
Injection Administration Techniques Rachel Nowak, PharmD Clinical Instructor, UWSOP Bartell Drugs...
46
Injection Administratio n Techniques Rachel Nowak, PharmD Clinical Instructor, UWSOP Bartell Drugs Clinical Coordinator January 29, 2010
-
Upload
laurence-lindsey -
Category
Documents
-
view
213 -
download
0
Transcript of Injection Administration Techniques Rachel Nowak, PharmD Clinical Instructor, UWSOP Bartell Drugs...

Injection Administration Techniques
Rachel Nowak, PharmDClinical Instructor, UWSOP
Bartell Drugs Clinical CoordinatorJanuary 29, 2010

Objectives Describe proper techniques for
administering injectable drugs Describe precautions to take when
administering injectable products Appreciate pharmacist role in
administering injectable medications

Vaccines 101

Immunity Passive Immunity
– Antibody produced by one human or other animal is transferred to another
– Temporary protection• Example: Immunity an infant receives from its mother
Active Immunity– Immune system is stimulated to produce cellular
and humoral immunity – Lasting protection
• Example: Survive infection from the disease causing organism

Basic MOA of Vaccines
Vaccinations produce active immunity.
Immune response and immunologic memory produced is similar to that caused by natural infection.
Comes without the risks of the actual disease and associated complications.

Classifications of Vaccines Live attenuated
– Attenuated or weakened form of disease-causing bacterium or virus
– Must replicate to be effective• Uncontrolled replication of the vaccine virus
can cause severe reactions - only occurs in patients with immunodeficiency
– Immune response is cellular & humoral– Circulating antibodies interfere – Usually produce immunity after one dose

Classifications of Vaccines
Inactivated– Inactivated form of bacterium or virus– Can’t replicate
• Can’t cause disease, even in immunodeficient patients
– Immune response primarily humoral– Less affected by circulating antibody than
live vaccines– Always requires more than one dose– Antibody titer decline over time

Immunization Procedures

Screening
Standard Questions– Do you have any drug/food allergies?– Do you have any chronic diseases?– What medications do you take?
Basic Vaccine Screening Questions Are you sick today? Are you allergic to latex? Do you have any allergies to any vaccine or
vaccine components? – Ex: Eggs, gelatin
Have you ever had a serious reaction after receiving a vaccine?
Have you had Guillian-Barre Syndrome in the past?
Is it possible that you could be pregnant? Breastfeeding?

Additional Vaccine Screening Questions
Do you have cancer, leukemia, AIDs, or any other immune system problem?
Do you take cortisone, prednisone, other steroids, anticancer drugs, or have you had radiation treatments?
In the past year, have you received a transfusion of blood or blood products or been given immune globulin or an antiviral medication?
Have you received any vaccinations in the past 4 weeks?

Consent Answer any questions patient may
have Patient needs to understand
benefits and risks of getting immunized and consent to vaccine administration.– If it is a child under 18, then parent or
guardian consent should be obtained

Vaccine Information Statements (VIS) Patient education sheets developed
by the CDC– Helps to explain the risks and benefits
of receiving a particular vaccine Federal law requires that VISs be used
for most vaccines when vaccinating patients
– Should be given before vaccine administered

Parts of a Syringe

Preparing Syringe Choose correct SYRINGE size
– If <0.5ml need low-dose syringe (1mL, 3mL)– Finely graduated syringe will ensure accurate amount– Fluzone (influenza) is 0.5mL dose– Pneumovax (pneumonia) is 0.5mL dose
Maximum volumes– Deltoid – No more than 0.5-1mL– Large muscle (gluteus medius)
• Adult – no more than 4mL• Child – no more than 1-2mL

Needle Lengths and Gauges

Preparing Needle
Choose correct needle LENGTH and GAUGE
Minimize tissue injury and SQ leakage Allow easy passage (23 vs. 25 gauge) Needle length depends on injection site
– Adults 5/8” vs. 1” vs. 1.5”– Children 5/8” vs. 1”– If less SQ fat, use smaller needle
Get Organized Get all supplies ready in advance
– ex: Band-Aid, alcohol pad, cotton ball, VIS
Double Check– Correct vaccine, dose, & expiration date– Go over screening/consent form with patient
Record– Vaccine name, manufacturer, lot number, expiration
date– Location of administration (L/R deltoid)– Provider administering the vaccine– Vaccine Information Sheet publication date

Administer the Vaccine Cleanse area with alcohol swab
– Allow alcohol to dry
Target – C technique and shoot (IM)– Bunch skin (SQ)
Inject – DO NOT Aspirate– Dart-like motion with steady pressure– Inject at:
• 90° angle for IM• 45° angle for SQ

