Influence of food on oestriol blood levels
5
Mutt&as, 6 (1984) 71-75 Elsevier 71 MAT 00309 Preliminary Report Influence of food on oestriol blood levels D. Englund, G. Heimer and E.D.B. Johansson Department of Obstetrics and Gvnaecolo~, Umversity Hospital, -Uppsala (Received 17 January 1984; accepted after revision 16 March 1984) (Key words: Oestriol, Blood levels of, Route of administration, Influence of food intake) The good clinical effect produced by oestriol administered in a single daily dose has been demonstrated by several investigators [3,5,7,9,11]. However, the findings are confusing in a way, since oestriol is known to be/short acting [l]. Oral oestriol raises the plasma oestriol concentration for about 4 h only [2,10] and it is rapidly metabolised to oestriol conjugates [lo]. Indeed, oestriol’s weak oestrogenicity has been attributed to its transient effect. To achieve a full oestrogenic effect, a prolonged increase in plasma oestriol con- centration is essential, since the nuclear binding time of oestriol is short and a minimum of 6 h is necessary for full oestrogen receptor stimulation [l]. Despite the rapid metabolism of oestriol, Rauramo et al. [8] have reported high blood levels of oestriol as long as 12 h after a single oral dose. One possible reason for this could be deconjugation of oestriol ‘and enterohepatic recirculation, bringing about a prolonged elevation of the plasma oestriol level. To test this hypothesis, oestriol was given orally in the morning after overnight fasting. No food was allowed until 4 h after the ingestion of oestriol, whereupon its ingestion could be expected to induce gall bladder activity and produce oestriol conjugates available for deconjugation and enterohepatic recirculation. The significance of food ingestion was also assessed by intravaginal oestriol administration, In one trial, oestriol was given in the morning followed by a meal 4 h later, and in another oestriol was inserted vaginally in the evening and no meal was given until the following morning. Three healthy, menopausal women who were not cholecystectomized volunteered to participate in the study. A 10 mg dose of oestriol (Leo AB, Sweden) was given once orally and 1 mg of oestriol (Leo AB, Sweden) was administered intravaginally once a day for a 16-day treatment period. In all three cases, venous blood samples were drawn off at frequent intervals via an indwelling catheter over a 24-h period. Plasma oestriol levels were determined by a specific radioimmunoassay technique ]21. Correspondence fo: Dr. D. Englund, Department of Obstetrics and Gynaecology, University Hospital, Uppsala, Sweden. 0378-5122/84/$03.00 0 1984 Elsevier Science Publishers B.V.
Transcript of Influence of food on oestriol blood levels

Mutt&as, 6 (1984) 71-75 Elsevier
71
MAT 00309
Preliminary Report
Influence of food on oestriol blood levels
D. Englund, G. Heimer and E.D.B. Johansson Department of Obstetrics and Gvnaecolo~, Umversity Hospital, -Uppsala
(Received 17 January 1984; accepted after revision 16 March 1984)
(Key words: Oestriol, Blood levels of, Route of administration, Influence of food intake)
The good clinical effect produced by oestriol administered in a single daily dose has been demonstrated by several investigators [3,5,7,9,11]. However, the findings are confusing in a way, since oestriol is known to be/short acting [l]. Oral oestriol raises the plasma oestriol concentration for about 4 h only [2,10] and it is rapidly metabolised to oestriol conjugates [lo].
Indeed, oestriol’s weak oestrogenicity has been attributed to its transient effect. To achieve a full oestrogenic effect, a prolonged increase in plasma oestriol con- centration is essential, since the nuclear binding time of oestriol is short and a minimum of 6 h is necessary for full oestrogen receptor stimulation [l].
Despite the rapid metabolism of oestriol, Rauramo et al. [8] have reported high blood levels of oestriol as long as 12 h after a single oral dose. One possible reason for this could be deconjugation of oestriol ‘and enterohepatic recirculation, bringing about a prolonged elevation of the plasma oestriol level.
To test this hypothesis, oestriol was given orally in the morning after overnight fasting. No food was allowed until 4 h after the ingestion of oestriol, whereupon its ingestion could be expected to induce gall bladder activity and produce oestriol conjugates available for deconjugation and enterohepatic recirculation.
