Integrated Care Malissa McEntire, Manager of Integrated Health Care Traylor Rains, Director of...
27
Integrated Care Malissa McEntire, Manager of Integrated Health Care Traylor Rains, Director of Policy and Planning Jackie Shipp, Director of Community Based Services Presented on August 8, 2014
-
Upload
conrad-norton -
Category
Documents
-
view
218 -
download
2
Transcript of Integrated Care Malissa McEntire, Manager of Integrated Health Care Traylor Rains, Director of...
Integrated CareMalissa McEntire, Manager of Integrated Health CareTraylor Rains, Director of Policy and PlanningJackie Shipp, Director of Community Based Services
Presented on August 8, 2014
Integrated Care
The systematic coordination of general and behavioral healthcare. Integrating mental health, substance abuse, and primary care services produces the best outcomes and proves the most effective approach to caring for people with multiple healthcare needs.
Hogg Foundation for Mental Health, Connecting Body & Mind: A Resource Guide to Integrated Health Care in Texas and the U.S., www.hogg.utexas.edu

Why Integrated Care???• Individuals with serious mental illness are dying 25 years
earlier than the general population
• Average age of death is 53
• Substance use disorders and the Person-Centered Healthcare Home a 2010 report by B. Mauer finds that those with co-occurring MH/SUD were are greater risk.
• Average age of death is 45
People with SMI are Dying of Preventable Causes (NASMHPD)
Higher Rates of Modifiable Risk Factors: Smoking Alcohol consumption Poor nutrition, obesity Lack of exercise Unsafe sexual
behaviors IV drug use Residence in group
care facilities and homeless shelters
Vulnerability Due to Higher Rates of: Homelessness Victimization/
trauma Poverty Incarceration Social isolation
1.9 million youth, ages 12-17 (8% of the population) have had a major depressive episode Were more than twice as
likely to have engaged in illicit drug use
18-25 year olds, nearly 35% experienced a mental illness the previous year. Illicit drug use 21.5% Alcohol use 22.1%
Significant number of children in child welfare receiving psychotropic medications with no coordinated system of care to monitor appropriate utilization.
What About The
Children???
Common Childhood Health Problems Obesity Diabetes Hypertension Asthma Preventive care
This may be the first generation in which kids have a shorter lifespan than their
parents.
U.S. Sick Care VS. Health Care
• 45% of Americans have one or more chronic conditions
• Over half of these people receive their care from 3 or more physicians
• Treating these conditions account for 75% of direct medical care in the US
In large part due to the fact that money doesn’t start flowing into the U.S. healthcaresystem until after you become sick.
SOONERCAREHealth Homes
A strategy to build a system of care to improve health, enhance access and quality and control costs for members with SMI or SED.
Oklahoma Health Homes

What Is A Health Home?A place where individuals can
come throughout their lifetimes to have their health care needs identified and to receive the medical, behavioral and social supports they need, coordinated in a way that recognizes all of their needs as an individual, not just patients.
BackgroundSection 2703 of the Affordable Care Act (Public Law 11-148), creates a new opportunity for states to support improved integration of care for individuals with chronic conditions.
Through the establishment of section 1945 of the Social Security Act, this provision is an important opportunity for states to address and receive additional federal support for the enhanced integration and coordination of primary, acute, behavioral health, and long-term services and supports for persons across the lifespan with chronic illness.
Overall, it provides an opportunity for states to build a person-centered care delivery model that focuses on improving outcomes and disease management for enrollees with chronic conditions.
Background on Health Homes, November 16, 2010http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD10024.pdf
Background of Health Homes Quality Measures, January 15, 2013http://www.medicaid.gov/Federal-Policy-Guidance/Downloads/SMD-13-001.pdf
Frequently asked questions about Health Homeshttp://www.medicaid.gov/State-Resource-Center/Medicaid-State-Technical-Assistance/Health-Homes-Technical-Assistance/Downloads/Health-Homes-FAQ-5-3-12 2.pdf

