Inherited Surfactant Disorders - Associates in Newborn Medicine
12
DOI: 10.1542/neo.9-10-e458 2008;9;e458-e467 NeoReviews W. Adam Gower, Susan E. Wert and Lawrence M. Nogee Inherited Surfactant Disorders http://neoreviews.aappublications.org/cgi/content/full/neoreviews;9/10/e458 located on the World Wide Web at: The online version of this article, along with updated information and services, is Online ISSN: 1526-9906. Illinois, 60007. Copyright © 2008 by the American Academy of Pediatrics. All rights reserved. by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, it has been published continuously since 2000. NeoReviews is owned, published, and trademarked NeoReviews is the official journal of the American Academy of Pediatrics. A monthly publication, by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.org Downloaded from
Transcript of Inherited Surfactant Disorders - Associates in Newborn Medicine

DOI: 10.1542/neo.9-10-e458 2008;9;e458-e467 NeoReviews
W. Adam Gower, Susan E. Wert and Lawrence M. Nogee Inherited Surfactant Disorders
http://neoreviews.aappublications.org/cgi/content/full/neoreviews;9/10/e458located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Online ISSN: 1526-9906. Illinois, 60007. Copyright © 2008 by the American Academy of Pediatrics. All rights reserved. by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village,it has been published continuously since 2000. NeoReviews is owned, published, and trademarked NeoReviews is the official journal of the American Academy of Pediatrics. A monthly publication,
by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from
Inherited Surfactant DisordersW. Adam Gower, MD,*
Susan E. Wert, PhD,†
Lawrence M. Nogee, MD‡
Author Disclosure
Drs Gower, Wert, and
Nogee have disclosed
support by the
Eudowood
Foundation, the
National Institutes of
Health (HL 54703 to
LMN), and the
Hartwell Foundation
(WAG). This
commentary does not
contain a discussion
of an unapproved/
investigative use of a
commercial product/
device.
Objectives After completing this article, readers should be able to:
1. Recognize the clinical presentations resulting from inherited disorders of surfactantmetabolism.
2. Describe the roles of surfactant protein (SP)-B, adenosine triphosphate-bindingcassette member A3 (ABCA3), and SP-C in surfactant function and metabolism.
3. Evaluate infants for suspected inherited surfactant disorders and recognize thelimitations of such studies.
4. Delineate how rare disorders can provide insights into normal metabolism and thepathogenesis of more common illnesses.
AbstractInherited disorders of surfactant metabolism are rare causes of respiratory disease innewborns but are associated with significant morbidity and mortality. This reviewoutlines the molecular basis and pathophysiology of the three currently identifiedsingle-gene disorders of surfactant metabolism as well as the clinical presentations andevaluation of potentially affected infants. Implications for the understanding ofnormal surfactant metabolism and the potential roles of surfactant dysfunctionmutations in more common neonatal disorders, such as respiratory distress syndrome,also are discussed.
IntroductionPulmonary surfactant is the mixture of lipids and specific proteins that reduces surfacetension at the air-liquid interface and prevents end-expiratory atelectasis. Lack of pulmo-nary surfactant due to decreased production from pulmonary immaturity is the principalcause of respiratory distress syndrome (RDS) in preterm infants. RDS is a relatively
common disorder, affecting more than 50% of infants bornat 30 weeks’ or less gestation, but modern methods ofrespiratory support and exogenous surfactant replacementtherapy have aided in keeping mortality from RDS low.Surfactant deficiency also may result from genetic mecha-nisms that disrupt the production of key proteins importantin surfactant function and metabolism. Although thesesingle-gene disorders are rare, their associated morbidityand mortality are very high. Thus, recognition of thesedisorders is important to counsel families properly concern-ing prognosis, and because they are genetic in origin, recur-rence risk. In addition, the study of these disorders hasoffered insight into normal aspects of surfactant metabolismand can provide clues to genes that may be important ininfluencing the risk for RDS in preterm infants. In this
*Eudowood Division of Pediatric Respiratory Sciences, Department of Pediatrics, Johns Hopkins University School of Medicine,Baltimore, Md.†Divisions of Neonatology and Pulmonary Biology, Department of Pediatrics, Cincinnati Children’s Hospital Medical Center &University of Cincinnati College of Medicine, Cincinnati, Ohio.‡Eudowood Neonatal Pulmonary Division, Department of Pediatrics, Johns Hopkins University School of Medicine, Baltimore,Md.
Abbreviations
ABCA3: adenosine triphosphate-binding cassettemember A3
DPPC: dipalmitoyl phosphatidylcholineDSPC: disaturated phosphatidylcholineILD: interstitial lung diseasePC: phosphatidylcholinePG: phosphatidylglycerolRDS: respiratory distress syndromeSP: surfactant proteinTTF-1: thyroid transcription factor-1
Article respiratory disorders
e458 NeoReviews Vol.9 No.10 October 2008 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

article, we review the known inherited disorders of sur-factant metabolism, focusing on their clinical features,diagnosis, and implications for lung biology.
Surfactant Function, Components, andMetabolismPulmonary surfactant is synthesized by alveolar type IIcells of the lung and stored within lamellar bodies, whichare lysosomally derived organelles specific to these cells.Structurally, lamellar bodies consist of well-organizedconcentric rings of lipid membrane surrounding anelectron-dense core, as observed by electron microscopy.Surfactant is secreted by exocytosis after fusion of thelamellar body with the plasma membrane. Surfactantmay be either recycled through type II cells or catabo-lized by alveolar macrophages. Phosphatidylcholine(PC) (also known as lecithin) is the principal phospho-lipid in surfactant needed for lowering of surface tension,in particular, dipalmitoyl PC (DPPC) or disaturated PC(DSPC), which accounts for approximately half of sur-factant by weight. Precisely how surfactant becomes en-riched for DSPC is not known.
