Inheritance of fragile X to - Journal of Medical Genetics · as well as the Sherman paradox, could...
8
7 Med Genet 1992; 29: 794-801 Inheritance of the fragile X syndrome: size of the fragile X premutation is a major determinant of the transition to full mutation Dominique Heitz, Didier Devys, Georges Imbert, Christine Kretz, Jean-Louis Mandel Abstract The fragile X mental retardation syn- drome is caused by unstable expansion of a CGG repeat. Two main types of muta- tion have been categorised. Clinical expression is associated with the pres- ence of the full mutation, while subjects who carry only a premutation do not have mental retardation. Premutations have a high risk of transition to full mu- tation when transmitted by a female. We have used direct detection of the muta- tions to characterise large families who illustrate the wide variation in pene- trance which has been observed in dif- ferent sibships (a feature often called the Sherman paradox). A family originally found to show tight genetic linkage between the factor 9 gene and the fragile X locus was reanalysed, confirming the original genotype assignments and the observed linkage. The size of premu- tations was measured by Southern blot- ting and by using a PCR based test in 102 carrier mothers and this was correlated with the type of mutation found in their offspring. The risk of transition to full mutation was found to be very low for premutations with a size increase (A) of about 100 bp, increasing up to 100% when the size of premutation was larger than about 200 bp, even after taking into ac- count (at least partially) ascertainment bias. These results confirm and extend those reported by Fu etal(1991) and Yu ct a) (1992) and explain the Sherman para- dox. The low risk of transition to full mutation of small premutations leads to the prediction that carriers of such alleles may be more frequent in the population than was previously expected for fragile X carriers, and we have indeed observed a premutation in a man with no a priori risk. Possible mechanisms that could account for the sex biased expan- sion of the CGG repeat are discussed in relation to the absence of such bias in expansion at the myotonic dystrophy locus. (J Med Genet 1992;29:794-801) The fragile X syndrome is the most common inherited cause of mental retardation.' Segre- gation studies have previously shown the unique characteristics of its mode of inherit- ance.2 It was estimated that 20% of males carrying the mutation have no phenotypic expression; these were called normal transmit- ting males. Among carrier females, 55% were found to express the fragile site, and one third to have mental impairment in addition. How- ever, daughters of normal transmitting males appeared to have little or no phenotypic expression. Even more curious was the obser- vation that penetrance was low (- 18%) in brothers of NTMs, and high (> 80%) in brothers of affected males, a phenomenon often called the Sherman paradox. This led to a clustering of NTMs in certain sibships and of affected patients in others, even within the same family. It has recently been shown that the fragile X mental retardation syndrome is caused by elongation of a small target DNA fragment, containing a repeat of the trinucleo- tide CGG -5 located in a 5' exon of the FMR-1 gene6 in Xq27.3. We have proposed that muta- tions can be classified as two main types, according to the size of the elongation (A), its stability in somatic cells, and the methylation status of nearby restriction sites.37 Premu- tations are characterised by an elongation of 70 to about 500 bp, show little or no somatic heterogeneity, and the nearby restriction sites are not methylated in males or on the active X chromosomes of females (but are methylated on the inactive X chromosome). Premutations do not appear to cause mental retardation, and their carriers show very low or absent expres- sion of the fragile site.7 They are typically found in normal transmitting males and in their daughters (although some daughters of a carrier female may also have a premutation). The full fragile X mutation is characterised by an elongation (A) of more than 600 to 700 bp, often shows important somatic heterogeneity, and nearby sites are methylated on both active and inactive X chromosomes. In a study of 63 fragile X families, all males and 53% of females carrying a full mutation were found to have mental retardation.7 Al- though the distinction between premutation and full mutation appears clear at the cellular level, we have found that about 15% of sub- jects who have a full mutation are in fact mosaics and also have cells with a premu- tation.7 Such mosaic subjects may be more mildly affected than persons with a full muta- tion only. This is supported by the finding that FMR-1 mRNA is present in leucocytes of mosaic patients but not of patients with fully methylated mutations.8 The transition from premutation to full mu- tation (or to mosaic status) appears to occur LGME/CNRS, INSERM U184, Institut de Chimie Biologique, 11 rue Humann, 67085 Strasbourg Cedex, France. D Heitz D Devys G Imbert C Kretz J-L Mandel Correspondence to Dr Mandel. Received 8 June 1992. Accepted 17 June 1992. This paper is dedicated to the memory of Isabelle Oberle. 794 on April 7, 2020 by guest. Protected by copyright. http://jmg.bmj.com/ J Med Genet: first published as 10.1136/jmg.29.11.794 on 1 November 1992. Downloaded from
Transcript of Inheritance of fragile X to - Journal of Medical Genetics · as well as the Sherman paradox, could...