Required Health Home Activities Provide comprehensive care management; Provide care coordination; Provide health promotion; Coordinate transitional care from inpatient to other
settings Refer and link to community supports; Provide individual and family support; Use health information technology to link services.
Wagner, E.H. (2000). The role of patient care teams in chronic disease management. British Medical Journal.
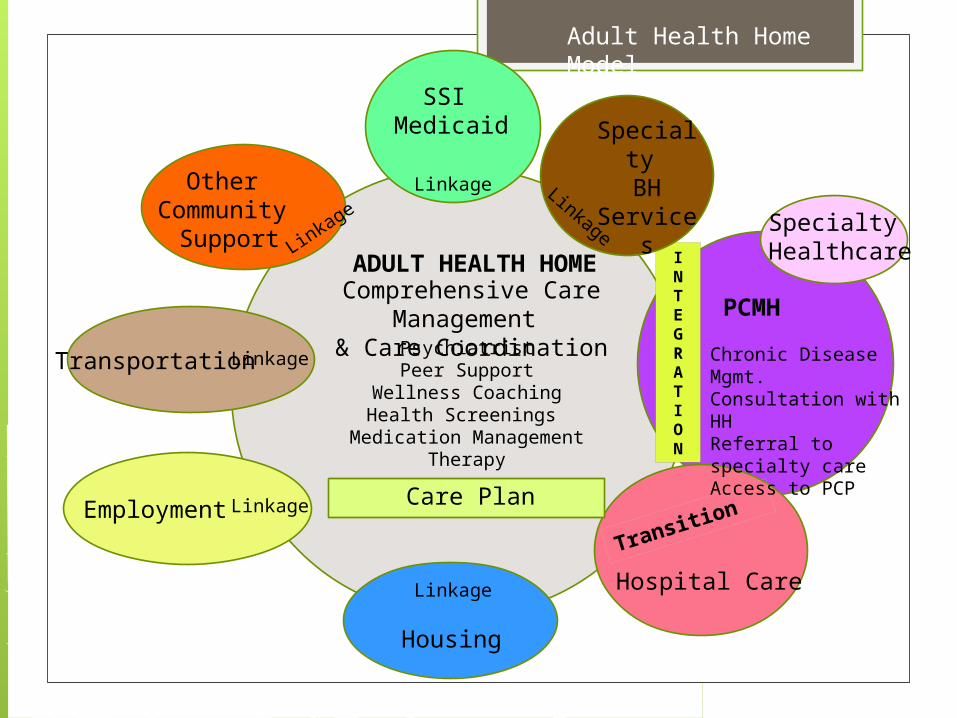
ADULT HEALTH HOMEComprehensive Care
Management & Care Coordination
INTEGRATION
PCMH
Chronic Disease Mgmt.Consultation with HHReferral to specialty careAccess to PCP
Hospital Care
Linkage
SSI Medicaid
Linka
ge
Other Community
Support
LinkageTransportation
Employment
Housing
PsychiatristPeer Support
Wellness CoachingHealth Screenings
Medication ManagementTherapy
Specialty Healthcare
Transition
Specialty BH
Services
Linkage
Linkage
Linkage
Care Plan
Adult Health Home Model
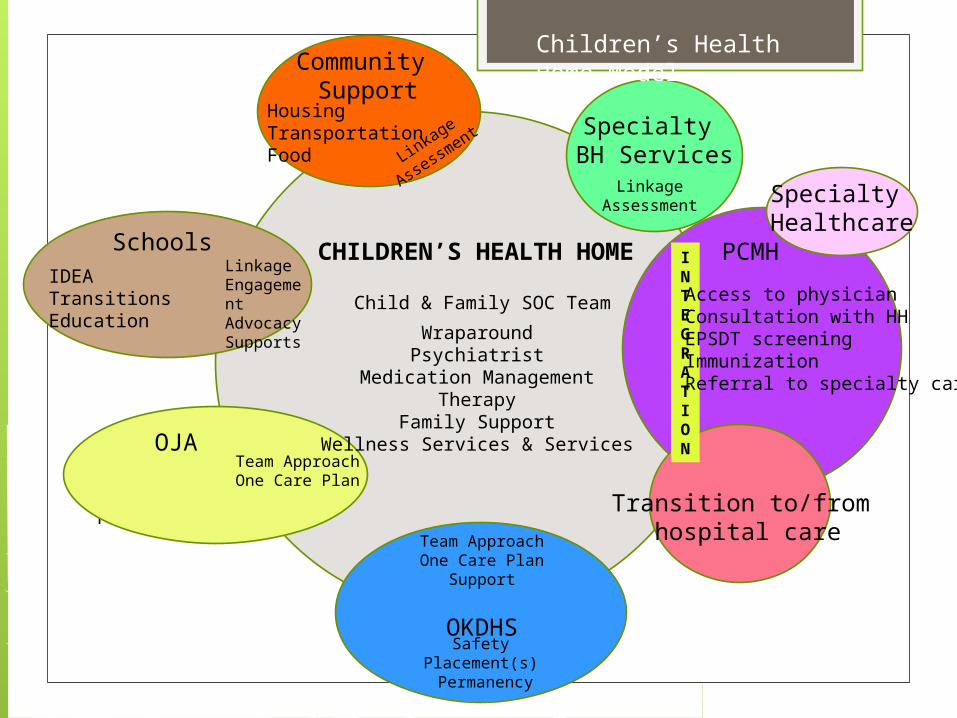
CHILDREN’S HEALTH HOME
Child & Family SOC Team
INTEGRATION
PCMH
Access to physicianConsultation with HHEPSDT screeningImmunizationReferral to specialty care
Transition to/from hospital care
LinkageAssessment
Specialty BH ServicesLin
kage
Assessm
ent
Community Support
HousingTransportationFood
LinkageEngagementAdvocacySupports
Schools
Community Safetyplacement
OJATeam ApproachOne Care Plan
Team ApproachOne Care Plan
Support
OKDHSSafety
Placement(s) Permanency
WraparoundPsychiatrist
Medication ManagementTherapy
Family SupportWellness Services & Services
IDEATransitionsEducation
Specialty Healthcare
Children’s Health Home Model

