
INSTITUTIONAL FACTORS CONTRIBUTING TO POOR …
98
INSTITUTIONAL FACTORS CONTRIBUTING TO POOR PERFORMANCE OF EMPLOYEES IN THE DELIVERY OF HEALTH SERVICES AT MBEYA DISTRICT COUNCIL
Transcript of INSTITUTIONAL FACTORS CONTRIBUTING TO POOR …

i
INSTITUTIONAL FACTORS CONTRIBUTING TO POOR
PERFORMANCE OF EMPLOYEES IN THE DELIVERY OF
HEALTH SERVICES AT MBEYA DISTRICT COUNCIL

ii
INSTITUTIONAL FACTORS CONTRIBUTING TO POOR
PERFORMANCE OF EMPLOYEES IN THE DELIVERY OF
HEALTH SERVICES AT MBEYA DISTRICT COUNCIL
By
Benadetha Teddy
A Dissertation Submitted in Partial Fulfilment of the Requirements for Award
of the Degree of Master of Public Administration and Management of
Mzumbe University
2019

i
CERTIFICATION
We, the undersigned, certify that we have read and hereby recommend for
acceptance by the Mzumbe University, a dissertation titled “Institutional Factors
Contributing to Poor Performance of Employees in the Delivery of Health
Services at Mbeya District Council” in fulfillment of the requirements for award of
the degree of Master of Public Administration and Management of Mzumbe
University.
____________________________________________
Major supervisor
____________________________________________
Internal examiner
____________________________________________
External Supervisor
Accepted for the Board of the school of Public Administration and Management
(SOPAM)
___________________________________
DEAN

ii
DECLARATIONANDCOPYRIGHT
I, Benadetha Teddy, declare that this Thesis is my own original work and it has not
been presented and will not be presented to any other university for a similar or any
other degree award.
Signature …………………………...
Date ……………………………
©
This dissertation is a copyright material protected under the Berne Convention, the
Copyright Act 1999 and other international and national enactment, in that behalf, on
the intellectual property. It may not be reproduced by any means in full or in part,
except for short extracts in fair dealings, for research or private study, critical
scholarly review or discourse with an acknowledgement, without the written
permission of Mzumbe University, on behalf of the author.

iii
ACKNOWLEDGEMENTS
It is not possible to acknowledge by using names of all those who have contributed in
one way or another to the completion of this study. Though, I would like to use this
opportunity to express my special gratitude to all of them. Therefore, I will mention
only a few of them.
First am grateful to the almighty God the creator of heaven and earth for all the love,
guidance and support that he has been giving me all this time.
I am also very grateful to the major supervisor, Dr. Dominick K. Muya, who read
commented comprehensively on countless drafts. His comments and criticisms have
contributed to the cleansing of this work.
I am also very thankful to the staff of the Mbeya District Council who kindly assisted
me in getting enough information to write my Master’s Thesis. Many thanks goes to
the office of Human resource and administration department and the department of
Health who have countless assisted me in getting enough data from employees and
head of departments.
I am gratefully to my lovely parents and siblings for their financial and moral support
throughout the whole period of my study and their encouragement.
Lastly, I would like to express my special appreciations to my colleagues in 2017-
2019 MPA programs for their support and encouragements throughout the entire
course of my studies.

iv
DEDICATION
I dedicate this work to my lovely parents Mr. and Mrs. Kabigi and my lovely
brothers Thomas and Abednego Teddy Kabigi.

v
ABBREVIATIONS
APA - American Psychological Association
CSRP - Civil Service Reform Program
CSSM - Child Survival and Survival & Safe Motherhood Program
DC - District Council
EPI - Expanded Programme of Immunization
GOT - Government of Tanzania
HR - Human Resource
HRM - Human Resource Management
IMCI - Integrated Management of Childhood Illness
LGA’S - Local Government Authorities
MDC - Mbeya District Council
MNCH - Maternal Newborn and Child Health
OPRAS - Open Performance Appraisal System
PSRP - Public Service Reform Program
RCH - Reproductive and Child Health
RCHS - Reproductive and Child Health Section
SMI - Safe Motherhood Initiatives
SPSS - Statistical Package for Social Science

vi
ABSTRACT
The increased number of people accessing health services in the countries of the
Global South has raised a necessity to address the problem of poor performance of
employees in the delivery of health services in health facilities. Bearing the public
outcry with regard to the delivery of health services at Mbeya District Council
(MDC), this research explored: institutional factors contributing to poor performance
of employees in the delivery of health services using Mbeya District Council as a
glaring example. The study was guided by three research objectives which assessed
whether to poor performance of employees in the delivery of reproductive health-
care services in the health facilities had anything to do with the: existing rules and
regulations in health facilities, established norms and values in health facilities, as
well as with the level of knowledge on customer care and medical acquired by the
Human Resources for Health (HRH).The study utilized a descriptive case-study
design that combines both quantitative and qualitative research approaches from a
sample of 105 study participants. The study’s participants were selected using both,
purposive stratified sampling and simple random sampling techniques. It utilized
stratified random sampling to select a sample of 100 study participants among HRH.
It also included 5 key informants. The study relied on data obtained through the use
of structured questionnaires to collect quantitative information. It also utilized
interview guides and FGD guides for generating qualitative information. In the same
vein, the study relied on descriptive statistics in the analysis of quantitative data as
well as thematic analysis for the analysis of qualitative data.
The findings revealed various levels to which institutional factors such as normative,
regulative and the cognitive factors contribute towards poor performance of
employees in the delivery of reproductive health-care services in the health facilities.
However, the study observed that poor performance of public employees in the
department of health at the local government level is skewed more by individual
factors observed among HRH instead of institutional norms, rules and regulations.
Because of this, employees’ performance in the health department failed to meet
customers’ expectation and requirements. Breaking the performance analysis at other
indicator levels, study revealed that the health services provided by HRH are not
timely and accurately delivered to the patients; and the health care centers are not
fully equipped with the necessary medical facilities. The study concludes that the
increased good initiatives of building more health facilities throughout the country
should also be complimented with the institutional reforms to address poor
performance of HRH in delivery of health services. In this light, the study has
advanced a number of recommendations for improving performance of HRH in the
delivery of healthcare services.

i
TABLE OF CONTENTS
CERTIFICATION ........................................................................................................ i
DECLARATIONANDCOPYRIGHT .......................................................................... ii
ACKNOWLEDGEMENTS ........................................................................................ iii
DEDICATION ............................................................................................................ iv
ABBREVIATIONS ..................................................................................................... v
ABSTRACT ................................................................................................................ vi
LIST OF TABLES ...................................................................................................... vi
LIST OF FIGURE ...................................................................................................... vii
LIST OF APPENDICES ........................................................................................... viii
CHAPTER ONE ........................................................................................................ 1
PROBLEM SETTING ............................................................................................... 1
1.0 Introduction ............................................................................................................ 1
1.1 General introduction............................................................................................... 1
1.2 Background of the study ........................................................................................ 1
1.3 Statement of the problem ....................................................................................... 6
1.4 Research objectives ................................................................................................ 7
1.4.1 General objective ................................................................................................ 7
1.4.2 Specific objectives .............................................................................................. 7
1.5 Research Questions ................................................................................................ 7
1.6 Significance of the study ........................................................................................ 7
1.7 The scope of the study............................................................................................ 8
1.8 Limitations of the study ......................................................................................... 8
1.9 Organization of the study ....................................................................................... 9
CHAPTER TWO ..................................................................................................... 10
LITERATURE REVIEW ........................................................................................ 10
2.0 Introduction .......................................................................................................... 10
2.1 Definitions of terms used in this study ................................................................. 10
2.1.1 Health services .................................................................................................. 10
2.1.2Health service delivery ....................................................................................... 10
2.1.3 Performance ...................................................................................................... 11

ii
2.1.4 Employee performance ..................................................................................... 11
2.1.5 Poor employee performance ............................................................................. 11
2.1.6 Institution .......................................................................................................... 11
2.1.7 Institutional factors............................................................................................ 12
2.1.8 Rules and Regulations ....................................................................................... 12
2.1.9 Norms and values .............................................................................................. 12
2.1.10 Knowledge ...................................................................................................... 12
2.2 Theoretical Framework ........................................................................................ 12
2.2.1 Theory underpinning this study ........................................................................ 12
2.3 The concept of employee performance and institutional factors ......................... 15
2.3.1 Employee performance ..................................................................................... 15
2.3.2 Factors Affecting Employees’ Performance ..................................................... 16
2.3.3 Causes of Poor Performance in Delivering Health Services ............................. 18
Poor competencies and trainings: .............................................................................. 18
2.3.4 Concept of Health Service System in Tanzania ................................................ 19
2.3.5 The Concept of Reproductive and Child Health ............................................... 20
2.4 Institutional factors on employees’ performance in delivering health service .... 21
2.4.1 Regulative factors and employee performance in delivering health service..... 22
2.4.2 Rules and Regulations of RCH services in Tanzania........................................ 24
2.4.3 Normative factor and employee performance in delivering health service ...... 25
2.4.3.1 Norms in Health Service in Tanzania ............................................................ 27
2.4.4 Cultural cognitive factors and employee performance in delivering health
services ....................................................................................................................... 28
2.4.4.1 Skills Required for Health Providers of Reproductive and Child Health ...... 29
2.5 Empirical literature review ................................................................................... 30
2.6 Conceptual Framework ........................................................................................ 32
2.7 Research Gap ....................................................................................................... 33
CHAPTER THREE ................................................................................................. 34
RESEARCH METHODOLOGY ........................................................................... 34
3.0 Introduction .......................................................................................................... 34
3.1 Research Design ................................................................................................... 34

iii
3.2 Area of the study and Population ......................................................................... 35
3.3Population of the study ......................................................................................... 35
3.4 Unity of Analysis ................................................................................................. 35
3.5 Variables and measurement ................................................................................. 35
3.6 Sample size and Sampling Technique ................................................................. 36
3.6.1 Sample Size ....................................................................................................... 36
3.6.2 Sampling Technique.......................................................................................... 36
3.7 Data Collection Methods ..................................................................................... 37
3.7.1 Primary Data collection methods ...................................................................... 37
3.7.1.1 Interviews ....................................................................................................... 37
3.7.1.2 Questionnaire ................................................................................................. 38
3.7.2 Secondary Data Collection Methods ................................................................. 38
3.8 Validity and Reliability ........................................................................................ 38
3.8.1 Validity .............................................................................................................. 38
3.8.2 Reliability .......................................................................................................... 39
3.9 Data Analysis ....................................................................................................... 39
3.9.1 Content analysis ................................................................................................ 40
3.9.2 Descriptive statistical analysis .......................................................................... 40
3.10 Ethical Issues ...................................................................................................... 40
CHAPTER FOUR .................................................................................................... 42
DATA PRESENTATION AND DISCUSSION OF FINDINGS .......................... 42
4.1 Introduction .......................................................................................................... 42
4.2 Demographic characteristics of respondents (Personal Particulars): ................... 42
4.2.1 Distribution of respondents by Sex ................................................................... 42
4.2.2Distribution of respondents by Age ................................................................... 43
4.2.3 Distribution of respondents by Education level ................................................ 44
4.2.4 Distribution of respondents by Working Experience ........................................ 45
4.3 How Regulative Factors Contribute to Poor Performance of Employees in
delivering health services ........................................................................................... 46
4.3.1 Policies, rules, regulations and circulars of RCH are available at Health
centers………. ........................................................................................................... 46
iv
4.3.2 Health care employees are being regulated for proper provision of health
services. ...................................................................................................................... 47
4.3.3 RCH policies enhance employees in the health sectors to have good
performance................................................................................................................ 48
4.3.4The policies, rules and regulation in the health sector enable employees to have
positive attitudes towards the job ............................................................................... 49
4.3.5 Infants get vaccines on time after being born as the policies, rules and
regulations indicate. ................................................................................................... 50
4.3.6 Maternal and Mortality rate have been reduced to the large extent .................. 50
4.3.7: The RCH services are provided with free charge ............................................ 51
4.4 How norms and values contribute to poor performance of employee in delivering
health service. ............................................................................................................. 52
4.4.1: The RCH service providers are honest, professional and respect organization
employment policy ..................................................................................................... 53
4.4.2 The health sector employees work with the line managers so as to ensure that
the values and norms are adhered .............................................................................. 53
4.4.3 Employees in the health centers do implement new ideas so as to improve their
performance................................................................................................................ 54
4.4.4The value of the health sector/ministry do reflect the performance of the
employees ................................................................................................................... 55
4.4.5 Employee soft skills are reflected from organization value and determine the
future employee’s performance.................................................................................. 55
4.4.6 The health sector emphasizes on obtaining competent and experienced
employees so as to improve the employees’ performance ......................................... 56
4.5 How the level of knowledge of employees about performance contribute to poor
performance of employees. ........................................................................................ 56
4.5.1: Public health service employees’ knowledge and experience of delivering
reproductive and child health ..................................................................................... 57
4.5.2: The patients haveknowledge and are aware on RCH service delivery ............ 57
4.5.3 RCH employees have experiences that enable them to provide better service . 58
4.6 Employee performance ........................................................................................ 58

v
4.6.1 The health care centers are fully equipped with the necessary medical facilities.
.................................................................................................................................... 59
4.6.2 The treatments to the patients are provided timely, thus no delay. ................... 59
4.6.3The patient’s expectations and requirements are well met as per their needs. .. 60
4.6.4The services are provided timely and with accuracy to the patients .................. 61
4.6.5The customers are well listened and attended effectively .................................. 61
4.6.6 The available resources are well utilized to provide quality health services .... 62
4.6.7 The health employees report and attend on their duties on time....................... 63
CHAPTER FIVE ...................................................................................................... 64
SUMMARY, CONCLUSIONS AND POLICY IMPLICATIONS ...................... 64
5.0 Introduction .......................................................................................................... 64
5.1 Summary .............................................................................................................. 64
5.2 Conclusion ........................................................................................................... 65
5.3 Recommendations ................................................................................................ 66
5.4 Suggestions for Further Research ........................................................................ 66
REFERENCES ......................................................................................................... 68
APPENDICES .......................................................................................................... 77

vi
LIST OF TABLES
Table 3.1 variables measurement ............................................................................... 35
Table 3.2 Sample distribution .................................................................................... 36
Table 4.1: Distribution of respondents by Age ......................................................... 44
Table 4.2 Distribution of respondents by Education Level........................................ 45
Table4.3: Distribution of respondents by Working Experience................................. 46
Table 4.4: Availability of policies, rules, regulations and circulars........................... 46
Table 4.5 Regulations of health care workers ............................................................ 47
Table 4.6: Policies and employee performance ......................................................... 48
Table 4.7 attitude of health employees ...................................................................... 49
Table 4.8 Infants Vaccines ......................................................................................... 50
Table 4.9 Reduction of Mortality and maternal rate .................................................. 50
Table 4.10: provision of free service ......................................................................... 51
Table 4.11: RCH employees’ honest, professionalism and respect ........................... 53
Table 4.12 Team working .......................................................................................... 53
Table 4.13 Implementation of New ideas .................................................................. 54
Table 4.14 Values of RCH service delivery............................................................... 55
Table 4.15: Employees’ skills .................................................................................... 55
Table 4.16: Competent Employees ............................................................................ 56
Table 4.17 Employees’ knowledge and experience on RCH ..................................... 57
Table 4.18 Patients knowledge and awareness on RCH services .............................. 57
Table 4.19: RCH employees’ experience................................................................... 58
Table 4.20 Health centers equipments ....................................................................... 59
Table 4.21 The treatments to the patients are provided timely, thus no delay. .......... 59
Table 4.22 Patients Expectations ............................................................................... 60
Table 4.23: Provision of services ............................................................................... 61
Table 4.24: Customer are listened .............................................................................. 61
Table 4.25: Resource availability ............................................................................... 62
Table 4.26 Working on Time ..................................................................................... 63

vii
LIST OF FIGURE
Figure 2.1: Conceptual Framework............................................................................ 33
Figure 4.1 Distribution of respondents by sex: .......................................................... 43

viii
LIST OF APPENDICES
Appendix I:A questionnaire for employees ............................................................... 77
Appendix II:Interview guide ...................................................................................... 80
Appendix III:Organization structure .......................................................................... 81
Appendix IV:Mbeya dc map ...................................................................................... 82

1
CHAPTER ONE
PROBLEM SETTING
1.0 Introduction
1.1 General introduction
Employee best performance is a concern of any public or private organization. The
organizations do strive to explore how best they can improve employees’
performance in their organizations. Both public and private organizations in various
sectors are reported to underperform and end up getting adverse or disclaimer reports
due to various factors (Deadrick and Gardner, 1997). That observation raised
interests to examine the institutional factors contributing to poor performance of
public employees’ in the delivery of health-care services using Mbeya District
Council as a case. This introductory chapter contains background of the study,
statement of the problem, research objectives, research questions, significance of the
study, scope of the study, limitation of the study, conceptual framework of the study
and organization of the study.
1.2 Background of the study
Throughout the World, both, public and private sectors strive towards improving
performance of their employees’ for the sustainability of their organization. At the
conceptual level, employee performance has been defined differently. According to
Deadrick and Gardner (1997), identifies employee performance as the record of
outcome achieved for each job function during specific period of time. Also, Darden
&Babin (1994) assert that, employee performance as a rating system used in many
firms to agree on the abilities and output of an employee. It is also, the effective
achievement of responsibilities by a selected individual or individuals, as set and
measured by a supervisor of an organization, to pre-defined standards while
efficiently and effectively utilizing available resources within changing environment
(Mathias & Jackson, 2009). This study adopts the Muya’s (2018) definition of
employee performance which views performance as: a process and a result or
outcome as well that is influenced by several factors including behaviors’ (Inputs) of
either an individual or individuals as team as well as organization set-ups.

