Interferon-alpha as a treatment target in systemic lupus erythematosus
4
Joint Bone Spine 79 (2012) 113–116 Available online at www.sciencedirect.com Editorial Interferon-alpha as a treatment target in systemic lupus erythematosus article info Keywords: Systemic lupus erythematosus Interferon-alpha In this era of biological therapies and therapeutic monoclonal antibodies, interferon is a crucial treatment target for autoimmune diseases, including systemic lupus erythematosus (SLE) in partic- ular. The type I interferons are at the cross-roads between innate immunity and adaptive immunity, where they play a pivotal role not only in controlling viral infections, tumor cell growth, and angiogenesis [1], but also in initiating and perpetuating SLE and Sjögren’s syndrome. As early as 2003, Mary Crow suggested in an editorial for Arthritis and Rheumatism that interferon- may be a treatment target in SLE [2]. Since then, progress has been slow and cautious, given the antiviral and antitumoral effects of type 1 inter- ferons. However, several molecules have completed Phase I studies and are being evaluated in Phase II studies. In addition to human monoclonal antibodies against interferon-, promising approaches include antagonists of the interferon- receptor and blockade of the toll-like receptors (TLRs) sensitive to ssRNA or dsDNA (TLR-7 and TLR-9) such as nucleic acid analogs and tyrosine kinase inhibitors acting via the TLR signaling pathway. Finally, an original strategy consists in vaccination with a kinoid that induces the production of antibodies capable of neutralizing endogenous interferon-. 1. Rationale for targeting interferon- A 1979 study established that serum interferon- levels were elevated in patients with SLE [3]. Interferon- levels are also high in the cerebrospinal fluid of patients with neurological lupus manifes- tations. As with all cytokines, interferon- (13 different functional molecules encoded by at least 17 genes at 9p21) binds to a mem- brane receptor, triggering intracellular signal transduction after phosphorylation of the STAT-1 and STAT-2 proteins by the tyrosine kinases JAK-1 and TYK-2 [1]. STAT-1/STAT-2 and interferon regu- latory factor 9 (IRF-9) form a complex (interferon-stimulated gene factor 3, ISGF3), which binds to the nuclear DNA at the interferon- stimulated response element (ISRE) of the promoter region for interferon-sensitive genes. The result is either activation or inhi- bition of the transcription of these genes. The mRNAs produced by alternative splicing constitute the interferon signature, which can be evaluated by transcriptome analysis [4]. Many genes activated by interferons encode proteins involved in granulopoiesis [5]. In cross-sectional studies, 50% of adults with SLE had an interferon signature and this proportion was 80% or more in recent-onset pediatric SLE. A good overall correlation has been reported between the interferon score of peripheral blood cells and disease progres- sion as assessed based on the number of ACR classification criteria and on the SLEDAI and SLAM values [4,6,7]. Several genes induced by interferon- encode chemokines such as IP-10 (CXCL-10), MIP- 3 (CCL-19), and MCP-1 (CCL-2). Thus, the concentrations of these chemokines in the peripheral blood or urine may also reflect the overall activity of the disease and, more specifically, the poten- tial for renal disease progression (a possible biomarker for disease activity) [8,9]. Longitudinal studies are under way to evaluate the usefulness of these biomarkers, which are easier to use than RNA transcript measurements [10]. Interferon- overproduction in SLE is related to both genetic and environmental factors. Family studies showed type I inter- feron overproduction not only in patients with SLE, but also in their first-degree relatives. Genome-wide association studies demonstrated overrepresentation of several rare allelic variants in patients with SLE. About 25 susceptibility genes have been identi- fied to date (accounting for about 10% of the genetic determinism of SLE). Their allelic variants identified using single-nucleotide polymorphisms have individual odds ratios lower than 1.5, the only exception being the gene for interferon regulatory factor 5 (IRF-5), whose product is involved in TLR signal transduction and, probably to a lesser degree, in interferon- signal transduc- tion. Several products of SLE susceptibility genes are involved in innate immunity and, more specifically, in regulating the pro- duction of interferon-. In addition to IRF-5, examples include STAT-4 (signal transducer and activator of transcriptor 4), SPP-1 (osteopontin), IRAK-1 (interleukin-1 receptor-associated kinase, a serine/threonine protein kinase involved in TLR signal transduc- tion), and TREX-1 (3’ DNA