Integration of Basic-Clinical Sciences, PBL, CBL, and … software (IBM Corp., ... of Iowa College...
10
March 2016 ■ Journal of Dental Education 281 Predoctoral Dental Education Integration of Basic-Clinical Sciences, PBL, CBL, and IPE in U.S. Dental Schools’ Curricula and a Proposed Integrated Curriculum Model for the Future Satheesh Elangovan, BDS, ScD, DMSc; Shankar Rengasamy Venugopalan, BDS, DMSc, PhD; Sreedevi Srinivasan, BDS, ScD; Nadeem Y. Karimbux, DMD, MMSc; Paula Weistroffer, DDS, MS; Veerasathpurush Allareddy, BDS, MMSc, MBA, MHA, PhD Abstract: The integration of basic and clinical sciences in dental curricula enhances the application of basic science principles to clinical decision making and improves students’ critical thinking. The aim of this study was to define the characteristics of U.S. dental schools’ curricula with regard to level of course integration and degree of incorporation of problem-based and case-based learning. A second aim was to propose a dental curriculum that supports effective integration of courses and addresses some of the concerns facing academic dentistry. A survey was sent to 58 academic deans in U.S. dental schools. The survey included questions about integrating courses in the schools’ curricula and major changes in curricular structure or teaching pedagogy that respondents anticipated in the immediate future. A total of 31 schools responded to the survey, for a 53.4% response rate. The results showed that three-quarters of the responding schools still teach basic and clinical sciences separately, although 61.3% reported having an integrated curriculum. Among the responding schools, 16 had a PBL component integrated into their curricula (two had inte- grated PBL in all courses and 14 used a hybrid PBL approach). Two schools had CBL integrated in all courses, and ten had CBL integrated in >75% of courses. Only slightly more than half agreed that their curricula foster students’ thinking “outside the box.” Faculty shortages and lack of protected time and resources were the most frequent reasons given for a lack of integrated courses. The integrated model proposed in this article has the potential to provide a low stress environment for students and to address important issues like faculty shortages. Dr. Elangovan is Assistant Professor in Periodontics, University of Iowa College of Dentistry & Dental Clinics; Dr. Venugopalan is Assistant Professor in Orthodontics, University of Missouri-Kansas City School of Dentistry; Dr. Srinivasan is Assistant Professor in Orthodontics, University of Iowa College of Dentistry & Dental Clinics; Dr. Karimbux is Associate Dean for Aca- demic Affairs and Professor of Periodontics, Tufts University School of Dental Medicine; Dr. Weistroffer is Clinical Associate Professor in Periodontics, University of Iowa College of Dentistry & Dental Clinics; and Dr. Allareddy is Associate Professor in Orthodontics, University of Iowa College of Dentistry & Dental Clinics. Direct correspondence to Dr. Satheesh Elango- van, University of Iowa College of Dentistry & Dental Clinics, S464, 801 Newton Road, Iowa City, IA 52242; 319-335-7543; [email protected]. Keywords: dental education, curriculum, critical thinking, problem-based learning, case-based learning, basic sciences Submitted for publication 6/22/15; accepted 8/19/15 I n 1995, the Institute of Medicine (IOM) report Dental Education at the Crossroads: Challenges and Change emphasized the need for moderniza- tion of courses in dental education, elimination of redundancy, and implementation of integrated curri- cula. 1 The authors of that report defined an integrated dental curriculum as “an integrated basic and clinical science curriculum that provides clinically relevant education in the basic sciences and scientifically based education in clinical care.” The continuing need for innovation in dental curricula was empha- sized by a series of articles commissioned by the American Dental Education Association Commis- sion on Change and Innovation in Dental Education (ADEA CCI) and published in the Journal of Dental Education in the first decade of the twenty-first century. These articles were republished together in a collection titled Beyond the Crossroads: Change and Innovation in Dental Education. 2 One of the important goals of dental curricular design—affirmed in both the IOM report and ADEA CCI articles—is to incorporate a multidisciplinary theme supporting one common goal: to graduate knowledgeable, skilled dentists. 3 More often than
Transcript of Integration of Basic-Clinical Sciences, PBL, CBL, and … software (IBM Corp., ... of Iowa College...
March 2016 ■ Journal of Dental Education 281
Predoctoral Dental Education
Integration of Basic-Clinical Sciences, PBL, CBL, and IPE in U.S. Dental Schools’ Curricula and a Proposed Integrated Curriculum Model for the FutureSatheesh Elangovan, BDS, ScD, DMSc; Shankar Rengasamy Venugopalan, BDS, DMSc, PhD; Sreedevi Srinivasan, BDS, ScD; Nadeem Y. Karimbux, DMD, MMSc; Paula Weistroffer, DDS, MS; Veerasathpurush Allareddy, BDS, MMSc, MBA, MHA, PhDAbstract: The integration of basic and clinical sciences in dental curricula enhances the application of basic science principles to clinical decision making and improves students’ critical thinking. The aim of this study was to define the characteristics of U.S. dental schools’ curricula with regard to level of course integration and degree of incorporation of problem-based and case-based learning. A second aim was to propose a dental curriculum that supports effective integration of courses and addresses some of the concerns facing academic dentistry. A survey was sent to 58 academic deans in U.S. dental schools. The survey included questions about integrating courses in the schools’ curricula and major changes in curricular structure or teaching pedagogy that respondents anticipated in the immediate future. A total of 31 schools responded to the survey, for a 53.4% response rate. The results showed that three-quarters of the responding schools still teach basic and clinical sciences separately, although 61.3% reported having an integrated curriculum. Among the responding schools, 16 had a PBL component integrated into their curricula (two had inte-grated PBL in all courses and 14 used a hybrid PBL approach). Two schools had CBL integrated in all courses, and ten had CBL integrated in >75% of courses. Only slightly more than half agreed that their curricula foster students’ thinking “outside the box.” Faculty shortages and lack of protected time and resources were the most frequent reasons given for a lack of integrated courses. The integrated model proposed in this article has the potential to provide a low stress environment for students and to address important issues like faculty shortages.
