
Influenza Outbreaks in Long-Term Care: Practical Approaches to Prevention and Control
4
Influenza Outbreaks in Long-Term Care Practical Approaches to Prevention and Control A ccording to the National Nursing Home Survey, there are 16,000 certified nurs- ing homes and other long-term care facilities (LTCFs) in the United States, in which approxi- mately 1.5 million older adults reside. 1 The majority (88.3%) of nursing home and LTCF residents are 65 years of age and older; 45.2% are 85 years of age and older. 1 By the year 2030, it is anticipated that 20% of the United States population will be 65 years of age or older, 2 and almost 30 million of these persons will have functional limitations that may require long-term care. 3 The impact of influenza is particularly severe among the elderly. Although adults 65 years of age and older represent only 13% of the total US population, 4 they account for 63% of influenza-related hospitalizations due to bacte- rial infections and pulmonary, cardiovascular, and cerebrovascular complications 5 ; 90% of annual influenza-related deaths 6 ; and 64% of the total economic burden of influenza. 7 Influenza illness is thought to be the cause of excess mortality due to ischemic heart disease, cerebrovascular disease, and diabetes in adults 70 years of age and older during the winter months. 8 The disproportionate burden of influenza in the elderly is due at least in part to immu- nosenescence, the age-related decline in the immune system that leads to a reduced capacity to fight infection and to develop an adequate protective immune response to vaccine. 9-11 The phenomenon of immunosenescence is the rationale for development of a more immuno- genic influenza vaccine specifically for people 65 years of age and older. The vaccine, first available in the 2010-2011 influenza season, has 4 times the amount of antigen compared to previously available vaccines and was licensed on the basis of its ability to generate a more robust immune response among people in the 65-and-older age group. 12,13 ResIdenTs Of LTCfs ARe espeCIALLy VuLneRAbLe Elderly residents of LTCFs may experience even higher morbidity and mortality secondary to influenza and influenza-like illness (ILI) than community-dwelling elderly persons. 14 The elderly living in LTCFs often suffer not only from immunosenescence but also from debilitating chronic medical conditions that place them at higher risk of infection and complications. In addition, they are more likely to be exposed to influenza and ILI in the institutional setting. Viruses can be easily introduced and spread via exposure to newly admitted residents, shared caregivers, health care personnel, volunteers, and visitors who circulate between the community and the facility. 3,14-16 The closed environment and limited mobility of residents within the facility also contribute to the spread of infection. 3,14-16 Seasonal attack rates of ILI among residents of LTCFs vary considerably: During years in which no influenza epidemic occurs, an attack rate of 5%-20% is typical. In epidemic years, up to 70% of residents may become ill, and case- fatality rates may be as high as 30%. 16,17 befORe An OuTbReAk OCCuRs: VACCInATIOn Is key! Annual vaccination of all residents and staff in LTCFs is the most effective method currently available for reducing the morbidity and mor- tality associated with influenza infection. 9,16 Vaccinated residents of LTCFs who develop ILI often have milder illness of shorter duration than unvaccinated residents, and they are less likely to develop secondary complications or die as a result of their illness. 14,17 Even influenza vaccine that is a bad match for the circulating strain can attenuate symptoms, such as fever. 18 Vaccinating the staff against influenza can help prevent deaths in residents (Figure 1) 19-22 as well © Alloy Photography/Veer fACuLTy ReVIeweR stefan Gravenstein, Md, MpH Professor of Medicine and Health Services Policy and Practice Alpert Medical School of Brown University Clinical Director, Healthcentric Advisors Providence, Rhode Island Dear Colleague: Influenza remains the leading infectious cause of death from a virus for older adults in the United States. Many long-term care facilities experience outbreaks of respiratory illness but fail to recognize influenza as a source of additional hospitalizations, exacerbations of heart failure or emphysema, or heart attacks and strokes because the laboratory tests to prove they’re secondary to influenza typically aren’t ordered. In 2012, for example, outbreaks of influenza were occurring as late as May and early June, but would have been overlooked if such testing had not been done. Influenza vaccine can reduce the severity of outbreaks. The combined reduction in heart attacks and strokes realized by those vaccinated may be even greater than the reduced incidence of pneumonia. Getting nursing home residents vaccinated has become easier as long-term care facility policies have included influenza vaccination as part of the current standard of care. Continued on page 2
