Institute of Medicine Report on Nutrition Standards in Schools
16
AMERICAN ACADEMY OF PEDIATRICS Summer 2007 VIRGINIA CHAPTER VIRGINIA PEDIATRICS IS PROVIDED AS A SERVICE TO MEMBERS OF THE VIRGINIA CHAPTER AND THE VIRGINIA PEDIATRIC SOCIETY TO PROMOTE THE PROFESSION OF PEDIATRICS AND TO FURTHER BENEFIT THE CHILDREN WE SERVE. 2 Everyday Advocates and Heroes 5 FAMIS Introduces New Staying Healthy Web Pages 6 Growing Up Bilingual 8 Pediatric Endocrinology at UVa 8 29th Annual Pediatric Primary Conference 9 AAP 2007 Legislative Conference- SCHIP REAUTHORIZATION 9 DMAS Dual Use Period Extended 10 Unintended Consequences: The Impact of New Medicaid Citizenship Documentation Requirements on Virginia’s Children 13 Do You Have Questions About Tuberculosis? 14 New AAP Policy on Early Detection of Developmental and Behavioral Problems 15 “Prevent Blindness Mid-Atlantic Encourages Everyone to Add Vision to Back-to-School Health Check-List” 16 Prostate Cancer CME Conference inside this issue Continued on page 3 Institute of Medicine Report on Nutrition Standards in Schools Robert Gunther, MD, MPH, FAAP Vice President, Virginia Chapter-AAP The “obesity epi- demic” has been a growing concern in the United States. Childhood obesity places children at risk for serious lifelong health problems such as diabetes, and cardiovascular disease, hyperlip- idemia and hypertension. Poor food choices may lead to other concerns such as inadequate calcium intake and the potential for other nutrient defi- ciencies. Most research to date sites a number of issues in the rise of this overweight epidemic with concerns about what children are eating and how much they are exercising. The home is a major environmental component in determin- ing what children are eating. School is an additional significant environmen- tal component in determining what children are eating because children spend a major portion of their day at school and may consume 2 meals and additional snacks while there. The Child Nutrition and WIC Re- authorization Act passed in 2004 required that local schools develop a Wellness Policy which includes nutritional guidelines, physical activity goals, and other school based activi- ties. Schools across the country have been inconsistent with this policy. To help this process Congress directed the Center for Disease Con- trol to initiate a study with Institute of Medicine (IOM) “to review and make recommendations about nutri- tional standards for the availability, sale, content, and consumption of foods at school with attention on competitive foods.” The IOM concluded that feder- ally-reimbursed school nutrition programs should be the main source of nutrition at school and opportuni- ties for competitive foods should be limited. Their intent is to create an environment providing healthful foods and beverages offered on the school campus and those foods and beverages offered outside the feder- ally reimbursable school nutrition program will meet certain standards based mainly on the Dietary Guide- lines for Americans (DGA). Foods and beverages were divided into three groups based on their nutrient composition and its consis- tency with the DGA. Tier 1 foods and beverages provide at least one serving of fruit, vegetable, whole grains, or nonfat/ low fat dairy products. Examples of Tier 1 foods would include water without flavor- ing, additives, or carbonation, low fat or non fat milk, and 100% fruit
Transcript of Institute of Medicine Report on Nutrition Standards in Schools

AMERICAN ACADEMY OF PEDIATRICS Summer 2007VIRGINIA CHAPTER
VIRGINIA PEDIATRICS IS PROVIDED AS A SERVICE TO MEMBERS OF THE VIRGINIA CHAPTER AND THE VIRGINIA PEDIATRIC SOCIETY TO PROMOTE THE PROFESSION OF PEDIATRICS AND TO FURTHER BENEFIT THE CHILDREN WE SERVE.
2 EverydayAdvocatesandHeroes
5 FAMISIntroducesNewStayingHealthyWebPages
6 GrowingUpBilingual
8 PediatricEndocrinologyatUVa
8 29thAnnualPediatricPrimaryConference
9 AAP2007LegislativeConference-SCHIPREAUTHORIZATION
9 DMASDualUsePeriodExtended
10 UnintendedConsequences:TheImpactofNewMedicaidCitizenshipDocumentationRequirementsonVirginia’sChildren
13 DoYouHaveQuestionsAboutTuberculosis?
14 NewAAPPolicyonEarlyDetectionofDevelopmentalandBehavioralProblems
15 “PreventBlindnessMid-AtlanticEncouragesEveryonetoAddVisiontoBack-to-SchoolHealthCheck-List”
16 ProstateCancerCMEConference
inside this issue
Continued on page 3
Institute of Medicine Report on Nutrition Standards in Schools Robert Gunther, MD, MPH, FAAPVice President, Virginia Chapter-AAP
The “obesity epi-demic” has been a growing concern in the United States. Childhood obesity places children at risk for serious lifelong health problems such as diabetes,
and cardiovascular disease, hyperlip-idemia and hypertension. Poor food choices may lead to other concerns such as inadequate calcium intake and the potential for other nutrient defi-ciencies.
Most research to date sites a number of issues in the rise of this overweight epidemic with concerns about what children are eating and how much they are exercising. The home is a major environmental component in determin-ing what children are eating. School is an additional significant environmen-tal component in determining what children are eating because children spend a major portion of their day at school and may consume 2 meals and additional snacks while there.
The Child Nutrition and WIC Re-authorization Act passed in 2004 required that local schools develop a Wellness Policy which includes nutritional guidelines, physical activity goals, and other school based activi-ties. Schools across the country have
been inconsistent with this policy. To help this process Congress directed the Center for Disease Con-trol to initiate a study with Institute of Medicine (IOM) “to review and make recommendations about nutri-tional standards for the availability, sale, content, and consumption of foods at school with attention on competitive foods.”
The IOM concluded that feder-ally-reimbursed school nutrition programs should be the main source of nutrition at school and opportuni-ties for competitive foods should be limited. Their intent is to create an environment providing healthful foods and beverages offered on the school campus and those foods and beverages offered outside the feder-ally reimbursable school nutrition program will meet certain standards based mainly on the Dietary Guide-lines for Americans (DGA).