Dr. Elangovan is Assistant Professor in Periodontics, University of Iowa College of Dentistry & Dental Clinics; Dr. Venugopalan is Assistant Professor in Orthodontics, University of Missouri-Kansas City School of Dentistry; Dr. Srinivasan is Assistant Professor in Orthodontics, University of Iowa College of Dentistry & Dental Clinics; Dr. Karimbux is Associate Dean for Aca-demic Affairs and Professor of Periodontics, Tufts University School of Dental Medicine; Dr. Weistroffer is Clinical Associate Professor in Periodontics, University of Iowa College of Dentistry & Dental Clinics; and Dr. Allareddy is Associate Professor in Orthodontics, University of Iowa College of Dentistry & Dental Clinics. Direct correspondence to Dr. Satheesh Elango-van, University of Iowa College of Dentistry & Dental Clinics, S464, 801 Newton Road, Iowa City, IA 52242; 319-335-7543; [email protected].
Keywords: dental education, curriculum, critical thinking, problem-based learning, case-based learning, basic sciences
Submitted for publication 6/22/15; accepted 8/19/15
In 1995, the Institute of Medicine (IOM) report Dental Education at the Crossroads: Challenges and Change emphasized the need for moderniza-
tion of courses in dental education, elimination of redundancy, and implementation of integrated curri-cula.1 The authors of that report defined an integrated dental curriculum as “an integrated basic and clinical science curriculum that provides clinically relevant education in the basic sciences and scientifically based education in clinical care.” The continuing need for innovation in dental curricula was empha-sized by a series of articles commissioned by the
American Dental Education Association Commis-sion on Change and Innovation in Dental Education (ADEA CCI) and published in the Journal of Dental Education in the first decade of the twenty-first century. These articles were republished together in a collection titled Beyond the Crossroads: Change and Innovation in Dental Education.2
One of the important goals of dental curricular design—affirmed in both the IOM report and ADEA CCI articles—is to incorporate a multidisciplinary theme supporting one common goal: to graduate knowledgeable, skilled dentists.3 More often than

282 Journal of Dental Education ■ Volume 80, Number 3
were obtained from the ADEA Directory of Institu-tional Members and Association Officers (dim.adea.org). Additional contact information, when needed, was obtained by searching the websites of individual dental institutions.
Survey questions were designed to obtain in-formation about the overall integration of basic and clinical science courses in the schools’ predoctoral curricula and to assess the integration of problem-based, case-based, and interprofessional learning components. We asked about perceived challenges in integrating dental curricula as well. By using open-ended questions, we also attempted to elucidate information about major planned changes in schools’ curricula.
All data were exported to an SPSS dataset. Simple descriptive statistics were used to summa-rize survey responses. Two subset analyses were conducted for responses between schools that had some degree of problem-based learning (PBL) versus schools that did not and between schools that had <25% case-based learning (CBL) versus schools that had >75% CBL. Chi-square tests were used to determine statistically significant differences in re-sponses between the two groups across the subsets. In situations in which the assumptions of chi-square tests were not met, Fischer’s exact tests were used. For the global tests of association, a p-value of <0.05 was deemed to be statistically significant. All statis-tical analyses were conducted using SPSS Version 22.0 software (IBM Corp., New York, NY, USA).
ResultsA total of 31 schools’ academic deans out of the
58 contacted responded to the survey, for a response rate of 53.4%. Of these 31 schools, 16 had a PBL component integrated into their curricula: two had integrated PBL in all courses, and 14 used a hybrid PBL approach. Two schools had CBL integrated in all courses, and ten had CBL integrated in >75% of courses.
Responses to questions on current organiza-tion of curricula are summarized in Table 1. Overall, 45.2% of respondents had discipline-based courses with individual course directors; 22.6% had inte-grated course blocks with a single course director; 9.7% had integrated course blocks with multiple course directors from within the dental field; 25.8% had integrated course blocks with multiple course directors from multiple disciplines (including phy-
not, dental curricula end up being convoluted and disjointed, creating a heavy academic workload that lacks connections and clinical relevance.4 Traditional curricula are also blamed for taking a passive learn-ing approach, which may thwart critical thinking and discourage acquisition of lifelong learning abilities.4 Hendricson emphasized that most courses in predoctoral dental education in the United States are internally well organized but remain within their respective silos in the overall curriculum.5 This organization allows little time for students to make sense of the information taught in multiple back-to-back courses, which are offered mostly by different departments or units. In some universities, efforts have been made to break down these disciplinary silos to promote curricular coherence.6,7
The most recent comprehensive survey of North American predoctoral dental curricula was conducted in 2009, reporting results from 50 U.S. and five Canadian dental schools.8 The aim of our study was to contribute to the body of knowledge on evolving U.S. dental curricula by conducting a survey of dental schools regarding such characteristics as the extent of curricular integration and incorporation of interprofessional education. In addition, we sought to propose a model for an integrated dental curriculum that is both interdisciplinary and interprofessional in nature.