-
Upload
haymarket-media -
Category
Documents
-
view
213 -
download
1
description
Influenza Outbreaks in Long-Term Care: Practical Approaches to Prevention and Control
Transcript of Influenza Outbreaks in Long-Term Care: Practical Approaches to Prevention and Control

Influenza Outbreaks in Long-Term Care Practical Approaches to Prevention and Control
A ccording to the National Nursing Home Survey, there are 16,000 certified nurs-
ing homes and other long-term care facilities (LTCFs) in the United States, in which approxi-mately 1.5 million older adults reside.1 The majority (88.3%) of nursing home and LTCF residents are 65 years of age and older; 45.2% are 85 years of age and older.1 By the year 2030, it is anticipated that 20% of the United States population will be 65 years of age or older,2 and almost 30 million of these persons will have functional limitations that may require long-term care.3
The impact of influenza is particularly severe among the elderly. Although adults 65 years of age and older represent only 13% of the total US population,4 they account for 63% of influenza-related hospitalizations due to bacte-rial infections and pulmonary, cardiovascular, and cerebrovascular complications5; 90% of annual influenza-related deaths6; and 64% of the total economic burden of influenza.7 Influenza illness is thought to be the cause of excess mortality due to ischemic heart disease, cerebrovascular disease, and diabetes in adults 70 years of age and older during the winter months.8
The disproportionate burden of influenza in the elderly is due at least in part to immu-nosenescence, the age-related decline in the immune system that leads to a reduced capacity to fight infection and to develop an adequate protective immune response to vaccine.9-11 The phenomenon of immunosenescence is the rationale for development of a more immuno-genic influenza vaccine specifically for people 65 years of age and older. The vaccine, first available in the 2010-2011 influenza season, has 4 times the amount of antigen compared to previously available vaccines and was licensed on the basis of its ability to generate a more robust immune response among people in the 65-and-older age group.12,13
ResIdenTs Of LTCfs ARe espeCIALLy VuLneRAbLeElderly residents of LTCFs may experience even higher morbidity and mortality secondary to influenza and influenza-like illness (ILI) than community-dwelling elderly persons.14
The elderly living in LTCFs often suffer not only from immunosenescence but also from debilitating chronic medical conditions that place them at higher risk of infection and complications. In addition, they are more likely to be exposed to influenza and ILI in the institutional setting. Viruses can be easily introduced and spread via exposure to newly admitted residents, shared caregivers, health care personnel, volunteers, and visitors who circulate between the community and the facility. 3,14-16 The closed environment and limited mobility of residents within the facility also contribute to the spread of infection.3,14-16
Seasonal attack rates of ILI among residents of LTCFs vary considerably: During years in which no influenza epidemic occurs, an attack rate of 5%-20% is typical. In epidemic years, up to 70% of residents may become ill, and case-fatality rates may be as high as 30%.16,17
befORe An OuTbReAk OCCuRs: VACCInATIOn Is key!Annual vaccination of all residents and staff in LTCFs is the most effective method currently available for reducing the morbidity and mor-tality associated with influenza infection.9,16 Vaccinated residents of LTCFs who develop ILI often have milder illness of shorter duration than unvaccinated residents, and they are less likely to develop secondary complications or die as a result of their illness.14,17 Even influenza vaccine that is a bad match for the circulating strain can attenuate symptoms, such as fever.18
Vaccinating the staff against influenza can help prevent deaths in residents (Figure 1)19-22 as well
© Alloy Photography/Veer
fACuLTy ReVIeweRstefan Gravenstein, Md, MpH Professor of Medicine and Health Services Policy and Practice Alpert Medical School of Brown University Clinical Director, Healthcentric Advisors Providence, Rhode Island
Dear Colleague:
Influenza remains the leading infectious cause of death from a virus for older adults in the United States. Many long-term care facilities experience outbreaks of respiratory illness but fail to recognize influenza as a source of additional hospitalizations, exacerbations of heart failure or emphysema, or heart attacks and strokes because the laboratory tests to prove they’re secondary to influenza typically aren’t ordered. In 2012, for example, outbreaks of influenza were occurring as late as May and early June, but would have been overlooked if such testing had not been done.