repair exonuclease 1 also known as DNAse III, an enzyme capable of degrading DNA and therefore of blocking interferon induction via stimulation of TLR-9 or other cytosolic DNA receptors [11,12]). The environmental factors that stimulate interferon- produc- tion are nucleoprotein complexes (histones in nucleosomes and the ribonucleoproteins U-RNPs and Y-RNPs, i.e., Sm, U1-RNP, and SS- A/Ro52Kd or Ro60Kd) released during cell apoptosis and necrosis (e.g., keratinocytes damaged by ultraviolet radiation and lympho- cytes or neutrophils stimulated by various microorganisms such as the Epstein-Barr virus) [13] and microparticles released by neu- trophil extracellular traps (NETs) and very rich in nucleic acids and ribonucleoproteins [14,15]. Nucleic acids are potent interferon- inducers via TLR pathway activation (TLR-3 for dsRNA, TLR-7 for 1297-319X/$ – see front matter © 2011 Société franc ¸ aise de rhumatologie. Published by Elsevier Masson SAS. All rights reserved. doi:10.1016/j.jbspin.2011.10.013
-
Upload
olivier-meyer -
Category
Documents
-
view
216 -
download
0
Transcript of Interferon-alpha as a treatment target in systemic lupus erythematosus

E
I
a
KSI
aduinaSetcfamitTaco
1
ettmbpklfsibabb
1d
Joint Bone Spine 79 (2012) 113–116
Available online at
www.sciencedirect.com
ditorial
nterferon-alpha as a treatment target in systemic lupus erythematosus
r t i c l e i n f o
eywords:ystemic lupus erythematosusnterferon-alpha
In this era of biological therapies and therapeutic monoclonalntibodies, interferon is a crucial treatment target for autoimmuneiseases, including systemic lupus erythematosus (SLE) in partic-lar. The type I interferons are at the cross-roads between innate
mmunity and adaptive immunity, where they play a pivotal roleot only in controlling viral infections, tumor cell growth, andngiogenesis [1], but also in initiating and perpetuating SLE andjögren’s syndrome. As early as 2003, Mary Crow suggested in anditorial for Arthritis and Rheumatism that interferon-� may be areatment target in SLE [2]. Since then, progress has been slow andautious, given the antiviral and antitumoral effects of type 1 inter-erons. However, several molecules have completed Phase I studiesnd are being evaluated in Phase II studies. In addition to humanonoclonal antibodies against interferon-�, promising approaches
nclude antagonists of the interferon-� receptor and blockade of theoll-like receptors (TLRs) sensitive to ssRNA or dsDNA (TLR-7 andLR-9) such as nucleic acid analogs and tyrosine kinase inhibitorscting via the TLR signaling pathway. Finally, an original strategyonsists in vaccination with a kinoid that induces the productionf antibodies capable of neutralizing endogenous interferon-�.
. Rationale for targeting interferon-�
A 1979 study established that serum interferon-� levels werelevated in patients with SLE [3]. Interferon-� levels are also high inhe cerebrospinal fluid of patients with neurological lupus manifes-ations. As with all cytokines, interferon-� (13 different functional
olecules encoded by at least 17 genes at 9p21) binds to a mem-rane receptor, triggering intracellular signal transduction afterhosphorylation of the STAT-1 and STAT-2 proteins by the tyrosineinases JAK-1 and TYK-2 [1]. STAT-1/STAT-2 and interferon regu-atory factor 9 (IRF-9) form a complex (interferon-stimulated geneactor 3, ISGF3), which binds to the nuclear DNA at the interferon-timulated response element (ISRE) of the promoter region fornterferon-sensitive genes. The result is either activation or inhi-
ition of the transcription of these genes. The mRNAs produced bylternative splicing constitute the interferon signature, which cane evaluated by transcriptome analysis [4]. Many genes activatedy interferons encode proteins involved in granulopoiesis [5]. In297-319X/$ – see front matter © 2011 Société francaise de rhumatologie. Published by Eoi:10.1016/j.jbspin.2011.10.013
cross-sectional studies, 50% of adults with SLE had an interferonsignature and this proportion was 80% or more in recent-onsetpediatric SLE. A good overall correlation has been reported betweenthe interferon score of peripheral blood cells and disease progres-sion as assessed based on the number of ACR classification criteriaand on the SLEDAI and SLAM values [4,6,7]. Several genes inducedby interferon-� encode chemokines such as IP-10 (CXCL-10), MIP-3� (CCL-19), and MCP-1 (CCL-2). Thus, the concentrations of thesechemokines in the peripheral blood or urine may also reflect theoverall activity of the disease and, more specifically, the poten-tial for renal disease progression (a possible biomarker for diseaseactivity) [8,9]. Longitudinal studies are under way to evaluate theusefulness of these biomarkers, which are easier to use than RNAtranscript measurements [10].