Benefits of a Team! Effective chronic illness models generally rely on
multidisciplinary teams. Successful teams can provide critical elements
of care that doctors do not have the time or training to do.
Participation of medical specialists in consultative and educational roles contribute to better outcomes.
Wagner, E.H. (2000). The role of patient care teams in chronic
disease management. British Medical Journal.

The Health Home Team
An interdisciplinary team Person/Family Centered process Identifies strengths and needs Creates a unified plan Empowers persons towards self-management Coordinates the varied healthcare needs

Health Home Team Members
Adults
Physician Team Member
HH Director
Licensed Nurse Care ManagerBehavioral Health Case ManagerWellness Coach/Peer Specialist
Consulting Psychiatrist
Child and Family Team
Physician Team Member
Licensed Nurse Care ManagerBehavioral Health Care Coordinator
Family Support Provider
Consulting Psychiatrist
Role of Physician Team Member
Coordinates and cooperates with HH Case Manager and/or Nurse Care Manager in development of integrated care plan.
Consults with CMHC on-site HH psychiatrists as needed;
Supplies post visit follow-up and relays information back to HH;
Maintains a system to track referrals;
Coordinates the delivery of medical care services with all specialists, case manager and other medical providers;
Educates members on appropriately using medical resources such as emergency rooms.
Role of Physician Team Member(PCMH, FQHC, IHS, PCP)
Requirements for Children
Educates regarding the importance of immunizations and screenings, child physical and emotional development;
Links each child with screening in accordance with the EPSDT periodicity schedule;
Identifies children in need of immediate or intensive care management for physical health needs;
Provides opportunities and activities for promoting wellness and preventing illness, including the prevention of chronic physical health conditions; and
Assist HH care manager in developing wellness goals to be included in the comprehensive care plan.
Health Homes Core Set Values
• Person Centered
• Recovery based
• Wellness focused
• Family inclusion
• Cultural inclusion
The following core values should be considered in planning of integrated care.

