
Innovative Business Models in Global Healthcare - David Spellberg
26
Pharmaceutical Reference Pricing in the U.S. Delusion or a soon-to-be Reality? April 2016 Ilkka Anhava Ling Chen Huiyan Jin Emil Nedev David Spellberg Innovative Business Models in Global Healthcare – EMBA Course Spring 2016
-
Upload
david-spellberg -
Category
Healthcare
-
view
220 -
download
7
Transcript of Innovative Business Models in Global Healthcare - David Spellberg

Pharmaceutical Reference Pricing in the U.S.Delusion or a soon-to-be Reality?
April 2016
Ilkka AnhavaLing ChenHuiyan JinEmil NedevDavid Spellberg
Innovative Business Models in Global Healthcare – EMBA Course Spring 2016

- 2 -
Executive Summary
CMS will likely tweak Part B drug payment in near term to incentivize use of cheaper drugs
CMS will test other new Medicare drug payment systems over the next 5 years
However, near-term likelihood of reference pricing for Part B and/or D drugs is <25%
Significant biosimilar competition very soon
But, first US biosimilar priced only at 15% discount
Affordability may need to be addressed via other methods
Regardless, RA and Crohn’s on Chopping Block
Macular Degeneration also in Focus
Headwinds for Reference Pricing in Near Term
Most ophthalmologists prefer cheaper Avastin
But Avastin off-label issue remains a hurdle
18B potential Medicare savings over 10 years remain on table
Mixed performance in EU
Political gridlock and pharma lobby
Competing ideas (e.g., Medicare price negotiations)
- 3 -
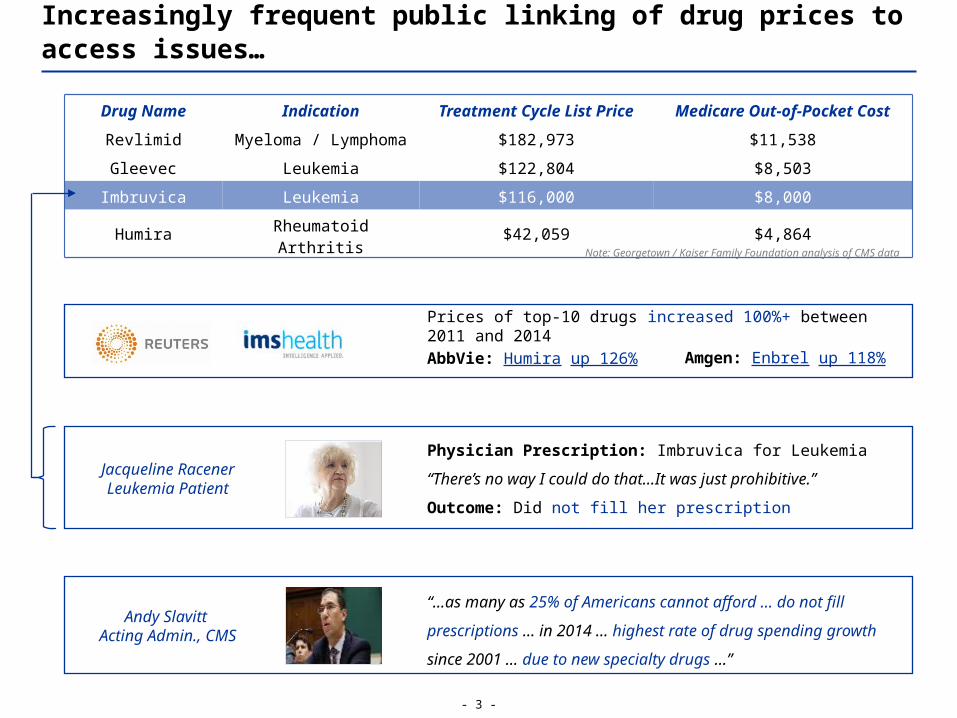
Increasingly frequent public linking of drug prices to access issues…
Physician Prescription: Imbruvica for Leukemia
“There’s no way I could do that…It was just prohibitive.”
Outcome: Did not fill her prescription
Drug Name Indication Treatment Cycle List Price Medicare Out-of-Pocket Cost
Revlimid Myeloma / Lymphoma $182,973 $11,538
Gleevec Leukemia $122,804 $8,503
Imbruvica Leukemia $116,000 $8,000
Humira Rheumatoid Arthritis $42,059 $4,864
“…as many as 25% of Americans cannot afford … do not fill
prescriptions … in 2014 … highest rate of drug spending growth
since 2001 … due to new specialty drugs …”
Jacqueline RacenerLeukemia Patient
Andy Slavitt Acting Admin., CMS
Note: Georgetown / Kaiser Family Foundation analysis of CMS data
Prices of top-10 drugs increased 100%+ between 2011 and 2014
AbbVie: Humira up 126% Amgen: Enbrel up 118%
- 4 -
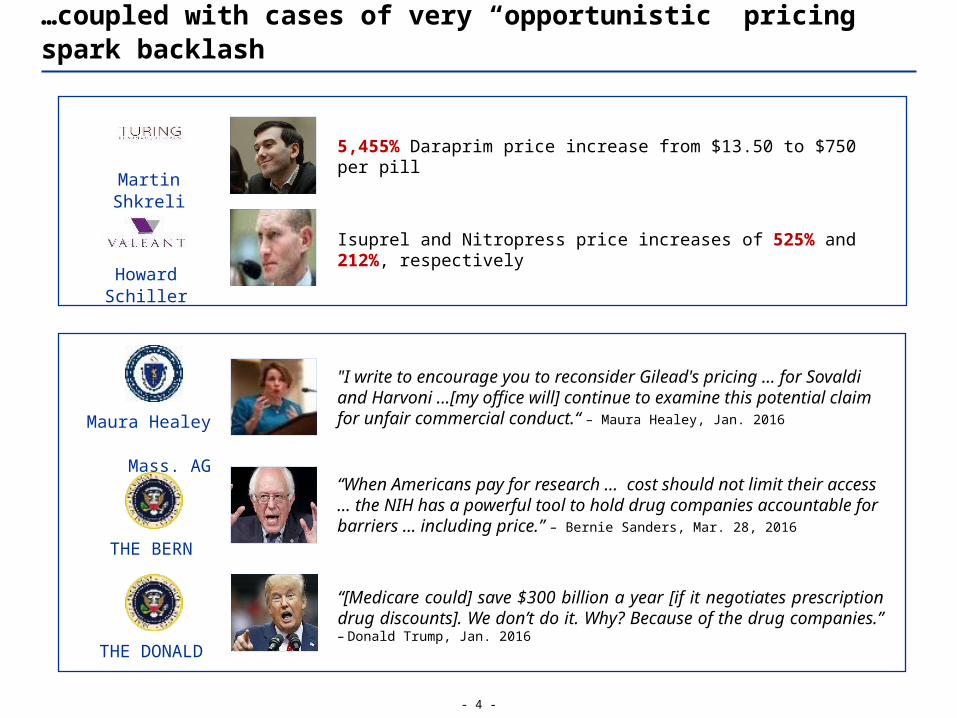
"I write to encourage you to reconsider Gilead's pricing … for Sovaldi and Harvoni ...[my office will] continue to examine this potential claim for unfair commercial conduct.“ – Maura Healey, Jan. 2016
“[Medicare could] save $300 billion a year [if it negotiates prescription drug discounts]. We don’t do it. Why? Because of the drug companies.” – Donald Trump, Jan. 2016
5,455% Daraprim price increase from $13.50 to $750 per pill
Isuprel and Nitropress price increases of 525% and 212%, respectively
…coupled with cases of very “opportunistic” pricing spark backlash
THE DONALD
Maura Healey Mass. AG