Interferon-� overproduction in SLE is related to both geneticand environmental factors. Family studies showed type I inter-feron overproduction not only in patients with SLE, but alsoin their first-degree relatives. Genome-wide association studiesdemonstrated overrepresentation of several rare allelic variants inpatients with SLE. About 25 susceptibility genes have been identi-fied to date (accounting for about 10% of the genetic determinismof SLE). Their allelic variants identified using single-nucleotidepolymorphisms have individual odds ratios lower than 1.5, theonly exception being the gene for interferon regulatory factor5 (IRF-5), whose product is involved in TLR signal transductionand, probably to a lesser degree, in interferon-� signal transduc-tion. Several products of SLE susceptibility genes are involved ininnate immunity and, more specifically, in regulating the pro-duction of interferon-�. In addition to IRF-5, examples includeSTAT-4 (signal transducer and activator of transcriptor 4), SPP-1(osteopontin), IRAK-1 (interleukin-1 receptor-associated kinase, aserine/threonine protein kinase involved in TLR signal transduc-tion), and TREX-1 (3’ DNA repair exonuclease 1 also known asDNAse III, an enzyme capable of degrading DNA and therefore ofblocking interferon induction via stimulation of TLR-9 or othercytosolic DNA receptors [11,12]).
The environmental factors that stimulate interferon-� produc-tion are nucleoprotein complexes (histones in nucleosomes and theribonucleoproteins U-RNPs and Y-RNPs, i.e., Sm, U1-RNP, and SS-A/Ro52Kd or Ro60Kd) released during cell apoptosis and necrosis(e.g., keratinocytes damaged by ultraviolet radiation and lympho-cytes or neutrophils stimulated by various microorganisms such
as the Epstein-Barr virus) [13] and microparticles released by neu-trophil extracellular traps (NETs) and very rich in nucleic acids andribonucleoproteins [14,15]. Nucleic acids are potent interferon-�inducers via TLR pathway activation (TLR-3 for dsRNA, TLR-7 forlsevier Masson SAS. All rights reserved.
114 Editorial / Joint Bone Spine 79 (2012) 113–116