Final Steps Do not recap needle Dispose of needle properly Apply pressure to injection site with cotton ball
(if necessary) Apply adhesive bandage Provide patient with immunization record &
Vaccine Information Statement (VIS) Record all necessary information Have patient remain under surveillance for
~15 minutes

Routes of Administration
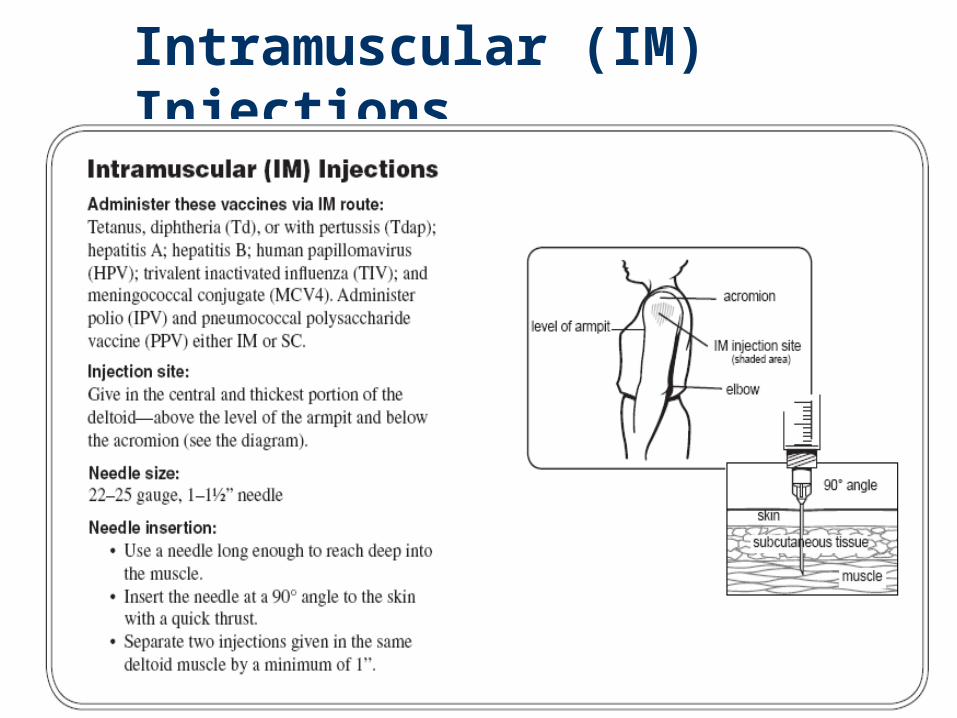
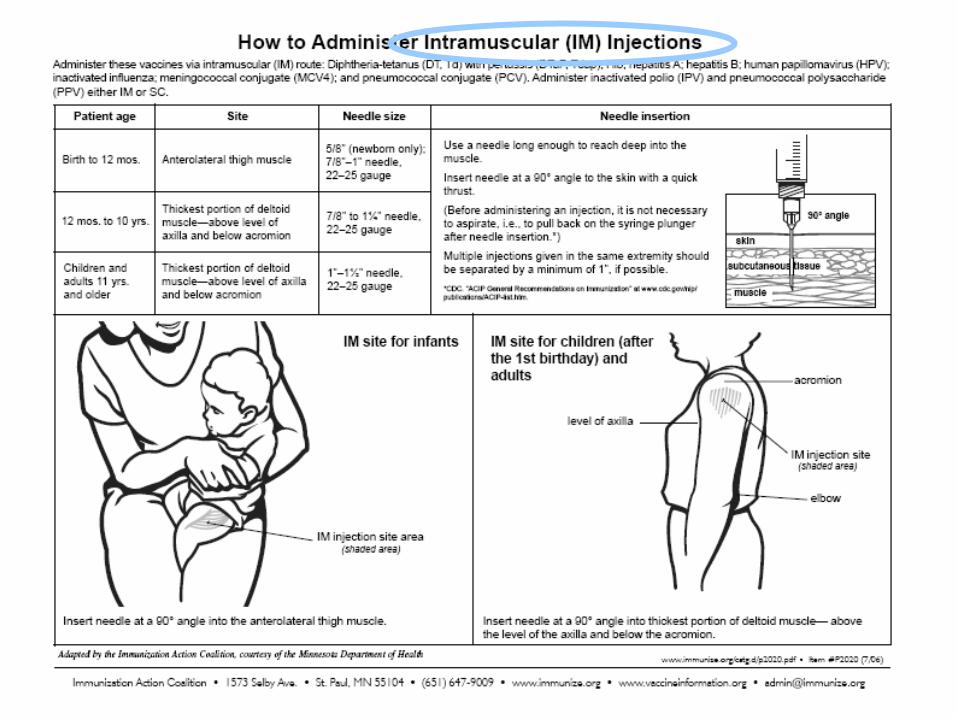
Intramuscular (IM) Injections