Martin Shkreli
Howard Schiller
“When Americans pay for research … cost should not limit their access … the NIH has a powerful tool to hold drug companies accountable for barriers … including price.” – Bernie Sanders, Mar. 28, 2016
THE BERN
- 5 -
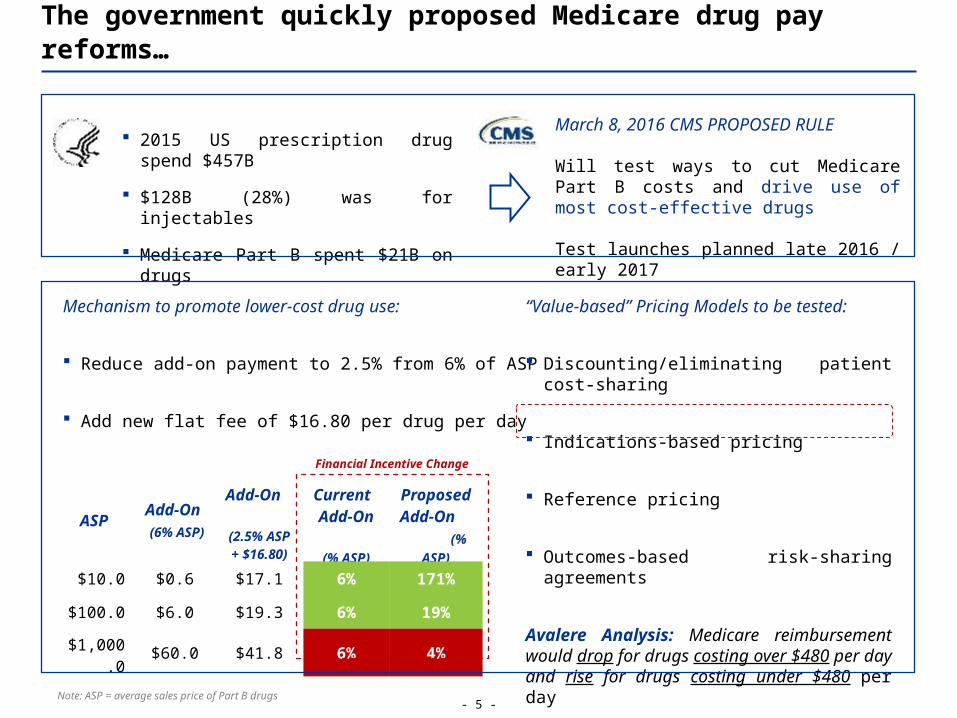
The government quickly proposed Medicare drug pay reforms…
March 8, 2016 CMS PROPOSED RULE
Will test ways to cut Medicare Part B costs and drive use of most cost-effective drugs Test launches planned late 2016 / early 2017
ASPAdd-On
(6% ASP)
Add-On
(2.5% ASP + $16.80)
Current Add-
On (%
ASP)
Proposed Add-On (%
ASP)
$10.0 $0.6 $17.1 6% 171%
$100.0 $6.0 $19.3 6% 19%
$1,000.0 $60.0 $41.8 6% 4%
2015 US prescription drug spend $457B
$128B (28%) was for injectables
Medicare Part B spent $21B on drugs
Mechanism to promote lower-cost drug use:
Reduce add-on payment to 2.5% from 6% of ASP
Add new flat fee of $16.80 per drug per day
“Value-based” Pricing Models to be tested:
Discounting/eliminating patient cost-sharing
Indications-based pricing
Reference pricing
Outcomes-based risk-sharing agreements
Avalere Analysis: Medicare reimbursement would drop for drugs costing over $480 per day and rise for drugs costing under $480 per day
Note: ASP = average sales price of Part B drugs
Financial Incentive Change

- 6 -
Reference Pricing – General Methodology Overview
“Clusters” usually based on cheapest drug in group
For drugs priced above the reference price, patient must pay the difference
Some countries (e.g., Belgium) require drugs to be priced below the reference price
…including reference pricing which is dreaded by the pharma industry
External Reference Pricing (ERP) – Use of prices of a medicine in one or several countries as a benchmark for setting or negotiating the price of the product in another country
$
Drug #1 Drug #2 Drug #3 Drug #4
Reference Group
ReferencePrice
$100 $200 $300 $400
Applicable to all drugs in group
Price #1 $300
Referenced Country
Price #2 $200
Price #3 $100
Drug
Group X
Referencing Country
Lowest Price
Methodology
Drug X Price $100
Note: Some countries use average instead of lowest prices and reference-price based on multiple countries

- 7 -
So far, reference pricing has achieved mixed results in Europe…
Belgian researchers found that reference groups reduce medication costs for poorer patients
? However, Italy, Sweden, and Denmark are moving away from reference pricing to price negotiations because of lack of evidence of savings
The real impact of ERP on drug costs is still not well understood; more studies are needed
‼ ERP programs vary by country (e.g., # of comparator countries, price benchmarks)
‼ ERP ignores cross-country variations in care needs, income and care costs
‼ Differences between public and actual prices are usually confidential
‼ Drug names, doses, pack sizes vary across countries
‼ ERP incentivizes international launch sequencing strategies by drug makers
1:1 comparisons are difficult and can impede access, especially in smaller/poorer countries
The “Good” … ?