7 Med Genet 1992; 29: 794-801
Inheritance of the fragile X syndrome: size ofthe fragile X premutation is a major determinantof the transition to full mutation
Dominique Heitz, Didier Devys, Georges Imbert, Christine Kretz,Jean-Louis Mandel
AbstractThe fragile X mental retardation syn-drome is caused by unstable expansion ofa CGG repeat. Two main types of muta-tion have been categorised. Clinicalexpression is associated with the pres-ence of the full mutation, while subjectswho carry only a premutation do nothave mental retardation. Premutationshave a high risk of transition to full mu-tation when transmitted by a female. Wehave used direct detection of the muta-tions to characterise large families whoillustrate the wide variation in pene-trance which has been observed in dif-ferent sibships (a feature often called theSherman paradox). A family originallyfound to show tight genetic linkagebetween the factor 9 gene and the fragileX locus was reanalysed, confirming theoriginal genotype assignments and theobserved linkage. The size of premu-tations was measured by Southern blot-ting and by using a PCR based test in 102carrier mothers and this was correlatedwith the type of mutation found in theiroffspring. The risk of transition to fullmutation was found to be very low forpremutations with a size increase (A) ofabout 100 bp, increasing up to 100% whenthe size of premutation was larger thanabout 200 bp, even after taking into ac-count (at least partially) ascertainmentbias. These results confirm and extendthose reported by Fu etal(1991) and Yu cta) (1992) and explain the Sherman para-dox. The low risk of transition to fullmutation of small premutations leads tothe prediction that carriers of suchalleles may be more frequent in thepopulation than was previously expectedfor fragile X carriers, and we have indeedobserved a premutation in a man with noa priori risk. Possible mechanisms thatcould account for the sex biased expan-sion of the CGG repeat are discussed inrelation to the absence of such bias inexpansion at the myotonic dystrophylocus.(J Med Genet 1992;29:794-801)
The fragile X syndrome is the most commoninherited cause of mental retardation.' Segre-gation studies have previously shown theunique characteristics of its mode of inherit-ance.2 It was estimated that 20% of males
carrying the mutation have no phenotypicexpression; these were called normal transmit-ting males. Among carrier females, 55% werefound to express the fragile site, and one thirdto have mental impairment in addition. How-ever, daughters of normal transmitting malesappeared to have little or no phenotypicexpression. Even more curious was the obser-vation that penetrance was low (- 18%) inbrothers of NTMs, and high (> 80%) inbrothers of affected males, a phenomenonoften called the Sherman paradox. This led toa clustering of NTMs in certain sibships andof affected patients in others, even within thesame family. It has recently been shown thatthe fragile X mental retardation syndrome iscaused by elongation of a small target DNAfragment, containing a repeat of the trinucleo-tide CGG -5 located in a 5' exon of the FMR-1gene6 in Xq27.3. We have proposed that muta-tions can be classified as two main types,according to the size of the elongation (A), itsstability in somatic cells, and the methylationstatus of nearby restriction sites.37 Premu-tations are characterised by an elongation of 70to about 500 bp, show little or no somaticheterogeneity, and the nearby restriction sitesare not methylated in males or on the active Xchromosomes of females (but are methylatedon the inactive X chromosome). Premutationsdo not appear to cause mental retardation, andtheir carriers show very low or absent expres-sion of the fragile site.7 They are typicallyfound in normal transmitting males and intheir daughters (although some daughters of acarrier female may also have a premutation).The full fragile X mutation is characterised byan elongation (A) of more than 600 to 700 bp,often shows important somatic heterogeneity,and nearby sites are methylated on both activeand inactive X chromosomes.
In a study of 63 fragile X families, all malesand 53% of females carrying a full mutationwere found to have mental retardation.7 Al-though the distinction between premutationand full mutation appears clear at the cellularlevel, we have found that about 15% of sub-jects who have a full mutation are in factmosaics and also have cells with a premu-tation.7 Such mosaic subjects may be moremildly affected than persons with a full muta-tion only. This is supported by the finding thatFMR-1 mRNA is present in leucocytes ofmosaic patients but not of patients with fullymethylated mutations.8The transition from premutation to full mu-
tation (or to mosaic status) appears to occur
LGME/CNRS,INSERM U184,Institut de ChimieBiologique, 11 rueHumann, 67085Strasbourg Cedex,France.D HeitzD DevysG ImbertC KretzJ-L Mandel
Correspondence toDr Mandel.Received 8 June 1992.Accepted 17 June 1992.
This paper is dedicated tothe memory of IsabelleOberle.
794
on April 7, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.11.794 on 1 Novem
ber 1992. Dow
nloaded from

Inheritance of the fragile X syndrome
only after transmission through the femalegermline, which fits with the pattern of in-heritance of phenotypic traits. In previousstudies37 we found an 80% overall risk oftransition. However, this was uncorrected forascertainment biases. A more accurate study ofthis risk and of the parameters affecting it is ofimportance both for genetic counselling pur-poses and as a test of the main hypothesesproposed to account for fragile X inheritance,and in particular for the Sherman paradox.Laird9 proposed that the fragile X mutationlocally blocks the reactivation, before oogene-sis, of a previously inactive X, and the failureto erase the imprint specific to an inactive Xchromosome (most likely DNA methylation)would account for the transition from a muta-tion with no phenotypic consequence (such asthat found in normal transmitting males or intheir daughters) to a mutation causing disease.Laird's hypothesis predicted that the observedprobability of such a transition should be only50% and it was proposed that the higher value,as well as the Sherman paradox, could beaccounted for by ascertainment biases, and bya small number of oogonial precursors at thetime of X inactivation.'0 The finding of abnor-mal methylation linked to the mutation caus-ing disease3 "'i3 appeared to support Laird'shypothesis. When the true nature of the muta-tion was shown, we suggested as an alternativepossibility that the sequence of the premu-tation could dictate the risk of transition to thefull mutation.3 Results were first presented bySutherland et al at the 5th X Linked MentalRetardation Workshop (August 1991) suggest-ing a strong positive correlation between thesize of the premutation in the female and therisk of a full mutation in the offspring.'4 Simi-lar results were reported by Fu er al'5 whilethis work was in preparation. We present herethe molecular findings in families which illus-trate well the Sherman paradox. Our resultsconfirm and extend those of Fu et al'5 and Yuet al,'4 as they are based on a larger populationand have been, at least in part, corrected forascertainment biases. The finding that smallpremutations have a low risk of transition tofull mutation suggests that carriers of premu-tations may be more frequent in the populationthan previously expected, and we have indeeddetected one in a person with no a priori risk.