Two low-molecular weight, extremely hydrophobicproteins, surfactant protein (SP) B and C, facilitate theadsorption of surfactant lipids to the air-liquid interfaceafter secretion and are essential for surfactant’s surfacetension-lowering properties. Both SP-B and SP-C arefound in varying amounts in the mammalian-derivedexogenous surfactants used to treat preterm babies whohave RDS. Surfactant also contains two larger, morehydrophilic, structurally related glycoproteins, SP-A andSP-D. These proteins are involved primarily in innateimmunity and immunomodulation, with more limitedroles in surface tension-lowering and metabolism. (1)Genetic diseases related to abnormalities in SP-A andSP-D production have not yet been reported.
Genetic Lung Disease Due to SP-B DeficiencySP-B is a 79-amino acid protein derived from a muchlarger precursor protein (proSP-B) encoded by a singlegene (SFTPB) on chromosome 2. Proteolytic cleavage ofamino- and carboxyterminal domains from proSP-Byields the mature form of SP-B found in the airspaces.The final processing steps are specific to type II cells andoccur in lamellar bodies or their immediate precursors.(2)(3)
SFTPB contains ten coding exons, with mature SP-Bencoded in exons 6 and 7. SP-B expression is regulateddevelopmentally, increasing dramatically in late gesta-tion. Sequences in the 5� untranslated region critical forthe developmental and cell-specific regulation of SP-B
have been identified, as have transcription factors neededfor its expression, most notably thyroid transcriptionfactor 1 (TTF-1) (also known as Nkx2.1). (4) Manycommonly occurring polymorphisms have been identi-fied in the SP-B gene, including one in the promoterregion that affects the level of SP-B gene transcription.(5) Another in exon 4 determines whether N-linkedglycosylation occurs in the aminoterminal domain of theproprotein (6) and, thus, may be functionally significant.An extensively characterized variable nucleotide tandemrepeat region in intron 4 may be associated with a risk forRDS in conjunction with other variables. (7)(8)
Complete deficiency of SP-B results in lethal neonatalrespiratory disease. (9) The usual phenotype is a terminfant who presents with symptoms and signs of respira-tory distress and diffuse lung disease radiographically,resembling RDS in preterm infants. The initial severity oflung disease can be variable, with some children havingrelatively mild symptoms in the first several postnataldays, while others have rapid onset of hypoxemic respi-ratory failure progressing to the need for extracorporealmembrane oxygenation. The disease is progressive, withonly transient improvement seen with surfactant replace-ment therapy and modest improvement with corticoste-roid treatment. Death from respiratory failure usuallyoccurs within 3 to 6 months despite maximal medicaltherapy, and lung transplantation is currently the onlyeffective treatment option. (10)(11) The disease is ex-tremely rare, although the exact incidence is unknown.
As an autosomal recessive disorder, mutations onboth alleles are necessary for an infant to be affected bySP-B deficiency. One particular frameshift mutation(121ins2) has been identified in multiple unrelated pa-tients who have the disorder. Approximately 1 in 1,000individuals of Northern European descent are carriers forthis mutation, which has accounted for approximately60% to 70% of the mutant SFTPB alleles identified to dateand likely has a common ancestral origin (founder ef-fect). (12)(13) Multiple other mutations, including alarge deletion, have been identified, all of which may becategorized as loss-of-function mutations. (10)(11)(14)(15) Some mutations allow for production ofproSP-B that is unable to be processed efficiently tomature SP-B, resulting in marked reduction or completeabsence of mature SP-B. Those children who have mu-tations that allow for some SP-B production (partialdeficiency) can survive well beyond the neonatal period,although they are the exception. (16)(17) Transientdeficiency in association with a mutation on only oneallele also has been recognized. (18) These observations,along with experiments using genetically engineered
respiratory disorders inherited surfactant disorders
NeoReviews Vol.9 No.10 October 2008 e459 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

mice in which SP-B production can be shut off, indicatethat a critical level of SP-B expression is needed fornormal lung function. (19) Thus, individuals whose abil-ity to produce SP-B is impaired due to genetic mecha-nisms, either because of a loss-of-function mutation onone allele or more common variants associated withdecreased SP-B gene expression, may be at higher risk forlung disease if other factors, such as prematurity orinflammation, further limit their SP-B production. SP-Bis, therefore, a reasonable candidate gene for susceptibil-ity to neonatal RDS as well as lung injury later in life.
Surfactant isolated from the lungs of SP-B-deficientinfants is abnormal in composition and is ineffective inlowering surface tension. (20) Incomplete processing ofSP-C from its precursor protein to the mature formresults in the secretion of large amounts of partiallyprocessed SP-C intermediates with hydrophilic epitopes.(11) Accordingly, surfactant from SP-B-deficient infantsis lacking in mature SP-C, and because the partiallyprocessed intermediates are not very surface-active, theyalso inhibit its function. (21) Phospholipid compositionalso is altered, with decreased amounts of PC and evenmore so of phosphatidylglycerol (PG). (20) Such sec-ondary alterations may be related to changes within theSP-B-deficient type II cell, which lacks normal lamellarbodies and contains disorganized, poorly lamellated ve-sicular inclusions. (22) The lack of normally formedlamellar bodies may account for the incomplete process-ing of SP-C as the final steps occur in lamellar bodies.These observations indicate a fundamental intracellularrole for SP-B (or proSP-B) in lamellar body biogenesisand surfactant packaging and at least partly explain therefractory nature to therapy. Incompletely processedSP-C may be a useful biomarker for diagnosis, but thesensitivity and specificity of such testing are currentlyunknown, and analyses are confined to research labora-tories.
