Interim Guidelines in the Management and Prevention of Ebola Virus Disease as of 12012014
79
-
Upload
arthur-dessi-roman -
Category
Health & Medicine
-
view
234 -
download
0
Transcript of Interim Guidelines in the Management and Prevention of Ebola Virus Disease as of 12012014

2RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Good newsTo date, the Philippines remains EVD-free.
2
All 24 samples tested in RITM were
NEGATIVE.
3 asymptomatics – negative
1 urolithiasis
19 malaria
1 hypertensive emergency
DEPARTMENT OF HEALTH
RESEARCH INSTITUTE FOR TROPICAL
MEDICINE
Interim Guidelines on the Management and Prevention of
Ebola Virus DiseaseIn consultation with
Philippine Society for
Microbiology and
Infectious Diseases
Arthur Dessi Roman, MD, MTM, FPCP, DPSMID
PSMID 36th Annual Convention
November 28, 2014
4RESEARCH INSTITUTE FOR TROPICAL MEDICINE
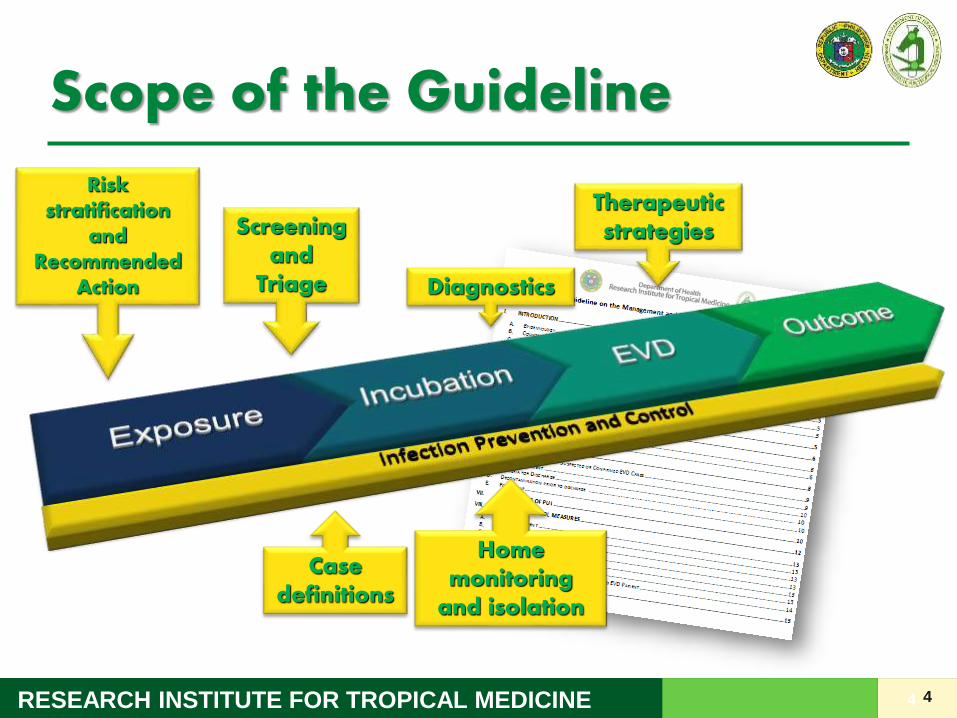
Scope of the Guideline
4
Risk stratification
and Recommended
Action
Screening and
Triage Diagnostics
Therapeutic strategies
Case definitions
Home monitoring
and isolation
5RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Objectives• To familiarize the participants with the process of screening
and triage for EVD
• To provide basic knowledge on the available diagnostics and therapeutic strategies for EVD
• To stratify the risk level for EVD transmission based on the nature of exposure of persons and provide recommendations for activities and monitoring
• To give an overview on infection control and prevention strategies in the management of EVD cases
5
6RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Disclaimer 1
6
Warning:Lecture NOT intended to make you intensivists.

7RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Disclaimer 2
7
Lecture NOT intended to make you a ONE-MAN EBOLA FIGHTING MACHINE
8RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Disclaimer 3
Ebola is an evolving disease.
Interim guidelines change as new information becomes available.
8
Keep yourself updated!

9RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Outline• Case definitions
• Laboratory testing
• Screening and triage
• Monitoring of PUI
• Clinical Management
9

10RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Outline• Case definitions
• Laboratory testing
• Screening and triage
• Monitoring of PUI
• Clinical Management
10

Case Definitions
11

12RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Person Under Investigation (PUI)
Any person who has resided in or traveled to any of the countries with ongoing widespread EVD transmission
in the past 21 days
OR
Any person who had significant contact with a suspect/probable/confirmed case in the past 21 days
12
Asymptomatic+
Epidemiologic risk factor

13RESEARCH INSTITUTE FOR TROPICAL MEDICINE 1313
14RESEARCH INSTITUTE FOR TROPICAL MEDICINE 14

15RESEARCH INSTITUTE FOR TROPICAL MEDICINE 15
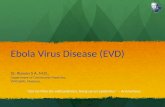
Site of the 2014 Western Africa Ebola outbreak

16RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Country Classification
16http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-
counts.html

17RESEARCH INSTITUTE FOR TROPICAL MEDICINE
What is significant contact?
Exposure to a suspect/probable/confirmed EVD case in at least one of the following ways:
• Sleeping in the same household
• Direct physical contact (while alive, during illness or after demise)
• Touched blood or body fluids during the illness;
• Touched the clothes/linen of the case during his or her illness;
• Being breastfed
• Direct handling of bats, rodents, or primates from disease-endemic areas
• Direct contact with specimens collected from an EVD patient or animal
• Has worked in a hospital where EVD cases are being treated.
17
18RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Suspect Case
• fever (actual or reported)
• headache
• nausea/ vomiting
• anorexia/loss of appetite
• intense fatigue
• Diarrhea
• abdominal pain
18
• muscle or joint pains
• difficulty swallowing or sore throat
• difficulty in breathing
• drowsiness or lethargy
• bleeding (from different sites such as gums, skin, eyes, urine, etc.)
• hiccups
PUI+
Signs and symptoms
19RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Probable EVD Case
Any suspected case evaluated by a clinician/epidemiologist having an epidemiological link with a confirmed case (where it was possible to collect specimen for laboratory confirmation).
OR
Any deceased suspected case (where it was not possible to collect specimen for laboratory confirmation) having an
epidemiological link with a confirmed case
19
20RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Laboratory Confirmed EVD Case
A suspected case with laboratory confirmation of infection with EVD.
20
Laboratory confirmation is done by the RITM Special
Pathogens Laboratory and Molecular Biology Laboratory.
The sample must test positive for the Ebolavirus antigen by
RT PCR.

21RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Discard/ Non-EVD Case
A suspected case with a negative laboratory result that was from a blood specimen collected
72 hours after onset of symptoms.
21
22RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Outline• Case definitions
• Laboratory testing
• Screening and triage
• Monitoring of PUI
• Clinical Management
22

23RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Laboratory testing for EVD
23
Antigen Antibodies
ELISA RT-PCR ELISA

24RESEARCH INSTITUTE FOR TROPICAL MEDICINE
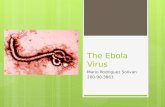
Martines et al. J Pathol 2014
Asymptomatic patients are not contagious!
Course of EVDNo virus before
symptoms

25RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Recommendation: EVD Testing
25
EVD test on admission
Confirmed EVD case
Positive YES
Done 72 hrs after onset of
illness?
Negative NO Asymptomatic?
Alternative Dx?
NO
Repeat EVD test 72 hrs after onset
of illnessPositive
YES
Non-EVD
Negative
26RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Outline• Case definitions
• Laboratory testing
• Screening and triage
• Monitoring of PUI
• Clinical Management
26

27RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Screening and Triage
To quickly identify people with a travel history to affected countries and provide proper home advice or
promptly isolate them if symptomatic
27
28RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Guidelines on Screening and Triage
• All health care facilities MUST designate a triage area.• Screen at all points of entry to health facility (to catch every patient
and visitors)• Train screening staff on what to say; e.g., Have you traveled
overseas in the last 21 days? Did you travel to (name countries with Ebola)?.
• Train screening staff on what to do when a PUI is identified (include contact numbers)
• Identify holding and isolation areas and who will perform further assessment of the patient.
• Ensure necessary precautions are observed.– Perform hand hygiene frequently– Follow standard precautions and wear the complete recommended
personal protective equipment (PPE) if there is any potential for contact with infectious blood and body fluids
28
29RESEARCH INSTITUTE FOR TROPICAL MEDICINE 29
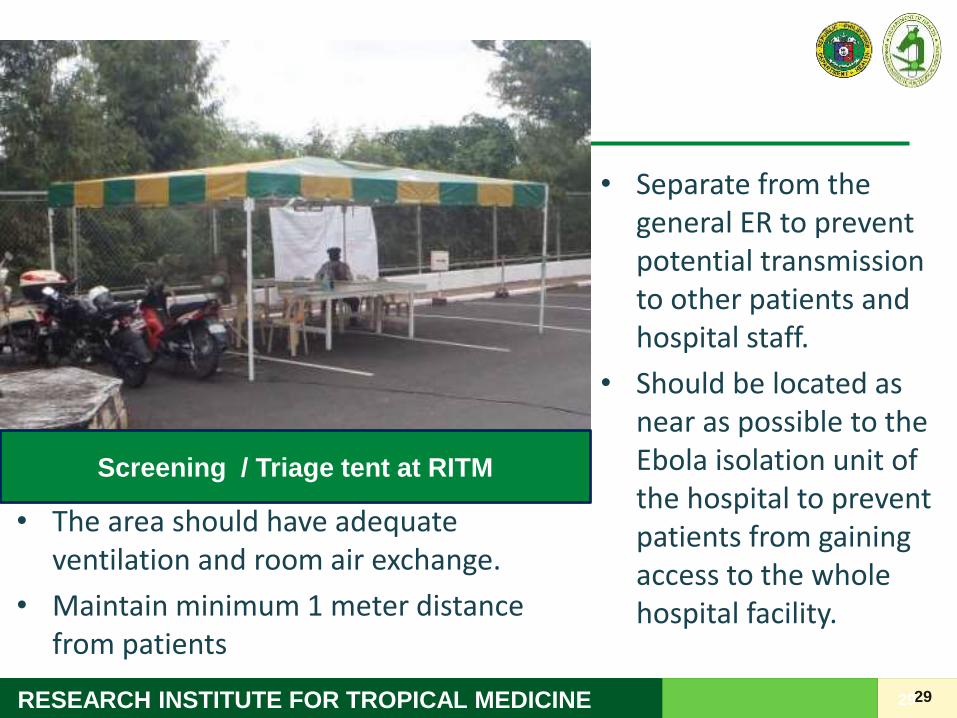
Screening / Triage tent at RITM
• Separate from the general ER to prevent potential transmission to other patients and hospital staff.
• Should be located as near as possible to the Ebola isolation unit of the hospital to prevent patients from gaining access to the whole hospital facility.
• The area should have adequate ventilation and room air exchange.
• Maintain minimum 1 meter distance from patients

30
Entrance to Isolation

31
Stairs going to isolation room

32RESEARCH INSTITUTE FOR TROPICAL MEDICINE 32Antechamber to isolation area

33

34

35
36RESEARCH INSTITUTE FOR TROPICAL MEDICINE 36

37RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Screening and Triage: Case
37
Travel
History
Contact
History
Fever or
other
symptoms
Assessment Testing for
EVD
Disposition
- - +Not considered for EVD No Treat per normal procedures
- + -PUI No Active monitoring for symptoms for 21 days
± Home quarantine based on risk level
+ - -PUI No Active monitoring for symptoms for 21 days
± Home quarantine based on risk level
+ + -PUI No Active monitoring for symptoms for 21 days
± Home quarantine based on risk level
- + +Suspect EVD Case Yes Admit to isolation room
Manage Appropriately
+ - +Suspect EVD Case Yes Admit to isolation room
Manage Appropriately
+ + +Suspect EVD Case Yes Admit to isolation room
Manage Appropriately
38RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Screening and Triage: Case
Amy and Gino, both 38, are a newly-wed couple who arrived home from an African adventure trip today. They started their trip 20 days ago and have visited the following countries: South Africa, Botswana, Liberia, Senegal. Amy came to the hospital seeking contraceptive advice.
38

39RESEARCH INSTITUTE FOR TROPICAL MEDICINE
PPE for Ebola• Repeated training is necessary
• Trained observer or “buddy” is
• Composed of:– Double gloves
– Boot covers
– Single-use impermeable (waterproof) gown or coverall
– Respirators (including either N95 respirators or powered air purifying respirator [PAPR])
– Single-use, full-face shield
– Hoods to ensure complete coverage of the head and neck
– Waterproof apron to cover the body up to the level of the calf.
39
40RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Who should wear PPE?• Persons who will have close contact with a person
with Ebola who has symptoms (e.g., doctors or nurses who will take care of Ebola patients)
• Persons who will have contact with patients withoutsymptoms (e.g., travelers without symptoms who are staying at home after returning from Ebola-affected countries)
40
Who should not wear PPE?

