
Innovative Uses of Geographic Information Systems Lance A. Waller Department of Biostatistics...
28
Innovative Uses of Geographic Information Systems Lance A. Waller Department of Biostatistics Rollins School of Public Health Emory University [email protected]
-
date post
22-Dec-2015 -
Category
Documents
-
view
214 -
download
0
Transcript of Innovative Uses of Geographic Information Systems Lance A. Waller Department of Biostatistics...
Innovative Uses of Geographic Information Systems
Lance A. WallerDepartment of Biostatistics
Rollins School of Public HealthEmory University
Outline
Why does the geography of immunization matter?
What is GIS?What does GIS do?What data do I have?What questions can I answer
with my data?
Why geography?
Is immunization coverage constant?
If you know where coverage is low, can you do something?
If you know where coverage is high, can you learn something?
What is GIS?
A “geographic information system” (GIS) links: Geographic features
Houses Census tracts
Attribute measurements Immunized (yes/no) Age Sociodemographics

Think of…
Map (locations) Table (attributes)
linked with
Each cell contains an attribute value
Objects on the map are features.
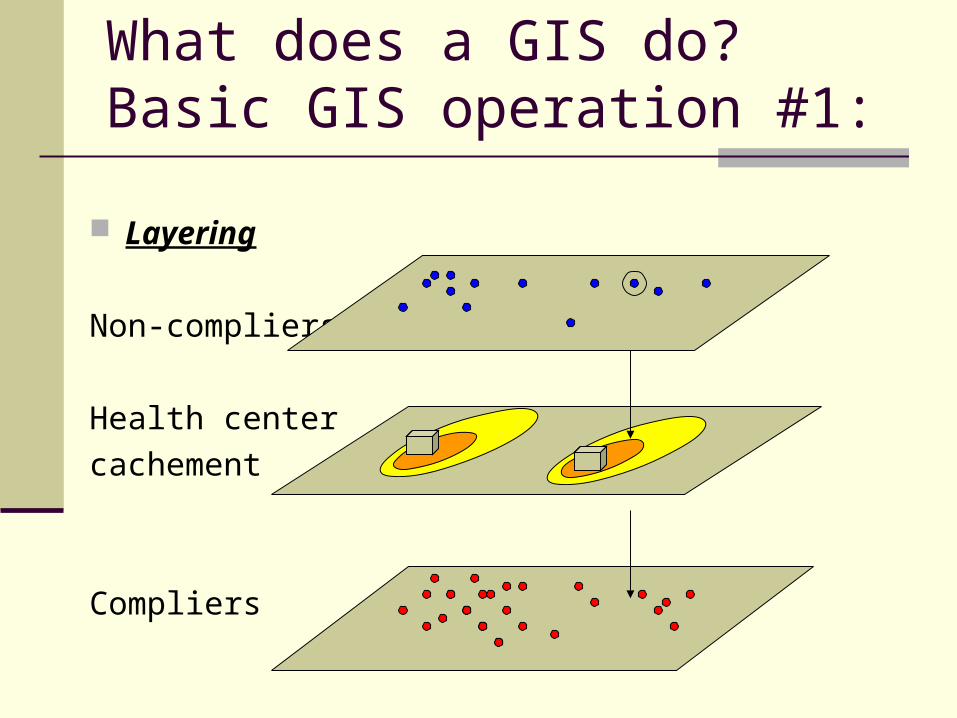
What does a GIS do?Basic GIS operation #1:
Layering
Non-compliers
Health centercachement
Compliers

