
Intake of Carrots, Spinach, and Supplements Containing...
7
Vol. 6, 887-892. Nm’e,nher 1997 Cancer Epidemiology, Biomarkers & Prevention 887 Intake of Carrots, Spinach, and Supplements Containing Vitamin A in Relation to Risk of Breast Cancer1 Matthew P. Longnecker,2 Polly A. Newcomb, Robert Mittendorf, E. Robert Greenberg, and Walter C. Willett Epidemiology Branch. National Institute of Environmental Health Sciences. Research Triangle Park. North Carolina 27709 IM. P. LI: Fred Hutchinson Cancer Research Center, Seattle, Washington 98104 lP. A. N.]; Department of Obstetrics and Gynecology, Pritzker School of Medicine, The University of Chicago. Chicago, Illinois (R. M.]: Norris Cotton Cancer Center, Dartmouth Hitchcock Medical Center, Lebanon, New Hampshire 03756 [E. R. G.l; and Departments of Nutrition and Epidemiology, Harvard School of Public Health. Channing Laboratory. Harvard Medical School. and Department of Medicine. Brigham and V/omens’ Hospital. Boston. Massachusetts t)2l 15 [W. C. W.] Abstract Intake of fruits, vegetables, vitamin A, and related compounds are associated with a decreased risk of breast cancer in some studies, but additional data are needed. To estimate intake of 3-carotene and vitamin A, the authors included nine questions on food and supplement use in a population-based case-control study of breast cancer risk conducted in Maine, Massachusetts, New Hampshire, and Wisconsin in 1988-1991. Multivariate- adjusted models were fit to data for 3543 cases and 9406 controls. Eating carrots or spinach more than twice weekly, compared with no intake, was associated with an odds ratio of 0.56 (95% confidence interval 0.34-0.91). Estimated intake of preformed vitamin A from all evaluated foods and supplements showed no trend or monotonic decrease in risk across categories of intake. These data do not allow us to distinguish among several potential explanations for the protective association observed between intake of carrots and spinach and risk of breast cancer. The findings are, however, consistent with a diet rich in these foods having a modest protective effect. Introduction Epidemiological data suggest that intake of fruits, vegetables, carotenoid vitamin A, or total vitamin A is associated with a lower risk of breast cancer ( 1-3), although not all evidence supports this (4-6). [Some carotenoids can be converted to vitamin A (retinol) in t’ivo; total vitamin A refers to the com- bined vitamin A activity of vitamin A precursors and preformed retinol.] Selected vegetables and carotenoids appear to prevent cancer in some laboratory studies (7, 8), and vitamin A plays a Received 2119/97: revised 6/I 1/97: accepted 6/27/97. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisemeiti in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Supported by USPHS Grants CA 47147 and CA 47305 from the National Cancer Institute, NIH. Department of Health and Human Services. 2 To whom requests for reprints should be addressed. role in regulating cell differentiation (9): thus, it is biologically plausible that these may prevent breast cancer in humans. Recent trials in men ( 10. 11 ), however, show supplementation with n-carotene or preformed vitamin A increasing risk of lung cancer in high-risk populations. and other data ( 12) indicate that associations with breast cancer attributed to n-carotene may be due to other aspects of a diet high in vegetables. These obser- vations highlight the need for additional study of the relation between fruits, vegetables. carotenoids, vitamin A, and breast cancer. When designing the questionnaire for a large population- based case-control study of breast cancer ( I 3). we selected a brief set of questions on intake of foods and supplements that could efficiently be used to classify subjects according to intake of f3-carotene and vitamin A. Here we present our results regarding risk of breast cancer in relation to intake of selected foods and supplements and estimated intakes of a-carotene and vitamin A. Materials and Methods Selection of Cases and Controls. Eligible subjects (cases and controls) met the following criteria: (a) female: (h) age less than 75 years; (c) resident of Maine, Massachusetts (outside of the Boston area), New Hampshire, or Wisconsin; (d telephone number listed in a telephone book or available through direc- tory assistance at the time of contact: (e) fluent in English: and (I) for subjects less than 65 years old, self-reported possession of a driver’s license. Detailed descriptions of the methods of this study are available elsewhere (13, 14). Cases were eligible if the diagnosis of invasive breast cancer was first reported to one of the four state-wide cancer registries during I 988 -1 99 1 . During the accrual period. 1 1,879 potentially eligible cases were reported to the four cancer registries. Of these, 28% were not eligible (14), leaving 8579 eligible cases, of whom 6888 (80%) were interviewed. The cancer registry record indicated histological confirmation of breast cancer in 98% of the interviewed cases. We selected controls less than 65 years old from state driver’s license lists and controls 65-74 years old from the Health Care Financing Administration’s list of Medicare ben- eficiaries. The driver’s license lists and the Health Care Financ- ing Administration lists were updated yearly. We excluded controls who reported a previous diagnosis of breast cancer. We identified 16,217 potential controls of whom 3 1% were not eligible (14). leaving 1 1,238 eligible controls. of whom 9.428 (84%) were interviewed. Data Collection. Trained study staff interviewed subjects for (on average) less than 25 mm by telephone using an identical protocol in all states. All interviewers collected data from both cases and controls. We did not tell the interviewers whether the subjects were cases or controls. and the interview began with a request that subjects not discuss their medical history until the end of the interview. The interviewers reported that they were on January 20, 2019. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
-
Upload
nguyendung -
Category
Documents
-
view
219 -
download
0
Transcript of Intake of Carrots, Spinach, and Supplements Containing...

Vol. 6, 887-892. Nm’e,nher 1997 Cancer Epidemiology, Biomarkers & Prevention 887
Intake of Carrots, Spinach, and Supplements Containing Vitamin A in
Relation to Risk of Breast Cancer1
Matthew P. Longnecker,2 Polly A. Newcomb,Robert Mittendorf, E. Robert Greenberg, andWalter C. Willett
Epidemiology Branch. National Institute of Environmental Health Sciences.