Influenza vaccine can reduce the severity of outbreaks. The combined reduction in heart attacks and strokes realized by those vaccinated may be even greater than the reduced incidence of pneumonia. Getting nursing home residents vaccinated has become easier as long-term care facility policies have included influenza vaccination as part of the current standard of care.
Continued on page 2

as ILI during periods of moderate influenza activity—even when there are high levels of vaccination among residents.21,22 In fact, protec-tion works best when both residents and staff are vaccinated. In 1 study, LTCFs where more than 89% of residents and 55% of staff were immunized were 60% less likely to experience an outbreak of ILI compared with LTCFs that did not achieve these vaccination rates in both residents and staff.23
However, influenza outbreaks are a con-sequence of more than poor vaccine uptake. Outbreaks continue to occur even in LTCFs in which most residents are vaccinated.24 Several factors, including immunosenescence, can cause failure of the influenza vaccine to provide opti-mal protection.9,16,25 For example, vaccination prevents laboratory-confirmed influenza in only about 30%-40% of elderly adults, compared with 70%-90% of young healthy adults, and standard-dose influenza vaccine is consistently less effective among adults 65 years of age
and older compared with adults 15-64 years of age.26,27
Despite an age-related decline in effective-ness of standard-dose vaccine, it still provides substantial protection. Therefore, since October 2005, the Centers for Medicare and Medicaid Services (CMS) has required nursing homes it certifies to offer influenza vaccine to all residents and to document the results.28 The requirements specify that each resident is to be vaccinated unless vaccination is contraindicated medically, the resident or legal representative refuses vac-cination, or the vaccine is not available because of shortages. This information must be reported as part of the CMS Minimum Data Set, which tracks LTCF health parameters.28
In addition, the Advisory Committee on Immunization Practices currently recommends annual vaccination against influenza for all per-sons 6 months of age and older,29 and Healthy People 2020 goals for seasonal influenza immu-nization are 90% for both residents of LTCFs
However, this isn’t enough to protect older residents from influenza.
Influenza prevention in long-term care settings requires a 3-pronged defense:
1. Vaccinate residents to help prevent disease, but also to improve outcomes should they become infected despite vaccination. Use standing orders to accomplish this goal.
2. Vaccinate staff. Staff are often the vector that brings influenza into a facility. Dedicated staff may feel they cannot be absent from work even when they are ill, so vaccinating them reduces the chance that they will become sick from influenza. Consider whether making annual influenza vaccination a condition of employment makes sense for your facility.
3. Monitor and test residents with respiratory illnesses for influenza when influenza arrives in your community. This will position the facility to start antiviral prophylaxis when someone has confirmed influenza to help keep others from becoming ill. Develop a policy for influenza monitoring and implementation of chemoprophylaxis, or adopt the one developed by the Centers for Disease Control and Prevention. Consider whether your facility’s pharmacy has adequate antiviral stock should you declare an outbreak and wish to provide chemoprophylaxis to residents and staff.
Think about the policies that are in place to vaccinate (standing orders), monitor (infection control, testing), and react (chemoprophylaxis, cohorting or canceling activities) to influenza in your facility. The best time to do this quick organizational check-up is before the start of the influenza season. Make sure families and staff know that influenza is an important disease that is readily preventable if everyone is vaccinated and understands the policies designed to keep it at bay.
Sincerely,
Stefan Gravenstein, MD, MPH
Continued from page 1
2 | Influenza Outbreaks in Long-Term Care
Figure 1. Vaccinating health care personnel against influenza can prevent deaths in residents of LTCFs.19-22
Res
iden
t m
ort
alit
y (%
)
a HCP = Health care personnel.