Foods and beverages were divided into three groups based on their nutrient composition and its consis-tency with the DGA. Tier 1 foods and beverages provide at least one serving of fruit, vegetable, whole grains, or nonfat/ low fat dairy products. Examples of Tier 1 foods would include water without flavor-ing, additives, or carbonation, low fat or non fat milk, and 100% fruit
�������virginia�pediatrics
VIRGINIA PEDIATRICS
Virginia Pediatrics
President’s Message
is a quarterly publication of the VA Chapter, American Academy of Pediatrics and the Virginia Pediatric Society. We welcome your opinions and ideas. Please send comments on articles, ideas for new articles, letters to the editor, suggestions for making Virginia Pediatrics more useful and address changes to:
Virginia Pediatrics2201 West Broad Street, Suite 205 • Richmond, Virginia 23220Phone: (804) 643-6631 • Fax: (804) 788-9987 • email: [email protected]
Jane Davis: Chapter Manager Mork Design: Newsletter Layout
Next Issue: Fall 2007Deadline for entries: August 5, 2007Publication of an advertisement in Virginia Pediatrics neither constitutes nor implies a guarantee or endorsement by Virginia Pediatrics or the VA-AAP / VPS of the product or service advertised or of the claims made for the product or service by the advertiser.
Continued on page 3
President’s MessageColleen A. Kraft, MD, FAAPPresident, Virginia Chapter, AAP
Spring has been a time of travel around the state and an opportunity to be a part of many different pedi-atric activities in every region. As Chapter President, I am honored to be a participant in so many of the great projects that pediatricians are doing around Virginia.
This past weekend, Dr. Rachel Rog-ers from Mountainview Pediatrics in Marion, Virginia, hosted a conference entitled “Expanding Your Comfort Zone, including Psychiatry as Part of Pediatrics.” Guest speakers included Dr. Bela Sood from the Virginia Treatment Center for Children and Dr. Roger Burket from the University of Virginia Department of Child Psychi-atry. Attendees included both pedia-tricians and mental health profession-als. The meeting was a first step in the discussion of increasing access to mental health services to children in Southwestern Virginia.
Earlier in the week, I joined Dr. Keith Derco and several Richmond pediatricians in a Pediatric practice management informal club that has met several times to discuss practice issues, ideas, and concerns. The group has shared some great ideas with regard to staffing, office design and flow, coding resources, benefits, and many other practice ideas. It is in these informal groups that ideas for Health Systems advocacy are started and supported.
Dr. Ralph Northam from Norfolk is taking Child Advocacy to an impor-tant level as he runs for Virginia State Senate. We need his voice as we encourage our elected leaders to make the right decisions for kids.
Drs. Rebecca Benton and Robert Gunther will be heading to Capitol Hill as part of the AAP Legislative Conference to talk with our federal legislators about SCHIP Reauthorization. SCHIP started in 1997, and is due to be reauthorized by September 30, 2007. SCHIP has been a tremendous opportunity for America to ensure that all of her children have health care coverage. Two thirds of all uninsured children are now eligible to enroll in Medicaid or SCHIP, and the AAP in addition to other advocacy organizations supports the SCHIP “Fair Plan,” which includes:
· Fully Fund. It is vital that Con-gress deliver on its pledge to children’s health coverage by pro-viding the full $50 billion in new
Everyday Advocates and Heroes

virginia�pediatrics����� ������
VIRGINIA PEDIATRICS
commission, which models the Medicare Payment Advisory Commission, would determine the adequacy of payment for Medicaid/SCHIP services.
· Reach Eligible Children. Con-gress should provide states with new tools, options, and financial support to cover more children.
· Promote Quality. Simply providing children with an insurance card, whether through SCHIP or Medicaid, is not suf-ficient. Health insurance must assure access to services needed for healthy development, includ-ing mental health and dental care. Congress should utilize the expertise of pediatricians to establish child health quality initiatives that reflect children’s unique needs.
We all have an opportunity to speak to our patients, families, and colleagues about the importance of the FAIR Plan and SCHIP reauthorization. Talking to everyone who can vote, everyone who can call their senator or congress-man to vote for this important reau-thorization, can make each and every one of us Everyday Advocates and Heroes.
Thanks for all you do and keep me posted on what is happening in your region of the Commonwealth!
Colleen Kraft, MD, FAAPPresident, Virginia Chapter,American Academy of Pediatrics
Continued from page 2
funds for SCHIP and Medicaid allowed for in the congressional budget resolutions.
· Act Now. SCHIP needs to be reauthorized before September 30, 2007, or our families risk disrup-tion of their coverage, and thus their access to health care.
· Improve Payment: AAP surveys report that Medicaid pays 58% of most private pay plans. As a result, pediatricians have to limit the number of Medicaid patients they care for, and patients find it difficult to access care from specialists. The National AAP is advocating for the formation of a Medicaid and SCHIP Payment Advisory Commission, which would advise Congress on physi-cian payment policies related to state Medicaid programs. This
juice. Tier 2 foods and beverages fall short of Tier 1, but they meet DGA for other nutrients such as fat and sodium. Examples of Tier 2 are baked chips, graham crackers, and animal crackers. The final group is all other foods that do not meet Tier 1 or Tier 2 standards. Tier 1 foods are recommended for use by all students as competitive foods and for use in school fundraisers. Tier 2 foods are recommended for use after school only for high school
students. Sports drinks (which did not meet Tier 1 or Tier 2 standards) are recommended only for high school students engaged in vigor-ous physical activity.
It remains to be seen how these guidelines are implemented. Pedi-atricians serving on School Health Advisory Boards and other con-sultative roles with schools should understand and encourage use of these guidelines in formulating and revising School Wellness Policy.
Institute of Medicine Report on Nutrition Standards in SchoolsContinued from page 1
Pediatricians may also find these guidelines useful to assist par-ents in creating their own “family wellness program”. The full IOM report is available at http://www.nap.edu .

�������virginia�pediatrics
VIRGINIA PEDIATRICS

virginia�pediatrics����� ������
VIRGINIA PEDIATRICS
FAMIS Introduces New Staying Healthy Web PagesThe Virginia Department of Medical Assistance Services unveiled a new Staying Healthy addition to the Family Access to Medical Insurance Security (FAMIS) website, www.famis.org, aimed at providing valuable informa-tion for families enrolled in the FAMIS programs or for anyone visit-ing the website.
The Staying Healthy section is com-prised of seven new pages of infor-mation specifically tailored to meet the needs of expectant mothers and parents of children from birth through age twenty-one. The introductory Staying Healthy web page has six clearly defined links that lead to the following pages: Prenatal Care, Infant & Toddler, Preschooler, “Big Kids,” Preteens & Teens, and Dental Care. Pages contain information on well-child checkups, immunizations, safety, nutrition, development, parent-ing, special health care needs, dental care, and more. Staying Healthy also contains five newly-designed well-child checkup schedules and two newly-designed book lists for parents to read to their children about “Stay-ing Healthy” and “Healthy Smiles.” There are downloadable calendars about FAMIS and “Baby’s First Year” and special month-by-month booklets on caring for your baby during the first year. The Staying Healthy pages also contain more than 200 health-related links and resources for parents and parents-to-be.
