Influence of Modern Radiological Techniques on Clinical Staging of
9
1196 ADVANcES IN RADIOLOGY Canad. Med. Ass. J. Dec. 21, 1968, vol. 99 12. LOUGHEED, W. M.: Unpublished data. 13. LOUGHEED, W. M., ELGIE, R... G. AND BARNETT, H. J. M: Canad. Med. Ass. J., 95: 1279, 1966. 14. MAKI, Y. AND NAKATA, Y.: On the cases with abnormal vascular network in the cerebral basal region. Paper presented at the 8th Symposium Neuroradiologicum, Paris, September 25-30, 1967. 15. MINAGI, H. AND NEWTON, T. H.: Radiology, 86: 100, 1966. 16. MIsHKIN, M. M.: Radiol. Olin. N. Amer., 5: 395, 1967. 17. MULLER, R. et aL: Neurology (Minneap.), 14: 136, 1964. 18. MYER, J. S., SHEEHAN, S. AND BAUER, R. B.: A.M.A. Arch. Neurol., 2: 27, 1960. 19. NISHIMOTO, A. AND KATOW, T.: A special type of cerebral vascular abnormality of the Japanese. Paper presented at the 8th Symposium Neuro- radlologicum, Paris, September 25-30, 1967. 20. NORTH, R. R. et al.: Neurology (Minneap.), 12: 810, 1962. 21. POTTER, J. M.: Brain, 82: 367, 1959. 22. RIISHEDS, J.: Canad. Med. Aas. J., 97: 151, 1967. 23. ROBINSON, R. W. et al.: J. A. M. A. 169: 1149, 1959. 24. ROCKETT, J. F. AND JOHNSON, T. H., JR.: Radiology, 90: 46, 1968. 25. SCHWARTZ, C. J. AND MITCHELL, J. R. A.: Brit. Med. .7., 2: 1057, 1961. 26. SHELDON, P.: Brit. .7. Radiol., 37: 526, 1964. 27. SIEKERT, R. G. AND MILLIKAN, C. H.: Arch. Intern. Med. (Chicago), 101: 872, 1958. 28. SUTTON, D. AND DAVIES, E. R.: Olin. Radiol., 17: 330, 1966. 29. WALLACE, S. et al.: Amer. .7. Roentgen., 101: 34, 1967. 30. WEIDNER, W., HANAFEE, W. AND MARKHAM, C. H.: Neurology (Minneap.), 15: 39, 1965. 31. YATES, P. 0. AND HUTCHINSON, E. C. Med. Re8. Couno. Spec. Rep. Ser. (London), 300: 1, 1961. Influence of Modern Radiological Techniques on Clinical Staging of Malignant Lymphomas J. W. DAVIDSON, M.R.C.P.(Glasg.), D.M.R.D.(Eng.)* and E. A. CLARKE, M.B., B.S.,t Toronto RADIOGRAPHIC procedures now form part of the routine pre-management investiga- tion of patients suffering from histologically proved malignant lymphoma. The importance of accurate pre-treatment staging according to the detected extent of disease, with respect to plan- ning of optimal therapy and accurate prognosis, is generally accepted.14' 15 Current figures for long-term survival suggest that failures of treat- ment in previous years may have been due to the presence and progression of occult disease which can now be revealed by modem investi- gative methods.'0 This communication is an ac- count of our experience at The Ontario Cancer Institute in the radiographic investigation of 392 patients suffering from malignant lympho- mas. The findings are interpreted in the light of more recent pathological concepts.'2 Their in- fluence with respect to clinical staging and the natural history of malignant lymphomas is dis- cussed. In the widely adopted system of pre-manage- ment assessment, recommended by an interna- tional committee on the staging of Hodgkin's disease,'8 the diaphragm is an important ana- This paper is based on a presentation to the Royal college of Physicians and Surgeons of Canada. Toronto, January 18-20,1968. This work was supported in part by Grant 41-15 from The Ontario cancer Treatment and Research Foundation. *Senior consultant in Diagnostic Radiology, The Ontario Cancer Institute, and Assistant Professor of Diagnostic Radiology, University of Toronto, Toronto, Ontario. tResearch Assistant In Diagnostic Radiology, The Ontario Cancer Institute. Reprint requests to: Dr. J. W. Davidson, The Princess Margaret Hospital, 500 Sherbourne Street, Toronto 5, Ontario. Clinical stag§ (. . .-.- Chest Radiography . ......Mediastinaljorn.graphy 11 ----lWhale Lung Skeletal Survey Diaphragm. . Inferior Vena Cavog.gpjjy .- Cisterna Chyli visualization ;:YiriPh§L2P.Y. ( . . Small Bowel studies .'lntravenous Pyelogram Extranodal TV Fig. 1.-Radiographic investigations in lymphoma. tomical line of demarcation for lymphomatous infiltration involving lymphatic structures. Pa- tients in clinical Stages I and II are those in whom the disease process involves lymph nodes on only one side of the diaphragm, and should disease be detected on the other side as well. they are advanced to Stage III. If structures outwith the lympho-reticular system are af- fected, the patient is placed in Stage IV. Similar concepts are applied to appraisal of lympho- sarcomas and reticulum cell sarcomas. The rele- vant radiographic procedures are illustrated in Fig. 1. Lymphography has proved the most valuable investigation for detecting occult dis- ease in pelvic and retroperitoneal lymph nodes. By outlining soft tissue abnormalities above the para-aortic nodes but still below the diaphragm, inferior vena cavography has proved a useful
Transcript of Influence of Modern Radiological Techniques on Clinical Staging of

1196 ADVANcES IN RADIOLOGY Canad. Med. Ass. J.Dec. 21, 1968, vol. 99
12. LOUGHEED, W. M.: Unpublished data.13. LOUGHEED, W. M., ELGIE, R... G. AND BARNETT, H. J.
M: Canad. Med. Ass. J., 95: 1279, 1966.14. MAKI, Y. AND NAKATA, Y.: On the cases with abnormal
vascular network in the cerebral basal region. Paperpresented at the 8th Symposium Neuroradiologicum,Paris, September 25-30, 1967.
