Inpatient violence and aggression: a literature review...Inpatient violence and aggression: a...
196
Inpatient violence and aggression: a literature review Report from the Conflict and Containment Reduction Research Programme Len Bowers Duncan Stewart Chris Papadopoulos Charlotte Dack Jamie Ross Husnara Khanom Debra Jeffery May 2011 Section of Mental Health Nursing Health Service and Population Research Institute of Psychiatry Kings College London
Transcript of Inpatient violence and aggression: a literature review...Inpatient violence and aggression: a...

Inpatient violence and
aggression: a literature
review
Report from the Conflict and Containment Reduction Research Programme Len Bowers Duncan Stewart Chris Papadopoulos Charlotte Dack Jamie Ross Husnara Khanom Debra Jeffery
May 2011 Section of Mental Health Nursing Health Service and Population Research Institute of Psychiatry Kings College London

1. BACKGROUND Mentally ill people in hospital sometimes behave aggressively. They may try to harm other patients, staff, property or themselves. In the UK, the National Audit of Violence found that a third of inpatients had been treatened or made to feel unsafe while in care [Royal College of Psychiatrists 2007]. This figure rose to 44% for clinical staff and 72% of nursing staff working in these units. Such aggression can result in injuries, sometimes severe, to patients or to staff, causing staff absence and hampering the efficiency of the psychiatric service. The ways in which aggressive behaviour is managed by staff is contentious and emotive, and there is little evidence or agreement about their effectiveness. This review aims to describe the available research literature on the prevalence, antecedents, consequences and circumstances of violence and aggression in psychiatric hospitals. Our previous research has focussed on how to reduce of conflict and containment on acute wards. By conflict we mean those things that threaten patient and staff safety, such as aggression, rule breaking, drug/alcohol use, absconding, medication refusal, self-harm/suicide etc. By containment we mean those things the staff do to prevent these things occurring, or reduce the amount of harm that occurs, such as giving extra medication, intermittent observation, constant observation, show of force, manual restraint, coerced injections of medication, seclusion, time out, locking of the ward door, and other security policies. This research indicates a complicated relationship between conflict behaviours and containment, and that the behaviour and attitudes of staff may influence both. It led to the development of the ‘City model’ describing the ways in which staff factors can reduce rates of conflict and containment on wards. Three processes are posited to create low conflict and containment: positive appreciation of patients (kindness), emotional self-regulation of anger and fear (tranquillity), and an effective structure of rules and routines for patients based upon an ethical (not punitive) stance (orderliness). In addition to an analysis of the research literature, therefore, each chapter considers the evidence for and against the City Model and suggests lessons for future research. 2. LITERATURE SEARCH Electronic searches of the main databases were conducted to locate studies of psychiatric inpatient aggression published in English between 1960 and 2009. Searches were conducted using the following databases: MEDLINE, PsychInfo, Cochrane Clinical Trials, EMBASE Psychiatry, CINAHL and DARE and the following keywords: (psychiat* or mental*) and (hospital or ward or inpatient or in-patient) and (aggressi* or violen*). No attempt was made to search for unpublished results. 4,353 references were identified. Papers from adolescent and geriatric services were excluded. Resulting titles and abstracts were then inspected for relevance. As the literature accumulated, further references were obtained by following up citations. A total of 997 hardcopy references were obtained. These were divided between five researchers for detailed review and data extraction. Under the supervision of the lead author, the researchers inspected the papers for relevance, eligibility and suitable

empirical data (quantitative or qualitative) which could be used for the review. The final number of studies included in the review was 424. A matrix (in Excel) was constructed with a number of headings including: methodology, sample, definitions and setting used in the article; the patient profiles (age, gender, ethnicity, diagnosis, treatment, marital status, family circumstances, previous psychiatric history, etc); the rates of occurrence; times and places or occurrence of the event; circumstances of event; antecedents and causes; relationships between types of adverse events; patient motivations; staff related factors and limitations. Each of the 424 articles was reviewed and analysed by extracting data/evidence for the relevant sections in the matrix. Additional information not directly fitting in the predefined categories, was collated in an ‘other findings’ column and processed separately. Definitions were provided for each item on the matrix to facilitate consistency of data extraction. The initial ten matrix entries for each researcher were cross checked for accuracy and correct interpretation by the lead author and another team member. Direct feedback was provided and emerging issues or problems discussed among the team. Progress with the data extraction phase of the review was monitored by regular individual and group meetings for a period of six months. Having extracted data onto the matrix, responsibility for analysis and write-up of specific sections of the review was divided among the team. This phase of the review took five months to complete. Written reports for each section were submitted to the lead author for feedback, revisions and final editing, before being combined into a single document.

3. THE INCIDENCE OF VIOLENCE AND AGGRESSION
3.1 The studies reviewed
At least one measure of the rate of aggression or violence could be calculated for 128 papers. In some cases data had been extracted from multiple publications which shared the same source data. These studies were only counted once in the analyses. One Canadian study of treatment resistant patients reported an event based rate of 3696% [Ehmann et al. 2001] which was substantially higher than any other study, so was excluded from further analysis as an extreme outlier. One study reported rates from three European cities (London, Modena and Athens)[Bowers et al. 2005]. The London data from this study was also reported elsewhere [Bowers et al. 2003], but data for the other two cities are analysed separately. The final sample was 122 studies. Sixty-seven of the studies (55%) were retrospective analyses of official incident records and/or patient notes, while 55 (45%) used descriptive data from other sources such as surveys, interviews and observation recording instruments designed for the study. Thirty-eight were case-control studies and six were classified as before and after studies. The studies were conducted in various types of setting, ranging from acute wards (n=37, 30%), forensic units (n=36, 30%) to psychiatric hospitals with a mix of ward types (n=40, 33%). In nine (7%) cases the type of ward was classified as ‘other’. Most studies were conducted in the USA (n=35, 29%) or UK (n=31, 26%). Other countries represented included Australia (n=14, 12%), Norway (n=6, 5%), Canada (n=5, 4%), Netherlands (n=5, 4%), Sweden (n=4, 3%), Italy (n=4, 3%), Germany (n=2, 2%), Israel (n=2, 2%) and Taiwan (n=2, 2%). The studies involved a total of 69,249 patients, with an average sample of 581.9 (SD=1,035.1) per patient-based study.
The definition of violence and aggression differed widely between studies. Types of violence recorded included physical violence, physical violence directed at staff only, verbal aggression, aggression towards objects, self-harm and sexual aggression. Almost all the studies included physical violence, but the inclusion of the other categories of violence and aggression varied. Where patients were responsible for more than one category of violence studies typically only recorded the most serious incident. These complexities meant that the review could not accurately describe rates for individual categories of violence.
3.2 Overall incidence
The incidence of violence was calculated for seven types of measure: patient based % (violent patients/sample*100), event based % (incidents/sample*100); events per 100 admissions per month (incidents per month/admissions per month*100); patients per 100 admissions per month (violent patients per month/admissions per month*100); events per 100 occupied bed days (incidents/total patient bed days*100); patients per 100 occupied bed days (violent patients/total patient bed days*100); and events per 100k population per year. The overall mean incidence of violence across all the studies was as follows: 32.4% (SD=19.6) of patients, 224.8 (SD=378.8) event based percentage, 182.8 (SD=366.8) events per 100 admissions per month, 26.2 (SD=18.0)

patients per 100 admissions per month, 3.14 (SD=5.4) events per 100 occupied bed days, 0.42 (SD=0.32) patients per 100 occupied bed days, and 122.2 (SD=138.6) events per 100k population per year.
A meta-analysis (with random effects) was conducted as an alternative method of calculating an overall rate of violence. This has the advantage of taking sample sizes into account. The analysis showed a combined rate of 30.7% (95% CI=28.4-33.0). However, the I-squared measure of heterogeneity was 98.7%, substantially higher than the 50% recommended as an indicator that combining studies for meta-analysis may be invalid [Perera & Heneghan 2008].
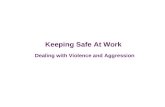
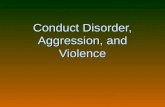
Kernel density plots show that the distribution of each variable was not normally distributed (Figures 1 to 6), with event based rates showing greater positive skew than patient based rates. For the purposes of statistical analysis in this report, patient and event rates were square root and log transformed respectively to reduce the influence of extreme scores.
0.0
05.0
1.0
15
.02
Den
sity
0 20 40 60 80 100
Kernel density estimateNormal density
kernel = epanechnikov, bandwidth = 7.1065
Figure 1: Distribution for patient based rate

0.0
01.0
02.0
03.0
04D
ensi
ty
0 500 1000 1500 2000
Kernel density estimateNormal density
kernel = epanechnikov, bandwidth = 51.7366
Figure 2: Distribution of event based rate
0.0
01.0
02.0
03.0
04.0
05D
ensi
ty
0 500 1000 1500 2000
Kernel density estimateNormal density
kernel = epanechnikov, bandwidth = 41.2450
Figure 3: Distribution of events per 100 admissions per month
0.0
05.0
1.0
15.0
2D
ensi
ty
0 20 40 60 80
Kernel density estimateNormal density
kernel = epanechnikov, bandwidth = 7.8351
Figure 4: Distribution of patients per 100 admissions per month
0.0
5.1
.15
.2D
ensi
ty
Kernel density estimateNormal density
kernel = epanechnikov, bandwidth = 1.2985
Figure 5: Distribution of events per 100 occupied bed days
0.5
11.
5D
ensi
ty
-.5 0 .5 1 1.5
Kernel density estimateNormal density
kernel = epanechnikov, bandwidth = 0.1573
Figure 6: Distribution of patients per 100 occupied bed days

3.3 Incidence by country and setting
Mean rates were calculated for countries and settings with at least two studies for each type of measure (Table 1). Unfortunately, there was insufficient data to enable comparable analysis of rates per 100 occupied bed days or per 100k population. Countries were also ranked for each measure (Table 2).
Table 1: Mean violence rates by country and measure
Country Patient based %
Event based %
Events per 100 adms per month
Patients per 100 adms per month
Events per 100 occ bed days
Patients per 100 occ bed days
Australia 36.85 150.72 109.67 31.58 9.09 0.63 Canada 32.61 81.46 36.27 18.77 0.70 0.40 Germany 16.06 Israel 16.73 Italy 20.28 27.47 8.99 8.21 Netherlands 24.99 186.69 220.21 31.79 3.50 0.56 Norway 33.47 471.85 460.78 32.47 10.19 Sweden 42.90 59.25 Taiwan 128.27 United Kingdom 41.73 303.49 170.73 32.97 2.25 0.35 Unites States 31.92 341.87 302.47 16.92 0.16 0.14
Analysis using one way ANOVAs showed that none of the comparisons were statistically significant. However, the highest proportion of violent patients was found in Sweden, the UK and Australia. The lowest patient based rates were from Germany, Israel and Italy. Despite having the highest proportion of patients involved in violence Sweden had one of the lowest event based rates, suggesting that violent patients in that country commit fewer violent acts than in others. The UK remained one of the countries with the highest event based rate, but while the USA had the second highest rate for this measure, it was sixth out of ten for patient based rates. The highest event based rate was for Norway, but this were influenced by one forensic study with a high level of violence (2069%)[Rasmussen and Levander 1996], although the study only measured physical violence towards staff in a forensic unit. Without this study the mean event based rate for Norway was 58.69, which was one of the lowest rates and comparable to Sweden. Italy had the fewest violent patients and events among the countries which had data available for both these measures. When rates were standardised by the number of admissions per month, the proportion of patients involved in violence was highest for Australia, UK, Norway and the Netherlands. Around a third of patients per 100 admissions from these countries had committed at least one violent act. Greater differentiation was apparent for standardised event based rates. Again Norway had the highest event based rate, reflecting the outlier in this country. The USA had the next highest rate followed by the Netherlands and UK. A mean rate per 100 occupied bed days could be calculated for only six countries. Nevertheless, Australia and Norway had by far the highest event based results for this measure (this time the outlier study from Norway could not be included in the calculations). Canada and the USA had the lowest rates. Norway and Australia also had the highest patient based rate per 100 occupied bed days, and the UK and US the lowest. International comparisons across these different
measures needs to be interpreted cautiously because the same studies did not contribute to each average score, the proportion of studies from different settings differed between the countries, the definition of violence varied and the number of studies from some countries was small. Table 2: Ranked mean violence rates by country (high to low)
Patient based %
Event based %
Events per 100 adms per month
Patients per 100 adms per month
Events per 100 occ bed days
Patients per 100 occ bed days
Australia 3 5 5 1 2 1 Canada 5 7 6 5 5 3 Germany 10 Israel 9 Italy 8 9 7 7 Netherlands 7 4 3 4 3 2 Norway 4 1 1 3 1 Sweden 1 8 Taiwan 6 United Kingdom 2 3 4 2 4 4 Unites States 6 2 2 6 6 5
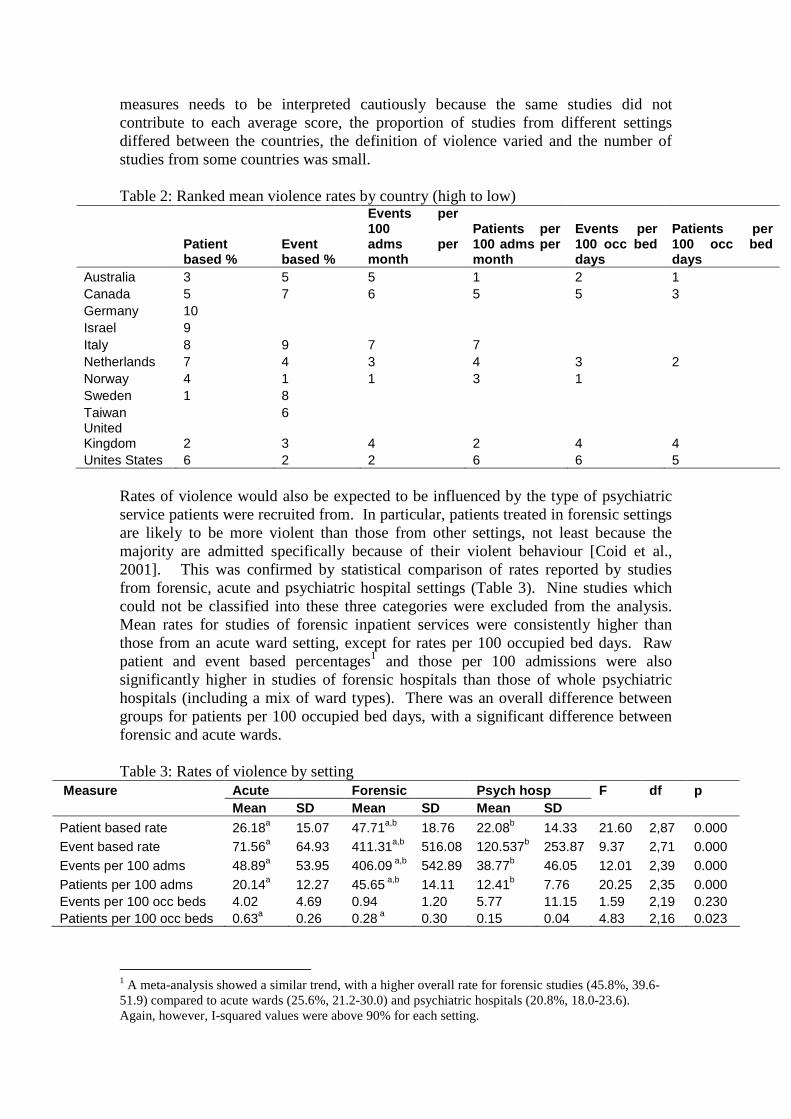
Rates of violence would also be expected to be influenced by the type of psychiatric service patients were recruited from. In particular, patients treated in forensic settings are likely to be more violent than those from other settings, not least because the majority are admitted specifically because of their violent behaviour [Coid et al., 2001]. This was confirmed by statistical comparison of rates reported by studies from forensic, acute and psychiatric hospital settings (Table 3). Nine studies which could not be classified into these three categories were excluded from the analysis. Mean rates for studies of forensic inpatient services were consistently higher than those from an acute ward setting, except for rates per 100 occupied bed days. Raw patient and event based percentages1 and those per 100 admissions were also significantly higher in studies of forensic hospitals than those of whole psychiatric hospitals (including a mix of ward types). There was an overall difference between groups for patients per 100 occupied bed days, with a significant difference between forensic and acute wards. Table 3: Rates of violence by setting
Measure Acute Forensic Psych hosp F df p Mean SD Mean SD Mean SD
Patient based rate 26.18a 15.07 47.71a,b 18.76 22.08b 14.33 21.60 2,87 0.000 Event based rate 71.56a 64.93 411.31a,b 516.08 120.537b 253.87 9.37 2,71 0.000 Events per 100 adms 48.89a 53.95 406.09 a,b 542.89 38.77b 46.05 12.01 2,39 0.000 Patients per 100 adms 20.14a 12.27 45.65 a,b 14.11 12.41b 7.76 20.25 2,35 0.000 Events per 100 occ beds 4.02 4.69 0.94 1.20 5.77 11.15 1.59 2,19 0.230 Patients per 100 occ beds 0.63a 0.26 0.28 a 0.30 0.15 0.04 4.83 2,16 0.023
1 A meta-analysis showed a similar trend, with a higher overall rate for forensic studies (45.8%, 39.6-51.9) compared to acute wards (25.6%, 21.2-30.0) and psychiatric hospitals (20.8%, 18.0-23.6). Again, however, I-squared values were above 90% for each setting.

Note: Means on the same row and sharing the same superscript letter differ significantly by p<0.05 (Scheffe test). Standardising measures by bed occupancy countered the trend indicated by basic rates or rates standardised by admissions. There were 26 studies which provided data to enable calculation rates per 100 occupied bed days (20 for patients, 24 for events), but there was no statistically significant difference between these and the remainder of studies in terms of setting (χ2
[3] =4.67, p=0.197), methodology (χ2[1] =0.32 p=0.570) or
definition (,χ2[3] =2.39, p=0.495).
The different results for occupancy based rates are likely to reflect insensitivity of this measure to patient throughput. The mean sample size for the forensic studies (152.8, SD=154.8) was significantly smaller than the studies from acute wards (632.4, SD=1088.0) and psychiatric hospitals (999.3, SD=1349.7)(F[2,107]=13.29, p=0.000). This would have provided forensic studies with a lower denominator for calculation of admissions based rates. However, the impact of a smaller sample on occupancy based rates was probably offset by a longer study period for forensic studies. The mean timeframe (in months) was 31.3 (SD=41.0) compared to 18.7 in acute services and 15.6 (SD=18.8) in psychiatric hospitals. This difference was statistically significant (F[2,106]=4.29, p=0.016), with a post-hoc Scheffe test indicating that forensic and acute ward studies differed significantly (p<0.05). These statistical comparisons of sample size and months were conducted with log transformed variables. Further (non-statistical) analysis was conducted to compare rates across both country and setting (Figures 7 to 10). In all countries with available data patient based percentages showed forensic services to have the highest rates of violence. Rates among forensic patients were highest in the UK and US and lowest in Australia, although the rate in all countries was over 40%. A similar pattern was found for acute patients, with the highest rates found for the UK, US and Netherlands and the lowest in Australia. However, a greater proportion of violent patients reported by studies of whole psychiatric hospitals were found in Australia, compared to the US and UK. Event based percentages were greatly higher in forensic studies from the UK and USA. Among the Australian studies the rate for forensic patients was much lower, and almost equal to the rate for psychiatric hospitals. The rate for acute patients was highest in the Netherlands. Fewer studies were available for comparisons of rates per 100 admissions. Only the UK had data available for both patient and event based rates and for each setting. As expected, the UK rates were much higher for studies of forensic patients, but there was greater differentiation between acute and general psychiatric hospitals for patient than event based rates per 100 admissions. The UK also had the highest rates for forensic studies compared to other countries. Australia had the lowest patient based rates for both forensic and acute studies. Patient and event based rates for acute services were highest in the Netherlands.
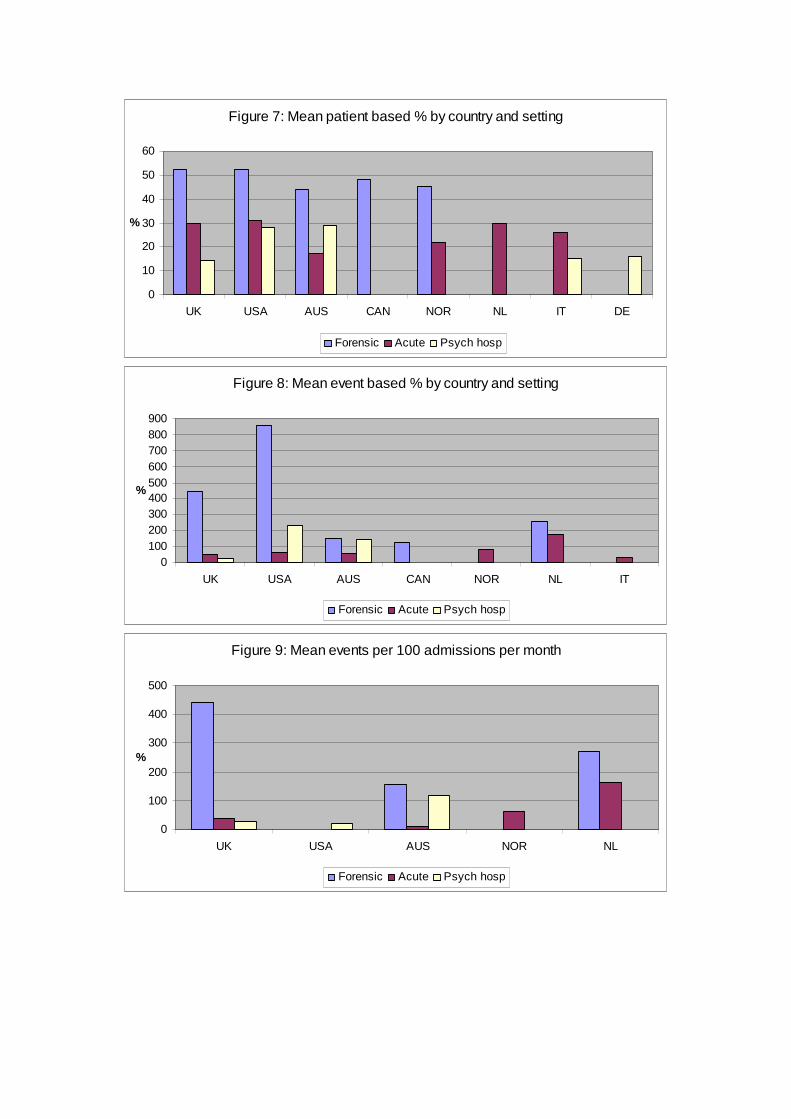
Figure 7: Mean patient based % by country and setting
0
10
20
30
40
50
60
UK USA AUS CAN NOR NL IT DE
%
Forensic Acute Psych hosp
Figure 8: Mean event based % by country and setting
0100200300400500600700800900
UK USA AUS CAN NOR NL IT
%
Forensic Acute Psych hosp
Figure 9: Mean events per 100 admissions per month
0
100
200
300
400
500
UK USA AUS NOR NL
%
Forensic Acute Psych hosp
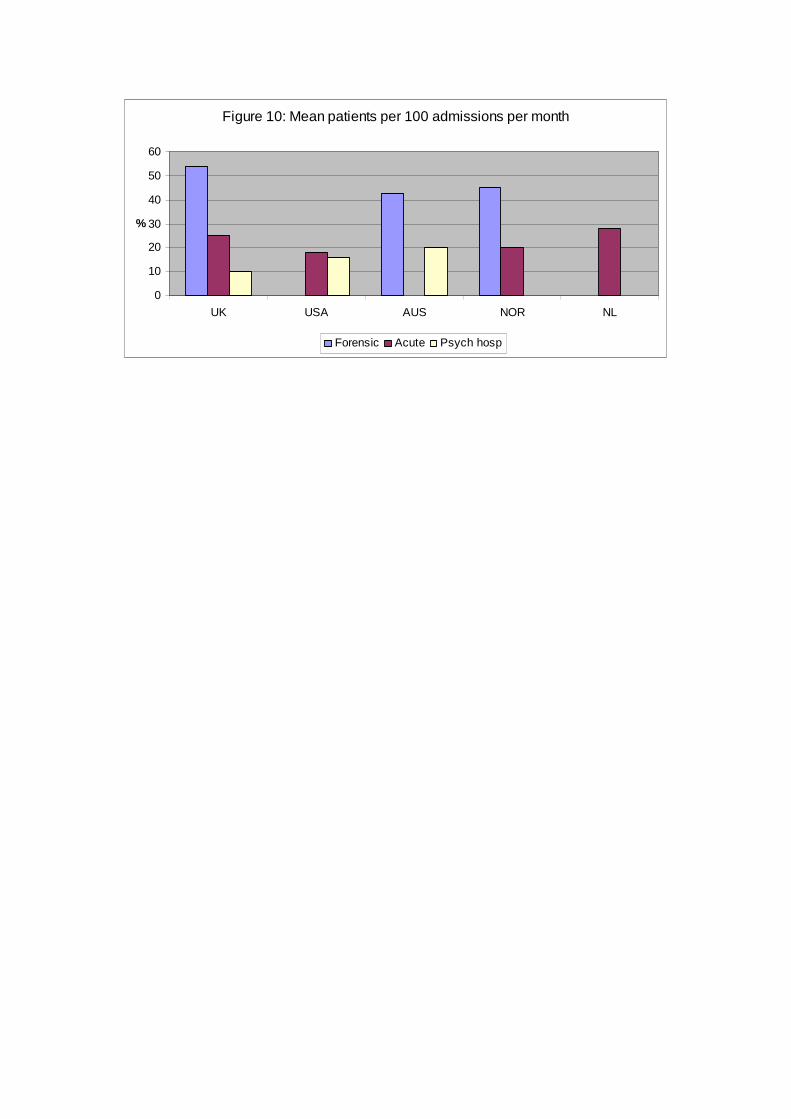
Figure 10: Mean patients per 100 admissions per month
0
10
20
30
40
50
60
UK USA AUS NOR NL
%
Forensic Acute Psych hosp

3.4 Definition The influence of definition on overall rates was tested as follows. The studies were classified by whether they included verbal aggression, physical violence, aggression towards objects and self-harm. Occasionally studies also included sexual aggression. The number of studies which measured each type of violence is shown in Table 4. The most common combinations were: verbal, physical, towards objects & self-harm; physical only; verbal, physical & towards objects. All the studies which defined violence or aggression (n=121) included physical violence, although in six studies this was against staff only. Fifty-nine percent of studies included verbal aggression and 36% included self-harm. Table 4: Definitions of violence/aggression Type of aggression N % Physical only 26 21.3 Physical only – directed at staff 6 4.9 Physical & towards objects 8 6.6 Physical, towards objects & self-harm 5 4.1 Physical & self-harm 4 3.3 Verbal & physical 8 6.6 Verbal, physical & sexual 2 1.6 Verbal, physical & towards objects 26 21.3 Verbal, physical, towards objects & sexual 2 1.6 Verbal, physical, towards objects & self-harm 30 24.6 Verbal, physical & self-harm 4 3.3 Not defined 1 0.8 The frequencies enabled four groups of studies to be compared: physical aggression, verbal, physical and towards objects, verbal, physical, towards objects and self-harm, and the remainder of studies (Table 5). Table 5: Rates of violence by definition
Measure Physical
Verbal, physical & objects
Verbal, physical, objects & self Other F P
Mean SD Mean SD Mean SD Mean SD Patient based rate 24.93 14.43 37.67 20.39 38.55 23.98 31.80 18.38 2.31 0.081 Event based rate 217.98 513.99 239.48 399.19 302.81 399.68 142.20 182.29 0.95 0.420 Events per 100 adms 269.45 675.83 103.19 76.99 231.46 336.3 146.08 238.85 0.29 0.831 Patients per 100 adms 25.46 16.16 31.08 16.73 21.44 18.05 24.52 22.55 0.59 0.625 Events per 100 occ beds 10.83a,b,c 5.58 0.71 a 0.64 1.55 b 2.23 1.91c 2.27 4.63 0.014 Patients per 100 occ beds 0.63 0.04 0.38 0.35 0.54 0.34 0.21 0.22 1.54 0.242
Note: Means on the same row and sharing the same superscript letter differ significantly by p<0.05 (Scheffe test). The standard deviations indicate large variations in rates within the groups, but there were no statistically significant difference for patient based rates, event based rates, events per 100 admissions or patients per 100 admissions. However, studies of

physical violence had higher event rates per 100 occupied be days than other categories of study. Studies were then classified by whether or not they included verbal aggression. Each measure of violence was then compared between the verbal (n=72) and non-verbal (n=49) aggression groups (Table 6). The results show only one statistically significant difference: patient based rates were higher when verbal aggression was included in the definition of violence. Table 6: Rates of violence by inclusion/exclusion of verbal aggression
3.5 Study methodology Sixty-seven of the studies (55%) collected incident data from official hospital records or nursing notes while 55 (45%) were observation studies (typically using SOAS or a similar instrument). Rates by these two methodologies were compared (Table 7). There were no significant differences for the patient based rate, event based rate, events per 100 admissions, patients per 100 admission or events per 100 occupied beds. However, observational studies had a significantly higher rate for patients per 100 occupied beds. Table 7: Rates by methodology Measure Official records Observational t p Mean SD Mean SD Patient based rate 32.15 19.76 33.20 19.78 0.33 0.743 Event based rate 264.78 462.42 180.57 254.10 0.01 0.994 Events per 100 adms 213.01 433.17 131.72 217.03 0.78 0.441 Patients per 100 adms 28.90 20.48 22.40 13.71 0.35 0.726 Events per 100 occ beds 4.01 7.17 2.27 2.60 0.01 0.995 Patients per 100 occ beds 0.20 0.21 0.60 0.28 3.58 0.002
Measure Without verbal aggression With verbal aggression t p
Mean SD Mean SD Patient based % 27.22 15.74 36.80 21.47 2.28 0.025 Event based % 191.30 400.82 240.72 361.97 1.37 0.175 Events per 100 adms 206.19 533.82 170.23 247.16 1.33 0.192 Patients per 100 adms 22.26 15.95 28.19 20.35 0.96 0.345 Events per 100 occ beds 4.66 6.30 1.64 2.07 1.135 0.269 Patients per 100 occ beds 0.34 0.26 0.45 0.34 0.611 0.549
3.6 Trends over time Studies were ordered by date of data collection. Where studies were conducted over two years the most recent was chosen for the purposes of the analysis. For studies covering more than two years, the midpoint was selected. However, no discernable trends over time were identified. 3.7 Repeated violence The studies commonly reported that a small sub-group of patients were responsible for the majority incidents. This was expressed a variety of ways: different proportions of patients were reported to account for different proportions of incidents. The lack of consistency in reporting makes it impossible to compare or aggregate across individual studies. Thirty-one studies provided enough information to calculate the proportion of violent patients who were involved in repeated incidents. This figure ranged from 12% to 81%, with a mean of 44.7% (SD=16.8). Studies from Australia (n=3) recorded a higher rate (59.9, SD=20.4) than the UK (41.2, SD=11.4) and USA (35.6, SD=21.1). Forensic studies reported a higher rate (54.0, SD=17.1) than those from acute settings (44.9, SD=17.9) and psychiatric hospitals (36.6, SD=12.6). The papers were examined for information allowing the calculation of a mean rate of violence per violent patient. This repeat rate was available for 65 studies. However, the analysis excludes one outlier study from Norway (mean incidents per violent patient=37.4), leaving a final sample of 64 for this section. The number of incidents per violent patient ranged from 1 to 21.1, with an overall mean of 4.2 (SD=3.6). A kernel density plot indicated that the variable was positively skewed and was log transformed for the purposes of statistical analysis.

0.0
5.1
.15
.2D
ensi
ty
0 5 10 15 20
Kernel density estimateNormal density
kernel = epanechnikov, bandwidth = 0.8567
Figure 11: Distribution of repeated violence
Countries with at least two studies reporting repeated violence were compared (Figure 5). Individual studies with high rates of repeated violence were found in Norway, UK and USA. Averages across countries ranged from: Canada (2.3, SD=1.4), Italy (2.3, SD=0.7), Taiwan (2.6, SD=0.5), UK (4.2, SD=3.5), Netherlands (4.3, SD=2.6), USA (4.4, SD=4.0). Australia (4.6, SD=1.5 and Norway (5.0, SD=4.4). However, a statistical comparison did not reach significance (F[7,45]=0.82, p=0.579). Repeated violence was also examined across settings (Figure 6). The mean rate was highest for forensic studies (5.4, SD=4.9), compared to acute wards (3.0, SD=2.1) and psychiatric hospitals (3.9, SD=2.8). This difference was not statistically significant (F[2,57]=1.76, p=0.181). As with rates of violence, studies were categorised into four groups based upon the definition of violence employed (n=64). The mean rate of repeated violence for studies of physical aggression was 5.6 (SD=9.1), 4.1 (SD=2.5) for studies of verbal, physical and aggression towards objects, 4.1 (SD=4.0) for studies verbal, physical, self-harm and aggression towards objects and self-harm, and 4.1 (SD=3.0) for the remainder of studies. There was no significant difference between the groups (F[3,60]=0.25; p=0.864).

Figure 12: Incidents per violent patient by country
0 2 4 6 8 10 12 14
A U SA U SA U SA U SA U SA U SA U SA U SA U SC A NC A NC A NC A NC A N
ITITIT
N LN LN L
N ORN ORN OR
TWTWU KU KU KU KU KU KU KU KU KU KU KU KU KU KU KU KU KU KU KU K
U SAU SAU SAU SAU SAU SAU SAU SA
Figure 13: Incidents per violent patient by setting
0 5 10 15 20 25
AAAAAAAAAAAAAAAAAAAAFFFFFFFFFFFFFFFFFFFFFPPPPPPPPPPPPPPPPPPP

The proportion of violent patients who were responsible for more than one incident was calculated for 31 studies. This figure ranged from 12% to 81% with a mean of 44.7 (SD=16.5). Again, the mean repeat rate was highest in forensic studies (54.0%, SD=17.1) than studies from acute (44.9%, SD=17.9) or psychiatric hospital settings (36.6%, SD=12.6). This did not quite achieve statistical significance (F[2,28]=2.82, p=0.078). The available studies were distributed across too many countries to allow analysis by country of origin. 3.8 Physical violence Although a comparative analysis by type of violence could not be conducted, it was possible to focus on physical violence because studies counting multiple categories of violence would be the least likely to undercount these incidents. Excluding studies which only measured physical violence, the proportion of incidents involving physical violence ranged from 6% to 93%, with a mean of 45.0% (SD=22.8). This was calculated for a sub-sample of 39 studies. It might be expected that this proportion would be lower for studies which included more categories of violence. The proportion of incidents involving physical violence for studies which measured two categories of violence was 52.6% (SD=22.7) and 54% (SD=21.8) for those which measured three categories. However, the proportion for studies reporting four categories of violence was significantly lower (32.1%, SD=16.6; F[2,34]=5.49, p=0.009). Comparison by definition also showed that studies which included verbal aggression, physical violence, aggression to objects and self-harm had the lowest rate (32.1%, SD=16.7; F[2,35]=4.76, p=0.015. Studies of physical violence only were combined with those for which it was possible to calculate a separate event or patient based rate for physical violence (n=50). Patient based rates for physical violence ranged from 4% to 55% with a mean of 22.5% (SD=13.0). Event based rates ranged from 1.4 to 2069.1 with a mean of 219.5 (SD=447.6). Without the 2069 outlier [Rasmussen and Levander 1996], the mean event based rate was 148.4 (SD=257.3). Comparison of patient based rate by setting revealed no significant difference (F[2,32]=1.04, p=0.366). The rate was 20.8% (SD=9.2) for acute wards, 27.9% (SD=18.3) for forensic wards and 19.1% (SD=12.7) for psychiatric hospitals. After dropping the outlier study, mean event based rates by setting were: 42.7 (SD=48.0) for acute wards, 39.7 (SD=25.3) for forensic wards and 99.9 (SD=156.1) for psychiatric hospitals. However, the differences were not statistically significant (F[2,19]=0.73, p=0.495). 3.9 Staff surveys of violence A separate analysis was conducted for studies which asked nurses and other clinical staff about their experiences of violence. This excluded service wide recording systems for violent incidents. To allow meaningful comparisons, only studies reporting the proportion of sampled staff experiencing violence were included. Where possible, rates for nurses and other staff were analysed separately.

Forty-two studies fulfilled these criteria. Most single country studies were from the USA (n=10; 24%) or the UK (n=10; 24%). Others were from: Australia (n=3; 7%), Taiwan (n=3; 7%), Canada (n=2; 5%), Japan (n=2; 5%), Sweden (n=2; 5%), Turkey (n=2; 5%), Belgium (n=1; 2%), Norway (n=1; 2%), Poland (n=1; 2%) and Switzerland (n=1; 2%). Two studies compared rates between the UK and Sweden, and one between the UK and USA. A further study compared the USA, UK, Canada and South Africa. The vast majority of studies were of multiple ward types or hospitals (n=32; 76%). A further four (10%) were from a mix of psychiatric inpatient and community staff, and only data for the former were included in the review if possible. Two studies were from acute ward settings and one from a forensic hospital. The setting was unspecified in three studies. Twenty studies (48%) were of physical violence only and three (7%) of verbal aggression only. Fifteen studies (36%) were of both verbal and physical aggression. The remainder included other types of violence or were unspecified. Half of the studies (n=20; 48%) surveyed psychiatric nurses, seven surveyed psychiatrists (17%), while 14 (33%) were of a mix of staff types (wherever possible, separate rates were calculated for nurses, psychiatrists and other clinicians). One study was of student nurses. In almost all cases (n=39; 93%) staff were asked about their own experiences, but in three studies the questions were about staff observations of violence on wards. The surveys usually asked about violence experienced during a staff member’s professional career (n=19; 44%) or events during the previous year (n=13; 31%). The others had various other reporting periods (n=8; 19%) and some were unspecified (n=6; 14%). Note that some studies included data for more than on time frame. Rates of violence by staff type and time period are shown in Figure 14. A greater proportion of nurses consistently reported experiencing violence during their career (79%), the previous year (62%) and where the timeframe was unclear (80%). Data for psychiatrists were only available for career based rates, but these were substantially lower (43%). It is more difficult to interpret rates reported for all ward or hospital staff, but the finding that they were lower than for nurses probably reflects the inclusion of psychiatrists.

Figure 14: Proportion of staff reporting violence by profession and time period
0
10
20
30
40
50
60
70
80
90
Ever Year Unspecified
%
Nurses Psychiatrists Mix
Some studies did not include an overall violence rate but presented survey results by violence type. A study from Taiwan reported that 35% of staff reported being the victim of physical violence during the previous year and 51% were verbally abused [Chen et al. 2009]. Over the course of a career, 83% of staff in another study had experienced verbal aggression and 51% physical violence [Hatch-Maillette et al. 2007]. For studies of nurses, rates tended to be higher for both types of aggression. Average career based rates were 71% for verbal aggression and 66% for physical violence. Over the previous year, mean rates were 84% and 77% respectively. Only one study of (trainee) psychiatrists reported rates by type and found 26% had been assaulted in the previous year and 54% threatened [Pieters et al. 2005]. Rates for the duration of residency were 72% and 56% respectively. Four studies reported international comparisons. UK nurses experienced higher rates of violence during the previous year than nurses from Sweden (71% vs 59%), and a non-significant difference remained for physical aggression only (43% vs 33%)[Nolan et al. 2001]. A second comparison of these countries [Lawoko et al. 2004] found the same, with UK nurses reporting higher rates of verbal or physical violence during their career (94% vs 84%) and during the previous year (73% vs 65%). The same study found a difference for psychiatrists in the same direction. Rates for UK psychiatrists were 94% over a career and 53% over a year, compared to 86% and 58% in Sweden. A comparison of US and UK psychiatrists also found rates to be marginally higher among the UK sample (rates over career: 20% vs 24%)[Hatti et al. 1982]. Finally, one study compared physical violence rates for nurses in the USA, UK, Canada and South Africa, although the mix of hospital settings from each country was very different [Poster 1996]. Rates of any assault were significantly higher in Canada (94%) than the UK (78%), USA (76%) and SA (51%).

3.10 Evidence for and against the City model The review of violence rates offered little information which was relevant to the City model. The studies reported wide ranging levels of violence, even within countries and settings. This variation is likely to reflect differences in nursing practice, at least to some degree, but further exploration was beyond the scope of this review which did not consider nursing interventions. 3.11 Points the City model has missed The analyses clearly show that raw rates of violence are highest in forensic services. This was found within and across countries. Different management strategies are likely to be needed for forensic patients, particularly as many have a history of violent behaviour and their stay in hospital is often much longer than the typical acute ward patient. The City model strives to reduce levels of conflict and containment to a minimum, but the extent of possible reductions may well differ by service typology. What seems a high level of containment in an acute ward may be the norm in a forensic setting. A small minority of patients were found to be responsible for multiple episodes of violence. This was a consistent finding, with no significant difference in the mean level of repeated violence between settings or countries. This has implications for the City model in the sense that targeted approaches to violence reduction may be more appropriate or effective than blanket strategies across the whole ward or hospital. This may mean changing the way in which violent behaviour is managed for these individuals or increasing efforts to tackle the root causes or triggers for violence if they are known. The level of violence and aggression reported by the studies suggests a high degree of tolerance among staff, not least because they are frequently the victims of patient violence and aggression. This is supported by the apparent gap between official incidents and actual levels of violence and aggression reported by many studies. This could be interpreted as evidence of positive appreciation among staff, but in the case of verbal abuse in particular a certain amount of putting up with aggression seems inevitable. However, this leaves the question of what is level of abuse is acceptable? At what point should nurses intervene and how? 3.12 Discussion Summary Of the 424 studies included in the violence review, at least one rate was calculable for 30% of them. Rates varied markedly by country, setting, and settings within countries. The proportion of patients involved in violence tended to be higher in the UK, Australia and Scandinavia. In terms of the number of incidents, at least two were reported per patient overall, with studies from Norway, the USA and UK reporting the highest rates. The UK also had relatively high levels of staff victims of violence. Forensic patients had the highest proportion of violent patients and highest rate of violent incidents, but there was no difference between studies of acute patients and
those from psychiatric hospitals. Within countries, rates also tended to be higher among forensic studies. All the studies included physical violence, but there was huge variation in the measurement of other types of violence. This makes comparisons across studies difficult. Statistical tests found a modest influence of definition on overall rates of violence. Studies confined to physical violence had higher rates of events per 100 occupied days while those which included verbal aggression had higher patient based rates. Whether studies relied upon official reports of incidents or used observational methods was not associated with rates of violence, except for patient rates per 100 occupied days. Forensic studies had the lowest proportion of physical violence only studies (see below), which may be one reason why overall rates were higher in this setting. The findings must be interpreted with care. The availability of data to calculate each measure of violence varied such that each comparison reported above included a different sub-set of studies. Only eleven studies included data for each of the six measures of violence. The distribution of violent incidents among the patient population was skewed, with a minority of patients usually responsible for a large proportion of the violence. On average, 45% of violent patients were involved in more than one incident with each violent patient responsible for four incidents. There was no pattern to repeated violence by country, setting or definition of violence. Lessons for future research Given the scale of the literature review, surprisingly few studies included data which could be used to calculate rates of violence. The results differed by the type of measure employed, with higher rates for forensic studies compared to acute wards disappearing when controlling for occupied bed days. It can be concluded that a higher proportion of forensic patients were violent and committed more violent acts, but acute wards admit many more patients, including violent ones. When viewed as a measure of exposure to risk, controlling for patient bed days takes account of these differences and suggests that the chances of a violent incident occurring in a forensic hospital is lower than for other psychiatric services. Such differences in the balance between the number of admissions and static patient population probably also explain a similar phenomenon observed for comparisons by country: some of those with high rates per 100 admissions (e.g. UK) had comparatively lower rates per 100 occupied bed days. An important complicating factor for the review was the variation in definitions of violence. This sometimes reflected different emphases in the papers. For example, six studies were specifically focussed on staff victims of patient assault. Comparisons between the studies indicated that differences in definition did not greatly influence overall rates of violence. However, within studies it was commonly reported that official incident reports under-reported the true extent of violence. There were also interactions between definition, methodology and setting. Cross tabulation of these variables showed that over twice the proportion of studies measuring physical violence only used official data rather than observational methods (69% vs 31%; χ2
[1] =3.74, p=0.053). By setting, forensic studies were significantly more likely to use official data sources than observational methods (72% vs 28%; χ2
[3] =9.44, p=0.024).

The balance between official data and observational methods was more even for studies of acute wards (46% vs 54%) and psychiatric hospitals (54% vs 46%). Studies from psychiatric hospitals more likely to include physical violence only (41%) than forensic (8%) and acute ward (24%) studies (χ2
[3] =11.53, p=0.009). From these complexities, it can be concluded that prospective studies of violence are preferable to retrospective analysis of official incident reports and this applies to studies from forensic services in particular. Studies which recruit patients across ward types in psychiatric hospitals currently under-represent verbal aggression, aggression to objects and self-harm. There remains, therefore, more research to be conducted in order for a more complete picture of violence among psychiatric inpatients to emerge.

4. THE ANTECEDENTS OF VIOLENCE AND AGGRESSION 4.1 The studies reviewed Seventy one studies provided live, prospective antecedent data. This data is derived from what was recorded about the reason why violence/aggression occurred. Therefore, it should in theory be an accurate account of why the incident occurred, rather than a subjective opinion or belief about why the incident occurred. Fifty-three of these papers reported antecedent proportion data that was able to be meta-analysed. Data source There were 11 different sources of antecedents data. The most predominant of these were ‘incident forms’ (n=35 studies used this method), followed by the ‘SOAS/SOAS-R’ (Staff Observation Aggression Scale) ([Nijman et al. 1999;Palmstierna and Wistedt 1987];(Nijman et al. 1999) instrument (n=16), qualitative follow-up interviews (which were carried out either immediately after the incident or soon after) (n=9), ‘ASAP’ (Assaulted Staff Action Program) (Flannery, 1999) (n=4), video recording (n=3), study-specific questionnaires (n=3), medical claim documents (n=2), official records (clinical, legal, and/or case records) (n=2), participant observation (n=1), and case studies (n=1). Countries Antecedent data was collected from 13 different countries. These were: USA (n=22 studies), UK (n=19), Australia (n=7), Norway (n=6), Sweden (n=4), Canada (n=4), Italy (n=3), Taiwan (n=2), and Denmark, Finland, Germany, Netherlands, and Singapore (all n=1). Study settings Twenty-six studies collected antecedent data from inpatient acute settings. Twenty-two studies collected data from a mixture of settings, 14 studies collected data from forensic settings, 6 from Psychiatric Intensive Care Units (PICU), 2 from Rehab units, and 1 study collected data within a veteran setting. Perspective Sixty-eight studies collected data based on represented the staff’s perspective of the antecedent (63 of which collected data solely from this perspective), 5 studies included data from the patients’ perspective (1 of which collected data solely from this perspective), and 3 exclusively from the perspective of the video camera. 4.2 Thematic analysis A thematic analysis of the antecedent data produced 59 distinct ‘lower-level’ themes which formed 9 higher-level themes: ‘patient-patient interaction’, ‘staff-patient interaction’, ‘patient conflict behaviours’, ‘external / personal themes’, ‘structural themes’, ‘patient behavioural cues’, ‘patient emotional / mood cues’, ‘patient symptoms’, and ‘no clear cause’ (see Table 1 for a full breakdown of these themes).


Table 1: Thematic analysis of antecedent
PATIENT-PATIENT INTERACTION
STAFF-PATIENT INTERACTION
PATIENT CONFLICT BEHAVIOURS
EXTERNAL / PERSONAL
STRUCTURAL ISSUES
PATIENT BEHAVIOURAL CUES
PATIENT EMOTIONAL / MOOD CUES
• Limiting patients’ freedoms
ENVIRONMENTAL ISSUES • Overcrowding • Confined
environment • Noisy ward • Patient found
weapons
MEDICATION RELATED CONTAINMENT • Medication
administration • Staff requesting patient
to take medication • Disputes over
medication ANY OTHER CONTAINMENT • Restraint • Seclusion • De-escalation • ECT
• Physical contact (1)
• Patient engaged in an activity (1)
• Intrusion into personal psychological or physical space
• Reaction to sexual approach
• Miscommunication (1)
• Victim doing something patient wanted stopped
• Competition • Retaliation • Patient victim
characteristics • Teased / bugged • Unspecified patient
provocation (1) • Unspecified
patient-patient conflict
• Unspecified patient-patient interaction
ANY OTHER STAFF-PATIENT INTERACTION • Unspecified patient
provocation (2) • Ordering patients • Intervening on fight or
argument • Caring for patient • Searching patients • Negative staff attitude • Physical contact (2) • Patient engaged in an
activity (2) • Miscommunication (2) • Staff too permissive • Unspecified staff-
patient interaction • Staff victim
characteristics • Staff error
• Absconding attempt
• Substance misuse
• Verbal aggression
• Threatening behaviour
• Self-harming
• Money issues • Visit from family
member or friend
• Receiving bad news
• Unresolved family problem
REGIME ISSUES • Inadequate
staffing levels • Admitted /
transferred / discharged
• Excessive sensory stimulation
• Lack of stimulation
• Agitation • Attention
seeking behaviour
• Increased motor activity
• Boisterousness • Confusion
• Anger • Sexual
frustration • Irritability • Tobacco
withdrawal • Anxiety
PA
TIE
NT
SY
MP
TO
MS
NO
CL
EA
R C
AU
SE

Patient-patient interaction Thirty-four studies (47.9%) reported this theme. This included 12 lower-level themes that related to an interaction between two or more patients as the reported antecedent to a violent incident (see table 2). One of the lower-level themes was ‘physical contact’ which was reported as an antecedent by one study [Mellesdal 2003]. They defined this antecedent as actual physical contact between two patients, or when an intrusion into the patient’s physical or psychological space occurs. Using the ‘Report Form for Aggressive Episodes’ data collection tool prospectively over a period of 3 years within a Norwegian inpatient psychiatric acute ward, they found that ‘physical contact’ was the antecedent of 73 out 981 incidents (7.4%).
Table 2: Patient-patient interactions as recorded antecedents of violent incidents
Lower-level antecedent theme Definition
N studies used this theme
% studies used this theme
Key differences across study background factors
Physical contact Physical contact between patient and victim
1 1.40% -
Intrusion into personal psychological or physical space
Another patient enters into the percieved psychological and/or physical space of another patient
4 5.60% -
Competition Two or more patients engaged in some type of competition between each other
1 1.40% -
Patient engaged in an activity*
Patient engaged in an activity 1 1.40% -
Reaction to sexual approach
One patient approaches another patient in a sexual manner
1 1.40% -
Victim doing something which patient wanted stopped
Victim of aggression/violence was engaging in a behaviour that the assailant wanted stopped
1 1.40% -
Retaliation The assailant retaliated on another patient 2 2.80% -
Patient victim characteristics
The assailant became violent/aggressive due to a characteristic of another patient
1 1.40% -
Teased/bugged The assailant was being teased or bugged by another patient
4 5.60% -
Miscommunication* A communication problem between patient and victim
5 6.90% -
Unspecified patient provocation*
Patient was provoked by another person. Specific type of provocation is not stated.
13 18.30% 5/13 UK-based studies, 7/12 sourced from SOAS/R, 5/12 within inpatient acute settings.
Unspecified patient-patient conflict
An unspecified type of conflict occurred between two or more patients
9 12.60% 6/9 sourced from incident forms
Unspecified patient-patient interaction
An unspecified type of interaction occurred between two or more patients
5 6.90% -
* These themes were also coded within patient-patient interaction

Four studies reported intrusion into personal psychological or physical space as an antecedent to violence. This included a case study of an aggressive schizophrenic patient at a public psychiatric hospital who committed violence after his personal space was invaded [Longo and Bisconer 2003]. Additionally, one study which evaluated aggressive incidents in the dining rooms at a American state forensic hospital, reported this theme in relation to patients cutting in line for food [Hunter and Love 1996]. Another study also showed evidence of this through the use a video camera system installed within a PICU [Crowner et al. 2005]. They stated that “the assailants in this study may have been especially sensitive to others moving too close”. Further, another study by revealed via a video camera system installed within a PICU that violence occurred after the assailant invaded the victim’s personal space by standing or pacing direct in front of the victim [Crowner et al. 1991]. This same study also reported ‘competition’ between patients over an (unspecified) object as antecedent to violence. Another lower-level patient-patient interaction antecedent of violence was ‘patient engaged in an activity’. This was reported in a study that aimed to increase the understanding of female aggression within Canadian inpatient forensic psychiatry settings [Nicholls et al. 2009]. After retrospectively reviewing official archive data, they found that female patients were more often engaging some sort of activity prior to acting out aggression than male patients. The antecedent ‘reaction to sexual approach’ was also only reported by one study [Harris and Varney 1986]. In this 10 year prospective study of assaults and assaulters on a US maximum security psychiatric unit, they found that 0.3% of staff (n not stated) and 0.5% (n not stated) of assaulters reported this as an antecedent of violence. A potentially overlapping theme to this was ‘victim doing something which patient wanted stopped’ which was reported by a study that examined PICU patients’ explanations of assaults [Crowner et al. 1995]. This theme was cited by assailants as the antecedent of 14.9% of violence incidents (n=20 from total n incidents = 134). This study also reported the antecedent ‘retaliation ’ which accounted for 9% of incidents (n=12). Retaliation was also reported by two other studies as an antecedent to 9.4% (n=79) assaults within a US-based forensic service [Quanbeck et al. 2007], as well as within a five month prospective study of aggression in a large UK NHS psychiatric hospital [Shepherd and Lavender 1999] who attributed it as antecedent for 12% of 130 incidents. This study also reported that in 6.9% of incidents, the assailant committed a violent act because of the (patient) victim’s characteristics. Four studies cited ‘teased / bugged’ as an antecedent to violence. This included a study which reported that assailants cited this theme for 18.6% of violent incidents (n=25) [Crowner et al. 1995], while another reported that 6.4% of staff and 0.5% of assailants reported this being teased/bugged as an antecedent to violence [Harris and Varney 1986]. Another study revealed that 5.9% (n=50) of assaults were due to ‘bothersome/annoying behaviour’, while 1.8% (n=15) of assaults were due to a fellow patient ‘talking/laughing’ at them [Quanbeck et al. 2007]. Furthermore, a four month study of violence in a UK psychiatric hospital found that patients being bugged for cigarettes was an antecedent to violence [Casseem 1984]. Five studies reported the antecedent ‘miscommunication’. This included a retrospective review of incidents in a UK psychiatric hospital in which 2% of 355 incidents were precipitated by ‘communication difficulties’ [Tobin et al. 1991]. Another study retrospectively examined 590 assaultive child/adolescent and adult patients (via ASAP) from
Massachusetts, and found that 1% of assaults (n=6, total n=615) were precipitated by a miscommunication [Flannery, Jr. et al. 2001],. Another US-based study, after examining video-camera footage of an inpatient psychiatric ward over 18 months, found that assailants became aggressive when they misunderstood the actions of their victims [Nolan et al. 2003]. A three year prospective study of a Norwegian inpatient psychiatric acute ward revealed that communication problems preceded 30% of 981 aggressive incidents and were reported to result in assaults in 55.4% of incidents [Mellesdal 2003]. They also reported that miscommunication was significantly more frequently involved within cases of female aggression (although no statistics were provided). Finally, this antecedent was reported for 7.9% of incidents (total n=1000) over a 13 month period within 3 UK-based psychiatric hospitals after reviewing hospital untoward incident forms [Powell et al. 1994]. The antecedent ‘unspecified patient provocation’ was reported by thirteen studies. This included a UK-based prospective study in which 6.9% out of 130 incidents were triggered by some sort of provocation [Shepherd and Lavender 1999]. Another study found that 46% of 35 assaults were preceded by an unspecified form of patient provocation [Crowner et al. 1991]’s, while a later study revealed 17.5% of 1000 incidents were preceded by unspecified provocation from other patients, relatives or visitors [Powell et al. 1994]. A prospective study of violent incidents in a UK forensic hospital in which 15% of 1144 incidents were due to “some sort of provocation” [Larkin et al. 1988]. A study of physical assaults in a psychiatric unit of an American general hospital revealed that 75.6% of 37 incidents involved mild or moderate verbal provocation [Edwards et al. 1988], while a study of aggressive behaviour on UK acute psychiatric wards where 11.4% of 264 incidents were due to unspecified provocation [Foster et al. 2007], and a study of aggression in a Northern Irish psychiatric female-only observation ward where staff interviews immediately after an aggressive incident revealed 7% of 208 incidents were explained by this theme [Cooper et al. 1983]. A 7-year Italian study of persistently assaultive inpatient acute psychiatric patients attributed this theme to 32.8% of 409 incidents [Grassi et al. 2006], while a prospective study of violence rates in a Danish psychiatric hospital and found that patients were responsible for provocation in only 8 (5.1% of total) violent acts [Benjaminsen et al. 1996]. Another study examined aggression among psychiatric inpatients in Australian rehabilitation wards, finding that 19.7% of 806 incidents were due to an unspecified type of provocation between patients [Cheung et al. 1996]. Furthermore, another study investigated aggressive behaviour on a Dutch acute psychiatric admissions ward and revealed that 14.4% of 164 incidents were attributed to this theme [Nijman et al. 1997]. A Swedish study revealed this theme in relation to crowding and aggressive behaviour on a PICU [Palmstierna et al. 1991], while another Swedish study examined assaults on staff by acute psychiatric inpatients showed that 10% of 137 incidents were attributed to this theme by [Omerov et al. 2002],. Overlapping with this theme was the antecedent ‘unspecified patient-patient conflict’. Nine studies reported this: a study of aggression and violence in three UK-based inpatient acute psychiatric wards which revealed that 14% of 221 incidents were preceded by this theme [Duxbury 2002]; a prospective study of a UK secure forensic ward in which 5.6% of 178 were triggered by this type of conflict [Mortimer 1995], and a study of precipitants of violence in a psychiatric inpatient setting in which 17.1% of 82 incidents were preceded by conflict with another patient [Sheridan et al. 1990]. Additionally, a retrospective review of incident forms within an UK psychiatric hospital showed that 17% of 355 incidents were due to ‘inter-patient friction’ [Tobin et al. 1991], while a prospective study of patient assaults in a Canadian psychiatric hospital revealed that 4.5% of 201 incidents were due to this theme [Cooper and Medonca 1991]. Furthermore, a study of four Taiwanese inpatient acute

psychiatric wards that revealed that 51.1% of 595 incidents were due to patient-patient conflict [Chou et al. 2001], while another study attributed 2.5% (n=21) of incidents to this theme [Quanbeck et al. 2007]. Finally, a prospective study of aggression in a UK psychiatric hospital and an American study of assaults in an inpatient acute psychiatric settings (using incident forms and follow-up interviews of patients and staff) also attributed incidents to this theme [Shepherd and Lavender 1999] [Conn and Lion 1983] The final lower-level patient-patient interaction theme was ‘unspecified patient-patient interaction’ which is defined an unspecified type of interaction between patients preceding a violence incident. This was referenced by five studies: a five year Italian study of the characteristics of violent behaviour in acute psychiatric in-patients in which 31% of 323 was attributed to this theme [Grassi et al. 2001]; a UK study of the management of psychiatric inpatient violence which revealed that 24% of 1515 incidents were triggered by an unspecified interaction with patients (or staff) [Gudjonsson et al. 2004]; an investigation of aggression in Canadian forensic psychiatry inpatients which found that this antecedent was found by 14.3% (n=9) of 65 female patients and 25.2% (n=116) of 461 male patients [Nicholls et al. 2009]; a study which revealed from patient follow-up interviews that 11% of 208 incidents were due to this theme [Cooper et al. 1983], and another study which attributed this theme to 20.1% (n=27) of 134 violent incidents [Crowner et al. 1995]. Finally, it is important to note that the antecedents ‘physical contact’, ‘patient engaged in an activity’, ‘miscommunication’, and ‘unspecified patient provocation’ were also coded under the higher-level theme of ‘staff-patient interaction’. This is because it was not possible to determine which kind of interaction (patient-patient or patient-staff) had taken place within the studies that reported these themes. Staff-patient interaction As can be seen in tables 1 and 3, this higher-level theme constituted 18 lower-level themes which were divided into four categories: 1. Limiting patients’ freedoms (1 theme), 2. Medication-related containment method (3 themes), 3. Any other containment (5 themes), and 4. ‘Any other containment methods’ (10 themes).
1. Limiting patients’ freedoms More than half of all papers (n=37) cited this theme as an antecedent to violence. This included many references to requests by patients being denied. In most instances (n=24/37) studies did not specify the type of requests that patients made which were denied [Benjaminsen et al. 1996;Cheung et al. 1996;Cheung et al. 1997;Conn and Lion 1983;Cooper and Medonca 1991;Duxbury 2002;Flannery, Jr. and Walker 2008;Flannery et al. 2006;Foster et al. 2007;Grassi et al. 2006;Gudjonsson et al. 2004;Harris and Varney 1986;Langsrud et al. 2007;Lim et al. 1991;Mellesdal 2003;Murray and Snyder 1991;Nicholls et al. 2009;Omerov et al. 2002;Omerov et al. 2004;Palmstierna et al. 1991;Powell et al. 1994;Quanbeck et al. 2007;Rasmussen and Levander 1996;Shepherd and Lavender 1999]. Seven studies referred to ‘setting limits/restrictions’ as an antecedent to violence: one found that 59% of 1090 incidents were due to limit setting [Mellesdal 2003]; a one year study of 40 incidents were due to ‘staff limits’ [Murray and Snyder 1991]’s, another found that 19.2% of 1000 were due to unspecified ‘clinical and legal restrictions’ [Powell et al. 1994], while four other studies reported limit setting as a precipitant to violence without reporting proportion-type data [Shepherd and Lavender 1999], [Hunter and Love 1996], [Lim et al. 1991], [Lanza 1988] .
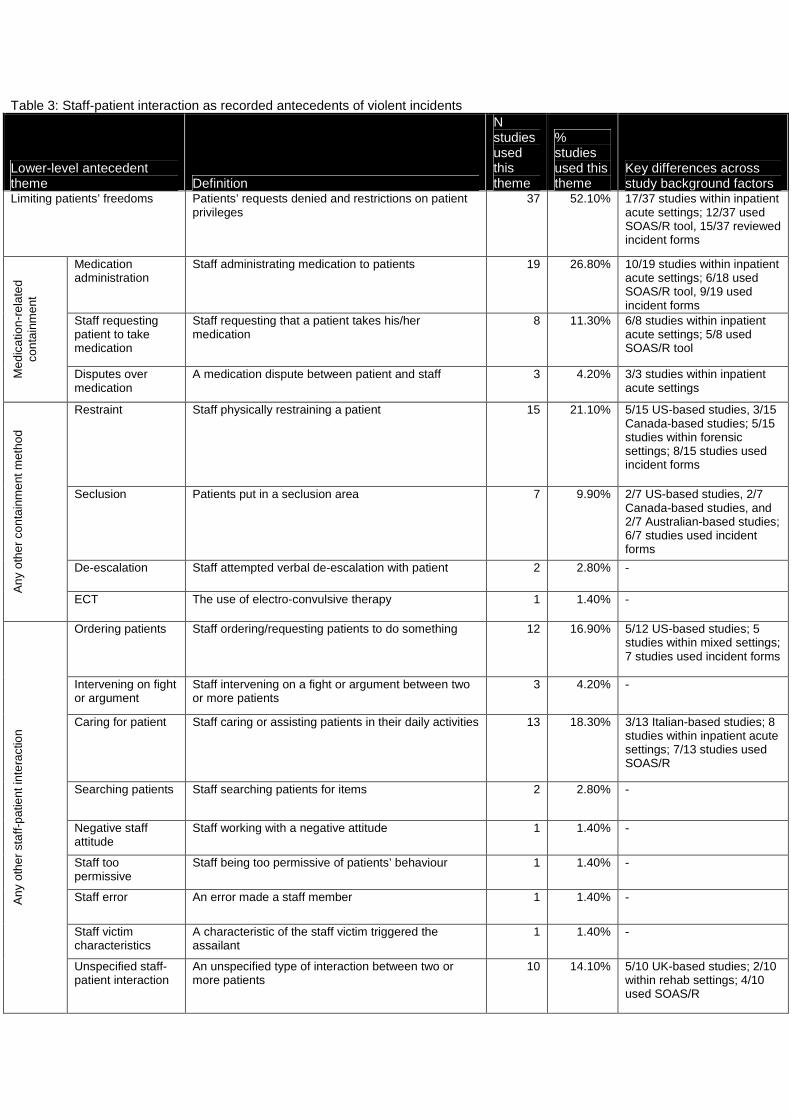
Table 3: Staff-patient interaction as recorded antecedents of violent incidents
Lower-level antecedent theme Definition
N studies used this theme
% studies used this theme
Key differences across study background factors
Limiting patients’ freedoms Patients’ requests denied and restrictions on patient privileges
37 52.10% 17/37 studies within inpatient acute settings; 12/37 used SOAS/R tool, 15/37 reviewed incident forms
Medication administration
Staff administrating medication to patients 19 26.80% 10/19 studies within inpatient acute settings; 6/18 used SOAS/R tool, 9/19 used incident forms
Staff requesting patient to take medication
Staff requesting that a patient takes his/her medication
8 11.30% 6/8 studies within inpatient acute settings; 5/8 used SOAS/R tool
Med
icat
ion-
rela
ted
cont
ainm
ent
Disputes over medication
A medication dispute between patient and staff 3 4.20% 3/3 studies within inpatient acute settings
Restraint Staff physically restraining a patient 15 21.10% 5/15 US-based studies, 3/15 Canada-based studies; 5/15 studies within forensic settings; 8/15 studies used incident forms
Seclusion Patients put in a seclusion area 7 9.90% 2/7 US-based studies, 2/7 Canada-based studies, and 2/7 Australian-based studies; 6/7 studies used incident forms
De-escalation Staff attempted verbal de-escalation with patient 2 2.80% -
Any
oth
er c
onta
inm
ent m
etho
d
ECT The use of electro-convulsive therapy 1 1.40% -
Ordering patients Staff ordering/requesting patients to do something 12 16.90% 5/12 US-based studies; 5 studies within mixed settings; 7 studies used incident forms
Intervening on fight or argument
Staff intervening on a fight or argument between two or more patients
3 4.20% -
Caring for patient Staff caring or assisting patients in their daily activities 13 18.30% 3/13 Italian-based studies; 8 studies within inpatient acute settings; 7/13 studies used SOAS/R
Searching patients Staff searching patients for items 2 2.80% -
Negative staff attitude
Staff working with a negative attitude 1 1.40% -
Staff too permissive
Staff being too permissive of patients’ behaviour 1 1.40% -
Staff error An error made a staff member 1 1.40% -
Staff victim characteristics
A characteristic of the staff victim triggered the assailant
1 1.40% -
Any
oth
er s
taff-
patie
nt in
tera
ctio
n
Unspecified staff-patient interaction
An unspecified type of interaction between two or more patients
10 14.10% 5/10 UK-based studies; 2/10 within rehab settings; 4/10 used SOAS/R