Definition of types of integrated care
Minimal collaboration: Mental health providers and primary care providers work in separate facilities, have separate systems, and communicate sporadically.
Basic collaboration at a distance: Primary care and behavioral health providers have a separate system at separate sites, but engage in periodic communication about shared patients/clients.
Basic collaboration on-site: Mental health and primary care professionals have separate systems but share the same facility. Proximity allows for more communication, but each provider remains in his or her own professional culture.
Close collaboration in a partly integrated system: Mental health professionals and primary care providers share the same facility and has some systems in common, such as scheduling appointments or medical records. Physical proximity allows for regular face-to-face communication and there is a sense of being part of a larger team treating shared patients/clients.
Close collaboration in a fully integrated system: The mental health provider and primary care providers are part of the same team.
1) Mental health or substance use services are provided in primary care (The client/patient receives mental health or substance abuse services as part of his or her regular primary care
2) Primary care services are provided in a mental health or substance use cline (The client receives basic primary care services within mental health or substance use disorders program. The program may be dual certified as a mental health and primary care clinic.)
Evolving Models of Behavioral Health Integration in Primary Care – 2010 (pgs., 13-15, Collins, Hewson, Munger, and Wade)
Health Home Core Set Measures
To support ongoing assessment of the effectiveness of the Health Home model, The Centers for Medicare & Medicaid Services has established a recommended Core Set of health quality measures.
• Adult Body Mass Index (BMI)• http://www.ncqa.org
• Screening for Clinical Depression and Follow-Up Plan• https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-In
struments/PQRS/MeasuresCodes.html• Plan All-Cause Readmission Rate
• http://www.ncqa.org• Follow-Up after Hospitalizations for Mental Illness
• http://www.ncqa.org• Controlling High Blood Pressure
• http://www.ncqa.org• Care Transition – Timely Transmission of Transition Record
• http://www.ma-assn.org• Initiation and Engagement of Alcohol and Other Drug Dependence
Treatment• http://www.ncqa.org
• Chronic Condition Hospitalization Admission Composite – Prevention Quality Indicator• http://qualityindicators.ahrq.gov/
Considerations for Health Homes Building relationships with physical health care
Primary care physicians Specialists Medical hospitals
Designing your space for integrated care Work flow for integrated care Choosing your team Facilitating communication
Staffings Huddles
Health Home Assignment
OHCA will attribute to Health Homes, SoonerCare members with a qualifying SMI/SED designation who have an existing relationship with the HH agency. Members will be notified via US mail service. Message will include: a brief description of Health Home services; a description of individuals’ options to choose
another Health Home; a process to opt out of enrollment in a HH; and encouragement to continue any existing
relationship with their primary care provider (PCP).
Health Home Assignment
Anticipated start date January 15, 2015 RFP Payment rates will be pmpm (per member
per month) For behavioral health information on
Oklahoma Healthcare Authority website, http://www.okhca.org/providers.aspx?id=406
For draft state plan amendment on OKHA, http://www.okhca.org/providers.aspx?id=12003
Resourceshttp://www.integration.samhsa.gov/
http://www.thenationalcouncil.org/topics/health-integration-and-wellness/
http://integrationacademy.ahrq.gov/atlas
http://nyshealthfoundation.org/resources-and-reports/resource/outreach-to-high-cost-individuals-best-practices-for-new-york-health-homes
http://www.chcs.org/
http://downloads.cms.gov/cmsgov/archiveddownloads/SMDL/downloads/SMD10024.pdf
http://www.medicaid.gov/Federal-Policy-Guidance/Downloads/SMD-13-001.pdf
http://www.medicaid.gov/State-Resource-Center/Medicaid-State-Technical-Assistance/Health-Homes-Technical-Assistance/Downloads/Health-Homes-FAQ-5-3-12 2.pd
ResourcesEvolving Models of Behavioral Health Integration in Primary Care – 2010 (pgs., 13-15, Collins, Hewson, Munger, and Wade)
Substance Use Disorders and the Person Centered Healthcare Home – 2010 (B. Mauer)
From SickCare to HealthCare to Health and Wellness: Evolution or Revolution? (David Mee-Lee, M.D. )