15. MINAGI, H. AND NEWTON, T. H.: Radiology, 86: 100,1966.
16. MIsHKIN, M. M.: Radiol. Olin. N. Amer., 5: 395, 1967.17. MULLER, R. et aL: Neurology (Minneap.), 14: 136,
1964.18. MYER, J. S., SHEEHAN, S. AND BAUER, R. B.: A.M.A.
Arch. Neurol., 2: 27, 1960.19. NISHIMOTO, A. AND KATOW, T.: A special type of
cerebral vascular abnormality of the Japanese.Paper presented at the 8th Symposium Neuro-radlologicum, Paris, September 25-30, 1967.
20. NORTH, R. R. et al.: Neurology (Minneap.), 12: 810,1962.
21. POTTER, J. M.: Brain, 82: 367, 1959.22. RIISHEDS, J.: Canad. Med. Aas. J., 97: 151, 1967.23. ROBINSON, R. W. et al.: J. A. M. A. 169: 1149, 1959.24. ROCKETT, J. F. AND JOHNSON, T. H., JR.: Radiology,
90: 46, 1968.25. SCHWARTZ, C. J. AND MITCHELL, J. R. A.: Brit. Med.
.7., 2: 1057, 1961.26. SHELDON, P.: Brit. .7. Radiol., 37: 526, 1964.27. SIEKERT, R. G. AND MILLIKAN, C. H.: Arch. Intern.
Med. (Chicago), 101: 872, 1958.28. SUTTON, D. AND DAVIES, E. R.: Olin. Radiol., 17: 330,
1966.29. WALLACE, S. et al.: Amer. .7. Roentgen., 101: 34, 1967.30. WEIDNER, W., HANAFEE, W. AND MARKHAM, C. H.:
Neurology (Minneap.), 15: 39, 1965.31. YATES, P. 0. AND HUTCHINSON, E. C. Med. Re8. Couno.
Spec. Rep. Ser. (London), 300: 1, 1961.
Influence of Modern Radiological Techniques on ClinicalStaging of Malignant Lymphomas
J. W. DAVIDSON, M.R.C.P.(Glasg.), D.M.R.D.(Eng.)* andE. A. CLARKE, M.B., B.S.,t Toronto
RADIOGRAPHIC procedures now form partof the routine pre-management investiga-
tion of patients suffering from histologicallyproved malignant lymphoma. The importance ofaccurate pre-treatment staging according to thedetected extent of disease, with respect to plan-ning of optimal therapy and accurate prognosis,is generally accepted.14' 15 Current figures forlong-term survival suggest that failures of treat-ment in previous years may have been due tothe presence and progression of occult diseasewhich can now be revealed by modem investi-gative methods.'0 This communication is an ac-count of our experience at The Ontario CancerInstitute in the radiographic investigation of392 patients suffering from malignant lympho-mas. The findings are interpreted in the light ofmore recent pathological concepts.'2 Their in-fluence with respect to clinical staging and thenatural history of malignant lymphomas is dis-cussed.
In the widely adopted system of pre-manage-ment assessment, recommended by an interna-tional committee on the staging of Hodgkin'sdisease,'8 the diaphragm is an important ana-
This paper is based on a presentation to the Royal collegeof Physicians and Surgeons of Canada. Toronto, January18-20,1968.This work was supported in part by Grant 41-15 fromThe Ontario cancer Treatment and Research Foundation.*Senior consultant in Diagnostic Radiology, The OntarioCancer Institute, and Assistant Professor of DiagnosticRadiology, University of Toronto, Toronto, Ontario.tResearch Assistant In Diagnostic Radiology, The OntarioCancer Institute.Reprint requests to: Dr. J. W. Davidson, The PrincessMargaret Hospital, 500 Sherbourne Street, Toronto 5,Ontario.
Clinical stag§
(.. .-.- Chest Radiography. ......Mediastinaljorn.graphy11
----lWhale LungSkeletal Survey
Diaphragm. . Inferior Vena Cavog.gpjjy.- Cisterna Chyli
visualization;:YiriPh§L2P.Y.
( . . Small Bowel studies
.'lntravenous Pyelogram
ExtranodalTV
Fig. 1.-Radiographic investigations in lymphoma.
tomical line of demarcation for lymphomatousinfiltration involving lymphatic structures. Pa-tients in clinical Stages I and II are those inwhom the disease process involves lymph nodeson only one side of the diaphragm, and shoulddisease be detected on the other side as well.they are advanced to Stage III. If structuresoutwith the lympho-reticular system are af-fected, the patient is placed in Stage IV. Similarconcepts are applied to appraisal of lympho-sarcomas and reticulum cell sarcomas. The rele-vant radiographic procedures are illustrated inFig. 1. Lymphography has proved the mostvaluable investigation for detecting occult dis-ease in pelvic and retroperitoneal lymph nodes.By outlining soft tissue abnormalities above thepara-aortic nodes but still below the diaphragm,inferior vena cavography has proved a useful

Canad. Med. Ass. J.Dec. 21, 1968, vol. 99 Advances in Radiology 1197
Fig. 2..Hodgkin's disease. (1) Large iliac nodes withdiffuse contrast pattern and filling defects. (2) Smallgranular nodes. (3) Hyperplastic nodes. (4) Normal nodes.
supplement to lymphographic study. Chestradiography, including tomography of themediastinum and whole lung, will accuratelydelineate disease within the thorax. All of theseinvestigations are commonly used, in the aboveorder, before pre-management staging of anypatient presenting with an apparently localizedlymphoma. However, it is apparent that carefulradiographie study of the small bowel may re-
veal mucosal or submucosal lesions in a numberof patients, indicating extra-nodal disease. Thisis also being more frequently recognized on ex¬cretion urograms and radiographie skeletalsurveys.