2
In that regard, there are behaviors that are performance oriented (solution focused),
and others which are performance blocking. Indeed, it should also be noted that one’s
assumptions and attitudes drives his/her behavior. As such, managers should
therefore be vested with attitudes which lead to greater motivation for performance
such as: Trust, honesty, openness, interest in individuals as persons, challenging,
encouraging, confidence, straightforward, value others, fairness and integrity (Muya,
ibid.)
Organization require highly performing individuals in order to meet their goals to
deliver the products and services they provide and finally to attain competitive
advantage. According to Fauzilah, et al (2011),the elements of employee
performance are personal, organizational, environmental, motivation, skill level,
aptitudes and role perceptions. Employee performance is important as it reveals
organization performance by designing employee performance criteria in order to
measure performance of organizations. Also the quality of employees is the
important aspect on the attainment of organization performance as employees are the
backbone of the organization services by the role of ensuring that organization
policies and programs are implemented efficiently and effectively.
The problem of poor performance of employees in public organizations according to
the Public Service commission (2007) is caused by the following factors; Lack of
capacity where in the organization there is imbalance between work volume and the
available resources. Which lead to the employees and management having to take
more responsibilities than they are able to manage. Also poor employee performance
is caused by work culture as there is no real pressure on them to perform. Another
cause is lack of resources; where there are few tool in performing day to day task that
lead to failure to meet the desired level of performance. Also poor performance of
employees is caused by lack of accountability, leadership and leadership style;
person to post mismatch; poor performance standard; role clarity and definition and
the management commitment.

3
According to Basaza, (2016) there are also other factors that affect employee
performance which are, remuneration of employees, job security, delegation,
working condition, fringe benefit and time of work. When there is poor employees’
performance in organization it will distract the performance of the organization. As it
can cost the great deal of money, time and energy. Sometimes some of the
employees who cannot be able to improve and adjust to their working environment
resign which lead to employee turnover and this affects the organization in terms of
cost and productivity, and it will also raise customer complaints over services and
products.
At the global level, there seems to be increased trend of poor performance among
employees working in public organizations(Nabukeera, Ali &Raja, 2014). In 1980s
and 1990s after liberalization, most organization in developing countries has
experienced growing competition from multinationals. And because of these
organizations must plan ways of becoming more responsive to customers’
expectations and to compete in global village (Karuhanga, 2010). According to
(Elzinga et al, 2009), in Africa for the past few decades the application of
performance management in public organizations is steadily increasing. Also in
Malaysia employee performance is considered as the agencies of the quality of
personnel which was held by the company and is a key drive in the ninth Malaysia
plan, while in Malawi employee performance is important as because it imitate the
government performance by planning employee performance quantity in order to
measure performance of the organization, and the quality of employee is the
important influence on performance (Fauzilah et al., 2011).
In Tanzania the problem of low employee performance in public organization can be
traced back soon after independence in 1960s when the government adopted the
socialist ideology. In which the government was the important factor in the economy
and society, including the provision of free social service and its basic functions.
These functions lead to the increase in number of employees from 89,745 in 1961 to
354,612 in 1993 (Kumburu, 2009). This means that the increase in number of
employees in public service was because the focus was on quantity rather than
quality of service. World Bank, (2003) approved that this was because of the poor

4
planning which lead into having a lot of employees who failed to attain their goals
and the goals of the organization.
Also the government was unable to maintain service delivery values, but also having
employees with low self-esteem, absenteeism and failure in discipline and ethical
conduct (Kumburu, 2009). Which the resulted to overstaffing, low salaries and
provision of few resources of basic services and crowding out of operational
spending which resulted in the dropping of real wage levels and quality of
government, collapse in service and a growth in maladministration and corruption
(Clarke & Wood, 2001). Due to these problems the government decided to take
initiatives so as to solve them, and one of the initiatives was to adopt Civil Service
Reform Program (CSRP) in 1991 with the objective of achieving the smaller,
affordable, well compensated, efficient and effective performing employees
(Caulfield, 2004). The government aimed at improving the performance of
employees who were engaged on other activities that will increase their income
rather than focusing on their work due to the low salaries that they were paid. This
was supported by (NORAD, 1995) who state that during the CSRP the government
also made the pay reform by enhancing the basic salary levels, developing
appropriate remuneration system to respond to the problem that existed.
According to Rugumyamheto (2005) The government of Tanzania also adopted the
Public Service Reform Program in 2000 where the employees were required to
improve their performance by adopting the mind set to serve customers with
efficiency, effectiveness and high standards of courtesy and integrity. Also the PSRP
included three phase which aimed at improving the performance of employees and
the public services, those phases were as follows, first phase was about instituting
performance management system in 2000 up to 2005, second phase was about
instituting a performance management culture from 2005 up to 2008, and the third
phase was about instituting quality improvement cycles from 2008up to 2010
(Rugumyamheto, 2005). These phases were about performance management which
lead to the introduction of the application of monitoring and evaluation both internal
and external which involved short term and long term constraints (Kumburu, 2009).
This system enhanced the development of a culture of accountability among public

5
servants and provision of incentives to monitor their own performances. It was also
argued that performance management works only if there is information and only if
there are real consequences to under performance (Rugumyamheto, 2005). Tanzania
Public Service Commission (TPSC), (2008) stated that there was also installation of
Open Performance Appraisal System (OPRAS) in 2005 that was the instrument used
to assess the individual performance of employees by their supervisors to the
achievement of quality public services. Also there was introduction of strategic
plans, action plans; clients service charters, service delivery survey and self-
assessment.
According to Ying (2012) employee performance is strongly related to
organizational performance, effective and efficient employee performance will
positively influence organizational performance. In order to organize organization
effectively, organizations must rethink how they hire, train and reward their
employees; therefore, employees could be encouraged to be competitive. This was
supported by Millar (2007) as cited by Ying, (2012) who built a framework of talent
management which consist of planning, recruiting, performance, learning, career
development, succession planning, compensation and measuring and reporting.
There is an important factor in human organization as the main strategy of
organization is to invest in employees. Organizations are seeking to develop,
motivate and increase performance of their employees in a variety of the human
resource applications (Gungor, 2011).
Also the Public Service Management and Employment Policy (1999), states that
every public service institution should have a system of evaluating performance of
all its employees. And each employee will have duties that include specific goals that
are measurable according to the expected result within 12 months. Responsibilities
and goals will be prepared by consultation with the employee and will show the
objectives of developing the employees’ skills as well as the objective of
implementation. Employees will be given feedback about their performance over a
period not exceeding six months and will be advised to be provided with assistance
to correct the deficiencies that will rise. After evaluating their performance
employees should be given the feedback of their performance if they performed

6
poorly they should be provided assistance and training, they should be awarded for a
better performance. Now days there are many organizations that are relying on
employees for success and competitiveness. As employees are the resources and
assets of an organization. But organizations have to figure out strategies of
identifying, encouraging, measuring, evaluating and improving and rewarding
employees’ performance. Though the organizations rely on employees for
performance, there are many local governments that still perform poorly in every
year and end up getting qualified report, adverse or disclaimer reports which is due to
poor performance of their employees. This is why this study will focus on finding
how institutional factors can contribute to poor performance of employees in
delivering health services in Mbeya Dc.
1.3 Statement of the problem
Academic, policy makers and performance technocrats in both public and private
sector continue to explore how best they can improve employees’ performance in
their organizations. This is because the higher the performance, the higher the way
how organization compete to develop in the global economy. Ideally, the
implementation of Tanzania public service management and employment policy
(1999) strived towards improved employees’ performance at various work
measurable according to the expected results within twelve months. However, in real
situation general observation show that employees underperform the work for
various reasons (Interviews with Director, HRH Mbeya DC, February 2019)
Many people think that under performance of employees in the public sector is
associated with: such as: ineffective leadership, organization culture, poor working
environment, poor or lack of motivation, training, rewards, communication,
promotion, personal problems norms and standards and behaviors (Arinanye, 2015;
Ying, 2012; Thao& Hwang 2010; Ngowi, 2014; Mbah, 2015; Landa 2018; Peter
2014). This initial perception fails to take into account on how institutional factors
such as (regulative, normative and cognitive) factors contribute to poor employees’
performance in delivery of health services. This is the gap filled by this study. This
essay, therefore, bridged that gap of knowledge.

7
1.4 Research objectives
1.4.1 General objective
The general objective of this study was to investigate how institutional factors
contribute to poor performance of public employees in delivering health services at
Mbeya DC.
1.4.2 Specific objectives
i. To determine how existing rules and regulations contribute to poor
performance of employees in delivering health service at Mbeya DC
ii. To find out how norms and values contribute to poor performance of
employee in delivering heath service at Mbeya DC
iii. To examine how the level of knowledge of employees about health
service delivery contribute to poor performance of employees.
1.5 Research Questions
i. How do the existing rules and regulations contribute to poor performance
of employees in delivering health services at Mbeya DC?
ii. How Does Norms and values contribute to poor performance of employee
in delivering health services at Mbeya DC?
iii. How does the level of knowledge employees about health service
contribute to poor performance of public employees in delivering health
services at Mbeya DC?
1.6 Significance of the study
This study will help Mbeya district council and other similar public institutions to
understand and know the institutional factors that contribute to poor performance of
public employees in delivering health services. To other researchers and scholars, the
outcome of this study is expected to become a fundamental source of literature
materials for future studies especially on the field of institutional factors. Also the
results of this study will be helpful to policy makers by providing valuable
information on the extent to which institutional factors contribute to poor
performance of employees when delivering health services. The study will also be
also helpful to other stakeholders of public organizations to become aware of how

8
institutional factors can contribute to poor performance of employees in delivering
services. It will also benefit employees of public institutions by improving their
performance towards their clients.
In addition to the above significances the study will be significantly important to the
researchers to gain analytical skills and experience in research methodology for a
successful accomplishment of the Master’s degree and career development
1.7 The scope of the study
This study did focus on investigating how institutional factors contributing to poor
performance of public employees in delivering health services. Despite the fact that
employee performance is the concern of all public organizations and institutions but
for the purpose of this study the focus was on the Local Government Authorities
(LGA’s) and only in Mbeya District that was used to represent other LGA’s in
Tanzania.
1.8 Limitations of the study
Despite reaching the study objectives there were some constrictions of the study,
including; a disappointing response from the research respondents, the research
respondents had a low response rate due to them being in hurry, being busy with
their job activities while others not being at their particular working places.
However, the researcher did a continuous follow-up to respondents thus enabling the
completion of the particular task.
Lack of funds, since the researcher was self-sponsored while getting research
materials that included pamphlets, journals together with internet bundles and data
collection movements required money, this led to completing of the research study in
a difficulty way.
Other major limitation confronted was lack of cooperation from the government
officials/employees in areas where data was collected, who some of them specifically
seemed unwilling to give out data and information for the study

9
1.9 Organization of the study
The study is organized into five chapters which are arranged as per guidelines for
writing dissertation. Chapter one presents the problem setting which include
introduction, background of the study, statement of the problem, objectives of the
study, research question, significance of the study, the scope of the study and
organization of the study.
Chapter two of this study presents the review of literature which consists of
conceptual definitions, empirical reviews, theoretical analysis, conceptual framework
and knowledge gap.
Chapter three of this study covers research methodology which includes research
design, study area, population of the study, sample and sampling techniques, data
collection methods, data analysis, data reliability and chapter summary.
Chapter four of this study represents the research findings and discussion of findings,
while chapter five provides the conclusion and recommendations. It ends with the list
of bibliography and appendices attached to this report.

10
CHAPTER TWO
LITERATURE REVIEW
2.0 Introduction
This chapter reviewed the literature from various sources in order to provide both,
theoretical and empirical literatures of the study. Within the theoretical lens, it
explained the conceptual definitions of the study and the applications in the context
of this study. It also critically analyzed empirical data related to the objectives of the
study as shown in Chapter One.
2.1 Definitions of terms used in this study
2.1.1 Health services
Health service involves the services that provide medical treatment and care to the
public or particular group. Health services consist of medical professionals,
organizations, and ancillary health care workers who provide medical care to those in
need. They serve patients, families, communities, and populations. They cover
emergency, preventative, rehabilitative, long-term, hospital, diagnostic, primary,
palliative, and home care (Unfried, 2003).Provision of health services refers to the
way inputs such as money, staff, equipment and drugs are combined to allow the
delivery of a series of interventions or health actions. Provision of health services is
the most visible and familiar product of the health care system (WHO, 2000).Access
to health services means the timely use of personal health services to achieve the best
health outcomes. It is a concept which measures the capacity of the health system to
reach the population without excluding part of it from receiving healthcare services.
Ensuring a high degree of access to healthcare improves people’s overall health
status, prolongs life expectancy and decreases health inequalities.
2.1.2Health service delivery
Health service delivery is defined as the provision or stipulation of the health
services by the health care centers to the individuals or the community for the
purpose of preventing and curing health problems, promoting maintenance of health
and well-being, or obtaining information about one’s health status (Marc D.
Gellman, 2013).