Genetic Lung Disease Due to ATP-bindingCassette Protein Member 3(ABCA3) DeficiencyABCA3 is a member of the ABC family of transporters,transmembrane proteins that hydrolyze adenosinetriphosphate to move substrates across biologic mem-branes. The protein is comprised of 1,704 amino acidsand contains 12 membrane-spanning domains and twonucleotide-binding domains. ABCA3 mRNA is ex-pressed in many tissues, including brain and kidney. Inthe lungs, it is expressed primarily in type II cells, withthe protein localized to the limiting membranes of lamel-lar bodies. (23) Other members of the ABCA subfamily
are involved in lipid transport, and mutations in ABCgenes are frequent causes of human genetic diseases. Forexample, ABCA1 transports cholesterol, and its gene ismutated in Tangier disease; ABCA4 transports phos-phatidylethanolamine, and its gene is mutated in a formof retinal degeneration; and ABCC7 is also known asCFTR, the gene mutated in cystic fibrosis. ABCA3 defi-ciency now has been recognized as the cause of lungdisease in both newborns who have an RDS-like pheno-type and older children and adults who have forms ofinterstitial lung disease (ILD). (24)(25)(26)
ABCA3 is located on chromosome 16, spans morethan 60,000 bases, and contains 30 coding exons. Morethan 90 different mutations have been reported inABCA3, distributed among all of the coding exons.Most mutations are “private” and unique to a givenfamily, and the degree of allelic heterogeneity has impor-tant implications for diagnostic genetic testing becausesequencing of all coding exons is needed to identifyaffected patients. ABCA3 deficiency is an autosomal re-cessive disorder. However, patients have been identifiedwho have a consistent phenotype and typical lung histo-pathology findings but only one identifiable mutation.(25)(26)(27) Such patients may have functionally signif-icant mutations in untranslated regions that were notexamined or could have major deletions, insertions, orrearrangements of ABCA3 that would not be detectedby usual approaches. Therefore, the sensitivity of genetictesting is less than 100% for all ABCA3 mutations.
Neonates who have ABCA3 deficiency may presentidentically as those who have SP-B deficiency, exhibitingsigns and symptoms of respiratory distress, pulmonaryhypertension, diffuse infiltrates radiographically, rapidprogression to hypoxemic respiratory failure, and deathdespite maximal medical therapy. Although initial studiesfocused on identifying ABCA3 mutations in newbornswho had very severe disease, more recent experienceindicates that the course of infants who have ABCA3deficiency is much more variable than that seen withthose who have SP-B deficiency. Affected infants whohave severe initial lung disease may show gradual im-provement and can be discharged from the hospital,although symptoms and signs of lung disease usuallypersist. Some affected infants have very mild or even nolung disease as neonates, presenting later with nonspe-cific findings, including failure to thrive and digital club-bing along with pulmonary signs and symptoms and adiagnosis of ILD. The finding of the same mutation, asubstitution of valine for glutamic acid in codon 292(E292V), in multiple unrelated older patients who haveILD suggests a genotype-phenotype correlation. (25)
respiratory disorders inherited surfactant disorders
e460 NeoReviews Vol.9 No.10 October 2008 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

Children who have milder forms of ABCA3 deficiencymay have mutations that allow for some ABCA3 func-tion, although this hypothesis has yet to be tested for-mally. Disease results from loss-of-function mutationsleading to absent or decreased ABCA3 expression, ab-normal trafficking of ABCA3 within the type II cell, ordecreased functional activity of ABCA3. (24)(28)(29)Because many affected children have mutations otherthan those that would be predicted to preclude ABCA3expression completely, therapies that improve traffickingof misfolded proteins through the endoplasmic reticu-lum or augment residual ABCA3 function may be ofbenefit. Glucocorticoids have been shown to increaseABCA3 expression in vitro, (30) although clinical studiesassessing their efficacy for this disorder have not beenperformed.
The precise role of ABCA3 in the lung and in surfac-tant metabolism is unknown. Because ABCA proteinstransport lipids, ABCA3 may act by transporting lipidsessential for surfactant function, such as DSPC, intolamellar bodies. Analysis of lung fluid obtained at thetime of lung transplantation in infants subsequentlydemonstrated to be ABCA3-deficient revealed markeddecreases in both DSPC and PG, consistent with thishypothesis. (31) The surface tension-lowering ability ofthe surfactant material isolated from ABCA3-deficientchildren was markedly reduced compared with materialobtained from control infants transplanted for pulmo-nary vascular disease or SP-B deficiency, which supports alack of functional surfactant as important in the patho-physiology of the lung disease resulting from ABCA3deficiency. (31) Although not a uniform finding, re-duced amounts of SP-B and impaired processing ofproSP-B to mature SP-B have been observed in associa-tion with ABCA3 deficiency, both in human infants andin a mouse model, which may aggravate surfactant defi-ciency further. (24)(25)(32) A role for ABCA3 in lamel-lar body biogenesis is supported by electron microscopicfindings in affected infants. Normal lamellar bodies areabsent or markedly reduced in number; instead, small,dense bodies that have eccentrically placed very electron-dense cores (giving a “fried-egg” appearance) are foundin the cytoplasm of type II cells. (22)(24)(26)
An estimate of the incidence of ABCA3 deficiency isnot available at this time. Given the relative frequencywith which this condition has been recognized since itsinitial description compared with SP-B deficiency, it isprobably the most common genetic cause of surfactantdeficiency. The population frequency of the ABCA3E292V mutation recently was estimated at 1 in 275individuals in two populations. (33) Because this muta-
tion has accounted for fewer than 10% of the mutantABCA3 alleles identified to date, the contribution ofABCA3 sequence variants to lung disease may be sub-stantial. Interestingly, the E292V mutation was enrichedin a cohort of relatively mature (�28 weeks’ gestation)infants who had RDS compared with controls, and in adifferent study, a specific ABCA3 haplotype was associ-ated with RDS risk. (33)(34) These findings support thehypothesis that ABCA3 variants may influence the riskfor RDS in preterm infants.