Material and methodsThe families were those analysed previously7with some new families included. Mutationswere analysed in EcoRI + EagI digests7 or, formore accurate sizing, in PstI digests8 separatedon 1-2% agarose gels and hybridised to probeStB12XX.'6 The A values are given by refer-ence to a base level corresponding to the mostcommon normal allele (29 repeats).PCR across the CGG repeats was performed
in a total volume of 50 jl with about 100 ng ofDNA, in the presence of 10 mmol/l Tris-HClpH 8-3, 50 mmol/l KC1, 20 mmol/l MgCl2,100 gmol/l dATP, 100 mmol/l dCTP,100 jmol/l dTTP, 100 pmol/l 7-deaza-dGTP,and 2 5 U of Ampli- Taq DNA polymerase.
Primers PF199: 5'ATCTTCTCTTCAGCC-CTGCTAGCG3' and PE138: 5'GCATG-AATTCGAGCATTTGATTTCCCACGC-CAC3' were added at a final concentration of0-5 jmol/l. These primers allow amplificationof a 600 bp fragment for a normal allele with 29CGG repeats. The reactions were heated at96°C for five minutes, followed by 35 cycles of0-5 minutes denaturation at 96°C, one minuteannealing at 60°C, four minutes of elongationat 72°C with a two second extention at eachcycle, and a final elongation of 10 minutes at72°C. Addition of 2% deionised formamideusually helped the amplification of DNA thatwas refractory to PCR across this region. A5 gl aliquot of the PCR reaction was loaded ona 2% agarose gel in buffer containing 5 to 10 ngof the 0 9 kb EagI-PstI fragment correspond-ing to the StB12.5 probe, and which serves asinternal marker for accurate size determi-nation. Another size marker (MspI digest ofpBR322) was added separately to each gel.After migration, the gel was treated for 20minutes in 1-5 mol/l NaCl, 0-5 mol/l NaOH,neutralised in 1-5 NaCl, 0-5 mol/l Tris-HClpH 7 2, 1 mmol/l EDTA, and blotted ontoHybond N + for one or two hours. The mem-brane was hybridised for six hours or more at42°C in the presence of 50% formamide toprobe StB12.5 (labelled by random priming),showing the PCR products and the 0 9kbreference band. Small premutations were alsosized on sequencing gels after PCR in thepresence of 32P-dCTP, as described by Fu etal.'5
ResultsTHE CLUSTERING PHENOMENON EXAMINED ATTHE DNA LEVELWe have systematically analysed fragile Xfamilies for the type of mutation, using thestrategy described by Rousseau et al.7 Inseveral large families, the Sherman paradoxwas well illustrated by the clustering of pre-mutations in some sibships and the clusteringof full mutations in others. In family A awoman with a rather small premutation(A= 120 bp), the sister of an affected male(with a full mutation), had seven normal chil-dren who inherited the premutation (with arange of A = 130 to 550 bp), and none with acharacteristic full mutation (figs 1 and 2). Itcan be seen that II-7 (lane 5) was one of therare cases where the diagnosis of premutationwas based solely on mutation size (A=550)and not on the presence of an unmethylatedpremutation, which is in general seen in EcoRI+ EagI digests. In this woman, the pattern ofX inactivation was extremely biased with verylittle of the 5-2 kb band indicative of the nor-mal inactive X. This could well account for thefailure to see the small expected amount ofmutated fragment on the active X chromosome(especially since unmethylated premutationsin this range tend to give fuzzy bands owing tosome degree of somatic instability). However,it cannot be eliminated that she had in fact asmall full mutation, as a homogeneous patternwith preferential inactivation of the mutated X
795
on April 7, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.11.794 on 1 Novem
ber 1992. Dow
nloaded from

Heitz, Devys, Imbert, Kretz, Mandel
Family A
1 2 3
DX: Nor Pre FullA(kb): 0-12
62 t3 L4 LS [I6 ( 7 8
Pre Pre Pre Pre Pre Pre Nor
0 20 013 0.18 0-22 0-12 0-55
11
III
DX:A(kb):
Nor Full1 7
Nor
DX: PreA(kb): 0-21
01
DX: FullA(kb): 1-1-2-0
02 03 04 5 06 07 08Pre Pre Pre Pre Pre Pre Pre0-17 0-21 0-20 0-24 0-17 0-15 0.23
t2 t3 #4 6W ZYL 8 0Full 'Me Mos' Full Nor Nor Nor Nor 'Me Mos' Nor
1-3 1.0-2-3 0-6-2 0 1.0
Figure I Pedigrees showing clustering ofpremutation within a sibship. Carriers of a premutation are indicated by adot. Half filled symbols correspond to cytogenetic expression on the right (hatched I to 3% fragile site, filled > 4%),and mental retardation on the left (hatched: mild MR, filled: moderate or severe MR). The symbol in III14 (familyA) corresponds to a prenatal diagnosis. The molecular diagnosis (DX) is indicated as normal (Nor), premutation(Pre), full mutation (Full), or mosaic (Mos or Me Mos, the latter corresponding to presence of partiallyunmethylated bands in the A = 0 5 to 1 kb range). The size increase over the normal size is represented by the Avalue (in kb).