11
2.1.3 Performance
Armstrong (2001) defined performance as behavior the way in which organizations,
teams and individuals get work done. Generally, performance is an accomplishment
of a given task measured against present known standards of accuracy, completeness,
cost and speed.
2.1.4 Employee performance
Employee performance is the successful completion of tasks by selected individual
or individuals, as set and measured by supervisor or organization, to pre-define
acceptable standard while efficiently and effectively utilizing available resource
within a changing environment (Mathias & Jackson, 2009).
The employee performance is usually regarded as the criteria standards for employee
behavior at work. These criteria contain much more than how an employee does the
work. Employees are rated on how well they do their jobs compared with a set of
standards determined by the employer. The employee performance is usually
evaluated by the level of execution, quality of work, level of creativity, amount of
consistent improvement, responsiveness to feedback, percentage of the task
completed on time and most being on time and on the required budget.
2.1.5 Poor employee performance
Poor employee performance refers to the failure by the employee to reach the
required targets or maintain the required employee performance standards that are
either measured qualitative or quantitative (Mathias & Jackson, 2009). It specifically
implies a failure to satisfactorily meet up the work requirements specified to the
particular employee as directed by the employer or the supervisor.
2.1.6 Institution
Institution is a shared rules and typefication that identify categories of social actors
and their appropriate activities or relationship (Barley & Tolbert, 1997). Also Meyer
and Jepperson (1991) defined institution as it comprises regulative, normative and
cultural cognitive elements that together with associated activities and resources
provide stability and meaning to social life. Institutions are multifaceted and durable

12
social structures that are made up of symbolic elements, social activities and material
resources.
2.1.7 Institutional factors
Institutional factors are the factors that govern how organizations should operate,
influence leadership styles and the performance of employees within the organization
and the overall organization performance. Institutions factors can be formal or
informal, formal institutions are raised from laws, regulations, rules and other
statements of formulating sanctions while informal institutions are raised form
interactions with formal institutions. Public organizations are formal institutions
governed by rules, regulations and procedures.
2.1.8 Rules and Regulations
In this study rules and regulations means frame of meaning which guide human
actions in an organization. These see to regulate or constrain behavior and it uses
type of coercive force in order to gain agreements.
2.1.9 Norms and values
In this study norms and values means authoritative standards which specify how
things should be done and define legitimate means to pursue valued ends. They also
impose not only constraints but also empower and enable social actions.
2.1.10 Knowledge
In this study knowledge means information and skills and acquired by employees
through education or experience. It also means understanding of facts and service
offered to customers.
2.2 Theoretical Framework
2.2.1 Theory underpinning this study
This study was guided by institutional theory. It is argued that institutions have
certain features in common, with each possessing an identity such as name,
objectives, a written constitution, a list of employees and methods of replacing and
recruiting new employees to ensure continuity. These like institutions have some
features in common like institutional objectives, the use of employees to achieve

13
goals, a form of structure to coordinate the people expected to achieve the objective
and changing environment to operate within (Glover &Masete 2006).
Institutional theory emphasize that modern organization depend on their environment
which can influence the development of formal organization structures. The theory
acknowledges the importance of economic and social factors that shape the system
and structures of organization (North, 1990; DiMaggio, 1983). Institution may hinder
or enhance performance in the organization. Institutional theory state that
organizational structures and process become institutionalized over time and these
have an effect on worker’s behavior and performance. The factors may include
economic, social, and political that constitute a structure of particular environment of
an organization that gives it a competitive advantage.
Oliver (1990) explained that the main concept of institutional theory is that
organization structure and process tend to acquire meaning and achieve stability in
their own right rather than on the basis of their effectiveness and efficiency. He also
mentioned that institutional theorist is interested in examining the organizational
structures and practices that have no economic or ethical purpose and therefore they
do not enhance performance in organization. Although scholars have different
emphasis on these factors elements and in level of analysis at which they work, they
all recognize the common subject that social behavior and associated resources are
anchored in rules and plans.
DiMaggio and Powell (1983) stated that organizations converge on similar activities,
behavior and practices which appear similar to like organizations. The appearance
change towards homogeneity is explained through isomorphic change theory which
identified three forces on the organizations: coercive, normative and mimetic.
Coercive evolves from political influence and legitimacy and conveyed through
policies, rules, procedure, regulations and external environment requirements.
Normative is associated with the professional values and mimetic is about mimic or
copying behaviors that is the result of organizational response to uncertainty.
Meyer & Rowan, (1997); Suchman, (1995) explained that institutional factors have
been theorized in literature to be potentially important determinant of performance in

14
an organization. As it suggests that performance increases legitimacy because it
indicates how well a firm is fulfilling its roles in society. Galbraith (2002) also said
that factors such as structure, strategy, culture, policies, practices and technology
play crucial role in the overall performance within organization. Institutional system
should be viewed as a class of element because institutionalized rules, standards and
norms do not come from one source but multiple environments which is shaped by
different actors. It is also accompanied by other changes like cultural elements,
multiplicity and diversity of organizational sources, markets, strategy, competitors
and customers (Scott, 1987).
It was argued that institutionalization involves the process through which members
of organization acquire values that go beyond the technical requirement of
organization tasks. No organization is completely free of values. This was also
supported by Selznick (1957) who argued that to institutionalize is to infuse with
value beyond the technical requirement of the task at hand. It is also induced by
selective recruiting of personnel, by establishing strong ties or alliance with outside
groups through processes like implicit alliances, sharing common values or co-
optation with local partners. Institutionalization is achieved when rules or procedures
are sanctified, when members of public institutions become semi-autonomous center
of power and develop their own vested interested and when administrative symbols
and ideologies exist.
Therefore, according to institutional theory, besides formal rules and procedures
institutional includes symbols, moral models and cognitive schemes. It provides
frames of meaning which guide human action and therefore are similar to cultural
systems. Institutionalization is a cognitive process that models the sense people give
to events or acts. Institutionalized myths are central of explanation as formal
structures should be understood as composed of myths and ceremonies influencing
the conduct of public administrators not only by influencing what they have but also
by shaping the imagination of actors about alternatives and solutions (Meyer &
Rowan, 1997).

15
2.3 The concept of employee performance and institutional factors
2.3.1 Employee performance
Employee performance plays an important role in organization performance, as
employee performance is what an employee does or does not do. As it is argued by
Gungor (2011) performance of employees includes quantity of output, quality of
outputs, timeliness of output, presence at work and cooperativeness. Good employee
performance has been linked with increased customer complaints and brand witching
and also employee performance is related to activities expected to be done by
employee and how those activities are executed. In many organizations Human
resources and directors assess employee performance of each worker on annually,
quarterly, monthly and weekly basis depend on organization strategy in order to help
employees identify suggested areas of improvement.
Employee performance is usually looked in terms of outcome, though it can also be
looked in terms of behavior (Armstrong, 2002). Kenney et al (1992) explained that
employee performance is measured against the performance standards set by
organization. Also there are numbers of measures that can be taken into
consideration when measuring performance of employees like using productivity,
efficiency, effectiveness, quality and performance measures (Ahuja, 19920). It is the
responsibility of human resource managers to set desired level of performance by
setting goals and standards against which individual performance can be measured.
Organizations ensure that their employees are contributing to producing high quality
products or services through the process of employee performance management.
Naharuddin and Sadegi (2013) stated that employee performance depends on the
willingness and openness of employees on doing their job. He also mentioned that by
having the willingness and openness of the employees in doing their job, it could
increase the employee’s productivity which also leads to the performance
improvement. Apart from employee skills and experience, necessary resources to
perform have to be made available for employees to perform like good working
environment, tools and materials. Foot & Hook, (2008) clarified that employees need
to be given the ability to contribute to the performance of the firm together with the

16
means and incentives to do so. They also argued that the management should work in
partnership with its employees for continuous and improved production through the
use of involvement and partnership practice. They further explained that organization
should try to maximize their employee’s contribution to the achievement of
organizational goals so that employees have the ability to add value through high
performance working while at the same time they directly benefit employees.
Managers should initiate activities which will help in improving employee’s
weakness like engaging in training and development exercise to attain the required
skills which will result in improved performance (Mbithe, 2012).Mbithe also argued
that some of employees’ strength should be rewarded hence motivating them to add
more effort on their work and improve their performance. Organizations which are
ignorant on employee performance might end up collapsing as managers do not
monitor their employee achievements which may not relate to the organizational
goals and objectives set.
The success of employees’ performance is based on some factors example physical
work environment, equipment, meaningful work, performance expectation, feedback
on performance, reward for good or bad performance, operating procedures,
knowledge, skills and attitude. Naharuddin and Sadegi, (2013) supported that there
are number of factors that may affect employees’ performance where each employee
may have different impact from different things at workplace. Also their attitude and
behavior can play an important role in their performance.
2.3.2 Factors Affecting Employees’ Performance
Team working
According to Aichouni (2005), a man cannot live on his own effort alone; he requires
the help of fellow man. The profit and non-profit making organization are
considering teamwork very important in their operations and especially in employee
performance and overall performance of the organization. Many organizations have
established the culture of teamwork that operate with high quality and speed in their
operation (Aichomi, 2005). In most organizations that has no culture of team work

17
there is poor performance because every individual employee is focusing on
achieving his own goals rather than team goals.
Performance appraisal
According to Peter and Waterson (2004) performance appraisal affect employee
performance. Performance system of an organization has to be maintained by
monitoring performance of employees through having periodic evaluations. And data
obtained from these has to be a part of critical component at internal staff decision
making like in retention, promotions and termination of employee (Bernadin, 2007).
Remuneration of employees
Remuneration of employees as significant impact on worker’s attitude and
performance in an organization since that it has most effective motivation techniques
once remuneration is not fulfilled to the employees they became demoralized
(Basaza, 2016). Good remuneration improves productivity and morale of employees
which lead to high employee performance. But poor remuneration affects
productivity.
Job security
Another factor is job security; some employees tend to underperform especially in
public organization because of the notion that to terminate the employees there
should be a procedure to follow than those who are in private organization because in
public organization job security is very observed thus affect the performance and
outcome of production in a given organization, under this scenario performance of
employees depends on the perception and readiness of employees in an organization.
According to Sanderson et al (2009), commented that public organizations are often
criticized for providing too much job security and failing to address
underperformance
Delegation
Delegation creates relation between superior and subordinate in work place, under
this fashion the delegated one may lead to unification of employees or destruction of
relations among the employees within an organization thus may lead to affect the
performance of employees in the aspect of production and psychological torture.

18
2.3.3 Causes of Poor Performance in Delivering Health Services
Poor competencies and trainings:
In most cases the health care sector is faced with poor performance due to the
employees having poor and inadequate level of competencies, which include lack of
enough health related knowledge, skills and competencies which all result to poor
performances in delivering the health services (Noe et al, 2010). In most case,
especially in Tanzania’s context in the hospital staffs usually provide poor services to
the customers (patients) due to lack of enough trainings or not being competent
enough to work in the health sector.
Insufficient funding:
In Africa’s context most of the health delivering is usually reported poor due to lack
of the funds that are directed in the health sector. According to Mathauer & Imhoff,
(2006) most of majority cases where the health sector has failed perform or failed to
deliver the intended outcomes the major cause has been found to be a lack of enough
funds which enable them the sector to employ well educated expertise, and enable
the health care centers to acquire enough medical facilities and utilities.
Lack of enough staffs:
Lack of enough skilled staffs and well competent employees has on the hand led to
the poor performance of the employees especially when the few available health
employees are supposed to attend a large group of people (Mathauer &Imhoff,
2006). In most African cases majority of the public hospitals have less staffs
especially those in remote areas. However, this challenge has heavily been
contributed by the underpayments and lack of necessary social services in the remote
areas.
Poor working environment:
Chan (2013) did suggest that the working environment in most health centers and
hospitals are poor thus leading to the poor performances of the overall sector at large.
In most case of Africa and especially Tanzania the working environment are poor
especially to the nurses and other lower ranked medical attendants, which highly
influence the poor performance of the sector as a whole.

19
Indicators of poor performance of employees in delivering health services
According to Hornby and Forte (1999) Indicator provides an indication of the
relative state of key determinants of efficiency and effectiveness in comparison to
norms of organizational activity. Also According to WHO (2007) Indicators are
markers of health status, service provision or resource availability, designed to
enable the monitoring of service performance or program goals. Also indicators are
measurements that have the power to summarize represent or reflect certain aspects
of the health of persons in a defined population. The following are the indicators of
poor employee performance in health service delivery.
Infrastructure
Bold et al (2011) states that, most health clinics ac basic infrastructure especially in
rural areas. Infrastructures like electricity which is necessary in operating health
equipment, clean water and sanitation facilities which is important for quality
services. He also argues that some of public hospitals lack medical equipment’s like
stethoscope, weighting scale and thermometers. In public hospitals there is also a
problem of stock-out of drugs.
Medical personnel
This indicator focuses with health staffs in public hospitals. Where the employees are
being characterized by the following; absence rate where many health workers are
not in the clinic during working hours. Also number of personnel’s in health sectors
is the crisis in Tanzania especially the lower level health services in which
dispensaries and health sectors have shortage of employees which lead to poor
performance in delivering reproductive and child health (URT, 2008).
2.3.4 Concept of Health Service System in Tanzania
The Tanzania’s health service system is designed to follow a specific government
structured pattern which specified in a hierarchy form. Which comprises form the
referral hospital (hosipitaliyarufaa) to the regional hospital to the district hospital to
the health centers and the finally the dispensaries (MoHSW, 2008). The system
works in a pyramidal shape where the referral hospitals are ranked highly to the top

20
and usually regarded as the final solutions for the medical issues before the patients
are referred to the national hospital.
Furthermore, the health service system has been structured into mainly four
categories that include the health promotion, preventive, curative care and the
rehabilitative care, which all these are to be done at all levels of the health care
centers (URT, 2015). This structure was designed to archive all the health sector
objectives, specially the overall objective which is to provide the essential quality,
affordable and sustainable health care services on the bases of equity and gender
equivalence.
2.3.5 The Concept of Reproductive and Child Health
According to Chaturvedi (2010), RCH program included the existing programs like
National Family Welfare Program and Child Survival and Survival & Safe
Motherhood Program (CSSM). He also states that RCH compose the family
planning, child survival and safe mother hood prevention/ management of
RIT/STD/AIDS (Maternal Health), Child health and adolescent health. Tanzania
government has prioritized reproductive and child health, adopting policies to inform
Reproductive, Maternal, newborn, child and adolescent health program by
developing the National Road Map Strategic plan to Improve Reproductive,
Maternal, Newborn, Child and adolescent Health in Tanzania (2016-2020) one Plan
II (Dutta, Slevin, Barker and Leahy-Madsen, 2015).
In 1974 maternal and child health services were introduced in Tanzania. In 1975 the
Expanded Program of Immunization (EPI) was launched to support immunization
facilities for vaccine preventable childhood. In 1989 the government adopted Safe
Motherhood Initiative (SMI) which was followed by the launch of the Global Safe
Motherhood Initiative in 1987 in Nairobi Kenya. Also the government of Tanzania
introduced Reproductive and Child Health Section (RCHS) within the Ministry of
Health and it developed a National Reproductive and Child Health Strategy (URT,
2008).

21
According to URT (2008) In 1996 GOT adopted the Integrated Management of
Childhood Illness (IMCI) approach for reduction of childhood morbidity and
mortality. Also GOT established different initiatives so as to address the problem
concerning of reproductive and child health which include maternal, newborn, child
and health. Also in 2003 the government established the National Program on
Prevention of Mother to Child HIV Transmission so as to reduce the number of
affected people in the country. And in 2005 the National Strategy on Infant and
Young Child Feeding and Nutrition (IYCF) was created so as to reduce the number
of children with malnutrion (URT, 2006).
The government of Tanzania also in 2008 introduced the program called National
Reproductive Health Cancers- Cervical Cancer Prevention and Control and Health
Sector Prevention and Response to Gender Based Violence. Also the government
decided to provide RCH services free of charge so as to improve accessibility and
availability of service to the people (URT, 2016). Therefore, the government of
Tanzania introduced all these programs so as to address all the problems that will be
associated with RCH services.
2.4 Institutional factors on employees’ performance in delivering health service
Institutional factors relate to structures within the organization. It includes rules,
policies, procedures, norms, shared beliefs and routines of behavior in an
organization. Scott (1995) revealed that institutions are social structures that have
obtained a high degree of resilience and they include cultural elements, normative
and regulatory factors. Institutional factors are important as they govern how
organizations should operate, influence leadership styles and the performance of
employees and organization. Institutions can be formal or informal, formal
institutions are raised from laws, regulations, rules and other statements of
formulating sanctions while informal institutions are raised form interactions with
formal institutions. Public organizations are formal institutions governed by rules,
regulations and procedures.