Genetic Lung Disease Due to SP-C Gene(SFTPC) MutationsRespiratory symptoms due to mutations in SFTPC usu-ally do not present in neonates. Affected infants are lesslikely to be encountered by neonatologists than thosewho have SFTPB or ABCA3 mutations. The first re-ported patient who had an SFTPC mutation was evalu-ated at birth due to a family history of ILD, but was notrecognized to be symptomatic until 6 weeks of age. (35)Mice engineered to be SP-C-deficient do not exhibitlung disease at birth, suggesting that SP-C is not criticalfor perinatal adaptation, although SP-C-deficient micedo develop lung disease with increasing age in a strain-dependent manner. (36) However, the presentation andnatural history of patients who have SFTPC mutations ishighly variable and includes newborns who have severe,rapidly evolving respiratory distress as well as adults whoexperience the onset of ILD in the fifth or sixth decade.(37) The highly variable natural history of the disordercomplicates interpretation of single-patient studies oftherapeutic interventions, such as therapeutic whole lunglavage and hydroxychloroquine. (38)(39) Lung trans-plantation may be considered in cases of severe progres-sive disease.
SP-C is encoded by a single small gene containing 6exons located on the short arm of chromosome 8. Theprimary translation product, proSP-C, undergoes exten-sive proteolysis to form the 35-amino acid hydrophobicmature SP-C molecule that is encoded in exon 2 of thegene. Most mutations identified to date are located in theregion of the gene encoding the carboxyterminal portionof proSP-C and only rarely involve the mature peptidedomain. A substitution of threonine for isoleucine incodon 73 (I73T) is the most commonly found mutation.(38)(40) In contrast to SP-B and ABCA3 deficiencies, amutation on one allele can result in lung disease, andfamilial cases exhibit an autosomal dominant pattern ofinheritance. Sporadic disease also may occur as the resultof apparent spontaneous de novo mutations in the SP-Cgene. (38)(40)
respiratory disorders inherited surfactant disorders
NeoReviews Vol.9 No.10 October 2008 e461 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

The pathophysiology of lung disease due to SFTPCmutations is complex and incompletely understood.SFTPC mutations are believed to result in misfoldedproSP-C, which can elicit the unfolded protein responseand accumulate in the endoplasmic reticulum of the typeII cells, resulting in cellular stress and apoptosis in a toxicgain-of-function mechanism. (41)(42)(43) Alterna-tively, misfolded proSP-C may be targeted for degrada-tion, and as proSP-C self-aggregates within the secretorypathway, causes wild type proSP-C to be degraded aswell, resulting in SP-C deficiency by a dominant negativemechanism. (41)(42)(43)(44) Whether the specific mu-tation determines which mechanism occurs in a givenpatient or each can occur at different times in the sameindividual, depending on the degree of SP-C gene ex-pression and other genetic and environmental factors, isunknown. The severity of lung disease cannot be pre-
dicted by the specific SFTPC muta-tion. Relatives of affected individu-als may carry the same mutationand remain asymptomatic. ABCA3may act as a disease-modifying genein this disorder, as indicated by in-fants heterozygous for both anABCA3 gene mutation and theSFTPC I73T mutation havingmore severe lung disease than fam-ily members who had the I73T mu-tation and were not carriers for anABCA3 mutation. (45)
PathologyLung histopathology findings in
patients who have SFTPB, ABCA3, and SFTPC muta-tions may include nonspecific changes of lung injurydue to prolonged mechanical ventilation and exposureto hyperoxia. More characteristic findings includemarked type II cell hyperplasia, foamy macrophages in theairspaces, and accumulation of granular, proteinaceous ma-terial in the distal airspaces (Fig. 1). (9)(11)(26)(38)(46)The latter finding is similar to that observed in adult patientswho have alveolar proteinosis, a disorder caused by accu-mulation of surfactant due to impaired macrophage func-tion as a result of autoantibodies directed againstgranulocyte-macrophage colony-stimulating factor. (47)Although the term “congenital alveolar proteinosis” hasbeen used to characterize these disorders, this terminologyis potentially misleading. The amount of proteinosis mate-rial observed varies and may even be absent, proteinosis isnot specific for the underlying gene disorder, and the mech-
anisms for proteinosis differ fromthose in adults. The term “surfactantdysfunction” has been used to en-compass all three disorders related togenetic mechanisms disrupting sur-factant function, which cannot bedistinguished from one another onthe basis of routine histopathologyalone. (48) Specific immunohisto-chemical stains may provide addi-tional information but currently areavailable primarily on a research ba-sis. (11)(24)(25) Electron micro-scopic findings (Fig. 2) can distin-guish between SP-B and ABCA3deficiency and may be diagnostic,and such studies should be per-formed on lung tissue obtained by
Figure 1. Histopathology of neonatal lung. A. Normal neonatal lung histology with thinalveolar septa and airspaces devoid of debris. B. Histopathology of the lung from a childwho had fatal SP-B deficiency demonstrates thickened alveolar septa and eosinophilic,lipoproteinaceous material intermixed with large foamy alveolar macrophages (arrow)filling the alveolar spaces. C. Histopathology of the lung from a child who had fatalABCA3 deficiency is similar to that for fatal SP-B deficiency, as shown in panel B. Originalmagnification is �10.
Figure 2. Electron microscopy of lamellar bodies in human alveolar type II cells. A.Well-developed, mature lamellar bodies (arrows) are found in alveolar type II cells from anormal lung. B. Large, disorganized, multivesicular bodies (arrows) are observed in alveolartype II cells from the lung of a child who had SP-B deficiency. C. Small, dense bodies thathave eccentrically placed, electron-dense inclusions, and tightly packed phospholipidlamellae (arrows) are observed in the alveolar type II cells from the lung of a child whohas ABCA3 deficiency. For panels A and B, original magnification is �5,000; for panel C,original magnification is �10,000.
respiratory disorders inherited surfactant disorders
e462 NeoReviews Vol.9 No.10 October 2008 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from
biopsy or autopsy from infants suspected of having one ofthese disorders. (22)(24)(26)
Other Genetic Causes of SurfactantDysfunctionHaploinsufficiency for the gene encoding TTF-1, eitheras a result of gene deletion or loss-of-function mutationson one allele, can cause a syndrome whose manifestationsinclude neonatal respiratory distress, recurrent pulmo-nary infection, hypothyroidism, and neurologic symp-toms. (49) Because TTF-1 is an important regulator ofSP-A, SP-B, and SP-C expression, neonatal lung diseasecould result from delayed expression of SP-B and SP-Cand chronic lung disease from reduced expression of allthree proteins. However, neurologic disease (benign fa-milial chorea) in the absence of any pulmonary diseasealso has been observed in association with TTF-1 haplo-insufficiency.