Five studies cited the request as patients wanting to leave the ward, including a UK-based 6 month study of assaults within an inpatient psychiatric hospital [Convey 1986]’s, a 12 month study of violent incidents in a Swedish inpatient psychiatric ward (in which 6 out 41 violent incidents were attributed to this request) [Omerov and Wistedt 1997], a study of assaults on staff within a locked UK-based inpatient psychiatric ward (11 out of 41 incidents) [Aiken 1984]’s, a study of aggressive behaviour on a Dutch acute psychiatric admissions ward [Nijman et al. 1997], and a four month study of violence in a UK psychiatric hospital [Casseem 1984]. Four studies stated that denying the patient discharge from the ward triggered violence, including a study of precipitants of violence in a US psychiatric inpatient setting (3 out of 82 incidents) [Sheridan et al. 1990], violence among psychiatric inpatients at a UK-based a locked acute ward and an ‘interim secure unit’ (2 out of 70 incidents and 7 out of 65 incidents respectively) [Agarwal and Roberts 1996], and two studies of Taiwanese inpatient acute psychiatric wards (37 out 595 incidents and 35 out of 529 incidents) [Chou et al. 2001];[Chou et al. 2002]. Requests related to cigarette smoking was cited by five studies as an antecedent to violence, including the two Chou studies (2001: 68 out of 595 incidents; 2002: 111 out of 529 incidents respectively), a prospective of UK secure forensic ward [Mortimer 1995]’s, a prospective study of aggression in a UK psychiatric hospital [Shepherd and Lavender 1999], and a study of patient assault in a large US-based neuropsychiatric facility [Lanza 1988]. Another patient request which was denied and led to violence was for ‘off the ward privileges’ which was cited by both Chou et al studies (2001: 11 out of 595 incidents; 2002: 70 out of 529 incidents). Two studies cited restrictions on food as antecedent to violence: a prospective study of a UK secure forensic ward [Mortimer 1995], and a study of aggressive incidents in dining rooms at an American state forensic hospital in which ‘denying patient extra portions of food’ was the reported antecedent to incidents 17% of times (denominator not stated) [Hunter and Love 1996]. Another study also cited restrictions upon patient’s demands for money (Mortimer, 1995), while a study on the impact of verbal abuse on inpatient acute psychiatric staff in Singapore found that ‘being denied a phone call’ was the antecedent of aggressive incidents on 10% of occasions (out of 42 incidents), while being denied discharge, leave or parole precipitated 14.3% of incidents [Yusuf et al. 2006].
2. Medication-related containment This category of antecedents was reported by a total of 29 (40.8%) studies as an antecedent to violence. It constituted three lower-level themes: administration of medication, staff
Unspecified patient provocation*
Patient was provoked by another person. Specific type of provocation is not stated.
13 18.30% 5/13 UK-based studies, 7/12 sourced from SOAS/R, 5/12 within inpatient acute settings.
Physical contact* Physical contact between patient and victim 1 1.40% -
Patient engaged in an activity*
Patient engaged in an activity 1 1.40% -
Miscommunication* A communication problem between patient and victim 5 6.90% -
* These themes were also coded within patient-patient interaction

requesting that the patient takes his/her medication, and disputes over medication. Nineteen studies (26.4%) reported administration of medication as an antecedent to violence [Grassi et al. 2006];[Manfredini et al. 2001];[Grainger and Whiteford 1993];[Omerov et al. 2004];[Grassi et al. 2001];[Walker et al. 1994];[Powell et al. 1994];[Gudjonsson et al. 2004];[Sheridan et al. 1990];[Murray and Snyder 1991];[Flannery et al. 2006];[Nicholls et al. 2009];[Duxbury 2002];[Cooper and Medonca 1991];[Lion et al. 1981];[Chou et al. 2002];[Chou et al. 2001];[Bowers et al. 2002] . This theme referred to any incident being precipitated by staff administering medication to patients. The lower-level antecedent theme ‘staff requesting that the patient takes his/her medication’ was cited by eight studies (11.3%), four of which provided proportions data of this antecedent. These included a study of aggressive behaviour in UK acute psychiatric wards in which this theme was attributed as antecedent to 12.5% of 264 incidents [Foster et al. 2007], a study of abuse in an inpatient acute ward in Singapore where 19% of 42 incidents [Yusuf et al. 2006], and a study of violence rates in a Danish psychiatric hospital where staff requesting patients to take their medication was an antecedent in 10.2% of 110 violent acts [Benjaminsen et al. 1996]. The lowest proportion of incidents attributed to this theme was reported for 6.8% of 512 incidents in two Norwegian acute psychiatric inpatient wards over a seven year period [Langsrud et al. 2007]. Four other studies which cited this theme as an antecedent of violence but did report proportion data: a study of violence in a Swedish inpatient psychiatric ward [Omerov and Wistedt 1997], a study of aggression among psychiatric inpatients in Australian rehabilitation wards [Cheung et al. 1996], a study of aggression in a Dutch acute psychiatric admissions ward [Nijman et al. 1997], and a study of crowding and aggressive behaviour on a Swedish PICU [Palmstierna et al. 1991]. The other medication-related lower-level theme was ‘medication disputes’. This was cited as an antecedent by three studies: a study of staff assaults within a locked UK-based inpatient psychiatric ward (9.8% of 41 incidents) [Aiken 1984], a three year study within a Norwegian inpatient psychiatric acute ward (5.2% of 981 incidents) [Mellesdal 2003], and a study of prevalence and precipitants of aggression within four Australian psychiatric inpatient units (3.1% of 394) [Barlow et al. 2000].
3. Any other containment method This category of antecedents was reported by a total of 20 (28.2%) as an antecedent to violence and constituted four lower-level antecedent themes: restraint, seclusion, de-escalation, and electro-convulsive therapy (ECT). Fifteen studies (21.1%) cited restraint as an antecedent to violence, including a study which attributed this antecedent to 70% of 88 incidents involving violent patients within a Norwegian inpatient acute psychiatric ward [Blomhoff et al. 1990]. Other considerably high proportions of incidents attributed to this antecedent were found in a study of workplace assaults on ethnic minority mental health care workers in a Los Angeles psychiatric unit (40.5% of 111 incidents) [Sullivan and Yuan 1995], a study of staff injuries sustained at a forensic mental Health Centre in Ontario (38% of 123 incidents) [Harris et al. 1986], and a 27 month study of assaults in a Canadian psychiatric hospital (35% of 201 incidents) [Cooper and Medonca 1991]’s. A 3 year study of an American maximum-security forensic hospital showed that 23% of 157 violent incidents resulting in staff injury involved the patient being restrained immediately before the assault occurred [Hillbrand et al. 1996], while a retrospective study of patient precipitants of violence within 10 public sector mental health

care facilities revealed that 15% of 193 violent incidents over a year were precipitated by restraint procedures [Flannery, Jr. et al. 2003]. A similar proportion of this antecedent was reported in a study of four Taiwanese inpatient acute psychiatric wards over a 7 month period (14.3% of 595 incidents) [Chou et al. 2001]’s. Lower reported proportions were reported to be 4.5% from 838 assaults, 3.2% from 529 incidents, and 2.7% from 1000 incidents ([Quanbeck et al. 2007];[Chou et al. 2002];[Powell et al. 1994]). Five other studies reported restraint as an antecedent to violence but did not report data on the proportion of incidents that it was attributable for: a retrospective study of patterns of aggression in an Australian forensic psychiatric hospital [Daffern et al. 2003], a study of violent incidents patterns in a general psychiatric hospital also reported restraint [Tam et al. 1996], a study on the development of the 'attacks' scale (attempted and actual assault scale) [Bowers et al. 2002], a review of staff assaults at an American state psychiatric hospital [Lion et al. 1981], and a study of violent incidents at a Norwegian maximum security forensic hospital [Rasmussen and Levander 1996]. Seclusion as an antecedent to violence was reported by seven studies (9.9%), two of which reported proportions data on this lower-level theme: a study which investigated injuries to psychiatric staff working in high security, rehabilitation, acute, and geriatric units in an Australian psychiatric hospital (7.3% of 328 incidents) [Grainger and Whiteford 1993], and a study of assaults in an American inpatient acute psychiatric setting (32 of 24 incidents) [Conn and Lion 1983]. Five other studies cited seclusion as an antecedent but did not report useable proportions data ([Daffern et al. 2003];[Nicholls et al. 2009];[Tam et al. 1996];[Lion et al. 1981];[Rasmussen and Levander 1996]). Two studies reported that the use of de-escalation was an antecedent to violence: a study in which reported that ‘attempting to calm an already aggressive patient’ was an antecedent to further violence in 22% of 1945 incidents [Rasmussen and Levander 1996], while a study of violence in a UK psychiatric hospital reported that one of the types of causes of violence included talking and reassuring an aggressive patient [Casseem 1984]. Finally, there was one mention of ECT as an antecedent of violence [Grainger and Whiteford 1993].
4. Any other staff-patient interaction Just over half of all papers (n=36) cited this theme as an antecedent to violence. The lower-level antecedent themes that it constituted were ‘ordering patients’, ‘intervening on fight or argument’, ‘caring for patient’, ‘searching patients’, ‘negative staff attitude’, ‘staff too permissive’, ‘unspecified staff-patient interaction’, ‘unspecified patient provocation’, ‘physical contact’, ‘patient engaged in an activity’, and ‘miscommunication’. The last four of these themes have also been included in the ‘patient-patient interaction’ higher-level theme as it was not possible to determine which kind of interaction (patient-patient or patient-staff) had taken place within the studies that reported these themes. Therefore, a description of these themes and the studies that cited them can be seen under the ‘patient-patient interaction’ report section. Twelve studies (16.9%) cited that ordering patients triggered violence, five of which reported data on the proportion of incidents that this antecedent counted towards. The highest proportion was reported to be by 14.3% from 42 incidents of verbal aggression that were triggered by staff advising patients to attend to their personal hygiene [Yusuf et al. 2006].Another study revealed that 14.1% of 838 assaults on staff occurred ‘after the assailant was directed to perform an activity by a staff member’ [Quanbeck et al. 2007]. A similar
proportion of incidents precipitated by this theme was reported to be 13% from 1945 incidents and 13% from 355 assaults ([Tobin et al. 1991]);[Rasmussen and Levander 1996]). Lower proportions included 5% of 40 assaults [Murray and Snyder 1991], a study which revealed that 16.8% of staff and 4.8% of assaulters reported that being ordered to do something triggered an incident [Harris and Varney 1986], and a UK-based study of aggression in a UK psychiatric hospital which reported that ‘insisting on an activity’ precipitated violence in 4.3% of 130 incidents [Shepherd and Lavender 1999]. Other studies also reported this lower-level theme as an antecedent of violence but did not report useable proportions data ([Longo and Bisconer 2003], [Sheridan et al. 1990], [Cooper and Medonca 1991], [Cheung et al. 1996] and [Lim et al. 1991]). Staff intervening on a fight or argument between two or more patients was an antecedent reported to be attributed to 14.3% of 328 incidents, 21% of 24 incidents, and 18% out of 203 [Grainger and Whiteford 1993]; [Conn and Lion 1983]; [Lion et al. 1981]. Thirteen studies reported that caring for patient was an antecedent to violence, ten of which reported the proportion of incidents that this antecedent was applied to. This included a study which reported that providing minimal or ‘hands-on’ care accounted triggered 36% of 111 incidents [Sullivan and Yuan 1995], a three month prospective survey study abusive incidents which found that 22.2% of 18 incidents in an adult psychiatric unit were due to a ‘service being provided’ [Yassi et al. 1998], and a study that revealed that providing care (which they define as feeding, dressing, and recreation) preceded 20.4% of 328 incidents at Australian psychiatric hospital [Grainger and Whiteford 1993]. Similar proportions were reported to be 19% of 1945 incidents [Rasmussen and Levander 1996] as well as by a study which found that during an 8 week period in an Australian rehabilitation unit, 19.1% of 477 incidents were preceded by theme [Cheung et al. 1997]. Smaller proportions were reported to be 10.2% of 512 incidents [Langsrud et al. 2007], 8% of 137 incidents [Omerov et al. 2002], 7.4% of 409 incidents [Grassi et al. 2006]), 7.1% of 323 incidents [Grassi et al. 2001] and 4.2% of 264 incidents [Foster et al. 2007]. A study by on day-night variation in aggressive behaviour within an Italian psychiatric inpatient unit over a five year period also reported this theme[Manfredini et al. 2001], as did another study who reported that “assaults also occurred when staff tried to help patients” [Lanza 1988],while another study reported that some assaults occurred after patients were fed or toileted [Lion et al. 1981]. The predominant definition of this theme was found by studies that used the SOAS tool who referred to ‘staff assisting patients activities of daily living’ ([Rasmussen and Levander 1996],[Cheung et al. 1997],[Langsrud et al. 2007],[Omerov et al. 2002],[Grassi et al. 2006],[Grassi et al. 2001],[Foster et al. 2007]) Two other studies [Yusuf et al. 2006];[Cooper and Medonca 1991] also revealed that staff searching patients was an antecedent to violence, although less frequently compared to other antecedents. Specifically, the former revealed that ‘checking for smoking’ triggered 8% of 42 incidents, while the latter found that staff taking something from a patient after searching them triggered 3.5% of 201 incidents. One study cited that negative staff attitude was an antecedent for 10.3% of 615 incidents [Flannery et al. 2006], while another found that staff being too permissive (including letting patients into the staff office) triggered 5.6% of 178 incidents in a UK secure forensic ward over 31 months [Mortimer 1995]. Astudy of aggression in a UK psychiatric hospital reported that a staff error precipitated violence in 1.7% of 130 incidents, and also reported that in 5.2% of incidents, the assailant committed a violent act because of the (staff) victim’s characteristics [Shepherd and Lavender 1999].
The final lower-level staff-patient interaction theme was ‘unspecified staff-patient interaction’ which is defined an unspecified type of interaction occurring between staff and patients that precedes a violence incident. This was cited by ten studies, three of which inferred that did not provide useable data regarding the proportion of incidents that this theme accounted for ([Manfredini et al. 2001], [Gudjonsson et al. 2004],[Shepherd and Lavender 1999]). The largest proportions were reported by to be (34.3% of 806 incidents and 69.9% of 477 incidents ([Cheung et al. 1996] and [Cheung et al. 1997] respectively), followed by a study which reported that 18% of 221 incidents were triggered by some sort of staff-patient interaction [Duxbury 2002]. It was also reported that 6.7% of 135 violent incidents at a UK-based ‘interim secure unit’ were due to an unspecified ‘staff-patient interaction’ [Agarwal and Roberts 1996], while a later study reported that this theme in relation to 2.2% of 595 incidents [Chou et al. 2001]. Another study revealed that that 0.2% of staff and 12% of assaulters reported staff-patient interaction as an antecedent to violence [Harris and Varney 1986], while a study of aggression in a Northern Irish psychiatric observation ward revealed that according to patients, 4% of 208 incidents were triggered by this theme, while according to staff, 6% of the 208 incidents were due to this theme [Cooper et al. 1983]. Patient-conflict behaviours Ten studies (14.1%) reported this theme. This included 5 lower-level themes of patient conflict behaviours that were reported antecedents to violence (see table 4). The lower-level theme was most frequently reported was ‘patient displaying threatening behaviour’. This conflict-behaviour was cited as an antecedent to violence by three studies with proportion data: an American study of violence among psychiatric inpatients in which 47% of 82 incidents were preceded by ‘hostile’ behaviour [Sheridan et al. 1990]; a study of battery incidents in a US-based maximum security hospital in which 10% of 221 battery incidents were due to some sort of threatening behaviour (including ‘provocative action’, ‘throwing an object at someone’, ‘destruction of property’, ‘threatening action’, ‘striking an inanimate object’, and ‘bizarre conduct’) [Dietz and Rada 1982]; and a study which found that ‘intimidation’ was an antecedent to 8.2% of 838 incidents within a US-based forensic service [Quanbeck et al. 2007]. Two other studies reference this theme: one which examined the predictors of violence within a Norwegian maximum security unit [Linaker and Busch-Iversen 1995], and another which examined PICU violence through the use of a video camera system in which violence occurred after the assaulter displayed ‘threatening gestures’ to the victim [Crowner et al. 1991].

Table 4: Patient conflict behaviours as recorded antecedents of violent incidents
Lower-level antecedent theme Definition
N studies used this theme
% studies used this theme
Key differences across study background factors
Threatening behaviour
Patient displaying threatening behaviour 5 6.90% 4/5 US-based studies; 2/5 studies within forensic settings
Substance misuse
Alcohol and/or drugs misuse 4 5.60% 4/4 studies used incident forms
Absconding attempt
An unsuccessful absconding attempt 3 4.20% 3/3 studies used incident forms
Verbal aggression
A patient being verbally aggressive 3 4.20% 3/3 studies within forensic settings
Self-harming
Patient engaged in self-harming 2 2.80% -
‘Substance misuse’ was cited as an antecedent by four studies: a study of violent incidents within three UK-based psychiatric hospitals in which this antecedent was attributed to 1.2% of 1000 incidents [Powell et al. 1994]’s, a study of aggression and violence in three UK-based inpatient acute psychiatric wards which revealed that 14% of 221 incidents were preceded by this theme [Duxbury 2002], a study of aggression in a UK psychiatric hospital which found that 1.7% of 130 incidents were triggered by substance misuse [Shepherd and Lavender 1999], and a study of prevalence and precipitants of aggression within four Australian psychiatric inpatient units which revealed that alcohol and drug use was an antecedent for 2.9% of 394 incidents of aggression [Barlow et al. 2000]. The conflict behaviours ‘absconding attempt’ and ‘verbal aggression’ were both cited as antecedents by three studies. The former was found to account for 7% of 1515 incidents, 5.4% of 1000 incidents, and 0.5% of 221 incidents ([Gudjonsson et al. 2004], [Powell et al. 1994], and [Dietz and Rada 1982] respectively), while the theme verbal aggression was reported to precede 8.2% of 221 incidents and 2.9% of 838 incidents [Quanbeck et al. 2007] - who specifically referred to patients making ‘cold threats’ and [Dietz and Rada 1982] - who referred to provocative and threatening talk respectively). Another study also cited ‘verbal threats’ as an antecedent to violence [Linaker and Busch-Iversen 1995]. Finally, a patient engaged in self-harming was shown to precipitate 7.4% of 1000 incidents over a 13 month period within three UK-based psychiatric hospitals [Powell et al. 1994], while a study of violence, also within a UK psychiatric hospital, revealed that 4% of 355 incidents were precipitated by this behaviour [Tobin et al. 1991]. External / personal issues This higher level theme was referred to as antecedents to violence by eight studies. It constituted three lower level themes: ‘money issues’, ‘visit from a family member or friend’, and ‘unresolved family problem’ (see table 5). Three studies referred to some sort of money issue precipitating a violent incident. This included a study of staff assaults within a locked UK-based inpatient psychiatric ward (3 out of 41 incidents were ‘over money and cigarettes’) [Aiken 1984], a study of three UK-based psychiatric hospitals (2.6% of 1000 incidents were
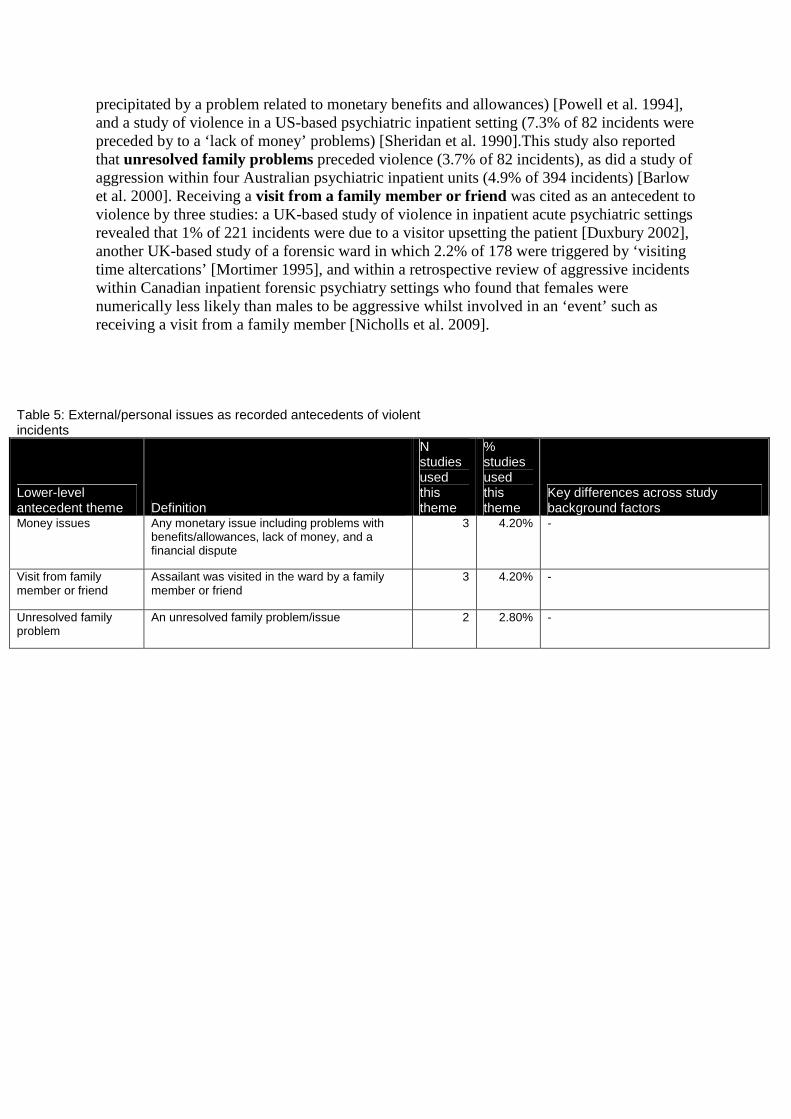
precipitated by a problem related to monetary benefits and allowances) [Powell et al. 1994], and a study of violence in a US-based psychiatric inpatient setting (7.3% of 82 incidents were preceded by to a ‘lack of money’ problems) [Sheridan et al. 1990].This study also reported that unresolved family problems preceded violence (3.7% of 82 incidents), as did a study of aggression within four Australian psychiatric inpatient units (4.9% of 394 incidents) [Barlow et al. 2000]. Receiving a visit from a family member or friend was cited as an antecedent to violence by three studies: a UK-based study of violence in inpatient acute psychiatric settings revealed that 1% of 221 incidents were due to a visitor upsetting the patient [Duxbury 2002], another UK-based study of a forensic ward in which 2.2% of 178 were triggered by ‘visiting time altercations’ [Mortimer 1995], and within a retrospective review of aggressive incidents within Canadian inpatient forensic psychiatry settings who found that females were numerically less likely than males to be aggressive whilst involved in an ‘event’ such as receiving a visit from a family member [Nicholls et al. 2009].
Table 5: External/personal issues as recorded antecedents of violent incidents
Lower-level antecedent theme Definition
N studies used this theme
% studies used this theme
Key differences across study background factors
Money issues Any monetary issue including problems with benefits/allowances, lack of money, and a financial dispute
3 4.20% -
Visit from family member or friend
Assailant was visited in the ward by a family member or friend
3 4.20% -
Unresolved family problem
An unresolved family problem/issue 2 2.80% -

Structural issues As can be seen in table 6, this higher-level theme was divided into two categories of 7 lower-level themes: 1. environmental issues (3 themes) and 2. regime issues (4 themes). Such structural issues were reported by 13 papers (18.1%) in total.
1. Environmental issues Three papers cited environmental issues as the antecedent of violence. This included the problem of overcrowding within wards which was cited as an antecedent by 1% of staff and 2.6% of assaulters (n not stated) in a longitudinal, prospective study of assaults in a US maximum security psychiatric unit [Harris and Varney 1986]. A study of prevalence and precipitants of aggression within four Australian psychiatric inpatient units found that 6.2% of 394 incidents of aggression were precipitated due a patient being in a confined environment [Barlow et al. 2000]. The other lower-level antecedent theme was ‘patient found weapons’ which was also cited by only one study who found that 2.8% of 178 incidents of violence in a UK secure forensic ward over 31 months were precipitated by this occurrence [Mortimer 1995].
2. Regime issues The latter study also revealed that inadequate staffing level was an antecedent in 14.6% of 178 incidents. A theme more frequently referenced as an antecedent was ‘excessive sensory
Table 6: Structural issues as recorded antecedents of violent incidents
Lower-level antecedent theme Definition
N studies used this theme
% studies used this theme
Key differences across study background factors
Overcrowding An over-crowded ward environment 1 1.40% -
Confined environment A confined ward environment 1 1.40% -
Env
ironm
enta
l iss
ues
Patient found weapons Assailant got access to objects that could be used as a weapon
1 1.40% -
Inadequate staffing levels
The level of staffing on ward was inadequate
1 1.40% -
Admitted/ transferred/ discharged
Assailant was in the process of being admitted, transferred or discharged from ward
4 5.60% 3/4 studies within mixed psychiatric settings; 3/4 studies used incident forms
Excessive sensory stimulation
Assailant was overly stimulated 4 5.60% 3/4 studies used incident forms
Reg
ime
issu
es
Lack of stimulation Assailant was under stimulated 2 2.80% 2/2 studies UK-based;2/2 studies within mixed psychiatric settings; 2/2 studies used incident forms

stimulation’. This was cited by a retrospective study of patient precipitants of violence in which during one year, 14.2% of 193 violent incidents within 10 public sector mental health care facilities were due to excessive sensory stimulation, [Flannery, Jr. et al. 2003] while a later study revealed a similar proportion of incidents were precipitated by this antecedent: 14.6% of 615 incidents over a 3 year period within a public mental health care system in Massachusetts [Flannery et al. 2006]. A retrospective 15 year analysis of the ‘Assaulted Staff Action Program’ used within the latter public mental health care system also cited this antecedent as a key precipitant to violence in child and adult assaultive patients [Flannery, Jr. and Walker 2008], while a 12 month study of violent incidents in a Swedish inpatient psychiatric ward also cited this theme (specifically that some violent acts were ‘activated by response to stimuli’) [Omerov and Wistedt 1997]. Linked to this theme was the antecedent ‘ lack of stimulation’, which a prospective study of aggression in a UK psychiatric hospital reported as an antecedent of 3.4% of 130 violent incidents [Shepherd and Lavender 1999]. The most frequently cited regime issue as antecedent to violence was being admitted, transferred, or discharged. Studies which cited this theme included a retrospective analysis of recorded reasons for 1000 incidents within 3 UK-based psychiatric hospitals over 13 months in which this theme accounted for 2% of incidents [Powell et al. 1994]; a study of violence precipitants in a psychiatric inpatient setting in which the ‘transfer of a patient’ accounted for 3.7% of 82 incident [Sheridan et al. 1990]; a study of staff assaults in a veteran’s psychiatric hospital in which ‘recent admission’ was cited as a trigger for 2.5% out of 40 incidents [Murray and Snyder 1991]; an Australian study of aggression prevalence and precipitants found that ‘patient admission status’ accounted for 9.6% of 394 incidents [Barlow et al. 2000]; while another study also reported this theme as an antecedent for 3.4% of 130 incidents [Shepherd and Lavender 1999]. Patient behavioural cues Nineteen studies (26.8%) reported this higher-level theme which included 5 lower-level themes of behavioural cues as reported antecedents to violence (see table 7). The lower-level theme by far the most frequently reported was ‘patient agitation’ which was referenced by 11 studies, three of which also provided useable proportion data on this theme: a study of staff injuries in a maximum-security forensic hospital (this antecedent was cited for 22% of 157 incidents [Hillbrand et al. 1996], a study of psychiatric inpatient violence (32% of 1515 incidents) [Gudjonsson et al. 2004], and a retrospective study of violent incidents on two PICUs over a course of one year (in which 55.4% of 116 incidents the patient had been ‘showing signs of unsettled behaviour’) [Coldwell and Naismith 1989]. Another study reported that this antecedent, in tandem with disturbed behaviour, accounted for 31% of 1000 incidents over a 13 month period within 3 UK-based psychiatric hospitals [Powell et al. 1994]. Other studies that cited this theme as an antecedent and which also did not report useable proportion data included a three month study of abusive incidents in an adult psychiatric unit which reported that health care workers involved in an ‘abusive event’ were not completely surprised by the event as they believed that the assailants were often agitated before incident occurred [Yassi et al. 1998]’s. Another was a 10 year prospective study of assaults and assaulters in a US maximum security psychiatric unit reported that 1.2% staff and 5.3% assaulters reported ‘building tension’ as antecedent of violence [Harris and Varney 1986]. A seven month prospective study on violent and aggressive incidents in Australian psychiatric units found

Table 7: Patient behavioural cues as recorded antecedents of violent incidents
Lower-level antecedent theme Definition
N studies used this theme
% studies used this theme
Key differences across study background factors
Agitation Patient showed signs of agitation or unsettled behaviour
11 15.50% 5/11 studies UK-based, 4/11 US-based, 2/11 Australia-based
Confusion Patient appeared confused 4 5.60% 2/4 Norway-based studies, 1/4 study used video camera footage
Increased motor activity The patient increased their motor activity e.g. increasing their pacing level
3 4.20% 3/3 studies used incident forms
Boisterousness Patient appeared animated, noisy, energetic, rowdy
2 2.40% 2/2 Norway-based studies,
Attention-seeking behaviour Patient behaviour that seeks the attention of others
1 1.40% --
that of the 752 incidents rated as ‘serious’ (from a total of 1,289 incidents), 82% were ‘preceded by a warning sign, commonly agitation’ [Owen et al. 1998], while in a different paper by the same authors (and based on the same data), agitation as a warning sign for recidivist aggressive patients [Owen et al. 1998]. Another study of precipitants of violence in a psychiatric inpatient setting reported that 75% of 73 aggressive patients showed signs of anxiety before the incident occurred [Sheridan et al. 1990], while a study of inpatient violence found that within a locked acute ward over a course of year, 58% of 70 incidents were precipitated by patients appearing as ‘agitated, irritable’ while a year later within an ‘interim secure unit’, 65% of 65 incidents were precipitated by these cues [Agarwal and Roberts 1996]. Finally, a study on the development of the 'attacks' scale (attempted and actual assault scale) stated that one of ‘the most common antecedents [to violent incidents] were agitated/disturbed behaviour’ (p. 108) [Bowers et al. 2002]. The next most frequently cited behavioural cue was ‘patient confused’ which one study reported to precipitate 40% of 40 incidents at a US-based veterans medical centre over the course of a year [Murray and Snyder 1991]. Another study of violence predictors within a Norwegian maximum security unit found that reported the presence patient confusion before violent event [Linaker and Busch-Iversen 1995]. In another study, after examining video-camera footage of an inpatient psychiatric ward over 18 months, assailants became aggressive after misunderstanding the actions of their victims and appearing confused [Nolan et al. 2003]. It has also been reported that that for patients in one of three Norwegian inpatient acute wards who had been involved in violent incidents, a high incidence of confusion was presented prior to the violent event [Almvik and Woods 1998]. This study and another [Linaker and Busch-Iversen 1995] also cited ‘boisterousness’ as a behavioural cue to violent incidents. The antecedent ‘increased motor activity’ was cited by three studies: one in which violence reports between 1992 and 1996 were retrospectively analysed in a Finnish forensic psychiatric hospital and ‘restlessness’ was attributed as antecedent in 55.5% of 616 incidents [WeizmannHenelius and Suutala 2000], another in which 49% of 82 incidents were
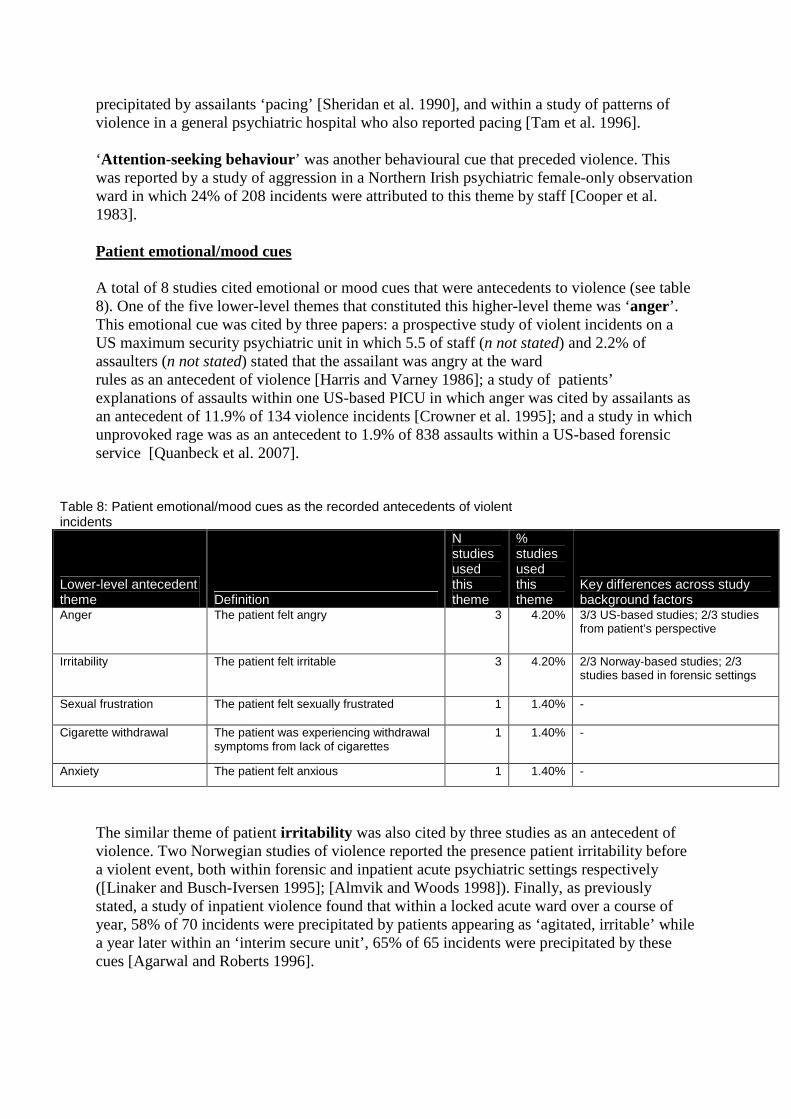
precipitated by assailants ‘pacing’ [Sheridan et al. 1990], and within a study of patterns of violence in a general psychiatric hospital who also reported pacing [Tam et al. 1996]. ‘Attention-seeking behaviour’ was another behavioural cue that preceded violence. This was reported by a study of aggression in a Northern Irish psychiatric female-only observation ward in which 24% of 208 incidents were attributed to this theme by staff [Cooper et al. 1983]. Patient emotional/mood cues A total of 8 studies cited emotional or mood cues that were antecedents to violence (see table 8). One of the five lower-level themes that constituted this higher-level theme was ‘anger’. This emotional cue was cited by three papers: a prospective study of violent incidents on a US maximum security psychiatric unit in which 5.5 of staff (n not stated) and 2.2% of assaulters (n not stated) stated that the assailant was angry at the ward rules as an antecedent of violence [Harris and Varney 1986]; a study of patients’ explanations of assaults within one US-based PICU in which anger was cited by assailants as an antecedent of 11.9% of 134 violence incidents [Crowner et al. 1995]; and a study in which unprovoked rage was as an antecedent to 1.9% of 838 assaults within a US-based forensic service [Quanbeck et al. 2007].
Table 8: Patient emotional/mood cues as the recorded antecedents of violent incidents
Lower-level antecedent theme Definition
N studies used this theme
% studies used this theme
Key differences across study background factors
Anger The patient felt angry 3 4.20% 3/3 US-based studies; 2/3 studies from patient’s perspective
Irritability The patient felt irritable 3 4.20% 2/3 Norway-based studies; 2/3 studies based in forensic settings
Sexual frustration The patient felt sexually frustrated 1 1.40% -
Cigarette withdrawal The patient was experiencing withdrawal symptoms from lack of cigarettes
1 1.40% -
Anxiety The patient felt anxious 1 1.40% -
The similar theme of patient irritability was also cited by three studies as an antecedent of violence. Two Norwegian studies of violence reported the presence patient irritability before a violent event, both within forensic and inpatient acute psychiatric settings respectively ([Linaker and Busch-Iversen 1995]; [Almvik and Woods 1998]). Finally, as previously stated, a study of inpatient violence found that within a locked acute ward over a course of year, 58% of 70 incidents were precipitated by patients appearing as ‘agitated, irritable’ while a year later within an ‘interim secure unit’, 65% of 65 incidents were precipitated by these cues [Agarwal and Roberts 1996].
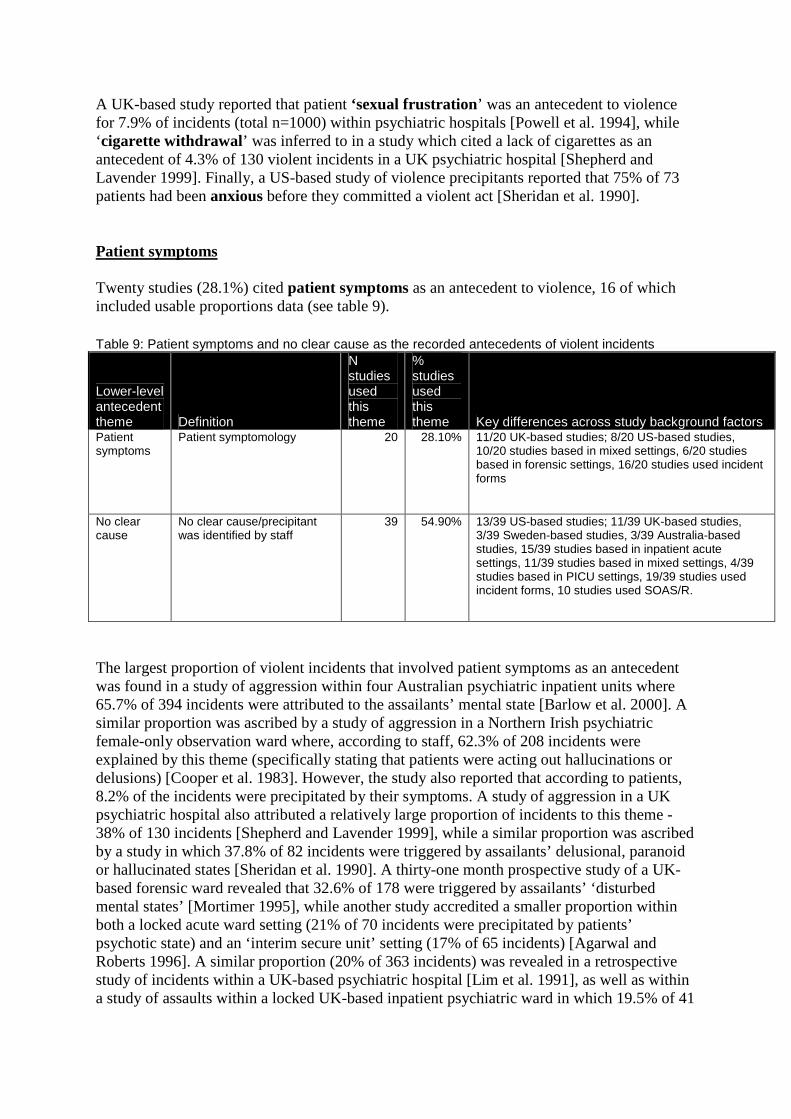
A UK-based study reported that patient ‘sexual frustration ’ was an antecedent to violence for 7.9% of incidents (total n=1000) within psychiatric hospitals [Powell et al. 1994], while ‘cigarette withdrawal’ was inferred to in a study which cited a lack of cigarettes as an antecedent of 4.3% of 130 violent incidents in a UK psychiatric hospital [Shepherd and Lavender 1999]. Finally, a US-based study of violence precipitants reported that 75% of 73 patients had been anxious before they committed a violent act [Sheridan et al. 1990]. Patient symptoms Twenty studies (28.1%) cited patient symptoms as an antecedent to violence, 16 of which included usable proportions data (see table 9). Table 9: Patient symptoms and no clear cause as the recorded antecedents of violent incidents
Lower-level antecedent theme Definition
N studies used this theme
% studies used this theme Key differences across study background factors
Patient symptoms
Patient symptomology 20 28.10% 11/20 UK-based studies; 8/20 US-based studies, 10/20 studies based in mixed settings, 6/20 studies based in forensic settings, 16/20 studies used incident forms
No clear cause
No clear cause/precipitant was identified by staff
39 54.90% 13/39 US-based studies; 11/39 UK-based studies, 3/39 Sweden-based studies, 3/39 Australia-based studies, 15/39 studies based in inpatient acute settings, 11/39 studies based in mixed settings, 4/39 studies based in PICU settings, 19/39 studies used incident forms, 10 studies used SOAS/R.
The largest proportion of violent incidents that involved patient symptoms as an antecedent was found in a study of aggression within four Australian psychiatric inpatient units where 65.7% of 394 incidents were attributed to the assailants’ mental state [Barlow et al. 2000]. A similar proportion was ascribed by a study of aggression in a Northern Irish psychiatric female-only observation ward where, according to staff, 62.3% of 208 incidents were explained by this theme (specifically stating that patients were acting out hallucinations or delusions) [Cooper et al. 1983]. However, the study also reported that according to patients, 8.2% of the incidents were precipitated by their symptoms. A study of aggression in a UK psychiatric hospital also attributed a relatively large proportion of incidents to this theme - 38% of 130 incidents [Shepherd and Lavender 1999], while a similar proportion was ascribed by a study in which 37.8% of 82 incidents were triggered by assailants’ delusional, paranoid or hallucinated states [Sheridan et al. 1990]. A thirty-one month prospective study of a UK-based forensic ward revealed that 32.6% of 178 were triggered by assailants’ ‘disturbed mental states’ [Mortimer 1995], while another study accredited a smaller proportion within both a locked acute ward setting (21% of 70 incidents were precipitated by patients’ psychotic state) and an ‘interim secure unit’ setting (17% of 65 incidents) [Agarwal and Roberts 1996]. A similar proportion (20% of 363 incidents) was revealed in a retrospective study of incidents within a UK-based psychiatric hospital [Lim et al. 1991], as well as within a study of assaults within a locked UK-based inpatient psychiatric ward in which 19.5% of 41
incidents were precipitated by paranoid and delusional beliefs [Aiken 1984]. This proportion was closely matched with a finding of 19% of 355 incidents being precipitated by patient psychosis in a retrospective study of incidents in a UK psychiatric hospital [Tobin et al. 1991], while another retrospective study of violence within 10 public sector mental health care facilities revealed that 18.7% of 193 violent incidents over a year were precipitated by an acute psychotic episode [Flannery, Jr. et al. 2003]. This antecedent was found to be slightly raised in another Flannery et al study three years later when 16.4% of 615 incidents were attributed to acute psychosis within a US-based public mental health care system [Flannery et al. 2006]. A study of a maximum-security forensic hospital in America found that in 17.2% of 157 incidents ‘florid psychotic behaviour was noted in pts before assault occurred’ [Hillbrand et al. 1996]’s, while another study of chronically assaultive patients attributed 14.3% of 838 incidents to patient symptoms [Quanbeck et al. 2007]. One study of violence within a UK-based inpatient acute psychiatric setting revealed that 13% of 221 incidents were preceded by this theme [Duxbury 2002]. This theme was also reported by a prospective study of assaults in a US-based forensic unit in which ‘voices and delusional thoughts’ were attributed as antecedents by 2.6% of staff and 3.1% of assaulters (n not stated) [Harris and Varney 1986]. Another study also reported this theme when they reported that 286 incidents (out of 1000) were preceded by patients in an ‘agitated, disturbed’ state within 3 UK-based psychiatric hospitals [Powell et al. 1994]. A study which retrospectively analysed data extracted from clinical and legal records over 51 month period in which patients with ‘command hallucinations’ (a hallucination in which a person perceives spoken orders or commands from an 'entity' within) were compared with those without such hallucinations for assaultive behaviour within a forensic medium secure unit [Rogers et al. 2002]. They found that out of 62 violent incidents, 18 command-hallucinators precipitated 74% of incidents while 10 non-command hallucinators precipitated for 26% of incidents. Further, a retrospective 15 year analysis of assaulted staff working within a public mental health care service within Massachusetts found that patients’ symptoms of psychosis precipitated 33% of sexual aggression incidents [Flannery, Jr. and Walker 2008]. Finally, a US-based and a UK-based study of inpatient violence cited patient symptoms as important antecedents of violence but did not report useable proportions data [Nolan et al. 2003] and [Casseem 1984] respectively. No clear cause Thirty nine studies (54.9%) reported that there was no clear cause to a violent incident (see table 9). Four of these studies did not report useable proportions data: a UK-based study of inpatient acute violence who reported from their semi-structured questionnaire that most staff did not recognise the antecedent of violence [Convey 1986], a case study of an aggressive schizophrenic patient in at a public psychiatric hospital in which some staff ‘perceived no apparent cause or warning signs’ [Longo and Bisconer 2003], a study which revealed that 58.6% of staff and 15.4% of assailants reported that ‘no reason’ or ‘unknown’ when enquired to the antecedent of incidents [Harris and Varney 1986], and a study of violent assaults in a large US-based neuropsychiatric facility who reported that ‘most assaults came without warning’ [Lanza 1988]. The largest proportion of incidents attributed to this theme was reported in a UK-based prospective study of violence in a forensic hospital in which 85% of 1144 incidents ‘arose spontaneously’ [Larkin et al. 1988].A US-based study of battery incidents in a maximum security hospital found that 77.3% of 221 incidents were attributed to this theme [Dietz and
Rada 1982]; while a study of aggression in a Northern Irish psychiatric female-only observation ward revealed a similar proportion - 75% of 208 incidents [Cooper et al. 1983], and a three month study of abusive incidents in an adult psychiatric unit in which 66.7% of 18 incidents had no reported cause [Yassi et al. 1998]. A preliminary evaluation of the first 90 days of the ‘Assaulted Staff Action Program’ in which 58.2% of 67 assaults were unprovoked [Flannery et al. 1991]; while a study of video camera recordings installed within a PICU revealed that 54.3% of 35 incidents did appeared that violence occurred after the assaulter invaded the victim’s personal space by standing or pacing direct in front of the victim were not preceded by a cue or warning [Crowner et al. 1991]. Lower proportions were reported in a retrospective study of violent incidents on two PICUs over a course of one year (in which 46.6% of 116 incidents patients were settled in the period immediately preceding the incident) [Coldwell and Naismith 1989],a five year Italian study of the characteristics of violent behaviour in acute psychiatric in-patients in which no cause was apparent for 44.6% of 323 incidents [Grassi et al. 2001]; an investigation of aggressive behaviour on a Dutch acute psychiatric admissions ward in which the provocation was not understood in 43.3% of 71 incidents [Nijman et al. 1997]’s; and an examination of inpatient aggression in Australian rehabilitation wards in which no apparent antecedents could be identified for 40.2% of 806 incidents [Cheung et al. 1996]. Similar proportions were cited in a 7-year study of persistently assaultive inpatient acute psychiatric patients (39.9% of 409 incidents) [Grassi et al. 2006], a Swedish study of aggressive behaviour on a PICU (38.7% of 119 incidents) [Palmstierna et al. 1991], a study of violence at a Norwegian maximum security forensic hospital (38% of 1945 incidents) [Rasmussen and Levander 1996], a study of violence within a UK-based psychiatric hospital (36.9% of 363 incidents) [Lim et al. 1991], a study of violent incidents in a UK psychiatric hospital (36.1% of 355 incidents) [Tobin et al. 1991], a prospective study of violence in an Australian rehabilitation unit (35% of 477 incidents) [Cheung et al. 1997], a study of aggression over the course of a year in a German psychiatric hospital (34.7% of 441 incidents) [Ketelsen et al. 2007], and a retrospective study of violence in a Finnish forensic psychiatric hospital (32.6% of 616 incidents) [WeizmannHenelius and Suutala 2000]. Five studies reported proportions falling between 20% and 30%: a study staff assaults among acute psychiatric inpatients (29.9% of 137 incidents) [Omerov et al. 2002], a study of assaults within American inpatient acute psychiatric settings (29.2% of 24 incidents) [Conn and Lion 1983], a UK-based study of aggression in acute psychiatric wards (26.5% of 264 incidents) [Foster et al. 2007], a UK-based study of aggression and violence in three inpatient acute psychiatric wards (25.8% of 221 incidents) [Duxbury 2002], and a study of assaults in a psychiatric unit within an American general hospital (24.3% of 37 incidents) [Edwards et al. 1988]. Lower proportions were reported by in a review of staff assaults at an American state psychiatric hospital (18.2% of 203 incidents) [Lion et al. 1981], a study of staff injuries in two Norwegian acute psychiatric inpatient wards over a seven year period (17.5% of 512 incidents) [Langsrud et al. 2007], a study of patient assaults in a Canadian psychiatric hospital (14.9% of 201 incidents) [Cooper and Medonca 1991], and a US-based study of precipitants to staff assaults over a 3 year period (12.2% of 615 incidents) [Flannery et al. 2006]. The lowest proportions were revealed in a study of patients’ explanations of assaults within one US-based PICU (9.7% of 134) [Crowner et al. 1995], a study on the impact of verbal abuse on staff at Singapore-based inpatient acute psychiatric wards (9.5% of 42 incidents) [Yusuf et al. 2006], a study of assaults within a US-based forensic service (8.6% of 838 incidents) [Quanbeck et al. 2007], a 12 month study of violent incidents in a Swedish inpatient psychiatric ward (8.3% of 24 incidents) [Omerov and Wistedt 1997], a study of events that preceded violent incidents within 3 UK-based psychiatric hospitals (7.9% of 1000 incidents) [Powell et al. 1994], a study of staff assaults within a locked UK-based inpatient psychiatric ward (7.3% of 41 incidents) [Aiken 1984], an investigation of staff

injuries working in high security, rehabilitation, acute, and geriatric units in an Australian psychiatric hospital (6.1% of 328 incidents) [Grainger and Whiteford 1993]’s and by study of staff assaults in a veteran’s psychiatric hospital (2.5% out of 40 incidents) [Murray and Snyder 1991]. 4.3 Meta analysis Fifty-three (74.6%) of the seventy-one papers with antecedent data also reported proportion data which was used in a series of meta-analyses of the following 14 high- and medium-level antecedent themes: ‘patient-patient interaction’, ‘staff patient interaction’ (which included ‘limiting patient freedoms’, ‘medication-related containment’, ‘all other containment’, and ‘any other staff-patient interaction’), ‘patient conflict behaviours’, ‘external / personal issues’, ‘structural issues’ (which included ‘environmental issues’ and ‘regime issues’), ‘patient behavioural cues’, ‘emotional / mood cues’, ‘patient symptoms’, and ‘no clear cause’. Only the medium-level theme ‘environmental issues’ was not meta-analysed as only two studies reported useable proportion data.
A formal statistical test for heterogeneity using the I² test (Higgins et al, 2003) was conducted using Stata v11. The heterogeneity and robustness of pooled proportions were also explored by conducting sensitivity analyses and a subgroup analysis of proportions based on incident forms only, and proportions within acute inpatient psychiatric settings. The subgroup analyses conducted were antecedent themes per psychiatric setting, per country, and per data source. When heterogeneity was found to be statistically significant, a random effects model was used. The overall combined pooled estimate results of the themes can be found in table 10. It shows that the antecedent theme which precipitates the highest proportion of violent and aggressive incidents is ‘staff-patient interaction’, followed by ‘patient behavioural cues’, ‘no clear cause’, ‘patient symptoms’, and ‘limiting patient freedoms’. The results of the subgroup analyses can be found in tables 11 (incident forms subgroup analysis) and 12 (acute inpatient
Table 10: Combined pooled estimate results of meta analyses of themes across all studies
High-level antecedent theme N of studies
Pooled proportion (%)
Pooled proportion <95% CI
Pooled proportion >95% CI
Rank of proportion
Patient-patient interaction 22 0.24 (24%) 0.17 0.3 5
Staff-patient interaction 41 0.39 (39%) 0.28 0.5 1
Patient conflict behaviours 8 0.1 (10%) 0.06 0.15 6
External / personal issues 7 0.03 (3%) 0.02 0.04 8
Structural issues 8 0.1 (10%) 0.05 0.16 6
Patient behavioural cues 7 0.38 (38%) 0.26 0.49 2
Emotional / mood cues 4 0.03 (3%) 0.01 0.05 8
Patient symptoms 15 0.28 (28%) 0.2 0.36 4
No clear cause 35 0.32 (32%) 0.24 0.41 3
psychiatric settings subgroup analysis) A full breakdown of the results of these themes across all studies is now presented. Patient-patient interaction As can be seen in Figure 1, 21 studies were included in the meta-analysis of this theme (Cooper et al’s 1983 study was entered twice as they provided antecedent data according to the patient and staff perspective). The overall pooled estimate was found to be 0.24 (95% CI= 0.17-0.30). The I² was 99.1% and significantly heterogeneous (p=.000). Sensitivity analyses were conducted to explore the robustness of this observation. After removing those studies whose proportion and 95% confidence interval were outliers (n = 2; Edwards et al, [1998] and Crowner et al [1995]), the recalculated pooled proportion size was reduced to 0.20 (95% CI= 0.13-0.28). The I² statistic remained at 99.1% and remained significantly heterogeneous (p=.000). Staff-patient interaction A total of 41 studies reported proportion data pertaining to staff-patient interactions and were included the meta-analysis. The pooled estimate was found to be 0.39 (95% CI=0.28-0.50) (see figure 2). The I² was 99.6% and significantly heterogeneous (p=.000). A sensitivity analysis was not required as no studies produced proportion sizes or confidence intervals considered to be outliers. Four medium-level themes under the umbrella of staff-patient interaction were also meta-analysed in order to examine which themes of interactions were producing the higher antecedent proportions. This included the theme ‘limiting patient freedoms’ which produced an overall pooled estimate of 0.25 (95% CI=0.18-0.31) across 27 studies (see figure 3). The I² was 99% and significantly heterogeneous (p=.000). The Langsrud et al (2007) study proportion was considered an outlier and was removed for a sensitivity analysis. The I² statistic decreased to 98.6% and remained significantly heterogeneous (p=.000), while the recalculated pooled proportion was 0.23 (95% CI=0.17-0.29). A meta-analysis of the theme ‘medication-related containment’ produced a pooled proportion size of 0.08 (95% CI = 0.06-0.09) across 21 studies (see figure 4). The I² was 90.8% and significantly heterogeneous (p=.000). The studies by Yusuf et al (2006) and Omerov et al (2002) were dropped for a sensitivity analysis as their proportions and 95% confidence intervals were considered outliers. This resulted in a recalculated pooled proportion size was 0.07 (95% CI = 0.06-0.09), while the I² increased to 91.2% and remained significantly heterogeneous (p=.000). As can be seen in figure 5, the theme ‘any other containment’ included a total of 13 studies which were entered in a meta-analysis. The overall pooled estimate was found to be 0.22 (95% CI =0.16-0.27). The I² was 98.4% and significantly heterogeneous (p=.000). For the sensitivity analysis, one study was removed as its proportion size was considered an outlier (Blomhoff et al, 1990). The pooled proportion size decreased to 0.18 (95% CI =0.13-0.23), while the I² statistic decreased to 98.2% and remained significantly heterogeneous (p=.000).