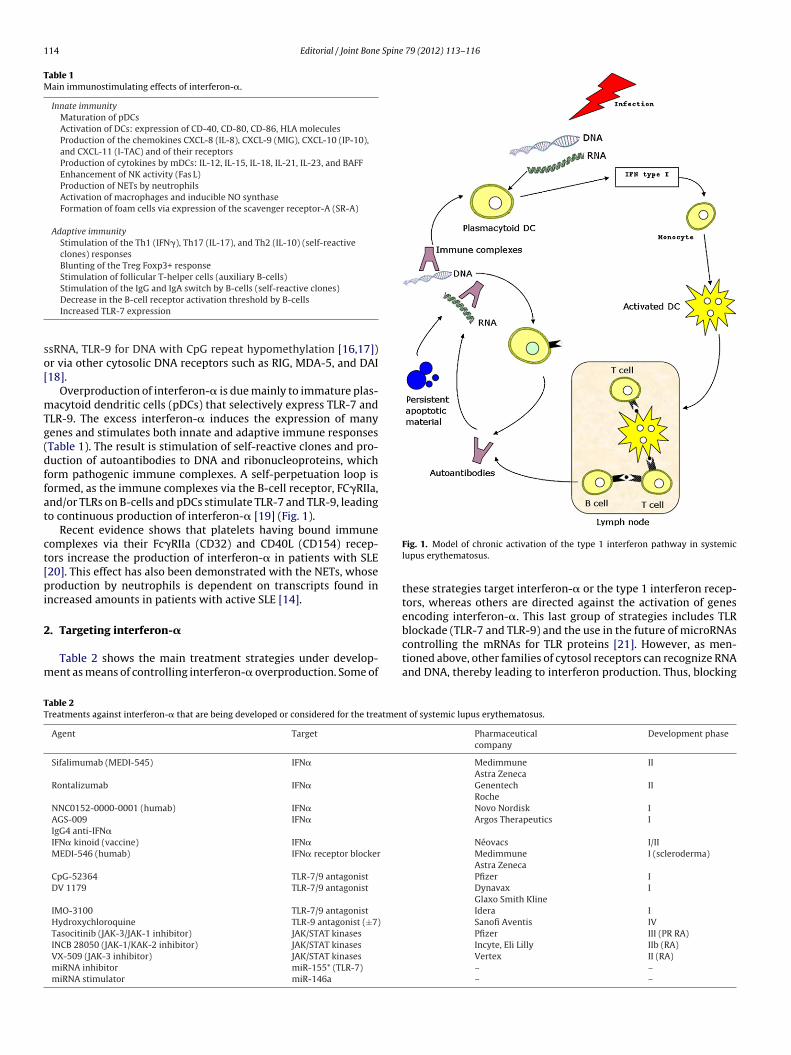
Table 1Main immunostimulating effects of interferon-�.
Innate immunityMaturation of pDCsActivation of DCs: expression of CD-40, CD-80, CD-86, HLA moleculesProduction of the chemokines CXCL-8 (IL-8), CXCL-9 (MIG), CXCL-10 (IP-10),and CXCL-11 (I-TAC) and of their receptorsProduction of cytokines by mDCs: IL-12, IL-15, IL-18, IL-21, IL-23, and BAFFEnhancement of NK activity (Fas L)Production of NETs by neutrophilsActivation of macrophages and inducible NO synthaseFormation of foam cells via expression of the scavenger receptor-A (SR-A)
Adaptive immunityStimulation of the Th1 (IFN�), Th17 (IL-17), and Th2 (IL-10) (self-reactiveclones) responsesBlunting of the Treg Foxp3+ responseStimulation of follicular T-helper cells (auxiliary B-cells)Stimulation of the IgG and IgA switch by B-cells (self-reactive clones)
so[
mTg(dffat
ct[pi
2
m
TT
Decrease in the B-cell receptor activation threshold by B-cellsIncreased TLR-7 expression
sRNA, TLR-9 for DNA with CpG repeat hypomethylation [16,17])r via other cytosolic DNA receptors such as RIG, MDA-5, and DAI18].
Overproduction of interferon-� is due mainly to immature plas-acytoid dendritic cells (pDCs) that selectively express TLR-7 and
LR-9. The excess interferon-� induces the expression of manyenes and stimulates both innate and adaptive immune responsesTable 1). The result is stimulation of self-reactive clones and pro-uction of autoantibodies to DNA and ribonucleoproteins, whichorm pathogenic immune complexes. A self-perpetuation loop isormed, as the immune complexes via the B-cell receptor, FC�RIIa,nd/or TLRs on B-cells and pDCs stimulate TLR-7 and TLR-9, leadingo continuous production of interferon-� [19] (Fig. 1).
Recent evidence shows that platelets having bound immuneomplexes via their Fc�RIIa (CD32) and CD40L (CD154) recep-ors increase the production of interferon-� in patients with SLE20]. This effect has also been demonstrated with the NETs, whoseroduction by neutrophils is dependent on transcripts found in
ncreased amounts in patients with active SLE [14].