MethodsThe study was granted exempt status after be-
ing reviewed by the University of Iowa Institutional Review Board (#201501727). A 17-item question-naire was developed by two of the authors (SE and VA). One faculty member (author PW), who leads interprofessional learning efforts at The University of Iowa College of Dentistry & Dental Clinics, re-viewed and edited the questionnaire for content and sequence. (The questionnaire is available from the corresponding author.) The survey was conducted using SurveyMonkey, an online survey portal.
The questionnaire was emailed in May 2015 to 58 associate deans for education or academic affairs at U.S. dental schools. Although there were more than 58 U.S. dental schools at the time, some newer institutions that have more than one campus had only one academic dean who managed identical curricula across campuses. In such cases, we counted those multiple campuses as one although they are separate institutions. The email addresses for the target group

March 2016 ■ Journal of Dental Education 283
to interprofessional education in 48.4% of respond-ing schools in their third year and in 45.2% in their fourth year. Two respondents mentioned that some amount of interprofessional education was integrated into their schools’ curricula in all years. There were no statistically significant differences in responses pertaining to integration of interprofessional educa-tion between institutions that had PBL or CBL or not.
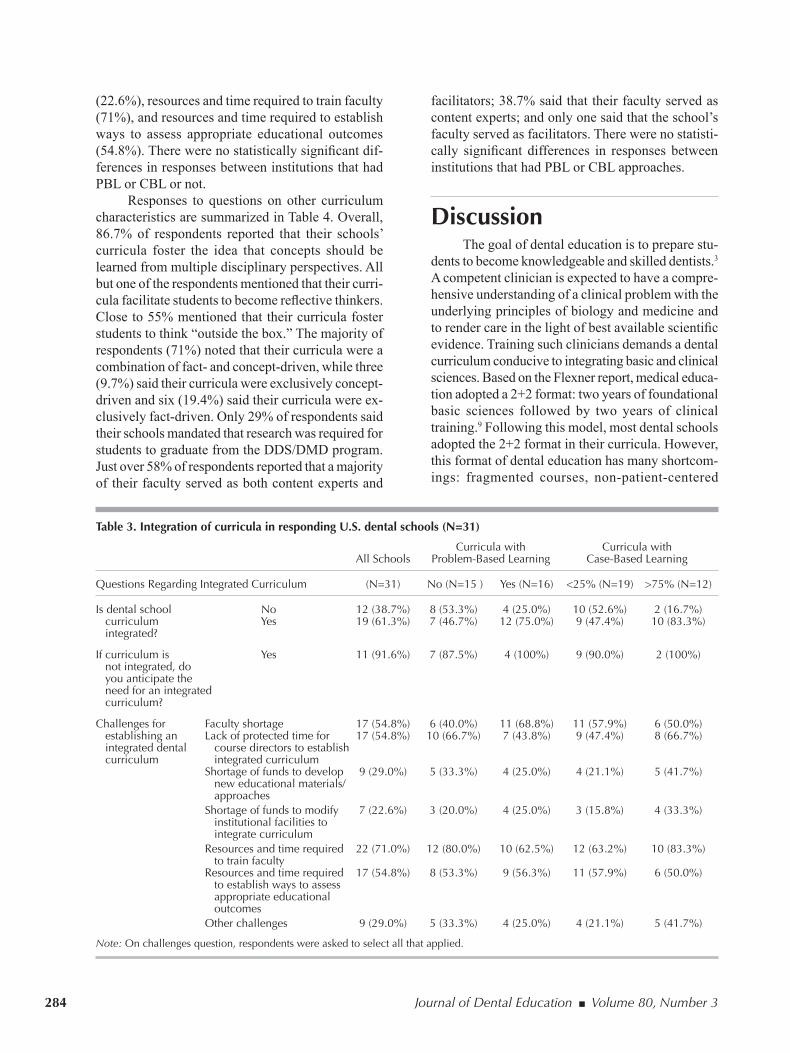
Responses to questions on integrated curri-cula are summarized in Table 3. Overall, 61.3% of responding schools reported having an integrated curriculum. Among those that did not have an in-tegrated curriculum, 57.9% said they anticipated a need for an integrated curriculum. Some of the chal-lenges reported in establishing an integrated dental curriculum included the following: faculty shortage (54.8%), lack of protected time for course directors to establish an integrated curriculum (54.8%), short-age of funds to develop new educational materials/approaches (29%), shortage of funds to modify in-stitutional facilities in order to integrate curriculum
sicians); and 74.2% exposed their students to bio-medical/basic science courses and clinical courses separately. There was no statistically significant difference in responses between PBL and non-PBL schools. Schools that had <25% CBL were more likely to have integrated course blocks with a single course director when compared to schools that had >75% CBL (36.8% versus 0; p=0.026). The majority of schools (84.2%) that had CBL in <25% of courses exposed their students to biomedical/basic sciences courses and clinical courses separately as compared to 58.3% of schools that indicated using CBL in >75% of courses. However, this association was not statistically significant.