The final medium-level staff-patient interaction theme to be meta-analysed was ‘any other staff-patient interaction’. This theme produced an overall pooled proportion size of 0.21 Figure 1: Meta analysis of 'Patient-Patient Interaction' – all studies
(95% CI =0.14-0.28) (see figure 6). The I² was 99.3% and significantly heterogeneous (p=.000). The proportion sizes reported by Edwards et al (1988) and Cheung et al (1997) were considered to be outliers and were removed for a sensitivity analysis. The I² statistic decreased to 97.8% and remained significantly heterogeneous (p=.000), while the recalculated pooled proportion decreased to 0.16 (95% CI=0.12-0.20). Patient conflict behaviours Eight studies reported proportion data pertaining to patient conflict behaviours as antecedents of incidents. A meta-analysis of these proportions revealed that the overall pooled estimate of this theme was 0.1 (95% CI=0.06-0.15) (see figure 7). The I² was 97.2% and significantly heterogeneous (p=.000). One study was removed for a sensitivity analysis as its proportion size was considered to be an outlier (Sheridan et al, 1990). This resulted in a recalculated overall pooled estimate of 0.08 (95% CI=0.04-0.11), and a similar I² value (96.8%) which was significantly heterogeneous (p=.000)
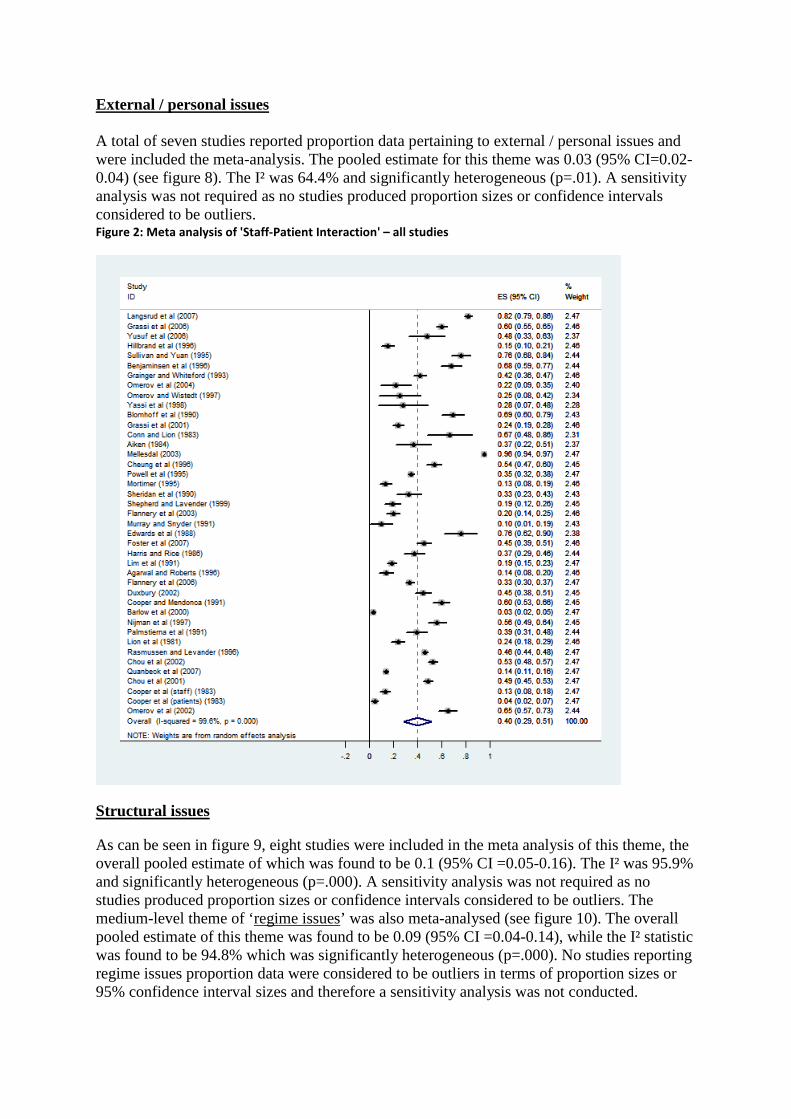
External / personal issues A total of seven studies reported proportion data pertaining to external / personal issues and were included the meta-analysis. The pooled estimate for this theme was 0.03 (95% CI=0.02-0.04) (see figure 8). The I² was 64.4% and significantly heterogeneous (p=.01). A sensitivity analysis was not required as no studies produced proportion sizes or confidence intervals considered to be outliers. Figure 2: Meta analysis of 'Staff-Patient Interaction' – all studies
Structural issues
As can be seen in figure 9, eight studies were included in the meta analysis of this theme, the overall pooled estimate of which was found to be 0.1 (95% CI =0.05-0.16). The I² was 95.9% and significantly heterogeneous (p=.000). A sensitivity analysis was not required as no studies produced proportion sizes or confidence intervals considered to be outliers. The medium-level theme of ‘regime issues’ was also meta-analysed (see figure 10). The overall pooled estimate of this theme was found to be 0.09 (95% CI =0.04-0.14), while the I² statistic was found to be 94.8% which was significantly heterogeneous (p=.000). No studies reporting regime issues proportion data were considered to be outliers in terms of proportion sizes or 95% confidence interval sizes and therefore a sensitivity analysis was not conducted.

Patient behavioural cues
Seven studies were included in the meta-analysis of patient behavioural cues precipitating violent / aggressive incidents. The results showed a pooled estimate size of 0.38 (95% CI = 0.26-0.49) (see figure 11). The I² was 97% and significantly heterogeneous (p=.000). No Figure 3: Meta analysis of 'Limiting patient freedoms' – all studies
NOTE: Weights are from random effects analysis
Overall (I-squared = 99.0%, p = 0.000)
Benjaminsen et al (1996)
Chou et al (2002)
Mellesdal (2003)
Chou et al (2001)
Palmstierna et al (1991)
Quanbeck et al (2007)
Nijman et al (1997)
Cheung et al (1997)
Aiken (1984)
Study
Flannery et al (2006)
Murray and Snyder (1991)
Duxbury (2002)
ID
Omerov et al (2002)
Rasmussen and Levander (1996)
Agarwal and Roberts (1996)
Mortimer (1995)
Grassi et al (2006)
Foster et al (2007)
Conn and Lion (1983)
Omerov and Wistedt (1997)
Yassi et al (1998)
Sheridan et al (1990)
Lim et al (1991)
Shepherd and Lavender (1999)
Powell et al (1995)
Langsrud et al (2007)
Yusuf et al (2006)
0.25 (0.18, 0.31)
0.51 (0.42, 0.60)
0.41 (0.37, 0.45)
0.53 (0.50, 0.56)
0.19 (0.16, 0.23)
0.39 (0.31, 0.48)
0.09 (0.07, 0.11)
0.32 (0.25, 0.39)
0.26 (0.22, 0.30)
0.27 (0.13, 0.40)
0.18 (0.15, 0.21)
0.10 (0.01, 0.19)
0.25 (0.19, 0.31)
ES (95% CI)
0.47 (0.38, 0.55)
0.03 (0.02, 0.04)
0.07 (0.03, 0.12)
0.08 (0.04, 0.12)
0.14 (0.11, 0.18)
0.28 (0.23, 0.33)
0.13 (-0.01, 0.26)
0.25 (0.08, 0.42)
0.06 (-0.05, 0.16)
0.28 (0.18, 0.38)
0.19 (0.15, 0.23)
0.07 (0.03, 0.11)
0.19 (0.17, 0.22)
0.65 (0.61, 0.69)
0.24 (0.11, 0.37)
100.00
3.61
3.83
3.85
3.85
3.64
3.87
3.72
3.83
3.35
%
3.86
3.61
3.78
Weight
3.66
3.89
3.82
3.83
3.85
3.79
3.37
3.08
3.54
3.59
3.83
3.82
3.87
3.83
3.40
0.25 (0.18, 0.31)
0.51 (0.42, 0.60)
0.41 (0.37, 0.45)
0.53 (0.50, 0.56)
0.19 (0.16, 0.23)
0.39 (0.31, 0.48)
0.09 (0.07, 0.11)
0.32 (0.25, 0.39)
0.26 (0.22, 0.30)
0.27 (0.13, 0.40)
0.18 (0.15, 0.21)
0.10 (0.01, 0.19)
0.25 (0.19, 0.31)
ES (95% CI)
0.47 (0.38, 0.55)
0.03 (0.02, 0.04)
0.07 (0.03, 0.12)
0.08 (0.04, 0.12)
0.14 (0.11, 0.18)
0.28 (0.23, 0.33)
0.13 (-0.01, 0.26)
0.25 (0.08, 0.42)
0.06 (-0.05, 0.16)
0.28 (0.18, 0.38)
0.19 (0.15, 0.23)
0.07 (0.03, 0.11)
0.19 (0.17, 0.22)
0.65 (0.61, 0.69)
0.24 (0.11, 0.37)
100.00
3.61
3.83
3.85
3.85
3.64
3.87
3.72
3.83
3.35
%
3.86
3.61
3.78
Weight
3.66
3.89
3.82
3.83
3.85
3.79
3.37
3.08
3.54
3.59
3.83
3.82
3.87
3.83
3.40
0-.2 0 .2 .4 .6 .8 1
sensitivity analysis was undertaken as no studies were considered outliers in terms of reported proportion sizes or confidence intervals. Patient emotional / mood cues As can be seen in figure 12, the theme included a total of four studies which were entered in a meta-analysis. The overall pooled estimate was found to be 0.03 (95% CI =0.01-0.05). The I² was 76.5% and significantly heterogeneous (p=.000). A sensitivity analysis was not conducted due to the small number of studies included in this analysis.

Patient symptoms A total of 16 studies reported proportion data pertaining to patient symptoms as an antecedent to violent and aggressive incidents. The pooled estimate for this theme was found to be 0.28 (95% CI=0.20-0.36 (see figure 13). The I² was 97.7% and significantly heterogeneous (p=.000). The proportion sizes reported by Barlow et al (2000) and Cooper et al (1988) were considered to be outliers and were removed for a sensitivity analysis. Removing these studies reduced the I² statistic to 84.1% and remained significantly Figure 4: Meta analysis of 'Medication-related containment' – all studies
heterogeneous (p=.000), while the recalculated pooled proportion decreased to 0.22 (95% CI=0.18-0.26). No clear cause The meta-analysis of this theme included a total of 35 studies which produced an overall pooled estimate of 0.32 (95% CI =0.24-0.41). The I² was 99.4% and significantly heterogeneous (p=.000). After removing those studies whose proportion and 95% confidence interval were outliers (n = 12; Grainger and Whiteford [1993], Omerov and Wistedt [1997], Yassi et al [1998], Aiken [1984], Powell et al [1995], Larkin et al [1988], Dietz and Rada [1982], Murray and Snyder [1991], Quanbeck et al [2007], Cooper et al [1983], Crowner et al [1991], and Flannery et al [1991]), the recalculated pooled proportion size was 0.31 (95% CI

= 0.26-0.36). The I² statistic decreased to 95.5% and remained significantly heterogeneous (p=.000). Figure 5: Meta analysis of 'Any other containment' – all studies

Figure 6: Meta analysis of 'Any other staff-patient interaction' – all studies

Figure 7: Meta analysis of 'Patient conflict behaviours' – all studies
Figure 8: Meta analysis of 'External / personal issues' – all studies

Figure 9: Meta analysis of 'Structural issues' – all studies
Figure 10: Meta analysis of 'Regime issues' – all studies

Figure 11: Meta analysis of 'Patient behavioural cues' – all studies
Figure 12: Meta analysis of 'Emotional / mood cues' – all studies

Figure 13: Meta analysis of 'Patient symptoms' – all studies

Figure 14: Meta analysis of 'No clear cause' – all studies
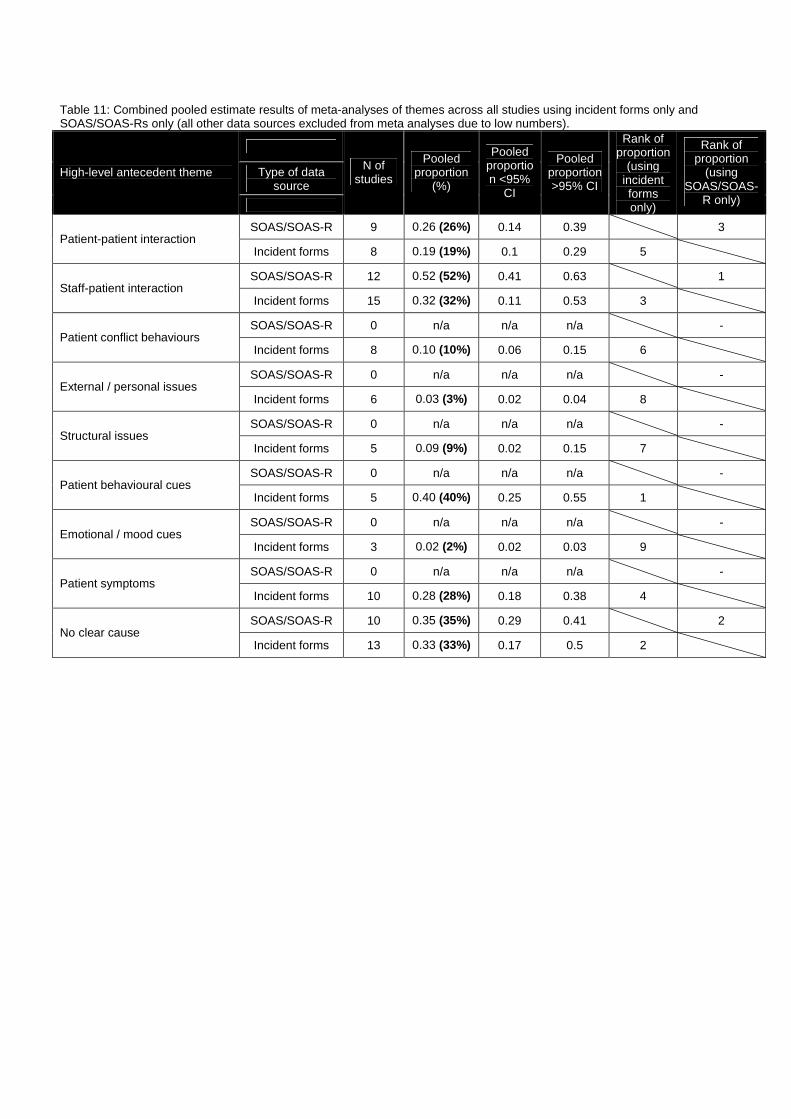
Table 11: Combined pooled estimate results of meta-analyses of themes across all studies using incident forms only and SOAS/SOAS-Rs only (all other data sources excluded from meta analyses due to low numbers).
Type of data source
High-level antecedent theme
N of studies
Pooled proportion
(%)
Pooled proportion <95%
CI
Pooled proportion >95% CI
Rank of proportion
(using incident forms only)
Rank of proportion
(using SOAS/SOAS-
R only)
SOAS/SOAS-R 9 0.26 (26%) 0.14 0.39 3 Patient-patient interaction
Incident forms 8 0.19 (19%) 0.1 0.29 5
SOAS/SOAS-R 12 0.52 (52%) 0.41 0.63 1 Staff-patient interaction
Incident forms 15 0.32 (32%) 0.11 0.53 3
SOAS/SOAS-R 0 n/a n/a n/a - Patient conflict behaviours
Incident forms 8 0.10 (10%) 0.06 0.15 6
SOAS/SOAS-R 0 n/a n/a n/a - External / personal issues
Incident forms 6 0.03 (3%) 0.02 0.04 8
SOAS/SOAS-R 0 n/a n/a n/a - Structural issues
Incident forms 5 0.09 (9%) 0.02 0.15 7
SOAS/SOAS-R 0 n/a n/a n/a - Patient behavioural cues
Incident forms 5 0.40 (40%) 0.25 0.55 1
SOAS/SOAS-R 0 n/a n/a n/a - Emotional / mood cues
Incident forms 3 0.02 (2%) 0.02 0.03 9
SOAS/SOAS-R 0 n/a n/a n/a - Patient symptoms
Incident forms 10 0.28 (28%) 0.18 0.38 4
SOAS/SOAS-R 10 0.35 (35%) 0.29 0.41 2 No clear cause
Incident forms 13 0.33 (33%) 0.17 0.5 2

Table 12: Combined pooled estimate results of meta-analyses of themes across all studies based within inpatient acute, forensic and other settings
Type of data source >95% CI High-level antecedent theme
N of studies
Pooled proportion
(%)
<95% CI
Rank of proportion (inpatient)
Rank of proportion (forensic)
Rank of proportion
(other)
Inpatient acute 10 0.27 (27%) 0.16 0.38 3 - -
Forensic 2 n/a n/a n/a - - - Patient-patient interaction
Other 10 0.22 (22%) 0.15 0.29 - - 5
Inpatient acute 20 0.49 (49%) 0.3 0.68 1 - -
Forensic 6 0.23 (23%) 0.1 0.39 - 2 - Staff-patient interaction
Other 14 0.34 (34%) 0.24 0.43 - - 2
Inpatient acute 3 0.03 (3%) 0.01 0.07 5 - -
Forensic 2 n/a n/a n/a - - - Patient conflict behaviours
Other 3 0.19 (19%) 0.06 0.33 - - 6
Inpatient acute 3 0.04 (4%) 0.01 0.08 9 - -
Forensic 2 n/a n/a n/a - - - External / personal issues
Other 2 n/a n/a n/a - - -
Inpatient acute 1 n/a n/a n/a - - -
Forensic 1 n/a n/a n/a - - - Structural issues
Other 6 0.09 (9%) 0.02 0.15 - - 7
Inpatient acute 1 n/a n/a n/a - - -
Forensic 2 n/a n/a n/a - - - Patient behavioural cues
Other 4 0.40 (40%) 0.29 0.57 - - 1
Inpatient acute 0 n/a n/a n/a - - -
Forensic 1 n/a n/a n/a - - - Emotional / mood cues
Other 3 0.05 (5%) 0.01 0.09 - - 8
Inpatient acute 3 0.33 (33%) -0.06 0.72 2 - -
Forensic 4 0.23 (23%) 0.14 0.32 - 2 Patient symptoms
Other 8 0.27 (27%) 0.18 0.37 - - 4
Inpatient acute 13 0.26 (26%) 0.17 0.35 4 - -
Forensic 5 0.48 (48%) 0.17 0.8 - 1 - No clear cause
Other 17 0.32 (32%) 0.24 0.41 - - 3

Table 13: Combined pooled estimate results of meta-analyses of themes across all UK and US-based studies (other countries excluded due to low numbers)
Country High-level antecedent theme
N of studies
Pooled proportion
(%)
<95% CI
>95% CI
Rank of proportion
(USA)
Rank of proportion
(UK)
UK 7 0.19 (19%) 0.12 0.26 4 Patient-patient interaction
USA 4 0.28 (28%) 0.04 0.52 4
UK 9 0.33 (33%) 0.23 0.42 1 Staff-patient interaction
USA 10 0.31 (31%) 0.2 0.42 3
UK 4 0.06 (6%) 0.01 0.11 6 Patient conflict behaviours
USA 3 0.24 (24%) 0.1 0.38 5
UK 4 0.02 (2%) 0.01 0.03 7 External / personal issues
USA 2 n/a n/a n/a -
UK 3 0.08 (8%) 0.01 0.16 5 Structural issues
USA 4 0.1 (10%) 0.03 0.18 7
UK 2 n/a n/a n/a - Patient behavioural cues
USA 3 0.32 (32%) 0.11 0.54 1
UK 2 n/a n/a n/a - Emotional / mood cues
USA 2 n/a n/a n/a -
UK 7 0.23 (23%) 0.18 0.29 3 Patient symptoms
USA 6 0.20 (20%) 0.16 0.25 6
UK 9 0.33 (33%) 0.06 0.6 1 No clear cause
USA 10 0.32 (32%) 0.2 0.44 1

4.4 Evidence for and against the City model One of the underlying assumptions of the City model is the way staff can directly influence the likelihood of conflict and containment levels, particularly through the way that they interact with their patients. Therefore, the finding of staff-patient interaction precipitating an estimated 40% of aggressive/violent incidents provides compelling evidence of this assumption, as does the finding of 59 out of 71 papers (83%) reporting some sort of staff-patient interaction as an antecedent to incidents. One of the key moderators of conflict and containment levels in the City model is the role of effective structure. This model component is supported by this review as limiting patients’ freedoms was found to frequently precipitate violence/aggression (an estimated 25% of incidents) and was reported by 37 papers in total (52%). The level and type of limits that are placed upon patient behaviour and conduct can be influenced by the structure of the ward which includes rules about restrictions on objects and behaviour. Further support of the importance of an effective structure is highlighted by the finding that regime issues such as inadequate staff-levels, boredom, and excessive sensory stimulation were reported by 10 papers as antecedents of violence/aggression (which were estimated to trigger 9% of incidents). The review also lends evidence to the importance of technical mastery in influencing the outcome of conflict and containment levels. This is because the review revealed that emotional/mood and, in particular, behavioural cues are presented by assailants prior to an incident occurring. Staff who are skilled in recognising such cues should be able to pre-empt and minimise the likelihood of an aggressive/violent incident from occurring. Further support for the importance of technical mastery is highlighted by the fact that carrying out containment methods, especially restraint, seclusion and de-escalation, can contribute to the likelihood of violent/aggressive incident occurring (non-medication related containment is estimated to precipitate 22% of incidents). If containment measures are carried out by effectively by staff, the likelihood of such a conflict event occurred can be reduced. 4.5 Points the City model has missed The City model does not explicitly include the role of patient-patient interaction in the production of conflict and containment outcomes. This theme was found to be an important precipitant to violence/aggression as it was reported by 34 of the 71 papers (48%) and was estimated to precipitate 24% of violent/aggressive incidents. The model also does not include a consideration of how issues that are external and personal to the patient (such as receiving bad news, family and money issues) may influence conflict and containment outcomes. The effect of patient symptoms (estimated to precipitate 28% of incidents and reported by 21 papers as an antecedent) and the physical environmental (such as overcrowding, a confined physical environment, noisiness) are also not included (although the latter was only reported by 3 papers). Although the effect of limiting patient freedoms on conflict and containment is influenced by the model’s components of effective structure and technical mastery, this review’s findings indicate that more explicit and direct consideration of this theme may be strengthen the model. Finally, the City model does not emphasise the inter-relationship that exists between conflict and containment. This relationship is emphasised by the finding of containment measures (such as medication, restraint, seclusion, de-escalation) being reported as

antecedents of violence/aggression by a total of 29 papers, while non-related medication containment was estimated to trigger 22% of incidents. 4.5 Discussion One of the clearest findings depicted in this review is that antecedents of violent and/or aggressive incidents are wide-ranging. This is underlined by the fact that there were in total 59 distinct lower-level antecedent themes across the 71 studies included in this review. Antecedents ranged from specific types of interactions between patients and patients, patients and staff, other conflict behaviours, issues relating to external source or of a personal nature, structural issues within wards, patient symptoms, and behavioural and emotional cues. However, it is important to consider that these themes and the extent to which they trigger incidents are predominantly staff-based constructions of reality. It is the psychiatric staff members who interpret their personal view of the incident and subsequently complete an incident form, a SOAS/R, a study questionnaire, a claim form, an assault form, and/or who are qualitatively interviewed. Sixty-three (89%) of the 71 studies reported antecedent data exclusively from the staff’s perspective of the incidents, while only five papers (7%) captured the patients’ perspective. Such a large disparity of perspectives underlines the importance of viewing this review’s findings as predominantly a representation of the staff’s views of antecedents, and that the true breadth and scope of antecedents of violence and aggression remains uncertain. A key reason for the existence of this disparity is that psychiatric wards are focusing on the staff’s recording of the antecedents of incidents. This is underscored by the finding that 8 out of the 11 different sources of antecedent data revealed in this review were exclusively staff-centred outcome measures such as incident forms and the SOAS/R. Participant observation was used by only one study [Murray and Snyder 1991], while video camera footage of incident was analysed by just three studies ([Crowner et al. 1991], [Crowner et al. 2005] and [Nolan et al. 2003]). Qualitative follow-up interviews of patients following an incident were carried out by five studies ([Aiken 1984], [Harris and Varney 1986], [Edwards et al. 1988], [Crowner et al. 1995], and [Cooper et al. 1983]) compared to nine studies which interviewed staff members. Studies that retrospectively analyse the antecedent data are only able to utilise what data is available to them. However, prospective studies have the opportunity to analyse the precipitating factors of an aggressive/violent incident from a patient’s perspective and should be encouraged to do so. Where possible, prospective studies should also utilise video camera footage, or retrospectively analyse existing video camera footage. Researchers may also find it useful to cross-check their interpretation of video-camera footage with the assailant, staff and/or witness as source of validation. This type of research is necessary in reducing the perspective disparity and augmenting our understanding of what triggers violence and aggression. Another advantage of involving patients in research studies interested in antecedents to violence/aggression is that they can elicit an understanding of how the patient felt prior to the incident occurring. Enhancing our knowledge of such cues may help staff become better at sensing or feeling a patient’s emotional state prior to an incident occurring, and lead to a greater psychological understanding. The current state of literature illustrates that a far greater level of reporting goes into understanding the behavioural cues prior to an incident – 20 studies reported assailants’ behavioural cues prior to an incident, but only 8 studies

reported assailants’ emotional cues. This disparity is likely to be a consequence of it being easier for staff to recognise a behavioural cue than an emotional cue prior to an incident, and also because such few studies consider the patient’s perspective in their examination of antecedents. Despite a greater emphasis within the literature on reporting what happened prior to the incident compared to how the assailant was feeling before an incident, many lower-level antecedent themes were infrequently reported (for example, assailants’ reaction to sexual approach, attention-seeking behaviour, physical contact between patients and/or staff, assailants finding potential weapons, being in a confined or over-crowded environment, competition between patients – all n=1). It is debateable as to whether the implication of this is that such antecedents are less important and less frequently triggers of aggression/violence, or whether they being under-reported. If the latter is considered true, then the root of the under-reporting may be the recording tools used by wards and research studies. For example, if a violent incident was triggered because two patients were being overly-competitive with each other while playing a computer game, this detail may be lost within a recording form such as the SOAS-R which has a pre-defined category of ‘provoked by other-patient’. Therefore, psychiatric staff should record the precipitating factors prior to a violent/aggressive incident in as much detail as possible so that the richness of the data can be preserved. This need is substantiated by the fact that 13 studies reported that the antecedent of violence/aggression was ‘patient provocation’ and that 15 studies reported that the antecedent was some form of unspecified staff-patient or patient-patient interaction. In keeping for the call of greater antecedent recording detail, one of the most salient findings was that more than half of the literature (n=37 papers) cited that limiting patients’ freedoms was a trigger of aggression/violence, yet the majority of these studies (n=24) did not specify what the nature of the requests/freedoms being denied. This may again be due to a low level of recording detail by ward staff, or a consequence of studies not providing further details despite its availability. The need for a greater understanding of what requests and freedoms are being denied is strongly emphasised by the meta-analysis finding of this theme being estimated to be antecedent of 25% of violent/aggressive incidents – a comparatively high estimate compared to the 12 other themes meta-analysed. Further support for the call of greater antecedent recording detail comes from the fact that 35 (49%) of the studies stated that in one of more incidents, no clear cause could be attributed an incident. Perhaps even more concerning, the results of meta-analyses revealed that there was no clear cause for an estimated 32% of incidents. This either implies that approximately 32% of incidents are unprovoked (which is unlikely), that staff are failing to recognise existent antecedent(s), or that staff are recognising the antecedent(s) but are not recording them. If staff are unsure about the antecedent(s) of an incident, they should attempt to reflect further, converse with any witnesses of the incident, and/or directly ask the assailant at an appropriate time after the incident. Another key point to be considered is that the sequence of antecedents could not be established from the data. Therefore, the data does not necessarily represent the immediate precursors to an incident, but instead what precipitating phenomena were perceived to be present at an unknown time point prior to an aggressive/violent incident. The meta-analyses of the antecedent themes estimated that staff-patient interactions are the most frequent types of antecedents (39% of all incidents involved a staff-patient interaction

antecedent). An examination of the medium-level staff-patient interaction themes revealed that limiting patients freedoms, either by placing some sort of restriction or denying a patient request, was the most frequent precursor of incidents. The other staff-patient interaction themes related to containment procedures and all other types of interactions such ordering patients, searching patients, and intervening on an argument or fight. This finding underscores the influence that staff have in making wards safe and efficacious environments. It also highlights that most violent incidents are preceded by the staff exercising their power over the patient. Therefore, prospective interventions aimed at reducing inpatient violence and aggression should include methods centred on enhancing staff-patient interactions, particularly in terms of finding better ways to manage patient requests and increasing staff’s technical mastery of containment procedures so that the risk of escalating an aggressive incident is not increased. It may also be important to reduce the real or perceived level of power differences that exist between staff and patients, either by giving patients more powers and freedoms, or staff exercising their position of power less liberally and only when the situation necessitates it. The behavioural cues associated with the expression of aggression was the second most frequently reported antecedent of violent incidents, with an estimated 38% of incidents precipitated the assailant displaying signs of agitation, attention-seeking behaviour, increased motor activity, boisterousness, and/or confusion. This is not an unexpected finding as it is likely that assailants will be displaying such cues just prior to an incident occurring. Further, as already stated, staff should find it easier to recognise such behavioural cues compared to emotional/mood cues prior to an incident. An implication of this finding is that staff the presentation of such cues should provide staff with an opportunity to be pre-empt an incident from occurring. The results of the meta-analyses also revealed that the approximately 1 in 4 aggressive/violent incidents are estimated to be triggered by a type of patient-patient interaction. This finding implies that it may be beneficial if staff encourage and support patients in positively interacting with other patients, such as helping them to appreciate each other and communicate with each other in positive and constructive ways. If conflicts arise, staff should find ways that de-escalate the conflict before an incident occurs, such as finding a resolution, offering a compromise, or, if necessary, removing them from each other’s vicinity. It is also important to consider that the heterogeneity of the meta-analyses was very high and therefore these results should be treated with caution This is demonstrated by the high I2 scores and the large confidence intervals, which were also present for each of the pooled estimates. It was anticipated that splitting the meta-analyses by setting, country, and, in particular, data source would significantly lower heterogeneity and tighten the confidence intervals, however the variability between the studies remained high. Filtering the data in this manner also did not produce any differences of note within the data. The fact that the pooled proportion estimates were relatively similar when incident forms were compared to the SOAS/R data collection tool implies that the high variability that exists is not due to the reliability of the data collection methods, but rather due to important differences across the studies (e.g. cultural differences, regime/practice differences etc).

5. THE CONSEQUENCES OF VIOLENCE AND AGGRESSION
5.1 The studies reviewed One hundred and eight studies provided live, prospective consequences data. This data is derived from what was recorded immediately after the violence/aggression occurred. Therefore, it should in theory be an accurate account of what happened after the incident occurred, rather than a subjective opinion or belief about what happened, or what occurred to beyond the immediate. Sixty-one of these papers reported counts on the outcomes and consequences of interest in this review, as well as a total incident count. Data source There were 13 different sources of consequences data. The most predominant of these were incident forms (n=46 studies used this method), followed by the ‘SOAS/SOAS-R’ (Staff Observation Aggression Scale) [Nijman et al. 1999;Palmstierna and Wistedt 1987] instrument (n=19), qualitative follow-up interviews (which were carried out either immediately after the incident or soon after) (n=14), official records (clinical, legal, and/or case records) (n=18), study-specific questionnaires (n=9), ‘OAS/MOAS’ ([Modified] Overt Aggression Scale) [Knoedler 1989] (n=9), ‘ASAP’ (Assaulted Staff Action Program) (Flannery, 1999) (n=8), video recording (n=3), participant/non-participant observation (n=2), the ‘Attacks’ scale [Bowers et al. 2002] (n=2), medical claim documents (n=1), case studies (n=1), the IES-R instrument (Impact of Events Scale - Revised) [Weiss and Marmar 1997] (n=1), and supervisory logs (n=1). Countries Consequences data was collected from 15 different countries. These were: USA (n=44 studies), UK (n=27), Australia (n=10), Sweden and Canada (both n=5), Italy (n=4), Norway (n=3), Germany and Netherlands (both n=2), and Denmark, Spain, Sri Lanka, Switzerland, New Zealand, and Bahrain (all n=1). Study settings Thirty-seven studies collected consequences data from inpatient acute settings and thirty seven studies collected data from mixed settings. Twenty-five studies collected data from forensic settings, 5 from Psychiatric Intensive Care Units (PICU), two from rehabilitation units and 2 from veteran settings. Perspective One hundred and five studies collected data based on represented the staff’s perspective of the consequence (103 of which collected data solely from this perspective), 3 studies included data from the perspective of the video camera (2 exclusively), one study analysed the patients perspective (as well as the staff’s perspective), and one study documented a researcher’s perspective. 5.2 Findings A thematic analysis of the consequences data produced 67 distinct ‘lower-level’ themes which formed 8 higher-level themes: ‘physical injury’, ‘severity of injury’, ‘containment/staff response’, ‘patient transferred/discharged’, ‘victim psychological outcome’, ‘victim
behavioural outcome’, ‘property/object damage’, and ‘no consequence’. Please see Table 1 for a full breakdown of these themes. Physical injury Sixty-one studies (56.5%) reported this higher-level theme as an outcome of violence/aggression. This included 19 lower-level themes that related to different types of physical injury for the assailant or victim(s) (see table 1). The majority of these studies (n=32) did not specify the nature of the physical injury as a consequence of violence/aggression [Abeyasinghe and Jayasekera 2003;Bowers et al. 2002;Carton and et al. 2003;Casseem 1984;Cheung et al. 1996;Cheung et al. 1997;Crowner et al. 1991;Crowner et al. 1994;Dietz and Rada 1982;Dowson et al. 1999;Flannery, Jr. 2008;Flannery, Jr. and Walker 2008;Grassi et al. 2001;Gudjonsson et al. 2004;Hamadeh et al. 2003;Helmuth 1994;Kennedy et al. 1995;Ketelsen et al. 2007;Larkin et al. 1988;Mellesdal 2003;Nijman et al. 1997;Nijman and Rector 1999;Palmstierna et al. 1991;Palmstierna and Wistedt 1987;Palmstierna and Wistedt 1995;Powell et al. 1994;Rasmussen and Levander 1996;Reid et al. 1985;Steinert et al. 1999;Stockman and Heiber 1980;Torpy and Hall 1993]. Twenty-eight studies specified the nature of the injury, including ‘head injuries’ which was reported as a consequence by seven studies. A retrospective study of two Norwegian acute psychiatric inpatient wards over a seven year period found that 38.1% of 507 violent/aggressive incidents resulted in head injuries [Langsrud et al. 2007]. Another retrospective study of injury reports over a five year period in a US-based, large, all-male, forensic hospital revealed that from 236 staff injuries, 70.7% of them were head injuries [Carmel and Hunter 1993]. The same authors also found in an earlier study of staff injuries within a state hospital that over the course of a year, 75.5% of all injuries sustained during a patient assault (49 injuries in total) resulted in head injuries, while 8.6% of all injuries sustained during containment procedures (86 injuries in total) resulted in head injuries [Carmel and Hunter 1989]. Another US-based retrospective study of injury reports, which aimed to replicate the previously referenced study, found that 39% of all injuries sustained during a patient assault (31 injuries in total) resulted in head injuries, while 20% of all injuries sustained during containment procedures (15 injuries in total) resulted in head injuries [Hanson and Balk 1992]. Another US-based study retrospectively examined data from the ‘Assaulted Staff Action Program’ (ASAP) and found that over a one year period, 7% of 193 staff assaults (within a mixture of psychiatric inpatient settings) resulted in head and back injuries [Flannery, Jr. et al. 2003]. A 15 year retrospective analysis of the same data source found that 10.2% of 460 staff assault incidents within acute psychiatric inpatient settings resulted in head and back injuries [Flannery, Jr. et al. 2007]. A 6 month prospective study of a female observation ward in a Northern Irish General Psychiatric Hospital found

Table 1: Thematic analysis of consequences
PHYSICAL INJURY CONTAINMENT/ STAFF RESPONSE
PATIENT TRANSFERRED/
DISCHARGED
VICTIM PSYCHOLOGICAL
OUTCOME
VICTIM BEHAVIOURAL
OUTCOME • Unspecified physical
injury • Head injury • Back/spine/trunk
injury • Injury to extremities • Facial/eye injury • Injury to limbs • Soft tissue/muscle
injury • Abdominal injury • Sprain/strain/
soreness • Scratched/cut/
grazed/nosebleed • Bump/ knock/ bruise • Bone injury • Serious open wound/
laceration • Burned • Loss of
consciousness/ concussion
• Biting injury • Pain lasted <10mins • Pain lasted >10mins • Headache
SE
VE
RIT
Y O
F IN
JUR
Y
• Seclusion • Manual restraint • Oral medication • Intra-muscular
medication • Time out/patient
removed from situation • Verbal de-escalation • Staff counselled
assailant after incident ended
• Mechanical restraint • Contacted police • Constant special
observation • Patient denied some of
their privileges • Ward doors locked • Patient detained in
hospital • Staff confronted patient • Nursing management
plan reviewed
• Transfer to higher security ward
• Transfer to jail • Transfer to another
hospital/unit • Transfer to PICU • Criminal reconviction/
prosecution
• Irritability • Muscle tenseness • Intrusive thoughts • Ruminated about
incident • Anger • Resentment • Staff fear of patient • Decreased job
satisfaction • Dreamt about
incident/ sleep disturbances
• Repression • Anxiety • Acute stress disorder • PTSD symptoms • Disruption in domain
of mastery • Disruption in domain
of attachment • Disruption in domain
of meaning
• Staff fatigue • Staff alcohol use • Staff smoked • Staff ate more/ lost
appetite • Staff resigned • Debriefing/review • Strained family
relationships • Counselling • Support group
meetings
PR
OP
ER
TY
/ O
BJE
CT
S D
AM
AG
E
NO
CO
NS
EQ
UE
NC
E

that out of 208 incidents, there was only one head injury sustained when a patient intentionally struck their head on a wall during a violent episode [Cooper et al. 1983]. Eight studies reported a ‘back/spine/trunk injury ’ as a consequence of an incident including six studies previously mentioned: one which revealed that 22.1% of 507 violent/aggressive incidents resulted in head injuries [Langsrud et al. 2007]; one which found that 13.3% and 6.7% of 236 staff injuries resulted in spinal and trunk injuries respectively [Carmel and Hunter 1993]; another which found that 12.2% of all injuries sustained during a patient assault (49 injuries in total) resulted in head injuries, while 16.2% of all injuries sustained during containment procedures (86 injuries in total) resulted in spinal injuries [Carmel and Hunter 1989]; the replication study which found that found that 29% of all injuries sustained during a patient assault (31 injuries in total) resulted in trunk injuries, while 67% of all injuries sustained during containment procedures (15 injuries in total) resulted in injuries to trunk or extremities [Hanson and Balk 1992]; another which revealed that 7% of 193 staff assaults (within a mixture of psychiatric inpatient settings) resulted in head and back injuries [Flannery, Jr. et al. 2003]; a 15 year retrospective analysis of the same data source found that 10.2% of 460 staff assault incidents within acute psychiatric inpatient settings resulted in head and back injuries [Flannery, Jr. et al. 2007]. A Canadian-based retrospective study of staff injuries in a 500 bed forensic psychiatric service found that over a seven year period, found that incidents that resulted in injuries to major joints (including the neck and back) were significantly more likely to result in lost work days than injuries to other body parts [Harris et al. 1986]. Finally, a UK-based study of staff from an inpatient acute psychiatric unit found that over the course of 6 months, face or trunk injuries were the result of having been slapped or punched [Whittington and Wykes 1989]. Five studies cited ‘injury to extremities ’ as a consequence of a violent/aggressive incident. A retrospective study of two Norwegian acute psychiatric inpatient wards over a seven year period found that 52.7% and 13.6% of 507 violent/aggressive incidents resulted in injuries to the upper and lower extremities respectively [Langsrud et al. 2007]. As previously mentioned, a US-based study found that while 67% of all injuries sustained during containment procedures (15 injuries in total) resulted in injuries to trunk or extremities [Hanson and Balk 1992]. The study of which the latter replicated also reported this theme: specifically that over the course of a year, 6.1% of all injuries sustained during a patient assault (49 injuries in total) resulted in injuries to the extremities, while 67.4% of all injuries sustained during containment procedures (86 injuries in total) resulted in injuries to the extremities [Carmel and Hunter 1989]. The same authors’ later study found that 9.3% of 236 staff injuries resulted in injuries to the extremities [Carmel and Hunter 1993]. Finally, a prospective study conducted at a 23 bedded US-based acute psychiatric female unit during a six month period reported that from 87 incidents, injuries occasionally included ‘contusions of an extremity’. One US-based study of patient assault cited facial and eye injuries as a consequence of violence [Lanza 1988] – specifically ‘numbness on parts of the face’, ‘black eyes’, and ‘eye injuries’. Another study retrospectively investigated staff injuries over a two year period in one Australian psychiatric hospital and found that 1.9% of 328 incidents resulted in eye injuries, while 0.4% of 328 incidents results in teeth being knocked out [Grainger and Whiteford 1993]. This study also specified injuries to

limbs as a consequence – specifically that 12.3% of 328 incident resulted in twisted limb injuries. The Canadian-based retrospective study of staff injuries in a 500 bed forensic psychiatric service found that over a seven year period, found that incidents that resulted in injuries to major joints (including knee injuries) were significantly more likely to result in lost work days than injuries to other body parts [Harris et al. 1986]. The two aforementioned ASAP studies also referred to this type of injury – specifically that 5.8% of 460 staff assault incidents within acute psychiatric inpatient settings resulted in bone/tendon/ligament injuries [Flannery, Jr. et al. 2007] and that 3% of 193 staff assaults (within a mixture of psychiatric settings) resulted in bone/tendon/ligament injuries [Flannery, Jr. et al. 2003]. Finally, a US-based 6 month prospective study of repeatedly assaultive psychiatric inpatients found that 21 of 497 recorded incidents resulted in ‘serious’ injuries such as severe lacerations, fractures, suspected fractures, burns or dislocations) [Convit et al. 1990]. Another specified type of injury from inpatient assaults were ‘soft tissue/muscle injuries ’. These injuries were cited by four studies including one case study of an aggressive and self-harming patient in a US-based psychiatric hospital who caused 25 injuries to nursing staff over a 39 month study period which included muscle injuries [Bisconer et al. 2006]. Both previously mentioned ASAP studies cited this injury type - specifically that 46.3% of 460 staff assault incidents within acute psychiatric inpatient settings resulted in soft tissue injuries [Flannery, Jr. et al. 2007] and that 52% of 193 staff assaults (within a mixture of psychiatric settings) resulted in soft tissue injuries [Flannery, Jr. et al. 2003]. An earlier study by the same lead author conducted a preliminary evaluation of ASAP and found that out of 67 reported assaults upon psychiatric nursing staff over a 90 day period, 34% resulted in soft tissue injuries [Flannery et al. 1991]. ‘Abdominal injuries ’ were also cited by two of the ASAP studies – specifically as an outcome for 0.4% of 193 assaults [Flannery, Jr. et al. 2003] and 1.8% of 460 assaults [Flannery, Jr. et al. 2007]. A number of studies did not explicitly specify the area of the physical injury, but did refer to sprains, strains, and/or soreness. This included a one year study of a US-based Veterans unit in which 12.5% of 40 incidents resulted in to sprains/strains [Murray and Snyder 1991], a study of patient assaults over a 27 month period in a Canadian psychiatric hospital reported that most of the 201 recorded violent/aggressive incidents resulted in lacerations, bruising and sprains [Cooper and Medonca 1991]. A US-based study of nursing staff characteristics related to patient assault reported that over a 1 year period, reported soreness as a consequence of violence [Lanza et al. 1991], while another US-based study of violence within a locked university-based short-term Forensic inpatient unit reported that 45% of staff injuries (n injuries or incidents not stated) resulted in sprains or strains [Lam et al. 2000]. A retrospective study of patterns of aggression in an Australian forensic psychiatric hospital reported that mild-moderate injuries such as bruises, sprains, or welts occurred in 20.3% of 197 incidents [Daffern et al. 2003], Nine studies cited a physical injury as being ‘scratched/cut/grazed/having a nose-bleed’. This included the previously mention Australian-based retrospective study which found that 20% of 328 incidents resulted in staff being scratched, cut or grazed over a two year period at a psychiatric hospital [Grainger and Whiteford 1993]. A 12 month study of violent incidents in a Swedish inpatient psychiatric ward revealed that in 9.8% of 41 violent incidents, staff suffered bruises or minor wounds [Omerov and

Wistedt 1997]. The previously cited US-based study of a Veterans unit found that 10% of incidents resulted in to scratches or cuts [Murray and Snyder 1991]. A prospective two year study of the nature of accidents in a 2400 patients from a US-based psychiatric hospital reported that the majority of the injury reports concerned trivial injuries such as cuts [Abbott 1978]. Another US-based study examined data from video cameras and incident reports over a 27 month period within one inpatient acute psychiatric ward and reported that from 149 incidents, there was 1 incident of a staff member suffering from a nose bleed after an incident, and that the rest of minor injuries suffered were predominantly scratches [Crowner et al. 1994]. A 15 year retrospective analysis of the ‘ASAP’ found that 12.4% of 460 staff assault incidents within acute psychiatric inpatient settings resulted in open wounds, scratches, or spitting incidents [Flannery, Jr. et al. 2007]. A US-based study of patient assault reported that most staff assaults were judged to be minor such as cuts and scratches [Lanza 1988]. A Canadian-based study of violent incidents patterns in a general psychiatric hospital also reported that 5% of injuries from 133 violent incidents resulted in scratches [Tam et al. 1996]. Finally, a previously cited US-based study of violence within a locked university-based short-term Forensic inpatient unit reported that 9% of staff injuries (n injuries or incidents not stated) resulted in abrasions or scratches [Lam et al. 2000]. The latter study was one of 11 studies that made referenced to bumps, bruises and/or knocks as a consequence of a violent/aggressive incident. It stated that 32% of staff injuries resulted contusions or bruises. As previously mentioned, a retrospective study of patterns of aggression in an Australian forensic psychiatric hospital reported that mild-moderate injuries such as bruises, sprains, or welts occurred in 20.3% of 197 incidents [Daffern et al. 2003]. Also previously mentioned, an Australian-based retrospective study found that 3.2% of 328 incidents resulted in staff being knocked or pushed to the floor over a two year period at a psychiatric hospital [Grainger and Whiteford 1993]. A 12 month study of violent incidents in a Swedish inpatient psychiatric ward revealed that in 9.8% of 41 violent incidents, staff suffered bruises or minor wounds [Omerov and Wistedt 1997], while a one year study of a US-based Veterans unit reported that 27.5% of 40 incidents resulted in to bruising [Murray and Snyder 1991]. A prospective two year study of the nature of accidents in a 2400 patients from a US-based psychiatric hospital reported that the majority of the injury reports concerned trivial injuries such as bruising [Abbott 1978], while a UK-based study which studied physical assaults in a psychiatric unit of a general hospital found that over a 12 month period 15 victims sustained mild bruising from 37 incidents [Edwards et al. 1988]. A study that preliminarily evaluated the data collected during ASAP’s first 90 days reported that the type of staff injury most often sustained were bruises with swelling (37% from 67 recorded assaults) [Flannery et al. 1991]. A UK-based exploratory study of coping strategies used by staff in an acute psychiatric inpatient unit following a patient assault reported that some assaults over a 3 week period resulted in bruises or swelling [Whittington and Wykes 1991]. As previously stated, a study of patient assaults over a 27 month period in a Canadian psychiatric hospital reported that most of the 201 recorded violent/aggressive incidents resulted in lacerations, bruising and sprains [Cooper and Medonca 1991]. Finally, a US-based study of nursing staff characteristics related to patient assault reported that over a 1 year period, most reported assaults were judged as minor, many of which were cuts, scratches, soreness, and/or bruises [Lanza et al. 1991]. Five of the aforementioned studies reported the total number of violent/aggressive incidents as well as the total

number of bumps/bruises/knocks from these incidents. From this data, a mean and standard deviation bumps, bruises and/or knocks data was calculated (see table 2).
Six studies reported a bone injury as a consequence to aggression/violence. This included a retrospective study of staff injuries over a two year period in one Australian psychiatric hospital in which 1.1% of 328 incidents resulted bone fractures or suspected fractures [Grainger and Whiteford 1993]. A retrospective study of two Swedish ‘psychosis wards’ reported that from the 7 (17%) incidents in which the staff member was seriously injured, the most serious injuries included a finger fracture and a fracture of the coccyx [Omerov et al. 2004]. lacerations and muscle injuries. Another study presented a case study of an aggressive and self-harming patient in a US-based psychiatric hospital who caused 25 injuries to nursing staff over a 39 month study period which included bone fractures [Bisconer et al. 2006]. Two of the aforementioned ASAP studies also referred to this type of injury – specifically that 5.8% of 460 staff assault incidents within acute psychiatric inpatient settings resulted in bone/tendon/ligament injuries [Flannery, Jr. et al. 2007], and that over a one year period, 3% of 193 staff assaults resulted in bone/tendon/ligament injuries [Flannery, Jr. et al. 2003]. Finally, a US-based 6 month prospective study of repeatedly assaultive psychiatric inpatients found that 21 of 497 recorded incidents resulted in ‘serious’ injuries including bone fractures and suspected fractures [Convit et al. 1990]. A serious open wound/laceration was reported to be a consequence of violence/aggression by six studies, including the latter study. Further, a case study of an aggressive and self-harming patient in a US-based psychiatric hospital was reported to cause an unspecified number of lacerations to staff [Bisconer et al. 2006]. Further, a retrospective examination of ASAP data found that 9% of 193 staff assaults over a one year period resulted in an open wound injury [Flannery, Jr. et al. 2003]. A Canadian-based, prospective 27 month study of patient assaults in a psychiatric hospital reported that most of the 201 recorded violent/aggressive incidents resulted in lacerations, bruising and sprains [Cooper and Medonca 1991]. Another US-based 6 month prospective study of severely disturbed female patients at a 23 bed psychiatric unit reported that out of 87 violent incidents, staff injuries were ‘primarily lacerations’ [Ionno 1983]. Finally, a prospective 6 month observational study of a female
Table 2: Bumps/bruises/knocks rate data
Study authors N Incidents N bumps/ bruises/knocks
% bumps/ bruises/knocks
Daffern et al (2003) 197 40 20.30%
Grainger & Whiteford (1993) 328 13 4%
Omerov & Wistedt (1997) 24 4 16.7%
Murray & Snyder (1991) 40 11 27.5%
Edwards et al (1988) 37 15 40.5%
Flannery et al (1991) 67 25 37.3%
Mean (SD) 115.5 (122) 18 (12.7) 15.6%

observation ward in a Northern Irish general psychiatric hospital reported one serious injury where a patient intentionally struck their head on wall and sustained a serious laceration but no fracture [Cooper et al. 1983]. Two studies reported that victims of the staff assaults suffered from burn injuries : one which retrospectively investigated staff injuries over a two year period in an Australian psychiatric hospital that found that 1.9% of 328 incidents resulted in this injury [Grainger and Whiteford 1993]; and one which prospectively studied of repeatedly assaultive inpatients which reported that 4.2% of 497 recorded incidents resulted in ‘serious’ injuries such as burns [Convit et al. 1990]. The former study also reported that 3.2% of 328 incidents were biting injuries and that 1.9% of 328 incidents resulted in a loss of consciousness or concussion. The aforementioned case study of an aggressive and self-harming patient in a US-based psychiatric hospital also reported concussion as a consequence of violence/aggression [Bisconer et al. 2006]. Four studies reported that the incurred physical injury resulted in less than 10 minutes of pain while two of these studies also reported that the injury resulted in more than 10 minutes of pain. Specifically, one study which examined aggression among psychiatric inpatients in Australian rehabilitation wards found that 7.6% of 806 incidents resulted in pain lasting up to 10 minutes only, and that 2.6% of these incidents resulted in pain lasting more than 10 minutes [Cheung et al. 1996]. A study of aggressive behaviour in UK acute psychiatric wards reported that 2.3% of 264 aggressive incidents resulted in pain for the victim that lasted less than 10 minutes incidents, whereas in 1.9% of these incidents the pain lasted beyond 10 minutes [Foster et al. 2007]. A retrospective study of two Norwegian acute psychiatric inpatient wards over a seven year period found that 59% of 507 violent/aggressive incidents resulted in injuries that resulted in less than 10 minutes of pain [Langsrud et al. 2007]. A retrospective study of two Norwegian acute psychiatric inpatient wards over a seven year period found that 38.1% of 507 violent/aggressive incidents resulted in head injuries [Langsrud et al. 2007], while a Swedish study which examined assaults on staff by acute psychiatric inpatients showed reported that in 95% of 137 incidents, the pain of any injury lasted less than 10 minutes [Omerov et al. 2002]. Developing a headache as a consequence of violence/aggression was cited by three studies. This included a one year study of a US-based Veterans unit in which 1 of the 40 incidents resulted in a headache for the victim [Murray and Snyder 1991]. Headaches were reported to be one of the most commonly reported symptoms immediately following an assault on staff at a UK-based acute psychiatric inpatient unit [Whittington and Wykes 1991] while, a US-based study of patient assault cited this symptom as a consequence of violence [Lanza 1988]. Severity of physical injury Thirty-two of the 61 studies which reported a physical injury as a consequence of violence/aggression also reported the severity of the reported injury. Twenty-three of these studies reported the number of physical injuries that were classed as minor, moderate, and/or as a serious injury (see Table 4) [Abeyasinghe and Jayasekera 2003;Brizer et al. 1988;Casseem 1984;Convit et al. 1990;Cooper et al. 1983;Crowner

et al. 1994;Daffern et al. 2003;Daffern et al. 2003;Edwards et al. 1988;Flannery, Jr. et al. 2007;Foster et al. 2007;Grainger and Whiteford 1993;Kennedy et al. 1995;Maier et al. 1994;Mellesdal 2003;Miller et al. 1993;Murray and Snyder 1991;Nijman and Rector 1999;Omerov et al. 2004;Omerov and Wistedt 1997;Palmstierna et al. 1991;Powell et al. 1994;Torpy and Hall 1993], while nine studies did not this breakdown ([Abbott 1978;Bisconer et al. 2006;Carton and et al. 2003;Cheung et al. 1996;Hodgkinson et al. 1984;Hunter and Love 1993;Joyal et al. 2008;Pearson et al. 1986;Whittington and Wykes 1991]. As can be seen in table 3, eighteen studies reported both the number of minor/moderate/serious injuries as well as the number of total recorded injuries. Table 4 examines the differences in rates across settings, country, and data source after controlling for the total number of violent/aggressive incidents and physical injuries per study.
Table 3: Severity of injuries rate data
N moderate severity (% of
injuries)
N serious severity
(% of injuries)
Study authors
N mild severity (% of
injuries)
Total injuries
recorded Setting Country Data source
Nijman & Rector (1999) 18 (100%) 18 Acute Netherlands
SOAS-R
Daffern et al (2003) 40 (100%) 40 Forensic Australia Incident forms
Grainger & Whiteford (1993) 36 (7.7%) 465 Acute Australia Incident forms
Omerov et al (2004) 15 (68%) 7 (32%) 22 Acute Sweden Interview
Omerov & Wistedt (1997) 16 (100%) 16 Acute Sweden Official records
Daffern et al (2003) 17 (100%) 17 Forensic Australia Incident forms
Mellesdal (2003) 21 (20%) 106 Acute Norway Official records
Powell et al (1994) 40 (22.7%) 176 Mix UK Incident forms
Kennedy et al (1995) 280 (80.9%) 66 (19.1%) 346 Forensic UK Incident forms
Maier et al (1994) 44 (10.7%) 412 Forensic USA OAS
Murray & Snyder (1991) 19 (70.3%) 5 (18.5%) 3 (11.1%) 27 Veterans USA Observation
Crowner et al (1994) 16 (89%) 1 (5.5%) 1 (5.5%) 18 Acute USA Video recording
Brizer et al (1995) 1 (100%) 1 Acute USA Video recording
Edwards et al (1988) 15 (100%) 15 Mix UK Interview
Convit et al (1990) 21 Not stated Acute USA Incident forms
Foster et al (1994) 13 2 Not stated Acute UK SOAS-R
Torpy & Hall (1993) 20 Not stated Forensic UK Incident forms
Abeyasinghe & Jayasekers (2003) 33 (68.8%) 15 (32.2%) 48 Acute Sri Lanka Study questionnaire
Flannery et al (2007) 170 (37%) 145 (31.5%) 65 (14.1%) 460 Acute USA ASAP
Miller et al (1993) 365 Not stated Mix Australia Incident forms
Palmstierna et al (1991) 31 (94%) 2 (6%) 33 PICU Sweden SOAS
Casseem (1994) 2 Not stated Mix UK Incident forms
Cooper et al (1983) 30 (96.7%) 1 (3.3%) 31 Mix UK Incident forms

Rates of physical injuries Thirty studies reported the total number of violent/aggressive incidents as well as the total number of the physical injuries resulting from these incidents. The mean number of violent/aggressive incidents among these studies was 548 (SD=679), and the mean number of physical injuries was 148 (SD=183). As can be seen in table 5, the mean number of violent/aggressive incidents per study was substantially higher within forensic studies compared to acute and other settings. It also shows that the mean number of physical injuries per study within forensic settings is slightly higher than in acute settings. However, the likelihood of experiencing a physical injury as a consequence of an incident is nearly twice as high within acute settings compared to forensic settings, but similar to mixed settings. The mean number of recorded incidents and physical injuries was found to similar across countries. However, the likelihood of experiencing a physical injury during an incident was revealed to be higher within Australia and other non-UK and non-USA countries. The mean number of physical injuries was more than twice the number within incident forms compared to the SOAS/R and other forms of data sources, while the mean number of physical injuries was also higher within incident forms compared to all other sources. However, the likelihood of experiencing a physical injury during an incident was revealed to be fairly similar across data sources.
Table 4: Injury severity rates
Grouping variable
Percentage of
mild injuries per incident
(SD) [n studies]
Percentage of moderate-
severity per incident (SD)
[n studies]
Percentage of serious injuries
per incident (SD)
[n studies]
Percentage of mild injuries per injury (SD)
[n studies]
Percentage of moderate-
severity per injury (SD) [n studies]
Percentage of serious
injuries per injury (SD) [n studies]
All studies 26% (18) [13] 11% (10) [5] 6% (6) [18] 85% (20) [13] 19% (30) [3] 35% (52) [13]
Setting: Acute (including PICU) 27% (21) [7] 5% (4) [3] 8% (7) [10] 80% (23) [7] 19% (18) [2] 48% (64) [8] Setting: Forensic 18% (12) [3] - 4% (3) [3] 94% (11) [3] - 15% (6) [2] Setting: Mix 27% (18) [2] 28% (-) [1] 2% (2) [3] 98% (2) [2] - 13% (14) [2]
Country: UK 28% (13) [3] 5% (-) [1] 3% (2) [6] 93% (10) [3] - 15% (10) [3] Country: USA 23% (21) [3] 7% (6) [3] 4% (2) [6] 65% (26) [3] 19% (13) [3] 28% (40) [5] Country: Australia 13% (11) [2] 28% (-) [1] 5% (8) [2] 100% (-) [2] - 8% (-) [1] Country: Any other 33% (21) [5] - 13% (8) [4] 86% (16) [5] - 64% (82) [4]
Data source: Incident forms 21% (7) [3] 28% (-) [1] 4% (4) [8] 93% (10) [3] - 13% (9) [4] Data source: SOAS/R 24% (14) [3] 5% (-) [1] 7% (9) [3] 87% (17) [3] - 19% (18) [2] Data source: Any other 30% (23) [7] 7% (6) [3] 7% (7) [7] 81% (24) [7] 19% (13) [3] 51% (68) [7]