The launch of the new Staying Healthy web pages coincided with Cover The Uninsured Week 2007, an initiative of the Robert Wood Johnson Foundation that seeks to highlight the plight of the uninsured in the United States. This year, Cover The Uninsured Week, ran from April 23-29, promoting the im-portance of the State Children’s Health Insurance Program (SCHIP), which Congress must reauthorize this year.
Covering the uninsured is a national problem, but it’s a local problem, too. Here in Virginia, we are working to find solutions and to help educate Vir-ginians about the options available to them. The Commonwealth of Virginia offers traditional medical assistance programs that cover pregnant women and children such as Medicaid and FAMIS Plus (children’s Medicaid), as well as SCHIP programs such as FAMIS MOMS and FAMIS that cover pregnant women and children who earn too much to qualify for Medicaid, but not enough to afford private health insurance. “The new Staying Healthy web pages are a nice compliment to the prenatal, well-child and preventa-tive services already offered by the FAMIS programs. It is important for families to know that FAMIS and FA-MIS Plus not only cover the medical care children need if they get sick or
hurt, but also the well-child preven-tive care children need to keep them healthy,” said Linda Nablo, Director of Maternal and Child Health at the Virginia Department of Medical Assis-tance Services. “FAMIS MOMS also provides prenatal care to help promote healthy birth outcomes.”
Nablo continued, “We are looking forward to Congress reauthorizing the SCHIP program with adequate funding so that we can continue to provide these vital services all the currently enrolled children and pregnant women and reach those remaining uninsured Virginians in the future.” To view the new Staying Healthy section of the FAMIS website or for more information about the FAMIS programs go to www.famis.org.
For more information go to the Medical Home Plus website at www.medicalhomeplus.org.

�������virginia�pediatrics
VIRGINIA PEDIATRICS
Growing Up Bilingual Joan Wabschall, RN, MSConsultant, Reach Out and Read Virginia
At a recent symposium on school readiness in Fairfax County, a mother stood up and told a room full of educa-tors that her pediatrician advised her not to speak Farsi at home with her child because it would result in brain damage to the child. It’s impossible to know whether this was a case of misunderstanding between the parent and the pediatrician, or if the pediatri-cian really lacked knowledge about dual language acquisition. Regardless of what actually happened during that parent-pediatrician interaction, the child ultimately lost the opportunity to become fluent in his native language and the ability to communicate with his own grandparents and others of his culture.
With the growing number of children in the United States who are exposed to two languages, more parents are asking their pediatricians for advice on how to best support dual language learning. What should families be told about raising a bilingual child? The following suggestions are summarized from an article written by Dr. Victoria Fierro-Cobas and Dr. Eugenia Chan.
Be consistent. Experts stress separat-ing the languages to make language acquisition easier for children. Parents need to decide on language strategies that emphasize boundaries between the languages and be consistent in enforc-ing the boundaries. The following are all strategies that can work to separate the spoken languages:
• Each parent consistently speaks only one language to the child.
• Both parents speak one language in the home and a second language is used at school.
• One language is used in both the home and school and the second language is used in the commu-nity.
With consistent exposure to two languages, the child will adapt and be able to differentiate which language to use in different situations.
Do what feels natural. If a par-ent prefers to use one language over another, encourage them to do so. It may be more natural for each parent to speak a different language (depending on their comfort level) to the child.
Keep the language developmen-tally appropriate. Regardless of the language being taught, adults should simplify their speech when talking to a child. If the child is learning two languages, the grammar of each language should be developmentally appropriate.
Keep the child interested in learning the language. Allow the child to feel “special” and proud that he is learning a second language. Encouragement and praise for using a second language goes a long way to motivate a child to learn a second language. Be careful not to ask the child to “show off” his language skills, however. This ap-proach may make him feel “different” or embarrassed and may deter his in-terest in learning the second language.
These suggestions are general guide-lines for development of almost any language. How should the pediatri-cian respond when the parent asks specific questions about bilingualism like the ones below?
Does bilingualism cause speech and language delays? No. Language de-
lays can certainly occur in bilingual children, but there is not a cause and effect relationship between bilin-gualism and language delays. In addition, learning a second language generally does not interfere with the development of a child’s first lan-guage.
Does learning two languages simultaneously interfere with a child’s cognitive development? No. Contrary to what researchers first reported, more recent studies show that second language acquisi-tion does not negatively affect a child’s intelligence.
In Reach Out and Read programs around the country, children and par-ents are being given multi-cultural books to take home as well as child-rens’ books written in other languag-es. Reach Out and Read embraces the concept that the priority should be to do what is best for the child and empower parents to read to their children. Some books in the Reach Out and Read catalog are available in twelve languages other than English and there are many bilingual titles as well.
Growing up bilingual and knowing two (or more!) languages should be an asset to the child, not a detri-ment. Bilingual children have the advantage of knowing two cultures, of being able to communicate with a wider variety of people, and of possible economic advantages in their future. Becoming bilingual is a special gift that parents can offer their child, and one that pediatricians can support as part of healthy child development.
Continued on page 7

virginia�pediatrics����� ������
VIRGINIA PEDIATRICS
Resources for Bilingual Families:
www.asha.org/speech/development/Bilingual-children.cfm
This page contains general informa-tion about bilingualism in children with links to specific information on speech and language development. It is sponsored by the American Speech-Language-Hearing Associa-tion (ASHA)
www.nethelp.no/cindy/biling-fam.html
This page is intended primarily as a place for bilingual parents to find in-formation and resources to help them raise their children as bilinguals.
If you are interested in learning more about how Reach Out and Read can help you make books part of a healthy childhood, visit www.reachoutandread.org or call Elli Sparks, Executive Director of Reach Out and Read Virginia at 804-521-0425. For information about the Reach Out and Read National Spanish Speaking Fami-lies Initiative, contact Dr. Gonzalo Paz-Soldan, Medical Director, Reach Out and Read Virginia, at 703-271-8109.
1 V. Fierro-Cobas and E. Chan. “Language development in bilingual children: A primer for pediatricians.” Contemporary Pediatrics, July 2001, pp 79-98.
2 Ben-Zeev S: Bilingualism and cognitive develop-ment, in Miller N (ed): Bilingualism and Language Disability: Assessment and Remediation. San Diego, College-Hill Press, 1984, pp. 55-60.