Children who have a phenotype consistent with aninherited surfactant disorder but in whom no causativemutations in SFTPB, ABCA3, or SFTPC were foundhave been reported, suggesting that mutations in othergenes in the surfactant metabolic pathway can result in asimilar phenotype. (26)(27)(48) Candidate genes in-
clude those encoding SP-A andSP-D and the enzymes needed toprocess proSP-B and proSP-C totheir mature forms. Mice engi-neered to lack expression of SP-Ddevelop lipid accumulations andemphysema. (50) These changeswere observed starting at about3 weeks after birth and progressedwith age, suggesting that human dis-ease due to SP-D deficiency may beunlikely to present in the neonatalperiod. Napsin A and cathepsin Hare enzymes expressed in type IIpneumocytes that have potentialroles in the processing of SP-B.(51)(52) Mutations in the genesencoding these proteins that dis-rupt their function might alter sur-factant composition and lead todysfunction and lung disease in thenewborn period.
Diagnostic EvaluationIt is not possible to distinguish ge-netic causes of surfactant deficiencyfrom treatable or transient causes of
neonatal respiratory disease such as RDS, retained fetallung liquid syndrome, or pneumonia purely on clinical orradiographic grounds. A lack of risk factors for RDS orinfection in a child who has diffuse parenchymal lungdisease should raise suspicion for an inherited surfactantdisorder, and a family history of severe neonatal lungdisease should prompt evaluation. Disease due to SP-Bdeficiency is relentlessly progressive; disease due toABCA3 deficiency may improve, but the symptoms usu-ally do not resolve and radiographs do not clear com-pletely. Newborns who have SFTPC mutations mayshow substantial improvement either with treatment oras a result of the natural history of the disease. In general,the longer that respiratory symptoms and diffuse radio-graphic changes persist without a cause established, thehigher the likelihood of an inherited surfactant disorder.
Analysis of lung fluid samples for surfactant compo-nents currently is only available in research laboratories.The sensitivity and specificity of such testing is unknown,both for distinguishing inherited surfactant disordersfrom other diseases and for indicating which gene isresponsible. Genetic analyses provide the most definitivemeans for establishing a specific diagnosis, and sequenceanalysis of all of the coding exons of SFTPB, ABCA3, and
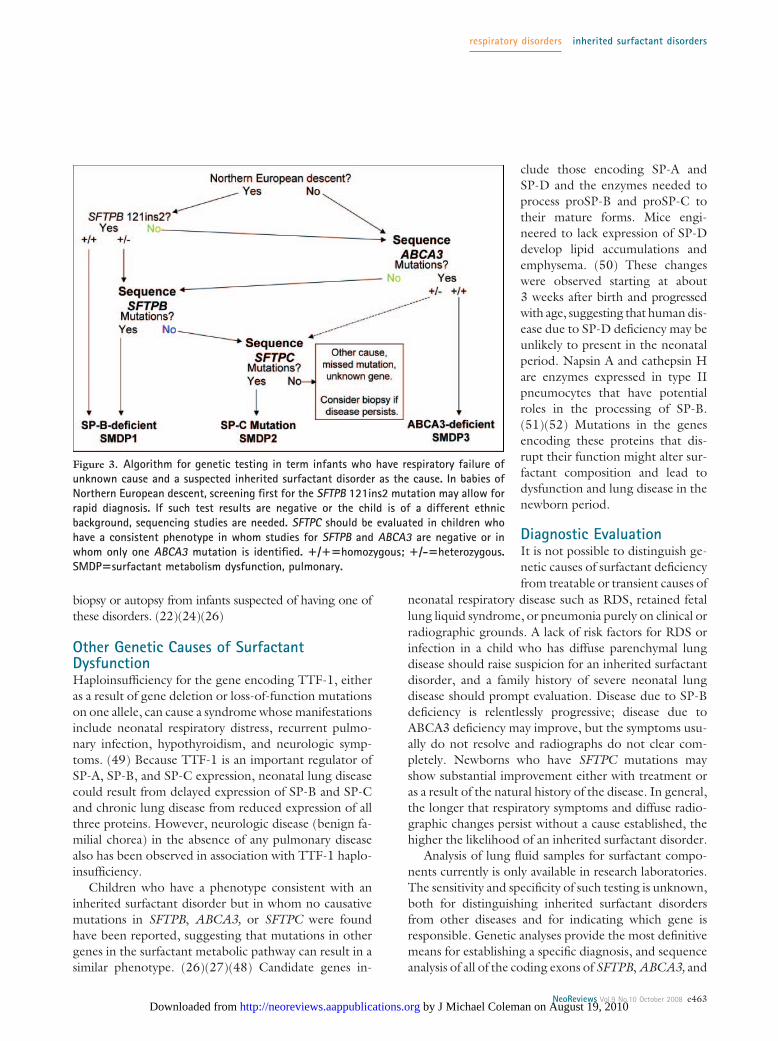
Figure 3. Algorithm for genetic testing in term infants who have respiratory failure ofunknown cause and a suspected inherited surfactant disorder as the cause. In babies ofNorthern European descent, screening first for the SFTPB 121ins2 mutation may allow forrapid diagnosis. If such test results are negative or the child is of a different ethnicbackground, sequencing studies are needed. SFTPC should be evaluated in children whohave a consistent phenotype in whom studies for SFTPB and ABCA3 are negative or inwhom only one ABCA3 mutation is identified. �/��homozygous; �/-�heterozygous.SMDP�surfactant metabolism dysfunction, pulmonary.
respiratory disorders inherited surfactant disorders
NeoReviews Vol.9 No.10 October 2008 e463 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

SFTPC is available through certified diagnostic laborato-ries in the United Staters and Europe. A positive resultmay obviate the need for lung biopsy. Limitations togenetic testing include cost and long turnaround times incritically ill or rapidly deteriorating infants for whom atimely diagnosis is needed for management decisions.The interpretation of genetic studies also may be diffi-cult, particularly when rare missense variants not previ-ously known to be associated with lung disease are found,or if an SFTPB or ABCA3 mutation is identified on onlyone allele.