22
2.4.1 Regulative factors and employee performance in delivering health service
According to Scott (2008) regulative pillar of institutionalization include rules, laws
and structures that seek to regulate or constrain behavior and it uses type of coercive
force in order to gain agreement. In order for the organization to constrain and
regularize behavior of employees they use this pillar. It is also argued that regulative
may include formal written rules, informal and unwritten code of conduct (Scott,
1995). Regulatory also processes rule setting, monitoring and sanctioning activities.
The process involves the capacity to establish rules, inspect others conformity to
them and manipulate sanctions rewards or punishment in an attempt to influence
behavior. Sanction process operate through informal mechanism which may include
shaming or shunning and through formalized and assigned actors like police and
courts.
Abbot et al (2001) informed that formalization of rule system is a continuum whose
values vary along three dimensions: obligation which means the extent to which
actors are bound to obey because their behavior is matter to scrutiny by external
parties; precision which involve the extent to which rules unambiguously specify the
required conduct; and delegation involves the extent to which third parties have been
granted authority to apply the rules and resolve disputes. Many types of regulation
enable and empower social actors and action, conferring licenses, special powers and
benefits to some type of actors. Actors in this study will mean top management,
employees, customers and shareholders. Regulatory process in private rely on
positive incentives like profits and increased returns while in public sector actors
uses negative sanctions like taxes, penalties and fines.
Dornbusch and Scott (1975) stated that force, sanctions and expedient responses are
central components of the regulatory pillar, but they are often tempered by the
existence of rules that justify the use of force. When coercive power is both
supported and constrained by rules it moves into the realms of authority as power is
institutionalized. Basing on economic point of view they emphasize the cost of
overseeing systems of regulation. Agency theory explained the expense and difficult
entailed in accurately monitoring performance relevance to contracts whether
23
implicit or explicit and in designing appropriate incentives (Milgrom& Robert,
1992).
Employment policies and laws may influence the size and the role of Human
Resource Management (HRM) within organizations. People with HRM role could
either be administrative or strategic level (Brewster et al, 2008). For example,
countries which have active trade unions, the HRM department can be expected to
take a limited role. When organization develops institutional rules, they rely to some
extent on normative and cognitive paths (Budhwar and Sparrow, 2002). As
normative approach related to the context of economy and political conditions,
cognitive emerges in the way actors perceive values, norms and symbols surrounding
the business like the way society perceive power, plays the role of affecting
managerial concepts of delegation, autonomy and participation and the status of
communication in the work place.
Also policies, rules, regulations and laws may help in shaping organization culture if
it is well documented. Munir, Perera and Braid, (2011) support that the role of top
management in shaping the organizational culture through their policies is well
documented. Top management can influence the manner in which organization can
undertake change by showing commitment and by creating supportive policies which
will also influence the performance strategies in the organization. Organization
cultures influences the beliefs and behavior of the employees and shape the attitude
of employees towards performance. When there is consistency in standard behavior
performance improvement and quality will increase. It will also increase
opportunities in HRM functions exist in recruiting and development policies,
incentive policies and flexible work system that involves employee participation
(Katou and Budhwar, 2010).
Individuals craft laws and rules that they believe will advance their interests, and
individual conforms to laws and rules because they seek the attendant rewards or
wish to avoid sanctions. Basing on this logic regulative pillar is the one around which
rational choice scholars gather. Rules must be interpreted and disputes must be
resolved, incentives and sanctions must be designed and will have unintended

24
effective, mechanism are required but they are expensive and will prove to be fallible
and conformity is one of many possible responses by those subject to regulative
institutions.
2.4.2 Rules and Regulations of RCH services in Tanzania
In Tanzania there are different rules and regulations that guide reproductive and child
health. According to URT (2008), reproductive and child health is guided by the
following; National Health policy (revised 2003), Health Sector Reform and Health
Sector Strategic Plan (2003-2007), Reproductive and Child Health Strategy (2005-
2010), National Road Map Strategic Plan (2006-2010), National Strategy for Growth
and Poverty Reduction (2005-2010) and the National Road Map Strategic Plan to
Accelerate Reduction of Maternal, New-born and Child Deaths. Therefore, basing on
these rules and regulations to monitor service delivery for Reproductive and Child
Health, public employees’ performance is supposed to be measured by considering
the reduction of maternal, New-born and Child deaths in Tanzania (URT, 2008).
National Road Map Strategic Plan to accelerate Reduction of Maternal New-born
and Child Deaths in Tanzania (2008-2015), One Plan. According to URT (2016) this
aimed at providing guidance on the implementation of Maternal New-born and Child
Health (MNCH) at different level of service delivery. In which the key indicators
included reducing the maternal mortality ratio to 193 per 100,000 live births by 2015,
also reducing the neonatal mortality to 19 per 1000 live births and reducing under-
five mortality rates to 54 per 1000 live births from levels in 2008 or before.
National Road Map Strategic Plan to improve Reproductive, Maternal, New-born,
Child and Adolescent Health in Tanzania (2016-2020), One Plan II. This was
introduced so as to reduce maternal, newborn, child and adolescence morbidity and
mortality by providing services with equity, which are provided by skilled attendants
in allowing environment and in an integrated manner along the continuum of care by
considering community and facilities (URT, 2016). This strategic plan covers
different areas of RCH services like maternal health, Newborn and Child Health,
Family Planning, prevention of Mother to child Transmission, immunization and
vaccine development, Reproductive health gender and reproductive health cancer.

25
Also the main objective of this strategy is to accelerate reduction of preventable
maternal, newborn, child and adolescent morbidity and mortality.
The National Development Vision 2025. One of the goals in 2025 Vision is to have
the access to quality reproductive health service for all individuals and reduction of
infant and maternal mortality
Tanzania National Health Policy Document of 2003.According to Mueenuddin and
Msuya (2012) the main goal of this policy was to reduce the burden of diseases,
maternal and infant mortality, and increase life expectancy through the provision of
adequate and equitable maternal and child health services, facilitates the promotion
of environmental health and sanitation promotion of adequate nutrition control of
communicable diseases and treatment of common conditions.
2.4.3 Normative factor and employee performance in delivering health service
Normative is mechanism that creates a pool of almost interchangeable individuals
who occupy similar position that may override variations in tradition and control that
might otherwise shape organizational behavior (DiMaggio& Powell, 1983).
Normative include factors like norms and values, expectations and roles that seek to
influence behavior (Scott, 2008). Norms specify how things should be done; they
define legitimate means to pursue valued ends. Values are conception of the
preferred or the desirable together with the construction of standards to which
existing structures or behaviors can be compared and assessed. Normative system
defines goals or objectives and designates appropriate way to pursue them (Blake
&Davis, 1964). As it is argued by Scott (1995) they prescribe rights, privileges,
responsibilities and duties of actors who are obliged to do so as the normative factor
is based on asking the question of “what is expected of me”. Normative also
emphasize that individual actions and behaviors are appropriate and expected of
various social roles and values and what norms are pertinent (Scott, 1987).
Some values and norms are applicable to all members of the collectivistic as others
apply only to selected type of actors or position. And those selected actors give rise
to the roles which include establishment of appropriate goals and activities for
particular individuals or special social position. These beliefs are not only

26
anticipation or predictions, but also prescription normative expectations regarding
how specified actors are supposed to behave. Roles can be formally designed and
emerge overtime through interactions, differentiated expectations developed to guide
behavior (Blau& Scott, 2003). Normative systems are viewed as imposing
constraints and social behavior but they also empower and enable social action. As
they confer rights, responsibilities, privileges, duties, mandates and licenses. Hughes
(1958) supports that power and mystique associated with these types of roles come
from the license they are given to engage in forbidden or fateful activities like
conducting physical examinations or sentencing individuals to death or prison.
Hanson (2001) argued that normative stems from values of professionalism where
professionalism is associated with the members of an organization and their desire to
maintain autonomy over work procedures and legitimization of their work, example
professional works or boards, on the job socialization and networking, training and
professional development, formal education and certification process accredited by
professional bodies. Professional norms are normally most influential pressure that
organization faces (DiMaggio & Powell, 1983). Hussain and Hoque (2002), argue
that the experience of professionals such as managers may also influence the design
and use of performance measurement system. According to Apospori (2008) there is
relationship between HRM practices and its environment from the inner institutional
level factors with primary focus on the status of HRM within organizations at
different level like strategic level, HRM position role and HRM practices. The
strategy level focuses on the clarity of HRM strategy in defining duties, jobs and
extent of alignment between HR strategy and business strategy. Validity of HRM
practice can be measured by the ability of HRM practice to develop employees to the
level of required for competition and the ability of HRM practice to improve
individual abilities and skills and motivate employees to exploit their potentials. Also
the HRM position role describes HR professional as partners with managers and
having a voice in setting business strategies, being considered and HR as an
investment asset.

27
Like in regulative system normative system can also evoke strong feelings. As
feelings associated with the trespassing of norms include a sense of shame or
disgrace, and a feeling from exemplary behavior lead to the feelings of respect and
honor. The conformity or violation of norms involves a large measure of self-
evaluation, high remorse or effects on self-respect. These emotions provide powerful
inducements to comply with prevailing norms. Helco (2008) insisted that human
being are supposed to be moral agents, as by virtue of being human they experience
existence as partaking in question of right and wrong. Human life is morally
implicated.
2.4.3.1 Norms in Health Service in Tanzania
The norms in the health services employees or the health sector as a whole are much
likely to similar to the norms, values and ethics of the public employees. In most
cases these norms vales and ethics are aimed to govern the employee to deliver good
performance in his or her area of work and hence neutralize or reduce the poor
performance that could result in the sector.
Respect all human right and be courteous; the employees should employees are
required to perform their duties diligently while respecting the human right so as to
enable an efficient performance without irrespective results (URT, 2015).
Accountability; in this case the employees should inculcate the notion of
accountability so as to ensure there is an adequate performance between the
individual employees and the health organization as a whole. Furthermore, the
employees should enhance the notion of transparency within the organization.
Avoid the conflicts of interest; the public employees are supposed to perform their
duties with honesty and fairly avoid the circumstances that will or may lead to the
conflicts of personal interest. If the conflicts of interest tend to occur the employees
should report to their superiors who are to decide upon the best course of action to
resolve the blunder.

28
2.4.4 Cultural cognitive factors and employee performance in delivering health
services
Cognition is the mental action or process of acquiring knowledge and understanding
it through thought and experience. In cultural cognitive individuals have perception
of social reality that come from their understanding of the way institutions have
internalized social perception (Welter, 2011). It involves people shared beliefs with
reference to what is generally taken for granted. Cultural cognitive emphasize
common schemas, frames and other symbolic representations that guide behavior
(Scott, 2008). Also cultural cognitive imitates the cognitive structure and social
knowledge shared by the people in a given country or region. Scott (2001) argued
that the cognitive elements of institution are shared conceptions that constitute the
nature of reality and frames through which meaning is made. Cultural cognitive
considers that internal processes are shaped by external or environmental cultural
framework. Individual behavior depends on interpretation of their context and
consensus within the group. As the group of reference contribute to the definition of
values, virtues and beliefs of the individuals (Scott, 1995).
Cultural cognitive mediate between the external world of stimuli and response of
individual is a collection of internalized symbolic representations of world.
According to Andrade (1984) in cognitive what a creature does is in large part a
function of the creature internal representation of its environment. They are cognitive
in that they provide important templates of framing individual perceptions and
decisions. Some of the beliefs and assumptions are explicit and relatively superficial
(Swidler, 1986) but others are deeply entrenched assumptions and the conceptions of
the way the world is as the soft-ware of the mind (Hofstede, 1991). The cultural
cognitive provides the foundation for normative prescriptions and regulative controls
as norms and rules must refer to institutionalized constituted entities. They can also
provide framework for order. In other words, cultural cognitive involves the process
of knowledge acquisition and processing which affect institutional learning.
Institutional responsiveness and adaptation are stimulated in both the regulative and
normative if communication mechanisms are in place to transfer the knowledge.

29
According to Kooiman et al, 2005; Ostrom, 1990 and Scott (2014), Institution is a
dynamic system that is continually subject to stressors that forces varying
characteristics including conflicts, acting within and external environment system.
The system must be flexible enough to adapt in order to minimize disruption from
stressors. No single factor of institution can function alone no does it dominate as
when there is balance in the system the capacity to adopt is high and the chances for
sustainability are greater. Strange and Sine 2002) supported that when the system
moves out of the balance it means the stressors are exerting force on one or more
factors or pillars and the adaptation to re-establish balance becomes necessary.
Example in recruitment there are different criteria used which are cultural bound of
the organization like education, past experience, personality trait and cognitive skills.
For example, in US the recruitment and selection criteria are perceived to be relevant
to the job and predictive of future performance. In Japan they base on the team
member’s favorable opinions about candidate, right temperament and personality. In
Arab countries they look at agreeableness, good interpersonal relations and
trustworthiness (Ali, 1989). In India belonging to the same group as the manager like
the same family or home land (Sinha, 1997). In collectivistic and high power
distance countries where ascribed social statusand social political connections are
more important than applicants merit and credentials (Budhwari and Khatri, 2001).
In Korea system places emphasis on the applicants’ socio economic background,
including family ties, school and birth place (Lee, 1999).
2.4.4.1 Skills Required for Health Providers of Reproductive and Child Health
The health care providers should well skilled and trained for them to venture and
yield an adequate performance in the health services delivery especially in the
reproductive health and child health. The employees or the health service providers
should be aware of the application of the family planning and should also enhance
and provide this education to the patients. Moreover, the health sector employees
should be aware of the overall gender norms and additionally the employees should
also be well trained on the reproductive measures and the caring measure so as to

30
improve the reproductive health services and the new born children’s health (URT,
2017).
2.5 Empirical literature review
There are few studies which have similar problem which have been conducted in
different places within and outside the country. The researcher therefore has
reviewed some of those studies which have been conducted regarding employee
performance in order to learn what they have found about factors affecting employee
performance and especially in delivering health services.
Mubyazi (2005), conducted a research on user charges in public health facilities in
Tanzania: effect on revenues, quality of services and people’s health-seeking
behavior for malaria illnesses in Korogwe district with the main objective of
establishing the influence of user charges at government health centers and
dispensary levels on revenue collection, quality of service, patient attendances for
malaria and other illness conditions and people’s health seeking behavior in general.
Data were collected through focus-group discussions with community members,
interviewing community leaders and health workers, field observations and review of
patient registers. However, in the findings he revealed that the quality of the health
services provided in most public owned health care centers is still low and thus a
need to ensure the health service providers to improve the health service delivery.
Shem and Ngassa (2015) in their study of Effects of training on employees’
performance found that on the job training have positive impact on the employee
performance because trained employees showed the willingness to continue working
while those who did not have on the job training were unwilling to continue working.
According to them training motivate employees and make them feel that
management appreciate their improved skills, and those employees feel the desire to
continue working effectively for the organization which positively impact their
performance. They have also found that orientation as one of training program is the
key determinant of employee performance because it helps new employees learn and
understand how organizations run business. They also figured that coaching has
influence on individual performance and organization performance as it helps

31
organization to improve their competitive position, maximize benefits and minimize
cost.
Kida (ESRF, 2012), conducted a research on provision and access of health services
in the urban health care market in Tanzania. This research was conducted in Kawe
ward (an urban ward) located in Dar es Salaam as the case study which is quite a
large ward that features both low and high density areas, respectively indicative of
richer and poorer populations, thus allowing for sampling across a wide
wealth/income range. The objective of this research was to find out if there is
existence of segmentation in the provision of health care services by the health care
providers in the urban health care market in Tanzania. The research was conducted at
three distinct levels: household level, health care facilities and municipal level. The
ward has varied infrastructure for health care, including both public and private
health care facilities at different levels. The results obtained from this research
showed that there is an existence of a two-way segmentation in the provision of
health care services; the upper segment serving the better off and the lower segment
serving mainly the poor which showed that these two segments of the health care
market have distinct institutional characteristics, distinct behaviors on the supply and
demand sides, as well as distinct competition pattern.
Thao and Whang (2010) in their study of factors affecting employee performance
found that Leadership, Motivation and training are the main factors that affect
employee performance. Leadership style affects employee performance through
leaders’ coach; empowerment or increase the employee participation and employee
will perform in a better way. Training is successful techniques for better employee
performance as it improves their competencies to be qualified for high technical and
international projects which enhance the organization competitive advantage in the
market and its sustainable development. Even though this study did not show how
working environment affects the employee performance which was one of their
hypotheses.

32
Mbah (2015), on his study of assessing motivation as a tool to enhance employee
performance found that employee motivation has an effect on the profitability of the
company, and a manager has to continuously design and put into action the dynamic
motivational structure which will be able to meet the desire of the employees. As
individuals have different needs and ambitions when they enter in the organization
and they are established as workers. Motivating employees will depend on managers’
ability to identify and satisfy his workers needs and ambitions. The researcher also
identified that when the manager has ability to show appreciation to workers who
performed well it help in increasing the degree of satisfaction and motivate the other
employees. The researcher also found that the poor relation and communication flow
between workers and the manager tends to demotivate employees, and then he
suggested that in order to keep employees motivated the manager should give chance
to good flow of information and ideas complimented with a possibility for feedback.
2.6 Conceptual Framework
Conceptual framework is an interconnected set of ideas (theories) about how
particular phenomenon functions or is related to its parts (Svinicki, 2010).
Conceptual framework aims at indicating the important area that will be covered by
the study. A researcher did need a good foundation that helped in collecting
necessary data. In this study conceptual framework did show the relationship
between independent variables and dependent variables. Regulative factors,
normative factors and cognitive factors are independent variables as their effective
occurrence can affect dependent variable which is employee performance that is
conceptualized by quality of service, productivity, efficiency and effectiveness of
organization and customer satisfaction.