3 Ibid, pp. 81-103
4 Saunders, G: Bilingual Children: Guidance for the Family. Clevedon, England, Multilingual Matters Ltd, 1982.
Growing Up Bilingual Continued from page 6

�������virginia�pediatrics
VIRGINIA PEDIATRICS
Pediatric Endocrinology at UVaRobert L. Chevalier, MD, FAAPProfessor and Chair, Department of Pediatrics, University of Virginia
We are pleased to announce that Dr. Mark DeBoer will be joining the Division of Pediatric Endocrinology this summer as Assistant Professor Dr. DeBoer was a pediatric resident at UVA, and has been a pediatric endocrine fellow at Oregon Health Sciences University for the past four years. His research interests are in the area of cachexia and weight control. He will be joining Division Chief Dr. William Clarke, and Dr. Alan Rogol who works part-time as Clinical Professor of Pediatrics.
Those of you who have attempted to get a non-urgent appointment with a pediatric endocrinologist are well aware of the shortage of these sub-specialists throughout the country. According to the American Board of Pediatrics, as of 2005, there were 1055 ever-certified pediatric endocrinolo-gists in the US (over 200 of these are over 60 years of age). This number in-cludes those who are retired, working in industry or working part-time. In 2007 there are less than 50 third-year fellows finishing their training and 77 academic positions open. Given the rise in the incidence of both Type 1 and Type 2 diabetes, and the increas-ing number of FDA approved indica-tions for the use of growth hormone in short children, it is no wonder that appointments are tight. We are pleased that over the past four years, four of our residents have entered pediatric endocrine fellowships (including Dr. DeBoer). This demonstrates the continued appeal of this challenging discipline, and the strengths of our training program.
In addition to physician faculty, the pediatric diabetes clinics at the Kluge Children’s Rehabilitation Center are staffed by nurse practitioners,
dieticians, and an educational consultant. Diabetes field clinics are held in Winchester, Fredericksburg, and Roanoke, while other pediatric endocrine problems such as short stature, disorders of puberty, and thyroid dysfunction are seen at the UVa Medical Center. Children with obesity are always seen first in the Children’s Fitness Clinic. Currently there are several pediatric endocrine clinics each week. Patient phone calls are managed by three full-time Pediatric Nurse Practitioners who have been trained to teach families about endocrine disorders and to adjust insulin and other medication doses. For appointments or referrals, please call 434-924-5897.
Research has been and will remain an important academic activity for our Division of Pediatric Endocrinology. Dr. Clarke is currently working in the area of accuracy of continuous glucose sensors and developing an artificial pancreas. He has also been involved in development of a bio-behavioral in-tervention (Blood Glucose Awareness Training) to help adults and parents of children with diabetes better anticipate high and low blood glucose levels.
Dr. Clarke was recently named the Robert M. Blizzard, Professor of Pedi-atric Endocrinology, Endowed Chair, in honor of the former Chairman of Pediatrics at UVa, and internationally-recognized expert in growth disorders of children. We hope that the expan-sion of the Division will enable us to better meet the needs of children with endocrine disorders, and of the pedia-tricians and family practitioners who care for them on a daily basis.
29th Annual Pediatric Primary Conference
The VCU Department of Pedi-atrics and the VCU Office of Continuing Professional Devel-opment and Evaluation Studies are proud to present the 29th Annual Pediatric Primary Conference – Pediatrics at the Beach that will take place July 20-22, 2007 at the new Hilton Oceanfront Hotel in Virginia Beach, Virginia. Three half-day sessions include important topics in the areas of Emergency Medicine, Primary Care and Developmental & Behavioral Pediatrics. This course is de-signed for physicians and other health care professionals who deliver primary care to children and adolescents.
This is a combined meeting with the Virginia Chapter, American Academy of Pediat-rics. Chapter members receive $100.00 off of the conference registration fee! Simply in-dicate that you are a Virginia Chapter member on your course registration form.
The Chapter will hold a Busi-ness Luncheon on Saturday, July 21, 2007 at 1:30 p.m. Please make plans for you and your family to join us for lunch!
For registration information please contact Natasha Williams at (804) 828-3640.
A brochure and on-line registra-tion is available at www.cmereg-istration.som.vcu.edu.

virginia�pediatrics����� ������
VIRGINIA PEDIATRICS
AAP 2007 Legislative Conference-SCHIP REAUTHORIZATION
DMAS Dual Use Period ExtendedImportant! DMAS has de-cided to continue Virginia Medicaid’s NPI/API Dual Use Period beyond May 23, 2007. DMAS is currently reviewing contingency plans and will issue a Medicaid Memo to providers well in advance of the mandatory NPI compliance date. Providers should continue to prepare for transition to use of the NPI/API and full NPI Compliance.
DMAS strongly encourages healthcare providers who have not yet shared their NPI with DMAS and other payors to do so immediately, and to begin send-ing claims with their NPI/API as soon as possible in order to work through any billing and payment issues prior to the end of the Dual Use extension.
For information and resolution to the most common NPI-related billing errors, please refer to http://www.dmas.virginia.gov/downloads/pdfs/pr-NPI_rel_er-ror_cd_1500.pdf.
June 1st – New Paper Claim Form Deadline
DMAS will accept the UB-92 and the CMS-1500 (12/90) only through May 31, 2007. Provid-ers must begin billing with the new UB-04 and the new CMS-1500 (08/05) on June 1, 2007. Old claim forms received by DMAS with a postmark of June 1, 2007, or later, will be denied. Providers may use either their legacy or NPI number on the new forms.
The 2007 AAP Legislative Confer-ence had Virginia representation from Dr. Colleen Kraft, Dr. Rebecca Ben-ton, and Dr. Bob Gunther. The attend-ees received training on advocacy and meeting with legislative offices. The schedule was intense and the training was excellent. It concluded with a visit to Capitol Hill and appointments with legislative offices. Federal advocacy is occurring on many levels including child mental health, safe and effective therapeutics for chil-dren, physician payment, and disas-ter preparedness. However, SCHIP (State Children’s Health Insurance Program) was the legislative focus of the meeting as SCHIP reauthorization is looming.
The AAP is recommending that Congress deliver on its pledge to children’s health coverage by fully funding the $50 billion in new funds for SCHIP and Medicaid (over the next 5 years) allowed for in the con-gressional budget resolutions. This amount will allow states to sustain their existing programs and reach a large portion of the uninsured chil-dren already eligible for SCHIP and Medicaid. There are over 150,000 uninsured children in Virginia. Con-gress must act promptly … by the end of September or services could be disrupted.