Although genetic testing is not inexpensive (currentlyapproximately United States $4,000 for all three genes),its costs, both in dollars as well as risks to the patient,should be kept in perspective relative to those of per-forming a lung biopsy and of prolonged intensive care.A sequential approach to genetic studies may be reason-able, screening first for the SFTPB 121ins2 mutation inbabies of Northern European descent, given its preva-lence in this subpopulation, followed by sequence anal-ysis for ABCA3 and SFTPC mutations (Fig. 3). If resultsof such studies are negative and the index of suspicionremains high for a surfactant metabolic disorder, studiesfor SFTPC mutations can be obtained. Children whopresent with lung disease after the neonatal periodshould be evaluated initially for SFTPC mutations andsubsequently for ABCA3 mutations if initial study resultsare unrevealing. SP-B deficiency is very unlikely in chil-dren presenting beyond the neonatal period, and testingfor SFTPB mutations is unlikely to be revealing and notcost-effective in older children, with very rare exceptions.Finally, in cases where results of genetic studies areunrevealing or ambiguous or when a more immediatediagnosis is needed, lung biopsy may be indicated.Guidelines for the handling and processing of such tissuehave been published. (53) In addition to routine histo-
logic studies, tissue should be prepared for electronmicroscopy.
SummaryInherited surfactant disorders are rare but importantcauses of neonatal mortality and morbidity. Considerableclinical overlap exists among the three known single-gene disorders, with the spectrum of disease rangingfrom severe neonatal respiratory failure to chronic respi-ratory symptoms in older children and adults; salientfeatures are summarized in the Table. These disordershave provided insights into normal surfactant metabo-lism and indicated that these genes may be involved inmore common lung diseases, such as RDS and broncho-pulmonary dysplasia. Mutations in genes encoding otherproteins important in surfactant function and metabo-lism may result in similar disease pictures.
ACKNOWLEDGMENTS. The authors wish to thanktheir collaborators, including Janine Bullard, MD(JHU); Timothy Weaver, PhD, and Jeffrey Whitsett,MD (Cincinnati Children’s Hospital); Aaron Hamvas,MD, and F. Sessions Cole, MD (Washington Univer-sity); and Michael Dean, PhD (NCI-Frederick).
References1. Kuroki Y, Takahashi M, Nishitani C. Pulmonary collectins ininnate immunity of the lung. Cell Microbiol. 2007;9:1871–18792. Weaver TE. Synthesis, processing and secretion of surfactantproteins B and C. Biochim Biophys Acta. 1998;1408:173–1793. Weaver TE, Conkright JJ. Function of surfactant proteins B andC. Annu Rev Physiol. 2001;63:555–5784. Bohinski RJ, Di Lauro R, Whitsett JA. The lung-specific surfac-tant protein B gene promoter is a target for thyroid transcriptionfactor 1 and hepatocyte nuclear factor 3, indicating common factorsfor organ-specific gene expression along the foregut axis. Mol CellBiol. 1994;14:5671–5681
Table. Inherited Surfactant Deficiency DisordersOMIM SMDP1 #265120 SMDP2 #610913 SMDP3 #610921
Locus SFTPB SFTPC ABCA3Chromosomal location 2p12-p11.2 8p21 16p13.3Protein SP-B SP-C ABCA3Inheritance Autosomal recessive Autosomal dominant or sporadic Autosomal recessiveMechanism Loss-of-function Dominant negative or toxic gain-of-function Loss-of-functionAge of onset Neonatal Infancy to adult > Neonatal Neonatal > ChildhoodClinical Syndrome RDS ILD > RDS RDS or ILDOutcome Fatal without transplant Variable Severe variable
ILD�interstitial lung disease, OMIM�Online Mendelian Inheritance in Man, www.ncbi.nlm.nih.gov/sites/entrez?db�OMIM, RDS�respiratory distresssyndrome, SMDP�surfactant metabolism dysfunction, pulmonary
respiratory disorders inherited surfactant disorders
e464 NeoReviews Vol.9 No.10 October 2008 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

5. Steagall WK, Lin JP, Moss J. The C/A(-18) polymorphism inthe surfactant protein B gene influences transcription and proteinlevels of surfactant protein B. Am J Physiol Lung Cell Mol Physiol.2007;292:L448–L4536. Wang G, Christensen ND, Wigdahl B, Guttentag SH, Floros J.Differences in N-linked glycosylation between human surfactantprotein-B variants of the C or T allele at the single-nucleotidepolymorphism at position 1580: implications for disease. Biochem J.2003;369:179–1847. Hallman M, Haataja R. Genetic basis of respiratory distresssyndrome. Front Biosci. 2007;12:2670–26828. Hamvas A, Wegner DJ, Trusgnich MA, et al. Genetic variantcharacterization in intron 4 of the surfactant protein B gene. HumMutat. 2005;26:494–4959. Nogee LM, de Mello DE, Dehner LP, Colten HR. Brief report:deficiency of pulmonary surfactant protein B in congenital alveolarproteinosis. N Engl J Med. 1993;328:406–41010. Nogee LM. Alterations in SP-B and SP-C expression in neo-natal lung disease. Annu Rev Physiol. 