The “Bad”

- 8 -
CMS’ Part B proposal already has stiff opposition from the pharma industry and providers
Political gridlock between a Republican Congress and a Democratic President + Pharma lobby
Estimating cost savings from reference pricing is difficult and makes gathering support harder
Most experts agree that the President can NOT make this change via executive order
Competing proposals seem more popular (e.g., Medicare price negotiation authority)
…and it is unlikely to fare better in the US if it ever sees the light of day
CMS’ viability tests of new payment models (incl. reference pricing) over next 5 years
Potential Longer-Term Lifeline for Medicare Drug Reference Pricing:

- 9 -
However, if reference pricing became a reality…
Note: Analysis performed and published by Avalere Health on April 7, 2016
Drug Name Indication Drug
MakerTotal 2014 Medicare Spending
# Medicare Users /
Year
Rituxan Rheumatoid Arthritis Genentech $1.5B 68,708
Lucentis Macular Degeneration Genentech $1.3B 141,606
Eylea Macular Degeneration Regeneron $1.3B 132,511
Neulasta Cancer Amgen $1.2B 98,519
Remicade Rheumatoid Arthritis Janssen $1.2B 59,748
Total $6.5B 501,092
Note: Analysis performed by CMS based on 2014 Medicare drug spending data
Specialty Aggregate Impact on Medicare Part B Drug Payment
Ophthalmology -18%
Oncology -14%
Rheumatology -6%
RA and MD drugs made up 25% of total $21B Part B drug spending on 1% of beneficiaries
High competition of largely equivalent drugs in both areas
RA and MD likely focus areas for reference pricing
Medicare could generate large savings on cancer, RA, and OP drugs
CMS will most likely not go after cancer first
RA and OP, however, will likely land on top of CMS’ priority list right away
RA = rheumatoid arthritisOP = ophthalmology
Impact Estimate of recent CMS Part B Proposal
Top-5 Drugs by Medicare Part B Spending in 2014
- 10 -
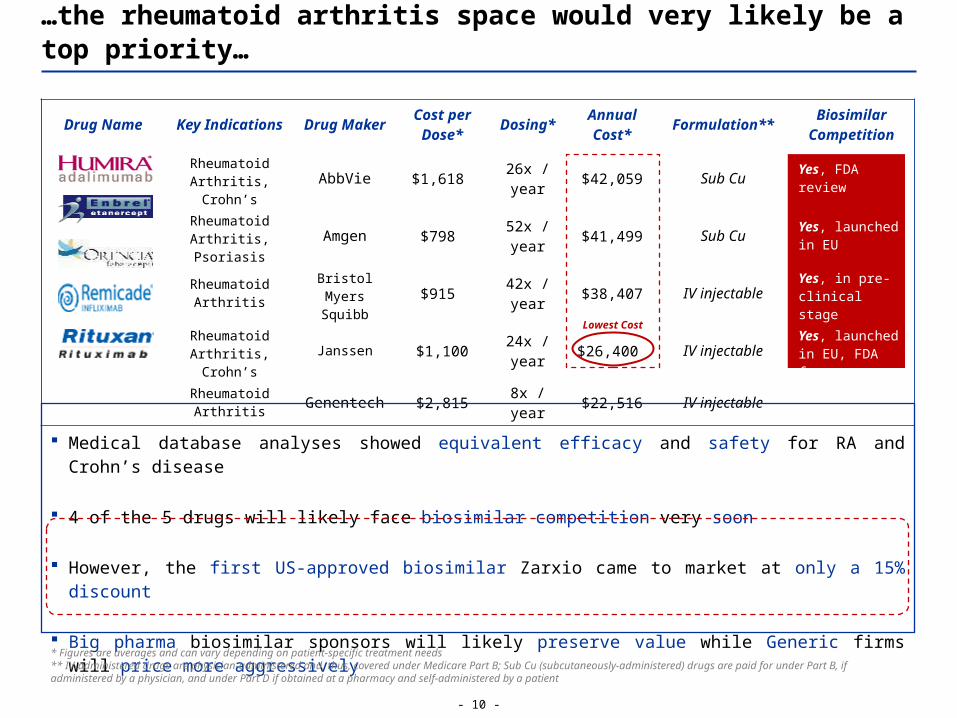
…the rheumatoid arthritis space would very likely be a top priority…
Drug Name Key Indications Drug Maker Cost per Dose* Dosing* Annual
Cost* Formulation** Biosimilar Competition
Rheumatoid Arthritis, Crohn’s AbbVie $1,618 26x / year $42,059 Sub Cu Yes, FDA review
Rheumatoid Arthritis, Psoriasis Amgen $798 52x / year $41,499 Sub Cu Yes, launched in
EU
Rheumatoid Arthritis
Bristol Myers Squibb $915 42x / year $38,407 IV injectable Yes, in pre-
clinical stage
Rheumatoid Arthritis, Crohn’s Janssen $1,100 24x / year $26,400 IV injectable Yes, launched in
EU, FDA favors
Rheumatoid Arthritis Genentech $2,815 8x / year $22,516 IV injectable Yes, EMA review
Medical database analyses showed equivalent efficacy and safety for RA and Crohn’s disease
4 of the 5 drugs will likely face biosimilar competition very soon
However, the first US-approved biosimilar Zarxio came to market at only a 15% discount
Big pharma biosimilar sponsors will likely preserve value while Generic firms will price more aggressively
Lowest Cost
* Figures are averages and can vary depending on patient-specific treatment needs** IV-administered drugs are physician-administered and, thus, covered under Medicare Part B; Sub Cu (subcutaneously-administered) drugs are paid for under Part B, if administered by a physician, and under Part D if obtained at a pharmacy and self-administered by a patient
- 11 -
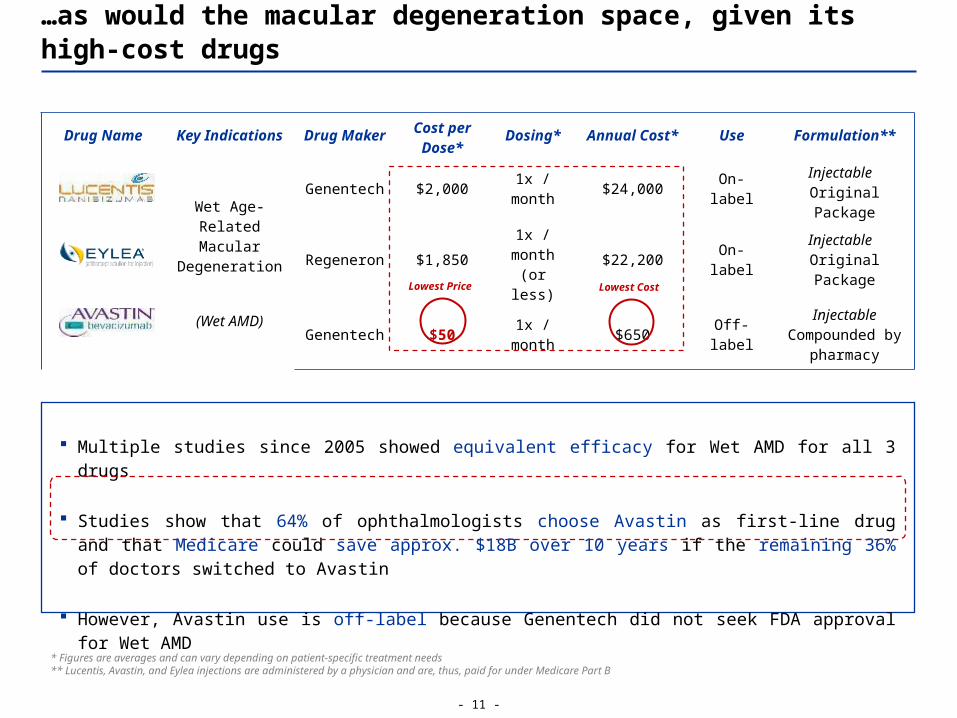
…as would the macular degeneration space, given its high-cost drugs
Drug Name Key Indications Drug Maker Cost per Dose* Dosing* Annual Cost* Use Formulation**
Wet Age-Related Macular
Degeneration
(Wet AMD)
Genentech $2,000 1x / month $24,000 On-label Injectable