Containment/staff response Half of all studies with consequences/outcomes data reported 15 different types of containment/staff responses in relation to violence/aggression (n=54, 50%). Thirty nine studies (36.1%) reported seclusion as a consequence of violence/aggression. Twenty two of these studies did not report the total number of seclusion episodes as well as the total number of violent/aggressive incidents. This included a US-based study of repeated inpatients assaults within a ‘Veterans’ hospital which found that measures such as seclusion, transfer to a maximum-security treatment program, or transfer to jail for confinement were used in 4.7 % of 422 assaults [Blow et al. 1999]. Another US-based study that investigated the relationship between psychopathy and violence in a forensic setting and reported that 17% of their patient sample were either secluded or restrained in the first 2 months of hospitalisation while 8.5% of their sample were either secluded or restrained in the last 2 months of hospitalisation [Heilbrun 1998]. Another US-based study that revealed that violent inpatients within acute settings are significantly more frequently secluded than non-violent patients [Krakowski and Czobor 1997]. An exploratory investigation into the nursing management of aggression in Australian acute psychiatric settings found that patients were secluded after 61% of incidents (although the total number of incidents was not reported) [Delaney et al. 2001], while a retrospective UK-based study of the management of psychiatric inpatient violence found that black patients were more likely than white patients to be secluded after a violent incident (however, these differences disappeared when other variables were considered), and that the strongest predictors of seclusion were the gender of patient, nurse being a target, patient being rated as agitated, extent of injury, age of patient and being on a civil section [Gudjonsson et al. 2004]. A US-based study of staff injuries
Table 5: Rates of physical injury
Grouping variable Mean (SD) Incidents [n studies]
Mean (SD) Physical Injuries
[n studies]*
Percentage of injuries controlling
for incidents (injuries N / Incident
N * 100) [n studies]*
All studies 521 (583) [61] 148 (183) [30] 37% (35) [30]
Setting: Acute (including PICU) 345 (408) [27] 166 (217) [13] 43% (44) [13] Setting: Forensic 907 (814) [16] 201 (199) [8] 23% (15) [8] Setting: Mix 441 (419) [15] 88 (77) [7] 40% (32) [7]
Setting: Any other 441 (384) [3] 20 (11) [2] 35% (46) [2]
Country: UK 501 (549) [19] 107 (127) [7] 29% (17) [7] Country: USA 690 (788) [15] 193 (198) [10] 35% (31) [10] Country: Australia 631 (448) [8] 134 (221) [4] 43% (66) [4] Country: Any other 362 (462) [19]] 135 (205) [9] 41% (37) [9]
Data source: Incident forms 716 (656) [25] 227 (170) [10] 34% (39) [10] Data source: SOAS/R 306 (236) [17] 131 (249) [6] 40% (45) [6]
Data source: Any other 457 (637) [19] 98 (151) [14] 37% (29) [14]
* = only studies which reported physical injuries were included in calculation

and violence in a forensic psychiatric setting reported that restraints were used were in 48% of seclusion episodes [Morrison et al. 2002], while the same lead author in an earlier 7 month, observational study of violent psychiatric inpatients at a public hospital reported that seclusion was used on a daily basis and that it was common for several patients to be in seclusion at the same time [Morrison 1990]. A UK-based study of physical assaults in a general hospital psychiatric unit revealed that ‘some degree of physical restraint or seclusion (with or without psychotropic drugs) was exercised after 24 incidents’ [Edwards et al. 1988], while another UK-based study found that the combined containment methods of medication, restraint and seclusion were used in 47% (n=103) cases within one acute psychiatric unit. A US-based study that examined the relationship of staffing to violence by patients in a forensic setting found that there were 2,720 (20.6%) instances of interventions to prevent attack such as seclusion and restraint [Carmel et al. 1991]. A Canadian study examining violence within forensic settings reported that the likelihood of female (77.8%) and male (63.3%) patients being placed in seclusion as a result of aggression differed, although not significantly [Nicholls et al. 2009]. A prospective, 9 month study of aggressive behaviour in a New Zealand-based acute psychiatric unit reported that all of the 80 aggressive patients (15% of the sample) were secluded at some point during their admission [El-Badri and Mellsop 2006]. Similarly, all violent patients in a US-based study of inpatient violence in a maximum security hospital were secluded for their actions [Dietz and Rada 1982]. Additionally, a retrospective study of reported incidents over a five and a half year period in a US-based general hospital and a nursing home found that following a violent incident, an intervention was used in 40% of cases which was most often seclusion, medication, medication and seclusion [Jones 1985]. Another US-based study of 6 case reports of psychiatric patients considered what the impact of therapist counter- transference was. They reported that the use of containment was seen to exaggerate the patients’ dangerousness as violence grew once in they were in seclusion [Lion and Pastermak 1973]. Another US-based, 6 month prospective study of severely disturbed female patients at a 23 bed acute psychiatric unit reported that seclusion was used more with psychotic patients than other patients [Ionno 1983]. A German study of aggressive behaviour among first admission patients with schizophrenia at a general psychiatric hospital reported 22% of these patients were placed in seclusion as a consequence of aggression during their admission [Steinert et al. 1999]. An Australian-based prospective, 7 month study of violent incidents within inpatient psychiatric settings reported that non-recidivist patients were more likely to be secluded after an incident [Owen et al. 1998]. A retrospective study of aggression in an Australian forensic psychiatric hospital that reported 253 seclusion episodes out of 197 incidents (128%) over the course of a year [Daffern et al. 2003].A study of 40 hospital wards in the USA and Canada were surveyed during specified periods for 1 year to document assaults by inpatients on staff or other pts. They revealed that about two thirds of all incidents led to seclusion or restraint [Reid et al. 1989]. Additionally, a UK-based study on the development of the 'attacks' scale (attempted and actual assault scale) revealed that within acute psychiatric services, only 2 incidents of seclusion were reported in response to violence (total number of incidents not stated) [Bowers et al. 2002]. Finally, 54% of violent patients in a forensic hospital were secluded in a 6 month prospective study [Larkin et al. 1988]. Sixteen studies reported the total number of seclusion episodes as well as the total number of violent/aggressive incidents. The highest rate of seclusion was reported by

a UK-based retrospective study of violent incidents on two PICUs in which 87% of 116 incidents resulted in the patient being secluded following an incident over a course of one year [Coldwell and Naismith 1989]. The next highest rate was substantially lower: 49% of 164 incidents in a Dutch acute psychiatric admissions ward over a 24 week period [Nijman et al. 1997]. Seclusion was used in 26% of 536 incidents over a 3 year period in a US-based medium secure unit [Parkes 2003], 25% of 264 incidents over a 10 month period in 5 UK-based acute wards [Foster et al. 2007], 20.6% of 331 incidents over a 6 month period in an Australian forensic psychiatric hospital [Daffern et al. 2003], 18% of 257 incidents over a 6 month period in a Canadian maximum security hospital [Joyal et al. 2008], 16% of 50 incidents over a 6 month period in three Australian forensic wards [Daffern et al. 2003], and 15% of 208 incidents over a 6 month period in a female observation ward within a Northern-Irish general psychiatric hospital [Cooper et al. 1983]. It was also used in 15% of 820 incidents over a 3 year period in a UK-based medium secure unit [Torpy and Hall 1993], 14% of 760 incidents in 24 Swiss-based acute psychiatric wards [Abderhalden et al. 2007], 13% of 512 incidents over a 7 year period in two Norwegian acute psychiatric wards [Langsrud et al. 2007], 13% of 441 incidents over a 1 year period in a German general psychiatric hospital [Ketelsen et al. 2007], 12% of 963 incidents in 2 UK-based forensic and 1 UK-based PICUs [Mills 1997], 6% of 1289 incidents over a 3 month period in 2 units located in an Australian primary psychiatric hospital and a 6 month period in 3 acute psychiatric units of an Australian general hospital [Owen et al. 1998], 4% of 2180 incidents in a UK-based medium secure unit [Gudjonsson et al. 2000] and 2% of 130 incidents over a 5 month period in a large NHS psychiatric hospital [Shepherd and Lavender 1999]. Seclusion rate Using the total number of seclusion episodes as well as the total number of violent/aggressive incidents reported in the above seventeen studies, a percentage statistic representing the likelihood of incident resulting in seclusion was calculated. Across all studies which reported at seclusion use (as well as the total number of violent/aggressive incidents), the mean percentage of this statistic was found to 20.89% (SD = 20.7) (see table 5). Table 6 also shows that that the mean number of seclusion episodes per study within forensic settings is slightly higher than in acute settings and more than twice as high compared to other settings. However, the likelihood of a patient experiencing seclusion as a consequence of an incident is more than twice as high within acute settings compared to forensic settings, and even higher compared to mixed settings. The mean number of recorded seclusion episodes and the likelihood of experiencing seclusion as a consequence of violence/aggression was found to be slightly lower within Australia compared to the UK and other countries. Additionally, both the mean number of recorded seclusion episodes and the likelihood of experiencing seclusion as a consequence of violence/aggression were found to be very similar between incident forms and SOAS/R data sources.

Another containment method in response to violence/aggression was manual restraint (non-mechanical) which was reported by twenty-three studies (21.3%), six of which did not report the total number of restraint episodes as well as the total number of violent/aggressive incidents [Gudjonsson et al. 2000] [Edwards et al. 1988] [Duxbury 2002] [Omerov et al. 2002] [Bowers et al. 2002] [Harris et al. 1986]. Eighteen studies did report the total number of physical restraint episodes as well as the total number of violent/aggressive incidents. The highest rate of manual restraint was reported to be 84% of 507 incidents over a seven year period in two Norwegian acute psychiatric inpatient wards [Langsrud et al. 2007]. The next highest rate of restraint was found to be 78% of 116 incidents over a course of a year within two UK-based PICUs [Coldwell and Naismith 1989], followed by 76% of 1144 incidents over a 6 month period within one UK-based forensic hospital [Larkin et al. 1988], 67% of 2180 incidents over a 17 year period in a UK- based medium secure unit [Gudjonsson et al. 2000], and 57% of 3874 incidents within UK-based general psychiatric units across 10 NHS trusts [Dowson et al. 1999]. Additionally, restraint was used in 38% of 130 incidents over a 5 month period within a large NHS psychiatric hospital [Shepherd and Lavender 1999], 38% of 477 incidents over an eight week period within 11 Australian-based psychiatric rehabilitation wards [Cheung et al. 1997], 36% of 981 incidents over a 4 year period within a UK-based forensic unit [Kennedy et al. 1995], 33% of 124 incidents over a 9 month period in a New Zealand-based acute psychiatric unit [El-Badri and Mellsop 2006] and 26% of 355 incidents over the course of a year within one UK-based general psychiatric hospital [Tobin et al. 1991]. Lower physical restraint rates were reported to be 21% of 409 incidents over a 7 year period within one Italian 15-bed acute inpatient unit [Grassi et al. 2006], 19% of 1289 incidents over a 3 month period in 2 units located in an Australian primary psychiatric hospital and a 6 month period in 3 acute psychiatric units of an Australian general hospital [Owen et al. 1998], 17% of 441 incidents over a 1 year period in a German general psychiatric hospital [Ketelsen et al. 2007], 17% of 963 incidents in 2 UK-based forensic and 1 UK-based PICUs [Mills 1997], and 12% of 820 incidents over a 3 year period in a UK-based medium secure unit [Torpy and Hall 1993]. The lowest reported physical restraints were reported to be 10% of 264 incidents over a 10 month period in 5 UK-based acute wards [Foster et al. 2007], 5% of 257 incidents over a 6
Table 6: Rates of seclusion
Grouping variable Mean (SD) Incidents [n studies]
Mean (SD) Seclusion episodes
[n studies]*
Percentage of seclusions controlling
for incidents (seclusion N / Incident N * 100)
[n studies]*
All studies 516 (584) [61] 76 (36) [16] 21% (21) [16]
Setting: Acute (including PICU) 345 (408) [27] 84 (21) [5) 38% (31) [5] Setting: Forensic 908 (814) [16] 90 (37) [7] 16% (7) [7] Setting: Mix 441 (419) [15] 42 (33) [4] 9% (6) [4]
Country: UK 501 (549) [19] 74 (44) [7] 23% (29) [7] Country: Australia 594 (474) [8] 65 (14) [3] 14% (7) [3]
Country: Any other 506 (639) [34] 83 (36) [6] 22% (14) [6]
Data source: Incident forms 716 (656) [25] 81 (48) [8] 22% (27) [8] Data source: SOAS/R 306 (236) [17] 75 (21) [5] 23% (15) [5]
Data source: Any other 457 (637) [19] 62 (13) [4] 17% (7) [4]
* = only studies which reported seclusion episodes were included in calculation
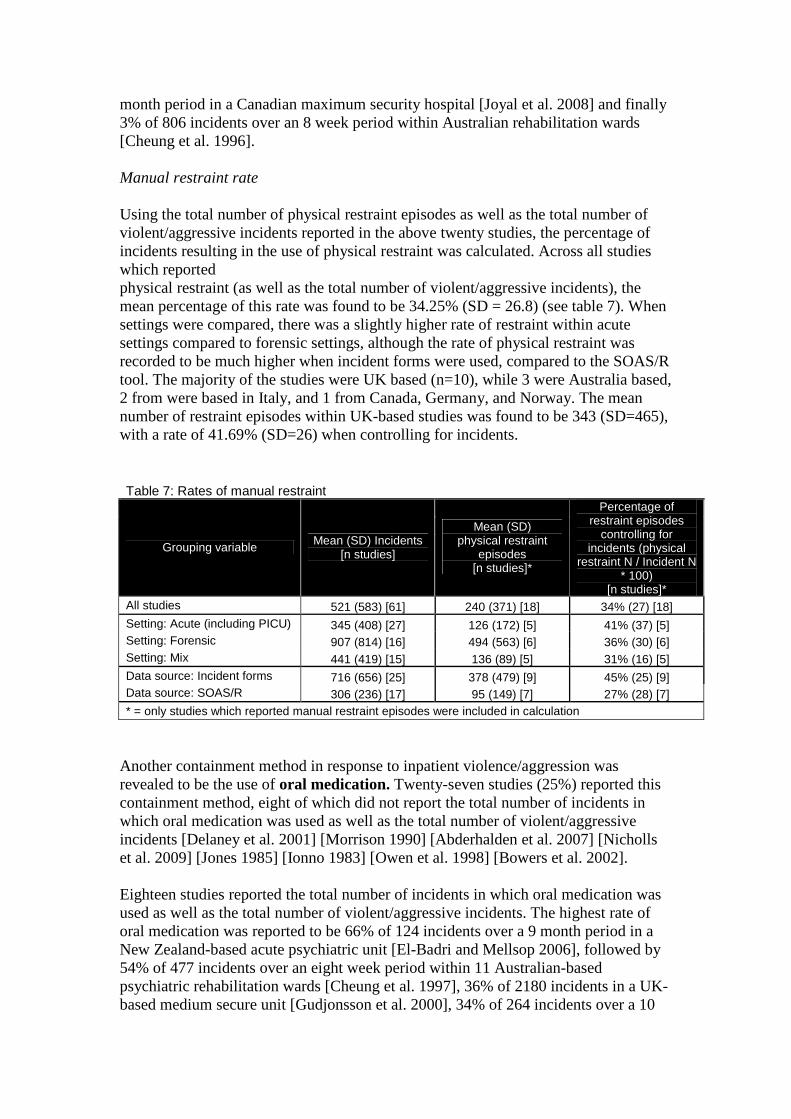
month period in a Canadian maximum security hospital [Joyal et al. 2008] and finally 3% of 806 incidents over an 8 week period within Australian rehabilitation wards [Cheung et al. 1996]. Manual restraint rate Using the total number of physical restraint episodes as well as the total number of violent/aggressive incidents reported in the above twenty studies, the percentage of incidents resulting in the use of physical restraint was calculated. Across all studies which reported physical restraint (as well as the total number of violent/aggressive incidents), the mean percentage of this rate was found to be 34.25% (SD = 26.8) (see table 7). When settings were compared, there was a slightly higher rate of restraint within acute settings compared to forensic settings, although the rate of physical restraint was recorded to be much higher when incident forms were used, compared to the SOAS/R tool. The majority of the studies were UK based (n=10), while 3 were Australia based, 2 from were based in Italy, and 1 from Canada, Germany, and Norway. The mean number of restraint episodes within UK-based studies was found to be 343 (SD=465), with a rate of 41.69% (SD=26) when controlling for incidents. Table 7: Rates of manual restraint
Grouping variable Mean (SD) Incidents [n studies]
Mean (SD) physical restraint
episodes [n studies]*
Percentage of restraint episodes
controlling for incidents (physical
restraint N / Incident N * 100)
[n studies]* All studies 521 (583) [61] 240 (371) [18] 34% (27) [18] Setting: Acute (including PICU) 345 (408) [27] 126 (172) [5] 41% (37) [5] Setting: Forensic 907 (814) [16] 494 (563) [6] 36% (30) [6] Setting: Mix 441 (419) [15] 136 (89) [5] 31% (16) [5] Data source: Incident forms 716 (656) [25] 378 (479) [9] 45% (25) [9] Data source: SOAS/R 306 (236) [17] 95 (149) [7] 27% (28) [7] * = only studies which reported manual restraint episodes were included in calculation
Another containment method in response to inpatient violence/aggression was revealed to be the use of oral medication. Twenty-seven studies (25%) reported this containment method, eight of which did not report the total number of incidents in which oral medication was used as well as the total number of violent/aggressive incidents [Delaney et al. 2001] [Morrison 1990] [Abderhalden et al. 2007] [Nicholls et al. 2009] [Jones 1985] [Ionno 1983] [Owen et al. 1998] [Bowers et al. 2002]. Eighteen studies reported the total number of incidents in which oral medication was used as well as the total number of violent/aggressive incidents. The highest rate of oral medication was reported to be 66% of 124 incidents over a 9 month period in a New Zealand-based acute psychiatric unit [El-Badri and Mellsop 2006], followed by 54% of 477 incidents over an eight week period within 11 Australian-based psychiatric rehabilitation wards [Cheung et al. 1997], 36% of 2180 incidents in a UK-based medium secure unit [Gudjonsson et al. 2000], 34% of 264 incidents over a 10

month period in 5 UK-based acute wards [Foster et al. 2007], 34% of 116 incidents over a course of a year within two UK-based PICUs [Coldwell and Naismith 1989], and 34% of 41 incidents within two Swedish ‘psychosis wards’ [Omerov et al. 2004]. The next highest rates were recorded as 28% of 1289 incidents over a 3 month period in 2 units located in an Australian primary psychiatric hospital and a 6 month period in 3 acute psychiatric units of an Australian general hospital [Owen et al. 1998], 25% of 221 incidents within one UK-based mental health unit that comprised of three acute wards [Duxbury 2002], 24% of 355 incidents over the course of a year within one UK-based general psychiatric hospital [Tobin et al. 1991], 21% of 806 incidents over an 8 week period within Australian rehabilitation wards [Cheung et al. 1996], and 21% of 130 incidents over a 5 month period within a large NHS psychiatric hospital [Shepherd and Lavender 1999]. Lower rates of oral medication use were reported to be 17% of 409 incidents over a 7 year period within one Italian 15-bed acute inpatient unit [Grassi et al. 2006], 16% of 257 incidents over a 6 month period in a Canadian maximum security hospital [Joyal et al. 2008], 13% of 981 incidents over a 4 year period within a UK-based forensic unit [Kennedy et al. 1995], and 13% of 24 incidents over a 12 month period in one Swedish inpatient psychiatric [Omerov and Wistedt 1997]. The lowest recorded rates were 9% of 507 incidents over a seven year period in two Norwegian acute psychiatric inpatient wards [Langsrud et al. 2007], 8% of 37 incidents over a a one year period in a UK-based psychiatric unit of a general hospital [Edwards et al. 1988], 7% of 137 incidents over a 3 year period within one Swedish-based acute psychiatric ward [Omerov et al. 2002], and 3% of 208 incidents over a 6 month period in a female observation ward within a Northern-Irish general psychiatric hospital [Cooper et al. 1983]. Oral medication rate Using the total number of oral medication episodes as well as the total number of violent/aggressive incidents reported in the above nineteen studies, the percentage of incidents resulting in the use of oral medication was calculated. Across all studies which reported oral medication restraint (as well as the total number of violent/aggressive incidents), the mean percentage of this rate was found to be 24% (SD = 16) (see table 8). When settings were compared, there was a slightly higher rate of oral medication within acute settings compared to forensic settings and mixed settings, while no differences of note were revealed when comparing data sources. The majority of the studies were UK based (n=9), while 3 were based in Sweden, 3 from Australia, 1 from Italy, Canada, New Zealand, Norway, and Sweden. The mean number of restraint episodes within UK-based studies was found to be 135 (SD=246), with a rate of 22% (SD=12) when controlling for incidents. Another medication-based containment method that was reported by the literature to be used in response to inpatient violence/aggression was intra-muscular medication. This was reported by fourteen studies (12.8%) reported this containment method, six of which did not report the total number of incidents in which intra-muscular medication was used as well as the total number of violent/aggressive incidents [Gudjonsson et al. 2004] [Tardiff 1983] [Abderhalden et al. 2007] [Steinert et al. 1999] [Bowers et al. 2002] [Turns and Gruenberg 1973] Omerov, Edman, & Wistedt 2002).

Table 8: Rates of oral medication
Grouping variable Mean (SD) Incidents [n studies]
Mean (SD) oral medication
episodes [n studies]*
Percentage of oral medication controlling
for incidents (oral medication N /
Incident N * 100) [n studies]*
All studies 521 (583) [61] 111 (183) [19] 24% (16) [19]
Setting: Acute (including PICU) 345 (408) [27] 45 (32) [9] 27% (18) [9] Setting: Forensic 907 (814) [16] 318 (406) [3] 22% (12) [3] Setting: Mix 441 (419) [15] 96 (152) [5] 17% (11) [5]
Data source: Incident forms 716 (656) [25] 179 (299) [6] 22% (13) [6] Data source: SOAS/R 306 (236) [17] 69 (51) [8] 25% (15) [8] Data source: Any other 457 (637) [19] 98 (151) [5] 26% (24) [5]
* = only studies which reported oral medication were included in calculation Six studies reported the total number of incidents in which intra-muscular medication was used as well as the total number of violent/aggressive The highest rates of intra-muscular medication were reported by the same lead author: 46% of 41 incidents within two Swedish ‘psychosis wards’ [Omerov et al. 2004], and 29% of 24 incidents over a 12 month period in a Swedish inpatient psychiatric ward [Omerov and Wistedt 1997]. Lower rates of intra-muscular medication included 16% of 441 incidents over a 1 year period in a German general psychiatric hospital [Ketelsen et al. 2007], 10% of 477 incidents over an eight week period within 11 Australian-based psychiatric rehabilitation wards [Cheung et al. 1997], 3% of 806 incidents over an 8 week period within Australian rehabilitation wards [Cheung et al. 1996], and 3% of 257 incidents over a 6 month period in a Canadian maximum security hospital [Joyal et al. 2008]. Intra-muscular medication rate Using the total number of intra-muscular medication episodes as well as the total number of violent/aggressive incidents reported in the above six studies, the percentage of incidents resulting in the use of intra-muscular medication was calculated. Across all studies which reported this containment method (as well as the total number of violent/aggressive incidents), the mean percentage of this rate was found to be 17.91% (SD = 17.1). Country, setting and data source comparisons were not calculated due to lack of study numbers. A total of sixteen studies (14.8%) reported time out/patient removed from the situation. Three of these studies did not report the number of time out episodes as well as the total number of violent/aggressive incidents [Kennedy et al. 1995] [Morrison 1990] [Bowers et al. 2002]. Of the 13 which did report these data, the highest reported rate of time out use was reported to be 45% of 181 incidents over an eight week period within 11 Australian-based psychiatric rehabilitation wards [Cheung et al. 1997], followed by 37% of 257 incidents over a 6 month period in a Canadian maximum security hospital [Joyal et al. 2008], and 27% of 806 incidents over an 8 week period within Australian rehabilitation wards [Cheung et al. 1996]. Other reported rates included 21% of 1289 incidents over a 3 month period in 2 units located in an Australian primary psychiatric hospital and a 6 month period in 3 acute psychiatric units of an Australian general hospital [Owen et al. 1998], 21% of 24 incidents over a 12 month period in one Swedish inpatient psychiatric [Omerov and

Wistedt 1997], 20% of 264 incidents over a 10 month period in 5 UK-based acute wards [Foster et al. 2007], 15% of 41 incidents within two Swedish ‘psychosis wards’ [Omerov et al. 2004], and 14% of 409 incidents within over a 7 year period within one Italian 15-bed acute inpatient unit [Grassi et al. 2006]. Lower rates of time out included 11% of 507 incidents over a seven year period in two Norwegian acute psychiatric inpatient wards [Langsrud et al. 2007], 7% of 164 incidents over a 24 week period in a Dutch-based acute psychiatric admissions ward [Nijman et al. 1997], 7% of 137 incidents over a 3 year period within one Swedish-based acute psychiatric ward [Omerov et al. 2002], and 5% of 130 incidents over a 5 month period within a large NHS psychiatric hospital [Shepherd and Lavender 1999]. The lowest reported rate of time out was found to be 4% of 2180 incidents over a 17 year period in a UK-based medium secure unit [Gudjonsson et al. 2000]. Time-out/patient removed from the situation medication rate Using the total number of time out episodes as well as the total number of violent/aggressive incidents reported in the above eight studies, the percentage of incidents resulting in the use of time-out was calculated. Across all studies which reported this containment method (as well as the total number of violent/aggressive incidents), the mean percentage of this rate was found to be 18.02% (SD = 12.4). The mean number of time-out episodes within acute-based studies (n=7) was 28.4 (SD = 25.3), while the average rate of use was found to be 13.6% (SD = 5.6). This data could not be meaningfully compared to forensic (n=2) and other settings (mixed settings: n=2; rehabilitation settings: n=2). The mean number of episodes recorded by SOAS/R was found to be 61.63 (SD = 68.8), while the average recorded rate of use was found to be 18.3% (SD = 12.6). This data source could not be meaningfully compared to other data sources due to lack of study numbers, while country comparisons were also not calculated for the same reason. Another frequently cited containment method was verbal de-escalation which was reported by 12 studies, 3 of which did not report the number of verbal de-escalation episodes and/or the total number of violent/aggressive incidents [Kennedy et al. 1995] [Ionno 1983] [Morrison 1990]. Of the nine studies which did report these data, the highest reported rate of verbal de-escalation in response to violence/aggression was reported to be 70% of 806 incidents over an 8 week period within Australian rehabilitation wards [Cheung et al. 1996]. This containment method was also used for 42% of 264 incidents over a 10 month period in 5 UK-based acute wards [Foster et al. 2007], 35% of 507 incidents over a 7 year period in two Norwegian acute psychiatric wards [Langsrud et al. 2007], 24% of 41 incidents within two Swedish ‘psychosis wards’ [Omerov et al. 2004], 24% of 409 incidents over a 7 year period within one Italian 15-bed acute inpatient unit [Grassi et al. 2006], 23% of 130 incidents over a 5 month period in one NHS psychiatric hospital [Shepherd and Lavender 1999], and 22% of 221 incidents within one UK-based mental health unit that comprised of three acute wards [Duxbury 2002]. Verbal de-escalation was least frequently used by two Swedish-based studies which reported that it was applied in 17% of 24 incidents over a 12 month period in one inpatient psychiatric [Omerov and Wistedt 1997], and applied in only 14% of 137 incidents over a 3 year period within one acute psychiatric ward [Omerov et al. 2002]. The overall mean number of verbal de-escalation episodes across the aforementioned nine studies was found to be 118 (SD = 176.9), while the mean rate of verbal de-escalation was found to be 30.1% (SD = 17.4).

It was reported by seven studies that staff counselled the assailant after the incident ended, four of which did not provide the number of episodes relating to this theme, as well as the total number of violent/aggressive incidents [Omerov et al. 2004] [Kennedy et al. 1995] [Owen et al. 1998] [Cheung et al. 1997]. The three studies which did report these data reported that it was used in 98% of 130 incidents over a 5 month period in a large NHS psychiatric hospital [Shepherd and Lavender 1999], in 47% of 355 incidents over the course of a year within one UK-based general psychiatric hospital [Tobin et al. 1991], and in 9% of 116 incidents over a course of a year within two UK-based PICUs [Coldwell and Naismith 1989]. The use of mechanical restraint as a containment strategy for violence/aggression was reported by nineteen studies (17.6%), five of which reported the total number of mechanical restraint episodes as well as the total number of violent/aggressive incidents. The highest reported rate of mechanical restraint was found to be 46.3% of 41 incidents within two Swedish ‘psychosis wards’ [Omerov et al. 2004], followed by 42% of 24 incidents over a 12 month period in one Swedish inpatient psychiatric involved the use of mechanical restraint [Omerov and Wistedt 1997]. Another study revealed that 24% of 441 incidents over a 1 year period in a German general psychiatric hospital resulted in mechanical restraint [Ketelsen et al. 2007], while 19.6% of 409 incidents over a 7 year period within one Italian 15-bed acute inpatient unit [Grassi et al. 2006] and 13% of 31 incidents over a 6 month period within one Italian-based acute psychiatric unit [Troisi et al. 2003] also resulted in this containment measure. Fifteen studies did not report the total number of mechanical restraint episodes as well as the total number of violent/aggressive incidents. This included a Danish study of inpatient acute setting violence which reported that violent patients were significantly more likely than non-violent patients to be restrained using a leather belt (55.4% vs. 8.9% respectively; OR=12.72, CI=6.83-23.61) [Benjaminsen et al. 1996]. A US-based study of violence in a forensic setting found that 39% of violent incidents resulted in the use of ambulatory restraints and that 13% of incidents resulted in ‘4 or 5 point restraints to the bed’ [Morrison et al. 2002], while another US-based study found that 17% of patients were either secluded or restrained in the first 2 months of hospitalisation, and that 8.5% were either secluded or restrained in the last 2 months of hospitalisation in a forensic hospital [Heilbrun 1998]. Also within the US, it was revealed that violent inpatient acute patients were significantly more frequently restrained or secluded than non-violent patients (F=17.24, p=.0001) [Krakowski and Czobor 1997], while a large-scale 2 month cross-sectional study of a State hospital system reported that violent patients were likely to have receive mechanical restraint during previous month [Tardiff 1983]. It was also reported in a qualitative study that this containment measure is used by nurses in order to effectively control the ward activities in the most efficient manner possible as they saw it, and that many staff prefer to deal with situations using physical restraints rather than taking the time to use verbal techniques [Morrison 1990]. Another US-based study which retrospectively analysed 6 years of ASAP data revealed that assaultive personality disorder patients were significantly more frequently required to be mechanically restrained than assaultive schizophrenic patients [Flannery et al. 2002], while a study examining the relationship of staffing to patient violence over a 56 month period within forensic settings incident reports found that in 36.8% of aggressive incidents, interventions to prevent attack such as seclusion and restraint were used by nursing staff [Carmel et al. 1991]. Another US-based forensic-based

study reported that controlling interventions such as mechanical restraint were used significantly more often for physical aggression towards staff compared to other types of incidents [Parkes 2003], while a German-based study of aggressive behaviour against the self and others among first admission patients with schizophrenia revealed that 5% of patients were mechanically restrained [Steinert et al. 1999]. Another US-based study reported that patients tried to resist transfer, had to be 'forcibly subdued', or that a 'violent struggle ensued' between patient and officers in 40% of cases within a maximum-security hospital [Dietz and Rada 1982]. Furthermore, a 1 year study of 40 hospital wards in the USA and Canada revealed that about two thirds of the all incidents led to seclusion or mechanical restraint [Reid et al. 1989]. Finally, a Swedish study that analysed 3 years of data within one Swedish-based acute psychiatric ward revealed that in 46% of 137 aggressive/violent cases, the patient had to be give compulsory intra-muscular medication or be immobilised [Omerov et al. 2002] Other containment responses including staff contacting the police which a UK-based study of 37 physical assaults in a psychiatric unit over a 12 month period reported [Edwards et al. 1988]. The latter was the only study to have reported that the assailant was denied some of their privileges (this occurred for 2 out of 25 assaultive patients). The use of constant special observation was reported by only one study which reported that violent patients were more likely to have been under constant special observation the month prior to the patients becoming violent [Tardiff 1983]. Staff locking the ward doors was reported by a US-based study of a staff murder that occurred within a State psychiatric hospital [Turns and Gruenberg 1973]. Only one study reported that the being detained as a consequence of violence – specifically that violent patients were found to be significantly more likely than non-violent patients to be detained in hospital than non-violent patients (58.5% vs. 22.4% respectively; OR=4.87, CI=2.75-8.66) [Benjaminsen et al. 1996], while a UK-based study of violence in an inpatient acute psychiatric unit reported the outcome of staff confronting the assailants – specifically that nurses were more willing to confront violent female patients on their own without colleague support, compared to violent male patients. Finally, an Australian-based study of aggression within acute psychiatric settings reported that an assailants’ nursing management plan was reviewed after 26% of violent incidents. Patient transferred or discharged Seven studies (6.5%) reported this type of outcome which consisted of 5 lower-level themes including violent/aggressive patients being transferred to a higher security ward including a US-based study of repeated assaults within a ‘Veterans’ inpatients unit which found that measures such as this and transfer to jail were used in 4.7 % of 422 assaults [Blow et al. 1999]. Being transferred to another hospital was a consequence of violence/aggression reported by four studies: one which reported this outcome for 31% of incidents (total incident N not reported) within Australian-based acute psychiatric settings [Delaney et al. 2001], and another an Australian-based study of violent incidents within inpatient psychiatric settings which reported that non-recidivist patients were more likely to be transferred to another hospital after becoming violent [Owen et al. 1998]. Additionally, a study of 40 hospital wards in the USA and Canada revealed that assailants who committed the most severe incidents

slightly more likely than other assailants to be transferred to another hospital or be discharged [Reid et al. 1989], while another study reported being transferred to another hospital in 10.7% of 2180 incidents within a UK-based medium secure unit [Gudjonsson et al. 2000]. The latter study also reported that in 0.02% (n=49) of 2180 incidents, the assailant was transferred to a psychiatric intensive care unit, while a one year study of a UK-based general psychiatric hospital also cited this theme [Tobin et al. 1991]. A German-based study of aggressive behaviour among first admission patients with schizophrenia at a general psychiatric hospital which reported that 17% of male assailants and 3% of female assailants were prosecuted for their aggressive behaviour during their admission [Steinert et al. 1999] Victim psychological outcome A total of 12 studies (11.1%) reported 16 types of psychological outcomes for the victim of a violent/aggressive incident. This included irritability which was reported to be one of the most commonly reported symptoms immediately following an assault on staff at a UK-based acute psychiatric inpatient unit [Whittington and Wykes 1991]. The latter study, which prospectively interviewed staff victims following a violent assault also reported muscle tenseness, anxiety, intrusive thoughts, and the staff ruminating about the incident as commonly reported symptoms. An earlier study by the same authors also reported muscle tenseness, intrusive thoughts and rumination about the incident [Whittington and Wykes 1989]. A UK-based study of assaults on staff in a locked inpatient acute psychiatric ward revealed that in 47% of 41 recorded staff assaults over a 6 month period, the staff victim felt a change in attitude toward the assailant - in particular anger at the patient for being 'allowed to get away with' their violent behaviour, changing to resentment and subsequently fear of patient [Aiken 1984]. This study also reported that two other victims felt that their job satisfaction had decreased because of the violence. One other study also reported staff anger towards the assailant as an outcome – a US-based study that preliminarily evaluated the data collected during ASAP’s first 90 days [Flannery et al. 1991]. The latter study also reported that the staff victims sleep disturbances about the incident, an outcome which was also reported by another US-based study that examined various characteristics related to assault over a 3 and a half month period in one large neuropsychiatric hospital [Lanza 1988], as well as a UK-based prospective study of verbal aggression towards psychiatric staff who reported that 43% of 68 staff victims dreamt about the incident [Adams and Whittington 1995]. The latter study also reported that 78% of the victims tried to repress the incident As well as the aforementioned Whittington and Wykes (1991) study, three other studies reported staff anxiety as an outcome of violence/aggression. An the study by the same authors [Whittington and Wykes 1989], as well as the Adams and Whittington (1995) study which asked staff victims to estimate their level of anxiety at the time of the incident using a 5-point Likert-type scale (0 = no anxiety to 5 = extreme anxiety). They revealed that the mean level of staff anxiety for inpatient staff was 1.75, while female staff reported higher levels of anxiety (2.26) than males (1.54), while anxiety was reportedly higher during threatening incidents (2.27) than during incidents involving purely verbal abuse (1.71) (although these figures include community psychiatric nurses whose mean anxiety scores were higher than inpatient staff). Another study examined aggression among psychiatric inpatients in Australian

rehabilitation wards and found that 35.2% of 806 incidents resulted staff feeling ‘shaken up’ [Cheung et al. 1996]. Another study which retrospectively examined ASAP data reported victims symptoms associated with acute stress disorder and post-traumatic stress disorder (PTSD) [Flannery and Walker 2001], while three other studies by the same lead author also reported the latter psychological outcome via retrospectively analysing ASAP data – specifically, that more female staff victims compared to male staff victims of severe threats experience PTSD-related symptoms at the time of the incident [Flannery, Jr. et al. 1995], that psychological trauma symptoms of physical, intrusive, and avoidant responses were frequently associated with staff assaults [Flannery, Jr. and Walker 2008], and that 53% of staff victims had physical arousal symptoms associated with their assault [Flannery et al. 2006]. A UK-based prospective study of verbal aggression towards psychiatric staff reported that 93% of 14 staff victims who completed the ‘Revised Impact of Events Scale’ experienced PTSD symptoms [Adams and Whittington 1995]. Experiencing ‘disruptions in mastery, attachment, and meaning’ were three other psychological outcomes all of which were reported by various Flannery studies. Flannery defines mastery as one's ability to reasonably shape one's environment, attachments as the caring and support of others, and meaning as the ability to make understandable sense out of what has happened. One study reported that disruptions of these domains were frequently recorded across all categories of assault reported via ASAP [Flannery and Walker 2001], while another study reported that more female staff victims compared to male staff victims of severe threats experience disruptions in the sense of mastery and meaning of the event at the time of the incident as well as one day later, and that these disruptions could potentially occur up to 10 days after the incident [Flannery, Jr. et al. 1995]. An earlier study that preliminarily evaluated ASAP found that 69% of staff victims regained a sense of mastery within 3-10 days of the incident [Flannery et al. 1991]. A 15 year analysis of ASAP data revealed that disruptions of ‘reasonable’ mastery, caring attachments, and purposeful meaning frequently associated with all categories of assault, although physical and sexual assaults, and verbal threats resulted in more frequent domain disruptions than nonverbal intimidation incidents [Flannery, Jr. and Walker 2008]. Additionally, 69.4% of assaulted staff were reported to frequently experience disruptions in their sense of mastery of the environment, 58.4% of staff victims experienced disruptions in their ability to understand or make meaningful sense of the incident [Flannery et al. 2006]. Victim behavioural outcome A total of 6 studies (5.6%) reported 9 different types of behavioural outcomes for the victim of a violent/aggressive incident. This included staff fatigue which was cited as an outcome by a UK-based exploratory study of coping strategies used by staff in an acute psychiatric inpatient unit soon after a patient assault [Whittington and Wykes 1991]. The latter study and an earlier 6 month study of acute inpatient staff injuries also reported that staff used alcohol, smoked, and increased appetite in the hours and first few days after an incident [Whittington and Wykes 1989]. An increase in appetite and strained family relationships were outcomes reported by a US-based
study that examined various characteristics related to assault over a 3 and a half month period in one large neuropsychiatric hospital [Lanza 1988]. Another type of behavioural outcome was resigning from their post which was cited by two studies – one which investigated staff assaults over a 6 month period in a UK-based locked acute psychiatric ward [Aiken 1984], and a study that preliminarily evaluated ASAP’S first 90 days which found that one employee left the their job as a result of being assaulted [Flannery et al. 1991]. A US-based study that prospectively studied violence and social structure on four acute and two ‘chronic’ wards reported that in contrast to the more peaceful wards, on violent wards there was usually no post-incident debriefing/review [Katz and Kirkland 1990]. Finally, a study that evaluated 90 days worth of ASAP data reported that, from 67 recorded staff assaults, 1 staff member was referred for counselling, while 7 staff victims attended support group meetings [Flannery et al. 1991]. Property / objects damage Fourteen studies (13%) reported damage to property/objects as an outcome of inpatient violence/aggression, 13 of which reported the number of total incidents as well as the number of incidents which resulted in property/objects damage, whereas one study did not [Ketelsen et al. 2007]. The highest rates of property/object damage were found to be 35% of 17 incidents over a 2 month period in a UK-based forensic hospital [Carton and et al. 2003], 26% of 323 incidents over a 5 year period in an Italian-based acute inpatient unit [Grassi et al. 2001], 20% of 197 incidents over a 1 year period in an Australian forensic psychiatric hospital [Daffern et al. 2003], and 20% of 164 incidents over a 24 week period in a Dutch acute psychiatric admissions ward [Nijman et al. 1997]. The next highest rate was found to be 16% of 135 incidents over a 2 year period within a UK-based forensic unit [Agarwal and Roberts 1996], followed by 12% of 419 incidents over a 5 month period in a large US-based state psychiatric hospital [Kraus and Sheitman 2004], and 11% of 820 incidents over a 3 year period in a UK-based medium secure unit [Torpy and Hall 1993]. Lower rates included 9% of 316 incidents over a 6 month period on 3 Australian-based forensic wards [Daffern et al. 2006], 9% of 1289 incidents over a 3 month period in 2 units located in an Australian primary psychiatric hospital and a 6 month period in 3 acute psychiatric units of an Australian general hospital [Owen et al. 1998], and 6% of 119 incidents over a 25 week period within one Swedish psychiatric intensive care unit [Palmstierna et al. 1991]. The lowest rates of property/object damage were 4% of 331 incidents over a 6 month period in an Australian forensic psychiatric hospital [Daffern et al. 2003], 2% of 264 incidents over a 10 month period in 5 UK-based acute wards [Foster et al. 2007], and 1% of 806 incidents over an 8 week period within Australian rehabilitation wards [Cheung et al. 1996]. Using the total number of property/damage episodes as well as the total number of violent/aggressive incidents reported in the above thirteen studies, the percentage of incidents resulting in property/objects damage was calculated. Across all studies which reported this theme, (as well as the total number of violent/aggressive incidents), the mean percentage of this rate was found to be 13.12% (SD = 9.9) (see table 9). When settings were compared, there was a slightly higher rate within
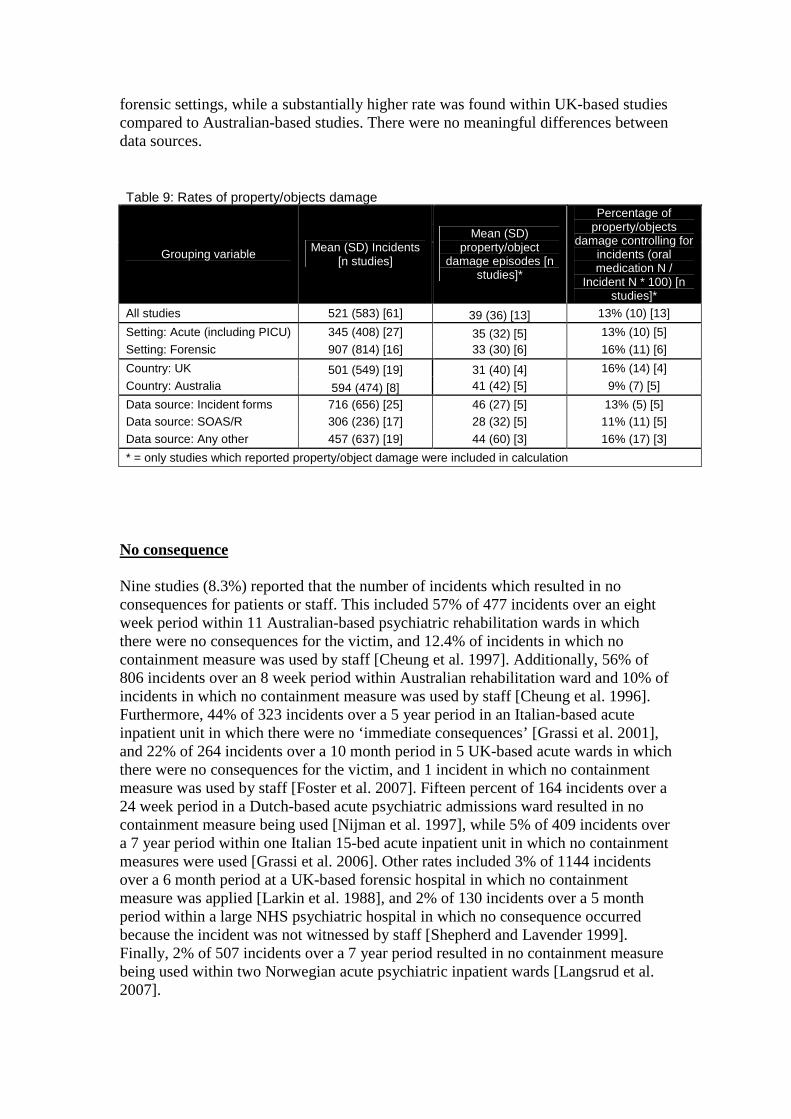
forensic settings, while a substantially higher rate was found within UK-based studies compared to Australian-based studies. There were no meaningful differences between data sources. Table 9: Rates of property/objects damage
Grouping variable Mean (SD) Incidents [n studies]
Mean (SD) property/object
damage episodes [n studies]*
Percentage of property/objects
damage controlling for incidents (oral medication N /
Incident N * 100) [n studies]*
All studies 521 (583) [61] 39 (36) [13] 13% (10) [13]
Setting: Acute (including PICU) 345 (408) [27] 35 (32) [5] 13% (10) [5]
Setting: Forensic 907 (814) [16] 33 (30) [6] 16% (11) [6]
Country: UK 501 (549) [19] 31 (40) [4] 16% (14) [4]
Country: Australia 594 (474) [8] 41 (42) [5] 9% (7) [5]
Data source: Incident forms 716 (656) [25] 46 (27) [5] 13% (5) [5] Data source: SOAS/R 306 (236) [17] 28 (32) [5] 11% (11) [5]
Data source: Any other 457 (637) [19] 44 (60) [3] 16% (17) [3]
* = only studies which reported property/object damage were included in calculation
No consequence Nine studies (8.3%) reported that the number of incidents which resulted in no consequences for patients or staff. This included 57% of 477 incidents over an eight week period within 11 Australian-based psychiatric rehabilitation wards in which there were no consequences for the victim, and 12.4% of incidents in which no containment measure was used by staff [Cheung et al. 1997]. Additionally, 56% of 806 incidents over an 8 week period within Australian rehabilitation ward and 10% of incidents in which no containment measure was used by staff [Cheung et al. 1996]. Furthermore, 44% of 323 incidents over a 5 year period in an Italian-based acute inpatient unit in which there were no ‘immediate consequences’ [Grassi et al. 2001], and 22% of 264 incidents over a 10 month period in 5 UK-based acute wards in which there were no consequences for the victim, and 1 incident in which no containment measure was used by staff [Foster et al. 2007]. Fifteen percent of 164 incidents over a 24 week period in a Dutch-based acute psychiatric admissions ward resulted in no containment measure being used [Nijman et al. 1997], while 5% of 409 incidents over a 7 year period within one Italian 15-bed acute inpatient unit in which no containment measures were used [Grassi et al. 2006]. Other rates included 3% of 1144 incidents over a 6 month period at a UK-based forensic hospital in which no containment measure was applied [Larkin et al. 1988], and 2% of 130 incidents over a 5 month period within a large NHS psychiatric hospital in which no consequence occurred because the incident was not witnessed by staff [Shepherd and Lavender 1999]. Finally, 2% of 507 incidents over a 7 year period resulted in no containment measure being used within two Norwegian acute psychiatric inpatient wards [Langsrud et al. 2007].

5.3 Evidence for and against the City model The findings of this review lend some indirect support of the City model. Direct support is minimal given that this review is examining the outcomes of violence and aggression, rather than the contributing factors. One source of indirect support for the City model comes from the containment/staff response findings. Specifically, these findings emphasise the importance of technical mastery and teamwork skill – two components of the model which play crucial a role in determining how effective staff are in delivering containment to violence. As the results of the antecedents review highlight, containment procedures such as restraint, seclusion, medication administration and verbal de-escalation may trigger more conflict when carried out poorly, and which have been clearly documented in this review to be highly frequently used in response to violence and aggression. The emotional regulation component is also indirectly supported by this review. This is because a number of studies and lower-level themes related to the psychological and behavioural outcomes of the victim, all of which were negative. Therefore, it can be argued that if staff become victims of an aggressive/violence incident, their ability to effectively regulate their emotional state during future interactions with patients may become compromised. For example, if a nurse who has recently been assaulted by a particular patient becomes angry and/or holds resentment toward the assailant (and potentially other patients), he/she may not carry be not keep their emotional state regulated and work as effective as possible. A staff victim who is suffering from such negative outcomes may also struggle to attain positive moral commitments, engage in effective team-working, and may have their psychiatric philosophy impaired temporarily or even permanently. One of the underlying assumptions of the City model is the way staff can directly influence the likelihood of conflict and containment levels, particularly through the way that they interact with their patients. This is potentially supported by the finding that that there are higher rates of seclusion and oral medication use in acute wards compared to forensic wards. These differences may be due to the inherent differences within the patient population, or they may reflect the differences in working style and practice across the two types of settings. If the latter is at least partially true, this would lend some support to the assumption that differences in staff are a key contributor to differences in conflict and containment rates. 5.4 Points the City model has missed One of the main focuses of this review is upon the nature and severity of the physical injuries which inpatient staff (and patients) experience as a result of violence and aggression. The impact of the physical injuries is an area which is not explicitly referred to within the City model. For example, if a key member of staff is not able to work for an extended period of time due to a serious physical injury, there may be repercussions on how the ward is run in general as well as the psychological

implications upon the rest of the team which may impact the staff’s ability to positively appreciate (if morale becomes poor), as well as the team’s ability to work effectively together. The impact of property and object damage is also not referred to within the City model. This may be because no consideration to the physical environment is explicitly referred to within the City model. If it is considered that a high-quality, functional physical environmental is an important component of a therapeutic and safe psychiatric ward (a theory which is supported by our transitions analysis and the antecedents review), then it is logical to assume that damage to properties and objects may produce an overall negative effect. It is also possible that staff and patients attach some psychological significance to certain personal objects which may upset them and trigger conflict (and containment) if they are damaged or destroyed. As stated earlier, this review highlighted some important differences in certain containment measures, as well as the rate and severity of physical injuries, within different inpatient settings. This has two possible implications. Firstly, if the likelihood of certain containment measures is setting-specific, then some consideration of setting type should be included in the City model. Secondly, if we deduce from the findings that acute wards are more dangerous than forensic wards (due to the comparatively higher injury rates and lower numbers of ‘mild’ injuries), then one potential explanation for the difference could be the predictability level of the patients’ behaviour. This is a reasonable assumption as the level of patient throughput is much higher within acute settings, and therefore staff have much less time to interact and learn about the patient including what his/her particular conflict triggers are, and how and when best to carry out containment measures. Therefore, the level of patient predictability may be an important addition to the City model. 5.4 Discussion Similarly to the antecedents review, one of the most discernable findings of this review is that the potential consequences and outcomes of inpatient violence/aggression are wide-ranging. This is underlined by the fact that there 8 higher-level themes incorporating a total of 67 distinct lower-level themes across the 108 studies in this review. The consequences ranged from the nature and severity of physical injuries, patient transfers/discharges, psychological and behavioural outcomes for the victims, and damage to property/objects. Another distinguishing finding is that a large proportion of the papers include data on the prospective/live consequences and outcomes that ensued immediately after the incident (approximately a quarter all of papers across the entire literature review included such information). More papers provided live consequences data than antecedents data, perhaps suggesting that studies are either slightly more interested in what happens to the patient/staff following the incident than what led to the incident, or that staff are focused more on documenting the consequence of an incident than the triggers of it. Another similarity to the antecedents review is that the types and rates of consequences and outcomes represented in this review are staff-based depictions of reality. It is the psychiatric staff members who interpret their personal view of the incident and subsequently complete an incident form, a SOAS/R, a study

questionnaire, a claim form, an assault form, and/or who are qualitatively interviewed. One hundred and three studies (95.3%) of the 108 studies reported consequences data exclusively from the staff’s perspective, while only one study captured the patient perspective. Such a large disparity of perspectives also implies that the true breadth and scope of the consequences and outcomes of violence and aggression remains uncertain. In order to bridge this gap, future studies interested in the consequences and outcomes of inpatient conflict should also use video camera footage as well as the patient interviews and questionnaires. The former method would be a useful objective tool for recording containment responses; however the latter methods would be the only mechanisms towards understanding the psychological consequences of the patient. It may also be useful to understand the wider consequences of inpatient conflict events such as violence and aggression by researching the consequences for the patient and staff witnesses as well as the patient and staff communities as a whole. Such research is necessary in reducing the perspective disparity and augmenting our understanding of what the consequences and outcomes of violence and aggression are, and what the resulting effects of such phenomena are. It may also be useful for staff to record in their incident forms the psychological consequences for the victims and assailants soon after the event, particularly if the process helps staff become more psychologically understanding of their patients and colleagues. Talking to the victims and assailants about how they are feeling soon after the incident will also show support and empathy for both the patient and staff communities. The most frequently reported type of consequence across all of the violence and aggression literature pertained to physical injuries. This predominantly regarded the types of injuries experienced by the staff victims of the assault. An extensive range of injury types and severity were cited implying that victims of assaults could experience any type of injury. Due to the lack of data necessary in calculating rates, it was not possible to accurately assess which types of injuries are most likely to occur during an incident. However, if the number of study citations of types of injuries is to be used as an indicator, then the most frequent type of injury may be head injuries which were referred to by 28 studies – by far the largest number of studies which specified an injury type. The next most frequent study citations were nine studies which reported scratches/cuts/nosebleeds/grazes, eight studies which reported injuries to the back/spine/trunk, six which reported a bone injury and 6 which reported a serious open wound or laceration. It is reasonable to expect that head injuries could be the most common type of injury experienced after an assault as it would be expected that punches to the face/head area would be a common method of assault. As head injuries can be potentially severe and traumatic, the obvious implication is that staff are trained in defending their heads effectively during an assault so that the risk of experiencing an injury is minimised. There was, however, enough data to calculate the mean rate of physical injuries controlling for total violent incidents. This was found to be 37% which can be interpreted to purport that for every three violent/aggressive incidents that a staff member is involved in, they are likely to be injured at least once. There are important clinical implications associated with this finding. Firstly, there is a clear need for staff to be well trained in how to non-harmful defensive techniques so that they can minimise their risk of injury during an assault. Secondly, it could be argued that a 37% injury rate is too high and that more could be done to de-escalate the patient and prevent the assault from occurring. Thirdly, if a staff member is injured, first aid
should be delivered as quickly and as effectively as possible so that the risk of the injury becoming worse is reduced and that the amount of recovery time that an injured staff member might need is minimised. This can be ensured if (a) wards regularly check to make sure that first aid boxes are always available and fully kitted and if (b) staff and patients take part in regular first aid training sessions so that anyone on the ward can be potentially be on hand to provide first aid to the victim. If this can be achieved, the morale of the entire ward community should be boosted. Another meaningful finding was the contrasting rates of injury by setting – specifically that staff involved in a violent/aggressive incident within acute settings are 20% more likely to be injured as a consequence compared to forensic settings. This implies that acute wards are more dangerous for psychiatric staff (and patients) than forensic wards. This raises a number of questions: Could it be that forensic wards are better prepared to deal with a violent incident than on an acute ward, perhaps due to better training in injury prevention and/or dealing with violent events? Perhaps they have higher levels of staffing which minimises the risk an individual nurse? Perhaps they have better management strategies? Another potential explanation for the difference could be the predictability level of the patients’ behaviour. This is a reasonable assumption as the level of patient throughput is much higher within acute settings, and therefore staff have much less time to interact and learn about the patient including what his/her particular conflict triggers are, and how and when best to carry out containment measures. The argument for acute wards being more dangerous for staff than forensic wards is further corroborated when injury severity rates are considered. This is because injuries were more likely to be considered ‘severe’ within acute settings compared to forensic settings (although only three forensic-based studies reported the required data) both when controlling for total violent/aggressive incidents and total number of physical injuries. Non-UK, USA or Australia-based studies produced substantially higher rates of severe injuries which tentatively suggests that psychiatric wards from these countries pose a comparatively greater danger to psychiatric staff. The second most frequently reported higher-level consequence theme was containment/staff response. A total of fifty-four studies cited 15 types of containment measures/staff responses to violent/aggressive incidents which is a considerable number and emphasises the possible range of measures at the staff’s disposal when facing aggression/violence and other conflicts. Despite the breadth of reported containment types, no studies in the review cited the use of intermittent observation which is considered surprising given that this measure has been previously documented to be one of the most frequently used within UK inpatient acute wards [Bowers 2009] and that it associates with reduced self-harm rates which may occur during patient violence/aggression [Bowers et al. 2008]. The most frequently cited containment measure was seclusion, which was cited by nineteen studies, followed by oral medication (27 studies), mechanical (19) and manual (18) restraint, time out/removed from the situation (16), intra-muscular medication (14) and verbal de-escalation. However, the overall most frequently used containment measure – in terms of rates – was found to be manual restraint (34%), followed by verbal de-escalation (30%), oral medication (24%), seclusion (21%), time out (18%) and intra-muscular medication (18%). However, it is important to take into account that these are estimates based upon available data, and that it is possible that other containment

measures for which a reliable rate could not calculated (due to low numbers of studies providing the necessary data) may be used as frequently. Seclusion, oral medication and manual restraint were the only containment measures which were able to be analysed and meaningfully compared across settings. These comparisons revealed that each of these measures were employed to a substantially greater degree within acute settings than forensic settings during or following violence/aggression. This adds evidence to the theory that acute psychiatric wards are less calm and safe places of recovery than forensic settings. There are a number of possible explanations for this difference. Firstly, nurses working with acute settings may be more reliant of such containment measures because they are not confident or effective as forensic nurses at verbally de-escalating a violent/aggressive patient. Another possibility is that there may be more conflict within acute wards in general. As conflict and containment have been showed to be correlated within acute psychiatric settings [Bowers 2009], this would logically result in the higher use of containment measures. Another potential explanation for the difference could be that forensic staff are better at predicting what might trigger a patient to become violent/aggressive than acute nurses due to a greater familiarity of their patients and therefore containment measures are not as necessary. The use of seclusion within inpatient psychiatric services was also found to be greater within the UK and USA compared to Australia for containing with violence/aggression. This supports the findings of a previous study which reviewed international seclusion rates within inpatient psychiatry also revealed that seclusion rates are lower within Australia (and New Zealand) than in the USA and UK [Janssen et al. 2008]. A methodological problem that surfaced during the thematic analysis was that most non-UK literature did not explicitly make a distinction between manual and mechanical restraint and instead only referred to ‘physical restraint’. This problem was addressed by making informed decisions on which type of restraint the study authors were most likely to be referring to, given the country in which the study took place and other implicit references to the type of restraint being measured. It is therefore clear that future studies must clearly state which type of restraint is being researched and that clear definitions provided, so that interpretations of such results are accurate and applied correctly. Twelve studies referred to the psychological outcome of the victim of violence and aggression, while only 6 referred to behavioural outcome of the victim. The reason why so few studies referred to such outcomes is because it often takes time for such outcomes to become apparent. This review examined live consequences data that were collected immediately or soon after the incident which would be unlikely to capture such outcomes. Therefore, studies which surveyed staff victims at a future time point would be much more likely to research such outcomes. Although it was not possible to meaningfully analyse the rates of these outcomes within this review (due to low study numbers and available data), it is interesting to note the large range of lower-level themes related to this outcome despite the limited number of studies captured by this review. The latter tentatively indicates the importance of such outcomes which may have short-term and long-term negative clinical and economical repercussions. It is recommended that staff are provided with ‘safe areas’ in which they can express such outcomes if and when they occur so that they can be helped by the appropriate support structures to recover more quickly and effectively.
Dissimilar to the antecedents review was that were very few studies (nine in total) which could not identify at least one type of consequence or outcome following a violent/aggressive incident. This is possibly because it is easier for staff to observe a consequence of an incident, compared to an antecedent of an incident. Another interpretation is that staff are more interested or focused in recording consequences-type data, perhaps due to common practice and custom.