. Targeting interferon-�
Table 2 shows the main treatment strategies under develop-ent as means of controlling interferon-� overproduction. Some of
able 2reatments against interferon-� that are being developed or considered for the treatmen
Agent Target
Sifalimumab (MEDI-545) IFN�
Rontalizumab IFN�
NNC0152-0000-0001 (humab) IFN�AGS-009IgG4 anti-IFN�
IFN�
IFN� kinoid (vaccine) IFN�MEDI-546 (humab) IFN� receptor blocker
CpG-52364 TLR-7/9 antagonistDV 1179 TLR-7/9 antagonist
IMO-3100 TLR-7/9 antagonistHydroxychloroquine TLR-9 antagonist (±7)Tasocitinib (JAK-3/JAK-1 inhibitor) JAK/STAT kinasesINCB 28050 (JAK-1/KAK-2 inhibitor) JAK/STAT kinasesVX-509 (JAK-3 inhibitor) JAK/STAT kinasesmiRNA inhibitor miR-155* (TLR-7)miRNA stimulator miR-146a
Fig. 1. Model of chronic activation of the type 1 interferon pathway in systemiclupus erythematosus.
these strategies target interferon-� or the type 1 interferon recep-tors, whereas others are directed against the activation of genesencoding interferon-�. This last group of strategies includes TLR
blockade (TLR-7 and TLR-9) and the use in the future of microRNAscontrolling the mRNAs for TLR proteins [21]. However, as men-tioned above, other families of cytosol receptors can recognize RNAand DNA, thereby leading to interferon production. Thus, blockingt of systemic lupus erythematosus.
Pharmaceuticalcompany
Development phase
MedimmuneAstra Zeneca
II
GenentechRoche
II
Novo Nordisk IArgos Therapeutics I
Néovacs I/IIMedimmuneAstra Zeneca
I (scleroderma)
Pfizer IDynavaxGlaxo Smith Kline
I
Idera ISanofi Aventis IVPfizer III (PR RA)Incyte, Eli Lilly IIb (RA)Vertex II (RA)– –– –

Spine
oieion
bctrstpAfipoup
itirobaafab4famutafptsctrmaaTwac[
P�acio
tit
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
Editorial / Joint Bone
nly the TLR-7/9 pathway may fail to suppress the production ofnterferon [22]. Most of the compounds listed in Table 2 are in thearly phases of development for SLE. The most advanced prelim-nary clinical results available as abstracts presented at meetingsr press releases are for either human monoclonal antibodies thateutralize interferon-� or the vaccine against interferon-�.
Rontalizumab is a humanized monoclonal antibody developedy Roche and Genentech. A Phase I study was done in the USA in 20enters in 60 patients with moderately active SLE requiring no morehan 20 mg of prednisone per day and no immunosuppressants. Theontalizumab doses ranged from 0.3 to 10 mg/kg intravenously orubcutaneously. Tolerance was satisfactory with no difference inhe infection rate compared to the placebo arm. During the study, 1atient had appendicitis and another was diagnosed with leukemia.bout 50% of the study patients had the interferon signature, which
aded in proportion to the rontalizumab dose, with the highest dosenducing the strongest response. Given the type of SLE in the studyatients and small sample size, the results do not constitute prooff efficacy on the clinical symptoms. A Phase II trial (ROSE) that isnder way in the USA, South America, and Europe will include 210atients with moderate-to-high disease activity.
Sifalimumab is a fully human monoclonal IgG1 againstnterferon-� that has been used both intravenously and subcu-aneously. Sifalimumab binds to specific amino acid residues ofnterferon-�-2a involved in binding to subunit-1 of the IFNAR1eceptor for interferons-� and -�. This event prevents formationf the interferon-�-2a/IFNAR1/2 heterotrimer. Sifalimumab alsoinds to the IFNAR2 receptor in the presence of interferon-�-2and prevents the internalization of interferon-�-2a. It partiallyntagonizes interferon-� and -� [23]. A multicenter randomizedour-arm Phase Ib trial tested three sifalimumab doses (0.3, 3,nd 10 mg/kg) in 161 patients with moderate-to-severe SLE (meanaseline SLEDAI, 10). Sifalimumab was given intravenously everyweeks for 26 weeks. At baseline, 75% of patients had an inter-
eron signature. The infection rates were similar in the treatmentrms and placebo arm (2.1 and 2.2 patients/year, respectively). Theain side effects were urinary tract infections, nausea, diarrhea,
pper airway infections, arthralgia, headaches, and a decline inhe hemoglobin level [24]. The patients with the highest SLEDAInd BILAG index values were also those with the strongest inter-eron signatures [25]. Inhibition of the interferon signature wasroportional to the sifalimumab dose and persisted throughout thereatment period in both the peripheral blood and the skin lesionamples [26]. Importantly, the SLEDAI decrease was not signifi-antly larger with the study drug than with the placebo. Antibodieso sifalimumab developed in 21% of patients. A Phase IIa multicenterandomized double-blind placebo-controlled trial with five treat-ent arms was conducted in 87 SLE patients (60% of Caucasians
nd 30% of blacks). Sifalimumab was given subcutaneously onceweek, once every 2 weeks, or once every 4 weeks, for 13 weeks.