Original Package
Regeneron $1,8501x /
month (or less)
$22,200 On-label Injectable Original Package
Genentech $50 1x / month $650 Off-label
Injectable Compounded by
pharmacy
Multiple studies since 2005 showed equivalent efficacy for Wet AMD for all 3 drugs
Studies show that 64% of ophthalmologists choose Avastin as first-line drug and that Medicare could save approx. $18B over 10 years if the remaining 36% of doctors switched to Avastin
However, Avastin use is off-label because Genentech did not seek FDA approval for Wet AMD
Lowest Price Lowest Cost
* Figures are averages and can vary depending on patient-specific treatment needs** Lucentis, Avastin, and Eylea injections are administered by a physician and are, thus, paid for under Medicare Part B

- 12 -
Our Call
CMS will likely tweak Part B drug payment in near term to incentivize use of cheaper drugs
o A model involving a lower ASP+% coupled with a fixed fee is a viable way of doing so
o CMS will test other new Medicare drug payment systems over the next 5 years
o Depending on these test results, CMS may or may not identify reference pricing as viable
The likelihood of reference pricing for all Part B and D drugs in the near term is <25% due to:
o Mixed performance in EU
o Political gridlock and pharma lobby
o Competing ideas (e.g., Medicare price negotiations) and methodologies (e.g., value-based pricing)
Longer term implementation depends on CMS pilot results and may be holistic or targeted
Appendix
Detailed Presentation & Sources
- 14 -
Executive Summary
Significant biosimilar competition in RA / Crohn’s spaces very soon
First US biosimilar launched at only 15% discount to reference product
Need for additional affordability improvement likely to persist
Regardless, RA and Crohn’s on Chopping Block
Macular Degeneration also in Focus
Headwinds for Reference Pricing in Near Term
2/3 ophthalmologists prefer cheaper Avastin to Eylea and Lucentis
Avastin off-label issue remains a hurdle to physician switching
Remaining savings potential for Medicare approx. $18B over 10 years
Mixed performance in EU with some countries abandoning system
Political gridlock and pharma lobby kill chances for action in near-term
Competing ideas (e.g., Medicare price negotiations) may have more legs
CMS will likely tweak Part B drug payment in near term to incentivize use of cheaper drugs
CMS will test other new Medicare drug payment systems over the next 5 years
Near-term likelihood of reference pricing for all Part B and/or Part D drugs is <25%

- 15 -
Increasingly frequent public linking of drug prices to access issues…
Source: Wall Street Journal (WSJ) article from December 31, 2015
Physician Prescription: Imbruvica
Patient Reaction: “There’s no way I could do that…It was just prohibitive.” – Jacqueline Racener
Outcome: Ms. Racener, a 76-year-old legal secretary, decided to not fill her prescription
Drug Name Indication List Price Medicare OOP Cost*
Revlimid Myeloma / Lymphoma $182,973 $11,538
Gleevec Leukemia $122,804 $8,503
Imbruvica Leukemia $116,000 $8,000
Zytiga Prostate Cancer $97,025 $7,227
Humira Rheumatoid Arthritis $42,059 $4,864
Enbrel Rheumatoid Arthritis $41,499 $4,872
Orencia Rheumatoid Arthritis $38,407 $4,413
“Surveys suggest that as many as 25% of Americans cannot afford … do not fill prescriptions
… spending on medicines increased 13% in 2014, compared to 5% for health care spending growth
overall, the highest rate of drug spending growth since 2001 … due to new specialty drugs —
drugs that account for nearly 33% of costs, but represent less than 1% of prescriptions.” – Nov.