Responses to questions on interprofessional education are summarized in Table 2. The vast majority of responding schools (90.3%) reported having interprofessional education integrated into their curricula. In 58.1% of the responding schools, students were exposed to interprofessional education in the first and second years. Students were exposed
Table 1. Organizational characteristics of curricula of responding U.S. dental schools (N=31)
Curricula with Curricula with All Schools Problem-Based Learning Case-Based Learning
Organization (N=31) No (N=15 ) Yes (N=16) <25% (N=19) >75% (N=12)
Fragmented courses with individual course 14 (45.2%) 7 (46.7%) 7 (43.8%) 10 (52.6%) 4 (33.3%) directors Integrated course blocks with a single course 7 (22.6%) 4 (26.7%) 3 (18.8%) 7 (36.8%) 0 director Integrated course blocks with multiple course 3 (9.7%) 0 3 (18.8%) 1 (5.3%) 2 (16.7%) directors from within the dental field Integrated course blocks with multiple course 8 (25.8%) 3 (20.0%) 5 (31.3%) 3 (15.8%) 5 (41.7%) directors from various disciplines (including physicians)Students exposed to biomedical/basic science 23 (74.2%) 11 (73.3%) 12 (75.0%) 16 (84.2%) 7 (58.3%) courses and clinical courses separately
Note: Percentages may not total 100% because of rounding.
Table 2. Interprofessional education (IPE) in curricula of responding U.S. dental schools (N=31)
Curricula with Curricula with All Schools Problem-Based Learning Case-Based Learning
IPE Characteristics (N=31) No (N=15 ) Yes (N=16) <25% (N=19) >75% (N=12)
Is IPE integrated into curriculum? No 3 (9.7%) 3 (20.0%) 0 3 (15.8%) 0 Yes 28 (90.3%) 12 (80.0%) 16 (100%) 16 (84.2%) 12 (100%)
During which years are students First 18 (58.1%) 8 (53.3%) 10 (62.5%) 10 (52.6%) 8 (66.7%) exposed to IPE? Second 18 (58.1%) 9 (60.0%) 9 (56.3%) 12 (63.2%) 6 (50.0%) Third 15 (48.4%) 8 (53.3%) 7 (43.8%) 9 (47.4%) 6 (50.0%) Fourth 14 (45.2%) 7 (46.7%) 7 (43.8%) 9 (47.4%) 5 (41.7%)
Note: On second question, respondents were asked to select all that applied.
284 Journal of Dental Education ■ Volume 80, Number 3
Table 3. Integration of curricula in responding U.S. dental schools (N=31)
Curricula with Curricula with All Schools Problem-Based Learning Case-Based Learning
Questions Regarding Integrated Curriculum (N=31) No (N=15 ) Yes (N=16) <25% (N=19) >75% (N=12)
Is dental school No 12 (38.7%) 8 (53.3%) 4 (25.0%) 10 (52.6%) 2 (16.7%) curriculum Yes 19 (61.3%) 7 (46.7%) 12 (75.0%) 9 (47.4%) 10 (83.3%) integrated?
If curriculum is Yes 11 (91.6%) 7 (87.5%) 4 (100%) 9 (90.0%) 2 (100%) not integrated, do you anticipate the need for an integrated curriculum?
Challenges for Faculty shortage 17 (54.8%) 6 (40.0%) 11 (68.8%) 11 (57.9%) 6 (50.0%) establishing an Lack of protected time for 17 (54.8%) 10 (66.7%) 7 (43.8%) 9 (47.4%) 8 (66.7%) integrated dental course directors to establish curriculum integrated curriculum Shortage of funds to develop 9 (29.0%) 5 (33.3%) 4 (25.0%) 4 (21.1%) 5 (41.7%) new educational materials/ approaches Shortage of funds to modify 7 (22.6%) 3 (20.0%) 4 (25.0%) 3 (15.8%) 4 (33.3%) institutional facilities to integrate curriculum Resources and time required 22 (71.0%) 12 (80.0%) 10 (62.5%) 12 (63.2%) 10 (83.3%) to train faculty Resources and time required 17 (54.8%) 8 (53.3%) 9 (56.3%) 11 (57.9%) 6 (50.0%) to establish ways to assess appropriate educational outcomes Other challenges 9 (29.0%) 5 (33.3%) 4 (25.0%) 4 (21.1%) 5 (41.7%)
Note: On challenges question, respondents were asked to select all that applied.
(22.6%), resources and time required to train faculty (71%), and resources and time required to establish ways to assess appropriate educational outcomes (54.8%). There were no statistically significant dif-ferences in responses between institutions that had PBL or CBL or not.