Research Triangle Park. North Carolina 27709 IM. P. LI: Fred HutchinsonCancer Research Center, Seattle, Washington 98104 lP. A. N.]; Department of
Obstetrics and Gynecology, Pritzker School of Medicine, The University of
Chicago. Chicago, Illinois (R. M.]: Norris Cotton Cancer Center, Dartmouth
Hitchcock Medical Center, Lebanon, New Hampshire 03756 [E. R. G.l; and
Departments of Nutrition and Epidemiology, Harvard School of Public Health.
Channing Laboratory. Harvard Medical School. and Department of Medicine.
Brigham and V/omens’ Hospital. Boston. Massachusetts t)2l 15 [W. C. W.]
Abstract
Intake of fruits, vegetables, vitamin A, and related
compounds are associated with a decreased risk of breastcancer in some studies, but additional data are needed.To estimate intake of �3-carotene and vitamin A, theauthors included nine questions on food and supplementuse in a population-based case-control study of breastcancer risk conducted in Maine, Massachusetts, NewHampshire, and Wisconsin in 1988-1991. Multivariate-adjusted models were fit to data for 3543 cases and 9406
controls. Eating carrots or spinach more than twiceweekly, compared with no intake, was associated with anodds ratio of 0.56 (95% confidence interval 0.34-0.91).Estimated intake of preformed vitamin A from all
evaluated foods and supplements showed no trend ormonotonic decrease in risk across categories of intake.These data do not allow us to distinguish among severalpotential explanations for the protective associationobserved between intake of carrots and spinach and riskof breast cancer. The findings are, however, consistentwith a diet rich in these foods having a modest protectiveeffect.
Introduction
Epidemiological data suggest that intake of fruits, vegetables,carotenoid vitamin A, or total vitamin A is associated with alower risk of breast cancer ( 1-3), although not all evidence
supports this (4-6). [Some carotenoids can be converted tovitamin A (retinol) in t’ivo; total vitamin A refers to the com-
bined vitamin A activity of vitamin A precursors and preformedretinol.] Selected vegetables and carotenoids appear to preventcancer in some laboratory studies (7, 8), and vitamin A plays a
Received 2119/97: revised 6/I 1/97: accepted 6/27/97.
The costs of publication of this article were defrayed in part by the payment of
page charges. This article must therefore be hereby marked advertisemeiti in
accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
� Supported by USPHS Grants CA 47147 and CA 47305 from the National
Cancer Institute, NIH. Department of Health and Human Services.2 To whom requests for reprints should be addressed.
role in regulating cell differentiation (9): thus, it is biologically
plausible that these may prevent breast cancer in humans.Recent trials in men ( 10. 1 1 ), however, show supplementationwith n-carotene or preformed vitamin A increasing risk of lungcancer in high-risk populations. and other data ( 12) indicate thatassociations with breast cancer attributed to n-carotene may bedue to other aspects of a diet high in vegetables. These obser-vations highlight the need for additional study of the relation
between fruits, vegetables. carotenoids, vitamin A, and breast
cancer.When designing the questionnaire for a large population-
based case-control study of breast cancer ( I 3). we selected abrief set of questions on intake of foods and supplements thatcould efficiently be used to classify subjects according to intake
of f3-carotene and vitamin A. Here we present our resultsregarding risk of breast cancer in relation to intake of selected
foods and supplements and estimated intakes of a-carotene and
vitamin A.
Materials and Methods
Selection of Cases and Controls. Eligible subjects (cases andcontrols) met the following criteria: (a) female: (h) age less than
75 years; (c) resident of Maine, Massachusetts (outside of the
Boston area), New Hampshire, or Wisconsin; (d� telephonenumber listed in a telephone book or available through direc-tory assistance at the time of contact: (e) fluent in English: and
(I) for subjects less than 65 years old, self-reported possessionof a driver’s license. Detailed descriptions of the methods ofthis study are available elsewhere (13, 14).
Cases were eligible if the diagnosis of invasive breastcancer was first reported to one of the four state-wide cancerregistries during I 988 -1 99 1 . During the accrual period. 1 1,879potentially eligible cases were reported to the four cancerregistries. Of these, 28% were not eligible (14), leaving 8579
eligible cases, of whom 6888 (80%) were interviewed. The
cancer registry record indicated histological confirmation ofbreast cancer in 98% of the interviewed cases.
We selected controls less than 65 years old from state
driver’s license lists and controls 65-74 years old from theHealth Care Financing Administration’s list of Medicare ben-
eficiaries. The driver’s license lists and the Health Care Financ-ing Administration lists were updated yearly. We excludedcontrols who reported a previous diagnosis of breast cancer. Weidentified 16,217 potential controls of whom 3 1% were noteligible (14). leaving 1 1,238 eligible controls. of whom 9.428
(84%) were interviewed.