2015
Jacqueline RacenerLeukemia Patient
Andy Slavitt Acting Admin., CMS
*Medicare OOP Cost:
Medicare patients who receive high-cost injectable / infusible drugs under Medicare Part B are still responsible for a part of the drug’s total cost out of their own pockets (i.e., OOP = out-of-pocket cost)
Note: Georgetown / Kaiser Family Foundation analysis of CMS data
The press is running more and more stories on patients who struggle with high drug costs …
… and government is not far behind

- 16 -
"I write to encourage you to reconsider Gilead's pricing structure for Sovaldi and Harvoni ...[my office will] continue to examine this potential claim for unfair commercial conduct.“ – Maura Healey, Jan. 2016
“[Medicare could] save $300 billion a year [if it negotiates prescription drug discounts]. We don’t do it. Why? Because of the drug companies.” – Donald Trump, Jan. 2016
“[I support free market principles but am] disgusted…what was done here [Turing, Valeant] was different. Perverse business practices were employed.“ – Rep. Carter R(GA), Feb. 2016
Action: 5,455% Daraprim price increase from $13.50 to $750 per pill
"So 5,000 paying bottles at the new price is $375,000,000 - almost all of it is profit and I think we will get three years of that or more…Should be a very handsome investment for all of us.'‘ – Martin Shkreli
Action: Isuprel and Nitropress price increases of 525% and 212%, respectively
“We are listening and changing…in a number of cases, we have been too aggressive.” – Howard Schiller (before Congress)
…coupled with cases of very “opportunistic” pricing spark backlash
THE DONALD
Maura Healey, Mass. AG
Rep. Buddy Carter R-GA
While drug price hikes are no rarity, two arguably excessive examples recently caused a huge public outcry …
… and brought the wrath of the federal and state governments and Presidential hopefuls upon the pharma industry
Martin Shkreli, Ex-CEO
Howard Schiller, CEO
“When Americans pay for research…high cost should not limit their access to it…the NIH has a powerful tool to hold drug companies accountable for barriers to access…including price.” – Bernie Sanders, Mar. 28, 2016
THE BERN

- 17 -
The government quickly proposed Medicare drug pay reforms…
March 8, 2016 CMS PROPOSED RULE
Test new ways to pay for Medicare Part B prescription drugs
Goal: Slow the growth of Medicare spending on Part B drugs while encouraging doctors to choose the most (cost-) effective treatments for their patients
CMS is accepting comments through May 9, 2016
ASPAdd-On (6% of
ASP)
Add-On (2.5%
of ASP + $16.80)
Current Add-On (%
of ASP)
Proposed Add-On (%
of ASP)
$5.00 $0.30 $16.93 6% 339%
$10.00 $0.60 $17.05 6% 171%
$100.00 $6.00 $19.30 6% 19%
$1,000.00 $60.00 $41.80 6% 4%
Prescription drug spending in the US totaled $457B in 2015
$128B (28%) was for drugs provided in hospitals and doctors’ offices (injectables)
Medicare Part B drug spending was $21 billion
Problem: Part B ASP+6% payment formula may create incentives for use of high-priced drugs
Promote use of lower-cost, clinically equivalent drugs by:
Reducing the add-on payment to 2.5% from 6% of ASP
Adding a new flat fee payment of $16.80 per drug per day
A recent HHS report decried yet another drug spending increase and CMS started looking for a solution …
… via proposing a change to current Part B drug payment … … as well as several “value-based” pricing strategies
Discounting or eliminating patient cost-sharing
Indications-based pricing
Reference pricing
Risk-sharing agreements based on outcomes
Test launches planned in late 2016 / early 2017
Avalere Analysis: Medicare reimbursement would drop for drugs costing over $480 per day and rise for drugs costing under $480 per day
Note: ASP = average sales price of Part B drugs
- 18 -
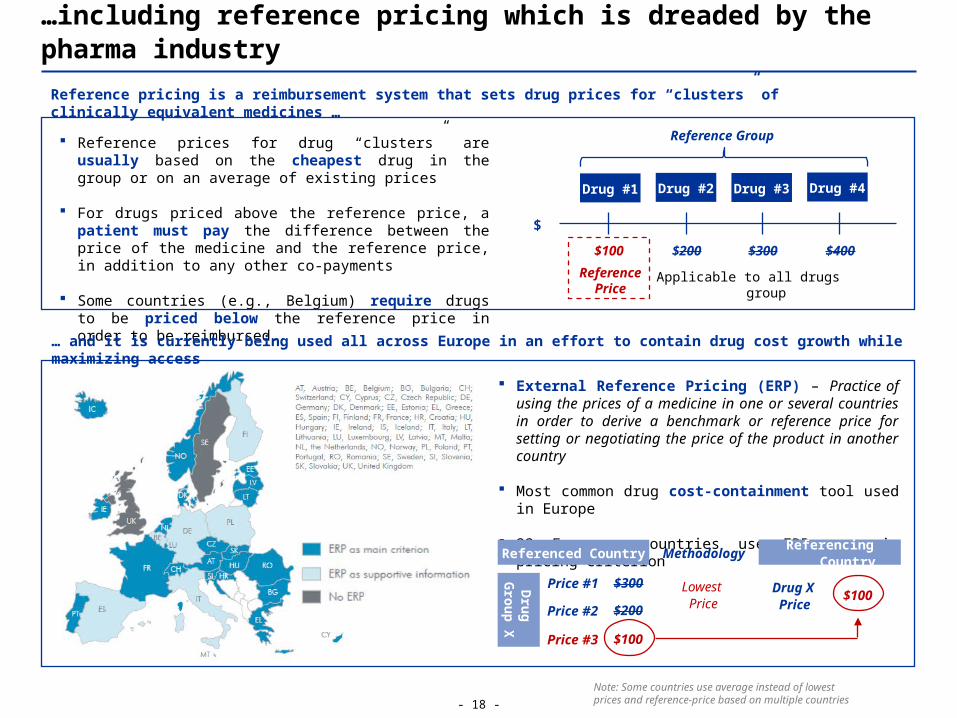
Reference prices for drug “clusters” are usually based on the cheapest drug in the group or on an average of existing prices
For drugs priced above the reference price, a patient must pay the difference between the price of the medicine and the reference price, in addition to any other co-payments
Some countries (e.g., Belgium) require drugs to be priced below the reference price in order to be reimbursed.
