
Inhibidores de PARP ¿Una realidad? ¿dónde y cuando? · tumor initiation BRCA1/2 are central...
24
Inhibidores de PARP ¿Una realidad? ¿dónde y cuando? Alberto Ocana Hospital Universitario Albacete Centro Regional Investigaciones Biomédicas CIC-Salamanca
Transcript of Inhibidores de PARP ¿Una realidad? ¿dónde y cuando? · tumor initiation BRCA1/2 are central...

Inhibidores de PARP
¿Una realidad?
¿dónde y cuando?
Alberto OcanaHospital Universitario AlbaceteCentro Regional Investigaciones BiomédicasCIC-Salamanca

DNA is continually exposed to endogenous and exogenous sources of damage, DNA repair pathways is required to maintain genomic integrity
Failure to repair DNA damage can result in a variety of genomic aberrations: point mutations, chromosomal translocations, and gain or loss of chromosomal segments or entire chromosomes.
These genomic alterations produce changes in cell physiology that drive tumor initiation
BRCA1/2 are central players in the homologous recombination (HR)repair pathway, and loss of BRCA1/2 or other genes in the HR pathway can confer an HR-deficient phenotype in breast, ovarian, prostate, and other tumor types
DNA repair mechanisms

Double-strand breaks (DSBs): non-homologous end joining (NHEJ)microhomology-mediated end joining (MHEJ) homologous recombination (HR) (BRCA1/2 mutations)
Single strand break: base excision repair (BER) (PARP1 inhibitors), nucleotide excision repair (NER) mismatch repair.
Redundancy

Response to platinum compoundsSomatic BRCA mut

PARP INHIBITORS IN BREAST CANCER
OlympiAD (NCT02000622)
FDA approves olaparib for germline BRCA-mutated metastaticbreast cancerOn January 12, 2018, the Food and Drug Administration granted regular approval to olaparib tablets (Lynparza, AstraZeneca Pharmaceuticals LP), a poly (ADP-ribose) polymerase (PARP) inhibitor, for the treatment of patients with deleterious orsuspected deleterious germline BRCA-mutated (gBRCAm), HER2-negative metastaticbreast cancer.


Randomization• previous use of chemotherapy for metastatic disease (yes vs. no)
• hormone-receptor status (hormone- receptor positive vs. triple negative)
• previous use of platinum-based therapy (yes vs. no)
Treatment design Randomly assigned, in a 2:1 ratio, to receive olaparib tab lets (300 mg twice daily) or standard therapy:
• capecitabine administered orally at a dose of 2500 mg per square meter of body-surface area daily (divided into two doses) for 14 days, repeated every 21 days;
• eribulin mesylate administered intravenously at a dose of 1.4 mg per square meter on day 1 and day 8, repeated every 21 days; or
• vinorelbine administered intravenously at a dose of 30 mg per square meter on day 1 and day 8, repeated every 21 days.
Crossover to olaparib was not permitted in this trial.
Inclusion Criteria
• HER2-negative metastatic breast cancer that was hormone-receptor positive or was triple negative.
• Patients had a confirmed deleterious or suspected deleterious germline BRCA mutation; central testing with BRACAnalysis (Myriad Genetics)
• Patients had received no more than two previous chemotherapy regimens for metastatic disease
• Patients with hormone-receptor– positive breast cancer had received at least one endocrine therapy
• Previous neoadjuvant or adjuvant treatment with platinum was allowed if at least 12 months had elapsed since the last dose.
• Previous treatment with platinum for metastatic disease was allowed if there was no evidence that disease progression had occurred during treatment.

• Median progression free survival olaparib compared with
standard therapy
(7.0 months vs. 4.2 months; HR 0.58; 95% CI, 0.43
to 0.80; P<0.001).
• The response rate was 59.9% in the olaparib group and
28.8% in the standard-therapy group.
• Grade 3 or higher adverse events was 36.6% in the
olaparib group and 50.5% in the standard-therapy group
• Treatment discontinuation due to toxic effects was 4.9%
and 7.7%, respectively.
Results




Results summary
Median progression-free survival was 2.8 months longer
Less toxic
Grade 3 or higher adverse events was 36.6% in the olaparib group and 50.5% in the standard-therapy group
Treatment discontinuation due to toxiceffects was 4.9% and 7.7%, respectively
FDA also granted marketing authorization for the BRACAnalysis CDx® test (Myriad Genetic Laboratories, Inc.)