Data Collection. Trained study staff interviewed subjects for
(on average) less than 25 mm by telephone using an identicalprotocol in all states. All interviewers collected data from both
cases and controls. We did not tell the interviewers whether thesubjects were cases or controls. and the interview began with arequest that subjects not discuss their medical history until the
end of the interview. The interviewers reported that they were
on January 20, 2019. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

888 Carrots, Spinach, and Breast Cancer Risk
3 The abbreviations used are: OR, odds ratio; Cl, confidence interval; RR, relative
risk; FFQ. food frequency questionnaire.
unaware of case or control status until the end of the interview
for 74% of cases and 90% of controls.Foods and supplements were selected for inclusion on the
questionnaire based on the proportion of between-subject var-iation in intake of (3-carotene or vitamin A they accounted for(15-17) and on their nutrient content. The first version of the
questionnaire asked, “How often, on average, did you eat
____________ two years ago?” The foods ascertained were:“half a raw carrot or carrot sticks,” “a serving of cooked
carrots,” “raw spinach, as in salad,” “a serving of cookedspinach,” “a serving of liver,” and “cold breakfast cereal.” The
type (brand name) of breakfast cereal eaten most often was alsoascertained. For supplements, we asked about ever use ofmultiple vitamins, vitamin A capsules, and cod liver oil. Foreach supplement, we ascertained whether the subject was tak-ing the preparation 2 years ago, and, if so, how often they tookthe preparation at that time. Total duration of use of each
preparation was also obtained, and for vitamin A supplements,we asked the amount contained in each dose.
After data collection began, we found that the median time
between case diagnosis and interview was 14 months. Thus,with a reference date for the dietary questions of “two years
ago,” for most cases, the interval between the reference dateand diagnosis date was less than 1 year. To address the possi-bility that breast cancer might affect diet, the reference date waschanged in 1990 from “two years ago” to “three years ago.”
Standard nutrient databases provided the vitamin A con-tent of cereals, liver, and cod liver oil (Ref. 18; nutrient data-base 2 1 ) and the /3-carotene content of carrots and spinach ( 19).The portion sizes assumed were identical to those for the
Willett questionnaire (20), i.e., raw carrots, #{189}carrot; cooked
carrots, #{189}cup; raw spinach, #{189}cup; cooked spinach, #{189}cup;cold breakfast cereal, I cup; and liver, 3.5 oz. We assumed that
multiple vitamins contained 5000 IU of preformed vitamin A
per pill; although �3-carotene now provides part of the vitaminA activity in multiple vitamins, this is a recent change.
Analysis. For the present analysis, we included cases if theirreference date was I year or more before their diagnosis (n
3543). Of these cases, 2396 (68%) had a reference date 2 yearsbefore interview, and 1 147 (32%) had a reference date 3 yearsbefore interview. Controls were included (n = 9406) unlesstheir reference date was unknown (n = 22). The average age atinterview was 58.6 years (SD, 1 1.9), and 74% of subjects were
aged 50 years or more. The average body mass index was 24.9kg/m2 (SD, 4.7), and 40.9% ofthe women had more than a highschool education. The vast majority (98.5%) were white. Their
average daily lifetime alcohol consumption (14) was 5.7 g/day(SD, 15.1).
For our statistical analysis, we defined categories of intake
of foods and nutrients based on distributions of intake among
cases and controls combined. in genera], we aimed to have thehighest intake category be extreme, yet not too sparse, and todefine categories in round numbers.
Menopausal status was assessed based on reported history
of menopause or bilateral oophorectomy, or, in the case ofhysterectomy, was imputed as described elsewhere (14).
ORs3 and their 95% CIs were estimated from multivariate
unconditional logistic regression models (21). The ORs ad-justed for age (5-year age groups) and state in logistic regres-sion models were virtually identical to those obtained after
stratifying on the same factors with the Mantel-Haenzel ap-
proach (results not shown). The factors (and number of cate-gories for each) included in the fully adjusted models were: age(10), state (4), age at first full-term pregnancy (5), parity (4),
body mass index (6), age at menarche (4), education (4), benign
breast disease (2), family history (2), menopausal status (2), age
at menopause (5), and lifetime alcohol intake (7). Additional
adjustment for use of oral contraceptives (as never used, used
<5 years ago, or used S + years ago), replacement estrogens (asduration of use), or for date of interview had no effect onresults, and therefore these variables were not included in the
fully adjusted models. Except as noted, subjects had to havecomplete data to be included in the analyses. For menopausal
status, family history, and benign breast disease, missing datawere represented as a category. All trend Ps presented are fortwo-sided tests with exposure represented as an ordinal van-
able; exposure was similarly represented when we evaluated
effect modification, which was considered noteworthy if the P
associated with the interaction term was less than 0.10.
Reliability Substudy. Seven hundred controls in Wisconsin
completed a mailed FFQ as part of another study (22). Of these,
642 were included in a reliability substudy; each had an energyintake within a plausible range (500-4000 kcal/day) and had
sufficiently complete FFQ data. The FFQ (20) was modified toassess diet 2 years before the interview. Spearman correlation
coefficients between frequency of consumption measured bythe interview questionnaire and the FFQ were: raw and cooked
carrots and spinach (combined), 0.58; cold breakfast cereal,0.71; liver, 0.58; multiple vitamins, 0.74; vitamin A supple-ments, 0.69; and cod liver oil, 0.37. The correlation between
estimates of intake from the interview and those based on theFFQ were a-carotene, 0.49; preformed vitamin A, 0.61 ; and
total vitamin A, 0.47. We also calculated the Spearman coef-
ficient between the combined frequency of intake of raw andcooked carrots and spinach from the interview and the com-bined frequency of intake of 28 vegetables on the FFQ; the r
was 0.40.
Results
Subjects who ate carrots or raw spinach once weekly or more
(52+ servings/year) had a decreased risk of breast cancer(Table 1), and in general, the OR decreased with more frequent
consumption of these foods. Intake of cooked spinach showeda similar pattern, but the associations were not as strong.