6. PROFILE OF VIOLENT AND AGGRESSIVE PATIENTS 6.1 The studies reviewed Of the 424 empirical studies included in the literature review, 75 (18%) papers made some sort of comparison between groups of patients as can be seen in Table 1. Table 1: types of comparison studies Type of Comparison N %
Aggressive vs. Non aggressive Random
29 38.67
Aggressive vs. Non aggressive Controls
7 9.33
Repeater/High vs. Single/Low 6 8
Repeater/High vs. Single/Low vs. Non aggressive Random
6 8
Repeater/High vs. Single/Low vs. Non aggressive Control
4 5.33
Other 23 30.67
Aggressive vs. Non-aggressive comparison studies From the 29 aggressive vs. non aggressive random group studies were excluded from the analysis if there was any missing data (Goldberg et al. 2007; Flannery et al. 1998; Daffern et al. 2008), if it was unclear whether the aggression had occurred on the ward when defining the groups (Abushua’leh et al. 2006; Margari et al. 2005) and if the demographic data was reported in terms of the number of aggressive incidents rather than the number of aggressive patients (Chou et al. 2001). From the aggressive vs. non aggressive control studies, 4 papers were excluded (Cheung et al. 1997; Ramussen et al. 1995; Doyle et al. 2006; Lanza et al. 1988) as they were comparing factors other than the patient demographics we were interested in. Ten papers reported more than one comparison. Where aggressive patients were split into those who had been physically aggressive versus verbally aggressive or aggressive against object (McNiel et al. 1988; Raja et al. 1997; Raja et al. 2005) the data was combined to produce one aggressive group for comparison. This was also the procedure for studies that compared persistently and transiently aggressive patient over the study period (Krakowski et al. 1989a; Krakowski et al. 1997). Some studies made further comparisons using a subset of patients from either the aggressive group (Barlow et al. 2000; Daffern et al. 2005) or the non aggressive group (Ketelsen et al. 2007). These extra comparisons were not included in the analysis. Two studies were excluded from the analysis (Krakowski et al. 1989b; Krakowski et al. 1999) as the non-aggressive group was matched to the aggressive group. A total of 34 studies (See Table 2) remained and were analysed in the present series of meta-analyses. Where available the following information was collected from each paper: patient demographics (for gender, ethnicity, marital status, diagnosis, history of

violence, suicide, drug abuse and admission type this was split into binary data, e.g. the proportions of patients in the aggressive and nonaggressive group that were male or female; for age and years of education continuous data was collected, e.g. means and standard deviations for each group), size of sample, type of ward, violence definition (verbal, physical against others, physical against objects, physical against self), and country. Data analysis A series of meta-analyses were performed on each demographic factor to estimate the common effect over several studies using STATA. For binary data the effect measure was the ratio of proportions of aggressive and non aggressive patients were calculated. For continuous data the observed differences in means between the two groups was calculated.

Author Country Setting Data Status Number Violence Definition
Measurement Duration Type of sample
Barlow et al. 2000 Australia Acute Gender, Diagnosis, No. previous admission
agg/nonagg 174/1096 VPOS SIR 18 months
Random
Blomhoff et al. 1990
Norway Acute Gender, Age, History of C & C
agg/nonagg 25/34 P SIR 12 months
Random
Coldwell et al. 1989
UK Forensic Age agg/nonagg 31/20 PO Patient notes 12 months
Random
Daffern et al. 2005 Australia Forensic Age, Gender, Diagnosis
agg/nonagg 105/127 VPO OAS 12 months
Random
Dietz et al. 1982 USA Forensic Age, Ethnicity, Years of education
agg/nonagg 64/147 P lead to seclusion
SIR 12 months
Random
Dolan et al. 2008 UK Forensic Age, Gender, Ethnicity, Marital status, Diagnosis
agg/nonagg 79/68 VP SIR Missing Random
Doyle et al. 2002 UK Forensic Age, Gender, Ethnicity, Marital status, Diagnosis
agg/nonagg 45/52 VP VRAG 3 months Random
Edwards et al. 1988
UK Mixed Marital status, Diagnosis, Admission type, History of C & C
agg/nonagg 25/25 P Interviews 12 months
Matched for Age and Gender
Fullam et al. 2008 UK Forensic Age, Yrs in education, medication
agg/nonagg 33/49 PO had to be instigated
SIR Missing Men/schizophrenics
Grassi et al. 2001 Italy Acute Age, Gender, Marital status, Diagnosis
agg/nonagg 116/1418 VPO SOAS 60 months
Random
Harris et al. 1983 USA Forensic Age, Yrs in education, Diagnosis, No. previous admissions
agg/nonagg 45/45 P SIR 60 months
Random

Hillbrand et al. 1996
USA Forensic Age, History of C & C agg/nonagg 79/79 P lead to injury
Patient notes 36 months
Random
Hoptman et al. 1999
USA Forensic Age, Ethnicity, Yrs. in education
agg/nonagg 60/123 P NOSIE 3 months Men
James et al. 1990 UK Acute Age, Gender, Ethnicity, Diagnosis, Admission type
agg/nonagg 64/216 POS SIR 15 months
Random
Karson et al. 1987 USA Research Age, Gender, Diagnosis, No. previous admissions, History of C & C
agg/nonagg 45/95 P Patient notes 135 months
Aggressive group had not responded well to neuroleptic treatment
Kennedy et al. 1995
UK Forensic Gender, Ethnicity, Diagnosis, History of C & C
agg/nonagg 27/54 PO 10+ incidents
SIRS 4 years Random
Ketelsen et al. 2007
Germany Mixed Age, Gender, Marital status, Diagnosis, Admission type, No. previous admission
agg/nonagg 171/2039 VPO SOAS 12 months
Random
Krakowski et al. 1989a
USA Mixed Diagnosis & History of C & C
agg/nonagg 77/40 VPO Patient notes 2 months Matched for age, sex, race and chronicity of illness
Krakowski et al. 1997
USA Mixed History of C & C, Admission type
agg/nonagg 75/62 P MOAS and Patient notes
26 months
Matched for Age, Gender, Ethnicity, Diagnosis, Length of stay
Lam et al. 2000 USA Acute Age, Gender, Ethnicity, Diagnosis, Admission type, History of C & C
agg/nonagg 76/314 P lead to injury
SIR 129 months
Random
Lanza et al. 1994 USA Veteran hospital
Ethnicity, Marital Status, Diagnosis
agg/nonagg 36/36 VP Patient notes Matched for Age and Gender

McKenzie et al. 2005
UK Forensic Age, Gender agg/nonagg 70/24 PO SIR 2 weeks Random
McNiel et al. 1988 USA Acute Age, Gender, Ethnicity, Marital status, Diagnosis, History of C & C
agg/nonagg 138/100 VPO Patient notes 3 days Involuntary patients
Mellesdal et al. 2003
Norway Acute Age, Gender, Diagnosis, Admission type
agg/nonagg 98/836 VP REFA 36 months
Some day patients, numbers not specified
Nijman et al. 1997 Netherlands Acute Age, Gender, Diagnosis, Admission type
agg/nonagg 31/31 VPO SOAS 6 months Random
Nijman et al. 2002 Netherlands Acute Age, Gender, Diagnosis, Admission type
agg/nonagg 31/58 VPOS SOAS 9 months Random
Noble et al. 1989 UK Mixed Ethnicity, Marital status, Employment status, Diagnosis, Admission type, No. of previous admissions, History of C & C
agg/nonagg 137/137 P Patient notes 144 months
Matched for Age, Gender and Ward
Oulis et al. 1996 Greece Acute Age, Gender, Diagnosis
agg/nonagg 32/104 VPOS MOAS 5 days Random
Raja et al. 2005 Italy PICU Age, Gender, Marital status, Yrs.in education, Diagnosis, Medication, Admission type, History of C & C
agg/nonagg 70/1322 P Morrison scale
72 months
Random
Raja et al. 1997 Italy PICU Age, Gender agg/nonagg 22/256 P Patient notes 13.5 months
Random

1Abbreviations used: agg, aggressive; nonagg, non aggressive; V, verbal aggression/threat; P, physical aggression against others; O, physical aggression against others; S, aggression against self; SIR, standard incident reports; VRAG, violence risk appraisal guide; OAS, overt aggression scale; SOAS, staff observation aggression scale; MOAS, modified overt aggression scale; NOSIE, nurses’ observation scale for inpatient evaluation; C & C, Conflict and Containment.
Soliman et al. 2001 UK Acute Age, Gender, Diagnosis, Medication, Admission type, History of C & C
agg/nonagg 49/280 PO SOAS 12 months
Random
Tardiff et al. 1982 USA Chronic Age, Gender, Diagnosis
agg/nonagg 384/4780 P NOSIE 3 months Random
Troisi et al. 2003 Italy Acute Age, Admission type agg/nonagg 20/20 VPOS MOAS 6 months Men
Walker et al. 1994 UK PICU Gender, Ethnicity, Diagnosis, History of C & C
agg/nonagg 16/32 P SIR 6 months Random

6.2 Results for all comparison studies Age From the 34 comparison studies 26 studies included information comparing the age of aggressive and non aggressive patients. Of these half reported no significant difference in age (Blomhoff et al. 1990; Daffern et al. 2005; Dietz et al. 1982; Dolan et al. 2008; Doyle et al. 2002; Fullam et al. 2008; Lam et al. 2000; McKenzie et al. 2005; McNeil et al. 1988; Mellesdal et al. 2003; Nijman et al. 2002; Oulis et al. 1996; Troisi et al 2003) whereas the other half found aggressive patients were significantly younger than non aggressive patients (Coldwell et al. 1989; Grassi et al. 2001; Harris et al. 1983; Hillbrand et al. 1996; Hoptman et al. 1996; James et al. 1990; Karson et al. 1987; Ketelsen et al. 2007; Nijman et al. 1997; Raja et al. 1997; Raja et al. 2005; Soliman et al. 2001; Tardiff et al. 1982). Eight papers were excluded from the meta-analysis as the ages were recorded as categorical data (James et al. 1990; McNiel et al. 1988; Oulis et al. 1996; Tardiff et al. 1982), means were not reported (Blomhoff et al. 1990; Troisi et al. 2003) or because standard deviations were not reported (Dietz et al. 1982; McKenzie et al. 2005). Figure 1 shows the difference between the mean ages of patients who had been aggressive and those who had not been aggressive during their inpatient stay. The findings show that the 1186 aggressive patients were significantly younger by - 0.32 years than the 7212 non aggressive patients (95% confidence intervals [CI], -0.39 to -0.25, z = 9.30, p < 0.001). However, this result was statistically heterogeneous (Q = 34.76, p < 0.08, I2 = 51.1%). Four studies were removed from the analysis as their samples were taken from selected groups (See Table 1: Fullam et al. 2008; Hoptman et al. 1996; Karson et al 1987; Mellesdal et al 2003). This reduced the amount of variability due to heterogeneity to less than 50% (I2 = 48.3) which suggests combining the studies is valid (See Perera & Heneghan, 2008). The result remained significant; the aggressive patients were significantly younger than the non aggressive patients (Standard Mean Difference [SMD] = -0.33, CI = -0.41 to -0.26, z = 8.64, p < 0.001). The meta-analysis was also run by setting to see if there were any differences between acute and forensic wards. Aggressive patients remained significantly younger than non aggressive patients on the 6 studies from acute wards (SMD = -0.24, CI = -0.35 to -0.13, z = 4.13, p < 0.001) and on the 8 studies from forensic wards (SMD = -0.33, CI = -0.46 to -0.21, z = 5.17, p < 0.001). However, the result within acute wards was statistically heterogeneous (Q = 13.87, p < 0.05, I2 = 60.9%) but not within forensic wards (Q = 6.07, p > 0.10, I2 = 0.00%).

Figure 1: Forest plot showing the differences in mean age between aggressive patients and non aggressive patients2
Gender Twenty-two studies included information comparing the gender of aggressive and non aggressive patients. Twenty-one of these reported no significant difference in the gender of aggressive to non aggressive patients (Barlow et al. 2000; Blomhoff et al. 1990; Daffern et al. 2005; Dolan et al. 2008; Doyle et al. 2002; Grassi et al. 2001; James et al. 1990; Karson et al. 1987; Kennedy et al. 1995; Ketelsen wt al. 2007; Lam et al. 2000; McKenzie et al. 2005; Mellesdal et al. 2003; Nijman et al. 1997; Nijman et al. 2002; Oulis et al. 1996; Raja et al. 1997; Raja et al. 2005; Soliman et al. 2001; Tardiff et al. 1982; Walker et al. 1994). McNiel et al. (1988) reported that men were significantly overrepresented in the group of pts exhibiting fear-inducing behaviour (verbal attacks on persons, threats to attack persons, and attacks on objects), whereas women were significantly overrepresented in the physically assaultive group. Blomhoff et al. 1990 was excluded from the meta-analysis as data were missing.
2 The black circle and horizontal line correspond to the standard mean difference (smd) between groups and 95% confidence intervals. The area around the black circle reflects the weight each study contributes in the meta-analysis.
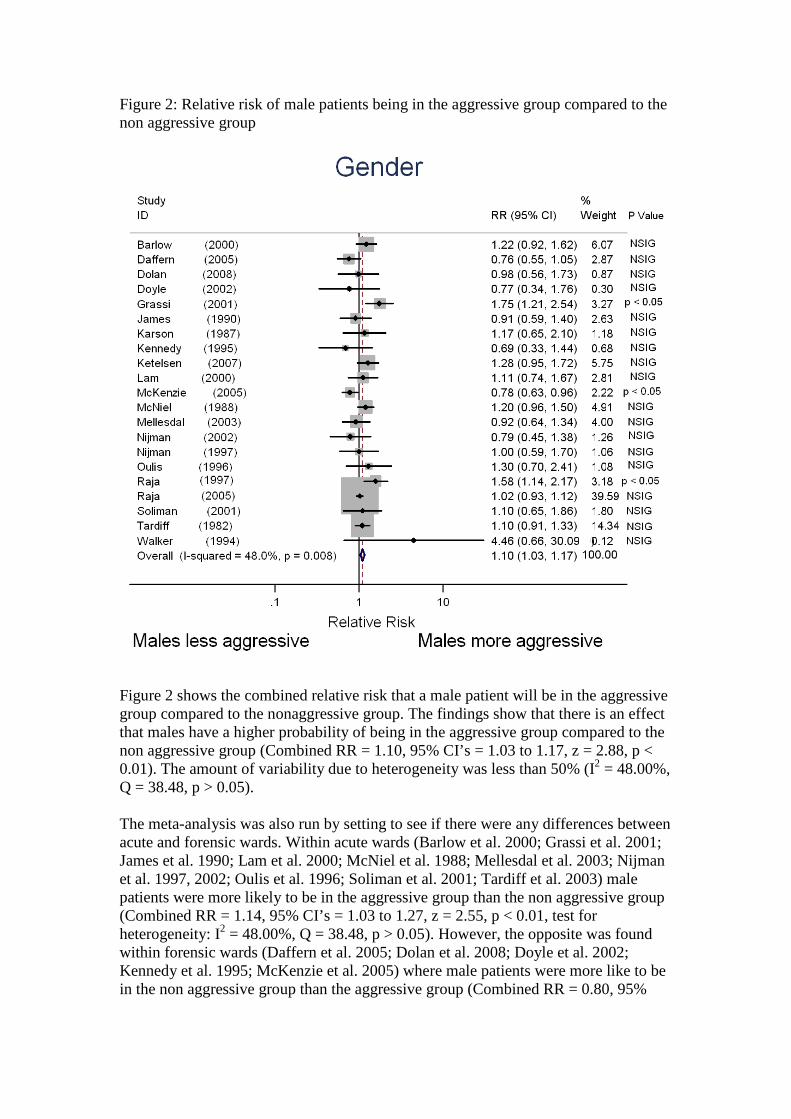
Figure 2: Relative risk of male patients being in the aggressive group compared to the non aggressive group
Figure 2 shows the combined relative risk that a male patient will be in the aggressive group compared to the nonaggressive group. The findings show that there is an effect that males have a higher probability of being in the aggressive group compared to the non aggressive group (Combined RR = 1.10, 95% CI’s = 1.03 to 1.17, z = 2.88, p < 0.01). The amount of variability due to heterogeneity was less than 50% (I2 = 48.00%, Q = 38.48, p > 0.05). The meta-analysis was also run by setting to see if there were any differences between acute and forensic wards. Within acute wards (Barlow et al. 2000; Grassi et al. 2001; James et al. 1990; Lam et al. 2000; McNiel et al. 1988; Mellesdal et al. 2003; Nijman et al. 1997, 2002; Oulis et al. 1996; Soliman et al. 2001; Tardiff et al. 2003) male patients were more likely to be in the aggressive group than the non aggressive group (Combined RR = 1.14, 95% CI’s = 1.03 to 1.27, z = 2.55, p < 0.01, test for heterogeneity: I2 = 48.00%, Q = 38.48, p > 0.05). However, the opposite was found within forensic wards (Daffern et al. 2005; Dolan et al. 2008; Doyle et al. 2002; Kennedy et al. 1995; McKenzie et al. 2005) where male patients were more like to be in the non aggressive group than the aggressive group (Combined RR = 0.80, 95%
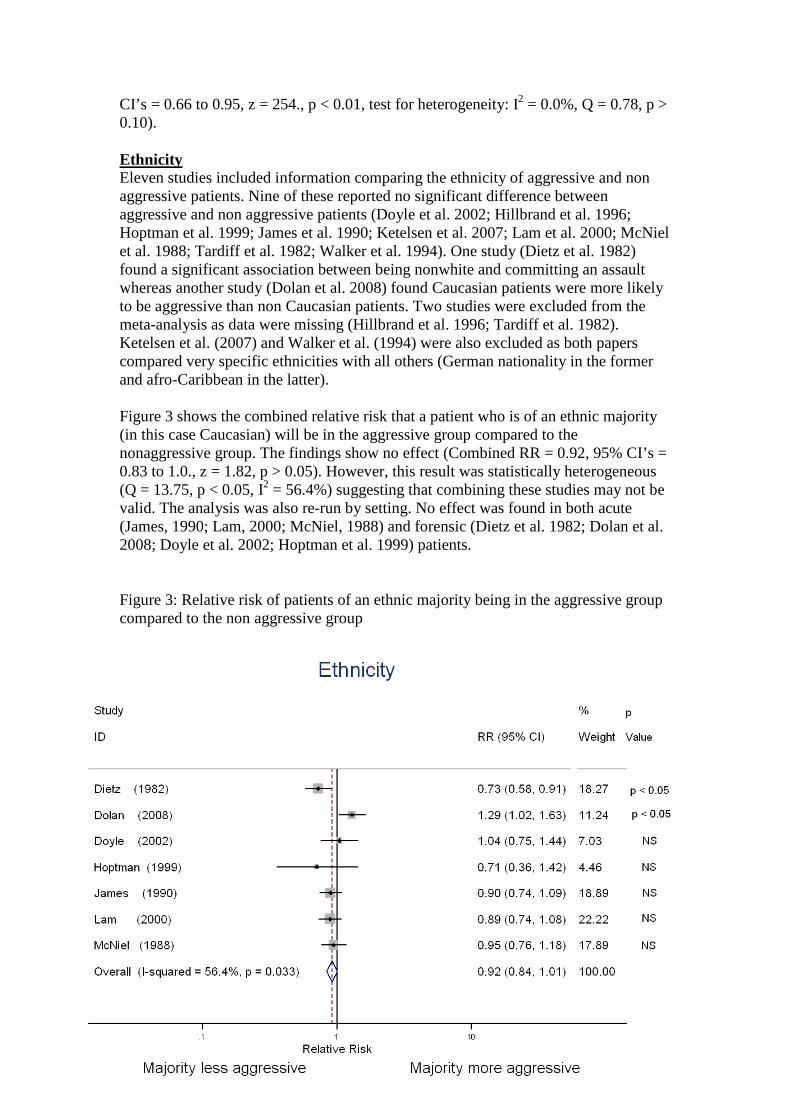
CI’s = 0.66 to 0.95, z = 254., p < 0.01, test for heterogeneity: I2 = 0.0%, Q = 0.78, p > 0.10). Ethnicity Eleven studies included information comparing the ethnicity of aggressive and non aggressive patients. Nine of these reported no significant difference between aggressive and non aggressive patients (Doyle et al. 2002; Hillbrand et al. 1996; Hoptman et al. 1999; James et al. 1990; Ketelsen et al. 2007; Lam et al. 2000; McNiel et al. 1988; Tardiff et al. 1982; Walker et al. 1994). One study (Dietz et al. 1982) found a significant association between being nonwhite and committing an assault whereas another study (Dolan et al. 2008) found Caucasian patients were more likely to be aggressive than non Caucasian patients. Two studies were excluded from the meta-analysis as data were missing (Hillbrand et al. 1996; Tardiff et al. 1982). Ketelsen et al. (2007) and Walker et al. (1994) were also excluded as both papers compared very specific ethnicities with all others (German nationality in the former and afro-Caribbean in the latter). Figure 3 shows the combined relative risk that a patient who is of an ethnic majority (in this case Caucasian) will be in the aggressive group compared to the nonaggressive group. The findings show no effect (Combined RR = 0.92, 95% CI’s = 0.83 to 1.0., z = 1.82, p > 0.05). However, this result was statistically heterogeneous (Q = 13.75, p < 0.05, I2 = 56.4%) suggesting that combining these studies may not be valid. The analysis was also re-run by setting. No effect was found in both acute (James, 1990; Lam, 2000; McNiel, 1988) and forensic (Dietz et al. 1982; Dolan et al. 2008; Doyle et al. 2002; Hoptman et al. 1999) patients. Figure 3: Relative risk of patients of an ethnic majority being in the aggressive group compared to the non aggressive group

Marital Status Seven studies included information comparing the marital status of aggressive and non aggressive patients. Two of these reported no significant difference between aggressive and non aggressive patients (Dietz et al. 1982; Doyle et al. 2002) and one (Dolan et al 2008) that did not report whether the differences between groups were significant. Three studies (Grassi et al. 2001; Raja et al. 2005; Ketelsen et al. 2007) found aggressive patients were significantly overrepresented as single compared to non aggressive patients. McNiel et al. (1988) reported that single people were significantly overrepresented in the group of pts exhibiting fear-inducing behaviour (verbal attacks on persons, threats to attack persons, and attacks on objects), whereas married patients were significantly overrepresented in the physically assaultive group. One study was excluded from the meta-analysis as data were missing (Dietz et al. 1982). Figure 4 shows the combined relative risk that a patient who is married will be in the aggressive group compared to the nonaggressive group. The findings show a significant effect (Combined RR = 0.72, 95% CI’s = 0.63 to 0.83., z = 4.70, p < 0.001, test for heterogeneity: I2 = 2.3%, Q = 5.12, p > 0.10) showing that married patients are more likely to be in the non aggressive group than the aggressive group. The analysis was also re-run by setting. A significant effect was found within acute and PICU wards (Grassi et al. 2001; McNiel et al. 1988; Raja et al. 2005) but not for forensic (Dolan et al. 2008; Doyle et al. 2002).
Figure 4: Relative risk of a married patient being in the aggressive group compared to the non aggressive group
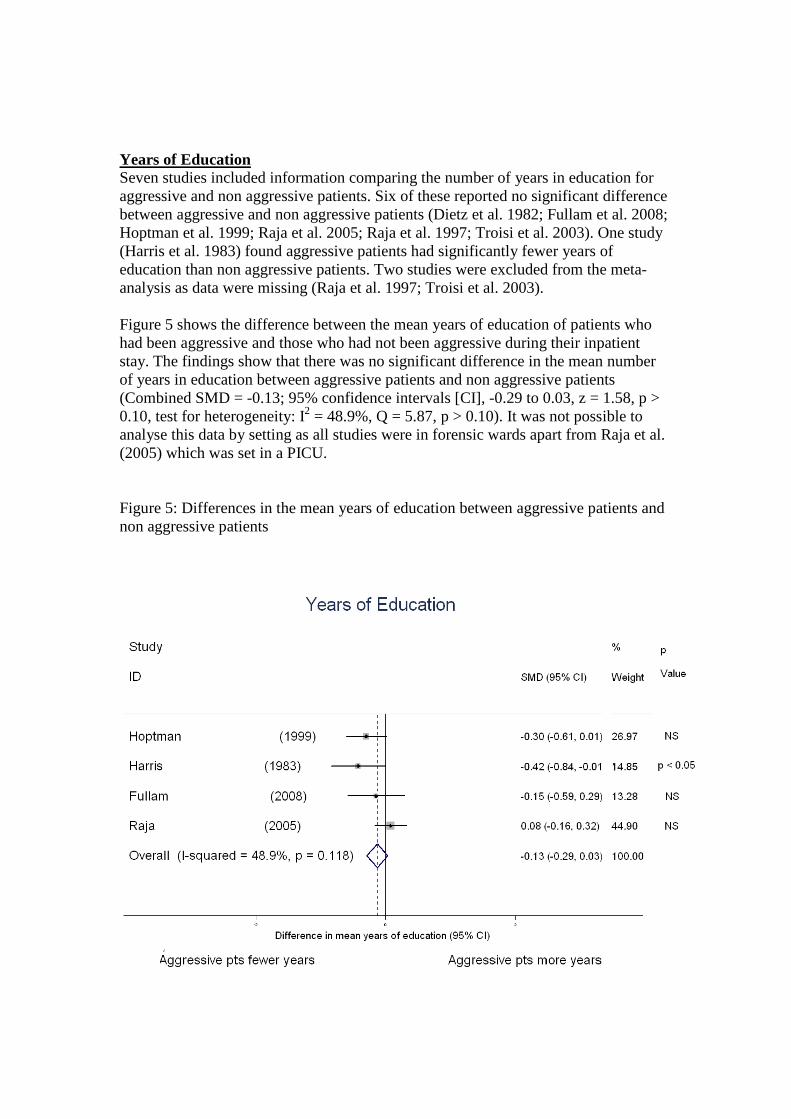
Years of Education Seven studies included information comparing the number of years in education for aggressive and non aggressive patients. Six of these reported no significant difference between aggressive and non aggressive patients (Dietz et al. 1982; Fullam et al. 2008; Hoptman et al. 1999; Raja et al. 2005; Raja et al. 1997; Troisi et al. 2003). One study (Harris et al. 1983) found aggressive patients had significantly fewer years of education than non aggressive patients. Two studies were excluded from the meta-analysis as data were missing (Raja et al. 1997; Troisi et al. 2003). Figure 5 shows the difference between the mean years of education of patients who had been aggressive and those who had not been aggressive during their inpatient stay. The findings show that there was no significant difference in the mean number of years in education between aggressive patients and non aggressive patients (Combined SMD = -0.13; 95% confidence intervals [CI], -0.29 to 0.03, z = 1.58, p > 0.10, test for heterogeneity: I2 = 48.9%, Q = 5.87, p > 0.10). It was not possible to analyse this data by setting as all studies were in forensic wards apart from Raja et al. (2005) which was set in a PICU. Figure 5: Differences in the mean years of education between aggressive patients and non aggressive patients

Diagnosis Nineteen studies included information comparing the diagnoses of aggressive and non aggressive patients. Nine of these reported no significant difference between aggressive and non aggressive patients (Dolan et al., 2008; Doyle et al. 2002; Hillbrand et al. 1996; Karson et al. 1987; Nijman et al. 1997; Nijman et al. 2002; Oulis et al. 1996; Raja et al. 1997; Walker et al. 1994). Six studies found that schizophrenia was more prevalent among the aggressive group (Barlow et al. 2000; Grassi et al. 2001; Harris et al. 1983; Mellesdal et al. 2003; Raja et al. 2005; Ketelsen et al. 2007). Tardiff et al. (1982) also found that nonparanoid schizophrenia was more prevalent in the aggressive group but that a diagnosis of paranoid schizophrenia was more likely in the non aggressive group. This study also reported that aggressive patients were more likely to have a diagnosis of psychotic organic brain syndrome, mental retardation or seizure disorders than non aggressive patients. McNiel et al. (1988) reported patients with mania were more likely to be physically aggressive whereas, Soliman et al. (2001) found a diagnosis of personality disorder predicted violence. Diagnoses that were found to be less prevalent in the aggressive group were bipolar and adjustment disorder (Barlow et al. 2000), depression (James et al. 1990) and substance abuse and affective disorders (Ketelsen et al. 2007). For the meta-analysis studies that included data about patient’s diagnoses were collated into three categories: schizophrenic (including schizoaffective etc.), affective (depression, mania etc) and other (personality disorder, organic brain syndrome etc.). Analyses were the made comparing the ratio of affective diagnoses compared to all other diagnoses in the aggressive and non aggressive group as well as comparing the ratio of schizophrenic diagnoses with all other diagnoses in both groups. Five studies were excluded from the analyses due to missing data (Hillbrand et al. 1996; Nijman et al. 1997; Raja et al. 1997), inaccurate data (Raja et al. 2005) or because co-morbid diagnoses were included (Soliman et al. 2001). Affective Vs All Other Diagnoses: Four studies of the 15 had just made the comparison between patients with schizophrenia versus all other diagnoses and so could not be included here (Harris et al. 1993; Karson et al. 1987; Nijman et al. 2002; Walker et al. 1994). Figure 6 shows the combined relative risk that a patient who is diagnosed with an affective disorder will be in the aggressive group compared to the nonaggressive group. The findings showed no significant effect (Combined RR = 0.94, 95% CI’s = 0.82 to 1.08., z = 0.87, p > 0.1, test for heterogeneity: I2 = 44.1%, Q = 17.9, p > 0.05) showing no difference in the probability that patients with and affective disorder will be aggressive or non aggressive. The analysis was also re-run by setting. There was also no significant effect within forensic wards or acute wards.

Figure 6: Relative risk of a patient diagnosed with an affective disorder being in the aggressive group compared to the non aggressive group
Schizophrenia Vs All Other Diagnoses: Two studies of the 15 had just made the comparison between patients with psychosis versus all other diagnoses and so were not be included here (Harris et al. 1993; Nijman et al. 2002). Figure 7 shows the combined relative risk that a patient who is diagnosed with a schizophrenia disorder will be in the aggressive group compared to the nonaggressive group. The findings showed a significant effect (Combined RR = 1.16, 95% CI’s = 1.10 to 1.22., z = 5.52, p < 0.001). However, this result was statistically heterogeneous (Q = 160.41, p < 0.05, I2 = 92.5%) and remained so when some outlier studies were removed. This suggests that in this case it may not be valid to combine these studies together. However, when the analysis was re-run by setting the effect remained significant within acute wards (Combined RR = 1.32, 95% CI’s = 1.21 to 1.44., z = 6.16, p < 0.001) but the test for heterogeneity was no longer significant (Q = 9.30, p > 0.1, I2 = 35.5%). No significant effect was found (Combined RR = 1.00, 95% CI’s = 0.90 to 1.11., z = 0.03, p > 0.1, test for heterogeneity: I2 = 4.4%, Q = 1.05, p > 0.10) within the two forensic wards (Dolan et al. 2008; Doyle et al. 2002).

Figure 7: Relative risk of a patient diagnosed with a schizophrenia disorder being in the aggressive group compared to the non aggressive group
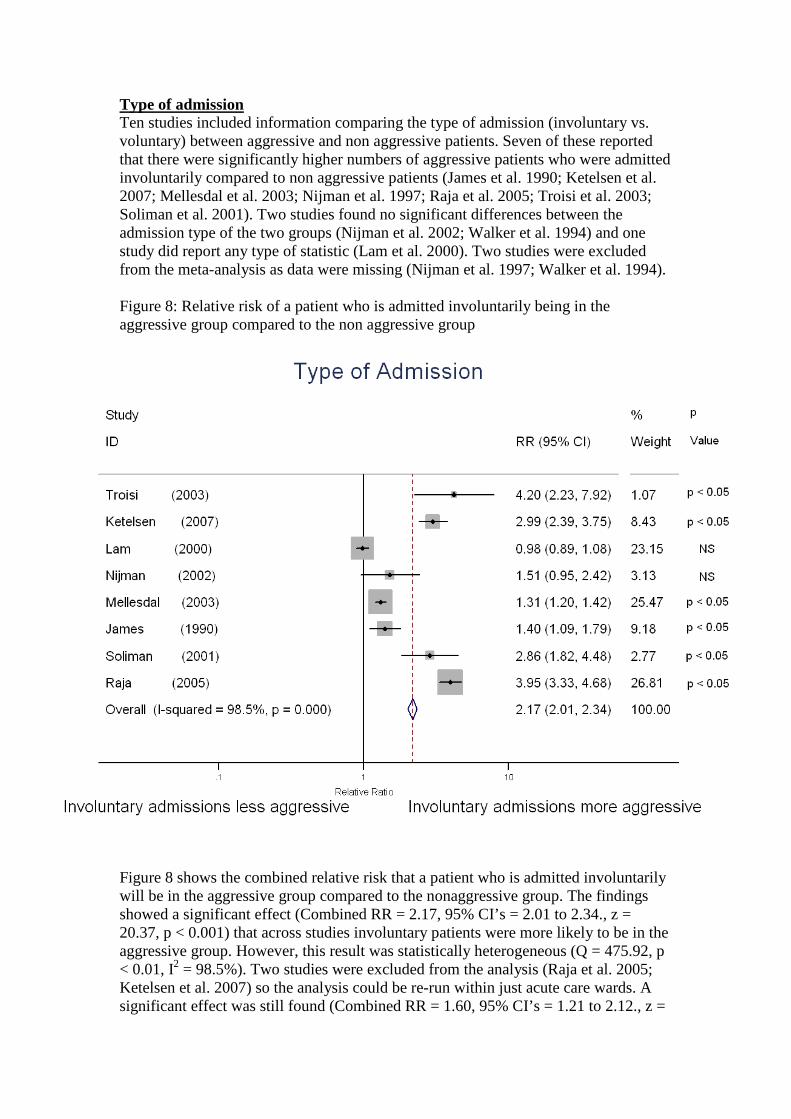
Type of admission Ten studies included information comparing the type of admission (involuntary vs. voluntary) between aggressive and non aggressive patients. Seven of these reported that there were significantly higher numbers of aggressive patients who were admitted involuntarily compared to non aggressive patients (James et al. 1990; Ketelsen et al. 2007; Mellesdal et al. 2003; Nijman et al. 1997; Raja et al. 2005; Troisi et al. 2003; Soliman et al. 2001). Two studies found no significant differences between the admission type of the two groups (Nijman et al. 2002; Walker et al. 1994) and one study did report any type of statistic (Lam et al. 2000). Two studies were excluded from the meta-analysis as data were missing (Nijman et al. 1997; Walker et al. 1994). Figure 8: Relative risk of a patient who is admitted involuntarily being in the aggressive group compared to the non aggressive group
Figure 8 shows the combined relative risk that a patient who is admitted involuntarily will be in the aggressive group compared to the nonaggressive group. The findings showed a significant effect (Combined RR = 2.17, 95% CI’s = 2.01 to 2.34., z = 20.37, p < 0.001) that across studies involuntary patients were more likely to be in the aggressive group. However, this result was statistically heterogeneous (Q = 475.92, p < 0.01, I2 = 98.5%). Two studies were excluded from the analysis (Raja et al. 2005; Ketelsen et al. 2007) so the analysis could be re-run within just acute care wards. A significant effect was still found (Combined RR = 1.60, 95% CI’s = 1.21 to 2.12., z =
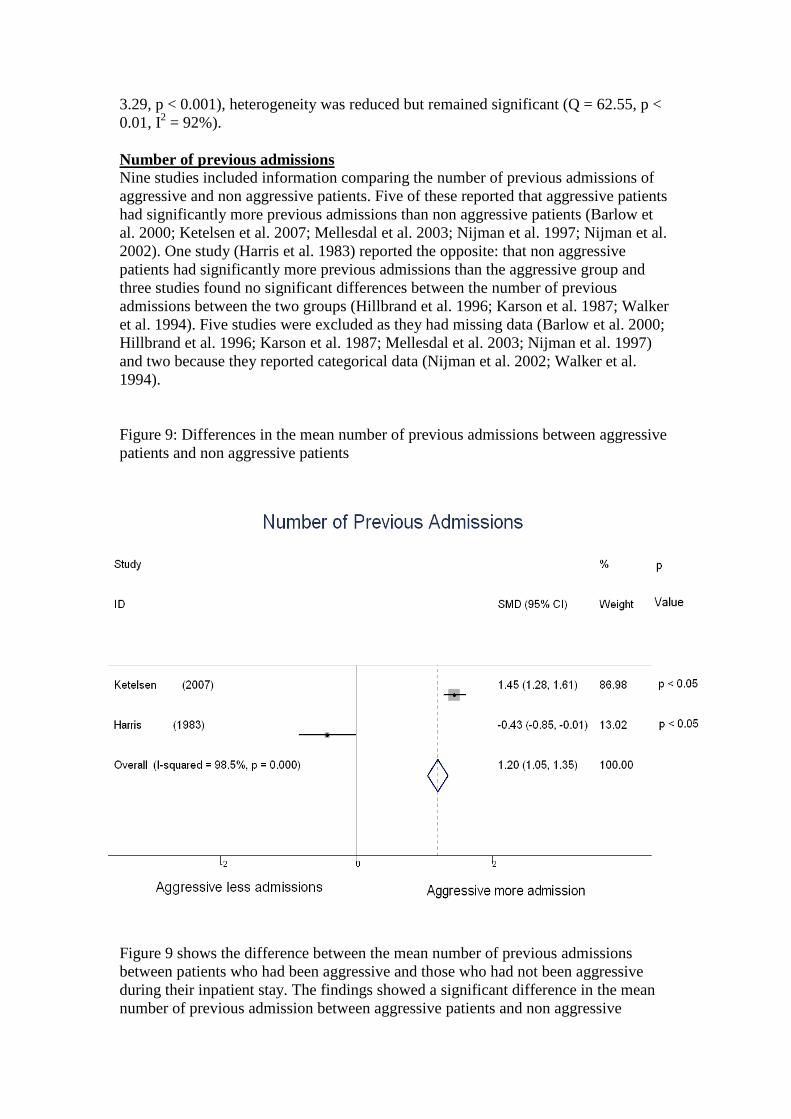
3.29, p < 0.001), heterogeneity was reduced but remained significant (Q = 62.55, p < 0.01, I2 = 92%). Number of previous admissions Nine studies included information comparing the number of previous admissions of aggressive and non aggressive patients. Five of these reported that aggressive patients had significantly more previous admissions than non aggressive patients (Barlow et al. 2000; Ketelsen et al. 2007; Mellesdal et al. 2003; Nijman et al. 1997; Nijman et al. 2002). One study (Harris et al. 1983) reported the opposite: that non aggressive patients had significantly more previous admissions than the aggressive group and three studies found no significant differences between the number of previous admissions between the two groups (Hillbrand et al. 1996; Karson et al. 1987; Walker et al. 1994). Five studies were excluded as they had missing data (Barlow et al. 2000; Hillbrand et al. 1996; Karson et al. 1987; Mellesdal et al. 2003; Nijman et al. 1997) and two because they reported categorical data (Nijman et al. 2002; Walker et al. 1994). Figure 9: Differences in the mean number of previous admissions between aggressive patients and non aggressive patients
Figure 9 shows the difference between the mean number of previous admissions between patients who had been aggressive and those who had not been aggressive during their inpatient stay. The findings showed a significant difference in the mean number of previous admission between aggressive patients and non aggressive

patients (Combined SMD = 1.20; 95% confidence intervals [CI], 1.05 to 1.35, z = 15.60, p < 0.001, test for heterogeneity: I2 = 98.5%, Q = 67.09, p < 0.001).
Patient Past History of Conflict Previous History of Violence: Six studies included information about patient’s previous history of violence for both the aggressive and non aggressive groups. All of these reported that aggressive patients were significantly more likely to have a history of previous violence (Blomhoff et al. 1990; Karson et al. 1987; Lam et al. 2000; Oulis et al. 1996; Soliman et al. 2001) or a significant association between violent behaviour in the community 2 weeks before admission and aggressive patient behaviour on the ward (McNiel et al. 1988). Figure 10 shows the combined relative risk that a patient with a previous history of violence will be in the aggressive group compared to the nonaggressive group. The findings showed a significant effect (Combined RR = 2.27, 95% CI’s = 1.90 to 2.69., z = 9.24, p < 0.001) that across studies patients with a history of violence were more likely to be in the aggressive group. However, this result was statistically heterogeneous (Q = 16.56, p < 0.01, I2 = 75.8%). Karson et al. (1987) was removed so the meta analysis could be rerun on studies from acute inpatient care. The effect remained significant (Combined RR = 2.37; 95% confidence intervals [CI], 1.97 to 2.86, z = 9.04, p < 0.001, test for heterogeneity: I2 = 80.3%, Q = 15.23, p < 0.01). History of self-destructive behaviour (suicidal behaviour, suicidal risk, self harm, suicide attempts): Six studies included information about patient’s previous history of self-destructive behaviour for both the aggressive and non aggressive groups. Hillbrand et al. (1996) found that aggressive patients were significantly more likely to have a history of self-destructive behaviour than non aggressive patients. Soliman et al. (2001) also found that aggressive patients were more likely to have a history of self-harm but no difference between whether the patients in each group had been admitted because of suicidal behaviour or intention. Raja et al. (2005) found suicidal risk to be significantly higher in physically aggressive patients compared to non aggressive patients and patients who were verbally aggressive or aggressive to objects. Similarly Tardiff et al. (1982) reported that aggressive patients were 3/4 times more likely to have attempted suicide than non aggressive patients. However, one study (McNiel et al. 1988) reported that suicidal patients were less likely than non suicidal patient to be aggressive on the ward.

Figure 10: Relative risk of a patient with a history of previous violence being in the aggressive group compared to the non aggressive group
Figure 11 shows the combined relative risk that a patient with a previous history of self-destructive behaviour will be in the aggressive group compared to the nonaggressive group. The findings showed a significant effect (Combined RR = 1.24, 95% CI’s = 1.03 to 1.50., z = 2.26, p < 0.05) that across studies patients with a history of self destructive behaviour were more likely to be in the aggressive group. However, this result was statistically heterogeneous (Q = 42.45, p < 0.01, I2 = 95.3%). This may be because each study took a different measure of self destructive behaviour. Hillbrand et al. (1996) looked at patient’s history of ‘self destructive behaviour’ but gave no definition for what behaviours this included. McNiel et al. (1988) measured patient’s suicidal behaviour while in hospital which included any threats, gestures or attempts. Soliman et al (1988) measured patient’s history of self-harm.
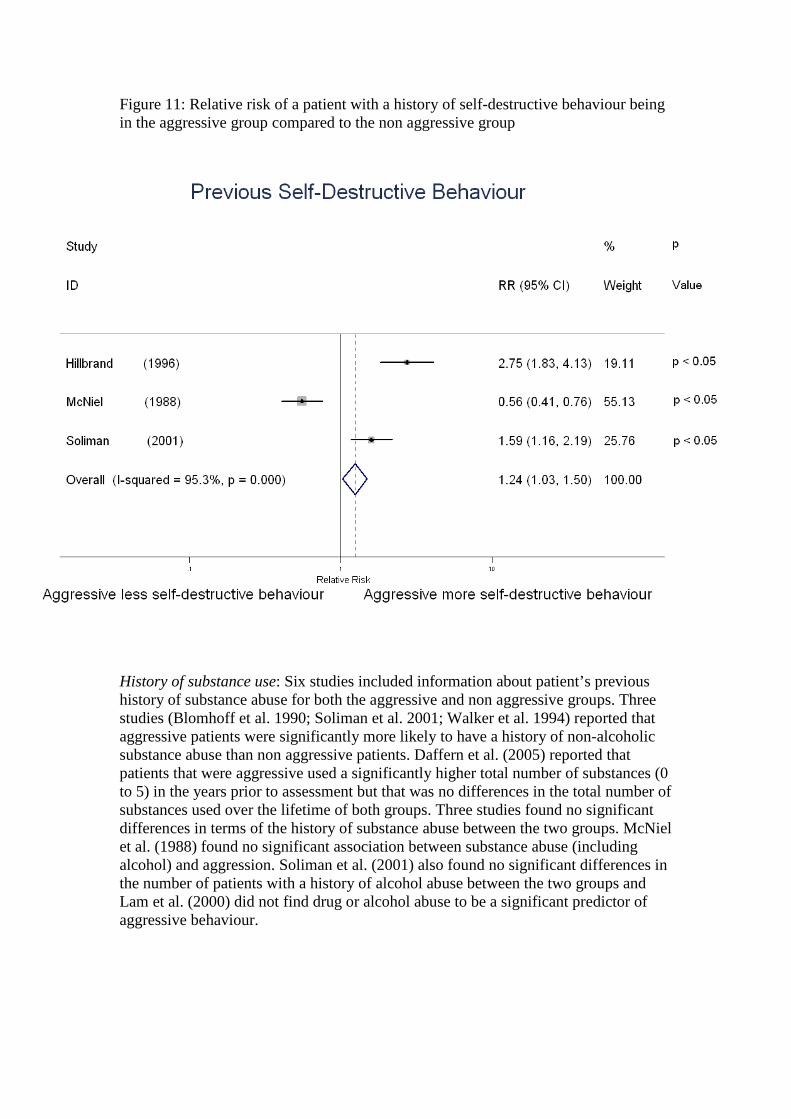
Figure 11: Relative risk of a patient with a history of self-destructive behaviour being in the aggressive group compared to the non aggressive group
History of substance use: Six studies included information about patient’s previous history of substance abuse for both the aggressive and non aggressive groups. Three studies (Blomhoff et al. 1990; Soliman et al. 2001; Walker et al. 1994) reported that aggressive patients were significantly more likely to have a history of non-alcoholic substance abuse than non aggressive patients. Daffern et al. (2005) reported that patients that were aggressive used a significantly higher total number of substances (0 to 5) in the years prior to assessment but that was no differences in the total number of substances used over the lifetime of both groups. Three studies found no significant differences in terms of the history of substance abuse between the two groups. McNiel et al. (1988) found no significant association between substance abuse (including alcohol) and aggression. Soliman et al. (2001) also found no significant differences in the number of patients with a history of alcohol abuse between the two groups and Lam et al. (2000) did not find drug or alcohol abuse to be a significant predictor of aggressive behaviour.

Figure 12: Relative risk of a patient with a history of substance abuse being in the aggressive group compared to the non aggressive group
Figure 12 shows the combined relative risk that a patient with a previous history of substance abuse will be in the aggressive group compared to the nonaggressive group. The findings showed a significant effect (Combined RR = 1.15, 95% CI’s = 1.00 to 1.31., z = 2.02, p < 0.05) that across studies patients with a history of substance abuse were more likely to be in the aggressive group. However, this result was statistically heterogeneous (Q = 21.19, p < 0.01, I2 = 76.4%). Findings suggest that when alcohol use is included there is little difference between the 2 groups, whereas the use of illicit drugs seems to be more likely within the aggressive group. The analysis was therefore re-run on just the studies that looked a patient’s history of previous illicit drug use. The results were no longer statistically heterogeneous (Q = 2.17, p > 0.1, I2 = 7.8%) and the significant effect remained (Combined RR = 2.09, 95% CI’s = 1.46 to 3.00., z = 4.03, p < 0.01). History of previous arrests or convictions for violent crime: Eight studies included information about patient’s criminal records in each group. Four studies found no difference between the records of the aggressive and non aggressive groups (Dolan et al. 2008; Doyle et al. 2002; Edwards et al. 1998; Fullam et al. 2008). Three studies found that the aggressive group were significantly more likely to have a criminal record (Daffern et al. 2005; Walker et al.1994) or a positive correlations between the number of assaults and arrest for violent offences. Harris et al. (1983) reported that
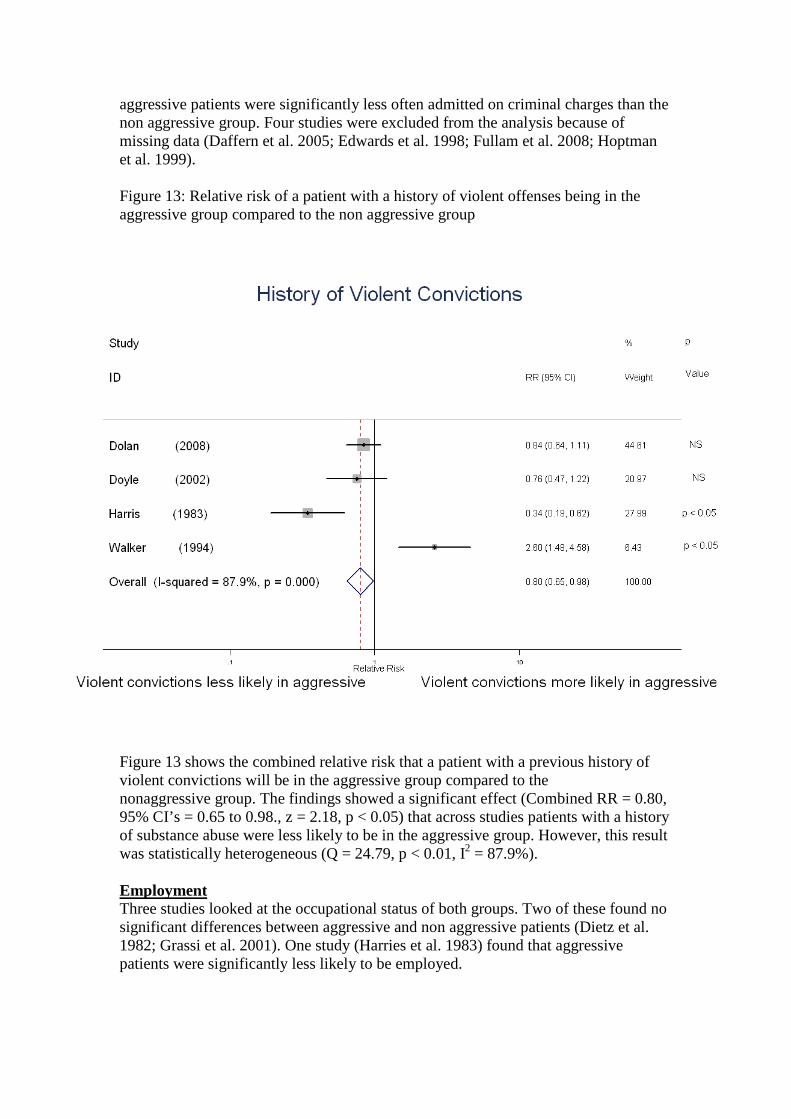
aggressive patients were significantly less often admitted on criminal charges than the non aggressive group. Four studies were excluded from the analysis because of missing data (Daffern et al. 2005; Edwards et al. 1998; Fullam et al. 2008; Hoptman et al. 1999). Figure 13: Relative risk of a patient with a history of violent offenses being in the aggressive group compared to the non aggressive group
Figure 13 shows the combined relative risk that a patient with a previous history of violent convictions will be in the aggressive group compared to the nonaggressive group. The findings showed a significant effect (Combined RR = 0.80, 95% CI’s = 0.65 to 0.98., z = 2.18, p < 0.05) that across studies patients with a history of substance abuse were less likely to be in the aggressive group. However, this result was statistically heterogeneous (Q = 24.79, p < 0.01, I2 = 87.9%). Employment Three studies looked at the occupational status of both groups. Two of these found no significant differences between aggressive and non aggressive patients (Dietz et al. 1982; Grassi et al. 2001). One study (Harries et al. 1983) found that aggressive patients were significantly less likely to be employed.

6.3 Results for high vs. low aggression comparison studies Inclusion criteria From the 6 repeater/high vs. single/low aggressive group studies one was excluded from the analysis as a large number of patients included were on outpatient wards (Fresan et al. 2005). Ten papers reported more than one comparison. Of these half (Barlow et al. 2000; Krakowski et al. 1989a, 1989b, 1997, 1999) made some sort of comparison between persistently aggressive and transiently aggressive patients. Mckenzie et al. (2005) was also included as patients within the aggressive group were analysed further based on their number of aggressive incidents. This left a total of 11 studies (See Table 3) to be analysed in the present series of meta-analyses. Where available the following information was collected from each paper: patient demographics (for gender, ethnicity, marital status, diagnosis, history of violence, suicide, drug abuse and admission type this was split into binary data, e.g. the proportions of patients in the aggressive and nonaggressive group that were male or female; for age and years of education continuous data was collected, e.g. means and standard deviations for each group), size of sample, type of ward, violence definition (verbal, physical against others, physical against objects, physical against self), and country.

Author Country Setting Data Status
(repeaters vs. single aggressors)
Number
Violence Definition
Measurement
Duration
Type of sample
1 Barlow et al. 2000
Australia Acute Age Multiple/Single
70/104 VPOS SIR 18 months
Random
2 Convit et al. 1990
USA Psychiatric Hospital
Age, Gender, Diagnosis
3+ / 1-2 70/243 P SIR 6 months
Random
3 Flannery et al. 2002
USA Other Age, Gender, Diagnosis, History of C & C
3+ / 1 61/566 VPO Sexual
ASAP 120 months
Random
4 Grassi et al. 2006
Italy Other Age, Gender, Marital Status, Education, Diagnosis, No of previous admissions, History of C & C
2+ / 1 65/95 VPOS SOAS 84 months
Random
5 Krakowski et al. 1989a
USA Special Unit
Age, Gender, Ethnicity, Diagnosis, History of C & C
Persistent/ Transient
38/39 VPO SIR 28 days
Consecutive admissions to special unit designed to manage assaultive behaviour
6 Krakowski et al. 1989b
USA Special Unit
Age, Gender, Ethnicity, Yrs of educations, History of C & C
2+/ 0-1 28/27 VPO SIR ? Schizophrenic admitted to special unit designed to manage assaultive behaviour

7 Krakowski et al. 1997
USA Admission wards
Age, Gender, Ethnicity, Diagnosis, Medication, Admission Type
Persistent/ Transient
34/43 P MOAS 28 days
Random
8 Krakowski et al. 1999
USA Admission wards
Age, Gender, Ethnicity, Diagnosis, Medication, History of C & C
Persistent/ Transient
44/52 VP MOAS 28 days
Schizophrenic
9 McKenzie et al. 2005
UK Forensic Age, Gender 10+ / 1-5 17/40 PO SIR 2 weeks
Random
10 Owen et al. 1998 Australia Mixed Age, Gender, Marital Status, Diagnosis, Medication, Type of admission, Previous admissions
20+ / 1 20/22 VPS Morrisons 7 month
Random
11 Rutter et al. 2004 UK Forensic Age, Gender, Admission type, Diagnosis, Ethnicity
25+ / <25 17/217 Unclear SIR 192 months
Random

Age From the 11 comparison studies all included information comparing the age of repeaters and single aggressors. Of these eight reported no significant difference in age (Barlow et al. 2000; Flannery et al. 2002; Grassi et al. 2006; Krakowski et al. 1989a, 1989b, 1997, 1999; McKenzie et al. 2005). Two studies found that patients who were repeatedly violent were significantly younger than less frequently aggressive patients (Owen et al. 1998; Rutter et al. 2004). Convit et al. (1990) found that female repeaters (3+) were significantly younger than single aggressors but there was no difference between males in either group. Five papers were excluded from the meta-analysis as the ages were recorded as the standard deviations or mean value were not reported (Barlow et al. 2000; Convit et al. 1990; Krakowski et al. 1989a; McKenzie et al. 2005; Rutter et al. 2004). Figure 14 shows the difference between the mean ages of patients who had been repeatedly aggressive and those who had been less aggressive during their inpatient stay. The findings showed no significant difference between the two groups (SMD = -0.08, 95% confidence intervals [CI], -0.23 to 0.07, z = 1.06, p > 0.1). The result was not statistically heterogeneous (Q = 6.54, p > 0.1, I2 = 23.5%). Figure 14: Differences in mean age between repeatedly aggressive patients and less frequently aggressive patients

Gender Ten of the studies included information comparing the gender of repeatedly aggressive and less frequently aggressive patients. Eight of these reported no significant difference in the gender of repeatedly aggressive and less aggressive patients (Flannery et al. 2002; Grassi et al. 2006; Krakowski et al. 1989a, 1989b, 1997, 1999; McKenzie et al 2005; Owen et al. 1998). Convit et al. (1990) and Rutter et al. (2004) both found that repeatedly aggressive patients were more likely to be females than males. Owen et al. (1998) was excluded from the meta-analysis as data. Figure 15 shows the combined relative risk that a male patient will be in the repeatedly aggressive group compared to the less frequently aggressive group. The findings show that there is an effect that males are less likely to be in the repeatedly aggressive group (Combined RR = 0.83, 95% CI’s = 0.75 to 0.93, z = 3.30, p < 0.01). However, the test for heterogeneity was significant (I2 = 56.7%, Q = 18.46, p < 0.05). Figure 15: Relative risk of a male being in the repeatedly aggressive group compared to the less aggressive group

Ethnicity Four studies included information comparing the ethnicity of repeatedly aggressive and less frequently aggressive patients. All of these reported no significant differences between the two groups of patients (Krakowski et al. 1989a, 1989b, 1997, 1999). Figure 16 shows the combined relative risk that a patient who is of an ethnic majority (in this case Caucasian) will be in the repeatedly aggressive group compared to the less frequently aggressive group. The findings show no significant effect (Combined RR = 0.79, 95% CI’s = 0.52 to 1.18, z = 1.15, p > 0.1). The result was not statistically heterogeneous (Q = 5.81, p > 0.1, I2 = 48.4%). Figure 16: Relative risk of a patient who belongs to an ethnic majority being in the repeatedly aggressive group compared to the less aggressive group

Marital Status Two studies included information comparing the marital status of repeatedly aggressive and less aggressive patients. Owen et al. (1998) found that repeatedly aggressive patients were more likely to be widowed than less frequently aggressive patients. Grassi et al. (2006) found no significant difference between the 2 groups (repeatedly violent group: 70.9% married; less frequently violent group: 66.3% married). There was not enough data to run a meta-analysis. Diagnosis Eight studies included information comparing the diagnoses of repeatedly aggressive and less aggressive patients. Seven of these reported no significant difference in the diagnoses of the two groups (Convit et al. 1990; Flannery et al, 2002; Grassi et al. 2006; Krakowski et al. 1989a, b, 1997, 1999). One study (Owen et al. 1998) reported that repeaters were more likely to suffer from organic brain syndrome or personality disorder. For the meta-analysis studies that included data about patient’s diagnoses were collated into three categories: schizophrenic (including schizoaffective etc.), affective (depression, mania etc) and other (personality disorder, organic brain syndrome etc.). Analyses were the made comparing the ratio of affective diagnoses compared to all other diagnoses in the repeatedly aggressive and less aggressive group as well as comparing the ratio of schizophrenic diagnoses with all other diagnoses in both groups. Three studies were excluded from the analyses due to missing data (Owen et al. 1998), or because all patients were either diagnosed with schizophrenia or schizoaffective disorder (Krakowski et al. 1989b, 1999). Schizophrenia Vs All Other Diagnoses: Figure 17 shows the combined relative risk that a patient who is diagnosed with a schizophrenic disorder will be in the repeatedly aggressive group compared to the less aggressive group. The findings showed no significant effect (Combined RR = 1.04, 95% CI’s = 0.95 to 1.14, z = 0.81, p > 0.1, test for heterogeneity: I2 = 26.3%, Q = 5.43, p > 0.10). Affective Vs All Other Diagnoses: Figure 18 shows the combined relative risk that a patient who is diagnosed with an affective disorder will be in the repeatedly aggressive group compared to the less aggressive group. The findings showed no significant effect (Combined RR = 0.70, 95% CI’s = 0.43 to 1.13, z = 1.46, p > 0.1). However the test for heterogeneity was significant (I2 = 65.5%, Q = 8.68, p < 0.05) questioning the validity of combining these studies.

Figure 17: Relative risk of a patient with schizophrenia being in the repeatedly aggressive group compared to the less aggressive group
Figure 18: Relative risk of a patient diagnosed with an affective disorder being in the repeatedly aggressive group compared to the less aggressive group

Patient Past History of Conflict Previous History of Violence: Three studies included information about patient’s previous history of violence for both the repeatedly aggressive and non aggressive groups. Grassi et al. (2006) found that repeated episodes occurred significantly more in patients with previous violent behaviour and Owen et al. (1998) reported that repeatedly aggressive patients were more likely to have a history of aggression (100%) compared to less aggressive patients (26%). Flannery et al. (2002) reported no significant difference in patient’s history of violence between the two groups. Figure 18 shows the combined relative risk that a patient with a previous history of violence will be in the repeatedly aggressive group compared to the less aggressive group. The findings showed a significant effect (Combined RR = 1.58, 95% CI’s = 1.45 to 1.73., z = 10.26, p < 0.001) that across studies patients with a history of violence were more likely to be in the repeatedly aggressive group aggressive group. However, this result was statistically heterogeneous (Q = 105.28, p < 0.01, I2 = 99.1%). Validity of data is questionable as only two studies are included in the analysis.