HCPa vaccinated HCP not vaccinated
10.0
13.6
11.2
5.2
17.0
22.4
15.3
6.0
0
5
10
15
20
25
Potter J, et al 19 Carman WF, et al 20 Hayward AC, et al 21 Lemaitre M, et al 22
6 LTCFs/arm N = 1059 pts
10 LTCFs/arm N = 1437 pts
22 LTCFs/arm N = 2604 pts 20 LTCFs/arm
N = 3483 pts
ns
0
10
20
30
40
50
60
70
80
90
100
76.9%
67.7%
52.4%
61.5%66.9%
Infl
uen
za v
acci
nat
ion
co
vera
ge
(%)
Health care personnel work setting
Hospital Physician office
Long-term care facility
Other work settinga
Overall
a Other work settings include dental offices, pharmacies, nonhospital laboratories, medical-related schools, emergency medical technician sites, and home medical-care sites.
Figure 2. Influenza vaccina-tion coverage among health care person-nel by work setting — United States, 2011–2012 influenza season.32 Rates of coverage continue to fall short of Healthy People 2020 target of 90% for HCP in all work settings,30 with the lowest rates among HCPs working in long-term care.
Healthy People 2020 goal = 90% for health care personnel30
and health care personnel.30 However, rates of vaccine coverage in these groups still fall short: In the 2005-2006 influenza season—the first year that immunization coverage was reported following the CMS requirement—only 72% of residents of LTCFs overall received influenza vaccine (with coverage varying from 49% to 87% among states).31 Further, in the 2011-2012 influenza season, only 52.4% of health care personnel working in LTCFs reported receiving influenza vaccine (Figure 2).32
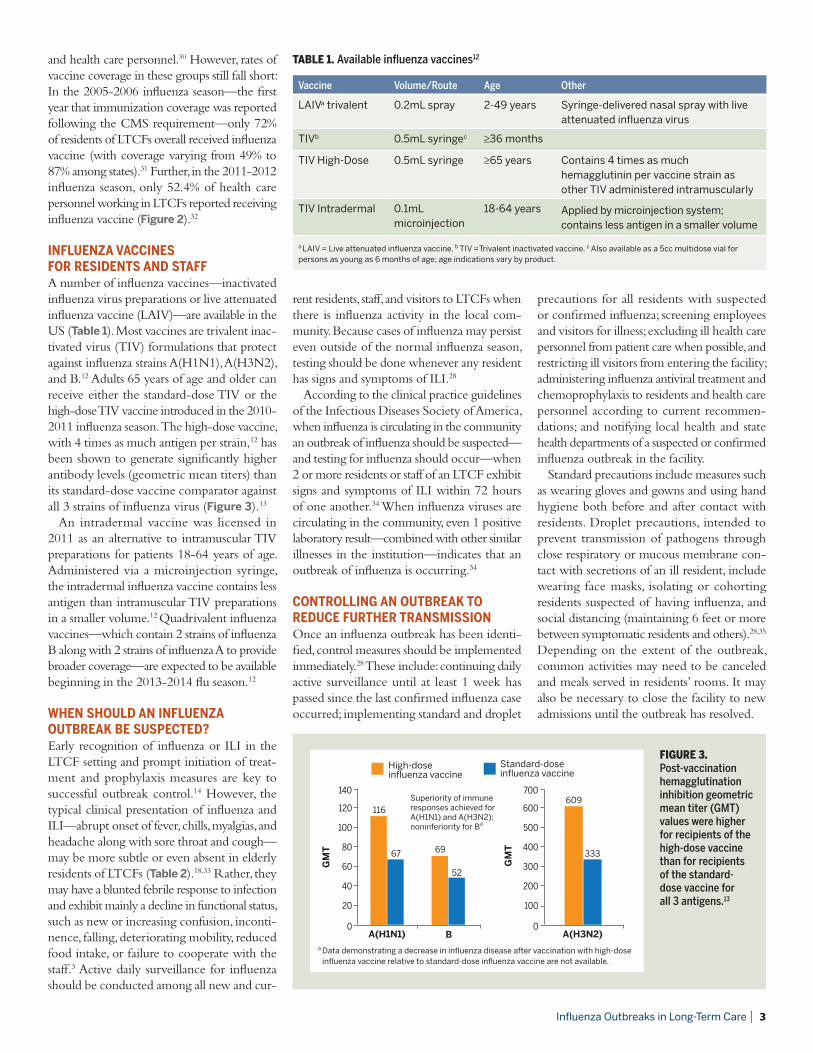
InfLuenzA VACCInes fOR ResIdenTs And sTAffA number of influenza vaccines—inactivated influenza virus preparations or live attenuated influenza vaccine (LAIV)—are available in the US (Table 1). Most vaccines are trivalent inac-tivated virus (TIV) formulations that protect against influenza strains A(H1N1), A(H3N2), and B.12 Adults 65 years of age and older can receive either the standard-dose TIV or the high-dose TIV vaccine introduced in the 2010-2011 influenza season. The high-dose vaccine, with 4 times as much antigen per strain,12 has been shown to generate significantly higher antibody levels (geometric mean titers) than its standard-dose vaccine comparator against all 3 strains of influenza virus (Figure 3).13
An intradermal vaccine was licensed in 2011 as an alternative to intramuscular TIV preparations for patients 18-64 years of age. Administered via a microinjection syringe, the intradermal influenza vaccine contains less antigen than intramuscular TIV preparations in a smaller volume.12 Quadrivalent influenza vaccines—which contain 2 strains of influenza B along with 2 strains of influenza A to provide broader coverage—are expected to be available beginning in the 2013-2014 flu season.12