-1--E! :
1
4 567J 8 9 10 11
;...I-1 2 3
-F
12
5 2 _
do ~ ~ ~- 2-8 -_ a
Figure 2 Analysis offamily A on a EcoRI+ EagI digest. Normalfragm2 8 kb (unmethylated on the active X) and 5-2 kb (methylated on the inaPremutations are best seen over the 2-8 kb band. The carrier female in lanfig 1A) does not show the four band pattern typical of premutations, owininactivation (the 5 2 kb band is only faintly visible) and may represent aborderline case between premutation and full mutation. Subjects in lanes Iunrelated to family A. A partial digest fragment is indicated by an asteris
is not infrequent in adult carriers of a fullmutation.17 This woman twice passed a full
r; mutation to her offspring (and no premu-tation). Another example of such clusteringwas that of family B (fig 1) with four normal
transmitting males known from pedigree or
DNA analysis. A fifth brother had a A of60 bp (tested by the more accurate PCR test)
13 14 15 (fig 3) and was later verified to correspond to48 repeats'5 at the limit between premutationand normal. He was tested for two microsatel-lite markers within 150kb of the fragile Xlocus (DXS458 and FRAXAC2)618 and wasfound to be identical to his NTM brothers,suggesting that he had in fact inherited thepremutated allele from his dead mother (unlessshe was homozygous for both polymorphicmarkers). Eight daughters in generation II allhad a premutation (in the A= 150 to 250 bprange); in the next generation, five childrenhad inherited a full mutation (in two cases with
'ents are the smallest fragment partially unmethylated)ctive X). and none had a premutation. One child (III 5)te 5 (II17 in with mild mental retardation was normal at theg to biased fragile X locus. The clustering was not always
and 8 are absolute, however, as shown by family C (figsk in lane 4. 4), where two sibships showed a mixture of
1
DX: PreA(kb): 0.14
Nr9 r10
Nor Nor
L1 2 d3 44
Family B
DX:Av(kb):
Full0-8
11
III
796
on April 7, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.11.794 on 1 Novem
ber 1992. Dow
nloaded from

Inheritance of the fragile X syndrome
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
- am_ _ - 0 9 kb
.-, .4-0*+6kb
Figure 3 PCR based assay for detection and sizing of premutations. The assay was performed as described inMaterial and methods. The 0 9 kb band corresponds to the internal control fragment loaded with the PCR product.The 0-6 kb fragment corresponds to the amplified product for a common allele with - 30 CGG repeats. Lanes 1 to 3correspond to a branch of a fragile Xfamily who had no a priori risk of having a mutation. The abnormal band hasa A of 80 to 90 bp (54 and 58 repeats respectively as measured on sequencing gels). Lanes 4 to 7 correspond to partof a family also shown in fig 7B. Lanes 9, 17, 19, and 23 correspond to subjects in family B (fig 1). In lane 17, themale Il had a - 60 bp A (48 repeats measured on sequencing gels) and may correspond to a high normal allele or asmall premutation (see text). Subjects in lanes 1, 5, and 20 have only normal alleles.
Family C
DX: (- W+ Nor Pre Nr PreA(kb): 0-1 6 0-11
1 2 * 3 *4 5 6 7 8; 9 10 ( )11 [12 *13
DX: Pre Nor Full Mos Nor Full Nor Nor Pre Nor Pre Pre FullA(kb): 0-42 2-5 0-25-3-1 1.5 0-20 0-25 0.35 1-0
DX: Nor Full NorA(kb): 2-3
Figure 4 A pedigree showing partial clustering of premutations. Same symbols as in fig 1. A fragile X site had beenobserved in 1% of cells in I 1 0, who was later found to be normal.
subjects with a premutation or a full muta-tion (or a mosaic pattern). It can be noted inthis family that the woman who had threechildren with a premutation and one with a fullmutation had a small (A= 110 bp) premu-tation. II 10, who was originally found to have1% of fragile X site, had inherited a normalhaplotype for flanking RFLPs, and was laterconfirmed to have no fragile X mutation.Finally the family who had originally showncomplete linkage between an RFLP at thecoagulation factor 9 locus and the fragile Xlocus'9 was also reanalysed (fig 5). All the sevendaughters of a normal transmitting male(A = 230 bp) had inherited premutations in theA = 230 to 310 bp range (fig 5B), while in thenext generation direct DNA analysis con-firmed the former genotype assignments, thatis, all the phenotypically normal children hadno mutation and all the 10 affected children,who had inherited the grandpaternal F9 allele,had a full mutation or were mosaics. No DNAwas available for direct mutation analysis forfive chorionic villi samples, but their statuswas deduced either from cytogenetic results(III-18 and III22) or from the F9-DXS52(Stl4) haplotype as they did not show recom-bination between these markers that flank thefragile X locus. It is of interest to note that inthis family there are no recombinants betweenF9 and FraX in 21 meiotic events (or 18 if one
takes only those who have a status establishedby direct DNA analysis or by cytogenetics). Atthe time of the original description there wereonly 15 non-recombinants. This confirms thestriking tight linkage, contrasting with the-20% recombination found between the twoloci in other families'220; the probability ofobserving this by chance is 0.821, about 1 in100. In fact this family was one of the threewhich accounted for most of the heterogeneityof recombination reported by Brown et al.2'
A PCR BASED TEST FOR THE ANALYSIS OFPREMUTATIONSIn order to characterise quickly and accuratelythe size of premutations, we have developed aPCR based test. Primers were chosen thatshould amplify a 600 bp normal fragment (forsubjects with the most frequent allele contain-ing 29 repeats). The extreme GC richness ofthe region (100% for the CGG repeat)prompted us to use 7-deaza-dGTP instead ofdGTP for the PCR reaction.'6 However, undersuch conditions, it is not possible to detect theDNA synthesised by fluorescence in the pres-ence of ethidium bromide. The reaction pro-ducts were thus analysed on agarose gel, blot-ted, and hybridised to a 900 bp probe(StB12.5) that includes the amplified segmentand contains 20 CGG repeats.3 An aliquot of
__ b_o 1 -40a-
do I m g pip_m _wio40
797
F.