…including reference pricing which is dreaded by the pharma industry
External Reference Pricing (ERP) – Practice of using the prices of a medicine in one or several countries in order to derive a benchmark or reference price for setting or negotiating the price of the product in another country
Most common drug cost-containment tool used in Europe
23 European countries use ERP as main pricing criterion
Reference pricing is a reimbursement system that sets drug prices for “clusters” of clinically equivalent medicines …
… and it is currently being used all across Europe in an effort to contain drug cost growth while maximizing access
$
Drug #1 Drug #2 Drug #3 Drug #4
Reference Group
ReferencePrice
$100 $200 $300 $400
Applicable to all drugs group
Price #1 $300
Referenced Country
Price #2 $200
Price #3 $100
Drug
Group X
Referencing Country
Lowest Price
Methodology
Drug X Price $100
Note: Some countries use average instead of lowest prices and reference-price based on multiple countries

- 19 -
So far, reference pricing has achieved mixed results in Europe…
Cost-savings to-date are questionable across Europe … … while pharma decries ERP’s impact on innovation
Belgian research found that reference groups lead to lower medication costs for poorer patients
However, Italy, Sweden, and Denmark are moving away from reference pricing to negotiations because of lack of evidence of savings
The real impact of ERP on cost reduction is still not well understood and more studies are needed
“Path dependence” – ERP programs vary by country (e.g., # of comparator countries, price benchmarks)
ERP ignores key market aspects such as health needs and cross-country variations in income and care costs
Differences between public and actual prices under confidential managed entry agreements are unknown
Drug names, doses, pack sizes vary across countries
These factors make 1:1 price comparisons difficult
Drug makers say ERP discourages incremental innovation by reducing revenues for R&D
Additionally, since reference pricing can severely cut into profitability, in some cases, drug makers may even cancel new drug launches altogether
While drug makers’ criticism may be politically charged, a decline in innovation is never positive
The “Good” … ?
The “Bad”
Barrier to Innovation
ERP has incentivized pharmaceutical companies to adopt international launch sequence strategies
They often delay or avoid launching new drugs in countries with lower prices, especially if they are markets referenced by countries with larger markets
Additionally, in countries referencing the lowest prices, drug makers may even discontinue supply
These profit-driven strategies can lead to access issues, especially in smaller/poorer countries
Barrier to Access
- 20 -
CMS’ Part B proposal already has stiff opposition from the pharma industry and providers:
“It is inappropriate for CMS to manipulate choice of treatment for cancer patients using heavy-handed reimbursement techniques.” – Dr. Allen Lichter, CEO of the American Society of Clinical Oncology
Political gridlock between a Republican Congress and a Democratic President coupled with a well-entrenched pharma lobby drop the chances for action in the near-term to close to zero:
"There's not much they [CMS/Obama administration] can do, that's the sad truth … so they're not gonna do much—but they're going to talk about it a lot.“ – Ira Loss, Founder of Washington Analysis
Estimating the cost savings from reference pricing has been very difficult (because they depend on exact pricing system specifications) which has made gathering support even harder
Most experts agree that the President can NOT make this change via executive order
Competing proposals have been more popular among proponents (incl. Presidential candidates), such as plans to allow Medicare to negotiate drug prices, which could save $15B-$54B/year*
…and it is unlikely to fare better in the US if it ever sees the light of day
Implementing reference pricing for Medicare would require Congressional approval which is unlikely …
CMS will be testing new payment models over the next 5 years which will determine with which approaches the agency will ultimately decide to move forward
Afterwards, the likelihood of adoption of reference pricing across all Part B drugs is <25%
… making CMS’ recent Part B proposal the only realistic way to such a pricing system in the long run
* Figures are estimates and based on early CBO/OMB scores
- 21 -
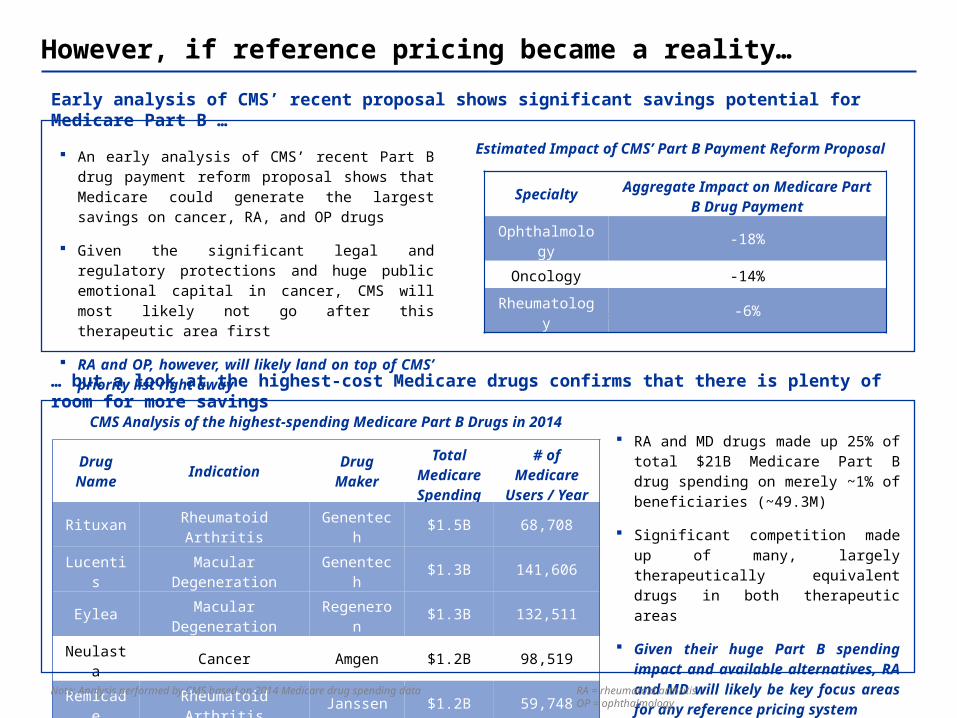
However, if reference pricing became a reality…
Drug Name Indication Drug
MakerTotal
Medicare Spending
# of Medicare
Users / Year
Rituxan Rheumatoid Arthritis Genentech $1.5B 68,708
Lucentis Macular Degeneration Genentech $1.3B 141,606
Eylea Macular Degeneration Regeneron $1.3B 132,511
Neulasta Cancer Amgen $1.2B 98,519
Remicade Rheumatoid Arthritis Janssen $1.2B 59,748
Total $6.5B 501,092
… but a look at the highest-cost Medicare drugs confirms that there is plenty of room for more savings
RA and MD drugs made up 25% of total $21B Medicare Part B drug spending on merely ~1% of beneficiaries (~49.3M)
Significant competition made up of many, largely therapeutically equivalent drugs in both therapeutic areas