Figure 18: Relative risk of a patient with a history of aggression being in the repeatedly aggressive group compared to the less aggressive group
History of suicide attempts: Only one study included information about patient’s previous history of suicide attempts for both the repeatedly aggressive and less aggressive groups. Krakowski et al. (1989a) found that a history of suicide attempts was more frequent in repeatedly aggressive patients (61.8%) than less aggressive patients (36.1%).
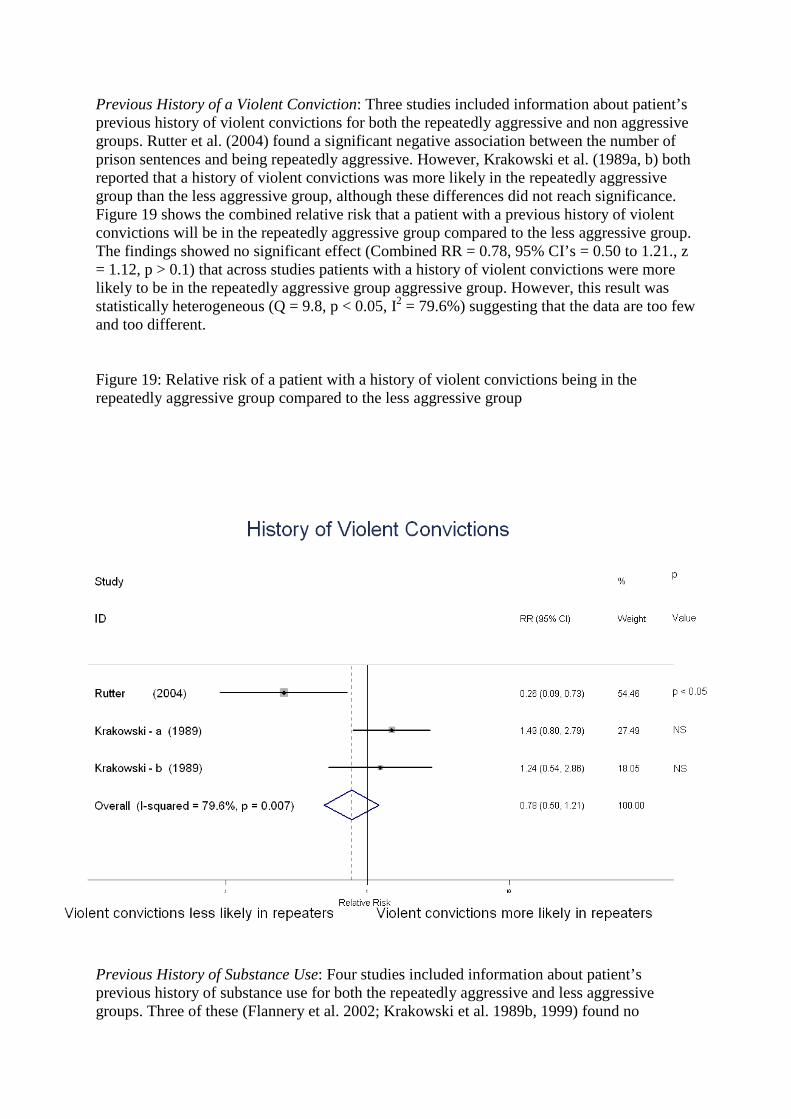
Previous History of a Violent Conviction: Three studies included information about patient’s previous history of violent convictions for both the repeatedly aggressive and non aggressive groups. Rutter et al. (2004) found a significant negative association between the number of prison sentences and being repeatedly aggressive. However, Krakowski et al. (1989a, b) both reported that a history of violent convictions was more likely in the repeatedly aggressive group than the less aggressive group, although these differences did not reach significance. Figure 19 shows the combined relative risk that a patient with a previous history of violent convictions will be in the repeatedly aggressive group compared to the less aggressive group. The findings showed no significant effect (Combined RR = 0.78, 95% CI’s = 0.50 to 1.21., z = 1.12, p > 0.1) that across studies patients with a history of violent convictions were more likely to be in the repeatedly aggressive group aggressive group. However, this result was statistically heterogeneous (Q = 9.8, p < 0.05, I2 = 79.6%) suggesting that the data are too few and too different. Figure 19: Relative risk of a patient with a history of violent convictions being in the repeatedly aggressive group compared to the less aggressive group
Previous History of Substance Use: Four studies included information about patient’s previous history of substance use for both the repeatedly aggressive and less aggressive groups. Three of these (Flannery et al. 2002; Krakowski et al. 1989b, 1999) found no

significant differences between the repeatedly aggressive and less aggressive patients. Krakowski et al. (1989a) did find that a history of drug abuse was significantly more frequent in repeatedly aggressive patients than the less aggressive patients group. Krakowski et al. (1989b) was excluded from the analysis because of missing data. Figure 20 shows the combined relative risk that a patient with a previous history of substance use will be in the repeatedly aggressive group compared to the less aggressive group. The findings showed a significant effect (Combined RR = 1.28, 95% CI’s = 1.04 to 1.59, z = 2.30, p < 0.05) that across studies patients with a history of drug use were more likely to be in the repeatedly aggressive group aggressive group. The results were not statistically heterogeneous (Q = 2.26, p > 0.1, I2 = 11.3%). Figure 20: Relative risk of a patient with a history of substance abuse being in the repeatedly aggressive group compared to the less aggressive group
History of arrest for violent crimes: Two studies provided information about the number of arrests for violent crime in both the repeatedly aggressive group and the less aggressive group (Krakowski 1989a, b). Neither of these reported significant differences between the two groups. Figure 21 shows the combined relative risk that a patient with a previous history of arrests for violent crimes will be in the repeatedly aggressive group compared to the less

aggressive group. The findings showed no significant effect (Combined RR = 1.04, 95% CI’s = 0.70 to 1.53, z = 0.19, p > 0.1) that across studies patients with a history of arrests for violent crimes were more likely to be in the repeatedly aggressive group aggressive group. The results were not statistically heterogeneous (Q = 0.08, p > 0.1, I2 = 0%). Figure 21: Relative risk of a patient with a history of arrests for violent crime being in the repeatedly aggressive group compared to the less aggressive group

Age at first hospitalisation Three papers included information about the ages of patient’s first hospitalisation for both aggressive groups (repeaters, single aggressors). Krakowski et al. (1989a) found that repeatedly aggressive patients were significantly younger at their first hospitalisation than less aggressive patients (16.2 vs. 19.1). Two studies reported no significant differences in the ages of the two groups (Grassi et al. 2006; Krakowski et al. 1989b. Krakowski et al. (1989a) was excluded from the meta-analysis as the standard deviations were not reported. Figure 22 shows the difference between the mean age at the first hospitalisation of patients who had been repeatedly aggressive and those who had been less aggressive during their inpatient stay. The findings showed no significant difference between the two groups (SMD = -0.10, 95% confidence intervals [CI], -0.37 to 0.18, z = 0.69, p > 0.1). The result was not statistically heterogeneous (Q = 0.16, p > 0.1, I2 = 0%).
Figure 22: Differences in mean age at the first hospitalisation between repeatedly aggressive patients and less frequently aggressive patients

Number of Previous Admissions Grassi et al. (2006) was the only study which compared the number of previous admissions in each group and found episodes of violence were positively associated with the number of previous admissions (19.68 vs. 3.42). Other Relevant Factors Krakowski et al (1989a,b) looked at neurological impairment within the two groups and found that repeatedly violent patients had more neurological impairments (particularly cerebellar signs) than the less aggressive group. This difference remained even when neuroleptic medications were controlled for. Krakowski et al. (1997) found repeatedly aggressive patients were more impaired in frontal lobe functioning and tended to show more dysfunction on motor integrative tasks. Some studies also found differences between the groups on the Brief Psychiatric Rating Scale (BPRS) and the Nurses’ Observation Scale for Inpatient Evaluation (NOSIE). Repeatedly violent patients had a greater impairment on the total BPRS score (Krakowski et al 1989a, 1999), and the Anergia (Krakowski et al 1989a), and the Hostility-suspiciousness subscales (Krakowski et al 1989a, 1999). Differences were also found on the NOSIE mean score and NOSIE (Krakowski et al 1989a, 1999), social subscale (Krakowski et al 1989a, 1999), and routine and temper subscales (Krakowski et al. 1999), which were both lower in the repeatedly violent group. Krakowski et al. (1997) showed less resolution of symptoms over the 4 weeks in the repeatedly violent patients than the less frequently violent patients. 6.4 Evidence for and against the City model The review of comparison studies of aggressive and non aggressive patients does not provide much information that is relevant to the City model. To some extent although differences between the two groups were significant, the overall effects were small suggesting that other factors included in the City Model (staff morale, technical mastery and team working skills, the physical environment of the ward, positive appreciation for the patients etc.) play a bigger role in causing aggressive behaviour. This was especially apparent in the repeatedly aggressive patients, where very few demographic factors distinguished them from less aggressive patients. These patients are responsible for multiple episodes of aggression so it is important to understand the triggers for this subset of patients or the variables that may be associated with this repetitive behaviour. 6.5 Points the City model has missed Patient characteristics such as age, gender, type of admission, marital status, diagnosis, and past history of conflict are not addressed in the existing model. Some of these factors may be used as part of a risk assessment. 6.6 Discussion In total, a relatively small number of comparison studies were found relative to the number of publications on impatient aggression (17.5%). The majority of publications instead tended to focus on the rate of aggressive incidents within wards, or the antecedents and consequences of aggression. The small number of comparison studies suggests that future research would

benefit from focusing on this type of research design. By comparing aggressive with non-aggressive patients important differences between the two populations may be highlighted. These differences may help staff improve predictions of which patients might become aggressive and enable steps to be taken to reduce an aggressive incident occurring. All but seven of the studies included had fewer than 100 patients in both the aggressive and non-aggressive groups and the demographics were not often the focus of the research. The small sample sizes included in the analysis will have impacted on the result because smaller studies were weighted as less significant. More prospective comparison studies are needed which should be designed on the basis of power analyses to calculate the minimum sample size required in order to detect an effect or a reliable difference between aggressive and non-aggressive patients. Despite these limitations, a number of demographic characteristics appear to be associated with an increased likelihood of inpatient aggression. These included being younger, male, involuntary admissions, not being married, a diagnosis of schizophrenia, a greater number of previous admissions, a history of violence, a history of self-destructive behaviour and a history of substance abuse. Interestingly, a history of previous violent convictions was associated with a decreased likelihood of inpatient aggression. We can be fairly confident that these results represent true effects as they have been estimated by combining the results of several studies. The effects are also more powerful than those reported in individual studies whose findings are sometimes mixed. The associations between demographic factors and aggression were fairly small and for some factors (involuntary admission, number of previous admissions, history of violence, history of self-destructive behaviour and history of previous convictions) the heterogeneity was high (I2 was greater than 50%) suggesting that combining the studies for these factors in particular may lead to less generalisable estimates. The high levels of heterogeneity found may be because psychiatric services can vary a great deal in terms of setting, routines, ward rules and atmosphere. It is also probable that levels of aggression are influenced more by factors other than patient demography. For example, these may include a patient’s current presentation e.g. whether or not they appear under the influence of alcohol or drugs; the symptoms they are currently displaying such as: fear, agitation, anger, confusion, excitement, suspiciousness or irritability; whether patients are having delusions and/or hallucinations; and their current attitude towards treatment and management. Contextual factors may also have a substantial impact upon the levels of aggression, for example whether the patient has a weapon available; the ward environment (i.e. levels of surveillance/visibility, ward door-locking policies, ward rules); the relationship and proximity between a victim and aggressor; and the extent of social support both within the ward with staff and patients and outside the ward with family and friends. Although we have identified a number of demographic factors that are associated with inpatient violence, the utility of these for an actuarial based risk assessment tool is questionable. The generally small effects found coupled with the heterogeneity between studies, suggest that any such instrument would be too inaccurate to be useful. Approaches based on short term prediction may prove to be more practically useful (Abderhalden et al., 2004; Ogloff & Daffern, 2006). There is a significant debate in the literature about the link between schizophrenia, substance misuse and violence in the community and this review is consistent with research which has found associations between these variables (Fazel et al., 2009). The mechanism of the link between substance use, schizophrenia and aggression is uncertain as they share a number of confounding risk factors such as male gender, younger age, increased suicide rate, non-adherence to treatment, higher levels of social deprivation. Common factor models suggest

the links are the result of shared risk factors such as genetics, antisocial personality disorder, socioeconomic status an impaired cognitive functioning. Secondary substance use models posit that there are certain reasons (self medication, alleviation of dysphoria) why having a diagnosis of schizophrenia increases the risk of substance misuse. Secondary psychiatric disorder models put forward the opposite argument that substance misuse leads to a diagnosis of schizophrenia in individuals who would not have developed the disorder had they not taken illicit substances. In addition there are bidirectional models that propose that either variable (schizophrenia, substance misuse) can increase the likelihood of the other co-occurring (for a review of the evidence for and against each model, see Mueser et al., 1998). Future research is needed that follows patients longitudinally to shed more light on the direction and relationships between aggression and the significant demographics identified here (age, gender, history of previous violence, history of substance misuse, type of admission, diagnosis, marital status). This in turn may provide useful information about which of these factors reliably predicts an aggressive patient. It may be possible to then start thinking about management strategies for these patients. What is it about a young, single, male admitted involuntarily with a diagnosis of schizophrenia and a history of previous violence, self-destructive behaviour and substance misuse that makes an aggressive incident more likely? Potentially the way in which staff make requests of a patient could be a potential antecedent of an aggressive incident. Requests may be perceived as demands and feel a lack of control over their environment or their actions. This may be attenuated by a lack of social support, and symptomology such as delusions and irritability.

7. THE TIME AND PLACE OF VIOLENT INCIDENTS 7.1 The studies reviewed The literature review on violence and aggression identified 78 papers which contained empirical data on the time and place of violent incidents. Most studies were from the USA (n=24) or the UK (n=22). Six were from Australia and three from Canada, Italy, New Zealand, Norway and Taiwan. Twenty studies were from acute wards, 22 from forensic services, and 34 from a mix of wards in psychiatric hospitals. Two were categorised as ‘other’. 7.2 Time of day Only studies which specified the time of day in which violent incidents occurred or reported the time of peaks in incident rates were included in this section (n=57). The time categories employed by these studies varied widely. These often reflected shift patterns specific to individual hospitals or were constructed for analytical convenience. This makes aggregating data across studies particularly difficult. Our approach was to categorise peaks of incidents by either shift or time interval. If data was available for both, only the time interval data (i.e. the most specific timing) was analysed. The time intervals with the best fit across all the studies were: 6:00-7.59, 8:00-11.59, 12:00-13.59, 14:00-17.59, 18:00-19.59, 20:00-21.59, 22:00-5.59 (night). These categories were applied with a degree of flexibility (plus or minus one hour) in order to capture all the available data. Data presented in the form of two shifts (day or night) or three shifts (morning, afternoon/evening and night) were also extracted, as were specific activities associated with peaks of incidents (e.g. mealtimes). The frequency of studies which reported peaks of violence within each time category or shift were calculated. Where studies reported two or more peaks of incidents during the day each was included in the calculations. It was much more difficult to examine actual rates of violence by shift or time. Studies typically mentioned times of peak rates of violence, rather than report rates across a complete 24 hour period. Therefore, insufficient data was available for this kind of analysis A total of 27 papers reported specific times of day when higher rates of violent incidents occurred. As Figure 1 shows, incidents tended to peak between 8am and 8pm, with none of the studies reporting a peak during the night. The most frequently reported peak of violence was between 8:00 and 11:59 (n=13), with a reduced frequency for each subsequent category thereafter. A further 30 studies reported high rates of violence during certain shifts (Figure 2). Again, no studies reported a peak during the night. In contrast to the time based analysis, most peaks were found in the afternoon/evening shift (n=15). However, studies restricted to analysis of violent incidents by shift may well have missed more subtle variations in the distribution of violence during the course of the day.

Figure 1: Peak times for violent incidents
0
2
4
6
8
10
12
14
6:00-7:59 8:00-11:59 12:00-13:59 14:00-17:59 18:00-19:59 20:00-21:59 22:00-5:59
Time
Fre
qu
ency
Figure 2: peak shifts for violent incidents
0
2
4
6
8
10
12
14
16
Day Morning Afternoon/evening Night
Shift
Fre
qu
ency

There was a difference by setting in the proportion of peak times for violence which occurred before midday, with studies from psychiatric hospitals reporting a higher percentage (63%) than acute (29%) and forensic (23%) services. Similarly for analysis by shift, 50% of peak times for violence were on a morning shift in the psychiatric hospital studies, compared to 33% in studies of acute wards and 17% in forensic studies. The timing of peaks in violence may be related to levels of patient activities on the ward, staff handover, medication round, meal times or waking time. These all place demands on patients which may trigger a violent incident. Ten papers specifically stated that meal times were high risk periods for violence. This was usually an association with mealtimes in general (n=8), but where papers were more specific they were not entirely consistent. One study from the USA found that violent incidents peaked sharply in the morning before breakfast, but rates of incidents were then fairly consistent throughout the day [Abbott 1978]. In contrast, a prospective study from Australia reported that fewer incidents occurred at lunchtime compared to the morning or evening periods [Owen et al. 1998]. Two forensic studies reported that staff handover times corresponded to high levels of violence and aggression. One was from Finland and found statistically significant higher rates of violence during 1-3pm which was the time for nursing handovers [Weizmann-Henelius and Suutala 2000]. The other identified the night-shift handover (9pm) as a particular risk period for violence [Gudjonsson et al. 1999] and was also the only study to report a peak of violence at medication times. In addition, a prospective survey of incidents in a psychiatric hospital found that a fifth of incidents occurred in the first hour of a shift [Yassi et al. 1998]. Explanations for these associations were less forthcoming. It may be that peak times for patient violence are related to activity demand changes, particularly when patients are requested to become active after a period of inactivity such as mealtimes [Depp 1976]. Alternatively, it has been suggested that more incidents occur in the early afternoon because nurses are least available to patients during this time and there is increased interaction between patients [Whittington and Wykes 1994]. This is supported by another study which found less violence during early morning and evening periods when staff were maximally available to patients [Fairlie and Brown 1994]. Weekends may have fewer incidents simply because they are less hectic than weekdays [Gudjonsson et al. 1999]. One analysis of mealtime incidents found a greater number to occur when patients were walking or standing in line (54%) compared to actually sitting in the dining room (35%)[Hunter and Love 1996]. Mealtimes involve most patients congregating in the same place which may create tension, on top of any irritability associated with hunger [Gudjonsson et al. 1999]. Most studies included both physical and verbal aggression, but no differences were reported in terms of the relative timing of these incidents. 7.3 Day of week Thirty-three studies reported the distribution of violent incidents by day of the week (Figure 3). Peak days for violence tended to be at the start of the week (Monday, Tuesday and Wednesday), with no studies reporting a peak on Saturday, although three reported a peak on Sunday. Some studies (n=9) compared weekdays to weekends and overwhelming found that violence was more prevalent during the former. However, it should also be noted that a fifth of the studies (n=7) reported no pattern to violence during the course of the week. The most

frequent category for studies of acute patients was Monday-Friday (n=3). For forensic studies the most frequent peaks were Monday and Tuesday (n=3 each) and for psychiatric hospitals it was Tuesday and None (n=4 each). One study reported frequencies by incident type [Bowers et al. 2006]. It found that property damage was less frequent on Wednesday and Friday, physical aggression to be lower on weekends and Wednesday, but no significant pattern for verbal aggression or self-harm. The most common explanation provided for differences by weekday concerned greater levels of association between patients and staff during the week compared to the weekend. Patients are involved in more activities, there is greater movement around the ward and higher staff levels so there is more interaction with staff and more staff around to notice and report incidents [Abbott 1978]. Other explanations for fewer incidents at weekends include patients having the option of not going to the dining room [Hunter and Love 1996], lower levels of patient activities [Carmel and Hunter 1989], and fewer procedures carried out and decisions made [Morken et al. 1999]. Explanations for the prevalence of violence on specific weekdays involved the routines of the ward or hospital. This included patients assembling to watch films [Dietz and Rada 1982], visiting days and unit meetings [Ionno 1983], and tension associated with ward rounds [Cooper et al. 1983]. One acute ward study found levels of verbal and physical aggression to be significantly more likely on the days before and after ward rounds [Bowers et al. 2006], when patients may anticipate or react to significant decisions about their care.
Figure 3: Peak days for violent incidents
0
1
2
3
4
5
6
7
8
9
10
Mon Tue Wed Thu Fri Sat Sun Mon-Fri Weekend None
Fre
qu
ency
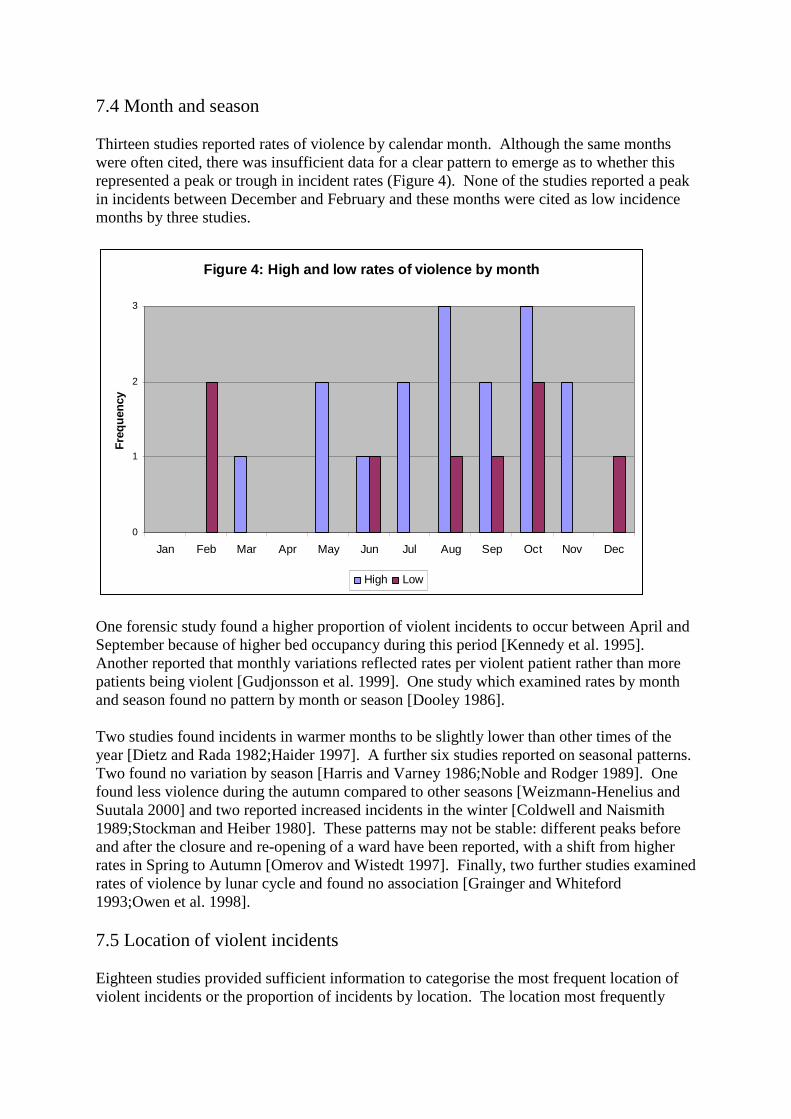
7.4 Month and season Thirteen studies reported rates of violence by calendar month. Although the same months were often cited, there was insufficient data for a clear pattern to emerge as to whether this represented a peak or trough in incident rates (Figure 4). None of the studies reported a peak in incidents between December and February and these months were cited as low incidence months by three studies.
Figure 4: High and low rates of violence by month
0
1
2
3
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Fre
qu
ency
High Low
One forensic study found a higher proportion of violent incidents to occur between April and September because of higher bed occupancy during this period [Kennedy et al. 1995]. Another reported that monthly variations reflected rates per violent patient rather than more patients being violent [Gudjonsson et al. 1999]. One study which examined rates by month and season found no pattern by month or season [Dooley 1986]. Two studies found incidents in warmer months to be slightly lower than other times of the year [Dietz and Rada 1982;Haider 1997]. A further six studies reported on seasonal patterns. Two found no variation by season [Harris and Varney 1986;Noble and Rodger 1989]. One found less violence during the autumn compared to other seasons [Weizmann-Henelius and Suutala 2000] and two reported increased incidents in the winter [Coldwell and Naismith 1989;Stockman and Heiber 1980]. These patterns may not be stable: different peaks before and after the closure and re-opening of a ward have been reported, with a shift from higher rates in Spring to Autumn [Omerov and Wistedt 1997]. Finally, two further studies examined rates of violence by lunar cycle and found no association [Grainger and Whiteford 1993;Owen et al. 1998]. 7.5 Location of violent incidents Eighteen studies provided sufficient information to categorise the most frequent location of violent incidents or the proportion of incidents by location. The location most frequently

reported as having the most number of incidents was the lounge or day room (27%), followed by bedrooms (23%), corridors (14%), nurse stations (14%) and unspecified common areas (14%). Twelve studies reported the proportion of violence incidents at each location (Figure 5). The mean percentage of incidents was similar for bedrooms, corridors, lounge and nurses office (between 24% and 28%), but dining areas and bathrooms had relatively low rates. Comparison of the seven acute and forensic studies showed that lounge and nurses office were the most frequent locations for the former, while the forensic studies typically reported more incidents in generic communal and lounge areas.
Figure 5: Location of violent incidents
0
5
10
15
20
25
30
Bathroom Bedroom Corridor Dining area Lounge Nurse office Ward door
Location
%
7.6 Evidence for and against the City model There is a clear link between the degree of patient association and levels of violence. In general, the more opportunity there is for interaction the greater the chance of violence occurring. This explains the fewer incidents reported at weekends when wards tend to be quieter and there are fewer activities for patients to engage in. Less stress, noise and bustle at weekends reduces the chances of aggression and violence occurring. These findings were reported by studies of both patient-patient and patient-staff violence and those which focussed on violence against staff only. Taken together, the best it is possible to conclude from the studies is that the routines and organisation of the ward can influence the rate of violent incidents. Mealtimes, staff handover and group activities area associated with an increased risk of violence. It may be possible to organise these interactions differently to reduce tension or opportunities to commit violent acts, but from the papers reporting violence against staff it does seem that patient-staff interactions can be associated with violence also. Of course, what all the papers lack is an assessment of the manner of the interaction between

staff and patients rather than simply the circumstances or frequency of it. A greater presence of nurses at some periods of the day may simply increase the opportunity for an aggressive patient to verbally or physically abuse them. On the other hand, there is evidence that staff presence reduces the risk of violence. For example, one multi-site study found lower levels of violence in a PICU, possibly reflecting the nurses’ expertise in handling aggressive behaviour, and overall levels of violence to be lower at times when staff are most available to patients [Fairlie and Brown 1994]. The notion that increased staff presence raises the risk of violence was further examined in the literature. Twelve studies examined the relationship between staffing levels and violence (surveys of nurses’ and patients’ perceptions of this issue were excluded). However, the collective findings are inconclusive. Three studies found no overall association between staffing and violence levels [Depp 1983;Lanza and Kayne 1997;Palmstierna and Wistedt 1995]. Four reported that more staff to be associated with greater violence [Bowers et al. 2009;Carmel et al. 1991;Morrison 1990;Owen et al. 1998] and another four found a negative association [Bowers et al. 2007;Chou et al. 2002;Fairlie and Brown 1994;Jones 1985]. In a further study, the relationship between staffing numbers and violence was negative for permanent staff but positive for temporary staff [James et al. 1990]. Whilst reporting no apparent relationship overall, one study found it to be positive for inter-patient violence but negative for patient-staff violence [Palmstierna and Wistedt 1995]. Another of the studies which found no overall effect reported differences in the direction of the relationship between staffing and violence between individual wards [Lanza and Kayne 1997]. 7.7 Points the City model has missed The City model does not include the kinds of temporal effects described here. However, the evidence from this review suggests that observed variations by time actually reflect aspects of service organisation. 7.8 Discussion Summary The evidence available in the literature suggests that time and place have some association with levels of violence on wards, but the way in which this happens is most likely to be related to the specific configuration of individual services. There is no compelling evidence for seasonal effects, but peaks in violence by time of week and day seem to correspond with particular events and activities on the wards. Incidents occur in most areas of the ward, but particularly in corridors, bedrooms, lounge areas and around nursing stations. Lessons for future research We know from the literature that small numbers of patients are responsible for the majority of violent incidents. In light of this, it is not clear how the findings for time and place should be interpreted. Are we to conclude that only certain patients are likely to find social situations stressful or difficult to cope with (e.g. mealtimes)? Perhaps patients with a propensity for violence deliberately plan attacks to occur at particular times and places. None of the studies address these issues.

Given the links between service organisation and violent incidents, as well as evidence of setting differences in the timing of violence, local assessment of the time and place of incidents may facilitate initiatives to reduce violence on wards. Such initiatives are unlikely to work unless more is understood about the nature and content interactions between patients and staff which occur at specific times and places. Further exploration of time and place by victim type (patient or staff) would be a useful and achievable starting place for future studies.

8. STAFF AND PATIENT PERCEPTIONS OF VIOLENCE AND AGGRESSION
8.1 The studies reviewed Sixty four papers were identified that address staff and patient attitudes and perceptions of aggression in inpatient psychiatry. 43 papers contained information on staff perceptions, 9 on patient perceptions and 12 had information on both staff and patient perceptions. Type of wards Seven studies collected data from acute settings, six from forensic settings, twenty four from more than one inpatient setting, two studies collected data from psychiatric intensive care units, twenty collected data from non specified wards (10 psychiatric hospital/institutions, 3 unspecified psychiatric units, 6 cross sectional surveys of staff) and five collected data from other types of wards (1 chronic long stay setting, 1 closed psychosis wards, 1 psychiatric unit in general hospital, 1 veterans medical centre, 1 psychiatric nurses’ college). Countries Data were collected from 14 different countries. These were: UK (24 studies), USA (n=19), Netherlands (n=6), Australia (n=5), Sweden (n=3), Canada (n=3), Switzerland (n=3), Taiwan (n=2), Spain, Turkey, Norway, Germany, South Africa and China (n=1). Data source There were five methods of data collection used. Data were collected from questionnaires (n= 41 studies), interviews (n=29), observations (n=2), focus groups (n=3) and video footage (n=1). Thirty papers employed quantitative methods of data collection, 27 used qualitative methods and 7 used a mixed methods approach. Sample The number of staff members who took part in these studies ranged from 4 to 3074 and the number of patients from 4 to 1386. 8.2 Method A thematic analysis of the staff and patient perceptions, attitudes and belief data produced 11 distinct ‘lower-level’ themes which formed 4 higher-level themes: perceptions of aggression, aggression facilitators, preventing aggression and reaction to aggression. These themes will now be discussed in terms of both staff and patient perceptions.

8.3 The function of aggression This section presents literature on psychiatric staff’s perceptions of the function of aggression. Quantitative findings Nine studies (Jansen et al, 1997; Jansen et al., 2006a, Jansen et al., 2006b; Jonker et al., 2008; Muro et al, 2002; Palmstierna and Barredal, 2006; Whittington and Higgins, 2002; Alderhalden et al., 2002; Whittington, 2002) quantitatively explore staff perceptions of the function of aggression by psychiatric patients. Jansen et al (1997) asked 274 psychiatric nurses to rate 60 descriptions of aggression (that had been generated during a qualitative study with nurses, Finnema et al 1994). A factor analysis of these ratings produced three distinct dimensions of aggression. Nurses perceived aggression as either a ‘normal’ reaction to feelings of anger, aggression as a ‘violent’ reaction or aggression as a ‘functional’ reaction. A follow up study surveying 618 psychiatric staff in the Netherlands (Jansen et al 2006a) investigated whether staff characteristics may underlie differences in perceptions of the function of aggression. Staff working with geriatric patients, on long stay wards, and those who used restraining interventions were found to agree with the ‘violent’ reaction attitude. Male nurses, those working daytime shifts and those working in geriatric psychiatry agreed that aggression was a ‘normal’ reaction. Female staff, those working in child and adolescent services, on short stay wards, those who worked on both day and evening shifts were the strongest predictor of perceiving aggression as ‘functional’ reaction. Nurses with more than 11 years of experience agreed less often than less experienced nurses that aggression was a functional behaviour. Using the Attitudes Toward Aggression Scale (ATAS) (Jansen et al, 2006a) which comprises five types of attitudes towards aggression; ‘offensive’, ‘communicative’, ‘destructive’, ‘protective’ and ‘intrusive’ attitudes, Jansen et al (2006b) investigated the attitudes of 1963 nurses internationally. Men were found to agree more with the ‘communicative’ scale than female nurses but less on the ‘destructive’ scale. Nurses who worked part time had lower scores than full time staff on the ‘offensive’, ‘destructive’, ‘protective’ and ‘intrusive’ attitudes. Using the same measure Jonker et al (2008) looked at the prevalence of each function of aggression amongst 113 nurses in the Netherlands. The highest scores were found for the view that patient aggression is ‘destructive’ and ‘offensive’, and lowest scores for the view that aggression is ‘protective’ and ‘communicative’. Three of these studies looked at differences in perceptions cross culturally. In the Jansen study UK nurses had the highest score for the ‘offensive’ and ‘intrusive’ attitude scales and the lowest scores for the ‘protective’ attitude scale on which the Norwegian nurses scored highest. UK, German and Norwegian nurses had higher scores on the ‘destructive’ scale than the Dutch or Swiss nurses. Alderhalden et al (2002) found that German nurses scored lower on aggression as ‘dysfunctional’ than nurses form other European countries who in turn scored lower than nurses from non-European countries and in this study German nurses scored higher on aggression as ‘functional’ scale than nurses from other European countries. In a comparison of UK and Chinese mental health nurses, Whittington and Higgins (2002) found that UK nurses agreed significantly more than the Chinese sample with the notion that aggression is something that can be tolerated, a notion that ties into viewing aggression as a ‘normal’ reaction. Five of the studies employed the Perception of Aggression Scale (POAS) (Jansen et al, 1997) to measure psychiatric staff perceptions of aggression. This measure also draws its statements from the original attitude inventory from the Finnema study. Muro et al (2002) administered

the POAS to 90 nursing students in Spain, 48.9% scored between strongly agree and agree with the perception that aggression is a ‘violent’ reaction; this figure was 0% and 6.7% for ‘normal’ reaction and ‘functional’ reaction. There was a significant difference between gender and perception of aggression as a ‘violent’ reaction with females in stronger agreement than males. Whittington (2002) investigated the ‘normal’ reaction to aggression attitude with 37 UK nurse. Nurses with 15 years or more experience agreed with this attitude more than nurses with less experience. This study also found that staff with lower burnout scores supported the view that violence is a ‘normal’ reaction more than those with higher burnout scores. Similarly, Whittington and Higgins (2002) found that attitudes regarding aggression as positive were related to a sense of personal accomplishment at work in a sample of mental health nurses in the UK and China. In contrast to Whittington (2002), Adberhalden et al (2002) found more experienced nurses had higher scores on the attitude that aggression is ‘dysfunctional’ than less experienced nurses. Older nurses also rated this function higher than younger colleagues. Diploma nurses scored lower on the aggression as ‘functional’ scale than nursing aids and students. Palmstierna and Barredal (2006) found that more agreement with aggression as a ‘protective’ measure was related to older age and more experience of aggression management training, and that male nurses with longer experience tended to regard aggression more negatively on the aggression as ‘dysfunctional’ factor. Qualitative findings Three papers qualitatively explore staff perceptions of the function of aggression. Finnema et al (1994) conducted interviews exploring the characterisation and perception of patient aggression by twenty four nurses working in a psychiatric hospital in the Netherlands. This study shows that nurses perceive and describe aggression in a number of ways. As well as negative views about aggression, most nurses acknowledged that aggression also has positive features. This is illustrated in respondents’ descriptions of aggression which included, ‘aggression as a way to express feelings’, ‘aggression as a way to get things done which would otherwise not have been done’. Five categories of aggression emerged from the definitions given by staff. These were definitions that contained a value statement, a form of aggression, feelings that aggression evokes, the function of aggression and consequences of aggression. Daffern and Howells (2009) conducted semi-structured interviews with psychiatric staff, and where possible with patients, at a personality disorder unit in the UK. They were asked to recall and describe an incident of aggression and these descriptions were scored for the presence or absence of a particular function as classified by the Assessment and Classification of Function (ACF) tool (Daffern et al., 2006). Incidents of aggression were viewed by staff and patients as multi functional with each incident containing a median of three functions. Most incidents involved the expression of anger (97%), 58% were expressed as tension reducing and as a means to enhance status or social approval and 42.42% had a demand avoidance function. A phenomenological study by Cutcliffe (1999) highlights the individualistic nature of nurses’ views about aggression. In relation to the same patients’ aggression one nurse stated ‘I would not consider his behaviour to be violent, It was his way of telling us that he is pissed off’ another nurse described this patients behaviour as, ‘I would say that is violent, sure…I report that as a violent outburst’. An interesting theme emerging from this study was the way nurses decided on what they regard as violent. Intent, the extent of the therapeutic relationship a

nurse has with a patient and the focus of the patients’ violence were described by staff. ‘What I report as violence depends upon my previous experience of violence’, ‘what defines something as violence is the intent’, ‘if I get the sense that the violence is pre-meditated, this makes it harder to be compassionate and empathetic’. 8.4 Staff expectation of aggression Quantitative findings Seven quantitative studies (Baxter et al., 1992; Chaimowitz and Moscovtich, 1991; Poster and Ryan, 1989; Schwartz and Park, 1999; Gordon et al., 1996; Collins, 1994; Poster, 1996) report upon staffs’ perceptions of the expectation of encountering aggression during their careers. These studies show that a number of mental health workers expect to encounter aggression during the course of their role caring for the mentally unwell and some feel that this is part of their job. Chaimowitz and Moscovtich surveyed 132 psychiatric residents in Canada about their experience of aggression by psychiatric patients, 40.2% of residents had been assaulted at least once during their training and 45.3% of those assaulted believed that being assaulted was part of the risks of psychiatric practice. Similarly, Schwartz and Park (1999) surveyed 517 psychiatric residents in America and 12% felt that being assaulted by patients is an inherent part of the profession. Four studies asked staff to rate whether they agreed or disagreed with the statement ‘staff working with mentally ill patients can expect to be physically assaulted at some point during their career’. Eighty five percent (n=263) of psychiatric nurses in Australia (Baxter et al., 1992), 75% of psychiatric staff in America (n=184) (Poster and Ryan, 1989), 56% of health care workers (n=40) providing care psychiatric inpatients in Australia (Gordon et al, 1996) and 73% of 999 nursing staff surveyed in the United States, Canada, UK and South Africa (Poster, 1996) agreed with the statement. Collins (1994) reported that before taking part in an intervention that addressed the prevention and management of aggressive behaviour 51% of psychiatric staff and students expected to be assaulted by patients in their career. Following training and education this figure decreased to 39% which the authors attribute to staff’s increased confidence and reduced anxiety following training. Qualitative findings Two qualitative studies (Chen et al., 2007; Delaney et al., 201) report staff perceptions of assaults as an inevitable part of a career in psychiatric care. Chen et al, (2007) interviewed thirteen staff victims of psychiatric inpatient assault. The interviews revealed that staff perceive aggression to be a common problem at work. In response to questions about the experience of aggression one member of staff said 'we prepared in our minds to encounter such events when we took the job as psychiatric nurse. It is very common to have such an assault in a psychiatric ward.' Another said, 'It was natural to be physically attacked as a psychiatric nurse.’ Staff who took part in focus groups conducted by Delaney et al (2001) discussed the expectancy of being assaulted. An interesting view raised during these discussions was that perhaps expecting to be a victim of aggression may in fact lead to being assaulted. This self fulfilling prophecy effect was described by one staff member as; ‘'Do we want to say acute nursing aggressive incidents will happen...that's a fact of life…'well actually no it's not part of the job, like it's not in my job description’ ...it's the general attitude...that we will get assaulted...but maybe if we looked at the other way that we shouldn't expect to get assaulted and it shouldn't happen...would that change things at all…Maybe...we are going to be assaulted...because we expect it to happen.’ This study also sheds light on the fact that although nurses expect to be assaulted, they don’t necessarily see if as part of their job to be on the receiving end of aggression.

8.5 Causes of aggression The characteristics of violent patients, staff characteristics, denying and the restriction of patients, environmental factors and interaction factors were identified by respondents as facilitators of aggressive behaviour. Patient factors Quantitative findings Six papers addressed the role of characteristics of violent patients in facilitating aggression (Chaplin et al., 2006a; Chaplin et al., 2006b; Gillig et al., 1998; Duxbury and Whittington, 2004; Duxbury et al., 2008; Duxbury, 2002) A study comparing the views of 32 staff and 54 patients regarding the causes of psychical aggression in a psychiatric unit reported that 50% of staff and 65% of patients cited patient psychosis as a major cause of physical aggression on the unit (Gillig et al.,1998). In three papers using The Management of Aggression and Violence Attitude Scale (MAVAS) to evaluate staff and patient perspectives of violence in mental health units (Duxbury and Whittington, 2004; Duxbury et al., 2008; Duxbury, 2002) staff viewed patient internal factors as causes of aggression. However, two of these papers compared staff and patient views (Duxbury, 2002; Duxbury and Whittington, 2004) and found that the ratings of agreement to the statement ‘patients are aggressive because they are ill’ were significantly lower for patients than for staff. The use of substances by patients is referred to by respondents in three of these studies. The use of drugs and alcohol was rated highly by staff and patients as causes of aggression in the study by Gillig. 43% of patients and 74% of staff believed patients using drugs or alcohol, patients who sell drugs and alcohol (35% v 49%) and patients who are intoxicated (44% v 77%) were major causes of physical aggression on the units. Interestingly, 33% of patients and 3% of staff believed that staff who use drugs and alcohol was a major cause of aggression. Patient intoxication as a cause of aggression was also reported in a large national audit study of 3074 staff and 1386 patients (Chaplin et al, 2006b). Sixty-one percent of nurses believed that there was trouble on the ward because of alcohol (compared to 25% of patients) and 72% of nurses said that they thought trouble on the ward was caused by drugs (compared to 29% of patients). However, in an audit study with 585 staff and 157 service users only 5% of staff and 7% of service users affirmed the question ‘is there trouble because of people getting drink?’ and only 4% of staff and 5% service users agreed that ‘there [is] trouble because of people taking drugs?’ (Chaplin et al, 2006a). Qualitative findings In six interview studies (De Neit et al., 2005; Duxbury and Whittington, 2004; Lanza, 1998; Kindy et al., 2005; Spokes et al., 2002; Finnema et al., 1994) nurses reported that psychotic symptoms are often precursors to aggression. Nurses in the study by Kindy cited characteristics of psychiatric and developmental disorders including impulsiveness, explosiveness and feeling superior to and antagonistic toward staff as contributing factors to the uncontrollability of the environment. Nurses in the study by Finnema described patient hallucinations, delusions and inability to express angry feelings in other ways as factors contributing to violence. In the study by De Neit nurses talked about not always being able to understand a patient’s reasons for their aggressive behaviour, and related this to the patient’s psychosis and impulsivity.

In a small interview study with 4 staff and 4 patients (Hinsby & Baker 2004), the patients talked about their unstable mental state as a reason for violence, this is illustrated in the following quote from a patient in the study; ‘When your mental state is all right you know the difference between right and wrong; even if you are angry you can control yourself. But when you are not stable and you are a paranoid schizophrenic, little things spark you off.’ However, in an interview study (Johnson et al., 1997) with twelve thought disordered patients only two attributed the cause of violence to internal factors, the patients in this study more frequently described external factors as reasons for their aggression. Ninety two patients were interviewed about their views on the causes of patient- to-patient and patient-to-staff aggression in a study by Fagan-Pryor et al. (2003). Internal factors including cognitive factors, feelings and symptoms were described by 33% of the patients as contributing to patient-to-patient aggression, and by 39% in relation to patient-to-staff aggression. Cognitive factors included, the aggressive patient thinking everyone is against him or her; feeling disrespected, not understanding why he or she is hospitalised and not being in the right frame of mind. Jealousy, anxiety, frustration, emotions not being right, ‘alcohol depression’, anger, boredom and irritability were examples of the feelings patients viewed as causing aggression. And symptoms included hallucinations; talking too much without stopping; losing control because one is not in touch with reality and incoherence. Meehan et al (2006) conducted focus groups with patients in a high secure forensic mental health facility to capture patient perceptions about the factors leading to aggressive behaviour. Personal characteristics of the patients emerged as a theme from the discussions. The impulsive and demanding nature of some patients was described as a source of tension in relationships between patients, and patients and staff. There was a perception that ‘some patients have a short fuse’ and they lose control very quickly which was attributed to illness factors. One patient described difficulties in controlling aggressive outbursts; ‘sometimes I’m ready to explode I get so annoyed with some of the other patients . . . and the staff too. It’s not easy to control myself but I have to control it.’ The use of drugs and alcohol by patients was described as contributing to violence in two studies (Spokes et al., 2002; McGeorge et al., 2000). In an audit study of psychiatric staff, patients and visitors from 42 NHS Trusts in the UK (McGeorge et al., 2000) staff reported that even when alcohol and drugs were not readily available on the wards, problems would occur when patients returned to the wards having consumed them off the premises. In free-text responses to questions about the triggers of aggression, 16% of patients and 29% of staff in the study by Chaplin et al (2006b) mentioned illegal drugs and alcohol. Other patient factors described as causes of violence include involuntary admission status, a history of violence as mentioned by staff (Delaney et al., 2001; Finnema et al., 1994) and patients (Omerov et al., 2004), and mix of patients with different diagnosis and mental health problems on the same ward (McGeorge et al., 2000; Quirk et al 2004). Staff factors Quantitative findings A survey of 263 psychiatric nurses using the Attitudes to Assault Questionnaire (Baxter et al., 1992) found that 70% of nurses agreed that behaviour and attitudes of staff can invite assaults from patients. In contrast, several studies (Bilgin & Buzlu, 2006; Poster & Ryan, 1994; Poster & Ryan, 1989) who administered the Attitudes Toward Patient Physical Assault Questionnaire (ATPPAQ) to psychiatric staff found a strong disagreement with statements pertaining to patient aggression being related to staff competency, skills and personality. For example, 78% of 162 Turkish psychiatric nurses (Bilgin & Buzlu, 2006) and 75% of 184 staff

working in a psychiatric hospital in the USA (Poster & Ryan, 1994) did not agree with the statements ‘staff members who are assaulted have personality traits that make them vulnerable to patient assaults’, ‘patient physical assault of a staff member is a result of performance deficiency’ (88.3% and 78% respectively), or ‘staff members who are physically assaulted are less competent clinically than staff who are not assaulted’ (80.9% and 92%). However, in this American sample male staff were significantly more likely than female staff to believe that assaulted staff had personality traits that made them vulnerable to assault (14% vs 5%). Qualitative findings Unlike the majority of the quantitative studies reported above, nine qualitative studies report that staff characteristics, behaviours and attitudes can lead to patient aggression. In a study conducted using semi structured interviews (Bond and Brimblecomb, 2003) with 102 English psychiatric nursing staff, 96.1% of staff reported that individual characteristics of staff increase the likelihood assault. Staff factors that were most frequently cited as increasing the risk of violence included a lack of skills including communication, understanding and attentiveness; personality characteristics including being overly opinionated, controlling, eager or shy; and attitudes including rudeness, sarcasm, belittling, ignoring and arguing. In a focus group study (Kumar et al, 2001) with six mental health service users who had experienced aggression reported that stressed staff, staff attitudes, being treated disrespectfully by staff and a decline in staff caring attitudes were all precipitants to violence. Omerov et al., (2004), interviewed patients who had been involved in violent incidents about the causes of their aggression, in 73% of the incidents patients considered that the violence was provoked by staff. Spokes et al., (2002) obtained views of 108 mental health nurses about the role of staff related factors in violence. The nursing staff interviewed believed that staff factors affect the likelihood of a violent incident occurring. Staff factors that were reported as affecting the likelihood of violence occurring included staff clinical skills, such as competency in the use of techniques such as distraction, interpersonal skills such as verbal and non-verbal communication, including providing explanations and being able to build rapport with patient; and personal characteristics including physical characteristics, personality traits and behaviours. Madden et al (1976) surveyed 115 psychiatrists about assaults by patients. 53% of respondents believed that they had provoked the patient into attacking them by making comments or interpretations that were received unfavourably by the patient and at times felt they had been too insistent that a patient confront upsetting material. Several of the psychiatrists reported that they did not particularly like the patient who assaulted them and might have projected this feeling to the patient. Other staff factors contributing to aggression that were reported in the qualitative literature included, professional elitism, staff disrespect for ethnic, racial and gender issues, competitive tensions among staff '...and we have a lot of pettiness among the treatment team, a lot of egos...my degree is better than yours, or I have more experience.' (Kindy et al., 2005), staff not being adequately trained, staff treating patients disrespectfully, staff not paying enough attention to patients (Bensley et al., 1995), staff allowing patients to antagonise each other (Quirk et al., 2004), deliberately provoking patients, not understanding and neglecting patients and being aggressive towards patients (Finnema et al., 1994).

Interaction factors Quantitative findings Using the Management of Aggression and Violence Attitude Scale with mental health nurses in Switzerland and UK Duxbury et al (2008) found that both samples of nurses agreed with the statements that ‘poor communication between staff and patients leads to patient aggression’ and ‘improved one to one relationships between staff and patients can reduce the incidence of aggression’. Using the same measure with staff and patients Duxbury (2002) recorded differences in opinion between these two groups with regard to interaction between staff and patients causing aggression. This view was supported by the patient scores on this statement however, staff did not view their interactions with patients to be problematic or a cause of patient aggression. Qualitative findings Eight qualitative studies (Duxbury & Whittington, 2004; Johnson et al., 1997; Fagan-Pryor et al., 2003; Meehan et al., 2006; Finnema et al., 1994; Spokes et al., 2004; De Neit et al., 2005; Duxbury, 2002) report that interaction between staff and patients can facilitate aggression. Duxbury and Whittington (2004) reported that poor communication, specifically staff failing to listen to patients, was commonly reported by patients as a precursor to aggression. 'People in here just want to be listened to'. ‘They don't seem to care. I don't think anyone trains them in how to deal with people. Staff seem to think once you are in here they do not need to bother’ ‘There is no respect. Just because we are patients they think they can tell us to shut up’. Interestingly, the staff in this study did not view communication with patients to be problematic. De Neit et al conducted a small qualitative study alongside a larger quantitative study with nurse who identified several causes of aggression. They reported that the mutual interaction between patients, interaction between patient and nurse and the so-called ‘social moments’ like drinking coffee and having dinner were often moments when aggression was initiated. Finnema et al (1994) interviewed twenty four Dutch psychiatric nurses about their perceptions of the causes of violence by patients. The respondents related aggression to an inadequate attitude of nursing staff including not listening to patients, deliberately provoking patients and interrupting patients. Meehan et al (2006) conducted focus groups with patients about the causes of aggression on the unit. A major theme to come out of these focus groups was that the way in which staff interacted with patients was a major source of dissatisfaction for the patients. Staff were perceived as adopting superior attitudes and controlling behaviours to enforce a strict hierarchy of authority rather than to assist in the delivery of therapeutic care: ‘you just get a lot of smart-arse comments from them [staff] and not much caring. Some of them [staff] act as if they’re in a prison, prison guards, walking around all day giving us an ear-full of what we can and cannot do’. There was also a feeling that staff lacked understanding about the problems associated with their illness and treated them with a distinct lack of empathy. The perceived lack of caring gave rise to thoughts of harming staff and retaliatory aggression. Denying, restricting and imposing rules on patients Quantitative findings Four quantitative studies (Gillig et al,. 1998; Ruben et al,. 1980; Schwartz, and Park, 1999; Lanza, 198) report that patient frustration borne out of actions such as limit and rule setting and refusing patient requests is a precipitant to aggression. Ruben et al., (1980) conducted a study with fifteen psychiatric residents who had been attacked by patients, 93.4% believed they had done something to trigger the attack; the most common reason was that they had

frustrated the patient who had attacked them. Frustrations that were listed included setting limits on patients, especially on issues around admission and discharge, carrying out physical examinations on patients who didn’t want them and making patients attend group therapy sessions. Refusal to satisfy a patient request and setting limits on patients were recorded as reasons for patient attacks on staff during a survey of 517 psychiatric residents (Schwartz & Park 1999). Nineteen percent thought they had been assaulted because they had refused a patient request and seventeen percent because they had set a limit on the patient. Gillig et al., (1998) reported that refusing a smoking requests, leave or discharge and forcing patients to take medication were common causes of physical aggression by patients reported by 32 nursing staff (which country?). In an audit survey of 184 psychiatric wards (what country?) 9% of the patients surveyed reported that staff inadvertently provoke violence by restricting their freedoms (Chaplin et al., 2006b). Qualitative findings Five interviews studies with staff (Finnema et al., 1994; Spokes et al., 2002; Madden et al., (1976); Secker et al., 2004; Chen et al., 2007) and one focus group study (Delaney et al., 2001) revealed that denying a patient something they have requested or limiting and restricting their freedom are often perceived as causes of aggression. Of the 108 mental health nurses interviewed about the causes of violence by Spokes et al, 9% of staff thought violence was related to staff employing limit-setting techniques with patients. Nurses in the study by Finnema described constantly imposing restrictive measures on patients, limitations among patients, the fact that patients are forced to conform to unit rules and the lack of freedom for patients to do what they want are causes of patient aggression. Madden et al, reports the views of clinicians that refusing to meet a patient's requests, setting too many limits on a patients as well as interestingly, not setting enough limits are triggers to patient violence. Secker et al interviewed 15 staff about the cause of 11 specific violent incidents that had occurred on a psychiatric ward in the UK. Themes that emerged from several of the incidents centred on staff denying patients’ requests, for example, requests to see a doctor, access to the office, access to a telephone, and requests to be discharged. In four of these studies (Spokes et al., 2002; Madden et al., (1976); Secker et al., 2004; Chen et al., 2007), administering medication or checking that patients have taken their medication was identified by staff as other triggers of patient aggression. Evidence from four qualitative studies with patients (Omerov et al., 2004; Johnson et al., 1997; Duxbury, 2002; Meehan et al., 2006; Bensley et al., 1995) support the role of frustration, denial, and medication in triggering aggression. Thirty seven (90%) patients in the study by Omerov who had perpetrated aggressive incidents considered that their violence had been provoked. In 73% of these incidents patients considered that the violence was provoked by staff often when permission was denied, for example to take part in an activity. In 34% of the incidents patients reported that the incident had occurred when medication was being given. Meehan et al (2006) conducted focus groups with 27 patients in a forensic setting to capture patient perceptions of the factors leading to aggressive behaviour. The inflexible and strict way in which staff enforce ward rules was perceived as a source of aggression. Frustration was expressed when staff appeared to override the rules and withdraw patients’ privileges for no apparent reason: ‘I was on the phone to my girlfriend, and ah I was on there for two minutes and they made me hang up, you’re allowed ten minute phone calls, you know, and I gave them a big heap of abuse.’ Ward procedures such as queuing at the office window to talk to staff were seen by patients as demeaning and the source of friction amongst patients. Staff were portrayed as ignoring frequent requests for assistance as ‘you’ve got to beg these people 26 [swear word] times before you get anything.’ Almost all of the

participants identified boredom as a source of frustration and medication was frequently blamed for taking control away from the patients resulting in outbursts of aggression: ‘. . . when they [nurses] try to give me something else I say ‘hold on mate that’s not my medication’. I have seen lots of arguments over medications that end up physical . . . you know . . . take-downs, seclusion, the lot.’ Patients in the study by Duxbury viewed themselves to be victims of the controlling style of nursing staff. Johnson reported that the policies that restricted patient freedom seemed linked to anger and aggressiveness. And patients in the study by Bensley believed that not enough explanation of the rules contributed to patient assaults. Environmental factors Quantitative findings Several studies report that the environment of the psychiatric hospital or ward can be conducive to patient aggression. Environmental factors such as the lack of adequate facilities (Chaimowitz & Moscovtich, 1991; Poster & Ryan, 1989), inadequate staff numbers (Poster & Ryan, 1989; Bilgin & Buzlu, 2006; Chaplin et al., 2006a) the use of bank and agency staff and overcrowding (Chaplin et al., 2006a) have been reported as contributing factors of aggression on inpatient wards. Using the Management of Aggression and Violence Attitude Scale (MAVAS) Duxbury et al., (2008) surveyed nurses in the UK and Switzerland about their views of the antecedents to violence, the UK respondents agreed with the statement that ‘Patients are aggressive because of the environment they are in’ while Swiss respondents disagreed. UK respondents were also more likely than the Swiss nurses to agree with the statement ‘If the physical environment were different, patients would be less aggressive’ although this did not achieve statistical significance. A lack of activities resulting in boredom and in turn aggression was cited by service users in an audit including 1386 patients as a cause of aggression (Chaplin et al., 2006b). Although 63% were satisfied with daytime activities and therapy, only 47% expressed satisfaction with evening activities and 41% with activities during the weekend. Qualitative findings The findings from several qualitative studies report that environmental factors play a role in facilitating inpatient aggression. Finnema et al., (1994) interviewed 24 nurses about their perception of patient aggression; a lack of privacy for patients, environmental factors specific to closed wards and lack of activities were cited as preceding factors to violence. The staff and patients interviewed in a study by Duxbury & Whittington (2004) deemed environmental factors to be problematic and precipitants to aggression; the nursing staff referred to the poor ward design and a bad atmosphere ‘We are fighting against a really difficult structural environment’. Currid (2008) conducted a phenomenological study with eight mental health nurses in London. Several of the participants linked insufficient staffing with the high rates of aggressive acts and believed that if there were more staff available to meet patients’ needs or to support the staff who were dealing with the aggressive patients, incidents would decrease. Staff in an audit study by Chaplin et al (2006a) also made the link between low staffing levels, lack of activities, boredom, and the potential for violence. The major concern among service users in this study was the lack of things to do. This is reflected in free-text responses, which indicated problems with boredom, dislike of being on the unit, lack of or cancelled activities, being locked up, and denial of access to money and cigarettes. Twelve patients were interviewed by Johnson et al (1997). A main theme to come out of the interviews was that patients felt that aspects of the environment were influential in
precipitating aggressive incidents and some of the participants perceived the aggressive incident to be justified because of the intolerable aspects of the environment. These included being confined behind locked doors, the inability to go outdoors and the lack of space and freedom, one patient stated ‘Well, when you’ve got up to 25 people living together in one locked up unit, sooner or later sparks are going to fly. If anyone expects anything else they should be locked up in here with us!’ Bensley et al (1995) interviewed 69 patients from eight high assault wards in the USA about factors they believed contributed to the assaults, in order of importance these were smoking and access to outdoors, not enough to do (boredom), overcrowding, noise, amount of food and lack of daytime access to bedrooms.
8.6 Preventing aggression Predicting aggression Quantitative findings Nurses in four studies express the belief that it is possible to predict patient aggression. Poster & Ryan (1989) report that 43% of the nurses they surveyed agreed that prediction of patient assault is within competence and ability of all psychiatric staff, similarly, 49% (n=132) of psychiatric residents attacked by patients in a study in Canada felt the attack could have been predicted (Chaimowitz and Moscovtich, 1991). Milius (1990) conducted a cross sectional survey with 43 mental health workers in the USA to assess that predictability of aggressive outbursts. Nurses were asked for their opinions on the predictability of aggressive behaviour and were asked to identify signals they would use to assess impending patient aggression. 88.4% of the nurses believed it was possible to predict that a patient was at risk of showing aggressive behaviour and 76.7% said imminent aggressive outbursts were predictable. The most cited predictors of inpatient aggression were; patient agitation (74% of nurses stated this), verbal hostility (53%), frustration (49%), non-compliance (49%) and family conflict (44%). Collins (1994) conducted a questionnaire study that assessed nurses’ attitudes about their ability to predict aggression before and after taking part in an educational programme. The nurses’ agreement with the statement ‘It is impossible to know when patients will become aggressive’ decreased following training, suggesting that through training and education nurses become more confident in their ability to predict aggression. Qualitative findings The majority of assaulted staff (n=40) in a study by Lanza (1983) believed there are certain important cues that can be predictive of assault. These included patients speaking in a loud voice and using demanding or threatening language, pacing, obstinance, using threatening gestures, withdrawal, refusing medication, irritability, hostility, anxiety, anger, inadequate number of staff, lack of male staff, high noise level and high activity level, situations in which staff are not in control of the ward, and overcrowding on the ward. Preventive measures Quantitative findings Bond and Brimblecomb (2003) surveyed 102 mental health nurses working in a range of settings about factors they perceive to make violence less likely. The responses focused around staff characteristics that could lessen the risk of assault. Seventy one percent of the nurses reported that good communication skills including body language, good use of voice and active listening made assault less likely. Sixty four percent felt that a calm manner, confidence and not over reacting could reduce the risk of assault and 37.8% cited human

relation skills such as likeability, humour, courtesy, empathy, warmth and 31.6% cited decisiveness, good organisational skills and having clear boundaries as factors that could make violence less likely. Chaimowitz, G. & Moscovtich, A. (1991) reported that 24.5% (n=132) of psychiatric residents who had been assaulted in psychiatric facilities in Canada believed that trained backup staff may have prevented the incident or rendered it less serious. Several quantitative studies report that training around aggression management isn’t always provided to all staff, and/or isn’t always perceived by staff as being adequate to meet their needs of dealing with aggression. Seventy seven percent of psychiatric staff and students surveyed by Collins (1994) agreed with the statements that ‘doing the wrong thing will make a bad situation [with a patient] worse’ and ‘someone who is good at recognising the signs can tell when a patient is becoming agitated’. However, many studies report that psychiatric staff do not receive adequate training for these purposes. Gordon et al (1996) reported that only over half of staff working in a psychiatric institution in Australia (n=40) believed they had sufficient training in dealing with assaultive behaviour. Chaplain et al (2006b) reported that even though 90% of the 3074 staff they surveyed had received training in the last 5 years to deal with aggression, almost 40% of these nurses did not receive this training until after they began working on psychiatric wards and 20% of the nurses reported that the training they had received was not adequate to equip them to manage violence. Baxter et al (1992) surveyed 263 nurses about their experiences of aggression, 87% believed that nurses should regularly attend workshops in aggression management, similarly 98% of 184 nurses surveyed by Poster & Ryan (1999) agreed that staff should be educated about prevention & management of assaultive behaviour as part of their in-service education. Qualitative findings Finnema et al (1994) asked 24 nurses working in a psychiatric hospital about the interventions they use to prevent and stop aggression. Talking to the patient, distracting the patient‘s attention, comforting the patient and giving unexpected reactions were mentioned as interventions used to prevent aggression as well as to stop it. Extra medication and locked seclusion were also mentioned. Chen et al (2007) interviewed 13 assaulted psychiatric nurses in Taiwan about their aggression prevention strategies. Responses included, pre-placement training, promotion of good practices such as taking precautionary awareness 'before entering the patient's room, be attentive to his condition.’ avoiding being alone, asking for the patient's consent, 'If a patient is unwilling to follow your orders, do not rush it'. 'Do not directly touch a patient without his consent.' and respecting the patient's human rights, 'keep a kind attitude; do not raise one's voice.' Roper and Anderson (1991) conducted interviews with nursing staff at one acute inpatient unit in America. Staff emphasised the importance of the structure of the ward milieu, maintaining routines of daily activities for patients as well as staff, keeping the environment as safe as possible by removing potentially harmful personal items from patients, removing the patient from potentially harmful events and situations, 'talking down the patient', or using chemical and/or physical restraints and regulating and supervising smoking as powerful constraints on harmful patient behaviour. Ten nurses working in psychiatric facilities in America were interviewed as a part of a phenomenological inquiry about nurses' experiences working in environments where there is a high risk of assault (Kindy et al, 2005). Nurses described taking personal precautionary measures to prevent violence through specialised education and training including therapeutic communication, body language, physical positioning, teamwork, methods of managing assaultive behaviour, noting client histories, observing patterns of behaviour and use of medications. Nurses also described the use of tangible devises such as walkie-talkies, cameras, seclusion rooms, restraints, mirrors and medications as fortifications against aggression.