Subjects who ate raw or cooked carrots and spinach more thantwice a week (105 + servings/year) had a 44% lower risk of
breast cancer (95% CI 9-66%). When subjects consuming 105or more servings/year were considered according to more finelydivided categories, the categories of intake (in servings/year)
and fully adjusted ORs (and 95% CIs) were: 105-156, 0.60
(0.37-0.98); 157-208, 0.64 (0.39-1.05); and 209+, 0.50(0.30-0.81). Repeating the analysis shown in Table 1 forcarrots and spinach combined after excluding subjects with nointake still showed a significant trend (P = 0.0007), with an ORfor the 105+ servings/day category of 0.82 (95% CI, 0.61-1 . 1 1). Further adjustment of the results for carrots and spinach
for intake of vitamin A supplements had essentially no effect on
results (data not shown). The reduction in risk associated withcarrots and spinach were independent (data not shown). We
also examined the relation of breast cancer risk with estimatedintake of $-carotene, based on use of carrots and spinach; theresults were similar to those for carrots and spinach (data notshown). The results in Table I from the fully-adjusted model
on January 20, 2019. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Table I ORs for breast cancer according to intake of carrots, spinach, breakfast cereal, and liver
Servings per yearTrend P
52-<105 105+None >0-<l2 12-<52
Carrots, raw
Cases 681 294 825 1028 615
Controls 1890 787 2044 2776 1727
OR” 1.00 1.03 1.04 0.91 0.85 0.004
CI” 0.88-1.22 0.92-1.18 0.81-1.02 0.75-0.97
MV-OR’ 1.00 1.02 0.99 0.87 0.81 0.0004
CI 0.85-1.21 0.87-1.14 0.76-0.99 0.70-0.93
Carrots, cooked
Cases 174 285 1197 1549 281
Controls 384 787 2968 4287 867
OR 1.00 0.74 0.78 0.71 0.63 0.0003
CI 0.58-0.93 0.64-0.95 0.59-0.87 0.50-0.80
MV-OR 1.00 0.71 0.76 0.70 0.62 0.0006
Cl 0.56-0.91 0.62-0.94 0.57-0.86 0.48-0.79
Spinach, raw
Cases 1804 732 728 177 39
Controls 4559 1909 1896 761 163
OR 1.00 0.94 0.95 0.59 0.65 0.0001
Cl 0.85-1.05 0.86-1.05 0.49-0.70 0.46-0.94
MV-OR 1.00 0.93 0.90 0.55 0.64 0.0001
CI 0.83-1.04 0.80-1.01 0.45-0.66 0.43-0.94
Spinach, cooked
Cases 1295 569 1092 498 35
Controls 3024 1550 2976 1625 117
OR 1.00 0.91 0.96 0.83 0.79 0.02
CI 0.81-1.03 0.87-1.06 0.73-0.95 0.53-1.17
MV-OR 1.00 0.93 0.97 0.85 0.88 0.07
CI 0.82-1.06 0.87-1.08 0.74-0.97 0.62-1.42
Carrots and spinach. raw and cooked
Cases 43 73 610 1002 1803
Controls 81 197 1486 2547 5078
OR 1.00 0.74 0.76 0.71 0.63 0.0001
CI 0.47-1.19 0.51-1.13 0.48-1.05 0.43-0.93
MV-OR 1.00 0.68 0.66 0.65 0.56 0.0001
CI 0.39-1.19 0.40-1.08 0.40-1.06 0.34-0.91
Breakfast cereal
Cases 728 146 357 710 1567
Controls 2097 447 1031 1888 3854
OR 1 .00 0.94 0.96 1 .00 1 .06 0.20
CI 0.76-1.16 0.83-1.12 0.88-1.13 0.95-1.18
MV-OR 1 .00 0.95 0.94 0.96 1 .02 0.60
CI 0.76-1.18 0.80-1.11 0.84-1.10 0.91-1.15
Liver x x”
Cases 1478 1223 659 162
Controls 4250 2821 1770 505
OR 1 .00 1 . I 2 0.94 0.85 0.17
CI 1.02-1.23 0.85-1.06 0.70-1.03
MV-OR 1.00 1.14 0.97 0.81 0.24
CI 1.03-1.26 0.86-1.09 0.66-1.00
‘, OR. OR adjusted for age and state.
b CI, 95% CI for OR immediately above.
‘ MV-OR, multivariate OR adjusted for age. state, age at the first full-term pregnancy, parity, body mass index, age at menarche, education, benign breast disease, age
at menopause, menopausal status, family history, and average lifetime alcohol intake. Number of cases and controls applies to age and state adjusted results.d A bar over results for adjacent categories means these categories were collapsed due to sparse data.
Cancer Epidemiology, Biomarkers & Prevention 889
differed little from those from the age- and state-adjusted mod-
els, a finding also true for all subsequent analyses.
Eating breakfast cereal was unrelated to relative risk; withsubjects consuming 105 or more servings per year furthersubdivided, ORs remained near one (Table I). Eating liver wasnot clearly associated with risk.