Is the magnitude of benefit large enough?
TDM1Pertuzumab+trastuzumabEverolimusPalbociclib…
Unmet disease
Is the magnitude of benefit large enough? ….Howcan activity be improved?...patients selection

Approved HRD Biomarkers for PARP Inhibitor Use: Germline and somatic BRCA Mutations
Under evaluation:
ONGOING COMBINATIONS



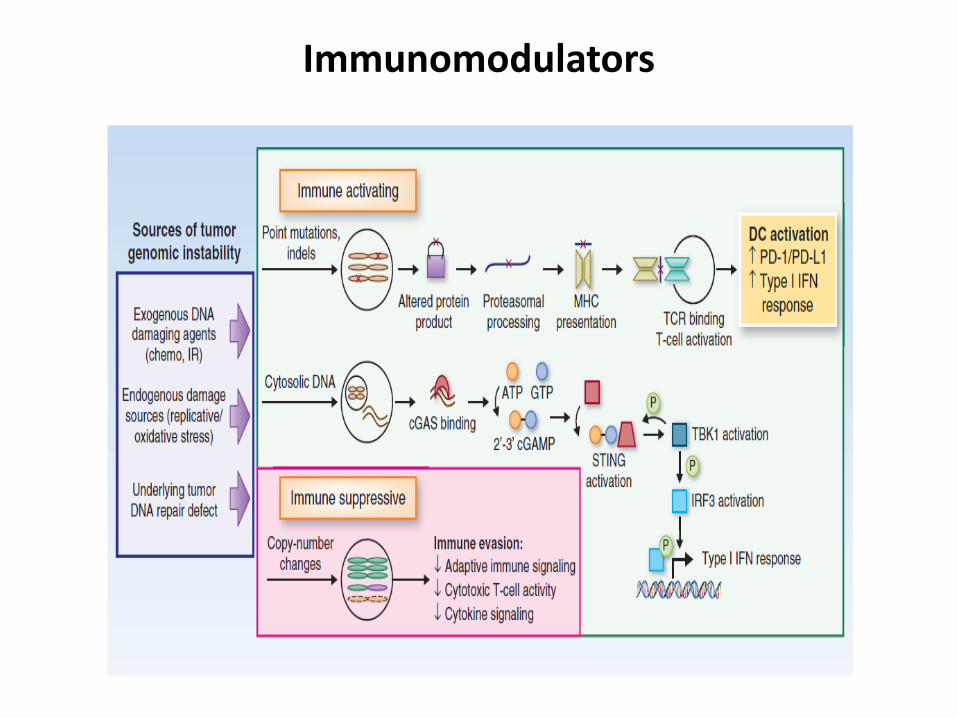
Immunomodulators

Take home message
On January 12, 2018,FDA approves olaparib for germline BRCA-mutatedmetastatic breast cancer: PFS 2.8 months
Limitations
PARP inhibitors have not been compared head-to-head against platinum.
In OlympiAD, prior platinum was allowed only if there was no PD on treatment as platinum was not allowed as one of the control groups.
Long standing side effects? late toxic effects is especially important for adjuvant setting where olaparib is currently evaluated (OlympiA trial) (NCT02032823)

Future options
Selection of patients: biomarkers of HR repair, triple negativetumors, response to platinum
Genetic instability more important than just presence of mutations at BRCA genes
In combination with other agents: immunomodulators?
Thanks for your attention















![Flyer PARP FAmily NP V01 - biolinks k.k.1].pdf · Tomorrow’s Reagents Manufactured Today® International Edition The PARP Family T highlight PRODUCT FLYER The PARP Family](https://static.fdocuments.us/doc/165x107/5cb9946788c993f37c8c0cfc/flyer-parp-family-np-v01-biolinks-kk-1pdf-tomorrows-reagents-manufactured.jpg)