In a study with veteran psychiatric patients in America (Fagan-Pryor et al, 2001) 92 patients were asked about their perceptions of effective interventions to prevent assaultive behaviour. These interventions were grouped into interventions to prevent patient to patient aggression and interventions to prevent patient to staff aggression. For the former type of aggression patients described individual interventions such as, walking away; good personal hygiene; staying with people who are like you; cooperative patient-staff interventions included, communicating better; understanding each other; getting to know each other and interventions by staff included, setting limits; having better or more staff to supervise or talk with patients; having patients with the same problem together; getting rid of patients who fight; Interventions for preventing patient to staff aggression included interventions by individual patients such as, trying to change the subject; not messing with other patients; talking with a health care professional; not arguing; recognizing that one has a mental illness and needs medication and help, cooperative patient-staff interventions such as, everyone forgiving the past and talking it out; and interventions by staff including being oneself; not making promises you cannot keep; not having an attitude; being more understanding; informing patients ahead of time of their rights, endless patience and understanding. Kumar et al, (2001) conducted focus groups with 6 psychiatric patients about their experience of violence on psychiatric units and their perceptions of how violence can be reduced. Views on approaches to reduce violence included increasing staff service user interaction, the recruitment of more staff and fewer agency staff, screen to recruit caring staff, staff should all be trained to diffuse tension, more grounds and environment should be designed to facilitate engagement between staff and service users and a system to address complaints and monitor incidents. In a study designed to explore the experiences and feelings of patients which precede incidents of aggression (Johnson et al 1997), 12 Canadian psychiatric patients were interviewed. Patients spoke about strategies that they employed to keep their feelings under control and prevent aggressive outbursts. These strategies included diversion, physical activity ‘I have two choices: one, act out, or two, go down and pump some weight . . . . or go for a jog or something like that.’, avoidance and talking to someone ‘If I get in difficulty, I know I can approach a nurse and get calmed down or at least have someone to talk to as a sounding board.’ Delaney et al (2001) conducted focus groups with nursing staff in Australia about nurse management of aggression, staff highlighted on-ward in-service education focusing on the management of aggression as important and relevant tool in managing aggression. Staff explained that in addition to providing information and skills enhancement this education promotes teamwork, peer support and sharing. It also addresses contextual issues and environmental factors associated with aggression. 'It is very important to do 'cause...it's probably the only time all year when the senior staff here get to get together and discuss how they feel about things and I think that is important.’ Spokes at al (2002) interviewed 108 staff about their perceptions of their colleagues training needs. The most common needs identified included crisis intervention and prevention training (n= 50), theoretical training (n= 33) and interpersonal skills training (n= 34). One mental health worker interviewed in a study by Conn & Lion (1983) who was seriously injured by a patient attack pointed out that nowhere in her training program had the topic of how to assess or manage dangerous patients had been discussed until after she was attacked. She felt that she might have unwittingly contributed to the assault because of her naiveté about dealing with potentially volatile patients.

8.7 Reaction to aggression Quantitative findings Ten studies (Lu et al., 2007; Gillig et al., 1998; Omerov et al., 2002; Lanza et al., 1991; Lanza, 1998; Haffke and Reid, 1983; Lanza, 1983; Baxter et al., 1992; Rees and Lehane, 1996; Collins, 1994) describe emotional and social reactions of staff following an experience of aggression. Among these studies, fear and anger were the most commonly reported staff reactions to aggression. Gillig reported that 16% of 32 nurses reported anger towards the patient who had assaulted them, Omervo found this figure to be around the third mark and Lu surveyed 106 nurses from Taiwan who repored that anger was the most common reaction amongst staff following an aggressive incident. In this study fear was described as the most common social reaction by these nurses. Omervo reported that 36% of male staff and 17% of female staff reported feelings of fear following an incident of violence, this difference between genders was significant with men becoming frightened more often than women who were significantly more likely to be surprised by the attack then men (30% vs. 6%). Staff in four studies reported that experiencing aggression by patients impacted upon their work. Forty three percent of the nurses in the study by Lu reported that they experienced discomfort in caring for the patient who had assaulted them. Gillig reported that 12% of the 32 nurses surveyed avoided contact with the patient who assaulted them, 15% wanted to leave their job and 18% wanted to change professional fields and Lanza (1988) reported that 27% of assaulted nurses said their view of the future had changed which included staff considering leaving nursing, changing their job, retiring early, working in a less dangerous setting and questioning the value of a job with these risks. Wanting revenge, negative physiological reactions, stress, hopelessness, feeling shocked and insulted and depressed were other staff reactions to aggression reported in these studies. Gillig et al (1997) also surveyed 54 patients about their reaction to the experience of aggression. Twenty six percent said they had trouble sleeping, 27% experienced a change in appetite, 33% suffered an increase of depression/sadness, 34%felt feelings of anger or rage, 22% avoided contact with other people, 21% wanted to leave hospital for good, 23% suffered with a physical illness. Four quantitative studies report on staff perceptions of blame for the violent incident. Baxter et al, (1992) collected the responses of 263 psychiatric nurses in Australia. Of these, 44% believed that nurses were unfairly blamed by others for provoking assaults upon themselves. Similarly, 58% of male nurses (n=34) working in a psychiatric hospital in the UK (Rees and Lehane, 1996) felt that blame for the aggressive incident had been attached to staff. They felt those on duty at the time were held responsible for the incident. All 34 males said they felt they had failed the victims, conversely all of the female members of staff (n=16) who had witnessed an aggressive event did not believe they had failed the victims. Chaimowitz and Moscovtich, (1991) and Schwartz and Park (1999) conducted studies with psychiatric residents in Canada and America respectively. Twenty five percent of the Canadian sample and 16% of the American sample believed that they had been responsible for the aggressive incident occurring. Qualitative findings Six studies (Currid, 2008; Kindy et al., 2005; Conn and Lion, 1983; Roper and Anderson, 1991; Chen et al., 2007; Lanza, 1983) qualitatively report the reaction of staff to experiencing aggression. In five of these studies staff discuss the impact aggression has on their work.
During one open interview study (Kindy et al., 2005) ten nurses who had experienced aggression on the wards described how the incident had left them feeling hypervigilant, distrustful and fearful which resulted in poor morale. Several participants expressed a desire to leave 'I’m looking for a new job. I’m finding that it’s just absolutely too much and I think it’s asking too much and it is not a safe environment. I’m worried about patient care. And that will in turn reflect on my license.' Nurses also reported feeling that they had an internal conflict regarding their nursing roles, 'When you’re at work and you get hit or punched, I don’t know. . .it just kind of takes, takes a little part of you. I didn’t feel like a nurse. I felt like uh, I felt like an underpaid correctional officer. I didn’t feel like this was nursing.’ In six qualitative studies staff described feelings of fear, anxiety and stress following an incident of aggression. Staff who took part in an in depth semi structured interview study to investigate workplace violence with staff working with schizophrenic patients in Taiwan described feeling, ‘worried, and scared‘, ‘fear of facing patients’ and experiencing ‘nightmares’. Other staff reactions recorded by these studies included anger, hopelessness “I don’t know what we are going to do with this patient,” “We have tried everything and he is still no better,” (Roper and Anderson, 1991) and denial “I don’t want to think about this” (Lanza, 1983). 8.8 Evidence for and against the City model Two studies in the theme ‘the function of aggression’ (Whittington, 2002 and Whittington and Higgins, 2002) found a relationship between the way staff perceive aggression and levels of burnout. Nurses in these studies who held more positive perceptions of aggression were less likely to experience burnout and had greater feelings of personal accomplishment with their work. This is evidence for the role of psychiatric philosophy. The capacity to understand aggression in psychological terms leads to positive attitudes and impacts which is displayed by staff feeling less burnt out when working with aggressive patients and experiencing feelings of personal accomplishment. A number of studies reported that staff characteristics, especially clinical skills and ability can influence patient aggression. This finding is in line with the model’s main assumption that staff can directly influence aggression in inpatient settings through their psychiatric philosophy, moral commitments to patients, the use of cognitive-emotional self management and technical mastery. Moreover, literature in the subtheme of ‘interaction’ pointed to the role of poor interaction between staff and patients as a contributing factor in the occurrence of aggression. A lack of understanding and respect by staff towards patients was reported as causing incidents which could be attributed to staff lacking positive appreciation of patients. The City model suggests that an effective structure on the ward including the way in which staff manage the restriction of patient behaviours, freedoms and the denial of patient requests can modify conflict. This review found that placing limits on patients, restricting their behaviours and denying requests were all perceived as antecedents to aggression by staff and patients. Importantly, several studies reported that the way staff manage these events can influence the occurrence of aggression. The study by Madden et al (1976) highlights the importance of staff managing these rules and restrictions consistently and in a fairly in order to reduce the potentially aggressive outcomes that can result, and Meehan et al (2006) reported that communication when dealing with such events as well as staff adhering to the rules in place are important factors in maintaining an effective structure and reducing the potential for conflict.

The role of training was a theme that was prominent throughout the literature. The City model identifies specialist training as an underlying mechanism for reducing aggression. This is supported in this review by the findings that, training increased staff ability to predict aggression (Collins, 1994), staff perceived that more trained staff could prevent aggression better (Chaimowitz and Moscovtich, 1991; Chen et al, 2007) and that training in aggression management was related to those staff who perceived aggression as protective, thus displaying an ability to understand aggression in a psychological way. 8.9 Points the City model has missed Although the role of staff characteristics is covered by the model in relation to skills and competencies, other characteristics such as demography, physical characteristics and personality are not addressed. Several studies reported that staff perceived personality to influence aggression and physical attributes were mentioned in one study (Spokes et al, 2002). In relation to a number of themes staff experience is perceived as influencing aggression. Although the City model acknowledges the role of experience in terms of training, experience in terms of length of tenure as a modifying factor in its own right has been missed. The ward environment was a theme in the literature that was believed by staff and patients as contributing to the occurrence of aggression. Environmental factors including a lack of activities and being in a locked environment were reported to facilitate aggression in several studies but the role of the ward or hospital environment has been missed by the City model. 8.9 Discussion From the review of literature on staff and patient perceptions of aggression four higher level themes were synthesised. These were ‘the perception of aggression’, ‘causes of aggression’, ‘preventing aggression’ and ‘reactions to aggression’. The first theme, ‘the perception of aggression’, reports on the way in which the function of psychiatric patient aggression is perceived by staff and the expectations that psychiatric staff have about encountering aggression. Aggression was perceived as having both negative and positive functions. A number of quantitative studies reported that staff variables such as gender, psychiatric setting, staff experience and working pattern may influence the perceptions staff have towards the function of aggression. The qualitative studies further illustrated the individualistic nature of judgements about the function of aggression. The findings that certain staff characteristics may influence staff perceptions of the function of aggression may give scope for aiming interventions at certain staff groups in an attempt to positively change their attitudes towards aggression. Understanding the way the nurses think about the function of aggression has important implications for clinical practice. The way in which nurses perceive aggression has important consequences for the way that incidents of aggression are dealt with and reported. For example, if aggression is perceived as normal or functional nurses may be less encouraged to intervene and to report these acts than if aggression is perceived as violent behaviour (Jansen et al, 1997). Alder et al (1983) believe that staffs’ general attitudes towards aggression are a key element in the management of aggressive incidents.

Nurses’ expectations of encountering aggression were addressed in the ‘expectation of aggression’ subtheme. These studies overwhelmingly showed that nurses’ believe they will be a victim of patient aggression during their careers, many nurses also felt that experiencing aggression was to be expected as part of the nursing role. However, one study (Collins, 1994) showed that through a training intervention, nurses’ expectation of being assaulted decreased. By equipping nurses with more skills and confidence to deal with aggressive situations, they felt more empowered and less expectant to be assaulted. This finding is interesting in terms of interventions that can be used in practice to increase staff confidence in dealing with aggression. This is even more important when considering an idea put forward by one of the nurses in the study by Cutcliffe (1999) who suggested that nurses holding the expectation of being assaulted could actually create the effect of a self fulfilling prophecy. Staff anxiety has been found as a major contributor to aggression and violence in clinical areas (Madden et al, 1983) and Levy & Hartocollis (1976) reported that staff feelings of inadequacy concerning their ability to handle a difficult situation with patients, when accompanied by frustration and anger, may scare a disturbed patient to the point of driving them to violence. Interventions could be targeted at helping nurses become more aware of the signals they give off when dealing with patients who have the potential to become aggressive and learn skills in managing their sensory outputs, such as voice, body language and posture, in such a way that it reduces the likelihood of a patient becoming fearful and acting out.
The second theme to come out of the literature dealt with the ‘causes of aggression’. Patient factors, staff factors, interaction, denying and restricting patients and environmental factors were all identified by staff and patients as antecedents to aggression. The nature of the patient group was described by both staff and patients as causing aggression. Staff believed that symptoms of patient illness, especially psychotic symptoms were strong contributing factors in aggressive acts by patients. Patients also described how they had difficulty in controlling their behaviour when they became unwell. The intoxication of patients through the use of drugs and alcohol was perceived to be another cause of aggression. Staff training in attending to symptomatic displays, encouraging discussion between staff and patients about how the patient is feeling, and limiting the ease of access to intoxicating substances are strategies that could be employed by hospitals and staff which have the potential to reduce aggression. In contrast to patient factors as antecedents of aggression, the second subtheme reported on the role of staff factors. Several of the quantitative studies reported that staff skills and competencies (or lack thereof) and staff personality can trigger aggressive incidents. The qualitative studies allowed further exploration into the specific qualities that may result in aggression. Staff perceptions of these factors included poor communication skills, being inattentive, uncaring and rude. Tying in with this subtheme is the ‘interaction’ antecedent. This subtheme includes staff and patient perceptions of the interaction that takes place on psychiatric units as a cause of aggression. These studies report that poor interactions between staff and patients, including staff not listening adequately to patients, social moments where there are groups of patients together and a lack of staff displayed empathy, can cause aggression. Theses themes highlight the importance of the staff role in the occurrence of aggression. Interventions aimed at reducing aggression on psychiatric wards should focus on ways to improve and enhance interactions between staff and patients. Increasing staff psychiatric philosophy to help them understand aggression in psychological terms instead of blaming patients may serve to increase empathy, increasing staff interaction skills through training in active listening and talking in a caring way may help to reduce the perceptions that staff are rude, inattentive and uncaring. The denial and restriction of patient behaviours including enforcing ward rules, refusing a request by a patient and limiting patient behaviour, were described by thirteen studies as contributing to aggression. In addition,
patients described the way in which staff communicated restrictions and denials had the potential to trigger aggression by patients. These studies highlight the importance of dealing with patient requests and enforcing ward rules in a transparent and consistent way. Patients described feeling frustrated when rules appeared too strict or when they felt they were being ignored by staff. Staff should be encouraged to show patients that their requests have been heard and give them a clear expectation of what will be done about the request and when. If these requests are inappropriate or unrealistic then staff should be consistent and clear in their explanations of why the request cannot be met or why the restrictions on behaviour are being imposed. The way in which these matters are dealt with by staff has great potential to inflame or dampen a potentially aggressive situation. Patients describe how staff take superior attitudes or are brisk with patients, things that may seem trivial to staff might seem a much more important issue to a patient, and this should be held in mind by staff. The environment of the psychiatric ward was described by eleven studies as a factor perceived as causing aggression by staff and patients. Specifically, overcrowding, lack of facilities and activities, inadequate staffing and lack of access to outside space. Changing structural aspects of the environment and increasing staff numbers is not easily achievable in most inpatient situations. However, boredom was reported by patients as causing aggression, and staff actions have the potential to lessen the patient experience of boredom. Staff can ensure that there are activities available for patients to take part in on the ward, that scheduled activities are not cancelled unless absolutely necessary, that they spend time with patients, engaging and conversing with them, and increase opportunities for patients to go outside when appropriate. The third theme to come out of the literature was ‘preventing aggression’. Staff ability to predict that an aggressive event will occur was the subject of the first subtheme. The majority of staff believed that it is possible to predict that an aggressive event will occur. Noticing a change in a patient’s behaviour was the most common way staff reported being able to predict aggression. Other cues to aggression included times when there is increased activity on the ward or overcrowding. If staff are able to foresee an aggressive event occurring then they have an opportunity to stop it, or limit the fallout. Being aware of each patient’s ‘normal’ behaviour provides staff with the ability to notice when this starts to change. Good communication between staff at handover of shift is important for information about a patient’s behaviour to be passed on to staff coming onto shift. Staff skills in deescalating situations are crucial at times when they feel a patient might start to become aggressive, knowing a patient well, knowing what might calm them down or distract them are essential for staff in successful de-escalation. The second subtheme ‘preventing aggression’ focused on the perceptions of staff about factors that could prevent aggression from arising. Positively communicating, using distraction techniques, taking precautionary measures before interacting with patients, keeping the ward calm and safe and displaying a caring manner were ways in which staff believed they could prevent patient aggression from occurring. In essence these are skills staff can use to calm a patient down. Medication is also mentioned in these studies as a way to prevent aggression from occurring. Although medication is often effective, by using the staff skills described above, potentially aggressive situations may be able to be prevented without turning to medication first. Staff training in the management of aggressive behaviour is essential in preventing aggression from occurring or escalating. A high percentage of staff in these studies did not believe they had received adequate training or training at an appropriate time in their career to enable them to deal successfully with aggressive patients.

Specific training needs identified by staff included training in identifying potentially aggressive situations, managing an aggressive situation, interpersonal skills and dealing with volatile patients. Equipping staff with the specific skills they need to have the confidence and skills to prevent and deal with aggression effectively should be at the forefront of clinical aims for nurses in psychiatric settings. The final theme in this review was the ‘reaction to aggression’. Most commonly staff victims of aggression felt angered and fearful. Following assault several studies report that nurses had difficulty in resuming their role of caring for the patients who were aggressive towards them. As discussed earlier with regard to the self fulfilling prophecy idea of aggression, if staff are fearful and angry towards patients they may exhibit behavioural cues which in turn put the patient on edge, escalating situations and creating more conflict. Staff should use techniques that allow them to control their own emotional reactions to situations so that none of these emotional cues are leaked to patients. Staff should be encouraged to form relationships with patients in order to gain a greater understanding of them and their behavioural motives. The ability to understand the patient separately from their behaviour, being realistic in expectations of the patient, understanding that there may be times when a patient needs to express anger or vent emotions, and the ability to view aggression as a product of the patient’s situation and diagnosis may reduce the staffs perceptions that an aggressive act is a personal attack on them and reduce experienced anger and fear. Conclusion This review looked at quantitative and qualitative studies which explored both staff and patient perceptions of aggression. By taking into consideration both types of methodologies this review allowed a rich exploration of the perceptions of these groups. In many cases the qualitative data allowed a deeper understanding of the findings presented by the numerical findings of the quantitative studies which in turn added statistical validity to many of the findings. Consideration of the views of both staff and patients gave an opportunity to explore perception of aggression from both sides of the nurse patient relationship. Fundamental to many of the themes presented in this review was the need for positive interaction between staff and patients. Interaction and communication between staff and patients, if done meaningfully and sincerely, can afford both groups better understanding of the behaviours, reasons and attitudes of one another. Many of the causes of aggression and the skills used in preventing and managing aggression were centred on communication and interaction. Spending time with patients, communicating and interacting positively can foster a greater understanding of patient needs, behaviours, motivations and individualities. Understanding and appreciation of patients are important skills staff should work towards, having the potential to make staff feel more positively about the function of patient aggression, reduce aggression that is triggered by staff related factors, prevent aggression from occurring though skills such as recognising changes in behavioural cues and, if and when aggression does occur, being able to maintain understanding and positive appreciation of the patient which can reduce the negative outcomes for both staff and patients.

9. REVIEW SUMMARY This review included 424 empirical studies of inpatient violence and aggression, published in English between 1960 and 2009. The findings are summarised below. Incidence Rates of violence and aggression could be calculated for 122 studies (30% of all those included in the literature review). Rates varied markedly by country, setting, and settings within countries. A higher proportion of forensic patients were violent and responsible for more violent incidents. However, acute wards admitted many more patients (including violent ones), and had higher rates per 100 occupied bed days. On balance, therefore, the risk of violence was greater on acute wards. On average, nearly half of incidents involved physical violence, and repeated incidents were common. The majority of nurses reported experiencing violence at least once during their career, but rates for psychiatrists were much lower. Antecedents The antecedents of violent and/or aggressive incidents were wide-ranging. Seventy-one studies reported antecedent data, from which nine categories of antecedent were identified: staff-patient interaction, patient behavioural cues (agitation, attention-seeking behaviour, increased motor activity, boisterousness, and confusion), no clear cause, patient symptoms, patient-patient interaction, patient conflict behaviours, structural issues, patient emotional/ mood cues and external/personal issues. However, most studies reported antecedent data exclusively from the perspective of staff, while only five papers captured the patients’ perspective. The data also suggest that a third of incidents are either unprovoked (which is unlikely), staff are failing to recognise antecedents, or staff are recognising antecedents but are not recording them. The true breadth and scope of antecedents of violence and aggression therefore remains uncertain. Consequences There were eight categories of consequences identified from 108 studies. These ranged from the nature and severity of physical injuries, use of containment (such as seclusion, medication or restraint), patient transfers/discharges, psychological and behavioural outcomes for the victims, and damage to property/objects. Again, the data overwhelming reflected staff reports of consequences, with a tendency to focus on injuries experienced by the staff victims of the assault. Overall, an injury is likely to occur in a third of violent/aggressive incidents that a staff member is involved in. Violent incidents within acute settings were 20% more likely to result in staff injury compared to forensic settings. Patient profile Sixty-three studies compared aggressive and non-aggressive patients. Meta analyses identified several patient factors associated with violence and aggression. Patients with a diagnosis of schizophrenia were more likely to be violent than patients with other diagnoses. Patients were also more likely to be violent if they were young, male, single, from an ethnic minority, and admitted a compulsory/formal admission.

Time and place Evidence from 78 studies found no consistent seasonal effects, but peaks in violence by time of day corresponded with specific events and activities on the wards (e.g. waking, medication rounds and meal-times). Weekends were usually quieter because of reduced association between patients and staff. Incidents occur in most areas of the ward, but particularly in corridors, bedrooms, lounge areas and around nursing stations. Patient and staff perspectives Sixty papers included data on staff and patient attitudes, perceptions and motivations of violence and aggression (38 staff, 9 patient and 13 both). These were organised into four themes: the perception of aggression, causes of aggression, preventing aggression and reactions to aggression. Aggression was perceived as having both negative and positive functions, and varied by staff variables such as gender, setting, experience and working pattern. Staff firmly believe they will be a victim of patient aggression at some point during their career, with may reporting that experiencing aggression was to be expected as part of the nursing role. Patient factors (especially psychotic symptoms), staff factors (e.g. lack of skills), denying and restricting patients and environmental factors (overcrowding, lack of facilities and activities, inadequate staffing and lack of access to outside space) were all identified by staff and patients as reasons for aggression. Most staff believed it possible to predict aggressive events before, usually by noticing a change in a patient’s behaviour.

10. Acknowledgement This report presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-0707-10081) and supported by the NIHR Mental Health Research Network. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
11. REFERENCES Studies included in the review
Abbott, A. 1978, "Accident and its correlates in a psychiatric hospital", Acta Psychiatrica Scandinavica, vol. 57, no. 1, pp. 36-48.
Abderbalden, C., Needham I., Friedli, T., Poelmans, J., & Dassen, T. 2002, "Perception of aggression among psychiatric nurses in Switzerland", Acta Psychiatr Scand, vol. 106, no. Suppl 412, pp. 110-117.
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Fischer, J. E., & Haug, H.-J. 2007, "Frequency and severity of aggressive incidents in acute psychiatric wards in Switzerland", Clinical Practice & Epidemiology in Mental Health, vol. 30.
Abderhalden, C., Needham, I., Dassen, T., Halfens, R., Haug, H. J., & Fischer, J. E. 2008, "Structured risk assessment and violence in acute psychiatric wards: randomised controlled trial", British Journal of Psychiatry, 193, pp. 44-50.
Abeyasinghe, R. & Jayasekera, R. 2003, "Violence in a general hospital psychiatry unit for men", Ceylon Medical Journal, vol. 48, pp. 45-47.
Abushua'leh, K. & bu-Akel, A. 2006, "Association of psychopathic traits and symptomatology with violence in patients with schizophrenia", Psychiatry Research no. 2-3, pp. 205-211.
Adams, J. & Whittington, R. 1995, "Verbal aggression to psychiatric staff: traumatic stressor or part of the job?", Perspectives in Psychiatric Care, vol. 2, no. 2, pp. 171-174.
Agarwal, M. & Roberts, M. 1996, "Violence among psychiatric inpatients at an Interim Secure Unit: changes in pattern over a two-year period.", Medicine, Science and the Law, vol. 36, no. 1, pp. 31-36.
Agervold, M. & Andersen, L. P. 2006, "Incidence and impact of violence against staff on their perceptions of the psychosocial work environment", Nordic Psychology, vol. 58, no. 3, pp. 232-247.
Aiken, G. J. M. 1984, "Assaults on staff in a locked ward: Prediction and Consequences", Medicine, Science and the Law, vol. 24, no. 3, pp. 199-207.
Alder, W., Kreeger, C., & Ziegler, P. 1983, "Patient violence in private psychiatric wards," in Assaults within psychiatric facilities, R. Lion & W. Reid, eds., Grune & Stratton, New York.
Almvik, R. & Woods, P. 1998, "The Broset Violence Checklist (BVC) and the prediction of inpatient violence: Some preliminary results.", Psychiatric Care, vol. 5, no. 6, pp. 208-211.
Arango, C., Barba, A. C., Gonzalez-Salvador, T., & Ordonez, A. C. 1999, "Violence in Inpatients With Schizophrenia: A Prospective Study", Schizophrenia Bulletin, vol. 25, no. 3, pp. 493-503.

Arnetz, J. & Arnetz, B. 2000, "Implementation and evaluation of a practical intervention programme for dealing with violence towards health care workers", Journal of Advanced Nursing, vol. 31, no. 3, pp. 668-680.
Augestad, L. B. & Vatten, L. V. 1994, "Five year risk of assault on employees in a psychiatric hospital", Safety Science, vol. 18, pp. 113-124.
Barlow, K., Grenyer, B., & Ilkiw-Lavalle, O. 2000, "Prevalence and precipitants of aggression in psychiatric inpatient units", Australian and New Zealand Journal of Psychiatry, vol. 34, pp. 967-974.
Baxter, E., Hafner, R. J., & Holme, G. 1992, "Assaults by patients: the experience and attitudes of psychiatric hospital nurses", Australian & New Zealand Journal of Psychiatry., vol. 26, no. 4, pp. 567-573.
Beauford, J. E., Dale, E., McNiel, E., & Binder, R. L. 1997, "Utility of the Initial Therapeutic Alliance in Evaluating Psychiatric patients' Risk of Violence", American Journal of Psychiatry, vol. 154:1272-1276.
Benjaminsen, S., GotzscheLarsen, K., Norrie, B., Harder, L., & Luxhoi, A. 1996, "Patient violence in a psychiatric hospital in Denmark. Rate of violence and relation to diagnosis", Nordic Journal of Psychiatry., vol. 50, no. 3, pp. 233-242.
Bensley, L., Nelson, N., Kaufman, J., Silverstein, B., & Shields, J. W. 1995, "Patient and staff views of factors influencing assaults on psychiatric hospital employees", Issues in Mental Health Nursing, vol. 16, no. 5, pp. 433-446.
Bensley, L., Nelson, N., Kaufman, J., Silverstein, B., Kalat, J., & Shields, J. W. 1997, "Injuries due to assaults on psychiatric hospital employees in Washington State", American Journal of Industrial Medicine., vol. 31, no. 1, pp. 92-99.
Bilgin, H. & Buzlu, S. 2006, "A study of psychiatric nurses' beliefs and attitudes about work safety and assaults in Turkey", Issues in Mental Health Nursing, vol. 27, pp. 75-90.
Binder, R. L. & McNiel, D. E. 1990, "The relationship of Gender to violent behavior in Acutely Disturbed Psychiatric Patients", Journal of Clinical Psychiatry, vol. 51(3): pp110-114.
Binder, R. L. & McNiel, D. E. 1994, "Staff gender and risk of assault on doctors and nurses", Bulletin of the American Academy of Psychiatry & the Law, vol. 22, no. 4, pp. 545-550.
Bisconer, S. W., Green, M., Mallon-Czajka, J., & Johnson, J. S. 2006, "Managing aggression in a psychiatric hospital using a behaviour plan: a case study", Journal of Psychiatric and Mental Health Nursing, vol. 13, pp. 515-521.
Bjorkdahl, A., Heilig, M., Palmstierna, T., & Hansebo, G. 2007, "Changes in the occurrences of coercive interventions and staff injuries on a psychiatric intensive care unit", Archives of Psychiatric Nursing , vol. 21, no. 5, pp. 270-277.
Blomhoff, S., Seim, S., & Friis, S. 1990, "Can prediction of violence among psychiatric inpatients be improved", Hospital and Community Psychiatry, vol. 41: 771-775.

Blow, F., Barry, K., Copeland, L., McCormick, R., Lehmann, L., & Ullman, E. 1999, "Repeated assaults by patients in VA hospital and clinical settings", Psychiatric Services, vol. 50, pp. 390-394.
Bond, K. & Brimblecombe, N. 2004, "Violent Incidents and Staff Views", Mental Health Nursing, vol. 23, no. 6, pp. 10-12 (cont on 17).
Bouras, N., Trauer, T., Rosen, B., & et al 1981, "Temporal patterns in ward disturbances among psychiatric patients", British Journal of Clinical Psychology, vol. 20, pp. 139-140.
Bouras, N., Trauer, T., & Watson, J. P. 1982, "Ward environment and disturbed behaviour", Psychological Medicine, vol. 12, pp. 309-319.
Brizer, D. A., Crowner, M. L., Convit, A., & Volavka, J. 1988, "Videotape Recording of Inpatient Assaults: A Pilot Study", American Journal of Psychiatry, vol. 145:6, p751-752.
Brock, G., Gurekas, V., Gelinas, A. F., & Rollin, K. 2009, "Use of a "secure room" and a security guard in the management of the violent, aggressive or suicidal patient in a rural hospital: a 3-year audit", Canadian Journal of Rural Medicine, vol. 14, no. 1, pp. 16-20.
Calabro, K., Mackey, T., & Williams, S. 2002, "Evaluation of training designed to prevent and manage patient violence", Issues in Mental Health Nursing, vol. 23, pp. 3-15.
Caldwell, M. 1992, "The incidence of PTSD among staff victims of patient violence", Hospital and Community Psychiatry, vol. 43, pp. 838-839.
Carmel, H., Tanke, E., & Yesavage, J. 1991, "Physican staffing and patient violence", Bulletin of the Academy of Psychiatry and the Law, vol. 19, p. 1.
Carmel, H. & Hunter, M. 1989, "Staff injuries from inpatient violence", Hospital and Community Psychiatry, vol. 40(1): 41-46.
Carmel, H. & Hunter, M. 1993, "Staff injuries from patient attack: five years' data", Bulletin of the American Academy of Psychiatry & the Law, vol. 21, no. 4, pp. 485-493.
Carmel, H. & Hunter, M. 1991, "Psychiatrists injured by patient attack", Bulletin of the American Academy of Psychiatry and law , vol. 19, pp. 309-316.
Carmel, M. D. & Hunter, M. 1990, "Compliance with training in managing assaultive behaviour and injuries from inpatient violence", Hospital and Community Psychiatry, vol. 41(5): 558-560.
Carr, V. J., Lewin, T. J., Sly, K. A., Conrad, A. M., Tirupati, S., Cohen, M., Ward, P. B., & Coombs, T. 2008, "Adverse incidents in acute psychiatric inpatient units: rates, correlates and pressures", Australian & New Zealand Journal of Psychiatry, vol. 42, no. 4, pp. 267-282.
Carton, G. & et al. 2003, "Reducing Violence in a Special Hospital", Nursing Standard, vol. 17, no. 5, pp. 29-31.
Casseem, M. 1984, "Violence on the Wards", Nursing Mirror, vol. 158, pp. 14-16.

Chaimowitz, G. A. & Moscovitch, A. 1991, "Patient assaults on psychiatric residents: the Canadian experience", Canadian Journal of Psychiatry, vol. 36, no. 2, pp. 107-111.
Chaplin, R., McGeorge, M., & Lelliott, P. 2006, "The National Audit of Violence: In-patient care for adults of working age", Psychiatric Bulletin, vol. 30, no. 12, pp. 444-446.
Chaplin, R., McGeorge, M., & Lelliott, P. 2006, "Violence on inpatient units for people with learning disability and mental illness: the experiences of service users and staff", British Journal of Developmental Disabilities, vol. 52 part 2, no. 103, pp. 105-115.
Chaplin, R., McGeorge, M., Hinchcliffe, G., & Shinkwin, L. 2008, "Aggression on psychiatric inpatient units for older adults and adults of working age", International Journal of Geriatric Psychiatry, vol. 23, no. 8, pp. 874-876.
Chen, S., Hwu, H., & Williams, R. 2005, "Psychiatric nurses' anxiety and cognition in managing psychaitric patients' aggression", Archives of Psychiatric Nursing, vol. 19, no. 3, pp. 141-149.
Chen, W. C., Wang, J. D., Lew-Ting, C. Y., Chiu, H. J., & Lin, Y. P. 2007, "Workplace violence on workers caring for long-term institutionalized schizophrenic patients in Taiwan", Journal of Occupational Health, vol. 49, no. 4, pp. 311-316.
Chen, W. C., Hwu, H. G., Kung, S. M., Chiu, H. J., & Wang, J. D. 2008, "Prevalence and determinants of workplace violence of health care workers in a psychiatric hospital in Taiwan", Journal of Occupational Health, vol. 50, no. 3, pp. 288-293.
Chen, W. C., Hwu, H. G., & Wang, J. D. 2009, "Hospital staff responses to workplace violence in a psychiatric hospital in Taiwan", International Journal of Occupational & Environmental Health, vol. 15, no. 2, pp. 173-179.
Cheung, P., Schweitzer, I., Tuckwell, V., & Crowley, K. C. 1996, "A Prospective Study of Aggression Among Psychiatric Patients in Rehabilitation Wards", Australian and New Zealand Journal of Psychiatry, vol. 30, pp. 257-262.
Cheung, P., Schweitzer, I., Tuckwell, V., & Crowley, K. C. 1997, "A prospective study of assaults on staff by psychiatric in-patients", Medicine, Science & the Law, vol. 37, no. 1, pp. 46-52.
Cheung, P., Schweitzer, I., Crowley, K., & Tuckwell, V. 1997, "Violence in schizophrenia: role of hallucinations and delusions.", Schizophrenia Research, vol. 26, pp. 181-190.
Cheung, P., Schweitzer, I., Crowley, K., & Tuckwell, V. 1997, "Aggressive behaviour in schizophrenia: the role of psychopathology.", Australian & New Zealand Journal of Psychiatry, vol. 31, pp. 62-67.
Chou, K. R., Lu, R. B., & Mao, W. C. 2002, "Factors relevant to patient assaultive behavior and assault in acute inpatient psychiatric units in Taiwan. [References]", Archives of Psychiatric Nursing., vol. 16, no. 4, pp. 187-195.
Chou, K., Lu, R., & Chang, M. 2001, "Assaultive Behavior by Psychiatric In-Patients and Its Related Factors", Journal of Nursing Research, vol. 9, no. 5, pp. 139-151.

Chukwujekwu, D. C. & Stanley, P. C. 2008, "The Modified Overt Aggression Scale: how valid in this environment?", Nigerian Journal of Medicine: Journal of the National Association of Resident Doctors of Nigeria.17(2):153-5, vol. 17, no. 2, pp. 153-155.
Coldwell, J. & Naismith, L. 1989, "Violent incidents on special care wards in a special hospital", Medicine, Science and the Law, vol. 29, pp. 116-123.
Cole, A. 2005, "Four in five nurses on mental wards face violence", British Medcial Journal, vol. 330, no. 7502, p. 1227.
Collins, J. 1994, "Nurses' attitudes towards aggressive behaviour, following attendance at 'The Prevention and Management of Aggressive Behaviour Programme'", Journal of Advanced Nursing, vol. 20, pp. 117-131.
Conn, L. & Lion, J. 1983, "Assaults in a university hospital," in Assualts Within a Psychiatric Facilities, J. Lion, ed., Grune & Stratton, New York, pp. 61-69.
Convey, J. 1986, "A Record of Violence", Nursing Times, vol. 82, no. 46, pp. 36-38.
Convit, A., Isay, D., Gadioma, R., & et al 1988, "Underreporting of physical assaults in schizophrenic inpatients", Journal of Nervous and Mental Disease, vol. 176, pp. 507-509.
Convit, A., Jaeger, J., Pin Lin, S., Meisner, M., & Volavka, J. 1988, "Predicting Assaultiveness in psychiatric inpatients: a pilot study", Hospital and Community Psychiatry, vol. 39, no. 4, pp. 429-434.
Convit, A., Isay, D., Otis, D., & Volavka, J. 1990, "Characteristics of repeatedly assaultive psychiatric inpatients", Hospital & Community Psychiatry., vol. 41, no. 10, pp. 1112-1115.
Cooper, A. & Medonca, J. 1991, "A prospective study of patient assaults on nurses in a provincial psychiatric hospital in Canada", Acta Psychiatrica Scandinavica, vol. 84, pp. 163-166.
Cooper, S. J., Brown, F. W. A., McLean, K. J., & King, D. J. 1983, "Aggressive behaviour in a psychiatric observation ward", Acta Psychiatrica Scandinavica, vol. 68(386-393).
Crichton, J., Callanan, T., Beauchamp, L., Giasson, M., & Tardiff, H. 1998, " Staff response to psychiatric inpatient violence: an international comparison", Psychiatric Care, vol. 5, no. 2, pp. 50-56.
Crichton, J. H. M. & Calgie, J. 2002, "Responding to Inpatient Violence at a Psychiatric Hospital of Special Security: A Pilot Project", Medicine, Science and the Law, vol. 42, no. 1, pp. 30-33.
Crowner, M., Peric, G., Stepcic, F., & Ventura, F. 1995, "Psychiatric Patients' Explanations for Assaults", Psychiatric Services, vol. 46, no. 6, pp. 614-615.
Crowner, M. C., Douyon, R., Convit, A., & Volavka, J. 1991, "Videotape Recording of Assaults on a State Hospital Inpatient Ward", Journal of Neuropsychiatry, vol. 3, no. 2, pp. 59-64.

Crowner, M. L., Peric, G., Stepcic, F., & Van Oss, E. 1994, "A comparison of videocameras and official incident reports in detecting inpatient assaults", Hospital and Community Psychiatry, vol. 45: 11 1144-1145.
Crowner, M. L., Peric, G., Stepcic, F., & Lee, S. 2005, "Assailant and victim behaviors immediately preceding inpatient assault", Psychiatric Quarterly, vol. 76, no. 3, pp. 243-256.
Currid, T. J. 2008, "The lived experience and meaning of stress in acute mental health nurses", British Journal of Nursing, vol. 17, no. 14, pp. 880-884.
Cutcliffe, J. 1999, "Qualified nurses' lived experience of violence perpetuated by individuals suffering from enduring mental health problems", International Journal of Nursing Studies, vol. 36, pp. 105-116.
Daffern, M., Mayer, M. M., & Martin, T. 2003, "A preliminary investigation into patterns of aggression in Australian forensic psychiatric hospital", The Journal of Forensic Psychiatry & Psychology, vol. 14, no. 1, pp. 67-84.
Daffern, M. & Howells, K. 2007, "Aggressive Behaviour in High-Risk Personality Disordered Inpatients During Prison and Following Admission to Hospital", Psychiatry Psychology & Law, vol. 14, no. 1, pp. 26-34.
Daffern, M., Howells, K., Ogloff, J., & Lee, J. 2005, "Individual characteristics predisposing patients to aggression in a forensic psychiatric hospital", Journal of Forensic Psychiatry & Psychology, vol. 16, no. 4, pp. 729-746.
Daffern, M., Mayer, M., & Martin, T. 2006, "Staff gender ratio and aggression in a forensic psychiatric hospital", International Journal of Mental Health Nursing, vol. 15, pp. 93-99.
Daffern, M., Howells, K., & Ogloff, J. 2007, "The interaction between individual characteristics and the function of aggression in forensic psychiatric inpatients", Psychiatry Psychology & Law, vol. 14, no. 1, pp. 17-25.
Daffern, M. & Howells, K. 2009, "The function of aggression in personality disordered patients", Journal of Interpersonal Violence, vol. 24, no. 4, pp. 586-600.
Daffern, M., Ogloff, J., & Howells, K. 2003, "Aggression in an Australian forensic psychiatric hospital.", British Journal of Forensic Practice., vol. 5, no. 4, pp. 18-28.
Daffern, M., Mayer, M. M., & Martin, T. 2004, "Environment contributors to aggression in two forensic psychiatric hospitals.", International Journal of Forensic Mental Health., vol. 3, no. 1, pp. 105-114.
Daffern, M., Ogloff, J. R. P., Ferguson, M., & Thomson, L. 2005, "Assessing risk for aggression in a forensic psychiatric hospital using the Level of Service Inventory-Revised: Screening Version", International Journal of Forensic Mental Health, vol. 4, no. 2, pp. 201-206.
Daffern, M., Ferguson, M., Ogloff, J., Thomson, L., & Howells, K. 2007, "Appropriate treatment targets or products of a demanding environment? The relationship between aggression in a forensic psychiatric hospital with aggressive behaviour preceding admission and violent recidivism", Psychology, Crime & Law, vol. 13, no. 5, pp. 431-441.

Daffern, M., Duggan, C., Huband, N., & Thomas, S. 2008, "The impact of interpersonal style on aggression and treatment non-completion in patients with personality disorder admitted to a medium secure psychiatric unit", Psychology, Crime & Law, vol. 14, no. 6, pp. 481-492.
Daffern, M., Howells, K., Stacey, J., Hogue, T., & Mooney, P. 2008, "Is sexually abusive behaviour in personality disordered inpatients analogous to sexual offences committed prior to hospitalization?", Journal of Sexual Aggression, vol. 14, no. 2, pp. 123-133.
Dawson, J., Johnson, M., Kehiayan, N., & et al 1988, "Response to patient assault: a peer support program for nurses", Journal of Psychosocial Nursing and Mental Health Services, vol. 26, pp. 8-15.
De Neit, G. J., Hutschemaekers, J. M., & Lendemeijer, B. H. H. G. 2005, "Is the reducing effect of the Staff Observation Aggression Scale owing to a learning effect? An explorative study", Journal of Psychiatric and Mental Health Nursing, vol. 12, pp. 687-694.
de Vogel, V. & de Ruiter, C. 2006, "Structured professional judgment of violence risk in forensic clinical practice: A prospective study into the predictive validity of the Dutch HCR-20", Psychology, Crime & Law, vol. 12, no. 3, pp. 321-336.
Decaire, M. W., Bedard, M., Riendeau, J., & Forrest, R. 2006, "Incidents in a psychiatric forensic setting: association with patient and staff characteristics", Canadian Journal of Nursing Research, vol. 38, no. 3, pp. 68-80.
Delaney, J., Cleary, M., Jordan, R., & Horsfall, J. 2001, "An exploratory investigation into nursing management of aggression in acute psychiatric settings", Journal of Psychiatric and Mental Health Nursing, vol. 8, pp. 77-84.
Delaney, K. R. & Johnson, M. E. 2006, "Keeping the unit safe: mapping psychiatric nursing skills", Journal of the American Psychiatric Nurses Association, vol. 12, no. 4, pp. 198-207.
Depp, F. 1983, "Assaults in a Public Mental Hospital", in Lion, J.and Reid, W.(Eds) Assaults Within psychiatric Facilities.Orlando: Grune and Stratton., vol. 21-45.
Depp, F. C. 1976, "Violent behaviour patterns on psychiatric wards", Aggressive Behaviour, vol. 2, pp. 299-306.
Dernevik, M., Grann, M., & Johansson, S. 2002, "Violent behavior in forensic psychiatric patients: Risk assessment and different risk-management levels using the HCR-20.", Psychology, Crime & Law, vol. 8, pp. 93-111.
Dibben, C., O'Shea, R., Chang, R., & Woodger, J. 2008, "Safety for psychiatrists--From trainee to consultant", Psychiatric Bulletin, vol. 32, no. 3, pp. 85-87.
Dietz, P. E. & Rada, R. T. 1982, "Battery Incidents and Batterers in a Maximum Security Hospital", Archives of General Psychiatry, vol. 39:31-34.
Dinakar, H. S. & Sobel, R. N. 2001, "Violence in the community as a predictor of violence in the hospital", Psychiatric Services, vol. 52, no. 2, pp. 240-241.

Dolan, M. & Fullam, R. 2007, "The validity of the Violence Risk Scale second edition (VRS-2) in a British forensic inpatient sample", Journal of Forensic Psychiatry & Psychology.Vol.18(3)()(pp 381-393), 2007. no. 3, pp. 381-393.
Dolan, M., Fullam, R., Logan, C., & Davies, G. 2008, "The Violence Risk Scale Second Edition (VRS-2) as a predictor of institutional violence in a British forensic inpatient sample", Psychiatry Research, vol. 158, no. 1, pp. 55-56.
Dooley, E. 1986, "Aggressive incidents in a secure hospital", Medicine, Science and the Law, vol. 26, pp. 125-130.
Dowson, J. H., Butler, J., & Williams, O. 1999, "Management of psychiatric in-patient violence in the Anglia region. Implications for record-keeping, staff training and victim support", Psychiatric Bulletin. , vol. 23, no. 8, pp. 486-489.
Doyle, M. 2002, "The validity of North American risk assessment tools in predicting inpatient violent behaviour in England", Legal and Criminological Psychology, vol. 7, pp. 141-154.
Doyle, M. & Dolan, M. 2006, "Evaluating the Validity of Anger Regulation Problems, Interpersonal style, and Disturbed Mental state for Predicting Inpatient Violence", Behavioral Sciences and the Law, vol. 24, pp. 783-798.
Duxbury J., Hahn, S., Needham I., & Pulsford, D. 2008, "The Management of Aggression and Violence Attitude Scale (MAVAS): a cross-national comparative study.", Journal of Advanced Nursing, vol. 62, no. 5, pp. 596-606.
Duxbury, J. & Whittington, R. 2005, "Causes and management of patient aggression and violence: staff and patient perspectives", Journal of Advanced Nursing, vol. 50, no. 5, pp. 469-478.
Edwards, J., Jones, D., Reid, W., & et al 1988, "Physical assaults in a psychiatric unit of a general hospital", American Journal of Psychiatry, vol. 145, pp. 1568-1571.
Ehmann, T. S., Smith, G. N., Yamamoto, A., McCarthy, N., Ross, D., Au, T., Flynn, S. W., Altman, S., & Honer, W. G. 2001, "Violence in treatment resistant psychotic inpatients", Journal of Nervous & Mental Disease., vol. 189, no. 10, pp. 716-721.
El-Badri, S. M. & Mellsop, G. 2006, "Aggressive behaviour in an acute general adult psychiatric unit", Psychiatric Bulletin no. 5, pp. 166-168.
Elbogen, E. B., Williams, A. L., Kim, D., Tomkins, A. J., & Scalora, M. J. 2001, "Gender and perceptions of dangerousness in civil psychiatric patients", Legal and Criminological Psychology, vol. 6, pp. 215-228.
Emmerson, B., Fawcett, L., Ward, W., Catts, S., Ng, A., & Frost, A. 2007, "Contemporary management of aggression in an inner city mental health service", Australasian Psychiatry, vol. 15, no. 2, pp. 115-119.
Evenson, R. C., Sletten, I. W., Altman, H., & Brown, M. L. 1974, "Disturbing Behavior: A Sudy of Incident Reports", Psychiatric Quarterly., vol. 48, no. 2, pp. 266-275.

Evershed, S., Tennant, A., Boomer, D., Rees, A., Barkham, M., & Watson, B. 2003, "Practice-based outcomes of dialectical behavior therapy (DBT) targeting anger and violence, with male forensic patients: a pragmatic and non-contemporaneous comparison.", Criminal Behaviour & Mental Health , vol. 13, pp. 198-213.
Fagan-Pryor, E. C., Haber, L. C., Dunlap, D., Nall, J. L., Stanley, G., & Wolpert, R. 2003, "Patients' views of causes of aggression by patients and effective interventions", Psychiatric Services., vol. 54, no. 4, pp. 549-553.
Fairlie, A. & Brown, R. 1994, "Accidents and incidents involving patients in a mental health service", Journal of Advanced Nursing, vol. 19, no. 5, pp. 864-869.
Farrell, G. 1999, "Aggression in clinical settings: Nurses' views-A follow-up study", Journal of Advanced Nursing, vol. 29, pp. 532-541.
Farrell, G. A., Bobrowski, C., & Bobrowski, P. 2006, "Scoping workplace aggression in nursing: findings from an Australian Study", Journal of Advanced Nursing, vol. 55, no. 6, pp. 778-787.
Ferguson, C. J., Averill, P. M., Rhoades, H., Rocha, D., Gruber, N. P., & Gummattira, P. 2005, "Social Isolation, Impulsivity and Depression as Predictors of Aggression in a Psychiatric Inpatient Population.", Psychiatric Quarterly, vol. 76, no. 2, pp. 123-137.
Ferns, T. & Meerabeau, L. 2008, "Verbal Abuse Experienced by Nursing Students", Journal of Advanced Nursing, vol. 61, no. 4, pp. 436-444.
Finnema, E. J., Dassen, T., & Halfens, R. 1994, "Aggression in Psychiatry: a Qualitative Study Focussing on the Characterisation and perception of Patient Agression by Nurses Working on Psychiatric Wards", Journal of Advanced Nursing, vol. 19:1088-1095.
Flannery Jr, R. B., Hanson, M., Penk, W., & Flannery, G. J. 1994, "Violence against women: Psychiatric patient assaults on female staff", Professional Psychology Research and Practice, vol. 25, no. 2, pp. 182-184.
Flannery, R., Fulton, P., Tausch, J., & et al 1991, "A program to help staff cope with psychological sequelae of assaults by patients", Hospital and Community Psychiatry, vol. 42, pp. 935-938.
Flannery, R. & Penk, W. 1993, "Cyclical variaitons in psychiatric patients-to-staff assaults: preliminary enquiry", Psychological Reports, vol. 72, p. 642.
Flannery, R., Hanson, M. A., Penk, W., Goldfinger, S., Pastva, G., & Navon, M. 1998, "Replicated declines in assault rates after implementation of the assaulted staff action program", Psychiatric Services, vol. 49, pp. 241-243.
Flannery, R., Schuler, A., Farley, E., & Walker, A. 2002, "Characteristics of assaultive psychiatric patients: ten year analysis of the Assaulted Staff Action Program (ASAP)", Psychiatric Quarterly, vol. 73, pp. 59-69.
Flannery, R., Rachlin, S., & Walker, A. 2002, "Characteristics of repetitively assaultive patients: Ten year analysis of the Assaulted Staff Action Program (ASAP)", International Journal of Emergency Mental Health, vol. 4, no. 3, pp. 173-179.

Flannery, R., Rachlin, S., & Walker, A. 2002, "Characteristics of assaultive patients with schizophrenia versus personaility disorder:Six year analysis of the Assaulted Staff Action Program (ASAP)", Journal of Forensic Sciences, vol. 47, no. 3, pp. 558-561.
Flannery, R. B., Jr., Hanson, M. A., & Penk, W. 1995, "Patients' threats. Expanded definition of assault", General Hospital Psychiatry., vol. 17, no. 6, pp. 451-453.
Flannery, R. B., Jr., Hanson, M. A., Penk, W. E., & Flannery, G. J. 1996, "Violence and the lax milieu?: preliminary data", Psychiatric Quarterly., vol. 67, no. 1, pp. 47-50.
Flannery, R. B., Jr., Hanson, M. A., Penk, W. E., Pastva, G. J., Navon, M. A., & Flannery, G. J. 1997, "Hospital downsizing and patients' assaults on staff", Psychiatric Quarterly, vol. 68, no. 1, pp. 67-76.
Flannery, R. B., Jr., Penk, W. E., Irvin, E. A., & Gallagher, C. 1998, "Characteristics of violent versus nonviolent patients with schizophrenia", Psychiatric Quarterly., vol. 69, no. 2, pp. 83-93.
Flannery, R. B., Jr., Irvin, E. A., & Penk, W. E. 1999, "Characteristics of assaultive psychiatric inpatients in an era of managed care", Psychiatric Quarterly., vol. 70, no. 3, pp. 247-256.
Flannery, R. B., Jr., Corrigan, M., Tierney, T., & Walker, A. P. 2000, "Time and risk of psychiatric patient assault: Ten year analysis of the ASAP.", Journal of healthcare safety, compliance and infection control, vol. 5, pp. 31-35.
Flannery, R. B., Jr., Hanson, M. A., & Rego, J. J. &. W. A. P. 2003, "Precipitants of psychiatric patient assault on staff: Preliminary empirical inquiry of the Assaulted Staff Action Program (ASAP)", International Journal of Emergency Mental Health, vol. 5, pp. 141-146.
Flannery, R. B., Jr., Juliano, J., Cronin, S., & Walker, A. P. 2006, "Characteristics of assaultive psychiatric patients: fifteen-year analysis of the Assaulted Staff Action Program (ASAP)", Psychiatric Quarterly, vol. 77, no. 3, pp. 239-249.
Flannery, R. B., Jr., Farley, E., Rego, S., & Walker, A. P. 2007, "Characteristics of staff victims of pschiatric patient assaults: 15-year analysis of the Assaulted Staff Action Program (ASAP)", Psychiatric Quarterly, vol. 78, no. 1, pp. 25-37.
Flannery, R. B., Jr., Marks, L., Laudani, L., & Walker, A. P. 2007, "Psychiatric patient assault and staff victim gender: fifteen-year analysis of the Assaulted Staff Action Program (ASAP)", Psychiatric Quarterly, vol. 78, no. 2, pp. 83-90.
Flannery, R. B., Jr. & Walker, A. P. 2008, "Characteristics of four types of patient assaults: fifteen-year analysis of the Assaulted Staff Action Program (ASAP) with EMS implications", International Journal of Emergency Mental Health., vol. 10, no. 3, pp. 177-184.
Flannery, R. B., Jr. & Walker, A. P. 2008, "Repetitively assaultive psychiatric patients: fifteen-year analysis of the Assaulted Staff Action Program (ASAP) with implications for emergency services", International Journal of Emergency Mental Health, vol. 10, no. 1, pp. 1-8.

Flannery, R. B. J. & Walker, A. P. 2001, "Characteristics of four types of patient assaults: Six year analysis of the Assaulted Staff Action Program (ASAP). [References]", International Journal of Emergency Mental Health., vol. 3, no. 4, pp. 211-216.
Flannery, R. B. J., Laudani, L., Levitre, V., & Walker, A. P. 2006, "Precipitants of psychiatric patient assaults on staff: Three-year empirical inquiry of the assaulted staff action program (ASAP)", International Journal of Emergency Mental Health, vol. 8, no. 1, pp. 15-22.
Flannery, R. B. J., White, D. L., Flannery, G. J., & Walker, A. P. 2007, "Time of psychiatric patient assaults: Fifteen-year analysis of the Assaulted Staff Action Program (ASAP)", International Journal of Emergency Mental Health, vol. 9, no. 2, pp. 89-96.
Flood, C., Bowers, L., & Parkin, D. 2008, "Estimating the costs of conflict and containment on adult acute inpatient psychiatric wards.", Nursing Economics, vol. 26, no. 5, pp. 325-330.
Foster, C., Bowers, L., & Nijman, H. 2007, "Aggressive behaviour on acute psychiatric wards: prevalence, severity and management", Journal of Advanced Nursing, vol. 58, no. 2, pp. 140-149.
Fottrell, E., Bewley, T., & Sqizzoni, M. 1978, "A Study of Aggressive and Violent Behaviour Among a Group of psychiatric In Patients", Medicine, Science and the Law, vol. 18, no. 1, pp. 66-69.
Fottrell, E. 1980, "A Study of Violent behaviour Among patients in psychiatric Hospitals", British Journal of Psychiatry, vol. 136, pp. 216-221.
Fresan, A., Apiquian, R., Fuente-Sandoval, C., Loyzaga, C., Garcia-Anaya, M., Meyenberg, N., & Nicolini, H. 2005, "Violent behavior in schizophrenic patients: Relationship with clinical symptoms.", Aggressive Behavior, vol. 31, pp. 511-520.
Friis, S. 1986, "Characteristics of a good ward atmosphere", Acta Psychiatrica Scandinavica, vol. 74, pp. 469-473.
Frueh, B., Knapp, R. G., Cusck, K. J., Grubaugh, A. L., Sauvageot, J. A., Cousins, V. C., Yim, E., Robins, C. S., Monnier, J., & Hiers, T. G. 2005, "Patients' Reports of Traumatic or harmful experiences Within the Psychiatric Setting", Psychiatric Services, vol. 56, no. 9, pp. 1123-1133.
Fullam, R. S. & Dolan, M. C. 193, "Executive function and in-patient violence in forensic patients with schizophrenia", British Journal of Psychiatry. no. 3, pp. 247-253.
Gebhardt, R. P. & Steinert, T. 1999, "Should severely disturbed psychiatric patients be distributed or concentrated in specialized wards? An empirical study on the effects of hospital organization on ward atmosphere, aggressive behavior, and sexual molestation", The Journal of the Association of European Psychiatrists., vol. 14, no. 5, pp. 291-297.
Gerberich, S. G., Church, T. R., McGovern, P. M., Hansen, H., Nachreiner, N. M., Geisser, M. S., Ryan, A. D., Mongin, S. J., Watt, G. D., & Jurek, A. 2005, "Risk factors for work-related assaults on nurses", Epidemiology, vol. 16, no. 5, pp. 704-709.

