Integrating the chronic-care model: implementation of ... · (SMA) program for gestational diabetes...
1
Karen Holder, FNP – Clinician Lead for Shared Medical Appointment; Kelly McCue, BS, MPH - Diabetes Program Coordinator; Jessica Chambers – Health Educator and Audrey Wall – Health Educator • A shared medical model is being implemented in a rural clinic. • Inclusion criteria: target population includes pregnant patients diagnosed with type 2 diabetes mellitus, gestational diabetes and patients at risk of developing gestational diabetes. • Exclusion criteria include a diagnosis of cognitive impairment, a psychiatric diagnosis of schizophrenia/psychosis and/or any behavioral problem which might interfere with group participation and discussion. • Session format: a 4-week curriculum (every other week) developed in collaboration with the healthcare provider and diabetes educator • Each session is 2- 2.5 hours and includes a prenatal visit with the healthcare provider; healthy snacks included • The team members involved in SMA include • Healthcare provider (lead) • Program coordinator (diabetes educator) • Two health coaches to co-facilitate the group • A medical assistant to assist with documentation and charting • The invitation is sent two weeks prior to the SMA session. • HIPPA and voluntary disclosure of personal medical info in a group will be addressed in each session. • Billing will be done individually for each patient as a CPT level 3 (99213) or 4 (99214) depending on the complexity of the medical decision making (AAFP, 2017). Methods • The Chronic Care Model (CCM) of disease management provides a useful framework for establishing group shared medical appointments. Background and Significance Format of Shared Medical Appointment • The goal of this study is to develop and implement a Shared Medical Appointment (SMA) program for gestational diabetes patients. • A group medical care model (SMA) is an important inter-disciplinary care delivery innovation to complement the individual medical visit. • SMAs focus on education for patients on their chronic disease and enhancement of self- management skills. Purpose • SMA model implementation date: March 31, 2017 • Review of literature demonstrates that SMA is an innovative practice model that: • increased patient satisfaction, • improved clinical outcomes/ health behaviors, • improved provider-patient relationships, • improved quality of life, • decreased emergency care visits, • decreased referrals to specialists, • improved medication adherence, • increased self-efficacy. •Outcomes to be measured: • Clinical outcomes: blood sugar, blood pressure and weight gain • Patient satisfaction and quality of life survey •Conclusion: It is anticipated that the SMA program will improve gestational diabetes-related clinical outcomes and quality of life and empower patients to learn how to better care for themselves. Summary/Implications American Academy of Family Physicians. (2017). Coding for group visits. Retrieved from http://www.aafp.org/practice- management/payment/coding/group-visits.html. American Diabetes Association. (2016). Standards of medical care in diabetes. Diabetes Care, 39(1). S1-112. Retrieved from http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf Improving Chronic Illness Care (n.d.). The chronic care model. Retrieved from http://www.improvingchroniccare.org/index.php?p=The_Chronic_Care_Model&s=2 Kirsh, S., Watts, S., Pascuzzi, K., O'Day, M.E., Davidson, D., Strauss, G., Kern, E., Aron, D.C. (2007). Shared medical appointments based on the chronic care model: a quality improvement project to address the challenges of patients with diabetes with high cardiovascular risk. Quality and Safety in Health Care, 16(5), 349-353. Retrieved from http://qualitysafety.bmj.com/content/16/5/349.long Kirsh, S.R., Lawrence, R.H. & Aron, D.C. (2008). Tailoring an intervention to the context and system redesign related to the intervention: case study of implementing shared medical appointments for diabetes. Implementation Science, 3, 34-48. doi: 10.1186/1748-5908-3-34 Millermaier, E., Neuwirth, Z., Noffsinger, E. & Prescott D. (2009). Shared medical appointments: a proven health care delivery model. Retrieved from: http://www.massmed.org/Continuing-Education-and-Events/Conference-Proceeding-Archive/Shared-Medical- Appointments--Harvard-PPT-(pdf)/ Stellefson, M., Dipnarin,e K., & Stopka, C. (2013). The chronic care model and diabetes management in US primary care settings: a systematic review. Preventing Chronic Disease, 10, 120180. doi: http://dx.doi.org/10.5888/pcd10.120180 Watts, S. A., Lawrence, R. H., & Kern, E. (2011). Diabetes nurse case management training program: enhancing care consistent with the chronic care and patient-centered medical home models. Clinical Diabetes, 29(1), 25-33. doi: http://dx.doi.org.libproxy.nau.edu/10.2337/diaclin.29.1.25 References Integrating the chronic-care model: implementation of shared medical appointments for patients with gestational diabetes College of Health & Human Services - School of Nursing - Northern Arizona University Despina Ciocanel, RN, BSN, MSBS, MADM Kirsch et al., 2007 Acknowledgments Improving Chronic Illness Care, n.d. Session Curriculum Activity Session 1. Introduction to gestational diabetes Diabetic A1c visuals Fetal and placenta models Session 2. Healthy eating in gestational diabetes Reading food labels Sugar in beverages models Session 3. Stress and exercise Types of physical exercises (short practice) Breathing exercise Session 4. After pregnancy Measuring blood sugar Delivery activity Millermaier et al., 2009 0 10 20 30 40 50 60 70 80 90 Overall Access to Care Overall Visits Overall Sensitivity to Patients Needs Wait Before Going to Exam Room Wait in Exam Room Likelyhood to Recommend Provider Likelyhood to Recommend Practice SMA Non-SMA
Transcript of Integrating the chronic-care model: implementation of ... · (SMA) program for gestational diabetes...