on April 7, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.11.794 on 1 Novem
ber 1992. Dow
nloaded from

Heitz, Devys, Imbert, Kretz, Mandel
A
Family D
II
11FIX:Dx:
iA(kb):
III d
FIX:Dx:
A(kb):
12 2 2 12Nor Full Full Full
2-0 1-5 0-9-2-2 12Mos
0*3-3*
2 1 12 2 1 11 12 1 12 12 2 2 2 2 1 12Mos Nor Full Mos Nor Nor Full (-) (+) Nor Full + (±) Full Nor -
0.5-3-0 2-3 0.2-3.1 0-9-2-6 1-5-3-3 1-6-2-8
0
-c
L~~~
Figure 5 (A) Segregation of the mutation in a family showing complete linkage between the fragile X and the coagulation factor IX gene. Thepedigree offamily D is presented in the upper panel. Symbols are as in fig 1. 1I18 had 5% fragile X site. The alleles at the TaqI RFLP in thecoagulation factor IX gene are indicated.'9 Five prenatal diagnoses had been performed in II 14, 15, 18, 19, and 22 using flanking probes in allcases, and cytogenetic analysis for II118 and 22. No recombination was detected between F9 and DXS52 in these five cases (which were fullyinformative for the markers). A spontaneous abortion occurred in II 14, while pregnancy was terminated in II 15, 18, and 19 because anaffected F9-DXS52 haplotype was found. III-22 who had the normal haplotype was confirmed to be fragile X negative after birth. + or -
corresponds to presence or absence offragile site, ( + ) or ( - ) corresponds to the genotype deducedfrom the F9-DXS52 haplotype. (B) Analysisof premutations in generations I and II. The premutations were analysed in a PstI digest hybridised to probe StB12XX.'6 This probe detects thepolymorphic CGG containing fragment 1060+ 70 bp (6 to 54 repeats) in normal subjects (range indicated by the bracket) and a constant band at1075 bp.
the StB12.5 insert was included in the loadingbuffer to provide an internal control band. Theblotting, hybridisation, and exposure stepscould be considerably shortened compared tostandard genomic blotting and results wereobtained in less than two days from the start ofthe PCR reaction (see Material and methods).While this work was completed, two otherPCR based tests were reported. A direct PCRtest developed by Fu et all5 allows even moreaccurate sizing of premutations on sequencinggels. A hybrid method similar to ours, butusing the CGG repeat itself as probe, was
reported by Pergolizzi et aP2 which also allowsdetection, in most cases, of full mutations.23Our procedure allows accurate sizing with
an estimated precision of 20 bp, that is, sevenCGG repeats (fig 3). This was especially ap-plied to the study of small premutations or
ambiguous cases. We could thus confirm thatan abnormal fragment first observed in EcoRI+ EagI digests in a man with no a priori riskand in his daughter had a size typical of a smallpremutation (A = 80 and A = 90 bp, fig 3, lanes2 and 3 corresponding to 54 and 58 repeatswhen measured as described by Fu et all5). It isalso obvious with this assay that large premu-tations (A> 200 bp) are already somaticallyunstable with a span of -50 bp (fig 3, lanes
10-12, 19, 23). This can also be detected as
fuzzy bands in Southern blots using PstI orEcoRI + EagI digests.
RELATIONSHIP BETWEEN SIZE OF PREMUTATIONIN THE MOTHER AND RISK OF TRANSITION TOFULL MUTATIONA correlation between the size of amplificationin a mother and the risk of inheritance of a
large and somatically unstable mutation in theoffspring has recently been reported by Yu etal'4 and Fu et all5 while our large data set wasbeing analysed. We measured size of premu-tations in mothers using the EcoRI + EagI di-gest described by Rousseau et al7 (fig 2) and inmost cases also in PstI digests5 14 (fig 5B). Themajority of these mothers were also analysed ina PCR assay, which is more accurate for mea-suring small premutations as the normal frag-ment is only 600 bp (compared to 2-8 kb in theEcoRI + EagI digest, and 1 kb in the PstI di-gest (fig 3)). In fact, except for the smallestpremutations, we found that measurement inthe EcoRI + EagI digest gave values in verygood agreement with those obtained with theother assays (as noted previously,24 a A value of200 bp corresponds to a differential migrationof - 5 mm in an EcoRI + EagI digest and
FIX: 1Dx: Nor
A(kb):
B
11
798
"--( .I... -1
- 1,- .. .4-
on April 7, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.11.794 on 1 Novem
ber 1992. Dow
nloaded from

Inheritance of the fragile X syndrome
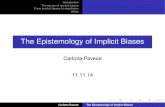
Offspring of mothers with premutations. Mothers have been grouped into classesaccording to the size of their premutation. The number of children with a premutation,full mutation, or who inherited the normal allele (as controlled by direct DNAanalysis) is indicated. Untested children are classified as normal or mentally retarded.In the FM-proband column, one affected proband was removed in each family.