The AAP recommends that services receive improved payment. Cur-rently the FAMIS program reimburses at Medicaid rates. These payment rates impact access to care as many physicians have limited the number of Medicaid patients making it difficult to access primary care and specialty care in many regions of the state. The access issue forces families to turn to
more expensive emergency rooms and urgent care centers for acute care.
Congress should provide states with new tools, options and financial sup-port to reach more eligible children. States should have options to cover pregnant women through SCHIP without relying on waivers, as well as providing SCHIP and Medicaid cover-age to those legal immigrant children and pregnant women who currently cannot be covered until they have been in the country for five years. Enroll-ment should be as simple as possible and accessible through other related programs such as school lunch and WIC. Virginia is doing better than many states with these issues.
Finally the AAP recommends that SCHIP promote quality by providing the full range of pediatric services in-cluding mental health and dental care. Virginia does provide outpatient and inpatient mental health services and dental services under SCHIP. Access is an issue in many areas of the state. Congress should establish a new child health quality initiative that reflects children’s unique needs and provides new data on the country’s success in meeting those needs.
Chapter members can contact their Representative and Senators about SCHIP and let them know that SCHIP has been an effective program in Vir-ginia. The need continues to exist for federal funding and support. Con-tact the AAP Department of Federal Affairs for additional information at [email protected].
�10�����virginia�pediatrics
VIRGINIA PEDIATRICS
Unintended Consequences: The Impact of New Medicaid Citizenship Documentation Requirements on Virginia’s Children
Among the requirements of the Deficit Reduction Act (DRA) of 2005 is a provision requiring documentation of citizenship and identity for all those applying for or renewing eligibility for Medicaid. This was added to prevent illegal immigrants from obtaining pub-lic benefits intended for U.S. citizens, a problem that has not been identified in Virginia. Instead, the new federal requirement has hampered Virginia’s ability to enroll eligible, uninsured children.
A study conducted by the Virginia Health Care Foundation (VHCF), in partnership with the Virginia Depart-ment of Medical Assistance Services (DMAS), has found that the new requirements have had a much broader impact than expected, adversely affect-ing thousands of citizen children since implementation last July. The unin-tended consequences include:
• A significant decrease in the num-ber of children enrolled in Medic-aid in Virginia;
• 4-6 month delays in obtaining Medicaid coverage for Virginia children;
• Inability of citizen children to ob-tain medical care; and
• A dramatic increase in emergency room utilization by those caught up in lengthy eligibility determina-tions
These requirements have also in-creased costs and administrative burdens to state and local government agencies, which have required addi-tional tax dollars.
350,000
355,000
360,000
365,000
370,000
375,000
380,000
385,000
390,000
Sep-0
4
Dec-0
4
Mar
-05
Jun-0
5
Sep-0
5
Dec-0
5
Mar
-06
Jun-0
6
Sep-0
6
Dec-0
6
Mar
-07
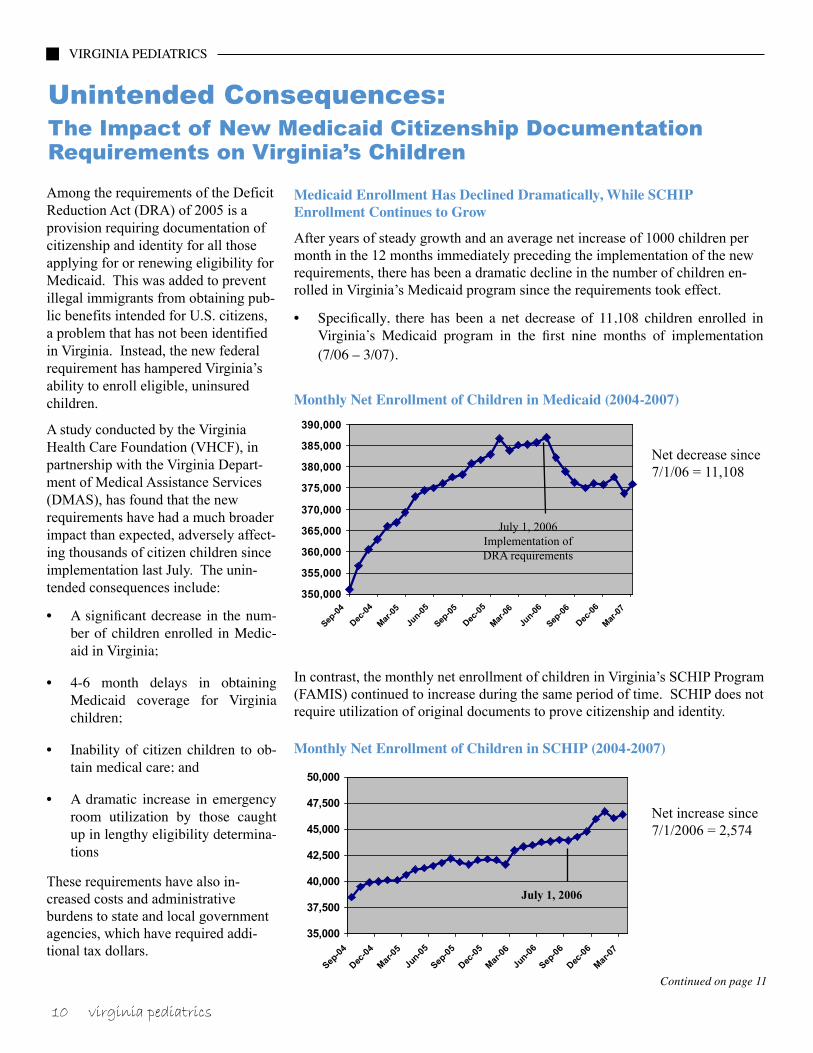
Medicaid Enrollment Has Declined Dramatically, While SCHIP Enrollment Continues to Grow
After years of steady growth and an average net increase of 1000 children per month in the 12 months immediately preceding the implementation of the new requirements, there has been a dramatic decline in the number of children en-rolled in Virginia’s Medicaid program since the requirements took effect.
• Specifically, there has been a net decrease of 11,108 children enrolled in Virginia’s Medicaid program in the first nine months of implementation (7/06 – 3/07).