wHen sHOuLd An InfLuenzA OuTbReAk be suspeCTed?Early recognition of influenza or ILI in the LTCF setting and prompt initiation of treat-ment and prophylaxis measures are key to successful outbreak control.14 However, the typical clinical presentation of influenza and ILI—abrupt onset of fever, chills, myalgias, and headache along with sore throat and cough—may be more subtle or even absent in elderly residents of LTCFs (Table 2).18,33 Rather, they may have a blunted febrile response to infection and exhibit mainly a decline in functional status, such as new or increasing confusion, inconti-nence, falling, deteriorating mobility, reduced food intake, or failure to cooperate with the staff.3 Active daily surveillance for influenza should be conducted among all new and cur-
rent residents, staff, and visitors to LTCFs when there is influenza activity in the local com-munity. Because cases of influenza may persist even outside of the normal influenza season, testing should be done whenever any resident has signs and symptoms of ILI.28
According to the clinical practice guidelines of the Infectious Diseases Society of America, when influenza is circulating in the community an outbreak of influenza should be suspected—and testing for influenza should occur—when 2 or more residents or staff of an LTCF exhibit signs and symptoms of ILI within 72 hours of one another.34 When influenza viruses are circulating in the community, even 1 positive laboratory result—combined with other similar illnesses in the institution—indicates that an outbreak of influenza is occurring.34
COnTROLLInG An OuTbReAk TO ReduCe fuRTHeR TRAnsMIssIOnOnce an influenza outbreak has been identi-fied, control measures should be implemented immediately.28 These include: continuing daily active surveillance until at least 1 week has passed since the last confirmed influenza case occurred; implementing standard and droplet
precautions for all residents with suspected or confirmed influenza; screening employees and visitors for illness; excluding ill health care personnel from patient care when possible, and restricting ill visitors from entering the facility; administering influenza antiviral treatment and chemoprophylaxis to residents and health care personnel according to current recommen-dations; and notifying local health and state health departments of a suspected or confirmed influenza outbreak in the facility.