Tested offspring Untested offspringA bpin mothers PM FM FM-proband N N MR
75-125 18 4 2 6 3 0125-175 7 15 9 22 1 1 5175-225 5 64 45 34 16 4225-275 0 33 24 15 2 2275-325 0 18 15 15 1 0325-375 0 2 1 1 1 0375-425 0 1 1 2 0 0425-475 0 5 3 0 1 0475-525 0 3 1 4 0 0
Total 30 145 101 99 35 11
9 mm in a Pst digest). On the basis of bothsize and methylation analysis, we divided off-spring into two classes: those with premutationand those with full mutation (table). All 30children with premutations had mothers witha premutation of A < 225, and for 18 of these,the mother's A was < 125 (in only two of these30 cases did the size of the premutation de-crease). In contrast, in mothers with aA > 225 bp, the transition to full mutation (ormosaic) occurred in all 62 children analysed.However, it was evident that our data sufferedfrom ascertainment bias in favour of childrenwith a full mutation, as indicated by the factthat in the sibships analysed 175 children hadinherited a mutated chromosome and only 99inherited the normal one (ratio 1-77 to 1). Totry to correct for this bias we subtracted fromeach family a single affected proband (assum-ing single ascertainment). Under these con-ditions, the mutated to normal ratio decreasedto 1-32 and the ratio of premutated to fullmutated was 0-3. This apparently incompletecorrection reflects in part the fact that 46 sibscould not be studied (of whom only 11 werementally retarded). Assuming that the propor-tion of premutations in the untested normalsibs is the same as in the tested ones, themutated to normal ratio would be 119. Thedifference from the expected ratio of 1 is mostprobably the result of multiple ascertainment
50
* PremutationEH Full mutation40
30
20
10
0
75-125 175-225 275-325 5375-425 475-525125-1 75 225-275 5325-375 5425-475
(8) (19) (36) (22) (11) (1) (1) (2) (2)
Size of premutation in bp (number of mothers in each size class)
Figure 6 Risk of transition to full mutation as a function of the size of premutationin the mother, after correction for ascertainment bias. Offspring with the abnormalallele were characterised as having the premutation or full mutation (the latter classincludes mosaics). One affected proband per family was removed (see text).
for some families. The effect of size of thepremutation on the type of mutation inheritedby the offspring (after this still partial correc-tion for ascertainment bias) is presented in fig6. It shows that for As of 75 to 125 bp, about90% of children inherit a premutation. Rareexamples of small premutations leading to fullmutation in the offspring are shown in fig 7.The smallest of these (lane 1, left panel) has
60 repeats as measured on a sequencing gelafter PCR. An about even risk was found forAs of 125 to 175 bp while, as stated above,premutations larger than 225 bp always led to afull mutation. It should be noted that very fewpremutations were found above 325 bp, whichis probably because, past 175 bp, a premu-tation is more likely to pass to a full mutationthan to have a moderate increase in size withinthe range of premutation.
DiscussionOur results confirm that the size of the premu-tation is a major (and perhaps the only) deter-minant of the risk of transition from premu-tation to full mutation.'415 We have analysed102 sibships from fragile X families whosemothers had a premutation, a sample sizelarger than that of Fu et all5 (30 sibships) or Yuet al'4 (60 sibships). We have tried to correctfor ascertainment bias, which favours affectedchildren and which was not taken into accountin the previous reports. Although our correc-tion appears still incomplete, it should result ina more accurate estimation of the risk of transi-tion from premutation to full mutation. Thisrisk would be about 10% for premutations
1 2 3 4
Q
5 6 7 8 9 10 11 12
52-_
e _ _-28-.-
Figure 7 Small premutations that had directly orindirectly led to a full mutation as visualised in anEcoRI+ EagI digest. In the family on the left, themother (lane 1) had a premutation (measured in PstIdigests) with a A of 90 bp (60 repeats were measured inthe direct PCR assay of Fu et al'5) while the daughtersin lanes 2 and 3 had larger premutations (A = 200 to300 bp; in lane 3, the abnormal allele is mostly on theinactive X), and the third daughter had a heterogeneousfull mutation. In the right panel, lanes 7, 11, 8 and 6correspond to lanes 4, 5, 6, and 7 respectively in fig 5.The premutation appears smaller in lane 6 because mostof it is on the inactive X (slightly above the 5-2 kbnormal band), which does not allow accurate sizing, andbecause this woman inheritedfrom her father a high'normal' allele (see fig 5, lane 7). Premutations have aA of 120, 115, 125, and 200 bp in lanes 6, 7, 8, and 10respectively.
0)a._
Co(0~0'a)Cu)
799
on April 7, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.11.794 on 1 Novem
ber 1992. Dow
nloaded from

Heitz, Devys, Imbert, Kretz, Mandel
with amplification (As) of 75 to 125 bp (corres-ponding to 55 to 70 repeats), about 50%between 125 and 175 bp (70 to 90 repeats), and>98% above 225 bp (105 repeats) which fitsremarkably well with the data of Fu et all5 andYu et al.14 Although this has important conse-quences in genetic counselling, since the riskof having affected children can vary considera-bly depending on premutation size, for a situa-tion with a low but measurable risk it willprobably be necessary to consider prenatalDNA diagnosis. It remains to be seen,however, whether different patterns ofinterspersed AGG units exist within the CGGrepeat,356 which might influence the risk oftransition to full mutation. It has been shownfor (CA)n microsatellites that imperfect tan-dem repeats are less polymorphic (that is, morestable) than perfect ones.25As already discussed by Fu et al,"5 these
findings account very well for the Shermanparadox and the clustering within sibships ofeither normal transmitting males (or unaffec-ted carriers) or ofmales or females with pheno-typic expression. After correction for ascer-tainment bias we found a 77% overall risk fortransition to full mutation, which fits well withthe 80% penetrance value found by Shermanet aP in fragile X families. The fact that about15% of carriers with premutations (or about10% of all carriers) in fragile X families have asmall amplification associated with a low riskof having affected children strongly suggeststhat their frequency in the general populationmight be about as high as that of carriers with aA of 150 to 300, who make up the majority ofpremutation carriers in fragile X families.Assuming that one male in 1500 has clinicalexpression of the fragile X syndrome, thefrequency of carrier females would be about 1in 600, assuming an 80% average risk of transi-tion to full mutation, but that figure may beconsiderably increased, to perhaps 1 in 400 ormore, if one takes into account women with asmall risk who do not belong (yet) to fragile Xfamilies. This is supported by the observationsof abnormal fragments of premutation size inspouses26 (fig 3, lanes 1, 2, 3) and in one CEPHfamily,'5 and raises the possibility of system-atic screening for such mutations in women ofchild bearing age in the general population.The 100% risk of transition of premutations