Basic GIS operation # 2:
Buffering Find areas
within a user-specified distance of:points linesareas
Buffers around an area
Buffers around a line feature
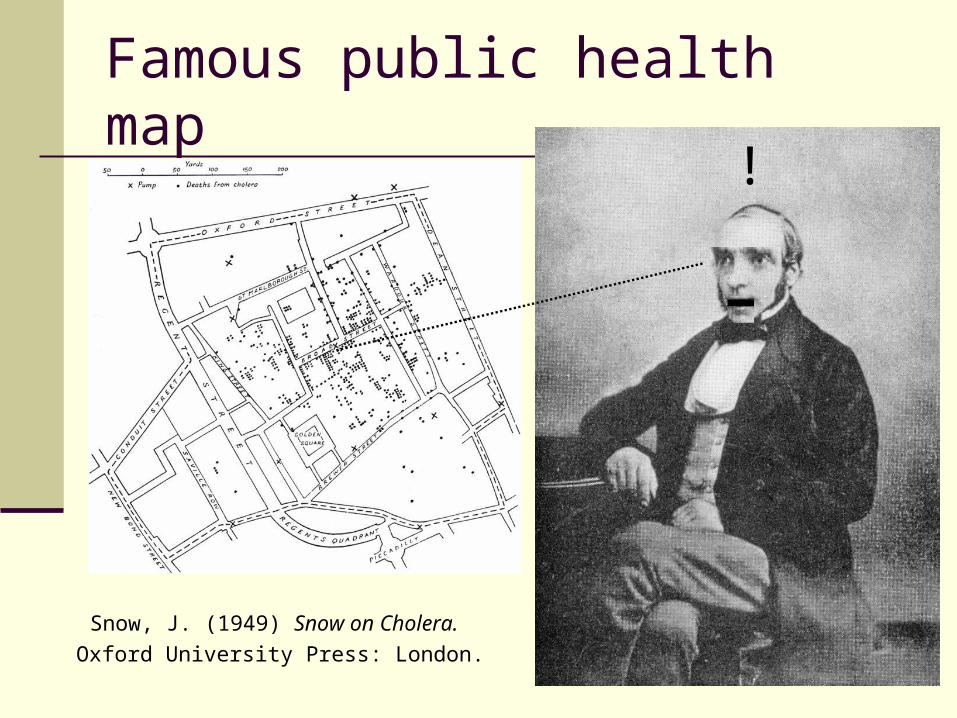
Famous public health map!
Snow, J. (1949) Snow on Cholera. Oxford University Press: London.
Wow! Can we do that?
Many introductions to GIS and public health essentially say:
“If John Snow could do it with shoe leather, ink, and paper, just imagine what we can do with a computer!”

Basic take-home figure
The Whirling Vortex of GIS analysis
The question you want to
answer
The data youneed to answerthat question
The data youcan get
The questionyou can
answer withthose data
Original source: Toxicologist EPA Region IV
GIS

What kind of questions?
Where is coverage the lowest?Where is coverage the highest?Outbreak size starting in high
coverage area?Outbreak size starting in low
coverage area?How could coverages impact the
course of an outbreak?Best response to current outbreak?
What kind of attributes?
CompliersResidence locationCensus region counts
Sociodemographic dataCensus summaries on age, race,
sex, income of census region residents
Some information on compliers’ sociodemographics

Additional attributes
NoncompliersResidence locationRegional counts
School dataSchool district
Health plan dataBilling provides residence
addressZIP codes?
Basic location types
Point dataLatitude and longitude(Seems) preciseDistance calculations
Regional dataCounts (cases/controls) from census regions