The significance of food ingestion was also assessed by intravaginal oestriol administration, In one trial, oestriol was given in the morning followed by a meal 4 h later, and in another oestriol was inserted vaginally in the evening and no meal was given until the following morning.
Three healthy, menopausal women who were not cholecystectomized volunteered to participate in the study. A 10 mg dose of oestriol (Leo AB, Sweden) was given once orally and 1 mg of oestriol (Leo AB, Sweden) was administered intravaginally once a day for a 16-day treatment period. In all three cases, venous blood samples were drawn off at frequent intervals via an indwelling catheter over a 24-h period. Plasma oestriol levels were determined by a specific radioimmunoassay technique ]21.
Correspondence fo: Dr. D. Englund, Department of Obstetrics and Gynaecology, University Hospital, Uppsala, Sweden.
0378-5122/84/$03.00 0 1984 Elsevier Science Publishers B.V.

12
The plasma levels of oestriol achieved after oral administration of 10 mg of oestriol and vaginal administration of 1 mg of oestriol, in the morning and evening respectively are presented in Figs. l-3. Fig. 1 shows an initial but short-lived rise in plasma oestriol concentration after the oral administration of oestriol with a return to almost the pretreatment level within 4 h.
Fig. 1 also illustrates a second rise in plasma oestriol immediately after a meal. The second peak is followed by slowly decreasing plasma oestriol levels.
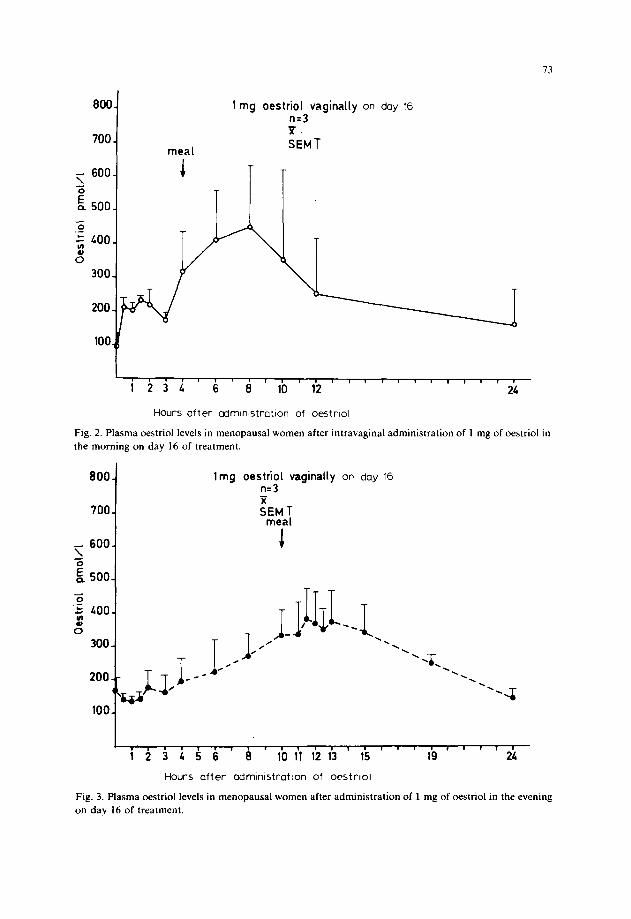
The effect of vaginal administration of 1 mg of oestriol in the morning is illustrated in Fig. 2. The initial increase in plasma oestriol was minimal as compared with that following oral administration, but a meal again induced a second rise in plasma oestriol.
Fig. 3 illustrates the quite different plasma oestriol pattern seen after administra- tion of 1 mg of oestriol in the evening. There was no initial peak, but slow increasing plasma oestriol levels during the overnight fasting period and a further, albeit minimal, increase after the morning meal were observed.
The results achieved in this study strengthen the hypothesis that enterohepatic recirculation of oestriol might have a significant bearing on the plasma levels of oestriol and hence its oestrogenicity. The generally accepted view of oestriol as a weak hormone is therefore open to further investigation.
In the case of the oral route, the amount of oestriol administered is possibly of
800. I
700. I I
600. i
meal
3
10 mg nqe;triol orally
I SEM T
Hours after admtnlstration of oestrlol
Fig. 1. Plasma oestriol levels in menopausal women after oral administration of 10 mg of oestriol.