Given their huge Part B spending impact and available alternatives, RA and MD will likely be key focus areas for any reference pricing system
Early analysis of CMS’ recent proposal shows significant savings potential for Medicare Part B …
An early analysis of CMS’ recent Part B drug payment reform proposal shows that Medicare could generate the largest savings on cancer, RA, and OP drugs
Given the significant legal and regulatory protections and huge public emotional capital in cancer, CMS will most likely not go after this therapeutic area first
RA and OP, however, will likely land on top of CMS’ priority list right away
Estimated Impact of CMS’ Part B Payment Reform Proposal
CMS Analysis of the highest-spending Medicare Part B Drugs in 2014
Note: Analysis performed and published by Avalere Health on April 7,, 2016
Specialty Aggregate Impact on Medicare Part B Drug Payment
Ophthalmology -18%
Oncology -14%
Rheumatology -6%
Note: Analysis performed by CMS based on 2014 Medicare drug spending data RA = rheumatoid arthritisOP = ophthalmology

- 22 -
…the rheumatoid arthritis space would very likely be a top priority…
Drug Name Key Indications Drug Maker Cost per Dose* Dosing* Annual
Cost* Formulation Biosimilar Competition
Rheumatoid Arthritis, Crohn’s AbbVie $1,618 26x / year $42,059 Injectable Yes, FDA review
Rheumatoid Arthritis, Psoriasis Amgen $798 52x / year $41,499 Injectable Yes, launched in
EU
Rheumatoid Arthritis
Bristol Myers Squibb $915 42x / year $38,407 Injectable Yes, in pre-
clinical stage
Rheumatoid Arthritis, Crohn’s Janssen $1,100 24x / year $26,400 Injectable Yes, launched in
EU, FDA favors
Rheumatoid Arthritis Genentech $2,815 8x / year $22,516 Injectable Yes, EMA review
While high-cost, high-volume RA products will likely face biosimilar competition in the US very soon …
… the resulting price drops may not be as huge as anticipated, leaving a need for further action
Despite a lack of head-to-head studies, medical database-based comparisons of these drugs showed equivalent efficacy and safety for RA and Crohn’s disease and Medicare currently covers all of them and leaves the choice to doctors and patients
4 of the 5 drugs will likely face biosimilar competition very soon which, many hope, will improve affordability for patients
However, the first US-approved biosimilar Zarxio came to market at only a 15% discount to its reference product Neupogen, indicating a much lower price reduction potential than the typical 40%+ for non-biologic generics
Big pharma biosimilar sponsors Pfizer (Remicade), Biogen (Enbrel), and Amgen (Humira) will likely focus on preserving value via moderate price discounts while Celltrion (Rituxan) and Mylan (Orencia) could make more of a dent pricing-wise
Lowest Cost
Pricing Wildcards
* Figures are averages and can vary depending on patient-specific treatment needs

- 23 -
…as would the macular degeneration space, given its high-cost drugs
Drug Name Key Indications Drug Maker Cost per Dose* Dosing* Annual Cost* Use Formulation
Wet Age-Related Macular
Degeneration
(Wet AMD)
Genentech $2,000 1x / month $24,000 On-label Injectable
Original Package
Regeneron $1,850 1x / month $22,200 On-label Injectable
Original Package
Genentech $501x /
month (or less)
$650 Off-labelInjectable
Compounded by Pharmacy
… which make them a prime target for price/cost reduction under a reference pricing system
Multiple studies since 2005 comparing Lucentis, Eylea, and Avastin (all of which have essentially the same mechanism of action) showed equivalent efficacy for Wet AMD for all 3 drugs
Medicare currently covers all 3 drugs and allows doctors and patients choose whichever medication they prefer
Recent surveys showed that 64% of ophthalmologists choose Avastin as first-line drug and a 2014 Health Affairs study showed that Medicare could save $18B over 10 years if the remaining 36% of doctors switched to Avastin
However, there is an off-label issue with Avastin which CMS would need to solve when defining the reference group for MD
o Avastin use is off-label because Genentech did not seek FDA approval for Wet AMD (Avastin is indicated for cancer)
o Hence, Avastin for Wet AMD is prepared by compounding pharmacies and does not come in an original package
MD is dominated by 3 therapeutically equivalent drugs that come with huge price differentials …
Lowest Price Lowest Cost
* Figures are averages and can vary depending on patient-specific treatment needs

- 24 -
Our Call
CMS will likely tweak Part B drug payment in near term to incentivize use of cheaper drugs
o A model involving a lower ASP+% coupled with a fixed fee is a viable way of doing so
o CMS will test other new Medicare drug payment systems over the next 5 years
o Depending on these test results, CMS may or may not identify reference pricing as viable
The likelihood of reference pricing for all Part B and D drugs in the near term is <25% due to:
o Mixed performance in EU
o Political gridlock and pharma lobby
o Competing ideas (e.g., Medicare price negotiations) and methodologies (e.g., value-based pricing)
Longer term (3+ years), reference pricing may be deemed viable if drug costs continue to rise and CMS’ pilot shows superiority vs. other methods (e.g., outcomes- or indication-based pay); CMS could apply reference pricing across the board or to certain high-cost therapeutic areas*.