Gerolamo, A. M. 2008, "Measuring adverse outcomes in inpatient psychiatry: the reliability of nurse recall", Archives of Psychiatric Nursing, vol. 22, no. 2, pp. 95-103.
Gillig, P. M., Markert, R., Barron, J., & Coleman, F. 1998, "A comparison of staff and patient perceptions of the causes and cures of physical aggression on a psychiatric unit", Psychiatric Quarterly, vol. 69, no. 1, pp. 45-60.
Goldberg, B. R., Serper, M. R., Sheets, M., Beech, D., Dill, C., & Duffy, K. G. 2007, "Predictions of aggression on the psychiatric inpatient service: self-esteem, narcissism, and theory of mind deficits", Journal of Nervous & Mental Disease. no. 5, pp. 436-442.
Goodykoontz, L. & Herrick, C. A. 1990, "Evaluation of an Inservice Education Program Regarding Aggressive Behavior in a Psychiatric Unit", The Journal of Continuing Education in Nursing, vol. 21, no. 3, pp. 129-133.
Gorden, J., Gorden, C., & Gardener, D. 1996, "A study of assaultive/aggressive behaviour on staff by patients/clients in psychiatric facilities", Journal of Occupational Health and Safety, vol. 12, no. 2, pp. 169-177.
Grainger, C. & Whiteford, H. 1993, "Assault on staff in psychiatric hospitals: a safety issue", Australian & New Zealand Journal of Psychiatry, vol. 27, no. 2, pp. 324-328.
Grassi, L., Peron, L., Marangoni, C., Zanchi, P., & Vanni, A. 2001, "Characterisitcs of violent behaviour in acute psychiatric inpatients: a 5 year Italian study", Acta Psychiatrica Scandinavica, vol. 104, pp. 273-279.
Grassi, L., Biancosino, B., Marmai, L., Kotrotsiou, V., Zanchi, P., Peron, L., Marangoni, C., Vanni, A., & Barbui, C. 2006, "Violence in psychiatric units: a 7-year Italian study of persistently assaultive patients", Social Psychiatry & Psychiatric Epidemiology, vol. 41, no. 9, pp. 698-703.
Gray, N. S., Hill, C., McGleish, A., Timmons, D., MacCulloch, M., & Snowdon, R. 2003, "Prediction of violence and self-harm in mentally disordered offenders: A prospective study of the efficacy of HCR-20, PCL-R, and psychiatric symptomatology.", Journal of Consulting & Clinical Psychology, vol. 71, no. 3, pp. 443-451.
Greenfield, T. K., McNiel, D. E., & Binder, R. L. 1989, "Violent behavior and length of psychiatric hospitalization", Hospital & Community Psychiatry, vol. 40, no. 8, pp. 809-814.
Grenade, G. & Macdonald, E. 1995, "Risk of physical assaults among student nurses", Occupational Medicine (Oxford), vol. 45, no. 5, pp. 256-258.
Grevatt, M., Thomas-Peter, B., & Hughes, G. 2004, "Violence, mental disorder and risk assessment: can structured clinical assessments predict the short-term risk of inpatient violence?", The Journal of Forensic Psychiatry and Psychology, vol. 15, no. 2, pp. 278-292.
Grube, M. 2007, "Gender differences in aggressive behavior at admission to a psychiatric hospital", Aggressive Behavior, vol. 33, no. 2, pp. 97-103Apr.
Gudjonsson, G., Rabe-Hesketh, S., & Szmukler, G. 2004, "Management of psychiatric inpatient violence: patient ethnicity and use of medication, restraint and seclusion", British Journal of Psychiatry, vol. 184, pp. 258-262.
Gudjonsson, G. H., Rabe-Hesketh, S., & Wilson, C. 1999, "Violent incidents on a medium secure unit over a 17-year period", Journal of Forensic Psychiatry, vol. 10, pp. 249-263.
Gudjonsson, G. H., Rabe-Hesketh, S., & Wilson, C. 2000, "Violent incidents in a psychiatric hospital. The target of assault and the management of incidents", Journal of Forensic Psychiatry, vol. 11, pp. 105-118.
Haffke, E. & Reid, W. 1983, "Violence Against mental Health Personnel in Nebraska", in Lion, J.and Reid, W.(Eds) Assaults Within psychiatric Facilities.Orlando: Grune and Stratton., vol. 91-102.
Hagen.D.Q., Mikolajczak, J., & Wright, R. 1972, "Aggression in Psychiatric Patients", Comprehensive Psychiatry, vol. 13(481-487).
Hahn, S., Needham I., Abderbalden, C., Duxbury J., & Halfens, R. 2006, "The effect of a training course on mental health nurses' atitudes on the reasons of patient aggression and its management", Journal of Psychiatric and Mental Health Nursing, vol. 13, pp. 197-204.
Haider, I. I. 1997, "Violence by psychiatric inpatients", Journal of the College of Physicians & Surgeons Pakistan., vol. 7, no. 4, pp. 170-172.
Haim, R. 2002, "Predictions made by psychiatrists and psychiatric nurses of violence by patients", Psychiatric Services, vol. 53, pp. 622-624.
Haller, R. M. & Deluty, R. H. 1990, "Characteristics of psychiatric inpatients who assault staff severely", Journal of Nervous & Mental Disease, vol. 178, no. 8, pp. 536-537.
Hamadeh, R. R., Al Alaiwat, B., & Al Ansari, A. 2003, "Assaults and nonpatient-induced injuries among psychiatric nursing staff In Bahrain.", Issues in Mental Health Nursing., vol. 24, no. 4, pp. 409-417.
Hanson, R. & Balk, J. 1992, "A replication study of staff injuries in a state hospital", Hospital and Community Psychiatry, vol. 43, no. 8, pp. 836-837.
Hardie, T. 1999, "Crowding and violent behaviour: the influence of patient density on violent and self-harming behaviour at a medium secure unit", Medicine, Science and the Law, vol. 39, pp. 161-166.
Harris, C. T. & Varney, G. W. 1986, "A ten-year study of assaults and assaulters on a maximum security psychiatric unit", Journal of Interpersonal Violence, vol. 1, pp. 173-191.
Harris, G., Rice, M. E., & M 1986, "Staff injuries sustained during altercations with psychiatric patients", Journal of Interpersonal Violence, vol. 1(2) : 193 - 211.
Hatch-Maillette, M. A., Scalora, M. J., Bader, S. M., & Bornstein, B. H. 2007, "A gender-based incidence study of workplace violence in psychiatric and forensic settings", Violence & Victims, vol. 22, no. 4, pp. 449-462.
Hatti, S., Dubin, W., & Weiss, K. 1982, "A study of circumstances surrounding patient assaults on psychiatrists", Hospital and Community Psychiatry, vol. 33, pp. 660-661.
Heilbrun, K. 1998, "Inpatient and post discharge aggression in mentally disordered offenders: The role of psychopathy", Journal of Interpersonal Violence, vol. 13, pp. 514-527.
Helmuth, R. 1994, "Nursing staff educational preparation and patient inflicted injuries in a 160 bed psychiatric hospital", Alaska Medicine, vol. 36, no. 4 (Dec), pp. 189-192.
Hesketh, K. L., Duncan, S., Estabrooks, C. A., Reimer, M. A., Giovannetti, P., Hyndman, K., & Acorn, S. 2003, "Workplace violence in Alberta and British Columbia hospitals.", Health Policy, vol. 63, pp. 311-321.
Hildebrand, M., De-Ruiter, C., & Nijman, H. 2003, "PCL-R Psychopathy Predicts Disruptive Behavior Among Male Offenders in a Dutch Forensic Psychiatric Hospital", Journal of Interpersonal Violence, vol. 18, no. 10, pp. 1-17.
Hillbrand, M. 1992, "Self-directed and other-directed aggressive behaviour in a foresnic sample", Suicide and Life-Threatening Behaviour, vol. 22, pp. 333-340.
Hillbrand, M., Foster, H. G., & Spitz, R. T. 1996, "Characteristics and cost of staff injuries in a forensic hospital", Psychiatric Services, vol. 47, no. 10, pp. 1123-1125.
Hills, D. 2008, "Relationships between aggression management training, perceived self-efficacy and rural general hospital nurses' experiences of patient aggression", Contemporary Nurse, vol. 31, no. 1, pp. 20-31.
Hinsby, K. & Baker, M. 2004, "Patient and nurse accounts of violent incidents in a Medium Secure Unit", Journal of Psychiatric and Mental Health Nursing, vol. 11, pp. 341-347.
Hodgins, S., Alderton, J., Cree, A., Aboud, A., & Mak, T. 2007, "Aggressive behaviour, victimisation and crime among severely mentally ill patients requiring hospitalisation", British Journal of Psychiatry, vol. 191, pp. 343-350.
Hodgkinson, P., Hillis, T., & Russel, D. 1984, "Assaults on Staff in psychiatric Hospitals", Nursing Times, vol. 80, no. 18, pp. 44-46.
Hodgkinson, P., McIvor, L. L., & Phillips, M. 1985, "Patient Assaults on Staff in a Psychiatric Hospital. A two year retrospective study", Medicine, Science and the Law, vol. 28, pp. 288-294.
Holden, B. & Gitlesen, J. P. 2008, "The relationship between psychiatric symptomatology and motivation of challenging behaviour: a preliminary study", Research in Developmental Disabilities., vol. 29, no. 5, pp. 408-413.
Hoptman, M. J., Yates, K. F., Patalinjug, M. B., Wack, R. C., & Convit, A. 1999, "Clinical prediction of assaultive behavior among male psychiatric patients at a maximum-security forensic facility.", Psychiatric Services, vol. 50, no. 11, pp. 1461-1466.
Hornsveld, R. H., Nijman, H. L., Hollin, C. R., & Kraaimaat, F. W. 2007, "Development of the Observation Scale for Aggressive Behavior (OSAB) for Dutch forensic psychiatric inpatients with an antisocial personality disorder", International Journal of Law & Psychiatry, vol. 30, no. 6, pp. 480-491.

Hornsveld, R. H. J., Nijman, H. L. I., & Kraaimaat, F. W. 2008, "Aggression control therapy for violent forensic psychiatric patients: First results", Psychology, Crime & Law, vol. 14, no. 1, pp. 1-18.
Huber, C. G., Lambert, M., Naber, D., Schacht, A., Hundemer, H. P., Wagner, T. T., & Schimmelmann, B. G. 2008, "Validation of a Clinical Global Impression Scale for Aggression (CGI-A) in a sample of 558 psychiatric patients", Schizophrenia Research, vol. 100, no. 1, pp. 342-348.
Huchzermeier, C., Bruss, E., Geiger, F., Kernbichler, A., & Aldenhoff, J. 2008, "Predictive validity of the psychopathy checklist: screening version for intramural behaviour in violent offenders-a prospective study at a secure psychiatric hospital in Germany", Canadian Journal of Psychiatry - Revue Canadienne de Psychiatrie, vol. 53, no. 6, pp. 384-391.
Hunter, M. E. & Love, C. C. 1993, "Types of weapons and patterns of use in a forensic hospital", Hospital and Community Psychiatry, vol. 44(11): 1082-1085.
Hunter, M. E. & Love, C. C. 1996, "Total Quality Management and the Reduction of Inpatient Violence and Costs in a Forensic Psychiatric Hospital", Psychiatric Services, vol. 47, no. 7, pp. 751-754.
Huss, M. T. & Zeiss, R. A. 2004, "Clinical assessment of violence from inpatient records: A comparison of individual and aggregate decision making across risk strategies.", International Journal of Forensic Mental Health, vol. 3, pp. 139-147.
Infantino, J. A. & Musingo, S. A. 1985, "Assaults and Injuries Among Staff with and without Training in Aggression Control techniques", Hospital and Community Psychiatry, vol. 36, no. 12, pp. 1312-1314.
Inoue, M., Tsukano, K., Muraoka, M., Kaneko, F., & Okamura, H. 2006, "Psychological impact of verbal abuse and violence by patients on nurses working in psychiatric departments", Psychiatry & Clinical Neurosciences., vol. 60, no. 1, pp. 29-36.
Ionno, J. 1983, "A Prospective Study of Assaultive Behaviour in Female Psychiatric Inpatients", in Lion, J.and Reid, W.(Eds) Assaults Within psychiatric Facilities.Orlando: Grune and Stratton. pp. 71-80.
Ireland, J. L. & Rowley, J. 7 A.D., "Sectioned offenders presenting with enduring mental illness: a study exploring behaviors indicative of bullying", Aggressive Behavior., vol. 33, no. 5, pp. 377-388.
Ireland, J. L. 2004, "Nature, extent and caused of bullying among personality-disordered patients in a high secure hospital", Aggressive Behavior, vol. 30, pp. 229-242.
Ireland, J. L. 2005, "Exploring Definitions of Bullying Among Personality Disordered Patients in a Maximum-Secure Hospital", Aggressive Behavior, vol. 31, pp. 359-373.
Ireland, J. L. & Bescoby, N. 2005, "Behavioural Assessment of Bullying Behaviour Among Personality Disordered Patients in a High Secure Hospital", Aggressive Behavior, vol. 31, no. 1, pp. 67-83.

Ireland, J. L. 2006, "Bullying Among Mentally-Ill Patients Detained in a High-Secure Hospital: An Exploratory Study of the Perceptions of Staff and Patients into How Bullying is Defined", Aggressive Behavior , vol. 32, no. 5, pp. 451-463.
Ito, H., Eisen, S., Sederer, L., Yamada, O., & Tachimori, H. 2001, "Factors affecting psychiatric nurses' intention to leave their current job", Psychiatric Services, vol. 52, no. 2, pp. 232-234.
James, D., Fineberg, N., Shah, A., & Priest, R. 1990, "An Increase in Violence on an Acute Psychiatric Ward: A Study of Associated Factors", British Journal of Psychiatry, vol. 156, pp. 846-852.
Jansen, G., Dassen, T., & Moorer, P. 1997, "The Perception of Aggression", Scandinavia Journal of Caring Sciences, vol. 1, pp. 51-55.
Jansen, G. J., Middel, B., Dassen, T. W., & Reijneveld, M. S. 1920, "Cross-cultural differences in psychiatric nurses' attitudes to inpatient aggression", Archives of Psychiatric Nursing. no. 2, pp. 82-93.
Jansen, G. J., Dassen, T. W. N., Burgerhof, J. G. M., & Middel, B. 2006, "Psychiatric nurses' attitudes towards inpatient aggression: Preliminary report of the development of Attitude Towards Aggression Scale (ATAS)", Aggressive Behavior, vol. 32, no. 1, pp. 44-53.
Johnson, B., Martin, M., Guha, M., & Montgomery, P. 1997, "The experience of thought- disordered individuals preceding an agressive incident", Journal of Psychiatric Nursing and Mental Health Services, vol. 4, no. 3, pp. 213-220.
Johnson, M. E. & Delaney, K. R. 2007, "Keeping the unit safe: the anatomy of escalation", Journal of the American Psychiatric Nurses Association, vol. 13, no. 1, pp. 42-52.
Johnston, R. & Lundy, B. W. 1982, "Disruptive behavior by hospitalized patients following movie viewing", Hospital & Community Psychiatry, vol. 33, no. 12, pp. 1015-1017.
Jones, M. K. 1985, "Patient Violence: report of 200 incidents", Journal of Psychosocial Nursing, vol. 23, no. 6, pp. 12-17.
Jones, N. T., Sheitman, B., Hazelrigg, M., Carmel, H., Williams, J., & Paesler, B. 2007, "Development of a clinical instrument to record sexual aggression in an inpatient psychiatric setting", Journal of Sexual Aggression, vol. 13, no. 1, pp. 51-58.
Jonker, E. J., Goossens, P. J. J., Steenhuis, I. H. M., & Oud, N. E. 2008, "Patient aggression in clinical psychiatry: Perceptions of mental health nurses", Journal of Psychiatric and Mental Health Nursing, vol. 15, no. 6, pp. 492-499.
Joyal, C. C., Gendron, C., & Cote, G. 2008, "Nature and frequency of aggressive behaviours among long-term inpatients with schizophrenia: a 6-month report using the modified overt aggression scale", Canadian Journal of Psychiatry - Revue Canadienne de Psychiatrie, vol. 53, no. 7, pp. 478-481.
Karson, C. & Bigelow, L. 1987, "Violent behaviour in schizophrenic inpatients", Journal of Nervous Mental Disorders, vol. 175, pp. 161-164.

Katz, P. & Kirkland, F. R. 1990, "Violence and Social Structure on Mental Hospital Wards", Psychiatry, vol. 53, no. 3, pp. 262-277.
Kennedy, J., Harrison, J., & Hillis, T. 1995, "Analysis of violent incidents in a regional secure unit", Medicine, Science and the Law, vol. 35, pp. 226-231.
Kennedy, M. G. 1993, "Relationship between psychiatric diagnosis and patient aggression", Issues in Mental Health Nursing., vol. 14, no. 3 (Sep), pp. 263-273.
Ketelsen, R., Zechert, C., Driessen, M., & Schulz, M. 2007, "Characteristics of aggression in a German Psychiatric hopsital and predictors of patients at risk", Journal of Psychiatric and Mental Health Nursing, vol. 14, pp. 92-99.
Kho, K., Sensky, T., Mortimer, A., & Corcos, C. 1998, "Prospective study into factors associated with aggressive incidents in psychiatric acute admissions wards", British Journal of Psychiatry, vol. 172, pp. 38-43.
Kiely, S., McCafferty, G., & McMahon, A. 1999, "Danger at work? - violence and mental health nursing", Mental health Practice, vol. 2, no. 7, pp. 4-5.
Kindy, D., Peterson, S., & Parkhurst, D. 2005, "Perilous work: Nurses' experiences in psychiatric units with high risks of assault", Archives of Psychiatric Nursing, vol. 19, no. 4, pp. 169-175.
Knowles, S. F., Coyne, S. M., & Brown, S. L. 2008, "Sex differences in aggressive incidents towards staff in secure services", Journal of Forensic Psychiatry & Psychology, vol. 19, no. 4, pp. 620-631.
Kohen, D. 2002, "Nurses' uniforms", Psychiatric Bulletin, vol. 26, no. 4, p. 156.
Krakowoski, M., Jaeger, J., & Volavka, J. 1988, "Violence and psychopathology: A longitudinal study", Comprehensive Psychiatry, vol. 29, pp. 174-181.
Krakowski M, Convit, A., Jaeger, J., Lin, S., & Volavka, J. 1989, "Neurological impairment in violent schizophrenic inpatients.", American Journal of Psychaitry, vol. 146, pp. 849-853.
Krakowski, M. & Czobor, P. 1997, "Violence in psychiatric patients: the role of psychosis, frontal lobe impairment, and ward turmoil", Comprehensive Psychiatry, vol. 38, no. 4 (Aug), pp. 230-236.
Krakowski, M., Czobor, P., & Chou, C. Y. 1999, "Course of Violence in Patients with Schizophrenia: Relationship to Clinical Symptoms", Schizophrenia Bulletin, vol. 25, no. 3, pp. 505-517.
Krakowski, M. I., Convit, A., Jaeger, J., Lin, S., & Volavka, J. 1989, "Inpatient violence: trait and state", Journal of Psychiatric Research, vol. 23, no. 1, pp. 57-64.
Kraus, J. E. & Sheitman, B. B. 2004, "Characteristics of Violent Behavior in a Large State Psychiatric Hospital", Psychiatric Services., vol. 55, no. 2, pp. 183-185.

Kumar, S., Guite, H., & Thornicroft, G. 2001, "Service Users' Experience of Violence within a Mental health System: A Study Using Grounded Theory Approach", Journal of mental Health, vol. 10, no. 6, pp. 597-611.
Lam, J. N., McNiel, D. E., & Binder, R. L. 2000, "The relationship between patients' gender and violence leading to staff injuries", Psychiatric Services., vol. 51, no. 9, pp. 1167-1170.
Lancee, W. J., Gallop, R., McCay, E., & Toner, B. 1995, "The relationship between nurses' limit-setting styles and anger in psychiatric inpatients", Psychiatric Services, vol. 46, no. 6, pp. 609-613.
Langsrud, K., Linaker, O. M., & Morken, G. 2007, "Staff injuries after patient-staff incidences in psychiatric acute wards", Nordic Journal of Psychiatry, vol. 61, no. 2, pp. 121-125.
Lanza, M. & Kayne, H. 1997, "Staffing of inpatient units and assault by patients", Journal of the American Psychiatric Nurses Association, vol. 3, no. 2, pp. 42-48.
Lanza, M. L. 1983, "The Reactions of Nursing Staff to Physical Assault by a Patient", Hospital of Community Psychiatry, vol. 34, no. 1, pp. 45-47.
Lanza, M. L. 1985, "How Nurses React to Patient Assault", Journal of Psychosocial Nursing, vol. 23, no. 6, pp. 6-11.
Lanza, M. L., Milner, J., & Riley, E. 1988, "Predictors of Patient Assault on Acute Inpatient Psychiatric Units: A Pilot Study", Issues in Mental Health Nursing, vol. 9, no. 3, pp. 259-270.
Lanza, M. L. 1988, "Factors Relevant to Patient Assault", Issues in Mental Health Nursing, vol. 9, no. 239, p. 257.
Lanza, M. L., Kayne, H. L., Hicks, C., & Milner, J. 1991, "Nursing Staff Characteristics Related to Patient Assault", Issues in Mental Health Nursing, vol. 12, no. 3, pp. 253-265.
Lanza, M. L. & Carifio, J. 1991, "Blaming the victim: complex (nonlinear) patterns of causal attribution by nurses in response to vignettes of a patient assaulting a nurse", Journal of Emergency Nursing, vol. 17, no. 5, pp. 299-309.
Lanza, M. L., Kayne, H. L., Pattison, I., Hicks, C., & Islam, S. 1994, "Predicting violence:nursing daignosis versus psychiatric diagnosis", Nursing Diagnosis, vol. 5, no. 4, pp. 151-157.
Lanza, M. L. & Kayne, H. L. 1995, "Patient Assault: A Comparison of Patient and Staff Perceptions", Issues in Mental Health Nursing, vol. 16, pp. 129-141.
Larkin, E., Silvester, M., & Jones, S. 1988, "A Preliminary Study of Violent Incidents in a Speical Hospital (Rampton)", British Journal of Psychiatry, vol. 153, pp. 226-231.
Lawn, S. & Pols, R. 2003, "Nicotine withdrawal: Pathway to aggression and assault in the locked psychiatric ward?", Australasian Psychiatry., vol. 11, no. 2, pp. 199-203.
Lawoko, S., Soares, J., & Nolan, P. 2004, "Violence towards psychiatric staff: a comparison of gender, job and environmental characteristics in England and Sweden", Work & Stress, vol. 18, no. 1, pp. 39-55.
Lee, H. K., Villar, O., Juthani, N., & Bluestone, H. 1989, "Characteristics and behaviour of patients involved in psychiatric ward incidents", Hospital and Community Psychiatry, vol. 40, no. 12, pp. 1295-1297.
Lehmann, L., McCormick, R., & Kizer, K. 1999, "A survey of assaultive behaviour in a Veterans Health Administration Centre", Psychiatric Services, vol. 50, pp. 384-389.
Lehmann, L., McCormick, R., & Kizer, K. 1999, "A survey of assaultive behaviour in a Veterans Health Administration Centre", Psychiatric Services, vol. 50, pp. 384-389.
LePage, J. P., DelBen, K., Pollard, S., McGhee, M., VanHorn, L., Murph, J., Lewis, P., Aboraya, A., & Mogge, N. 2003, "Reducing assaults on an acute psychiatric unit using a token economy: A 2-year follow-up", Behavioral Interventions., vol. 18, no. 3, pp. 179-190.
LePage, J. P., McGhee, M., Aboraya, A., Murphy, J., VanHorn, L., Pollard, S., & Dean, P. 2005, "Evaluating risk factors for violence at the inpatient unit level: combining young adult patients and those with mental retardation", Applied Nursing Research, vol. 18, no. 2, pp. 117-121.
Levy, P. & Hartocollis, P. 1976, "Nursing Aides and Patient Violence", American Journal of Psychiatry, vol. 133, no. 4, pp. 429-431.
Lim, L., Tobin, M., & Falkowski, W. 1991, "The characteristics of patients who display violent behaviour in a psychiatric hospital", British Journal of Clinical and Social Psychiatry, vol. 8, no. 1, pp. 12-18.
Linaker, O. M. & Busch-Iversen, H. 1995, "Predictors of Imminent Violence in Psychiatric Inpatients", Acta psychiatr.scand., vol. 92, no. 4, pp. 250-254.
Linhorst, D. M. & Scott, L. P. 2004, "Assaultive Behavior in State Psychiatric Hospitals: Differences Between Forensic and Nonforensic Patients. [References]", Journal of Interpersonal Violence., vol. 19, no. 8, pp. 857-874.
Lion, J. R. & Pastermak, S. A. 1973, "Countertransference Reactions to Violent Patients", American Journal of Psychiatry, vol. 130, no. 2, pp. 207-210.
Lion, R. J. & et al. 1981, "Underreporting of assaults on staff in a state hopsital", Hospital and Community Psychiatry, vol. 32 815-825, pp. 815-825.
Lipscomb, J., McPhaul, K., Rosen, J., Brown, J. G., Choi, M., Soeken, K., Vignola, V., Wagoner, D., Foley, J., & Porter, P. 2006, "Violence prevention in the mental health setting: the New York state experience", Canadian Journal of Nursing Research, vol. 38, no. 4, pp. 96-117.
Longo, D. A. & Bisconer, S. W. 2003, "Treatment of aggression for an adult diagnosed with schizophrenia at a public psychiatric hospital", Professional Psychology Research and Practice, vol. 34, no. 2, pp. 177-179.

Love, C. & Hunter, M. 1996, "Violence in public sector psychiatric hospitals. Benchmarking nursing staff injury rates", Journal of Psychosocial Nursing and Mental Health Services, vol. 34, no. 5, pp. 30-34.
Love, C. & Hunter, M. 1999, "The Atascadero State Hospital experience: engaging patients in violence prevention", Journal of Psychosocial Nursing and Mental Health Services, vol. 37, no. 9, pp. 32-36.
Lowe, T. 1992, "Characteristics of effective nursing interventions in the management of challenging behaviour", Journal of Advanced Nursing, vol. 17, pp. 1226-1232.
Lowenstein, M., Binder, R. L., & McNiel, D. E. 1990, "The relationship between admission symptoms and hospital assaults", Hospital and Community Psychiatry, vol. 41, no. 3, pp. 311-313.
Lu, C. H., Wang, T. F., & Liu, C. Y. 2007, "Psychiatric nurses' reactions to assault upon them by inpatients: A survey in Taiwan", Psychological Reports, vol. 100, no. 3, pp. 777-782.
Lucas, M. & Stevenson, D. 2006, "Violence and abuse in psychiatric in-patient institutions: a South African perspective", International Journal of Law & Psychiatry, vol. 29, no. 3, pp. 195-203.
Madden, D. J., Lion, J. R., & Penna, M. 1976, "Assaults on psychiatrists by patients", American Journal of Psychiatry, vol. 133, pp. 422-425.
Maier, G., Van Rybroek, G., & Mays, D. 1994, "A report on staff injuries and ambulatory restraints: dealing with patient aggression", Journal of Psychosocial Nursing and Mental Health Service, vol. 32, no. 11, pp. 23-29.
Manfredini, R., Vanni, A., Peron, L., La Cecilia, O., Smolensky, M. H., & Grassi, L. 2001, "Day-night variation in aggressive behavior among psychiatric inpatients", Chronobiology International., vol. 18, no. 3, pp. 503-511.
Margari, F., Matarazzo, R., Casacchia, M., Roncone, R., Dieci, M., Safran, S., Fiori, G., Simoni, L., & The EPICA Study Group 2005, "Italian validation of MOAS and NOSIE: a useful package for psychiatric assessment and monitoring of aggressive behaviours", International Journal of Methods in Psychiatric Research, vol. 14, no. 2, pp. 109-118.
McGeorge, M., Lelliott, P., Stewart, J., & Royal College of Psychiatrist Research Unit, L. 2001, "Managing Violence in Psychiatric Wards: Preliminary Findings of a Multi-centre Audit", Mental Health Care, vol. 31, no. 11, pp. 366-369.
McKenzie, B. & Curr, H. 2005, "Predicting violence in a medium secure setting: a study using the historical and clinical scales of the HCR-20", British Journal of Forensic Practice, vol. 7, no. 3, pp. 22-28.
McNiel, D., Binder, R., & Greenfield, T. 1988, "Predictors of violence in civilly committed acute psychiatric patients", American Journal of Psychiatry, vol. 145, no. 8, pp. 965-970.
McNiel, D., Lam, J., & Binder, R. 2000, "Relevance of interrater agreement to violence risk assessment.", Journal of Consulting & Clinical Psychology, vol. 68, no. 6, pp. 1111-1115.

McNiel, D., Gregory, A. L., Lam, J., Binder, R. L., & Sullivan, G. 2003, "Utility of decision support tools for assessing acute risk of violence.", Journal of Consulting & Clinical Psychology, vol. 71, no. 5, pp. 945-953.
McNiel, D. E. & Binder, R. L. 1989, "Relationship between preadmission threats and later violent behavior by Acute psychiatric inpatients", Hospital and Community Psychiatry, vol. 40, no. 6, pp. 605-608.
McNiel, D. E. & Binder, R. L. 1991, "Clinical Assessment of the Risk of Violence Among Psychiatric Inpatients", American Journal of Psychiatry, vol. 148, no. 10, pp. 1317-1321.
McNiel, D. E. & Binder, R. L. 1994, "The relationship between acute psychiatric symptoms, diagnosis, and short-term risk of violence", Hospital and Community Psychiatry, vol. 45, no. 2, pp. 133-137.
McNiel, D. E., Sandberg, D. A., & Binder, R. L. 1998, "The relationship between confidence and accuracy in clinical assessment of psychiatric patients potential for violence", Law & Human Behavior, vol. 22, no. 6, pp. 655-669.
Meehan, T., McIntosh, W., & Bergen, H. 2006, "Aggressive behaviour in the high-secure forensic setting: the perceptions of patients", Journal of Psychiatric and Mental Health Nursing, vol. 13, pp. 19-25.
Meehan, T., Fjeldsoe, K., Stedman, T., & Duraiappah, V. 2006, "Reducing aggressive behaviour and staff injuries: a multi-strategy approach", Australian Health Review, vol. 30, no. 2, pp. 203-210.
Mellesdal, L. 2003, "Aggression on a Psychiatric Acute Ward: A Three-Year Prospective Study", Psychological Reports, vol. 92, pp. 1229-1248.
Merecz, D., Rymaszewska, J., Moscicka, A., Kiejna, A., & Jarosz-Nowak, J. 2006, "Violence at the workplace--a questionnaire survey of nurses", European Psychiatry: the Journal of the Association of European Psychiatrists.21(7):442-50.
Mezey, G., Hassell, Y., & Bartlett, A. 2005, "Safety of women in mixed-sex and single-sex medium secure units: staff and patient perceptions", British Journal of Psychiatry, vol. 187, no. 6, pp. 579-582.
Middleby-Clements, J. L. & Grenyer, B. F. S. 2007, "Zero tolerance approach to aggression and its impact upon mental health staff attitudes", Austrailian and New Zealand Journal of Psychiatry, vol. 41, pp. 187-191.
Milius, A. C. 1990, "Experienced psychiatric nurses' prediction of inpatient aggression", Kansas Nurse, vol. 65, no. 10, pp. 1-10.
Miller, R., Zadolinnyj, K., & Hafner, J. 1993, "Profiles and Predictors of Assaultiveness for Different Psychiatric Ward Populations", Am J Psychiatry, vol. 150, no. 9, pp. 1368-1373.
Mills, A. 1997, "Incident reports in secure psychiatric hospitals", Nursing Standard, vol. 12, no. 6, pp. 34-35.

Morken, G., Linaker, O. M., & Langsrud, K. 1999, "Weekly and daily variations in patient-staff incidents in psychiatric acute wards", Nordic Journal of Psychiatry., vol. 53, no. 4, pp. 293-295.
Morken, G. & Linaker, O. M. 2000, "Seasonal variation of violence in psychiatric patients and the general population", European Journal of Psychiatry., vol. 14, no. 3, pp. 153-159.
Morrison, E., Morman, G., Bonner, G., Taylor, C., Abraham, I., & Lathan, L. 2002, "Reducing Staff Injuries and Violence in a Forensic Psychiatric Setting", Archives of Psychiatric Nursing, vol. XVI, no. 3, pp. 108-117.
Morrison, E. F. 1990, "Violent Psychiatric Inpatients in a Public Hospital", Scholarly Inquiry for Nursing Practice: An International Journal, vol. 4(1): 65-82.
Mortimer, A. 1995, "Reducing Violence on a Secure Ward", Psychiatric Bulletin, vol. 19, pp. 605-608.
Murray, G. & McKenzie, K. 1999, "The relationship between staff sickness levels and client assault levels in health service unit for people with an intellectual disability and severely challenging behaviour", Journal of applied research in intellectual disabilities, vol. 12, pp. 263-268.
Murray, M. G. & Snyder, J. C. 1991, "When staff are assaulted. A nursing consultation support service", Journal of Psychosocial Nursing & Mental Health Services., vol. 29, no. 7, pp. 24-29.
Myers, K. & Dunner, D. 1984, "Self and other directed violence on a closed acute care ward", Psychiatric Quarterly, vol. 56, pp. 178-188.
Needham, I., Abderhalden, C., Meer, R., Dassen, T., Haug, H., Halfens, R., & Fischer, J. 2004, "The effectiveness of two interventions in the management of patient violence in acute mental inpatient settings: report on a pilot study", Journal of Psychiatric and Mental Health Nursing, vol. 11, pp. 595-601.
Needham, I., Abderbalden, C., Dassen, T., Haug, H. J., & Fischer, E. 2002, "Coercive Procedures and Facilities in Swiss Psychiatry", Swiss Med Weekly, vol. 132, pp. 253-258.
Needham, I., Abderhalden, C., Haug, H. J., Dassen, T., Halfens, R. J. G., & Fischer, J. E. The effect of a training course in aggression management on the prevalence of aggression and coercive measures in inpatient psychiatric settings: A randomised controlled trial. 2004. Ref Type: Unpublished Work
Ng, B., Kumar, S., Ranclaud, M., & Robinson, E. 2001, "Ward crowding and incidents of violence on an acute psychiatric inpatient unit", Psychiatric Services., vol. 52, no. 4, pp. 521-525.
Nicholls, T. L., Ogloff, J., & Douglas, K. S. 2004, "Assessing risk for violence among male and female civil psychiatric patients: The HCR-12, PCL:SV and VSC", Behavioral Sciences and the Law, vol. 22, pp. 127-158.
Nicholls, T. L., Brink, J., Greaves, C., Lussier, P., & Verdun-Jones, S. 2009, "Forensic psychiatric inpatients and aggression: an exploration of incidence, prevalence, severity, and

interventions by gender", International Journal of Law & Psychiatry, vol. 32, no. 1, pp. 23-30.
Nijman, H., Allertz, W., Merckelbach, H., & Ravelli, D. 1997, "Aggressive Behaviour on an Acute Psychiatric Admissions Ward", European Journal of Psychiatry, vol. 11, no. 2, pp. 106-114.
Nijman, H., Merckelbach, H., Evers, C., Palmstierna, T., & Campo, J. 2002, "Prediction of Aggression on a Locked Psychiatric Amission Ward", Acta Psychiatrica Scandinavica, vol. 105, pp. 1-6.
Nijman, H. L., Merckelbach, H., & Campo, J. 1997, "Prevention of Aggressive Incidents on a Closed Psychiatric Ward", Psychiatric Services, vol. 48, no. 5, pp. 694-698.
Nijman, H. L. I. & Rector, G. 1999, "Crowding and aggression on inpatient psychiatric wards", Psychiatric Services., vol. 50, no. 6, pp. 830-831.
Noble, P. & Rodger, S. 1989, "Violence by Psychiatric In-patients", British Journal of Psychiatry, vol. 155, pp. 384-390.
Nolan, K. A., Czobor, P., Roy, B. B., Platt, M. M., Shope, C. B., Citrome, L. L., & Volavka, J. 2003, "Characteristics of assaultive behavior among psychaitric inpatients", Psychiatric Services, vol. 54, no. 7, pp. 1012-1016.
Nolan, K. A. & Volavka, J. 2006, "Video recording in the assessment of violent incidents in psychiatric hospitals", Journal of Psychiatric Practice, vol. 21, no. 1, pp. 58-63.
Nolan, K. A. & Citrome, L. 2008, "Reducing inpatient aggression: does paying attention pay off?", Psychiatric Quarterly, vol. 79, no. 2, pp. 91-95.
Nolan, K. A., Volavka, J., Czobor, P., Sheitman, B., Lindenmayer, J. P., Citrome, L. L., McEvoy, J., & Lieberman, J. A. 2005, "Aggression and psychopathology in treatment-resistant inpatients with schizophrenia and schizoaffective disorder", Journal of Psychiatric Research, vol. 39, no. 1, pp. 109-115.
Nolan, P., Dalender, J., Soares, J., Thomsen, S., & Arnetz, B. 1999, "Violence in mental health care: the experiences of mental health nurses and psychiatrists", Journal of Advanced Nursing, vol. 30(4) 934-941.
Ogloff, J. R. P. & Daffern, M. 2006, "The Dynamic Appraisal of Situational Aggression: An Instrument to Assess Risk for Imminent Aggression in Psychiatric Inpatients", Behavioral Sciences & the Law, vol. 24, no. 6, pp. 799-813.
Omerov, M. & Wistedt, B. 1997, "Mangageable violence in a new ward for acutely admitted patients", European Psychiatry: the Journal of the Association of European Psychiatrists., vol. 12, no. 6, pp. 311-315.
Omerov, M., Edman, G., & Wistedt, B. 2004, "Violence and threats of violence within psychiatric care - A comparison of staff and patient experience of the same incident", Nordic Journal of Psychiatry., vol. 58, no. 5, pp. 363-369.

Oulis, P., Lykouras, L., Dascalopoulou, E., & Psarros, C. 1996, "Aggression among psychiatric inpatients in Greece", Psychopathology., vol. 29, no. 3, pp. 174-180.
Owen, C., Tarantello, C., Jones, M., & Tennant, C. 1998, "Violence and Aggression in Psychiatric Units", Psychiatric Services, vol. 49, no. 11, pp. 1452-1456.
Owen, C., Tarantello, C., Jones, M., & Tennant, C. 1998, "Repetitively violent patients in psychiatric units", Psychiatric Services., vol. 49, no. 11, pp. 1458-1461.
Owen, C., Tarantello, C., Jones, M., & Tennant, C. 1998, "Lunar cycles and violent behaviour", Australian & New Zealand Journal of Psychiatry., vol. 32, no. 4, pp. 496-499.
Palmstierna, J., Huitfelt, B., & Wistedt, B. 1991, "The relationship of crowding and aggressive behaviour on a psychiatric intensive care unit", Hospital and Community Psychiatry, vol. 42, pp. 1237-1240.
Palmstierna, T. & Wistedt, B. 1989, "Risk Factors for Aggressive Behaviour are of Limited Value in Predicting the Violent Behaviour of Acute Involuntarily Admitted Patients", Acta Psychiatrica Scandinavica, vol. 81: 152-155.
Palmstierna, T., Lassenius, R., & Wistedt, B. 1989, "Evaluation of BPRS in relation to aggressive behaviour by acute involuntarily admitted patients", Acta Psychiatrica Scandinavica, vol. 79:313-316.
Palmstierna, T. & Wistedt, B. 1995, "Changes in the pattern of aggressive behaviour among inpateints with changed ward organization", Acta psychiatr.scand., vol. 91: 32-35.
Palmstierna, T. & Barredal, E. 2006, "Evaluation of the Perception of Aggression Scale (POAS) in Swedish nurses", Nordic Journal of Psychiatry, vol. 60, no. 6, pp. 447-451.
Parkes, J. 2003, "The nature and management of aggressive incidents in a medium secure unit", Medicine, Science & the Law, vol. 43, no. 1, pp. 69-74.
Pearson, M., Wilmot, E., & Padi, M. 1986, "A study of violent behaviour among in-patients in a psychiatric hospital", British Journal of Psychiatry, vol. 149, pp. 232-235.
Pieters, G., Speybrouck, E., de Gucht, V. +., & Joos, S. 2005, "Assaults by patients on psychiatric trainees: Frequency and training issues", Psychiatric Bulletin, vol. 29, no. 5, pp. 168-170.
Poster, E. & Ryan, J. 1989, "Nurses' attitudes toward physical assaults by patients", Archives of Psychiatric Nursing, vol. III, no. 6, pp. 315-322.
Poster, E. 1996, "A multinational study of psychiatric nursing staff's beliefs and concerns about work safety and patient assault", Archives of Psychiatric Nursing, vol. 10, no. 6, pp. 365-373.
Poster, E. & Ryan, C. 1994, "A Multiregional Study of Nurses' Beliefs and Attitudes About Work Safety and Patient Assault", Hospital and Community Psychiatry, vol. 45, no. 11, pp. 1104-1108.
Powell, G., Caan, W., & Crowe, M. 1994, "What events precede violent incidents in psychiatric hospitals?", British Journal of Psychiatry, vol. 165, pp. 107-112.
Price, T. B., David, B., & Otis, D. 2004, "The use of restraint and seclusion in different racial groups in an inpatient forensic setting", Journal of the American Academy of Psychiatry and the Law, vol. 32, no. 2, pp. 163-168.
Privitera, M., Weisman, R., Cerulli, C., Tu, X., & Groman, A. 2005, "Violence toward mental health staff and safety in the work environment", Occupational Medicine (Oxford), vol. 55, pp. 480-486.
Quanbeck, C., McDermott, B. E., Lam, J., Eisenstark, H., Sokolov, G., & Scoatt, C. L. 2007, "Categorization of Aggressive Acts Committed by Chrnoically Assaultive State Hospital Patients", Psychiatric Services, vol. 58, no. 4, pp. 521-528.
Quirk, A., Lelliott, P., & Seale, C. 2004, "Service users' strategies for managing risk in the volatile environment of an acute psychiatric ward", Social Science & Medicine., vol. 59, no. 12, pp. 2573-2583.
Rabinowitz, J. & Mark, M. 1999, "Risk factors for violence among long-stay psychiatric patients: National study.", Acta Psychiatrica Scandinavica, vol. 99, no. 5, pp. 341-347.
Raja, M. & Azzoni, A. 2005, "Hostility and violence of acute psychiatric inpatients", Clinical Practice and Epidemiology in Mental Health, vol. 1, no. 11.
Raja, M., Azzoni, A., & Lubich, L. 1997, "Aggressive and violent behaviors in a population of psychiatric inpatients", Social Psychiatry and Psychiatric Epidemiology, vol. 32, no. 7, pp. 428-434.
Rasmussen, K. & Levander, S. 1996, "Individual rather than situational characteristics predict violence in a maximum security hospital", Journal of Interpersonal Violence, vol. 11, no. 3, pp. 376-390.
Rasmussen, K., Lavender, S., & Sletvold, H. 1995, "Aggressive and nonaggressive schizophrenics: sympton profile and neuropsychological differences.", Psychology, Crime & Law, vol. 15, pp. 397-408.
Rauter, U. K., de-Nesner, A., & Grandfield, S. 1997, "Up in Smoke? Linking Patient Assaults to a Psychiatric Hospital's Smoking Ban", Journal of Psychiatric Nursing, vol. 35, no. 6, pp. 35-40.
Ray, C. L. & Subich, L. M. 1998, "Staff Assaults and Injuries in a Psychiatric Hospital as a Function of Three Attitudinal variables", Issues in Mental Health Nursing, vol. 19, no. 3, pp. 277-289.
Rees, C. & Lehane, M. 1996, "Witnessing violence to staff: a study of nurses' experiences", Nursing Standard., vol. 11, no. 13-15, pp. 45-47.
Reid, W., Bollinger, M., & Edwards, J. 1989, "Serious assaults by inpatients", Psychosomatics, vol. 30, pp. 54-56.

Richter, D. & Berger, K. 2006, "Post-traumatic stress disorder following patient assaults among staff members of mental health hospitals: A prospective longitudinal study", BMC Psychiatry.Vol.6, 2006.Article Number: 15.Date of Publication: 10 APR 2006., vol. 6.
Rinn, R. C. 1976, "Effects of nursing apparel upon psychiatric inpatients' behavior", Perceptual & Motor Skills, vol. 43, no. 3 pt 1, pp. 939-945.
Rix, G. 1987, "Staff sickness and its relaitonship to violent incidents on a regional secure psychiatric unit", Journal of Advanced Nursing, vol. 12, pp. 223-228.
Rix, G. & Seymour, D. 1988, "Violent incidents on a regional secure unit", Journal of Advanced Nursing, vol. 13: 746-751.
Rofman, E. S., Asjubazi, C., & Fant, E. 1980, "The Prediction of Dangerous Behaviour in Emergency Civil Commitment", American Journal of Psychiatry, vol. 137:1061-1064.
Rogers, P., Watt, A., Gray, N. S., MacCulloch, M., & Gournay, K. 2002, "Content of command hallucinations predicts self-harm but not violence in a medium secure unit", Journal of Forensic Psychiatry., vol. 13, no. 2, pp. 251-262.
Rogers, R., Ciula, B., & Cavanaugh, J. L. 1980, "Aggressive and socially disruptive behaviour among maximum security psychiatric patients", Psychological Reports, vol. 46(291-294).
Roitman, G., Orev, E., & Schreiber, G. 1990, "Annual rhythms of violence in hospitalized affective patients: correlation with changes in the duration of the daily photoperiod", Acta Psychiatrica Scandinavica., vol. 82, no. 1, pp. 73-76.
Roper, J. M. & Anderson, N. L. R. 1991, "The interactional dynamics of violence part 1: An Acute Psychiatric Ward", Archives of Psychiatric Nursing, vol. 5(4): 209-215.
Rosenthal, T. L., Edwards, N. B., Rosenthal, R. H., & Ackerman, B. J. 1992, "Hospital violence: site, severity, and nurses' preventive training", Issues in Mental Health Nursing, vol. 13, pp. 349-356.
Roy, S., Herrera, J., Parent, M., & Costa, J. 1987, "Violent and nonviolent schizophrenic patients: Clinical and developmental characteristics.", Psychological Reports, vol. 61, pp. 855-861.
Ruben, I., Wolkon, G., & Yamamoto, J. 1980, "Physical attacks on psychiatric residents by patients", Journal of Nervous Mental Disorders, vol. 168, pp. 243-245.
Rutter, S., Gudjonsson, G., & RabeHesketh, S. 2004, "Violent incidents in a medium secure unit: The characteristics of persistent perpetrators of violence", Journal of Forensic Psychiatry & Psychology., vol. 15, no. 2, pp. 293-302.
Ruzic, K., Franciskovic, T., Sukovic, Z., Zarkovic-Palijan, T., Buzina, N., Roncevic-Grzeta, I., & Petranovic, D. 2008, "Predictors of aggressiveness in schizophrenic patients treated in inpatient forensic institutions", Collegium Antropologicum, vol. 32, no. 2, pp. 331-337.
Ryan, J. & Poster, E. 1989, "The assaulted nurse: Short-term and long-term responses", Archives of Psychiatric Nursing, vol. 3, no. 6, pp. 323-331.
Schwartz, T. & Park, T. 1999, "Assaults by patients on psychiatric residents: A survey and training recommendations", Psychiatric Services, vol. 50, no. 3, pp. 381-383.
Secker, J., Benson, A., Balfe, E., Lipsedge, M., Robinson, S., & Walker, J. 2004, "Understanding the social context of violent and aggressive incidents on an inpatient unit", Journal of Psychiatric and Mental Health Nursing, vol. 11, pp. 172-178.
Serper, M., Beech, D. R., Harvey, P. D., & Dill, C. 2008, "Neuropsychological and symptom predictors of aggression on the psychiatric inpatient service", Journal of Clinical & Experimental Neuropsychology: Official Journal of the International Neuropsychological Society, vol. 30, no. 6, pp. 700-709.
Serper, M. R., Goldberg, B. R., Herman, K. G., Richarme, D., Chou, J., Dill, C. A., & Cancro, R. 2005, "Predictors of aggression on the psychiatric inpatient service", Comprehensive Psychiatry., vol. 46, no. 2, pp. 121-127.
Shader, R., Jackson, A., Harmatz, J., & et al 1977, "Patterns of violent behaviour among schizophrenic patients", Diseases of the Nervous System, vol. 38, pp. 13-16.
Shepherd, M. & Lavender, T. 1999, "Putting aggression into context: An investigation into contextual factors influencing the rate of aggressive incidents in a psychiatric hospital", Journal of Mental Health. , vol. 8, no. 2, pp. 159-170.
Sheridan, M., Henrion, R., Robinson, L., & Baxter, V. 1990, "Precipitants of violence in a psychiatric inpatient setting", Hospital and Community Psychiatry, vol. 41, no. 7, pp. 776-780.
Sjostrom, N., Eder, D. N., Malm, U., & Beskow, J. 2001, "Violence and its prediction at a psychiatric hospital", European Psychiatry: the Journal of the Association of European Psychiatrists., vol. 16, no. 8, pp. 459-465.
Smith, C. & McKay, L. 1965, "The open psychiatric ward and its vicissitudes", American Journal of Psychiatry, vol. 121, pp. 763-767.
Soares, J. & Lawoko, S. 2000, "The nature, extent and determinants of violence against psychiatric personnel", Work & Stress, vol. 14, no. 2, pp. 105-120.
Soliman, A. & Reza, H. 2001, "Risk factors and correlates of violence among acutely ill adult psychiatric inpatients", Psychiatric Services, vol. 52, no. 1, pp. 75-80.
Spokes, K., Bond, K., Lowe, T., Jones, J., Illingworth, P., Brimblecombe, N., & Wellman, N. 2004, "HOVIS-The Hertfordshire/Oxfordshire Violent Incident Study", Journal of Psychiatric and Mental Health Nursing no. 9, pp. 199-209.
Steinert, T., Wolfle, M., & Gebhardt, R. P. 2000, "Measurement of violence during in-patient treatment and association with psychopathology.", Acta Psychiatric Scandinavica, vol. 102, pp. 107-112.
Steinert, T., Wiebe, C., & Gebhardt, R. P. 1999, "Aggressive behavior against self and others among first-admission patients with schizophrenia", Psychiatric Services., vol. 50, no. 1, pp. 85-90.

Steinert, T., Eisele, F., Goeser, U., Tschoeke, S., Uhlmann, C., & Schmid, P. 2008, "Successful interventions on an organisational level to reduce violence and coercive interventions in in-patients with adjustment disorders and personality disorders", Clinical Practice & Epidemiology in Mental Health, vol. 4, no. 27.
Stockman, C. L. J. & Heiber, P. 1980, "Incidents in hospitalised forensic patients", Victimology, vol. 5(175-192).
Sullivan, C. & Yuan, C. 1995, "Workplace assaults on minority health and mental health care workers in Los Angeles", American Journal of Public Health, vol. 85, no. 7, pp. 1011-1014.
Swinton, M. & Hopkins, R. 1996, "Violence and Self-injury", Journal of Forensic Psychiatry, vol. 7, no. 3, pp. 563-569.
Tam, E., Engelsmann, F., & Fugere, R. 1996, "Patterns of violent incidents by patients in a general hospital psychiatric facility", Psychiatric Services, vol. 47, no. 1, pp. 86-88.
Tardiff, K. & Koenigsberg, H. 1985, "Assaultive behaviour among psychiatric outpatients", American Journal of Psychiatry, vol. 142, pp. 960-963.
Tardiff, K. 1983, A survey of assault by chronic patients in a state hospital system in Lion, J. and Reid, W.(Eds) Assaults Within psychiatric Facilities. Orlando: Grune and Stratton..
Thomas, C., Bartlett, A., & Mezey, G. C. 1995, "The extent and effects of violence among psychiatric in-patients", Psychiatric Bulletin, vol. 19, pp. 600-604.
Thomas, M., Ekland, E., Griffin, M., & et al 1990, "Intrahospital relocation of psychiatric patients and effects on aggression", Archives of Psychiatric Nursing, vol. 4, pp. 154-160.
Tobin, M., Lim, L., & Falkowshi, W. 1991, "How do we manage violent behavior", British Journal of Clinical and Social Psychiatry, vol. 8, no. 1, pp. 19-23.
Torpy, D. & Hall 1993, "Violent incidents in a Secure Unit", Journal of Forensic Psychiatry, vol. 4, no. 3, pp. 517-544.
Troisi, A., KUstermann, S., Di-Genio, M., & Siracusano, A. 2003, "Hostility during admission interview as a short term predictor of aggression in acute psychiatric make inpatients", Journal of Clinical Psychiatry, vol. 64, pp. 1460-1464.
Turns, D. & Gruenberg, E. 1973, "An attendant is murdered: The state hospital responds", Psychiatric Quarterly, vol. 47, no. 4, pp. 487-494.
Tyrer, P., Cooper, S., Herbert, E., Duggan, C., Crawford, M., Joyce, E., Rutter, D., Seivewright, H., O'Sullivan, S., Rao, B., Cicchetti, D., & Maden, T. 2007, "The Quantification of Violence Scale: A simple method of recording significant violence", International Journal of Social Psychiatry, vol. 53, no. 6, pp. 485-497.
Uzun, O. Perceptions and Experiences of Nurses in Turkey about Verbal Abuse in Clinical Settings. Journal of Nursing Scholarship 35, 81-85. 2003. Ref Type: Generic
Vanderslott, J. 1998, "A study of violence towards staff by patients in an NHS Trust Hospital", Journal of Psychiatric and Mental Health Nursing, vol. 5, pp. 291-298.
Waldheter, E. J., Jones, N. T., Johnson, E. R., & Penn, D. L. 193, "Utility of social cognition and insight in the prediction of inpatient violence among individuals with a severe mental illness", Journal of Nervous & Mental Disease. no. 9, pp. 609-618.
Walker, Z., Seifert, R., & Walker, Z. 1994, "Violent Incidents in a Psychiatric Intensive Care Unit", British Journal of Psychiatry, vol. 164: 826-828.
Watts, D. 2003, "The prediction of violence in acute psychiatric units", International Journal of Forensic Mental Health, vol. 2, pp. 173-180.
Wazome, E. G. 1988, "A study of aggressive and violent behaviour among a group of psychiatric in-patients in Kenya", East African Medical Journal, vol. 65, no. 6, pp. 360-365.
Weizmann-Henelius, G. & Suutala, H. J. O. 2000, "Violence in a Finnish forensic psychiatric hospital", Nordic Journal of Psychiatry., vol. 54, no. 4, pp. 269-273.
Werner, P. D., Yesagave, J. A., Becker, J. M. T., Brunsting, D. W., & Issacs, J. S. 1983, "Hostile words and assaultive behaviour on an acute in-patient psychiatric unit", Journal of Nervous and Mental Disease, vol. 171(385-387).
Whittington, R. 2002, "Attitudes toward patient aggression amongst mental health nurses in the 'zero tolerance' era: associations with burnout and length of experience", Journal of Clinical Nursing, vol. 11, pp. 819-825.
Whittington, R. & Higgins, L. 2002, "More than zero tolerance? Burnout and tolerance for patient aggression amongst mental health nurses in China and the UK", Acta Psychiatr Scand, vol. 106, no. Suppl. 412, pp. 37-40.
Whittington, R. & Wykes, T. 1989, "Aggression: Invisible injury", Nursing Times, vol. 85, no. 42, pp. 30-32.
Whittington, R. & Wykes, T. 1991, "Coping Strategies used by staff following assault by a patient: an exploratory study", Work & Stress, vol. 5, no. 1, p. -37.
Whittington, R. & Wykes, T. 1992, "Staff strain and social support in a psychiatric hospital following assault by a patient", Journal of Advanced Nursing, vol. 17, pp. 480-486.
Whittington, R. & Wykes, T. 1994, "Violence in psychiatric hospitals: are certain staff prone to being assaulted", Journal of Advanced Nursing, vol. 19, pp. 219-225.
Whittington, R. & Wykes, T. 1994, "An observational study of associations between nurse behavior and violence in psychiatric hospitals", Journal of Psychiatric and Mental Health Nursing, vol. 1, pp. 85-92.
Whittington, R. & Wykes, T. 1996, "An evaluation of staff training in psychological techniques for the management of patient aggression", Journal of Clinical Nursing, vol. 5, pp. 257-261.
Whittington, R. & Wykes, T. 1996, "Aversive stimulation by staff and violence by psychiatric patients", British Journal of Clinical Psychology, vol. 35, pp. 11-20.
Woods, P., Ashley, C., Kayto, D., & Heusdens, C. 2008, "Piloting violence and incident reporting measures on one acute mental health inpatient unit", Issues in Mental Health Nursing, vol. 29, no. 5, pp. 455-469.
Wynn, R. & Bratlid, T. 1998, "Staff's experiences with patients' assaults in a norwegian psychiatric university hospital: A pilot study", Scandinavian Journal of Caring Sciences., vol. 12, no. 2, pp. 89-93.
Yassi, A., Tate, R., Cooper, J., Jenkins, J., & Trottier, J. 1998, "Causes of staff abuse in health care facilities. Implications for prevention", American Association of Occupational Health Nurses (AAOHN) Journal, vol. 46, pp. 484-491.
Yesavage, J., Werner, P., Becher, J., & et al 1981, "Inpatient evaluation of aggression in psychiatric patients", Journal of Nervous Mental Disorders, vol. 169, pp. 299-302.
Yesavage, J. A. 1983, "Bipolar Illness: Correlates of dangerous in-patient behaviour", British Journal of Psychiatry, vol. 143, pp. 554-557.
Yesavage, J. A. 1983, "Inpatient violence and the schizophrenic patient", Acta Psychiatrica Scandinavica, vol. 67, pp. 353-357.
Yusuf, F., Hendriks, M. M., Eng, T. S., Kandasamy, R., R, Selvarani, S., & Huang, P. H. 2006, "The impact of verbal abuse on staff working in the psychiatric wards", Singapore Nursing Journal, vol. 33, no. 3, pp. 31-36.
Other references Abderhalden, C., Needham, I., Miserez, B., Almvik, R., Dassen, T., Haug, H. et al. 2004, "Predicting inpatient violence in acute psychiatric wards using Broset-Violence-Checklist: a multicentre prospective cohort study", Journal of Psychiatric and Mental Health Nursing, vol. 11, pp. 422-427. Coid, J., Kahtan, N., Gault, S., Cook., A., Jarman, B. 2001, "Medium secure forensic psychiatric services: comparison of seven English health regions", British Journal of Psychiatry, vol. 178, pp. 55-61.
Fazel, S., Gulati, G., Linsell, L., Geddes, J.R., Grann, M. 2009, Schizophrenia and Violence: Systematic Review and Meta-Analysis. PLoS Medicine, vol 6(8): e1000120.
Higgins, J., Thompson S, Deeks, J., Altman, D.G. 2003, "Measuring inconsistency in meta-analyses", British Medical Journal, vol. 327, pp. 557-560.
Mueser, K. T., Drake, R. E., Wallach, M.A. 1998, "Dual diagnosis: a review of etiological theories", Addictive Behaviors, vol. 23, pp. 717-734. Ogloff, J. R. P. & Daffern, M. 2006, "The Dynamic Appraisal of Situational Aggression: An Instrument to Assess Risk for Imminent Aggression in Psychiatric Inpatients", Behavioral Sciences & the Law, vol. 24, pp. 799-813.

Perera, R. & Heneghan, C, 2008, "Interpreting meta-analysis in systematic reviews", Evidence Based Medicine, vol. 13, pp. 67-69.
Royal College of Psychiatrists 2007, Healthcare Commission National Audit of Violence 2006-7. London: Royal College of Psychiatrists.