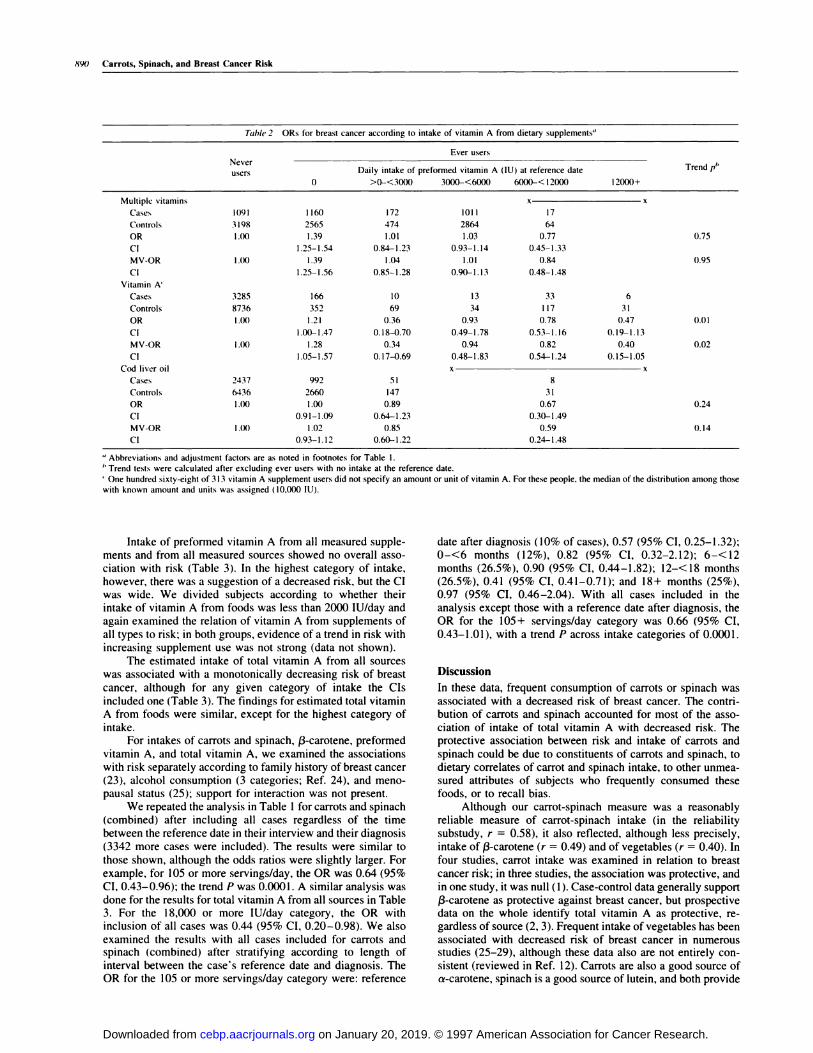
For multiple vitamins, cod liver oil, and especially vitaminA supplements, subjects in the highest category of intake had a
decreased risk of breast cancer, but relatively few people took
large doses, and the CIs were wide (Table 2). When the results
for vitamin A supplements were further adjusted for intake of
a-carotene, the findings were essentially unaltered. A protec-tive association of vitamin A supplement use was suggested,
regardless of duration of use. For multiple vitamins or cod liveroil, duration of use was unrelated to risk. Among ever users ofmultiple vitamins or vitamin A supplements who were not usersat the reference date, risk was increased. This was likely an
artifact due to study design (see “Discussion”).
on January 20, 2019. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
890 Carrots, Spinach, and Breast Cancer Risk
Table 2 ORs for breast c ancer according to intake of vitamin A from dietary supplements”
Never
users
Ever users
0
Daily intake of preformed vitamin A (lU) at reference date
>0-<3000 3000-<6000 6000-< I 2000 12000+
Trend pI,
Multiple vitamins
Cases 1091 1160
x
172 1011 17
Controls 3 198 2565 474 2864 64
OR 1(X) 1.39 1.01 1.03 0.77 0.75
Cl 1.25-1.54 0.84-1.23 0.93-1.14 0.45-1.33
MV-OR l.()0 1.39 1.04 1.01 0.84 0.95
Cl 1.25-1.56 0.85-1.28 0.90-1.13 0.48-1.48
Vitamin A’
Cases 3285 166 10 13 33 6
Controls 8736 352 69 34 117 31
OR 1.0’) 1.21 0.36 0.93 0.78 0.47 0.01
Cl I .00- 1 .47 0. I 8-0.70 0.49-1 .78 0.53- 1 . I 6 0. 19- 1 . I 3
MV-OR l.()0 1.28 0.34 0.94 0.82 0.40 0.02
Cl
Cod liver oil
Cases 2437
1.05-1.57
992
0.17-0.69 0.48-1.83 0.54-1.24
x
0.15-1.05
51 8
Controls 6436 2660 147 31
OR I .00 1 .00 0.89 0.67 0.24
CI 0.91-1.09 0.64-1.23 0.30-1.49
MV-OR 1(X) 1.02 0.85 0.59 0.14
CI 0.93-I . I 2 0.60-1 .22 0.24-1.48
“ Abbreviations and adjustment factors are as noted in footnotes for Table I.I, Trend tests were calculated after excluding ever users with no intake at the reference date.
‘ One hundred sixty-eight of 3 13 vitamin A supplement users did not specify an amount or unit of vitamin A. For these people. the median of the distribution among those
with known amount and units was assigned ( 10,000 lU).
Intake of preformed vitamin A from all measured supple-ments and from all measured sources showed no overall asso-
ciation with risk (Table 3). In the highest category of intake,however, there was a suggestion of a decreased risk, but the CIwas wide. We divided subjects according to whether their
intake of vitamin A from foods was less than 2000 lU/day andagain examined the relation of vitamin A from supplements of
all types to risk; in both groups, evidence of a trend in risk withincreasing supplement use was not strong (data not shown).
The estimated intake of total vitamin A from all sourceswas associated with a monotonically decreasing risk of breast
cancer, although for any given category of intake the CIs
included one (Table 3). The findings for estimated total vitaminA from foods were similar, except for the highest category of
intake.For intakes of carrots and spinach, a-carotene, preformed
vitamin A, and total vitamin A, we examined the associations
with risk separately according to family history of breast cancer(23), alcohol consumption (3 categories; Ref. 24), and meno-pausal status (25); support for interaction was not present.