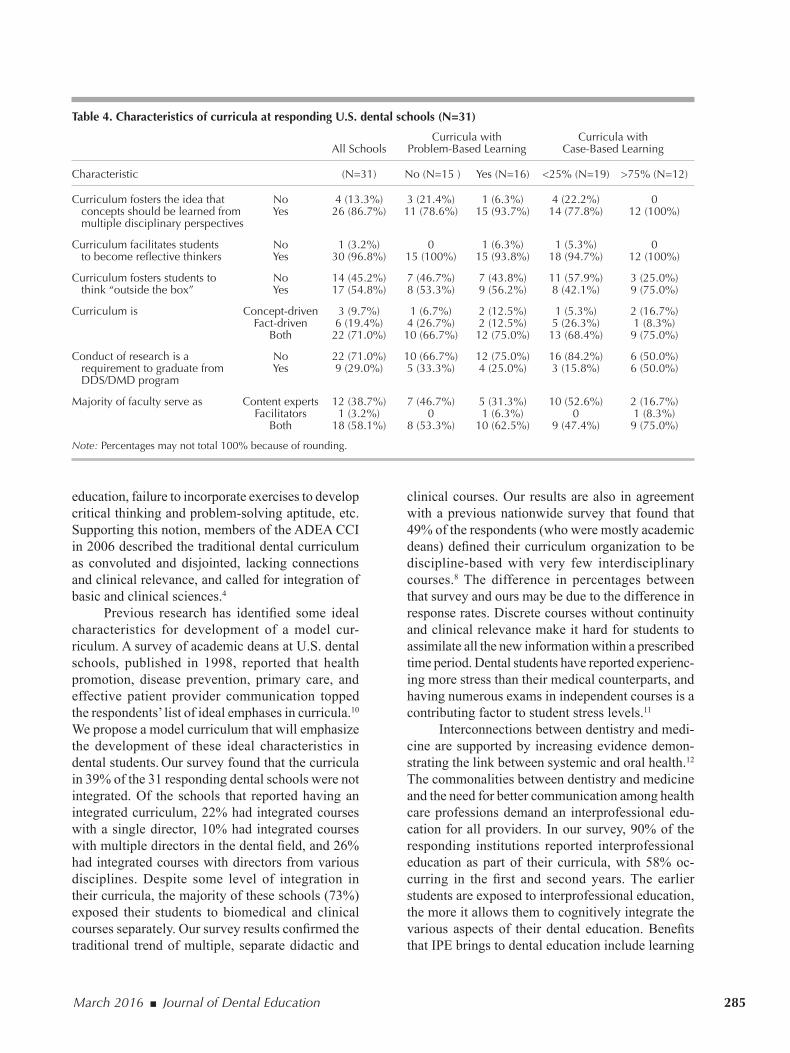
Responses to questions on other curriculum characteristics are summarized in Table 4. Overall, 86.7% of respondents reported that their schools’ curricula foster the idea that concepts should be learned from multiple disciplinary perspectives. All but one of the respondents mentioned that their curri-cula facilitate students to become reflective thinkers. Close to 55% mentioned that their curricula foster students to think “outside the box.” The majority of respondents (71%) noted that their curricula were a combination of fact- and concept-driven, while three (9.7%) said their curricula were exclusively concept-driven and six (19.4%) said their curricula were ex-clusively fact-driven. Only 29% of respondents said their schools mandated that research was required for students to graduate from the DDS/DMD program. Just over 58% of respondents reported that a majority of their faculty served as both content experts and
facilitators; 38.7% said that their faculty served as content experts; and only one said that the school’s faculty served as facilitators. There were no statisti-cally significant differences in responses between institutions that had PBL or CBL approaches.
Discussion The goal of dental education is to prepare stu-
dents to become knowledgeable and skilled dentists.3 A competent clinician is expected to have a compre-hensive understanding of a clinical problem with the underlying principles of biology and medicine and to render care in the light of best available scientific evidence. Training such clinicians demands a dental curriculum conducive to integrating basic and clinical sciences. Based on the Flexner report, medical educa-tion adopted a 2+2 format: two years of foundational basic sciences followed by two years of clinical training.9 Following this model, most dental schools adopted the 2+2 format in their curricula. However, this format of dental education has many shortcom-ings: fragmented courses, non-patient-centered
March 2016 ■ Journal of Dental Education 285
clinical courses. Our results are also in agreement with a previous nationwide survey that found that 49% of the respondents (who were mostly academic deans) defined their curriculum organization to be discipline-based with very few interdisciplinary courses.8 The difference in percentages between that survey and ours may be due to the difference in response rates. Discrete courses without continuity and clinical relevance make it hard for students to assimilate all the new information within a prescribed time period. Dental students have reported experienc-ing more stress than their medical counterparts, and having numerous exams in independent courses is a contributing factor to student stress levels.11
Interconnections between dentistry and medi-cine are supported by increasing evidence demon-strating the link between systemic and oral health.12 The commonalities between dentistry and medicine and the need for better communication among health care professions demand an interprofessional edu-cation for all providers. In our survey, 90% of the responding institutions reported interprofessional education as part of their curricula, with 58% oc-curring in the first and second years. The earlier students are exposed to interprofessional education, the more it allows them to cognitively integrate the various aspects of their dental education. Benefits that IPE brings to dental education include learning
education, failure to incorporate exercises to develop critical thinking and problem-solving aptitude, etc. Supporting this notion, members of the ADEA CCI in 2006 described the traditional dental curriculum as convoluted and disjointed, lacking connections and clinical relevance, and called for integration of basic and clinical sciences.4
Previous research has identified some ideal characteristics for development of a model cur-riculum. A survey of academic deans at U.S. dental schools, published in 1998, reported that health promotion, disease prevention, primary care, and effective patient provider communication topped the respondents’ list of ideal emphases in curricula.10 We propose a model curriculum that will emphasize the development of these ideal characteristics in dental students. Our survey found that the curricula in 39% of the 31 responding dental schools were not integrated. Of the schools that reported having an integrated curriculum, 22% had integrated courses with a single director, 10% had integrated courses with multiple directors in the dental field, and 26% had integrated courses with directors from various disciplines. Despite some level of integration in their curricula, the majority of these schools (73%) exposed their students to biomedical and clinical courses separately. Our survey results confirmed the traditional trend of multiple, separate didactic and
Table 4. Characteristics of curricula at responding U.S. dental schools (N=31)
Curricula with Curricula with All Schools Problem-Based Learning Case-Based Learning
Characteristic (N=31) No (N=15 ) Yes (N=16) <25% (N=19) >75% (N=12)
Curriculum fosters the idea that No 4 (13.3%) 3 (21.4%) 1 (6.3%) 4 (22.2%) 0 concepts should be learned from Yes 26 (86.7%) 11 (78.6%) 15 (93.7%) 14 (77.8%) 12 (100%) multiple disciplinary perspectives
Curriculum facilitates students No 1 (3.2%) 0 1 (6.3%) 1 (5.3%) 0 to become reflective thinkers Yes 30 (96.8%) 15 (100%) 15 (93.8%) 18 (94.7%) 12 (100%)