Standard precautions include measures such as wearing gloves and gowns and using hand hygiene both before and after contact with residents. Droplet precautions, intended to prevent transmission of pathogens through close respiratory or mucous membrane con-tact with secretions of an ill resident, include wearing face masks, isolating or cohorting residents suspected of having influenza, and social distancing (maintaining 6 feet or more between symptomatic residents and others).28,35 Depending on the extent of the outbreak, common activities may need to be canceled and meals served in residents’ rooms. It may also be necessary to close the facility to new admissions until the outbreak has resolved.
69
52
0
20
40
60
80
100
120
GM
T
BA(H1N1)
High-dose influenza vaccine
Standard-dose influenza vaccine
116
67
140
0
100
200
300
400
500
600
GM
T
A(H3N2)
609
333
700Superiority of immune responses achieved for A(H1N1) and A(H3N2); noninferiority for Ba
Table 1. Available influenza vaccines12
Vaccine Volume/Route Age Other
LAIVa trivalent 0.2mL spray 2-49 years Syringe-delivered nasal spray with live attenuated influenza virus
TIVb 0.5mL syringec ≥36 months
TIV High-Dose 0.5mL syringe ≥65 years Contains 4 times as much hemagglutinin per vaccine strain as other TIV administered intramuscularly
TIV Intradermal 0.1mL microinjection
18-64 years Applied by microinjection system; contains less antigen in a smaller volume
a LAIV = Live attenuated influenza vaccine. b TIV =Trivalent inactivated vaccine. c Also available as a 5cc multidose vial for persons as young as 6 months of age; age indications vary by product.
Influenza Outbreaks in Long-Term Care | 3
Figure 3. Post-vaccination hemagglutination inhibition geometric mean titer (GMT) values were higher for recipients of the high-dose vaccine than for recipients of the standard-dose vaccine for all 3 antigens.13
a Data demonstrating a decrease in influenza disease after vaccination with high-dose influenza vaccine relative to standard-dose influenza vaccine are not available.

InfLuenzA OuTbReAks In LTCfs ARe COsTLy Influenza outbreaks within LTCFs carry con-siderable human and economic costs. Direct costs include hospitalization of residents with loss of per diem bed payments plus additional expenses for patient care, including ambulance calls and emergency room and physician visits. Indirect costs include outbreak control mea-sures (influenza testing, antiviral treatment, and prophylactic medications for residents and staff), additional staff time, concurrent staff sick time, as well as documentation, inspections, and reporting to comply with regulations.
The reputation of the facility may also be at risk, with the perception of diminished quality of care. By increasing the potential for catastrophic disability (defined as a loss of 3 or more basic activities of daily living, such as dressing, eating, personal hygiene, and ambu-lation), weight loss, pressure ulcers, infections, and loss of functional independence, influenza represents a substantial financial burden for the facility and has a major negative effect on quality of life for residents of LTCFs.36-39
Prevention of influenza outbreaks via mea-sures such as comprehensive annual immuni-zation of residents and staff, combined with active surveillance and prompt recognition and control when outbreaks do occur, can help reduce the human and economic costs of influenza in long-term care.
RefeRenCes
1. Jones AL, Dwyer LL, Bercovitz AR, Strahan GW. The National Nursing Home Survey: 2004 overview. Vital Health Stat. 2009;13(167):1-155.
2. US Census Bureau. The older population in the United States: 2010 to 2050. http://www.census.gov/prod/2010pubs/p25-1138.pdf. Accessed December 3, 2012.
3. High KP, Bradley SF, Gravenstein S, et al; Infectious Diseases Society of America. Clinical practice guideline for the evaluation of fever and infection in older adult residents of long-term care facilities: 2008 update by the Infectious Diseases Society of America. J Am Geriatr Soc. 2009;57(3):375-394.
4. US Department of Health & Human Services Administration on Aging. US population by age: July 1, 2010. US population totals by age group and sex in the 2010 and 2000 censuses. http://www.aoa.gov/Aging_Statistics/Census_Population/census2010/Index.aspx. Accessed December 3, 2012.
5. Thompson WW, Shay DK, Weintraub E, et al. Influenza-associated hospitalizations in the United States. JAMA. 2004;292(11):1333-1340.