with > 100 repeats to a disease causing fullmutation during female transmission is verydifficult to reconcile with Laird's hypothesis ofa correlation with the X inactivation status, asthe latter would predict a maximum risk of50°/0.9 1 Laird's hypothesis would still be ten-able, however, if in oogonial precursors aselection was occurring which would result inpreferential survival of cells with the premu-tation on the inactive X. We have observedsuch a selection (albeit with an extendedcourse of time) in leucocytes of female carriersof a full mutation, but not in carriers of apremutation.'7 However, it is formally possiblethat oogonial precursors would be criticallydependent on FMR-1 function and thatexpansion of about 100 repeats could impairfunction of the FMR- 1 gene, either through
modification of the protein (if the repeat istranslated) or by decreasing stability of themRNA.This obligatory and sex biased expansion,
with catastrophic consequences, appears toshow a major difference from myotonic dys-trophy, where expansions of similar size canoccur in both sexes."729 As the full mutation infragile X is correlated with abnormal methyla-tion of nearby sites, and the CGG repeat itselfis able to be methylated (although it has notbeen experimentally shown that it is indeedmethylated in a full mutation), while the CTGrepeat is unable to be methylated, it is tempt-ing to propose that methylation could be thebasis for the difference between the two dis-eases, if it were a cause rather than a conse-quence of the large expansion. We have pro-posed earlier3 that methylation could modifythe secondary structure of the CGG repeat,interfere with replication processes, and in-duce a greater instability. A second unsolvedquestion is whether large expansion really oc-curs during female meiosis or very early inembryogenesis. In the latter case, one wouldhave to suppose a sex imprint (not necessarilylinked to female X inactivation) in the FMR-1region which would distinguish between apremutation on a paternally or maternally de-rived X. This question is raised by the puz-zling case of 'mosaics' who have cells witheither a full or premutation."8 In the firstalternative (meiotic expansion) some postcon-ception processes (sister chromatid exchangefor instance) could lead both to shortening ofthe repeat and loss of methylation. However,this is in apparent contradiction to the veryrare occurrence of extensive shortening in off-spring from females with a full mutation7 (andin the rare event recorded, one cannot excludethat the mother was a 'mosaic' and the off-spring with a premutation had inherited an Xchromosome that originally carried a premu-tation). Thus it seems that the second alternat-ive (expansion being mostly a postconceptionalevent) is at least as attractive, especially asheterogeneity of the full mutation (by somaticmutation) is already present early in fetal lifeand further mutation may be much reducedpostnatally.-0 We suggest as one possibilitythat abnormal methylation could occur veryearly in embryogenesis on the maternally de-rived chromosome carrying a premutation,with a frequency which depends on the size ofthe premutation (that is, of the methylabletarget). This would lead to expansion to fullmutation and stabilisation of the methylation.That abnormal methylation (of the full muta-tion) occurs very early is suggested by thefinding that in chorionic villi the full mutationis in general (but not always) methylated,whereas the normal inactive X is in generalunmethylated at the FMR- 1 CpG island.'0Undermethylation ofCpG islands on the inac-tive X in chorionic villi is well known, and isattributed to the later timing of the methyla-tion process with respect to the earlier differ-entiation of trophoblasts." 32 Methylation pat-terns may, however, be obscured by existencein early embryogenesis of both methylation
800
on April 7, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.11.794 on 1 Novem
ber 1992. Dow
nloaded from

Inheritance of the fragile X syndrome
and demethylation activity.3"3 It is obviousthat these questions will be difficult to analysedirectly in humans, and solutions may come
from comparison with molecular patterns
observed at other X linked or autosomal fragilesites, or at loci such as that for myotonicdystrophy, and by trying to find or establishanimal (murine) models which mimic thevarious features of unstable expansion of suchrepeats.
We thank our clinical colleages for referringfragile X families, V Biancalana for providingblots of the families, F Rousseau for participa-tion in the initial stage of this work, A Stauband F Ruffenach for oligonucleotide synthesis,and J M Lafontaine and A Landman for pho-tography. This work was supported byINSERM/CNAMTS, the CHRU of Stras-bourg, the Ministere de la Recherche et de laTechnologie (MRT) (to JLM), and theAssociation Frangaise contre les Myopathies(AFM).
Sherman S. Recognition of the fragile X or Martin-Bellsyndrome. In: Hagerman RJ, Silverman AC, eds. FragileX syndrome: diagnosis, treatment and research. Baltimore:The Johns Hopkins University Press, 1991:69-97.
2 Sherman SL, Jacobs PA, Morton NE, et al. Further segre-
gation analysis of the fragile X syndrome with specialreference to transmitting males. Hum Genet 1985;69:289-99.
3 Oberle I, Rousseau F, Heitz D, et al. Instability of a 550 bpDNA segment and abnormal methylation in fragile Xsyndrome. Science 1991;252:1097-102.
4 Yu S, Pritchard M, Kremer E, et al. Fragile X genotype
characterized by an unstable region of DNA. Science1991;252:1 179-81.
5 Kremer EJ, Pritchard M, Lynch M, et al. Mapping ofDNAinstability at the fragile X to a trinucleotide repeat se-
quence p(CGG)n. Science 1991;252:1711-4.6 Verkerk AJ, Pieretti M, Fu YH, et al. Identification of a
gene (FMR-1) containing a CGG repeat coincident with a
breakpoint cluster region exhibiting length variation infragile X syndrome. Cell 1991;65:905-14.