33
Figure 2.1: Conceptual Framework
Source; Researcher’s Design, (2019)
2.7 Research Gap
Based on theoretical review and literature from earlier studies review in this study,
there are different factors that affect or contribute to employee performance in public
organizations regarding to what have been envisage from various studies. Those
factors include motivation, intrinsic and extrinsic rewards, leadership styles,
communication, training, promotions, performance management system, and
organization structure and organization culture. However, in most of public
organizations in Tanzania seem to be facing the problem of poor performance among
employees that lead to poor organization performance. Although various studies have
shown different measures on what public organizations need to do so as to overcome
the problem of low employee performance, there is no study that have tried to
identify how institutional factors contribute to poor performance of employee in
delivering health services. Therefore, this study tried to fill that gap.
INDEPENDENT VARIABLES DEPENDENT VARIABLE
REGULATIVE
Rules and regulations
Policy and procedures
NORMATIVE
Norms
Values
COGNITIVE
Knowledge and skills
Employee’s performance

34
CHAPTER THREE
RESEARCH METHODOLOGY
3.0 Introduction
This chapter contains Research design, area of the study, study population, unit of
analysis, variables and their measurements, sample size and sampling techniques,
types and sources of data, data collection methods, validity issues and data analysis
methods.
3.1 Research Design
This study was a case study design. The design gives explanation of the phenomenon
in depth and is a method used to narrow down a very broad area of research to make
it small so as to be manageable per resource available to the researcher. This design
was chosen by a researcher because it is relevant specific to the content of area of
study and will permit a thorough study of the problem. Claire et al (1962) defined a
research design as the arrangement of conditions for collection and analysis of data
in manner that aims to combine relevance to research purpose with the economy in
the procedure. Concerning this view, the researcher investigated institutional factors
contributing to poor employee performance in delivering health services in Mbeya
District Council and the findings of this study are limited generalization to other
councils.
This study used both qualitative and quantitative approach. The study adopted
qualitative approach because it did help the researcher in the assessment of employee
performance and provide the answers to the organization through the in depth
investigation and analysis of personal experiences (beliefs, opinions, motivations and
practices of individual respondents on the institutional factors and employee
performance. And quantitative approach was adopted where quantitative data was
collected in order to explain the relationship between institutional factors and
employee performance.

35
3.2 Area of the study and Population
The study was conducted at Mbeya district council which is one of the eight districts
in Mbeya region and is located at the North West of Tanzania. This area is selected
due to time factor and the accessibility of the information that will be needed to
complete the research and also cost saving for a researcher. This study included both
employees from top management and lower level employees and inpatients and
outpatients.
3.3Population of the study
The population of this study included all public employees especially those working
or indirectly involved to the health service delivery in the case of Mbeya district
council and outpatients and inpatients who were admitted at different Health centers.
Most of the information was collected from normal employees and patients who
were involved directly in this study.
3.4 Unity of Analysis
The focus of this study is to investigate the contribution of institutional factors
contributing to poor employee performance in health service delivery. Therefore, the
unity of analysis was an institution which is Mbeya DC at Mbeya region.
3.5 Variables and measurement
Table 3.1: variables measurement
Variable Description Measurement
Employee
performance
Provision of quality of the health
services and health sector customer
(patients) satisfaction
measured by using ordinal
measurement through a five
interval Likert scale
Regulative factors The present rules and regulations on
whether they lead to a poor performance
of the employees
measured by using five interval
Likert scale
Normative factors Present norms and values on whether
the lead to poor performance of
employees
measured by using five interval
Likert scale
Cultural Cognitive
factors
The present individuals perceptions and
beliefs on the health services delivery to
the employee performance
measured by using five interval
Likert scale
Source; Researcher’s idea

36
3.6 Sample size and Sampling Technique
3.6.1 Sample Size
Omary (2011) stated that a sample is a small portion of population selected for
observations and analysis. A sample size is a small portion that presents a whole
population (Kothari, 2009). Also bailey defined that sample is a group of hopefully
representative of population intended to study and from which one derives
generalization about population. For any study to provide reliable result it should
have enough sample size to reduce the chance of errors. When there is large sample
size there is probability of having true finding. Huysamen (1991) proclaimed that
there are many criteria that are used to determine the size of the sample which
includes population variability, purpose of the study, time for the study, research
approach, method used in the study and availability of the respondents. This study
did have 105 respondents which is 30% of the study population.
Table 3.2: Sample distribution
Category Population Sample Sampling Technique
DMO 1 1 purposive
RCH CODINATOR 1 1 purposive
DNO 6 1 purposive
Medical doctor 10 2 purposive
Clinical officers 30 10 Simple random sampling
Nurse Assistances 45 25 Simple random sampling
Nurses 40 15 Simple random sampling
Medical attendants 50 20 Simple random sampling
Patients 300 30 Simple random sampling
Total 483 105
Source; Mbeya DC
3.6.2 Sampling Technique
Sampling is the process of selecting a number of individual for a study in such a way
that individual selected represent the large group from where they are selected
(Mugenda & Mugenda, 2003). Kothari (1990) stated that sampling is a procedure in
which a researcher decides about the technique to be used in selecting the items for
sample. This study used two sampling technique that included purposive sampling
technique and simple random technique.

37
a) Purposive Sampling
Omary (2011) explained that purposive sampling involves picking unit most relevant
or knowledgeable in the subject matter and study it. According to Kothari (1999)
purposive sampling is the method used purposely to pick up people whom the
researcher thinks and regards to have adequate knowledge of the available
information regarding the nature of the target group or population and the important
feature which can be used to make a close judgement on research. The purposive
sampling was used by researcher to select five (5) respondents where the selected 5
respondents were on the managerial and administrative positions in health
department in MDC. The purpose of using this technique was to obtain the special
information regarding institutional factors and employee performance.
b) Simple random sampling
Simple random sampling is a technique where all possible subset of a population
more accurately of sampling frame are given an equal probability of being selected
(Bhattacherjee, 2012).This method was utilized because respondents had the same
and independent chance of being selected, and it was used to select samples from
each population. This technique was used to select 100 respondents from health
department employees, in patients and outpatients.
3.7 Data Collection Methods
In collecting data both primary and secondary data collection methods were used to
obtain information from respondents and other sources.
3.7.1 Primary Data collection methods
Mbogo et al (2012) stated that Primary data are information gathered directly from
the field surveys. Primary data collection methods were used by researcher to collect
data from the field where by interviews and questionnaires were utilized.
3.7.1.1 Interviews
Interview is a selected set of a questions administered through verbal communication
in a face to face communication between interviewer and interviewee (Kothari,
2004). This study utilized interview to collect data from 5 respondents who are on
the administrative and management positions in the health sector and who are

38
experienced and have more information about institution and employee performance.
This method was used because it is important source of getting information and it
gives respondents freedom to ask in case of need. Yin (2003) said that interview tool
is very important source of getting information and it is helpful in handling case
study related matters. An interview guide was attached in appendix II.
3.7.1.2 Questionnaire
A questionnaire is a data collection method used to gather data over a large numbers
of respondents (Kombo& Tromp, 2006). A questionnaire was used to obtain
information from 100 respondents who were from different segments including those
who are working under the health sector (health service providers) and the citizens
receive reproductive and child health services within the Mbeya district council. This
compliment and supplement information obtained from interview and documentary
review. This method was used by a researcher so as to obtain consistency of
responses to the questions asked in repeated measurement (Carmines & Zeller,
1979). The samples of questionnaire are attached in Appendix I.
3.7.2 Secondary Data Collection Methods
Secondary data are information gathered from other previous studies like published
materials and information from books, journals and newspapers and raw data and
unpublished summaries. The researcher did use documentary review in order to
access accurate and reliable data regarding to institutional factors and how they
contributing to poor public employee performance in delivering health services. In
this study data was collected from books and references about employee
performance, institutional factors and health service delivery, also use periodical,
published papers, articles, journals, thesis, dissertations organization meetings
minutes and employee performance reports.
3.8 Validity and Reliability
3.8.1 Validity
Refers to the extent in which research instrument measures what they are intended to
measure (Oso&Onen, 2005). It is concerned mostly with the questionnaires
consistency of respondents to the questions asked repeated measurement. That is
39
why the researcher of this study identified the validity of data analyzing the
consistency of the respondents to the given question. In this study researcher tested
data collection tools through pilot study before conducting the study.
3.8.2 Reliability
Refers to consistency measure produce the same results across time and across
observers (Patton, 2002). Is the degree to which the observed variable measures the
true value and its error free. Reliability deals with the consistency of measurement in
research. Reliability tend to answer the question of consistency, that is does the
measure as a whole and do the items comprising the measure, give the same kind of
results when used under the same circumstance. Therefore, in this study the
researcher to ensured reliability was used questionnaires and interview to the
respondents so as to identify if there were the same answers.
3.9 Data Analysis
Kothari (2004) defined data analysis as the computation of certain measures along
with searching for patterns of relationship that exist among data group. This study
will use both qualitative and quantitative data analysis. Qualitative data analysis is
the analysis of qualitative data like text data that are obtained from interview and is
heavily dependent on the researcher’s analytic and integrative skills and personal
knowledge of the social context where data is collected. Qualitative analysis is based
on sense making and understanding phenomenon rather than predicting or explaining
(Bhattacherjee, 2012). Qualitative data analysis involves content analysis, grounded
theory analysis and hermeneutic analysis.
Quantitative data analysis consists of numeric values from which description such as
mean, median, mode and standard deviations will be made (Kombo& Tromp, 2006).
It will require a number of closely related operations like estimation of categories,
application of these categories to raw data through coding, tabulation and drawing
statistical inferences quantitative data analysis involve both descriptive statistical
analysis and inferential statistical analysis.
This study used content analysis for qualitative data and descriptive statistical
analysis for quantitative data.

40
3.9.1 Content analysis
This study analyzed data by using content analysis because of its qualitative nature as
the study did involve both independent variables which include regulative factors,
normative factors and cultural cognitive factors and the dependent variable which
involve employee performance. Content analysis procedures was used where by the
data was transcribed and summarized in a way that lead to the formation of large
themes of information to be reflected by data. The emerging themes or chunks of
information was compared, merged and described and their meaning was assigned in
a manner that addresses research objectives and research questions (Cresswell,
2007). The narrative style was used to describe the emerging theme and pattern of
data that reflect experiences of respondents with regards to institutional factors
contributing to poor performance of employee in delivering health services.
3.9.2 Descriptive statistical analysis
It refers to statistically describing, aggregating and presenting the constructs of
interest or associations between the constructs (Bhattacherjee, 2012). This study
analyzed quantitative data using descriptive data analysis that was summarized,
coded and analyzed by Statistical Package for Social Science (SPSS). The
descriptive analysis techniques that were used are mean, median, standard deviation
and percentages andwere presented in tables, graphs and pie chart.
3.10 Ethical Issues
Ethical consideration is a way a researcher should describe how she /he will ensure
that ethical issues or requirements are upheld in the study (Knight, 2003). The
researcher has to consider ethical issues during the whole process of research starting
from problem setting, data collection and data analysis. In this study the researcher
considered the following issues;
Voluntary participation in which respondents were not forced to participate in the
study and the researcher did advise whomever did not wanted to participate to
withdraw at any time they want to; respondents were informed about the purpose,
procedures and consequences of their participation in the study before they make
decisions to participate; also respondents were not required to provide for the name

41
or any other form that identify a person by name; respondents were also assured that
the information they provide was not to be used for other purpose than being used for
the study; literature and other sources of empirical evidence were acknowledge and
cited by using American Psychological Association (APA); and lastly in order to
facilitate data collection process, letters of introduction were obtained from the
Directorate of Research and Postgraduate Studies (DPRS) at Mzumbe University.

42
CHAPTER FOUR
DATA PRESENTATION AND DISCUSSION OF FINDINGS
4.1 Introduction
This chapter presents and discusses the empirical findings from the study that
investigated the institutional factors contributing to poor performance of the public
employee in delivering health services, using Mbeya district council as a case study.
The analysis involved a well collected data from a total of 105 respondents from
different categories mostly the public employees, management through the
questionnaire and the customers who access health service within those health
facilities located in Mbeya district council. A total of 100 well-structured
questionnaires were distributed to the sampled population and 5 respondents were
interviewed. However, 100 questionnaires were well answered and the
questionnaires from the respondents were collected back successfully and all 5
interview respondents were successfully interviewed.
4.2 Demographic characteristics of respondents (Personal Particulars):
The research study did establish demographic information profile of the research
respondents to determine their personal particulars based on their Sex/Gender, their
levels of education, Age, occupations and their respective working experience in the
Mbeya district council.
4.2.1 Distribution of respondents by Sex
The distribution of sex was assessed in the study as one of the demographic
characteristics of the respondents, since the gender disparity concept has proved to be
a very significant notion in the development scenario and ensuring balance within the
community and in public organizations. Furthermore, sex was assessed in this study
to determine perceptions of the respondents basing on their respective gender. As
figure 4.1 shows, all the 100 sampled research respondents did indicate their gender,
whereas 47 of the respondents’ equivalent to 47 percent were female respondents
while 53 research respondents were male respondents indicating a 53 percent of the
researched respondents.

43
This particular finding implies that within the Mbeya district council the gender
inequality is not high. This is to say both men and women have equal employment
opportunities and equal access to the health services, thus minimizing the presence of
gender inequality.
Figure 4.1 Distribution of respondents by sex:
Source; Field Data, 2019
4.2.2Distribution of respondents by Age
The distribution of the respondents by their age was assessed in the study as one of
the personal particulars of the researched respondents so as to determine the group or
range of age of majority of the public employees specifically within the Mbeya
district council.
As table 4.1 shows, all of the 100 studied research respondents did indicate their
respective age groups as specified in the questionnaire, that is equal to 100 percent of
the researched respondents, whereas 10 percent of the researched respondents that 10
in actual number were aged less than 25 years of age that is the young adults group,
24 of the respondents that is equivalent to 24 percent of the respondents were age
grouped between 26 years to 35 years which can be also categorized as the young
47%
53%
sex
female male

44
adults group. Furthermore 38 of the studied respondents were aged between 36 years
to 45years of age this is equivalent to 38 percent of the entire researched respondents,
18 of the researched respondents were age grouped between 46 years to 55 years of
age that is equivalent to 18 percent of the studied respondents, lastly 10 of the
studied respondents were age grouped above 56 years of age that is equivalent to 10
percent of the studied respondents.
These findings on the age of the respondents simply indicate that within the Mbeya
district council most of the public health services stakeholders (i.e. the employees
and the customers) have an age range of 36 years and 45 years which indicated a
matured adult age group which is the appropriate age and the most effective age.
Table 4.1: Distribution of respondents by Age
Categories Frequency Percent
less than 25 years 10 10.0
26-35 years 24 24.0
36-45 years 38 38.0
46-55 years 18 18.0
56 years and above 10 10.0
Total 100 100.0
Source: Field Data, 2019
4.2.3 Distribution of respondents by Education level
As table 4.2 presents, all the 100 sampled research respondents did indicate their
levels of education that is 100 percent of the researched respondents, whereas 3
individuals equaling to 3 percent of the entire respondents were PHD level educated,
on the other hand 18 of the researched respondents that is equivalent to 18 percent
were Master’s degree level educated while bachelor degree holders were 33 in actual
number that is equivalent to 33 percent of the studied respondents. Furthermore,
diploma level employees were 23 in actual number that is equivalent to 23 percent,

45
14 researched respondents were certificate level educated that is equivalent 14
percent, lastly 9 of the respondents that is 9 percent indicated others who specifically
notified less educated mostly secondary educated.
These findings on the level of education specifically signify that within the Mbeya
district council most of the public health services users and employees are
satisfactorily educated that is to say their education level distribution is ideal and can
yield an adequate performance in delivering the health services.
Table 4.2 Distribution of respondents by Education Level
Categories Frequency Percent
PHD 3 3.0
Masters 18 18.0
Bachelor 33 33.0
Diploma 23 23.0
Certificate 14 14.0
Others 9 9.0
Total 100 100.0
Source: Field Data, 2019
4.2.4 Distribution of respondents by Working Experience
As per table 4.3 confirms, all of the 100 studied respondents did indicate their
respective working experience, which is 100 percent response of the respondents,
whereas 30 of the researched respondents that is 30 percent of the entire studied
respondents had an experience of less than 5 years, 39 percent of the studied
respondents that is 39 respondents in actual numbers had an experience of between 5
years to 10years. On the other hand, 25 of the researched respondents’ equivalent to
25 percent had an experience of 11 years to 16 years. Lastly 6 respondents that is
equivalent to 6 percent of the respondents had an experience of 17 years and above
which are the elite group and the most experienced group within the Mbeya district
Council.