Karen Holder, FNP – Clinician Lead for Shared Medical Appointment; Kelly McCue, BS, MPH - Diabetes Program
Coordinator; Jessica Chambers – Health Educator and Audrey Wall – Health Educator
• A shared medical model is being implemented in a rural clinic.
• Inclusion criteria: target population includes pregnant patients diagnosed with type 2 diabetes mellitus, gestational diabetes
and patients at risk of developing gestational diabetes.
• Exclusion criteria include a diagnosis of cognitive impairment, a psychiatric diagnosis of schizophrenia/psychosis and/or any
behavioral problem which might interfere with group
participation and discussion.
• Session format: a 4-week curriculum (every other week) developed in collaboration with the healthcare provider and
diabetes educator
• Each session is 2- 2.5 hours and includes a prenatal visit with
the healthcare provider; healthy snacks included
• The team members involved in SMA include
• Healthcare provider (lead)
• Program coordinator (diabetes educator)
• Two health coaches to co-facilitate the group
• A medical assistant to assist with documentation and charting
• The invitation is sent two weeks prior to the SMA session.
• HIPPA and voluntary disclosure of personal medical info in a group will be addressed in each session.
• Billing will be done individually for each patient as a CPT level 3 (99213) or 4 (99214) depending on the complexity of the
medical decision making (AAFP, 2017).
Methods
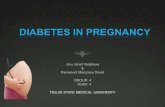
• The Chronic Care Model (CCM) of disease
management provides a useful framework for
establishing group shared medical
appointments.
Background and Significance
Format of Shared Medical Appointment
• The goal of this study is to develop and
implement a Shared Medical Appointment
(SMA) program for gestational diabetes patients.
• A group medical care model (SMA) is an
important inter-disciplinary care delivery
innovation to complement the individual
medical visit.
• SMAs focus on education for patients on their
chronic disease and enhancement of self-
management skills.
Purpose
• SMA model implementation date: March 31, 2017
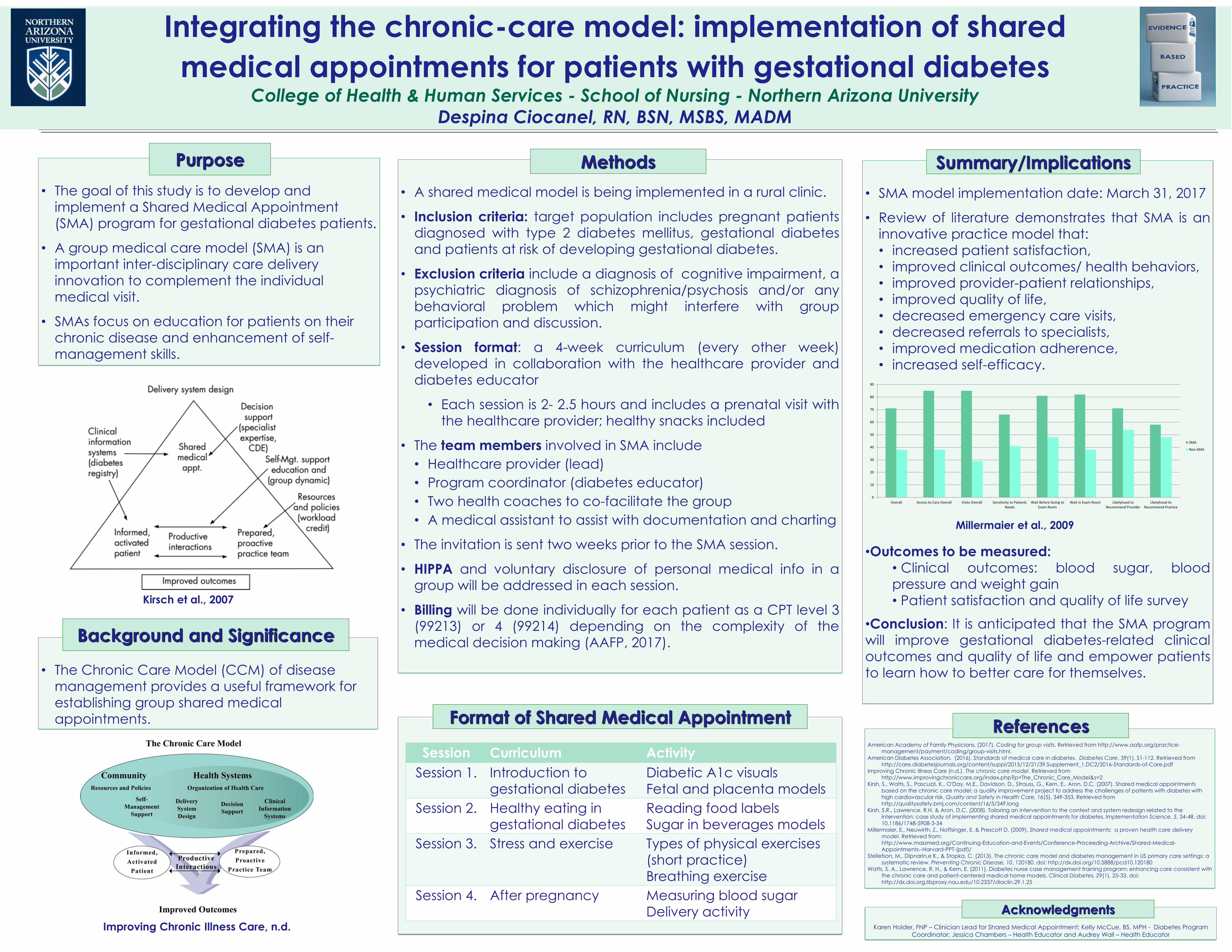
• Review of literature demonstrates that SMA is an
innovative practice model that:
• increased patient satisfaction,
• improved clinical outcomes/ health behaviors,
• improved provider-patient relationships,
• improved quality of life,
• decreased emergency care visits,
• decreased referrals to specialists,
• improved medication adherence,
• increased self-efficacy.
•Outcomes to be measured:
• Clinical outcomes: blood sugar, blood pressure and weight gain
• Patient satisfaction and quality of life survey
•Conclusion: It is anticipated that the SMA program will improve gestational diabetes-related clinical
outcomes and quality of life and empower patients
to learn how to better care for themselves.
Summary/Implications