Any complications?
Maxcy (1926): Endemic typhus fever in Montgomery, AL
Where is “where”?Which location for each case?
Maxcy, K.F. (1926) “An epidemiological study of endemic typhus (Brill’s disease) in the Southeastern United States with special reference to its mode of transmition.” Public Health Reports 41, 2967-2995.
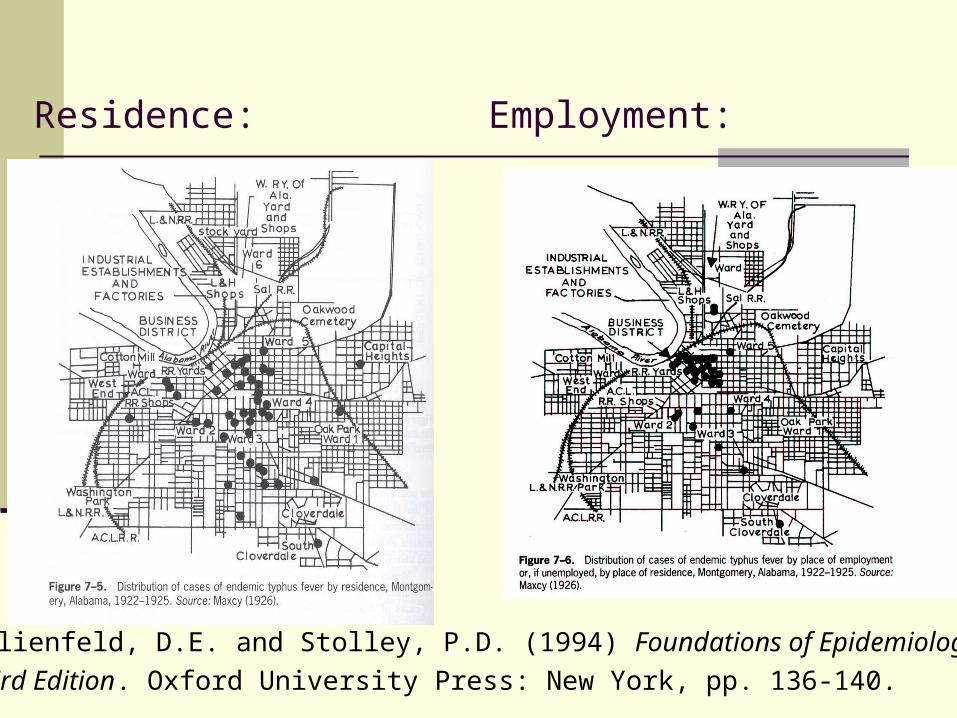
Residence:
Lilienfeld, D.E. and Stolley, P.D. (1994) Foundations of Epidemiology, Third Edition. Oxford University Press: New York, pp. 136-140.
Employment:
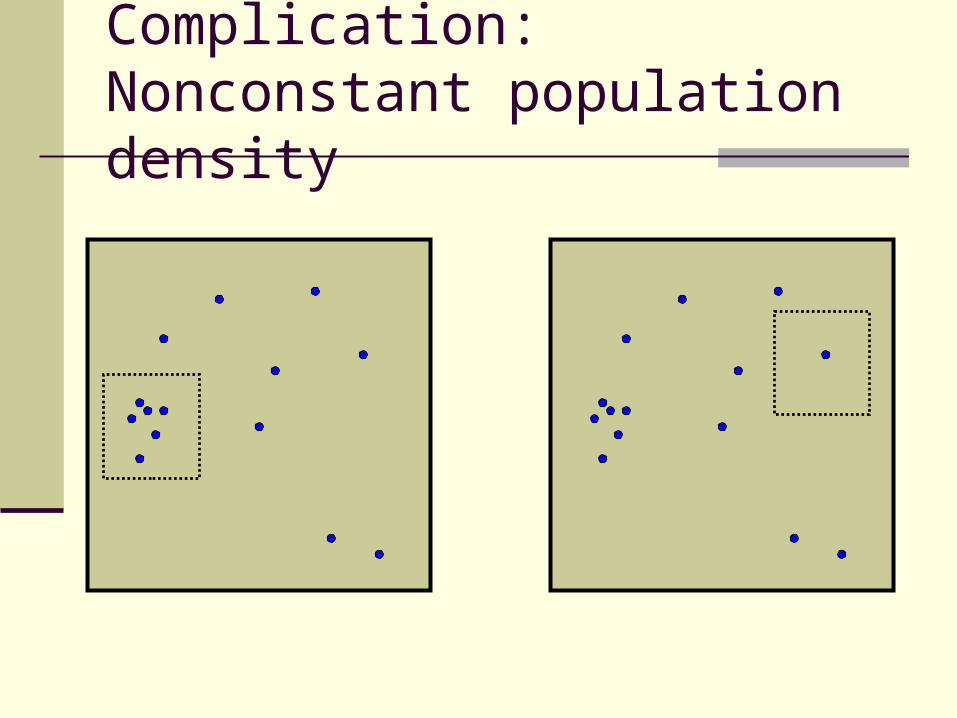
Complication: Nonconstant population density