Lymphographic Findings and
their SignificanceThe method of performing lymphography and
the appearance of normal lymph nodes are nowwell known.7,8'20 Disordered architecture dueto lymphoma, a reflection of abnormal cellularity,is revealed by displacement and compression ofradiopaque contrast-filled sinusoids within af¬fected lymph nodes. A typical example is il¬lustrated in the lymphadenogram of a youngman who complained of "lumps in the left groin"of two years' duration (Fig. 2). On biopsy of one
of these swellings, an enlarged lymph node in¬filtrated with Hodgkin's granuloma was found.By the more recently introduced classification ofLukes and his colleagues,10'11 in which thenatural history of Hodgkin's disease is related toits pathological picture, the cellularity indicatedthe mixed nodular type of the disease. The mostcommonly recognized radiographie image oflymphomatous infiltration in lymph nodes adja¬cent to the site of biopsy is indicated by thenumber 1 in Fig. 2. Radiopaque ultra-fluidlipiodol gives a fine linear pattern, with smallradiolucent filling defects, in markedly enlargedlymph nodes. Small irregular granular nodes de-picting disease in the left para-aortic chain are
outlined at a higher level (2). The lymphglands in the right para-aortic chain (3) showslight enlargement with an even distribution ofthe contrast material indicating hyperplasia. Thesize and configuration of the glands in the rightiliac region (4) are within normal limits.
Indirect evidence which helps to identify lym¬phomatous infiltration of nodes with less obviousradiographie appearances may be revealed byvisualization of lymphatic trunks and the cis-terna chyli. A male patient, aged 19 years, com¬
plained of a lump on the left side of the neckwhich had been present for three months. Thelymphangiogram (Fig. 3a) shows displacementto the right of the cisterna chyli by an adjacentsoft-tissue mass. On the lymphadenogram alone(Fig. 3b), irregular lymphoid aggregates seen
in the upper para-aortic region are not sufficientevidence for diagnosis of lymphomatous infil¬tration. However, in this instance, visualization
(a) (b)Fig. 3a..Lymphangiogram: cisterna chyli displaced to
the right at level of D-12 L-l. Fig. 3b..Lymphadeno¬gram: irregular lymphoid aggregates in the upper para-aortic region.

1198 Advances in Radiology Canad. Med. Ass. J.Dec. 21, 1968, vol. 99
of both vessels and lymph glands provides use¬
ful complementary evidence of lympho-reticularabnormality in the high subdiaphragmaticregion.Although in the majority of patients there are
few indications for a second biopsy, we nowhave 31 cases in whom histological examinationof lymph nodes from sites opacified by lympho-graphy allows comparison of the radiographiecontrast pattern with the pathology. Such studiesindicate that even distribution of radiopaqueultra-fluid lipiodol throughout the lymph nodes,giving a pattern more granular than normal, is a
reflection of lymphocytic and/or histiocytic pro¬liferation. Filling defects within the contrastpattern (as illustrated in the left iliac region at(1) of Fig. 2) indicate increasing pleomorphismwith areas of fibrous tissue, necrosis and/oraggregates of atypical reticular or neoplasticcells. Most nodes affected by lymphoma are en¬
larged, but normal or small glands showingalteration in pattern may also indicate ab¬normality, particularly in those patients withlymphocyte depletion, now classified as diffusefibrosis, or the reticular type of Hodgkin's dis¬ease. Thus, the radiographie appearances fol¬lowing lymphography in patients with lymphomareflect disordered architecture secondary to al¬tered cellularity.As cellular proliferation occurs in Hodgkin's
disease with lymphocytic and/or histiocyte pre-dominance, in lymphosarcoma, reticulum cellsarcoma, granulomas, infective conditions andnon-specific hyperplasia, these cannot be dif-ferentiated on the basis of alteration in the dis¬tribution of radiopaque contrast material in thesinusoids of the lymph nodes. However, in anypatient in whom the diagnosis of a malignantlymphoma has been made by biopsy, the radio¬logist may accurately detect the presence andextent of disease, and has the advantage ofsurveying a large portion of the lympho-reticularsystem. If lymphographic findings are inter-preted in the light of the histological diagnosis,accurate in vivo appraisal can be made of thedistribution of the types of disease in the areas
opacified by lymphography.4The "Second-Look" Lymphogram13As contrast material persists within the lymph
nodes for up to one year, they may be keptunder surveillance by repeat radiographs at in¬tervals and comparison of the appearances withthe original lymphogram may be made. This isof value in gauging the response to therapy bynoting shriiikage or enlargement of the involvedglands on these follow-up films.
In approximately 10% of patients with lym-
(a) (b)Fig. 4a..Slightly enlarged "hyperplastic" nodes, all
areas. Fig. 4b..Larger nodes with filling defects.
phomas, radiographie appearances are regardedas doubtful. These are reported as suspicious bythe radiologist, but are recorded as negative inthe context of clinical staging. Review by repeatradiographs is undertaken at three-monthly in¬tervals to detect alteration in the contrast pat¬tern which may indicate progressive lymphomarequiring therapy. If most of the contrast ma¬terial has disappeared and active disease is sus¬
pected, repeat lymphogram is indicated. Theopacified para-aortic and pelvic nodes of a
young woman presenting with Hodgkin's diseasein the neck are shown in Fig. 4a. In 1966 thesenodes were considered to be hyperplastic, pos¬sibly due to early diffuse abnormality. Repeatexamination after nine months shows enlarge¬ment of many of these lymph nodes with a
break-up in the contrast pattern (Fig. 4b). Fil¬ling defects in lymph nodes are seen in both thepelvic and para-aortic regions. These findingsindicate progressive Hodgkin's disease, and suchinvestigation may prove a useful addition to thesurveillance of patients with lymphoma.