6. Centers for Disease Control and Prevention (CDC). Esti-mates of deaths associated with seasonal influenza—United States, 1976-2007. MMWR. 2010;59(33):1057-1062.
7. Molinari NM, Ortega-Sanchez IR, Messonnier ML, et al. The annual impact of seasonal influenza in the US: measuring disease burden and costs. Vaccine. 2007;25(27):5086-5096.
8. Reichert TA, Simonsen L, Sharma A, et al. Influenza and the winter increase in mortality in the United States, 1959-1999. Am J Epidemiol. 2004;160(5):492-502.
9. Reber AJ, Chirkova T, Kim JH, et al. Immunosenescence and challenges of vaccination against influenza in the aging population. Aging Dis. 2012;3(1):68-90.
10. Targonski PV, Jacobson RM, Poland GA. Immunosenescence: role and measurement in influenza vaccine response among the elderly. Vaccine. 2007; 25(16):3066-3069.
11. Aspinall R, Del Giudice G, Effros RB, Grubeck-Loebenstein B, Sambhara S. Challenges for vaccination in the elderly. Immun Ageing. 2007;4:9.
12. CDC. Prevention and control of influenza with vaccines: rec-ommendations of the Advisory Committee on Immunization Practices (ACIP)—United States, 2012-13 influenza season. MMWR. 2012;61(32);613-618.
13. Falsey AR, Treanor JJ, Tornieporth N, Capellan J, Gorse GJ. Randomized, double-blind controlled phase 3 trial compar-ing the immunogenicity of high-dose and standard-dose influenza vaccine in adults 65 years of age and older. J Infect Dis. 2009;200(2):172-180.
14. Arden NH. Control of influenza in the long-term care facility: a review of established approaches and newer options. Infect Control Hosp Epidemiol. 2000;21(1):59-64.
15. Bradley SF; Long-Term-Care Committee of the Society for Healthcare Epidemiology of America. Prevention of influenza in long-term-care facilities. Infect Control Hosp Epidemiol. 1999;20(9):629-637.
16. Gravenstein S, Davidson HE. Current strategies for manage-ment of influenza in the elderly population. Clin Infect Dis. 2002;35(6):729-737.
Brought to you as an educational service by Sanofi Pasteur Inc.
MKT25569-1 1/13
17. Patriarca PA, Weber JA, Parker RA, et al. Efficacy of influenza vaccine in nursing homes: reduction in illness and com-plications during an influenza A (H3N2) epidemic. JAMA. 1985;253(8):1136-1139.
18. Gravenstein S, Pop-Vicas A, Ambrozaitis A. The 2009 A/H1N1 pandemic influenza and the nursing home. Med Health R I. 2010;93(12):382-384.
19. Potter J, Stott DJ, Roberts MA, et al. Influenza vaccination of health care workers in long-term-care hospitals reduces the mortality of elderly patients. J Infect Dis. 1997;175(1):1-6.
20. Carman WF, Elder AG, Wallace LA, et al. Effects of influenza vaccination of health-care workers on mortality of elderly people in long-term care: a randomised controlled trial. Lancet. 2000;355(9198):93-97.
21. Hayward AC, Harling R, Wetten S, et al. Effectiveness of an influenza vaccine programme for care home staff to prevent death, morbidity, and health service use among residents: cluster randomised controlled trial. BMJ. 2006;333(7581):1241-1246.
22. Lemaitre M, Meret T, Rothan-Tondeur M, et al. Effect of influenza vaccination of nursing home staff on mortality of residents: a cluster-randomized trial. J Am Geriatr Soc. 2009;57(9):1580-1586.
23. Shugarman LR, Hales C, Setodji CM, Bardenheier B, Lynn J. The influence of staff and resident immunization rates on influenza-like illness outbreaks in nursing homes. J Am Med Dir Assoc. 2006;7(9):562-567.
24. Drinka PJ, Gravenstein S, Langer E, Krause P, Shult P. Mortality following isolation of various respiratory viruses in nursing home residents. Infect Control Hosp Epidemiol. 1999; 20:812-815.