Monthly Net Enrollment of Children in Medicaid (2004-2007)
35,000
37,500
40,000
42,500
45,000
47,500
50,000
Sep-0
4
Dec-0
4
Mar
-05
Jun-
05
Sep-0
5
Dec-0
5
Mar
-06
Jun-
06
Sep-0
6
Dec-0
6
Mar
-07
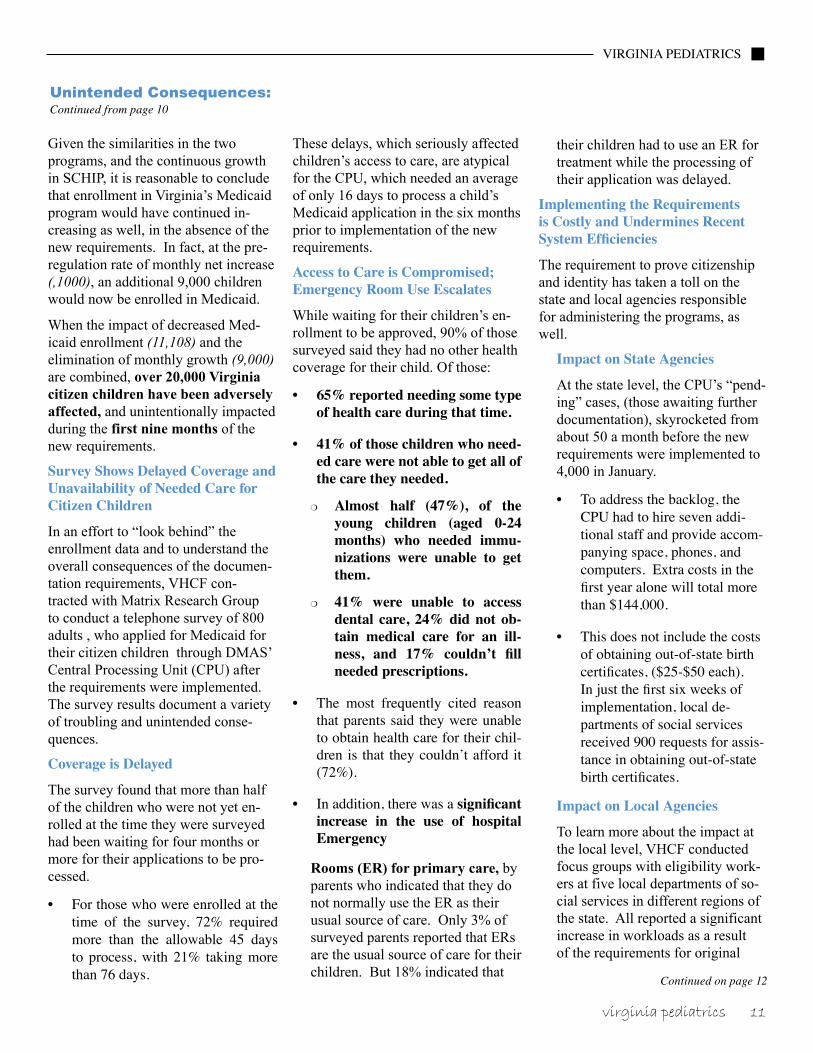
In contrast, the monthly net enrollment of children in Virginia’s SCHIP Program (FAMIS) continued to increase during the same period of time. SCHIP does not require utilization of original documents to prove citizenship and identity.
Monthly Net Enrollment of Children in SCHIP (2004-2007)
Net increase since 7/1/2006 = 2,574
Net decrease since7/1/06 = 11,108
July 1, 2006Implementation ofDRA requirements
July 1, 2006
Continued on page 11
virginia�pediatrics����� 11�����
VIRGINIA PEDIATRICS
Given the similarities in the two programs, and the continuous growth in SCHIP, it is reasonable to conclude that enrollment in Virginia’s Medicaid program would have continued in-creasing as well, in the absence of the new requirements. In fact, at the pre-regulation rate of monthly net increase (,1000), an additional 9,000 children would now be enrolled in Medicaid.
When the impact of decreased Med-icaid enrollment (11,108) and the elimination of monthly growth (9,000) are combined, over 20,000 Virginia citizen children have been adversely affected, and unintentionally impacted during the first nine months of the new requirements.
Survey Shows Delayed Coverage and Unavailability of Needed Care for Citizen Children
In an effort to “look behind” the enrollment data and to understand the overall consequences of the documen-tation requirements, VHCF con-tracted with Matrix Research Group to conduct a telephone survey of 800 adults , who applied for Medicaid for their citizen children through DMAS’ Central Processing Unit (CPU) after the requirements were implemented. The survey results document a variety of troubling and unintended conse-quences.
Coverage is Delayed
The survey found that more than half of the children who were not yet en-rolled at the time they were surveyed had been waiting for four months or more for their applications to be pro-cessed.
• For those who were enrolled at the time of the survey, 72% required more than the allowable 45 days to process, with 21% taking more than 76 days.
These delays, which seriously affected children’s access to care, are atypical for the CPU, which needed an average of only 16 days to process a child’s Medicaid application in the six months prior to implementation of the new requirements.
Access to Care is Compromised; Emergency Room Use Escalates
While waiting for their children’s en-rollment to be approved, 90% of those surveyed said they had no other health coverage for their child. Of those:
• 65% reported needing some type of health care during that time.
• 41% of those children who need-ed care were not able to get all of the care they needed.
m Almost half (47%), of the young children (aged 0-24 months) who needed immu-nizations were unable to get them.
m 41% were unable to access dental care, 24% did not ob-tain medical care for an ill-ness, and 17% couldn’t fill needed prescriptions.
• The most frequently cited reason that parents said they were unable to obtain health care for their chil-dren is that they couldn’t afford it (72%).
• In addition, there was a significant increase in the use of hospital Emergency
Rooms (ER) for primary care, by parents who indicated that they do not normally use the ER as their usual source of care. Only 3% of surveyed parents reported that ERs are the usual source of care for their children. But 18% indicated that
their children had to use an ER for treatment while the processing of their application was delayed.
Implementing the Requirements is Costly and Undermines Recent System Efficiencies
The requirement to prove citizenship and identity has taken a toll on the state and local agencies responsible for administering the programs, as well.
Impact on State Agencies
At the state level, the CPU’s “pend-ing” cases, (those awaiting further documentation), skyrocketed from about 50 a month before the new requirements were implemented to 4,000 in January.
• To address the backlog, the CPU had to hire seven addi-tional staff and provide accom-panying space, phones, and computers. Extra costs in the first year alone will total more than $144,000.
• This does not include the costs of obtaining out-of-state birth certificates, ($25-$50 each). In just the first six weeks of implementation, local de-partments of social services received 900 requests for assis-tance in obtaining out-of-state birth certificates.
Impact on Local Agencies
To learn more about the impact at the local level, VHCF conducted focus groups with eligibility work-ers at five local departments of so-cial services in different regions of the state. All reported a significant increase in workloads as a result of the requirements for original
Unintended Consequences: Continued from page 10
Continued on page 12

�1������virginia�pediatrics
VIRGINIA PEDIATRICS
documentation of citizenship and identity.