Results: Lymphography and StagingResults of 412 lymphograms performed on 392
patients are shown in Table I. Examinations innew patients may be classed as initial or pre-management lymphograms and those in patientswho have had previous therapy, as reassessmentlymphograms. Although the latter are of con¬siderable value in the management of recur¬
rences, only the former apply to pre-treatmentstaging. Although the findings are of similarsignificance in patients with lymphosarcomas andreticulum cell sarcomas, emphasis in this pre¬sentation is on Hodgkin's disease, because of thelarger number of examinations performed.

Canad. Med. Ass. J.Dec. 21, 1968, £ol. 99 Advances in Radiology 1199
TABLE I..Results op 412 Lymphograms in Patients with Histo¬logically Proved Lymphomas (March 1968)
Total number %lymphograms Abnormal Normal Suspicious abnormal
Total lymphograms in study: 412.Total patients: 392.Repeat lymphograms: 20.
TABLE III..Hodgkin's Disease: Influence ofLymphogbaphy on New Stage I Patients
Alteretding site stage
. 9
. 0
. 0
. 1
Total. 10 9 3150
Table II depicts the alteration in clinicalstaging of new patients with Hodgkin's diseasefollowing lymphography. In 38% of patients inclinical Stage I, occult lymphomatous infiltra¬tion was found, and the pre-management stageadvanced. Similarly in Stage II patients, ab¬normal lymphograms were present in 43% ofpatients with increase in pre-treatment assess¬ment to Stage III. It should be noted that twoof the abnormal lymphograms in Stage I and onein Stage II gave no advancement in staging, asthe extent of disease on the lymphogram wassimilar to the clinical findings. In those new pa¬tients in whom clinical evidence of lymphadeno¬pathy on both sides of the diaphragm, or extra-nodal disease, was apparent, i.e Stage III or
more, only 20 lymphograms have been per¬formed. These patients are not routinely ex¬
amined, as the clinical evidence already indi¬cates that extensive dissemination has occurred.
TABLE II..Hodgkin's Disease: Influence op Lymphography inStaging op New Patients
Initial Study Lymphograms
Total. 123 63 40 20
*Note: In two Stage I patients and one Stage II patient, abnormallymphography has not advanced staging.
More detailed analysis of the influence oflymphography on Stage I patients with Hodg¬kin's disease is presented in Table III. Of 12patients presenting with disease in the groin, 9were shown to have further involvement of ad¬jacent groups of lymph nodes on the same sideof the diaphragm and the stage was subse¬quently altered from I to II. Of 33 patients pre¬senting with the disease above the diaphragm,24 in the neck and 9 in the axilla, para-aorticlymph node involvement was diagnosed in 9instances raising the pre-management stage toIII. Thus, in Stage I Hodgkin's disease, radio¬graphie diagnosis of clinically occult abnor¬mality in lymph nodes on the opposite side of
the diaphragm has been made in 18% of pa¬tients. Similarly, in 53 patients with clinicalStage II disease (Table IV), in 44 of whom thedisease presented in the neck, 23 were found tohave involvement of nodes on the opposite sideof the diaphragm, requiring an advance to StageIII in 43% of these cases. The higher incidenceof abdominal involvement in patients with moreadvanced disease is again a reflection of the in¬ereased accuracy of pre-management assessmentfollowing lymphography.
TABLE IV..Hodgkin's Disease: Influence ofLymphography on New Clinical Stage II Patients
Accuracy of LymphographyThis may be gauged by comparison of the
histological and radiological diagnosis in thosepatients in whom surgical biopsy was performedat the site of opacified lymph nodes. Table Vshows that in 25 abnormal lymphograms it wasconfirmed that the radiographie appearanceswere due to Hodgkin's disease. Two patients inwhom the lymphographic findings were regard¬ed as suspicious were both found to have Hodg¬kin's disease in the questionable nodes. Onefalse-negative examination came to light. Thusthe lymphographic appearances have proved ex-
TABLE V..Hodgkin's Disease: Accuracy ofLymphography (240 Patients)
Surgical biopsy ofopacified lymph nodes
Lymphographic diagnosis Positive
Abnormal.25Suspicious. 2Normal. 1
Total. 28
Negative

1200 Advances in Radiology Canad. Med. Ass. J.Dec. 21, 1968, vol. 99
Fig. 5..Lymphosarcoma. (1) Enlarged "lace-pattern"nodes. (2) Paravertebral opacified nodes. (3) Deviatedrvc
tremely accurate in the detection of lymphoma¬tous infiltration, and as one might expect, false-negative examinations are evidence of the limi¬tations of the radiographie method in compari¬son with histological examination.
Inferior Vena CavographyAs a supplement to lymphography, inferior
vena cavography may give additional informa¬tion which can alter the clinical stage. In thepresence of radiographically normal or doubtfullymph nodes in the para-aortic regions, espe¬cially in their upper extent, opacification of theinferior vena cava may reveal its displacement orindentation. This finding is useful indirect evi¬dence of adjacent soft-tissue abnormality. Grossdeviation of the inferior vena cava to the right,indicating an extensive adjacent soft tissue mass,is shown in Fig. 5. This patient had presentedwith a lymphosarcoma in the neck two yearspreviously, and had been well during the inter¬
val following local radiotherapy. Diffusely granu¬lar enlarged lymph nodes are seen in the lowerpara-aortic regions (Fig. 5, at 1). At a higherlevel, a paravertebral mass consisting of lymphnodes which are irregularly and partially opaci¬fied is seen (at 2). The opaque inferior vena
cava (at 3) reveals a more extensive soft-tissuemass than that seen on the lymphogram. Sucha finding may be of particular importance inexamining the high subdiaphragmatic region,and in a small number of cases may be the onlyindicator of adenopathy around the porta hepa-tis or celiac axis.