American Academy of Family Physicians. (2017). Coding for group visits. Retrieved from http://www.aafp.org/practice-
management/payment/coding/group-visits.html. American Diabetes Association. (2016). Standards of medical care in diabetes. Diabetes Care, 39(1). S1-112. Retrieved from
http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf Improving Chronic Illness Care (n.d.). The chronic care model. Retrieved from
http://www.improvingchroniccare.org/index.php?p=The_Chronic_Care_Model&s=2 Kirsh, S., Watts, S., Pascuzzi, K., O'Day, M.E., Davidson, D., Strauss, G., Kern, E., Aron, D.C. (2007). Shared medical appointments
based on the chronic care model: a quality improvement project to address the challenges of patients with diabetes with high cardiovascular risk. Quality and Safety in Health Care, 16(5), 349-353. Retrieved from http://qualitysafety.bmj.com/content/16/5/349.long
Kirsh, S.R., Lawrence, R.H. & Aron, D.C. (2008). Tailoring an intervention to the context and system redesign related to the intervention: case study of implementing shared medical appointments for diabetes. Implementation Science, 3, 34-48. doi: 10.1186/1748-5908-3-34
Millermaier, E., Neuwirth, Z., Noffsinger, E. & Prescott D. (2009). Shared medical appointments: a proven health care delivery
model. Retrieved from: http://www.massmed.org/Continuing-Education-and-Events/Conference-Proceeding-Archive/Shared-Medical-
Appointments--Harvard-PPT-(pdf)/ Stellefson, M., Dipnarin,e K., & Stopka, C. (2013). The chronic care model and diabetes management in US primary care settings: a
systematic review. Preventing Chronic Disease, 10, 120180. doi: http://dx.doi.org/10.5888/pcd10.120180 Watts, S. A., Lawrence, R. H., & Kern, E. (2011). Diabetes nurse case management training program: enhancing care consistent with
the chronic care and patient-centered medical home models. Clinical Diabetes, 29(1), 25-33. doi: http://dx.doi.org.libproxy.nau.edu/10.2337/diaclin.29.1.25
References
Integrating the chronic-care model: implementation of shared
medical appointments for patients with gestational diabetes College of Health & Human Services - School of Nursing - Northern Arizona University
Despina Ciocanel, RN, BSN, MSBS, MADM
Kirsch et al., 2007
Acknowledgments
Improving Chronic Illness Care, n.d.
Session Curriculum Activity
Session 1. Introduction to
gestational diabetes
Diabetic A1c visuals
Fetal and placenta models
Session 2. Healthy eating in
gestational diabetes
Reading food labels
Sugar in beverages models
Session 3. Stress and exercise Types of physical exercises
(short practice)
Breathing exercise
Session 4. After pregnancy Measuring blood sugar
Delivery activity
Millermaier et al., 2009
0
10
20
30
40
50
60
70
80
90
Overall Access to Care Overall Visits Overall Sensitivity to PatientsNeeds
Wait Before Going toExam Room
Wait in Exam Room Likelyhood toRecommend Provider
Likelyhood toRecommend Practice
SMA
Non-SMA