46
These findings on the working experience of the respondents specifically signify that
within the Mbeya district council, most of the employees in the public health services
have an even distribution of working experience and that the public organizations do
provide equal opportunities of employment to the individuals.
Table4.3: Distribution of respondents by Working Experience
Categories Frequency Percent
less than 5 years 30 30.0
5-10 years 39 39.0
11-16 years 25 25.0
17 and above 6 6.0
Total 100 100.0
Source: Field Data, 2019
4.3 How Regulative Factors Contribute to Poor Performance of Employees in
delivering health services
To administer the first objective that involved identifying how rules and regulations
contribute to poor performance of public sector employees in delivering health
service in Mbeya district council, a set of 7 statements were used so as to extract the
data from the respondents. These statements were provided to be answered in a
Likert scale form that is in a set of strongly agree, agree, neutral, disagree and
strongly disagree.
4.3.1 Policies, rules, regulations and circulars of RCH are available at Health
centers
Table 4.4: Availability of policies, rules, regulations and circulars
Responses Frequency Percent
Strongly agree 36 36.0
Agree 43 43.0
Neutral 15 15.0
Disagree 5 5.0
Strongly disagree 1 1.0
Total 100 100.0
Source; Field Data, 2019

47
From the table 4.4 findings reveal that policies, rules, regulations and circulars are
available in health service hospitals and are understood well adhered by the
employees. This is approved by the 36 percent of the respondents strongly agreeing
to the statement. Furthermore 43 percent of the studied respondents agree and 15
percent were neutral. However, 5 of the studied respondents did not agree with the
matter1 of the respondents strongly disagreed.
These findings reveal that the rules and regulations are available in hospitals and are
understood well and adhered by the employees and not contributing to the poor
performance of employees.
4.3.2 Health care employees are being regulated for proper provision of health
services.
Table 4.5 Regulations of health care workers
Responses Frequency Percent
Strongly agree 30 30.0
Agree 44 44.0
Neutral 15 15.0
Disagree 11 11.0
Total 100 100.0
Source; Field Data, 2019
As on the table 4.5, findings revealed that majority of the respondents agreed (such
as 44 percent agree and 30 percent strongly agreed) that the employees’ behaviors
are being regulated by the management of the health care providers and thus cannot
lead or contribute to poor performance of the employees. However, 15 percent of the
respondents were neutral and 11 percent of the respondents disagree with the
statement.
Also, during the interview, one respondents remarked that:
“……. the policies, rules, regulations and circulars about RCH
services are available in our Hospitals, and we are adhering to them
when we are providing services to the patients…”
(Interview with Respondent A: April, 2019)

48
These findings reveal that RCH employees are aware with the policies, rules and
regulations that are available at Mbeya DC hospitals. And those policies are the one
that provides them guidance on what they should achieve and at what time. Some of
these rules that researcher has found in Mbeya DC health centers are National Health
Policy and reproductive and child health policy, Tanzania Development Vision 2025,
and Millennium Development Goals.
4.3.3 RCH policies enhance employees in the health sectors to have good
performance.
Table 4.6: Policies and employee performance
Responses Frequency Percent
Strongly agree 9 9.0
Agree 30 30.0
Neutral 37 37.0
Disagree 23 23.0
Strongly disagree 1 1.0
Total 100 100.0
Source; Field Data,2019
From the Table 4.6, the findings revealed that the RCH policy enhances the RCH
service provider to have good performance. This is approved by the 9 percent of the
respondents strongly agreeing to the statement. Furthermore 30 percent of the studied
respondents agree despite 37 percent being neutral. However, 23 percent of the
studied respondents disagree with the matter and 1 percent of the respondents
strongly disagreed.
Also, during the interview, one of the respondents remarked that;
“……. the available RCH services rules, regulations and policies has
enabled us to perform well on different goals, as they give us
guidelines on what we should do as service providers…”
(Interview with respondent B: April, 2019)
These findings of the study from both questionnaires and interviews reveal that the
RCH policy enhances the RCH employees to perform well, and thus it does not
contribute to the poor performance of employees in delivering health services. This is

49
because the RCH policies and other rules and regulations provide the directions on
what goals should be achieved after certain period of time. This was supported by the
National Road Map Strategic Plan to accelerate Reduction of Maternal Newborn and
Child Deaths in Tanzania (2008-2015) which provided guideline to the RCH service
providers to reduce the maternal mortality ratio to 193 per 100,000 live births by
2015. This goal was achieved by health service providers of which it indicates that
there was good performance in public health sectors, though they did not eradicate
entirely the deaths of mother and child (URT, 2008).
4.3.4The policies, rules and regulation in the health sector enable employees to
have positive attitudes towards the job
Table 4.7 Attitude of health employees
Responses Percent Frequency
Strongly agree 26 26.0
Agree 39 39.0
Neutral 24 24.0
Disagree 10 10.0
Strongly disagree 1 1.0
Total 100 100.0
Source; Field data, 2019
As on the table 4.7, findings revealed that majority of the respondents agreed (39
percent agree and 26 percent strongly agreed) that health services policy, rules and
regulation helps employees to have positive attitudes towards the job and thus cannot
lead or contribute to poor performance of the employees. However, 24 percent of the
respondents were neutral and 10 percent of the respondents disagree with the
statement while 1 percent strongly disagreed.

50
4.3.5 Infants get vaccines on time after being born as the policies, rules and
regulations indicate.
Table 4.8 Infants Vaccines
Responses Frequency Percent
Strongly agree 7 7.0
Agree 41 30.0
Neutral 30 41.0
Disagree 22 22.0
Total 100 100.0
Source; Field Data, 2019
As on the table 4.8 above, findings revealed that some of the respondents agreed (41
percent agree and 7 percent strongly agreed) that infants obtain vaccines at time soon
after they are born. However, 30 percent of the respondents were neutral and 22
percent of the respondents disagree with the statement.
On this particular statement finding imply that respondents have different opinions
on whether the infants are being given vaccines after they are born.
Also, during the interview, one the respondents stated that;
“….... Infants and children under-age of 5 are being given different
vaccines after they are being born and when they continue to grow so
as to prevent them in being affected by different diseases…….”
(Interview with respondent C: April, 2019)
4.3.6 Maternal and Mortality rate have been reduced to the large extent
Table 4.9:Reduction of Mortality and maternal rate
Responses Frequency Percent
Strongly agree 28 28.0
Agree 35 35.0
Neutral 23 23.0
Disagree 10 10.0
Strongly disagree 4 4.0
Total 100 100.0
Source; Field Data, 2019

51
As on the table 4.4.6 above, findings revealed that majority of the respondents agreed
(35 percent agree and 28 percent strongly agreed) that maternal and mortality rate
have been reduced compared to previous decades where there was high rate of infant,
maternal mortality rate. However, 23 percent of the respondents were neutral and 11
percent of the respondents disagree with the statement while 4 percent strongly
disagreed.
Also, during the interview, one the respondents said that;
“……. Maternal and mortality rate have been reduced at our hospitals
compared to before where there was a lot of deaths of infants and
maternal…….”
(Interview with respondent E: April, 2019).
The findings revealed that mortality and maternal rate have been reduced in Mbeya
Dc because citizens have been told during different seminars to give birth in
hospitals instead of giving birth at their places. Different policies, laws, rules and
regulations are addressing the problem the reduction of maternal and mortality rate.
These laws emphasize health service providers to focus on reducing mortality and
maternal rate improving RCH services.
4.3.7: The RCH services are provided with free charge
Table 4.10: provision of free service
Responses Frequency Percent
Strongly agree 32 32.0
Agree 43 43.0
Neutral 18 18.0
Disagree 7 7.0
Total 100 100.0
Source; Field Data 2019
From the table 4.10 findings reveal that RCH services are being provided with free of
charge to citizens. This is approved by the 32 percent of the respondents strongly
agreeing to the statement. Furthermore 43 percent of the studied respondents agree
and 18 percent were neutral. However, 7 of the studied respondents disagreed.
Furthermore, on the interview’s side all the 5 interviewed respondents suggested that

52
the public organizations should ensure and strategize for improving the employee
performance through ensuring there are proper rules and regulations that will monitor
and control the employee to yield an adequate performance. Where one of the
respondents said that;
“……. Hospitals in Mbeya DC do provide free RCH services to the
people who access their services, though there are some of the
challenges regarding to delivery of RCH service……”
(Interview with respondent D: April 2019)
These findings reveal that the RCH services are being provided freely to the citizens
and it is not a contributing factor to the poor performance of employees. This goes in
line with the URT (2008), which state that the Government of Tanzania in 1994
started to provide free RCH services to the citizens, where they are not required to
pay anything for them to get service in the hospital. Even though the government
have provided free RCH service to the people there are equipment that the pregnant
women are required to buy so that will be used when they are delivering a bay. This
matter hinders the poor women who cannot afford to buy that equipment to access
services.
4.4 How norms and values contribute to poor performance of employee in
delivering health service.
To administer the second objective that involved finding out how norms and values
contribute to poor performance of employee in delivering heath service within the
Mbeya District, a set of 7 statements were used so as to extract the data from the
respondents. These statements were provided to be answered in a likert scale form
that is in a set of strongly agree, agree, neutral, disagree and strongly disagree.

53
4.4.1: The RCH service providers are honest, professional and respect
organization employment policy
Table 4.11: RCH employees’ honest, professionalism and respect
Responses Frequency Percent
Strongly agree 6 6.0
Agree 5 25.0
Neutral 39 39.0
Disagree 24 24.0
Strongly disagree 26 6.0
Total 100 100.0
Source; Field Data, 2019
From the table 4.11 findings reveal that RCH employees are not very honest,
professional and respect organization employment policy and RCH policies. This is
approved by majority of the studied respondents not complying with the statement.
Where by 50 percent of the respondents disagreed (24 percent disagree and 26
percent strongly disagree) to the statement. Furthermore 39 percent of the studied
respondents were neutral while 11 percent of the studied respondents agreed.
These findings reveal that the RCH employees are not honest, not professional and
do not respect organization employment policy thus contributing factor to the poor
performance of employees.
4.4.2 The health sector employees work with the line managers so as to ensure
that the values and norms are adhered
Table 4.12 Working with line Managers
Responses Frequency Percent
Strongly agree 24 24.0
Agree 28 28.0
Neutral 29 29.0
Disagree 11 11.0
Strongly disagree 8 8.0
Total 100 100.0
Source; Field Data, 2019

54
As on the table 4.12, findings revealed that majority of the respondents agreed (28
percent agree and 24 percent strongly agreed) that the health sector employees work
with the line managers so as to ensure that the values and norms are adhered and thus
cannot lead or contribute to poor performance of the employees. However, 29
percent of the respondents were neutral and 11 percent of the respondents disagree
with the statement while 8 percent strongly disagreed.
This shows that there is team working at Mbeya Dc health department as employees
work well with employees from other department so as to provide service to the
people. Also other employees including nurses, doctors and clinical officers from
other departments works together with RCH department in delivering service to
women, children and adolescents.
4.4.3 Employees in the health centers do implement new ideas so as to improve
their performance
Table 4.13 Implementation of New ideas
Responses Frequency Percent
Strongly agree 33 33.0
Agree 44 44.0
Neutral 16 16.0
Disagree 7 7.0
Total 100 100.0
Source; Data field, 2019
From the table 4.13 findings reveal that employees in the health centers do
implement new ideas so as to improve their performance. This is approved by the 33
percent of the respondents strongly agreeing to the statement. Furthermore 44
percent of the studied respondents agree and 16 percent were neutral. However, 7 of
the studied respondents disagreed.
Also, during the interview, one the respondents said that;
“……. I use new ideas in delivering health services so as to achieve
goals that I have been assigned and this helped me to provide better
service to the patients as I focus on finding the best in me to serve
people…….”
(Interview with Respondent C: April, 2019)

55
These findings reveal that the employees in the health centers do implement new
ideas so as to improve their performance and thus an employee performance.
4.4.4The value of the health sector/ministry do reflect the performance of the
employees
Table 4.14 Values of RCH service delivery
Responses Frequency Percent
Strongly agree 36 36.0
Agree 32 32.0
Neutral 10 10.0
Disagree 21 21.0
Strongly disagree 1 1.0
Total 100 100.0
Source; Field data 2019
As on the table 4.14 above, findings revealed that majority of the respondents agreed
(32 percent agree and 36 percent strongly agreed) that the value of the health
sector/ministry do reflects the performance of the employees and this implies that it
cannot lead or contribute to poor performance of the employees. However, 10
percent of the respondents were neutral and 21 percent of the respondents disagree
with the statement while 1 percent strongly disagreed.
4.4.5 Employee soft skills are reflected from organization value and determine
the future employee’s performance
Table 4.15: Employees’ skills
Responses Frequency Percent
Strongly agree 19 19.0
Agree 32 32.0
Neutral 40 40.0
Disagree 9 9.0
Total 100 100.0
Source; Field Data, 2019
As on the table 4.15, findings revealed that majority of the respondents agreed (32
percent agree and 19 percent strongly agreed) that the employee soft skills are
reflected from organization value and determine the future employee’s performance
and this implies that it cannot lead or contribute to poor performance of the

56
employees. However, 40 percent of the respondents were neutral while 9 percent
disagreed.
4.4.6 The health sector emphasizes on obtaining competent and experienced
employees so as to improve the employees’ performance
Table 4.16: Competent Employees
Responses Frequency Percent
Strongly agree 18 18.0
Agree 41 41.0
Neutral 25 25.0
Disagree 15 15.0
Strongly disagree 1 1.0
Total 100 100.0
Source; Field Data, 2019
As on the table 4.16 above, findings revealed that majority of the respondents agreed
(41 percent agree and 18 percent strongly agreed) that the health sector emphasize on
obtaining competent and experienced employees so as to improve the employees’
performance and thus this factor cannot contribute to poor performance of the
employees. However, 25 percent of the respondents were neutral and 15 percent of
the respondents disagree with the statement while 1 percent strongly disagreed.
Moreover, on the interview’s side findings suggest that majority of the studied
respondents suggested that there should be proper following of ethics and conducts
by the employees so as to enable them achieve an adequate performance in their
respective working fields and enhancing a proper delivery of the health services.
4.5 How the level of knowledge of employees about performance contribute to
poor performance of employees.
To administer the third objective that involved examining how the knowledge of
employees about performance contribute to poor performance of employees Mbeya
district, a set of 3 statements were used so as to extract the data from the respondents.
These statements were provided to be answered in a Likert scale form that is in a set
of strongly agree, agree, neutral, disagree and strongly disagree.
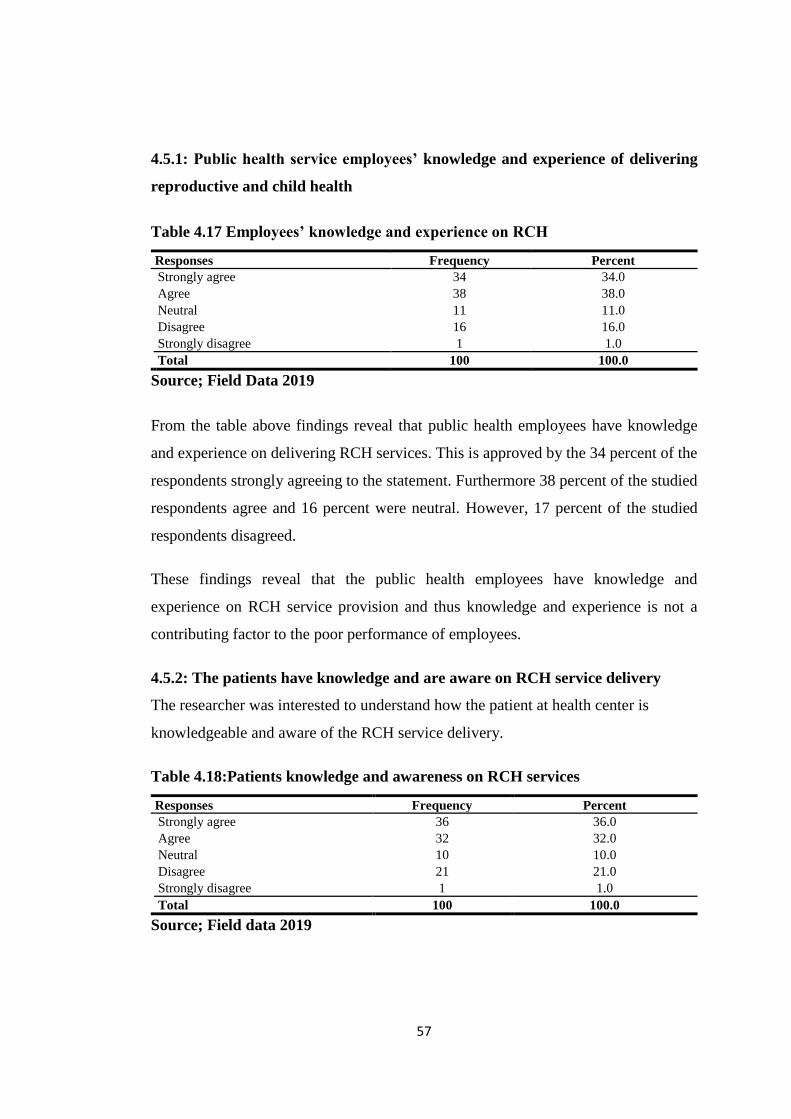
57
4.5.1: Public health service employees’ knowledge and experience of delivering
reproductive and child health
Table 4.17 Employees’ knowledge and experience on RCH
Responses Frequency Percent
Strongly agree 34 34.0
Agree 38 38.0
Neutral 11 11.0
Disagree 16 16.0
Strongly disagree 1 1.0
Total 100 100.0
Source; Field Data 2019
From the table above findings reveal that public health employees have knowledge
and experience on delivering RCH services. This is approved by the 34 percent of the
respondents strongly agreeing to the statement. Furthermore 38 percent of the studied
respondents agree and 16 percent were neutral. However, 17 percent of the studied
respondents disagreed.
These findings reveal that the public health employees have knowledge and
experience on RCH service provision and thus knowledge and experience is not a
contributing factor to the poor performance of employees.
4.5.2: The patients have knowledge and are aware on RCH service delivery
The researcher was interested to understand how the patient at health center is
knowledgeable and aware of the RCH service delivery.
Table 4.18:Patients knowledge and awareness on RCH services
Responses Frequency Percent
Strongly agree 36 36.0
Agree 32 32.0
Neutral 10 10.0
Disagree 21 21.0
Strongly disagree 1 1.0
Total 100 100.0
Source; Field data 2019