Chest Radiography Plus TomographyIn gauging the extent of disease within the
thorax, tomography is now a routine supplementto plain P.A. and lateral chest radiographs. Fig.6 shows widening of the upper mediastinalshadow in a young woman presenting withHodgkin's disease in the neck. A few doubtfulsmall opacities are demonstrated within the lungfields. Tomographic cut at 11 cm. from the tabletop more clearly delineates the large paratra-cheal nodes (Fig. 7). In addition, gross sub-carinal disease is evident, with pressure on themain bronchi. Several small nodular opacities(arrows) are seen in each lung. As these are
often of low density in Hodgkin's disease,19 theymay best be shown by tomography.
Fig. 6 Fig. 7Fig. 6..Wide mediastinal shadow in Hodgkin's disease.
Fig. 7..11-cm. tomograph subcarinal mass.lung nodules.
The results of 82 such examinations in new
patients with lymphomas are shown in TableVI. In 44 of these examinations, additional dis¬ease was demonstrated which could not be seen
on the plain radiographs. In 15 patients this was
subcarinal, and unilateral involvement of thelung hilum, which may frequently be obscuredby the size of the mediastinal mass, was notedin a further 15 instances. Lung infiltration was
detected in eight patients, in four of whom thiscould not be seen on plain radiographs. In onlysix patients with mediastinal disease, no infor¬mation additional to that on the chest radio-
Canad. Med. Ass. J.Dec. 21, 1968, vol. 99
Advances in Radiology 1201
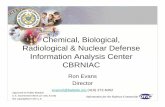
TABLE VI..Mediastinal Tomography in 82 Patients
InitialstudiesReassessment
36 Abnormal. 1319 Normal. 14
6 Plain film negative,tomogram positive. 1
34 Information additional to plainfilm. 10
10 Sub-carinal disease. 53 Parenchymal lung disease.6
10 Hilar node disease. 51 Bone disease. 06 Post-lymphographic opaque
nodes. 03 No additional information.3
graphs was obtained. Thus, the influence oftomography on accurate pre-management stag¬ing is evident.
ExTRA-NODAL DlSEASEThe importance of detecting lymphoma out-
with the lymph nodes is now increasingly ap¬parent because of its role in the latest concept ofstaging.21 Careful examination of the gastro¬intestinal tract may detect visceral disease. Thealtered appearance of the small bowel on an
A.P. radiograph of the abdomen, 45 minutes afterthe ingestion of barium, is shown in Fig. 8.Gross abnormality of contour and calibrethroughout the jejunum and ileum and a largepost-bulbar duodenal ulcer crater are seen. Thesefindings were the result of extensive mural in¬volvement of the duodenum and small bowelwith reticulum cell sarcoma.
Infiltration of the kidneys may be detectedon excretion urography. Richmond et al.,17 in a
series of 696 autopsies in patients with lym¬phoma, found an overall incidence of renal in¬volvement of 33%. This varied from 13% inHodgkin's disease to 63% in lymphosarcoma.Radiographie skeletal surveys may also showextra-nodal disease, namely bone involvement,in about 10% of patients. The spine has beenfound to be the most frequent site of the lytic,osteoblastic or mixed lesions caused by the lym-phomas.Radiographic Procedures and theNatural History of Hodgkin's Disease
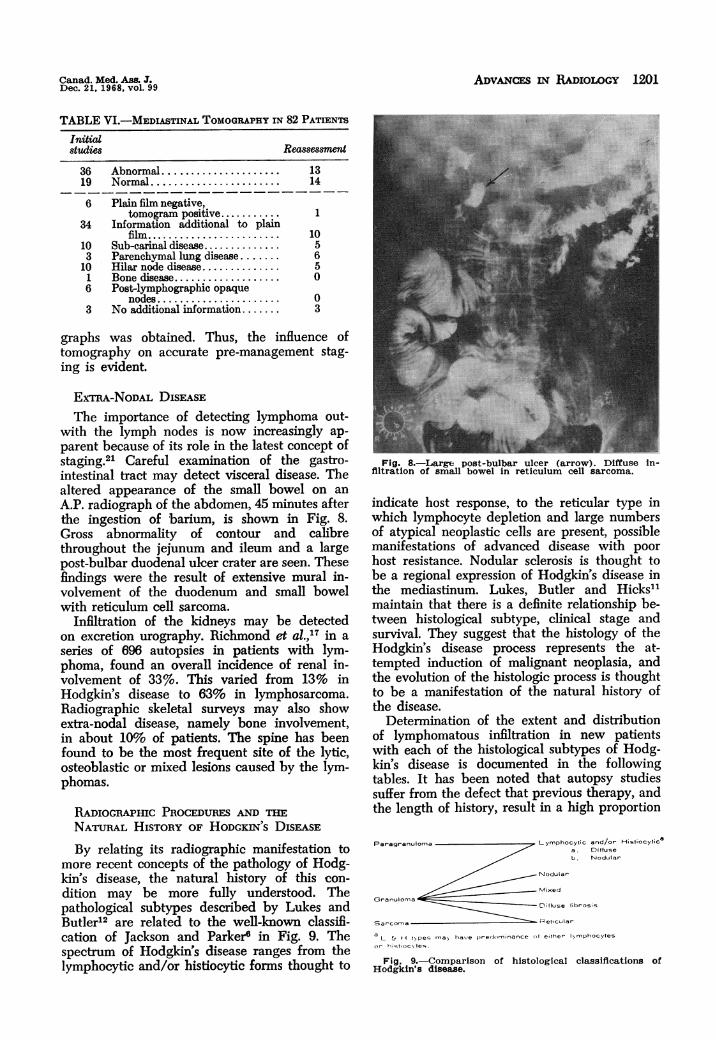
By relating its radiographic manifestation tomore recent concepts of the pathology of Hodg¬kin's disease, the natural history of this con¬dition may be more fully understood. Thepathological subtypes described by Lukes andButler12 are related to the well-known classifi¬cation of Jackson and Parker6 in Fig. 9. Thespectrum of Hodgkin's disease ranges from thelymphocytic and/or histiocytic forms thought to
Fig. 8..Large post-bulbar ulcer (arrow). Diffuse in¬filtration of small bowel in reticulum cell sarcoma.