Complications with regions
Counts lose some resolution...
4 1
21
1 2
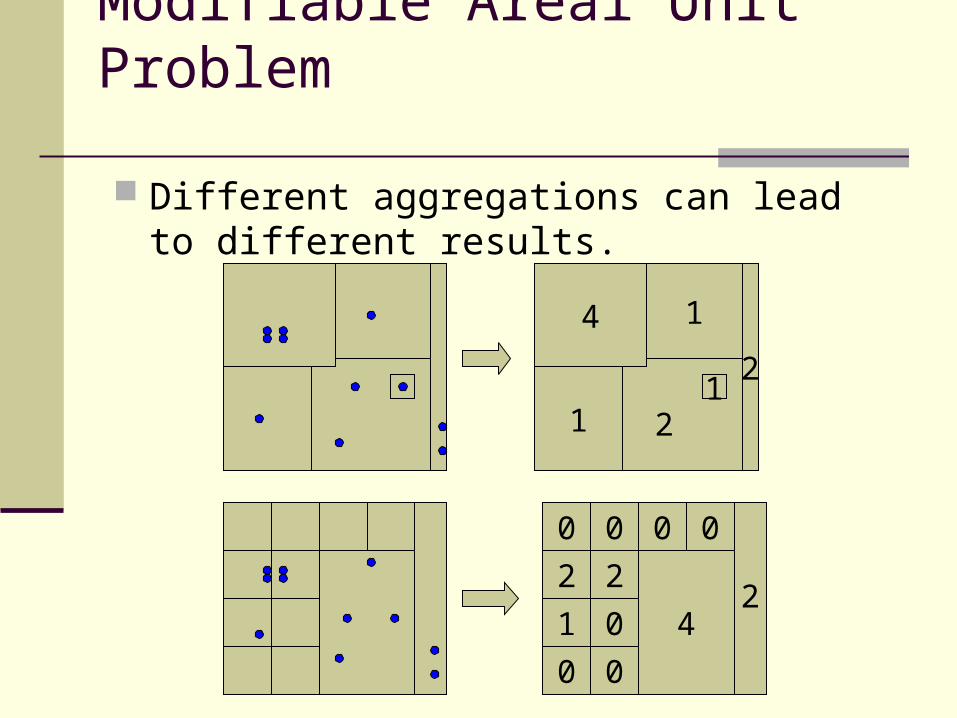
Modifiable Areal Unit Problem
Different aggregations can lead to different results.
4 1
21
1 2
2
0 0 0 0
2
1
0
2
0
0
24
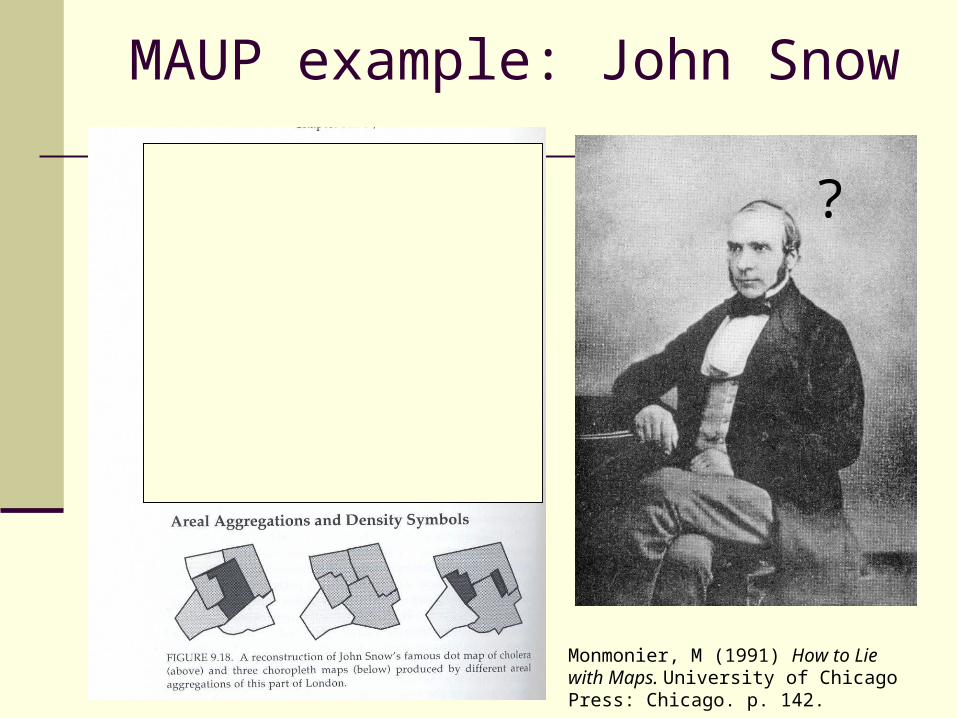
MAUP example: John Snow
Monmonier, M (1991) How to Lie with Maps. University of Chicago Press: Chicago. p. 142.
?
What questions can I ask?
Point locations Interesting/uninteresting clusters Interesting: clusters of non-
compliers away from clusters of compliers
Regional counts Interesting/uninteresting raised
counts Interesting: Less coverage than
“expected”
Point locations
Treat locations as spatial point process
Spatial “intensity” (average number of events per unit area)
Think of intensity as a surfaceCompare intensity of compliers to
intensity of non-compliers.Peaks and valleys in same places?