We repeated the analysis in Table 1 for carrots and spinach
(combined) after including all cases regardless of the timebetween the reference date in their interview and their diagnosis
(3342 more cases were included). The results were similar tothose shown, although the odds ratios were slightly larger. For
example, for 105 or more servings/day, the OR was 0.64 (95%CI, 0.43-0.96); the trend P was 0.0001. A similar analysis wasdone for the results for total vitamin A from all sources in Table3. For the 18,000 or more lU/day category, the OR with
inclusion of all cases was 0.44 (95% CI, 0.20-0.98). We alsoexamined the results with all cases included for carrots andspinach (combined) after stratifying according to length ofinterval between the case’s reference date and diagnosis. TheOR for the 105 or more servings/day category were: reference
date after diagnosis (10% ofcases), 0.57 (95% CI, 0.25-1.32);
0-<6 months (12%), 0.82 (95% CI, 0.32-2.12); 6-<12months (26.5%), 0.90 (95% CI, 0.44-1.82); l2-<18 months(26.5%), 0.41 (95% CI, 0.41-0.71); and 18+ months (25%),0.97 (95% CI, 0.46-2.04). With all cases included in the
analysis except those with a reference date after diagnosis, theOR for the 105+ servings/day category was 0.66 (95% CI,0.43-1.01), with a trend P across intake categories of 0.0001.
Discussion
In these data, frequent consumption of carrots or spinach was
associated with a decreased risk of breast cancer. The contri-bution of carrots and spinach accounted for most of the asso-
ciation of intake of total vitamin A with decreased risk. Theprotective association between risk and intake of carrots and
spinach could be due to constituents of carrots and spinach, todietary correlates of carrot and spinach intake, to other unmea-sured attributes of subjects who frequently consumed thesefoods, or to recall bias.
Although our carrot-spinach measure was a reasonablyreliable measure of carrot-spinach intake (in the reliabilitysubstudy, r = 0.58), it also reflected, although less precisely,intake of (3-carotene (r = 0.49) and of vegetables (r 0.40). In
four studies, carrot intake was examined in relation to breast
cancer risk; in three studies, the association was protective, andin one study, it was null (1). Case-control data generally supportf3-carotene as protective against breast cancer, but prospectivedata on the whole identify total vitamin A as protective, re-gardless of source (2, 3). Frequent intake of vegetables has beenassociated with decreased risk of breast cancer in numerousstudies (25-29), although these data also are not entirely con-
sistent (reviewed in Ref. 12). Carrots are also a good source ofa-carotene, spinach is a good source of lutein, and both provide
on January 20, 2019. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 891
Table 3 ORs for bre ast cancer a ccording to intake o f vitamin A, for preformed vitamin A. and for total vitamin A, ac cording to source””
Daily Intake in IUTrend P
0 >0-<3000 3000-<6000 6000-< I 2000
Preformed vitamin A
12000-< I 8000 I 800()+
All measured supplements”
Cases
Controls
OR
CI
MV-OR
All measured sources
Cases
Controls
OR
Cl
MV-OR
CI
2169
5547
1.00
1.00
385
1144
1.00
1.00
187
528
0.98
0.81-1.18
1.04
0.85-1.26
1856
4580
1.07
0.94-1.22
1.09
0.94-I .26
964 56
2710 161
1.02 0.97
0.91-1.14 0.70-1.34
1.01 0.88
0.90-1.13 0.63-1.25
813 431
2260 1233
0.95 0.88
0.82-1.09 0.75-1.04
1.06 0.97
0.90-1 .25 0.8 1-1 . I 7
27
105
0.75
0.49-1.17
0.71
0.45-1.14
41
126
0.86
0.59-1.26
0.96
0.64-I .44
6
36
0.46
0.19-1.11
0.40
0.15-1.06
14
59
0.61
0.33-1.11
0.64
0.33-I .23
0.48
0.28
0.001
0.21
Total vitamin A
All measured foods
Cases
Controls
OR
CI
MV-OR
Cl
All measured sources
Cases
Controls
OR
Cl
MV-OR
CI
21
40
1.00
1.00
18
34
1.00
1.00
2735
7154
0.75
0.43-1.30
0.65
0.29-1.46
1873
4766
0.77
0.42-1.42
0.76
0.31-1.87
593 176
1625 545
0.67 0.60
0.38-1.16 0.34-1.06
0.56 0.48
0.25-1.28 0.21-1.1 1
717 835
1862 2420
0.72 0.64
0.39-1.33 0.35-1.18
0.74 0.68
0.30-1.83 0.27-1.67
x
14
35
0.80
0.35-1.86
0.73
0.26-2.07
80
230
0.64
0.33-1.23
0.64
0.25-1.63
x
7
90
0.36
0.16-0.80
0.37
0.13-1.07
0.002
0.0(X)7
0(5)01
0.0049
“ Abbreviations and adjustment factors are as noted in footnotes for Table 1.b For the exposure variables that include intake from supplements, the results are also adjusted for past use of multiple vitamins and vitamin A supplements.
fiber (18, 19). Freudenheim et a!. (12) used a complete diet
assessment in a case-control study and found lower risk ofbreast cancer with greater intake of /3-carotene and lutein,independent of total vegetable intake. Disentangling the effects
of specific vegetables or nutrients with a short food list likeours, however, is not possible.
On the whole, our measure of preformed vitamin A intakewas not strongly related to risk. Supplement users taking larger
doses, however, had lower risk, albeit with wide CIs. In threeprospective studies (5, 25, 30), subjects in the highest dose
category of vitamin A supplements had a reduced risk of breastcancer. Supplement users, however, differ from nonusers innumerous ways (3 1 ); therefore, whether use of vitamin A
supplements accounts for the inverse association is not clear.Furthermore, other constituents of the vitamin A-containingsupplements could affect risk.
Comparisons of intake of n-carotene and vitamin A re-ported prospectively and retrospectively among breast cancer
cases and controls (32, 33) suggest that recall bias probablydoes not account for the associations observed in the present
study. The response rates in the present study (>80% for cases
and for controls) indicate that selection bias, if any, was un-likely to have greatly affected the findings. We used our reli-ability substudy data to examine the relation of energy intake
assessed by FFQ to items assessed by interview. Energy intakewas neither strongly related to intake of carrots and spinach
combined (Spearman r = 0.12) nor to intake of supplementalvitamin A (Spearman r < 0.01). These correlations suggest that
energy intake was unlikely to have substantially confounded
our results. Women who used multiple vitamins or vitamin Asupplements but who were not users at the reference dateappeared to be at increased risk of breast cancer. Use of theseagents in response to a diagnosis of breast cancer may explain
the finding.