indicate host response, to the reticular type inwhich lymphocyte depletion and large numbersof atypical neoplastic cells are present, possiblemanifestations of advanced disease with poorhost resistance. Nodular sclerosis is thought tobe a regional expression of Hodgkin's disease inthe mediastinum. Lukes, Butler and Hicks11maintain that there is a definite relationship be¬tween histological subtype, clinical stage andsurvival. They suggest that the histology of theHodgkin's disease process represents the at¬
tempted induction of malignant neoplasia, andthe evolution of the histologic process is thoughtto be a manifestation of the natural history ofthe disease.
Determination of the extent and distributionof lymphomatous infiltration in new patientswith each of the histological subtypes of Hodg¬kin's disease is documented in the followingtables. It has been noted that autopsy studiessuffer from the defect that previous therapy, andthe length of history, result in a high proportion
Paragranuloma Lymphocytic and/or Histiocytica. Diffuseb. Nodular
Granuloma
Fig. 9..Comparison of histological classiflcations ofHodgkin's disease.

1202 Advances in Radiology Canad. Med. Ass. J.Dec. 21, 1968, vol. 99
TABLE VII..Hodgkin's Disease: Lymphocytic andHistocytic Type. Distribution of Abnormal Lymph
Nodes
18
TABLE IX..Hodgkin's Disease, Mixed Type:Distribution of Abnormal Lymph Nodes
Number of MediastinalPresenting site patientsLow neck. 20Peripheral. 13Mediastinum. 1Systemic. 1
Total. 36
13510
19
Abdominaldisease
15
of generally distributed lymphocyte-depletedforms of the disease.3 The radiographic pro¬cedures have the advantage of in vivo visualiza¬tion of a large portion of the lympho-reticularsystem. The distribution and type of disease maybe estimated in new patients, as well as in thosein whom a breakdown follows previous therapy.Our findings in 32 new patients with the lym¬
phocytic and histiocytic form of Hodgkin's dis¬ease are shown in Table VII. Twenty clinicalpresentations were in sites classified as peri¬pheral, namely groin, axilla or high neck. Al¬though only two of these patients had involve¬ment of the mediastinum, 10 were found bylymphography to have abdominal disease. Simi¬larly, of 11 patients whose disease presented inthe low neck, 7 were found to have lymphoma¬tous infiltration in the para-aortic nodes. Thus,disease in the neck or axilla with concomitantoccult lymphoma below diaphragm was a fre¬quent occurrence.
In patients with Hodgkin's disease of nodularsclerosing type (Table VIII), in contrast to thelymphocytic and histiocytic forms, a much higherincidence of mediastinal involvement was re¬vealed. Of 22 patients with disease in the neck,enlarged mediastinal nodes were demonstratedin 18. Only 3 patients out of the 29 had diseasein the peripheral gland groups, and all werefound to have mediastinal disease. No patientin this category presented with disease in thegroin. Therefore, in nodular sclerosis, 25 of 29new patients had detectable mediastinal disease,and 14 of these were found to have involvementof abdominal lymph nodes.In Hodgkin's disease of mixed type (Table
IX), 15 of 36 new patients were found to have
TABLE VIII..Hodgkin's Disease, Nodular Scleros¬ing Type: Distribution of Abnormal Lymph Nodes at
Time of Initial Assessment
Number of MediastinalPresenting site patients disease
Low neck. 22Peripheral. 3Mediastinum. 2Systemic. 2
Total. 29
Abdominal
18322
25 14
abdominal disease and 19 showed enlargedmediastinal nodes. Analysis of the presentingand involved sites gave numbers which appearto fall somewhere between those of the lympho¬cytic and histiocytic, and the nodular sclerosingforms of Hodgkin's disease.The overall picture of the patterns of dis¬
tribution in each pathological subtype of Hodg¬kin's disease is shown in Table X. Of 103 pa¬tients, only 6 were diagnosed as presenting withone of the lymphocyte depletion forms of thedisease and 5 of those were found to have ab¬dominal node involvement. This small numbermay support the pathological concept that lym¬phocyte depletion occurs in advanced andgeneralized disease, a finding more common atautopsy than on presentation. It can be seenthat a peripheral distribution and involvementof abdominal and cervical nodes was the com¬mon finding in the lymphocytic and histiocyticforms of Hodgkin's disease. In nodular sclerosis,a predilection for a central distribution in themediastinum, neck and abdomen was evident.