he side effects were the same as in the Phase Ib trial. The once-a-eek regimen induced a 40% decrease in the interferon signature
s evaluated using proteomics. In this preliminary study, no clini-al benefits were recorded during the 3-month observation period27].
Anti-interferon vaccination using the IFN-K kinoid is at thehase I/II stage and is therefore not yet available [28]. Interferon--2b is injected in combination with the KLH carrier protein anddjuvant to induce the production of anti- interferon-� antibodiesapable of neutralizing the effects of all 13 subtypes of endogenousnterferon-� without interfering with the activity of interferon-�r � [29].
Thus, more than 30 years after learning that interferon con-ributes to the pathophysiology of SLE, we will soon know whethernhibiting this cytokine is a valid therapeutic strategy. Transla-ional research must be slow and cautious, since the crucial role
[
79 (2012) 113–116 115
for interferons in protecting against infections and tumors must bepreserved in order to minimize the risk of serious adverse eventsthat might limit the development of these innovative treatments[30].
Disclosure of interest
The author declares that he has no conflicts of interest concern-ing this article.
References
[1] Meyer O. Interferons and autoimmune disorders. Joint Bone Spine2009;76:464–73.
[2] Crow MK. Interferon-alpha: a new target for therapy in systemic lupus erythe-matosus? Arthritis Rheum 2003;48:2396–401.
[3] Hooks JJ, Moutsopoulos HM, Geis SA, et al. Immune interferon in the circulationof patients with autoimmune disease. N Engl J Med 1979;301:5–8.
[4] Baechler EC, Batliwalla FM, Karypis G, et al. Interferon-inducible gene expres-sion signature in peripheral blood cells of patients with severe lupus. Proc NatlAcad Sci USA 2003;100:2610–5.
[5] Bennett L, Palucka AK, Arce E, et al. Interferon and granulopoiesis signatures insystemic lupus erythematosus blood. J Exp Med 2003;197:711–23.
[6] Obermoser G, Pascual V. The interferon-alpha signature of systemic lupus ery-thematosus. Lupus 2010;19:1012–9.
[7] Petri M. Update on anti-phospholipid antibodies in SLE: the Hopkins’ LupusCohort. Lupus 2010;19:419–23.
[8] Bauer JW, Petri M, Batliwalla FM, et al. Interferon-regulated chemokines asbiomarkers of systemic lupus erythematosus disease activity: a validationstudy. Arthritis Rheum 2009;60:3098–107.
[9] Bauer JW, Baechler EC, Petri M, et al. Elevated serum levels of interferon-regulated chemokines are biomarkers for active human systemic lupuserythematosus. PLoS Medicine 2006;3:2274–84.
10] Fu Q, Chen X, Cui H, et al. Association of elevated transcript levels of interferon-inducible chemokines with disease activity and organ damage in systemiclupus erythematosus patients. Arthritis Res Ther 2008;10:R112.
11] Moser KL, Kelly JA, Lessard CJ, et al. Recent insights into the genetic basis ofsystemic lupus erythematosus. Genes Immun 2009;10:373–9.
12] Delgado-Vega AM, Alarcon-Riquelme ME, Kozyrev SV. Genetic associationsin type I interferon related pathways with autoimmunity. Arthritis Res Ther2010;12:S2.
13] Harley JB, James JA. Everyone comes from somewhere: systemic lupuserythematosus and Epstein-Barr virus induction of host interferon andhumoral anti-Epstein-Barr nuclear antigen 1 immunity. Arthritis Rheum2010;62:1571–5.
14] Garcia-Romo GS, Caielli S, Vega B, et al. Netting neutrophils are major inducersof type I IFN production in pediatric systemic lupus erythematosus. Sci TranslMed 2011;3:73ra20.