• Eligibility workers reported that they are taking more phone calls, and that the calls last longer. They indicate parents call repeatedly to check on the status of their applications, and to ask for help in finding care for their sick children during the delays in enrollment.
These difficulties are reflected in the dramatic change in Medicaid appli-cants’ experience with the application process. The survey found that 40% of respondents reported the Medicaid application process to be difficult, compared to only 8% in a similar sur-vey conducted in 2004.
• Getting paperwork together (36%), obtaining answers to questions (24%), and under-standing what was needed (22%), were the most frequent-ly identified difficulties.
Conclusion
Unfortunately, the requirement for original documentation of citizenship and identity has resulted in unin-tended, adverse consequences. While waiting for their health coverage to be approved, Virginia children have gone without needed medical care, includ-ing care for illness or injury, immuni-zations, dental care and prescription medications. All evidence indicates that these are US citizen children, born in US hospitals, with more than two-thirds born in Virginia.
The new requirements have also had a serious impact on state and local agen-cies responsible for administering the Medicaid program, and have under-mined Virginia’s previously successful
efforts to simplify and streamline application procedures.
Virginia’s impressive progress in en-rolling eligible children in the Med-icaid program is being diminished by these requirements, and the health of thousands of Virginia’s most vulner-able children is threatened.
For more information, please con-tact:
Judith CashDeborah OswaltThe Virginia Health Care Foundation Services(804) 828-5804
Cindi JonesVirginia Department of Medical Assistance(804) 786-4626
Unintended Consequences: Continued from page 11
1 The survey sample was drawn from approxi-mately 3000 adults who applied for Medicaid for their children after July 1, 2006. It included 509 adults whose children were enrolled at the time of the survey, and 291 adults who had applied during the same period, but whose children were not yet enrolled. Except where noted, there were no sig-nificant differences in the responses of the sample groups.
2. The survey targeted those who reported that their children were U.S. citizens. Matrix used several methods to confirm citizenship, including a ques-tion asking for the name of the U.S. hospital in which a child was born. 93% of respondents were able to respond to this question without difficulty. Given the challenges of obtaining original docu-ments (31% were born in a state other than Vir-ginia), and the delays in processing applications, a portion of the survey group was not enrolled in Medicaid at the time of the survey. At this point, 80% have been approved, and the remaining cases are pending while parents and caseworkers work through the costly, time-consuming process of ob-taining original documentation.
Do you know aPediatrician who is not a member of
the Virginia Chapter?
YOU are the most valuable link to reaching
potential members.
Please encourage your colleagues to become active members in the Virginia Chapter.
Visit our Web site:
www.virginiapediatrics.org

virginia�pediatrics����� 1������
VIRGINIA PEDIATRICS
®
The Southeastern National Tuber-culosis Center (SNTC) operates a 24-hour HOTLINE for health care professionals. If you have questions about LTBI, active TB, diagnosis, treatment, or other aspects of the disease, call 1-800-4TB-INFO. You can also make a non-urgent medical consultation request (http://sntc.medicine.ufl.edu/MCS.aspx) from our website. SNTC is a CDC-funded project housed at the University
of Florida and the AG Holley TB Hospital in Lantana, Florida. The SNTC provides TB-related educa-tion and training to eleven south-eastern states, Puerto Rico, and the Virgin Islands. In addition, SNTC staff provides expert TB medical consultation services and techni-cal assistance to the southeastern region. Please visit the SNTC website http://sntc.medicine.ufl.edu for more information about TB and the SNTC.
Southeastern National Tuberculosis Center University of Florida 1329 SW 16th Street, Room 5174Gainesville, Florida 32608888-265-SNTC (7682)
Do You Have Questions About Tuberculosis?

�1������virginia�pediatrics
VIRGINIA PEDIATRICS
New AAP Policy on Early Detection of Developmental and Behavioral ProblemsMost health care providers attempt to identify children with developmental and behavioral problems in order to ensure that patients receive the enor-mous benefits of early intervention. Unfortunately, 70% of pediatricians rely on informal milestone checklists. These lack reliability, validity, accura-cy or scoring criteria. The result is that only one-fourth of children eligible for early intervention services actually receive them.
To address this problem the American Academy of Pediatrics (AAP) issued a new policy statement (Pediatrics, July, 2006) that calls for enhanced developmental surveillance. Surveil-lance includes eliciting and addressing parents’ concerns at every well visit. Most suitable for this task is Parents’ Evaluation of Developmental Status (www.pedstest.com), a 10 question measure that indicates, based on evi-dence, when to refer, screen further, advise parents, or reassure.
But, surveillance also involves rou-tinely monitoring milestones and screening periodically, and again, us-ing quality tools is absolutely essential for accurate detection. A new measure can help with these additional recom-mendations, Parents’ Evaluation of Developmental Status: Developmental Milestones (PEDS:DM). The PEDS:DM is for children birth to age eight and consists of 6 to 8 questions per visit, one per developmental domain: fine motor, gross motor, social-emo-tional, self-help, expressive language, receptive language, and for older chil-dren, reading and math. Parents can answer these on their own or provid-ers can elicit the skills directly from children (but parent report saves time and is equally accurate). Each question serves as a screen for the domain from which it is derived and problematic
performance is tied to a cutoff at the 16th percentile or below (the point below which children have great dif-ficulty with regular curricula). Stan-dardized and validated on more than 1600 children around the US, who participated from health care settings as well as day care centers and pre-schools, the PEDS:DM has sensitivity and specificity across domains as well as age ranges of 83% to 84%, well within standards for screening tools.
There are many interesting features to this measure. It consists of a book of laminated forms, one for each age range, which parents complete with a dry erase marker. The 6 – 8 questions per form are written at the high first grade level and answered, via multiple choice, and in less than 5 minutes. Parents are then encouraged (option-ally) to read to their child a short story that is presented in the book on the opposite page. The stories focus on child development and positive par-enting practices (such as talking and reading to your baby, giving toddlers choices, making clean-up time into a game, etc.). Since parents are known to learn about child developmental through assessment, the fact that the PEDS:DM actively promotes healthy development and parenting is exciting as are the accompanying photographs and drawings that reflect the diverse ethnicities within American society. In addition, the PEDS:DM manual contains photo-copiable parent educa-tion handouts, a list of links helpful for finding local services, and referral letter templates (all are also download-able at www.pedstest.com).
