis factor-alpha in hepatic ischemia-reperfusion injury: studies in tumor necrosisfactor-alpha gene knockout mice. HEPATOLOGY 2004;39:412–421.
50. Selzner M, Rudiger HA, Selzner N, Thomas DW, Sindram D, Clavien PA.Transgenic mice overexpressing human Bcl-2 are resistant to hepatic isch-emia and reperfusion. J Hepatol 2002;36:218–225.
HEPATOLOGY, Vol. 40, No. 4, 2004 HONG ET AL. 941