73
800
700 meal
1 mg oestriol vaginally on day 16 n=3 I. SEMT
I,,,,,,,,,,,,,,,,,,,,,,,, 1 2 3 4 6 8 10 12 24
Hours after cdmlnlstratlon of oestrlol
Fig. 2. Plasma oestriol levels in menopausal women after intravaginal administration of 1 mg of oestriol in the morning on day 16 of treatment.
800 lmg oestriol vaginaily on day 16 n-3
< 600.
‘0 & 500-
.2 ; 400.
cs 300-
200.- ‘< I-
100. rrr
I,,,,,,,,.,,,,,,,,,,,,,,,, 123456 8 10 11 12 13 15 19 24
Hours after admInIstratIon of oestrlol
Fig. 3. Plasma oestriol levels in menopausal women after administration of 1 mg of oestriol in the evening on day 16 of treatment.
74
significant importance, since at high dosage the enterohepatic recirculation produces a more pronounced second peak than at low dosage.
The phenomenon of enterohepatic recirculation enhances oestriol’s potency, since the receptor binding time is prolonged and its full oestrogenic effect can be induced.
This study confirms earlier findings indicating that the absorption of oestriol is more effective by the vaginal than the oral route [lo], the difference being main- tained during long-term treatment and the induction of mature vaginal epithelium. A difference was also revealed between the effect of daytime and evening insertion of pessaries. Insertion is possibly more usual in the evening, but earlier studies have reported only daytime results [4,6,10].
As shown in Figs. 2 and 3, daytime vaginal insertion produces an earlier oestriol peak than evening insertion. The difference may be ascribable to faster metabolism resulting from the intake of food and the induction of enterohepatic recirculation.
Vaginal insertion of pessaries in the evening can therefore result in greater oestrogenicity due to a more prolonged increase in the plasma oestriol level, which may possibly result from slower metabolism during the long overnight fast.
Conclusions
The route of administration and eating habits seem to be significant as regards plasma oestriol levels during oestriol treatment, since enterohepatic recirculation may possibly exert a vital influence. It would therefore seem that, inter alia, the spacing of meals and probably also the fat content of the food ingested should be investigated more extensively, since the results reported here are based on a very small series.
References
1 Clark JH, Peck EJ, Anderson JN. Estrogen receptor binding: relationship of estrogen induced responses. J Toxic01 Environ Health 1976; 1: 561.
2 Enghmd DE, Elansson KB, Johansson EDB. Bioavailability of oestriol. Acta Endocrinol 1982; 99: 136-140.
3 Haskins AL, Moszkowshi EF, Whitelock VP. The estrogenic potential of estriol. Am J Obstet Gynecol 1968; 1: 665.
4 Haspels AA, Luisi M, Kocovic PM. Endocrinological and clinical investigations in post-menopausal women following administration of vaginal cream containing oestriol. Maturitas 1981; 3: 321-327.
5 Heuser HP, Staemmler HJ. Histological investigations into the effect of oestriol succinate on the corpus uteri in postmenopausal women. Arzneim-Forsch Drug Res 1973; 23: 558-562.
6 Keller PI. Oestrogens, gonadotropins and prolactin after intravaginal administration of oestriol in post-menopausal women. Maturitas 1980; 3: 47-53.
7 Myhre E. Endometrial responses to different estrogens. In: Lauritzen C, Van Keep PA, eds. Estrogen therapy. The benefits and risks. Frontiers of Hormone Research 5. Basel: S. Karger, 1978; 126-144.
8 Rauramo L, Punnonen R, Kaihola HL, Gronroos M. Serum oestriol, oestrone and oestradiol concentrations during oral oestriol succinate treatment in ovariectomized women. Maturitas 1978; 1: 71-78.
9 Schiff I, Wentworth B, Koos B, Ryan KJ, Tulchinsky D. Effect of oestriol administration on the hypogonadal women. Fertil Steril 1978; 30: 278-282.
10 Schiff I, Tulchinsky D, Ryan KJ, Kadner S, Levitz M. Plasma estriol and its conjugates following oral and vaginal administration of estriol to postmenopausal women: correlations with gonadotropin levels. Am J Obstet Gynecol 1980; 138: 1137-1141.
11 Tzingounis V, Aksu MF, Greenblatt RB. Oestriol in the management of the menopause. J Am Med Assoc 1978; 239: 1638-1641.