Subcutaneous (SQ) Injections

Self-Injection Teaching:Insulin Advise patients to wash hands Have patient confirm type of insulin on bottle label Roll vial or pen in palms, if appropriate Show patients in counseling where to read dose on
syringe and appropriate amount to draw– Ensure using best syringe for dose Inject at 90° angle for SQ insulin Injecting into the subcutaneous fat of the belly most
common– Site should be approximately 2 inches from belly button Rotate sites – avoid formation of fatty deposits or scarring

Insulin Injection Sites Alternate sites include the back of the
arms, thighs, and buttocks– Slower onset with alternate sites
Self-Injection Teaching: Insulin Go over insulin storage
– Generally insulin not in use should not be stored in fridge
– Extreme temperatures and excess agitation should be avoided
Discard dates – Important to go over how long insulin can be
stored at room temperature Insulin inspection Mixing of Insulins Proper disposal of sharps

Self-Injection Teaching
Pen devices/ insulin cartridges:– Deliver insulin subcutaneously through a needle.– All a little different and might require extra
teaching time– In specific patient populations these devices
have been demonstrated to improve:• accuracy of administration • adherence
– Requires needle to be left embedded in skin for at least 5 seconds after plunger depressed

Managing Adverse Reactions

Vasovagal Syncope (Fainting) Be aware of patient behavior Have patient sit before
administration Lay patient down if necessary Check airway, breathing and vital
signs
Anaphylaxis
Rare but potentially fatal Occurs within 15 minutes Call 911 Lay patient down, check airway,
breathing, vital signs Be prepared and ready to administer
epinephrine (Epipen)

Delayed Adverse Reactions Child – fever, fussy, crying, injection
site Adult – injection site discomfort Symptomatic relief
– Fluids– Pain medications
• No aspirin for children• Acetaminophen (Tylenol)• Ibuprofen (Advil, Motrin)

Reporting Adverse Reactions Vaccine Adverse
Event Reporting System (VAERS)
Required for:- Rare, serious or unexpected events

Emergency Plan and Training Access to Emergency Medical
Services (EMS) – phone on hand Be prepared for adverse reactions
– CPR trained staff– Necessary medications on hand– Have patient remain under
surveillance after administration

Universal Precautions
Controlling Infection Transmission

Be Prepared
Control infection transmission– Use universal precautions
– Proper cleaning and disposal of waste Anticipate adverse effects
Assure patient safety– Know your equipment
– Establish quality procedures– Practice good technique
Protect Yourself:Use Universal Precautions Infection control guidelines
designed to protect workers from exposure to diseases spread by blood and certain body fluids
Assume all patients to be infectious for blood-borne diseases

Universal Precautions Apply To: Blood semen vaginal secretions synovial fluid
cerebrospinal fluid
pleural fluid peritoneal fluid pericardial fluid amniotic fluid
Universal precautions should be applied to all body fluids when it is difficult to identify the
specific body fluid or when body fluids are visibly contaminated with blood.

Universal Precautions DO NOT necessarily apply to: feces nasal secretions sputum sweat
tears urine vomit saliva (except in
the dental setting)
But, you must still be mindful of transmitting infectious material.
They may not carry blood-borne illness, but they do carry viruses and bacteria.

Universal Precautions
Wear gloves if likely to touch body substances or mucous membranes– Latex or non-latex– Monitor for allergies
Wear eye protection if likely to be splashed
Wear lab coat or gown if likely to be soiled

Universal Precautions Place needles in special
containers (Sharps Container)
Place soiled articles in plastic bag for disposal
Place soiled linen in laundry bag

Pharmacists Role

Pharmacist Role Dispensing versus administration Makes sense for:
– Vaccinations– Teaching patients to self-inject
• Insulin and glucagon• Increasing availability of self-injection
products– Allergic reactions, migraine, MS, infertility
Proper training required
Why are immunizations
so important? Profession:
– Establishes the role of the pharmacist Patients:
– Pharmacists are easily accessible Population:
– Preventing disease

For More Information APhA: Pharmacy-Based Immunization
Delivery Certificate Program – www.pharmacist.com
Center for Disease Control – Vaccines– http://www.cdc.gov/vaccines
Vaccine Adverse Event Reporting System– http://vaers.hhs.gov


