15] Hakkim A, Furnrohr BG, Amann K, et al. Impairment of neutrophil extracellulartrap degradation is associated with lupus nephritis. Proc Natl Acad Sci USA2010;107:9813–8.
16] Richez C, Blanco P, Rifkin I, et al. Role for toll-like receptors in autoim-mune disease: the example of systemic lupus erythematosus. Joint Bone Spine2011;78:124–30.
17] Baccala R, Hoebe K, Kono DH, et al. TLR-dependent and TLR-independentpathways of type I interferon induction in systemic autoimmunity. Nat Med2007;13:543–51.
18] Kontaki E, Boumpas DT. Innate immunity in systemic lupus erythematosus:sensing endogenous nucleic acids. J Autoimmun 2010;35:206–11.
19] Ronnblom L, Alm GV, Eloranta ML. The type I interferon system in the devel-opment of lupus. Semin Immunol 2011;23:113–21.
20] Duffau P, Seneschal J, Nicco C, et al. Platelet CD154 potentiates interferon-alphasecretion by plasmacytoid dendritic cells in systemic lupus erythematosus. SciTransl Med 2010;2:47ra63.
21] Zhou H, Huang X, Cui H, et al. miR-155 and its star-form partner miR-155*cooperatively regulate type I interferon production by human plasmacytoiddendritic cells. Blood 2010;116:5885–94.
22] Barrat FJ, Meeker T, Chan JH, et al. Treatment of lupus-prone mice with a dualinhibitor of TLR7 and TLR9 leads to reduction of autoantibody production andamelioration of disease symptoms. Eur J Immunol 2007;37:3582–6.
23] Riggs JM, Cibotti R, Liang M, et al. Mechanism of action of sifalimumab, ahuman neutralizing IFN alpha specific monoclonal antibody. Ann Rheum Dis2011;70:123.
24] Petri M, Wallace DJ, Spindler A, et al. Sifalimumab, a fully human anti-interferon-alpha monoclonal antibody in subjects with systemic lupuserythematosus (SLE): results of a phase 1B randomized, placebo-controlled,
dose-escalation intravenous study. Ann Rheum Dis 2011;70:125.25] Morehouse C, Liu Z, Higgs BW, et al. A type I IFN gene signature is used tomeasure PD and correlates with both IFN protein and two instruments used toassess disease activity at baseline in systemic lupus erythematosus in a phase1B clinical trial. Ann Rheum Dis 2011;70:78.

1 Spine
[
[
[
[
[
E-mail address: [email protected]
16 Editorial / Joint Bone
26] Yao Y, Richman L, Higgs BW, et al. Neutralization of interferon-alpha/beta-inducible genes and downstream effect in a phase I trial of an anti-interferon-alpha monoclonal antibody in systemic lupus erythematosus. Arthritis Rheum2009;60:1785–96.
27] Merrill JT, Chindalore V, Box J, et al. Results of a randomized, placebo-controlled,phase 2A study of sifalimumab, an anti-inerferon-alpha monoclonal antibody,administered subcutaneously in subjects with systemic lupus erythematosus.Ann Rheum Dis 2011;70:314.
28] Houssiau F, Raskhov R, Hachulla E, et al. Therapeutic against IFN alpha in lupuspatients: a phase I-II clinical study of IFN kinoid. Ann Rheum Dis 2011;70:738.
29] Zagury D, Le Buanec H, Mathian A, et al. IFNalpha kinoid vaccine-induced neu-
tralizing antibodies prevent clinical manifestations in a lupus flare murinemodel. Proc Natl Acad Sci USA 2009;106:5294–9.30] Dupuis S, Jouanguy E, Al-Hajjar S, et al. Impaired response to interferon-alpha/beta and lethal viral disease in human STAT1 deficiency. Nat Genet2003;33:388–91.
79 (2012) 113–116
Olivier Meyer ∗
Service de rhumatologie, CHU Bichat, 46, rueHenri-Huchard, 75018 Paris, France
∗ Corresponding author. Tel.: +33 1 40 25 74 03;fax: +33 1 42 29 06 88.
5 October 2011
Available online11 December 2011