58
As on the table 4.18, the findings of the study revealed that majority of the
respondents agreed (32 percent agreed and 36 percent strongly agreed) that the
patients have knowledge and awareness on RCH services. Since they are
knowledgeable and aware of it, this cannot lead or contribute to poor performance of
the employees at the health centers. However, 10 percent of the respondents were
neutral and 21 percent of the respondents disagree with the statement while 1 percent
strongly disagreed. Also the 21 percent of patients who disagreed on being aware
about RCH service delivery revealed that there were no enough seminars and
educations to citizens about RCH services.
4.5.3 RCH employees have experiences that enable them to provide better
service
Table 4.19: RCH employees’ experience
Responses Frequency Percent
Strongly agree 59 9.0
Agree 12 12.0
Neutral 20 20.0
Disagree 9 59.0
Total 100 100.0
Source; Field Data, 2019
From the table above findings reveal that the human resources do have experiences
that enable them to provide service to the people. This is approved by the 59 percent
of the respondents strongly agreed to the statement that Human resources have
experiences that enable them to identify employees who will be performing well.
Furthermore 20 percent of the studied respondents were neutral. However, 12 of the
studied respondents agreed with the statement while 9 strongly disagreed.
4.6 Employee performance
To administer the employee performance in Mbeya district council, a set of 7
statements were used so as to extract the data from the respondents. These statements
were provided to be answered in a Likert scale form that is in a set of strongly agree,
agree, neutral, disagree and strongly disagree.

59
4.6.1 The health care centers are fully equipped with the necessary medical
facilities.
Table 4.20 Health Centre equipment’s
Responses Frequency Percent
Strongly agree 4 4.0
Agree 11 11.0
Neutral 11 11.0
Disagree 30 30.0
Strongly disagree 44 44.0
Total 100 100.0
Source; Field data, 2019
From the table 4.20 findings reveal that majority of the respondents do not concur
with the health care centers being fully equipped with the necessary medical facilities
that is 44 percent of the studied respondents strongly disagreed with presence of the
medical facilities in the health care centers while 30 percent of the studied
respondents also disagreed with the statement. Furthermore 11 percent were neutral
while the other 11 percent agreed and 4 percent also strongly agreed with presence of
medical facilities.
These findings imply that majority of the health care centers are not well equipped
with the necessary medical facilities and thus implying a lower or poor performance
of the health center and the employees at large.
4.6.2 The treatments to the patients are provided timely, thus no delay.
Table 4.21The treatments to the patients are provided timely, thus no delay.
Responses Frequency Percent
Strongly agree 6 6
Agree 8 8
Neutral 9 9
Disagree 34 34
Strongly disagree 43 43
Total 100 100
Source; Field Data, 2019

60
From the table 4.21 findings reveal that majority of the respondents do not concur
with the treatments to the patients being timely and with no delay, specifically 43
percent of the studied respondents strongly disagreed with the treatments to the
patients being timely and with no delay while 38 percent of the studied respondents
also disagreed with the statement. Furthermore 9 percent were neutral while 8
percent agreed and 6 percent also strongly agreed with the statement.
These findings imply that majority of the treatments to the patients are not timely and
always on delay s and thus implying a poor performance of the public employees in
the health service delivery.
4.6.3The patient’s expectations and requirements are well met as per their
needs.
Table 4.22 Patients Expectations
Responses Frequency Percent
Strongly agree 11 11
Agree 4 4
Neutral 25 25
Disagree 29 29
Strongly disagree 31 31
Total 100 100
Source; Field Data, 2019
From the table 4.22 findings reveal that majority of the respondents do not
correspond with the statement the patient’s expectations and requirements are well
met as per their needs, specifically 31 percent of the studied respondents strongly
disagreed with patient’s expectations and requirements being well met as per their
needs while 29 percent of the studied respondents also disagreed with the statement.
Furthermore 25 percent were neutral while 4 percent agreed and 11 percent also
strongly agreed with the statement.
These findings imply that majority of the patient’s expectations and requirements are
not well met as per their needs and thus implying a poor performance of the public
employees in the health service delivery.

61
4.6.4The services are provided timely and with accuracy to the patients
Table 4.23: Provision of services
Responses Frequency Percent
Strongly agree 1 1
Agree 5 5
Neutral 16 16
Disagree 43 43
Strongly disagree 35 35
Total 100 100
Source; Field Data, 2019
From the table above findings revel that majority of the respondents do not concur
with the services are provided timely and with accuracy to the patients, specifically
35 percent of the studied respondents strongly disagreed with the services are
provided timely and with accuracy to the patients while 43 percent of the studied
respondents also disagreed with the statement. Furthermore 16 percent were neutral
while 5 percent agreed and 1 percent also strongly agreed with the statement.
These findings imply that majority of the services are not provided timely and with
no accuracy to the patients and thus implying a poor performance of the public
employees in the health service delivery.
4.6.5The customers are well listened and attended effectively
Table 4.24: Customer are listened
Responses Frequency Percent
Strongly agree 5 5
Agree 6 6
Neutral 19 19
Disagree 20 20
Strongly disagree 50 50
Total 100 100
Source; Field Data 2019
From the table 4.24 findings revel that majority of the respondents do not concur
with the customers are well listened and attended effectively, specifically 50 percent
of the studied respondents strongly disagreed with the customers being well listened
and attended effectively while 20 percent of the studied respondents also disagreed

62
with the statement. Furthermore 19 percent were neutral while 6 percent agreed and
5 percent also strongly agreed with the statement.
These findings imply that majority of the customers are not well listened and
attended effectively and thus implying a poor performance of the public employees
in the health service delivery.
4.6.6 The available resources are well utilized to provide quality health services
Table 4.25: Resource availability
Responses Frequency Percent
Strongly agree 6 6
Agree 5 5
Neutral 13 13
Disagree 46 46
Strongly disagree 30 30
Total 100 100
Source; Field Data, 2019
From the table 4.25 findings revel that majority of the respondents do not concur
with the available resources being well utilized to provide quality health services,
specifically 30 percent of the studied respondents strongly disagreed with the
available resources being well utilized to provide quality health services while 46
percent of the studied respondents also disagreed with the statement. Furthermore 13
percent were neutral while 5 percent agreed and 6 percent also strongly agreed with
the statement.
These findings imply that majority of the available resources are not well utilized to
provide quality health services and thus implying a poor performance of the public
employees in the health service delivery.

63
4.6.7 The health employees report and attend on their duties on time
Table 4.26 Working on Time
Responses Frequency Percent
Strongly agree 15 15
Agree 15 15
Neutral 31 31
Disagree 39 39
Total 100 100
Source; Field Data, 2019
From the table above findings revel that majority of the respondents do not agree
with the health employees report and attend on their duties on time, specifically 39
percent of the studied respondents disagreed with the health employees report and
attend on their duties on time. Furthermore 31 percent were neutral while 15 percent
agreed and 15 percent also strongly agreed with the statement.
These findings imply that majority of the health employees do not report and attend
on their duties on time and thus implying a poor performance of the public
employees in the health service delivery. Furthermore, majority of the interviewed
respondents suggested that for the employees to efficiently effectively perform in the
working areas and especially in the health delivery section the employees should be
well treated and motivated for work furthermore there should be a provision of
incentives and increase in the salaries, which all together may trigger off the
employees to perform better

64
CHAPTER FIVE
SUMMARY, CONCLUSIONS AND POLICY IMPLICATIONS
5.0 Introduction
This chapter comprised of a summary of the findings made as a result of the data
analyzed. Furthermore, the chapter has made some conclusions based on the study
and on the findings. Suggestions for areas of further research have also been
outlined. Finally, the chapter draws certain recommendations to on the overall
scenario of institutional factors and their contributions to public employee
performance in delivering health services.
5.1 Summary
The study findings revealed that 47 percent of the studied respondents were female
respondents while 53 percent of the studied respondents were male respondents.
Furthermore, on the age groups findings indicated that majority of the respondents
were aged between 36 years to 45 years of age (38 percent) which are mostly the
matured adults while 10 percent were less than 25 years, 24 percent were aged
between 26 years to 35 years of age, 18 percent of the respondents were aged
between 46 to 55 years and lastly 10 percent of respondents were above 56 years of
age. Moreover, findings revealed on the education level majority of the respondents
that is 33 percent were bachelor degree holders 23 percent were diploma level 18
percent had masters, 14 percent had a certificate level of education and lastly 3
percent had PHD level of education. On the experience level 39 percent of the
respondents had an experience between 5 to 10 years, 30 percent were less than 5
years while 25 percent of the respondents were experienced between 11 years to 16
years and lastly 6 percent of the respondents that is equivalent to 4 respondents were
above 17 years experienced.
On the other hand, findings revealed that the existing rules and regulations do not
contribute to poor performance of public sector employees in delivering health
service and furthermore these rules and regulations have proved to be the key pillars
for the effective employee’s performance. On the second objective that involved
finding out how the norms and values contribute to poor performance of employee in

65
delivering heath service, the study findings revealed that most of these normative
factors are agreed by most of the respondents to contribute to the employee
performance and not leading to the poor performance. Lastly findings showed that
the level of knowledge about performance among the employees does contribute to
employee performance since it enables them to recruit efficient employees in the
organization. However, the employee performance is still proved to be low
particularly in the delivering of health services which further brings a notion that the
institutional factors have a very low influence on the poor performance of the
employees but relatively other external factors may be the major causes of poor
performance to the public employees in delivering health services.
5.2 Conclusion
In concluding, the study revealed that all of the three institutional factors studied
such as normative factors, regulative factors and the cultural cognitive factors have
proved have contribution at various levels on the poor performances of employees in
delivering health services. However, the study observed that poor performance of
public employees in the department of health at the local government level is caused
more by individual factors observed among HRH instead of institutional norms, rules
and regulations. Furthermore, the study outcomes have revealed that the employee
performance is low thus it is a notion for the top administrators and management to
enhance a high performance from the employees especially in the health sector.
Moreover, the findings did prove that the employees do not meet their customers’
expectation and requirements to a distinctive extent thus it is urged that the
managerial and administrators should take a keen note on this. On the other hand,
study revealed that the health services provided are not timely and accurate to the
patients; health care centers are not fully equipped with the necessary medical
facilities; customers (patients) are not well listened and attended. Thus the public
organization specifically the Mbeya district council should take a keen note on this
matter to enhance a good performance strategy and enable an adequate performance
to the employee in delivering the health services.
66
5.3 Recommendations
According to the findings the study does recommend that, the management of the
organization particularly the Mbeya district council and other similar type of
governmental institutions should take keen note on the overall institutional factors
contributing to poor performance of employees and their appliances in the
application of proper management of the organization and yielding a proper
performance for the employees and the organization as a whole.
However, the organization’s management needs to explore the best performance
strategies which are likely to work with the particular organization structure and
improve their operational and standard performance and increase the level of
application of those strategies that are already in play. The organization’s top
management should also improve the organization’s structure and their level of
support, especially on the human factor such as training of staff, proper
communication systems, and financial constraints which are both related to become
challenges for the performance of employees.
5.4 Suggestions for Further Research
The study assessed the institutional factors contributing to the poor employee
performance in delivering health services a case of Mbeya district council in Mbeya
Region. Thus similar studies should focus in the following concerns.
Firstly, the study recommends similar type of studies on different geographical
locations since different case studies would yield different results and outcome of the
study. Furthermore, since the study found out that the institutional factors are not the
key reasons for poor performance of the public employees in the delivering of health
services. Thus the study does recommend an analysis on the factors contributing to
the poor employee and organization performance in a case study public organizations
and also private entities.
Lastly the study focused on the institutional factors specifically the norms and
values, rules and regulations and the level of knowledge of the human resource
officers on the employee performance. Thus other study should specifically focus on

67
these institutional factors as individually how they affect the employee’s and
organization performance.

68
REFERENCES
Abbott, A. (2007). Time Matters on Theory and Methods. Chicago IL: University of
Chicago Press.
Abonm, N. D., (2011). The Role of Motivation on Employee Performance in the
Public Sector: A Case of the University for Development Studies-Wa
Campus- Kwame Nkurumah University of Science.
Ahuja, K., (2006). Personnel Management. (3rd Ed) New Delhi, India. Kalyani
Publishers.
Ali, A. (1989). A Comparative Study of Managerial Beliefs About Work in the Arab
States’. Advances in International Comparative Management, 4: 95-112.
Apospori, E., Nikandrou, L., Brewster, C., and Papalexandris, N. (2008).HRM and
Organisation Performance in Northern and southern Europe.The International
Journal of Human Resource Management, 19(7), pp. 1187-1207.
Arinanye, R. T. (2015). Organizational Factors Affecting Employee Performance at
the Collage of Computing and Information Science (COCIS).Unpublished
Master Dissertation, Makerere University.
Armstrong, M. (2001).Human Resource Management Practice. London: Kogan Page
Publishers
Armstrong, M. (2002).A Handbook of Human Resource Management Practice.10th
edition. London: Kogan Page.
Barley S.R., and Tolbert P.S. (1997). Institutionalization and Structuration: Study
the Links between action and institution. Organization Studies.
Bhattacherjee, A. (2012). Social Science Research: Principles, Methods and
Practices. Florida: Creative Common Attribution-Non Commercial-Share
Alike 3.0 Unported License.
Binjabi, H. (2014). Exploration of the Impact of Institutional Factors on Actors in
the Implementation of Effective High Performance Work System. Published