A single scoring template is laid on top of the completed PEDS:DM form to reveal correct and incorrect answers. These are then transferred to a one-page longitudinal growth chart that
remains in the patient record. Over time, the growth chart builds a graph of children’s developmental strengths and weaknesses.
The second section of the PEDS:DM Family Book contains supplemen-tary measures (also laminated) that together with (optionally) Parents’ Evaluation of Developmental Status are helpful in fully complying with the AAP’s new policy. The supple-mentary tools include: the Modified Checklist of Autism in Toddlers (M-CHAT) recommended by the AAP at 18 and 24 months; the Pictorial Pediatric Symptom Checklist-17 (a screen for depression, attention, and conduct problems in older children); the Brigance Parent-Child Interac-tions Scale (to determine whether parenting style is likely to lead to healthy development); the Family Psychosocial Screen (a measure of parental depression and other risk factors); the Safety Word Inventory and Literacy Screener (SWILS) (a measure of school skills for older children); and the Vanderbilt ADHD Scale (a diagnostic measure of atten-tion, hyperactivity and impulsivity). The PEDS:DM manual suggests when to use supplementary measures, since not all are needed at any single well-visit.
In terms of electronic applications, PEDS (the measure eliciting and ad-dressing parents’ concerns), and the (optional) M-CHAT are already avail-able online. The site can be used with or without integration with electronic medical records. The PEDS:DM will be added to the website by late Sum-mer, 2007.
A Spanish language version of the PEDS:DM should be available this
Continued on page 15

virginia�pediatrics����� 1������
VIRGINIA PEDIATRICS
“Prevent Blindness Mid-Atlantic Encourages Everyone to Add Vision to Back-to-School Health Check-List”As parents and children begin planning for back-to-school, one important item must be added to the checklist – a vision screening or an eye exam. Problems with vision can have a profoundly negative impact on a child’s learning ability. And, a vision screening or eye exam may be the only way to detect a lifelong, vision-threatening condition known as amblyopia (lazy eye).
Untreated vision problems in children can lead to permanent vision loss, as well as learning difficulties and developmen-tal delays. Studies show that less than 15% of children have had a professional eye exam before starting school. While Prevent Blindness Mid-Atlantic recommends that every child has an exam from an eye care professional before they begin school, a vision screening identifies children most in need of an eye examination by detecting potential problems with their vision.
Prevent Blindness Mid-Atlantic’s nationally certified children’s vision screening program addresses the need for an effective screening by providing a standardized method of checking a child’s acuity and, for those nine years old and younger, a stereopsis test. The screening protocol stresses the importance of observation for behavior and signs that a child may be having difficulty seeing, as well as the impor-tance of the use of approved charts for acuity screening. In addition to those components, stereopsis screening is key to preventing blindness because it identifies children at risk for amblyopia.
According to the National Eye Institute, amblyopia is the most common cause of visual impairment in childhood. As the brain develops and receives diminished images from the affected eye, it begins to suppress those images and favor
the unaffected eye. If this condition persists, the weaker eye may become functionally blind. Early detection means that a child’s amblyopia and its underlying cause can most often be treated, ensuring that the child begins and continues his or her school career with the benefits of good vision. “The most frightening aspect of amblyopia is that a child may have it and not even know it,” said Tim Gresham, President and CEO of Prevent Blindness Mid-Atlantic. “The child grows up believing that how they see is how everyone else sees.”
“We can’t emphasize enough how important it is to have a child’s vision checked early on,” added Gresham. “When detected early, treatment of amblyopia can be highly successful!” Prevent Blindness Mid-Atlantic’s vision screening certification is tailored for school and pediatric nurses, as well as community volunteers, and is an effective way of identifying children who potentially have vision problems, including amblyopia. Still, it is important to let parents know that because not all screen-ings are standardized and because a screening cannot replace a comprehensive eye exam, seeing an eye care professional should be part of their child’s health care plan.
Prevent Blindness Mid-Atlantic, formerly Prevent Blind-ness Virginia, is the only local non-profit health organiza-tion solely dedicated to the detection and prevention of early-stage vision problems and proudly serves Virginia, Maryland and Washington, DC. For more information or to make a contribution to the sight-saving fund, call toll-free (888)790-2020 or visit us on the web at www.TheEyeSite.org.
summer (PEDS and the M-CHAT are already published in Spanish and PEDS has been translated into many other languages). Vanderbilt Universi-ty is trialing PEDS plus the PEDS:DM via a waiting room computer kiosk.
Also of note, the PEDS:DM was creat-ed with items from several of the Brig-ance Diagnostic Inventories. Albert Brigance and his publisher, Curricu-lum Associates, along with Ellsworth
& Vandermeer Press have jointly agreed to donate a portion of PEDS:DM sales to the American Academy of Pediatrics’ Section on Developmental and Behavioral Pediatrics in support of its website devoted to helping health care providers learn about screening and surveillance, www.dbpeds.org including other screening tools. More information on PEDS and the PEDS:DM, including slide shows and other
training materials, can be found at www.pedstest.com/dm.
For more information contact Frances Page Glascoe, Professor of Pediatrics Vanderbilt University, Editor, Ameri-can Academy of Pediatrics, Section on Developmental-Behavioral, Pediatrics’ Newsletter www.dbpeds.org at [email protected].
New AAP Policy on Early Detection of Developmental and Behavioral Problems
Continued from page 14
�1������virginia�pediatrics
VIRGINIA PEDIATRICS
Virginia Chapter, American Academy of Pediatrics& The Virginia Pediatric Society2201 West Broad Street, Suite 205Richmond, VA 23220
Prostate Cancer CME Conference
The VCU Massey Cancer Center and the Office of Continuing Professional Development and Evaluation Studies presents Controversies and Updates in the Management of Prostate Cancer to be held September 29, 2007 at the Jefferson Hotel in Richmond, Virginia. This course is designed for physicians and other health care professionals who deliver care to patients with prostate cancer. This conference will cover the latest issues and updates in the management of prostate cancer in the areas
of surgery, radiation therapy, systematic therapies, imaging and the economics of prostate cancer. Plenary sessions and case discussions will enhance your opportunity to learn more about this condition.
The course registration fee is $150.00 for physicians and $100.00 for physicians-in-training. For more information call 828-3640 or to register on-line go to www.cmeregistration.som.vcu.edu.
Calendar of Events
July 20-22 page 8
29th Annual Pediatric Primary Conference
July 27 -29 page 5
Strong Roots for a Healthy Future Conference
September 29 Prostate Cancer CME Conference
October 12-14Pediatrics at Williamsburg 2007 ConferenceWilliamsburg LodgeWilliamsburg, VA