7 Rousseau F, Heitz D, Biancalana V, et al. Efficient andreliable direct diagnosis of the fragile X mental retard-ation syndrome. N Engl Med 1991;325:1673-81.
8 Pieretti M, Zhang F, Fu YH, et al. Absence of expression ofthe FMR-1 gene in fragile X syndrome. Cell 1991;66:817-22.
9 Laird CD. Proposed mechanism of inheritance and expres-
sion of the human fragile-X syndrome of mental retard-ation. Genetics 1987;117:587-99.
10 Laird CD, Lamb MM, Thorne JL. Two progenitor cellsfor human oogonia inferred from pedigree data and the X-inactivation imprinting model of the fragile X syndrome.Am Hum Genet 1990;46:696-719.
11 Vincent A, Heitz D, Petit C, Kretz C, Oberle I, Mandel JL.Abnormal pattern detected in fragile X patients by pulsedfield gel electrophoresis. Nature 1991;349:624-6.
12 Bell MV, Hirst MC, Nakahori Y, et al. Physical mappingacross the fragile X: hypermethylation and clinicalexpression of the fragile X syndrome. Cell 1991;64:861-6.
13 Heitz D, Rousseau F, Devys D, et al. Isolation of sequencesthat span the fragile X and identification of a fragile X-relatedCpG island. Science 1991;251:1236-9.
14 Yu S, Mulley J, Loesch D, et al. Fragile X syndrome:unique genetics of the heritable unstable element. AmJ7Hum Genet 1992;50:968-80.
15 Fu YH, Kuhl DPA, Pizzuti A, et al. Variation of the CGGrepeat at the fragile X site results in genetic instability:resolution of the Sherman paradox. Cell 1991;67:1047-58.
16 McConlogue L, Brow MAD, InnisMA. Structure-inde-pendent DNA amplification by PCR using 7-deaza-2'-deoxyguanosine. Nucleic Acids Res 1988;16:9869.
17 Rousseau F, Heitz D, Oberle I, Mandel JL. Selection inblood cells from female carriers of the fragile X syndrome:inverse correlation between age and proportion of activeX chromosomes carrying the full mutation. J Med Genet1991;28:830-6.
18 Richards RI, Holman K, Kozman H, et al. Fragile Xsyndrome: genetic localisation by linkage mapping of twomicrosatellite repeats FRAXACI and FRAXAC2 whichimmediately flank the fragile site. J Med Genet1991;28:818-23.
19 Camerino G, Mattei MG, Mattei JF, Jaye M, Mandel JL.Close linkage of fragile X-mental retardation syndrome tohaemophilia B and transmission through a normal male.Nature 1983;306:701-4.
20 Arveiler B, Oberle I, Vincent A, Hofker MH, Pearson PL,Mandel JL. Genetic mapping of the Xq27-q28 region:new RFLP markers useful for diagnostic applications infragile X and hemophilia B families. Am 7 Hum Genet1988;42:380-9.
21 Brown WT, Gross A, Chan C, et al. Multi-locus analysis ofthe fragile X syndrome. Hum Genet 1988;78:201-5.
22 Pergolizzi RG, Erster SH, Goonewardena P, Brown T.Detection of full fragile X mutation. Lancet 1992;339:271-2.
23 Erster SH, Brown WT, Goonewardena P, Dobkin CS,Jenkins EC, Pergolizzi RG. PCR analysis of fragile Xmutations. Hum Genet (in press).
24 Rousseau F, Heitz D, Biancalana V, Oberle I, Mandel JL.On some technical aspects of direct DNA diagnosis of thefragile X syndrome. Am J Med Genet 1992;43:197-207.
25 Weber JL. Informativeness of human (dC-dA)n.(dG-dt)npolymorphisms. Genomics 1990;7:524-30.
26 Macpherson J, Harvey J, Curtis G, et al. A reinvestigationof thirty three fragile(X) families using probe StB12.3.Am J Med Genet 1992;43:905-12.
27 Fu YH, Pizzuti A, Fenwick RG, et al. An unstable tripletrepeat in a gene related to myotonic muscular dystrophy.Science 1992;255:1256-8.
28 Mahadevan M, Tsilfidis C, Sabourin L, et al. Myotonicdystrophy mutation: an unstable CTG repeat in the 3'untranslated region of the gene. Science 1992;255:1253-5.
29 Brook JD, McCurrach ME, Harley HG, et al. Molecularbasis of myotonic dystrophy: expansion of a trinucleotide(CTG) repeat at the 3' end of a transcript encoding aprotein kinase family member. Cell 1992;68:799-808.
30 Devys D, Biancalana V, Rousseau F, Boue J, Mandel JL,Oberle I. Analysis of full fragile X mutations in fetaltissues and monozygotic twins indicate that abnormalmethylation and somatic heterogeneity are establishedearly in development. Ann J Med Genet 1992;43:208-16.
31 Migeon BR, Wolf SF, Axelman H, Kaslow DC, SchmidtM. Incomplete X chromosome dosage compensation inchorionic villi of human placenta. Proc Natl Acad SciUSA 1985;82:3390-4.
32 Migeon BR. Insights into X chromosome inactivation fromstudies of species variation, DNA methylation and repli-cation, and vice versa. Genet Res 1990;56:91-8.
33 Migeon BR, Holland MM, Driscoll DJ, Robinson JC.Programmed demethylation in CpG islands duringhuman fetal development. Somatic Cell Mol Genet1991;17:159-68.
34 Frank D, Keshet I, Shani M, Levine A, Razin A, Cedar H.Demethylation of CpG islands in embryonic cells. Nature1991;351:239-41.
801
on April 7, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.11.794 on 1 Novem
ber 1992. Dow
nloaded from