69
Thesis submitted for Degree of Doctor of Philosophy. London; Brunel
University
Boselie, P.(2002). Human Resource Management. Work Systems and
Performance:ATheoretical-Empirical Approach. Rotterdam: Tinbergen
Institute
Brewster, C., Wood G., and Brookes M., (2008).Similarity, Isomorphism or
duality?Recent Survey Evidence on Human Resources Policies of
Multinational Corporations.British Journal Management. 19(4), pp 320-342.
Budhawari, P. S, and Sparrow, P. R (2002).An Integrative framework for
Understanding Cross National Human Resource Management
Practices.Human Resource Management Review, 12(3), pp.377-403.
Budhawiri, P. S., and Khatri, N. (2001).A Comparative Study of Human Resource
Practices in Britain and India.International Journal of Human Resource
Management, 12(5): 800-826
Byars, L.L and Rue, L.W. (1987).Human Resource
Management.Homewood,IL:Irwin.
Carmines, B. and Zeller, A. (1979).Primary and Secondary Data Collection
Methods. U.S: Macmillan.
Carrell, M.R. Elbert, N.E., Hatfield, R.D., Grobler, P.A., Marx, M. and Van der
Schyf, S. (1999).Human Resource Management in South Africa. Upper
Saddle River, NJ: Prentice-Hall
Cascio, W.F., (1998). Managing Human Resources: Productivity, Quality of Work
Life, Profits. (5thed). New York, NY: John Wiley.
Claire, S., Jahoda, M., and Deutsch, M. (1962).Research Methods in Social Relations
3rd ed. Holt, Reinhart and Winston.
Dimaggio, P. J. (1983). State Expansion and Organization Field.In Organization
Theory and Public Policy.Beverly Hills; CA Sage.
70
Dimagio, P., and Powell, W., (1983).The Iron Cage’ Institution Isomorphism and
Collective Rationality in Organizational Fields.American Sociological
Review, 48:147-60.
Dornbursch, S. M., and Scott R. W. (1975).Evaluation and Exercise of Authority.San
Francisco; Jossey –Bass.
Elzinga, T., Abronda, B., and Kluijtmans, F. (2009).Behavioral Factors Influencing
Performance Management Systems’ Use.International Journal of
Productivity and Performance Management.Vol 58(6), pp 508-522.
Erasmus, B., Swanepoel, B., Schenk, H., Van der Westhuizen, E. and Wessel J.S.
(2005).South African Human Resource Management for the Public Sector.
Cape Town: Juta.
Evance, P., Pucik, V. &Barsoux, J. L., (2002).The Global Challenge: Framework for
International Human Resource Management. Boston; McGraw-Hill.
Fauzilah, (2011).The Effect of Motivation on Job Performance of State Government
Employees in Malaysia.International Journal of Humanities and Social
Science Vol 1 No. 4: April 2011 pp 147-154.
Foot, M. & Hook C., (2008).Introducing Human Resource Management (5th Ed).
Pearson Education Limited: Prentice Hall.
Gilbrait, J.R., (2002). Designing Organizations: An Executive Guide to Strategy,
Structure and Process. San Francisco: Jossey-Bass.
Gungor, P. (2011). The Relationship between Reward Management System and
Employee Performance.Procedia Social and Behavioral Sciences, 1510-
1520.
Hofstede, G., (1991). Culture and organization: Software of the Mind. New York:
McGraw-Hill

71
Hope Sr, K.R (2003), Employee perceptions of leadership and performance
management in the Botswana public service, Public Personnel Management,
Washington: Summer. Vol 32, Iss. 2
Hughes, E. C. (1958). Men and their Work. Glencoe; IL Free Press
Hussain, M. M., and Hoque, Z. (2002). Understanding Non-Financial Performance
Measurement Practices in Japanese Bank; A New Institutional Sociology
Perspective. Accounting, Auditing and Accountability Journal, 15(2), pp 162-
183.
Karuhanga, B. N., (2010). Challenges of Performance Management in Universities
in Uganda.International Research Symposium in Service Management. Le
Meridiem Hotel, Mauritius, 24-27th Aug 2010. ISSN pp 1694-0938.
Kenney et al, (1992).Management Made East. (1st Ed). South Carolina: Oman
Publisher.
Kombo, D. K. and Tromp D. L. (2006). Proposal and Thesis Writing: An
Introduction. Nairobi; Pauline Publisher.
Kooiman, J., Bavinck, M., Jentoft, S. and Pullin, R. (2005).Fish for Life; Interactive
Governance for Fisheries.MARE Publication Series. Amsterdam:
Amsterdam University Press.
Kothari, C. R. (1990). Research Methodology: Methods and Techniques 2nded. New
Delhi: New Age International (P) Ltd.
Kothari, C. R. (2009). Research Methodology: Methods and Techniques. New Delhi:
New Age International Publishers.
Kothari, C. R., (2004). Research Methodology; Methods and Techniques(2nded.).
New Delhi: New Age International.
Kumburu, N. P. (2009). Civil Service Reform and Human Resource Status in Central
Government: The Case of President Office Public Service Management in
Tanzania. Journal of Cooperative and Business studies (JCBS) Vol 1No. 1

72
Landa, E. (2018). Influence of Training on Employee Performance in Public
Institution in Tanzania.International Journal of Human Resource Studies,
Micro think Institute ISSN 2162-3058 Vol 8.No. 2.http://www. researchgate.
net. Retrieved on Dec 5th, 2018.
Lee, H. C. (1999). Transformation of Employment Practices in Korean Business.
International Studies of Management and Organization 28(4):26-39.
Lepold, J. (2008). Human Resource in Organizations. Financial Times Press.
Mathias, R and Jackson, H (2009).Human Resource Management, Mason, OH, USA,
South-Western Cengage Learning
Mbah, T. (2015).Assessing Motivation as a Tool to Enhance Employee
Performance.Centria University of Applied Science: Scandinavia.
Mbithe, M. N., (2012). Determinants of Employee Performance in the Public
Universities; A Case of University of Nairobi Kenya. Unpublished Master
Thesis.
Mbithe, M.N. (2012). Determinants of Employee Performance in the Public
Universities: A Case of the University of Nairobi, Kenya. Master’s Thesis,
University of Nairobi Kenya.
Meyer J.W., and Jepperson R.L. (2000). The actors of Modern Society: The Cultural
Construction of Social Agency. Social Logical Theory
Meyer, J.W., and Rowan, B., (1991). Institutionalized Organization: Formal
Structure as Myth and Ceremony.In W.W. Powell and P.J. Dimaggio
(Eds).The New institutionalism in Organizational Analysis (41-62). Chicago:
University of Chicago Press.
Mugenda, O., and Mugenda A., (2003).Research Methods: Quantitative and
Qualitative approaches. Nairobi: ACTS Press.

73
Nabukeera, M., Ali, B., and Raja, N. B. (2015).Performance Evaluation of Public
Service Institutions (C&S) Framework.World Journal of Social Science; Vol
2, No. 1: 2015 pp 1-25. http://wiss.scie.edupress.com.
Naharuddin, N.M. and Sadegi, M. (2013).Factors of Work Environment that Affect
Employees Performance: A Case Study of Miyazu Malaysia. Journal of
Independence Research and Studies, Vol 2, No. 2 (April 2013) 66-78.
Ngowi, P. A. (2014). Assessment of Employee Performance in Commercial Banks in
Tanzania: A Case of Stan Bick Bank Tanzania. Unpublished Master
Dissertation, Open University Tanzania.
North, D. C., (2005). Understanding the Process of Economic Change.Princeton;
Princeton University place.
North, D., (1990). Institution, Institutional Change and Economic
Performance.Cambridge University Press.
Oliver, C., (1997). Sustainable Competitive Advantage: Combining Institutional and
Resource Based Views. Strategic Management Journal, 18:697-713.
Oso, W. Y., and Onen, D. (2005).A Handbook for Beginning Researchers (2nd
Edition).Kampla: Mkerere University Printer
Ostrom, E., (1990). Governing the Commons: The Evolution of Institution for
Collective Action. New York: Cambridge University Press.
Patton, M. Q. (2001), Qualitative Evaluation and Research Methods (3rded.).
Newbury Park, CA: Sage Publication.
Peter, C. G. (2014). Impact of Promotion to Employees Performance at Dar-es -
Salaam City Council.Unpublished Master Dissertation, Mzumbe University.
Rugumyamheto, J. (2005). Reforming the Public Service in Tanzania: A Critical
Prerequisite to Economic Growth, Wealth, Creation and Poverty Reduction.

74
Paper presented at 26th AAPAM Annual Roundtable Conference White Sands
Hotel, Mombasa Kenya.
Salem, H., (2003). Organization Performance Management and Measurement.
Beirut, The Lebanese Experience.
Schacter, M: (1999). Means, Ends, Indicators: Performance Measurement in the
Public Sector, Institute on Governance, Ontario
Scott, R. W. (1987). The Adolescence of Institutional Theory.Administrative Science,
QuarterlyVol 32: No 4. Pp 493-511. http://links.jstor.org/sici=0001-
8392%28198712%2932%3A4%3C493%3ATAOIT%3E2.0.CO%3B2-Q.
Retrieved on Nov 26, 2018.
Scott, r. w. (1995).Institution and Organizations.Ideas Interest and Identities. Oaks:
Sage; 2014/2, Vol. 17, pp 136-140. http://www.cirn-int.info/article-
E_MANA_172_0136—w-richard-scott-1995-institutions.htm Retrieved on
Dec, 12th 2018.
Scott, R. W. (2008). Institution and Organization; Ideas and Interest 3rd edition.Los
Angeles, CA; Sage Publication.
Scott, W. R., (1995 & 2001, 2004). Institutions and Organizations. Thousand Oaks,
C, Sage.
Scott, W. R., (2014). Institutions and Organizations- Ideas, Interest and Identities,
4th Ed). Thousand Oaks, CA: Sage Publication Inc.
Selznick, P., (1957). Leadership in Administration. New York: Harper and Row
Shem, J. M., Ngussa B. M (2015). Effects of Training on Employee performance: A
Case Study of Institution of Higher Learning in Arusha City, Tanzania.
Volume 6 2319-7064
Sinha, J. B. P., (1997). A Cultural Perspective on Organization Behavior in India. In
Earley P. C. and Erez, M. (eds) New Perspective on Organizational

75
Industrial/ Organizational Psychology. San Francisco; CA: The New
Lexington Press.
Strange, D., and Sine, W. (2002).Interorganizational Institutions. In the Blackwell
Companion to organizations, ed. Joel A.C. Baum, 497-519. Oxford, UK:
Blackwell.
Suchman, M. C., (1995). Localism and Globalism in Institutional Analysis: The
Emergence of Contractual Norms in Venture Finance. In The Institutional
Construction of Organizations: International and Longitudinal Studies, 39-
63, W. Richard Scott, and Soren Christensen, ed. Thousand Oaks, CA: Sage.
Svinicki, M. D. (2010). A Guide Book on Conceptual Frameworks for Research in
Engineering Education.University of Texas.
Swidler, A., (1986). Culture in Action: Symbols and strategies. American
Sociological Review, 51, pp. 273-286.
Tanzania Public Service Commission, (2008).Improvement of the Efficiency and
Effectiveness of Public Service as an Essential Component of Development
Efforts; An Overview of Tanzania Experience. A Paper Presented in a
Workshop for Enhancing Leadership Capacity Development of the African
Public Service Commission. Kampala, Uganda.
Thao, L. T. T and Hwang, C., (2010). Factors Affecting Employees Performance
Evidence from Petro Vietnam Engineering Consultancy. Vietnam: J. S.C.
Thompson, H (2005). What a Performance; Human Resources, London
United Republic of Tanzania, (1999).Sera
yaMenejimentinaAjiraKatikaUtumishiwaUmma. Dar es Salaam:
MkukinaNyota Publishers.
Welter, F., (2011). Contextual Entrepreneurship- Conceptual Challenges and Ways
Forward. Entrepreneurship: Theory & Practice 35, no 1:165-185

76
Welter, F., and David, S., (2011). Institutional Perspective on Entrepreneurial
Behaviour in Challenging Environments. Journal of Small Business
Management 49 no 1:107-125
Yin, R. K. (2003).Case Study Research Design and Methods. Oaks, CA: Sage
Publication.
Ying, Z. Y., (2012). The Impact of Performance Management System on Employee
performance. Work Place Employee Relation Survey.

77
APPENDICES
APPENDIX I
A QUESTIONNAIRE FOR EMPLOYEES
Dear Respondents,
I am Benadetha Teddy a student of Mzumbe University (MU) pursuing a Master
degree in Public Administration and Management. The questionnaire is intended to
help the researcher obtain information on the institutional factors contributing to poor
performance of public employees in delivering health services a case of Mbeya DC.
The purpose of this study is to generate information for improving public sector
employees, it is purely academic and information given will be treated with the
highest degree of confidential. You have been selected as a key respondent for this
study. Kindly, complete the questionnaire to enable the researcher complete the
study. Please tick the answer which represents your opinion.
I appreciate your participation in this effort.
Section A: Personal Particulars
Please circle or tick (√)the appropriate number or fill where applicable.
1 SEX
Female Male
1 2
2 AGE
Less than 25 years 26-35 years 36-45 years 46-55 years 56 years and above
1 2 3 4 5
3 EDUCATION LEVEL
PhD Masters Bachelor Diploma Certificate Other specify
1 2 3 4 5 6
4 YEARS OF EXPERIENCE
Less than 5 years 5-10 years 11-16 years 17 and above
1 2 3 4

78
From question 1-44, tick or circle the number that best indicates your opinion on the
question using the following scale:
SCALE 1 2 3 4 5
Strongly agree Agree Neutral Disagree Strongly disagree
SECTION B: REGULATIVE FACTORS SA A N D SD
1. How rules and regulations contribute to poor performance of
public sector employees in delivering health service
1 2 3 4 5
2. Policies, rules, regulations and circulars of RCH are available at
Health centres
1 2 3 4 5
3. Health care employees are being regulated for proper provision of
health services.
1 2 3 4 5
4. RCH policies enhance employees in the health sectors to have
good performance
1 2 3 4 5
5. Infants get vaccines on time after being born as the policies, rules
and regulations indicate.
1 2 3 4 5
6. Maternal and Mortality rate have been reduced to the large extent 1 2 3 4 5
7. The RCH services are provided with free charge 1 2 3 4 5
SECTION C: NORMATIVE FACTORS
8. The RCH service providers are honest, professional and respect
organization employment policy
1 2 3 4 5
9. The health sector employees work with the line managers so as to
ensure that the values and norms are adhered
1 2 3 4 5
10. Employees in the health centres do implement new ideas so as to
improve their performance
1 2 3 4 5
11. The value of the health sector/ministry do reflects the
performance of the employees
1 2 3 4 5
12. Employee soft skills are reflected from organization value and
determine the future employees performance
1 2 3 4 5
13. The health sector emphasize on obtaining competent and
experienced employees so as to improve the employees
performance
1 2 3 4 5
14. SECTION D: CULTURAL COGNITIVE FACTORS 1 2 3 4 5
14. Public health service employees’ knowledge and experience of
delivering reproductive and child health.
1 2 3 4 5
15. The patients have knowledge and are aware on RCH service
delivery.
1 2 3 4 5
16. RCH employees have experiences that enable them to provide
better service
1 2 3 4 5
17. SECTION E: EMPLOYEE PERFORMANCE 1 2 3 4 5
18. The health care centres are fully equipped with the necessary
medical facilities.
1 2 3 4 5
19. The treatments to the patients are provided timely, thus no delay. 1 2 3 4 5
20. The patient’s expectations and requirements are well met as per
their needs.
1 2 3 4 5
21. The services are provided timely and with accuracy to the patients 1 2 3 4 5
22. The customers are well listened and attended effectively 1 2 3 4 5
23. The available resources are well utilized to provide quality health
services
1 2 3 4 5
24. The health employees report and attend on their duties on time 1 2 3 4 5

79
26. Please comment on the overall performance of public employees in delivering
health services at Mbeya DC?
…………………………………………………………………………………………
27. What should be done to improve the employee performance in delivering health
services?
…………………………………………………………………………………………
Thank you very much for your participation

80
APPENDIX II
INTERVIEW GUIDE
1. Are there any policies, rules, regulations and circulars that relate to RCH
services in health centres?
2. Are the policies, rules, regulations and circulars provide guidelines on how to
reduce maternal and mortality ratio?
3. Do the RCH services being provided to citizens free of charges as per
directions of policies?
4. Do the employees have skills and experience that enable them to perform and
deliver well RCH services?
5. Are the employees provided enough resources they need to effectively
perform their duties?
6. How often do you meet with your employees to discuss different issues that
affect their performance?
7. How do you determine that subordinates accomplish their tasks?
8. In your opinion what do you think is the overall performance of employees in
delivering the health services
9. What can be done to improve their performance?

81
APPENDIX III
ORGANIZATION STRUCTURE
MBEYA DISTRICT COUNCIL
DED
LEGAL UNITY PROCUMENT
UNIT
INTERNAL
AUDITOR
PLANNING
ECONOMY
AND
STATISTICS
HR and
Administrat
ion
Finance
supplies and
trade
Education,
vocation
and
training
Land, water
natural
resources and
environment
Agriculture
livestock and
environment
WARD
EXECUTIVE
VILLAGE
EXECUTIVE
Health Works Community
development

82
APPENDIX IV
MBEYA DC MAP


