The results of our reliability substudy are consistent with
other data (16, 17) that show a large portion of variation inintake of carotenoids and vitamin A is accounted for with a
short list of foods. In a study based on use of diet records for4 weeks (17), intake of carrots accounted for 58% of among-
subject variation in intake of carotene, intake of liver accountedfor 74% of variation in intake of preformed vitamin A from
foods, and use of supplements accounted for 88% of variationin intake of total vitamin A. Nevertheless, our brief dietary
assessment allowed only imprecise measures of nutrient intake,and thus true underlying associations, if any, would have been
underestimated.Many substances in vegetables have anticarcinogenic ac-
tivity in animal models (7, 34). Although high-dose supple-
mentation with �3-carotene has been associated with an in-creased risk of lung cancer ( 10, 1 1 ), diets rich in fruits,vegetables, and carotenoids are consistently associated with
reduced risk of lung and other cancers (29, 35). Animal and
epidemiological evidence is mounting that several specific flu-trients thought to be protective against cancer do not fullyaccount for the protective effect of vegetables (7, 12. 36).
In summary, these data show a protective associationbetween intake of carrots and spinach and risk of breast cancer
although they do not allow us to distinguish among several
on January 20, 2019. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

892 Carrots, Spinach, and Breast Cancer Risk
potential explanations for the relation. The findings are, how-ever, consistent with a diet rich in these foods having a modestprotective effect against breast cancer.
Acknowledgments
The authors are grateful to Miao-Jung Chen, Donna Li, and Rebecca Darden for
computer programming.
References
I . Steinmetz. K. A.. and Potter, J. D. Vegetables, fruits. and cancer prevention:
a review. J. Am. Diet Assoc., 96: 1027-1039, 1996.
2. Hunter, D. J., and Willett, W. C. Diet, body size. and breast cancer. Epidemiol.
Rev., 15: 110-132. 1993.
3. Hunter, D. J., and Willett, W. C. Nutrition and breast cancer. Cancer Causes
Control, 7: 56-68. 1996.
4. Byers. T. Nutritional risk factors for breast cancer. Cancer (Phila.). 74:288-295, 1994.
5. Kushi. L. H.. Fee. R. M., Sellers, T. A., Theng. W.. and Folsom. A. R. Intakeof vitamins A, C. and E and postmenopausal breast cancer. The Iowa Women’s
Health Study. Am. J. Epidemiol.. 144: 165-174, 1996.
6. Verhoeven, D. T. H.. Assen, N.. Goldbohm, R. A., Dorant. E., van’t Veer, P..Sturmans, F.. Hermus, R. J. J., and van den Brandt, P. A. Vitamins C, and E,
retinol, beta-carotene and dietary fibre in relation to breast cancer risk: a pro-
spective cohort study. Br. J. Cancer, 75: 149-155. 1997.
7. Wattenberg. L. W. Inhibition of carcinogenesis by minor dietary constituents.
Cancer Res., 52 (Suppl.): 2085s-2091s, 1992.
8. Krinsky, N. I. Effects of carotenoids in cellular and animal systems. Am. J.
Clin. Nutr.. 53: 238s-.246s, 1991.
9. Moon, R. C. Vitamin A, retinoids, and breast cancer. Adv. Exp. Med. Biol.,
364: 101-107, 1994.
10. The alpha-tocopherol. beta carotene cancer prevention study group. Theeffect of vitamin E and beta carotene on the incidence of lung cancer and other
cancers in male smokers. N. EngI. J. Med., 330: 1029-1035, 1994.
I 1. Omenn, G. S., Goodman, G. E.. Thornquist. M. D.. Balmes, J., Cullen, M. R..Glass. A., Keogh, J. P., Meyskens. F. L.. Valanis, B.. Williams, J. H., Barnhan,
S.. and Hammar, S. Effects of a combination of beta-carotene and vitamin A on
lung cancer and cardiovascular disease. N. EngI. J. Med.. 334: 1 150-1 155. 1996.
12. Freudenheim, J. L., Marshall, J. R., Vena, J. E., Laughlin. R.. Brasure. J. R..Swanson. M. K., Nemoto. T.. and Graham, S. Premenopausal breast cancer riskand intake of vegetables. fruits, and related nutrients. J. NatI. Cancer. Inst., 88:
340-348. 1996.
13. Newcomb, P. A., Storer, B. E., Longnecker. M. P.. Mittendorf, R.,
Greenberg. E. R.. Clapp. R. W., Burke, K. P.. Willett. W. C., and MacMahon. B.
Lactation and a reduced risk of premenopausal breast cancer. N. EngI. J. Med.,
330: 81-87, 1994.
14. Longnecker, M. P., Newcomb, P. A., Mittendorf. R., Greenberg. E. R.. Clapp,
R. W., Bogdan, G. F., Baron, J., MacMahon, B.. and Willett, W. C. Risk of breast
cancer in relation to lifetime alcohol consumption. J. Natl. Cancer Inst., 87:
923-929, 1995.
15. Romieu, I., Stampfer, M. J., Stryker. W. S., Hemandez, M.. Kaplan, L.,
Sober, A., Rosner, B., and Willett, W. C. Food predictors of plasma beta-carotene
and alpha-tocopherol: validation of a food-frequency questionnaire. Am. J. Epi-demiol., 131: 864-876, 1990.