25. Goodwin K, Viboud C, Simonsen L. Antibody response to influenza vaccination in the elderly: a quantitative review. Vaccine. 2006;24(8):1159-1169.
26. Monto AS, Ansaldi F, Aspinall R, et al. Influenza control in the 21st century: optimizing protection of older adults. Vaccine. 2009;27(37):5043-5053.
27. Legrand J, Vergu E, Flahault A. Real-time monitoring of the influenza vaccine field effectiveness. Vaccine. 2006;24(44-46):6605–6611.
28. CDC. Interim guidance for influenza outbreak management in long-term care facilities. http://www.cdc.gov/flu/profes-sionals/infectioncontrol/ltc-facility-guidance.htm. Accessed December 3, 2012.
29. CDC. Recommended adult immunization schedule—United States, 2012. MMWR. 2012;61(4):1-7.
30. Healthy People 2020. 2020 topics & objectives: immu-nization and infectious diseases. http://www.healthy-people.gov/2020/topicsobjectives2020/objectiveslist.aspx?topicid=23. Accessed December 3, 2012.
31. Bardenheier BH, Wortley P, Ahmed F, Hales C, Shefer A. Influ-enza immunization coverage among residents of long-term care facilities certified by CMS, 2005-2006: the newest MDs quality indicator. J Am Med Dir Assoc. 2010;11(1):59-69.
32. CDC. Influenza vaccination coverage among health-care personnel—2011–12 influenza season, United States. MMWR. 2012;61(38):753-757.
33. Smith PW, Bennett G, Bradley S, et al. Society for Healthcare Epidemiology of America (SHEA)/ Association for Profes-sionals in Infection Control (APIC) guideline: infection prevention and control in the long-term care facility, July 2008. Infect Control Hosp Epidemiol. 2008;29(9):785-814.
34. Harper SA, Bradley JS, Englund JA, et al; Expert Panel of the Infectious Diseases Society of America. Seasonal influenza in adults and children—diagnosis, treatment, chemopro-phylaxis, and institutional outbreak management: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2009;48(8):1003-1032.
35. CDC. Infection control measures for preventing and control-ling influenza transmission in long-term care facilities. www.cdc.gov/flu/professionals/infectioncontrol/pdf/longterm-care.pdf. Accessed December 3, 2012.
36. Ferrucci L, Guralnik JM, Pahor M, Corti MC, Havlik RJ. Hospital diagnoses, Medicare charges, and nursing home admissions in the year when older persons become severely disabled. JAMA. 1997;277(9):728-734.
37. Barker WH, Borisute H, Cox C. A study of the impact of influenza on the functional status of frail older people. Arch Intern Med. 1998;158(6):645-650.
38. Gozalo PL, Pop-Vicas A, Feng Z, Gravenstein S, Mor V. Effect of influenza on functional decline. J Am Geriatr Soc. 2012;60(7):1260-1267.
39. Fried TR, Bradley EH, Williams CS, et al. Functional disability and health care expenditures for older persons. Arch Intern Med. 2001;161(21):2602-2607.
Table 2. Biologic changes with age related to clinical presentation of influenza.18
Biologic change with age Clinical effect
Reduced IL-6a Reduced fever, less efficient viral clearance
Impaired mucociliary function in respiratory tract
Reduced cough, less efficient viral clearance and mucus clearance
Reduced TNF-ab Less malaise
Delayed increase in inflammatory cytokines
Fewer symptoms at disease onset
Delayed decline in inflammatory cytokines
Longer period during which inflammatory cytokines produce a prothrombotic state (risk for thromboembolic stroke, myocardial infarction)
Reduced T-cell help Reduced protection from vaccine, reduced longevity of protection from vaccine
Reduced nutrition Reduced physiologic reserve, more difficult rehabilitation
Brain aging Greater likelihood of delirium, sleep and appetite disturbance with cytokine storm
a IL-6 = interleukin-6. b TNF-a = tumor necrosis factor alpha.


