Curriculum fosters students to No 14 (45.2%) 7 (46.7%) 7 (43.8%) 11 (57.9%) 3 (25.0%) think “outside the box” Yes 17 (54.8%) 8 (53.3%) 9 (56.2%) 8 (42.1%) 9 (75.0%)
Curriculum is Concept-driven 3 (9.7%) 1 (6.7%) 2 (12.5%) 1 (5.3%) 2 (16.7%) Fact-driven 6 (19.4%) 4 (26.7%) 2 (12.5%) 5 (26.3%) 1 (8.3%) Both 22 (71.0%) 10 (66.7%) 12 (75.0%) 13 (68.4%) 9 (75.0%)
Conduct of research is a No 22 (71.0%) 10 (66.7%) 12 (75.0%) 16 (84.2%) 6 (50.0%) requirement to graduate from Yes 9 (29.0%) 5 (33.3%) 4 (25.0%) 3 (15.8%) 6 (50.0%) DDS/DMD program
Majority of faculty serve as Content experts 12 (38.7%) 7 (46.7%) 5 (31.3%) 10 (52.6%) 2 (16.7%) Facilitators 1 (3.2%) 0 1 (6.3%) 0 1 (8.3%) Both 18 (58.1%) 8 (53.3%) 10 (62.5%) 9 (47.4%) 9 (75.0%)
Note: Percentages may not total 100% because of rounding.
286 Journal of Dental Education ■ Volume 80, Number 3
collected data from 50 U.S. dental schools.8 While our findings cannot therefore be taken as representa-tive of U.S. dental education in general, the data from our sample are suggestive, providing at least some indication of curricular developments over the past five years, including the continuing need for greater integration of the basic and clinical sciences.
Proposed Integrated Curriculum Model
It is evident from our survey that curricular integration in U.S. dental schools varies significantly. These findings underscore the need for a novel cur-riculum that allows integration of basic and clinical sciences seamlessly and prepares students to face real-life challenges. We are proposing a model for a dental curriculum that allows for integration at the macro (program) and micro (courses) level (Figure 1). This model has the potential to eliminate unwant-ed redundancy and also provides clinically relevant information to students from early on in their training. Other advantages of this type of integrated curricu-lum are listed in Table 5. It has several differences from the conventional discipline-based curriculum.
The curriculum that we are proposing has three major blocks: 1) Systems Biology and Medicine, 2) Health Care Concepts and Technology, and 3) Dental Sciences. All three blocks involve patient-centered learning with a knowledge domain from various disciplines (Figure 1). Students will be exposed to all three blocks during their first and second years. With regard to time allotment, in the first year, emphasis will be placed on the first two blocks, while emphasis will be placed on dental sciences in the second year.
The Systems Biology and Medicine (SBM) block encompasses a knowledge domain from basic and clinical sciences, such as cellular and molecular biology, anatomy and embryology, physiology and biochemistry, pharmacology, diagnosis and radiol-ogy, microbiology and pathology, general medicine, and nursing. In the SBM block, students will learn about organ systems with a focus on integrated knowledge domain from different areas. For ex-ample, the cardiovascular system will have learning material from anatomy, physiology and biochemistry, associated pathological conditions, their link to oral health, and the pharmacology of drugs to treat various disease conditions. Students will also have real-life patient cases pertaining to that organ system to di-agnose and treatment plan under the supervision of a
to be collaborative, working as a team player, better understanding of the oral-systemic connection, and comprehending the referral and insurance systems on a much more global scale. Despite the presence of interprofessional education, the majority of dental schools still keep the basic sciences separate from the clinical sciences, according to our survey results.
Indisputably, critical thinking and problem-solving are essential components of dental training. Of the institutions that responded to our survey, 87% reported that their curricula foster learning concepts from multiple disciplinary perspectives, and 97% reported that their curricula facilitate students to become reflective thinkers. Only slightly more than half of the respondents agreed that their curriculum fosters thinking “outside the box” in students, and a large majority of responding institutions did not require students to conduct some form of research as part of their curricular requirements.
PBL is a teaching methodology that fosters self-directed learning and allows students to acquire knowledge with an analytical approach to solve a clinical problem. In 2001, Hendricson and Cohen noted the traditional surgical-restorative dominance in dental education and the skepticism in academic dentistry for change from lectures to PBL format as reasons for lack of enthusiasm in incorporating PBL.13 This reluctance may be changing since almost half of the respondents to our survey reported that their dental curricula incorporate some form of PBL. CBL is another teaching methodology that allows for effective integration of biomedical sciences and multidisciplinary courses with a clinical focus.14 We also know that multidisciplinary teaching is most ef-fective when it is made relevant to clinical practice. It allows for the engagement of faculty and students in critical thinking as they apply their knowledge to the management of clinical problems.15 Despite clear evidence that the CBL approach improves clinical skills,16 our survey found that only a few institutions utilize CBL to its maximum benefit.