41RESEARCH INSTITUTE FOR TROPICAL MEDICINE
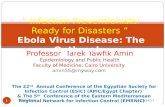
Martines et al. J Pathol 2014
No virus before
symptoms
Asymptomatic patients are not contagious!
Why?
42RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Outline• Case definitions
• Laboratory testing
• Screening and triage
• Monitoring of PUI
• Clinical Management
42
43RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of PUIs
Active monitoring
43
Active monitoring through direct observation (actual patient visit)
DOH personnel (such as members of the Regional Surveillance Units) will actively communicate with the PUIs and perform the twice daily assessment for the presence of symptoms and fever,
rather than relying solely on individuals to self-monitor and report symptoms if they develop
Direct active monitoring

44RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of PUIs
Quarantine
44
separation of a symptomatic individual reasonably believed to be infected with EVD from those not
infected to prevent spread of the disease
Isolation
separation and restriction of the movement of healthy people who were exposed to a contagious disease to
see if they become sick
45RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of PUIs
Home quarantine
45
staying at home and limiting
unnecessary travel or contact with the general community

46RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of PUIs
Home quarantine
46
To prevent the possible spread if the person
becomes sick with Ebola during travel.
To avoid unnecessary exposure to other local
diseases that may mimic some symptoms of
EVD
Audience participation:
These patients are asymptomatic.
Why do you have to separate themselves???
47RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of PUIs
Home quarantine
47
Includes restricted public activities

48RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of PUIs
• PUI symptomatic SUSPECT isolate admit
• Isolation precaution at once
– Isolate yourself inside a room
– No kissing, hugging or laying of hands
– Avoiding contact with body fluids
– Immediately place all used clothes and linen in a plastic bag . DO NOT dispose of this yourself, but inform DOH regarding its disposal.
– Inform DOH immediately.

49RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of PUIsThe following persons are NOT at risk of getting Ebola:
• Those who have been in a country with widespread Ebola transmission (Guinea, Liberia, Sierra Leone) or Mali
– Since MORE THAN 21 days ago
– with no symptoms of Ebola since leaving any of these countries.
• Aircraft or ship crew members who did not leave the immediate area of the airplane/ship and had no direct contact with anyone from the community during the entire time that they were present in a country with widespread Ebola virus transmission
• Contact with a healthy person with NO symptoms who had contact with a person with Ebola.
• Contact with a person with Ebola BEFORE the person developed symptoms.
• Those who have been in places WITHOUT widespread Ebola transmission (e.g. Spain, Texas, New York).

50RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of PUIsPeople with LOW (BUT NOT ZERO) risk:
NO direct contact with body fluids from a person with Ebola.
Brief proximity, such as being in the same room for a brief period of time, with a person with Ebola who has symptoms.
Traveled on an aircraft with a person with Ebola who has symptoms.
People with MODERATE RISK:
Direct contact, while using appropriate PPE, with a person with Ebola who has symptoms, or with the person’s body fluids.
Directly took care of patients in other healthcare settings.
With close contact in households, healthcare facilities, or the community, WITHOUT appropriate PPE, with a person with Ebola who
has symptoms. Close contact means being within approximately 3 feet (1 meter) of a person with Ebola for a long time.
People at HIGH RISK:
Exposed to blood or body fluids of a person with Ebola who has symptoms, through broken skin (like a wound or a needle prick) or
mucus membranes (such as splashes to the eyes, nose or mouth).
Exposed to the blood or body fluids (including but not limited to feces, saliva, sweat, urine, vomit, breast milk, and semen) of a
person with Ebola with symptoms while not wearing appropriate PPE.
Processed blood or body fluids of a person with Ebola who has symptoms without appropriate PPE or standard biosafety
precautions.
Direct contact with a dead body without appropriate PPE
Those who live in the immediate household and provide direct care to a person with Ebola who has symptoms.

51RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of PUIsRISKLEVEL
RECOMMENDED ACTIONS Other comments
Monitoring Travel
Restrictions
Restricted
Public Activities
Home quarantine
NO risk No No No No Not PUIsConsult physician for the diagnosisand management of other non-Eboladiseases if symptoms develop.
LOW risk Yes--Active monitoring in
general; Direct active for special
conditions *
No No No No restrictions including work.
MODERATErisk
Yes—direct active
Conditional Conditional Conditional Imposition of restrictions will depend on certain factors**
HIGH risk Yes—directactive
Yes Yes Yes Non-congregate public activities while maintaining a 3-foot distance from others may be permitted (e.g. jogging)
* Special conditions include (1) healthcare workers caring for symptomatic Ebola patients while wearing appropriate PPE and (2) for travellers on an aircraft with, and sitting within 3 feet of, a person with Ebola**Factors include: intensity of exposure (e.g., daily direct patient care versus intermittent visits to an Ebola treatment unit); point of time in the incubation period (risk falls substantially after 2 weeks); complete absence of symptoms; compliance with direct active monitoring; the individual's ability to immediately recognize and report symptom onset, self-isolate, and seek medical care; and the probability that the proposed activity would result in exposure to others prior to effective isolation.
52RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Outline• Case definitions
• Laboratory testing
• Screening and triage
• Monitoring of PUI
• Clinical Management
52
53RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Lessons Learned: Clinical Care
• In West Africa, limited clinical evaluations and essentially no laboratory testing due to the lack of any infrastructure to support this.
53
Ribner BS. Treating patients with Ebola virus infections in the US: lessons
learned. Presented at IDWeek, October 8, 2014. Philadelphia PA
Wolz A. Face to Face with Ebola — An Emergency Care Center in
Sierra Leone. N Engl J Med 2014; 371:1081-1083.

54RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Lessons Learned: Clinical Care
• Case fatality rate: 90% 70.8-74% 50% 37%
• Fever is the most common symptom
• Predominance of gastrointestinal symptoms
• Bleeding is rare
• Patients with <100,000 EBOV copies per mL had a lower case fatality rate than those with ≥10 million EBOV copies per mL (33% vs. 94%, P = 0.003).
54
1 WHO Ebola Response Team. N Engl J Med 2014;371:1481-1495.2 Schieffelin, J.S., et al., Clinical Illness and Outcomes in Patients with
Ebola in Sierra Leone. New England Journal of Medicine. 0(0): p. null.
55RESEARCH INSTITUTE FOR TROPICAL MEDICINE
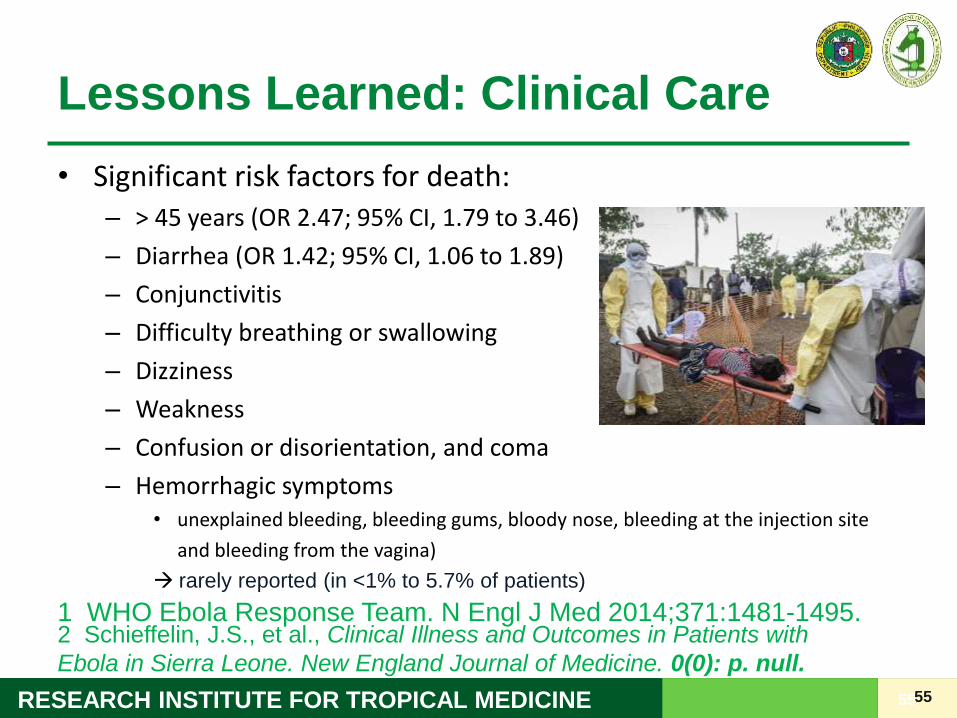
Lessons Learned: Clinical Care
• Significant risk factors for death:– > 45 years (OR 2.47; 95% CI, 1.79 to 3.46)
– Diarrhea (OR 1.42; 95% CI, 1.06 to 1.89)
– Conjunctivitis
– Difficulty breathing or swallowing
– Dizziness
– Weakness
– Confusion or disorientation, and coma
– Hemorrhagic symptoms• unexplained bleeding, bleeding gums, bloody nose, bleeding at the injection site
and bleeding from the vagina)
rarely reported (in <1% to 5.7% of patients)
55
1 WHO Ebola Response Team. N Engl J Med 2014;371:1481-1495.2 Schieffelin, J.S., et al., Clinical Illness and Outcomes in Patients with
Ebola in Sierra Leone. New England Journal of Medicine. 0(0): p. null.

56RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Lessons Learned: Clinical Care
• Laboratory findings associated with a fatal outcome
– Elevated levels of BUN, AST and creatinine
• Significant findings among EVD+ patients:
– Hyponatremia (127.32 SD 0.84)
– Hypokalemia (3.67 SD 0.11)
– Hypocalcemia (7.84 SD 0.15)
– Albumin (3.34 SD 0.10)
56
Schieffelin, J.S., et al., Clinical Illness and Outcomes in Patients with Ebola
in Sierra Leone. New England Journal of Medicine. 0(0): p. null.

58RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Lessons Learned: Clinical Care
• The Emory team observation of 2 patients:
– Severe hypovolemia low serum albumin and vascular leak with third spacing.
• Fluid losses in their patients were 5-10 L/day.
– Electrolyte losses were significant :• Low Na, K+, Ca++
• Lead to arrhythmias required IV and oral electrolyte correction
– Nutritional depletion was evident as well.
58
Ribner BS. Treating patients with Ebola virus infections in the US: lessons learned. Presented
at IDWeek, October 8, 2014. Philadelphia PA

59RESEARCH INSTITUTE FOR TROPICAL MEDICINE 59
It’s not all Ebola!
Acute febrile illness
+
Travel to (West) Africa
60RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Differential Diagnoses
• Malaria, Malaria, Malaria
• Typhoid fever
• Shigellosis
• Cholera
• Leptospirosis
• Plague
• Rickettsiosis
• Relapsing fever
• Meningitis
• Hepatitis
• Other viral hemorrhagic fevers
Source: WHO, 2014

61RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Other Tests
• Complete blood count with platelet count
• Biochemical tests – PT, PTT, ALT, AST, BUN, creatinine, Na, K, Ca
• Blood typing
• Chest X-ray
• Malarial smear
Reference: WHO, 2014; MSF VHF Manual, 2008

62RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Important
• Make sure that your institution is prepared to perform such tests.
– Is a protocol in place?
62

63RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Important
Reality check:
• Is your laboratory willing/ready to dedicate separate equipment or lab area to process EVD samples?
• Are your MedTechs willing/ready to do it?
• If there are spills, is your lab willing to close down for hours to decontaminate
63
64RESEARCH INSTITUTE FOR TROPICAL MEDICINE
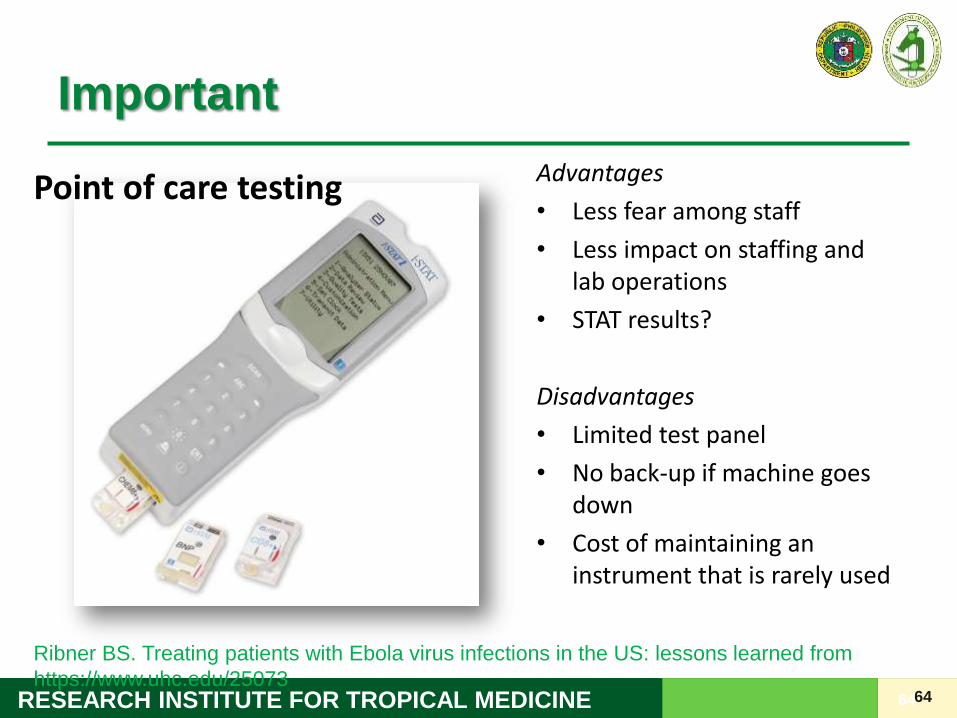
Important
Advantages
• Less fear among staff
• Less impact on staffing and lab operations
• STAT results?
Disadvantages
• Limited test panel
• No back-up if machine goes down
• Cost of maintaining an instrument that is rarely used
64
Point of care testing
Ribner BS. Treating patients with Ebola virus infections in the US: lessons learned from
https://www.uhc.edu/25073

65RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Treatment
• Objective: To provide optimal care to the patient with maximal protection of the health care personnel
• No FDA-approved vaccines or medicines (e.g., antiviral drug) available for Ebola.
• Treatment is mainly supportive and symptomatic.
– Fluid balance
– Nutrition
– Managing hemorrhagic complications

66RESEARCH INSTITUTE FOR TROPICAL MEDICINE
“Advanced” Supportive Treatment
• Maintaining adequate fluid balance– Providing IV fluid replacement and maintenance
• D5-containing fluids
• Plain crystalloid solution (LR or NSS)
– Fluid replacement should be adjusted to the hydration status and fluid requirement of the patient
• Emory’s caveat: No IV is to be started on patients unless the patient is in emergent need of volume replacement or reasonably expected to require IV medication.

67RESEARCH INSTITUTE FOR TROPICAL MEDICINE
“Advanced” Supportive Treatment
• Balancing electrolytes– Monitor Na, K, Ca, q3 days or as necessary
– IV or oral correction
– WOF: arrhythmias, weakness, paresthesia, ileus (may limit PO intake)

68RESEARCH INSTITUTE FOR TROPICAL MEDICINE
“Advanced” Supportive Treatment
• Management of hemorrhagic complications
– Transfusion of blood or blood components for severe bleeding and coagulation abnormalities
• May perform universal blood transfusion

69RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Supportive Treatment
• NUTRITIONAL SUPPORT, parenteral feeding (may include glutamine) when warranted
• Maintaining blood pressure with pressors
• Antipyretic and analgesics for fever and pain. DO NOT use aspirin or other nonsteroidal anti-inflammatory agents
• Anti-emetic against vomiting
• Anxiolytics to combat anxiety
• Monitoring of kidney function and renal replacement therapy if needed.
70RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Supportive Treatment
• Oxygen support if needed.
• Aggressive ventilatory support and invasive procedures (intubation and mechanical ventilation, etc.) may put healthcare workers at a much greater risk for exposure to the virus due to aerosolization.
• Performance of aerosol generating procedures (nebulization, BiPAP, suctioning, sputum induction) is highly discouraged.

71RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Other Treatments
• Antibiotics for superimposed or concomittant bacterial infections. – For CA-infections, ceftriaxone/ertapenem may be used. For HA-
infections, piperacillin-tazobactam or meropenem
– Secondary peritonitis and sepsis due to the loss of mucosal integrity and bacterial translocation(1) add metronidazole?
• Empiric co-artem administration if malarial smear cannot be done.
1 Kreuels, B., et al., A Case of Severe Ebola Virus Infection Complicated by Gram-
Negative Septicemia. New England Journal of Medicine
72RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Monitoring of Ebola tests
• Repeat Ebola antigen ELISA or RT - PCR test 72 hours after resolution of symptoms.
• If still positive, repeat the test every 3 days until 2 negative tests.
72

73RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Criteria for Discharge
Patients SHOULD ONLY be discharged if ALL of the following conditions are fulfilled:
• Two negative ELISA antigen tests
• Asymptomatic for at least 72 hours
73

74RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Follow-up
• Follow-up one week after discharge
• Repeat CBC and other blood tests that were abnormal.
74

75RESEARCH INSTITUTE FOR TROPICAL MEDICINE
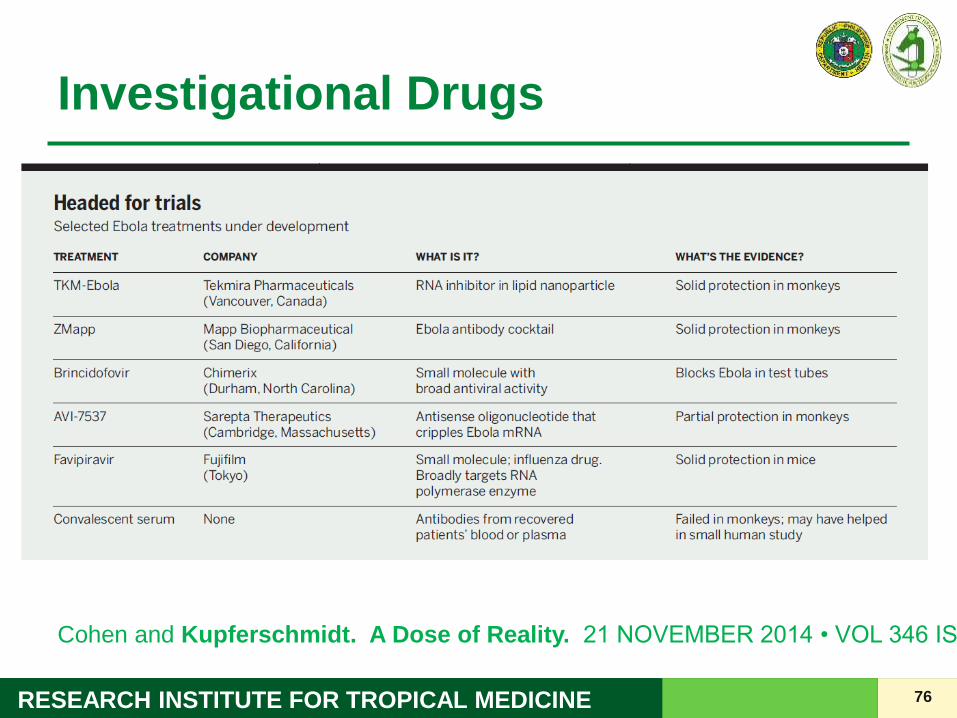
Investigational Drugs
• There have been no clinical trials of drugs in humans infected with Ebola virus
• Drugs have been used either in animal models in experimental trails and/or in individual people
• Clinical trials in humans naturally infected or exposed are needed to determine efficacy
76RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Investigational Drugs
Cohen and Kupferschmidt. A Dose of Reality. 21 NOVEMBER 2014 • VOL 346 ISSUE 6212

77RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Things to ponder on…
• In the clinical management of EVD, the patient may benefit more from the care of an intensivist/critical care specialist more than the expertise of an ID physician
• Remember that we are treading the unknown here…
– Notice: Clinical management in most guidelines is just ONE paragraph!
– There are many questions and issues that even experts do not have an answer.
77

78RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Things to ponder on…
• Balance between patient care and safety of HCWs
– How aggressive are you willing to go in your respective institutions?
• Intubate?
• Dialyse?
• Surgical procedures?
78

79RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Summary
79
• Efficient screening and triage is important.
• Home quarantine and monitoring strategies depend on the risk level for EVD transmission.
• Cornerstone of management in EVD is “advanced” supportive therapy which include:– Fluid and electrolyte balance
– Management of hemorrhagic complications
– Other supportive treatment including nutritional support and malaria management
• Novel treatments still warrant further investigation.
• Balance between patient care and healthcare worker safety should be achieved.
• Institutions should be ready to handle specific issues that may arise in the course of management in EVD via a multidisciplinary approach.

80RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Thank you!
80