16. Byers. T., Marshall. J.. Fiedler, R., Zielezny. M.. and Graham, S. Assessing
nutrient intake with an abbreviated dietary interview. Am. J. Epidemiol., 122:41-50, 1985.
17. Stryker. W. S., Salvini, S., Stampfer. M. J.. Sampson. L.. Colditz. G. A.. andWillett, W. C. Contributions of specific foods to absolute intake and between-
person variation ofnutrientconsumption. J. Am. Diet. Assoc., 91: 172-178, 1991.
18. Schakel, S. F., Sievert, Y. A., and Buzzard, I. M. Sources of data for
developing and maintaining a nutrient database. J. Am. Diet. Assoc.. 88: 1268-
1271, 1988.
19. Mangels, A. R., Holden, J. M.. Beecher, G. R., Forman, M. R., and Lanza,E. Carotenoid content of fruits and vegetables: an evaluation of analytic data.
J. Am. Diet. Assoc., 93: 284-296, 1993.
20. Willeu, W. C., Sampson. L., Browne, M. L., Stampfer, M. J., Rosner, B.,
Hennekens, C. H., and Speizer. F. E. The use of a self-administered questionnaire
to assess diet four years in the past. Am. J. Epidemiol.. 127: 188-199. 1988.
21. SAS Institute, Inc. Statistical analysis system. Cary, NC: SAS Institute. Inc.,
1987.
22. Coates, R. J., Serdula, M. K., Byers, T., Mokdad, A.. Jewell, S., Leonard.
S. B., Ritenbaugh, C., Newcomb, P., Mares-Perlman. J.. Chavez, N.. and Block,G. A brief, telephone-administered food frequency questionnaire can be useful for
surveillance of dietary fat intakes. J. Nutr., 125: 1473-1483, 1995.
23. Ambrosone, C. B., Graham, S., Marshall, J. R., Hellman, R., Nemoto, T., and
Freudenheim, J. L. Dietary antioxidants and breast cancer risk: effect modifica-
tion by family history. Adv. Exp. Med. Biol., 366: 439-440, 1994.
24. Mayne, S. T., Graham, S., and Zheng, T. Dietary retinol: prevention or
promotion of carcinogenesis in humans? Cancer Causes Control, 2: 443-450,
1991.
25. Hunter, D. J., Manson, J. E., Colditz, G. A.. Stampfer, M. J.. Rosner. B.,Hennekens, C. H., Speizer, F. E., and Willett, W. C. A prospective study of the
intake of vitamins C, E, and A and the risk of breast cancer. N. EngI. J. Med., 329:234-240. 1993.
26. Holmberg. L., Ohlander, E. M., Byers. T., Zack. M.. Wolk, A.. Bergstrom, R..
Bergkvist, L., Thurfjell. E., Bruce, A.. and Adami. H. 0. Diet and breast cancer
risk. Arch. Intern. Med., 154: 1805-1811, 1994.
27. Yuan, J-M., Wang, Q-S., Ross, R. K., Henderson, B. E., and Yu, M. C. Dietand breast cancer in Shanghai and Tianjin, China. Br. J. Cancer. 71: 1353-1358.
1995.
28. Trichopoulou, A., Katsouyanni, K., Stuver, S., Tzala, L., Gnardellis, C.,
Rimm, E., and Trichopoulos, D. Consumption of olive oil and specific food
groups in relation to breast cancer risk in Greece. J. NatI. Cancer Inst., 87:
110-116, 1995.
29. Block, G., Patterson, B., and Subar, A. Fruit, vegetables, and cancer preven-
tion: a review of the epidemiological evidence. Nutr. Cancer, 18: 1-29, 1992.
30. Rohan, T. E., Howe, G. R., Friedenreich, C. M., Jam, M., and Miller. A. B.
Dietary fiber. vitamins A, C. and E. and risk of breast cancer: a cohort study.Cancer Causes Control, 4: 29-37, 1993.
31. Slesinski, M. J., Subar, A. F., and KaIsle, L. L. Dietary intake of fat. fiber and
other nutrients is related to the use of vitamin and minced supplements in theUnited States: the 1992 National Health Interview Survey. J. Nutr., 126: 3001-
3008, 1996.
32. Friedenreich, C. M., Howe, G. R., and Miller, A. B. Recall bias in the
association of micronutrient intake and breast cancer. J. Clin. Epidemiol.. 46:1009-1017. 1993.
33. Giovannucci, E., Stampfer, M. J., Colditz, G. A., Manson, J. E., Rosner,
B. A., Longnecker, M., Speizer. F. E., and Willett, W. C. A comparison of
prospective and retrospective assessments of diet in the study of breast cancer.
Am. J. Epidemiol., 137: 502-51 1, 1993.
34. Steinmetz. K. A., and Potter, J. D. Vegetables, fruit, and cancer. II. Mech-
anisms. Cancer Causes Control, 2: 427-442, 1991.
35. Ziegler, R. G., Mayne, S. T., and Swanson, C. A. Nutrition and lung cancer.Cancer Causes Control, 7: 157-177, 1996.
36. Wine, J. S., Longnecker. M. P.. Bird, C. L., Lee, E. R., Frankl, H. D., andHaile, R. W. Relation of vegetable, fruit, and grain consumption to colorectal
adenomatous polyps. Am. J. Epidemiol., 144: 1015-1025, 1996.
on January 20, 2019. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1997;6:887-892. Cancer Epidemiol Biomarkers Prev M P Longnecker, P A Newcomb, R Mittendorf, et al. A in relation to risk of breast cancer.Intake of carrots, spinach, and supplements containing vitamin
Updated version
http://cebp.aacrjournals.org/content/6/11/887
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/6/11/887To request permission to re-use all or part of this article, use this link
on January 20, 2019. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from


