In our survey, 25% of the responding 31 dental schools reported having integrated course blocks with interdisciplinary instructors that included physicians. An even smaller number of schools reported having integrated course blocks organized by a group of interdisciplinary dental faculty members.
A limitation of this survey study is the low response rate, collecting information from less than half of the current 65 U.S. dental schools. This lower response also complicates our attempt to compare our results with those of the Haden et al. study, which

March 2016 ■ Journal of Dental Education 287
performance was integration of basic and clinical sci-ences with an emphasis on a patient-centered problem.
In a traditional dental curriculum, knowledge domains in the SBM block occur in independent courses directed by individual faculty members, not encouraging the learners to integrate the informa-tion and not providing time for them to assimilate what was learned. In our proposed curriculum, by contrast, students receive integrated information from different knowledge domains and apply the learned knowledge to solve a real-life patient case concurrently. This approach requires faculty mem-bers from different disciplines to come together to concept map the knowledge domain and integrate them, thereby helping students to appreciate the
faculty member. This model provides an opportunity for students to understand a clinical problem through basic sciences, thereby allowing them to cognitively integrate all the knowledge domains.
An observational study conducted in Dutch medical schools comparing the diagnostic perfor-mance of students trained in conventional, problem-based, and integrated medical curricula found that the students trained in the integrated and problem-based frameworks made more accurate diagnoses than the students trained in the conventional curriculum.17 The second- and third-year students in an integrated curriculum were also superior to their second- and third-year counterparts trained in other curricula. That study concluded that the key to accurate diagnostic
Figure 1. Proposed integrated and interdisciplinary dental curriculum model

288 Journal of Dental Education ■ Volume 80, Number 3
these patient cases, they will acquire knowledge in the disciplines of dental sciences: preventive and interceptive dentistry (pedodontics and orthodontics), restorative dentistry (operative, prosthodontics, and endodontics), and surgical dentistry (oral surgery and periodontics). For example, students will be pre-sented with a case of an adult patient with a history of systemic problems and a mutilated dentition with decayed, missing, and sensitive teeth. Through such cases, students will learn to identify problems and understand the restorative and surgical approaches to treat the patient. A traditional dental curriculum includes fragmented courses in the dental sciences and expects students to integrate, on their own, the information learned in the preclinical years to treat patients during the clinical years. Unlike the con-ventional curriculum, our proposed one is patient-centered, and the various avenues of knowledge are acquired through a patient case.
Our proposed curriculum has many advantages. Strategically pooling the existing basic and clinical courses into blocks (as shown in Figure 1) will allow students to gain knowledge in a low-stress, stream-lined fashion with the utmost clinical applicability. Currently, when students are registered for multiple courses concurrently, their focus is more likely to be on the successful completion of course requirements and examinations, rather than on the understanding and application of the learned concepts. A recent systematic review reported that examinations and grades are an important academic factor causing stress in dental students, generating fears of failing and being unable to catch up in the overcrowded dental curriculum.18 Instead of weeks- or months-
connection between basic biology and medicine and its impact on systemic and oral health. When basic science courses such as human physiology or biochemistry are linked with clinical situations, it will improve the student’s appreciation of the need to understand the basic sciences. Providing such an environment may also nurture students’ interest in basic or translational research. A block type curricu-lum will give the directors enough time and space to incorporate case-based discussions from year one of the curriculum. This strategy is in line with Garvey et al.’s argument, back in 2000, for exposing dental students to patient-oriented curricula from year one.14
The Health Care Concepts and Technology (HCCT) block will focus primarily on public health and the integrated knowledge domain from various disciplines as shown in Figure 1. The aims of this block are to expose dental students to the concepts of evidence-based practice of dentistry, help them identify knowledge gaps in the etiology of patho-logical conditions, and develop research projects grounded in scientific principles to address those knowledge gaps. This will help students to develop critical thinking and problem-solving abilities with a translational focus.
In the third block, on dental sciences, students will be introduced to patient cases with dental prob-lems in pediatric, adolescent, adult, and geriatric age groups. Concurrently, they will perform laboratory exercises in the disciplines of restorative dentistry (operative, prosthodontics, and endodontics). Stu-dents will learn to evaluate the patient as a whole, collect diagnostic records, identify problems, and develop a comprehensive treatment plan. Through
Table 5. Potential advantages of the proposed curriculum model
Advantages
Organization will provide opportunity for continuous reinforcement of basic science concepts in a clinically applicable fashion.
The resulting low stress learning environment will be more conducive to developing critical thinking and problem-solving skills.
A group of directors from various fields will bring different perspectives to a block that will be truly interdisciplinary, interprofessional, and applied in nature.
Pooling all relevant courses into a block will reduce unwanted redundancy in the curriculum.
Due to fewer blocks versus multiple courses, structure will allow easy monitoring of curricular activities and allow for changes to be made more easily.
Case-based clinically relevant basic science information will likely kindle students’ interest in basic as well as translational science.
Structure may ease faculty shortage problem.