Discussion
"Inguinal nodes, axillary nodes, and cervicalnodes can be felt. Nobody can feel iliac nodesor retroperitoneal nodes, the so-called aortic-abdominal nodes, through the aMominal wall,and evaluate them with any degree of ac¬
curacy."5 The advantages of lymphography andtomography are the visualization of the lympha¬tic structures in the retroperitoneal regions andmediastinum. It should be emphasized that lym¬phographic findings have been interpreted withfull knowledge of the clinical presentation andhistological diagnosis from biopsy. The identifi¬cation on radiographs of extensive lymphomatousinfiltration by demonstration of enlarged lymphnodes with a foamy pattern is relatively simple.On the other hand, the significance of abnormali¬ties of distribution of contrast medium in smal¬ler lymph glands is fraught with difficulty.Demonstration of adequate filling on the lym¬phangiogram is a prerequisite to accurate inter¬pretation, as is knowledge of factors affectinglymph node size and morphology such as pre¬vious radiotherapy, chemotherapy including

Canad. Med. Ass. J.Dec. 21. 1968, vol. 99 Advances in Radiology 1203
Total. 15 13 10 4256320 28 11 49 55 74 0
Presenting site in bold figures.Sites of disease after pre-management assessment (including clinical examination and investigation).
103
steroid administration, regional sepsis, skinchanges, and the age and sex of the patient.
In this series, the influence of lymphographyon pre-management staging of patients withHodgkin's disease is in close agreement with thefindings of Lee.9 Of 28 of his patients withHodgkin's disease in the neck in clinical StageI, four were shown to have occult lymphomatousinvolvement of the abdominal nodes. Thirty-oneper cent of his patients in Stage Ila and 88%of those in Stage Hb had abnormal lympho¬grams from the lower extremities. In this seriesof 24 Stage I patients with disease presenting inthe neck, five were shown to have occult ab¬dominal disease, and of the total number of 33patients in Stage I presenting with disease abovethe diaphragm with cervical or axillary adeno-pathy, nine were found to have radiographic evi¬dence of para-aortic node involvement. Includingthose with disease presenting in the groin, theoverall increase in accuracy of assessment follow¬ing lymphography was 38%. Similarly, the influ¬ence of lymphography in patients in clinical StageII has been to advance the staging in 46% ofcases. It is of interest that the accuracy of themethod for the detection of lymphoma is similarto that of Abrams, Takahashi and Adams1 whofound an overall diagnostic accuracy of 81% inlymphographic studies performed on 206 patients.In lymphosarcoma and reticulum cell sarcoma,the demonstration of diffuse abnormalitythroughout the lympho-reticular system asso¬
ciated with a clinically localized presentation,has proved of similar value in pre-managementassessment.
Experience at The Ontario Cancer Instituteis at variance with that of Brickner, Boyer andPerry,2 who found only 3 positive lymphogra¬phic studies in 50 cases of Stages I and IlaHodgkin's disease. From their experience in re-
viewing 71 lymphograms, these authors recog¬nized that although a great number of abnor¬malities can be demonstrated with lymphangio-graphy, these are not necessarily significant inthe evaluation of the patient at hand. In thepresent study, demonstration of clinically occultdisease in a highly significant percentage ofboth Stage I and Stage II patients with Hodg¬kin's disease has proved of particular value bothin prognosis and planning of therapy.
Radiographic studies have revealed patternsof distribution of the lymphomatous processthroughout lympho-reticular structures whichmay add considerably to our knowledge of thenatural history of Hodgkin's disease in particu¬lar and of the other lymphomas as well. Thesefindings agree with the concept that nodularsclerosis appears to be a regional expression ofHodgkin's disease in the mediastinum. It is tobe noted that a significant difference in distri¬bution between the lymphocytic and histiocyticand the nodular sclerosing forms of Hodgkin'sdisease has been found in new patients. It ispossible that progression from these two basicvarieties of disease occurs to produce, with in¬creasing pleomorphism, the mixed type with a
pattern of distribution intermediate between theother two. With further progression, and de¬creasing host resistance, the eventual terminalstage of a diffusely distributed, lymphocyte-de-pleted, fibrous or reticular Hodgkin's disease,the common autopsy finding, may ensue.
Evaluation of the lymphographic pattern inindividual nodes in terms of the underlyinghistological abnormality confirms that variationsin the types of Hodgkin's disease may be foundin different regions of the body at any one time.Radiographic demonstration of homogeneousarchitecture in one lymph node or group ofglands, and filling defects in an adjacent node or

1204 A.v.cEs i. RADIOLOGY Canad. Mei. Ass. 3.vol. 99
group, suggests that lymphocytic and/or histio-cytic proliferative fonns and mixed disease mayco-exist. In the lymphadenogram illustrated (Fig.2), mixed nodular Hodgkin's disease was foundat biopsy in external iliac nodes which showedenlargement with filling defects in fairly evenlydistributed contrast medium. At higher levels,filling defects were not seen and the evenlydistributed coarse granular pattern was similarto that found in those forms of the diseaseshowing lymphocyte proliferation. It is possiblethat the development of the mixed pattern is amanifestation of the length of exposure and hostresponse to the etiological agent, and that adja-cent lymph nodes are displaying earlier involve-ment by a disease process spreading by con-tiguity. An alternative explanation could beregional variability in the response of peri-pheral and centrally placed lymph nodes to theattempted induction and progression of the neo-plastic process. Similar considerations may applyto nodular sclerosing Hodgkin's disease, in whichless florid radiographic changes in the upperpara-aortic nodes may be evident in the pres-ence of gross mediastinal abnormality. The im-plications of these combined pathological andradiological studies of patients with lymphomasare apparent in furthering the understanding oftheir natural history which still remains un-known. The prognostic significance of such find-ings, and their influence on future concepts instaging and in evaluating the effects of currenttherapeutic endeavour, must await further ex-perience.