Monte Carlo simulation Simulate data sets under null
hypothesis (e.g., constant coverage rate).
See if observed data (actual compliers) appear “unusual”.
To compare intensities, split all locations into compliers and non-compliers at random, find out how high peaks, how low valleys can get.
Most GIS packages will not do this, but it is a very handy tool in spatial statistics.
Regions
Compare observed counts to “expected” counts.
Some basic point process results extend to counts (counts of points in regions).
Constant coverage rate (perhaps age-adjusted) again a common way of obtaining “expected” counts.
Monte Carlo simulation for significance.

Related work
Cancer registries: North American Association of Central Cancer Registries (NAACCR) report on GIS (Wiggins 2002)
Birth outcome registries Public Health/Bioterrorism/Syndromic
Surveillance Similarities:
Registry data Differences:
Infectious vs. chronic outcome Urgency of temporality

Conclusion
Best work a collaboration betweenGeographersGISersEpidemiologistsStatisticians
Get the best data you can to answer the questions you want.

Handy references
Wiggins L (Ed). Using Geographic Information Systems Technology in the Collection, Analysis, and Presentation of Cancer Registry Data: A Handbook of Basic Practices. Springfield (IL): North American Association of Central Cancer Registries, October 2002, 68 pp.
Cromley, E.K. and McLafferty, S.L. (2002) GIS and Public Health. The Guilford Press.
Bailey and Gatrell (1995) Interactive Spatial Data Analysis. Longman.
Waller and Crawford (2004) Applied Spatial Statistics for Public Health Data. Wiley.
What kind of software?
Statistical Software(SAS, S+ Spatial Stats)Spatially and/or visually challenged
Subject-specificSpaceStat/GeoDaSaTScanGS+ClusterSeerWinBUGS/GeoBUGSXGOBI/XGvisR (many nice spatial modules, must write code, quality control?)Link to GIS S+/ArcView 3.x SAS Bridge to ArcGIS 8.x
Commercial GIS Software(ArcView, Mapinfo)Statistically challenged
Extensions (Analysts)$$$, limited capability Packages by scientific user good, but basic Scripts and MacrosUser-contributed
Often do not give numerical output


