2004;66:601–62311. Nogee LM, Wert SE, Proffit SA, Hull WM, Whitsett JA. Allelicheterogeneity in hereditary surfactant protein B (SP-B) deficiency.Am J Respir Crit Care Med. 2000;161:973–98112. Hamvas A, Trusgnich M, Brice H, et al. Population-basedscreening for rare mutations: high-throughput DNA extraction andmolecular amplification from Guthrie cards. Pediatr Res. 2001;50:666–66813. Tredano M, Cooper DN, Stuhrmann M, et al. Origin of theprevalent SFTPB indel g. 1549C � GAA (121ins2) mutationcausing surfactant protein B (SP-B) deficiency. Am J Med Genet A.2006;140:62–6914. Tredano M, Griese M, de Blic J, et al. Analysis of 40 sporadic orfamilial neonatal and pediatric cases with severe unexplained respi-ratory distress: relationship to SFTPB. Am J Med Genet A. 2003;119:324–33915. Wegner DJ, Hertzberg T, Heins HB, et al. A major deletion inthe surfactant protein-B gene causing lethal respiratory distress.Acta Paediatr. 2007;96:516–52016. Ballard PL, Nogee LM, Beers MF, et al. Partial deficiency ofsurfactant protein B in an infant with chronic lung disease. Pediat-rics. 1995;96:1046–205217. Dunbar AE 3rd, Wert SE, Ikegami M, et al. Prolonged survivalin hereditary surfactant protein B (SP-B) deficiency associated witha novel splicing mutation. Pediatr Res. 2000;48:275–78218. Klein JM, Thompson MW, Snyder JM, et al. Transient surfac-tant protein B deficiency in a term infant with severe respiratoryfailure. J Pediatr. 1998;132:244–24819. Melton KR, Nesslein LL, Ikegami M, et al. SP-B deficiencycauses respiratory failure in adult mice. Am J Physiol Lung Cell MolPhysiol. 2003;285:L543–L54920. Beers MF, Hamvas A, Moxley MA, et al. Pulmonary surfactantmetabolism in infants lacking surfactant protein B. Am J Respir CellMol Biol. 2000;22:380–39121. Li J, Ikegami M, Na CL, et al. N-terminally extended surfac-tant protein (SP) C isolated from SP-B-deficient children has re-duced surface activity and inhibited lipopolysaccharide binding.Biochemistry. 2004;43:3891–389822. Edwards V, Cutz E, Viero S, Moore AM, Nogee L. Ultrastruc-ture of lamellar bodies in congenital surfactant deficiency. Ultra-struct Pathol. 2005;29:503–50923. Mulugeta S, Gray JM, Notarfrancesco KL, et al. Identification
of LBM180, a lamellar body limiting membrane protein of alveolartype II cells, as the ABC transporter protein ABCA3. J Biol Chem.2002;277:22147–2215524. Brasch F, Schimanski S, Muhlfeld C, et al. Alteration of thepulmonary surfactant system in full-term infants with hereditaryABCA3 deficiency. Am J Respir Crit Care Med. 2006;174:571–58025. Bullard JE, Wert SE, Whitsett JA, Dean M, Nogee LM.ABCA3 mutations associated with pediatric interstitial lung disease.Am J Respir Crit Care Med. 2005;172:1026–103126. Shulenin S, Nogee LM, Annilo T, Wert SE, Whitsett JA, DeanM. ABCA3 gene mutations in newborns with fatal surfactant defi-ciency. N Engl J Med. 2004;350:1296–130327. Somaschini M, Nogee LM, Sassi I, et al. Unexplained neonatalrespiratory distress due to congenital surfactant deficiency. J Pedi-atr. 2007;150:649–65328. Cheong N, Madesh M, Gonzales LW, et al. Functional andtrafficking defects in ABCA3 mutants associated with respiratorydistress syndrome. J Biol Chem. 2006;281:9791–980029. Matsumura Y, Ban N, Ueda K, Inagaki N. Characterizationand classification of ATP-binding cassette transporter ABCA3 mu-tants in fatal surfactant deficiency. J Biol Chem. 2006;281:34503–3451430. Yoshida I, Ban N, Inagaki N. Expression of ABCA3, a causativegene for fatal surfactant deficiency, is up-regulated by glucocorti-coids in lung alveolar type II cells. Biochem Biophys Res Commun.2004;323:547–55531. Garmany TH, Moxley MA, White FV, et al. Surfactant com-position and function in patients with ABCA3 mutations. PediatrRes. 2006;59:801–80532. Cheong N, Zhang H, Madesh M, et al. ABCA3 is critical forlamellar body biogenesis in vivo. J Biol Chem. 2007;282:23811–2381733. Garmany TH, Wambach JA, Heins HB, et al. Population anddisease-based prevalence of the common mutations associated withsurfactant deficiency. Pediatr Res. 2008;63:645–64934. Karjalainen MK, Haataja R, Hallman M. Haplotype analysis ofABCA3: association with respiratory distress in very prematureinfants. Ann Med. 2008;40:56–6535. Nogee LM, Dunbar AE 3rd, Wert SE, Askin F, Hamvas A,Whitsett JA. A mutation in the surfactant protein C gene associatedwith familial interstitial lung disease. N Engl J Med. 2001;344:573–57936. Glasser SW, Detmer EA, Ikegami M, Na CL, Stahlman MT,Whitsett JA. Pneumonitis and emphysema in sp-C gene targetedmice. J Biol Chem. 2003;278:14291–1429837. Nogee LM. Genetics of pediatric interstitial lung disease. CurrOpin Pediatr. 2006;18:287–29238. Brasch F, Griese M, Tredano M, et al. Interstitial lung diseasein a baby with a de novo mutation in the SFTPC gene. Eur RespirJ. 2004;24:30–3939. Rosen DM, Waltz DA. Hydroxychloroquine and surfactantprotein C deficiency. N Engl J Med. 2005;352:207–20840. Cameron HS, Somaschini M, Carrera P, et al. A commonmutation in the surfactant protein C gene associated with lungdisease. J Pediatr. 2005;146:370–37541. Beers MF, Mulugeta S. Surfactant protein C biosynthesis andits emerging role in conformational lung disease. Annu Rev Physiol.2005;67:663–696
respiratory disorders inherited surfactant disorders
NeoReviews Vol.9 No.10 October 2008 e465 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