March 2016 ■ Journal of Dental Education 289
that responded to our survey, courses were still fragmented with multiple course directors. In nearly 75% of the responding schools, students are exposed to basic science and clinical courses separately. By contrast, our findings suggest that interprofessional learning is being widely incorporated. Although chal-lenges exist in implementing a curriculum that better integrates the basic and clinical sciences, we believe that, in the long run, an integrated curriculum like the one proposed in this article not only offers a highly clinically relevant education for students but also has the potential to address some of those challenges.
AcknowledgmentsThe authors would like to thank the respondents
to our survey.
DisclosureThe authors report no conflicts of interest with
respect to this study.
REFERENCES1. Feld MJ, ed. Dental education at the crossroads: challenges
and change. An Institute of Medicine report. Washington, DC: National Academies Press, 1995.
2. American Dental Education Association Commission on Change and Innovation in Dental Education. Beyond the crossroads: change and innovation in dental education. Washington, DC: American Dental Education Association, 2010.
3. Howard KM, Stewart T, Woodall W, et al. An integrated curriculum: evolution, evaluation, and future direction. J Dent Educ 2009;73(8):962-71.
4. Pyle M, Andrieu SC, Chadwick DG, et al. The case for change in dental education. J Dent Educ 2006;70(9):921-4.
5. Hendricson WD. Changes in educational methodologies in predoctoral dental education: finding the perfect intersec-tion. J Dent Educ 2012;76(1):118-41.
6. Stark JS. On defining coherence and integrity in the cur-riculum. Res Higher Educ 1986;24(4):433-6.
7. Briggs CL, Patston PA, Knight GW, et al. Fitting form to function: reorganization of faculty roles for a new dental curriculum and its governance. J Dent Educ 2013;77(1): 4-16.
8. Haden NK, Hendricson WD, Kassebaum DK, et al. Cur-riculum change in dental education, 2003-09. J Dent Educ 2010;74(5):539-57.
9. Flexner A. Medical education in the United States and Canada: a report to the Carnegie Foundation for the Ad-vancement of Teaching. Bulletin no. 4. Boston: Updyke, 1910.
10. Graber DR, O’Neil EH, Bellack JP, et al. Academic deans’ perceptions of current and ideal curriculum emphases. J Dent Educ 1998;62(11):911-8.
11. Murphy RJ, Gray SA, Sterling G, et al. A compara-tive study of professional student stress. J Dent Educ 2009;73(3):328-37.
long courses, a one- or two-year block will provide some breathing room for students, allow them to assimilate information, and apply it in a creative and analytical fashion. Furthermore, having blocks that encompass multiple disciplines will allow multiple faculty members from different areas of dentistry and beyond to come together to design and implement a truly interdisciplinary training program. If the case scenarios are developed by a team of basic science and clinical faculty members from different disci-plines, they will integrate the knowledge domains and bring unique perspectives. It will also be an ideal platform to incorporate interprofessional education, including representatives from other health care pro-fessions (such as nursing, pharmacy, and medicine) in the block course design.
In addition to curricular restructuring, we propose to evaluate a student’s cognitive integration through written examinations using case presentation and problem-solving type questions. In our model, there is enough flexibility for a more formative type of evaluation throughout years one and two and a summative evaluation by the end of year two. This structure should result in a low-stress learning envi-ronment, allowing students to be creative with their focus shifted to critical thinking and problem-solving rather than reception, memorization, and regurgita-tion of the information that occurs on most current examinations.
There are also challenges in integrating dental curricula. When the respondents to our survey were asked to rate these challenges, we found that a lack of resources and time required to train faculty topped the list, followed by faculty shortage, lack of protected time to accomplish curriculum change, and short-age in resources. Other challenges included coming up with newer strategies to assess credit hours for students and proper acknowledgment of faculty con-tribution and efforts within the team. Though such challenges exist, we believe that a truly integrated, interdisciplinary, and interprofessional dental cur-riculum will provide excellent experiences for our students and ultimately produce clinical leaders in our field.
ConclusionAs we expected, our survey found extensive
variation in curricular structures across U.S. dental schools, but the need for greater integration in dental curricula persists. In close to half of the 31 schools

290 Journal of Dental Education ■ Volume 80, Number 3
16. Prystowsky JB, DaRosa DA, Thompson JA. Promoting collaborative teaching in clinical education. Teach Learn Med 2001;13(3):148-52.
17. Schmidt HG, Machiels-Bongaerts M, Hermans H, et al. The development of diagnostic competence: comparison of a problem-based, an integrated, and a conventional medical curriculum. Acad Med 1996;71(6):658-64.
18. Alzahem AM, van der Molen HT, Alaujan AH, et al. Stress amongst dental students: a systematic review. Eur J Dent Educ 2011;15(1):8-18.
12. Barnett ML. The oral-systemic disease connection: an update for the practicing dentist. J Am Dent Assoc 2006;137(Suppl):5S-6S.
13. Hendricson WD, Cohen PA. Oral health in the 21st cen-tury: implications for dental and medical education. Acad Med 2001;76(12):1181-207.
14. Garvey MT, O’Sullivan M, Blake M. Multidisciplinary case-based learning for undergraduate students. Eur J Dent Educ 2000;4:165-8.
15. Behar-Horenstein LS, Dolan TA, Courts FJ, Mitchell GS. Cultivating critical thinking in the clinical learning environment. J Dent Educ 2000;64(8):610-5.