Summary Radiographic findings in 392 patientswith malignant lymphomas confirm
the value of bilateral lower extremity lymphographyand mediastinal tomography in delineating clinicallyoccult lymphomatous infiltration. Of 123 new pa-tients with Hodgkin's disease, 21 of 50 in clinicalStage I and 24 of 53 in clinical Stage II were foundto have abnormal lymphograms. Of clinical Stage Ipatients, 38% were advanced to Stage II or IIIfollowing lymphography, of whom 18% presentingin the neck or axilla were shown to have clinicallysilent disease in the peri-aortic nodes. Similarly, in43% of patients in clinical Stage II, occult abnor-mality was demonstrated within the lympho-reticularsystem.
Pre-treatment radiographic findings, in each ofthe histological subtypes of Hodgkin's disease de-scribed by Lukes, provide further evidence thatnodular sclerosis is a regional manifestation of dis-ease of mediastinal origin. In new patients, a highlysignificant difference in distribution of involvementbetween the nodular sclerosing and the lymphocyticand histiocytic types of Hodgkin's disease suggeststhat two basic disease processes exist, and that pro-gression occurs from these to the mixed and lym-phocyte-depleted forms.
Re'8ume' Les constatations radiographiques chez392 malades souffrant de lyrnphome
maim confirment Ia valeur des lymphographies bi-Iat6rales des membres inf6rieurs et de la tomogra-phie m6diastinale pour pr6ciser cliniquement i'm-filtration lymphomateuse occulte. Sur 123 nouveauxmalades atteints de maladie de Hodgkin, 21 sur 50du stade clinique I et 24 sur 53 du stade II avajentdes lymphogrammes anormaux. Apr.s lymphogra-phie, 38% des malades qui 6taient auparavant con-sid6r6s comme appartenant au stade clinique Ifurent consid6r6s comme appartenant au stade II ouIII et 18% qui avaient une atteinte au cou ou auniveau des aisselles, pr6sentaient des signes silen-cieux de Ia maladie au niveau des ganglions p6ri-nortiques. De m.me, chez 43% des malades qui en6taient au stade clinique II, on a d6montr6 des ano-malies latentes dans le syst.me lympho-r6ticulaire.
Les constatations radiographiques pr6-th6rapeu-tiques, dans chacun des sous-types histologiques deIa maladie de Hodgkin d6crits par Lukes, ont fournide nouvelles preuves que Ia scl6rose ganglionnaireest une manifestation r6gionale ayant une originemddiastinale. Une diff6rence tr.s marqu6e dans lar6partition des r6gions atteintes, chez de nouveauxmalades, entre la scl6rose nodulaire et les typeslymphocytaire et histiocytaire de la maladie deHodgkin permettent de croire que deux processuspathologiques fondamentaux existent et que leur6volution s'effectue . partir des formes mixtes et desformes lymphocytop6niques.
The authors wish to thank Dr. Robert J. Lukes andJ. B. Lippincott Co. for the use of Fig. 9. The contribu-tions of Miss Ruth MacLean, who typed this manuscript,and of Mrs. Gaettens, Department of Photography, Prin-cess Margaret Hospital, are gratefully acknowledged.
REFERENCES
1. ABRAMS, H. L., TAKAHASHI, M. AND ADAMS, D. F.:Cancer C1.emothsr. Rep., 52: 157, 1968.
2. BRIcKNER, T. J., JR., BOYER, C. W., JR. AND PERRY,R. H.: Radiology, 90: 52 1968.
3. BROWN, T. C. B.: Personal communication.4. DAvIDsoN, J. W. AND CLARKE, E. A.: The significance
of the lymphographic appearances in Hodgkin'sdisease. In: Proceedings of the 2nd InternationalCongress on Lymphology. Miami, March 15-20.1968, edited by M. I. Viamonte, Jr. In press.
5. FIscHER, H. W.: In discussion. Cancer Chernother.Rep., 52: 202, 1968.
6. JACKSON, H., JR. AND PARKER, F., JR.: New Eng. J.Med., 231: 35, 1944.
7. KINMONTH, J. B.: Clin. Sci., 11: 13, 1952.8. KINMONTH, J. B., TAYLOR, G. W. AND HARPER, R. K.:
Brit. Med. J., 1: 940. 1955.9. LEE, B. J.: Cancer Chemother. Rep., 52: 205, 1968.
10. LUKES, R. J.: Amer. J. Roentgen., 90: 944, 1963.11. LUKES, R. J., BUTLER, J. J. AND HIcKS, B. B.: Cancer,
19: 317, 1966.12. LUKES. R. J. AND BUTLER, J. J.: Cancer Res., 26: 1063,
1966.13. PEREZ-TAMAYO, R., THORNBURY, J. R. AND ATKINSON,
R. J.: Amer. J. Roentgen., 90: 1078, 1963.14. PETERS, M. V.: Ibi4., 63: 299, 1950.15. PETERS, M. V., ALISON, R. B. AND BUSH, R. S.:
Cancer, 19: 308, 1966.16. PETERS, M. V. et al.: The value of locating occult dis-
ease in the treatment of Hodgkin's disease. In:Progress in lymphology: Proceedings of the Inter-national Symposium on Lymphology, Zurich, 1966,edited by A. Riittimann, Georg Thieme Verlag KG,Stuttgart, 1966, p. 119.
17. RICHMOND, J. et al.: Amer. ,T. Med., 32: 184. 1962.18. ROSENBERG, S. A.: Cancer Res., 26: 1310, 1966.19. STRICKLAND, B.: Brit. ,T. Radiol., 40: 930, 1967.20. WALLACE, S. et al.: Radiology, 76: 179, 1961.21. PETERS, M. V.: A clinical classification of the malig-
nant lymphomas related to the course of the dis-ease. In: Proceedings of the 2nd InternationalCongress on Lymphology, Miami, March 15-20,1968. edited by M. I. Viamonte, Jr. In press.