* MD is a likely candidate given how much cheaper Avastin is vs. the other two available products (Lucentis and Eylea)
- 25 -
Bloomberg “Valeant, Turing Slammed as Shkreli Calls Congress ‘Imbeciles’ “ – Feb. 4, 2016
Houston Chronicle “'Handsome' profit was seen in big drug price increase” – Feb. 2, 2016
CNBC “Gilead may face legal action if it doesn’t cut drug prices” – Jan. 27, 2015
CMS Medicare Drug Spending Dashboard, December 21, 2015
Politico “Trump backs Medicare negotiating drug prices” – Jan. 25, 2015
NCBI “Reimbursement of pharmaceuticals: reference pricing versus health technology assessment” – Aug. 28. 2010
MedicalXpress “No clear path to lowered drug prices” – Mar. 16, 2016
NYT “U.S. to Test Ways to Cut Drug Prices in Medicare” – Mar. 8, 2016
US News “Medicare to Experiment With New Drug Pricing for Doctors” – Mar. 8, 2016
WSJ “U.S. Officials Propose Test Program Aimed at Lowering Medicare Drug Costs” – Mar. 8, 2016
Generics and Biosimilars Initiative Journal “Reference pricing systems in Europe: characteristics and consequences” – 2012
FiercePharma “Valeant, Turing slammed for price hikes during congressional hearing” – Feb. 4, 2015
Chicago Tribune “Why do doctors choose a $2,000 cure when a $50 one is just as good?” – Dec. 11, 2015
CostHelper Macular Degeneration
American Academy of Ophthalmology “Avastin, Eylea and Lucentis – What’s the Difference?” – Jul. 20, 2015
HealthLine “Rheumatoid Arthritis Patients Bear Heavy Cost Burden for Biologic Drugs” – Apr. 25, 2016
Consumer Reports “Treating Rheumatoid Arthritis Are Biologic Drugs Right for You?”
CMS Newsroom “CMS proposes to test new Medicare Part B prescription drug models to improve quality of care and deliver better value for Medicare beneficiaries” – Mar. 8, 2016
CreativCeutical “Overview of External Reference Pricing in Europe” – May 31, 2014
Journal of Market Access & Health Policy “Overview of external reference pricing systems in Europe” – Aug. 2015
Merrill Lynch - Pricing and Politics 2016 Report, Dec. 17, 2015
ISPOR Cost Description of RA Drugs
RA Warrior on RA Treatment Comparison Study Results
Reuters “Novartis launches first US biosimilar drug at 15% discount – Sept. 3, 2015
FierceBiotech “Amgen's Humira biosimilar nears FDA nod, but legal hurdles remain” – Jan. 26, 2016
FierceBiotech “Samsung and Biogen win first EU approval for an Enbrel copycat” – Jan. 19, 2016
PR Newswire “Hospira launches first biosimilar monoclonal antibody (mAb) Inflectra™ (infliximab) in major European markets” – Feb. 16, 2015Generics and Biosimilars Initiative “Celltrion submits rituximab biosimilar application to EMA “ – Nov. 11, 2015
PMLive “Mylan buys into six biosimilars, including Orencia candidate” – Jan. 11, 2016
SOURCES
Avastin.com website
Eylea.us website
Rituxan.com website
Humira.com website
Remicade.com website
Orencia.com website
Enbrel.com website
MedPAC.gov
CBO.gov
Drugchannels.net
Evaluate Pharma & Deloitte RA Space Landscape Overviews, 2015
Reuters “Exclusive: Makers took big price increases on widely used drugs”, April 5, 2016
CMS Blog on Drug Affordability – Nov. 5, 2015
Healthcare Payer News, December 22, 2015Avalere Health analysis of recent CMS Part B Proposed Rule, April 7, 2016
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-sheets-items/2015-12-21.html
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-03-08.html
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-03-08.html
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-03-08.html
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-03-08.html
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-03-08.html
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-03-08.html
http://www.gabionline.net/Biosimilars/News/Celltrion-submits-rituximab-biosimilar-application-to-EMA
http://www.gabionline.net/Biosimilars/News/Celltrion-submits-rituximab-biosimilar-application-to-EMA



