42. Bridges JP, Wert SE, Nogee LM, Weaver TE. Expression of ahuman surfactant protein C mutation associated with interstitiallung disease disrupts lung development in transgenic mice. J BiolChem. 2003;278:52739–5274643. Mulugeta S, Nguyen V, Russo SJ, Muniswamy M, Beers MF.A surfactant protein C precursor protein BRICHOS domain mutationcauses endoplasmic reticulum stress, proteasome dysfunction, andcaspase 3 activation. Am J Respir Cell Mol Biol. 2005;32:521–53044. Wang WJ, Mulugeta S, Russo SJ, Beers MF. Deletion of exon4 from human surfactant protein C results in aggresome formationand generation of a dominant negative. J Cell Sci. 2003;116:683–69245. Bullard JE, Nogee LM. Heterozygosity for ABCA3 mutationsmodifies the severity of lung disease associated with a surfactantprotein C gene (SFTPC) mutation. Pediatr Res. 2007;62:176–17946. Tredano M, Griese M, Brasch F, et al. Mutation of SFTPC ininfantile pulmonary alveolar proteinosis with or without fibrosinglung disease. Am J Med Genet A. 2004;126:18–2647. Trapnell BC, Whitsett JA, Nakata K. Pulmonary alveolar pro-teinosis. N Engl J Med. 2003;349:2527–253948. Deutsch GH, Young LR, Deterding RR, et al. Diffuse lung
disease in young children: application of a novel classificationscheme. Am J Respir Crit Care Med. 2007;176:1120–112849. Pohlenz J, Dumitrescu A, Zundel D, et al. Partial deficiencyof thyroid transcription factor 1 produces predominantly neuro-logical defects in humans and mice. J Clin Invest. 2002;109:469–47350. Yoshida M, Whitsett JA. Alveolar macrophages and emphy-sema in surfactant protein-D-deficient mice. Respirology. 2006;11(suppl):S37–S4051. Brasch F, Ochs M, Kahne T, et al. Involvement of napsin A inthe C- and N-terminal processing of surfactant protein B in type-IIpneumocytes of the human lung. J Biol Chem. 2003;278:49006–4901452. Ueno T, Linder S, Na CL, Rice WR, Johansson J, Weaver TE.Processing of pulmonary surfactant protein B by napsin and cathep-sin H. J Biol Chem. 2004;279:16178–1618453. Langston C, Patterson K, Dishop MK, et al. A protocol for thehandling of tissue obtained by operative lung biopsy: recommen-dations of the chILD pathology co-operative group. Pediatr DevPathol. 2006;9:173–180
respiratory disorders inherited surfactant disorders
e466 NeoReviews Vol.9 No.10 October 2008 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

NeoReviews Quiz
5. Pulmonary surfactant is a mixture of lipids and specific proteins that reduces surface tension at the air-liquid interface and prevents end-expiratory atelectasis of the lung. Of the following, the principalconstituent of surfactant needed for lowering surface tension is:
A. Cholesterol.B. Phosphatidylcholine.C. Phosphatidylethanolamine.D. Phosphatidylglycerol.E. Sphingomyelin.
6. Surfactant protein B (SP-B) is a low-molecular weight, hydrophobic protein that facilitates the adsorptionof surfactant lipids to the air-liquid interface after secretion, essential for surface tension-loweringproperties of the surfactant. Genetic lung disease from SP-B deficiency is a rare, autosomal recessivedisorder that results in progressive hypoxemic respiratory failure and death by 3 to 6 months of age. Of thefollowing, the most common genetic mutation related to the SP-B gene in infants of Northern Europeandescent involves:
A. Frameshift mutation (121ins2).B. Nucleotide tandem repeats in intron 4.C. Polymorphism in exon 4.D. Polymorphism in promoter region.E. Thyroid transcription factor-1.
7. Adenosine triphosphate (ATP)-binding cassette (ABC) transporters are transmembrane proteins thathydrolyze ATP to move substrates across biologic membranes. Mutations in ABC genes are frequent causesof human genetic diseases. Of the following, the deficiency of ABCA3 protein is most likely to cause:
A. Cystic fibrosis.B. Hypothyroidism.C. Interstitial lung disease.D. Retinal degeneration.E. Tangier disease.
8. Surfactant protein C (SP-C) is a low-molecular weight, hydrophobic protein, derived by proteolysis of itsprecursor, proSP-C, the primary translational product of a gene located on chromosome 8. SP-C genemutations can cause genetic lung disease. Of the following, the most accurate statement regarding geneticlung disease from SP-C gene mutations is that:
A. Lung histopathology reveals hypoplasia of type II alveolar epithelial cells.B. Most familial cases exhibit an autosomal recessive pattern of inheritance.C. Most mutations occur in the carboxy-terminal portion of proSP-C.D. Respiratory symptoms typically manifest in the perinatal period.E. Severity of lung disease can be predicted by specific SP-C gene mutations.
respiratory disorders inherited surfactant disorders
NeoReviews Vol.9 No.10 October 2008 e467 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

DOI: 10.1542/neo.9-10-e458 2008;9;e458-e467 NeoReviews
W. Adam Gower, Susan E. Wert and Lawrence M. Nogee Inherited Surfactant Disorders
& ServicesUpdated Information
s;9/10/e458http://neoreviews.aappublications.org/cgi/content/full/neoreviewincluding high-resolution figures, can be found at:
Permissions & Licensing
http://neoreviews.aappublications.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://neoreviews.aappublications.org/misc/reprints.shtml
Information about ordering reprints can be found online:
by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from